An evidence-based review of yoga as a complementary intervention for patients with cancer
11
Psycho-Oncology Psycho-Oncology 18: 465–475 (2009) Published online 26 September 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pon.1411 Review An evidence-based review of Yoga as a complementary intervention for patients with cancer Kelly B. Smith and Caroline F. Pukall Department of Psychology, Queen’s University, Kingston, Ont., Canada Abstract Objective: To conduct an evidence-based review of yoga as an intervention for patients with cancer. Specifically, this paper reviewed the impact of yoga on psychological adjustment among cancer patients. Methods: A systematic literature search was conducted between May 2007 and April 2008. Data from each identified study were extracted by two independent raters; studies were included if they assessed psychological functioning and focused on yoga as a main intervention. Using a quality rating scale (range 5 9–45), the raters assessed the methodological quality of the studies, and CONSORT guidelines were used to assess randomized controlled trials (RCTs). Effect sizes were calculated when possible. In addition, each study was narratively reviewed with attention to outcome variables, the type of yoga intervention employed, and methodological strengths and limitations. Results: Ten studies were included, including six RCTs. Across studies, the majority of participants were women, and breast cancer was the most common diagnosis. Methodological quality ranged greatly across studies (range 5 15.5–42), with the average rating (M 5 33.55) indicating adequate quality. Studies also varied in terms of cancer populations and yoga interventions sampled. Conclusions: This study provided a systematic evaluation of the yoga and cancer literature. Although some positive results were noted, variability across studies and methodological drawbacks limit the extent to which yoga can be deemed effective for managing cancer-related symptoms. However, further research in this area is certainly warranted. Future research should examine what components of yoga are most beneficial, and what types of patients receive the greatest benefit from yoga interventions. Copyright r 2008 John Wiley & Sons, Ltd. Keywords: cancer; oncology; yoga; systematic review; psychological functioning Introduction Receiving a diagnosis of cancer and undergoing treatment is associated with high emotional distress and lowered psychological and physical quality of life [1]. The most common symptoms experienced by patients with cancer are pain, anxiety, depres- sion, and fatigue, which may continue even after the treatment has ended [1]. The National Institutes of Health has identified the need for research to specify what patients are at risk for cancer-related symptoms such as emotional distress, and what treatments can best address such symptoms [1]. Many patients with cancer turn to complemen- tary and alternative medicine (CAM) techniques to help manage their symptoms [2,3]. CAM encom- passes a broad array of heterogeneous treatments, ranging from herbal medicine to yoga. Yoga has recently undergone empirical investigation as a potentially beneficial intervention for patients with cancer. An ancient Eastern tradition, the Indian form of yoga encompasses various domains, including ethical disciplines (e.g. non-harm in actions and words), physical postures, and spiritual practices, with the goal of uniting the mind, body, and spirit for health and self-awareness [4,5]. In Western cultures, yoga is most often associated with physical poses (i.e. asanas), breath control (i.e. pranayama), and meditation (i.e. dyhana) [6]. Fifteen million adults are estimated to have used yoga in their lifetime in the United States, with almost half using yoga to promote wellness, prevent health problems, or manage a specific health condition [7]. Recent studies suggest that yoga is beneficial for reducing certain symptoms in a number of conditions, including asthma, carpal tunnel syndrome, multiple sclerosis, anxiety, and depression [8–12]. Research also indicates that yoga is successful in generating the relaxation response among healthy participants [e.g. 13]. * Correspondence to: Department of Psychology, Queen’s University, 62 Arch Street, Kingston, Ont., Canada K7L 3N6. E-mail: [email protected] Received: 18 February 2008 Revised: 17 May 2008 Accepted: 22 May 2008 Copyright r 2008 John Wiley & Sons, Ltd.
Transcript of An evidence-based review of yoga as a complementary intervention for patients with cancer
Psycho-OncologyPsycho-Oncology 18: 465–475 (2009)Published online 26 September 2008 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pon.1411
Review
An evidence-based review of Yoga as a complementaryintervention for patients with cancer
Kelly B. Smith� and Caroline F. PukallDepartment of Psychology, Queen’s University, Kingston, Ont., Canada
Abstract
Objective: To conduct an evidence-based review of yoga as an intervention for patients with
cancer. Specifically, this paper reviewed the impact of yoga on psychological adjustment among
cancer patients.
Methods: A systematic literature search was conducted between May 2007 and April 2008.
Data from each identified study were extracted by two independent raters; studies were
included if they assessed psychological functioning and focused on yoga as a main intervention.
Using a quality rating scale (range5 9–45), the raters assessed the methodological quality of
the studies, and CONSORT guidelines were used to assess randomized controlled trials
(RCTs). Effect sizes were calculated when possible. In addition, each study was narratively
reviewed with attention to outcome variables, the type of yoga intervention employed, and
methodological strengths and limitations.
Results: Ten studies were included, including six RCTs. Across studies, the majority of
participants were women, and breast cancer was the most common diagnosis. Methodological
quality ranged greatly across studies (range5 15.5–42), with the average rating (M5 33.55)
indicating adequate quality. Studies also varied in terms of cancer populations and yoga
interventions sampled.
Conclusions: This study provided a systematic evaluation of the yoga and cancer literature.
Although some positive results were noted, variability across studies and methodological
drawbacks limit the extent to which yoga can be deemed effective for managing cancer-related
symptoms. However, further research in this area is certainly warranted. Future research
should examine what components of yoga are most beneficial, and what types of patients
receive the greatest benefit from yoga interventions.
Copyright r 2008 John Wiley & Sons, Ltd.
Keywords: cancer; oncology; yoga; systematic review; psychological functioning
Introduction
Receiving a diagnosis of cancer and undergoingtreatment is associated with high emotional distressand lowered psychological and physical quality oflife [1]. The most common symptoms experiencedby patients with cancer are pain, anxiety, depres-sion, and fatigue, which may continue even after thetreatment has ended [1]. The National Institutes ofHealth has identified the need for research tospecify what patients are at risk for cancer-relatedsymptoms such as emotional distress, and whattreatments can best address such symptoms [1].Many patients with cancer turn to complemen-
tary and alternative medicine (CAM) techniques tohelp manage their symptoms [2,3]. CAM encom-passes a broad array of heterogeneous treatments,ranging from herbal medicine to yoga. Yoga hasrecently undergone empirical investigation as apotentially beneficial intervention for patients with
cancer. An ancient Eastern tradition, the Indianform of yoga encompasses various domains,including ethical disciplines (e.g. non-harm inactions and words), physical postures, and spiritualpractices, with the goal of uniting the mind, body,and spirit for health and self-awareness [4,5]. InWestern cultures, yoga is most often associatedwith physical poses (i.e. asanas), breath control (i.e.pranayama), and meditation (i.e. dyhana) [6].Fifteen million adults are estimated to have usedyoga in their lifetime in the United States, withalmost half using yoga to promote wellness,prevent health problems, or manage a specifichealth condition [7]. Recent studies suggest thatyoga is beneficial for reducing certain symptoms ina number of conditions, including asthma, carpaltunnel syndrome, multiple sclerosis, anxiety, anddepression [8–12]. Research also indicates thatyoga is successful in generating the relaxationresponse among healthy participants [e.g. 13].
