
Cholesterol catabolism as a therapeutic target in Mycobacterium tuberculosis
Upload
independentCategory
view
4download
0
AA
CSDa
*§
LIo�
Bap2sapMtajlubsoagcsmawv5d32iwCada
Ke
GASTROENTEROLOGY 2010;xx:xxx
ARTICLE IN PRESS
4-Gene Signature Predicts Survival of Patients With Resecteddenocarcinoma of the Esophagus, Junction, and Gastric Cardia
HRISTOPHER J. PETERS,* JONATHAN R. E. REES,‡ RICHARD H. HARDWICK,§ JAMES S. HARDWICK,�
ARAH L. VOWLER,¶ CHIN–ANN J. ONG,* CHUNSHENG ZHANG,� VICKI SAVE,# MARIA O’DONOVAN,** DORIS RASSL,‡‡
EREK ALDERSON,§§ CARLOS CALDAS,� � and REBECCA C. FITZGERALD,* on behalf of the Oesophageal Cancer Clinicalnd Molecular Stratification (OCCAMS) Study Group
MRC Cancer Cell Unit, Hutchison-MRC Research Centre, Cambridge, United Kingdom; ‡Department of Surgery, Bristol Royal Infirmary, Bristol, United Kingdom;Cambridge Oesophago-Gastric Centre, **Department of Pathology, Addenbrookes Hospital, Cambridge, United Kingdom; �Molecular Profiling, Merck Researchaboratories, North Wales, Pennsylvania; ¶Bioinformatics Core, Cambridge Research Institute, Cambridge, United Kingdom; #Department of Pathology, Royal
nfirmary of Edinburgh, Edinburgh, United Kingdom; ‡‡Department of Pathology, Papworth Hospital, Papworth, United Kingdom; §§University of Birmingham Collegef Medical and Dental Sciences, School of Cancer Sciences, Academic Department of Surgery, Queen Elizabeth Hospital, Birmingham, United Kingdom; and
�Department of Oncology and Cancer Research UK Cambridge Research Institute, University of Cambridge, Li Ka Shing Centre, Cambridge, United KingdomT6entgriAwpwerta
phcepcn7n
CCjsStttu
BA
SIC–
ALI
MEN
TARY
TRA
CT
ACKGROUND & AIMS: The incidence of esophagealnd junctional adenocarcinoma has increased 6-fold in theast 30 years and 5-year survival remains approximately0%. Current staging is limited in its ability to predicturvival which has ramifications for treatment choices. Theim of this study was to generate and validate a molecularrognostic signature for esophageal adenocarcinoma.ETHODS: Gene expression profiling was performed and
he resulting 42,000 gene signatures correlated with clinicalnd pathologic features for 75 snap-frozen esophageal andunctional resection specimens. External validation of se-ected targets was performed on 371 independent casessing immunohistochemistry to maximize clinical applica-ility. RESULTS: A total of 119 genes were associatedignificantly with survival and 270 genes with the numberf involved lymph nodes. Filtering of these lists resulted inshortlist of 10 genes taken forward to validation. Four
enes proved to be prognostic at the protein level (deoxy-ytidine kinase [DCK], 3=-phosphoadenosine 5=-phospho-ulfate synthase 2 [PAPSS2], sirtuin 2 [SIRT2], and tripartite
otif-containing 44 [TRIM44]) and were combined to cre-te a molecular prognostic signature. This 4-gene signatureas highly predictive of survival in the independent external
alidation cohort (0/4 genes dysregulated 5-year survival,8%; 95% confidence interval [CI], 36%–80%; 1–2/4 genesysregulated 5-year survival, 26%; 95% CI, 20%–32%; and–4/4 genes dysregulated 5-year survival, 14%; 95% CI, 4%–4% (P � .001). Furthermore, this 4-gene signature was
ndependently prognostic in a multivariable model togetherith the existing clinical TNM staging system (P � .013).ONCLUSIONS: This study has generated a clinicallypplicable prognostic gene signature that indepen-ently predicts survival in an external validation cohortnd may inform management decisions.
eywords: Esophageal Adenocarcinoma; Prognostic Mark-rs; Gene Expression Profiling.
he incidence of esophageal and gastroesophagealjunctional (GEJ) adenocarcinoma has increased
-fold in the past 30 years, making it the most commonsophageal malignancy in the Western world.1 Unfortu-ately, 5-year survival remains less than 8% for all pa-ients diagnosed1 and only 18%–23% for patients under-oing surgery.2 It is staged using the internationallyecognized TNM system,3 although this has limited abil-ty to stratify patients according to their likely outcome.lthough patients with advanced stage tumors clearly doorse than those with earlier disease, most patientsresent late (T3N1) and even within this group there areide variations in survival. The highly invasive nature of
sophageal surgery and the toxic nature of neoadjuvantegimens make it important to find better ways to selectreatment. Complex management decisions require moreccurate prognostic information.
In other epithelial tumors molecular signatures haveroven to be prognostic. In breast cancer gene signaturesave been shown to predict survival4,5 and response tohemotherapy6 with good external validation.7,8 Insophageal adenocarcinoma the application of molecularrognostic signatures is less advanced. Genome-wideomparison of gene transcript levels in esophageal ade-ocarcinomas produced a signature that could predict5% of lymph node–positive and 41% of lymph node–egative cases, although the signature did not outper-
Abbreviations used in this paper: ADCY9, adenylate cyclase 9;5AR1, complement component 5a receptor 1; CI, confidence interval;T, cycle threshold; DCK, deoxycytidine kinase; GEJ, gastroesophageal
unction; MNT, MAX binding protein; mRNA, messenger RNA; NEU4,ialidase 4; OCCAMS, Oesophageal Cancer Clinical and Moleculartratification; PAPSS2, 3=-phosphoadenosine 5=-phosphosulfate syn-hase 2; PLK-1, polo-like kinase 1; REMARK, Reporting Recommenda-ions for Tumour Marker Prognostic Studies; SIRT2, sirtuin 2; TMA,issue microarray; TRIM44, tripartite motif-containing 44; UBE2d2,biquitin-conjugating enzyme E2D 2.
© 2010 by the AGA Institute0016-5085/$36.00
doi:10.1053/j.gastro.2010.05.080

feeatv
nmsscktrATtrtcctcfgp
attnmvvighRrsbf
w9e2CvLa
t1aClrrtAtwcR4Sn
srRmSdnatw
cuwspMtaCcogMndvioTdtviapBt
BA
SIC–
ALIM
ENTA
RY
TRA
CT
2 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
orm current clinical staging and has not been validatedxternally.9 Similarly, comparison of gene transcript lev-ls from patients who responded to neoadjuvant therapynd those who did not respond identified 86 differen-ially expressed genes, but again the findings were notalidated externally.10
In general, although the breast cancer prognostic sig-atures have been well validated the same is not true ofost molecular predictors of outcome. No molecular
ignatures have been incorporated into formal TNMtaging, although some have gained a place in nationalancer guidelines.11 It has been proposed that a biomar-er of prognosis should be sensitive, specific, cost effec-ive, fast, robust against variability, and better than cur-ent clinical parameters.12 The US Food and Drugdministration and National Institute of Standards andechnology have proposed 5 steps of biomarker valida-
ion: preclinical exploration, clinical assay and validation,etrospective longitudinal validation, prospective valida-ion, and demonstration of benefits in cancer out-omes.13,14 Other reviews looking at predictors of out-ome have reiterated the need for external validation andhe development of a test that has general clinical appli-ability,15–18 whereas the Reporting Recommendationsor Tumour Marker Prognostic Studies (REMARK)uidelines suggested the requirements for reportingrognostic biomarker studies.19
Although work continues to better stratify esophagealnd GEJ adenocarcinomas by more detailed characteriza-ion of clinical and pathologic features,20 –22 the oppor-unity to generate a robust and practical molecular prog-ostic signature remains. This study aimed to generate aolecular prognostic signature that could predict sur-
ival in esophageal and GEJ adenocarcinoma and then toalidate this signature externally at the protein level in anndependent cohort of patients, in keeping with recentuidelines.12–14,19 This is in contrast to other projects thatave used large gene signatures applied at the messengerNA (mRNA) level, which depend on analysis in expert
eference laboratories.7,8 We hope that the combined pre-entation of data from generation and clinically applica-le external validation will act as a useful framework foruture work on prognostic signatures in other cancers.
Materials and MethodsGeneration of Molecular PrognosticSignatureAfter appropriate ethical approval, tumor samples
ere collected and snap-frozen in liquid nitrogen from1 patients undergoing potentially curative resections forsophageal and GEJ adenocarcinoma between 1992 and000 at the Bristol Royal Infirmary in Bristol, UK (D.A.).linical data, including survival, were collected from re-iew of the medical records (J.R.E.R., ethical approvalREC 04/Q2006/28). The frozen sections were cut and
ll primary diagnoses were confirmed by an expert gas- arointestinal pathologist (V.S.). RNA was extracted from0� 15-�m sections of the frozen specimen using Trizolccording to the manufacturer’s instructions (Invitrogen,arlsbad, CA). Amplification was performed via a very
ow input amplification and labeling technique using 2ounds of a modified mouse Moloney leukemia virus–everse transcription mediated reverse-transcription pro-ocol23 or a 2� UniAmp protocol using a modification ofmbion’s 2-round MessageAmp II kit (Applied Biosys-
ems, Inc, Foster City, CA). Resulting RNA was labeledith cyanine dyes and competitively hybridized with a
ommon control RNA (Human Universal ReferenceNA; Stratagene, La Jolla, CA) to a custom-made Agilent4K 60-mer oligo-microarray (Agilent Technologies,anta Clara, CA) using previously described tech-iques.24,25
After competitive hybridization, the 2-color arrays werecanned and fluorescence intensities for each probe wereecorded. Ratios of transcript abundance (experimentalNA to common control RNA) were obtained after nor-alization and correction of the array intensity data (see
upplementary Materials and Methods). Gene expressionata analysis was performed on the 75 samples withormalized data using Rosetta Resolver gene expressionnalysis software (version 6.0; Rosetta Biosoftware, Seat-le, WA) and MATLAB software (version 7.0.4; Math-orks, Natick, MA).The expression array data were correlated with out-
ome and the histopathologic features of the tumorsing a Pearson correlation coefficient, and the resultsere plotted as a histogram. The clinical data for all the
amples then were randomized, and the process was re-eated with the results plotted on the same histogram (aonte Carlo simulation).26 Because there were 40,600
ranscripts on the array, 16,449 of which were variablecross at least 10 samples, it was found that one Montearlo simulation produced a stable and smooth plot
lose to the theoretical curve. Genes that were positivelyr negatively correlated with the clinical features to areater degree than the random distribution of theonte Carlo simulation were considered potentially sig-
ificant. This identified 2 sets of genes, one associatedirectly with survival (with time considered a continuousariable) and the other associated with the number ofnvolved lymph nodes (a feature known to be predictivef outcome and therefore a surrogate of survival20 –22).hese lists were filtered by a number of criteria to pro-uce a short list of the targets to take forward to valida-ion (see Supplementary Materials and Methods). Toalidate the expression array data 4 targets were assessedn the 32 patients for whom there was RNA remainingfter the expression profiling experiment using real-timeolymerase chain reaction (ABI Prism 7900HT; Appliediosystems, Inc). The average cycle threshold (CT) of the
arget (2 technical replicates) was subtracted from the
verage CT of 3 housekeeping genes identified from the
lpptpds
WaogABU(h
itpfr7aEdinocitHwivctttccat
0Co0ttq
trvC(u
(wpitap3a1pswsctpte7ou
Cawfmtlcff(limnar[t
BA
SIC–
ALI
MEN
TARY
TRA
CT
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 3
ARTICLE IN PRESS
iterature27 (glyceraldehyde-3-phosphate dehydrogenase,olymerase (RNA) II (DNA directed) polypeptide, andhosphoglycerate kinase; 2 technical replicates of each)o create a delta CT. The median delta CT of the poorrognosis group then was compared with the medianelta CT of the good prognosis group for each target toee if there was a difference in expression.
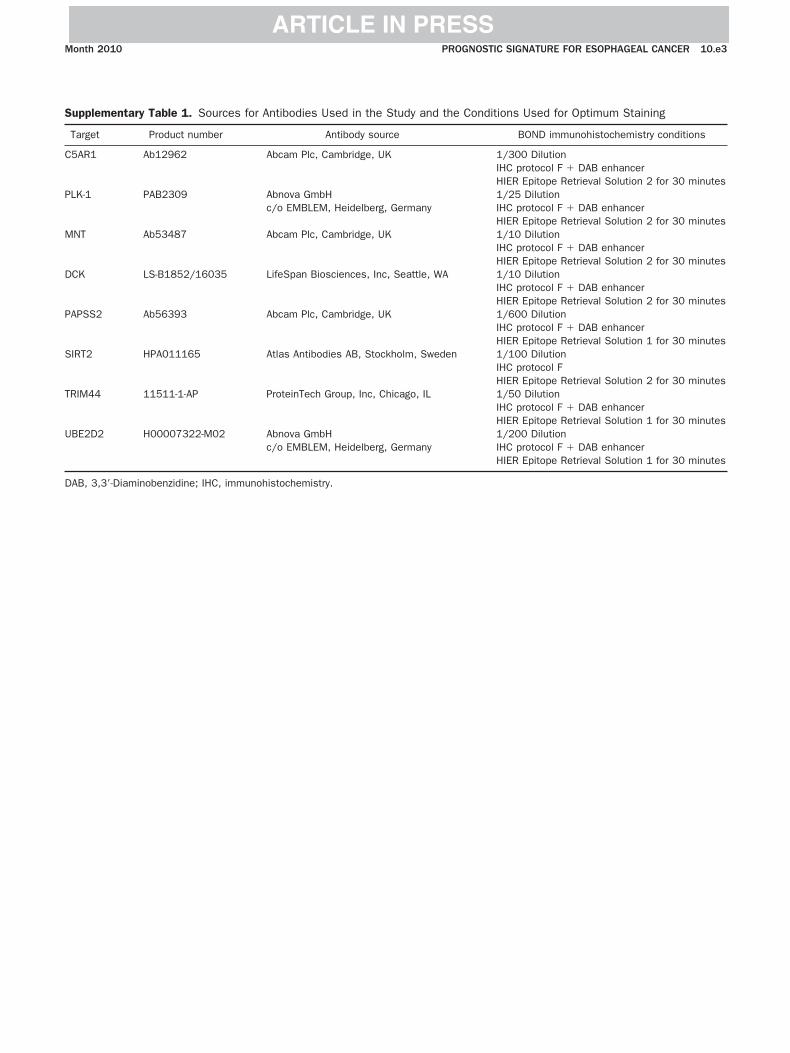
Validation of Molecular Prognostic Signaturevia ImmunohistochemistrySpecificity of all antibodies was confirmed by
estern blotting, which included both positive and neg-tive controls (data not shown). Antibodies then wereptimized with positive control cell blocks and esopha-eal tissue before application to the tissue microarrays.ll immunohistochemistry was performed using theond System (Leica Microsystems, Ltd, Milton Keynes,K) according to the manufacturer’s recommendations
C.J.P. and C.-A.J.O., for antibody sources and immuno-istochemistry conditions see Supplementary Table 1).Internal validation aimed to determine if the genes
dentified from the expression array study were prognos-ic at the protein level in the generation dataset. This waserformed using tissue microarrays (TMAs) constructedrom the formalin-fixed, paraffin-embedded tissue de-ived from the original Bristol cohort (V.S.). Forty-five of5 cases had formalin-fixed tissue available from therchive; triplicate cores were included from each case.xternal validation aimed to prove that the signatureerived in the first part of the study was prognostic in an
ndependent cohort of esophageal and GEJ adenocarci-omas. H&E slides and the corresponding blocks werebtained for 371 patients who underwent potentiallyurative surgery at 1 of the 5 Oesophageal Cancer Clin-cal and Molecular Stratification (OCCAMS) centers con-ributing to this project (ethical approval MREC 07/0305/52, see Acknowledgment section). The TMAsere constructed in triplicate in the same way as the
nternal validation dataset with all original diagnoseserified by 2 histopathologists in the host institution,onfirmed by a further expert gastrointestinal his-opathologist (V.S., M.D., and D.R.). Comparisons be-ween groups were made using the chi-square test andhe Mann–Whitney U test. Loss of some cores duringutting and staining of the TMAs means the number ofases analyzed did not reach the maximum of 45 internalnd the 371 external validation patients represented inotal on the arrays for each antibody.
