Marital Quality, Acculturation, and Communication in Mexican ...
Upload
independentCategory
view
0download
0
Community Dent Oral Epidemiol 2001; 29: 107–19 Copyright C Munksgaard 2001Printed in Denmark . All rights reserved
ISSN 0301-5661
Rodrigo Marino1, Geoff W. Stuart2,F. A. Clive Wright3, I. Harry Minas2Acculturation and dental healthand Steve Klimidis2
1School of Health, The University of NewEngland Armidale, NSW, 2Victorianamong Vietnamese living in Transcultural Psychiatry Unit, Melbourne,Victoria, 3Dental Health Services Victoria,Melbourne, Victoria, AustraliaMelbourne, Australia
Marino R, Stuart GW, Wright FAC, Minas IH, Klimidis S: Acculturation and den-tal health among Vietnamese living in Melbourne, Australia. Community DentOral Epidemiol 2001; 29: 107–19. C Munksgaard, 2001
Abstract – Objectives: To describe the relationship between acculturation and oralhealth status, oral health knowledge and frequency of dental visits in subjects ofVietnamese background, 18 years or older, living in Melbourne, Australia. Meth-ods: Oral health status was measured using the DMFS index. Oral health knowl-edge was estimated by responses to six specific oral preventive measures: brush-ing, flossing, use of fluorides, diet, and dental visits. Dental visits was measuredby the number of visits in the 12 months prior to the survey. Acculturation wasmeasured along two dimensions, psychological and behavioural, using the Psycho-logical-Behavioural Acculturation Scale. Data were analysed using multivariateanalysis to identify the combined effect of eight predictors (age, gender, occupa-tional status, education, reason for migration, proportion of life in the host coun-try, behavioural acculturation and psychological acculturation) against the depen-dent variables. Results: The analysis was conducted on a sample of 147 subjectsand showed significant interactions between the acculturation variables and three Key words: acculturation; dental visits; oral
health; oral health knowledge; Vietnameseoutcome measures: dental caries, knowledge of preventive measures and dentalpopulationsvisits. Results indicated that acculturation was an important intervening variable.Rodrigo Marino, School of Health, UniversityPsychological acculturation was strongly related to the three oral health out-of New England, Armidale, NSW 2351,comes, although the effect of behavioural acculturation was also apparent re-Australia
garding dental status. Conclusions: This study offers several insights for under- Tel: 61 2 6773 3746standing the mechanisms by which acculturation impacts oral health status. Inter- Fax: 61 2 6773 3666
e-mail: rmarino/metz.une.edu.auventions that simplify the cultural influence of immigrant groups by focusing onsocio-demographic differences and even immigration variables to define risk Submitted 10 September 1999; acceptedgroups might not produce predicted changes in oral health status. 30 May 2000
Although there is a solid link between how an indi-vidual thinks, acts and feels, and the culture whichnurtured him or her, it is also the case that whenthe cultural environment changes, the individualmay change as well (1). This process of change isreferred to as ‘‘acculturation’’. Defined by Redfieldet al. (2), ‘‘acculturation’’ refers to a complex pro-cess whereby a group – as a result of its continuousexposure to a cultural system that is significantlydifferent from the original – modifies its socialnorms, attitudes, values and behaviours, and char-acteristics of the culture of origin, or the cultures in
107
which people were socialised or where they havehad extreme life experiences (3).
The process has been described as taking placealong two different and independent dimensionsdefined as behavioural, and psychological (2, 4–6).Behavioural acculturation is related to culturallearning and the adoption of the most observable,external aspects of the dominant culture, includingsocial skills, language usage, life styles, and theability to ‘‘fit in’’ or negotiate aspects of the newsociocultural reality (3–5, 7–9).
The second dimension, psychological accultura-

Marino et al.
tion, consists of a more complex process which re-flects the degree of consensus with defined norms,basic values, ideologies, beliefs, attitudes and pref-erences of the majority of the group (4, 5, 7, 10, 11).
Some authors (6) have indicated that reports onimmigrant health may have reached erroneousconclusions as they have ignored the importance ofthe issue of variability within the minority popula-tion under consideration. These reports have ob-scured individual differences by operationally de-fining culture or ethnicity as a dichotomous vari-able (overseas-born against national-born), countyof birth, race (White, Black, etc.), language spokenat home or length of residence, thus, obscuring thepossible ways in which culture may operate, rarelygiving any consideration to the heterogeneity thatexists within the sample of migrant subjects (12).
It has been suggested that differences in accultur-ation may play a crucial role in areas such as men-tal health and/or deviant behaviours, use of healthservices, maternal and child health, drugs, alcoholand tobacco consumption, HIV knowledge, practic-es and beliefs, and risk of circulatory and heartdisease. These studies have strongly suggested, orclearly established, that differences in the level ofacculturation contribute to explaining the relation-ship between health and culture, and can createbarriers for health care for migrants. Level of accul-turation will generally be a good marker for shiftsin health-related knowledge, attitudes, beliefs andpractices, all of which may influence health statusand health service use and clinical outcomes.
The majority of these studies concluded that fo-cusing only on migrants’ socio-economic status,such as level of education, occupational status, orlanguage barriers, when formulating health pro-motion, disease prevention or treatment ap-proaches, rather than focusing on cultural factors,can be a major cause of failure to establish individ-ual differences between and within groups, duringthe process of acculturation, and can directly affecthealth outcomes.
Three studies have examined the effect of accul-turation on oral health and preventive behaviours(13, 14, 15). Ismail & Szpunar (13) presented across-sectional analysis of the prevalence of dentalcaries and periodontal disease, as well as the useof dental services. Three hundred and ninety-fivelow acculturated dentate Mexican-Americans, 12 to74 years of age were compared with 1894 dentateMexican-American who had high acculturationstatus (acculturation was measured by the modi-fied Cuellar scale [11]). They found that those with
108
low acculturation had a high mean number of de-cayed and missing teeth, compared to those withhigh acculturation status. Comparisons of perio-dontal data showed that those with low accultura-tion had a significantly higher prevalence of gin-givitis than those with higher acculturation status.Mexican-Americans with low acculturation werealso significantly less likely to have dental insur-ance or to have visited the dentist as frequently asthose who were highly acculturated.