* Correspondence to:Department of Psychology,Queen’s University, 62 ArchStreet, Kingston, Ont.,Canada K7L 3N6. E-mail:[email protected]
Received: 18 February 2008
Revised: 17 May 2008
Accepted: 22 May 2008
Copyright r 2008 John Wiley & Sons, Ltd.

To date, a number of studies have incorporatedyoga into larger intervention programs aimed atpatients with cancer. For example, Mindfulness-Based Stress Reduction (MBSR) programs includeyoga as one of the mind–body techniques designedto reduce stress. Speca et al. [14] conducted arandomized controlled trial (RCT) of MBSRamong 90 patients with various forms of cancer.After the seven-week intervention, the treatmentgroup reported significantly less mood disturbanceand reduced stress in comparison with the wait-listcontrol group. Other studies using an MBSRapproach have found positive effects on sleep,anxiety, quality of life, and spiritual growth, andon physical parameters such as lowered bloodpressure and altered cortisol levels [15–18]. Theseresults are promising and suggest that MBSRprograms are beneficial for patients with canceron several psychological and physical outcomes.However, it is not clear what component(s) of theseprograms may be responsible for inducing change.Recently, studies investigating yoga as a com-
plementary intervention for various populations ofcancer patients have emerged in the literature. Todate, one systematic review has focused on yogainterventions for people with cancer [19], and atleast one non-systematic review has been published[20]. The literature searches for these previousreviews occurred in November 2003 and March2005, respectively; as such, they do not includeseveral studies that have since been completed.Furthermore, previous reviews have not calculatedthe effect sizes associated with primary outcomes,and the quality of studies included by Bower et al.[20] was not systematically assessed. The purposeof the current paper was to systematically reviewthe literature examining yoga as an intervention forpersons with cancer. Specifically, this paper aimedto review recent literature examining the impact ofyoga on psychological adjustment among cancerpatients. In addition, the methodological quality ofthe studies was coded systematically and the effectsizes were calculated when possible.
Methods
Literature search
The literature search was conducted between May2007 and April 2008. The following databases weresearched using the combined terms of yoga, cancer,and neoplasm: EMBASE; PsycINFO; PsycARTI-CLES; Psychology: A SAGE Full-Text Collection;Medline; The Cochrane Library; Cochrane Data-base of Systematic Reviews; The Complementaryand Alternative Medicine Evidence Online (CA-MEOL) database; The Database of Abstracts ofReviews of Effects (DARE); and Dissertations andTheses. No language restrictions were set during
the search. The reference lists of all identifiedarticles and the table of contents of the Interna-tional Journal of Yoga Therapy were also reviewed.In addition, the web sites of the AmericanPsychosomatic Society (APS) and the AmericanSociety of Clinical Oncology (ASCO) weresearched to identify recent work in this area.Finally, authors who had published or presentedon the topic of yoga and cancer were contacted viaemail to obtain information on recently publishedor in-press articles.
Study inclusion criteria
To be included in this review, studies were requiredto include at least one group of participants with adiagnosis of cancer. Studies were included if theyassessed psychological functioning as a measure ofoutcome (e.g. quality of life). In addition, studieshad to examine yoga as a main intervention;studies that included yoga as part of a largerintervention program (e.g. MBSR), and/or thosethat did not provide findings specific to yoga, werenot included [for a systematic review of MBSR forcancer see 21]. No restrictions were imposed on thetype of study included in the review. However, onlyfull research papers were included; studies forwhich only abstracts were available were not used.Furthermore, unpublished studies (e.g. disserta-tions) were included only if they had not beensubsequently published.Using these criteria, 10 articles were identified by
the primary author for inclusion in the review, andone article [22] was brought to our attentionthrough discussion. Although an increased lengthof follow-up was documented in one article [23],this paper appeared to be based on the samedata as another [24]. As such, only the peer-reviewed article was included in this review; thiswas done in order to reduce bias that would resultif multiple publications of the same data wereincluded [25]. Thus, 10 studies were included in thereview.
Data extraction
Information was extracted from each study using aform that was based on a template developed bythe Center for Reviews and Dissemination (CRD)[25]. Information regarding study characteristics(e.g. target population), methodological factors(e.g. study design), outcome variables, data analy-sis, and results was extracted from each study toensure that inclusion criteria were met and to aid inthe quality rating process described below. All datawere extracted independently by each author andsubsequently combined.
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon
466 K. B. Smith and C. F. Pukall

Quality rating system
Using the measure developed by Suydam [26],the quality of each study was evaluated on thefollowing dimensions: (1) significance of theproblem; (2) clarity of the definition of theproblem; (3) adequacy of design; (4) adequacy ofcontrol variables; (5) adequacy of sample selection;(6) reliability and validity of measures; (7) validityof data analysis; (8) appropriateness of interpreta-tions and generalizations; and (9) adequacy of theresearch report. Each dimension was rated using a5-point Likert scale from 1 (poor) to 5 (excellent),and a total quality score was created by summingthe ratings for each dimension (range5 9–45;higher scores indicated greater methodologicalquality). This rating system and approach has beenused previously in health psychology review articles[e.g. 27]. Each author independently rated eachstudy, and total scores for each study were thencompared. If a discrepancy of more than fourpoints for any one study was found, the scores werediscussed and the article was subsequently re-rated.The final quality score for each study represents theaverage of the two rater’s scores.In addition, each RCT was evaluated using the
guidelines and checklist of the ConsolidatedStandards of Reporting Trials (CONSORT) State-ment 2001 [28,29]. The 22-item checklist was usedto examine whether specific information wasreported in the reviewed RCTs. Subsequently, ascore out of 21 was created to indicate how closelyCONSORT guidelines were followed in the report-ing of each study; item 11 was not included in thisscore, as the nature of the RCTs evaluated made itimpossible for participants to be blinded. Inaddition, half points were given when studiesincluded one part of a multi-component item. Eachauthor independently evaluated the RCTs, andCONSORT ratings were subsequently compared.Any discrepancies were discussed, and a finalCONSORT score for each RCT was calculated.
Statistical calculations
Effect sizes were calculated using Cohen’s d statisticfor studies that: (1) based their findings oncalculated group means; and (2) included treatmentand control groups. For the majority of thesestudies, Cohen’s d was calculated using thereported post-intervention means from the treat-ment and control groups and a pooled standarddeviation. One study [i.e. 22] only reported mid-intervention means; in this case, Cohen’s d wascalculated using these means and a pooled stan-dard deviation. Data for the effect sizes wereextracted by the primary author and calculatedusing the Statistical Package for Social Sciences(SPSS), Version 14.0.
Results
Six published RCTs [22,24,30–33], two non-con-trolled studies (one unpublished) [34,35], and oneprogram evaluation study [36] were located. Onepublished study indirectly compared yoga with twoother treatment groups, yet no direct between-group comparisons were made [37]. This paper wastherefore treated as a non-controlled trial in thepresent review.
