
ankylosing spondylitis
189
THE UTILITY OF RHUS TOX IN “ANKYLOSING SPONDYLITIS” By DR. MAMATA GIDNAVAR Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore In partial fulfillment of the requirement for the award of the degree of DOCTOR OF MEDICINE IN HOMOEOPATHY (HOMOEOPATHIC MATERIA MEDICA) Under the guidance of Dr. S. S. DIVATE M.D. (HOM) PROFESSOR AND GUIDE DEPARTMENT OF HOMOEOPATHIC MATERIA MEDICA BHARATESH HOMOEOPATHIC MEDICAL COLLEGE & HOSPITAL, BELGAUM – 590016 2009
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ankylosing spondylitis

THE UTILITY OF RHUS TOX IN
“ANKYLOSING SPONDYLITIS”
By
DR. MAMATA GIDNAVAR
Dissertation
Submitted to the
Rajiv Gandhi University of Health Sciences,
Karnataka, Bangalore
In partial fulfillment of the requirement for the award of the degree of
DOCTOR OF MEDICINE
IN HOMOEOPATHY
(HOMOEOPATHIC MATERIA MEDICA)
Under the guidance of Dr. S. S. DIVATE M.D. (HOM)
PROFESSOR AND GUIDE
DEPARTMENT OF HOMOEOPATHIC MATERIA MEDICA
BHARATESH HOMOEOPATHIC MEDICAL COLLEGE & HOSPITAL, BELGAUM – 590016
2009

DECLARATION BY THE CANDIDATE
I here by declare that this dissertation / thesis entitled THE
UTILITY OF RHUS TOX IN “AKYLOSING SPONDYLITIS " is a
bonafide and genuine research work carried out by me under the guidance
of Dr. S. S. DIVATE M.D (HOM), Professor and Guide, Department of
Homoeopathic Materia Medica, Bharatesh Homoeopathic Medical
College & Hospital, Belgaum.
Date: DR. MAMATA GIDNAVAR
Place: Belgaum

CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled THE UTILITY OF
RHUS TOX IN “AKYLOSING SPONDYLITIS " is a bonafide research
work done by DR. MAMATA GIDNAVAR in partial fulfillment of the
requirement for the degree of DOCTOR OF MEDICINE
(HOMOEOPATHY) in Homoeopathic Materia Medica.
Date:
Place: Belgaum
Dr. S. M. DIVATE M.D. (HOM) Professor and Guide,
Department of Materia Medica,
Bharatesh Homoeopathic
Medical College & Hospital,
Belgaum- 590016.

ENDORCEMENT BY THE HOD, PRINCIPAL/HEAD OF
THE INSTITUTION
This is to certify that the dissertation entitled THE UTILITY OF
RHUS TOX IN “AKYLOSING SPONDYLITIS " is a bonafide research
work done by DR. MAMATA GIDNAVAR under the guidance of
Dr. S. S. DIVATE M.D. (HOM) Professor and Guide, Department of Materia
Medica, Bharatesh Homoeopathic Medical College and Hospital
Belgaum.
Dr. S. M. ANGADI M.D. (HOM.) DR. S. B. KONKANI M.D. (HOM.)
Professor, Guide, HOD of Principal
Department of Materia Medica Bharatesh Homoeopathic
Bharatesh Homoeopathic Medical College and Hospital
Medical College and Hospital Belgaum- 590016
Belgaum-590016
Date: Date:
Place: Belgaum Place: Belgaum

COPYRIGHT
Declaration By The Candidate
I hereby declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall have the rights to preserve, use and disseminate
this dissertation in print or electronic format for academic / research
purpose.
Date: DR. MAMATA GIDNAVAR
Place:
© Rajiv Gandhi University of Health Sciences, Karnataka.

ACKNOWLEDGEMENT
An endeavour of this work is the result of contributions from several quarters.
First and foremost, I am thankful to God for bestowing upon me patience and
fortitude to complete this work. A journey is easier when you travel together.
Interdependence is certainly more valuable than dependence. This dissertation is a
result of hard work during which I have collaborated with many people for which I
have great regards and wish to extend my warmest thanks to all those who have
helped me in this endeavour.
I wish to express my heartfelt gratitude to reverend teacher and Guide
Dr.S.S.Divate,M.D.(Hom), Professor, Dept of Homoeopathic Materia Medica, Bharatesh
Homoeopathic Medical College & Hospital, Belgaum under whose supervision this
work of dissertation has been accomplished. It was only due to his patient guidance,
constant encouragement, inspiration and meticulous attention that I have been able to
complete this study.
I owe a great debt of gratitude to Dr. Shrikant Konkani,M.D.(Hom) Principal,
Bharatesh Homoeopathic Medical College & Hospital, Belgaum who is a pallor of
ingenious knowledge and wisdom in himself.
I express my sincere thanks to Dr, S. M. Angdi, M.D.(Hom), H.O.D. of
Homoeopathic Materia Medica whose invaluable help, stimulating suggestions and
encouragement helped me to go ahead with my thesis. He has always been available
whenever I needed his advise has been valuable during the preparation of this thesis.
With a deep sense of reverence, I extend my heartfelt obligations to our
beloved Dr. Raveendra Nadhan, M.D. (Hom), Bharatesh Homoepathic Medical College,
Hospital and Post Graduate Institute, Belgaum for his unflinching support and
constant encouragement during the course.
I owe my sincere thanks and gratitude to Dr. D.H. Ajgaonkar,M.D.(Hom), P.G.
co-ordinator, of this institution for their valuable timely guidance and suggestions
when ever and what ever needed.

I thank Dr. P.A. Choudhary,M.D.(Hom), Dept of Repertory,
Dr.Ramdas,M.D.(Hom), Department Organon of Medicine of this institution.
I wish to express my warm and sincere thanks to the staff of Department of
Materia Medica, Dr. C.J. Desai, M.D(Hom), Dr. D.S. Varoor, M.D(Hom),
Dr.Jairaj,M.D(Hom), Dr. Anand, M.D(Hom) and Dr.Lingaraj, M.D(Hom) for their support
and numerous fruitful discussions.
My special appreciation goes to my esteemed teacher Dr. Shahala
Nadaf,M.D(Hom) who has been my mentor, throughout the period of my study.
I express my gratitude towards the Management of Bharatesh
Homoeopathic Medical College & Hospital, Belgaum, for providing seat in post
graduate course in homoeopathy and freedom granted to me in availing all the
institutional facilities to carry out the study.
The most overwhelming enthusiasm, good will, love and affection have
generously come from Chairman, Institute, Teaching and Non-teaching staff, Medical
officers and Hospital staff for which I shall remain always indebted to them.
My deepest gratitude goes to my parents, husband, children, brothers,
teachers and friends for their unflagging love and support throughout this period.
Several colleagues have added to the luster of this dissertation, so it suffices
here to note my gratitude to Dr. Sudharshan Jinagond , Dr. Yogesh, Dr. Abhijeet, Dr.
Nandkumar, Dr. Mahantesh, Dr.Renuka, Dr. Varsha, Dr. Jaiprakash and Dr. Shivaji..
I express my sincere thanks to Mr. Umesh S.P. UniSys IT Solutions, and Sai
Xerox & DTP Centre, Belgaum for helping in completing the manuscript of this
dissertation.
I apologize, if I fail to mention those names that have equal efforts in this
work either directly or indirectly, I remain grateful to them in this regard.
I also thank the patients for their kind cooperation.
Dr. Mamata Gidnavar

LIST OF ABBREVIATIONS USED
AMA American Medical Association
AP Anteroposterior
Ars. alb Arsenicum Album
AS Ankylosing Spondylitis
Bell Belladonna
Br. Asthma Bronchial Asthma
Ca Carcinoma
CRP C- Reactive Protein
CT Computed Tomography
DISH Diffuse Idiopathic Skeletal Hyperostosis
DM Diabetes Mellitus
DRE Diagnosis-related estimates
EA Enteropathic Arthritis
EMG Electromyography
ESR Erythrocyte Sedimentation Rate
F Female
GI GastroIntestinal
GU Genitourinary
H/W House wife
HLA Human Leucocyte Antigen
HNP Herniated nucleus pulposus
HTN Hypertension
IBS Irritable Bowel Syndrome
IgA Immunoglobulin A
IPD Indoor patient department
JCA Juvenile Chronic Arthritis
Kali Mur Kali Muraticum
Kali Sulph Kali Sulphuricum
Lach Lachesis
Led. Ledum Pal
LS Lumbar spine
Lyco Lycopodium

M Male
MRI Magnetic resonance Imaging
Nat. M Natrum Muraticum
Nit. Ac Nitric Acid
NSAID Nonsteroidal Anti-Inflammatory Drugs
OA Osteoarthritis
OPD Out patient department
PsA Psoriatic Arthritis
Puls Pulsatilla
RA Rheumatoid Arthritis
ReA Reactive Arthritis
Rhod Rhodendron
Rhus. T Rhus Toxicodendron
ROM Range of motion
SAPHO Synovitis-acne-pustulosis-hyperostosis-osteomyelitis
Sep Sepia
SI Sacroiliac
SLR Straight leg raising
SpAs Spondyloarthropathies
Staphs Staphysagria
Sulph Sulphur
TB Tuberculosis
Tub. Tuberculinum
URTI Upper Respiratory Tract Infection
U-SpA Undifferentiated Spondyloarthropathies

ABSTRACT
BACKGROUND
Ankylosing spondylitis is a long term disease that causes inflammation of
joints between the vertebral bones and the joints between the spine and the pelvis. It
eventually causes the affected spinal bones to join together and results in restricted
movements, such as peripheral arthritis and iritis. Sacroiliac joints are usually the first
to be involved and as a rule they are bilaterally involved within six months from the
onset of the disease. Sacroilitis produces sciatica – like pain, radiating down to one or
both thighs.
AS though a constitutional disorder, is clinically characterized by acute
exacerbations. The homoeopathic materia medica is a vast treasure house of remedies,
which when prescribed on the basis of totality help in treating any condition
effectively. The acute exacerbations, can be controlled with the presenting acute
totality Rhus tox, a well proved homoeopathic remedy has a wide spread sphere of
action, especially on the locomotory system. This present study is taken up to study
the efficacy of Rhus tox in managing the ankylosing spondylitis.
Thus the present study is taken up to study the utility of Rhus tox in
Ankylosing spondylitis.AS is prototype of the seronegative spondoarthritis group is a
chronic inflammatory arthritis with a progressive stiffening and fusion of the axial
skeleton.
The exact etiology of AS is still unknown. The familial nature of AS has been
stressed for many years and a genetic basis for this has been provided by the
discovery between 88 and 96% of patients with AS. It occurs in 1% of patients who
carry HLA B27 and is postulated that environmental factors, specifically carriage of
GI or GU micro-organisms, acts as triggering factors in individuals rendered

genetically susceptible by cell surface expression of the HLA B27 coded
polypeptides.
In more recent years, the frequency of this articular disorder increasing still
more as advances in modern medical science have led to a more prolonged life
expectations for humans. Homoeopathy being a holistic science treats the patient
effectively without any side effects.
OBJECTIVES
The following objectives were fixed up for the study:
1. To study the clinical spectrum of Ankylosing spondylitis.
2. To study the role and efficacy of Rhus tox and to evaluate the role of Rhus tox
in assessing the intensity of symptoms, frequency of remission and progress of
disease.
METHODS
The subjects for the study were taken from the OPD/IPD and village campus,
peripheral clinics and regular camp visits of Bhartesh Homoeopathic Medical College
and Hospital, Belgaum. Subjects were selected on the basis of inclusion and exclusion
criteria which are elaborated in the study. Sample of 30 size were considered by
simple random sampling procedure. All the cases were taken proforma. The drugs
were selected on the basis of the constitution and underlying miasms. Acute drugs
were also administered to provide symptomatic relief during acute exacerbation.
Routine blood investigations with ESR as required, HLA B27 and X-ray
investigations were the main parameters to confirm the diagnosis and to assess the
response to treatment. The inclusion criteria for cases of AS were diagnosed
clinically with articular manifestation like hip pain, stiffness low back pain and
limited joint motions in the low back.The exclusion criterias were the extra articular

manifestation, progressive disease with deformities and secondary to any other
systemic diseases with gross pathology.
The following parameters were fixed according to type of response obtained
after treatment:-
a) Recovered – patient has shown remarkable positive response to the treatment
and the considerable improvement helped them to perform their regular chores
effectively.
b) Improved – feeling of mental and physical well being along with the
disappearance of the old symptoms and considerable reduction in the
appearance of new complaints.
c) Not Improved – initial response but lots of suffering continued inspite of
administering the drugs. No reduction of complaints even after defined period
of treatment.
RESULTS
Out of 30 cases, 6 cases recovered accounting 20%, 13 cases improved
accounting 43.33% and 11 cases did not improve accounting 36.66%.
INTERPRETATION AND CONCLUSION
In the present study, out of 30 patients, 6 patients recovered, 13 patients
improved and 11 patients did not improve. The miasmatic background in most of the
cases was found to be psoro-syco-syphilitic. Hence it can be concluded that AS is tri
miasmatic. The X-ray changes of the AS were found in most of the cases along with
HLA B27 positive. Here the utility of Rhus tox proved its efficacy. The constitutional
remedies used were Lycopodium, Natrum mur, Calc carb, Sulphur, Phosphorus,
Aurum met, Sepia and Pullsatilla. The intercurrent remedies used were Thuja,

Medorrhinum, Tuberculinum, Mercurius and Syphillinum. Most of the cases were in
their initial stages.
The homoeopathic medicines found to be efficacious in reducing the mobility
and bring about significant improvement. The constitutional medicine, in addition to
alleviating the present ailments brings about the general well being of the patients.
The utility of Rhus tox is found efficacious in management of AS more speedily and
with less aggravations i.e. mildly, gently and permanently. In most of the cases there
are improvent, hence homoeopathy has good therapeutic scope in the management of
AS with use of Rhus tox.
The scope varies in every individual case depending upon the clinical
presentation, whether there are reversible or irreversible structural changes, the
underlying pathology and progress of disease. It was seen from the study that earlier
the cases were detected better were the results.
KEY WORDS
Seronegative spondoarthritis; Vertebral bones; Low back pain; Syphilis; Remedy;
Constitutional; Ankylosing spondylitis; Sciatica; Sacroilitis.

TABLE OF CONTENTS
CHAPTER PARTICULARS PAGE NO
1. INTRODUCTION 1-9
2. OBJECTIVES 10
3. REVIEW OF LITERATURE 11-104
4. METHODOLOGY 105-110
5. RESULTS 111-119
6. DISCUSSION 120-122
7. CONCLUSION 123
8. SUMMARY 124-126
9. BIBLIOGRAPHY 127-131
ANNEXURE-I- CASE PROFORMA 132-139
ANNEXURE-II- GRAPHS 140-142
ANNEXURE-III - MASTER CHART 143-146
ANNEXURE-IV – SYNOPSIS OF CASES 147-154

LIST OF TABLES
SR. NO. TABLES PAGE NO.
1. Age Incidence 111
2. Sex Incidence 112
3. Past History 113
4. Family History 114
5. Presenting complaints 115
6. Miasmatic background 116
7. Acute remedy 117
8. Incidence of Intercurrent Remedy 118
9. Results of treatment 118

LIST OF FIGURES
FIGURE NO.
FIGURE PAGE NO.
1. Leonard Trask 12
2. Vertebral column 20
3. Lateral view of vertebral column 22
4. Lumbar vertebra 23
5. Spine 26
6. Spinal cord 27
7. Sacrum 30
8. Anterior sacroiliac ligament 31
9. Posterior sacroiliac ligament 32
10. Sacrotuberous ligament 33
11. Angle of femoral neck 35

12. Bones of hip 42
13. Blood vessels of hip 43
14. Bursa of hips 45
15. Intervertebral disc 46
16. Simplified view of muscles 47
17. a. Biomechanics of hip 50
b. Biomechanics of hip 51
18. Classic areas of inflammation of spondyloarthropathy
54
19. Spine in Ankylosing spondylitis 61

LIST OF GRAPHS
SR. NO. GRAPHS PAGE NO.
1. Incidence of AS with reference to HLA-B27 60
2. Age Incidence 140
3. Sex Incidence 140
4. Presenting Complaints 141
5. Miasmatic Background 141
6. Acute Remedies 142
5. Result of treatment 142


Introduction

INTRODUCTION
Research is the backbone of any science. No science can progress unless and
until sincere efforts are made in all fields. Research is the basic foundation of science
and a scientific method of thinking according to a set of rules .It generates new
information which can be applied for means of solution for the problem we are facing
with. Today’s medicine is an evidence based medicine besides the subject
improvement other parameters need to be evolved as to measure objectively,
quantitatively and qualitatively what Homoeopathy the medical system especially
seeks to achieve.
Life is the journey. When it becomes hard and long. Homoeopathy is the oasis
where we can quench our thirst. We can drink from this fountain of youth—the
benefits will flow through us like an inward spiral joining mind, body and spirit until
it reaches the soul, our very core, our Vital Force, our spirit like dynamic. There it
swirls like a river, engulfing all we have experienced, in all our lives, connecting to
our collective unconscious and bringing us peacefully to the ebb and flow of life
where we are joined with the rest of the world as one living breathing organism all
wind, fire, earth, metal and water......1
A new curiosity and enthusiasm to learn about this autoimmune disease
ankylosing spondylitis finally have stimulated the considerable investigation that this
common and significant condition deserves.
The classical homoeopathy is highly individualised therapeutic approach and
success is often indirectly assessed by the changes in the system and general health
status of individual .Scientifically speaking this subjective evaluation is less valid and

reliable. Modern research has started to uncover a fascinating set of complex,
biophysical and biochemical processes. Further work lead to more fundamental
understanding of cartilage and connection tissues in general.
This research provides a fresh understanding of disease, mechanism of action
of our drug and will provide new tools for disease management. We use the scientific
method to discover facts and will provide new tools for disease management. We use
the scientific method to discover facts and their inter-relationship and allow the
application of this new knowledge in practical settings.
A physician must think scientifically and develop scientific attitude towards
patient’s management and research. Such attitude is useful in assessing new
approaches to management of patients .The need of this dissertation is to study in
depth and a thorough research work should be done which is helpful in reducing
prevalence under our homoeopathic management effectively. The potential benefits
hazards and discomfort of old method should be weighed against the advantages of
rational art of healing.
The understanding of the AS has undergone a sea change with the
advancement in the medical science .It is sufficient to establish that the patient is
suffering from AS, but needs further study. The modern physician is an alert clinician
who anticipates the problem before hand and institutes intervention planning as sound
clinical footings, incorporating latest developments in medical science.
One purpose of studying a disease is to gain insight concerning its causation.
In few of requirements for continuing education for licensure and relicensure, as well
as the emphasis on the certification a review over the arthritic condition is essential.

Since the time of Hahnemann, Homoeopathy is an identified system among
different systems of medicines having astonishing results in various difficult diseases
without harmful effects. Results are not occasional, accidental are by fully scientific
in accordance with the principles and laws. Still our development in the field of
scientific world through homoeopathy giving authentication as that of modern
systems of medicine which is required distressed and attended for vast acceptance of
Homoeopathic systems. We must realize that Homoeopathy is our identity, our
dignity. We selected Homoeopathy to serve people because we found it most useful
and affective even when our patients are disappointed by other systems of their
choices. Our practice confirms this truth again and again .We must realise the truth
and accept a challenge to establish this fact in the minds of our people. I have made
attempt for the same under the topic of Ankylosing spondylitis.
We need other dimensions of physical, mental and spiritual support in life if
we want to lead a holistic, well-rounded existence with a satisfactory quality of life.
The following thesis is essentially aimed at supplementing that noble medical role by
sharing some experiences by means of taking this nagging sensation in one stride in
the best interest of our patient.
Ankylosing spondylitis was probably first recognised as a disease which was
different from Rheumatoid arthritis by Galen as early as the second century AD;
however skeletal evidence of the disease (ossification of joints and enthuses primarily
of the axial skeleton, known as archaeological dig that unearthed the skeletal remains
of a 5000 year- old Egyptian mummy with the evidence of “bamboo spine” An
autoimmune disease known to be associated with tissue type HLA B27, affecting
facet joints between vertebrae together causing spine to become increasingly rigid.

Ankylosing spondylitis is long term disease that causes inflammation of joints
between the spinal bones and the joints between the spine and the pelvis. It eventually
causes the affected spinal bones to join together.
The cause of ankylosing spondylitis is unknown, but gene problems seem to
play role. The majority of people with Ankylosing spondylitis have gene called HLA
B27. There are theories on its link with some bacterial infection as a triggering factor.
The disease most frequently begins between age 20 and 40, but may begin before age
10. It affects more males than females. Risk factors include a family history of
ankylosing spondylitis and male gender. Ankylosing spondylitis is a systemic
rheumatic disease and is one of the seronegative spondyloarthropathies. About 90% of
patients express the HLA B27 genotype. Tumour necrosis factor-alpha (TNF α) and
IL-1 are also implicated in ankylosing spondylitis. Although specific autoantibodies
cannot be detected, its response to immunosuppressive medication has promoted its
classification as an autoimmune disease. The disease always begins in the sacroiliac
joints, and then extends upwards to involve the lumbar, thoracic and often cervical
spine. The articular cartilage, synovia and ligaments show chronic inflammatory
changes and eventually becomes ossified.
The classical Homoeopathy is highly individualized therapeutic approach and
success is often indirectly assessed by the changes in the system and general health
status of individual. Scientifically speaking this subjective evaluation is less valid and
reliable. This research will provide a fresh understanding of disease, mechanism of
action of Rhus tox will provide new tools for disease management. We use scientific
method to discover facts and their inter-relationships and allow the application of this
new knowledge in practical settings. A physician must think scientifically and

develop scientific method, attitude towards patient’s management. The need of this
dissertation is to study in depth and a thorough research work should be done which is
helpful in reducing prevalence under our homoeopathic management effectively .Such
attitude is useful in assessing new approach’s to management of patient. The potential
benefits hazards and discomfort of old method should be weighed against the
advantages of rational art of healing.
The understanding of Ankylosing spondylitis has undergone a sea of change
with the advancement in the medical science. It is sufficient to establish that patient is
suffering from Ankylosing spondylitis but needs further investigation. The modern
physician is alert clinician who anticipates the problem before hand and institutes
intervention planning as sound clinical footings, incorporating latest developments in
medical science.
One purpose of studying Ankylosing spondylitis is to gain insight concerning
its causation. In few of requirements for continuing education for licensure and
relicensure, as well as the emphasis on the certification and recertification a review
over the Ankylosing spondylitis condition is essential. Since the time of Hahnemann,
Homoeopathy is an identified system among different medicines having astonishing
results in various difficult diseases without harmful effects. Results are not
occasional, accidental or by chance but fully scientific, in accordance with principles
and laws. Still our development in field of scientific world through Homoeopathy
giving authentication as that of modern systems of medicine which is required
distressed and attended for vast acceptance of Homoeopathy system. We must realise
that Homoeopathy is our identity, our dignity. We selected Homoeopathy to serve
people because we found that Homoeopathy was useful and effective even when our

patients are disappointed by other systems of their choice. Our practice confirms the
truth again and again. We must realise this truth and accept a challenge to establish
this fact in the minds of our people. I have made attempt for the same under the topic
of Utility of Rhus tox in Ankylosing spondylitis.
We need other dimensions of physical, mental and spiritual support in life if
we want to lead a holistic, well-rounded existence with a satisfactory quality of life.
The following thesis is essentially aimed at supplementing that noble medical role by
sharing some experiences by means of taking this nagging sensation in one stride in
the best interest of our patients. Learning to live with pain is something that is thrust
on many of us. Such are the ways of cosmic force that moves men and matter, but the
charm lies in minimising its negativity impact while optimising all other elements of
day to day living. Needless to say we are the best person to advice the patient on the
art and science of living without pain. Medicine is an ever changing science as new
research and clinical experience broaden our knowledge, changes in the mode of
treatment and drug therapy is required.
Our school of Homoeopathy proposes a holistic approach to health care. The
word holistic comes from the Greek ‘halos’ meaning ‘whole’ i.e viewing the person
and his well being from every possible perspective. There is no doubt that the Holistic
approach is all encompassing. However it needs multidisciplinary health care system,
and requires a shift in roles and task among different professionals involved .The
western medicine felt the need that degree of specialization of different organs is
essential, but we Homoeopaths take the person as a whole. Since, we consider and
take care of physical, social, psychological and spiritual needs of our patients the
focus on Homoeopathy has helped us to realise that there are other models of health

care aspects from Western medicine and that each model has a different conceptual
framework, which must evaluated on a scientific basis. Our holistic approach
involves:
1. Responding to the person as a whole (body, mind and spirit) with in the
context of his environment.
2. Willingness to use wide range of interventions
3. An emphasis on a participatory relationship rapport between doctor and a
patient.
4. An awareness of the impact of the health of the patient.
“The perfection of our, the only healing art and the weal of the patients appear
well to deserve that the physicians take to requisite pains to procure for his medicines
the proper, the greatest possible efficacy.”2
The aim of this thesis is to adapt to this transition field of Ankylosing
spondylitis. So to bridge the gap in a meaningful manner. The amalgam of prevalent
medical applications, when incorporated in the light of homoeopathic principles,
beings about uniformity in the treatment planning of each individual case and using
Dr.Hahnemanns most perfected method. This facilitates the smooth interaction among
medical professionals as a rational and scientific basis, with uniformity in expression.
At the same time it maintains our great tradition of healing art in the purest form, and
provides an ample room and flexibility for every homoeopathic physician in his
individual professional judgement in every individual case in question.

