Acquired C1-inhibitor deficiency and lymphoproliferative disorders: A tight relationship
10
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor deficiency and lymphoproliferative disorders: A tight relationship. Crit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2013.02.004 ARTICLE IN PRESS ONCH-1713; No. of Pages 10 Critical Reviews in Oncology/Hematology xxx (2013) xxx–xxx Acquired C1-inhibitor deficiency and lymphoproliferative disorders: A tight relationship Roberto Castelli a,b , Andrea Zanichelli c , Marco Cicardi c , Massimo Cugno a,b,∗ a Department of Pathophysiology and Transplantation, Internal Medicine Section, University of Milan, Milan, Italy b Department of Medicine, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy c Dipartimento di Scienze Cliniche Luigi Sacco, Università degli Studi di Milano, Milano, Italy Accepted 14 February 2013 Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 2. Historical background and pathophysiology of acquired c1-inhibitor deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 3. Clinical characteristics of acquired C1-inhibitor deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 3.1. Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 3.2. Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 3.3. Course . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 3.4. Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 4. Link between acquired angioedema and lymphoproliferative disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Conflicts of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Reviewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Biography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Abstract Angioedema due to the acquired deficiency of C1-inhibitor is a rare disease known as acquired angioedema (AAE), which was first described in a patient with high-grade lymphoma and is frequently associated with lymphoproliferative diseases, including expansion of B cell clones producing anti-C1-INH autoantibodies, monoclonal gammopathy of uncertain significance (MGUS) and non-Hodgkin lymphoma (NHL). AAE is clinically similar to hereditary angioedema (HAE), and is characterized by recurrent episodes of sub-cutaneous and sub-mucosal edema. It may affect the face, tongue, extremities, trunk and genitals. The involvement of the gastrointestinal tract causes bowel sub-occlusion with severe pain, vomiting and diarrhea, whereas laryngeal edema can be life-threatening. Unlike those with HAE, AAE patients usually have late-onset symptoms, do not have a family history of angioedema and present variable response to treatment due to the hyper-catabolism of C1-inhibitor. Reduced C1-inhibitor function leads to activation of the classic complement pathway with its consumption and activation of the contact system leading to the generation of the vasoactive peptide bradykinin, which increases vascular permeability and induces angioedema. Lymphoprolipherative diseases and AAE are tightly linked with either angioedema or limphoprolyferation being the first symptom. Experi- mental data indicate that neoplastic tissue and/or anti-C1-inhibitor antibodies induce C1-inhibitor consumption, and this is further supported by the observation that cytotoxic treatment of the lymphoproliferative diseases associated with AAE variably reverses the complement impairment and leads to a clinical improvement in angioedema symptoms. © 2013 Elsevier Ireland Ltd. All rights reserved. Keywords: C1-inhibitor deficiency; Acquired angioedema; Lymphoproliferative disease; Auto-antibodies; Complement ∗ Corresponding author at: Department of Pathophysiology and Transplantation, Section of Internal Medicine, Via Pace 9, 20122 Milan, Italy. Tel.: +39 02 55035340; fax: +39 02 50320742. E-mail address: [email protected] (M. Cugno). 1040-8428/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.critrevonc.2013.02.004
Transcript of Acquired C1-inhibitor deficiency and lymphoproliferative disorders: A tight relationship

O
C
123
45
A
ipAewlCc
mta©
K
T
1h
ARTICLE IN PRESSNCH-1713; No. of Pages 10
Critical Reviews in Oncology/Hematology xxx (2013) xxx–xxx
Acquired C1-inhibitor deficiency and lymphoproliferative disorders:A tight relationship
Roberto Castelli a,b, Andrea Zanichelli c, Marco Cicardi c, Massimo Cugno a,b,∗a Department of Pathophysiology and Transplantation, Internal Medicine Section, University of Milan, Milan, Italy
b Department of Medicine, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italyc Dipartimento di Scienze Cliniche Luigi Sacco, Università degli Studi di Milano, Milano, Italy
Accepted 14 February 2013
ontents
. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Historical background and pathophysiology of acquired c1-inhibitor deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Clinical characteristics of acquired C1-inhibitor deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.1. Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.2. Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.3. Course . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.4. Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Link between acquired angioedema and lymphoproliferative disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Conflicts of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Reviewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Biography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
bstract
Angioedema due to the acquired deficiency of C1-inhibitor is a rare disease known as acquired angioedema (AAE), which was first describedn a patient with high-grade lymphoma and is frequently associated with lymphoproliferative diseases, including expansion of B cell clonesroducing anti-C1-INH autoantibodies, monoclonal gammopathy of uncertain significance (MGUS) and non-Hodgkin lymphoma (NHL).AE is clinically similar to hereditary angioedema (HAE), and is characterized by recurrent episodes of sub-cutaneous and sub-mucosal
dema. It may affect the face, tongue, extremities, trunk and genitals. The involvement of the gastrointestinal tract causes bowel sub-occlusionith severe pain, vomiting and diarrhea, whereas laryngeal edema can be life-threatening. Unlike those with HAE, AAE patients usually have
ate-onset symptoms, do not have a family history of angioedema and present variable response to treatment due to the hyper-catabolism of1-inhibitor. Reduced C1-inhibitor function leads to activation of the classic complement pathway with its consumption and activation of theontact system leading to the generation of the vasoactive peptide bradykinin, which increases vascular permeability and induces angioedema.
Lymphoprolipherative diseases and AAE are tightly linked with either angioedema or limphoprolyferation being the first symptom. Experi-ental data indicate that neoplastic tissue and/or anti-C1-inhibitor antibodies induce C1-inhibitor consumption, and this is further supported by
he observation that cytotoxic treatment of the lymphoproliferative diseases associated with AAE variably reverses the complement impairment
nd leads to a clinical improvement in angioedema symptoms.Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
2013 Elsevier Ireland Ltd. All rights reserved.
eywords: C1-inhibitor deficiency; Acquired angioedema; Lymphoproliferative di
∗ Corresponding author at: Department of Pathophysiology and Transplantation,
el.: +39 02 55035340; fax: +39 02 50320742.E-mail address: [email protected] (M. Cugno).
040-8428/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.critrevonc.2013.02.004
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
sease; Auto-antibodies; Complement
Section of Internal Medicine, Via Pace 9, 20122 Milan, Italy.

