Acoustic analysis of voice quality with or without false vocal fold displacement after cordectomy
10
INTRODUCTION It is commonly accepted that early glottic cancers can be treated either surgically or with radiotherapy. During the past 10 years, the latter was considered the treatment of choice because of the high cure rate and the good voice preservation achieved. 1 Radio- therapy, however, has disadvantages such as dryness, inflammation, the long time required for application, and oncogenetic potential. Among the surgical tech- niques, laser surgery gives better functional results compared to laryngofissure due to the more rapid healing processes, 2-4 but it is not always available. To improve the poor functional results obtained after conventional cordectomy, some authors have tried to resurface the mucosal defect using different tech- niques. 5-7 We usually close the surgical defect using a mucosal flap obtained from the false omolateral vo- cal cord. 8 The aim of the present study was to evalu- ate if the operation of replacing the excised cord is truly effective on voice quality compared to the cordectomy alone. MATERIALS AND METHODS Patient population A total of 14 patients, 12 males and 2 females, un- derwent conventional cordectomy with external ap- proach for T1aN0M0 squamous cell carcinomas of the glottis. The surgical technique consisted of sub- Journal of Voice Vol. 15, No. 1, pp. 131-140 © 2001 The Voice Foundation Acoustic Analysis of Voice Quality with or without False Vocal Fold Displacement After Cordectomy *Giulia Bertino, *Anna Bellomo, †Franco E. Ferrero, *and Alfio Ferlito *Department of Otolaryngology—Head Neck Surgery, University of Udine, udine, Italy; †Institute of Phonetic and Dialectology, national Research Council (CNR) of Padua, Padua, Italy Summary: Conventional cordectomy by means of a laryngofissure is one of the therapeutic options for treatment of early glottic cancer. To improve the poor voice quality related to this kind of operation, many authors have developed dif- ferent techniques to repair the mucosal defect. We analyzed voice quality acoustically and compared it after cordectomy alone and after cordectomy with the reconstruction of the vocal cord in a group of 14 patients affected by T1 glot- tic carcinoma. All the patients underwent postoperative speech therapy. Three pa- tients who underwent cordectomy with reconstruction showed the presence of diplophonia, while two patients without reconstruction showed the presence of bitonality. The differences of the acoustic parameters (jitter, shimmer, harmonic- to-noise ratio) between the two groups of patients were not statistically signifi- cant. Reconstruction of the vocal cord does not seem to improve voice quality af- ter cordectomy even in combination with postoperative speech therapy. Key Words: Cordectomy—Laryngeal cancer—Voice quality—Acoustic analysis. Accepted for publication January 14, 2000. Address all correspondence and reprint requests to Alfio Fer- lito, MD, Department of Otolaryngology—Head Neck Surgery, University of Udine, Viale Venezia 410, 33100 Udine, Italy. e-mail: [email protected] 131
-
Upload
independent -
Category
Documents
-
view
8 -
download
0
Transcript of Acoustic analysis of voice quality with or without false vocal fold displacement after cordectomy
INTRODUCTION
It is commonly accepted that early glottic cancerscan be treated either surgically or with radiotherapy.During the past 10 years, the latter was consideredthe treatment of choice because of the high cure rateand the good voice preservation achieved.1 Radio-therapy, however, has disadvantages such as dryness,inflammation, the long time required for application,and oncogenetic potential. Among the surgical tech-niques, laser surgery gives better functional resultscompared to laryngofissure due to the more rapid
healing processes,2-4 but it is not always available. Toimprove the poor functional results obtained afterconventional cordectomy, some authors have tried toresurface the mucosal defect using different tech-niques.5-7 We usually close the surgical defect usinga mucosal flap obtained from the false omolateral vo-cal cord.8 The aim of the present study was to evalu-ate if the operation of replacing the excised cord istruly effective on voice quality compared to thecordectomy alone.
