
self adjustment mahasiswa pascasarjana dengan cerebral palsy
Upload
independentCategory
view
3download
0
http://cre.sagepub.com/Clinical Rehabilitation
http://cre.sagepub.com/content/24/7/639The online version of this article can be found at:
DOI: 10.1177/0269215510367974
2010 24: 639 originally published online 8 June 2010Clin RehabilTeixeira Fonseca
Marina de Brito Brandão, Marisa Cotta Mancini, Daniela Virgínia Vaz, Ana Paula Pereira de Melo and Sérgiowith cerebral palsy: a randomized controlled trial
Adapted version of constraint-induced movement therapy promotes functioning in children
Published by:
http://www.sagepublications.com
can be found at:Clinical RehabilitationAdditional services and information for
http://cre.sagepub.com/cgi/alertsEmail Alerts:
http://cre.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cre.sagepub.com/content/24/7/639.refs.htmlCitations:
What is This?
- Jun 8, 2010 OnlineFirst Version of Record
- Jun 28, 2010Version of Record >>
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from

Clinical Rehabilitation 2010; 24: 639–647
Adapted version of constraint-induced movement ther-apy promotes functioning in children with cerebral palsy:a randomized controlled trialMarina de Brito Brandao Graduate Program in Rehabilitation Sciences, Universidade Federal de Minas Gerais, MarisaCotta Mancini Occupational Therapy Department, Universidade Federal de Minas Gerais, Daniela Virgınia Vaz PhysicalTherapy Department, Universidade Federal de Minas Gerais, Ana Paula Pereira de Melo Occupational Therapist and SergioTeixeira Fonseca Physical Therapy Department, Universidade Federal de Minas Gerais, Brazil
Received 30th November 2009; returned for revisions 12th January 2010; revised manuscript accepted 25th January 2010.
Objective: To evaluate the effects of constraint-induced movement therapy on
the use of the affected arm and on daily functioning in children with hemiplegic
cerebral palsy.
Design: A single-blinded randomized clinical trial.
Subjects: Sixteen children with cerebral palsy randomized to intervention (n¼ 8,
4 males, 4 females, mean age 5 years and 6 months) and control groups (n¼ 8,
4 males, 4 females, mean age 6 years and 7 months).
Interventions: Non-affected arm of intervention group was restricted for 10 hours/
day and the affected arm intensively trained for 3 hours/day for two weeks. The
intervention protocol included one week of bimanual functional training following
constraint therapy. The control group maintained usual rehabilitation throughout the
intervention period.
Main measures: Pediatric Evaluation of Disability Inventory (self-care domain) and
an adapted version of the Jebsen–Taylor test were administered before and after
intervention, and at one month follow-up. General linear models tested differences
in gain scores and the number needed to treat estimated relative effectiveness of
intervention protocol for functional skills and independence in self-care.
Results: Results are reported for 15 children who completed assessments and
intervention. Higher gains were observed in the intervention group for functional
skills and independence post intervention (dfunctional skills¼ 1.61, P¼ 0.0134;
dindependence¼1.37; P¼ 0.0001) and follow-up (dfunctional skills¼ 2.08, P¼ 0.004;
dindependence¼ 0.85; P¼ 0.0016). No group difference in manual dexterity gains was
observed. Low indices of number needed to treat (1.75 and 2.33) illustrate clinical
relevance of intervention.
Conclusions: The protocol associating constraint-induced movement therapy and
bimanual functional training was effective in promoting daily living functioning
among children with cerebral palsy.