To gather out from our boundless literature the multitude of facts relating to
the action and uses of our medicine, to shift the true form the false, has been a most
formidable task. To aid in this undertaking, I supply my self with all available works
treating upon this disease , in all schools of medicine. It is with this problem of clear
differentiation in mind that we submit these studies of cases pertaining to AS and
because of primary importance of these fold basis for preserving homoeopathically,
we to say little about the fearful diagnostic tags. Let me close with Hahnemann’s own
words concerning homoeopathy: I demand no faith at all, and do not demand that
anybody should comprehend it. Neither do I comprehend it. It is enough , that it is
fact and nothing else. Experience alone declares it, and I believe more in experience
than in my own intelligence. But who will arrogate to himself the power of weighing
the invisible forces that have hither to been concealed in the inner blossom of nature,
when they are brought out of the crude state of apparently dead matter through a new,
hitherto undiscovered agency, such as potentizing by long continued trituration and
succession. But he who will not allow himself to be convinced of this and who will
not, therefore, imitate what I now teach after many years ,trial and experience . He
who is not willing to imitate it exactly, can leave this greatest problem of our art
unsolved, he can also leave the most important chronic diseases uncured ,as they have
remained unhealed, indeed up to the time of my teaching .I have no more to say about
this. It seemed to me my duty to publish the great truths to the world that needs them,
uncontrolled as to whether people can compel themselves to follow them exactly or
not .If it is not done with exactness, let no one boast to have imitated me, nor expect a
good result.3 Try out these advanced methods for yourself, gain experience with
them, and you will become a true classical Hahnemannian Homoeopath , beloved by
all patients. This following work has been done with care and while it may approach

the perfection we hope it may prove of benefit in picking out the symptom of this
disease in relation to the individualizing the case.
The following steps are taken for evolving at the time of treatment :
1. Detailed case taking according to proforma specially rearranged for Ankylosing
spondylitis
2. Analysis of symptoms
3. Evaluation of symptoms
4. Repertorization to evolve the group of similar drugs
5. Miasmatic repertorization to confirm this miasmatic diagnosis.
6. To study the clinical spectrum of Ankylosing Spondylitis.
7. To study role and efficacy of Rhus tox and to evaluate the role of Rhus tox in
assessing the intensity of symptoms, frequency of remission and progress of
disease.

Objectives

AIMS AND OBJECTIVES
The following objectives were fixed up for the study:
1. To study the clinical spectrum of Ankylosing spondylitis.
2. To study the role and efficacy of Rhus tox and to evaluate the role of Rhus tox
in assessing the intensity of symptoms, frequency of remission and progress of
disease.

Review of Literature

REVIEW OF LITERATURE
HISTORICAL REVIEW
Ankylosing spondylitis (AS) is a systemic inflammatory disease that results in
ossification of joints and entheses primarily of the hip, spine, and peripheral joints.
The first signs of AS were first unearthed in the skeletal remains of a 5000 year–old
Egyptian mummy. The first description of AS in the literature was in 1559 by Realdo
Colombo and first account of the changes to the bones was given in 1669 by Bernard
Connor. Sir Benjamin Brodie in 1818 was the first to note that iritis accompanied
spondylitis. Charles Fagge and Carl von Rokitansky also reported similar findings of
AS in cadaveric specimens and patients. However, the first well–known description of
AS was reported by W. von Bechterew from Russia in 1883. Others, such as Adolph
Strumpell from Germany in 1897 and Pierre Marie from France in 1898 were also
among the first to offer a classic description of AS. Therefore, AS is also known as
Bechterew Disease or Marie–Strumpell Disease.4
The anatomist and surgeon Realdo Colombo described what could have been
the disease in 1559 and the first account of pathologic changes to the skeleton
possibly associated with AS was published in 1691 by Bernard Connor.
It was recognized as distinct from rheumatoid arthritis by Hippocrates as early
as the second century. Egyptian mummies have been found with ankylosing changes
to their skeleton.5(997pp)

“It was not until he [Trask] had exercised for some time that he could perform
any labor and that his neck and back have continued to curve drawing his head
downward on his breast.”
This account became the first documented case of AS in the united States,
since its indisputable description of inflammatory disease characteristics of AS, and
the hallmark of deforming injury in AS. It has been suggested that AS was first
recognized as a disease which was different from rheumatoid arthritis by Galen as
early as the second century A.D however, skeletal evidence of the disease
(ossification of joints and entheses primarily of the axial skeleton, known as "bamboo
spine") was first discovered in an archaeological dig that unearthed the skeletal
remains of a 5000-year–old Egyptian mummy with evidence of "bamboo spine".
In 1858, David Tucker published a small booklet which clearly described a
patient by the name of Leonard Trask who suffered from severe spinal deformity
subsequent to AS. In 1833 Trask fell from a horse, exacerbating the condition and
resulting in severe deformity.
In 1973 the association between AS and the gene HLA B27
was found.
It has been identified as the condition which Saint Banus
(355-395 AD) suffered from (named Father Palm Tree in
local language due to his stooped posture), forcing him to
eat and sleep standing for 18 years. A disease much like AS
has been found naturally in prehistoric crocodiles, monkeys.
CLASSIFICATION OF DISEASES OF JOINTS
Fig. 1: Leonard Trask

Infectional arthritis
• Acute (streptococcus, staphylococcus, gonococuss)
• Chronic (tubercle bacillus)
Probably inflectional
• Rheumatic fever
• Rheumatoid arthritis (arthropathic arthritis, proliferative arthritis, chronic
infectious arthritis)
• Ankylosing spondylitis (Marie-Stumpell disease)
• Psoriatic arthritis
Toxic arthritis associated with various infections.
Degenrative arthritis e.g.lumbar spondylosis (oestioarthritis, hypertrophic arthritis)
Arthritis associated with metabolic diseases
• Gout
• Other metabolic diseases
Neuropathic joints
• Tabes dorsalis
• Syringomyelia
Neoplasms of joints (cyst, xantoma, hemangioma,gaint cell tumor, synovioma)
Traumatic arthritis
• Direct trauma
• Indirect trauma (secondary to postural strain)
Systematic disease manifestation

• 1.Serum sickness
• 2. haemophilia
• 3. Intermittent hydrarthosis
• 4. Pulmonary osteoarthropathy
• 5. Hysterical joints
Local joint disturbances
• Aseptic necrosis
• Osteochondritis dissecans
• Osteochondromatosis
• Pigmented villonodular synovitis6
The spondyloarthropathies are a group of conditions which share similar
clinical features. Classification criteria permit separation of the conditions, allow
better targeting of therapies, better measurement of outcomes, and better prognostic
information. Early diagnosis remains problematic, but validated criteria for
established disease are now emerging.
Histopathology and histochemistry are providing a better understanding of the
underlying process of inflammatory arthritis in spondyloarthropathy and other
inflammatory arthritides. Early disease, however, continues to challenge current
criteria. Sophisticated imaging with magnetic resonance imaging is being increasingly
used and is proving useful for early diagnosis as well as helping to understand the
pathophysiology of disease. Juvenile idiopathic arthritis continues to provide
problems and criteria have recently been modified to allow a greater clinical utility
and inclusion of more patients. Poststreptococcal reactive arthritis appears to be a
heterogeneous clinical entity, with a group looking more like rheumatic fever and a
group with spondyloarthropathy traits. It may be that the association is not

streptococcal, but is a throat infection. Currently available criteria for psoriatic
arthritis have been evaluated in a large cohort. Four of the criteria performed well
with high specificity and sensitivity whereas the other two had moderate specificity
and low sensitivity. It was shown that rheumatoid factor positivity does not exclude a
diagnosis of psoriatic arthritis--the single most important clinical feature of this
condition being the presence of psoriasis.
The spondyloarthropathy classification criteria continue to be an area of
development. This is most apparent in juvenile arthritis and psoriatic arthritis. The
latter is currently undergoing intense scrutiny to develop classification criteria and
outcome measures.
CLASSIFICATION OF SPONDYLOARTHROPATHY (SpA)
THE EUROPEAN SPONDYLOARTHROPATHY STUDY GROUP (ESSG)
According to the ESSG criteria, for a patient to be classified as having SpA, he
or she has to satisfy one of two entry criteria: Inflammatory spinal pain or synovitis
that is either asymmetric or predominantly in the lower limbs.7
Inflammatory back pain: Back pain is common among the general population.
However, "inflammatory" back pain is much less common. Back pain is considered
inflammatory if four of the following five criteria are found:
Onset of back discomfort before the age of 40 years
Insidious onset
Persistence for at least three months
Associated with morning stiffness
Improvement with exercise
Asymmetrical synovitis: predominantly of the lower limbs is manifested by soft tissue
swelling, warmth over a joint, joint effusion, and reductions in both active and passive
range of motion. As with inflammatory spinal pain, the symptoms are worse after a
period of rest. It is clear the HLA is strongly associated with the SpAs. Yet prevalence
of HLA B27 varies widely in different racial and ethnic clusters around the world.8
Additional criteria: If a patient has one or both of the entry criteria listed above, he or
she should then be evaluated for the presence of one or more of the following
features:
Positive family history
Psoriasis
Inflammatory bowel disease
Urethritis, cervicitis, or acute diarrhea within one month before arthritis
Buttock pain alternating between buttocks
Enthesopathy
Plain film radiographic evidence of sacroiliitis
Importantly, blood tests, including an assessment for the presence of HLA-
B27, are not part of the ESSG criteria; in addition, only the sacroiliac joints need to be
evaluated radiographically.
The term spondyloarthritis (formerly spondyloarthropathy), is used to refer a
group of disorders that includes ankylosing spondylitis (AS), undifferentiated
spondyloarthritis, reactive arthritis (ReA), and the arthritis and spondylitis that may
accompany psoriasis and inflammatory bowel diseases.
Seronegative spondyloarthropathy:
Spondylarthropathy are inflammatory conditions affecting the spine and
occasionally other joints. The condition is often characterized by back pain but the

severity of the symptoms can vary greatly. Seronegative spondylarthropathy is
where the blood does not have a certain antibody (rheumatoid factor) which enables
it to be distinguished from rheumatoid arthritis. Seronegative spondylarthropathies
includes ankylosing spondylitis, psoriatic arthritis and Reiter's syndrome.
Seronegative spondyloarthropathies comprise a group of inflammatory
arthritides, which consists of:
ankylosing spondylitis,
psoriatic arthritis,
reactive arthritis (Reiter's syndrome),
enteropathic arthritis, and
undifferentiated spondyloarthropathy.
All of them share common laboratory, clinical, and imaging findings, with
characteristic involvement of the sacroiliac joints, spine, and, to various degrees,
peripheral joints. For many years, conventional radiography was the mainstay for
definitive diagnosis of sacroiliitis and for follow-up of the anatomic changes in the
spine, peripheral joints, and entheses. Conventional radiographs remain the imaging
investigation of choice; however, they are unable to detect early inflammatory
changes of sacroiliitis, which are important for establishing a diagnosis without delay.
Other imaging modalities, such as computed tomography, bone scintigraphy,
magnetic resonance imaging, and ultrasonography have improved the capabilities of
detecting early disease and became useful adjuncts to plain films. In addition, they
also have enabled more accurate detection of pathology at various anatomic sites of
the musculoskeletal system predominantly involved in spondyloarthropathies. This
article will review and highlight the role of each of these modalities in the assessment

of the axial and peripheral skeleton in seronegative spondyloarthropathies.
CLASSIFICATION OF SPONDYLOARTHROPATHIES
It is a member of the group of the spondyloarthropathies with a strong genetic
predisposition. Complete fusion results in a complete rigidity of the spine, a condition
known as bamboo spine. Although Hippocrates described a condition identical to
modern disease, it was not until the separate description Bechterew, Strumpell and
Marie at the end of the 19th century.9
Condition that overlap to form the seronegative spondylarthritides and their
common features
Types of seronegative spondyloarthrides
Ankylosing spondylitis
Psoriatic arthritis
Enteropathic arthritis(associated with ulcerative colitis, crohn’s disease and
whipple’s disease.)
Retier’s syndrome /Reactive arthropathy
Behcet’s syndrome
Common features
Negative tests from rheumatoid factor
Absence of rheumatoid nodules
Inflammatory peripheral arthritis
Radiological sacroilitis
Tendency to familial aggregation
ANATOMY
A thoroughly detailed study of anatomy of the spine, hip and peripheral joints,
is a need to treat the illness. Thus basics of AS starts from how the spine is developed
structurally. Generally the physician interested in the pain is not inclined to read essay
on anatomy, they are more interested in the bottom line how do I treat it? However
we need an understanding of anatomy to appreciate which elements of the spine is
inflamed and thus become painful, so as to prescribe treatment on a rational basis.
Modern research has revealed the leading contenders for previously but still the cause
is unknown, only hypothesis have been proposed like linked with genetic
predisposition.
In ankylosing spondylitis (AS), the whole spine can be affected, but symptoms
usually begin in the low back. To understand how ankylosing spondylitis can cause
your spinal bones to fuse, you should have a basic understanding of how your spine
works.
As you can see from the image below, your back, or spine, is made up of
many parts. First, we're going to look at the bone structures. Your backbone, also
called your vertebral column, helps support a lot of your body weight, and it protects
your spinal cord. You have 33 vertebrae (bones) that make up the vertebral column. In
the image, they're labeled as "Vertebral Body."
Your spine is divided into regions: there's your neck (cervical spine), mid-
back (thoracic spine), and low back (lumbar spine). At the bottom of your spine, you
also have the sacrum and the coccyx, which is commonly called your tailbone. Again,
AS generally starts in the lumbar spine and works its way up to the cervical spine.

The vertebrae in your neck are labeled C1-C7, meaning that you have seven
vertebrae in that region. Most adults have 12 vertebrae in the thoracic spine (T1-T12),
which goes from your shoulders to your waist. Then there are five vertebrae in your
low back (L1-L5).
Below your lumbar region, your sacrum is made up of five vertebrae between
the hipbones. By the time you're an adult, these five bones have fused into one bone.
The coccyx is made of small fused bones at the very tail of your spine (hence the
tailbone).
In between your vertebrae, you have intervertebral discs (also labeled on the
image). These act like pads or shock absorbers for your spine as it moves. Each disc is
made up of a tire-like outer band called the annulus fibrosus and a gel-like inner
substance called the nucleus pulposus.
Together, the vertebrae and the discs provide a protective tunnel (the spinal
canal) to house the spinal cord and spinal nerves. These nerves run down the center of
the vertebrae and exit to various parts of the body, where they help you feel and
Fig. 2: Vertebral column

move. With ankylosing spondylitis, your spinal nerves can be pinched (also known as
impinged or compressed) by the extra bone that develops as a result of AS.
Your spine also has facet joints, which are on the posterior side (back) of your
vertebrae. These joints (like all joints in your body) help facilitate movement and are
very important to your flexibility. The joints are covered by cartilage that protects
your bones as you move. In ankylosing spondylitis, the cartilage can be destroyed—
inflammation and chemicals released by the inflammation can destroy it. The cartilage
can then be replaced by scar tissue.10
Your back also has muscles, ligaments, tendons, and blood vessels. Muscles
are strands of tissues that act as the source of power for movement. Ligaments are the
strong, flexible bands of fibrous tissue that link the bones together, and tendons
connect muscles to bones and discs. Blood vessels provide nourishment. These parts
all work together to help you move.
The Skeletal System serves many important functions; it provides the shape
and form for our bodies in addition to supporting, protecting, allowing bodily
movement, producing blood for the body, and storing minerals. The number of bones
in the human skeletal system is a controversial topic. Humans are born with about 300
to 350 bones, however, many bones fuse together between birth and maturity. As a
result an average adult skeleton consists of 208 bones. The number of bones varies
according to the method used to derive the count. While some consider certain
structures to be a single bone with multiple parts, others may see it as a single part
with multiple bones. There are five general classifications of bones. These are Long
bones, Short bones, Flat bones, Irregular bones, and Sesamoid bones. The human
skeleton is composed of both fused and individual bones supported by ligaments,

tendons, muscles and cartilage. It is a complex structure with two distinct divisions.
These are the axial skeleton and the appendicular skeleton. The Skeletal System
serves as a framework for tissues and organs to attach themselves to. This system acts
as a protective structure for vital organs. Major examples of this are the brain being
protected by the skull and the lungs being protected by the rib cage.
Located in long bones are two distinctions of bone marrow (yellow and red).
The yellow marrow has fatty connective tissue and is found in the marrow cavity.
During starvation, the body uses the fat in yellow marrow for energy. The red marrow
of some bones is an important site for blood cell production, approximately 2.6
million red blood cells per second in order to replace existing cells that have been
destroyed by the liver. Here all erythrocytes, platelets, and most leukocytes form in
adults. From the red marrow, erythrocytes, platelets, and leukocytes migrate to the
blood to do their special tasks.
Another function of bones is the storage of certain minerals. Calcium and
phosphorus are among the main minerals being stored. The importance of this storage
"device" helps to regulate mineral balance in the bloodstream. When the fluctuation
of minerals is high, these minerals are stored in bone; when it is low it will be
withdrawn from the bone.11
Lumbar Spine:
Physicians use a code to number each of the
24 vertebrae in the spine. The low back officially
begins with the lumbar region of the spine directly
below the cervical and thoracic regions and directly
Fig. 3: Lateral view of vertebral column

above the sacrum. The lumbar vertebrae, L1-L5, are most frequently involved in back
pain because these vertebrae carry the most amount of body weight and are subject to
the largest forces and stresses along the spine.
The true spinal cord ends at approximately the L1 level, where it divides into
many different nerve roots that travel to the lower body and legs. This collection of
nerve roots is called the "cauda equina," which means horse's tail and describes the
continuation of the nerve roots at the end of the spinal cord.12
Vertebrae:
The vertebral body is a thin ring of dense cortical bone. The vertebral body is
shaped like an hourglass, thinner in the center with thicker ends. Outer cortical bone
extends above and below the superior and inferior ends of the vertebrae to form rims.
The superior and inferior endplates are contained within these rims of bone.
Pedicles:
The pedicles are two short rounded processes that extend posteriorly from the
lateral margin of the dorsal surface of the vertebral body. They are made of thick
cortical bone. The vertebrae surround and protect the spinal cord, a column of nerves
running down from the brain. Peripheral nerves branch off from the spinal cord and
Fig. 4: Lumbar vertebra

with their roots passing through the vertebrae, extend all over the body. As a result,
pain from a back problem may also travel to other parts of the body
Laminae:
The laminae are two flattened plates of bone extending medially from the
pedicles to form the posterior wall of the vertebral foramen. The Pars Interarticularis
is a special region of the lamina between the superior and inferior articular processes.
A fracture or congenital anomaly of the pars may result in a spondylolisthesis.
Intervertebral Discs
Intervertebral discs are found between each vertebra. The discs are flat, round
structures about a quarter to three quarters of an inch thick with tough outer rings of
tissue called the annulus fibrosis that contain a soft, white, jelly-like center called the
nucleus pulposus. Flat, circular plates of cartilage connect to the vertebrae above and
below each disc. Intervertebral discs separate the vertebrae, but they act as shock
absorbers for the spine. They compress when weight is put on them and spring back
when the weight is removed. Intervertebral discs make up about one-third of the
length of the spine and constitute the largest organ in the body without its own blood
supply. The discs receive their blood supply through movement as they soak up
nutrients. The discs expand while at rest allowing them to soak up nutrient rich fluid.
When this process is inhibited through repetitive movement, injury or poor posture,
the discs become thinner and more prone to injury. This may be a cause of the gradual
degeneration of the structure and function of the disc over time.

Facet Joints
Joints between the bones in our spine are what allow us to bend backward and
forward and twist and turn. The facet joints are a particular joint between each
vertebral body that help with twisting motions and rotation of the spine. The facet
joints are part of the posterior elements of each vertebra. Each vertebra has facet
joints that connect it with the vertebrae above and the vertebrae below in the spinal
column. The surfaces of the facet joints are covered with smooth cartilage that help
these parts of the vertebral bodies glide smoothly on each other. A facet joint joins
each pair of vertebra (i.e., the one above to the one below). Like hinges, the facet
joints guide the movement of the spine, while also stabilizing the vertebral column.
Ideally, the joints in the spine are lined up so that the back can twist and bend with
little friction between the vertebrae. Between each pair of vertebrae lies a flat,
circular inter-vertebral disc. The outer part of the disc, the annulus, is strong and
hard. The inner portion, the nucleus pulposus is soft and absorbs shocks to the spine
during movement
Ligamentum Flavum:
The ligamentum flavum is a strong ligament that connects the laminae of the
vertebrae. The term "flavum" is used to describe the yellow appearance of this
ligament in its natural state. The ligamentum flavum serves to protect the neural
elements and the spinal cord and stabilize the spine so that excessive motion between
the vertebral bodies does not occur. It is the strongest of the spinal ligaments and
often has a thinner middle section. Together with the laminae, it forms the posterior
wall of the spinal canal.

Spine anatomy:
The human spine is a complex structure that provides both mobility (so you
can bend and twist) and stability (so you can remain upright all day). The normal
spine has an “S” –like curve when looked at from the side. This curvature allows for
even distribution of weight. The “S” curve helps a healthy spine withstand stress.
Ultimately, this interdependence among all sections of the spine, plus the competing
demands of mobility and stability make the spine vulnerable to injury and
deterioration due to ageing.
The spine features three natural curves, the cervical (neck) curve, the thoracic
(middle back) curve and lumbar (lower back) curve. The thoracic spine is made up of
the 12 vertebrae in the upper back and each thoracic vertebra is attached to a rib. The
lumbar spine is made up of the next 5 vertebrae. The lower lumbar region. Finally,
below the lumbar region are 5 fused vertebrae of the sacrum and the 5 fused vertebrae
of the coccyx
Fig. 5: Spine

The spinal cord is part of the central nervous system of the human body. It is a
vital pathway that conducts electrical signals from the brain to the rest of the body
through individual nerve fibers. The spinal cord is a very delicate structure that is
derived from the ectodermal neural groove, which eventually closes to form a tube
during fetal development. From this neural tube, the entire central nervous system,
our brain and spinal cord, eventually develops. Up to the third month of fetal life, the
spinal cord is about the same length as the canal. After the third month of
development, the growth of the canal outpaces that of the cord. In an adult the lower
end of the spinal cord usually ends at approximately the first lumbar vertebra, where it
divides into many individual nerve roots (L1).
Spinal Canal:
Fig. 6: Spine cord

The spinal canal is the anatomic casing for the spinal cord. The bones and
ligaments of the spinal column are aligned in such a way to create a canal that
provides protection and support for the spinal cord. Several different membranes
enclose and nourish the spinal cord and surround the spinal cord itself. The outermost
layer is called the "dura mater," which is a Latin term that means "hard mother,"
indicating that early anatomists had at least a rudimentary sense of humor. The dura is
a very tough membrane that encloses the brain and spinal cord and prevents
cerebrospinal fluid from leaking out from the central nervous system. The space
between the dura and the spinal canal is called the "epidural space". This space is
filled with tissue, vessels and large veins. The epidural space is important in the
treatment of low-back pain, because it is into this space that medications such as
anesthetics and steroids are injected in order to alleviate pain and inflammation of the
nerve roots.13
Vertebra:
A vertebra (plural: vertebrae) is an individual bone in the flexible column that
defines vertebrate animals, e.g. humans. The vertebral column encases and protects
the spinal cord, which runs from the base of the cranium down the dorsal side of the
animal until reaching the pelvis. From there, vertebra continue into the tail.
Vertebrae are defined by regions. Cervical vertebrae are those in the neck area,
and can range from a single vertebra in amphibians, to seven in most mammals and
reptiles, and as many as 25 in swans or 76 in the extinct plesiosaur Elasmosaurus. The
dorsal vertebrae range from the bottom of the neck to the top of the pelvis. Dorsal
vertebrae attached to ribs are called thoracic vertebrae, while those without ribs are
called lumbar vertebrae. The sacral vertebrae are those in the pelvic region, and range

from one in amphibians, to two in most birds and modern reptiles, or up to 3 to 5 in
mammals. When more than one sacral vertebrae are fused into a single structure, it is
called the sacrum. The synsacrum is a similar fused structure found in birds that is
composed of the sacral, lumbar, and some of the thoracic and caudal vertebra, as well
as the pelvic girdle. Caudal vertebra compose the tail, and the final few can be fused
into the pygostyle in birds, or into the coccygeal or tail bone in chimpanzees or
humans.
Sacro-iliac Joint :
There is without a doubt a connection between chronic fixations in the
Sacroiliac Joint Anatomy, and hip arthritis. Every case of hip arthritis that I find has a
concommitent SIJ fixation. However, what we haven't yet discovered is whether the
SIJ fixation causes the hip arthritis, or the hip arthritis the SIJ fixation. Chicken and
egg. Sacroiliac joint anatomy (SI or sacro-iliac) is quite unlike any other joint in the
body, because the joint surfaces are covered by two different kinds of cartilage. Like
all true joints, there is cartilage on both sides of the SI joint surfaces, but the articular
surfaces have both hyaline cartilage (glassy) and fibro cartilage (spongy) surfaces that
rub against each other. No other joints have this feature!
The joint also has many large ridges and depressions that fit together like the
pieces in a puzzle. Unlike most other joints, the Sacroiliac Joint Anatomy is not
designed for large movements. The rocking movements made with every step are in
fact very small. The SI joint usually only moves about two to four millimeters during
weight bearing and forward flexion. It is a "viscoelastic joint", meaning that its major
movement comes from giving or stretching. Furthermore, it is common for the SI
joint to become even more stiff and actually lock, usually due to injury, but also due

to prolonged sitting, for example. This explains why manipulation is the treatment of
choice for the very painful SI joint syndrome.
Normal Sacrum Fused sacrum
The S-I joint can be thought of as the bottom joints of the spine relating to the
hip bones, The sacrum(bottom of the spine) relates on each side to the ilia (hip bones)
to form the sacroiliac joints. The ilia accept the femoral shafts of the lower extremities
to form the hip joints. Therefore, as a person walks with reciprocal motion of the legs,
the S-I joints also reciprocally move. There are muscles and ligaments that transverse
the S-I joint in the front and the back, all of which can be causes of pain and
inflammation if these joints are in dysfunction. The sacroiliac joint or SI joint is the
joint between the sacrum, at the base of the spine and the ilium of the pelvis, which
are joined by ligaments. It is a strong, weightbearing synovial joint with irregular
elevations and depressions that produce interlocking of the two bones. The human
body has two sacroiliac joints: a left and a right joint that often match individually but
are highly variable from person to person.The sacroiliac joints are two paired "kidney
bean" or L-shaped synovial joints that have minimal motion (2-18 degrees, which is
debatable at this time), that are formed between the articular surfaces of the sacrum
Fig. 7: Sacrum

and the ilium bones. The two sacroiliac joints move together as a single unit and are
considered bicondylar joints (where the two joint surfaces move correlatively
together). The joints are covered by two different kinds of cartilage; the sacral surface
has hyaline cartilage and the ilial surface has fibrocartilage. The stability of the SIJs
are maintained mainly through a combination of both bony structure and very strong
intrinsic and extrinsic ligaments. As we age the characteristics of the sacroiliac joint
change. The joint's surfaces are flat or planar in early life but as we start walking, the
sacroiliac joint surfaces develop distinct angular orientations (and lose their planar or
flat topography.) They also develop an elevated ridge along the ilial surface and a
depression along the sacral surface. The ridge and corresponding depression, along
with the very strong ligaments, increase the sacroiliac joints' stability and makes
dislocations very rare. The fossae lumbales laterales ("dimples of Venus") correspond
to the superficial topography of the sacroiliac joints.
Ligaments
The anterior sacroiliac ligament consists of
numerous thin bands, which connect the anterior
surface of the lateral part of the sacrum to the
margin of the auricular surface
Fig. 8: Anterior sacroiliac ligament

