Active management of third stage of labor: evidence versus practice
9
Acta Obstetricia et Gynecologica. 2009; 88: 1252–1260 ORIGINAL ARTICLE Active management of third stage of labor: evidence versus practice OLUFEMI T. OLADAPO 1 , OLUWAROTIMI I. AKINOLA 2 , ADENIRAN O. FAWOLE 3 , ADEWALE S. ADEYEMI 4 , OMOLOLU ADEGBOLA 5 , OLABISI M. LOTO 6 , ADETOKUNBO O. FABAMWO 2 , MOSES O. ALAO 7 & JOHN O. SOTUNSA 1 for the Nigerian AMTSL Group 1 Maternal and Fetal Health Research Unit, Department of Obstetrics & Gynecology, Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun State, Nigeria, 2 Department of Obstetrics & Gynecology, Lagos State University Teaching Hospital, Ikeja, Lagos State, Nigeria, 3 Department of Obstetrics & Gynecology, University College Hospital, Ibadan, Oyo State, Nigeria, 4 Department of Obstetrics & Gynecology, LAUTECH Teaching Hospital, Osogbo, Osun State, Nigeria, 5 Department of Obstetrics & Gynecology, Lagos University Teaching Hospital, Idi-Araba, Lagos State, Nigeria, 6 Department of Obstetrics, Gynecology and Perinatology, Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Osun State, Nigeria, and 7 Department of Obstetrics & Gynecology, Federal Medical Centre, Abeokuta, Ogun State, Nigeria Abstract Objective. To determine the correct use of active management of third stage of labor (AMTSL) (using the full complement of existing standard definitions) and compare the outcomes of third stage of labor in women who received AMTSL (according to these definitions) with those who did not. Design. Observational, cross-sectional survey. Setting. Seven tertiary centers in southwest Nigeria. Population. Women undergoing non-instrumental vaginal deliveries. Methods. Prospective direct observa- tions of childbirth procedures. AMTSL was defined according to Cochrane review, ICM/FIGO (International Confederation of Midwives/International Federation of Gynecology and Obstetrics), and WHO (World Health Organization) recommenda- tions. Main outcome measures. Use of AMTSL and its components and outcome of third stage of labor. Results. There was a high rate of compliance with most of the individual components of AMTSL. The use of AMTSL varied widely with the definition applied and tended to decrease with increasing strictness of the criteria (Cochrane review: 88.9%; ICM/FIGO: 42%; WHO: 1.8%). The frequencies of adverse labor outcomes were generally low (postpartum hemorrhage (PPH): 4.9%; severe PPH: 0.8%; retained placenta: 1.9%; uterine inversion: 0.0%). Frequencies of PPH, postpartum anemia, and mean blood loss among women who received AMTSL according to the Cochrane review definition were significantly lower than for those who did not (p < 0.05). There was no significant difference between any of the outcomes for women who received AMTSL according to the ICM/FIGO definition and those who did not. Conclusions. The survey reveals substantial definition-dependent variation in the providers’ adherence to recommended AMTSL practices. The clinical implications of the current practice in this population suggest the need for randomized comparison of various AMTSL packages to determine their comparative effectiveness in the prevention of PPH. Key words: Postpartum hemorrhage, active management, evidence-based medicine Introduction Postpartum hemorrhage (PPH) is an important cause of maternal mortality, accounting for about a quarter of maternal deaths worldwide (1). The burden of this childbirth complication is further compounded by the non-availability of safe blood and blood products for the management of women in dire need and the unfavorable premorbid hemoglobin profile of women in resource-poor settings. Of the various causes of Correspondence: Olufemi T. Oladapo, Maternal and Fetal Health Research Unit, Department of Obstetrics and Gynecology, Olabisi Onabanjo University Teaching Hospital, P.M.B. 2001 Sagamu, Ogun State, Nigeria. E-mail: [email protected] (Received 19 December 2008; accepted 12 August 2009) ISSN 0001-6349 print/ISSN 1600-0412 online Ó 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS) DOI: 10.3109/00016340903280958 Acta Obstet Gynecol Scand Downloaded from informahealthcare.com by HINARI For personal use only.