The staining of each core on the TMA was scored fromto 3 by 1 of 2 researchers blinded to outcome (C.J.P. and.-A.J.O.). Samples then were characterized as havingverexpression (score, 2–3) or underexpression (score,–1) of the target. The aim was to develop a signature
hat could be applied robustly in a binary way for eacharget (positive or negative), rather than one that used a
uantitative component requiring greater standardiza- pion of techniques (eg, using real-time polymerase chaineaction). These categories then were compared with sur-ival using Kaplan–Meier plots and a log-rank Mantel–ox test. A backward stepwise Cox regression model
entry probability, 0.05; removal probability, 0.10) wassed for multivariable analysis.
ResultsDemographics of Generation DatasetGood quality normalized gene expression data
Gene Expression Omnibus accession number GSE19417)ere generated from tumor tissue specimens for 75 of 91atients (Table 1). For 16 of 91 patients the RNA was of
nsufficient quality or quantity for robust analysis. Sixty-wo percent (n � 47) of patients were male with a mediange of 67 years (range, 35– 81 y). Forty-seven percent ofatients had esophageal or Siewert type I tumors (n �6), 11% had junctional or Siewert type II tumors (n � 8),nd 25% had tumors in the cardia or Siewert type III (n �2). The Siewert classification was not known for 25% ofatients (n � 19), but this group did not otherwiseignificantly differ in demographics from the patients inhom the Siewert classification was known (data not
hown). Ninety-five percent of patients (n � 71) werehemotherapy-naive, in keeping with the historical na-ure of this cohort. The median follow-up period for allatients was 20 months (range, 0.5–137 mo), althoughhis increased to 89 months for survivors. There was novidence of a difference between the demographics of the5 patients for whom normalized expression data werebtained and the 16 patients for whom there were noseable expression data (data not shown).
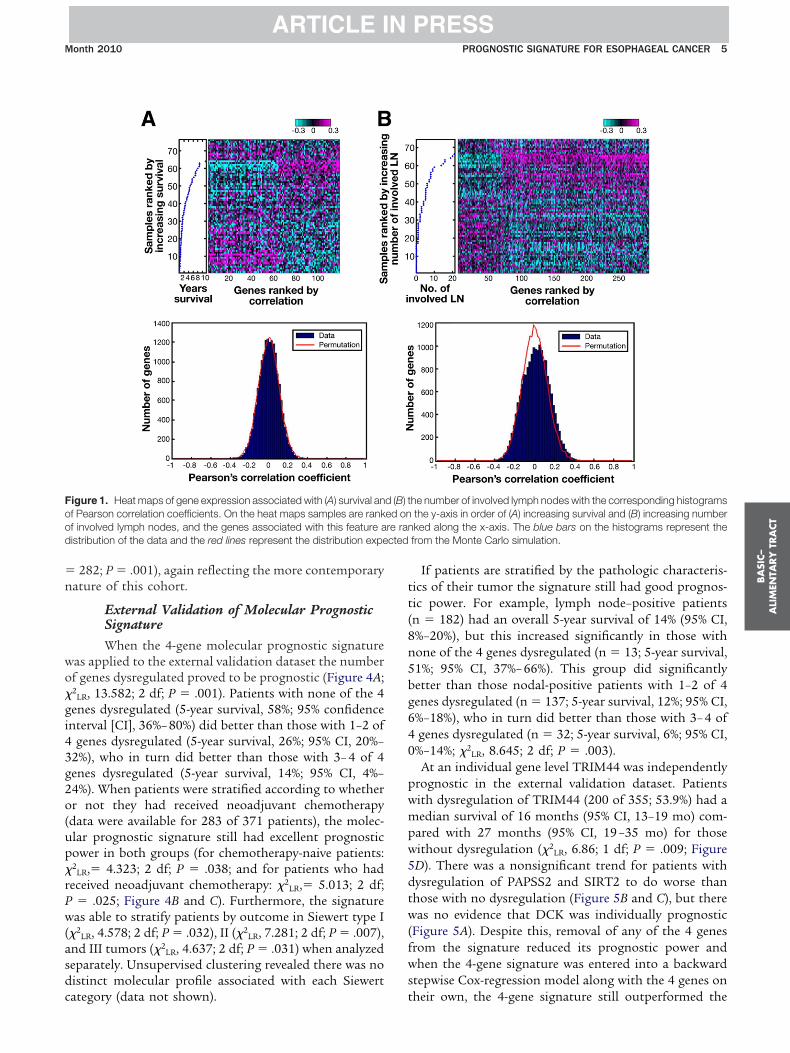
Identification of Prognostic Genes From theExpression ArrayThe Pearson correlation followed by a Monte
arlo simulation identified 119 genes that were associ-ted with survival and 270 genes that were associatedith the number of involved lymph nodes, a pathologic
eature known to be prognostic (Figure 1 and Supple-entary Table 2). The Monte Carlo simulation suggested
hat the potential false discovery rate was higher in theist associated with survival compared with the list asso-iated with the number of involved lymph nodes; there-ore, both lists were taken forward when selecting targetsor validation. These genes were filtered by several criteriaSupplementary Materials and Methods), resulting in aist of 10 for validation. Four of these were selected tonternally validate at the RNA level using real-time poly-
erase chain reaction; 2 were up-regulated in poor prog-osis tumors (tripartite motif-containing 44 [TRIM44]nd adenylate cyclase 9 [ADCY9]) and 2 were down-egulated (deoxycytidine kinase [DCK] and sialidase 4NEU4]). In all 4 cases real-time polymerase chain reac-ion showed the expected difference in expression (Sup-
lementary Figure 1).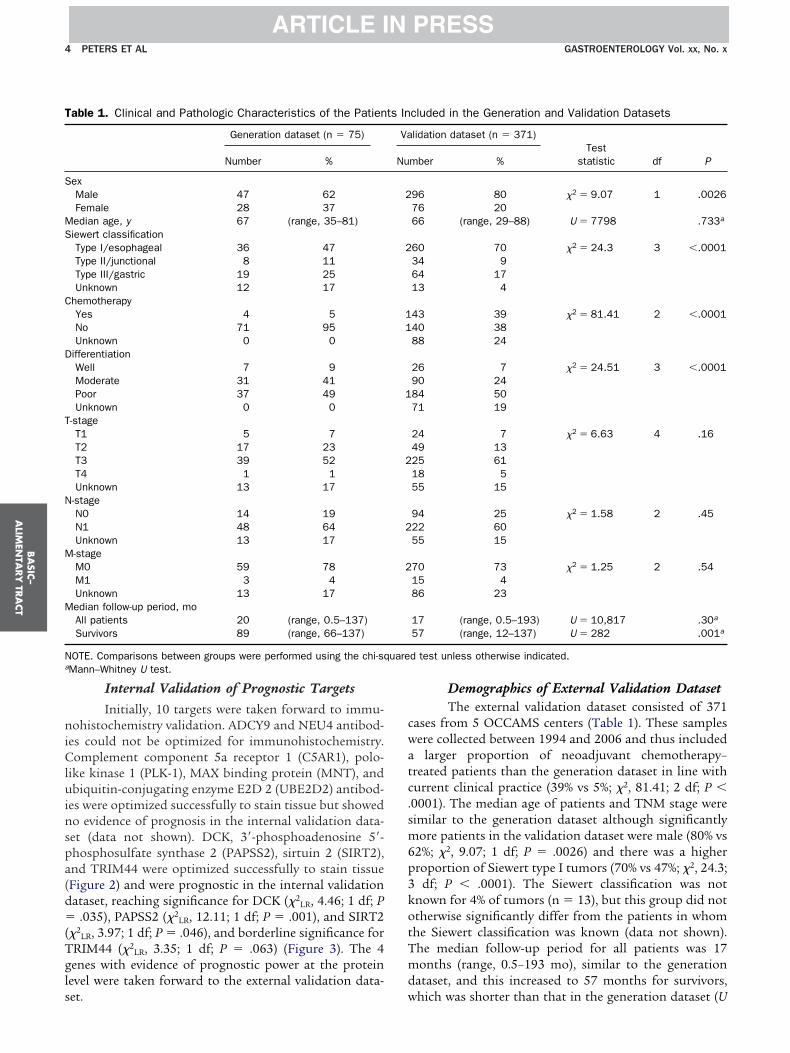
niCluinspa(d�(Tgls
cwatc.sm6p3kotTmd
T
S
MS
C
D
T
N
M
M
N uarea
BA
SIC–
ALIM
ENTA
RY
TRA
CT
4 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
Internal Validation of Prognostic TargetsInitially, 10 targets were taken forward to immu-
ohistochemistry validation. ADCY9 and NEU4 antibod-es could not be optimized for immunohistochemistry.omplement component 5a receptor 1 (C5AR1), polo-
ike kinase 1 (PLK-1), MAX binding protein (MNT), andbiquitin-conjugating enzyme E2D 2 (UBE2D2) antibod-
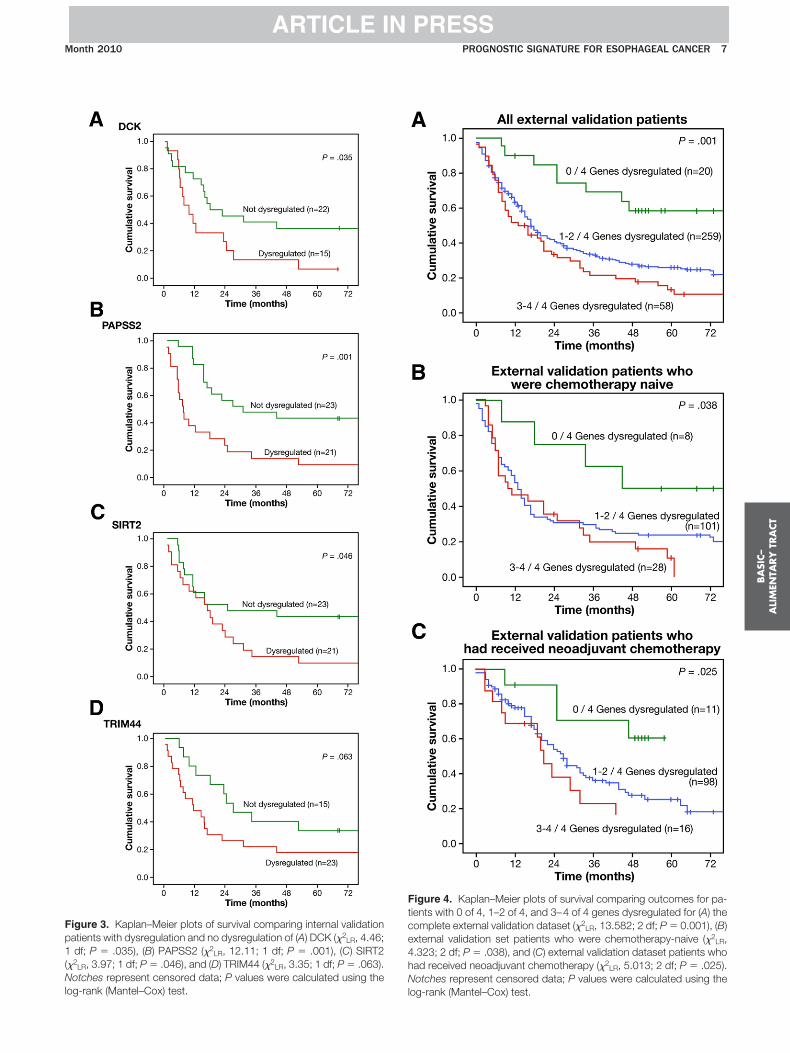
es were optimized successfully to stain tissue but showedo evidence of prognosis in the internal validation data-et (data not shown). DCK, 3=-phosphoadenosine 5=-hosphosulfate synthase 2 (PAPSS2), sirtuin 2 (SIRT2),nd TRIM44 were optimized successfully to stain tissueFigure 2) and were prognostic in the internal validationataset, reaching significance for DCK (�2
LR, 4.46; 1 df; P.035), PAPSS2 (�2
LR, 12.11; 1 df; P � .001), and SIRT2�2
LR, 3.97; 1 df; P � .046), and borderline significance forRIM44 (�2
LR, 3.35; 1 df; P � .063) (Figure 3). The 4enes with evidence of prognostic power at the proteinevel were taken forward to the external validation data-
able 1. Clinical and Pathologic Characteristics of the Patien
Generation dataset (n � 75)
Number %
exMale 47 62Female 28 37edian age, y 67 (range, 35–81)iewert classificationType I/esophageal 36 47Type II/junctional 8 11Type III/gastric 19 25Unknown 12 17
hemotherapyYes 4 5No 71 95Unknown 0 0
ifferentiationWell 7 9Moderate 31 41Poor 37 49Unknown 0 0
-stageT1 5 7T2 17 23T3 39 52T4 1 1Unknown 13 17
-stageN0 14 19N1 48 64Unknown 13 17-stageM0 59 78M1 3 4Unknown 13 17edian follow-up period, moAll patients 20 (range, 0.5–137)Survivors 89 (range, 66–137)
OTE. Comparisons between groups were performed using the chi-sqMann–Whitney U test.
et. w
Demographics of External Validation DatasetThe external validation dataset consisted of 371
ases from 5 OCCAMS centers (Table 1). These samplesere collected between 1994 and 2006 and thus included
larger proportion of neoadjuvant chemotherapy–reated patients than the generation dataset in line withurrent clinical practice (39% vs 5%; �2, 81.41; 2 df; P �0001). The median age of patients and TNM stage wereimilar to the generation dataset although significantly
ore patients in the validation dataset were male (80% vs2%; �2, 9.07; 1 df; P � .0026) and there was a higherroportion of Siewert type I tumors (70% vs 47%; �2, 24.3;
df; P � .0001). The Siewert classification was notnown for 4% of tumors (n � 13), but this group did nottherwise significantly differ from the patients in whomhe Siewert classification was known (data not shown).he median follow-up period for all patients was 17onths (range, 0.5–193 mo), similar to the generation
ataset, and this increased to 57 months for survivors,
cluded in the Generation and Validation Datasets
lidation dataset (n � 371)Test
statistic df Pmber %
96 80 �2 � 9.07 1 .002676 2066 (range, 29–88) U � 7798 .733a
60 70 �2 � 24.3 3 �.000134 964 1713 4
43 39 �2 � 81.41 2 �.000140 3888 24
26 7 �2 � 24.51 3 �.000190 2484 5071 19
24 7 �2 � 6.63 4 .1649 1325 6118 555 15
94 25 �2 � 1.58 2 .4522 6055 15
70 73 �2 � 1.25 2 .5415 486 23
17 (range, 0.5–193) U � 10,817 .30a
57 (range, 12–137) U � 282 .001a
d test unless otherwise indicated.
ts In
Va
Nu
2
2
11
1
2
2
2
hich was shorter than that in the generation dataset (U
�n
wo�gi43g2o(up�rPw(asdc
tt(8n5bg640
pwmpw5dtw(fws
Food cted
BA
SIC–
ALI
MEN
TARY
TRA
CT
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 5
ARTICLE IN PRESS
282; P � .001), again reflecting the more contemporaryature of this cohort.
External Validation of Molecular PrognosticSignatureWhen the 4-gene molecular prognostic signature
as applied to the external validation dataset the numberf genes dysregulated proved to be prognostic (Figure 4A;2
LR, 13.582; 2 df; P � .001). Patients with none of the 4enes dysregulated (5-year survival, 58%; 95% confidencenterval [CI], 36%– 80%) did better than those with 1–2 of
genes dysregulated (5-year survival, 26%; 95% CI, 20%–2%), who in turn did better than those with 3– 4 of 4enes dysregulated (5-year survival, 14%; 95% CI, 4%–4%). When patients were stratified according to whetherr not they had received neoadjuvant chemotherapydata were available for 283 of 371 patients), the molec-lar prognostic signature still had excellent prognosticower in both groups (for chemotherapy-naive patients:2
LR,� 4.323; 2 df; P � .038; and for patients who hadeceived neoadjuvant chemotherapy: �2
LR,� 5.013; 2 df;� .025; Figure 4B and C). Furthermore, the signatureas able to stratify patients by outcome in Siewert type I
�2LR, 4.578; 2 df; P � .032), II (�2
LR, 7.281; 2 df; P � .007),nd III tumors (�2
LR, 4.637; 2 df; P � .031) when analyzedeparately. Unsupervised clustering revealed there was noistinct molecular profile associated with each Siewert
igure 1. Heat maps of gene expression associated with (A) survival anf Pearson correlation coefficients. On the heat maps samples are rankf involved lymph nodes, and the genes associated with this feature aistribution of the data and the red lines represent the distribution expe
ategory (data not shown). t
If patients are stratified by the pathologic characteris-ics of their tumor the signature still had good prognos-ic power. For example, lymph node–positive patientsn � 182) had an overall 5-year survival of 14% (95% CI,%–20%), but this increased significantly in those withone of the 4 genes dysregulated (n � 13; 5-year survival,1%; 95% CI, 37%– 66%). This group did significantlyetter than those nodal-positive patients with 1–2 of 4enes dysregulated (n � 137; 5-year survival, 12%; 95% CI,%–18%), who in turn did better than those with 3– 4 ofgenes dysregulated (n � 32; 5-year survival, 6%; 95% CI,
%–14%; �2LR, 8.645; 2 df; P � .003).