Interosseous sacroiliac ligament:
The Interosseous Sacroiliac Ligament lies deep to the posterior ligament, and
consists of a series of short, strong fibers connecting the tuberosities of the sacrum
and ilium. The major function of the interosseous sacroiliac ligament is to keep the
sacrum and ilium together and therefore prevent abduction or distraction of the
sacroiliac joint. This is performed by the nearly horizontal direction of the fibers
running perpendicular from the sacrum to the ilium.
Posterior sacroiliac ligament : Articulations of pelvis. Posterior view. (Short post.
sacroiliac ligament labeled at upper left; long post.
sacroiliac ligament labeled at center right.)
The posterior sacroiliac ligament is situated in a
deep depression between the sacrum and ilium
behind; it is strong and forms the chief bond of
union between the bones.
It consists of numerous fasciculi, which pass between the bones in various
directions. The upper part (short posterior sacroiliac ligament) is nearly horizontal in
direction, and pass from the first and second transverse tubercles on the back of the
sacrum to the tuberosity of the ilium.
The lower part (long posterior sacroiliac ligament) is oblique in direction; it is
attached by one extremity to the third transverse tubercle of the back of the sacrum,
and by the other to the posterior superior spine of the ilium.
Fig. 9: Posterior sacroiliac ligament

Sacrotuberous ligament: Articulations of pelvis, anterior view, with greater sciatic
foramen (labeled in red) and its boundaries.
The sacrotuberous ligament (great or
posterior sacrosciatic ligament) is situated at
the lower and back part of the pelvis. It is flat,
and triangular in form; narrower in the
middle than at the ends. It runs from the
sacrum (the lower transverse sacral tubercles,
the inferior margins sacrum and the upper
coccyx) to the tuberosity of the ischium.
The membranous falciform process of the
sacrotuberous ligament was found to be
absent in 13% of cadavers. When present it extends towards the ischioanal fossa
travelling along the ischial ramus and fusing with the obturator fascia. The
sacrotuberous ligament contains the coccygeal branch of the inferior gluteal artery.
The lower border of the ligament was found to be directly continuous with the
tendon of origin of the long head of the Biceps femoris in approximately 50% of
subjects. Biceps femoris could therefore act to stabilise the sacroiliac joint via the
sacrotuberous ligament.
If the pudendal nerve becomes entrapped between this ligament and the
sacrospinous ligament causing perineal pain, the sacrotuberous ligament is surgically
severed to relieve the pain.
Fig. 10: Sacrotuberous ligament

The anterior ligament may be described as just a slight thickening of the
anterior joint capsule. The anterior ligament is certainly not as strong and well defined
as are the posterior ligaments.
The posterior sacroiliac (SI) ligaments can be further divided into short
(intrinsic) and long (extrinsic). The dorsal interosseous ligaments are very strong
ligaments. This ligament is even stronger than bone; such that the pelvis will usually
fracture before the ligament tears. The dorsal sacroiliac ligament runs perpendicular
from just behind the articular surfaces of the sacrum to the ilium and function to keep
the sacroiliac joint from distracting or opening. The extrinsic sacroiliac joint
ligaments, the sacrotuberous and sacrospinous ligaments, limit the amount the sacrum
flexes (or nutates).16
The ligaments of the sacroiliac joint become loose during pregnancy due to the
hormone relaxin; this loosening allows widening of the pelvic joints during the
birthing process, especially the related symphysis pubis. The long SI ligaments may
be palpated in thin persons for pain and compared from one side of the body to the
other; however, the reliability and the validity of comparing ligaments for pain have
currently not been shown. The short ligaments (e.g. interosseous) cannot be assessed,
since they are located deep inside the pelvis.
The acetabulum is oriented inferiorly, laterally and anteriorly, while the
femoral neck is directed superiorly, medially, and anteriorly.
The transverse angle of the acetabular inlet can be determined by measuring
the angle between a line passing from the superior to the inferior acetabular rim and
the horizontal plane; an angle which normally measures 51° at birth and 40° in adults,
and which affects the acetabular lateral coverage of the femoral head and several

other parameters. The sagittal angle of the acetabular inlet measures 7° at birth and
increases to 17° in adults.
Femoral neck angle:
The angle between the longitudinal axes of the femoral neck and shaft, called
the caput-collum-diaphyseal angle or CCD angle, normally measures approximately
150° in newborn and 126° in adults (coxa norma). An abnormally small angle is
known as coxa vara and an abnormally large angle as coxa valga. Because changes in
shape of the femur naturally affects the knee, coxa valga is often combined with genu
varum (bow-leggedness), while coxa vara leads to genu valgum (knock-knees).
Fig. 11: The angles of femoral neck
Changes in trabecular patterns due to altered CCD angle. Coxa valga leads to
more compression trabeculae, coxa vara to more tension trabeculae.
Changes in CCD angle is the result of changes in the stress patterns applied to
the hip joint. Such changes, caused for example by a dislocation, changes the
trabecular patterns inside the bones. Two continuous trabecular systems emerging on
auricular surface of the sacroiliac joint meander and criss-cross each other down
through the hip bone, the femoral head, neck, and shaft.

In the hip bone, one system arises on the upper part of auricular surface to
converge onto the posterior surface of the greater sciatic notch, from where its
trabeculae are reflected to the inferior part of the acetabulum. The other system
emerges on the lower part of the auricular surface, converges at the level of the
superior gluteal line, and is reflected laterally onto the upper part of the acetabulum.
In the femur, the first system lines up with a system arising from the lateral
part of the femoral shaft to stretch to the inferior portion of the femoral neck and
head. The other system lines up with a system in the femur stretching from the medial
part of the femoral shaft to the superior part of the femoral head.
On the lateral side of the hip joint the fascia lata is strengthened to form the
iliotibial tract which functions as a tension band and reduces the bending loads on the
proximal part of the femur capsule.
The capsule attaches to the hip bone outside the acetabular lip which thus
projects into the capsular space. On the femoral side, the distance between the head's
cartilaginous rim and the capsular attachment at the base of the neck is constant,
which leaves a wider extracapsular part of the neck at the back than at the front. The
strong but loose fibrous capsule of the hip joint permits the hip joint to have the
second largest range of movement (second only to the shoulder) and yet support the
weight of the body, arms and head.
The capsule has two sets of fibers: longitudinal and circular. The circular
fibers form a collar around the femoral neck called the zona orbicularis. The
longitudinal retinacular fibers travel along the neck and carry blood vessels.

Blood and nerve supply:
The hip joint is supplied with blood from the medial circumflex femoral and
lateral circumflex femoral arteries, which are both usually branches of the deep artery
of the thigh (profunda femoris), but there are numerous variations and one or both
may also arise directly from the femoral artery. There is also a small contribution
from a small artery in the ligament of the head of the femur which is a branch of the
posterior division of the obturator artery, which becomes important to avoid avascular
necrosis of the head of the femur when the blood supply from the medial and lateral
circumflex arteries are disrupted (e.g. through fracture of the neck of the femur along
their course).
The hip has two anatomically important anastomoses, the cruciate and the
trochanteric anastomoses, the latter of which provides most of the blood to the head of
the femur. These anastomoses exist between the femoral artery or profunda femoris
and the gluteal vessels.
Muscles of the hip:
The hip muscles act on three mutually perpendicular main axes, all of which
pass through the center of the femoral head, resulting in three degrees of freedom and
three pair of principal directions: Flexion and extension around a transverse axis (left-
right); lateral rotation and medial rotation around a longitudinal axis (along the thigh);
and abduction and adduction around a sagittal axis (forward-backward); and a
combination of these movements (i.e. circumduction, a compound movement in
which the leg describes the surface of an irregular cone). It should be noted that some
of the hip muscles also act on either the vertebral joints or the knee joint, that with

their extensive areas of origin and/or insertion, different part of individual muscles
participate in very different movements, and that the range of movement varies with
the position of the hip joint. Additionally, the inferior and superior gemelli may be
termed triceps coxae together with the obturator internus, and their function simply is
to assist the latter muscle.
The movement of the hip joint is thus performed by a series of muscles which
are here presented in order of importance with the range of motion from the neutral
zero-degree position indicated:
Extension or retroversion (20°): gluteus maximus (if put out of action, active standing
from a sitting position is not possible, but standing and walking on a flat surface is);
dorsal fibers of gluteus medius and minimus; adductor magnus; and piriformis.
Additionally, the following thigh muscles extend the hip: semimembranosus,
semitendinosus, and long head of biceps femoris.
Flexion or anteversion (140°): iliopsoas (with psoas major from vertebral column);
tensor fascia latae, pectineus, adductor longus, adductor brevis, and gracilis. Thigh
muscles acting as hip flexors: rectus femoris and sartorius.
Abduction (50° with hip extended, 80° with hip flexed): gluteus medius; tenso fascia
latae; gluteus maximus with its attachment at the fascia lata; gluteus minimus;
piriformis; and obturator internus.
Adduction (30° with hip extended, 20° with hip flexed): adductor magnus with
adductor minimus; adductor longus, adductor brevis, gluteus maximus with its
attachment at the gluteal tuberosity; gracilis (extends to the tibia); pectineus,

quadratus femoris; and obturator externus. Of the thigh muscles, semitendinosus is
especially involved in hip adduction.
Physiology:
Like most joints, the SI joints' function includes some shock absorption for the
spine, along with torque conversion, allowing the transverse rotations that take place
in the lower extremity to be transmitted up the spine. The SI joint, like all lower
extremity joints, provides a "self-locking" mechanism (where the joint occupies or
attains its most congruent position, also called the close pack position) that helps with
stability during the push off phase of walking. The joint locks (become close pack) on
one side as weight is transferred from one leg to the other, and through the pelvis, the
body weight is transmitted from the sacrum to the hip bone.
The motions of the sacroiliac joints are:
Anterior innominate tilt of both innominate bones on the sacrum (where the
left and right move as a unit). Posterior innominate tilt of both innominate bones on
the sacrum (where the left and right move together as a unit). Anterior innominate tilt
of one innominate bone while the opposite innominate bone tilts posteriorly on the
sacrum (antagonistic innominate tilt) which occurs during gait
The Skeletal System serves many important functions; it provides the shape
and form for our bodies in addition to supporting, protecting, allowing bodily
movement, producing blood for the body, and storing minerals. The number of bones
in the human skeletal system is a controversial topic. Humans are born with about 300
to 350 bones, however, many bones fuse together between birth and maturity. As a
result an average adult skeleton consists of 208 bones. The number of bones varies

according to the method used to derive the count. While some consider certain
structures to be a single bone with multiple parts, others may see it as a single part
with multiple bones. There are five general classifications of bones. These are Long
bones, Short bones, Flat bones, Irregular bones, and Sesamoid bones. The human
skeleton is composed of both fused and individual bones supported by ligaments,
tendons, muscles and cartilage. It is a complex structure with two distinct divisions.
These are the axial skeleton and the appendicular skeleton.
The Skeletal System serves as a framework for tissues and organs to attach
themselves to. This system acts as a protective structure for vital organs. Major
examples of this are the brain being protected by the skull and the lungs being
protected by the rib cage.
Located in long bones are two distinctions of bone marrow (yellow and red).
The yellow marrow has fatty connective tissue and is found in the marrow cavity.
During starvation, the body uses the fat in yellow marrow for energy. The red marrow
of some bones is an important site for blood cell production, approximately 2.6
million red blood cells per second in order to replace existing cells that have been
destroyed by the liver. Here all erythrocytes, platelets, and most leukocytes form in
adults. From the red marrow, erythrocytes, platelets, and leukocytes migrate to the
blood to do their special tasks.
Another function of bones is the storage of certain minerals. Calcium and
phosphorus are among the main minerals being stored. The importance of this storage
"device" helps to regulate mineral balance in the bloodstream. When the fluctuation
of minerals is high, these minerals are stored in bone; when it is low it will be
withdrawn from the bone.

Human synovial joint composition :
Joints are structures that connect individual bones and may allow bones to
move against each other to cause movement. There are two divisions of joints,
diarthroses which allow extensive mobility between two or more articular heads, and
false joints or synarthroses, joints that are immovable, that allow little or no
movement and are predominantly fibrous. Synovial joints, joints that are not directly
joined, are lubricated by a solution called synovia that is produced by the synovial
membranes. This fluid lowers the friction between the articular surfaces and is kept
within an articular capsule, binding the joints with taut tissue.
Understanding how the different layers of the hip are built and connected can
help you understand how the hip works, how it can be injured, and how challenging
recovery can be when this joint is injured. The deepest layer of the hip includes the
bones and the joints. The next layer is made up of the ligaments of the joint capsule.
The tendons and the muscles come next.
The important structures of the hip can be divided into several categories.
These include
• Bones and joints
• Ligaments and tendons
• Muscles
• Nerves
• Blood vessels
• Bursae
• Bones and Joints

The bones of the hip are the femur (the thighbone) and the pelvis. The top end
of the femur is shaped like a ball. This ball is called the femoral head. The femoral
head fits into a round socket on the side of the pelvis. This socket is called the
acetabulum.
The femoral head is attached to the rest of the femur by a short section of bone
called the femoral neck. A large bump juts outward from the top of the femur, next to
the femoral neck. This bump, called the greater trochanter, can be felt along the side
of your hip. Large and important muscles connect to the greater trochanter. One
muscle is the gluteus medius. It is a key muscle for keeping the pelvis level as you
walk.
Articular cartilage is the material that covers the ends of the bones of any
joint. Articular cartilage is about one-quarter of an inch thick in the large, weight-
bearing joints like the hip. Articular cartilage is white and shiny and has a rubbery
consistency. It is slippery, which allows the joint surfaces to slide against one another
without causing any damage. The function of articular cartilage is to absorb shock and
provide an extremely smooth surface to make motion easier. We have articular
Fig. 12: Bones of the hip

cartilage essentially everywhere that two bony surfaces move against one another, or
articulate.
In the hip, articular cartilage covers the end of the femur and the socket
portion of the acetabulum in the pelvis. The cartilage is especially thick in the back
part of the socket, as this is where most of the force occurs during walking and
running.
Blood Vessels:
Traveling along with the nerves are the large vessels that supply the lower
limb with blood. The large femoral artery begins deep within the pelvis. It passes by
the front of the hip area and goes down toward the inner edge of the knee. If you place
your hand on the front of your upper thigh you may be able to feel the pulsing of this
large artery.
The femoral artery has a deep branch, called the profunda femoris (profunda
means deep). The profunda femoris sends two vessels that go through the hip joint
capsule. These vessels are the main blood supply for the femoral head. As mentioned
Fig. 13: Blood vessels of hip

earlier, the ligamentum teres contains a small blood vessel that gives a very small
supply of blood to the top of the femoral head.
Other small vessels form within the pelvis and supply the back portion of the
buttocks and hip.14
Bursae:
Where friction occurs between muscles, tendons, and bones there is usually a
structure called a bursa. A bursa is a thin sac of tissue that contains fluid to lubricate
the area and reduce friction. The bursa is a normal structure. The body will even
produce a bursa in response to friction.
Think of a bursa like this. If you press your hands together and slide them
against one another, you produce some friction. In fact, when your hands are cold you
may rub them together briskly to create heat from the friction. Now imagine that you
hold in your hands a small plastic sack that contains a few drops of salad oil. This
sack would let your hands glide freely against each other without a lot of friction.
A bursa that sometimes causes problems in the hip is sandwiched between the
bump on the outer hip (the greater trochanter) and the muscles and tendons that cross
over the bump. This bursa, called the greater trochanteric bursa, can get irritated if the
iliotibial band (discussed earlier) is tight. Another bursa sits between the iliopsoas
muscle where it passes in front of the hip joint. Bursitis here is called iliopsoas
bursitis. A third bursa is over the ischial tuberosity, the bump of bone in your buttocks
that you sit on. Many powerful muscles connect to and cross by the hip joint making
it possible for us to accelerate quickly during actions like running and journey.

SPINE BIOMECHANICS
We briefly touch upon spine biomechanics and estimates of muscle forces
about the spine because this area of research is critical to ergonomics and whole body
biomechanics and is a heavily studied area. There are a number of reasons for
studying spine biomechanics, among these:
• Spine disorders are the most prevalent cause of chronic disability.
• Annual prevalence of AS is one in 250 people.
• HLA B27 antigen has been found in the blood of 95% of patients with AS.
• Environmental factors such as genitourinary or bowel infections acting as
triggers in the genetically predisposed individuals.
• Synovitis producing hyperplasia and accumulation of mononuclear
inflammatory cells is seen in the spine sacroiliac joint and costo-vertebral
joints leading to erosion, destruction of cartilage.
Fig. 14 : Bursa of hips

To better understand how muscle loads are placed on the spine, we need to
know some reference of anatomy. First consider the bony anatomy of the spine as
illustrated above.
• The major vertebra within the spine are grouped as cervical, thoracic and
lumbar. There are soft cartilaginous disks between each vertebra, that are
named appropriately enough intervertebral disks. A schematic of an
intervertebral disc is shown below:
• It is typically a problem with the disk that occurs when people complain of
low back pain. The disk contains an interior gel, the nucleus pulposus, and an
outer layer of laminated concentric rings formed primarily of type I collagen.
Typically severe lower back pain associated with numbness occurs when the
nucleus pulposus is "squeezed out" through the annulus fibrosus and places
pressure on the spinal cord. Although there is evidence that excessive loads
experimentally can cause disk prolapse, the clinical relationship is much more
complex and may involve genetic predispositions as well. Still, it is widely
theorized that excessive loads on the disks can cause damage, namely fissures
in the disk, that over time lead to disk degeneration and prolapse. Thus,
understanding the compressive loads on the spine is of critical importance for
Fig. 15 : Intervertebral disc

understanding the etiology of low back pain. To estimate spinal compression
loads, we also need to know something of spinal muscle anatomy.
• Spinal Muscles: The musculature of the spine is complex and is divided into 5
major classifications by location:
• Posterior Wall Musculature: erector spinae of paravertebral muscles
• Respiratory or Intercostal Muscles: between ribs
• Abdominal Wall Muscles: intertransversus, interior and exterior obliques,
rectus abdominus
• Superficial Trunk Muscles - broad muscles including the rhomboids,
latissimus dorsi, pectoralis, and trapezius
• Lower Trunk Muscles: transversis abdominus
A simplified view of muscles affecting the spine are shown below:
Fig. 16: Simplified view of muscles

Biomechanics of the Hip:
This section is not intended to be a comprehensive analysis of the forces
acting on the proximal femur and the acetabulum. It is, however, important to the
success of total hip arthroplasty that one understands the factors influencing both the
direction and magnitude of forces acting upon the femoral head. The forces exerted on
the hip have their biological expression in the form of the femur and acetabulum,
particularly in the location and orientation of the trabecular pattern. The forces
exerted on the prosthetic femoral head in a properly performed total hip replacement
will be very similar in both direction and magnitude.
Of all the species in the animal kingdom, only birds and man habitually use a
bipedal gait. Even the larger primates use a quadripedal ambulation mode for most of
their activity. When the weight of the body is being borne on both legs, the center of
gravity is centered between the two hips and its force is exerted equally on both hips.
Under these loading conditions, the weight of the body minus the weight of both legs
is supported equally on the femoral heads, and the resultant vectors are vertical.
When the hips are viewed in the sagittal plane and if the center of gravity is
directly over the centers of the femoral heads, no muscular forces are required to
maintain the equilibrium position, although minimal muscle forces will be necessary
to maintain balance. If the upper body is leaned slightly posteriorly so that the center
of gravity comes to lie posterior to the centers of the femoral heads, the anterior hip
capsule will become tight, so that stability will be produced by the Y ligament of
Bigelow. Therefore, in symmetrical standing on both lower extremities, the
compressive forces acting on each femoral head represent approximately one-third of
body weight.

In a single leg stance, the effective center of gravity moves distally and away
from the supporting leg since the nonsupporting leg is now calculated as part of the
body mass acting upon the weight-bearing hip. Since the pillar of support is eccentric
to the line of action of the center of gravity, body weight will exert a turning motion
around the center of the femoral head. This turning motion must be offset by the
combined abductor forces inserted into the lateral femur. In the erect position, this
muscle group includes the upper fibers of the gluteus maximus, the tensor fascia lata,
the gluteus medius and minimus, and the pyriformis and obturator internus. The
combined resultant vector of the abductor group can be represented by the line of
action M in Figure below. Since the effective lever arm of this resultant force (BO) is
considerably shorter than the effective lever arm of body weight acting through the
center of gravity (OC), the combined force of the abductors must be a multiple of
body weight. The vectors of force K and force M produces a resultant compressive
load on the femoral head that is oriented approximately 16° obliquely, laterally, and
distally. The orientation of this resultant vector is exactly parallel to the orientation of
the trabecular pattern in the femoral head and neck.
The effect of this combined loading of body weight and the abductor muscle
response required for equilibrium results in the loading of the femoral head to
approximately 4 times body weight during the single leg stance phase of gait. This
means that in normal walking the hip is subjected to wide swings of compressive
loading from one-third of body weight in the double support phase of gait to 4 times
body weight during the single leg support phase. The factors influencing both the
magnitude and the direction of the compressive forces acting on the femoral head are
• The position of the center of gravity;

• The abductor lever arm, which is a function of the neck-shaft angle;
• The magnitude of body weight.
Shortening of the abductor lever arm through coxa valga or excessive femoral
anteversion will result in increased abductor demand and therefore increased joint
loading. If the lever arm is so shortened that the muscles are overpowered, then either
a gluteus minus lurch (the center of gravity is brought laterally over the supporting
hip) or a pelvic tilt (Treridelenburg gait) will occur.
Forces on the hip with sideways limping. Note the reduction of vector M and
R even though K is unchanged. R is also more vertically oriented.15
Since the loading of the hip in the single leg stance phase of gait is a multiple
of body weight, increases in body weight will have a particularly deleterious effect on
the total compressive forces applied to the joint. The effective loading of the joint can
be significantly reduced by bringing the center of gravity closer to the center of the
femoral head. Sideways limping, however, requires acceleration of the body mass
laterally, its deceleration during the stance phase of gait, and then its acceleration
back to the midline or even to the other side as the single leg stance phase changes to
the opposite extremity. This requires considerable energy consumption and is a much
Fig. 17.a: Biomechanics of hip

less efficient means of ambulation than the normal situation in which the hip is
subjected to these considerable forces. Another effect of sideways limping is that the
resultant vector becomes more vertical because the center of gravity is acting in a
more vertical direction, and therefore the bending moment the femoral neck is
increased.
Another mechanism for reducing the resultant load on the femoral head is the
use of a walking stick in the opposite hand. Since some of its force is transferred to
the walking stick through the hand, the effective load of body weight is thus reduced
in two ways:
• The effective load of body weight is reduced;
• Since the turning moment around the femoral head is reduced, the abductor
demand is also reduced. 17
Fig. 17.b: Biomechanics of hip

ANKYLOSING SPONDYLITIS
Ankylosing spondylitis (AS, from Greek ankylos, bent; spondylos, vertebrae),
previously known as Bechterew's disease, Bechterew syndrome, and Marie Strümpell
disease, a form of Spondyloarthritis, is a chronic, inflammatory arthritis and
autoimmune disease. It mainly affects joints in the spine and the sacroilium in the
pelvis, causing eventual fusion of the spine.
Ankylosing Spondylitis A chronic progressive inflammatory disease of the spine,
sacroiliac joints, and paravertebral soft tissues. It is characterised by early sacroiliac
joint involvement, followed by ossification of the annulus fibrosusand surrounding
connective tissue, along with arthritic changes in the intervertebral joints, which
results in bony ankylosing of the spine. Peripheral joints may also be involved. The
disease occurs predominantly in young adult males and is often associated with the
presence of the HLA-B27 antigen, absence of rheumatoid factor in the serum, and
lack of rheumatoid nodules.18
Ankylosis.(n) Abnormal fixation, stiffness, immobility and consolidation of a joint.
This may result from bony, cartilaginous, or fibrous tissue overgrowth.
Ankylosing spondylitis belongs to a group of seronegative
spondyloarthropathies. A chronic form of arthritis, AS is estimated to affect 1.4 % of
the general population. Severity of the disease varies among individuals as well as
remission and exacerbation periods. Ankylosing spondylitis primarily affects the
spine and hip joints causing progressed bone fusion including fusion of the
costovertebral joints, erosion, destruction of the vertebral endplates, osteophytes,
subchondral sclerosis, squaring of vertebral bodies, ossification of the intervertebral

disc, narrowing of joints, and osteoporosis. Fusion of the spine mainly occurs at the
lumbar level with progression cranially to the cervical spine. Enthesopathy, or
inflammation of bone attachment to tendons, ligaments, and joint capsules also
occurs. The spine adopts a long bone persona and is easily susceptible to fracture. As
the spine undergoes chronic inflammation, the patient develops a more pronounced
curvature to lessen the severity of pain. The result is a fixed flexion deformity of the
spine or otherwise referred to as a "bamboo spine" when viewed radiographically.
Such an irregular posture contributes to a loss of horizontal gaze, physiologically
incorrect sagittal contour, physical embarrassment, respiratory restriction, and a
higher risk for trauma.
THE SPONDYLOARTHROPATHIES
The spondyloarthropathies (SpAs) encompass a group of clinical syndromes
that are linked in terms of disease manifestations and in terms of genetic
susceptibility. The clinical subsets most commonly recognized are ankylosing
spondylitis, reactive arthritis, psoriatic arthritis and enteropathic arthritis.8
In addition, there is sizeable population of patients that does not fit into one of
these distinct diagnostic categories but shares some of common clinical features. The
syndrome associated with this subset is termed undifferentiated SpA, which over time
may evolve into classical pattern such as AS but which may remain in an
undifferentiated pattern.
Family studies in which there are multiple individuals with an SpA have
emphasized some of the commonality between the four distinct subsets .The
impression from such studies is that there is shared common path of immunogenetic
susceptibility upon which various genetic and environmental influences lead to

characteristic clinical subsets. Thus, if enteropathic arthritis occurs in such a family,
in another family it may be psoriatic arthritis. In this sense, the SpAs seem to “breed
true”. It should be recognized, that some distinct feature can be clinically very close in
their manifestations (e.g. guttate psoriasis and keratodermia blennorrhagica), making
simple discrimination sometimes difficult.
There are several common features in family of SpAs, which at once link them
and serve to distinguish them from the other major contributor to chronic
polyarthritis, RA. The arthropathies have a strong predilection for spine, in
particularly the sacroiliac joints, There is shared predilection for new bone formation
Fig. 18

at sites of chronic inflammation, with joint ankylosis as a consequence. When
peripheral arthritis occurs, it is commonly lower extremity and asymmetrical. There is
predilection for the sites of tendon insertion into bone (enthese), so that enthesis
becomes one of the most specific clinical manifestations of SpAs.The basis for the
target organ involvement has invoked biomechanical factors, innervation, local
vascularity and bone marrow derived inflammatory mediators, but the precise
mechanism for this relationship remains in completely defined.
Whatever the reason, inflammation in the enthesis and contiguous subchondral
bone as a characteristic feature of this arthritis, and the appearance of this
inflammation on MRI is distinct enough to lead some investigators to use such
imaging for diagnostic purposes.
Predilection for ocular inflammation, particularly acute anterior uveitis, is
common feature of all subsets and indeed is considered by some to be a member of
SpA in its own right because it may occur in the same susceptible populations of
patients even in the absence of joint involvement. Finally all subsets have an
association with the class I HLA B27 allele, with the strength of the association
varying somewhat between them. Increasingly, diagnostic criteria are being used that
emphasizes the clinical common features, namely inflammatory spinal pain or
asymmetrical, lower extremity synovitis. There are several distinctive features that
differentiate the SpA from rheumatoid arthritis (RA), the other main contributor to the
differential diagnosis of chronic polyarthritis in the table below. These include sex
predilection, HLA association, pattern of joint involvement, and presence of
rheumatoid factor, which becomes the serologic borderline between seropositive
disease (RA) and seronegative disease (SpA).

