
Angell, B. & Bolden, G. (2015). Justifying medication decisions in mental health care:...
13
Justifying medication decisions in mental health care: Psychiatrists' accounts for treatment recommendations Beth Angell a, * , Galina B. Bolden b a School of Social Work and the Institute for Health, Health Care Policy, and Aging Research, Rutgers, The State University of New Jersey, United States b School of Communication and Information, Rutgers, the State University of New Jersey, United States article info Article history: Available online 29 April 2015 Keywords: United States Psychiatry Mental health Assertive community treatment Accounts Conversation analysis Medical recommendations Shared decision-making abstract Psychiatric practitioners are currently encouraged to adopt a patient centered approach that em- phasizes the sharing of decisions with their clients, yet recent research suggests that fully collabo- rative decision making is rarely actualized in practice. This paper uses the methodology of Conversation Analysis to examine how psychiatrists justify their psychiatric treatment recommen- dations to clients. The analysis is based on audio-recordings of interactions between clients with severe mental illnesses (such as, schizophrenia, bipolar disorders, etc.) in a long-term, outpatient intensive community treatment program and their psychiatrist. Our focus is on how practitioners design their accounts (or rationales) for recommending for or against changes in medication type and dosage and the interactional deployment of these accounts. We find that psychiatrists use two different types of accounts: they tailor their recommendations to the clients' concerns and needs (client-attentive accounts) and ground their recommendations in their professional expertise (au- thority-based accounts). Even though psychiatrists have the institutional mandate to prescribe medi- cations, we show how the use of accounts displays psychiatrists' orientation to building consensus with clients in achieving medical decisions by balancing medical authority with the sensitivity to the treatment relationship. © 2015 Published by Elsevier Ltd. 1. Introduction Within psychiatry, medications are considered a cornerstone of treatment; yet the process by which treatment decisions are made is poorly understood. On the basis of field recordings of actual psychiatric visits, this study analyzes how psychiatrists justify their psychiatric treatment recommendations to clients. We find that psychiatrists use two different types of accounts: they tailor their recommendations to the clients' concerns and needs (client-atten- tive accounts) and ground their recommendations in their profes- sional expertise (authority-based accounts). Even though psychiatrists have the institutional mandate to prescribe medica- tions, we show how the use of accounts displays psychiatrists' orientation to building consensus with clients in achieving medical decisions by balancing medical authority with the sensitivity to the treatment relationship. 1.1. Patient-centered care in psychiatry A growing body of literature points to the importance of patient-centered care in the field of community mental health, mirroring trends in many areas of medicine (Institute of Medicine Committee on Quality of Health in America (2006); President's New Freedom Commission on Mental Health, 2003). Patient- centeredness, often described as a philosophy rather than a formalized model of care, emphasizes two key ideas. First, it highlights the importance of treatment relationships in which providers understand and respond to their clients' needs, values, and preferences, and from these understandings, come to a mutual understanding of the problems and issues under consid- eration (Epstein et al., 2005). This component of patient-centered care parallels the concept of a “therapeutic alliance” or working relationship, which has long been considered a cornerstone of successful treatment in both psychiatry and psychotherapy (e.g., Norcross, 2002; Priebe et al., 2011). A second core component of the patient-centered care philos- ophy encourages the practitioner to invite the patient to take an active role in making medical decisions through a collaborative * Corresponding author. School of Social Work, 536 George St., New Brunswick, NJ 08901, United States. E-mail address: [email protected] (B. Angell). Contents lists available at ScienceDirect Social Science & Medicine journal homepage: www.elsevier.com/locate/socscimed http://dx.doi.org/10.1016/j.socscimed.2015.04.029 0277-9536/© 2015 Published by Elsevier Ltd. Social Science & Medicine 138 (2015) 44e56
Transcript of Angell, B. & Bolden, G. (2015). Justifying medication decisions in mental health care:...

lable at ScienceDirect
Social Science & Medicine 138 (2015) 44e56
Contents lists avai
Social Science & Medicine
journal homepage: www.elsevier .com/locate/socscimed
Justifying medication decisions in mental health care: Psychiatrists'accounts for treatment recommendations
Beth Angell a, *, Galina B. Bolden b
a School of Social Work and the Institute for Health, Health Care Policy, and Aging Research, Rutgers, The State University of New Jersey, United Statesb School of Communication and Information, Rutgers, the State University of New Jersey, United States
a r t i c l e i n f o
Article history:Available online 29 April 2015
Keywords:United StatesPsychiatryMental healthAssertive community treatmentAccountsConversation analysisMedical recommendationsShared decision-making
* Corresponding author. School of Social Work, 536NJ 08901, United States.
E-mail address: [email protected] (B. Angell
http://dx.doi.org/10.1016/j.socscimed.2015.04.0290277-9536/© 2015 Published by Elsevier Ltd.
a b s t r a c t
Psychiatric practitioners are currently encouraged to adopt a patient centered approach that em-phasizes the sharing of decisions with their clients, yet recent research suggests that fully collabo-rative decision making is rarely actualized in practice. This paper uses the methodology ofConversation Analysis to examine how psychiatrists justify their psychiatric treatment recommen-dations to clients. The analysis is based on audio-recordings of interactions between clients withsevere mental illnesses (such as, schizophrenia, bipolar disorders, etc.) in a long-term, outpatientintensive community treatment program and their psychiatrist. Our focus is on how practitionersdesign their accounts (or rationales) for recommending for or against changes in medication type anddosage and the interactional deployment of these accounts. We find that psychiatrists use twodifferent types of accounts: they tailor their recommendations to the clients' concerns and needs(client-attentive accounts) and ground their recommendations in their professional expertise (au-thority-based accounts). Even though psychiatrists have the institutional mandate to prescribe medi-cations, we show how the use of accounts displays psychiatrists' orientation to building consensuswith clients in achieving medical decisions by balancing medical authority with the sensitivity to thetreatment relationship.
© 2015 Published by Elsevier Ltd.
1. Introduction
Within psychiatry, medications are considered a cornerstone oftreatment; yet the process by which treatment decisions are madeis poorly understood. On the basis of field recordings of actualpsychiatric visits, this study analyzes how psychiatrists justify theirpsychiatric treatment recommendations to clients. We find thatpsychiatrists use two different types of accounts: they tailor theirrecommendations to the clients' concerns and needs (client-atten-tive accounts) and ground their recommendations in their profes-sional expertise (authority-based accounts). Even thoughpsychiatrists have the institutional mandate to prescribe medica-tions, we show how the use of accounts displays psychiatrists'orientation to building consensus with clients in achieving medicaldecisions by balancing medical authority with the sensitivity to thetreatment relationship.
George St., New Brunswick,
).
1.1. Patient-centered care in psychiatry
A growing body of literature points to the importance ofpatient-centered care in the field of community mental health,mirroring trends in many areas of medicine (Institute of MedicineCommittee on Quality of Health in America (2006); President'sNew Freedom Commission on Mental Health, 2003). Patient-centeredness, often described as a philosophy rather than aformalized model of care, emphasizes two key ideas. First, ithighlights the importance of treatment relationships in whichproviders understand and respond to their clients' needs, values,and preferences, and from these understandings, come to amutual understanding of the problems and issues under consid-eration (Epstein et al., 2005). This component of patient-centeredcare parallels the concept of a “therapeutic alliance” or workingrelationship, which has long been considered a cornerstone ofsuccessful treatment in both psychiatry and psychotherapy (e.g.,Norcross, 2002; Priebe et al., 2011).
A second core component of the patient-centered care philos-ophy encourages the practitioner to invite the patient to take anactive role in making medical decisions through a collaborative

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e56 45
partnership with the provider (Epstein et al., 2005). Inclusion of thepatient or client is often referred to as shared decision making(SDM), and this component in particular has been promoted in thefield of psychiatry as a critically important direction for oper-ationalizing foundational values of choice, self-determination, andempowerment (Drake and Deegan, 2009). SDM is conceptualizedas a collaborative process wherein both clinician and patient shareinformation about risks, benefits, preferences, and values related toa health care decision. From this bidirectional exchange, patientand clinician should each be prepared to engage in deliberation andshared responsibility regarding the final decision, which theymutually agree to implement (Barry and Edgman-Levitan, 2012;Charles et al., 1999).
Although SDM is promoted widely as a philosophy and style ofpractice, recent research suggests that it is only partially actualizedin mental health treatment (Matthias et al., 2012; Salyers et al.,2012; Woltmann and Whitley, 2010). Observational studies ofpsychiatric practice show that even when clients and providersagree nominally upon treatment decisions, the process that leads tothis agreement tends to omit important components of SDM, suchas discussion of alternatives and negotiation about the client's rolein making the decision (Matthias et al., 2012; Salyers et al., 2012).Research that inquires about client preferences for shared decisionmaking suggests that many desire a more participatory role andperceive that acquiescence to their providers is both expected andnaturalized within the psychiatric setting (Woltmann and Whitley,2010).
