Angiosarcoma of the heart
7
Angiosarcoma of the Heart* D. LUKE GLANCY, M.D., JORGE B. MORALES, JR., M.D. and WILLIAM C. ROBERTS, M.D., F.A.C.C. Bethesda, Maryland and Washington, D. C. NorosA~coMA is a rare, malignant tumor A that most often occurs in the skin and sub- cutaneous tissue, including breast, but that may arise from any blood vessel. When it originates in the heart, obstruction to filling of the right- sided cardiac chambers by a large right atria1 tumor, or extensive pericardial invasion, or both, almost uniformly occurs. This report describes a patient with primary cardiac angiosarcoma and summarizes the clinicopathologic features in previously reported patients with angiosar- coma of the heart. REPORT OF PATIENT A 35 year old Negro woman who died on Feb. 9, 1967, had been well until two months earlier when oc- cipital headaches appeared. These recurred daily and became progressively more severe. Cough, chills and fever appeared one week before death, and vomit- ing and mental obtundity were present on the day of death, when she was admitted to Providence Hospital. Examination disclosed stupor, slurred speech, nuchal rigidity, early papilledema and vertical and horizontal nystagmus. There were no precordial murmurs or abnormal sounds, and there was no evidence ofcardio- megaly or peripheral edema. Dullness to percussion and diminished breath sounds were noted over the right hemithorax. The temperature was 99.8” F., pulse 112/min. and blood pressure 140/80 mm. Hg. An electrocardiogram showed sinus tachycardia and nondiagnostic ST-T wave changes. Chest roentgen- ogram (Fig. 1) revealed a prominent right cardiac border, diffuse, finely nodular infiltration of both lungs and a right pleural effusion. On Lumbar puncture the opening pressure was 36 cm. cerebrospinal fluid, which was xanthochromic and contained 1,200 erythrocytes and 70 leukocytes (90 per cent polymorphonuclear cells) per cu. mm., 140 mg. protein and 70 mg. glucose per 100 ml. The pa- tient had a generalized seizure 45 minutes later, fol- lowed by coma and slow (lO,/min.) Cheyne-Stokes type respirations, and she died. AUTOPSY Numerous tumor nodules were present in the sub- epicardial adipose tissue (Fig. 1). The larger ones in- vaded the underlying myocardium of all four cardiac chambers and the overlying parietal pericardium, thus producing obliterative tumor pericarditis. A 6 by 6 by 5 cm. mass of tumor in the anterolateral right atrial wall had caused the bulging right cardiac border on roentgenogram. It involved epicardium, myo- cardium and endocardium and projected as a 2 by 2 by 2 cm. mass into the right atria1 cavity (Fig. 1). Large subepicardial tumor deposits surrounded the pulmonary trunk, the ascending aorta enclosed by pericardium and both atria; they also infiltrated the atrial septum. A 1.5 cm. tumor nodule was present in each cere- bellar hemisphere, and smaller ones were present in the midbrain. In both lungs there were diffuse, miliary metastases, most of which were less than 0.5 cm. in diameter. Tumor also was found in the ovaries, uterus, spleen, liver, thyroid gland, kidney and lymph nodes (paratracheal, periaortic and retro- peritoneal). The skin was normal. Histologicall), the tumor in some areas consisted of large, thin-walled, vascular spaces filled with blood, and in other areas it consisted mainly of sheets of spindle-shaped cells (Fig. 2). Both histologic pat- terns often were present in the same tumor nodule, as well as intermediate patterns containing small vascu- lar spaces. COMMENTS The clinical and pathoanatomic features in 40 previously reported patientslL40 with angiosar- coma of the heart are summarized in Table I. In each the heart was considered the site of the primary tumor, but in 26 this was not unequivo- cally established since extracardiac tumor also was present. As in the present patient, how- ever, the largest mass of tumor in each was in the heart, and the cardiac findings were similar, both clinically and pathologically, in those with * From the Laboratory of Pathology, Clinic of Surgery, National Heart Institute, National Institutes of Health, Bethesda, Md., and the Department of Pathology, Providence Hospital, Washington, D. C. Address for reprints: William C. Roberts, M.D., Laboratory of Pathology, Clinic of Surgery, National Heart In- stitute, National Institutes of Health, Department of Health, Education and Welfare, Bethesda, Md. 20014. VOLUME 21, MARCH 1968 413
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Angiosarcoma of the heart

Angiosarcoma of the Heart* D. LUKE GLANCY, M.D., JORGE B. MORALES, JR., M.D. and WILLIAM C. ROBERTS, M.D., F.A.C.C.