CONTRAST OF RHEUMATOID ARTHRITIS & SPONDYLOARTHROPATHY
Feature Rheumatoid
arthritis
Ankylosing
spondylitis
Entropathic
arthritis
Psoriatic
arthritis
Reactive
arthritis
Male/female
ratio
1:3 3:1 1:1 1:1 10:1
HLA
association
DR4 HLA B27 HLA B27
(axial)
HLA B27
(axial)
HLA B27
Joint pattern Symmetric,
Peripheral
Axial Axial and
peripheral
Axial and
asymmetric
peripheral
Axial and
asymmetric
peripheral
Sacroiliac 0 Symmetric Symmetric Asymmetric Asymmetric
Syndesmophyte 0 Smooth,
marginal
Smooth,
marginal
Coarse,
nonmarginal
Coarse,
nonmarginal
Eye Scleritis Iritis +/- 0 Iritis or
conjunctivitis
Skin Vasculitis 0 0 0 Keratoderma
Rheumatoid
factor
80% 0 0 0 0
HLA =human leukocyte antigen.

Furthermore, it is common for the SI joint to become even more stiff and
actually lock, usually due to injury, but also due to prolonged sitting, for example.
This explains why manipulation is the treatment of choice for the very painful SI joint
syndrome.
Orthopaedic surgeons, researching arthritis in knees and hips make the
following statement: Mechanical factors, including joint instability and malalignment,
contribute to the progressive degeneration that characterizes hip and knee arthritis.
Mobilization may also be useful for keeping the joint loose using certain specific
exercises and stretches that are important in the rehabilitative phase of the treatment.
Normal upper sacrum, sacroiliac joint and presacral soft tissues is involved.
The positioning of the cadaver during preparation of the cadaver has induced a slight
malalignment of the sacroiliac joints. These joints carry a true diarthrodial synovial
joint anteriorly and a complex array of dense ligaments posteriorly. The joints are
covered anteriorly by the iliacus muscle which in turn is bounded anteriorly by the
psoas major muscle. The iliolumbar nerve trunk and blood vessels are firmly stretched
over the (anterior) convexity of the ala. The lower poles of the ganglia, arteries and
veins are embedded in the fat filling the wide SI foramina, between them is the
vestige of the SI disc. Posteriorly the sacral canal contains the S2 ganglia and the
terminating thecal sac.
FACTORS PREDISPOSING
HLA B27
The major histocompatibility complex (MHC), on the short arm of
chromosome 6 in humans in one of the most polymorphic regions of the human

genome. This is particularly so for the B locus, which constitutes part of the class1
MHC genes in this complex. There are more than 200 different alleles at this locus
of which B27 is one As with all HLA alleles, there is codominant expression of B
locus genes, so that most individuals who are “B27 positive” are heterozygous for the
B locus and there appears to be little clinical or prognostic significance associated
with the less common homozygous B27 state. The conventional role of class1HLA
antigens is to present a processed peptide to the T-cell receptor of a specific CD8+
cytotoxic T cell, there by initiating an immune response against the pathogen from
which that peptide was derived by intracellular proteolysis and processing. This
function places the HLA antigens in a critical role in host defense against pathogens.
Three hypothesis have been put forward:
• HLA B27 acts as a receptor site for an infective agent.
• HLA B27 is a marker for an immune response gene that determines susceptibility
to an environmental cause.
• HLA B27 may induce tolerance to foreign antigens with which it cross-reacts.
The offspring of an individual with HLA B27 have 50% of chance of carrying
the same antigen.19
The role of class I HLA antigen in pathogenesis is supported by the fact that
HLA-B27 transgenic mice spontaneously develop arthritis, skin, gut and
genitourinary lesions. There are clues that infections play a role, with part of the
organism which are structurally similar to the HLA molecule triggering cross-reactive
antibody formation. AIDS is increasing the prevalence of reactive arthritis and
spondylytis is sub-Sharan Africa even in the absence of HLA B27. The types of
arthritis that follow a precipitating infection are called reactive arthritis. The

specialized immune systems of the gut and genitourinary mucous membranes may
also play causal role, perhaps reacting to local infections or to antigens which cross
the damaged mucosa.20
Aetiology:
The tendency to develop ankylosing spondylitis is believed to be genetically
inherited, and the majority (nearly 90%) of patients with ankylosing spondylitis are
born with the HLA-B27 gene. Blood tests have been developed to detect the HLA-
B27 gene marker and have furthered our understanding of the relationship between
HLA-B27 and ankylosing spondylitis. The HLA-B27 gene appears only to increase
the tendency of developing ankylosing spondylitis, while some additional factor(s),
perhaps environmental, are necessary for the disease to appear or become expressed.
For example, while 7% of the United States population have the HLA-B27 gene, only
1% of the population actually have the disease ankylosing spondylitis. In Northern
Scandinavia (Lapland), 1.8% of the population have ankylosing spondylitis while
24% of the general population have the HLA-B27 gene. Even among HLA-B27-
positive individuals, the risk of developing ankylosing spondylitis appears to be
further related to heredity. In HLA-B27-positive individuals who have relatives with
the disease, their risk of developing ankylosing spondylitis is 12% (six times greater
than for those whose relatives do not have ankylosing spondylitis).28
Recently, two more genes have been identified that are associated with
ankylosing spondylitis. These genes are called ARTS1 and IL23R. These genes seem
to play a role in influencing immune function. It is anticipated that by understanding
the effects of each of these known genes researchers will make significant progress in
discovering a cure for ankylosing spondylitis.21

Epidemiology:
Ankylosing spondilitis is also called as Strumpell and Marie, it was described
at the end of 19th century.27 It occurs in both the sexes but milder in female. The sex
ratio suggests that (M:F = 10:1). The prevalence in different ethnic groups is related
to the frequency of HLA-B27 in these populations shown in the figure below.
Graph 1: Incidence of Ankylosing spondilitis with reference to HLA-B27
Pathology:
The early histological changes in the synovial joints resemble rheumatoid
arthritis, but with less prominent lesions of the surface layers. The most important
effects are in the cartilaginous joints. Bony ankylosis is more frequent and the
sacroiliac joints often become fused. The apophyseal joints are involved and the discs
show replacement of the nucleus pulposus, the annulus fibrosus and parts of the
vertebral body by vascular fibrous tissue without any evidence of marked
inflammatory changes. In the spine, the lesion is in the ligamentous attachment to
bone (the enthesis) and this is characteristic of the disorder. 29
50%
8%
14%
8%
8%
0.50%
0.50%
0.50%
5%
1%
1%
1%
1%
0.50%
0.50%
0.50%
Haida Indians
White Americans
Finns
English
Germans
Japanese
Black Africans
Aboringines Ankylosing spondylitis
HLA‐B27

As the disease extends up to the intervertebral joints, there is ‘squaring’ of the
vertebral bodies and calcification of the annulus fibrous giving the characteristic
syndesmophytes which fuse to form the classic ‘bamboo spine’. This is caused by
inflammation of the anterior corners of the vertebrae which extends into the outer
layers of the annulus fibrosus.
Fig. 19: Spine in ankylosing spondylitis
Calcification of the inter-vertebral ligaments occurs. At this stage, there is
osteoporosis of the vertebra, and fractures of the spine after minor trauma can occur.
Other cartilaginous joints, such as the sternomanubrial joint and symphysis pubis, can
be affected with erosions and bony ankylosis.
http://w w w .medindia.net/patients/patientinfo/Images/anky losing_spondy lit is . g i f

Clinical features:
A gradual onset of low backache often with bilateral sciatic radiation as far as
knees, worse on waking and eased by exercise, occurring in young male is the
classical presentation of disease.24
The following features suggest inflammatory, not mechanical, low back pain
• The disease most commonly begins between 16 and 40 years of age.
• insidious and persistent discomfort for months with constitutional disturbances,
• Morning stiffness, the pain usually disturbs the sleep and stiffness after
immobility.
• Improvement of pain and stiffness with exercise.
In late stages of the disease there may be reduction in spinal pain as the axial
skeleton becomes ankylosed. Involvement of the costovertebral joints may result in
chest pain and, later, decreased chest expansion.
Other historic features that suggest the disease include common associations
such as eye disease, tendonitis, and a family history of low back pain, inflammatory
bowel disease, or psoriasis.25
The patient complains of back pain especially in the early sages when there
may be tenderness over the sacro-iliac joints. Later, examination will show abnormal
rigidity of the spine, reduced chest expansion and fixation of the hip joints. In
untreated cases, a flexion deformity of the spine ie, Kyphosis, lordosis, scoliosis,
asymmetry and range of motion is disturbed.26

Diagnosis is often delayed, symptoms being ascribed to lumbar disc disease.
In spondylitis, spinal mobility is limited in all directions in contrast to disc prolapse,
hen lateral flexion is usually normal. The lumbar spine becomes flattened and the
normal lordosis is lost. Sarco-iliac tenderness may be present. In an advanced case,
the diagnosis is usually decided on the posture, gait and limitation of back
movements. Only a few patients exhibit marked kyphosis and spinal rigidity.
Peripheral joints are involved in about a quarter of patients, and involvement
of the hip is important because of the functional implications. Sometimes, pain and
tenderness at thesite of tendinous insertions can be prominent feature, with the back,
pelvic brim and ischial tuberosities being characteristic sites. Several joints are
involved, usually the large joints of the lower limb frequently in an asymmetric
fashion.
The chest may also be involved. However, chest expansion is more difficult ot
measure, chest involvement usually is pronounced only later in the course of the
illness.
Although primarily an articular disease of the axial and peripheral skeleton,
other organs may be involved.
Extra-articular features of ankylosing spondylitis
• Malaise and weight loss
• Iritis
• Apical pulmonary fibrosis
• Amyloidosis
• Cardiac involvement

a. Aortic regurgitation
b. Conduction defects
• Neurological features
a. Spinal fractures
b. Cauda equine syndrome
Laboratory findings:
HLA-B27 gene is present in approximately 90% of patienst with AS. A mild
normochromic, normocytic anemia may be present. Patients with severe disease may
show an elevated talkaline phosphatase level. Rheumatoid factor and antinuclear
antibodies are largely absent. In cases with restriction of chest wall motion, decreased
vital capacity and increased functional residual capcity are common, but airflow
measurements are normal and ventilatory function is usually well maintained. The
ESR is raised while the disease is active.
At the level of joint histopathology, sites of chronic inflammation in the
former are associated with erosions but in the latter are associated with new bone
formation. This suggests a fundamental difference in the cytokine profile in the
microenvironment of the joint, and although there is some evidence that SpAs reflect
more of a type 2T helper cell (Th2) cytokine profile as opposed to the (Th1) profile
of RA.
• Bone mineral density and osteoporosis in Ankylosing Spondylitis
• Analysis of posture in patients with Ankylosing Spondylitis
• Sagittal balance of the spine in Ankylosing Spondylitis
• Planning the restoration of view and balance in Ankylosing Spondylitis.22

Diagnosis:
• A history of inflammatory back pain
• Limitation of motion of the lumbar spine in both the sagittal and frontal planes.
• Limited chest expansion, relative to standard values for age and sex.
• Definite radiographic sarcoiliitis.
Treatment
There is no definitive treatment for AS. Several nonsteroidal anti-
inflammatory drugs (NSAIDs) have proved effective in reducing the pain and
stiffness of AS and are commonly used.
Mostly conservative treatment which consists of rest, drugs, hot packs, spinal
exercises, traction, corset and education regarding the prevention of back pain.
Alternative Treatments
The National Institutes of Health defines complementary and alternative
medicine (CAM) as a group of diverse medical and health care systems, practices, and
products that are not presently considered to be a part of conventional medicine. CAM
therapies used alone are often referred to as "alternative". 23
Americans spend more than $1 billion a year on nontraditional treatments for
arthritis. The reasons for seeking CAM treatments vary – many people want relief
from pain and suffering that traditional medications have not provided; they hope to
avoid potentially serious side effects associated with such medications; and certain
conventional medical and surgical treatments cost more than many of us can afford.

Although there has been no rigorous scientific evidence to support the use of
CAM by people with ankylosing spondylitis (AS) and its related diseases, some
patients have benefited from such treatments.
Acupuncture
The exact way in which acupuncture works on the body remains unclear, but
stimulation of acupuncture points by puncturing the skin with hair-thin needles may
lead to release by the brain and spinal cord of opium-like molecules that help relieve
pain.
Enough research suggests that acupuncture relieves pain in some people, and
is safe if performed by a trained professional using sterile or disposable needles. More
scientific studies are underway to help determine its effect on various forms of
arthritis.
Treatments may be time-consuming and expensive, although some health plans cover
a certain number of acupuncture treatments per year for a variety of conditions.
Chiropractic Treatment
Some people with spondylitis swear by regular chiropractic sessions, but
doctors do not recommend this treatment for us. "Anyone with limited spinal mobility
due to [spondylitis] should avoid manipulation of their back or neck by chiropractors
and masseurs because it can be dangerous," claims Dr. Muhammad Asim Khan,
rheumatologist, researcher, and AS patient. Dr. Khan explains that chiropractic
treatments have sometimes inadvertently led to spinal fractures and neurological
complications, especially in people with fusion (extra bone growth) due to
spondylitis.

Massage
Many people with spondylitis find therapeutic massage very helpful, and if
done carefully, it can be a beneficial tool for pain relief and stress reduction. If a
massage therapist is aware of a person's spondylitis and understands the disease and
any potential manipulation issues, gentle massage can help promote well being. It
may provide temporary relief of pain or stiffness, and in some cases improve
flexibility because of the increased blood circulation. "In all my years of experience
as a physical therapist, I have never known massage to worsen the symptoms of
inflammation in a patient with AS. Deep tissue mobilization is nearly always
welcomed by those with AS and is usually given in combination with passive
stretches and ultrasound, heat or ice,".
Yoga Therapy
Yoga has been practiced for over 5,000 years and can greatly benefit people
with spondylitis under the instruction of a knowledgeable instructor who can tailor the
program to the individual.
DIET'S EFFECT ON SPONDYLITIS SYMPTOMS
In recent years many specialized diets have gained popularity among some
people with arthritis. To date, none of these claims have been substantiated by
rigorously controlled studies. That said, some people find that certain foods trigger
changes in symptoms - either for the better or the worse. If you find yourself noticing
this type of pattern, try keeping a food diary for a few weeks to find out if indeed
what you eat makes a difference or if you have food sensitivities.

Whether a person is affected by a chronic illness or not, there are some
straightforward guidelines that if followed, would lead to improved health and well-
being for almost everyone.
• Both calcium and alcohol affect the strength of the bones, and it is a well known
fact that people with spondylitis are already at higher risk for osteoporosis, a
dangerous thinning of the bones that can lead to fractures. Following a diet with
adequate amounts of calcium and vitamin D will help reduce the risk of
osteoporosis. Alcoholic beverages can also weaken bones. Consuming more than
two alcoholic drinks per day increases a person's chances of developing weakened
bones. In addition, alcohol mixed with certain medications can cause serious side-
effects to the gastro-intestinal tract and to major organs such as the liver and the
kidneys.
Experts agree that there are basic guidelines to good nutrition, which are:
• Eat a variety of foods that make you feel good - avoid those that do not.
• Eat plenty of vegetables, fruits, and whole-grain products.
• Use fat (especially saturated fat found in animal products), cholesterol, sugar,
and salt in moderation.
• Drink 8-10 glasses of water a day.
• Most people receive daily requirements of vitamins and minerals by eating a
well-balanced diet, but others need to take vitamin supplements.
• Avoid alcohol or foods that can interact with your medication. Talk with your
doctor and/or pharmacist about potential interactions.

Radiologic Findings
Erosions are much less than seen with other spondyloarthropathies. The
synovial portion of the SI joint, i.e. the anteroinferior 1/2 to 2/3 of the joint, ankyloses
first, follwed by the ligamentous portion. Ankylosis of the posterosuperior
ligamentous portion is considered to look like a "star."
Other findings you might see in the pelvis, if you're not overwhelmed by those
SI joints and a glimpse of the spine, are ossification of ligamentous attachments in the
iliac crests and ischial tuberosities, classically giving a purported "whiskered" look.
That sounds cute doesn't it. Looks just kind of fuzzy to me. The symphysis pubis can
show tiny "serrated" erosions like the SI joints, before it ankyloses. Purportedly,
~25% of ankylosing sponylitis eventually has symphysis pubis involvement.

HOMOEOPATHIC CONCEPT OF HEALTH, DISEASE, CURE AND
APPROACH TO THE DISEASE
Hahnemann explained in the aphorism 11 as “It is only this spiritual, self
acting (automatic) vital force every where present in the organism, that is primarily
deranged by the dynamic influence upon it of the morbific agent inimical to life, it is
only the vital principle, deranged to such an abnormal state, that can furnish the
organism with disagreeable sensations, and incline it to the irregular processes which
we call disease; for as a power invisible in itself and only cognizable by its effects on
the organism, its morbid derangement only makes itself known by the manifestation
of disease in the sensation and functions of those parts of the organism exposed to the
senses of the observer and the physician, that is by morbid symptoms and in no other
way can it make itself known.
Homoeopathy not only deals with the disease but the person as a whole.
Disease are nothing more than alteration in the site of the health of the individual
which expresses themselves with morbid signs and symptoms. This is where the
approach of homoeopathy varies from modern method of patient cure. Much stress
and value is placed on homoeopathic physician when his duty is not only to treat the
desire but to deal with this whole person to define problem of the patient and to
formulate the totality based on which the remedy should be selected using “the law of
similar”30
The biological concept of disease as elaborated above stands accepted in
Homoeopathy. The study of disease however, the homoeopathic physician as is
already indicated considers the individual response on the greater importance from the

standpoint of the selection of curative remedy and is guided by the totality of
symptoms.
Hahnemann explained the cause of disease in the aphorism 5 as “a chronic
maism which is fundamental cause for every disease”. Further he explains about it in
the aphorism no.8 as “after removal of all the symptoms of the disease and of the
entire collection of the perceptible phenomena, there should or could remain anything
else besides health, or that the morbid alteration in the interior could remain
uneradicated”.
He has further stated in aphorism no. 12 as “it is morbidly affected vital
energy alone that produces diseases, so that the morbid phenomena perceptible to our
senses express at the same time all the internal change, that is to say, the whole
morbid derangement of the internal dynamics”.
He has explained in the aphorism no 17 “ the practitioner ,therefore only
needs to take away the totality of the disease signs and has removed the entire
disease”.
He has explained in the aphorism no 78 “the true natural chronic diseases are
those that arise from a chronic miasm, which when left to themselves, unchecked by
the employed of those remedies that are specific for them, always go on increasing
and growing worse, not with standing the best mental and corporeal regimen and
torment the patient to the end of his life with ever aggravated suffering”.
In the aphorism 79 ”Syphilis alone has been to some extent known as such a
chronic miasmatic disease which when uncured ceases only with the termination of
life. Sycosis (the condylomatous disease) equally ineradicable by the vital force

without proper medicinal treatment was not recognized as a chronic miasmatic
disease of peculiar character, which it nevertheless undoubtedly is and the physician
imagined they had cured it when they had destroyed the growths upon the skin , but
the persisting dyscrasia occasioned by it escaped their observation”.
In aphorism 80 Hahnemann “incalculably greater and more important that the
two chronic miasm just named, however is chronic miasm of psora. The monsterous
internal chronic maism-the psora, the only fundamental cause and producer of all the
other numerous . I may say innumerable nervous debility, hysteria, hypochondriasis,
mania, melancholia, imbecility, madness, epilepsy and convulsions of all sorts,
softening of bones(rachits), scoliosis and kyphosis, caries, cancer, fungus heamatodes,
neoplasms, gout, haemorrhides, jaundice, cyanosis, dropsy, amenorrhoea,
haemorrhage
from stomach, nose, lungs, bladder and womb. Asthma and ulceration of
lungs, impotence and barrenness,of migraine, deafness, cataract, amaurosis, urinary
calculus, paralysis, defects of the senses and pains of thousands of kinds, etc figure in
systematic works on the pathology as peculiar, independent diseases.
Dr.Kent31 states disease as “Disorder of the activities of the internal man, a
lack of harmony or lack of balance, which gives forth the signs and symptoms by
which we recognize disease. These sensation constitute the language of the disorder.
Further he explains as “only the vital principle thus disturbed can give to the organism
its abnormal sensations and incline it to the irregular actions to which we call
disease”. Morbid disturbances can be perceived solely by means of expression of the
disease in the sensations and actions. For him symptoms are language of sickness, at
the level of mind, emotions and body.

