African Newsletter - on Occupational Health and Safety
28
African Newsletter Volume 11, number 3, December 2001 on Occupational Health and Safety GLOBALIZATION
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of African Newsletter - on Occupational Health and Safety
African NewsletterVolume 11, number 3, December 2001
on Occupational Health and Safety
GLOBALIZATION

African Newsletter onOccupational Health andSafety
Volume 11, number 3, December2001Globalization and its effects onoccupational health and safety
Published bythe Finnish Institute of Occupational HealthTopeliuksenkatu 41 a AFIN-00250 Helsinki, Finland
in collaboration with the ILO-FINNIDAAfrican Safety and Health Project,INT/89/M16/FIN
Guest Editor in ChiefSuvi Lehtinen
Guest EditorMarianne Joronen
Guest Linguistic EditorSheryl S. Hinkkanen
Layout of the cover pageTuula Solasaari-Pekki
The Editorial Board is listed (as of 31December 1994) on the back page.A list of contact persons in Africa is also onthe back page.
This publication enjoys copyright underProtocol 2 of the Universal CopyrightConvention. Nevertheless, short excerpts ofarticles may be reproduced without authori-zation, on condition that source is indicated.For rights of reproduction or translation,application should be made to the FinnishInstitute of Occupational Health, Office ofInformation and International Affairs,Topeliuksenkatu 41 a A, FIN-00250Helsinki, Finland.
The African Newsletter on OccupationalHealth and Safety homepage address is:http://www.occuphealth.fi/eng/info/anl/
The next issue of the African Newsletter willcome out at the end of April 2002. Thetheme of the issue 1/2002 is Violence atwork.
Photograph of the cover page: M. Lintunen /Photo Gallery of the Department of InternationalDevelopment Cooperation
© International Labour Organisation, 2001© Finnish Institute of Occupational Health, 2001
Printed publication:ISSN 0788-4877On-line publication:ISSN 1239-4386Printed in Finland byEdita, Helsinki
The responsibility for opinions expressed in signed articles, studies andother contributions rests solely with their authors, and publication does notconstitute an endorsement by the International Labour Office or the FinnishInstitute of Occupational Health of the opinions expressed in it.
Contents
Editorial 55H. Holkeri
Mobilizing to protect worker’s health:The WHO Global Strategy onOccuphealth Health and Safety 56G. Goldstein, R. Helmer, M. Fingerhut
New challenges and oppurtunities for occupationalsafety and health (OSH) in a globalized world 61A. López-Valcárcel
External relations of the European Unionare a global commitment 64K. LeichnitzIOHA
Effects of globalization on working women 66R. LoewensonZIMBABWE
Guidelines on Occupational Safety and Health 68Management Systems (ILO-OSH 2001)S. Machida, P. Baichoo
Globalization and its effects on occupational healthand safety: focus on chemical safety at workplaces 70M. AmweeloNAMIBIA
Work in the Global Village 72S. LehtinenFINLAND
Use of pesticides and personal protective equipment byapplicators in a Kenyan district 74J.A. HanshiKENYA
Fifth Network Meeting of the WHO CollaboratingCentres in Occupational Health 77S. LehtinenFINLAND
Follow-up meeting on indicators and profilesin Chiang Mai, Thailand 78S. Lehtinen, FINLAND

The emergence of new technologiesand expansion of trade and finan-cial regimes have accelerated the
speed of globalization. True, globalizationhas made markets more open and inclu-sive. However, the improved interconnect-edness and economic dimension of glo-balization are often over-emphasized.
The record of globalization is mixed:some countries have been able to take ad-vantage of market economy, when othershave become more marginalized, disinte-grated, and impoverished. Market forcesand economic growth have not been ableto guarantee social justice, employment,and development to all.
As industrialized countries are facing thechallenge of maintaining their welfare sys-tems and high levels of employment, indeveloping countries and economies intransition ensuring employment and social security are evenmore acute and critical for daily survival, as well as for socialand political stability. For this reason, there is a need to elabo-rate the ways structural changes in global economy have af-fected societies and quality of life, including workers and work-ing conditions.
The number of poor has increased in absolute terms duringthe second half of the 1990s in almost all regions of the world.The financial crisis in South East Asia spread to other conti-nents and some developing countries have recovered slowly.Technological advancement further deepens the gap in knowl-edge, wealth, and opportunities.
In the North, health and safety of workers are mainly relatedto their age, gender, and a type of profession, when in the Southpoverty forces people to work in the informal economy with-out supervision and work safety guarantees. Poor nutrition,long working hours and exposure to chemicals and work-re-lated accidents make the status of workers in developing coun-tries unequal compared to ones in wealthier societies. In theformal sector, globalization leads to subcontracting and flexi-bilization, which may cause further compromising health andsafety standards of the poor. The HIV/AIDS epidemic is erod-ing the human resource capacity by killing labour force from
all sectors and causing a major burden onthe basic health care systems.
Globalization can be argued to have ledto a democracy deficit with a huge gapbetween ordinary citizens and the deci-sion-makers. Yet, new global informationnetworks and the rise of civil society allaround the world have enhanced the ex-change of knowledge and universaliza-tion of ethical and moral values. Theawareness and consensus of social stand-ards and rights of labour force have in-creased. More than ever, individuals havethe power to move mountains and influ-ence global policy-making, also concern-ing the issues of labour.
The right to collective bargaining andfreedom of association are crucial forfunctioning labour market and contributeto good governance at national and inter-
national levels. Trade unions already have a long history asdefenders of human rights and decent working conditions andtheir role needs to be recognized and appreciated. Today, ag-ricultural, domestic, and migrant workers also have the rightto be included in the social dialogue.
Governments need more co-operation and partnerships withregional and international organizations, but also with civilsociety actors to alleviate poverty and harmonize minimumlabour standards and safety for workers. The private sectorand investors should include into their ethical code a supportfor safe and healthy work environment. Nationally, legal frame-work, policies, service delivery, and access to education aremeans to ensure the realisation of human rights. International-ly, the rights-based approach to development needs a particu-lar focus on occupational health and safety of the poor.
Globalization and its effects onoccupational health and safety
Harri HolkeriPresident of the 55th General Assembly ofthe United Nations
Global occupational healthchallenges, and the relationto globalizationConditions at work, and especially oc-cupational health and safety have im-proved substantially during the past fewdecades in many parts of the world.
But the overall global situation re-mains poor. Working conditions for themajority of workers do not meet theminimum standards and guidelines setby the International Labour Organisa-tion (ILO) and the World Health Organ-ization for occupational health, safetyand social protection. As an example themajority of the world’s workforce is stillnot served by competent occupationalhealth services.
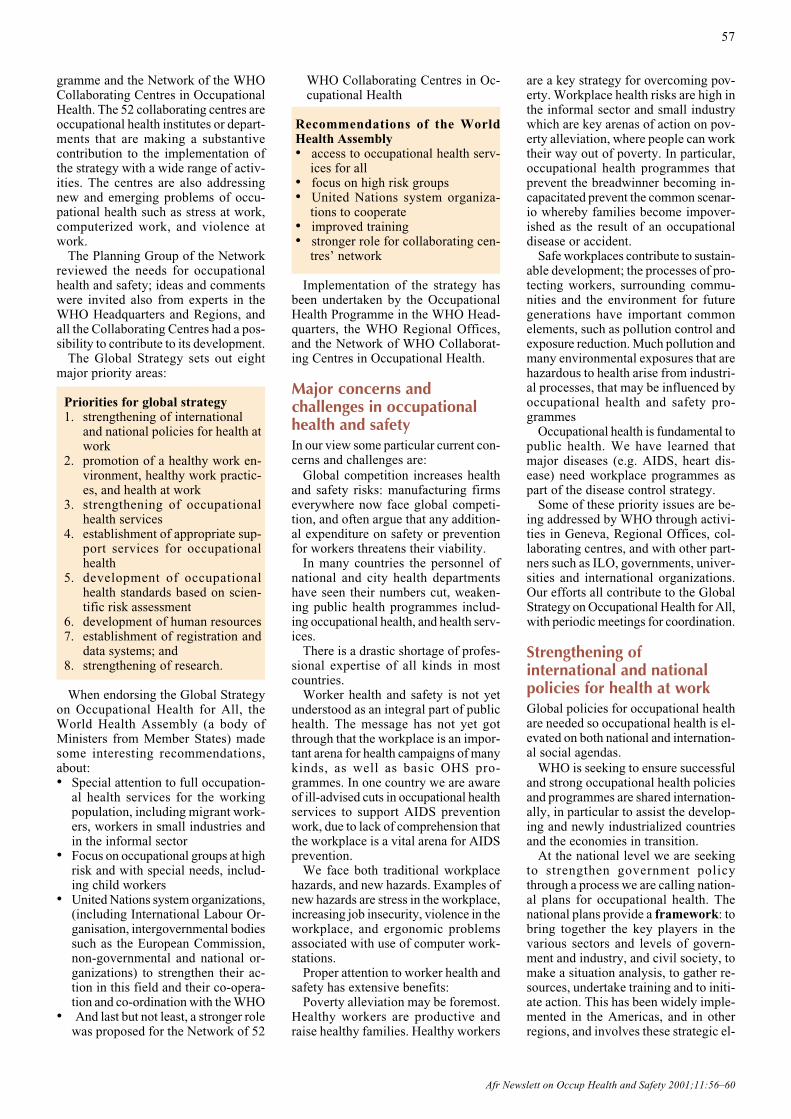
As a result the global burden of oc-cupational disease and injury remains
unacceptably high, on a par with theburden from malaria. Yet occupationalhealth programmes receive only a tinyfraction of the resources devoted tocombating malaria.
Major traditional occupational healthneeds still prevail among the globalworkforce. In addition, due to the rapidchanges in economic structures, tech-nologies and demography, new occu-pational health needs have appeared.Globalization has deep-going effects onthe working life and the conditions ofwork everywhere in the world.
Growing internationalization, globalcompetition, changes in the regulatorystrategies, major changes in enterprisestructures and associated technologychanges must now be taken into con-sideration in policies affecting workinglife. A great fear is that more flexible
labour policies may lead to a weaken-ing of commitment to occupationalhealth and safety programmes. Thestress of global competition may leademployers to view the prevention ofoccupational injuries and protection ofworkers’ health not as an integral partof quality management, but as a barrierto trade.
Freer trade as part of globalization hasalready led to a number of adverse oc-cupational health impacts:
Globalization and occupationalhealth: Some problems• pesticides that are banned in cer-
tain countries are still sold in oth-ers, causing hazards for agricultur-al workers and consumers
• machines that are obsolete in somecountries, and often in a poor orhazardous condition, are transferredto low income countries
• free trade zones are being devel-oped, where occupational healthand environmental legislation isoften poor and where hazardous orstrenuous production processes areconcentrated.
Purpose of articleThis article reviews the work carried outto implement the World Health Organ-ization Global Strategy on Occupation-al Health for All, and considers somekey issues affecting its implementation.
What is the Global Strategy?An overviewThe need for a global strategy on occu-pational health was recognized at thebeginning of the 1990s. The initiativeto develop a strategy was undertaken bythe WHO Occupational Health Pro-
The WHO Global Strategy onOccupational Health and Safety
G. Goldstein, R. Helmer, M. FingerhutWHO
Figure 1: Global burden of disease (Occupational causes)* These estimates from Murray and Lopez, 1996 are currently (October 2001) under revision
Mobilizing to protect worker’s health:
Afr Newslett on Occup Health and Safety 2001;11:56−60
56
gramme and the Network of the WHOCollaborating Centres in OccupationalHealth. The 52 collaborating centres areoccupational health institutes or depart-ments that are making a substantivecontribution to the implementation ofthe strategy with a wide range of activ-ities. The centres are also addressingnew and emerging problems of occu-pational health such as stress at work,computerized work, and violence atwork.
The Planning Group of the Networkreviewed the needs for occupationalhealth and safety; ideas and commentswere invited also from experts in theWHO Headquarters and Regions, andall the Collaborating Centres had a pos-sibility to contribute to its development.
The Global Strategy sets out eightmajor priority areas:
Priorities for global strategy1. strengthening of international
and national policies for health atwork
2. promotion of a healthy work en-vironment, healthy work practic-es, and health at work
3. strengthening of occupationalhealth services
4. establishment of appropriate sup-port services for occupationalhealth
5. development of occupationalhealth standards based on scien-tific risk assessment
6. development of human resources7. establishment of registration and
data systems; and8. strengthening of research.
When endorsing the Global Strategyon Occupational Health for All, theWorld Health Assembly (a body ofMinisters from Member States) madesome interesting recommendations,about:• Special attention to full occupation-
al health services for the workingpopulation, including migrant work-ers, workers in small industries andin the informal sector
• Focus on occupational groups at highrisk and with special needs, includ-ing child workers
• United Nations system organizations,(including International Labour Or-ganisation, intergovernmental bodiessuch as the European Commission,non-governmental and national or-ganizations) to strengthen their ac-tion in this field and their co-opera-tion and co-ordination with the WHO
• And last but not least, a stronger rolewas proposed for the Network of 52
WHO Collaborating Centres in Oc-cupational Health
Recommendations of the WorldHealth Assembly• access to occupational health serv-
ices for all• focus on high risk groups• United Nations system organiza-
tions to cooperate• improved training• stronger role for collaborating cen-
tres’ network
Implementation of the strategy hasbeen undertaken by the OccupationalHealth Programme in the WHO Head-quarters, the WHO Regional Offices,and the Network of WHO Collaborat-ing Centres in Occupational Health.
Major concerns andchallenges in occupationalhealth and safetyIn our view some particular current con-cerns and challenges are:
Global competition increases healthand safety risks: manufacturing firmseverywhere now face global competi-tion, and often argue that any addition-al expenditure on safety or preventionfor workers threatens their viability.
In many countries the personnel ofnational and city health departmentshave seen their numbers cut, weaken-ing public health programmes includ-ing occupational health, and health serv-ices.
There is a drastic shortage of profes-sional expertise of all kinds in mostcountries.
Worker health and safety is not yetunderstood as an integral part of publichealth. The message has not yet gotthrough that the workplace is an impor-tant arena for health campaigns of manykinds, as well as basic OHS pro-grammes. In one country we are awareof ill-advised cuts in occupational healthservices to support AIDS preventionwork, due to lack of comprehension thatthe workplace is a vital arena for AIDSprevention.
We face both traditional workplacehazards, and new hazards. Examples ofnew hazards are stress in the workplace,increasing job insecurity, violence in theworkplace, and ergonomic problemsassociated with use of computer work-stations.
Proper attention to worker health andsafety has extensive benefits:
Poverty alleviation may be foremost.Healthy workers are productive andraise healthy families. Healthy workers
are a key strategy for overcoming pov-erty. Workplace health risks are high inthe informal sector and small industrywhich are key arenas of action on pov-erty alleviation, where people can worktheir way out of poverty. In particular,occupational health programmes thatprevent the breadwinner becoming in-capacitated prevent the common scenar-io whereby families become impover-ished as the result of an occupationaldisease or accident.
Safe workplaces contribute to sustain-able development; the processes of pro-tecting workers, surrounding commu-nities and the environment for futuregenerations have important commonelements, such as pollution control andexposure reduction. Much pollution andmany environmental exposures that arehazardous to health arise from industri-al processes, that may be influenced byoccupational health and safety pro-grammes
Occupational health is fundamental topublic health. We have learned thatmajor diseases (e.g. AIDS, heart dis-ease) need workplace programmes aspart of the disease control strategy.
Some of these priority issues are be-ing addressed by WHO through activi-ties in Geneva, Regional Offices, col-laborating centres, and with other part-ners such as ILO, governments, univer-sities and international organizations.Our efforts all contribute to the GlobalStrategy on Occupational Health for All,with periodic meetings for coordination.
Strengthening ofinternational and nationalpolicies for health at workGlobal policies for occupational healthare needed so occupational health is el-evated on both national and internation-al social agendas.
WHO is seeking to ensure successfuland strong occupational health policiesand programmes are shared internation-ally, in particular to assist the develop-ing and newly industrialized countriesand the economies in transition.
At the national level we are seekingto strengthen government policythrough a process we are calling nation-al plans for occupational health. Thenational plans provide a framework: tobring together the key players in thevarious sectors and levels of govern-ment and industry, and civil society, tomake a situation analysis, to gather re-sources, undertake training and to initi-ate action. This has been widely imple-mented in the Americas, and in otherregions, and involves these strategic el-
Afr Newslett on Occup Health and Safety 2001;11:56–60
57

