
Diesel or LPG engine Pneumatic or Superelastic Tyres 4000 ...

A prognostic model for prolonged event-free survival after autologous or
allogeneic blood or marrow transplantation for relapsed and refractory
Hodgkin’s disease
T Hahn1,6, M Benekli1,6, C Wong2, KB Moysich3, A Hyland3, AM Michalek2, A Alam1, MR Baer1,B Bambach4, MS Czuczman1, M Wetzler1, JL Becker5 and PL McCarthy1
1Department of Medicine, Roswell Park Cancer Institute, Buffalo, New York, USA; 2Department of Education, Roswell Park CancerInstitute, Buffalo, New York, USA; 3Department of Epidemiology, Roswell Park Cancer Institute, Buffalo, New York, USA;4Department of Pediatrics, Roswell Park Cancer Institute, Buffalo, New York, USA; and 5Laboratory Medicine, Roswell ParkCancer Institute, Buffalo, New York, USA
Summary:
There are several prognostic models for Hodgkin’s disease(HD) patients, but none evaluating patient characteristicsat time of blood and marrow transplantation (BMT).We developed a prognostic model for event-free survival(EFS) post-BMT based on HD patient characteristicsmeasured at the time of autologous (auto) or allogeneic(allo) BMT. Between 1/1991 and 12/2001, 64 relapsedor refractory HD patients received an auto (n¼ 46) orallo (n¼ 18) BMT. A multivariate prognostic model wasdeveloped measuring time to relapse, progression or death.Median follow-up was 51.7 months; median EFS forauto and allo BMT was 36 and 3 months, respectively(P¼ 0.001). Significant multivariate predictors of shorterEFS were chemotherapy-resistant disease, KPS o90 andX3 chemotherapy regimens pre-BMT. Patients with twoto three adverse factors had significantly shorter EFS at 2years (58 vs 11% in auto; 38 vs 0% in allo BMT patients).Despite a selection bias favoring auto BMT, the modelwas valid in both auto and allo BMT groups. We wereable to differentiate patients at high vs low risk foradverse outcomes post-BMT. This prognostic model mayprove useful in predicting patient outcomes and identifyinghigh-risk patients for novel treatment strategies. Valida-tion of this model in a larger cohort of patients iswarranted.Bone Marrow Transplantation (2005) 35, 557–566.doi:10.1038/sj.bmt.1704789Published online 24 January 2005Keywords: prognostic model; Hodgkin’s disease; auto-logous BMT; allogeneic BMT
Relapsed or refractory Hodgkin’s disease (HD) patientshave a poor prognosis with standard salvage chemother-apy, yielding a cure rate of 20% or less.1–4 High-dosetherapy followed by autologous blood or marrow trans-plantation (auto BMT) has become a standard treatmentfor patients refractory to or relapsing after inductiontherapy.5–17 The role of allogeneic BMT (allo BMT)in relapsed or refractory HD has not been fully deter-mined,18–26 although the existence of a graft-versus-lymphoma (GVL) effect has been suggested.20–25
Prognostic models based on presentation features in HDpatients have been proposed for predicting the outcome.26–35
These models have proven quite useful for predicting theoutcome in newly diagnosed HD patients, however, not allHD patients have these prognostic factors evaluated atdiagnosis, which can be difficult to obtain in patientsreferred for BMT often years after diagnosis. There havebeen three prognostic scoring systems reported in the last 3years for auto BMT patients. Stiff et al36 developed aprognostic score based on 72 patients treated from 1990 to1995 in the SWOG 9011 trial of cyclophosphamide,etoposide and carmustine vs cyclophosphamide, etoposideand total body irradiation as conditioning for auto BMT.Significant multivariate predictors of overall survival (OS)were 42 prior regimens, relapse in a previously radiatedfield and extranodal disease. Patients with two to threeadverse factors had a significantly inferior OS compared tothose with zero to one factor (38 vs 60%, P¼ 0.05).Moskowitz et al37 proposed a two-step risk-adapted
treatment strategy for 65 relapsed and refractory HDpatients enrolled from 1994 to 1998, of whom 57 underwentauto BMT at the Memorial Sloan-Kettering Cancer Center(MSKCC) based on a prognostic model of factorsevaluated at the initiation of salvage chemotherapy. Thethree prognostic factors identified by the MSKCC modelwere B symptoms at the time of salvage chemotherapy,extranodal involvement at the time of salvage chemo-therapy and CR duration o1 year or primary refractorydisease. Patients with zero to one adverse factors hadsignificantly superior EFS (83%) compared to those withtwo (27%) or three (10%) adverse factors (Po0.001).
