
Overcoming Skin Problems in Jejunostomy and Ileostomy by ...

JOURNAL OF THE EXPERIMENTAL ANALYSIS OF BEHAVIOR
AN OPERANT APPROACH TO REHABILITATION MEDICINE:OVERCOMING LEARNED NONUSE BY SHAPING
EDWARD TAUB, JEAN E. CRAGO, Louis D. BURGIO, THOMAS E. GROOMES,EDWIN W. COOK, III, STEPHANIE C. DELUCA, AND NEAL E. MILLER
UNIVERSITY OF ALABAMA AT BIRMINGHAM, YALE UNIVERSITY, ANDTHE ROCKEFELLER UNIVERSITY
A new approach to the rehabilitation of movement, based primarily on the principles of operantconditioning, was derived from research with deafferented monkeys. The analysis suggests that acertain proportion of excess motor disability after certain types of injury involves a learned suppressionof movement and may be termed learned nonuse. Learned nonuse can be overcome by changing thecontingencies of reinforcement so that they strongly favor use of an affected upper extremity in thechronic postinjury situation. The techniques employed here involved 2 weeks of restricting movementof the opposite (unaffected) extremity and training of the affected limb. Initial work with humans hasbeen with chronic stroke patients for whom the approach has yielded large improvements in motorability and functional independence. We report here preliminary data suggesting that shaping withverbal feedback further enhances the motor recovery.
Key words: shaping, training, restriction, somatosensory deafferentation, stroke, rehabilitation med-icine, impaired movement, monkeys, humans
This article describes a new approach to therehabilitation of movement in physical medi-cine. It is based in its essential features on theprinciples of operant conditioning. It is fittingthat it appear in a tribute to Joseph V. Brady,because he persuasively endorsed the relevanceand importance of applying the principles ofthe experimental analysis of behavior to newareas and in this way strongly influenced thedevelopment of this work.
It is appropriate that this article appear in a tribute toJoseph V. Brady, because the basic approach that it rep-resents stems from research carried out with monkeys givensomatosensory deafferentation in a laboratory of the In-stitute for Behavioral Research (IBR) in Silver Spring,Maryland. Joe Brady was first a member of the Board ofDirectors of IBR and then Chairman of the Board. Theanimal rights group, People for the Ethical Treatment ofAnimals (PETA), tried to gain custodianship of the colonyof deafferented monkeys; if they had succeeded, it wouldhave set a dangerous legal precedent that would have hadserious adverse effects on the future ability to conductanimal research in the United States. As Chairman of theIBR Board of Directors and, thus, the main representativeof the owner of the monkeys, Joe Brady was subjected toan enormous amount of pressure to release the monkeysto PETA or agents that it designated. Some, but not all,of this pressure consisted of a petition demanding thisaction signed by a majority of the members of Congress,attempts at persuasion by direct contact by more than onehalf dozen members of Congress, attempts by NIH toconvince him to accede to the political pressure, and thevery negative reaction of his own university to his involve-ment in the situation. Nevertheless, Joe Brady, recognizingthe importance of the case for the future integrity of the
Experiments with Deafferented Monkeys
Although the present approach is funda-mentally behavioral, the original observationswere made in the context of studies of theneurophysiology of motor control and the roleof sensory feedback in movement and learning.The spinal nerves, which are fundamental forthese functions, emerge from the spinal cordin two roots. The dorsal root is sensory. Thus,
animal-research enterprise, responded by saying, to quotehim, "They will get those monkeys over my dead body."As a result, the monkeys were preserved so that significantexperiments could be carried out (Pons et al., 1991; Rau-sell, Cusick, Taub, & Jones, 1992). These experimentswill not be described here because their subject matter isnot directly relevant to the main theme of this paper, butthere is widespread recognition of their potential practicalimportance for the fields of cortical plasticity and physicalrehabilitation (Barinaga, 1992; Palca, 1991; Stephens,1991). Thus, Joe Brady resisted pressure that very fewcould have withstood, and thereby achieved a significantvictory for animal research on several levels. However, hisrole in this incident is largely unknown. He is an unsunghero. It is hoped that this account will help to some extentto begin to rectify this situation.
This work was supported in part by a grant from theCenter for Aging, University of Alabama at Birmingham.We thank Samuel L. Stover, Director, and Hugh S. Gainer,Administrator, Spain Rehabilitation Center, University ofAlabama at Birmingham for their help in implementingthe study. Address correspondence and reprint requests toEdward Taub, Psychology Department, University of Al-abama at Birmingham, 201 Campbell Hall, Birmingham,Alabama 35294.
281
1994, 61, 281-293 NUMBER 2 (MARCH)
EDWARD TAUB et al.
by severing all of the dorsal roots innervatinga limb, one can eliminate all sensation fromthat limb involved in the support of ongoingbehavior sequences while leaving the motorinnervation intact over the ventral root. In themonkey, when a single forelimb in a monkeyis deafferented, the animal stops making useof it in the free situation (Knapp, Taub, &Berman, 1958; Lassek, 1953; Mott & Sher-rington, 1895; Twitchell, 1954).
However, it was found to be possible toinduce a monkey to use the deafferented limbby three general types of behavioral tech-niques. One type involved restriction of move-ment of the intact upper extremity through theuse of a device that left the deafferented limbfree (Knapp, Taub, & Berman, 1963; Stein &Carpenter, 1965). Use of the deafferented limbwould usually begin within an hour of em-placing the restriction device, typically for pos-tural support while the animal was in a sittingposition. Within several hours, the limb couldtypically be used, although somewhat clum-sily, for a wide variety of activities, includingambulation, climbing, and thumb-forefingerprehension of small objects.When the restriction device was left in place
for 1 or 2 days, removal of the device resultedin a remarkable reversion to nonuse of thedeafferented limb. Even though the animalshad used their limbs quite well for a widevariety of purposes when their intact arms weresecured in the restriction device, the animalssuddenly stopped using their deafferented ex-tremities as soon as the device was removedand use of the intact limb was permitted. How-ever, when the animals were left in the intact-limb restriction device for a longer period oftime, as short as 3 days for 1 animal, the useof the deafferented limb persisted after the de-vice was removed. There was no apparentdiminution of range or quality of movementafter device removal, and this level of use con-tinued for the remainder of the animals' lives,which in one case was over 4 years (Taub,1976, 1977, 1980).A second behavioral method for overcoming
the inability to use a single deafferented limbis the application of procedures for traininguse of that limb. In initial work, conditioned-response techniques were employed for en-abling the animals to make a variety of move-ments with the deafferented limb, includingphasic forelimb flexion (Knapp et al., 1958,
1963; Taub, Bacon, & Berman, 1965; Taub& Berman, 1963,1968), grasp (Taub, Ellman,& Berman, 1966), forelimb flexion on a fixed-ratio schedule of reinforcement (Taub, Wil-liams, Barro, & Steiner, 1978), sustained limbflexion (Taub, 1976, 1977), and compensationfor progressively increasing loads on the arm(Taub, 1976, 1977; Wylie & Tyner, 1981,1989). However, generalization to natural set-tings never occurred (Taub, 1976, 1977). Themovements that were trained in the condition-ing chamber were never observed in the colonyenvironment. This lack of generalization wasclearly similar to the results obtained by re-moval of the restriction device from the intactlimb after insufficiently long periods of time.A third, even more effective training method
for inducing recovery of motor function wasfound to be shaping, in which a desired motoror behavioral objective is approached in smallsteps, by successive approximations (e.g.,Morgan, 1974; Panyan, 1980; Risley & Baer,1973; Skinner, 1938, 1968). With shapingtechniques, the animals not only learned toemploy a single deafferented limb in the train-ing situation, but its use also generalized tothe normal environment as well.The actions shaped included (a) pointing at
visual targets (Taub, Goldberg, & Taub, 1975)and (b) prehension in juveniles deafferentedon day of birth (Taub, Perrella, & Barro, 1973)and prenatally (Taub, Perrella, Miller, &Barro, 1975) who had never exhibited anyprehension previously. In both cases, shapingpermitted an almost complete reversal of themotor disability, which progressed from totalabsence of the target behavior to very good(although not normal) performance.
