Addressing Alcohol and Drug Addiction Among People With Mental Retardation in Nonaddiction Settings:...
22
71 Journal of Social Work Practice in the Addictions, 9:71–90, 2009 Copyright © Taylor & Francis Group, LLC ISSN: 1533-256X print/1533-2578 online DOI: 10.1080/15332560802646547 WSWP 1533-256X 1533-2578 Journal of Social Work Practice in the Addictions, Vol. 9, No. 1, January 2009: pp. 1–35 Journal of Social Work Practice in the Addictions Addressing Alcohol and Drug Addiction Among People With Mental Retardation in Nonaddiction Settings: A Need for Cross-System Collaboration Cross-System Collaboration E. Slayter and S. A. Steenrod ELSPETH SLAYTER, PHD, MSW, and SHELLEY A. STEENROD, PHD, LICSW Assistant Professors, School of Social Work, Salem State College, Salem, Massachusetts, USA People with mental retardation (MR) and addiction are an espe- cially vulnerable population, yet evidence-based approaches to substance abuse (SA) treatment for this group are limited. Research suggests that SA-related services for this population are most likely received in nonaddiction settings that are generally focused on provision of mental health services to populations with MR and that might be unequipped for this work. This fact, com- bined with documented challenges to cross-system collaboration, suggests the potential for discontinuities in care for people with MR and SA. Recommendations for SA screening and a framework for cross-system collaboration are presented with specific recommen- dations for the ways in which social workers in both MR and SA service settings can promote positive client outcomes. KEYWORDS cross-system collaboration, mental retardation, nonaddiction service settings, substance abuse treatment, treat- ment access Since the era of deinstitutionalization, increased exposure to community life for people with mild to moderate mental retardation (MR) has, for some, included access to alcohol and illicit drugs and thus the potential for developing alcohol addiction, drug addiction, or both (Burgard, 2000; Christian & Poling, Received May 24, 2007; accepted February 8, 2008. Address correspondence to Elspeth Slayter, School of Social Work, Salem State College, Alumni Hall, Room 1B, 352 Lafayette Street, Salem, MA 01970, USA. E-mail: [email protected]
-
Upload
salemstate -
Category
Documents
-
view
2 -
download
0
Transcript of Addressing Alcohol and Drug Addiction Among People With Mental Retardation in Nonaddiction Settings:...
71
Journal of Social Work Practice in the Addictions, 9:71–90, 2009Copyright © Taylor & Francis Group, LLC ISSN: 1533-256X print/1533-2578 onlineDOI: 10.1080/15332560802646547
WSWP1533-256X1533-2578Journal of Social Work Practice in the Addictions, Vol. 9, No. 1, January 2009: pp. 1–35Journal of Social Work Practice in the Addictions
Addressing Alcohol and Drug Addiction Among People With Mental Retardation
in Nonaddiction Settings: A Need for Cross-System Collaboration
Cross-System Collaboration E. Slayter and S. A. Steenrod
ELSPETH SLAYTER, PHD, MSW, and SHELLEY A. STEENROD, PHD, LICSW
Assistant Professors, School of Social Work, Salem State College, Salem, Massachusetts, USA
People with mental retardation (MR) and addiction are an espe-cially vulnerable population, yet evidence-based approaches tosubstance abuse (SA) treatment for this group are limited.Research suggests that SA-related services for this population aremost likely received in nonaddiction settings that are generallyfocused on provision of mental health services to populations withMR and that might be unequipped for this work. This fact, com-bined with documented challenges to cross-system collaboration,suggests the potential for discontinuities in care for people with MRand SA. Recommendations for SA screening and a framework forcross-system collaboration are presented with specific recommen-dations for the ways in which social workers in both MR and SAservice settings can promote positive client outcomes.
KEYWORDS cross-system collaboration, mental retardation,nonaddiction service settings, substance abuse treatment, treat-ment access
Since the era of deinstitutionalization, increased exposure to community lifefor people with mild to moderate mental retardation (MR) has, for some,included access to alcohol and illicit drugs and thus the potential for developingalcohol addiction, drug addiction, or both (Burgard, 2000; Christian & Poling,
Received May 24, 2007; accepted February 8, 2008.Address correspondence to Elspeth Slayter, School of Social Work, Salem State
College, Alumni Hall, Room 1B, 352 Lafayette Street, Salem, MA 01970, USA.E-mail: [email protected]

72 E. Slayter and S. A. Steenrod
1997; Clarke & Wilson, 1999; Edgerton, 1967, 1986). Although population-based substance abuse (SA) prevalence estimates are unavailable, it is esti-mated that approximately 2% of the community-based population with MRuse SA treatment services (Larson, Lakin, Anderson, & Kwak, 1999).Addiction has been identified as a concern that may impede communityinclusion in employment (Cocco & Harper, 2002; Horwitz, Kerker, Owens,& Zigler, 2000; U.S. Surgeon General, 2002). Guidelines about how com-munity-based clients with MR should be assisted when making choicesabout alcohol and drug use are especially challenging in light of the needto simultaneously foster self-determination and engage in risk manage-ment (Simpson, 1998; Slayter, 2007). Population-specific barriers to SAtreatment complicate this reality (Lottman, 1993; National Association onAlcohol, Drugs, and Disability [NAADD], 1999; Slayter, 2006; Tyas & Rush,1993). A better understanding of how to best serve populations with MRand co-occurring SA is especially important to the field of social work as“clinical management . . . may be particularly problematic, and these(individuals) have the potential to consume large amounts of health careresources,” among other concerns (Strain, Buccino, Brooner, Schmidt, &Bigelow, 1993, p. 585).
The scant literature on this topic examines SA among people with MRin three distinct groups: people with MR in general; people with MR andmental illness (MI); and people with a “triple diagnosis,” of MR, MI, and SA.Substantial research and evaluation have resulted in the development ofspecialized mental health services for people with cooccurring MR andMI (Reiss & Aman, 1997). Little is known, however, about how to bestaddress alcohol or drug addiction among people with MR with or withoutcooccurring MI (Campbell, Essex, & Held, 1994; McGillivray & Moore, 2001;Westermeyer, Kemp, & Nugent, 1996; Westermeyer, Phaobtong, & Neider,1988). Given the dearth of MR-specific SA treatment knowledge and special-ized programming across the United States, and the high rate of psychopa-thology present in this population, addiction is most likely to be identifiedin outpatient mental health counseling settings. Indeed, the literature sug-gests that SA appears to be a greater concern for people with MR than MI(Fotheringham, Abdo, Ouelette-Kuntz, & Wolfgarth, 1993; Slayter, 2006;Strain et al., 1993). Compared to SA programs, outpatient mental healthcounseling settings might not be fully equipped to either screen, assess, ortreat SA problems. Further, different treatment goals, interventionapproaches, and overall case management philosophies in the MR andaddiction treatment service sectors can cause confusion at administrative,case management, and clinical levels (Degenhardt, 2000; Miranda, 1999;Rivinus, 1988; Slayter, 2007).
To best support those with MR and SA, social workers in nonaddictionsettings must have the ability to conduct population-specific screenings andengage in “bridging” conversations with their colleagues in addiction

Cross-System Collaboration 73
settings to bring about effective intervention. This article provides socialworkers in nonaddiction settings with the tools to engage in both processes.To set a foundation for these activities, we first define MR and comment onthe potential risks and consequences of SA in this population. We thensummarize existing knowledge about the prevalence of SA among differentpopulations of people with MR to show that SA treatment for this popula-tion is likely to be received in nonaddiction settings. After a brief review ofthe known barriers to SA treatment experienced by people with MR, we dis-cuss current knowledge about SA screening, assessment, and intervention inthis population. Finally, we conclude with a basic framework for socialworkers in nonaddiction settings to improve cross-system collaborationwhen working with a client with MR and SA.