Received 10 August 2004; accepted 16 September 2004Published online 24 January 2005
Correspondence: Dr T Hahn, Department of Medicine, Roswell ParkCancer Institute, Elm and Carlton Streets, Buffalo, New York 14263,USA; E-mail: [email protected] two authors contributed equally to this work
Bone Marrow Transplantation (2005) 35, 557–566& 2005 Nature Publishing Group All rights reserved 0268-3369/05 $30.00
www.nature.com/bmt

Josting et al38 developed a prognostic score based on therelapse characteristics of 422 eligible relapsed HD patientsfrom the German Hodgkin’s Lymphoma Study Group(GHSG) treated between 1988 and 1998 with salvagechemotherapy plus autologous transplant (n¼ 140) vssalvage chemotherapy alone (n¼ 228) vs salvage radiationtherapy alone (n¼ 54). Significant multivariate adversepredictors of OS and freedom from second failure (FF2F)were o12 months from the end of induction therapy torelapse, stage III or IV at relapse, and hemoglobino12 g/dlin males or o10.5 g/dl in females at relapse. Relapsed HDpatients o60 years old with a KPS X90 and zero, one, twoor three of these factors treated with autologous transplanthad an OS of 100, 73, 55 and 50%, respectively (Po0.0001).We intended to develop a prognostic model for event-
free survival based on factors measured at the time oftransplant rather than at salvage therapy that would beapplicable to both autologous and allogeneic BMTpatients. In the current study, we also present ourvalidation of the MSKCC prognostic model in our autoand allo BMT patient population. The model presentedherein may allow for more rapid validation using auto-logous and allogeneic transplant registry data.
Patients and methods
Patients
A total of 64 patients with relapsed or refractory HDunderwent auto and/or allo BMT at the Roswell ParkCancer Institute between January 1991 and December 2001.Standard eligibility criteria included agep60 for allo BMT,p70 for auto BMT and adequate cardiac, pulmonary,hepatic and renal function. A total of 68 BMT procedureswere performed (18 allo BMT and 50 auto BMT). Fourpatients received two transplants at our center during thistime period, all of whom had an allo BMT after a failedauto BMT. To avoid violating the statistical assumption ofindependent samples, only one transplant per patient (thesecond BMT) was included in the analysis; therefore, fourfirst auto BMTs were excluded from the analysis, yielding64 transplants on 64 patients. Of the 64 patients, 11 hadprior transplants (see Table 1), seven of which wereperformed at other centers. Only transplants performed atRPCI were included and analyzed in this study. A sensitivityanalysis of the multivariate model was conducted, in whichthe study population was restricted to the first BMTpatients only (see results section). All allo BMT patientshad HLA-matched (at A, B and DRB1 antigens) related(n¼ 16) or unrelated (n¼ 2) donors. All patients receivedmyeloablative conditioning regimens. All patients weretreated on multiple Institutional Review Board approvedprotocols and signed informed consent. All individualpatient data presented in this report have been de-identified.