Transcript of Active management of third stage of labor: evidence versus practice

Acta Obstetricia et Gynecologica. 2009; 88: 1252–1260
ORIGINAL ARTICLE
Active management of third stage of labor: evidence versus practice
OLUFEMI T. OLADAPO1, OLUWAROTIMI I. AKINOLA2, ADENIRAN O. FAWOLE3,ADEWALE S. ADEYEMI4, OMOLOLU ADEGBOLA5, OLABISI M. LOTO6,ADETOKUNBO O. FABAMWO2, MOSES O. ALAO7 & JOHN O. SOTUNSA1 for the NigerianAMTSL Group
1Maternal and Fetal Health Research Unit, Department of Obstetrics & Gynecology, Olabisi Onabanjo UniversityTeaching Hospital, Sagamu, Ogun State, Nigeria, 2Department of Obstetrics & Gynecology, Lagos State UniversityTeaching Hospital, Ikeja, Lagos State, Nigeria, 3Department of Obstetrics & Gynecology, University College Hospital,Ibadan, Oyo State, Nigeria, 4Department of Obstetrics & Gynecology, LAUTECH Teaching Hospital, Osogbo, OsunState, Nigeria, 5Department of Obstetrics & Gynecology, Lagos University Teaching Hospital, Idi-Araba, Lagos State,Nigeria, 6Department of Obstetrics, Gynecology and Perinatology, Obafemi Awolowo University Teaching HospitalComplex, Ile-Ife, Osun State, Nigeria, and 7Department of Obstetrics & Gynecology, Federal Medical Centre, Abeokuta,Ogun State, Nigeria
AbstractObjective. To determine the correct use of active management of third stage of labor (AMTSL) (using the full complement ofexisting standard definitions) and compare the outcomes of third stage of labor in women who received AMTSL (according tothese definitions) with those who did not. Design. Observational, cross-sectional survey. Setting. Seven tertiary centers insouthwest Nigeria. Population. Women undergoing non-instrumental vaginal deliveries. Methods. Prospective direct observa-tions of childbirth procedures. AMTSL was defined according to Cochrane review, ICM/FIGO (International Confederationof Midwives/International Federation of Gynecology and Obstetrics), and WHO (World Health Organization) recommenda-tions. Main outcome measures. Use of AMTSL and its components and outcome of third stage of labor. Results. There was ahigh rate of compliance with most of the individual components of AMTSL. The use of AMTSL varied widely with thedefinition applied and tended to decrease with increasing strictness of the criteria (Cochrane review: 88.9%; ICM/FIGO: 42%;WHO: 1.8%). The frequencies of adverse labor outcomes were generally low (postpartum hemorrhage (PPH): 4.9%; severePPH: 0.8%; retained placenta: 1.9%; uterine inversion: 0.0%). Frequencies of PPH, postpartum anemia, and mean blood lossamong women who received AMTSL according to the Cochrane review definition were significantly lower than for those whodid not (p < 0.05). There was no significant difference between any of the outcomes for women who received AMTSLaccording to the ICM/FIGO definition and those who did not. Conclusions. The survey reveals substantial definition-dependentvariation in the providers’ adherence to recommended AMTSL practices. The clinical implications of the current practice inthis population suggest the need for randomized comparison of various AMTSL packages to determine their comparativeeffectiveness in the prevention of PPH.
Key words: Postpartum hemorrhage, active management, evidence-based medicine
Introduction
Postpartum hemorrhage (PPH) is an important causeof maternal mortality, accounting for about a quarterof maternal deaths worldwide (1). The burden of this
childbirth complication is further compounded by thenon-availability of safe blood and blood products forthe management of women in dire need and theunfavorable premorbid hemoglobin profile of womenin resource-poor settings. Of the various causes of
Correspondence: Olufemi T. Oladapo, Maternal and Fetal Health Research Unit, Department of Obstetrics and Gynecology, Olabisi Onabanjo UniversityTeaching Hospital, P.M.B. 2001 Sagamu, Ogun State, Nigeria. E-mail: [email protected]
(Received 19 December 2008; accepted 12 August 2009)
ISSN 0001-6349 print/ISSN 1600-0412 online � 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS)DOI: 10.3109/00016340903280958
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.

PPH, uterine atony is the most common and theleading cause of maternal death resulting from thiscomplication. Because of the inability to predictwomen who may develop this complication, interven-tions to prevent postpartum bleeding from uterineatony (atonic PPH) are directed at all women duringchildbirth.An evidence-based intervention for the prevention
of atonic PPH is the active management of thirdstage of labor (AMTSL), which has been promotedglobally as part of efforts to reduce maternal mortalityespecially in developing countries (2). AMTSL asa preventive intervention greatly reduces the needfor additional interventions and expensive and fre-quently unavailable resources needed to managehemorrhage (3). While there is general agreementon the beneficial effects of AMTSL, its componentsand their definitions are less clear. This is reflectedin the rapid evolution of internationally recom-mended guidelines on AMTSL over the last fewyears. A Cochrane review described the interventionas a package comprising of administration of pro-phylactic uterotonics after birth, early cord clampingand cutting, and placental delivery by controlledcord traction (4). Recent joint recommendationsby the International Confederation of Midwives/International Federation of Gynecology and Obstet-rics (ICM/FIGO) include the following components:administration of uterotonic agent within one minutefollowing delivery of the baby, controlled cord trac-tion, and uterine massage after placental delivery(5,6); while in the ‘WHO recommendations for theprevention of postpartum hemorrhage’ (7), delayedcord clamping was added to the components recom-mended by ICM/FIGO to accommodate recent evi-dence suggesting beneficial effects of delayed cordclamping to the baby.In spite of the efforts to standardize, update, and
disseminate AMTSL practices worldwide, the extentof practice in areas where they are most needed isunclear. In Nigeria, for instance, the adoption andproper practice of this intervention at all levels ofhealthcare delivery is doubtful in view of the contri-bution of PPH to the national maternal mortalityfigures (8). Although a survey of Nigerian obstetri-cians reported a high adoption and practice rate ofAMTSL (9), it is uncertain whether the same ratewould be recorded through direct observation ontheir labor wards and to what extent the recom-mended components are adhered to. Objective assess-ment of the prevailing AMTSL practices in the lightof current evidence and recommendations wouldguide health professionals and policy makers in theirreview of evidence-based strategies for reduction ofmaternal mortality due to PPH in this setting. In view
of the challenges faced in translating research evi-dence into clinical practice in low resource settings,it is also imperative to examine the clinical conse-quences of current AMTSL practices in order tojustify the advocated changes in related policies andregulations. It is within this framework that we con-ducted a multicenter study of providers’ practices inthe third stage of labor in tertiary obstetric centers insouthwest Nigeria.The aim of this study was to specifically examine
the proportion of deliveries where AMTSL (using thefull complement of existing standard definitions) wascorrectly used in the tertiary institutions in this region,assess how frequently the individual components ofAMTSL were used, identify practices in third stageof labor that did not conform to existing definitionsof AMTSL, and compare the outcomes of thirdstage of labor of women who received the full com-plement of AMTSL (according to different defini-tions) with those who did not.
