
A Randomized Controlled Trial on the Effectiveness of a Classification-Based System for Sub-acute...
10
RANDOMIZED TRIAL SPINE Volume 37, Number 16, pp 1347–1356 ©2012, Lippincott Williams & Wilkins Spine www.spinejournal.com 1347 A Randomized Controlled Trial on the Effectiveness of a Classification-Based System for Subacute and Chronic Low Back Pain Adri T. Apeldoorn, PhD,*† Raymond W. Ostelo, PhD ,*‡ Hans van Helvoirt, MA,§ Julie M. Fritz, PhD, Dirk L. Knol, PhD,* Maurits W. van Tulder, PhD ,*‡ and Henrica CW de Vet, PhD* Study Design. A randomized controlled trial. Objective. To assess the effectiveness of Delitto’s classification– based treatment approach compared with usual physical therapy care in patients with subacute or chronic low back pain. Summary of Background Data. No trial has evaluated this approach in patients with subacute and chronic low back pain. Methods. Before randomization, all patients were classified by research physical therapists according to a modified version of Delitto’s classification–based system. Randomization was computer- generated, with centralized allocation concealment. The statistician and the physical therapists were unblinded. Patients and assistants who collected follow-up questionnaires were blinded. Follow-up assessments were completed at 8, 26, and 52 weeks. The primary analysis was performed according to the intention-to-treat principle, using multilevel analysis. The main outcomes were global perceived effect, disability (Oswestry Disability Index, 0–100), and pain intensity (Numerical Rating Scale, 0–10). Secondary outcomes were quality of life, fear-avoidance beliefs, and psychosocial status. Results. A total of 156 patients were included (classification-based group, n 74; usual physical therapy group, n 82). There were no statistically significant differences between the treatment groups for any of the outcomes at any of the follow-up time points. After 8 weeks, patients in the classification-based group had greater global F or care providers, it is often not possible to make a spe- cific pathoanatomical diagnosis reliably for patients with low back pain (LBP). Consequently, 85% to 95% of patients with LBP are diagnosed by their general practitio- ner as having nonspecific LBP. 1 Given this absence of diagnos- tic precision, and the limited evidence that basing treatment on a specific etiology improves outcomes, most clinicians use pattern recognition and patient profiling in an attempt to optimize treatment outcomes. 2 One of the attempts is a classification-based treatment approach initially developed by Delitto et al 3 and subsequently updated using more recent research. 4 This approach is based on the identification of specific findings from a patient’s his- tory, clinical presentation, and physical examination that are integrated into a classification algorithm. This algorithm is thought to help clinicians identify the treatment most likely to benefit the patient. Two randomized controlled trials (RCTs) have investigated the effectiveness of this approach. Both studies reported slightly more favorable outcomes for the classification-based approach than other physical therapy management strategies in patients with acute and subacute LBP and mild to severe disability. 5 ,6 The aim of this study was to determine whether the effectiveness of this classification- based approach was generalized to another health care sys- tem, other clinicians, and another population. In this study, we compared classification-based treatment with usual physi- cal therapy care in patients with subacute (6–12 wk) and chronic (12 wk) LBP. From the *Department of Epidemiology and Biostatistics and the EMGO + Institute for Health and Care Research, VU University Medical Centre, Amsterdam, the Netherlands; †Medical Centre Alkmaar, Alkmaar, the Netherlands; ‡Department of Health Sciences and the EMGO + Institute for Health and Care Research, Faculty of Earth and Life Sciences, VU University, Amsterdam, the Netherlands; §Medical Back Neck Centre, The Hague, the Netherlands; and Department of Physical Therapy, University of Utah, and Intermountain Health Care, Salt Lake City, UT. Acknowledgment date: July 12, 2011. First revision date: December 10, 2011. Acceptance date: January 30, 2012. The manuscript submitted does not contain information about medical device(s)/drug(s). The Netherlands Organisation for Health Research and Development grant funds were received to support this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. Address correspondence and reprint requests to Adri T. Apeldoorn, PhD, Department of Epidemiology and Biostatistics and the EMGO Institute for Health and Care Research, VU University Medical Centre, Van der Boechorststraat 7, 1081 BT Amsterdam, the Netherlands; E-mail: [email protected] perceived effect scores; adjusted odds ratio of 1.01 (95% confidence interval [CI], 0.31 to 3.28), and higher adjusted Oswestry Disability Index and Numerical Rating Scale scores; mean adjusted differences of 0.48 points (95% CI, −4.59 to 3.63) and 0.49 points (95% CI, −1.34 to 0.37) respectively, but all differences were statistically nonsignificant. Conclusion. The classification-based system used in this study was not effective for improving physical therapy care outcomes in a population of patients with subacute and chronic low back pain. Key words: low back pain, classification, physical therapy guidelines, subgroups, randomized controlled trial. Spine 2012; 37:1347–1356 DOI: 10.1097/BRS.0b013e31824d9f2b Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of A Randomized Controlled Trial on the Effectiveness of a Classification-Based System for Sub-acute...

RANDOMIZED TRIAL
SPINE Volume 37, Number 16, pp 1347–1356©2012, Lippincott Williams & Wilkins
Spine www.spinejournal.com 1347
A Randomized Controlled Trial on the Effectiveness of a Classifi cation-Based System for Subacute and Chronic Low Back Pain
Adri T. Apeldoorn , PhD,*† Raymond W. Ostelo , PhD , * ‡ Hans van Helvoirt , MA,§ Julie M. Fritz , PhD , � Dirk L. Knol , PhD , * Maurits W. van Tulder , PhD , * ‡ and Henrica CW de Vet , PhD *
Study Design. A randomized controlled trial. Objective. To assess the effectiveness of Delitto’s classifi cation–based treatment approach compared with usual physical therapy care in patients with subacute or chronic low back pain. Summary of Background Data. No trial has evaluated this approach in patients with subacute and chronic low back pain. Methods. Before randomization, all patients were classifi ed by research physical therapists according to a modifi ed version of Delitto’s classifi cation–based system. Randomization was computer-generated, with centralized allocation concealment. The statistician and the physical therapists were unblinded. Patients and assistants who collected follow-up questionnaires were blinded. Follow-up assessments were completed at 8, 26, and 52 weeks. The primary analysis was performed according to the intention-to-treat principle, using multilevel analysis. The main outcomes were global perceived effect, disability (Oswestry Disability Index, 0–100), and pain intensity (Numerical Rating Scale, 0–10). Secondary outcomes were quality of life, fear-avoidance beliefs, and psychosocial status. Results. A total of 156 patients were included (classifi cation-based group, n � 74; usual physical therapy group, n � 82). There were no statistically signifi cant differences between the treatment groups for any of the outcomes at any of the follow-up time points. After 8 weeks, patients in the classifi cation-based group had greater global
For care providers, it is often not possible to make a spe-cifi c pathoanatomical diagnosis reliably for patients with low back pain (LBP). Consequently, 85% to 95%
of patients with LBP are diagnosed by their general practitio-ner as having nonspecifi c LBP. 1 Given this absence of diagnos-tic precision, and the limited evidence that basing treatment on a specifi c etiology improves outcomes, most clinicians use pattern recognition and patient profi ling in an attempt to optimize treatment outcomes. 2
One of the attempts is a classifi cation-based treatment approach initially developed by Delitto et al 3 and subsequently updated using more recent research. 4 This approach is based on the identifi cation of specifi c fi ndings from a patient’s his-tory, clinical presentation, and physical examination that are integrated into a classifi cation algorithm. This algorithm is thought to help clinicians identify the treatment most likely to benefi t the patient. Two randomized controlled trials (RCTs) have investigated the effectiveness of this approach. Both studies reported slightly more favorable outcomes for the classifi cation-based approach than other physical therapy management strategies in patients with acute and subacute LBP and mild to severe disability. 5 , 6 The aim of this study was to determine whether the effectiveness of this classifi cation-based approach was generalized to another health care sys-tem, other clinicians, and another population. In this study, we compared classifi cation-based treatment with usual physi-cal therapy care in patients with subacute (6–12 wk) and chronic (�12 wk) LBP.