Study characteristics
The descriptive characteristics of the 10 reviewedstudies are presented in Table 1. The number ofparticipants ranged from 13 to 398. Based on thesix studies that reported average age, the mean ageof participants was 52.37 years. The majority ofparticipants (directly reported in 8 of 10 studies)were women. Only three studies reported specificethnic breakdown of their participants [33–35]. Intwo of these studies, the majority of participantswere Caucasian [34,35]. With regard to diagnosis,six of the studies focused exclusively on breastcancer, and this type of cancer was present in 85%of participants sampled by Culos-Reed et al. [24].The majority of studies (9 of 10) included patientswho were concurrently receiving other forms oftreatment at the time of participation, and 6 of thestudies reported on participants’ past treatmentstatus. Information regarding concurrent and pasttreatments of the reviewed samples is also pre-sented in Table 1.
Quality ratings and effect sizes
The psychological outcome variables, quality rat-ings of the studies, CONSORT ratings (whenapplicable), and effect sizes (when calculated) arepresented in Table 2. The quality ratings of thestudies ranged from 15.5 to 42. The mean qualityrating was 33.55, indicating an adequate score [27],and the average CONSORT rating score was 12.5.Effect sizes were calculated for each study that
included a control group condition and reportedbetween-group findings using mean values. Usingthese criteria, effect sizes were calculated for four ofthe studies using post-intervention means[24,30,32,33], and for one study using mid-inter-vention means [22]. Only one of these studiesreported effect sizes within its article [33]; however,as it reported effect sizes based on adjusted estimatechange scores, Cohen’s d effect sizes were calcu-lated in the present review.Given the large number of psychological vari-
ables included in these five studies, effect sizes werecalculated for total scores of the measures whenavailable. In some cases, mean values were onlyprovided for significant between-group findings[e.g. 24]; when this occurred, effect sizes could not
Evidence-based review of Yoga for cancer 467
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon

Tab
le1.
Study
des
crip
tive
char
acte
rist
ics
Stu
dy
Desi
gn
Inte
rven
tio
nS
am
ple
Can
cer
typ
e
Co
ncu
rren
t
treatm
en
tP
ast
treatm
en
t
Tim
esi
nce
past
treatm
en
t
Co
ntr
ol
Tre
atm
en
t
Ban
erje
e
etal
.[3
0]
RC
TY
oga
.90
min
clas
ses
for
6w
eeks
.N
um-
ber
of
clas
ses/
wee
kN
/A.
Hom
epra
ctic
een
cour
-
aged
n5
58
wom
en.
Age
rang
e
30–70.
Mag
e5
44
Bre
ast
(Sta
ge
II–III
)
Rad
iatio
nth
erap
y(a
llw
om
en;
n5
58)
Che
moth
erap
y(n
528)
Surg
ery
(all
wom
en;n
558)
N/A
Support
ive
coun
selin
g/lig
ht
exer
cise
(n5
23)
Bla
nket
al.
[31]
RC
TIy
enga
rY
oga
.2
clas
ses/
wee
kfo
r8
wee
ks.
Cla
ss
dur
atio
nN
/A.H
om
epra
c-
tice
enco
urag
ed
n5
18
wom
en.
Age
rang
e
48–69.M
age
N/A
Bre
ast
(Sta
ge
I–III
)
Ant
i-es
troge
nor
arom
atas
e
inhi
bito
rho
rmona
lth
erap
y
(all
wom
en;n
518)
Surg
ery
(all
wom
en;
n5
18).
Che
moth
erap
y(5
0%
).R
adia
-
tion
ther
apy
(ove
r60%
).
Rec
ons
truc
tive
surg
ery
(n5
2)
N/A
(sur
geries
).
3m
ont
hs–3ye
ars
(che
moth
erap
y/ra
dia
-
tion
ther
apy)
Wai
t-lis
t
(n5
9)
Car
son
etal
.
[34]
NC
TY
oga
.of
Aw
aren
ess
Pro
gram
.120
min
clas
s/w
eek
for
8
wee
ks.H
om
epra
ctic
e
enco
urag
ed
n5
13
wom
en.
Age
rang
e
44–75.
Mag
e5
59
Bre
ast
(met
asta
tic)
Che
moth
erap
y(n
57).
Ant
i-
dep
ress
ants
(n5
N/A
)
N/A
N/A
No
cont
rol
group
Cohe
net
al.
[32]
RC
TT
ibet
anY
oga
.7
wee
kly
sess
ions
.Cla
ssdur
atio
nN
/
A.H
om
epra
ctic
e
enco
urag
ed
n5
39,24
wom
en.A
ge
rang
eN
/A.M
age
551
Lym
pho
ma
(Sta
geI–
IV)
Che
moth
erap
y(n
59)
Che
moth
erap
y(n
530)
12
mont
hsor
less
Wai
t-lis
t
(n5
19)
Cul
os-
Ree
det
al.[2
4]
RC
TY
oga
.75
min
clas
s/w
eek
for
7w
eeks
.
n5
38,95%
wom
en.A
ge
rang
eN
/A.M
age
551.1
8
Bre
ast
(85%
).
Oth
erty
pes
N/A
.
None
N/A
Min
imum
3m
ont
hsW
ait-
list
(n5
18)
Jose
ph
[37]
NC
Ta
Yoga
.90
min
clas
s
2tim
es/w
eek.
Dur
atio
n
of
pro
gram
N/A
n5
125.
Gen
der
ratio
N/A
.A
ge
rang
eN
/A.
Mag
e
N/A
N/A
Dai
lyra
dia
tion
ther
apy
N/A
N/A
TM
(n5
25)
Gro
upth
erap
y
(n5
50)
Moad
elet
al.
[33]
b
RC
TH
atha
Yoga
spec
ific
to
bre
ast
canc
erpat
ient
s.
90
min
clas
s/w
eek
for
12
wee
ks.H
om
epra
ctic
e
enco
urag
ed
n5
128
wom
en.
Age
rang
e
28–75.M
age
554.8
1
Bre
ast
(Sta
ge
I–IV
)
Che
moth
erap
y(a
tbas
elin
e
527%
;3
mont
hsf/u
533%
).
Rad
iatio
nth
erap
y(a
tbas
elin
e
510%
;3
mont
hsf/u
510%
).
Ant
i-es
troge
nth
erap
y(a
t
bas
elin
e5
30%
;3
mont
hsf/
u5
41%
)
Mas
tect
om
y(3
1%
).
Lum
pec
tom
y(5
3%
).
Mas
tect
om
yan
d
lum
pec
tom
y(1
1%
).
N/A
Wai
t-lis
t
(n5
44)
Rag
have
ndra
et
al.[2
2]
RC
TY
oga
.30
min
clas
s.N
um-
ber
of
clas
ses
N/A
.
Leng
thof
yoga
pro
gram
N/A
.H
om
epra
ctic
e
requi
red
n5
62
wom
en.