The discrepancy between the prevailing ideology of SDM andthe practice of medication management as described in thepsychiatric literature thus requires greater exploration. Studieswhich examine the perspectives of providers report that clini-cians express concerns about risk management, their colleagues'disapproval, and pessimism regarding their clients' capacities formaking sound decisions (Mahone et al., 2011; Seale et al., 2006).These perspectives accord with sizeable literature illustratingthat those patients who are least likely to adhere to treatmentand who exhibit disagreement with their providers about clinicalneeds are those with lower “insight,” or awareness of their illness(Carter, 2003; Olfson et al., 2006). With such clients, providersoften feel obliged to adopt a paternalistic approach by usingmethods of persuasion and even coercion (Brodwin, 2013). Cli-ents may also, at times, accept providers' suggestions out ofrespect to their expertise, deference to their institutional au-thority, and desire to align with and maintain relationships withproviders, who often represent a conduit to needed resources(Angell et al., 2014).
In recognition that patient-centered practice has provenchallenging across a variety of fields of medicine, Pilnick andDingwall (2011) suggest that this is because provider-clientasymmetry is embedded in the institution of medicine and, infact, functional to its effective operation (Pilnick and Dingwall,2011). From this point of view, the accountability with whichphysicians are vested places major constraints upon collaborativedecision-making. Indeed, such approaches may be in fact unde-sirable or poorly received by patients because they underminethe social order that is taken for granted by all parties in amedical encounter. In this sense, shared decision making ap-proaches could be resisted as much by clients, who seek medicalexpertise to deal with a problem, as by providers, who are so-cialized to exercise authority. In psychiatry this argument is,however, complicated by the fact that some persons with mentalillness do not necessarily “seek” services, but are pressured toaccept them (Pescosolido et al., 1998). When clinicians view a
client's resistance to a psychiatric treatment recommendation asa by-product of the illness itself, they may deem that exercisingauthority (and, at times, paternalism) is justified to ensure apatient-centered and clinically effective approach.
Exercise of clinician authority in treatment decisions does notautomatically connote a unilateral model in which patients arepassive recipients of physician recommendations, however. Forexample, research conducted from an interactional perspectivedemonstrates that providers may modify their treatment recom-mendations in response to patient resistance (Hudak et al., 2011;Stivers, 2007; Toerien et al., 2013). In this way, as Toerien et al.(2013) argue, “authority is, at least somewhat, influenced andtempered by the actions of the patient” (p. 874). In treatments forchronic conditions, moreover, participation in decisionmakingmaymore fruitfully viewed as a process which may unfold over thecourse of an encounter, or even multiple encounters (Say et al.,2006) and, in the case of psychiatric disorders, is inextricably tiedto the context of an ongoing therapeutic relationship (Matthiaset al., 2013). In this sense, everyday psychiatric practice mayinhabit a middle ground between the egalitarian process idealizedin SDM and the starkly authoritarian model of medicine to whichSDM was designed to respond.
Understanding how such communicative processes unfold inactual interactions between psychiatric providers and their clientsrequires methods that capture these processes in situ. The meth-odology of Conversation Analysis (deployed here) enables us tosee how practitioners' arguments for treatment decisions aredesigned in ways that both enact their decision-making authorityand, at the same time, are responsive to client's preferences andconcerns.
1.2. Prior conversation analytic research on treatment decisions
Conversation Analysis has been used extensively to examinethe organization of activities that comprise medical visits, suchas, patients' problem presentation, medical history taking,physical examination, delivery of diagnostic and prognostic news,and negotiation of treatment recommendations (e.g., Heritageand Maynard, 2006). This research has identified and describedsystematic ways in which patients and medical providersparticipate in medical decisions (Collins et al., 2005). A number ofstudies into treatment recommendation sequences have shownthat even though it is medical providers who ordinarily maketreatment recommendations, patients are actively involved inthis stage of a medical consultation in that they are in a positionto accept (or reject) the doctor's proposals (Koenig, 2011; Stivers,2005b, 2006) and may even pressure physicians for particulartreatments (Gill, 2005; Stivers, 2007). In other words, treatmentdecision-making is a bilateral process in which patients are moreor less actively involved (Collins et al., 2005). These studies havealso documented the fact that, if the patient does not accept amedical recommendation explicitly (e.g., by remaining silentfollowing the proposal formulation, which is a form of passiveresistance, or by questioning the proposal, a form of activeresistance), medical providers may pursue acceptance of theirrecommendation by using a variety of conversational practices(Costello and Roberts, 2001; Koenig, 2011; Roberts, 1999; Stivers,2005a, b). One of such documented practice is to account e i.e., toprovide rationales, justifications, or explanations e for a treat-ment recommendation.
The sociological interest in accounts and accounting is longstanding, in large part because accounts offer insight intomembers'common-sense reasoning about their world e what they see as

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e5646
accountable (i.e., in need of correction, justification, or explanation)and what sorts of accounts are seen as legitimate and intelligible(e.g., Antaki, 1994; Buttny, 1993; Harr�e et al., 1985; Orbuch, 1997;Scott and Lyman, 1968; Shotter, 1984). An examination of ac-counting episodes gives access to participants' understandings ofsocial norms for acting and reasoning e for instance, in medicine,what medical providers and patients may see as “good reasons” fortheir medical decisions. Given the prominence of accounts andaccounting in medicine, surprisingly few studies have examinedproviders' use of accounts in interactions with their patients (Parry,2009). (For a study of patients' accounts, see Halkowski, 2006.)Prior research in this area has analyzedwhen accounts are proffered(and less systematically what sorts of accounts they are) and foundthat physicians' accounts play a role in two medical activities:providing a diagnosis and proposing a treatment plan. When doc-tors provide accounts or explanations for their diagnosis, theybalance their medical authority with accountability, suggestingthat patients are capable of understanding medical matters(Per€akyl€a, 1998). Physicians' accounts may be used prospectively e
to build agreement and reduce incipient patient resistance to asensitive diagnosis (Maynard, 2004) and to pre-justify a particulartreatment recommendation (Costello and Roberts, 2001; Hudaket al., 2011). They may also be offered retrospectively e to justifya proposed treatment in the face of patients' (active or passive)resistance (Costello and Roberts, 2001; Koenig, 2011; Roberts, 1999;Stivers, 2005a, b).
While this research has provided valuable insights intocommunicative processes through which medical treatment de-cisions are achieved in interaction, up to now, a majority of thiswork has examined primary care visits (e.g., Gill, 2005; Koenig,2011; Stivers, 2005b, 2006, 2007) and a small number of spe-cialty care settings, such as, oncology, neurology, and diabetes(e.g., Collins et al., 2005; Koenig et al., 2014; Roberts, 1999;Toerien et al., 2011, 2013). Furthermore, most of the studieshave focused on treatment recommendations in acute rather thanchronic care visits. The present study begins to fill the gaps in ourunderstanding of the treatment recommendation phrase byexploring the interactional processes involved in treatment de-cision making in ongoing, long-term psychiatric care, adding to asmall but growing body of conversation analytic literature onpsychiatry (e.g., Bergmann, 1992; McCabe et al., 2013, 2002;Quirk et al., 2012).
1.3. The setting: assertive community treatment
This study examines communication in an assertive communitytreatment (ACT) program, a commonly used team model of inten-sive case management for people with serious and prolongedpsychiatric disorders such as schizophrenia and bipolar disorder(Allness and Knoedler, 2003; Stein and Santos,1998). ACT programsprovide intensive, comprehensive community-based support via aninterdisciplinary treatment team, frequently including socialworkers, nurses, psychologists, and a psychiatrist. Several featuresof the model are distinct from traditional psychiatric treatment.First, treatment plans are tailored to client needs, incorporatingmedicationmanagement, training in everyday life tasks, supportivepsychotherapy, and assistance with gaining disability benefits andhousing. Second, many services are provided primarily via mobileoutreach (clients' homes, workplaces, etc.), rather than in an office-based setting, to encourage more accurate assessment of needs andto obviate the need for clients to transfer learned skills to a novelenvironment. Third, ACT programs provide services in a time-unlimited manner, and thus treatment relationships are
frequently carried out over multiple years or even decades. Finally,a hallmark of the model is the assertiveness of efforts to offer ser-vices to clients, even if they exhibit reluctance or ambivalenceabout treatment.
Within the ACT model, as in psychiatric treatment moregenerally, medications are a cornerstone of treatment and areprovided via a long-term relationship with a psychiatrist, who isoften employed directly by the program. Within the particulartreatment model studied here (assertive community treatment),psychiatric appointments are scheduled at regular intervals aspart of the program's comprehensive medication support func-tion, which frequently includes procurement and daily deliveryof medications to clients in addition to prescribing and moni-toring activities (Allness and Knoedler, 2003). While the explicitpurpose of these appointments is medication management,psychiatrists working within ACT tend to adopt a generalistorientation to treatment that involves discussing with clientslifestyle issues (such as living arrangements, family relation-ships, and work activities) in addition to the medicationregimen. Because of the variable course of serious mental dis-orders, psychiatry appointments serve to monitor the client'sstability and responses to medication, and to make adjustmentsto the medications in order to optimize the client's capacity tocope with the illness and pursue personally determined psy-chosocial goals. The paper will analyze how interactional prac-tices of accounting are used by psychiatrists to advance the goalof achieving consensus with clients about such medicationadjustments.
