
Adipokines as emerging depression biomarkers: A systematic review and meta-analysis
10
Adipokines as emerging depression biomarkers: A systematic review and meta-analysis Andr e F. Carvalho a, * , Davi Q.C. Rocha a , Roger S. McIntyre b, c , Lucas M. Mesquita a , Cristiano A. K € ohler d , Thomas N. Hyphantis e , Paulo M.G. Sales a , Rodrigo Machado-Vieira f, g, h , Michael Berk i, j, k a Translational Psychiatry Research Group, Faculty of Medicine, Federal University of Ceara, Fortaleza, CE, Brazil b Departments of Pharmacology and Psychiatry, University of Toronto, Toronto, ON, Canada c Mood Disorders Psychopharmacology Unit, University of Toronto, Toronto, ON, Canada d Memory Research Laboratory, Brain Institute (ICe), Federal University of Rio Grande do Norte (UFRN), Natal, RN, Brazil e Department of Psychiatry, Medical School, University of Ioaninna, Ioaninna, Greece f National Institute of Mental Health (NIMH), Bethesda, USA g Laboratory of Neuroscience, LIM-27, Department and Institute of Psychiatry, University of S~ ao Paulo, USP, Brazil h Center for Interdisciplinary Research in Applied Neuroscience (NAPNA), USP, Brazil i IMPACT Strategic Research Centre, School of Medicine, Deakin University, Geelong, Vic., Australia j Florey Institute of Neuroscience and Mental Health, Australia k Orygen Youth Health Research Centre, University of Melbourne, Parkville, Vic., Australia article info Article history: Received 27 June 2014 Received in revised form 6 August 2014 Accepted 7 August 2014 Keywords: Major depressive disorder Meta-analysis Adiponectin Leptin Resistin Biomarkers abstract Adiponectin, leptin and resistin may play a role in the pathophysiology of major depressive disorder (MDD). However, differences in peripheral levels of these hormones are inconsistent across diagnostic and intervention studies. Therefore, we performed meta-analyses of diagnostic studies (i.e., MDD sub- jects versus healthy controls) and intervention investigations (i.e., pre-vs. post-antidepressant treatment) in MDD. Adiponectin (N ¼ 1278; Hedge's g ¼0.35; P ¼ 0.16) and leptin (N ¼ 893; Hedge's g ¼0.018; P ¼ 0.93) did not differ across diagnostic studies. Meta-regression analyses revealed that gender and depression severity explained the heterogeneity observed in adiponectin diagnostic studies, while BMI and the difference in BMI between MDD individuals and controls explained the heterogeneity of leptin diagnostic studies. Subgroup analyses revealed that adiponectin peripheral levels were significantly lower in MDD participants compared to controls when assayed with RIA, but not ELISA. Leptin levels were significantly higher in individuals with mild/moderate depression versus controls. Resistin serum levels were lower in MDD individuals compared to healthy controls (N ¼ 298; Hedge's g ¼0.25; P ¼ 0.03). Leptin serum levels did not change after antidepressant treatment. However, heterogeneity was significant and sample size was low (N ¼ 108); consequently meta-regression analysis could not be performed. Intervention meta-analyses could not be performed for adiponectin and resistin (i.e., few studies met inclusion criteria). In conclusion, this systematic review and meta-analysis underscored that relevant moderators/confounders (e.g., BMI, depression severity and type of assay) should be controlled for when considering the role of leptin and adiponectin as putative MDD diagnostic biomarkers. © 2014 Elsevier Ltd. All rights reserved. 1. Introduction Current diagnostic practice for major mental disorders, including major depressive disorder (MDD) is based on the clus- tering of symptoms and other clinical features (Pizzagalli, 2011). MDD is frequently not properly recognized in diverse ‘real world’ clinical settings (Craven and Bland, 2013; Kessler et al., 2007; Lake and Baumer, 2010; Yan et al., 2013). This delay in diagnosis hinders early treatment intervention, leading to worse outcomes due to the * Corresponding author. Department of Clinical Medicine, Federal University of Cear a, Faculty of Medicine, Rua Prof. Costa Mendes, 1608, 4 andar, 60430-040, Fortaleza, CE, Brazil. Tel./fax: þ55 8532617227. E-mail addresses: [email protected], [email protected] (A.F. Carvalho). Contents lists available at ScienceDirect Journal of Psychiatric Research journal homepage: www.elsevier.com/locate/psychires http://dx.doi.org/10.1016/j.jpsychires.2014.08.002 0022-3956/© 2014 Elsevier Ltd. All rights reserved. Journal of Psychiatric Research xxx (2014) 1e10 Please cite this article in press as: Carvalho AF, et al., Adipokines as emerging depression biomarkers: A systematic review and meta-analysis, Journal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychires.2014.08.002
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Adipokines as emerging depression biomarkers: A systematic review and meta-analysis

lable at ScienceDirect
Journal of Psychiatric Research xxx (2014) 1e10
Contents lists avai
Journal of Psychiatric Research
journal homepage: www.elsevier .com/locate/psychires
Adipokines as emerging depression biomarkers: A systematic reviewand meta-analysis
Andr�e F. Carvalho a, *, Davi Q.C. Rocha a, Roger S. McIntyre b, c, Lucas M. Mesquita a,Cristiano A. K€ohler d, Thomas N. Hyphantis e, Paulo M.G. Sales a,Rodrigo Machado-Vieira f, g, h, Michael Berk i, j, k
a Translational Psychiatry Research Group, Faculty of Medicine, Federal University of Ceara, Fortaleza, CE, Brazilb Departments of Pharmacology and Psychiatry, University of Toronto, Toronto, ON, Canadac Mood Disorders Psychopharmacology Unit, University of Toronto, Toronto, ON, Canadad Memory Research Laboratory, Brain Institute (ICe), Federal University of Rio Grande do Norte (UFRN), Natal, RN, Brazile Department of Psychiatry, Medical School, University of Ioaninna, Ioaninna, Greecef National Institute of Mental Health (NIMH), Bethesda, USAg Laboratory of Neuroscience, LIM-27, Department and Institute of Psychiatry, University of S~ao Paulo, USP, Brazilh Center for Interdisciplinary Research in Applied Neuroscience (NAPNA), USP, Brazili IMPACT Strategic Research Centre, School of Medicine, Deakin University, Geelong, Vic., Australiaj Florey Institute of Neuroscience and Mental Health, Australiak Orygen Youth Health Research Centre, University of Melbourne, Parkville, Vic., Australia
a r t i c l e i n f o
Article history:Received 27 June 2014Received in revised form6 August 2014Accepted 7 August 2014
Keywords:Major depressive disorderMeta-analysisAdiponectinLeptinResistinBiomarkers
* Corresponding author. Department of Clinical MeCear�a, Faculty of Medicine, Rua Prof. Costa MendesFortaleza, CE, Brazil. Tel./fax: þ55 8532617227.
E-mail addresses: [email protected](A.F. Carvalho).
http://dx.doi.org/10.1016/j.jpsychires.2014.08.0020022-3956/© 2014 Elsevier Ltd. All rights reserved.
