ANALGESICS IN ENDODONTICS - mgumst
335
. 1 1 ANALGESICS IN ENDODONTICS Dr Prachi Mital Department of Conservative Dentistry and Endodontics 2 Introductio n Origin of pain Analgesics NSAIDs NSAIDs in dentistry Opioids Drug interactions Analgesic strategy Conclusion CONTENTS 3 Introduction • Dental pain is one of the main reason for patient to visit Endodontist. • Management of dental pain with anxiety during or after treatment remains a big challenge. 4 • “ An unpleasant sensory and emotional experience associated with acute or potential tissuse damage or described in terms of such damage”. - IASP DEFINITION OF PAIN 5 • Type of pain:- a. Nociceptive pain b. Neuropathic pain a. Peripheral sensitization b. Central sensitization c. Heterotopic pain Odontogenic Pulp dentin complex Periradicular tissues Non odontogenic Musculoskeletal pain Neuropathic pain Neurovascular pain Pyschogenic pain 6
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ANALGESICS IN ENDODONTICS - mgumst
.
1
1
ANALGESICS IN
ENDODONTICS
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
2
Introduction
Origin of pain
Analgesics NSAIDs
NSAIDs in dentistry
Opioids Drug
interactions
Analgesic strategy
Conclusion
CONTENTS
3
Introduction
• Dental pain is one of the
main reason for patient
to visit Endodontist.
• Management of dental
pain with anxiety
during or after
treatment remains a big
challenge.
4
• “An unpleasant
sensory and emotional
experience associated
with acute or potential
tissuse damage or
described in terms of
such damage”. - IASP
DEFINITION OF PAIN
5
• Type of pain:-
a. Nociceptive pain
b. Neuropathic pain
a. Peripheral sensitization
b. Central sensitization
c. Heterotopic pain
Odontogenic
Pulp dentin complex
Periradicular tissues
Non
odontogenic
Musculoskeletal pain
Neuropathic pain
Neurovascular pain
Pyschogenicpain
6
.
2
7
“ The skill of the clinican is oftenjudged primarily by their successor failure of pain control” .
-cohen, pathway of pulp
▪ Toothache is the most
common pain entity
occurring in facial
region.
▪ Usually acute in nature.
DENTAL PAIN
8
TRIGEMINAL PAIN SYSTEM
9 10
ANALGESIC
Opioid Non opioid
Antipyretic- analgesic or NSAIDS are commonly employed for dental pain because tissue injury and inflammation due to tooth abscess, caries, etc is major cause of acute dental pain
11
• Analgesic is a drug that selectively relieves pain by
acting in the CNS or on peripheral pain mechanisms,
without significantly altering consciousness.
• Analgesics relieves pain as symptoms without affecting
its cause .
NON-NARCOTIC ANALGESICS
•Management of endodontic pain is multifactorial and directed at reducing peripheral and central components of hyperalgesia through combined endodontic procedures
and pharmacotherapy.
✓Include – I) NSAIDsII) Acetaminophen
12

.
3
Non Steroidal Anti Inflammatory Drugs
Analgesic, antipyretic and anti-
inflammatory action
A drug of choice in treating
odontogenicpain
Act primarily on peripheral
pain mechanism
Don’t depress CNS
Don’t produce physical
dependence
13
CLASSIFICATION
➢A. Nonselective COX inhibitors (traditional NSAIDs) :-
1. Salicylates :- Aspirin
2. Propionic acid derivatives :- Ibuprofen, Naproxen,
Ketoprofen ,Flurbiprofen.
3. Anthranilic acid derivative :- Mephenamic acid.
4. Aryl-acetic acid derivative :- Diclofenac,
Aceclonfenac.
5. Oxicam derivatives :- Piroxicam , Tenoxicam.
6. Pyrrolo-pyrrole derivatives :- Ketorolac.
14
7. Indole derivatives :- Indomethacin
8. Pyrazolone derivatives :- Phenylbutazone ,
Oxyphenbutazone.
15
➢Preferntial COX-2 inhibitor :- Nimesulide ,Meloxicam.
➢Selective COX-2 inhibitor :- Celecoxib, Etoricoxib, Parecoxib
➢Analgesic – antipyretics with poor anti-inflammatory action:-1. Paraminophenol derivative :- Paracetamol .
2. Pyrazolone derivatives :- Metamizol, propiphenzone..
3. Benzoxazocine derivative :- Nefopam.
16
Mechanism of action :-
➢Depression of cyclo oxygenases activity.
➢ Decreasing of prostagladins synthesis in peripheral tissue and in CNS.
➢ Decreasing of sensitivity of nerve endings and depression of transmission impulses on the level of CNS
structure.
17
Arachidonic Acid
COX -1 COX -2
Prostaglandins Thromoboxane Prostaglandins
GI Mucosal protection Hemostasis Mediate pain ,
inflammation ,fever
Cyclo oxygenase
InducibleConstitutive
18
.
4
Beneficial Actions Due To PG Synthesis
Inhibition
Analgesia : prevention of pain nerve ending sensitization.
Anti –pyretic.
Anti- inflammatory.
Anti – thrombotic.
19
-KD Tripathi 2nd Edition20
21
Non selective COX inhibitors
22
✓ Aspirin :-• Aspirin is acetylsalicylic acid.
• It is the oldest analgesic- anti-inflammatory drug .
✓Mechanism of action :-• Aspirin inhibits COX irreversibly by acetylating
serine residues ; return of COX activity depends on synthesis of fresh enzyme.
✓Dosage:-• Anti inflammatory action – 3-5gm/day or 100
mg/kg/day• Analgesic:- 0.3-0.6 gm (low dose)
23 24

.
5
Anti-inflammatory doses produce syndrome called
salicyalism- dizziness, tinnitus, reversible
impairment of hearing ,mental confusion
25
Serious toxicity seen at serum
salicylate levels > 50mg/dl
More common in children
Treatment :-• External cooling • I.V fluid with Na+,
K+, glucose.• Gastric lavage→
remove absorbed drug
• haemodialysis_→remove absorbed
drug
26
Contraindications
•Peptic ulcers
•Bleeding disorder
•Hypersensitivity against NSAID
•<12 years of children
•Liver disease
•Pregnancy and lactation
•Chickenpox or influenza
27 28
Propionic acid derivatives
29
Ibuprofen
•Prototype of contemporary NSAIDs.
• Has a well-documented efficacy and safety profile.
•Largely metabolized in liver by hydroxylation and excreted in urine as well as bile.
Dose :- 400-600 mg TDS
30

.
6
31
Aryl Acetic Acid Derivatives
Diclofenac sodium
Inhibits PG synthesis reversibly.
Reduces neutrophils
chemotaxis and
superoxide
production
at inflammatory site.
Has good tissue
penetrability→
concentration in joints
and other sites of
inflammation it is
maintained for longer
period extending
therapeutic effect. 33
Dose -50mg BD ;75 mg i.m
USES
In tooth ache.
In rheumatoid and osteoarthritis.
Post- traumatic & post-operative inflammatory conditions → provide
quick relief of pain and wound edema.
Ankylosing spondylitis
SIDE EFFECTS
Epigastric pain
Nausea
Headache
Dizziness
34 35
Oxicam derivatives
36
Piroxicam
Long acting NSAIDs
Anti inflammmatory , good analagesic-
antipyretic actions.
Mechanism :-reversible
inhibitory of COX.
Lowers PG concertation in
synovial fluid and inhibit platelet aggregation→
prolonging bleeding time.
Inhibits inflammation in diverse ways , either :-
1.Decreases production of IgM rheumatoid factor
2.Reduces leucocyte chemotaxis.
37
.
7
1. As short term analgesic or as long term anti inflammatory drug in rheumatoid and osteoarthritis.
2. Acute gout.
3. Musculoskeletal injury.
1.Heart burn
2.Nausea
3.Anorexia
Doses :- 20 mg BD followed by 20 mg OD.
38
Pyrrolo-Pyrrole Derivatives
39
Novel NSAID – potent analgesic and anti inflammatory activity.
In post operative pain – equals efficacy of morphine but is free of opioids side effects .
Mechanism :- inhibits PG synthesis & relieves pain by peripheral mechanism.
Dose :- 10-20mg 6 hourly
Ketorolac :-
40
Uses :1. In postoperative dental and acute muscloskeletal pain.
2. Also for renal colic, migraine , pain due to bony metastasis.
-For short term , moderate pain management :-
given orally in dose of 10-20 mg 6 hourly In postoperative dental pain ketorolac has been rated superior to aspirin (650mg ) , paracetamol (600mg )
& equivalent to ibuprofen 400mg .
-Continuous use for more than 5 days is not recommended
41
42
Preferntial COX-2 Inhibitors
43

.
8
Sulfonamide derivatives
Weak inhibitor of PG synthesis
Used as short lasting inflammatory drug in patients with asthma,
bronchospasn, intolerance to aspirin
Dose – 100mg BD
Nimesulide :-
44
Selective COX-2 Inhibitors:- ( Coxibs)
45
•Introduction of selective inhibitors of COX-2 offered potential for both analgesic and anti-inflammatory benefits
and reduced GI irritation.
•COX-2 levels are increased in inflamed human dental pulp, and a COX-2 inhibitor is analgesic in patients with
endodontic pain.
Do not affect COX-1 function, do not inhibit platelet aggregation, but reduce PGI₂ production → exert prothrombotic influence → enhance CV risk.
46 47
• Currently 3 selective COX-2 inhibitor are available in india –
# Celecoxib# Etoricoxib# Parecoxib
• Rofecoxib and Valdecoxib have been withdrawn for increasing CV risk.
• Contraindications– Patient with history of ischemic heart disease / hypertension/cardiac failure/ cerebrovascular disease
48
• Should be used only in patients at high risk of peptic ulcer, perforation or bleeds.
• If selected → administered in the lowest dose for short period of time .
49
ANALGESICS ANTIPYRETICS
WITH ANTI-INFLAMATORY

.
9
50
Paracetamol (acetaminophen ) :-
• One of the most commonly used drugs.
• Analgesic and antipyretic drug.
• Actions :- Central analgesic action →It raises pain threshold ,
but has weak peripheral anti inflammatory component.
• Normal dose :- safe (> 10g or >150mg/kg -adults)
• Higher dose :- causes liver toxicity→ acute liver failure
51
• Mechanism :- Poor inhibitor of PG synthesis in
peripheral tissues but more active on COX in brain.
• It has negligible anti inflammatory action.
Uses
• Best to be used as antipyretic.
• As Analgesic for headache, musculoskeletal pain, toothache, → anti inflammatory action not required.
52
Acute paracetamol poisoning
• Occur specially in small children→ having low hepatic glucuronnide conjugating ability.
• Fatality is common with >250 mg/kg.
• Early manifestations :- nausea, vomiting, abdominal pain, liver tenderness.
• After 12-18 hours:- centri lobular hepatic necrosis, hypoglycemia.
• After 2days :- jaundice occurs
53
• Treatment :-
• Early treatment :- vomiting can be induced or gastric
lavage done.
• N-acetylaysteine infused i.v or given orally .→ prevents
hepatic glutathione and prevents binding of toxic
metabolite to other cellular constituents.
54 55
Nsaids In Dentistry

.
10
56
Mild-to-moderate pain with little inflammation :-
paracetamol or low dose ibuprofen given.
Acute but short lasting pain or postextraction :-ketorolac, diclofenacsodum or aspirin given. Gastric intolerance
to NSAIDs :-paracetamol or etoricoxib given.
57
• History of asthma or anaphylactoid reaction to aspirin CoX-2 inhibitors.
• Pediatric patients Paracetamol, aspirin, ibuprofen.
• Pregnancy Paracetamol, aspirin .
• Hypertensive, diabetic ischaemic heart disease , epileptic drug interaction can occur with NSAIDs should be considered and physician consultation.
58 59
Drug Interaction with NSAIDs
60
Diuretics : Diuresis
Beta-blockers : Anti-hypertensive effect
ACE inhibitors : Anti-hypertensive effect
Anticoagulant : Risk Of GI bleed
Alcohol: Risk Of GI bleed
Cyclosporine : Nephrotoxicity
Corticosteroids : Risk Of GI bleed
61
OPIOID
ANALGESICS

.
11
62
Two type of alkaloid
Phenanthrenederivatives
Morphine‘
Codeine
Thebaine
Benzoisoquinoline
derivatives
Papaverine
Nosacapine
• Opium – dark brown, resinous material obtained from poppy ( Papaver somniferum).
63
Opioid receptors
64
• Opioid exert their actions by interacting with specific
receptors present on neurons in the CNS & periphery
tissues.
• Opioid receptors are divided into 3 types :-
• Kappa (κ)
• Delta (δ)
• mu (μ)
65
• Opioids ligands
interact with
different opioid
receptors as agonists,
partial agonists or
competitive
anatagonists.
66
Opiod Receptor Activation
Response Mu-1 Mu-2 Kappa Delta Sigma
Analgesia
Respiratory depression
Euphoria
Dysphoria
Decrease GI motility
Physical Dependence
Mania, hallucination
67
Opioid receptor transducer
mechanisms

.
12
68
• All opioid receptors are G- protein coupled receptors
situated on prejunctional neurons.
• Cause inhibotry modulation.
Decrease release of junctional
Transmitter such as
noradrenaline, dopamine,
GABA, glutamate.
69
Principal alkaloid in opium
Considered as Prototype Drug
Rarely prescribed orally because most
of drug is metabolized in liver
before reaching systemic circulation
Freely crosses placenta and can
affect the foetus more than mother.
70
• It produces relief of pain in a dose that usually does not
alter other functions of CNS.
• Indications :-
• Moderate dose- relieves continuous , dull pain
• High dose- relieves sharp, intermittent pain caused by
trauma
• Dose :- 10-15mg oral/i.m; 2-6 mg i.v; 2-3 mg epidural.
71
Pharmacological actions
72
Analgesic
•Strong analgesic- most effective in most kind of acute & chronic pain.
•Suppression of pain perception is selective ,without affecting other sensation or producing proportionate generalized CNS depression ( contrast GA _)
Sedation
•Drowsiness .•Higher dose can produce sleep and coma.•No anticonvulsant action.
Mood and subjective effects:-
•Has calming effect, feeling of detachment, lack of initiative, inability to concentrate.
•Patient in pain or anxiety & addictive perceive it as pleasurable
73

.
13
74
Codeine
75
• Methyl –morphine occurs naturally in opium.
• Most commonly used opioid.
• Combined with acetaminophen for oral
administration.
• 60 mg of codeine has analgesic strength of 650 mg
of acetaminophen or 200 mg of ibuprofen.
Codeine NSAIDsAnalgesic activity increases.
Dose :-0.5-1mg/kg 4-6 hourly
76
Fentanyl
77
• 80 to 100 times more potent than morphine.
• Peak analgesic effect is reached in 5 minafter IV injection.
• Indications :-
• Used exclusively in Anaesthesia in injectable form.
• Respiratory depression alone as well in combination with Droperidol.
• Transdermal fentanyl→ for management of persistent chronic pain .
78
DOSE: 100-200 µg i.v(FENT, FENDROP 50µg/ml)
Transdermal patch -25 µg/hr
79
Pethidine (Meperidine)
.
14
80
• Equal analgesic efficacy to morphine & some properties
like Atropine.
• Indications :-
▪ As substitute to morphine .
▪ In pre anesthetic medication.
▪ In asthmatics patients→ causes less histamine release
• DOSE : 50-100 mg i.m/ orally
81
Tramadol
82
• Centrally acting analgesic .
• Weak agonist of all type of
opioid receptors.
• Indicated :-
▪ Moderate to severe pain.
▪ Short lasting pain due to diagnostic procedures, surgery
etc.
▪ Chronic pain including cancer pain
83
• Dose :- 50-100 oral/ i.m /slow
i.v infusion(4-6 hourly).
• Injected i.v 100mg tramadol is
equianalgesic to 10 mg i.m
morphine.
84
Opioid In Dentistry
85
• Narcotic (opioid) analgesics are extremely
effective in reducing acute dental and
postoperative pain.
• Hydrocodone, oxycodone, codeine, and
occasionally meperidine are the narcotics used to
treat dental pain.
Opioid analgesics
can be used
NSAIDs are less effective

.
15
86
• Gender is another interesting genetic factor associated with
altered opioid responsiveness. Several studies have reported
that women demonstrate significantly greater analgesia to
kappa opioids than men.
87
Opioid Dosing Regimens
For Dental Pain
88
Codeine should be the first to consider.Next opioid
to consider is
oxycodone
89
• Meperidine a synthetic opioid, is chemically distinct
from codeine and oxycodone.
• Meperidine for dental pain should be reserved for
patient who is allergic to morphine and codeine
derivatives, but who still requires an opioid.
90
Opioid
Most powerful analgesic
Relieve any type of pain
Act mainly at level of cortex, CNS
Produce addiction
NSAIDs
Mild analgesics
Relieve mild type of pain
Act mainly at levels of thalamus & hypothalamus
No addiction
91
Combination analgesics

.
16
92
• To enhance the analgesic benefit is to combine two (or
more) drugs with different mechanisms of action.
No pain relief
Increased analgesia effect because the drugs act through dissimilar mechanisms
93
Analgesic Selection
94
• Acetaminophen-opioid combinations are the drugs of
choice for moderate to severe pain when NSAIDs are
contraindicated.
Opioids (Codeine 60mg )
Paracetamol(600-650 mg)
Very effective analgesia in post-operative pain patients.
Doxylamine (5mg)
Increases analgesia effect
95
96 97
Analgesic use in pregnancy or lactation

.
17
98
American Geriatrics Society
Recommendations for
Choosing Medications
99
• Use the least invasive route to give medication.
• Start low and go slow.
• Nonsteroidal anti-inflammatory drugs should be used
with caution due to side effects.
• Opioid analgesics are effective for relieving moderate to
severe pain.
100
• Combination of an NSAID with acetaminophen provides
effective pain control in both
postsurgical and postendodontic patients.
• Pharmacologic therapy is most effective when combined with
nonpharmacologic therapy.
101
Conclusion
•From a dentists’ perspective, we are able to choose from a
plethora of medications to provide patients with pain relief,
but trying to judge the relative efficacy of analgesics is not
easy.
•One must remember that the best means of managing pain is
to remove the source of pain as quickly as possible.
102
• Essentials of medical pharmacology –K.D. Tripathi
• Pathways of the pulp-cohen• Endodontics –Ingle • Australian dental journal medication
supplement-2005• AAE; A “3D” Approach for Treating Acute
Pain;winter 2015• Current concepts of analgesics in dental pain
management; Monika Kaushik, Atul Kaushik;Indian Journal of Dental Education; Volume 5 Number 2, April - June 2012
103
• Drug Therapy in Dental Practice: Nonopioidand Opioid Analgesics;Daniel E. Becker, James C. Phero; 52:140–149 2005.
• Evaluation of NSAIDs for treating post-endodontic pain;A systematic review;Andreaholstein, kenneth m. Hargreaves &richardniederman; 2002, 3, 3–13
.
18
104
THANKYOU
105
106 107
108 109

.
19
110 111
112 113
114 115
.
20
116 117
118 119
120 121
.
1
1
Antibiotics In Endodontics
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
2
•Introduction
•History
•Classification
•Uses Of Antibiotics In Endodontics
•Antimicrobial Agents Used In Endodontics
•Recent Advances
•Conclusion
•References
CONTENTS
INTRODUCTION
•In Oral cavity over 700 species of micro organisms belonging to 11 divisions have been Identified.
•In essence endodontic infection is infection of root canal system and micro organisms play a tremendous
role in pulpal and periapical disease.
3
•Ultimate goal of endodontic treatment is to remove as many micro-organisms and their by products
from root canal space by using various antimicrobial agents to provide a environment free of
microorganisms .
•Antibiotics have revolutionized entire health care system including both medicine and dentistry.
• Paradigm shift occurred since the discovery of Penicillin by Alexander Fleming in 1928.
4
5
•Mixtures with antimicrobial properties utilized in treatment of infections were described over 2,000
years ago.
•Traditionally, plant materials and extracts, honey, moldy soybean curd, warm earth rich in molds and
fungi were used to treat infections.
6
.
2
•Physician Paul Ehrlich laid down foundation of idea of antibiotics by introducing term “magic
bullets” for a chemical that would attach itself togerm and kill it.
•Jean Paul Vuillemin used the term “antibiosis” that means “against life” for early antibacterial
drugs.
7 8
Antibiosis was first described in 1877 by Louis Pasteur and Robert Koch.
9
• Chemical structure• Mechanism of action• Type of organisms against which primarily active• Spectrum of activity • Type of action
12
CLASSIFICATION
Chemical structure
• Sulfonamides and related drugs: Sulfadiazine and others, Sulfones—Dapsone (DDS),
Paraaminosalicylic acid(PAS).
• Quinolones: Nalidixic acid, Norfloxacin, Ciprofloxacin, etc.
•β-lactam antibiotics: Penicillins, Cephalosporins, Monobactams, Carbapenems.
13
• Tetracyclines: Oxytetracycline, Doxycycline, etc.
• Nitrobenzene derivative: Chloramphenicol.
•Aminoglycosides: Streptomycin,Gentamicin, Neomycin
•Macrolide antibiotics: Erythromycin, Clarithromycin, Azithromycin
14

.
3
• Lincosamide antibiotics: Lincomycin, Clindamycin.
• Polypeptide antibiotics: Polymyxin-B, Colistin, Bacitracin, Tyrothricin.
•Glycopeptides: Vancomycin, Teicoplanin
• Nitroimidazoles: Metronidazole, Tinidazole.15
•Nicotinic acid derivatives: Isoniazid,Pyrazinamide, Ethionamide.
•Polyene antibiotics: Nystatin,Amphotericin-B, Hamycin.
• Azole derivatives: Miconazole,Clotrimazole, Ketoconazole, Fluconazole.
• Others: Rifampin, Spectinomycin, Sod. fusidate, Cycloserine, Viomycin, Ethambutol, Thiacetazone,
Clofazimine, Griseofulvin. 16
Mechanism of action
17
Spectrum of activity
18
Type of action
19
Problems That Arise With The Use Of Antimicrobial Agents
Toxicity• Local irritancy:• Systemic toxicityHypersensitivity reactionsDrug resistance• Natural resistance• Acquired resistanceSuperinfectionNutritional deficienciesMasking of an infection
22

.
4
24
Uses of Antibiotics in Endodontics
25
•Pulp capping
• Irrigant
•Intra Canal medicament
• Obturating material containing antibiotics
•Reimplantation
• Regenerative endodontics
•Signs of systemic involvement, • Immunosuppressed patients• Bacteremia
Local uses Systemic uses
26
Systemic Antimicrobial Agents Most Frequently Used In Endodontics
•Recent recommendations warrant mention, according to a new report by the American Dental Association for
proper prescription of antibiotics in case of endodontic infection.
29
Indications for Adjunctive Antibiotics
30
Conditions NOT Requiring Adjunctive Antibiotics
31

.
5
PenicillinErythromycinClindamycinClarithromycinAzithromycinTetracyclineDoxycyclineCiprofloxacinMetronidazole
35 36
penicillin
37
•first antibiotic to be used clinically in 1941.
•Originally obtained from fungusPenicillium notatum but present source is a high
yielding mutant of P. chrysogenum.
38
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329
•
•Also the first choice drug for prophylaxis of local wound infection as well as distant infection
(endocarditis) following dental surgery in susceptible patients
40
Amoxicillin is one of the most frequentlyused antibiotics for treatment of dental
infections.
41
•Oral absorption is better
•Food does not interfere with absorption
•Higher and more sustained blood levels are produced.
•Incidence of diarrhea is lower.
Advantages

.
6
Augmentin-combination of amoxicillin with clavulanate
Clavulanate is a competitive inhibitor of betalactamaseenzyme produced by bacteria to inactivate penicillin + cell wall synthesis inhibition by amoxicillin
Both gram positive and gram negative
usual oral dosage for amoxicillin with clavulanate is 1,000 mg loading dose followed by 500 mg every eight hours for five to seven days
42
Obtained from Streptomyces clavuligerus .Called a ‘suicide’ inhibitor, it gets
inactivated after binding to the enzyme.
Adverse effects
•Same as for amoxicillinalong with tolerance is poorer—especially in
children.
•Other side effects are Candida stomatitis/vaginitis and rashes.
•Some cases of hepaticinjury have been reported with the combination.
44
45
Trade Names
46
47
ERYTHROMYCIN
•Isolated from Streptomyces erythreus in 1952and is widely employed, mainly as an alternative
to penicillin.
•Quite frequently prescribed in dentistry.
48
.
7
Adverse effects
•Mild-to-severe epigastric pain is experienced by many patients, especially children on
oral therapy.
•Diarrhea is occasional.
•Very high doses of erythromycin have causedreversible hearing impairment.
52
Interaction
•Inhibits hepatic oxidation of many drugs.
•Clinically significant interactions are—rise in plasma levels of theophylline, carbamazepine,
valproate, warfarin, terfenadine, astemizole and cisapride
53
•Second choice drug to Penicillins for periodontal/ periapical abscesses, necrotizing ulcerative gingivitis, postextraction infections,
gingival cellulitis, etc.
•Particularly valuable for patients allergic to penicillins, or those with penicillin resistant
Infections.
Uses
54 55
•Not active against gram negative anaerobes involved in polymicrobial orodental infections.
•Being bacteriostatic, less effective than Penicillins in eradicating dental infections
caused by penicillin-sensitive bacteria.
limitations
56
Trade Names
57
.
8
58
Clarithromycin•Antimicrobial spectrum of is similar to erythromycin.
• More acid stable thanerythromycin, and is rapidly absorbed.
• Oral bioavailability is ~50% due to first pass metabolism, food delays absorption.
59
61
Azithromycin
•Expanded spectrum, improved pharmacokinetics, better tolerability and drug interaction profiles.
•Remarkable pharmacokinetic properties are acid stability, rapid oral absorption, marked tissue
distribution and intracellular penetration.However, absorption is decreased by food.
62
63
•Can be used in orodental infections in place of erythromycin, particularly in patients not
tolerating the latter.
64

.
9
65
Trade Names
66
68
Clindamycin
69
70 71
Doses Of Systemic Antibiotics

.
10
72 80
81
Agents Locally Used In Endodontics
•TAP - Triple Antibiotic Paste •MTAD •Tetraclean•Ledermix Paste •Odontopaste•Pulpomixine•Septomixine Forte •Medicated Gutta Percha •Scaffolds Containing Antibiotics
82
TAP –Triple Antibiotic Paste
83
•First used by Sato et al., now commercially available as 3-MIX.MP
•Employed under the concept of “Lesion sterilization and tissue repair therapy” for treating
immature teeth with endodontic Infection.
85
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329

.
11
•Hoshino et al. recommended metronidazole(500 mg) minocycline (100mg) and
ciprofloxacin (200mg) at 1:1:1 ratio for 3mix formulation.
•Later modified by Takushige et al. as metronidazole, minocycline and ciprofloxacin
mixed in a ratio of 3:3:1
87
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329
88
(a) Pre-operative radiograph showing large periapical lesion with respect to #11 and #21. (b) 4 weeks after placement of triple antibiotic intra-canal medicament.
(c) Increased bone density at the periradicluar region 10 months post-obturation.(d) Radiograph taken 18 months post-obturation
89
(a) Greenish intrinsic stain caused by triple antibiotic paste after 10 month post-obturation recall visit. (b) Greenish stain more evident after tooth preparation. (c) Masking the discoloration with all ceramic crowns
91
MTAD
92
Part-A (liquid)
•4.25% citric acid •0.5% polysorbate 80 (Tween 80)
Part-B (powder)
3% doxycycline hyclate
•Tong et al. showed by adding Nisin to MTAD it enhanced its effectiveness against E. Faecalis
biofilm
•Davis et al. done an in vitro study and concluded that 2% chlorhexidine and 5.25%
Naocl both exhibited less antimicrobial effectiveness against E. Faecalis
than Biopure MTAD
94
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329

.
12
95
(A) Preoperative periapical radiograph showing tooth #8 with an open apex and periapical radiolucency. (B) Postoperative periapical radiograph following regenerative endodontic procedure and placement of MTA
96
(A) Periapical radiograph taken at 1 year recall showing continued root thickening and apical closure. (B) Periapical radiograph taken at 4-year recall with complete apical closure. (C) Photograph taken at 4-year recall showing no discoloration of right maxillary central incisor
97
Tetraclean
Antibiotic Acid Detergent
•Differs from MTAD by the concentration of doxycycline (50mg/ml) and type of detergent
polypropylene glycol.
• More effective than MTAD against endodontic pathogen E. Faecalis in planktonic culture and
mixed species in in-vitro biofilm.
98
Pappen FG, Shen Y, Qian W, Leonardo MR, Giardino L, Haapasalo M. Int Endod J. 2010;43(6):528-35.
99
Odontopaste
developed in Australia [Australian Dental Manufacturing, Kenmore Hills, Old Australia].
•Contains zinc-oxide based root canal paste with Clindamycin hydrochloride 5% and 1%
Triamcinolone acetonide
•Bacteriostatic and prevents bacterial repopulation in the root canal system.
•Steroid reduces post operative pain and inflammation.
100
.
13
102
Ledermix paste
3.2% Demeclocycline Hcl
Steroid 1% Tramcinoloneacetomide
Polyethylene glycol base.
•Uses both as pulp capping agent and as an intracanal medicament.
•Steroids mainly reduce inflammation and pain, while antibiotics limit the infection by microbes .
• A modification is available in cement form consisting of 0.7% triamcinolone, 3%
demecloycline and calcium salts, used for pulp capping, pulpotomy procedure and also as a
liner for hypersensitive dentin 103
•Advantagewater soluble rinsed out easily and does not
cause any systemic side effect.
•Study by Thong et al., showed the incidence of replacement resorption was significantly lower in
the teeth treated with ledermix paste, when compared with calcium treated teeth
104
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329
•Kim et al. studied discoloration caused by ledermix paste when used as an intracanal
medicament and found this is mainly because of presence of tetracycline in the formulation.
•It was suggested that if paste is placed in canal below the CEJ, it reduced staining effects
105
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329
106
•Present clinical study aimed to investigate the effectiveness of Ledermix paste as intracanal
medicament in symptomatic teeth using the eugenol as control.
•Ledermix is a better intra canal medicament than eugenol in reducing postoperative pain in symptomatic teeth during root
canal therapy.•Ledermix acts quicker than eugenol in reducing symptoms that is within 72 h Postoperative pain and tenderness were
completely controlled, both with Ledermix and eugenol within 2 weeks
•No adverse systemic reactions found in any patients while using Ledermix.
107
Medicated Gutta percha

.
14
•Howard Martin introduced medicated gutta percha containing 10% Iodoform and 10% tetracycline
impregnated gutta percha (TGP) intended toreduce growth of bacteria inside the
obturated root canal.
•Prevent colonization of bacteria on gutta percha points and within root canals
108
Balasubramaniam R, Jayakumar S. Antibiotics in endodontics - A concise review. International Journal of Applied Dental Sciences 2017; 3(4): 323-329
109
•Act as a reservoir of that is capable of diffusing onto Surface of gutta percha thereby inhibiting colonization
of bacteria on gutta percha points and within root canal System.
• Tetracycline is capable of coalescing within dentinal tubules to inhibit long term microbial growth.
•These medicated gutta percha points are site Specific, Surface acting antimicrobial gutta percha points.
110
Recent Advances
111
•Nanoparticles have been found to have a broad spectrum of antimicrobial activity and less
incidence of microbial resistance development than antibiotics.
•Nanoparticles range from 1- 100 nm in size.
112
•Nano silver, gold, zinc oixde, magnesium oxide, calcium oxide and titanium oxide have been
extensively analysed and studied.
117
•combination of nano-particles with photosensitizer molecules has emerged as
a new interdisciplinary research field.
Simplified Jabłoński diagram showing the generation of reactive oxygen species (ROS) by a photosensitizer(PS) following absorption of light, intersystem crossing and Type-I and -II mechanisms.In antimicrobial photodynamic therapy (PDT), the resulting ROS are able to kill bacteria and fungi as illustrated on the right.

.
15
118
•Nanodiamond gutta percha composite (NDGP) embedded with nanodiamond amoxicillin (ND-
AMC) conjugates, which can reduce likelihood of root canal re-infection and enhance
treatment outcomes .
•Nanosilver coated gutta percha was introduced in 2008 by Iranian researchers to prevent bacterial
colonization in root canal space
119
•Bottino MC et al. suggested the use of the polymer based antibiotic containing electrospun scaffolds may act as an antimicrobial drug delivery system for regenerative endodontics. As the scaffolds degrade over time, it does
not require to be removed.
120
conclusion
121
•Since discovery of antibiotics eight decades ago, safe use of antibiotics has revolutionized treatment of diseases, transforming once deadly diseases into
manageable health problems.
•However, the phenomenon of bacterial resistance, caused by use and abuse of antibiotics and
simultaneous decline in research and development of new antimicrobial agents, is now threatening to take
us back to pre-antibiotic era.
•A fundamentally changed view of antibiotics is required and needs to be immediately
addressed
122
References
123

.
16
124
T
H
A
N
K
Y
O
U

.
1
BIOCOMPATIBILITY AND TISSUE REACTIONS TOWARDS BIOMATERIALS
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
Contents
•INTRODUCTION
•HISTORICAL BACKGROUND
•TEST USED TO MEASURE BIOCOMPATIBILITY
•TISSUE REACTIONS TOWARDS BIOMATERIAL
•CONCLUSION
•REFERENCES
Tissue reactions towards biomaterial
Any substance or combination of substances, other than drugs, synthetic or natural in origin, which can be used for any period of time, which augments or replaces partially or totally any tissue, organ or function of the body, in order to maintain or improve the quality of life of the individual
Definition of biomaterials
-American National Institute of Health
A Biomaterial is any substance that has been engineered to interact with biological systems for a medical purpose - either a therapeutic (treat, augment, repair or replace a tissue function of the body) or a diagnostic one.
Amalgam
Swerdlow and Stanley (1962) reported that the pulp response to amalgam placement is due tocondensation pressure.
•Little pulpal response is elicited when cavity isprepared with high-speed air-water spray techniqueHowever, when cavity is restored with amalgam thepressures of condensation will intensify the responseBoremark and associates (1968) showed thatradioactive mercury reached the pulp in humans after6 days if no cavity liner was used.

.
2
•Implantations tests show that low copper amalgams are well tolerated, but high copper amalgam cause severe reaction.
•Liners are suggested to avoid pulpal reaction.
•Amalgam based on gallium rather than mercury have been developed that are free of mercury.
• Reduced number of odontoblasts
• Dilated capillaries
• Slight to severe inflammatory cell infiltration in the odontoblast layer
Pulp Reactions
Pulp reaction 1 month after application of an amalgam filling. Dilated blood vessels close to the predentin; otherwise, no noteworthy alterations. Distance between pulp and cavity is 0.52 mm
CYTOTOXICITY OF METALS AND DENTAL CASTING ALLOYS
•A study of 43 metal salts, using the colony formation method and two types of cells (fibroblasts and osteoblast like cells), revealed that IC50 depends on the types of metallic elements, their chemical states, and their elemental concentrations•IC50 for the salts with highest toxicity (greater than 10-5mol/L) were CdCl2, VCl3, AgNO3, HgCl2, SbCl3, BeSO4, and InCl3.
•Relatively high-toxicity salts—HgCl, Ti(NO3)3, TINO3, GaCl3, CuCl2, MnCl2, CoCl2, ZnCl2, NiCl2, SnCl2, IrCl4, CuCl, RhCl3, Pb(NO3)2, Cr(NO3)3, and Bi(NO3)3—had IC50s below 10-4 mol/L for each cell line
•Various studies have shown that copper is more toxic thangold, palladium, and titanium. However, this result may bemisleading since copper is more susceptible to corrosion.
•Thus, analyses of cytotoxicity test results should also consider relative corrosion rates of specific elements in various solutions including artificial saliva.
Local toxicity and tissuecompatibility
Dental Ceramics

.
3
Cell Cultures
•Silicon oxide ceramics found to be nontoxic in different cell culture assays (agar overlay test, Millipore filter test, MTT test) when tested on gingival fibroblasts.
•Erbium oxide, used for coloring dental ceramics, also proved to be nontoxic.
•Zirconium oxide ceramics were nontoxic in various cell cultures (human gingival fibroblasts, 3T3 cells, L-929 cells)
Gingival Reactions
•Silicon oxide ceramics are innocuous for the gingiva.
•On various occasions, gingival inflammations adjacent to metal ceramic crowns have been reported. However, this situation should be attributed to the alloy rather than to the ceramic
Pulp Reactions
•Postoperative sensitivities have been observed in a fewcases after the (adhesive) luting of ceramics (inlays, crowns) . However, these complaints could primarily have been caused by luting resin rather than ceramic.
Mutagenicity and Carcinogenicity
•Aluminum oxide ceramics have generated no teratogenic or mutagenic effects in animals, nor were they found to affect fertility.
•Calcium phosphate ceramic was neither carcinogenic nor teratogenic in animal experiments
•Zirconium oxide ceramic reveals a considerablyhigher level of radioactivity compared with aluminum oxide and silicon oxide ceramic.
• However, activity concentration of modern zirconium oxide ceramics is below the administrative threshold values.
Zinc Phosphate Cement
•If zinc phosphate is used instead of ZOE to cement a crown or inlay, the phosphate cement is forced into the dentinal tubules
•After 3-4 days, it creates a wide spread three dimensionalinflammatory lesion involving all the coronal pulp tissue.
•A young tooth with wide – open dentinal tubules is more susceptible to intense response than an older tooth, which has produced sclerotic and reparative dentin that block’s the tubules.
•Zinc phosphate cements elicits strong to moderate cytotoxic reactions that decrease with time after setting Leaching of zinc ions and a low pH is cause of these effects
•Initial pH on setting is 2 at 2 minutes
•Best protection against phosphoric acid penetration is provided by coating the dentin with two coats of an appropriate varnish, a dentin-bonding agent, or a thin wash of calcium hydroxide.
•These procedures eliminate 90% of the severity of the adverse pulp responses, making them similar to those of polycarboxylate cement

.
4
Polycarboxylate cements
•Causes slight to moderate response after 3 days.
•Recommended only in cavities with intact dentin.
Zinc Oxide Eugenol cements
•ZOE is recommended as a nontoxic reference substance in respective
•Cox CF et al 1987 stated that eugenol from ZOE fixes cells, depresses cell respiration and reduces nerve transmission with direct contact
•May form a temporary seal against bacterial invasion.
•Inhibits the synthesis of prostaglandin and leukotriens(anti-inflammatory).
•Interaction of eugenol with vallinoid receptors on nerve cells playing an important role in nociception.
Glass Ionomer Cement
•When GIC first introduced, the pulpal response were classified as bland, moderate, less irritating than silicate cement, zinc phosphate cement
•Blandness of GIC is attributed to absence of strong acids of toxic monomers.
•Polyacrylic acid and polyacids are much weaker than phosphoric acid and possess higher molecular weight that limit their diffusion through dentinal tubules to the pulp.
•Tobias and other (1978), found that glass ionomer cements were less irritating than zinc phosphate cement, equivalent in irritancy to polycarboxylate cement and more irritating than zinc oxide cement.
•If there is less than 0.5-mm residual dentin or a pulp exposure, an appropriate lining of calcium hydroxide should be placed prior to placement of a glass ionomer
calcium hydroxide
•Was introduced to endodontics as a direct pulp-capping agent (Hermann 1920).• Molecular weight – 74.08 g/mol• Dissociation coefficient of Ca(OH) - (0.17)•Low solubility in water•high pH (approximately 12.5–12.8)•In contact with aqueous fluids, dissociates into calcium and hydroxyl ions.
.
5
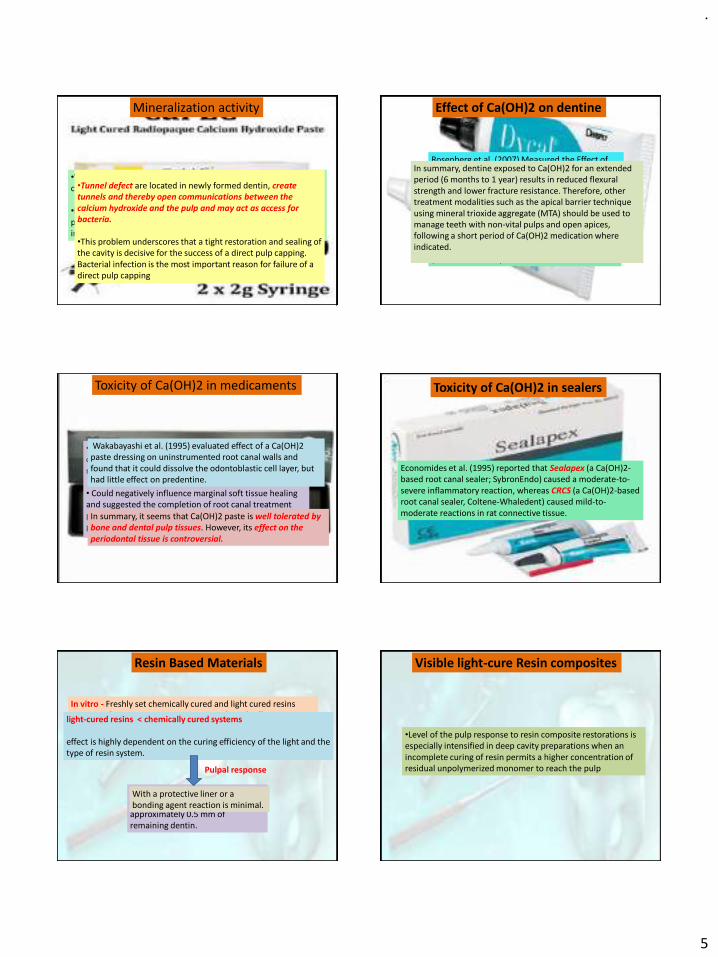
Mineralization activity
•When used as a pulp-capping agent and in apexification, a calcified barrier may be induced by calcium hydroxide.
•Because of the high pH a superficial layer of necrosis occurs in the pulp to a depth of up to 2 mm Beyond this layer, only a mild inflammatory response is seen
•Tunnel defect are located in newly formed dentin, create tunnels and thereby open communications between the calcium hydroxide and the pulp and may act as access for bacteria.
•This problem underscores that a tight restoration and sealing of the cavity is decisive for the success of a direct pulp capping. Bacterial infection is the most important reason for failure of a direct pulp capping
Effect of Ca(OH)2 on dentine
Rosenberg et al. (2007) Measured the Effect of Ca(OH)2 on the micro tensile fracture strength (MTFS) of teeth and found that it was reduced by almost 50% following 7–84 days of application.
A study of bovine dentine maintained in Petri dishes for 5 weeks concluded that Ca(OH)2reduced fracture strength by 32%(White et al. 2002).
In summary, dentine exposed to Ca(OH)2 for an extended period (6 months to 1 year) results in reduced flexural strength and lower fracture resistance. Therefore, other treatment modalities such as the apical barrier technique using mineral trioxide aggregate (MTA) should be used to manage teeth with non-vital pulps and open apices, following a short period of Ca(OH)2 medication where indicated.
Toxicity of Ca(OH)2 in medicaments
•Ca(OH)2 has been reported to have a detrimental effect on periodontal tissues when used as an intracanal medicament
• Could negatively influence marginal soft tissue healing and suggested the completion of root canal treatment prior to the removal of cementum as might occur during periodontal therapy
Wakabayashi et al. (1995) evaluated effect of a Ca(OH)2paste dressing on uninstrumented root canal walls and found that it could dissolve the odontoblastic cell layer, but had little effect on predentine.
In summary, it seems that Ca(OH)2 paste is well tolerated by bone and dental pulp tissues. However, its effect on the periodontal tissue is controversial.
Toxicity of Ca(OH)2 in sealers
Economides et al. (1995) reported that Sealapex (a Ca(OH)2-based root canal sealer; SybronEndo) caused a moderate-to-severe inflammatory reaction, whereas CRCS (a Ca(OH)2-based root canal sealer, Coltene-Whaledent) caused mild-to-moderate reactions in rat connective tissue.
Resin Based Materials
In vitro - Freshly set chemically cured and light cured resins cause moderate cytotoxic reactions in cultured cells over 24 to 72 hours of exposure
light-cured resins < chemically cured systems
effect is highly dependent on the curing efficiency of the light and the type of resin system.
Low to moderate after 3 days whenthey were placed in cavities with approximately 0.5 mm of remaining dentin.
Pulpal response
With a protective liner or a bonding agent reaction is minimal.
Visible light-cure Resin composites
•Level of the pulp response to resin composite restorations is especially intensified in deep cavity preparations when an incomplete curing of resin permits a higher concentration of residual unpolymerized monomer to reach the pulp
.
6
•A more conservative cavity preparation with incremental placement of the resin composite is highly recommended to minimize the pulp response.
•No pulp damage is to be expected if resin-based composites or adhesives are applied in shallow or medium cavities, even after prior acid-etching of the dentin (total etch/total bonding technique).
•In these situations, adhesives may serve as sealants and thus as protection against potentially penetrating bacteria
•In deep cavities, however, especially if microexposure of the pulp cannot be excluded, the use of a calcium hydroxide preparation applied on the deepest part of the cavity is still recommended.
•If a calcium hydroxide suspension is used for this purpose, then it should be covered by suitable glass ionomer cement.
Bioceramics
Refer to biomaterials that are used in direct contact with
living tissue in the medical and dental field. Various types
of bioceramics that are available in medicine and dentistry.
Bioactivity of the materials refers to its ability to create a
hydroxyapatite layer when in contact with tissue fluid rich
in calcium and phosphate. This property allows the material
to be highly biocompatible, osteoinductive,
osteoconductive, and contributes to its sealing ability.
Bioceramic cements
1)Biodentine
2)MTA
3)MTA Angelus
4)ERRM Putty, ERRM Paste, and iRoot FS
Biodentine
•“Biodentine” a calcium silicate based product which became commercially available in 2009 (Septodont) and thatwas specifically designed as a “dentine replacement” material.
•Has a wide range of applications includingendodontic repair (root perforations, apexification, resorptive lesions, and retrograde filling material in endodonticsurgery) and pulp capping and can be used as a dentine replacement material in restorative dentistry
Microleakage
Koubi et al. were the first to assess in vitro marginal integrity of restorations based on aged calcium silicate cement and resin-modified glass ionomer cement
They explained the good marginal integrity of Biodentine as compared to GIC due to ability of calcium silicate materials to form hydroxyapatite crystals at the surface. These crystals might have the potential to increase sealing ability, especially when formed at interface of Material with dentinal walls.
Only disadvantage was related to the operating time that was determined to be longer than the resin modified GIC

.
7
Biocompatibility of Biodentine
Han and Okiji compared Biodentine and white ProRoot MTA in terms of Ca and Si uptake by adjacent root canal dentine andobserved that both materials formed tag-like structures. Theobserved that dentine element uptake was more prominentfor Biodentine than MTA.
In another study by Laurent et al. Biodentine was found to significantly increase TGF-B1 secretion from pulp cells. TGF is a growth factor whose role in angiogenesis, recruitment of progenitor cells, cell differentiation, and mineralization has been high Lighted in recent research.
•In a study performed by Zhou et al. where Biodentinewas compared with white MTA (ProRoot) and glassionomer cement (FujiIX) using human fibroblasts, both whiteMTA and Biodentine were found to be less toxic compared toglass ionomer during the 1- and 7-day observation period.
•Cell adhesion and growth were determined to be more favorablein MTA and Biodentin compared to glass ionomer.
•A recently published article of Biodentine, assessed theproliferative, migratory, and adhesion effect of differentconcentrations of the material on human dental pulp stemcells (hDPSCs) obtained from impacted third molars .
•Biodentine favorably affected healing when placed directly in contact with the pulp by enhancing the proliferation, migration, and adhesion of human dental pulp stem cells, confirming the bioactive and biocompatible characteristics of the material
Biodentine as a vital pulp treatment material
•First study to demonstrate induction of effective dentinal repair was done by Tran et al. where material was applied directlyon mechanically exposed rat pulps. structure induced by Ca(OH)2 contained several cell inclusions, also called tunnel defects.
•On the contrary, dentine bridge formation induced by Biodentine showed a pattern well-localized at the injury site.
•Quality of the formed dentine was also much more favorable compared to calcium hydroxide.
•Complete dentinal bridge formation and absence of an inflammatory response were observed as majorfinding
Due to its superior sealing potential, there is no risk of microleakage which may cause the pulp to become infected or necrotic and jeopardize the success of vital treatment procedures
Laurent et al. done a study by Using an entire human toothculture model, they showed that, upon application on theexposed pulp, Biodentine had the potential to significantlyincrease TGF-B1 secretion from pulp cells and induce an earlyform of reparative dentin synthesis
MTA
Following the introduction of bioceramic materials into clinical endodontics, mineral trioxide aggregate (MTA) has become recognized as the gold-standard material for a variety of clinical situations and is perhaps closest to the ideal reparative material, due to its excellent physicochemical and biological properties
BiocompatibilityMutagenicity
•Ames mutagenicity test was used to assess the mutagenicity of MTA . •Results of this study determined that MTA is not mutagenic

.
8
Vascular Effect
•Investigation on rabbit ear chambers evaluatedthe effect of MTA on microcirculation.
• Investigation showed that 4 weeks after MTA placement, microcirculation was completely restored, and new vessels were formed
•Torabinejad et al have shown that freshly mixed and set MTA and amalgam are less cytotoxic than Super EBA or IRM.
A recent investigation examined the effect of MTA and CH on 3T3fibroblast cells and showed that MTA has a significantly shorter duration of cytotoxicity in comparison to CH
Cell Cultures
Neurotoxicity and Neurologic Effects
With murine cerebral cortical cells, neurotoxic effects of MTA, Diaket, amalgam, and Super EBA were compared on both glial and neuronal cultures. Results showed that all of the materials except MTA are toxic in either freshly mixed or set conditions.
PDL fibroblasts show an osteogenic phenotype, which reflects up-regulation of the expression of alkaline phosphatase, osteonidogen, osteonectin, and osteopontin. Twenty-four–hour cured MTA shows a more favorable response to PDL fibroblast cell types than freshly mixedMTA
Another investigation compared WMTA, Sealapex on macrophages and gingival fibroblasts . Only WMTA showed no adverse effect on the viability of either cell line and not increased the release of prostaglandin E2 (PGE2).
Initial human studies showed that MTA induced less inflammation, hyperemia and necrosis, better formation of odontoblastic layer and create a thicker dentin bridge, compared to calcium hydroxide.
ERRM Putty, ERRM Paste, iRoot FS •Majority of studies concluded that ERRM has minimal in vitro cytotoxicity, Similar to MTA
•Recently, an in vivo study was performed comparing MTA and ERRM Putty, as root-end filling material, using CBCT and micro-CT. Results showed that ERRM Putty achieved a better tissue healing response adjacent to resected root-end surface histologically and a superior healing tendency compared to MTA, when detected by CBCT and micro-CT . Superior performance by ERRM Putty may be due to its better mineralized tissue inductive/conductive properties.

.
9
BioaggregateSealing ability and bond strength of Bioaggregate
•Comparable to MTA and higher than silver amalgam when used as a root-end filling.
In in vitro studies, Bioaggregate also showed higher porosityand fewer cracks at the cement–dentine interface in comparisonwith Biodentinepush-out bond strength values were lower than to MTA.
Calcium-enriched mixture cement(CEMC) and MTA have a similar ability to induce osteoblastic/odontoblastic differentiation, enhance the expression of mineralization-related genes, promote dentine bridge formation in vital pulp, and stimulate cementum deposition when used as root-end filling material
Calcium-enriched mixture cement
•Antimicrobial activity of CEMC against Enterococcus faecalis is comparable to Ca(OH)2 and greater than MTA, because it contains more potent bacterial inhibitors than CSC-based materials.• Antifungal effect of CEMC is comparable to MTA
•Favourable biological response in contactwith MTA and CEM •Studies of complete pulpotomy treatment using CEM, MTA, and
CH have shown that CEM group exhibited lower inflammation,improved quality/thickness of calcified bridge, superior pulp vitality status and morphology of odontoblast cells, compared to CH. no significant differences were identified in comparison to MTA.
Pulpal reactions
Periradicular tissue reactions
An animal study demonstrated that both CEM cement and MTA induced periradicular tissue healing regeneration, including the production of cementum and new bone, when used as root-end filling biomaterials
Microleakage studies
•A study of CEM microleakage and its comparison with IRM and MTA as root-end filling materials in various environments has been done.• Results have shown that the highest sealing ability was seen in CEM, then MTA and the least seal was in IRM.
.
10
TheraCalTheracal
• Ca2+ released from TheraCal serves as a bioactive signaling molecule, which promotes the process of pulpal tissue repair.
•After 28 days, induces complete dentine bridge and mild inflammation when used for direct pulp capping in primate teeth.
•Well-tolerated by immortalized odontoblast- like cells.
•However, cellular proliferation induced by TheraCal is lower than that of Biodentine and MTA.
•Has antibacterial activity against Streptococcus mutans lower than MTA and higher than Biodentine.
BIOCERAMIC SEALERS AND HYBRID BIOCERAMIC SEALERS
CALCIUM
SILICATE BASED
• iRoot SP
• EndoSequence
BC Sealer
MTA BASED
• MTA-Fillapex
• Endo CPM sealer
• MTA-Angelus
• ProRoot Endo Sealer
CALCIUM PHOSPHATE
BASED
• Sankin apatite root
canal sealer(I,II,III)
• Capseal (I,II)
SOLUBILITY
•According to ANSI/ADA Specification 57, solubility is the loss of mass during a period of immersion in water following setting Should not exceed 3% by mass
• Both iRoot SP and MTA-Fillapex are highly soluble, 20.64% and14.89%, respectively, which does not meet ANSI/ADArequirements
• EndoSequence BC was reported to be practically insoluble which is in accordance with ANSI/ADA specifications.
• H.-M. Zhou, Y. Shen, W. Zheng, L. Li, Y.-F. Zheng, and M. Haapasalo,“Physical properties of 5 root canal sealers,” J Endod,vol.39,no.10,pp.1281–1286,2013.
• R. Viapiana, D. L. Flumignan, J. Camilleri, and M. Tanomaru-Filho, “Physicochemical and mechanical properties of zirconium oxide and niobium oxide modified Portland cement-based experimental endodontic sealers,” Int Endod J,vol.47,no.5,pp.437– 448,2014
CROWN DISCOLOURATION
• K. Ioannidis, I. Mistakidis, P. Beltes, and V. Karagiannis, “Spectrophotometric analysis of crown discoloration induced by MTA- and ZnOE-based sealers,” J Appl Oral Sci,vol.21,no.2,pp.138–144,2013.
• SPECTROPHOTOMETRIC ANALYSIS OF CROWN DISCOLORATION INDUCED BY MTA AND ZNOE-BASED SEALERS
• Application of MTA Fillapex in tooth crowns resulted in minimal color alterations, while Roth 811 induced severe discoloration, in vitro.
• IN VITRO COMPUTER ANALYSIS OF CROWN DISCOLOURATION FROM COMMONLY USED ENDODONTIC SEALERS
Sankin apatite III results in the least discolouration nine months after application as compared with AH26, Endofill, Tubli -Seal, and zinc oxide eugenol sealers.
• M. Partovi, A. H. Al- Havvaz, and B. Soleimani, “In vitro computer analysis of crown discoloration from commonly used endodontic sealers,” Aust Endod J,vol.32, no.3,pp.116–119,2006.
BIOCOMPATIBILITY
• EndoSequence BC, iRoot SP, and MTA-Fillapex showed moderate toxicity when freshly mixed; however, cytotoxicity reduced over time until being completely set.
• S. Bilginer, T. Esener, F. S ¨ oylemezoglu, and A. M. Tiftik, “The investigation of biocompatibility and apical microleakage of tricalcium phosphate based root canal sealers,” J Endod,vol.23,no.2,pp.105–109,1997.
.
11
• Sankin apatite type II and type III were found to be more biocompatible than either type I or Grossman’s sealer
• Capseal I and Capseal II sealers have been shown to produce less tissue irritation and less inflammation compared to other sealers.
• D. Mukhtar-Fayyad, “Cytocompatibility of new bioceramic based materials on human fibroblast cells (MRC-5),”Oral Sur Oral Med Oral Pathol Oral Radiol Endod,vol.112,no.6,pp.e137–e142,2011
• T. E. Bryan, K. Khechen, M. G. Brackett et al., “In vitro osteogenic potential of an experimental calcium silicate-based root canal sealer,”J Endod,vol.36,no.7,pp.1163– 1169,2010
BOND STRENGTH
iRoot SP AH Plus MTA Fillapex
• The bond strength of EndoSequence BC Sealer was compared to AH Plus in the presence and absence of a smear layer, finding that the dislocation resistance of EndoSequence BC Sealer was equal to that of AH Plus and with no significant effect on the smear layer
• B.Sagsen, Y. Ust¨un, S.Demirbuga , and K.Pala,“Push-out bond strength of two new calcium silicate-based endodontic sealers to root canal dentine,” Int Endod J,vol.44, no.12,pp.1088–1091,2011.
• N.Shokouhinejad, H.Gorjestani, A.A.Nasseh, A.Hoseini and A. R. Shamshiri, “Push-out bond strength of gutta-percha with a new bioceramic sealer in the presence or absence of smear layer,” Australian Endodontic Journal,vol.39, no.3,pp.102–106,2013.
Endo-CPM sealer MTA Fillapex AH Plus(8.265 MPa) (2.041 Mpa)
•CPM sealer is advantageous when a post preparation is required
• E. Assmann, R. K. Scarparo, D. E. B¨ottcher, and F. S. Grecca, “Dentin bond strength of two mineral trioxide aggregate-based and one epoxy resin-based sealers,”Journal of Endodontics,vol. 38,no.2,pp.219–221,2012
(3.034 Mpa)
ANTIMICROBIAL PROPERTIES
• iRoot SP sealer had a high pH value (11.5) even after setting but that its antibacterial effect was greatly diminished after seven days
H.Zhang,Y.Shen,N.D.Ruse,and M.Haapasalo,“Antibacterial activity of endodontic sealers by modified direct contact test against Enterococcus faecalis,” J Endod,vol.35,no. 7,pp.1051–1055,2009.
• The pH of the Endo CPM suspension was greater than that of MTA-Fillapex(>11); however, the bacterial inhibition zone produced by MTA-Fillapex was greater than that produced by Endo CPM .
• Nevertheless, neither sealer was able to sustain its antibacterial activity after setting despite their initial high pH levels.
R.D.Morgental, F.V.Vier-Pelisser, S.D.Oliveira, F.C.Antunes, D. M. Cogo, and P. M. P. Kopper, “Antibacterial activity of two MTA-based root canal sealers,” Int Endod J,vol.44,no.12,pp.1128–1133,2011.
MICROLEAKAGE
✓ AH Plus and Sealapex were the most resistant against bacterial leakage. Active GP and the MTA-based materials (Endo CPM
Sealer and MTAS) were less resistant to coronal leakage
The MTA-based sealers had the most leakage.
Oliveira ACM, Tanomaru JMG, Faria-Junior N, Tanomaru-Filho M. Bacterial leakage in root canals filled with conventional and MTA-based sealers. Int Endod J 2011;44: 370–5

.
12
Stereomicroscopic dye leakage measurement of six different root canal sealers
Zinc oxide eugenol based sealer, Sealapex, AH Plus, MTA Plus, EndoRez, Endosequence BC. All the specimens were examined under stereomicroscope for microleakage ✓ The Endosequence BC group showed the least dye leakage and
the highest leakage was seen in Zinc oxide Eugenol based sealer
Srinidhi V. Ballullaya et al.Journal of Clinical and Diagnostic Research. 2017 Jun, Vol-11(6)
• ENDOSEAL MTA is a paste-type root canal sealer based on pozzolan cement that has excellent physical and biological properties of MTA
ENDOSEAL MTA
✓Exhibit not only Against Gram-negative bacteria but also exhibited substantial antimicrobial activity to E. faecalis incomparison with Endosequence BC sealer which exhibits weak antibacterial effect on all bacteria studied.
ANTIBACTERIAL PROPERTIES
Lim ES, Park YB, Kwon YS, Shon WJ, Lee KW, Min KS. Physical properties and biocompatibility of an injectable calcium-silicate-based root canal sealer: in vitro and in vivo study. BMC oral health 2015;15(1):129.
X-ray fluorescence analysis Greater profile and greater quantities of oxide compounds such as Al2O3, Fe2O3, Mgo, Na2O, NiO, and SO2 in comparison with Endosequence BC sealer
➢ Exhibit strong antimicrobial activity.
Lim ES, Park YB, Kwon YS, Shon WJ, Lee KW, Min KS. Physical properties and biocompatibility of an injectable calcium-silicate-based root canal sealer: in vitro and in vivo study. BMC oral health 2015;15(1):129.
TOOTH DISCOLOURATION
In vitro studies comparing Endoseal MTA to both AH Plus and conventional MTA (ProRoot; Dentsply, Tulsa, OK, USA)
•Less discoloration than conventional MTA
•No significant difference in brightness change or total color change when compared to AH Plus and control.
Lee DS, Lim MJ, Choi Y, Rosa V, Hong CU, Min KS. Tooth discoloration induced by a novel mineral trioxide aggregate-based root canal sealer. European journal of dentistry 2016;10(3):403-407.
BIOCOMPATIBILITY
da Silva EJ, Zaia AA, Peters OA. Cytocompatibility of calcium silicate-based sealers in a three-dimensional cell culture model. Clinical oral investigations. 2017 Jun 1;21(5):1531-6.
.
13
Biocompatibility of nanoparticles as biomaterials in dentistry
Silver nanoparticles
•To avoid the build-up of biofilms over composites and in restorations margins, AgNPs are incorporated into composite resins•Zhang et al. studied the biocompatibility of AgNPs as restorative materials.
•AgNPs were incorporated at 0.05% by mass into a primer and an adhesive, which were then tested for human gingival fibroblast viability.
•Incorporation of AgNPs did not induce any cytotoxicity andsubstantially enhance the antibacterial potency of the primer and the adhesive.
•Tschoppe et al. investigated in vitro effects of HAP NP toothpastes on remineralization. Samples were obtained from bovine incisors. A quarter of all specimens were covered with acid-resistant varnish, which served as controls
•Increased remineralization of dentin and enamel was observed with toothpastes containing HAP NPs compared with amine fluorid toothpastes
Hydroxyapatite nanoparticles
•Various studies showed that HAP NPs can stimulate cell proliferation to a considerable extent and can contribute to periodontal tissue regeneration
Dabbagh et al. analyzed the effect of polyethylene glycol (PEG)- coated maghemite NPs (PEG-MNPs) in the treatment of dentin hypersensitivity. These NPs blocked the dental tubules via an external magnetic field because of their superparamagnetic properties
•Priyadarshini et al. analyzed in vitro and ex vivo effects of novel PCL nanocapsules (nano-PCL) loaded with CHX in various ratios compared with unloaded nanocapsules.
• A ratio of 125:50 of nano-PCL-CHX in SEM as well as transmission electron microscopy (TEM) showed deeper diffusion and retention of CHX within dentin tubules ex vivo and in vitro.
• Thus, this study revealed a novel nanosized drug delivery system for demineralized surfaces of dentin and resin dentin interfaces .
Polymeric nanoparticles in dentistry
Chitosan nanoparticle
•Early enamel carious lesions can also be remineralized by the use of CSNPs . CSNPs have also shown success in endodontic treatment because of their antibacterial.
•Compared with calcium hydroxide, CSNPs showed amarked reduction in Enterococcus faecalis.Highantimicrobial effects on biofilms of Streptococcus mutans were also observed .
Bioactive Bioglass
•At present, researchers in the field of biomaterials are focusing on tissue engineering and tissue regeneration. One of the accessible materials is bioactive glass (BAG)
•Originally, BAG was commercially trademarked as Bioglass 45S5

.
14
GUTTA PERCHA
Using Resilon or Gutta-percha cones implanted into the dorsal connective tissue of rats, Onay et al. have shown that both materials induced a moderate to severe inflammatory reaction at 1-week time point, which decreased at 8-week observation time point and Bodrumlu et al. have shown that Resilon or gutta-percha cones exhibited less inflammation after the first post-operative week, which subsided by the 60th day
However, in the present study, quantitative measurement showed, at 60 days and over time, suggests that long-term biocompatibility of Resilon, despite validated, is inferior to gutta-percha control.
Conditioning (etching) agents
•Before a resin composite or a GIC restorative material is placed, surface contaminants must be removed to permit the micro mechanical attachment or the ionic exchange of the dental material with the tooth structure.
•Brannstrom and Nordenvall (1977) noted no significant difference between dentinal surface conditioned for 15 seconds and those conditioned for 2 seconds and thus recommended shorter conditioning times.
•Brannstrom (1981), showed that conditioning of dentin and removal of smear layer allows the ingress of bacteria and the outward flow of dentinal fluid within the tooth – material inter facial region resulting in biofilm formation that interfaces withadhesion.
•Some scientists recommend that smear layer showed remain but in modified form, where as some other propose that the smear layer be completely removed
•Bowen and colleagues (1982) introduced mordanting solution (acidified ferric oxalate), that appeared to dissolve the original smear layer and replace it with a more uniform ‘artificial’ (altered) smear layer.
•With the use of less concentrated acids with higher molecular weights and shorter time intervals for conditioning, pulp response is minimized.