From the * Department of Epidemiology and Biostatistics and the EMGO + Institute for Health and Care Research, VU University Medical Centre, Amsterdam, the Netherlands; †Medical Centre Alkmaar, Alkmaar, the Netherlands ; ‡ Department of Health Sciences and the EMGO + Institute for Health and Care Research, Faculty of Earth and Life Sciences, VU University, Amsterdam, the Netherlands ; § Medical Back Neck Centre, The Hague, the Netherlands; and � Department of Physical Therapy, University of Utah, and Intermountain Health Care, Salt Lake City, UT .
Acknowledgment date: July 12, 2011. First revision date: December 10, 2011. Acceptance date: January 30, 2012.
The manuscript submitted does not contain information about medical device(s)/drug(s).
The Netherlands Organisation for Health Research and Development grant funds were received to support this work.
No benefi ts in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Address correspondence and reprint requests to Adri T. Apeldoorn, PhD, Department of Epidemiology and Biostatistics and the EMGO Institute for Health and Care Research, VU University Medical Centre, Van der Boechorststraat 7, 1081 BT Amsterdam, the Netherlands; E-mail: [email protected]
perceived effect scores; adjusted odds ratio of 1.01 (95% confi dence interval [CI], 0.31 to 3.28), and higher adjusted Oswestry Disability Index and Numerical Rating Scale scores; mean adjusted differences of 0.48 points (95% CI, − 4.59 to 3.63) and 0.49 points (95% CI, − 1.34 to 0.37) respectively, but all differences were statistically nonsignifi cant. Conclusion. The classifi cation-based system used in this study was not effective for improving physical therapy care outcomes in a population of patients with subacute and chronic low back pain. Key words: low back pain , classifi cation , physical therapy guidelines , subgroups , randomized controlled trial . Spine 2012 ; 37 : 1347 – 1356
DOI: 10.1097/BRS.0b013e31824d9f2b
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1347BRS204963.indd 1347 21/06/12 11:25 AM21/06/12 11:25 AM

RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
1348 www.spinejournal.com July 2012
METHODS The methods used in this study have been described in detail elsewhere. 7 The Medical Ethics Committee of the VU Univer-sity Medical Centre in Amsterdam approved this study.
PATIENTS AND SETTING Participants were recruited by physical therapists from 21 pri-vate physical therapy clinics in the city of Amsterdam and the surrounding (rural) area ( < 50-km radius). Inclusion criteria were LBP as the primary complaint, with or without associated leg pain, age between 18 and 65 years, current episode longer than 6 weeks, and ability to read and write Dutch. Exclusion criteria were known or suspected specifi c LBP ( e.g., cauda equina compression, fractures), severe radicu-lopathy, spondylolisthesis (grade 2 or more), serious comor-bidity ( e.g., metastases, AIDS, cerebrovascular accident), psychopathology, lumbar spinal surgery in the previous year, more than 1 low back operation, more than 1 year of absence from work due to LBP, currently pregnant or given birth in the past 3 months, inability to attend 6 or more regular physi-cal therapy appointments, moderate complaints about 1 or more items of the Urogenital Distress Inventory (UDI-6, Short Form), 8 , 9 or inability to demonstrate any LBP symptoms dur-ing mechanical examination.
Examination and Classifi cation Algorithm Potentially eligible patients were referred to 1 of 4 research physical therapists who were not involved in providing intervention. They evaluated eligibility, obtained written informed consent, collected baseline questionnaires, and conducted a clinical examination in the private practice that the patient attended. All clinical features outlined in Part 1 of Figure 1 were assessed in each patient. On the basis of their clinical presentation, patients could fi t 1, more than 1, or none of the classifi cation categories, that is , direction-specifi c exercises, manipulation, or stabilization exercises. When a patient met the criteria of direction-specifi c exer-cises and another classifi cation category, direction-specifi c exercises were preferred. In cases in which the patient met the criteria of manipulation and stabilization exercises or none of the classifi cation categories, extra criteria were used to categorize the patient (see Part 2 of Figure 1 ). The classifi cation algorithm is based on an updated version of the algorithm by Fritz et al 4 and modifi ed to fi t into the Dutch health care system and the typical practice patterns of Dutch physical therapists. Following the suggestion of Stanton et al , 10 patients who meet the subgrouping crite-ria in any of the hierarchical boxes in the fi rst part of the algorithm received the label “clear classifi cation”. Patients were given the label “unclear classifi cation” if additional criteria in the bottom box of the classifi cation algorithm were needed.
Randomization Procedure After the examination, an independent researcher random-ized each patient to the intervention or control group, using computer-generated preprepared randomization lists.
Treatment After randomization, the patient was scheduled for his or her fi rst treatment session as soon as possible in the clinic he or she attended. In each clinic, at least 1 physical therapist was instructed about the classifi cation system, and at least 1 physical therapist was instructed about the usual physical therapy care procedure, depending on preference and expertise. The physical therapists providing treatment on the basis of the classifi cation algorithm were not allowed to provide usual physical therapy care for patients included in this trial and vice versa. For both treatment groups, decisions about the frequency and the number of sessions were left to the discretion of the physical therapist.
Usual Physical Therapy Group Patients assigned to usual physical therapy care received indi-vidually tailored treatment according to the current Dutch LBP guidelines. 11 , 12
Classifi cation-Based Treatment Group Patients assigned to the classifi cation-based group were treated according to their primary classifi cation category ( i.e., direc-tion-specifi c exercises, spinal manipulation, or stabilization exercises) for a minimum of 4 weeks. After this period, the physical therapist was allowed to change treatment strategy according to the current Dutch LBP guidelines. 11 , 12 Full details of the interventions and criteria to change the treatment strategy in the fi rst 4 weeks are provided in the protocol. 7
Contrast Between Interventions The key distinction between the 2 treatment groups was the use of a standardized examination protocol and related treat-ment protocols in the classifi cation-based group compared with the usual physical therapy group. It was expected that examination techniques varied in the latter group, 13 , 14 and a wide range of treatment goals and strategies was used.
Blinding The statistician, research physical therapists, and the treating physical therapists were aware of the treatment allocation but were not involved in the data collection. The administrative assistants who collected all follow-up questionnaires were blinded for the patient’s group assignment. Every attempt was made to keep patients blinded to treatment allocation.
Measurements The baseline questionnaire included sociodemographic character-istics ( Table 1 ) and all primary and secondary outcome measures. The primary outcomes were assessed at 8, 26, and 52 weeks after the start of treatment and the secondary outcomes were assessed only at 52 weeks, all by means of postal questionnaires.
