An "Ecological" Approach to the Obesity Pandemic
7
Education and debate An “ecological” approach to the obesity pandemic Garry Egger, Boyd Swinburn The increasing prevalence of obesity in many countries means that it should now be considered a pandemic. 1 One estimate from Australia suggests that over the past decade the average adult has been adding 1 gram a day to body weight. 2 This has occurred in the face of increasing knowledge, awareness, and education about obesity, nutrition, and exercise. It has been suggested that a paradigm shift is necessary if future progress is to be made. 3 Traditionally, weight gain was thought of as caused by eating too much or exercising too little, or both (changes in weight = energy intake - energy expendi- ture). This led to the search for small deficiencies in energy metabolism such as a reduced thermic effect of food to explain obesity. 4 Treatment was dominated by calorie counting, and public health messages extolled people to balance their intake and output. This paradigm has changed with the increasing under- standing of the dynamic relations between energy stores, appetite mechanisms, and energy metabolism and of the wider recognition of nutrient partitioning. 56 From studies which have shown that fat balance is equivalent to energy balance, 7 the fat balance equation was developed (rate of change of fat stores = rate of fat intake - rate of fat oxidation). 5 This equation is more dynamic than the original static equation and reflects energy balance under normal conditions of free access to foods. Because fat intake and oxidation are not closely balanced, 8 this approach does not need metabolic abnormalities or genetic mutations to explain weight gain. Indeed, the differences in body fat between people living in the same environment could be better described as normal physiological variation. This paradigm is more helpful in explaining changes in body fat within an individual over time, but it does not account for the wider influences within and around individuals on obesity. An ecological model The model presented in figure 1 proposes three main influences on equilibrium levels of body fat—biological, behavioural, and environmental—mediated through energy intake or energy expenditure, or both, but moderated by physiological adjustments during periods of energy imbalance. The level of body fat is seen not as a “set point” like a thermostat fixed on an exact temperature but as a “settling point” that depends on the net effects of the other components of the model and that changes as they change. This places obesity in an ecological context which calls for more than simple education about risk factors and needs a collaborative strategy with the multiple sectors which impact on the problem. 9 Mediators The ecological model uses total energy as mediator; for most conditions of human living it is interchangeable with fat energy. Fat intake is an important determinant of total energy intake, and for output, total energy expenditure is a major determinant of fat oxidation. Energy intake—Dietary fat is very energy dense and has a limited effect on suppressing appetite and enhancing fat oxidation. 10 This makes reducing dietary fat an obvious choice for reducing total energy to treat or prevent obesity. A reduction in dietary fat with an Summary points Current strategies are not containing the obesity pandemic A shift is needed away from the traditional view of obesity as a personal disorder that requires treatment An ecological approach regards obesity as a normal response to an abnormal environment, rather than vice versa This approach resembles the classical epidemiological triad used in successfully controlling other epidemics Understanding, measuring, and altering the “obesogenic” environment is critical to success Mediators Influences Behaviour Biology Environment Energy intake Energy expenditure Physiological adjustment Equilibrium fat stores – + = Moderators Fig 1 An ecological paradigm for understanding overfatness and obesity School of Human Movement, Deakin University, Melbourne, Australia Garry Egger, adjunct professor of health sciences Department of Community Health, University of Auckland, Auckland, New Zealand Boyd Swinburn, senior lecturer Correspondence to: Garry Egger, Centre for Health Promotion and Research, PO Box 313, Balgowlah, NSW 2093, Australia (eggergj@ozemail. com.au). BMJ 1997;315:477–80 477 BMJ VOLUME 315 23 AUGUST 1997
Transcript of An "Ecological" Approach to the Obesity Pandemic

Education and debate
An “ecological” approach to the obesity pandemicGarry Egger, Boyd Swinburn
The increasing prevalence of obesity in many countriesmeans that it should now be considered a pandemic.1
One estimate from Australia suggests that over the pastdecade the average adult has been adding 1 gram a dayto body weight.2 This has occurred in the face ofincreasing knowledge, awareness, and education aboutobesity, nutrition, and exercise. It has been suggestedthat a paradigm shift is necessary if future progress isto be made.3
Traditionally, weight gain was thought of as causedby eating too much or exercising too little, or both(changes in weight = energy intake − energy expendi-ture). This led to the search for small deficiencies inenergy metabolism such as a reduced thermic effect offood to explain obesity.4 Treatment was dominated bycalorie counting, and public health messages extolledpeople to balance their intake and output. Thisparadigm has changed with the increasing under-standing of the dynamic relations between energystores, appetite mechanisms, and energy metabolismand of the wider recognition of nutrient partitioning.5 6
From studies which have shown that fat balance isequivalent to energy balance,7 the fat balance equationwas developed (rate of change of fat stores = rate of fatintake − rate of fat oxidation).5 This equation is moredynamic than the original static equation and reflectsenergy balance under normal conditions of free accessto foods. Because fat intake and oxidation are notclosely balanced,8 this approach does not needmetabolic abnormalities or genetic mutations toexplain weight gain. Indeed, the differences in body fatbetween people living in the same environment couldbe better described as normal physiological variation.This paradigm is more helpful in explaining changesin body fat within an individual over time, but it doesnot account for the wider influences within and aroundindividuals on obesity.