At an individual gene level TRIM44 was independentlyrognostic in the external validation dataset. Patientsith dysregulation of TRIM44 (200 of 355; 53.9%) had aedian survival of 16 months (95% CI, 13–19 mo) com-
ared with 27 months (95% CI, 19 –35 mo) for thoseithout dysregulation (�2
LR, 6.86; 1 df; P � .009; FigureD). There was a nonsignificant trend for patients withysregulation of PAPSS2 and SIRT2 to do worse thanhose with no dysregulation (Figure 5B and C), but thereas no evidence that DCK was individually prognostic
Figure 5A). Despite this, removal of any of the 4 genesrom the signature reduced its prognostic power andhen the 4-gene signature was entered into a backward
tepwise Cox-regression model along with the 4 genes on
he number of involved lymph nodes with the corresponding histogramsthe y-axis in order of (A) increasing survival and (B) increasing numberked along the x-axis. The blue bars on the histograms represent thefrom the Monte Carlo simulation.
d (B) ted onre ran
heir own, the 4-gene signature still outperformed the

ig
spCtstciopctistp(aemsp
4vmpasfvsa3tv
tltfsSv
toche
BA
SIC–
ALIM
ENTA
RY
TRA
CT
6 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
ndividual genes, there was no 2-way interaction betweenenes (data not shown).
When TNM stage, differentiation, resection margintatus, neurovascular invasion, and the 4-gene molecularrognostic signature were entered into a multivariableox regression model, the 4-gene signature remained in
he final model along with T- and N-stage (P � .013),howing its independent prognostic power (Supplemen-ary Table 3). Furthermore, the log likelihood ratio de-reases when the 4-gene molecular prognostic signatures added to the model, showing it improves the fit withutcome. If the signature was a marker of an existingathologic feature (such as differentiation) or only appli-able in a certain stage of tumor it would not remain inhe final model. A prognostic index was created by enter-ng T-stage, N-stage, and the 4-gene molecular prognosticignature into a Cox regression model and then addinghe regression co-efficient (�) for each factor to create arognostic score that takes into account all 3 features
model 1). This process was repeated with just T-stagend N-stage (model 2). When model 1 and model 2 werentered together into a backward stepwise Cox regressionodel, model 1 (containing the molecular prognostic
ignature) remains (P � .0001), showing its improved
Figure 2. Examples 0, 1�, 2�, and 3� scoring from immunohis
rognostic power over the current pathologic system. i
DiscussionThis study generates and externally validates a
-gene molecular prognostic signature that predicts sur-ival in an entirely independent cohort of patients. Thisethodology, involving internal and external validation,
rovides a robust framework for future similar projectsnd follows the published guidelines on generating suchignatures.12–14 Furthermore, this prognostic signatureor esophageal and junctional adenocarcinoma has beenalidated externally. Previously published data havehown that methylation,28 the number of copy numberberrations,29 and the expression of the microRNA mir-7530 can be linked to prognosis in esophageal and junc-ional adenocarcinoma, but none of this work has beenalidated externally.
The molecular prognostic signature was validated athe protein level for 2 reasons. The availability of forma-in-fixed, paraffin-embedded tissue was far greater thanhat of fresh-frozen samples. This meant that movingrom the RNA to the protein level for the validation stepsignificantly increased the size of the validation cohort.econd, although the use of immunohistochemistry foralidation of our signature reduced the number of genes
mistry staining of TMAs for DCK, PAPSS2, SIRT2, and TRIM44.
n our system compared with those selected at the RNA
Fp1(Nl
Ftce4hN
BA
SIC–
ALI
MEN
TARY
TRA
CT
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 7
ARTICLE IN PRESS
igure 3. Kaplan–Meier plots of survival comparing internal validationatients with dysregulation and no dysregulation of (A) DCK (�2
LR, 4.46;df; P � .035), (B) PAPSS2 (�2
LR, 12.11; 1 df; P � .001), (C) SIRT2�2
LR, 3.97; 1 df; P � .046), and (D) TRIM44 (�2LR, 3.35; 1 df; P � .063).
otches represent censored data; P values were calculated using the
og-rank (Mantel–Cox) test. ligure 4. Kaplan–Meier plots of survival comparing outcomes for pa-ients with 0 of 4, 1–2 of 4, and 3–4 of 4 genes dysregulated for (A) theomplete external validation dataset (�2
LR, 13.582; 2 df; P � 0.001), (B)xternal validation set patients who were chemotherapy-naive (�2
LR,.323; 2 df; P � .038), and (C) external validation dataset patients whoad received neoadjuvant chemotherapy (�2
LR, 5.013; 2 df; P � .025).otches represent censored data; P values were calculated using the
og-rank (Mantel–Cox) test.

laefhrfesStmsdpgirNic
gctgrmctnasidtaniBci
rsmtlinptatti
Fp0(Nlog-rank (Mantel–Cox) test.
BA
SIC–
ALIM
ENTA
RY
TRA
CT
8 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
evel, this was offset by the significant gains in clinicallypplicability and robustness. The scoring of paraffin-mbedded, formalin-fixed samples as positive or negativeor 4 antibodies is reproducible and straightforward in aospital pathology setting using existing facilities. Weealized there was a high chance that genes identifiedrom the expression array would be false positives but thexternal validation of the 4 genes in the final signatureuggests that this is not the case for TRIM44, PAPSS2,IRT2, and DCK. The protein level validation is in con-rast to other signatures that use gene expression at the
RNA level, a more variable feature that requires greatertandardization of techniques to allow comparison ofata from different days, laboratories, and types of sam-le (fresh, snap-frozen, fixed, and so forth). Some of theenes identified from the expression profiling but notncluded in the 4-gene protein signature are oncologicallyelevant (eg, NEU4,31 UBE2D2,32 MNT,33 PLK1,34 andEU431) and worthy of future investigation. This might
nclude the generation of new antibodies, where suitableommercial products are not available.
It is clear that the validation dataset differed from theeneration dataset in a number of ways (most notablyhemotherapy, Siewert classification, and differentia-ion), nonetheless, this did not affect the ability of the 4enes to predict outcome. This heterogeneity of datasetseflects the different populations that the signature
ight be applied to; and it could be argued that the moreontemporary validation dataset is a better reflection ofhe current population of patients with esophageal ade-ocarcinoma. Furthermore, differences in the generationnd validation datasets would serve to make it harder tohow the worth of this signature, rather than falselymproving its prognostic power. Although the generationataset was largely chemotherapy-naive owing to its his-orical nature (93%), it was shown that the signature waspplicable to a population of patients who had receivedeoadjuvant chemotherapy (n � 125; Figure 4C). This
ncreases the robustness and applicability of the findings.ecause none of the patients in this study had receivedhemoradiotherapy or adjuvant chemotherapy it will bemportant to assess this population in future work.
All 4 genes in the signature have interesting biologicaloles. Up-regulation of TRIM44 was associated withhorter life expectancy in the present study. TRIM44 is a
ember of a protein family involved in the ubiquitina-ion pathway,35 other members of which have establishedinks to cancer.36 The region of chromosome 11 contain-ng TRIM44 is also a locus of amplification in head andeck squamous cell cancer.37 DCK is involved in thehosphorylation of several deoxyribonucleosides andheir nucleoside analogues, and its deficiency is associ-ted with resistance to antiviral and anticancer chemo-herapeutic agents in pancreatic cancer,38 consistent withhe fact that down-regulation conferred a poor prognosis
igure 5. Kaplan–Meier plots of survival comparing external validationatients with dysregulation and no dysregulation of (A) DCK (�2
LR,.038; 1 df; P � .85), (B) PAPSS2 (�2
LR, 1.91; 1 df; P � .17), (C) SIRT2�2
LR, 1.97; 1 df; P � .16), and (D) TRIM44 (�2LR, 6.86; 1 df; P � .009).
otches represent censored data; P values were calculated using the
n our study. PAPSS2 is a bifunctional enzyme with both

apiLslpmgpmspgmtba
lepwsrTlwnlTatTdSdIo
s5snattcgotpngsa
gcwt
tmb4tb(itwefp
aG1
1
1
1
BA
SIC–
ALI
MEN
TARY
TRA
CT
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 9
ARTICLE IN PRESS
denosine triphosphate and adenosine 5=-phosphosul-hate kinase activity, which was highlighted by compar-
ng malignant and nonmalignant colorectal cell lines.39
oss of PAPSS2 was a poor prognostic sign in the presenttudy, consistent with the observation that complete de-etion or inactivation of PAPSS2 has been reported inrostate cancer cell lines and xenografts.40 SIRT2 has aitotic checkpoint function and may be a potential tar-
et of anticancer drugs.41 It was down-regulated in poorrognosis tumors consistent with the fact that it nor-ally promotes cell death when they are under severe
tress and overexpression can mediate a delay in cellularroliferation.42 It will be important to determine if theseenes are simply biomarkers of poor outcome or areechanistically important and thus might represent po-
ential therapeutic targets. None of these 4 genes haseen identified previously as prognostic in esophagealnd junctional adenocarcinoma.
We noted that individually DCK did not appear to beinked to survival in the external validation dataset. How-ver, when a 4-gene signature containing DCK was com-ared using a Cox regression model with a 3-gene signature,here DCK was removed, it was found that the 4-gene
ignature outperformed one containing only 3 genes andemained in the final model (data not shown). In contrast,RIM44 was of only borderline significance at the protein
evel in the relatively small generation cohort (Figure 3), butas the only one of the 4 targets to be individually prog-ostic in the larger validation cohort (Figure 5). This high-
ights the importance of external validation becauseRIM44 was one of the most significantly correlated genest the RNA level (P � 6.58 � 10�05). It is interesting to notehat when one gene is dysregulated it most commonly isRIM44 (57% of the time). However, when 3 genes areysregulated the most common combination is PAPSS2,IRT2, and DCK (41% of this group). This shows thatifferent genes have different roles to play in the signature.t will be important to assess the relative importance of eachf the genes in future large prospective studies.
This 4-gene molecular prognostic signature makes it pos-ible to identify a cohort of patients with a 5-year survival of8%, which is remarkable for this disease. Although pro-pective evaluation is required it might be possible to avoideoadjuvant chemotherapy in this group. Equally, knowingpatient has a very good chance of survival might influence
he decision to go ahead with an esophagectomy in a pa-ient who was otherwise considered borderline in terms ofomorbidity or clinical staging information. Although thisroup represents a small proportion of the population (6%verall and 9% of neoadjuvant chemotherapy–treated pa-ients) this is not surprising when we consider that mostatients with this disease will have a poor outcome. It is alsooteworthy that even patients staged T3N1 but with 0 of 4enes dysregulated have a 5-year survival of 50% (data nothown). Equally, the signature identifies a population with
very poor prognosis, a 5-year survival of just 14%. This
roup (17% of the overall cohort and 22% of neoadjuvanthemotherapy–treated patients) may do poorly regardless ofhat treatment they receive and therefore might be spared
he morbidity of surgery and/or chemotherapy.A multicenter prospective study will be required to fur-
her validate this molecular prognostic signature and deter-ine whether it can be applied to preoperative endoscopic
iopsies. It also will be interesting to determine if any of thegenes can predict response to chemotherapy. We envision
hat once prospectively validated it will be possible to com-ine the 4-gene signature with other clinical characteristicseg, age, TNM stage, differentiation) to provide a prognosticndex to guide management decisions. We would expecthat this index would subdivide patients into several groupsith significantly different outcomes. Equally, the knowl-
dge of which of these 4 genes are dysregulated may informuture targeted treatment, improving outcomes for the veryoor prognosis group.
Supplementary Material
Note: To access the supplementary materialccompanying this article, visit the online version ofastroenterology at www.gastrojournal.org, and at doi:0.1053/j.gastro.2010.05.080.
References
1. Cancer stats. Cancer Research UK 2009. Available from: URL:http://info.cancerresearchuk.org/cancerstats/. Accessed De-cember 1, 2009.
2. Allum WH, Stenning SP, Bancewicz J, et al. Long-term results ofa randomized trial of surgery with or without preoperative chemo-therapy in esophageal cancer. J Clin Oncol 2009;27:5062–5067.
3. Sobin I, eds. TNM classification of malignant tumours. 6th ed.Hoboken, NJ: John Wiley and Sons, Inc, 2002.
4. van ’t Veer LJ, Dai H, van de Vijver MJ, et al. Gene expressionprofiling predicts clinical outcome of breast cancer. Nature 2002;415:530–536.
5. Paik S, Shak S, Tang G, et al. A multigene assay to predictrecurrence of tamoxifen-treated, node-negative breast cancer.N Engl J Med 2004;351:2817–2826.
6. Straver ME, Glas AM, Hannemann J, et al. The 70-gene signatureas a response predictor for neoadjuvant chemotherapy in breastcancer. Breast Cancer Res Treat 2010;119:551–558.
7. van de Vijver MJ, He YD, van’t Veer LJ, et al. A gene-expressionsignature as a predictor of survival in breast cancer. N Engl J Med2002;347:1999–2009.
8. Fan C, Oh DS, Wessels L, et al. Concordance among gene-expression-based predictors for breast cancer. N Engl J Med2006;355:560–569.
9. Lagarde SM, Ver Loren van Themaat PE, Moerland PD, et al.Analysis of gene expression identifies differentially expressedgenes and pathways associated with lymphatic dissemination inpatients with adenocarcinoma of the esophagus. Ann Surg Oncol2008;15:3459–3470.
0. Schauer M, Janssen KP, Rimkus C, et al. Microarray-based re-sponse prediction in esophageal adenocarcinoma. Clin CancerRes 2010;16:330–337.
1. Benowitz S. Revised guidelines signal that gene expression pro-files are coming of age. J Natl Cancer Inst 2008;100:916–917.
2. Ludwig JA, Weinstein JN. Biomarkers in cancer staging, progno-
sis and treatment selection. Nat Rev Cancer 2005;5:845–856.
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
R
CCr
A
(tPH(MHBIUcSaR
Bdhl
C
F
RcodTC
BA
SIC–
ALIM
ENTA
RY
TRA
CT
10 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
3. Pepe MS, Etzioni R, Feng Z, et al. Phases of biomarker develop-ment for early detection of cancer. J Natl Cancer Inst 2001;93:1054–1061.
4. Barker PE. Cancer biomarker validation: standards and process:roles for the National Institute of Standards and Technology(NIST). Ann N Y Acad Sci 2003;983:142–150.
5. Moons KG, Royston P, Vergouwe Y, et al. Prognosis and prog-nostic research: what, why, and how? BMJ 2009;338:b375.
6. Royston P, Moons KG, Altman DG, et al. Prognosis and prognosticresearch: developing a prognostic model. BMJ 2009;338:b604.
7. Altman DG, Vergouwe Y, Royston P, et al. Prognosis and prognosticresearch: validating a prognostic model. BMJ 2009;338:b605.
8. Moons KG, Altman DG, Vergouwe Y, et al. Prognosis and prog-nostic research: application and impact of prognostic models inclinical practice. BMJ 2009;338:b606.
9. McShane LM, Altman DG, Sauerbrei W, et al. REporting recom-mendations for tumour MARKer prognostic studies (REMARK).Br J Cancer 2005;93:387–391.
0. Peters CJ, Hardwick RH, Vowler SL, et al. Generation and valida-tion of a revised classification for oesophageal and junctionaladenocarcinoma. Br J Surg 2009;96:724–733.
1. Korst RJ, Rusch VW, Venkatraman E, et al. Proposed revision ofthe staging classification for esophageal cancer. J Thorac Car-diovasc Surg 1998;115:660–669.
2. Pedrazzani C, de Manzoni G, Marrelli D, et al. Nodal staging inadenocarcinoma of the gastro-esophageal junction. Proposal of aspecific staging system. Ann Surg Oncol 2006;14:299–305.