Bethesda, Maryland and Washington, D. C.
NorosA~coMA is a rare, malignant tumor A that most often occurs in the skin and sub- cutaneous tissue, including breast, but that may arise from any blood vessel. When it originates in the heart, obstruction to filling of the right- sided cardiac chambers by a large right atria1 tumor, or extensive pericardial invasion, or both, almost uniformly occurs. This report describes a patient with primary cardiac angiosarcoma and summarizes the clinicopathologic features in previously reported patients with angiosar- coma of the heart.
REPORT OF PATIENT
A 35 year old Negro woman who died on Feb. 9, 1967, had been well until two months earlier when oc- cipital headaches appeared. These recurred daily and became progressively more severe. Cough, chills and fever appeared one week before death, and vomit- ing and mental obtundity were present on the day of death, when she was admitted to Providence Hospital.
Examination disclosed stupor, slurred speech, nuchal rigidity, early papilledema and vertical and horizontal nystagmus. There were no precordial murmurs or abnormal sounds, and there was no evidence ofcardio- megaly or peripheral edema. Dullness to percussion and diminished breath sounds were noted over the right hemithorax. The temperature was 99.8” F., pulse 112/min. and blood pressure 140/80 mm. Hg. An electrocardiogram showed sinus tachycardia and nondiagnostic ST-T wave changes. Chest roentgen- ogram (Fig. 1) revealed a prominent right cardiac border, diffuse, finely nodular infiltration of both lungs and a right pleural effusion.
On Lumbar puncture the opening pressure was 36 cm. cerebrospinal fluid, which was xanthochromic and contained 1,200 erythrocytes and 70 leukocytes (90 per cent polymorphonuclear cells) per cu. mm., 140 mg. protein and 70 mg. glucose per 100 ml. The pa- tient had a generalized seizure 45 minutes later, fol- lowed by coma and slow (lO,/min.) Cheyne-Stokes type respirations, and she died.
AUTOPSY Numerous tumor nodules were present in the sub-
epicardial adipose tissue (Fig. 1). The larger ones in- vaded the underlying myocardium of all four cardiac chambers and the overlying parietal pericardium, thus producing obliterative tumor pericarditis. A 6 by 6 by 5 cm. mass of tumor in the anterolateral right atrial wall had caused the bulging right cardiac border on roentgenogram. It involved epicardium, myo- cardium and endocardium and projected as a 2 by 2 by 2 cm. mass into the right atria1 cavity (Fig. 1). Large subepicardial tumor deposits surrounded the pulmonary trunk, the ascending aorta enclosed by pericardium and both atria; they also infiltrated the atrial septum.
A 1.5 cm. tumor nodule was present in each cere- bellar hemisphere, and smaller ones were present in the midbrain. In both lungs there were diffuse, miliary metastases, most of which were less than 0.5 cm. in diameter. Tumor also was found in the ovaries, uterus, spleen, liver, thyroid gland, kidney and lymph nodes (paratracheal, periaortic and retro- peritoneal). The skin was normal.
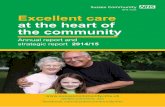
Histologicall), the tumor in some areas consisted of large, thin-walled, vascular spaces filled with blood, and in other areas it consisted mainly of sheets of spindle-shaped cells (Fig. 2). Both histologic pat- terns often were present in the same tumor nodule, as well as intermediate patterns containing small vascu- lar spaces.
COMMENTS
The clinical and pathoanatomic features in 40 previously reported patientslL40 with angiosar- coma of the heart are summarized in Table I.
In each the heart was considered the site of the primary tumor, but in 26 this was not unequivo- cally established since extracardiac tumor also was present. As in the present patient, how- ever, the largest mass of tumor in each was in the heart, and the cardiac findings were similar, both clinically and pathologically, in those with
* From the Laboratory of Pathology, Clinic of Surgery, National Heart Institute, National Institutes of Health, Bethesda, Md., and the Department of Pathology, Providence Hospital, Washington, D. C.
