ACEs Mapping Survey Report - Alaska Children's Trust
55
ACEs Mapping Survey Report Prepared for: Alaska Children’s Trust September 2014
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of ACEs Mapping Survey Report - Alaska Children's Trust

ACEs Mapping Survey Report
Prepared for: Alaska Children’s Trust
September 2014

ACES Mapping Survey Report
Prepared for: Alaska Children’s Trust
Prepared by:
Juneau � Anchorage
Funding provided by:
Alaska Children’s Trust Alaska Mental Health Trust Authority
Rasmuson Foundation
September 2014

Table of Contents
Executive Summary ..................................................................................................... 1 Key Findings and Themes ........................................................................................... 1
Survey Purpose, Methodology and Reporting ........................................................... 3 Survey Respondents .................................................................................................... 4
Professional Roles ........................................................................................................ 4 Length of Involvement with ACEs ............................................................................... 4 Organizations Represented ......................................................................................... 5 Service Locations ........................................................................................................ 6 Program Focus ............................................................................................................ 7 Work Priorities ............................................................................................................ 9 Follow-up Desired ..................................................................................................... 10 Current ACEs Projects ............................................................................................... 10
Impact of ACEs on Practitioners ............................................................................... 12 Strategies and Measures ........................................................................................... 16 Needs of the Field ..................................................................................................... 19
Frequently Asked Questions ...................................................................................... 19 Barriers to Trauma-Informed Care ............................................................................. 21 Access to ACEs-related Services ................................................................................. 24 Resources Needed .................................................................................................... 26 Improving Statewide Systems ................................................................................... 30
Appendix 1 – Survey Participants ............................................................................. 34 Appendix 2 – Current ACEs-related Projects ............................................................ 36 Appendix 3 – ACEs Strategies and Measures ........................................................... 41 Appendix 4 – Survey Questions ................................................................................ 50
Special acknowledgment to University of Maine Cooperative Extension for sharing their state mapping-survey and results.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 1
Executive Summary
The Alaska Children’s Trust designed and fielded a survey to capture baseline data about individuals and
organizations whose work incorporates concepts and tools associated with Adverse Childhood Experiences
(ACEs). The survey is an initial step toward better alignment and coordination of these efforts locally,
regionally and statewide.
Of 81 total survey respondents, 62 answered most or all the survey questions. Respondents include program
managers/administrators, service providers, trainers, researchers/educators, and other professionals. They
represent 39 identified organizations or agencies and an unknown number of other entities involved in ACEs-
related work.
Key Findings and Themes
Survey respondents are passionate about ACEs.
• Respondents provided detailed and often lengthy answers to ten open-ended questions about their
activities in addition to substantial other information.
• Almost uniformly, survey respondents believe ACEs is very important and that both awareness and
use of ACEs principles should expand significantly.
• Respondents argued often for expansion of trauma-informed care and education to raise awareness
and increase adoption of ACEs-related approaches.
There appears to be no broad consensus about what, specifically, constitutes “ACEs-related work.”
• For example, many respondents view their involvement in ACEs as pre-dating the 1997 study that
popularized the term. It is not clear from the survey responses whether practitioners tend to see
themselves as engaged in an ACEs-driven strategy or whether they view ACEs primarily as a useful
perspective or component within a more traditional approach, such as violence intervention or
therapeutic services.
• ACEs is a broad and pervasive field. Strategies associated with ACEs encompass prevention,
intervention, training, and treatment, and all four may be pursued at the child, adult, family, and
community levels. Nearly all respondents, even those who also provide therapeutic services and
screening, said they are engaged in training/education, making that the most common ACEs-related
program activity.
• Although all the respondents use ACEs in their work, many expressed a need for more information
about the design, implementation and communication of ACEs-related strategies.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 2
Although most respondents say their organizations partner with other programs, survey results indicate the ACEs field as a whole in Alaska lacks a collaborative approach based on mutually reinforcing activities and collection of quality data that addresses similar outcomes in a coordinated network.
• Strategies vary widely, and there seems to be limited common vocabulary used to describe similar
approaches.
• When asked what kinds of questions need to be answered about ACEs, a number of respondents said
questions about the goals and next steps for expanding the field in Alaska.
• Measurement approaches appear to reflect the needs of individual organizations or specific grants,
which is an impediment to assessing broader needs and impacts.
• Suggestions for changes in statewide systems addressed a wide variety of goals including:
o Changes in thinking and overall priorities o Changes to/expansion of Medicaid o More program funding, especially for prevention and intervention o Less bureaucracy and better collaboration
• When asked what resources are needed to support individual and community activities, most
respondents said they need funding, tools, training, and materials to expand awareness and
understanding of ACEs and to support their own programs. Few mentioned better coordination
among core practitioners.
(See Appendix 3 for detailed survey responses regarding strategies and measures.)
Tribal organizations are not widely represented in the survey responses.
• Only three respondents identified themselves as representing a tribal organization. Several others said
they work for Alaska Native regional nonprofits, but only two respondents listed their place of
employment as one of the 15 organizations represented on the Board of Directors of the Alaska
Native Tribal Health Consortium (ANTHC). One other respondent works for ANTHC, itself.
• Survey results suggest tribal organizations interpret ACEs broadly to include cultural and multi-
generational impacts.
There is considerable variation in the way respondents feel ACEs has affected their work.
• Learning about ACEs has had profound effects on some practitioners, changing the way they
understand and respond to clients, families and funders.
• Others said they view ACEs as a confirmation of what they already knew or suspected.
• A third group of respondents said ACEs changed the way they design training and, especially, tailor
communications.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 3
Survey Purpose, Methodology and Reporting
The survey was designed and fielded by a committee supported by the Alaska Children’s Trust (ACT) to
collect information about organizations, programs, and activities associated with the field of Adverse
Childhood Experiences (ACEs) in Alaska. The committee consisted of members from First Alaskans Institute,
Alaska Mental Health Trust Authority, Mat-Su Health Foundation, Recover Alaska, Alaska Child Trauma Center,
and the Alaska Mental Health Board. This report was prepared by McDowell Group, an Alaska research and
consulting firm. It summarizes the survey results and identifies major themes.
The survey was fielded on the SurveyMonkey website, initially during February of 2014 and again in May
2014 to expand participation. A variety of individuals and organizations engaged in ACE’s-related work were
invited to participate. Twenty-six questions addressed ACEs-related activities of the respondents and the
respondents’ organizations, where applicable. Sixty-two respondents answered most or all the questions. This
includes 46 representatives of 39 different organizations or agencies, and 16 other respondents who did not
identify their places of employment. An additional five respondents provided partial answers.
Many of the survey respondents took time to provide detailed answers to questions about how ACEs affects
their work, how they incorporate it, barriers to providing ACEs-related care, needs of the field, and other
complex issues. This report discusses major themes and findings from the research. ACT will undertake more
detailed analysis of the implications of individual answers.
Because the survey is not statistically representative (respondents were not randomly selected), readers must
use their own judgment as to the degree to which answers to individual questions represent the field broadly
or narrowly. The primary value of this type of research lies in the insights that may be gained from individual
experiences and perceptions reported by the respondents, rather than the percentage of respondents who
said one thing or another.
The survey results provide a baseline of information for future updates and expansion. ACT will use the data
for ongoing reference and analysis in its efforts to encourage and support the ACEs field statewide.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 4
Survey Respondents
This section of the report summarizes data provided by the respondents about their professional roles and the
roles of their organizations. In the report tables, the number of people answering a particular question is
shown in the heading following the letter “n”.
Professional Roles
Respondents represent a mix of ACEs practitioners, and many are involved in more than one capacity. Seven
in ten are responsible for a program, and four in ten provide direct services.
What is your professional role? (Multiple responses allowed)
n=67 %
Program manager/administrator 70%
Service provider 39
Researcher/professor 19
Trainer 19
Other 22
“Other” includes the following:
• Clinical services and supervision
• Funder
• Health and Social Services planner
• High school nurse and family planning ANP
• Infant learning program
• Public health nurse
• Epidemiologist
• State system administrator
• Tribal judge
• Victim advocate
Length of Involvement with ACEs
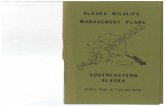
Eighty percent of respondents have performed ACEs-related work for 3 years or more. Since the CDC/Kaiser
Permanente study that defined ACEs was first reported in 1998, respondents who said they have been doing
ACEs-related work for more than 20 years are referring to work that is recognized as ACEs-related, but was
not labeled as such prior to 1998.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 5
How many years have you been doing this work? (n=62)
Organizations Represented
Not every respondent specified her or his place of employment. Those who did represent 39 different
organizations. (This counts five different divisions or programs of the Alaska Department of Health and Social
Services (DHSS), and the department as a whole, as separate organizations.)
AK Child & Family AK Mental Health Trust Authority Alaska CARES (2 respondents) Alaska Child Trauma Center at ACMHS Alaska Children's Alliance Alaska Children's Trust Alaska Department of Education and Early
Development Alaska Department of Health and Social
Services (DHSS) DHSS/Division of Juvenile Justice DHSS/Division of Behavioral Health (2
respondents) DHSS/Division of Public Health/Alaska Family
Violence Prevention Project DHSS/Homer Public Health Center DHSS/Office of Children’s Services Alaska Mental Health Board/Advisory Board on
Alcoholism and Drug Abuse Alaska Native Tribal Health Consortium Anchorage Community Mental Health Services
(2 respondents) Boys & Girls Clubs Alaska
Child Welfare Academy Co-Occurring Disorders Institute Fairbanks Regional Public Health First Alaskans Institute Haven House Homer High School Justice for Native Children Kawerak, Inc. Kodiak Area Native Association Mat-Su Health Foundation Mat-Su Services for Children and Adults North Star Behavioral Health Hospital REACH Inc. SeaView Community Services (2 respondents) Sound Alternatives South Peninsula Hospital Community Health
Services Southcentral Foundation Sprout Family Services The All-Alaska Pediatric Partnership University of Alaska Anchorage (3 respondents) United Way of Mat-Su Women In Safe Homes
13
16
8
10
15
0
2
4
6
8
10
12
14
16
18
< 3 3 to 5 6 to 10 11 to 20 > 20
Number of Respondents
Number of Years in ACEs-‐related Work

ACEs Mapping Survey Report McDowell Group, Inc. � Page 5
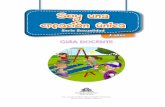
Most respondents represent organizations that employ 20 or fewer people. The larger organizations are
regional nonprofits or state agencies.
Respondents’ Organizations by the Number of ACEs-related Employees*
*Note: these figures include some duplication and represent a rough estimate. Several respondents provided different numbers of employees for the same organization.
Accounting for duplicate employment figures provided by some respondents, survey results suggest there are
at least 1,000 individuals engaged in ACEs-related work in Alaska at approximately 59 unique organizations.
Type of Organization Represented by Respondents
Organization Type
# Respondents
Approximate # Unique
Organizations
Non-profit Organization 32 29
State Agency 14 14*
Educational Institutions 6 6
Tribal Agency 6 6
Businesses 3 3
Foundations 1 1
Totals 62 59**
* Includes 5 individual DHSS components counted as separate agencies. ** An actual count is not available because some respondents did not provide the name of their organization. This total is inferred from other information provided in the survey.
29
16
8
2 3
0
5
10
15
20
25
30
35
1 to 5 6 to 20 22 to 50 51 to 100 > 100
Number of Organiza=ons
Number of ACE's-‐related Employees

ACEs Mapping Survey Report McDowell Group, Inc. � Page 6
Service Locations
Most respondents serve clients statewide or in the Railbelt. Northern and Western Alaska are the most lightly
represented.
What borough(s) / region(s) do you serve? (Multiple responses allowed)
n=62 # Serving
Statewide 27
Municipality of Anchorage 12
Kenai Peninsula Borough 11
Matanuska-Susitna Borough 8
Aleutians East Borough 6
Nome Census Area 4
Fairbanks North Star Borough 3
Northwest Arctic Borough 3
Valdez-Cordova Census Area 3
Dillingham Census Area 2
Haines Borough 2
Hoonah-Angoon Census Area 2
Juneau City and Borough 2
Ketchikan Gateway Borough 2
Kodiak Island Borough 2
Lake and Peninsula Borough 2
Petersburg Census Area 2
Skagway Municipality 2
Yakutat City and Borough 2
Aleutians West Census Area 1
Bethel Census Area 1
Bristol Bay Borough 1
North Slope Borough 1
Prince of Wales-Hyder Census Area 1
Sitka City and Borough 1
Wade Hampton Census Area 1
Wrangell City and Borough 1
Denali Borough 0
Southeast Fairbanks Census Area 0
Yukon-Koyukuk Census Area 1

ACEs Mapping Survey Report McDowell Group, Inc. � Page 7
Program Focus
Respondents represent program areas and activities that extend well beyond behavioral health.
What is your program area of focus? (Multiple responses allowed)
n=67 %
Mental health 49%
Advocacy 41
Child welfare 28
Early care and education 28
Substance abuse 26
Training 26
Home visiting 17
Community development 12
Education (K-12) 12
Healthcare provider/hospital 12
Research 10
Public health 10
Public safety 9
Corrections 6
Primary health care 6
Government (any level) 6
Education (postsecondary) 4
Public health nursing 4
University 4
Faith based organizations 3

