An interactive videodisc-based smoking cessation program: Prototype development and pilot test
12
Pergamon Computers in Human Behavior, Vol. 10, No. 3, pp, 347-358, 1994 Copyright 0 1994 Elsevier Science Ltd F’rinted in the USA. All rights reserved 0747-5632/94 $6.00 + .OO An Interactive Videodisc-Based Smoking Cessation Program: Prototype Development and Pilot Test John Noel/, Anthony Big/an, Don Hood, and Barbara Britz Oregon Research lnsfitufe Abstract - The development and pilot testing of an interactive videodisc-based smoking cessation program (IVD-SCP) are described. Designed for use in outpatient medical settings, the IVD-SCP was created in response to the needfor eficacious, low-cost alternatives for assisting physicians in delivering smoking cessation interventions. Based on a successful intervention that utilized a linear video and nurse-counselon the system takes advantage of the “teachable moment” that occurs when a physician advises a patient to stop smoking. After receiving a brief (30-s) message on the advisability of stopping smoking, the patient is directed by the physician to use the IVD-SCP Only a touchscreen monitor and printer are visible. Activated by a touch on the screen, the system presents a complete intervention, tailored to the individual user’s characteristics and needs, and ends by printing a personalized quit plan. Pilot-tested with 27 patients in family practice medical ofJices, the IVD-SCP was well received by patients. Ratings of the system’s utility and ease of use were high, and 70% of the users set quit dates, although none were abstinent at 3 months postintervention. INTRODUCTION In response to the need for alternative, cost-effective mechanisms for encouraging smoking cessation, we have developed a stand-alone kiosk-style smoking cessa- tion program using an interactive videodisc-based system designed for use in med- ical settings. Cigarette smoking continues to be the leading preventable cause of Requests for reprints should be addressed to John Noell, Oregon Research Institute, 1899 Willamette Street, Eugene, OR 97401. 347
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of An interactive videodisc-based smoking cessation program: Prototype development and pilot test

Pergamon Computers in Human Behavior, Vol. 10, No. 3, pp, 347-358, 1994
Copyright 0 1994 Elsevier Science Ltd F’rinted in the USA. All rights reserved
0747-5632/94 $6.00 + .OO
An Interactive Videodisc-Based Smoking Cessation Program: Prototype
Development and Pilot Test
John Noel/, Anthony Big/an, Don Hood, and Barbara Britz
Oregon Research lnsfitufe
Abstract - The development and pilot testing of an interactive videodisc-based smoking cessation program (IVD-SCP) are described. Designed for use in outpatient medical settings, the IVD-SCP was created in response to the needfor eficacious, low-cost alternatives for assisting physicians in delivering smoking cessation interventions. Based on a successful intervention that utilized a linear video and nurse-counselon the system takes advantage of the “teachable moment” that occurs when a physician advises a patient to stop smoking. After receiving a brief (30-s) message on the advisability of stopping smoking, the patient is directed by the physician to use the IVD-SCP Only a touchscreen monitor and printer are visible. Activated by a touch on the screen, the system presents a complete intervention, tailored to the individual user’s characteristics and needs, and ends by printing a personalized quit plan. Pilot-tested with 27 patients in family practice medical ofJices, the IVD-SCP was well received by patients. Ratings of the system’s utility and ease of use were high, and 70% of the users set quit dates, although none were abstinent at 3 months postintervention.
INTRODUCTION
In response to the need for alternative, cost-effective mechanisms for encouraging smoking cessation, we have developed a stand-alone kiosk-style smoking cessa- tion program using an interactive videodisc-based system designed for use in med- ical settings. Cigarette smoking continues to be the leading preventable cause of
Requests for reprints should be addressed to John Noell, Oregon Research Institute, 1899 Willamette Street, Eugene, OR 97401.
