
A systematic review of the effectiveness of naltrexone in the maintenance treatment of opioid and...
13
A systematic review of the effectiveness of naltrexone in the maintenance treatment of opioid and alcohol dependence Hendrik G. Roozen a,b, * , Ranne de Waart a , Danielle A.W.M. van der Windt c , Wim van den Brink d,e , Cor A.J. de Jong a,f , Ad J.F.M. Kerkhof b,g a Novadic-Kentron, Network for Addiction Treatment Services, Roosendaal/Sint-Oedenrode, The Netherlands b Department of Clinical Psychology, Vrije Universiteit, Amsterdam, The Netherlands c Institute for Research in Extramural Medicine and Department of General Practice, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands d The Amsterdam Institute for Addiction Research (AIAR), Amsterdam, The Netherlands e Academic Medical Centre (AMC)/University of Amsterdam, The Netherlands f Nijmegen Institute for Scientist-Practitioners in Addiction (NISPA), Nijmegen, The Netherlands g Research Institute Psychology and Health (P&H), Utrecht, The Netherlands Received 15 April 2005; received in revised form 28 October 2005; accepted 4 November 2005 Abstract This systematic review summarises evidence of the effectiveness of naltrexone (NTX) and the added value of psychosocial treatment in the maintenance treatment of opioid and alcohol dependence. Studies were selected through a literature search conducted in March 2004. Seven opioid and seventeen alcohol studies were identified. When possible, meta-(regression) analyses were performed. There is lack of evidence about the effectiveness of NTX in the maintenance treatment of opioid dependence. There is evidence for the effectiveness and applicability of NTX in the management of alcohol dependence. The opioid studies combined NTX with a variety of psychosocial interventions, which plagued the evaluation of their value. Concomitant psychosocial interventions used in the alcohol studies were mainly cognitive behavioural, which seems to be more effective than NTX combined with supportive therapy. Available data do not allow firm conclusions regarding the added effect of psychosocial interventions. However, the 0924-977X/$ - see front matter D 2005 Elsevier B.V. and ECNP. All rights reserved. doi:10.1016/j.euroneuro.2005.11.001 * Corresponding author. Novadic-Kentron, Network for Addiction Treatment Services, Roosendaal, Streuvelslaan 18, 4707 CH Roosendaal, The Netherlands. Tel.: +31 165 597300; fax: +31 165 560375. E-mail address: [email protected] (H.G. Roozen). KEYWORDS Systematic review; Naltrexone; Alcohol; Opioid; Psychosocial treatment; Meta-analysis European Neuropsychopharmacology (2006) 16, 311 — 323 www.elsevier.com/locate/euroneuro
Transcript of A systematic review of the effectiveness of naltrexone in the maintenance treatment of opioid and...
www.e l sev i e r . com/ loca te /eu roneu ro
A systematic review of the effectiveness ofnaltrexone in the maintenance treatmentof opioid and alcohol dependence
Hendrik G. Roozen a,b,*, Ranne de Waart a, Danielle A.W.M. van der Windt c,Wim van den Brink d,e, Cor A.J. de Jong a,f, Ad J.F.M. Kerkhof b,g
a Novadic-Kentron, Network for Addiction Treatment Services, Roosendaal/Sint-Oedenrode, The Netherlandsb Department of Clinical Psychology, Vrije Universiteit, Amsterdam, The Netherlandsc Institute for Research in Extramural Medicine and Department of General Practice, Vrije Universiteit Medical Centre,Amsterdam, The Netherlandsd The Amsterdam Institute for Addiction Research (AIAR), Amsterdam, The Netherlandse Academic Medical Centre (AMC)/University of Amsterdam, The Netherlandsf Nijmegen Institute for Scientist-Practitioners in Addiction (NISPA), Nijmegen, The Netherlandsg Research Institute Psychology and Health (P&H), Utrecht, The Netherlands
Received 15 April 2005; received in revised form 28 October 2005; accepted 4 November 2005
0924-977X/$ - see front matter D 200doi:10.1016/j.euroneuro.2005.11.001
* Corresponding author. Novadic-KenThe Netherlands. Tel.: +31 165 597300
E-mail address: hendrik.roozen@no
KEYWORDSSystematic review;Naltrexone;Alcohol;Opioid;Psychosocialtreatment;Meta-analysis
Abstract This systematic review summarises evidence of the effectiveness of naltrexone(NTX) and the added value of psychosocial treatment in the maintenance treatment of opioidand alcohol dependence.Studies were selected through a literature search conducted in March 2004. Seven opioid and
seventeen alcohol studies were identified. When possible, meta-(regression) analyses wereperformed. There is lack of evidence about the effectiveness of NTX in the maintenancetreatment of opioid dependence. There is evidence for the effectiveness and applicability ofNTX in the management of alcohol dependence. The opioid studies combined NTX with a varietyof psychosocial interventions, which plagued the evaluation of their value. Concomitantpsychosocial interventions used in the alcohol studies were mainly cognitive behavioural, whichseems to be more effective than NTX combined with supportive therapy. Available data do notallow firm conclusions regarding the added effect of psychosocial interventions. However, the
European Neuropsychopharmacology (2006) 16, 311—323
5 Elsevier B.V. and ECNP. All rights reserved.
tron, Network for Addiction Treatment Services, Roosendaal, Streuvelslaan 18, 4707 CH Roosendaal,; fax: +31 165 560375.vadic-kentron.nl (H.G. Roozen).
H.G. Roozen et al.312
data suggest that a combination of naltrexone with cognitive behavioural relapse preventiontherapy is beneficial in alcohol dependent patients.D 2005 Elsevier B.V. and ECNP. All rights reserved.
1. Introduction
Naltrexone (NTX), an opioid antagonist, blocks intrinsicproperties of psychoactive substances that act on the M,K, and D opioid receptor sites by competitive occupation.It is ascertained that alcohol acts on the opioid receptorsites. By blocking these sites, NTX prevents the reinforcingeffects of alcohol consumption (O’Brien et al., 1996). Themetabolic pattern of NTX predominantly involves thereduction of NTX into 6-B-hydroxy naltrexone (6-B-nal-trexol; Wall et al., 1981). The long acting properties ofNTX are mainly due to this metabolite, which has anelimination half-life (T1/2) of approximately 13 h comparedto the parent drug with a T1/2 value of 4 h. The dose-related antagonism on both subjective and objectiveresponses has been subject to some research, althoughthese findings are based on small samples (Resnick et al.,1974; Verebey, 1981). NTX and 6-h-naltrexol are doseproportional (linear increase) in terms of AUC and Cmax
over the range of 50 to 200 mg. A bio-equivalence wasdemonstrated after 100-mg single doses (Meyer et al.,1984). Despite the excellent pharmacological (blocking)properties, in practice NTX treatment is often hamperedby dropout, non-compliance and consequently relapsesinto opioid or alcohol abuse (Rothenberg et al., 2002;Tucker et al., 2004).
However, evidence is scant regarding the questionwhether and which type of psychosocial intervention shouldbe combined with NTX treatment in order to optimise itseffectiveness.
First and foremost, the current study was conducted tounfold and update the effectiveness of NTX. To summarisethe available (recent) evidence on the effectiveness of NTX,in the maintenance treatment of alcohol and opioiddependence, a systematic (meta-analytic) review was con-ducted with the following aims:
1. to study the effects of NTX compared to placebo in themaintenance treatment of opioid and alcohol depen-dence;
2. to study whether combining NTX with psychosocialtreatment is more effective than treatment with NTXalone.
2. Experimental procedures
2.1. Criteria for considering studies for this review
Randomised (placebo) controlled trials (RCTs) and controlledclinical trials (CCTs) with NTX maintenance treatment wereincluded. When group allocation in a trial was determinedrandomly, the study could be labelled as an RCT. If therandomisation procedure was unclear, but considered asrandomised (e.g. double-blind study), the trial was assumedto be a CCT.
RCTs and CCTs had to include participants with alcoholor opiate abuse or dependence (DSM-III-R or DSM-IV)between 18 and 75 years of age. Only RCTs and CCTs inoutpatient settings were included to diminish clinicalheterogeneity. Specific populations (populations such asfederal probationers, prisoners and healthcare profes-sionals) were omitted as the outcomes may be biased.RCTs and CCTs had to report data on at least one of thefollowing outcome measures: (1) relapse rates, withrelapse defined as drinking at least four alcoholic drinksfor women, five for men on an occasion or single day;and (2) (continuous) abstinence, confirmed by urinesamples, blood samples or self-reports. When data oncontinuous abstinence was not available, abstinencepercentage (i.e. the proportion of participants abstinentduring the follow-up period) was included; (3) frequencyof substance abuse (percentage of drinking days or daysusing drugs); (4) time to first relapse and (5) time to firstdrink. It must be noted that relapse is the most sensitiveoutcome measure linked to the assumed mechanisms ofNTX’s action, which is the reduction of the reinforcingpleasure when drinking alcohol (Volpicelli et al., 1997;Littleton and Zieglgansberger, 2003) or when usingopioids.
2.2. Search strategy for identification of studies
Relevant RCTs meeting the inclusion criteria were identifiedby:
1. A computer-aided search using the following data-bases: Pubmed, EMBASE, PsychINFO and the CochraneControlled Trials Register (CCTR). All databases weresearched from the date of commencement. The searchwas conducted in March 2004, using the first twostages of the search strategy recommended in theCochrane Handbook (Appendix V of Section V) andpublished by Alderson et al. (2004). This strategy wasrun in conjunction with combinations of the followingkeywords: naltrexone, alcohol abuse, substance abuse,drug abuse, alcohol(-)related disorder(s), opioid(-)re-lated disorder(s), opiate(-)related disorder(s), alcoholdependence and opioid dependence. Only RCTs thatwere published in the English language were included.
2. Reference checking of identified trials and reviews.
2.3. Methods of the review
Two reviewers (RdW and HGR) independently assessed themethodological quality and extracted the data from theincluded trials. The criteria list for experimental studies(RCTs and CCTs), issued by the Cochrane Drugs andAlcohol Group, was used to assess the methodologicalquality (personal communication, M. Ferri, 2003) The fullcriteria list with operationalisations is available on
NTX’s effectiveness in treatment of opioid and alcohol dependence 313
request from the corresponding author. The guidelines ofthe Cochrane Drug and Alcohol Group consider six criteriaincluding randomisation (range 0—2), allocation conceal-ment (range 0—6), blinding (range 0—3), inclusion of allpatients in the analysis (range 0—3), similarity of baselinecharacteristics (range 0—1) and equal treatment ofgroups (range 0—1). A total score was computed bysumming the scores of all six criteria (range 0—16). Lowquality was defined by a 0—8 score, and high quality by 9(N 50%) or higher.