Address for reprints: William C. Roberts, M.D., Laboratory of Pathology, Clinic of Surgery, National Heart In- stitute, National Institutes of Health, Department of Health, Education and Welfare, Bethesda, Md. 20014.
VOLUME 21, MARCH 1968 413

414 Glancy, Morales and Roberts
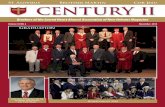
FIG. 1. .4bove, chest roentgenogram and heart. Upper left, anteroposterior projection, taken with the patient supine, shows generalized cardiac enlargement, prominence of the right cardiac border and right ventricular outflow tract, finely nodular infiltrates in both lungs, and a right pleural effusion. Lower left, anterior surface of the heart after removal of the adherent parietal pericardium. A large right atria1 tumor (R.A.) caused the prominent right cardiac border on roentgenogram. Large masses of epicardial tumor surround the aorta (.40.) and pulmonary trunk (P.T.), and smaller nodules are in the right (R.V.) and left (L.V.) ventricular epicardium. Upper right, the free walls of the right atrium and right ventricle. A partially hemorrhagic tumor, 6 cm. in diameter, involves the right atria1 epicardium, myo- cardium and endocardium and projects into the right atria1 cavity just above the tricuspid valve (T.V.). Lower right, the intracavitary projection of the tumor shown at upper right measures 2 cm. in diameter.
FIG. 2. Opposite page, photomicrographs of the cardiac angiosarcoma. Upper left, epicardial tumor nodule with both cel- lular areas and large vascular spaces (X 25). Upper right, large vascular spaces separated by cords of endothelial cells (X 160). Lower left, spindle-shaped cells with inconspicuous vascular spaces between them. This histologic pattern is indistinguishable from that of Kaposi’s sarcoma (X 251). Lower right, high power photomimograph of the tumor cells (X 628). All sections stained with hematoxylin and eosin.
THE AMERICAN JOURNAL OF CARDIOLOGY

Angiosarcoma of the Heart 415
VOLUME 21, MARCH 1968

416 Glancy, Morales and Roberts
and those without extracardiac tumor. The an- giosarcomas were described under a variety of names : angiosarcoma, 1,10,12.13,16,18,19,21,25.21-29,
31 1 p5 p37 1 4o angioendothelial sarcoma,24 hemangio- sarcoma,23 endothelioma,ll hemangioendotheli- oma 4,34,3g malignant hemangioendothelioma,3*20v 38 I-leInangioendotheliosarcoma, 8 315 217 ,22,26 heman-
gioendothelioblastoma,14 malignant hemangio- blastoma,5 hemangioreticuloendothelioma,g telangiectatic and cavernous spindle-cell sarcoma2 and primary Kaposi’s sarcoma of the heart.6 s7 b30 ,32 ZG Judged by the histologic fea- tures in published photomicrographs, “primary Kaposi’s sarcoma of the heart” (Table I, Cases 6, 7, 31 and 33) is identical to primary cardiac angiosarcoma (Fig. 2) and in the absence of cutaneous manifestations of Kaposi’s sarcoma should be classified as angiosarcoma.
CLINICAL FEATURES
The clinical features in the 41 patients with cardiac angiosarcoma were remarkably uniform (Table I). All were adults, and 35 were under age 50 years (range 22 to 68, average 40 years); 29 were men. Of the 37 patients for whom ade- quate clinical information was available, 32 had evidence of obstruction to filling of the right- sided cardiac chambers. All 32 had cardiome- galy. Dyspnea was described in 23, systemicven- ous distention in 19, hepatomegaly in 17, edema in 16, cyanosis in 11, diminished cardiac sounds in 11, systemic arterial pulse pressures of 25 mm. Hg or less in 6, pulsus paradoxus in 5 and syn- cope in 4 of the 32 patients. Venous distention, edema and cyanosis were at times limited to the head and upper trunk. A few reports simply stated that the patient had superior vena caval obstruction or cardiac tamponade without listing each sign and symptom. Orthopnea, paroxy- smal nocturnal dyspnea, pulmonary alveolar edema, pulsus alternans and other manifesta- tions of left-sided cardiac failure rarely occurred.