Afr Newslett on Occup Health and Safety 2001;11:56–60
58
ements:
Strategic elements of national plan• improved quality of the work envi-
ronment (primary prevention)• regulatory policy and legislation• workers’ health promotion• delivery of comprehensive health
services
This involvement of government inthe preparation of a national plan doesnot prejudice the primary responsibili-ty of the employer for health and safetyat work, but rather it complements theemployer’s efforts.
A model national programme for de-veloping occupational health based onthe WHO Global Strategy would in-clude the following:
Model national programme• updating of legislation and stand-
ards• definition and strengthening of the
role of the competent authority• emphasis on the primary responsi-
bility of the employer for health andsafety
• tripartite collaboration betweengovernment, employers and tradeunions
• education, training and informationavailable to employers and work-ers
• development of occupational healthservices
• analytical and advisory services• research• registration systems of occupational
accidents, diseases and exposures• collaboration between employers
and workers at the workplace andenterprise level.
The national occupational health sys-tem to implement this programme isrealized at the level of the enterprise andat the local level in the form of OHSprovided by occupational health teamsin collaboration with employers andworkers.
Promotion of a healthy workenvironment, healthy workpractices and health at workBetter health requires that improve-ments be made simultaneously to thework environments, work practices, andorganization of work. Most hazardousconditions at work are in principle pre-ventable and the primary preventionapproach is the most cost-effective strat-egy for their elimination and control.
Primary prevention means that haz-
ards are engineered out of the work-place production process and environ-ment. Reliance is NOT placed primari-ly on training workers to avoid hazards,or the use of protective clothing anddevices such as ear-plugs.
This commitment to primary preven-tion means that intensive actions forbetter work environments are requiredin virtually every country.
Criteria and actions for the planningand design of healthy and safe workenvironments that are conducive tophysical, psychological and social well-being need to be considered. We havemany activities underway that covermany issues in different environments,from guidelines on prevention of pesti-cide hazards, to reduction of dust, tomental health issues such as workplace“mobbing”, and human factors and er-gonomics. Countries are encouraged toinclude in their national occupationalhealth programmes a strong element forimprovement of the physical and psy-chological work environment.
Does it work? Evidence is availablefrom some countries on highly positivecost-effectiveness of occupationalhealth programmes in view of health,work ability, productivity and economyat the national and enterprise levels.Thus, development of occupationalhealth and safety can be seen as an in-vestment, not as an economic burden.
So why is improvement in workingconditions so difficult? We have all ourrational arguments that occupationalhealth programmes improve health,work ability, productivity and economy,and are highly cost-effective. We arguethat most hazardous conditions at workare in principle preventable and the pri-mary prevention approach is the mostcost-effective strategy for their elimi-nation and control.
We suggest there is a need to advo-cate.
Advocacy is a key health promotionactivity for overcoming major barriersto public health and occupational health.The barriers addressed by advocacy arepoor living and working conditions,rather than individual or behaviouralbarriers. The modern use of the termadvocacy gained momentum from theOttawa Charter on Health Promotion:“Political, economic, social, cultural,environmental, behavioural and biolog-ical factors can all favor health or beharmful to good health. Health promo-tion aims at making these conditionsfavorable through advocacy forhealth”.
There is a common public health met-aphor about “upstream” versus “down-
stream” work, that talks about expen-sive rescue services hard at work drag-ging drowning people from a river.They never pause to look upstream tosee why people are falling in the river,because they are so busy. Those whoare rescued are grateful for the servic-es, and conversely, a lot of politicallydamaging fuss would result if impor-tant people should be left to drown.
Some people may advocate that fenc-es might be constructed upstream to stoppeople falling in; however, decision-makers are reluctant to act. Fences maydisrupt the view, and fences lack theglamour of ambulances and dramaticrescue routines. Perhaps most impor-tantly, fences do their job when noth-ing happens, while a rescue provides agreat photo opportunity for a politician.
There are many unfenced rivers inpublic health, and quite a number ofthose that are fenced have fences thattopple under the slightest pressure.Fences such as curbs on pollution, pol-icies to ensure improved housing, wa-ter and sanitation, or improved work-place safety are coveted, long-standinggoals in public health, and remain farfrom being realized. Advocacy has akey role in building and maintainingpublic health fences, and it is essentialto shape the social and political climate.
The tactics and strategies of advoca-cy and lobbying are not easily describedin terms of programmes. This is becauseadvocates need to adopt the same set ofopportunist, responsive, imaginative,flexible, dramatic and above all news-worthy tactics that are the stuff of allsuccessful public opinion, political andcommercial campaigning.
Historically, many types of healthand safety reform have been imple-mented in the wake of a disaster. Stra-tegic use of the media can promote ahealthy work environment, especially inthe aftermath of a major workplace dis-aster. At these times newspaper editorsare inclined to place stories on occupa-tional health – or the lack thereof – onthe front page, and politicians may beprepared to back new occupationalhealth initiatives and legislation. Nor-mally, stories on occupational health onthe front page, or politicians who sup-port occupational health measures sim-ply do not occur. But in the aftermathof a disaster there is a rare opportunity:occupational health workers who areprepared, who contact the media andexplain their plans, who engage politi-cians with specific reforms and safetymeasures etc. have a chance to succeedin advancing their agendas in workplacehealth and safety.
59
Afr Newslett on Occup Health and Safety 2001;11:56−60
The WHO Offices in the Western Pa-cific, European and Americas regionshave been particularly successful indeveloping effective workplace healthpromotion programmes that focus onprimary prevention. In these initiativesthe hazards associated with the com-bined effects of lifestyle factors andoccupational exposures are identifiedand minimised. Health promotion thatintroduces healthy lifestyles and sup-ports the maintenance of such lifestyleswith appropriate information, counsel-ling and educational measures is under-taken as part of the OHS programme.
Effective health promotion is essen-tial where adoption of appropriateworking practices by the worker is need-ed, for example, a choice to use personalprotective devices. Occupational healthpersonnel require training and educa-tion in health promotion to enable themto implement it as a part of their occu-pational health practice.
Experience in workplace health pro-motion has shown that competitionsand awards are valuable in engagingenterprises in OHS activities. Firms andenterprises achieve valuable publicityand a boost in staff morale through com-peting to become the most healthy andcaring company.
Occupational health and safety grewup in the environment of the large fac-tory and enterprise, and we are only nowlearning how to carry it out in smallenterprises and the informal sector. In-termediary organizations – whichmay be NGOs, universities and techni-cal schools, or private consultancies thatspecialise in OHS – play an importantrole in working with employers, self-
employed workers, and sometimes di-rectly with workers.
A good example of workplace healthpromotion, from the Western PacificRegion, is the Project on Healthy Work-places in Small and Medium-Scale En-terprises in Vietnam. All sectors at na-tional, provincial, local and individualworkplace levels were involved in anational workshop in 1998 to launch theproject. In the Hai Phong City project asurvey and needs assessment were un-dertaken by the steering committee, andcriteria for health promoting workplac-es were developed with participation ofemployers. Implementation was moni-tored, and good results were demon-strated: that is, the working conditionsimproved.
Healthy workplaces in small andmedium scale enterprises in HaiPhong, VietnamRESULTS• installation of insulation against
heat• better ventilation• control measures for dust and tox-
ic gases• provision of adequate personal pro-
tective clothing• reduced noise• improved lighting• addition of equipment to lift heavy
loads• upgrading of staff facilities• promotion of sports• enhancement of surrounding envi-
ronment• construction of sheds to house bi-
cycles and motorbikes• establishment of an awards system
for health and safety
Strengthening ofoccupational health services(OHS)In many developing and newly indus-trialized countries no more than 5–10%of the working population have accessto competent occupational health serv-ices in spite of the evident needs. In sev-eral industrialized countries access islimited to less than 20–50% of work-ers.
Modern occupational health servicesdraw from each relevant profession, dis-cipline or science – be it biomedical orenvironmental – all the required ele-ments and integrate them into a com-prehensive multidisciplinary approachaimed at the protection and promotionof workers’ health. Actions relate bothto assessing the risks of the work envi-ronment, to ensuring preventive actions
to reduce risks of workers, and to pro-viding treatment and compensation forworkers experiencing illness or injury.Disciplines relevant for occupationalhealth services include occupationalmedicine and nursing, occupationalhygiene, work physiology and physio-therapy, ergonomics, safety and workpsychology.
In South Africa, partners in the WHO-ILO Joint Effort for OccupationalHealth and Safety in Africa have foundthat integrated training of occupation-al health professionals – the nurses,safety officers, environmental healthofficers, inspectors – is best. That is, thestaff are trained together, as a team, towork as a team. Otherwise experiencehas shown they may not work well to-gether once they are graduated and inemployment in their own professionalniche.
A majority of African countries arenow partners in this WHO-ILO JointEffort initiative to intensify co-ordina-tion of occupational health and safetyactivities. The challenges are indeedlarge. Clinicians in one African coun-try, for example, report the ongoingoccurrence of acute silicosis, showingthat extremely high exposures to silicadust persist even to this day.
Other major activities of the JointEffort in Africa include the strengthen-ing of a system for surveillance of oc-cupational respiratory diseases (SORD-SA); research on silicosis incidence andimplementation of interventions; andthe creation of an occupational healthwebsite and listserver for Africa.
Development of humanresources for occupationalhealthOccupational health is a broad expertactivity that utilizes the basic knowledgeof several disciplines, such as medicine,chemistry, physics, toxicology, physi-ology, psychology and safety technol-ogy, and functions in a multidisciplinarymanner. High-quality occupationalhealth clearly requires appropriate train-ing of personnel in these fields.
In many industrialized countries, suf-ficient numbers of occupational medi-cal experts have been trained to provideone physician per 2 000–3 000 work-ers and about one nurse per 1 000–2 000workers (with a wide range of varia-tion). Many European countries andthose of North America, as well as Aus-tralia and Japan, have established spe-cialist or diploma curricula for occupa-tional health and some countries requirespecialization or diploma as a condition

Afr Newslett on Occup Health and Safety 2001;11:56–60
60
for the right to carry out occupationalhealth practices. Special training in oc-cupational health is available for nurs-es in most countries.
The training of specialists other thanthe medical experts for the multidisci-plinary occupational health team ismuch less systematically organized.Special curricula for occupational hy-giene are available in six Europeancountries and in the United States andCanada. WHO has defined the profileof an occupational hygienist on the ba-sis of defined areas of knowledge in aneffort to promote international harmo-nization of training curricula. Trainingof physiotherapists specialized in occu-pational health is also available in somecountries while the special training ofoccupational psychologists is rare. Formany Western European countries, thetraining of safety engineers is well or-ganized. There is a universal shortageof both expert resources and training indeveloping and newly industrializedcountries in the South. This is due tothree main reasons:
a) lack of effective legislation andlack of requests from authoritiesand employers make the employ-ment opportunities for such expertsminimal
b) in the absence of requests, the vo-cational training institutions anduniversities have not organized anddeveloped curricula for the train-ing of experts in occupationalhealth
c) in some instances, where trainingis available, it is too limited, forexample, oriented to clinical occu-pational medicine only.
Equally important is the awarenessand knowledge of managers and fore-men of the key principles of occupation-al health because they make decisionsabout several aspects of work that de-termine health and safety. And of courseawareness, knowledge and skills arealso needed by the workers and the self-employed for appropriate safety andhealth behaviour and for adopting safeworking practices.
WHO is supporting many types oftraining through its collaborating cen-tre network, for example a global sur-vey of competencies and curricula.
Plan to implement thestrategyCountry offices and collaborating cen-tres constitute important WHO assets inall countries and regions of the world.WHO is committed to mobilize thesein implementing all elements of the glo-
bal strategy. Some important aspects ofthe implementation plan involve:
The partnership with ILO is strong.In the face of increasing encouragementfrom countries, WHO and ILO areforming specific partnership pro-grammes at all levels in all kinds of oc-cupational health activities, such as theILO-WHO Global Elimination of Sili-cosis campaign, and the Joint Effort inAfrica.
WHO’s most high-profile, successfuland acclaimed programmes involvedthe eradication of diseases such assmallpox, guinea-worm and polio. Weare going to use the silicosis elimina-tion campaign as a flagship to raise theprofile of not just silicosis but many is-sues of occupational health and safety.
The case for more attention to occu-pational health and safety is compelling.A major goal is to share with our globalpartners rational arguments based on theglobal burden of disease study, demon-strations of cost-effectiveness of occu-pational health programmes, and otheranalytical tools that demonstrate thepriority of occupational health pro-grammes.
Finally, we propose that occupation-al health can benefit from building coa-litions with organizations and pro-grammes concerned with sustainabledevelopment, poverty alleviation, envi-ronmental protection, infectious diseas-es, social justice, women’s health, etc.These major development challengescan only be successfully addressed if theconditions of working life for all peo-ple are improved.
References
Murray C, Lopez A. Eds. The Global Burden ofDisease. Harvard University Press. 1996.
WHO, 1996. Global Strategy on OccupationalHealth for All. WHO, Geneva.
Globalization of the economy has inten-sified over the recent years and, togeth-er with the development of the new in-formation and telecommunicationstechnology, it is bringing about radicalchanges in society, comparable to thoseproduced during the industrial revolu-tion. Occupational safety and healthcannot ignore those changes. And, inthis context, the greatest challenge forthe countries of the region is the trans-formation of the difficulties involved inadapting to the new situation into op-portunities for the future developmentof occupational safety and health.
Harmonising standards:labour standards andproduct standardsOne of the most important impacts thateconomic integration and the liberali-sation of international trade have hadon occupational safety and health isundoubtedly that of the harmonisationof standards.
In talking about occupational safetyand health standards, we are in fact re-ferring to two distinct types of stand-ards.
First, there are the standards concern-ing labour. They define the general con-ditions of occupational safety and healthin the workplace. The objective in har-monising this type of standard is to pre-vent “social dumping”; i.e. prevent thecomparative advantages that are derivedfrom lower production costs at the ex-pense of inferior working conditions inthe enterprise. By harmonising thesestandards, we are also seeking socialintegration within the process of eco-nomic integration and liberalisation, insuch a way that the economic growth,achieved through economic integrationand liberalisation, is accompanied bysocial progress.
Second are the standards concerning
A. López-ValcárcelILO
Greg Goldstein, Richard Helmer,Marilyn FingerhutOccupational and EnvironmentalHealthWorld Health Organization20, avenue AppiaCH-1211 Geneva 27Switzerland
E-mail: [email protected]