Galan et al. (14) evaluated the medical and den-tal status and drug utilisation patterns of CanadianInuit elders. They described the poorly fitting den-tures, the poor oral hygiene, the high levels oftooth decay and periodontal disease of these Inuitelders as the profile for a population undergoingcultural transition (or acculturation). However, thisconcept was not defined or operationalised apartfrom a brief statement about their ‘‘cultural transi-tion’’ regarding use of clothing, housing and food.
More recently, Spolsky et al. (15) described thedental caries experience of a Hispanic sample fromLos Angeles. They concluded that caries experiencewas significantly related to acculturation. Thosewho were highly acculturated had a better dentalstatus when compared to those who were less ac-culturated.
The most common approach to studying the ef-fect of acculturation on health has been to define amigrant group along ethnic or racial lines, select ordevelop some measure of the acculturation con-struct, and then use this as an independent vari-able, relating it to the health variables under in-vestigation. Most of the scales used to measure ac-culturation have been assessments of languagecompetence. Other measures which have beenused include preference for the original culture orhost culture, access to the new culture as measuredby exposure to the media, friends, social contacts,generational status and place of birth. Few scales,and none of those used in the oral health studies,measured the contents of this new experience interms of new cultural values, preferences or identi-fication (7, 10, 16, 17).
Failure to measure the psychological dimensionof acculturation may represent a key limitationwhen relating acculturation to health. An under-standing of immigrants’ use and knowledge of thehost country’s language is important, but their mo-tivation, socio-cultural beliefs and habits may beeven more central to the framing of appropriatehealth policies. This may include the developmentof health preventive program, the planning of cul-

Acculturation and dental health
turally appropriate and effective health services,and the development of health promotion activitiesand appropriate strategies to meet particular oralhealth needs.
Over the past two decades there has been a sub-stantial expansion of the non-English speakingbackground (NESB) population living in Australia(18). One of the fastest growing groups is the Viet-namese. From 1986 to 1996 the Vietnamese popula-tion in Australia almost doubled, reaching a totalof 150 839 persons (19). While Sydney has thelargest Vietnamese population in Australia (39.3%of the total Vietnamese population lives in Syd-ney), Melbourne has registered the highest increasein Vietnamese population since 1986 (51.5%). TheVietnamese-born population represents more than10% of the total population in some suburbs ofSydney and Melbourne.
The primary objective of this article is to examinethe roles of the two major dimensions of accultura-tion (behavioural and psychological) as factors in-fluencing oral health status, oral health knowledgeand behaviours in a sample of Vietnamese back-ground adults living in a suburban, multiethniccommunity of Melbourne.
Its central innovation was the incorporation ofthe concept of acculturation in this inquiry, by theadministration of a valid measure of acculturation,the psychological behavioural acculturation scale(P-BAS) (20), to the sample. This scale, togetherwith other demographic variables, was used toconstruct an explanatory model of oral health out-comes, and to address the diversity that may existin oral health status in a migrant population.
Material and methods
This study focused on Vietnamese born peopleolder than 18 years of age, living in Melbourne,Victoria, and comprised people from a Vietnamesebackground registered as patients of a CommunityHealth Centre.
Three bilingual research assistants helped in thefield work. They telephoned potential participants,explained the project, and invited individuals toparticipate by attending the Community HealthCentre (CHC) during March and the first week ofApril, 1995. If the person agreed to participate anappointment was made for an interview and clin-ical examination. When the subjects arrived at theCHC, they were asked to complete two surveyforms in a dedicated area of the waiting room.First, the Psychological Behavioural Acculturation
109
Scale (P-BAS) (20), and second, a questionnaire onself-assessed oral health status, utilisation of oralhealth services, oral hygiene practices and oralhealth knowledge. Following the completion ofthese questionnaires and forms the subjects re-ceived an oral examination, which consisted of anassessment of dental and periodontal status.
The Psychological-Behavioural AcculturationScale (P-BAS) is a self-administered questionnairecontaining sixty-six items ordered into two mainareas, which cover behavioural acculturation andpsychological acculturation. The behavioural sec-tion consists of 15 items in a multiple choice for-mat, including language proficiency and use (with-in the family, with friends, as a child, and at work),social contacts and use and preference of languagein the media. Answers were in a multiple choiceformat, coded from 1 to 5 with 1 representing theimmigrant (Vietnamese) pole and 5 the host society(Australian)/host society language (English) pole.The middle score, 3, indicated an integration ofboth poles with denial of neither. The psychologi-cal scale was based on Kluckhohn & Strodtbeck’s(21) value orientation theory (See Table 1), and con-sisted of 45 items designed to measure the five val-ue orientation domains – three items for each ofthe three possible variations in each domain. Eachof the 15 variations represents one subscale of thepsychological scale. Thus, the psychological accul-turation scale is composed of 15 value subscales.Subjects were asked to rate on a 5-point scale theextent of their agreement with the statements, from
Table 1. Value Orientation Model with alternative solutionsa
Value orientation Variation
Human nature Good(What is the character of human Mixed
nature?) BadPerson/nature Mastery over nature(What is the relation of man to Harmony with
nature?) natureSubjugation to nature
Time Future(What is the temporal focus of Present
human life?) PastActivity Being(What is the modality of human Being in becoming
activity?) DoingRelational Lineal(What is the modality of person’s Collateral
relationship to others?) Individual
a Modified from Kluckhohn & Strodtbeck (21).

Marino et al.
complete agreement (1) to complete disagreement(5).
The questionnaire was constructed in English,translated into Vietnamese, and back-translatedinto English, following Brislin’s (22) recommenda-tions. Another independent translator carried outthe back translation. Both translators were Viet-namese-born, had tertiary education and were flu-ently bilingual. The final version of the Vietnameseform of the questionnaire was decided by groupconsensus. Its psychometric properties were testedusing a probability sample of Vietnamese back-ground subjects (nΩ187) and Anglo-Celtic Austra-lians (nΩ196) living in Melbourne. Reliability wasassessed using Cronbach’s alpha coefficient for in-ternal consistency. In the Vietnamese sample, the15 value subscales and the behavioural accultura-tion scale had alpha coefficients ranging from 0.55to 0.92. In the Anglo-Celtic sample three of the fif-teen value subscales did not reach the 0.50 thresh-old. The remaining twelve subscales satisfied theacceptable minimum of 0.50, ranging from 0.50 to0.81 (20). According to several authors (23, 24, 25,26) alpha coefficients of 0.50 or above were judgedto be appropriate to demonstrate internal consis-tency, especially for shorter scales. Low reliabilitiesshould also be considered as a trade-off betweenlength of the scale and the need for short scales.The behavioural scale had an alpha of 0.79.