Treatment
Four patients did not receive any salvage therapy prior toBMT. All others were treated with etoposide-, or platinum-based salvage chemotherapy regimens and/or radiation
therapy at the discretion of the referring physician. Patientswere prioritized to receive an auto BMT and only receivedan allo BMT after a failed auto BMT or in the setting of ahigh risk of relapse at the discretion of the transplant teamand contingent on the availability of a suitable donor.Myeloablative conditioning regimens for patients under-
going allo BMT included thiotepa 450mg/m2� 2 days andcarboplatin 400mg/m2� 4 days (TtCp) (n¼ 12),39 thiotepa300mg/m2� 2 days and 1000-1200 cGy TBI over 3 days(TtTBI) (n¼ 3),39 busulfan 1mg/kg every 6 h for 16 dosesand cyclophosphamide 50mg/kg� 2 days (BuCy) (n¼ 1),40
etoposide 1800mg/m2� 1 day, cyclophosphamide 60mg/kg� 3 days and TBI 1000 cGy in 5 fractions over 3 days(n¼ 1),41 or fludarabine 25mg/m2� 5 days and melphalan70mg/m2� 2 days (n¼ 1).42 Auto BMT patients receivedetoposide 2400mg/m2� 1 day, cyclophosphamide 1800mg/m2� 4 days, and BCNU 600mg/m2� 1 day (VCB)(n¼ 28),43 TtCp with the above schedule (n¼ 10), TtTBIwith the above schedule (n¼ 4), thiotepa 300mg/m2� 3days and cyclophosphamide 60mg/kg� 3 days (n¼ 2)39 orBuCy as busulfan 1mg/kg every 6 h for 16 doses andcyclophosphamide 50mg/kg� 2 or 4 days (n¼ 2).40,44
Conditioning regimen-related toxicity (RRT) was gradedaccording to published criteria.45
Graft-versus-host disease (GVHD) prophylaxis for pa-tients undergoing allo BMT consisted of combinations ofcyclosporine (CSA) and methotrexate (n¼ 4),46 CSA, metho-trexate and methylprednisone (MP) (n¼ 1),47 CSA and MP(n¼ 3),48 or CSA, MP and OKT3 (n¼ 10)49 based on theinstitutional protocols available at the time of BMT. CSAwas switched to FK506 in three patients due to CSA toxicity.Acute GVHD was defined according to standard criteria.50–51
Statistical considerations
The primary outcome was event-free survival (EFS) aftertransplant. Progression-free survival (PFS), overall survival(OS) and regimen-related toxicity (RRT) were analyzed assecondary end points. Analysis of variance (ANOVA) ofindependent samples was performed to compare means andthe w2 test (with Fisher’s exact test, where applicable) wasused to compare proportions. Tests of significance weretwo-sided, with Po0.05 considered statistically significant.All analyses were conducted using the intent-to-treatprinciple. Kaplan–Meier survival curves were calculatedfrom the date of hematopoietic stem cell infusion (day 0).52