Dr.Boenninghausen32 opines that diseases as, “The invisible, morbid
mutation in man’s internal change in condition perceptible to our senses in the
external (complex of symptoms), from before eyes of creative omnipotence, what we
call disease: but only the totality of symptoms is the slide of the disease, which in
turned to the disciple of healing; and what he needs to know for the purpose of cure”.
Dr.Richards33 opines disease as “It may be concealed that every disease is
dependent on an alteration in the interior of organism. But the alteration is only
guessed at by the understanding in a dim and illusionary manner from what the
morbid symptom reveal concerning it, and the exact nature of this inner invisible
alteration cannot be ascertained in any reliable manner. The invisible morbid
alteration in the interior and the alteration in the health perceptible to our senses
together constitute to the eye of creative omnipotence, what we term disease”.
Dr. Charles J.Hemple said that “Disease is totality of the effect by which an
organism which has been specifically adapted, or prepared for their reception”.
Dr. Allen34 Quotes “The character of the maism yields the character to the
disease or the form of illness”.
Dr. C.A. Gutierrez tells “chronic disease is a modification of the vital
dynamism, leading to the creation of a special state called susceptibility; when we
neutralize this state, we cause it to lose its essential modality, i.e. its driving force. In
the patient we should recognize two perfectly defined facets; on one hand the illness,
which is only is only the vital dynamism neutralizes or denatured by something which
produces a pure modification, giving rise to susceptibility, and which Hahnemann
called the maism, and on the other hand, the human being in his environment which

colored by a series of modalities, permits us to catalogue the individual case of
sickness”.
Dr.Hahnemann35 regarding the three explains “Psora is the most universal,
most destructive and yet most misapprehended chronic miasmatic disease which for
many thousands of years has disfigures and tortured mankind, and during the last
centuries has become the mother of all the thousands of incredibly various acute and
chronic (nonveneral) diseases by which the whole civilized human race on the
inhabitated globe is being more and more afflicted. It is most infectious , most general
of all the chronic miasms. At least 7/8th of all the chronic maladies spring from it as
their only source, while the remaining 1/8th springs from syphilis and sycosis or from
a combination of two of these miasmatic chronic diseases or from a combination of
three of them (which is rare)”.
He explains regarding Syphilis that it began to raise its dreadful head in 1493.
It only passes into a tedious malady difficult to cure, when it is complicated with
Psora, the second chronic miasm, which is more widely spread than the fig wart
disease, and which for 31/2 centuries has been the source of many other chronic
aliments, is the miasm of venereal disease proper, the chancre disease.
He explains regarding Sycosis, as being that miasm which has produced by far
the fewest chronic diseases, and has only been dominant from time to time. The fig
wart disease, during the French war, was treated in an inefficient and injurious
manner, internally with mercury, because it was considered homogenous with the
venereal chancre disease. After the violent treatment of fig warts by allopathic
physicians, we often find developed Psora complicated with Sycosis, when the Psora,
as is often the case, was latent before in the patient. At times, when a badly treated

case of venereal chancre disease has proceeded, both these miasma are conjoined in
threefold complication with syphilis.
Dynamisation;
C.M.Boger36 Dynamism, until lately laughed out of court, is about to rend
asunder its mockers before the whole world and it is high time to realize that it is not a
thing apart, but an essential factor of our very nature and life and must be reckoned
with if we would practice medicine. They are intended to condition him, elevate the
profession and benefit the community. Actually we see the reverse; want of logic,
incoherence and prideful selfishness. If there be lack harmony, among us, our
foundations cannot be very secure and no amount of subtle reasoning can make them
so, hence we have no right to call ourselves scientist much less artist. If science or art
holds anything at all for the benefit of man, by that much is medicine concerned
therein. These being true how are we going to disassociate the dynamics of action
from action itself. Preposterous as the idea is, it is just what is being attempted in
everyday practice.
The real homoeopathic physician is such a specialist; he makes materiamedica
and the exemplification of the law his being. Thus and only thus can he make cures
that are impossible to the old line physician and there by justify a separate existence it
must be his aim to do things and do them well; no other course is honestly possible
under the law, which like all natural laws is exacting in its demands. And knows no
compromise.
The first step in the study of Homoeopathic science is not always the same,
but as obvious things make the strongest appeal many convert have been made after
seeing or experiencing the power of similia. Such clinical demonstrations keep for

you a perennial interest because each new hopes, the greatest of all aids to curing.
Every problem solved opens the way for other better work. This is in itself not only a
source of satisfaction to all concerned, but a mental exercise in which all the powers
of thought are concentrated upon finding and applying the suitable remedy.36
A new mode of Dynamisation:
Dr. B.K.Sarkar2 Again, there are people who have read 6th edition of organon
(unfortunately, the translation of the 6th edition is at many defective and does not
represent Hahnemannian thinking) and still frown on Hahnemann’s writing on the
matters and those have taken ideas with prejudiced ‘minds’ have given unfair trials,
and left their efforts in the midst and did not come to any conclusions and so all have
again gone to the same old erroneous practice. These are the people who ‘cry’ to
make Homoeopathy more scientific, as if Homoeopathy is not scientific and there are
‘gaps’ in Homoeopathy, because they cannot understand and make people understand
our Master. I have read those ‘cries’ of our learned bosses in Journals. My humble
request to them is “be scientific minded first and then make Homoeopathy more
scientific”. When other ‘so called’ sciences are borrowing ideas from our Master’s
pen, what further proof do they want to make Homoeopathy “more scientific”. Is
science for scientists or scientists for science? Brothers! Better change your outward
makeup and look at your real face in the mirror. It will give you more pleasure than
pain. If you are not getting results. it is your defeat and it is the greatest defeat as you
cannot win the hearts of the suffering “Souls”.
Health:
Man has the will and the understanding and the house which he lives in is his
body. The organs are not the man .The man is prior to the organs. The order of

sickness as well as the order of cure is from man to his organs. The real sick man is
prior to the sick body. A man is sick prior to localization of disease. When we wait for
localization, the results of disease have rendered the patient incurable. Symptoms are
but the language of nature, talking out, as it were, and showing as clearly as the
daylight, the internal nature of sickman or woman. Crude drugs cannot heal the sick
and that what changes they effect are not real but only apparent. Tissue changes are
the body and are the results of the disease, they are not the disease. The bacteria are
the results of the disease. The disease cause is more subtle. The remedy, which will
produce on healthy man similar symptoms, is the master of the situation, is the
necessary antidote, will overcome the sickness, restore the will and understanding to
order and cure the patient. Man consists in what he thinks and what he loves and there
is nothing else in man.
The physician has to’ perceive’ in the disease that which is to be cured, and
that is through ‘totality of symptoms’. He has to perceive the nature of remedy .
Experiences has only a confirmatory place. It cannot take the place of science and
truth. All true diseases of the economy flow from centre to circumference. All miasms
are true diseases. The active cause is within, and apparent cause of sickness is
without. If a man has no deep miasmatic influence, outer causes will not affect them.
Homoeopathy has two parts ; the science of homoeopathy is the art of homoeopathy.
One has to learn the art of homoeopathy to prepare himself for the application of the
science of homoeopathy. Vital force is constructive and formative in its thing in the
universe has its aura. Every star and planet has it. The remedy to be Homoeopathic
must be similar in quality and similar in action to the disease cause . As soon as the
internal economy is deprived in any manner of its freedom, death is threatening;
where freedom is lost, death is sure to follow. Potency should suit the varying

susceptibility of sick man. Any more than just enough to supply the susceptibility is a
surplus and dangerous. Human race has been greatly disordered in the economy
because of surplus drug taking. Primitive cause is not in the bacteria. Bacteria
themselves have a cause to appear and survive. Over sensitive patients are actually
poisoned by inappropriate administration of potentized medicines. Their chronic
maisms are complicated with chronic drugging and its effect upon vital force. The
physician who can only hold in his memory the symptoms of a disease or remedy will
never succeed as a homoeopath. The majority of such who call themselves
homoeopaths at the present time, are perfectly incompetent to examine a patient, and
therefore incompetent to examine homoeopathy. It is impossible to test homoeopathy
without learning how to get the disease image so before eyes that the homoeopathic
remedy can be selected. At the present day, there is almost no such thing as an
unprejudiced mind. Do not prescribe until you have found the remedy that is similar
to the whole case, even although it is clear in your mind that one remedy may be more
similar to one particular group of symptoms and another remedy to another group.37
The life and composition of cells is complex nature. The composition of
animal protoplasm is capable of analysis, yet there is in each cell and its life function
that which is beyond our comprehension and defies analysis. We cannot as yet fathom
the reason why a human ovum takes on growth and development only when the
spermatozoa imbed itself deep in its innermost nuclei. We only know that it possesses
some hidden vital function that compels it to develop and grow. The power of each
life to develop from the single ovum into its own ego, unfolding and expressing itself
forever in its own way and individuality, never varying from the ideal that is once
stamped, to carry out its perfection all the powers of adult life, distinguishing it from
all other created species, is a marvel until we comprehend the principle of the vital

force or the energy permeating all created things. That power, although defying
analysis, nevertheless continues all through life as a mysterious manifestation of the
vital functions. It is the close study of these vital functions that becomes the chief
study of the physician. In order to obtain a thorough knowledge of these vital
functions we must study them in their manifestations during health. From the earliest
period of its existence growth is manifest from within the cell out; it is never observed
growing from without in. The point most vital to observe is the course and the
direction of its expression always from within outward. This is true in embryonic state
and always maintained as long as life exists. This is equally true in the specialization
of functions. The special organs are developed and their functions maintained by the
expression of the vital energy as the life giving principle. All expression of the mind
are such manifestations. Indeed, it is the expression of the vital force in and through
the mind and intellect that has a very great influence in the functioning of all life and
the special organs. In health all expressions of vital force may be expressed by perfect
functioning of all parts of the body by the sense of general well-being.38
Health is that balanced condition of the living organism in which the integral,
harmonious performance of the vital functions tends to the preservation of the
organism and the normal development of the individual.39
Cure:
Dr Kent says homoeopathy always demands for cure, the remedy that
provokes symptoms most like those to be cured. But the most like of all often is the
disease poison itself; not in its crude condition, but changed y preparation and
potentization; rendered inert for mischief, and only potent for good. You have heard
in a Compton Burnett Lecture that, where old school is using disease products,

rendered “similar” by preparation, it is being forced into what Hahnemann was forced
into and taught one hundred years ago. That is to say……. They have to change their
polypharmacy for the single remedy. They have to adopt his single dose, to evoke
vital reaction; repeated as symptoms demand. To realize that he is correct when he
contended that it is only the reaction of vital force against drug or against disease, that
is curative. That disease is merely the rebellion of vital force against noxious agent,
inimical to life and that cure comes from the stimulated reaction of vital force against
diseases. They experience also his initial aggravation sometimes of great severity,
because they lack his experience in the preparation, the administration, and the dosage
of homoeopathic remedies; which differ entirely from those of the old school37.
Health is restored after the removal of all symptoms, then only than is all disease
removed.
Hahnemann this way distinguishes between disease itself and its causes,
manifestation, and products and then show at once that sphere of homoeopathy is
limited to functional changes from which the phenomena of disease arise. Thus
homoeopathy operates only in the dynamic sphere. Directly, homoeopathy has
nothing in common with the physical cause or product of disease, but secondarily it is
related, here is the place where surgery may have its functions, yet many of the
tangible effects may remain. If these effects are too far advanced, they may be
removed. If this is not done, it stands to reason that the best effects of the remedy will
not primarily within the range of similia, and therefore not the objective of
homoeopathic treatment, the morbid process from which they arise or to which they
lead is under the control of homoeopathic treatment, This medication may control and
retard the development of pathological conditions. Thus tumors may be retarded or
completely arrested, and absorption increased, and finally the disappearance of the

growth; secretions or excretions increased or decreased, ulcer healed; but all this is
secondary to the real cure which takes place solely in the dynamic sphere, restoring
the patient to health and harmonious functioning of this whole being by the dynamic
influence of the symptomatically similar remedy.39
As Stuart Close has well said, that real field of homoeopathy is to those
agents which effect the organism as to health in ways not governed by chemistry,
mechanics or hygiene, but those capable of producing ailments similar to those found
in the sick.
Fincke has shown that in the development and growth of the child much can
be done to make this symmetrical, for the child is peculiarly under the influence of
the laws of assimilation, here the laws of similia have pre-eminence, for the child is
peculiarly under the influence of the laws of action and reaction as applied to the
action of similar remedy in its development and growth. The homoeopathic principle
is not used in another field of what might be called extreme emergency, but rather we
use what may be called a principle of palliation.

MIASMATIC APPROACH OF ANKYLOSING SPONDYLITIS
Miasm interpretation varies in degenerative joint disorders depending upon the
presentation or stages. Depending upon the expression available it can be identified
Psoric, structural changes.
Miasm is interpreted by the family history and past history. This also is
appreciated as predisposition. In the back ground of this current presentation of
degenerative joint disorders has to be understood. Miasm dominant at this phase may
be analyzing the present symptoms. This may be pertaining to this presentation only.
But this attains momentum from the fundamental miasm.
Miasm is always expressed by the signs and symptoms that the patient
produces. These permit the individual expression of the characteristic of miasm which
allow us to determine, recognize and handle out patients individually.
Dr. Ortega Proceso stand that “The natural healing force inside the human
body, in its integral completeness, represent of the universe acting on one point and
with the inherent purpose of preserving what has been created i.e. of enabling it to
continue-the specific objective which the human intellect can deduce from all that
exists, all things.”
Man’s natural healing power is undoubtedly undermined, caused to
deteriorate, and lessened as a restorative or reconstructive force by the presence of a
miasmatic condition-a profound and indelible stamp permanently imprinted on the
being by repeated perversions, excesses or deficiencies in its functioning.

Psora is perturbation of nutrition; sycosis compels it to accumulate debris
which should be eliminated, and syphilis causes it to degenerate. Since all of these
conditions can act as the true causes of all imbalances etiology for every degenerative
disease.
According to C.G.Jung human unconsciously pursue an archetype, a sort of
pattern of self, through accumulation of qualities establishing in the transcendent
realm a pattern which in the future will be of use to animist, spiritual, or organic
groupings. In other words, individual today are tracing-by virtue of rather indefinable
functions-the somewhat esoteric shapes of other existences.
Life as a succession of perfectly linked phenomena constitutes an order whose
result is persistence, i.e. affirmation. Disorder is negentropy or negative entrophy. The
miasm is disorder, a profound form of entrophic disorder which can scarcely be held
in check by the preservative vital force; and if it is greatly augmented and complicated
by another sycosis-syphilis, it can easily burst through the dike opposed to it by the
natural healing power, the destruction becomes evident, and the individual is headed
for death-with what is, from the medical point of view, a degenerative disease.
PSORA: Effects occur at the level of protecting envelops with the touch of
hypersensitivity & reativity metabolism nutrition glands, endothelial system, cardio
vascular system, nervous system, disorders represent with reversible functional
disturbances. Incoordinatiion and imbalance of function on account of induced
changes of control persist. Adverse environments act as mere accelerators.
In the early stages when only a subjective feeling is available and
investigations prove negative the available picture suggests of predominantly Psora.
Neuralgic pains usually better by quiet rest and warmth. Often worse motion.

Psora the sympathetic overactive express the labile hypertension under
emotional stress, blood pressure, with secondary effect on kidneys, dry skin, altered
fat, protein metabolism, ovarian imbalance, functional menstrual problems. Acrid
non-infective leucorrhoea with emotional background imbalance in general make-up,
malabsorption, malnutrition allergic response, spasm with emotional, hysterical
functional origin, vicarious, congestive haemorrhage.
SYPHILIS: A whole miasmatic disease expression terminates in the phase
characterized by destruction all over and at all levels. Homoeopathic physician with
right appreciation promotes reversal of disease. Over stimulated and exhausted system
under continued adverse environmental inputs leads to total loss of controls at
intellectual, emotional, and physical levels. Progressive loss of valves of life leads to
lack of discriminative intelligence, intelligence, perception, thinking and decision
making worst feeling of-anger, hate, envy, jealousy, suspicion leading to paranoid
traits with violent outbursts.
Stitching, shooting or lancinating pains in the periosteum or long bones of the
upper or lower extremities. Worse at night or approach of night, worse change of
weather; by cold and damp. Feet become deformed because legs cannot take weight
of body in osteoarthritis signifying combination of miasms.
Miasm express in the level of physical as cracks, fissures, ulceration which
destruction, abscess carries, explosive inflammation with toxaemia, malignant rapid
spread, necrosis with crippling deformities, ostoeoporotic changes and fractures, deep
disfigured scar formation, atrophy, degeneration of tissues, vessels, aneurysm,
ischemic attacks, calcium deposition, damage of myelin sheath, organic degenerative
states.

According Homoeopathy treatment is needed for the patient not for the
disease. This system considers the organism as a whole treatment starts from the
collection of data the case taking. Mostly person are victims of osteoarthritis. They
will not have much attention from the expected ones. From the detailed homoeopathic
case taking itself they will have a feeling that this physician will given enough
attention for them. It will boost up their confidence so the improvement will start
form this point.
SYCOSIS: Over stimulated responsive system with failed arrested activity, activity,
loss of control leads to inefficient aberrant immune responses and metabolic
maladjustments. Miasm engulfs severe refractory anaemia, weakness disproportionate
aggravation by suppression of discharges, fatigue with slowness, indolence, altered
mental expression, slow registration of sensory inputs, inadequate interpretation, with
paranoid ideas, guilt, feeling of insecurity which are mostly seen in majority geriatric
patients.
According to Hahnemann’s concept of chronic diseases joint disorders with
stiffness and early morning aggravation are expressions of sycotic miasm. As phyllip
Speight writes in comparison of Chronic miasms, arthritic-deformans is Sycotic.
Pains in joint or muscles are of shooting or tearing type. Pains in fingers or
small joints. Slow progress of inflammatory process. Recovery is slow. Oedema and
lack of heat may be present. Worse at approach of storm or a damp, humid
atmosphere and falling barometer or becoming cold. Stiffness and soreness especially
lameness is very characteristic of sycosis. Worse stooping, bending or beginning to
move.

THE UTILITY OF RHUS TOX IN ANKYLOSING SPONDYLITIS
Common name: Poison ivy; poinson oak.40
Natural order : Anacardiaceae.
Habitat : North America. Grows in woods and along fences on low ground.
Part Used : Tincture of the fresh leaves gathered at sunset just before flowering.
Active Principles : Toxicodendric acid; Toxicodendrol.
Physiological action:
Farrington H. says if applied locally to the skin , Rhus tox. is an irritant and
causes itching and vesicular eruption on the skin which may extend to the mucous
membranes where it produces edematous swelling, dryness, rawness and burning.
When taken internally or inhaled there are colicky pains in the abdomen worse at
night, diarrhoea, tenesmus, bloody stools and urine, and fever which is often typhoid
or intermittent in character; pains of a rheumatoid type in fibrous structures, joints and
lumbar region, ameliorated by heat and aggravated by rest. Fatal results have not
followed any case of poisoning recorded.
General characteristics :
Antipsoric, rheumatoid, paretic and typhoidal conditions due to exposure to
cold and dampness; from getting wet; from overexertion and straining ; from trauma.
Left sided complaints ; or extending from left to right). Restlessness; anxiety; fear;
mild disposition, irritability. Impatience; absent mindedness; confusion; forgetfulness,
sadness, discouragement; suspiciousness; impulse to commit suicide; aversion to
company; delirium; unconsciousness; prostration. Aversion to the open air. Thirst.
Jerking of muscles; trembling.

Sensations: dryness of mucous membranes ; heaviness, numbness; tingling;
numbless of single parts; of affected parts; coldness of affected parts. Pains. As if
sprained, as if torn loose; pressing; bruised soreness; aching; stitching; burning.
Paralysis. Haemorrhage, periodicity. Septic infection; phlegmonous inflammation;
suppuration; carbuncle; gangrene; inflammation of lymphatic glands. Eruptions:
moist; fine vesicular; pustular; eczematous; crusty; erysipelatous. Worse: morning;
night; after midnight; in repose; on beginning to move while lying down; exertion;
cold; becoming cold; cold drinks ; bathing; wet weather; change of weather; open air;
touch. Better : continued motion; change of position; motion of the affected part; after
sweating; hot applications; warm covering; pressure.
Rhus toxicodendron is indigenous to North America but was brought to
England in 1640. The earliest record of its use as a medicine was in 1798. Its
poisonous effects were noted by a Doctor Dufresnoy of Valenciennes, in the case of a
young man who was cured of a vesicular eruption of six years’ duration by being
accidentally exposed to the volatile emanations of the plant. Dufresnoy and others
used it successfully in rheumatism, paralysis, amaruosis and certain forms of chronic
skin disease. Hahnemann and his followers have made extensive provings,
establishing it as one of the principal polychrests.
The active principles of Rhus tox are toxicondendrol, a fixed oil, and a volatile
substance known as “ toxicodedric acid”, which is given off from the plant in greatest
amount after the sun goes down, in damp or cloudy weather and in the warm days of
June and July. Its poisonous effects are augmented if the victim is warm and sweaty
when exposed. It is a remarkable fact that these peculiarities were brought out in the
provings and have become important modalities through clinical experience.
Although many persons are immune, some are so susceptible to the action of
the volatile principle of Rhus tox, that merely passing to the leeward of the paint will
precipitate a violent attack of poisoning.
Two varieties of Rhus tox. are recognized, one growing in the form of shrub
with erect, comparatively smooth and slender stem, seldom reaching more than four
feet in height, and known as poison oak; the other known as foison ivy or Rhus
radicans, a climbing vine with thick tortuous stem, heavily fringed with brownish
rootlets by which it clings to its host.
In spite of the fact that the two varieties may spring from one and the same
root stock and their morphology seems to be due merely to habit, they differ
somewhat in pathogenetic action and clinical usefulness. But since they are so nearly
identical in action, they are treated as one remedy, - Rhus tox. And their differences
noted briefly at the close of this lesson.
The leading characteristics of Rhus are lameness, stiffness, anxiety and
restlessness; fevers of typhoidal type; phlegmonous inflammation; paretic conditions;
aggravation from cold and dampness, repose and over – exertion; amelioration by
heat and continued motion.
Around these central features may be grouped all the many and varied phases
of this powerful and useful polychrest. Common colds, influenza, rheumatism,
neuritis, typhoid, intermittent and eruptive fevers, septic infections and erysipelas are
among the many ailments that it will curve.
Rhus stands next to Arnica as a vulnerary and often follows that remeday in
the after effects of injuries. But, since it has an especial affinity for fasciae,

aponeuroses and the sheaths and fibrous prolongations of muscles, rather than the
musclar tissues themselves, it is most useful in the after effects of sprains, lifting of
heavy objects and strenuous effort such as running and swimming. If indicated after
contusion, it is because the fibrous tissues have been injured – tissues which do not
fall within the sphere of Arnica.
Rhus has cured more cases of arthritis, both acute and chronic, than any other
remedy. It is not usually suitable in cases that develop suddenly from exposure to dry
cold wind, as are Aconite and Belladonna, but more to the acute pains and stiffness
following a thorough drenching in a rain storm, sleeping on damp ground, from being
chilled while perspiring or after strenuous physical effort. The patient needing Rhus is
more susceptible to exposure when his skin is moist. Moisture seems to be an
essential factor favoring the production of Rhus symptoms.
In acute arthritis the joints become smooth, shining and edematous with little
or no redness. The stitching, tearing pains force the patient to move although motion
may be excruciatingly painful. After moving a while, the pains and stiffness abate and
he stops and tries to rest. However, his respite is but short lived for the pains return
with renewed severity and he must move again. This is repeated until he is exhausted.
At times he feels as though the flesh were being torn from the bones, or the bones
scraped. Often there is numbness and tingling in the affected members and a sensation
of on-coming paralysis.
In chronic arthritis there is less swelling but much stiffness and lameness,
often with contractures in the structures about eth joints. The patient is a veritable
barometer. Every change in the weather increases his suffering, especially if a change
to wet weather. He hugs the stove by day and piles on the covers as night. After long

sitting his joints grow sore and stiff so that motion is very difficult, but soon they
limber up after he walks a while.
However, the Rhus patient cannot walk very far. He lacks endurance and soon
tires. He becomes weak and exhausted from slight effort and must lie down.
Weakness and prostration and a feeling of helplessness are of frequent occurrence in
acute Rhus poisoning and appear early in the provings.
Nash says about Rhus Tox41. Pains running down the limbs in streaks, with
every stool. Lumbago from sleeping on damp sheets, or ground; on getting wet while
perspiring; pains, strain, etc., worse while at rest; on beginning to move; better when
gets in motion and by pressure. Stiffness and aching, bruised pains in small of back;
when siting still or when lying; better from motion or lying upon something hard.
Pains in back compelling to move constantly in bed. Lameness in back as if strained
or after straining. Great restlessness, cannot lie long in one position, changes often
with temporary relief, tosses about continually. Lamensess and stiffness on beginning
to move after rest; on getting up ni the a.m.> by continued motion.
Stupor and mild, persistent delirium; continually tossing about, with
labourious dreams. Modalities: < when quietly sitting or lying and on beginning to
move; wet, cold weather; lifting or straining; getting wet when perspiring. > by
continued motion, by warmth, dry air or weather; lying on hard floor (backache).
Muscular rheumatism, sciatica, left side (col.); aching in left arm, with heart disease.
Great sensitiveness to open air; putting the hand from under the bed cover
brings on the cough (Bar., Hep.) Back; pain between the shoulders on swallowing.