ACEs Mapping Survey Report McDowell Group, Inc. � Page 8
Survey responses did not suggest an obvious gap in services for a particular age group.
What age group(s) do you serve? (Multiple responses allowed)
n=64 %
High school (14-18 years) (addressing individual needs ) 70%
High school (14-18 years) (focusing on parental roles) 55
Early childhood (Birth to 3 years) 62
Pre-K & kindergarten (4-5 years) 65
Elementary school (6-11 years) 62
Middle school (12-13 years) 67
College age (19-23 years) (addressing individual needs) 58
College age (19-23 years) (focusing on parental roles) 44
Other adults (24-59 years) 56
Elders (60+) 47
Prenatal family support 27
N/A 8
Although only 20 percent of respondents said their own professional role includes training, more than 80
percent work for organizations that either engage, or plan to engage, in training. Partnering with other
programs is also a common strategy.
What ACEs-related activities has your organization pursued? (Multiple responses allowed)
n=62 In the Past Current or Planned
Training/education 85% 83%
Partner with other programs 55 63
Prevention 49 50
Therapeutic services 43 45
Screening 39 45
Write grant 31 30
Evaluate service 23 31
Develop program 22 41
Research 19 25
Funding for programs/services 14 22
N/A 2 0

ACEs Mapping Survey Report McDowell Group, Inc. � Page 9
Work Priorities
Respondents’ top priorities typically involve the needs of individual victims of ACEs or efforts to prevent it.
The table shows the number of people who identified each area as their first, second, or third highest priority
and the average overall score when each rating of first priority is assigned a value of 1, each rating of second
priority a value of 2, and so on, through thirteenth priority (a value of 13).
From this list, please rank your top priorities in relation to your work. (Lower average score indicates higher overall priority)
n=66 # Choosing
as First Priority
# Choosing as Second
Priority
# Choosing as Third Priority
Average Score
Overall Protective factor/resilience/healthy coping measures
25 11 11 2.4
Prevention 22 16 8 2.5
Trauma-informed care 26 15 6 2.7
Child welfare 22 7 7 3.1
Personal violence 18 8 7 3.8
Mental illness 19 8 3 4.3
Substance use 13 8 5 4.5
Education measures 7 3 8 5.6
Community violence 8 4 6 5.6
Chronic disease 4 1 4 6.7
Health care efficiency and/or cost 3 1 4 7.4
Work productivity 1 1 5 7.4
Crime 3 2 5 7.5
Please rate the importance of advancing ACEs understanding and prevention in Alaska. n=50 %
Very important 77%
High importance 19
Moderate importance 4
Low importance 0
Not at all important 0

ACEs Mapping Survey Report McDowell Group, Inc. � Page 10
Follow-up Desired
Would you like to receive more information about ACEs, or participate in any future statewide ACEs initiatives we develop?
n=48 %
Yes 94%
No 6
Respondents who said they want to be more involved provided contact information.
What sort of follow-up information are you interested in? (Multiple responses allowed)
n=45 %
Reports 94%
Planning opportunities 89
Writing opinion-editorial and/or news articles 43
How to become a member of ACEs speakers bureau 36
Interviews to share more about my experiences 26
Current ACEs Projects
COULD YOU GIVE US A COMPREHENSIVE LIST OF ALL THE ACES PROJECT(S) YOU'RE CURRENTLY WORKING ON?
Following is a summary of the types of projects currently being pursued. Appendix 2 provides a detailed list
of projects sorted by type of organization.
Training and Education Projects
This is by far the most common activity among ACEs-related organizations, pursued by tribal agencies,
educational institutions, nonprofit service providers, and state agencies alike. Many organizations conduct
presentations and trainings on ACEs concepts, prevention and therapeutic/diagnostic tools. Other current
projects include resource guides, screening/assessment tools, policy/procedure revisions, clearinghouse
functions, group/community discussions, and tribal/community empowerment strategies.
Provision of Therapeutic Services
Current services include assessments, counseling (for victims and families), advocacy, case management, and
trauma response/intervention

ACEs Mapping Survey Report McDowell Group, Inc. � Page 11
Program Development and Evaluation
Eleven respondents reported new programs in development. These include programs to help strengthen
youth’s ability to cope with traumatic situations, especially in early childhood, a community-based discussion
project to address collective impact and historic traumas, integrating ACEs into healthcare delivery, and other
strategies. State funding has been provided to several trauma-informed partner organizations for early
childhood mental health (ECMH) projects.
Only one respondent reported a formal assessment or consumer research related to trauma-informed care.
Partnerships among Programs
Several respondents mentioned the Alaska ACEs Initiative to build community awareness, informed systems
and focused interventions. Several others said they are involved in the Homer Prevention Project, a
collaboration to combat teen suicide. Other partnerships include:
• A variety of presentations and trainings, including train-the-trainer
• Working with the state Infant Learning Program on ACEs reporting and evaluation
• Various collaborations to facilitate prevention or service delivery, including breaking down service silos to improve family access
• A potential pilot program to implement an ACE screening tool
Prevention, Screening, and Early Intervention
These include home-based intervention and support programs as well as broader efforts to promote trauma-
informed care. Screening projects include addressing childhood trauma in hospital admissions, mental and
behavioral health assessments, and primary healthcare, and steps to train front-line juvenile-justice, behavioral
health, domestic violence and other staff in trauma-informed care, including use of intimate partner violence
(IPV) screening.
Research
Only two individuals and one state agency described current research projects that focus on ACE’s. One is a
regional behavioral-health-environment scan that includes childhood trauma. One respondent said research is
needed to address the relationship between epigenetics and ACEs prevention.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 12
Impact of ACEs on Practitioners
IN WHAT WAYS HAS LEARNING ABOUT THE ACES STUDY AFFECTED/CHANGED YOUR WORK?
Learning about ACEs has had profound effects on some practitioners, changing the way they understand and
respond to clients, families and funders. Others say they view ACEs as a confirmation of what they already
knew or suspected. Finally, a third group of respondents says ACEs changed the way they train and
communicate.
Changed my thinking, increased my understanding
• Changed how I view chronic illness; inspiration to do better with care of children who have experienced trauma.
• Given me more understanding about trauma in my patients.
• Helped us to see the bigger picture of the work we do on children exposed and address this within a resiliency
framework.
• I understand better, through the training, how so many experiences can be helped to be growing times or at least
made less devastating. As a foster parent, I saw how my own attitudes made a difference in the emotional and
physical outcomes for children and their families. Now, in my EI work, it is even more crucial to be aware of the ACEs
work. Children's development is often shaped by negative experiences so profoundly.
• Increased compassion. Understanding the cause of some of the disruption to the child's development resulting in more
effective strategies for helping the child and the family develop and grow.
• Increased understanding with workers and clients.
• It has given me a place to focus that is way upstream - which is hopeful.
• It has made me even more committed to ensuring we do a better job of intervening when abuse has occurred and
empowering families to break the cycle of abuse.
• It has made me more sensitive to clients with multiple/serial traumas. These are some of the most challenging cases I
work with because there is no specific index trauma to focus on as one does with many PTSD cases. Also, with younger
clients, there are huge developmental impacts that the school system writes off as disciplinary issues instead of the
symptoms that they truly are. I am hopeful we will be able to discuss some of these topics at teacher in-service
trainings. The school system and principals seem to be stuck in 70's behavioral approaches to discipline that are not
recognizing why ACEs kids behave as they do and pass them off as "spec-ed." or discipline problems.
• It has placed a greater emphasis on prevention.
• It has provided an in-depth understanding of the potential "root cause" of very complex issues of child abuse and
neglect. It provides focus.
• More understanding of families who come into contact with the child welfare system.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 13
• Provides a better way to argue for the cost effectiveness of preventative and early intervention programs with policy
makers and funders. Provides a way to target those programs to the individuals who are at highest risk. Decreases the
"blaming" that tends to focus on populations who are not meeting societal expectations (obese, depressed, in jail,
etc.). Helps focus interventions.
• Recognition of importance of primary prevention to reduce multiple negative ripple impact over life course.
• Research based info to share with families- I can articulate better now that I have information to back it up.
• Data resulting from involvement since 2005 has led to early childhood initiative plus linked with national networks of
like-minded and focused researchers and providers.
• I learned about ACEs and trauma-informed work prior to beginning work in the field. The program I attended was
trauma-informed and utilized reflective supervision. I will admit it has been challenging to transition into working at a
community health agency after experiencing trauma-informed environments. This has influenced me to advocate and
educate any chance I get for trauma informed and ACEs education.
Validated my thoughts/feelings/assumptions
• It has given me permission to take time in the place where I intuitively and personally and professionally knew it
needed to be prioritized, but the system I work in did not acknowledge, never mind validate that. (It still feels slow to
actually walk the talk).
• ACEs helped to put numbers behind information and validate what we have known for a long time. It has made it
easier for people to understand the need for urgency in this area.
• Confirmed what I already know since my ACES score is 8.
• Far greater attention to early experiences in patients’ lives. It verified a view of health and mental health that I came to
hold when I was in residency over 20 years ago - the data wasn't there then - now it is and I feel more confident
screening/discussing with people I see. I give some related talks - key theme is we need to move upstream (way) with
interventions if we want to really impact health for future generations.
• Helps to support the case for more funding and planning to on prevention and earlier intervention.
• Immensely! Child therapists knew for a long time that child abuse has devastating impact on children and families, the
ACES study was confirmatory to this opinion.
• It confirmed a lot that I already suspected, but it provided a very powerful tool for understanding my work and for
making an impact, especially with those who have not seen child maltreatment as a priority.
• It has confirmed much of what I suspected for many years.
• It has refreshed my knowledge of how the body responds during times of stress.
• It primarily gave us a new model to use when explaining our long held conviction that the public health and other
societal problems in the Native community stem from long-standing historic traumas and other colonial impacts. It

ACEs Mapping Survey Report McDowell Group, Inc. � Page 14
may have also broadened our perspective to include more physical health effects (e.g., cancer) to the list of symptoms
of colonialism we already knew about.
• It provides the science to support what we know from our work. It provides a clear and concrete connection between
childhood trauma and lifetime consequences. It gives us a tool to communicate to the public. It is very hard to argue
with. It also reminds us of the importance of meaningful intervention and early intervention.
• It simply supplied already firmly held beliefs and anecdotal experience with the credibility of diligent scientific study.
• Strengthened it. There is a concrete reason for individuals cycling through services -- once we address their trauma
history - we see improvement in their lives. It has also shaped how we implement services at the program level. Our
hospital is also seeking to implement a trauma informed treatment system/environment.
• These data give solid scientific background to what has been known for years. It gives another tool to demonstrate the
effects of early trauma.
• Validated what I have learned anecdotally, trauma affects people negatively lifelong in every aspect of their life. In my
field, reducing child abuse directly correlated to reduced ACE scores with better outcomes for people lifelong.
Changed our training/ways of communicating
• ACEs is helping with framing some of the trauma that is experienced by some children and youth for staff in their day
to day work. Training for staff and volunteers is a key consideration.
• As I stated earlier, we are in the beginning stages of implementation and have just completed the ACEs training for
four of our sites. We will continue to review data to assess the effectiveness of TIC implementation
• Easier to communicate potential impact of Early Intervention on tangible long-term health issues. Influencing change
in curriculum for graduate students.
• I talk to staff and kids about ACEs and what happened to them and why they are self-medicating, acting out, not
coming to school; depressed.
• It changes the way that we relate to families and children, and it changes the way that our employees understand the
way that their own trauma has impacted them.
• It has helped staff see the link between childhood trauma and the effects later in life. It has helped staff plan treatment
more thoughtfully.
• It has helped when developing an economic argument for investing in early childhood. It has helped focus our program
mission on prevention. It has brought light to the necessity to continually train front line staff in ACE's and it has
increased my sensitivity as a manager to some of my staff's projected experiences (knowing that many of us have
experienced out own ACE.)
• More important than the ACEs information for our practice, has been the information about how to implement trauma
informed care. Adapting language from Linda Chamberlain's booklets for parents to use with our adults with chronic
disease population helps the groups relax and stop blaming themselves for being obese or having diabetes.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 15
• The ACEs study and other research related to trauma has helped shape our agency's organizational goals. We've
formally adopted trauma informed care principals and the ARC (Attachment, Self-Regulation and Competency) model
of care.
• The ACEs study is not the first, nor the last, study that demonstrates the role trauma plays in human outcomes. Where
the ACE study has been most effective is in making trauma a public health issue and broadening the conversation
about trauma-informed care beyond behavioral health. The ACEs study's greatest strength is that it broadens the
conversation. Its primary challenge is that it can sometimes cause folks to oversimplify solutions to what is the most
complex problem confronted by human beings.
Other
• The ACE Study’s stated evidence provides clear indicators of the nation’s need to focus preventive efforts on issues of
abuse. It does not however inform of methodologies and processes which serve as a viable answer. It would seem to
serve our State well to focus on researching what builds protective factors and resiliency skills to increase a person’s
ability to deal effectively with the issues of domestic violence, abuse, and neglect; to study aspects of cutting-edge
trauma therapies and to understand culturally appropriate strategies. It is proven individuals who resolve their own
history of childhood abuse develop resiliency that reduces the likelihood they will abuse their own children. The focus
needs to be on what effectively assists individuals in healing. The ACE study is lacking in addressing individual or
community impacts. For example there is no mention of culture or culturally appropriate strategies for healing,
mentoring and bringing people back into a way of living that affirms cultural norms. In addition to the State’s need to
expand a focus on effective methodologies and programs, it is highly recommended they come to acknowledge and
recognize cultural engagement as a protective factor against child abuse. The ACE Survey in itself, while designed for
use with adults, has been inappropriately administered by organizations to children. The graphic and triggering nature
of the questions are seen to be potential for harm. In our view, if administering this tool to teenagers or younger
children it would be critical to have a trained professional available to intervene if needed. There is a possibility to have
the questions trigger those answering them and not having immediate support could create more harm.
• Not at all. The issues raised in the ACE's study have been incorporated in competent clinical programming for many
years.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 16
Strategies and Measures
This section summarizes information about respondents’ theories of change and the measures used for
tracking and evaluating them. Verbatim answers are listed in Appendix 3.
WE'RE INTERESTED IN LEARNING MORE ABOUT YOUR 'THEORY OF CHANGE.' HOW DO YOU SEE THE WORK YOU DO (PERSONALLY OR AS AN ORGANIZATION) IMPACTING THE COMMUNITY YOU SERVE? FOR EXAMPLE, HOW DO YOU SEE YOUR WORK REDUCING ACES OR INCREASING RESILIENCY?
AS A FOLLOW-UP QUESTION, WHAT OUTCOME MEASURES AND RESULTS DO YOU TRACK TO MONITOR THE PROGRESS OF YOUR ACES WORK?
A little more than two-thirds of the respondents (43 of 62) addressed both strategies and measures, and they
identified several broad types of change activities, including:
• Screening
• Training of practitioners and trauma victims
• Working therapeutically/restoratively at three levels: individuals, families and communities
• Providing information and support at three levels: individuals, families and communities
• Intervention
• Prevention
• Research and planning
• Advocacy
More consistent use of terminology would help amplify overall impact and assist in communicating with
policy makers and the public. When describing their activities and programs, many respondents referred to
“trauma-informed” care and “resilience.” Beyond that, however, they employed a wide variety of conceptual
language to talk about ACEs. This lack of common terminology may reflect a relatively new, rapidly evolving
field engaged in experimentation and/or limited dialogue among practitioners.
One third of respondents did not provide information on their theories of change, and of those who did, one
quarter have no established measurement system. Several respondents specifically mentioned needing help
measuring impacts. Answers to the theory-of-change question further suggest that a number of practitioners
are not familiar with the “cause-and-effect” approach to program design inherent in the theory-of-change
framework. Lack of familiarity with theories of change and measurement systems may be another indication
of an evolving field.
Relatively few of the strategies described seem aimed at paradigm shifts or policy change. Respondents did
not talk about how change might be accomplished over time, nor was there much mention of how to create
fundamental infrastructure to support ACEs prevention at the community or organizational level.
Because respondents’ descriptions of their strategies and measures were so different from one another,
McDowell Group summarized those descriptions to make them somewhat easier to compare. Each line of the
table on the next two pages paraphrases a single respondent’s answers to survey questions about 1) his/her