Introduction
Constraint-induced movement therapy is consid-ered to be one of the most effective techniques
Address for correspondence: Marisa Cotta Mancini, GraduateProgram in Rehabilitation Sciences, School of PhysicalEducation, Physical Therapy and Occupational Therapy,Universidade Federal de Minas Gerais (UFMG), Av.Antonio Carlos 6627, Campus Pampulha, Belo Horizonte-MG, Brazil 31270-910. e-mail: [email protected]
� The Author(s), 2010.Reprints and permissions: http://www.sagepub.co.uk/journalsPermissions.nav 10.1177/0269215510367974
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from

used in rehabilitation to improve the use of theaffected upper extremity in patients with neuromo-tor dysfunctions.1–3 The constraint-induced move-ment therapy protocol involves intensive trainingof the affected arm, restriction of the non-affectedarm and use of behavioural methods aimed at pro-moting compliance of patients to the interventionprotocol.4 It was originally developed to treatadults with hemiplegia.5 Recently, it is beingused to improve manual function of childrenwith cerebral palsy.6–8
Positive results on the use of constraint-inducedmovement therapy in children are reported. Acrossover experimental design conducted byDeLuca et al.7 evaluated the manual function ofchildren with cerebral palsy treated with a proto-col of intensive training for 6 hours associatedwith restriction during all day for 21 days,compared with children who maintained routinephysiotherapy and occupational therapy. Theintervention group demonstrated superiorimprovements in the amount and quality of useof the affected arm, as well as in the use of thislimb in functional activities, compared with theroutine intervention group.In a randomized controlled trial, Charles et al.8
tested the efficacy of an adapted version of con-straint-induced movement therapy for childrenwith cerebral palsy aged 4–8 years. This modifiedversion involved intensive training for 6 hours aday for 10 days. The restriction was used onlyduring training hours. Children from the interven-tion group demonstrated significant improvementsin manual dexterity tests, which were maintainedin a six-month follow-up.8 Moreover, children’scaregivers reported increased amount and qualityof use of the affected arm after the intervention.Similarly, Eliasson et al.6 conducted a controlledclinical trial and documented superior improve-ments in bimanual function in children aged 18months to 4 years treated for two months withan adapted version of constraint-induced move-ment therapy.Several studies on the use of the constraint-
induced movement therapy in children with hemi-plegia have documented positive effects on qualityand amount of use of the affected arm, and on theinvolvement of the affected arm on manualtasks.6,7 To date, no study has demonstrated theimpact of constraint-induced movement therapy
protocols on children’s daily functioning. Onereason for the lack of evidence of functionalgains might be attributed to the fact that con-straint-induced movement therapy is exclusivelyfocused on the training of the affected arm.9
However, most daily functional activities requirethe use of both hands. In addition, improvementin performance of daily activities is often thedesired outcome identified by parents and childrenwith cerebral palsy. It is not known whetherchanges in unilateral arm use will result inimprovements in the performance of bimanualdaily living activities. According to Eliasson,10
hand function is a dynamic phenomenon thatmay be changed by practice. However, trainingneeds to be specific to the characteristics of theintended outcomes. Thus, in order to meet func-tional goals, especially those that require the use ofboth hands, it may be necessary to implement abimanual training, which provides demands foruse of the affected arm in conjunction with thenon-affected arm.10,11 The inclusion of a func-tional bimanual training following constraint ther-apy traditional protocols may be necessary toimprove cerebral palsy children’s daily activityperformance, specially those that require bimanualuse. The objective of the present study was to eval-uate the effects of a modified constraint-inducedmovement therapy protocol associated withbimanual functional training on the performanceof daily activities and independence to performfunctional self-care tasks in children with hemiple-gic cerebral palsy.
Methods
A randomized clinical trial was conducted with 16children with hemiplegic cerebral palsy. Samplesize calculation was based on effects obtainedfrom Taub et al.12 Participants were recruitedfrom occupational therapy services in a local reha-bilitation centre. To participate in the study, chil-dren should have a medical diagnosis of spastichemiplegic cerebral palsy and should be able tocomprehend simple verbal commands and executeactivities proposed during intervention. Childrenwith associated pathologies or movement disor-ders, or who had been submitted to surgeries
640 M de Brito Brandao et al.
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from

or botulinum toxin injections during the sixmonths prior to the beginning of the study wereexcluded from the sample.
The University’s Institutional Research EthicsCommittee approved this study (protocol 041/6).Parents signed an informed consent form allowingparticipation of their child. Participants were ran-domly allocated into intervention and controlgroups by draw of sealed envelopes. The interven-tion group was submitted to an adapted con-straint-induced movement therapy protocol andthe control group received regular occupationaltherapy sessions once a week. This study tookplace during school holidays in order not to inter-fere with children’s participation at school.
The adapted constraint-induced movement ther-apy protocol consisted of 3 hours of upper extrem-ity training on every weekday for two weeks (10out of 12 consecutive days), in association with theimmobilization of the non-affected arm during theentire day. After this period, the restriction wasremoved and children took part in sessions offunctional training of bimanual activities relevantto their daily context.
A resting splint to restrict wrist and fingersmovements was custom-made for each child ofthe intervention group in the day before the begin-ning of intervention. In addition to the splint, chil-dren from the experimental group used a sling torestrict the movements of the non-affected elbowand shoulder. Children and parents receivedinstructions on the use of immobilization duringawake hours throughout the two weeks of con-straint-induced movement therapy, for an averageof 10 hours a day. The restriction was removedonly for bathing or use of public transportation.Parents received a logbook in which they regis-tered the amount of use of the restriction anddescribed any improvements or difficultiesobserved in the performance of typical activitiesat home.