3. Shannon K, inventor. Method for linear mRNA amplification. USpatent 6,132,997. October 17, 2000.
4. Hughes TR, Mao M, Jones AR, et al. Expression profiling usingmicroarrays fabricated by an ink-jet oligonucleotide synthesizer.Nat Biotechnol 2001;19:342–347.
5. Marton MJ, DeRisi JL, Bennett HA, et al. Drug target validationand identification of secondary drug target effects using DNAmicroarrays. Nat Med 1998;4:1293–1301.
6. Metropolis N, Ulam S. The Monte Carlo method. J Am Stat Assoc1949;44:335–341.
7. Rubie C, Kempf K, Hans J, et al. Housekeeping gene variability innormal and cancerous colorectal, pancreatic, esophageal, gas-tric and hepatic tissues. Mol Cell Probes 2005;19:101–109.
8. Brock MV, Gou M, Akiyama Y, et al. Prognostic importance ofpromoter hypermethylation of multiple genes in esophageal ad-enocarcinoma. Clin Cancer Res 2003;9:2912–2919.
9. Pasello G, Agata S, Bonaldi L, et al. DNA copy number alterationscorrelate with survival of esophageal adenocarcinoma patients.Mod Pathol 2009;22:58–65.
0. Mathe EA, Nguyen GH, Bowman ED, et al. MicroRNA expression insquamous cell carcinoma and adenocarcinoma of the esophagus:associations with survival. Clin Cancer Res 2009;15:6192–6200.
1. Yamanami H, Shiozaki K, Wada T, et al. Down-regulation ofsialidase NEU4 may contribute to invasive properties of humancolon cancers. Cancer Sci 2007;98:299–307.
2. Wu CH, Sahoo D, Arvanitis C, et al. Combined analysis of murineand human microarrays and ChIP analysis reveals genes associ-ated with the ability of MYC to maintain tumorigenesis. PLoSGenet 2008;4:e1000090.
3. Hurlin PJ, Zhou ZQ, Toyo-oka K, et al. Deletion of Mnt leads todisrupted cell cycle control and tumorigenesis. EMBO J 2003;22:4584–4596.
4. Jang YJ, Kim YS, Kim WH. Oncogenic effect of Polo-like kinase 1expression in human gastric carcinomas. Int J Oncol 2006;29:589–594.
5. Nisole S, Stoye JP, Saib A. TRIM family proteins: retroviral restric-tion and antiviral defence. Nat Rev Microbiol 2005;3:799–808.
6. Urano T, Saito T, Tsukui T, et al. Efp targets 14-3-3 sigma forproteolysis and promotes breast tumour growth. Nature 2002;
417:871–875. R7. Jarvinen AK, Autio R, Kilpinen S, et al. High-resolution copynumber and gene expression microarray analyses of head andneck squamous cell carcinoma cell lines of tongue and larynx.Genes Chromosomes Cancer 2008;47:500–509.
8. Sebastiani V, Ricci F, Rubio-Viqueira B, et al. Immunohistochem-ical and genetic evaluation of deoxycytidine kinase in pancreaticcancer: relationship to molecular mechanisms of gemcitabineresistance and survival. Clin Cancer Res 2006;12:2492–2497.
9. Franzon VL, Gibson MA, Hatzinikolas G, et al. Molecular cloningof a novel human PAPS synthetase which is differentially ex-pressed in metastatic and non-metastatic colon carcinoma cells.Int J Biochem Cell Biol 1999;31:613–626.
0. Hermans KG, van Alewijk DC, Veltman JA, et al. Loss of a smallregion around the PTEN locus is a major chromosome 10 alter-ation in prostate cancer xenografts and cell lines. Genes Chro-mosomes Cancer 2004;39:171–184.
1. Inoue T, Hiratsuka M, Osaki M, et al. The molecular biology ofmammalian SIRT proteins: SIRT2 in cell cycle regulation. CellCycle 2007;6:1011–1018.
2. North BJ, Verdin E. Mitotic regulation of SIRT2 by cyclin-depen-dent kinase 1-dependent phosphorylation. J Biol Chem 2007;282:19546–19555.
Received March 1, 2010. Accepted May 26, 2010.
eprint requestsAddress requests for reprints to: Rebecca Fitzgerald, MRC Cancer
ell Unit, Hutchison/MRC Research Centre, Box 197 Hills Road,ambridge, CB2 0XZ, United Kingdom. e-mail:[email protected]; fax: (44) 1223-763-296.
cknowledgmentsThe Oesophageal Cancer Clinical and Molecular Stratification
OCCAMS) Study Group is a multicenter UK collaboration. In additiono the listed authors, OCCAMS members involved in this study were. M. Safranek, N. Carroll, and S. Dwerryhouse (Addenbrookesospital, Cambridge, UK); S. J. Darnton and R. S. Steyn
Birmingham Heartlands, Birmingham, UK); J. Going and M.cKernan (Glasgow Royal Infirmary, Glasgow, UK); R. Stuart (Rossall Hospital, Glasgow, UK); M. Moorghen, J. Blazeby, and C. P.arham (Bristol Royal Infirmary, Bristol, UK); and C. Rajaguru, N.
mrit, and N. Maynard (Oxford Radcliffe Hospitals NHS Trust, Oxford,K). All OCCAMS Study Group members participated in the dataollection and approved the final version of the manuscript. K. A.erikawa, H. Dai, M. D. Ferguson, G. Y. Tokiwa, M. M. McWhorter,nd L. E. Carlini assisted in the expression profiling at Merckesearch Laboratories.Microarray data are available from the National Center for
iotechnology Information’s Gene Expression Omnibus publicatabase, accession number GSE19417. Available at:ttp://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?token�
fanlgcymycgupi&acc�GSE19417.
onflicts of interestThe authors disclose no conflicts.
undingThis study was funded by the Medical Research Council. Merck
esearch Laboratories performed the expression profiling as part of aollaborative research agreement. The funding source had no influencen the study design, collection and analysis of data, interpretation ofata, the writing of the report, or the decision to submit for publication.his work was supported by the National Institute for Health Researchambridge Biomedical Research Centre and the National Cancer
esearch Institute Cambridge Experimental Cancer Medicine Centre.
fpsersepbwmbto
isb.3fvwvtflct
dbpr
h(rpscTlKmtdgwcS
afnle(t(trac
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e1
ARTICLE IN PRESS
Supplementary Materials and Methods
Normalization of Expression ArraysNormalization of the expression arrays was per-
ormed by determining if array intensity of reporterrobes correlated with quality control parameters such aspike-in controls, 3’ bias slope, especially if those report-rs are C-rich. If these criteria were met the correlatedeporters were used as a template. This left 75 of 91amples with good quality normalized data. The averagexpression level (log [ratio]) of all reporters in the tem-late was calculated for each experiment to get the meaniased level of each experiment, and a linear regressionas performed between each gene on the array and theean biased level across all the experiments with the
iased effect then subtracted. Samples that did not meethe criteria were not included in the final analysis (16f 91).
Creating a Short List of Targets forValidationThe 270 genes associated with the number of
nvolved lymph nodes and the 119 genes associated withurvival were filtered by selecting those that appeared onoth lists (n � 18) and those with a P value of less than
0001 for their association with the clinical feature (n �3 from the number of involved lymph nodes list, n � 7rom the survival list), leaving a long list of 58 targets foralidation. The Monte Carlo simulation showed thereas a higher probability of false positives from the sur-
ival list (false discovery rate, 100%; representing the facthat any of the genes could have been associated with theeature by chance) when compared with the lymph nodeist (false discovery rate, 56%), thus we preferentially in-luded more genes from the lymph node list for valida-
ion. It should be noted that the genes selected as pre- licting the number of involved lymph nodes also coulde shown to predict survival (data not shown). The highotential false discovery rates highlight the need forobust external validation of any target taken forward.
For each of these 58 genes, tumors were scored asaving relative increased, decreased, or neutral expression
defined as a 1.5-fold increase or decrease in normalizedatio compared with the group average). Kaplan–Meierlots then were generated to correlate each gene withurvival, and a log-rank Mantel–Cox test was used toompare the up-regulated and down-regulated groups.7
he groups then were assessed to determine their corre-ation with the number of involved lymph nodes using aruskal–Wallis test (the data were not distributed nor-ally). To determine the range of expression for each of
he 58 genes the variance was calculated from the rawata. Gene accession numbers then were linked to theene symbol, and function if known. Statistical analysisas performed using SPSS version 15.0 (SPSS, Inc, Chi-
ago, IL) and Prism Version 3.0 (GraphPad Software, Inc,an Diego, CA).
The initial 58 genes in the long list then were rankedccording to a number of criteria. These included theollowing: (1) being associated both with survival and theumber of involved lymph nodes; (2) having a P value of
ess than 1 � 10�4 for the correlation of expression withither survival or the number of involved lymph nodes;3) having a significant difference between groups inerms of survival or the number of involved lymph nodesP � .05); (4) having a variance of expression of greaterhan 0.1; (5) having a biologically interesting role (ie,elated to the cell cycle, inflammation, differentiation,nd so forth); and (6) having antibodies available. Thisreated a list of 10 targets for validation at the protein
evel.
Sp(
10.e2 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Figure 1. Box and whisker plots of the average deltaoor prognosis tumors), (B) ADCY9 (up-regulated in poor prognosis tu
down-regulated in poor prognosis tumors).
CT for the good and poor prognosis groups for (A) TRIM44 (up-regulated inmors), (C) NEU4 (down-regulated in poor prognosis tumors), and (D) DCK
S
C
P
M
D
P
S
T
U
D
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e3
ARTICLE IN PRESS
upplementary Table 1. Sources for Antibodies Used in the Study and the Conditions Used for Optimum Staining
Target Product number Antibody source BOND immunohistochemistry conditions
5AR1 Ab12962 Abcam Plc, Cambridge, UK 1/300 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 2 for 30 minutes
LK-1 PAB2309 Abnova GmbHc/o EMBLEM, Heidelberg, Germany
1/25 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 2 for 30 minutes
NT Ab53487 Abcam Plc, Cambridge, UK 1/10 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 2 for 30 minutes
CK LS-B1852/16035 LifeSpan Biosciences, Inc, Seattle, WA 1/10 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 2 for 30 minutes
APSS2 Ab56393 Abcam Plc, Cambridge, UK 1/600 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 1 for 30 minutes