Age
rang
e
30–70.M
age
N/A
Bre
ast
(Sta
ge
II–III
)
Che
moth
erap
y(a
llw
om
en;
n5
62)
Mas
tect
om
y(a
llw
om
en;
n5
62).
Rad
ioth
erap
y
(n5
38)
N/A
Support
ive-
ex-
pre
ssiv
eco
un-
selin
g/co
pin
g
educ
atio
n
468 K. B. Smith and C. F. Pukall
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon

be calculated for the non-significant findings. Anaverage effect size was not calculated across studiesdue to the small number of effect sizes and to thevariation between studies with respect to outcomevariables and interventions. Using Cohen’s recom-mendations, effect sizes were considered to be small(0.20), medium (0.50), or large (0.80) [38].
Description of studies
The remaining results section focuses on a narra-tive description of the reviewed studies. Studies aregrouped below by type (e.g. RCT). Within eachgroup, individual studies are described in terms oftheir targeted intervention, outcomes, andstrengths and limitations.
Randomized controlled trials
Blank et al. [31] published the first RCT examiningyoga as a primary intervention for cancer patients.Women with breast cancer were randomized toeither a wait-list control group (n5 9) or to anintervention group (n5 9) that consisted of parti-cipation in an eight-week Iyengar yoga programand the completion of a self-report measure duringweek six. The sessions involved a discussion period,seated meditation, asanas (including standing,seated, and inverted postures), and a final relaxa-tion pose (i.e. savasana). The self-report compo-nent evaluated reasons for participation, stress,levels of effort during class, body image, andperceptions regarding the impact of yoga onawareness.Given that no outcome reports are provided for
the control group, no formal statistics wereconducted, and no information is provided regard-ing potential differences in group characteristics, itis difficult to assess whether changes reported bythe treatment group are associated with theintervention. However, 88% of the interventiongroup reported improved body image and feelingmore relaxed in their daily lives, and 63% reportedincreased mood and reduced anxiety. Womenprovided a number of reasons for choosing toparticipate in the study, including a desire toimprove health and stress-management abilities.When asked on a scale of 1 (unlikely) to 10(extremely likely) how likely they were to practiceyoga after the completion of the study, the averageresponse with regard to home practice and practicein formalized classes was 6.2 and 5.5, respectively.Cohen et al. [32] examined Tibetan yoga,
consisting of breathing, visualization, mindfulness,and postures, in a seven-week intervention forpatients with lymphoma. Group assignment wasdetermined through the process of minimization,with participants assigned to either the yogatreatment (n5 20) or wait-list control (n5 19)group. Patients completed well-validated measuresR
ose
nbau
m
etal
.[3
6]
Pro
gram
Eval
.
Res
tora
tive
Yoga
.
2cl
asse
s/w
eek.
Cla
ss
dur
atio
nN
/A
n5
398,66%
wom
en.A
ge
rang
e25–75
or
more
.M
age
N/A
Bre
ast
Pro
stat
e
Lym
pho
ma
Leuk
emia
Oth
er
Med
ical
(i.e
.ch
emoth
erap
y;
imm
unoth
erap
y;ra
dia
tion;
sur-
gery
).O
ther
(e.g
.ex
erci
se;
support
group
s)(n
s5
N/A
)
N/A
N/A
No
cont
rol
group
.Pro
-
gram
sno
t
com
par
ed.
War
ner
[35]
NC
TA
rtof
Livi
ngPro
gram
.
Dai
lycl
ass
for
8day
s
rang
ing
from
3–5
h.5-
wee
ksm
aint
enan
ceper
iod
n5
26
wom
en.
Age
rang
e
35–78.
Mag
e5
54.2
1
Bre
ast
(Sta
ge
0–III
)
Surg
ery
(n5
1).
Rec
ons
truc
-
tive
surg
ery
(n5
1)
(occ
urre
d
dur
ing
mai
nten
ance
per
iod).
Rad
iatio
nth
erap
y(n
52).
Horm
ona
lth
erap
y(n
510)
Mas
tect
om
y(n
57).
Lum
-
pec
tom
y(n
513).
Mas
tect
-
om
yan
dlu
mpec
tom
y(n
55).
Rec
ons
truc
tive
surg
ery
(n5
10).
Che
moth
erap
y
(n5
15).
Rad
iatio
nth
erap
y
(n5
16)
1–36.3
mont
hs(s
ur-
gery
)21
day
s–35.4
mont
hs(c
hem
oth
er-
apy)
1day
–29.1
mont
hs(r
adia
tion
ther
apy)
No
cont
rol
group
RC
T,ra
ndom
ized
contr
olle
dtr
ial;
NC
T,non-c
ontr
olle
dtr
ial;
N/A
,not
avai
lable
(stu
dy
did
not
report
);Eva
l.,ev
aluat
ion;F/
U,fo
llow
-up;
TM
,tr
ansc
enden
tal
med
itat
ion;
Mag
e,m
ean
age
show
nin
year
s.a T
his
study
was
trea
ted
asnon-c
ontr
olle
din
the
pre
sent
revi
ew.
bT
his
study
asse
ssed
par
tici
pan
tsat
bas
elin
ean
d1-,
3-,
and
6-m
onth
follo
w-u
pin
terv
als.
How
ever
,only
bas
elin
ean
d3-m
onth
follo
w-u
pdat
aar
ere
port
edin
the
ori
ginal
articl
e.