The 3-hour daily intervention protocol waschosen to facilitate the implementation of thistechnique in the clinical setting. It followed thestudy of Sterr et al.13 which observed improve-ments in the motor function of adults withstroke after the implementation of the constraint-induced movement therapy using a 3-hour dailytraining. The 3-hour protocol allowed structuringthe intervention activities in such a way as to
maintain the functional relevance of the activities(including eating activities) as well as the interestof the children. Children from the interventiongroup were individually assisted by an experiencedoccupational therapist. To stimulate the use of theaffected upper extremity in play and daily livingactivities, children were involved in specific activ-ities of fine motor tasks, which included stackingsmall blocks, pegboard, playdough, among others,as well as arts activities, board games, gross motorgames and functional tasks (food preparation,eating, cleaning, dressing, etc). Each task wasplanned in accordance with shaping procedures2,12
with progression of complexity achieved by chang-ing the activities’ demands of speed, dexterity andversatility. Positive verbal feedback and rewards(e.g. stickers, collectables, small toys and choco-lates) were used to motivate the child to use theaffected extremity.
After the end of the constraint-induced move-ment therapy protocol the restriction of the non-affected arm was discontinued and training ofbimanual function was initiated. The trainingwas undertaken in order to favour consolidationof abilities that emerged during the constrainttherapy period, helping the children to incorporatethe use of the affected arm in the performance ofbimanual activities that were relevant to their dailyroutines. The training consisted of three 45-minutedaily sessions during one week.
Children from the control group maintainedtheir regular routines of occupational therapy.They received one treatment session of 45 minuteseach week. Sessions were functionally oriented andincluded training of bimanual activities and sen-sory stimulation.
Before the beginning of data collection, twoinvestigators were trained to use all the assessmentinstruments and reliability coefficients were calcu-lated (inter-examiner coefficients ranged between0.86 and 0.98; intra-examiner coefficients rangedbetween 0.98 and 0.99). All assessments were per-formed one week before the beginning of interven-tion (pre-intervention measure), one week after theend of intervention (post-intervention measure)and one month after the end of the intervention(follow-up measure) by an examiner blinded as tothe children’s groups (intervention or control).
Information regarding the socioeconomic charac-teristics of the families was obtained for each child.
Adapted CIMT promotes functioning 641
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from
The Gross Motor Function Classification System14
and theManualAbility Classification System15wereused for functional classification. Children werethen assessed with manual tasks adapted from theJebsen–Taylor Hand Function Test (JTHF)16,17 andwith the Pediatric Evaluation Disability Inventory(PEDI).18,19
Three manual tasks adapted from the Jebsen–Taylor Hand Function Test16,17 were used to eval-uate manual dexterity: (1) picking-up two pencils,two correction fluid bottles and two erasers andputting them in a can, (2) stacking four woodencheckers, (3) picking-up five round containers(diameter 4.8 cm, height 10.6 cm). Children wereinstructed to complete each task as fast as theycould. Time to complete each task and the totaltest time were analysed. Intra-rater reliability coef-ficients of the Jebsen–Taylor Hand Function Testtasks assessment ranged from 0.86 to 0.99.Children’s functioning in activities of daily
living was assessed with the Pediatric Evaluationof Disability Inventory. The test consists of a semi-structured interview with parents regarding func-tional skills and caregiver assistance to performself-care, mobility and social function tasks.18,19
In the present study, only functional skills andcaregiver assistance scales of the self-care domainwere assessed. The raw scores were transformedinto scaled scores.18,19 Intra-rater reliability coeffi-cients varied from 0.98 to 0.99.
Statistical analysisDescriptive statistics with means, standard devi-
ations and frequency counts were used to charac-terize participants in relation to age, sex, family’ssocioeconomic status, gross motor function andmanual function classifications.Gain scores for all dependent variables were
obtained by subtracting pre-intervention scoresfrom post-intervention and follow-up scores.Because of the unbalanced number of participantsin the two groups, differences in gain scoresbetween groups were analysed with general linearmodels. The models included one independentfactor (group), one repeated measure (assessment)and an interaction factor (assessment� group).Groups were compared with regard to manualdexterity, use of the affected upper limb anddaily functioning. When results showed significant
main effects, pre-planned contrasts were used toidentify bivariate differences. The level of signifi-cance was set to a¼ 0.05. Statistical analyses wereperformed with SUPERANOVA.