Precordial pain, often typically pericarditic in type, was present in 23 of 34 patients, and peri- cardial friction rubs were heard in 8 of 32 sub- jects (Table I). Temperatures over 100” F. were recorded in 16 of 22 patients whose temper- ature was stated. Of 30 patients, 13 had cough and 8, including 2 without pulmonary metas- tases, had hemoptysis. The combination of fever, hemoptysis and evidence of a pericardial effusion led to a diagnosis of tuberculosis in at least 5 patients. ’
X-ray and Electrocardiographic Findings: All 28
patients with chest roentgenograms had cardio- megaly. In 20 the enlargement was general- ized, and often the cardiac silhouette was globu- lar and massive; in 7 generalized enlargement was present, but the most striking finding was a prominent right cardiac border (Fig. 1); in 1 the right ventricular outflow tract was promi- nent. In addition, chest roentgenograms dem- onstrated pulmonary metastases in 4 patients and rib metastases in 3. All but 1 of 24 patients had electrocardiographic abnormalities : ST-T wave changes, which were usually nonspecific but were occasionally typical of pericarditis, in 1.5 patients; low QRS voltage in 13; right axis de- viation in 5 ; supraventricular arrhythmias in 4; right bundle branch block in 2; QRS changes suggesting an old myocardial infarct in 2 ; and in 2 patients changes suggesting a recent myocar- dial infarct, which was found at necropsy in 1 of them.
Clinical Diagnosis and Prognosis: A malignant, primary cardiac tumor was suspected clinically in 12 patients, and this diagnosis was supported by a positive biopsy of bone, lung or the primary tumor in 4 patients, by finding tumor cells in pericardial fluid in 1, by visualizing the tumor by pneumopericardium in 1 and by venous angio- cardiogram in 1. The duration of symptoms from their onset until death was nine months or less in 29 of the 33 patients in whom this interval could be determined. Each of the 4 patients (Table I, Cases 15, 22, 25, 28) who lived longer than nine months after the onset of symptoms had a biphasic illness, and it is possible that the initial phase in them was unrelated to angiosarcoma.
PATHOANATOMIC FEATURES
Site of Primary Tumor: The pathoanatomic features in the 41 patients were even more uni- form than the clinical features. The site of the primary tumor was the right side of the heart (al- most always the right atrium) or the pericardium (usually the epicardium) in all but 1 patient (Table I, Case 4), and her left atria1 tumor was an incidental autopsy finding. In each of the other patients, tumor involved the right atrium (Fig. 1) ; this chamber almost invariably was the one most extensively involved. Right atria1 intracavitary projections of tumor were usually present, and measured up to 12 cm. in diameter In 17 patients tumor obstructed one orbothvenae cavae, or the tricuspid valvular orifice, or both. The epicardium was involved by tumor in all but
THE AMERICAN JOURNAL OF CARDIOLOCY

Angiosarcoma of the Heart
1 patient (Table I, Case 14). At times only the it contained hemorrhagic fluid in 24, serous epicardium over a right atria1 tumor was in- fluid in 1 and was normal in 2. Pericardial vaded, but usually there was extensive invasion tumor most often limited right ventricular filling of the epicardium and subepicardial adipose by producing hemopericardium with tampon- tissue, and in at least 11 patients, the heart was ade, but ventricular constriction by a thick layer encased by a layer of tumor over 1 cm. thick. of epicardial tumor was probably another mech- The pericardial cavity was obliterated by tumor, anism, and each of these mechanisms at times or organized hemorrhage, or both, in 13 patients; coexisted with vena caval obstruction.