61
Afr Newslett on Occup Health and Safety 2001;11:60–63
product safety. As tariffs areeliminated or reduced, as iscurrently occurring with theregional economic integrationagreements and with the sign-ing of multilateral trade agree-ments in the framework of theWorld Trade Organisation(WTO), non-tariff technicalbarriers acquire more signifi-cance in international trade(1). Technical standards, particularlythose related to product safety, couldblock international trade as effectivelyas high tariffs did in the past, and forthat reason harmonisation of productsafety standards has become a prereq-uisite for economic integration.
This harmonisation has in fact alreadyhad a positive impact on the develop-ment of occupational safety and health(OSH) in many countries.
In many European countries, OSH hasbenefited as the result of these countriesjoining the European Union (EU). Thatwas not only due to the application ofEuropean Directives related to the so-cial policy areaa – aimed at harmonisa-tion in the framework of progress ofoccupational safety and health condi-tions – but also due to the efforts madeto achieve a single market (2). To guar-antee the free flow of products and toavoid having to invoke safety reasonsthat could impede free circulation,measures were taken so that only “safeproducts” could be traded. In doing so,the safety of a product has become anindispensable condition for its trade andfree circulation. At the same time, as theworker is the user of many of theseproducts (substances, machinery, equip-ment), establishing a system that guar-antees the safety of products purchasedby the employer and used by the work-er means, in fact, an important contri-bution to the progress of OSH.
In the case of Mexico, NAFTA’sb side
agreements introduced an interesting(an innovative) approach to the devel-opment of occupational safety andhealth. The Agreement on Labour Co-operation considers that the nationallegislation of the three NAFTA mem-ber countries (Canada, Mexico andUSA) contains the basic principles ofworker protection. Therefore, theAgreement does not oblige the partiesto modify their national legislation inthis regard, but requires them to guar-antee the effective application of theirlegislation. In addition, it creates an in-stitutional scheme to ensure compliancewith these obligations, and it also es-tablishes a special system for disputeresolution in cases related to the lack ofeffective enforcement of OSH, childlabour, and minimum wage labourstandards (3).
But the most far-reaching process re-garding harmonisation of safety prod-uct standards is probably taking placewithin the new agreement on Techni-cal Barriers to Trade (TBT, signed in1994 within the Uruguay Round ofGATT) (4)c. The harmonising strategyof the TBT/1994 is based on adherenceof the national standards to internation-al standards, and in the transparency ofthe standard setting process (1). Formany developing countries adaptationto the TBT/1994 will require profoundreorganisation of their standard settingsystems and institutions; but this effortwill bring about a double benefit: bet-
New challenges and opportunities foroccupational safety and health (OSH)
in a globalized world
ter opportunities for exportingtheir products, and a signifi-cant improvement in the safe-ty.
Occupational safetyand health (OSH) andcompetitivenessWith the elimination of tariffbarriers, less state interventionin economic matters and the
globalization of the economy, marketsare becoming more and more transpar-ent and an enterprise that wants to stayin the market is forced to continuouslyimprove its competitiveness.
Three factors can be seen as determin-ing the competitiveness of an enterprise:its capacity for innovation, the qualityof its products and its productivity. Itis, therefore, not surprising that thesethree factors have become a true obses-sion for the modern enterprise thatwants to remain competitive and thus,survive in the global economy.
The search for new relationships withclients and suppliers, as factors for pro-ductivity, is nothing new in businessstrategy. What is new, however, in thisera of globalization, is the emergenceof a new culture concerning the natureof the relationship between the enter-prise and its workers. This new culturecan be summarised by the words “thereis a need to invest in the worker”, bothin their training and in the improvementof their working conditions. Thus, OSHis beginning to be seen by many enter-prises not only as a legal requirementbut also as a means of improving pro-ductivity.
Another determining factor for com-petitiveness is the quality of the prod-ucts. Over the years concepts and pro-grammes such as quality control, qual-ity circles, total quality, and quality as-surance, have gained ground. But in the
Phot
o by
M-L
. Kilj
unen

Afr Newslett on Occup Health and Safety 2001;11:60–63
62
context of international trade, one usu-ally frequently refers to the internationalquality management standards, ISO9000, that over a short period have be-come the most well known ISO stand-ards. Customers are starting to demandthat enterprises obtain ISO 9000 regis-tration, and the number of enterprisesall over the world obtaining this certifi-cation has escalatedd (5).
Although the ISO 9000 series doesnot explicitly cover the issue of OSH,they show many of the links that existbetween OSH and quality. Thus, a pro-gramme for the management of thequality of an enterprise has to ensurethe safety of the production processes.On the other hand, there is a similaritybetween the nature of the safety prob-lems and the quality problems (e.g.shortcomings, errors). Besides, there arealso similarities between the solutionsand organisational structures that, with-in the limits of the enterprise, both safe-ty and quality apply (e.g. documenta-tion, workers’ participation, criteria fortraining, motivation and qualification).Finally, quality has to be built into theworkstation. Therefore, ergonomics isan essential factor to be taken into con-sideration. If the operator has appropri-ate conditions with regard to tempera-ture, lighting, cleanliness, workload,etc., the probability of human error de-creases significantly. As a result, manyenterprises now consider their policiesfor improving working conditions as akey element in their policies for improv-ing quality.
To reach high levels of quality, thefact of having appropriate technologyis not sufficient; nor is it sufficient tohave highly trained workers. The highlevels of quality required today can onlybe reached if the enterprise can alsocount on workers who are willing andinterested in achieving it. Therefore,concepts such as motivation, participa-tion and co-operation are becoming soimportant in the management of mod-ern enterprises. Thus also the impor-tance of investing in the OSH of theworker in order to improve both quali-ty and productivity.
The third factor that determines com-petitiveness is the capacity for innova-tion. Many of the characteristics of awork environment that favour innova-tion can also be found in safe andhealthy work environments. It has beensaid, for example, that creativity bloomswhere the work atmosphere is relaxedor even playful, where conflicts amongpersonnel are at a minimum, and wherethe worker enjoys ample freedom in themanner in which he performs his work.
All of these are also characteristic ofgood OSH conditions.
Occupational safety andhealth (OSH) and theenvironmentFollowing the success of ISO 9000, theInternational Standards Organisationhas also developed a series of environ-mental management standards, ISO14000. These standards have appearedat a time of increased interest by con-sumers for environmentally-friendlyenterprises and products. In this context,it seems that the new series will favourinternational trade, as the ISO 9000standards did.
Although the ISO 14000 series doesnot directly deal with OSH issues, theywill probably have a positive impact onthe management of OSH in the work-place, due to the link that exists betweenthe work environment and the environ-ment in general.
This link is especially clear when weconsider the handling of chemicals. Thestandards and handling requirements forthe environmentally-sound manage-ment of chemicals are similar to thoserequired by OSH for the safe use ofchemicals at the workplace.
The problems faced by chemical safe-ty are enormous, not only as regards theprotection of the environment but alsowith respect to the prevention of occu-pational risks. At a meeting of expertsorganised by the ILO (6), it was esti-mated that the number of chemicalsavailable on the market was approxi-mately 80,000; and that 5 to 10 per cent(i.e. 4,000 to 8,000) of those should beconsidered hazardous.
Classification of chemicals, accord-ing to the type and degree of their haz-ards, is a key element of any chemicalsafety policy. Another key element iscorrect labelling, to reduce the risks as-sociated with not using them correctly.Standards related to the classificationand labelling of chemicals are in factproduct safety standards and are, there-fore, subject to the requirements of har-monisation inseparable from the liber-alisation of international trade. A draftproposal prepared by the Co-ordinatingGroup for the Harmonisation of Chem-ical Classification Systems is alreadyavailable on the Web (7).
In fact, one of the Agenda 21 objec-tives (UNCED – United Nations Con-ference on Environment and Develop-ment, Rio de Janeiro, 1992) is the es-tablishment of a globally harmonisedsystem of classification and labelling ofchemicals. According to the Agenda,
this system will not only serve to im-prove the control of chemical hazards,but will also favour the development ofinternational trade. Agenda 21 consid-ers, moreover, that collaboration be-tween UNEP, ILO and WHO within theframework of the IPCS (InternationalProgramme for Chemical Safety)should be reinforced and become thenucleus for international co-operationin the environmentally-sound manage-ment of toxic chemicals (8).
A major concern related to interna-tional trade is the export of dangerouschemicals whose use has been prohib-ited or severely restricted in the export-ing country itself. Several United Na-tions agencies have adopted internation-al standards to ensure that the import-ing country, appropriately informed,may make a sound decision regardingthe eventual acquisition of such prod-ucts.
Thus, UNEP has introduced provi-sions for Prior Informed Consent (PIC)in its London Guidelines (9); and FAO,the principle of Information and Previ-ous Consent in its International Con-duct Code for the Distribution and Useof Pesticides (10). Similarly, the ILO(Convention No. 170, on ChemicalProducts -1990) (11) calls for commu-nication between exporting and import-ing countries when hazardous chemicalshave been prohibited for OSH reasons.In addition, a joint FAO/UNEP pro-gramme has been launched for the op-eration of the PIC procedures for chem-icals all over the world.
New codes of conductadopted by the enterpriseA final issue to consider is the growthof consumer action against enterprisesthat do not have adequate environmen-tal or social behaviour. This situation isleading companies to adopt voluntarycodes of conduct.
In today’s world where informationflows at high speed, where increasedcompetition is increasing consumerpower, and where state control of en-terprises is lessening, a significantchange is occurring in the demands ofthe consumers from enterprises. Theyare beginning to demand not only priceand quality, but also specific codes ofconduct with respect to the environ-ment, workers and the community ingeneral.
One of the codes of conduct worthhighlighting is the chemical industry’sinitiative, called “Responsible Care”.This is a public and voluntary commit-ment by the chemical industry to im-