ARTICLE IN PRESSONCH-1713; No. of Pages 10
2 Oncol
1
coatwaCppdlmp([
cCuhbapCftitci
oTiu(ctiMaalpibtss[
At
rp
2a
aCldCCtC[
tppCdfawc1losCcncpatc
ClafiwCarwIas
R. Castelli et al. / Critical Reviews in
. Introduction
The clinical characteristics of acquired C1-inhibitor defi-iency or acquired angioedema (AAE) are similar to thosef hereditary C1-inhibitor deficiency known as hereditaryngioedema (HAE), except for the later onset of symptoms,he absence of a family history, and the potential associationith lymphoproliferative diseases and/or anti-C1-inhibitor
uto-antibodies [1,2]. Scattered reports describe acquired1-inhibitor deficiency associated with nonhematologic neo-lasm, infections or autoimmune diseases, whereas 14% ofatients with acquired C1-inhibitor deficiency have no otherisease [2]. The symptoms include recurrent, self-limitingocal swelling located in the subcutaneous tissues (which
ay be disfiguring), the upper airways (which may causeossibly fatal laryngeal edema), and the gastrointestinal tractwhich induces bowel obstruction and severe abdominal pain)2–4].
A deficiency in C1-inhibitor leads to the activation of thelassic complement pathway and consumption of C1, C2 and4 components; furthermore, the contact system becomesnstable and prone to generate kallikrein, which cleavesigh-molecular-weight kininogen (HK) and thus releasesradykinin, the mediator of the increased vascular perme-bility [5–10]. The release of bradykinin is facilitated by thelasmin [11] generated during edema attacks in patients with1-inhibitor deficiency [10,12]. The mechanisms responsible
or the consumption of C1-inhibitor and the massive activa-ion of the classic complement pathway have been extensivelynvestigated [1,13–15], and the initial experiments indicatedhat C1-inhibitor and/or the classic complement pathway areonsumed by neoplastic lymphatic tissues; moreover, C1-nhibitor can be cleaved/inactivated by its auto-antibody.
The majority of patients carry an underlying B cell dis-rder which is thought to cause C1-inhibitor consumption.hese disorders range from the production of anti-C1-
nhibitor auto-antibodies to monoclonal gammopathy ofncertain significance (MGUS) and non-Hodgkin lymphomaNHL) [16,17]. The relationship between pathological B celllones and C1-inhibitor deficiency is easily identified whenhe clone produces auto-antibodies that cleave/inactivate C1-nhibitor, but it is not immediately obvious in the case of
GUS or NHL. Under these conditions, the presence of cause-effect relationship between the pathological clonend C1-inhibitor consumption is supported by: (1) the preva-ence of MGUS and NHL extraordinarily higher in AAEatients compared to the general population [16,18]; (2)solated reports showing various degrees of reversal of theiochemical and/or clinical abnormalities of AAE upon theherapeutically induced remission of NHL [18–20]; and (3)ome experimental evidence suggesting that lymphatic tis-ues from AAE patients absorb or consume C1-inhibitor1,13–15].
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
We here review the pathophysiological mechanisms ofAE by concentrating on the relationship between it and
he associated B cell disorders, and underline the potential
wwe
ogy/Hematology xxx (2013) xxx–xxx
eversal of complement abnormalities after treating the lym-hoproliferative disease.
. Historical background and pathophysiology ofcquired c1-inhibitor deficiency
An acquired C1-inhibitor deficiency resulting inngioedema symptoms was first described in 1972 byaldwell et al. [1], who observed it in a patient with a
ymphoproliferative disorder. In 1986, Jackson et al. [13]iscovered an autoreactive immunoglobulin G against1-inhibitor in a patient with angioedema and acquired1-inhibitor deficiency. These and other findings indicated
hat the pathogenetic mechanism underlying acquired1-inhibitor deficiency may be related to autoimmunity
21,22].Initial experiments indicated that C1-inhibitor and/or
he classic complement pathway were consumed by neo-lastic lymphatic tissues. Schreiber et al. [14] described aatient with lymphoproliferative angioedema and acquired1-inhibitor deficiency whose complement profile revealedepletion of the first component of complement. It wasound that the patient’s peripheral blood mononuclear cellsnd a suspension of cells taken from pulmonary infiltrateere both capable of depleting the first component of
omplement and its inhibitor from homologous plasma. In979, Hauptmann et al. studied a patient with an extensiveymphosarcoma of the spleen (without the involvement ofther lymphoid organs) and hypogammaglobulinemia pre-enting the characteristic complement profile of acquired1-inhibitor deficiency [15]. Functional and immunochemi-al studies revealed extremely low C1-inhibitor levels, whichormalized after splenectomy together with the complementomponents. In vitro tests showed that lymphosarcoma tissueieces or cells were capable of interacting with complementnd reduced hemolytic activity. These findings showed thatumor cells were responsible for the abnormalities of theomplement system.
Geha et al. [23] found that some patients with acquired1-inhibitor deficiency and paraproteins had immunoglobu-
ins against the idiotypic determinants of the M components,nd these idiotype/anti-idiotype immune complexes mightx C1q and consume C1-inhibitor. However, these findingsere not subsequently confirmed. As auto-antibodies against1-inhibitor were first found in an otherwise healthy patient,cquired C1-inhibitor deficiency was divided into two sepa-ate forms (paraneoplastic type I, which is mainly associatedith lymphoproliferative disease, and auto-immune type
I caused by C1-inhibitor auto-antibodies), evidence thatutoimmunity and lymphoproliferation can co-exist in theame patients lead to abandon this distinction [24].
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
A number of studies have investigated the mechanism byhich auto-antibodies consume C1-inhibitor. Experimentsith linearized peptides suggest that these antibodies bind
pitopes around the reactive center of C1-inhibitor [25]. This

ARTICLE IN PRESSONCH-1713; No. of Pages 10
Oncology/Hematology xxx (2013) xxx–xxx 3
bmCliiitHao[
bmocsholiaoKmmCts[ibff
3d
3
in1trttuotfAa
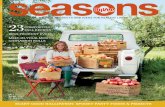
Fig. 1. Angioedema of the left foot in a patient with acquired C1-inhibitordeficiency and lymphoproliferative disease. This patient had high levelsof D-dimer as previously described in patients with such conditions [32].However, the presence of foot edema, lymphoproliferative disease and highlevels of D-dimer induced the physicians to rule out the diagnosis of deepvein thrombosis and pulmonary embolism by performing leg compressionu
rtcogi
3
yf
dimca
R. Castelli et al. / Critical Reviews in
inding could either create a steric impairement to the for-ation of C1-inhibitor-protease complexes and/or convert1-inhibitor into a substrate for proteases accounting for
arge amounts of a cleaved inactive form of C1-inhibitor thats detected in the serum of most patients with acquired C1-nhibitor deficiency [21,22]. Zuraw and Curd demonstratedn vitro that the cleavage mainly depends on the activation ofhe contact system and not on the complement system [22].owever, a preeminent role of plasmin in C1 inhibitor cleav-
ge has also been claimed based on the molecular weightf the cleaved form after incubation of plasma with plasmin21].