Please cite this article in press as: CarvalhoJournal of Psychiatric Research (2014), http:
a b s t r a c t
Adiponectin, leptin and resistin may play a role in the pathophysiology of major depressive disorder(MDD). However, differences in peripheral levels of these hormones are inconsistent across diagnosticand intervention studies. Therefore, we performed meta-analyses of diagnostic studies (i.e., MDD sub-jects versus healthy controls) and intervention investigations (i.e., pre-vs. post-antidepressant treatment)in MDD. Adiponectin (N ¼ 1278; Hedge's g ¼ �0.35; P ¼ 0.16) and leptin (N ¼ 893; Hedge's g ¼ �0.018;P ¼ 0.93) did not differ across diagnostic studies. Meta-regression analyses revealed that gender anddepression severity explained the heterogeneity observed in adiponectin diagnostic studies, while BMIand the difference in BMI between MDD individuals and controls explained the heterogeneity of leptindiagnostic studies. Subgroup analyses revealed that adiponectin peripheral levels were significantlylower in MDD participants compared to controls when assayed with RIA, but not ELISA. Leptin levelswere significantly higher in individuals with mild/moderate depression versus controls. Resistin serumlevels were lower in MDD individuals compared to healthy controls (N ¼ 298; Hedge's g ¼ �0.25;P ¼ 0.03). Leptin serum levels did not change after antidepressant treatment. However, heterogeneitywas significant and sample size was low (N ¼ 108); consequently meta-regression analysis could not beperformed. Intervention meta-analyses could not be performed for adiponectin and resistin (i.e., fewstudies met inclusion criteria). In conclusion, this systematic review and meta-analysis underscored thatrelevant moderators/confounders (e.g., BMI, depression severity and type of assay) should be controlledfor when considering the role of leptin and adiponectin as putative MDD diagnostic biomarkers.
© 2014 Elsevier Ltd. All rights reserved.
dicine, Federal University of, 1608, 4� andar, 60430-040,
AF, et al., Adipokines as emer//dx.doi.org/10.1016/j.jpsychi
1. Introduction
Current diagnostic practice for major mental disorders,including major depressive disorder (MDD) is based on the clus-tering of symptoms and other clinical features (Pizzagalli, 2011).MDD is frequently not properly recognized in diverse ‘real world’clinical settings (Craven and Bland, 2013; Kessler et al., 2007; Lakeand Baumer, 2010; Yan et al., 2013). This delay in diagnosis hindersearly treatment intervention, leading to worse outcomes due to the
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002
A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e102
dysregulation of several measureable pathophysiological pathwaysin the central nervous system, including but not limited to adysfunctional activation of the hypothalamic-pituitary adrenal(HPA) axis (Pariante and Lightman, 2008), inflammation (Goldet al., 2013) and the generation of oxidative and nitrosative stress(O&NS) (Moylan et al., 2013). Despite this, there are currently novalidated peripheral biomarkers for the diagnosis, treatment se-lection and response prediction in MDD (Breitenstein et al., 2014).The development of biomarkers for MDD and their incorporationinto clinical practice promises to revolutionize the landscape ofhealth care.
Since the discovery of leptin by Zhang et al. (1994), its role inmetabolism and homeostasis has been extensively investigated(Berman et al., 2013; Licinio et al., 2004; Paz-Filho et al., 2008;Zhang et al., 1994). It is increasingly recognized that the adiposetissue is not an inert tissue devoted to energy storage, rather beinga metabolically active endocrine organ capable of secreting anumber of bioactive products referred to as ‘adipokines’, whichinclude adiponectin (Maeda et al., 1996), leptin, and resistin(Steppan et al., 2001). Adipokines are also secreted by diverse tis-sues, including but not limited to macrophages, myocytes, andpancreatic cells (Arnoldussen et al., 2014). The adipocyte-braincrosstalk is mediated to a large extent by adipokines and this cir-cuit plays a pathophysiological role beyond obesity and car-diometabolic conditions (Nakamura et al., 2013; Paz-Filho et al.,2010). Leptin influences neurotransmitters such as dopamine(Ishibashi et al., 2012) and impacts gray matter plasticity (Londonet al., 2011). Consequently, a putative role for leptin, adiponectinand resistin in the pathophysiology of neuropsychiatric conditionsassociated with metabolic abnormalities, including MDD hasemerged (vide infra) (Diniz et al., 2012; Liu et al., 2012; Lu et al.,2006; Weber-Hamann et al., 2007; Yamada et al., 2010).
Adiponectin is a polypeptide that regulates glucose levels aswell as fatty acid breakdown (Yildiz et al., 2004). It is exclusivelysecreted by adipocytes as an abundant adipose-derived serumprotein. Adiponectin exerts insulin-sensitizing and either inflam-matory or anti-inflammatory effects (Kwon and Pessin, 2013; Wanet al., 2014). AdipoR1 and AdipoR2, the cognate adiponectin re-ceptors, are expressed in discrete brain areas related to moodregulation, including the hippocampus (Liu et al., 2012). Adipo-nectin exerts antidepressant-like effects in the social-defeat stressanimal model of depression (Liu et al., 2012). Adiponectin hap-loinsufficiency blunts glucocorticoid-mediated negative feedbackon the HPA axis (Liu et al., 2012). Notwithstanding that plasmalevels of adiponectin are negatively correlated with obesity, waistcircumference and visceral fat in humans, metabolically healthyobese subjects have peripheral levels of adiponectin similar to leanindividuals (Arita et al., 2012; Cohen et al., 2011; Doumatey et al.,2012). Some reports point to higher adiponectin serum levels inMDD subjects compared to healthy controls (Jow et al., 2006), whileother investigators found either lower levels (Cizza et al., 2010;Zeman et al., 2010) or unaltered (Kotan et al., 2012) peripherallevels in MDD individuals versus controls.
Leptin circulates as a 16-kDa protein, and is the product of the obgene. It is mainly synthesized by adipose tissue in proportion topercentage body fat (Zupancic and Mahajan, 2011). This peptide istransported across the bloodebrain barrier by a saturable processto exert its central effects (Zupancic and Mahajan, 2011). Leptin hasantidepressant and anxiolytic activities in rodents (Liu et al., 2010).Diet-induced obesity in mice is associated with an impaired anti-depressant response to leptin which is related to a blunted leptin-induced increment in hippocampal BDNF levels compared to micefed a standard diet (Yamada et al., 2011). The antidepressant ac-tivity of leptin may result from its modulatory effect upon the HPAaxis. In food-deprived ob/obmice, systemic administration of leptin
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
lowers corticosterone levels and prevents the induction of CRHsynthesis in the paraventricular nucleus (PVN) (Huang et al., 1998).Leptin levels were associated with an elevated risk of depressiononset in older men with a significant amount of visceral fat(Milaneschi et al., 2012). Several studies have found lower serumleptin levels in individuals with MDD compared to healthy controls(Jow et al., 2006; Kraus et al., 2001), whereas other studies inwomen with MDD found that plasma leptin levels were signifi-cantly increased (Esel et al., 2005; Rubin et al., 2002; Zeman et al.,2009). Similarly, some studies reported that leptin levels are vari-ously increased (Esel et al., 2005; Kraus et al., 2002) or not changedby antidepressant treatment (Kraus et al., 2002; Schilling et al.,2013). Lastly, some studies suggest that leptin may be abiomarker of risk for de-novo depression (Pasco et al., 2008).
The protein resistin is related to insulin resistance in rodents(Schwartz and Lazar, 2011). Some studies found elevated peripheralresistin levels in human obesity (Degawa-Yamauchi et al., 2003;Owecki et al., 2011), whereas other investigations found resistindown-regulated in obesity (Way et al., 2001). The findings relatingresistin to MDD are inconsistent across studies. Lower resistinserum levels in individuals withMDD compared to healthy controlsare reported (Aliyazicioglu et al., 2011a), but not replicated(Papakostas et al., 2013). In addition, resistin levels were positivelycorrelated with cortisol levels in MDD patients (Weber-Hamannet al., 2007). Furthermore, there was a significant decrease inresistin serum levels in patients receiving antidepressant treatmentwho remitted from depression (Weber-Hamann et al., 2007).
In order to clarify the inconsistent findings on the associationsbetweenperipheral levels of adiponectin, leptin and resistin both asputative diagnostic as well as treatment response biomarkers inMDD, we performed a meta-analysis of the available evidence. Wehypothesized that there would be significant heterogeneity be-tween studies (for example, related to age, body mass index andgender). Therefore, this review also aimed to identify potentialconfounders. As far as we know no previous meta-analyses hadbeen published on the role of akipokines as depression biomarkers.