Construct validity was examined for the behav-ioural scale in terms of hypothesised associationswith demographic variables identified from the lit-erature: length of contact with the Australian cul-ture, extent of exposure to the mainstream culture,measured by level of education reached, income,age of the initial contact with the host culture, andgender. Four of these were found to be significantlycorrelated with the behavioural acculturationscore: a) length of contact with the Australian cul-ture (rΩ0.47; P∞0.001); b) extent of exposure to themainstream culture (rΩ0.43; P∞0.001); c) income asa measure of access to the mainstream society (rΩ0.34; P∞0.001); d) age at initial contact with thehost culture (rΩ0.36; P∞0.001). One variable, gen-der, was found to be non-significantly correlatedwith acculturation. A specific validation for thepsychological scale assessed whether the scalecould differentiate between Anglo-Celtic and Viet-namese on their responses to the value subscales.A stepwise discriminant function analysis was per-formed using the 14 value orientation scores andeach of the three items on the ‘‘doing’’ subscale topredict ethnic group membership. There was a
110
significant separation between groups from 6 pre-dictors (F (6,307)Ω38.42 P∞0.001). Using this proce-dure, 77% of the cases were correctly identified.Variables that maximised the discrimination be-tween ethnic groups were: linear relation, collateralrelation, present time, control over nature, harmo-ny with nature orientations, and two items on thedoing-scale (20).
Socio-demographic information included in theanalyses were age, sex, occupation and education.Income, marital status and religion were not in-cluded in analyses because most subjects had lowincomes (less than A$ 15 000) and marital statuswas found to be highly correlated with age. Reli-gion was also removed due to the lack of variancein this variable. Age was grouped into five agegroups. Occupation was classified into threegroups: 1 ‘Working’, 2 ‘Students’, and 3 ‘Notworking’.
Participants were classified according to educa-tional level reached in Australia and in their origi-nal country: 1 ‘Primary level’, which included alllevels from no formal education to complete pri-mary education; 2 ‘Some secondary’, which includ-ed incomplete secondary education; 3 ‘Secondarycomplete or trade education’; and 4 ‘Tertiary edu-cation’, those who had completed university de-grees or were university students.
Two immigration variables were included in theanalysis, namely, ‘proportion of life in Australia’and ‘reason for immigration’. Because all migrantshave lived a part of their life in their countries oforigin before migration, actual length of residencewill vary according to the subject’s age and age ofarrival. Length of residence was considered a poorindicator of the effect of contact with the main-stream society. An index, [(Current year – year ofarrival)/age] made up of the respondent’s lengthof residence and actual age was computed to repre-sent the proportion of life spent in Australia (27).‘Reason for immigration’ was grouped into 3 cate-gories; 1 ‘Family’ including those who arrived asa child and those migrating for family reunion; 2‘Political’ which included those whose main reasonfor migration was political including refugees; and3 ‘Other’, all other reasons, such as, economic, edu-cation, etc. The acculturation scores (behaviouraland psychological) were also included in this anal-ysis.
Three oral health measures were used as the de-pendent variables: dental status, recency of dentalvisits, and preventive dental health knowledge. Toassess the dental status, the DMFS index was used.

Acculturation and dental health
Clinical examinations were performed by one den-tal examiner (RM) in a dental surgery at the CHC,using well-established method of data collection(28, 29). The clinical assessment was carried out inthe dental clinic using standard dental light. Teethwere neither cleaned nor dried before the examina-tion, but debris obscuring the visual inspection oftooth surfaces was removed using the dentalprobe. No dental radiographs were taken.
Patterns of dental attendance were investigatedby asking participants the interval since their lastdental visit. In order to facilitate interpretation ofthe data, use of services was grouped accordingto the following criteria: group 1 were those whohad visited the dentist within the last 12 months,group 2 were those who had not visited the den-tist in the last 12 months, including those whohad never been to the dentist. From the oralhealth interview, six questions were selected toconstruct the oral health knowledge index: tooth-brushing, flossing, two items regarding fluoride,use and exposure, visits to the dentist, and diet.Using the Goldsmith et al. approach (30), an oralknowledge index was created. Each response op-tion was dichotomised as ‘0’Ωincorrect or ‘1’Ωcor-rect, with subjects assigned one point for eachcorrect oral health knowledge answer. Responseswere summed to form the oral health knowledgeindex, scored from 0 (no knowledge) to 6 (goodknowledge). Following the practice used bySchwarz & Lo (31) and Spencer et al. (32), ‘‘Donot know’’ and items not answered were taken asan indication of inability to answer the questionand scored as incorrect.
Results were analysed first using a one-way anal-ysis of variance (ANOVA) to examine the main ef-fects of selected socio-demographic variables ondental caries history and oral health knowledge. Inthe event of differences between groups using AN-OVA, a Tukey’s Honestly Significant Differencestest was performed. To better understand the rela-tionship between the combination of socio-demo-graphic variables and the acculturation scores withoral health outcomes, the relationships werestudied using automatic interaction detection pro-cedures (AID) (33), using the KnowledgeSEEKERsoftware program (34). KnowledgeSEEKER is amultivariate stepwise decision making procedurewhich selects combinations of independent vari-ables that best separate groups on the basis of sta-tistical significance. This is a method for partition-ing data into homogeneous groups which allowsthe identification of combinations of predictors and
111
non-linear relations between them and the out-come variable (34, 35).
A detailed explanation of this method will not beattempted here, however, in order to better inter-pret the results it must be noted that Knowl-edgeSEEKER splits data sets into new, homoge-neous subsets of data (nodes) (35). At each node allpredictor variables are considered to further splitthe node. The node of best partition is based onthe selection of that variable which produces thehighest level of significance. This process continuesuntil no more significant splits can be found (35).To determine if the relationship between the out-come variable and the independent variable wassignificant, the significance level was set at 0.20, theexploration level. This method resulted in a‘‘bushy’’ decision tree. In the next step, in order toavoid association patterns that may be found bychance, the resulting tree was pruned back untilthe significance level of the lowest branch waslower than 0.01. This method has been shown tobe robust under cross validation when the nominaltype I error is set at the 0.01 confidence level (33).However, it suffers a limitation common to step-wise methods in that it does not examine the con-tribution of all variables to prediction.