MATERIALS AND METHODS
Patient populationA total of 14 patients, 12 males and 2 females, un-
derwent conventional cordectomy with external ap-proach for T1aN0M0 squamous cell carcinomas ofthe glottis. The surgical technique consisted of sub-
Journal of VoiceVol. 15, No. 1, pp. 131-140© 2001 The Voice Foundation
Acoustic Analysis of Voice Quality with or withoutFalse Vocal Fold Displacement After Cordectomy
*Giulia Bertino, *Anna Bellomo, †Franco E. Ferrero, *and Alfio Ferlito
*Department of Otolaryngology—Head Neck Surgery, University of Udine, udine, Italy; †Institute of Phonetic and Dialectology, national Research Council (CNR) of Padua, Padua, Italy
Summary: Conventional cordectomy by means of a laryngofissure is one of thetherapeutic options for treatment of early glottic cancer. To improve the poorvoice quality related to this kind of operation, many authors have developed dif-ferent techniques to repair the mucosal defect. We analyzed voice qualityacoustically and compared it after cordectomy alone and after cordectomy withthe reconstruction of the vocal cord in a group of 14 patients affected by T1 glot-tic carcinoma. All the patients underwent postoperative speech therapy. Three pa-tients who underwent cordectomy with reconstruction showed the presence ofdiplophonia, while two patients without reconstruction showed the presence ofbitonality. The differences of the acoustic parameters (jitter, shimmer, harmonic-to-noise ratio) between the two groups of patients were not statistically signifi-cant. Reconstruction of the vocal cord does not seem to improve voice quality af-ter cordectomy even in combination with postoperative speech therapy. KeyWords: Cordectomy—Laryngeal cancer—Voice quality—Acoustic analysis.
Accepted for publication January 14, 2000.Address all correspondence and reprint requests to Alfio Fer-
lito, MD, Department of Otolaryngology—Head Neck Surgery,University of Udine, Viale Venezia 410, 33100 Udine, Italy.e-mail: [email protected]
131

perichondrial removal of the true vocal cord with theupper line of incision passing in the Morgagni’s ven-tricle and the lower line located 5 mm below the in-ferior side of the vocal cord. Only 1 patient under-went extended cordectomy (with the inferior line ofincision passing 1 cm below the vocal cord). The vo-cal process of the arytenoid was left intact in all thepatients. In seven patients the mucosal defect was al-lowed to heal spontaneously, whereas in the otherseven we replaced the defect by means of a mucosalflap obtained from the false omolateral vocal cord8
(Figure 1).The mucosa of the false vocal fold is freed from the
inner perichondrium of the thyroid cartilage andshifted downward at the level of the inferior marginof incision. The false vocal fold should reach the lev-el of the opposite true vocal fold at least in the ante-rior part to reduce airflow escape during phonation asmuch as possible. The right position of the false vo-cal fold can be easily verified intraoperatively. Themucosal flap is then sutured to the subglottic mucosawith a reabsorbable suture. The tension of the suturemust not be too strong because the mucosa can belacerated or the false vocal fold can lose its shape.Reconstruction was casually determined except forthe patient who underwent extended cordectomy. Infact, in this case reconstruction was not possible be-cause of the large surgical defect.
Tracheotomy was not required for any patient. Thepatients were extubated in the operating room and
could eat normally 2 to 3 days after the operation. Allpatients were allowed to leave the hospital on theseventh postoperative day and received antibioticsfor 10 days. Aerosol therapy with steroids wasmaintained twice on a daily basis for 8 to 10 daysafter dismissal. The healing process was monitoredwith serial monthly videolaryngostroboscopies usinga 90° rigid Karl Storz endoscope, an Atmos Endo-Stroboscope, a Karl Storz Endovision 539 videocamera, and a JVC TM-20PSN color video monitor.All the patients underwent speech therapy starting 1month after the operation and had an average of 20lessons (from 10 to 40 lessons). The aim of voice re-habilitation was to reduce the phonatory effort and totry to establish a good glottic closure so that the pa-tient would acquire greater intelligibility and reducehoarseness.
Speech samplesSix months after the end of speech therapy the
voices of the subjects were recorded with a ShureSM58 microphone and a Sanio Model MW737F taperecorder. Every patient was asked to produce thevowel /a/ for 3 seconds and to produce three differentlevels of intensity (loud = max, medium = med, soft= min) with the vowel /a/ repeated three times at eachlevel of intensity. Maximum phonation time (MPT)was calculated asking each patient to produce thevowel /a/ as long as possible at a comfortable level ofintensity for three times. The best of the three trialswas chosen.
132 GIULIA BERTINO ET AL
Journal of Voice, Vol. 15, No. 1, 2001
FIGURE 1. Left cordectomy with reconstruction8. The glottic defect is reconstructed, shifting thefalse vocal cord at the level of the controlateral true vocal cord. L = left; R = right.
R L R L R L
Tumor

At the same time, a short conversation with thespeech therapist was also recorded for each patient.Voice quality and some vocal characteristics, such asdyplophonia, bitonality, and “falsetto” voice werethen subjectively assessed by a group of trained lis-teners who did not know the patients.