Evidence-based review of Yoga for cancer 469
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon
of distress, anxiety, depression, fatigue, and sleepquality at baseline and at one-week, one-month,and three-month follow-up periods. However, dueto a lack of significant group-by-time interactions,the post-intervention data were averaged across allfollow-ups. In this study, the treatment and controlgroups were equivalent on demographic character-istics and baseline measures.Although no significant post-treatment differ-
ences were reported between groups on themeasures of distress, anxiety, mood, and fatigue,significant improvements on most aspects of sleepquality were reported for the intervention group.As shown in Table 2, a large effect size wasassociated with overall sleep quality, whereas smalleffect sizes were noted for the remaining outcomes.The authors suggest that the lack of significantfindings for the various psychological measurescould be due to several factors, including the
generally low levels of distress at baseline andfollow-up in their sample [32]. In comparison withthe reviewed RCTs that demonstrated large effectsizes and significant between-groups differences onmeasures of anxiety and depression [e.g. 22,30],Cohen et al.’s sample was less likely to be receivingconcurrent medical treatment. In fact, the majorityof participants in this study were not receivingtreatment, whereas all participants in Banerjee etal.’s and Raghavendra et al.’s studies (outlinedbelow) were concurrently receiving radiotherapyand chemotherapy, respectively; perhaps this mayaccount for differences noted across some ofthe RCTs.Culos-Reed et al.’s [24] study included 38 cancer
patients who were not currently undergoing anyform of treatment. The majority of participants hadbreast cancer; other cancer types were not reported.Patients were randomly assigned to either a wait-list
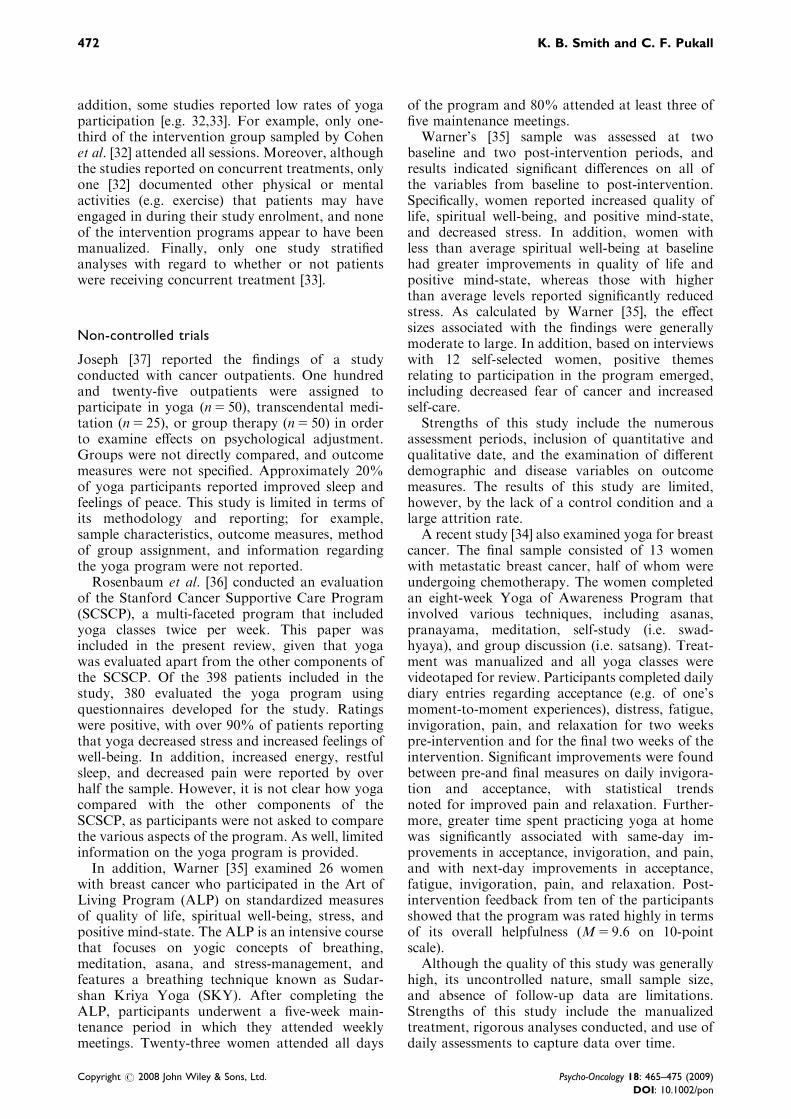
Table 2. Outcomes and results of reviewed studies
Study Quality rating CONSORT score Outcomesa Effect size
Banerjee et al. [30] 34.5 12.5 Anxiety 4.67
Depression 7.44
Stress 2.25
Blank et al. [31] 27.5 3.5 Stress —
Effort level —
Awareness —
Carson et al. [34] 39 — Daily diary —
Cohen et al. [32] 39.5 16.5 Distress 0.04
Anxiety 0.04
Depression 0.17
Fatigue 0.00
Sleep quality 0.98
Culos-Reed et al. [24] 38 13 Mood 0.74
Quality of life 0.83b
Stress —
Joseph [37] 15.5 — N/A
Moadel et al. [33] 42 15 Quality of life 0.28
Fatigue 0.05
Spiritual well-being 0.39
Mood 0.27
Raghavendra et al. [22] 36 14.5 Anxiety 1.34
Depression 1.31
Symptom distress 1.24
Quality of life 1.51
Rosenbaum et al. [36] 24.5 — Quality of life —
Warner [35] 39 — Quality of life —
Spiritual well-being —
Stress —
Mood —
N/A, not available (study did not report). Effect size shown for all studies except Raghavendra et al.’s is Cohen’s d, calculated for the total score of a measure (when
available) using the following formula: d 5 (post-interventionM1)-(post-interventionM2)/pooled SD. Effect size shown for Raghavendra et al.’s study is Cohen’s d, calculated
for the total score of a measure using the following formula: d 5 (mid-interventionM1)–(mid-interventionM2)/pooled SD. Quality rating possible range 5 9–45.
CONSORT score possible range 5 0–21.aOnly psychological outcomes are shown.bEffect size shown pertains to the emotional function aspect of quality of life.
470 K. B. Smith and C. F. Pukall
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon

(n5 18) or a seven-week yoga treatment condition(n5 20) that included supine breathing, asanas, andsavasana. Patients completed standardized psycho-logical measures assessing mood, stress, and qualityof life at pre- and post-intervention. Both groupswere equivalent in terms of demographic character-istics, and analyses accounted for baseline scoreswhen comparing groups on the post-interventionmeasures. Following the intervention, patients inthe yoga group reported significant improvementsin emotional functioning and quality of life incomparison with control patients. In addition, therewas a statistical trend toward improvement for thetreatment group on several measures, includingoverall mood disturbance and cognitive function.The estimated effect sizes associated with this studywere large (Table 2), suggesting that statisticallysignificant findings may have resulted with a largersample size.Furthermore, Moadel et al. [33] conducted a
RCT investigating the effectiveness of yoga forwomen with breast cancer. Women were of variousethnicities, and almost half were receiving medicaltreatment for cancer. Participants were stratified bymedical treatment type (e.g. chemotherapy) andwere then randomly assigned to a yoga treatment(n5 84) or wait-list control (n5 44) condition.Although patients were assessed on standardizedmeasures of quality of life (e.g. social well-being),distressed mood, fatigue, and spiritual well-being atbaseline and one-, three-, and six-month intervals,only baseline and three-month data are reported inthe article.The study investigators conducted a series of
intent-to-treat analyses to assess the predictivevalue of the treatment conditions on the outcomevariables. In comparison with the yoga group,control patients experienced a greater decrease insocial well-being over time. In addition, secondaryanalyses conducted only with patients not receivingchemotherapy (treatment group, n5 45; controlgroup, n5 26) demonstrated that yoga participantsreported greater quality of life, increased emotional,social, and spiritual well-being, and less distressafter the intervention in comparison with controls.Given that 31% of the intervention patients did notattend any of the yoga classes, the authors alsoexamined predictors of class attendance. Womenwho attended class less frequently were more likelyto be fatigued, younger, receiving radiotherapy, andnot receiving anti-estrogen therapy. In addition, aninteraction was noted between adherence to theyoga program and baseline levels of distress:patients with the lowest levels of baseline distressexperienced decreased distress with high adherence,and greater distress with no adherence to theprogram. As shown in Table 2, estimated effectsizes for this study were generally small.Two recent RCTs conducted in India examined
yoga for women with breast cancer. One examined
a six-week yoga program, including asanas, pra-nayama, and relaxation for women with breastcancer who were concurrently receiving radio-therapy [30]. Participants were randomly assignedto a yoga treatment (n5 35) or supportive counsel-ing (n5 23) condition, and were assessed both pre-and post-intervention on standardized measures ofanxiety, depression, and perceived stress. In com-parison with pre-treatment levels, self-reportedanxiety, depression, and stress decreased for thewomen who underwent the yoga intervention,whereas anxiety and depression scores increasedfor controls. Analyses indicated that these changeswere significantly different between groups.The second RCT from India compared breast
cancer patients who received a yoga program,including asanas, pranayama, meditation, andrelaxation (n5 28) with those who received sup-portive counseling and education (n5 34) [22]. Allpatients were concurrently receiving chemother-apy, and were assessed pre-, mid-, and post-chemotherapy on standardized measures of anxi-ety, depression, and quality of life and on a non-standardized measure of symptom (both physicaland psychological) distress. Only mid-interventionmeans are reported in the paper; however, partici-pants in the yoga group reported significantly lessanxiety, depression, and distress and significantlyhigher quality of life as compared with the controlgroup. Within this study, yoga participants wereexpected to practice a minimum of three hours perweek, although adherence data are not reportedwithin the paper. Estimated effect sizes for thesetwo studies are shown in Table 2 and were large.