Eight variables (4 socio-demographic, 2 immigra-tion and 2 acculturation) were used to classify thecases into subgroups according to the oral healthoutcomes under study. To further isolate the effectof acculturation on the dependent variables, fiveadditional analyses were performed, one using ageas the only predictor, another adding the set of soc-io-demographic predictors without the accultura-tion variables, and another with behavioural accul-turation only. A fourth model added psychologicalacculturation only and a fifth added, both types ofacculturation. This was done to determine theunique contribution of this set of measures (age,socio-demographic, acculturation) on oral healthoutcomes, given the limitation of stepwise modelselection outlined above
Results
Of the valid contacts made 158 resulted in ap-pointments, which represents a response rate of39%. The present analysis was conducted on 147Vietnam-born subjects who had complete informa-tion. More than 50% were under 35 years of age(55.8%). A total of 94 (63.9%) participants were fe-male and 53 (36.1%) were males.

Marino et al.
Data on occupation showed that about half(49.0%) of the participants were not working or notworking outside the home. About 20% of the parti-cipants reported employment in paid jobs. Of thosewho reported their occupation (nΩ29) about a thirdwere labourers or a related occupation, few wereinvolved in professional or para-professional occu-pations. Distribution by level of education indi-cated that the majority of participants had less thancompleted secondary education (nΩ68; 46.2%); an-other 39 subjects (26.5%) had completed secondaryeducation and 23 or 15.6% had some tertiary edu-cation.
Nearly 10% of the sample arrived in Australiabefore 1980; 48.3% during the 1980s, and 41.2% af-ter 1990. In assessing immigration history, we alsoemployed a measure of the proportion of their livesthat the immigrants had lived in Australia (27). Inthis sample, more than half of the subjects hadlived less than two-fifths (0.40) of their lives inAustralia. The majority of subjects in the samplearrived under the family reunion category (51.3%)and another (29.7%) for political reasons, which didnot necessarily entail a formal refugee status.
The socio-demographic profile of the sample re-sembled that of the broader Vietnamese com-munity living in Australia, in terms of their settle-ment and demographic characteristics. No differ-ences were found in terms of age, level of Englishproficiency, citizenship or income. Differences wereapparent, however, by level of education (this sam-ple had lower levels of formal education) andparticipation in the labour force (higher number ofsubjects not in the labour force in this sample). Thissample also had a higher percentage of females,more subjects in the family reunion migration cat-egory, a higher number of Buddhists, less Chris-tians and fewer with no religion. (36). This varia-tion was acceptable given that the study was notan epidemiological survey, but a study of the rela-tionship between acculturation and oral health.
Total scores for behavioural acculturation rangedfrom 1 to 5, with a total score of 1 indicating mini-mum acculturation. In the present sample scoresranged from 1.19 and a maximum score of 4.63.The mean behavioural acculturation score was 2.36(s.d. 0.84). The overall distribution was skewed to-ward higher acculturation scores.
The psychological acculturation scores obtainedwere standardised towards the Anglo-Celtic meanto facilitate their interpretation (20). An hypotheti-cal Anglo-Celtic sample would have a mean psy-chological acculturation score of 0.00 (s.d. 1.00).
112
The standardised mean psychological accultura-tion score of the Vietnamese sample was ª1.52 (s.d.1.11), with a range from minus ª4.67 to 1.36.
The DMFS values ranged from 0 to 128, with amean of 27.80 (S.D. 26.11) surfaces affected. Eightsubjects (5.1%) had no history of caries experience(DMFSΩ0) and only one participant as fully eden-tulous (DMFSΩ128). Separate bivariate analyses ofthe DMFS and DMFT indices were carried outusing each of the socio-demographic (age, gender,level of education, and occupation status) and im-migration (proportion of life in Australia andreason for immigration) variables. The DMFS scorediffered significantly when stratified by differentage groups, occupational status, level of educationand proportion of life in Australia, while therewere no significant differences between meanDMFS score by reason for immigration or gender.There was a significant increase in the mean DMFSas age increased, showing a significant ANOVA atP∞0.01 [F(4,150)Ω20.20]. Statistically significantdifferences were also present by level of education.Post-hoc comparisons showed that those with lessthan secondary education had a significantlyhigher DMFS index (DMFSΩ37.89) than any othereducation group [F(3,131)Ω3.23; P∞0.05]. Analysisof groups according to their occupational statuswas also significantly related to DMFS [F(2,136)Ω8.50; P∞0.01] and students had a lower meanDMFS score than any of the other groups whenpairwise comparisons were applied. Proportion oftime lived in Australia, grouped into 5 categorieswas also a significant predictor of DMFS [F(4,135)Ω2.94, P∞0.05]. Pairwise comparisons indicated thatthose with the highest proportion of life in Austral-ia had a lower DMFS (DMFSΩ12.92) compared tothose with the smallest proportion (DMFSΩ32.29).By level of acculturation, only the behaviouralscores reached levels of statistical significance. Be-havioural acculturation score was negatively corre-alted with DMFS (rΩª0.33; P∞0.01).
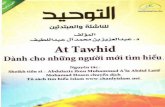
Using multivariate analysis several combinationsof socio-demographic and acculturation variableswere significant predictors of the DMFS score.However, when occupational status was entered asthe first split, together with the other predictors,this accounted for 44% of the variance (h2Ω0.4365)(see Fig. 1).
Those who were students or workers had, as anaverage, significantly lower DMFS (18.25) thanthose not working outside home (34.04) [F(1,137)Ω16.00; P∞0.01]. When considering these two occu-pational groups independently, the students or

Acculturation and dental health
Fig. 1. Pruned decision tree showing the predictive model for dental caries history.
workers subgroup was further split by level of psy-chological acculturation. Those with a mediumlevel of acculturation had significantly higherDMFS scores (24.40) than those in the low or highacculturation categories [F(2,64)Ω3.96; P∞0.05].Among those who were in the medium acculturat-ed subgroup, age was the next split. Those youngerthan 35 years of age had an average DMFS scoreof 14.76. If, however, the subjects were 35 or olderthe mean DMFS score was 39.33. This differencewas statistically significant [F(1,27)Ω18.46; P∞0.01].