Acoustic analysisThe nine sustained /a/ vowels of each of the 14
subjects were analyzed by Kay Elemetrics Multi-speech 3700 software after the digitalization at 50kHz/16 bit of analog signals (by Kay Elemetrics CSL4300 hardware) to perform a reliable voiced parame-ters extraction [i.e., jitter, shimmer and harmonic-to-noise ratio (HNR)].These signal files were alsodownsampled to 12.5 kHz to produce the followingdiagrams:9
1. spectrogram (SPG) at FFT-1024 points rangingbetween 0 and 5 kHz
2. long-term averaged (LTA) power spectrum atFFT-1024 points (narrowband)
3. linear prediction formant spectrum envelope(LPC) at 14 poles on a 200-ms frame length.
Results of the acoustic analysis were reported on agraph (Figure 2) illustrating (from top to bottom andfrom left to right) the waveform of the nine vowels/a/, the narrowband SPG, and the nine spectral sec-tions of narrowband LTA on which was superim-posed the LPC. The mean values of the voicing para-meters for the three different levels of intensity ofphonation were reported in Tables 2 and 3.
The differences of the voicing parameters and ofMPT between the two groups were statistically ana-lyzed using the t-test for unpaired samples.
RESULTS
Table 1 shows the clinical profile of the 14 patientswho underwent cordectomy with or without recon-struction. The patients’ ages ranged from 62.7 to 84.6years (with a mean of 70.5 years, median 66.8 years)for the patients that underwent conventional cordec-tomy, and from 44.8 to 84.6 years (with a mean of63.7 years, median 62.6 years) for the patients whohad reconstruction of the vocal cord.
No major complications due to any of the two sur-gical procedures were observed. Three cervical em-physemas developed through the vertical thyrotomybut neither of them caused any dyspnea and theywere resolved through the use of a lightly compres-sive dressing.
The development of small posterior granulomaswas observed in 5 (35.7%) patients, 4 reconstructed(cases SR, BM, AA, CL, Table 2), and 1 not recon-structed (case RL, Table 3). They resorbed sponta-neously in 3 months in 4 patients (28.5%), while in 1female patient (7.1%) the granuloma was removedsurgically after 3 months (case BM, Table 2). In threepatients (21.4%), one reconstructed (case SR, Table2) and two not reconstructed (cases MS and GF,Table 3), an anterior synechia appeared; no patientunderwent surgical excision.
Table 2 illustrates the results of the acoustic analy-sis of the patients who underwent cordectomy withreconstruction for the three different degrees of in-tensity of phonation. A physiological decrease of theF0 values together with the diminishing of thephonatory effort (intensity) was observed. The meanvalues of jitter were always greater than the normalvalue (�1%). Shimmer values were more than twicethe normal value (0.4 dB). The only exception is caseBM, who showed almost normal shimmer values. Allthe patients with positive values of HNR showed agood prominence of the first harmonics from noise,while patients with negative values of HNR showedthe preponderance of noise on harmonics.
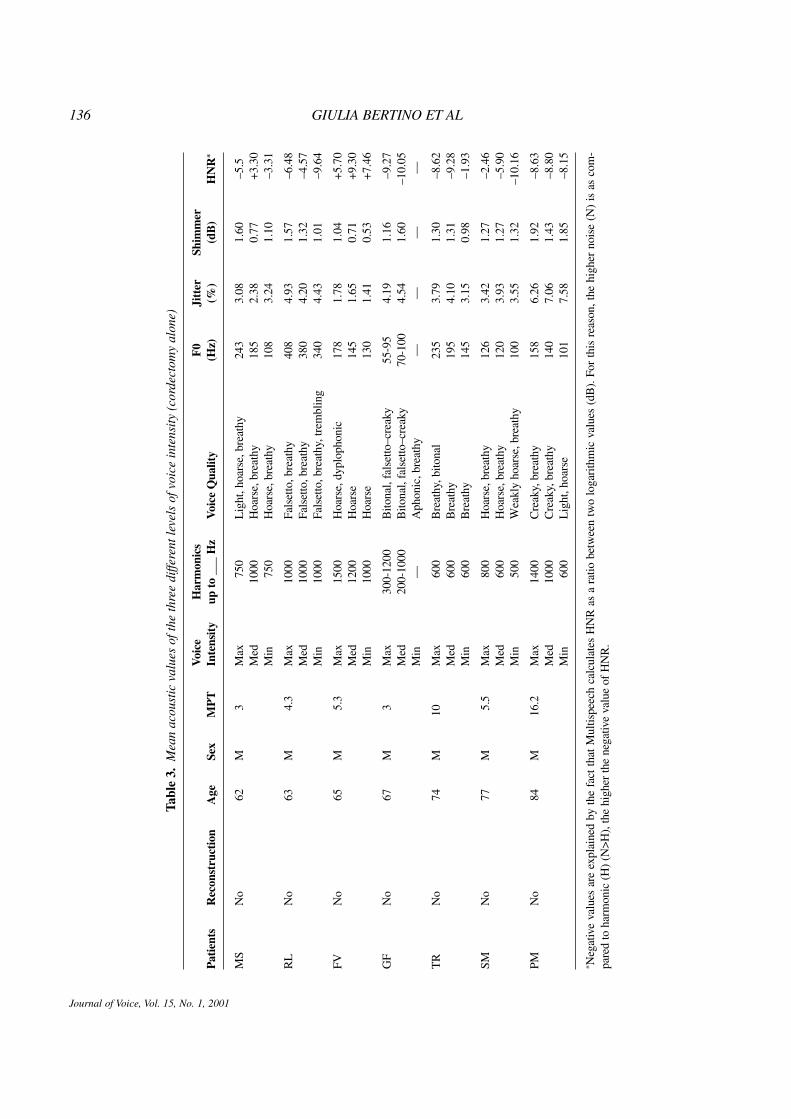
Table 3 reports the results of the acoustic analysisof the patients who underwent cordectomy alone.