Strengths and limitations
In general, the methodological quality of the RCTswas high (Table 2). With the exception of Blank etal. [31], standardized measures were administeredpre- and post-treatment, and baseline and post-intervention comparisons between the treatmentand control groups were reported in the majority ofstudies. Overall, the articles provide importantdetails regarding the type of yoga administered andthe various components of the interventions.However, a limiting factor in four of the reviewedRCTs is the lack of long-term data; similarly, thelength of time between pre- and post-interventionwas not specified in the study conducted byBanerjee et al. [30] and it is not clear from theRaghavendra et al. [22] study whether participantshad been administered the yoga intervention inconjunction with previous medical treatments. Incontrast, a strength of Cohen et al.’s [32] andMoadel et al.’s [33] studies is the inclusion of three-month follow-up assessments. Furthermore,although Cohen et al. [32] deemed their samplesize adequate for power and error control, smallsample sizes were common among the RCTs. In
Evidence-based review of Yoga for cancer 471
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon
addition, some studies reported low rates of yogaparticipation [e.g. 32,33]. For example, only one-third of the intervention group sampled by Cohenet al. [32] attended all sessions. Moreover, althoughthe studies reported on concurrent treatments, onlyone [32] documented other physical or mentalactivities (e.g. exercise) that patients may haveengaged in during their study enrolment, and noneof the intervention programs appear to have beenmanualized. Finally, only one study stratifiedanalyses with regard to whether or not patientswere receiving concurrent treatment [33].
Non-controlled trials
Joseph [37] reported the findings of a studyconducted with cancer outpatients. One hundredand twenty-five outpatients were assigned toparticipate in yoga (n5 50), transcendental medi-tation (n5 25), or group therapy (n5 50) in orderto examine effects on psychological adjustment.Groups were not directly compared, and outcomemeasures were not specified. Approximately 20%of yoga participants reported improved sleep andfeelings of peace. This study is limited in terms ofits methodology and reporting; for example,sample characteristics, outcome measures, methodof group assignment, and information regardingthe yoga program were not reported.Rosenbaum et al. [36] conducted an evaluation
of the Stanford Cancer Supportive Care Program(SCSCP), a multi-faceted program that includedyoga classes twice per week. This paper wasincluded in the present review, given that yogawas evaluated apart from the other components ofthe SCSCP. Of the 398 patients included in thestudy, 380 evaluated the yoga program usingquestionnaires developed for the study. Ratingswere positive, with over 90% of patients reportingthat yoga decreased stress and increased feelings ofwell-being. In addition, increased energy, restfulsleep, and decreased pain were reported by overhalf the sample. However, it is not clear how yogacompared with the other components of theSCSCP, as participants were not asked to comparethe various aspects of the program. As well, limitedinformation on the yoga program is provided.In addition, Warner [35] examined 26 women
with breast cancer who participated in the Art ofLiving Program (ALP) on standardized measuresof quality of life, spiritual well-being, stress, andpositive mind-state. The ALP is an intensive coursethat focuses on yogic concepts of breathing,meditation, asana, and stress-management, andfeatures a breathing technique known as Sudar-shan Kriya Yoga (SKY). After completing theALP, participants underwent a five-week main-tenance period in which they attended weeklymeetings. Twenty-three women attended all days
of the program and 80% attended at least three offive maintenance meetings.Warner’s [35] sample was assessed at two
baseline and two post-intervention periods, andresults indicated significant differences on all ofthe variables from baseline to post-intervention.Specifically, women reported increased quality oflife, spiritual well-being, and positive mind-state,and decreased stress. In addition, women withless than average spiritual well-being at baselinehad greater improvements in quality of life andpositive mind-state, whereas those with higherthan average levels reported significantly reducedstress. As calculated by Warner [35], the effectsizes associated with the findings were generallymoderate to large. In addition, based on interviewswith 12 self-selected women, positive themesrelating to participation in the program emerged,including decreased fear of cancer and increasedself-care.Strengths of this study include the numerous
assessment periods, inclusion of quantitative andqualitative date, and the examination of differentdemographic and disease variables on outcomemeasures. The results of this study are limited,however, by the lack of a control condition and alarge attrition rate.A recent study [34] also examined yoga for breast
cancer. The final sample consisted of 13 womenwith metastatic breast cancer, half of whom wereundergoing chemotherapy. The women completedan eight-week Yoga of Awareness Program thatinvolved various techniques, including asanas,pranayama, meditation, self-study (i.e. swad-hyaya), and group discussion (i.e. satsang). Treat-ment was manualized and all yoga classes werevideotaped for review. Participants completed dailydiary entries regarding acceptance (e.g. of one’smoment-to-moment experiences), distress, fatigue,invigoration, pain, and relaxation for two weekspre-intervention and for the final two weeks of theintervention. Significant improvements were foundbetween pre-and final measures on daily invigora-tion and acceptance, with statistical trendsnoted for improved pain and relaxation. Further-more, greater time spent practicing yoga at homewas significantly associated with same-day im-provements in acceptance, invigoration, and pain,and with next-day improvements in acceptance,fatigue, invigoration, pain, and relaxation. Post-intervention feedback from ten of the participantsshowed that the program was rated highly in termsof its overall helpfulness (M5 9.6 on 10-pointscale).Although the quality of this study was generally
high, its uncontrolled nature, small sample size,and absence of follow-up data are limitations.Strengths of this study include the manualizedtreatment, rigorous analyses conducted, and use ofdaily assessments to capture data over time.