Learned Nonuse and OvercomingLearned Nonuse
Substantial neurological injury usually leadsto a shock-like phenomenon, whether at thelevel of the spinal cord (spinal shock) or brain(diaschisis or cortical shock). With regard todeafferentation, the elimination of somatosen-sory input results initially in a reduction inthe background level of excitation within thespinal cord that maintains neurons in a sub-liminal state of readiness to respond. This ef-fect is most marked in the deafferented seg-ments of the spinal cord, where the depressedcondition of motoneurons greatly elevates thethreshold for incoming excitation necessary to
282

OVERCOMING LEARNED NONUSE
produce movement. The early postsurgical spi-nal shock also may be partly due to activeinhibitory processes. As time elapses followingdeafferentation, recovery processes, which areat present incompletely understood, raise thebackground level of excitability of motoneu-rons so that movements can once again, at leastpotentially, be expressed. The period of spinalshock lasts from 2 to 6 months in monkeysfollowing forelimb deafferentation (Taub,1977; Taub & Berman, 1968).
Several converging lines of evidence suggestthat nonuse of a single deafferented limb is alearning phenomenon involving a conditionedsuppression of movement (Taub, 1977, 1980).The restraint and training techniques ap-peared to be effective because they altered thecontingencies of reinforcement, thereby en-abling the learned nonuse to be successfullyovercome. Thus, immediately after operation,the monkeys cannot use a deafferented limb;recovery from spinal shock requires consid-erable time. An animal with one deafferentedlimb tries to use that extremity in the imme-diate postoperative situation, but it cannot.Continued attempts to use the deafferentedlimb often lead to painful and otherwise aver-sive consequences such as incoordination andfalling, as well as to loss of food objects, and,in general, to failure of any activity attemptedwith the deafferented limb. The resultant pun-ishment leads to a conditioned suppression ofattempts to use the limb. Moreover, the animalgets along quite well in the laboratory envi-ronment on three limbs; thus, these patternsof behavior are therefore positively reinforcedand as a result are strengthened. The tendencynot to use the deafferented extremity persists,and consequently the monkeys never learn that,several months after operation, the limb hasbecome potentially useful.When the movements of the intact limb are
restricted several months after unilateral deaf-ferentation, the contingencies of reinforcementare changed dramatically. The animal eitheruses the deafferented limb or it cannot withany degree of efficiency feed itself, move about,or carry out a large portion of its normal ac-tivities of daily life. This change in the con-tingencies of reinforcement "overcomes" thelearned nonuse of the deafferented limb andinduces the animal to use it. However, if themovement-restricting device is removed a shorttime after the early display of operant move-
ment, the newly learned use of the deafferentedlimb acquires little strength and is, therefore,quickly overwhelmed by the well-learned ten-dency not to use the limb. If the movement-restriction device is left on for several days orlonger, however, use of the deafferented limbacquires strength and is then able to competesuccessfully with the learned nonuse of thatlimb in the free situation. The learned nonuseformulation has received direct experimentalsupport from two studies (Taub, 1977, 1980).
Shaping had several advantages over theconditioned-response training employed in ourearlier work that enabled generalization of newuse of the deafferented limb to the free situ-ation: (a) There was the obvious advantage ofa slow, step-wise procedure that could grad-ually lead an organism from a rudimentaryinitial response level to more complex re-sponses. By allowing the extent of progress todetermine the amount of time spent at eachstep, behavioral requirements did not exceedbehavioral capacity excessively; thus, the like-lihood of failure was reduced. (b) The re-sponses being shaped more closely resembledthose carried out in daily life in complexityand functional significance than did the typeof simple and artificial movements adopted forconvenience in the conditioning situations. (c)The shaping series took place over a muchlonger period of time and involved much moretraining than was the case in the conditioned-response situations.Shaping stands partway between our earlier
conditioned-response training and restrictingmovement of the intact limb, both conceptuallyand empirically, in its ability to enable gen-eralization from the experimental interventionto the natural environment. Although shapingand intact-limb restriction represent two dif-ferent approaches to the rehabilitation ofmovement, they are not mutually exclusive;indeed, from the outset they appeared to bepotentially complementary. These two pro-cedures were not employed jointly in the re-search with monkeys; however, it seemed rea-sonable to attempt this approach in the workwith human stroke patients described below.The mechanism of learned nonuse is de-
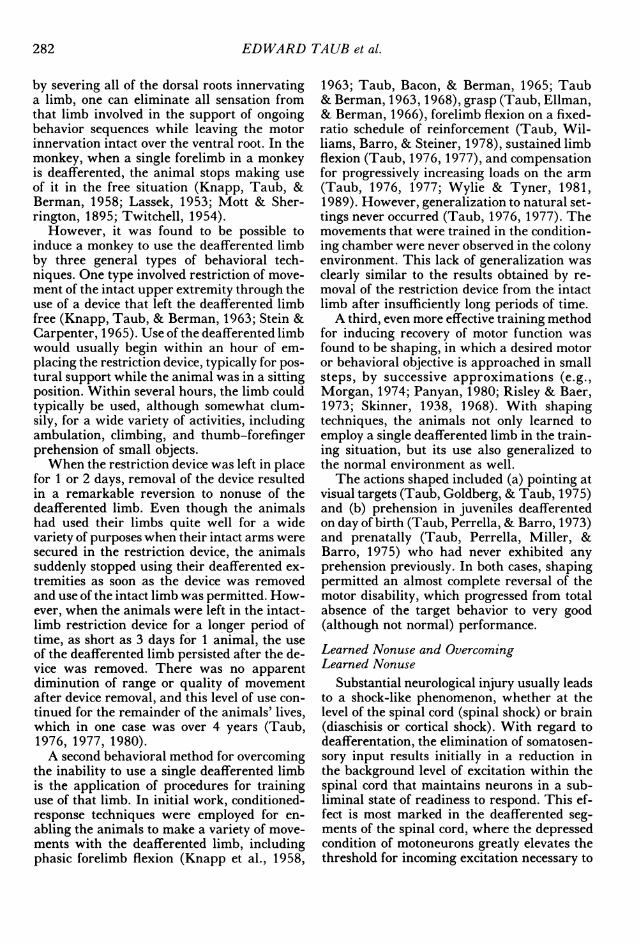
picted schematically in Figure 1, and themethod by which techniques that overcomelearned nonuse operate is presented in Figure2. These models explain the motor phenomenathat follow forelimb deafferentation in mon-
283
EDWARD TAUB et al.
DEVELOPMENT OF LEARNED NONUSE
Fig. 1. Schematic model for development of learned nonuse. After Tries (1991).
keys. However, they are meant as more generalformulations that also apply to other situationsin which excess disability develops.
During the course of this century, severalinvestigators have found that a behavioraltechnique could be employed in nonhuman an-imals to improve substantially a motor deficitresulting from neurological damage (Cham-bers, Konorski, Liu, Yu, & Anderson, 1972;Lashley, 1924; Ogden & Franz, 1917; Tower,1940; Yu, 1980). There may thus be someinteresting parallels in terms of the possibleparticipation of a learned nonuse mechanismin the masking of the behavioral capacity ac-tually present both after pyramidotomy andother motor lesions and after unilateral deaf-ferentation.