For those not working outside home (nΩ72), agewas the next best split. With subjects younger than35 years, the group was further split by level ofbehavioural acculturation. Those with a lower levelof behavioural acculturation also had a signifi-cantly higher DMFS scores (24.56 vs. 7.64)[F(1,137)Ω16.0; P∞0.01]. This suggests that thosenot working outside the home with a high level ofbehavioural acculturation, not only had an averageDMFS nearly one third of the score for the rest ofthat age group, but when compared to students orworkers in the same age group they had almosthalf the DMFS of those younger than 35. In fact,they had the lowest DMFS score.
Turning to the multivariate analysis, severalmodels were tested in an attempt to overcome thelimitations of the stepwise knowledgeSEEKER pro-cedure, while capitalising on its ability to identify
113
interactions between variables that predict oralhealth outcomes. As outlined in the Methods sec-tion, variables were grouped into subsets for thepurpose of modelling. Age was always included inthe models tested. The model with age alone ex-plained 35% of the variance (h2Ω0.3467), the socio-demographic model accounted for 39% of the vari-ability (h2Ω0.3935), the model which included psy-chological acculturation and the socio-demogra-phic variables accounted for 41% of the variability(h2Ω0.4098), and the model which included behav-ioural acculturation together with socio-demogra-phic variables accounted for 42% of the variability(h2Ω0.4199). Thus, acculturation scores did not addstrongly to the prediction of dental caries history(See Table 2).
Regarding dental caries prevention knowledgescore, about 19% of the subjects did not answer anyquestion correctly. However, most of the partici-pants (nΩ49) gave two correct answers (33.8%),and 42 subjects (29.0%) indicated one correct an-swer. The mean dental caries prevention knowl-edge score was 1.52 (s.d. 1.0). Bivariate analysisshowed that dental caries prevention knowledgewas significantly related to two socio-demographicvariables (age and occupational status), but not toany of the immigration variables. Respondents inthe youngest age group had significantly moreknowledge than any other age group [F(4,135)Ω

Marino et al.
Table 2. Percentage of variance in oral health outcome explained by different subsets of predictors, including the full set ofpredictors
Independent variable
% variation in% variation % variation in dental visit
Predictor in DMFSa knowledgea recencya
Age only 34.67 6.90 2.79Socio-demographic and immigration plus age 39.35 15.33 7.56Behavioural acculturation only plus socio-demographic and immigration
and age 41.99 15.33 7.56Psychological acculturation only plus socio-demographic and immigration
and age 40.98 20.58 13.74Full model 43.62 24.41 13.74
a h2.
2.67; P∞0.05]. Regarding occupational status, stu-dents had a higher level of knowledge than anyother group [F(2,134)Ω7.58; P∞0.01]. Regarding ac-culturation scores, only behavioural acculturationreached levels of statistical significance (P∞0.01).
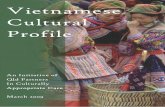
Fig. 2. Pruned decision tree showing the predictive model fororal health knowledge.
114
With regard to oral health knowledge scores, inthe multivariate analysis, using KnowledgeSEEK-ER (see Fig. 2), psychological acculturation hadthe most significant split [F(3,140)Ω5.52; P∞0.01].Those who had medium level of acculturation hadsignificantly lower knowledge scores (0.73) thanthose in the low (1.60) and high (1.62) acculturationcategory [F(2,140)Ω5.52; P∞0.01]. For the high psy-chological acculturated group, if they wereyounger than 25 years of age had an averageknowledge score of 2.03. If, however, the subjectswere 25 or older the mean score was of 1.45[F(1,110)Ω7.92; P∞0.01].
The older group could be further split by propor-tion of life in Australia. Proportion of life in Aus-tralia was grouped in 3 categories, which exhibiteda non linear distribution of knowledge score thatranged form 1.62 in those who had the largest pro-portion of their life in Australia to a mean score of0.75 in those who had between 27 and 32% of theirlife in Australia [F(2,77)Ω4.02; P∞0.05]. For subjectswith a proportion of life in the host country shorterthan 27%, level of education was the next signi-ficant split. Those with complete primary educa-tion or lower had lower scores (1.34) than thosewith higher levels of education (1.89) [F(1,46)Ω3.96;P∞0.05]. The lower education group could be sepa-rated by age groups. Those in the with the 25 to34 years of age group had lower knowledge scores(0.85), than those older than 35 years of age(knowledge scoresΩ1.75) [F(1,27)Ω10.77; P∞0.01].
The model presented in Fig. 2 explains 24% (h2Ω0.24) of the variance in dental caries preventionknowledge and suggests interactions between psy-chological acculturation, age, proportion of life inAustralia and level of education. The model withage alone explained 7% of the variance (h2Ω

Acculturation and dental health
0.0690), the full socio-demographic model ac-counted for 15% of the variability (h2Ω0.1533), themodel which included psychological acculturationand the socio-demographic variables accounted for21% of the variability (h2Ω0.2058). The model withthe socio-demographic and behavioural accultura-tion did not improve the previous full socio-demo-graphic model (see Table 2).
More than 40% of the subjects (42.1%) had beento the dentist in the 12 months prior to thestudy. About half of the sample had not been tothe dentist for more than 12 months, and 8 subjects(5.5%) had never been to the dentist. The last twogroups plus those who did not know when theyhad last been (nΩ4; 2.8%) were put into one cat-egory for the multivariate analysis. Bivariate anal-ysis showed that none of the socio-demographicvariables were significantly associated with dentalvisits. Subjects’ proportion of life in Australia andbehavioural acculturation were significantly re-lated to use of oral health services in the bivariateanalysis, but psychological acculturation was not.Those who had not visited the dentist in the 12months previous to the survey had as an averagea shortest proportion of their lives in Australia thanthose who had visited the dentists [F(1,136)Ω5.97;P∞0.02] and those who visited the dentist in the 12months previous to the survey had as an averagea higher level of behavioural acculturation thanthose who had not visited the dentist in the previ-ous 12 months [F(1,141)Ω4.47; P∞0.05].
The multivariate analysis showed that age hadthe most significant effect on visits to dentist(c2(1)Ω3.91; P∞0.05). For subjects younger than 35years, 35% had been to the dentist in the 12 monthsprevious to the examination, while 51.7% of thoseolder than 34 years had been to the dentist in the12 months prior to the collection of data.
No other split was significant for those youngerthan 35 years. In the older group, proportion of lifein Australia produced the next most significantsplit. For subjects whose proportion of life spent inAustralia was less than 21%, a higher proportionreported visits to the dentist in the previous 12months than in the complementary group (70.4%versus 36.4%) (c2(1)Ω6.88; P∞0.01). For the shorterproportion of life group the remaining variableswere not statistically significant to further split thenode.