2. Data and method
The data were collected in 2009e2010 in an established ACTprogram in a mid-sized city. The data corpus used for this anal-ysis consists of 36 audio-recorded naturally-occurring in-teractions between clients and a team psychiatrist, each between15 and 45 min long. Treatment relationships are well-establishedin this program, with clients having been in the program for 12years, on average.
The research protocol received Institutional Review Boardapproval and was likewise approved by the research reviewboard of the organization that housed the ACT program. Aconvenience sample of 36 clients was recruited by distributingstudy information sheets to clients during case managementappointments and in the waiting area of the program. Clientswho expressed interest in participating were instructed toattend drop-in meeting hours with research staff to completeinformed consent procedures. Data were gathered via audio-recording one case management appointment and one medi-cation check appointment with the team psychiatrist, whoprovided primary psychiatric services to all clients in the pro-gram (only the psychiatry appointment recordings were used inthe analysis presented here). Informed consent was obtainedfrom both client and provider participants, which includedpermission for the relevant provider to tape the session as itoccurred.
The audio-recorded consultations were analyzed using Con-versation Analysis, an inductive methodology that examines theorganization of social interaction, including how conversational-ists accomplish social actions in their interactions with others(Sidnell and Stivers, 2013). Audio-recordings of the psychiatricvisits were transcribed following the standard conversation an-alytic transcription conventions (Hepburn and Bolden, 2013). Allnames and other identifiers on the transcripts are pseudonyms.

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e56 47
In accordance with conversation analytic methods, sequences ofinteractions in which psychiatrists and clients discuss possiblechanges in psychiatric medications were identified and thenanalyzed case by case in order to elucidate recurrent interactionalpractices through which participants reach treatment decisions.For this article, we examined composition and sequential featuresof practitioners' justificatory accounts for their treatment rec-ommendations. The data excerpts included in the article arerepresentative of the corpus and were selected for their clarity;multiple instances of all analytic categories were found in thedata. Instances of accounting for treatment recommendationswere found in all consultations where a medication decision (achange in dose or type of medication) was discussed (24 out of 36visits).
3. Analysis
3.1. Observations on the overall organization of medication checkvisits
The psychiatric visits analyzed for this study have an explicitinstitutional agenda as “medication check” appointments. Whileother topics are typically discussed (e.g., the client's living ar-rangements, family relationships, and work activities), the medicalagenda is evident throughout the visit (cf. Robinson, 2004). Giventhe great heterogeneity between clients and across the course ofthe illness, the psychiatrist may take a more or less active role indirecting the interactional agenda, depending on whether theclient is exhibiting symptoms (e.g., actively hallucinating) orcognitive impairments that affect their participation in the inter-action. Early in a typical visit, the psychiatrist asks a series ofprobing questions into “how things are” e how the client is feeling,thinking, sleeping, etc. These questions e not unlike history takingin other kinds of medical interactions e serve to evaluate (amongother things) how well the medications are working, both thera-peutically to control the client's psychiatric symptoms and in termsof the harmful side effects.
Following this diagnostic evaluation stage, possible changesin the treatment plan e i.e., whether (and how) to modify dosesor types of medication the client takes e may be discussed. Inour data, these discussions are ordinarily extensive and may takeup a significant portion of the visit. If in acute primary careencounters, the treatment phase may consist of two turns e thephysician's recommendation followed by the patient's briefacceptance (Stivers, 2006) e in the medication check appoint-ments in our corpus this is never the case. While much moreresearch is needed to analyze the organization of the treatmentphase of a psychiatric visit (Bolden and Angell, 2015), somepreliminary observations will help situate the findings presentedhere.
A number of different trajectories are possible, depending onwho (the psychiatrist or the client) initiates the discussion of apossible medication change. First, following the diagnostic ques-tioning phase of the visit, the psychiatrist may begin to build a casefor a medication change. The psychiatrist may formulate her eval-uation of how well the client is doing in a way that prepares theground for a particular recommendation. The psychiatrist may thenfloat the idea of a medication change by, for example, explainingthe therapeutic effects of a particular medication (cf. Toerien et al.,2013). Once this information is provided, the psychiatrist maypropose a medication change and solicit (more or less directly) theclient's in-principle agreement to the change. The psychiatrist maythen consult the client's medical records (e.g., test results,
medication history, etc.) and propose a specific implementationplan (such as, the exact dosages and timeline for implementing thechange). The client's acceptance of the plan is then sought and maybe explicitly solicited (and re-solicited) at multiple points. Alter-natively, the client may be the one who initiates the discussion of amedication change by, for example, directly requesting a change inthe regimen or, less directly, by reporting a medication side effectproblem. These requests may occur at the beginning of the visit orlater, during the treatment discussion. The client's request mayinstigate diagnostic questioning, and the psychiatrist will eventu-ally respond by either rejecting the request or proposing somealternative plan (e.g., re-evaluating the situation at a subsequentvisit or reducing the dosage rather than eliminating the drugaltogether). An acceptance of the alternative plan is then soughtfrom the client.
These observations about the unfolding of treatment discus-sions reveal that, even though in this setting the psychiatrist isinstitutionally authorized to make medication decisions, partici-pants orient to achieving consensus about the treatment plan. Tothis end, the psychiatrist employs an array of interactionalpractices to account for, justify, and explain a particular course oftreatment. Our analysis shows that the psychiatrist's accounts aredeployed in the following interactional contexts: First, accountsare provided when a psychiatrist's proposal is met with active orpassive resistance from the client (Koenig, 2011; Stivers, 2005b,2006), i.e., when the client does not (immediately) accept thepsychiatrist's proposal but instead remains silent (passive resis-tance) or questions or rejects the proposal (active resistance). Insuch cases, accounts may be used to pursue acceptance of thepsychiatrist's treatment proposal (see Excerpt 2 and Excerpt 5below). Second, accounts are given to ground a refusal of a clientrequest (cf. Robinson and Bolden, 2010; Schegloff, 2007), such as,a request for a new medication or a medication dose decrease(see Excerpt 1, Excerpt 3, Excerpt 4, and Excerpt 6 below). Third,accounts may be given by the psychiatrist in an attempt toforestall an incipient resistance to an upcoming proposal of amedication change (especially, an increase in dosage of antipsy-chotic medications which is often resisted by clients) during thediagnostic evaluation stage or as part of building a case for anupcoming recommendation (cf. Costello and Roberts, 2001) (seeExcerpt 7 below). In the interests of space, here we only examineaccounts given as part of the medication regimen discussion;accounts produced in the diagnostic stage of the visit are subjectof a separate manuscript.
3.2. Two types of psychiatrists' accounts
In this section, we introduce two broad types of accounts psy-chiatrists may employ to forge agreement about a medication planwith the client. These are: client-attentive accounts, which displayan orientation to the client's medical concerns or emotional needs(cf. Hudak et al., 2011); and professional authority based accounts,which draw upon an asymmetry between the two parties withrespect to professional expertise and institutional legitimacy (cf.Pilnick and Dingwall, 2011).
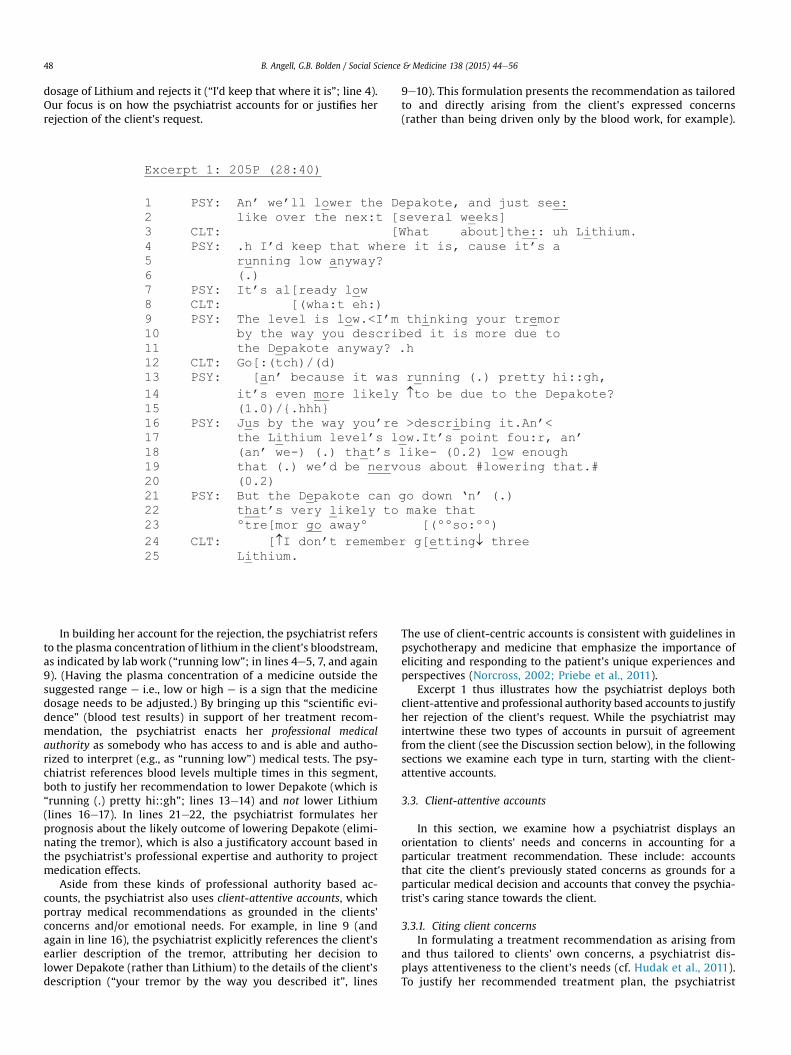
The interactional deployment of these two types of accounts isillustrated in Excerpt 1. Earlier in the consultation, the client (CLT)had complained of an uncomfortable tremor, a common side effectof several medications. Near the end of the visit, the psychiatrist(PSY) summarizes the plan of action (lines 1e2), which is to lowerthe dose of a mood stabilizing medication (Depakote). In line 3, theclient asks about anothermood stabilizingmedication she is taking,Lithium. The psychiatrist treats the inquiry as a request to lower the
B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e5648
dosage of Lithium and rejects it (“I'd keep that where it is”; line 4).Our focus is on how the psychiatrist accounts for or justifies herrejection of the client's request.