ACEs Mapping Survey Report McDowell Group, Inc. � Page 17
theory of change (labeled “ACEs Strategy,” 2) the measures used, and 3) the type of organization
represented. A striking aspect of the table is the wide variety of both strategies and measures.
ACEs Strategy Type of Measure Type of Organization
Screening Symptom Acuity Rating Scale, Trauma Symptom Checklist for Children Business
Acknowledge trauma, build resiliency School behavior/performance Educational Institution
Training for practitioners None Educational Institution
Education, focus on supports and prevention
Changes in knowledge and attitudes Educational Institution
Education for practitioners None Educational Institution
Strategic analysis In development Foundation
Intervene in cycle of violence. Increase resiliency. Follow-up referrals
None Non-profit Organization
Community awareness, change culture, "informed systems", mitigate trauma, reduce transgenerational transmission.
In development Non-profit Organization
Reduce trauma associated with child maltreatment
Parent survey, trauma symptom checklist Non-profit Organization
Client education Client success attaining behavioral/lifestyle goals Non-profit Organization
Educating families about supports and child development None Non-profit Organization
Advocacy and outreach for healing through traditional dialogue techniques
Specific to different initiatives Non-profit Organization
Prevention Not ACEs-specific Non-profit Organization
Working with children and clients to increase resiliency Repeat OCS involvement Non-profit Organization
Helping individuals and families to improve overall mental and physical health
CAF Assessment Scale, ongoing improvement. Post-discharge interviews with parents.
Non-profit Organization
Recognize need and provide trauma-informed care
Increased engagement and graduation of children
Non-profit Organization
Increase resiliency Client feedback Non-profit Organization
Supporting individual parent-child relationships within families
Life Skills Progression, Parents as Teachers survey. Also risk-factors checklist.
Non-profit Organization
Screening Confirm documentation Non-profit Organization
Therapeutic approaches to build resiliency AST/CSR, client feedback Non-profit Organization
Strengthening parent-child relationships None Non-profit Organization

ACEs Mapping Survey Report McDowell Group, Inc. � Page 18
Family support, family and community education
Participant feedback, community efforts/assessment materials
Non-profit Organization
Trauma-informed social services Functional improvement in children, families, community and school. Monitor Transitional Aged Youth.
Non-profit Organization
Exploring ACEs causal role in BH problems. Supporting prevention activities. Promoting recovery and resiliency.
For behavioral health recipients - CSR, CBCL, TSCC, TSCYC, DECA For early education service recipients - DECA, ASQSE, ECRS
Non-profit Organization
Various programs Program-specific data and tools Non-profit Organization
Family services and community programs to promote resiliency None Non-profit Organization
Intervention and prevention Progress on treatment plan (symptom reduction) Non-profit Organization
Individual psychotherapy Client feedback Non-profit Organization
Education leads to better decisions and prevention Perception of training quality State Agency
Support collaboration and planning In development State Agency
Education # trained, perception of training quality State Agency
Strategies for effective training of educators, providers, community
# trained State Agency
Educating practitioners In development State Agency
Raising awareness to generate system change
Population BH indicators State Agency
Build resiliency, reduce unhealthy behaviors
Population BH indicators State Agency
Building capacity in programs and communities to respond effectively to trauma and to build protective/resiliency factors
Population BH and other indicators. Program-specific measures, perceptions of training quality
State Agency
Exploring primary prevention Program-specific data State Agency
Educating practitioners, supporting trauma-informed treatment services
Program-specific data, BH population data State Agency
Acknowledging impact, trauma response, prevention, assessment of functionality
Pre-post tests for training. Measures of individual functionality. State Agency
Incorporating ACEs into restorative justice In development State Agency
Social change: build trust, acknowledge trauma, manage impacts, prevent future abuse
Reports from participants/communities Tribal Agency
Family-centered support and education
Monitor child behavior/relationships at program entry, annually, and at exit Tribal Agency
Training for providers In development Tribal Agency

ACEs Mapping Survey Report McDowell Group, Inc. � Page 19
Needs of the Field
Frequently Asked Questions
WE ARE GOING TO BE COMPILING A LIST OF FREQUENTLY ASKED QUESTIONS. WHAT QUESTIONS DO YOU HAVE, OR HAVE YOU HEARD FROM OTHERS, ABOUT ACES?
The most common questions offered by respondents involved specific guidance for addressing ACEs in the
field. Many respondents also asked about expanding the ACEs field in Alaska, including what the goals and
next steps should be. Other questions addressed ACEs prevention, training, measurement, and the
mechanisms by which ACEs affects people.
Preventing ACEs
• Folks are interested in knowing more about interventions that specifically target reduction in adverse experiences.
• How does the study of ACES translate into prevention?
• We have been taught over and taught over about the ACE study and it's effects. We need to spend more time on the
prevention of ACE and on what to do about it once it's identified.
Training
• How can we get more training for staff and teachers?
• How do the ACES experience of a caregiver affect their ability to adequately care for their child?
• Many people we talk to express at least some familiarity with ACEs. Some do need to start from the beginning for an
ACEs 101 style introduction, but not too many; and other than the "What's ACEs" style questions, I don't recall any
other specific questions people have asked us about ACEs.
Measurement
• How can we know when what we are doing is actually making a difference?
• What is the best way to measure the outcomes of programs trying to address ACEs?
How ACEs affect people
• "Why do some people do ok despite being exposed to numerous ACEs?" "What is different for them?"
• How has the cultural oppression and intrusion of western culture on Tribal cultures contributed to individual ACES?
• How does ACES affect a child's ability to be focuses in school?