Material and methods
Study setting
The study was an observational, cross-sectionalsurvey in the obstetric units of all public tertiarycare institutions in southwest Nigeria. These institu-tions were Olabisi Onabanjo University TeachingHospital (OOUTH), Sagamu; University CollegeHospital (UCH), Ibadan; Lagos University Teach-ing Hospital (LUTH), Lagos; Ladoke AkintolaUniversity of Technology Teaching Hospital(LAUTECHTH), Osogbo; Lagos State UniversityTeaching Hospital (LASUTH), Lagos; ObafemiAwolowo University Teaching Hospital Complex(OAUTHC), Ilesa; and Federal Medical Centre(FMC), Abeokuta. These hospitals serve as referralcenters for private, primary, and secondary healthcare facilities within the region. Obstetric servicesare provided to both high- and low-risk pregnantwomen by nurse/midwives, postgraduate residentdoctors undergoing specialist obstetric training, andconsultant obstetricians.The investigation was conducted by prospective
direct observations of childbirth procedures at indi-vidual centers by assigned and trained clinicians whoare familiar with the existing and current standarddefinitions of AMTSL. The processes of the manage-ment of third stage of labor among non-instrumentalvaginal deliveries conducted over a period of 14 hoursper day (7 a.m. to 9 p.m.) were documented. Usinga standardized data capture sheet, demographiccharacteristics such as age, parity, gestational age at
Active management of third stage of labor 1253
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.

delivery, booking status, hemoglobin concentrationin labor or at the last antenatal visit, and previoushistory of PPH were obtained through a review ofthe parturients’ case files. Data on labor character-istics such as its nature of onset and duration, useof oxytocin for augmentation during the course oflabor, time of birth, and fetal birth-weight wererecorded. The components of AMTSL were observedand any practice(s) at variance with the existing defi-nitions were noted. The outcome of third stage oflabor with respect to estimated postpartum bloodloss, use of additional uterotonics to stop or preventfurther bleeding (in the form of either infusion orbolus injection), placenta retention, and postpartumhemoglobin concentration were also documented.No personal identifier of parturients or labor atten-dants was recorded. Written informed consent wasobtained from the parturients in the admissionroom of the labor ward. Institutional approval wasobtained from the ethical review boards of all par-ticipating institutions.
Sample size determination
The minimum sample size required for the studywas estimated to be 384 using the formula n = p(1 – p)(Za/d)
2, where n is the sample size, Za is the stan-dard normal deviate (set at 1.96 for 95% confi-dence level), d is the desired degree of accuracy(taken as 0.05), and p is the estimate of the rate ofcorrect use of AMTSL among the target population(which was assumed to be 50% in the absence of apre-existing estimate) (10). Adjustment for a 10%rate of invalid/erroneous entries yielded a final sam-ple size of 427.All women undergoing non-instrumental vaginal
deliveries at the designated tertiary care centers dur-ing the period of the study were eligible for the study.Using the available statistics at each center, the aver-age number of non-instrumental vaginal deliveriesduring each month at each center was estimated apriori. To achieve the desired sample size for thestudy, the number of deliveries to be observed ateach center was determined by the proportional allo-cation ratio method (i.e. the total number of deliveriesobserved at each center was in accordance with therelative proportion of its monthly non-instrumentalvaginal deliveries). Deliveries that were observed wereselected by the systematic random sampling method(every third eligible parturient) during the period ofthe study until the estimated sample size for the centerwas achieved. Observations of deliveries were carriedout concurrently at all the centers over a period ofthree months.
Definitions of AMTSL
Three definitions of AMTSL were considered in thisstudy. The definitions are as described in theCochrane review (4), the joint statement by ICM/FIGO on the prevention of PPH (5), and ‘WHOrecommendations for the prevention of postpartumhemorrhage’ (7).
(1) The definition of AMTSL as described by theCochrane review includes the following inter-locking interventions:
(i) Administration of prophylactic uterotonic(defined as the administration of anyuterotonic concurrently with the deliveryof the anterior shoulder of the baby orimmediately after the delivery of the fetusbut before the delivery of the placenta).
(ii) Early cord clamping and cutting.(iii) Controlled cord traction for delivery of the
placenta.
(2) The definition of AMTSL as promoted by ICM/FIGO includes the following components:
(i) Administration of uterotonic agent (pref-erably 10 IU of oxytocin via intramuscularinjection) within one minute following thedelivery of the fetus.
(ii) Controlled cord traction (defined as thegentle pulling of the clamped umbilicalcord, with upward, manual support ofthe uterus) as a means of delivering theplacenta.
(iii) Immediate uterine massage followingdelivery of the placenta and palpation ofthe uterus to assess the need for continuedmassage every 15 minutes over the next2 hours. For the purpose of this study,assessment of this component was limitedto observation of immediate uterine mas-sage following delivery of the placenta.
(3) The definition of AMTSL as recommended byWHO includes the three components above plusdelayed cord clamping (regarded as cord clamp-ing after three minutes of birth).