In building her account for the rejection, the psychiatrist refersto the plasma concentration of lithium in the client's bloodstream,as indicated by lab work (“running low”; in lines 4e5, 7, and again9). (Having the plasma concentration of a medicine outside thesuggested range e i.e., low or high e is a sign that the medicinedosage needs to be adjusted.) By bringing up this “scientific evi-dence” (blood test results) in support of her treatment recom-mendation, the psychiatrist enacts her professional medicalauthority as somebody who has access to and is able and autho-rized to interpret (e.g., as “running low”) medical tests. The psy-chiatrist references blood levels multiple times in this segment,both to justify her recommendation to lower Depakote (which is“running (.) pretty hi::gh”; lines 13e14) and not lower Lithium(lines 16e17). In lines 21e22, the psychiatrist formulates herprognosis about the likely outcome of lowering Depakote (elimi-nating the tremor), which is also a justificatory account based inthe psychiatrist's professional expertise and authority to projectmedication effects.
Aside from these kinds of professional authority based ac-counts, the psychiatrist also uses client-attentive accounts, whichportray medical recommendations as grounded in the clients'concerns and/or emotional needs. For example, in line 9 (andagain in line 16), the psychiatrist explicitly references the client'searlier description of the tremor, attributing her decision tolower Depakote (rather than Lithium) to the details of the client'sdescription (“your tremor by the way you described it”, lines
9e10). This formulation presents the recommendation as tailoredto and directly arising from the client's expressed concerns(rather than being driven only by the blood work, for example).
The use of client-centric accounts is consistent with guidelines inpsychotherapy and medicine that emphasize the importance ofeliciting and responding to the patient's unique experiences andperspectives (Norcross, 2002; Priebe et al., 2011).
Excerpt 1 thus illustrates how the psychiatrist deploys bothclient-attentive and professional authority based accounts to justifyher rejection of the client's request. While the psychiatrist mayintertwine these two types of accounts in pursuit of agreementfrom the client (see the Discussion section below), in the followingsections we examine each type in turn, starting with the client-attentive accounts.
3.3. Client-attentive accounts
In this section, we examine how a psychiatrist displays anorientation to clients' needs and concerns in accounting for aparticular treatment recommendation. These include: accountsthat cite the client's previously stated concerns as grounds for aparticular medical decision and accounts that convey the psychia-trist's caring stance towards the client.
3.3.1. Citing client concernsIn formulating a treatment recommendation as arising from
and thus tailored to clients' own concerns, a psychiatrist dis-plays attentiveness to the client's needs (cf. Hudak et al., 2011).To justify her recommended treatment plan, the psychiatrist

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e56 49
may cite an issue mentioned by the client as problematic,which may involve reusing the words the client used indescribing the problem. This sort of “overt linking” to the cli-ent's own words may increase pressure on the client to affiliatewith the psychiatrist's position (Parry et al., 2014; Per€akyl€a,1995).
In Excerpt 1 (introduced in the previous section), the psy-chiatrist explicitly references the client's formulations of con-cerns in pursuit of the client's acquiescence to a treatment plan.As noted above, the client asks about lowering Lithium (line 3),and the psychiatrist rejects the request (line 4) and then accountsfor her rejection by referring to the blood tests (lines 4e5). Whenthe client does not respond (see the short gap in line 6), thisaccount is re-iterated twice (lines 7 and 9). The psychiatrists thenshifts her line of argument, and explicitly references the client'searlier description of the tremor, attributing her decision tolower Depakote rather than Lithium to the details of the client'sdescription (“your tremor by the way you described it”, lines9e10). (Note that Lithium and Depakote each may produce handtremors as side effects; Canning et al., 2012). In overlap with theclient's response (which indicates some kind of acknowledge-ment but is barely audible on the recording; line 12), the psy-chiatrist extends her account by bringing up the Depakote bloodlevels (“running (.) pretty hi::gh”; line 13). The client again failsto respond to this explanation (see the 1.0 s gap in line 15), andthe psychiatrist extends her turn to again reference the client'sdescription of the tremor (“just by the way you're describing it”;line 16). So here we can see how the psychiatrist shifts from anaccount grounded in her medical authority to a client-attentiveone in an attempt to secure the client's support for a particularmedication decision.
Excerpt 2 provides another illustration of this practice. Earlierin the visit from which this excerpt is taken, the client com-plained about hearing voices that remind him to do daily tasks(e.g., brush his teeth, take showers, etc.), and the psychiatrist hadproposed raising Lithium and Zyprexa dosages. Even though theclient initially agreed with the plan (data not shown), when thepsychiatrist again suggests raising Zyprexa (lines 1e2; 4e5), theclient remains silent (see the gaps in lines 3 and 6), which couldindicate the client's resistance to the proposed raise. The psy-chiatrist goes on to justify her recommended course of treatmentby formulating a potential positive outcome of the medication on
the client's symptoms (lines 7e10). In her justification, the psy-chiatrist explicitly cites the client's earlier descriptions of the“reminders” and the “voices” (“reminders in your head” and “thevoices you are describing”; lines 9e10), thus formulating herrecommendation as directly responsive to the client's statedconcerns.
Thus, in both of the discussed excerpts, the psychiatrist de-ploys accounts that present her medication treatment plan asarising from and tailored to the client's own presented concerns.These accounts are proffered in environments where the clientmay be seen as (passively) resisting the psychiatrist recommen-dation for or against a particular medication change. We now turnto accounts that convey the psychiatrist's caring for the client'swell-being.
3.3.2. Enacting a caring stance towards the clientIn psychiatry, it is commonly acknowledged that a positive
working relationship with clients is essential for promotingtheir cooperation in treatment plans (Blackwell, 1997;Turkington et al., 2006). Psychotherapy research has shownthat certain practitioner attributes and behaviors are successfulin fostering effective psychotherapy relationships, and amongthese are empathic communication and what psychotherapyresearchers term “positive regard,” which refers to projectingwarmth and caring toward the client through both behaviorand attitude (Farber and Doolin, 2011). Our analysis documentshow psychiatrists' enactment of concern for the clients' well-being, which often index the psychiatrist's knowledge of theclient's long-term history, may be deployed to justify theirmedication decisions and to pursue consensus about a treat-ment plan.