An ecological modelThe model presented in figure 1 proposes three maininfluences on equilibrium levels of body fat—biological,behavioural, and environmental—mediated throughenergy intake or energy expenditure, or both, butmoderated by physiological adjustments duringperiods of energy imbalance. The level of body fat isseen not as a “set point” like a thermostat fixed on anexact temperature but as a “settling point” thatdepends on the net effects of the other components ofthe model and that changes as they change. This placesobesity in an ecological context which calls for more
than simple education about risk factors and needs acollaborative strategy with the multiple sectors whichimpact on the problem.9
MediatorsThe ecological model uses total energy as mediator; formost conditions of human living it is interchangeablewith fat energy. Fat intake is an important determinantof total energy intake, and for output, total energyexpenditure is a major determinant of fat oxidation.
Energy intake—Dietary fat is very energy dense andhas a limited effect on suppressing appetite andenhancing fat oxidation.10 This makes reducing dietaryfat an obvious choice for reducing total energy to treator prevent obesity. A reduction in dietary fat with an
Summary points
Current strategies are not containing the obesitypandemic
A shift is needed away from the traditional view ofobesity as a personal disorder that requirestreatment
An ecological approach regards obesity as anormal response to an abnormal environment,rather than vice versa
This approach resembles the classicalepidemiological triad used in successfullycontrolling other epidemics
Understanding, measuring, and altering the“obesogenic” environment is critical to success
Mediators
Influences
BehaviourBiology Environment
Energyintake
Energyexpenditure
Physiologicaladjustment
Equilibriumfat stores
– +=
Moderators
Fig 1 An ecological paradigm for understanding overfatness andobesity
School of HumanMovement, DeakinUniversity,Melbourne,AustraliaGarry Egger,adjunct professor ofhealth sciences
Department ofCommunity Health,University ofAuckland,Auckland, NewZealandBoyd Swinburn,senior lecturer
Correspondence to:Garry Egger,Centre for HealthPromotion andResearch, PO Box313, Balgowlah,NSW 2093,Australia([email protected]).
BMJ 1997;315:477–80
477BMJ VOLUME 315 23 AUGUST 1997

otherwise free choice of food promotes a modest weightloss which is initially less than that from a conventionallow energy diet.11 However, the longer term results aresimilar,12 and the reduced fat regimen seems easier tomaintain.13 All weight loss programmes suffer fromrebound weight gain, probably partly because ofphysiological defences against weight loss,14 but ulti-mately weight loss is limited by the high settling point offat stores for people living in an environment thatpromotes obesity. To keep fat stores below this pointoften requires considerable effort, which is difficult tomaintain in an unsupportive “obesogenic” environment.
At a population level, it seems that dietary fat andenergy intake have not fallen as fast as energy output.15
The result is a large energy imbalance, leading to obes-ity. On the input side of the equation, the strategy ofreducing dietary fat within the diet (that is, changingthe foods eaten and the composition of meals) seems amore realistic approach than reducing total energy(decreasing the size and frequency of meals). Largereductions in the fat content of the modern diet seemunlikely, and they may not be necessary for apopulation based approach, as small changes made bya large percentage of the population often show up asgreater improvements in a population’s disease indexthan do large shifts made by only a few people.16
Energy expenditure—The intensity of physical activityrequired for optimal oxidation of fat is controversial.Relative fat utilisation is higher during activity of mod-erate intensity such as walking, but absolute energy useis higher during vigorous exercise such as running. Ithas thus been suggested that vigorous exercise resultsin greater absolute fat oxidation.17 This may be true foraerobically fit people, but unfit people tend to oxidiseless fat at all levels of intensity. Hence, vigorous
exercise—even if it could be carried out—is not likely toresult in as much fat oxidation in unfit people as activ-ity of more moderate intensity which can becomfortably sustained for longer periods. Obesepeople are usually unfit, and so moderately intensephysical activity should be recommended for them.
As with fat intake, population benefits are morelikely to come from modest increases in activity of lowor moderate intensity in many people than fromincreases in high intensity exercise in a few. Indeed,part of the secular increase in obesity is probablyattributable to modest, population-wide reductions inphysical activity of low to moderate intensity or toreduction in “incidental movement” due to theintroduction of labour saving technology.18
ModeratorsPhysiological adjustment refers to the metabolic and,
in some cases, behavioural changes that follow adisequilibrium in energy balance and that minimiselarge fluctuations in body weight. For example, inresponse to a negative energy balance, initially appetitemay increase or physical activity may decrease14; then,with weight loss, fat oxidation and resting metabolicrate may decline until a new energy balance isachieved.19 Physiological adjustment may be more vig-orous in some people, as a result of biological factorssuch as sex, age, or genetic makeup.20
One implication of this is that frequent plateaus, orslowing of weight losses over time, are a normalphysiological response to energy disequilibrium.14
Adjustments seem to be more vigorous in response toweight loss than weight gain, especially in lean individu-als,21 and they may also be more vigorous after rapid,rather than slow, changes. Hence the need toconcentrate on long term loss of fat rather than shortterm, and usually temporary, loss of weight. Thisquestions the ethics of programmes that advertise largeweight losses in short periods.
InfluencesBiological influences—Biological factors known to
influence body fat levels include age, sex, hormonal fac-tors, and genetics,22 all of which have been considered tobe unalterable. The identification of the ob gene and itsproduct leptin in 1994 caused widespread optimismabout unlocking the cause of obesity and developingsuccessful treatments.23 A greater understanding ofappetite control will undoubtedly come from researchon leptin, but no major effect of single gene defects hasyet been identified, and it is likely that the genetic influ-ences on body fat levels are polygenic.