Primary Outcome Measures Pain intensity during the previous week was measured on an 11-point Numerical Rating Scale (NRS, 0 � “no pain” to 10 � “worst imaginable pain”). Functional status was measured with the 10-item Oswestry Disability Index (ODI), version 2.1a 15 , 16 (score range, 0–100), with higher scores indicating lower
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1348BRS204963.indd 1348 21/06/12 11:25 AM21/06/12 11:25 AM

RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
Spine www.spinejournal.com 1349
functional status. Global perceived effect (GPE) was measured by self-assessment on a 7-point Likert scale ranging from com-pletely recovered to worse than ever. This was dichotomized a priori into success (completely recovered and much recov-ered) and nonsuccess (slightly recovered to worse than ever).
Secondary Outcome Measures Fear-avoidance beliefs were measured with the Fear-Avoidance Beliefs Questionnaire Activity (score range, 0–24) section and Fear-Avoidance Beliefs Questionnaire Work section (score range, 0–42), 17 with higher scores indicating an increased level of fear-avoidance beliefs. Psychosocial status was assessed with the Örebro Musculoskeletal Pain Screening Questionnaire (ÖMPSQ, score range, 0–210), 18 with higher scores indicating greater risk of prolonged recovery from LBP. General health
status was evaluated with the 36-Item Short Form Health Survey. 19 , 20 Scores can be aggregated into 2 higher-order scores; the Physical Component Summary and the Mental Component Summary (score range, 0–100), with higher scores indicating better functioning. Responders to treatment were evaluated for the NRS and the ODI according to an a priori defi ned cutoff value (�30% improvement from baseline). 21
Sample Size Sample size calculations were based on detecting a clinically relevant difference using results of the studies of Brennan et al 6 and Fritz et al 5 and were performed for the 3 primary outcomes (for all: power 0.90; 2-sided � 0.05). We calculated that 68 patients were needed per group. Anticipating a poten-tial dropout of 10%, we aimed at 75 patients per group.
Figure 1. The classifi cation-based system for patients with LBP (�6 wk) used in this RCT. DP indicates directional preference; FABQW, Fear-Avoidance Beliefs Questionnaire Work; ROM, range of motion; SLR, straight leg raise; BLLS, Beighton Ligamentous Laxity Scale; ASLR, active straight leg raise; LBP, low back pain; RCT, randomized controlled trial; FABQA, Fear-Avoidance Beliefs Questionnaire Activity.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1349BRS204963.indd 1349 21/06/12 11:25 AM21/06/12 11:25 AM
RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
1350 www.spinejournal.com July 2012
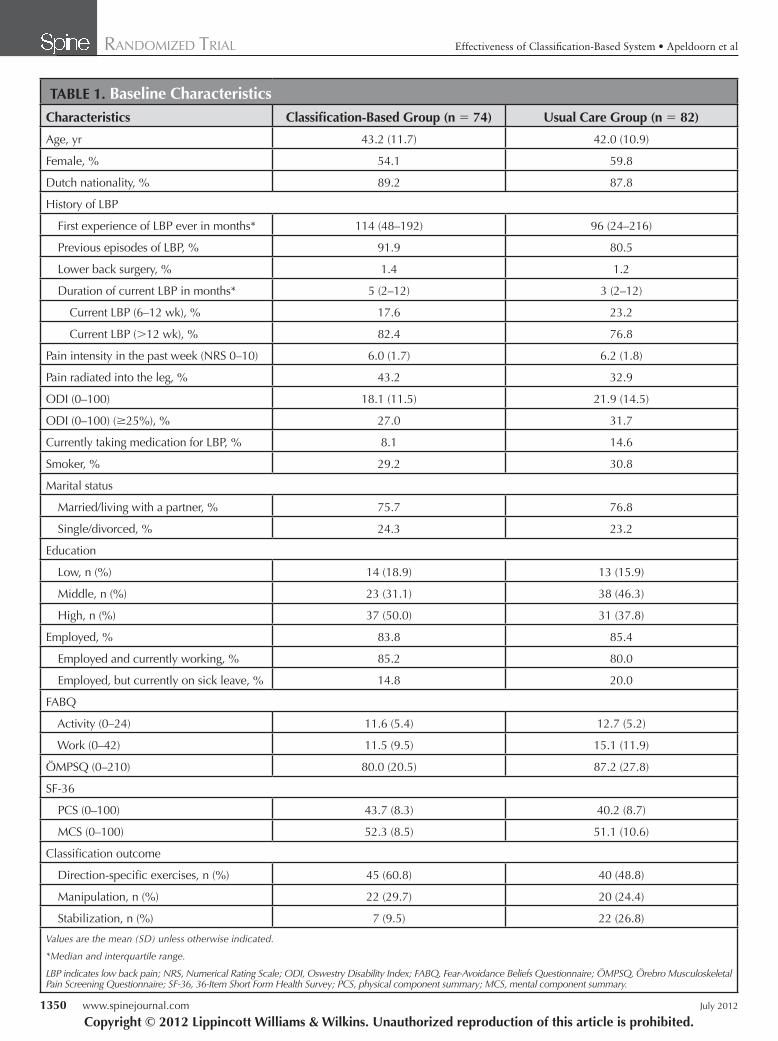
TABLE 1. Baseline Characteristics Characteristics Classifi cation-Based Group (n � 74) Usual Care Group (n � 82)
Age, yr 43.2 (11.7) 42.0 (10.9)
Female, % 54.1 59.8
Dutch nationality, % 89.2 87.8
History of LBP
First experience of LBP ever in months* 114 (48–192) 96 (24–216)
Previous episodes of LBP, % 91.9 80.5
Lower back surgery, % 1.4 1.2
Duration of current LBP in months* 5 (2–12) 3 (2–12)
Current LBP (6–12 wk), % 17.6 23.2
Current LBP (�12 wk), % 82.4 76.8
Pain intensity in the past week (NRS 0–10) 6.0 (1.7) 6.2 (1.8)
Pain radiated into the leg, % 43.2 32.9
ODI (0–100) 18.1 (11.5) 21.9 (14.5)
ODI (0–100) ( � 25%), % 27.0 31.7
Currently taking medication for LBP, % 8.1 14.6
Smoker, % 29.2 30.8
Marital status
Married/living with a partner, % 75.7 76.8
Single/divorced, % 24.3 23.2
Education
Low, n (%) 14 (18.9) 13 (15.9)
Middle, n (%) 23 (31.1) 38 (46.3)
High, n (%) 37 (50.0) 31 (37.8)
Employed, % 83.8 85.4
Employed and currently working, % 85.2 80.0
Employed, but currently on sick leave, % 14.8 20.0
FABQ
Activity (0–24) 11.6 (5.4) 12.7 (5.2)
Work (0–42) 11.5 (9.5) 15.1 (11.9)
ÖMPSQ (0–210) 80.0 (20.5) 87.2 (27.8)
SF-36
PCS (0–100) 43.7 (8.3) 40.2 (8.7)
MCS (0–100) 52.3 (8.5) 51.1 (10.6)
Classifi cation outcome
Direction-specifi c exercises, n (%) 45 (60.8) 40 (48.8)
Manipulation, n (%) 22 (29.7) 20 (24.4)
Stabilization, n (%) 7 (9.5) 22 (26.8)
Values are the mean (SD) unless otherwise indicated.