The next significant predictor, for those with thelargest proportion of life in Australia, was psycho-logical acculturation. This split showed that theproportion of subjects with lower levels of psycho-
115
logical acculturation who had been to the dentistin the previous 12 months, was four times smallerthan the proportion of the high psychologically ac-culturated group. In fact, this group presented thelowest proportion of visits to the dentists in theprevious 12 months of all participants. Those withhigh psychological acculturation had an equivalentproportion to those with the shortest proportion oflife in Australia (72.7% vs. 70.4%) (c2(1)Ω10.01;P∞0.01).
The model presented in Fig. 3 indicates thatusing the level of acculturation in addition to theset of socio-demographic variables, explained 14%(h2Ω0.1374) of the variance in visits to the dentist.To further explore the effect of acculturation on vis-its to the dentist, three additional analyses wereperformed, one using age as the only predictor ofvisits to the dentist. This model explained less than3% of the variability (h2Ω0.0279). The full socio-demographic model, without the acculturationvariables, explained 7.6% (h2Ω0.0756) of the vari-ability. The model which added behavioural accul-turation to the socio-demographic model did notimprove the previous one. Finally, the model withthe psychological acculturation score only and thefull socio-demographic set of variables explainedthe same amount of variance as the first complete
Fig. 3. Pruned decision tree showing the predictive model forvisits to the dentist in the previous 12 months.

Marino et al.
model (both acculturation variables available forselection), that is 14% (h2Ω0.1374) of the variability(see Table 2).
Discussion
The use of an analytic strategy free from restrictiveassumptions, demonstrates that acculturation in-teracts with occupation, age, level of education andimmigration variables and appears to be a sensibleaddition to these socio-demographic variables inexplaining oral health measures, particularly oralhealth knowledge and visits to the dentist. In eachof the final models (see Table 2), the results indi-cated that acculturation variables added a signi-ficant explanation to the variance in the oral healthoutcome under study. This is demonstrated by thefact that the models without acculturation ex-plained less than those with acculturation. Theseresults indicate that the contribution of accultura-tion to the final model cannot be substituted withsocio-demographic or immigration history vari-ables. These provide evidence of the unique contri-bution of acculturation in explaining the variabilityin oral health knowledge, visits to the dentist andto a lesser extent dental caries history.
Acculturation, either psychological or behav-ioural, was related to all three oral health outcomesmeasured; dental caries history, knowledge of pre-ventive measures for dental caries and frequencyof visits to the dentist. Overall, those with higheracculturation had not only a lower number of teethaffected with caries history, but they were alsomore likely to have used oral health services in the12 months prior to the study, and had a betterknowledge of ways of preventing dental caries. Inthe present study, the mediating role of accultura-tion was found to be mainly via psychological ac-culturation (core cultural values), but also throughthe traditionally measured external aspects of ac-culturation, such as language use, food, clothing(behavioural acculturation). This would indicatethat acculturation should be seriously consideredin the future, when studying oral health in migrantgroups, as it added to the amount of variance ac-counted for by standard socio-economic indices,particularly for oral health knowledge and dentalvisits. Regarding dental status, the acculturation ef-fect was less apparent but still improved themodel.
Psychological acculturation was operationalisedas the degree to which the target group approachesthe defined value orientations of members of the
116
dominant group. For this particular group, threevalue orientations maximised the discriminationbetween ethnic groups: people to nature orienta-tion; time orientation; and relational orientation(20). This suggests that if an individual, because ofthe endorsement of these values, feels less in con-trol of his/her health (people to nature orienta-tion), or if the subject does not have a future timeperspective of her/his actions, there may be noreason to engage in long-term goals or time con-suming activities in the present. Furthermore, re-garding the relational orientation, if the personthinks in a more hierarchical relational way, thedentist would be ‘‘the one who knows’’ (37), and itshould not be surprising that the less acculturated,who tended to go less to the dentist, had lowerknowledge of preventive measures. However, it isalso possible that subjects who have less fullyadopted the predominant culture’s core values(those less acculturated) may be less aware of avail-able services, or may make greater use of alterna-tive or traditional systems of health care.
Language has been related to the likelihood ofusing preventive services, that is, immunisation,mammographies, pap smear programs and com-munity-based services, with migrant subjects lesslikely to use those services, particular those whodo not speak the host society language (38, 39). Inanother study, oral health knowledge was also re-lated to the ability to speak the host society lan-guage (40). In the present study, language was notassessed directly, but as an aspect of behaviouralacculturation. This study measured behavioural ac-culturation combined with information on abilityto read and speak English; use of Vietnamese lan-guage with parents, children, spouses, parents; eth-nicity of social contacts; and media preference. Be-havioural acculturation was a significant predictoronly for dental caries status. This effect of behav-ioural acculturation on dental caries is consistentwith the findings of Ismail & Szpunar (13) andSpolsky et al. (15) results, who used acculturationscales based on language items.
The present results showed that this sample ofVietnamese background people had generallybetter dental health than the broader Australianpopulation. However, within the Vietnamesegroup acculturation led to an even better oralhealth outcome, which indicates that the protectiveeffect of the original cultural values might bestrengthened. Those who are more behaviourallyacculturated may reach an even higher level of oralhealth than less acculturated individuals. Also, if a

Acculturation and dental health
person has language access to the mainstream me-dia, where oral health messages are usually com-municated, they may be more aware of the main-stream culture’s advancements in oral health pre-ventive and restorative care.
Another interesting outcome concerns the nonlinear effect of acculturation on dental status. Ourresults suggest that those in the moderately psy-chologically acculturated group tended to have ahigher DMFS index, while lower or higher accultu-rated groups had generally better oral health. Theconclusion to be drawn from this is that both theoriginal culture and the receiving mainstream cul-ture offer protective effects against dental diseases.A similar effect of psychological acculturation wasfound regarding caries prevention knowledge. Inthis case, those in the moderately acculturatedgroup emerged as the least informed.
These findings lend support to the ‘‘cultural mar-ginality model’’, which proposes that the partially-acculturated individual, who is alienated fromtheir traditional culture, but not yet integrated intothe dominant culture, will be the most affected(41), producing an inverted U-shape relationship.This cultural marginality model supports Dur-ward & Wright’s findings (42) regarding the effectof Western dietary habits on migrants’ oral health.They attributed the high prevalence of dental cariesin Vietnamese adolescent to the adoption of West-ern dietary habits. In terms of acculturation, thissuggests that the moderately psychologically accul-turated may have adopted some aspects of theWestern diet (i.e. junk food, sweets, beverages),without full appreciation of its consequences, orthe adoption of other preventive aspects of themainstream diet and Western oral hygiene prac-tices.