There are also important sex differences in fat stor-age.24 The differences between the sexes are apparentearly in life, become greatest with the onset of menses,then tend to decrease with the changes in hormonestatus in postmenopausal women.25 Fat loss and main-tenance of lower equilibrium fat stores also becomesmore difficult with age.26 Finally, there is increasing evi-dence of racial influences on energy balance.27 Thesebiological influences explain much of the variance inbody fat in individuals within a given environment, butthey do not explain the large population increaseswhich represent the epidemic itself.
Behavioural influences—Behavioural factors typicallythought to influence obesity are “sloth” and “gluttony,”
Education and debate
478 BMJ VOLUME 315 23 AUGUST 1997
which imply a potential for willful control over theforces affecting body weight. Behaviours are the resultof complex psychological factors, including habits,emotions, attitudes, beliefs, and cognitions developedthrough a background of learning history. Biologicaland environmental influences also affect behaviour,and, in turn, energy balance. Cognitive factors(willpower based on knowledge, for example) may haveonly a minor effect on eventual behaviour, and thisexplains the limitations of education in the treatmentand prevention of obesity. However, the causes andeffects of behavioural factors do have to be con-sidered,28 and interventions to deal with these shouldbe a part of any overall strategy.
Environmental influences—Environment can bebroadly categorised into “macro” (of the widerpopulation) and “micro” (with close proximity to theindividual). In general, the macro-environment deter-mines the prevalence of obesity in a population and themicro-environment, along with biological and behav-ioural influences, determines whether an individual isobese. The environmental influences on the amount andtype of food eaten and the amount and type of physicalactivity taken are vast and underrated; table 1 showssome examples. A close examination of specificmacro-environmental sectors (such as the fitness indus-try or the food service industry) or micro-environmentalsettings (such as the local gym or the workplace) willreveal many more interconnecting environmental influ-
ences than those listed. For example, food safety regula-tions, policies of food manufacturers, costs of cookingoils, and the availability of training programmes for foodcaterers can affect the choice, price, and quality of foodat the work canteen.
Environmental influences represent the publichealth arm of the obesity problem. If the macro-environment is obesogenic, obesity will become moreprevalent and programmes aimed at influencingindividual behaviour can be expected to have only alimited effect. Historically, epidemics have beencontrolled only after environmental factors have beenmodified. Similarly, reductions in population levels ofobesity seem unlikely until the environments whichfacilitate its development are modified. Yet this is oftenneglected in obesity management (as it was initiallywith tobacco control). Environmental change, such asregulation of the food industry or changes in buildingdesign, is likely to be unpopular. Although somechanges may be overt, others—such as reductions of fatin the meat supply—may be more surreptitious.
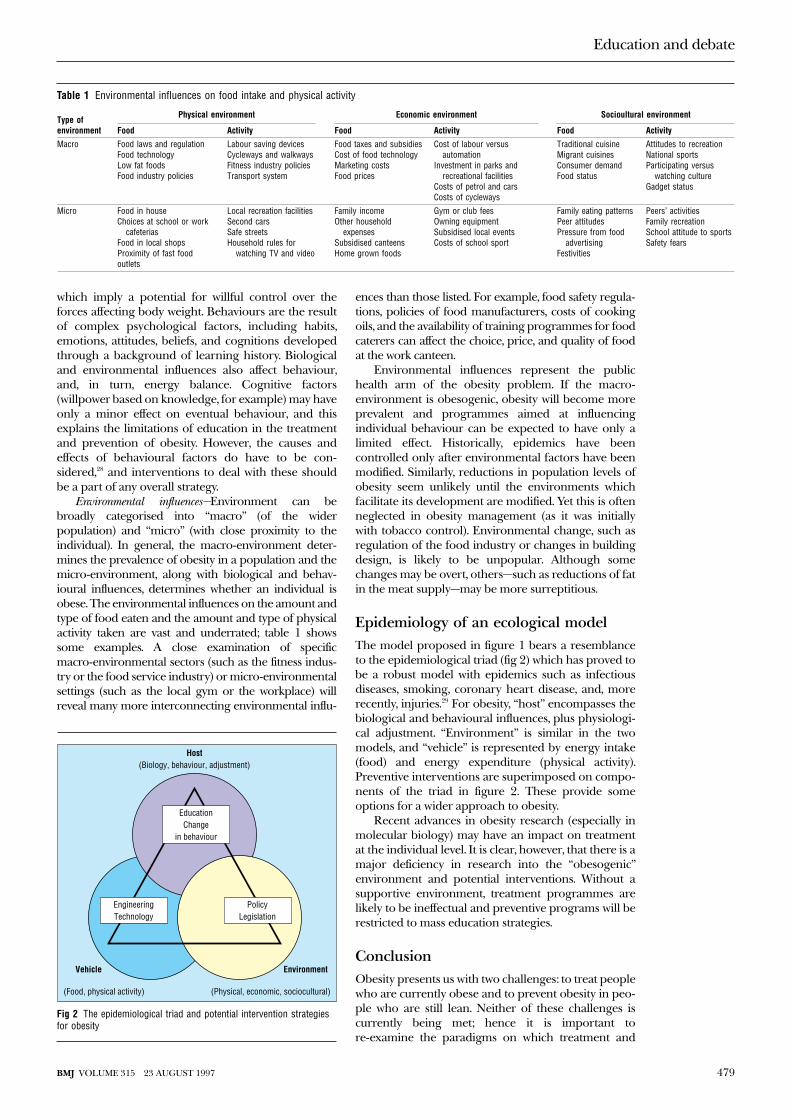
Epidemiology of an ecological modelThe model proposed in figure 1 bears a resemblanceto the epidemiological triad (fig 2) which has proved tobe a robust model with epidemics such as infectiousdiseases, smoking, coronary heart disease, and, morerecently, injuries.29 For obesity, “host” encompasses thebiological and behavioural influences, plus physiologi-cal adjustment. “Environment” is similar in the twomodels, and “vehicle” is represented by energy intake(food) and energy expenditure (physical activity).Preventive interventions are superimposed on compo-nents of the triad in figure 2. These provide someoptions for a wider approach to obesity.