472 K. B. Smith and C. F. Pukall
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon

Discussion
This review described and evaluated ten studiesthat examined yoga as an intervention for psycho-logical symptoms in cancer patients. A number ofpositive results were found; however, the variabilityacross studies and some methodological drawbackslimit the extent to which yoga can be deemedeffective for managing psychological symptomsassociated with cancer.Overall, significant improvements were seen in
patients participating in RCT yoga programs onmeasures of sleep [e.g. 32], quality of life [e.g.24,33], and levels of stress [e.g. 24,30]; thesefindings were paralleled in non-controlled trials[e.g. 35–37]. Improvements in mood were alsonoted in five of the six RCTs [e.g. 22,24,30,31,33].With regard to non-controlled trials, increasedenergy and acceptance was noted among breastcancer patients in Carson et al.’s [34] study.However, results varied across the reviewedstudies. For example, while Culos-Reed et al.[24] found statistical trends toward improvementsin mood among cancer patients who had under-gone a seven-week yoga program, no significantdifferences in mood were found among lymphomapatients who had participated in seven weeks ofTibetan yoga [32]. Similarly, although Warner [35]found significant increases in quality of life amongwomen with breast cancer in a non-controlledtrial, only social well-being was significantlypredicted by participation in the RCT yogaintervention among breast cancer patients inanother study [33].Certainly, given its recent emergence in the
literature, research examining yoga among cancerpatients is preliminary. Conclusions stating thatyoga is an effective therapy for cancer patientsare also preliminary, yet promising. Despitemethodological issues, the review of the studiessuggests that some psychological benefits mayresult from yoga. Further research into thisintervention is warranted, especially since highsatisfaction rates were reported in some studies[e.g. 31,34]. Yoga is currently being offered as partof complementary treatment for cancer at majorcenters [36,39], and it is important for research toexamine this popular form of mind–body disciplineamong patients with and without cancer.The state of research investigating yoga for
cancer patients is similar to that examining yogawith other populations. For example, in theirreview of yoga for the treatment of anxiety,Kirkwood et al. [12] concluded that research resultswere encouraging, yet preliminary. However, re-search with non-cancer populations has found apositive effect of yoga on mood in older patientswith mild depression [e.g. 40], and on sleepoutcomes in older patients [41] and in patientswith insomnia [42]. In one study, when inpatients
with melancholic depression received either SKY,imipramine, or electroconvulsive therapy (ECT),patients in the SKY and imipramine groups hadcomparable reductions in depressive symptoms(although less so than those in the ECT group)[11]. To this end, the authors concluded that SKYmay be a potential alternative to medication forpatients with melancholic depression, althoughthey acknowledged that the research was prelimin-ary and that larger scale studies are needed.Importantly, this study documented that noadverse side effects (e.g. confusion, cardiovascularsymptoms) were associated with SKY, suggestingthat yoga techniques may be a safe and effectivemethod for improving mood. To date, littleresearch has examined this form of yoga amongpatients with cancer, and information on contra-indications for yoga with cancer populations islacking; this suggests potential avenues for futureresearch.
Limitations of current study
One limitation of the present review is that only fullresearch papers were included. While this proce-dure was followed in order to properly assess andrate the quality of the research, previous reviewpapers focusing on mind–body interventions forcancer have been criticized for excluding abstracts[e.g. 43]. Similarly, this review does not includefindings from studies that were never, or have notyet been, published. Thus, the reviewed studies maynot be representative of all of the research that hasexamined the effectiveness of yoga for cancer, andcaution regarding the file-drawer effect is war-ranted [44]. In addition, the number of studiesidentified in this review was small and limited thestatistical analyses that could be conducted.
Conclusions and directions for future research
The preliminary results reviewed in this paper arepromising, and positive feedback reported bypatients indicates that yoga may have value as aclinical intervention. Although further researchand high-quality studies with controlled condi-tions are needed in this area, this review indicatesseveral avenues for future research. First, giventhe various types of cancer and the differentexperiences that patients may face as a result oftheir diagnosis, research should attempt to specifywhat patients may benefit from yoga. Forexample, the study by Moadel et al. [33] suggestedthat yoga may have differential effects on psycho-logical adjustment for breast cancer patients whoare or are not concurrently receiving medicaltreatment. Similarly, as the majority of studiesincluded women with breast cancer, research isneeded to examine the use of yoga among malecancer and female non-breast cancer patients. In
Evidence-based review of Yoga for cancer 473
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon

addition, although positive psychological effectsof yoga have been noted among cancer patients, itis not clear what aspect of the intervention may beresponsible for such improvements. Studies havedemonstrated that yoga can generate the relaxa-tion response among healthy subjects, and thatpranayama is successful at increasing immunefunction among patients with cancer [13,45].Presumably, yoga may influence outcomesthrough various pathways such as relaxation,and through increased coping, acceptance, self-efficacy, and physical health. As such, teasingapart the active ingredients of yoga treatmentswill be important in future studies. Finally, asvarious forms of yoga exist, it will be valuable tounderstand what type(s) are best indicated forpatients with cancer.
Acknowledgements
K. B. Smith was supported by a Canada GraduateScholarship from the Social Sciences and HumanitiesResearch Council of Canada (SSHRC). This paper standsin partial fulfillment of K. B. Smith’s PhD requirements. Wewould like to thank Drs Patricia Minnes and Sheryl Frenchfor their helpful comments on this manuscript. The authorshave no potential financial or personal conflicts of interest todisclose in relation to this work.
References
1. Patrick DL, Ferketich SL, Frame PS et al. NationalInstitutes of Health State-of-the-Science ConferenceStatement: symptom management in cancer: pain,depression, and fatigue, July 15–17, 2002. J Natl CancerInst 2003;95:1110–1117.
2. Molassiotis A, Fernadez-Ortega P, Pud D et al. Use ofcomplementary and alternative medicine in cancerpatients: a European survey. Ann Oncol 2005;16:655–663.
3. Bernstein BJ, Grasso T. Prevalence of complementaryand alternative medicine use in cancer patients. Oncol-ogy 2001;15:1267–1272.
4. Iyengar BKS. Light on Life. Raincoast Books: Vancou-ver, 2005.
5. Collins C. Yoga: intuition, preventive medicine, andtreatment. J Obstet Gynecol Neonatal Nurs 1998;27:563–568.
6. Feuerstein G. The Shambhala Guide to Yoga. Shambha-la: Boston, 1996.
7. Saper RB, Eisenberg DM, Davis RB, Culpepper L,Phillips RS. Prevalence and patterns of adult yoga use inthe United States: results of a national survey. AlternTher Health Med 2004;10:44–49.
8. Garfinkel MS, Singhal A, Katz WA, Allan DA,Reshetar R, Schumacher HR. Yoga-based interventionfor carpal tunnel syndrome. J Am Med Assoc 1998;280:1601–1603.
9. Oken BS, Kishiyama S, Zajdel D et al. Randomizedcontrolled trial of yoga and exercise in multiplesclerosis. Neurology 2004;62:2058–2064.
10. Vedanthan PK, Kesvalu LN, Murthy KC et al. Clinicalstudy of yoga techniques in university students withasthma: a controlled study. Allergy Asthma Proc 1998;19:3–9.
11. Janakiramaiah N, Gangadhar BN, Naga VenkateshaMurthy PJ, Harish MG, Subbakrishna DK, Veda-murthachar A. Antidepressant efficacy of SudarshanKriya Yoga (SKY) in melancholia: a randomizedcomparison with electroconvulsive therapy (ECT) andimipramine. J Affect Disord 2000;57:255–259.