.
15
Dentin Bonding
• Strength of bonds to Enamel > Dentin
• Because of its composition (being both organic and inorganic) wetness, and lower mineral content
• Because the dentinal tubules and their resident odontoblasts are extensions of the pulp, bonding to dentin also involves biocompatibility issues.
• After being cut dentin is covered by 1- to 2-μm layer of organic and inorganic debris named as smear layer
Numerous acids, including phosphoric, hydrochloric, citric and lactic acids have been used to remove the smear layer.
Effect of these acids on pulp tissuesdepends on a number of factors
Degree of etching
Strength of the acid
Remaining dentin thickness
A dentin thickness of 0.5 mm has proved adequate. According to Usage tests effects of acids have shown phosphoric, pyruvic, and citric acids produce moderate pulpal inflammatory responses, resolves after 8 weeks.
Conclusion-All acid solutions used removed superficial smear layer, increasing the width of dentinal tubule apertures to greater or lesser degrees. When observing the fractured surface, acid solutions provided a mean demineralization in depth of dentinal tubules of 9.83 µm, except for maleic acid.
Bonding Agents
Longer-term in vitro studies - components of the bonding agents may penetrate up to 0.5 mm of dentin and cause significant suppression of cellular metabolism for up to4 weeks after application.
Hydroxyethyl methacrylate (HEMA)
may penetrate up to 0.5 mm of dentin and cause significantsuppression of cellular metabolism for up to 4 weeks after application.
A hydrophilic resin contained in several bonding systems is at least 100 times less cytotoxic in tissue culture than Bis-GMA.
If the dentin in the floor of the cavity preparation is thin (<0.1mm) there is some evidence HEMA is cytotoxic in vivo
Release of matrix metalloproteinases (MMPs) from dentin by virtue of its interaction with the acid components. Application of an MMP inhibitor, such as chlorhexidine has beenshown to minimize this effect and has been recommended for maintaining the durability of the dentin bond.

.
16
•These agents contain peroxides•Peroxides can penetrate the intact enamel and reach the pulp.
Bleaching agents
•Occurrence of tooth sensitivity is very common with the use of these agents.•Bleaching agents will also damage the gingiva, if not isolated properly.
Adverse effects and drawbacks of Dental restorative materials
Conclusion
•Biocompatibility of a dental material depends on its composition, location, and interactions with oral cavity.
•Metal, ceramic, and polymer materials elicit different biological responses because of differences in composition.
•Furthermore, diverse biological responses to these materials depend on whether they release their components and whether those components are toxic, immunogenic, or mutagenic at the released concentrations.
•Dental restorative materials interact continuously with the oral environment. From the time of placement they are subjected to constant degradation, both mechanical and chemical. One cannot assume that the placed restoration material remains stable during function. On the contrary, it undergoes relentless change.
•When addressing the question of biocompatibility, the clinician should consider the properties of the materials in the hostile oral environment, rather than the inert material itself, taking into account that all dental materials keep on changing and reacting while functioning.
References

.
17

.
1
BIOFILM IN ENDODONTICS
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENTS
◦ INTRODUCTION
◦ DEFINITION
◦ COMPOSITION OF BIOFILM
◦ DEVELOPMENT OF BIOFILM
◦ CLASSIFICATION OF ENDODONTIC BIOFILMS
◦ BIOFILM IDENTIFICATION TEHNIQUES
◦ ERADICATION OF BIOFILM
◦ CONCLUSION
INTRODUCTION
▪Endodontic disease is a biofilm-mediated infection, and primary aim in the management of endodontic disease is the elimination of bacterial biofilm from the root canal system.
▪ It is important to apply the biofilm concept to endodontic microbiology to understand the pathogenic potential of the root canal microbiota as well as to form the basis for new approaches for disinfection.
◦ Biofilm is a mode of microbial growth where dynamic communities of interacting sessile cells are irreversibly attached to a solid substratum, as well as each other, and are embedded in a self made matrix of extracellular polymeric substance(EPS) -Ingle
◦ Biofilm is defined as a community of microcolonies in an aqueous solution that is surrounded by a matrix of glycocalyx, which also attaches the bacterial cells to a solid substratum. -Grossman
DEFINITION
Biofilms grow virtually everywhere, in almost any environment where there is a combination of • Moisture• Nutrient supply• Surface
Sites include:• Natural materials above and
below ground• Metals and plastics• Medical implant materials• Plant and body tissue
Staph aureus Biofilm on a
catheter
Candida albicans biofilm
on dental implant
Biofilms are characterized by:
• Surface attachment• Extracellular matrix of polymeric substances• Structural heterogenicity• Genetic diversity• Complex community interactions

.
2
• The ability to self-organize
Autopoiesis
• Resist environmental perturbations
Homeostasis• Effective
in association than in isolation
Synergy
• Respond to environmental changes as a unit rather than as single individuals
Communality
BASIC CRITERIA FOR A BIOFILM
Caldwell DE, Atuku E, Wilkie DC, Wivcharuk KP, Karthikeyan S, Korber DR. Germ theory vs. community theory in
understanding and controlling the proliferation of biofilms. Advances in dental research. 1997 Apr;11(1):4-13.
◦ Composed primarily of microbial cells and glycocalyx like matrix( extracellular polymeric substance)
◦ Fully developed biofilm is described as heterogenous arrangement of microbial cells on a solid surface
The Root Canal BiofilmEditors: Chávez de Paz, Luis E., Sedgley, Christine M., Kishen, Anil (Eds.)
COMPOSITION OF BIOFILM
• Basic structural unit of a biofilm is the microcolonies or cell cluster formed by the surface adherent bacterial cells
◦ It is composed of
- 85% matrix (polysaccharides, proteins, nucleic acids and salts)
- 15% bacterial cells
• A fully hydrated biofilm appears like a mushroom / tower shape.
◦ Water channels are primitive circulatory system in biofilms, establish connection between microcolonies
✓ -facilitate exchange of material between bacterial cells and bulk fluid
✓ -Coordinate functions in a biofilm community
MATRIX
A glycocalyx matrix made up of extracellular polymeric substance (EPS) surrounds the microcolonies and anchors the bacterial cells to the substrate
Functions:✓Maintains the integrity of biofilms✓Prevents dessication✓Resists antimicrobial agents✓Creates a nutritionally rich environment✓Acts as a buffer and retains extracellular enzymes
◦ Quorum sensing is a bacterial cell-to-cell communication system, using chemical signaling molecules
◦ Quorum sensing is mediated by low molecular weight molecules- autoinducers eg competence-stimulating peptide (CSP) which is important to co-ordinate gene expression.
QUORUM SENSING

.
3
• Symbiosis
• Virulence• Antibiotic
production• Motility• Sporulation
• Bioflm formation
◦ Specific quorum sensing genes have also been implicated in the biofilm forming ability of E. fecalis (e.g., S-ribosylhomocysteinelyase [luxS]).
DEVELOPMENT
Stage 1 Formation of conditioning layer
◦ Biofilm formation occurs in three stages
Stage 2 Planktonic bacterial cell attachment
Stage 3 & 4Bacterial growth and biofilm maturationDetachment of biofilm microcolonies
Phase 1 (transport of microbe to the substrate surface)Phase 2 (initial non-specific microbial-substrate adherence phase)Phase 3 (specific microbial-substrate adherence phase)
➢The earliest stage of biofilm formation involves the adsorption of macromolecules in the planktonicphase to the surface, leading to the formation of a conditioning film.
➢On tooth surfaces, the conditioning film is comprised of proteins and glycoproteins from saliva and gingival crevicular fluid, and some secreted microbial products.
➢This conditioning film is always formed prior to the arrival of microorganisms and selectively promotes adhesion of certain microorganisms.
STAGE 1 Formation of conditioning layer
• Phase 1 (transport of microbe to the substrate surface)
• The nature of initial bacteria-substrate interaction is determined by physicochemical properties such as surface energy and charge density.
• The bacteria adhere to a substrate by bacterial surface structures such as fimbriae, pili, flagella, and EPS (glycocalyx).
• Bridges are formed between the bacteria and the conditioning film by these bacterial structures.
STAGE 2 Planktonic bacterial cell attachment
Phase 2 (initial non-specific microbial-substrate adherence phase)
◦Molecular-specific interactions between bacterial surface structures and substrate become active.
◦ These bridges are a combination of electrostatic attraction, covalent and hydrogen bonding, dipole interaction, and hydrophobic interaction.
P. gingivalis, Streptococcus mitis, Streptococcus salivarius, P. intermedia, Streptococcus mutans are some of the oral bacteria possessing surface structures

.
4
Phase 3 (specific microbial-substrate adherence phase)
◦ With the help of polysaccharideadhesin or ligand formation which binds to receptors on the substrate, specific bacterial adhesion with a substrate is produced.
➢The third stage involves multiplication and metabolism of attached microorganisms that ultimately will result in a structurally organized mixed microbial community.
➢During this stage the inherent characteristics of the microorganisms and the nature of the microenvironment influence growth and succession of microorganisms in the biofilm.
Stage 3 Bacterial growth and biofilm maturation
◦ Recognition between a suspended cell and a cell already attached to substratum- co-adhesion
◦ Genetically distinct cells recognize and clump together - co- aggregation
◦ Involves the deattachment of biofilmmicroorganisms into their surroundings which are of two types –
seeding dispersal by hydrolysis and
clumping dispersal by erosion (simple detachment in single/ sloughing-massive
Stage 4Detachment of biofilm microcolonies
BIOFILM FORMATION
CLASSIFICATION OF ENDODONTIC BIOFILMS
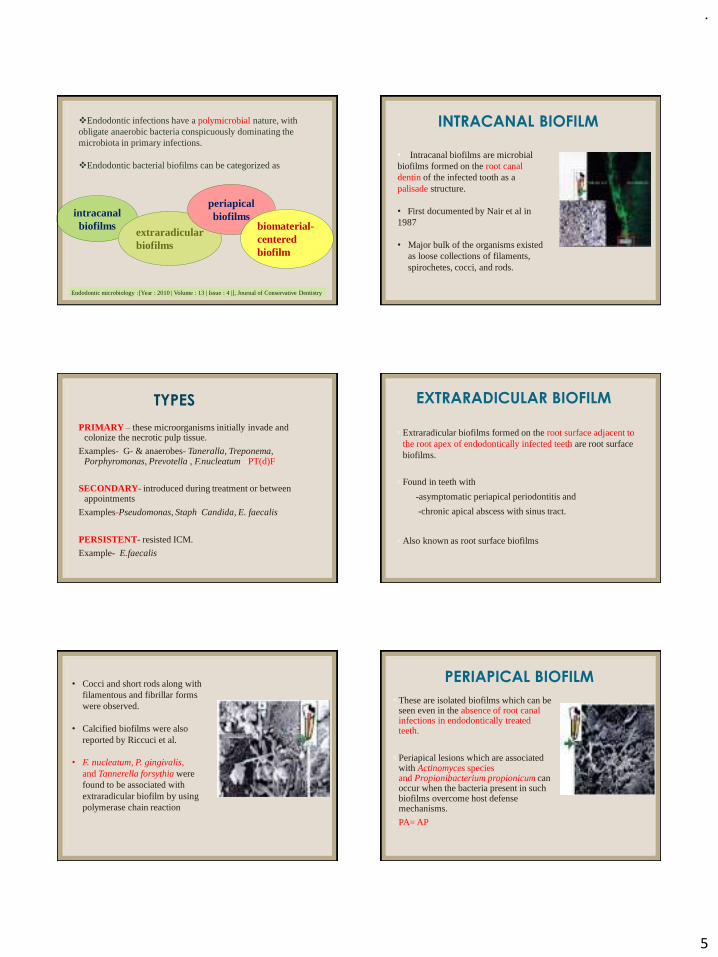
.
5
intracanalbiofilms
❖Endodontic infections have a polymicrobial nature, with obligate anaerobic bacteria conspicuously dominating the microbiota in primary infections.
❖Endodontic bacterial biofilms can be categorized as
extraradicularbiofilms
periapicalbiofilms
biomaterial-centeredbiofilm
Endodontic microbiology :[Year : 2010 | Volume : 13 | Issue : 4 |], Journal of Conservative Dentistry
• Intracanal biofilms are microbial biofilms formed on the root canal dentin of the infected tooth as a palisade structure.
• First documented by Nair et al in 1987
• Major bulk of the organisms existed as loose collections of filaments, spirochetes, cocci, and rods.
INTRACANAL BIOFILM
TYPES
PRIMARY – these microorganisms initially invade and colonize the necrotic pulp tissue.
Examples- G- & anaerobes- Taneralla, Treponema, Porphyromonas, Prevotella , F.nucleatum -PT(d)F
SECONDARY- introduced during treatment or between appointments
Examples-Pseudomonas, Staph, Candida, E. faecalis
PERSISTENT- resisted ICM.
Example- E.faecalis
◦ Extraradicular biofilms formed on the root surface adjacent to the root apex of endodontically infected teeth are root surface biofilms.
◦ Found in teeth with
-asymptomatic periapical periodontitis and
-chronic apical abscess with sinus tract.
◦ Also known as root surface biofilms
EXTRARADICULAR BIOFILM
• Cocci and short rods along with filamentous and fibrillar forms were observed.
• Calcified biofilms were also reported by Riccuci et al.
• F. nucleatum, P. gingivalis, and Tannerella forsythia were found to be associated with extraradicular biofilm by using polymerase chain reaction
◦ These are isolated biofilms which can be seen even in the absence of root canal infections in endodontically treated teeth.
◦ Periapical lesions which are associated with Actinomyces species and Propionibacterium propionicum can occur when the bacteria present in such biofilms overcome host defensemechanisms.
◦ PA= AP
PERIAPICAL BIOFILM

.
6
◦ Foreign body-centered biofilm is found when bacteria adhere to an artificial biomaterial surface and form biofilm structures. It is also known as biomaterial-centeredinfection.
◦ E. faecalis, Str. sanguinis, Streptococcus pyogenes, Staphylococcus aureus form biofilm on GP points.
BIOMATERIAL CENTERED BIOFILM◦ A study investigated the initial biofilm-forming ability of
root canal isolates on gutta percha in vitro.
◦ E.faecalis and S. sanguinis biofilms were significantly thicker than others
◦ P.gingivalis and P.intermedia did not form biofilms on gutta percha
◦ Suggests that gram positive facultative anaerobes have the ability to colonize and form extracellular matrices on gutta percha points.
◦ Serum plays a crucial role in biofilm formation.
Takemura N, Noiri Y, Ehara A, Kawahara T, Noguchi N, Ebisu S. Single species biofilm‐forming
ability of root canal isolates on gutta‐percha points. European journal of oral sciences. 2004
Dec;112(6):523-9.
A- biofilm on gutta perchaB- E.faecalis on biofilm
BIOFILM IDENTIFICATION TECHNIQUES
.
effective antimicrobial
therapy
understanding the disease initiation and progression
Accurate identification
of micro-organisms
Biofilm models and methods of biofilm assessment , Endodontic Topics 2012, 22, 58–78 Anil Kishen &
Markus Haapasalo
thickness (mono-layered or
multilayered)
number and type of
microorganism,
vitality (dead/living cells) of the resident microbial population,
age
structure (homogeneous, irregular, dense, porous),
BIOFILM ASSAYS
surface topography (peaks and valleys) of
biofilms
BIOFILM ASSAYS

.
7
Different techniques such as
◦ (i) Microbiological culture techniques,
◦ (ii) Calorimetric techniques,
◦ (iii) Microscopic techniques,
◦ (iv) Physical methods,
◦ (v) Biochemical methods, and
◦ (vi) Molecular methods are used to study biofilm assays.
◦ The biofilm formed on a substrate can be quantified directly by the Colony Forming Units (CFU) of the viable bacteria adhering to the surface
◦ Several protocols recommend the removal of biofilm bacteria from the substrate by a sonication or centrifugation process.
◦ In such cases, the CFU is usually determined from the supernatant obtained after the sonication/centrifugation procedure
MICROBIOLOGIC CULTURE TECHNIQUE
◦ However, the CFU may only detect bacteria that are able to initiate cell division at a sufficient rate to form colonies and whose growth requirements are supported by the culture medium used.
◦ It is a semi-quantitative method based on dye uptake by the bacterial cells in a biofilm
◦ In this assay, after the bacterial biofilm is stained with a dye (e.g. crystal violet), it is disrupted using a known quantity of alcohol or a surfactant (sodium dodecyl sulfate) and the intensity of the eluted dye is measured using a spectrophotometer
CALORIMETRIC TECHNIQUE
◦ This is an easy assay that allows the rapid quantification of biofilm bacteria.
• However, this test may sometimes be difficult to interpret because the absorbance/optical density measured is a reflection of the number of bacteria and is not a true indicator of the EPS in the biofilm structure.
◦ Light microscopy is the fundamental technique used for biofilm assays
◦ It is a relatively inexpensive, simple to use, rapid, and readily available method.
MICROSCOPIC TECHNIQUE

.
8
◦ In the microscopic method, the bacterial biofilm is stained with a suitable dye that is fluorescent (e.g. propidium iodide) or non-fluorescent in nature (e.g. safranin).
◦ The biofilm slime may be stained with Alcian blue, a phthalocyanine dye that stains acidic mucopolysaccharides and glycosaminoglycans in the EPS
• Scanning Electron Microscopy (SEM) and Transmission Electron Microscopy (TEM) have been effective workhorses in biofilm analyses for many years.
• High resolution electron microscopy has been employed for the morphological and structural characterization of microbial biofilms.
• The main disadvantage with these techniques is the need for extensive sample preparation steps such as fixation, dehydration, freeze- or critical point-drying, and sputtering. These treatments can deeply affect the original biofilm morphology
SEM images of a) E. faecalis cells adhering to root canal dentin b) multi-layered biofilm of E.faecalis on root canal dentin
• CLSM is a particularly important biofilm analysis technique that is restricted to 50–200-mm-thick biofilm structures.
• Green fluorescent protein (GFP) tagging of certain bacterial strains such as Pseudomonas aeruginosa is utilized to study biofilm formation.
◦ CLSM reconstruction of E. faecalis biofilm
◦ Left: the biofilm has received no treatment
◦ Right: the biofilm has been subjected to Light Activated Disinfection with methylene blue and laser
• Fluorescence in situ hybridization (FISH) technique uses probes to target specific 16S rRNA sequences in bacteria.
• It is applied for the simultaneous analysis of the spatial distribution of both Gram positive and Gram-negative bacteria in biofilms.
• FISH is a recognized tool for the specific and sensitive identification of target organisms within complex microbial communities.
• Visualization of FISH labeled cells in biofilms can be carried out by fluorescent microscopy and CLSM
.
9
The ultrastructure of (A) a typical
mature biofilm of E. faecalis on root
canal dentine after 6 weeks under (B) LM, (C) CLSM, and (D) SEM.
Kishen A, George S, Kumar R. Enterococcus faecalis‐mediated biomineralized biofilm formation on root canal dentine in vitro. Journal of Biomedical Materials Research Part A: An Official Journal of The Society for Biomaterials, The Japanese Society for Biomaterials, and The Australian Society for Biomaterials and the Korean Society for Biomaterials. 2006 May;77(2):406-15.
◦ The difference in the fine adjustment settings of microscope can be used to calculate the thickness
◦ The substrate can be weighed before biofilm growth (with the assumption that no substrate solubilization occurred during biofilm formation) and then cleaned, dried, and weighed again in order to record the dry biofilm weight.
PHYSICAL METHODS: THICKNESS, WEIGHT, AREA AND DENSITY MEASUREMENTS
If both wet and dry weight measurements on the same biofilm sample are performed, the approximate density may be determined by assuming that the volume of the biofilm sample is the same as the water volume estimated as the wet weight minus the dry weight
DENSITY=VOLUME OF THE BIOFILM
VOLUME= WET WEIGHT-DRY WEIGHT
◦ Microbial biomass denotes the total number of microbes in a given area.
◦ The measurement of microbial biomass is considered to be a rapid method and includes measurements of the wet or dry weight of the entire biofilm, measurements of the cell contents, measurements of the cellular activities or viable cells,
BIOCHEMICAL METHODS: BIOMASS AND EXTRACELLULAR MATRIX (ECM)
◦ Adenosine triphosphate (ATP) bioluminescence is widely used to determine the metabolic activity of a bacterial population.
◦ One method that is used for the early detection of viable bacteria is based on metabolic activity.
◦ Molecular biological techniques have provided a great deal of genetic information on biofilm bacteria.
◦ Enzyme-linked immunosorbent assay (ELISA) is a very sensitive method used to detect the presence of antigens or antibodies of interest in a sample.
◦ ELISA can be used for quantitative analysis.
◦ ELISA may be used to quantify the population of a particular bacterium in a mixed biofilm.
MOLECULAR BIOLOGICAL METHODS
.
10
◦ Polymerase chain reaction (PCR) is a method that allows exponential amplification of short DNA sequences.
◦ This method of analysis is mostly used as a qualitative tool for detecting the presence or absence of a particular bacterial DNA.
◦ RT-PCR enables both detection and quantification of one or more specific sequences in a DNA sample.
• Microbiologic studies for identification of the species participating in endodontic infections can be chronologically divided into five generations on the basis of the different strategic approaches used
◦ Atomic force microscopy (AFM) has been applied recently to study the forces of interaction between bacteria cells and between bacteria cells and substrates
MISCELLANEOUS ADVANCED TECHNIQUES • Fourier Transform Infra-Red
(FTIR) spectroscopy has been applied to characterize the chemical composition of mature biofilm structures.
• FTIR spectroscopy can be used for the qualitative and quantitative analysis of the chemical constituents on a biofilm structure
• Nuclear magnetic resonance (NMR) is a powerful analytical tool and has been applied to study the constituents of bacterial biofilm.
• NMR spectroscopy techniques has been used as a non-invasive method to obtain metabolic information of bacterial cells.
Kishen A, Haapasalo M. Biofilm models and methods of biofilm assessment. Endodontic Topics. 2010 Mar;22(1):58-78.
NMR 3D structure of
E. faecalis
ERADICATION OF BIOFILM
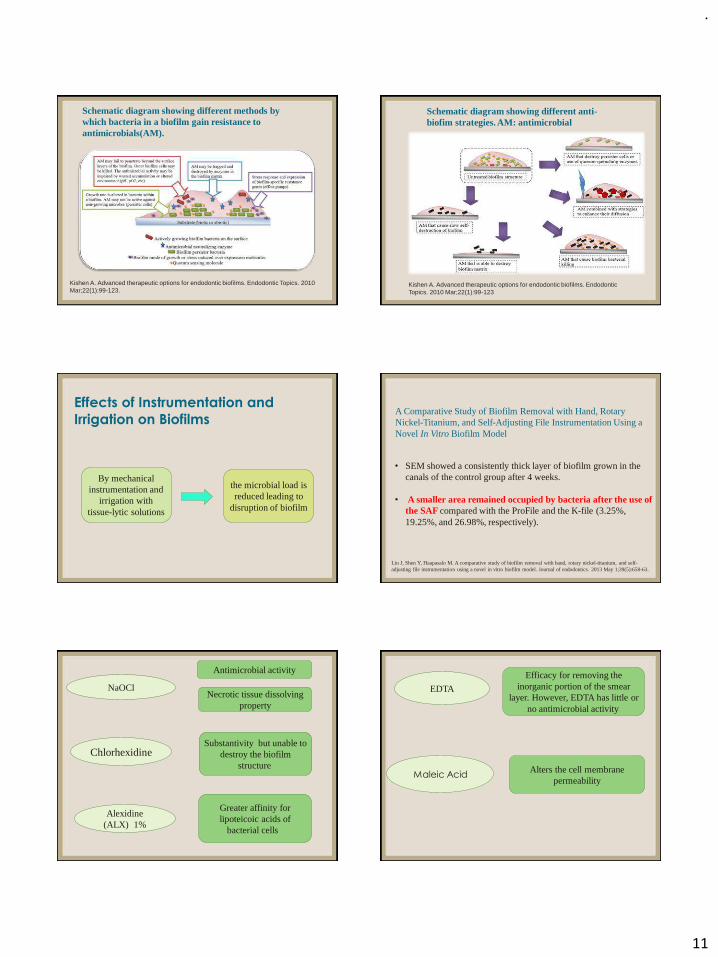
.
11
Kishen A. Advanced therapeutic options for endodontic biofilms. Endodontic Topics. 2010 Mar;22(1):99-123.
Schematic diagram showing different methods by which bacteria in a biofilm gain resistance to antimicrobials(AM).
Schematic diagram showing different anti-biofim strategies. AM: antimicrobial
Kishen A. Advanced therapeutic options for endodontic biofilms. Endodontic Topics. 2010 Mar;22(1):99-123
By mechanical instrumentation and
irrigation with tissue-lytic solutions
the microbial load is reduced leading to
disruption of biofilm
Effects of Instrumentation and
Irrigation on Biofilms A Comparative Study of Biofilm Removal with Hand, Rotary Nickel-Titanium, and Self-Adjusting File Instrumentation Using a Novel In Vitro Biofilm Model
• SEM showed a consistently thick layer of biofilm grown in the canals of the control group after 4 weeks.
• A smaller area remained occupied by bacteria after the use of the SAF compared with the ProFile and the K-file (3.25%, 19.25%, and 26.98%, respectively).
Lin J, Shen Y, Haapasalo M. A comparative study of biofilm removal with hand, rotary nickel-titanium, and self-adjusting file instrumentation using a novel in vitro biofilm model. Journal of endodontics. 2013 May 1;39(5):658-63.
NaOCl
Antimicrobial activity
Necrotic tissue dissolving property
Chlorhexidine
Alexidine(ALX) 1%
Greater affinity for lipoteicoic acids of
bacterial cells
Substantivity but unable to destroy the biofilm
structure
EDTA
Efficacy for removing the inorganic portion of the smear
layer. However, EDTA has little or no antimicrobial activity.
Maleic AcidAlters the cell membrane
permeability

.
12
Spratt et al. evaluated the effectiveness of NaOCl (2.25%), 0.2% chlorhexidine gluconate (CHX), 10% povidone iodine, 5 ppm colloidal silver, and phosphate-buffered saline (PBS) solution (as control) against five root canal isolates including Prevotella intermedia, Peptostreptococcus micros, Streptococcus intermedius, Fusobacterium nucleatum, and E. faecalis.
Spratt DA, Pratten J, Wilson M, Gulabivala K. An in vitro evaluation of the antimicrobial efficacy
of irrigants on biofilms of root canal isolates. Int Endod J 2001;34:300-7.
NaOCl was the most effective antimicrobial, followed by the iodine
solution.Tetraclean
Is a mixture of doxycycline hyclatepresent at a lower concentration than MTAD, an acid, and detergents, has
the ability to eliminate microorganisms and smear layer in
dentinal tubules of infected root canals with a final 4-min rinse.
It has been shown to be as effective as NaOCl and superior to CHX against Enterococcus fecalis and mixed plaque bacteria in planktonicand biofilm states
QMiX is a mixture of CHX,
EDTA and a detergent
BioPure MTADis a mixture of 3%
doxycycline, 4.25% citric acid and 0.5%
Tween 80
Has been described as a universal irrigating solution.Torabinejad et al. have shown that MTAD removes the smear layer safely; also, it is effective against E. faecalis and it can eliminate bacteria in human root canals that had been infected by whole saliva.
Prabhakar et al., showed complete inhibition of bacterial growth by MTAD in a 3 week old biofilm .
In contrast, some studies have concluded that MTAD did not have good antibacterial activity against E. fecalis
Prabhakar, J.; Senthilkumar, M.; Priya, M.S.; Mahalakshmi, K.; Sehgal, P.K.; Sukumaran, V.G. Evaluation of antimicrobial efficacy of herbal alternatives (Triphala and green tea polyphenols), MTAD, and 5% sodium hypochlorite against Enterococcus faecalis biofilm formed on tooth substrate: An in vitro study. J. Endod. 2010, 36, 83–86.
NaOCl in different concentrations
Studies have show that the antimicrobial activity is not concentration dependent, but tissue dissolution and biofilm disruption are concentration dependent
Clegg et al. evaluated the effectiveness of three concentrations of NaOCl (6%, 3%, and 1%), 2% CHX, and BioPure MTAD on apical dentin biofilms in vitro.
Clegg MS, Vertucci FJ, Walker C, Belanger M, Britto LR. The effect of exposure to irrigant solutions on
apical dentine biofilms in vitro. J Endod 2006;32:434-7.
6% NaOCl was the only irrigant capable of both rendering the bacteria nonviable and
physically removing the biofilm
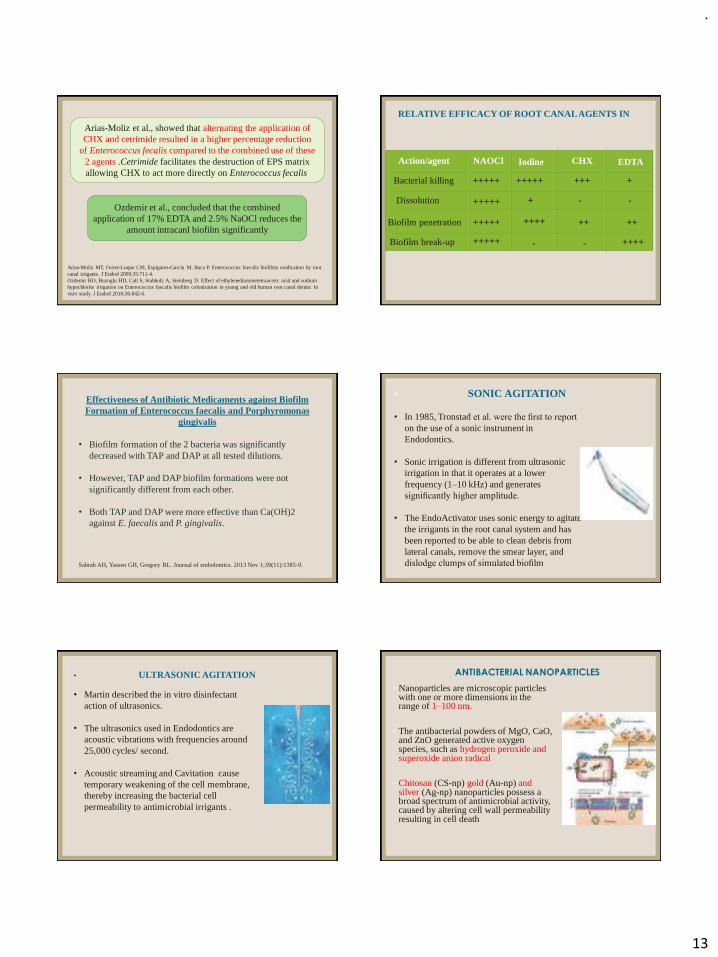
.
13
Arias-Moliz et al., showed that alternating the application of CHX and cetrimide resulted in a higher percentage reduction
of Enterococcus fecalis compared to the combined use of these 2 agents .Cetrimide facilitates the destruction of EPS matrix allowing CHX to act more directly on Enterococcus fecalis
Arias-Moliz MT, Ferrer-Luque CM, Espigares-García M, Baca P. Enterococcus faecalis biofilms eradication by root canal irrigants. J Endod 2009;35:711-4. Ozdemir HO, Buzoglu HD, Calt S, Stabholz A, Steinberg D. Effect of ethylenediaminetetraacetic acid and sodium hypochlorite irrigation on Enterococcus faecalis biofilm colonization in young and old human root canal dentin: In vitro study. J Endod 2010;36:842-6.
Ozdemir et al., concluded that the combined application of 17% EDTA and 2.5% NaOCl reduces the
amount intracanl biofilm significantly
Action/agent NAOCl Iodine CHX EDTA
Bacterial killing
Dissolution
Biofilm penetration
Biofilm break-up
+++++
+++++
+++++
+++++
+++++
+
+
++++
+++
++ ++
++++
- -
--
RELATIVE EFFICACY OF ROOT CANAL AGENTS IN
Effectiveness of Antibiotic Medicaments against Biofilm Formation of Enterococcus faecalis and Porphyromonas
gingivalis
• Biofilm formation of the 2 bacteria was significantly decreased with TAP and DAP at all tested dilutions.
• However, TAP and DAP biofilm formations were not significantly different from each other.
• Both TAP and DAP were more effective than Ca(OH)2 against E. faecalis and P. gingivalis.
Sabrah AH, Yassen GH, Gregory RL. Journal of endodontics. 2013 Nov 1;39(11):1385-9.
• SONIC AGITATION
• In 1985, Tronstad et al. were the first to report
on the use of a sonic instrument in Endodontics.
• Sonic irrigation is different from ultrasonic irrigation in that it operates at a lower frequency (1–10 kHz) and generates significantly higher amplitude.
• The EndoActivator uses sonic energy to agitate the irrigants in the root canal system and has been reported to be able to clean debris from lateral canals, remove the smear layer, and dislodge clumps of simulated biofilm
• ULTRASONIC AGITATION
• Martin described the in vitro disinfectant action of ultrasonics.
• The ultrasonics used in Endodontics are acoustic vibrations with frequencies around 25,000 cycles/ second.
• Acoustic streaming and Cavitation cause temporary weakening of the cell membrane, thereby increasing the bacterial cell permeability to antimicrobial irrigants .
◦ Nanoparticles are microscopic particles with one or more dimensions in the range of 1–100 nm.
◦ The antibacterial powders of MgO, CaO, and ZnO generated active oxygen species, such as hydrogen peroxide and superoxide anion radical
◦ Chitosan (CS-np),gold (Au-np) and silver (Ag-np) nanoparticles possess a broad spectrum of antimicrobial activity, caused by altering cell wall permeability resulting in cell death
ANTIBACTERIAL NANOPARTICLES

.
14
combat microorganism
resistance
very small sizes
antimicrobial activity
very good reactivity
a large surface-area-to-mass ratio
BIOACTIVE GLASS
The antibacterial mechanism of BAG has been attributed to a combination of several factors including:(i) a high pH;
(ii) an increase in osmotic effects;and(iii)Ca/P precipitation
• However, when compared with Ca(OH)2,BAG showed significantly less antibacterial effects .
• In addition, BAG application did not effectively prevent recontamination of instrumented root canals.
Zehnder M, Luder HU, Schätzle M, Kerosuo E, Waltimo T. A comparative study on the disinfection potentials of bioactive glass S53P4 and calcium hydroxide in contra-lateral human premolars ex vivo. Int Endod J 2006: 39: 952–
958.
◦ Also termed as Light Non-Coherent Photoactivated Disinfection
◦ It is a two-step procedure
◦ Step 1: photosensitization of the infected tissue
◦ Step 2:irradiation of the photosensitized tissue, which would generate a toxic photochemistry on the target cell, leading to cell lysis.
ANTIMICROBIAL PHOTODYNAMIC THERAPY Different PSs are used in dentistry including methylene blue (MB),
toluidine blue O (TBO), indocyanine green (ICG) and curcumin
George & Kishen demonstrated a 97.7% success rate in killing Enterococcus faecalis compared to 30% human fibroblast dysfunction following Methylene blue-mediated APDT
George S, Kishen A. Advanced noninvasive light activated disinfection: assessment of cytotoxicity on fibroblast
versus antimicrobial activity against Enterococcus faecalis. J Endod 2007: 33: 599–602.
LASER-ASSISTED ROOT CANAL DISINFECTION
◦ Infrared lasers such as CO2, Nd:YAG, diode, and Erbium lasers have been used for endodontic disinfection.
◦ Their antimicrobial effects are the result of a photothermal interaction (i.e. resulting in a localized increase in temperature) with the target provided enough absorption of radiation takes place.

.
15
Meire MA et al compared the antimicrobial efficacy of two high power lasers (Nd:YAG and Er:YAG) and two commercial antimicrobial photodynamic therapy (APDT) systems with that of NaOCl action on E. faecalis biofilms grown on dentine discs.
▪ NaOCl was the most effective in biofilm elimination, while Er:YAG laser treatment also resulted in high reductions in viable counts.
▪ The use of both APDT systems resulted in a weak reduction in the number of E. faecalis cells.
▪ Nd:YAG irradiation was the least effective.
Meire MA, Coenye T, Nelis HJ, De Moor RJ. Evaluation of Nd: YAG and Er: YAG irradiation, antibacterial photodynamic therapy and sodium hypochlorite treatment on Enterococcus faecalis biofilms. International Endodontic Journal. 2012 May;45(5):482-91.
PHOTON-INITIATED PHOTOACOUSTIC STREAMING (PIPS)
◦ PIPS is based on the direct shock wave generated by an Er:YAG laser in the liquid irrigant.
◦ When activated in a limited volume of fluid,the high absorption of the Er:YAG wavelength in water, combined with the high peak power derived from the short pulse duration results in a photomechanical phenomenon
◦ Peters et al. studied the efficacy of laser-activated and ultrasonically activated root canal disinfection with conventional irrigation, specifically their ability to remove
3-week-old in vitro bacterial biofilm formed on root canal
walls.
• Activated disinfection did not completely remove bacterial biofilms from the apical third of the root canal.
• However, laser activation generated more negative bacterial samples and left less apical bacteria/biofilm than ultrasonic
activation.
NONEQUILIBRIUM PLASMA
• Exists at atmospheric pressure and room temperature and does not inflict thermal damage to nearby objects.
• The preliminary results of nonequilibrium plasma against endodontic bacteria in planktonic culture and biofilms have been promising.
Pan J, Sun K, Liang Y, Sun P, Yang X, Wang J, Zhang J, Zhu W, Fang J, Becker KH. Cold plasma therapy of a tooth root canal infected with Enterococcus faecalis biofilms in vitro. Journal of endodontics. 2013 Jan 1;39(1):105-10.
OZONE
Ozone (O3) is an energized, unstable gaseous form of oxygen that readily dissociates back into oxygen (O2), liberating a reactive form of oxygen, the singlet oxygen (O1).
The singlet oxygen is capable of oxidizing cells & It has been suggested that ozone accomplishes its antimicrobial efficacy without developing drug resistance.
It is applied to oral tissues in the forms of ozonated water, ozonated olive oil and oxygen/ozone gas.
• The bactericidal properties of ozone are well recognized and have shown to reduce the level of viable E. Faecalis in dentine tubules.
• Several endodontic pathogens including E. faecalis are rendered nonviable upon exposure to 2 and 4 ppm (mg/L) ozone in water
.
16
Hems RS, Gulabivala K, Ng YL, Ready D, Spratt DA. An in vitro evaluation of the ability of ozone to kill a strain of Enterococcus faecalis. Int Endod J 2005: 38: 22–29.
Hems et al. evaluated the potential of ozone as an antibacterial agent using Enterococcus (E.) faecalis as a test species. Different interaction times ranging from 30 sec to 240 sec were applied to both cultures.Ozone was used both as gasiform (produced by Pure zone device), and aqueous (optimal concentration 0.68 mg/L).
• Ozone in solution was antibacterial against E. faecalis after 240 sec treatment.
• The antibacterial efficacy of ozone was not
comparable with that of sodium hypochlorite under the conditions tested in this study
ENZYMES
• Enzymatic irrigation was introduced by Niazi and coworkers
• Evaluated the effectiveness of 1% trypsin and 1% proteinase K, with or without ultrasonic activation, on a multi-species biofilm.
• Trypsin with ultrasonic activation was able to effectively kill both aerobic and anaerobic bacteria and has the capability of disrupting the biofilm
Niazi, S.A.; Clark, D.; Do, T.; Gilbert, S.C.; Foschi, F.; Mannocci, F.; Beighton, D. The effectiveness of enzymic irrigation in removing a nutrient-stressed endodontic multispecies biofilm. Int. Endod. J. 2014, 47, 756–768.
• Lactobacillus plantarum ( L. plantarum ) is a probiotic that is known to have antiinflammatory and anti-biofilm effect.
• Bacterial cell wall components especially LTA inhibit Streptococcus mutans, E. faecalis, and Staphylococcus aureus biofilm formation by controlling gene expression, quorum sensing, and inhibiting exopolysaccharides production.
Ahn KB, Baik JE, Park OJ, Yun CH, Han SH. Lactobacillus plantarum lipoteichoic acid inhibits biofilm formation of Streptococcus mutans . PLoS One 2018;13:e0192694
LACTOBACILLUS PLANTARUM LTA MICROBUBBLE EMULSION
• Halford et al., were the first to employ a microbubble
emulsion to enhance the effect of sonic and ultrasonic agitation of sodium hypochlorite.
• Essentially, the technique employs unstable gas-filled
microbubbles that expand when exposed to ultrasonic waves.
• In addition, it may also generate reactive oxygen species to exhibit an antibacterial effect.
Halford, A.; Ohl, C.D.; Azarpazhooh, A.; Basrani, B.; Friedman, S.; Kishen, A. Synergistic effect of microbubble emulsion and sonic or ultrasonic agitation on endodontic biofilm in vitro. J. Endod. 2012, 38, 1530–1534.
• Microbubble emulsion in combination with ultrasonic agitation was shown to be superior than with sonic agitation.
• This approach appears clinically interesting and warrants further research
HERBAL AND ENZYME ALTERNATIVES
• Natural polyphenols are present in a variety of plants.
• Polyphenols are well known for their antimicrobial activity.
• Anacardic acid (found in the liquid extract of cashew nut shells) has been shown to exhibit antimicrobial activity against Streptococcus mutansand Staphylococcus aureus
• Other eg. Curcumin, Morinda citrifolia (MCJ), TriphalaKishen A. Advanced therapeutic options for endodontic biofilms. Endodontic Topics. 2010 Mar;22(1):99-123
.
17
There were no significant differences in the antimicrobial properties of Triphala and 2.5% and 5% NaOClsolutions.
An In Vitro Comparison of the Antibacterial Efficacy of Triphala with Different Concentrations of Sodium Hypochlorite, Iran Endod J. 2014 Fall; 9(4): 287–289.
Triphala powder was dissolved in 10% dimethylsulfoxid to prepare an irrigation solution at a concentration of 5 mg/ml. Different concentrations of NaOCl were prepared by dilution of 5.25% solution with sterile water without preservatives.
Evaluation of Antimicrobial Efficacy of Herbal Alternatives (Triphala and Green Tea Polyphenols), MTAD, and 5% Sodium Hypochlorite against Enterococcus faecalis Biofilm Formed on Tooth Substrate: An In Vitro Study
• Maximum inhibition was observed by 5% NaOCl followed by MTAD compared with Triphala and GTP.
• NaOCl and MTAD achieved 100% killing of E. faecalis at 2 minutes, whereas Triphala and GTP took 6 minutes.
Prabhakar J, Senthilkumar M, Priya MS, Mahalakshmi K, Sehgal PK, Sukumaran VG. Evaluation of antimicrobial efficacy of herbal alternatives (Triphala and green tea polyphenols), MTAD, and 5% sodium hypochlorite against Enterococcus faecalis biofilm formed on tooth substrate: an in vitro study. Journal of Endodontics. 2010 Jan 1;36(1):83-6.
Propolis (bee glue) has antibacterial, antifungal, antiviral and anti-inflammatory action.
Carbajal Mejia JB. 2014. Antimicrobial effects of calcium hydroxide, chlorhexidine, and propolis on Enterococcus faecalis and Candida albicans. J Investig Clin Dent. 5(3): 194–200.Kayaoglu G, Omurlu H, Akca G, Gurel M, Gencay O 2011. Antibacterial activity of Propolis versus conventional endodontic disinfectants against Enterococcus faecalis in infected dentinal tubules. J Endod. 37(3): 376–381.
• Reduction in E. faecalis CFUs did not differ between CHX and propolis
• Propolis was more effective than Ca(OH)2 against E. faecalis but did not exceed that of CHX
CONCLUSION
• The root canal biofilm is a very complex, organized entity.
• Within root canal systems, the complexity is not only related to the nature of the biofilm, but also the complex anatomy, which houses tissue along with biofilms and removal of such biomasses is as relevant as being able to kill bacteria in biofilms.
• Future studies should offer due credence to the complexity of the microbial biofilm and to re-evaluate removal of the biomass from the root canals in addition to evaluating the action of novel antimicrobial agents on complex biofilms.

.
1
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
•In the pursuit of looking good, man has always
tried to beautify his face.
•Since alignment and appearance of teeth
influence personality, they have received
considerable attention.
•Tooth discoloration varies in etiology
appearance localization, severity and adherence
to tooth structure.
2
•Causes of tooth staining must be carefully
assessed for better prediction of rate and degree
to which bleaching will improve tooth color,
since some stains are more responsive to
process than others.
3 4
5 6

.
2
7
Most susceptible - during the II trimerster
in utero to roughly 8 years after birth.
Severity of the stains depends on the time, duration
and the dosage of the drug and also the type of
tetracycline.
• Chlortetracycline (Aureomycin): Gray-brown
• Dimethylchlortetracycline (Ledermycin): Yellow
• Doxycycline (Vibramycin): Does not cause staining
• Oxytetracycline (Terramycin): Yellow
8
9 10
I-Light yellow or gray stain
II-Yellow-brown or deeper gray
stain
III-Brownish-yellow or blue-gray
stain with distinctive banding
11 12

.
3
•May arise endemically from naturally occurring water
supplies or from fluoride delivered in mouth rinses, tablets
or toothpastes as a supplement.
•High concentration of fluoride in excess of 1ppm is
believed to cause a metabolic alteration in the
ameloblasts resulting in defective matrix and
improper calcification
13
Mild- brown pigmentation
Moderate- flat gray or white
flakes
Pitting- dark pigmentation
with surface defects14
15 16
Based on chemistry of the discoloration – Nathoo 1997
•N1 type dental stain: The chromogens binds to the tooth
surface to cause tooth discoloration.
•N2 type dental stain : The chromogen changes color after
binding to the tooth.
•N3 type dental stain : The prechromogens binds to the
tooth and under goes a chemical reaction to cause a stain.
17
Scaling and polishing of the teeth removes many extrinsic
stains. For more stubborn extrinsic discoloration and
intrinsic stain, a variety of tooth whitening options are
available today.
Currently available tooth whitening options are:
1. Office bleaching procedures.
2. At home bleaching kits.
3. Composite veneers.
4. Porcelain veneers.
5. Whitening toothpastes
The lightening of color of the tooth through the application
of a chemical agent to oxidize the organic pigmentation in
the tooth.
The use of a chemical agent, sometimes in combination with
heat, to remove tooth discolorations.
Extracoronal bleaching (external bleaching)- The
use of a chemical agent on the outside of a tooth to remove
discoloration from tooth structures; most frequently used
agents are hydrogen peroxide and urea (Carbamide)
peroxide.
-Grossman 12th edi
-AAE Glossary of Endodontic Terms 201218
.
4
19
The lightening of the color of a tooth through
the application of a chemical agent to oxidize
the organic pigmentation in the tooth is
referred to as bleaching.
-Sturdevant
20
•Vital teeth were also bleached as early as 1868, by
means of oxalic acid or Pyrozone and later with
hydrogen peroxide.
• In Fisher1911 use of concentrated hydrogen peroxide
with a heating instrument or a light source for tooth
bleaching.
21
•Furthermore, in the late 1960s, a successful home-
bleaching technique was established when Dr. Bill
Klusmier, an orthodontist, instructed his patients to use an
“over-the counter” oral antiseptic, which contained 10%
carbamide peroxide delivered via a custom-fitting
mouth tray at night.
• Dr. Klusmier found that this treatment not only
improved gingival health but also
whitened teeth.
22
•Subsequently, Proxigel (a mixture of 10% carbamide
peroxide, water, glycerin, and carbopol)
was marketed.
• Haywood and Heymann (1989) described a home-
bleaching technique in their article, “Nightguard vital
bleaching”, and an at-home bleaching product “White and
Brite™” was introduced.
23
•“Over-the-counter” (OTC) bleaching agents were first
launched in U.S in 1990s, containing lower
concentrations of hydrogen peroxide or carbamide
peroxide and sold directly to consumers
for home use.
• Finally current in-office bleaching technique typically
uses different concentrations of hydrogen peroxide,
between 15% and 40%, with or without light and in
presence of rubber dam isolation.
24

.
5
25 26
27
•Clear, colorless, odorless liquid, stored in amber
colored bottles.
•Various concentration of this agent are available but
30- 35% stabilized solution of H2O2(superoxol)
are most common.
• Stored in refrigerated container where it retains
sufficient potency for appro 3-4 months.
28
29
•Also known as urea hydrogen peroxide, carbamyl
peroxide,perhydrol urea (3-45%).
•A bi-functional derivative of carbonic acid
• Available in the concentration range of 3 to 45%.
• Popular commercial preparations contain about 10%
carbamide peroxide
•Mean Ph of 5 to 6.5.
30
.
6
31
•15% carbamide peroxide solution (CPS) yields
5.4% hydrogen peroxide and 20% solution yields
7% hydrogen peroxide.
•35% carbamide peroxide gel is available as Quickstart
(DenMat, Lompoc, CA) and 45% gel as Opalescence
Quick (Ultradent Products, South Jordan, UT).
32
33
•When fresh contains about 95% perborate
corresponding to 9.9% of available oxygen.
•Sodium perborate is stable when dry.
S.P + H2O S.M.Borate + H2O2
S.P + H2O2 S.M.Borate + H20 + O2
34
Three types of sodium perborate preparations
are available:
•Monohydrate
•Trihydrate
•Tetrahydrate
35 36
•Based on oxidation of bleaching
material.
•Oxidation-reduction reaction that takes place in
bleaching process is known as
REDOX REACTION.
•Oxidizing agent has a free radical with unpaired
electrons, which it gives up, becoming reduced.
•Reducing agent (i.e. the substance being
bleached) accepts electrons and
becomes oxidized.

.
7
37 38
39
•Pt education and informed consent
• Careful diagnosis
a)Visual examination
b)Behavioral history
c)Medical history
d)Determining soundness of individual teeth
•Record keeping with photographs and
shade selection
40
•Preparation of patient
Protective draping and eye wear
41
Application of orabase/vaseline on labial and lingual tissues and vaseline on lips
Rubber dam of heavy gauze is used punched holes –smaller in size
42
•Oral prophylaxis
Prophy-Jet 30 (Dentsply)

.
8
43
Bleaching
Vital
In office Night guard
Nonvital
In officeWalking bleach
44
45
IN OFFICE BLEACHING
Wash the etching solution
After 10 secs Chalky white appearance46
47 48

.
9
49
•Great heat is generated during bleaching which can
•result in tooth sensitivity.
•Causes tooth dehydration
•Uncomfortable for patient
•Slower in action
DISADVANTAGES OF
CONVENTIONAL BLEACH
LIGHT
50
51
•high intensity light, which was used as a heat
source, is replaced with conventional halogen units,
plasma arc lamps, LED lights, Xeno halogen
lights and lasers.
ADVANTAGES
• Time factor(fast result)
• Avoids problems of home bleaching
DISADVANTAGES
• Caustic nature of 35-50% HP
• Increased in office time
• Dehydration of teeth resulting in false light shade
• Expensive52
53 54
.
10
55
•A true laser is delivered to chemical agent
•488nm WL, Blue light, absorbed by dark stains
•Action is to stimulate the catalyst in the chemical.
Adv: •No thermal effect,
•Less dehydration of enamel,
•Less time(10sec/tooth)
56
57
•10,600nm
• Invisible infrared light, energy is emitted
in the form of heat
• Directly interacts with catalyst/peroxide
• Deeper penetration
58
59
•830 and 980 nm
•Ultra fast 3-5 sec to activate bleaching agent
Adv: •Produce no heat
60
•Accelerates activation of H2O2 in whitening gels
which typically contain 30% to 35% H2O2
concentration.
•In reaction to absorption of photon, H2O2breaks down
into particle of water and radical
of oxygen.
.
11
61
•Free radical oxygen chemically reduces larger
organic-pigmented molecules (chromophores) in
enamel matrix into smaller, less pigmented
constituents by rapid oxidation.
• These compounds that originally have double bonds
and long carbon chains are subsequently reduced to
smaller carbon chains and hydroxyl groups, which
eliminate discoloration.
62
63
•Uses 6-7.5% HP gel
•Two cycles of 5 min
64
•Mixed to get good consistency
•A 2-3 mm layer of freshly mixed gel should
be applied to all the labial surfaces of teeth
in smile zone and lipped over to cover the
incisal edges and extend slightly lingually
or palatally.
•Activation with or without light source
depends on bleaching system used.
65
•Gel is left in place for a length of time
dependent on the system and
cocentration of HP used, usually about
10mins, but can range from 3-20
mins at a time.
•Gel is suctioned off teeth using
high volume suction, rinsed , wiped
using damp gauze before being
lightly dried.
66
•Application and activation procedure is repeated one more
time before final washing and drying of the teeth.
Power bleaching procedures usually involve three
10-minute passes.
• Surrounding mucosa are examined for blanching or areas
of redness indicating H202 seepage through
isolation.
• Areas of damage should be thoroughly washed with
copious amounts of water before application of a
neutralizing agent, such as vitamin E, usually supplied
within the bleaching kits.
.
12
67
•Polishing with a diamond polishing paste gives a
high lustre.
• Application of a neutral colorless fluoride gel.
• Final shade assessment and postoperative photographs.
• Patients should be given postoperative instructions.
68
69
Introduced by Dr. Van Haywood and Dr. Harald
Haymann in 1989.
70
•After an initial consultation with the dentist, a mouth
guard or tray is made for the patient to bleach teeth
at home.
• Pt. is given bleaching materials (normally 10%
carbamide peroxide) to take home together with a
bleaching protocol.
• Pt. applies bleaching material into tray.
•Tray with the material is worn for several hours during the
day or at night depending on patient's schedule, while the
teeth lighten.
71
•NightguardVital Bleaching
• Matrix bleaching
• Dentist-assisted / prescribed
home-applied bleaching
• Dentist-supervised at-home
bleaching
• At-home bleaching
Various names
72
Clinical examination of all teeth
Pre-existing shade evaluation
Alginate impression
of the arch to
be taken

.
13
73
Model prepared
Block resin applied on
the labial surface of the
teeth to be bleached to
form a small reservoir
for the bleaching agent.
74
Fabrication of bleaching tray
is done using BIOSTAR
Place the model on the
base section of vacuum
tray forming machine.
Ensure that plastic sheet
is properly placed over
model.
75
Plastic sheet is now more
easily removed from press.
Scalloping tray On
buccal/facial surface of
model using a heated scalpel
blade. Tray trimmed 1mm
above gingival margin.
Polishing of tray is done
gently with a special soft
cotton wheel. Finished tray
placed back on cast to
prevent distortion.
76
BRUSHING FLOSSING
Bleaching material is placed
on buccal surfaces of tray
77
Gentle finger pressure is
applied to tray to improve
retention and suction while
removing excess material at
same time.
STORAGE
78
instruct patient that this procedure should be
performed 3-4 hours per day or over night. Recall
patient every 2 weeks to monitor stain
lightening.10% carbamide peroxide is used for
this technique ,this can be later increased to
16%,or up to 20% as per case reqirements.
.
14
79 80
•Gingival irritation
•Soft tissue irritation.
•Altered taste sensation
•Tooth thermal sensitivity
81 82
Active treatment
Fluoride toothpaste
Neutral sodium fluoride gel
Potassium nitrate-fluoride
gel
Passive treatment
Remove excess
material is.
bleaching gel with a lower
concentration
Reduce treatment
time
83 84

.
15
85 86
Procedure
•Should be freshly mixed and applied directly to enamel
surface for 5min at 1-min interval.
•On completion of bleaching solution is neutralized with a
baking soda solution and copious irrigation with water.
•Bleached surface should be poolished with cuttle disc and a
prophylactic paste.
•Procedure may have to be repeated 2 or 3 times before
desired shade is obtained.
87 88
•Insoluable in water.
•Consequently varnish is not prematurely washed off the
teeth by saliva.
• Contains 6% carbamide peroxide when
Applied, it releases oxygen , which gently
lightens stains. Once dried, its concentration is about
five times higher
89
Available as standing tube with brush and
dispensing dish for single use
90
Brushing and flossing of teeth before
application of varnish

.
16
91
Drying with blotting
Paper
Applying protective
Gel
92
Vivastyle paint on is applied
directly to teeth with
a brush and allowed to dry
for 30 seconds
93
Dried varnish remains on the
teeth for 20 minutes
and is subsequently removed with
a toothbrush.
Once daily for 20 min. over a period of 14 days.
Twice daily for 20 min. over a period of 7 days .
94
Advantages
•Professional tooth whitening
without a tray
•Smooth integration into daily
schedule
•Gentle application
•Touching up of previously
whitened teeth
95 96
Whitening strips(The Trayless Approach to
Tooth Whitening)
Thin,flexible polyethylene strips coated one side with
a film of H2O2 Worn for 30mins , twice a day.

.
17
97
Duration6% coated H2O2 worn over 14 days
10% coated H2O2 worn over 10 days
Adv•No tray is needed
•Less visible
•No gagging, salivation, speech problem, jaw joint
problem.
•More convenient & compatible
98
99
•Darkening and loss of translucency may follow loss
of vitality, both before and subsequent to endodontic
therapy.
•In case of Acute trauma
• Seepage of toxins from a necrotic pulp
• Staining form medicaments, cements, metal posts ,
or the optical effects of dehydration
100
Successful bleaching depends upon two
important criteria-
•Root canal obturation must be complete. In
order to prevent an endodontic failure
root canal system must be filled in
three dimensions
•Remaining tooth structure must be intact
101
Intracoronal bleaching
•Material is sealed into access cavity during in-office visits and
requires frequent changing of dressings.
• Walking Bleaching Technique: Sodium perborate and water
sealed into the tooth .
• Modified intracoronal bleaching technique : Various
increasing hydrogen peroxide concentrations and sodium
perborate is used.
• Intracoronal bleaching using thermocatalytic technique or
other forms of heat or heating instruments
102
Open chamber bleaching
•Combining intra- and extracoronal bleaching; material
is applied into the pulp chamber directly and retained
with a home bleaching matrix.
• Inside/Outside technique with bleaching tray using
different concentrations of Carbamide peroxide.

.
18
103
Closed chamber bleaching
•Bleaching material is placed on external surfaces of
tooth.
• Power bleaching using 35% hydrogen peroxide
• Nightguard Vital Bleaching using 10%, 15% or 20%
applied only to
non-vital tooth in tray
104
INDICATIONS
Discoloration of pulp chamber
origin
Dentin discolorations
Discolorations not amenable to
extra coronal bleaching
CONTRAINDICATIONS
Superficial enamel discolorations
Defective enamel formation
Presence of caries
Discolored composite restoration
Severe dentin loss
105 106
Familiarize the patients with
possible causes of discoloration.
Evaluate tooth color with shade
guide
Isolate the tooth with rubber dam
107
Cavit and GIC
base at least 2
mm thick to
cover the
endodontic
obturation.
108
Remove all restorative material
from access cavity to a level just
below labial gingival margin
Apply at least 2mm of protective
cement barrier ,such as zinc
phosphate cement ,GIC,
intermediate restorative materials
Material is placed at correct depth
snugly, using a flat plastic or
endodontic plugger

.
19
109
Prepare walking bleach paste by
mixing sodium perborate and
inert liquid , such as water etc.
Pack the pulp chamber with
paste. remove excess liquid by
tamping with a cotton pellet.
Carefully pack temporary filling
at least 3mm thick, to ensure a
good seal
110
PRE AND POST OPERATIVE
111 112
113 114

.
20
115 116
117
.
1
Blood
disorders
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENTS
• Introduction
• Red blood cell and its disorders
• White blood cell and its disorders
• Platelet and its disorders
• Coagulation disorders
• Anticoagulant-Related Coagulopathies
• Disease-Related Coagulopathies
• Conclusion
INTRODUCTION
• William Harvey- father of physiology discovered bloodcirculated through the body in 1628.
• Blood is fluid connective tissue present in circulatorysystem
• FLUID OF LIFE- because it carries oxygen from lungsto all parts of the body and carbon dioxide from all partsof the body to the lungs.
• Erythrocytes or red blood cells are the non nucleatedformed elements in the blood.
RED BLOOD CELL AND ITS DISORDERS Variations in the number of red blood cells
❑ Physiological variations
A. Increase in RBC:
1. Age
2. Sex
3. High altitude
4. Muscular exercise
5. Emotional conditions
6. Increase environmental temperature
7. After meals

.
2
B. Decrease in RBC:
1. High barometric pressures
2. After sleep
3. Pregnancy
❑ Pathological variation:
1. Polycythemia
2. Anemia
RED BLOOD CELL DISORDERS
• Erythrocytoses
• Polycythemia vera
• Anemia
✓ Iron deficiency anemia
✓Anemia owing to hemolysis
✓Sickle cell anemia
✓Erythroblastosis fetalis
✓Thalassemia
✓Pernicious anemia
✓Aplastic anemia
Erythrocytoses
• A conditions with an increase in circulating red blood cells (RBCs), characterized by a increased hemoglobin level.
• 2 types- relative and absolute
• Relative polycythemia: Occur as a result of loss of fluidwith hemoconcentration of cells.
-Seen in: vomiting, diarrhea or loss of electrolytes with accompanying loss of water.
-Increase in number of RBC is only relative to the totalblood volume.
• Absolute erythrocytoses
• Primary polycythemia: True idiopathic increase in the number of circulating RBC and of the hemoglobin level.
- Bone marrow with an inherited increased proliferative activity.
• Secondary polycythemia: known etiology
• Absolute increase in RBC mass resultant to enhancedstimulation of RBC production.
• Bone marrow anoxia – pulmonary dysfunction, high altitude, CO poisoning.
• Production of an erythropoietic stimulating factor- drugs and chemicals such as coal-tar, mercury, iron, bismuth.
POLYCYTHEMIA VERA
• Chronic stem cell disorder with an insidious onsetcharacterized as a panhyperplastic, malignant and neoplasticmarrow disorder.
• Absolute increase in the number of circulating RBC and in the total blood volume because of uncontrolled RBC production.
• Accompanied by increase in WBC and platelet production.
.
3
Clinical Manifestations
• Asymptomatic
• Pruritis
• Vertigo
• Gastrointestinal pain
• Headache
• Paresthesias, fatigue, weakness,
• visual disturbances, tinnitus,
Oral Manifestations
• Erythema (red-purple color) of mucosa,
• Glossitis,
• Erythematous & edematous gingiva
• Spontaneous gingival bleeding
Laboratory findings
• RBC- normochromic normocytic- >10,000.000/cubic mm
• HEMOGLOBIN: >20gm/dl
• PLATELETS- 400,000-800,000/dl
• BONE MARROW- hypercellular, megakaryocytes are increased
Case Report A 65 year old male patient
mobility present in relation to all the teeth, red inflammed gingiva with loss of stippling which bled profusely on slight provocation, generalized recession, gingival enlargement, attrition and root caries present in relation. Orthopantogram(OPG) showed generalized horizontal bone loss extending upto two third of root surface of almost all the teeth present
TREATMENT
• Phlebotomy
• Chemotherapy
• Radioactive phosphorus
Oral health consideration:
• Clinically significant bleeding may paradoxically require platelet transfusion
• Tranexamic acid can be used
• Adjustment of any concomitant antiplatelet and/oranticoagulant therapy
When to initiate the dental procedures proposed inPolycythemia Vera patientsThe dental surgeon should consult with the primary carephysician or hematologist to obtainA. Clearance for implementing the ProceduresB. Advice about
a. Excessive bleedingb. Complications that may be affected by oral healthcare,such as increased risk of blood clotsc. Recent changes in medications, under medical advice orotherwise
d. Recently experienced changes in the patient/client’s medicalcondition

.
4
ANEMIA
• Anemia refers to reduction in
1. Red blood cell count
2. Hemoglobin content
3. Packed cell volume
• It can also be defined as a lowered ability of the bloodto carry oxygen.
Etiologic classification of Anemia:1. Loss of blood:• Acute posthemorragic anemia
• Chronic posthemorrhagic anemia
2. Excessive destruction of RBC:a) Extra corpuscular causes: Antibodies, Infection(malaria),
• Splenic sequestration and destruction•Drugs, chemicals and physical agents
b) Intracorpuscular haemolytic disease
1) Hereditary
• Disorder of glycolysis, abnormalities in RBC membrane.
• Abnormalities in synthesis of globin
2) Acquired – lead poisonong
3. Impaired blood production resulting from deficiency of substances essential for erythropoiesis
a. Iron deficiency
b. Deficiency of vitamin B12 , folic acid and Protein deficiency
4. Inadequate production of mature erythrocytesa) Deficiency of erythroblasts
b) Pure red cell aplasia
c) Infiltration of bone marrow- Leukemia, lymphoma, Multiple myeloma
d) Endocrine abnormality- myxedema
e) Chronic renal disease
f) Chronic inflammatory disease
g) Cirrohisis of liver
Anemia owing to blood loss- Iron deficiency anemia
• Iron deficiency is defined as a reduction in total body ironto an extent that iron stores are fully exhausted and somedegree of tissue iron deficiency is present.
• Females are mostly affected.
for iron- infancy, childhood,
Etiology
• Chronic blood loss
• Inadequate dietary intake
• Faulty iron absorption
• Increased requirements pregnancy.
Clinical Manifestations
• Chronic fatigue
• Pallor of the conjunctiva, lips, and oralmucosa;
• Brittle nails with spooning, cracking,
• Splitting of nail beds, koilonychia
• Palmar creases
• Palpitations
• Shortness of breath, numbness
• Bone pain
Oral Manifestations
• Angular cheilitis,
• Glossitis with different degrees of atrophyof fungiform and filliform papillae
• Pale oral mucosa
• Oral candidiasis
• Recurrent aphthous stomatitis
• Erythematous mucositis
• Burning mouth
.
5
Treatment
• Oral iron supplementation - Ferrous sulfate.
• High protein diet.
Oral Health Considerations
• Low hemoglobin levels - physician consultation prior to surgical treatment.
• If Hemoglobin is less than 8 gm/dL, general anesthesia should be avoided.
• Narcotic use should be limited.
• Increased risk for ischemic heart disease
Plummer-Vinson Syndrome/ Paterson-Kelly syndrome
• Rare syndrome , middle-aged white women
• Classic triad : Dysphagia,
Iron deficiency anemia
Upper esophageal webs or strictures.
Etiopathogenesis :
• Unknown - iron deficiency.
• Malnutrition,
• Genetic predisposition and Autoimmune processes.
Treatment: Iron supplementation
Anemia Owing to Hemolysis
• Normal RBC life span - 90 to 120 days.
• Hemolytic diseases result in anemia if the bone marrow isthe prematurelynot able to replenish adequately
destroyed RBCs.
• Either inherited or acquired.
3 mechanism for accelerated destruction of RBCs:
1. Molecular defect inside the red cell
2. Abnormality in membrane structure and function
3. Environmental factor- mechanical trauma
Clinical Manifestations
• Signs and symptoms depend on the mechanism that leads to red cell destruction.
• Acute back pain,
• Renal failure.
• Fatigue
• Loss of stamina
• Breathlessness
• Tachycardia
• Hemoglobinuria
• Physical findings : jaundice of skin and mucosae, splenomegaly
Oral Manifestations
• Pallor or jaundice of oral mucosa,
• Paresthesia of mucosa, and,
• Hyperplastic marrow spaces in the mandible, maxilla, and facial bones
Laboratory findings:
• An elevated reticulocyte count is the most usefulindicator of hemolysis, reflecting erythroid hyperplasiaof the bone marrow.
Sickle Cell Disease/Sickle Cell Anemia
• Hereditary type of chronic hemolytic anemia transmitted as a mendalian dominant, nongender linked characteristic.
• Exclusively in blacks and in whites of Mediterranean origin.
• A concordance exists between the prevalence of malaria andHbS
HbA is genetically altered to produce HbS,
Substituition of valine for glutamine at the sixth position of theβ globin chain

.
6
• Reduces both their plasticity and lifetime from the normal 120 days average down to 14 days.
• This results in the underlying anemia and hypertrophic bone marrow.
• In heterozygote- 40% of hemoglobin is HbS
• In homozygote- nearly all hemoglobin is HbS
• Common in females, before the age of 30 years
• Cerebrovascular accidents/ strokes,
• Aplastic crises leading to severe anemia,
• chronic leg ulcers,
• Hematuria,
• Aseptic osteonecrosis,
• Retinitis leading to blindness
• Splenic sequestration,
• Renal failure
• Acute chest syndrome - fever, cough, sputum production, dyspnea,or hypoxia.
Clinical Manifestations Oral Manifestations
• Significant bone change in dental radiograph
• Mild to severe generalized osteoporosis
• Loss of trabeculation of the jaw bone
• Enamel hypomineralization
• Increased overjet and overbite
• Pallor of the oral mucosa
• Delayed eruption of the teeth
• Pulpal necrosis
• High arched palate and dental caries
Smooth tongue
Orthopantomograph showing massive resorption in lowerborder of mandible.horizontal trabeculation creating a "ladder-like effect.
Radiographic features
• HAIR – ON – END: perpendiculartrabeculations radiating outward fromthe inner table.
• Outer table of bone may appear absentand the diploe thickened.
• Generalized osteoporosis
• Enlarged medullary cavities with thincortices
Dental considerations
The initial evaluation of the patient must include a thorough history and physical examination.Increased susceptibility to dental infections. Delayed eruption and hypoplasia of the dentition secondary to their general underdevelopment.Hard tissue changes are conspicuous: hypercementosis may develop, and bone marrow hyperplasia with apparent osteoporosis of the jaw, increased radiolucency resulting from the decreased number of trabeculae observed on the dental radiographs.