DEFINING MENTAL RETARDATION
MR is a “disability characterized by significant limitations both in intellectualfunctioning and in adaptive behavior as expressed in conceptual, social,and practical adaptive skills” that manifests before the age of 21 (AmericanAssociation on Mental Retardation, 2008, p. 1). Although many use the termdevelopmental disability (DD) when referring to the MR diagnosis, it isimportant to recognize that these are diagnostically distinct diagnoses,although most people with MR meet the diagnostic criteria for DD (Larson,2001). DD conditions manifest before a person attains age 22 and result insubstantial functional limitations in three or more areas of major life activity(Developmental Disabilities Act of 1984). A diagnosis of MR is also diagnosti-cally distinct from MI, which is defined as “severe disturbances of behavior,mood, thought process and/or social and interpersonal relationships” (TheArc, 2001a, p. 1). Less than 1% (0.78%) of the noninstitutionalized U.S. pop-ulation is estimated to have MR based on self-report and proxy data fromthe National Health Interview Survey’s Disability Panel (NHIS–D) whichsuggests that in 1994, more than 4 million noninstitutionalized people withMR lived in the United States (Larson, 2001). A majority of this populationlives in community-based, noninstitutional settings and might be most atrisk for SA conditions (Sturmey, Reyer, Lee, & Robeck, 2003).
RISKS AND CONSEQUENCES OF SUBSTANCE ABUSE
People with MR experience all of the risks and consequences of addictionthat are experienced by the general population—family strife, employmenttroubles, and problems with the law—but risks and consequences can beheightened for this population. For example, the potential for a person withmild to moderate MR to develop an SA problem might be related to “feelings

74 E. Slayter and S. A. Steenrod
of being different from their peers” (Linna et al., 1999, p. 81) or awareness oftheir capabilities as compared to others (Miranda, 1999). Because “impairmentin social functioning is a central feature of the substance-use condition,” peoplewith MR might be at risk due to functional impairment in activities of daily liv-ing, including self-care (Alverson, Alverson, & Drake, 2001, p. 3) A reduction inthe ability to care for oneself may have ramifications for community involve-ment in the areas of employment or social activities. Given these concerns, SAmight be an important factor in limiting inclusion of people with MR—a centralgoal of disability policy in the United States.
Because a significant percentage of people with MR take prescribed psy-chotropic medications, further risk in functional impairment can result from thenegative consequences of mixing alcohol or illicit drugs with prescribed medi-cations (Borthwick-Duffy & Eyman, 1990). It is estimated that between 15% and50% of all people with MR use prescribed psychotropic medications (Reiss &Aman, 1997; Santosh, 1999). The potential for life-threatening reactions result-ing from concurrent use of prescribed psychotropic medications (especiallyanticonvulsants) and SA is a major concern (The Arc, 2001a; Rivas, 2001). In amedical commentary on this issue, it is noted:
Neurological disorders sometimes associated with MR pose special prob-lems relative to alcohol use. Motor deficits of cerebral palsy are mark-edly worsened by various substances of abuse, including alcohol. Thesynergistic effect of alcohol with anticonvulsants for patients withseizure disorders can present additional problems: severe mental confu-sion, sedation, toxic levels, dementia, coma and death. We have seenoverdosage of anticonvulsant medication associated with use of unpre-scribed drugs in epileptic persons and alcohol withdrawal can cause orexacerbate seizures. (Rivinus, 1988, p. 19)
With respect to the behavioral correlates of SA, given the well-documentednexus between alcohol or other drug use and criminal behavior, peoplewith MR and SA conditions might also be at greater risk of being influencedby negative role models, possibly leading to criminal justice involvement(McGillivray & Moore, 2001; Simpson, 1998). Some small-scale, localizedstudies have noted that people with MR who engage in SA might exhibitbehavioral disturbances such as aggression, fire-setting, window-breaking,tantrums, and self-destructive acts (Rivinus, 1988; Westermeyer et al., 1988).These acts can increase the risk of arrest or incarceration. Given that a lackof population-specific services exist both in and out of correctional settings,prevention and treatment of SA in community settings is especially important.People with MR have been found to be at increased risk of victimization(e.g., sexual assault, financial victimization, larceny) and it is posited thatSA contributes to this (Pack, Wallander, & Browne, 1998; Petersilia, 2000;Walkup, Sambamoorthi, & Crystal, 1999).
Cross-System Collaboration 75
PREVALENCE OF SUBSTANCE ABUSE AMONG PEOPLE WITH MENTAL RETARDATION
Little is known about the prevalence, course, and scope of SA in popula-tions with MR (McGillicuddy, 2006). Nonetheless, two U.S.-based studiesprovide SA treatment utilization rates for large-scale groups. First, in anationally representative study of the noninstitutionalized population withMR, past-year SA treatment utilization was reported by 2.2% of people sur-veyed (Larson et al., 1999). Second, in an examination of Medicaid billingrecords for a national sample of people with MR diagnoses, 2.6% of bothinstitutionalized and noninstitutionalized individuals had received atleast one past-year addiction-related service (Slayter, 2006). Beyond thesepopulation-based estimates of SA treatment utilization among people withMR, two different sets of studies identify people with MR and SA in bothcommunity-based and mental health-oriented counseling settings.