Data management and analysis
Completed data forms were reviewed by the investi-gator at each center and later sent to a central collatingcenter for analysis. Centrally collated data was codedand analyzed using the Epi Info 2002 statistical soft-ware (11). The frequency distribution and summarystatistics (where applicable) of parturients observed
1254 O.T. Oladapo et al.
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.
was computed. The proportion of women for whomAMTSL was correctly used according to the abovedefinitions was calculated. Similarly, the proportionof women who received individual components ofAMTSL was determined. The outcomes of thirdstage of labor were compared between parturientswho had the full complement of AMTSL (accordingto each definition) and those who did not. Categoricalvariables were compared with the c2 or Fisher’s exacttest while continuous variables were compared withthe t-test. Differences were considered statisticallysignificant when p < 0.05.
Results
Characteristics of observed deliveries
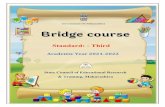
Using the pre-specified selection criteria, a totalof 486 non-instrumental vaginal deliveries wereobserved between April and June 2008 at the sevensites. Table I shows the characteristics of the observeddeliveries and those of the parturients. The volumeof deliveries in these facilities varied considerably,ranging from low-volume facilities with less than1,000 deliveries a year to high-volume facilities witha volume of more than 5,000 deliveries a year. Theproviders who managed the deliveries included mid-wives, interns, and resident doctors. The majority ofthe parturients were between the ages of 20 and34 years (mean 29.9 years, SD 4.8), received ante-natal care at the respective study site, and deliveredtheir babies at term. About two-fifths of them werehaving their first delivery and only 2.1% were grand-multiparae. A small fraction of the women had expe-rienced PPH in their previous delivery.
Use of uterotonic drugs
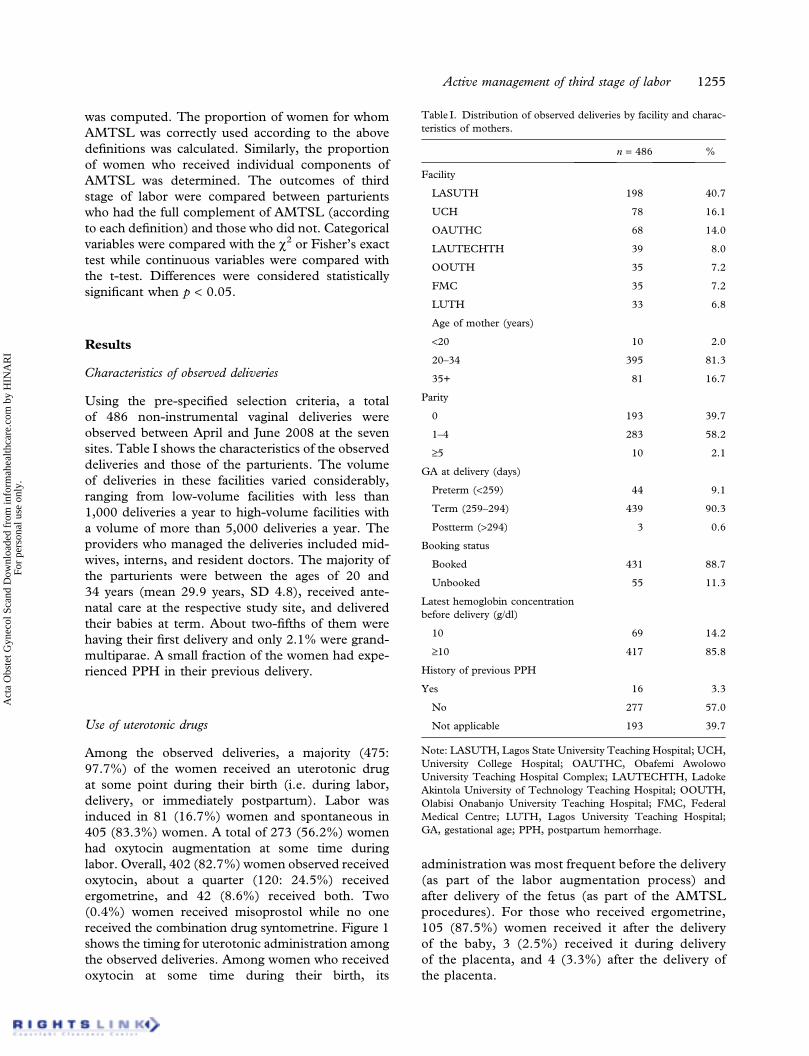
Among the observed deliveries, a majority (475:97.7%) of the women received an uterotonic drugat some point during their birth (i.e. during labor,delivery, or immediately postpartum). Labor wasinduced in 81 (16.7%) women and spontaneous in405 (83.3%) women. A total of 273 (56.2%) womenhad oxytocin augmentation at some time duringlabor. Overall, 402 (82.7%) women observed receivedoxytocin, about a quarter (120: 24.5%) receivedergometrine, and 42 (8.6%) received both. Two(0.4%) women received misoprostol while no onereceived the combination drug syntometrine. Figure 1shows the timing for uterotonic administration amongthe observed deliveries. Among women who receivedoxytocin at some time during their birth, its
administration was most frequent before the delivery(as part of the labor augmentation process) andafter delivery of the fetus (as part of the AMTSLprocedures). For those who received ergometrine,105 (87.5%) women received it after the deliveryof the baby, 3 (2.5%) received it during deliveryof the placenta, and 4 (3.3%) after the delivery ofthe placenta.