63
Afr Newslett on Occup Health and Safety 2001;11:60–63
prove its performance with respect tosafety, health and the environment.Employers associations in 45 countrieshave already adopted the “ResponsibleCare” programme, among them twoAfrican countries, Morocco and SouthAfrica (12)e.
Another voluntary initiative that isgetting a lot of attention is that of the“Corporate social responsibility”, a con-cept that is generally understood as thecommitment of the enterprise to be fairto all its stakeholders, and specially itsemployees. In a recent opinion poll12,000 European consumers were inter-viewed on their attitudes to the role ofbusiness (13). Seventy per cent of themsaid that a company’s commitment tosocial responsibility is important whenbuying a product or a service. More-over, the issue European consumerscare about most is the protection ofworkers’ health and safetyf.
Recognising the existence of a rangeof OSH management-related interna-tional and national voluntary pro-grammes, and also the ISO standards onquality and environment management,the ILO has recently adopted Guidelineson occupational safety and health man-agement systems ILO-OSH 2001 (14).These guidelines carry no legal obliga-tion, and emphasize concepts such ascontinual improvement, employers’leadership and commitment, and work-ers’ participation.
The successful enterprise in this timeof globalization can no longer afford tobe a faceless institution that does noth-ing more than sell the right product atthe right price. But it will have to presentitself with a more personalised image,expressing explicit moral judgementswhen dealing with its own employees,the community and society at large (15).Moreover, a product or a workplace thatis seen as unsafe by clients or the com-munity, will inevitably affect the imageof the enterprise, and will reduce itscompetitiveness.
Bibliography
1. Kenneth SL. 1994. Health and safety regu-lations. (Kluwer Law and Taxation Publish-ers, 1994, Boston).
2. EUR-LEX, 2001. Directory of Communitylegislation in force (EU, 2001, Brussels).http://europa.eu.int/eur-lex/en/lif/reg/en_register_05202010.html
3. NAFTA. 1993. Agreement on labour co-op-eration between Canada, Mexico and USA:ht tp: / /www.sice.oas .org/ t rade/naf ta/naftatce.asp#labor
4. WTO, 2001. Agreement on technical barri-ers to trade. GATT 1994 (WTO, Geneva2001): http://www.wto.org/english/tratop_e/tbt_e/tbtagr_e.htm
5. ISO, 2000. The ISO Survey of ISO 9000 and
ISO 14000 Certif icates (ISO, 2000,Geneva):http://www.iso.ch/iso/en/iso9000-14000/pdf/survey10thcycle.pdf
6. ILO, 1987. Report of a Meeting of Expertson Harmful Substances in Work Establish-ments (ILO, 1987, Geneva)
7. ILO/IOMC, 2001. Globally Harmonised Sys-tem for the Classification and Labelling ofChemicals (GHS). Draft Integrated Proposal(ILO/IOMC, 2001, Geneva):http://mirror/public/english/protection/safework/ghs/ghsfinal/index.htm
8. UN, 1992. United Nations. UNCED. Agenda21 (New York, 1992)http://www.un.org/esa/sustdev/agenda21text.htm
9. UNEP, 1989. London Guidelines for the ex-change of information on chemicals in in-ternational trade. (UNEP, Geneva, 1989):http://irptc.unep.ch/pic/longuien.htm
10. FAO, 1990. International Code of Conducton the Distribution and Use of Pesticides(FAO, 1990, Rome):http:/ /www.fao.org/waicent/FaoInfo/Agr icul t /AGP/AGPP/Pes t ic id /Code/PM_Code.htm
11. ILO, 1990. C170 Chemicals Convention(ILO, 1990, Geneva, ):h t t p : / / i l o l e x . i l o . c h : 1 5 6 7 / s c r i p t s /convde.pl?C170
12. ICCA, 2001. ICCA Responsible Care StatusReport 2000:http://www.icca-chem.org/rcreport/
13. CSR. 2000. European Survey of Consumer’sAttitudes towards Corporate Social Respon-sibility (CSR Europe, November 2000, Lon-don):http://www.csreurope.org/csr_europe/Ac-tivities/activitiesframes. htm?content=Dialogue/Mori.htm
14. ILO, 2001. Guidelines on occupationalsafety and health management systems.(ILO, 2001, Geneva):http://www.ilo.org/public/english/protec-tion/safework/managmnt/guide.htm
15. The Economist. 1995. Saints and sinners(The Economist, June 24th 2001. London)
López-Valcárcel A. 1996. Occupationalsafety and health in the framework of the eco-nomic globalisation. (ILO, 1996, Lima).Available only in Spanish: http://www.ilolim.org.pe/spanish/260ameri/publ/docutrab/dt-26/index.shtml
Explanatory notes:
a) The fact that most EU Directives related tothe area of social policy are OSH Directives(approximately 66% of them) is a clear in-dication of the high status of OSH withinthe EU.
b) The North American Free Trade Area(NAFTA) signed by Canada, Mexico and theUSA, in 1993, has two side agreements: TheAgreement on Environmental Co-operation;and the Agreement on Labour Co-operation.
c) One of the fifty-three agreements of the Uru-guay Round GATT was the agreement es-tablishing the World Trade Organisation(WTO), an institution that is to, among otherissues, deal with the dispute settlement un-der the Uruguay Round agreements, includedthe TBT/1994. Members of the WTO agreeto conform their domestic laws to implementthe Uruguay Round GATT agreements. At
the end of 1999, WTO had 135 members,among them 39 African Countries.
d) According to the ISO Survey of ISO 9000and ISO 14000 Certificates, at December2000 there were 408,631certifications of en-terprises to ISO 9000, in 158 countries, ofthose 30 were African. On the other hand,six of these thirty countries had more thanone hundred certifications: South Africa3,454; Egypt 468; Tunisia 196; Kenya 173;Mauritius 131; and Zimbabwe 103.
e) In the case of Morocco, Responsible Carewas adopted by the Fédération de la Chimieet de la Parachimie (FCP), on 1998. In thecase of South Africa, the initiative wasadopted by the Chemical and Allied Indus-tries Association (CAIA), on 1994.
f) 70% of the consumers answered that “Pro-tecting the health and safety of its workers”was an important area for the companies tosupport; while 68% of them consider “En-suring products do not harm the environ-ment” was also an important area for thecompanies to support.
Alberto López-ValcárcelSenior Occupational Safety andHealth SpecialistSafeWork ProgramInternational Labour Office4, route des Morillons1211 Geneva [email protected]
64
Afr Newslett on Occup Health and Safety 2001;11:64–65
IntroductionWhen we see the term “glbalization” wemay also see the many people who areprotesting in front of conference cen-tres where so-called globalization meet-ings take place. It is not my intention tocomment on this kind of activities. Irather wish to point out that globaliza-tion could be a useful concept e.g. whenoccupational health and safety becomesinvolved.
There are already many activities onglobal level to improve occupationalhealth and safety; such as the ILO Safe-Work Programme (1).
Another example is the so-calledPhare Programme which has been de-veloped by the European Union. Thequestion may now be: Why referring toa European programme in the Asian-Pacific and African Newsletter? In thefollowing text I am trying to give an an-swer.
Phare: a programme of theEuropean UnionThe Phare Programme is the EuropeanUnion’s initiative which provides grantfinance to support the process of eco-nomic transformation of Central andEastern European Countries (2). Phareprovides know-how including policyadvice and training; occupational healthand safety projects are part of Phare.
The overall objective of Phare is tohelp the candidate countries to join theEuropean Union. The programme isthus “accession-driven”, concentratingthe support on priorities which help thecandidate countries to fulfil the mem-bership criteria, which require: The can-didate country has achieved stability of
institutions guaranteeing democracy,the rule of laws, human rights respectfor and protection of minorities; theexistence of a functioning market econ-omy.
European Union cooperateswith African, Caribbean andPacific CountriesThe initiatives of the European Unionare not restricted to European pro-grammes. In the year 2000 the Europe-an Commission presented a major re-orientation of its development policywhich also included the cooperationwith African, Caribbean and PacificCountries ACP (3). This cooperation isbased on the Cotonou Agreement,which is according to the EU Commis-sion’s opinion, the most ambitious andcomprehensive agreement between de-veloped and developing countries (3).The basic objective is to promote andexpedite the economic, cultural and so-cial development of the ACP States andto consolidate and diversify their rela-tions with the European Union in a spiritof solidarity and mutual interest. TheCotonou Agreement was signed in June2000 in the capital of Benin, which isthe origin for the informal name of theagreement. The wide-ranging partner-ship is based on equality between thesignatories, respect for their sovereign-ty and mutual interest and interdepend-ence.
The European Union is committed tohelping the ACP Countries becomemore active members in the internation-al economic and trade system. That, ithopes, will encourage other countriesand international business to establishcloser relations with ACP partners,
boosting investment and the transfer oftechnology and know-how.
Occupational Health and Safety In-stitutions interested in further details ofthe Cotonou Agreement should contactin their country the respective ministry(e.g. ministry of labour, ministry ofhealth). They may also contact the Eu-ropean Commission in Brussels (Bel-gium) at: http://europa.eu.int/comm/world. The European Commission hasdelegations in most countries around theworld; the addresses can be found at:h t t p : / / e u r o p a . e u . i n t / c o m m /external_relations/repdel/index.htm.
It has to be clear for all of us that thedecisions about funding of projects willbe made by the officials of the nationalgovernments and the European Com-mission. But they may consider in theirdecisions also the advice given by pro-fessional occupational safety and healthinstitutions of the respective country.
Example of a project fundedby PhareAs an example for funding of occupa-tional health and safety by the Europe-an Commission, I refer to the aforementioned Phare Programme. There, Ihad the opportunity to manage in a Cen-tral European Country a project called“train-the-trainer”.
The terms of reference of the projectwere pre-determined by the responsiblenational ministry and the EuropeanCommission. According to this agree-ment, the task of the Consultants Teamwas:• Preparing a tailor-made programme• Training of occupational medical,occupational hygiene and occupationalsafety staff under consideration of the
are a global commitment
K. LeichnitzIOHA
External Relations ofthe European Union
Afr Newslett on Occup Health and Safety 2001;11:64–65
65
following subcomponents:– Training of 30 future trainers (na-
tional experts from the Central Eu-ropean Country) in the Central Eu-ropean Country
– Training of 12 future trainers (na-tional experts from the Central Eu-ropean Country) in two Western Eu-ropean Countries
– Elaboration of an occupational safe-ty and health (OH&S) agenda for thecourses; organizing and carrying outof local refresher courses
– Elaboration and organizing the vis-its of institutions, plants, manufac-turers and laboratories in WesternEuropean Countries
– Establishing a library and preparingand issuing of practical textbooks,manuals, guidelines and learningmaterials on OH&S.
The project team consisted of fivetrainers from different Western Euro-pean countries and five trainers from theCentral European country. Preparatorymeetings and training courses altogether
lasted 80 days.The training was structured as fol-
lows: Presentations including case stud-ies; discussions; practical demonstra-tions; visits to workplaces; visits to lab-oratories; individual and group exercis-es.
Contents of the training programme:Basis was the WHO publication “Oc-cupational Hygiene in Europe – Devel-opment of the Profession” (4). This in-cluded courses on the legal basis ofOH&S (ILO and WHO Documents,European Directives, ISO Standards),exposure assessment at workplaces,quality assurance, toxicology, classifi-cation and labelling of substances, lim-it values, biological monitoring, preven-tive measures, control measures (meansand technology to reduce or eliminateoccupational hazards), risk assessment,cost/benefit, indoor air quality (sickbuilding syndrome), entry into confinedspaces, ergonomics, statistics, environ-mental protection.
Kurt LeichnitzPresident of the InternationalOccupational Hygiene Associa-tion (IOHA)Am Waldrand 42D-23627 Gross GroenauGermanyE-mail:[email protected]
Concluding remarksThe European Union’s (EU) support inworld affairs is on the increase. The EUhas a number of foreign objectives. Thefirst is to establish a stable Europe; partof it is the Phare Programme which isan initiative to provide grant finance tosupport the process of economic trans-formation of Central and Eastern Euro-pean Countries. Financial support to oc-cupational health and safety projects ispart of Phare. In the year 2000 the Eu-ropean Commission presented a re-orientation of its development policywhich included the cooperation withAfrican, Caribbean and Pacific Coun-tries; this may result in supporting alsoin these countries occupational healthand safety projects.
References
1. Somavia J. Decent Work, Safe Work. Asian-Pacific Newsletter on Occupational Healthand Safety 1999;6:59.
2. European Commission: Guidelines for PhareProgramme Implementation in candidatecountries for the period 2000–2006. Novem-ber 1999.
3. European Commission: The European Un-ion and the World, 2001 (ISBN 92-828-8260-8).
4. WHO Regional Office for Europe. Occupa-tional Hygiene in Europe – Development ofthe Profession, 1991 (European OccupationalHealth Series No. 3).
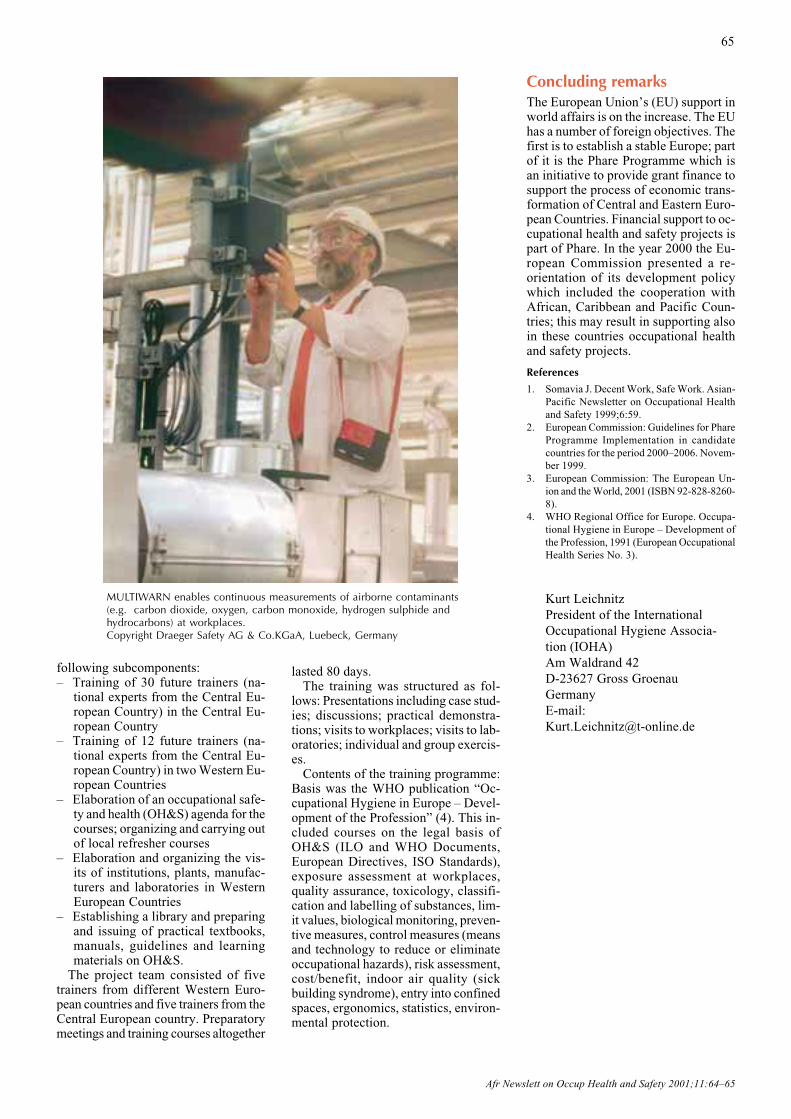
MULTIWARN enables continuous measurements of airborne contaminants(e.g. carbon dioxide, oxygen, carbon monoxide, hydrogen sulphide andhydrocarbons) at workplaces.Copyright Draeger Safety AG & Co.KGaA, Luebeck, Germany
Afr Newslett on Occup Health and Safety 2001;11:66–67
66
Impacts of globalization onwomen’s workDuring the past two decades the worldtrade has tripled and global trade in serv-ices has increased more than 14-fold (1).Not all are benefiting from this change.Globalization under liberalized marketshas generally benefited the industrial-ized or strong economies and margin-alized the weak economies (1,2,3).Hence, despite optimistic assertions of‘an end to poverty’ in the 21st century,and adequate knowledge and technolo-gy to achieve this, poverty and inequal-ity have in fact increased in many partsof the world (1).
Women are among those with thepoorest social and economic status inmany countries of the world, and amongthose with the weakest control over di-recting resources towards their needs.Households headed by women, estimat-ed to be one third of the total world-wide, are many times more likely to bepoor than those headed by men, and thenumber of such households has in-creased following the introduction ofstructural adjustment and liberalisationprogrammes (2,4). Gender disparities insocial outcomes exist across regions,countries, socio-economic groups andage groups (5,6). These disparities havebeen widened, rather than bridged, byglobalization, in part owing to thechanges in women’s access to and qual-ity of work.
Firstly, women work longer hours.Women work on average one to threetimes longer than men in the same soci-ety, whatever the number of hours menput in (6). The dual burden of house-hold work and work in other produc-tive spheres places the greatest stress on
poor women, whose social support is theweakest (7,8). Women also spend a sig-nificant amount of time informally trad-ing surplus produce. This domestic andsocial work is generally not valued aspart of the domestic product, and thusassumes an invisible status and com-mands little investment in improvedconditions.
Women often work in undercapital-ized and insecure production activitieswith inadequate access to credit, land,marketing and extension services, train-ing and other inputs. In Zimbabwe, forexample, 90–92% of workers in the in-formal sector are women (8).
Whilst there is generally legal protec-tion for gender equity in formal employ-ment, in practice, women continue tobe generally employed in low-skill, low-paying jobs, in casual or non-permanentforms of employment, in jobs whereunionization rates are low, and in cer-tain sectors – e.g. agriculture, the tex-tile and garment industry, food process-ing, domestic work, market activitiesand social services. The work that wom-en do is of-ten heavy,m o n o t o n -ous, ergono-mically un-sound, andinvolves lit-tle controlover thepace or con-tent of thework (9).Women areoften regard-ed as supple-m e n t a r ywage-earn-
ers rather than as workers in their ownright. Reproductive health responsibil-ities (and the extent to which these areexclusively borne by women) are oftena de facto constraint in hiring or invest-ing in women workers, with employersregarding this as an added cost, even ifthe law sets no specific barriers to this(10).
The twin processes of globalizationand marginalization described earlierhave produced unequal effects on thispattern of female employment. On theone hand, the global spread of genderand human rights agendas, the enhance-ment of gender equity in employmentlaw and the widening of employmentopportunities in non-traditional spheresof employment have brought morewomen into the workforce. On the oth-er hand, there is evidence that much ofthe new formal employment for wom-en is in poor-quality work and assem-bly line processes with weak options foradvancement, and that in the main,women have experienced a growth ininsecure, casual employment. Women
Effects of globalization onworking women
R. LoewensonZimbabwe
“Women are half the world’s population, receive one tenth of theworld’s income, account for two thirds of the world’s working hours
and own only one hundredth of the world’s property.”
Phot
o by
K. H
onka
salo
International Labour Organisation