Community Settings
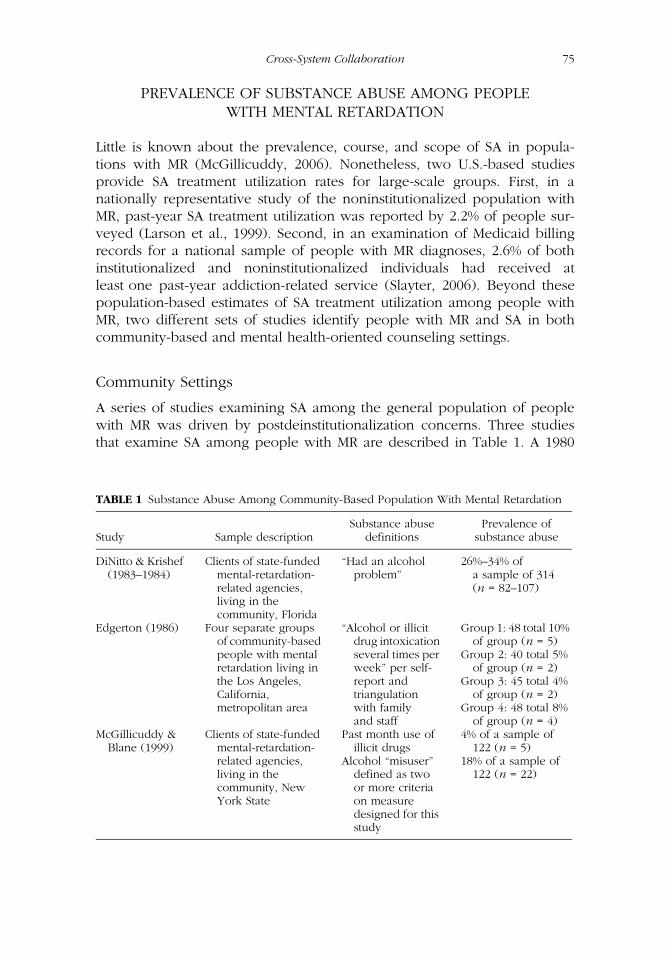
A series of studies examining SA among the general population of peoplewith MR was driven by postdeinstitutionalization concerns. Three studiesthat examine SA among people with MR are described in Table 1. A 1980
TABLE 1 Substance Abuse Among Community-Based Population With Mental Retardation
Study Sample descriptionSubstance abuse
definitionsPrevalence of
substance abuse
DiNitto & Krishef (1983–1984)
Clients of state-funded mental-retardation-related agencies, living in the community, Florida
“Had an alcohol problem”
26%–34% of a sample of 314 (n = 82–107)
Edgerton (1986) Four separate groups of community-based people with mental retardation living in the Los Angeles, California, metropolitan area
“Alcohol or illicit drug intoxication several times per week” per self-report and triangulation with family and staff
Group 1: 48 total 10% of group (n = 5)
Group 2: 40 total 5% of group (n = 2)
Group 3: 45 total 4% of group (n = 2)
Group 4: 48 total 8% of group (n = 4)
McGillicuddy & Blane (1999)
Clients of state-funded mental-retardation-related agencies, living in the community, New York State
Past month use of illicit drugs
4% of a sample of 122 (n = 5)
Alcohol “misuser” defined as two or more criteria on measure designed for this study
18% of a sample of 122 (n = 22)

76 E. Slayter and S. A. Steenrod
survey of 314 community-based people with MR in Florida found that between26% and 34% “had an alcohol problem” (DiNitto & Krishef, 1983–1984).In another longitudinal study on the after-effects of deinstitutionalizationamong 181 Californians with MR, the presence of SA conditions and SA-related consequences were noted in several case vignettes (Edgerton, 1967,1986). Later, a substudy on the specific topic of SA looked at individualswith MR living in four group home placements. Depending on the group,between 4% and 10% of the people in each setting were reported to haveSA-related problems (Edgerton, 1986).
Despite little available knowledge about the prevalence of SA orapproaches to treating it, during the 1980s and 1990s agencies working withpeople with MR began to address SA by providing prevention programming(McCarver & Craig, 1974; Meyers, Branch, & Lederman, 1988; Rivinus, 1988;Selan, 1976; Sengstock, Vergason, & Sullivan, 1975; Small, 1980; Wenc, 1980).A study by McGillicuddy and Blane (1999) presents carefully collected evi-dence regarding the prevalence of SA among a sample of 122 communitymembers with MR in Buffalo, New York, who were categorized into groups ofnonusers (abstainers), alcohol or other drug users, and misusers. Using mea-sures of alcohol or other drug consumption patterns developed for the pur-poses of the study, 18% of the entire group surveyed were found to be alcoholmisusers and 4% were reported lifetime users of illicit drugs. Notably, mari-juana use was more common among people with MR who were misusers ofalcohol versus those who only used or abstained from drinking alcohol.
Mental Health Service Settings
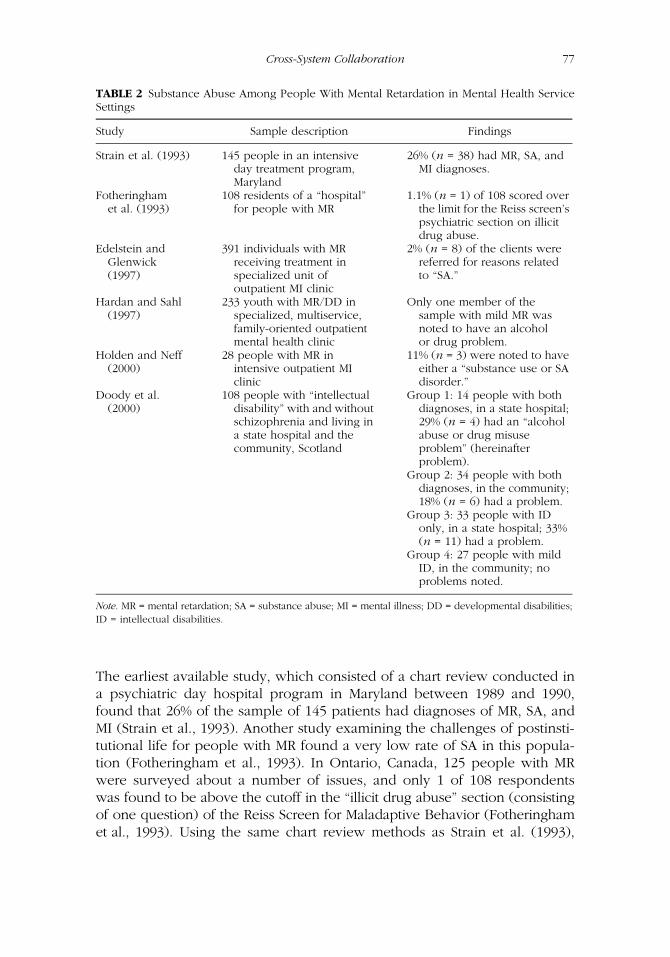
The presence of people with MR and SA who are receiving services in mentalhealth service settings has been documented in several smaller scale, localizedstudies, although this research does not specifically address the efficacy of anyparticular screening, assessment, intervention, or aftercare model for this popu-lation. Ten studies examining the prevalence of people with MR and SA whopresent with cooccurring MI in mental health settings are reviewed here.
A study by Slayter (2006) on a national sample of Medicaid beneficia-ries with MR indicates that there was a higher likelihood of the presence ofserious and persistent MI among people with MR and SA as compared topeople with MR only. In this study, people with MR and SA were morelikely than their counterparts with SA alone to have diagnoses of schizo-phrenia, affective psychoses, paranoid states, and long-term depression.
Nine other small empirical studies identify SA among subpopulations ofpeople with MR (or DD, or both, as noted herein) in small, community-based settings who are already identified as being at risk due to theircooccurring MI problems. These studies, although they vary in their researchmethods and their definitions of MI and SA, suggest a higher likelihood ofinvolvement of such individuals in nonaddiction settings (see Table 2).
Cross-System Collaboration 77
The earliest available study, which consisted of a chart review conducted ina psychiatric day hospital program in Maryland between 1989 and 1990,found that 26% of the sample of 145 patients had diagnoses of MR, SA, andMI (Strain et al., 1993). Another study examining the challenges of postinsti-tutional life for people with MR found a very low rate of SA in this popula-tion (Fotheringham et al., 1993). In Ontario, Canada, 125 people with MRwere surveyed about a number of issues, and only 1 of 108 respondentswas found to be above the cutoff in the “illicit drug abuse” section (consistingof one question) of the Reiss Screen for Maladaptive Behavior (Fotheringhamet al., 1993). Using the same chart review methods as Strain et al. (1993),
TABLE 2 Substance Abuse Among People With Mental Retardation in Mental Health ServiceSettings
Study Sample description Findings
Strain et al. (1993) 145 people in an intensive day treatment program, Maryland
26% (n = 38) had MR, SA, and MI diagnoses.
Fotheringham et al. (1993)
108 residents of a “hospital” for people with MR
1.1% (n = 1) of 108 scored over the limit for the Reiss screen’s psychiatric section on illicit drug abuse.
Edelstein and Glenwick (1997)
391 individuals with MR receiving treatment in specialized unit of outpatient MI clinic
2% (n = 8) of the clients were referred for reasons related to “SA.”