.
7
sickle cell may cause intrinsic bluish ,brown ,or green discoloration which can be corrected by endodontic procedure followed by bleaching.Preventive dental care is important to lessen the need for radical treatment requiring general anaesthesia (GA).Pulpal symptoms are common in the absence of any obvious dental disease.Surgical procedures should be carried out under antibiotic coverage.Wherever possible, the dental treatment should be carried out under local anaesthesia.
Dental considerationsLaboratory findings
• RBC- may reach a level of 1,000,000 cells per cubic mm.• Decreased hemoglobin level.• High reticulocyte count-Anemia• Increased marrow response.• Elevated lactic dehydrogenase and decreased levels of
hepatoglobin- confirms hemolysis
Blood smear:
• Typical sickle- shaped RBCs seen
Treatment :
• Management of vaso-occlusive crisis
• Management of chronic pain syndrome
• Management of chronic hemolytic anemia
• Prevention and treatment of infections
• Management of the complications.
Oral Health Considerations:
• Amoxicillin was the most commonly chosen antibiotic
• Maintaining good oral hygiene, routine care needed,
• Aggressive treatment of oral infection,
• Avoidance of long, stressful dental visits
Erythroblastosis fetalis
• Congenital hemolytic anemia due to Rh incompatibilityresults from the destruction of fetal blood brought aboutby a reaction between maternal and fetal blood factors.
Pathogenesis
• EF is essentially due to inheritance by the fetus of a blood factor fromthe father that acts as a foreign antigen to the mother.
Transplacental transfer of this antigen, transplacental leaks of RBC
From the fetus to the mother
Immunization of the mother, formation of antibodies which
When transferred back to the fetus by the same route
Produce fetal hemolysis
Clinical features• Some infants are stillborn.
• Anemia with pallor
• Jaundice
• Compensatory erythropoiesis
• Fetal hydrops
Oral manifestation
• Deposition of blood pigments in the enamel and dentin
• Ground sections- positive test for bilirubin
• Intrinsic stains
• Enamel hypoplasia
• Rh hump

.
8
Laboratory findings
• RBC count decreased, large number of normoblasts or nucleated red cells
• Icterus index high
• Positive direct coombs test on cord blood
Treatment
• At present, Rh-negative mothers are being given anti-Dgamma globulin to prevent immunization
Thalassemias
• Thalassemia is a group of genetic disorders ofhemoglobin synthesis characterized by a disturbance ofeither alpha (α) or beta (β) hemoglobin chain production.
• An estimated 900,000 births are expected to occur in thenext 20 years with clinically significant thalassemiadisorders
• First described by Thomas B Cooley in 1925.
• Thalassa means ‘sea’in Greek.
Pathogenesis:
• Normal adult hemoglobin (HbA)- heme is conjugated to globin.
• Globin- 2 pairs of α chain and β chain.
In thalassemia group of anemias,
• Heterogenous group- diminished synthesis of α chain and β chain ofhemoglobinA.
• Thalassemia α- deficient synthesis of α chain.
• Thalassemia β – deficient synthesis of β chain.
- an excess of α- chains, producing ‘unstable hemoglobins’.
Damage the erythocytes → vulnerability to destruction
• FESSAS BODIES: Intracellular inclussion bodies,leads to increased erythrocyte hemolysis andsevere ineffective hematopoiesis.
2 other forms of thalassemia major thatrepresent α- thelasemia are:
Hemoglobin H disease- very mild form
Hemoglobin Bart’s disease- with hydrops fetalis,in which infants are stillborn or die shortly afterbirth
Clinical Manifestations
• Occurs within the first 2 years of life.
• Siblings are commonly affected.
• Yellowish pallor of the skin
• Fever, chills, malaise,
• Generalized weakness
• Splenomegaly and hepatomegaly
• RODENT FACIES- develops mongoloid features due toprominence of the cheeks, protrusion of the maxillaryanterior teeth, depression of the bridge of the nose.
Oral manifestation
• Unusual prominance of the premaxilla
• Anemic pallor observed
Laboratory findings
• Hypochromic microcytic
• RBC- exhibiting Poikilocytosis and Anisocytosis.
• Safety pin cells and nucleated RBCs in the circulating RBCis also a characteristic feature.
• WBC- frequently elevated.
• Bone marrow- cellular hyperplasia with large number ofimmature, primitive and stem form of RBCs.
• Supravital staining- Methyl blue demonstrate inclusion bodies.
.
9
Radiographic findings
• RIB- WITHIN- A- RIB: noted in middle and anteriorportion of the ribs. Long linear density within oroverlapping the medullary space of the rib and runningparallel to its long axis.
• HAIR- ON- END appearance.
• SALT AND PEPPER EFFECT: peculiar trabeculae patternof maxilla and mandible, apparent coarsening of sometrabeculae and the blurring and disappearance of others.
Treatment
• Blood transfusion- temporary remission
• Bone marrow transplantation.
The main oral manifestations of thalassemia are Class II malocclusion,Maxillary protrusion, High caries index, severe gingivitis. Any dental surgical procedure for such patients should be done under antibiotic cover and immediately after transfusion. Caution should be exercised in thalassemia patients due to complications related to compromised immunity and cardiovascular issues.Multidisciplinary approach involving dental surgeon, haematologist and orthodontist is the best advised approach.
Dental considerations
Anemia Owing to Decreased Production ofRBCs
Megaloblastic (Pernicious) Anemia and VitaminB12 (Cobalamin) Deficiency
• It is adult form of anemia that is associated with gastricatrophy and a loss of intrinsic factor production in gastricsecretions.
• Rare congenital autosomal recessive form.
• Autoimmune disease resulting from autoantibodiesdirected against intrinsic factor (a substance needed toabsorb vitamin B12 from the gastrointestinal tract) andgastric parietal cells.
• Vitamin B12 → erythrocyte – maturing factor.
Clinical Manifestations
Hematologic
Neurologic
Psychiatric
Megaloblastic (macrocytic) anemia
Pancytopenia (leukopenia, thrombocytopenia)
Paresthesias, tingling and numbness of hands and feet
Peripheral neuropathy
Muscle weakness
Impaired sense of smell
Syncope
FatigueIrritability, personality changes
Mild memory impairment
Depression
Cardiovascular increased risk of myocardial infarction and stroke
Oral Manifestations
• Burning sensation in the tongue, lips, buccalmucosa, and other mucosal sites.
• The tongue is generally inflammed often describedas ‘beefy red’in color.
• Characteristically with the glossitis, glossodynia andglossopyrosis there is gradual atrophy of thepapillae tongue that eventuates in a smooth or baldtongue → Hunter’s glossitis or Moeller’s glossitis.
• Fiery red appearance of the tongue may undergoperiods of remission, recurrent attacks are common.
• Dysphagia and taste alterations have been reported.
.
10
Laboratory findings
• BLOOD: RBC count is seriously decreased, often to 1,000,000 or less per cubic mm.
-Macrocytosis is one of the chief characteristic feature, althoughpoikilocytosis or variation in shape of cells present.
- pear or tear drop shape erythrocytes are present.
- increased hemoglobin content.
- mild to moderate thrombocytopenia is noticed.
• SERUM: Indirect bilirubin may be elevated.
serum lactic dehydrogenase is markedly increased.
↓- serum potassium, cholesterol and alkaline phosphatase
• BONE MARROW- hypercellular and show trilineage differentiation.
TREATMENT:
• Weekly intramuscular injections of 1,000 μg of vitamin B12 for the initial 4 to 6 weeks, followed by 1,000 μg per week indefinitely.
• Delayed treatment permits progression of the anemia and neurological complication
Aplastic Anemia
• Aplastic anemia (AA) is a rare blood dyscrasia in whichperipheral blood pancytopenia results from reduced orabsent blood cell production in the bone marrow andnormal hematopoietic tissue in the bone marrow has beenreplaced by fatty marrow.
• Environmental exposures, such as to drugs, viruses, andtoxins, are thought to trigger the aberrant immuneresponse in some patients, but most cases are classified asidiopathic
2 chief forms:
• Primary aplastic anemia: unknown etiology.
young adults, develops rapidly and terminates fatally.
FANCONI’S SYNDROME: congenital, sometimes familial,aplastic anemia is associated with other congenital defectsincluding bone abnormalities, microcephaly, hypogenitalismand generalized olive brown pigmentation of the skin.
• Secondary aplastic anemia- known etiology
Exposure of the patient to various drugs or chemicalsubstances or to radiant energy in the form of x-rays, radium orradioactive isotopes.
Clinical Manifestations
• Pancytopenia
• Anemia→ such as fatigue and malaise, chest pain, orshortness of breath.
• More sudden onset of bleeding caused bythrombocytopenia, manifest as increased bruising, evidentby purpura and petechiae, and epistaxis or gingivalbleeding.
• Leukopenia, particularly neutropenia, can result in fever andinfection.
• Preceded by infections by hepatitis viruses, EBV, HIVparvovirus, mycobacterial infections.
Oral Manifestations
• Hemorrhage,• Candidiasis,• Viral infections,• Gingival bleedings
Laboratory findings
• RBC- diminished as low as 1,000,000 cells per cubic mm• ↓ in hemoglobin level.• A paucity of granulocytes, monocytes and reticulocytes is
found.• Prolonged bleeding time• Tourniquet test is positive.

.
11
Treatment
• Blood transfusions to correct anemia and thrombocytopenia
• Immunosuppression with antithymocyte globulins andcyclosporine is effective at restoring blood cell production
• Neutropenia leads to an increased susceptibility to infection,
• Thrombocytopenia leads to bruising and mucosal bleeding.
• Neutropenic fevers must be treated aggressively withparenteral, broad-spectrum antibiotics.
• Antifungal therapy should be added
• Attention to details of oral hygiene and hand washing andavoidance of minor injuries or casual exposure to infectiousagents can reduce the risk of serious complications.
Dental considerations
WHITE BLOOD CELLS AND ITS DISORDERS
• White blood cells (WBCs), alsocalled leukocytes or leucocytes, are the cells of theimmune system that are involved in protecting the bodyagainst both infectious disease and foreign invaders.
• All white blood cells are produced and derived frommultipotent cells in the bone marrow known ashematopoietic stem cells.
• Leukocytes are found throughout the body, including theblood and lymphatic system
• 2 types: granulocytes and agranulocytes
Variations in the number of white blood cells
❑PHYSIOLOGICALVARIATIONS:
• Age
• Sex
• Diurnal variations
• Exercise
• Emotional condition
• Pregnancy
• Sleep
❑PATHOLOGICALVARIATIONS• Leukopania• Leukocytosis• Neutrophilia• Eosinophilia• Basophilia• Monocytosis• Lymphocytosis• Leukemia
Disorders
• Leukocytosis
• Leukopenia
• Agranulocytosis
• Neutropenia
• Chediak – Higashi Syndrome
• Acute Leukemia
• Chronic leukemia
.
12
LEUKOCYTOSIS• Defined as abnormal increase in the number of circulating
WBCs.
• Considered to be a manifestation of the reaction of the bodyto a pathologic situation.
• It may also occur after exercise, convulsions such asepilepsy, emotional stress, pregnancy, anesthesia, andepinephrine administration.
• There are five principal types of leukocytosis:
1. Neutrophilia (the most common form)
2. Lymphocytosis
3. Monocytosis
4. Eosinophilia
5. Basophilia
in new born, during labor, after exercise,Neutrophilia
• Physiologic-convulsions
• Acute infections- certain bacilli, fungi, viruses, parasites.
• Inflammatory conditions- Gout, Burns, Vascular disease, Hypersensitivity reactions
• Intoxications- Uremia, Poisoning by chemicals and drugs- lead, mercury.
• Acute hemorrhage
• Acute hemolysis
• Polycythemia, myelotic leukemia.
Eosinophilia
• Allergic disorders- bronchial asthma, hay fever
• Skin disease- phemphigus, erythema multiforme
• Scarlet fever,
• Parasitic infection- malaria.
• Diseases of the hemopoietic system- chronic myeloidleukemia, polycythema vera, hodgkins disease, perniciousanemia
• Following irradiation
• Sarcoidosis, rheumatoid arthritis.
Basophilia
• Splenectomy
• Blood disease- CML, polycythemia vera, hodgkin’s
anemia
• Infection- smallpox, chickenpox
• After injection of foreign proteins
Lymphocytosis
• Acute Infections- infectious mononucleosis,
• Chronic Infections- tuberculosis, syphilis,
• Lymphocytic leukemia, lymphosarcoma
• Hemopoietic disorders- lymphocytosis,
• Mumps, german measles, thyrotoxicosis.
Monocytosis
• Bacterial infections- tuberculosis, SABE, syphilis,
• Protozoal and Rickettsial- malaria, typhus, kala-azar
• CML, hodgkin’s disease, multiple myeloma
• Lipid storage disease- Gaucher’s disease
• Granulomatous disease- sarcoidosis, ulcerative colitis
• Collagen vascular disease- lupus erythematosus,rheumatoid arthritis.

.
13
Agranulocytosis
(Neutropenia/Granulocytopenia)
• Serious disease involving the WBC and is characterized bydecrease in the number of circulating granulocytes.
• The terms agranulocytosis, neutropenia, andgranulocytopenia are commonly used interchangeably for areduced quantity of leukocytes.
Types:
• Primary Agranulocytosis- unknown etiology
• Secondary Agranulocytosis- known etiology.
ETIOLOGY• Antineoplastics,
• Antibiotics,
• Anticonvulsants,
• Antiinflammatories,
• Antithyroid agents,
• Diuretics, and
• Phenothiazines
Kostmann syndrome is a group of diseases that affectmyelopoiesis, causing a congenital form of neutropenia ,usually without other physical malformations.
- manifests in infancy with life-threatening bacterial infections
Drugs → hapten
Induce Antibody formation
Destroy granulocytes or form immune complexes
Bind to neutrophils
Destroy them
Clinical features
• Occur at any age- particularly among adults
• Women are more affected.
• High fever, chills, sore throat,
• Malaise, weakness
• Skin appears pale and anemic,
• Presence of infections
• Regional lymphadenitis,
• Complication- Generalized sepsis.
Oral manifestations
• Necrotizing ulceration of the oral cavity, tonsils and pharynx particularly gingiva and palate.
• Necrotic ulcers are covered by gray or even blackmembrane.
• No purulent discharge are noted.• Excessive salivation.• Oral surgical procedures are contraindicated.
Laboratory findings
• WBC are often below 2000 cells per cubic mm• Almost complete absence of granulocytes or
PMNs.• RBC and platelet counts are normal
Treatment
• Recognition and withdrawal of the causative drugs
• Oral hygiene should be meticulous to foster an immaculate oral environment.
Cyclic Neutropenia
• Cyclic neutropenia is a rare hematologic disorder,characterized by repetitive episodes of fever, mouth ulcers,and infections attributable to recurrent severe neutropenia.
• Characterized by periodic or cyclic diminution in circulatingPMNs as a result of bone marrow maturation arrest.
• Neutropenia recurs with a regular periodicity of 21 days,persists for 3 to 5 days, and is characterized by infectiousevents that are usually less severe than in severe chronicneutropenia.
• Autosomal dominant cyclic neutropenia is caused by amutation of the gene for neutrophil elastase, ELA2, locatedat 19p13.3

.
14
Clinical features
• Occurs at any age, infants or young adults.
• Symptoms are milder
• Fever, malaise, sore throat, stomatitis
• Regional lymphadenopathy
• Headache, arthritis,
• Cutaneous infections,
• conjunctivitis.
Oral manifestations
• Severe gingivitis
• Stomatitis with Ulceration
• Isolated painful ulcers- lasts for 10-14 days , heals with scarring.
• With return of the neutrophil count to normal, gingiva appears normal
Radiographic features
• Mild to severe loss of superficial alveolar bone.
• Prepubertal periodontitis- in children, loss of bone aroundmultiple teeth.
• No specific treatment
• Splenectomy may be beneficial.
Treatment
Chédiak-Higashi Syndrome
• Chediak-Higashi syndrome (CHS) is a rare autosomalrecessive immunodeficiency disorder characterized byabnormal intercellular protein transport.
• Described by Steinbrinck in 1948, Chediak in 1952 andHigashi in 1954.
• Epstein – Barr virus
Clinical Manifestations
• Immune deficiency
• Oculocutaneous albinism
• Neurologic features- peripheral neuropathy,
• Recurrent infections, and
• Easy bruisability and bleeding
• Abnormalities can be found in the hematopoietic tissues, hair, ocular pigment, skin, adrenal and pituitary glands, gastrointestinal organs, peripheral nerves, and elsewhere.
• Infections are caused by S. aureus, S. pyogenes.
Oral manifestation• Ulceration of the oral mucosa,
• Severe gingivitis and glossitis
• Periodontal breakdown
Laboratory findings
• Exhibit giant abnormal granules in the peripheral circulating leukocytes and in the marrow precursors.
• Granules represent abnormal lysosomes bear resemblanc to toxic granulations and Dohle bodies.
• Pancytopenia may be present.
.
15
Treatment
• No specific treatment
• Most of the therapy available in CHS is symptomatic, suchas childhood immunizations and antibiotics for infections.
Oral Health Considerations
• When oral surgical procedures are planned, excessiveoperative blood loss should be anticipated secondary toqualitive defects in platelet function.
• Intramuscular injections should be avoided.
• Patients often have photophobia and may be sensitive to thebright operatory lights.
• Patients can be encouraged to bring sunglasses to dentalappointments.
Leukemia
• Leukemia is a disease characterized by the progressiveoverproduction of WBCs which usually appear in thecirculating blood in an immature form.
• Leukemic cells multiply at the expense of normalhematopoietic cell lines, resulting in marrow failure,altered blood cell counts, and, when untreated, death frominfection, bleeding, or both.
Leukemia is classified into:
• Lymphoid (lymphoblastic, lymphocytic) leukemia- involvingthe lymphocytic series.
• Myeloid (myelogenous) leukemia- involving progenitor cellsthat gives rise to terminally differentiated cells of the myeloidseries (erythrocytes, granulocytes, monocytes, platelets).
Classification may be modified to indicate the course of thedisease- acute –survival is less than 6 months
subacute- survival is between acute and chronic
chronic- survival of over 1 year
Etiology
• Combination of environmental and genetic factors.
• Certain syndromes are associated with an increased risk. These genetic disorders include the following:
❖Down syndrome
❖ Bloom syndrome
❖ Neurofibromatosis
❖Ataxia- telangiectasia syndrome
❖Klinefelter syndrome
❖Fanconi's anemia
❖Myelodysplasia syndromes
• Certain types of leukemia show specific chromosomalabnormalities.
• Chronic myeloid leukemia has a genetic alterationcalled the Philadelphia chromosome which represents atranslocation of the chromosomal material between thelong arms of chromosomes 22 and 9.
• Exposure to pesticides, benzene, and benzene likechemicals, Ionizing radiation has been associated with anincreased risk of developing leukemia.
• EBV, Polyoma virus, Human T-cell leukemia virus- 1(HTLV-1) is known to be associated.
ACUTE LEUKEMIA
Acute Lymphocytic/Lymphoblastic Leukemia• ALL is the clonal proliferation of lymphoid cells that
have undergone maturational arrest in earlydifferentiation.
Acute Myelogenous (Nonlymphocytic)Leukemia• AML is a heterogeneous clonal disorder of hematopoietic
progenitor cells (“blasts”) that lose the ability todifferentiate normally and to respond to normal regulatorsof proliferation.

.
16
Clinical features of acute leukemia
• Weakness,
• Fever, headache
• Generalized swelling of lymph node
• Petechial or ecchymotic hemorrhages in the skin and mucous membrane
• Anemia
• Spleen, liver and kidney become enlarged owing to leukemic infiltration.
• Hemorrhage
CHRONIC LEUKEMIA
Chronic Myelogenous leukemias
• Less pronounced marrow failure than acute leukemias.
• Indolent course, median age of 53 years at diagnosis.
• Risk factors: older age, male gender, and exposure toionizing radiation and benzene and benzene-containingproducts.
• Most patients with CML have an acquired mutation calledthe Philadelphia chromosome that results from atranslocation between chromosomes 9 and 22, producingthe Bcr-Abl abnormal gene → causes the excess WBCstypical of CML.
Chronic Lymphocytic Leukemia
• CLL results from the slow accumulation of clonal Blymphocytes in 95% of patients.
• Median age at diagnosis of CLL is 65 years• Etiology: unknown, although an abnormality of
chromosome 12 is noted• Lymphocytosis >5,000/mL for a month, with at least 30%
of nucleated marrow granulocytes being well-differentiated lymphocytes, in an adult is diagnostic forCLL.
Clinical features
• Develop insidiously that the disease may be present formonths or even several years before the symptoms lead todiscovery.
• Anemic pallor
• Lymph node enlargement
• Splenomegaly, hepatomegaly
• Enlargement of the salivary gland and tonsils
• Xerostomia
Oral manifestations
• Gingivitis, gingival hyperplasia
• Hemorrhage, petechiae and ulceration of the mucosa
• Rapid loosening of the tooth due to necrosis of the PDL
• Destruction of the alveolar bone
• Oral mucositis, exfoliative cheilitis
• Infection with herpes and candida
Treatment• Chemotherapy
• Radiation therapy
• Corticosteroids
• If bcr-abl fusion is identified- Tyrosine kinase inhibitor is appropriate.
• Supportive care
• Optimal oral hygiene care
.
17
Dental considerations Dental considerations PLATELET AND ITS DISORDERS
• Platelets or thrombocytes are small colorless, nonnucleated and moderately refractive bodies.
• Considered to be fragments of cytoplasm
• Spherical or rod shaped, becomes oval or disc shaped when inactivated.
Properties:
1. Adhesiveness
2. Aggregation
3. Agglutination
Normal count and its variation
• Normal platelet count- 2,00,000-4,00,000/cu mm of blood
❑Physiological variation
• Age
• Sex
• High altitude
• After meals
❑Pathological variation
Thrombocytopenia-• acute infections,•acute leukemia,•aplastic and pernicious anemia,•chickenpox,•smallpox,•splenomegaly,•scarlet fever, typhoid,•tuberculosis
Thrombocytosis-
• allergic conditions,
• hemorrhage,
• bone fracture,
• surgical operations,
• splenectomy,
• rheumatic fever,
• trauma.
Thrombocythemia-
• carcinoma,
• chronic leukemia,
• hodgkin’s disease
Platelet Disorders
• Platelet disorders may be divided into two categories by etiology— congenital and acquired
.
18
Purpura
• Purpura is defined as a purplish discoloration of the skinand mucous membrane due to spontaneous extravasationof blood.
•Symptoms rather than a disease entity.
Classification:
• Nonthrombocytic purpura
• Thrombocytic purpua
a) Primary or essential purpura
b) Secondary or symptomatic purpura
Bleeding disorders due to Nonthrombocytopenic purpura
Autoimmune
• Allergic purpuras
• Drug- induced vascular purpuras
Infections
• Bacterial- typhoid fever, scarlet fever, tuberculosis
• Viral- smallpox, influenza, measles
• Rickettsial- typhus
• Protozoal- malaria, toxoplasmosis
Structural malformations
• Hereditary hemorrhagic telangiectasia, Ehlers- Danlos syndrome, Osteogenesis Imperfecta, scurvy.
Thrombocytic purpura
• Abnormal reduction in the number of circulating blood platelets.
• Patient develops focal hemorrhages in to various tissues and organs, including skin and mucous membranes.
2 basic forms-
• Primary- unknown etiology
• Secondary- known etiology
Clinical features:
• Spontaneous appearance of purpuric orhemorrhagic lesions of the skin which varyin size – tiny red pinpoint petechiae to largepurplish ecchymoses.
• Massive hemartomas
• Bruising tendency
• Epistaxis
• Hematuria
• Malena
• Complications- intracranial hemorrhage,hemiplagia.
Oral manifestations
• Severe and profuse gingival bleeding
• Hemorrhage may be spontaneous
• Petechiae- palate
• Ecchymosis
Laboratory findings
• Platelet count is usually below 60,000 platelets/cubic mm
• Bleeding time is prolonged
• Coagulation time- normal
Treatment
• No specific treatment
• Splenomegaly
• Corticosteroids
• Oral surgical procedures are contraindicated until thedeficiency has been compensated.
.
19
Thrombocytopathic purpura
• A group of rare disease of unknown etiology.
referable to• Patient manifests a bleeding tendencyqualitative defects in the blood platelets.
• Platelet count is usually normal.
• Defective platelet aggregation.
Clinical features
• Severe bleeding tendency and bruise easily after only minor trauma.
• Spontaneous ecchymoses• Epistaxis• Bleeding into GIT are frequent• Menstrual bleeding is severe- may require blood
transfusion
Oral manifestation
• Spontaneous gingival bleeding• Mucosal ecchymosis• Excessive and prolonged bleeding from extraction socket
Laboratory findings
• Platelet count- nearly normal
• Bleeding time- is either normal or prolonged
• Normal capillary plugging is impaired
Treatment
• Conventional hemostatic agents
• Blood transfusion
Thrombocythemia/ Thrombocytosis
• Condition characterized by an increase in the number of circulating blood platelets.
• 2 types:
• Primary- unknown etiology
• Secondary- occur after traumatic injury, inflammatoryconditions, surgical procedures, parturition.
- may be due to the overproduction of proinflammatorycytokines such as IL-1, IL-6, IL-11, that occurs in chronicinflammatory, infective, and malignant states.
Clinical features
• No gender or age predilection is seen
• Bleeding tendency in spite of the fact that their plateletcount is elevated.
• Epistaxis
• Bleeding into- Genitourinary tract and CNS
Oral manifestations
• Spontaneous gingival bleeding
• Excessive and prolonged bleeding
Laboratory findings
• Platelet count is increased
• Clotting time, PT, clot retraction and tourniquet test- allare normal
Treatment
• Radioactive phosphorus
• Blood transfusion
• Corticosteroids
• Aspirin, heparin

.
20
Congenital coagulopathies
Hemophilia
• Blood disease characterized by prolonged coagulation time andhemorrhagic tendencies.
• Hereditary disease, defect being carried by x-chromosome,
• Transmitted as a gender-linked Mendelian recessive trait.
• Occurs only in males, transmitted through an unaffected daughter to a grandson.
Etiology
• Hemophilia A- Plasma Thromboplastinogen (AHG factor VIII)
• Hemophilia B- Plasma Thromboplastin component (PTC factor IX)
• Hemophilia C- Plasma Thromboplastin antecedent (PTA factor XI)
Hemophilia A
• A deficiency of F VIII, the antihemophilic factor, isinherited as an X-linked recessive trait that affects males.The trait is carried in the female without clinical evidenceof the disease.
Clinical signs:
• hematomas, hemarthroses, hematuria,
• gastrointestinal bleeding, and
• bleeding from lacerations
• head trauma or spontaneous intracranial bleeding
• Joint synovitis, hemophilic arthropathies
• Intramuscular bleed and pseudotumors
Hemophilia B
• Due to PTC deficiency also known as Christmas disease.• 2 forms- apparently normal levels of the inactive protein
and another in which there is deficient level of thecoagulant factor.
Hemophilia C
• Mild disorder seen in pedigrees of Jewish descent; it istransmitted as an autosomal dominant trait.
• Bleeding symptoms do occur but are usually mild.
Oral manifeststions
• Gingival Hemorrhage- massive and prolonged
• Pseudotumor
Laboratory findings
• Prolonged coagulation time
• Bleeding time- normal
• PTT is prolonged
Treatment
• Preoperative transfusion of whole blood
• Administration of antihemophilic factor
• Protected from traumatic injuries
Endodontic considerationsIf done carefully, endodontic treatment usually does not pose any significant risk of bleeding. It is usually preferred over extraction.Nerve blocks like inferior alveolar block, lingualinfiltration are usually contraindicated until and unless the factor levels are raised above 30% by replacement therapy, else extravasation of blood in the oropharyngeal area or in the pterygoid plexus can be life threatening. Acetaminophen and narcotics are preferably used for postoperative pain .

.
21
. Endodontic considerationRubber dam usage is mandatory as expected. Notches may be placed in buccal and lingual surfaces with a fissure bur into which clamp prongs will fit tightly.
It is imperative that the working length of root canals is maintained during endodontic treatment.Avoiding instrumentation through the periapex is of prime importance in endodontic therapy
Apex locators should be preferably used for measuring workinglength of the canal to minimise the need for intra oral periapical(IOPA) radiographs as repeated placement of film can lead to injuryand bleeding in the lingual mucosa.
Endodontic considerationsSodium hypochlorite should be used for irrigation in all casesfollowed by use of calcium hydroxide paste to control bleeding.
Severe hemophiliacs endodontic treatment (taking into consideration the question of LA discussed previously) can be usually carried out under antifibrinolytic cover (usually tranexamic acid).
Intracanal injection of LA solution containing adrenaline or topical application (using paper points) of adrenaline 1:1000 may be useful to minimize bleeding
Endodontic considerationsEven cotton rolls may cause mucosal bleeding and should be wetted before removal. High speed vacuum evacuators and saliva ejectors can also cause trauma to the floor of mouth and thus lead to haematoma formation. They should be placed by resting them on a gauze swab in the floorof the mouth.
Identification of the Dental Patient with a
Bleeding Disorder
• Begins with a thorough review of the medical history.
• A family history of bleeding problems may help to identifyinherited disorders of hemostasis.
• Past history of bleeding following surgical procedures, includingdental extractions, can help identify a risk.
• Identification of medications with hemostatic effect-coumarinanticoagulants, heparin, aspirin.
• Active medical conditions, including hepatitis or cirrhosis, renaldisease, hematologic malignancy, and thrombocytopenia, maypredispose patients to bleeding problems.
Conclusion
• A wide array of disorders of blood and hemostasisencountered in internal medicine has manifestations inthe oral cavity and the facial region.
that all clinicians are aware of the and oral manifestations of blood
• It is importantphysiopathologydisorders .
• Dental surgeons should carefully obtain the patient’s
clinical history and information about particular featuresso that they can plan any dental treatment such that it isappropriate to the patient’s limitations and needs.

.
22
References
• Guyton and Hall, textbook of medical physiology, 11th
edition.
• K. sembulingam, Essentials of medical physiology, 3rd
edition.
• Burket’s oral medicine, 11th edition.
• Shafer’s textbook of oral pathology, 6th edition.
• Oral and maxillofacial pathology, 3rd edition, Neville

.
1
CASTING DEFECTS
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENTS▪ Introduction
▪Classification
▪ Types of casting defects✓ Distortion✓ Surface roughness✓ Porosity✓ Incomplete casting✓ Discoloration
▪Conclusion
▪References
2
INTRODUCTION
▪ The dental profession has used precision-type castings for the most part of century.
▪ Using the lost wax technique, Taggart in 1907 developed a process for making castings used in restoration of prepared teeth.
3
▪ An unsuccessful casting results in considerable trouble and loss of time.
▪ Casting procedure is technique sensitive.
▪ Proper sequence of all steps is essential for obtaining correct desirable casting.
4
WAXES IN DENTISTRY
▪ Wax has been a valuable commodity for many decades in dentistry.
▪ They have a versatile role to play in conservative as well as prosthetic dentistry.
5
▪ May be composed of natural and synthetic waxes, gums, fats, fatty acids, oils, natural and synthetic resins, and pigments.
▪ The particular working characteristics of each wax are achieved by blending the appropriate natural and synthetic waxes, resins and other additives.
6

.
2
7DENTAL WAXES
PATTERN PROCESSING IMPRESSION
CASTING
BASEPLATE
BOXING
UTILITY
STICKY
CORRECTIVE
BITE REGISTRATION
INLAY
INLAY WAX▪ Used to prepare patterns which replicates the casting .
▪ Composition:✓Paraffin : promotes moldability of wax below its melting temp.✓Carnauba : decrease flow at mouth temp.
✓Ceresin : increase the melting range✓Beeswax✓Gum dammar : improve smoothness in molding, doesnot flake
✓Synthetic wax✓Colorants
8
▪ A/C to ADA specification no. 4
Inlay wax : Type I (Medium) : Direct technique
Type II (Soft) : Indirect technique
9
▪ Properties of Inlay wax :
• Melting range : 23°C - 40°C
• Thermal expansion : 0.7% above 20°C
• Volumetric contraction : 0.35% when cooled from 37°C to 25°C
• Flow : Type I - not more than 1% at 37°CType II – not more than 1% at 30°C
10
11
CASTING DEFECTS
12

.
3
▪ Defects in castings can be classified under five headings a/c to Coombe:
1) Distortion
2) Surface roughness and irregularities
3) Porosity
4) Incomplete or missing detail
5) Discolouration
13
DISTORTION
▪ Any marked distortion of the casting is probably related to distortion of the wax pattern.
▪ Some distortion of the wax pattern occurs as the investment hardens around it.
14
▪WHY??
• Release of stresses in pattern due to:
1. Contraction on cooling2. Occluded gas bubbles
3. Change of shape of wax during moulding4. From manipulation, carving and removal
• Wax not at uniform temp. when inserted in cavity
• Wax not held under uniform pressure during cooling
15
Configuration of the patternType of the wax
Thickness
▪ Distortion as the thickness of the pattern
Distortion as the setting expansion of the investment
Factors that influence distortion
16
▪PREVENTION
✓By proper manipulation of wax:
Minimal carving force & change in temp.Minimal storage of pattern
17
SURFACE ROUGHNESS & IRREGULARITIES
▪ The surface of a dental casting should be an accurate reproduction of the surface of the wax pattern from which it is made.
▪ Excessive roughness or irregularities on the outer surface of the casting necessitate additional finishing and polishing.
18

.
4
• Defined as relatively finely spaced surface imperfections whose height, width, and direction establish the predominant surface pattern.
Surface Roughness
• Refer to isolated imperfectionssuch as nodules, that don’t characterize the total surface area.
Surface Irregularity
19CAUSES
• Air bubbles on the pattern
• Water films causing ridges & veins on the surface
• Too rapid heating resulting in fins or spines
• Under heating causing incomplete elimination of wax
• Inappropriate water/powder ratio
• Prolonged heating
• Temperature of alloy too high
• Casting pressure too high
• Foreign bodies
• Impact of molten alloy
• Pattern position
20
PREVENTION
• Use of Vacuum Investing Technique
• Vibrate during & after mixing
• Use of wetting agent to reduce surface tension of wax pattern
• Air dry the wetting agent as excess water will dilute investment, causing irregularities
• The mold should be heated gradually
• Heat the ring for sufficient period of time to remove carbonaceous residue
• Water/powder ratio should be accurate
21 22
POROSITY
▪ Porosity may occur both within the interior region of a casting and on the external surface.
▪ The latter is a factor in surface roughness, but also it is generally a manifestation of internal porosity.
23
▪ Not only does the internal porosity weaken the casting but also if it extends to the surface, it may be a cause for discoloration.
▪ If severe:➢ can produce leakage at the tooth-restoration interface
➢ secondary caries
24

.
5
POROSITY
Solidification Shrinkage
Trapped Gas Residual air
Localized Shrinkage Porosity
Microporosity
Suck Back Porosity
Pin Hole Porosity
Gas Inclusions
Subsurface Porosity
Back Pressure Porosity
Phillips’; Science of dental material ; 10thedition
25
LOCALIZED SHRINKAGE POROSITY
▪ These are large irregular voids usually found near the sprue-casting junction.
▪ Occurs when cooling sequence is incorrect & the sprue freezes before the rest of the casting.
26
▪ During a correct cooling sequence, sprue should freeze last.
Helps molten metal to flow into mold to compensate for the shrinkage of the casting as it solidifies
27
CAUSES REMEDY28
▪ Incomplete feeding of molten metal during solidification shrinkage
▪ Thin sprue & absence of reservoir
▪ Incorrect sprue attachment and angulation
▪ Sprue of adequate diameter▪ Flaring at point of sprue
attachment
▪ Maintaining adequate flow of alloy
▪ Presence of reservoir
▪ Sprue attached at thickest portion and 45° angulation
29
MICROPOROSITY
▪ Fine irregular voids within the casting
▪ Seen when the casting freezes too rapidly
▪ Rapid solidification occurs when the mold or casting temperature is too low
▪ This type of defect is not detectable unless the casting is sectioned
30
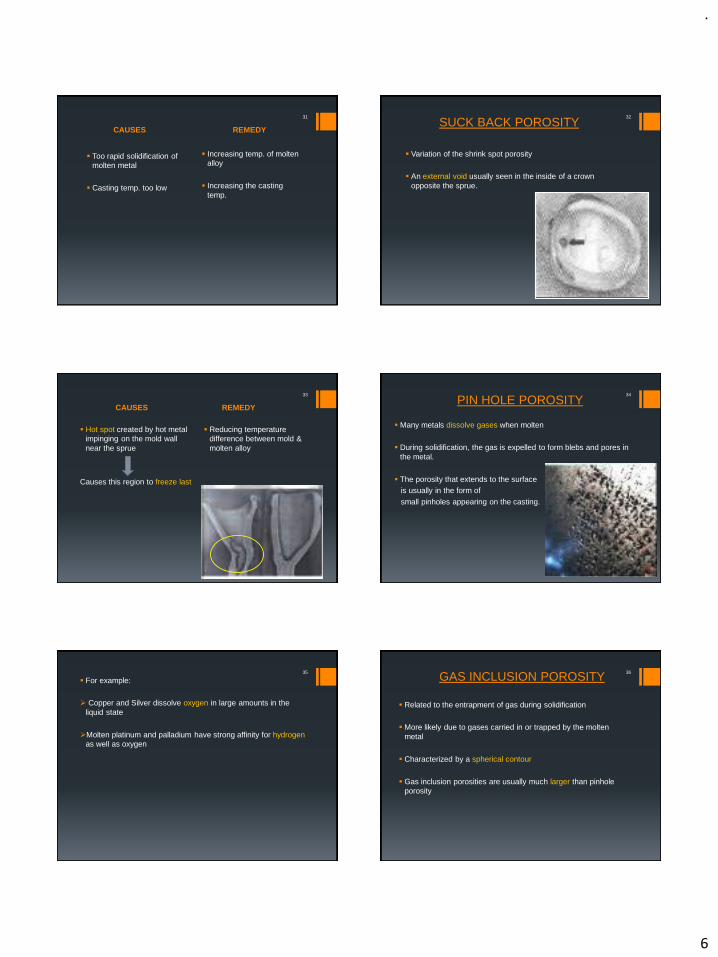
.
6
CAUSES REMEDY
31
▪ Too rapid solidification of molten metal
▪ Casting temp. too low
▪ Increasing temp. of molten alloy
▪ Increasing the casting temp.
SUCK BACK POROSITY
▪ Variation of the shrink spot porosity
▪ An external void usually seen in the inside of a crown opposite the sprue.
32
CAUSES REMEDY
33
▪ Hot spot created by hot metal impinging on the mold wall near the sprue
Causes this region to freeze last
▪ Reducing temperature difference between mold & molten alloy
PIN HOLE POROSITY
▪ Many metals dissolve gases when molten
▪ During solidification, the gas is expelled to form blebs and pores in the metal.
▪ The porosity that extends to the surfaceis usually in the form of
small pinholes appearing on the casting.
34
▪ For example:
➢ Copper and Silver dissolve oxygen in large amounts in the liquid state
➢Molten platinum and palladium have strong affinity for hydrogenas well as oxygen
35 GAS INCLUSION POROSITY
▪ Related to the entrapment of gas during solidification
▪ More likely due to gases carried in or trapped by the molten metal
▪ Characterized by a spherical contour
▪ Gas inclusion porosities are usually much larger than pinhole porosity
36

.
7
37
CAUSES REMEDY
38
▪ Gas incorporated during casting procedure due to :
➢Use of poorly adjusted torch flame
➢Use of oxidizing flame
➢Proper adjustment and positioning of torch
➢Use of reducing zone
CAUSES REMEDY
39
SUBSURFACE POROSITY
▪ Caused by the simultaneous nucleation of solid grains and gas bubbles at the first moment the metal freezes at the mould walls.
▪ Controlling the rate at which the molten metal enters the mould
• It also occurs due to entrapped gases in molten alloy
• Ryge et al reported that subsurface & microporosities are reduced by the use of a sufficiently long sprue & a melt temperature of 100˚C-150˚C above the melting point of alloy.
• Leinfelder et al reported that long sprues are preferable for thick castings while short sprues are beneficial for thin castings i.e. the sprue design should be related to the surface area-to-volume ratio of castings.
Journal of dental rest.; Jan 1981; vol 60; no1; page 59-67
40
BACK PRESSURE POROSITY
▪ Caused by the inability of the air in the mold to escape through the pores in the investment
▪ Appears as large concave depressions on inner surface of casting
▪ Results in a porous casting with rounded short margins
41
CAUSES REMEDY42
▪ Less porous, dense investing material
▪ Vacuum investing producing increase in mold density
▪ Improper wax elimination, clogging of mold with residual carbon
▪ Low casting temp. and pressure
▪ Use of porous investment material
▪ Adequate liquid/powder ratio
▪ Proper wax burn out
▪ Adequate casting temp. and pressure administered

.
8
INCOMPLETE CASTINGS
▪ Occasionally, only a partially complete casting or perhaps no casting at all, is found.
▪ The obvious cause is that molten alloy has been prevented, in some manner, from completely filling the mold
▪ It manifests in 2 forms :
✓Rounded margins✓Partial/No casting
44
CAUSES REMEDY
45
Rounded margins
▪ Incomplete wax elimination during burnout leaving behind CO that creates strong reducing environment. Produces shiny round margins
▪ Inadequate casting pressure
▪ Proper time and temp. utilized during wax burnout
▪ Proper casting force applied
Incomplete casting resulting from incomplete wax elimination is characterized by rounded margins &
shiny appearance
46
CAUSES REMEDY
47
Partial/No casting
▪ Obstructed flow of molten alloy due to blockage of ingate
▪ High viscosity of molten alloy due to insufficient heating
▪ Inadequate casting pressure
▪ Insufficient venting of air from mold creating back pressure preventing filling of mold
▪ Debris properly cleaned from sprue channel
▪ Casting temp. atleast 150° above melting point of alloy
▪ Adequate casting force
▪ Backpressure overcome by sufficient casting pressure
DISCOLOURATION▪ Casting may acquire certain discolouration due to incorrect
procedure which then becomes difficult to remove
▪ These include:✓Carbon inclusions✓Copper contamination✓Sulphur contamination✓Mercury contamination✓Wax residues
48
▪Carbon inclusions
➢Improperly adjusted torch flame
➢Carbon containing investment or crucible
▪ Carbon tends to get absorbed on surface of alloy causing formation of visible inclusions
49

.
9
50
Non combustion zone
Combustion zone Reducing zone
Oxidizing zone
▪Copper contamination
➢If casting held by steel tongs and placed in pickling solution
remnant copper creates galvanic cell
Copper deposition on casting metal
Permanent discolouration
51
Avoided byuse of steel tongs to hold
casting during pickling
▪Sulphur contamination
➢Sulphur content of torch flame causes black casting
➢Prolonged heating of casting : disintegration of investment & formation of sulphur compounds
▪Mercury contamination
➢Casting placed close to amalgam dies or scrap
52 Black Casting:
▪ Occurs due to :
➢Overheating the investment above 7000c
Causes it to decompose liberating Sulphur or Sulphur compounds
They readily combine with the metals in alloy forming a sulphide film
Gives a dark casting which cannot be cleaned by pickling
53
CONCLUSION
▪ Casting defects are often difficult to characterize due to the intrinsic complexity of casting process.
▪ Proper identification of a particular defect is the prerequisite to correcting and controlling the quality of castings.
54
▪ Defects in castings can be avoided by strict observance of procedures governed by certain fundamental rules and principles.
▪ With present techniques and continuous advancements, casting failures should be the exception, not the rule.
55

.
10
REFERENCES
▪ Phillips sciences of dental materials- Anusavice 10th ed.
▪ Fundamentals of fixed prosthodontics- Shillinburg
▪ Contemporary fixed prosthodontics- Rosensteil
▪ Textbook of operative dentistry- Vimal K Sikri
▪ Journal of dental rest.; Jan 1981; vol 60; no1; page 59-67
▪ Journal of American Dental Association, Leinfelder ;1997
56

.
1
CAVITY PREPARATION FOR COMPOSITE RESTORATIONS
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENTS
Introduction Objectives of composite cavity preparation Differences between composite and amalgam cavity preparation Principles of cavity preparation Types – Conventional
Bevelled conventionalModifiedBox – onlyFacial / Lingual slot
Related articles Conclusion
INTRODUCTION
Skinner in 1959 wrote “The esthetic quality of a restoration may be as
important to the mental health of the patient as the biological & technological qualities of a restoration are to his physical or dental health ”.
The search for an ideal esthetic material for restoring teeth has resulted in significant improvement in both esthetic materials and techniques for using them.
Composite restorations have revolutionized restorative dentistry due to their conservative nature, adhesive bonding and patient appeal. The adhesive bonding ability makes it unnecessary to remove tooth structure for retention, prevention, and convenience. Successful restorations can be done with less precise preparations.
With paradigm shift from retentive restorations to conservative restorations, there is an increasing emphasis on minimally invasive cavity preparations.
OBJECTIVES
Removing the fault, defect, old material, or friable tooth structure
Creating prepared enamel margins of 90 degrees or greater (>90 degrees usually preferable)
Creating 90-degree (or butt joint) cavosurface margins on root surfaces.
DIFFERENCES BETWEEN CAVITY PREPARATION OF COMPOSITE RESTORATION WITH THAT OF AMALGAM
Less outline extension (adjacent suspicious
or at-risk areas [grooves or pits] may be
“sealed” rather than restored)
An axial or pulpal wall (or both) of varying
depth (not uniform)
Incorporation of an enamel bevel at some areas (the width of which is dictated by the need for secondary retention or esthetics)
Tooth preparation walls being rough (to increase the surface area for bonding)
Possible use of a diamond stone (to increase the roughness of the tooth preparation walls)
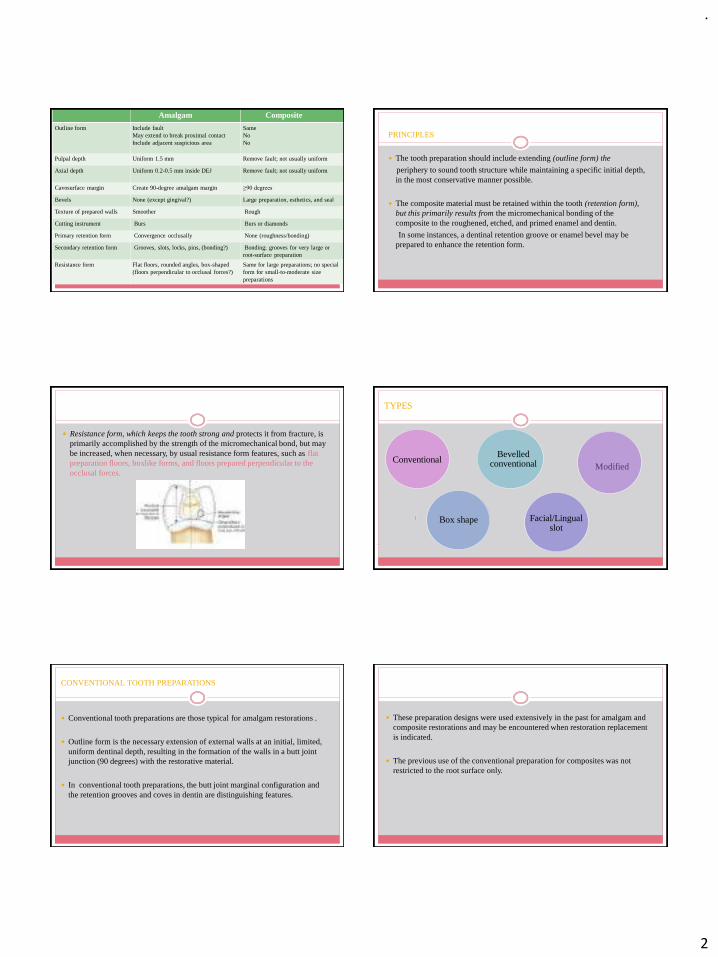
.
2
Amalgam Composite
Outline form Include fault May extend to break proximal contact Include adjacent suspicious area
SameNoNo
Pulpal depth Uniform 1.5 mm Remove fault; not usually uniform
Axial depth Uniform 0.2-0.5 mm inside DEJ Remove fault; not usually uniform
Cavosurface margin Create 90-degree amalgam margin ≥90 degrees
Bevels None (except gingival?) Large preparation, esthetics, and seal
Texture of prepared walls Smoother Rough
Cutting instrument Burs Burs or diamonds
Primary retention form Convergence occlusally None (roughness/bonding)
Secondary retention form Grooves, slots, locks, pins, (bonding?) Bonding; grooves for very large orroot-surface preparation
Resistance form Flat floors, rounded angles, box-shaped (floors perpendicular to occlusal forces?)
Same for large preparations; no special form for small-to-moderate size preparations
PRINCIPLES
The tooth preparation should include extending (outline form) the
periphery to sound tooth structure while maintaining a specific initial depth, in the most conservative manner possible.
The composite material must be retained within the tooth (retention form), but this primarily results from the micromechanical bonding of the composite to the roughened, etched, and primed enamel and dentin.
In some instances, a dentinal retention groove or enamel bevel may be prepared to enhance the retention form.
Resistance form, which keeps the tooth strong and protects it from fracture, is primarily accomplished by the strength of the micromechanical bond, but may be increased, when necessary, by usual resistance form features, such as flat preparation floors, boxlike forms, and floors prepared perpendicular to the occlusal forces.
TYPES
Bevelledconventional Modified
Facial/Lingual slot
Conventional
Box shape
CONVENTIONAL TOOTH PREPARATIONS
Conventional tooth preparations are those typical for amalgam restorations .
Outline form is the necessary extension of external walls at an initial, limited, uniform dentinal depth, resulting in the formation of the walls in a butt joint junction (90 degrees) with the restorative material.
In conventional tooth preparations, the butt joint marginal configuration and the retention grooves and coves in dentin are distinguishing features.
These preparation designs were used extensively in the past for amalgam and composite restorations and may be encountered when restoration replacement is indicated.
The previous use of the conventional preparation for composites was not restricted to the root surface only.
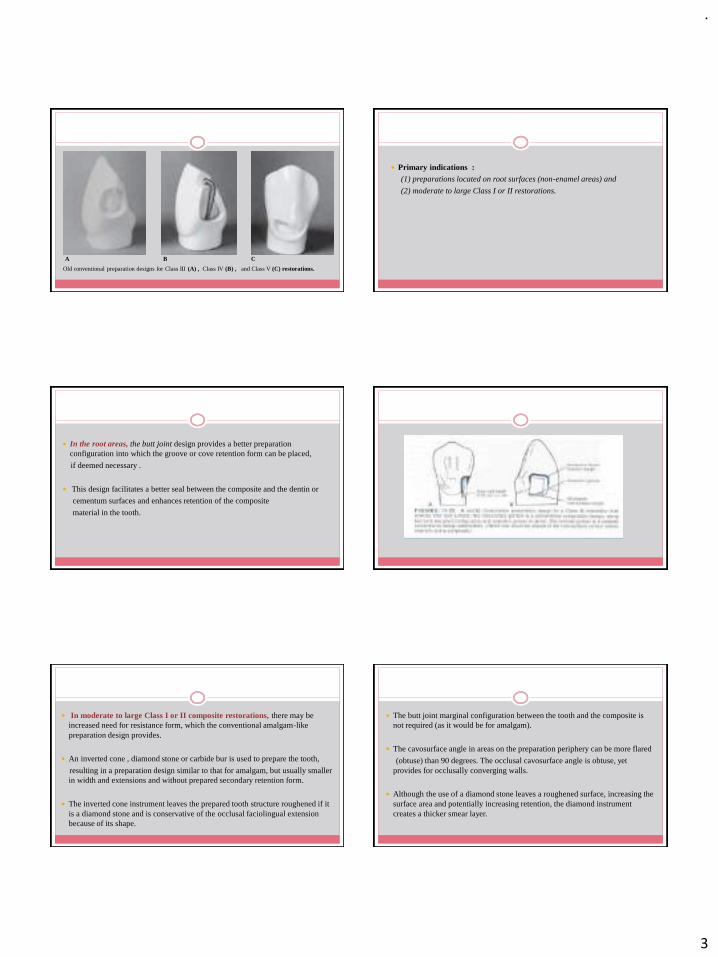
.
3
Old conventional preparation designs for Class III (A) , Class IV (B) , and Class V (C) restorations.
A B C
Primary indications :(1) preparations located on root surfaces (non-enamel areas) and
(2) moderate to large Class I or II restorations.
In the root areas, the butt joint design provides a better preparation configuration into which the groove or cove retention form can be placed,
if deemed necessary .
This design facilitates a better seal between the composite and the dentin or
cementum surfaces and enhances retention of the composite
material in the tooth.
In moderate to large Class I or II composite restorations, there may be increased need for resistance form, which the conventional amalgam-like preparation design provides.
An inverted cone , diamond stone or carbide bur is used to prepare the tooth,
resulting in a preparation design similar to that for amalgam, but usually smaller in width and extensions and without prepared secondary retention form.
The inverted cone instrument leaves the prepared tooth structure roughened if it is a diamond stone and is conservative of the occlusal faciolingual extension because of its shape.
The butt joint marginal configuration between the tooth and the composite is not required (as it would be for amalgam).
The cavosurface angle in areas on the preparation periphery can be more flared
(obtuse) than 90 degrees. The occlusal cavosurface angle is obtuse, yet provides for occlusally converging walls.
Although the use of a diamond stone leaves a roughened surface, increasing the surface area and potentially increasing retention, the diamond instrument creates a thicker smear layer.

.
4
Because of the similarity of the Class I or II conventional compositepreparation to an amalgam tooth preparation, many operators prefer its usewhether the Class I or II preparation is for a large posterior composite
or for restoring a new, smaller carious lesion.
Because conservation of tooth structure is important, it should be preparedwith as little faciolingual extension as possible and should not routinely beextended into all pits and fissures on the occlusal surface where sealants maybe otherwise indicated.
The box-like form increases the negative effects of the C-factor.
BEVELED CONVENTIONAL
Beveled conventional tooth preparations are similar to conventional preparations in that the outline form has external boxlike walls, but with some beveled enamel margins.
The preparation may be accomplished with a diamond stone or bur.
The principles of conventional outline form with the limited initial depth of the axial and pulpal walls are followed.
Indications :-
when a composite restoration is used to replace an existing restoration (usually amalgam) exhibiting a conventional tooth preparation design with enamel margins
to restore a large carious lesion
❖ This design is most typical for Classes III, IV, and V restorations
FIGURE- Beveled conventional preparation designs for Class III (A and B), Class IV (C and D), and Class V (E and F) restorations.
Usually all of the old material is removed, providing increased bonding potential, not only to enamel, but also to dentin.
Sometimes the old restorative material may be only partially removed if the remaining material is judged acceptable (radiographically negative for caries, with symptomless tooth pulp).
Leaving old amalgam material may result in a poor esthetic result as it may show through the overlying composite material.
To facilitate better marginal sealing and bonding, some accessible enamel margins may be beveled and acid etched.
ADVANTAGE OF ENAMEL BEVEL
the ends of the enamel rods (exposed by beveling) are more effectively etched than otherwise occurs when only the sides of the enamel rods are exposed to the acid etchant.
Ends of enamel rods (A) are more effectively etched, producing deeper microundercutsthan when only the sides of enamel rods are etched (B).

.
5
Also, the increase in etched surface area results in a stronger enamel-to-resin bond, which increases retention of the restoration and reduces
marginal leakage and marginal discoloration.
Incorporation of a cavosurface bevel may enable the restoration
to blend more esthetically with the coloration of the surrounding tooth
structure.
Even recognizing these advantages, bevels are not usually placed on theocclusal surfaces of posterior teeth or other areas of potential heavycontact because a conventional preparation design already producesend-on etching of the enamel rods by virtue of the enamel rod directionon occlusal surfaces.
Bevels also are not placed on proximal margins if such beveling results inexcessive extension of the cavosurface margins.
The beveled conventional preparation design is rarely used for posteriorcomposite restorations.
bevel
bevel
Four groups of 15 teeth each were prepared for a class 5 composite resin restoration with the cervical margins finished as follows:
a butt joint margin 1) <1 mm from the CEJ, 2) >1.5 mm from the CEJ
a beveled margin 3) < 1 mm from the CEJ, 4) >1.5 mm from the CEJ
The teeth were acid etched, bonded and restored with a microfilled composite resin and evaluated for cervical microleakage by Ca45 autoradiography.
The butt joint margins placed less than 1 mm from the CEJ had significantly more
microleakage than the other groups, indicating that all enamel margins of a class 5
composite resin restoration should be beveled to decrease microleakage
regardless of their location relative to the CEJ.
DIRECT ADHESIVE RESTORATION OF ANTERIOR TEETH:
PART 1. FUNDAMENTALS OF EXCELLENCE
E.M.de Araújo Jr, L.N. Baratieri, S. Monteiro Jr, L.C.C. Vieira, M.A.C. Andrada P P
Objective: To present an innovative approach for direct restorations with composite resin in anterior teeth. Emphasis is placed on minimally invasive preparation and esthetics.
Cavosurface bevels are not necessary for retention and/or esthetics.
EFFECT OF LIGHT SOURCE POSITION AND BEVEL PLACEMENT ON FACIAL MARGIN ADAPTATION OF RESIN-BASED COMPOSITE RESTORATIONS
D.C. Hoelscher, W.A. Gregory, J.B. Linger, F.E. Pink American Journal of Dentistry 2000 (13:171–175)
The nonbeveled restorations leaked more than the beveled restorations. In
the beveled specimens, facial light curing resulted in less microleakage as
compared to lingual cure and concluded that Facial bevels with facial
light curing can reduce microleakage in Class III composite resin restorations.
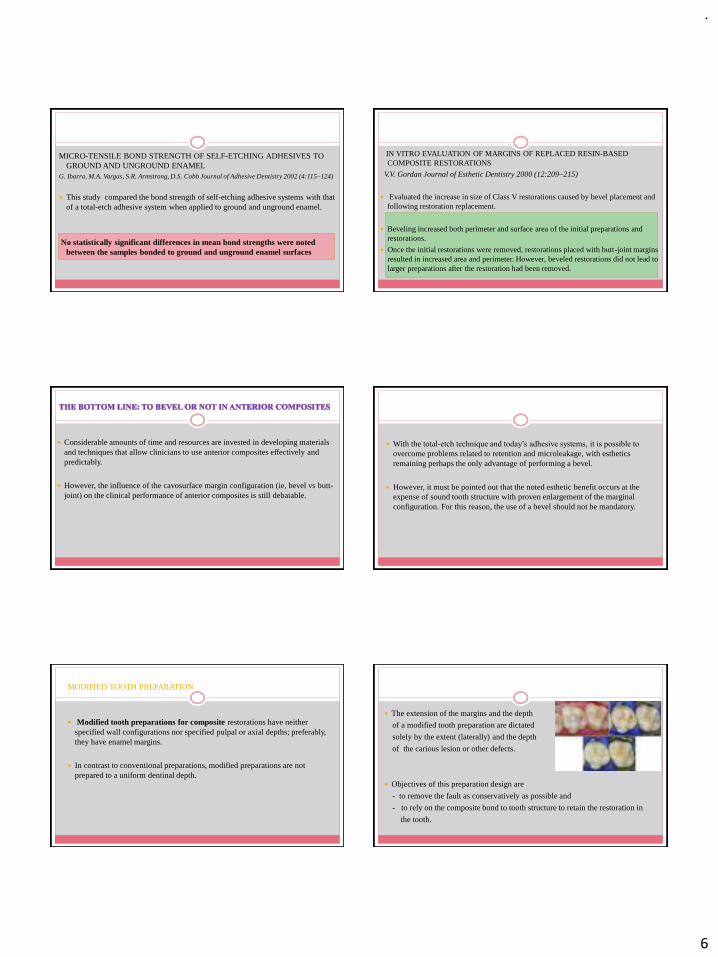
.
6
MICRO-TENSILE BOND STRENGTH OF SELF-ETCHING ADHESIVES TO GROUND AND UNGROUND ENAMEL
G. Ibarra, M.A. Vargas, S.R. Armstrong, D.S. Cobb Journal of Adhesive Dentistry 2002 (4:115–124)
This study compared the bond strength of self-etching adhesive systems with that of a total-etch adhesive system when applied to ground and unground enamel.
No statistically significant differences in mean bond strengths were noted between the samples bonded to ground and unground enamel surfaces
IN VITRO EVALUATION OF MARGINS OF REPLACED RESIN-BASED COMPOSITE RESTORATIONS
V.V. Gordan Journal of Esthetic Dentistry 2000 (12:209–215)
Evaluated the increase in size of Class V restorations caused by bevel placement and following restoration replacement.
Beveling increased both perimeter and surface area of the initial preparations and restorations.
Once the initial restorations were removed, restorations placed with butt-joint margins resulted in increased area and perimeter. However, beveled restorations did not lead to larger preparations after the restoration had been removed.
Considerable amounts of time and resources are invested in developing materials and techniques that allow clinicians to use anterior composites effectively and predictably.
However, the influence of the cavosurface margin configuration (ie, bevel vs butt-joint) on the clinical performance of anterior composites is still debatable.
With the total-etch technique and today’s adhesive systems, it is possible to
overcome problems related to retention and microleakage, with esthetics remaining perhaps the only advantage of performing a bevel.
However, it must be pointed out that the noted esthetic benefit occurs at the expense of sound tooth structure with proven enlargement of the marginal configuration. For this reason, the use of a bevel should not be mandatory.
MODIFIED TOOTH PREPARATION
Modified tooth preparations for composite restorations have neither specified wall configurations nor specified pulpal or axial depths; preferably, they have enamel margins.
In contrast to conventional preparations, modified preparations are not prepared to a uniform dentinal depth.
The extension of the margins and the depth
of a modified tooth preparation are dictated
solely by the extent (laterally) and the depth
of the carious lesion or other defects.
Objectives of this preparation design are
- to remove the fault as conservatively as possible and
- to rely on the composite bond to tooth structure to retain the restoration in
the tooth.