TABLE I Cardiac Angiosarcoma: Clinical and Pathologic Data in 41 Cases
r-p---- Clinical Features -7 Pathoanatomic Features--------, RV Duration Venous or
ChSC Inflow Peri- Fever Heart of Symp- Peri- Valvular No. Obstruc- cardial Chest (>lOO” Hemop- on toIns Primary cardial Obstruction Extracardiac
(Ref. ) Age/Sex don Rub Pain F.) tysis x-ray bo. ) Site Cavity by Tumor Metastases
1’ 22/M 22 44/M 33 62/F 44 45/F 56 44/M 66,’ 26/M 7” i 30/M 88 40,‘M
9” 46/M 10’0 60/M 11” 45/M 12’2 47/M
13’3 27/M 14’4 54/M
15’5 23/F 1616 46/M 17” 26/M 18’0 45/F
19’” 27/M 20’0 25/‘M 2120 33/M 222’ 37/M 23* 46/M 2423 32/F 252’ 35/M 2625 47/M 27%~ 45/M 281’ 29/F 29es 38/M 3029 59/F 318” 43/M
+ 0 0
0 0 0 0
0 0
0 0
0
0 0
: 0
:
:
0 0 0
0
0 0
+
0
: 0
+ + 0
0 0
:
0
0 0
+
:
0
:
: 0
i- +
T + +
0
i +
: + 0
+
+ + +
0
+ 0
+
+ 0
:'
:
: f
+
. .
+
i 0
0
:
0
: 0
0
0 0
0
0 0
0 0
: 0
:
+ 0 0
+
0 0
+
0
0 0
GE GE GE GE
4 1.5 6
t 6’ 2 1.5 9
GE GE
: 1.2 2
GE 5 GE 8
GE ?21, ?7
RVO 2.5 R 2
R GE GE GE R GE GE
GE R R
4 4
?23, ?3 8 2
?24, ?5 5 1.2
?15,?8 8
GE
GE R
5 6
GE 0.3 3
GE GE R
0.3 5 1 5 2
P Hem0. RA Oblit. RA Herrlo. LA N0*ltld P Helllo. RA Oblit. RA Hemo. P Oblit.
vc L WC L, CNS 0 L, B, LN, Om 0 0 WC L. Liv. TV L, Liv., LN, Om WC, WC, TV 0 WC L, Liv., S, B, K.
Pan., T, A 0 L, Liv., LN, B 0 LN
PorRA Oblit. RA Henlo. RA HeIrlo. P, RA, or Hem0.
RV
WC 0 0 L, LN, SM
svc, IVC, PV 0 SVC, WC, TV, 0
RVI SVC, WC, TV 0 0 L, Liv., K. A, B
P Oblit. RA, RV, or Normal
TV RA Nemo. RA or RV Oblit. RA or RV Oblit. RA Hema.
0 L, Pr. SVC. IVC. TV, L
RA NeIllO. RA Oblit. RA Hema.
cs 0 svc 0 0 svc 0 0 0 SVC, ?TV IVC, ?SVC 0 0
0 L, Liv., LN, A L, Liv., B, LN L. s CNS, Liv., A. B 0 0
L, Liv., LN L 0 L, Liv., B, A L
RA RA RA
RA P RA P RA or RV RA PorRA RA P RA RA RA RA P RA RA RA
Hemo. Oblit. Hemo. HetrIo.
HeIll0. Hem0. Oblit. S.Zt-OUS Oblit. Hemo. Hemo. Helllo. Hemo. Herrlo. Hemo. Oblit.
tv, IVC 0
L L 0 L, Liv. 0 L, LN 0 0 L, LN L, ov. L, CNS, Ov., U,
S, Liv., T, K, LN
323’ 39/F 33h2 .a1 38iM 34* 38iF svc
0 LSV 0 0 0 0 0
35as 52:F 36’6 43/M 3737 25/M 38= 33/M 3939 68/M 4010 26/F 41* 35/F
(Ref.) = reference describing the patient; + = present; 0 = absent; . = insufficient information; A = adrenal gland; B = bone; CNS = brain; CS = coronary sinus; GE = generalized enlargement; Herno. = hemopericardium; IVC = inferior vena cava; K = kidney; L = lung and/or oleura: Liv. = liver: LA = left atrium: LN = Ivmuh nodes: LSV. = left subclatian vein: Oblit. = obliterated: Om. = ornentum:
. .
Ov. = ovary; P = pericardium; Pan. = panc&s; Pr. =. _ prostate; Pb = pulmonary veins; R = p;ominent right cardiac border; RA = righi atrium; RV = right ventricle; RVI = right ventricular infundibulum; RVO = prominent right ventricular outflow tract; S = spleen; Serous = xrous effusion; SM = skeletal muscle; SVC = superior vena cava; T = thyroid; TV = tricuspid valve; U = uterus; VC = vena cava.