This is the third remedy of our so called restless trio the other two are Acon.,
and Ars. This restlessness of Rhus is on account of the aching pain and soreness
which is temporarily relieved by movement. There is also an internal uneasiness
which is purely nervous which causes the patient to want to be on the move, even
when there is no particular pain present; but not nearly to the degree that we find it
under Aconite and Arsenicum.
As in Bryonia, so in Rhus, the leading characteristic is found in its modality.
The aggravation on movement, in the former, is no less marked than the aggravation
when quiet of the latter. The patient tosses and turns from side side with Rhus. The
same as with Aconite and Arsenicum. With Rhus. The change relieves, while with eth
other two it does not. In Bryonia, the more the patient moves the more the suffers,
while with Rhus, the more and longer he moves the better he feels, until he is
exhausted. In acute affections, constant movement seems to be the patients only relief.
With chronic diseases like chronic rheumatism the patient must move, suffers on first
beginning to move, but as he continues to move, or as he express it, “gets limbered
up,” he feels better. But he cannot long lie comfortably in either the acute or chronic
trouble, for the aching comes on and he must move even if it does hurt him at first.
The pains causing the restlessness of Rhus are not so agonizing as they are under
Aconite and Arsenicum, nor is the prostration so great as under Arsenicum nor the
excitement so great as under Aconite.
Swollen around the ankles after sitting too long, particularly in traveling.
Powerlessness of lower limbs; cannot draw them up. Lameness, stiffness, and
paralyzed sensation in joints, from sprains, over-lifting or over – stretching.
Rheumatic tension, drawing, tearing in limbs during rest. Lameness, stiffness and pain

on first moving after rest or on getting up in the morning; relieved by constant motion.
Rheumatic tension, drawing, tearing in limbs during rest. Lameness, stiffness and pain
on first moving after rest or on getting up in the morning; relieved by constant motion.
Aching pains in legs; must change position every moment. Labourious dreams of
excessive bodily exertion, as running, wading in the snow, hurrying and the life.
Restless at night, has no change position frequently. Complaints from getting wet in
the rain when over heated or perspiring. Pains as if sprained; ailments from spraining
or straining, lifting, particularly from reaching up high for things.
Complaints worse while at rest; after midnight; before storms, or on rising
from a seat or bed; on beginning to move after quiet; from getting wet and in wet
weather. Bad effects from sprains, bruises , etc. Bad effects from getting wet in a rain
storm while sweating or over – heated.
Richard Hughes42 says that the rheumatoid pains described by Dr. Phillips as
occurring in Rhus poisoning are seen in an especial degree in the provers of the drug.
From Rhus venenata the joints, as well as the fibrous tissues, were affected –
especially the knees, ankles, feet, and hands; but there was no genuine synovial
swelling, as with Bryonia and Pulsatilla. It is chiefly to these rheumatoid pains that
Hahnemann’s well-known observation belongs, that unlike those of Bryony, the are
most violent when the part affected is an a state of perfect rest. He extends the
statement, indeed, to the symptoms produced by the drug generally; and the recent
provings of Rhus venenata support his statement.
Rhus has thus come to occupy a high place in homoeopathi therapeutics
amongst the remedies for rheumatism. It is not often indicated in rheumatic fever. It
would be so where, as in a case mentioned by Dr. Bayes, restlessness and constant

desire to change the position were present. Dr. Phillips also say that “in the after stage
of acute rheumatic fever, when aconite may have been employed, and when the
temperature has fallen to 100°, or below it, and where the patient still suffers from
wearing stiffness, and aching in the neighbouthood of the joints, rhus is positively
ionvaluable:. But in various subacute and chronic rheumatic affections it is a most
precious remedy, especially when they can be traced to a wetting. Herein it resembles
Dulcamara, the differs from Acornite and Bryonia, whose local rheumatic symptoms
are rather such as drug cold produces. Its action is mainly, if notentirely, upon the
fibrous tissues – tendons, fasciae, sheaths of nerves, and c. – and perhaps the muscles.
I do not think that it controls the rheumatic affections of the synovial membranes, but
only those of the ligaments external to the capsules of the joints. Nor do I think that is
acts upon the nerves themselves. Its undoubted value in rheumatic sciatica depends, I
take it upon its influence on the fibrous sheath of the nerve, which is so often the seat
of the pain. It is powerless in pure neuralgia here or elsewhere. It is certainly the best
remedy pect that here the lumber fascia is the part affected rather than the actual
muscles. It is thus especially indicated when lumbago and sciatica are present
together. In rheumatic lameness of the lower extremities, depending largely cures. In
all these maladies the characteristic features, “worse at rest, relieved by motion,” are
of immense weight in determining our choice of Rhus. Dr. Neidhard has added the
important observation that on first moving after rest the pains are increased. It is not
until the parts have been moved for some little time that relief ensues. With Bryony,
on the other hand, the longer the movement continues, the worse the pains become;
and with Rhododendron, as we have seen, movement relieves from the first. Dr.
Carroll Dunham has drawn out these characteristics of the pains of Rhus in a which
you will find in the first volume of his Lectures. “The rheumatic symptoms of the

drug,” he says, “come on with severity during repose, and they increase as long as the
patient remains quiet, until, at length, their severity compes him to move. New, on
first attempting to move, he finds himself very stiff, and the very first movement is
exceedingly painful. But as he continues to move, however, the stiffness is relieved
and the pains decidedly decrease, the patient feeling much better.” He goes on to paint
out that this improvement does not continue indefinitely; for weariness readily comes
on in such patients, and then rest is at first grateful, only after a while to be disturbed
by a recurrence of the aching pain. As chronic rheumatisms of muscles, ligaments,
and fascia are generally of this character, Rhus is by far the most frequently indicated
remedy for them, and in my hands has made many a cure.
The action of Rhus on the white fibrous tissues has led to its being used in the
treatment of sprains. Hahnemann says, - “I have recognized in these latter years that
Rhus is the best specific against the consequences of muscular strains and
contusions”. He does not say what relation it bears to Arnica. It is very valuable in
ankylosing spondilytis.
Henry B.43 says that this powerful drug was first introduced into English
practice by Dr. Alderson, of Hull, in 1793; who successfully treated some cases of
Paralysis, Dyspepsia, many Stomach complaints, and Gout, with the powdered leaves
of the plant. Dr. A. Duncan, however, gave it in large doses, and failed to cure –
observing that it only acted as as a gentle laxative. This might be accounted for in
consequence of the clumsy mode of administration. The powdered leaves were, of
course, dried, and the medicinal properties lost in most cases; while in a few it acted
with immense power, producing Convulsions, and many untoward symptoms. Thus a
very valuable medicine was cast aside as dangerous and useless, for the simple reason

that the physicians of the period did not know how to use it. Now Hahnemann has
come to the rescue. Thanks to his beautiful mode of preparation, we posses, in Rhus, a
remedy of immense value, daily and hourly used by Homoeopathic practitioners, with
almost unvarying success when properly selected and administered. It seems to have a
powerful action on the cerebro-spinal system, both sensitive and motor; also the
Ganglionic nerves. Its salutary effects on the human body are especially manifested
during a state of rest. Its action on the ligments, tendons, serous mucous membranes,
and the skin, is now tolerably well ascertained. According to recorded experience,
Rhus will be found useful under the following conditions: - Acute and chronic
rheumatism, with or without swelling of the parts. Sufferings caused by a heavy
shower of rain, when in a state of perspiration; Evil consequences of bathing in cold
water, or wet feet during the menses; Straining of tendons or single muscles; swelling
and induratino of the glands in the parotid region; paralysis of the extremities;
Vesicular and Phlegmonous Erysipelas; Pemphigus; Moist eruptions on the hairy
scalp; impetigo; swelling of the head and face; inflammation of the eyelids; some
states of typhoid and typhus fever.
Neck and back: Pain and stiffness in the cervical region; pains in the dorsal region,
and across the loins, as from a strain; pains in back as if bruised ; tearing beween the
scapulae; swelling of the axillary and parotid glands.
Upper extremities: Tearing , burning in the shoulder, with lameness of the arm;
Burning, pricking below the axilla; Burning and itching pustules; Coldness
Insensibility of the arm; Vesciles on the wrists; smarting cracks on the back of the
hands.

Lower extremities: Sensation as if the joins were sprained; Aching pain in the hip-
joints at every step; Paralysis of the lower limbs; Cramp in the calves; Cramp-like
pressure in the legs; Heaviness in the legs; Painless swelling of the feet; Inflammation
and swelling of the instep ( erysipelatous), with vesicles and pimples; Red Blotches
on the balls of the toes; Heels red, painful.
Characteristic of Rhus Tox. The Rheumatism of Rhus Tox. Is characterized by
rigidity and pain on first moving the joints after rest. Motion relieves the pain; but
frequently the pains are greatly increased during rest, and when warm in bed.
Notwithstanding this, rest is absolutely necessary to promote the curative action.
Dr. Neidhard states, that the Rheumatism cured by Rhus is as follows:
“Rigidity; Paralytic, weakness of the joints; stinging in the tendons and muscles;
Swelling and redness about the joints, especially the hip and wrist. ( The greatest
rigidity and pain are felt on frist moving the joint after rest, and on awaking in the
morning).
Farrington44 say the chief member of the Anacardiaceae, namely, the poison-
ivy or Rhus toxicodendron. It is complementary to Bryonia, a fact discovered by
Hahnemann in his experience with an epidemic of war typhus, during which he
treated many cases, losing but two; the success he then gained was acknowledged on
all sides. Rhus tox. Bears an inimical relation to Apis mellifica. Although the
symptoms of the two are superficially similar, for some reason which I cannot
explain, these drugs do not follow each other well.
We find Rhus tox. Forming the centre of a very large group of medicines. If
we were to study them al comparatively. We will study the action of Rhus on the
fibrous tissues. The are also including tissue the aponeuroses and tendons of muscles,

the ligaments about joints and the connective tissue. No remedy has a more prodound
action on the fibrous tissues than has Rhus tox. First of all, I wil speak of its action on
the tendons of muscles. We find Rhus useful whenever these tendons are inflamed,
whether it be from over-exertion or from a sudden wrenching, as in the case of sprain.
We find, also that we may give Rhus in other affections arising from over – exertion.
For example, if a musician from prolonged performing on wind instruments suffers
from pulmonary hemorrhages. Rhus will be his remedy. If from violent exertion a
patient is seized with paralysis, his trouble may yield to Rhus tox. In sprains, Calcarea
ostrearum follows when Rhus has relieved, but failed to cure.
Arnica acts more on the muscular tissue than on the ligaments. Henc, we
would find it indicated when, as a result of long exertion, there is a great soreness of
the muscle. The patient feels as if he had been pounded. It has not that strained feeling
of Rhus. When a joint is clearly sprained, Arnica is not the best remedy, unless there
is considerable inflammation of the soft parts other than the ligaments.
Arsenicum is to be thought of for the effects of over – exertion, particularly if
that exertion consists in climbing steep hills and mountains. Here you have the effects
of breathing rarefied air as well as those of the exertion. It is also useful for
inflammation and soreness in enarthrodial joints from concussion, as, for instance,
when the head of the femur is jammed violently into its socket.
The general characteristic, however, which helps you to decide for Rhus in all
these cases is this: the patient has relef of his symptoms by continued motion, while
he experiences aggravation on beginning to move. The reason for this symptom is that
the fibrous tissues become timbered up as the patient continues to move.

There is somewhat of an exception to this characteristic, and that is in that
painful disease known as lumbago. I find that in the beginning of this affection Rhus
is the remedy, whether the patient is better from motion or not. The symptoms calling
for Rhus are great pains on attempting to rise, stiff neck of rheumatic origin from
sitting in a draught, rheumatic pains in the interscapular region, better from warmth
and worse from cold. There may also be constrictive pains in the dorsal muscles,
relived form bending backward.
In rheumatism Rhus is incdicated, not so much in the inflammatory form as in
the rhueumatic diathesis, when the characteristic modality just mentioned is present,
and when there is aggravation during damp weather, or from dwelling in damp places.
Another peculiarity of Rhus is that prominent projections of bones are sore to the
touch, as for example, the cheek-bones. This shows you that Rhus affects the
periosteum. Still another characteristic is that the patient cannot bear the least
exposure to cool air.
Farrington EA.45 says about Rhus Tox. Involves the fibrous tissues nad sheaths of
the muscles. Rheumatism after exposure to wet, especially when overheated or
perspiring. Relief from moving about. Bryonia Copious effusion. Muscular
rheumatism. Lacks the excitement of chamomilla. Relief by continued motion, while
aggravation on beinning to move. Aggravation during damp weather or from dwelling
in a damp place; the patient cannot bear the least exposure to cool air. Prominent
projections of the bones are sore to the touch.
Calcarea Ostrearum - Rheumatic affections, caused by working in water.
Rheumatism of the muscles of the back and shoulders, after the failure of Rhus.

Causticum - Joints are stiff and tendons shortened, drawing the limbs out of
shape. Articulation of the jaw particularly involved. Worse from cold and relieved by
warmth. Restlessness at night. Worse weather.
Chamomilla - Feverishness and excitement.pains drive the patient out of the
bed and compel him to walk about. Stitching pains jump from place to place, worse in
the ankles and knees, and leave a sense of weakness. Sweat does not relieve him, but
his pains are better after sweat. The patient is corss and excitable.
Colchicum - Begins in one joint and travels thence to another, or in one side of
the body and then flies to the other. The pains are worse in the evening. The joints are
extremely sensitive to touch and the slightest motion. The patient is extremely
irritable. Metastasis of rheumatism to the chest. The sensation, as if the chest were
being squeezed in a vise. Pulsatilla - The patient is mild and tearful. The erratic paints
do not leave any weakness.
Dulcamara - Aggravation from cold, damp weather or from changes from hot
to cold weather, especially if these changes are sudden. Calcarea Phos. - In women –
joints ache in every change of weather. Kali Bichromicum - Rheumatism of the
smaller joints – particularly of the finger and wrists, in spring or summer weather
when there are cool days or nights. Gastric and rheumatic symptoms alternate.
Kali Carb. - Stubborn rheumatism. Sharp stitching pains. 3 am aggravation.
Lumbago. Rananculus Bulb. - Inter-costal rheumatism. Worse in damp weather and
particularly from a change of weather or change of temperature.
Ledum - The pains travel upward worse from warmth of the bed and
ameliorated by cold applications. Drawing pains in the joints aggravated by wine. The

muscles feel sore, as if out of place. Pains in the joints, extended from feet upwards.
Worse from covering up.
Rhododendron - Susceptibility to changes in the weather and to electric
changes in the atomosphere. Pains in the limbs especially in the bones of forearms,
hands and feet. Numbness. Formication.
Carroll Dunham46 says about Rhus Tox, in the region of the neck and back
we find stiffness of the nape and entire neck, with tensive pain and crying out on
moving. The sacral region is stiff when he moves, but pains when sitting, as if he had
been stooping and bending the back too much. Stitching and pressing pains.
In the extremities we have, most frequently, sticking pains. They may occur in
all parts. Also tearing pains, aggravated by hard labor. When felt of, the bones feel
sore. The salient osseous processes, condyles, olecranon, etc, are sore to pressure.
Drawing pains are frequent. They go from the elbow to the hand. In Dr.
Joslin’s proving of Rhus radicans a pain is described as following the ulnar nerve. I
have twice met this in patients and relieved it permanently with a dose of Rhus
redicans. Tensive pain; aching and pains as it luxated are common under Rhus. They
affect all parts of the extremities and all the joints.
Besides the above pains and sensation there is a feeling of creeping,
formication and numbness as if the fingers were asleep. This is allied to the paralysis.
Also a sensation of great weakness in the limbs; a trembling of the arms and fingers
on moderate exertion; a heaviness and lassitude of the lower extremities so that one
can hardly move. There is painless and lassitude of the feet at evening, evidently
oedematous. Also swelling and pain of the axillary glands.

Dr Hering 47 says it has its action on neck, back, lower limbs. Stiff neck, with
painful tension when moving. Pains in shoulders and back, with stiffness as from a
sprain. Curvature inflamed, even myelitis; from getting wet or sleeping on damp
ground.Pains in small of back, better lying upon something hard. Lumbago.
Tearing and burning in shoulder, arm lame, worse in cold, wet weather, in bed
and at rest. Axillary glands suppurating. Hot swelling of hands in evening. Rhagader
on back of hand. Warts on hands. Swelling of the fingers. Hang-nails.
Coxaligia; involuntary limping; pains felt mostly in knee and worse from
overexertion; pain worse at night. Spasmodic twitching in limbs when stepping out.
Sciatica right side, dull, aching by rubbing and formication.
Paroxysmal pains in legs from getting wet, especially when warm and sweaty.
Cramps in legs and feet, must walk about.Ulcers: on lags, discharging profusely; on
dropsical legs, discharging serum. Swollen about ankles after too long sitting; feet
swell in evening. Intolerable itching of legs and feet at night; old rash.
Swelling and stiffness of joints from sprains, over lifting, or over stretching.
Rheumatoid pains in limbs: also with numbness and tingling; joints weak or stiff, or
stiff, or red, shining swellings of joints, stitches when touched; worse on beginning to
move: after I2 P.M and in wet, damp weather or places; better from continued motion.
Tearing pains in limbs, during rest.
Dr Phatak48 says, this remedy is irritating to the Skin, esp. of face, scalp,
genitals; affects the fibrous tissue, ligaments and joints causing Rheumatic
Symptoms; it is an infective agent producing Typhoid-Like Fever. Affections of
Nerves and Spinal Cord give rise to Paretic Effects. Glands are swollen, hot and

painful; indurated; suppurating. Symptoms appear on the left side or go from left to
right. Pains are tearing, Shooting, <at Night, Cannot Rest in any position. Parts feel
sore, bruised and stiff. Pain as if the flesh was torn loose from the bone. Dislocative
sensation. Mucous discharges are acrid, rusty red, like meat water; musty; causing
eruptions. Infection, septicemia, carbuncles in early stage. Cellulites; inflammation
and swelling of the long bones; scraping, gnawing, tearing in periosteum.
Rheumatism in cold season. Post-operation complications. Hemiplegia, right side;
sensation as if gone to sleep. Infantile pox. Stricture after inflammation. Soreness of
prominent projections of bones. Paralysis after unwanted exertion, after parturition.
Boils, abscesses.
Worse from exposure to wet, Cold air draft. Chilled when hot or sweaty.
Uncovering parts-head, etc. Beginning of Motion. Rest. Before Storm. Sprain. Over-
exertion. After Midnight. Blows; jar. Riding. Ice. Cold drink. Side lain on. Better after
Continued motion. Heat. Hot bath; if heated. Warm wrapping Rubbing. Nosebleed.
Holding affected part, abdomen, head, etc. stretching limbs. Change of position.
Warm dry weather.
Stiff neck, with painful tension when moving. Interscapular pain, <
swallowing. Contractive or breaking backache, > hard pressure; lying on something
hard; walking about or bending backwards. Lumbago. Coccyx aches into thighs.
Numbness, and prickling in limbs. Arms nervous and shaky. Paralytic pains in
elbows. Rhagades on back of hands. Plams are dry, hot, and cracked; washing causes
burning. Pains down back of thighs <stools; Legs feel dead, wooden. Cramps in
claves. Involuntary limping. Soreness of condyles of the bones. Limbs stiff,
paralysised. Hot painful swelling of the joints. Pricking like pins in the tip of fingers
and palms when grasping. Pain along ulnar nerve. Ulcers; on legs ;gangrenous; runs
bloody water; on dropsical legs. Itching of lags and feet. Ankles swollen after too
Long sitting and long standing; feet swell in the evening. Paraplegia; after
parturition, sexual excess; fevers. As if walking on needles.
Allen.H.C.49 describes pains as if sprained; as if a muscle or tendon was torn
from its attachment; as if bones were scraped with a knife; worse after midnight and
in wet, rainy weather affected parts sore to touch. Lamness, stiffness and pain or first
moving after rest, or on getting up in the morning, >by walking or continued motion.
Back pain between the shoulders on swallowing pain and stiffness in small of back <
sitting or lying, > by motion or lying on something hard. Muscular rheumatism,
sciatica, left side; aching in left arm, with heart disease.
Vermeulen50 describes. Back- pain between scapulae on swallowing
>warmth, <cold. Pain and stiffness in small of back; >motion or lying on something
hard; <while sitting as after long stooping stiffness of nape of neck as if it is been
lying in an uncomfortable position and painful tension when moving. Contractive
backache, or as if back would break, >hard pressure, lying on hard, moving about or
bending backward. Aching in coccyx thighs. Pain in the cervical muscles, as if asleep,
or as if head had been too long in an unaccountable position, esp toward evening.
Stitches inback,> bending back, < bending forward. Cutting in sacrum when standing
and bending backwards .PAINS IN THE BACK COMPELLING HIM TO MOVE
CONSTANTLY IN BED. In Extremities-Hot, painful swelling of joints. Tearing
pains in tendons, ligaments and fasciae. Rheumatic pains spread over a large suface at
nape of neck, loins, and extremities; > motion [Agar.].Soreness of condyles of bones.
Limbs stiff, paraysed. Pain along ulnar nerve. Sciatica; <cold, damp weather, at night.

Numbness and formication, after overwork and exposure. Paralysis; trembling after
exertion. Tenderness about knee-joint. Loss of power in forearm and fingers; crawling
sensation in the fingertips. Tingling in feet. 2Arms nervous and trembling [L].
paralitic pains in elbows. Rhagades on back of hands. Palms; dry, hot, cracked and
sore; washing=burning. Pain down back of thighs, <stools. Legs feel dead, wooden.
Cramps in calves; 7in legs and feet, must walk about, esp. at night. Involuntary
limping. Pricking like pins in fingertips and palms when grasping. Ulcers; on legs;
gangrenous; discharge of bloody water; on dropsical legs. Itching of legs and feet.
Ankles awollen after sitting too long; feet swell in the evening. Paraplegia; after
parturition; sexual excess; fevers. As if walking on needles. 5Rheumatic gnawing
pains, & desire to move the limbs frequently, which >. Limbs on which he lies fall
asleep; 7esp. arms. Pains in the bones of the legs at night; must constantly move them.
5Stiff and paralysed sensation in joints from sprains. Over lifting and overstretching.
Lameness. Stiffness and pain on first moving after rest, or on getting up in the
morning; > constant motion. Sprained pain in arm when carried far upward and
backward. Swelling of hands; of fingers. Tingling pain in shafts of tibia at night when
feet are covered, & constant necessity to move legs, preventing sleep. Sprained pain
in feet in morning on rising. Drawing like paralysis in feet when sitting. Tension as
from shortening of the 0..muscles. Powerlessness of the lower limbs; cannot draw
them up.

Methodology

METHODOLOGY
The present study was conducted in the Bharatesh Homoeopathic Medical
College and Hospital – Belgaum. During the period of 1st August 2007 to 31st July
2009.
This study consist of 30 patients of Ankylosing spondylosis, attending OPD,
IPD, village camps and peripheral clinics of Bharatesh Homoeopathic Medical
College and Hospital – Belgaum were selected at random irrespective of their age,
sex, socio – economic status and occupation. These cases make the material for the
present study.
The inclusion and exclusion criteria for the present study are as follows.
Inclusion Criteria:
Cases of Ankylosing spondylitis will be diagnosed clinically with articular
manifestation.
• Hip pain and stiffness.
• Low back pain that is worse at night, in the morning or after inactivity.
• Stiffness and limited motion in the low back.
Exclusion Criteria:
• Extra articular manifestation
• Progressive disease with deformities
• Ankylosing spondylitis secondary to any other systematic disease with gross
pathology will be excluded.

Case taking was done according to the scheme of model case format with a
special emphasis on ascertaining the following points.
1. History of present complaints :
The complaints along with the duration have been recorded with a special
reference to the age of on set, nature, duration and progress.
Special criteria for the diagnosis of Ankylosing spodylitis have been included
to spot out the complaints in a more systematic and perfect order. Also considered the
significant impairments of patients in various aspects like occupational,
environmental along with destructive tendencies, and considered regarding whether
the patients has got the difficulty in morning, position, motion to elicit the causative
factor, to know the influence of the environmental factors, to unify the system and
pattern of approach in the homoeopathy. Modalities are considered and recorded.
2. Past history:
It is recorded with special reference first illness after birth vaccination past
disorders in chronological order with the nature of treatment and the result.
3. Family history :
A detailed family history was taken to find the incidence of an acute and
chronic disease which becomes important in framing the evolution of miasms in the
patient. A detailed family history of both paternal and maternal side is recorded.
4. Personal history :
All the generalities of the patient are recorded with special reference to
physical built (constitution), thermal, seasonal and atmospheric, diurnal and postural
modalities, diet, appetite, the desire, aversions, food habits, thirst, micturation, bowel

movement, perspirations, sleep, dreams, menses (in women), hobbies, mental
reactions and the findings of observations regarding the behavior of the patient as well
as physical examination are also recorded.
5. Life space investigations :
The significant events in the life and the effects of such events on the
constitution of the patient are recorded in order to demonstrate the role of miasm and
the role of exciting factors and early malnutrition and other factors whichcontribute in
the progress of Ankylosing spondylitis.
6. General physical examination :
The positive findings of the built, nourishment and vital data along with
congenital anomalies if present were recorded.
7. Systemic examination :
Positive finding from all the system were recorded with a special emphasis to
locomotor system. Detailed locomotor system findings were recorded under different
headings
8. Laboratory investigation :
The study requires few investigations
• Routine blood investigation with ESR
• HLA B27
• X-ray(lumbar region)
• Other higher investigations as required like CT Scan and MRI.

9. Diagnosis :
Diagnosis of Ankylosing spondylitis is done on the basis of case history and
clinical findings.
10. Steps for homoeopathic prescription :
a. Analysis of symptoms :
The cases were taken by the guidelines laid by Dr Hahnemann
in the Organon of Medicine 6th edition. The symptoms of the patient
were grouped into various categories like mental generals physical
generals and particulars.
b. Evaluation :
After analyzing the symptoms into various categories like pain
–continuous /intermittent / morning /afternoon /night rest/ better after
exercise / any other.
Stiffness- always /morning /night.
Muscle spasm.
Restriction of movements and pain radiating to other parts
Were evaluated to give value or rank according to the order of their
importance.
c. Repertorization :
To aid in the selection of a suitable remedy, repertorisation
according to Kent, and Murphy. Repertorisation with synthesis was done for
all cases. Characteristic particular considered at the final stage of
repertorisation.

d. Miasmatic diagnosis:
Miasmatic diagnosis is done using the knowledge acquired from the
book ‘Miasmatic Diagnosis’‐Banerjee, Speight, Ortega.
e. Selection of the medicine:
Reportorial result, rare, peculiar, uncommon symptoms and
miasmatic diagnosis of the patient were considered for selecting the
constitutional medicines, acute medicine on sector totality and intercurrent
remedy was selected on symptomatology, follow‐well relation and miasmatic
predominance.
f. Potency and repetation:
Starting with 200th potency in single dose the medicine was
repeated only when there was no further improvement higher potencies in
acute cases. 1M were restored to only after exhausting the lower potencies
but intercurrent was started with 1M in single dose according to the need of
the case
g. Acute remedies :
In cases where the intensity of symptoms were unbearable to the
patient and demanded immediate relief acute, short acting medicines were
prescribed.
h. Constitutional remedies :
The constitution of the patient was thoroughly investigated and the
miasmatic tendencies were identified. Based on these observations the
constitutional drug selected.
i Intercurrent remedies :

These remedies are used in 1M potencies for clearing the miasmatic
block in cases where the improvement of patient makes no progress or
comes to stand sill stage even after repeating the constitutional remedy in
higher potency.
10. Follow up criteria:
Patients shall be reviewed every fortnight for the first two months and later every
month for the remaining period of study or may be called as per the demand of particular
case. New case is taken only during the period. 1st August ‐2007 to 31st July‐2009. No new
cases will be taken after July 2009 but the cases will be followed up for the period of six
months.
11. Para‐meters :
The following para‐meters were fixed according to type of the response obtained
after the treatment.
a. Recovered – Feeling of mental and physical well being with disappearance of all the
symptoms and signs for more than six months.
b. Improved – Feeling of mental and physical well beings with marked disappearance
of symptoms and signs for a period less than six months.
c. Not‐improved –
No relief of symptoms and signs even after sufficient period of treatment.
Results

OOBBSSEERRVVAATTIIOONNSS AANNDD RREESSUULLTTSS
The study was conducted on 30 cases of Ankylosing spodylitis, irrespective of their age, sex & socio economic status.
1. Age Incidence
Statistical study was conducted to identify the age group with the highest
incidence of Ankylosing spondylitis.
Table No 1: Age Incidence
Sr. No. Age group No. of Patients Percentage
1. 10-20 4 13.33 %
2. 21-30 14 46.66 %
3. 31-40 7 23.33 %
4. 41-50 5 16.66 %
Total 30 100%
As shown in the above chart the maximum incidence seen in the age group 21-
30 i.e 46.66% in 14 cases. In 31-40 age group the incidence was 23.33%. i.e in 7
cases. Between the age group 41-50 i.e 16.66% in 5 cases. And in the age group 10-20
years i.e 13.33% in 4 cases.