2. Material and methods
2.1. Study selection
2.1.1. Search strategyArticles for review were identified from the PubMed/MEDLINE,
EMBASE, and Web of Science databases from inception to January12, 2014. The standardized search algorithms are detailed inSupplementary Material S1. Search terms included ‘akipokines’,‘leptin’, ‘adiponectin’ and ‘resistin’ cross-referenced with ‘depres-sion’, ‘major depressive disorder’ and ‘depressive’. This searchstrategy was augmented by manual searches were performed onreference lists of included articles. We also tracked citations ofincluded articles and relevant reviews using Google Scholar. Au-thors were contacted to provide additional data when necessary.We followed the Preferred Items for Reporting of Systematic Reviewsand Meta-Analyses (PRISMA) statement (Moher et al., 2009).
2.1.2. Identification of eligible studiesEligible articles included original studies in any language which
measured leptin, adiponectin and/or resistin levels in plasma orserum in patients with major depressive disorder and healthycontrols (diagnostic studies), or measured these adipokines atbaseline and after a trial with a standard antidepressant agent(referred hitherto as intervention studies). Eligible studies includedparticipants who fulfilled Diagnostic and Statistical Manual ofMental Disorders (DSM) or International Classification of Diseases(ICD) criteria for MDD based on a validated structured or semi-
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002

A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e10 3
structured clinical interview (e.g., Structured Clinical Interview forDSM-IV [SCID-I] (Frist et al., 1996), Composite International Diag-nostic Interview [CIDI] (Wittchen, 1994), Diagnostic InterviewSchedule [DIS] (Robins et al., 1981)) or a screening instrument. Caseseries or case reports were excluded. Studies including MDD par-ticipants with co-morbid major mental disorders (e.g., substanceuse disorders or anxiety disorders) were excluded from this review.Finally, studies involving bipolar disorder participants on depres-sive episodes were also excluded from this review.
Two investigators independently reviewed the articles foreligibility. If either deemed an article as potentially eligible basedon title/abstract screening, then a full-text review was performed.Final decisions regarding eligibility were made by consensusfollowing the full-text review.
2.2. Data extraction
For each study, data were independently extracted by two au-thors (DQCR and LMM) and entered in a standardized form. Dis-crepancies were resolved by consensus. The following variableswere extracted: (1) mean and standard deviation of leptin, adipo-nectin and/or resistin serum levels for each group; (2) de-mographic, clinical and treatment characteristics (including age,gender distribution, body mass index (BMI), scores on MDD ratingscales, depression subtype, previous treatments, type of antide-pressant treatment, depression severity, differences in mean BMIbetween MDD individuals and healthy controls); (3) type of assay(ELISA or RIA) and (4) study design (e.g., caseecontrol or trial).
When an included study measured serum or plasma levels ofadiponectin, leptin and/or resistin at different time points, weconsidered the last available observation.When an eligible study didnot provide extractable data, corresponding authorswere contacted.
2.3. Quantitative analyses
Meta-analytical calculations were carried out using Compre-hensive Meta-Analyses version 2.0 (CMA 2.0) with statistical sig-nificance set at P � 0.05.
Random effects models was used to estimate effect sizes usingHedge's g (±95% Confidence intervals; 95CI) on the difference be-tween each adipokine (i.e., adiponectin, leptin and/or resistin)levels between MDD individuals and healthy controls (diagnosticstudies), or the difference between each adipokine serum levelsbefore and after antidepressant treatment (intervention studies).Heterogeneity between studies were assessed through the Q sta-tistic. Publication bias was assessed by funnel plot asymmetry in-spection and the Egger test (Egger et al., 1997). Whenever theheterogeneity between studies was not significant, fixed effectsmodels were used to estimate Hedge's g.
Weevaluated thepotentialmoderatingeffectsof clinicalvariables(depression severity, whether the diagnosis was performed througha semi-structured interview, overall sample BMI, mean BMI differ-ence between MDD individuals and controls), socio-demographicfactors (% of female in overall sample; difference in % of females be-tweenMDD individuals and controls) and type of assay (ELISAversusRIA).We also conducted subgroup analyses. To investigatewhether aparticular study determined the summary measure in each meta-analysis, sensitivity analyses were performed.
3. Results
3.1. Search results and study characteristics
Of 1185 unique references, 1120 were excluded after title/ab-stract screening. Sixty five references were selected for full-text
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
review. Finally, 23 original studies were included in the system-atic review (Fig. 1). Please see Tables S1A and S1B for a descriptionof primary reasons for exclusion (Supplementary Material). Theauthors of meeting abstracts were electronically contacted by theauthors. Characteristics of the included diagnostic (i.e., MDD in-dividuals vs. healthy controls) and intervention studies are pre-sented in Supplementary Tables S2A and S2B (SupplementaryMaterial), respectively. Primary data which could be extracted inmeta-analyses are depicted in Tables S3A (diagnostic studies) andS3B (intervention studies). Please see supporting on-line materialin the journal's web site for reference lists of excluded (i.e., afterfull-text review) as well as included studies. Diagnostic meta-analyses were performed for adiponectin (9 studies; N ¼ 1278),leptin (11 studies; N ¼ 893) and resistin (2 studies; N ¼ 298) (videinfra). Papakostas et al. (2013) reported a pilot and a replicationstudy; for each study resistin data could be extracted (diagnosticmeta-analysis). Standard meta-analyses techniques were per-formed to control for heterogeneity (meta-regression and subgroupanalyses) for the adiponectin and leptin diagnostic meta-analyses.There were few included studies for the resistin diagnostic meta-analysis. Therefore, these results should be considered exploratory.
3.2. Publication bias
After inspection of funnel plots of the diagnostic meta-analyses(Supplementary Fig. 1), there was no evidence of publication biasfor adiponectin (Egger's intercept¼ �6.15; 95% CI ¼ �14.09 to 1.79,P ¼ 0.10), leptin (Egger's intercept ¼ 3.07; 95% CI ¼ �7.10 to 13.2,P ¼ 0.51) or resistin (Egger's intercept ¼ 5.23; 95% CI ¼ �38.01 to48.49, P ¼ 0.36).
3.3. Meta-analysis of diagnostic studies
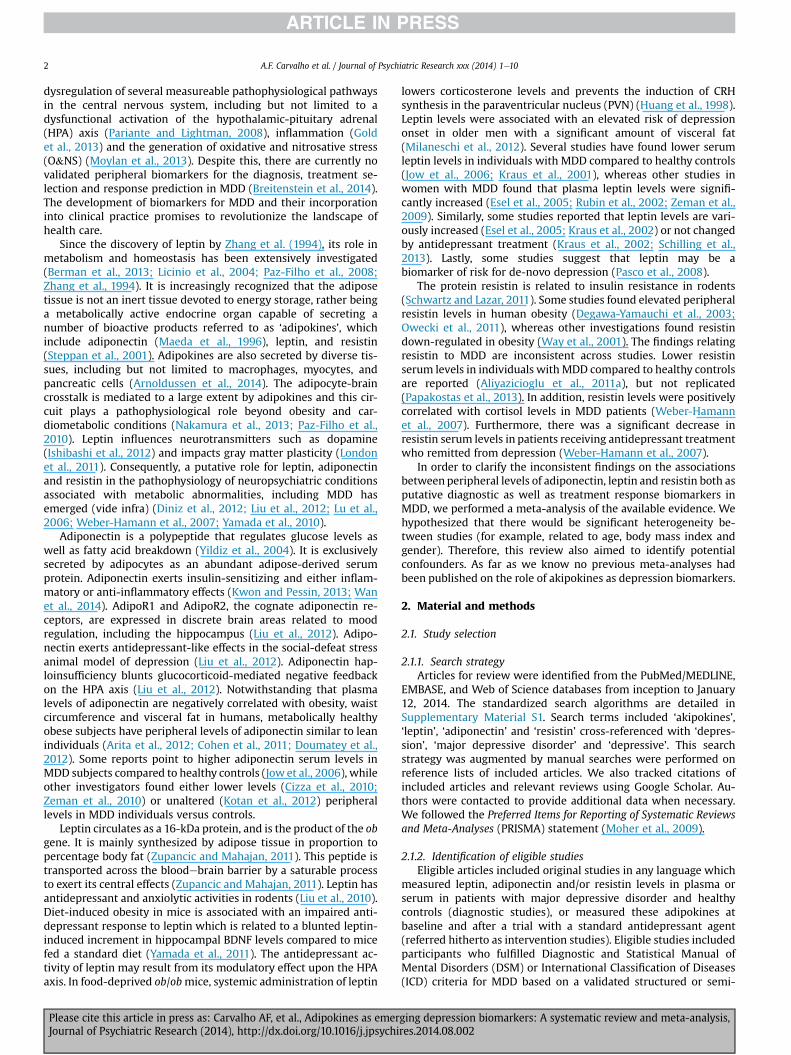
Significant heterogeneity between studies included for theadiponectin diagnostic meta-analysis was observed (Q ¼ 96.3;df ¼ 8; P < 0.001). A significant summary difference in adiponectinperipheral levels between MDD individuals and controls was notobserved (Hedge's g ¼ �0.35, P ¼ 0.16) (Fig. 2).