Recent advances in obesity research (especially inmolecular biology) may have an impact on treatmentat the individual level. It is clear, however, that there is amajor deficiency in research into the “obesogenic”environment and potential interventions. Without asupportive environment, treatment programmes arelikely to be ineffectual and preventive programs will berestricted to mass education strategies.
ConclusionObesity presents us with two challenges: to treat peoplewho are currently obese and to prevent obesity in peo-ple who are still lean. Neither of these challenges iscurrently being met; hence it is important tore-examine the paradigms on which treatment and
EducationChange
in behaviour
EngineeringTechnology
PolicyLegislation
Environment
Host(Biology, behaviour, adjustment)
(Food, physical activity) (Physical, economic, sociocultural)
Vehicle
Fig 2 The epidemiological triad and potential intervention strategiesfor obesity
Table 1 Environmental influences on food intake and physical activity
Type ofenvironment
Physical environment Economic environment Socioultural environment
Food Activity Food Activity Food Activity
Macro Food laws and regulationFood technologyLow fat foodsFood industry policies
Labour saving devicesCycleways and walkwaysFitness industry policiesTransport system
Food taxes and subsidiesCost of food technologyMarketing costsFood prices
Cost of labour versusautomation
Investment in parks andrecreational facilities
Costs of petrol and carsCosts of cycleways
Traditional cuisineMigrant cuisinesConsumer demandFood status
Attitudes to recreationNational sportsParticipating versus
watching cultureGadget status
Micro Food in houseChoices at school or work
cafeteriasFood in local shopsProximity of fast foodoutlets
Local recreation facilitiesSecond carsSafe streetsHousehold rules for
watching TV and video
Family incomeOther household
expensesSubsidised canteensHome grown foods
Gym or club feesOwning equipmentSubsidised local eventsCosts of school sport
Family eating patternsPeer attitudesPressure from food
advertisingFestivities
Peers’ activitiesFamily recreationSchool attitude to sportsSafety fears
Education and debate
479BMJ VOLUME 315 23 AUGUST 1997

prevention programmes are based. The modelpresented here suggests that the driving force for theincreasing prevalence of obesity in populations is theincreasingly obesogenic environment rather than any“pathology” in metabolic defects or genetic mutationswithin individuals. A paradigm shift to understandingobesity as “normal physiology within a pathologicalenvironment” signposts the directions for a wider pub-lic health approach to the obesity pandemic.
1 James WPT. Epidemiology of obesity. Int J Obesity 1992;16(suppl 2):S23-6.2 Magnus P, Bennett S. Trends in cardiovascular risk factors in Australia.
Med J Aust 1994;161:519-27.3 Hawks SR, Richins P. Toward a new paradigm for the management of
obesity. J Health Educ 1994;25:147-53.4 Ravussin E, Swinburn B. Energy metabolism in obesity. In: Stunkard AJ,
Wadden TA, eds. Obesity: theory and therapy. 2nd ed. New York: Raven,1992:97-124.
5 Swinburn B, Ravussin E. Energy balance or fat balance? Am J Clin Nutr1993;57(suppl):766-71S.
6 Stubbs RJ. Macronutrient effects on appetite. Int J Obesity 1995;19(suppl5):S11-9.
7 Flatt JP. Importance of nutrient balance in body weight regulation. DiabMet Rev 1988;4:571-81.
8 Schutz Y, Flatt JP, Jequier E. Failure of dietary fat intake to promote fatoxidation: a factor favouring the development of obesity. Am J Clin Nutr1989;50:307-14.
9 Kickbush I. Approaches to an ecological base for public health. HealthPromotion 1989;4:265-8.
10 Westrate JA. Fat and obesity. Int J Obesity 1995;19(suppl 5):S38-43.11 Lissner L, Heitman BL. Dietary fat and obesity: evidence from epidemi-
ology. Eur J Clin Nutr 1995;49:79-90.12 Prewitt TE, Schmeisser D, Bowen PE, Aye P, Dolecek TA, Langenberg P, et
al. Changes in body weight, body composition, and energy intake inwomen fed high- and low-fat diets. Am J Clin Nutr 1991;54:304-10.
13 Lyon X-H, Di Vetta V, Milton H, Schutz Y. Compliance to dietary advicedirected towards increasing the carbohydrate to fat ratio of the everydaydiet. Int J Obesity 1995;19:260-9.
14 Prentice AM, Goldberg GR, Jebb SA, Black AE, Murgatroyd PR.Physiological responses to slimming. Proc Nutr Soc 1991;50:441-58.