Overall, results of this study on current dentalstatus, show a more encouraging situation thanthat described by other reports on the oral healthof migrant groups in Australia (42–46). However,an acculturation perspective helps to explain partof this inconsistency, as these apparent contradic-tions may arise as a result of which group of mi-grants is studied. No randomly selected epidemio-logical sample of Vietnamese immigrants has yetbeen studied in Australia, and previous studieshave concentrated on groups living under partic-ularly extreme conditions, for example refugeecamps (44, 45) or recently arrived refugees, whenindividuals are isolated from both cultures (47–50).Participants in this study also represented a rela-tively homogeneous social group. Socio-demogra-
117
phic effects were to some extent reduced by focus-sing on one particular suburb of Melbourne. Also,in terms of other enabling factors such as physicalaccess to services, and regular sources of oralhealth care, as Health Card Holders this grouplived close to oral health services and was entitledto free health treatment, including dentistry, whichmay have positively affected their oral health out-comes relative to recently arrived refugees.
From an acculturation inquiry perspective, theseresults strengthen the bidimensional conception ofthe acculturation construct – behavioural and psy-chological. They encourage more in depth study ofthe relationship between (oral) health and accultur-ation, as well as the relationship between healthand socio-demographic and immigration variables.This is a way of increasing understanding of therole of acculturation in health issues and im-proving the accuracy of the prediction of higherrisk groups by adding acculturation as a predictor.
Knowledge of psychological and behavioural ac-culturation levels may provide some guidance forprogram contents and suggests that different ap-proaches may be required to address the culturalneeds of those less psychologically and behav-iourally acculturated. This is because, using accul-turation as a predictor, it is possible to identifywhich cultural aspects are responsible for whichoutcomes, and which knowledge, behaviours orclinical outcome offer most room for improvement.With this information, particular oral conditionsand populations can be more effectively targetedwhich may increase the cost efficiency of themeasure.
The information derived from such an approachcould be used to avoid large dental care expendi-ture for those segments of the populations at lowrisk and those for whom caries preventive serviceswould be only of marginal value. For example, theeffects of psychological acculturation on visits tothe dentist showed that those less psychologicallyacculturated were the least likely to use oral healthcare services in the 12 months previous to thestudy (see Fig. 3). This suggests that increased ef-forts should be directed to identify subjects in thisgroup than in any other. However, without the useof an acculturation variable, this effect would nothave been apparent and this high risk group wouldnot be or would be ill-detected, misleading conclu-sions of the possible effect of proportion of life inthe host society as the mediating factor for oralhealth status.
These findings support the contention that differ-

Marino et al.
ences in cultural expectation, in addition to socio-demographic or behavioural acculturation, mayhelp to explain the inability to reach the same oralhealth outcome in individuals from different cul-tural/ethnic backgrounds. In a multicultural coun-try, individuals might experience emotional, eco-nomic or language barriers, which need to be takeninto account. But a central difference would be theunderstanding of the process through which a mi-grant broadens his or her world and constructs hisor her actions and expectations in the light of his/her interaction with the original and the receivingculture values. Focusing only on linguistic or socio-economic dimensions does not cover the meaningof being an immigrant in a host culture. On thecontrary, the present findings suggest the need todirect efforts to find particular elements in bothcultures that are effective and lead to a positiveoral health outcome. These findings would alsosuggest that increasing the number of bilingual(Vietnamese/English) staff and practitioners, byitself, may not result in increased use of oral healthcare service, as the effects of culture on health is-sues may involve more complex social and culturalprocesses (51). Thus, focusing only on the languageaspect of acculturation may not produce the ex-pected change in oral health outcome.
Acknowledgements
We would also like to thank and acknowledge the assistanceof the Richmond Community Health Centre during thefieldwork and our colleagues at the Victorian TransculturalPsychiatry Unit and the School of Dental Science, The Uni-versity of Melbourne who offered advice and guidancethrough the course of the research.
References
1. Berry JW, Triandis J, Olmedo E. Assessment of accultura-tion. In: Lonner WJ, Berry JW, eds. Fields methods incross-cultural research. SAGE Publication Ltd; 1986. p.291–349.
2. Redfield R, Linton R, Herskovits MJ. Memorandum forthe study of acculturation. Am Anthropol 1936;38:149–52.
3. Ramırez M. Recognising and Understanding diversity:multiculturalism and the Chicano movement in psychol-ogy. In: Martınez JL, Mendoza RH, editors. Chicanopsychology. 2nd edn. New York: Academic Press; 1980.p. 343–53.
4. Searle W, Ward C. The prediction of psychological andsociocultural adjustment during cross-cultural transi-tions. Int J Intercult Relat 1990;14:449–64.
5. Berry JW. Acculturation and adaptation in a new society.Int Migrat 1992;30:69–85.
118
6. Olmedo EL. Acculturation: a psychometric perspective.Am Psychol 1979;34:1061–70.
7. Szapocznik J, Scopetta MA, Kurtines W. Aranalde MA.Theory and measurement of acculturation. Interam JPsychol 1978;12:113–30.
8. Taft R. The Psychological Adaptation of Soviet Immi-grants in Australia. In: Kim YY, Gudykunst W, editors.Cross-cultural adaptation: current approaches. BeverlyHills: SAGE; 1987. p.150–67.
9. Ward C, Kennedy A. Where’s the culture in cross-cultur-al transition? J Cross Cult Psychol 1993;24:221–49.
10. Miranda MR, Castro FG. Culture distance and success inpsychotherapy with Spanish-speaking Clients. In: Martı-nez JL, Mendoza RH, editors. Chicano psychology. 2ndedn. New York: Academic Press; 1980. p. 249–62.
11. Cuellar I, Harris LC, Jasso R. An acculturation scale forMexican American normal and clinical populations.Hisp J Behav Sci 1980;2:199–217.
12. Olmedo EL, Martınez JL, Martınez SR. Measure of accul-turation for Chicano adolescents. Psychol Rep 1978;42:159–70.
13. Ismail AI, Szpunar SM. Oral health status of Mexican-Americans with low and high acculturation status:findings from Southwestern HHANES, 1982–84. J PublicHealth Dent 1990;50:24–31.