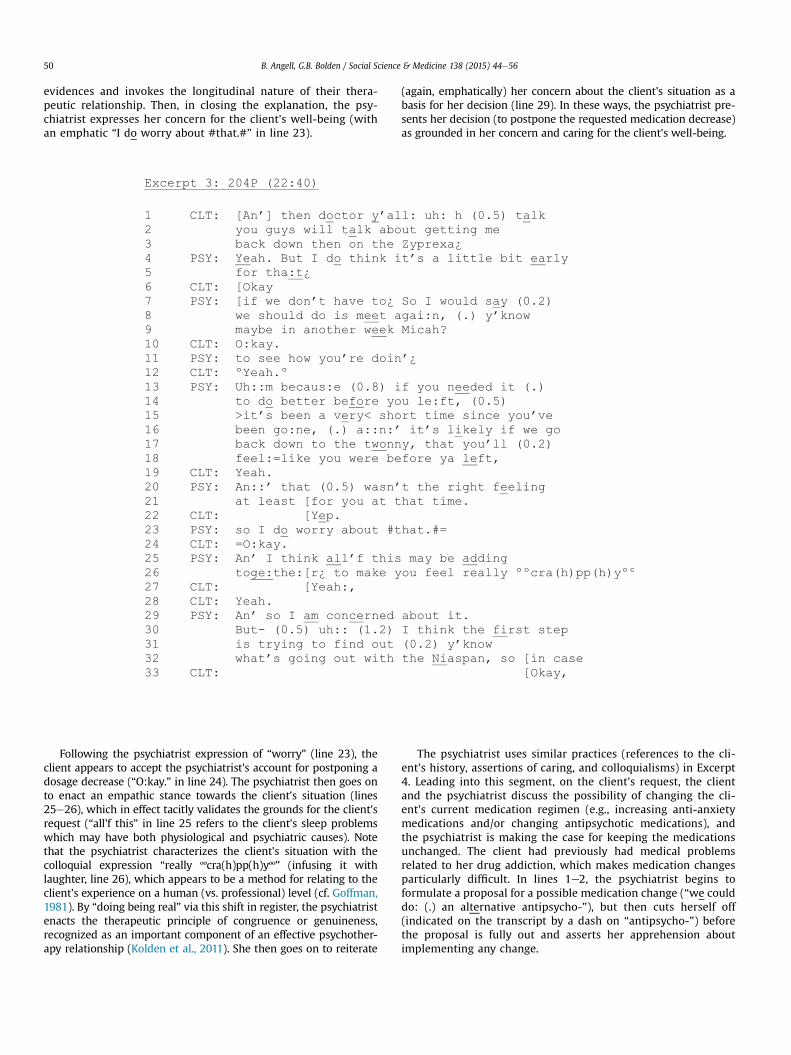
Assertions of caring may be used to counter medicationchanges proposed by clients. In Excerpt 3, the client requests areduction in Zyprexa, an antipsychotic medication, to a level hehad been on previously (lines 1e3). The psychiatrist says that it istoo soon, thereby rejecting the request for the time being (lines4e5). Even though the client agrees with the psychiatrist's planto assess the situation at a later time (lines 6e12), the psychia-trist goes on to justify the postponement by projecting that areduction will cause the client to feel worse, as he had before themost recent increase (lines 13e21). This reference to the client'spast psychiatric status and life events (e.g., him “leaving”)
B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e5650
evidences and invokes the longitudinal nature of their thera-peutic relationship. Then, in closing the explanation, the psy-chiatrist expresses her concern for the client's well-being (withan emphatic “I do worry about #that.#” in line 23).
Following the psychiatrist expression of “worry” (line 23), theclient appears to accept the psychiatrist's account for postponing adosage decrease (“O:kay.” in line 24). The psychiatrist then goes onto enact an empathic stance towards the client's situation (lines25e26), which in effect tacitly validates the grounds for the client'srequest (“all'f this” in line 25 refers to the client's sleep problemswhich may have both physiological and psychiatric causes). Notethat the psychiatrist characterizes the client's situation with thecolloquial expression “really ººcra(h)pp(h)yºº” (infusing it withlaughter, line 26), which appears to be a method for relating to theclient's experience on a human (vs. professional) level (cf. Goffman,1981). By “doing being real” via this shift in register, the psychiatristenacts the therapeutic principle of congruence or genuineness,recognized as an important component of an effective psychother-apy relationship (Kolden et al., 2011). She then goes on to reiterate
(again, emphatically) her concern about the client's situation as abasis for her decision (line 29). In these ways, the psychiatrist pre-sents her decision (to postpone the requested medication decrease)as grounded in her concern and caring for the client's well-being.
The psychiatrist uses similar practices (references to the cli-ent's history, assertions of caring, and colloquialisms) in Excerpt4. Leading into this segment, on the client's request, the clientand the psychiatrist discuss the possibility of changing the cli-ent's current medication regimen (e.g., increasing anti-anxietymedications and/or changing antipsychotic medications), andthe psychiatrist is making the case for keeping the medicationsunchanged. The client had previously had medical problemsrelated to her drug addiction, which makes medication changesparticularly difficult. In lines 1e2, the psychiatrist begins toformulate a proposal for a possible medication change (“we coulddo: (.) an alternative antipsycho-”), but then cuts herself off(indicated on the transcript by a dash on “antipsycho-”) beforethe proposal is fully out and asserts her apprehension aboutimplementing any change.

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e56 51
In justifying her inclination to keep the medications unchanged,the psychiatrist enacts a caring stance towards the client: “I'd feelYnervous ºas hell about changing anything.º” (lines 2e3). Whileproducing this account, the psychiatrist shifts into a conspiratorial e“betweenyouandme”e toneofvoice (note thedownwardpitchshift,marked by the arrow, and a quiet voice, marked by the degree signs)and colloquial register (“as hell”). Again, this expression of the psy-chiatrist's own apprehension resonates with the notion of genuine-ness (“doingbeing real”), believedbypsychotherapy researchers tobeessential to an effective therapeutic relationship (Kolden et al., 2011).Following the client's endorsement of the psychiatrist's reservations(“I know” in line 4), the psychiatrist extends her account with afurther, upgraded enactment of a caring stance, again using a collo-quial expression (“scary (.) as a:ll get out”; line 6) to formulate herfeelings about the change. The psychiatrist then enacts an empathicstance towards the client by invoking the client's troubling history(“what you've been through. (.) over the last- (.) coupla years.”; lines7e9). By bringing up the past, the psychiatrist claims to know andremember what the client has “been through,” thereby using theirlong-term relationship as a resource in the service of strengtheningher argument for not changing the medications.
In this section, we have examined a range of client-attentive ac-counts a psychiatrist may deploy in an attempt to foster agreementwith the client about a treatment plan. We have seen that these ac-countsmay be used in environments when consensus is in question:to overcome clients' (active or passive) resistance to a medicationchange recommendation (as in Excerpt 2) and to justify rejecting aclient's request for a medication change (Excerpt 1, Excerpt 3, andExcerpt 4). Client-centric accounts may be used in combinationwithother practices that rely on and invoke the psychiatrist's professionalexpertise, as discussed in the following section.
3.4. Professional authority based accounts
Psychiatrists may account for their treatment recommendationsby grounding their decisions in their professional expertise, usingthe disparity in medical knowledge and professional training be-tween the client and the clinician as a resource (cf. Per€akyl€a, 1998).In justifying their recommendations, psychiatrists may enact theirprofessional expertise by making a prognosis about the client'sfuture state in light of a proposed treatment plan and by catego-rizing the client's experiences as either “normal” or symptomatic oftheir mental illness. Psychiatrists' enacted expertise thus becomes asource of leverage in convincing the client to take part in a pro-posed treatment plan (Blackwell, 1997).
3.4.1. Prognostic formulationsDiagnostic and prognostic evaluations are the hallmark of the
asymmetry that persists between provider and client expertise in
medical settings: Clients' subjective experiences are elicited andinterpreted through a medical lens to produce an authoritativeassessment (e.g., Maynard, 1991; Pilnick and Dingwall, 2011). In thesetting studied here, clients' psychiatric diagnoses are already wellestablished, yet diagnostic assessments of changes in psychiatricstatus are continually rendered and updated. This process involveswhat Longhofer and Floersch (2004) term medication effect in-terpretations, inwhich providers judge towhat degreemedicationsare optimized. As mentioned above, medication check appoint-ments typically begin with a series of probing questions into howthe client is doing (similar to history taking in other kinds ofmedical interactions). On the basis of the client's responses andother available evidence (such as blood tests, reports from otherteam members, etc.), the psychiatrist proffers a diagnostic andprognostic evaluation of the client's current status and then uses itas grounds for subsequent treatment recommendations.
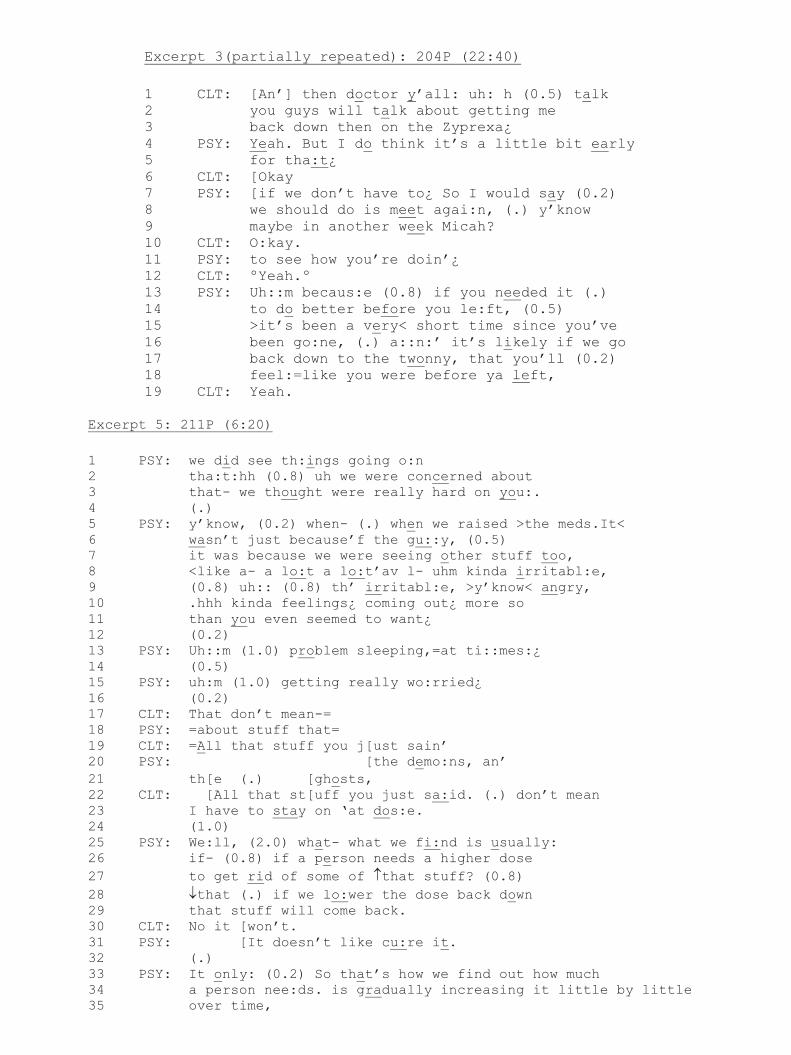
As the instances below show, psychiatrists' recommendations foror against a particular treatment decision may be justified by pro-jectionsof their (beneficial orharmful) consequences. Suchprojectionsare often formulatedwith references to the client's psychiatric historyand previousmedication changes. For instance, in Excerpt 3 (analyzedabove; a partial transcript is reproduced below), the client requests amedication dosage reduction (lines 1e3), and the psychiatrist rejectsthe request (lines 4e5) and suggests reassessing the situation at a latertime (lines 6e12). The psychiatrist then produces an account for thepostponement by formulating a likely negative outcome to therequesteddosage reduction: “you'll feel:¼ likeyouwerebeforeya left”(lines 17e18). The client agrees with the account (“Yeah” in line 19).