Table I. Distribution of observed deliveries by facility and charac-teristics of mothers.
n = 486 %
Facility
LASUTH 198 40.7
UCH 78 16.1
OAUTHC 68 14.0
LAUTECHTH 39 8.0
OOUTH 35 7.2
FMC 35 7.2
LUTH 33 6.8
Age of mother (years)
<20 10 2.0
20–34 395 81.3
35+ 81 16.7
Parity
0 193 39.7
1–4 283 58.2
‡5 10 2.1
GA at delivery (days)
Preterm (<259) 44 9.1
Term (259–294) 439 90.3
Postterm (>294) 3 0.6
Booking status
Booked 431 88.7
Unbooked 55 11.3
Latest hemoglobin concentrationbefore delivery (g/dl)
10 69 14.2
‡10 417 85.8
History of previous PPH
Yes 16 3.3
No 277 57.0
Not applicable 193 39.7
Note: LASUTH, Lagos State University Teaching Hospital; UCH,University College Hospital; OAUTHC, Obafemi AwolowoUniversity Teaching Hospital Complex; LAUTECHTH, LadokeAkintola University of Technology Teaching Hospital; OOUTH,Olabisi Onabanjo University Teaching Hospital; FMC, FederalMedical Centre; LUTH, Lagos University Teaching Hospital;GA, gestational age; PPH, postpartum hemorrhage.
Active management of third stage of labor 1255
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.
Components and use of AMTSL by different definitions
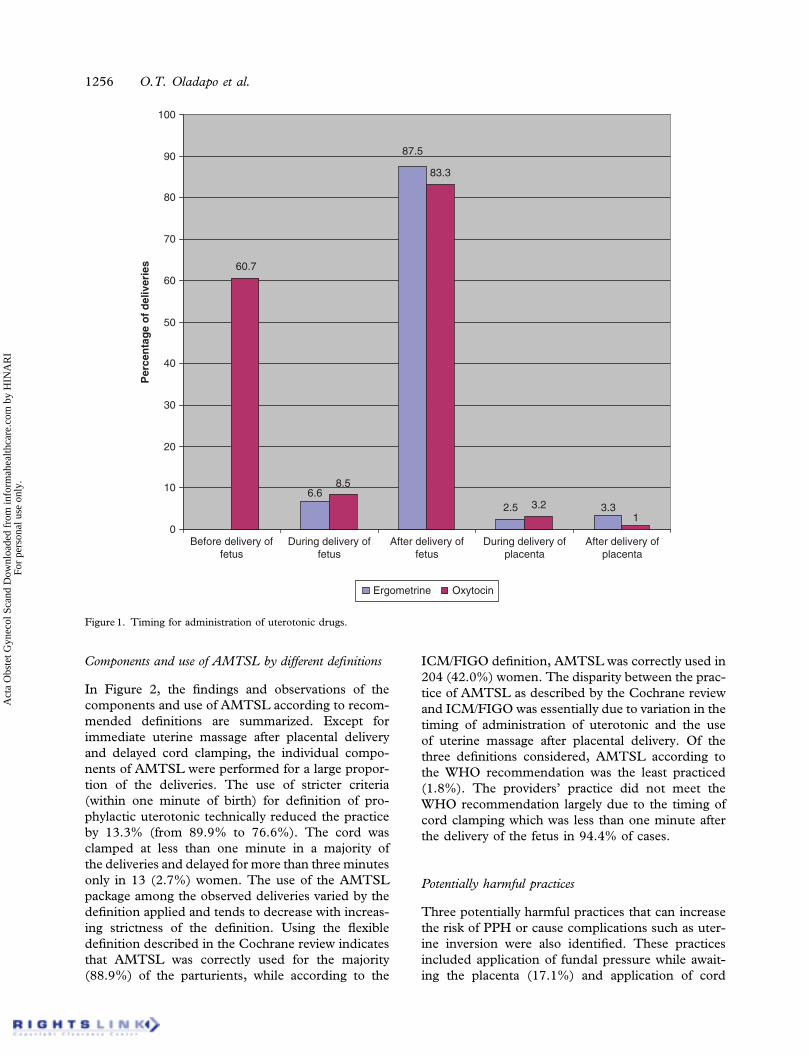
In Figure 2, the findings and observations of thecomponents and use of AMTSL according to recom-mended definitions are summarized. Except forimmediate uterine massage after placental deliveryand delayed cord clamping, the individual compo-nents of AMTSL were performed for a large propor-tion of the deliveries. The use of stricter criteria(within one minute of birth) for definition of pro-phylactic uterotonic technically reduced the practiceby 13.3% (from 89.9% to 76.6%). The cord wasclamped at less than one minute in a majority ofthe deliveries and delayed for more than three minutesonly in 13 (2.7%) women. The use of the AMTSLpackage among the observed deliveries varied by thedefinition applied and tends to decrease with increas-ing strictness of the definition. Using the flexibledefinition described in the Cochrane review indicatesthat AMTSL was correctly used for the majority(88.9%) of the parturients, while according to the
ICM/FIGO definition, AMTSL was correctly used in204 (42.0%) women. The disparity between the prac-tice of AMTSL as described by the Cochrane reviewand ICM/FIGO was essentially due to variation in thetiming of administration of uterotonic and the useof uterine massage after placental delivery. Of thethree definitions considered, AMTSL according tothe WHO recommendation was the least practiced(1.8%). The providers’ practice did not meet theWHO recommendation largely due to the timing ofcord clamping which was less than one minute afterthe delivery of the fetus in 94.4% of cases.
Potentially harmful practices
Three potentially harmful practices that can increasethe risk of PPH or cause complications such as uter-ine inversion were also identified. These practicesincluded application of fundal pressure while await-ing the placenta (17.1%) and application of cord
6.6
87.5
2.5 3.3
60.7
8.5
83.3
3.21
0
10
20
30
40
50
60
70
80
90
100
Before delivery offetus
During delivery offetus
After delivery offetus
During delivery ofplacenta
After delivery ofplacenta
Per
cen
tag
e o
f d
eliv
erie
s
Ergometrine Oxytocin
Figure 1. Timing for administration of uterotonic drugs.