347

348 Noell, Biglan, Hood, and Britz.
morbidity and mortality in the United States (U.S. Public Health Service, 1990). Approximately 439,000 Americans die each year from smoking-related illness, about 1,200 deaths per day (Glantz & Parmley, 1991). There are now over 30,000 studies linking cigarette smoking to increased mortality and morbidity from a number of diseases including heart disease, lung cancer, chronic obstructive lung disease, and peptic ulcer (National Heart, Lung, and Blood Institute, 1977; U.S. Public Health Service, 1979, 1984). Despite knowledge of the health consequences of cigarette smoking, 29.1% of U.S. adults continue to smoke (U.S. Public Health Service, 1989), and the spontaneous cessation rate is less than 3% (Russell et al., 1979). While public health campaigns have been successful in changing the pub- lic’s attitudes about smoking and most smokers (80%) would like to quit (U.S. Public Health Service, 1989), smoking cessation programs that are effective, eco- nomical, and accessible are still needed.
Multisession group programs typically produce abstinence in only 1520% of participants at one-year follow-up (Glasgow & Lichtenstein, 1987; McFall, 1978; Pechacek, 1979). While multicomponent behaviorally based programs appear some- what more effective (Glasgow & Bernstein, 1981; Lichtenstein & Mermelstein, 1984), these programs at best achieve about 30% long-term cessation. Those tobac- co cessation intervention programs that have been effective have generally been relatively intensive and costly interventions directed towards motivated volunteers in hospitals, university settings, and community health organizations (Glasgow & Lichtenstein, 1987). Such programs reach only a small portion of the general pub- lic and will not achieve the broader public health impact that is needed (Lichtenstein & Glasgow, in press; National Cancer Institute, 1991).
According to Ockene (1987b), 70% of U.S. smokers are seen in medical care settings each year. Thus, 38 million smokers could be given smoking cessation assistance and/or advice as part of their regular medical care, if this opportunity were fully realized (Ockene, 1987b). When physicians do advise patients to quit smoking, they generally provide little in the way of behavioral intervention: They either provide simple advice to quit (sometimes with printed materials) or offer a prescription such as nicotine chewing gum or nicotine patch (Ockene, 1987a, 1987b; Thompson et al., 1988). There is now evidence that brief physician advice can have a meaningful impact on quit rates (Kottke et al., 1988; Ockene, 1987a; Pederson, 1982). Although the overall effect size may be modest, broad implemen- tation of brief physician intervention would result in significant public health impact (Wilson et al., 1987).
Although brief advice-to-quit strategies may be useful, there is evidence that more intensive and more frequent patient-physician interactions result in larger effects (Fagerstrom, 1984; Kottke et al., 1988; Wilson et al., 1987). Unfortunately, heavy demands on physicians’ office time have thus far rendered this approach unworkable in practice. Consequently, only a small proportion of physicians go beyond providing brief advice to stop smoking (Ockene, 1987a).
Primary care settings are at the intersection of clinical and public health approaches to smoking cessation (Lichtenstein & Glasgow, in press). Large num- bers of smokers can be accessed, motivated, and offered personalized assistance. If effective smoking cessation interventions in medical settings are to be widely implemented, however, the delivery system must minimize demands on physician or support staff time, require minimal physician training, be of low cost, and be efficacious and effective (Hollis, Lichtenstein, Mount, Vogt, & Stevens, 1991).

ND smoking cessation 349
Interactive videodisc (ND)-based programs hold the promise of being a signifi- cant development in efforts to assist people in changing high-risk health behaviors. Videodiscs have proven to be quite effective in educational settings (Hasselbring et al., 1987; Kelly et al., 1987). The use of IVD-based curricular materials, as com- pared to traditional print and video materials, has resulted in increased academic scores and increased rates of learning (Hasselbring et al., 1987). The ability to pre- sent activities that branch according to performance has resulted in the production and use of IVD-based education in many fields, from medicine (Hatless, 1986) to military training (McGrane, Allely, & Toth, 1990).
IVD systems that combine a videodisc player with a computer and touch-sensi- tive display screen are able to respond to patient requests virtually instantaneously. Such touchscreen systems provide users (even computer-shy users) with an intu- itively simple and nonthreatening mechanism for indicating choices and exercising control of the program. IVD systems, which allow the user to control what material is presented and in what order, are quite different from linear video systems (i.e., videotapes played with a video cassette recorder) where the observer is passive.
The computer is a key component; it can use information provided by users to determine which parts of the video to show. Fast access to any portion of the video program (usually less than one second) under computer control means that IVD systems can tailor presentations imperceptibly. The use of an instantaneous logical branching process to tailor the intervention to the characteristics of the user causes the intervention to appear essentially seamless, despite the presence of numerous alternative intervention tracks.