The low levels of C1-inhibitor due to its consumptiony pathological lymphatic tissue or its auto-antibody-ediated inactivation are associated with hyper-activation
f the complement or contact system, which may furtheronsume C1-inhibitor [26]. The contact and fibrinolyticystems are slightly activated during remission but greatlyyper-activated during acute attacks [10]. The incidentalver-activation of the contact system may initiate a cascadeeading to the generation of bradykinin, which mediates thencrease in vasopermeability that leads to angioedema. Thectivation of the contact system begins with the activationf factor XII, which activates pre-kallikrein to kallikrein.allikrein further activates factor XII and acts on high-olecular-weight kininogen releasing bradykinin, the mainediator of increased vascular permeability [27]. Moreover,1-inhibitor not only inhibits complement, the contact sys-
em and fibrinolysis, but also coagulation [28–31], whicheems to be activated in patients with C1-inhibitor deficiency7,32,33]. Experimental evidence showing that thrombinncreases vascular permeability [34–36] and can be inhibitedy C1-inhibitor [32], particularly at endothelial surface [33],urther supports the role of C1-inhibitor deficiency in edemaormation.
. Clinical characteristics of acquired C1-inhibitoreficiency
.1. Presentation
The typical symptom of both hereditary and acquired C1-nhibitor deficiency is angioedema, a recurrent, self-limiting,on-pitting, non-pruritic edema that completely resolves in–5 days [2,37–39]. Angioedema affects the subcutaneousissue, the gastrointestinal mucosa, and the mucosa of upperespiratory tract. Angioedema of the skin causes deformitieshat may involve the face, genitals, buttocks, and extremi-ies. Urticaria is usually absent, although transient and mildrticarial eruptions (erythema marginatum) may herald thevert swelling. Cutaneous angioedema creates discomfort
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
o patients, and can impair social life if it deforms theace (Fig. 1), or affects the function of hands and feet [2].bdominal attacks due to edema of the bowel wall are char-
cterized by vomiting, colicky abdominal pain and, more
oitc
ltrasonography and spiral computed tomography of the chest.
arely, diarrhea [40]. These symptoms usually revert spon-aneously within two days if not treated. Dysphagia, voicehanges and respiratory stridor are signs of the involvementf the upper airways and may precede asphyxia due to laryn-eal edema. This condition is life-threatening and requiresmmediate emergency therapy [2].
.2. Diagnosis
Clinical suspicion should be confirmed by laboratory anal-ses [41]. Table 1 shows the clinical and laboratory criteriaor a diagnosis of C1-inhibitor deficiency.
The typical biochemical picture of acquired C1-inhibitoreficiency is low plasma levels of C1-inhibitor function, C1-nhibitor antigen, C4 and C1q, with normal levels of C3. A
inority of patients have normal C1q levels. Antigen con-entrations of complement components (C1-inhibitor C4, C3nd C1q) are usually measured by means of radial immun-diffusion or nephelometry. C1-inhibitor functional activity
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
s measured by quantifying the capacity of plasma to inhibithe esterase activity of a fixed amount of C1s on a specifichromogenic substrate or by an immunoenzymatic assay [2].

ARTICLE IN PRESSONCH-1713; No. of Pages 10
4 R. Castelli et al. / Critical Reviews in Oncol
Table 1Clinical and laboratory markers for the diagnosis of acquired C1-inhibitordeficiencies.
Clinical markers-Self-limiting, non-inflammatory subcutaneous angioedema without
hives, recurrent and lasting for more than 12 hours-Self-remitting recurrent adominal pain without organic etiopathology
lasting for more than six hours-Recurrent laryngeal edemaLaboratory markers-C1-inhibitor antigen levels <50% of normal at two separate
measurements-C1-inhibitor functional levels <50% of normal at two separate
measurements-C1q levels <50% of normal at two separate measurements*
-Auto-antibodies against C1-inhibitor can be detected asimmunoglobulins preventing C1-inhibitor function or bindingC1-inhibitor.
Atpcdtita[ais[
3
Caawespdeataw
3
vt
(lwac[tlaifatwatabpsd
CtlBpiftp
t
casdamlodrsrotpmadisappearance of angioedema symptoms after chemother-
* In some cases C1q levels can be normal.
ny patient with acquired C1-inhibitor deficiency should beested for C1-inhibitor auto-antibodies [38], which may beresent in patients with AAE and induce C1-inhibitor hyper-atabolism [17,42–44]. C1-inhibitor auto-antibodies can beetected as immunoglobulins that prevent C1-inhibitor func-ion or bind C1-inhibitor. In the first assay, immunoglobulinssolated from serum block C1-inhibitor activity measured ashe inhibition of the conversion of synthetic substrates thatre specific for its target proteases [45]. In 1987, Alsenz et al.46] developed a solid-phase enzyme-linked immunosorbentssay (ELISA) for detecting immunoglobulins binding to C1-nhibitor coated on micro-titer plates, a simple and highlyensitive method that is still used with slight modifications42,43].
.3. Course
The course and prognosis of angioedema due to acquired1-inhibitor deficiency depends on the underlying diseasend the availability of appropriate therapy for life-threateningngioedema. Although angioedema attacks usually resolveithout treatment, patients are exposed to the risk of laryngeal
dema [38]. The frequency of attacks varies widely betweenubjects (from rare attacks to several events per year or evener month), and may also vary in the same subject at differentisease stages [2]. It has been reported that one patient experi-nced severe angioedema symptoms for five years that endedbruptly for no apparent reason [16]. Successful treatment ofhe underlying disease can resolve the angioedema symptomsnd biochemical abnormalities, but treatment responses varyidely [18,38].
.4. Therapy
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
The therapy of AAE follows two lines: (1) the pre-ention/reversal of the symptoms of angioedema; and (2)reatment of the associated disease [47–50].
ape
ogy/Hematology xxx (2013) xxx–xxx
Whatever the mechanism of C1-inhibitor consumptioncleavage by auto-antibodies or absorption by neoplasticymphatic tissue), the reduced C1-inhibitor levels in patientsith AAE induce the hyperactivation of the complement
nd contact systems, and this leads to further C1-inhibitoronsumption [26]. The hyper-consumption of C1-inhibitor44] explains why AAE patients are usually resistant tohe treatment normally used in cases of HAE [2]. For theong-term prevention of angioedema recurrences, patientsre currently treated with attenuated androgens (whichncrease C1-inhibitor synthesis and aminopeptidase Punction, an enzyme involved in bradykinin catabolism) andntifibrinolytic agents, which inhibit the enzyme plasminhat facilitates bradykinin production [10,43,50,51]. Patientsith acquired C1-inhibitor deficiency respond better to
ntifibrinolytic agents (which seem to be well tolerated) thano attenuated androgens [38,49]. Although antifibrinolyticgents are potentially prothrombotic, no increased throm-otic risk has ever been documented. Short- and long-termrophylaxis with C1-inhibitor concentrates has also beenuccessfully used in AEE patients, albeit at generally higheroses than those used to treat HAE [38,52].