.
7
Modified preparation designs for Class III (A and B), Class IV (C and D),and Class V (E and F) restorations
Modified tooth preparations conserve more tooth structure because retention is obtained primarily by micromechanical adhesion to the surrounding enamel and underlying dentin, rather than by preparation of retention grooves or coves in dentin.
Round burs or diamond stones may be used for this type of preparation, resulting in a marginal design similar to a beveled preparation; however, less tooth structure is removed in the internal portions of the preparation.
• Often, the preparation appears to have been “scooped out” rather than having
the distinct internal line angles characteristic of a conventional preparation design.
Indications for the initial restoration of smaller, cavitated, carious lesions usually
surrounded by enamel and
for correcting enamel defects.
They can be successful for larger restorations as well .
However, for the restoration of large carious lesions, wider bevels or flares and retention grooves, coves, or locks may be indicated in addition to the
retention afforded by the adhesive procedures.
BOX-ONLY TOOTH PREPARATION
This design is indicated when only the proximal surface
is faulty, with no lesions present on the occlusal surface.
A proximal box is prepared with an inverted cone or round
diamond stone or bur held parallel to the long axis of the tooth crown.
• The instrument is extended through the marginal ridge in a gingival direction.
• The initial proximal axial depth is prepared 0.2 mm inside the dentinoenameljunction.
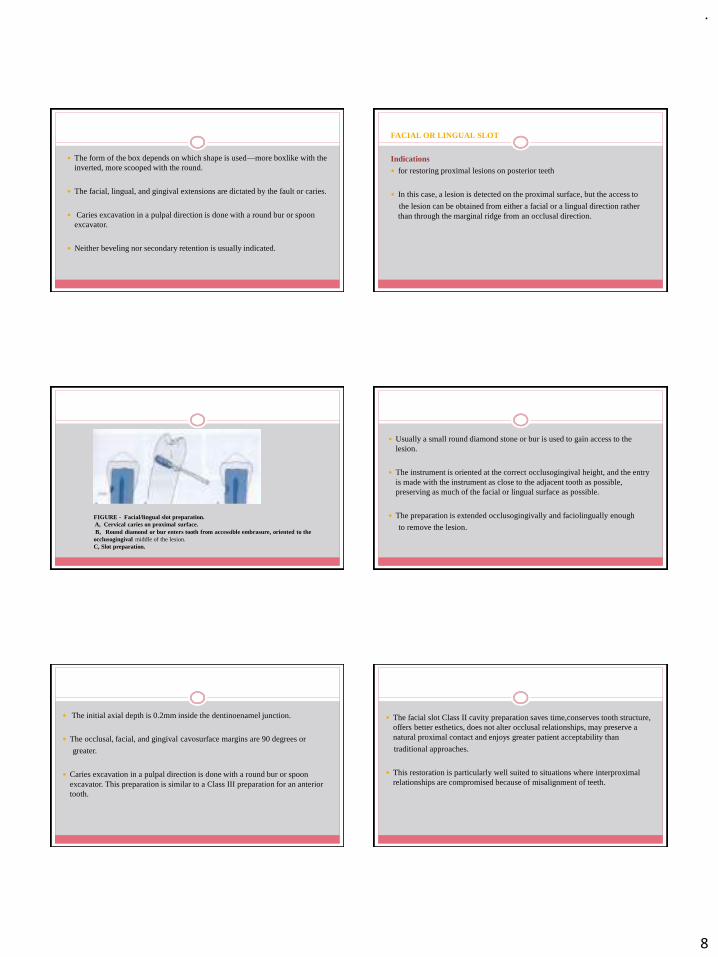
.
8
The form of the box depends on which shape is used—more boxlike with the inverted, more scooped with the round.
The facial, lingual, and gingival extensions are dictated by the fault or caries.
Caries excavation in a pulpal direction is done with a round bur or spoon excavator.
Neither beveling nor secondary retention is usually indicated.
FACIAL OR LINGUAL SLOT
Indications
for restoring proximal lesions on posterior teeth
In this case, a lesion is detected on the proximal surface, but the access to
the lesion can be obtained from either a facial or a lingual direction rather than through the marginal ridge from an occlusal direction.
FIGURE - Facial/lingual slot preparation.A, Cervical caries on proximal surface.B, Round diamond or bur enters tooth from accessible embrasure, oriented to the
occlusogingival middle of the lesion. C, Slot preparation.
Usually a small round diamond stone or bur is used to gain access to the lesion.
The instrument is oriented at the correct occlusogingival height, and the entry is made with the instrument as close to the adjacent tooth as possible, preserving as much of the facial or lingual surface as possible.
The preparation is extended occlusogingivally and faciolingually enough
to remove the lesion.
The initial axial depth is 0.2mm inside the dentinoenamel junction.
The occlusal, facial, and gingival cavosurface margins are 90 degrees or
greater.
Caries excavation in a pulpal direction is done with a round bur or spoon excavator. This preparation is similar to a Class III preparation for an anterior tooth.
The facial slot Class II cavity preparation saves time,conserves tooth structure, offers better esthetics, does not alter occlusal relationships, may preserve a natural proximal contact and enjoys greater patient acceptability than
traditional approaches.
This restoration is particularly well suited to situations where interproximalrelationships are compromised because of misalignment of teeth.
.
9
Effect of Cavity Design on the Strength of Direct Posterior Composite Restorations: An Empirical and FEM Analysis
V. Susila Anand , C. Kavitha, and C. V. Subbarao
International Journal of dentistry , 2011
Two cavity preparation designs, a conventional box and a new minimally invasive
concave shaped cavity with 4° taper, were studied with two composite restorative
materials, Restofill and Esthet-X.
Materials and Methods
Two split stainless steel (s.s) moulds with suitable plungers were fabricated using prototype designing with Pro E software.
box design. concave design.
The four corners of the moulds were focused for 10 s each with the curing tip to ensure adequate curing.
The final increment was covered with a mylar strip during curing
Every 2 mm increment of composite was cured with QTH curing light with an intensity of 400 mW/cm2 for 40 s.
Twenty samples were prepared for each design, 10 for each material.
The material was condensed into the moulds using Teflon-coated composite condensers
Empirical Testing The composite samples were loaded under compression in a universal testing
machine .
The load at fracture was noted and the compressive strength calculated.
FEM
Abaqus 6.7 3-D models of the moulds .
Statistical Analysis
t-test was done to analyze the statistical significance of the results.
Levene’s test of Equality of variances and t-test for equality of means was done for intra- and intergroup comparisons of strength values.
The stress level at the tooth-restoration interface in the optimized design was reduced significantly compared with the conventional design, irrespective of the bonding condition .
The conservative design (concave shape) had better strength (twofold on an average) than conventional design irrespective of the type of material.
Results
Cavities with large cavosurface angle , which are considered to lead to low stress concentrations near the free surface, were found to have better marginal integrity in a finite element study using axisymmetric models .P. Hubsch, J. Middleton, and J. Knox, “The influence of cavity shape on the stresses in composite dental
restorations: a finite element study,” Computer Methods in Biomechanics and Biomedical Engineering, vol. 5, no. 5, pp. 343–349, 2002.
In another study using shape optimization technique, it was found that the optimized design showed significant (24%) improvement in the resistance against debonding under compressive load compared with the traditional design .H. Li, X. Yun, J. Li et al., “Strengthening of a model composite restoration using shape optimization: a
numerical and experimental study,” Dental Materials, vol. 26, no. 2, pp. 126–134, 2010.

.
10
A more recent study compared the survival of restorations placed in saucer-shaped cavities to that of restorations placed in tunnel preparations .
After a mean service life of 28.8 and 30.3 months, the proportion of the tunnel and saucer-shaped restorations survived was 46% and 76%, respectively. Moreover, saucer-shaped restorations showed lower caries development than the tunnel restorations after an observation period of 24 months.
P. Horsted-Bindslev, B. Heyde-Peterson, P. Simonson, and V. Baelum, “Tunnel or saucer-shaped restorations: a survival analysis,” Clinical Oral Investigations, vol. 9, no. 4, pp. 233–
238, 2005.
CONCLUSION
In general, the development of caries removal techniques in restorative dentistry is progressing towards a more biological and conservative direction.
This has been made possible with better understanding of the aetiology, development and prevention of dental caries, the emergence of new caries removal techniques and advances in dental restorative materials.
In particular, the development of reliable adhesive technology in the oral cavity, which led the way to a minimal cavity preparation concept, has given a great impetus to the current thinking in this area.
The coming decades will continue to see shifts in the approach to caries removal techniques, cavity preparation and restoration techniques based on rational clinical and scientific principles.
TAKE HOME MESSAGE
✓A dentist must be familiar with the different cavity designs for a composite restoration .
✓ Should be able to clinically assess the type of design to be used based on skillful judgment taking into account the condition of the tooth and the type of material to be used.
✓ Updating one’s knowledge to the recent advances and developments is
important .
Only the wisest and stupidest of men never change . - Confucius

.
1
Ceramic veneers
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
contentS
◦ Introduction
◦ Indications and contraindications
◦ Advantages and Disadvantages
◦ Tooth preparation, impression , provisionalization
◦ Try in and adhesive luting procedure
◦ Choice of restorative material and technique
◦ Post op instruction
DEFINITION
◦ A veneer is a layer of tooth-colored material that is applied to a tooth to restore localized or generalized defect and intrinsic discolorations.
(Sturdevant's Art & Science of Operative Dentistry 7th Edition)
Constructing a veneer (without regard to the material) and bonding it to etched tooth structure is referred to as “laminating” (Faunce FR)
A porcelain laminate veneer is an extremely thin shell of porcelain applied directly to tooth structure
(McLaughlin G).
LAMINATE AND VENEER ????
Laminates are used to restore the original color of the tooth,
Veneers are used to change the original color of the tooth to make it look more natural.
Sandesh M Mayekar , Shades of a colour – illusion or reality?. DCNA. January 2001, 45 (1) 155 -173.
HISTORY
◦ 1930s- Porcelain veneers were introduced by Dr Charles Pincus to enhance an actor’s appearance for close-ups in movie industry.
◦ 1975 - Rochette introduced the use of silane coupling agent with porcelain laminate veneers in repairing fractured incisors
◦ 1983- Porcelain as a material for veneering was first reported by Horn
Indications for porcelain veneers
◦ Type I: moderate tooth discolorations/color corrections:
Tetracycline, Fluorides, Amelogenesis imperfecta
◦ Type II: anatomical malformations/corrections of position:
Type IIa Conoid teeth
Type IIb Diastemma
Type IIc Incisal edge lengthening
◦ Type III: extensive damage/changes in form:
Type IIIa Extensive coronal fractures
Type IIIb Congenital and acquired malformations

.
2
◦ Moderate discolorations, such as tetracycline staining, fluorosis, devitalized teeth
◦ Teeth darkened by age which are not conducive to vital bleaching
◦ Surface defects
◦ Replacement of missing or fractured parts of the teeth.
◦ Closing of diastemas
◦ rotated or malpositioned teeth
◦ Short teeth
◦ Agenesis of the lateral incisor
◦ Progressive wear pattern. If sufficient enamel remains and the desired increase in length is not excessive, porcelain veneers can be bonded
◦ Functionally sound metal ceramic or all‐ceramic crowns with
unsatisfactory color
Contraindications
◦ Certain tooth-to-tooth habits like bruxing or clenching, or other para-functional habits such as pencil chewing or ice crushing.
◦ little or no enamel for bonding
extended veneer restorations or ceramic crown may be the preferable treatment.
◦ Class III and end‐to‐end bites
◦ Poor oral hygeine
◦ Deciduous teeth and teeth that have been excessively fluoridated may not etch effectively
◦ Severe crowding
◦ Extreme bleaching‐resistant
discolorations, such as deep tetracycline or amalgam staining, or discolored devitalized teeth.
more opaque high‐strength ceramics
such as lithium disilicate,aluminumoxide, or zirconium oxide is indicated.
ADVANTAGES
◦ better shade control and long term stability of the chosen shade.
◦ Highly acceptable tensile bond strength
17.9 to 22.1 Mpa
6.2–9.7 Mpa (composite veneer)
◦ Inherent porcelain strength that permits reshaping teeth
Porcelain veneers are themselves fragile but once bonded to enamel, the restoration develops high tensile and shear strengths.
◦ Extremely good biocompatibility with gingival tissues
◦ Long lasting For example, a 5 year clinical study of 186 porcelain veneers placed in 61 patients showed a survival rate of 98.4%
◦ Resistance to stain
◦ Exceptional resistance to wear and abrasion.
◦ More resistant to deleterious effects of solvents
◦ Resistant to absorption of fluids
◦ Surface luster retention
◦ Lack of radiopacity

.
3
DISADVANTAGES
◦ The color cannot be easily modified once bonded in position.
◦ Irreversibility of preparation
◦ Level of difficulty of fabrication and placement,
◦ time involved and expense.
◦ Fragility
◦ Technical difficulties in avoiding overcontours and obtaining closely fitted porcelain/enamel margins.
◦ Margins- brittle and difficult to finish.
◦ Lower reparability
◦ Susceptibility to pitting by certain topical fluoride treatments. Stannous fluoride paste should be avoided
CLINICAL TECHNIQUE FOR SHADEMATCHING
◦ The dentist should try to take shades in a room free from wall coverings and decorations highly saturated with color.
◦ If the patient is wearing bright colors, they should be offset by using a relatively neutral colored apron like pale blue apron, since this color is most restful to the operator's cones.
◦ The patient's lipstick should be removed.
◦ Dentists should remove all tinted glasses before matching colors.
15
◦ WHEN-This should be done before beginning treatment, at a session when the teeth have not been dried out for any period of time.
◦ WHERE It should be done inside the operatory using color corrected light (Durotest “power plus” or Phillips color corrected), outside in daylight, and inside using incandescent light. And finally, reconsider the shade after the enamel has been prepared
16
WHEN WHERE AND HOW TO RECORD SHADE
◦HOW-Shade guides such as the Vita porcelain shade guide, are not ideal for veneers because they are too thick and are composed of several different layers including opaques.
◦ The best method is to have ceramist construct several trial laminates made from an impression of your patient’s teeth. Thus, several samples of different shade
choices can be offered.
17
Classification of tooth preparation for anterior veneers
◦ Class 0: no preparation
◦ Class 1: window preparation
veneers ends below incisal edge
◦ Class 2: feather‐edged preparation
technique
Veneer extends to the incisal edge; there is no reduction of the incisal edge.
.
4
◦ Class 3: bevel preparation (bevel/small butt joint)
Buccopalatal bevel; there is reduction of the incisal edge.
◦ Class 4: overlapping preparation of incisal edges (incisal overlap)
Reduction of the incisal edge and palatal extension of the preparation.
◦ Class 5: butt joint preparation
Incisal reduction of ≥2 mm, 90° lingual marginal finish.
Interproximal preparation includes the contact areas.
◦ Class 6: full veneer preparation (complete veneer, ¾ veneer)
Interproximal and palatal preparation extension,
palatal deep chamfer or rounded shoulder preparation.
hybrid between veneer and all‐ceramic crown.
Mandibular veneers: special considerations
◦ Not enough tooth structure remaining after the horizontal and vertical reduction.
◦ weak at the incisolabial junction,
sufficiently reduced and rounded to allow the veneer to be thick enough in that area
◦ greater maintenance for mandibular veneers in patients with heavy occlusal demands
◦ If discoloration is the reason it is advised to try bleaching first
◦ Incisal edge of mandibular anteriors is usually the most visible part of the veneer.
◦ Sufficient incisal reduction is needed to ensure a normal incisal edge appearance for that patient
TO REDUCE OR NOT
Depends on
(a) the thickness of the veneer needed for covering or reshaping,
(b) the degree of anticipated retention of the veneer
(c) recognition of how the increased thickness of the veneered tooth will change its appearance, structure, alignment, and function.
Most patients need to have about 50% of the labial and some proximal enamel removed in order not to overbuild the teeth being veneered.
◦WHEN TO CONSIDER REDUCTION
if no preparation
◦ distinct overcontouring at cervical and proximal tooth surfaces
◦ higher clinical failure rates due to an increase in microbial plaque accumulation.

.
5
CONTRAINDICATIONS TO REDUCTION
◦ The size of the pulp.
◦ The patient’s psychological state and feelings about tooth reduction or veneers
IF REDUCING, HOW MUCH?
◦ Depends on relative position of the tooth in the arch.
◦ ideally margins of the preparation should have enough enamel left to ensure an adequate seal.
◦ The gingival finish line should be epigingival or ≤0.5 mm subgingival to the
gingival margin
◦SUBGINGIVAL MARGIN
◦ In case of discolouration
◦ problem
dentin bonding provides less bond strength
difficult to achieve ideal dry bonding conditions with rubber dam insulation at subgingival veneer margins
◦ surgical crown‐lengthening procedure may be indicated (deeper than 0.5 mm
subgingivally)
◦ The best alternative for deeply stained teeth is the use of more opaque ceramic materials than porcelain.
◦ Monolithic lithiumdisilicate offers higher opacity for pressable (e.g. IPS e.maxPress) and CAD/CAM fabricated (e.g. Emax CAD) veneer
◦ In extreme discoloration cases, highly opaque zirconium oxide veneers might be an alternative to crown
BASIC PRINCIPLES OF TOOTH REDUCTION
➢ Reduction bur with caliberated diamond ring were used
➢ depth control based on the preexisting tooth surface
➢ excessive amount of enamel is reduced,
➢ risking dentin exposure
➢Diagnostic waxup restoring the original volume of tooth should be used as reference for tooth reduction
➢use of slightly tapered round bur in association with silicon indexes of additive waxup will allow economic reduction

.
6
TOOTH PREPARATION TECHNIQUE
Graded tooth reduction
◦ The minimal thickness for a porcelain laminate veneer is 0.3 to 0.5 mm. The required uniform reduction can be achieved by following an orderly progression of-
Labial reduction
Interproximal extension
Sulcular extension
Incisal or occlusal modification
Lingual reduction
31
ARMAMENTARIUM
Veneer preparation kit
Depth cuttersLVS 1-.3MM
LVS 2- .5MM
Two grit diamond burs
Labial reduction
◦ In most instances the needed reduction will be 0.5 mm, obtained by using the LVS‐1.
◦ Small teeth such as the mandibular incisors only require 0.3 mm reduction using LVS‐2.
◦ The appropriate LVS diamond depth cutter is selected and gently drawn across the labial surface of the tooth from mesial to distal. This will develop the depth cuts as horizontal grooves, leaving a raised strip of enamel in between
◦ The remaining enamel is then reduced to the depth of these initial cuts using a coarse diamond (LVS-3 or -4).
◦ The labial surface is axially reduced by 0.3–0.5 mm. Cervically, a shallow chamfer (0.5 mm) is prepared epigingival.
34
Proximal preparation
Proximal preparation is devided into
◦ Gingivoproximal area, which extends gingivally from the interdental contact area
◦ Direct proximal contact area, which is located in the incisal 2/3rd of the proximal surface
Gingivoproximal Preparation
◦ Care must be taken to avoid penetration into the dentogingival complex as well as the cementoenamel junction,
◦ The bur is held almost 60 degrees to the axial inclination and gently pushed towards the palate to create a dogleg gingivoproximal extension
◦ Depending on the facial convexity of the incisors, their depth can alter.
◦ It is usually kept supragingival.

.
7
◦The type of margin is preferably a chamfer form in this particular area.◦Depth of chamfer◦ chamfer is kept too deep then the
replacing porcelain will be thicker
◦ color-adjustment options will be limited when a heavy chamfer is used
◦ Although thin chamfer may produce improved color control, it is impractical because its thin porcelain margin makes it vulnerable in the dental laboratory or even in the dentist's chair.
◦ prefers medium chamfer that allows color adjustments and yet has a porcelain margin of adequate thickness.
◦ They can be placed subgingivally and more palatally in cases that display severe discoloration or diastema closure
◦Depth of Extension◦ The palatine extension of the
gingivoproximal area is related to the required color change and the visibility of the area.
◦ Usually distinct color difference between restoration and tooth requires deeper preparations towards the palate.
Interproximal Preparation
◦ Preferably, the interproximal margin should stay short of the contact area.
◦ Using the same round-end tapered fissure diamond bur, the gingivoproximal reduction is continued by uprighting the angle of the bur vertically into the proximal area
◦ Bur held parallel with the long axis of the tooth and parallel to the mid-line.
◦ The proximal margin on teeth that are free from color alteration or with "discreet discoloration" should be hidden by the preparation made far enough into the contact area so that the proximal wall will end 0.25 mm facial to the actual contact area
◦Whenever possible, it is best to preserve the contact area,
◦ an anatomical feature that is difficult to reproduce
◦ try-in procedures are simplified and save clinical adjustments of the contact areas
◦ Bonding and finishing procedures are thereby simplified and
◦ easier toothbrushing and dental flossing is made possible

.
8
Breaking the Contact
◦ closing a diastema or changing the shape or position of a group of teeth,
◦ the existence of caries, defects or preexisting composite fillings
Magne and Douglas classified preparation depth –
short-Veneer extend only to facial margin
medium- Extend into 50 % interdental area
Long-Veneer covers entire interdental area
◦ "medium wrapping" was the preferred choice The margin can be hidden, and extending the preparations into the contact area can provide a better, more stable seat for cementation.
◦ wraparound laminates can provide improved stress distribution within the restoration when it is subjected to incisal loading
Incisal preparation
◦ Window preparation
◦ Incisal lapping
Incisal Overlap
◦ porcelain is stronger and produces a positive seat during the cementation process.
◦ The esthetic characteristics of the porcelain veneer are more easily handled and controlled by the dental technician
◦ To improve the translucency of the veneer, a 1 mm incisal reduction is suggested with rounded line angles
◦ This preparation reduces stress concentration within the veneer by distributing the occlusal load over a widersurface
◦ The bur is held 90 degrees to the incisal edge and the necessary preparation is done

.
9
Window preparation◦ IN-VITRO STUDY
◦ increased risk of cohesive fracture due to the maximum stress placed on the veneer caused by incisal overlap design was demonstrated.
◦ window design prepared entirely into the enamel was resistant to axial stress
◦ concluded that the most conservative type of veneer or window preparation was the treatment of choice when strength was the first priority
◦ Maxillary canines in a patient with canine guided lateral guidance.
Cohesive fracture
◦ Due to the greater stress at the incisal edge of the veneer, clinical cohesive ceramic fractures can occur
◦ Photo-elastic studies have shown that by providing a wide vertical stop to resist loads by covering the incisal edge lessens the stress concentration in them.
◦ 1.5-2.0 mm reduction
◦ This will not only enhance the mechanical resistance but the esthetics as well.
Highton R, Caputo AA, Matyas JA. A protoelastic study of stress on porcelain laminate preparations. J Prosthetic Dent 1987;58:157-161.
Butt Joint
◦ Instead of a chamfer margin that may weaken the final restoration a flat shoulder should be used at the incisal edge.
◦ This will place 2.00-2.5 mm down from the incisal on the lingual surface
◦ creating a pleasing length, form and incisal characterization, allowing the ceramist much more flexibility.
◦ The butt joint preparation is simpler and consumes less time than the tooth preparation with palatal chamfer, and the master cast can be used for a precise palatal finish line
Tensile Forces
◦ If the ceramic is exposed to tensile loads it is more susceptible to failure.
◦ In a study of veneers with 2 mm of unsupported incisal ceramic and butt joint configuration, it was found that the incidence of fractured ceramic veneers was reduced to zero.
◦ The strongest veneers that remain intact for the longest period of time are those with 2.0 mm of unsupported incisal ceramic and butt joint ceramic veneers.
◦ Placing a palatal chamfer does not increase the strength.
◦ Ease of tooth preparation, veneer fabrication, insertion and bonding are some of the clinical advantages of a butt joint preparation.
Lingual preparation
◦ Magne et al showed that Palatal concavity proved to be an area of stress concentration
◦ The area of the cingulum presents the lowest tensile strength
◦ therefore be considered as an ideal location of porcelain-bonded restoration margin
◦ Margin Placement
◦ should preferably not finish at the concavity but rather it should be placed either above the concavity or below on the smooth convex area of the cingulum so that they will be subject to low tensile forces

.
10
◦ The round-ended fissure diamond bur should be held parallel to the long axis of the tooth while preparing the lingual side.
◦ should form a slight chamfer, 0.5 mm deep
◦ The finish line should preferably be about one-fourth the way down the lingual surface about 1.0mm from the centric contacts
◦ Care should be given not to locate this finishing line on the palatal concavity.
The direction of enamel rods varies from the incisal third to the cingulum.
increasing angle to the horizontal from 30° to more than 50°
This imposes a specific design of porcelain-bonded restoration finish line according to its location.
In the cingulum areaA butt margin or long chamfer cutting enamel rods at 90° is ideal for strong bonding,
In the incisal third, a mini-chamfer remains the best margin configuration
Temporaries
Class 4–6 preparations
(a) Teeth that have been extensively reduced and sensitivity exists,
(b) open contacts that could allow movement of the teeth,
(c) reduced teeth are too esthetically compromised for comfort
methods:
(1)direct composite veneers, directly on the non‐etched surface of the prepared
tooth;
(2) direct composite veneers, directly on a 1–2 mm etched surface of the prepared tooth
(3) direct composite veneers using a vacuform or silicone matrix made on a preoperative plaster model
(4) direct acrylic veneers using methyl methacrylate self‐cure acrylic
(5) indirect composite/acrylic temporaries, which are fabricated in the laboratory
IMPRESSION
◦ One step double mix impression technique
◦ Gingival cord of small diameter is placed into the bottom of sulcus
◦ This will remain in place during impression taking
◦ Gingival cord of large diameter placed into the entrance of sulcus with bimanual technique
◦ It is carried out 5-10 mins before impression taking
Deflection cord is removed immediately followed by injection of light body into sulcus
Insertion of tray loaded with heavy body

.
11
Placement of veneers
◦Try‐in
◦ each of the veneers is tried in individually, beginning with the most distal veneer
◦ After that each veneer should be placed on one by one.
◦ usually done posterior to anterior, except the centrals and laterals which should be placed centrals first, then laterals
◦ check the collective fit and relationship of one veneer to another, especially in the contact areas.
◦ Assess the shade and modify it as necessary.
◦ A good initial test is to place one veneer in position with glycerin on the tooth and compare that veneer to a shade tab of the selected shade.
◦ If the veneer color is unsatisfactory, use try‐in pastes that do not polymerize,
or place a small portion of the luting composite on the veneer and then reset the veneer on the prepared tooth to check the color.
◦ If patient is not happy with the shade, try the veneer with a lighter or darker shade of try‐in paste or composite until the right one is found
Final insertion
Soft tissue control.
◦ Gingival retraction cord should be placed
◦ Ideally, a rubber dam is the best way to secure overall moisture control.
◦ However, in subgingival margins it is either impossible or impractical to precisely seat the veneers with a rubber dam in place.
Cleaning and etching
◦ Apply 10 % HF for 90 sec to the inner surface and rinsed
◦ The precipitates remain after acid application ,
◦ Even abundant rinsing proves insufficient to clean
Handheld using flat ended instruments with sticky wax
◦ These residues removed by placing the restoration in ultrasonic bath (in 95% alcohol, acetone, distilled water) for 4-5 min
SILANATION
◦ One‐component adhesive silane is a easiest way to silanate
◦ 2-component silane systems will polymerize to an unreactive polysiloxane and therefore it must be used within a few hours
◦ Applied for 1 min and then air dried to thus allowing solvent to evaporate completely

.
12
◦ Drying the inside of the veneer, with "warm air" (possibly with a small hair dryer) will enhance the effect of the silane.
◦ Heating to 100°C (Using hair dryer or oven for 1 min) results in bond strength double
Enamel etching
◦ etched with 37% phosphoric acid (e.g. Total‐Etch, Ivoclar Vivadent,),
◦ dentin for 15 s
◦ enamel for 40 s
◦ sprayed with water for 15 s, and dried.
◦ If the patient contaminates this etched enamel surface with saliva, the surface must be re‐etched for
10 s, washed, and dried again
Adhesive application◦ The primer is applied over the exposed dentin area, left in place for 30 seconds and than very gently
dried until the carrier of the primer evaporates.
◦ This time should be extended if the carrier of the primer is water based, or shortened if it is alcohol or
acetone based
◦ Preferably it should be executed with a hair-dryer, the air from the air syringe can always be
contaminated
◦ Once the glossy appearance of the primer is achieved , than the adhesive can be applied on both the
dentin and the enamel with a brush
◦ adhesive is not light cured at this time
Bonding ◦ A light-curing luting composite is preferred for cementation
◦ A longer working time compared with dual cure or chemically curing materials is the major advantage of light curing
◦ if no color adjustments are needed, a transparent luting composite should be used
◦ The resin is applied with a brush to the inner part of the restoration.
Placement
◦ Generally, the distal‐most veneers in the posterior should be seated and
polymerized first, followed by the next mesial‐most veneer until the canines.
Next, seat central incisor veneers together, then the laterals, and finally, the canines.
◦ The adjacent teeth should be separated with matrix strips during both acid etching and insertion so the cement does not lock in or adhere to the adjacent tooth .
◦ Immediately remove excess cement in all marginal areas with foam pellets.
◦ Ten seconds of light polymerization at the incisal edge ensures stabilization of the veneer while other veneer surfaces should be covered with instruments or finger.
◦ Remove residual interproximal cement gently with foam pellets, dental floss, and Superfloss (Oral‐B) without dislocating the veneer
.
13
Polymerization◦ After excess is removed
◦ To avoid the development of an oxygen-inhibited layer at the margins, an oxygen inhibition material, such as deox (Ultradent) or glycerin, should be applied prior to the final polymerization
◦ Then each tooth's veneer is light polymerized for 60 to 90 seconds on all surfaces.
◦ Refine occlusion with microthin articulating film, 0.02 mm (AccuFilm II, Parkell),
PATIENT INSTRUCTIONS
✓Do's • Use a soft toothbrush with rounded bristles, and floss as you do with
natural teeth. • Use a less abrasive toothpaste and one that is not highly
fluoridated. • Use a soft acrylic mouth guard when involved in any form of
contact sport. • Ensure routine cleaning.
✓Don'ts • Avoid food or drinks that may contain coloring. • Do not use alcohol
and some medicated mouthwashes because they have the potential to affect the resin bonding material during the early phase (the first 48 hours). • Avoid hard
foods, chewing on ice, eating ribs and biting hard confectionaries and candy. •
Avoid extremes in temperature.
74
CONCLUSION◦ Perfect smile improves the self confidence, personality; social life and
have psychological effect on improving self image with enhanced self esteem of the patient
◦ New emerging concepts in esthetic dentistry with regards to materials, technology and public awareness has made veneers on demand
◦ The objective of cosmetic dentistry must be to provide the maximum improvement in esthetic with minimum trauma to the dentition.
75

.
1
DENTAL COMPOSITES
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
2
Introduction
History
Composition
Classification of composites
Properties of composite
3
Types of composites
Recent advances of composite
Finishing and polishing
Sandwich technique
Conclusion
References
INTRODUCTION
• The search for an ideal esthetic material for restoring teeth has resulted in significantly improvements in esthetic materials and techniques.
• Composites and acid etch technique represent two major advances.
• Composite resins are a class of mature and well established restorative materials that have their own indication in anterior and posterior teeth.
4INTRODUCTI
ON
• Dental composites have continued to evolve with the development of smaller particle sizes, better bonding systems, curing refinements and sealing systems.
5
DEFINITION
Composite—
“In materials science, a solid formed from two or more distinct phases (e.g., filler particles dispersed in a polymer matrix) that
have been combined to produce properties superior to or intermediate to those of the individual constituents”
-Philips
6

.
2
DEFINITION
Dental Composite—
“Highly cross-linked polymeric materials reinforced by a dispersion of glass, crystalline or resin filler particles and/or short fibers bound to the matrix by a coupling agents”
7
• Esthetic consideration are primary factors for seeking dental treatment.
• In 1959, Skinner quoted-
“ The esthetic quality of a restoration may be as important to
the mental health of patient as the biological and technical qualities of restoration are to his physical or dental health”
8
HISTORY• In the middle of the 20th century, in 1873 Thomas Fletcher
introduced the first tooth- colored filing materials, silicate cement .
• In the early 1940s, German chemists developed the first acrylic resins, but it was not marketed until the late 1940s because of World War II.
• The first dental acrylic resin product was introduced in 1948 in United States.
9 10
1950s, adhesive dentistry began with acid-etch
technique.
In 1962, Bowen developed a new type of composite material-
bisphenol-A glycidyl dimethacrylate(bis-GMA) , a monomer that forms a
cross-linked matrix
INDICATION OF COMPOSITES
Class I, II, III, IV, V, VI
11
Core buildups Sealants and preventive resin restorationsEsthetic enhancement procedures Veneering metal crowns/bridgePeriodontal splinting Non carious lesions Composite inlays
Contraindications of composites
• Isolation
• Occlusion
• Subgingival area/root surface
• Poor oral hygiene
• High caries index
• Habits (bruxism)
• Operator abilities
12

.
3
ADVANTAGES
1. Esthetic
2. Conservation of tooth structure
3. Less complex when preparing the tooth
4. Insulative,having low thermal conductivity.
5. Used almost universally
6. Bonded to tooth structure
7. Repairable
8. No corrosion
9. No health hazard
10. Cheaper then porcelain
13
DISADVANTAGES
1. Polymerization shrinkage→ leading to gap formation.
2. Technique sensitive
3. Higher coefficient of thermal expansion
4. Difficult, time consuming
5. Increased occlusal wear
6. Low modulus of elasticity
7. Lack of anticariogenic property
8. Staining Costly
14
COMPOSITION
Resin Matrix
Coupling Agent Fillers
15
COMPOSITION
Activator-Initiator system
Pigments
Optical modifiers
Color stabilizers
16
Other Components
17
RESIN MATRIX
“A plastic resin material that forms a continuous phase upon curing and binds the reinforcing filler particles”
-Philips➢ Aromatic or aliphatic dimethacrylate monomers:-• Bis-GMA
• Urethane-dimethacrylate (UDMA)
➢ Diluent monomers• Triethylene glycol dimethacrylate (TEGDMA)
• EGDMA
• HEMA
18
.
4
RESIN MATRIX
19
Form highly cross-linked,Strong, rigid, and durable polymer
structures
• Bis-GMA• UDMA
Polymerization shrinkage → low as 0.9%
Highly viscous and are difficult to blend and manipulate
RESIN MATRIX
20
-Bis-GMA
-UDMA
-TEGDMA
- HEMA
Varying proportions of
diluent monomers are blended for incorporating enough filler
The greater theProportion of these
“diluting” monomers,
the greater thePolymerization
shrinkage and the greater the risk of
eventualleakage in marginal
gaps
RESIN MATRIX
• Alternatives to TEGDMA are-
- Monomethacrylates and
-Acrylates such as –hydroxypropyl methacrylate
-isobornyl acrylate.
-Bicyclic cyclopropyl-acrylates
• Bicyclic cyclopropyl-acrylates undergo a radical ring-opening polymerization under formation of a 1,5-substituted ring-opened unit, and are more reactive.
• Therefore exhibit lower volume shrinkage during their polymerization.
21
FILLER “Inorganic, glass, and/or organic-resin particles that are dispersed in a resin matrix to increase rigidity, strength, and wear resistance, to decrease thermal expansion, due to water sorption, and reduce
polymerization shrinkage”
-Philips
➢ Material used :-
1. Borosilicate “hard glass”,
fused quartz, aluminum silicate, lithium aluminum silicate
Barium and strontium are the
most common elements used in fill
22
FILLER ➢ Filler loading:- from 50 - 86 % by weight
-35 to 71 % by volume
➢ Particle size distribution of filler :-
• Packing fraction for close-packed spherical structures of uniform-size is approximately 74% by volume.
• On insertion of smaller particles among the larger spheres, the void space can be reduced.
23
FILLER ➢ Fillers can provide the following benefits:-1. Reinforcement of the matrix resin resulting in increased hardness and
strength.
2. Reduction in polymerization shrinkage:- Increased filler loading reduces curing shrinkage in proportion to filler volume fraction.
3. Reduction in thermal expansion and contraction:- Increased filler loading decreases the overall coefficient of thermal expansion of the composite because glass and ceramic fillers thermally expand and contract less than do polymers.
4. Reduction in water sorption, softening and staining
5. Improved workability by increasing viscosity:- more filler, the thicker is the paste.
6. Increased radiopacity and diagnostic sensitivity
24

.
5
FILLER Important factors with regard to fillers that determine the properties and clinical application of composite –
• Amount of filler added
• Size of particles and distribution
25
Filler Size
• Determines the surface smoothness.
• Larger particles = rougher surface
• Composites are most often classified by the filler size.
Filler Content
• As the filler content increases, the resin content decreases
• Hardness and abrasion resistance increases
COUPLING AGENTS
“A bonding agent applied to filler particles to ensure chemical
bonding to resin matrix”
-Philips
26
Filler particle
Resin matrix
BOND
COUPLING AGENTS
“A bonding agent applied to filler particles to ensure chemical bonding to
resin matrix”
➢ Types of coupling agent used:-
1. Organosilane such as gamma methacryloxy propyl trimethoxy silane.
2. Titanates
3. Zirconates
➢ Organosilane methacrylate groups form covalent bonds with the resin when it is polymerized, thereby completing the coupling process.
27
COUPLING AGENTS
➢Function of coupling agent:-
1. Bind filler particles to resin.
2. Improved physical and mechanical properties
3. Inhibit leaching by preventing water from penetrating along the filler-resin interface.
28ACTIVATION/INITIATI
ON SYSTEM
• Activator- “Source of energy used to activate an initiator and produce free radicals.”
• Initiator- “A free radical−forming chemical used to start the
polymerization reaction”.
-Philips
➢ Free radicals can be generated by chemical activation or by external energy activation (heat, light, or microwave)
29
CHEMICALLY ACTIVATED (SELF-CURE) RESINS
Chemically activated resins are supplied as two pastes,
1. Benzoyl peroxide initiator
2. An aromatic tertiary amine activator (e.g., N, N-dimethyl-p-toluidine)
30
Amine Benzoyl peroxide
Form free radicals, and addition polymerization is
initiated
.
6
CHEMICALLY ACTIVATED (SELF-CURE) RESINS
31
➢ Advantages:-
1. Convenience and simplicity: no equipment needed, hazard-free
2. Long-term storage stability
3. Manipulation of working/ setting time by varying proportions
4. Degree of cure equal throughout material if mixed properly
5. Marginal stress buildup during curing is much lower than for photocured resins owing to relatively slower rates of cross-link formation
CHEMICALLY ACTIVATED (SELF-CURE) RESINS
32
➢Disadvantage :-
1. During mixing it is almost impossible to avoid incorporating air into the mix, thereby forming pores that weaken the structure and trap oxygen, which inhibits polymerization during curing.
2. No control over the working time after the two components have been mixed. Therefore both insertion and contouring must be completed quickly once the resin components are mixed.
3. Aromatic amine accelerators oxidize and turn yellow with time—i.e., color instability.
PHOTO-CHEMICALLY ACTIVATED (LIGHT-CURE) RESINS
“Particle-filled resin consisting of a single paste that becomes polymerized through the use of a photosensitive initiator system (typically camphorquinone and an amine) and a light-source activator (typically visible blue light)”
- Philips
• Supplied as a single paste contained in a lightproof syringe.
• The free radical initiating system, consisting of a photosensitizer and an amine initiator.
33 34
Exposure to light in the blue region
Produces an excited state of the
photosensitizer
Interacts with the amine
Form free radicals that initiate
addition polymerization
PHOTOCHEMICALLY ACTIVATED (LIGHT-CURE) RESINS
• Camphorquinone (CQ) is a commonly used photosensitizer that absorbs blue light with wavelengths between 400 and 500 nm.
• Organic aliphatic amine initiator:- Dimethyl-amino-ethyl methacrylate (DMAEMA)
35
PHOTOCHEMICALLY ACTIVATED (LIGHT-CURE) RESINS
➢Advantages :-1. No mixing needed: thus low porosity, less staining, stronger.
2. No aromatic amine accelerator: thus greatly improved color stability.
3. “Command” setting (upon exposure to an intense blue light). This means that working time is controlled, at will, by the clinician.
4. Small increments of composite can be polymerized at a time allowing the use of multiple shades within a single restoration and accommodating for shrinkage within each increment as opposed to bulk shrinkage.
36
.
7
PHOTOCHEMICALLY ACTIVATED (LIGHT-CURE) RESINS
➢Disadvantages :-
1. Limited cure depth: necessary to build up in layers of about 2 mm.
2. Marginal stress buildup during curing is much higher than in self-cured resins. This is due to faster cross-linking and thus reduced time for chains to slide among themselves and relax interfacial stress build-up due to cure shrinkage.
3. Mildly sensitive to normal room illumination (thus a crust will form when exposed too long to an examination light).
4. Special lamp is needed to photoinitiate curing.
5. Cure is affected by additives such as ultraviolet absorbers for color stabilization, fluorescent dyes for clinical aesthetics, or excessive inhibitor concentration. 37
DUAL-CURED RESINS
“Dental composite that contains both chemically activated and light-activated components to initiate polymerization and
potentially overcome the limitations of either the chemical or light-cure systems when used alone.”
-Philips
• Consist of two light-curable pastes, one containing benzoyl peroxide and the other containing an aromatic tertiary amine accelerator.
• Formulated to set up very slowly when mixed via the self-cure mechanism.
38
DUAL-CURED RESINS
➢Advantage:-1. Assurance of completion of cure throughout, even if photocure is inadequate.
➢Disadvantage:-1. Porosity caused by the required mixing.
2. lessŠcolor stability than with the photocure resins.
3. Air inhibition and porosity.
➢ Indication :-Dual-cure materials are intended for any situation that does not allow sufficient light penetration to produce adequate monomer conversion—example, cementation of bulky ceramic inlays.
39
INHIBITORS:
• Inhibitors are added to the resin to minimize or prevent spontaneous or accidental polymerization of monomers.
• A typical inhibitor is butylated hydroxytoluene (BHT) used in concentration of 0.01 wt%.
• Inhibitors have a strong reactivity potential with free radicals.
40INHIBITORS:
• Inhibitors have two functions:
1. Extend the resin’s storage life
2. Ensure sufficient working time.
41
OPTICAL MODIFIERS
• Dental composites must have visual shading and translucency for a natural appearance.
• Shading is achieved by adding pigments usually metal oxide particles-Titanium dioxide ,Aluminum oxide in minute quantities(0.001-0.007%wt)
• These are added to make the translucency of filler particle similar to the tooth structure.
• Darker shades and greater opacities have a decreased depth of light curing ability.
42
.
8
CLASSIFICATION OF COMPOSITES
43
CLASSIFICATION
➢ SKINNER’S (10th ed) :-
1. Traditional composites (Macrofilled): 8-12µm
2. Small particle filled composite: 1-5µm
3. Microfilled composite: 0.04 – 0.4 µm
4. Hybrid composite : 0.6 – 1 µm
44
CLASSIFICATION ➢ANUSAVICE (11th edition)
45
CLASSIFICATION ➢ANUSAVICE (11th edition)
46
CLASSIFICATION ➢ STURDEVANT
Classification of composites based on the filler particle size
1. Megafill- in this one or two large glass inserts 0.5 to 2 mm in size are placed into composites at points of occlusal contact.
2. Macrofill- particle size range between 10 to 100 µm in diameter
3. Midifill - particle size range between 1 to 10 µm in diameter, also called traditional or conventional composites.
4. Minifill- particle size range between 0.1 to 1 µm in diameter
5. Microfill- particle size range between 0.01 to 0.1 µm
6. Nanofill- particle size range between 0.005 to 0.01 µm
47
CLASSIFICATION ➢Marzouk’s Generation:-
1. First Generation:- consists of macro-ceramic reinforcing phases in an appropriate resin matrix.
• Has highest mechanical properties
• High surface roughness
2. Second generation- consists of colloidal and micro-ceramic phases in a continuous phase
• Exhibit best surface texture
• Have unfavorable properties of strength and cofficient of thermal expansion
48

.
9
3 Third generation:- hybrid composite with combination of macro and micro colloidal particles
• Ratio of 75:25
• Properties compromises between first and second generation
4. Fourth generation:- hybrid type with heat cured, irregularly shaped, highly reinforced composite macro particles with reinforcing phase of micro ceramics.
• Technique sensitive
• Prerequisites for their successful use-
a) Concentration of dispersed micro ceramics must be equal in pre polymerized particles and in polymerizable organic matrix to ensure their uniform distribution
b) Bonding between continuous organic matrix and partially organic complex reinforcing particles should be strong cohesive bond
49
5. Fifth generation:- hybrid system with continuous resin phase with reinforced micro-ceramic and macro, spherical,highly reinforced heat cured compoiste particle.
• Improved workability
• Have good surface texture
6. Sixth generation:- hybrid types, continuous phase is reinforced with a combination of micro-cermaics and agglomerates of sintered micro-ceramics
• Exhibit highest percentage of reinforcing articles
• Exhibit best mechanical properties
• Wear and surface rexture similar to 4th generation
• Exhibit least shrinkage
50
CLASSIFICATION ➢ CRAIG:
1. TYPE I:
i. Class 1 – Macrosized particles – 8-25µ
ii. Class 2 – Mini size particles – 1-8µ
iii. Class 3 – Micro size particles – 0.04-0.2µ
iv. Class 4 – Blend of macro and micro – 0.04-10µ
2. TYPE II
i. Class 1: Macrosized 10-20µ (organic particles in unreinforced resin matrix).
ii. Class 2: Macrosize unreinforced particles 10- 20µ (organic in reinforced resin matrix 0.04- 0.2µ organic)
51
CLASSIFICATION
➢ Based on polymerization method:
• Self-curing
• UV light curing
• Visible light curing
• Dual curing
52
CLASSIFICATION
➢ Matrix Classification System:-
• Bis GMA
• UDMA
• Combination of both
53
CLASSIFICATION
➢ Based on inorganic loading:-
• Heavy filler material :- 75%
• Lightly filler material:- 66%
➢Based on consistency:-
• Light body:- flowable
• Medium body:-homogenous microfills,macrofills, midfills.
• Heavy body:- packable hybrid
54
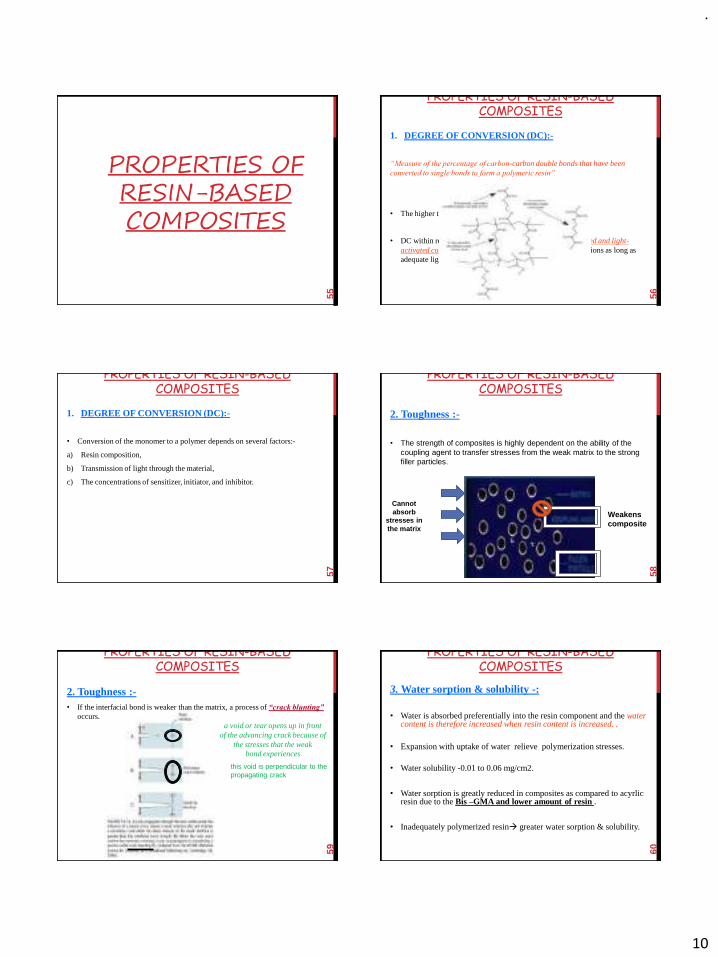
.
10
PROPERTIES OF RESIN-BASED COMPOSITES
55
PROPERTIES OF RESIN-BASED COMPOSITES
1. DEGREE OF CONVERSION (DC):-
“Measure of the percentage of carbon-carbon double bonds that have been converted to single bonds to form a polymeric resin”
• The higher the DC →the better the strength, wear resistance.
• DC within resins does not differ between chemically activated and light-activated composites containing the same monomer formulations as long as adequate light curing.
56
PROPERTIES OF RESIN-BASED COMPOSITES
1. DEGREE OF CONVERSION (DC):-
• Conversion of the monomer to a polymer depends on several factors:-
a) Resin composition,
b) Transmission of light through the material,
c) The concentrations of sensitizer, initiator, and inhibitor.
57
PROPERTIES OF RESIN-BASED COMPOSITES
2. Toughness :-
• The strength of composites is highly dependent on the ability of the coupling agent to transfer stresses from the weak matrix to the strong filler particles.
58
Cannot absorb
stresses in the matrix
Weakens composite
PROPERTIES OF RESIN-BASED COMPOSITES
2. Toughness :-• If the interfacial bond is weaker than the matrix, a process of “crack blunting”
occurs.
59
a void or tear opens up in frontof the advancing crack because of
the stresses that the weakbond experiences
this void is perpendicular to thepropagating crack
PROPERTIES OF RESIN-BASED COMPOSITES
3. Water sorption & solubility -:
• Water is absorbed preferentially into the resin component and the water content is therefore increased when resin content is increased. .
• Expansion with uptake of water relieve polymerization stresses.
• Water solubility -0.01 to 0.06 mg/cm2.
• Water sorption is greatly reduced in composites as compared to acyrlicresin due to the Bis –GMA and lower amount of resin .
• Inadequately polymerized resin→ greater water sorption & solubility.
60

.
11
PROPERTIES OF RESIN-BASED COMPOSITES
3. Water sorption & solubility :-
• If the stress is greater than the bond strength, the resulting debond is referred to as HYDROLYTIC BREAKDOWN.
• Microfills and flowable have greater water sorption.
61
PROPERTIES OF RESIN-BASED COMPOSITES
4. Thermal properties-:
• CTE of composite is approximately three times higher than normal tooth structure.
• This can be reduced by adding more filler content.
• Microfill composites show more cofficient of thermal expansion because of presence of more polymer content.
62
PROPERTIES OF RESIN-BASED COMPOSITES
5. Wear (volume loss by abrasion and other mechanisms):-
• Wear rate differences of 10 to 20 μm/year for posterior composites is studied, well this wear rate still amounts to 0.1 to 0.2 mm more than enamel over 10 years.
• Two principal mechanisms of composite wear:-
A. Two-body wear:- based on direct contact of the restoration with an opposing cusp or with adjacent proximal surfaces. It is related to the higher force levels exerted by the opposing cusp or forces transferred to proximal surfaces.
B. Three-body wear:- simulates loss of material in non-contacting areas, most probably owing to contact with food as it is forced across the occlusalsurfaces
63
PROPERTIES OF RESIN-BASED COMPOSITES
5. Wear (volume loss by abrasion and other mechanisms):-
• The loss of material caused by direct wear in areas of tooth-to-tooth contact appears to be greater than that of three-body abrasion by food in non-contact areas.
• Composites with smaller filler particles size (1 μm or less), high in concentration, and well bonded to the matrix are the most resistant to wear.
64PROPERTIES OF RESIN-BASED
COMPOSITES
6. Curing shrinkage and shrinkage stress:-
• “Curing shrinkage arises as the monomer is converted to polymer and the free space it occupies reduces.”
• The polymerization shrinkage and resultant stress can be affected by:-
i. Total volume of the composite material,
ii. Type of composite,
iii. Polymerization speed,
iv. Ratio of bonded/nonbonded surfaces or the conguration of the tooth preparation (C-factor).
65
Configuration factor / C factor
• “It is the ratio of bonded surfaces to the unbonded surfaces in a tooth preparation”
• Higher the C-factor, greater is the potential for bond disruption from polymerization effects.
66
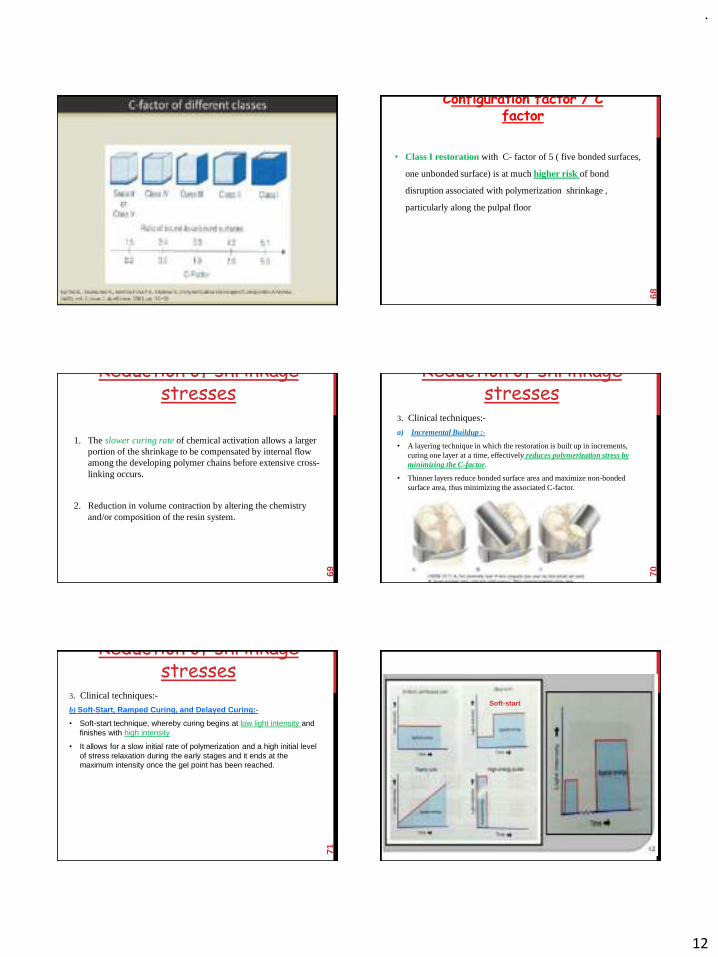
.
12
67
Configuration factor / C factor
• Class I restoration with C- factor of 5 ( five bonded surfaces,
one unbonded surface) is at much higher risk of bond
disruption associated with polymerization shrinkage ,
particularly along the pulpal floor
68
Reduction of shrinkage stresses
1. The slower curing rate of chemical activation allows a larger portion of the shrinkage to be compensated by internal flow among the developing polymer chains before extensive cross-linking occurs.
2. Reduction in volume contraction by altering the chemistry and/or composition of the resin system.
69
Reduction of shrinkage stresses
3. Clinical techniques:-
a) Incremental Buildup :-
• A layering technique in which the restoration is built up in increments, curing one layer at a time, effectively reduces polymerization stress by minimizing the C-factor.
• Thinner layers reduce bonded surface area and maximize non-bonded surface area, thus minimizing the associated C-factor.
70Reduction of shrinkage
stresses3. Clinical techniques:-
b) Soft-Start, Ramped Curing, and Delayed Curing:-
• Soft-start technique, whereby curing begins at low light intensity and finishes with high intensity
• It allows for a slow initial rate of polymerization and a high initial level of stress relaxation during the early stages and it ends at the maximum intensity once the gel point has been reached.
71 72
Soft-start

.
13
73 74
Thank You
75
GOOD MORNING TYPES OF
COMPOSITES
76CONVENTIONAL
COMPOSITES
• Also known as – Traditional or macrofilled composites.
• Filler:- finely ground amorphous silica or quartz.
77
CONVENTIONAL COMPOSITES
• The average particle size of conventional composites was approx
8-12 um.
➢ Filler loading:- 70-80% by wt, 60-70% by volume.
➢ Indications:-
• Used in class II and IV restorations.
78
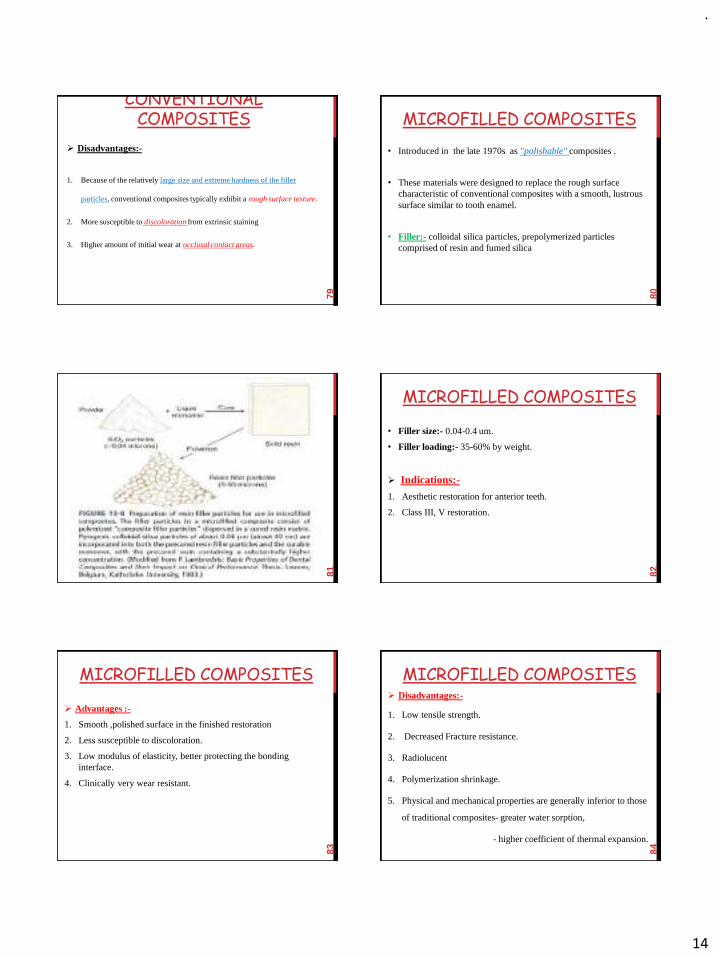
.
14
CONVENTIONAL COMPOSITES
➢ Disadvantages:-
1. Because of the relatively large size and extreme hardness of the filler
particles, conventional composites typically exhibit a rough surface texture.
2. More susceptible to discoloration from extrinsic staining
3. Higher amount of initial wear at occlusal contact areas.
79
MICROFILLED COMPOSITES
• Introduced in the late 1970s as "polishable" composites .
• These materials were designed to replace the rough surface characteristic of conventional composites with a smooth, lustrous surface similar to tooth enamel.
• Filler:- colloidal silica particles, prepolymerized particles comprised of resin and fumed silica
80
81
MICROFILLED COMPOSITES
• Filler size:- 0.04-0.4 um.
• Filler loading:- 35-60% by weight.
➢ Indications:-
1. Aesthetic restoration for anterior teeth.
2. Class III, V restoration.
82
MICROFILLED COMPOSITES
➢ Advantages :-
1. Smooth ,polished surface in the finished restoration
2. Less susceptible to discoloration.
3. Low modulus of elasticity, better protecting the bonding interface.
4. Clinically very wear resistant.
83
MICROFILLED COMPOSITES➢ Disadvantages:-
1. Low tensile strength.
2. Decreased Fracture resistance.
3. Radiolucent
4. Polymerization shrinkage.
5. Physical and mechanical properties are generally inferior to those
of traditional composites- greater water sorption,
- higher coefficient of thermal expansion.
84

.
15
• Diamond burs, rather than fluted tungsten-carbide burs, are recommended for trimming microfilledcomposites so as to minimize the risk of chipping.
85
Scanning electron micrograph of polished surface of a conventional
composite (x300).
Scanning electron micrograph of polished surface of a microfill
composite (x300).
HYBRID COMPOSITES
• In an effort to combine the favorable physical and mechanical
properties characteristic of conventional composites with the
smooth surface typical of the microfill composites, the hybrid
composites were developed.
• Hybrid composites are formulated with mixed filler systems
containing both microfine (0.01 to 0.1 μm) and fine (0.1 to 10
μm) particle fillers
86
HYBRID COMPOSITES
• Filler:- colloidal silica and ground particles of glass containing heavy metals.
• Filler loading:- 75-85% by weight.
• Filler size:- 0.4-1 um.
• Indications :-
1. Restoring incisal edges and small non-contact occlusalcavities.
2. Anterior restorations, including class IV sites.
87
HYBRID COMPOSITES ➢ Advantages :-
1. Smaller microfiller sizes increase the surface area → increases the viscosity.
2. Because of the relatively high content of inorganic fillers, the physical and mechanical characteristics are generally superior to those of conventional composites.
3. The presence of sub-micrometer sized microfiller particles interspersed among the larger particles provides a smooth "patina-like" surface texture in the finished restoration
88
HYBRID COMPOSITES
➢Disadvantages :-
1. Resins lose their high polish over time with the development of a rougher surface, reducing their suitability for esthetically demanding cases.
89
FLOWABLE COMPOSITES • A modification of the small-particle composite and hybrid
composite results in the flowable composites, which have become popular since 1995.
• Resins typically have a lower viscosity through a reduced filler loading, which enables the resin to flow readily, spread uniformly, intimately adapt to a cavity form, and produce the desired dental anatomy.
90

.
16
FLOWABLE COMPOSITES • Filler size :- 0.6-1 um.
• Filler content :- 30-55 % by wt.
➢Indications :-1. Class I,II,III,IV,V restorations
2. Pit-and-fissure sealants
3. Marginal repair materials,
4. Infrequently, as the first increment placed as a liner under hybrid or packable composite.
5. Core build up
91
Because they can flow into small crevice defects along restoration margins, some dentists refer to flowable resins as
“DENTAL CAULK.”
FLOWABLECOMPOSITES
➢Advantages :-
1. Ease of use.
2. Favorable wettability.
3. Less sticky during handling than microfills and hybrids.
➢Disadvantages :-
1. Low strength
2. Exhibit much higher polymerization shrinkage.
3. Higher susceptibility to wear
92
PACKABLE COMPOSITES
• Also known as “Condensable composites.”
• Based on new concept called PRIMM ( polymer rigid inorganic
matrix material).
• Packable composites are designed to be inherently more viscous
to afford a "feel" upon insertion, similar to that of amalgam.
93
PACKABLE COMPOSITES
94
Packable/condensable characteristics are derived from the inclusion of elongated, fibrous filler particles of about
100 μm in length and/or rough-textured surfaces or branched geometries that tend to interlock and resist flow
It causes the uncured resin to be stiff and resistant to slumping yet moldable under the force of
amalgam condensers (“pluggers”).
PACKABLE COMPOSITES
• Packable Composites were development in an attempt to accomplish two goals:
1. Easier restoration of a proximal contact, and
2. Handling properties similar to amalgam.
95
NANO COMPOSITES • Also known as “Nano-composites or Nanohybrid Composites”.
• Sir Richard Feynman in 1959 coined the term like “nano” .
• This discovery was a landmark for advances in dental composites. The introduction of nanotechnology led to the discovery of nano-filler particles.
• Nanofills and nanohybrids are the two different types of more commonly available nano-composites.
96

.
17
NANO COMPOSITES 1. Nanofill composites :-
• These contain nanometer sized particles (1-100nm) throughout the resin matrix.
• Contains high filler load in order to obtain strength and wear resistance similar to that of microhybrid composite resins.
• The nanofill type of composites, are formed by a combination of:
(a) Nanomers, which are nanosized mono-dispersed, non-aggregated silica filler particles in the size range of 20-75nm and
(b) Nanoclusters, which are agglomerations of combination of zirconia-silica and silica nanomeric particles.
97
NANO COMPOSITES 2. Nanohybrids Composites :
• Consists of large particles (0.4-5 microns) with added nanometer sized particles. Thus they are hybrid and not true nanofilledcomposites.
• The surface of nanohybrid becomes gradually dull after a few years of clinical service because of its large size particles.
98
NANO COMPOSITES
• Various commercially available brands of nanocompositesinclude:-
1. Filtek Supreme XTE Universal Restorative (3M ESPE),
2. Premise (Kerr/Sybron, Orange, CA),
3. IPS Empress Direct & Tetric N-Ceram (both Ivoclar Vivadent).
99
RECENT ADVANCEMENT IN
COMPOSITES
100
ANTIBACTERIAL RESIN COMPOSITES
• Composites that offer antibacterial properties are promisingsince several studies have shown that greater amount ofbacteria and plaque accumulate on the surface of resincomposite than on the surface of other restorative material /enamel surface.
• In resin composite materials the addition of an antibacterialcomponent can be achieved through modifications made to thefiller particles or the resin matrix
• Imazato et al 1994 incorporated anon-releasing newlysynthesized monomer MDPB with anti-bacterial properties intoresin composite
101
ANTIBACTERIAL RESIN COMPOSITES
• The strategies that have provided resin composites possessing antibacterial activity can be divided into two main groups:
1. Released soluble antimicrobial agent or,
2. Stationary non-released antibacterial agent
102