ACEs Mapping Survey Report McDowell Group, Inc. � Page 20
Addressing ACEs in the field
• From providers: "What if I ask about ACEs and people fall apart? Will this trigger their own trauma?"
• Should the ACEs questionnaire be used with children/teens? Or is it only for adults?
• If someone has high ACE score, are they doomed? What, if anything, can they (and others) do to mitigate the negative
impact of high ACE scores?
• The difference between single-event trauma and complex trauma as it relates to resiliency.
• I think the question I hear the most often is: why doesn't everybody with a high a score have these problems? What
makes them so resilient? Perhaps it's our American fascination with exceptionalism, but it also poses important
questions about what helps protect children and what helps adults to heal.
• Many folks seem to feel that they don't know what to do to help children, youth and families who have been exposed
to trauma to increase resiliency. Needs to be more information with simple strategies to demystify trauma so that
people do not feel that they are unable to help individuals impacted by trauma.
• What's the difference between single event trauma and complex trauma as it relates to resiliency?
• We often hear people ask about other types of trauma that aren't on the basic screening tool. How do we screen in a
way that is sensitive and supportive? How can we apply this to our own staff and acknowledge vicarious trauma? How
can we share the message in a hopeful way? Can Alaska conduct a large-scale ACE study?
• We know the study/information, what are people doing with it? (Two responses)
• Where's the best place to start - with high schoolers before they become parents, with parents who are asking for help
now or right from the beginning with brand new first time parents?
Expanding the Field
• Is the goal to provide from a trauma-informed perspective only or to change the agency environments to being trauma
informed as well? Will there be more support to make agency wide changes?
• The big challenge for Alaska is how to safely bring this into highly traumatized communities in a culturally relevant
and acceptable manner.
• Is there going to be an ACES study focused on Alaska Natives in this state?
• I would like to know about community wide efforts (other than Walla Walla) that have focused on ACEs.
• What next?
• "So now what?" "What do we DO about it?"
• Why don't politicians know about this?
• Why is this just now coming to light?
• Why should I teach SEL (Social Emotional Learning) as a teacher? I have enough to teach.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 21
Barriers to Trauma-Informed Care
WHAT BARRIERS HAVE YOU EXPERIENCED IN PROVIDING ACES RELATED CARE?
Along with lack of resources and funding and lack of widespread understanding of how ACEs works,
respondents noted barriers such as:
• Tying access to trauma-informed care to health and behavioral symptoms, rather than the underlying childhood experiences.
• Matching client needs with appropriate levels of care
• Access to practical tools and training
• Fear of asking/talking about trauma on the part of both clients and service providers
• Fragmented efforts to address ACEs
The practice of making access to care contingent on health or behavioral symptoms, rather than on the childhood experiences that are the underlying cause
• Access to systems of care is typically based on inclusion criteria associated with dysfunction or disorder. It is the
subsequent adaptations to adverse experiences (behavioral, health, academic, etc.) that trigger access to care, rather
than exposure to adversity and the risk associated with such exposure. An ACE informed system of care would go
beyond an understanding of the relationship between problematic outcomes and exposure - to an analysis of the risk
elevation associated with exposure and intervention aimed at intercepting problematic adaptive processes to prevent
problematic outcomes.
• Generally, we wait too long, until problems are severe, to provide support to people in need. Prevention and early
intervention are a hard sell, even though it pays big dividends financially and morally. Many professionals are not
trauma- informed and lack training in early brain development.
Finding an appropriate level of care to meet client need
• Given the prevention focus of services, connecting children and youth experiencing difficulties with an appropriate level
of care can be a challenge. Boys & Girls Clubs works to partner with a variety of other human service agencies to
facilitate on-site work at Clubs.
• Many providers use behavioral interventions that may not work with individuals impacted by trauma and then
discharge or deny services to those individuals when they do not respond. Youth who have extreme behaviors related
to trauma (aggression, self-harm, running) are frequently sent outside Alaska for treatment.
Lack of practical tools
• Good research, but few tools have been developed to put it into practice.
• Prevention is difficult. Deciding upon where to focus efforts, getting the powers that be to decide it is a priority.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 22
Access to training
• Staff have not had training on SEL and how to teach this for K-12.
• The training has been in Anchorage, and with a small staff it is difficult to release staff for out of town training.
Recently, a webinar was offered (Trauma 101), and real time instruction (like PESI, e.g.) would really help those of us
with small travel and training budgets.
• Educating everyone and having the capacity to follow-up with further care.
• Shifting an organizational culture, getting all staff trained and sustaining the change has been challenging, although
well worth the effort. It's always a work in progress because of staff turnover.
Fear of asking about trauma
• A major barrier I see among health care professional is the fear that asking about ACEs will "open a can of worms" -
the data does not support this concern - rather it suggests that asking is meaningful to a patient and may have some
therapeutic benefit.
• It is heavy to talk about. People respond differently. Unless there is a focus on hope and resilience, it can be
disheartening and triggering for people.
• Some families have routinely been "burned" by governmental agencies. They've experienced judgment and punishment
which has made them leery of getting involved with our program.
• The traumas that people suffered in their childhood, and the historic traumas that led to societal scale problems in the
Native community (and other communities) as well as new retraumatization episodes that are the results of historic
trauma, are so personal in nature, so intimate, that very few people actually want to talk about them. Dialogues
around trauma, ACEs, adverse collective experiences, etc. can be difficult to get off the ground - people don't want to
open up, they don't want to believe it's a safe space for conversation. We have techniques and dialogue models that
can help us to get around these barriers - but they are still barriers.
Lack of time, staff, resources and general knowledge of the fundamental nature of ACEs
• I don't provide direct care. The barrier we have faced in helping organizations to provide ACEs related care is the time
commitment to train staff adequately and getting administrators and Boards to prioritize it, given all of the other
things on their plate.
• Lack of education of other health care entities about ACEs and lack of belief by health care providers in ACES.
• Lack of interest/knowledge related to importance and potential far-reaching impact of adverse childhood experiences.
Fatalism that once bad things have happened there is no point in trying to address.
• Lack of knowledge as to next steps once ACEs identified - what intervention/treatment works.
• Too many folks think children "bounce back" and that they don't need long term help with events. Not enough folks
understand the long-term physical, emotional and social implications of not helping families through PTSD, domestic
violence aftermath and growing up with mentally ill parents.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 23
• Lack of resources available in rural Alaska to do age-specific support for children particularly; lack of understanding by
school teachers about the impact of ACES on a child's behavior & ability to learn in rural Alaska.
• Lack of understanding of brain development. Concerned that ACEs is just the next "shiny" thing that grabs our
attention.
• Not having enough resources (providers) who are trauma informed and can provide trauma informed interventions.
• Screening tools. Training for staff on screening for ACE's.
• The workload, work environment, paperwork and supervision. There seems to always be a budget crisis and the
certainty of employment appears questionable. The agency environment is often crisis oriented making it challenging
to work in alternative ways. Supervisors appear to be under so much pressure that supervision is pressured (somewhat
"flyby") and inconsistent. While paperwork is necessary and important, it is so extensive that it takes time away from
the reason we are being funded.
• Time. Lack of support to prioritize within the state system (in Public Health Nursing) just yet, so we have to do much of
this as volunteers--ok for some, but we need more prioritization of this work some of the needed referral sources are
severely lacking in our community, like substance abuse services.
• Time and audience.
• Time to shape the policy and practice.
Funding
• Being able to connect with the people we perceive may need it most. Lack of resources in the community to meet the
need. Consistency in approach - programs are started and funded for a period of time and then go away. Programs
come and go and there's no consistency for the long term. These programs take time to measure change and often
just when we start to see change, funds are cut and programs are gone. Healthy Families is a great example of that.
Much of the ACEs work relates back to much of the ASSETS work from years ago. We need a funding commitment for
more than 10 years. How long did it take to collect the ACEs info? We need a long term plan and commitment to the
next generation.
• Funding.
• No funding for brief interventions after someone completes the questionnaire. Brief intervention for mental health does
not have a billable code. This questionnaire would have to be administered in an intake or treatment setting and not
as a screening tool.
Other
• Figuring out how to implement questionnaire with b-3 services.
• Fragmented efforts. Duplication of effort. Not listening to those people in the state that have been doing this work for
10 years or more.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 24
Access to ACEs-related Services
ARE THERE ANY PLACES, POPULATIONS, ETC. THAT YOU HAVE DIFFICULTY REACHING THAT COULD BENEFIT FROM ACES-RELATED WORK?
Many respondents said rural Alaska does not have adequate access to services. Others identified demographic
populations such as adult Medicaid patients, foster families, families with young children, and recent
immigrants.
Rural Alaska
• Aleutians.
• I am mostly in rural Alaska where multigenerational trauma & oppression is so common that every individual living in
a village needs to be trained not only on recognizing ACES, but how to adjust their response/management to address
ACES impacts.
• I would think we would really want to get the news out to rural and village Alaska.
• In my work often the rural and remote communities in Alaska that can benefit but have trouble accessing services or
funding for prevention.
• It will be important to engage the tribal communities in this effort.
• It's chronically difficult to reach people living in Bush villages - logistically difficult. Even if they're willing, the weather
might not be, and ticket prices are prohibitively high for many people in these communities, so travel monies are a
must if you want to pull together people from many different villages.
• More remote rural Alaska.
• The rural areas of the state with limited resources need to be addressed. Cannot just plug in what was done in other
states around ACEs to these folks. Business community is just getting exposed to this information.
• The Russian Old Believer communities on the Kenai are difficult to access.
• Villages.
• Yes, many. Definitely CHAs and BHAs in rural villages. Also, it is not my area of work currently, but it seems to me that
immigrant and refugee populations in Alaska are sorely underserved in this area (and almost never brought into these
planning conversations), despite high degrees of war related and other traumas and potential insight into individual,
family, cultural, and community level protective factors. Additionally, some of the DV/SV shelters in the state have
received training on trauma informed care, but could use more training. The number of children in shelters is very high
and not all have really strong children's programming to help children understand and heal.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 25
All other
• Absolutely, but we can't force people to accept services. There's never enough funding, so I think we need to start with
those populations that are more receptive and accessible to build programs that can then show data and evidence
that they make a difference to hopefully stabilize funding.
• Adult Medicaid patients are not eligible for diabetes self-management education coverage in Alaska at this time.
• Foster families when the child is repeatedly moved from home to home in the system. Getting information and
returned phone calls and e-mails from OCS.
• I work with families with very young children, which is an advantage. When kids are at more "difficult" ages, pre-teen
and teens, they have often been so neglected that connecting with them is more work. Flex School in Homer is a great
example of a school-based way of dealing with such issues.
• Much community work does not yet reach some of our highest risk population, and many do not "come to us" and as
PHNs, we are no longer building relationships over time through home visiting and even regular immunizations where
disclosure became easy. New providers of some of this work (e.g. PAT, Head Start home visitors) say they do not get
the support and training to feel confident with the highest risk. Again, private providers. How to infuse in schools--we
have WIDESPREAD understanding in our school district, but teachers, like providers, have full schedules and see this as
an "extra thing.”
• People who have experienced domestic violence and in primary care settings. While we are working towards this, it is
challenging.
• Refugee/immigrant communities, particularly those from war-torn communities, secondary to language and cultural
barriers, and few resources for outreach.
• Tanana Chiefs Conference providers and administration.
• Teachers! They need to know how SEL is the biggest contributor to drop outs, mental health issues and you really start
to see that in 7-9th then the kids are gone/ check out/drop out.
• There is a need statewide.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 26
Resources Needed
Resources to Support Individual Efforts
WHAT RESOURCES WOULD HELP YOU PERSONALLY CARRY OUT ACE-RELATED ACTIVITIES?
Training and information were mentioned most often by a large margin. Also identified were a need for
specific systems, tools and research that can be used to address ACEs; more opportunities for networking;
and more funding in general.
Additional training, education, workshops, etc.
• Continued educations, training and resources on utilizing ACEs.
• Curriculum review help.
• Free and more accessible education about ACES and what to do with them.
• I have a clear understanding of the statistical impact of 4+ ACE on clients/patients wellbeing. I need more training in
outcome-based methods to guide treatment planning.
• I have only read the original study, therefore anything related to ACES would help.
• I think access to a variety of training and technical assistance would be helpful at this time.
• I think more training on how to present about ACEs to other people, as well as additional literature on the community-
level effects of individual ACEs. Well, and money of course.
• I would like more training on the data and on the behavioral and biological mechanisms of how trauma affects health
and family dynamics. I would like more training on what trauma informed care looks like at a very detailed level in
primary care, pediatrics, women's health care, emergency room, behavioral health, dental, social services, etc. I would
like the chance to practice in some of these settings. I would also like a very simple, user-friendly, beautiful handout or
card that could assist patients or others to understand ACEs. Dr. Chamberlain's newest publication for parents is very
good for that, but is more focused on parenting than on general health. Perhaps a version that looks at effects on
health would be useful.
• Might be useful if there were a study specific to Alaska showing the cost of not treating ACES. We can make the case
using ACES data from the national website, but it might be helpful to raise the level of concern and the willingness to
invest resources and energy.
• More education and supervision on specific evidenced based treatments to continue building skills. Trauma informed
supervision. Trauma informed agency orientation.
• More statewide training opportunities for workers from the medical, education, and medical sectors.
• SEL learning in the classroom K-12.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 27
• Tools for training informational tools we could personalize and print and share support for addressing vicarious
trauma sharing the information with the general public in a way that gets them to care and feel connected to it
(mastering the "why this matters to you" piece to the average person).
Handouts, websites, brochures, etc.
• Central website to promote communication between partners in Alaska.
• Easily utilized informational handouts, power point slides to educate others.
• Handouts on resiliency and tools to share 1:1 and in presentations help with designing evaluation at all levels of the