Hardan and Sahl (1997)
233 youth with MR/DD in specialized, multiservice, family-oriented outpatient mental health clinic
Only one member of the sample with mild MR was noted to have an alcohol or drug problem.
Holden and Neff (2000)
28 people with MR in intensive outpatient MI clinic
11% (n = 3) were noted to have either a “substance use or SA disorder.”
Doody et al. (2000)
108 people with “intellectual disability” with and without schizophrenia and living in a state hospital and the community, Scotland
Group 1: 14 people with both diagnoses, in a state hospital; 29% (n = 4) had an “alcohol abuse or drug misuse problem” (hereinafter problem).
Group 2: 34 people with both diagnoses, in the community; 18% (n = 6) had a problem.
Group 3: 33 people with ID only, in a state hospital; 33% (n = 11) had a problem.
Group 4: 27 people with mild ID, in the community; no problems noted.
Note. MR = mental retardation; SA = substance abuse; MI = mental illness; DD = developmental disabilities;ID = intellectual disabilities.

78 E. Slayter and S. A. Steenrod
another study focused on referral source and presenting problem at intakefor 391 individuals with MR in a specialized unit of an outpatient clinic (Edel-stein & Glenwick, 1997). Results suggested that 2% of the clients were referredfor reasons related to SA. A majority of these cases came from a referral initi-ated by what was termed a “legal agency,” although it is unclear what thismeans (Edelstein & Glenwick, 1997, p. 5). A similar study focused on 233 ado-lescents with MR and DD who were served in a specialized, multiservice, andfamily-oriented mental health clinic. A review of medical and social servicecharts for a 12-month period suggested that only one member of the samplewith mild MR had an alcohol or other drug problem (Hardan & Sahl, 1997).
Slightly higher rates were noted in a 2000 chart review-based study onoutpatient MI interventions for people with MR. Data were gathered for a12-month period for 28 people (Holden & Neff, 2000). Of these people, 11%(n = 3) were found to have either a “substance use or SA disorder” (Holden &Neff, 2000, p. 29). Another chart review study examined a sample of 108Scottish and Irish people with “intellectual disability” (another term for men-tal retardation), some of whom had a diagnosis of schizophrenia (Doody,Thomson, Miller, & Johnstone, 2000). The sample was categorized into fourgroups. Nearly a fourth (24%; n = 4) of people with both MR and MI whowere living in a state hospital were found to have an SA problem. In the sec-ond group (n = 34) of people with MR and MI living in the community, 18%(n = 6) were found to have an SA problem. In the third group of 33 peoplewith MR but not MI living in a state hospital, 33% (n = 11) were found to havean SA problem. Finally, in the fourth group of 27 people with mild MR livingin the community, no SA problems were noted. Results suggested “previousalcohol abuse and drug misuse occur more often in patients in the StateHospital than those in the community” (Doody et al., 2000, p. 132).
Although the prevalence of SA service need among clients with MR inboth community-based settings and mental health service settings variesaccording to these studies, given the potential for increased risk that SA posesto this population, especially regarding involvement with legal authorities,low prevalence is not a de facto argument for ignoring the problem. Further,although these studies do provide some evidence of SA as a concern in twopopulations with MR, they do not provide empirical analysis of barriers totreatment or advance practice knowledge around effective interventionapproaches. A review of the literature on these topics is presented next.
ACCESS TO TREATMENT FOR PEOPLE WITH MENTAL RETARDATION
Less than 25% of the general population in need of SA treatment actuallyaccesses it, with a higher demand for treatment than capacity to meet it(McAuliffe, Woodworth, Zhang, & Dunn, 2002; National Survey on Drug

Cross-System Collaboration 79
Use and Health, 2005). Three reasons are cited for this gap: poor benefitcoverage for SA treatment, reliance on self-help models versus treatmentservices, and the stigma of having an SA problem (Mark, Buck, Dilionardo,Coffey, & Chalk, 2003). Stigma plays a role in treatment access as peoplemight fear the consequences of seeking such help or receiving services.Aside from the standard challenges to accessing SA treatment faced by thegeneral population, it is posited that people with MR face additional barriers.Although in theory the Americans with Disabilities Act of 1990 has func-tioned to increase the responsibility of SA treatment programs toaccommodate people with disabilities, many people with disabilities,including those with MR, are not able to access treatment (NAADD, 1999).
The U.S. Surgeon General’s (2002) report on health disparities amongpeople with MR suggests that people with MR have poorer health in manyareas, including behavioral health, and notes that people with MR have moredifficulty accessing appropriate and quality health care when compared tothe general population. This might relate, in part, to the fact that people withMR are unlikely to seek health care of their own volition (Horwitz, Kerker,Owens, & Zigler, 2000). Guardianship issues can further exacerbate thisproblem, as people with MR might not have legal power to make their owndecisions about accessing treatment. Further, navigating the confusing worldof behavioral health insurance benefits can also function as a barrier.
Access to SA treatment is also a concern for people with MR. A study ofurban U.S. SA providers that examined access to treatment for this populationfound that although SA treatment programs expressed willingness to servepeople with MR, most had little experience in doing so (Lottman, 1993). Lackof staff expertise in serving this population was thought to be the strongestbarrier to their access to SA treatment. In their commentary on the topic,Prout and Strohmer (1998) concluded, “accessibility in theory does not nec-essarily equate to service utilization in practice” (p. 119). Treatment researchon the general population has established that people with cooccurring SAand MI conditions benefit from “concurrent” treatment (where both condi-tions are treated together in the same setting) as opposed to “sequential”treatment, where one condition is treated “first,” but whether this applies topopulations with MR is unclear (Drainoni & Bachman, 1995; Onken, 1997).
Little empirical evidence is available regarding actual levels of access toSA treatment for people with MR (Lottman, 1993; Slayter, 2006; Tyas &Rush, 1993). Slayter’s (2006) study of treatment utilization among 9,848Medicaid beneficiaries with and without MR found that 24.5% of all peoplewith MR and SA initiated treatment, and of these, only half (52.6%)remained in treatment for at least 1 month. Both of these rates were statisti-cally lower than for those with SA alone. Adolescents were most likely toinitiate (start) and engage (remain for at least 1 month) in SA treatment, fol-lowed by adults and elders. In these analyses, the presence of a serious MIappeared to be a pathway to accessing treatment in outpatient mental

80 E. Slayter and S. A. Steenrod
health settings, further supporting the idea that services to this populationmight be more likely to be received in nonaddiction-oriented service set-tings regardless of the appropriateness of this setting for individual treat-ment needs and program capabilities.
Although the research reported here has not addressed the issue ofcooccurring MI and SA conditions among people with MR, it does suggestthat people with MR require behavioral health treatment that is tailored totheir specific needs and realities—services that are often not available dueto the dearth of clinicians with expertise in working with people with MR(DesNoyers-Hurley, Tomasulo, & Pfadt, 1998; VanderSchie-Bezyak, 2003).Whether people with MR and SA are accessing treatment of this nature is asyet undetermined. Researchers in the area of mental health treatment forpeople with MR have “emphasized the need for specialist, interdisciplinarycommunity-based and accessible” services for this population (Bouras,Cowley, Holt, Newton, & Sturmey, 2003, p. 439). Yet, this discussion hasjust begun with respect to SA treatment for this population. A review ofexisting knowledge of SA treatment for people with MR is presented next.