1256 O.T. Oladapo et al.
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.
traction without manual support (9.1%) and withouthaving administered any uterotonic drug (2.3%).
Use of AMTSL according to different definitionsand outcome of third stage of labor
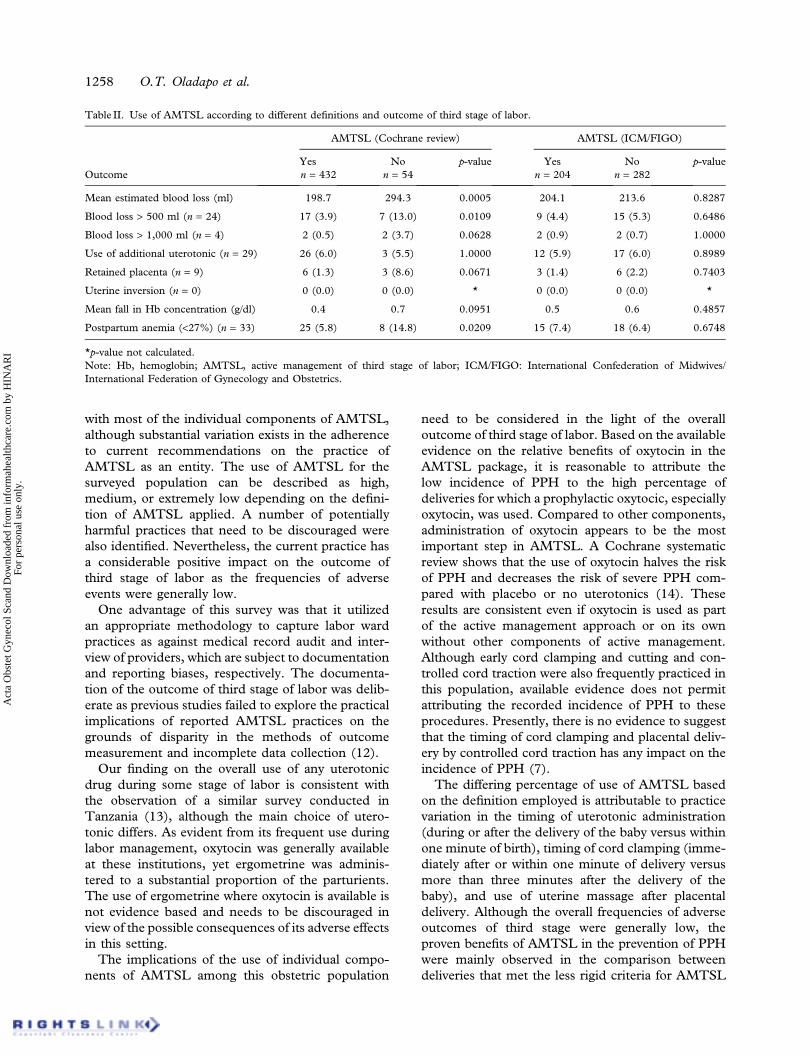
Of all the observed deliveries, 24 (4.9%) were com-plicated by blood loss in excess of 500 ml (PPH) and4 (0.8%) by blood loss in excess of 1,000 ml (severePPH). Estimated blood loss ranged between 100 mland 2 liters with a mean of 209.4 ml. Thirty-threewomen (6.8%) had postpartum anemia (Hb < 9 g/dl).Twenty-nine women (13.6%) required additionaluterotonic in addition to the prophylactic uterotonicto prevent or stop excessive blood loss. Nine cases(1.9%) of retained placenta and no case of uterineinversion were recorded.Table II shows the comparison of the outcomes of
third stage of labor between women who receivedAMTSL (according to different definitions) and thosewho did not. The mean blood loss and frequencies of
PPH and postpartum anemia (Hb < 9 g/dl) were sig-nificantly lower among those who received the fullcomplement of AMTSL as described by the Cochranereview than those who did not (p < 0.05). In thecomparison of the outcomes of women who receivedthe full complement of AMTSL according to theICM/FIGO definition and those who did not, nosignificant difference was found between any of theparameters (p > 0.05). Comparison of outcomes ofthose who received the full complement of AMTSLaccording to the WHO definition with those who didnot could not be made due to the small numbers.
Discussion
This survey describes the rates of use of an inexpen-sive and simple intervention in a region whereenforcement of clinical policies is flexible and adher-ence to recommended guidelines is sometimes guidedby factors other than providers’ knowledge of whatworks. The findings show a high rate of compliance
89.9
76.6
94.4
2.7
89.3
62.6
88.9
42
1.8
0
10
20
30
40
50
60
70
80
90
100
Prophylacticuterotonic
Cord clamping Controlled cordtraction
Uterinemassage
AMTSL
Per
cen
tag
e o
f d
eliv
erie
s
Prophylactic uterotonic(Cochrane review)
Prophylactic uterotonic(ICM/FIGO)
Cord clamping within 1 min
Cord clamping > 3 min
Controlled cord traction
Uterine massage
AMTSL (Cochrane review)
AMTSL (ICM/FIGO)
AMTSL (WHO)
Figure 2. Components and use of AMTSL according to different definitions.Note: AMTSL, active management of third stage of labor; ICM/FIGO: International Confederation of Midwives/International Federation ofGynecology and Obstetrics; WHO, World Health Organization.