2. Sex incidence:
Statistical study was conducted to identify the Sex incidence with the highest
of Ankylosing spodylitis.
Table No 2: Sex Incidence
Sr. No. Sex No. of Patients Percentage
1. Male 20 66.66%
2. Female 10 33.34%
Total 30 100%
The above table shows statistical study of sex incidence in 30 patients with
Ankylosing spondylitis. As per the study, maximum sex incidence seen in male i.e 20
cases accounting 66.66% of total and minimum incidence of 33.34% of the total who
where males in 10 cases.
3. Past History:
Statistical study was conducted to identify the past history of the patient
suffering from Ankylosing spondilitis to know the highest incidence.

Table No.3 Past History
Sl. No. Past History No of cases Percentage
1. Typhoid 06 20.00%
2. Jaundice 03 10%
3. Joint complaints 03 10%
4. Respiratory complaints 06 20.00%
5. Haemorrhoids 01 03.33%
6. HTN 05 16.66%
7. Malaria 01 03.33%
8. Chicken pox 02 06.66%
9. Measles 02 06.66%
10. Skin eruptions 03 10.00%
11. Peptic ulcer 04 13.33%
12. Others 02 06.66%
Above table shows maximum incidence in 06 patients of Typhoid accounting
of 20.00% of the total. 03 patients are having joint complaints accounting 10% of the
total.06 patients are having respiratory complaints accounting 20.00% of the total. 1
patient is having haemorrhoides and malaria accounting 03.33% each of the total.

HTN in 5 patients accounting 16.66% of the total. 2 patients are having chicken pox
and measles accounting 6.66% each.
4. Family History
Statistical study was conducted to identify the incidence of disease in the
family was analysed.
Table No 4: Family History
Sr. No Family History No of Subjects Percentage
1 Joint complaints 17 56.66%
2 HTN 2 6.66%
3 DM 2 6.66%
4 Bronchail asthama 2 6.66%
5 CVS 2 6.66%
6 Kochs 2 6.66%
7 Paralysis 2 6.66%
8 Haemorrhides 1 3.33%
Total 30 100%
30 cases were taken to have a statistical study of their family history. The
study carried out on the 30 patients, showed 17 patients had family history of joint

pain which accounted for 56.66% of total. 02 patients were having family history
HTN accounted to 6.66% of the total. 02 patients were having family history of DM,
accounted to 6.66% of the total. 02 patients were having family history of bronchial
asthma were accounted to 6.66% of the total.02 patients were having family history
of CVS, accounted to 06.67% of the total.02 patient have family history of Kochs
accounted to 6.66% of the tota02 patients were having F/H of paralysis accounted to
6.66% .
5. Presenting Complaints:
The statistical study shows that the highest incidence of presenting
complaints.
Table No 5: Presenting Complaints
Sr. No Presenting
Complaints
No of Patients Percentage
1 Low back pain 14 46.66%
2 Stiffness 8 26.66%
3 Limitation in chest
expansion
3 10.00%
4 Constitutional
symptoms
2 6.66%
5 Improvement in
pain by exercise
3 10.00%

The above table shows statistical study of presenting complaints in 30 patients
the study shows 14 patients presented with low backache accounting to 46.66% of the
total.8 patients had stiffness accounting for 26.66%. Of the total 03 patients each
presented with limitation in chest expansion accounting for 10.00%, of the total.02
patients presented with constitutional symptoms accounting for 6.66%. Of the total.03
patients presented with improvement in pain by exercise accounting for 10.00% of the
total.
6. Miasmatic Background:
Statistical study of 30 cases were done to know the miasmatic background of
the patient.
Table No 6: Miasmatic Background
Sr. No Miasmatic
Background
No of Patients Percentage
1 Psoro-sycotic 3 10.00%
2 Psoro-syphilitic 10 33.33%
3 Psoro-syco-syphilitic 17 56.66%
In this study 56.66%of patient had psoro-syco-syphilitic miasmatic
background, 33.33% of patient had psoro-syphilitic and 10% of patients had psoro-
sycotic.

7. Acute Remedies:
The statistical study of 30 cases was done to know the acute remedies used in
Ankylosing spondylitis..
Table No. 7: Acute Remedies
Sr. No Acute/ Sectoral Remedies No of cases Percentage
1 Rhus Tox 17 56.66%
2 Bryonia 04 13.33%
3 Kali Bich 04 13.33%
4 Causticum 02 06.67%
5 Dulcamara 02 06.67%
6 Chammomila 01 03.33%
The most commonly prescribed acute remedy in this study was Rhus Tox
.Other remedies are Bryonia, Kali bich, Causticum, Dulcamara, Chammomilawhich
had also produced a good response. Rhus Tox was given in 17 cases, Bryonia in 4
cases, Kali bich in 4 cases, Causticum in 2 cases, Dulcamara in 2 cases, and
Chammomila in 1 case.

8. Incidence of Intercurrent remedies:
Statistical study was conducted to identify the incidence of intercurrent
remedies used for the treatment of Eczema with their highest incidence.
Table No. 8: Incidence of Intercurrent Remedies
Sr. No Intercurrent remedy No of cases Percentage
1 Tuberculinum 5 16.66%
2 Sulphur 2 6.66%
Out of 30 patients Tuberculinum was prescribed as a intercurrent remedy in
16.66% of total i.e 5 cases. Sulphur was prescribed as a intercurrent remedy in 6.66%
of total i.e 2 cases.
9. Results of the Treatment:
The statistical study shows that utility of Rhus Tox in the treatment of
Ankylosing spondylitis with highest incidence.
Table No. 9 : Results of the Treatment
Sr. No Result No of cases Percentage
1 Recovered 06 20.0%
2 Improved 13 43.33%
3 Not-improved 11 36.66%

Out of 30 cases 20% showed recovery i.e 6 cases. 43.33% of total cases
showed improvement i.e 13 cases and 36.66% of total cases showed no improvement
i.e 11 cases.

Discussion

DDIISSCCUUSSSSIIOONN
Ankylosing spondylitisis is an auto immune disease known to be
associated with tissue type HLAB 27, affecting facet joints between vertebrae
together causing spine to become increasingly rigid.
The critical evaluation of the 30 cases of the present study, shows that the
cause of the disease is unknown. The family history is one of the factors
accountable The results of various observations are discussed below under
different headings.
1. Age incidence:
The maximum incidence seen in the age group 21-30 i.e 46.66% in 14
cases. In 31-40 age group the incidence was 23.33%. i.e in 7 cases. Between the
age group 41-50 i.e 16.66% in 5 cases. And in the age group 10-20 years i.e
13.33% in 4 cases.
2. Sex Incidence:
Statistical study shows the sex incidence in 30 patients with
Ankylosing spondylitis. As reviewed in the literature male are more prone to
have Ankylosing spondylitis. As per the study, maximum sex incidence seen in
male i.e 20 cases accounting 66.66% of total and minimum incidence of 33.34%
of the total who where males in 10 cases.
3. Past History:

The maximum incidence in 06 patients of Typhoid accounting of 20.00% of
the total. 03 patients are having joint complaints accounting 10% of the total.06
patients are having respiratory complaints accounting 20.00% of the total. 1 patient is
having haemorrhoides and malaria accounting 03.33% each of the total. HTN in 5
patients accounting 16.66% of the total. 2 patients are having chicken pox and
measles accounting 6.66% each.
4. Family History:
30 cases were taken to have a statistical study of theirfamily history. The
study carried out on the 30 patients, showed 17patients had family history of joint
pain which accounted for 56.66% . of total. 02 patients were having family history
HTN accounted to 6.66% of the total. 02 patients were having family history of DM,
accounted to 6.66% of the total. 02 patients were having family history of bronchial
asthma were accounted to 6.66% of the total.02 patients were having family history
of CVS, accounted to 06.67% of the total.02 patient have family history of Kochs
accounted to 6.66% of the tota02 patients were having F/H of paralysis accounted to
6.66% .
5. Presenting Complaints:
The statistical study of presenting complaints in 30 patients, shows 14 patients
presented with low backache accounting to 46.66% of the total.8 patients had stiffness
accounting for 26.66%. Of the total 03 patients each presented with limitation in chest
expansion accounting for 10.00%, of the total. 02 patients presented with
constitutional symptoms accounting for 6.66%. Of the total.of the total.03 patients
presented with improvement in pain by exercise accounting for 10.00% of the total.
6. Miasmatic Background:

In this study 56.66%of patient had psoro-syco-syphilitic miasmatic
background, 33.33% of patient had psoro-syphilitic and 10% of patients had
psoro-sycotic.
7. Acute/Sectoral Remedies :
The most commonly prescribed acute remedy in this study was Rhus Tox.
Other remedies are Bryonia, Kali bich, Causticum, Dulcamara, Chammomila which
had also produced a good response. Rhus Tox was given in 17 cases, Bryonia in 4
cases, Kali bich in 4 cases, Causticum in 2 cases, Dulcamara in 2 cases, and
Chammomila in 1 case.
8. Incidence of Intercurrent Remedies:
Out of 30 patients Tuberculinum was prescribed as a intercurrent remedy in
16.66% of total i.e 5 cases. Sulphur was prescribed as a intercurrent remedy in 6.66%
of total i.e 2 cases.
When the action of the well indicated constitutional remedy gets blocked and
the patient fails to respond to further medication, the obstacles in the way of to cure
has looked for. When this analysis pointed to a miasmatic block, an antimiasmatic
prescription has cleared the way for the constitutional medicine to act in many of the
cases.
9. Result of treatment:
Out of 30 cases 20% showed recovery i.e 6 cases. 43.33% of total cases
showed improvement i.e 13 cases and 36.66% of total cases showed no improvement
i.e 11 cases

Conclusion

CCOONNCCLLUUSSIIOONN
This study enables us to draw some valid conclusions. They are :
1) The highest incidence of Ankylosing spondylitis was most common in the age
group 21-30 i.e 46.66% in 14 cases.
2) In this study the maximum incidence of male i.e 20 cases accounting 66.66%
of total and minimum incidence of 33.34% of the total who where females in
10 cases.
3) The maximum incidence of patient had family history of joint pains, most
common 17 cases i.e. 56.66% .next highest presentation was HTN in 2 casec
i.e. 6.66%. .
4) The most common miasmatic background was psora-syco-syphilitic which
was 56.66% of total, followed by psora-syphilitic in 33.33% of total; psoric
and psora-sycotic was 10.00% of total each.
5) The result has been satisfactory with 13 cases improved i.e.43.33% of total; 06
cases recovered i.e. 20% of total & 11cases did not improve 36.66 % of total.
So the present study has been a confirming one wherein according to the
tenets placed in Organon of Medicine, it has been clearly mentioned that in such
instances the totality taken into consideration with holistic approach, these cases can
be treated effectively.

Summary

SSUUMMMMAARRYY
Low back pain is one of the common ailments to man. Ankylosing spondylitisis is one
of the cause for low back pain and if not diagnosed and treated early, leads to chronic pain
and long term disability and resulting in the increase of personal suffering and health care
costs. Therefore, through this study, an attempt has been made to find out the effectiveness
of homoeopathic medicines in the management of acute pain and the long term
constitutional treatment as required for Ankylosing spondylitis and utility of Rhus Tox in
most of the cases. In this study, 30 cases of Akylosing spondylitis irrespective of both the
sexes between the age group 15‐47 yrs which satisfied the inclusion and exclusion criteria
were considered.
The most common age for AS in this study is found 21‐30 yrs age group and the next
common in age group of 31 – 40yrs.
In this study, the sex incidence showed a male predominance than females.
In this study of 30cases the statistical study of the mode of presentations were low
back pain in 14cases, next in order was stiffness in 8cases followed by limitation of chest
expansion in 3cases, improvement in pain after exercise in 3cases and constitutional
symptoms in 2cases.
In this study of 30 cases the family history with which the patients presented were
17cases had joint complaints, HTN, DM, Bronchial asthma, CVS, Kochs, Paralysis, and
Hemorrhoids in 2 cases.
In this study of 30 cases the presenting complaints was digged up which showed that
14 patients had low back pain, 8 cases had stiffness, 3 cases had limitation of chest
expansion, 2 had constitutional symptoms and 3 had improvement in pain after exercise.

The maximum incidence of past history of typhoid in 06 patients, 03 patients
are having joint complaints. 06 patients are having respiratory complaints. 1 patient is
having haemorrhoides and malaria each of the total. HTN in 5 patients of the total. 2
patients are having chicken pox and measles each.
30 cases were taken to have a statistical study of their family history. 17
patients had family history of joint pain. 02 patients were having family history HTN.
02 patients were having family history of DM.. 02 patients were having family history
of bronchial asthma. 02 patients were having family history of CVS. 02 patient have
family history of Kochs. 02 patients were having family history of paralysis.
The statistical study of presenting complaints in 30 patients showed 14
patients presented with low backache. 8 patients had stiffness, 03 patients each
presented with limitation in chest expansion.02 patients presented with constitutional
symptoms.03 patients presented with improvement in pain by exercise.
In the study of miasmatic background, 17 patients had psoro-syco-syphilitic
miasmatic background, 10 patients had psoro-syphilitic and 3 patients had psoro-
sycotic.
The most commonly prescribed acute remedy in this study was Rhus Tox.
Other remedies are Bryonia, Kali bich, Causticum, Dulcamara, Chammomilawhich
had also produced a good response. Rhus Tox was given in 17 cases, Bryonia in 4
cases, Kali bich in 4 cases, Causticum in 2 cases, Dulcamara in 2 cases,and
Chammomila in 1 case.

Out of 30 patients Tuberculinum was prescribed as a intercurrent remedy in 5
cases. Sulphur was prescribed as a intercurrent remedy in 2 cases.
Out of 30 cases 6 showed recovery. 13 cases showed improvement and 11
cases showed no improvement.
Bibliography
BIBLIOGRAPHY
1. Luc De Schepper. Achieving and maintaining the similimum. New Delhi:B.Jain
publishers; 2006, 356pp.
2. BK Sarkar. Commentry on organon of medicine. New Delhi: B.Jain publishers;
1998, 611pp.
3. Hahnemann. Chronic diseases. New Delhi: B.Jain Publishers; 1997, 124pp.
4. http://en/wikipedia.org/wiki/ankylosingspondilitis
5. Souhami RL. Text book of Medicine. New York: Churchill Livingstone; 1990,
997pp.
6. Carthy MC and Frassica. Disease of Jionts, pathololgoy of bone nad joints
disorders with clinical radiographic correction. Philadelphia : W.B. Saunders
Company ; 1988, 317-332pp.
7. Cecil. Textbook of Medicine. 22nd Ed., California : WB Saunders; 1998.1654pp.
8. http://www.medalreg.com/irh/medal/ch22/ch22.21/ch22.21.07.php
9. Souhami and Moxham. Text Book Of Medicine. New York: Churchill
Livingstone ; 1990, 997,998,999pp.
10. Chaurasia BD. Human anatomy regional and applied. Vol.2, New Delhi: CBS
Publishers ; 1990.

11. Romanes BJ. Conningham’s Manual of practical Anatomy. 15th Ed., Vol 2.
Oxford : Medical Publishers; 2004.
12. www.spineuniversity.com,3/1/06.
13. Bellenir, K. Health Reference Series: Back & Neck Disorder Sourcebook. Detroit,
MI: Omnigraphics, Inc.; 1997.
14. Cole and Hering. Low back pain handbook. Vol.1, a guide for practicinig
clinician. 2nd Ed., Oxford: Elsevier Publisher; 1996.
15. Unswarth A. Biomechanics of articulations and derangement in disease. New
York: Churchill Livingstone; 1993.
16. Mercer. Orthopaedic Surgery. 9th Ed., Oxford : Arnold ; 1993. 982pp.
17. Demeter S, Gunnar BJA, George SM. Disability evaluation. New York: Mosby;
1993. 278pp.
18. Stanely Hoppenfeld AND Michael Zeide, Orthopaedic Dictionary, J.B.Lippincott
Company ; Philadelphia.
19. Souhami RL, Moxham J. Text book of medicine. Edinburgh: Churchill
Livingstone; 1990, pg no.997,998,999pp.
20. Kumar &Clark. Clinical Medicine. Fifth Edition, New Delhi: Jaypee Publishers;
1991, 548,549pp.
21. http://www.medicinenet.com/ankylosing_spondylitis/article.htm
22. Biomechanical Considerations http://www.chipsbooks.com/ankylos.htm

23. U.O.di Reumatologia, Policlinico Univrsitario G. Martino, Messina.
24. Steinberg ME. The hip and its disorders. Philadephia: W.B. Saunders Company ;
1991, 509pp.
25. Vakil RJ, Golwalla AF and Golwalla SA. A Textbook of Symptoms and Physical
Signs. Mumbai: MPP Pvt. Ltd. 1997, 206pp.
26. Ogilvie C, Evans CC. Chamberlain’s symptoms and signs in clinical medicine.
12th Ed., UK: Butterworth Publishers; 1986, 209pp.
27. Davidson’s Principles and practice of Medicine 19th Ed. Churchill Livingstone :
An imprint of Elsevier Science Limited.
28. Macnab I, McCulloch J. Backache. 2nd Ed., Baltimore: Williams and Wilkins;
2003. 109pp.
29. Harisons Principles of Internal Medicine. 15th Ed., New York: McGraw-Hill pvt.
Ltd.; 2002, 1949pp.
30. SAMUEL HAHNEMANN, ORGANON OF MEDICINE,6TH EDITION ,B JAIN
PUBLISHER
31. Kent JT. Lectures of homoeopathic philosophy. New Delhi: B Jain Publishers;
1993, 20,137,150pp.
32. Bradford TL. The lesser writings of CMF, Von Boenninghausen translated by
Tafel LH., New Delhi: B.Jain Publishers; 1988, 285pp.

33. Hughes R. Principles and practice of Homoeopathy. New Delhi: B.Jain
Publishers; 1999, 40-41pp.
34. Allen JH. The chornic miasms. New Delhi: B.Jain Publishers; 1998, 5-41pp.
35. Hahnemann S. The Chronic diseases their peculiar nature and their homoeopathic
cure. New Delhi: B.Jain Publishers; 2002, 35-163pp.
36. Boger CM. The philosophy of Healing. New Delhi: B.Jain Publishers; 1999.
37. Kent JT. Lectures on HOmoeoapthic philosophy. New Delhi: B.Jain Publishers;
1999.
38. Robert HA. The principles and art of cure by homoeoapthy. New Delhi: B.Jain
Publishers; 2003.
39. Close S. The genius of Homoeopathy. New Delhi: Indian Books and Periodicals
Publishers; 2001.
40. Farrington Harvey. Homoeopathy and Homoeopathic prescribing. New Delhi:
B.Jain publishers; Reprint 1999, 73,74pp.
41. Nash E.B. Expended works of Nash compiled by Shivraman 1st Ed., New Delhi:
B’ Jain Pub. Printed by UTFC; Pg. 677, 678, 1995.
42. Richard Hughes LRCP Ed. “A Manual of Pharmacodynamics. 6th Ed. New Delhi:
B. Jain Publishers; Pg. 782-83, 2001.
43. Henry B. The outlines of material medica by Henry B. New Delhi: B Jain ; pg.
305-8, Reprint 1997.

44. Farrington E.A. Lectures on Clinical Materia medica. New Delhi: B. Jain
Publishers Pvt Ltd; 1991 pg. 253,54.
45. Farrington EA. Comparative materia medica. New Delhi: B.Jain Publishing Pvt.
Ltd. 2003 to 2007. Reprinted.
46. Carroll Dunham- lectures on matcria medica 5th edition New Delhi .B.J
Publisheoher Pg: 133, 134
47. C Hering condensed M.M Report ed. 1997 4-B: Jain Publ Pg: 809 New
Delhi.
48. Dr. S.R Phatak, Materia medica of Homeopathic medicine 2nd edition New
Delhi, B Jain Publishes PV. ltd. 1999, 604PP
49. H.C.Allen Keynotes rearranged and classified ninth edition; New Delhi Indian
books and publishers.
50. Frans Vermeulen. Concordant materia medica 2001 Emryss, The Neitherlands
publications 826pp.


Annexure - I

ANNEXURE-I : CASE TAKING PROFORMA
BHARATESH HOMOEOPATHIC MEDICAL COLLEGE & HOSPITAL,
BELGAUM
DEPARTMENT OF HOMOEOPATHIC MATERIA MEDICA
UTILITY RHUS TOX. IN THE TREATEMENT OF ANKYLOSING
SPONDILITIS
UNDER THE GUIDANCE OF DR.S S.DIVATE.
DOCTOR INCHARGE: DR. MAMATA GIDNAVAR.
SL NO : OPD NO : IPD NO:
NAME OF THE PATIENT :
AGE: SEX: RELIGION:
MARITAL STATUS:
OCCUPATION :
ADDRESS :
PHONE :
D.O.A : D.O.D :
DIAGNOSIS: 1.NOSOLOGICAL:
2. REMEDIAL :
MIASMATIC DIAGNOSIS:
REMEDY : ACUTE/ CONSTITUTIONAL/ INTER-CURRENT
RESULTS :
IMPROVED /NOT IMPROVED /RECOVERED
SIGNATURE OF THE SIGNATURE OF THE
GUIDE: H.O.D :

I) CHIEF COMPLAINTS WITH DURATION:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
II) HISTORY OF PRESENT COMPLAINTS:
a) ORIGIN/PROBABLE CAUSE:
• Pain : Continuous/ intermittent/ Morning / Night/ Rest/ Exercise/ any other
• Stiffness: Always/ morning / night
• Numness and lower extremities : Always / occasionally / whole of lower limb/
any other.
• Muscle spasm:
• Restriction of movements of chest/ back/ hips/ any other :
• Pain radiating to the thigh/ thoracic region / neck
• Modalities
• Any other complaints/ concomitant
III) PAST HISTORY (WITH TREATMENT ADOPTED)
Any history of trauma , tuberculosis, dysentery, malaise, sore throat, fever, iritis,
urethritis or any other illness.