The number needed to treat (NNT) was used asan index of the clinical relevance of the interven-tion to produce gains in daily functioning(Pediatric Evaluation of Disability Inventory self-care scale). The number needed to treat indicatesthe number of patients that should be treated toobtain one positive outcome due to intervention.20
Changes greater than two standard error of mea-surement (SEM)21 in the two self-care scales of thePediatric Evaluation of Disability Inventory wereconsidered indicative of positive clinically relevantresult. Calculation of the number needed to treat isbased on the number of positive outcomes in theintervention group (Pi), number of subjects in theintervention group (Ti), number of positive out-comes in the control group (Pc) and number ofparticipants in the control group (Tc), accordingto the following formula:
NNT ¼1
ðPi=TiÞ � ðPc=TcÞ
Results
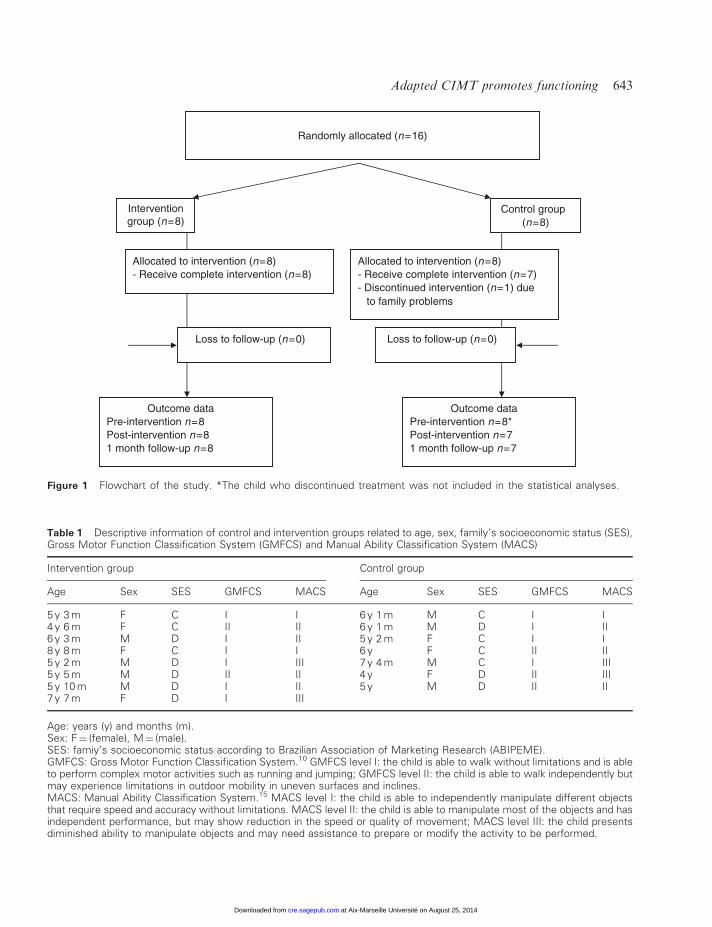
Figure 1 shows the flow diagram of the study.Among 16 children selected for the study, onechild from the control group discontinued thestudy because of family problems. Thus, therewere eight children in the intervention group andseven in the control group.
Table 1 provides information on children’s age,sex, gross motor function and manual functionclassification, as well as family’s socioeconomicstatus. There were no significant differencesbetween groups (P40.05) for any of the descrip-tive variables.
Table 2 shows the mean scores and standarddeviations of measures related to manual dexterityand daily functioning, in the intervention and con-trol groups, at pre-intervention, post-interventionand one-month follow-up assessments.
Use of the affected upper extremityNo significant differences between groups in the
Jebsen–Taylor Hand Function Test gain scoreswere found.
642 M de Brito Brandao et al.
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from
Randomly allocated (n=16)
Interventiongroup (n=8)
Control group (n=8)
Outcome dataPre-intervention n=8Post-intervention n=81 month follow-up n=8
Outcome dataPre-intervention n=8*Post-intervention n=71 month follow-up n=7
Loss to follow-up (n=0) Loss to follow-up (n=0)
Allocated to intervention (n=8)- Receive complete intervention (n=8)
Allocated to intervention (n=8)- Receive complete intervention (n=7)- Discontinued intervention (n=1) due
to family problems
Figure 1 Flowchart of the study. *The child who discontinued treatment was not included in the statistical analyses.