*Median and interquartile range.
LBP indicates low back pain; NRS, Numerical Rating Scale; ODI, Oswestry Disability Index; FABQ, Fear-Avoidance Beliefs Questionnaire; ÖMPSQ, Örebro Musculoskeletal Pain Screening Questionnaire; SF-36, 36-Item Short Form Health Survey; PCS, physical component summary; MCS, mental component summary.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1350BRS204963.indd 1350 21/06/12 11:25 AM21/06/12 11:25 AM
RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
Spine www.spinejournal.com 1351
a P value of less than 0.05 (2-tailed) was considered signifi -cant. Continuous data were analyzed using SPSS 18.0 (SPSS Inc., Chicago, IL) and dichotomized data were analyzed using STATA 11.1 (StataCorp LP, College Station, TX) software.
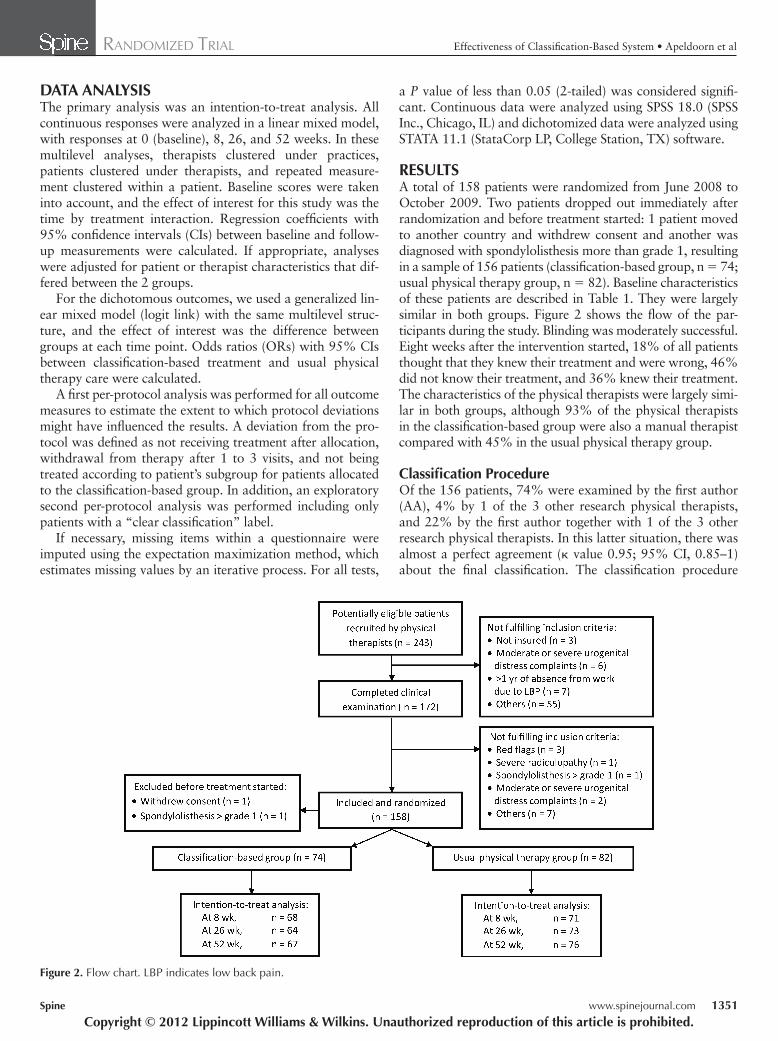
RESULTS A total of 158 patients were randomized from June 2008 to October 2009. Two patients dropped out immediately after randomization and before treatment started: 1 patient moved to another country and withdrew consent and another was diagnosed with spondylolisthesis more than grade 1, resulting in a sample of 156 patients (classifi cation-based group, n � 74; usual physical therapy group, n � 82). Baseline characteristics of these patients are described in Table 1 . They were largely similar in both groups. Figure 2 shows the fl ow of the par-ticipants during the study. Blinding was moderately successful. Eight weeks after the intervention started, 18% of all patients thought that they knew their treatment and were wrong, 46% did not know their treatment, and 36% knew their treatment. The characteristics of the physical therapists were largely simi-lar in both groups, although 93% of the physical therapists in the classifi cation-based group were also a manual therapist compared with 45% in the usual physical therapy group.
Classifi cation Procedure Of the 156 patients, 74% were examined by the fi rst author (AA), 4% by 1 of the 3 other research physical therapists, and 22% by the fi rst author together with 1 of the 3 other research physical therapists. In this latter situation, there was almost a perfect agreement ( κ value 0.95; 95% CI, 0.85–1) about the fi nal classifi cation. The classifi cation procedure
DATA ANALYSIS The primary analysis was an intention-to-treat analysis. All continuous responses were analyzed in a linear mixed model, with responses at 0 (baseline), 8, 26, and 52 weeks. In these multilevel analyses, therapists clustered under practices, patients clustered under therapists, and repeated measure-ment clustered within a patient. Baseline scores were taken into account, and the effect of interest for this study was the time by treatment interaction. Regression coeffi cients with 95% confi dence intervals (CIs) between baseline and follow-up measurements were calculated. If appropriate, analyses were adjusted for patient or therapist characteristics that dif-fered between the 2 groups.
For the dichotomous outcomes, we used a generalized lin-ear mixed model (logit link) with the same multilevel struc-ture, and the effect of interest was the difference between groups at each time point. Odds ratios (ORs) with 95% CIs between classifi cation-based treatment and usual physical therapy care were calculated.
A fi rst per-protocol analysis was performed for all outcome measures to estimate the extent to which protocol deviations might have infl uenced the results. A deviation from the pro-tocol was defi ned as not receiving treatment after allocation, withdrawal from therapy after 1 to 3 visits, and not being treated according to patient’s subgroup for patients allocated to the classifi cation-based group. In addition, an exploratory second per-protocol analysis was performed including only patients with a “clear classifi cation” label.