Statistical pooling was performed for subsets of studiesthat were clinically sufficient homogeneous with respect topopulation, interventions and outcome assessment. Statis-tical heterogeneity was assessed by visually inspectingforest plots, and quantified with the Q-test (v2). Studyresults were considered heterogeneous when p V0.05.Meta-analyses were performed for medium term (N 4 andV 16 weeks) and long term (N 16 and V 32 weeks)treatment effect (Van Tulder et al., 2003, adapted). PooledRisks Differences (RD) were computed for dichotomousoutcomes (relapse rate, abstinence) and Weighted MeanDifferences (WMD) for continuous outcomes (percentagedrinking days per time period, time to first relapse andtime to first drink), along with 95% Confidence Intervals(CI) using the random effects model. For dichotomousoutcomes the number needed to treat (NNT) was alsocomputed.
A qualitative analysis was also performed using a four-level rating system for the strength of the scientificevidence (Van Tulder et al., 2000):
1. Strong evidence—provided by generally consistent find-ings in multiple high quality RCTs.
2. Moderate evidence—provided by generally consistentfindings in one high quality RCT and one or more lowquality RCTs or by generally consistent findings inmultiple low quality RCTs.
3. (A) Limited evidence—only one RCT (either high or lowquality); (B) Conflicting evidence—inconsistent findingsin multiple RCTs.
4. No evidence—no RCTs.
Generally consistent findings were defined as 75% ormore of the studies having statistically significant findings inthe same direction.
Subgroup analyses were carried out to analyse thepotential influence of the type of co-intervention on theefficacy of NTX: individual or group psychotherapy. Meta-regression analysis was used to determine the statisticalsignificance of subgroup effects. Weighted and unweight-ed linear regression analyses were carried out usingindividual RCTs as the unit of analysis (dependentvariable). The inverse of the variance (1/S.E.2) was usedto weigh effect estimates of individual RCTs. The type ofco-intervention was introduced in the model as indepen-dent variable.
To estimate the effect of (non-)compliance on out-come we calculated, where possible, the magnitude ofthe linear relationship between effect size (RD fordichotomous outcomes and WMD for continuous outcomes)and treatment retention by Spearman’s non-parametriccorrelation.
3. Results
3.1. Study selection: NTX in opioid studies
After consulting Pubmed, EMBASE, PsychINFO and CCTR 119,275, 149 and 65 publications, including duplicates, wereidentified respectively. Only seven placebo-controlled trialson maintenance treatment of opioid dependence met theselection criteria and were included in the review (Brahenet al., 1977; Guo et al., 2001; Hollister, 1978; Lerner et al.,1992; Mello et al., 1981; San et al., 1991; Shufman et al.,1994).
3.2. Study selection: NTX in alcohol studies
The search via Pubmed, EMBASE, PsychINFO and CCTRyielded 136, 461, 101 and 165 publications, including dupli-cates, respectively. The first selection was based on titles,keywords and abstracts. Initially, 27 studies were selected.
After reading the full articles, three studies wereexcluded because the studies encompassed experimentssuch as cue reactivity assessment during the study (Montiet al., 1999; Monti et al., 2001; Rohsenow et al., 2000). Onestudy did not report on at least one of the outcome measuresof interest and was therefore excluded (Monterosso et al.,2001). Another study was excluded, because it used aninpatient treatment of 21 days (Knox and Donovan, 1999). Arecent study by Oslin et al. (2003) used participants of threeaggregated studies containing one included study (Kranzleret al., 2000), an excluded study (Monterosso et al., 2001) andunpublished data, and was left out. Furthermore, a studyused a nested sequence of 3 randomised trials and wasexcluded because the first 10 months were not placebo-controlled (O’Malley et al., 2003). Three studies wereexcluded because the studies reported data from an earlierpublished parent trial: Cramer et al. (2003) derived datafrom Krystal et al. (2001), Oslin et al. (2002) used data fromOslin et al. (1997a) and Monterosso et al. (2001); Pettinati etal. (2000) used data from the study of Volpicelli et al. (1992).
Finally, a total of 17 discrete placebo-controlled trials onalcohol dependence were included (Ahmadi and Ahmadi,2002; Anton et al., 1999; Balldin et al., 2003, Chick et al.,2000; Gastpar et al., 2002; Guardia et al., 2002; Heinala etal., 2001; Kiefer et al., 2003; Kranzler et al., 2000; Krystalet al., 2001; Latt et al., 2002; Lee et al., 2001; Morris et al.,2001; O’Malley et al., 1992; Oslin et al., 1997b; Volpicelli etal., 1992, 1997). Furthermore, two follow-up studies wereincluded, Anton et al. (2001), a follow-up study of Anton etal. (1999), and O’Malley et al. (1996), a follow-up study ofO’Malley et al. (1992). The study of O’Malley et al. (1995)was also included, which used data from two trials (O’Malleyet al., 1992; Volpicelli et al., 1992).
3.3. Methodological quality
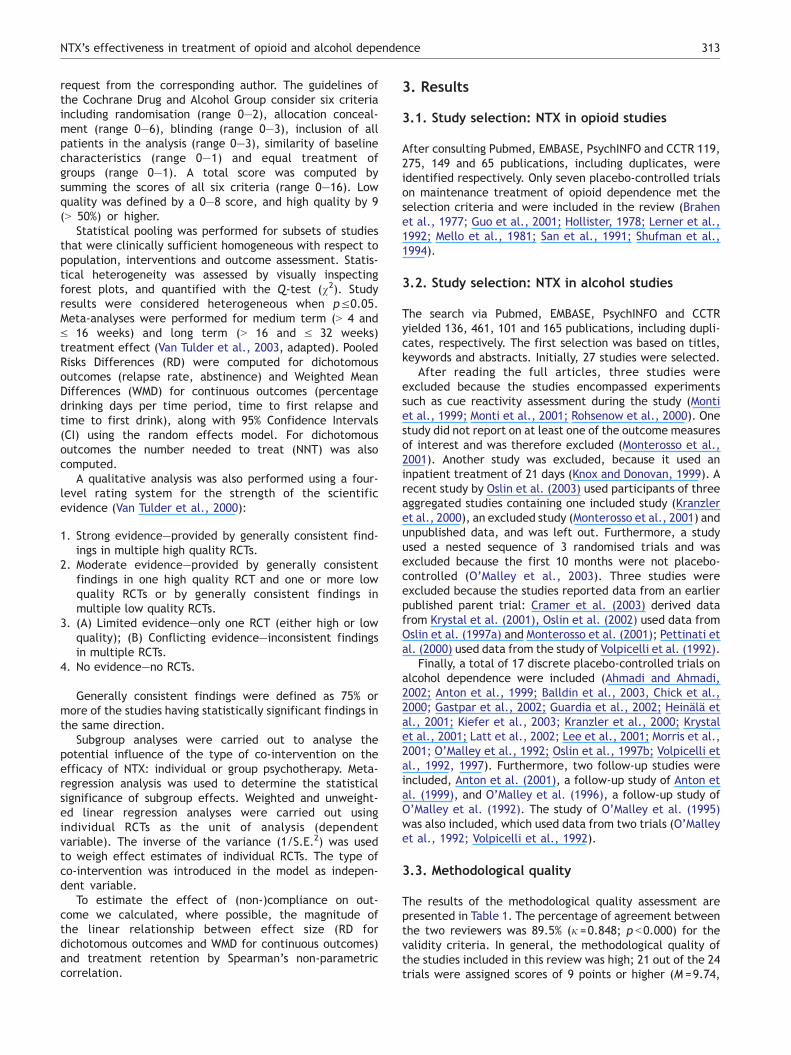
The results of the methodological quality assessment arepresented in Table 1. The percentage of agreement betweenthe two reviewers was 89.5% (j =0.848; p b0.000) for thevalidity criteria. In general, the methodological quality ofthe studies included in this review was high; 21 out of the 24trials were assigned scores of 9 points or higher (M =9.74,
Table 1 Methodological quality assessment of 7 studies inthe treatment of opioid dependence and 17 studies in thetreatment of alcohol dependence
First author, year 1 2 3 4 5.1 5.2 Total
Opioid studiesBrahen et al., 1977 1 3 3 0 0 1 8Guo et al., 2001 2 3 3 0 1 1 10Hollister, 1978 1 3 3 0 0 0 7Lerner et al., 1992 2 3 3 0 0 1 9Mello et al., 1981 1 3 3 2 1 1 11San et al., 1991 1 3 3 0 1 1 9Shufman et al., 1994 1 3 3 0 1 1 9
Alcohol studiesAhmadi and Ahmadi,2002
1 3 3 0 1 1 9
Anton et al., 1999 2 3 3 2 1 1 12Balldin et al., 2003 2 6 3 0 1 0 12Chick et al., 2000 1 3 3 0 1 0 8Gastpar et al., 2002 1 3 3 0 1 1 9Guardia et al., 2002 1 3 3 3 1 1 12Heinala et al., 2001 1 3 3 2 1 0 10Kiefer et al., 2003 2 6 3 0 1 1 13Kranzler et al., 2000 1 3 3 0 1 1 9Krystal et al., 2001 1 3 3 0 1 1 9Latt et al., 2002 2 3 3 0 1 1 10Lee et al., 2001 1 3 3 0 1 1 9Morris et al., 2001 1 3 3 0 1 1 9O’Malley et al., 1992 1 3 3 3 0 1 11Oslin et al., 1997b 1 3 3 0 1 1 9Volpicelli et al., 1992 1 3 3 2 1 1 12Volpicelli et al., 1997 2 6 3 0 1 1 13
The following Cochrane quality criteria were defined: (1)Randomisation (score: 2, 1 or 0); (2) Allocation concealment(score: 6, 3 or 0); (3) Blinding (score: 3, 1 or 0); (4) Inclusion of allpatients in the analysis (score: 3, 2 or 0); (5) Other criteria: (5.1)similarity of the groups at the start of the trial (score: 1 or 0); (5.2)groups were treated equally (aside from the experimentalintervention (score: 1 or 0)). Two follow-up studies (Anton,1996; O’Malley et al., 1996) and the study of O’Malley et al.(1995) were excluded from methodological quality assessment.
H.G. Roozen et al.314
S.D.=1.63, range 7—13). The methodological quality of thealcohol studies was somewhat higher (M =10.00, S.D.=1.69)than the opioid studies (M =9.00, S.D.=1.29), but thisdifference was not statistically significant. Frequentlyencountered problems were a lack of (information about)concealment of the randomisation, and the fact that inmany studies not all patients who were randomised wereincluded in the (ITT) analysis.
3.4. Opioid studies: effectiveness of NTX
The seven studies on opioid dependence showed wideheterogeneity in population, intervention, and outcomeassessment. Therefore statistical pooling was not legiti-mate. Four studies reported on abstinence rates verified byurinalysis (Guo et al., 2001, Lerner et al., 1992, San et al.,1991; Shufman et al., 1994).
On the medium term, two studies reported no statisti-cally significant difference on abstinence between NTX and
placebo (Lerner et al., 1992; San et al., 1991). Two otherstudies reported differences in abstinence rates in favour ofNTX (Guo et al., 2001; Shufman et al., 1994), but in only onetrial this difference was statistically significant (Guo et al.,2001).
Long-term effects of NTX were only reported in twostudies (Guo et al., 2001; San et al., 1991). One studyshowed a statistically significant difference in favour of NTXregarding abstinence rates (Guo et al., 2001). One studyreported no significant difference on the long term (San etal., 1991).