IRT2 HPA011165 Atlas Antibodies AB, Stockholm, Sweden 1/100 DilutionIHC protocol FHIER Epitope Retrieval Solution 2 for 30 minutes
RIM44 11511-1-AP ProteinTech Group, Inc, Chicago, IL 1/50 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 1 for 30 minutes
BE2D2 H00007322-M02 Abnova GmbHc/o EMBLEM, Heidelberg, Germany
1/200 DilutionIHC protocol F � DAB enhancerHIER Epitope Retrieval Solution 1 for 30 minutes
AB, 3,3=-Diaminobenzidine; IHC, immunohistochemistry.

S
GT
SCPU
NAPHP
LS
CVM
NVLIUFLBP
A
ATHFZnA
E
T
ND
N
MP
T
10.e4 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Table 2. The 270 Genes Associated With the Number of Involved Lymph Nodes and the 119 GenesAssociated With Survival
Alternative names Accession number
Correlation withnumber ofinvolved LN
P valuefor association
enes associated with number of involved lymph nodesRIM44 TRIM44, DIPB, DIPB, HSA249128, HSA249128, MC7, MC7,
MGC3490, MGC3490NM_017583 0.477611 6.58E-05
IRT2 SIRT2, SIR2L, SIR2L, SIR2L2, SIR2L2, sirtuins NM_012237 0.547886 2.79E-065AR1 C5R1, (C5A), C5A, C5AR, C5AR, CD88, CD88 NM_001736 0.457444 1.45E-04LK1 PLK1, PLK, STPK13 HSS00056704 0.544843 3.25E-06BE2D2 UBE2D2, (UBC4), (UBC4_5), E2(17)KB2, E2(17)KB2, PUBC1,
PUBC1, UBC4/5, UBC4, UBCH5B, UBCH5BNM_181838 0.405883 8.76E-04
EU4 NEU4, MGC102757, MGC18222, MGC18222 NM_080741 0.410348 7.58E-04DCY9 ADCY9, AC9 NM_001116 0.434387 3.35E-04APSS2 PAPSS2, (SK2), ATPSK2 HSS00023134 �0.366539 .002892SS00095627 HSS00095627 0.523903 8.88E-06NPLA2 PNPLA2, 1110001C14Rik, 1110001C14Rik, ATGL, ATGL, TTS-
2.2, TTS-2.2NM_020376 0.50994 1.68E-05
OC401021 Contig38918_RC 0.475423 7.19E-05T3GAL4 ST3GAL4, (SAT3), (STZ), CGS23, CGS23, FLJ11867, FLJ11867,
IV, NANTA3, NANTA3, SAT3, SIAT4, SIAT4, SIAT4C, SIAT4C,ST3Gal, ST3Gal_IV, ST3GalIV, ST3GalIV, STZ
NM_006278 0.471308 8.46E-05
AMK1 CAMK1, CaMK1a, CAMKI, CAMKI, MGC120317, MGC120318 NM_003656 0.448481 2.02E-04PS33A VPS33A, FLJ22395, FLJ22395, FLJ23187, FLJ23187 NM_022916 0.443585 2.41E-04S4A6A MS4A6A, 4SPAN3, 4SPAN3.2, 4SPAN3.2, 4SPAN3, CD20-L3,
CD20L3, CD20L3, CDA01, CDA01, LOC64166, MGC22650,MGC22650, MS4A6, MS4A6, MST090, MST090, MSTP090,MSTP090
NM_152851 0.440783 2.67E-04
OXA1 NOXA1, FLJ25475, NY-CO-31, p51NOX, p67PHOX, SDCCAG31 AF039697 0.438385 2.91E-04PREB3 VPREB3, 8HS20, 8HS20, N27C7-2, N27C7-2 NM_013378 0.429783 3.94E-04OC253039 AL117474 �0.42865 4.10E-04TGB6 AL359053 �0.427223 4.30E-04NC93B1 UNC93B1, MGC126617, UNC93, UNC93, UNC93B, UNC93B NM_030930 0.425623 4.55E-04LJ32312 FLJ32312, MGC126729, MGC126755 NM_144709 �0.425265 4.60E-04OC285479 LOC285479 XM_211908 0.419516 5.59E-04BS1 BBS1, BBS2L2, BBS2L2, FLJ23590, FLJ23590, MGC51114 NM_024649 0.418792 5.73E-04OLR3A POLR3A, hRPC155, hRPC155, Hs.44003, RPC1, RPC1,
RPC155, RPC155Contig51732_RC 0.418611 5.77E-04
POE APOE, AD2, AD2, apoprotein, apoprotein, LOC281004,MGC1571, MGC1571
NM_000041 0.417808 5.92E-04
DM ADM, (PAMP), AM,proAM-N20 AL359337 �0.413245 6.89E-04MED9 TMED9, gp25L2, Hs.279929, HSGP25L2G, HSGP25L2G NM_017510 0.413202 6.90E-04SPBP1 HSPBP1 NM_012267 0.413107 6.92E-04GD2 FGD2, LOC221472, MGC71330, MGC71330, ZFYVE4, ZFYVE4 NM_173558 0.412676 7.02E-04YG11B ZYG11B, FLJ13456 AB051517 0.411991 7.18E-04bla 3076 AB029326 0.409266 7.85E-04SPH ASPH, BAH, BAH, CASQ2BP1, CASQ2BP1, HAAH, HAAH, JCTN,
JCTN, JUNCTATE, Junctin, LOC56921NM_032468 �0.407741 8.25E-04
FCBP1 EFCBP1, (STIP1), 10, Hs.302754, NECAB1, NECAB1, STIP-1,STIP-1
NM_022351 0.404807 9.07E-04
SPAN5 TSPAN5, 2810455A09Rik, 4930505M03Rik, NET-4, NET-4,TM4SF9, TM4SF9, TSPAN-5, TSPAN-5
NM_005723 �0.404661 9.11E-04
OM1 NOM1, C7orf3, LOC93130 AF107455 �0.403396 9.49E-04YM DYM, DMC, DMC, FLJ20071, FLJ20071, FLJ90130, FLJ90130,
SMC, SMCNM_017653 0.403193 9.55E-04
EDD9 NEDD9, (P105), CAS-L, CAS-L, CASL, CASL, dJ49G10.2,dJ49G10.2, dJ761I2.1, dJ761I2.1, HEF1, HEF1, Hs.80261,neural
NM_006403 0.402829 9.66E-04
YBBP1A MYBBP1A, (P160), (PAP2), P160, PAP2 NM_014520 0.400353 .001046IP5K2A PIP5K2A, PIP5K-II_alpha, PIP5KII-alpha, PIP5KII-alpha, PIPK,
PIPKNM_005028 0.399648 .001069
RAF2 TRAF2, (TRAP), Hs.373508, MGC:45012, MGC_45012, TRAP, NM_145718 0.398564 .001106
TRAP3, TRAP3 Contig6654_RC �0.397581 .001141
S
CCKKM
SMCS
BP
CMPMUULTCFCMBS
ES
LPT
N
P
A
TRMCM
PP
P
AKI
A
P
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e5
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
20orf52 C20orf52, bA353C18.2, bA353C18.2, MGC111180 NM_080748 0.396959 .00116414orf128 C14orf128, MGC15504 NM_032751 0.396248 .00119IAA1912 AB067499 0.395771 .001208DELR2 KDELR2, ELP-1, ERD2.2 BC027714 0.395325 .001225GRN1 MGRN1, (CD41B), (GP2B), (ITGA2B), CD41B, GP2B, Hs.32316,
ITGA2B, KIAA0544, RNF156AB011116 0.395197 .00123
KIL SKIL, Hs.198292, SNO, SNO, SnoA, SnoA, SnoN, SnoN NM_005414 0.394197 .001269GC24665 MGC24665 NM_152308 �0.393201 .00130817orf28 C17orf28, (DMC1), DMC1 NM_030630 0.392935 .001319LC38A2 SLC38A2, (PRO1068), (SAT2), ATA2, KIAA1382, PRO1068,
SAT2, SNAT2NM_018573 �0.391714 .00137
CAS1 BCAS1, AIBC1, AIBC1, NABC1, NABC1 NM_003657 0.389446 .001469RKACA PRKACA, Calpha, cPKA, Hs.169269, MGC48865, MGC48865,
PKACA, PKACANM_002730 0.388681 .001504
A11 CA11, CA-RP, CA-RP_XI, CARP2, CARP2, XI NM_001217 0.388231 .001525GC4093 MGC4093 NM_030578 0.38384 .001742KIA PKIA, PRKACN1, PRKACN1 NM_006823 �0.38251 .001813ED28 MED28, 1500003D12Rik, DKFZP434N185, EG-1, EG1, magicin AK024944 0.382161 .001832AP1L1 UAP1L1, LOC91373 AK074143 0.380657 .001916SP45 USP45, MGC14793 Contig36457_RC �0.380194 .001943PHN3 LPHN3, CIRL3, Hs.21917, KIAA0768, LEC3 AK094703 �0.379075 .002008SPAN6 TSPAN6, T245, T245, TM4SF6, TM4SF6, TSPAN-6, TSPAN-6 NM_003270 �0.379076 .002008DK8 CDK8, Hs.397734, K35 L23311 �0.378821 .002023MR1 FMR1, (FRAXA), FMRP, FMRP, FRAXA, MGC87458, MGC87458 NM_002024 �0.378834 .002023D52 CD52, CDW52, CDW52 NM_001803 0.378806 .002024VP MVP, (LRP), LRP, VAULT1, VAULT1 NM_017458 0.377499 .002104CDIN3 BCDIN3, FLJ20257 NM_019606 0.376054 .002196LC38A2 SLC38A2, (PRO1068), (SAT2), ATA2, ATA2, KIAA1382,
KIAA1382, PRO1068, SAT2, SNAT2, SNAT2NM_018976 �0.375269 .002247
LN ELN, (WBS), (WS), elastin, SVAS, WBS AF086171 0.374653 .002288TK16 STK16, FLJ39635, FLJ39635, KRCT, KRCT, MPSK, MPSK,
MPSK1, PKL12, PKL12, TSF1, TSF1NM_003691 0.371494 .002508
OC253982 LOC253982 NM_181718 0.36999 .00262CDHGA10 PCDHGA10, PCDH-GAMMA-A10, PCDH-GAMMA-A10 NM_018913 0.369939 .002624REM2 TREM2, TREM-2, TREM-2, Trem2a, Trem2a, Trem2b, Trem2b,
Trem2c, Trem2cNM_018965 0.368281 .002752
PDC1 NPDC1, (CAB), (CAB1), CAB-, CAB-, CAB-1, CAB-1, CAB, CAB1,DKFZP586J0523, DKFZP586J0523, Hs.105547
NM_015392 0.36813 .002764
CDHGA12 PCDHGA12, CDH21, CDH21, FIB3, FIB3, KIAA0588, KIAA0588,PCDH-GAMMA-A12, PCDH-GAMMA-A12
NM_003735 0.36804 .002771
RTS-1 ARTS-1, A-LAP, ALAP, APPILS, ARTS1, ERAAP, ERAP1,KIAA0525, PILSAP
NM_016442 0.367835 .002787
MEPAI TMEPAI, (STAG1), PMEPA1, PMEPA1, STAG1 NM_020182 0.367475 .002816PL15 RPL15, (RPL10), EC45, MGC88603, RPL10, RPLY10, RPYL10 AF087974 �0.367465 .002817VP MVP, (LRP), LRP, VAULT1, VAULT1 NM_005115 0.36738 .002824ENPC2 CENPC2, (140 kilodalton), 2, C, CENPC, centromere hCT2307059 0.36723 .00283611S1 M11S1, GPIAP1, GPIAP1, GPIP137, GPIP137, p137, p137GPI,
p137GPINM_005898 0.366652 .002883
CBD2 PCBD2, DCOH2, DCOH2, DCOHM, DCOHM, DKFZP566K1946 NM_032151 0.366142 .002925EA15 PEA15, (HMAT1), (MAT1), (PED), HMAT1, HUMMAT1H,
HUMMAT1H, MAT1, MAT1H, MAT1H, PEA-15, PEA-15, PEDNM_003768 0.365901 .002946
CDHGA8 PCDHGA8, KIAA0327, KIAA0327, PCDH-GAMMA-A8, PCDH-GAMMA-A8
NM_032088 0.365878 .002947
TPBD1B ATPBD1B, FLJ10349 NM_018066 0.365503 .002979LC2 KLC2, FLJ12387, FLJ12387, Hs.280792, Klc2 NM_022822 0.365296 .002997
L-10 IL10, (TGIF), CSIF, CSIF, IL-10, IL-10, IL-10M1, IL10A, IL10A,MGC126450, MGC126451, TGIF
NM_000572 0.364947 .003027
LDH9A1 ALDH9A1, (ALDH4), (ALDH7), (E3), ALDH4, ALDH7, ALDH9,ALDH9, E3, TMABA-DH, TMABADH, TMABADH
NM_000696 0.364659 .003051
CDHGA4 PCDHGA4, PCDH-GAMMA-A4, PCDH-GAMMA-A4 NM_018917 0.364431 .003071
S
C
FR
M
CPPC
AATSC
DAP
S
P
G
PHLPKLCC
S
AXDPLPG
PLFF
LZDLEH
10.e6 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
LMN CLMN, calmin, calmin, FLJ12383, FLJ12383, KIAA1188,KIAA1188
NM_024734 0.364292 .003083
AM76A FAM76A, MGC34648, RP3-426I6.1 Contig47078_RC �0.364286 .003084NF41 RNF41, MGC45228, MGC45228, NRDP1, NRDP1, SBB103,
SBBI03, SBBI03NM_005785 0.363775 .003129
AP1LC3A MAP1LC3A, LOC84557, MAP1ALC3, MAP1ALC3, MAP1BLC3,MAP1BLC3
NM_032514 0.363392 .003163
14orf92 C14orf92, KIAA0737, KIAA0737 NM_014828 0.362612 .003233EX26 PEX26, FLJ20695, Hs.5420, PEX26M1T, Pex26pM1T HSS00298727 0.362534 .00324CDHGB2 PCDHGB2, MGC126854, PCDH-GAMMA-B2, PCDH-GAMMA-B2 NM_018923 0.362219 .003269DK5RAP1 CDK5RAP1, (C42), C20orf34, C20orf34, C42, CDK5RAP1.3,
CDK5RAP1.3, CDK5RAP1.4, CDK5RAP1.4, CGI-05, CGI-05,dJ1187J4.4, HSPC167, HSPC167, LOC51654
NM_016082 0.362115 .003279
L833402 AL833402 0.361351 .00335TG4A ATG4A, APG4A, AUTL2 NM_178271 �0.361002 .003383BX18 TBX18, Hs.381297 BC040697 0.360941 .003389LC44A2 SLC44A2, CTL2, DKFZp666A071, PP1292 NM_020428 0.360714 .00341YLN2 CYLN2, (CLIP), CLIP-115, CLIP-115, CLIP, CLIP2, CLIP2,
Hs.104717, KIAA0291, KIAA0291, MGC11333, MGC11333,WBSCR4, WBSCR4, WSCR4, WSCR4
NM_032421 0.359826 .003496
YNLL2 DYNLL2, Dlc2, MGC17810 NM_080677 0.359628 .003516SB6 ASB6, FLJ20548, FLJ20548, MGC1024, MGC1024 NM_177999 0.3596 .003518RKAB1 PRKAB1, (AMPK), ampk, AMPK, AMPKbeta1, HAMPKb,
HAMPKb, MGC17785, GC17785NM_006253 0.358918 .003586
TEAP3 STEAP3, 2, dudlin, dudlin, FLJ10829, STMP3, STMP3, TSAP6,TSAP6
NM_018234 �0.358897 .003588
CDHGB1 PCDHGB1, MGC119466, MGC119467, MGC119469, PCDH-GAMMA-B1, PCDH-GAMMA-B1
NM_018922 0.358708 .003607
JA12 GJA12, CX46.6, CX46.6, Cx47, Cx47, Hs.100072,MGC105119, MGC105119, PMLDAR, PMLDAR
NM_020435 0.358516 .003626
IGT PIGT, CGI-06, CGI-06, LOC51604, MGC8909, MGC8909 NM_015937 0.358066 .003672SA9761 HSA9761 NM_014473 0.357763 .003703OC442125 LOC442125, FLJ35473 hCT1785631.2 0.357344 .003746CDHGB6 PCDHGB6, PCDH-GAMMA-B6, PCDH-GAMMA-B6 NM_018926 0.357266 .003754IAA0258 hCT1832087.1 0.356815 .003802OC149448 BC015894 0.356593 .003825UL4B CUL4B, KIAA0695, KIAA0695 NM_003588 0.356073 .00388DH1 CDH1, Arc-1, Arc-1, CDHE, CDHE, E-cadherin, ECAD, ECAD,
LCAM, LCAM, UVO, UVONM_004360 �0.355964 .003892