The behavior of the F0, jitter, shimmer, and HNRvalues was similar to that of the group of patientswith reconstruction.
The difference of the acoustic parameters (jitter,shimmer, HNR) between the two groups of patientswas not statistically significant, as was the differencein MPT. Figures 3-5 show the results of the t-test per-formed for jitter, shimmer, and HNR, respectively.
On videolaryngostroboscopy all the patients with ahigh fundamental frequency were shown to use theglottic level more often, while patients using a supra-glottal mechanism of phonation tended to use lowerfundamental frequencies, regardless of the surgicaltechnique used.
ACOUSTIC ANALYSIS OF VOICE QUALITY 133
Journal of Voice, Vol. 15, No. 1, 2001

134 GIULIA BERTINO ET AL
Journal of Voice, Vol. 15, No. 1, 2001
FIGURE 2. Graph of the acoustic analysis performed (see text).
Table 1. Clinical profile of the patients considered
Mean/MedianSex
Procedure No. Patients Age (years) Male Female
Cordectomy alone 7 70.5/66.8 7 —
Cordectomy with reconstruction 7 63.7/62.6 5 2

ACOUSTIC ANALYSIS OF VOICE QUALITY 135
Journal of Voice, Vol. 15, No. 1, 2001
Tabl
e 2.
Mea
n ac
oust
ic v
alue
s of
the
thre
e di
ffere
nt le
vels
of v
oice
inte
nsity
(co
rdec
tom
y w
ith r
econ
stru
ctio
n)
Voi
ceH
arm
onic
sF
0Ji
tter
Shim
mer
Pat
ient
sR
econ
stru
ctio
nA
geSe
xM
PT
Inte
nsit
yup
to
___
Hz
Voi
ce Q
ualit
y(H
z)(%
)(d
B)
HN
R*
SRY
es45
M10
Max
1000
Lig
ht,h
oars
e–dy
plop
honi
c25
02.
952.
71–8
.06
Med
500
Lig
ht,h
oars
e–dy
plop
honi
c23
01.
752.
30–4
.77
Min
250
Bre
athy
,hoa
rse–
dypl
opho
nic
215
3.65
2.05
–11.
54
BM
Yes
54F
10.2
Max
2500
Lig
htly
pre
ssed
,dyp
loph
onic
221
1.61
0.52
+9.1
9M
ed20
00L
ight
ly p
ress
ed,d
yplo
phon
ic17
51.
580.
35+7
.01
Min
1000
Lig
htly
bre
athy
,dyp
loph
onic
150
1.90
0.57
+4.9
3
BC
Yes
58M
24.5
Max
1000
Hoa
rse,
crea
ky–d
yplo
phon
ic11
33.
771.
30–4
.01
Med
1000
Hoa
rse,
crea
ky–d
yplo
phon
ic11
58.
341.
49–2
.27
Min
1000
Hoa
rse,
crea
ky–p
ulse
d11
37.
811.
86–5
.51
AA
Yes
64M
3M
ax12
50B
reat
hy23
01.
960.
65+3
.93
Med
750
Bre
athy
160
3.62
0.70
+4.2
5M
in50
0B
reat
hy13
53.
990.
84+2
.60
MV
Yes
71F
9.2
Max
2000
Fals
etto
,bre
athy
395
1.87
1.02
–2.6
5M
ed15
00L
ight
,hoa
rse,
brea
thy
305
2.06
0.92
+1.4
8M
in10
00H
oars
e,br
eath
y23
82.
681.
27–5
.25
TL
Yes
75M
9M
ax10
50C
reak
y,br
eath
y,w
avin
g88
3.93
1.25
–12.