Interventions also should be responsive to the needs of varied subpopulations who are attempting to quit smoking and who are doing so within very different social contexts. Evidence of such differences lies in the fact that while African Americans are more likely to attempt to quit than Caucasians (40% vs. 34%), they are much less likely to maintain abstinence at 3 months (12% vs. 20%) (U.S. Public Health Service, 1989). Similarly, it seems that the context for women who quit is different than men. For example, the annual rate of change in the quit ratio for African American males is much higher than for African American females (1.15% vs. 0.27%) (U.S. Public Health Service, 1989). Younger smokers and older smokers may need to deal with different issues. Interventions that demonstrate sen- sitivity to differences in the social context surrounding the quit experience for each subpopulation (e.g., by showing people who are similar in race/ethnicity) and that offer components (e.g., testimonials) designed to address those differences appear likely to be more effective (McGuire, 1969, 1981).
Other media-based approaches to smoking cessation have been tried, such as print materials and audio cassettes (e.g., Danaher & Lichtenstein, 1978). Such pro- grams have had limited success. Additionally, computer-based programs have also been developed (Schneider, 1986; Schneider, Walter, & O’Donnell, 1990). Originally offered via Electronic Information Exchange System (EIES) and then CompuServe, computerized electronic information services, the on-line smoking cessation program significantly increased cessation rates. The primary drawback of such on-line approaches (which require a computer, modem, and telephone line) is the limited number of people reached. The limitations on what can be presented via on-line services is also problematic. Most services have limited abilities to transmit more than simple character-based (i.e., text) screens. Full-motion animated graphics or video require a greater bandwidth than is currently available via telephone lines.

350 Noell, Biglan, Hood, and Britz
The primary advantages of IVD are the captivating medium (video) and auto- matic branching, which allows the intervention content to be tailored to the values and concerns of the individual. Because individual concerns about smoking cessa- tion differ greatly, a comprehensive program that covers all concerns would be extremely long. By asking about the concerns of the user, the IVD system can cus- tomize the content of intervention material (e.g., testimonials and quit tips), stress- ing those aspects having greatest salience. For example, for those people particu- larly concerned with weight gain following cessation, the system could offer rele- vant advice and information, potentially including tips on exercise and diet pro- grams (as appropriate for the individual’s physical condition and desires). Identification with the on-screen models (people modeling healthy behaviors and giving testimonials) may be enhanced using IVD, since the characteristics of the user determine which models are presented. By showing individuals acting in ways that reduce risk and discussing their desire to avoid high-risk behavior, video mate- rial may affect perceived norms and produce a more desirable normative context. Depicting models that are similar to the target audience and showing the modeled behavior being reinforced are two important factors that have been shown to increase the probability that the behavior will be imitated (Bandura, 1969).
Video materials can model attitudinal statements that support the learning of needed skills and support activities, such as engaging in cognitive rehearsal or role play, as an adjunct to the video material. Videos generally hold audience interest better than the typical didactic (lecture) presentation and provide educational advantages over didactic presentations and printed material. For example, videos can show dynamic transformations, using motion sequences (either live or via ani- mation), such as smoke infiltrating a building. Through the use of video it also is possible to show targeted behaviors in realistic settings. Messages can be presented in an appealing, cohesive manner that incorporates interesting and attractive indi- viduals with music, images, and relevant topics.
Another potential advantage is that IVD can be sensitive to the patient’s motiva- tional level or stage of change (DiClemente et al., 1991). The system can ascertain whether the patient most needs - or is interested in - motivation-enhancing mes- sages or strategies and tips to help with quitting. An important feature of IVD sys- tems, as opposed to passive linear video presentations, is that they can increase attention by requiring frequent responses from the user (Holland, 1960) and by providing material contingent on the user’s choices.