*Present patient. t Died of rheumntic mitral stenosis. Angiosarcoma an incidental necropsy finding. $ Died suddenly of hemopericardium with tamponade. Dyspnea for one year and cardiac murmur probably due to cardiac disease other than
angiosarcoma.
VOLUME 21, MARCH 1968

418 Glancy, Morales and Roberts
Metastatic Tumors: Metastases were present in 27 patients and occurred in the lung in 25 of them. Pleural &fusions were present in at least 24 patients, and were bilateral in 14 and hemor- rhagic in 16. Benign hepatic hemangiomas were described in 5 patients. Widely metasta- sizing angiosarcomas, however, not uncommonly have a “benign” histologic appearance in some or all portions of the tumor,41-43 and it is likely that many of the hepatic hemangiomas were in fact angiosarcomatous metastases. Brain me- tastases were found in only 2 of the 40 previously reported patients with cardiac angiosarcoma (Table I). We have found reports of brain me- tastases in only 2 patients with angiosarcomas originating in extracardiac sites,44*45 and brain metastases have not been reported in patients with cutaneous Kaposi’s sarcoma. Cerebellar and midbrain metastases caused the present pa- tient’s death before significant cardiac dysfunc- tion developed.
Incidence: Although it is a rare tumor, angio- sarcoma may be the most common primary malignant tumor of the heart. It originates in the heart about as frequently as does rhabdo- myosarcoma, and probably more frequently than does fibrosarcoma, reticulum-cell sarcoma, or lymphosarcoma. Angiosarcomas accounted for 23 of the 177 malignant primary cardiac tumors summarized in reviews through 1959.46-48 In addition, there have been at least 6 patients with metastases to the heart from angiosarcomas originating elsewhere,41 S .45 ,4g-51 and 1 of them49 both clinically and pathologi- cally closely resembled the patients listed in Table I. Cardiac metastases also have been re- ported in patients with Kaposi’s sarcoma and typical cutaneous involvement.33
SUMMARY
The clinical and pathoanatomic features in a 35 year old woman with angiosarcoma of the heart are described, and the findings in previ- ously reported patients with cardiac angiosar- coma are summarized. Obstruction to filling of the right-sided cardiac chambers by hemoperi- cardium with tamponade, constriction of the ventricles by a thick layer of epicardial tumor, vena caval or tricuspid valvular obstruction, or a combination of these mechanisms was almost uniformly present in the previously reported pa- tients. The present patient’s right atrium and epicardium were massively invaded by tumor, but she died of metastases to the brain, an un-
usual finding in patients with angiosarcoma, b+ fore significant cardiac dysfunction de\ eloped.
1. REDTENRACHER, L. Ein Fall van .\nyiosar~orna pericardii. Wien h-lin. Wschnschr., 2: 214, 1889.
2. G~~DEL, A. Zur Kenntnis der prim&rrn Herzgesch- wiilste. Zentralbl. Herz. u. G~fzsskr., 14: 99, 1922.
3. HEWER, T. F. and KEMP, R. P. Malignant heman- gio-endothelioma of the heart: Report of a case. J. Path. @ Bact., 43: 511, 1936.
4. GROSS, P. and ENGLEHARI., C. E. Primary ht-man- gio-endothelioma of the heart: Report of a case. Am. J. Cancer, 30: 102, 1937.
5. SCHEIDEGGER, S. Malignes H~mangioblastom des Perikards. (Beitrag zur Frage der Deckzellengesch- wiilste.) Frankfurt. Ztschr. Path., 51 : 286, 1937-S.
6. CHOISSER, R. M. and RAMSEY, E. M. zlngiore- ticuloendothelioma (Kaposi’s disease) of the heart. Am. J. Path., 15: 155, 1939.
7. WELLER, G. L., JR. The clinical aspects of cardiac involvement (right auricular tumor) in idiopathic hemorrhagic sarcoma (Kaposi’s disease). ‘4?v?. Znt. Med., 14: 314, 1940.
8. JUCKER, P. Die Diagnose der primgren BBsartigen Geschwiilste des Perikards und der das Perikard infiltrierenden Herzwandtumoren. Bericht uber zwei an der Basler Medizinischen Klinik beobach- teten prim;ire Perikardsarkome. Ztschr. Xlin. Med., 139: 208, 1941.