Prognoses of harmful consequences of amedication changemaybeused to bolster the psychiatrist's argument when other kinds of ac-counts aremetwith resistance. Excerpt5 is a rare instance inwhich theclient overtly rejects the psychiatrist's justification for a treatmentdecision. Prior to this segment, the client had requested a sharpdecrease in the dose of his antipsychoticmedications, arguing that therecentraiseshadbeenunfounded.Thepsychiatristrejectedtherequestand isnowattemptingto justifyherdecision tokeepthemedicationsatthe current level. In her account, she uses a number of different inter-actionalpracticeswehavediscussed, includingenactingacaringstancetowards theclient (“th:ings…werereallyhardonyou:”; lines1e3)andciting evidence in support of the diagnostic assessment of the client'spast state (as irritable, angry, problem sleeping, and “really wo:rried”;lines 8e15) in a client-attentive way, which treads on the client'sepistemic territory (“more so than you even seem to want¿”; lines10e11). Once the client begins a response that clearly projects arejectionof thepsychiatrist's account (lines 17 and19), the psychiatristextends her turn (in competitionwith the client's) to amend the list ofsymptoms (whichmight be seen as falling into a category of “normal”behavior) to include more obviously medically actionable items:worrying about “the demo:ns, an’ the (.) ghosts” (lines 20e21).

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e56 53
The client, however, persists in rejecting the psychiatrist'sexplanation as a valid reason for keeping the medications at thecurrent dosage (lines 22e23). In response, in lines 25e29, thepsychiatrist produces another type of account in which sheformulates a likely possible outcome of lowering the dose: “ifwe lo:wer the dose back down that stuff will come back” (lines28e29). While this prognostic formulation is directly applicableto the client's current situation, the account is produced ingeneric terms (in reference to “a person”; line 26) and invokesthe psychiatrist's medical authority as a representative of theinstitution (the use of the “institutional we”; lines 25 and 28)(Angell & Bolden, in press; Drew and Heritage, 1992). So here, inthe face of open resistance from the client, the psychiatristmoves from a client-attentive, particularized reasoning to anaccount that is entirely within the psychiatrist's epistemicdomain. The client again rejects this reasoning (line 30), andthe psychiatrist continues with an institutional, medicalexplanation of how antipsychotic medications work (lines31e35). In the two excerpts above, then, the psychiatrist uses
both her medical authority and the history of the therapeuticrelationship with the client to piece together seeminglydisparate pieces of information about the client into a coherentaccount of medication effects so as to justify a treatmentrecommendation.
3.4.2. Categorizing clients' experiences in psychiatric termsOne central issue in psychiatry is whether a behavior or a set
of behaviors is a psychiatric symptom (controlled/treatable withmedications) or whether it falls within a range of “normal”behaviors that are not subject to medical treatment (cf. Antakiet al., 2005). The process of medicalization occurs at an inter-actional level when physicians or other medical authoritiesadopt a medical frame to interpret and act on a particularbehavior. Conversely, classification or reclassification of aquestionable or deviant behavior as normal is termed deme-dicalization (Conrad, 1992). In building a case for a particularmedical regimen, a psychiatrist may formulate behaviors theclients report (or that she observes directly) in ways that convey(explicitly or tacitly) this distinction. Behavior formulations relyon what Sacks (1972a, b) called “membership categorization
analysis”: They are selected for their association with a partic-ular identity category (“psychiatric patient” vs. “normal per-son”) in the service of the implemented action (i.e., justifying aparticular medical decision). Thus, behavior descriptions can be“normalized” when the psychiatrist argues against prescribing(or increasing) a medication or, alternatively, “medicalized”when the argument is made for the necessity of a medication(or dosage increase).
Excerpt 6 illustrates the use of normalization of a clientconcern as an account for declining the client's medicationchange request. Prior to Excerpt 6, the client requested an in-crease in Prozac to address depression and anxiety. The psychi-atrist has been building a case against this increase by assertingthat what the client experiences is not a clinical depression thatcan be addressed with more Prozac (data not shown). In line 1,the psychiatrist again rejects the request, explaining that thedecision is complicated by the fact that the client is goingthrough withdrawal from stimulants, which she had beenabusing (and needs “more clea:n time”; line 2).
In lines 6e7, the psychiatrist refers to the client as “somebodycoming off: (0.2) stimulants,” thereby putting the client into themembership category of recovering addicts (and tacitly rejectingthe applicability of the “clinical depression” label). In this way,the symptoms are normalized (any person coming off drugswould feel this way) and separated from a treatable/psychiatriccondition. The psychiatrist goes on to describe the client's ex-periences as “crashi:ng” (line 9), which again invokes a drugwithdrawal problem (i.e., an activity categorically bound to “drugaddicts”).
The psychiatrist may also formulate the client's behavior ascomparable with other people suffering from a mental illness(and thus medically actionable) in order to justify a medicationincrease. In Excerpt 7, the psychiatrist begins to build a case forraising the dosage of Zyprexa (lines 11e13). In lines 1e8, thepsychiatrist suggests that the voices the client has complainedabout earlier in the visit (data not shown) are part of thesymptoms of his schizoaffective disorder. In building her case fora medication increase, the psychiatrist compares the client toother people with this disorder who “c:ycle” (line 6) or “havecycles of symptoms” (line 8).

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e5654
In this section, we have analyzed ways in which a psychiatristenacts her professional expertise in accounting for her treatmentrecommendations. In these types of accounts, the client's individ-ual experiences are recast as generic or typical of a particularpopulation, and the psychiatrist's authoritative access to thisgeneralized professional knowledge is used as leverage to justify aparticular treatment recommendation. The analysis shows thatauthority based accounts may be used prospectively to build a casefor a medication increase (Excerpt 7) and retrospectively in thecourse of rejecting the patient's request for a medication change(Excerpt 3, Excerpt 5, and Excerpt 6). These accounts bolster thepsychiatrist's recommendation for or against a particular medicalregimen and are rarely challenged by clients (but see Excerpt 5).
4. Discussion
In long-term psychiatric treatment, medication management isan ongoing process in which drug type and dosage are adjustedperiodically to address changes in psychiatric symptoms andmedication side effects. In this paper, we have shown that, eventhough the psychiatrist is granted the institutional authority tomake medication decisions, she routinely justifies her recommen-dations to the clients using a variety of accounts to achieveconsensus about the treatment plan. First, client-attentive accountsdisplay the psychiatrist's attentiveness and caring for the client andinclude accounts that present the treatment recommendation asfitted to the client's stated needs and concerns (Excerpt 1 andExcerpt 2) and express caring and concern for the client's well-being (Excerpt 3 and Excerpt 4). The analysis has shown howattentiveness to personal and relational aspects of client-providercommunication, an important component of both psychotherapyand psychiatric treatment (Norcross, 2002; Priebe et al., 2011),represents a resource that may be deployed interactionally injustifying treatment plans.
A second type of accounts used to justify medication treatmentrecommendations relies upon the psychiatrist's medical authorityand expertise. Physician authority is thought to be an Americancultural phenomenon that traditionally resulted in patientcompliance, obviating the need for justification and persuasion bythe physician (Starr, 1982). As medicine has shifted to a patient-centered ideology, however, practitioners increasingly mustattempt to develop consensus with their patients (see also
Per€akyl€a, 1998). Accounts for treatment recommendations thatcontain discussions of medical tests (e.g. plasma levels), prognosticprojections (Excerpt 3 and Excerpt 5), and categorical ascriptions ofclients' symptoms (Excerpt 6 and Excerpt 7) invoke the scientificauthority of the practitioner as an expert, while also displayingproviders' orientation to getting patients to understand and agreeto the proffered recommendation.