Significant heterogeneity between studies included for theleptin diagnostic meta-analysis was shown (Q ¼ 96.3; df ¼ 11;P < 0.001). No differences in leptin peripheral levels betweensubjects with MDD and healthy controls was verified (Hedge'sg ¼ �0.018; P ¼ 0.93) (Fig. 2).
As there was no significant heterogeneity between studiesincluded in the resistin diagnostic meta-analysis, a fixed effectsmodel was applied. Resistin levels were significantly lower in in-dividuals with MDD compared to healthy controls (Hedge'sg ¼ �0.25; P ¼ 0.03).
3.3.1. Meta-regression analysesSince there was significant heterogeneity observed between
studies included in the adiponectin and leptin diagnostic meta-analyses, meta-regression analyses were performed to verifypossible influence of moderator variables.
For adiponectin, differences in peripheral levels between par-ticipants with MDD and healthy volunteers were significantlymoderated by differences in the percentage of female participantsacross studies (i.e., MDD group minus control group) (Table 1).Greater differences in the percentage of females were reflected by alower difference between adiponectin levels among MDD in-dividuals and controls. Differences in adiponectin serum levelsbetween MDD individuals and controls were also significantlymoderated by depression severity (Table 1; Fig. 3). More severedepression was associated with higher differences in adiponectinperipheral levels between MDD subjects and healthy volunteers.
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002

Fig. 1. PRISMA flow diagram of study selection process.
A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e104
There was a significant moderator effect of overall sample BMIacross leptin diagnostic studies (Table 1; Fig. 3). A higher overallsample BMI was associated with a significantly higher difference inleptin serum levels between MDD patients and healthy controls. Asimilar pattern was observed for differences in BMI between MDDindividuals and healthy controls.
3.3.2. Subgroup analysesSubgroup analyses were also performed to control for hetero-
geneity between studies for the adiponectin and leptin diagnosticmeta-analyses.
For adiponectin, there was a significant influence of the type ofassay (RIA versus ELISA). When adiponectin serum levels weremeasured with RIA, significantly lower peripheral levels of adipo-nectin were observed in participants with MDD compared tohealthy controls (Fig. 4). Importantly, significant heterogeneitybetween studies which had measured adiponectin levels with RIAwas not verified (Q ¼ 2.13; df ¼ 3; P ¼ 0.51).
Notwithstanding leptin peripheral levels did not differ betweenMDD individuals with severe depression versus healthy controls,but were significantly higher for participants with mild/moderateMDD compared to controls (Fig. 4). Significant heterogeneity wasno longer observed for studies which had included participantswith mild/moderate MDD (Q ¼ 2.13; df ¼ 4; P ¼ 0.30).
3.3.3. Sensitivity analysesSensitivity analyses were carried out for the adiponectin and
leptin diagnostic meta-analyses to determine whether each
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
individual study had an independent influence in the summaryeffect size measure. These analyses revealed that the removal ofeach individual study did not alter the overall direction of thefindings for each diagnostic meta-analysis (see SupplementaryFig. 2A and 2B).
3.4. Qualitative systematic review of intervention studies
Few intervention studies met inclusion criteria for systematicreview (see Supplementary Table S2B) andmeta-analyses could notbe performed for either adiponectin or resistin. While a meta-analysis could be performed for leptin (SupplementaryTable S3B), there was a high and significant degree of heteroge-neity in the performedmeta-analysis (data available upon request).Overall, there was no difference in leptin peripheral levels before orafter antidepressant treatment (Supplementary Fig. 3).
There were three intervention studies for adiponectin. A studyincluded 34 participants with severe DSM-IV MDD (Pinar et al.,2008). These subjects received a 30-day maprotiline (150 mg/day)trial. By the end of the trial, participants had a significant increase inbody weight and insulin resistance. Adiponectin levels significantlydecreased compared to baseline (29.66 ± 5.64 to 24.00 ± 6.26,P < 0.001). In the second study, after receiving placebo for six days,MDD participants were randomized to either amitriptyline (n¼ 24;up to 150 mg/day) or paroxetine (n ¼ 11; up to 40 mg/day) for 35days. No significant differences in adiopnectin serum levels afterantidepressant treatment were observed compared to baseline(Weber-Hamann et al., 2007). A third study in 43 hospitalized
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002
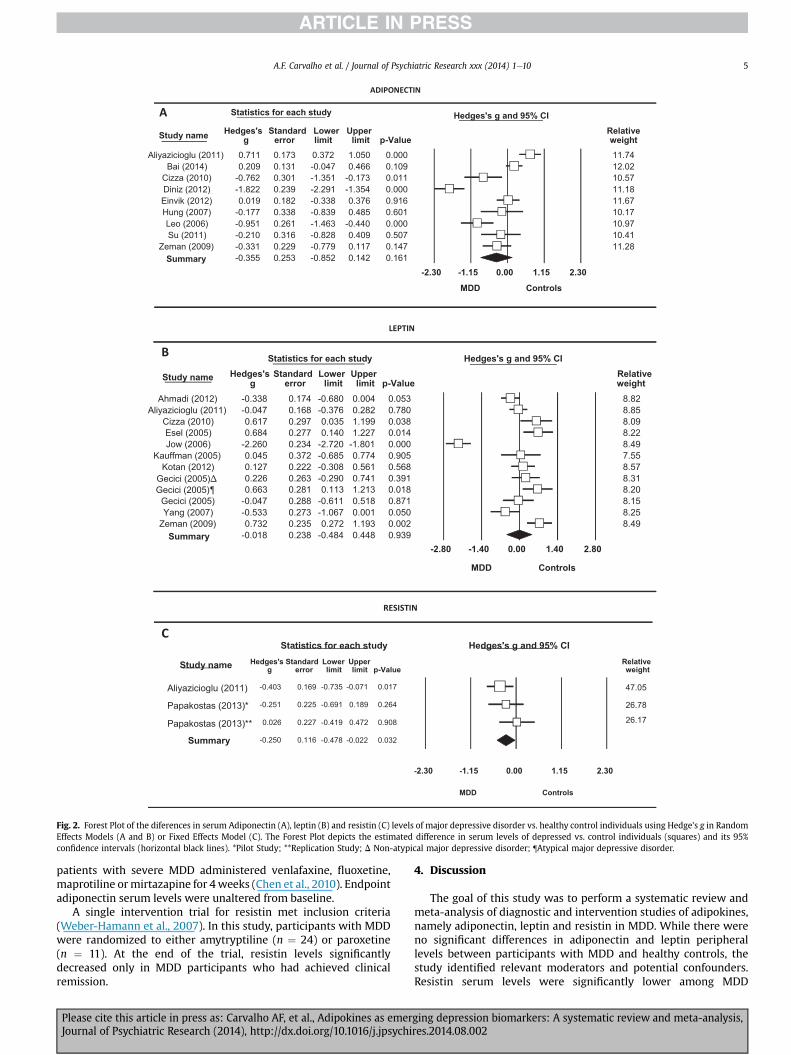
Fig. 2. Forest Plot of the diferences in serum Adiponectin (A), leptin (B) and resistin (C) levels of major depressive disorder vs. healthy control individuals using Hedge's g in RandomEffects Models (A and B) or Fixed Effects Model (C). The Forest Plot depicts the estimated difference in serum levels of depressed vs. control individuals (squares) and its 95%confidence intervals (horizontal black lines). *Pilot Study; **Replication Study; D Non-atypical major depressive disorder; ¶Atypical major depressive disorder.