15 Prentice AM, Jebb SA. Obesity in Britain: gluttony or sloth? BMJ 1995;311:437-9.
16 Rose G. The strategy of preventive medicine. Oxford: Oxford UniversityPress, 1992.
17 Glasser GA. Burning carbohydrate to lose fat. Sports Med Digest1995;March:5.
18 James WPT. A public health approach to the problem of obesity. Int JObesity 1995;19 (suppl 3):S37-46.
19 Liebel RL, Rosenbaum M, Hirsch J. Changes in energy expenditureresulting from altered body weight. N Engl J Med 1995;332:621-8.
20 Heitmann BL, Lissner L, Sorensen TI, Bengtsson C. Dietary fat intakeand weight gain in women genetically predisposed for obesity. Am J ClinNutr 1995;61:1213-7.
21 Keys A, Brozek J, Kenschel A, Mickelsen O, Taylor HL. The biology ofhuman starvation. Vol 1, Minneapolis: University of Minnesota Press,1950.
22 Katahn M, McMinn MR. Obesity: a biobehavioral point of view. Ann NYAcad Sci 1990;602:189-204.
23 Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Posi-tional cloning of the mouse obese gene and its human homologue.Nature 1994;372:425-32.
24 Frisch RE. The right weight: body fat, menarche and fertility. Proc Nutr Soc1994;53:113-29.
25 Rebuffe-Scrive M, Enk L, Crona N, Lonnroth P, Abrahamsson L, Smith U,et al. Fat cell metabolism in different regions in women: effect ofmenstrual cycle, pregnancy and lactation. J Clin Invest 1985;75:1973-6.
26 Bourdin M, Pastene J, Germain M, Lacour JR. Influence of training, sex,age and body mass on the energy costs of running. Eur J Appl Physiol1993;66:439-44.
27 Tuten C, Petosa R, Sargent R, Weston A. Biracial differences in physicalactivity and body composition. Obesity Res 1995;3:313-8.
28 Brownell KD, Wadden TA. Etiology and treatment of obesity:understanding a serious, prevalent, and refractory disorder. J Consult ClinPsychol 1992;60:505-17.
29 Hadden W. Advances in the epidemiology of injuries as a basis for publicpolicy. Public Health Rep 1980;95:411-21.
(Accepted 17 February 1997)
How to read a paperPapers that report drug trialsTrisha Greenhalgh
“Evidence” and marketingIf you prescribe drugs, the pharmaceutical industry isinterested in you and is investing a staggering sum ofmoney trying to influence you. The most effective wayof changing the prescribing habits of a clinician isthrough personal representatives (known in Britain as“drug reps” and in North America as “detailers"), whotravel round with a briefcase full of “evidence” insupport of their wares.1
Pharmaceutical “reps” do not tell nearly as manylies as they used to (drug marketing has become analtogether more sophisticated science), but they havebeen known to cultivate a shocking ignorance of basicepidemiology and clinical trial design when it suitsthem.2 It often helps their case, for example, to presentthe results of uncontrolled trials and express them interms of before and after differences in a particularoutcome measure.3 The recent correspondence in theLancet and BMJ on placebo effects should remind youwhy uncontrolled before and after studies are the stuffof teenage magazines, not hard science.4-12
Making decisions about treatmentSackett and colleagues have argued that before givinga drug to a patient the doctor should:
x identify, for this patient, the ultimate objective oftreatment (cure, prevention of recurrence, limitation offunctional disability, prevention of later complications,reassurance, palliation, relief of symptoms, etc);
Summary points
Pharmaceutical “reps” are now much moreinformative than they used to be, but they mayshow ignorance of basic epidemiology andclinical trial design
The value of a drug should be expressed in termsof safety, tolerability, efficacy, and price
The efficacy of a drug should ideally be measuredin terms of clinical end points that are relevant topatients; if surrogate end points are used theyshould be valid
Promotional literature of low scientificvalidity (such as uncontrolled before and aftertrials) should not be allowed to influencepractice
Education and debate
This is the sixthin a series of 10articlesintroducingnon-experts tofinding medicalarticles andassessing theirvalue
Unit forEvidence-BasedPractice and Policy,Department ofPrimary Care andPopulationSciences, UniversityCollege LondonMedical School/Royal Free HospitalSchool of Medicine,WhittingtonHospital, LondonN19 5NFTrisha Greenhalgh,senior lecturer
BMJ 1997;315:480–3
480 BMJ VOLUME 315 23 AUGUST 1997

x select the most appropriate treatment, using allavailable evidence (this includes considering whetherthe patient needs to take any drug at all); andx specify the treatment target (to know when to stoptreatment, change its intensity, or switch to some othertreatment).13
For example, in treating high blood pressure, the doc-tor might decide that:x the ultimate objective of treatment is to prevent(further) target organ damage to brain, eye, heart, kid-ney, etc (and thereby prevent death);x the choice of specific treatment is between the vari-ous classes of antihypertensive drug selected on thebasis of randomised, placebo controlled and compara-tive trials—as well as non-drug treatments such as saltrestriction; andx the treatment target might be a phase V diastolicblood pressure (right arm, sitting) of less than90 mm Hg, or as close to that as tolerable in the face ofdrug side effects.
If these three steps are not followed (as is often thecase—for example in terminal care), therapeutic chaoscan result.