In this article we have documented how e and in what inter-actional contexts e psychiatrists account for their treatment rec-ommendations. The analysis has shown that different kinds ofaccounts may be used within the same action sequence (andsometimes within the same turn), which raises the question ofwhether there is orderliness to their deployment. The data showthat the psychiatrist may shift between different types of accounts(e.g., from conveying a caring stance towards the client to usingprofessional expertise to formulate a prognosis), especially whentheir accounts are met with some kind of resistance from the client(e.g., Excerpts 1, 3 and 5). Note that client-centric accounts may bemore vulnerable to resistance in that they tread on the client'sepistemic domain (by addressing clients' own experiences; seeExcerpt 5), while accounts that are based on professional authoritye especially as expressed through the language of “scientific” tests,etc. e are less so. On the other hand, clinicians may see accountsthat cite medical evidence as opaque to clients (e.g., Excerpt 1), andthus not as effective in explaining the bases for their treatmentdecisions. The choice of a particular account type appears to besensitive a number of different issues, including the local sequentialcontext (the course of action in progress), the available medicalevidence (e.g., blood tests), the client's displayed competencies inthe relevant domain, the history of the client-psychiatrist rela-tionship, etc. Further research is needed to sort out the consider-ations involved in deploying particular kinds of accounts, theirsequencing, and their fittedness to the course of action beingimplemented through them. As it stands, however, the article ex-tends our limited understanding of the complex nature of treat-ment decision making in psychiatry and chronic care moregenerally.
While this analysis is one of the first efforts to characterizetreatment recommendations in psychiatry using recordings ofactual psychiatric visits, several limitations of the study should beacknowledged. Although assertive community treatment is awidely used treatment model for people with serious mental

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e56 55
illness, the analysis presented here focuses only upon one program,and as such, only features the practices of a single psychiatristemployed by that program. Thus, our findings warrant furtherstudy with a wider spectrum of types of psychiatric practice andmultiple practitioners. In addition, the use of audio recordings forexamining face-to-face interactions is limiting because partici-pants' non-vocal conduct and embodied activities (such as workingwith medical records), which are undoubtedly important featuresof clinical interaction, are unavailable to the analysts.
The paper has shown that accounts, whether designed toaccentuate attentiveness to client needs or medical authority, aredeployed as part of a negotiation process in which the clinicianresponds to client concerns, anticipates and counters resistance,ultimately leading to a client accepting or agreeing a treatmentrecommendation so that a corresponding treatment plan may beimplemented. Analyzing the resources used by practitioners in thisnegotiation process, as we have done here, provides insight intohow psychiatric providers pursue agreement on medication de-cisions that accord with their own professional opinions, yet aresensitive to the client's concerns, needs, and illness trajectories (cf.Koenig et al., 2014).
The use of accounts to convince clients to accept a profferedtreatment recommendation is arguably a form of persuasion thatconforms poorly to the idealized vision of collaborative, delibera-tive decision making endorsed by the shared decision makingmovement. In this sense, the current study adds to a growingliterature that suggests that this idealized view shared decisionmaking is distant from standard psychiatric practice (Matthiaset al., 2012; Quirk et al., 2012; Salyers et al., 2012) and may evencontradict fundamental principles of the social order of medicine(Pilnick and Dingwall, 2011). Whether psychiatric practice can orshould find ways to increase client control in decision makingcannot be determined by studies such as this one. However, if, asMatthias et al. (2013) argue, what matters most is that decisions arecarried out in the context of a trusting partnership between clientand clinician, this study provides an illustration of how caring yetauthoritative decisions might look in practice. We show howpractices of accounting enable practitioners to tailor justificationsof their treatment recommendations to the client's preferences andknowledge about treatments; and concomitantly, to extend op-portunities for clients to exercise agency (i.e. to accept, reject, andquestion the accounts) even as practitioners enact their authorityas prescribers.
Acknowledgements
This study was funded by the Center on Adherence and SelfDetermination (CASD) (NIMH P20MH085981). We particularlywish to thank CASD director Patrick Corrigan and co-investigatorColleen Mahoney for her part in study design and data collection.We also thank Jeffrey Robinson, members of the Rutgers UniversityConversation Analysis Laboratory (RUCAL), and two anonymousreviewers for feedback on earlier versions of the manuscript.
References
Allness, D.J., Knoedler, W.H., 2003. A Manual for ACT Start-up: Based on the PACTModel of Community Treatment for Persons with Severe and Persistent MentalIllnesses: National Alliance for the Mentally Ill (NAMI).
Angell, B., Bolden, G.B., 2015. Team work in action: building grounds for psychiatricmedication decisions in assertive community treatment. In: O'Reilly, M.,Lester, J. (Eds.), Handbook of Adult Mental Health: Discourse and ConversationStudies. Palgrave Macmillan, London (in press).
Angell, B., Matthews, E., Barrenger, S., Watson, A.C., Draine, J., 2014. Engagementprocesses in model programs for community reentry from prison for peoplewith serious mental illness. Int. J. Law Psychiatry 37 (5), 490e500.
Antaki, C., 1994. Explaining and Arguing: The Social Organization of Accounts. Sage,
London.Antaki, C., Barnes, R., Leudar, I., 2005. Diagnostic formulations in psychotherapy.
Discourse Stud. 7, 627e647.Barry, M.J., Edgman-Levitan, S., 2012. Shared decision making d The Pinnacle of
patient-centered care. N. Engl. J. Med. 366, 780e781.Bergmann, J.R., 1992. Veiled morality: notes on discretion in psychiatry. In: Drew, P.,
Heritage, J. (Eds.), Talk at Work: Interaction in Institutional Settings. CambridgeUniversity Press, New York, pp. 137e162.
Blackwell, B.E., 1997. Treatment Compliance and the Therapeutic Alliance. HarwoodAcademic Publishers.
Bolden, G.B., Angell, B., 2015, July 3e5. The organization of the treatment recom-mendation phase in psychiatric visits. In: Paper Presented at the 5th Interna-tional Conference on Conversation Analysis & Clinical Encounters,Loughborough, UK.
Brodwin, P., 2013. Everyday Ethics: Voices from the Front Line of CommunityPsychiatry. University of California Press.
Buttny, R., 1993. Social Accountability in Communication. Sage, Newbury Park, CA.Canning, J., Burton, S., Hall, B., 2012. Lithium and valproate-induced tremors. Ment.
Health Clin. 1, 19.Carter, M., 2003. The relationship of a self-reported assessment of need in mental
illness to insight. J. Ment. health 12, 81e89.Charles, C., Gafni, A., Whelan, T., 1999. Decision-making in the physicianepatient
encounter: revisiting the shared treatment decision-making model. Soc. Sci.Med. 49, 651e661.
Collins, S., Drew, P., Watt, I., Entwistle, V., 2005. ‘Unilateral’ and 'bilateral' practi-tioner approaches in decision-making about treatment. Soc. Sci. Med. 61,2611e2627.
Conrad, P., 1992. Medicalization and social control. Annu. Rev. Sociol. 18, 209e232.Costello, B.A., Roberts, F., 2001. Medical recommendations as joint social practice.
Health Commun. 13, 241e260.Drake, R., Deegan, P., 2009. Shared decision making is an ethical imperative. Psy-
chiatr. Serv. 60, 1007e1007.Drew, P., Heritage, J., 1992. Analyzing talk at work: an introduction. In: Drew, P.,
Heritage, J. (Eds.), Talk at Work: Interaction in Institutional Settings. CambridgeUniversity Press, New York, pp. 1e65.
Epstein, R.M., Franks, P., Fiscella, K., Shields, C.G., Meldrum, S.C., Kravitz, R.L., et al.,2005. Measuring patient-centered communication in patientephysician con-sultations: theoretical and practical issues. Soc. Sci. Med. 61, 1516e1528.
Farber, B.A., Doolin, E.M., 2011. Positive regard. Psychotherapy 48, 58e64.Gill, V.T., 2005. Patient “demand” for medical interventions: exerting pressure for
an offer in a primary care clinic visit. Res. Lang. Soc. Interact. 38, 451e479.Goffman, E., 1981. Forms of Talk. University of Pennsylvania Press, Philadelphia.Halkowski, T., 2006. Realizing the illness: patients' narratives of symptom discov-
ery. In: Heritage, J., Maynard, D.W. (Eds.), Communication in Medical Care:Interaction between Primary Care Physicians and Patients. Cambridge Univer-sity Press, Cambridge, England, pp. 86e114.
Harr�e, R., Clarke, D.D., Decarlo, N., 1985. Motives and Mechanisms: An Introductionto the Psychology of Action. Methuen, New York.
Hepburn, A., Bolden, G.B., 2013. The conversation analytic approach to transcrip-tion. In: Sidnell, J., Stivers, T. (Eds.), The Handbook of Conversation Analysis.Blackwell, Oxford, pp. 57e76.