A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e10 5
patients with severe MDD administered venlafaxine, fluoxetine,maprotiline ormirtazapine for 4weeks (Chen et al., 2010). Endpointadiponectin serum levels were unaltered from baseline.
A single intervention trial for resistin met inclusion criteria(Weber-Hamann et al., 2007). In this study, participants with MDDwere randomized to either amytryptiline (n ¼ 24) or paroxetine(n ¼ 11). At the end of the trial, resistin levels significantlydecreased only in MDD participants who had achieved clinicalremission.
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
4. Discussion
The goal of this study was to perform a systematic review andmeta-analysis of diagnostic and intervention studies of adipokines,namely adiponectin, leptin and resistin in MDD. While there wereno significant differences in adiponectin and leptin peripherallevels between participants with MDD and healthy controls, thestudy identified relevant moderators and potential confounders.Resistin serum levels were significantly lower among MDD
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002

Table 1Meta-regression of included studies.
Variable Variable type d.f. Point estimate(b)
95% CI of b Value of p % of Tau2
explained (R2)
Adiponectin% Females difference (MDD-controls) Continuous 6 0.063 0.020 to 0.105 0.004 46.74% Females in sample Continuous 11 0.018 �0.009 to 0.013 0.186 N/ASample age Continuous 8 �0.024 �0.055 to 0.006 0.115 N/AAge difference (MDD-controls) Continuous 8 0.054 �0.079 to 0.186 0.429 N/ASample BMI Continuous 8 �0.020 �0.233 to 0.193 0.856 N/ABMI difference (MDD-controls) Continuous 8 0.122 �0.487 to 0.730 0.695 N/ADepression severity Categorical
(Mild/Moderate vs. Severe)5 �1.274 �2.026 to �0.522 0.001 73.73
Semi-structured interview Categorical(No vs. Yes)
8 �0.168 �1.291 to 0.955 0.769 N/A
Type of assay Categorical(ELISA vs. RIA)
7 0.071 �1.163 to 1.305 0.910 N/A
Leptin% Females difference (MDD-controls) Continuous 11 �0.001 �0.071 to 0.070 0.986 N/A% Females in sample Continuous 11 0.018 �0.009 to 0.044 0.186 N/ASample age Continuous 10 0.056 �0.003 to 0.115 0.064 N/AAge difference (MDD-controls) Continuous 10 �0.023 �0.209 to 0.163 0.812 N/ASample BMI Continuous 11 0.325 0.182 to 0.469 <0.001 66.39BMI difference (MDD-controls) Continuous 11 0.336 0.113 to 0.559 0.003 43.56Depression severity Categorical
(Mild/Moderate vs. Severe)8 �0.805 �2.072 to 0.463 0.213 N/A
Semi-structured interview Categorical(No vs. Yes)
11 0.247 �0.892 to 1.387 0.670 N/A
Type of assay Categorical(ELISA vs. RIA)
11 0.427 �0.543 to 1.398 0.388 N/A
d.f.: Degrees of freedom; B is the non-standardized regression coefficient of each linear regression, representing the slope of each model; 95% CI is the confidence interval forthe true B coefficient; N/A: Not applicable, since only a portion of the studies was included. Significant results are in bold.
A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e106
participants compared to healthy volunteers. However, this meta-analysis included relatively few participants and only threestudies published in two separate reports (Aliyazicioglu et al.,2011b; Papakostas et al., 2013). Although this meta-analysis sug-gests that resistin holds promise as a relevant diagnostic biomarkerfor MDD, more studies are necessary.
4.1. Meta-analysis of diagnostic studies
There are important obstacles for the translation of valid bio-markers to routine clinical practice not only for MDD, but for psy-chiatric disorders at large (Breitenstein et al., 2014; Stuart andBaune, 2014). This fact contrasts with other fields in medicine,where biomarker guided therapy is a clinical reality. For example,some guidelines now advocate the use of B-type natriuretic peptideto guide the treatment of heart failure (Troughton et al., 2014).However, a recent influential meta-epidemiological survey claimsthat biomarker studies in cardiology have been subjected to sig-nificant bias (Tzoulaki et al., 2013). Therefore, aspects of studydesign and selective reporting of the data need to be consideredwhen interpreting evidences across biomarker studies. The con-founders and moderators identified in the present meta-analysesopen important aspects which should be considered when inter-preting individual data across reviewed studies (vide infra).Another important question is the validity of a unitary MDD diag-nosis, which is not based in brain mechanisms of disease (Insel,2014). For example, atypical and melancholic forms of MDD havesubstantial neurobiological and clinical dissimilarities (Gold et al.,2013). The HPA axis appears hyperactive in melancholic depres-sion, while this stress system is relatively hypoactive in atypicaldepression (Gold and Chrousos, 2013). Exogenous leptin down-regulates CRH expression in PVN neurons (Huang et al., 1998).Interestingly, Gecici and colleagues found leptin serum levels spe-cifically elevated in atypical MDD (Gecici et al., 2005). Therefore,one could argue that leptin may play a pathophysiological role in
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
the down-regulation of the HPA axis in atypical depression. Futurestudies of diagnostic biomarkers in MDD should consider sepa-rating these canonical depression subtypes (i.e., melancholic vs.atypical).
The difference between adiponectin levels between MDD in-dividuals and controls was influenced by differences in genderdistribution between MDD participants and controls as well as bydepression severity. A well known gender dimorphism in adipo-nectin serum levels have been reported, with women presentingsignificantly higher levels (Weber-Hamann et al., 2007). The dif-ference in adiponectin between MDD individuals and controls waspositively associated with depression severity. There are at leasttwo plausible explanations for this finding. First, adiponectinshould be directly involved in the pathophysiology of depression,and therefore differences in serum levels would become apparentat more severe depression (Liu et al., 2012). Another possibility isthatMDD participants withmore severe depressionmay havemoreco-morbid metabolic abnormalities, which indirectly could explainhigher differences in adiponectin levels betweenMDD subjects andhealthy volunteers (Kahl et al., 2012). Subgroup analyses revealedthat adiponectin serum levels were significantly lower in MDDindividuals compared to healthy controls when measured throughRIA (although overall effect sizes were relatively small), but notthrough ELISA. Therefore, assay properties like sensitivity and inter-and intra-assay coefficients of variability should be considered. Inall studies the RIA kit was provided by LINCO Res., Mo., USA(sensitivity: 1 ng/ml intra- and inter CV 3.1 and 6.4%, respectively).However, ELISA kits varied across studies. Consistently, there was ahigher heterogeneity across studies. Test properties could not bereliably obtained for all studies.
Body mass index and differences in body mass index betweenMDD participants and controls to a large extent explained theheterogeneity in results across leptin diagnostic studies. A recentpopulation-based study demonstrated that the interaction be-tween leptin and abdominal obesity was associated with a high risk
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002

Fig. 3. (A) Meta-regression on depression severity (mild/moderate vs. severe) vs. difference in adiponectin levels between patients and healthy controls (effect size, Hedge's g); (B)Meta-regression on overall sample BMI vs. difference in leptin levels between MDD patients and healthy controls (effect size, Hedge's g); (C) Meta-regression on BMI differencesbetween MDD patients and controls vs. difference in leptin serum levels between MDD patients and controls.