9. DA CUNHA MOTTA, L. Hemangio reticulo-endo- thelioma. Ann. Fat. med. &a Pa&, 17: 627, 1941.
10. AEGERTER, E. E. and PEALE, A. R. Kaposi’s sar- coma. A critical survey. Arch. Path., 34: 413, 1942.
11. REISINGER, J. A., PEKIN, T. J. and BLUMENTHAL, B. Primary tumor of the inferior vena cava and heart with hemopericardium and alternation of the ven- tricular complexes in the electrocardiogram Ann. Znt. Med., 17: 995 1942.
12. LANGE, H. F. and CHRISTIANSEN, T. Hemoperi- cardium-angiosarcoma cordis. A case of primary heart tumor, diagnosed intra vitam. Acta med. scandinav., 127: 107, 1947.
13. GREENBERG, M. and ANGRIST, ‘2. Primary vascular tumors of the pericardium : A report of two cases. Am. Heart J., 35: 623, 1948.
14. AMSTERDAM, H. J., GRAYZEL, D. M. and LOURIA, A. L. Hemangio-endothelioblastoma of the heart. Am. Heart J., 37: 291, 1949.
15. L~~BSCHITZ, K., LUNDSTEEN, E. and FORCHHAMMER, E. Primary malignant heart tumor diagnosed in vivo with the aid of artificial pneumopericardium. Radiology, 52: 79, 1949.
16. TATSUMI, T., NAGATOMO, T. and KASHIWAI, K. An autopsy case of primary heart tumor. Gann, 40: 174,1949.
17. GLASSY, F. J. and MASSEY, F. C. Primary heman- gio-endothelial sarcoma of the heart. Am. J. Med., 8: 544, 1950.
18. TACKET, H. S., JONES, R. S. and KYLE, J. W. Pri- mary angiosarcoma of the heart. Am. Heart J., 39:912,1950.
19. BRUZZONE, P. L. and GUGLIELMINI, G. Immagini anatomo-radiologiche cistosimili de1 diaframma
THE AMERICAN JOURNAL OF CARDIOLOGY

Angiosarcoma of he Heart
di destra e dell’angolo cardio-frenico (pseudo- ernia de1 diaframma e angiosarcoma de1 cuore). Minerva med., 1: 968, 1951.
20. BLANCHARD, .\. J. and HETHERINCTON, II. Malig- nant hemangioendothelioma of the heart. Canad. M. A. J., 66: 147, 1952.
21. SCHWAR.~~, N. 13. and LODER, M. Primary tumor of the heart. AVeu? York J. Med., 52: 2658, 1952.
22. DELOACH, J. F. and HAYNES, J. W. Secondary tumors of the heart and pericardium. Review of the subject and report of one hundred and thirty-seven cases. A.M.A. Arch. Int. Med., 91: 224, 1953.
23. SCHWARZKOPF, H. and GAB, H. Primares Haman- giosarkom im Gebiet der rechten Kranzarterie. Frankfurt. Ztschr. Path., 64: 483, 1953.
24. BRANDENBURG, R. 0. and EDWARDS, .I. E. Cardiac sarcoma: Report of a case and comparison with a case of metastatic carcinoma of the pericardium. PTOC. Staff. Meet,.. Mayo Clin., 29: 437, 1954.
25. FLORANGE, W. Uber die Beobachtung eines angio- plastischen Sarkoms des Perikards; zugleich ein Beitrag zur Frage des ausgangsortes der Sarkome des Herzbeutels. Zentralbl. allg. Path., 91: 413, 1954.
26., CHENG, T. 0. and SUTTON, D. C. Primary heman- gioendotheliosarcoma of heart, diagnosed by angiocardiography: Review of the literature and report of a case. Circulation, 11: 456, 1955.
27. GROSSE-BROCKHOFF, F. and SCHREIBER, H. W. Angiosarkom des Herzbeutels. Ztschr. Rreislauf-
forsch., 44: 866, 1955. 28. GROOM, D. Electrocardiogram of the month. J.
South Carolina M. A., 52: 10, 1956. 29. KURASHOVA, M. V. and KOGAN, R. P. [.4ngiosar-
coma of the Heart.] Klin. med., 34(11): 77, 1956. Abstr. in Abstr. Soviet Med., 2-B: 352, 1958.