AMD9L SAMD9L, C7orf6, C7orf6, FLJ39885, FLJ39885, Hs.319825,KIAA2005, KIAA2005
NM_152703 0.355647 .003926
POC1 NM_001645 0.355636 .003927M_063557 XM_063557 �0.355354 .003958NAJB2 DNAJB2, HSJ1, HSJ1, HSPF3, HSPF3 NM_006736 0.355227 .003972CDHGC4 PCDHGC4, MGC119489, PCDH-GAMMA-C4, PCDH-GAMMA-C4 NM_018928 0.355021 .003994MO4 Contig50755_RC 0.354865 .004012APD5 PAPD5, TRF4-2 Contig41078_RC �0.354823 .004016ALNT10 GALNT10, DKFZP586H0623, DKFZp586H0623, FLJ00205,
FLJ00205, FLJ11715, FLJ11715, GalNAcT10, GalNAcT10,pp-GalNAc-T10, pp-GalNAc-T10
NM_017540 0.354771 .004022
CDHGA3 PCDHGA3, PCDH-GAMMA-A3, PCDH-GAMMA-A3 NM_018916 0.354465 .004056OC221955 LOC221955 NM_139179 0.354108 .004096UT8 FUT8, alpha1-6_FucT, MGC26465, MGC26465 NM_004480 �0.353894 .00412ARP2 FARP2, (FIR), FIR, FRG, FRG, KIAA0793, KIAA0793, PLEKHC3,
PLEKHC3NM_014808 0.353198 .004199
OC152485 AL117519 �0.353003 .004222YG11BL ZYG11BL, C9orf60, Hzyg, RP11-545E17.4, ZYG NM_006336 0.351828 .004359DX43 DDX43, DKFZp434H2114, DKFZp434H2114, HAGE, HAGE NM_018665 0.351775 .004366OC91137 LOC91137 NM_138773 0.351663 .004379PHA4 EPHA4, HEK8, SEK, TYRO1 Contig47294_RC �0.351284 .004424
NRPUL2 HNRPUL2, DKFZp762N1910 AL834470 0.351119 .004444
S
E
PHHULSPSNCSC
DMZ
S
FA
P
A
PPTUE
G
CCPZH
LPSCCDP
H
PI
L
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e7
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
XOSC5 EXOSC5, hRrp46p, hRrp46p, LOC56915, MGC12901,MGC12901, p12B, p12B, RRP41B, RRP41B, RRP46, RRP46,Rrp46p, Rrp46p
NM_020158 0.350598 .004508
CDHGB7 PCDHGB7, ME6, ME6, PCDH-GAMMA-B7, PCDH-GAMMA-B7 NM_018927 0.350531 .004516SS00368544 HSS00368544 �0.35052 .004517SS00181268 HSS00181268 0.350178 .004559TS2D UTS2D, (URP), U2B AK090630 0.349959 .004586OC493754 AK054923 0.349734 .004614DC3 SDC3, KIAA0468, SDCN, SDCN, SYND3, SYND3 NM_014654 0.348681 .004748CDHGA11 PCDHGA11, PCDH-GAMMA-A11, PCDH-GAMMA-A11 NM_032092 0.348636 .004753LC25A27 SLC25A27, FLJ33552, UCP4 Contig23761_RC �0.348129 .004819DUFC2 NDUFC2, B14.5B, B14.5b, NADHDH2, NADHDH2 NM_004549 0.347986 .0048371QG C1QG, C1q-C, C1q-C, C1QC, C1QC, FLJ27103, FLJ27103 NM_172369 0.347614 .004886LC22A2 SLC22A2, (OCT2), MGC32628, MGC32628, OCT2 NM_003058 0.347339 .004922CL21 CCL21, 6Ckine, 6Ckine, CKb9, CKb9, ECL, ECL, Exodus-2,
MGC34555, MGC34555, SCYA21, SCYA21, SLC, SLC, TCA4,TCA4
NM_002989 0.346423 .005045
LOC440850 XM_173072 �0.346343 .005056OM3Z DOM3Z, DOM3L, DOM3L, NG6, NG6 NM_005510 0.345459 .005176FSD1 MFSD1, FLJ14153, FLJ14153, UG0581B09, UG0581B09 NM_022736 0.345059 .005232NF473 ZNF473, DKFZP434N043, Hs.59255, HZFP100, KIAA1141,
ZFP100, ZN473hCT12197.3 0.344717 .00528
ENST00000300223 ENST00000300223 0.344631 .005292PSB1 SPSB1, SSB-1, SSB1 NM_025106 0.344256 .005345
RPS26 hCT23582.2 0.343554 .005446GA FGA, Fib2, Fib2, MGC119422, MGC119423, MGC119425 NM_021871 �0.343359 .005474DPGK ADPGK, 2610017G09Rik, 2610017G09Rik, ADP-GK, ADP-GK,
DKFZP434B195, DKFZP434B195NM_031284 �0.342736 .005565
CDHGA6 PCDHGA6, PCDH-GAMMA-A6, PCDH-GAMMA-A6 NM_018919 0.342609 .005584BE501035 BE501035 �0.34253 .005596
BTB1 ABTB1, BPOZ, BPOZ, EF1ABP, EF1ABP, MGC20585,MGC20585, PP2259, P2259
NM_032548 0.342363 .00562
CDHGB5 PCDHGB5, PCDH-GAMMA-B5, PCDH-GAMMA-B5 NM_018925 0.342335 .005625CDHGB3 PCDHGB3, PCDH-GAMMA-B3, PCDH-GAMMA-B3 NM_018924 0.342285 .005632IMM10 TIMM10, TIM10, TIM10, TIM10A, IM10A NM_012456 0.341926 .005686NQ9433 UNQ9433 NM_207413 0.341851 .005697NTPD8 ENTPD8, GLSR2492, GLSR2492, NTPDase-8, NTPDase-8,
NTPDase8, UNQ2492, UNQ2492NM_198585 0.341489 .005752
IMAP6 GIMAP6, DKFZp686A01175, DKFZp686A01175, FLJ22690,FLJ22690, hIAN2, hIAN2, IAN6, IAN6
NM_024711 0.340758 .005863
18orf17 C18orf17, FLJ33761, HsT2697 AK074875 0.34056 .00589421orf71 C21orf71, PRED21 AF086441 �0.340127 .005961CDHGA1 PCDHGA1, PCDH-GAMMA-A1, PCDH-GAMMA-A1 NM_018912 0.340088 .005968NF668 ZNF668, FLJ13479, FLJ13479, FLJ14492, FLJ14492 NM_024706 0.339909 .005996FE HFE, (HH), (HLA-H), dJ221C16.10.1, HFE1, HFE1, HH, HLA-H,
MGC103790, MGC103790,NM_139002 0.339839 .006007
FLJ36208 AK093527 0.339194 .006109OC388795 LOC388795 Contig55248_RC �0.338999 .00614OP5 POP5, (RPP2), (RPP20), HSPC004, HSPC004, RPP2, RPP20 NM_015918 0.338727 .006184HC2 SHC2, SCK, SHCB, SLI AB001451 0.338578 .00620814orf172 C14orf172, FLJ40452, FLJ40452 NM_152307 0.338559 .006211CNJ CCNJ, bA690P14.1, bA690P14.1, FLJ10895 NM_019084 �0.338484 .006224LST DLST, DLTS, DLTS, Hs.296348, MIRTD NM_001933 0.33834 .006247CDHGC5 PCDHGC5, PCDH-GAMMA-C5, PCDH-GAMMA-C5 NM_018929 0.338047 .006295
Contig27623_RC 0.337768 .006341MGA2 HMGA2, BABL, BABL, HMGI-C, HMGI-C, HMGIC, HMGIC, LIPO,
LIPONM_003483 �0.337533 .00638
CDHGA2 PCDHGA2, PCDH-GAMMA-A2, PCDH-GAMMA-A2 NM_018915 0.337514 .006383TM2B ITM2B, ABRI, ABRI, BRI, BRI, BRI2, BRI2, BRICD2B, BRICD2B,
E25B, E25B, E3-16, E3-16, FBD, FBDNM_021999 0.33751 .006384
OC442515 hCT1783331.1 0.337454 .006393

S
LAP
HN
PSP
M
V
KSMTASPMRA
C
W
BhPAD
LZPMP
DS
MMhMSP
E
P
HLH
10.e8 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
OC286404 hCT2257040 0.336973 .006474CBD4 ACBD4, FLJ13322, FLJ13322, HMFT0700, HMFT0700 NM_024722 0.33695 .006477CDHGB4 PCDHGB4, (CDH20), CDH20, FIB2, FIB2, PCDH-GAMMA-B4,
PCDH-GAMMA-B4NM_003736 0.336922 .006482
SU79303 HSU79303, ZNF581, NM_013301 0.336672 .006524DUFB2 NDUFB2, AGGG, AGGG, CI-AGGG, CI-AGGG, MGC70788,
MGC70788NM_004546 0.336656 .006527
CDHGA7 PCDHGA7, PCDH-GAMMA-A7, PCDH-GAMMA-A7 NM_018920 0.336634 .006531USD1 SUSD1, bA4O1.1, DKFZP761E1824, RP11-4O1.1, RP11-4O1.1 NM_022486 0.335994 .00664IK3CG PIK3CG, (PI3K), p110gamma, PI3CG, PI3CG, PI3K, PI3Kgamma,
PI3Kgamma, PIK3, PIK3Contig36042_RC 0.335751 .006682
SR1 MSR1, (MSR), MSR-1, phSR1, phSR1, phSR2, phSR2, SCARA1,SCARA1, SR-A, SR-A
NM_002445 0.335543 .006718
APB VAPB, ALS8, ALS8, LOC55820, VAMP-B, VAMP-B, VAMP-C,VAMP-C, VAP, VAP-B, VAP-B, VAP-C, VAP-C, VAPC
Contig18780_RC �0.335402 .006743
IBRA KIBRA, KIAA0869 NM_015238 0.333966 .006997BDSP SBDSP, CGI-97-like BC010183 0.33391 .007007AP2 MAP2, MAP2A, MAP2B, MAP2C AK055674 0.333679 .007049
CF15 TCF15, EC2, EC2, PARAXIS, PARAXIS NM_004609 0.333654 .007054DORA3 ADORA3, A3AR, A3AR, AD026, bA552M11.5, RP11-552M11.7 NM_000677 0.333337 .007111CD5 SCD5, ACOD4, FADS4, FLJ21032, HSCD5, SCD2, SCD4 Contig2339_RC �0.333064 .007161OP5 POP5, (RPP2), (RPP20), HSPC004, HSPC004, RPP2, RPP20 BM995033 0.332734 .007222UC2 MUC2, (MLP), Hs.315, MLP NM_002457 0.332326 .007298PS26 hCT23517.2 0.332166 .007328RHGDIB ARHGDIB, (D4), D4, GDIA2, GDIA2, GDID4, GDID4, Ly-GDI, Ly-
GDI, LYGDI, LYGDI, RAP1GN1, RAP1GN1NM_001175 0.332114 .007338
8orf20 C8orf20, FLJ22246, FLJ22246, FLJ22277, FLJ22277, PP432,PP432, REEP4, REEP4
NM_025232 0.331873 .007383
TIP hCT16728 0.331424 .007468Contig52994_RC �0.331331 .007486
AT4 BAT4, D6S54E, D6S54E, G5, G5 NM_033177 0.331209 .007509CT1970919 hCT1970919 0.331114 .007528TPN21 PTPN21, Hs.155693, PTPD1, PTPRL10 AK056249 0.330802 .007588DAM15 ADAM15, MDC15, MDC15 NM_003815 0.330712 .007605ATF1 DATF1, (DIO1), DIO1, dJ563E14.1, FLJ11265, Hs.155313,
KIAA0333HSS00138473 �0.330577 .007632
OC440111 HSS00340376 0.330309 .007684NF226 ZNF226, LOC51595 NM_015919 0.330219 .007701CDHGA9 PCDHGA9, PCDH-GAMMA-A9, PCDH-GAMMA-A9 NM_018921 0.32993 .007758BD1 MBD1, (PCM1), CXXC3, CXXC3, PCM1, RFT, RFT NM_015847 0.329635 .007817DGFRB PDGFRB, CD140B, CD140B, JTK12, JTK12, PDGF-R-beta, PDGF-
R-beta, PDGFR, PDGFR, PDGFR1, PDGFR1NM_002609 0.329561 .007831
J122O8.2 DJ122O8.2, FLJ21130, MGC104253 NM_020466 0.329146 .007914PG3A SPG3A, (GBP3), AD-FSP, AD-FSP, ATL1, ATLASTIN, atlastin1,
FSP1, FSP1, GBP3, LOC51062, SPG3, SPG3NM_181598 0.329114 .007921
GC10812 NM_031425 0.328926 .007958GC50273 MGC50273 NM_214461 0.328541 .008036CT1838320.1 hCT1838320.1 �0.327911 .008165YD88 MYD88, Hs.82116 NM_002468 0.327909 .008166MG1 SMG1, 61E3.4, ATX, KIAA0421, LIP Contig575_RC �0.327705 .008208CDHGA5 PCDHGA5, (ME3), CDH-GAMMA-A5, CDH-GAMMA-A5, ME3,
PCDH-GAMMA-A5, PCDH-GAMMA-A5NM_018918 0.327572 .008235
PHB2 EPHB2, (ERK), DRT, DRT, EPHT3, EPHT3, ERK, HEK5, Hek5,MGC87492, MGC87492, Tyro5, Tyro5
NM_017449 �0.327535 .008243
CGF3 PCGF3, (RNF3), DONG1, DONG1, FLJ36550, FLJ36550,MGC129615, MGC40413, MGC40413, RNF3, RNF3A, RNF3A
NM_153250 �0.327391 .008273
S1BP3 HS1BP3, ETM2, FLJ14249 NM_022460 0.327356 .008281OC56901 LOC56901, FLJ26118, NUOMS NM_020142 0.327287 .008295ARS2 HARS2, bA379J5.3, bA379J5.3, bA555E18.1, bA555E18.1,
C20orf88, C20orf88, DUEB, DUEB, MGC119131,NM_080820 0.327162 .008321
MGC41905, MGC41905

S
L
RSM
M
ZCC
C
LFPT
RLD
P
RLR
P
AHFMZCSLHLS
SA
CCCMDS
GMD
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e9
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
TBP3 LTBP3, (LTBP2), DKFZP586M2123, DKFZP586M2123, LTBP-3,LTBP-3, LTBP2, pp6425, pp6425,
NM_021070 0.32651 .008459
LOC134145 AK055604 0.326395 .008483NF184 RNF184, FLJ10546, FLJ10546, KIAA1585, KIAA1585 NM_018133 �0.326248 .008515LC7A11 SLC7A11, CCBR1, XCT Contig55727_RC �0.32619 .008527GC19604 MGC19604, MGC74760 NM_080665 0.326171 .008531
Contig52960_RC 0.326129 .00854AP3K8 MAP3K8, (COT), (EST), (FLJ10486), c-COT, c-COT, COT, EST,
ESTF, ESTF, FLJ10486, TPL-2, Tpl-2, TPL2, TPL2NM_005204 �0.324997 .008786
NF613 ZNF613, FLJ13590, FLJ13590 NM_024840 0.324954 .008795ARD6 CARD6, CINCIN1, CINCIN1 NM_032587 0.324927 .008801UEDC1 CUEDC1, (FLJ20739), DKFZp547L163, DKFZp547L163,
FLJ20739, LOC404093Contig51726_RC 0.324698 .008852
HRDL2 CHRDL2, BNF1, BNF1, CHL2, CHL2, DKFZP586N2124,DKFZp586N2124, FKSG37, FKSG37
NM_015424 0.324538 .008887
OC389182 HSS00337272 0.324523 .008891LJ32206 FLJ32206 NM_152497 0.323847 .009042roSAPiP2 ProSAPiP2, KIAA0775, TBKBP1 NM_014726 0.323597 .009098NFSF13B TNFSF13B, BAFF, BAFF, BLYS, BLYS, delta, TALL-1, TALL-1,
TALL1, TALL1, THANK, THANK, TNFSF20, TNFSF20, ZTNF4,ZTNF4
NM_006573 0.323569 .009105
AB3C RAB3C, LOC115827 NM_138453 0.323476 .009126OC285628 AL389942 �0.323318 .009162GKA DGKA, (DAGK), DAGK, DAGK1, DAGK1, DGK-ALPHA, DGK-alpha,
Hs.169153, Hs.172690, MGC12821, MGC12821,MGC42356, MGC42356
NM_001345 0.323053 .009222
IK3CG PIK3CG, (PI3K), p110gamma, PI3CG, PI3CG, PI3K, PI3Kgamma,PI3Kgamma, PIK3, PIK3
NM_002649 0.322993 .009236
APGEF5 RAPGEF5, GFR, KIAA0277, LOC285936, MR-GEF, REPAC NM_012294 0.322904 .009257EPRE1 LEPRE1, GROS1, GROS1, P3H1, P3H1 NM_022356 0.322537 .009341OM1 ROM1, ROM, ROM-1, ROM, ROSP1, ROSP1, TSPAN23,
TSPAN23NM_000327 0.32238 .009378