Afr Newslett on Occup Health and Safety 2001;11:66–67
67
have been a primary target for employ-ment in new export processing zonejobs in the textile, microelectronic andchemical sectors, but women have alsolost these jobs as they have shifted tomore value added, skilled and morehighly regulated employment(11,12,13,14). There has been an in-crease in out-contracted home-basedwork. While en-abling women to meettheir domestic duties more easily, thissort of work disguises the employmentrelationship and shifts liability for work-ing conditions to the women. Manymore women have been brought intotrading and informal sector work in en-terprises that are poorly regulated andexcluded from support systems. In ad-dition, women’s household tasks, it hasbeen noted, take an increasingly longertime as water supplies dry up, forestsbecome degraded, transport becomesmore inconsistent and expensive, andcompetition for scarce resources inten-sifies.
The phenomenon of women respond-ing to an economic squeeze by work-ing harder and longer is not confined todeveloping countries. A study in theUSA found that the percentage of work-ing women holding two or more paidjobs rose from 2.2% in 1970 to 5.9% in1989, at the same time as the percent-age of men holding two jobs fell by0.6% (6). While this may increase theeconomic contribution and importanceof women, it may also increase the lev-el of stress and its health consequenc-es.
Occupational healthoutcomesWomen’s occupational health in thecurrent process of globalization reflectsthese shifts in employment, where in-adequate regulatory and inspection sys-tems combine with employment inse-curity and poor control over work toundermine hazard control. Moreover,new demands for household caring inthe face of declining access to socialservices mean increased domestic bur-dens.
Much of the occupational morbidityexperienced by women is not detectedor reported in occupational health sys-tems. Against a background of 50-foldunder-reporting of occupational diseasein sub-Saharan Africa, for example(15), women work in sectors – such asagriculture, textile work and small en-terprises – where under-reporting islikely to be even higher.
Women may face chronic healthproblems at work that interact with and
exacerbate illness caused by the workthey do in the home and in caring fordependants. At the same time, women’spoor health status arising from poor diet,inadequate vitamin intake, and poor liv-ing and social conditions may increasetheir risks of work-related cancers orchemical toxicity (3,16). Multiple ex-posures are exacerbated by the longhours of work and the multiple part-timejobs many women have.
Women’s work is often characterizedby a high level of demands, with littlecontrol over the nature and content ofthe work. They are often drawn intounfair conflict and choice over the pos-itive health gains of being employed andthe negative health impacts of the waythat work is organized. Women havebeen hired as flexible labour in an in-flexible work organization, a situationthat can lead to digestive disorders,sleep difficulties and musculoskeletalproblems (9,6,17).
More importantly, this lack of con-trol over the work process and the roleswomen are expected to play enhance orimpede their ability to prevent and man-age work-related risks.
It may thus be argued that, with inad-equate recognition from social, scien-tific and insurance systems, women bearmany of the health costs of current pro-duction and market policies. As a ‘si-lent epidemic’ this may have short-termyields, but may also create long-termcosts for development. Such costs maybe manifest in uncontrolled populationgrowth, high infant and child mortali-ty, poor socialization of and social un-derdevelopment of children, increasedpoverty, ineffective agriculture, foodinsecurity and high levels of sexually-transmitted disease. Conversely, invest-ing in women generates returns inhealth, social and intergenerational de-velopment, in a manner that has greaterpotential to reach the most vulnerablegroups. Indeed, the analysis of women’swork-related health is a strong testimo-ny to the fact that there is an urgent glo-bal imperative to make the structure andquality of growth as critical a develop-ment issue as its quantity.
This article is an abridged and edited ver-sion of: Loewenson R. Women’s Occupa-tional Health in Globalization and Devel-opment. Am J Ind Med. 36:34–42, 1999,Wiley-Liss, Inc., a subsidiary of John Wiley& Sons, Inc., USA. Published with the per-mission of Wiley -Liss.
References
1. UNDP. Human Development Report 1996,
Oxford University Press, New York 1996.2. Onimode B. (ed) The IMF, the World Bank
and the African Debt Vols 1 and 2, Zed Press,London 1989.
3. Pearce N, Matos E. Industrialisation andhealth in occupational cancer in developingcountries, IARC Publications No 129, Lyon1994.
4. Cliff J. Destabilisation, adjustment and theimpact on Women, Paper presented to theZCTU/UZ Economics Department workshopon Structural Adjustment and Health,Harare, February 1991.
5. Jhamba T. Mortality determinants in Zim-babwe: policy implications, University ofZimbabwe Mimeo, Harare, Zimbabwe 1994.
6. Smyre P. Women and Health. Women andWorld Development Series. 1992.
7. Zimbabwe Women’s Bureau. We Carry aHeavy Load. Part II. Triple-R Printers,Harare, 1994.
8. Johal R, Keyvanshad S, Lisker D. Zimba-bwe gender issues information sheet No 1.43.World Bank, July Africa Region. 1993.
9. Kothari U, Nababsing V. Gender and Indus-trialisation, Editions de l’Ocean Indien,Mauritius 1996.
10. Jirira OK. Southern African Political andEconomic Monthly, 1990 April pp 19–23.
11. Fuentes A, Ehrenreich B. Women in the Glo-bal Factory. Boston 1994.
12. SATUCC. Report of the follow up regionaltrade union workshop on Export ProcessingZones, Environment and Sustainable Devel-opment, Pretoria, May 3–5, 1997.
13. ILO. Economic and Social Effects of Multi-national Enterprises in Export ProcessingZones. Geneva 1988.
14. US Department of Labour Bureau of Inter-national Standards. 1989–1990. Worker’srights in Export Processing Zones. USA.
15. World Health Organization / OGIEH. Glo-bal burden of disease and injury due to oc-cupational factors, Geneva 1996.
16. Koblinsky M, Campbell O, Harlow S.Mother and more: a broader perspective onwomen’s health from Koblinsky M, TimyanJ, Gay J. (eds) The Health of Women: a glo-bal perspective, Westview Press, Boulder,USA 1992.
17. Loewenson R. The health impact of chang-ing patterns of large scale agricultural pro-duction: the Zimbabwean farmworker, PhDthesis, London University 1989.
Bibliography
Commonwealth Secretariat (1989) EngenderingAdjustment for the 1990’s, Commonwealth Sec-retariat Publications, London, 1989.
Klitzman S, Silverstein B, Punnett L, Mock A.A Women’s Occupational Health Agenda for the1990s in New Solutions 1990(1);1:7–17.
Dr Rene LoewensonTARSC47 Van Praagh Ave.HarareZimbabwe

Afr Newslett on Occup Health and Safety 2001;11:68–69
68
BackgroundAs a result of the ever-increasing paceof worldwide liberalization of trade andeconomies, as well as technologicalprogress, the number of occupationalaccidents and diseases are increasing inmany developing countries. It is esti-mated that every year over 1.2 millionworkers are killed due to work-relatedaccidents and diseases and 250 millionoccupational accidents and 160 millionwork-related diseases are occurring.The economic loss related to these ac-cidents and diseases is estimated toamount to 4% of world gross nationalproduct.
After the successful introduction ofthe “systems” approach to managementby the International Organization forStandardization (ISO) through its serieson Quality Management (ISO 9000 se-ries) and Environmental Management(14000 series) during the early 1990s,there was a view that the same approachcould be used for managing occupation-al safety and health at the organizationallevel. The possible initiation of work todevelop an ISO standard on OSH Man-agement Systems was discussed at anISO International Workshop on OSH-MS Standardization in 1996. The work-shop formed the view that the ISOshould discontinue its respective effortsand that the International Labour Organ-isation (ILO), because of its tripartitestructure, would be a more appropriatebody than ISO to elaborate internation-al guidance documents for the establish-ment and implementation of effectiveoccupational safety and health manage-ment systems.
In the light of the Workshop conclu-sion, the Occupational Safety andHealth Branch (now: SafeWork) of theILO, in co-operation with the Interna-tional Occupational Hygiene Associa-tion (IOHA), started in 1998 with theidentification of key OSH-MS elementsin existing standards. The first step was
Guidelines on Occupational Safety and HealthManagement Systems
S. Machida, P. BaichooSafeWork, ILO
to review existing OSH managementsystem standards and guidance docu-ments. Based on this review, commonelements of OSH management systemswere identified and the draft Guidelineswere prepared. Over a period of nearlytwo years, the draft was systematicallyreviewed by international experts, andimproved continuously.
At the end of 1999, the British Stand-ards Institution (BSI), an ISO memberbody, launched an official proposal forthe establishment of a new field of tech-nical activity Occupational health andsafety management, with a view to de-veloping an ISO standard. This compet-ing initiative by the ISO to on-goingILO work encountered strong interna-tional opposition and a campaign to stopthe ISO work. This resulted in the fail-ure of the BSI proposal in favour of theILO.
The final draft ILO document wassubmitted for comments to ILO constit-uents in January 2001. The ILO Guide-lines on occupational safety and healthmanagement systems (ILO-OSH 2001)were adopted at a tripartite Meeting ofexperts in April 2001. The ILO Gov-erning Body approved the publicationof the Guidelines in June 2001. TheGuidelines will be published in Octo-ber 2001.
ILO Guidelines on OSHManagement Systems(ILO-OSH 2001)ILO-OSH 2001 provides a unique in-ternational model, compatible with oth-er management system standards andguides. It is not legally binding and notintended to replace national laws, regu-lations and accepted standards. It re-flects ILO values such as tripartism andrelevant international standards includ-ing the Occupational Safety and HealthConvention, 1981 (No. 155) and theOccupational Health Services Conven-tion, 1985 (No. 161). Its application
does not require certification, but it doesnot exclude certification as a means ofrecognition of good practice if this isthe wish of the country implementingthe Guidelines.
The ILO Guidelines encourage theintegration of OSH-MS with other man-agement systems and state that OSHshould be an integral part of businessmanagement. While integration is de-sirable, flexible arrangements are re-quired depending on the size and typeof operation. Ensuring good OSH per-formance is more important than for-mality of integration. As well as this,ILO-OSH 2001 emphasizes that OSHshould be a line management responsi-bility at the organization,
The guidelines provide guidance forthe implementation on two levels – na-tional (Chapter 2) and organizational(Chapter 3).
National occupational safety andhealth management systemframeworkAt the national level, they provide forthe establishment of a national frame-work for occupational safety and health(OSH) management systems, preferablysupported by national laws and regula-tions. Action at the national level in-cludes the nomination of (a) competentinstitution(s) for OSH-MS, the formu-lation of a coherent national policy andthe establishment of a framework for aneffective national application of ILO-OSH 2001, either by means of its directimplementation in organizations or itsadaptation to national conditions andpractice (by national guidelines) andspecific needs of organizations in ac-cordance with their size and nature ofactivities (by tailored guidelines).
The National Policy for OSH-MSshould be formulated by competentinstitution(s) in consultation with em-ployers’ and workers’ organizations,and should consider:
(ILO-OSH 2001)

69
Afr Newslett on Occup Health and Safety 2001;11:68−69
Action forimprovementPreventive andcorrective actionContinual improvement
EvaluationPerformancemonitoring andmeasurementInvestigationAuditManagement review
Planning &implementationInitial reviewSystem planning,development andimplementationOSH objectivesHazard prevention
OrganizingResponsibility &accountabilityCompetence & trainingOSH documentationCommunication
PolicyOSH policyWorker participation
• Promote OSH-MS as part of overallmanagement
• Promote voluntary arrangements forsystematic OSH improvement
• Avoid unnecessary bureaucracy, ad-ministration and costs
• Support by labour inspectorate, safe-ty and health and other services
The functions and responsibilities ofimplementing institutions should beclearly defined as well. Figure 1 (be-low) of the Guidelines describes the el-ements of the national framework forOSH managements systems. It showsthe different ways in which ILO-OSH2001 may be implemented in a mem-ber State.
The occupational safety and healthmanagement system in theorganizationChapter 3 of ILO-OSH 2001 deals withthe occupational safety and health man-agement system at the organizationallevel. The Guidelines stress that com-pliance to national laws and regulationsis the responsibility of the employer.ILO-OSH 2001 encourages the integra-tion of OSH management system ele-ments into overall policy and manage-ment arrangements, as well as stressingthe importance that at the organization-al level, OSH should be a line manage-ment responsibility, and should not beseen as a task for OSH departments and/or specialists.
The OSH management systems in theorganization has five main sectionswhich follow the internationally accept-ed Deming cycle of Plan-Do-Check-Act, which is the basis to the “system”approach to management. These sec-tions are namely Policy, Organizing,Planning and implementation, Evalua-tion and Action for improvement (seeFigure 2 above).
Figure 1. Elements of the national framework for OSH management systems
Policy contains the elements of OSHpolicy and worker participation. It is thebasis of the OSH management systemas it sets the direction for the organiza-tion to follow. Organizing contains theelements of responsibility and account-ability, competence and training, docu-mentation and communication. It makessure that the management structure isin place, as well as the necessary respon-sibilities allocated for delivering theOSH policy. Planning and implemen-tation contains the elements of initialreview, system planning, developmentand implementation, OSH objectivesand hazard prevention. Through the in-itial review, it shows where the organi-zation stands concerning OSH, and usesthis as the baseline to implement theOSH policy. Evaluation contains theelements of performance monitoring
and measurement, investigation ofwork-related injuries, ill-health, diseas-es and incidents, audit and managementreview. It shows how the OSH manage-ment system functions and identifiesany weaknesses that need improvement.It includes the very important elementof auditing, which should be undertak-en for each stage. Persons independentof the activity being audited should con-duct audits. This does not necessarilymean third party auditors. Action forimprovement includes the elements ofpreventive and corrective action andcontinual improvement. It implementsthe necessary preventive and correctiveactions identified by the evaluation andaudits carried out. It also emphasizes theneed for continual improvement of OSHperformance through the constant de-velopment of policies, systems andtechniques to prevent and control work-related injuries, ill-health, diseases andincidents.
For further information on ILO-OSH 2001, please contact us at:SafeWork – Infocus Programme on
Safety and Health at Work andthe EnvironmentInternational Labour Office4, route des MorillonsCH-1211 Geneva 22, SwitzerlandTel: + (41 22) 799 6715Fax: + (41 22) 799 6878E-mail: [email protected]://www.ilo.org/safeworkFor purchase, please contact:[email protected]
Seiji Machida, Pavan Baichoo, ILO
Figure 2. The main sections and their elements of the OSH management system in theorganization.
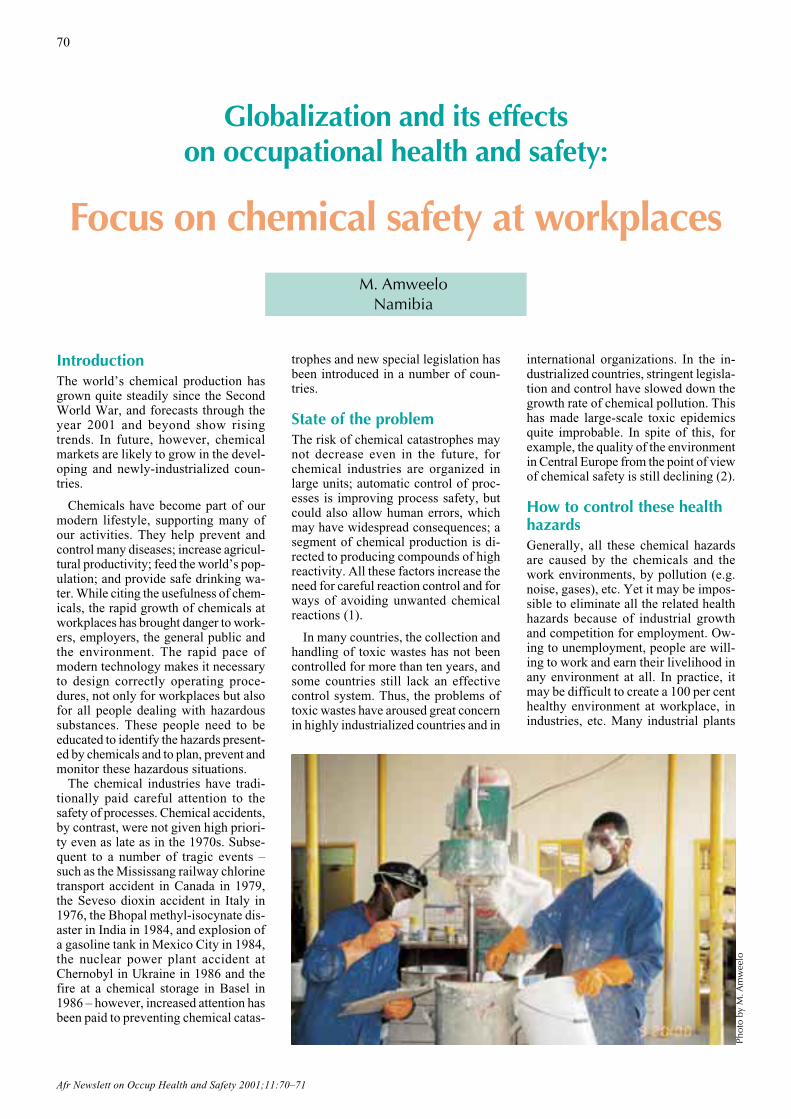
Afr Newslett on Occup Health and Safety 2001;11:70–71
70
IntroductionThe world’s chemical production hasgrown quite steadily since the SecondWorld War, and forecasts through theyear 2001 and beyond show risingtrends. In future, however, chemicalmarkets are likely to grow in the devel-oping and newly-industrialized coun-tries.
Chemicals have become part of ourmodern lifestyle, supporting many ofour activities. They help prevent andcontrol many diseases; increase agricul-tural productivity; feed the world’s pop-ulation; and provide safe drinking wa-ter. While citing the usefulness of chem-icals, the rapid growth of chemicals atworkplaces has brought danger to work-ers, employers, the general public andthe environment. The rapid pace ofmodern technology makes it necessaryto design correctly operating proce-dures, not only for workplaces but alsofor all people dealing with hazardoussubstances. These people need to beeducated to identify the hazards present-ed by chemicals and to plan, prevent andmonitor these hazardous situations.
The chemical industries have tradi-tionally paid careful attention to thesafety of processes. Chemical accidents,by contrast, were not given high priori-ty even as late as in the 1970s. Subse-quent to a number of tragic events –such as the Mississang railway chlorinetransport accident in Canada in 1979,the Seveso dioxin accident in Italy in1976, the Bhopal methyl-isocynate dis-aster in India in 1984, and explosion ofa gasoline tank in Mexico City in 1984,the nuclear power plant accident atChernobyl in Ukraine in 1986 and thefire at a chemical storage in Basel in1986 – however, increased attention hasbeen paid to preventing chemical catas-
trophes and new special legislation hasbeen introduced in a number of coun-tries.
State of the problemThe risk of chemical catastrophes maynot decrease even in the future, forchemical industries are organized inlarge units; automatic control of proc-esses is improving process safety, butcould also allow human errors, whichmay have widespread consequences; asegment of chemical production is di-rected to producing compounds of highreactivity. All these factors increase theneed for careful reaction control and forways of avoiding unwanted chemicalreactions (1).
In many countries, the collection andhandling of toxic wastes has not beencontrolled for more than ten years, andsome countries still lack an effectivecontrol system. Thus, the problems oftoxic wastes have aroused great concernin highly industrialized countries and in
international organizations. In the in-dustrialized countries, stringent legisla-tion and control have slowed down thegrowth rate of chemical pollution. Thishas made large-scale toxic epidemicsquite improbable. In spite of this, forexample, the quality of the environmentin Central Europe from the point of viewof chemical safety is still declining (2).
How to control these healthhazardsGenerally, all these chemical hazardsare caused by the chemicals and thework environments, by pollution (e.g.noise, gases), etc. Yet it may be impos-sible to eliminate all the related healthhazards because of industrial growthand competition for employment. Ow-ing to unemployment, people are will-ing to work and earn their livelihood inany environment at all. In practice, itmay be difficult to create a 100 per centhealthy environment at workplace, inindustries, etc. Many industrial plants
Globalization and its effectson occupational health and safety:
Focus on chemical safety at workplacesM. Amweelo
Namibia
Phot
o by
M. A
mw
eelo