30. CONTREARAS, R. Angiosarcoma de Kaposi pri- mario de1 corazbn; revision de la literatura y de- scripcibn de1 sexto case. Arch. Inst. cardiol. M&co, 27: 463, 1957.
31. KOGAN, R. P. [Tumors of Heart.] Arkh. Pat., 19 (1): 66, 1957. Abstr. in Excerpta med. sect. 76, 5: 703,1957.
32. GELFAND, M. Kaposi’s hemangiosarcoma of the heart. Brit. Heart J., 19: 290, 1957.
33. LOTHE, F. and MURRAY, J. F. Kaposi’s sarcoma: Autopsy findings in the African. Acta Unio inter- nat. cancum., 19: 429, 1962.
34. CRENSHAW, J. F., DOWLING, E. A. and CRESSWELL, W. F., JR. Primary hemangio-endothelioma of the heart. Ann. Znt. Med., 50: 1289, 1959.
35. HARRIS, H. R. Angiosarcoma of the heart. J. Clin. Path., 13: 205, 1960.
36. MCNALLEY, M. C., KELBLE, D., PRYOR, R. and
37
31 ‘1
BLOUN~, S. G., JR. Angiosarcoma of the heart, Report of a case and review of the literature. Am. Heart J., 65: 244, 1963.
WRIGHT, R. P., JR., MCCALL, M. M. and \\~I~NGEK. N. K. Primary atria1 tumor. Evaluation of clinical findings in ten cases and review of the literature. Am. J. Cardiol., 11 : 790, 1963.
38. BERLOV, G. A. and PIGAREV, Yu. G. [,\ peculiar form of systemic tumour-like angiomatosis (ma- lignant hemangioendothelioma of the pericar- dium, angiomatous polyp of the endocardium and progressive hemangiomatosis of the liver).] Arkh. Pat., 26(8): 74, 1964.
39. ROBINSON, D. S. and MACHANIC, P. B. Hemangio- endothelioma of the heart. J.B.,W.A., 183: 1026, 1964.
40. LUKASH, W. M., SCHNEIDER, P. J. and SENNETT, C. 0. Angiosarcoma presenting as acute rheu- matic pancarditis. J.A.M.A., 193: 975, 1965.
41. SHENNAN, T. Histologically non-malignant an- gioma with numerous metastases. J. Path. @ Bact., 19: 139, 1914.
42. ROBINSON, J. M. and CASTLEMAN, B. Benign me- tastasizing hemangioma. Ann. Surg., 104: 453, 1936.
43. STOUT, A. P. Hemangio-endothelioma: X tumor of blood vessels featuring vascular endothelial cells. Ann. Surg., 118: 445, 1943.
44. NESBITT, S., MARK, P. F. and ZIMMERMAN, H. M. Disseminated visceral idiopathic hemorrhagic sar- coma (Kaposi’s disease): Report of a case with necropsy findings. Ann. Int. Med., 22: 601, 1945.
45. TIBBS, D. Metastasizing hemangiomata: A case of malignant haemangio-endothelioma. Brit. .I. Surg., 40: 465, 1952-3.
46. WHORTON, C. M. Primary malignant tumors of the heart: Report of a case. Cancer, 2: 245, 1949.
47. BRUCKER, E. A., JR. and GLASSY, F. J. Primary reticulum-cell sarcoma of the heart with review of the literature. Cancer, 8: 921, 1955.
48. SOMERS, K. and LOTHE, F. Primary lymphosar- coma of the heart: Review of the literature and report of 3 cases. Caruer, 13: 449, 1960.
49. GRAYSON, R. R. Hemangioendotheliosarcoma of the ileum with metastases to the right auricle, rupture of the heart, and hemopericardium at least 10 days before death: A case report. Ann. Int. Med., 41: 151, 1954.
50. BOURNE, M. S., COOK, T. A. and WILLIAMS, G. Hemangiosarcomatosis: Two cases presenting as haematological problems. &it. M. J., 2: 275, 1965.
51. CRYMES, T. and TAYLOR, R. G. Angiosarcoma metastatic to the tongue: Report of a case. J. Oral Surg., 24: 63, 1966.
VOLUME 21, MARCH 1968