12. Kirkwood G, Rampes H, Tuffrey V, Richardson J,Pilkington K. Yoga for anxiety: a systematic review ofthe research evidence. Br J Sports Med 2005;39:884–891.
13. Telles S, Reddy SK, Nagendra HR. Oxygen consump-tion and respiration following two yoga relaxationtechniques. Appl Psychophy Biof 2000;25:221–227.
14. Speca M, Carlson LE, Goodey E, Angen M. Arandomized, wait-list controlled clinical trial: the effectof a mindfulness meditation-based stress reductionprogram on mood and symptoms of stress in canceroutpatients. Psychosom Med 2000;62:613–622.
15. Carlson LE, Speca M, Patel KD, Faris E. One year pre-post intervention follow-up of psychological, immune,endocrine, and blood pressure outcomes of mindfulness-based stress reduction (MBSR) in breast and prostatecancer outpatients. Brain Behav Immun 2007;21:1038–1049.
16. Carlson LE, Speca M, Patel KD, Goodey E. Mind-fulness-based stress reduction in relation to quality oflife, mood, symptoms of stress and levels of cortisol,dehydroepiandrosterone sulfate (DHEAS) and melato-nin in breast and prostate cancer outpatients. Psycho-neuroendocrinology 2004;29:448–474.
17. Garland SN, Carlson LE, Cook S, Lansdell L, Speca M.A non-randomized comparison of mindfulness-basedstress reduction and healing arts programs for facilitat-ing post-traumatic growth and spirituality in canceroutpatients. Support Care Cancer 2007;15:949–961.
18. Shapiro SL, Bootzin RR, Figueredo AJ, Lopez AM,Schwartz GE. The efficacy of mindfulness-based stressreduction in the treatment of sleep disturbance inwomen with breast cancer: an exploratory study.J Psychosom Res 2003;54:85–91.
19. Research Council for Complementary Medicine Centrefor Review and Dissemination (2005, June 27). Cancer(general): yoga. Retrieved August 26, 2007 from http://www.rccm.org.uk/cameol/Default.aspx.
20. Bower JE, Woolery A, Sternlieb B, Garet D. Yoga forcancer patients and survivors. Cancer Control 2005;12:165–171.
21. Smith JE, Richardson J, Hoffman C, Pilkington K.Mindfulness-based stress reduction as supportive ther-apy in cancer care: systematic review. J Adv Nurs2005;52:315–327.
22. Raghavendra RM, Nagarathna R, Nagendra HR et al.Effects of an integrated yoga programme on chemother-apy-induced nausea and emesis in breast cancerpatients. Eur J Cancer Care 2007;16:462–474.
23. Culos-Reed S, Carlson LE, Daroux LM, Hately-AldousS. Discovering the physical and psychological benefits ofyoga for cancer survivors. Int J Yoga Ther 2004;14:45–52.
24. Culos-Reed SN, Carlson LE, Daroux LM, Hately-Aldous S. A pilot study of yoga for breast cancersurvivors: physical and psychological benefits. Psycho-Oncology 2006;15:891–897.
25. Centre for Reviews and Dissemination (2001, March).Undertaking systematic reviews of research on effective-ness: CRD’s guidance for those carrying out or commis-sioning reviews (Report 4, 2nd ed.). Retrieved May 20,2007 from http://www.york.ac.uk/inst/crd/report4.htm.
26. Suydam MN. An instrument for evaluating experimen-tal educational research reports. J Educ Res 1968;61:200–203.
474 K. B. Smith and C. F. Pukall
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon

27. Skultety KM, Zeiss A. The treatment of depression inolder adults in the primary care setting: an evidence-based review. Health Psychol 2006;25:665–674.
28. Moher D, Schulz KF, Altman D. The CONSORTstatement: revised recommendations for improving thequality of reports of parallel-group randomized trials.J Am Med Assoc 2001;285:1987–1991.
29. Altman DG, Schulz KF, Moher D et al. The revisedCONSORT statement for reporting randomized trials:explanation and elaboration. Ann Intern Med 2001;134:663–694.
30. Banerjee B, Vadiraj HS, Ram A et al. Effects of anintegrated yoga program in modulating psychologicalstress and radiation-induced genotoxic stress in breastcancer patients undergoing radiotherapy. Integr CancerTher 2007;6:242–250.
31. Blank SE, Kittel J, Haberman MR. Active practice ofIyengar Yoga as an intervention for breast cancersurvivors. Int J Yoga Ther 2003;13:51–59.
32. Cohen L, Warneke C, Fouladi RT, Rodriguez MA,Chaoul-Reich A. Psychological adjustment and sleepquality in a randomized trial of the effects of a TibetanYoga intervention in patients with lymphoma. Cancer2004;100:2253–2260.
33. Moadel AB, Shah C, Wylie-Rosett J et al. Randomizedcontrolled trial of yoga among a multiethnic sample ofbreast cancer patients: effects on quality of life. J ClinOncol 2007;25:4387–4395.
34. Carson JW, Carson KM, Porter LS, Keefe FJ, Shaw H,Miller JM. Yoga for women with metastatic breastcancer: results from a pilot study. J Pain SymptomManage 2007;33:331–341.
35. Warner AS. Exploration of psychological and spiritualwell-being of women with breast cancer participating inthe Art of Living Program. Unpublished doctoraldissertation, Institute of Transpersonal Psychology, 2006.
36. Rosenbaum E, Gautier H, Fobair P et al. Cancersupportive care, improving the quality of life for cancerpatients: a program evaluation report. Support CareCancer 2004;12:293–301.
37. Joseph CD. Psychological supportive therapy for cancerpatients. Indian J Cancer 1983;20:268–270.
38. Cohen J. A power primer. Psychol Bull 1992;112:155–159.39. DiStasio SA. Integrating yoga into cancer care. Clin J
Oncol Nurs 2008;12:125–130.40. Manjunath NK, Telles S. Assessing depression follow-
ing two ancient Indian interventions: effects of yogaand ayurveda on older adults in a residential home.J Gerontol Nurs 2007;33:17–23.
41. Manjunath NK, Telles S. Influence of yoga andayurveda on self-rated sleep in a geriatric population.Indian J Med Res 2005;121:683–690.
42. Khalsa SBS. Treatment of chronic insomnia with yoga:a preliminary study with sleep–wake diaries. ApplPsychophys Biof 2004;29:269–278.
43. Proulx K. Integrating mindfulness-based stress reduc-tion. Holistic Nurs Practice 2003;17:201–208.
44. Rosenthal R. The ‘file drawer problem’ and tolerancefor null results. Psychol Bull 1979;86:638–641.
45. Kochupillai V, Kumar P, Singh D et al. Effect ofrhythmic breathing (sudarshan kriya and pranayam)on immune functions and tobacco addictions. Ann NYAcad Sci 2005;1056:242–252.
Evidence-based review of Yoga for cancer 475
Copyright r 2008 John Wiley & Sons, Ltd. Psycho-Oncology 18: 465–475 (2009)
DOI: 10.1002/pon