Active management of third stage of labor 1257
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.
with most of the individual components of AMTSL,although substantial variation exists in the adherenceto current recommendations on the practice ofAMTSL as an entity. The use of AMTSL for thesurveyed population can be described as high,medium, or extremely low depending on the defini-tion of AMTSL applied. A number of potentiallyharmful practices that need to be discouraged werealso identified. Nevertheless, the current practice hasa considerable positive impact on the outcome ofthird stage of labor as the frequencies of adverseevents were generally low.One advantage of this survey was that it utilized
an appropriate methodology to capture labor wardpractices as against medical record audit and inter-view of providers, which are subject to documentationand reporting biases, respectively. The documenta-tion of the outcome of third stage of labor was delib-erate as previous studies failed to explore the practicalimplications of reported AMTSL practices on thegrounds of disparity in the methods of outcomemeasurement and incomplete data collection (12).Our finding on the overall use of any uterotonic
drug during some stage of labor is consistent withthe observation of a similar survey conducted inTanzania (13), although the main choice of utero-tonic differs. As evident from its frequent use duringlabor management, oxytocin was generally availableat these institutions, yet ergometrine was adminis-tered to a substantial proportion of the parturients.The use of ergometrine where oxytocin is available isnot evidence based and needs to be discouraged inview of the possible consequences of its adverse effectsin this setting.The implications of the use of individual compo-
nents of AMTSL among this obstetric population
need to be considered in the light of the overalloutcome of third stage of labor. Based on the availableevidence on the relative benefits of oxytocin in theAMTSL package, it is reasonable to attribute thelow incidence of PPH to the high percentage ofdeliveries for which a prophylactic oxytocic, especiallyoxytocin, was used. Compared to other components,administration of oxytocin appears to be the mostimportant step in AMTSL. A Cochrane systematicreview shows that the use of oxytocin halves the riskof PPH and decreases the risk of severe PPH com-pared with placebo or no uterotonics (14). Theseresults are consistent even if oxytocin is used as partof the active management approach or on its ownwithout other components of active management.Although early cord clamping and cutting and con-trolled cord traction were also frequently practiced inthis population, available evidence does not permitattributing the recorded incidence of PPH to theseprocedures. Presently, there is no evidence to suggestthat the timing of cord clamping and placental deliv-ery by controlled cord traction has any impact on theincidence of PPH (7).The differing percentage of use of AMTSL based
on the definition employed is attributable to practicevariation in the timing of uterotonic administration(during or after the delivery of the baby versus withinone minute of birth), timing of cord clamping (imme-diately after or within one minute of delivery versusmore than three minutes after the delivery of thebaby), and use of uterine massage after placentaldelivery. Although the overall frequencies of adverseoutcomes of third stage were generally low, theproven benefits of AMTSL in the prevention of PPHwere mainly observed in the comparison betweendeliveries that met the less rigid criteria for AMTSL
Table II. Use of AMTSL according to different definitions and outcome of third stage of labor.
AMTSL (Cochrane review) AMTSL (ICM/FIGO)
Yes No p-value Yes No p-valueOutcome n = 432 n = 54 n = 204 n = 282
Mean estimated blood loss (ml) 198.7 294.3 0.0005 204.1 213.6 0.8287
Blood loss > 500 ml (n = 24) 17 (3.9) 7 (13.0) 0.0109 9 (4.4) 15 (5.3) 0.6486
Blood loss > 1,000 ml (n = 4) 2 (0.5) 2 (3.7) 0.0628 2 (0.9) 2 (0.7) 1.0000
Use of additional uterotonic (n = 29) 26 (6.0) 3 (5.5) 1.0000 12 (5.9) 17 (6.0) 0.8989
Retained placenta (n = 9) 6 (1.3) 3 (8.6) 0.0671 3 (1.4) 6 (2.2) 0.7403
Uterine inversion (n = 0) 0 (0.0) 0 (0.0) * 0 (0.0) 0 (0.0) *
Mean fall in Hb concentration (g/dl) 0.4 0.7 0.0951 0.5 0.6 0.4857
Postpartum anemia (<27%) (n = 33) 25 (5.8) 8 (14.8) 0.0209 15 (7.4) 18 (6.4) 0.6748
*p-value not calculated.Note: Hb, hemoglobin; AMTSL, active management of third stage of labor; ICM/FIGO: International Confederation of Midwives/International Federation of Gynecology and Obstetrics.
1258 O.T. Oladapo et al.
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.