Acute attacks are treated by the infusion of plasma-derived1-inhibitor despite the variable degree of resistance and
he need for high doses [2,37]. By overcoming the prob-em of accelerated C1-inhibitor catabolism, the bradykinin2 receptor antagonist icatibant is a promising alternative tolasma-derived C1-inhibitor for patients with acquired C1-nhibitor deficiencies. It is already an established treatmentor acute HAE attacks, and we have successfully used thisreatment in eight patients with AAE resistant to C1-inhibitorlasma concentrates [53].
Table 2 summarizes the pharmacological approaches tohe prevention/treatment of AAE symptoms.
Treatment of the associated disease by means ofhemotherapy or other cytoreduction (radiotherapy, surgery,nd antibodies to specific cell populations) or immuno-uppressive treatment may not only control the underlyingisease, but also relieve the clinical symptoms ofngioedema and variably reverse the biochemical abnor-alities [18–20,54,55]. The therapeutic approaches to
ymphoproliferative diseases are the same in patients withr without C1-inhibitor deficiency. However, C1-inhibitoreficiency with frequent angioedema attacks that do notesponding to conventional AAE treatment should be con-idered a sign of active lymphoproliferative disease possiblyequiring cytoreductive therapy. In a previous study, webserved the reversal of complement abnormalities andhe remission of angioedema symptoms in two NHLatients treated with chemotherapy, and one patient witharginal splenic lymphoma undergoing splenectomy [8],
nd other groups have also reported a reduction in, or the
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
py, with an improvement in complement parameters inatients with AAE associated with lymphoproliferative dis-ase [15,19,20,54,55] (Table 3).

Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
ARTICLE IN PRESSONCH-1713; No. of Pages 10
R. Castelli et al. / Critical Reviews in OncoloTa
ble
2Ph
arm
acol
ogic
al
appr
oach
es
to, i
ndic
atio
ns
for,
and
pote
ntia
l sid
e
effe
cts
of
prev
entio
n/tr
eatm
ent o
f
acqu
ired
angi
oede
ma
(AA
E)
sym
ptom
s.
Tre
atm
ent
Mec
hani
sm
of
actio
n
Indi
catio
ns
Adv
anta
ges
Side
effe
cts
Com
men
ts
Plas
ma
deri
ved
hum
an
C1-
inhi
bito
rR
epla
cem
ent o
f
the
defic
ient
prot
ein
Acu
te
atta
cks
Phys
iolo
gica
l rep
lace
men
t
Pote
ntia
l tra
nsm
issi
on
ofbl
ood-
born
e
infe
ctio
nsV
aria
ble
degr
ee
ofre
sist
ance
and
the
need
for
high
dose
sSh
ort-
and
long
-ter
m
prop
hyla
xis
of
acut
e
atta
cks
Rap
id
mec
hani
sm
of
actio
n
Ant
i-fib
rino
lytic
agen
tsIn
hibi
tion
of
fibri
noly
sis
and
brad
ykin
in
gene
ratio
nL
ong-
and
shor
t-te
rm
prop
hyla
xis
Ora
l adm
inis
trat
ion
Pote
ntia
l thr
ombo
phili
a
Mor
e ef
ficac
ious
than
andr
ogen
deri
vativ
esT
reat
men
t of
acut
e
cuta
neou
s
and
muc
osal
atta
cks
Dia
rrhe
a
And
roge
n
deri
vativ
es
Enh
ance
men
t of
C1-
inhi
bito
r
synt
hesi
san
d
amin
opep
tidas
e
Pfu
nctio
n
Lon
g-
and
shor
t-te
rm
prop
hyla
xis
Low
dire
ct
cost
; ora
lad
min
istr
atio
nV
irili
satio
n,
men
stru
alir
regu
lari
ties,
hepa
ticto
xici
ty, h
yper
tens
ion
Nee
d
for
med
ical
follo
wup
to
redu
ce
side
effe
cts
Rec
ombi
nant
kalli
krei
n
inhi
bito
r(e
calla
ntid
e)
Kal
likre
in
inhi
bitio
n
Acu
te
atta
cks
Subc
utan
eous
adm
inis
trat
ion
Rar
e
anap
hyla
ctic
reac
tions
Bra
dyki
nin
anta
goni
st(i
catib
ant)
Ant
agon
ism
ofbr
adyk
inin
B2
rece
ptor
sA
cute
atta
cks
Alte
rnat
ive
to
plas
ma
C1-
inhi
bito
r;
subc
utan
eous
adm
inis
trat
ion
Loc
al
disc
omfo
rt
atin
ject
ion
site
Lim
ited
dura
tion
ofac
tion.
Furt
her
stud
ies
inA
AE
are
need
ed
All
poss
ible
trea
tmen
ts
are
off-
labe
l.
CitIlcetasim
uwcomwppsrao
4l
dTthta(aalfdaTatrwfidfCal
gy/Hematology xxx (2013) xxx–xxx 5
Rituximab, a chimeric mouse/human monoclonal anti-D20 antibody, targets B cells and has been used successfully
n autoimmune disorders such as rheumatoid arthritis, sys-emic lupus erythematosus [56–58], and pemphigus [59,60].t has also been investigated in cases of aggressive and indo-ent NHL as a single agent or in combination with standardhemotherapy regimens [61–65]. Given the rarity of the dis-ase, no controlled clinical trials have systematically assessedhe efficacy and safety of rituximab in AAE patients but annalysis of the published data shows that 14 patients haveo far been treated with rituximab, which led to a clinicalmprovement in 12, and the reversal of complement abnor-
alities in 10 [66–71] (Table 4).Despite that absence of controlled clinical trials of rit-
ximab in patients with acquired C1-inhibitor deficiency,e believe it to be reasonable to use rituximab in the
ase of selected patients experiencing multiple episodesf angioedema who fail to respond to conventional treat-ents, and (in combination with chemotherapy) in patientsith high-grade lymphoproliferative disease or active lym-homas. In addition it seems reasonable to use rituximab inatients with severe and otherwise uncontrolled angioedemaymptoms associated with lymphoproliferative disease notequiring per se conventional chemotherapy treatments, suchs patients with MGUS or indolent lymphomas with no signsf active disease.
. Link between acquired angioedema andymphoproliferative disease
AAE is frequently associated with lymphoproliferativeisorders of B cell lineage ranging from MGUS to NHL.hree studies by our group have previously demonstrated
hat patients with acquired C1-inhibitor deficiency are atigher risk of developing NHL than the general popula-ion [16–18]. A lymphoproliferative disease may be presentt the onset of AAE symptoms, or may develop thereafterin our experience, between three months and seven yearsfter) [18]. The most frequent lymphoproliferative diseasessociated with acquired C1-inhibitor deficiency is indolentymphoma. According to the WHO classification, the mostrequent histotypes in patients with acquired C1-inhibitoreficiency are nodal and splenic marginal zone lymphomas,nd lymphoplasmocytic lymphomas/Waldeström’s disease.he association with these histotypes is similar to that of otherutoimmune diseases such as cryoglobulinemia, or rheuma-oid arthritis [72,73], these observations suggest that theisk of developing lymphoproliferative diseases in patientsith acquired C1-inhibitor deficiency is not generic but con-ned to specific histotypes. As these NHL subtypes developuring the post-antigen exposure stages of lymphocyte dif-
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
erentiation, it can be argued that the immunocomplexes of1-inhibitor and C1-inhibitor auto-antibodies may play a roles antigenic drivers in the genesis of autoimmunity-relatedymphomas [18,26].