89M
ed80
0C
reak
y,br
eath
y,w
avin
g95
4.81
1.67
–10.
21M
in50
0C
reak
y,br
eath
y10
14.
511.
70–1
0.31
CL
Yes
84M
6.3
Max
700
Hoa
rse,
brea
thy
146
4.07
1.16
–6.7
7M
ed50
0H
oars
e,br
eath
y13
53.
411.
25–1
0.14
Min
400
Hoa
rse,
brea
thy
101
5.14
1.37
–8.7
3
* Neg
ativ
e va
lues
are
exp
lain
ed b
y th
e fa
ct th
at M
ultis
peec
h ca
lcul
ates
HN
R a
s a
ratio
bet
wee
n tw
o lo
gari
thm
ic v
alue
s (d
B).
For
this
rea
son,
the
high
er n
oise
(N
) is
as
com
-pa
red
to h
arm
onic
(H
) (N
>H),
the
high
er th
e ne
gativ
e va
lue
of H
NR
.
136 GIULIA BERTINO ET AL
Journal of Voice, Vol. 15, No. 1, 2001
Tabl
e 3.
Mea
n ac
oust
ic v
alue
s of
the
thre
e di
ffere
nt le
vels
of v
oice
inte
nsity
(co
rdec
tom
y al
one)
Voi
ceH
arm
onic
sF
0Ji
tter
Shim
mer
Pat
ient
sR
econ
stru
ctio
nA
geSe
xM
PT
Inte
nsit
yup
to
___
Hz
Voi
ce Q
ualit
y(H
z)(%
)(d
B)
HN
R*
MS
No
62M
3M
ax75
0L
ight
,hoa
rse,
brea
thy
243
3.08
1.60
–5.5
Med
1000
Hoa
rse,
brea
thy
185
2.38
0.77
+3.3
0M
in75
0H
oars
e,br
eath
y10
83.
241.
10–3
.31
RL
No
63M
4.3
Max
1000
Fals
etto
,bre
athy
408
4.93
1.57
–6.4
8M
ed10
00Fa
lset
to,b
reat
hy38
04.
201.
32–4
.57
Min
1000
Fals
etto
,bre
athy
,tre
mbl
ing
340
4.43
1.01
–9.6
4
FVN
o65
M5.
3M
ax15
00H
oars
e,dy
plop
honi
c17
81.
781.
04+5
.70
Med
1200
Hoa
rse
145
1.65
0.71
+9.3
0M
in10
00H
oars
e13
01.
410.
53+7
.46
GF
No
67M
3M
ax30
0-12
00B
itona
l,fa
lset
to–c
reak
y55
-95
4.19
1.16
–9.2
7M
ed20
0-10
00B
itona
l,fa
lset
to–c
reak
y70
-100
4.54
1.60
–10.
05M
in—
Aph
onic
,bre
athy
——
——
TR
No
74M
10M
ax60
0B
reat
hy,b
itona
l23
53.
791.
30–8
.62
Med
600
Bre
athy
195
4.10
1.31
–9.2
8M
in60
0B
reat
hy14
53.
150.
98–1
.93
SMN
o77
M5.
5M
ax80
0H
oars
e,br
eath
y12
63.
421.
27–2
.46
Med
600
Hoa
rse,
brea
thy
120
3.93
1.27
–5.9
0M
in50
0W
eakl
y ho
arse
,bre
athy
100
3.55
1.32
–10.
16
PMN
o84
M16
.2M
ax14
00C
reak
y,br
eath
y15
86.
261.
92–8
.63
Med
1000
Cre
aky,
brea
thy
140
7.06
1.43
–8.8
0M
in60
0L
ight
,hoa
rse
101
7.58
1.85
–8.1
5
* Neg
ativ
e va
lues
are
exp
lain
ed b
y th
e fa
ct t
hat
Mul
tispe
ech
calc
ulat
es H
NR
as
a ra
tio b
etw
een
two
loga
rith
mic
val
ues
(dB
). F
or t
his
reas
on,t
he h
ighe
r no
ise
(N)
is a
s co
m-
pare
d to
har
mon
ic (
H)
(N>H
),th
e hi
gher
the
nega
tive
valu
e of
HN
R.

The analysis of voice quality showed that one pa-tient (case GF) was totally aphonic at the minimum(min) intensity, while at the other two intensities ofphonation he showed the presence of a falsetto voice.This was one of two cases that presented an anteriorsynechia.
Another case (RL), showed the presence of falset-to voice. This was the patient who underwent ex-tended cordectomy.