Heritage, J., Maynard, D.W. (Eds.), 2006. Communication in Medical Care: Interac-tion between Primary Care Physicians and Patients. Cambridge University Press,New York.
Hudak, P.L., Clark, S.J., Raymond, G., 2011. How surgeons design treatmentrecoommendations in orthopaedic surgery. Soc. Sci. Med. 73, 1028e1036.
Institute of Medicine Committee on Quality of Health in America, 2006. Improvingthe Quality of Health Care for Mental and Substance Use Conditions. NationalAcademies Press Report, Washington, DC, pp. 77e139.
Koenig, C.J., 2011. Parient resistance as agency in treatment decisions. Soc. Sci. Med.72, 1105e1114.
Koenig, C.J., Wingard, L.M., Sabee, C., Olsher, D., Vandergriff, I., 2014. Managingpatient-centered communication across the Type 2 diabetes illness trajectory: agrounded practical theory of interactional sensitivity. J. Appl. Commun. Res. 42,244e267.
Kolden, G.G., Klein, M.H., Wang, C.-C., Austin, S.B., 2011. Congruence/genuineness.Psychotherapy 48, 65e71.
Longhofer, J., Floersch, J., Jenkins, J.H., 2004. Medication effect interpretation andthe social grid of management. Soc. Work Ment. Health 1, 71e89.
Mahone, I.H., Farrell, S., Hinton, I., Johnson, R., Moody, D., Rifkin, K., et al., 2011.Shared decision making in mental health treatment: qualitative findings fromstakeholder focus groups. Archives Psychiatric Nurs. 25, e27ee36.
Matthias, M.S., Salyers, M.P., Frankel, R.M., 2013. Re-thinking shared decision-making: context matters. Patient Educ. Couns. 91, 176e179.
Matthias, M.S., Salyers, M.P., Rollins, A.L., Frankel, R.M., 2012. Decision making inrecovery-oriented mental health care. Psychiatric Rehabilitation J. 35, 305e314.
Maynard, D.W., 1991. Interaction and asymmetry in clinical discourse. Am. J. Sociol.97, 448e495.
Maynard, D.W., 2004. On predicating a diagnosis as an attribute of a person.Discourse Stud. 6, 53e76.
McCabe, R., Healey, P.G.T., Priebe, S., Lavelle, M., Dodwell, D., Laugharne, R., et al.,2013. Shared understanding in psychiatrist-patient communication: associationwith treatment adherence in schizophrenia. Patient Educ. Conseling 93, 73e79.
McCabe, R., Heath, C., Burns, T., Priebe, S., 2002. Engagement of patients withpsychosis in the consultation: conversation analytic study. Br. Med. J. 325,

B. Angell, G.B. Bolden / Social Science & Medicine 138 (2015) 44e5656
1148e1151.Norcross, J.C. (Ed.), 2002. Psychotherapy Relationships that Work: Therapist Con-
tributions and Responsiveness to Patients. Oxford University Press.Olfson, M., Marcus, S.C., Wilk, J., West, J.C., 2006. Awareness of illness and non-
adherence to antipsychotic medications among persons with schizophrenia.Psychiatr. Serv. 57, 205e211.
Orbuch, T.L., 1997. People's accounts count: the sociology of accounts. Annu. Rev.Sociol. 23, 445e478.
Parry, R., 2009. Practitioners' accounts for treatment actions and recommendationsin pshysiotherapy: when do they occur, how are they structured, what do theydo? Sociol. Health Illn. 31, 835e853.
Parry, R., Land, V., Seymour, J., 2014. How to communicate with patients aboutfuture illness progression and end of life: a systematic review. BMJ Support.Palliat. Care 00, 1e11.
Per€akyl€a, A., 1995. AIDS Conselling: Institutional Interaction and Clinical Practice.Cambridge University Press, Cambridge.
Per€akyl€a, A., 1998. Authority and accountability: the delivery of diagnosis in primaryhealth care. Soc. Psychol. Q. 61, 301e320.
Pescosolido, B.A., Gardner, C.B., Lubell, K.M., 1998. How people get into mentalhealth services: stories of choice, coercion and “muddling through” from “first-timers”. Soc. Sci. Med. 46, 275e286.
Pilnick, A., Dingwall, R., 2011. On the remarkable persistence of asymmetry indoctor/patient interaction: a critical review. Soc. Sci. Med. 72, 1374e1382.
President's New Freedom Commission on Mental Health, 2003. TransformingMental Health Care in America. SMA-03-3832, Rockville, MD.
Priebe, S., Dimic, S., Wildgrube, C., Jankovic, J., Cushing, A., McCabe, R., 2011. Goodcommunication in psychiatry e a conceptual review. European Psychiatry 26,403e407.
Quirk, A., Chaplin, R., Lelliott, P., Seale, C., 2012. How pressure is applied in shareddecisions about antipsychotic medication: a conversation analytic study ofpsychiatric outpatient consultations. Sociol. Health Illn. 34, 95e113.
Roberts, F., 1999. Talking about Treatment: Recommendations for Breast cancerAdjuvant Therapy. Oxford University Press, New York.
Robinson, J.D., 2004. The sequential organization of “explicit” apologies in naturallyoccurring English. Res. Lang. Soc. Interact. 37, 291e330.
Robinson, J.D., Bolden, G.B., 2010. Preference organization of sequence-initiatingactions: the case of explicit account solicitations. Discourse Stud. 12, 501e533.
Sacks, H., 1972a. An initial investigation of the usability of conversational materialsfor doing sociology. In: Sudnow, D.N. (Ed.), Studies in Social Interaction. FreePress, New York, pp. 31e74.
Sacks, H., 1972b. On the analyzability of stories by children. In: Gumperz, J.J.,
Hymes, D. (Eds.), Directions in Sociolinguistics: The Ethnography of Commu-nication. Holt, Rinehart & Winston, New York, pp. 329e345.
Salyers, M.P., Matthias, M.S., Fukui, S., Holter, M.C., Collins, L., Rose, N., et al., 2012.A coding system to measure elements of shared decision making during psy-chiatric visits. Psychiatr. Serv. 63, 779e784.
Say, R., Murtagh, M., Thomson, R., 2006. Patients' preference for involvement inmedical decision making: a narrative review. Patient Educ. Couns. 60, 102e114.
Schegloff, E.A., 2007. Sequence Organization in Interaction: A Primer in Conversa-tion Analysis. Cambridge University Press, Cambridge.
Scott, M.B., Lyman, S.M., 1968. Accounts. Am. Sociol. Rev. 33, 46e62.Seale, C., Chaplin, R., Lelliott, P., Quirk, A., 2006. Sharing decisions in consultations
involving anti-psychotic medication: a qualitative study of psychiatrists' ex-periences. Soc. Sci. Med. 62, 2861e2873.
Shotter, J., 1984. Social Accountability and Selfhood. Blackwell, Oxford.Sidnell, J., Stivers, T. (Eds.), 2013. The Handbook of Conversation Analysis. Blackwell,
Oxford.Starr, P., 1982. The Social Transformation of American Medicine. Basic Books.Stein, L.I., Santos, A.B., 1998. Assertive Community Treatment of Persons with Se-
vere Mental Illness. WW Norton & Co.Stivers, T., 2005a. Non-antibiotic treatment recommendations: delivery formats and
implications for patient resistance. Soc. Sci. Med. 60, 949e964.Stivers, T., 2005b. Parent resistance to physicians' treatment recommendations: one
resource for initiating a negotiation of the treatment decision. Health Commun.18, 41e74.
Stivers, T., 2006. Treatment decisions: negotiations between doctors and parents inacute care encounters. In: Heritage, J., Maynard, D.W. (Eds.), Communication inMedical Care: Interaction between Primary Care Physicians and Patients.Cambridge University Press, Cambridge, England, pp. 279e312.
Stivers, T., 2007. Prescribing under Pressure: Parent-physician Conversations andAntibiotics. Oxford University Press, New York.
Toerien, M., Shaw, R., Duncan, R., Reuber, M., 2011. Offering patients choices: a pilotstudy of interactions in the seizure clinic. Epilepsy & Behav. 20, 312e320.
Toerien, M., Shaw, R., Reuber, M., 2013. Initiating decision-making in neurologyconsultations: 'recommending' versus 'option-listing' and the implications formedical authority. Sociol. Health Illn. 35, 878e890.
Turkington, D., Kingdon, D., Weiden, P.J., 2006. Cognitive behavior therapy forschizophrenia. Am. J. Psychiatry 163, 365e373.
Woltmann, E.M., Whitley, R., 2010. Shared decision making in public mental healthcare: perspectives from consumers living with severe mental illness. PsychiatricRehabil. J. 34, 29.












![The American Legion [Volume 138, No. 3 (March 1995)]](https://static.fdokumen.com/doc/165x107/631d437e6c6907d36801aec2/the-american-legion-volume-138-no-3-march-1995.jpg)