.
18
ANTIBACTERIAL RESIN COMPOSITES
• A soluble agent is gradually released over time, discharging the antibacterial agent from the bulk of the material.
• Although an antibacterial effect is achieved, the agent’s
release has several disadvantages:
1. An adverse influence on the mechanical properties of the base material,
2. The release of the agent possibly generating a porous structure,
3. Time limited efficacy, and
4. Possible toxicity to the adjacent tissues given that the rate of diffusion can be difficult to monitor
103
ORMOCER• Ormocer is an acronym for “organically modified ceramics”.
• First time introduced in 1998 by Dr Herbert Wolters.
• Ormocer materials contain inorganic-organic co-polymers in addition to the inorganic silanated filler particles.
• Organic, reactive monomers are bound to an inorganic -Si-O-Si-network.
104
105
ORMOCER• Ormocers basically consist of three components – organic and
inorganic portions and the polysiloxanes.
• The proportions of those components can effect the mechanical, thermal and optical qualities of the material:
1. The organic polymers influence the polarity, the ability to cross link, hardness and optical behavior.
2. The glass and ceramic components (inorganic constituents) are responsible for thermal expansion and chemical stability.
3. The polysiloxanes influence the elasticity, interface properties and processing
106
ORMOCER➢ Indicated in-
• All types of restorations, for esthethic veeners, repairing porcelain or acrylic facing.
➢ Contraindicated in –
• Patients with known allergy to methacrylates, phenol, TEGDMA.
➢ Commercial name-
• “Denite” and “Admira,” Voco ;
• “Ceram-X,” Dentsply
107
108

.
19
COMPOMERS• Polyacid Modified Composite Resin is known as COMPOMER.
• As proposed by Krejci (1992), the acronym ‘ compomer” was
created by combing the words composite and glass ionomer.
COMPOSITE + GLASS IONOMER = COMPOMER
109
COMPOMERS• COMPOSITION :-
• Resin matrix: Dimethacrylate monomers with two carboxylic
group present in their structure
• Filler: Reactive silicate glass containing filler
• Photoinitiators and Stabilizers
• There is no water in composition and ion leachable glass is
partially silanized to ensure bonding to matrix
110
COMPOMERS➢ Indication:-
• Pit and fissure sealant
• Restoration of primary teeth
• Liners and bases
• Core build up material
• For class III & V lesions
• Cervical erosion / abrasion
• Repair of defective margins in restorations
• Sealing of root surfaces for over dentures
• Reterograde filling material.
111
COMPOMERS
➢Contraindications:-
• Class IV carious lesions
• Large areas of labial surfaces
• Class II cavities where conventional cavity is prepared
• Lost cusp areas
• Under full crown or PFM crowns.
112
COMPOMERS➢Drawback:-
1. Use of bonding system mandatory
2. Insignificant release of fluoide
3. Lower wear resistant than regular composites.
➢Commercial names of compomers :-
• Compoglass (Vivadent-ivoclar)
• Dyract (Dentsply Caulk,Milford,Delaware)
• F2000 (3M-Espe,St.Paul,Minnesota)
113
GIOMERS
• The name "Giomer" is a hybrid of the words "glass ionomer"
and "composite” .
• Introduced by Shofu Inc. (Kyoto, Japan) in 2000.
• GIOMER is a new group of direct restorative materials and
adhesives that comprises Pre-Reacted Glass-ionomer (PRG)
114
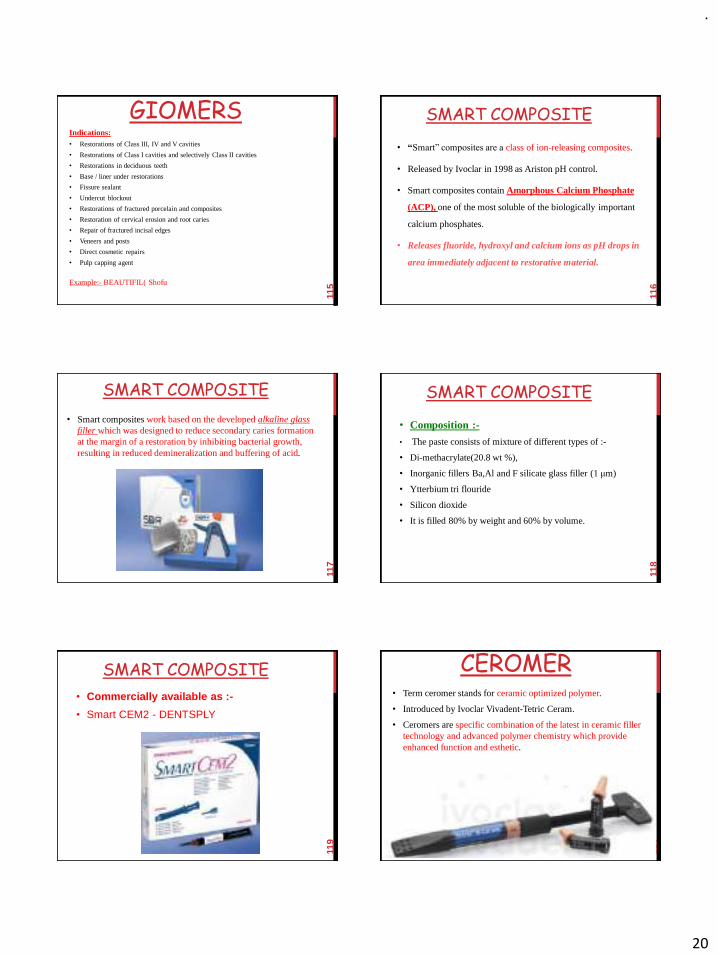
.
20
GIOMERS Indications:• Restorations of Class III, IV and V cavities
• Restorations of Class I cavities and selectively Class II cavities
• Restorations in deciduous teeth
• Base / liner under restorations
• Fissure sealant
• Undercut blockout
• Restorations of fractured porcelain and composites
• Restoration of cervical erosion and root caries
• Repair of fractured incisal edges
• Veneers and posts
• Direct cosmetic repairs
• Pulp capping agent
Example:- BEAUTIFIL( Shofu
115
SMART COMPOSITE
• “Smart” composites are a class of ion-releasing composites.
• Released by Ivoclar in 1998 as Ariston pH control.
• Smart composites contain Amorphous Calcium Phosphate
(ACP), one of the most soluble of the biologically important
calcium phosphates.
• Releases fluoride, hydroxyl and calcium ions as pH drops in
area immediately adjacent to restorative material.
116
SMART COMPOSITE
• Smart composites work based on the developed alkaline glass filler which was designed to reduce secondary caries formation at the margin of a restoration by inhibiting bacterial growth, resulting in reduced demineralization and buffering of acid.
117
SMART COMPOSITE
• Composition :-
• The paste consists of mixture of different types of :-
• Di-methacrylate(20.8 wt %),
• Inorganic fillers Ba,Al and F silicate glass filler (1 μm)
• Ytterbium tri flouride
• Silicon dioxide
• It is filled 80% by weight and 60% by volume.
118
SMART COMPOSITE
• Commercially available as :-
• Smart CEM2 - DENTSPLY
119
CEROMER• Term ceromer stands for ceramic optimized polymer.
• Introduced by Ivoclar Vivadent-Tetric Ceram.
• Ceromers are specific combination of the latest in ceramic filler technology and advanced polymer chemistry which provide enhanced function and esthetic.
120

.
21
CEROMER
• It consist of fine particle ceramic filler which are closely packed
and embedded in advance organic polymer matrix.
• The paste of ceromer contain barium, aluminum fluoride and
silicate glass fillers with silicone dioxide and calcium silicate glass
in di-methacrylate monomer filler contents is 80% by weight.
• The particle size varies from 0.04-3 μm.
121
CEROMER
➢Indications :-
• ClassI and II posterior restorations(stress bearing areas)
• ClassIII and IV anterior restorations
• ClassV restorations ,cervical caries, root erosion,
abfraction, wedge-shaped defects
• Inlays/onlays with extraoral post-tempering
122
BIOACTIVE COMPOSITES• BioACTIVE-RESTORATIVE is a highly esthetic, bioactive
composite that delivers all the advantages of glass ionomers in a
strong, resilient, resin matrix that will not chip or crumble.
• It chemically bonds to teeth, seals against microleakage,
releases more, calcium, phosphate and fluoride and is more
bioactive than glass ionomers, and is more durable and fracture
resistant than composite
123
BIOACTIVE COMPOSITES
• Bioactive formulations :-
• ACP (amorphous calcium phosphate)-2000
• ACP + BIS-GMA /TEGDMA/HEMA with Zirconyl methacrylate
• Fluorinated Bis-GMA analogues
• Liquid crystalline monomers
124
125
BIOACTIVE COMPOSITES
➢ Commercially available as :-• ACTIVA- Bioactive restorative –Pulpdent
➢ Key Features:• Natural esthetics – Highly polishable• Tough, resilient, fracture and wear resistant,
absorbs shock• Releases and recharges calcium, phosphate and
fluoride• Chemically bonds – Seals against microleakage• No sensitivity• Moisture tolerant – Simplified technique
126

.
22
SILORANE:
127
• The name of this material class
refers to its chemical composition
from Siloxanes and Oxirans.
• Introduced by Guggenburger and
Weinmann in 2000.
• It comprised of ring-opening
monomers that provide for low
polymerization shrinkage.
SILORANE:• Siloranes are polymerized by a cationic reaction in contrast to
methaycrylates, which crosslink via radicals.
• The photoinitiator system is based on three components: light absorbing camphor chinon, an electron donor (eg amine) and an idonium salt.
128
SILORANE:➢ Advantages:-1. Have lower shrinkage
2. Longer resistance to fading and
3. Less marginal discoloration.
➢ Indication:-• Class I
• Class II
• May be used together with glass ionomer cements or resin-modified glass ionomer cements, as cavity liners or bases.
129
STIMULI RESPONSIVE COMPOSITE
• Stimuli-responsive materials possess properties that may be considerably changed in a controlled fashion by external stimuli.
• Such stimuli may be for example changes of temperature, mechanical stress, pH, moisture, or electric or magnetic fields .
130
SELF HEALING COMPOSITE
• Self-repairing or self-healing synthetic materials are reported
showing some similarities to resin-based dental material; it was
the epoxy resin composite
• If a crack occurs in the epoxy composite material, some of the
microcapsules are destroyed near the crack and release the
resin.
• The resin subsequently fills the crack and reacts with a Grubbs
catalyst dispersed in the epoxy composite, resulting in a
polymerization of the resin and repair of the crack
131
FIBRE REINFORCED COMPOSITE
• Conventional dental composite (white fillings) and glass fibres
are combined to give the same level of strength and flexibility.
• The fibers are typically long thin strands of glass fibre that are
aligned as meshes or strips depending on their requirement
• The main advantage of these fibre reinforced composite was
they can be used in both direct and indirect restorations
132
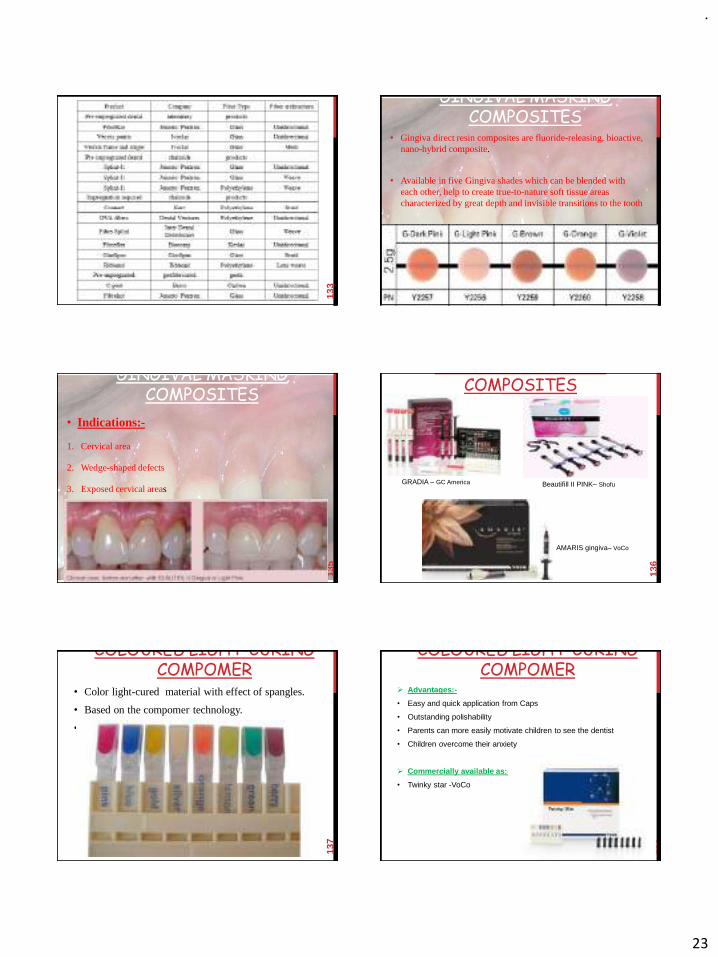
.
23
133
GINGIVAL MASKING COMPOSITES
• Gingiva direct resin composites are fluoride-releasing, bioactive, nano-hybrid composite.
• Available in five Gingiva shades which can be blended with each other, help to create true-to-nature soft tissue areas characterized by great depth and invisible transitions to the tooth
134
GINGIVAL MASKING COMPOSITES
• Indications:-
1. Cervical area
2. Wedge-shaped defects
3. Exposed cervical areas
4. Aesthetic correction of gingival recession
5. Primary splinting
6. Ability to mask exposed crown margins to improve aesthetic.
135
GINGIVAL MASKING COMPOSITES
136
GRADIA – GC America Beautifill II PINK– Shofu
AMARIS gingiva– VoCo
COLOURED LIGHT-CURING COMPOMER
• Color light-cured material with effect of spangles.
• Based on the compomer technology.
• Available in eight attractive colors with glitter effect
137
COLOURED LIGHT-CURING COMPOMER
➢ Advantages:-
• Easy and quick application from Caps
• Outstanding polishability
• Parents can more easily motivate children to see the dentist
• Children overcome their anxiety
➢ Commercially available as:-
• Twinky star -VoCo
138

.
24
139
Thank you
140
Good Morning
DENTAL COMPOSITE
SPART-III
141
RECENT
ADVANCES OF
DENTAL
COMPOSITES
142
Omnichroma• Single shade of composite.
• Its uniformly sized supra-nano spherical fillers (260nm spherical SiO2-ZrO2) allow OMNICHROMA to match every one of the 16 VITA classical shades.
143
MRP: $99.99
Omnichroma• Single shade of composite.
• Its uniformly sized supra-nano spherical fillers (260nm spherical SiO2-ZrO2) allow OMNICHROMA to match every one of the 16 VITA classical shades.
144

.
25
Omnichroma➢How it works:-
• Most composites depend on the chemical color of the dyes and pigments added to the resin material to emulate certain shades of human teeth.
• OMNICHROMA’s Smart Chromatic Technology is the first use of structural color in composite dentistry as the main color mechanism.
• As ambient light passes through the spherical fillers in OMNICHROMA, they generate red to yellow structural color, the natural colors found in all human teeth.
145
Omnichroma➢How it works:-
• The red-to-yellow color combines with the reflected color of the surrounding tooth to create a seamless match.
• This technology eliminates the need for pigments or dyes, and the result is an unprecedented color-matching ability combined with excellent mechanical properties and high polishability
146
147
Omnichroma• Advantages :-
1. Universal use.
2. Shade matches both before and after bleaching
3. High polishability
4. Highest wear resistance
5. High compressive strength
148
SANDWICH
TECHNIQUE
149
SANDWICH TECHNIQUE
• Developed by McLean.
• Also known as “ laminate” or “bilayer technique”.
150

.
26
SANDWICH TECHNIQUE
“The sandwich of glass ionomer cement, dental adhesive and composite resin is an effective technique that optimally combines the desirable properties of the restorative materials.”
• In the sandwich technique, the GI is placed as a liner or base, followed by placement of a resin composite to provide an aesthetic restoration of the remaining cavity.
151
152
Sandwich Technique
Open technique
Close technique
SANDWICH TECHNIQUE• In the open technique, the GI is used to replace the dentin and
also fill the cervical part of the box, which results in a part of the GI being exposed to the oral environment.
• Use the “open sandwich” technique when there is no remaining
enamel at the gingival margin.
153
SANDWICH TECHNIQUE
• In the closed technique, the dentin is covered by the GI, which is in turn completely covered by the overlaying composite.
• Use the “closed sandwich” technique when there is remaining
enamel at the gingival margin.
154
SANDWICH TECHNIQUE
➢ Indications:
• Class I, Class II, Class III and Class V lesions
• Deep posterior restorations
• Extensive, bulky posterior restorations
• Posterior restorations with sub-gingival interproximal preparations that are difficult to isolate or where no enamel remains.
155
SANDWICH TECHNIQUE
➢Clinical benefits:
• Reduced post-operative sensitivity
• Pulpal protection from irritation
• Fluoride release over time
• Helps in prevention of demineralization
• Rapid placement and curing of a single bulk layer
• Aesthetics
• Radiopacity
156

.
27
Insertion of composites • Different designs of increment placement:-
1. Three increment design:-
• one flat increment at gingival & occlusal wall & two oblique increments both at proximal box occlusal box.
• 1st increment thinner than 1.00mm.
157
Insertion of composites 2. Horizontal layering design:-
• Small increments placed horizontally one above the other, starting from gingival wall to occlusal wall.
• The horizontal placement technique utilizes composite resin layers, each <2.0 mm thick.
158
Insertion of composites 3. Oblique layering technique:-
• The oblique technique is accomplished by placing a series of wedge-shaped composite increments.
• Each increment is photocured twice, first through the cavity walls and then from the occlusal surface, to direct the vectors of polymerization toward the adhesive surface
159
Insertion of composites 4. Vertical layering technique:-
• Place small increments in vertical pattern starting from one wall, i.e., buccal or lingual and carried to another wall.
• Start polymerization from behind the wall, i.e., if buccal increment is placed on the lingual wall, it is cured from outside of the lingual wall.
160
This reduces gap at gingival wall which is formed due to polymerization shrinkage, hence
postoperative sensitivity and secondary caries
Insertion of composites 5. Stratified layering technique:-
• The stratified layering technique was schemed and oriented to the development of functional and anatomic restoration applying the “esthetic”
composite resin restorative materials that include shades of dentin and enamel as well as various translucencies and intensive colors.
• It involves placing dentin shades of composite resin with a higher chroma in the middle of the preparation and placing a lower chroma resin close to the cusp walls.
• The enamel layer is placed following the contours established by the dentin layers and it varies in thickness depending on the desired effect.
161
Insertion of composites 6. Centripetal buildup technique:-• This technique offers a number of advantages when composite resin
posterior restorations are indicated.
• This technique employs thin metal matrix bands and wooden wedges eliminating the need for transparent matrix bands.
162

.
28
Insertion of composites 6. Centripetal buildup technique:-• An important benefit of the procedure is offered by the centripetal buildup
steps first by creating a very thin proximal layer .
• Once the second step of the procedure is completed and peripheral composite envelope is created, the cavity is managed as a simple Class I cavity.
• The centripetal buildup technique is very conservative with preservation of sound tooth structure; it is not time-consuming and it is easy to implement.
163
Insertion of composites 7. Successive cusp buildup technique:-• Here, individual cusps are restored one at a time up to the level of
the occlusal enamel.
• Small sloping increments are applied to each corner of the cavity in turn and manipulation is kept to a minimum, to avoid folding voids into the material.
164
Insertion of composites 8. Three-site technique:-• This is a layering technique that is associated with the use of a clear matrix
and reflective wedges.
• First, the curing light is directed through the matrix and wedges in the attempt to guide the polymerization vectors toward the gingival margin thus preventing any gap formation.
• Then, wedge-shaped composite increments are placed.
165
BIOCOMPATIBILITY OF COMPOSITES
• The biocompatibility of restorative materials usually relate to the effects on the pulp from two aspects:
1. The inherent chemical toxicity of the material and
2. The marginal leakage of oral fluids.
166
BIOCOMPATIBILITY OF COMPOSITES
• Various components may be released from resin composite restorations into the oral environment.
• According to a national survey of adverse reactions to dental materials in the UK, dental resins are the main cause of adverse reactions in dental technicians, and more than 12% of adverse reactions in patients are related to resin-based dental materials.
167
BIOCOMPATIBILITY OF COMPOSITES
• Unpolymerized monomers can be leached into saliva and cause adverse reactions .
• Inadequately cured composite materials at the floor of a cavity can serve as a reservoir of diffusible components that can induce long-term pulp inflammation.
• Adequately polymerized composites are relatively biocompatible because they exhibit minimal solubility, and unreacted species are leached in very small quantities.
168
The inherent chemical toxicity of the material

.
29
BIOCOMPATIBILITY OF COMPOSITES
• According to some studies, it is suggested that formaldehyde, which is a by-product of polymerization, may be responsible for oral lickenoid reactions.
169
BIOCOMPATIBILITY OF COMPOSITES
• The marginal leakage might allow bacterial ingrowth, and these microorganisms may cause secondary caries or pulp reactions.
• Marginal leakage also leads to accumulate of substrate leading to interfacial staining
• Therefore, the restorative procedure must be designed to minimize polymerization shrinkage and marginal leakage.
170
The marginal leakage of oral fluids
BIOCOMPATIBILITY OF COMPOSITES
• Bis–GMA/TEGDMA-based composite resins and 4-META/MMA-based resin cements show better biocompatibility compared to 2-hydroxy-ethyl-methacrylate (HEMA) containing resin modified glass ionomer.
• Calcium hydroxide containing products are the materials of choice to be placed in direct contact with the pulp, prior to placement of restorative resins.
171
BIOCOMPATIBILITY OF COMPOSITES
• There are some reports about the estrogenicity of bisphenol A, a precursor of bis-GMA.
• Bisphenol A was first shown to be estrogenic in 1938, using ovariectomized rats by (Dodds and Lawson, 1938) and then by the other researchers.
172
Bisphenol A Toxicity
BIOCOMPATIBILITY OF COMPOSITES
• BPA and other endocrine-disrupting chemicals (EDCs) have been shown to cause reproductive anomalies, especially in the developmental stages of fetal wildlife.
• BPA has recently also been shown to exhibit antiandrogenicactivities, which may prove to be detrimental in organ development.
173
Bisphenol A Toxicity
FINISHING OF COMPOSITES
• Optimal finishing and polishing of resin-based composites is a very important step in the completion of a restoration.
• Residual surface roughness can encourage bacterial growth, which can lead to a myriad of problems including secondary caries, gingival inflammation, and surface staining.
174

.
30
FINISHING OF COMPOSITES
• To examine the effect of several significant factors on the finish and polish of a composite restoration:
1. Environment,
2. Delayed versus immediate finish,
3. The types of materials, and
4. Surface coating and sealing.
175
FINISHING OF COMPOSITES
• Environment involves whether the process of finishing and polishing should be performed in a wet or dry field in the mouth.
• Finishing in a dry field with the finishing equipment mounted on a slow-speed handpiece allows for better visualization of the restoration margins.
176
1. Environment
FINISHING OF COMPOSITES
• Studies have shown that a dry polishing technique results in an increase in marginal leakage, possibly because of heat production, which can disturb the marginal sealing ability of the adhesive resins.
• The clinician should finish the restoration in an environment where the margins are clearly discernible and where minimal heat is generated.
177
1. Environment
FINISHING OF COMPOSITES
• Elapsed time may also have an effect on surface characteristics and resistance to leakage that develops.
• Studies have shown that delayed finishing can actually increase marginal leakage and has no effect on surface characteristics compared with immediate finishing.
178
2. Elapsed time between curing of the composite and finishing and polishing
FINISHING OF COMPOSITES
• Almost all composite restorations should be finished and polished shortly after placement during the same appointment, although the finishing should be delayed for approximately 15 minutes after curing.
179
2. Elapsed time between curing of the composite and finishing and polishing
FINISHING OF COMPOSITES
• A variety of materials and devices can be used to finish and polish composite restorations.
• Coarse to ultrafine aluminum oxide discs can be applied to areas with difficult access around the proximal surfaces or in embrasures.
• Tungsten carbide burs or fine diamond tips can be used to adjust occlusal surfaces and blend the composite to the surfaces of the teeth.
180
3. Types of materials and devices

.
31
FINISHING OF COMPOSITES
• An important step in finishing and polishing is the application of a bonding agent or a surface sealer.
181
4. Surface coating and sealing
FINISHING OF COMPOSITES
• Contouring the composite restoration requires skill and knowledge.
• Usually a slight excess of material is present that must be removed to provide final contour and smooth finish.
• Coarse diamond instruments used for removing gross excess.
• Twelve bladed finishing burs or special fine diamond finishing instruments can be used.
182
FINISHING OF COMPOSITES
• Difference between finishing of Microfill composites and Hybrid composites :-
183
Microfill composites
• It posses a surface luster similar to that of tooth enamel.
• Difficult to detect finished margins.
• Contain less inorganic filler→finishing burs tends to clog and need periodic debridement
Hybrid composites
• Exhibit an opaque appearance during dry finishing.
• Preparation margin easily distinguishable.
CONCLUSION• Composites have acquired a prominent place among
the filling materials employed in direct techniques.
• Their considerable aesthetic possibilities give rise to a variety of therapeutic indications, which continue to grow as a result of the great versatility of the presentations offered.
184
CONCLUSION
• Nonetheless, it should not be forgotten that they are highly technique-sensitive, hence the need to control certain aspects: correct indication, good isolation, choice of the right composite for each situation, use of a good procedure for bonding to the dental tissues and proper curing are essential if satisfactory clinical results are to be achieved.
185
REFERENCES• Art and Science of operative dentistry; Sturdevant.
• Science of Dental Material;Philips
• Textbook of operative dentistry; Vimal k Sikri
• Textbook of operative dentistry; Marzouk
• Craig RG: chemistry,composition and properties of composite reins.
• Recent Advances in Composite – A Review P.Benly et al /J. Pharm. Sci. & Res. Vol. 8(8), 2016, 881-883
186

.
32
REFERENCES• Trends in restorative composites research: what is in the future?
Mariel Soeiro MAAS, Yvette ALANIA, et al. Braz. Oral Res. 2017;31(suppl):e55.
• Murray PE,et al; bacterial microleakage and pulp inflammation associated with various restorative,Dent Mater,18:470-478.2002
• Incremental techniques in direct composites; Veeramachaneni Chandrasekhar,Laharika Rudrapati,Vijetha Badami;journal of conservative dentistry;vol 20;6;2017;386-391.
187
188
Thank You

.
1
DENTAL
CARIES
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENTS
PART-1
• Introduction
• Definition of caries
• Epidemiology
• Etiology of caries
• Theories of caries
• Classification of caries
2
DENTAL CARIES
➢‘Caries’ derived from Latin word meaning ‘rot’ or ‘decay’.
➢ It is one of the most common of all diseases
➢ A major cause of loss of tooth
3
• Major oral disease which hinders the achievement and maintenance of good health in all age groups.
• Dental caries is a chronic disease that progresses slowly in most of the people which results from an ecological imbalance between tooth minerals and oral environment.
4
• At present, It is affecting 60-90% of school children and the vast majority of adults.
• Most prevalent oral disease in several Asian and Latin American countries.
5
• Easily the most negligent disease because initialcarious lesions lack signs & symptoms and so the patient is left unaware of it for long.
• The patient only reports to the dentist after experiencing pain, thus making caries a chronic disease.
6
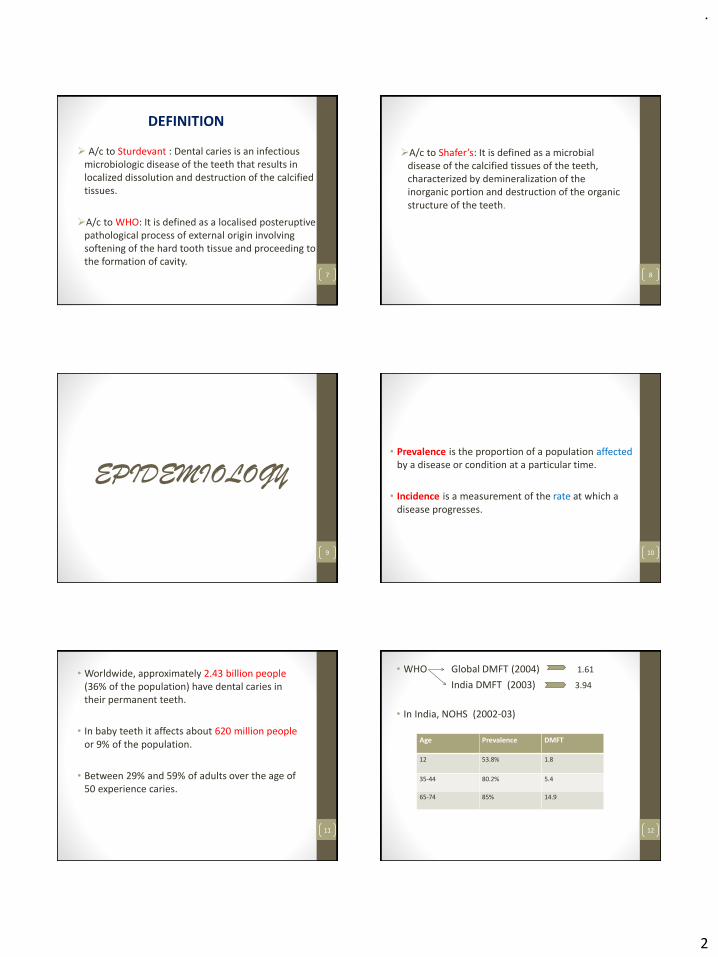
.
2
➢ A/c to Sturdevant : Dental caries is an infectious microbiologic disease of the teeth that results in localized dissolution and destruction of the calcified tissues.
➢A/c to WHO: It is defined as a localised posteruptivepathological process of external origin involving softening of the hard tooth tissue and proceeding to the formation of cavity.
7
DEFINITION
➢A/c to Shafer’s: It is defined as a microbial disease of the calcified tissues of the teeth, characterized by demineralization of the inorganic portion and destruction of the organic structure of the teeth.
8
EPIDEMIOLOGY
9
• Prevalence is the proportion of a population affectedby a disease or condition at a particular time.
• Incidence is a measurement of the rate at which a disease progresses.
10
• Worldwide, approximately 2.43 billion people (36% of the population) have dental caries in their permanent teeth.
• In baby teeth it affects about 620 million people or 9% of the population.
• Between 29% and 59% of adults over the age of 50 experience caries.
11
• WHO Global DMFT (2004) 1.61
India DMFT (2003) 3.94
• In India, NOHS (2002-03)
12
Age Prevalence DMFT
12 53.8% 1.8
35-44 80.2% 5.4
65-74 85% 14.9

.
3
ETIOLOGY
13
Two hypotheses concerning the pathogenicity of plaque in the etiology of caries:
✓Non specific plaque hypotheses
Promotes the presence of potential pathogens in plaque and assumes all accumulations of plaque are pathogenic.
✓Specific plaque hypotheses
It is based on the observation that plaque is assumed to be pathogenic only when signs of disease are present.
- Sturdevant14
15
Dentalplaque
diet
tooth
caries
16
17
Formation of plaque
18
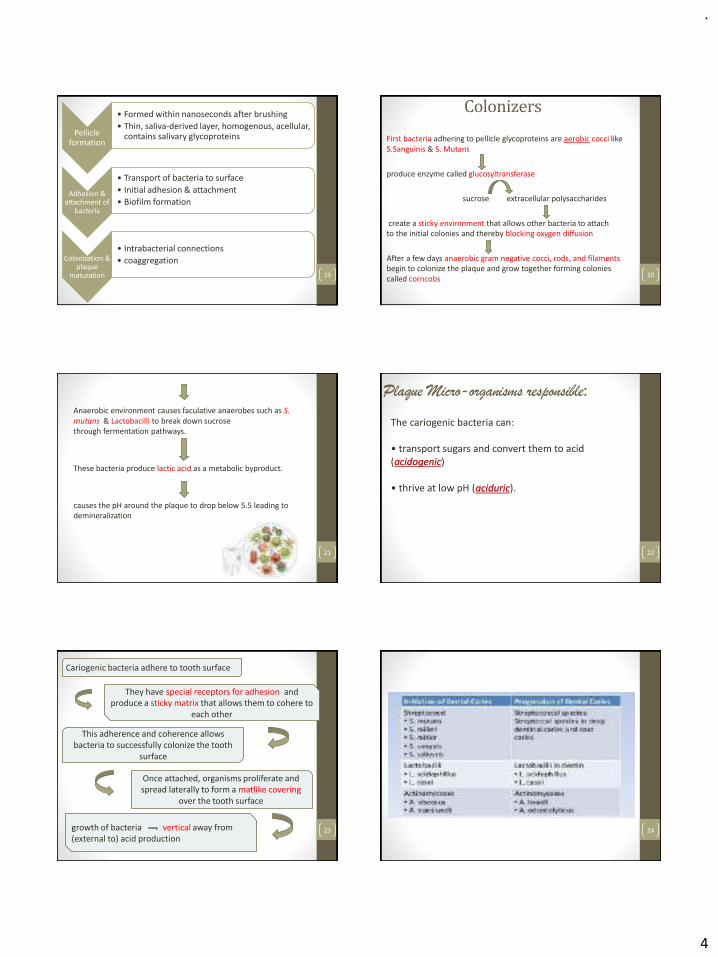
.
4
Pellicle formation
• Formed within nanoseconds after brushing
• Thin, saliva-derived layer, homogenous, acellular, contains salivary glycoproteins
Adhesion & attachment of
bacteria
• Transport of bacteria to surface
• Initial adhesion & attachment
• Biofilm formation
Colonization & plaque
maturation
• Intrabacterial connections
• coaggregation
19
Colonizers
First bacteria adhering to pellicle glycoproteins are aerobic cocci like S.Sanguinis & S. Mutans
produce enzyme called glucosyltransferase
sucrose extracellular polysaccharides
create a sticky environment that allows other bacteria to attach to the initial colonies and thereby blocking oxygen diffusion
After a few days anaerobic gram negative cocci, rods, and filaments begin to colonize the plaque and grow together forming colonies called corncobs
20
Anaerobic environment causes faculative anaerobes such as S. mutans & Lactobacilli to break down sucrose through fermentation pathways.
These bacteria produce lactic acid as a metabolic byproduct.
causes the pH around the plaque to drop below 5.5 leading to demineralization
21
Plaque Micro-organisms responsible:
22
The cariogenic bacteria can:
• transport sugars and convert them to acid (acidogenic)
• thrive at low pH (aciduric).
23
Cariogenic bacteria adhere to tooth surface
They have special receptors for adhesion and produce a sticky matrix that allows them to cohere to
each other
This adherence and coherence allows bacteria to successfully colonize the tooth
surface
Once attached, organisms proliferate and spread laterally to form a matlike covering
over the tooth surface
growth of bacteria vertical away from (external to) acid production
24
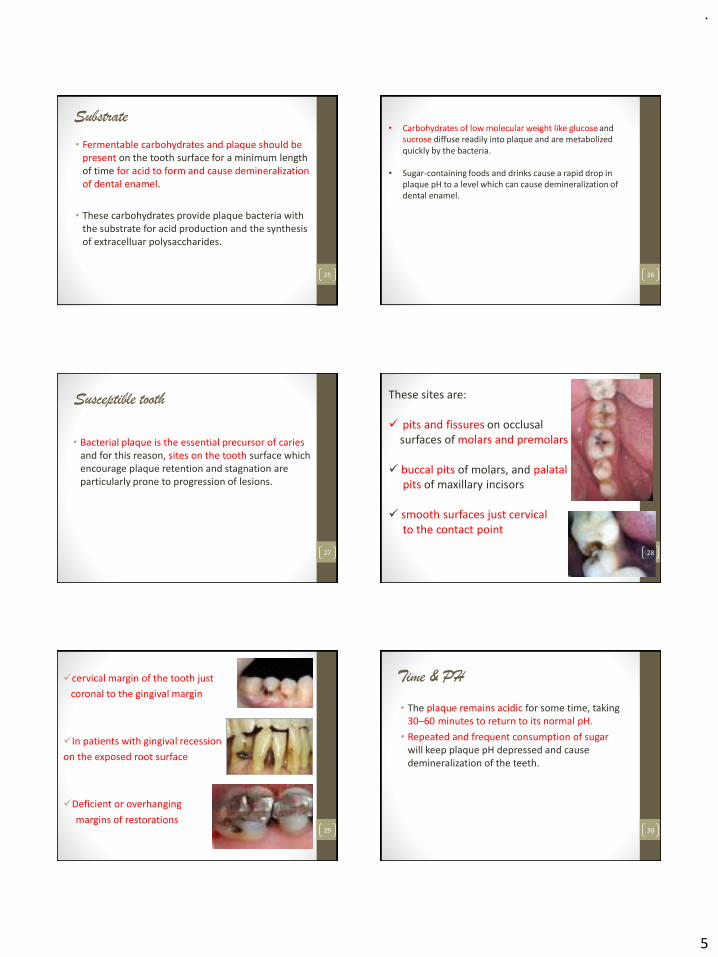
.
5
Substrate
• Fermentable carbohydrates and plaque should be present on the tooth surface for a minimum length of time for acid to form and cause demineralization of dental enamel.
• These carbohydrates provide plaque bacteria with the substrate for acid production and the synthesis of extracelluar polysaccharides.
25 26
• Carbohydrates of low molecular weight like glucose and sucrose diffuse readily into plaque and are metabolized quickly by the bacteria.
• Sugar-containing foods and drinks cause a rapid drop in plaque pH to a level which can cause demineralization of dental enamel.
Susceptible tooth
• Bacterial plaque is the essential precursor of caries and for this reason, sites on the tooth surface which encourage plaque retention and stagnation are particularly prone to progression of lesions.
27
These sites are:
✓ pits and fissures on occlusalsurfaces of molars and premolars
✓ buccal pits of molars, and palatal pits of maxillary incisors
✓ smooth surfaces just cervicalto the contact point
28
✓cervical margin of the tooth just
coronal to the gingival margin
✓In patients with gingival recession
on the exposed root surface
✓Deficient or overhanging
margins of restorations29
Time & PH
• The plaque remains acidic for some time, taking 30–60 minutes to return to its normal pH.
• Repeated and frequent consumption of sugar will keep plaque pH depressed and cause demineralization of the teeth.
30

.
6
• Critical pH: The pH at which any particular saliva ceases to be saturated with calcium and phosphorous is referred to as critical pH.
• Under normal conditions, the critical pH ranges from 5 - 5.5 & below this value, the inorganic material of tooth may dissolve.
31 32
• The change in plaque pH may be represented graphically over a period of time following a glucose rinse. Such a graph is called a ‘Stephan curve’ after the person who first described it in 1944.
Saliva
1. Composition of saliva :
• Inorganic calcium and phosphorus show variation, depending upon the rate of salivary flow.
• Oral enzyme called amylase or ptyalin
degradation of starches
• Parotid saliva > amylase content
33
2. Buffer capacity of saliva:
• Bicarbonate in saliva diffuses into the dental plaque to neutralize the acid formed by microorganisms.
• higher the flow rate greater will be its buffering capacity
3. Quantity of saliva:
• Reduced salivary flow due to pathological conditions or
use of antisialagogues.
34
4. Viscosity of saliva:
• Comes from the mucin content, derived from the submandibular, sublingual and minor salivary glands
• patients with an abundant, thin, watery saliva exhibit rampant caries.
5. Antibacterial properties:
• Presence of lysozymes, salivary peroxidase system and immunoglobulins like IgA
35 36
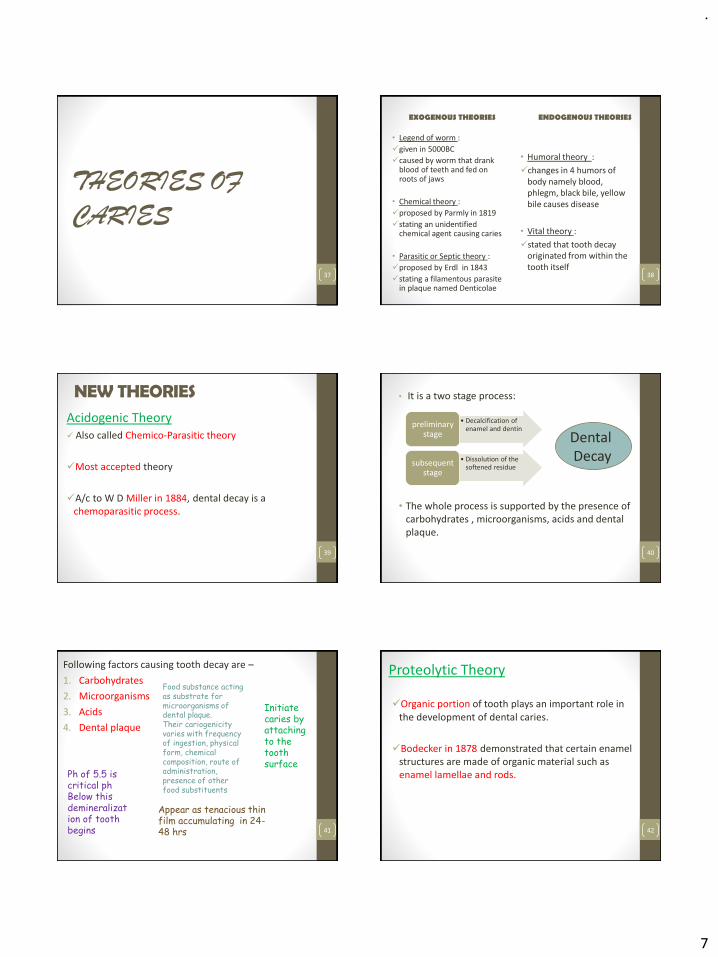
.
7
THEORIES OF
CARIES
37
EXOGENOUS THEORIES
• Legend of worm :
✓given in 5000BC
✓caused by worm that drank blood of teeth and fed on roots of jaws
• Chemical theory :
✓proposed by Parmly in 1819
✓stating an unidentified chemical agent causing caries
• Parasitic or Septic theory :
✓proposed by Erdl in 1843
✓stating a filamentous parasite in plaque named Denticolae
ENDOGENOUS THEORIES
• Humoral theory :
✓changes in 4 humors of body namely blood, phlegm, black bile, yellow bile causes disease
• Vital theory :
✓stated that tooth decay originated from within the tooth itself
38
NEW THEORIESAcidogenic Theory ✓ Also called Chemico-Parasitic theory
✓Most accepted theory
✓A/c to W D Miller in 1884, dental decay is a chemoparasitic process.
39
• It is a two stage process:
• The whole process is supported by the presence of carbohydrates , microorganisms, acids and dental plaque.
40
• Decalcification of enamel and dentin
preliminary stage
• Dissolution of the softened residue
subsequent stage
DentalDecay
Following factors causing tooth decay are –
1. Carbohydrates
2. Microorganisms
3. Acids
4. Dental plaque
41
Food substance acting as substrate for microorganisms of dental plaque.Their cariogenicityvaries with frequency of ingestion, physical form, chemical composition, route of administration, presence of other food substituents
Initiate caries by attaching to the tooth surface
Ph of 5.5 is critical phBelow this demineralization of tooth begins
Appear as tenacious thin film accumulating in 24-48 hrs
Proteolytic Theory
✓Organic portion of tooth plays an important role in the development of dental caries.
✓Bodecker in 1878 demonstrated that certain enamel structures are made of organic material such as enamel lamellae and rods.
42

.
8
• Microorganisms produce proteolytic enzymes that destroy the organic matrix of enamel lamellae or rod sheath.
• Which means proteolysis occurs as the first event in further progression of bacterial invasion + demineralization of tooth causing caries
43
Proteolysis Chelation Theory ✓Proposed by Schatz et al in 1955
✓This theory Suggests that caries occur by simultaneous events of proteolysis + chelation.
✓Destruction of Removal of calcium
organic portion of by forming soluble
tooth by proteolytic chelates.
micro-org.
Caused by oral caused by breakdown
bacteria products44
✓It considers dental caries to be a bacterial destruction of teeth where the initial attack is essentially on the organic components of enamel.
✓The breakdown products of this organic matter have chelating properties and thereby dissolve minerals in enamel.
45
CLASSIFICATION
46
1. Depending on nature of attack2. Depending on progression of
caries3. Depending on surfaces involved4. Based on direction of caries
attack5. Based on number of surfaces
involved6. G V Black’s classification7. Based on location of lesion8. Based on tissue involved
47
APSDNBLT – DPS Bilkul Acha Nhi LgTa Nature of Attack
a) Primary caries
✓ Incipient: initial
✓ First attack on tooth surface
b) Secondary caries
✓ Recurrent
✓Occurs on margins or walls of existing restorations 48

.
9
Progression of caries
49
a) Acute Caries
✓ Rapidly invading process✓ Involves several teeth✓ Lesions are soft + light coloured✓Usually pulp is involved at early stage
b) Chronic caries
✓Lesions are long standing
✓Fewer teeth in number
✓Pain is not a common feature
✓Dark brown and leathery decalcified dentin
50
caries
51
Surfaces Involved
52
➢Pit & Fissure caries
➢Smooth surface caries
Direction of caries
Forward caries
• Proceeds from enamel to dentin
• Lesion is triangle in shape with base of triangle at enamel surface + apex towards dentin
Backward caries
• Proceeds from DEJ towards enamel surface
• Triangle shaped with base at DEJ + apex towards enamel surface
53
Number of surfaces involved
54
Simple : only one surface is involved by caries
Compound : 2 surfaces are involved
Complex : more than 3 surfaces involved

.
10
G V Black’s classification
55
• Later, Simon added Class VI to G V Black’s classification
Class VI: carious lesions occuring on cusp tips of molars, premolars & cuspids
56
Location of Lesion
57
Pit & Fissure caries
• The long and narrow orifice prevents visual and tactile examination.
• caries expands as it penetrates the enamel but have a small entry site.
• They have a cross-section of
inverted V.
58
Smooth surface caries
• Less favourable site for plaque attachment.
• Lesions have a broad area of origin and a conical extension.
• Path of ingress is parallel to the enamel rods.
• It has a cross-section of V shape
with a wide area of origin
with apex towards DEJ.
59
Root caries
• Root surfaces become exposed to the oral environment by gingival recession and are susceptible to caries.
• commonly seen in older people.
• Clinically both active (soft) and arrested or slowly progressing lesions (hard or leathery) are seen.
• Active lesions are usually close to the gingival margin.
60

.
11
Tissue involved
61
Senile caries
• Caries associated with ageing
• Almost exclusively seen on
root surface
62
Residual caries
• Demineralized and infected tissue left by a dentist during cavity preparation.
• darkly staining
• hard or dry and
crumbly in texture.
63
Recurrent caries
64
• primary caries next to a filling caused by the biofilm at the tooth surface or surface of any cavity.
• These are a consequence of leakage between the filling and the tooth.
Rampant caries
• Multiple active carious lesions occurring in the same patient, frequently involving surfaces of teeth that are usually caries-free.
• seen in mouths where there is a sudden marked reduction in salivary flow (hyposalivation).
65
• Conditions required for diagnosis of rampant caries:
1. Lesions > 10 in number
2. New carious lesion in 6-10 months
3. Development of caries in otherwise caries immune surfaces
4. Extensive loss of tooth structure particularly dentin even though enamel shows little defect
5. Soft, ivory coloured dentinal consistency
66
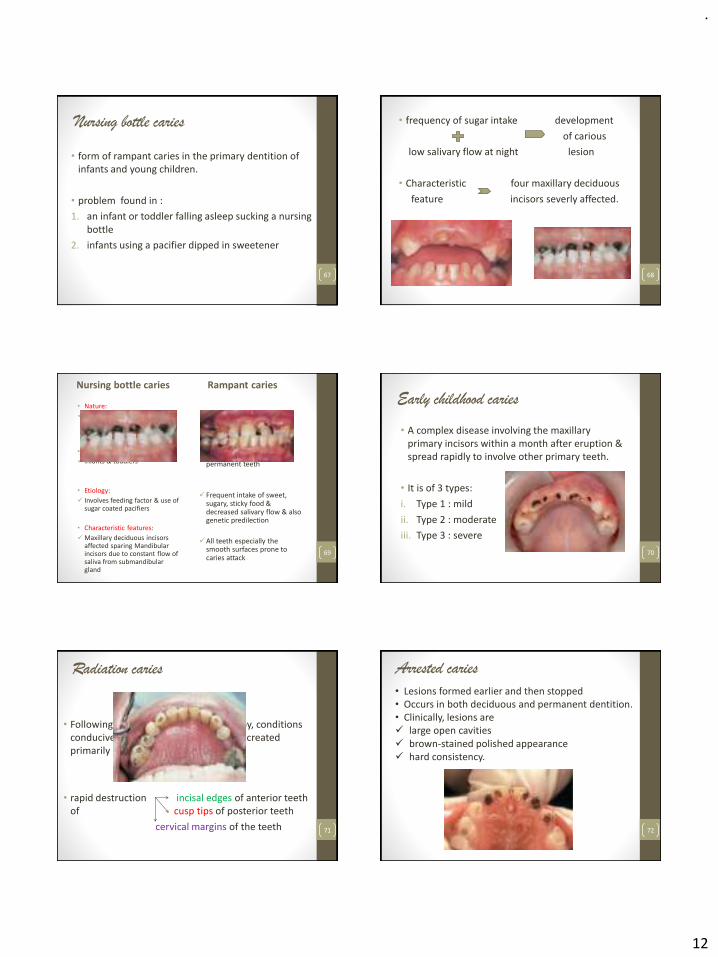
.
12
Nursing bottle caries
• form of rampant caries in the primary dentition of infants and young children.
• problem found in :
1. an infant or toddler falling asleep sucking a nursing bottle
2. infants using a pacifier dipped in sweetener
67
• frequency of sugar intake development
of carious
low salivary flow at night lesion
• Characteristic four maxillary deciduous
feature incisors severly affected.
68
Nursing bottle caries
• Nature:
✓Acute generalized spread & pulpal involvement in selected teeth
• Age:
✓ infants & toddlers
• Etiology:
✓ Involves feeding factor & use of sugar coated pacifiers
• Characteristic features:
✓Maxillary deciduous incisors affected sparing Mandibular incisors due to constant flow of saliva from submandibular gland
Rampant caries
✓Acute generalized spread & pulpal involvement in all teeth
✓all ages + both primary and permanent teeth
✓Frequent intake of sweet, sugary, sticky food & decreased salivary flow & also genetic predilection
✓All teeth especially the smooth surfaces prone to caries attack
69
Early childhood caries
• A complex disease involving the maxillary primary incisors within a month after eruption & spread rapidly to involve other primary teeth.
• It is of 3 types:
i. Type 1 : mild
ii. Type 2 : moderate
iii. Type 3 : severe
70
Radiation caries
• Following radiotherapy or chemotherapy, conditions conducive to a rapid onset of caries are created primarily by the shortage of saliva.
• rapid destruction incisal edges of anterior teeth of cusp tips of posterior teeth
cervical margins of the teeth 71
Arrested caries
72
• Lesions formed earlier and then stopped• Occurs in both deciduous and permanent dentition.• Clinically, lesions are ✓ large open cavities ✓ brown-stained polished appearance ✓ hard consistency.

.
13
73
GOOD MORNING DENTAL
CARIES
74
CONTENTS
PART-2
• Histology of caries
• Caries diagnosis
• Caries prevention
• Summary
• References
75
HISTOLOGY OF
CARIES
76
•Caries of enamel
•Caries of dentin
•Caries of cementum
77
CARIES OF ENAMEL• Microscopically 4 zones are seen in caries of enamel:
1. Translucent zone
2. Dark zone
3. Body of lesion
4. Surface zone
78
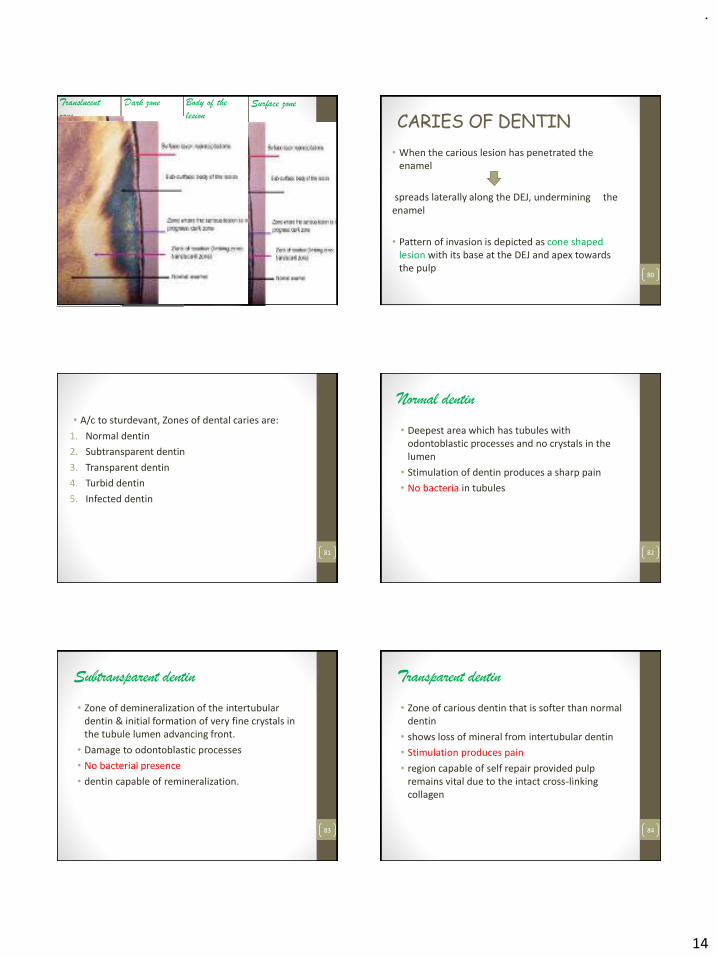
.
14
79
Translucent
zone
• Deepest zone
• advancing front of the enamel lesion
• Structurelessappearance
Dark zone
• Immediateabovetranslucent zone
• Appears dark
• Loss of crystalline structure
Body of the
lesion
• maximum dimineralization
• positively bifringent
• largest zone exhibiting enhanced striae of retzius.
Surface zone
• Relatively unaffected
• first sites of bacterial entry into carious lesion
• Thinner in active lesions
• Partial dimineralization = 10% mineral loss
CARIES OF DENTIN
• When the carious lesion has penetrated the enamel
spreads laterally along the DEJ, undermining the enamel
• Pattern of invasion is depicted as cone shaped lesion with its base at the DEJ and apex towards the pulp
80
• A/c to sturdevant, Zones of dental caries are:
1. Normal dentin
2. Subtransparent dentin
3. Transparent dentin
4. Turbid dentin
5. Infected dentin
81
Normal dentin
• Deepest area which has tubules with odontoblastic processes and no crystals in the lumen
• Stimulation of dentin produces a sharp pain
• No bacteria in tubules
82
Subtransparent dentin
• Zone of demineralization of the intertubulardentin & initial formation of very fine crystals in the tubule lumen advancing front.
• Damage to odontoblastic processes
• No bacterial presence
• dentin capable of remineralization.
83
Transparent dentin
• Zone of carious dentin that is softer than normal dentin
• shows loss of mineral from intertubular dentin
• Stimulation produces pain
• region capable of self repair provided pulp remains vital due to the intact cross-linking collagen
84
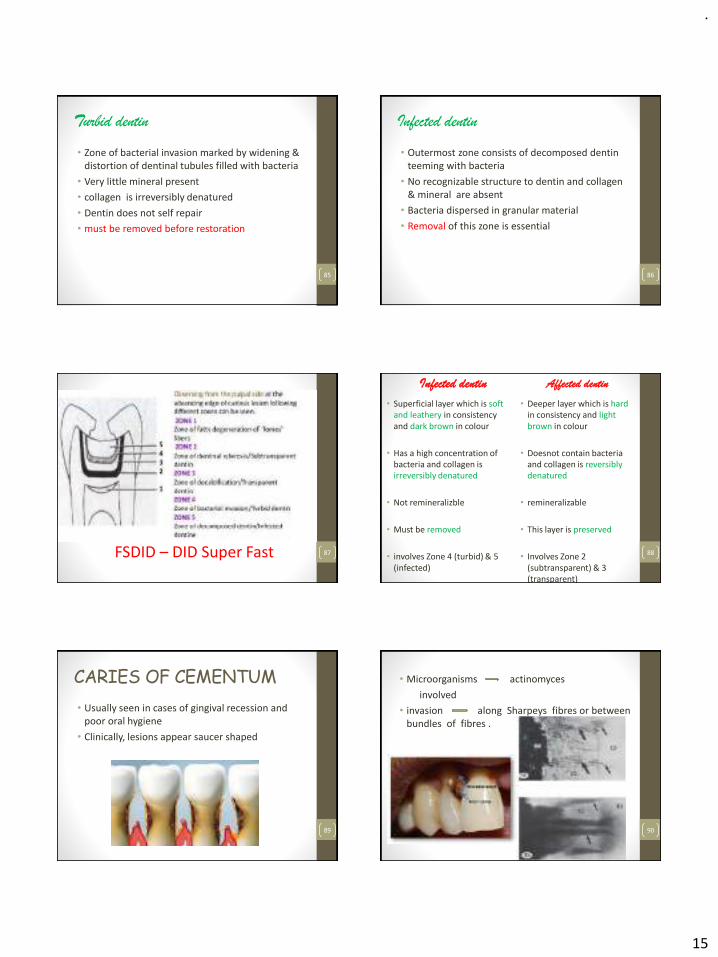
.
15
Turbid dentin
• Zone of bacterial invasion marked by widening & distortion of dentinal tubules filled with bacteria
• Very little mineral present
• collagen is irreversibly denatured
• Dentin does not self repair
• must be removed before restoration
85
Infected dentin
• Outermost zone consists of decomposed dentin teeming with bacteria
• No recognizable structure to dentin and collagen & mineral are absent
• Bacteria dispersed in granular material
• Removal of this zone is essential
86
87FSDID – DID Super Fast
Infected dentin
• Superficial layer which is soft and leathery in consistency and dark brown in colour
• Has a high concentration of bacteria and collagen is irreversibly denatured
• Not remineralizble
• Must be removed
• involves Zone 4 (turbid) & 5 (infected)
Affected dentin
• Deeper layer which is hardin consistency and light brown in colour
• Doesnot contain bacteria and collagen is reversibly denatured
• remineralizable
• This layer is preserved
• Involves Zone 2 (subtransparent) & 3 (transparent)
88
CARIES OF CEMENTUM
• Usually seen in cases of gingival recession and poor oral hygiene
• Clinically, lesions appear saucer shaped
89
• Microorganisms actinomyces
involved
• invasion along Sharpeys fibres or between bundles of fibres .
90

.
16
CARIES
DIAGNOSIS
91
• The word diagnosis is derived from a Greek word “dia” meaning “through” and “gnosis” meaning “knowledge”.
• Thus ‘to diagnose’ implies that it is only through knowledge about the disease that a diagnosis can be established.
92
• Diagnosis can be defined as an art and science that results from the synthesis of scientific knowledge, clinical experience, intuition & common sense.
93
• In dentistry, caries being the major cause of all the progressive diseases, correct and early diagnosis of caries is of utmost importance to the clinician as well as the patient.
94
• The PRIMARY OBJECTIVE of caries diagnosis is to identify those lesions that require surgical (restorative) treatment, those that require nonsurgical treatment, and those persons who are at high risk for developing carious lesions.
• The process of caries diagnosis involves both risk assessment and the application of diagnostic criteria to determine the disease state.
95
• Caries diagnosis implies deciding whether a lesion is active, progressing rapidly or slowly or whether already arrested.
• Diagnosing caries is equally important as treating the caries to prevent misdiagnosis and confusion over the patient’s oral health condition.
96

.
17
Diagnostic aids❖Visual & Tactile inspection
* Conventional method
Visual examination
Tactile examination
*Advances in visual method
A) Illumination
i) Optical caries monitor
ii) Fiberoptic transillumination
iii) Digital fiberoptic transillumination
iv) Quantitative laser fluoroscence
vi) DIAGNOdent
vii) Ultrasound imaging
B) Dye penetration method
97
❖Radiographic diagnosis
* Conventional
* Digital radiographic methods
❖Electrical conductance methods
❖Recent advances
98
Visual & tactile inspection• Most commonly used & conventional method of dental
examination
• dentist detects the presence of caries and diseases in the mouth via sight (visual inspection) or touch (usually using a dental explorer).
• Pre-requisites : clean & dried tooth surface under adequate light source
99
Clinical indications of enamel dissolution and demineralization are :
• “Tackiness” on the surfaces of the tooth.
• Discontinuity of the enamel
• Discolouration:o White spots on clean, dry, illuminated teeth (Active, non- cavitated) ‘disappears on wetting surface’
o Yellow tinge due to erosion of enamel and greater exposure of underling dentine
o Black/brown areas, especially along pits and fissures (Inactive, non-cavitated)
o Yellow/orange/tan/light brown appearance of roots100
• Penetration of tooth surface by explorer.
• Loss of translucency and lustre of tooth surface
• Exposure of dentine and/or pulp
(Ismail, 2004)101
• On probing:
✓Active, cavitated lesions soft or leathery
✓Inactive, cavitated lesions shiny and hard
• Progression to formation of cavity:
active, cavitated > inactive, non-cavitated > healthy surfaces
102
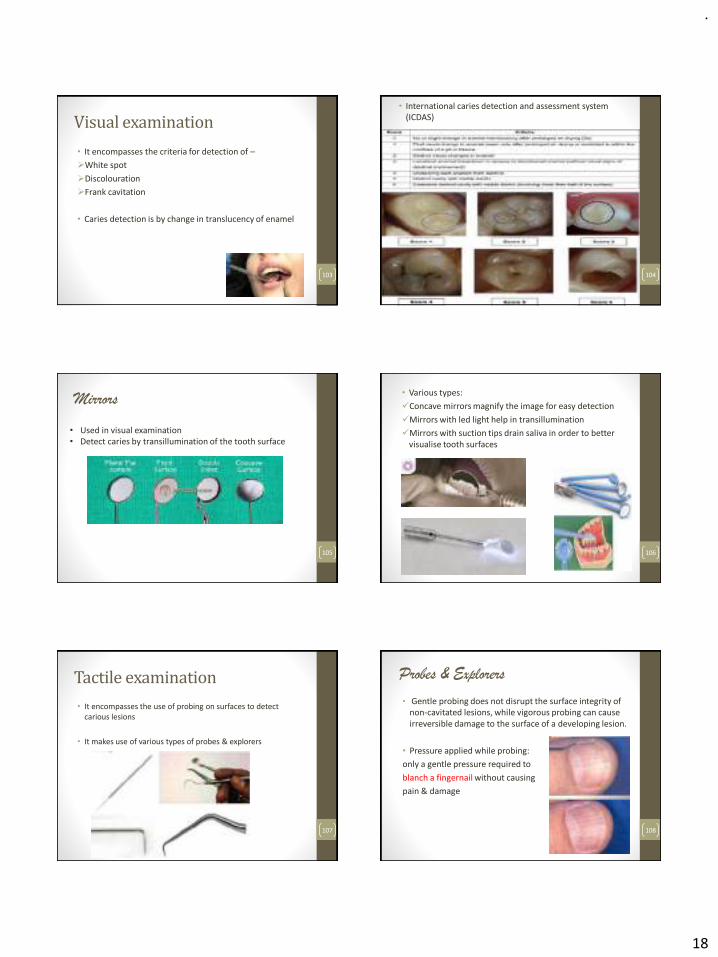
.
18
Visual examination
• It encompasses the criteria for detection of –
➢White spot
➢Discolouration
➢Frank cavitation
• Caries detection is by change in translucency of enamel
103
• International caries detection and assessment system (ICDAS)
104
Mirrors
105
• Used in visual examination• Detect caries by transillumination of the tooth surface
• Various types:
✓Concave mirrors magnify the image for easy detection
✓Mirrors with led light help in transillumination
✓Mirrors with suction tips drain saliva in order to better visualise tooth surfaces
106
Tactile examination
• It encompasses the use of probing on surfaces to detect carious lesions
• It makes use of various types of probes & explorers
107
Probes & Explorers
• Gentle probing does not disrupt the surface integrity of non-cavitated lesions, while vigorous probing can cause irreversible damage to the surface of a developing lesion.
• Pressure applied while probing:
only a gentle pressure required to
blanch a fingernail without causing
pain & damage
108
.
19
Various explorers used:
• Most common explorer used is No. 17 explorer, also known as a 'shepherd's hook'.
• Used to check for assessment of anterior surfaces and facial & lingual surfaces of posteriors & irregular restorative margins 109
• Orban’s explorer no. 23 used specific for detecting proximal lesions
110
111
Disadvantages
• Excessive probing force may produce irreversible traumatic defects in potentially remineralizable lesions
• May transmit cariogenic bacteria in
the mouth
• Binding of the tip may also occur due
to non-carious reasons like:
✓Shape of fissure
✓Sharpness of explorer
✓Force of application
✓Path of explorer placement112
Visible light methods
• Optical caries monitor
• Fiber-optic transillumination (FOTI)
• Digital Image fiber-optic transillumination (DIFOTI)
• Quantitative light/laser-induced fluorescence (QLF).
113
Optical Caries Monitor :
• Principle : in white spot carious lesion, scattering is stronger than in sound enamel surface
• Light is transported through a fiber bundle to the tip of handpiece.
• Tip placed against the tooth surface and reflected light is collected by different fibers of the same tip
114