METHODS
Development of the IVD Program
Program content. The Interactive Videodisc Smoking Cessation Program (IVD- SCP) was modeled on a nurse-presented self-help intervention of proven efficacy (Hollis et al., 1991; Lichtenstein & Hollis, in press). The nurse-based intervention was tested as part of a large (N > 2,700) randomized trial. All subjects received a 30-s physician advice message to quit and supporting print materials. In addition to physician advice alone (plus a nurse-delivered pamphlet), a second condition tested the efficacy of physician advice plus a nurse-presented self-help cessation program (utilizing a linear smoking cessation video). The self-help group received an expired air carbon monoxide assessment (a measure of smoking rate), viewed a lo-

ND smoking cessation 351
min (linear) video, received “stop smoking” printed materials (some mailed), were given encouragement by the nurse-counselor to set a quit date, and received a fol- low-up phone call.
At 3-month follow-up, self-reported abstinence in the nurse-assisted intervention (11 .O%) was significantly better than reported abstinence in the advice-only condi- tion (6.2%). At one-year follow-up, the proportion of participants reporting contin- uous abstinence at both 3 and 12 months was still significantly (p < .Ol) higher (7.1%) for the nurse-assisted intervention when compared to advice only (3.9%). In each of these analyses nonrespondents were conservatively counted as smokers.
The protocol the nurse used to present information (including the linear video), answer questions, and solicit the patient to set a quit-smoking date was used as the basis for designing the IVD-SCP. A flowchart of the resulting program is shown in Figure 1. Most of the video used in the videodisc program was obtained from the linear videotape used by the nurse (Quitting oy1 Your Own; Biglan & Noell, 1987). The process used to create the original video was similar to that described in Biglan, James, LaChance, Zoref, and Joffe (1988). Some additional video footage was added to replicate the nurse’s activities.
Graphic screens for menus and data entry (e.g., where users type in their names and the quit date they want to set) were generated separately (using a desktop
Bars*
+ Work Breaks*
-_* DriakiogCoffee*
+ Talking on Phone*
other SmokeIx Phone Hotline
l These segments are matched to UK user on basis of mcdehg and branching variables (see text)
Figure 1. Program logic flowchart. ‘These segments are matched to the user on basis of modeling and branching variables (see text).

352 Noell, Biglan, Hood, and Britz
computer video production system), recorded on videotape, and edited into the master tape. The resulting tape was transferred to a plastic direct-read-after-write (DRAW) videodisc at Crawford Post-production Services (Atlanta).
Software development. SuperCard (Silicon Beach Software, Inc.) was used to cre- ate the computer program for controlling the videodisc player. Similar to HyperCard, SuperCard was chosen because of its ease of use. The inevitable trade- off between ease of use and power is compensated for by the ability to invoke external commands and functions (XCMDs and XFCNs) written in more powerful languages (e.g., Pascal or C) as necessary. For example, the personalized quit-plan generated by the IVD-SCP was written in Pascal, as it exceeded the report-generat- ing capabilities of SuperCard. When used with touchscreens that emulate mouse input, SuperCard obviates the need to develop independent device-drivers to han- dle touchscreen input. Creating SuperCard cards with “buttons” (i.e., screen areas sensitive to mouse inputs) allows direct mapping of touches to the on-screen cards.
Hardware platform. A unique, low-cost hardware configuration was used for this program. The IVD-SCP includes a Macintosh Classic computer (2-megabyte RAM, 40-megabyte hard disk), a Pioneer 4200 videodisc player, a Hewlett- Packard DeskWriter printer, and a 13-in. Panasonic TV/monitor (NTSC), equipped with a touchscreen from Information Strategies, Figure 2 illustrates the configura- tion. A critical point to note is that all of the video seen by the user is generated by the videodisc player. No video is generated directly by the computer. Generating
[Computer and laserdisc pla er are not vlslble to end-user. t;
Figure 2. Hardware configuration for IVD-SCP.

ND smoking cessation 353
video images through the computer would have necessitated purchase of a video board capable of generating computer (RGB) images and combining them with the videodisc player’s NTSC image format. With the exception of text generated by the character generator in the videodisc player (providing 11 lines of 20 characters each), all images are stored on the videodisc.
One implication of this approach is that any computer which has a serial (RS- 232) port and some way of accepting touchscreen input (e.g., a second serial port, an ADB port, or a parallel port) can be used to control the system, potentially reducing overall costs greatly. Eliminating the need for a computer that accepts video/graphics overlay boards and using an NTSC monitor rather than RGB moni- tors have allowed us to assemble complete interactive systems (including printer and cabinet) for less than $4,000.