Three of the seven patients who underwent cordec-tomy with reconstruction showed the presence of dy-plophonia (see Table 2), while two of the seven pa-
ACOUSTIC ANALYSIS OF VOICE QUALITY 137
Journal of Voice, Vol. 15, No. 1, 2001
FIGURE 3. Result of the t-test performed for jitter values. cl = confi-dence level; df = degrees of freedoms; sd = standard deviation.
FIGURE 4. Result of the t-test performed for shimmer values.
cl
cl
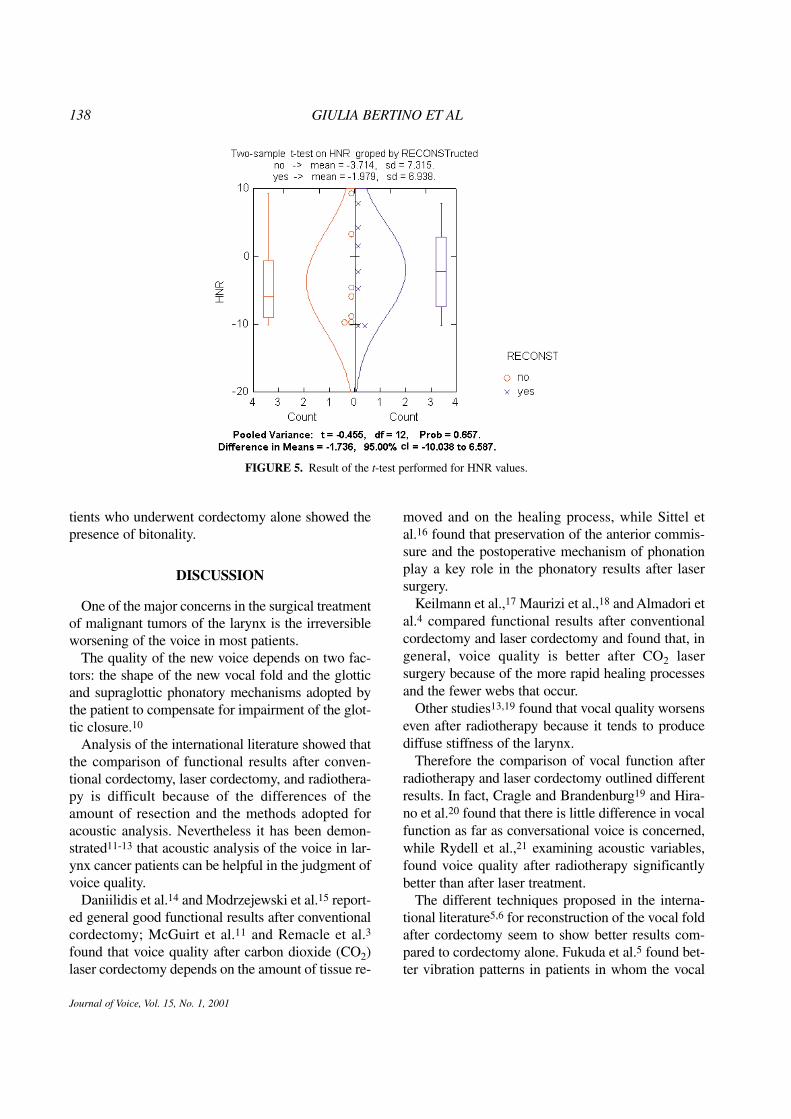
tients who underwent cordectomy alone showed thepresence of bitonality.
DISCUSSION
One of the major concerns in the surgical treatmentof malignant tumors of the larynx is the irreversibleworsening of the voice in most patients.
The quality of the new voice depends on two fac-tors: the shape of the new vocal fold and the glotticand supraglottic phonatory mechanisms adopted bythe patient to compensate for impairment of the glot-tic closure.10
Analysis of the international literature showed thatthe comparison of functional results after conven-tional cordectomy, laser cordectomy, and radiothera-py is difficult because of the differences of theamount of resection and the methods adopted foracoustic analysis. Nevertheless it has been demon-strated11-13 that acoustic analysis of the voice in lar-ynx cancer patients can be helpful in the judgment ofvoice quality.
Daniilidis et al.14 and Modrzejewski et al.15 report-ed general good functional results after conventionalcordectomy; McGuirt et al.11 and Remacle et al.3
found that voice quality after carbon dioxide (CO2)laser cordectomy depends on the amount of tissue re-
moved and on the healing process, while Sittel etal.16 found that preservation of the anterior commis-sure and the postoperative mechanism of phonationplay a key role in the phonatory results after lasersurgery.
Keilmann et al.,17 Maurizi et al.,18 and Almadori etal.4 compared functional results after conventionalcordectomy and laser cordectomy and found that, ingeneral, voice quality is better after CO2 lasersurgery because of the more rapid healing processesand the fewer webs that occur.