SUBSTANCE ABUSE TREATMENT FOR PEOPLE WITH MENTAL RETARDATION
Empirical evidence is lacking with respect to appropriate SA screeningtools, assessment instruments, or treatment curricula and modalities for pop-ulations with MR. Three publications provide basic guidance. First, in 1998,the Substance Abuse and Mental Health Services Administration (SAMHSA)published a Treatment Improvement Protocol (TIP) addressing SA amongpeople with “cognitive disability”—which includes both people with MRand people with traumatic brain injury (Moore, 1998). This document is use-ful as an orientation tool for professionals new to working with people witheither MR or SA. Significant emphasis is placed on the need to remove phys-ical and communication-related barriers to treatment, the need to screen fordisability in addiction settings, and the need to develop an understanding ofthe client’s level of acceptance of his or her disability.
Second, a recent book published by the National Association of theDually Diagnosed reviews much of the same material presented in the TIP,but also adds a discussion of SA treatment approaches for other populationswith disabilities, such as people with traumatic brain injury (Sturmey et al.,2003). The third recommended publication presents the results of an expertconsensus panel of 93 MR-focused mental health clinicians commenting onSA treatment for this population (Rush & Frances, 2000). As a whole, theseclinicians suggest the importance of bolstering the “circles of support” forpeople with MR (i.e., family members and staff in group homes). In addition,a focus on the use of relapse prevention planning, general SA education, and

Cross-System Collaboration 81
managing the environment for safety is recommended, in conjunction withtherapy, social and communication skills development, and applied behav-ior analysis to reduce problem behaviors and increase functional skills.Across these three documents, specific suggestions are made with respect toassessment, treatment planning, and the process of counseling, althoughcounseling recommendations appear to focus on the use of individualsessions.
Taken together, these documents provide a useful framework for socialworkers to screen for SA in people with MR in nonaddiction settings. Oneuseful screening tool that has been validated with populations with MR isthe Reiss Screen for Maladaptive Behaviors. However, it might be difficult toobtain outside of specialized MR service settings (Reiss & Valenti-Hein,1994). Otherwise, social workers should approach SA screening in this pop-ulation as they would for any client by addressing a range of medical, psy-chiatric, and social concerns, remaining alert to the potential for distorteddiagnostic concerns (Owen, 1999). Another important issue not raised bythese publications is the need to use accessible language that reduces thechance for biased answers as a result of acquiescence, as the MR populationis at high risk for providing socially desirable responses in interview settings(Matikka & Vesala, 1997). For this reason, corroboration of data is vital tothe screening process, suggesting the need for conversations with collateralsources such as group home staff, family members, or other treatment pro-viders, provided permission from the client has been obtained.
As with many clients, one starting point might include an assessment ofthe ways in which alcohol or drug use impacts relationships with significantothers. For example, have family members or friends expressed concernabout SA? Have important relationships been impaired as a result of sub-stance use? Inquiries about the incidence of intoxication are important,examining whether, for example, recreational activities center around get-ting and using substances as well as recovering from use. Obtaining abroader picture of the client’s regular social setting is important. For exam-ple, social workers can determine whether the client’s immediate peergroup encourages SA, whether the client is reluctant to attend social eventswhere substances will not be present, or whether they have been victimizedin such a setting when under the influence of substances. Especially impor-tant for risk assessment is a determination of whether the client uses alcoholor other drugs along with prescribed medication and whether rates ofintake appear to be unsafe given those prescriptions and given existinghealth conditions. Many people with MR are employed in either integratedor sheltered work settings. Consideration of whether the client has experi-enced job-related problems as a result of SA can be instructive. Has the clientmissed work or been late due to use of substances? Additionally, socialworkers should explore for any potential problems the client has had withauthority figures, with police, or with the juvenile or criminal justice system.

82 E. Slayter and S. A. Steenrod
Should the screening process suggest the need for further intervention,social workers in nonaddiction settings would likely refer clients to specialtySA settings for a more in-depth assessment. Existing gold standard assess-ment tools such as the Addiction Severity Index have not been validatedwith populations with MR and the scant available recommendations aboutassessment made in the literature are often based on anecdotal clinicalexperiences and, therefore, are not reviewed in detail here (Small, 1980;Wenc, 1980). Regarding assessment, the consensus is that the use of writingis contra-indicated, which suggests the need for verbal administration ofexisting assessment instruments that could be modified to address compre-hension challenges among people with MR. Social workers in nonaddictionsettings should consider the need to collaborate with and possibly engagein cross-training with SA clinicians to create an accessible and accurateassessment process.
Once assessment is completed, social workers in both types of settingsneed to collaborate in planning the treatment process. The consensus ofthe authors of the three suggested documents is that treatment plansshould be strengths-based, but not static. Several treatment approachesmight need to be explored before finding a suitable one. Given the poten-tial need for disability-specific accommodation in the treatment process,clinicians should explain clients’ rights under the public accommodationmandates of the Americans with Disabilities Act of 1990. Clinicians areencouraged to design explicit behavioral contracts with consequencestailored to realistic potential accomplishments. The treatment planningprocess should also include a mandatory assessment of any medicationscurrently used by the client.
Treatment recommendations in these publications also appear to bebased on clinicians’ personal observations and views as well as empiricalevidence from research populations with disabilities that did not includeMR, such as traumatic brain injury (Campbell et al., 1994). Although there isa strong evidence base for both the assessment and treatment of MI amongpeople with MR, it is unclear whether clinical approaches used with thatpopulation can be adapted to address SA as well. Once engaged in thecounseling process, the publications suggest that sessions should be flexiblein duration and timing. During counseling sessions, clinicians are encouragedto use simple language, to assess comprehension of all terms, and to use“concrete” terminology instead of metaphors. Further, the authors posit thatclients with cognitive disabilities may benefit from expressive therapy orrole-playing, although this does not appear to be based on empirical datagathered from people with MR. Clinicians are also counseled to systemati-cally review what has been learned and to link this to the next stage oftreatment or aftercare. The publications’ recommendations also emphasizethe need for cross-system collaboration and coordination to address infor-mation sharing and funding challenges. Especially important to this process

Cross-System Collaboration 83
is the need to develop an understanding of each system’s theoreticalapproach to treatment as well as knowledge of the services rendered.
Overall, there was consensus across the three documents about usingsimple, concrete language as well as reinforcement and consequence-oriented approaches (as compared to cognitive-behavioral or classical con-ditioning approaches, supportive counseling, or psychotherapy). Althoughnot empirically based, these recommendations on SA treatment approachesfor people with MR should be considered by clinicians in both addictionand nonaddiction settings to find the right mix in fostering cross-system col-laboration to support clients’ goals and outcomes.
Given the dearth of knowledge about how to treat SA in this popula-tion and that people with MR and SA are being reported in the literature asbeing served primarily in mental health treatment settings, it is likely thatmost people with MR will be seen by clinicians who are not familiar withtheir needs (VanderSchie-Bezyak, 2003). In turn, this could cause therereferral of clients and a discontinuity in patient care as people may oftenbe sent to a series of treatment providers who are not trained in the appro-priate clinical approaches (Chaplin, 2004).
RECOMMENDATIONS FOR SOCIAL WORKERS IN NONADDICTION SETTINGS
Social workers in nonaddiction settings can best support people with MRand SA by engaging in a two-step process. First, these workers should famil-iarize themselves with basic SA screening approaches and utilize the sug-gested screening techniques referenced earlier. Second, social workersshould engage in efforts to foster cross-system collaboration around specificclient needs. The four-part framework presented here is intended to supportsocial workers in taking the next steps in this process (see Table 3).