Afr Newslett on Occup Health and Safety 2001;11:70–71
71
are very old; the layouts were notplanned or designed to clear out or re-move all unhealthy substances, materi-als, gases, etc. On the basis of the exist-ing arrangements and layouts, how-ever, management can take certain con-trol measures after studying or survey-ing the various operations and effluents.Control of potential health hazards canthen be planned, and action should betaken:• to eliminate the health hazards by
redesigning the layouts• to isolate operations and effluents
and to keep workers away from oth-ers
• to ensure the use of proper personalprotective equipment by workers.
It is the management’s responsibilityto reduce all the health hazards and toprotect workers from risk in the workenvironment. It is also the legal obliga-tion of the workers to use the personalprotective equipment.
Transport of hazardoussubstancesThe supplier and transporter of hazard-ous substances shall ensure that themarking, labelling and storage of haz-ardous substances for safe transport,especially the labelling of the transportvehicle and storage of the hazardoussubstances during transport, are in ac-cordance with existing legislation, or ifsuch legislation is not in place, in ac-cordance with the recommendations onthe transport of hazardous substances ordangerous goods made by the UnitedNations.
Storage of hazardoussubstancesAt all times, hazardous substances shallbe stored in such a manner that they donot pose a risk to the health and safetyof employees or other persons, nor anyrisk of contamination of the environ-ment, due to seepages, leakage, fire oraccidental release. Areas designated forthe storage of hazardous substancesshall be isolated from other activitiesand shall be clearly marked with appro-priate warning signs.
Handling of hazardous wasteHazardous waste and deposits shall beremoved at intervals, by methods appro-priate to the type of hazard in question.Following their collection, contami-nants shall be disposed of in a way thatposes no risk to the health of any per-son or to the environment, and in ac-
cordance with applicable statutory pro-visions and regulations.
Fire fightingRapid industrialization and urbanizationhave resulted in the phenomenal growthof industries and also in the importa-tion of hazardous materials. The result-ing increases in manufacture, storage,handling, transportation and waste dis-posal have meant fire, explosion andtoxic hazards of different degree.
A disastrous situation can arise either“on site”, at the manufacturing site it-self, or “off site”, away from the pro-duction or process location, such asduring transportation by land (rail orroad), sea or air. In all of these cases,the land-based fire departments, indus-trial fire brigades and other trainedgroups are invariably summoned totackle any emergency situation involv-ing fire, explosion or environmentalpollution. Hence it is essential that fireservice officers, as well as those respon-sible for the management of such dis-astrous situations, are conversant withthe likely emergencies that can occurwhile manufacturing, handling, storingor transporting hazardous substances,and know how to deal with such emer-gencies.
Emergency planningCarefully thought out emergency plansfor all hazardous industrial operationsshould be readily available for imme-diate application in order to stop or min-imize the risk involved in an incidentcaused by dangerous substances beforethe situation gets out of hand. Suchplans should specify the following:
Notification and alerting proceduresOn-scene-coordinator (OSC)Spill control and clean-up proce-duresProcedures for disposal of the con-taminantEvacuation proceduresIdentification of public relations per-sonnelIdentification of the resource inven-tory method.
Finally, the plan should be tested in aknock-up situation involving dangeroussubstances to prove how far it is practi-cal in the event of an actual incident.
Discussion and conclusionsThere is a global shortage of trainedmanpower in the field of chemical safe-ty. The availability of expert manpow-er is, however, a prerequisite for all con-
trol strategies. It is important tostrengthen programmes developing thetraining of various categories of experts.
Education and information concern-ing chemical safety – for the public, tar-get groups and decision-makers – arepoorly developed. New, systematicmethodologies for effective actions inthis area should be developed. Further-more, owing to the increased quantityof dangerous substances transported andsubsequently handled in industries,safety considerations have taken on di-mensions which are strenuous for eco-nomically strained nations. This, there-fore, necessitates a relatively simple andinexpensive safety approach to reduce,if not replace, the sophistication re-quired to maintain safety and efficien-cy in the industries of such nations. Sim-ple, easy to understand safety rules andregulations should be introduced, en-forced properly, and seen to be en-forced.
At both national and regional levels,monitoring and surveillance pro-grammes for following up the most im-portant toxic exposures and for assess-ing health and environmental risksshould be established and coordinated.
References
1. Rasmussen B. Unwanted chemical reactionsin the chemical process industry. In: Pro-ceedings of World Conference ChemicalAccidents, Rome, July 1987:388–91.
2. Del Bino B. Community environmentalpolicy: Priority for prevention. In: Proceed-ings of World Conference Chemical Acci-dents, Rome, July 1987:10–1.
African Newsletter on Occupational Healthand Safety 1988/2.
Labour Act, 1992 (No. 6 of 1992), Govern-ment Gazatte of the Republic of Namibia.
Regulation 176 of the regulations on theHealth and Safety of the Employees at Work,made in accordance to the Labour Act, 1992(No. 6 of 1992) May 1995.
Moses AmweeloMinisterMinistry of Works, Transportand CommunicationPrivate Bag 133416719 Bell StreetSnyman CircleWINDHOEKNAMIBIA

Afr Newslett on Occup Health and Safety 2001;11:72–73
72
In mid-October 2001, altogetherabout 170 experts from 40 differ-ent countries, from every cornerof the world, gathered in Helsin-ki to the Work in the Global Vil-lage Conference. More than 90communications were presentedand the most prominent keynotespeakers had accepted the invi-tation to share their data, viewsand experience on the major chal-lenges of globalization. This in-ternational gathering providedone forum for the exchange ofinformation and for developingnew ideas on how to solve thepossible problems of globaliza-tion, and how to promote produc-tive interaction and collaborationin the world. These efforts areneeded now more than ever.
The International Conferenceon Work in the Global Villagewas opened by Ms. Tarja Fila-tov, Minister of Labour, Finland.In her opening speech, shestressed the importance of bothinternational collaboration aswell as the need for national ac-tivities and measures in facing thechallenges posed by globalization. It isworthwhile to analyse also in this Con-ference, how globalization will affectemployment, and to try and find solu-tions for productive developments inthis field, she said.
Dr. Osmo Soininvaara, Minister ofSocial Services emphasized the need forstudying the impacts of globalization onthe health of the working people. Hepointed out that this is no longer the timeto ponder whether we are for or againstglobalization. Rather, we need to askwhat kind of globalization we want. Itis of utmost importance that the serviceprovision system for occupationalhealth and safety be strengthened in or-der to ensure that the most productivepopulation in all societies, the working-aged people, have access to effectiveand competent occupational health serv-ices.
most important targets of thedeclaration is to halve the pro-portion of those 1.2 billion peo-ple living in extreme poverty bythe year 2015, said H.E., Mr.Harri Holkeri, President of the55th General Assembly of theUnited Nations, in his openingpresentation. Economic growthdoes not reduce poverty auto-matically. Studies (e.g. WID-ER; ILO) prove that in manycountries the impacts of glo-balization are mixed. Nationaland international policies andactions are mutually supportivemeasures in reducing poverty.Poverty is a multidimensionalphenomenon, and thereforealso the alleviation measuresneed numerous forms. The lackof education is closely relatedto poverty. Therefore, one wayto alleviate poverty is to in-crease education. At the inter-national level, improved man-agement of globalization anddevelopment finance can sup-port country-driven processes.Partnerships with civic organi-
zations, including the private sector, atall these levels are a necessity. The al-leviation of poverty throughout theworld is a realistic goal.
Groups that deserve specialattentionThe Government, employers and theworkforce are joining forces in the pro-motion of a safe and healthy work en-vironment, said Dr. Dulce Estrella-Gust of the Occupational Safety andHealth Center, The Philippines. Themotives vary from achieving higher pro-ductivity and efficiency to promotingthe basic human rights of workers. Alsomultinational companies are helping tospread some positive developments.Despite all the developments, the vastmajority of workers in small and medi-um-sized enterprises, in the informal
Work in the Global VillageS. LehtinenFINLAND
The conference Work in the Global Villagegathered about 170 participants to share
data, information and knowledge about theeffects of globalization.
Professor Jorma Rantanen, on be-half of the Finnish Institute of Occupa-tional Health and the Organizing Com-mittee of the Conference, concluded thatduring the past few months the discus-sion on globalization has become moreand more important. He called uponnew fresh ideas on how to ensure theminimum level of working conditionsto all working people throughout theworld.
Alleviation of poverty as abasis for all other activitiesOne year ago, the Heads of State andthe Governments adopted the Millen-nium Declaration in the UN. One of the
Photo by S. Hiltunen

Afr Newslett on Occup Health and Safety 2001;11:72−73
73
sector and agriculture, as well as mi-grant workers, female workers and childlabourers remain outside effective Oc-cupational Safety and Health (OSH)protection. In order to improve the sit-uation, concerted action is needed atinternational and regional, national, cor-porate, sectoral and community levels,she said.
Models and good practicesThe media reports us some negative in-fluences of globalization daily, saidProfessor Jerry Jeyaratnam whentalking about the development of meth-ods and models and good practices.Globalization must also have beneficialeffects, or else it would not continue togrow and exist. E.g. many multination-als can provide the same kind of occu-pational health and safety services fortheir employees in developing countriesas they do in industrialized countries.The ensuring of global uniformity inoccupational health care is not solely theduty of the multinationals, but also leg-islative control is needed from interna-tional agencies in the UN, as well ascommitment from the governments ofthe developing countries. The questionof double standards should be givenserious thought, because the needs ofworkers and their health are exactly thesame in the industrialized countries asin the developing world.
Country profiles – a basis forimprovement in OH&SA special session addressed the need forcountry profiles to determine the statusof occupational health and safety incountries that are in various phases ofdevelopment. The further developmentof policies for occupational health andsafety is nevertheless increasingly basedon information steering. Such a policyis critically dependent on up-to-dateinformation on the current status ofhealth and safety, the exposures andrisks threatening health, and informa-tion on the consequences of such expo-sures at individual and population lev-els. Such information is also crucialwhen setting priorities for further de-velopment, identifying the need for ac-tions, including the development of ca-pacities and infrastructures, and attract-ing partners and allies to join the devel-opment work. Appropriate indicatorsystems can also be used for compar-ing the needs for policies in differentparts of the world, and for recognizingthe impact of health and safety actions.Country reports were presented from
Kenya, Nepal, the Philippines, Sri Lan-ka, Tanzania, Thailand and Vietnam.Several countries are now shifting theemphasis of OH&S to workers in SMEsand the informal sector, which form themajority of the world’s labour force.OH&S issues related to agriculturalwork were also given priority status inmany presentations. Novel approachesare needed to address these large seg-ments of the labour force that usuallyhave remained underserved with regardto OH&S, if served at all. The prioritylists of many countries stressed the im-portance of strengthening the reportingsystems on work accidents and occu-pational diseases.
The preparation of the country pro-files requires a thorough description ofthe OH&S structures in the countries,as well as the collection of as detaileddata on various indicators as possible.This will allow the setting of prioritiesfor actions at the national level, as wellas the setting of objectives for concert-ed activities for better working condi-tions.
The new National Plan of Thailand,effective in January 2002, will expandOH&S to workers in agriculture and theinformal sector, including 1 million inhome-based industries. The priorities inVietnam will include women at work,and people working in agriculture andin small enterprises. Agriculture andSMEs were in fact reported as priori-ties in all countries presenting countrypapers.
A very well organized national OH&Sinformation network has been estab-
lished in Vietnam during the past fewyears. The membership of nearly 200organizations includes several minis-tries, employers’ organizations, tradeunions and universities. Regional sub-networks have been established in HoChi Minh City and Danang; the preven-tion of silicosis has received special at-tention.
In Thailand, a unique arrangement ofcollaboration between government min-istries and Thai university institutionsallows the government to identify aca-demic capabilities when planning andimplementing new projects and activi-ties. A Thai Directory of academic in-stitutions with OH&S capacities hasbeen prepared.
The country profiles were discussedfurther in another workshop on 18 Oc-tober 2001 in Helsinki. The follow-upof the March country profile and indi-cator meeting took place on 12 Novem-ber 2001 in Chiang Mai, Thailand. Thework on profiles and indicators contin-ues.
Suvi LehtinenFinnish Institute of OccupationalHealthTopeliuksenkatu 41 a AFIN-00250 HelsinkiFinlandE-mail:[email protected]
The workshop on country profiles and indicators took place in Helsinki on 18 October 2001.
Phot
o by
T. P
ääkk
önen