Operation. The IVD-SCP system is a self-contained turnkey system that is com- pletely automatic; when turned on it presents a screen saying “Please touch screen to begin.” When touched, the system begins presenting the intervention. If at any time the user fails to touch the screen when prompted, the system waits 30 s and then displays a message saying that if the screen is not touched within 60 s the pro- gram will return to the beginning. Thus, if a patient leaves the program midway, the IVD-SCP resets itself in preparation for the next user.
The exact path followed through the program depends on the choices made by the user (see flowchart in Figure 1). However, all users see the humorous opening vignette, which is designed to reduce negative reactance (Brehm, 1966). After a brief introduction, the user is asked to indicate his or her readiness to quit (i.e, stage of change), using the “contemplation ladder” of Biener and Abrams (1991). This question marks the first branching point. A number of decision points follow, allowing users to tailor their own program.
A key feature of the program is that it presents on-screen models (e.g., as in tes- timonials) matched to the user. This is accomplished by using data on age, gender, and smoking rate provided by users in response to on-screen questions. Whenever advice from “ex-smokers” is appropriate, the program selects a matching model to deliver the testimonial. All testimonials use the words of actual ex-smokers, and regardless of demographics and smoking rate, each user hears the same words in a given testimonial (e.g., the testimonial on the importance of setting a specific quit date), although the person speaking those words may be an actor using a real ex- smoker’s words.
Ultimately, all smokers are led to a point where they are asked if they are willing to commit to quitting. If they answer affirmatively, they are asked if they are will- ing to prepare a quit plan, which includes setting a quit date. If they indicate readi- ness to prepare a quit plan, they see an on-screen keyboard and are asked to type their names by touching the letters on the keyboard. Each touch of a letter causes that letter to appear (using the character generator function of the videodisc player) in a window on the screen. (No video is generated by the computer itself, avoiding the need for expensive graphic overlay cards.)
The IVD-SCP presents a current calendar (determined by the computer’s built- in clock/calendar function) and asks the user to set a quit date within the next 4-5 weeks by touching the chosen day. Finally, the IVD-SCP prints a quit plan, which includes the user’s name, the coping tips they chose as most helpful, the American Lung Association telephone hotline number, and a calendar with the quit date circled.

354 Noel& Biglan, Hood, and Britz
In order to test user satisfaction with this type of system, subjects are asked three questions upon exiting the program:
1. How helpful was the program? 2. Would they recommend the program to others? 3. How easy was it to use?
Following these questions, the program presents a closing collage of positive images and motivational music. In this pilot test, no further contact with the IVD system occured.
Pilot Testing
Setting. Pilot testing of the IVD-SCP system was done in two branches of a fam- ily practice/internal medicine clinic in Eugene, Oregon. The protocol was similar to that used in the original nurse-based intervention (Hollis et al., 1991). At one clinic, a single provider gave patients identified as smokers a brief message about the importance of stopping smoking and then urged the patient to try out the IVD-SCP. At the other branch, three providers referred patients to the IVD- SCP. The IVD-SCP was placed in whatever exam room was not being used for other purposes that day. Each morning the physician’s assistant rolled the IVD system cart into the appropriate exam room and turned the IVD-SCP on. The system remained on until the end of the day, when it was switched off. Subjects were not observed during use, although the computer recorded all choices, as well as start and finish times. Subjects were free to leave at any point during the course of the program. All subjects were informed, in writing, that their use or nonuse of the program would have no bearing on their medical care and that none of the medical staff would see any of the information resulting from the patient’s use of the program.
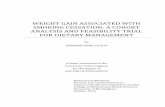
Subjects. A total of 27 adult smokers (10 males and 17 females) were referred by their providers to the IVD-SCP. Age distribution and smoking rate, by gender, are shown in Figure 3.
A) Subject Distribution by Age and Gender
T z : : 0
19-21 22-25 26-30 31-35 36-40 41-45 46-50 51-60 61+
nge 6) Smoking Rate by Gender
9
; $6 05 E4 13
2
:, cl0 11-14 15-19 20-24 25-29 30+
Cigarettes per Day
Figure 3. Subject characteristics.