CDH1 PCDH1, Hs.115642, MGC45991, MGC45991, PC42, PC42,PCDH42, PCDH42
NM_002587 0.322355 .009383
RRDC1 ARRDC1, MGC40555, MGC40555, RP11-48C7.5 NM_152285 0.322331 .009389SS00383658 HSS00383658 0.322266 .009404LJ23560 FLJ23560 NM_024685 0.322243 .009409SRA NM_012331 0.322239 .009411NF426 ZNF426, MGC2663, MGC2663 NM_024106 0.322132 .00943520orf133 C20orf133, dJ631M13.5, dJ631M13.5, RP11-189J1.1 Contig31913_RC 0.321955 .009477PECC1 SPECC1, FLJ36955, HCMOGT-1, HCMOGT-1, NSP NM_152904 0.32176 .009523OC284215 AK098180 0.321687 .00954SZFP36 hCT19106.3 �0.321164 .009664OC441220 LOC441220 ENST00000297321 0.3211 .00968OAT1 SOAT1, (ACAT), (ACAT1), (SOAT), ACACT, ACACT, ACAT, ACAT1,
RP11-215I23.2, SOAT, STAT, STATNM_003101 0.320871 .009734
LC2A14 SLC2A14, GLUT14, GLUT14 Contig26461_RC �0.320501 .009824BTB2 ABTB2, DKFZP586C1619, DKFZP586C1619 NM_145804 0.320493 .009826
Contig39391_RC �0.320447 .009837ENTA2 CENTA2, cent-b, cent-b, Hs.415471, HSA272195, HSA272195 NM_018404 0.320413 .009845LTB CLTB, Hs.380749, LCB, LCB NM_007097 0.320364 .009857OL4A4 COL4A4, CA44, CA44 NM_000092 0.320332 .009865DH1 MDH1, MDH-s, MDHA, MGC:1375, MGC_1375, MOR2 Contig48371 �0.320316 .009868GCR13 DGCR13, DGS-H L77565 0.319881 .009975NAPAP SNAPAP, SNAPIN, SNAPIN NM_012437 0.319826 .009988
Correlation withsurvival
enes associated with survivalNT MNT, MAD6, MAD6, MXD6, MXD6, ROX, ROX NM_020310 0.521739 9.82E-06
CK DCK, MGC117410 NM_000788 0.444598 2.33E-04
S
U
PS
KF
GTSA
R
IGCFKCS
U
ZAS
LTA
FXG
FDW
K
BAK
HPBM
A
CZ
HO
10.e10 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
BE2D2 UBE2D2, (UBC4), (UBC4_5), E2(17)KB2, E2(17)KB2, PUBC1,PUBC1, UBC4/5, UBC4, UBCH5B, UBCH5B
NM_181838 �0.355205 .003974
APSS2 PAPSS2, (SK2), ATPSK2 HSS00023134 0.336878 .00649EC14L2 SEC14L2, (TAP), C22ORF6, C22orf6, Hs.198667, KIAA1186,
KIAA1186, KIAA1658, KIAA1658, MGC65053, MGC65053,SPF, SPF, TAP
NM_012429 �0.457293 1.45E-04
IAA1447 KIAA1447, FLJ23058 NM_024696 0.43851 2.90E-04NBP4 FNBP4, DKFZp779I1064, DKFZp779I1064, FBP30, FBP30,
KIAA1014, KIAA1014NM_015308 0.418487 5.79E-04
OSR2 GOSR2, GS27, GS27, MEMBRIN, MEMBRIN NM_004287 �0.41209 7.16E-04CF15 TCF15, EC2, EC2, PARAXIS, PARAXIS NM_004609 �0.406177 8.68E-04ERAC1 SERAC1, (FLJ30544), FLJ14917, FLJ14917, FLJ30544 NM_032861 0.405813 8.78E-04RTS-1 ARTS-1, A-LAP, ALAP, APPILS, ARTS1, ERAAP, ERAP1,
KIAA0525, PILSAPNM_016442 �0.405387 8.90E-04
AB3IP RAB3IP, FLJ14660, FLJ14660, FLJ22548, FLJ22548,MGC71495, MGC71495, RABIN3, RABIN3
NM_022456 0.39724 .001153
FNGR1 IFNGR1, CD119, CD119, IFN-gammaRalpha, IFNGR, IFNGR NM_000416 0.392012 .001357NB5 GNB5, DKFZP586O1922, GB5, GB5 NM_016194 �0.385298 .0016671orf176 C1orf176, FLJ11445, FLJ13183, FLJ21144 NM_022774 �0.384361 .001715ABP4 FABP4, A-FABP, A-FABP, ALBP, aP2 NM_001442 �0.382318 .001823IAA0195 KIAA0195 NM_014738 0.382213 .00182914orf128 C14orf128, MGC15504 NM_032751 �0.380964 .001898CD5 SCD5, ACOD4, FADS4, FLJ21032, HSCD5, SCD2, SCD4 Contig2339_RC 0.380283 .001937
Contig55201_RC 0.379526 .001982SP15 USP15, KIAA0529, KIAA0529, MGC74854, MGC74854,
UNPH4, UNPH4NM_006313 0.377405 .00211
NF596 ZNF596, FLJ36123, FLJ36123, LOC169270 NM_173539 0.375166 .002254MPH AMPH, AMPH1, AMPH1 NM_001635 �0.370012 .002618OCS6 SOCS6, STATI4, STATI4, (SOCS4), (STAT4), CIS4, CIS4, Cish4,
HSPC060, HSPC060, LOC9306, SOCS4, SSI4, SSI4, STAI4,STAI4, STAT4
NM_004232 0.369996 .002619
OC146517 Contig55562_RC �0.369474 .002659CF3 TCF3, E2A, E2A, E47, ITF1, ITF1 NM_003200 0.367743 .002795BCC10 ABCC10, (MRP7), EST182763, EST182763, FLJ00002,
FLJ00036, MRP7, SIMRP7, SIMRP7NM_033450 0.36396 .003112
LJ90396 FLJ90396, MGC126179, MGC126180 NM_153358 �0.362902 .003207RCC4 NM_003401 �0.362691 .003226KAP1 GKAP1, FKSG21, FKSG21, FLJ25469, FLJ25469, GKAP42,
GKAP42, RP11-162J2.1NM_025211 0.362516 .003242
LJ23235 FLJ23235 NM_024943 �0.3625 .003243LNB14 DLNB14 NM_198489 0.36156 .00333HSC1 WHSC1, KIAA1090, KIAA1090, MMSET, MMSET, NSD2, NSD2,
REIIBP, REIIBP, TRX5, TRX5NM_133330 0.360931 .00339
IAA0319L KIAA0319L, FLJ14225, KIAA1837, KIAA1837, PKD1-like, PKD1-like, PP791, PP791, RP4-765A10.3
NM_024874 0.358755 .003602
HMT2 BHMT2, FLJ20001, FLJ20001 NM_017614 �0.358552 .003623RL5 Contig6113_RC �0.357946 .003684IAA1912 AB067499 �0.35721 .00376
Contig42954_RC 0.356223 .003864SS00383658 HSS00383658 �0.354939 .004003PCDC PPCDC, FLJ14585, MDS018 NM_021823 �0.354152 .004091C007356 BC007356 �0.35293 .00423S4A4A MS4A4A, (MS4A4), (MS4A7), 4SPAN1, CD20-L1, CD20L1,
HDCME31P, LOC51338, MGC22311, MS4A4NM_016650 �0.351948 .004345
LDH18A1 ALDH18A1, GSAS, GSAS, MGC117316, P5CS, P5CS, PYCS,PYCS
NM_002860 0.351392 .004411
21orf18 C21orf18, C21orf27, C21orf27 NM_017438 0.351281 .004425NF248 ZNF248, (KIAA0137), bA162G10.3, bA162G10.3, KIAA0137,
LOC57209NM_021045 0.35123 .004431
SS00095627 HSS00095627 �0.350903 .004471
SGEPL1 OSGEPL1, LOC64172 NM_022353 �0.350738 .004491
S
PTZ
C
LMM
NCGFP
PPFFCPCD
CRZ
S
CD
O
N
UE
LSBGLCMKLP
C
LT
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e11
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
EX26 PEX26, FLJ20695, Hs.5420, PEX26M1T, Pex26pM1T HSS00298727 �0.35062 .004505IA1 NM_022173 0.349835 .004602MYND11 ZMYND11, BRAM1, BRAM1, BS69, BS69, Hs.145894,
MGC111056, MGC111056, PRKCBP1L1, RP11-486H9.1NM_006624 0.349615 .004629
OMMD1 COMMD1, C2orf5, C2orf5, MGC27155, MGC27155, MURR1,MURR1
NM_152516 �0.349212 .00468
RRC34 LRRC34, MGC27085, MGC27085 NM_153353 0.348706 .004744BTD1 MBTD1, FLJ20055, FLJ20055, SA49P01, SA49P01 NM_017643 �0.346029 .005098SMB MSMB, (MSP), (PSP), IGBF, IGBF, MSP, MSPB, MSPB, PN44,
PN44, PRPS, PRPS, PSP-94, PSP-94, PSP, PSP57, PSP57,PSP94, PSP94
NM_002443 0.345843 .005124
GFRAP1L1 NGFRAP1L1, MGC104434 Contig36448_RC 0.342415 .005613TBP2 CTBP2, Hs.171391, ribeye NM_001329 0.341825 .005701PD2 GPD2, GDH2, mGPD, mGPDH Contig53191_RC 0.340702 .005872AM14A FAM14A, MGC44913, MGC44913, TLH29, TLH29 NM_032036 �0.340679 .005876IK3CG PIK3CG, (PI3K), p110gamma, PI3CG, PI3CG, PI3K, PI3Kgamma,
PI3Kgamma, PIK3, PIK3NM_002649 �0.340417 .005916
ARP6 PARP6, LOC56965, LOC56966 NM_020213 0.339747 .006021NLDC1 PNLDC1, dJ195P10.2, dJ195P10.2, FLJ40240, FLJ40240 NM_173516 0.338999 .00614LJ16231 ENST00000334095 �0.338888 .006158RMD4B FRMD4B, 6030440G05Rik, GRSP1, KIAA1013 HSS00209863 �0.338535 .006215EP4 CEP4, Cep135, FLJ13621, Hs.287583, KIAA0635 NM_014645 0.338087 .006288CDHB4 PCDHB4, PCDH-BETA4, PCDH-BETA4 NM_018938 0.33799 .006304A5BL CA5BL, Hs.31535, LOC340591, PRO2325 HSS00380435 0.337671 .006357GCR2 DGCR2, (IDD), DGS-C, DGS-C, IDD, KIAA0163, KIAA0163, LAN,
LAN, SEZ-12, SEZ-12NM_005137 0.337071 .006457
GI-115 CGI-115 NM_016052 �0.335848 .006665AB28 RAB28, MGC41862, MGC41862 NM_004249 �0.335575 .006712NF236 ZNF236, ZNF236A, ZNF236A, ZNF236B, ZNF236B NM_007345 0.335233 .006772
Contig27623_RC �0.335222 .006774T8SIA1 ST8SIA1, GD3S, GD3S, I, SIAT8, SIAT8, SIAT8A, SIAT8A,
ST8Sia, ST8SIA-I, ST8Sia_I, ST8SiaI, ST8SiaINM_003034 �0.335194 .006779
18orf55 C18orf55, HSPC154, HSPC154 NM_014177 0.335039 .006806HDDS DHDDS, (CIT), (CPT), CIT, CPT, DS, DS, FLJ13102, FLJ13102,
HDS, HDS, Hs.225160NM_024887 �0.334722 .006862
CRL OCRL, (INPP5F), (NPHL2), INPP5F, LOCR, LOCR, NPHL2, OCRL1,OCRL1
NM_000276 �0.334719 .006863
DUFC2 NDUFC2, B14.5B, B14.5b, NADHDH2, NADHDH2 NM_004549 �0.334223 .006951Contig52994_RC 0.334063 .00698
VRAG NM_003369 �0.333955 .006999PN3 EPN3, FLJ20778, FLJ20778 NM_017957 �0.333742 .007038
Contig49806_RC �0.33273 .007223OC130355 hCT1647780.3 �0.332542 .007258LBP SLBP, (HBP), HBP NM_006527 0.332515 .007263ATF BATF, B-ATF, B-ATF, SFA-2, SFA-2 NM_006399 �0.332417 .007281SDM1 GSDM1, FKSG9, FKSG9, FLJ39120, FLJ39120, GSDM, GSDM NM_178171 �0.331933 .007372OC440782 HSS00093016 �0.331551 .0074448orf36 C8orf36, FLJ32440, MMS21, NSE2 NM_173685 �0.331484 .007457S4A6E NM_139249 �0.331407 .007472IAA1731 KIAA1731, FLJ40913 AK057804 0.330221 .007701PHN3 LPHN3, CIRL3, Hs.21917, KIAA0768, LEC3 AK094703 0.329496 .007844VRL3 PVRL3, (PRR3), DKFZP566B0846, DKFZP566B0846,
FLJ90624, FLJ90624, nectin-3, nectin-3, PPR3, PPR3, PRR3,PVRR3, PVRR3
NM_015480 0.328973 .007949
20orf12 C20orf12, bA189K21.8, bA189K21.8, C20orf84, C20orf84,dJ568F9.2, dJ568F9.2, DKFZp781J2425, DKFZp781J2425,FLJ10600, FLJ10600, FLJ30892, FLJ30892
NM_018152 0.328575 .008029
OC401220 XM_211972 �0.328527 .008039REM2 TREM2, TREM-2, TREM-2, Trem2a, Trem2a, Trem2b, Trem2b, NM_018965 �0.32839 .008067
Trem2c, Trem2c
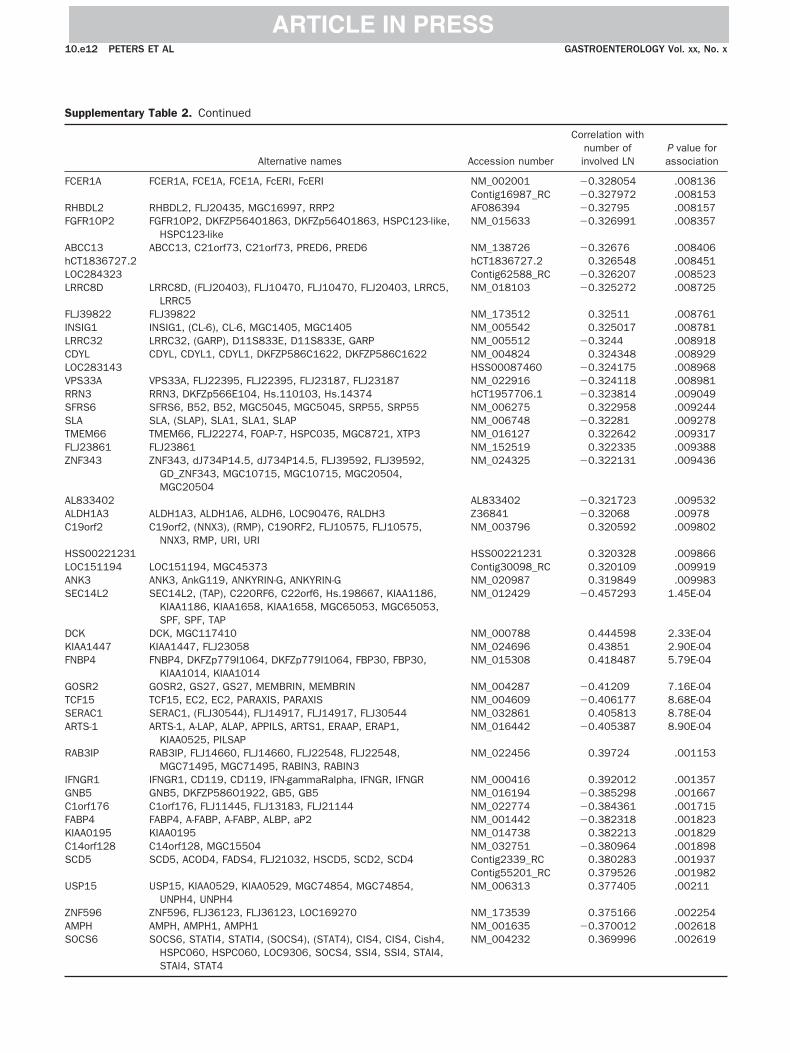
S
F
RF
AhLL
FILCLVRSSTFZ
AAC
HLAS
DKF
GTSA
R
IGCFKCS
U
ZAS
10.e12 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
CER1A FCER1A, FCE1A, FCE1A, FcERI, FcERI NM_002001 �0.328054 .008136Contig16987_RC �0.327972 .008153
HBDL2 RHBDL2, FLJ20435, MGC16997, RRP2 AF086394 �0.32795 .008157GFR1OP2 FGFR1OP2, DKFZP564O1863, DKFZp564O1863, HSPC123-like,
HSPC123-likeNM_015633 �0.326991 .008357
BCC13 ABCC13, C21orf73, C21orf73, PRED6, PRED6 NM_138726 �0.32676 .008406CT1836727.2 hCT1836727.2 0.326548 .008451OC284323 Contig62588_RC �0.326207 .008523RRC8D LRRC8D, (FLJ20403), FLJ10470, FLJ10470, FLJ20403, LRRC5,
LRRC5NM_018103 �0.325272 .008725
LJ39822 FLJ39822 NM_173512 0.32511 .008761NSIG1 INSIG1, (CL-6), CL-6, MGC1405, MGC1405 NM_005542 0.325017 .008781RRC32 LRRC32, (GARP), D11S833E, D11S833E, GARP NM_005512 �0.3244 .008918DYL CDYL, CDYL1, CDYL1, DKFZP586C1622, DKFZP586C1622 NM_004824 0.324348 .008929OC283143 HSS00087460 �0.324175 .008968PS33A VPS33A, FLJ22395, FLJ22395, FLJ23187, FLJ23187 NM_022916 �0.324118 .008981RN3 RRN3, DKFZp566E104, Hs.110103, Hs.14374 hCT1957706.1 �0.323814 .009049FRS6 SFRS6, B52, B52, MGC5045, MGC5045, SRP55, SRP55 NM_006275 0.322958 .009244LA SLA, (SLAP), SLA1, SLA1, SLAP NM_006748 �0.32281 .009278MEM66 TMEM66, FLJ22274, FOAP-7, HSPC035, MGC8721, XTP3 NM_016127 0.322642 .009317LJ23861 FLJ23861 NM_152519 0.322335 .009388NF343 ZNF343, dJ734P14.5, dJ734P14.5, FLJ39592, FLJ39592,
GD_ZNF343, MGC10715, MGC10715, MGC20504,MGC20504
NM_024325 �0.322131 .009436
L833402 AL833402 �0.321723 .009532LDH1A3 ALDH1A3, ALDH1A6, ALDH6, LOC90476, RALDH3 Z36841 �0.32068 .0097819orf2 C19orf2, (NNX3), (RMP), C19ORF2, FLJ10575, FLJ10575,
NNX3, RMP, URI, URINM_003796 0.320592 .009802
SS00221231 HSS00221231 0.320328 .009866OC151194 LOC151194, MGC45373 Contig30098_RC 0.320109 .009919NK3 ANK3, AnkG119, ANKYRIN-G, ANKYRIN-G NM_020987 0.319849 .009983EC14L2 SEC14L2, (TAP), C22ORF6, C22orf6, Hs.198667, KIAA1186,