Please cite
this article
in press
as: C
astelli R
, et
al. A
cquired C
1-inhibitor deficiency
and lym
phoproliferative disorders:
A tight
relationship.C
rit R
ev O
ncol/Hem
atol (2013),
http://dx.doi.org/10.1016/j.critrevonc.2013.02.004
AR
TIC
LE
IN P
RE
SS
ON
CH
-1713;
No.
of Pages
10
6
R.
Castelli
et al.
/ C
ritical R
eviews
in O
ncology/Hem
atology xxx
(2013) xxx–xxx
Table 3Clinical and complement parameters in acquired angioedema (AAE) patients with lymphoproliferative disease treated with chemotherapy or immunochemotherapy.
Author Patients Associatedhemopathy
Chemotherapy Pre-chemotherapyC1-INHAg/function/anti-C1-INH
Post-chemotherapyC1-INHAg/function/anti-C1-INH
Clinicalimprovement
Duration offollow-up
Jung M [19] 1 Chronic lymphocyticleukemia
Chlorambucil + danazol NA/83% (duringdanazol)/NA
NA/100%/NA Yes NA
2 Chronic lymphocyticleukemia
Fludarabine,CyC + rituximab
6.7 mg/dL/1%/NA NA/120%/NA Yes NA
3 Lymphocyticlymphoma
Cyc + danatrol NA/4%/NA NA/NA/NA Yes NA
Guilarte M [20] 1 Follicular lymphoma Chlorambucil(0.2 mg/kg/d) and PDN
10 mg/dL/45%/NA 12 mg/dL/55%/NA Yes 8 months
Castelli R [18] 1 Waldestromlymphoplasmocyticlymphoma
R-CHOP 31%/<5%/IgM 500 U/mL 115%/116%/IgM60 U/mL
Yes 3 year
2 Follicular lymphoma CEOP/fludarabine/Cyc <1%/<1%/0 109%/90%/0 Yes 4 year3 Splenic marginal zone
lymphomaSplenectomy NA NA Yes 2 years
Healy C [54] 1 Follicular lymphoma CVP 2.54 mg/dL/NA/NA 3 mg/dL/NA/NA Yes 40 monthsRossi D [55] 1 Anaplastic CD30+
large B celllymphoma
Yes Reduced/NA/NA Normalized/NA/NA Yes NA
CYC: cyclophosphamide; R-CHOP: rituximab-cyclophosphamide-vincristine and prednisone; NA: not available; CVP: cyclophosphamide-vincristine and prednisone; CEOP: Cyclophosphamide-Etoposide-Prednisolone-Vincristine.

Please cite
this article
in press
as: C
astelli R
, et
al. A
cquired C
1-inhibitor deficiency
and lym
phoproliferative disorders:
A tight
relationship.C
rit R
ev O
ncol/Hem
atol (2013),
http://dx.doi.org/10.1016/j.critrevonc.2013.02.004
AR
TIC
LE
IN P
RE
SS
ON
CH
-1713;
No.
of Pages
10
R.
Castelli
et al.
/ C
ritical R
eviews
in O
ncology/Hem
atology xxx
(2013) xxx–xxx
7
Table 4Clinical and complement parameters in acquired angioedema (AAE) patients treated with rituximab.
Author Patients Associated hemopathy orconcomitant disease
Frequency ofattacks
Pre-rituximab C1-inhibitorAg/function/anti-C1-inhibitor
Post-rituximabC1-inhibitorAg/function/anti C1inhibitor
Clinicalefficacy
Durationoffollow-up
Lam DH [67] 1 Marginal zone lymphoma;coronary artery disease
NR 2 mg/dL/20%/NA Normalization C1-INHAg
Yes 8 months
Branellec A [66]
1 N0 Twice monthly 139 mg/L/5 U/mL/IgM 2320 U 227 mg/L/16.1 U/mL/IgM760 U
Yes 6 months
2 Marginal zone lymphoma Every 8–10 days 96 mg/L/5.4 U/mL/IgM 271 U 202 mg/L/13.3 U/mL/IgM378 U
Yes NR
3 MGUS IgA � Monthly 170 mg/L/2.7 U/mL/IgA 339 U 103 mg/L/NA/NA Yes 6 months4 MGUS IgG 2 attacks/year 144 mg/L/4.9 U/mL/IgG
1000 U155 mg/L/4.1 U/mL/IgG1170 U
Yes 5 years
5 No Repeated 80 mg/L/NA/IgM 317 U 89 mg/L/3.7 U/mL/IgM696 U
Yes 6 months
6 MGUS IgG � Monthly 16 mg/L/<2/IgM positive 92 mg/L/<2/IgM positive No 3 years7 Marginal zone lymphoma NR 81 mg/L/ND/undetectable NA/NA/undetectable No 17 months
Sánchez-Cano D [70] 1 Sjögren’s syndrome 3/month 016 U/mL/32%/IgM 578 U NA – NA – IgM 346 U Yes 11 months
Levi M [68]1 None 3/month <0.5 U/mL/<0.25 U/mL/IgG
positiveNearnormal/>0.5 U/mL/NA
Yes 12 months
2 Follicular B cell lymphoma 3/month <0.5 U/mL/<0.25 U/mL/NA Nearnormal/>0.5 U/mL/NA
Yes 12 months
3 None 3/month <0.5 U/mL/<0.25 U/mL/NA Nearnormal/>0.5 U/mL/NA
Yes 12 months
Ziakas PD [69] 1 Monoclonal IgMnephrosclerosis
5–6/year Low/40%/Positive NA/NA/NA Yes NR
Hassan A [71]1 MGUS IgM k 6–8/month C4 (0.06 g/L, normal:
0.10–0.40 g/L)C1-INH functional levelsimproved to 3.1 U/mL
Yes 24 months
C1-INH antigen: 0.08 g/L(n.v.: 0.21–0.34 g/L); C1-INHfunctional levels: 2.0 U/mL(n.v.: 17.2–27.4 U/mL)
MGUS: monoclonal gammopathy of uncertain significance; Ag: antigen; NR: not reported; NA: not available.