TABLE 3 Systemic Differences Between Mental Retardation and Substance Abuse TreatmentSystems
DomainMental retardation
service systemSubstance abuse treatment system
Philosophy of care Holistic and supportive Prescriptive and confrontational
Obligation to client Long term TemporaryValues/lexicon Human rights,
self-determinationGetting “real,” breaking
down denial systemsConfidentiality policies Communication between care
providers encouraged to facilitate collaboration (case management, service coordination)
Communication between care providers limited by strict confidentiality laws to protect against stigma

84 E. Slayter and S. A. Steenrod
First, reliance on service coordination and collaboration is vital—butmight not come naturally to social workers in either the MR or SA systems,given differences in treatment paradigms between these two service sec-tors. An analysis of some of the philosophical and practical characteristicsof each system illuminates the potential issues that might make collabora-tion difficult. The MR field employs a holistic model designed to enhancethe quality of life for individuals with MR with the goal of self-determina-tion and participation in community-based life. This is evidenced by thewide range of services offered to MR individuals, including service coordi-nation, community support, residential support, facility support, individualsupport, community day support, employment support, family support,and respite care. In contrast, the SA system has a more limited mandate tooffer services that are specific to the prevention, intervention, treatment,and recovery of SA. Although other life domains, such as housing oremployment, might be considered in a select number of specialized SAprograms, this is not true of the majority. Further, the treatment modelemployed by SA systems may be prescriptive and confrontational in nature.This philosophical “culture clash” between the MR and SA systems mightinhibit collaboration.
Second, the obligation to individuals with both MR and SA might varybetween the systems. For example, clients with MR are lifelong consumersof the MR system provided they meet the eligibility criteria for such services.Some services might be provided directly by state MR authorities, whereasothers are provided via contract with public or private-sector programs. Thefact remains, however, that once MR eligibility status has been determined,ongoing services are usually ensured for life. A case management model isthen employed to enhance and coordinate services. In contrast, clients ofthe SA system receive services from public or private SA agencies thatprovide temporary and episodic treatment based on three eligibility compo-nents: diagnostic criteria, financial or insurance coverage, and availabilityof a treatment slot. State SA authorities neither maintain client lists nordetermine eligibility for services. A lack of awareness of MR and SA casemanagers and clinicians of each system’s mandated obligations and respon-sibilities can result in frustration and confusion when making referralsacross systems.
Third, the lexicons of both systems vary according to their history, corevalues, and professional beliefs.
For example, for reasons that are beyond the scope of this article, theMR system is organized to support community inclusion within the guise ofa human rights framework, which encourages personal choice, indepen-dence, and dignity (Trent, 1995). In marked contrast, the SA system oftenworks with court-mandated or involuntary clients. For example, in 2002,36% of all SA treatment admissions were referred from the criminal justicesystem (Drug and Alcohol Services Information System [DASIS], 2004). In
Cross-System Collaboration 85
this context, SA treatment has historically included “tough love” techniquesdesigned to interrupt entrenched denial systems concerning the behaviorand consequences of abuse and dependence. A potential result of these con-flicting values can range from misunderstandings and confusion in serviceprovision to a deep distrust between the MR and SA systems (Slayter, 2007).
Another variable that might challenge collaboration between the MRand SA systems is the confidentiality practices of the SA system. To protectthe identity of individuals seeking alcohol and drug treatment and to pro-mote treatment-seeking behavior, strict federal regulations have inhibitedthe release of information to other service providers (Confidentiality ofAlcohol and Drug Abuse Patient Records, 1987). Therefore, MR providersmight feel frustrated by attempts to collaborate with SA providers if they areinformed that they cannot share information regarding individual clients.
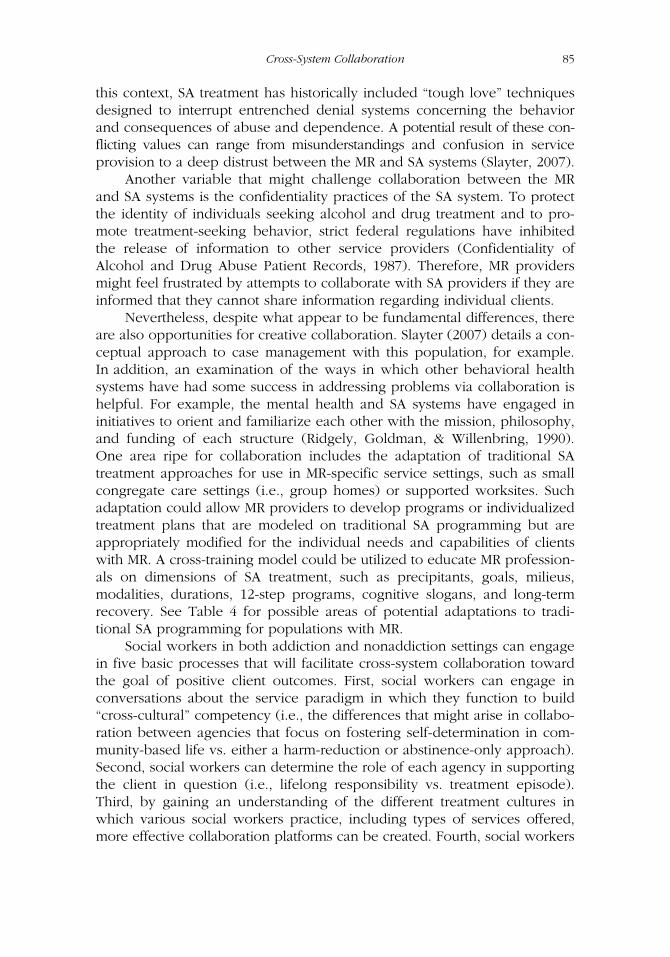
Nevertheless, despite what appear to be fundamental differences, thereare also opportunities for creative collaboration. Slayter (2007) details a con-ceptual approach to case management with this population, for example.In addition, an examination of the ways in which other behavioral healthsystems have had some success in addressing problems via collaboration ishelpful. For example, the mental health and SA systems have engaged ininitiatives to orient and familiarize each other with the mission, philosophy,and funding of each structure (Ridgely, Goldman, & Willenbring, 1990).One area ripe for collaboration includes the adaptation of traditional SAtreatment approaches for use in MR-specific service settings, such as smallcongregate care settings (i.e., group homes) or supported worksites. Suchadaptation could allow MR providers to develop programs or individualizedtreatment plans that are modeled on traditional SA programming but areappropriately modified for the individual needs and capabilities of clientswith MR. A cross-training model could be utilized to educate MR profession-als on dimensions of SA treatment, such as precipitants, goals, milieus,modalities, durations, 12-step programs, cognitive slogans, and long-termrecovery. See Table 4 for possible areas of potential adaptations to tradi-tional SA programming for populations with MR.
Social workers in both addiction and nonaddiction settings can engagein five basic processes that will facilitate cross-system collaboration towardthe goal of positive client outcomes. First, social workers can engage inconversations about the service paradigm in which they function to build“cross-cultural” competency (i.e., the differences that might arise in collabo-ration between agencies that focus on fostering self-determination in com-munity-based life vs. either a harm-reduction or abstinence-only approach).Second, social workers can determine the role of each agency in supportingthe client in question (i.e., lifelong responsibility vs. treatment episode).Third, by gaining an understanding of the different treatment cultures inwhich various social workers practice, including types of services offered,more effective collaboration platforms can be created. Fourth, social workers
86 E. Slayter and S. A. Steenrod
will need to negotiate information-sharing approaches that respect theneeds of their clients and the requirements of all agency types involved.Finally, social workers have the opportunity to think outside of the box in“starting where the client is” to create responsive intervention approachesthat will foster client well-being in the long run.