Experiments with Human Patients After StrokeBecause the mechanism of learned nonuse
is behavioral in nature, it was reasoned thatit ought to be independent of the source andnature of an injury, coming into operationwhenever the appropriate contingencies of re-inforcement exist in the early postinjury pe-riod. For example, stroke in humans oftenleaves patients with an apparently permanentloss of function in an upper extremity, al-though the limb is not paralyzed. In addition,the motor deficit is almost always unilateral.These factors are similar to the situation that
exists after unilateral forelimb deafferentationin monkeys. Therefore, it seemed reasonableto formulate a formal protocol for simplytransferring the techniques used for convertinga useless limb into one that could be used ex-tensively from unilaterally deafferented mon-keys to human patients after stroke (Taub,1980).
Preliminary application of one of the con-ditioned-response paradigms developed in pri-mate deafferentation research to human strokepatients had taken place previously with somesuccess (Halberstam, Zaretsky, Brucker, &Guttman, 1971; Ince, 1969). Subsequently,Wolf and co-workers (Ostendorf & Wolf, 1981;Wolf, Lecraw, Barton, & Jann, 1989) took thelimb-restriction portion of the published pro-tocol (but not the training component) andapplied it to chronic stroke and traumatic-brain-injury patients. The results were prom-ising. They stimulated the next research effort(Taub et al., 1993), which made some modi-fications in the research design and added atraining aspect (Taub, 1980) to the treatmentof patients.The subjects were chronic stroke patients
who had experienced cerebrovascular acci-dents from 1 to 18 years earlier. Patients withthis degree of chronicity, according to the tra-ditional belief of the field, have presumablyreached a plateau in their motor recovery and
284
OVERCOMING LEARNED NONUSE
OVERCOMING LEARNED NONUSE
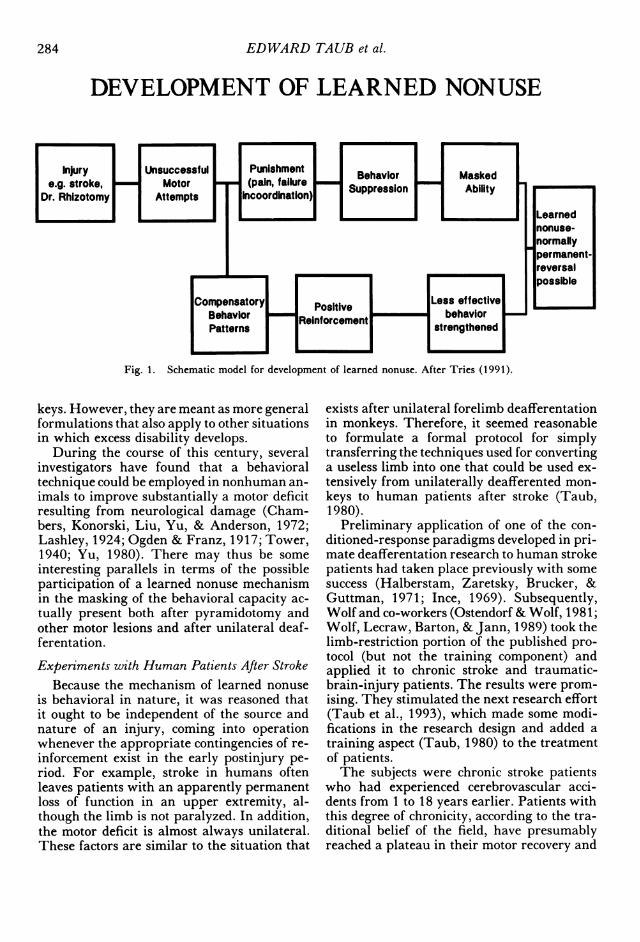
Fig. 2. Schematic model of mechanism for overcoming learned nonuse.
will not exhibit any further improvement forthe rest of their lives. The focal criterion forinclusion in the study was the ability to extendat least 20° at the wrist and 100 at the fingers.
Nine persons who met the study's inclusioncriteria (Taub et al., 1993) were assigned bya random process to either an experimentalgroup (4 subjects) or to an attention-compar-ison group (5 subjects). The subjects in thetwo groups were closely matched in initial mo-tor ability and did not diverge significantly inmajor demographic characteristics or in chro-nicity (median 4.1 years for the restraint group;median 4.5 years for the comparison group).
For the experimental group, the unaffectedlimb was secured in a resting hand splint andwas then placed in a sling; the affected armwas left free. The restraint was to be worn atall times during waking hours except whenspecific activities were being carried out (e.g.,excretory functions, naps, and situations inwhich balance might be compromised). A be-havioral contract was drawn up for each sub-ject, and in each case he or she agreed to spendapproximately 90% of waking hours in re-straint. The restraint devices were worn for12 days. On each of the 8 weekdays duringthis period, patients spent 7 hr at the reha-bilitation center and were given a variety oftasks to be carried out by the paretic upperextremity for 6 hr (e.g., eating lunch with a
fork and spoon; throwing a ball; playing dom-inoes, Chinese checkers, or card games; writingon paper or on a chalk board; pushing a broom;using the Purdue Dexterity Board; taking theMinnesota Rate of Manipulation Test). Noexplicit training of any kind, including shap-ing, was given; the subjects simply practicedthe tasks repeatedly. The purpose was pri-marily to provide experience and overtrainingin use of the affected limb.The procedures given to the comparison
group were designed to focus attention on theinvolved extremity. This was accomplished inthree ways. First, patients were told (duringfour periods on separate days) that they hadmuch greater motor ability with their affectedextremity than they were exhibiting; they wereexhorted to focus attention at home on usingthe affected extremity in as many new activitiesas possible. Examples were given, and recordkeeping was required and monitored. Second,patients received two sessions (labeled physicaltherapy) that involved only those activities thatrequired neither active movement nor limber-ing of the involved limb. Third, patients weregiven self-range-of-movement exercises to carryout at home for 15 min a day. In these exer-cises, the affected extremity was passivelymoved into a variety of positions by the unaf-fected extremity.Two laboratory tests of motor function were
285
EDWARD TAUB et al.
administered to experimental and comparisonsubjects just before and immediately after their2-week intervention period. One test consistedof simple limb movements, half without func-tional end points (Wolf et al., 1989). The otherwas composed of more complex tasks involvingcomplete activities of daily living (McCullochet al., 1988). To summarize the findings ofTaub et al. (1993), there were significantchanges in the motor ability of the subjectswhose uninvolved extremity was restricted, andthese changes were large. The mean perfor-mance time of the experimental subjects de-creased 38% on the first test and 28% on thesecond. The subjects also exhibited substantialincreases in measures of quality of movementand functional ability in the two tests. Therewere particularly large improvements on thetwo tasks that assessed strength. In the 1 ex-perimental subject given specific strengthtraining, ability to lift weights by flexion atthe shoulder increased 808.9%, and gripstrength increased 275%. In contrast, the per-formance of the comparison group was notsignificantly changed at their postinterventiontesting on any of these parameters.A third instrument, the Motor Activity Log
(MAL), provided information about motorfunction in the normal environment, thus ad-dressing the critical issue of generalization.This log consists of ratings of 14 common andimportant activities of daily life from suchfunctional areas as feeding, dressing, andgrooming. The comparison subjects did notimprove on this scale in relation to the yearpreceding their entry into the project. In con-trast, the movement-restriction subjects im-proved almost 2.5 rating steps (out of 6). Therewas virtually no overlap in the records of thetwo groups during treatment or during thefollow-up period. Moreover, the treatmentgains of the experimental subjects were fullymaintained 2 years after the completion of the2 weeks of treatment.The improvement of the movement-restric-
tion patients in MAL scores in part reflectsbetter quality of movement and in part reflectsthe fact that these patients were able to trans-late the improvements made in the laboratoryinto mastery of a large range of daily activitiesthat they had not previously been able to carryout with the affected arm. The new activitiesincluded brushing teeth, combing hair, picking
up a glass of water and drinking, eating witha fork or spoon, and writing, among others.There was a mean increase of 97.1% in thenumber of activities on the MAL that the pa-tients reported they could carry out 1 monthafter restraint compared to the period beforetreatment. The comparable change for thecomparison subjects was 14.5%. The differ-ence between groups on this measure was sta-tistically significant after the interventions (Utest, p < .01) but not before.