3.5. Opioid studies: compliance of NTX
There was no statistically significant or relevant relationshipbetween the effect size, which was calculated for eachincluded study and treatment retention over the studies.
3.6. Opioid studies: concomitant psychosocialtreatments
The co-interventions in the treatment of opioid dependencewidely varied, which complicated the evaluation of theadditional effect of these co-interventions. In four studiesonly NTX was provided (Brahen et al., 1977; Guo et al.,2001; Hollister, 1978; San et al., 1991). In one study operantanalysis through reinforcement combined with NTX wasanalysed (Mello et al., 1981). In some other studies apsychosocial treatment, such as individual counselling,(supportive) group therapy and behavioural therapy wasprovided as a co-intervention (Lerner et al., 1992; Shufmanet al., 1994). In sum, it was not possible to analyse thebenefits of the included co-interventions for the opioidstudies.
3.7. Alcohol studies: effectiveness of NTX (mediumterm)
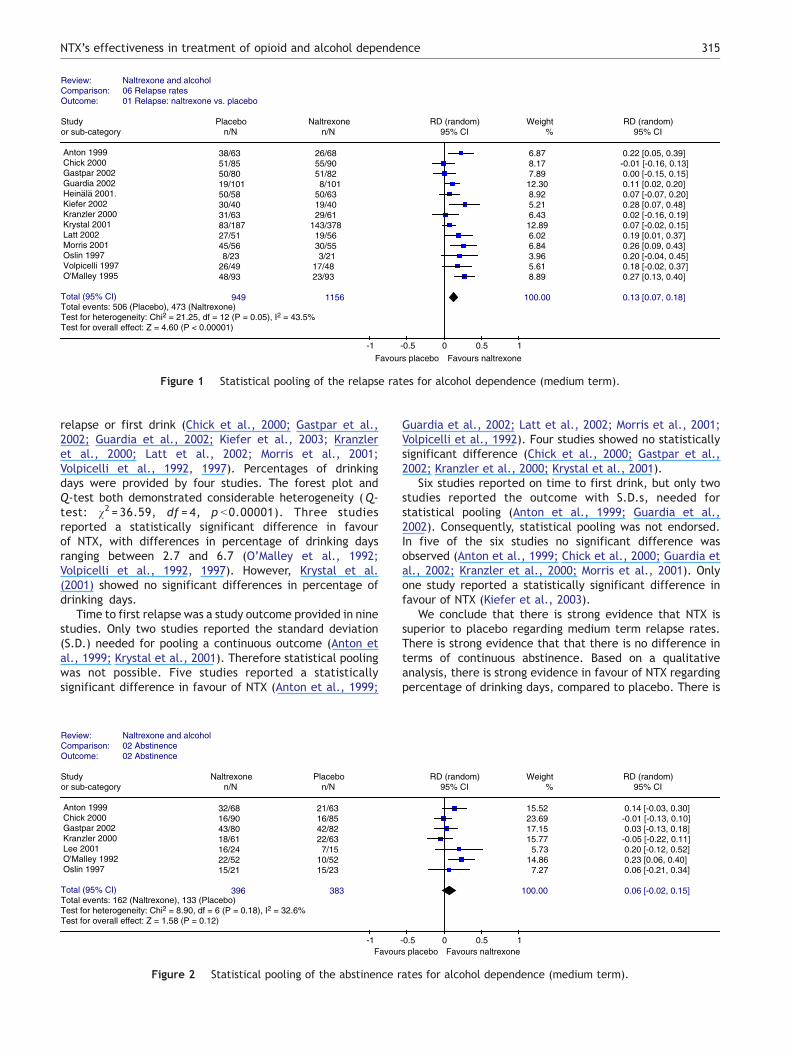
Relapse rates were reported by almost all studies (exceptfor Ahmadi and Ahmadi, 2002; Balldin et al., 2003; Lee etal., 2001). Three studies displayed the relapse rates infigures (Chick et al., 2000; Heinala et al., 2001; Kiefer etal., 2003). These outcome rates were assessed throughgraphical inspections. Fourteen studies provided sufficientdata regarding relapse rates. Studies showed sufficientclinical homogeneity. The Q-test showed statistical hetero-geneity [v2=21.25, df =12, p =0.05 (Fig. 1)], but the forestplot did not show a wide variation in effect sizes andconfidence intervals. Therefore, we calculated an overalleffect estimate. The pooled difference in relapse rate was13% in favour of NTX [(95% CI) 7% to 18%; NNT=8 (Fig. 1)].
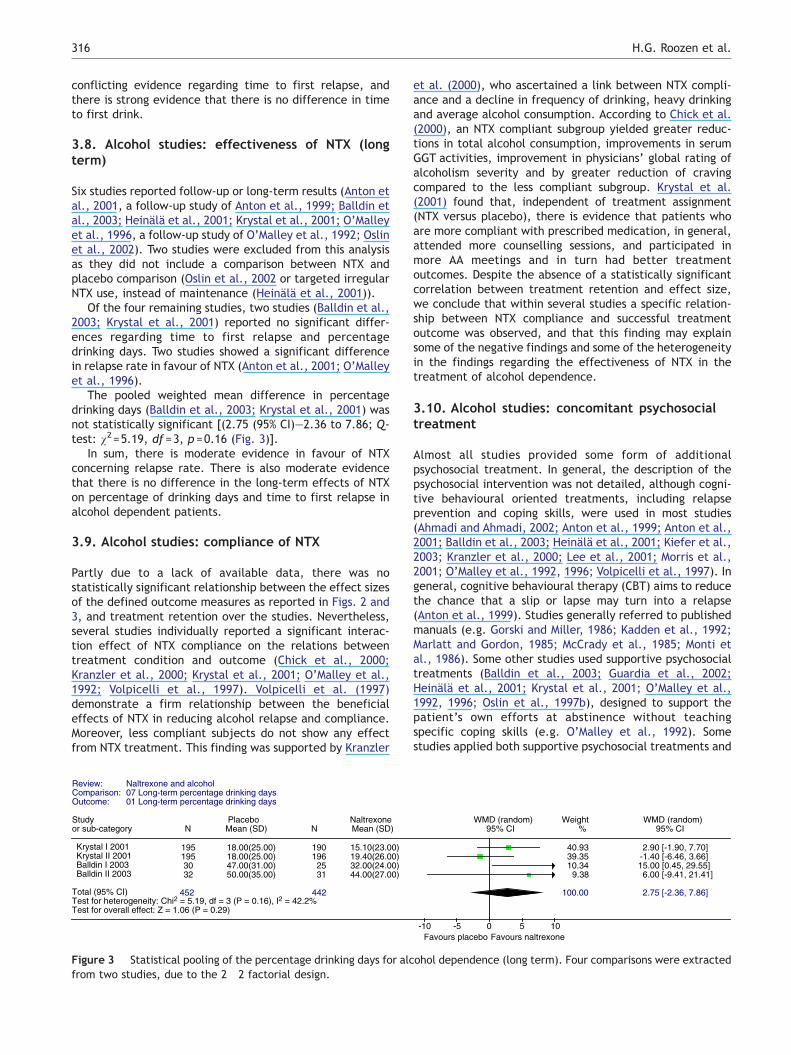
Seven studies reported on continuous abstinence (Antonet al., 1999; Chick et al., 2000; Gastpar et al., 2002;Kranzler et al., 2000; Lee et al., 2001; O’Malley et al., 1992;Oslin et al., 1997a,b). Both the forest plot and Q-testshowed no significant statistical heterogeneity. The pooleddifference in the proportion of participants remainingabstinent was 6% and not significant [(95% CI) � 2% to15%, p =0.12, Q-test: v2=8.90, df =6, p =0.18 (Fig. 2)].
Several studies did not provide the standard deviation(S.D.) on one or more continuous outcome: time to first
Review: Naltrexone and alcoholComparison: 06 Relapse rates Outcome: 01 Relapse: naltrexone vs. placebo
Study Placebo Naltrexone RD (random) Weight RD (random)or sub-category n/N n/N 95% CI % 95% CI
Anton 1999 38/63 26/68 6.87 0.22 [0.05, 0.39] Chick 2000 51/85 55/90 8.17 -0.01 [-0.16, 0.13] Gastpar 2002 50/80 51/82 7.89 0.00 [-0.15, 0.15] Guardia 2002 8/10119/101 12.30 0.11 [0.02, 0.20] Heinala 2001. 50/58 50/63 8.92 0.07 [-0.07, 0.20] Kiefer 2002 30/40 19/40 5.21 0.28 [0.07, 0.48] Kranzler 2000 31/63 29/61 6.43 0.02 [-0.16, 0.19] Krystal 2001 83/187 143/378 12.89 0.07 [-0.02, 0.15] Latt 2002 27/51 19/56 6.02 0.19 [0.01, 0.37] Morris 2001 45/56 30/55 6.84 0.26 [0.09, 0.43] Oslin 1997 8/23 3/21 3.96 0.20 [-0.04, 0.45] Volpicelli 1997 26/49 17/48 5.61 0.18 [-0.02, 0.37] O'Malley 1995 48/93 23/93 8.89 0.27 [0.13, 0.40]
Total (95% CI) 949 1156 100.00 0.13 [0.07, 0.18]Total events: 506 (Placebo), 473 (Naltrexone)Test for heterogeneity: Chi2 = 21.25, df = 12 (P = 0.05), I2 = 43.5%Test for overall effect: Z = 4.60 (P < 0.00001)
-1 -0.5 0 0.5 1
Favours placebo Favours naltrexone
.. ..
Figure 1 Statistical pooling of the relapse rates for alcohol dependence (medium term).
NTX’s effectiveness in treatment of opioid and alcohol dependence 315
relapse or first drink (Chick et al., 2000; Gastpar et al.,2002; Guardia et al., 2002; Kiefer et al., 2003; Kranzleret al., 2000; Latt et al., 2002; Morris et al., 2001;Volpicelli et al., 1992, 1997). Percentages of drinkingdays were provided by four studies. The forest plot andQ-test both demonstrated considerable heterogeneity (Q-test: v2 = 36.59, df = 4, p b0.00001). Three studiesreported a statistically significant difference in favourof NTX, with differences in percentage of drinking daysranging between 2.7 and 6.7 (O’Malley et al., 1992;Volpicelli et al., 1992, 1997). However, Krystal et al.(2001) showed no significant differences in percentage ofdrinking days.
Time to first relapse was a study outcome provided in ninestudies. Only two studies reported the standard deviation(S.D.) needed for pooling a continuous outcome (Anton etal., 1999; Krystal et al., 2001). Therefore statistical poolingwas not possible. Five studies reported a statisticallysignificant difference in favour of NTX (Anton et al., 1999;
Review: Naltrexone and alcoholComparison: 02 Abstinence Outcome: 02 Abstinence
Study Naltrexone Placeboor sub-category n/N n/N
Anton 1999 32/68 21/63 Chick 2000 16/90 16/85 Gastpar 2002 43/80 42/82 Kranzler 2000 18/61 22/63 Lee 2001 16/24 7/15 O'Malley 1992 22/52 10/52 Oslin 1997 15/21 15/23
Total (95% CI) 396 383Total events: 162 (Naltrexone), 133 (Placebo)Test for heterogeneity: Chi2 = 8.90, df = 6 (P = 0.18), I2 = 32.6%Test for overall effect: Z = 1.58 (P = 0.12)
-1 Favour
Figure 2 Statistical pooling of the abstinence r
Guardia et al., 2002; Latt et al., 2002; Morris et al., 2001;Volpicelli et al., 1992). Four studies showed no statisticallysignificant difference (Chick et al., 2000; Gastpar et al.,2002; Kranzler et al., 2000; Krystal et al., 2001).