A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e10 7
for depression (Milaneschi et al., 2014). Therefore, low leptinsignaling rather than low leptin levels per se could be related toMDD pathophysiology. Leptin levels were significantly elevated inpatients with mild/moderate depression when compared tohealthy controls. This finding might be explained by a loweroccurrence of visceral obesity and metabolic abnormalities in lessseverely depressive patients (Kahl et al., 2012). Therefore, leptinmay act as a compensatory mechanism. Once a more severe dis-order is established with accompanying metabolic abnormalities,central resistance to leptin may ensue (Yamada et al., 2011). Indeed,in the metabolic syndrome, sensitivity to leptin rather than
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
absolute leptin levels appear to be the predominant driver; thesame may be true in depression and requires confirmation (Ungerand Scherer, 2010). However, it should be emphasized that thesummary effect size of the difference between peripheral levels ofleptin of patients withmild-to-moderateMDD and healthy controlswas relatively small (i.e., Hedge's g ¼ 0.317).
Our exploratory meta-analysis revealed that resistin levelsare lower in MDD participants compared to healthy controls. Thisresult should be regarded as exploratory. Furthermore, the overalleffect size of this difference was small. Resistin wassignificantly correlated with free cortisol levels in one study
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002
Fig. 4. (A) Forest Plot of the diferences in serum Adiponectin levels of MDD vs. healthy control individuals using Hedge's g in Random Effects Model grouped by Type of Assay. TheForest Plot depicts the estimated difference in serum levels of depressed vs control individuals (squares) and its 95% confidence intervals (horizontal black lines). (B) Forest Plot ofthe diferences in serum Leptin levels of MDD vs. Control individuals using Hedge's g in Random Effects Model grouped by Depression Severity. The Forest Plot depicts the estimateddifference in serum levels of depressed vs control individuals (squares) and its 95% confidence intervals (horizontal black lines).
A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e108
(Weber-Hamann et al., 2007). Therefore, relatively low resistinlevels may play a compensatory role (i.e., to override HPA activa-tion). However, more studies are necessary to clarify the patho-physiological role of resistin in MDD and to estimate its validity as aputative diagnostic depression biomarker.
4.2. Systematic review of intervention studies
Few intervention studies met inclusion criteria for this sys-tematic review. Therefore, we could not control for heterogeneity(for example, in the leptin intervention meta-analysis). Includedtrials used different antidepressants (Moosa et al., 2003; Schillinget al., 2013). Antidepressants differ in the likelihood of inducingweight gain and metabolic abnormalities (Serretti and Mandelli,2010). For example, Shilling and colleagues had demonstratedthat leptin serum levels increased during mirtazapine andamitriptyline treatment, but not following treatment with eitherparoxetine or venlafaxine (Schilling et al., 2013). Furthermore, formirtazapine-treated patients the increase in leptin levels washigher for remitters compared to non-remitters (Schilling et al.,2013). This finding suggests that leptin may be also a marker formetabolic abnormalities associated with antidepressant treatment.However, the utility of adipokines for response prediction in MDDremains inconclusive. A leptin exploratory meta-analysis indicated
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
that leptin blood levels did not change after antidepressant treat-ment. Due to the few studies available and the high heterogeneityof findings, additional well-designed studies are required beforedefinitive conclusions can be drawn.
4.3. Limitations
While this study could identify moderators and confoundersacross leptin and adiponectin diagnostic studies it is possible thatother unmeasured factors could also explain the observed hetero-geneity. For example, Wong and colleagues demonstrated a 25-foldvariation in plasma leptin levels across the day with significantnocturnal increases (Wong et al., 2004). Therefore, the precise timeof blood sampling might have influenced the data. Furthermore,the BMI might not be an accurate proxy for metabolic abnormal-ities. A recent cohort study suggests that metabolically healthyobesity is not associated with a higher risk of depression (Hameret al., 2012). The presence of co-morbid metabolic disturbancescould not be controlled for. Prior exposure of included MDD pa-tients to antidepressant treatments (and different antidepressantdrugsmay have distinct effects upon blood levels of adipokines) arenot reported in included studies, and could not be controlled for.Finally, there were relatively very few including Asian samples,while several of the included studies did not provide reliable
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002

A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e10 9
information on sample distribution across ethnic groups. Therefore,we could not compare adipokine levels between Asian andCaucasian samples. This is of particular interest giving the fact thesome pharmacogenetic findings in MDD differ across these pop-ulations (Niitsu et al., 2013; Porcelli et al., 2012).
5. Conclusions and future research directions
In conclusion, these meta-analyses provide evidence that theinitial enthusiasm regarding the possible utility of adiponectin andleptin as diagnostic depression biomarkers is not justified. Ourfindings underscore the need for a more uniform methodology infuture studies (i.e., a better control of confounders like BMI,depression severity and type of assay) to estimate the potentialvalidity of these adipokines as emerging depression biomarkers.Few studies were performed on the potential utility of adipokinesas treatment predictor biomarkers. Future studies should considerthe dissimilar propensity of different antidepressants to induceweight change and metabolic abnormalities. In keeping with thisview, adipokines may be included in multi-assay panels of MDDbiomarkers in the near future (Breitenstein et al., 2014; Papakostaset al., 2013).
Role of funding source
None.
Contributions
AFC, DQCR, LMM, PMGC, CAK and RSM designed the study. AFC,CAK and PMGC analyzed the data. AFC, RMV, CAK, RSM and MBwrote the paper. All authors contributed to and had approved thefinal version.
Conflicts of interest
The authors declare no competing financial interests relevant tothe present work.
Acknowledgments
AFC was supported by a research scholarship from ConselhoNacional de Desenvolvimento Científico e Tecnol�ogico (Brazil; Level2). MB is supported by a NHMRC Senior Principal ResearchFellowship 1059660.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.jpsychires.2014.08.002.
References
Aliyazicioglu R, Deger O, Kural BV, Hocaoglu C, Colak M, Yucesan FB. The rela-tionship between the peroxisome proliferator-activated receptor gamma 2 genepolymorphism, lipids and adipokines in patients with major depression. TurkKlin Tip Bilim Derg 2011a;31:1065e72.
Aliyazicioglu R, Deger O, Vanizor Kural B, Hocaoglu C, Colak M, Balaban Yucesan F.The relationship between the peroxisome proliferator-activated receptorgamma 2 gene polymorphism, lipids and adipokines in patients with majordepression. Turkiye Klinikleri J Med Sci 2011b;31:1065e72.
Arita Y, Kihara S, Ouchi N, Takahashi M, Maeda K, Miyagawa J, et al. Paradoxicaldecrease of an adipose specific protein, adiponectin in obesity, 1999. BiochemBiophys Res Commun 2012;425:560e4.
Arnoldussen IA, Kiliaan AJ, Gustafson DR. Obesity and dementia: adipokinesinteract with the brain. Eur Neuropsychopharmacol: J Eur Coll Neuro-psychopharmacol 2014. http://dx.doi.org/10.1016/j.euroneuro.2014.03.002[Epub Ahead of Print].
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
Berman SM, Paz-Filho G, Wong ML, Kohno M, Licinio J, London ED. Effects of leptindeficiency and replacement on cerebellar response to food-related cues. Cere-bellum (London, England) 2013;12:59e67.
Breitenstein B, Scheuer S, Holsboer F. Are there meaningful biomarkers of treatmentresponse for depression? Drug Discov Today 2014.
Chen Y-C, Lin W-W, Chen Y-J, Mao W-C, Hung Y-J. Antidepressant effects on insulinsensitivity and proinflammatory cytokines in the depressed males. MediatInflamm 2010.