CONCLUSION
Individuals with MR and cooccurring SA are an especially vulnerable popu-lation at increased risk for a variety of negative consequences. The evidencesuggests that SA-related services for this population might be most likely tobe received in nonaddiction settings that are unequipped to serve andsupport such clients. The distinct lack of evidence-based practices for thispopulation, combined with the reality of challenges to cross-system collabo-ration, presents a call to action to social workers in both types of settings tofoster client-specific cross-system collaboration and evaluation of theseefforts. Social work clinicians collaborating across the MR and SA servicesectors can, in the long run, best serve this population by documentingwhat does and does not work. Recommendations for collaboration, such as
TABLE 4 Adaptations of Traditional Substance Abuse Programming for Populations withMental Retardation
Domain General population Population with mental retardation
Precipitant to treatment
Leverage from loved ones or authority figures
Pressure and/or acquiescence to loved ones or authority figures
Treatment goal Abstinence Harm reduction (more in line with self-determination)
Treatment milieu Substance abuse treatment facility
Family residence, group home, or substance abuse treatment facility, as appropriate
Primary treatment model
Group Group treatment (“holistic treatment”) possibly supplemented by individual and home-based services
Length of time in session
Up to 50 min Shorter based on attention span assessment, possibly 20 min twice per treatment period
Use of 12-step programs
Expected/strongly encouraged
Strongly encouraged with modifications including visual queues, vetting of sponsors
Use of slogans: “Keep it simple” or “One day at a time”
Helpful to reinforce treatment process with these slogans on a regular basis
Extremely helpful to reinforce treatment process in accessible language
Long-term recovery plan
Managed by individual in recovery
Managed by individuals and their “circles of support”
Cross-System Collaboration 87
those made earlier, should also be empirically tested and reported toimprove the services to this important population group.
REFERENCES
Alverson, H., Alverson, M., & Drake, R. (2001). Social patterns of substance useamong people with dual diagnoses. Mental Health Services Research, 3, 3–14.
American Association on Mental Retardation. (2008). Fact sheet: Frequently askedquestions about mental retardation. Washington, DC: Author. RetrievedOctober 17, 2008, from http://www.aamr.org/Policies/mental_retardation.shtml
The Arc. (2001a). Fact sheet: Mental retardation and mental illness. Washington,DC: Author.
The Arc. (2001b). Managed care and long-term services for people with mentalretardation. Washington, DC: Author.
Borthwick-Duffy, S., & Eyman, R. (1990). Who are the dually diagnosed? AmericanJournal on Mental Retardation, 94, 586–595.
Bouras, N., Cowley, A., Holt, G., Newton, J., & Sturmey, P. (2003). Referral trends ofpeople with intellectual disabilities and psychiatric disorders. Journal of Intel-lectual Disability Research, 47, 439–446.
Burgard, J. (2000). Prevalence and treatment of substance abuse in the mentally retardedpopulation: An empirical review. Journal of Psychoactive Drugs, 32, 293–298.
Campbell, J., Essex, E., & Held, G. (1994). Issues in chemical dependency treat-ment and aftercare for people with learning differences. Health and SocialWork, 19, 63.
Chaplin, R. (2004). General psychiatric services for adults with intellectual disabilityand mental illness. Journal of Intellectual Disability Research, 48, 1–10.
Christian, L., & Poling, A. (1997). Drug abuse in persons with mental retardation:A review. American Journal on Mental Retardation, 102, 126–136.
Clarke, J., & Wilson, D. (1999). Alcohol problems and intellectual disability. Journalof Intellectual Disability Research, 43, 135–139.
Cocco, K., & Harper, D. (2002). Substance use in people with mental retardation:A missing link in understanding community outcomes? Rehabilitation CounselingBulletin, 46, 34–42.
Confidentiality of Alcohol and Drug Abuse Patient Records, 42 C.F.R., Part 2 (1987).Degenhardt, L. (2000). Interventions for people with alcohol use disorders and an
intellectual disability: A review of the literature. Journal of Intellectual andDevelopmental Disabilities, 25, 135–146.
DesNoyers-Hurley, A., Tomasulo, D., & Pfadt, A. (1998). Individual and group psy-chotherapy approaches for persons with mental retardation and developmentaldisabilities. Journal of Developmental and Physical Disabilities, 10, 365–386.
The Developmental Disabilities Act of 1984, Pub. L. No. 98–527 (1984).DiNitto, D., & Krishef, C. (1983–1984). Drinking patterns of mentally retarded per-
sons. Alcohol Health and Research World, 8, 40–42.Doody, G., Thomson, P., Miller, P., & Johnstone, E. (2000). Predictors of admission
to a high-security hospital of people with intellectual disability with and with-out schizophrenia. Journal of Intellectual Disability Research, 44, 130–137.
88 E. Slayter and S. A. Steenrod
Drainoni, M., & Bachman, S. (1995). Overcoming treatment barriers to providingservices for adults with dual diagnosis: Three approaches. Journal of DisabilityPolicy Studies, 6, 43–55.
Drug and Alchol Services Information System (DASIS). (2004). In brief: Substanceabuse treatment admissions referred by the criminal justice system: 2002.Arlington, VA: Office of Applied Studies, SAMHSA; Synectics for ManagementDecisions, Inc.; and Research Triangle Park, NC: RTI. July 30, 2004.
Edelstein, T., & Glenwick, D. S. (1997). Referral reasons for psychological services foradults with mental retardation. Research in Developmental Disabilities, 18, 45–59.
Edgerton, R. (1967). Cloak of competence—Stigma in lives of mentally retarded.Rehabilitation Literature, 28, 383–385.
Edgerton, R. (1986). Alcohol and drug use by mentally retarded adults. AmericanJournal of Mental Deficiency, 90, 602–609.
Fotheringham, J., Abdo, K., Ouelette-Kuntz, H., & Wolfgarth, A. (1993). Survey ofcommunity adjustment of previously institutionalized developmentally disabledpersons. Canadian Journal of Psychiatry, 38, 641–648.
Hardan, A., & Sahl, R. (1997). Psychopathology in children and adolescents withdevelopmental disorders. Research in Developmental Disabilities, 18, 369–382.
Holden, P., & Neff, J. A. (2000). Intensive outpatient treatment of persons withmental retardation and psychiatric disorder: A preliminary study. Mental Retar-dation, 38, 27–32.
Horwitz, S., Kerker, B., Owens, P., & Zigler, E. (2000). The health status and needs ofindividuals with mental retardation. New Haven, CT: Department of Psychol-ogy, Yale University and Special Olympics, Inc.
Larson, S. (2001). Prevalence of mental retardation and developmental disabilities:Estimates from the 1994/1995 National Health Interview Survey DisabilitySupplements. American Journal on Mental Retardation, 106, 231–252.
Larson, S., Lakin, C., Anderson, L., & Kwak, N. (1999). Characteristics of and serviceuse by persons with MR/DD living in their own homes or with family mem-bers: NHIS-D analysis. MR/DD Data Brief, 3, 1–12.