In interviews, each of the restraint patientsstated that they were capable of a greatly ex-panded range of activities. They reported thatthey had made major gains in what was, ineffect, functional independence. This is con-sistent with the results from the MAL. In themost dramatic case, motor improvement wasgreat enough to permit part-time clerical em-ployment. One of this subject's main tasks wasanswering the phone with the unaffected handand writing messages with the affected hand.She was thus able to relieve a self-reporteddepressed state because she previously "hadnothing to do except spend most of my daysstaring at the four walls of my apartment."
Shaping As a Means of Facilitating OvercomingLearned Nonuse in Human Chronic StrokePatients
In monkeys, restriction of the intact limband shaping had been used independently toimprove motor function after unilateral fore-limb deafferentation. With human chronicstroke patients, unaffected limb restriction hadbeen combined with practice of use of the af-fected limb, but no explicit training of limbmovement had been given. It seemed reason-able to combine shaping with limb restrictionas complementary and possibly synergistictechniques for overcoming learned nonuse.This approach is being carried out in currentwork.A battery of approximately 30 tasks was
developed with a preliminary shaping plan foreach. The actual subset of tasks selected foruse with each subject depended on (a) specificjoint movements that exhibited the most pro-nounced deficit, (b) the joint movements thatstaff members felt had the greatest potentialfor improvement, and (c) subject preferenceamong tasks that had similar potential for pro-ducing specific improvements. The three tasks
286
OVERCOMING LEARNED NONUSE
100
90
80a 70
60
0) 50C)c 40co 30C,)'~ 20
10
01 5 10 15 20 1 5 10 15 20 1 5 10 15
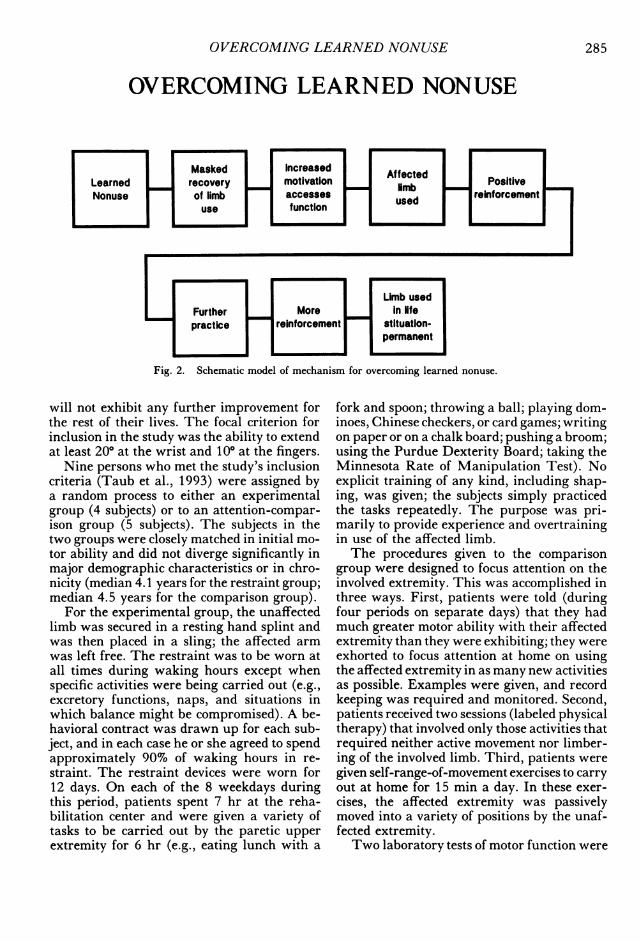
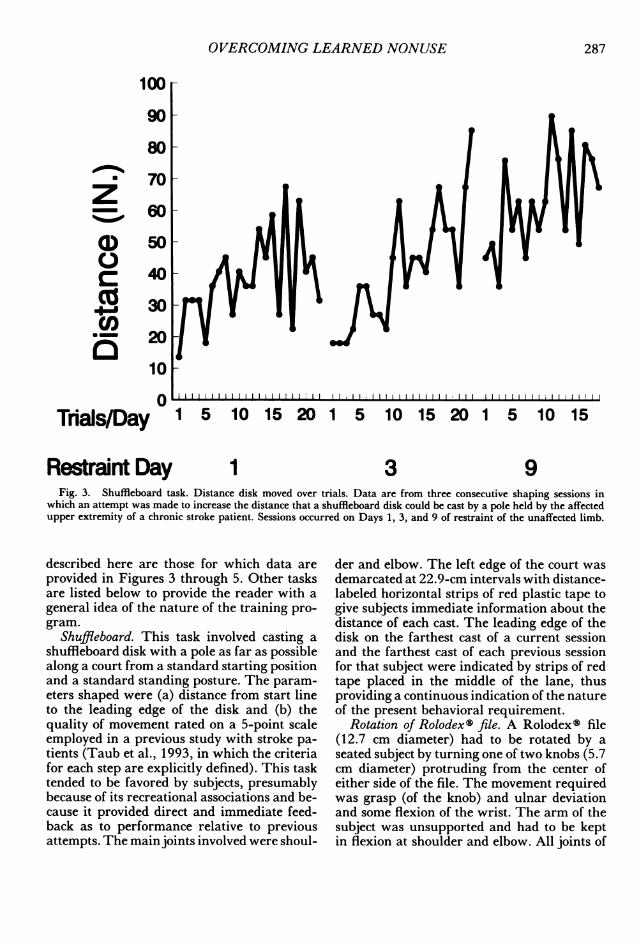
1 3 9Fig. 3. Shuffleboard task. Distance disk moved over trials. Data are from three consecutive shaping sessions in
which an attempt was made to increase the distance that a shuffleboard disk could be cast by a pole held by the affectedupper extremity of a chronic stroke patient. Sessions occurred on Days 1, 3, and 9 of restraint of the unaffected limb.
described here are those for which data areprovided in Figures 3 through 5. Other tasksare listed below to provide the reader with ageneral idea of the nature of the training pro-gram.
Shuffleboard. This task involved casting ashuffleboard disk with a pole as far as possiblealong a court from a standard starting positionand a standard standing posture. The param-eters shaped were (a) distance from start lineto the leading edge of the disk and (b) thequality of movement rated on a 5-point scaleemployed in a previous study with stroke pa-tients (Taub et al., 1993, in which the criteriafor each step are explicitly defined). This tasktended to be favored by subjects, presumablybecause of its recreational associations and be-cause it provided direct and immediate feed-back as to performance relative to previousattempts. The main joints involved were shoul-
der and elbow. The left edge of the court wasdemarcated at 22.9-cm intervals with distance-labeled horizontal strips of red plastic tape togive subjects immediate information about thedistance of each cast. The leading edge of thedisk on the farthest cast of a current sessionand the farthest cast of each previous sessionfor that subject were indicated by strips of redtape placed in the middle of the lane, thusproviding a continuous indication of the natureof the present behavioral requirement.
Rotation of RolodexS file. A Rolodexs file(12.7 cm diameter) had to be rotated by aseated subject by turning one of two knobs (5.7cm diameter) protruding from the center ofeither side of the file. The movement requiredwas grasp (of the knob) and ulnar deviationand some flexion of the wrist. The arm of thesubject was unsupported and had to be keptin flexion at shoulder and elbow. All joints of
Tnals/Day
Restraint Day
287

EDWARD TAUB et al.
c
CO)I-
F-
21
18
15L-
U1)
~12
Z ~9Trials/Day
/.