ND smoking cessation 355
Procedures. Patients identified as smokers by their provider were asked to try the IVD-SCP. They were escorted to the room with the IVD-SCP and given an informed consent statement to read. If they consented to use the system, they signed the informed consent statement and were given a short questionnaire covering general health factors (e.g., amount of exercise each week, consump- tion of foods high in fats), demographics (including SES measures), and smok- ing status.
After completing the questionnaire (and indicating their willingness to be recon- tacted), patients activated the IVD-SCP by touching the screen. On-screen prompts directed patients to enter a code number (as listed on their questionnaire) to enable correlation of information obtained from the questionnaire with information obtained from the IVD-SCP Patients were free to leave at any point.
Those subjects who set a quit date while using the IVD program and who gave permission for recontact (on the written questionnaire) were called 3-5 months after their quit date and asked if they actually had attempted to quit and, if so, were they still abstinent. No further contact occurred.
In preliminary tests, it became apparent that subjects did not distinguish between the baseline questionnaire and the body of the intervention when both were administered, in succession, by the IVD kiosk. As we wished to assess reac- tions to the IVD intervention specifically, we tried to avoid confusion between assessment and intervention by administering the baseline questionnaire in written form, although a computerized version was available. An additional reason for using the written version was to preserve the methodology used in the nurse-deliv- ered intervention so that IVD subjects could be compared to subjects from the nurse-delivered version.
RESULTS
Overall, smokers who used the IVD-SCP were willing to complete the program, and the majority set quit dates (see Table 1). Indeed, the proportion of smokers willing to actually set quit dates (70%) compares quite favorably with the propor- tion of smokers who set quit dates in the model nurse-assisted intervention (30%; Hollis et al., 1991). Of the 19 smokers who set quit dates, 17 (89%) gave permis- sion for recontact. We were able to recontact 14 of 17 (82%). Of the 14 smokers recontacted, 11 (79%) reported a quit attempt. However, none of the 14 was absti- nent at follow-up.
Table 1. Subject Characteristics and Program Use by Gender
Agreed to use program Finished complete program Time to finish program Readiness to quit (IO-point scale) Set quit date Agreed to follow-up Reached for follow-up Attempted quit/abstinent @ 3 months No. of cravings tips viewed No. of situations tips viewed
Males
$90%) ,?-= 21.4, SD = 2.27 X= 7.9, SD= 1.85 6 (60%) 6 6 4/o X= 2.4, SD = 1.8 X= 2.0, SD= 1.5
Females
Z(94%) x= 20.1, SD = 2.60 X= 7.3, SD = 2.77 13 (76%) 11 8 7/o X= 1.6, SD = 0.9 X= 1.8, SD= 1.0

356 Noell, Biglan, Hood, and Britz
Users expressed general satisfaction with the program (see Figure 4), with most indicating the program was useful, easy to use, and worthy of recommenda- tion to others. The number of coping-with-cravings tips viewed varied widely, ranging from zero to the maximum possible, six. Both males and females viewed slightly fewer dealing-with-difficult-situation tips, on average, than coping-with- cravings tips.
DISCUSSION
The use of IVD-based smoking cessation programs appears promising. In this pilot test, subjects were more likely to set a quit date (70%) than in the nurse-delivered intervention on which it was modeled (30%; Hollis et al., 1991). Of those who set quit dates, the number that actually attempted to quit was also high when compared to the nurse-delivered intervention (79% vs. 50%). However, none of the 14 sub- jects who were recontacted were abstinent. Given that a typical quit rate is 5-15% (Glasgow & Lichtentstein, 1987; Hollis et al., 1991), only one to three abstinent subjects would have been expected. Statistically, there is no significance to the absence of successful quitters in a sample of 14 subjects, although it would have been more encouraging to have found one or more successful quitters.
The low cost of the hardware platform and the ability to amortize development costs over a number of sites makes the IVD-SCP quite cost competitive with other approaches for encouraging smoking cessation. IVD is not a “magic bullet,” nor is the system described above intended as a completely stand-alone intervention. The physician’s sanction and advice, which also communicates personalized concern to the patient, undoubtedly increases the efficacy of the intervention. However, the relatively low cost of using IVD systems (less than $4,000 each for the configura- tion described herein) compares very favorably to personnel costs using a live interventionist. The cost, when combined with advantages such as sensitivity to stage of change, consistency in delivery of the intervention, and ease of dissemina- tion, makes IVD systems very attractive.