work the awareness of secondary trauma and methods for self-care while working in a system (or certain layers of
supervision at least) who are not sensitive to the impact of working in this arena I have my own ACEs that both
motivate me and sometimes get in my way--I have great tools, but still need support from my workplace to be at my
best.
• Materials about ACEs and resiliency written for adults with chronic illnesses and adults with addictions.
• Public domain training materials, including those tailored to diverse communities and circumstances. Expanded
professional network of people interested and knowledgeable about this. Expanded referral network of resources to
help those impacted by ACEs.
• Screening tools for home visitors with evaluations.
• Well put together slide shows and learning materials.
Systems/tools
• A comprehensive system or program for serving customers who experience/d trauma. System that has tools and
training for our providers to support their customers.
• Research and evidence-based practices that have solid research behind them.
• Some specific strategies and tools when dealing with various ACEs that can be used by clinicians.
Networking
• I'd like our agency to have the opportunity to directly participate in state wide initiatives such as this one. The
opportunities to network, share ideas and stay abreast of the direction that the state is headed is helpful.
• More collaboration with OCS and the early childhood mental health community.
• Names of providers providing trauma interventions.
More funding
• Additional funding sources.
• Additionally staff to support the work.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 28
• Funding for more community based training in a series approach (based on community readiness) so communities can
truly heal & have the support needed to make changes.
• Funding. (Two responses)
• More money always comes to mind... for training, gas for home visits, programs and so on. If our state became an at
risk state, then children could be helped long before the damage took a toll of 50% delay in their development.
Resources to Support Community Activities
WHAT RESOURCES WOULD HELP YOUR COMMUNITY CARRY OUT ACE-RELATED ACTIVITIES?
Information, training and more funding were the three types of resources most often identified.
More community awareness/information
• Access to information about the study, information about how to modify practice based on this information and
additional capacity within communities to serve people and children with complex trauma related to ACEs.
• Broader understanding in the general community and particularly with funding sources about ACES.
• Community wide education.
• Education for general population and legislators.
• Education! Being able to blanket our community with the information, so everyone understands how the things that
happen in a child's life will have long-term impacts for them and society. I would love to see an intensive investment in
one community, clearly defined, with all partners working together toward the same goal. I worry that by trying to
make ACEs changes on a large scale, it will turn out like so many other efforts. Pick one or two pilot communities and
work out all the kinks and show the results, so others want to participate.
• Greater awareness for those both in the behavioral health field and the greater community.
• Greater community education tied to ACEs appropriate interventions and activities. When faced with issues tied to
mental health, child welfare, and juvenile delinquency, too much of the public discussion ends up involving
oversimplified solutions. The issues are complex, so are the solutions. Resourcing solutions up front is cheaper than
chasing problems with bits of money throughout the lifespan.
• Statewide policy and legislation that promotes an ACEs informed approach to health and education.
• More media attention and social awareness would be helpful.
• We feel that community dialogue is an effective means of healing from traumas like ACEs, but communities need help
to come together in a safe respectful space before those conversations can happen. Train the trainer style workshops to
help community members conduct dialogues within their own or other communities can be one way to help the
community achieve that safe respectful stance; but that needs money, and master trainers as well.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 29
Handouts, websites, brochures, etc.
• Guides, tools, training and informational materials, innovative examples from other communities, funding for evidence
based TI practices.
• It'd be helpful for this ACEs project to develop a website that is available to the public, containing resource information
(upcoming trainings, research articles, etc.).
• Maybe an Alaska ACES website with links to resources - for families, for schools, for individuals, for policy makers...
Maybe there could be a provider listing too: those who had met some type of trauma expertise in their services.
• Same comment as last sentence above regarding a handout. Someone who can do ACEs trainings in Kodiak and train
a trainer there, especially someone who can work with local Tribal and other cultural leaders so they present the
information in a way that is very culturally relevant. I don't work in schools anymore, but I would love to see more
support for staff training in schools, training of School District officials, support to implement aces informed discipline
policies, $ for all of this and for counselors and social workers in the schools. Also, the community in Anchorage and
many places in Alaska is very diverse culturally and linguistically. These ACEs related resources and activities need to be
available in multiple languages.
• Short educational materials regarding what ACEs is.
More training
• Education and training.
• More parenting classes in many different formats and time frames.
• More specifically trained early childhood mental health providers who understand both early childhood and trauma
informed care.
• Teacher training, and outreach to the Community Prevention Coalition.
• Training and consultation funding.
More funding
• A grant specific to ACEs education, prevention and treatment.
• Additional funding.
• Collaborative Funding - it is difficult to apply for multiple small grants versus one.
• Financial Support for Early Home Visiting.
• Funding to do trauma-informed training such as Sanctuary for the entire community.
• Funding. (Two responses)
• More money to provide programs, training, better pay for the staff so there is less turn over, materials and fees for use
of gyms and pools, equipment for outdoor ed.
Other
• Easy referral/drop referral for substance abuse, educating parents.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 30
Improving Statewide Systems
ARE THERE ANY CHANGES TO STATEWIDE SYSTEMS (E.G., MEDICAID REGULATIONS, ALASKA DEPARTMENT OF HEALTH & SOCIAL SERVICES FUNDING OR PROGRAMMING, ACCREDITATION) THAT WOULD HELP PROMOTE ACES WORK IN YOUR COMMUNITY?
Suggestions for changes in statewide systems tended to address one of four areas:
• Changes in thinking and overall priorities
• Changes to/expansion of Medicaid
• More program funding, especially for prevention and intervention
• Less bureaucracy and better collaboration
Change in thinking and priorities
• A paradigm shift from what is wrong with you to what has happened to you.
• Trauma informed needs to be the norm statewide.
• More focus. Being made a high priority.
• I'm not sure what needs to change there - we don't really work within the public health arena per se. However, greater
recognition of ACEs and resiliency within the state medical system would be supremely beneficial to advancing
ACEs-related work.
• DHSS could focus more on this instead of just doing a routine DV screening at each patient visit.
• OCS is the most non-trauma-informed entity we work with. The way that the child and family are perceived and
treated only re-traumatizes those they serve. They do not communicate with children or families in trauma sensitive
ways. I don't know what would help. Prevention funding from DHSS would be helpful. It would be great to be able to
bill Medicaid for child advocacy center services (forensic interviews and family interventions). If statewide systems
modeled trauma informed practices within their own systems.
• Well of course we need a single payer to take away health inequities, which still hold much of all this in place as a root
cause. There was a panel of state directors at the TIC conference a couple of years ago---for them to work together
over time would surely help Medicaid reimbursement for non-drug interventions i.e. stress management, yoga and
alternative therapies, a few non-licensed providers who are doing this work). In general, letting community self-
determination have an influence on agency priorities, like we are promoting with our local Community Health
Improvement Plan, based on data and community driven. It's all about the system listening to people and
responding....that's the essential paradigm shift, believing that all behavior is purposeful, rather than needing
people to adapt to our systems.
• The first thing I would suggest is a panel of people with scientific background - understanding of both epidemiology
and developmental biology. The research on the impact of ACEs and early experiences in particular is coming out
rapidly. These studies will guide translation research and implementation. This panel would include outside experts - it
could guide/inform service development/ assessment/ Medicaid regulations etc.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 31
• Analysis of the risk pathways associated with adverse exposure point to the need to target intervention earlier (not
just developmentally, but etiologically.) For example, in the world of alcohol abuse, a starting point is understanding
the role that trauma plays as a driver of substance abuse (self-medication, attempt at affect regulation, attempt to
numb or avoid negative feelings memories etc.) This is a starting point. An end point would be to intervene with those
who experience adversity and are showing early signs of maladaptive coping (drinking) to prevent the development of
full-blown substance abuse. How to do that. That is a question that is tough to discuss in a survey.
• Specific teaching and information for Alaska Native families, communities and individuals--putting in a cultural
context.
• As noted earlier, there continue to be system gaps that prevent at-risk families and individuals from obtaining basic
services: help meeting basic needs, parenting classes, care management, peer supports, peer navigation, resiliency
development, etc.
Changes/expansion of Medicaid
• It would be helpful to have more programs available for "at-risk" families that do not qualify for Medicaid; an
increased number of mental health programs providing family therapy; increased resources focused on young children;
increased awareness in primary care community about ACEs and need for screening and intervention; and
collaboration across all programs.
• EPSDT changes that are funded would go a long way to improving the system. Many efforts already going on in
the state being supported by a broad range of agencies and groups - no need to reinvent the wheel just roll up your
sleeves and help.
• Medicaid - Early Intervention/Infant Learning Program expanded Medicaid services, so every program could have an
Infant Mental Health practitioner. Funding for Parents as Teachers Programs.
• Medicaid coverage for diabetes, self-management, education for adults.
• Medicaid expansion access to support services.
• Medicaid expansion to cover more people for routine health care. Reimbursement for preventive screening, counseling
and health education/promotion. More investment in prevention and resiliency supports (and trauma-informed care).
More work related to racism, sexism and general de-stigmatization of complex social issues (substance abuse,
behavioral health, intentional injury, violence prevention).
• We will see the same challenges we have seen with domestic violence regarding the need to be able to have
reimbursement codes for assessment and counseling.
• All Alaskan children and their families (esp. Girls and women of reproductive age), no matter what, should have access
to healthcare and social services. This means Medicaid expansion, more funding for community based health
centers that provide care to immigrants and refugees who do not yet qualify for Medicaid, more
health/behavioral health professional pipelines for students from rural Alaska to ease the shortage of providers.
We need universal, free preschool (Oklahoma did it). We need more high-quality, subsidized day care. We need more
school-based clinics. We need law enforcement and court official training to include a trauma informed focus.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 32
• New Medicaid funding codes for brief intervention in mental health. New Medicaid codes for screening or tools used
to promote ACEs.
• Payment reform is needed to support behavioral health interventions; Medicaid care settings; Medicaid
reimbursement needs to fund the total cost of completing comprehensive assessments of children that allow for
interviews with additional sources beyond parents including school etc. and others.
• Would like to see Medicaid regulations more consistently fund and promote best practices, at times providers
choose to do things pro bono as non-billable services in order to best serve the clients. I hope that Alaska DHSS works
closely with providers on this initiative in a proactive manner versus taking a top down approach, announcing changes
or new directives. There is an opportunity for this to be a positive community collaboration that includes direct care
providers and those in the field doing the work. For example, this survey to gather feedback is a great start.
• Allow for family support and counseling to be reimbursable-can't help a child without helping the family.
More funding
• Front-end education and prevention. Alaska does not devote enough resource up front tied to prenatal through 0-5
years children and their parents and other caregivers.
• Fund programs to provide Early Intervention when kids and families are at risk, rather than having to wait for
Federal guidelines that put Part C kicking in when there is 50% delay. We shouldn't have to wait until the damage is
probably not remediable.
• Funding for evidence-based/evidence informed interventions.
• Funding support.
• Funding to allow mental health integration into primary care; and requirements for all teachers and administrators,
OCS, and juvenile corrections workers to be trained in providing trauma-informed educational services.
• More funding for prevention efforts!
• There needs to be a way to bill/fund services that would fall under prevention.
Less bureaucracy
• Decreasing and/or streamlining paperwork to support client care as a priority. Funding to increase security of
providers and agencies in order to decrease crisis orientation and support working towards trauma informed agencies
including self-care. This could potentially assist in decreasing rates of turnover and cost agencies less money in the long
term. Perhaps grant funding to cover a consultant or other means of ongoing support to agencies to shift to trauma
informed.
• Less government programs and bureaucracy. Simplified Social Services - more people centered than documentation
centered. Take away the state Dividend and use it to fund education, mental health services and roads to Western and
Northwestern Alaska. Our current system of state government and funding encourages entitlement and kills individual
responsibility and motivation. The Alaska Housing Authority needs a foundational overhaul.
• Most systems need to be revamped to have better collaboration and less barriers.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 33
Other
• Accreditation: adding trauma/resiliency to CEU's for doctors, nurses, school teachers, counselors etc.
• ICD code for Aces for health care providers, 504 in schools for ACEs, counselors/therapist that are in schools, groups
that meet during school time and teach tools for SEL, Big Brother. Big sisters/mentors for high schoolers.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 34
Appendix 1 – Survey Participants
Sixteen survey respondents did not identify themselves. Following are those who did:
Anne Dennis-Choi AK Child & Family
Katie Baldwin AK Mental Health Trust Authority
Adam Muhr Alaska CARES
Cathy Baldwin-Johnson Alaska CARES
Joshua Arvidson Alaska Child Trauma Center at ACMHS
Pam Karalunas Alaska Children's Alliance
Trevor Storrs Alaska Children's Trust
Sharon Fishel Alaska Department of Education and Early Development
Barbara Murray Alaska Department of Health and Social Services
Brita Bishop Alaska Department of Health and Social Services
Sara Clark Alaska Department of Health and Social Services
Shirley Pittz Alaska Department of Health and Social Services
Stacy Toner Alaska Department of Health and Social Services
Linda Chamberlain Alaska Family Violence Prevention Project
Patrick Sidmore Alaska Mental Health Board/Advisory Board on Alcoholism and Drug Abuse
Laura Avellaneda-Cruz Alaska Native Tribal Health Consortium
Mark Erickson Alaska Psychiatric Institute
Dee Foster Anchorage Community Mental Health Services
Jerry Jenkins Anchorage Community Mental Health Services
William Hurr Boys & Girls Clubs Alaska
Tammy Sandoval Child Welfare Academy
Aaron Clements Co-Occurring Disorders Institute
Paula Ciniero Fairbanks Regional Public Health
Kyle Wark First Alaskans Institute
Jessica Lawmaster Haven House
Sharon Gorman Homer High School
Sharon Whytal Homer Public Health Center
Diane Payne Justice for Native Children
Traci McGarry Kawerak, Inc.
Joanna McFarlin Kodiak Area Native Association
Melissa Kemberling, PhD Mat-Su Health Foundation
Jean Kincaid MSSCA
David J. Sperbeck, PhD North Star Behavioral Health Hospital
Kristen Spencer REACH Inc.
John Craig Williamson SeaView Community Services
PJ Hatfield-Bauer SeaView Community Services
Stephen Sundby, PhD Sound Alternatives