.
20
115
Fibre-Optic Transillumination :
• provides an intense light beam that is transmitted through a fiberoptic cable to a specially designed probe to permit the use of transillumination on the proximal surfaces of posterior teeth
116
Digital Imaging Fibre-Optic Transillumination :
• combining FOTI with a digital CCD camera.
• Areas of demineralized enamel or dentin scatter light and incipient caries appear darker in the resultant image
117
Quantitative Laser Fluorescence (QLF) :
• 1929 first described by Benedict
• aid in the detection of occlusal caries.
• machine emits light with a wavelength of 655 nm transported through a fibre bundle to the tip of a handpiece
• tip is placed against the tooth surface and rotated & the laser light penetrates the tooth.
• The received light is measured and its intensity is an indication of the size and depth of lesion.
• Tooth is seen on a computer monitor as fluorescent green and dark areas indicate mineral loss or white spot the carious lesion.
118
Laser Light
DIAGNO-dent :
• first introduced in 1998 by Hibst and Gal
• diagnosis of occlusal caries in adjunct to visual and radiographic examination.
• a variant of QLF system
• uses a simple laser diode to compare the reflection wavelength
• Carious tooth structure exhibits fluorescence proportionate to the degree of caries, resulting in elevated scale readings on the display
119 120
.
21
DIAGNO-dent Pen :
• advancement made in the DIAGNOdent technology.
• DIAGNOdent pen 2190 detects fissure and smooth surface caries accurately
121
Ultrasound method
• detecting early carious lesions on smooth surfaces
• makes the use of sound waves with frequency
• An ultrasonic probe is used which sends and receives longitudinal waves to and from the surface of the tooth.
• Initial white spot lesions no or weak surface echoes
• sites with visible cavitation echoes of higher amplitude
122
Dye penetration method
123
• Various dyes available for staining are:
124
Radiographic examination
125
IOPA
Bitewing
• A minimum of 30%-40% demineralization of the tooth surface is required to appear for radiographic detection.
• The actual depth of penetration of caries is clinically deeper than it appears on radiograph.
126
.
22
Digital radiographic methods
• Digital image enhancement
• Digital subtraction radiography
• Tuned-aperture computed tomography (TACT).
➢Digital detectors
• Charged couple device (CCD)
• Complementary metal oxide semiconductor
• Photo Stimulable Phosphor plate (PSP).
127
Electrical Current Method
• Electrical conductance measurement
• Electrical impedance measurement
128
Electrical Conductance Measurement :
• principle : demineralized tooth has more pores filled with water or saliva, and this is more conductive than intact tooth surface.
• first proposed by Magitot in 1878.
• the amount of demineralization, the electrical conductivity through enamel.
• Demineralized sites and sites with high pore volume and cavities can be detected by measuring the conductance.
129 130
Site specific Surface specific
This technique has two methods of application:
Two instruments based on the difference in electrical conductance of carious and sound enamel developed:
Vanguard electronic caries detector
• It used a current of 25 Hz.
• Measured conductance converted to an ordinary scale of 0–9.
• Moisture and saliva removed by a continuous stream of air to prevent surface conductance.
Caries meter
• It uses a current of 400 Hz.
• Measured conductance converted to four coloredlights.
• Green: No caries
• Yellow: Enamel caries
• Orange: Dentin caries
• Red: Pulpal involvement131
Electronic Impedance Measurement :
• measure of degree at which an electric circuit resists electric current flow when a voltage is applied across two electrodes.
• Caries tissue has a lower impedance than sound tooth.
• It is also known as electronic caries monitor
132

.
23
Newer technologies
1. Multiphoton imaging
2. Infrared fluorescence
3. Infrared thermography
4. Terahertz imaging
5. Optical coherence tomography
6. Polarized Raman spectroscopy
7. Modulated (frequency-domain) infrared photothermal radiometry
133
Multiphoton imaging
• Uses infrared light
• Collects information from carious lesion upto depth of 500 microns
134
Optical Coherence Tomography (OCT)
• Form of imaging technology which utilises light waves to provide high resolution morphological depth images.
• In the OCT scan of carious lesion , high intensity signals are present deeper into the tooth, suggesting the presence of a carious lesion.
• This is because demineralisation increases tooth porosity and opens up more space within the tooth matrix, allowing scattered light to penetrate deeper into the enamel.
135 136
Polarised Raman Spectroscopy (PRS)
• It also makes use of light scattering
• Acts on the principle of Raman effect
• It is able to detect changes in the biochemical signature of a tooth based on the state of demineralisation and remineralisation
137
Caries Activity Tests
• Several caries activity tests have been developed to help detect the presence of oral conditions associated with increased risk of caries.
138

.
24
Caries susceptibility tests
• Snyder’s colorimetric test
• Enamel solubility test
• Dewar test
• Fosdick calcium dissolution test
• Salivary reductase test
• Ora test
Caries activity tests
• Lactobacillus colony count test
• Streptococcus mutans level in saliva
• S. Mutans screening tests
– Plaque-tooth pick method
– Saliva/tongue blade method
– S. Mutans adherence method
– S. Mutans dip-slide method
– S. Mutans replicate technique
• Alban test
• Dewar test
• Swab test
• Salivary buffer capacity test
139
Lactobacillus Colony Count Test
• Principle involved: Estimation of the number of acidogenic and aciduric bacteria in the patient saliva by counting the number of colonies appearing on Tomato peptone agar plates (pH 5.0) after inoculation with a sample of saliva.
• Advantages
• Useful for monitoring the effectiveness of restorative dentistry.
• Simple to carry out.
• Useful as a screening test for caries activity in large groups.140
Streptococcus Mutans Level in Saliva
• Principle involved: Measures the number of S.mutanscolony forming units per unit volume of saliva and plaque samples from sites such as occlusal fissures and proximal areas.
• Incubation done on Mitis Salivarius + high concentration of sucrose(20%) + U Bacitracin (MSB)
• Advantage: Useful in caries management as S.mutans are main causative agents.
141
Calorimetric Snyder Test
• Principle involved: Measures the ability of salivary microorganisms to form organic acid from a carbohydrate medium.
• Medium - an indicator dye “Bromocresol green”, changes colour from green to yellow when pH changes from 5.4 to 3.8.
• Indirectly measures the number of both aciduric and acidogenic organisms in saliva.
142
Salivary Buffer Capacity Test
• Principle involved: Buffer capacity can be Quantities using either a pH meter or colour indicators.
• measures the number of milliliters of acid required to lower the pH of saliva through an arbitrary pH interval (6 to 7).
143
Salivary Reductase Test (Susceptibility Test)
• Principle involved: Measures the activity of the reductaseenzyme present in salivary bacteria, using a dye Diazo-resorcinol.
• The evaluation is based on the color change
• Advantage: Quick results, as no incubation period is required.
144
.
25
Caries diagnosis for pits & fissures
• The active, uncavitated lesion is white, often with a matt surface.
• The corresponding inactive lesion may be brown.
• The enamel lesion visible on a dry tooth
surface is in outer enamel.
• The lesion visible on a wet
surface is all through
enamel and into dentine.
145
• The factors for pit & fissure caries diagnosis are:
(1) softening at the base of the pit or fissure
(2) opacity surrounding the pit or fissure, indicating undermining or demineralization of the enamel
(3) softened enamel that may be flaked away by the explorer.
Cavitation means that extensive enamel demineralization has lead to destruction of the walls of the pit or fissure and bacterial invasion has occurred.
146
Noncavitated (caries-free):
✓No radiolucency below occlusal enamel
✓Deep grooves may be present
✓Superficial staining may be present in grooves
✓Mechanical binding of explorer may occur
Cavitated (diseased):
✓Chalkiness of enamel on walls and base of pit or fissure
✓Softening at the base of a pit or fissure
✓Brown-grey discoloration under enamel adjacent to pit or fissure
✓Radiolucency below occlusal enamel
147
Caries diagnosis for smooth surface
• Incipient caries consists of opaque, chalky white areas (white spots) that appear when the tooth surface is dried.
• The diagnosis is confirmed when the affected area is rehydrated (wetted) and the chalky area partially or totally disappears.
148
Caries diagnosis for Root surfaces
• Discoloration is associated with remineralization.
• The darker the discoloration, the greater the remineralization.
• Progressing root caries is primarily detected by the presence of softness and cavitation.
149
Caries diagnosis for proximal surfaces
Non-cavitated:
✓Surface usually intact
✓Opacity of proximal enamel may be present
✓Radiolucency may be present
✓Opaque area may be seen in enamel by transillumination
Cavitated:
✓Surface broken, detectable visually or tactilely
✓Marginal ridge may be discoloured
✓Opaque area in dentin on transillumination
✓Radiolucency is present150
.
26
CARIES
PREVENTION
151
• The primary goal of a caries prevention program should be to reduce the numbers of cariogenic bacteria.
152
At professional level
• Diet counselling
• Fluoride exposure
➢ Fluoride varnishes
• Salivary stimulants
• Antimicrobial agents
• Caries control restorations
➢ Pit & fissure sealants
➢ Atraumatic restorative treatment
At patient level
• Oral hygiene methods
• Xylitol gums
• Tooth mousse
153
Caries prevention at Professional level
154
Diet Counselling
• Goal of dietary counselling : reduce the frequency of sucrose ingestion in between the meals.
155
• Vipeholm Study concluded that :
➢ carbohydrate mainly sugar, caries activity
➢caries risk greater- sugar consumed retained in tooth surface
➢caries activity greatest when sugar consumed between meals
➢varies widely between individuals
➢withdrawal of sugar rich foods decreased caries activity rapidly
➢high concentration-prolong retention- caries activity increased
➢clearance time of sugar correlates closely with caries activity
156

.
27
• Turku Sugar Study concluded that :
➢Fructose was less cariogenic than Sucrose
➢Xylitol was non cariogenic & even anticariogenic
157
• The Dental Health Diet Score
➢A simple scoring procedure that can disclose a potential dietary problem that is likely to adversely affect a patient‘s dental health.
➢Diet counselling is given to the patient according to the diet score obtained from the test.
159
Fluoride Exposure
• Fluoride in trace amounts increases the resistance of tooth structure to demineralization and is therefore a particularly important consideration for caries prevention.
160
• Fluorides exert their anticaries effect by three different mechanisms:
➢First: greatly enhances the precipitation of fluorapatiteinto tooth structure from saliva making enamel more acid-resistant.
➢Second: incipient, non-cavitated, carious lesions are remineralized by the same process.
➢Third: fluoride has antimicrobial activity.
In low concentrations, it inhibits the enzymatic production of glucosyltransferase, reducing bacterial adhesion.
161
Fluoride varnish
• Varnishes provide a high uptake of the fluoride ion into enamel
• Contains 5% sodium fluoride
• Most cost-effective means of delivery of fluoride to teeth
• Effective bactericidal and caries prevention agent
163
• Fluoride varnish deposits large amounts of fluoride on demineralized enamel surface.
• Calcium fluoride precipitates on the surface and fluorapatite is formed.
• Less soluble under
acidic conditions
& more resistant
to demineralization 164

.
28
• Commercially available varnishes
165
Rs. 6560/-
5 bottle kit157$
69$
The general technique for fluoride varnish use is:
Teeth surface is dried
Thin layer of fluoride varnish
Applied onto the teeth.
After application, a yellow film
remains on the teeth
Patients are asked to avoid eating for several hours and
then avoid brushing until the next morning.
166
Advantages:
• fluoride varnish sets when contacting moisture, thorough isolation of the area is not required.
• Only toothbrushing, rather than prophylaxis, is necessary before application.
Disadvantage:
• a temporary change in tooth color may occur
167 168
Salivary Stimulants
• Normal salivary flow : 1 – 1.5L average daily
• Range of normal flow : 0.1-0.2mL/min
• Lack of saliva greatly increases the incidence of caries.
• Various Saliva stimulants available:
✓Chewing gums
✓paraffin waxes
✓Sialagogues like pilocarpine
✓Artificial saliva
169 170
Artificial saliva: comes in several forms
✓ oral spray✓ oral rinse✓ Gel✓ Swabs✓ dissolving tablets

.
29
• Contents include combination of water and the following:
✓Carboxymethylcellulose sodium: increases viscosity and helps lubricate the oral cavity.
✓Glycerin: acts as a lubricant reducing moisture loss and protect the mouth from mechanical trauma.
✓Minerals: phosphates, calcium, and fluoride can help protect and strengthen teeth
✓Xylitol: believed to increase saliva production and protect teeth from bacteria and decay.
✓Other ingredients: also contain preservatives to maintain shelf life and flavoring agents to give them a pleasant taste.
171
Antimicrobial Agents
172
Caries Control Restorations
• The most effective method for control of the progression of active, cavitated lesions.
• The term caries control refers to an operative procedure in which multiple teeth with acute threatening caries are treated by:
(1) Removing the infected tooth structure
(2) Medicating the pulp, if necessary
(3) Restoring the defects with a temporary material
173
• Indications :
(1) the caries is extensive enough to soon involve the pulp
(2) Removing nidus of caries infection in the patient's mouth
(3)tooth having extensive carious involvement that cannot be permanently restored because of questionable pulpal prognosis.
174
175
Temporary/amalgam restoration
Base/liner
Atraumatic Restorative Treatment
• ART is based on modern knowledge about minimal intervention, minimal invasion & minimal cavity preparation for carious lesion
• Procedure is based on
removing carious tissues using the
hand instruments alone
& restoring the cavity with
adhesive restorative material
• Material of choice is
Type VIII Glass Ionomer cement.176
.
30
• Why GIC?
➢the ability to bond chemically to enamel and dentin
➢biocompatibility with pulpal tissue
➢good cavity seal
➢ease of use and low costs
• GICs having surface antibacterial properties :
✓Fuji IX GP (GC America, Alsip, Ill.)
✓Fuji Plus (GC America)
✓Ketac Molar (3M ESPE Dental AG, Seefeld, Germany)
177
Indications
• Small cavities
• Cavities accessible to hand instruments
• Public health programs
Contraindications
• Swelling, abscess or fistula near the tooth
• Exposed pulp
• Cavities inaccessible to hand instruments
• Tooth painful for long time with chronic inflammation of pulp
178
Advantages
• Requires minimal cavity preparation & conserves sound tooth tissues
• Need for L.A. reduced due to painless procedure
• No electrically driven & expensive dental equipment
• Simpilfies infection control as only hand instruments are used
179
Hand instruments• Mouth mirror
• Explorer
• Tweezer
• Spoon excavator
• Dental hatchet
• Applier/carver
• Mixing pad & spatula
180
Pit & Fissure Sealants• Sealants have three important preventive effects:
✓mechanically fill pits and fissures with an acid-resistant resin
✓deny MS and other cariogenic organisms their preferred habitat
✓render pits and fissures easier to clean by tooth brushing and mastication
181 182
Indications & contraindications for use of sealants :
.
31
• Materials of choice :
✓Glass Ionomer Cement
Type IV : Pit & Fissure sealant
Type IX : Pediatric GIC
183
Rs. 2095/-
✓Polymerized resins
Generations first : polymerized with UV light
eg: Nuvalite (dentsply)
second: self cure/ chemical cure resins
eg: Concise White (3M)
third: light cured with visible light
eg: Helioseal
fourth: fluoride releasing sealnts
eg: Seal Right (Pulpdent) 184
Caries prevention at patient level
185
Oral Hygiene
• Plaque free tooth surfaces do not decay!
• Plaque removal aids:
✓ dental floss
✓ tooth brushing
✓mouth rinses
186
187
Xylitol Gums• Xylitol is a natural five-carbon sugar obtained from birch
trees.
• MS cannot metabolize xylitol.
• Xylitol reduces MS by altering their metabolic pathways and enhances remineralization and helps arrest dentinal caries.
• Recommended use: patient asked to chew a piece of xylitol gum after eating or snacking for 5 to 30 minutes.
188
.
32
Tooth Mousse • Developed by scientists at the Melbourne Dental School
at the University of Melbourne and GC Corporation in Japan.
• First oral health product to contain the peptide complex CPP-ACP (casein phosphopeptide amorphous calcium phosphate)
189
• It is a water-based creme containing Recaldent which is derived from the milk protein, casein.
• Bio-available calcium and phosphate, without fluoride
• Applied topically to teeth and gums to provide extra protection for teeth, to help neutralize acid challenges from bacteria and other acid sources.
190
191 192
Summary
• Combating caries has always been a major challenge for dentists around the world.
• Diagnosis, prevention, and treatment of dental caries must be the foremost objectives of operative dentistry.
• Patient education and motivation in the prevention and treatment of dental caries must be stressed.
• Research efforts in understanding the caries process; maximizing the benefits of fluoride use and perhaps, developing anticaries vaccines must be continued. 193
• The clinical treatment of carious teeth must be accomplished expeditiously, judiciously, and appropriately.
• Advanced carious lesions should be treated without delay to minimize the potential of adverse pulpal reaction and to provide time for assessment of the pulpal response to therapy.
194

.
33
References
195 196
THANK YOU
.
1
DENTAL PULP
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
Contents Introduction.
Development of tooth.
Anatomy of pulp.
Histological zones of pulp.
Innervation of pulp.
Functions of pulp.
Age related changes of pulp.
Systemic factors affecting pulp.
Genetic and developmental disorders affecting pulp.
Conclusion.
2
The Dental Pulp
INTROUDCTION
❑ The Pulp is a soft connective tissue that occupies the central part of the teeth.
❑ It is mesenchymal in origin .
❑ Made of connective tissue; contains nerves and blood vessels.
Consists of specialized
3
DEFINITIONS
The dental pulp is the soft connective tissue that supports the dentin.
- Ten Cate’s
Dental pulp is a connective tissue uniquely situated within the rigid encasement of mineralized dentin.
- Seltzer -3rd
edition
4
Anatomy of dental pulp
Pulp organ is composed of-
1) coronal pulp
2)radicular pulp
5
Coronal pulp
❑ It occupies the pulp chamber of the crown.
❑ In young teeth-resembles the shape of the outer dentin.
It has six surfaces.
Consists of Pulp horns.
It constricts at the cervical region where it continues as the radicular pulp.
6
.
2
Radicular pulp❑ It 0ccupies the root canal of tooth.
Anterior tooth-single
Posterior teeth-multiple.
The radicular portions of the pulp is continuous with
the periapical tissues through apical foramen.
As age advances the width of the radicular pulp is reduced ,and so is the apical foramen.
❑ It vary in size,shape,number.
7
GENERAL FEATURES
Total of 52 pulp organs - 32 in the permanent
- 20 in the primary teeth.
Total pulp volume-0.38cc.
Mean volume of single adult human pulp-0.002CC
Maxillary- first molar -0.068cc (maximum)
-lateral incisor-0.011cc(minimum)
Mandibular –first molar -0.053cc (maximum)
-central incisor-0.006cc (minimum)
Each of these organs has a shape that conforms to
that of the respective tooth.
8
DEVELOPMENT
Beginning of the tooth development -6th week of intrauterine life.
Oral epithelium - Two layers :
1)Basal layer of epithelial cells.
2)Surface layer of flattened epithelial cells.
9
DEVELOPMENTDevelopment is divided into four stages:
1)Bud stage.
2)Cap Stage.
3)Early bell Stage.
4)Late bell stage.
10
BUD STAGE
11
Oral ectoderm
Dental lamina
Developing tooth bud
Condensing ectomesenchyme
▪Initialstage–resembling small bud
▪Rapid thickening ofepithelial cells occur.
▪Area of condensation immediately belowenamel organ is the dental lamina.
▪Epithelial cells of dental lamina proliferate.12
Ectomesenchymalcondensation surrounding thetooth bud & the dental papillais the tooth sac.
Dental lamina & dental sacare not well defined at thisstage.
Dental lamina forms – dentin& pulp.
Dental sac forms-cementum& periodontal ligament.

.
3
▪ Rhythmic circadian cell division resulting in an unequal proliferation of some of the epithelium.
▪ Deep surface of the bud invaginate & several
layers become apparent.
1. Inner dental epithelium(tall columnar).
2. Outer dental epithelium(short epithelial cells).
13
CAP STAGE
Dental lamina
Stellate reticulum
epithelium
▪ In the centre, the cells become separated.
▪ These cells are called the Stellate Reticulum.or enamel
pulp.
▪ At around 8th week condensation of connective tissue
under the inner dental epithelium- future dental pulp.
▪ Cells in the dental papilla at first - large rounded or
polyhedral, with pale cytoplasm.
▪ As the pulp matures the cells take on the spindle shape.
14
Due to continued uneven growth of enamel organ it acquires a bell shape
4 layers :
1. Inner enamel epithelium
2. Stratum intermedium
3. Stellate reticulum
4. Outer enamel epithelium
EARLY BELL STAGE
Outer enamel epithelium
Stellate reticulumStratum intermediumInner enamel epithelium
Dental papilla
Differentiation of epithelial and mesenchymalcells into ameloblast and odontoblast.
Differentiation of odontoblast: Accomplished by interaction of cells and signaling molecules mediated through basal lamina and extra cellular matrix.
Exchange between epithelial and mesenchyme takes place across membrane known as Basal lamina.
16
Characterized by the commencement of mineralization & root formation.
Dental lamina that connects the tooth organ: disintegrates.
The boundary between the inner epithelium & odontoblasts outline the future DEJ.
Junction between inner and outer epithelia-future CEJ.
Formation of dentin occurs first as a layer along the future DEJ.
17
LATE BELL STAGE
Collapsed stellate
reticulumAmeloblasts
Outer enamel
epithelium
Dental sac
Odontoblast
Developing
pulp
18
After 1st layer of dentin is formed, ameloblasts laydown enamel over the dentin .
The cervical portion of enamel organ gives rise toHERS.
The most peripheral cells of the dental papilla enlarge and become organized along the basement membrane.
These newly differentiated cells are called odontoblast.
Dental papilla at this point: Dental pulp.
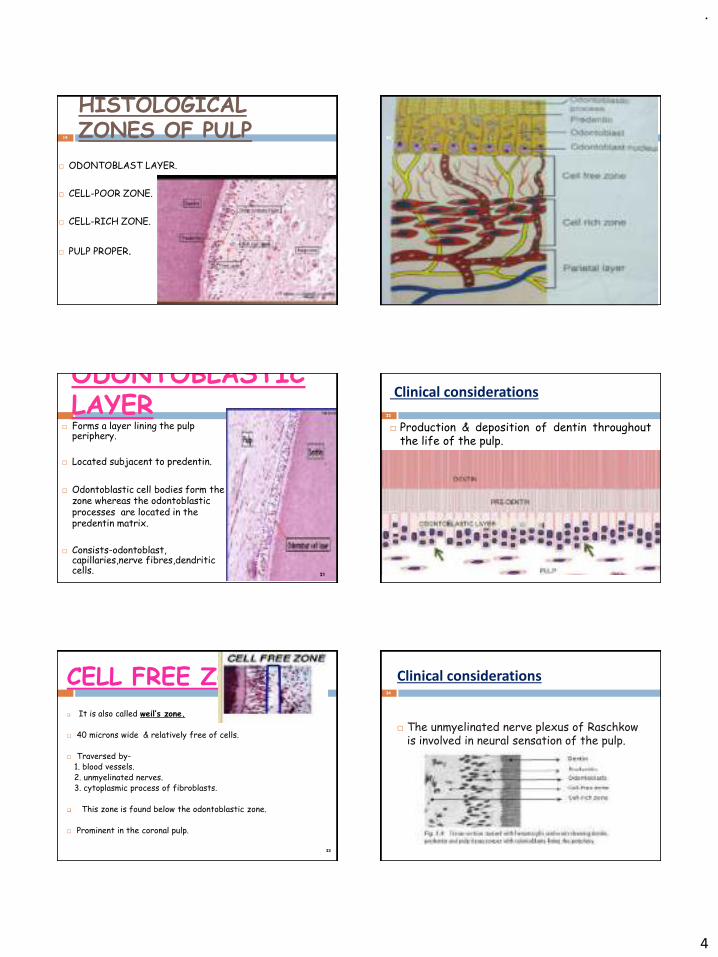
.
4
HISTOLOGICAL ZONES OF PULP
ODONTOBLAST LAYER.
CELL-POOR ZONE.
CELL-RICH ZONE.
PULP PROPER.
19 20
ODONTOBLASTIC LAYER
Forms a layer lining the pulp periphery.
Located subjacent to predentin.
Odontoblastic cell bodies form the zone whereas the odontoblasticprocesses are located in the predentin matrix.
Consists-odontoblast, capillaries,nerve fibres,dendriticcells.
21
Clinical considerations
Production & deposition of dentin throughoutthe life of the pulp.
22
CELL FREE ZONE
❑ It is also called weil’s zone.
40 microns wide & relatively free of cells.
Traversed by-1. blood vessels.2. unmyelinated nerves.3. cytoplasmic process of fibroblasts.
❑ This zone is found below the odontoblastic zone.
Prominent in the coronal pulp.
23
Clinical considerations
The unmyelinated nerve plexus of Raschkowis involved in neural sensation of the pulp.
24

.
5
CELL RICH ZONE
Lies next to sub odontoblastic zone.
Cell density :High in the coronal pulp
Contains high density of fibroblasts, undifferentiated mesenchymal cells, immune cells.
Zone formed due to migration of cells from pulpproper.
25
Clinical considerations
Serves as a reservoir for replacement ofdestroyed dentin producing cells.
26
PULP CORE
❑ It is central region of the pulp.
Principal cells-odontoblasts,fibroblasts,undifferentiatedectomesenchymal cells,macrophages.
Circumscribed by cell-rich zone.
27
Clinical considerations
During pulpal injury , the capillaries permit the seepage of blood proteins into pulpal tissue thereby increasing the osmotic pressure & resulting in stagnation of fluid i.e edema occurs.
28
29
CONTENTS OF THE PULP.
Cells of the pulp
◼ Odontoblasts◼ Fibroblasts◼ Undifferentiated mesenchymal cells◼ Macrophages◼ Lymphocytes ◼ Dendritic cells
Fibres and ground substances
Arteries
Lymphatic vessels
Nerves
30

.
6
Derived from ectomesenchymal cells.
❑ A Peripheral area of the pulp where the
odontoblasts reside is termed odontogenic zone.
Arranged in Palisading pattern cells one tall
columnar forming a layer of 3 to 5 cells in depth.
Shape may vary cornal pulp- columnar(more in no)
midportion – cuboidal(few in no)
Apical region – Flattened(less in no)
ODONTOBLASTS31
32
` No. of odontoblast correspond to
the no. of dentinal tubules.
They have active synthetic phase-
cell organelles are more prominent
and a resting phase.
Has large nucleus containing upto
four nucleoli.
Shape of the odontoblastsreflect-functional activity of the cell.
During active phase-cells show increase in endoplasmic reticulum ,golgi apparatus and secretory vesicles.
Life span of odontoblast is equal to that of the vital tooth.
They are end cells i.e once differentiated ,cannot redivide.
Extends into the dentinal tubule about 0.5- 0.7 mm.
Main function is the- production of dentin.-secretion of ground substance and collagen (type I).
33
Odontoblast process
Odontoblastic process begins at the neck of the cell.
Also known as dentinal fibres,Tome’s fibres.
Odontoblastic process coordinates the formation of peritubular dentin.
They are usually devoid of major cytoplasmic organelles.
34
FIBROBLAST Basic cell of pulp.
Originate from undifferentiated mesenchymal cells.
Greatest no. of cells in the pulp.
More in the coronal pulp.
Its function is to maintain and form pulp matrix(collagen and ground substances).
In young pulp,actively synthesizes matrix.37
In old age-flattened spindle shaped cells with dense nuclei.
It has the cabability of ingesting and degrading collagen.
They are responsible for the increase in size of the denticles.
Concentrated in the cell rich zone .
◼Dual function• Elaboration of ground substance &
collagen fibers.• Degradation of collagen & deposition
of calcified tissues
36
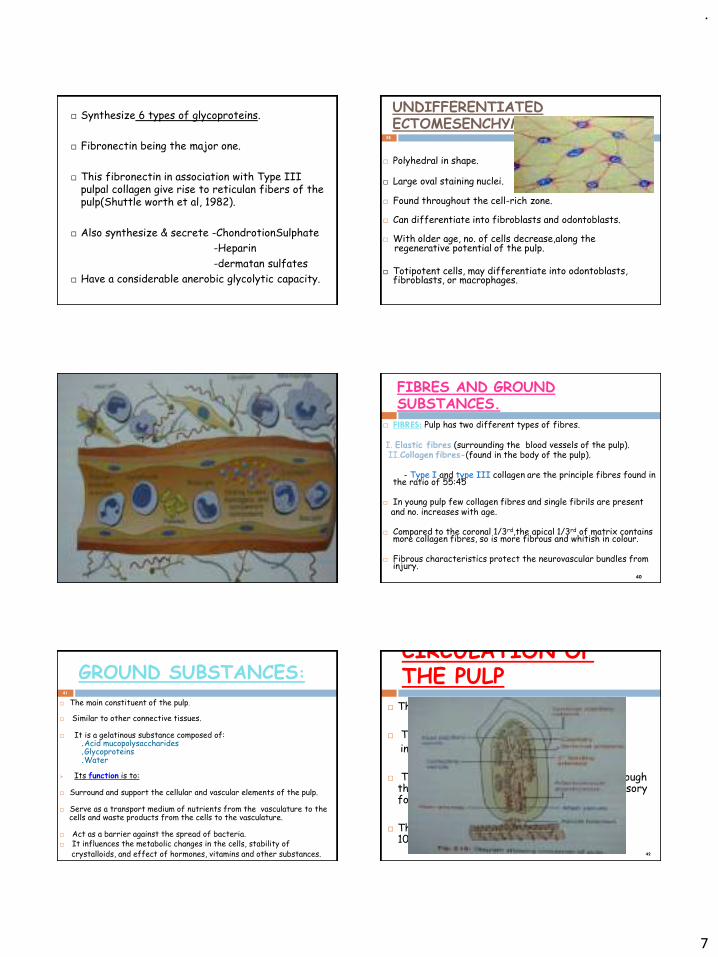
.
7
Synthesize 6 types of glycoproteins.
Fibronectin being the major one.
This fibronectin in association with Type III pulpal collagen give rise to reticulan fibers of the pulp(Shuttle worth et al, 1982).
Also synthesize & secrete -ChondrotionSulphate
-Heparin
-dermatan sulfates
Have a considerable anerobic glycolytic capacity.
UNDIFFERENTIATED ECTOMESENCHYMAL CELLS:
Polyhedral in shape.
Large oval staining nuclei.
Found throughout the cell-rich zone.
Can differentiate into fibroblasts and odontoblasts.
With older age, no. of cells decrease,along theregenerative potential of the pulp.
Totipotent cells, may differentiate into odontoblasts, fibroblasts, or macrophages.
38
Widely distributed in connective tissue
Occur in small groups in relation to blood vessels.
Seldom found in the normal pulp but routinely found in chronically inflamed pulps.
Significant role in inflammatory reactions as the granules of mast cells contain heparin, an anticoagulant & histamine
39
MAST CELLS FIBRES AND GROUND SUBSTANCES.
FIBRES: Pulp has two different types of fibres.
I. Elastic fibres (surrounding the blood vessels of the pulp).II.Collagen fibres-(found in the body of the pulp).
- Type I and type III collagen are the principle fibres found in the ratio of 55:45
In young pulp few collagen fibres and single fibrils are present and no. increases with age.
Compared to the coronal 1/3rd,the apical 1/3rd of matrix contains more collagen fibres, so is more fibrous and whitish in colour.
Fibrous characteristics protect the neurovascular bundles from injury.
40
GROUND SUBSTANCES:41
The main constituent of the pulp.
Similar to other connective tissues.
It is a gelatinous substance composed of:.Acid mucopolysaccharides.Glycoproteins.Water
➢ Its function is to:
Surround and support the cellular and vascular elements of the pulp.
Serve as a transport medium of nutrients from the vasculature to thecells and waste products from the cells to the vasculature.
Act as a barrier against the spread of bacteria. It influences the metabolic changes in the cells, stability of
crystalloids, and effect of hormones, vitamins and other substances.
CIRCULATION OF THE PULP
The pulp organ is extensively vascularized.
They are supplied by the superior and theinferior alveolar arteries.
The blood vessels gain entry into the pulp through the apical foramen and at times through accessory foramen.
The largest arteries in human pulp are 50-100micrometer- In diameter.
42
.
8
CIRCULATION OF THE PULP
The arterioles on entering the pulp show a reduction in thickness of vesselwall musculature and therefore luman size increases.
Pulpal blood flow is more rapid than in most area of the body.
The flow of blood in asterioles - 0.3-1mm/sec
Venules – 0.15mm/secCapilaries – 0.08mm/sec
43
MAXILLARY
ARTERY
MANDIBULAR
(FIRST)
PTERYGOID
(SECOND)
PTERYGOPALATINE
(THIRD)
INFERIOR ALVEOLAR
DENTAL BRANCHES
MENTALARTERY
INCISIVEARTERY
INFRAORBITALARTERY
ANTERIOR SUPERIOR
ALVEOLAR ARTERY
POSTERIOR SUPERIOR
ALVEOLAR ARTERY
MOLARS
PREMOLARSCANINES
LOWER LIP
AND CHIN
LOWER
INCISORS
INCISORS CANINES
MOLARS PREMOLARS
44
INNERVATION OF PULP
Dental pulp contains sensory and motor fibers.
Nerve fibers- mylelinated & unmyelinated, enter thetooth through the apical foramen.
Two types of nerve fibers-
Myelinated afferents
◼ Aα fibres.◼ Aβ fibers.◼ Aγ fibres.◼ Aδ fibers.
Unmyelinated C fibers
◼ Afferents or◼ Autonomic
45 46
Fiber Myelination Location Of Terminals
Pain Characeterstics
Stimulation Threshold
A-Delta
Yes Pulp-dentin junction(odontoblastic & subodontoblastic zones)
Sharp, pricking but bearable (fast & momentary).
Relatively low
C No Near blood vessels throughout the pulp
Continuous , aching, throbbing,lessbearable (than a delta).
Relatively high
‘Plexus of Raschkow’ -This layer contain both A and C fibres.
A fibers- largest diameter-fastest conduction.
C fibers-smallest diameter-slowest conduction.
Larger the diameter- faster the conduction.
80% of the nerves of the pulp are C Fibers & rest are A delta fibers.
47
A, Odontoblasts; B, Cell-free zone of Weil; C, Nerve plexus of
Raschkow
48
.
9
49
STIMULUS A Delta (LOW THRESHOLD)
C (HIGH THRESHOLD)
Intrapulpal pressure changes
Sudden-nervecompression
Increased Response Increased Response
Prolonged-nervecompression
Decreased Response(may block pain impulses)
Resistant to pressure increase(impulses will continue)
50
RESPONSES OF PULPAL ‘A’ AND
‘C’ NERVE FIBERSTO SPECIAL STIMULI
FUNCTIONS OF DENTAL PULP
INDUCTIVE.FORMATIVE.NUTRITIVE.PROTECTIVE.DEFENSE.
51
INDUCTIVE
It induces oral epithelial differentiation into dental lamina and enamel organ.
It also induces the enamel organ to differentiate into a particular type of tooth morphology.
52
FORMATIVE
The cells of Pulp induces dentin formation.
This involves formation of primary and secondary dentin.
The primary dentin is tubular and regularly arranged-Formed before root closure. Secondary dentin contain fewer tubules and is formed after root closure.
53
NUTRITIVE Dental pulp maintains the vitality
of dentin by providing O2 and nutrients to the odontoblasts.
Also provides continuing source of dentinal fluid.
Nutrition is made possible by rich peripheral capillary network.
54

.
10
PROTECTIVE
Pulp helps in recognition of stimuli like heat,cold,pressure,chemicals by way of sensory nerve fibres.
Vasomotor innervation controls the muscular wall of blood vessels.This regulates the blood volume and rate of blood flow and hence the intrapulpal pressure.
55
DEFENSIVE (OR) REPARATIVE Pulp has remarkable reparative
abilities.
It responds to irritation by producing reparative dentin and mineralizing affected dentinaltubules.
Mild to moderate irritation results in continued peritubulardentin formation, sclerosis and intratubular calcifiction-(Tublarsclerosis).
56
When irritated they contribute to one or moredefense functions◼ Dentinal pain
◼ Smear layer
◼ Tubular sclerosis
◼ Irritation(reparative) dentin formation
◼ Inflammation of connective tissue
57
AGE RELATED CHANGES
Reduction in size. Reduction in vascular, neural & cellular contents. Increase in fibrous matrix.
Some degree of mineralization- Pulp stones
◼ Single vs. groups.◼ True (dentine-like that may be lamellated) vs. false
(bone-like).◼ Free vs. attached.
Snow storm calcification◼ Tiny spicules throughout the pulp.
58
Age changes that have been reported to occur
in the pulp and dentin are :
Increases
Number & thickness of collagen fibers.
Dentinal sclerosis
Pulp stones and dystrophic calcification.
Decreases
Cellular components ,blood vessels and nerves.
Size & volume of the pulp due to continued secondary & reparative dentin formation.
59
Aging effects the reduction in number of cells (Symons,1967) of the pulp possibly as a consequence of reduced circulation.
Fibro blasts changesFibroblast exhibit less perinuclear cytoplasm,
long thin cytoplasmic processes.
Cell organelles like RER, mitochondria are smallerGolgi complex rarely found.Significant decrease in regenerable cellsDecreased oxygen uptake(Fisher et al, 1959)
60
CHANGES IN CELLULAR COMPONENTS
.
11
Odontoblasts changes Undergo degeneration
Vacuoles increases
61
FIBROSIS-Bundles of collagen fibres
Accumulation of both
- Diffuse fibrillar components
With age pulp becomes more fibrosis.
Fiber bundles may appear arranged longitudinally in the radicular pulp and more diffuse in coronal pulp.
Collagen accumulation also occurs in some older pulp.
Increase in fibers in the pulp organ is gradual and generalized.
62
External trauma such as dental caries (or) deep restorations cause a localized fibrosis (or) scarring effect.
Increase in collages fibers decrease in the size of the pulp. ( With age collagen fibers increase in length &
diameter).
Vascular changes occur in aging pulp.
Aging pulp-mature collagen accumulates.
63
Crab Grass Effect:
As the pulp chamber becomes narrower with age, the collagens inability to disintegrate to accommodate the smaller lumen results in fibrosis, a congestion could be called as a Crabgrass effect.
64
Pulp Stones(denticles)
Appearing in either or both coronal and root portions of the pulp organ.
Develop in teeth that appear to be normal in other respects.
Asymptomatic unless they impinge on nerves(or)blood vessels.
Seen in functional as well as embedded uneruptedteeth.
65
Pulp stonesClassification
1. True denticles
2. False denticles
3. Diffuse calcifications
66
.
12
Pulp stones
True denticles
True denticles are similar in structure to dentin.
They have dental tubules and contain processes of the odontoblasts.
Usually located close to the apical foramen.
Development of true denticles is caused by the inclusion of remnants of the epithelial root sheath with in the pulp.
67
False denticles
They do not exhibit dentinal tubules.
They appear as concentric layers of calcified tissue.
Some cases these calcification sites appear within a bundle of collagen fibers.
Some cases they appear in pulp free of collagen Accumulations.
68
Some arise around blood vessels.
In the center of calcified tissue there may be remnants of necrotic and calcified cells.
Eventually fill substantial parts of pulp chamber.
69
Diffuse Calcifications Appear as irregular calcific deposits in the pulp tissue,
following collagenous fiber bundles, blood vessels.
Sometimes they develop into larger mass, persist as calcified spicules.
These calcifications are usually found in the root canal and less often in coronal area.
These calcification surrounds blood vessels.
These calcifications may be classified as dystrophic calcification
70
Increase in peritubular dentin(Bradford, 1960).
Occlusion of dentinal tubules with apatite crystals.
Odontoblasts lining the sclerotic dentin become reduced in number & disappear.
2 patterns of dentinal tubule mineralizationContinuous growth of peritubular dentin.Intratubular crystal deposition.
71
DENTINAL
SCLEROSIS
Sclerosis of dentin is also initiated by dentalcaries,slow external irritations such as abrasion,attrition & erosion.
This sclerosis constitutes the initial defense ofthe pulp against dental caries.
72
.
13
INTRA PULPAL PRESSURE
The pulp blood pressure is directly related to the capillary blood pressure.
Measurement ranges from <1 to 100 mg Hg.
Intra pulpal pressure can apparently be
modified by changes in arterial blood
pressure, by increased venous pressure
and other factors over short intervals.
73
IntrapulpalpressureNormal pulp tissue pressure :5.5mm Hg.In empty inflamed pulp :16.3mm Hg.At the exposure site :50 mm Hg.When the exposure siteis necrotic :5-15 mmHg.
-Seltzer (3rd edition)
74
CHANGES DUE TO INFLAMMATION:
ACUTE INFLAMMATION:
Release of chemical mediator
Vasodilation
Increase in capillary permeability
Increase interstitial fluid
Increased pulpal pressure
75
CHRONIC INFLAMMATION:
Pulpal pressure slowly decreases.
SEVERE INFLAMMATION:
Closed lymphatic vessels Persistent increase in interstial fluid Increase in pulpal pressure Pulpal necrosis
76
SYSTEMIC FACTORS AFFECTING THE PULPI. SYSTEMIC VIRAL INFECTIONS.
HERPES VIRUS INFECTION:
Etiologic factor of pulpal necrosis.
Viral eruption patterns may include peripheral nerve ending in the pulp and PDL leading to pain and possibly to pulpal necrosis or internal resorption.
RUBELLA:
Rubella infections and their effect on the dental pulp may begin in the 1st trimester of pregnancy when the mother contracts rubella, causing cytopathic effects in the ameloblasts of primary teeth in the developing embryo.
77
PAGET’S DISEASE:
The radiographic appearance shows pulpal obliteration on the mandibular 3rd molar, there were signs of internal resorption of dentin.This pulpal tissue had the mosaic pattern that was present in the bone and cementum. The radicular region of the pulp displayed dystrophic calcification.
Location of the terminal apical ending is sometimes difficult to be established during endodontic treatment.
78

.
14
HIV:
HIV has been found in the dental pulp and in the periradicular lesions of pulpal origin.
79
GENETIC AND DEVELOPMENTAL DISORDERS OF THE DENTAL PULP.
HYPOPHOSPHATEMIC RICKETS:
Radiographic findings show the extension of pulp horns to DEJ.
Large pulp horns.
TAURODONTISM:
Presence of abnormally large pulp chambers and shortened root canal systems.
Endodontic treatment is difficult due to potential for additional root canal system and difficulty in locating canal orifices.
80
81
DENS IN DENTE:
Increased risk of bacteria induced pulpal necrosis.
Prophylactic placement of sealant is indicated.
DENS EVAGINATUS:
It is a localized outgrowth of ameloblast that appears clinically
as a globule of enamel and may be reminiscent of an accessory
cusp.This outgrowth contains enamel,dentin and pulp.
The clinical significance of this disorder is that the relatively
narrow shelf of enamel, once penetrated, often leads to pulpal
exposure.
AMELOGENESIS IMPERFECTA: Increased pulpal calcification as well as the
disturbances in the enamel formation.
GAUCHER’S DISEASE: Periapical replacement resorption- Periapical
cementum is replaced with Gaucher’s cells and fibrous tissue.
Slow and uniform apical resorption without producing the complication of pulpal necrosis, electric pulp testing in such cases;gave positive responses.
82
CONCLUSSION
The preservation of a healthy pulp during operative
procedures and successful management in cases of diseases
are two of most important challenge to the
clinical dentist.
83
Refernces
ORBAN’S Oral histology and embryology.
TEN CATE’S Oral Histology.
Dental Pulp:Seltzer& Bender.-3rd edition.
Pathways of Pulp :Cohen.
Textbook of Endodontics:Nisha Garg.
INGLE’S Endodontics.
84

.
15
85
.
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
1
DENTINCONTENT
Introduction
Definition
Physical Property Of Dentin
Development
Composition
Life Cycle Of Odontoblast
Structure Of Dentin (Histology)
Types Of Dentin
Dentin Pulp Complex
Age and Functional Changes
2
INTRODUCTIONDENTIN
Determines shape of crown and number and size
of the roots.
Connective tissue of mesodermal origin.
• Physically and chemically closely resembles bone.(
organic content -35% and inorganic content-65%)
3
o Dentin is considered vital tissues as they contain living
protoplasm.
o Act as a protector for pulp and overlying enamel.
Derived from latin word “dentinum”.
Synonym of dentin---- “substantia eburnea” ,’’eber
dentis”
4
5
5
A mineralized tissue that forms the bulk of the crown and root of the tooth, giving the root its characteristics forms, surrounds coronal and radicular pulp, forming the wall of pulp
chambers and root canals ,composition is approximately 67% inorganic 20%organic and 13% of water.
AMERICAN ASSOCIATION OF ENDODONTICS
(2012)
According to Sturdevant’s
“Specialised connective tissue of
mesodermal origin,formed from the dental
papilla of the tooth bud.”
According to Tencates
“ The hard tissue portion of the pulp-dentin
complex and forms the bulk of the tooth “
6

.
2
Parameters of dentin
DENSITY 2.14g/cm-3
Thermal Conductivity 0.57Wm-1k-1
Compressive Strength 297Mpa
Ultimate Tensile Strength 98Mpa
Stiffness(Young’s Modulus) 11.7Gpa
Specific Heat 0.30Cal/g/k
Coefficient of thermal expansion
8.3ppmK-1
Knoop Hardness no. 70 kg/mm2
Thermal Diffusivity 0.0018-0.0026 cm2s-1
7
Physical property of dentin
Dentin is yellow in color
It is harder than bone and softer than enamel
It elastic property higher than enamel. Which resist dentin fracture
Enamel
Dentin
Pulp
8
TOOTH DEVELOPMENT
9
DEVELOPMENT
Fig:Early dentin formation during the bell satge of tooth development.
From the apex of the tooth, dentin formation spreads down the slopes
of the cusp
10
11
Molecular signaling during tooth crown development , expression sites of
transcription factor and signaling molecule
DENTINOGENSIS
Dentin formation begins in the late bell stage.
• Dental papilla is the formative organ.
• Begins at the cusp tips.
• Formed by cells called odontoblasts.
• Odontoblasts differentiate from ectomesenchymal cells.
INITIAL MANTLE DENTIN FORMATION A) PRE-EXISTING GROUND SUSTANCE OF DENTAL PAPILLA B)
TRANSITIONAL FORM OF MANTLE DENTIN FORMATION 1) GROUND SUSTANCE AND LIPIDSN2) MINERALISATION
FRONT C) CONTINUING DENTINOGENSIS
12

.
3
ODONTOBLAST DIFFERENTIATION
The differentiation is brought about by expression of signaling molecules and growth factors in the
cells of inner enamel epithelium.
As odontoblasts differentiate they change from ovoid to columnar.
13
Nuclei becomes basally oriented at this stage.
Length increases to appx. 40 µm, but width remains constant(7 um).
Proline appears in RER and Golgi apparatus.
Nucleus moves away from the basement
membrane-reversal of polarity.
14
Once the formation of predentin at cuspal or incisal
edge begins, the differentiation takes place apically in dental papilla.
Initially daily increments of 4 micrometre is formed.
Once teeth erupts, formation slows down to 1
micrometre per day.
The root dentin formation requires proliferation of
Hertwig’s epithelial root sheath
15
16
Schematic representation of the cells bordering pulp ,golgi bodies,
Rough endoplasmic reticulum
17
Epithelial cells
Differentiation
A B
D
C
E
F
G
Odontoblast differentiation. The undifferentiated ectomesenchymal cell (A) of the dental papilla divides (B), with its mitoticspindle perpendicular to the basal lamina (pink line). A daughter cell (C), influenced by the epithelial cells and molecules they produce (D),differentiates into an odontoblast (E). Another daughter cell (F), not exposed to this epithelial influence, persists as a subodontoblast cell (G).This cell has been exposed to all the determinants necessary for odontoblastformation except the last.
Fully differentiated odontoblast
18

.
4
Matrix mineralization
Odontoblasts differentiate in the preexisting ground substance of dental papilla.
First sign of dentin formation is appearance of distinct, large-diameter collagen fibrils(0.1 – 0.2 µm) called von Korff’s fibers
.
The fibers consist of collagen type III.
Originate deep among the odontoblasts, extend towards inner enamel epithelium, and fan out in structureless ground substance immediately below epithelium.
19
Odontoblasts continue to increase in size.
Produce collagen type I fibrils that orient parallel
to the future dentinoenamel junction.
In this way a layer of mantle appears.
The odontoblasts develop a cell process, the odontoblasts process or Tome’s fiber, which is left behind in the forming dentin matrix as the
odontoblast move towards the pulp.
20
MATRIX MATURATION Influx of ground substance in the intercellular
spaces which forms predentin.
Matrix vesicles bud off from the bases of major cell processes.
In late bell stage limiting membranes disappear
and apatite crystals appear in cytoplasm matrix, functioning as sites of mineralization.
21
Matrix Calcification
Odontoblast is a key element in mineralization.
Produce matrix, control transport and release of calcium.
Buds produced by them, exhibit spicule shaped
crystallite, which appear centrally , spread peripherally.
22
FORMATION OF ROOT DENTIN
The epithelial cells of Hertwig’s root sheath initiate the differentiation of odontoblasts that form root
dentin.
Space between initial collagen and cells is filled with amorphous ground substance and fine, fibrillar, non-collagenous matrix which is a hyaline layer of 10
micrometre.
23
• Initial collagen fibres deposited lie approximately
parallel to dentinocemental junction.
• Radicular odontoblasts develop branches which loop in umbrella fashion -granular layer (Tome’s).
• Radicular dentin forms at a slower rate than coronal
dentin.
24

.
5
PATTERN OF MINERALIZATIONTWO PATTERN
Globular calcification-deposition of crystals in
discrete areas of matrix. With continued crystal growth, globular masses
are formed that enlarge and fuse to form a single
calcified mass.
Best seen in mantle dentin
Llinear calcification-
When the rate of formation is slow, mineralization front appears more uniform and the process is said to be linear.
In circumpulpal dentin both patterns are seen.
25
Difference between coronal dentin and root dentin
CORONAL DENTIN RADICULAR DENTIN
Location is crown Lies in root
Formation begins in late cap
stage
Later stages
Rate of formation high Slower pace
IEE differentiate odontoblasts Hertwig’s root sheath
More dentinal tubules Less DT than crown
Larger odontoblast- larger DT
diameter
Smaller cells and DT diameter
Less frequent major and terminal
branches
More frequent branches
S-shaped DT Almost straight DT
Less formation of sclerotic dentin More sclerosis
Granular layer of tomes absent Granular layer of tomes present26
compositions
Inorganic(75%) Organic(20%) Water(5%)
Hydroxyapatite Collagenous Non collagenous
Phosphate
Carbonate Dentin phosphoprotein
Calcium Gla protein
Proteoglycan
Acid proteins
Growth factors
Lipids
Proteins
• Type I Collagen
• The constituents of ground
substance are :
• Proteoglycans-
Chondroitin sulphates
• Decorin and Biglycan
• Glycoproteins-Dentin
sialoprotein (DSP)
• Osteonectin
• Osteopontin
• Phosphoproteins-
Dentin
phosphoproteins(DPP
)
• Gamma
craboxyglutamate
containing proteins
• Phospholipids
• Type III and Type V
collagen
27
Life cycle of odontoblast
28
Occurs in four stages :
1. Prepolarizing stage
2. Polarizing stage
3. Secretory stage
4. Resting stage
Prepolarizing stage Cells bordering the basement membrane are
pleomorphic.
Protoplasmic processes extend from cell mass.
Central mass dominated by nucleus.
Endoplasmic Reticulum is most abundant of all organelles.
Free ribosomes, mitochondria and Golgi apparatus are present.
29
Polarising stage
Cells at crest of papilla are first to become oriented.
Cell bodies are in close proximity.
Cells are cuboidal and later columnar in shape.
Polar positioning of nucleus.
Microtubules, microfilament, secretary vesicles seen.
Smaller collateral branches of the major processes extend.
30

.
6
Distal segment consists of classic terminal
web dominated by a fibrillar network.
Supranuclear cytoplasm houses Golgi complex, RER, mitochondria, membrane
bound vesicles and other organelles.
31
Secretary stage
32
Cells continue to lengthen and the organelles hypertrophy occurs and secretion of collagen.
7 cytoplasm zones seen-
1. Terminal web
2. Distal RER
3. The process
4. Golgi apparatus
5. Supranuclear ER
6. Nuclear
7. Infranuclear zone
Presecretary granules containing dense mass seen.
They get condensed becoming secretary granules and migrate to odontoblast surface and are
released into intercellular space to form collagen.
33
RESTING STAGE
Activities associated with matrix formation and calcification are suspended.
Shortening of the odontoblast to low
columnar or cuboidal.
Reduction in organelle production until functional demands are imposed on them.
34
Histological structure of dentin
Dentinal tubules
Odontoblasts
Incremental growth lines
Granular layer of Tomes
Junctions of dentin
35
Dentinal tubules
36
A circular duct in the dentin matrix that contains
an odontoblastic process and fluid.
Diameter--3-4μm at its pulpal end 1μm DEJ.
The number ranges from 20,000 to 75,000.
Course follows a gentle curve in the crown, less so
in roots where it resembles a gentle “S” shape.
Diagram illustrating curvature,size,and distance
betwwen dentinal tubules in human outer (A),mid(b),and inner dentin(c), (d) follows line of least resistance to reach the pulp

.
7
Ratio b/w outer and inner surface of dentin is 5:1
50,000 to 90,000 per sq mm at pulpal surface of
dentin.
Diameter at DEJ is .5-.9um, pulp 2-3um.
Average density in radicular dentin is less than that in cervical dentin.
Major branches occur more in root dentin.
37
Contents of dentinal tubules
Odontoblastic processes
Dentinal fluid
Nerve fibers
Lamina lamitans
38
Odontoblastic process Are the cytoplasmic extensions of the
odontoblasts.
Resides in peripheral pulp at pulp predentin
border and their process extend into the
dentinal tubules.
Larger in diameter near the pulp (3-4um) and
taper to (1 um) into dentin.
Approx 7um in diameter and 40um in length.
Occasionally mitochondria micro vesicles and
coated vesicles are also seen
39
Dentinal fluidAn intratubular and extracellular fluid that is thought to be an ultra filtrate of
blood from the terminal pulpal capillaries. It diffuses through the space
around the odontoblastic process and possibly through the intracellular
structure of the odontoblast itself prior to entering the dentinal tubule and
continuing a slow outward movement under a pressure gradient and
eventually leaving the tooth through dentinal tubules.
“According to AAE”(2012)
40
Between the odontoblastic process and the
peritubular dentin, a space known as periodontoblastic
space and this space contains the dentinal fluid.
Free fluid 1% of superficial dentin but about 22% of total
volume of deep dentin.
Flow of the fluid is outwards from pulp
Higher calcium and lower sodium content.
41
NERVE FIBRES
Small number of axons pass between odontoblasticcell bodies to enter the
dentinal tubules.
Penetrate as far as 100 microns.
Most numerous in areas of pulp horns.
Lie in a groove along the surface of the odontoblast
process.
42

.
8
Pain fibres in pulpA-delta fibres C fibres
1 Conduction velocity speed of
electrical impusle
As many as eight
smaller terminal feed
into one larger
myelinated parent
fibres to produce
greater velcity
0.4-2
2 Diameter(um) 2-5 .3-1.2
3 Myelinated Yes No
4 Location of terminals Superficial ; terminal in
the dentin tubule s in
dentinoblastic and
subdentinoblastic
Probably near the blood
vessels through out the pulp
5 Pain characterstics Sharp ,pricking and
unpleasant but
bearable
Throbbing ,aching,and less
bearable
6 Stimulation threshold Relative low High threshold
43
Incremental growth lines
Cyclic process of dentinogenesis, alternating periods of activity and rest, are registered as fine lines.
Incremental deposition-4µm per day.
These run at right angles to dentinal tubules and
mark linear pattern of dentin deposition in an inward and rootward direction and are known as incremental lines of von Ebner.
44
Contour lines of owen
Result from a coincidence of secondary curvatures between neighboring dentinal tubules.
More pronounced and represent normal physiologic alterations in the pattern of
mineralization, occurring at regular intervals.
neonatal line
• Neonatal line - exceptionally wide line found in
teeth at the border of dentin formed before and after birth.
• It typifies the changes in physiology occurring at
birth (nutritional, hormonal, etc).
• Seen in primary teeth and first permanent molars.
46
TOME’S GRANULAR LAYER
47
When root dentin is viewed under transmitted light in
ground sections, a granular layer appears just below the surface of dentin.
This layer is known as Tome’s granular layer.
The granules increase from CEJ to the apex of the tooth.
DENTOENAMEL JUNCTION Junction between the enamel and the dentin.
Has a scalloped pattern.
DEJ is a series of ridges of spikes, which increases the adherence between dentin and enamel.
Ridges are more pronounced in coronal dentin, where occlusal stresses are greatest.
Convexities are on enamel surface and concavities on dentinal surface.
48

.
9
DENTOCEMENTAL JUNCTION
Thin hyaline layer which presents peripheral to
tomes granular layer.
More mineralised and helps in cementing cementum to dentin.
Known to be a product of HERS.
Limits the instrumentation during root canal treatment.
49
CEMENTUM,
DENTIN
DENTIN PULPAL JUNCTION
Mainly formed by the odontoblasts of the pulp.
Odontoblasts are joined by junctional complexes between them.
50
PREDENTIN
Unmineralized organic matrix situated between
the odontoblast layer and mineralized dentin.
Located adjacent to pulp tissue.
2-6µm wide.
All odontoblasts are separated from dentin by a layer of predentin throughout the life of the cell.
52
PRIMARY DENTIN
53
• Mantle Dentin
– First formed dentin in crown underlying DEJ.
– Outer / most periphery part.
– 20 µm in thickness.
– Fibers are perpendicular to
DEJ.
– Von Korrf’s fibers are present.
– Less mineralized than
circumpulpal dentin.
CIRCUMPULPAL DENTIN
Forms remaining dentin / bulk of the tooth.
Represents all the dentin formed before root completion.
Collagen fibers are much smaller in diameter(0.05) and more
closely packed.
Contains more mineral than
mantle dentin.
54
SECONDARY DENTIN
55
• Narrow band of dentin bordering the pulp.
• Represents dentin formed after root completion.
• Contains fewer tubules than primary dentin.
• Not formed uniformly- greater amounts on roof and floor
of coronal pulp chamber.
• Protects pulp from exposure in older teeth.
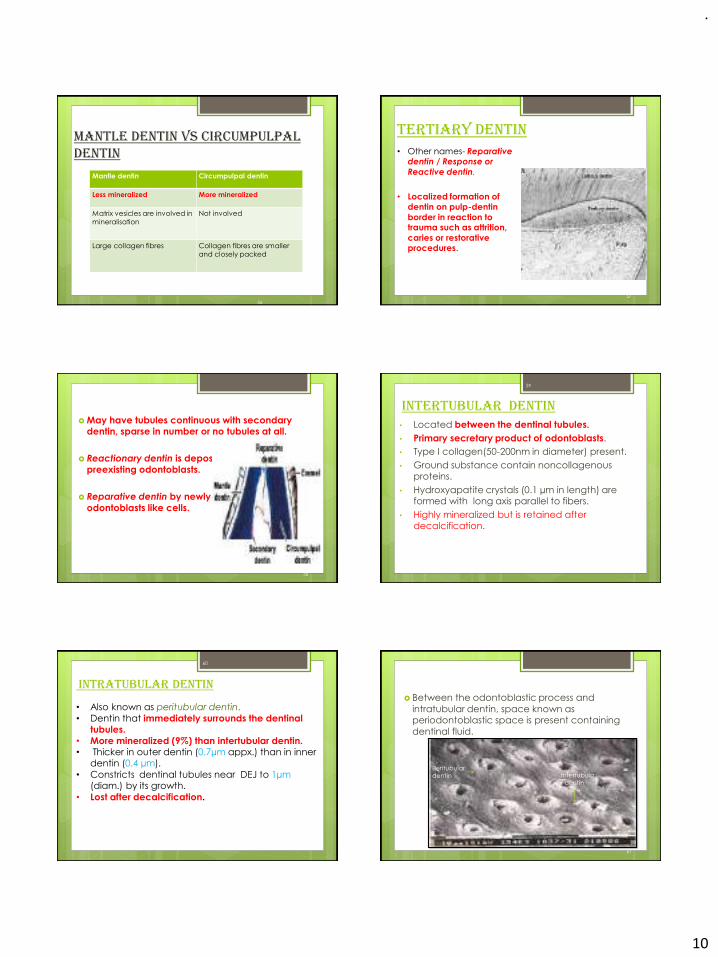
.
10
Mantle dentin vs circumpulpaldentin
Mantle dentin Circumpulpal dentin
Less mineralized More mineralized
Matrix vesicles are involved in
mineralisation
Not involved
Large collagen fibres Collagen fibres are smaller
and closely packed
56
Tertiary Dentin
57
• Other names- Reparative dentin / Response or
Reactive dentin.
• Localized formation of dentin on pulp-dentin
border in reaction to trauma such as attrition,
caries or restorative procedures.
May have tubules continuous with secondary dentin, sparse in number or no tubules at all.
Reactionary dentin is deposited by preexisting odontoblasts.
Reparative dentin by newly formed
odontoblasts like cells.
58
Intertubular Dentin• Located between the dentinal tubules.
• Primary secretary product of odontoblasts.
• Type I collagen(50-200nm in diameter) present.
• Ground substance contain noncollagenousproteins.
• Hydroxyapatite crystals (0.1 µm in length) are formed with long axis parallel to fibers.
• Highly mineralized but is retained after decalcification.
59
Intratubular Dentin
• Also known as peritubular dentin.
• Dentin that immediately surrounds the dentinal tubules.
• More mineralized (9%) than intertubular dentin.• Thicker in outer dentin (0.7µm appx.) than in inner
dentin (0.4 µm).
• Constricts dentinal tubules near DEJ to 1µm (diam.) by its growth.
• Lost after decalcification.
60
Between the odontoblastic process and
intratubular dentin, space known as periodontoblastic space is present containing
dentinal fluid.
61
Peritubular
dentin Intertubula
r dentin