Surrogate end pointsA surrogate end point may be defined as a variablewhich is relatively easily measured and which predicts arare or distant outcome of either a toxic stimulus (suchas a pollutant) or a therapeutic intervention (a drug, sur-gical procedure, piece of advice, etc) but which is notitself a direct measure of either harm or clinical benefit.The growing interest in surrogate end points in medicalresearch, and particularly by the pharmaceuticalindustry, reflects two important features of their use:x they can considerably reduce the sample size, dura-tion, and, therefore, cost, of clinical trials; andx they can allow treatments to be assessed insituations where the use of primary outcomes would beexcessively invasive or unethical.
In the evaluation of pharmaceutical products, com-monly used surrogate end points include:x pharmacokinetic measurements (for example,concentration-time curves of a drug or its activemetabolite in the bloodstream);x in vitro (laboratory) measures such as the meaninhibitory concentration of an antimicrobial against abacterial culture on agar;x macroscopic appearance of tissues (for example,gastric erosion seen at endoscopy);x change in levels of (alleged) serum markers ofdisease (for example, prostate specific antigen14 );x radiological appearance (for example, shadowingon a chest x ray film).
But surrogate end points have some drawbacks.Firstly, a change in the surrogate end point does notitself answer the essential preliminary questions: “whatis the objective of treatment in this patient?” and “what,according to valid and reliable research studies, is thebest available treatment for this condition?” Secondly,the surrogate end point may not closely reflect thetreatment target—in other words, it may not be valid orreliable. Thirdly, overreliance on a single surrogate endpoint as a measure of therapeutic success usuallyreflects a narrow clinical perspective. Finally, surrogate
end points are often developed in animal models ofdisease, since changes in a specific variable can bemeasured under controlled conditions in a welldefined population. However, extrapolation of thesefindings to human disease is likely to be invalid.15-17
The features of an ideal surrogate end point areshown in the box. If the “rep” who is trying to persuadeyou of the value of the drug cannot justify the endpoints used, you should challenge him or her toproduce additional evidence.
One important example of the invalid use of a sur-rogate end point is the CD4 cell count in monitoringprogression to AIDS in HIV positive subjects. TheCONCORDE trial was a randomised controlled trial
PETERBROWN
Features of the ideal surrogate end point
• The surrogate end point should be reliable,reproducible, clinically available, easily quantifiable,affordable, and show a “dose-response” effect (thehigher the level of the surrogate end point, the greaterthe probability of disease)• It should be a true predictor of disease (or risk ofdisease) and not merely express exposure to acovariable. The relation between the surrogate endpoint and the disease should have a biologicallyplausible explanation• It should be sensitive—a “positive” result in thesurrogate end point should pick up all or mostpatients at increased risk of adverse outcome• It should be specific—a “negative” result shouldexclude all or most of those without increased risk ofadverse outcome• There should be a precise cut off between normaland abnormal values• It should have an acceptable positive predictivevalue—a “positive” result should always or usuallymean that the patient thus identified is at increasedrisk of adverse outcome• It should have an acceptable negative predictivevalue—a “negative” result should always or usuallymean that the patient thus identified is not atincreased risk of adverse outcome• It should be amenable to quality control monitoring• Changes in the surrogate end point should rapidlyand accurately reflect the response to treatment. Inparticular, levels should normalise in states ofremission or cure
Education and debate
481BMJ VOLUME 315 23 AUGUST 1997

comparing early and late start of treatment withzidovudine in patients who were HIV positive but clini-cally asymptomatic.18 Previous studies had shown thatstarting treatment early led to a slower decline in theCD4 cell count (a variable which had been shown tofall with the progression of AIDS), and it was assumedthat a higher CD4 cell count would reflect improvedchances of survival.
However, the CONCORDE trial showed that,although CD4 cell counts fell more slowly in the treat-ment group, the three year survival rates were identicalin the two groups. This experience confirmed a warn-ing that was issued earlier by authors suspicious of thevalidity of this end point.19 Subsequent research in thisfield has attempted to identify a surrogate end pointthat correlates with real therapeutic benefit—that is,delayed progression of asymptomatic HIV infection toclinical AIDS, and longer survival time after the onsetof AIDS.20 21 Using multiple regression analysis, investi-gators in the USA found that a combination ofmarkers (percentage of CD4:C29 cells, degree offatigue, age, and haemoglobin concentration) was thebest predictor of progression.20
Other examples of surrogate end points whichhave seriously misled researchers include ventricularpremature beats as a predictor of death from seriouscardiac arrhythmias,22 23 blood concentrations ofantibiotics as a predictor of clinical cure of infection,24
and plaques seen on magnetic resonance imaging inmonitoring the progression of multiple sclerosis.25
Before surrogate end points can be used in themarketing of pharmaceuticals, those in the industrymust justify the utility of these measures by showing aplausible and consistent link between the end pointand the development or progression of disease. Itwould be wrong to suggest that the pharmaceuticalindustry develops surrogate end points with the delib-erate intention to mislead the licensing authorities andhealth professionals. However, the industry does, theo-retically, have a vested interest in overstating its case onthe significance of these end points. Given that much ofthe data relating to the validation of surrogate endpoints are not currently presented in published clinicalpapers, and that the development of such markers isoften a lengthy and expensive process, one author hassuggested setting up a data archive that would pooldata across studies.26
How to get evidence out of a drug repAny doctor who has ever given an audience to a “rep”who is selling a non-steroidal anti-inflammatory drugwill recognise the argument that “this NSAID reducesthe incidence of gastric erosion in comparison to itscompetitors.” The question to ask the rep is not “whatis the incidence of endoscopic signs of gastric erosionin volunteers who take this drug?” but “what is the inci-dence in clinical practice of potentially life threateninggastric bleeding in patients who take this drug?” Otherquestions, collated from recommendations in Drug andTherapeutics Bulletin27 and other sources,1 3 are listedbelow.