ACEs Mapping Survey Report McDowell Group, Inc. � Page 35
PeggyEllen Kleinleder South Peninsula Hospital Community Health Services
Katherine Gottlieb Southcentral Foundation
Jillian Lush Sprout Family Services
Stephanie Monahan The All Alaska Pediatric Partnership
Stephanie Allen United Way of Mat-Su
Erin Kinavey University of Alaska
Rhonda M. Johnson University of Alaska
Mary Dallas Allen University of Alaska
Cheryl DeWitt Women In Safe Homes

ACEs Mapping Survey Report McDowell Group, Inc. � Page 36
Appendix 2 – Current ACEs-related Projects
For organizations that reported multiple projects, the organization is assigned a number in the right-hand
column, and each project is reported on a separately. For example, Educational Institution 1 reported three
projects and is therefore represented on three different lines of the table. Organizations reporting a single
project have no number.
If Alaska were to launch a collective-impact1 project for ACEs statewide, action teams might be formed for
each type of project in order to compile all the work going on in that area. For example, a training/education
action team would work to assemble the key players pursuing training/education strategies and try to
coordinate their efforts around specific, data-driven goals.
Graph/Figure Heading: Example 4
Type of Project Current Projects Type of
Organization
Develop a program
We're pursuing a grant to host a Fish Camp to gather our people together (in an Alaska Native space, on the land, working with food) to begin to work through their own personal traumas, and our collective cultural traumas, in a healing environment - and simultaneously train them to go back home to host these types of conversations there. This project loosely follows in the style of our Alaska Native Dialogues on Racial Equity efforts.
Non-profit Organization 12
Develop a program
We recently worked with the Epicenter at the Alaska Native Tribal Health Consortium (ANTHC) on an ACEs-related think tank providing feedback on a project the Kodiak Area Native Association (KANA) is planning (around integrating ACEs work into their health care program in Kodiak). That think tank prompted ANTHC and KANA to postpone their study while they gather more community input. FAI (my organization) has offered to help them gather than community input through dialogues as well as potentially hosting some trainings so KANA people can gather more information themselves. We may also help with other aspects of the project as needed.
Non-profit Organization 12
Develop a program
One of the projects we have in development is a "Truth and Reconciliation Commission" for Alaska, echoing similar efforts in South Africa to talk about apartheid, or in Canada to talk about the First Nations' experience with boarding schools. These sorts of community-wide and community-led discussions will inevitably bring up collective and historic traumas that will touch on ACEs-related issues.
Non-profit Organization 12
Develop a program
AK Child & Family recruited a doctoral student intern to facilitate consumer focus groups (youth we serve) to incorporate the consumer voice/feedback. The youth completed a project called Photovoice.
Non-profit Organization 3
Develop a program
SMART Moves: Helping children and youth to make positive choices when faced with challenges tied to alcohol and other drugs, healthy dating relationships, and interpersonal conflict.
Non-profit Organization 7
Develop a program
Power Hour: Homework help and tutoring to help support children and youth in their academic endeavors.
Non-profit Organization 7
Develop a program
Project Learn: High-yield learning activities (academic enrichment) that takes the academic to a practical level and includes a range of activities from puzzles and games to science, technology, engineering, and math (STEM) activities.
Non-profit Organization 7
Develop a program
Triple Play / Healthy Habits: Helping children and youth learn about the importance of physical activity and nutrition in their lives.
Non-profit Organization 7
Develop a Developmental Trauma Disorder Field Trial. Non-profit
1 “Unlike most collaborations, collective impact initiatives involve a centralized infrastructure, a dedicated staff, and a structured process that leads to a common agenda, shared measurement, continuous communication, and mutually reinforcing activities among all participants.” (From the article, “Collective Impact” by John Kania and Mark Kramer, published in the Stanford Social Innovation Review, Winter 2011.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 37
program Organization 8 Develop a program Early Childhood Learning Network Trauma Training/Tech Transfer. Non-profit
Organization 8 Develop a program
Triple P Positive parenting Early Screening and detection - community services linkages (Help Me Grow).
Non-profit Organization 9
Develop a program
Built trauma informed care requirements into new projects (capital development for transition age youth. State Agency 2
Develop a program Designing steps to create a trauma-informed community. State Agency 3
Develop a program Planning for system changes. State Agency 4
Develop a program
The Infant Learning Program provides home visiting and related services to children birth to three referred by the child protection system. State Agency 6
Develop a program
For the next three years the Early Childhood Comprehensive Systems grant will be focusing on "improving developmental trajectories for infants and young children by fostering safe and nurturing relationships and mitigating the effects of toxic stress and trauma". Using a collective impact approach, ECCS efforts will work with local communities to address these issues.
State Agency 6
Develop a program
We are co-facilitating an Anchorage based Early Childhood Protective Services Collaborative that brings together agencies serving young children and their families in the Anchorage area who are in the child protection system.
State Agency 6
Evaluate Service AK Child & Family has completed Organizational Assessments on the Adoption of Trauma Informed Care Practice and has developed agency goals that are linked to the results/feedback from these internal assessments.
Non-profit Organization 3
Fund programs/services Exploring how to incorporated ACEs into funding system. Non-profit
Organization 6
Fund programs/services
We are funding several early childhood mental health (ECMH) projects: ECMH Consultation in early care and learning programs, ECMH Learning Network (training and reflective practice groups), Alaska Pyramid Partnership (training and coaching early childhood programs) ECMH conference, and ECMH systems development. All of the efforts are led by trauma-informed partners.
State Agency 6
Partner with other programs Homer Prevention Project - KPBSD Suicide Prevention in high schools. Educational
Institution Partner with other programs Coordination of ACEs related presentations at professional meeting(s). Educational
Institution 1 Partner with other programs
We are working directly with CAPTA referrals. We also have families not involved with OCS who have ACES.
Non-profit Organization
Partner with other programs
Working with the other local providers (DV/SA, Primary Care, School) in prevention and provision of services.
Non-profit Organization
Partner with other programs
We are working with the State Infant Learning Program Office (assigned intern) to look into ACE reporting/evaluating.
Non-profit Organization 10
Partner with other programs We have talked with partners about being a pilot for an ACE screening tool. Non-profit
Organization 10 Partner with other programs We collaborate and work with coalition on ACEs related projects. Non-profit
Organization 11 Partner with other programs We partner with early childhood on projects and support groups. Non-profit
Organization 11 Partner with other programs We're involved in the Alaska ACEs Initiative. Non-profit
Organization 12 Partner with other programs
Partner of the AK ACES Initiative Leader in developing statewide Train the Trainer program focused on brain development, ACEs and resiliency.
Non-profit Organization 6
Partner with other programs Alaska ACE initiative, Recover Alaska & Trust related. State Agency
Partner with other programs
New DBH Partnership Project, recently supported funding for secondary trauma training for school counselors and for state staff, etc.). State Agency 2
Partner with other programs Local collaboration to break down silos for families we serve. State Agency 3
Partner with other programs
Participate in Homer Prevention Project, one of whose implementation groups is tasked with raising local awareness on ACEs. State Agency 3
Partner with other programs
Co-present as a Green Dot trainer (where we infuse TIC principles, since the GDot model seems one small lens/cameo for this approach. State Agency 3

ACEs Mapping Survey Report McDowell Group, Inc. � Page 38
Partner with other programs Partnership with the Homer Prevention Project. State Agency 5
Partner with other programs
In development: building capacity and systems for trauma informed care among healthcare providers at one regional tribal health organization, KANA, + supporting them to do ACES education and community dialogues. Eventually, ACEs screening and research and intervention in that health care organization.
Tribal Agency 1
Prevention We have an Infant Learning Program providing Trauma Informed services to prevent the re-occurrence of ACE's in childhood after children have been referred through CAPTA.
Non-profit Organization 10
Prevention We provide lots of preventative strengths based programs and support groups to prevent ACE's in our region.
Non-profit Organization 10
Prevention
Our CEO serves on the Board for NACBH (National Association for Children's Behavioral Health) and the focus for the past 2 years at the Technical Meeting/Conference has been trauma informed care. We have had representation from clinical, management and training departments at the meetings. http://www.nacbh.org/PubDocs/TechnicalMeeting2013_ProgramMaterials.pdf
Non-profit Organization 3
Prevention Home-based early intervention services with families/caregivers who have a children birth to three (Infant Learning Program) who may have delays in any area of development.
Non-profit Organization 5
Research
I have published research previously in the area of the ethology/biology of familial relationships. My view is that at present there are gaps between ACEs research and epigenetics on the one hand and how we can more effectively prevent ACEs on the other. Otherwise I give some talks on ACEs and related work and screen for and discuss ACEs in my clinical work. I am resuming some research related work that I have published in peer reviewed journals in the past - and screening in clinic work with referral/ some talks of informative nature.
State Agency
Research Ongoing research. State Agency 4
Research I am conducting a Mat-Su Behavioral Health Environmental Scan that includes a focus on prevention and treating childhood trauma. Other
Screening We are using ACE as a mandate to train our BH/SA/DVSA staff and inform our treatment planning. We have two staff trained in TIC, and hope to have all staff trained as soon as practicable depending on availability of training.
Non-profit Organization
Screening We have been screening for ACE scores in our mental health assessments. This helps inform therapists in their treatment of children and youth.
Non-profit Organization
Screening We use ACEs to influence our work as a health care provider (primary care and behavioral health programs) through our screening, training, and program development.
Non-profit Organization
Screening ACMHS uses the Alaska Screening Tool with all its clients. Non-profit Organization 2
Screening Early childhood screening with follow-up support to parents/caregivers to provide education regarding child development and availability to answer questions anytime.
Non-profit Organization 5
Screening DJJ is in the beginning stages of implementing TIC and as a part of the implementation all line staff are trained on the ACEs. (x3) State Agency
Screening Behavioral Health System -- implemented ACEs screening for all individuals in our services to guide assessment and treatment planning decisions. State Agency 1
Screening IPV screening of every 1:1 adult encounter in our direct service provision. State Agency 3
Screening
All children who are admitted to our acute hospital facilities undergo comprehensive assessment of their pertinent psychosocial history which emphasizes the role of childhood trauma in the development of their personality, behavioral, emotional, and cognitive functioning.
Other
Therapeutic services I provide psychotherapy to individuals, couples and families. Non-profit
Organization Therapeutic services
We respond to child abuse cases. We serve survivors of violence to address lifetime impact of ACEs.
Non-profit Organization 11
Therapeutic services
A dedicated counselor provides therapeutic mental health services to our clients.
Non-profit Organization 2

ACEs Mapping Survey Report McDowell Group, Inc. � Page 39
Therapeutic services
Advocates assist clients with short term and long term advocacy and assistance.
Non-profit Organization 2
Therapeutic services
Case management focuses on interventions with clients suffering repeat victimizations, such as housing, emergency financial assistance, and understanding the patterns of violence and victimizations across generations.
Non-profit Organization 2
Therapeutic services
Advocates respond 24 hours a day to provide emergent crisis response to victims of sexual violence (adults and children).
Non-profit Organization 2
Therapeutic services Running a Child Trauma Center. Non-profit
Organization 8
Training/education Incorporating into Master’s program. Educational Institution
Training/education We have trained OCS staff in the ACE study and its implications for child welfare.
Educational Institution
Training/education Serving as Advisory Board member for Training program related to FASDs. Educational Institution 1
Training/education Integration of ACEs related content into graduate public health curriculum. Educational Institution 1
Training/education Education staff working with children and families Non-profit Organization
Training/education Including ACEs information in trainings. Non-profit Organization
Training/education ACEs slide included in two presentations on Diabetes planned for May 2014 for RNs and CNAs in LTC.
Non-profit Organization 1
Training/education ACEs information and resiliency information included in monthly Diabetes Self-Management Education for patients with diabetes.
Non-profit Organization 1
Training/education We have a prenatal-K Parents as Teachers Home Visiting Program focused on reducing specific ACE's.
Non-profit Organization 10
Training/education We provide training on ACEs. Non-profit Organization 11
Training/education We offer parenting classes. Non-profit Organization 11
Training/education
AK Child & Family was chosen by the National Council for Community Behavioral Healthcare, through a competitive application process, to participate in the 2012 Adoption of Trauma Informed Care Practices Learning Community. This included face to face learning at the 42nd and 43rd National Council Conferences in Chicago and Las Vegas; web and phone based education; consultation and technical assistance from national experts. Goals included: develop a trauma informed workforce, improve screening/assessment for trauma, increase consumer engagement, implement trauma informed best practices suited to the organizational environment, create safe environments that avoid re-traumatization and increase community involvement and utilize data to sustain/continue the improvement process. We are currently alumni of this learning community and continue to be actively involved with the group.
Non-profit Organization 3
Training/education AK Child & Family’s training department provides statewide training services that are funded in part through a State of Alaska grant. Trauma trainings have been offered.
Non-profit Organization 3
Training/education AK Child & Family is continuing to revise internal documents (example – policies and procedures; consumer handbook; etc.) to incorporate trauma informed care language and practices.
Non-profit Organization 3
Training/education
On-going consultation and training. Training for early child care providers to support positive social and emotional development practices. Training on early childhood mental health assessment and intervention. The Alaska Child Trauma Center is a regional training hub for the SAMHSA-supported National Complex Trauma Training Network and the lead agency for the Alaskan Trauma-Informed Care Statewide Training Initiative.
Non-profit Organization 4

ACEs Mapping Survey Report McDowell Group, Inc. � Page 40
Training/education
ACMHS is a certified ARC Training Site. The Alaska Child Trauma Center also works in partnership with Office of Children’s Services and provides behavioral health assessments to children entering child protective services custody in Anchorage.
Non-profit Organization 4
Training/education Alaska Child Trauma Center; ARC (Attachment, Self-Regulation and Competency Development; a framework for working with complex traumatized youth).
Non-profit Organization 4
Training/education We offer connections to a variety of community resources, networking with other parents, access to Infant Mental Health consultation, etc.
Non-profit Organization 5
Training/education Conduct ACEs 101 trainings. Non-profit Organization 6
Training/education Participated in national discussions on how ACEs is being utilized. Non-profit Organization 6
Training/education Statewide Trauma Training Initiative. Non-profit Organization 8
Training/education SAMHSA CAT II National Complex Trauma Training Initiative. Non-profit Organization 8
Training/education Trauma Informed Services Training for Hospitals in Alaska. Non-profit Organization 9
Training/education
Training on ACEs that is tailored to the target audience such as educators, suicide prevention, substance abuse and prevention; we have a major focus on universal education and trauma-informed parenting as the pathway to prevention.
State Agency
Training/education Training statewide as a partner with the ANTHC Domestic Violence Initiative Grant. State Agency
Training/education We are training all providers to implement trauma informed (responsive) services. State Agency 1
Training/education Co-led a community conversation on TIC. State Agency 3 Training/education Frequent in-house staff discussions on how to apply TIC strategies internally. State Agency 3
Training/education Display we created for multiple use at health fair tables, PHN events. Infusing recent MAPP community health assessment with ACES language. State Agency 3
Training/education Presentations to interested groups. State Agency 4
Training/education Training around the state. At the moment we are doing a lot of ACEs-related training with schools and our training usually has a focus such as ACEs specific to schools, or suicide prevention or alcohol issues.
State Agency 5
Training/education
We facilitate the Strengthening Families Protective Factors Framework project (a child abuse and neglect prevention strategy). There are several early care and learning programs receiving training and coaching on this approach through state funding. Training is provided to the community providers regarding this model upon request.
State Agency 6
Training/education The Alaska Early Childhood Coordinating Council has been trained on trauma and is discussing the role of the AECCC in mitigating the effects of toxic stress and trauma.
State Agency 6
Training/education Tribal community empowerment to end silence & denial about child sexual abuse - building skills & understanding to support victims in healing from multigenerational trauma.
Tribal Agency
Training/education Offer presentations on ACEs to audiences that request them (typically tribal health organizations). Tribal Agency 1
Training/education
Incorporate ACEs into trainings on DV/SV for healthcare organizations and other audiences. Prevention of ACEs via training providers and administrators in DV/SV integrated education, screening, and response in healthcare, behavioral health, and social services.
Tribal Agency 1
Training/education Making information on DV/SV and child maltreatment-related resources more accessible to families and service providers via creating a resource guide. Tribal Agency 1