Six studies reported on time to first drink, but only twostudies reported the outcome with S.D.s, needed forstatistical pooling (Anton et al., 1999; Guardia et al.,2002). Consequently, statistical pooling was not endorsed.In five of the six studies no significant difference wasobserved (Anton et al., 1999; Chick et al., 2000; Guardia etal., 2002; Kranzler et al., 2000; Morris et al., 2001). Onlyone study reported a statistically significant difference infavour of NTX (Kiefer et al., 2003).
We conclude that there is strong evidence that NTX issuperior to placebo regarding medium term relapse rates.There is strong evidence that that there is no difference interms of continuous abstinence. Based on a qualitativeanalysis, there is strong evidence in favour of NTX regardingpercentage of drinking days, compared to placebo. There is
RD (random) Weight RD (random) 95% CI % 95% CI
15.52 0.14 [-0.03, 0.30] 23.69 -0.01 [-0.13, 0.10] 17.15 0.03 [-0.13, 0.18] 15.77 -0.05 [-0.22, 0.11] 5.73 0.20 [-0.12, 0.52]
14.86 0.23 [0.06, 0.40] 7.27 0.06 [-0.21, 0.34]
100.00 0.06 [-0.02, 0.15]
-0.5 0 0.5 1s placebo Favours naltrexone
ates for alcohol dependence (medium term).
H.G. Roozen et al.316
conflicting evidence regarding time to first relapse, andthere is strong evidence that there is no difference in timeto first drink.
3.8. Alcohol studies: effectiveness of NTX (longterm)
Six studies reported follow-up or long-term results (Anton etal., 2001, a follow-up study of Anton et al., 1999; Balldin etal., 2003; Heinala et al., 2001; Krystal et al., 2001; O’Malleyet al., 1996, a follow-up study of O’Malley et al., 1992; Oslinet al., 2002). Two studies were excluded from this analysisas they did not include a comparison between NTX andplacebo comparison (Oslin et al., 2002 or targeted irregularNTX use, instead of maintenance (Heinala et al., 2001)).
Of the four remaining studies, two studies (Balldin et al.,2003; Krystal et al., 2001) reported no significant differ-ences regarding time to first relapse and percentagedrinking days. Two studies showed a significant differencein relapse rate in favour of NTX (Anton et al., 2001; O’Malleyet al., 1996).
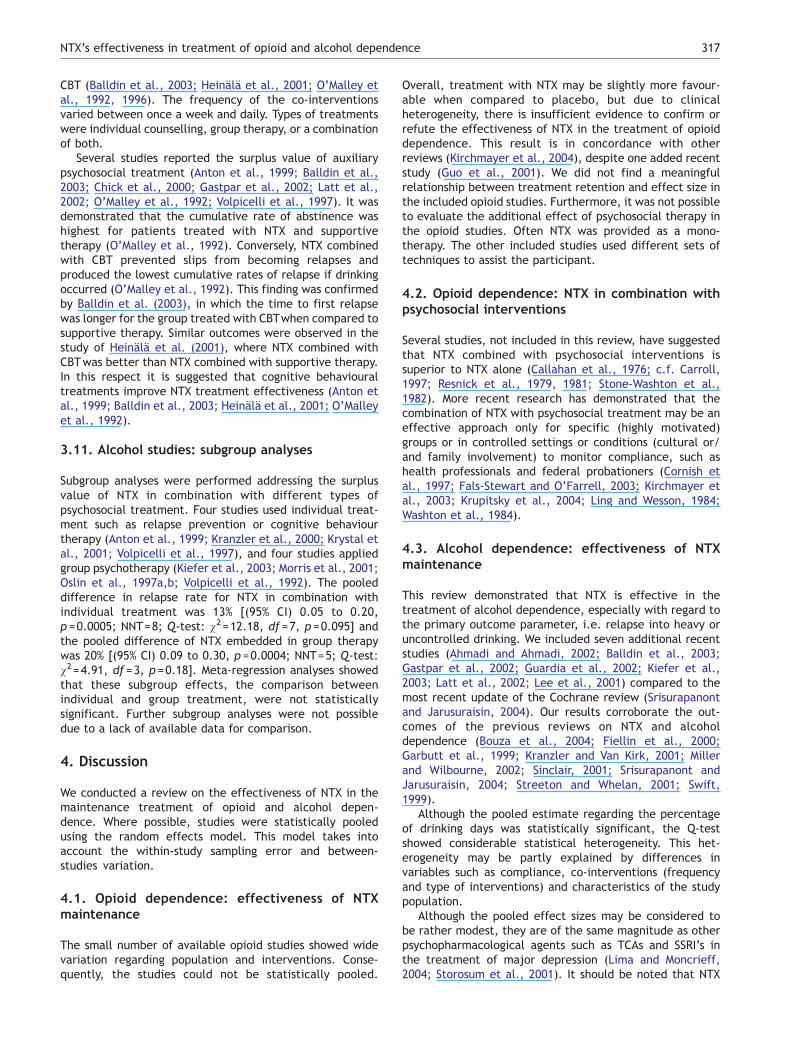
The pooled weighted mean difference in percentagedrinking days (Balldin et al., 2003; Krystal et al., 2001) wasnot statistically significant [(2.75 (95% CI)—2.36 to 7.86; Q-test: v2=5.19, df =3, p =0.16 (Fig. 3)].
In sum, there is moderate evidence in favour of NTXconcerning relapse rate. There is also moderate evidencethat there is no difference in the long-term effects of NTXon percentage of drinking days and time to first relapse inalcohol dependent patients.
3.9. Alcohol studies: compliance of NTX
Partly due to a lack of available data, there was nostatistically significant relationship between the effect sizesof the defined outcome measures as reported in Figs. 2 and3, and treatment retention over the studies. Nevertheless,several studies individually reported a significant interac-tion effect of NTX compliance on the relations betweentreatment condition and outcome (Chick et al., 2000;Kranzler et al., 2000; Krystal et al., 2001; O’Malley et al.,1992; Volpicelli et al., 1997). Volpicelli et al. (1997)demonstrate a firm relationship between the beneficialeffects of NTX in reducing alcohol relapse and compliance.Moreover, less compliant subjects do not show any effectfrom NTX treatment. This finding was supported by Kranzler
Review: Naltrexone and alcoholComparison: 07 Long-term percentage drinking days Outcome: 01 Long-term percentage drinking days
Study Placebo Naltrexoneor sub-category N Mean (SD) N Mean (SD)
Krystal I 2001 195 18.00(25.00) 190 15.10(23.00) Krystal II 2001 195 18.00(25.00) 196 19.40(26.00) Balldin I 2003 30 47.00(31.00) 25 32.00(24.00) Balldin II 2003 32 50.00(35.00) 31 44.00(27.00)
Total (95% CI) 452 442Test for heterogeneity: Chi2 = 5.19, df = 3 (P = 0.16), I2 = 42.2%Test for overall effect: Z = 1.06 (P = 0.29)
Figure 3 Statistical pooling of the percentage drinking days for alcfrom two studies, due to the 2�2 factorial design.
et al. (2000), who ascertained a link between NTX compli-ance and a decline in frequency of drinking, heavy drinkingand average alcohol consumption. According to Chick et al.(2000), an NTX compliant subgroup yielded greater reduc-tions in total alcohol consumption, improvements in serumGGT activities, improvement in physicians’ global rating ofalcoholism severity and by greater reduction of cravingcompared to the less compliant subgroup. Krystal et al.(2001) found that, independent of treatment assignment(NTX versus placebo), there is evidence that patients whoare more compliant with prescribed medication, in general,attended more counselling sessions, and participated inmore AA meetings and in turn had better treatmentoutcomes. Despite the absence of a statistically significantcorrelation between treatment retention and effect size,we conclude that within several studies a specific relation-ship between NTX compliance and successful treatmentoutcome was observed, and that this finding may explainsome of the negative findings and some of the heterogeneityin the findings regarding the effectiveness of NTX in thetreatment of alcohol dependence.
3.10. Alcohol studies: concomitant psychosocialtreatment
Almost all studies provided some form of additionalpsychosocial treatment. In general, the description of thepsychosocial intervention was not detailed, although cogni-tive behavioural oriented treatments, including relapseprevention and coping skills, were used in most studies(Ahmadi and Ahmadi, 2002; Anton et al., 1999; Anton et al.,2001; Balldin et al., 2003; Heinala et al., 2001; Kiefer et al.,2003; Kranzler et al., 2000; Lee et al., 2001; Morris et al.,2001; O’Malley et al., 1992, 1996; Volpicelli et al., 1997). Ingeneral, cognitive behavioural therapy (CBT) aims to reducethe chance that a slip or lapse may turn into a relapse(Anton et al., 1999). Studies generally referred to publishedmanuals (e.g. Gorski and Miller, 1986; Kadden et al., 1992;Marlatt and Gordon, 1985; McCrady et al., 1985; Monti etal., 1986). Some other studies used supportive psychosocialtreatments (Balldin et al., 2003; Guardia et al., 2002;Heinala et al., 2001; Krystal et al., 2001; O’Malley et al.,1992, 1996; Oslin et al., 1997b), designed to support thepatient’s own efforts at abstinence without teachingspecific coping skills (e.g. O’Malley et al., 1992). Somestudies applied both supportive psychosocial treatments and
WMD (random) Weight WMD (random) 95% CI % 95% CI
40.93 2.90 [-1.90, 7.70] 39.35 -1.40 [-6.46, 3.66] 10.34 15.00 [0.45, 29.55] 9.38 6.00 [-9.41, 21.41]
100.00 2.75 [-2.36, 7.86]
-10 -5 0 5 10 Favours placebo Favours naltrexone
ohol dependence (long term). Four comparisons were extracted
NTX’s effectiveness in treatment of opioid and alcohol dependence 317
CBT (Balldin et al., 2003; Heinala et al., 2001; O’Malley etal., 1992, 1996). The frequency of the co-interventionsvaried between once a week and daily. Types of treatmentswere individual counselling, group therapy, or a combinationof both.
Several studies reported the surplus value of auxiliarypsychosocial treatment (Anton et al., 1999; Balldin et al.,2003; Chick et al., 2000; Gastpar et al., 2002; Latt et al.,2002; O’Malley et al., 1992; Volpicelli et al., 1997). It wasdemonstrated that the cumulative rate of abstinence washighest for patients treated with NTX and supportivetherapy (O’Malley et al., 1992). Conversely, NTX combinedwith CBT prevented slips from becoming relapses andproduced the lowest cumulative rates of relapse if drinkingoccurred (O’Malley et al., 1992). This finding was confirmedby Balldin et al. (2003), in which the time to first relapsewas longer for the group treated with CBTwhen compared tosupportive therapy. Similar outcomes were observed in thestudy of Heinala et al. (2001), where NTX combined withCBTwas better than NTX combined with supportive therapy.In this respect it is suggested that cognitive behaviouraltreatments improve NTX treatment effectiveness (Anton etal., 1999; Balldin et al., 2003; Heinala et al., 2001; O’Malleyet al., 1992).