Other studies13,19 found that vocal quality worsenseven after radiotherapy because it tends to producediffuse stiffness of the larynx.
Therefore the comparison of vocal function afterradiotherapy and laser cordectomy outlined differentresults. In fact, Cragle and Brandenburg19 and Hira-no et al.20 found that there is little difference in vocalfunction as far as conversational voice is concerned,while Rydell et al.,21 examining acoustic variables,found voice quality after radiotherapy significantlybetter than after laser treatment.
The different techniques proposed in the interna-tional literature5,6 for reconstruction of the vocal foldafter cordectomy seem to show better results com-pared to cordectomy alone. Fukuda et al.5 found bet-ter vibration patterns in patients in whom the vocal
138 GIULIA BERTINO ET AL
Journal of Voice, Vol. 15, No. 1, 2001
FIGURE 5. Result of the t-test performed for HNR values.
cl

fold was reconstructed with displacement of the ven-tricular fold compared to those who underwent lasertreatment. Unfortunately their analysis is based onvideolaryngostroboscopic examination only, so noacoustic data exist that might provide a better objec-tive evaluation of voice quality. Milutinovic6 foundthat patients in whom the vocal fold was reconstruct-ed with a myomucosal flap had better glottic closure,MPT values, and sonographic patterns than thosethat underwent cordectomy alone or those treated byradiation therapy, but Milutinovic used the Yanagi-hara classification only. While better phonodynamicparameters can be explained in terms of the thicknessof the flap, the truth of the sonographic results is un-dermined by the nonhomogeneous numbers of pa-tients compared in the three groups. Perhaps a largergroup of patients with vocal fold reconstructionwould have revealed a more scattered pattern of dis-tribution of the degree of hoarseness.
In the majority of cases in our study, we were ableto obtain a socially acceptable voice, however, thevoice quality achieved must be considered worsethan a normal voice.
In one case (GF, Table 3) the objective evaluationof F0 and the judgment of voice quality were in con-trast. In fact, this case showed a low F0 while the pa-
tient’s voice was subjectively assessed as a falsettovoice. This may be due to the fact that his superiorharmonics have a higher energy compared to the F0which is creaky (see Figure 2).
Unfortunately, as demonstrated by statistical analy-sis of the acoustic parameters, our method of recon-struction of the excised vocal fold, although similar tothat reported by Fukuda et al.,5 neither improved thehealing process, as we observed more granulomas inthis group of patients, nor did it favor the creation ofa satisfactory new vocal cord. Nevertheless, in agree-ment with the data of Fukuda et al.5 and Milutinovic,6
we found clearly better MPT values in the group ofreconstructed patients, even if these values were notstatistically significant (Figure 6).
Therefore, the functional results depended on thephonatory mechanisms adopted by the patients aftersurgery, regardless of the surgical technique adopted.In fact, we did not find any correlation between theglottic position of the displaced false vocal fold andthe presence of a glottic pattern of phonation; in oth-er words, not all the reconstructed patients showed aglottic pattern of phonation, while some unrecon-structed patients used this kind of pattern. For thisreason we believe that speech therapy, when startedas soon as possible after surgery, can be useful both
ACOUSTIC ANALYSIS OF VOICE QUALITY 139
Journal of Voice, Vol. 15, No. 1, 2001
FIGURE 6. Result of the t-test performed for MPT values.
cl

to guide the acquisition of a good phonatory patternand to prevent a possible ankylosis of the arytenoids.Unfortunately, we have no data to confirm the real ef-ficacy of voice rehabilitation because we did notmake a comparison between rehabilitated and nonre-habilitated patients, but in our opinion these kinds ofpatients cannot reach satisfactory voice qualities bythemselves. In fact, the entire pneumophonic coordi-nation mechanism has to be rehabilitated.
CONCLUSIONS
Although the best surgical techniques are used, thevoice quality after cordectomy is never the same asthat of healthy people. One should consider that agood result has been achieved when the voice quali-ty after the operation is similar to the voice qualitybefore the operation.
The phonatory mechanism adopted by the patientsafter surgery is the most important factor in deter-mining the quality of the new voice. For this reasonthe need for postoperative voice rehabilitation has tobe assessed in every patient because well-directedvoice therapy is helpful in the acquisition of the mosteffective phonatory mechanism.
REFERENCES
1. Mendenhall WM, Parsons JT, Stringer SP, Cassisi NJ, MillionRR. Radiation therapy. In Ferlito A, ed. Neoplasms of the lar-ynx. Edinburgh: Churchill Livingstone, 1993:517-528.