.
1 2 4 5 1 2 3 1 2 1 1 1 2 3 4
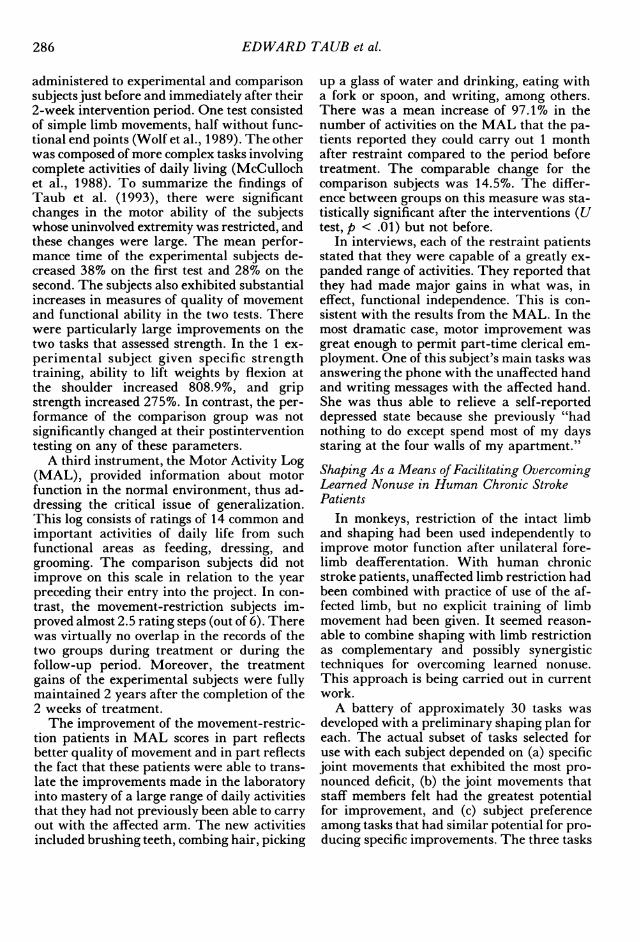
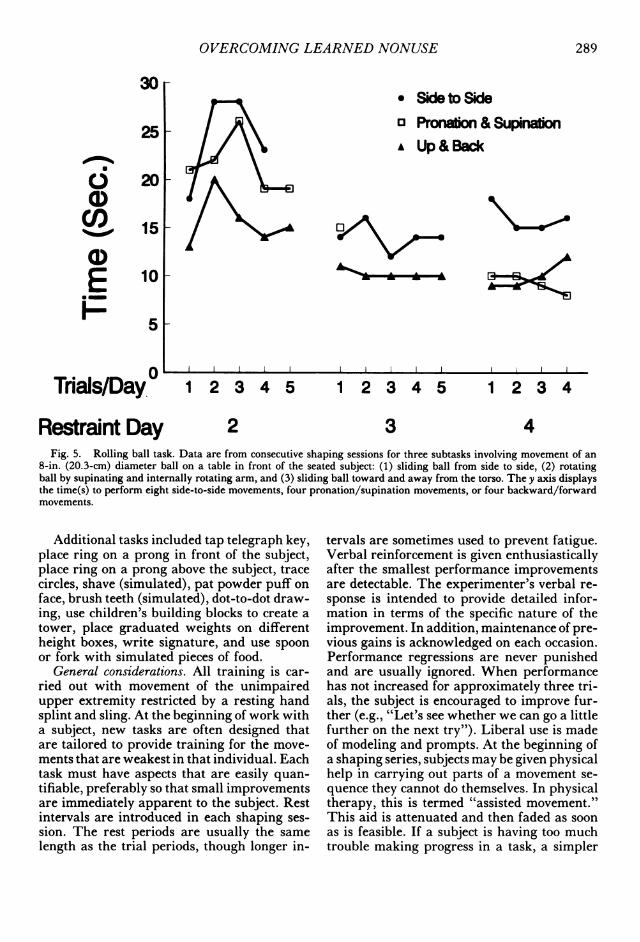
Restraint Day 3 4 7 8 9Fig. 4. Rolodexg task. Data are from consecutive shaping sessions involving an attempt to increase the number
of rotations per 1-min trial of a knob that turned a circular card file.
the arm were involved in the activity. A thinpiece of red tape secured across the radius ofthe knob was continued (with an interruption)onto the frame of the file. A trial began withthe segments of tape on the knob and framelined up; the completion of one rotation wasindicated when the two segments were againlined up. The experimenter informed the sub-ject of performance progress by counting com-plete rotations out loud. The parameters shapedwere (a) number of rotations per minute and(b) quality of movement. Although the limitingfactor in performance tended to be the abilityto make the appropriate movements at thewrist, difficulty frequently was encountered inkeeping the arm maintained in shoulder flex-ion for a period of 1 min.Moving a ball. The hand of a seated subject
grasped the soft top of an inflatable plastic ball(20.3 cm diameter) placed on a table surfacedirectly in front of the subject at a distancethat required the arm to be fully extended.Talcum powder was spread lightly on the tablesurface to decrease friction. One subtask re-
quired the subject to slide the ball from sideto side with the arm fully extended at the elbowfrom one edge of a table (1.2 m diameter) tothe other for four repetitions of both move-
ments. Subtask 2 involved grasping the ballwith the arm in full pronation (palm down),fully extended at the elbow and in approxi-mately 700 flexion at the shoulder, and thenrotating the ball back and forth four times bymoving into 30° to 40° supination, returningto full pronation and then moving the ball inthe opposite direction by internally rotatingthe shoulder till the fifth digit was uppermoston the ball. Subtask 3 required the subject toslide the ball backward till the arm was in 900flexion at the elbow and then forward to theoriginal fully extended position. The param-eters shaped were (a) time to accomplish thefour cycles of movement, (b) amount of supi-nation and internal rotation at the shoulder(for Subtask 3), and (c) quality of movement.The three subtasks were sometimes carried outin the same session and sometimes in separatesessions. They involved activity at all joints.