If necessary, missing items within a questionnaire were imputed using the expectation maximization method, which estimates missing values by an iterative process. For all tests,
Figure 2. Flow chart. LBP indicates low back pain.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1351BRS204963.indd 1351 21/06/12 11:25 AM21/06/12 11:25 AM
RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
1352 www.spinejournal.com July 2012
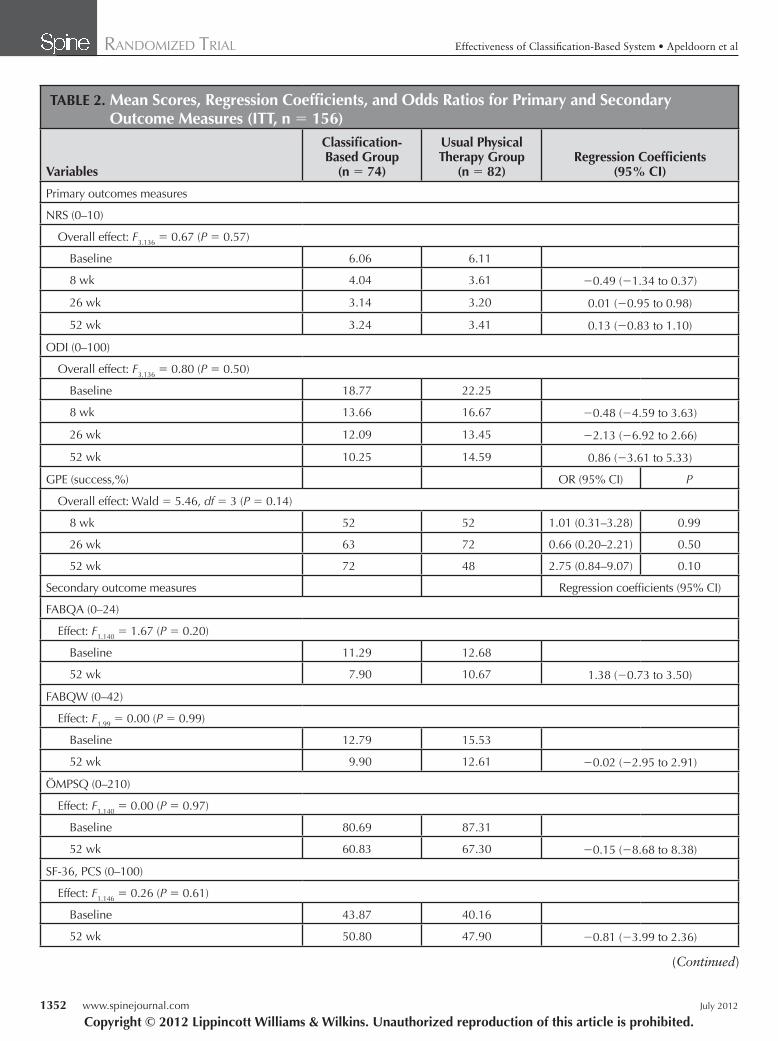
TABLE 2. Mean Scores, Regression Coeffi cients, and Odds Ratios for Primary and Secondary Outcome Measures (ITT, n � 156)
Variables
Classifi cation-Based Group
(n � 74)
Usual Physical Therapy Group
(n � 82)Regression Coeffi cients
(95% CI)
Primary outcomes measures
NRS (0–10)
Overall effect: F 3.136 � 0.67 ( P � 0.57)
Baseline 6.06 6.11
8 wk 4.04 3.61 − 0.49 ( − 1.34 to 0.37)
26 wk 3.14 3.20 0.01 ( − 0.95 to 0.98)
52 wk 3.24 3.41 0.13 ( − 0.83 to 1.10)
ODI (0–100)
Overall effect: F 3.136 � 0.80 ( P � 0.50)
Baseline 18.77 22.25
8 wk 13.66 16.67 − 0.48 ( − 4.59 to 3.63)
26 wk 12.09 13.45 − 2.13 ( − 6.92 to 2.66)
52 wk 10.25 14.59 0.86 ( − 3.61 to 5.33)
GPE (success,%) OR (95% CI) P
Overall effect: Wald � 5.46, df � 3 ( P � 0.14)
8 wk 52 52 1.01 (0.31–3.28) 0.99
26 wk 63 72 0.66 (0.20–2.21) 0.50
52 wk 72 48 2.75 (0.84–9.07) 0.10
Secondary outcome measures Regression coeffi cients (95% CI)
FABQA (0–24)
Effect: F 1.140 � 1.67 ( P � 0.20)
Baseline 11.29 12.68
52 wk 7.90 10.67 1.38 ( − 0.73 to 3.50)
FABQW (0–42)
Effect: F 1.99 � 0.00 ( P � 0.99)
Baseline 12.79 15.53
52 wk 9.90 12.61 − 0.02 ( − 2.95 to 2.91)
ÖMPSQ (0–210)
Effect: F 1.140 � 0.00 ( P � 0.97)
Baseline 80.69 87.31
52 wk 60.83 67.30 − 0.15 ( − 8.68 to 8.38)
SF-36, PCS (0–100)
Effect: F 1.146 � 0.26 ( P � 0.61)
Baseline 43.87 40.16
52 wk 50.80 47.90 − 0.81 ( − 3.99 to 2.36)
(Continued)
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1352BRS204963.indd 1352 21/06/12 11:25 AM21/06/12 11:25 AM

RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
Spine www.spinejournal.com 1353
that focus on these exercises. However, no information was collected whether these patients were actually treated with direction-specifi c exercises. In the classifi cation-based group, 53% of the patients received usual physical therapy care according to the current Dutch LBP guidelines after classifi -cation-based treatment, and this occurred after a median of 4.0 weeks (interquartile range, 2.8–5.0 wk).
Intention-to-Treat Analysis Compared with baseline, both treatment groups reported a signifi cant improvement at any of the follow-up time points regarding pain and functional status ( P < 0.001). At 8 weeks, the adjusted mean changes in NRS and ODI scores were 2.0 (95% CI, 1.4–2.6) and 5.1 (95% CI, 2.1–8.1), respectively, in the classifi cation-based group and 2.5 (95% CI, 1.9–3.1) and 5.6 (95% CI, 2.7–8.4), respectively, in the usual physi-cal therapy group. For GPE, the usual care group reported a large drop in success between 26 and 52 weeks (overall effect: Wald � 6.03, df � 2 [ P � 0.05]), a change that was not seen in the intervention group (overall effect: Wald � 3.66, df � 2 [ P � 0.16]) ( Table 2 ). Multilevel analyses adjusted for the type of care provider (physical or manual therapist) showed no signifi cant differences between the 2 groups for any
classifi ed 54% as direction-specifi c exercises (n � 85), 27% as manipulation (n � 42), and 19% as stabilization exercises (n � 29). For 6 patients, a senior educator of the Mechanical Diagnosis and Therapy Institute (MDT or McKenzie method) (HvH) was consulted to make a fi nal decision. For 6 patients who were allocated to classifi cation-based treatment, the clas-sifi cation was considered provisional, and a fi nal classifi ca-tion was made in discussion with the physical therapist who treated the patient on subsequent visits. The percentages of patients meeting the criteria of 0, 1, 2, or 3 subgroups using only the fi rst part of the algorithm were 24%, 60%, 14%, and 2%, respectively. The percentage of patients meeting the criteria of a “clear classifi cation” was 74.4% (n � 116). In most cases (70%), the physical therapist was moderate to very satisfi ed with the classifi cation algorithm decision and the related treatment protocol.
Contrast Between the 2 Interventions In the usual physical therapy group, 16% of the patients who were classifi ed into the manipulation subgroup were treated with manipulations, and 10% who were classifi ed into the direction-specifi c exercise subgroup were treated by a physi-cal therapist who had completed 2 or more McKenzie courses
TABLE 2. (Continued)
Variables
Classifi cation-Based Group
(n � 74)
Usual Physical Therapy Group
(n � 82)Regression Coeffi cients
(95% CI)
SF-36, MCS (0–100)
Effect: F 1.141 � 0.37 ( P � 0.54)
Baseline 52.12 50.73
52 wk 53.35 50.96 1.00 ( − 2.25 to 4.25)
OR (95% CI) P
NRS (�30% improvement from baseline, %)
Overall effect: Wald � 1.74, df � 3 ( P � 0.63)
8 wk 59 73 0.54 (0.17–1.70) 0.29
26 wk 74 74 0.98 (0.30–3.16) 0.97
52 wk 77 74 1.16 (0.37–3.69) 0.80
ODI (�30% improvement from baseline, %)
Overall effect: Wald � 2.61, df � 3 ( P � 0.46)
8 wk 36 45 0.70 (0.19–2.57) 0.59
26 wk 78 71 1.43 (0.37–5.47) 0.60
52 wk 81 68 1.95 (0.51–7.40) 0.33
Values presented are model estimates of linear mixed-effects models with a random intercept and adjusted for baseline and type of care provider (manual or physical therapist). Regression coeffi cients can be interpreted as mean differences between interventions at a certain follow-up moment compared with baseline. Positive values favor the classifi cation-based group.