14. Galan D, Odlum O, Grymonpre R, Brecx M. Medical anddental status of a culture in transition, the case of theInuit Elderly of Canada. Gerodontol 1993;10 44–50.
15. Spolsky VW, Atchison KA, Marcus M. The dental cariesexperience of a Hispanic sample in Los Angeles. J DentRes 1996;75(Special):186 (Abst 1351).
16. Szapocznik J, Scopetta MA, Aranalde MA, Kurtines W.Cuban value structure: treatment implications. J Coun-sult Clin Psychol 1978;46:961–70.
17. Betancourt H, Regeser S. The study of culture, ethnicity,and race in American psychology. Am Psychol 1993;48:629–37.
18. Australian Bureau of Statistics. Census-1991 Ethnic pack-age on hard copy. ABS. Catalogue No. 2803.2. Canberra:Australian Government Publishing Services; 1993.
19. Viviani N. Vietnamese in Sydney and Melbourne in 1996;some preliminary results from the census. People andPlaces 1997;5:54–7.
20. Marino R, Stuart GW, Minas H. Acculturation of valuesand behaviour: a study of Vietnamese immigrants. Mea-surement and Evaluation in Counseling and Develop-ment 2000;43:21–41.
21. Kluckhohn, F, Strodtbeck, F. Variations in value orienta-tion. Westport (CT): Greenwood Press; 1973.
22. Brislin RW. Back-translation for Cross-Cultural Research.J Cross Cult Psychol 1970;1:185–216.
23. Davies AR, Ware J. Measuring health perception in thehealth insurance experiment. Santa Monica (CA): TheRand Corporation; 1981.
24. Nunnally JC. Psychometric theory. 2nd edn. New York:McGraw-Hill Book Co; 1978.
25. Helmstadter GC. Principles of psychological measure-ment. London: Methuen, & Co., Ltd; 1966.
26. Streiner DL, Norman GR. Health measurement scales.Oxford: Oxford University Press; 1989.
27. Marın G, Sabogal F, Vanoos Marın B, Otero-Sabogal R,Perez-Stable EJ. Development of a short acculturationscale for Hispanics. Hisp J Behav Sci 1987;9;183–205.
28. World Health Organization. Oral Health Surveys: BasicMethods. 3rd end. Geneva: WHO; 1987.
29. National Center For Health Statistics. NHANES III oral

Acculturation and dental health
health examination. training manual. Rockville (MD):NCHS; 1987.
30. Goldsmith JM, Dielaman TE, Kirscht JP, Israel BA. Mech-anism of psychological effects on health: the role of socialintegration, coping style and health behavior. HealthEduc Qtrly 1988;15:151–73.
31. Schwarz E, Lo ECM. Dental health knowledge and atti-tudes among the middle-aged and the elderly in HongKong. Community Dent Oral Epidemiol 1994;22:358–63.
32. Spencer AJ, Wright FAC, Brown DF, Hammond RH,Lewis JM. A socio-dental study of adult periodontalhealth; Melbourne, 1985. Community Dental HealthMonograph Series; Number Five. Melbourne: The Uni-versity of Melbourne; 1988.
33. McKenzie DP, McGorry PD, Wallace CS, Low LH, Copo-lov DL, Singh BS. Constructing a minimal diagnostic de-cision tree. Meth Informatic Med 1993; 32: 161–6.
34. Firstmark Technologies. KnowledgeSEEKER User’sGuide. Ottawa: Firstmark Technologies; 1990.
35. Biggs D, DeVille B, Suen E. A Method of choosingmultiway partitions for classification and decision trees.J App Stat 1991;18:49–62.
36. Bureau of Immigration and Population Research. Com-munity Profiles 1991 Census. Vietnamese-born. Canber-ra: Australian Government Publishing Services; 1994.
37. Williams SA, Ahmend IA, Hussain P. Ethnicity, healthand dental care-perspectives among British Asians: 1.Dent Update 1991;18:154–61.
38. Andersen R, Zelman Lewis S, Giachello AL, Aday LA,Chiu G. Access to medical care among the Hispanicpopulation of the Southwestern United States. J HealthSoc Behav 1981;22:78–89.
39. National Health Strategy. Enough to make you sick: howincome and environmental affect health. Research PaperNo. 1. Canberra: Australian Government Publishing Ser-vices; 1992.
40. Bedi R, Uppal RD. The oral health of minority ethnic
119
communities in the United Kingdom. Br Dent J 1995;179:421–5.
41. Neff JA, Hoppe SK. Race/Ethnicity, Acculturation andpsychological distress: fatalism and religiosity as culturalresource. J Comm Psychol 1993;21:3–20.
42. Durward CS, Wright FAC. The dental health in Indo-Chi-nese and Australian-born adolescents. Aust Dent Jour1989;34:233–9.
43. Wright FAC, Spencer AJ. Oral status and service utiliza-tion of 5–6 years old children of migrant parents. J IntAssoc Dent for Children 1980;11:13–8.
44. McAllan LH. A survey of the gingival health of Indo-Chinese child refugees. Part I. Aust Dent J 1988;33:37–42.
45. McAllan LH. A survey of the gingival health of Indo-Chinese child refugees. Part II. Aust Dent J 1988;33:91–5.
46. Durward CS, Wright FAC. Dental knowledge, attitudes,and behaviors of Indochinese and Australian-bornadolescents. Community Dent Oral Epidemiol 1989;17:14–8.
47. Berry JW, Kim U, Minde T, Mok D. Comparative studiesof acculturative stress. Int Migrat Rev 1987;21:491–511.
48. Mavreas V, Bebbington P, Der G. The structure and valid-ity of acculturation. Soc Psychiatry Epidemiol 1989;24:233–40.
49. Cheng LRL. Cultural considerations in the treatment ofcraniofacial malformations in African-Americans. CleftPalate J 1990;27:294–300.
50. Sodowsky GR, Wai Ming Lai E, Plake BS. Moderatingeffects of sociocultural variables on acculturation atti-tudes of Hispanics and Asian-Americans. J Counsel Dev1991;70:194–204.
51. Chesney AP, Chavira JA, Hall RP, Gary HE. Barriers tomedical care of Mexican-Americans: the role of socialclass, acculturation and social isolation. Med Care1982;20 883–91.
Copyright © 2022 FDOKUMEN