Table 1 Descriptive information of control and intervention groups related to age, sex, family’s socioeconomic status (SES),Gross Motor Function Classification System (GMFCS) and Manual Ability Classification System (MACS)
Intervention group Control group
Age Sex SES GMFCS MACS Age Sex SES GMFCS MACS
5 y 3 m F C I I 6 y 1 m M C I I4 y 6 m F C II II 6 y 1 m M D I II6 y 3 m M D I II 5 y 2 m F C I I8 y 8 m F C I I 6 y F C II II5 y 2 m M D I III 7 y 4 m M C I III5 y 5 m M D II II 4 y F D II III5 y 10 m M D I II 5 y M D II II7 y 7 m F D I III
Age: years (y) and months (m).Sex: F¼ (female), M¼ (male).SES: famiy’s socioeconomic status according to Brazilian Association of Marketing Research (ABIPEME).GMFCS: Gross Motor Function Classification System.10 GMFCS level I: the child is able to walk without limitations and is ableto perform complex motor activities such as running and jumping; GMFCS level II: the child is able to walk independently butmay experience limitations in outdoor mobility in uneven surfaces and inclines.MACS: Manual Ability Classification System.15 MACS level I: the child is able to independently manipulate different objectsthat require speed and accuracy without limitations. MACS level II: the child is able to manipulate most of the objects and hasindependent performance, but may show reduction in the speed or quality of movement; MACS level III: the child presentsdiminished ability to manipulate objects and may need assistance to prepare or modify the activity to be performed.
Adapted CIMT promotes functioning 643
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from
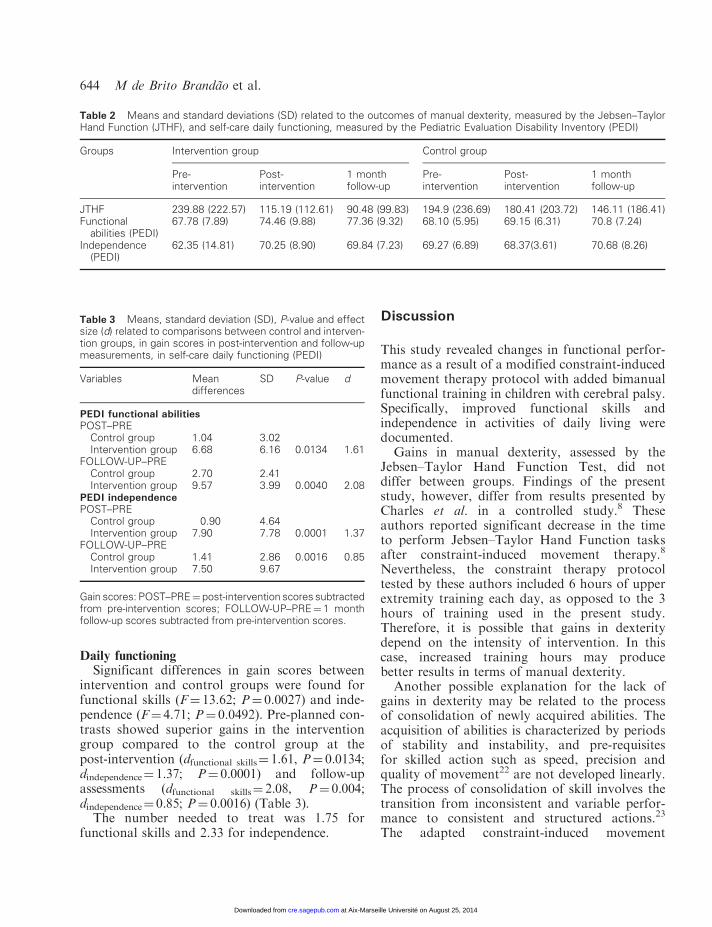
Daily functioningSignificant differences in gain scores between
intervention and control groups were found forfunctional skills (F¼ 13.62; P¼ 0.0027) and inde-pendence (F¼ 4.71; P¼ 0.0492). Pre-planned con-trasts showed superior gains in the interventiongroup compared to the control group at thepost-intervention (dfunctional skills¼ 1.61, P¼ 0.0134;dindependence¼ 1.37; P¼ 0.0001) and follow-upassessments (dfunctional skills¼ 2.08, P¼ 0.004;dindependence¼ 0.85; P¼ 0.0016) (Table 3).The number needed to treat was 1.75 for
functional skills and 2.33 for independence.
Discussion
This study revealed changes in functional perfor-mance as a result of a modified constraint-inducedmovement therapy protocol with added bimanualfunctional training in children with cerebral palsy.Specifically, improved functional skills andindependence in activities of daily living weredocumented.