Afr Newslett on Occup Health and Safety 2001;74–76
74
IntroductionGlobalization is a process that involvestransformation of a given national econ-omy into a more sophisticated econo-my. African countries, among the so-called developing nations, have beencaught by globalization unaware.
According to the joint WHO and FAOstatement of 1 February 2001 (1), “Pos-sible causes of low quality of pesticidescan include both poor production andformulation and the inadequate selec-tion of chemicals. In many pesticideproducts, for example the active ingre-dient concentration are outside interna-tionally accepted tolerance limits,” saidDr. David Heymann, Executive Direc-tor of WHO’s communicable diseaseactivities. “In addition, poor qualitypesticides may be contaminated withtoxic substances or impurities.”
The growing demand for enhancedfood productivity to meet the needs ofthe global population has led to the useof sophisticated agricultural technolo-gy in which pesticides play a crucialrole.
Pesticides can be classified accordingto the types of pests which they destroy.Thus, there are, e.g. insecticides, fungi-cides, herbicides, rodenticides and mol-luscicides. Aside from their benefits,many pesticides have the potential toharm human health.
The use of pesticides is steadily in-creasing. Pest resistance to pesticides insome developing countries, and aggres-sive marketing are among the causes forthe growing use.
According to Kaoneka andAk’habuhaya (2), in 1998 the world-wide use of pesticides amounted toabout 8 million tonnes, while the figurein 1988 was only 3 million tonnes. In
total, developing countries accountedfor approximately 30% of all pesticideuse. Because pesticide formulationshave changed, calculations of theamounts used do not reveal the wholepicture. Modern formulations are ap-plied in much lesser amounts now; onlymilligrams per hectare, as compared tograms per hectare in the past.
Agricultural workers are the largestoccupational group in developing coun-tries. Nkurlu (3) reported that 90% ofthe population of Southern Africancountries are gainfully employed in theagricultural sector. Farmers have spe-cial health problems arising from theagricultural pesticides they use, whichare believed to have adverse effects onthe health of farmers and on the envi-ronment.
Kenya is an agricultural country.About 80% of the population dependson farming as the basic livelihood. Gen-erally, farming includes the cultivationof crops and animal husbandry. Thecrops cultivated include cash crops (e.g.coffee, tea), food crops (e.g. maize,beans),flowers and vegetables. Animalhusbandry involves the tending of cat-tle and poultry. Pesticides are used inall these ventures.
The most serious occupational healthhazard among the agricultural popula-tion is exposure to a great variety ofsynthetic pesticides, mainly chlorinat-ed hydrocarbons and organophospho-rus compounds. The risks of pesticides– acute or long-term effects – are notunderstood by potential pesticide users.
A study on pesticide use and safetyawareness in Githunguri, Kiambu dis-trict, where the population and agricul-tural characteristics are similar to thoseof the current study, revealed that morethan 95% of the farmers used pesticides
extensively (4). The greatest risks ofexposure were found to be among wom-en and children. The study further es-tablished that the community’s aware-ness of safety was limited.
Pesticides may enter the body orally,by inhalation or through the skin. Themost important route of absorption isvia the skin, especially if the chemicalin question is sprayed on a windy day.Pesticides have been associated withdifferent types of cancer. They maycause genetic damage to an unborn childas well as abortion or malformation.They may also damage the brain, kid-neys and other vital organs if the levelof exposure exceeds the burden that thebody of the immediate user can toler-ate.
Studies have been conducted to inves-tigate effect of organophosphorus pes-ticides. A study carried out in Japanamong a sample of 7,435 people repre-senting the Japanese farming populationwho use pesticides found that 74 hadoptic autonomic contraction dynamicsof the pupil in reaction to light stimuli,and a high residual level of organophos-porous was found in their blood (5). Ex-posure to organophosphorus pesticidesmay cause other neurological effects,too.
Chemical safety is paramount in or-der to control the potential adverse ef-fects of chemicals. Primary preventionis the only effective way to combat theproblems associated with chemicals. Aset of principal tools for primary pre-vention has been compiled. It includesenhancing the knowledge of exposedworkers with regard to the safe handlingof chemicals (6).
VN Kimani and MA Mwath conduct-ed a case study in a Kenyan rural agri-cultural community (Githunguri loca-
Use of pesticides andpersonal protective equipment
by applicators in a Kenyan district
J.A. HanshiKENYA
Afr Newslett on Occup Health and Safety 2001;11:74–76
75
tion) in order to assess the knowledge,attitudes and practices concerning thesafe handling of agro-chemical pesti-cides. This study revealed that 95% ofthe farmers use pesticide extensively.These farmers had a rather limitedknowledge of the relevant safety issues(4).
A study conducted among Indonesianfarmers found that spraying caused sub-stantial pesticide exposure to the farm-ers. Signs and symptoms occurred sig-nificantly more often during the spray-ing season than outside the sprayingseason. The number of spray operationsper week, the use of hazardous pesti-cides, and the skin and clothes beingwetted with the spray solution weresignificantly and independently associ-ated with the number of signs and symp-toms. The study concluded that farm-ers in the tropics could not wear fullprotective gear because of the unfavour-able hot climate.
The frequency of spraying should bereduced by means of widespread train-ing in integrated pest management. Thelicensing and selling of most hazardouspesticides should be regulated.
The acute and chronic toxic effectsof pesticides may occur at the workplace(manufacturing, packing, mixing andspraying) or through accidental expo-sure – eating or drinking contaminatedfood. Acute pesticide poisoning is un-acceptably common, although it is im-possible to give precise figures for thenumber of cases on a worldwide scale.Almost all cases of acute pesticide poi-soning occur in the developing world,even though it uses only 25% (7) of theworld’s production of pesticides. Mostfarmers make extensive use of pesti-cides sold over the counter, therebycausing the farmers to be exposed to avariety of farm pesticides unnecessari-ly.
Aim and objectiveThis study was done in order to assessfarmers’ safe handling of pesticideswith regard to their knowledge, attitudesand practices.
A cross-sectional survey was con-ducted using a simple multiple close-ended questionnaire. The questionswere posed to the respondents by meansof an interview, and the author record-ed the responses.
The survey questions inquired into thetypes of pesticides being used in orderto:1. assess the farmers’ knowledge re-
garding the route of exposure to pes-ticides
2. identify the types of personal protec-tive equipment used
3. determine attitudes underlying thefailure to use personal protectiveequipment
4. assess the prevalence of symptomsassociated with pesticide poisoning.
Study districtGarissa district is one of the three dis-tricts forming North-eastern province.The district covers an area of 43,931 sq.km, which is about 7.45% of the totalarea of the country. The backbone ofthe district’s economy is a nomadic wayof life. The concept of farming was in-troduced along the freshwater Tana Riv-er. The full potential of agricultural pro-duce was realised shortly after the cul-tivation of fields started to be practisedin the district of this study around 1988.The types of produce grown range frompawpaw, passion fruits and bananas totomatoes and other crops.
Farming is practised along the river.Farmers are highly exposed not only torisks arising from pesticide use but alsoto those caused by reptiles in the water(the river is widely populated by croco-diles). Crocodiles are a constant men-ace at the riverbanks.
Farmers’ profileSmallholders form about 98% of allfarmers; large-scale farmers compriseonly 2% of the total. These groups aremostly found within central and Sankuridivisions. The indigenous communitydominates farming activity.
There are about 3,200 families withfarms under irrigation and 5,500 farmsdepend on rainfall. At the time of thestudy, most of the farmers were suffer-ing from floods caused by El Niño in-duced rains; thus many were unavaila-ble for interviews. Thus a sample ofonly 30 persons was available for inter-views.
Only people working the land andwho were believed to have been ex-posed to agricultural chemicals (pesti-cides) – i.e. potential applicators – wereincluded in the study. It was assumedthat applicators are more exposed thanother people working in a treated area.Applicators might be exposed to pesti-cide residues or their degradation prod-ucts, which in certain conditions can beeven more dangerous.
The following groups, who are notpotential applicators of pesticides, wereexcluded from the survey:• agricultural extension workers (em-
ployees of the Ministry of Agricul-
ture)• relatives of the potential worker or
relatives of those included in thesample population
• pump attendants.The study had some practical limita-
tions:1. The work to conduct interviews on
the farms was brought to a standstillby the flood caused by El Niño (No-vember 1997–February 1998).
2. Though the questionnaire was spe-cific, the study was not comprehen-sive, the prime reason being theomission of biological monitoring(blood samples for analysis) becausethe necessary reagents were notavailable in the Provincial GeneralHospital. The measurement ofcholinesterase inhibition from bloodsamples was not considered neces-sary because most of the pesticidesreportedly used by the farmers werecarbamate insecticides.
3. The study was demanding in mone-tary terms (e.g. the costs of transport,processing the report and photocop-ying).
ResultsThe farms included in the study wereselected through simple random sam-pling and had 35 persons, only 30 ofwhom were interviewed while five wereexcluded on the basis of the exclusioncriteria applied.
The mean age of the 30 respondentsinterviewed was 23 years. Thus, withreference to the questionnaire, youngadults between 15 and 20 years of agedominated the sample.
All persons interviewed (100%) weremales. 83% of the respondents had noformal education while only 17% hadattended various classes at primaryschool. On assessing their knowledgeas far as the use of pesticide is con-cerned, all of the respondents were ableto mention at least one purpose of pes-ticides, i.e. to kill insects.
On the basis of the responses, thetypes of insecticides used most fre-quently by the farmers were as follows:30% used Sherpa (pyrethroid); 47%used lanate (carbamate); 17% used kel-thane (organochorine compound) and6% used furadan (carbamate).
All of the farmers interviewed got thepesticides they applied from privatechemists.
Half of the respondents had been us-ing pesticides for a period of 5 years ormore; 17% had been using the samefarm chemical for 3–4 years; 30% hadbeen using some pesticide for 1–2 years;