ITT indicates intention-to-treat; CI, confi dence interval; NRS, Numerical Rating Scale; ODI, Oswestry Disability Index; GPE, global perceived effect; OR, odds ratio; FABQA, Fear-Avoidance Beliefs Questionnaire Activity; FABQW, Fear-Avoidance Beliefs Questionnaire Work; ÖMPSQ, Örebro Musculoskeletal Pain Screening Questionnaire; SF-36, 36-Item Short Form Health Survey; PCS, physical component summary; MCS, mental component summary.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1353BRS204963.indd 1353 21/06/12 11:25 AM21/06/12 11:25 AM
RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
1354 www.spinejournal.com July 2012
physical therapy care. We hypothesized that patients would benefi t most from classifi cation-based treatment; however, we found no support for this hypothesis.
The somewhat different results between our study and that of Fritz et al 5 should be considered in the light of several differ-ences in the designs of the studies. Probably, most important is the difference in patient selection criteria. The classifi cation-based treatment approach was originally tested on patients with acute symptoms and disability scores of more than 30 on the ODI (range, 0–100). 3 Delitto et al 3 based acuteness on a criterion related to the severity of disability rather than days since onset and reported that the majority of patients categorized in that manner have an ODI score between 40 and 60. The study by Fritz et al 5 included patients with a short duration of LBP and moderate to severe disability (mean ODI score at baseline of 43). In contrast, 79% of our participating patients had chronic LBP (�12 wk), and the mean ODI score for all patients at baseline was 20. We did not include patients with acute LBP because the Dutch LBP guidelines discourage physical therapy in the acute phase of LBP. Another difference between the study of Fritz et al 5 and this study was the use of slightly different classifi cation algorithms. We did not include
primary or secondary outcome measure ( Table 2 ). For all out-come measures, the intraclass correlation coeffi cients within physical therapy practices were almost zero and varied within physical therapists between almost zero and 0.14, indicating no practice-specifi c effect and a minor therapist-specifi c effect. Patients allocated to the classifi cation-based group attended fewer treatment sessions compared with those in the usual physical therapy group after 1 year (mean difference, 4.6; 95% CI, 0.7–8.5; P � 0.02), but this difference was not sig-nifi cant after the initial 8-week study period (mean difference, 1.3; 95% CI, − 0.2 to 2.8; P � 0.08).
For the intention-to-treat and the following analyses, only the missing items of the ÖMPSQ were imputed (2.2%) pro-vided that at least 75% of the questionnaire was completed.
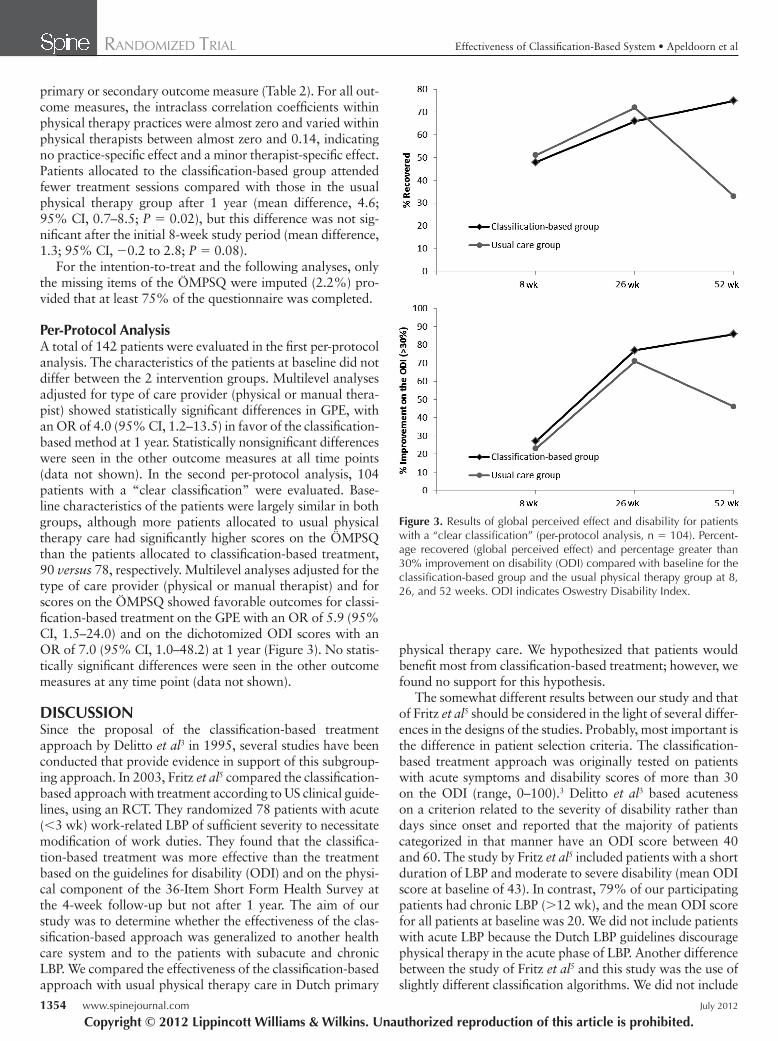
Per-Protocol Analysis A total of 142 patients were evaluated in the fi rst per-protocol analysis. The characteristics of the patients at baseline did not differ between the 2 intervention groups. Multilevel analyses adjusted for type of care provider (physical or manual thera-pist) showed statistically signifi cant differences in GPE, with an OR of 4.0 (95% CI, 1.2–13.5) in favor of the classifi cation-based method at 1 year. Statistically nonsignifi cant differences were seen in the other outcome measures at all time points (data not shown). In the second per-protocol analysis, 104 patients with a “clear classifi cation” were evaluated. Base-line characteristics of the patients were largely similar in both groups, although more patients allocated to usual physical therapy care had signifi cantly higher scores on the ÖMPSQ than the patients allocated to classifi cation-based treatment, 90 versus 78, respectively. Multilevel analyses adjusted for the type of care provider (physical or manual therapist) and for scores on the ÖMPSQ showed favorable outcomes for classi-fi cation-based treatment on the GPE with an OR of 5.9 (95% CI, 1.5–24.0) and on the dichotomized ODI scores with an OR of 7.0 (95% CI, 1.0–48.2) at 1 year ( Figure 3 ). No statis-tically signifi cant differences were seen in the other outcome measures at any time point (data not shown).