10
288
OVERCOMING LEARNED NONUSE
30[* Sideto Sideo Pronao & SupnationA Up& Back
25[
? 20U1)cO 15
UL)E 10
H~5
Trials/Day.0
IL
0v_
1 2 3 4 5 1 2 3 4 5 1 2 3 4
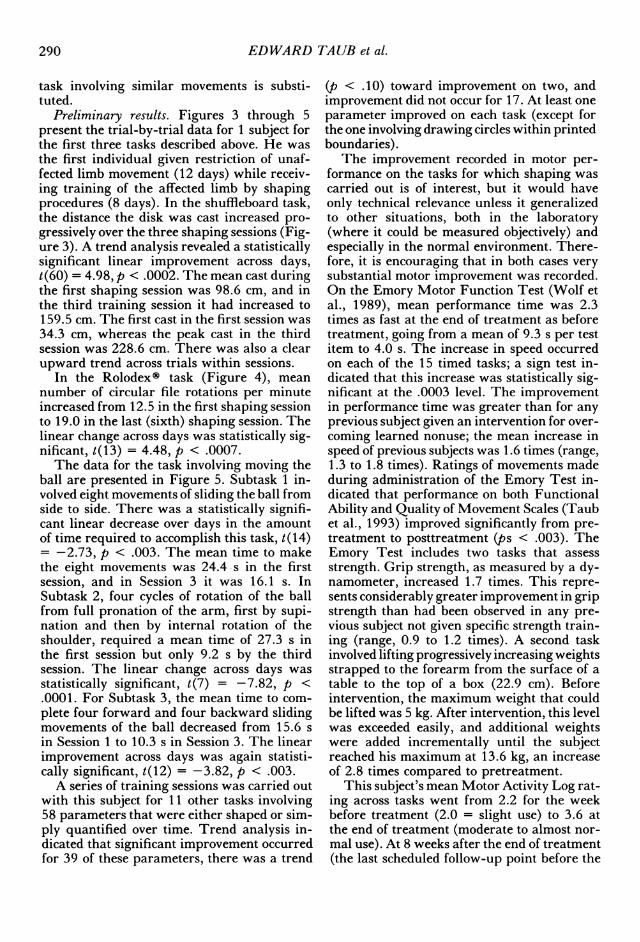
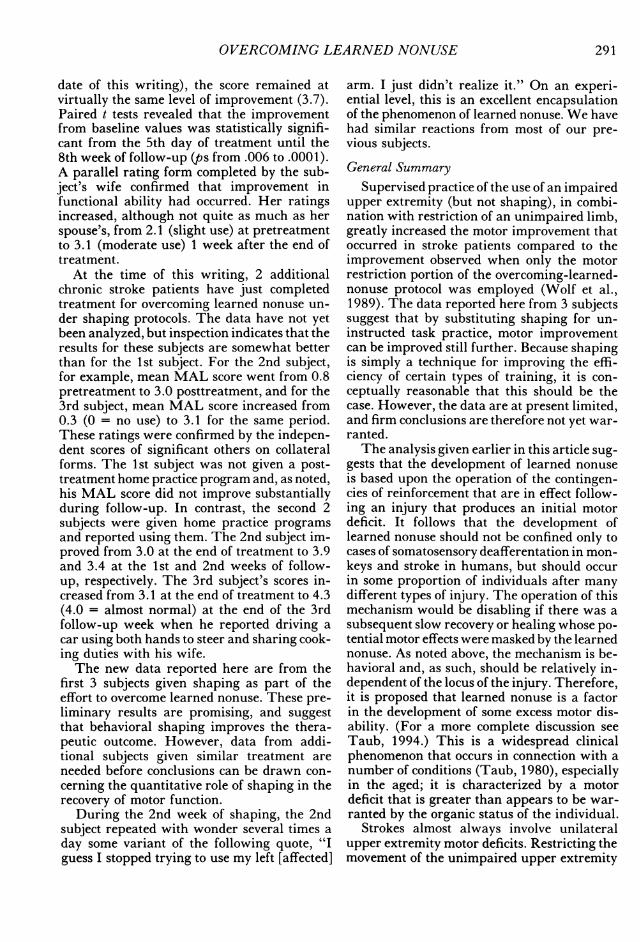
Restraint Day 2 3 4Fig. 5. Rolling ball task. Data are from consecutive shaping sessions for three subtasks involving movement of an
8-in. (20.3-cm) diameter ball on a table in front of the seated subject: (1) sliding ball from side to side, (2) rotatingball by supinating and internally rotating arm, and (3) sliding ball toward and away from the torso. The y axis displaysthe time(s) to perform eight side-to-side movements, four pronation/supination movements, or four backward/forwardmovements.
Additional tasks included tap telegraph key,place ring on a prong in front of the subject,place ring on a prong above the subject, tracecircles, shave (simulated), pat powder puff onface, brush teeth (simulated), dot-to-dot draw-ing, use children's building blocks to create atower, place graduated weights on differentheight boxes, write signature, and use spoonor fork with simulated pieces of food.
General considerations. All training is car-ried out with movement of the unimpairedupper extremity restricted by a resting handsplint and sling. At the beginning of work witha subject, new tasks are often designed thatare tailored to provide training for the move-ments that are weakest in that individual. Eachtask must have aspects that are easily quan-tifiable, preferably so that small improvementsare immediately apparent to the subject. Restintervals are introduced in each shaping ses-sion. The rest periods are usually the samelength as the trial periods, though longer in-
tervals are sometimes used to prevent fatigue.Verbal reinforcement is given enthusiasticallyafter the smallest performance improvementsare detectable. The experimenter's verbal re-sponse is intended to provide detailed infor-mation in terms of the specific nature of theimprovement. In addition, maintenance of pre-vious gains is acknowledged on each occasion.Performance regressions are never punishedand are usually ignored. When performancehas not increased for approximately three tri-als, the subject is encouraged to improve fur-ther (e.g., "Let's see whether we can go a littlefurther on the next try"). Liberal use is madeof modeling and prompts. At the beginning ofa shaping series, subjects may be given physicalhelp in carrying out parts of a movement se-quence they cannot do themselves. In physicaltherapy, this is termed "assisted movement."This aid is attenuated and then faded as soonas is feasible. If a subject is having too muchtrouble making progress in a task, a simpler
289
EDWARD TAUB et al.
task involving similar movements is substi-tuted.
Preliminary results. Figures 3 through 5present the trial-by-trial data for 1 subject forthe first three tasks described above. He was
the first individual given restriction of unaf-fected limb movement (12 days) while receiv-ing training of the affected limb by shapingprocedures (8 days). In the shuffleboard task,the distance the disk was cast increased pro-
gressively over the three shaping sessions (Fig-ure 3). A trend analysis revealed a statisticallysignificant linear improvement across days,t(60) = 4.98, p < .0002. The mean cast duringthe first shaping session was 98.6 cm, and inthe third training session it had increased to159.5 cm. The first cast in the first session was34.3 cm, whereas the peak cast in the thirdsession was 228.6 cm. There was also a clearupward trend across trials within sessions.
In the Rolodexg task (Figure 4), mean
number of circular file rotations per minuteincreased from 12.5 in the first shaping sessionto 19.0 in the last (sixth) shaping session. Thelinear change across days was statistically sig-nificant, t(13) = 4.48, p < .0007.The data for the task involving moving the
ball are presented in Figure 5. Subtask 1 in-volved eight movements of sliding the ball fromside to side. There was a statistically signifi-cant linear decrease over days in the amountof time required to accomplish this task, t(14)=-2.73, p < .003. The mean time to makethe eight movements was 24.4 s in the firstsession, and in Session 3 it was 16.1 s. InSubtask 2, four cycles of rotation of the ballfrom full pronation of the arm, first by supi-nation and then by internal rotation of theshoulder, required a mean time of 27.3 s inthe first session but only 9.2 s by the thirdsession. The linear change across days was
statistically significant, t(7) = -7.82, p <.0001. For Subtask 3, the mean time to com-
plete four forward and four backward slidingmovements of the ball decreased from 15.6 s
in Session 1 to 10.3 s in Session 3. The linearimprovement across days was again statisti-cally significant, t(12) = -3.82, p < .003.A series of training sessions was carried out
with this subject for 11 other tasks involving58 parameters that were either shaped or sim-ply quantified over time. Trend analysis in-dicated that significant improvement occurredfor 39 of these parameters, there was a trend
(p < .10) toward improvement on two, andimprovement did not occur for 17. At least oneparameter improved on each task (except forthe one involving drawing circles within printedboundaries).
The improvement recorded in motor per-formance on the tasks for which shaping wascarried out is of interest, but it would haveonly technical relevance unless it generalizedto other situations, both in the laboratory(where it could be measured objectively) andespecially in the normal environment. There-fore, it is encouraging that in both cases verysubstantial motor improvement was recorded.On the Emory Motor Function Test (Wolf etal., 1989), mean performance time was 2.3times as fast at the end of treatment as beforetreatment, going from a mean of 9.3 s per testitem to 4.0 s. The increase in speed occurredon each of the 15 timed tasks; a sign test in-dicated that this increase was statistically sig-nificant at the .0003 level. The improvementin performance time was greater than for anyprevious subject given an intervention for over-coming learned nonuse; the mean increase inspeed of previous subjects was 1.6 times (range,1.3 to 1.8 times). Ratings of movements madeduring administration of the Emory Test in-dicated that performance on both FunctionalAbility and Quality of Movement Scales (Taubet al., 1993) improved significantly from pre-treatment to posttreatment (ps < .003). TheEmory Test includes two tasks that assessstrength. Grip strength, as measured by a dy-namometer, increased 1.7 times. This repre-sents considerably greater improvement in gripstrength than had been observed in any pre-vious subject not given specific strength train-ing (range, 0.9 to 1.2 times). A second taskinvolved lifting progressively increasing weightsstrapped to the forearm from the surface of atable to the top of a box (22.9 cm). Beforeintervention, the maximum weight that couldbe lifted was 5 kg. After intervention, this levelwas exceeded easily, and additional weightswere added incrementally until the subjectreached his maximum at 13.6 kg, an increaseof 2.8 times compared to pretreatment.