Afr Newslett on Occup Health and Safety 2001;11:74–76
76
while only 3% had been using somepesticide for less than 1 year.
As to the farmers’ knowledge of theroutes of exposure to pesticides in hu-mans, 90% knew the routes of exposurewhile the remaining 10% did not knowthe routes of exposure to pesticides.
82% identified inhalation as a routeof pesticide entry into the human body;11% knew of skin absorption as a routeof pesticide entry and 7% knew of in-gestion as a route of pesticide entry.
The results on the farmers’ use ofpersonal protective equipment revealedthat 83% did not use any personal pro-tective equipment (PPE) and 17% diduse PPE.
All 17% of the interviewees who re-ported that they use PPE said that theyonly wore (improvised) masks. Theyreported wearing the masks in order tosafeguard their health.
83% who said that they did not usePPE gave the following reasons for theirfailure to do so: 40% of the respond-ents said it is very hot to use PPE; 36%confessed that it is too expensive topurchase PPE; and 24% did not knowthe importance of PPE.
77% of the respondents had experi-enced short-term illness as a result ofusing some pesticide, while 23% had notfallen sick since they started using pes-ticides.
14% had experienced eye irritation asa negative effect of pesticide use; 35%had had a skin problem; and 27% hadhad difficulties in breathing as a resultof pesticide exposure.
DiscussionAll of the farmers use pesticides of var-ying classes on their farms. The resultsof this study are similar to those of astudy conducted in Githunguri in 1995,which revealed that 95% of the farmersmake extensive use of agrochemicalpesticides.
The practice of the farmers in thissurvey was very poor, since 83% didnot use PPE. This low rate of PPE use,and the resulting unsafe use of pesti-cides, is assumed to be the reason forsome of the complaints reported by therespondents. Statistically, 77% of thefarmers had fallen ill, at one time oranother, probably owing to unsafe useof pesticides; this has led to impairedhealth among the farmers interviewed.
On assessing the farmers’ attitudes tothe use of PPE, many (40%) of the farm-ers who reported not using PPE blamedthe climate, i.e. the high temperaturesmake it very hot for them to use PPE.36% said that lack of purchasing power
has made it impossible for them to putthe use of PPE into practice. However,24% of the respondents reported hav-ing no idea of the importance of PPE.
The Pest Control Products Board hasbanned or restricted the use of severalpesticides in Kenya. Among these areold compounds containing chlorine(chlordane, heptachlor), toxaphene andmethylbromide.
The World Health Organization(WHO) has recently published a list ofpesticides that persist in the environ-ment (persistent organic pollutants).These include aldrin, dieldrin, chlorda-ne, dioxin, DDT, endrin, furans, hep-tachlor, hexachlorobenzene, mirex,polychlorinated biphenyls and toxa-phene.
ConclusionThe use of personal protective equip-ment among the farmers interviewedwas not common (83% do not use PPE).This is a high proportion and indicatesthe need for advice on good workingpractices.
It would be extremely important tocontinue the study on the remainingfarms. To do so would require that fundsbe made available.
Recommendations1. There should be a system for con-
trolling the sale of pesticides over thecounter so that farmers are not un-necessarily exposed to a variety orcertain classes of farm chemicals.
2. Agricultural Department (authorityanswerable to the Ministry of Agri-culture) should generally increasethe availability of information, edu-cation and communications on thesafe use of pesticides.
3. Agricultural Department should cre-ate awareness among farmers of thetoxicity of pesticides, and should ad-vise farmers to report accidents to thenearest clinic.
4. Farm members should consider thebest method of getting personal pro-tective equipment, at an affordablecost.
5. Agricultural Department should en-sure that, through simulation exer-cises, farmers are trained in the im-portance of personal protectiveequipment and how to use suchequipment.
6. Farmers should be encouraged toobserve good working practices; i.e.spraying down wind, not sprayingwhen the wind velocity is too low.
7. Intensive research should be con-
ducted in order to improve the levelof farmers’ knowledge, attitudes andpractices in the district.
References
1. WHO/FAO press release in Thursday, Feb-ruary 2001. (Amount of poor quality pesti-cides sold in developing countries alarminglyhigh.).
2. Kaoneka BS, Ak’habuhaya JL. Pesticidemanagement in developing countries. AfrNewsletter on Occup Health and Safety2000;10(1):21–2.
3. Nkurlu JI. Workplace exposure of womento chemicals. Afr Newsletter on OccupHealth and Safety 1999;10(2):37–8.
4. Kimani VN, Mwathi MN. Agriculture ex-posure and health implication in Githungurilocation, Kenya. East Afr Med Journal.Kenya, Dept of Comm Health, Universityof Nairobi, August 1995;72(8):531–5.
5. Ishikawa S. Opthalmopathy due to environ-mental toxic substances especially intoxica-tion by organophosphorus pesticides. Deptof opthalmology, School of Med, KitasatoUniversity, Nippon Ganka Gakka Zashi, Ja-pan., 1996;6:417–23.
6. ILO convention 170, safety in the use ofchemicals at work.
7. World Health Organisation (WHO) Generalchemical safety 46th year No. 5 Sept. – Oct.1993. (No. 1).
Bibliography
Guoly, Wang BJ Leece, Wang JD. Prevalenceof dermatosis and skin sensitization associatedwith use of pesticides in fruit farmers of South-ern Taiwan. Occup Environ Med 1996;53:27–31.
Stokes L, Stark A, Marshal E. Narany. A neuro-toxicity among pesticides applicants exposed toarganophosphales. England, October1995;52:48–53.
Kishi M, Hirschhorn N, Djajadisastra M,Satterlee LN, Strowman S, Dilts R. Relationshipof pesticide spraying to signs and symptoms inIndonesian farmers. Scand J Work EnvironHealth, Finland, 1995;2(2):124–33.
Sivatoganatharic, Gnanachandran S, Lewis J,Fernando M. Protective measure use and symp-toms among agro-pesticide applicators in Sri-Lanka. Soc Sci Med 1995;40:4431–6.
Jama Aden HanshiPublic Health OfficerMinistry of HealthP.O. Box 30IsioloEastern ProvinceKenya
77
Afr Newslett on Occup Health and Safety 2001;11:77
The Fifth Meeting of the Network ofWHO Collaborating Centres in Occu-pational Health was organized on 13-15 November 2001 in Chiang Mai,Thailand. Dr. Pakdee Pothisiri, Direc-tor General of the Ministry of PublicHealth, Thailand, opened the meetingand wished all participants warmly wel-come. He also stressed that occupationalhealth is as important to developingcountries as to industrialized ones. Heemphasized that the problems in worklife have become increasingly morecomplex, requiring more exchange ofinformation and sharing of experiencesto be solved. He also pointed out howimportant the role of the Network ofCollaborating Centres in OccupationalHealth has been from the very begin-ning of its establishment in Moscow,Russian Federation, later through thenetwork meetings organized in Beijing,China, Bogota, Colombia, Helsinki,Finland, and now in Chiang Mai, Thai-land.
The meeting gathered close to 60 par-ticipants from 39 Collaborating Centres,WHO Headquarters and Regions, ILO,as well as from NGOs. Altogether 24countries were represented.
Dr. Mike Repacholi, Dr. Marilyn Fin-gerhut, and Dr. Greg Goldstein of theWHO Headquarters had participated inpreparing the meeting programme. Thepractical arrangements were carried outby Dr. Wilawan Juengprasert and hercolleagues from the Thai Ministry ofPublic Health. Everything ran smooth-ly, and the participants were well takencare of, as regards both the businessmatters and the social programme. Itseems that although all the other previ-ous meetings have been very well or-ganized, the Thai colleagues surpassedthe previous records. Warm thanks aredue to all the Organizers of the FifthNetwork Meeting!
The agenda of the meeting consisted
Fifth Network Meeting ofthe WHO Collaborating Centres
in Occupational Health
of an overview of the WHO, ILO, andNGO Programmes, a presentation of theactivities of the WHO Regions relatedto the WHO Global Strategy on Occu-pational Health for All, as well as pa-pers on the impact of WHO/ILO Glo-bal Strategy activities, with special at-tention to the Programme for Elimina-tion of Silicosis. In addition, severalpapers focused on the impact of the col-laborating centre activities. A specialsession was dedicated to studies describ-ing the global/national burden of dis-ease. Much development work is stillneeded to make the calculations moreaccurate. Several posters described thesuccess stories of occupational healthand safety advances in various coun-tries.
The joint work plan of the WHOHeadquarters, Regions, and the Collab-orating Centres, to implement the WHOGlobal Strategy on Occupational Healthfor All, was discussed in three workinggroups. The contributions, commit-ments and interests of the Collaborat-ing Centres and discussions in the threeworking groups were integrated into onework plan that was then further devel-oped to respond to the challenges of thechanging work life in all corners of theworld. In all, 15 Task Forces on vari-ous aspects of work life were estab-lished. These will continue the work ina coordinated way so that the results canbe checked and evaluated in the SixthNetwork Meeting in two years.
The specific conclusions and recom-mendations of the Meeting dealt withthe continuous need to emphasize thepriority position of occupational health,both on the national and internationalagendas, the growing need for occupa-tional health and safety in all countries,and the further development of well-functioning and universally availableinfrastructures, particularly occupation-al health services, and sufficient and
well-trained human resources for occu-pational health. In addition, the need forresearch in the field of occupationalhealth and safety was recognized, es-pecially as a basis for the practical ap-plication of research results to improveworking conditions at the workplacelevel. Gathering reliable informationabout the status of occupational healthand safety in the countries was alsoemphasized. This information can beused to develop further the content ofoccupational health and safety pro-grammes in the countries, and it can toa certain extent be used to benchmarkand guide developments at the interna-tional level. WHO/HQ efforts for thecalculation of the global burden of oc-cupational injuries and diseases waswelcomed. The collection of data onnational as well as local occupationalhealth and safety indicators should beimproved further. The country occupa-tional health and safety profiles will beone of the main tasks on the work planfor the next few years. All Collaborat-ing Centres were encouraged to takepart in this effort.
In addition to the scientific and prac-tical papers given at the meeting, oneof the aims – the enthusiastic exchangeof ideas and information and the shar-ing of knowledge and expertise – wasrealized in all sessions of the Meeting.This was a truly stimulating event, andpoints to continuing collaboration inensuring Occupational Health for All.
Suvi LehtinenFinnish Institute of OccupationalHealthTopeliuksenkatu 41 a AFIN-00250 HelsinkiFinlandE-mail:[email protected]
S. Lehtinen, FINLAND
Afr Newslett on Occup Health and Safety 2001;11:78
78
Themes of the African Newsletterin 2002
1/2002 Violence at workplaces (manuscripts by 15 February 2002)2/2002 Occupational health and safety networks and the Internet (manuscripts by 30 May 2002)3/2002 Work-related diseases and their prevention (manuscripts by 30 September 2002)
Readers are encouraged to submit manuscripts focusing on above themes. Articles on other topics in the field of occupa-tional health and safety are also welcomed. Please send your manuscript to:
Suvi LehtinenEditor in ChiefAfrican Newsletter on Occupational Health and SafetyFinnish Institute of Occupational HealthTopeliuksenkatu 41 a AFIN-00250 Helsinki, FinlandE-mail: [email protected]
The first preparatory meeting on devel-oping national and local profiles in oc-cupational health and safety was organ-ized by the Ministry of Public Health,Thailand, and the Finnish Institute ofOccupational Health on 6–7 March2001 in Chiang Mai, Thailand. Alto-gether 35 participants, representing sev-eral ministries, universities and healthagencies, attended the meeting. As aresult of the lively discussions and keeninterest of all participants to continuethe development of OH&S indicatorsfurther, a follow-up procedure wasagreed upon. The first follow-up stepwas the 18 October 2001 workshop inHelsinki, where the Thai colleagues, Dr.Twisuk Punpeng and Dr. Somkiat Sir-iruttanapruk presented their communi-ty profiles in occupational health andsafety for the Lamphoon province. Itwas a most successful presentation, andgot a lot of positive feedback from theother participants. The Workshop wasattended by representatives from ninecountries, namely China, Kenya, Nepal,the Philippines, South Africa, Sri Lan-ka, Tanzania, Thailand, and Vietnam.
Follow-up meeting on indicators and profilesin Chiang Mai, Thailand
Such wide participation was made pos-sible by the funding from the FinnishMinistry for Foreign Affairs, WHO andILO.
In March 2001, it was also decidedthat a follow-up meeting be organizedin mid-November 2001. This meetingtook place on 12 November 2001 inChiang Mai, Thailand, and it was at-tended by the same persons and organ-izations as the first preparatory meet-ing. Dr. Twisuk Punpeng, Dr. WilawanJuengprasert and Dr. Somkiat Sirirut-tanapruk of the Ministry of PublicHealth, together with many other col-leagues, had organized an effectivemeeting to follow up the developmentsin preparing the profiles. At this timethe main focus was on provincial andlocal community profiles. In their pres-entations, the representatives of Pitsan-ulok, Lamphoon and Khon Kaen prov-inces described the situation in their re-spective provinces. The rapid assess-ment methods were also introduced anddiscussed, and there was interest in theaudience to carry out rapid assessmentsin order to increase the amount of in-
formation on various specific questionsof occupational health and safety. Inaddition, also the results of the Work inthe Global Village Conference held on15–17 October 2001, and the results ofthe 18 October Helsinki Workshop werebriefly high-lighted.
In the 18 October Workhops, the Ken-yan country profile was described by MrFranklin K. Muchiri of the Directorateof Occupational Health and Safety Serv-ices, Nairobi; the South African reportwas given by Dr Gopolang Sekobe ofthe Ministry of Health of South Africa;Tanzania was represented by Mr H. I.Kitumbo who also gave the report onthe Tanzanian occupational health andsafety situation.
It was agreed that a second follow-upbe organized in November 2002 in con-nection with the International Sympo-sium to be organized by the FIOH onthe topic of young people and work life.
Suvi LehtinenE-mail:[email protected]
Afr Newslett on Occup Health and Safety 2001;11:79
79
University of Michigan /Fogarty International Center Grant
Applications are hereby invited for bur-sary supported post-graduate study ORfocussed research training of up to 3months duration in Environmental orOccupational Health at the Universityof Michigan, USA.
MASTERS OR DOCTORALPROGRAMMESThe University of Michigan offers Mas-ters of Science (MS), Masters of PublicHealth (MPH), and Doctorates (PhD orDrPH) in Environmental Health Scienc-es (including Air Pollution, Water Qual-ity, Management of Hazardous Wastes,Risk Assessment), Occupational Medi-cine, Industrial Hygiene, OccupationalHealth Nursing Occupational SafetyEngineering, Toxicology, and Environ-mental and Occupational Epidemiolo-gy. Distinct preference will be given toapplications for study of environmen-tal health sciences and occupationalhygiene, but applications for study inthe other disciplines listed above willalso be considered. Masters Degrees areusually completed in 3 to 4 terms ofstudy over a 1 ˚ to 2 year period. Per-sons pursuing a PhD typically completeat least 2 years of course-work beforeturning to dissertation work requiring 2to 3 additional years of research. Mas-ter theses and PhD dissertations are ex-pected to be based on research conduct-ed in Southern Africa. Supervision ofstudents conducting research projectswill be shared between US and SouthAfrican advisors.
This grant will provide 1 ˚ to 2 yearsof support per student, including a sti-pend, health insurance, tuition and
transatlantic airfare. Funding is from aFogarty International Center grant. Thisprogramme does NOT provide funds forthe conduct of the actual research, how-ever, UM and local supervisors will as-sist the student in accessing researchfunding. Over the five-year period ofthe grant, a minimum of three studentswill be trained at either masters or doc-toral levels.
SHORT-TERM FOCUSSEDRESEARCH TRAINING (UPTO THREE MONTHSDURATION)Areas of expertise of University ofMichigan Faculty available to collabo-rate with applicants include preferential-ly Environmental Health Sciences (in-cluding Air Pollution, Water Quality,Management of Hazardous Wastes,Risk Assessment), Occupational Medi-cine, Industrial Hygiene, Toxicology,and Environmental and OccupationalEpidemiology. Consideration will alsobe given to Occupational Health Nurs-ing and Occupational Safety Engineer-ing.
This grant will provide up to threemonths support per successful appli-cant, including a stipend, health insur-ance, and transatlantic airfare. Twoawards are expected to be made in thefirst year of the grant.
ELIGIBILITYApplicants must be citizens of SADCnations, must hold a bachelors degreeand, for the short-term research train-
ing, must be involved in an existing re-search project.
CLOSING DATESApplications must be submitted to theUniversity of Michigan and to the Na-tional Centre for Occupational Health(NCOH). Strong preference will be giv-en to complete applications received nolater than 1 March 2002. However, ap-plications after this date will be consid-ered. If awarded, the earliest possibledate for commencing graduate studieswill be September 2002. Commence-ment dates for short-term programmescould be earlier depending on availa-bility of UM faculty. Applicants canexpect notification of status no later than30 June 2002.
Application forms and additional in-formation about the programme areavailable from:
Claudina NogueiraNational Centre for OccupationalHealthP.O. Box 4788Johannesburg 2000SOUTH AFRICA
email: [email protected]: + 011 712-6469fax: + 011-720-6608
To support environmental and occupational healthtraining and research in the Southern African
Development Community (SADC) Region
Afr Newslett on Occup Health and Safety 2001;11:79

Chief Inspector of FactoriesCommissioner of Labour andSocial SecurityDepartment of Labour andSocial SecurityPrivate Bag 0072GaboroneBOTSWANA
Samir Ragab SeliemEgyptian Trade Union FederationOccupational Health andSafety Secretary90 Elgalaa StreetCairoEGYPT
Z. GezahegneHead/workers’ Working ConditionsResearch and Education DivisionMinistry of Labour andSocial AffairsP.O.Box 2056Addis AbabaETHIOPIA
Commissioner of LabourMinistry of Trade Industry andEmploymentCentral Bank BuildingBanjulGAMBIA
Franklin K. MuchiriDirectorate of OccupationalHealth and Safety ServicesP.O.Box 34120NairobiKENYA
Noel J. MkhumbaInformation and DocumentationCentreP.O.Box 344Capital City Lilongwe 3MALAWI
Contact persons/country editors Editorial Board
as of 31 December 1994
Chief Inspector of FactoriesCommissioner of Labour and SocialSecurityBOTSWANA
Mebratu GebeyehuHead, Labour Inspector DepartmentMinistry of Labour andSocial AffairsETHIOPIA
T.F. BruceChief Inspector of FactoriesMinistry of Labour and Social WelfareGHANA
S. BalgobinChief Inspector of FactoriesMinistry of Labour and IndustrialRelationsMAURITUS
Chief Inspector of FactoriesMinistry of LabourSIERRA LEONE
Chief Inspector of FactoriesMinistry of Labour and SocialSecuritySUDAN
Jukka TakalaDirectorSafeWork, Global Programme onSafety, Health and EnvironmentInternational Labour OfficeSWITZERLAND
Jorma RantanenDirector GeneralFinnish Institute of OccupationalHealthFINLAND
N.A. ArogundadeAssistant Director of FactoriesFederal Ministry of Employment,Labour and ProductivityPrivate Mail Bag 12576147, Broad StreetLagosNIGERIA
Peter H. MavusoHead of CIS National CentreP.O.Box 198MbabaneSWAZILAND
Ministry of Labour andYouth DevelopmentFactories InspectorateP.O.Box 9014Dar es SalaamTANZANIA
Obua PaulOccupational Health andHygiene DepartmentMinistry of LabourP.O.Box 4637KampalaUGANDA