Gains in manual dexterity, assessed by theJebsen–Taylor Hand Function Test, did notdiffer between groups. Findings of the presentstudy, however, differ from results presented byCharles et al. in a controlled study.8 Theseauthors reported significant decrease in the timeto perform Jebsen–Taylor Hand Function tasksafter constraint-induced movement therapy.8
Nevertheless, the constraint therapy protocoltested by these authors included 6 hours of upperextremity training each day, as opposed to the 3hours of training used in the present study.Therefore, it is possible that gains in dexteritydepend on the intensity of intervention. In thiscase, increased training hours may producebetter results in terms of manual dexterity.
Another possible explanation for the lack ofgains in dexterity may be related to the processof consolidation of newly acquired abilities. Theacquisition of abilities is characterized by periodsof stability and instability, and pre-requisitesfor skilled action such as speed, precision andquality of movement22 are not developed linearly.The process of consolidation of skill involves thetransition from inconsistent and variable perfor-mance to consistent and structured actions.23
The adapted constraint-induced movement
Table 3 Means, standard deviation (SD), P-value and effectsize (d) related to comparisons between control and interven-tion groups, in gain scores in post-intervention and follow-upmeasurements, in self-care daily functioning (PEDI)
Variables Meandifferences
SD P-value d
PEDI functional abilitiesPOST–PRE
Control group 1.04 3.02Intervention group 6.68 6.16 0.0134 1.61
FOLLOW-UP–PREControl group 2.70 2.41Intervention group 9.57 3.99 0.0040 2.08
PEDI independencePOST–PRE
Control group �0.90 4.64Intervention group 7.90 7.78 0.0001 1.37
FOLLOW-UP–PREControl group 1.41 2.86 0.0016 0.85Intervention group 7.50 9.67
Gain scores: POST–PRE¼ post-intervention scores subtractedfrom pre-intervention scores; FOLLOW-UP–PRE¼ 1 monthfollow-up scores subtracted from pre-intervention scores.
Table 2 Means and standard deviations (SD) related to the outcomes of manual dexterity, measured by the Jebsen–TaylorHand Function (JTHF), and self-care daily functioning, measured by the Pediatric Evaluation Disability Inventory (PEDI)
Groups Intervention group Control group
Pre-intervention
Post-intervention
1 monthfollow-up
Pre-intervention
Post-intervention
1 monthfollow-up
JTHF 239.88 (222.57) 115.19 (112.61) 90.48 (99.83) 194.9 (236.69) 180.41 (203.72) 146.11 (186.41)Functional
abilities (PEDI)67.78 (7.89) 74.46 (9.88) 77.36 (9.32) 68.10 (5.95) 69.15 (6.31) 70.8 (7.24)
Independence(PEDI)
62.35 (14.81) 70.25 (8.90) 69.84 (7.23) 69.27 (6.89) 68.37(3.61) 70.68 (8.26)
644 M de Brito Brandao et al.
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from
therapy protocol used in this study may have ini-tially promoted instability in performance thatallowed the emergence of new motor skills notyet sufficiently consolidated to be performed in afaster and more precise way at the end of thestudy. Longer follow-ups would be required toverify possible later gains in manual dexterity inchildren submitted to the adapted constraint-induced movement therapy protocol.
The most important result of the present studyis related to the observed improvements in dailyfunctioning. Gains in functional skills and in inde-pendence to perform activities of daily living weresignificantly superior in the intervention group atthe post-intervention and follow-up assessments.Functional training after constraint therapy pro-tocol may have played an important role inimprovements of functioning. Boyd et al.1 pointout the importance of offering practice of activitiesof daily living to individuals with hemiplegia inorder to promote skill acquisition in relevant activ-ities. Although constraint-induced movement ther-apy protocols generally involve the use offunctional activities of self-care and play, theseactivities are performed exclusively with theaffected extremity while the non-affected arm isrestricted. Therefore, the bimanual functionaltraining following the constraint-induced move-ment therapy traditional protocol was specificallyintroduced to favour incorporation of abilitiesacquired during constraint therapy into functionalactivities of daily living. Results indicate that theassociation of the two intervention strategiesresulted in gains of independence and self-careskills in children with spastic hemiplegia.
The number needed to treat was calculated inorder to document the clinical relevance of con-straint-induced movement therapy. The lowvalues of number needed to treat indicate thatfew patients need to be treated in order to obtainpositive results after intervention.20 Thus, theseresults suggest that constraint-induced movementtherapy associated with bimanual functional train-ing is an effective clinical strategy, compared withtraditional rehabilitation intervention, to promotefunctional gains in children with cerebral palsy.