ACEs Mapping Survey Report McDowell Group, Inc. � Page 41
Appendix 3 – ACEs Strategies and Measures
WE'RE INTERESTED IN LEARNING MORE ABOUT YOUR 'THEORY OF CHANGE. HOW DO YOU SEE THE WORK YOU DO (PERSONALLY OR AS AN ORGANIZATION) IMPACTING THE COMMUNITY YOU SERVE? FOR EXAMPLE, HOW DO YOU SEE YOUR WORK REDUCING ACES OR INCREASING RESILIENCY?
Service Providers
• (Nonprofit) 1. Shifting the mental health system from a descriptive (symptoms, problems, disorders) to an etiological
(trauma, development, social/attachment/relational, functional, resiliency/recovery) oriented system. An
understanding of the role of adverse experiences as a sometimes causal, and often contributory factor in behavioral
health problems is essential to the development of a more humane and effective behavioral health system that better
promotes recovery. 2. Working with various service systems and communities to understand the role that everyone can
play in preventing traumatic experiences, mitigating the impact of traumatic experiences when they occur, and using a
better understanding of the impact of trauma to better promote recovery and foster resiliency. Helping systems
understand that while trauma treatment provided by specialists is one important component of an effective and
systematic response to trauma, that trauma-informed care is something that can be practiced by all committed
persons in all human serving systems to improve outcomes.
• (Clinical Services Business) A comprehensive and accurate analysis of the child's trauma background is essential to
understanding and recognizing the formative factors responsible for their presenting clinical problems, social
dysfunction, personality pathology, and emotional dysregulation. Clinical interventions should account for and be
customized to children’s' backgrounds in order to be effective, relevant, and ultimately generalizable to their
community and family of origin. Recognizing adverse childhood experiences and emotional traumas is crucial in
eventually tracing current pathology to its roots. As such, interventions can be developed for children that will help
them tolerate their contrary feelings, overcome adversity, solve problems, and improve their ability to navigate around
future potential adversity.
• (Nonprofit) (We provide) prevention services from a positive youth development platform looking to make an impact in
the outcome areas of character and leadership, healthy lifestyles, and academic success. These outcomes do not occur
in a vacuum, but require staff and volunteers to build connections with youth based on their strengths, interests, and
needs and provide opportunities for them to learn and grow building key social and emotional skills, increasing
resiliency. (Our locations) are in the places where children and youth need us most, working to reach those who are in
poverty, experiencing academic difficulty, those experiencing family stress and dysfunction, as well as youth who have
entered the child welfare system or the juvenile justice system.
• (Tribal Agency) Community & individual ownership of solutions to ending violence, protecting children and ending
denial about abuse takes place by working with communities and individuals at their SPECIFIC level of readiness. Social
change happens in Tribal communities when individuals are able to collectively build trust, acknowledge the impact of
historical trauma & work together to manage the impacts of trauma & prevent future abuse & violence.
• (Nonprofit) Early childhood intervention, child abuse prevention.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 42
• (Nonprofit) I typically work from the trans theoretical model of change due to interning in primary care and addictions.
When working with clients who have experienced trauma, there are a number of treatments however, I start with
safety concerns and instilling hope. At later stages I encourage them to explore what has changed for them as they
increase awareness and any potentially larger meaning they derive from it. Sometimes this will have to do with
preventing the cycle from continuing; protecting themselves and how they may be able to help others in their family in
preventing trauma. Since I provide psychotherapy, the change begins at an individual level however, my perspective is
that as individuals change or heal, that healing or change impacts their family and in turn the community.
• (Nonprofit) In our work with youth we believe we have an incredible opportunity to not only impact the family system
but we also hope to assist the young person in following a more positive/healthy life trajectory. This may include
improving overall mental and physical health, breaking the cycle of abuse in subsequent generations, etc. We believe
by helping individuals and families there is a corresponding favorable impact on the community at large in which these
individuals live, work and attend school.
• (Nonprofit) Increasing resiliency is the primary focus of our agency's advocacy and therapeutic counseling approaches.
• Nonprofit) More effective intervention to break the cycle and reduce ACEs for future generations, as well as to increase
resiliency.
• (Tribal Agency) Our role is to provide family centered services, embedding developmentally appropriate activities within
the family's daily routines and natural environments. In turn we hope to support parent resiliency, build social
connections, share resources for times of need, educate families about parenting and child development (research
based theories and practices), and help build children's social emotional well-being.
• (Nonprofit) Our screenings and discussions with clients around ACEs continues to inform direction and treatment for
the children we serve. This tool serves to validate children's concerns and also informs areas of resiliency to be
explored. We believe that having focused information concerning clients’ needs and history can help provide assistance
in directing services. This information seems to point to better client care and therefore positive change for the future.
• (Nonprofit) Our Theory of Change is that Change happens within the context of relationships, moment by moment.
We work within the complex system of the family to ensure that dyads (parent-child) are supported every day.
Primarily, we work through building up the parents’ capacity to prevent ACE's and to promote the healthy
development of children.
• (Nonprofit) Our work reduces the chances that children will be traumatized by abuse again. Increases opportunities for
children to be safe and get treatment for past trauma.
• (Nonprofit) Personally, I see myself as a change agent, and work to ameliorate the psychological and emotional
impact of ACEs using CBT, DBT, and PET types of therapies to build resiliency.
• (Nonprofit) Promoting understanding working with children and clients, and increasing resiliency and outcomes post-
intervention.
• (Nonprofit) Providing strengths based support, education and access to the families we work with. Engaging in
visionary community conversations and collaborating with other professionals. Bringing information to the community
to create investment and buy-in. Collecting data to support and inform our work.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 43
• (Nonprofit) Pursuing trauma informed Department of Health and Social Services including DBH, DJJ, DPA and OCS.
• (Nonprofit) We're still learning how to provide trauma informed care. We're also learning how to recognize when ACEs
are a variable in the child and family's life.
• (Nonprofit) Working to reduce trauma associated with the process of an investigation of child maltreatment for the
child and family, working to prevent trauma associated with child maltreatment within the community, family etc.
Training/Education/Technical Assistance
• (DHSS/DPH/Alaska Family Violence Prevention Project) Education is the stepping-stone to other effective strategies---
changes in policies, practices etc. We use a "resiliency sandwich" so that we start and end with resiliency when talking
about ACEs. Our work with ACEs and shifted our approach in interpersonal violence overall to use a strengths-based,
resiliency framework.
• (Tribal Agency) 1.) For the KANA project, training the providers, staff, and administrators in trauma informed care
and culturally informed care is essential for helping those who have been traumatized. By creating a safe environment,
patients' trauma is not exacerbated and staff are more skilled at helping patients to understand the health effects and
parenting effects of their trauma and helping them to get referrals for needed services or simply reach out to their own
support networks. By doing the community pieces, we believe that this will strengthen social networks, which increases
safety nets for kids and decreases family risk factors. Further, talking about and healing from trauma in a community
context is a more Alaska Native way to do this work--hearing and hearing others, and strengthening the support of
the community is essential for cultural and family well-being. 2.) If people know the basics about ACEs and some
efforts to reduce ACEs, they can bring this awareness into their own agencies and communities and tribes and the
work they already do. That is the basic goal of responding to requests for presentations and training 3.) Exposure to
domestic violence is the ACE that is most predictive of other ACEs, so it is essential to address domestic violence,
especially moms who are experiencing domestic violence, in order to reduce children's exposure. Through the training
we offer to healthcare organizations on the patient safety card approach, we are increasing the opportunities for
women and girls to learn about what a healthy relationship is, what an unhealthy relationship is, that abuse is not
their fault, that there is help out there for them, that relationships affect their health and their children's health, and
how to get help. It also gives them an opportunity to talk with a healthcare provider to do risk reduction and to
increase their opportunities for safety for themselves and their children. It also addresses closely the risks during
pregnancy and early childhood, because we know that abuse during the perinatal and early childhood period can be
even more damaging to long-term health than the ACEs that children can remember. 4.) The long-term behavioral
and health effects of ACEs can be mitigated by receiving early and appropriate help. The goal of the resource guide is
to facilitate this.
• (Educational Institution) Having child-welfare workers better informed about ACE, they can better serve families who
come into the system by helping them to connect to healing providers. Once ACEs are identified, child welfare can help
to enhance the families’ resiliency.
• (Nonprofit) Helping families identify their supports (both formal and informal) so they know who to turn to in times of
trauma. Also providing families with developmental information so they can gauge where their child(ren) should be to
avoid parental stress from their child either not meeting expectations or anticipating upcoming challenges with new