3.11. Alcohol studies: subgroup analyses
Subgroup analyses were performed addressing the surplusvalue of NTX in combination with different types ofpsychosocial treatment. Four studies used individual treat-ment such as relapse prevention or cognitive behaviourtherapy (Anton et al., 1999; Kranzler et al., 2000; Krystal etal., 2001; Volpicelli et al., 1997), and four studies appliedgroup psychotherapy (Kiefer et al., 2003; Morris et al., 2001;Oslin et al., 1997a,b; Volpicelli et al., 1992). The pooleddifference in relapse rate for NTX in combination withindividual treatment was 13% [(95% CI) 0.05 to 0.20,p =0.0005; NNT=8; Q-test: v2=12.18, df =7, p =0.095] andthe pooled difference of NTX embedded in group therapywas 20% [(95% CI) 0.09 to 0.30, p =0.0004; NNT=5; Q-test:v2=4.91, df =3, p =0.18]. Meta-regression analyses showedthat these subgroup effects, the comparison betweenindividual and group treatment, were not statisticallysignificant. Further subgroup analyses were not possibledue to a lack of available data for comparison.
4. Discussion
We conducted a review on the effectiveness of NTX in themaintenance treatment of opioid and alcohol depen-dence. Where possible, studies were statistically pooledusing the random effects model. This model takes intoaccount the within-study sampling error and between-studies variation.
4.1. Opioid dependence: effectiveness of NTXmaintenance
The small number of available opioid studies showed widevariation regarding population and interventions. Conse-quently, the studies could not be statistically pooled.
Overall, treatment with NTX may be slightly more favour-able when compared to placebo, but due to clinicalheterogeneity, there is insufficient evidence to confirm orrefute the effectiveness of NTX in the treatment of opioiddependence. This result is in concordance with otherreviews (Kirchmayer et al., 2004), despite one added recentstudy (Guo et al., 2001). We did not find a meaningfulrelationship between treatment retention and effect size inthe included opioid studies. Furthermore, it was not possibleto evaluate the additional effect of psychosocial therapy inthe opioid studies. Often NTX was provided as a mono-therapy. The other included studies used different sets oftechniques to assist the participant.
4.2. Opioid dependence: NTX in combination withpsychosocial interventions
Several studies, not included in this review, have suggestedthat NTX combined with psychosocial interventions issuperior to NTX alone (Callahan et al., 1976; c.f. Carroll,1997; Resnick et al., 1979, 1981; Stone-Washton et al.,1982). More recent research has demonstrated that thecombination of NTX with psychosocial treatment may be aneffective approach only for specific (highly motivated)groups or in controlled settings or conditions (cultural or/and family involvement) to monitor compliance, such ashealth professionals and federal probationers (Cornish etal., 1997; Fals-Stewart and O’Farrell, 2003; Kirchmayer etal., 2003; Krupitsky et al., 2004; Ling and Wesson, 1984;Washton et al., 1984).
4.3. Alcohol dependence: effectiveness of NTXmaintenance
This review demonstrated that NTX is effective in thetreatment of alcohol dependence, especially with regard tothe primary outcome parameter, i.e. relapse into heavy oruncontrolled drinking. We included seven additional recentstudies (Ahmadi and Ahmadi, 2002; Balldin et al., 2003;Gastpar et al., 2002; Guardia et al., 2002; Kiefer et al.,2003; Latt et al., 2002; Lee et al., 2001) compared to themost recent update of the Cochrane review (Srisurapanontand Jarusuraisin, 2004). Our results corroborate the out-comes of the previous reviews on NTX and alcoholdependence (Bouza et al., 2004; Fiellin et al., 2000;Garbutt et al., 1999; Kranzler and Van Kirk, 2001; Millerand Wilbourne, 2002; Sinclair, 2001; Srisurapanont andJarusuraisin, 2004; Streeton and Whelan, 2001; Swift,1999).
Although the pooled estimate regarding the percentageof drinking days was statistically significant, the Q-testshowed considerable statistical heterogeneity. This het-erogeneity may be partly explained by differences invariables such as compliance, co-interventions (frequencyand type of interventions) and characteristics of the studypopulation.
Although the pooled effect sizes may be considered tobe rather modest, they are of the same magnitude as otherpsychopharmacological agents such as TCAs and SSRI’s inthe treatment of major depression (Lima and Moncrieff,2004; Storosum et al., 2001). It should be noted that NTX

H.G. Roozen et al.318
studies in alcohol dependent patients were virtually allsupported by non-pharmaceutical sources and thus have asmaller likelihood of selective publication of only positivestudies.
4.4. Compliance with NTX treatment
To evaluate compliance, we estimated the relationshipbetween effect size and treatment retention. In general,studies reported on treatment retention and not directly onNTX compliance. In addition, the studies that did report onNTX compliance used a wide variety of methods to measurecompliance, such as pill-count, the inclusion of riboflavin inNTX capsules, and self-reports. Furthermore, the reportedcompliance rates were measured at different follow-upperiods and using different statistical methods.
Analyses of compliance measured, as the relationshipbetween treatment retention and effect size, yielded nopositive results. These negative findings may be due todaggregation biasT or decological fallacyT (Morgenstern,1982), as the relationship with participant averages acrosstrials may deviate from the relationship for participantswithin trials, and without individual data cannot beinvestigated (Thompson and Higgins, 2002). Indeed, severalindividual studies did report statistically significant findings(Chick et al., 2000; Kranzler et al., 2000; Krystal et al.,2001; O’Malley et al., 1992; Volpicelli et al., 1997).Consequently, we conclude that NTX compliance probablyis pivotal for successful alcohol treatment. It should benoted, however, that the relationship between complianceand outcome might be confounded by baseline differencesbetween compliant and non-compliant patients.
4.5. NTX in combination with psychosocialinterventions in alcohol treatment
It is suggested that there is added value of auxiliarypsychosocial treatment, and therefore NTX treatmentsshould be delivered in concert with psychosocial interven-tions (Srisurapanont and Jarusuraisin, 2004). Nearly allstudies on NTX embedded NTX in a cognitive-behaviouraloriented program. A systematic exploration of the influenceof psychosocial co-intervention was hindered by sketchydescriptions of these treatments. Consequently, the contentof CBT and supportive therapy was often unclear. Neverthe-less, based on the current data, there is some evidence thatthe combination of NTX with CBT is somewhat moreeffective than NTX combined with supportive therapy. NTXand CBT both target to prevent slips from becoming relapsesand therefore might have synergistic effects, but it is notpossible to draw firm conclusions on the possible auxiliarybenefits of these psychosocial interventions.
Nowadays, cognitive-behavioural interventions, such asteaching coping skills and relapse prevention are consideredas top-ranked treatment modalities (Miller and Wilbourne,2002). It should be noted, however, that some groups, suchas older adults, appear to respond well to a medicallyoriented program that is rather supportive and individua-lised (Oslin et al., 2002).
Subgroup analyses suggested a difference in effect infavour of NTX when combined with group therapy. The
difference between group therapy and individual or othertreatment was, however, not statistically significant. Themeta-regression analysis was hindered by the lack ofstatistical power (only four studies per subgroup).
4.6. Long-term effects of NTX
In general, the studies reported on the medium-term effects(i.e. 12—13 weeks) of NTX. Evaluations of placebo controlledNTX maintenance programs on the long term are ratherscant, especially for opioid studies. Due to insufficient data,no firm conclusions can be drawn with regard to the effectsof NTX after discontinuation. However, it is tempting toargue that NTX, just like other medications such asantipsychotics and antihypertensives, does not foster sus-tained remission after discontinuation, as chronic disordersneed continuous treatment (McLellan, 2002). This wouldsuggest that NTX should be prescribed over a long period oftime.
4.7. Methodological quality
In general, the methodological quality of the includedstudies just exceeded the threshold of 50% (N 8). In moststudies the scores regarding methodological quality weresuppressed due to inadequate description of randomisation,intention-to-treat analysis, and allocation concealmentcriteria. Furthermore, many studies showed dropout rates,which exceeded the threshold of 20%. The loss to follow-upand the high dropout rates (attrition bias) produce asubstantial problem, as retention itself is often one of theprimary outcomes.
All included opioid studies fulfilled the criterion of anadequate blinding. It should be noted, however, thatblinding of patients in an opioid NTX-placebo trial is virtuallyimpossible. Participants can easily trace their allocatedcondition by a heroin challenge test. NTX was approved bythe FDA based on its pharmacological efficacy without anypositive double-blind studies because of the above-men-tioned blinding problems. A third condition (no treatment)can be added to resolve some of the methodological issue.
4.8. Limitations of this review
This review has a few important limitations. We did notconsult the authors to receive either additional informationon methodological aspects of their study, or additional(statistical) information when it was not reported in theirstudies. Supplementary information on methodologicalassessment might have resulted in (slightly) higher methodscores. The number of studies that provided statistical dataneeded to perform quantitative analyses limited the actualperformed analyses, as we had to eliminate several studiesfrom the meta-analyses due to a lack of available data orbecause the standard deviations (S.D.s) were not provided.Therefore, the results might be slightly skewed and thismight attenuate the validity of the conclusions.
In general, the performed meta-analyses were based onintention to treat (ITT) analyses, although several studiesdid not report ITT data suitable to conduct statisticalanalyses. We often chose to extract reported outcomes
NTX’s effectiveness in treatment of opioid and alcohol dependence 319
based on smaller sample sizes than the initial number ofrandomised participants (Chick et al., 2000; Gastpar et al.,2002; Guardia et al., 2002; Krystal et al., 2001). This mighthave resulted in improved outcomes in favour of NTX. Dueto inclusion of other studies in the analyses this limitationis not substantial and probably does not affect theconclusions.
4.9. Safety of NTX
Exploring the literature, we encountered several publica-tions dealing with safety issues, which may be important foruse of NTX in regular clinical practice. There are threeremarks to make.
It must be noted that NTX itself has virtually no abusepotentials and is not characterised by tolerance. It has beenargued that NTX has the capacity to produce dose relatedhepatocellular injury. Nevertheless, there is virtually noevidence that NTX causes clinically significant liver diseaseor exacerbates, even at high doses, serious pre-existing liverdisease (Brewer and Wong, 2004).
Currently, there are some reports of serious adverseevents and even deaths, which are attributed to rapiddetoxification procedures (Dyer, 1998; Kaye et al., 2003;Pfab et al., 1999; Roozen et al., 2002; San et al., 1995).It is important to note that NTX has no approval for rapidopioid detoxification in the US and EC, though it has beenused for that purpose. The method is surrounded with avariety of opinions, as there is lack of agreement aboutthe treatment and evidence on the long term (Singh andBasu, 2004).