with those that did not. The lack of significant dif-ferences in the recorded outcomes between deliveriesin which AMTSL was practiced according to ICM/FIGO recommendations compared to others suggestsminimal contribution of uterine massage to the effec-tiveness of AMTSL as an intervention. This deduc-tion is supported by the lack of strong evidence forthe reduction of PPH by inclusion of uterine massageto AMTSL. In a Cochrane review, Hofmeyr et al.showed that the frequency of PPH was generallylow regardless of whether uterine massage was per-formed after AMTSL or not (15). Although a rel-atively simple procedure, uterine massage at quarterhourly intervals for two hours, as recommended byICM/FIGO, may be inconvenient to both womenand labor attendants. Its benefits therefore need tobe demonstrated to outweigh this shortcoming inlarge randomized trials that evaluate priority out-comes of third stage of labor. Although the impactof AMTSL practice in this population according tothe WHO recommendation could not be assesseddue to its low frequency, it is unlikely to be differentfrom that of ICM/FIGO because the main difference(delayed cord clamping) between the two recom-mendations has not been shown to influence theincidence of PPH.The limitations of this survey include its descriptive
nature, which limits the inferences derivable fromcomparisons, the confinement of data collection toa certain period of the day (thus excluding practices inthe early morning hours when labor attendants areunlikely to strictly adhere to protocol), and themethod used for estimating postpartum blood loss.Data collection was restricted to a feasible period thatpermitted observation by the same observer in orderto maintain the internal validity of the study. Althoughit may be argued that blood loss is often underesti-mated by the method employed, it is important torealize that interventions for combating hemorrhageby labor attendants in this setting and other similarsettings are dependent on this method of assessmentof blood loss.In conclusion, the survey reveals substantial defi-
nition-dependent variation in the adherence of pro-viders to the AMTSL practices recommended byinternational health bodies. The current practicesin these institutions mostly conform to the earliestand least stringent recommendation on AMTSLand are at wide variance with the most recent guide-line. The gap between current guideline and practicemay reflect the time it takes for the adaptation, adop-tion, and dissemination of internationally recom-mended guidelines by the Nigerian health ministryto the various health institutions. This gap can bebridged by making available resources such as the
Cochrane Library and WHO Reproductive HealthLibrary to all providers involved in managing preg-nant women at these institutions. However, the clin-ical implications of the use of AMTSL accordingto different definitions question the stringency ofAMTSL criteria and call for randomized comparisonof various AMTSL packages in order to determinetheir comparative effectiveness in the prevention ofPPH. The findings of such a study would providethe basis for introduction of new guidelines for pre-vention of PPH and justify the resources that would beexpended in translating current evidence into clinicalpractice in low resource settings.
Acknowledgements
The contributions of Drs. A. Akadri, O. Ayoola-Sotubo (OOUTH), B.A. Olofinbiyi, A. Adewumi(OAUTHC), Y. Oshodi, A. Adegboyega (LASUTH),O. Atanda (LAUTECHTH), O. Bamgbopa (FMC),O.M. Akindele, and A.A. Okunowo (OAUTHC)with respect to data collection are acknowledged.
Disclosure of interest: No conflict of interestdeclared.
References
1. AbouZahr C. Antepartum and postpartum hemorrhage. In:Murray CJ, Lopez AD (eds). Health dimensions of sex andreproduction: the global burden of sexually transmitted dis-eases, HIV, maternal conditions, perinatal disorders, andcongenital abnormalities. Boston, MA: Harvard UniversityPress, 1998. pp. 172–4.
2. Lalonde A, Daviss BA, Acosta A, Herschderfer K. Postpartumhemorrhage today: ICM/FIGO initiative 2004-2006. Int JGynecol Obstet. 2006;94:243–53.
3. Fullerton JT, Frick KD, Fogarty LA, Fischel JD, Vivio DM.Active management of third stage of labor saves facility costsin Guatemala and Zambia. J Health Popul Nutr. 2006;24:540–51.
4. Prendiville WJ, Elbourne D, McDonald S. Active versusexpectant management in the third stage of labor. CochraneDatabase Syst Rev. 2000;(3):CD000007.
5. International Confederation of Midwives and InternationalFederation of Gynecology and Obstetrics. International jointpolicy statement: management of third stage of labor toprevent postpartum hemorrhage. J Obstet Gynecol Can2003;25:952–3.
6. International Confederation of Midwives and InternationalFederation of Gynecology and Obstetrics. Internationaljoint policy statement: FIGO/ICM global initiative to pre-vent postpartum hemorrhage. J Obstet Gynecol Can.2004;26:1100–2.
7. World Health Organization. WHO recommendations forthe prevention of postpartum hemorrhage. Geneva: WHODepartment of Reproductive Health and Research, 2007.
8. Federal Ministry of Health. Fact sheet on safe motherhood.Abuja: FMOH, 2005.
Active management of third stage of labor 1259
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.

9. Oladapo OT, Fawole AO. Adoption and practice of evidence-based obstetric care among Nigerian obstetricians. J ObstetGynaecol. 2007;27:279–81.
10. Centers for Disease Control and Prevention (CDC), FamilyHealth International (FHI), In: World Health Organization(WHO). Sample size and power. Wingo PA, Higgins JE,Rubin GL, Zahniser SC(eds). An epidemiologic approach toreproductive health. Geneva: World Health Organization,1994. pp. 151–200.
11. Centers for Disease Control and Prevention (CDC), WorldHealth Organization. Epi Info 2002. In: Database and sta-tistics software for public health professionals. Atlanta, GA:Centers for Disease Control and Prevention, 2002.
12. Festin MR, Lumbiganon P, Tolosa JE, Finney KA,Ba-Thike K, Chipato T, et al. International survey on
variations in practice of the management of the third stageof labor. Bull World Health Organ. 2003;81:286–91.
13. U.S. Agency for International Development, Prevention ofPostpartum Hemorrhage Initiative, Support, Analysis andResearch in Africa. Facility-based management of third stageof labor and community perception and actions on post-partum haemorrhage: Findings from a national survey inTanzania. Washington, DC: POPHI, 2006.
14. Elbourne DR, Prendiville WJ, Carroli G, Wood J,McDonald S. Prophylactic use of oxytocin in the thirdstage of labor. Cochrane Database Syst Rev. 2001;(4):CD000201.
15. Hofmeyr GJ, Abdel-Aleem H, Abdel-Aleem MA. Uterinemassage for preventing postpartum hemorrhage. CochraneDatabase Syst Rev. 2008;16(3): CD006431.
1260 O.T. Oladapo et al.
Act
a O
bste
t Gyn
ecol
Sca
nd D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y H
INA
RI
For
pers
onal
use
onl
y.