ARTICLE IN PRESSONCH-1713; No. of Pages 10
8 Oncol
ialpqMpctasplpcwspwscgi
5
iapaslhaobtpsalcdecccrsitic
C
R
tC
R
[
[
[
[
[
[
[
R. Castelli et al. / Critical Reviews in
The prevalence of MGUS in patients with acquired C1-nhibitor deficiency is 35%, which is much higher than itspproximately 3% prevalence in the general population agedess than 70 years [74]. A study by our group has shown thatatients with MGUS and C1-inhibitor auto-antibodies fre-uently have the same heavy and light chain histotypes [18].GUS progresses to multiple myeloma as frequently in AAE
atients as in the general population [18]. Evidence that the Momponents detected in these patients frequently correspondo the C1-inhibitor auto-antibodies, and that patients withuto-antibodies may develop lymphoproliferative diseasesuggests that a single B cell clonal disorder with differentotential clinical evolutions underlies AAE. Furthermore, asymphoproliferative diseases may appear in AAE patients,atients with confirmed C1-inhibitor deficiency should belosely monitored for their development. For all patientsith angioedema due to acquired C1-inhibitor deficiency, we
uggest to perform annually a first level screening for lym-hoproliferative diseases based on complete blood cell countith differential leukocyte count, serum protein electrophore-
is, chest X ray and abdominal ultrasound, along with aomplete physical examination. Additional tests should beuided by clinical suspicion or abnormal laboratory find-ngs.
. Conclusions
Although the etiology of acquired C1-inhibitor deficiencys still partially unclear, the majority of patients presentn underlying B cell disorder, which ranges from the sim-le production of C1-inhibitor auto-antibodies to MGUSnd NHL. The most frequent histotypes are nodal andplenic marginal zone lymphomas and lymphoplasmocyticymphomas/Waldeström disease. The association with suchistotypes is similar to that of other autoimmune diseasesnd, as they develop during the post-antigen exposure stagesf lymphocyte differentiation, the immunocomplexes formedy auto-antibodies and C1-inhibitor may play a role inhe genesis of autoimmunity-related lymphomas. Lympho-roliferative disease may be present at the onset of AAEymptoms or may develop thereafter, thus AAE representsn example of the strict link between autoimmunity andymphoproliferation. Blocking autoreactive or neoplastic Bell proliferation is a pivotal step in the treatment of theisease. It has been shown that curing the associated dis-ase by means of chemotherapy and/or immunosuppressionan resolve angioedema symptoms and normalize the bio-hemical defects. However, AAE symptoms and pathologicalomplement parameters may reappear at the time of a recur-ence of the malignancy. In any case, patients with AAEhould be closely monitored because of its potential evolution
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
nto lymphoproliferative disease. It is still debated whetherhe exacerbation of angioedema symptoms in patients withndolent lymphoma is a sign of active disease requiringytoreductive treatment.
[
ogy/Hematology xxx (2013) xxx–xxx
onflicts of interest
The authors have no conflicting interests to disclose.
eviewer
Teresa Caballero, MD, PhD, Senior consultant, Hospi-al Universitario La Paz, Allergy Department, Paseo de laastellana 261, ES-28046 Madrid, Spain.
eferences
[1] Caldwell JR, Ruddy S, Schur PH, Austen KF. Acquired C1-inhibitor deficiency in lymphosarcoma. Clinical Immunology andImmunopathology 1972;1:39–52.
[2] Agostoni A, Aygören-Pürsün E, Binkley KE, et al. Hereditary andacquired angioedema: problems and progress proceedings of the thirdC1 esterase inhibitor deficiency workshop and beyond. Journal ofAllergy and Clinical Immunology 2004;114(Suppl. 3):S51–131.
[3] Longhurst H, Cicardi M. Hereditary angio-oedema. Lancet2012;379:474–81.
[4] Kaplan AP. C1 inhibitor deficiency: hereditary and acquired forms.Journal of Investigational Allergology and Clinical Immunology2001;11:211–9.
[5] Cugno M, Nuijens J, Hack E, et al. Plasma levels of C1-inhibitor complexes and cleaved C1-inhibitor in patients withhereditary angioneurotic edema. Journal of Clinical Investigation1990;85:1215–20.
[6] Schapira M, Silver LD, Scott CF, et al. Prekallikrein activation and high-molecular-weight kininogen consumption in hereditary angioedema.New England Journal of Medicine 1983;308:1050–3.
[7] Cugno M, Cicardi M, Bottasso B, et al. Activation of the coagulationcascade in C1-inhibitor deficiencies. Blood 1997;89:3213–8.
[8] Nussberger J, Cugno M, Amstutz C, Cicardi M, Pellacani A, AgostoniA. Plasma bradykinin in angio-oedema. Lancet 1998;351:1693–7.
[9] Nussberger J, Cugno M, Cicardi M. Bradykinin-mediated angioedema.New England Journal of Medicine 2002;347:621–2.
10] Cugno M, Cicardi M, Agostoni A. Activation of the contact systemand fibrinolysis in autoimmune acquired angioedema: a rationale forprophylactic use of tranexamic acid. Journal of Allergy and ClinicalImmunology 1994;93:870–6.
11] Kleniewski J, Blankenship DT, Cardin AD, Donaldson V. Mechanismof enhanced kinin release from high molecular weight kininogen byplasma kallikrein after its exposure to plasmin. Journal of Laboratoryand Clinical Medicine 1992;120:129–39.
12] Cugno M, Hack CE, de Boer JP, Eerenberg AJ, Agostoni A, Cicardi M.Generation of plasmin during acute attacks of hereditary angioedema.Journal of Laboratory and Clinical Medicine 1993;121:38–43.
13] Jackson J, Sim RB, Whelan A, Feighery C. An IgG autoantibody whichinactivates C1-inhibitor. Nature 1986;323(6090):722–4.
14] Schreiber AD, Zweiman B, Atkins P, et al. Acquired angioedema withlymphoproliferative disorder: association of C1-inhibitor deficiencywith cellular abnormality. Blood 1976;48:567–80.
15] Hauptmann G, Petitjean F, Lang JM, Oberling F. Acquired C1-inhibitordeficiency in a case of lymphosarcoma of the spleen. Reversal of com-plement abnormalities after splenectomy. Clinical and ExperimentalImmunology 1979;37:523–31.
16] Cicardi M, Zingale LC, Pappalardo E, Folcioni A, Agostoni A. Autoan-
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
tibodies and lymphoproliferative diseases in acquired C1-inhibitordeficiencies. Medicine 2003;82:274–81.
17] Cicardi M, Beretta A, Colombo M, Gioffre D, Cugno M, AgostoniA. Relevance of lymphoproliferative disorders and of anti-C1-inhibitor

ARTICLE IN PRESSONCH-1713; No. of Pages 10
Oncolo
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
R. Castelli et al. / Critical Reviews in
autoantibodies in acquired angio-oedema. Clinical and ExperimentalImmunology 1996;106:475–80.
18] Castelli R, Deliliers DL, Zingale LC, Pogliani EM, Cicardi M.Lymphoproliferative disease and acquired C1-inhibitor deficiency.Haematologica 2007;92:716–8.