Despite the positive outcomes in the use ofconstraint-induced movement therapy in the treat-ment of motor function disorders,6–8 the adequacyof this technique and its procedures should be
carefully considered for the paediatric popula-tion.3 High intensity of training and restrictionof the non-affected hand can result in frustrationand irritability. In the present study, reduced train-ing time and behavioural techniques to motivateuse of the restriction were implemented to mini-mize discomfort. It was noticed a progressiveadaptation to the procedures of the intensive train-ing and the use of the restriction happenedthroughout children’s daily routine. In the begin-ning of the intervention, children showed irritabil-ity with the use of the restriction, however, as theystarted observing gains in daily functioning withthe affected hand they were able to accept andmanage with the restriction procedures.
Adaptations in the intervention protocol wereimplemented to favour children and parents’ com-pliance to treatment. Modifications were based onevidence provided by Sterr et al.13 The authorscompared the effects of constraint-induced move-ment therapy protocols of 3 and 6 hours of func-tional training on upper extremity function ofadults with hemiplegia. Although the more inten-sive protocol produced better results, the 3-hourprotocol was also effective in promoting signifi-cant improvements in motor function.13 In thepresent study, the 3-hour daily protocol, associ-ated with the subsequent functional training, wassufficient to promote gains in functional skills andin independence in self-care activities.
Despite the observed effects, some limitations ofthe present study should be considered. The firstlimitation is related to the differences of intensity inthe protocols provided for the intervention andcontrol groups. While the intervention group wassubmitted to 3 hours of practice a day, the controlgroup received one 45-minute therapy session perweek. According to Dromerick,24 to determine theefficacy of constraint-induced movement therapy,control and intervention groups should receive thesame intensity of treatment. Otherwise, any posi-tive results could be attributed to differences inintensity and not to the type of intervention. Inthe present study, it was not possible to alter theroutine occupational therapy service to provide thecontrol group with the same intensity of treatmentas the constraint-induced movement therapygroup. Nevertheless, Taub and Uswatte25 pointedout that the high intensity of treatment is a uniquecharacteristic of constraint-induced movement
Adapted CIMT promotes functioning 645
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from

therapy protocols and that comparison betweentraditional intervention and constraint therapygroups should be performed according to their spe-cific features. It is possible that part of the effectsobserved in the intervention group could be attrib-uted to the higher intensity of the protocol.However, the effect of intensity in different typesof intervention needs to be investigated in futurestudies. Another limitation of the study is relatedto the length of follow-up. Since learning and skillacquisition take place continuously, it would beimportant to monitor gains obtained after theintervention protocol for a longer period of time.However, longer follow-ups could have resulted inexperimental losses, affecting the internal validityof the study. Finally, the relatively small number ofparticipants may have limited the generalization ofresults. Future studies with a larger group of chil-dren from a wide range of age and varied manualabilities repertoire would be useful to determine theefficacy of this intervention protocol for childrenwith hemiplegia.This clinical trial documented positive effects of
an adapted constraint-induced movement therapyprotocol associated with bimanual functionaltraining of activities on daily functioning of chil-dren with spastic hemiplegia. These findings mayadd to existing evidence on effects of constraint-induced movement therapy in children with cere-bral palsy and reinforce the use of this techniquein the clinical practice of rehabilitation profes-sionals. The present study also suggests specificadaptations to the original constraint-inducedmovement therapy protocol, which promotesfunctional gains.
Clinical messages
� Adaptations in the constraint-inducedmovement therapy protocol for a paediatricpopulation reducing the total time of inter-vention from 6 to 3 hours/day was effectivein promoting gains in self-care functioningin children and families to the intervention.
� The adapted protocol of constraint-inducedmovement therapy associated with bimanualintensive training promoted improvements indaily functioning in children with hemiplegia.
AcknowledgementsWe would like to thank Associacao Mineira de
Reabilitacao (AMR), Belo Horizonte (Brazil) forcollaborating with this study. Funding for thisstudy was provided by Conselho Nacional deDesenvolvimento Cientıfico e Tecnologico(CNPq) and by Fundacao de Apoio a Pesquisado Estado de Minas Gerais (FAPEMIG), Brazil.
References
1 Boyd RN, Morris ME, Graham HK. Managementof upper limb dysfunction in children with cerebralpalsy: a systematic review. Eur J Neurol 2001; 8:150–66.
2 Taub E, Uswatte G, Pidikiti R. Constraint-inducedmovement therapy: a new family of techniqueswith broad application to physical rehabilitation –a clinical review. J Rehabil Res Dev 1999; 36: 237–51.
3 Charles J, Gordon AM. A critical review of con-straint-induced movement therapy and forced usein children with hemiplegia. Neural Plast 2005; 12:245–61.