Warnings have been issued regarding the overdose riskfollowing NTX discontinuation in the treatment of opioiddependent patients. Receptor hypersensitivity followed bytolerance reduction could increase the risk of a fatalheroin overdose (Lesscher et al., 2003). However, aretrospective study showed no significant difference inoverdose deaths between a naltrexone-exposed and anon-exposed group of deaths (Arnold-Reed et al., 2003).Conversely, a recent large longitudinal study, based ondata from 12 trials, ascertained that individuals wholeave pharmacotherapies for opioid dependence experi-ence higher overdose and death rates compared withthose in treatment. Accordingly, naltrexone treatmentpatients should be warned about heroin overdose risks(Digiusto et al., 2004; Ritter, 2002).
4.10. Options to increase the effectiveness of NTX
Several strategies and hypotheses have been brought up inthe literature, in which NTX compliance is subject ofdebate. Recently, Weiss (2004) suggested three strategiesto improve the effectiveness of pharmacotherapy in thetreatment of patients with alcohol and drug dependence:(1) interventions that can be used by the clinician inindividual sessions, (2) the inclusion of external reinforce-ments (positive and negative contingencies) and involve-ment of family members or significant others and (3)medication prescribing and dosing strategies.
Individual sessions should focus on a collaborativeapproach to create a treatment plan that addresses the
cost/benefit ratio of improved outcome by NTX. Patientswho are adherent are considered as acting on a consensualagreed-upon plan that they have had a part in designing, orat least as accepting the importance of performing therecommended treatment actions (DiMatteo and DiNicola,1982). In this respect interventions aimed at enhancingmedication adherence should specifically target thepatient’s beliefs and attitudes concerning the illness andmedication and should not be in conflict with subjects’personal goals (Patel and David, 2004).
A second option concerns the inclusion of externalreinforcements. Linked to the Community ReinforcementApproach (CRA), an adjunctive instructional program forimproving compliance can be used (Azrin and Teichner,1998). It can be employed to encourage taking NTX undersupervision (of significant others) to increase treatmentadherence (Meyers and Smith, 1995; Roozen et al., 2003). Inaddition, Contingency Management (CM; Higgins et al.,2004) can enhance compliance and increase the effective-ness of NTX (Carroll et al., 2001; Carroll et al., 2002; Prestonet al., 1999). Both CRA and CM are based on the learningtheory derived from the operant reinforcement approachdesignated by Skinner (1938). NTX fits well in this frame-work as NTX directly competes with positive reinforcementinduced by the use of opioids and alcohol.
A third opportunity is aimed to increase the likelihood oftaking NTX. bPill-countQ or medication usage skills foreffectiveness program (e.g. MUSE-P) can improve medica-tion compliance through a feedback system. Feedback isgiven by medication bottles with micro-electronic monitorcaps that record the date and time of each opening anddisplay the number of hours passed since the previousopening (Cramer, 1998; Cramer and Rosenheck, 1999). Apharmacological route, as a dosing strategy, to governadequate plasma concentrations of NTX seems to be theinsertion of NTX implants or depots (Carreno et al., 2003;Foster et al., 2003; Garbutt et al., 2005; Kranzler et al.,2004) to treat both alcohol and opioid use disorders.
4.11. Predictors of NTX’s effectiveness
Recently, there is an increase in interest to predict theeffectiveness of NTX, which is important to explain thevariability in outcome in the current literature. It isascertained that genetic polymorphism programming thel-opioid receptor might play a pharmacogenetic role in thedifferential response to an antagonist (Oslin et al., 2003,Oswald et al., 2004). Other alcohol studies on predictors ofclinical effectiveness of NTX suggest that participants withan older age, high levels of alcohol craving, a strong familyhistory of alcohol use disorders, high levels of somaticdistress, and low educational level are more likely to benefit(e.g. Flannery et al., 2003; O’Malley et al., 1996; Oslin etal., 2002; Monterosso et al., 2001; Volpicelli et al., 1995).
Studies on opioids showed that young participants, a lowlevel of dependence, employment, being married, andlength of NTX therapy were related to better outcome(Greenstein et al., 1983; McGregor et al., 2002). A highscore on cluster-B personality disorders and polydrug use isassociated with relapse in NTX opioid treatment (Roozen etal., 2003).
H.G. Roozen et al.320
4.12. Conclusions and recommendations for futureresearch
We conclude that NTX, at least based on the pharmacolog-ical profile, is a viable agent in substance use disordersincluding opioids and alcohol. Blinding problems in theclassic way and insufficient data afflict the assessment ofeffectiveness in opioid dependence. Therefore, up to now,there is insufficient evidence to support maintenancetreatment in opioid dependent patients. In contrast, thisreview confirms the effectiveness of NTX in the mainte-nance treatment of alcohol dependence.
In general practice, it is crucial that patients take NTXas prescribed in order to control safety issues and toevaluate the effectiveness of NTX, properly. Therefore it iswarranted to pursue avenues of research to preventdropout and to ameliorate treatment compliance. Futurestudies on both alcohol and opioid disorders ought to seekthe identification of the cognitive-motivational rationale(adherence) concerning the NTX treatment regimen. Incombination with reports on side effects, craving andurinalyses on both NTX and its active metabolite (i.e. 6-b-naltrexol) related to alcohol consumption or opioidmetabolites (i.e. 6-monoacetylmorphine) may providemore awareness into the potential mechanisms of actionof NTX, in terms of discontinuation, relapse, and resumingalcohol or opioid use.
More RCTs with longer treatments are recommended,particularly because addiction is viewed as a chronicrelapsing disease (Leshner, 1997; McLellan, 2002; Van denBrink and van Ree, 2003). Finally, to gain more informationon the effects of NTX after discontinuation longer follow-upperiods are needed.
References
Ahmadi, J., Ahmadi, N., 2002. A double blind placebo-controlledstudy of naltrexone in the treatment of alcohol dependence.German J. Psychiatry 5 (4), 85–89.
Alderson, P., Green, S., Higgins, J.P.T. (Eds.), 2004. MEDLINE highlysensitive search strategies for identifying reports of randomizedcontrolled trials in MEDLINE, Cochrane Reviewers’ Handbook4.2.2 [updated March 2004]; Appendix 5b, The Cochrane Library,Issue 3. John Wiley and Sons, Ltd., Chichester, UK.
Anton, R.F., 1996. New methodologies for pharmacological treat-ment trials for alcohol dependence. Alcohol., Clin. Exp. Res. 20,3A–9A (Suppl.).
Anton, R.F., Moak, D.H., Waid, L.R., Latham, P., Malcolm, R.J., Dias,J.K., 1999. Naltrexone and cognitive behavioral therapy for thetreatment of outpatient alcoholics, results of a placebo-con-trolled trial. Am. J. Psychiatry 156 (11), 1758–1764.
Anton, R.F., Moak, D.H., Latham, P.K., Waid, L.R., Malcolm, R.J.,Dias, J., Roberts, J.S., 2001. Posttreatment results of combiningnaltrexone with cognitive-behavior therapy for the treatment ofalcoholism. J. Clin. Psychopharmacol. 21 (1), 72–77.
Arnold-Reed, D.E., Hulse, G.K., Hansson, R.C., Murray, S.D., O’Neil,G., Basso, M.R., Holman, C.D., 2003. Blood morphine levels innaltrexone-exposed compared to non-naltrexone-exposed fatalheroin overdoses. Addict. Biol. 8 (3), 343–350.
Azrin, N.H., Teichner, G., 1998. Evaluation of an instructionalprogram for improving medication compliance for chronicallymentally ill outpatients. Behav. Res. Ther. 36 (9), 849–861.
Balldin, J., Berglund, M., Borg, S., Mansson, M., Bendtsen, P.,Franck, J., et al., 2003. A 6-month controlled naltrexone study,combined effect with cognitive behavioral therapy in outpatienttreatment of alcohol dependence. Alcohol., Clin. Exp. Res. 27(7), 1142–1149.
Bouza, C., Angeles, M., Ana, M., Maria, A.J., 2004. Efficacy andsafety of naltrexone and acamprosate in the treatment of alcoholdependence: a systematic review. Addiction 99 (7), 811–828.
Brahen, L.S., Capone, T.,Wiechert, V., Desiderio, D., 1977. Naltrexoneand cyclazocine. Arch. Gen. Psychiatry 34, 1181–1184.
Brewer, C., Wong, V.S., 2004. Naltrexone: report of lack ofhepatotoxicity in acute viral hepatitis, with a review of theliterature. Addict. Biol. 9 (1), 81–87.
Callahan, E., Rawson, R., Glazer, M., McCleave, B., Arias, R., 1976.Comparison of two naltrexone treatment programs: naltrexonealone versus naltrexone plus behavior therapy. NIDA Res. Monogr.9, 150–157.
Carreno, J.E., Alvarez, C.E., Narciso, G.I., Bascaran, M.T., Diaz, M.,Bobes, J., 2003. Maintenance treatment with depot opioidantagonists in subcutaneous implants: an alternative in thetreatment of opioid dependence. Addict. Biol. 8 (4), 429–438.
Carroll, K.M., 1997. Integrating psychotherapy and pharmacother-apy to improve drug abuse outcomes. Addict. Behav. 22 (2),233–245.
Carroll, K.M., Ball, S.A., Nich, C., O’Connor, P.G., Eagan, D.A.,Frankforter, T.L., et al., 2001. Targeting behavioral therapies toenhance naltrexone treatment of opioid dependence: efficacy ofcontingency management and significant other involvement.Arch. Gen. Psychiatry 58 (8), 755–761.
Carroll, K.M., Sinha, R., Nich, C., Babuscio, T., Rounsaville, B.J., 2002.Contingency management to enhance naltrexone treatment ofopioid dependence: a randomized clinical trial of reinforcementmagnitude. Exp. Clin. Psychopharmacol. 10 (1), 54–63.
Chick, J., Anton, R., Checinski, K., Croop, R., Drummond, D.C.,Farmer, R., et al., 2000. A multicentre randomized double-blindplacebo controlled trial of naltrexone in the treatment ofalcohol dependence or abuse. Alcohol Alcohol. 35 (6), 587–593.
Cornish, J.W., Metzger, D., Woody, G.E., Wilson, D., McLellan, A.T.,Vandergrift, B., OTBrien, C.P., 1997. Naltrexone pharmacother-apy for opioid dependent federal probationers. J. Subst. AbuseTreat. 14 (6), 529–534.
Cramer, J., 1998. Medication use by the elderly: enhancing patientcompliance in the elderly Role of packaging aids and monitoring.Drugs Aging 12, 7–15.
Cramer, J., Rosenheck, R., 1999. Enhancing medication compliancefor people with serious mental illness. J. Nervous Mental Dis.187, 52–54.
Cramer, J., Rosenheck, R., Kirk, G., Krol, W., Krystal, J., 2003.Medication compliance feedback and monitoring in a clinicaltrial: predictors and outcomes. Value Health 6 (5), 566–573.