.
11
Interglobular Dentin
Areas of unmineralized or hypo mineralized dentin where
zones of mineralization fail to fuse.
Prevalent in people with vitamin D deficiency or
exposure to high levels of fluoride at time of dentin formation.
More freq. in circumpulpal dentin .
Dentinal tubules pass uninterruptedly.
No peritubular dentin exists where tubules pass
through unmineralized areas.
62
63
Dentin pulp complex
• Dentin and pulp are embryologically,
histologically, and functionally the same tissue and
therefore are considered as a complex.
• Both have a common origin i.e. Dental Papilla,
which is derived from neural crest cells.
64
Pulp and dentin function as a unit.
Odontoblasts are located in periphery of pulp tissue,
with extensions into dentin.
Dentin would not exists unless produced by odontoblasts, and pulp is dependent on protection
provided by dentin and enamel.
Impacts on dentin may affect pulpal components, and disturbances in pulp will in turn affect quantity and
quality of dentin produced.
65
Innervation of dentin pulp complex Dental pulp is innervated richly.
Nerves enter pulp through apical foramen, along with afferent blood vessels, and together from neurovascular
bundle.
Each nerve fiber provides at least 8 terminal branches.
They form an extensive plexus of nerves in cell free zone in crown portion of tooth known as subodontoblasticplexus of Raschkow.
66
In coronal portion the myelinated axons lose their myelin coating.
No synaptic relation between axons and odontoblast
processes.
Intratubular nerves characteristically contain
neurofilaments, neurotubules, numerous mitochondria, and many small vesicular structures.
67
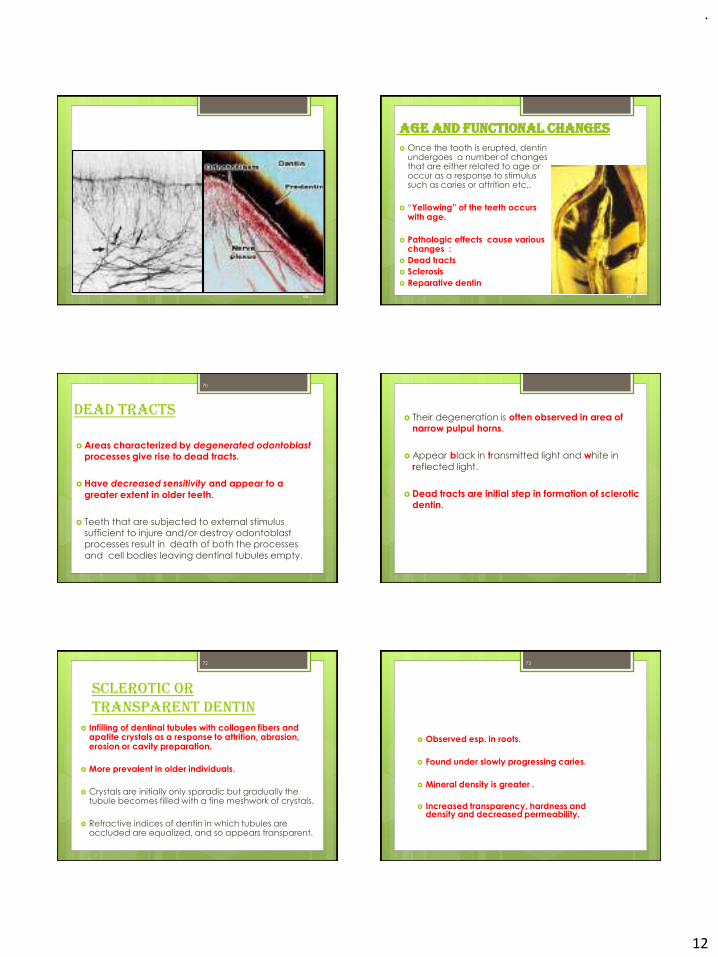
.
12
68
Age and Functional changes Once the tooth is erupted, dentin
undergoes a number of changes that are either related to age or occur as a response to stimulus such as caries or attrition etc,.
“Yellowing” of the teeth occurs with age.
Pathologic effects cause various changes :
Dead tracts
Sclerosis
Reparative dentin
69
Dead tracts
Areas characterized by degenerated odontoblastprocesses give rise to dead tracts.
Have decreased sensitivity and appear to a
greater extent in older teeth.
Teeth that are subjected to external stimulus sufficient to injure and/or destroy odontoblastprocesses result in death of both the processes
and cell bodies leaving dentinal tubules empty.
70
Their degeneration is often observed in area of narrow pulpul horns.
Appear black in transmitted light and white in
reflected light.
Dead tracts are initial step in formation of sclerotic dentin.
71
Sclerotic or transparent dentin
Infilling of dentinal tubules with collagen fibers and apatite crystals as a response to attrition, abrasion, erosion or cavity preparation.
More prevalent in older individuals.
Crystals are initially only sporadic but gradually the tubule becomes filled with a fine meshwork of crystals.
Refractive indices of dentin in which tubules are occluded are equalized, and so appears transparent.
72
Observed esp. in roots.
Found under slowly progressing caries.
Mineral density is greater .
Increased transparency, hardness and density and decreased permeability.
73
.
13
Reparative dentin
If by extensive abrasion, erosion, caries, or operative procedures the odontoblast processes
are exposed or cut, odontoblasts die or survive depending on intensity of injury.
If they survive dentin that is produced is
reactionary or reparative dentin.
Reactionary dentin - Existing odontoblasts recover and continue to form dentin.
74
Reparative dentin - New calcified tissue is formed by newly differentiated “odontoblast like cells”.
Has fewer and more twisted tubules than normal dentin.
Dentin forming cells are often included in osteodentin esp. in response to rapidly progressing caries.
TGF-beta is involved in production of tubular dentin and BMP is involved in production of osteodentin.
75
Interglobular dentin, incremental lines with
varying mineral content seen.
Dentin phosphophoryn is absent.
Growth factors like Nestin and Notch protein which are expressed in young odontoblasts and
subodontoblastic layer during odontogenesis, are absent in adult tissue, but are re-expressed during reparative dentin formation.
76
77
A) Normal and reparative dentin , B) Reparative dentin , C) decrease in
number of tubules , D) cells inclusion , E) irregular and twisted tubules ,
combination types
References❖ Ten Cate’s Oral Histology Development, Structure,
and Function Antonio Nanci : 7th edition
❖ Orban’s Oral Histology and Embryology : 12th
edition
❖ Phillips’ Sciences of Dental Materials : 11th edition
❖ Sturdevant’s Art and Science of Operative Dentistry : 5th edition
❖ Pathways of the pulp: Cohen: 10th edition;
78 79

.
1
1
ENDODONTIC EMERGENCIES AND IT’S MANAGEMENT
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
2
CONTENTS•Introduction•Definition•Classification•Drug therapy •Pre-treatment emergencies and management
PART – 2•Traumatic injuries•Intertreatment emergencies and management•Post-treatment emergencies and management•Managing emergencies in Covid -19 era•Conclusion•References
•Endodontic emergencies infringe on a tight, planned
schedule of a dentist as well as a of patient and tend to
upset the day for everyone including patient,
dentist and staff.
•Nevertheless they are practice builders as a dentist if often
judged by swiftness he sees a patient in pain, and his skill is
judged by speed by which he can alleviate pain.
•It is but natural that a patient in pain must be rendered
painless and comfortable as soon as possible. 3
INTRODUCTION
•Aim of emergency endodontic treatment is to relieve pain
and control any inflammation or infection that may be
present. Although insufficient time may prevent ideal
treatment from being carried out, the procedures followed
should not prejudice any final treatment plan.
•Nearly 90% of patients seeking emergency dental treatment
have symptoms of pulpal or periapical disease.
4
Definition
Occurrence of severe pain and / or swelling
following an endodontic treatment appointment,
requiring an unscheduled visit and active
treatment.
-Watson and Foud –1992
5 6
According to Grossman
.
2
According to Walton or Torabinejad
Pretreatment emergencies
Inter appointment emergencies
Post obturation emergencies
7
According to Gutmann
•Vital pulps
Reversible pulpitis
Irreversible pulpitis with localized symptoms
Irreversible pulpitis – symptoms not localized.
•Necrotic pulps
•Acute alveolar abscess
Localized swelling 8
According to surveys of board certified endodontists by Dorn and associates in 1977 and 1990 and by Lee in 2009 there are seven clinical presentations that are considered endodontic emergencies:
9 10
1. Irreversible pulpitis with
normal periapex
2. Irreversible pulpitis with
symptomatic apical
periodontitis
3. Necrotic pulp with
symptomatic apical
periodontitis, with no swelling
4. Necrotic pulp, fluctuant
swelling, with drainage
through the canal
5.Necrotic pulp, fluctuant
swelling, with no drainage
through the canal
6. Necrotic pulp, diffuse facial
swelling, with drainage
through the canal
7. Necrotic pulp, diffuse facial
swelling, with no drainage
through the canal
EMERGENCY ENDODONTIC MANAGEMENT
11 12
LOCAL ANAESTHETIC CONSIDERATIONS
Nonvital tooth No need of LA
Vital tooth LA mandatory
Hot tooth Bupivacaine
Traumatic tooth (involving enamel and dentin)
No need of LA
Trauma involving pulp LA mandatory

.
3
13
Non-Narcotic Analgesics: Nonsteroidal Anti-Inflammatory Analgesics and Acetaminophen
14
•Major analgesic drug class for treating endodontic
pain is non-narcotic drugs, consisting of the non steroidal
anti-inflammatory analgesics (NSAIDs) and
acetaminophen.
•In randomized placebo controlled endodontic studies have
demonstrated significant analgesic benefits for patients treated
with flurbiprofen, flurbiprofen/tramadol, intracanal
ketorolac, IM ketorolac, intraoral ketorolac, piroxicam,
mefanamic acid, aspirin, diclofenac, ketoprofen, ibuprofen
and ibuprofen/acetaminophen
•SYNGCUK KIM, KARIN J. HEYERAAS, SIVAKAMI R. HAUG. Pharmacologic Management of Endodontic Pain. John I. Ingle , Leif Bakland and Craig Baumgartner, editor. Ingle’s ENDODONTICS, 6th ed. Singapore: 2008. p. 118-50.
15
•For moderate to severe pain
relief, ibuprofen, an NSAID, has
been found to be superior to
aspirin (650 mg) and
acetaminophen (600 mg) with or
without codeine (60 mg). Also
ibuprofen has fewer side effects
than combinations with opioid.
Maximal dose of 3.2 g in a 24-
hour period should not be
exceeded.
•SYNGCUK KIM, KARIN J. HEYERAAS, SIVAKAMI R. HAUG. Pharmacologic Management of Endodontic Pain. John I. Ingle , Leif Bakland and Craig Baumgartner, editor. Ingle’s ENDODONTICS, 6th ed. Singapore: 2008. p. 118-50.
16
•Aspirin’s side effects include gastric distress,
nausea and gastrointestinal ulceration. In addition, its
analgesic effect is inferior to that of ibuprofen, 400 mg.
When NSAIDs and aspirin are contraindicated, such as in
patients for whom gastrointestinal problems, acetaminophen
is preferred analgesic.
•A recommended maximum
daily dose of 4 g of acetaminophen is currently in force, and
a further reduction of this dosage has been proposed to
reduce chance of acetaminophen-related liver toxicity
•SYNGCUK KIM, KARIN J. HEYERAAS, SIVAKAMI R. HAUG. Pharmacologic Management of Endodontic Pain. John I. Ingle , Leif Bakland and Craig Baumgartner, editor. Ingle’s ENDODONTICS, 6th ed. Singapore: 2008. p. 118-50.
17
•Good analgesic effect combined with additional anti-
inflammatory benefit make NSAIDs, especially ibuprofen
drug of choice for acute dental pain in absence of any
contraindication to their use.
•If NSAID alone does not have a satisfactory effect in
controlling pain then addition of an opioid may provide
additional analgesia.
•SYNGCUK KIM, KARIN J. HEYERAAS, SIVAKAMI R. HAUG. Pharmacologic Management of Endodontic Pain. John I. Ingle , Leif Bakland and Craig Baumgartner, editor. Ingle’s ENDODONTICS, 6th ed. Singapore: 2008. p. 118-50.
18
Ketorolac TROMETHAMINE
•Ketorolac is used for the short-
term treatment of moderate to
severe pain in adults. It is usually
used before or after medical
procedures or after surgery.
•Reducing pain helps you
recover more comfortably so
that you can return to your
normal daily activities.
•Do not take more
than 40 milligrams in a
24-hour period and
not more than 5 days.
•SYNGCUK KIM, KARIN J. HEYERAAS, SIVAKAMI R. HAUG. Pharmacologic Management of Endodontic Pain. John I. Ingle , Leif Bakland and Craig Baumgartner, editor. Ingle’s ENDODONTICS, 6th ed. Singapore: 2008. p. 118-50.
.
4
19
•In case of severe dental
pain I.M inj of Dicloran
75 mg should be
Prescribed.
22
•I.M inj. of dexamethasone on preoperative and Postreatment
endodontic pain after endodontic instrumentation or obturation
(IM injection of 1.0 mL of dexamethasone (4 mg/mL))
significantly reduces both pain incidence and severity.
•Intraosseous 40 mg of methylprednisolonen.
•Oral dose - 48 mg of methylprednisolone per
day for 3 days and by extrapolation 10 to 12 mg of
dexamethasone per day for 3 days should provide significant
posttreatment pain relief.
Steroid
23
•SYNGCUK KIM, KARIN J. HEYERAAS, SIVAKAMI R. HAUG. Pharmacologic Management of Endodontic Pain. John I. Ingle , Leif Bakland and Craig Baumgartner, editor. Ingle’s ENDODONTICS, 6th ed. Singapore: 2008. p. 118-50.
24
Premedication
•Following diagnosis, consideration should be given
to use of pre-operative medication to reduce pain
and inflammation at treatment site.
•Concept of using NSAIDs and corticosteroids as
premedication is largely based on reducing the
amount of prostaglandin in the inflamed pulp
25
Irreversible pulpitis with an acute apical periodontitis
Preoperative administration of an NSAID (e.g.
ibuprofen 800mg or flurbiprofen 100mg)
possibly with tramadol (50mg) or
acetaminophen (500 mg) augmentation for the
next 2 days;
26
Recent recommendations warrant mention, according to a new report by the American Dental Association for proper prescription of antibiotics in case of endodontic infection.
.
5
27
Indications for Adjunctive Antibiotics
28
Conditions NOT Requiring Adjunctive
Antibiotics
29
Acute Reversible Pulpitis
32
33
Mild to moderate inflammatory condition of pulp caused by noxious stimuli in which pulp is
capable of returning to uninflammed state
following removal of stimuli.
Clinical characteristics
Quick, sharp, shooting momentary tooth pain suggesting involvement of A-delta fibers. Sensitivity to mild discomfort. Pain is traceable to
stimulus such as cold water or a draft of air.
34

.
6
Causative factors
Recent history of pulp capping
Exposed restorations
Incipient caries or rapidly advancing carious lesions.
Orthodontic tooth movement
Periodontal disease
History of trauma
Recent restorations
35 36
Treatment
•Palliative treatment such as
placement of a zinc-oxide eugenol cement as a
temporary sedative filling is
indicated. If the pain
persists after several days,
pulp tissue should be
extirpated.
37
Subjective symptoms:
•Pain which is sharp, lasts a
few seconds and disappears
on removal of stimulus.
•Does not occur
spontaneously.
•Although paroxysms of
pain are of short duration
they may continue for
months . 38
Dental examination
•May reveal caries, large
restorations, fracture
and deep wear facets,
recently placed
restorations, exposed
dentin.
39
Pulp vitality tests: •Thermal tests: helps to locate
offending tooth. Cold test is
preferable.
•Percussion, palpation and
radiographs give normal status.
•Electric pulp test may give a
slightly early response
40
Treatment:
•Removal of noxious stimuli normally suffices.
•If a recent restoration has a high point, recontouring the high
spot will relieve the pain.
•If persistent painful episodes occur following cavity
preparation one should remove the restoration and place a
sedative dressing such as zinc oxide eugenol.
•If symptoms do not subside then pulpal inflammation should
be regarded
.
7
Acute Irreversible Pulpitis
A persistent
inflammatory
condition of pulp,
symptomatic/
non-symptomatic,
caused by noxious
stimuli
41
•Patient describes pain that lasts for minutes to hours,
or is spontaneous or disturbs sleep or occurs when
bending over, then patient will require pulpectomy
rather than palliative treatment.
•Symptoms can be localized or non-localized. Non-
localized pulpitis poses one of the most difficult and
challenging problem to practitioner since patient
cannot identify offending tooth.
42
•Pulpectomy followed by insertion of a medicated
cotton pellet
•Place a temporary filling.
•Prescribe analgesics if necessary. Premedications or post medication with antibiotic is indicated if the patient is
medically compromised.
•If there is no sufficient time for pulpectomy,
pulpotomy is indicated.
Treatment
43
Acute Apical Periodontitis
•An acute condition that
occurs before alveolar
bone is resorbed.
•One of the most
difficult emergency
condition to treat is
acute pulpitis with apical
periodontitis due to
difficulty in achieving
required depth of
anesthesia in such cases.
44
•complain of tooth feeling elevated in socket or
inability to chew on particular tooth.
•Diagnosis is usually simple tooth is tender on
percussion.
•A radiograph of tooth may appear normal or exhibit
a thickening of periodontal ligament space or show a
small periapical radiolucency
45
Causative factors
Occlusal trauma
Irreversible pulpitis
46
.
8
47
Treatment
•Removal of causative factors.
•If associated with non vital tooth, initiate
endodontic therapy.
•Occlusion should be relieved.
•During endodontic therapy, heavy doses of
anesthesia may be required to attain required
depth of aneshesia.
•Prescribe analgesics and anti-inflammatory
drugs.
Pulp Necrosis
•Rarely causes an
emergency
procedure.
•However
patient may notice
a swelling and
request emergency
treatment.
48
Treatment
•Proper treatment for pulp necrosis is canal debridement.
•No anesthetic is necessary in most instances but in some cases
there are still enough pain receptors to cause discomfort during
the procedure.
•Ensure removal of all necrotic tissue and thorough irrigation
of the canals is required. 49 50
Acute Alveolar Abscess: Acute periapical abscess
•Localized collection
of pus in alveolar
bone of root apex of
a tooth following
death of pulp, with
extension of
infection through
apical foramen into
periapical tissue.
52
Local symptom
•Tenderness of tooth remove by continuous slight
process.
•Throbbing sever pain with swelling of overlying
soft tissue with or wothout tooth
mobility.
•When swelling become extensive ,it result into
cellulitis and patients facial changes.
53

.
9
Where to expect swelling from which tooth???
54
Ludwig's angina
•Potentially life-threatening cellulitis or
connective tissue infection, of the floor
of mouth, usually occurring in adults
with concomitant dental infections.
•usually develops in
immunocompromised
persons
•Bilateral involvement of
submandibular, sublingual and
submental spaces 55
•Involves appropriate antibiotic medications,
monitoring and protection of airway in severe
cases, and, where appropriate, urgent ENT
surgery, maxillofacial surgery and/or
dental consultation to incise and
drain collections.
• Antibiotic of choice is from the penicillin
group
56
Treatment
•Infiltration anesthesia -
contraindicated
Forcing anesthetic
solution into an
acutely inflammed
and swollen area
localized
acidic pH
57
58
Acute episode may result from
•Conduction or block anesthesia may be
administered
•Test cavity tests for any remaining, vital pulp that
could require anesthesia and initiates emergency
quickly, without waiting for anesthesia to
take effect.
59
.
10
Procedure
•Access opening stabilize the tooth with finger pressure or
impression compound (high speed)
•Irrigate profusely
•Instrument within 1 mm of root apex.
60
•Frequently, a purulent exudate escapes into chamber and
indicates that root canal is patent and draining. (dry within
canal due to the apical contriction preventing the
inflammatory products from draining
through the tooth)
•To relieve this problem, a procedure called ‘apical trephination’ is followed.
61
•Aspiration using any mild suction devices such as a wide gauge
needle placed in the saliva ejector will give sufficient negative
pressure which aids in establishing drainage through the canal.
•Leave the tooth open.
•Advice the patient to use warm saline rinses for 3 minutes each
hour.
•Prescribe analgesics or antibiotics if indicated and necessary.
62
Gutmann describes various modalities of treatment for localized or diffuse
swellings associated with acute alveolar abscess.
63
• no need for incision and drainage. Advice warm saline rinses in addition to root canal therapy
swelling is slight and
localized
• incise and drainswelling is soft, extensive
and fluctuant
64
• antibiotic coverage and aggressive removal of any necrotic tissue in the pulp canal system
Diffused swelling, where there is
generalised tissue edema or cellulitis
• Consider antibiotics and advice hot saline rinsesIf tissue swelling is
non fluctuant
65

.
11
•Initial stages - sterile water and
saline (NaOCl - clumping debris)
•When patency through apex is
maintained NaOCL may be used
for further canal preparation.
•For further appointments, an
alternating solutions of NaOCL
and hydrogen peroxide is
recommended.
Irrigants used in treating acute abscess
66
Incision and Drainage
67
Rationale for I & D
•Decreases number of bacteria
•Reduces tissue pressure
•Alleviates pain/trismus
•Improves circulation
•Prevents spread of infection
•Alters oxidation-reduction
potential 68
Trephination – Apical and surgical
Apical
•Accomplished by
placing a No.15 to 25
K file beyond confines
of apex.
69
Surgical
•Rarely indicated.
•However it is a reliable
procedure to manage pain when
all other methods have failed.
•Indicated when severe pain is
due to increase in intracortical
pressure in periradicular tissues,
when apical trephination has
failed.
70
Acute Periodontal Abscess
71

.
12
•Often mistaken
for an acute
alveolar abscess
as periodontal
abscess causes
pain and
swelling.
Etiology •Usually an
exacerbation of
infection with
pus formation in
an existing deep
infrabony
pocket.
72
Treatment
•Vital pulp - periodontal therapy
•When the pulp is abnormal and vital - tooth is treated as if
for acute irreversible pulpitis.
•If the pulp is necrotic - treat as if for acute alveolar abscess.
•In any case, emergency periodontal treatment must be done
simultaneously otherwise, the patient will not be relieved of the
pain and swelling.
73
HOT TOOTH
74
•A tooth that is difficult to anesthetize.
•There is special class of sodium channels on C fibers,
known as tetradotoxin resistant (TTXr).
•Sodium channel expression shifts from TTX-sensitive to
TTXr during neuro inflammatory reactions, and the TTXr
resistant sodium channels play a role in
sensitizing C fibers.
•These sodium channels - resistant –lignocaine & is 5 times
more resistant to anesthetic than TTX
sensitive channels. 75
Treatment
•Bupivacaine
•Supplementary
injections
76
CRACK TOOTH SYNDROME
77

.
13
A fracture plane of unknown depth
and direction passing through tooth
structure, if not already involving, may
progress to communicate with the pulp
and/or periodontal ligament
•History of pain on release of biting on
a particular tooth, often occurring with
food having small, harder particles in
them.
78
VISUAL INSPECTION:
Transillumination
79
Magnifying loupes
Dyes-methylene
blue
Tooth slooth
80
Cracks in vital teeth
Urgentcare:
immediate
reduction of
tooth from its
occlusion by
selective grinding
cracks not involving pulp
•Compromised portion removed-
occlusal adjustment, cuspal
protection.
•Restoration-Composite -Pinned
amalgam-Cast restoration
•Full coverage restoration- as
permanent treatment
81
Crack involves pulp-causes pulpal
inflammation &
necrosis- RCT is
advised followed by
full coverage
restoration.
As a rule of thumb,
if crack involves a
root canal, extract the
tooth.
If crack involves
pulp chamber only,
RCT and restore
82
Cracks in root filled or nonvital teeth
Treatment
Location of crack-even surgical exposing of crack is done
and removal of source of pain(infection)- followed by
full coverage restoration if tooth can be saved.
In case if crack is vertical - involving entire root –
extraction is preferred.
83

.
14
REFERRED PAIN
84
•May be initiated from inflamed pulp,other parts of body on
same side or in close proximity to another tooth
Eg: infection of max ant teeth- referred to ocular pain, mandi
molars to back of ear.
•Pain from other parts of body- referred to tooth.
•Otitis media- refer pain- mandibular molars, tmj dysfunction-
toothache.
•Accurately determine origin of pain – radiograph is often
useful here and in any case if pulpal pain is diagnosed – start
with routine endodontic treatment.
85
86
THANK YOU
TRAUMATIC INJURIES
87
Endodontic treatment may be required as a
result of traumatic injury.
Most common endodontic emergencies are
a)Crown fracture.
b) Root fracture
c) Avulsion
88
CROWN FRACTURE
•If a green stick # of crown is present and crown
segment doesn’t shear off under pressure, a steel
band is cemented around the tooth.
•Relieve the occlusion- eliminates pain & re-
evaluate status pulp later
89

.
15
INVOLVING PULP:
•Fractures involving enamel, dentin & pulp are called
‘complicated crown” fractures by Andreasen & class 3 by
Ellis.
•Degree of pulp exposure--- pinpoint exposure to total
unroofing of coronal pulp.
•Initial reaction - hemorrhage - inflammatory response -
destructive (necrotic) / proliferative (polyp)
90
TREATMENTDepends on maturity
of the pulp
91
FOLLOW – UP AND PROGNOSIS: Acceptable results of evaluation following pulpotomy should
be all of the following
No clinical signs
or symptoms
No evidence of
periradicular
pathologies
No evidence of
resorption –
internal / external
Evidence of
continued root
formation in
developing tooth
92
ROOT FRACTURE:
DESCRIPTION: fracture
involves the root only;
cementum , dentin, and
pulp.
INCIDENCE: account
2% of all dental injuries
93
DIAGNOSIS
•Missed in conventional radiographs
•With conventional radiograph… 90 degree angulation
if fracture diagonal missed
•Additional film angulation of 45 degree + 90 degree -
reveal root fracture.
94
Management
95
SPLINTING:
•Repositioning the coronal
fragment
•Semirigid splinting ---
favour healing
•splinting for 4 wks

.
16
96
TREATMENT OF CORONAL FRAGMENT
97
•Most simplistic
•Fracture site located more coronally on
root - new apex which is wide and
open.
•Establishment of working length
radiographically
•Conventional apexification
•Calcium hydroxide - 3 to 12 months
for barrier formation
•MTA - immediate restoration
98
TREATNG CORONAL FRAGMENT & REMOVAL OF APICAL
FRAGMENT
99
•Signs and symptoms of non-healing after
coronal RCT.
•SWELLING / radiolucent area at
site / apically.
•Assuming coronal fragment stable - surgical removal of apical
fragment.
•68% success rate
•Notable mobility of coronal fragment - implant through
coronal fragment & into bone = endosseous implant.
100
TREATING CORONAL & APICAL FRAGMENTS AT
SAME TIME
101
•Difficult to get apical seal when endodontically treating only
coronal fragment.
•To achieve this seal --- treatment of both coronal & apical
fragment simultaneously which is almost impossible.
•low success rate
•Favorable approximation of fragments - intra radicular splint --
- rigid type of post (cobalt – chromium alloy [vitallium])
.
17
102
REMOVING THE CORONAL FRAGMENT & TREATING THE
APICAL SEGMENT
103
•Coronal fragment attached only by gingiva
•Acceptable crown :root ratio 1:1 (for planning post
and core)
•Endodontic treatment of apical segment .
•Followed by crown lengthening --- orthodontic/
periodontal
•Placement of appropriate crown.
104
SEQUELE OF ROOT FRACTURE Extrusive Luxation
•Displacement of tooth in
coronal direction results in
partial avulsion.
•Tooth – mobile &
continually traumatized by
contact with opposing
tooth - premature occlusion
•Radiographically -
“empty” radiolucent space
105
•Immediate treatment – repositioning the
tooth & stabilizing by flaxible splint for 2wks.
•Definitive treatment –vitality test RCT -
NECROSIS/ INFLAMATORY ROOT
RESORPTION SEEN
106
Lateral Luxation
•Traumatic injury - displacement of tooth
labially , distally or mesially --- lateral
luxation.
•Very painfull - premature occlusion e.g :
max.incisor pushed palatally.
•Crown makes contact long before centric
occlusion.
•Treatment plan depends on - presence or
absence of apical displacement at the time
of injury. 107

.
18
LATERAL LUXATION WITHOUT APICAL DISPLACEMENT:
•Teeth pushed only in facial / lingual direction with apical
root remaining in its original position within socket.
•Teeth loose enough – slight digital pressure to reposition
tooth.
•Some sulcular bleeding - typically seen
108
•If there is no widening of PDL space as confirmed
by radiographs - good prognosis - endodontic
treatment may not be necessary.
•Tooth is initially unresponsive to EPT and cold
test.
109
LATERAL LUXATION WITH APICAL DISPLACEMENT:
110
•Tooth is frequently pushed palatally / lingually and firmly
located in its new position.
•Tooth will elicit dull metallic sound on percussion.
•palpating alveolar bone --- reveal new location of apex.
111
112
•Radiographically – PDL space widened around
midportion and coronal portion of root.
•If apex moved out of its original position - damage to
neurovascular bundle.
•Negative response to cold and EPT .
•Closed apex cases - advice endodontic treatment
Treatment
•Repositioning the tooth in its socket
•Splinting --- 3 to 4 weeks
•Prognosis good --- if endodontic treatment
done when indicated.
113

.
19
TOOTH AVULSION/ EXARTICULATION
114
•Incidence – 3% of all dental injuries
•True dental emergency – timely attention to replantation could
save tooth.
•Sports and automobile accidents - frequent causes.
•Examine - tooth is replanted before coming to dental office.
•Record the time of avulsion.
115
Storage media
116 117
Management of Avulsed Teeth with an Extraoral Dry Time
of Less Than 60 Minutes
118
Management of Avulsed Teeth with an Extraoral Dry Time of More Than
60 Minutes
IMMEDIATE TREATMENT
•Radiographs --- fracture of alveolar bone
•Socket --- foreign bodies and debris - scrape gently
from bony walls.
•Blood clot – gently suctioned and irrigated with
saline
119
.
20
•Avulsed tooth --- debris
gently rinsed off
•Do not hold in hands ---
always use some twizer /
forceps to hold tooth
•Gently and slowly insert
into socket --- aneasthesia
may not be necessary.
120
•Check the alignment - no hyperocclusion .
•Mobility - splinting recommended
•Splinting should left for 1 to 2 wks
121
•Initial antibiotic course,
tetanus prevention & RCT
( after 10 to 14 days).
•Calcium hydroxide is
recommended as an
intracanal medicament –
2 wks during RCT.
122
DURING ENDODONTIC TREATMENT
123
Flare – ups
124
Definition :An acute exacerbation of peri radicular pathosis after initiation or continuation of root canal treatment.
-American Association of Endodontics(1998)
125

.
21
•Studies reports 1.8-3.2 %
flare-ups
•Characterized by
development of pain,
swelling or both, following
endodontic intervention.
126
•Causative factors of comprise mechanical, chemical, and/or
microbial injury to pulp or periradicular tissues, during root
canal treatment.
•Regardless of type of injury, intensity of inflammatory
response is directly proportional to intensity
of tissue injury.
•Higher in teeth with periradicular lesions as compared to
teeth with vital pulps and normal
periradicular tissues. 127
128
Contributing factors:
•Inadequate debridement
•Debris extrusion
•Over instrumentationSecondary apical
periodontitis
129
•Tenderness to percussion immediately after the treatment was initiated.
•Causes throbbing,
gnawing, pounding
pain.
•Cause is over instrumentation but
may also occur due to over medication,
forcing debris into periapex.
•Sympathomitic pain relief: access
cavity opened, saline irrigation and use
of corticosteriod-antibiotic paste as an
intracanal medicament – pt recalled
later for completion of endo
treatment.
130
PREVENTION
•Canals are normally
instrumented too close to
apex in an attempt to
completely clean canal.
•A intracanal
medicament+antibiotic
coverage.
131
.
22
Endodontic emergencies: Your medication may be the cause J Conserv Dent. 2009 Apr-Jun; 12(2): 77–79. Promila Verma
• Formaldehyde-containing
medications, various
compounds containing arsenic
and paraformaldehyde used as
pulp devitalizers.
• Such agents have some
clinical benefit, although soft
and hard tissue necrosis occurs
if they are not confined to
pulp.
132
Treatment & Prevention Of Flareups
133
•Occlusal reduction.
•Antibiotic prophylaxsis
•Leaving tooth open for complete drainage- 20 min – complete
removal of pulp tissue and debris -followed by
closed dressing
•Calcium hydroxide therapy: intra canal dressing
(Disadvantages: Unable to kill enterococcus species which is
commonly associated with failed r.c.t.)
•Antibiotics & Analgesics(releive pain) Corticosteroids –
antiinflammatory action.
134
Hypochlorite accident
135
•Refers to any event in which sodium hypochlorite
extruded beyond apex of a tooth and patient immediately
manifests a combination of some of
following symptoms:
•Severe immediate pain
•Swelling
•Profuse bleeding both interstitially and through the tooth.
136
Causes :
•Forceful injection of Naocl
due to wedging of the
irrigating needle into the
root canal.
•Irrigating a tooth with a
large apical foramen, apical
resorption or an
immature apex.
Features :
•Edema and ecchymosis,
accompanied by tissue
necrosis, paraesthesia and
secondary infection.
•Although most patients
recover within 1-2 weeks.
Long-term paraesthesia
and scarring have been
reported.
137

.
23
•Immediate aspiration
•Cold pack over the affected area.
•Regional block anesthesia administered.
•Monitor tooth for the next half hour. Bloody exudation from
Canal, Remove the fluid with high volume suction to encourage
further drainage. If drainage is persistent consider
leaving tooth open.
Management
138
•Antibiotic coverage to prevent secondary infection
•Analgesics prescribed
•Corticosteroids – inflammatory process
•Home care instructions: Cold compress to minimize pain
and swelling.
•Subsequently warm compresses to encourage healing.
139
•Bend the irrigating needle at centre to confine tip of needle
to higher/coronal levels of
root canal.
•Never bind the needle in the canal
•Oscillate needle in and out to ensure that tip is free to express
irrigant with out resistance
•express the irrigant slowly and gently
Prevention :
140
ASPIRATION / INGESTION OF ENDODONTIC INSTRUMENTS
141
•Can be a clinical disaster ending up in life threatening
situations or ending up in the need of major surgery to
remove instrument.
•Grossman had aptly stated (1955) that if an instrument
is swallowed by patient , dentist is likely to be
confronted lawsuite.
142
•Aspiration of endodontic
hand instruments happens
only when rubber dam is not
in place.
•High power suction along
with rubber dam help in
preventionof aspiration of
instruments.
143

.
24
PERFORATION
144
An artificial opening in the tooth or root,
created by clinician during entry to the canal
system or by a biologic event such as
pathologic resorption or caries that results in
communication between the root canal and
periodontal tissues.
145
146
Time
•Time elapsed between seal of
perforation and its inception -
Important in determining
prognosis - immediate treatment -
better prognosis.
Size of perforation
•smaller the defect better is
prognosis
147
Coronal third furcation management
Materials
Cavit, amalgam,
calcium
hydroxide, GIC,
MTA, Biodentin
148
Barrier technique:
•Artificial barrier (floor) using either calcium
sulphate and hydroxyapatite .
•improves sealing ability & provides successful barrier against its
over extension.
Calcium hydroxide:
•Control bleeding
•Placed in the area of perforation and left for at least few days
will leave the area dry and allow for inspection of perforation.
149
MIDROOT PERFORATIONS
.
25
150
•Lateral perforation at
midroot level tends to
occur in curved canals
when a ledge has formed
or along inside curvature
of root as canal is
straightened out.
•MB canal of lower molar
151
STRIPPING
•A “lateral”perforation
caused by Over
instrumentation through a
thin wall of root & mostly
happens along inside
curvature of root as canal is
straightened out.
•Distal wall of mesial roots in
mandibular 1 st molars.
152
•Recognition:Sudden appearance of blood or complaint
from patient.
•Access is difficult, Repair- unpredictable.
•Prognosis is poor. Lack of tooth structure & integrity of
wall may eventually lead to fractures & microleakage due
to inability to seal perforation.
153
Two Step method to repair midroot perforations
154
•Root canals are first obturated, then the defect is repaired
surgically.
•Removal of excess GP using a hot spatula & then cold
burnishing the site.
To Prevent Stripping:
•Anticurvature filing
•Maintaining mesial pressure.
•Careful use of rotary instruments inside the canal
155
APICAL PERFORATIONS
.
26
156
Due to….
•Not negotiating a curved canal or..
•Not establishing WL & over
instrumentation.
•Instrumentation beyond apical
confines.
157
POST ENDODONTIC TREATMENT
158
UNDEROBTURATION
ETIOLOGY-
•Natural barrier in canal
•Ledge
•Insufficient flaring
•Poorly adapted master cone
• Inadequate condensation
pressure
TREATMENT-
•Removal and retreatment 159
OVERFILLING
Can either gutta percha or
sealer
Etiology-
•Sequel of over instrumentation
•Uncontrolled condensation pressure
•Inflammatory resorption
•- incomplete development of root
•- open apex
160
TREATMENT:
•Sealer – no treatment required as it removed from
body by action of macrophages.
•Gutta percha – re- rct / apical surgery followed by
retrograde filling
161
Analgesics and Antibiotics

.
27
162 163
Dental trauma management in covid – 19 era
164
•If teeth require splinting - use of a composite resin using
self-etching adhesive or a resin-modifed glass ionomer
cement. This would minimise use of the 3-in-1 syringe and
in turn reduce aerosol Production.
•Splint removal - by sectioning the wire splint using pliers or
wire cutters between restorations. Composite buttons will
remain on tooth but can be removed at a later date,
remaining sections of wire or rough sections of composite
can be lightly polished with hand abrasive strips and discs or
abrasive discs in a slow handpiece to remove any sharp edges.
165
•Managing complicated crown fractures - Rubber dam
should be applied, once isolated exposed pulp can be
assessed for either a direct pulp cap or a partial
pulpotomy to limit amount of aerosol generation, as
length of instrumentation is unlikely to be prolonged in
reaching healthy pulp tissue . Once healthy pulp tissue is
exposed, haemostasis can be aided by a sterile cotton
wool pledget soaked in sodium
hypochlorite or saline.
166
•Exposed healthy tissue can then be covered with
non-setting calcium hydroxide or bioceramic materials
such as mineral trioxide aggregate or calcium silicate-
based materials . This can then be overlaid with glass
ionomer cement or a composite restoration using a
self etching adhesive without creation of
further aerosol.
169
There is no harm in hoping for the best as long as you are prepared for the worst.
—Stephen King
CONCLUSION
•More than 80% of pts who reports to dental , clinic are with
emergency symptoms with endodontically related pain.
Therefore the knowledge, skill for the treatment of these
endodontic emergencies is highly required for
every clinician.

.
28
170
•An accurate diagnosis and effective treatment of acute
situations are an important responsibility and priviledge
of dental practice.
•Effective caring and management of endodontic
emergencies not only represents a service to the public,
which the dentist can be proud of but also enhaces the
positive image of dentistry.
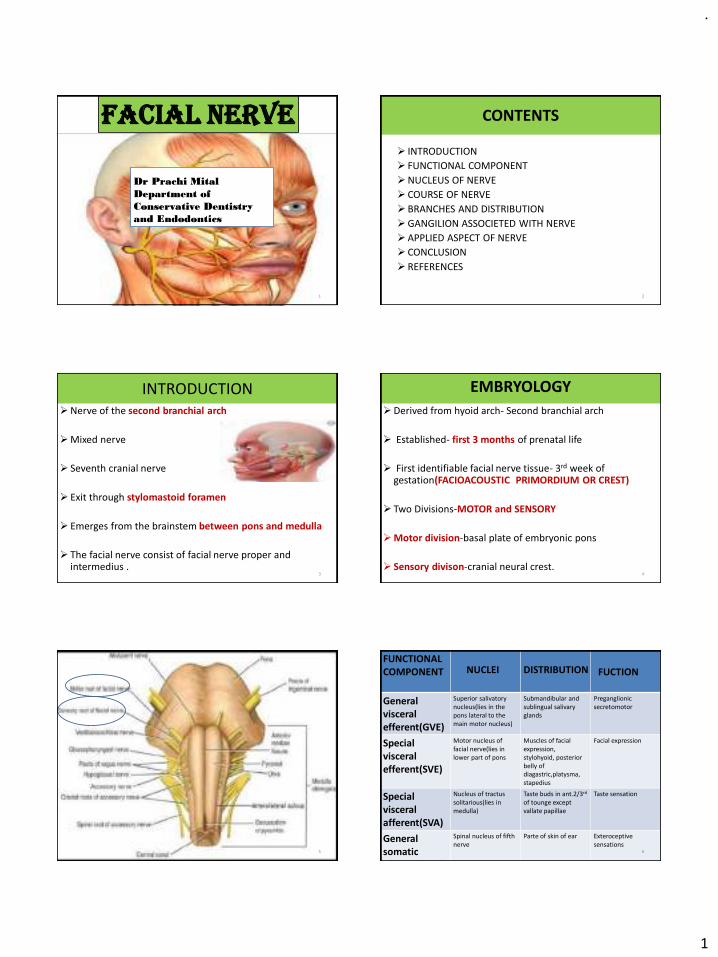
.
1
Facial nerve
1
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENTS
➢ INTRODUCTION
➢ FUNCTIONAL COMPONENT
➢NUCLEUS OF NERVE
➢ COURSE OF NERVE
➢ BRANCHES AND DISTRIBUTION
➢GANGILION ASSOCIETED WITH NERVE
➢ APPLIED ASPECT OF NERVE
➢ CONCLUSION
➢ REFERENCES
2
INTRODUCTION➢Nerve of the second branchial arch
➢Mixed nerve
➢ Seventh cranial nerve
➢ Exit through stylomastoid foramen
➢ Emerges from the brainstem between pons and medulla
➢ The facial nerve consist of facial nerve proper and intermedius .
3
EMBRYOLOGY
➢Derived from hyoid arch- Second branchial arch
➢ Established- first 3 months of prenatal life
➢ First identifiable facial nerve tissue- 3rd week of gestation(FACIOACOUSTIC PRIMORDIUM OR CREST)
➢ Two Divisions-MOTOR and SENSORY
➢Motor division-basal plate of embryonic pons
➢ Sensory divison-cranial neural crest.4
5
General visceral efferent(GVE)
Superior salivatorynucleus(lies in the pons lateral to the main motor nucleus)
Submandibular and sublingual salivary glands
Preganglionicsecretomotor
Special visceral efferent(SVE)
Motor nucleus of facial nerve(lies in lower part of pons
Muscles of facial expression, stylohyoid, posterior belly of diagastric,platysma, stapedius
Facial expression
Specialvisceral afferent(SVA)
Nucleus of tractussolitarious(lies in medulla)
Taste buds in ant.2/3rd
of tounge except vallate papillae
Taste sensation
General somatic afferent(GSA)
Spinal nucleus of fifth nerve
Parte of skin of ear Exteroceptivesensations
FUNCTIONAL COMPONENT NUCLEI DISTRIBUTION FUCTION
6

.
2
NUCLEUS OF FACIAL NERVE
7 8
COURSE OF NERVE
EXTRACRANIAL COURSE
INTRACRANIAL COURSE
9 10
EXTRACRANIAL COURSE
EXTRACRANIAL COURSE
11
BRANCHES AND DISTRIBUTION
A. Within facial canal 1.Greater petrosalnerve 2.Nerve to stapedius3.Chorda tympani
B. At stylomastoidforamen exit 1.Posterior auricular 2.Digastric 3.Stylohyoid
C.Terminalbranches with in parotid gland 1.Temporal 2.Zygomatic 3.Buccal 4.Marginal mandibular 5. cervical
D.communicationbranches with adjacent cranial nerve
12
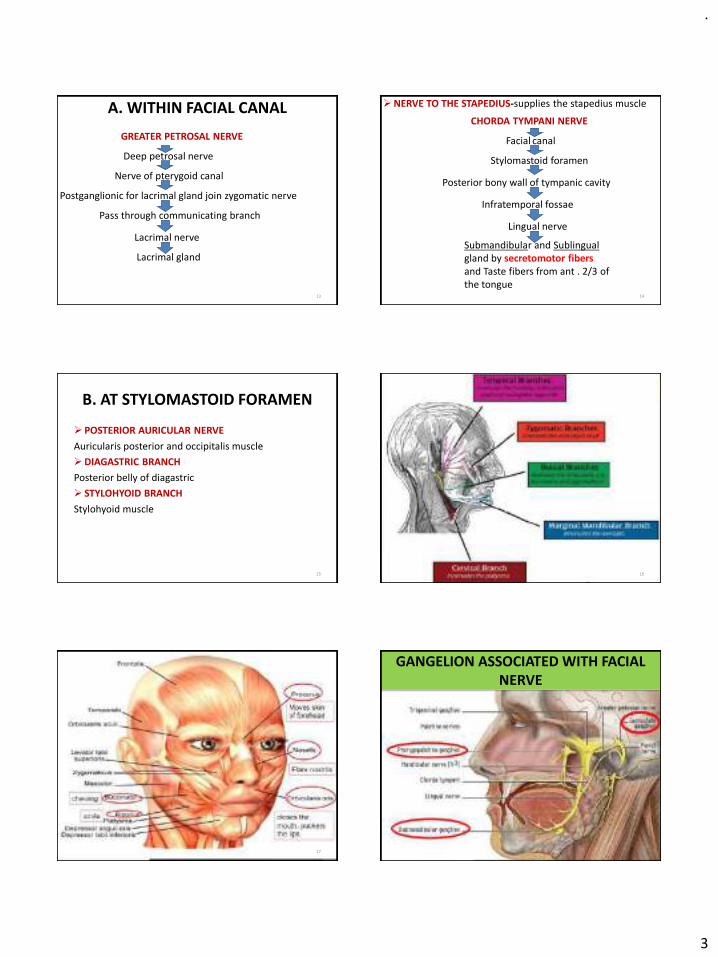
.
3
A. WITHIN FACIAL CANAL
Deep petrosal nerve
Nerve of pterygoid canal
Postganglionic for lacrimal gland join zygomatic nerve
Pass through communicating branch
Lacrimal nerve
Lacrimal gland
GREATER PETROSAL NERVE
13
➢NERVE TO THE STAPEDIUS-supplies the stapedius muscle
14
CHORDA TYMPANI NERVE
Facial canal
Stylomastoid foramen
Posterior bony wall of tympanic cavity
Infratemporal fossae
Lingual nerve
Submandibular and Sublingual gland by secretomotor fibersand Taste fibers from ant . 2/3 of the tongue
B. AT STYLOMASTOID FORAMEN
➢ POSTERIOR AURICULAR NERVE
Auricularis posterior and occipitalis muscle
➢DIAGASTRIC BRANCH
Posterior belly of diagastric
➢ STYLOHYOID BRANCH
Stylohyoid muscle
15 16
17
GANGELION ASSOCIATED WITH FACIAL NERVE
18

.
4
19
Facial muscle function
20
Zygomaticus major Smiling and laughing
Levator labii superioris,Levatorangulii oris
Sadness
Depressor anguli oris Grief
Dilator naris ,Depressor septi Anger
Corrugator supercilli,Procerus Frowning
Platysma Horror,terror and fright
Frontalis Surprise
Mentalis Doubt
Risorius Grinning
Zygomaticus minor Contempt
Orbicularis oris Closing the mouth
Orbicularis oculi Closing the eyelid
Buccinator,Orbicaris oris Whistling
FACIAL NERVE FUNCTION
GENICULATE GANGLION
➢It is a sensory ganglion
➢Located on first band offacial nerve
➢Taste fibers present innerve are peripheralprocess of pseudounipolarneurons present ingeniculate ganglion.
21
SUBMANDIBULAR GANGLION
➢Sensory root-branches from lingual nerve ➢Sympathetic root-branch from plexus around facial artery➢Secretomotor root-superior salivatory nucleus Facial
nerveCorda tympaniJoins the lingual nerve
➢Distribution-submandibular,sublingual,Ant. lingual gland
22
PTERYGOPALATINE GANGLION
➢Secretomotor root
Lacrimatory nucleus Nervous intermedius Facial nerveGeniculate ganglionGreater petrosal and
deep petrosal nerve
Nerve of pterygoid canal
➢Distribution -Mucous glands of Nose,paranasalsinuses,palate,nasopharynx,
23
AGE CHANGES
Chorda tympani exit through stylomastoid foramen
Chorda typani exit through proximal to stylomastoidforamen
Nerve trunk is more anterior or lateral on exit through stylomastoid foramen
Nerve trunk is lesser anterior and deeper
Nerve more superficial over angle of mandible
Nerve less superficial over angle of mandible
24
CHILD ADULT

.
5
25
TESTING OF FACIAL NERVE BRANCHES APPLIED ASPECT
26
SUPRANUCLEAR AND INFRANUCLEAR LESION
27
ETIOLOGY OF FACIAL NERVE PALSY
➢ Birth
➢ Trauma
➢ Infections
➢Metabolic
➢Neoplastic
➢ Iatrogenic
➢ Idiopathic
28
29
➢Two types of facial palsy
▪ Immediate type-Occurs within minutes of injection with recovery period of 3 hours or less▪ Delayed type-Occurs within several hours to saveraldays,while recovery may expand from 24
hours to saveral months
➢Causes▪ Direct accidental anesthesia of one or more branches of nerve. This is possible when an intraglandularinjection of the anesthetic solution occurs.
30

.
6
BELLS PALSY
31
➢First described by CHARLESBELL
➢Most common cause of facialparalysis
➢Sex-No difference exists
➢Age-Highest in persons aged15-45 years
32
FEATURES➢Unilateral involvement➢Inability to smile,close eye or raise eyebrow(BELLS PHENOMENON)➢Whisting impossible➢Drooping of corner of mouth➢Inability to close eyelid(Bells sign)➢ Inability to wrinkle forehead➢Loss of blinking reflex➢Slurred speech➢Mask like appearance of face➢Lost/Alteration of taste
33
DIAGNOSIS
➢ Based on CLINICAL PRESNTATION
➢ ELECTROMYOGRAPHY-Confirm the presence of nerve damage
➢MRI AND CT-Eliminate other structural causes of pressure on the facial nerve
34
MANAGMENT
➢Medical
CORTICOSTEROIDS-PREDNISOLONE 1mg/kg/day 7-10days
ANTIVIRAL DRUGS-ACYCLOVIR 400mg 5Times/day
➢ Surgical
Facial nerve decompression
➢ EYE LUBRICATION
Eye patch and lubricants(HYPROMELLOSE DROPS)
Are used to prevent drying of the cornea.
35
FACIAL NERVE PALSY IN NEWBORN
➢Mastoid process is absent in newborn and stylomastoidforamen is superficial.
➢Manipulation of baby’s head during delivery may damage the seventh nerve.
➢Leads to paralysis of facial muscles especially the buccinator,required for sucking the milk
36

.
7
CROCODILE TEARS SYNDROME
➢ Also called(BOGORADS REFLEX,PAROXYSMAL LACRIMATION).
➢ Following facial nerve injury, the regenerating nerve fibersundergo synkinesis or misdirected to ultimately innervate the lacrimal gland instead of the submandibular gland.
➢ TREATMENT-(BOTULINUM TOXIN INJECTION)
37
RAMSAY-HUNT SYNDROME
38
CONCLUSION
➢ Surgeons have to pay attention to minimize the risk of complication during parotidectomy.
➢ The best means of reducing iatrogenic facial nerve injury, in parotid surgery, still remains a clear understanding of the anatomy, good surgical technique with the use of multiple anatomic landmarks.
39
➢ Pre-operative discussion and consent for surgery, tailored according to the age and health of the patient as well as the behavior of the tumor, are mandatory.
➢ Furthermore, the patient has to be informed about the cosmetic sequelae of the incision and all patients have to be told that facial nerve paralysis or paresis is possible and can be partial or total, temporary or permanent.
40
REFERENCES
➢Gray's Anatomy By Richard Drake, A. Wayne Vogl, Adam W. M. Mitchell.
➢A.K. Datta Essentials Of Human Anatomy Head And Neck. 4th Edition
➢B D CHAURASIA’S Human Anatomy. Volume 3 Edition 4th
➢Atlas Of Anatomy Edited By Anne M. Gilroy, Brian R.Macpherson, Lawrence M. Ross
➢ Monheim’s Local Anaesthesia And Pain Control In Dental Practice
41 42
THANKYOU
.
1
LOCAL ANAESTHESIACOMPLICATIONS
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
CONTENT
◼ Introduction
◼ History
◼ Definition
◼ Desirable properties
◼ Mechanism of action of L.A
◼ Factors affecting L.A action
◼ Classification
◼ Composition of L.A
◼ Systemic effects of LA
◼ Contraindications of LA
◼ Vasocontrictors
◼ Clinical aspects
◼ Complications
◼ Future Directions
◼ Conclusion
CONTENT
INTRODUCTION
Joseph A et al,pharmacology of Local Anesthetics used in oral surgery ,Anesthesia:Oral and Maxillofacial clinics of North America;Volume 25, Issue 3, Pages 453-466 (August 2013)
The efforts of human kind to find the means to control pain presents as one of the greatest challenges in medicine. Pain is the phenomenon wisely instituted by nature as a warning sign of a condition that may be detrimental to our bodies.
Pain-free operating is of obvious benefit to the patient, it also helps the operator as treatment can be performed in a calm, unhurried manner.
DEFINITION
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013,Animprint of Elsevier.
Local anesthesia is defined as a loss of sensation in a circumscribed area of the body caused by a
depression of excitation in nerve endings or an inhibition of the conduction process in peripheral
nerves.
DESIRABLE PROPERTIES
◼ Non irritating.
◼ No permanent alteration of nerve structure.
◼ Low systemic toxicity.
◼ Must be effective ( injected or applied locally)
◼ Short onset of anaesthesia.
◼ Long duration of action.
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013,Animprint of Elsevier.

.
2
◼ Potency sufficient to give complete anesthesia.
◼ Free from producing allergic reactions.
◼ Stable in solution and readily undergo biotranformation in
the body.
◼ Sterile and capable of being sterlized.
DESIRABLE PROPERTIES
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013,Animprint of Elsevier.
◼ ACETYLCHOLINE THEORY
MECHANISM OF ACTION OF LOCAL ANESTHESIA
http://cnx.org/resources/09ab17c9199ed6fb925c5fae201df4bcfac9b846/Figure_35_02_01.jpg
◼ CALCIUM DISPLACEMENT
THEORY◼ SURFACE CHARGE THEORY
◼ MEMBRANE EXPANSION THEORY
◼ SPECIFIC RECEPTOR THEORY
SMS Audio Call
Factor Action affected Description
pKa Onset Lower pKa = more rapid onset of action, more uncharged molecules present to diffusethrough nerve sheath.
Lipid solubility Anesthetic potency Increased lipid solubility = increased potency
Protein binding Duration Increased protein binding allows anesthetic cations to be more firmly attached to protein located at receptor sites, thus duration of action is increased
Non-nervous tissue diffusibility
Onset Increased diffusibility = decreased time of onset
Vasodilator activity
Anesthetic potency and duration
Greater vasodilator activity = increased blood flow to region = rapid removal of anesthetic molecules from injection site, thus decreased anesthetic potency and decreased duration
FACTORS AFFECTING LOCAL ANESTHETIC ACTION
CLASSIFICATION
◼ BASED ON DURATION OF ACTION:
1)Ultra Short acting anesthetics (less than 30mins)
2)Short acting anesthetics(45 to 75 mins)
3)Medium acting anesthetics (90-150 mins)
4)Long acting anesthetics (180 mins or longer)
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
Based on the chemistry
Esters Quinilones
e.g. centbucridine
Amides
e.g. Articaine
LidocaineBupivacaine Mepivacaine ,prilocaine
Paraaminobenzoice.g. Procaine
Cloroprocaine Propoxycaine
Benzoice.g. Butacaine
Cocaine Benzocaine Tetracaine Piperocaine
PHARMACOLOGY
◼ UPTAKE• Degree of vasoactivity
• Vasodilating properties.
• Procaine is a potent vasodilator.
• Cocaine - only L.A having vasoconstriction action
• Vasodilatation - the rate of absorption of L.A. intothe blood .duration and depth of anesthesia.
Joseph A et al,pharmacology of Local Anesthetics used in oral surgery ,Anesthesia:Oral and Maxillofacial clinics of North America;Volume 25, Issue 3, Pages 453-466 (August 2013)

.
3
◼ ORAL ROUTE• Except cocaine , L.A are absorbed poorly , if at all from the
G.I.tract• 72% OF drug undergoes significant hepatic first pass effect.
◼ TOPICAL ROUTE• Applied to intact skin- No anesthetic action.• Damaged or sunburn skin- anesthetic effect• EMLA-can be used on intact skin
PHARMACOLOGY
Joseph A et al,pharmacology of Local Anesthetics used in oral surgery ,Anesthesia:Oral and Maxillofacial clinics of North America;Volume 25, Issue 3, Pages 453-466 (August 2013)
PHARMACOLOGY COMPOSITION
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
◼ Local anesthetic drug –eg lignocaine . 21.3 mg/ml
◼ Vasopressor drug - eg adrenaline.1:80,000, 1:20,0000
◼ Reducing agent - eg Sodium meta bisulfite. 0.4-0.5mg
◼ Preservative – eg Methyl paraben.0.1%
◼ For isotonicity – Normal Saline . 6mg
◼ Diluting agent – Distilled water
SYSTEMIC EFFECTS
◼ CNS• Easily crosses blood brain barrier.
• Causes CNS depression at low doses.
Blood level• 0.5-4μg/ml
• 4.5-7μg/ml
• > 7.5μg/mi
Effect
- Anticonvulsant action, direct depression
Increase in seizure threshold.
- Preseizure signs and symptoms caused by
depression of inhibitory neuron
- Tonic clonic seizure.
entire blokage of inhibitory neuron.Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
◼ CVS
• Causes myocardial depression.
• Produces peripheral vasodilation and hypotension.
• Maximum dose-
4.4 mg/kg body weight (plain)
7 mg/kg body weight (with adrenaline)
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
SYSTEMIC EFFECTS
◼ RESPIRATORY SYSTEM
◼ Dual effect.
◼ Low doses- direct relaxant action on bronchial smooth muscles.
◼ High doses- Respiratory arrest as a result of CNSdepression
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
SYSTEMIC EFFECTS
49
Notes
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
Main unwanted effectsPlasma half-life
Tissue penetration
DurationOnsetDrug
Rarely used, only as spray for upper respiratory tract
Cardiovascular and CNS effects due to block of amine uptake
~1hGoodMediumMediumCocaine
No longer usedCNS: restlessness, shivering, anxiety, occasionally convulsions followed by respiratory depression
CVS: bradycardia and decreased cardiac output, vasodilatation, which can cause cardiovascular collapse
<1hPoorShortMediumProcaine
(2-4%)
Widely used for local anaesthesia .Also used i.V. For treating ventricular arrhythmias mepivacaine is similar
Less tendency to cause CNS effects
~2hGoodMediumRapidLignocaine (lidocaine)
(2%)
Widely used because of long duration of action.Ropivacaine is similar, with less cardiotoxicity
As lingocaine, but greater cardiotoxicity
~2hModerateLongSlowBupivacaine
(0.5%)
Widely used, not for obstetric analgesia because of risk of neonatal methaemoglobinaemia
No vasodilator activity, can cause methaemoglobinaemia
~2hModerateMediumMediumPrilocaine

.
4
CONTRINDICATIONS
◼ ABSOLUTE• Local anaesthetic allergy
• Bisulfite allergy
◼ RELATIVE• Atypical plasma cholinesterase
• Methemoglobinemia
• Significant cardiovascular, liver or renal disease.
Malamed F Stanley,pg-1,Chapter I, Neurophysiology, Handbook of local anesthesia,Sixth edition,2013, An imprint of Elsevier.
VASOCONSTRICTOR
◼ Need for vasoconstrictor• ↑ absorption of L.A into CVS → removal from injection
site• Rapid diffusion of L.A from inj site → ↓ duration of
action & depth of anesthesia.
• Higher plasma level of L.A → ↑ risk of toxicity
• ↑ bleeding at inj site.
Fonseca J Raymond,Chapter 3; Local aneasthetics,Vol 1: Anesthesia and pain control, Dentoalveolar Surgery, Practice Managment, Implant Surgery, oral and maxillofacial Surgery,pg- 35-55,vol 1,2nd edition,2009, Saunders,Elsevier
◼ Addition of vasoconstrictor• Constriction of blood vessels → ↓ tissue perfusion
• Slow absorption into CVS → low anesthetic blood level→ ↓risk of toxicity.
• Higher volume of L.A around nerve → ↑ duration ofaction
• ↓ bleeding at inj site
Fonseca J Raymond,Chapter 3; Local aneasthetics,Vol 1: Anesthesia and pain control, Dentoalveolar Surgery, Practice Managment, Implant Surgery, oral and maxillofacial Surgery,pg- 35-55,vol 1,2nd edition,2009, Saunders,Elsevier
VASOCONSTRICTOR
CLINICAL ASPECTS
Max dose of lidocaine without adrenaline is = 300mgMax dose of LA with adrenaline = 500mg Max safe dose of adrenaline =0.2mg/visit
2% Lignocaine= 2g in 100 ml2000mg in 100 ml
20 mg in 1ml - 1 mg= 1/20 500mg=1/20500= 25ml can be given safely for a normal pt
Adrenaline present in vials is in conc. of 1:200,000
1ml=1/200,000=0.005mg
0.005mg-1ml
As MRD-0.2mg , so for normal pt- 0.2 mg=1/0.0050.2= 40ml of LA can beadministered safely
Outline
Local Complications
Paresthesia
Hematoma
Pain onInjectionFacial Nerve Paralysis
Infection
Trismus
NeedleBreakageSoft TissueInjury
Edema
OcularComplications
Outline
Systemic Complications
Overdose Allergy
Introduction
Predisposing Factors
Clinical Manifestations
Management

.
5
Local Complications
Rare because of using of disposableneedles.
Needle Breakage
Causes:1. Bending of the needle.
2. Sudden unexpected movement of thepatient.
3. Entire length of the needle inserted into the softtissue.
4. Use of the smaller needles ( e.g. 40 gauge )
Needle Breakage
Prevention:1. Use large-gauge needles,specially
with Inferior Alveolar Nerve and Posterior Superior Alveolar Nerve.
2. Use long needles.
3. Do not inserta needle into tissues to its hub.
4. Do not redirect a needle once it isinserted into tissue.
Needle Breakage
Management :➢ When a needle breaks (visible):
1. Stay calm.2. Instruct the patient not to move and let his
mouth open.
1. If the fragment visible, remove it with hemostator a Magill intubation forceps.
➢ When a needle breaks ( not-visible):1. No incision or probing.2. Calmly inform the patient.3. Referral Oral Surgeon, take radiograph and
determine if it is superficial, remove or leave it and flow up?!!
Needle Breakage
❖Amaurosis “temporary blindness“.
❖Mydriasis “Pupillarydilation”
❖Ptosis “droopyeyelid”
❖Diplopia “doublevision”
Ocular Complications
.
6
❖Causes :
Ocular Complications
Inadvertent arterial injection with retrograde blood flow
❖Causes :❖Orbital injection :
Inadvertent injection into the orbit throughthe inferior orbital fissure.
Ocular Complications
❖Prevention :❖ Aspiration before actual injection.
❖ Inject slowly.
❖Treatment :❖ Reassure the patient that it is transient.
❖ Cover the affected eye with gauze dressing.
❖Refer patients to an ophthalmologist for evaluation if it last more than 6 hours
❖ Regular follow-up
Ocular Complications
Paresthesia
Causes :➢ Trauma to the nerve.
➢ Local Anesthesia solution contaminated by alcohol or sterlizing solution near a nerve produce irritation, resulting edema and increased pressure in the region of the nerve leading to paresthesia.
➢ Insertion of a needle inside a foramen.
➢ Hemorrhage-increased pressure-paresthesia.
Paresthesia
Prevention :➢ Propercareand handling to injection control and
cartridge.
➢ Management :➢ Most paresthesiaresolvewithin 8 weekswithout
treatment.➢ Sequences of management:
➢ Reassuring the patient.
➢ Examine the patientand follow up each 2 months.➢ If sensory deficit is still more than 1 year, consultation
withneurologist and oralsurgeon.
Occurwhen anesthesia is introduced intodeep lobe of the parotid gland.
Facial Nerve Paralysis
.
7
Facial Nerve Paralysis
Causes :◦ Transient FNP caused by local anesthesia into capsule of
the parotid gland, which is located at posterior border ofthe mandibular ramus.
◦ Usually it occur during Inferior Alveoar Nerve Block orVazirani-Akinosi Nerve Block.
Facial Nerve Paralysis
Prevention :
➢ Proper care and handlingtoinjection control and cartridge.
➢ Management :
1. Reassuring thepatient.
2. Contact lenses should be removed.
3. An eye patched should beapplied to affected eye or manually close the lower eyelid periodically to keep the cornealubricated.
Most common : Trauma to muscles or blood vessels ininfratemporal fossa.
Pain and difficult of opening often after posterior superioralveolaror inferioralveolarnerve block.
Onset 1-6 dayspost-treatment.
Trismus
Causes :
➢ Trauma to the muscles or blood vessels inthe
infratemporal fossa.
➢ Local Anesthesia solution contaminated byalcohol or cold sterlizing solution produce irritation of the muscles.
➢ Low-grade infection.
Trismus
Prevention :1. Use sharp, sterile, disposable needle.
2. Proper care and handling to injection controland cartridge.
3. Atraumatic injection and avoid repeating of it.
Trismus
Management :➢ Heat therapy.➢ Warm saline rinse.➢ Analgesic, Aspirin 325 mg.➢ Muscle relaxant if necessary,
Diazepam 10 mg bid➢ Physiotherapy for 5 min. each3-4
hours.➢ If there is infection,antibiotic
described for 7 days.
➢ Improvement start within 2-3daysand recovery range 4-20weeks.
➢ Surgical intervention in somecases.
Trismus

.
8
Trauma to the lip or the tonguecaused by biting or chewing these tissue while still anesthetized, specially withchildren.
Soft-Tissue Injury
Prevention :◦ A cotton roll placed between the lips and the teeth.
◦ Warn the patient.
◦ Self-adherent warning sticker.
Soft-Tissue Injury
Management:◦ Analgesic forpain.
◦ Antibiotic if there is infection.
◦ Warm saline rinse to aid in decreasing the swelling.
◦ Petroleum jelly to cover the lesion and minimize theirritation.
Soft-Tissue Injury
The effusion of the blood into extravascular spaces can result from inadvertently injecting a bloodvessel.
Casued by nicking to the artery or vein.
Most occurwith IANB and PSA nerve block.
7 to 14 days the hematoma will be presented.
Hematoma
Prevention :1. Knowledge of normal anatomy.2. Use shorter needle for PSA nerve block.3. Minimize the number of the needle penetration.4. Neveruse a needle as a probe in the tissue.
Management:1. Direct pressure applied on to the site of bleeding.
2. Applycold moist towels to affected area each 20 min. every hour.
3. Advice the patient about soreness and limitation of themouth opening possibility.
Hematoma
Causes :1. Careless injection and callous attitude “ Palatal Injection
always hurt”.
2. Dull of the needle because of multiple injection.
3. Rapid deposition of the local anesthetic solution.
Pain on Injection

.
9
Prevention :◦ Adhere to proper techniques
of injection, both anatomicaland psychological.
◦ Sharp needles.
◦ Topical anesthetic.
◦ Inject slowly.
◦ Temperature of the solution.
Pain on Injection
Causes :◦ Contamination of the needle, now become rarely after
introduction of the sterile disposable needle and glasscartridge.
Management:◦ Antibiotic, penicillin 250 mg qid.
Infection
Causes :1. Trauma.
2. Infection.
3. Allergy, angioedema.
4. Hemorrhage.
5. Injection of irritatingsolution(alcohol, coldsolution).
Edema
Management :1. Minimal degree edema --- just analgesic for pain
and will resolve in several days.
2. If large degree edema and sign andsymptom of infection--- antibiotic should be prescribed.
Edema Systemic Complications Systemic Complications
Overdose Allergy
Introduction
Predisposing Factors
Clinical Manifestations
Management

.
10
◦ Overdose reaction is occurring when the drug access tothe circulatory system.
◦ Normally there is constant absorption of the drug from its site of admission into the circulatory system and a steady removal from the blood by theliver.
Overdose
➢Patient Factors: Age :
old people – increasing the half-life of the drug in circulation blood.
Weight
Medications : Meperidine”narcotic analgesic”,
phenytoin”anticonvalsun”, quinidine”antidysrhythmatic”,anddesipramine”antidepressant” – increase localanesthesia blood level, because of protein binding competition.
Predisposing Factors
➢Patient Factors:
Gender :
Renal function during pregnancy may impaired leading to increase local anesthesia blood level.
In adult women the seizure threshold is 5.8 mg\kg, in newborn 18.4, in the fetus 41.9 mg\kg.
Presence of disease :
Hepatic , renal dysfunction and congestive heart failure decrease liver perfusion – increase amide local anesthesia blood level.
➢Patient Factors:
Genetics :
Deficiency in enzyme serum pseudocholinesterase – responsible for biotransformation of ester localanesthesia.
Mental attitude Concentration Dose Vasoactivity
➢:
Route of administration Rate of injection :
Slow (60-seconds) IV administration percartridge (36 mg) .
Vasculratiy of the injection site
Vasoconstrictors
Drug Factors
1. Use aspirationsyringe.
2. Use a needle no smaller than 25 gauge.
3. Aspirate in at least two planes before injection.
4. Slowly injectingthe anesthetic.
Prevention

.
11
1. Talkativeness .
2. Apprehension.
3. Excitability.
4. Slurred speech.
5. Stutter.
Clinical Manifestation
1. Sweating.
2. Vomiting.
3. Failure to follow commands.
4. Elevated blood pressure, heart and respiratory rate.
5. Tonic-clonic seizure in highly overdose.
6. CNS depression, MyocardiacDepression and cardiac arrest.
Clinical Manifestation
1. Mild Overdose:1. Slow onset (>5 minutes)2. Slow onset (>15 minutes)
2. Severe Overdose:1. Rapid onset (within 1
minute)2. Slow onset (5 to15
minutes)
Management
1. Basic Emergency Management:1. Position.
2. Circulation.
3. Airway.
4. Breathing.
5. Definitive Care.
P-C-A-B-D
1. Mild Overdose: “Patient conscious”◦ Slow onset (>5 minutes): P-C-A-B
Reassure the patient.
Administer oxygen via nasal canal.
Monitor and record vital signs.
IV anticonvulsants (diazepam 5 mg\min.
or midazolam 1 m\min.) “optional”
Emergency medical assistance before patientdischarge.
1. Mild Overdose: “Patientconscious”◦ Slow onset (>15 minutes)
P-C-A-B
Reassure thepatient.
Administer oxygen via nasalcanal.
Monitor and record vitalsigns.
IV anticonvulsants (diazepam 5 mg\min. or midazolam 1 m\min.) “manadatory”
Emergency medical assistancebefore patientdischarge.