4 Morris DM, Taub E, Mark VW. Constraint-induced movement therapy: characterizing theintervention protocol. Eur Medicophys 2006; 42:257–68.
5 Wolf SL, Winstein CJ, Miller JP et al. Effect ofconstraint-induced movement therapy on upperextremity function 3 to 9 months after stroke: theEXCITE randomized clinical trial. JAMA 2006;296: 2095–104.
6 Eliasson AC, Krumlinde-Sundholm L, Shaw K,Wang C. Effects of constraint-induced movementtherapy in young children with hemiplegic cerebralpalsy: an adapted model. Dev Med Child Neurol2005; 47: 266–75.
7 Deluca S, Echols K, Law CR, Ramey SL. Intensivepediatric constraint-induced therapy for childrenwith cerebral palsy: randomized controlled, cross-over trial. J Child Neurol 2006; 21: 931–38.
8 Charles J, Wolf SL, Schneider JA, Gordon AM.Efficacy of a child-friendly form of constraint-induced movement therapy in hemiplegic cerebralpalsy: a randomized control trial. Dev Med ChildNeurol 2006; 48: 635–42.
9 Charles J, Gordon AM. Development of hand-armbimanual intensive training (HABIT) for improvingbimanual coordination in children with hemiplegiccerebral palsy. Dev Med Child Neurol 2006; 21:931–38.
646 M de Brito Brandao et al.
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from
10 Eliasson AC. Bimanual training for children withunilateral CP: is this something new? Dev MedChild Neurol 2007; 49: 806.
11 Eliasson AC. Improving the use of hands in dailyliving activities: aspects of treatment of childrenwith cerebral palsy. Phys Occup Ther Pediatr2005; 25: 37–60.
12 Taub E, Ramey SL, Deluca S, Echols K. Efficacyof constraint-induced movement therapy for chil-dren with cerebral palsy with asymmetric motorimpairment. Pediatrics 2004; 113: 305–12.
13 Sterr A, Elbert T, Berthold I, Kolbel S,Rockstroh B, Taub E. Longer versus shorter dailyconstraint-induced movement therapy of chronichemiparesis: an exploratory study. Arch Phys MedRehabil 2002; 83: 1374–77.
14 Palisano R, Rosenbaum P, Walter S, Russell D,Wood E, Galuppi B. Development and validationof a gross motor function classification system forchildren with cerebral palsy. Dev Med ChildNeurol 1997; 39: 214–23.
15 Eliasson AC, Krumlinde Sundholm L,Rosblad B et al. The Manual Ability ClassificationSystem (MACS) for children with cerebral palsy:scale development and evidence of validity andreliability. Dev Med Child Neurol 2006; 48:549–54.
16 Taylor N, Sand PL, Jebsen RH. Evaluation ofhand function in children. Arch Phys Med Rehabil1973; 54: 129–35.
17 Vaz DV, Mancini MC, Fonseca ST, Vieira DS,Pertence AEM. Muscle stiffness and strength andtheir relation to hand function in children withhemiplegic cerebral palsy. Dev Med Child Neurol2006; 48: 728–33.
18 Haley SM, Coster WJ, Ludlow LH,Haltiwanger JT, Andrellos PJ. Pediatric evaluationof disability inventory: development, standardiza-tion and administration manual. Boston: NewEngland Medical Center, 1992.
19 Mancini MC. Inventario de avaliacao pediatrica deincapacidade (PEDI) – manual da versao brasileiraadaptada. Belo Horizonte: Ed. UFMG, 2005.
20 Dalton GW, Keating JL. Number needed totreat: a statistic relevant for physical therapists.Phys Ther 2000; 80: 1214–19.
21 Kerlinger FN. Foundations of behavioral research,third edition. New York: Holt, Rinehart andWinston, 1986.
22 Shumway-Cook A, Woollacot MH. Motor control:theory and practical applications, second edition.Baltimore: Lippincott Williams & Wilkins, 2001.
23 Manoel EJ, Conolly KJ. Variability and the devel-opment of skilled actions. Int J Psychophysiol1995; 19: 129–47.
24 Dromerick AW. Evidence-based rehabilitation:the case for and against constraint-induced move-ment therapy. J Rehabil Res Dev 2003; 40: vii–ix.
25 Taub E, Uswatte G. The case for CI therapy.J Rehabil Res Dev 2003; 40: xiii–xv.
Adapted CIMT promotes functioning 647
at Aix-Marseille Université on August 25, 2014cre.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN




