A) How helpful was this program?
Very Some Not Much Not at all
B) Would you recommend this program?
ZO/_c---/ 15- _ lo- _ 5- 0/-‘
Yes Maybe No
C) How easy was it to use?
Very Easy Easy Hard Very Hard ’
Figure 4. Satisfaction with program.

IVD smoking cessation 357
The ultimate efficacy of the IVD approach will remain in question until a larger scale trial is conducted. Thus, an important research question yet to be answered is the extent to which IVD interventions can deliver stand-alone interventions effec- tively. Health education centers in clinics, schools, and worksites are just a few of the sites where stand-alone IVD interventions might be placed. Additional content areas beyond smoking cessation, such as diet, exercise, and substance use, also need to be evaluated.
REFERENCES
Bandura, A. (1969). Principles of behavior modification. New York: Holt, Rinehart, & Winston. Biener, L., & Abrams, D. B. (1991). The contemplation ladder: Validation of a measure of readiness
to consider smoking cessation. Health Psychology, 10, 360-365. Biglan, A., James, L. E., LaChance, P. A., Zoref, L., & Joffe, J. (1988). Videotaped materials in a
school-based smoking prevention program. Preventive Medicine, 17,559-584. Biglan, A., Noell, J. (Authors), & Independent Video Service (Producer). (1987). Quitting on your
own [Videotape]. Eugene: Oregon Research Institute. Brehm, J. W. (1966). A theory of psychological reactance. New York: Academic Press. Danaher, S. G., & Lichtenstein, E. (1978). Become an ex-smoker: With this book you can. Englewood
Cliffs, NJ: Prentice Hall. DiClemente, C. C., Prochaska, J. O., Fairhurst, S. K., Velicer, W. F., Velasquez, M. M., & Rossi, J. S.
(1991). The process of smoking cessation: An analysis of precontemplation, contemplation and preparation stages of change. Journal of Clinical and Consulting Psychology, 59,295-304.
Fagerstrom, K. 0. (1984). Effects of nicotine chewing gum and follow-up appointments in physician- based smoking cessation. Preventive Medicine, 13,5 17-527.
Glantz, S. A., & Parmley, W. W. (1991). Passive smoking and heart disease: Epidemiology, physiolo- gy, and biochemistry. Circulation, 83, 1-12.
Glasgow, R., & Lichtenstein, E. (1987). Long-term effects of behavioral smoking cessation interven- tions. Behavior Therapy, 18,297-324.
Glasgow, R. E., & Bernstein, D. D. (1981). Behavioral treatment of smoking behavior. In L. A. Bradley & C. K. Prokop (Eds.), Medical psychology: A new perspective. New York: Academic Press.
Harless, W. G. (1986). An interactive videodisc drama: The case of Frank Hall. Journal of Computer- Based Instruction, 13, 113-l 16.
Hasselbring, T., Sherwood, B., Bransford, J., Fleenor, K., Griffith, D., & Goin, L. (1987). An evalua- tion of a level-one instructional videodisc program. Journal of Educational Technology Systems, 16,151-169.
Holland, J. G. (1960). Teaching machines: An application of principles from the laboratory. Journal of the Experimental Analysis of Behavior, 34, 19-22.
Hollis, J. H., Lichtenstein, E., Mount, K., Vogt, T. M., & Stevens, V. J. (1991). Practical smoking ces- sation interventions for medical settings: Minimizing demands upon physicians. Preventive Medicine, 20,497-507.
Kelly, B., Camine, D., Gersten, R., & Grossen, B. (1987). The effectiveness of videodisc instruction in teaching fractions to learning-disabled and remedial high school students. Journal of Special Education Technology, 8,5-17.
Kottke, T. E., Battista, R. N., DeFriese, G. H., & Brekke, M. L. (1988). Attributes of successful smok- ing cessation interventions in medical practice: A meta-analysis of 39 controlled trials. Journal of the American Medical Association, 250,2883-2889.