IV) FAMILY HISTORY (WITH RELATIONSHIP)
PATTERNAL SIDE MATERNAL SIDE
A. FATHER A. MOTHER
IMMIDIATE RELATIONS
A. BROTHERS
B. SISTERS
C. CHILDRENS
Complaints:
Joint pains / Bronchial asthma / HTN/ DM/ haemorrhoides / Kochs/ any other
V) PERSONAL HISTORY
ASSIMILATIONS
a) DIET: VEG MIXED
b) APPETITE :
c) THIRST:
d) DESIRES: salty/ sweet/ sour/ fried
e) AVERSIONS: salty/ sweet/ sour/ fried
ELIMINATIONS
h) BOWELS : Regular / Irregular / Satisfactory/ Unsatisfactory
j) PERSPIRATION: Site/ odour/ character/ stain/ Moderate/ scanty/ profuse
k) MENSTURATION:
l) SUPPRESION OF ELIMINATION: (IF ANY)
m) HABITS: SMOOKING ALCOHOL TOBACCO
DRUGS
o) ADDICTIONS:
p) SLEEP :
q) DREAM:
THERMAL REACTION
r) SEASONAL PREFERENCE ANDAFFECTION: summer/ winter/ rainy
s) COVERING: Yes/ No
t) FAN/A.C/OPEN AIR PREFERENCES:
u) BATH: HOT/COLD/LUKE WARM
v) FOOD AND DRINKS: HOT/LUKE WARM/COLD
w) MENSTURAL HISTORY ASSOCIATED COMLAINTS:
x) OBSERVATIONS MADE (IF ANY):
y) LIFE SPACE/ MENTAL/ REACTIONS:
X) EXAMINATION:
GENERAL PHYSICAL EXAMINATION
1. VITAL SIGNS
a. TEMPRATURE:
b. PULSE RATE _____________ beats/min.
c. RESPIRATORY____________ rate /min.
d. BLOOD PRESSURE__________mm of Hg.
2. BUILT (FRAME): SMALL MEDIUM LARGE
3. ANAEMIA:
4. HEIGHT:
5. WEIGHT:

6. GAIT;
7. PALLOR CYANOSIS ICTERUS CLUBBING
PEDAL ODOEMA LYMPHADENOPATHY
8. HAIR AND SCALP :
9. FACE:
10. EYES/VISION:
11. EAR/HEARING:
12. NOSE/SMELL:
13. MOUTH/LIPS/TOUNGE/ORAL CAVITY/ GUMS/TEETH:
14. EXTREMITIES: UPPER LIMB/ LOWER LIMB
15. VERTEBRAL COLUMN:
16. JOINTS:
17. NECK:
SYSTEMIC EXAMINATION:
1. RESPIRATORY SYSTEM:
INSPECTION/ PALPATION/ PERCUSSION/ AUSCULTATION:
2. CARDIOVASCULAR SYSTEM:
INSPECTION:/ PALPATION/ PERCUSSION/ AUSCULTATION:
3. CENTRAL NERVOUS SYSTEM:
VERTEBRAL COLUMN: INSPECTION/ PALPATION
4. ABDOMEN:
INSPECTION:/ PALPATION/ PERCUSSION/ AUSCULTATION:

EXAMINATION OF THE LOCOMOTOR SYSTEM:
1. INSPECTION : Spinal part involvement/ swelling / deformity/ wasting of
muscles
2. PALPATION: Temperature of local part / tenderness/ corroboration of the
findings of inspection/ any swelling
XI) INVESTIGATIONS:
BLOOD
a. HB%: __________
b. TC: ____________
c. DC: Neutrophils
Eosionophils
Lymphocytes
Monocytes
d. ESR:
e. X-RAY
f. HLA B27 : Antigen
g. ANY OTHER INVESTIGATIONS:
XII) NOSOLOGICAL DIAGNOSIS:
XIII) TOTALITY OF SYMPTOMS:
XIV) ANALYSIS OF SYMPTOMS:
XV) EVALUATION OF SYMPTOMS:
XVI) REPERTORIAL TOTALITY:
XVII) MIASMATIC ANALYSIS:
XVIII) REMEDY ANALYSIS:
XIX) CONSTITUTION

XX) MIASMATIC REPERTORISATION TAB
Sr No SYMTOMS PSORA SYCO SYPH
1
2
3
4
5
6
1
2
3
4
5
6
1
2
3
456
TOTAL
PHYSICAL GENERALS
PARTICULAR SYMPTOMS
MENTAL GENERALS
FINAL MIASMATIC DIAGNOSIS:
XXI) GENERAL MANAGEMENT (DIET, REGIMENT, ETC,)
XXII) HOMOEOPATHIC TREATEMENT:
FIRST PRESCRIPTION:
XXIII) FOLLOW-UP CRITERIA:
DATE FOLLOW UP REMEDY

Annexure -II

ANNEXURE – II GRAPHS
AGE INCIDENCE
SEX INCIDENCE
0
2
4
6
8
10
12
14
10‐20 yrs 21‐30 yrs 31‐40 ysr 41‐50 yrs
67%
33%
Male
Female
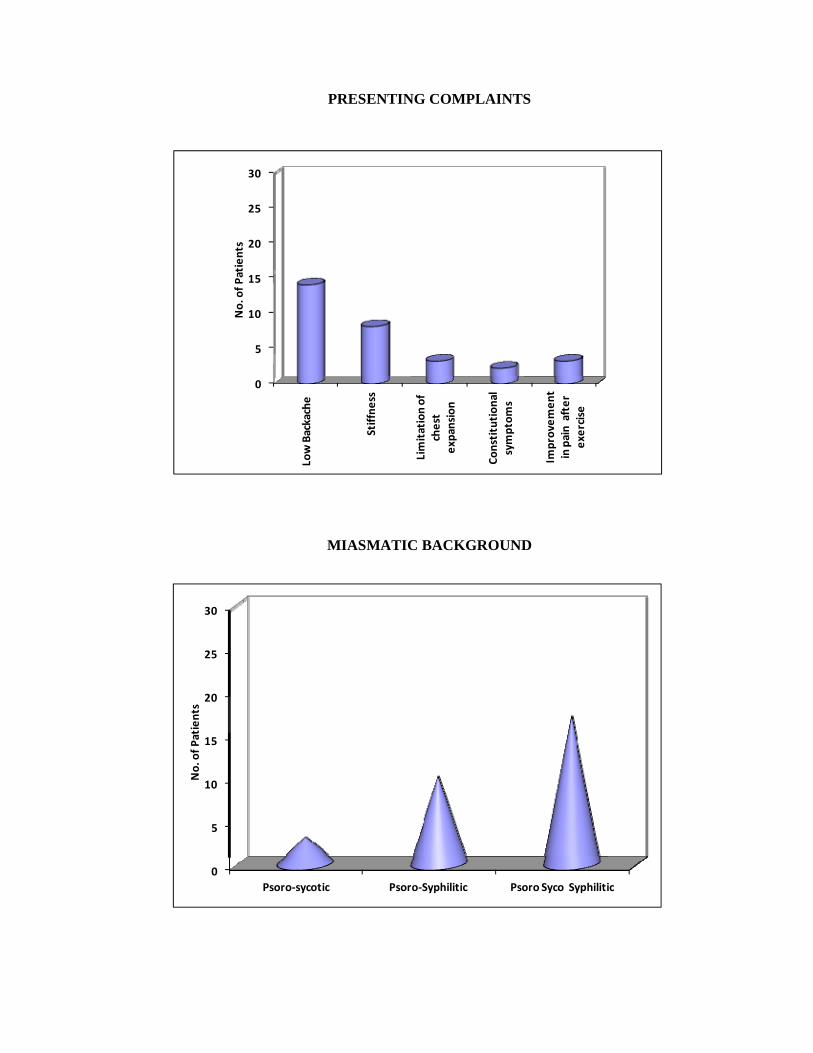
PRESENTING COMPLAINTS
MIASMATIC BACKGROUND
0
5
10
15
20
25
30
Low Backache
Stiffne
ss
Limitation of
chest
expansion
Constitution
al
symptom
s
Improvem
ent
in pain after
exercise
No. of P
atients
0
5
10
15
20
25
30
Psoro‐sycotic Psoro‐Syphilitic Psoro Syco Syphilitic
No. of P
atients

ACUTE REMEDIES
RESULT OF TREATMENT
0
5
10
15
20
25
30
Rhus.Tox Bryonia Kali.bich Causticum Dulcamara Chamomilla
No. of P
atients
0
5
10
15
20
25
30
Recovered Improved Not improved
No. of P
atients

Annexure - III


AANNNNEEXXUURREEIIIIII:: MMAASSTTEERR CCHHAARRTT
Remedial diagnosis Sl. No.
Name Age Sex Occ Presenting complaints
Associated Complaints
Past history
Family history Acute
Remedy Constitutio
nal Remedy
Inter currant Remedy
Miasm Result
1. Mr. SSN
28 M Engineer Pain in low back Lt knee joint pain
Headache Pain in knee joint
F‐ AR M‐ Rheumatism Rhus. Tox Lyc Tub
Psoro‐syco‐
syphilitic
Recovered
2. Mr. NBN
27 M Engineer Back pain on rising
GI disturbance Haemorrhoides
F‐ BrA M‐ HTN Rhus. Tox Lyc ‐
Psoro‐syco‐
syphilitic
Improved
3. Mr. PGG
29 M Business Pain in low back From prolong sitting
Dull mental feeling
Jaundice F‐ DM M‐ HTN Bry Thuja ‐
Psoro‐sycotic
Improved
4. Mrs. NGG
31 F h/w Pain in back Leg pain T/N
Haemorrhoides Haemorrhoides
F‐ DM M‐ HTN Bry Nat.mur ‐
Psoro‐sycotic
Improved
5. Mr. RPR
29 M Clerk Pain in low back Drawing, stitching
HTN Typhoid No significant family history Kali. bich.
Aurum mat.
‐ Psoro‐sycoitic
Improved
6. Mrs. RJS
28 F House made
Pain in low back T/N, legs
Dyspnoea Similar complaints 4 yrs back
M‐ HTN
Rhus. Tox Sepia ‐
Psoro‐syco‐
syphilitic
Improved

Remedial diagnosis Sl. No.
Name Age Sex Occ Presenting complaints
Associated Complaints
Past history
Family history Acute
Remedy Constitutio
nal Remedy
Inter currant Remedy
Miasm Result
7. Mrs. S.b.s
38 f HW Pain in low back Rt.ankle joint pain
eructation HTN F‐joint pain M‐HTN
Rhus Tox Sulp. Sulp.‐ Psoro—‐ syphilitic
Improved
8. Mrs. M.pT
43 M Manager Pain in low back Burning in spots
URTI URTI M‐ HTN CAUST. PHOS. ‐
Psoro‐syco‐
syphilitic
Improved
9. Mrs A.B.B
29 F HW Pain in back before menses while sitting
Pain hip to knee UTI F‐HTN M‐HTN Bryonia Lachesis ‐
Psoro‐syco‐
syphilitic
Recovered
10. Mr R.S.S
39 M Govt. service
LBP, stiffness and pain radiating downward.
Distention of stomach
Burning micturatio
n
No significant history Kali bich Lyc. ‐
Psoro‐syco‐
syphilitic
Recovered
11. Mr D.P.P
19 M Student LBP, burning sensation of spine
Headache Chicken pox
F – HTN M – TB Rhus. Tox Gels. ‐
Psoro‐syco‐
syphilitic
Improved
12. Mr. BPN
23 M Attender Low backache, Rheumatic pain
Thoughts of disease, despair of recovery
Typhoid M‐ DM Rhus. Tox Sulph. ‐
Psoro‐syco‐
syphilitic
Not Improved
13. Mr. PRP
30 M Service Low backache, T/N in LL
Mild yielding, fear something
bad
HTN, similar
complain
F‐Br. Asthma Rhus.tox Cal.carb ‐
Psoro‐syco‐
syphilitic
Not Improved
14. Mrs.TRR
28 F House made
Backpain Rheumatic Recurrent tonsillitis
NAD F‐died of CA throat Bryonia Lyc Thuja
Psoro‐syco‐
syphilitic
Recovered

Remedial diagnosis Sl. No.
Name Age Sex Occ Presenting complaints
Associated Complaints
Past history
Family history Acute
Remedy Constitutio
nal Remedy
Inter currant Remedy
Miasm Result
15. Mr. PTT
44 M Manager
Backpain, Sadness of disease
Neck pain NAD Rhus. Tox Aur. Mat Tub
Psoro‐ syphilitic
Not improved
16. Mr. PRN
35 M Business Backpain in cold air A/F alcoholic beverages, Headache
Typhoid F‐TB Bryoniya Nux.V ‐
Psoro‐ syphilitic
Not Improved
17. Mrs. NPS
28 F Teacher Back pain, extremities pain
Headache Jaundice F‐HTN Rhus.tox Puls. ‐
Psoro‐syco‐
syphilitic
Recovered
18. Mrs. CPR
21 F H/W Pain in lumbar region in morning, chill
during
Pain in rectum and swelling
HTN F‐Peptic ulcer M‐HTN Rhus. Tox Sepia Tub
Psoro‐syco‐
syphilitic
Improved
19. Mr. APR
29 M Business Pain in lower back, sacral region
Eye recurrent agglutination
NAD F‐Cirrhosis of liver
Rhus. Tox Sulph. ‐ Psoro‐ syphilitic
Recovered
20. Mr. SRR
30 M Clerk Pain in lower back Fear of lonelyness
Recurrent tonsillitis
F‐DM M‐HTN
Cali.Bich Nat.mur ‐ Psoro‐ syphilitic
Not Improved
21. Mr. HSP
31 M Laundry Backpain, Cursing and swearing
DM, Headache
M‐Br.asthma Bell. Caust. ‐
Psoro‐syco‐
syphilitic
Not improved
22. Mr. APK
21 M Student Backpain, Sciatica Measles, URTI
F‐Backpain M‐HTN Rhus. Tox Ars. Alb Tub
Psoro‐syco‐
syphilitic
Improved

Remedial diagnosis Sl. No.
Name Age Sex Occ Presenting complaints
Associated Complaints
Past history
Family history Acute
Remedy Constitutio
nal Remedy
Inter currant Remedy
Miasm Result
23. Mr. AVR
28 M Taxi driver
Low back pain as if sprain with stiffness
Irritable easily, indifferent
Jaundice F‐ HTN M‐ Flatulence
RhusTox. Nux V. Tub Psoro‐ syphilitic
Improved
24. Mr. APR
28 M Bus Driver
Low back pain with stiffness
Nervousness HTN F‐HTN M‐Knee joint pain
Rhus. Tox Sepia ‐ Psoro‐ syphilitic
Not Improved
25. Mr. RBD
25 M Field officer
Spinal stiffness, formication sensation
Fastidious, desire for company
HTN Duodenal ulcer
F‐ Operated for peptic ulcer M‐ HTN
Rhus. Tox Ars.alb ‐ Psoro‐ syphilitic
Improved
26. Mr. AKT
22 M Tailor Backache with tingling
Distension abdomen
Typhoid F – DM M‐ HTN Calc.flour Lyc ‐
Psoro‐syco‐
syphilitic
Not improved
27. Mrs. RCM
30 F Housewife
Backache bodyache Talkative suicidal thoughts
Pneumonia F – TB M‐ DM
Colcy. Nat. sulph Tub Psoro‐ syphilitic
Not Improved
28. Mrs. RSM
24 F H/w Backpain spinal stiffness
Bleeding gums, contraction sensation
Gastric ulcer
F‐ Flatulence M‐DM Kali. Bich Alumna
Psoro‐ syphilitic
Improved
29. Mr. DTD
28 M Govt. Service
Backpain burning, sciatica
A/F – Business failure
Skin eruption
F‐HTN Rhus tox Lach. ‐
Psoro‐syco‐
syphilitic
Not Improved
30. Mrs. PNK
27 F H/w Pain in lower extremities
Expressive, egoistic, talk+
Amoebic dysentery
F‐Br. Asth M‐Myoma of Uterus
Rhus tox Lyc Sulph Psoro‐syco‐
syphilitic
Not Improved


Annexure - IV

ANNEXURE – IV : SYNOPSIS OF THE CASES
1. Mr. CSN aged 25 yrs male presented with pain in back, stiffness early morning.
He had headache. Had past history of left knee joints. Family History of Father
suffering from Allergic Rhinitis & Mother from Rheumatism. He was diagnosed
as a case of as Ankylosing Spondylitis. The miasmatic diagnosis was Psora-Syco-
Syphilitic based on all the above data Lycopodium was selected as constitutional
remedy & Rhus tox as acute remedy & Tuberculinum as intercurrent remedy. The
patient recovered.
2. Mr. NBN. age 27yrs male presented with back pain on rising in the morning. He
complained about calf pain & cramps, GI disturbance and flatulence. He had past
history of Hemorrhoides & HTN father suffered from Bronchial Asthma and
mother is HTN & DM. He was diagnosed as a case of as Ankylosing Spondylitis.
Miasmatic diagnosis was Psoro-Syco-Syphilitic. From above data Rhux tox was
given as an acute medicine and Lycopodium was presented as constitutional
medicine & the patient was improved.
3. Mr. PGG age 29, male, with complaints of lumbar pain from prolonged sitting &
shifting kind pain, Anxiety about health, dull feeling mentally. He had wart on
neck. Had past history of Jaundice and pneumonia, his mother is HTN and father
DM. Case was diagnosed as Ankylosing Spondylitis. Miasmatic diagnosis was
Psora-Sycoti. Bryonia was given as acute medicine. Thuja was given as a
constitutional remedy. Patient improved.

4. Mrs. NGG age 31yrs, came with complaints of back pain, leg pain & tingling
numbness some times. She had Irritability at trifles, Her father is having problem
of Hemorrhoides. The case was diagnosed as Ankylosing Spondylitis. Miasmatic
diagnosis was Psora-Sycotic. Bryonia was acute remedy and Nat. mur was
prescribed as constitutional remedy. Patient improved.
5. Mr. RPR age 29yrs, male came with the complaints of pain in low back. drawing
stitching type, stiffness & HTN. He had a past history of typhoid, malaria. He had
no significant family history. He was diagnosed as a case of Ankylosing
Spondylitis. Miasmatic diagnosis was Psora-Sycotic. Kali bich was given as an
acute remedy & Aurum met as constitutional remedy. The patient improved.
6. Mrs. RJS aged 28yrs. Female came with the complaints of pain in low back,
tingling numbness of legs & dyspnoea. She had similar complaints four years
back. Her mother was hypertensive. Miasmatic diagnosis was Psoro-Syphitic.
Rhus.tox was given as acute remedy & Sepia as a constitutional remedy. Patent
improved.
7. Mrs. SBS aged 38 yrs, female came with complaint of low back pain, sciatica. She
was a case of primary infertility and complaint of eructation . she had past history
of HTN & pain in right ankle joint. Her father had joint pain &mother HTN. She
was diagnosed as Ankylosing Spondylitis. Miasmatic diagnosis was Psoro-
Syphilitic. Rhus tox was given as acute remedy and Kali.bich as constitutional
remedy and sulphur as intercurrent remedy. Patient improved.
8. Mr. MPT age 43 yrs male came with the complaint of back pain on slight
exertion, morning stiffness, having burning pain in spots on rubbing. In the past he
was having upper respiratory tract infection. In the family history mother was

HTN. He was diagnosed as a case of Ankylosing spondilitis. Miasmatic diagnosis
was Psora-Syco-Syphilitic. Causticum was acute remedy and Phosphorous was
constitutional remedy. Patient improved.
9. Mrs. ABB, 29 yrs F, came with c/o LBP before menses, sitting while. Better by
rising in morning. She was having pain in hip to knee. She had past history of
recurrent urinary tract infection. In her family history her father, M & brother are
suffering from HTN. She was diagnosed as case of Ankylosing spondilytis and
her miasmatic diagnosis was Psora-Syco-Syphilitic Bryonia was given as acute
remedy, Lachesis as constitutional medicine. The patient recovered.
10. Mr. RRS , 39 yrs M, came with c/o LBP with stiffness and pain radiating
downwards. He was having wart on his face recurrent burning micturation. There
is no significant family history. He was diagnosed as a case of Ankylosing
spondilytis and his miasmatic diagnosis was Psora-Syco-Syphilitic Kali bich. was
given as acute remedy. Lycopodium was prescribed as constitutional medicine.
The patient recovered.
11. Mr. DPP aged 19 yrs M, came with C/o LBP burning sensation in spine. Also
complained of headache. In the past he suffered from chicken pox. His Father -
HTN and Mother – Kochs elder brother DM. he was diagnosed as case of
Ankylosis spondilytis. The miasmatic diagnosis was Psora-Syco-Syphilitic. Rhus
tox was acute remedy. Gelsem was constitutional remedy. The patient improved.
12. Mr. BPN age 23 years Male, with C/o bhack pain, rheumatic. He also complained
of thoughts of disease, despair of recovery. In the past he suffered from typhoid,
family history – Mother – DM, HTN, sister had Ca breast. He was diagnosed as
case of ankylosis spondilytis. Rhus tox. Was acute remedy given and Sulphur as

constitutional remedy and Thuja as intercurrent remedy. Miasmatic diagnosis is
Psora-Syco-Syphilitic Patient did not improved.
13. Mr. PRP age 30 yrs, Male came with complaint of low back pain extending to
right lower leg. Tingling numbness and he complained mild, yielding fear
something bad. Family history – Father – Asthma. He was diagnosed as a case of
Ankylosing spondylitis. Miasmatic diagnosis was Psora-Syco-Syphilitic. Rhus tox
was given as acute remedy and Calcarea carb as constitutional. The case did not
improve.
14. Mrs. TRR, age 28 yrs, female came with low back pain and Rheumatic kind of
pain. No significant past history. Father died due to carcinoma of throat. Family
history – Mother – knee pain. She was diagnosed. Miasmatic diagnosis was Psora-
Syco-Syphilitic. Bryonia was given as acute remedy and Lycopodium as
constitutional and Thuja as intercurrent remedy. The patient recovered.
15. Mr. PTT aged, 44 yrs, Male came with complaint of back pan, < night sitting >
motion during, and pressure and complaint of sadness of disease. He had a history
of neck pain in past. No significant family history. He was diagnosed as a case of
ankylosis spondilitis. Miasmatic diagnosis was Psora-Syphilitic. Rhus tox was
given as acute remedy and Aurum-met as constitutional remedy Tuberculinum as
intercurrent remedy. The case did not improved.
16. Mr. PRN, Age 35 yrs, Male came with complaint of back pain on cold air, < from
lifting. The patient had ailments from alcoholic beverages. Headache. In the past
he had suffered from Kochs. He was diagnosed as a case of ankylosing
spondilytis. Miasmatic diagnosis was Psora-Syphilitic. Bryonia was given as acute
remedy and Nux-v as constitutional. The case did not improved.

17. Mrs. NPS age, 28 yrs, female came with complaint of back pain and stiffness. She
also complained of Headche. In the past she had suffered from jaundice and
chicken pox. Her father is suffering form HTN. She was diagnose ankylosing
spondilitis. Miasmatic diagnosis was Psora-Syco-Syphilitic. Rhus tox was given
as acute remedy and Pulsatilla as constitutional. The patient recovered.
18. Mrs. CPR age 21 yrs, female came with complaint of pain in lumbar region in
morning chill during. She also complained of pain in rectum. She is known HTN.
Family history – Father – peptic ulcer and Mother – HTN. She was diagnosed
case of Ankylosing spondilitis. Miasmatic diagnosis was Psora-Syco-Syphilitic.
Rhus tox was given as acute remedy and Sepia as constitutional and Tub as
intercurrent remedy. The patient improved.
19. Mr. APR, age 29yrs, male came with complaint of low back pain and sacral
region. Eye recurrent agglutination. No significant past history. In his family
father suffered from cirrhosis of liver. He was diagnosed as case of lumbar
spondylosis and miasmatic diagnosis was Psora-Syphilitic. Rus. Tox was given as
acute remedy and Tub. as intercurrent. The patient recovered.
20. Mrs. SPR, age 30 yrs female, came with complaint of pain in low back, fear of
loneliness. Past history – recurrent tonsilitis, family history – Father Diabetes
mellitus, mother – HTN. She was diagnosed as case of Ankylosing spondilitis and
Miasmatic diagnosis was Psora-Syphilitic. Kali.bich was given as acute remedy
and Nat.mur as constitutional. The patient not improved.
21. Mrs. HSP, 31 yrs, Back pain, < pressure, night, patient was always cursing and
swearing. Past history diabetes mellitus and headache. Family history- Mother had
Br. Asthma. She was diagnosed as case of Ankylosing spondilitis and Miasmatic

diagnosis was Psora-Syco- Syphilitic. Belladonna was given as acute remedy and
Causticum as constitutional. The patient did not improved.
22. Mr. APK, 21 years male, came with complaint of backpain, < evening cold air,
night. Associated with fever. Past history with measles and upper respiratory tract
infection. Family history of father had back pain mother was HTN. He was
diagnosed as case of Ankylosing spondilitis and Miasmatic diagnosis was Psora-
Syphilitic. Rhus.tox was given as acute remedy and Sepia as constitutional
remedy Tuberculinum as intercurrent remedy. The patient not improved.
23. Mr. AVR, 28 yrs male, came with the complaint of low back pain and pain as if
sprain with stiffness in the back. Also patient was irritable easily, indifferent to
every thing, nervous. He is known HTN. In the past patient had extensive skin
eruption on the legs. In his family history father was HTN and mother was
suffering from pain in knee joint. He was diagnosed as case of Ankylosing
spondilitis and Miasmatic diagnosis was Psora-Syphilitic. Rhus.tox was given as
acute remedy and Lycopodium as constitutional remedy Tuberculinum as
intercurrent remedy. The patient not improved.
24. Mr. APR 23 yrs male came with the complaint of low back pain, with eye
complains with stiffness of back which increased by rest. Patient was nervous
having past history of HTN, in the family father had HTN, and mother had knee
joint pain. He was diagnosed as case of Ankylosing spondilitis and Miasmatic
diagnosis was Psora-Syphilitic. Rhus.tox was given as acute remedy and
Causticum as constitutional. The patient not improved.
25. Mr. RBD age, 25 yrs male came with the complaint of stiffness and fatigue,
formication sensation. Anxious about health fastidious and desires for company.

He had HTN in the past. And in his family father was operated for perforated
duodenal ulcer and mother had HTN. He was diagnosed as case of Ankylosing
spondilitis and Miasmatic diagnosis was Psora-Syphilitic. Rhus.Tox was given as
acute remedy and Ars.alb as constitutional. The patient not improved.
26. Mr. AKT age 22 yrs male came with complaint of low pack pain tingling
numbness in back, neck pain with distension in abdomen. With his past history of
eruption over the legs and he had suffered form typhoid. In family mother had
diabetic mellitus and father was HTN. He was diagnosed as case of Ankylosing
spondilitis and Miasmatic diagnosis was Psora-Syco-Syphilitic. Calc.flour was
given as acute remedy and Lyco as constitutional. The patient not improved.
27. Mrs. RCM aged 30 yrs, Female came with complaint of low back pain and sciatic
and was fastidious, talkative, sucidal thoughts. She had past history of typhoid,
measles. Her family history tells us that her father had asthma and he had suffered
from TB and mother was diabetic mellitus. She was diagnosed as case of
Ankylosing spondilitis and Miasmatic diagnosis was Psora-Syphilitic. Colocynth
was given as acute remedy and Nat.sulph as constitutional and Tub. as intercurrent
remedy. The patient not improved.
28. Mrs. RSN, age 24 yrs, female came with the complaint of back pain, spinal
stiffness and sciatica. She was also having tendency of bleeding gums. She
suffered in the past from typhoid and gastric ulcer. Her mother had diabetes
mellitus and father had flatulence dyspepsia. She was diagnosed as case of
Ankylosing spondilitis and Miasmatic diagnosis was Psora-Syphilitic. Kali.bich
was given as acute remedy and Almina as constitutional. The patient improved.
29. MR. DTD age 28 yrs male came with the complaint of low back pain and pain
radiating to the legs. Ailments from business failure. He was irritable and hatred
to express feelings. He had past history of skin eruption over trunk. In his family
father had HTN. He was diagnosed as case of Ankylosing spondilitis and
Miasmatic diagnosis was Psora-Syco-Syphilitic. Rhus. Tox was given as acute
remedy and Lachesis as constitutional. The patient not improved.
30. Mrs. PNK age 27 female came with low back ache, restricted movements, pain in
the lower extremities, and was not expressive. Use to talk very fast and was
egoistic. In the past she had amoebic dysentery. In her family father had bronchial
asthma and mother had myoma of uterus and was diabetic. She was diagnosed as
case of Ankylosing spondilitis and Miasmatic diagnosis was Psora-Syco-
Syphilitic. Rhus.tox was given as acute remedy and Lycopodium as constitutional
remedy Sulphur as intercurrent remedy. The patient not improved.