19] Jung M, Rice L. Unusual autoimmune nonhematologic complicationsin chronic lymphocytic leukemia. Clinical Lymphoma, Myeloma andLeukemia 2011;11(Suppl. 1):S10–3.
20] Guilarte M, Luengo O, Nogueiras C, et al. Acquired angioedemaassociated with hereditary angioedema due to C1-inhibitor deficiency.Journal of Investigational Allergology and Clinical Immunology2008;18:126–30.
21] Jackson J, Sim RB, Whaley K, Feighery C. Autoantibody facilitatedcleavage of C1-inhibitor in autoimmune angioedema. Journal of Clin-ical Investigation 1989;83:698–707.
22] Zuraw BL, Curd JG. Demonstration of modified inactive firstcomponent of complement C1-inhibitor in the plasmas of C1-inhibitor-deficient patients. Journal of Clinical Investigation 1986;78:567–75.
23] Geha RS, Quinti I, Austen KF, Cicardi M, Sheffer A, Rosen FS.Acquired C1-inhibitor deficiency associated with antiidiotypic anti-body to monoclonal immunoglobulins. New England Journal ofMedicine 1985;312:534–40.
24] D’Incan M, Tridon A, Ponard D, et al. Acquired angioedema with C1-inhibitor deficiency: is the distinction between type I and type II stillrelevant? Dermatology 1999;199:227–30.
25] He S, Tsang S, North J, Chohan N, Sim RB, Whaley K. Epitope mappingof C1-inhibitor autoantibodies from patients with acquired C1-inhibitordeficiency. Journal of Immunology 1996;156:2009–13.
26] Cugno M, Castelli R, Cicardi M. Angioedema due to acquired C1-inhibitor deficiency: a bridging condition between autoimmunity andlymphoprolipheration. Autoimmunity Reviews 2008;8:156–9.
27] Cugno M, Zanichelli A, Foieni F, Caccia S, Cicardi M. C1 inhibitor defi-ciency and angioedema: molecular mechanisms and clinical progress.Trends in Molecular Medicine 2009;15:69–78.
28] Davis AE, 3rd, Lu F, Mejia P. C1-inhibitor, a multi-functional serineprotease inhibitor. Thrombosis and Haemostasis 2010;104:886–93.
29] Van Nostrand WE, McKay LD, Baker JB, Cunningham DD. Functionaland structural similarities between protease nexin I and C1-inhibitor.Journal of Biological Chemistry 1988;263:3979–83.
30] Cugno M, Bos I, Lubbers Y, Hack CE, Agostoni A. In vitro interac-tion of C1-inhibitor with thrombin. Blood Coagulation and Fibrinolysis2001;4:253–60.
31] Caccia S, Castelli R, Maiocchi D, Bergamaschini L, Cugno M. Inter-action of C1-inhibitor with thrombin on the endothelial surface. BloodCoagulation and Fibrinolysis 2011;7:571–5.
32] Cugno M, Zanichelli A, Bellatorre AG, Griffini S, Cicardi M. Plasmabiomarkers of acute attacks in patients with angioedema due to C1-inhibitor deficiency. Allergy 2009;64:254–7.
33] van Geffen M, Cugno M, Lap P, Loof A, Cicardi M, van Heerde W.Alterations of coagulation and fibrinolysis in patients with angioedemadue to C1-inhibitor deficiency. Clinical and Experimental Immunology2012;167:472–8.
34] Garcia JGN, Siflinger-Birnboim A, Bizios R, Del Vecchio PJ, FentonII JW, Malik AB. Thrombin induced increase in albumin per-meability across the endothelium. Journal of Cellular Physiology1986;128:96–104.
35] Garcia JGN, Pavalko FM, Patterson CE. Vascular endothelial cell acti-vation and permeability responses to thrombin. Blood Coagulation andFibrinolysis 1995;6:609–26.
36] Siller-Matula JM, Schwameis M, Blann A, Mannhalter C, Jilma B.Thrombin as a multi-functional enzyme. Focus on in vitro and in vivoeffects. Thrombosis and Haemostasis 2011;106:1020–33.
37] Agostoni A, Cicardi M. Hereditary and acquired C1-inhibitor defi-
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
ciency: biological and clinical characteristics in 235 patients. Medicine1992;71:206–15.
38] Zingale LC, Castelli R, Zanichelli A, Cicardi M. Acquired C1-inhibitor deficiency: presentation, diagnosis, course and conventional
[
gy/Hematology xxx (2013) xxx–xxx 9
management. Immunology and Allergy Clinics of North America2006;26:669–90.
39] Di Leo E, Nettis E, Montinaro V, et al. Acquired angioedemawith C1-inhibitor deficiency associated with anticardiolipin antibod-ies. International Journal of Immunopathology and Pharmacology2011;24:1115–8.
40] Bork K, Staubach P, Eckardt AJ, Hardt J. Symptoms, course, andcomplications of abdominal attacks in hereditary angioedema dueto C1-inhibitor deficiency. American Journal of Gastroenterology2006;101:619–27.
41] Frazer-Abel A, Giclas PC. Update on laboratory tests for the diagnosisand differentiation of hereditary angioedema and acquired angioedema.Allergy and Asthma Proceedings 2011;32(Suppl. 1):S17–21.
42] Spath PJ, Wuthrich B, Matter L, Loos M, Alsenz J. Acquiredangioedema and anti-C1-inhibitor autoantibody. Archives of InternalMedicine 1989;149:1213–6.
43] Cicardi M, Bisiani G, Cugno M, Spath P, Agostoni A. AutoimmuneC1-inhibitor deficiency: report of eight patients. American Journal ofMedicine 1993;95:169–75.
44] Melamed J, Alper CA, Cicardi M, Rosen FS. The metabolism of C1-inhibitor and C1q in patients with acquired C1-inhibitor deficiency.Journal of Allergy and Clinical Immunology 1986;77:322–6.
45] Jackson J, Feighery C. Autoantibody-mediated acquired deficiency ofC1-inhibitor. New England Journal of Medicine 1988;318:122–3.
46] Alsenz J, Bork K, Loos M. Autoantibody-mediated acquired deficiencyof C1-inhibitor. New England Journal of Medicine 1987;316:1360–6.
47] Castelli R, Zanichelli A, Cugno M. Therapeutic options for patientswith angioedema due to C1-inhibitor deficiencies: from pathophy-siology to the clinic. Immunopharmacology and Immunotoxicology2013;35:181–90.
48] Caballero T, Baeza ML, Cabanas R, et al. Consensus statement onthe diagnosis, management, and treatment of angioedema mediatedby bradykinin. Part I. Treatment, follow-up, and special situations.Journal of Investigational Allergology and Clinical Immunology2011;21:333–47.
49] Caballero T, Baeza ML, Cabanas R, et al. Consensus statement onthe diagnosis, management, and treatment of angioedema mediatedby bradykinin. Part II. Treatment, follow-up, and special situa-tions. Journal of Investigational Allergology and Clinical Immunology2011;21:422–41.