KIAA1186, KIAA1658, KIAA1658, MGC65053, MGC65053,SPF, SPF, TAP
NM_012429 �0.457293 1.45E-04
CK DCK, MGC117410 NM_000788 0.444598 2.33E-04IAA1447 KIAA1447, FLJ23058 NM_024696 0.43851 2.90E-04NBP4 FNBP4, DKFZp779I1064, DKFZp779I1064, FBP30, FBP30,
KIAA1014, KIAA1014NM_015308 0.418487 5.79E-04
OSR2 GOSR2, GS27, GS27, MEMBRIN, MEMBRIN NM_004287 �0.41209 7.16E-04CF15 TCF15, EC2, EC2, PARAXIS, PARAXIS NM_004609 �0.406177 8.68E-04ERAC1 SERAC1, (FLJ30544), FLJ14917, FLJ14917, FLJ30544 NM_032861 0.405813 8.78E-04RTS-1 ARTS-1, A-LAP, ALAP, APPILS, ARTS1, ERAAP, ERAP1,
KIAA0525, PILSAPNM_016442 �0.405387 8.90E-04
AB3IP RAB3IP, FLJ14660, FLJ14660, FLJ22548, FLJ22548,MGC71495, MGC71495, RABIN3, RABIN3
NM_022456 0.39724 .001153
FNGR1 IFNGR1, CD119, CD119, IFN-gammaRalpha, IFNGR, IFNGR NM_000416 0.392012 .001357NB5 GNB5, DKFZP586O1922, GB5, GB5 NM_016194 �0.385298 .0016671orf176 C1orf176, FLJ11445, FLJ13183, FLJ21144 NM_022774 �0.384361 .001715ABP4 FABP4, A-FABP, A-FABP, ALBP, aP2 NM_001442 �0.382318 .001823IAA0195 KIAA0195 NM_014738 0.382213 .00182914orf128 C14orf128, MGC15504 NM_032751 �0.380964 .001898CD5 SCD5, ACOD4, FADS4, FLJ21032, HSCD5, SCD2, SCD4 Contig2339_RC 0.380283 .001937
Contig55201_RC 0.379526 .001982SP15 USP15, KIAA0529, KIAA0529, MGC74854, MGC74854,
UNPH4, UNPH4NM_006313 0.377405 .00211
NF596 ZNF596, FLJ36123, FLJ36123, LOC169270 NM_173539 0.375166 .002254MPH AMPH, AMPH1, AMPH1 NM_001635 �0.370012 .002618OCS6 SOCS6, STATI4, STATI4, (SOCS4), (STAT4), CIS4, CIS4, Cish4,
HSPC060, HSPC060, LOC9306, SOCS4, SSI4, SSI4, STAI4,NM_004232 0.369996 .002619
STAI4, STAT4

S
LTA
FXG
FDW
K
BAK
HPBM
A
CZ
HOPTZ
C
LMM
NCGFP
PPFFCPCD
CRZ
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e13
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
OC146517 Contig55562_RC �0.369474 .002659CF3 TCF3, E2A, E2A, E47, ITF1, ITF1 NM_003200 0.367743 .002795BCC10 ABCC10, (MRP7), EST182763, EST182763, FLJ00002,
FLJ00036, MRP7, SIMRP7, SIMRP7NM_033450 0.36396 .003112
LJ90396 FLJ90396, MGC126179, MGC126180 NM_153358 �0.362902 .003207RCC4 NM_003401 �0.362691 .003226KAP1 GKAP1, FKSG21, FKSG21, FLJ25469, FLJ25469, GKAP42,
GKAP42, RP11-162J2.1NM_025211 0.362516 .003242
LJ23235 FLJ23235 NM_024943 �0.3625 .003243LNB14 DLNB14 NM_198489 0.36156 .00333HSC1 WHSC1, KIAA1090, KIAA1090, MMSET, MMSET, NSD2, NSD2,
REIIBP, REIIBP, TRX5, TRX5NM_133330 0.360931 .00339
IAA0319L KIAA0319L, FLJ14225, KIAA1837, KIAA1837, PKD1-like, PKD1-like, PP791, PP791, RP4-765A10.3
NM_024874 0.358755 .003602
HMT2 BHMT2, FLJ20001, FLJ20001 NM_017614 �0.358552 .003623RL5 Contig6113_RC �0.357946 .003684IAA1912 AB067499 �0.35721 .00376
Contig42954_RC 0.356223 .003864SS00383658 HSS00383658 �0.354939 .004003PCDC PPCDC, FLJ14585, MDS018 NM_021823 �0.354152 .004091C007356 BC007356 �0.35293 .00423S4A4A MS4A4A, (MS4A4), (MS4A7), 4SPAN1, CD20-L1, CD20L1,
HDCME31P, LOC51338, MGC22311, MS4A4NM_016650 �0.351948 .004345
LDH18A1 ALDH18A1, GSAS, GSAS, MGC117316, P5CS, P5CS, PYCS,PYCS
NM_002860 0.351392 .004411
21orf18 C21orf18, C21orf27, C21orf27 NM_017438 0.351281 .004425NF248 ZNF248, (KIAA0137), bA162G10.3, bA162G10.3, KIAA0137,
LOC57209NM_021045 0.35123 .004431
SS00095627 HSS00095627 �0.350903 .004471SGEPL1 OSGEPL1, LOC64172 NM_022353 �0.350738 .004491EX26 PEX26, FLJ20695, Hs.5420, PEX26M1T, Pex26pM1T HSS00298727 �0.35062 .004505IA1 NM_022173 0.349835 .004602MYND11 ZMYND11, BRAM1, BRAM1, BS69, BS69, Hs.145894,
MGC111056, MGC111056, PRKCBP1L1, RP11-486H9.1NM_006624 0.349615 .004629
OMMD1 COMMD1, C2orf5, C2orf5, MGC27155, MGC27155, MURR1,MURR1
NM_152516 �0.349212 .00468
RRC34 LRRC34, MGC27085, MGC27085 NM_153353 0.348706 .004744BTD1 MBTD1, FLJ20055, FLJ20055, SA49P01, SA49P01 NM_017643 �0.346029 .005098SMB MSMB, (MSP), (PSP), IGBF, IGBF, MSP, MSPB, MSPB, PN44,
PN44, PRPS, PRPS, PSP-94, PSP-94, PSP, PSP57, PSP57,PSP94, PSP94
NM_002443 0.345843 .005124
GFRAP1L1 NGFRAP1L1, MGC104434 Contig36448_RC 0.342415 .005613TBP2 CTBP2, Hs.171391, ribeye NM_001329 0.341825 .005701PD2 GPD2, GDH2, mGPD, mGPDH Contig53191_RC 0.340702 .005872AM14A FAM14A, MGC44913, MGC44913, TLH29, TLH29 NM_032036 �0.340679 .005876IK3CG PIK3CG, (PI3K), p110gamma, PI3CG, PI3CG, PI3K, PI3Kgamma,
PI3Kgamma, PIK3, PIK3NM_002649 �0.340417 .005916
ARP6 PARP6, LOC56965, LOC56966 NM_020213 0.339747 .006021NLDC1 PNLDC1, dJ195P10.2, dJ195P10.2, FLJ40240, FLJ40240 NM_173516 0.338999 .00614LJ16231 ENST00000334095 �0.338888 .006158RMD4B FRMD4B, 6030440G05Rik, GRSP1, KIAA1013 HSS00209863 �0.338535 .006215EP4 CEP4, Cep135, FLJ13621, Hs.287583, KIAA0635 NM_014645 0.338087 .006288CDHB4 PCDHB4, PCDH-BETA4, PCDH-BETA4 NM_018938 0.33799 .006304A5BL CA5BL, Hs.31535, LOC340591, PRO2325 HSS00380435 0.337671 .006357GCR2 DGCR2, (IDD), DGS-C, DGS-C, IDD, KIAA0163, KIAA0163, LAN,
LAN, SEZ-12, SEZ-12NM_005137 0.337071 .006457
GI-115 CGI-115 NM_016052 �0.335848 .006665AB28 RAB28, MGC41862, MGC41862 NM_004249 �0.335575 .006712NF236 ZNF236, ZNF236A, ZNF236A, ZNF236B, ZNF236B NM_007345 0.335233 .006772
Contig27623_RC �0.335222 .006774

S
S
CD
O
N
UE
LSBGLCMKLP
C
LT
F
RF
AhLL
FILCL
N
10.e14 PETERS ET AL GASTROENTEROLOGY Vol. xx, No. x
ARTICLE IN PRESS
upplementary Table 2. Continued
Alternative names Accession number
Correlation withnumber ofinvolved LN
P value forassociation
T8SIA1 ST8SIA1, GD3S, GD3S, I, SIAT8, SIAT8, SIAT8A, SIAT8A,ST8Sia, ST8SIA-I, ST8Sia_I, ST8SiaI, ST8SiaI
NM_003034 �0.335194 .006779
18orf55 C18orf55, HSPC154, HSPC154 NM_014177 0.335039 .006806HDDS DHDDS, (CIT), (CPT), CIT, CPT, DS, DS, FLJ13102, FLJ13102,
HDS, HDS, Hs.225160NM_024887 �0.334722 .006862
CRL OCRL, (INPP5F), (NPHL2), INPP5F, LOCR, LOCR, NPHL2, OCRL1,OCRL1
NM_000276 �0.334719 .006863
DUFC2 NDUFC2, B14.5B, B14.5b, NADHDH2, NADHDH2 NM_004549 �0.334223 .006951Contig52994_RC 0.334063 .00698
VRAG NM_003369 �0.333955 .006999PN3 EPN3, FLJ20778, FLJ20778 NM_017957 �0.333742 .007038
Contig49806_RC �0.33273 .007223OC130355 hCT1647780.3 �0.332542 .007258LBP SLBP, (HBP), HBP NM_006527 0.332515 .007263ATF BATF, B-ATF, B-ATF, SFA-2, SFA-2 NM_006399 �0.332417 .007281SDM1 GSDM1, FKSG9, FKSG9, FLJ39120, FLJ39120, GSDM, GSDM NM_178171 �0.331933 .007372OC440782 HSS00093016 �0.331551 .0074448orf36 C8orf36, FLJ32440, MMS21, NSE2 NM_173685 �0.331484 .007457S4A6E NM_139249 �0.331407 .007472IAA1731 KIAA1731, FLJ40913 AK057804 0.330221 .007701PHN3 LPHN3, CIRL3, Hs.21917, KIAA0768, LEC3 AK094703 0.329496 .007844VRL3 PVRL3, (PRR3), DKFZP566B0846, DKFZP566B0846,
FLJ90624, FLJ90624, nectin-3, nectin-3, PPR3, PPR3, PRR3,PVRR3, PVRR3
NM_015480 0.328973 .007949
20orf12 C20orf12, bA189K21.8, bA189K21.8, C20orf84, C20orf84,dJ568F9.2, dJ568F9.2, DKFZp781J2425, DKFZp781J2425,FLJ10600, FLJ10600, FLJ30892, FLJ30892
NM_018152 0.328575 .008029
OC401220 XM_211972 �0.328527 .008039REM2 TREM2, TREM-2, TREM-2, Trem2a, Trem2a, Trem2b, Trem2b,
Trem2c, Trem2cNM_018965 �0.32839 .008067
CER1A FCER1A, FCE1A, FCE1A, FcERI, FcERI NM_002001 �0.328054 .008136Contig16987_RC �0.327972 .008153
HBDL2 RHBDL2, FLJ20435, MGC16997, RRP2 AF086394 �0.32795 .008157GFR1OP2 FGFR1OP2, DKFZP564O1863, DKFZp564O1863, HSPC123-like,
HSPC123-likeNM_015633 �0.326991 .008357
BCC13 ABCC13, C21orf73, C21orf73, PRED6, PRED6 NM_138726 �0.32676 .008406CT1836727.2 hCT1836727.2 0.326548 .008451OC284323 Contig62588_RC �0.326207 .008523RRC8D LRRC8D, (FLJ20403), FLJ10470, FLJ10470, FLJ20403, LRRC5,
LRRC5NM_018103 �0.325272 .008725
LJ39822 FLJ39822 NM_173512 0.32511 .008761NSIG1 INSIG1, (CL-6), CL-6, MGC1405, MGC1405 NM_005542 0.325017 .008781RRC32 LRRC32, (GARP), D11S833E, D11S833E, GARP NM_005512 �0.3244 .008918DYL CDYL, CDYL1, CDYL1, DKFZP586C1622, DKFZP586C1622 NM_004824 0.324348 .008929OC283143 HSS00087460 �0.324175 .008968
OTE. Genes taken forward to validation are highlighted in bold.
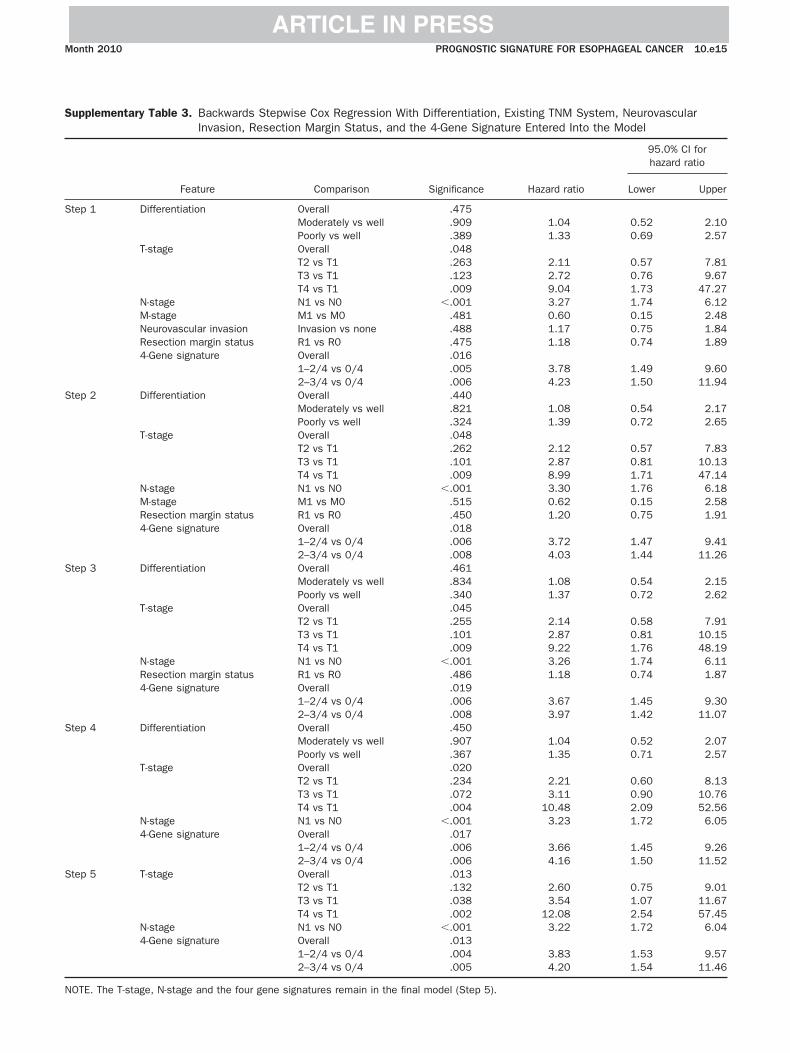
S
S
S
S
S
S
N
Month 2010 PROGNOSTIC SIGNATURE FOR ESOPHAGEAL CANCER 10.e15
ARTICLE IN PRESS
upplementary Table 3. Backwards Stepwise Cox Regression With Differentiation, Existing TNM System, NeurovascularInvasion, Resection Margin Status, and the 4-Gene Signature Entered Into the Model
Feature Comparison Significance Hazard ratio
95.0% CI forhazard ratio
Lower Upper
tep 1 Differentiation Overall .475Moderately vs well .909 1.04 0.52 2.10Poorly vs well .389 1.33 0.69 2.57
T-stage Overall .048T2 vs T1 .263 2.11 0.57 7.81T3 vs T1 .123 2.72 0.76 9.67T4 vs T1 .009 9.04 1.73 47.27
N-stage N1 vs N0 �.001 3.27 1.74 6.12M-stage M1 vs M0 .481 0.60 0.15 2.48Neurovascular invasion Invasion vs none .488 1.17 0.75 1.84Resection margin status R1 vs R0 .475 1.18 0.74 1.894-Gene signature Overall .016
1–2/4 vs 0/4 .005 3.78 1.49 9.602–3/4 vs 0/4 .006 4.23 1.50 11.94
tep 2 Differentiation Overall .440Moderately vs well .821 1.08 0.54 2.17Poorly vs well .324 1.39 0.72 2.65
T-stage Overall .048T2 vs T1 .262 2.12 0.57 7.83T3 vs T1 .101 2.87 0.81 10.13T4 vs T1 .009 8.99 1.71 47.14
N-stage N1 vs N0 �.001 3.30 1.76 6.18M-stage M1 vs M0 .515 0.62 0.15 2.58Resection margin status R1 vs R0 .450 1.20 0.75 1.914-Gene signature Overall .018
1–2/4 vs 0/4 .006 3.72 1.47 9.412–3/4 vs 0/4 .008 4.03 1.44 11.26
tep 3 Differentiation Overall .461Moderately vs well .834 1.08 0.54 2.15Poorly vs well .340 1.37 0.72 2.62
T-stage Overall .045T2 vs T1 .255 2.14 0.58 7.91T3 vs T1 .101 2.87 0.81 10.15T4 vs T1 .009 9.22 1.76 48.19
N-stage N1 vs N0 �.001 3.26 1.74 6.11Resection margin status R1 vs R0 .486 1.18 0.74 1.874-Gene signature Overall .019
1–2/4 vs 0/4 .006 3.67 1.45 9.302–3/4 vs 0/4 .008 3.97 1.42 11.07
tep 4 Differentiation Overall .450Moderately vs well .907 1.04 0.52 2.07Poorly vs well .367 1.35 0.71 2.57
T-stage Overall .020T2 vs T1 .234 2.21 0.60 8.13T3 vs T1 .072 3.11 0.90 10.76T4 vs T1 .004 10.48 2.09 52.56
N-stage N1 vs N0 �.001 3.23 1.72 6.054-Gene signature Overall .017
1–2/4 vs 0/4 .006 3.66 1.45 9.262–3/4 vs 0/4 .006 4.16 1.50 11.52
tep 5 T-stage Overall .013T2 vs T1 .132 2.60 0.75 9.01T3 vs T1 .038 3.54 1.07 11.67T4 vs T1 .002 12.08 2.54 57.45
N-stage N1 vs N0 �.001 3.22 1.72 6.044-Gene signature Overall .013
1–2/4 vs 0/4 .004 3.83 1.53 9.572–3/4 vs 0/4 .005 4.20 1.54 11.46
OTE. The T-stage, N-stage and the four gene signatures remain in the final model (Step 5).
Copyright © 2022 FDOKUMEN




