Lichtenstein, E., & Glasgow, R. E. (in press). Smoking cessation: What have we learned over the past decade? Journal of Consulting and Clinical Psychology.
Lichtenstein, E., & Hollis, J. (in press). Health care provider referral to a smoking cessation clinic: Who follows through? The Journal of Family Practice.
Lichtenstein, E., & Mermelstein, R. J. (1984). Review of approaches to smoking treatment strategies: Behavior modification strategies. In J. D. Matarozzo, S. M. Weiss, J. A. Herd, N. E. Miller, & S. M. Weiss (Eds.), Behavioral health: A handbook of health enhancement and disease prevention (pp. 695-712). New York: Wiley.

358 Noell, Biglan, Hood, and Britz
McFall, R. M. (1978). Smoking cessation research. Journal of Consulting and Clinical Psychology, 46,703-712.
McGrane, W. L., Allely, E. B., & Toth, F. J. (1990). The use of interactive media in HIV/AIDS pre- vention in the military community. Military Medicine, X5,235-240.
McGuire, W. J. (1969). Attitudes and attitude change. In G. Lindzey & A. Aronson (Eds.), Handbook of social psychology. Reading, MA: Addison-Wesley.
McGuire, W. J. (1981). Theoretical foundations of campaigns. In R. E. Rice & W. J. Paisley (Eds.), Public communication campaigns. Beverly Hills, CA: Sage.
National Cancer Institute. (1991). Strategies to control tobacco use in the United States: A blueprint for public health action in the 1990’s (DHHS Publication No. 92-3326). Washington, DC: U.S. Government Printing Office.
National Heart, Lung, and Blood Institute. (1977). Respiratory diseases: Task force report on preven- tion, control and education (DHEW Publication No. NIH 77-1248). Washington, DC: U.S. Government Printing Office.
Ockene, J. K. (1987a). Physician-delivered interventions for smoking cessation: Strategies for increasing effectiveness. Preventive Medicine, 16,723-737.
Ockene, J. K. (1987b). Trends in smoking intervention. In Smoking and health: A national status report (DHHS Publication No. CDC 87-8396). Washington, DC: U.S. Government Printing Office.
Pederson, L. L. (1982). Compliance with physician advice to quit smoking: A review of the literature. Preventive Medicine, 11,7 l-84.
Russell, M. A. H., Wilson, C., Taylor, C., & Baker, C. D. (1979). Effect of general practitioners’ advice against smoking. British Medical Journal, 2,231-235.
Schneider, S. J. (1986). Trial of an on-line behavioral smoking cessation program. Computers in Human Behavior, 2,277-286.
Schneider, S. J., Walter, R., & O’Donnell, R. (1990). Computerized communication as a medium for behavioral smoking cessation treatment: Controlled evaluation. Computers in Human Behavior, 6, 141-151.
Thompson, R. S., Michnich, M. E., Friedlander, L., Gilson, B., Grothaus, L. C., & Storer, B. (1988). Effectiveness of smoking cessation interventions integrated into primary care practice. Medical Care, 26,62-76.
U.S. Public Health Service. (1979). Smoking and health: A report of the Surgeon General (DHEW Publication No. PHS 79-50066). Washington, DC: U.S. Government Printing Office.
U.S. Public Health Service. (1982). Smoking and health: A report of the Surgeon General (DHEW Publication No. PHS 82-50179). Washington, DC: U.S. Government Printing Office.
U.S. Public Health Service. (1984). The health consequences of smoking: A report of the Surgeon General (DHHS Publication No. CDC 84-50205). Washington, DC: U.S. Government Printing Office.
U.S. Public Health Service. (1989). Reducing the health consequences of smoking: A report of the Surgeon General (DHHS Publication No. CDC 89-8411). Washington, DC: U.S. Government Printing Office.
U.S. Public Health Service. (1990). The health benefits of smoking cessation: A report of the Surgeon General (DHHS Publication No. CDC 90-8416). Washington, DC: U.S. Government Printing Office.
Wilson, D. M. C., Lindsay, E. A., Best, J. A., Gilbert, J. R., Wilms, D. G., & Singer, J. (1987). A smoking cessation intervention for family physicans. Canadian Medical Association Journal, 137, 613-619.