DISCUSSION Since the proposal of the classifi cation-based treatment approach by Delitto et al 3 in 1995, several studies have been conducted that provide evidence in support of this subgroup-ing approach. In 2003, Fritz et al 5 compared the classifi cation-based approach with treatment according to US clinical guide-lines, using an RCT. They randomized 78 patients with acute (�3 wk) work-related LBP of suffi cient severity to necessitate modifi cation of work duties. They found that the classifi ca-tion-based treatment was more effective than the treatment based on the guidelines for disability (ODI) and on the physi-cal component of the 36-Item Short Form Health Survey at the 4-week follow-up but not after 1 year. The aim of our study was to determine whether the effectiveness of the clas-sifi cation-based approach was generalized to another health care system and to the patients with subacute and chronic LBP. We compared the effectiveness of the classifi cation-based approach with usual physical therapy care in Dutch primary
Figure 3. Results of global perceived effect and disability for patients with a “clear classifi cation” (per-protocol analysis, n � 104). Percent-age recovered (global perceived effect) and percentage greater than 30% improvement on disability (ODI) compared with baseline for the classifi cation-based group and the usual physical therapy group at 8, 26, and 52 weeks. ODI indicates Oswestry Disability Index.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1354BRS204963.indd 1354 21/06/12 11:25 AM21/06/12 11:25 AM

RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
Spine www.spinejournal.com 1355
useful for “clear classifi cation” patients with subacute and chronic LBP in the long term. However, these results must be interpreted very cautiously. Importantly, we did not design or power our study for this subgroup analysis in advance, and as such, outcomes of subgroup analysis may be particularly unreliable. 27 Besides, it is not clear why the differences were not signifi cant at 8 and 26 weeks.
Ideally, a classifi cation algorithm should classify patients into 1 subgroup only. In this study, using only the fi rst part of the algorithm, 24% of all patients did not meet any of the subgroups and 16% met more than 1 subgroup. These fi nd-ings are consistent with those of Stanton et al . 10 They found that 25% of all patients did not meet any subgroup and 25% met more than 1 subgroup, although they used a different ver-sion of the classifi cation algorithm and recruited only patients with acute and subacute LBP with ODI scores above 20. Therefore, we agree with Stanton et al 10 that the classifi cation algorithm needs further refi nement.
The following 3 suggestions could potentially improve the performance of the system. First, centralization instead of directional preference might be a better criterion for the classifi cation of direction-specifi c exercises. Recently, Werneke et al 28 found that although centralization was an important factor for predicting functional outcome when patients were treated with direction-specifi c exercises, directional prefer-ence on its own was not. Second, available research supports the infl uence of key psychological factors ( e.g. , depression, catastrophizing) on treatment outcome. 29 These data state that more research is needed to explore whether incorpo-rating key psychological factors in a classifi cation-based approach leads to more positive outcomes. There is a reason to think that this might be more important for patients with chronic LBP with generally higher prevalence of psychologi-cal factors than for those with acute or subacute LBP. Third, more research is needed to further improve and validate the clinical prediction rule for the classifi cation of stabilization exercises. The rule for this classifi cation has been established in 1 derivation study, 30 but has not been validated and should not be considered ready for clinical application. Furthermore, this derivation study used a longitudinal cohort study design, whereas an RCT is the right approach to identify modifi ers to treatment. 23
LIMITATIONS Contrary to the original algorithm 3 and the algorithm used in the study of Fritz et al , 5 we did not include the subgroup traction. However, we do not think that this has infl uenced our results signifi cantly, because only 3 patients (2%) had signs of nerve root compression and thus met the modifi ed criteria for patients who might benefi t from traction. 31 We attempted to provide optimal training and guidance for our treating physical therapists in the classifi cation-based group; however, this support may have been insuffi cient for optimal competence and may therefore have caused an underestima-tion of the effectiveness of the direction-specifi c exercises and consequently also of the classifi cation-based treatment approach.
the subgroup traction because the Dutch LBP guidelines dis-courage traction in patients with LBP. Furthermore, we modi-fi ed the version used by Fritz et al 5 on the basis of updated evidence. 4 For example, we used the broader operational defi nition directional preference instead of centralization to classify patients in the subgroup direction-specifi c exercises. 22 Because directional preference identifi es a broader category of patients, this likely shifted more patients into a classifi ca-tion of direction-specifi c exercises compared with the study of Fritz et al . 5 Another difference was in comparison treat-ment. Although both studies compared classifi cation-based treatment with clinical guidelines-based treatment, including the advice to remain active, Fritz et al 5 treated their patients with low-stress aerobic exercises and general muscle recondi-tioning, whereas in our study, patients received personalized, individually tailored sessions.
Another RCT that provides support for the classifi cation-based approach was that by Brennan et al . 6 They included 123 patients with acute and subacute LBP and a mean ODI score of 43 at baseline. All patients were classifi ed accord-ing to the classifi cation algorithm and randomized to receive direction-specifi c exercises, manipulation or stabilization exer-cises, regardless of their subgroup. Outcomes were compared between patients who had received “matched treatment” (according to the classifi cation category) and “unmatched” (nonclassifi cation) treatment. Brennan et al 6 found a statis-tically signifi cant, but small, reduction in disability, favoring the matched treatment group after 4 and 52 weeks. However, because the study was designed to validate the subgrouping used ( i.e. , to examine the effectiveness of the classifi cation-based approach to target treatments compared with the use of the same treatments but not matched to patients) 23 and not the classifi cation-based approach compared with another cur-rent approach, these results do not directly compare with the results of our RCT.
Interestingly, for GPE and the dichotomized ODI scores, patients allocated to the classifi cation-based approach showed an improvement during the total period of 52 weeks, whereas patients treated according to usual physical therapy care deteriorated in the last 26 weeks. We do not have a clear explanation for these fi ndings. One potentially relevant fac-tor is that most patients in the classifi cation-based group received instruction booklets. This written instruction may have improved the patients’ knowledge about their LBP prob-lem, 24 their adherence to the clearly defi ned protocol-led exer-cises, 25 , 26 and/or their feeling of control. The use of exercise instruction booklets is not a common practice in the Nether-lands, and therefore we did not administrate this in the usual physical therapy group.
Another fi nding of interest is that the results of a secondary per-protocol analysis for patients with a “clear classifi cation” (patients who could be classifi ed using only the fi rst part of the classifi cation algorithm) were slightly in favor of the clas-sifi cation procedure compared with the usual physical ther-apy care on the outcome measures GPE and the dichotomized ODI score (�30% improvement) at 52 weeks. This could be an indication that the classifi cation-based approach might be
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1355BRS204963.indd 1355 21/06/12 11:25 AM21/06/12 11:25 AM

RANDOMIZED TRIAL Effectiveness of Classifi cation-Based System • Apeldoorn et al
1356 www.spinejournal.com July 2012
CONCLUSION The classifi cation-based treatment approach used in this study did not improve outcome in a population of patients with subacute and chronic LBP. To assess whether the classi-fi cation-based treatment approach is effective, we suggest fur-ther refi nement of the classifi cation algorithm or evaluation of the approach in a subgroup of patients who clearly meet the classifi cation algorithm criteria.
➢ Key Points
In an RCT, Delitto’s classifi cation-based system showed statistically signifi cant improvement on disability and return to work in patients with acute LBP compared with usual physical therapy care after 4 weeks but not after 1 year.
In the present RCT, a modifi ed version of this classi-fi cation-based treatment approach was compared with usual physical therapy care in patients with subacute and chronic LBP.
There were no statistically signifi cant diff erences between the treatment groups on any of the primary and secondary outcomes at 8, 26, and 52 weeks.
This trial suggests that the classifi cation-based system used in this study does not improve usual physical therapy care outcomes for this population.
References 1. Waddell G . Subgroups within “nonspecifi c” low back pain .