.
12
1. Severe Overdose: “Patient unconscious”◦ Rapid onset (within 1 minute) P-C-A-B
Protect the patient.
Immediately summon emergencymedical assistance.
Continue Basic life support (BLS)
IV anticonvulsants (diazepam 5 mg\min. or midazolam 1 m\min.) “if seizures protract more than 4 min.”
1. Severe Overdose: “Patient unconscious”◦ Slow onset (5 to 15 minutes) P-C-A-B
IV anticonvulsants (diazepam 5 mg\min. or
midazolam 1 mg\min.) and oxygen administration.
Immediately summon emergency medicalassistance.
Continue Basic life support (BLS).
Vasopressor and IV fluid is recommended for management of hypotension.
◦ Hypersensitive state, acquired through exposure to a particular allergen.
◦ Allergic reactions cover a broad spectrum odd clinical manifestations ranging from mild and delayed response occurring as long as 48 hours after exposure to allergen, to immediate and threatening reaction develop within seconds ofexposure.
Allergy
◦ Sodium Bisulfite: Antioxidant in vasoconstrictor local
anesthesia. 1984 has been excluded.
◦ Epinephrine.
◦ Latex.
◦ Topical Anesthesia: Mostly ester. Preservatives containing such as
methylparaben, ethylparaben, orpropylparaben.
Predisposing Factors Clinical Manifestation
Dermatological reaction
Generalized anaphylaxis
Respiratoryreactions
◦ Dermatological reaction:
Urticaria
Angioedema
Clinical Manifestation

.
13
◦ Respiratory reactions:
Bronchospasm: Respiratory distress Dyspnea Wheezing Flushing Cyanosis Perspiration Tachycardia Anxiety
Laryngeal edema: Extension of edema to the
larynx Life threatening emergency.
Clinical Manifestation
◦ Generalized Anaphylaxis:
Skin reactions Smooth muscle spasm of gastrointestinal
and genitourinary tracts andbronchospasm.
Respiratory distress.
Cardiovascular collapse.
Treatment of the entire reaction may be terminated rapidly, but hypotension and laryngeal edema may persist for hours to days.
Clinical Manifestation
◦ Skin reaction:
Delayed reaction.
Immediatereaction.
◦ Respiratory reaction:
Bronchospasm.
Laryngeal edema.
◦ Generalized anaphylaxis:
Signs of allergypresent.
No signs of allergypresent.
Management
◦ Skin reaction: Delayed reaction:
P-C-A-B
Oral histamine blocker 50 mg diphenhydramine or 10 mg chlorpheniramine, one tab at 6h for 3-4 days.
Observation for 1 hour.
Medical consultation.
If patient feels drowsiness,not allowed to leave the clinic.
Management
◦ Skin reaction: immediate reaction:
P-C-A-B
Epinpherine 0.3 mg IM.
IM histamine blocker 50 mg diphenhydramine or 10 mgchlorpheniramine.
Medical consultation
Observation for 1 hour.
Prescribe Oral histamine blocker 3 days.
Management ◦ Respiratory reaction: Bronchospasm :
P-C-A-B
Administer oxygen at flow 5-6 liters\min.
Epinpherine 0.3 IM or Bronchodilator “albuterol” , dose repeated 10-15 min. if needed.
Observation for 1 hour.
IM histamine blocker 50 mg diphenhydramine or 10mg chlorpheniramine.
Medical consultation Prescribe Oral histamine blocker 3 days.

.
14
◦ Respiratory reaction: Laryngeal Edema : “unconscious patient”
P-C-A-B Epinepherine 0.3 IM, dose repeated 10-15 min.
Activate Emergency Medical Services.
IM histamine blocker 50 mg diphenhydramine
or 10 mg chlorpheniramine. Corticosteroid IM or IV (100
mg Hydrocortisone sodium succinate to inhibit and decrease edema. Perform cricothyrotomy.
◦ Generalized Anaphylaxis : Signs of allergy present : “unconscious patient”
P-C-A-B.
Summon medical assistance.
Epinpherine 0.3 IM, dose repeated 10-15 min.
Administer oxygen.
Monitor vital signs, recorded every 5 min.
IM histamine blocker and Corticosteroid IM or IV “ If clinical improvement noted increased blood pressure, decreasedbronchospasm”.
◦ Generalized Anaphylaxis :
No signs of allergy present : “unconscious patient”
P-C-A-B
Summon medical assistance.
Administer oxygen.
Monitor vital signs, recorded every 5 min.
Addition management, on arrival of the emergency medical personnel depend on the cause of the loss of consciousness.
CASE PRESENTATION
This is a complication of extra oral hematoma formation in the mandibular buccal and lower eyelid region along with subconjunctivalhemorrhage following PSAN block administration for the root canal treatment of upper right maxillary first molar.
In the present case, the patient was advised to take analgesics (acetaminophen).
Application of ice pack for 20 minutes 4 to 8 times a day.
Anti-inflammatory medication containing trypsin and chymotrypsin.
Eye drop containing naphazoline and phenyl ephrine.
Any dental treatment in the involved region should be avoided until the symptoms and signs resolve.
The swelling and discoloration of the involved region got gradually subsided in 15 days.
FUTURE DIRECTION OF LOCAL
ANESTHETICS

.
15
BUFFERED LOCAL ANESTHESIA
MICROPARTICULATE FORMULATIONS
Fonseca J Raymond,Chapter 3; Local aneasthetics,Vol 1: Anesthesia and pain control, Dentoalveolar Surgery, Practice Managment, Implant Surgery, oral and maxillofacial Surgery,pg- 35-55,vol 1,2nd edition,2009, Saunders,Elsevier
REVERSAL OF LOCAL ANESTHESIA
◼ Formulation of phentolamine mesylate (OraVerse)
◼ a-adrenergic antagonist
◼ 1.7 ml cartridges containing 0.4 mg phentolamine mesylate.
Joseph A et al,pharmacology of Local Anesthetics used in oral surgery ,Anesthesia:Oral and Maxillofacial clinics of North America; Volume 25, Issue 3, Pages 453-466 (August 2013)
ELECTRONIC DENTAL ANESTHESIA
Joseph A et al,pharmacology of Local Anesthetics used in oral surgery ,Anesthesia:Oral and Maxillofacial clinics of North America; Volume 25, Issue 3, Pages 453-466 (August 2013)
Fonseca J Raymond,Chapter 3; Local aneasthetics,Vol 1: Anesthesia and pain control, Dentoalveolar Surgery, Practice Managment, Implant Surgery, oral and maxillofacial Surgery,pg- 35-55,vol 1,2nd edition,2009, Saunders,Elsevier
ELECTRONIC DENTAL ANESTHESIA
SINGLE TOOTH ANESTHESIA/COMPUDENT
Orrett E. Ogle,et al Advances in Local Anesthesia in Dentistry Dent Clin N Am 55 (2011) 481–499

.
16
INTRAOSSEOUS INJECTION, STABIDENT
Orrett E. Ogle,et al Advances in Local Anesthesia in Dentistry Dent Clin N Am 55 (2011) 481–499
ConclusionAdministration of a local anesthetic can be associated with complications of adverse events and so medical history of the patients should routinely be evaluated in details.
While administrating anesthesia, the painless injection should be performed, avoiding intravascular or intramuscular or direct trauma to the nerve.
New developments should be followed by the practitioners to reduce possible complications associated with the local anesthesia.
Take home message…..
In order to minimize the possible complications, visualization of the regional anatomy, numerous aspirations while injection, and aspiration on at least two planes before administration local anesthetic should be performed.
It is only with a thorough understanding of pharmacology and anatomy that clinicians have the basic clinical foundation to enhance the care of patients.
References:
1. Stanley F. Malamed. Handbook of local anesthsia. 5th edition. Page 285-332.
2. Sean G. Boynes, Zydnia Echeverria, Mohammad Abdulwahab. Ocular ComplicationsAssociated with Local Anesthesia Administration in Dentistry. Dent Clin N Am 54(2010) 677–686
3. Ngeow WC, Shim CK, Chai WL. Transient loss of power of accommodation in one eyefollowing inferior alveolar nerve block: report of two cases. J Can Dent Assoc2006;72:927–31.
4. Penarrocha-Diago M, Sanchis-Bielsa JM. Opthalmologic complications after intraorallocal anesthesia with articaine. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2000;90:21–4.
5. Lee C. Ocular complications after inferior alveolar nerve block. Hong Kong Med Diary2006;11:4–5.
6. Van der Bijil P, Meyer D. Ocular complications of dental local anesthesia. SADJ1998;53:235–8.
7. Goldenberg AS. Transient diplopia as result of block injections. Mandibular andposterior superioralveolar.N Y State Dent J 1997;63:29–31.
THANK YOU…..!!!!!
.
1
MANAGEMENT OF HORIZONTAL ROOT FRACTURES
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
Content
INTRODUCTION
ETIOLOGY
CLASSIFICATION OF ROOT FRACTURES
HORIZONTAL ROOT FRACTURE-
SUB-CLASSIFICATON
CLINICAL EXAMINATION
RADIOGRAPHIC EXAMINATION
Contents
PULPAL STATUS
MANAGEMENT
FOLLOW UP
HEALING IN ROOT FRACTURES
CONCLUSION
INTRODUCTION
✓ Traumatic injuries to a tooth can vary in severity from a simple enamel infraction to a complete ex-articulation of tooth (avulsion).
✓ Among these injuries, tooth fracture (crown fractures, crown-root fractures and root fractures) are considered to be the third most common cause of tooth loss.
Andreasen FM, Andreasen JO, Cvek M. Root fractures. In: Textbook and Color Atlas of Traumatic Injuries to Teeth
Root fractures
Horizontal/ transverse root
fractures
Vertical root fractures
.
2
Definition-
Horizontal root fractures are intra-alveolar fractures extending through the entire root—through the cementum, dentin, and pulp and presenting as being either transverse or oblique.
The root fracture will produce new sections of the root, which are termed fragments. These fragments are designated as being the coronal fragment and the apical fragment, with the space between these fragments referred to as the diastasis.
✓ Most affected age range:
primary teeth 3-4 years(less common owing to the elasticity of alveolar bone)
permanent teeth 11-20 years
More common in males than females.
✓ Root fractures are uncommon in teeth with incomplete root development and those in various stages of eruption .
✓ Although the outcome of treatment of a root fracture is generally favourable (60–80% cases), complications such as pulpal necrosis, radicular resorption and pulpal canal obliteration can arise.
✓ Root fracture account for 0.5 to 7% of the injuries affecting the permanent dentition.
✓ Root fracture are clinically challenging as their management may involve interdisciplinary / mulitidisciplinary treatment approach.
✓ Maxillary central incisors are most commonly involved, making up 80% of the cases.
Andreasen FM, Andreasen JO, Cvek M. Root fractures. In: Textbook and Color Atlas of Traumatic Injuries to Teeth
CLASSIFICATION-
Further classified on the basis of:
1) The number of fractures lines (simple, multiple and comminuted)
Horizontal root fractures
2)The location of the fracture line (cervical, middle, or apical)
3) The position of the coronal segment (displaced and not displaced)
Horizontal Root Fracture
Caliskan and Pehlivan, in an assessment of 56 root fractures, showed that fracture of the middle third was the commonest, equivalent to 57% of the cases, followed by fracture of the apical (34%) and cervical (9%) thirds.
Prithviraj, Bhalla HK, Vashisht R, Regish KM, Suresh P. An Overview
of Management of Root Fractures. Kathmandu Univ Med J 2014;47(3):222-30

.
3
Horizontal root fractures
4) The extent of the fracture (partial and total)
Based on relation with alveolar crest level-
Depending on the position of the fracture line, transverse root fractures can also be classified into three zones as follows:
Zone 1 – extends from the occlusal/incisal edge to the alveolar bone crest.
A review of root fractures: Diagnosis,treatment and prognosis.Dent Update 2011; 38: 615–628
Horizontal root fractures
Zone 2 – extends from the alveolar bone crest to 5 mm below.Zone 3 – extends from 5 mm below the alveolar bone crest to the apex of the root.
Root fracture
Physical trauma
Parafunctionalhabits
Traumatic occclusion
E
TI
O
L
O
GY
CLINICAL PRESENTATION
Slightly extruded depending on the severity of the dislocation.
Crown will become discolored with varying shades of brown and gray.
Fracture line is more coronal on the labial aspect, extending more apically towards the lingual aspect, with the coronal fragment of the tooth typically being displaced more lingually.
EXTRUDED AND DISCOLORED
FRACTURED CENTRAL INCISOR
Clinical examination
Coronal fragment has varying degrees of mobility and percussion sensitivity.
Fractures in the apical-third of the root do not show signs of displacement or mobility.
In cervical third fractures extending below crestalbone, the crown is usually present with minor mobility owing to attachement of periodontal fibers to the portion of root that has fractured off with the crown.
FRACTURE SLIGHTLY BELOW CRESTAL BONE
LINGUALLY
.
4
With fracture line above the crestal bone, the crown is usually extremely mobile or dislodged.
On palpation – tenderness is present over the root
Bleeding from gingival sulcus and tooth is tender on percussion.
If # is not apparent initially, it may become apparent days or weeks later as the patient complains of sensitivity to biting pressure.
GINGIVAL SULCUS BLEEDING
Radiographic examination
Radiographic examination is indispensable for the confirmation of intraalveolar root fractures.
The conventional periapical radiograph, two additional periapicalradiographs (one with a positive angulation of 15° to the fracture line and the second with a negative angulation of 15° to the fracture line) should be exposed.
The normal
projection
angle is
parallel to the
fractured
surface
Decrease or
Increase of the
projection
angle
Fracture line in
multiple root
fracture
Resulting in a
single
transverse line
on the
radiograph
Results in an
elipsoid
fracture line
Shows an
irregular shape
on the
radiograph
SINGLE TRANSVERE ELLIPSOIDAL IRREGULAR
Radiographic examination
Other suggested protocols to visualize the fracture line accurately are:
✓ Processing three-angled radiographs at 45°, 90° and 110°.
✓ A steep occlusal exposure along with two conventional periapical bisecting-angle exposures.
Recent advances include the use of CBCT to visualize root fractures.
Prognosis
The factors that influence healing and prognosis are as follows:
✓ Status of the pulp
✓ Position and mobility of coronal segment after trauma
✓ Position of the fracture line
✓ Treatment time
✓ Communication with the oral environment
✓ Age

.
5
Status of the pulp
A vital pulp and positive pulp sensibility at the time of injury are positively related to faster healing and hard tissue repair of the fracture.
Pulp in the apical segment of the fractured tooth is vital in almost all cases.
Pulpal Status
Pulpal status is one of the most important parameters in deciding the treatment plan.
There is a higher incidence of necrosis among teeth that are traumatized but not fractured.
Initially, sensibility and vitality testing may give negative results due to transient or permanent pulpal damage inflicted by trauma.
A routine follow-up is required.
More recently, pulse-oximeter is recommended to evaluate the pulpal status of a recently traumatized tooth because of better sensitivity and specificity.
Coronal fragment becomes nonvital only 20% to 24% of the time.
If the vitality of the tooth does not recover within 6 to 8 weeks, the coronal fragment should be considered nonvital
Apical fragment remains vital in majority of the cases.
Position & mobility of coronal segment after trauma
Increased dislocation and mobility results in a decreased prognosis.
In concussion, a high rate of hard-tissue healing is observed in while in cases of luxation, healing with connective tissue is high.
Position of the fracture line
The chance of healing with calcified tissue and survival is poorest when the fracture line is very close to the gingival crevice.
Zachrisson and Jacobsen observed that the location of the fracture line does not influence the outcome, except for fractures that occur too close to the alveolar bone crest (as the tooth support is compromised).
Zachrisson BU, Jacobsen I. Long-term prognosis of 66 permanent anterior teeth with root fracture. Scand J Dent Res
1995
A/c to LOUIS H. BERMAN,
Apical fractures-(24% to 34% success).
Coronal third fracture with extensive mobility of the coronal fragment=2-9%
A Clinical Guide to Dental Traumatology LOUIS H. BERMAN, LUCIA BLANCO, AND STEPHEN COHEN

.
6
Treatment time
Immobilization should be done as soon as possible for an optimum consolidation and repair across the fracture line.
Optimal repositioning and use of passive flexible splint favours healing.
Communication with the oral environment
If communication develops between the gingival sulcus and the fracture site the prognosis is poor because of bacterial contamination.
Andreasen, J. O., Andreasen, F. M., Mejare, I., & Cvek, M. (2004). Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development,
fracture type, location of fracture and severity of dislocation. Dental Traumatology, 20(4), 192–202.
Age
Young age and immature root formation are increasingly related to pulpal healing and hard tissue formation at the fracture site due to the increased size of pulp and vascularity.
Andreasen, J. O., Andreasen, F. M., Mejare, I., & Cvek, M. (2004). Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development,
fracture type, location of fracture and severity of dislocation. Dental Traumatology, 20(4), 192–202.
Management of horizontal
root fracture
Clinical management of a horizontal root fracture depends on different variables :
✓ Pulpal vitality status
✓ Mobility of the coronal fragment
✓ Location of the root fracture
✓ Stage of root formation
Management
Treatment is usually directed at repositioning and stabilizing the coronal fragment in its correct position and monitoring the tooth for an extended period for pulp vitality.
Management of root fractures can be divided into treatment of:
1. Apical-third
2. Middle-third and
3. Cervical-third fractures

.
7
Apical third fracture
In the case of apical-third fractures of the root, there is usually no mobility and the tooth may be asymptomatic.
Apical segment of a transversely fractured tooth remains vital in most of the cases.
Watch and observe policy is advocated.
Apical third fracture
If the pulp undergoes necrosis in the apical fragment, surgical removal of the apical fragment is indicated.
Pulp necrosis develops in the coronal segment owing to its displacement but occurs in only about 25% of cases.
Middle third fracture
Repositioning of the coronal fragment and immobilization through fixation to the neighbouring teeth by means of a semi-rigid or rigid splint.
Maintain the splint for 2–3 months.
The advocated splinting methods include the use of stainless-steel wire resin-based composite splints or titanium trauma splints (TTS).
Treatment options may becategorized as follows:
1) Repositioning the fractured segment and splinting
Indicated when-
Horizontal root fracture with a diastasis of 0.1 mm.
Pulp with cold-induced sensibility, absence of dental mobility or periapical changes and non-discolored crown.
A semi-rigid splinting is performed with an orthodontic wire bonded to the labial surfaces of the maxillary anterior teeth using composite resin.
Versiani MA, de Sousa CJ, Cruz-Filho AM, Perez DE, Sousa-Neto MD Clinical management and subsequent healing of teeth with horizontal root fractures. Dent Traumatol 2012
Treatment options
2) Disinfection and obturation of the coronal segment only
If pulp necrosis develops, the apical fragment remains vital in approximately 99% of cases, while the pulp tissue on the cervical fragment can develop necrosis with consequent formation of granulation tissue between the fragments.
Endodontic treatment is performed only in the coronal segment. An apexificationprocedure of this segment should be performed before obturation of the root canal.

.
8
Horizontal root fracture of the
left upper central incisor.
Worliknglength of
cervical fragment.
Radicular canal from cervical
fragment endodonticallyobturated
without overfilling
Periapicalradiograph
after 3 years of follow-up
Versiani MA, de Sousa CJ, Cruz-Filho AM, Perez DE, Sousa-Neto MD Clinical management and subsequent healing of teeth with horizontal root fractures. Dent Traumatol 2012
Treatment options
3) The third category of cases may be - of complete pulp necrosis, when endodontic treatment should be performed in both the apical and the coronal fragments.
4) If both the segments are misaligned, fourth treatment option should be considered
that is the-surgical removal of the apical portion.
Versiani MA, de Sousa CJ, Cruz-Filho AM, Perez DE, Sousa-Neto MD Clinical management and subsequent healing of teeth with horizontal root fractures. Dent Traumatol 2012
Treatment options
5) Intraradicular splintingAids in treating both coronal and apical fragments when they are well aligned.
The technique involves connecting the tooth fragments through the root canal using a metal pin together with a root canal sealer.
Steel pins, titanium endodontic implants, prefabricated titanium dowels, posts, and ceramic, silver, or alloy cast dowels and posts have been used for intraradicular splinting
Management of Horizontal Root Fracture in the Middle Third via Intraradicular Splinting Using a Fiber Post.Case reports in dentistry 2016
(a)
(b)
(c) (d) (e)
(f) (g)
Management of Horizontal Root Fracture in the Middle Third via Intraradicular Splinting Using a Fiber
Post.Case reports in dentistry 2016
(h) (i)
(j) (k) (l)

.
9
Treatment options
6) Removal of the apical segment and stabilization of the coronal segment with endodontic implants. Indicated in compromised alveolar support cases and both the fragments are displaced wide apart.
Feldman, advocated the use of endodontic stabilizers as a means of stabilizing and retaining seemingly non-retainable teeth.
The coronal segment is stabilized with the use of chrome cobalt pin as the implant material.
An endodontic stabilizer is used in conjunction with surgical intervention and bone grafting.
Mittal S, Kumar T, Aggarwal V, Bansal R, Kaur D.Endodontic stabilizers for treating mid root fractures. J Interdiscip Dentistry 2011
Treatment options
➢ The endodontic stabilizer increases the root anchorage in the bone by the extension of the artificial material beyond the limit of the alveolar socket within the limits of the alveolar bone and thus helps in stabilizing the teeth with compromised alveolar support.
CERVICAL THIRD ROOT FRACTURES
❖ Poor prognosis because of:
1. Exposure of pulp to oral environment
2. Short mobile coronal fragment therefore difficult to immobilize.
❖ Treatment options are decided upon by:
1. The position of the fracture line,
2. Length of the remaining root segment and the presence or absence of a coronal segment.
CERVICAL THIRD ROOT FRACTURES
❖ Chances of healing with calcified tissue is poorest in cervical-third fractures.
❖ A longer splinting period of 6 months to 1 year is required because of the mobility of the coronal segment.
Cervical 3rd root fracture
Coronal segment lost
Coronal segment intact
Fracture line below the alveolar crest
Fracture line above the level of alveolar crest
Fracture above the alveolar crest level
Coronal segment intact
Reattachment:
Reattachment of fractured segment can
be done by light transmitting or fibre-reinforced posts and
resin-based composite material
Coronal segment lost
Post crown with subgingival margins or false
shoulder
In cases where exposure of crown margins is required,
a simple gingivoplasty or an apical positioned flap surgery is performed.

.
10
Fracture line below level of alveolar crest
To convert the subgingival fracture to a supragingival fracture line:
✓ Gingivectomy
✓ Surgical or Orthodontic extrusion of apical fragment is necessary.
If the remaining root structure is long enough to support subsequently
applied restoration
Fracture portion extracted and
subsequent crown placement is done There is need to convert the subgingival fracture to a supragingival
fracture line
✓ Crown lengthening
✓ Gingivectomy, Apically positioned flap
✓ Surgical or Orthodontic extrusion of apical fragment
If the remaining root structure is not enough to support subsequently applied restoration
Crown lengthening
Crown lengthening is performed if the fracture line is not more than 1–2 mm below the alveolar bone crest.
Removal of 1–2 mm of crestal bone adjacent to the deepest part of the fracture and restoring the normal sulcus depth of 2 mm.
It usually leads to apical shifting of gingival margin which may compromise aesthetics.
Periodontal and osseous recontouring allows exposure of the fracture margin and sufficient root surface to give an acceptable restorative finish line.
Orthodontic extrusion
Also known as forced eruption, orthodontic eruption, vertical extrusion or assisted eruption.
When fracture line extends deeply in the interproximal or labial surface (up to 6 mm below the alveolar crest) and when crown lengthening would be unaesthetic.
For a successful extrusion and post-treatment restoration, the distance from the fracture line to the apex should not be less than 12 mm and a crown root ratio of approximately 50:50 must be obtained.
Orthodontic extrusion
This technique involves application of traction forces to the tooth, causing vertical extrusion of the root and marginal apposition of crestal bone.
The gingiva, epithelial attachment, and newly formed crestal bone are also extruded, along with the tooth, leading to a coronal shift of the marginal gingiva.

.
11
Pre -extrusion post-extrusion with the help of modified hawley’s appliance
A review of root fractures: Diagnosis,treatment and prognosis.Dent Update 2011; 38: 615–628
Orthodontic extrusionForced Surgical Extrusion
➢ Indication: Severe luxation of the fractured root.
➢ The tooth is carefully extruded to the required position by marginal luxation and stabilized by interdental suturing and surgical dressing.
➢ If the fracture line is more apical on the labial side , a rotation of 180°is given before fixation.
Tooth Fragment v/s Composite restorations
Using the original fragment to restore crown and crown– root fractures presents some advantages over composite restorations:
1. The technique is generally faster, economical and less complicated
2. More aesthetic restoration could be attained particularly by conserving the original translucency and contours
3. The restored tooth is more resistant to stain and abrasion than a resin restoration.
Vital Root Submergence
Indicated in young individuals where the above mentioned treatment alternatives can not be carried out and the remaining apical portion of injured tooth does not reach the criteria of 1:1 crown-root ratio and barely support a future permanent prosthetic build-up.
Prevents or retards resorption of the alveolar process and maintains the dimension of the alveolar process.
Follow –up-
Clinical and radiographic examination should be done at 3, 6, 12 months and yearly thereafter.
Patients should be advised to use of a soft brush and 0.2% chlorhexidinerinse which prevents accumulation of plaque and debris and helps in maintaining good oral hygiene.
Healing in root fractures
Indicators of favourable outcomes following treatment of root fractures include:
➢ Asymptomatic status
➢ Positive response to pulp testing
➢ Continuing root development in immature teeth
➢ Signs of repair between fractured segments and
➢ Absence of apical periodontitis.

.
12
Healing in root fractures
❑ According to the Andreasen and Hjorting- Hansen, root fracture can show healing in following ways:
Healing with calcified tissue
Healing with interposition of connective tissue
30% cases
43% cases
Healing with interproximal bone and connective tissues
Healing by interposition of granulation tissue
Signs of inflammation and pulp necrosis
5% cases
GRANULATION TISSUE
BONE DEPOSITION
CACIFIC BARRIER
THIN CONNECTIVE
TISSUE
Not only can intraalveolar root fractures have different types of healing, they can also have various types of sequelae, such as:
-Pulp canal obliteration
-Internal resorption
-External resorption
-Loss of crestal bone
INTERNATIONAL ASSOCIATION OF DENTAL TRAUMA GUIDELINESCLINICAL EXAMINATION
RULE OUT MAXILLOFACIAL; ALVEOLAR FRACTURE AND CROWN FRACTURES
PERFORM NEUROLOGICAL EVALUATION AND RULE OUT POSSIBLE CRANIAL NERVE INJURIES
PERFORM MOBILITY, PALPATION PERCUSSION AND VITALITY TESTS; RADIOGRAPHIC ASSESSMENT
VITALITY TEST POSITIVEIF NEGATIVE, SPLINT, WAIT,AND REPEAT
SPLINT AND KEEP ON FOLLOWUP
P
R
O
T
O
C
OL
.
13
NEGATIVE EVEN AFTER 6-8 WEEKS
Treat the coronal fragment
endodontically
Treat the coronal fragment and
surgicallyremove the apical fragment.
PERFORM SPLINTING OF CORONAL FRAGMENTS IF NOTABLE MOBILITY IS THERE (NO MORE THAN 4 WEEKS)
Treat both the coronal and apical
(Fragments if in proper approximation)
Remove the coronal fragment and
endodontically treatthe apical fragment
NEGATIVE VITALITY TEST
Intra-radicular splints
Signs of non
healing
FOLLOW-UP AT 3, 6, 12 MONTHS
PERFORM ENDODONTIC TREATMENT
Apical fragment is restorableand will result in an acceptable
crown-to-root ratio after acrown is fabricated (at least 1:1)
If apical fragment is non-restorable
Crown lengthening
Orthodontic extrusion
Forced Surgical Extrusion
Apical endodontic treatment and crown
placement afterwards
FOLLOW-UP AT 3, 6, 12 MONTHS
Signs of Non-Healing
EXTRACTION
Remove the coronal fragment and
endodontically treatthe apical fragment
Conclusion (1/2)
A functional and aesthetic outcome following treatment is achieved by a combined therapy, including restorative, endodontic, prosthodontic, periodontal and orthodontic therapies.
The clinician should have a thorough knowledge of aetiological cause of fracture, classic signs and symptoms of fracture, availability and applicability of diagnostic methods, differential diagnosis, and factors determining the prognosis, so as to arrive at an appropriate diagnosis and design a suitable treatment protocol.
A regular follow-up of teeth is required to evaluate the success of treatment,
The pros and cons of a tedious and long conservative therapy should always be weighed against the option of extraction and replacement with other fixed prosthesis.
EXIT KARDU MAMEX
THANKYOU

.
1
1
NONCARIOUS TOOTH
LESION AND ITS
MANAGEMENT Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
2
CONTENTS
➢Introduction
➢Attrition
➢Abrasion
➢Erosion
➢Abfraction
➢Localized Non- Hereditary Enamel Hypocalcification
3
➢Localized Non- Hereditary Dentin Hypolpasia
➢Localized Non- Hereditary Dentin Hypocalcification
➢Fracture lines
➢Amelogenesis imperfecta
➢Dentinogenesis imperfecta
➢References
➢conclusion
INTRODUCTION
4
✓Teeth play a significant role in mastication, phonetics and
esthetics.
✓Dental structure is a mineralized tissue that undergoes a
dynamic process of remineralization and demineralization
in oral cavity.
5
✓In response to chemical challenges and mechanical adversities,
such as erosion, abrasion, attrition, and abfraction, irreversible
loss of mineral components from dental tissue occurs.
✓However, in most cases, a combination of factors results
in tooth surface loss and poses diagnostic and
etiological challenges.
6
Tooth surface loss’ or ‘tooth wear’ refers to the pathological loss of tooth tissue by a disease
process other than dental caries.
-Eccles, 1982

.
2
Although decay is the usual cause of tooth destruction necessitating
operative procedures , it has been estimated that
25% of tooth destruction does not originate from a carious process .
7
Etiology of the non carious tooth surface lesions include
•Attrition• Abrasion•Erosion•Abfraction•Localized Non- Hereditary Enamel Hypocalcification•Localized Non- Hereditary Dentin Hypolpasia•Localized Non- Hereditary Dentin Hypocalcification•Fracture lines•Amelogenesis imperfecta•Dentinogenesis imperfecta
8
ATTRITION
Attrition is defined as the loss of enamel, dentin, or restoration by tooth-to-tooth contact
-Pindborg, 1970
Defined as the mechanical wear of the incisal or occlusal surface as a result of functional or parafunctional movements of
mandible (tooth to tooth contacts).
-Sturdevant.
9
It is an age dependent ,continuous process usuallyphysiologic.
-Marzouk
10
Attrition can predispose to or precipitate any of the following
✓Proximal surface attrition (Proximal surface facets)
11
✓Occluding surface attrition ( Occlusal wear)
➢If loss is severe & accomplished in
a relatively short time
➢If the loss occurs over a long period
12

.
3
If the loss is severe & accomplished in a relatively
short time
no chance for alveolar bone to erupt occlusally to compensate for
occlusal tooth loss & therefore vertical loss might be imparted to face
overclosure during mandibular functional movements & strainareas on stomatognathic system
13
If loss occurs over a long period
Alveolar bone can grow occlusally, bringing teeth to their original
occlusal termination i.e vertical dimension loss will be
confined to teeth but not imparted to face
14
CLINICAL PRESENTATION
✓Flattened occlusal surfaces
✓ degree of wear in both arches is normally equal
✓presence of hypertrophic masseter is a warning
sign of the impact of bruxism
15
✓TMJ problems can be elicited especially by over closure
situation ( will overstretch the joint ligaments ).
✓When surface attrition is slower & compensated by deposition of secondary & tertiary dentin, then there will be no pulpal
exposure but when attrition is faster than
dentine deposition leading to direct pulpal exposure.
16
✓Pulpally involved teeth
✓Para functional activities ,( bruxism)
➢Endodontic therapy /extraction
➢Protecting occlusal splints
17
✓Occlusal equilibration should be performed by
➢Selective grinding
➢creating adequate overlap between working inclines to prevent further cheek biting
➢Any exposed sensitive dentin should be protected
18

.
4
Restorations are only needed in the following situations:
✓Progressive loss of tooth structure is observed
compromising the tooth strength .
✓Noticeable loss of vertical dimension
✓Caries ,if present
✓A tooth is cracked or endodontically treated
19
RESTORATIVE TREATMENT
✓Less severe anterior wear can be treated with adhesive
composite resin.
Strassler HE, Kihn PW, Yoon R. Conservative treatment of the worn dentition with adhesive composite resin. Contemp Esthet Restor Pract. 1999
20
When the wear is more severe, a number of treatment modalities are available.
Ibsen RL, Ouellet DF. Restoring the worn dentition. J Esthet Dent. 1992;4:96-101.
✓In some cases, incisal edges can be restored to original vertical dimension with direct composite resin.
Strassler HE, Kihn PW, Yoon R. Conservative treatment of the worn dentitionwith adhesive composite resin. Contemp Esthet Restor Pract. 1999)
✓Bonded porcelain veneers have been used to treat incisal wear
21
✓Hemmings and coworkers reported on restoration of severe anterior wear with composite restoration including
reestablishment of occlusal vertical dimension and reported a 89.4% success at 30 months.
Hemmings KW, Darbar UR, Vaughan S. Tooth wear treated with direct composite restorations at an increased vertical )dimension: results at 30 months. J Prosthet Dent. 2000;83:287-293.
22
✓Adhesive cast metal restorations have also been used to
replace missing tooth structure.
Nohl FS, King PA, Harley KE, et al. Retrospective survey of resinretained cast-metal palatal veneers for the treatment of anterior palatal tooth wear. Quintessence Int. 1997
✓In cases where occlusion is severely altered by attrition only
treatment choice may be a reconstruction withcrowns and bridges
Stewart B. Restoration of the severely worn dentition using a systematized approach for a predictable prognosis. Int J Periodontics Restorative Dent. 1998;18:46-57.)
23
✓Most involved treatment modality is regaining lost vertical dimension
✓It gives an estimate up to what should be height of
worn clinical crowns be increased
✓ Amount of V.D. lost is estimated .
24

.
5
✓Hence , if a substantial increase in dimension is to be
considered (>2mm), it is wise to build a temporary restoration or removable occlusal splint that can be easily adjusted through
subsequent addition or removal of material .
25
✓An acrylic splint ( as a stabilization splint) may be necessary
to protect dentition from further damage due to attrition
and this is frequently only treatment required to
prevent further tooth tissue loss .
26
Endodontic considerations
✓In certain cases intentional endodontic therapy has to be performed in hypererupted
teeth or drifted teeth worn that have to reduced
drastically that pulp is certain to be
involved.
27
TREATMENT STRATEGIES
FOR DENTINAL
HYPERSENSITIVITY
28
Nerve desensitizationAnti-inflammatory
agents
Covering or plugging
dentinal tubulesLasers
Restorative materials
29 30
ABRASION
✓Abrasion is the loss of tooth substance from factors other than tooth contact.
-Pindborg, 1970
✓Abnormal tooth surface loss resulting from direct frictional forces between the teeth and external objects or from frictional
forces between contacting teeth components in the presenceof abrasive medium.
-Sturdevant 5 th edition

.
6
31 32
CAUSES OF ABRASION
33
IATROGENIC CAUSES
34
Notching in right central
incisor caused by improper
use of bobby pins
Tooth brush abrasion results in a
horizontal cervical notches on the
buccal surfaces of exposed
radicular cementum and dentin .
35
THE CLINICAL SIGNS AND
SYMPTOMS OF ABRASION
36
surface of the lesion is extremely smooth and
polished and seldom has any plaque
accumulation or caries activity
in it .
Probing or stimulating lesion can
elicit pain .
Hypersensitivity may be intermittent in
character appearing and disappearing at
occasional or frequently repeated
periods .

.
7
37
TREATMENT MODALITIES
38
Diagnose the cause
of the presented
abrasion
Avoidance or
counteraction of
causes
detailed history
should be taken
Instituting proper
oral hygiene
measures.
39
If the lesions are multiple, shallow( not exceeding 0.5 mm in
dentin) and wide no need to restore them
exceeds 0.5 mm into dentin
restoration is performed
40
If restoration is not indicated for a lesion, then :
Edges of defect should be eradicated to a smooth
Tooth surface then should be treated by fluoride
solution
to improve caries resistance
If the involved teeth extremely sensitive:Desensitize the exposed dentin before restoration
41
RESTORING CERVICAL
ABRASIONS
42
restoration is indicated when-
✓Caries, if present
✓Sensitivity is present
✓Esthetically objectionable
✓Contributes to a periodontal problem
✓When the depth of defect is found to be close to pulp

.
8
43
Restorative materials-
44
✓High modulus restorative materials are unable to flex in
cervical regions when tooth structure is deformed under
occlusal load and therefore restorative materials
can be displaced from cavity .
Heymann HO, Sturdevant Jr, Baynes S ,JADA,122(2) 41-57
45
✓An intermediate material with reduced elastic modulus may function as a stress absorbing layer and
improve marginal sealing
Kemp-Scholte CM ,Davidsson,CL complete marginal seal of class V resin composite restorations affected by increased flexibility .JDR 1990 ;69:1240 -3
46
CONCLUSION-
✓Retention levels at 2 years were 90% for F2000, 90% for DyractAP, 89% for Compoglass F, 84% for Elan, and 95% for Vitremer
restorations. No statistically significant differences were found among materials after 2 years for any
evaluation category
Two-year clinical evaluation of four polyacidmodified resin composites and a resin-modified glass-ionomer cement in Class V abrasion/erosion lesions. Ermiş RB.. Quintessence Int. 2002 Jul- Aug;33(7):542-8
47
5-year clinical performance of resin composite versus resin modified glass ionomer restorative system in non-carious cervical lesions. Franco Eb, Benetti A , SK Ishikiriama,SL Santiago,JRP Lauris
CONCLUSION -
✓After 5 years of evaluation clinical performance of resin modified glass ionomer restorations was superior to resin composite
restorations.
48
EROSION
✓Loss of surface tooth structure by chemical action in
continued presence of demineralizing agents.
-Sturdevant- 5 th edition
✓Erosion is loss of dental hard tissues by chemical
action not involving bacteria
-Eccles, 1982

.
9
49
Most predominant oral pathologic changes
50
Multiple factors have been theorized for its pathogenesis-
✓Mechanical factors
✓Chemical factors
51
Clinical presentation-
Extensive loss of buccal andocclusal tooth structure
Occlusal view of maxillary dentition
exhibiting concave dentin depressions
surrounded by elevated rims of enamel
52
Multiple cupped out depressions
corresponding to the cusp tips
Extensive loss of enamel and
dentin on Buccal surface of
maxillary bicuspids.
53
Perimylosis-
✓Decalcification of teeth caused by exposure to gastric acid in patients with chronic vomiting as
may occur in anorexia or bulimia
54
Eating disorders-
✓Anorexia
✓Bulimia nervosa
✓Rumination
✓Chronic alcoholism
.
10
55
✓ Any food substance with a critical pH value of less than 5.5 can become a corrodent and
demineralize teeth
( Stephan RM, JADA 1940) ,( Gray JA, J Dent Res 1962) ,(Zero DT. Cariology. Dent Clin North Am 1999)
✓As reported by Lussi corrosive potential of an acidic drink does
not depend exclusively on its ph value, but also is strongly
influenced by its buffering capacity of the acid and by
frequency and duration of ingestion.
Lussi A. Dental erosion: clinical diagnosis and case histor taking. Eur J Oral Sci 1996
56
PROTOCOL FOR PREVENTION
OF PROGRESSION OF EROSION
57
✓Diminish the frequency and severity of acid challenge
✓Treating underlying medical disorder or disease
✓Enhance defense mechanisms of body:
✓Enhance acid resistance, remineralization and
rehardening of the tooth surfaces.
GERD ,anorexia ,bulimia →
refer to a
physician/psychologists
Daily use topical flouride at home.
Fluoride application in office- 2-4 times
a year, flouride varnish recommended.
58
✓Improve chemical protection
✓Mechanical protection
✓Monitor stability
• Neutralize acids in mouth dissolving sugar free
antacid tablets 5 times a day ,particularly after an
intrinsic or extrinsic acid challenge.
• Dietary components- hard cheese ( provides Ca
and PO4), held in mouth after acidic challenge.
•Composites and direct bonding where
appropriate.
•Occlusal guard /Acrylic splint in the form of
stabilization splint
•By use of casts /photos to document tooth
wear status.
• Regular recall examinations to review diet,
oral hygiene methods, compliance with
medications, topical flouride and splint usage.
59
RESTORATION
✓Metallic restorations should be the choice of material if
restoration indicated .
✓Tooth colored materials may also be used with minimal or
no tooth preparation, with assumption that restoration may
require periodic replacement
60
ABFRACTION
✓Abfraction means ‘to break away’
-Braem et al.,1992
✓Rupture of chemical bond between hydroxyapetite crystals is
termed as Abfractures
-Grippo JO,1991: Levitch LC , Bader JD, Heymann HO ,1994

.
11
61
✓When tooth is loaded in long axis forces are dissipated with
minimal stress on enamel and dentin
✓If direction of force changes laterally ,teeth are flexed
towards both sides
✓compresssive ↔ tensile
reaches to fatigue limit
Abfractures occurs62
✓Most commonly in cervical regions
of tooth
✓Resulting defect has a smooth surface
✓Also known as Idiopathic erosion
Lee WC, Eakle WS, J Prosthet Dent 52(3): 374-380, 1984
63
✓Stresses that concentrate to produce abfractions in teeth
usually are transmitted by occlusal loading forces .
✓Occlusal interferences, premature contacts, habits of bruxism
and clenching all may act as stressors
Whitehead SA, Wilson NHF, Watts DC. J Esthet Dent 2000),(Pintado MR, DeLong R, Ko C, Sakaguchi RL, Douglas WH. Correlation J Prosthet Dent 2000
64
Monitoring abfraction lesions-
A novel method of determining the activity of abfraction lesions
over time - Scratch test
Kaidonis JA.The tooth wear :view of anthropologists ,Clin Oral Investing 2008
65
Restoration
✓Tyas recommended the RMGIC should be the
first preference
Tyas MJ,the class V lesion –aetiology ,restoration,Aust. Dental Journal.1995
✓use of microfilled resin composite (low modulus of
elasticity ) as it will flex with tooth and not
compromise retention
Vandelwalle and Vigil ( Gen Dent 1997)
66
Occlusal adjustments
✓Occlusal adjustment may involve
➢Reducing heavy contacts
➢Removing premature contacts
Piotrowski BT JADA 2001 and Ichim IP Dent Mater 2007
.
12
67
✓Occlusal splints
68
CLINICAL DIFFERENTIATION
OF EROSIVE LESIONS FROM
OTHER TYPES OF TOOTH
WEAR
69 70
71
FRACTURE LINES
72
✓Physical trauma
✓Occlusal prematurities
✓Repetitive heavy and stressful chewing
✓Resorption weakened teeth
✓Iatrogenic dental treatment
.
13
73
FIVE TYPES OF LONGITUDINAL FRACTURES
✓Craze line
✓Fractured cusp
✓Cracked tooth
✓Vertical root
✓Split tooth
74
Cracked tooth
✓Described as acute pain that resultsduring mastication (or release) of small hard food
substances and also exacerbates with cold.
Cameron CE,JADA,1964 : American Association of Endodontists,2008
75
TWO MAIN GROUPS OF CRACKED TEETH :
Tooth infarctions
Craze lines
Cuspal fractures
Cracked teeth
Vertical root fractures
76
Clinical test
✓Patient bites onto the moist cotton roll
and on release the pain will often be quite noticeable .
77
Etiology
✓Excessively large and incorrectly designed
restorations.
✓Use of pins for supporting large restorations
esp. self threading and friction locked.
✓Abrasion ,erosion ,caries ,along with age
changes in dentin.
✓Biting onto hard objects ,bruxism and
clenching, wedging effect.
78
Clinical examination
✓Begins with the chief complaint i.e. pain on chewing, elevated
sensitivity to cold food and sweets.
✓Absence of carious etiology trigger a suspicion of infarction.
✓Visual examination by Transillumination and Dyes
(methylene blue).
✓Any existing restoration in tooth should be removed to reveal
infarction lines.
.
14
79
✓Removal of restoration and highlighting with dye to detect crack
80
✓Use of optic light source to identify an infarction.
✓Beam of light does not cross the infarction.
81
Treatment
✓Not clear whether all teeth with infarction require root
canal therapy, it depends on extent of fracture .
✓Treatments designed to bind infarcted segments of
teeth together that includes use of adhesives, full
coverage crowns .
82
LOCALIZED NONHEREDITARY
ENAMEL HYPOPLASIA
83 84
.
15
85
LOCALIZED NONHEREDITARY
ENAMEL HYPOCALCIFICATION
86
87
LOCALIZED NON HEREDITARY
DENTIN HYPOPLASIA
88
89
LOCALIZED NON-HEREDITARY
DENTIN HYPOCALCIFICATION
90

.
16
91
AMELOGENESIS IMPERFECTA
92
93 94
95
Case report
✓An 8-year-old patient referred to Reference Centre of Rare Diseases,
Paris. Her medical and familial history revealed no etiologic explanation
and main complaint was extreme sensitivity to
hot and cold
96
Oral clinical exam showed
✓A mixed dentition, with eruption of permanent incisors and
first molars.
✓Hypomineralized AI was diagnosed.
✓Enamel was dark yellow in permanent teeth and brown in
primary teeth.
✓Panoramic radiograph showed a reduction in
the enamel thickness
.
17
97
Multidisciplinary treatment objectives taken into account at this
age were:
✓Preservation of tooth integrity and vitality of permanent teeth
emerged in the oral cavity
✓Non-invasive rehabilitation that allowed evolution during growth
✓Restoration of smile aesthetics
✓Normalization of oral function (mastication, respiration,
swallowing)98
99
DENTINOGENESIS
IMPERFECTA
100
101 102
CONCLUSION
✓Tooth surface loss and the resulting non-carious lesions are
issues that can be difficult to diagnose correctly and treat
successfully.
✓The etiology of tooth surface loss can be determined
by reviewing the potential causes for each patient and by
observing the pattern of wear, as the loss is exhibited in different
patterns and on different surfaces of the teeth for varying types of
tooth surface loss.
✓Determining the etiology and preventing further tooth surface
loss,which requires using proper preventive methods,good
management, and the appropriate restorations, is necessary for
restorations to be
successful.

.
18
103
References
104
THANK YOU
.
1
Problems in achieving pain control
Dr Prachi Mital
Department of
Conservative Dentistry
and Endodontics
Contents
✓Introduction✓History of pain✓Theories of pain
✓Pain Management
✓Problems in achieving pain control✓Future trends in pain control✓Conclusion✓References
•Problem of managing pain and anxiety in the practice of dentistry is significant one.
•Pain introduced by dental treatment can usually be minimised and entirely prevented through thoughtful
patient management and judicious use of techniques of pain control.
Introduction
•According to Monheims- Pain is defined as unpleasant
emotional experience usually initiated by a noxious stimulus and transmitted over a specialised neural network to Central nervous
system where it is interpreted as such
Definition
• According to Dorlands medical dictionary defined as a more
or less localized sensation of discomfort, distress
or agony resulting from the stimulation
of specialised nerve endings.
History of pain
• Greek word poin-means penalty
• Latin word poena- Punishment from God
• Aristotle first to distinguish five physical senses. Considered pain to be “passion of the sole”

.
2
Neurophysiology of painTransduction
Perception
Modulation
Trasmission
THEORIES OF PAIN
✓Specificity theory
✓Pattern theory
✓Gate control theory
Gate control theory
✓Melzack & Wall, 1965
✓Substantia Gelatinosa (SG) in dorsal horn ofspinal cord acts as a ‘gate’.
✓If A-beta neurons are stimulated – SG is activated which closes the gate to A-delta & C neurons
✓If A-delta & C neurons are stimulated – SG is blocked which closes the gate to A-beta neurons
✓Gate - located in the dorsal horn of the spinal cord
✓Smaller, slower n. carry pain impulses
✓Larger, faster n. fibers carry other sensations
.
3
✓Impulses from faster fibers arriving @ gate inhibit pain impulses (acupuncture/pressure, cold, heat, chem.
skin irritation).
Orofacial pain fibers
Etiological classification of pain

.
4
Based on onset, duration and quality of pain
Pain Management:
✓Blocking the path of pain impulses
✓Removing the cause
✓Raising the pain threshold
✓Cortical depression
✓Psychosomatic Methods
.
5
PROBLEMS IN ACHEIVING PAIN CONTROL
✓Local anesthetics (LA) are the safest and most effectivedrug in medicine for the prevention and
management of pain.
✓If LA are so effective, then whydo we encounter problems achieving profound pulpal
anesthesia? Where do these problems happen? and how can inadequate pulpal anesthesia
be prevented or corrected?
✓More common in the mandible:
8.2% - incisors11.5% - canines30.5% - premolars55.3% - molars
✓Maxillary teeth
19% - lateral incisors20% - canines
15% - first premolars 17% - first molars
-HANDBOOK OF LOCAL ANESTHESIA, SEVENTH EDITION
•Failure of LA injection can be classified as
✓Operator dependent
• Choice of technique and solution• Poor technique
✓Patient dependent
• Anatomical• Pathological• Psychological.
Choice of techniqueChoice of solution
.
6
Poor technique
✓Most likely defect in technique is faulty needle placement
✓Speed at which the solution is deposited There is evidence in
the surgical literature that the success of some techniques is increased with slower injection speeds
Rucci F S, Pippa P, Boccaccini A, Barbagli R. Effect of injection speed on anaesthetic spread during maxillary block using the orthogonal two-needle technique. Eur J Anaesth 1995; 12: 505-511.
Maxillary Incisors, Canines, and Premolars
•Primary Techniques for Pulpal Anesthesia:
✓ One or two maxillary anterior teeth - Infiltration
✓Multiple anterior teeth - Anterior superior alveolarnerve block
✓Premolar teeth - Middle superior alveolar nerveblock
In 15% of adults 15% of this 15%
Why do we miss?
Have exceedingly thick bone in this area minimizing the success of
infiltration anesthesia
cortical plate of bone overlying the maxillary anterior teeth will be
thicker than normal
maxillary canine (20%) central incisor
underinsertion of the needle with deposition of the anesthetic
solution below the apex of the tooth.
root apex of a CI is locatedunder cartilage and bone of the nasal
cavity, minimizingsuccess of infiltration anesthesia.
Another reason for anesthetic failure following infiltration
possible solutions
✓anterior superior alveolar nerve block
provides pulpal anesthesia to the maxillary incisor, canine, and in most premolar teeth.
✓Use of a buffered LA solution
✓Infiltration anesthesia using (buffered) articaine hydrochloride.
✓Intranasal local anesthetic mist for pulpal anesthesia of maxillary
nonmolar teeth.
$527.99
.
7
Maxillary Molars
✓Most used technique – infiltration
✓When treatment includes several maxillary molar teeth – PSA nerve block
Why do we miss?
✓Radicular anatomy of the maxillary first and
second molars
✓Thickness of the cortical plate of bone overlying the molar teeth
palatal root of a molar deviates (“flares”) more toward midline than usual—most injected LA
will successfully block two buccal roots but not palatal root.
possible solutions
✓PSA provides pulpal anesthesia to maxillary molar
teeth regardless of anatomy of their roots
✓Use of a buffered LA solution.
✓Supplemental anesthesia
Mandibular Teeth
Incisors, Canines, and Premolars
✓Primary Technique for Pulpal Anesthesia - infiltrationanesthesia with a rather low success rate
✓IANB - most often used for any and all treatment
of mandibular teeth.
Why do we miss
✓IANB has a rather high failure rate in mandibular incisors, canines, and premolars
✓lack of definitive and consistent anatomy from patient to patient

.
8
infiltration
thickness of the cortical plate of bone in mandible
possible solutions
✓Incisive nerve block When multiple mandibular nonmolar
teeth are being treated
✓use of a buffered LA solution
✓Buccal infiltration of (buffered) articaine
Mandibular molars
✓ Primary Technique for Pulpal Anesthesia
IANB - most commonly used
Possible solutions✓Slow administration of LA solution has been
shown a higher success rate
✓use of a buffered LA solution
✓Supplemental injection techniques, including PDL injection, intraseptal injection, and intraosseous injection
.
9
✓Buccal infiltration of (buffered) articaine as a supplement to a previously administered IANB
Kanaa JM, Whitworth JM, Corbett IP, Meechan JG. Articaine buccal infiltration enhances the effectiveness of lidocaine inferior alveolar nerve block. Int Endod J. 2009;42:238–246.
✓Buccal infiltration of (buffered) articaine at apex of mandibular molar to be treated as sole technique of anesthesia
has been demonstrated to be quite successful
Robertson D, Nusstein J, Reader A, Beck M, McCartney M. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J Am Dent Assoc. 2007;138:1104–1112.
Individual variations in the position of nerves and foramina
Accessory nerve supply
Barriers to anaesthetic
diffusion
Anatomical causes of failure ofanaesthesia
Accessory nerve supply
✓Accessory nerve supply can lead to failure of anaesthesia following both infiltration and regional block methods.
✓Pulpal supply to upper molar teeth may arise from the greater palatine nerves and a buccal infiltration is unlikely to affect
transmission by this source.
✓Similarly maxillary anterior teeth can receive innervation from naso-palatine nerve.
✓Solution for both these cases is a palatal injection.
✓When removing third molar teeth despite an apparently
effective lingual block distolingual gingivais not anaesthetised.
✓This accessory supply is readily countered by injecting just distolingual to third molar.
✓A classic example is failure of inferior alveolar or mentaland incisive nerve blocks to anaesthetise
a lower central incisor.
✓Alternatively, an infiltration, intraligamentary or intraosseous injection may be administered
at outset in this area.
✓first molar can obtain supply from both posterior and middle
superior alveolar nerves a posterior superior alveolarnerve block may be unsuccessful

.
10
Barriers to anaesthetic diffusion
✓Thick cortical plate of mandibular alveolus
✓First molar region in adult maxilla occasionally presents a similar problem because of thick zygomatic buttress
can prevent passage of anaesthetic todental apices.
✓Solution to this problem is to inject mesial and distal to first molar away from buttress
Pathological causes of failure ofanaesthesia
•Buccal infiltrations in maxilla are possible with mouth closed.
•To anaesthetise palatal tissues –inject toward the palate through the mesial and distal gingival papillae from buccal side.
•To achieve inferior alveolaranaesthesia - use Akinosi technique
✓Trismus
✓anatomical changes because of trauma or surgery
Inflammation
✓low tissue pH in areas of inflammation affects activity of LA solution by decreasing concentration of the unionised
(lipophilic) fraction which diffuses
✓through nerve sheaths.
✓Similarly areas of inflammation have an increased blood supply due to vasodilatation and this might increase
anaesthetic ‘wash-out’.
.
11
✓However, these answers do not explain the failure ofregional block techniques where the solution may be deposited 4
or 5 cm from area of inflammation.
✓Most plausible explanation is that inflammation makes nerves hyperalgesic.
Rood J P, Pateromichelakis S. Local anaesthetic failures due to an increase in sensory nerve impulses from inflammatory sensitization. J Dent 1982; 3: 201-206.
possible solutions
✓Supplemental Local Anesthesia
➢By increasing the dose of LA one could expose a greater
length of IAN and increase the likelihood of conduction blockade.
➢Increased dosage would also help to block population of TTX-resistant sodium channels that may be elevated in
inflamed state .
✓By using an anesthetic with a lower pKa, such as 3%mepivacaine, one could decrease the potential for ion trapping.
This would increase the concentration of local anesthetic molecules in the base form necessary for diffusionacross the nerve membrane, enhancing blockade
and increasing onset of anesthesia.
✓supplemental anesthesia includes Intraligamentary, intraosseous , intrapulpal injection.
Adjunctive Drugs or Techniques
✓Reduction of PGE2 could be accomplished with either NSAIDS or steroids, injectable NSAID, ketoroloac, tromethamine, when
injected intraorally or intramuscularly, produces significant analgesia in patients with severe odontogenic pain prior to
definitive treatment.
✓Ibuprofen in a liquid gel formulation (e.g. Advil LiquidGel A (White-Hall Robbins, Madison, NJ))
may have similar effects.
Gallatin E, Reader A, Nist R, Beck M. Pain reduction in untreated irreversible pulpitis using an intraosseous injection of Depo-Medrol. J Endod 2000: 26: 633–638.
✓In patients with a diagnosis of irreversible pulpitis, a double-blinded, randomized clinical trial showed that, for
7 day period preceding endodontic therapy, subjects that received an intraosseous injection of managing
LA failures 40mg methylprednisolone experienced significantly less pain and requiredsignificantly less pain medication than those
receiving the placebo .Psychological causes of failure
.
12
✓There are undoubtedly patients who do not do well with local anaesthesia but in whom the local anaesthetic
appears to have been effective.
✓This may be because of fear and apprehension. In such patients use of sedative techniques can be helpful as successful
anaesthesia is easier to achieve in the relaxed patient.
✓Benzodiazepines offer added bonus of reducing local anaesthetic toxicity which is useful when multiple
injections are being administered.
Strategies for the Patient With a ‘‘Hot’’ Tooth
✓When one considers the challenges of local anesthesiain dentistry, mandibular teeth pose most
severe challenge.
✓When the clinician is confronted with the case of a severe irreversible pulpitis in which the conventional IANB using 2%
lidocaine with 1:100,000 epinephrine achieveslip numbness but not pulpal anesthesia
possible solutions
Mandibular Buccal Infiltration
Injection with Articaine
✓Mannitol
Combination of 0.5 M mannitol and lidocaine with epinephrine in Inferior Alveolar Nerve Blocks exhibits higher
anesthetic efficiency compared to lidocaine and epinephrine alone
Ronald Wolf, Al Reader, Mike Bek. Anesthetic efficacy of combination of 0.5 M mannitol and lidocaine with epinephrine in IANB: A prospective randomized –singleblind study. Anesthetprog Winter. 2011;58(4):157-165.
In conclusion, the present meta analysis showed that in patients receiving dental therapy, buffered local anesthetics are more effective than non-buffered solutions when used for mandibular or maxillary anesthesia. Buffering local anesthetics has 2.29 times greater likelihood of achieving successful anesthesia.

.
13
Supplemental intraseptal injection of 2% lidocaine and buccalinfiltration of 4% articaine achieved profound pulpalanaesthesia in 69% of patients when the inferior alveolar nerveblock failed. Recommendations can be given to dentalpractitioners to use infiltration of 4% articaine in conjunctionwith intraseptal injection of 2% lidocaine to anaesthetize thelower molar teeth when inferior alveolar nerve block fails
broad arrows in show the ‘blunderbuss’ approach to the tooth which has proved resistant to local anaesthesia in the past
The flow diagrams for management of failure in maxilla
Future trends in pain control
✓Longer- and ultra-long-acting local anesthetics
➢Naturally occurring site-1 selective sodium Channel blockers➢New local anesthetic delivery systems➢Novel Adjutants of Local Anesthetics
✓Light-Activated, Light-Inactivated Local Anesthesia
Naturally Occurring Site-1 Selective Sodium Channel Blockers
✓Similar to the “traditional” LA Tetrodotoxin (TTX), saxitoxin (STX), and neosaxitoxinNeoSTX) are selective sodium
channel blockers
✓these compounds can act in a synergisticmanner with traditional LA
.
14
✓NeoSTX and TTX provide longer durations of anesthesia than traditional LA. When TTX is administered in combination
with bupivacaine and epinephrine, significant increases in duration are noted. Additionally, these compounds
are devoid of cardiotoxicity (NeoSTX) and have minimal myotoxicity and
neurotoxicity (TTX).
New Local Anesthetic Delivery Systems
✓Nanoparticles and liposome microparticleshave been used to enhance both the duration and
the safety of LA.
Novel Adjutants of Local Anesthetics
✓Magnesium has received considerable attention as
a LA adjuvant in recent years.
✓Addition of magnesium to LA provides a longer duration of anesthesia, lowers patient pain scores and in some
studies, lowers Opioid requirements when used
in combination with bupivacaine.
Light-Activated, Light-Inactivated Local Anesthesia
✓A new option, developed by researchers at University of California, Berkeley, University of Munich, and University of
Bordeaux involves a novel LA that can be switched on and off with the use of different wavelengths of light,
potentially allowing much finer control of exactly which nerves it blocks
✓Chemically, quaternary ammonium azobenzene–quaternary ammonium (QAQ) resembles
lidocaine. ✓Ability to provide location-specific pain control without additional
involvement of motor nerves would be a welcome addition tothe management of patients with chronic pain syndromes.
Further as most dental treatments are not associated with postoperative pain, the ability to “switch off”
anesthesia at the end of treatment would be
appreciated by most dental patients.

.
15
Conclusion
✓The pain in endodontics has various dimensions and their causes may be similar or may even vary, but for effective management
of endodontic pain removal of causative factors and treatment methods should be taken into proper
consideration to help the patient get relievedof unpleasant sensation of pain.
✓Once a definitive diagnosis is obtained, the primary approach of pain management is through rational pharmacotherapy.
Future directions include innovations in routes of pharmacotherapy that will not only augment efficacyof medication but also allow for combination therapy
with fewer adverse effects and greater prolongation of relief.
✓Future directions will also involve evidence-basedinterprofessional collaboratives that provide both
pharmacologic paradigms as well as nonpharmacologicmodalities for optimal pain relief.
References
THANK YOU