This subject's mean Motor Activity Log rat-ing across tasks went from 2.2 for the weekbefore treatment (2.0 = slight use) to 3.6 atthe end of treatment (moderate to almost nor-mal use). At 8 weeks after the end of treatment(the last scheduled follow-up point before the
290
OVERCOMING LEARNED NONUSE
date of this writing), the score remained atvirtually the same level of improvement (3.7).Paired t tests revealed that the improvementfrom baseline values was statistically signifi-cant from the 5th day of treatment until the8th week of follow-up (ps from .006 to .000 1).A parallel rating form completed by the sub-ject's wife confirmed that improvement infunctional ability had occurred. Her ratingsincreased, although not quite as much as herspouse's, from 2.1 (slight use) at pretreatmentto 3.1 (moderate use) 1 week after the end oftreatment.
At the time of this writing, 2 additionalchronic stroke patients have just completedtreatment for overcoming learned nonuse un-der shaping protocols. The data have not yetbeen analyzed, but inspection indicates that theresults for these subjects are somewhat betterthan for the 1st subject. For the 2nd subject,for example, mean MAL score went from 0.8pretreatment to 3.0 posttreatment, and for the3rd subject, mean MAL score increased from0.3 (0 = no use) to 3.1 for the same period.These ratings were confirmed by the indepen-dent scores of significant others on collateralforms. The 1st subject was not given a post-treatment home practice program and, as noted,his MAL score did not improve substantiallyduring follow-up. In contrast, the second 2subjects were given home practice programsand reported using them. The 2nd subject im-proved from 3.0 at the end of treatment to 3.9and 3.4 at the 1st and 2nd weeks of follow-up, respectively. The 3rd subject's scores in-creased from 3.1 at the end of treatment to 4.3(4.0 = almost normal) at the end of the 3rdfollow-up week when he reported driving acar using both hands to steer and sharing cook-ing duties with his wife.The new data reported here are from the
first 3 subjects given shaping as part of theeffort to overcome learned nonuse. These pre-liminary results are promising, and suggestthat behavioral shaping improves the thera-peutic outcome. However, data from addi-tional subjects given similar treatment areneeded before conclusions can be drawn con-cerning the quantitative role of shaping in therecovery of motor function.
During the 2nd week of shaping, the 2ndsubject repeated with wonder several times aday some variant of the following quote, "Iguess I stopped trying to use my left [affected]
arm. I just didn't realize it." On an experi-ential level, this is an excellent encapsulationof the phenomenon of learned nonuse. We havehad similar reactions from most of our pre-vious subjects.General Summary
Supervised practice of the use of an impairedupper extremity (but not shaping), in combi-nation with restriction of an unimpaired limb,greatly increased the motor improvement thatoccurred in stroke patients compared to theimprovement observed when only the motorrestriction portion of the overcoming-learned-nonuse protocol was employed (Wolf et al.,1989). The data reported here from 3 subjectssuggest that by substituting shaping for un-instructed task practice, motor improvementcan be improved still further. Because shapingis simply a technique for improving the effi-ciency of certain types of training, it is con-ceptually reasonable that this should be thecase. However, the data are at present limited,and firm conclusions are therefore not yet war-ranted.The analysis given earlier in this article sug-
gests that the development of learned nonuseis based upon the operation of the contingen-cies of reinforcement that are in effect follow-ing an injury that produces an initial motordeficit. It follows that the development oflearned nonuse should not be confined only tocases of somatosensory deafferentation in mon-keys and stroke in humans, but should occurin some proportion of individuals after manydifferent types of injury. The operation of thismechanism would be disabling if there was asubsequent slow recovery or healing whose po-tential motor effects were masked by the learnednonuse. As noted above, the mechanism is be-havioral and, as such, should be relatively in-dependent of the locus of the injury. Therefore,it is proposed that learned nonuse is a factorin the development of some excess motor dis-ability. (For a more complete discussion seeTaub, 1994.) This is a widespread clinicalphenomenon that occurs in connection with anumber of conditions (Taub, 1980), especiallyin the aged; it is characterized by a motordeficit that is greater than appears to be war-ranted by the organic status of the individual.
Strokes almost always involve unilateralupper extremity motor deficits. Restricting themovement of the unimpaired upper extremity
292 EDWARD TAUB et al.
in these cases is an obvious procedure to helpovercome the learned suppression of movementunderlying learned nonuse. However, whenthe motor deficit is bilateral or involves thelower extremities, constraint of function mayoften not be as simply applied as restriction ofan unimpaired arm. Thus, in bilateral andlower extremity conditions, shaping may as-sume even greater importance as a means ofovercoming learned nonuse than followingstroke.
In our laboratory, stroke patients are se-lected for study on the basis of whether theyhave more than a minimum ability to extendthe wrist (200) and fingers (100), but who makelittle use of the affected extremity. This in-cludes 20% to 25% of the chronic stroke pop-ulation with motor deficit (Wolf & Binder-Macloud, 1983). To date, every one of the 7subjects who have met this criterion have ex-hibited large improvements in the use of theaffected limb in the normal environment whengiven treatment for overcoming learned non-use. The percentage of stroke patients who donot meet this criterion, but who would alsobenefit from this therapeutic approach, is atpresent unknown. It would presumably not beas high as in the current work, but at leastsome of these patients might also be helped.Following stroke and traumatic brain injury,overcoming learned nonuse has been used withsuccess in clinical situations (Desai, 1991;Tries, 1989, 1991; N. Birbaumer, personalcommunication, 1993; S. L. Wolf, personalcommunication, 1993).
REFERENCES
Barinaga, M. (1992). The brain remaps its own con-tours. Science, 258, 216-218.
Chambers, W. W., Konorski, J., Liu, C. N., Yu, J., &Anderson, R. (1972). The effects of cerebellar lesionsupon skilled movements and instrumental conditionedreflexes. Acta Neurobiologiae Experimentalis, 32, 721-732.
Desai, V. (1991, March). Report on functional utilityscore change in nine chronic stroke or closed headinjury patients receiving a training program for over-coming learned nonuse as part of a multimodality treat-ment program. In N. E. Miller (Chair), Overcominglearned nonuse and the release of covert behavior as a newapproach to physical medicine. Symposium conducted atthe meeting of the Association for Applied Psycho-physiology and Biofeedback, Dallas.
Halberstam, J. L., Zaretsky, H. H., Brucker, B. S., &Guttman, A. (1971). Avoidance conditioning of mo-tor responses in elderly brain-damaged patients. Ar-
chives of Physical Medicine and Rehabilitation, 52, 318-328.
Ince, L. P. (1969). Escape and avoidance conditioningof response in the plegic arm of stroke patients: Apreliminary study. Psychonomic Science, 16, 49-50.
Knapp, H. D., Taub, E., & Berman, A. J. (1958). Effectof deafferentation on a conditioned avoidance response.Science, 128, 842-843.
Knapp, H. D., Taub, E., & Berman, A. J. (1963).Movements in monkeys with deafferented forelimbs.Experimental Neurology, 7, 305-315.
Lashley, K. S. (1924). Studies of cerebral function inlearning: V. The retention of motor areas in primates.Archives of Neurology and Psychology, 12, 249-276.