Linna, S., Moilanen, I., Ebeling, H., Piha, J., Kumpulainen, K., Tamminen, T., et al.(1999). Psychiatric symptoms in children with intellectual disability. EuropeanJournal of Child and Adolescent Psychiatry, 8, 77–82.
Lottman, T. (1993). Access to generic substance abuse services for persons withmental retardation. Journal of Alcohol and Drug Education, 39, 41–55.
Mark, T., Buck, J., Dilionardo, J., Coffey, R., & Chalk, M. (2003). Medicaid expendi-tures on behavioral health care. Psychiatric Services, 54, 188–194.
Matikka, L., & Vesala, H. (1997). Acquiescence in quality-of-life interviews withadults who have mental retardation. Mental Retardation, 35, 75–82.
McAuliffe, W., Woodworth, R., Zhang, C., & Dunn, R. (2002). Identifying substanceabuse treatment gaps in substate areas. Journal of Substance Abuse Treatment,23, 199–208.
McCarver, R., & Craig, E. (1974). Placement of the retarded in the community: Prognosis& outcome. International Review of Research in Mental Retardation, 7, 145–207.
McGillicuddy, N. (2006). A review of substance use research among those withmental retardation. Mental Retardation and Developmental DisabilitiesResearch Reviews, 12, 41–47.
Cross-System Collaboration 89
McGillicuddy, N., & Blane, H. (1999). Substance use in individuals with mentalretardation. Addictive Behaviors, 24, 869–878.
McGillivray, J., & Moore, M. (2001). Substance use by offenders with mild intel-lectual disability. Journal of Intellectual and Developmental Disability, 26,297–310.
Meyers, A., Branch, L., & Lederman, R. (1988). Alcohol, tobacco, and cannabis useby independently living adults with major disabling conditions. InternationalJournal of the Addictions, 23, 671–685.
Miranda, J. de. (1999, Fall). Policy, accessibility and disability: Barriers to substanceabuse services. Impact: Feature Issues on Alcohol and Drug Abuse Services forPersons With Developmental Disabilities, 4.
Moore, D. (1998). TIP 29: Substance abuse disorder treatment for people with physicaland cognitive disability. Washington, DC: Substance Abuse and Mental HealthServices Administration.
National Association on Alcohol, Drugs, and Disability. (1999). Access limited:Substance abuse services for people with disabilities: A national perspective.Washington, DC: Author.
National Survey on Drug Use and Health. (2005). National household survey ondrug use and health. Washington, DC: Substance Abuse and Mental HealthServices Administration.
Onken, L. (1997). Treatment of drug-dependent individuals with comorbid mentaldisorders (NIDA Research Monograph 172). Rockville, MD: National Instituteon Drug Abuse.
Owen, P. (1999). A guide to treatment approaches: Linking people with quality pro-grams. In University of Minnesota Institute on Community Inclusion (Ed.),Impact: Feature issue on alcohol and drug abuse services for people with develop-mental disabilities. Minneapolis, MN: Institute on Community Inclusion.
Pack, R., Wallander, J., & Browne, D. (1998). Health risk behaviors of African Americanadolescents with mild mental retardation: Prevalence depends on measurementmethod. American Journal on Mental Retardation, 102, 409–420.
Petersilia, J. (2000). Invisible victims. Human Rights, 27, 9–12.Prout, H., & Strohmer, D. (1998). Issues in mental health counseling with persons
with mental retardation. Journal of Mental Health Counseling, 20, 112–121.Reiss, S., & Aman, M. (1997). The international consensus process on psychophar-
macology and intellectual disability. Journal of Intellectual Disability Research,41, 448–445.
Reiss, S., & Valent-Hein, D. (1994). Development of a psychopathology rating scalefor children with mental retardation. Journal of Consulting and Clinical Psy-chology, 62, 28–33.
Ridgely, M., Goldman, H., & Willenbring, M. (1990). Barriers to the care of personswith dual diagnoses: Organizational and financing issues. Schizophrenia Bulletin,16, 123–132.
Rivas, L. (2001). Controversial issues in the diagnosis of narcissistic personalitydisorder: A review of the literature. Journal of Mental Health Counseling, 23,22–35.
Rivinus, T. (1988). Alcohol use disorder in mentally retarded persons. PsychiatricAspects of Mental Retardation, 7, 19–21.
90 E. Slayter and S. A. Steenrod
Rush, J., & Frances, A. (2000). Expert consensus guidelines for the use of treatmentof psychiatric and behavioral problems in mental retardation. American Journalon Mental Retardation, 105, 159–228.
Santosh, P. (1999). Psychopharmacotherapy in children and adults with intellectualdisability [Review]. The Lancet, 354, 231.
Selan, B. (1976). Psychotherapy with the mentally retarded. Health & Social Work,1, 73–85.
Sengstock, W., Vergason, G., & Sullivan, M. (1975). Considerations and issues in adrug abuse program for the mentally retarded. Education and Training of theMentally Retarded, 10, 138–143.
Simpson, M. (1998). Just say “no”? Alcohol and people with learning difficulties.Disability and Society, 13, 541–555.
Slayter, E. (2006). Establishing a baseline: Substance abuse treatment among Medic-aid beneficiaries with mental retardation. Unpublished doctoral dissertation,The Heller School for Social Policy and Management, Brandeis University,Waltham, Massachusetts.
Slayter, E. (2007). Balancing the dignity of risk with risk management: A casemanagement framework for people with substance abuse and co-occurring mentalretardation. Families in Society: A Journal of Contemporary Human Services, 8, 4.
Small, J. (1980). Emotions anonymous: Counseling the mentally retarded substanceabuser. Alcohol Health and Research World, 5, 46.
Strain, E., Buccino, D., Brooner, R., Schmidt, C., & Bigelow, G. (1993). The triplydiagnosed: Patients with major mental illness, cognitive impairment and sub-stance abuse. Journal of Nervous and Mental Disease, 181, 585–587.
Sturmey, P., Reyer, H., Lee, R., & Robeck, A. (2003). Substance-related disorders inpersons with mental retardation (R. Fletcher & W. Gardner, Eds.). Kingston,NY: NADD Press.
Trent, J. (1995). Inventing the feeble mind: A history of mental retardation in theUnited States. Berkeley: University of California Press.
Tyas, S., & Rush, B. (1993, May). The treatment of disabled persons with alcoholand drug problems: Results of a survey of addiction services. Journal of Studieson Alcohol, 54, 275–282.
U.S. Surgeon General. (2002). Closing the gap: A national blueprint to improve thehealth of persons with mental retardation. Washington, DC: U.S. Health andHuman Services Administration.
VanderSchie-Bezyak, J. (2003). Service problems and solutions for individuals withmental retardation and mental illness. Journal of Rehabilitation, 69, 53–58.
Walkup, J., Sambamoorthi, M., & Crystal, S. (1999). Characteristics of persons withmental retardation and HIV/AIDS: Infection in a state Medicaid population.American Journal on Mental Retardation, 104, 356–363.
Wenc, F. (1980). Special issue: The multidisabled: In focus: The developmentallydisabled substance abuser. Alcohol Health and Research World, 5, 42–46.
Westermeyer, J., Kemp, K., & Nugent, S. (1996). Substance disorder among personswith mild mental retardation. American Journal on Addictions, 5, 23–31.
Westermeyer, J., Phaobtong, T., & Neider, J. (1988). Substance use and abuseamong mentally retarded persons: A comparison of patients and a surveypopulation. American Journal of Drug and Alcohol Abuse, 14, 109–123.