2. Pia F, Gonella ML, Boggero R, Ponzo S, Giordano C. Valu-tazione obiettivo-strumentale della funzionalita glottica resid-ua dopo cordectomia tradizionale e cordectomia CO2 laser.Acta Otorhinolaryngol Ital. 1994;14:329-338.
3. Remacle M, Lawson G, Jamart J, Minet M, Watelet JB, DelosM. CO2 laser in the diagnosis and treatment of early cancer ofthe vocal fold. Eur Arch Otorhinolaryngol. 1997;254:169-176.
4. Almadori G, Ottaviani F, D’Alatri L, Carriero E, Modica V,Paludetti G. Risultati funzionali dopo cordectomia inlaringofissura e in microlaringoscopia con laser CO2. ActaOtorhinolaryngol Ital. 1998;18:16-22.
5. Fukuda H, Tsuji DH, Kawasaki Y, Kawaida M, Sakou T. Dis-placement of the ventricular fold following cordectomy. AurisNasus Larynx. 1990;17:221-228.
6. Milutinovic Z. Composite myo-mucosal reconstruction of thevocal fold. Eur Arch Otorhinolaryngol. 1995;252:119-122.
7. Silver CE. Conservation surgery for glottic cancer. In SilverCE, Ferlito A, eds. Surgery for cancer of the larynx and relat-ed structures, 2nd ed. Philadelphia: WB Saunders, 1996:65-121.
8. Sala O, Sala T. Testo-Atlante a colori di ORL. Padua, Italy:Piccin, 1996:389.
9. Ferrero FE, Accordi M, Accordi D, de Filippis C, Staffieri A.Semiologia avanzata della funzione vocale. In Logopedia eFonochirurgia. Relazione ufficiale XXXIII CongressoSIFEL, Abano Terme. Acta Phoniatr Lat. 1998;20:33-58.
10. Lengo M, Castagna G. Fisiopatologia vocale. In Riabili-tazione funzionale, chirurgica e logopedica dopo interventidi laringectomia parziale, sub-totale e totale. Tavola Roton-da 79° Congresso S.I.O. e Chir. Cerv. Fac., Sorrento. ActaOtorhinolaryngol Ital. 1992;12:209-220.
11. McGuirt WF, Blalock D, Koufman JA, Feehs RS. Voiceanalysis of patients with endoscopically treated early laryn-geal carcinoma. Ann Otol Rhinol Laryngol. 1992;101:142-146.
12. Bertino G, Bellomo A, Miani C, Ferrero F, Staffieri A. Spec-trographic differences between tracheal-esophageal andesophageal voice. Folia Phoniatr Logop. 1996;48:255-261.
13. Lehman JL, Bless DM, Brandenburg JH. An objective as-sessment of voice production after radiation therapy forstage I squamous cell carcinoma of the glottis. OtolaryngolHead Neck Surg. 1998;98:121-129.
14. Daniilidis J, Nikolaou A, Symeonidis V. Our experience inthe surgical treatment of T1 carcinoma of the vocal cord. JLaryngol Otol. 1990;104:222-224.
15. Modrzejewski M, Olszewski E, Strek P, Wszolek W, Zielin-ska J. Effectiveness of classical chordectomy in the treat-ment of cancer of the glottis. Auris Nasus Larynx. 1998;25:59-66.
16. Sittel C, Eckel HE, Eschenburg C. Phonatory results afterlaser surgery for glottic carcinoma. Otolaryngol Head NeckSurg. 1998;119:418-424.
17. Keilmann A, Bergler W, Artzt M, Hörmann K. Vocal func-tion following laser and conventional surgery of small ma-lignant vocal fold tumours. J Laryngol Otol. 1996;110:1138-1141.
18. Maurizi M, Paludetti G, Carriero E, D’Abramo G, AlmadoriG. Risultati clinici dopo cordectomia in laringofissura e inmicrolaringoscopia con laser CO2. Acta OtorhinolaryngolItal. 1997;17:289-297.
19. Cragle SP, Brandenburg JH. Laser cordectomy or radiother-apy: cure rates, communication, and cost. Otolaryngol HeadNeck Surg. 1993;108:648-654.
20. Hirano M, Hirade Y, Kawasaki H. Vocal function followingcarbon dioxide laser surgery for glottic carcinoma. Ann OtolRhinol Laryngol. 1985;94:232-235.
21. Rydell R, Schalén L, Fex S, Elner Å. Voice evaluation beforeand after laser excision vs. radiotherapy of T1A glottic car-cinoma. Acta Otolaryngol (Stockh). 1995;115:560-565.
140 GIULIA BERTINO ET AL
Journal of Voice, Vol. 15, No. 1, 2001