Lassek, A. M. (1953). Inactivation of voluntary motorfunction following rhizotomy. Journal of Neuropathol-ogy and Experimental Neurology, 3, 83-87.
McCulloch, K., Cook, E. W., III, Fleming, W. C., Novack,T. A., Nepomuceno, C. S., & Taub, E. (1988). Areliable test of upper extremity ADL function. Archivesof Physical Medicine and Rehabilitation, 69, 755.
Morgan, W. G. (1974). The shaping game: A teachingtechnique. Behavior Therapy, 5, 271-272.
Mott, P. W., & Sherrington, C. S. (1895). Experimentsupon the influence of sensory nerves upon movementand nutrition of the limbs. Proceedings of the RoyalSociety of London, 57, 481-488.
Ogden, R., & Franz, S. I. (1917). On cerebral motorcontrol: The recovery from experimentally producedhemiplegia. Psychobiology, 1, 35-50.
Ostendorf, C. G., & Wolf, S. L. (1981). Effect of forceduse of the upper extremity of a hemiplegic patient onchanges in function. Journal of the American PhysicalTherapy Association, 61, 1022-1028.
Palca, J. (1991). Famous monkeys provide surprisingresults. Science, 257, 1789.
Panyan, M. V. (1980). How to use shaping. Lawrence,KS: H & H Enterprises.
Pons, T. P., Garraghty, P. E., Ommaya, A. K., Kaas, J.H., Taub, E., & Mishkin, M. (1991). Massive cor-tical reorganization after sensory deafferentation in adultmacaques. Science, 252, 1857-1860.
Rausell, E., Cusick, C. G., Taub, E., & Jones, E. G.(1992). Chronic deafferentation in monkeys differ-entially affects nociceptive and nonnociceptive path-ways distinguished by specific calcium-binding pro-teins and down-regulates gamma-aminobutyric acidtype A receptors at thalamic levels. Proceedings of theNational Academy of Sciences, 89, 2571-2575.
Risley, T. R., & Baer, D. M. (1973). Operant behaviormodification: The deliberate development of behavior.In M. Caldwell & H.N. Riccuiti (Eds.), Review ofchilddevelopment research: vol. 3. Development and social ac-tion (pp. 283-329). Chicago: University of ChicagoPress.
Skinner, B. F. (1938). The behavior of organisms. NewYork: Appleton-Century-Crofts.
Skinner, B. F. (1968). The technology of teaching. NewYork: Appleton-Century-Crofts.
Stein, B. M., & Carpenter, M. W. (1965). Effects ofdorsal rhizotomy upon subthalamic dyskinesia in themonkey. Archives of Neurology, 13, 567-583.
Stephens, T. (1991). Brain reorganization puzzle in Sil-ver Spring monkeys. The Journal of NIH Research, 3,45-48.
Taub, E. (1976). Motor behavior following deafferen-
OVERCOMING LEARNED NONUSE 293
tation in the developing and motorically mature mon-key. In R. Herman, S. Griliner, H. J. Ralston, P. S.G. Stein, & D. Stuart (Eds.), Neural control of loco-motion (pp. 675-705). New York: Plenum Press.
Taub, E. (1977). Movement in nonhuman primates de-prived of somatosensory feedback. Exercise and sportssciences reviews (Vol. 4, pp. 335-374). Santa Barbara,CA: Journal Publishing Affiliates.
Taub, E. (1980). Somatosensory deafferentation re-search with monkeys: Implications for rehabilitationmedicine. In L. P. Ince (Ed.), Behavioral psychology inrehabilitation medicine: Clinical applications (pp. 371-401). New York: Williams & Wilkins.
Taub, E. (1994). Overcoming learned nonuse: A newapproach to treatment in physical medicine. In J. G.Carlson, A. R. Seifert, & N. Birbaumer (Eds.), Inter-national perspectives on applied psychophysiology (pp.185-220). New York: Plenum Press.
Taub, E., Bacon, R., & Berman, A. J. (1965). Theacquisition of a trace-conditioned avoidance responseafter deafferentation of the responding limb. Journal ofComparative and Physiological Psychology, 58, 275-279.
Taub, E., & Berman, A. J. (1963). Avoidance condi-tioning in the absence of relevant proprioceptive andexteroceptive feedback. Journal of Comparative andPhysiological Psychology, 56, 1012-1016.
Taub, E., & Berman, A. J. (1968). Movement andlearning in the absence of sensory feedback. In S. J.Freedman (Ed.), The neuropsychology of spatially ori-ented behavior (pp. 173-192). Homewood, IL: Dorsey.
Taub, E., Ellman, S. J., & Berman, A. J. (1966). Deaf-ferentation in monkeys: Effect on conditioned graspresponse. Science, 151, 593-594.
Taub, E., Goldberg, I. A., & Taub, P. B. (1975). Deaf-ferentation in monkeys: Pointing at a target withoutvisual feedback. Experimental Neurology, 46, 178-186.
Taub, E., Miller, N. E., Novack, T. A., Cook, E. W., III,Fleming, W. D., Nepomuceno, C. S., Connell, J. S.,& Crago, J. E. (1993). Technique to improve chronicmotor deficit after stroke. Archives of Physical Medicineand Rehabilitation, 74, 347-354.
Taub, E., Perrella, P. N., & Barro, G. (1973). Behav-ioral development following forelimb deafferentationon day of birth in monkeys with and without blinding.Science, 181, 959-960.
Taub, E., Perrella, P. N., Miller, E. A., & Barro, G.(1975). Diminution of early environmental controlthrough perinatal and prenatal somatosensory deaf-ferentation. Biological Psychiatry, 10, 609-626.
Taub, E., Williams, M., Barro, G., & Steiner, S. S.(1978). Comparison of the performance of deaffer-ented and intact monkeys on continuous and fixed ratioschedules of reinforcement. Experimental Neurology, 58,1-13.
Tower, S. S. (1940). Pyramidal lesion in the monkey.Brain, 63, 36-90.
Tries, J. (1989). EMG biofeedback for the treatmentof upper-extremity dysfunction: Can it be effective?Biofeedback and Self-Regulation, 14, 21-53.
Tries, J. M. (1991, March). Learned nonuse: A factorin incontinence. In N. E. Miller (Chair), Overcominglearned nonuse and the release of covert behavior as a newapproach to physical medicine. Symposium conducted atthe meeting of the Association for Applied Psycho-physiology and Biofeedback, Dallas.
Twitchell, T. E. (1954). Sensory factors in purposivemovement. Journal of Neurophysiology, 17, 239-254.
Wolf, S. L., & Binder-Macloud, S. A. (1983). Electro-myographic biofeedback applications to the hemiplegicpatient: Changes in upper extremity neuromuscularand functibnal status. Journal of the American PhysicalTherapy Association, 63, 1393-1403.
Wolf, S. L., Lecraw, D. E., Barton, L. A., & Jann, B. B.(1989). Forced use of hemiplegic upper extremities toreverse the effect of learned nonuse among chronicstroke and head-injured patients. Experimental Neu-rology, 104, 125-132.
Wylie, R. M., & Tyner, C. F. (1981). Weight-liftingby normal and deafferented monkeys: Evidence forcompensatory changes in ongoing movements. BrainResearch, 219, 172-177.
Wylie, R. M., & Tyner, C. F. (1989). Performance ofa weight-lifting task by normal and deafferented mon-keys. Behavioral Neuroscience, 108, 273-282.
Yu, J. (1980). Neuromuscular recovery with trainingafter central nervous system lesions: An experimentalapproach. In L. P. Ince (Ed.), Behavioral psychology inrehabilitation medicine: Clinical applications (pp. 402-417). Baltimore, MD: Williams and Wilkins.
Copyright © 2022 FDOKUMEN




