J Rheumatol 2005 ; 32 : 395 – 6 . 2. Kent P , Keating J . Do primary-care clinicians think that nonspecifi c
low back pain is one condition ? Spine 2004 ; 29 : 1022 – 31 . 3. Delitto A , Erhard RE , Bowling RW . A treatment-based classifi -
cation approach to low back syndrome: identifying and staging patients for conservative treatment . Phys Ther 1995 ; 75 : 470 – 85 .
4. Fritz JM , Cleland JA , Childs JD . Subgrouping patients with low back pain: evolution of a classifi cation approach to physical ther-apy . J Orthop Sports Phys Ther 2007 ; 37 : 290 – 302 .
5. Fritz JM , Delitto A , Erhard RE . Comparison of classifi cation-based physical therapy with therapy based on clinical practice guidelines for patients with acute low back pain: a randomized clinical trial . Spine 2003 ; 28 : 1363 – 71 .
6. Brennan GP , Fritz JM , Hunter SJ , et al. Identifying subgroups of patients with acute/subacute “nonspecifi c” low back pain: results of a randomized clinical trial . Spine 2006 ; 31 : 623 – 31 .
7. Apeldoorn AT , Ostelo RW , van Helvoirt H , et al. The cost-effectiveness of a treatment-based classifi cation system for low back pain: design of a randomised controlled trial and economic evaluation . BMC Musculoskelet Disord 2010 ; 11 : 58 .
8. Uebersax JS , Wyman JF , Shumaker SA , et al. Short forms to assess life quality and symptom distress for urinary incontinence in women: the Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Continence Program for Women Research Group . Neurourol Urodyn 1995 ; 14 : 131 – 9 .
9. van der Vaart CH , de Leeuw JR , Roovers JP , et al. De invloed van urine-incontinentie op de kwaliteit van leven bij thuiswonende Nederlandse vrouwen van 45–70 jaar [The infl uence of urinary incontinence on the quality of life in community-dwelling, 45–70 year-old women in the Netherlands] . Ned Tijdschr Geneeskd 2000 ; 144 : 894 – 7 .
10. Stanton TR , Fritz JM , Hancock MJ , et al. Evaluation of a treatment-based classifi cation algorithm for low back pain: a cross-sectional study . Phys Ther 2011 ; 91 : 496 – 509 .
11. Heijmans WFGL , Hendriks HJM , van der Esch M , et al. KNGF-richtlijn manuele therapie bij lage-rupijn [National practice guide-lines for manual therapy in patients with low back pain] . Ned Tijdschr Fysiother 2003 ; 113 : 1 – 12 .
12. Bekkering GE , Hendriks HJM , Koes BW , et al. KNGF-richtlijn fysiotherapie bij lage-rupijn [National practice guidelines for physi-cal therapy in patients with low back pain] . Ned Tijdschr Fysiother 2005 ; 115 : 1 – 32 .
13. Foster NE , Thompson KA , Baxter GD , et al. Management of nonspecifi c low back pain by physiotherapists in Britain and Ire-land. A descriptive questionnaire of current clinical practice . Spine 1999 ; 24 : 1332 – 42 .
14. Kent PM , Keating JL , Taylor NF . Primary care clinicians use vari-able methods to assess acute nonspecifi c low back pain and usually focus on impairments . Man Ther 2009 ; 14 : 88 – 100 .
15. Fairbank JC . Use and abuse of Oswestry Disability Index . Spine 2007 ; 32 : 2787 – 9 .
16. Fairbank JC , Pynsent PB . The Oswestry Disability Index . Spine 2000 ; 25 : 2940 – 52 .
17. Waddell G , Newton M , Henderson I , et al. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability . Pain 1993 ; 52 : 157 – 68 .
18. Linton SJ , Hallden K . Can we screen for problematic back pain? A screening questionnaire for predicting outcome in acute and sub-acute back pain . Clin J Pain 1998 ; 14 : 209 – 15 .
19. McHorney CA , Ware JE Jr , Raczek AE . The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs . Med Care 1993 ; 31 : 247 – 63 .
20. van der Zee K , Sanderman R , Heyink J . De psychometrische kwalit-eiten van de MOS 36-item Short Form Health Survey (SF-36) in een Nederlandse populatie [The psychometric properties of the SF-36 in a Dutch population] . Tijdschr Soc Gez 1993 ; 71 : 183 – 91 .
21. Ostelo RW , Deyo RA , Stratford P , et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change . Spine 2008 ; 33 : 90 – 4 .
22. Werneke MW . “Centralization” and “directional preference” are not synonymous . J Orthop Sports Phys Ther 2009 ; 39 : 827 – 8 .
23. Kent P , Hancock M , Petersen DH , et al. Clinimetrics corner: choos-ing appropriate study designs for particular questions about treat-ment subgroups . J Man Manip Ther 2010 ; 18 : 147 – 52 .
24. Coudeyre E , Givron P , Vanbiervliet W , et al. Un simple livret d’information peut contribuer à réduire l’incapacité fonctionnelle de patients lombalgiques subaigus et chroniques. Étude contrôlée randomisée en milieu de rééducation [The role of an information booklet or oral information about back pain in reducing disabil-ity and fear-avoidance beliefs among patients with subacute and chronic low back pain. A randomized controlled trial in a rehabilita-tion unit] . Ann Readapt Med Phys 2006 ; 49 : 600 – 8 .
25. Henrotin YE , Cedraschi C , Duplan B , et al. Information and low back pain management: a systematic review . Spine 2006 ; 31 : E326 – 34 .
26. Escolar-Reina P , Medina-Mirapeix F , Gascon-Canovas JJ , et al. Self-management of chronic neck and low back pain and relevance of information provided during clinical encounters: an observational study . Arch Phys Med Rehabil 2009 ; 90 : 1734 – 9 .
27. Brookes ST , Whitely E , Egger M , et al. Subgroup analyses in ran-domized trials: risks of subgroup-specifi c analyses; power and sam-ple size for the interaction test . J Clin Epidemiol 2004 ; 57 : 229 – 36 .
28. Werneke MW , Hart DL , Cutrone G , et al. Association between directional preference and centralization in patients with low back pain . J Orthop Sports Phys Ther 2011 ; 41 : 22 – 31 .
29. Nicholas MK , Linton SJ , Watson PJ , et al. Early identifi cation and management of psychological risk factors (“yellow fl ags”) in patients with low back pain: a reappraisal . Phys Ther 2011 ; 91 : 737 – 53 .
30. Hicks GE , Fritz JM , Delitto A , et al. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program . Arch Phys Med Rehabil 2005 ; 86 : 1753 – 62 .
31. Fritz JM , Thackeray A , Childs JD , et al. A randomized clinical trial of the effectiveness of mechanical traction for sub-groups of patients with low back pain: study methods and rationale . BMC Musculoskelet Disord 2010 ; 11 : 81 .
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204963.indd 1356BRS204963.indd 1356 21/06/12 11:25 AM21/06/12 11:25 AM



![Manipulative therapy and/or NSAIDs for acute low back pain: Design of a randomized controlled trial [ACTRN012605000036617]](https://static.fdokumen.com/doc/165x107/6332cf92576b626f850d96f1/manipulative-therapy-andor-nsaids-for-acute-low-back-pain-design-of-a-randomized.jpg)
