x See representatives only by appointment. Choose tosee only those whose product interests you, andconfine the interview to that product
x Take charge of the interview. Do not hear out arehearsed sales routine but ask directly for theinformation belowx Request independent published evidence fromreputable, peer reviewed journalsx Do not look at promotional brochures, which maycontain unpublished material, misleading graphs, andselective quotationsx Ignore anecdotal “evidence,” such as the fact that amedical celebrity is prescribing the productx Using the STEP acronym, ask for evidence in fourspecific areas:
Safety—the likelihood of long term or serious sideeffects caused by the drug (remember that rare butserious adverse reactions to new drugs may bepoorly documented)Tolerability—best measured by comparing thepooled withdrawal rates between the drug and itsmost significant competitorEfficacy—the most relevant dimension is how theproduct compares with your current favouritePrice—should take into account indirect as well asdirect costs
x Evaluate the evidence stringently, paying particularattention to the power (sample size) andmethodological quality of clinical trials, and the use ofsurrogate end points. Do not accept theoreticalarguments in the drug’s favour ("longer half life,” forexample) without direct evidence that this translatesinto clinical benefit
Checklist for evaluating information providedby a drug company
• Does this material cover a subject which interests meand is clinically important in my practice?• Has this material been published in independentpeer reviewed journals? Has any significant evidencebeen omitted from this presentation or withheld frompublication?• Does the material include high-level evidence suchas systematic reviews, meta-analyses, or double-blindrandomised controlled trials against the drug’s closestcompetitor given at optimal dosage?• Have the trials or reviews addressed a clearlyfocused, important and answerable clinical questionwhich reflects a problem of relevance to patients? Dothey provide evidence on safety, tolerability, efficacyand price?• Has each trial or meta-analysis defined the conditionto be treated, the patients to be included, theinterventions to be compared and the outcomes to beexamined?• Does the material provide direct evidence that thedrug will help my patients live a longer, healthier,more productive, and symptom-free life?• If a surrogate outcome measure has been used, whatis the evidence that it is reliable, reproducible, sensitive,specific, a true predictor of disease, and rapidly reflectsthe response to therapy?• Do trial results indicate whether (and how) theeffectiveness of the treatments differed and whetherthere was a difference in the type or frequency ofadverse reactions? Are the results expressed in termsof numbers needed to treat, and are they clinically aswell as statistically significant?• If large amounts of material have been provided bythe representative, which three papers provide thestrongest evidence for the company’s claims?
Education and debate
482 BMJ VOLUME 315 23 AUGUST 1997

x Do not accept the newness of a product as an argu-ment for changing to it. Indeed, there are goodscientific arguments for doing the opposite28
x Decline to try the product via starter packs or byparticipating in small scale, uncontrolled “research”studiesx Record in writing the content of the interview andreturn to these notes if the “rep” requests anotheraudience
In conclusion, it is often more difficult than you arebeing led to believe to weigh the potential benefits of adrug against its risks to the patient and cost to the tax-payer.29 The difference between the science of criticalappraisal and the pharmaceutical industry’s wellrehearsed tactics of marketing and persuasion shouldbe borne in mind when you are considering “evidence”presented by those with a commercial conflict ofinterest.
I am grateful to Dr Andrew Herxheimer for advice on thisarticle.
1 Shaughnessy AF, Slawson DC. Pharmaceutical representatives. BMJ1996;312:1494-5.
2 Bardelay D. Visits from medical representatives: fine principles, poorpractice. Prescrire International 1995;4:120-2.
3 Bero LA, Rennie D. Influences on the quality of published drug studies.Int J Health Technology Assessment 1996;12:209-37.
4 Kleijnen J, de Craen AJ, van Everdingen J, Krol L. Placebo effect indouble-blind clinical trials: a review of interactions with medications.Lancet 1994;344:1347-9.
5 Joyce CR. Placebo and complementary medicine. Lancet 1994;344:1279-81.
6 Laporte JR. Figueras A. Placebo effects in psychiatry. Lancet1994;344:1206-9.
7 Johnson AG. Surgery as a placebo. Lancet 1994;344:1140-2.8 Thomas KB. The placebo in general practice. Lancet 1994;344:1066-7.9 Chaput de Saintonge DM. Herxheimer A. Harnessing placebo effects in
health care. Lancet 1994;344:995-8.10 Gotzsche PC. Is there logic in the placebo? Lancet 1994;344:925-6.11 Rothman KJ. Placebo mania. BMJ 1996;313:3-4.12 McQuay H, Moore A, Double DB, Georgiou A, Korkia P. Placebo mania.
BMJ 1996;313:1008-9.13 Sackett DL, Haynes RB, Guyatt GH, Tugwell P. Clinical epidemiology—a
basic science for clinical medicine. London, Little, Brown, 1991:187-248.14 Bostwick DG, Burke HB, Wheeler TM, Chung LW, Bookstein R, Pretlow
TG, et al. The most promising surrogate endpoint biomarkers for screen-ing candidate chemopreventive compounds for prostatic adenocarci-noma in short-term Phase II clinical trials. J Cell Biochem 1994;56(suppl19):283-9.