50] Kanani A, Schellenberg R, Warrington R. Urticaria and angioedema.Allergy, Asthma and Clinical Immunology 2011;7(Suppl. 1):S9.
51] Drouet C, Désormeaux A, Robillard J, et al. Metallopeptidase activ-ities in hereditary angioedema: effect of androgen prophylaxis onplasma aminopeptidase P. Journal of Allergy and Clinical Immunology2008;121:429–33.
52] Bork K, Witzke G. Long-term prophylaxis with C1-inhibitor (C1 INH)concentrate in patients with recurrent angioedema caused by hereditaryand acquired C1-inhibitor deficiency. Journal of Allergy and ClinicalImmunology 1989;83:677–82.
53] Zanichelli A, Bova M, Coerezza A, Petraroli A, Triggiani M, Cicardi M.Icatibant treatment for acquired C1-inhibitor deficiency: a real-worldobservational study. Allergy 2012;67:1074–7.
54] Healy C, Abuzakouk M, Feighery C, Flint S. Acquired angioedema innon-Hodgkin’s lymphoma. Oral Surgery, Oral Medicine, Oral Pathol-ogy, Oral Radiology and Endodontics 2007;103:e29–32.
55] Rossi D, Gaidano G. Anaplastic large cell lymphoma and acquiredangioedema: a novel association? Annali Italiani di Medicina Interna2002;17:143–5.
56] Vossenkper A, Lutalo PM, Spencer J. Translational mini-review serieson B cell subsets in disease. Transitional B cells in systemic lupus ery-thematosus and Sjogren’s syndrome: clinical implications and effectsof B cell-targeted therapies. Clinical and Experimental Immunology
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
2012;167:7–14.57] Ramos-Casals M, Sanz I, Bosch X, Stone JH, Khamashta MA. B-cell-
depleting therapy in systemic lupus erythematosus. American Journalof Medicine 2012;125:327–36.

ARTICLE IN PRESSONCH-1713; No. of Pages 10
1 Oncol
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
B
MCiMiMtssh
0 R. Castelli et al. / Critical Reviews in
58] Boumans MJ, Thurlings RM, Yeo L, et al. Rituximab abrogates jointdestruction in rheumatoid arthritis by inhibiting osteoclastogenesis.Annals of the Rheumatic Diseases 2012;7:108–13.
59] Kim JH, Kim YH, Kim MR, Kim SC. Clinical efficacy of differentdoses of rituximab in the treatment of pemphigus: a retrospective studyof 27 patients. British Journal of Dermatology 2011;165:646–51.
60] Horváth B, Huizinga J, Pas HH, Mulder AB, Jonkman MF. Low-doserituximab is effective in pemphigus. British Journal of Dermatology2012;166:405–12.
61] Zwick C, Murawski N, Pfreundschuh M. German High-GradeNon-Hodgkin Lymphoma Study Group. Rituximab in high-grade lym-phoma. Seminars in Hematology 2010;47:148–55.
62] Sousou T, Friedberg J. Rituximab in indolent lymphomas. Seminars inHematology 2010;47:133–42.
63] McLaughlin P, Grillo-López AJ, Link BK, et al. Rituximab chimericanti-CD20 monoclonal antibody therapy for relapsed indolent lym-phoma: half of patients respond to a four-dose treatment program.Journal of Clinical Oncology 1998;16:2825–33.
64] Coiffier B, Haioun C, Ketterer N, et al. Rituximab (anti-CD20 mono-clonal antibody) for the treatment of patients with relapsing orrefractory aggressive lymphoma: a multicenter phase II study. Blood1998;92:1927–32.
65] Maloney DG. Anti-CD20 antibody therapy for B-cell lymphomas. NewEngland Journal of Medicine 2012;366:2008–16.
66] Branellec A, Bouillet L, Javaud N, et al. Acquired C1-inhibitordeficiency: 7 patients treated with rituximab. Journal of ClinicalImmunology 2012;32:936–41.
67] Lam DH, Levy NB, Nickerson JM, Gruenberg DA, Lansigan F.Acquired angioedema and marginal zone lymphoma. Journal of Clini-cal Oncology 2012;30:e151–3.
68] Levi M, Hack CE, van Oers MH. Rituximab-induced elimination ofacquired angioedema due to C1-inhibitoribitor deficiency. AmericanJournal of Medicine 2006;119:e3–5.
69] Ziakas PD, Giannouli S, Psimenou E, Evangelia K, Tzioufas AG,
Please cite this article in press as: Castelli R, et al. Acquired C1-inhibitor dCrit Rev Oncol/Hematol (2013), http://dx.doi.org/10.1016/j.critrevonc.2
Voulgarelis M. Acquired angioedema: a new target for rituximab?Haematologica 2004;89:ELT13.
70] Sánchez-Cano D, Callejas-Rubio JL, Lara-Jiménez MA, López-Trascasa M, Cicardi M, Ortego-Centeno N. Successful use of rituximab
iLB
ogy/Hematology xxx (2013) xxx–xxx
in acquired C1-inhibitor deficiency secondary to Sjogren’s syndrome.Lupus 2008;17:228–9.
71] Hassan A, Amarger S, Tridon A, Ponard D, Souteyrand P, D’IncanM. Acquired angioedema responding to rituximab. Acta Dermato-Venereologica 2011;91:733–4.
72] Monti G, Pioltelli P, Saccardo F, et al. Incidence and characteristics ofnon-Hodgkin lymphomas in a multicenter case file of patients with hep-atitis C virus-related symptomatic mixed cryoglobulinemias. Archivesof Internal Medicine 2005;165:101–5.
73] Dias C, Isenberg DA. Susceptibility of patients with rheumatic diseasesto B-cell non-Hodgkin lymphoma. Nature Reviews Rheumatology2011;7:360–8.
74] Fremeaux-Bacchi V, Guinnepain MT, Cacoub P, et al. Prevalenceof monoclonal gammopathy in patients presenting with acquiredangioedema type 2. American Journal of Medicine 2002;113:194–9.
iography
Massimo Cugno MD, is an associate professor of Internaledicine at the University of Milan. He is the chief of theenter for the study of complement at the Maggiore Hospital
n Milan. He graduated “cum laude” from the University ofilan in 1982. He completed his post-graduated speciality
n Hematology and Internal Medicine at the University ofilan. He is involved in research on prognostic, therapeu-
ic and biological aspects of hematological disorders. Thecientific work was conducted mainly in the field of protea-ic systems, coagulation, fibrinolysis and complement. Heas published around 150 original papers (130 in journals
eficiency and lymphoproliferative disorders: A tight relationship.013.02.004
ncluded in PubMed, some of excellence as New Engl J Med,ancet, J Clin Invest, Am J Hum Genet, Circulation, andlood).