Digiusto, E., Shakeshaft, A., Ritter, A., O’Brien, S., The NEPODResearch Group, 2004. Serious adverse events in the AustralianNational Evaluation of Pharmacotherapies for Opioid Depen-dence (NEPOD). Addiction 99 (4), 450–460.
DiMatteo, M.R., DiNicola, D.D., 1982. Achieving Patient Compliance:The Psychology of Medical Practitioner’s Role. Pergamon Press,New York.
Dyer, C., 1998. Addict died after rapid opiate detoxification. BMJ316, 170.
Fals-Stewart, W., O’Farrell, T.J., 2003. Behavioral family counselingand naltrexone for male opioid-dependent patients. J. Consult.Clin. Psychol. 71 (3), 432–442.
Fiellin, D.A., Carrington Reid, M., O’Connor, P.G., 2000. Newtherapies for alcohol problems: application to primary care.Am. J. Med. 108 (3), 227–237.
Flannery, B.A., Poole, S.A., Gallop, R.J., Volpicelli, J.R., 2003.Alcohol craving predicts drinking during treatment: an
NTX’s effectiveness in treatment of opioid and alcohol dependence 321
analysis of three assessment instruments. J. Stud. Alcohol 64(1), 120–126.
Foster, J., Brewer, C., Steele, T., 2003. Naltrexone implants cancompletely prevent early (1-month) relapse after opiate detox-ification: a pilot study of two cohorts totalling 101 patients witha note on naltrexone blood levels. Addict. Biol. 8 (2), 211–217.
Garbutt, J.U.C., West, S.L., Carey, T.S., Lohr, K.N., Crews, F.T.,1999. Pharmacological treatment of alcohol dependence. JAMA281 (14), 1318–1325.
Garbutt, J.C., Kranzler, H.R., O’Malley, S.S., Gastfriend, D.R.,Pettinati, H.M., Silverman, B.L., Loewy, J.W., Ehrich, E.W.,Vivitrex Study Group, 2005. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence: a random-ized controlled trial. JAMA 293, 1617–1625.
Gastpar, M., Bonnet, U., Boning, J., Mann, K., Schmidt, L.G.,Soyka, M., et al., 2002. Lack of efficacy of naltrexone in theprevention of alcohol relapse: results from a German multi-center study. J. Clin. Psychopharmacol. 22 (6), 92–98.
Gorski, T.T., Miller, M.M., 1986. Staying Sober: Guide to RelapsePrevention. Herald House, Independence Mo.
Greenstein, R.A., Evans, B.D., McLellan, A.T., O’Brien, C.P., 1983.Predictors of favorable outcome following naltrexone treat-ment. Drug Alcohol Depend. 12 (2), 173–180.
Guardia, J., Caso, C., Arias, F., Gual, A., Sanahuja, J., Ramirez, M.,et al., 2002. A double-blind placebo-controlled study ofnaltrexone in the treatment of alcohol-dependence disorder:results from a multicenter clinical trial. Alcohol., Clin. Exp. Res.26 (9), 1381–1387.
Guo, S., Jiang, Z., Wu, Y., 2001. Effectiveness of naltrexonehydrochloride for preventing relapse among opiate-dependentpatients after detoxification. Hong Kong J. Psychiatry 11 (4),20–28.
Heinala, P., Alho, H., Kiianmaa, K., Lonnqvist, J., Kuoppasalmi, K.,Sinclair, J.D., 2001. Targeted use of naltrexone without priordetoxification in the treatment of alcohol dependence: afactorial double-blind placebo controlled trial. J. Clin. Psycho-pharmacol. 21 (3), 287–292.
Higgins, S.T., Heil, S.H., Lussier, J.P., 2004. Clinical implications ofreinforcement as a determinant of substance use disorders.Annu. Rev. Psychol. 55, 431–461.
Hollister, L.E., 1978. Clinical evaluation of naltrexone treatment ofopiate-dependent individuals Report of the national researchcouncil committee on clinical evaluation of narcotic antagonists.Arch. Gen. Psychiatry 35, 335–340.
Kadden, R., Carroll, K., Donovan, D., Cooney, N., Monti, P., Abrams,D., et al., 1992. Cognitive-Behavioral Coping Skills TherapyManual: A Clinical Research Guide for Therapists TreatingIndividuals with Alcohol Abuse and Dependence (NIAAA Mono-graph Series Vol. 3 NIH Publications No 92-1985). US GovernmentPrinting Office, Washington DC.
Kaye, A.D., Gevitz, C., Bosscher, H.A., Duke, J.B., Frost, E.A.,Richards, T.A., et al., 2003. Ultrarapid opiate detoxification: areview. Can. J. Anaesth. 50, 663–671.
Kiefer, F., Jahn, H., Tarnaske, T., Helwig, H., Briken, P., Holzbach, R.,et al., 2003. Comparing and combining naltrexone and acampro-sate in relapse prevention of alcoholism: a double-blind placebo-controlled study. Arch. Gen. Psychiatry 60 (1), 92–99.
Kirchmayer, U., Davoli, M., Verster, A., 2003. Naltrexone mainte-nance treatment for opioid dependence. Cochrane DatabaseSyst. Rev. 2, CD001333.
Kirchmayer, U., Davoli, M., Verster, A., 2004. Naltrexone mainte-nance treatment for opioid dependence. The Cochrane Library,Issue 1. Update Software, Oxford.
Knox, P.C., Donovan, D.M., 1999. Using naltrexone in inpatientalcoholism treatment. J. Psychoact. Drugs 31 (4), 373–388.
Kranzler, H.R., Van Kirk, J., 2001. Effectiveness of naltrexone andacamprosate for alcoholism treatment: a meta-analysis. Alco-hol., Clin. Exp. Res. 25 (9), 1335–1341.
Kranzler, H.R., Modesto-lowe, V., Van Kirk, J., 2000. Naltrexone vs.nefazodone for treatment of alcohol dependence: a placebo-controlled trial. Neuropsychopharmacology 22 (5), 493–503.
Kranzler, H.R., Wesson, D.R., Billot, L., Drug Abuse SciencesNaltrexone Depot Study Group, 2004. Naltrexone depot fortreatment of alcohol dependence: a multicenter, randomized,placebo-controlled clinical trial. Alcohol., Clin. Exp. Res. 28 (7),1051–1059.
Krupitsky, E.M., Zvartau, E.E., Masalov, D.V., Tsoi, M.V., Burakov,A.M., et al., 2004. Naltrexone for heroin dependence treatmentin St. Petersburg, Russia. Subst. Abuse Treat. 26, 285–294.
Krystal, J.H., Cramer, J.A., Krol, W.F., Kirk, G.F., Rosenheck, R.A.,Veterans Affairs Naltrexone Cooperative Study 425 Group, 2001.Naltrexone in the treatment of alcohol dependence. N. Engl. J.Med. 345 (24), 1734–1739.
Latt, N.C., Jurd, S., Houseman, J., Wutzke, S.E., 2002. Naltrexonein alcohol dependence: a randomized clinical trial of effec-tiveness in a standard clinical setting. Med. J. Aust. 176 (11),530–534.
Lee, A., Tan, S., Lim, D., Winslow, R.M., Wong, K.E., Allen, J., etal., 2001. Naltrexone in the treatment of male alcoholics—aneffectiveness study in Singapore. Drug Alcohol Rev. 20 (2),1993–1999.
Lerner, A., Sigal, M., Bacalu, A., Shiff, R., Burganskim, I., Gelkopf,M., 1992. A naltrexone double blind placebo controlled study inIsrael. Isr. J. Psychiatry Relat. Sci. 29 (1), 36–43.
Leshner, A.I., 1997. Addiction is a brain disease and it matters.Science 278 (5335), 45–47.
Lesscher, H.M., Bailey, A., Burbach, J.P., Van Ree, J.M., Kitchen, I.,Gerrits, M.A., 2003. Receptor-selective changes in mu-delta- andkappa-opioid receptors after chronic naltrexone treatment inmice. Eur. J. Neurosci. 17 (5), 1006–1112.
Lima, M.S., Moncrieff, J., 2004. Drugs versus placebo for dysthymia.The Cochrane Library, Issue 1. Update Software, Oxford.
Ling, W., Wesson, D.R., 1984. Naltrexone treatment for addictedhealth-care professionals: a collaborative private practiceexperience. J. Clin. Psychiatry 45 (9 Pt. 2), 46–48.
Littleton, J., Zieglgansberger, W., 2003. Pharmacological mechan-isms of naltrexone and acamprosate in the prevention of relapsein alcohol dependence. Am. J. Addict. 12 (Suppl 1), S3–S11.
Marlatt, G.A., Gordon, J.R. (Eds.), 1985. Relapse Prevention. NYGuilford Press, New York.
McCrady, B.S., Dean, L., DuBreuil, E., Swanson, W., 1985. Theproblem drinkers project: a programmatic application of social-learning-based treatment. In: Marlatt, G.A., Gordon, J.R. (Eds.),Relapse Prevention: Maintenance Strategies in the Treatment ofAddictive Behaviors. Guilford Press, New York, pp. 417–471.
McGregor, C., Ali, R., White, J.M., Thomas, P., Gowing, L., 2002. Acomparison of antagonist-precipitated withdrawal under anes-thesia to standard inpatient withdrawal as a precursor tomaintenance naltrexone treatment in heroin users: outcomesat 6 and 12 months. Drug Alcohol Depend. 1, 68 (1), 5–14.
McLellan, A.T., 2002. Have we evaluated addiction treatmentcorrectly? Implications from a chronic care perspective. Addic-tion 97 (3), 249–252.
Mello, N.K., Mendelson, J.H., Kuehnle, J.C., Sellers, M.S., 1981.Operant analysis of human heroin self-administration and theeffects of naltrexone. J. Pharmacol. Exp. Ther. 216, 45–54.
Meyer, M.C., Straughn, A.B., Lo, M.W., Schary, W.L., Whitney, C.C.,1984. Bioequivalence dose-proportionality and pharmacokineticsof naltrexone after oral administration. J. Clin. Psychiatry 45,15–19.
Meyers, R.J., Smith, J.E., 1995. Clinical Guide to Alcohol Treat-ment: The Community Reinforcement Approach. Guilford Press,New York.
Miller, W.M., Wilbourne, P.L., 2002. Mesa Grande: a methodologicalanalysis of clinical trials of treatments for alcohol use disorders.Addiction 97 (3), 265–277.
H.G. Roozen et al.322
Monterosso, J.R., Flannery, B.A., Pettinati, H.M., Oslin, D.W.,Rukstalis, M., O’Brien, C.P., Volpicelli, J.R., 2001. Predictingtreatment response to naltrexone: the influence of craving andfamily history. Am. J. Addict. 10 (3), 258–268.
Monti, P.M., Abrams, D.B., Binkoff, J.A., Zwick, W.R., 1986.Interpersonal skills and substance abuse: theoretical and prac-tical considerations. In: Hollin, C.R., Trower, P. (Eds.), Handbookof Social Skills Training: Clinical Applications and New Directions.Pergamon, New York.
Monti, P.M., Rohsenow, D.J., Hutchison, K.E., Swift, R.M., Mueller,T.I., Colby, S.M., et al., 1999. Naltrexone’s effect on cue-elicitedcraving among alcoholics in treatment. Alcohol., Clin. Exp. Res.23 (8), 1386–1394.