15 Gøtzsche P, Liberati A, Torri V, Rosetti L. Beware of surrogate outcomemeasures. Int J Health Technology Assessment 1996;12:238-46.
16 Lipkin M. Summary of recommendations for colonic biomarker studiesof candidate chemopreventive compounds in Phase II clinical trials.J CellBiochem 1994;56(suppl 19):94-8.
17 Kimbrough RD. Determining acceptable risks: experimental andepidemiological issues. Clin Chem 1994;40:1448-53.
18 CONCORDE Co-ordinating Committee. CONCORDE MRC/ANRSrandomised double-blind controlled trial of immediate and deferredzidovudine in symptom-free HIV infection. Lancet 1994;343:871-81.
19 Jacobson MA, Bacchetti P, Kolokathis A et al. Surrogate markers for sur-vival in patients with AIDS and AIDS related complex treated with zido-vudine. BMJ 1991;302:73-8.
20 Blatt SP, McCarthy WF, Bucko-Krasnicka B, Melcher GP, Boswell RN,Dolan J, et al. Multivariate models for predicting progression to AIDS andsurvival in HIV-infected patients. J Infect Dis 1995;171:837-44.
21 Tsoukas CM, Bernard NF. Markers predicting progression of HIV-relateddisease. Clin Microbiol Rev 1994;7:14-28.
22 Epstein AE, Hallstrom AO, Rogers WJ, Liebson PR, Seals AA, AndersonJL, et al. Mortality following ventricular arrhythmia suppression by encai-nide, flecainide and moricizine after myocardial infarction. JAMA 1993,270, 2451-55.
23 Lipicky RJ, Packer M. Role of surrogate endpoints in the evaluation ofdrugs for heart failure. J Am Coll Cardiol 1993;22(suppl A):179-84.
24 Hyatt JM, McKinnon PS, Zimmer GS, Schentag JJ. The importance ofpharmacokinetic/pharmacodynamic surrogate markers to outcome.Focus on antibacterial agents. Clin Pharmacokinetics 1995;28:143-60.
25 Interferon beta-1b—hope or hype? Drug Ther Bull 1996;34:9-11.26 Aickin M. If there is gold in the labelling index hills, are we digging in the
right place? J Cell Biochem 1994;56(suppl 19):91-3.27 Getting good value from drug reps. Drug Ther Bull 1983;21:13-5.28 Ferner RE. Newly licensed drugs. BMJ 1996;313:1157-8.29 Risk:benefit analysis of drugs in practice. Drug Ther Bull 1995;33:33-5.
When I use a word ...Buyers and sellers
These articles about words elicit an interesting postbag. I haverecently been asked by F J Langfield of Frenchay in Bristol if I canremind him of the word for the inverse of a monopoly. Amonopoly is defined in the Oxford English Dictionary as “thecondition of having no competitor in the sale of some commodityor in the exercise of some trade or business.” What then do youcall the condition in which you have no competitor in thepurchase of some commodity?
Well monopoly comes from two Greek words, ìïíïò (monos)single and ðùëåù (poleo) I sell—monopoly, one seller. So what wewant is a word meaning one buyer. Attic Greek had more thanone word meaning I buy, but the relevant one is ï’øùíåù(opsoneo), and the word we want is monopsony.
Monopsony was first coined in the 1930s, but in contrast tomonopoly it is used almost exclusively by economists. Forinstance, in an article entitled “How to Pay for the NationalHealth Service” (Roy Soc Health J 1971;91:217-21) Michael HCooper, a social economist, defined a monopsony as “a consumerso large that it can exert pressure on price merely by the threat ofwithdrawing its custom.” One familiar instance is the governmentas a purchaser of healthcare. Other current or past examples ofmonopsonies, or at least oligopsonies, include the diamond trade,dominated by de Beers as both buyer and seller, the tobaccoindustry, and academic specialist book publication.
Opsonins are substances that combine with bacteria or otherforeign cells, making them more susceptible to phagocytosis. Tounderstand the genesis of the term opsonins (which we now callmembers of the complement group), we must explore the originsof ï’ øùíåù more closely. It originally meant to buy ï’´øïí (opson),cooked meat or fish, non-staple food as opposed to bread,consequently anything eaten with bread to give it flavour, andhence seasoning or sauce. So, as Shaw put it in the preface to hisplay The Doctor’s Dilemma (1906), “the white corpuscles orphagocytes which attack and devour disease germs for us do theirwork only when we butter the disease germs appetisingly forthem with a natural sauce which Sir Almroth [Wright] namedopsonin [in Proc Roy Soc 1903;72:366].” According to Wright’salter ego in the play, Sir Colenso Ridgeon, “To inject a vaccineinto a patient without first testing his opsonin is as near murderas a respectable practitioner can get.” An opinion on which heseems to have had a monopoly.
Jeff Aronson, clinical pharmacologist, Oxford
We welcome filler articles up to 600 words on topics such asA memorable patient, A paper that changed my practice, My mostunfortunate mistake, or any other piece conveying instruction,pathos, or humour. If possible the article should be supplied ona disk.
The articles in this series are excerpts from How toRead a Paper: the Basics of Evidence Based Medicine.The book includes chapters on searching theliterature and implementing evidence basedfindings. It can be ordered from the BMJPublishing Group: tel 0171 383 6185/6245; fax0171 383 6662. Price £13.95 for UK members,£14.95 for non-members.
Education and debate
483BMJ VOLUME 315 23 AUGUST 1997