Cizza G, Nguyen VT, Eskandari F, Duan Z, Wright EC, Reynolds JC, et al. Low 24-houradiponectin and high nocturnal leptin concentrations in a case-control study ofcommunity-dwelling premenopausal women with major depressive disorder:the Premenopausal, Osteopenia/Osteoporosis, Women, Alendronate, Depres-sion (POWER) study. J Clin Psychiatry 2010;71:1079e87.
Cohen SS, Gammon MD, Signorello LB, North KE, Lange EM, Fowke JH, et al. Serumadiponectin in relation to body mass index and other correlates in black andwhite women. Ann Epidemiology 2011;21:86e94.
Craven MA, Bland R. Depression in primary care: current and future challenges. CanJ Psychiatry 2013;58:442e8.
Degawa-Yamauchi M, Bovenkerk JE, Juliar BE, Watson W, Kerr K, Jones R, et al.Serum resistin (FIZZ3) protein is increased in obese humans. J Clin EndocrinolMetab 2003;88:5452e5.
Diniz BS, Teixeira AL, Campos AC, Miranda AS, Rocha NP, Talib LL, et al. Reducedserum levels of adiponectin in elderly patients with major depression.J Psychiatr Res 2012;46:1081e5.
Doumatey AP, Bentley AR, Zhou J, Huang H, Adeyemo A, Rotimi CN. Paradoxicalhyperadiponectinemia is associated with the Metabolically Healthy Obese(MHO) Phenotype in African Americans. J Endocrinol Metab 2012;2:51e65.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by asimple, graphical test. BMJ 1997;315:629e34.
Esel E, Ozsoy S, Tutus A, Sofuoglu S, Kartalci S, Bayram F, et al. Effects of antide-pressant treatment and of gender on serum leptin levels in patients with majordepression. Prog Neuro-Psychopharmacol Biol Psychiatry 2005;29:565e70.
Frist MB, Spitzer RL, Gibbon M, Williams J. Structured clinical interview for DSM-IVAxis I disorders e Patient Edition (SCID-I/P, version 2.0). New York: BiometricsResearch Department, New York Pychiatric Institute; 1996.
Gecici O, Kuloglu M, Atmaca M, Tezcan AE, Tunckol H, Emul HM, et al. High serumleptin levels in depressive disorders with atypical features. Psychiatry ClinNeurosci 2005;59:736e8.
Gold PW, Chrousos GP. Melancholic and atypical subtypes of depression representdistinct pathophysiological entities: CRH, neural circuits, and the diathesis foranxiety and depression. Mol Psychiatry 2013;18:632e4.
Gold PW, Licinio J, Pavlatou MG. Pathological parainflammation and endoplasmicreticulum stress in depression: potential translational targets through the CNSinsulin, klotho and PPAR-gamma systems. Mol Psychiatry 2013;18:154e65.
Hamer M, Batty GD, Kivimaki M. Risk of future depression in people who are obesebut metabolically healthy: the English longitudinal study of ageing. Mol Psy-chiatry 2012;17:940e5.
Huang Q, Rivest R, Richard D. Effects of leptin on corticotropin-releasing factor(CRF) synthesis and CRF neuron activation in the paraventricular hypothalamicnucleus of obese (ob/ob) mice. Endocrinology 1998;139:1524e32.
Insel TR. The NIMH Research Domain Criteria (RDoC) Project: precision medicinefor psychiatry. Am J Psychiatry 2014;171:395e7.
Ishibashi K, Berman SM, Paz-Filho G, Lee B, Robertson C, Mandelkern MA, et al.Dopamine D2/D3 receptor availability in genetically leptin-deficient patientsafter long-term leptin replacement. Mol Psychiatry 2012;17:352e3.
Jow GM, Yang TT, Chen CL. Leptin and cholesterol levels are low in major depressivedisorder, but high in schizophrenia. J Affect Disord 2006;90:21e7.
Kahl KG, Greggersen W, Schweiger U, Cordes J, Balijepalli C, Losch C, et al. Preva-lence of the metabolic syndrome in unipolar major depression. Eur Arch Psy-chiatry Clin Neurosci 2012;262:313e20.
Kessler RC, Merikangas KR, Wang PS. Prevalence, comorbidity, and service utiliza-tion for mood disorders in the United States at the beginning of the twenty-firstcentury. Annu Rev Clin Psychol 2007;3:137e58.
Kotan Z, Sarandol E, Kirhan E, Ozkaya G, Kirli S. Serum brain-derived neurotrophicfactor, vascular endothelial growth factor and leptin levels in patients with adiagnosis of severe major depressive disorder with melancholic features. TherAdv Psychopharmacol 2012;2:65e74.
Kraus T, Haack M, Schuld A, Hinze-Selch D, Koethe D, Pollmacher T. Body weight,the tumor necrosis factor system, and leptin production during treatment withmirtazapine or venlafaxine. Pharmacopsychiatry 2002;35:220e5.
Kraus T, Haack M, Schuld A, Hinze-Selch D, Pollmacher T. Low leptin levels butnormal body mass indices in patients with depression or schizophrenia.Neuroendocrinology 2001;73:243e7.
Kwon H, Pessin JE. Adipokines mediate inflammation and insulin resistance. FrontEndocrinol 2013;4:71.
Lake CR, Baumer J. Academic psychiatry's responsibility for increasing the recog-nition of mood disorders and risk for suicide in primary care. Curr Opin Psy-chiatry 2010;23:157e66.
Licinio J, Caglayan S, Ozata M, Yildiz BO, de Miranda PB, O'Kirwan F, et al. Pheno-typic effects of leptin replacement on morbid obesity, diabetes mellitus,hypogonadism, and behavior in leptin-deficient adults. Proc Natl Acad Sci U S A2004;101:4531e6.
Liu J, Garza JC, Bronner J, Kim CS, Zhang W, Lu X-Y. Acute administration of leptinproduces anxiolytic-like effects: a comparison with fluoxetine. Psychophar-macology 2010;207:535e45.
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002

A.F. Carvalho et al. / Journal of Psychiatric Research xxx (2014) 1e1010
Liu J, Guo M, Zhang D, Cheng SY, Liu M, Ding J, et al. Adiponectin is critical indetermining susceptibility to depressive behaviors and has antidepressant-likeactivity. Proc Natl Acad Sci U S A 2012;109:12248e53.
London ED, Berman SM, Chakrapani S, Delibasi T, Monterosso J, Erol HK, et al. Short-term plasticity of gray matter associated with leptin deficiency and replace-ment. J Clin Endocrinol Metab 2011;96:E1212e20.
Lu XY, Kim CS, Fraser A, ZhangW. Leptin: a potential novel antidepressant. Proc NatlAcad Sci U S A 2006;103:1593e8.
Maeda K, Okubo K, Shimomura I, Funahashi T, Matsuzawa Y, Matsubara K. cDNAcloning and expression of a novel adipose specific collagen-like factor, apM1(AdiPose most abundant Gene Transcript 1). Biochem Biophys Res Commun1996;221:286e9.
Milaneschi Y, Simonsick EM, Vogelzangs N, Strotmeyer ES, Yaffe K, Harris TB, et al.Leptin, abdominal obesity, and onset of depression in older men and women.J Clin Psychiatry 2012;73:1205e11.
Milaneschi Y, Sutin AR, Terracciano A, Canepa M, Gravenstein KS, Egan JM, et al. Theassociation between leptin and depressive symptoms is modulated byabdominal adiposity. Psychoneuroendocrinology 2014;42:1e10.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematicreviews andmeta-analyses: the PRISMA statement. PLoSMed 2009;6:e1000097.
Moosa MYH, Panz VR, Jeenah FY, Joffe BI. African womenwith depression: the effectof imipramine and fluoxetine on body mass index and leptin secretion. J ClinPsychopharmacol 2003;23:549e52.