ACEs Mapping Survey Report McDowell Group, Inc. � Page 44
skills. Providing parents with developmental information so they can provide their child(ren) with ample learning
opportunities.
• (DHSS – Fairbanks Regional Public Hospital) Education leads to better decision-making and hopefully better choices
and prevention.
• (Educational Institution) Improving training awareness impact of providers.
• (Nonprofit) Most of the material we present in the Diabetes Self-Management Education is designed to increase
resiliency. Framing it in just a little bit of trauma informed care language helps participants have compassion for
themselves and others.
• (Nonprofit) SCF creates programs, services, trainings for our customer owners. For example, The Family Wellness
Warriors Initiative (FWWI) is a statewide education and training project developed to prevent domestic violence, child
sexual abuse, and child maltreatment. The program focuses on Alaska Native families who experience the highest
incidence of any group in a state where reports of child maltreatment have increased 107% in the past decade with
close to half of all reports of child abuse and neglect substantiated. The ability to counter abuse has never been more
needed or more important than today. FWWI’s vision is to break the cycle of abuse in Alaska in this generation. The
program is unique in that it attacks these problems by preventing their occurrence, or reoccurrence, rather than
dealing with them after harm has been inflicted. FWWI was developed by Alaska Native leaders to incorporate the
values, strengths, and beliefs of Native cultures. It is sponsored by and receives support from Southcentral Foundation
(SCF), the Alaska Native Regional Health Care organization serving Anchorage, the Mat-Su Borough, and the
Anchorage Service Unit. The program started in 1999 and has trained nearly 2,000 people since then. Further, our
customer owners told us they want change in the behavioral health system. We are in the process of aligning all of our
BH programs with the SCF Nuka System of Care. Combined, these two efforts will create many opportunities for our
customer owners to enjoy healthier lives, reduced ACEs and stronger factors to support their lives going forward. In
summary, customer owners drive the change in programs, services, and trainings.
• (State Agency) Raising awareness system change.
• (Educational Institution) Recognizing socio-ecological framework, working with others to impact individual,
interpersonal, community and policy levels of change. Increased recognition. Additional supports. More prevention.
Broad-based Approaches
• (DHSS) Our theory of change is that knowledge is empowering but it must be delivered in a way that is relevant to
the specific audience (so presentation to educators is very different than health care providers or community etc.) and
that we need to start and end with resiliency and prepare people who work with this by addressing the issue of
secondary trauma, front and center.
• (DHSS/DBH) Acknowledging their impact on individuals in behavioral health services helps us to change the trajectory
for families. Developing trauma responsive systems. Addressing ACEs in our prevention programs to guide our
communities in building resiliency. On-going assessment of individuals’ functionality and improvements for the
individual supports.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 45
• (DHSS/DJJ) DJJ's mission is based on Restorative Justice and several years ago we implemented strength based
practice. The ACEs and will continue to enhance and strengthen our work with youth and families. (Two responses)
• (DHSS/OCS) For our state to address the issues of ACES and increase resiliency, several components are critical:
community awareness and commitment; easily accessible support in places where families naturally show up; trauma-
informed services across education, primary care, mental health and family support sectors; and efficient and effective
systems of care. The majority of the projects listed above focus on building capacity in programs and communities, so
they are more prepared to meet families and children where they are, build on protective factors, strengthen resiliency
and address issues as early as possible.
• (DHSS/Homer Public Health Center) We included ACES info in our first local CHA in 2010 to begin to make the
connection for all readers, even though we didn't have any local references. Currently, at the individual level, by
educating each person on the pervasiveness of violence in AK communities; community level, sharing the ACEs study as
a reference in trauma-informed conversations and in prevention work, and as a reference during Green Dot trainings I
co-lead; systems level, keeping the work at the forefront as we consider health equity issues in assessment and
updating our Community Health Improvement Plan I think we are still at the level of raising awareness--demonstrated
to be occurring in the results of our 2nd recent CHA--not yet able to measure change at health outcomes level. I think
we are changing the dialog to "what happened to you instead of what's wrong with you" at every opportunity.
• (DHSS) My work is supporting ACE reduction/increasing resiliency in several ways: by educating and training
professionals so that they will work more effectively with individuals who have been impacted by trauma, through
system development activities to support trauma informed policies or approaches and through funding treatment
services and supports that are trauma informed and work to increase individual and family resiliency.
Prevention
• (DHSS/DBH) The work we fund enhances community protective factors, across the lifespan, for all residents. There is
often a special focus building resiliency, preventing substance abuse, suicide prevention, interpersonal violence
prevention, FASD prevention and health promotion.
• (Nonprofit – Alaska Children’s Trust) Theory of change has three dimensions: (1) Community Awareness, (2) Informed
Systems, & (3) Focused Interventions. Community Awareness: increase awareness of the impacts of trauma and
resiliency on brain development, reduce shame, mobilize local resources, promote prevention and change cultural
norms. Informed Systems: systems are aware of the impact of trauma and resiliency on brain development/influence
who we become in the future and respond in ways that support resiliency, healing and support. Focused Interventions:
mitigate trauma, improve direct outcomes with high risk populations and reduce trans generational transmission.
• (Nonprofit – MSSCA) We are but a tiny drop in this bucket of reducing ACEs or increasing resiliency, but if we can start
with the parent and child to strengthen that relationship and provide better understanding while enhancing that
child's development for future success, we have had an impact for that child and family. People in this field understand
ACEs but we need to share this information with the broader population - churches, community employers &
employees, high school students, PTAs, etc. And it needs to be presented in a variety of formats, TV ads, newspapers,
radio, formal presentations, informal social media, whatever ways people are connecting.
• (Nonprofit – Sound Alternatives) We are working toward prevention and changing environments that generate ACEs.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 46
Other
• (Nonprofit) The primary model we center our theory of change around is dialogue. For thousands of years, Alaska
Native people have utilized stories, discussions, and even powerful silences, to great effect in healing from trauma,
building resiliency, and bonding as a community. We seek to reactivate that traditional methodology in newly initiated
discussion spaces, using story, presentations of personal experience, and tone-setting to create a space where people
can open up about their deep-seated emotional distress, find comfort in the group and in bringing to light long-buried
wrongs, and help others find their own voice. The model has proven very effective in our ANDORE dialogues, and we
have begun to adapt it to ACEs-related dialogues.
• (Foundation) The research I do will impact where the Mat-Su Health Foundation puts its money and resources in our
community.
• (DHSS - Alaska Psychiatric Institute) We’ve learned a great deal about the prevalence of ACEs, their impact on health
and are rapidly developing an understanding of the biology underlying ACEs. It is generally now understood that
primary prevention is crucial. This is where we are lagging - translational work. There is a lot more that can be done
here but this requires looking quite a bit further upstream than generally is the case.
• (Educational Institution) Yes--students and staff are surprised to hear, "It's not what is wrong with you, it’s what
happened to you." there is a cause for this and ways to work with ACEs/resiliency.
• (State Agency - AMHTA) Supporting improved collaboration and planning efforts to maximize impact statewide.
• (Nonprofit) The Early Intervention work Infant Learning does directly works on family strengths, identifying resiliency
factors in the family and their support system. We help families identify and enhance what is there in their lives already
and make plans to connect them with even more help in their community. We also work to establish self-sustaining
community programs that will help everyone grow more resilient, so folks in need are better supported.
AS A FOLLOW-UP QUESTION, WHAT OUTCOME MEASURES AND RESULTS DO YOU TRACK TO MONITOR THE PROGRESS OF YOUR ACES WORK?
Following are approaches being used or considered to evaluate 1) training quality 2) service quality, including
the extent to which trauma-informed care is incorporated into systems and services, and 3) client impacts.
• 1.) We will use a pre-and post-evaluation of the trauma informed care training and systems/policy changes at KANA.
Tools are not yet selected, but there are validated tools already in existence for measuring knowledge, attitudes, and
behaviors around trauma; for evaluating the trauma informed nature of facilities and systems and policies; and for
evaluating the cultural humility and cultural awareness of staff. These are the things we will look at changing in the
initial phase. In the screening/research phase of the project, we will be looking at Health record data linked with Ace
data to understand the correlation and will watch this to see if it changes when patients get help. That is, we will be
able to use health record data to understand whether trauma informed care decreases the negative effects of ACEs.
Some examples might include hospitalizations, asthma attacks, blood sugar management, ER admissions, self-
reported substance abuse and depression, STIs, etc. This, however, is years and multiple approvals down the road. 2.)
Nothing formal for tracking results of presentations that meet ad-hoc requests 3.) We have a structured evaluation of
the DV/SV project, which focuses primarily on changes in policy and practice within healthcare organizations.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 47
• Able to self-regulate emotions and stay in school for the day the year; focus on learning.
• As part of the TIC implementation we have been tracking Incident Reports and restraints. We will be meeting with the
Research team to determine the outcome measures and results DJJ will be utilizing.
• At AK Child & Family we use the 240 item Child and Adolescent Functional Assessment Scale (CAFAS) to conduct
ongoing assessments of how students function around 8 life domains. We measure rate of improvement from
admission to discharge; and we also conduct post discharge interviews of parents/guardians at 6, 12, and 18 months
after discharge from our services.
• Boys & Girls Clubs measures outcomes tied to social/emotional skills, conflict resolutions skills, and academic
commitment.
• BRFSS, YRBS, NSDUH, TEDS, NOMS, SUICIDE RATES, DJJ Data Corrections data. OCS Data when available. DBH ACEs
data.
• Clients receive surveys after initial service provision and then a 4 to 6 week follow up survey is conducted to determine
if initial services helped to ameliorate effects of trauma. Client feedback is actively sought regarding all counseling
services to determine if counseling is having desired outcomes - based on client's express needs at the time of intake.
• Currently, AST/CSR, along with client feedback. Hoping the NCTSN webinars may address outcome measures that will
guide future treatment.
• Currently, we monitor our ACEs screening by checking to see if documentation is recorded in client charts.
• Difficult to capture -- we know improvements in individual functionality and we pre and posttest individuals who take
our training.
• Evaluations for trainings.
• Feedback from program participants, documentation of community efforts, community assessment materials, data
from agencies and systems. We are interested in learning how to screen for ACEs with our clientele!
• Follow up with referrals to services such as mental health and medical services.
• For behavioral health recipients - CSR, CBCL, TSCC, TSCYC, DECA. For early education service recipients - DECA,
ASQSE, ECRS.
• FWWI uses a program evaluation tool. SCF employs a data team for BH and we are in the process of creating the
measures to track the progress of our BSD redesign.
• Immunizations rates. Breastfeeding rates access to primary care provider within the medical home child maltreatment
rates.
• Increase engagement and graduation of children who experience and live with families with ACEs.
• Involved in implementing Nurse Family Partnership program - data from this will start coming in within the next year
or so.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 48
• Our division tracks a number of population-level indicators around the focus areas mentioned above. These measures
are being tracked through statewide survey instruments, i.e. YRBS, BRFSS, PRAMS, etc.
• Our work focuses on training so our performance measures track the number of people trained. Because we are doing
training primarily at events organized by other organizations, the evaluation of the actual training is handled by the
event coordinators.
• Placement stabilization for children in custody as well as measuring functional improvement for children serve in areas
of family, community and school. Also, monitoring progress of Transitional Aged Youth towards service/treatment
goals.
• Primarily through reports from participants/communities about change & improved outcomes for children when adults
are supportive & protective.
• Recidivism of families with OCS involvement.
• Right now, our evaluation focuses on the number of people we train.
• Symptom Acuity Rating Scale, Trauma Symptom Checklist for Children.
• Symptom reduction as evidenced by progress on the treatment plan.
• The ACEs work we've done so far has mostly involved advocacy and outreach, participating in think tanks, hosting
dialogues, etc. Our advocacy and outreach work hasn't involved direct measurement of outcomes as such; think tanks
and other dialogues we've hosted produced notes and documentation that we can use in developing new programs
and reports. Future work, such as the Fish Camp project, will produce similar sets of notes, as well as a formal Toolkit
that others will be able to use to host their own dialogues (we used this model for another of our projects on racial
equity). Progress of this sort of dialogue work can be measured in how many conversations continue to be held in new
communities, but we haven't currently done much formal assessment (like survey work, etc.) to measure the desired
outcomes of our dialogue work - i.e., decreased inequity in racial issues, decreased ACEs or improved resilience to ACEs,
etc. We may yet engage in that sort of survey work in the future; the Institute did conduct an 'attitudinal survey' some
time ago, that looked at Native quality of life issues, but that wasn't performed in direct connection to ACEs work (it
could, however, be used as a baseline for future work, and a follow-up survey in a few years could be used to assess
progress).
• The client's self-report.
• The ECCS Project identified approximately 60 indicators to measure the well-being of young children in our state.
These indicators are updated as information becomes available. The individual ECMH projects, ILP and Strengthening
Families all have unique outcomes associated with their programs ranging from improved behaviors and development
for young children to increased protective factors for parents. We also collect training information- numbers training,
helpfulness to practice, etc.
• Varies - most have performance indicators specific to the project, and some also track ACE exposure. Also, BH system
now has some ACE info built into AKAIMS so we can look at program types and ACE exposure.
• Varies by project. Curriculum and Training efforts are assessed by knowledge and attitude change.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 49
• We currently use the Life Skills Progression, the Parents as Teachers satisfaction survey, the Parents as Teachers Parent
Reflection Survey and a Risk Factors Check List in the Infant Learning Program state-wide database. We have talked
about specific ACE screening tools (as they are coming out) and how we are hoping to be a pilot project for them. We
have access to so many children living through ACE's NOW - so we are hoping to prevent ACE's or promote resiliency
NOW.
• We do not track things related directly to ACES, rather we monitor child outcomes (positive social relationships,
acquiring and using knowledge and skills, and taking actions to meet their own needs), at entry, annually, and when
exiting from our program.
• We have 4 sites trained on ACEs and will be completing training for the other 4 sites in the next six months. We will be
meeting with the DJJ Research team to determine how we will measure and track progress in the next month.
• We track participants' success in reaching behavioral goals that they set for themselves r/t diabetes self-management
and healthy lifestyles.

ACEs Mapping Survey Report McDowell Group, Inc. � Page 50
Appendix 4 – Survey Questions
1. Do you currently utilize ACEs to influence or direct your work?
2. What is your professional role? [Check all that apply] - Service Provider, Researcher/Professor, Trainer,
Program Manager/Administrator, Other
3. How long have you been doing this work?
4. What type of organization do you represent?
5. In your organization, approximately how many people, including yourself, currently deal with ACEs-
related projects?
6. What is your program area of focus? [Check all that apply] - Advocacy, Business, Child Welfare,
Corrections, Community Development, Early Care and Education, Education K-12, Education
Postsecondary, Faith-based Organization, Government, Mental Health, Home Visiting, Public Health
Nursing, Primary Care, Public Health, Public Safety, Substance Abuse, Research, Training, University,
Healthcare Provider/Hospital, Other
7. From this list, please rank your top priorities in relation to your work. - Chronic disease, Substance
use, Crime, Mental Illness, Child welfare, Healthcare efficiency and/or cost, Work productivity,
Education measures, Personal violence, Protective factor/resilience/healthy coping measures,
Prevention, Trauma-informed care, Other
8. What borough(s) / region(s) do you serve?
9. Please indicate primary communities you serve
10. What age group(s) do you serve?
11. What ACEs-related activities have you implemented in the PAST? [Check all that apply] - Therapeutic
services, Develop program, Write grant, Partner with other programs, Evaluate service, Fund
programs/services, Training/education, Research, Screening, Prevention, Other
12. What ACEs-related activities are you engaged in CURRENTLY? [Check all that apply] - Therapeutic
services, Develop program, Write grant, Partner with other programs, Evaluate service, Fund
programs/services, Training/education, Research, Screening, Prevention, Other
13. Could you give us a comprehensive list of all the ACEs project(s) you're currently working on? -
Open-Ended Response
14. We're interested in learning more about your 'theory of change.' How do you see the work you do
(personally or as an organization) impacting the community you serve? For example, how do you see
your work reducing ACEs or increasing resiliency? - Open-Ended Response

ACEs Mapping Survey Report McDowell Group, Inc. � Page 51
15. As a follow-up question, what outcome measures and results do you track to monitor the progress of
your ACEs work? - Open-Ended Response
16. In what ways has learning about the ACEs study affected/changed your work? - Open-Ended
Response
17. We are going to be compiling a list of Frequently Asked Questions. What questions do you have, or
have you heard from others, about ACEs? - Open-Ended Response
18. What barriers have you experienced in providing ACEs related care? - Open-Ended Response
19. Are there any places, populations, etc. that you have difficulty reaching, that could benefit from
ACEs-related work? - Open-Ended Response
20. What resources would help you PERSONALLY carry out ACE-related activities? - Open-Ended
Response
21. What resources would help your COMMUNITY carry out ACE-related activities? - Open-Ended
Response
22. Are there any changes to statewide systems (e.g., Medicaid regulations, Alaska Department of Health
& Social Services funding or programming, accreditation) that would help promote ACEs work in
your community? - Open-Ended Response
23. Please rate the importance of advancing ACEs understanding and prevention in Alaska.
24. Would you like to receive more information about ACEs, or participate in any future statewide ACEs
initiatives we develop?
25. What sort of follow-up information are you interested in? [Check all that apply] - Reports, Planning
opportunities, Writing opinion-editorial and/or news articles, Interviews to share more about my
experiences, How to become a member of ACEs Speakers Bureau, Other
26. Based on your experience, who else should we contact to learn more about ACEs-related work in
Alaska, and to invite to collaborate with us on future ACEs-related activities in Alaska? Please provide
their name, agency (if applicable), and any known contact information. If you don't want to share
someone's name or contact info with us without their permission, please at least send them the link
to this survey so we have an opportunity to hear from them and learn about how they're working
with ACEs in Alaska. - Open-Ended Response