Monti, P.M., Rohsenow, D.J., Swift, R.M., Gulliver, S.B., Colby, S.M.,Mueller, T.I., et al., 2001. Naltrexone and cue exposure withcoping and communication skills training for alcoholics: treat-ment process and 1-year outcomes. Alcohol Clin Exp Res. 25 (11),1634–1647.
Morgenstern, H., 1982. Uses of ecological analysis in epidemiologicresearch. Am. J. Public Health 72, 127–130.
Morris, P.L., Hopwood, M., Whelan, G., Gardiner, J., Drummond, E.,2001. Naltrexone for alcohol dependence: a randomized con-trolled trial. Addiction 96 (11), 1565–1573.
O’Brien, C.P., Volpicelli, L.A., Volpicelli, J.R., 1996. Naltrexonein the treatment of alcoholism: a clinical review. Alcohol 13,35–39.
O’Malley, S.S., Jaffe, A.J., Chang, G., Schottenfeld, R.S., Meyer,R.E., Rounsaville, B., 1992. Naltrexone and coping skills therapyfor alcohol dependence. A controlled study. Arch. Gen. Psychi-atry 49 (11), 881–887.
O’Malley, S.S., Croop, R.S., Wroblewski, J.M., Labriola, D.F.,Volpicelli, J.R., 1995. Naltrexone in the treatment of alcoholdependence: a combined analysis of two trials. Psychiatr. Ann.25 (11), 681–688.
O’Malley, S.S., Jaffe, A.J., Chang, G., Rode, S., Schottenfeld, R.,Meyer, R.E., Rounsaville, B., 1996. Six month follow-up ofnaltrexone and psychotherapy for alcohol dependence. Arch.Gen. Psychiatry 53 (3), 217–224.
O’Malley, S.S., Rounsaville, B.J., Farren, C., Namkoong, K., Wu, R.,Robinson, J., O’Connor, P.G., 2003. Initial and maintenancenaltrexone treatment for alcohol dependence using primary carevs. specialty care: a nested sequence of 3 randomized trials.Arch. Intern. Med. 163 (14), 1695–1704.
Oslin, D., Liberto, J.G., O’Brien, J., Krois, S., Norbeck, J.,1997a. Naltrexone as an adjunctive treatment for olderpatients with alcohol dependence. Am. J. Geriatr. Psychiatry5 (4), 324–332.
Oslin, D., Liberto, J.G., O’Brien, J., Krios, S., 1997b. Tolerability ofnaltrexone in treating older alcohol-dependent patients. Am. J.Addict. 6, 266–270.
Oslin, D.W., Pettinati, H., Volpicelli, J.R., 2002. Alcoholismtreatment adherence: older age predicts better adherence anddrinking outcomes. Am. J. Geriatr. Psychiatry 10 (6), 740–747.
Oslin, D.W., Berrettini, W., Kranzler, H.R., Pettinati, H., Gelernter,J., Volpicelli, J.R., O’Brien, C.P., 2003. A functional polymor-phism of the mu-opioid receptor gene is associated withnaltrexone response in alcohol-dependent patients. Neuropsy-chopharmacology 28 (8), 1546–1552.
Oswald, L.M., McCaul, M., Choi, L., Yang, X., Wand, G.S., 2004.Catechol-O-methyltransferase polymorphism alters hypothalam-ic-pituitary-adrenal axis responses to naloxone: a preliminaryreport. Biol. Psychiatry 55 (1), 102–105.
Patel, M.X., David, A.S., 2004. Medication adherence: predictivefactors and enhancement strategies. Psychiatry 3 (10), 41–44.
Pettinati, H.M., Volpicelli, J.R., Pierce, J.D., OTBrien, C.P., 2000.Improving naltrexone response: an intervention for medicalcompliance in alcohol dependent patients. J. Addict. Dis. 19(1), 71–83.
Pfab, R., Hirtl, C., Zilker, T., 1999. Opiate detoxification underanesthesia: no apparent benefit but suppression of thyroidhormones and risk of pulmonary and renal failure. J. Toxicol.,Clin. Toxicol. 37, 43–50.
Preston, K.L., Silverman, K., Umbricht, A., DeJesus, A., Montoya,I.D., Schuster, C.R., 1999. Improvement in naltrexone treatmentcompliance with contingency management. Drug Alcohol De-pend. 54 (2), 127–135.
Resnick, R.B., Volavka, J., Freedman, A.M., Thomas, M., 1974.Studies of EN-1639A (naltrexone): a new narcotic antagonist.Am. J. Psychiatry 131 (6), 646–650.
Resnick, R.B., Schuyten-Resnick, E., Washton, A.M., 1979. Narcoticantagonists in the treatment of opioid dependence: review andcommentary. Compr. Psychiatry. 20 (2), 116–125.
Resnick, R.B., Washton, A.M., Stone-Washton, N., 1981. Psycho-therapy and naltrexone in opioid dependence. NIDA Res. Monogr.34, 109–115.
Ritter, A.J., 2002. Naltrexone in the treatment of heroin depen-dence: relationship with depression and risk of overdose. Aust.N. Z. J. Psychiatry 36 (2), 224–228.
Rohsenow, D.J., Colby, S.M., Monti, P.M., Swift, R.M., Martin,R.A., Mueller, T.I., et al., 2000. Predictors of compliancewith NTX among alcoholics. Alcohol., Clin. Exp. Res. 24 (10),1542–1549.
Roozen, H.G., de Kan, R., van den Brink, W., Kerkhof, A.J.F.M.,Geerlings, P.J., 2002. Dangers involved in rapid opioid detoxifi-cation while using opioid antagonists: dehydration and renalfailure. Addiction 97 (8), 1071–1073.
Roozen, H.G., Kerkhof, A.J.F.M., Van den Brink, W., 2003. Experi-ences with an outpatient relapse program (Community Rein-forcement Approach) combined with naltrexone in thetreatment of opioid-dependence: effect on addictive behaviorsand the predictive value of psychiatric comorbidity. Eur. Addict.Res. 9, 53–58.
Rothenberg, J.L., Sullivan, M.A., Church, S.H., Seracini, A.,Collins, E., Kleber, H.D., Nunes, E.V., 2002. Behavioral naltrex-one therapy: an integrated treatment for opiate dependence.J. Subst. Abuse Treat. 23 (4), 351–360.
San, L., Pomarol, G., Peri, J.M., Olle, J.M., Cami, J., 1991. Follow-up after a six-month maintenance period on naltrexone versusplacebo in heroin addicts. Br. J. Addict. 86, 983–990.
San, L., Puig, M., Bulbena, A., Farre, M., 1995. High risk ofultrashort noninvasive opiate detoxification. Am. J. Psychiatry.152, 956.
Shufman, E.N., Porat, S., Witztum, E., Gandacu, D., Bar-Hamburger,R., Ginath, Y., 1994. The effectiveness of naltrexone inpreventing reabuse of heroin after detoxification. Biol. Psychi-atry 35, 935–945.
Sinclair, J.D., 2001. Evidence about the use of naltrexone and fordifferent ways of using it in the treatment of alcoholism. AlcoholAlcohol. 36 (1), 2 –10.
Singh, J., Basu, D., 2004. Ultra-rapid opioid detoxification: currentstatus and controversies. J. Postgrad. Med. 50 (3), 227–232.
Skinner, B.F., 1938. The Behavior of Organisms: An ExperimentalAnalysis. Prentice Hall, Englewood Cliffs, NJ.
Srisurapanont, M., Jarusuraisin, N., 2004. Opioid antagonists foralcohol dependence (Cochrane Review). The Cochrane LibraryIssue 1. Update Software, Oxford.
Stone-Washton, N., Resnick, R.B., Washton, A.M., 1982. Naltrexoneand psychotherapy. NIDA Res. Monogr. 41, 505–507.
Storosum, J.G., Elferink, A.J., van Zwieten, J., van den Brink, W.,Gersons, B.P., van Strik, R., Broekmans, A.W., 2001. Short-termefficacy of tricyclic antidepressants revisited: a meta-analyticstudy. Eur. Neuropsychopharmacol. 11 (2), 173–180.
Streeton, C., Whelan, G., 2001. Naltrexone a relapse preventionmaintenance treatment of alcohol dependence: a meta-analysis of randomized controlled trials. Alcohol Alcohol. 36(6), 544–552.

NTX’s effectiveness in treatment of opioid and alcohol dependence 323
Swift, R.M., 1999. Drug therapy for alcohol dependence. N. Engl. J.Med. 340 (19), 1483–1490;Thompson, S.G., Higgins, J.P., 2002. How should meta-regressionanalyses be undertaken and interpreted? Stat. Med. 21 (11),1559–1573.
Tucker, T., Ritter, A., Maher, C., Jackson, H., 2004. Naltrexonemaintenance for heroin dependence: uptake, attrition andretention. Drug Alcohol Rev. 23 (3), 299–309.
Van den Brink, W., van Ree, J.M., 2003. Pharmacological treatmentsfor heroin and cocaine addiction. Eur. Neuropsychopharmacol.13 (6), 476–487.
Van Tulder, M.W., Ostelo, R., Vlaeyen, J.W.S., Linton, S.J., Morley,S.J., Assendelft, W.J.S., 2000. Behavioral treatment for chroniclow back pain. A systematic review within the framework of theCochrane back review group. Spine 25 (20), 2688–2699.
Van Tulder, M.W., Furlan, A., Bouter, L.M., Bombardier, C.,The Editorial Board of the Cochrane Back Review Group,2003. Updated method guidelines for systematic reviews inthe Cochrane collaboration back review group. Spine 28,1290–1299.
Verebey, K., 1981. The clinical pharmacology of naltrexone:pharmacology and pharmacodynamics. NIDA Res. Monogr. 28,147–158.
Volpicelli, J.R., Alterman, A.I., Hayashida, M., O’Brien, C.P., 1992.Naltrexone in the treatment of alcohol dependence. Arch. Gen.Psychiatry 49, 876–880.
Volpicelli, J.R., Clay, K.L., Watson, N.T., O’Brien, C.P., 1995.Naltrexone in the treatment of alcoholism: predicting responseto naltrexone. J. Clin. Psychiatry 56 (Suppl 7), 39–44.
Volpicelli, J.R., Rhines, J.S., Volpicelli, L.A., Alterman, A.I.,O’Brien, C.P., 1997. Naltrexone and alcohol dependence. Roleof subject compliance. Arch. Gen. Psychiatry 54, 737–742.
Wall, M.E., Brine, D.R., Perez-Reyes, M., 1981. Metabolism anddisposition of naltrexone in man after oral and intravenousadministration. Drug Metab. Dispos. 9 (4), 369–375.
Washton, A.M., Gold, M.S., Pottash, A.C., 1984. Naltrexone inaddicted physicians and business executives. NIDA Res. Monogr.55, 185–190.
Weiss, R.D., 2004. Adherence to pharmacotherapy in patients withalcohol and opioid dependence. Addiction 99, 1382–1392.




