Moylan S, Maes M, Wray NR, Berk M. The neuroprogressive nature of majordepressive disorder: pathways to disease evolution and resistance, and thera-peutic implications. Mol Psychiatry 2013;18:595e606.
Nakamura K, Fuster JJ, Walsh K. Adipokines: a link between obesity and cardio-vascular disease. J Cardiol 2013.
Niitsu T, Fabbri C, Bentini F, Serretti A. Pharmacogenetics in major depression: acomprehensive meta-analysis. Prog Neuro-Psychopharmacol Biol Psychiatry2013;45:183e94.
Owecki M, Miczke A, Nikisch E, Pupek-Musialik D, Sowinski J. Serum resistin con-centrations are higher in human obesity but independent from insulin resis-tance. Experimental and clinical endocrinology & diabetes: official journal. GerSoc Endocrinol Ger Diabetes Assoc 2011;119:117e21.
PapakostasGI, SheltonRC, KinrysG,HenryME, BakowBR, Lipkin SH, et al. Assessmentof a multi-assay, serum-based biological diagnostic test for major depressivedisorder: a pilot and replication study. Mol Psychiatry 2013;18:332e9.
Pariante CM, Lightman SL. The HPA axis in major depression: classical theories andnew developments. Trends Neurosci 2008;31:464e8.
Pasco JA, Jacka FN, Williams LJ, Henry MJ, Nicholson GC, Kotowicz MA, et al. Leptinin depressed women: cross-sectional and longitudinal data from an epidemi-ologic study. J Affect Disord 2008;107:221e5.
Paz-Filho G, Esposito K, Hurwitz B, Sharma A, Dong C, Andreev V, et al. Changes ininsulin sensitivity during leptin replacement therapy in leptin-deficient pa-tients. Am J Physiol Endocrinol Metab 2008;295:E1401e8.
Paz-Filho G, Wong ML, Licinio J. The procognitive effects of leptin in the brain andtheir clinical implications. Int J Clin Pract 2010;64:1808e12.
Pinar M, Gulsun M, Tasci I, Erdil A, Bolu E, Acikel C, et al. Maprotiline inducedweight gain in depressive disorder: changes in circulating ghrelin and adipo-nectin levels and insulin sensitivity. Prog Neuro-Psychopharmacol Biol Psy-chiatry 2008;32:135e9.
Pizzagalli DA. Frontocingulate dysfunction in depression: toward biomarkers oftreatment response. Neuropsychopharmacol: Official Publ Am Coll Neuro-psychopharmacol 2011;36:183e206.
Porcelli S, Fabbri C, Serretti A. Meta-analysis of serotonin transporter gene promoterpolymorphism (5-HTTLPR) association with antidepressant efficacy. Eur Neu-ropsychopharmacol: J Eur Coll Neuropsychopharmacol 2012;22:239e58.
Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of mental healthdiagnostic interview schedule. Its history, characteristics, and validity. Arch GenPsychiatry 1981;38:381e9.
Please cite this article in press as: Carvalho AF, et al., Adipokines as emerJournal of Psychiatric Research (2014), http://dx.doi.org/10.1016/j.jpsychi
Rubin RT, Rhodes ME, Czambel RK. Sexual diergism of baseline plasma leptin andleptin suppression by arginine vasopressin in major depressives and matchedcontrols. Psychiatry Res 2002;113:255e68.
Schilling C, Gilles M, Blum WF, Daseking E, Colla M, Weber-Hamann B, et al. Leptinplasma concentrations increase during antidepressant treatment withamitriptyline and mirtazapine, but not paroxetine and venlafaxine: leptinresistance mediated by antihistaminergic activity? J Clin Psychopharmacol2013;33:99e103.
Schwartz DR, Lazar MA. Human resistin: found in translation from mouse to man.Trends Endocrinol Metab: TEM 2011;22:259e65.
Serretti A, Mandelli L. Antidepressants and body weight: a comprehensive reviewand meta-analysis. J Clin Psychiatry 2010;71:1259e72.
Steppan CM, Bailey ST, Bhat S, Brown EJ, Banerjee RR, Wright CM, et al. The hor-mone resistin links obesity to diabetes. Nature 2001;409:307e12.
Stuart MJ, Baune BT. Chemokines and chemokine receptors in mood disorders,schizophrenia, and cognitive impairment: a systematic review of biomarkerstudies. Neurosci Biobehav Rev 2014;42C:93e115.
Troughton R, Michael Felker G, Januzzi Jr JL. Natriuretic peptide-guided heart failuremanagement. Eur Heart J 2014;35:16e24.
Tzoulaki I, Siontis KC, Evangelou E, Ioannidis JP. Bias in associations of emergingbiomarkers with cardiovascular disease. JAMA Intern Med 2013;173:664e71.
Unger RH, Scherer PE. Gluttony, sloth and the metabolic syndrome: a roadmap tolipotoxicity. Trends Endocrinol Metab: TEM 2010;21:345e52.
Wan Z, Mah D, Simtchouk S, Klegeris A, Little JP. Globular adiponectin induces apro-inflammatory response in human astrocytic cells. Biochem Biophys ResCommun 2014;446:37e42.
Way JM, Gorgun CZ, Tong Q, Uysal KT, Brown KK, Harrington WW, et al. Adiposetissue resistin expression is severely suppressed in obesity and stimulated byperoxisome proliferator-activated receptor gamma agonists. J Biol Chem2001;276:25651e3.
Weber-Hamann B, Kratzsch J, Kopf D, Lederbogen F, Gilles M, Heuser I, et al. Resistinand adiponectin in major depression: the association with free cortisol andeffects of antidepressant treatment. J Psychiatr Res 2007;41:344e50.
Wittchen HU. Reliability and validity studies of the WHOeComposite InternationalDiagnostic Interview (CIDI): a critical review. J Psychiatr Res 1994;28:57e84.
Wong ML, Licinio J, Yildiz BO, Mantzoros CS, Prolo P, Kling M, et al. Simultaneousand continuous 24-hour plasma and cerebrospinal fluid leptin measurements:dissociation of concentrations in central and peripheral compartments. J ClinEndocrinol Metab 2004;89:258e65.
Yamada N, Katsuura G, Ochi Y, Ebihara K, Kusakabe T, Hosoda K, et al. Impaired CNSleptin action is implicated in depression associated with obesity. Endocrinology2011;152:2634e43.
Yamada N, Katsuura G, Ochi Y, Ebihara K, Kusakabe T, Satoh N, et al. Depression inobesity: implication for pathophysiological role of endogenous leptin. Obes Rev2010;11:91.
Yan ZY, Gu MJ, Zhong BL, Wang C, Tang HL, Ling YQ, et al. Prevalence, risk factorsand recognition rates of depressive disorders among inpatients of tertiarygeneral hospitals in Shanghai, China. J Psychosom Res 2013;75:65e71.
Yildiz BO, Suchard MA, Wong ML, McCann SM, Licinio J. Alterations in the dynamicsof circulating ghrelin, adiponectin, and leptin in human obesity. Proc Natl AcadSci U S A 2004;101:10434e9.
Zeman M, Jirak R, Jachymova M, Vecka M, Tvrzicka E, Zak A. Leptin, adiponectin,leptin to adiponectin ratio and insulin resistance in depressive women. Neu-roendocrinol Lett 2009;30:387e95.
Zeman M, Jirak R, Vecka M, Zak A, Macasek J, Tvrzicka E, et al. Leptin, adiponectinand leptin to adiponectin ratio in depressive women. Atheroscler Suppl2010;11:159.
Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloningof the mouse obese gene and its human homologue. Nature 1994;372:425e32.
Zupancic ML, Mahajan A. Leptin as a neuroactive agent. Psychosom Med 2011;73:407e14.
ging depression biomarkers: A systematic review and meta-analysis,res.2014.08.002




