Differences in survival between the prognostic factor riskgroups were determined by the log rank test. Survival waslast updated on 1/15/2004. For EFS, all patients areincluded in the analysis and were censored only at the timeof last follow-up if disease progression did not occur; eventswere disease relapse, progression or death due to any cause.For PFS, all patients were included in the analysis and werecensored at the time of last follow-up if disease progressiondid not occur or at death if disease progression did notoccur; events were disease relapse or progression. For OS,all patients were included in the analysis and were censoredat the time of last follow-up; events were death due to anycause. No patients developed a secondary malignancypost-BMT. Landmark analysis at 2 years post-BMT wasperformed to provide a comparison with other reported
PreBMT prognostic factors in HDT Hahn et al
558
Bone Marrow Transplantation
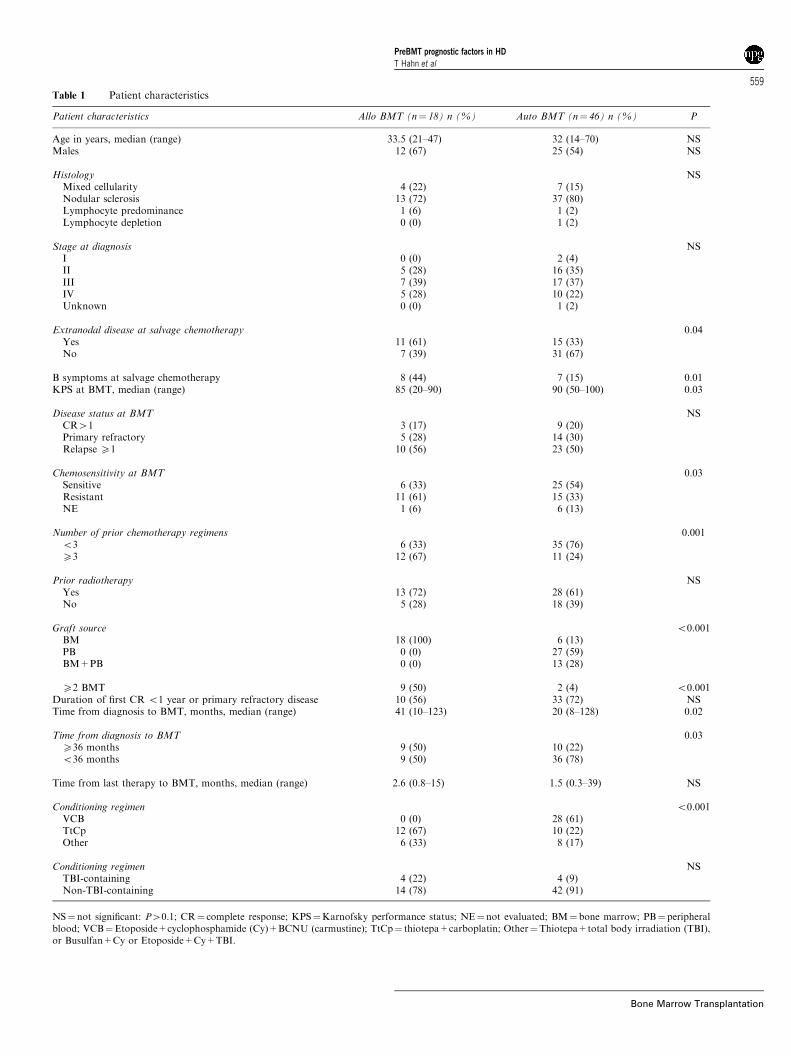
Table 1 Patient characteristics
Patient characteristics Allo BMT (n¼ 18) n (%) Auto BMT (n¼ 46) n (%) P
Age in years, median (range) 33.5 (21–47) 32 (14–70) NSMales 12 (67) 25 (54) NS
Histology NSMixed cellularity 4 (22) 7 (15)Nodular sclerosis 13 (72) 37 (80)Lymphocyte predominance 1 (6) 1 (2)Lymphocyte depletion 0 (0) 1 (2)
Stage at diagnosis NSI 0 (0) 2 (4)II 5 (28) 16 (35)III 7 (39) 17 (37)IV 5 (28) 10 (22)Unknown 0 (0) 1 (2)
Extranodal disease at salvage chemotherapy 0.04Yes 11 (61) 15 (33)No 7 (39) 31 (67)
B symptoms at salvage chemotherapy 8 (44) 7 (15) 0.01KPS at BMT, median (range) 85 (20–90) 90 (50–100) 0.03
Disease status at BMT NSCR41 3 (17) 9 (20)Primary refractory 5 (28) 14 (30)Relapse X1 10 (56) 23 (50)
Chemosensitivity at BMT 0.03Sensitive 6 (33) 25 (54)Resistant 11 (61) 15 (33)NE 1 (6) 6 (13)
Number of prior chemotherapy regimens 0.001o3 6 (33) 35 (76)X3 12 (67) 11 (24)
Prior radiotherapy NSYes 13 (72) 28 (61)No 5 (28) 18 (39)
Graft source o0.001BM 18 (100) 6 (13)PB 0 (0) 27 (59)BM+PB 0 (0) 13 (28)
X2 BMT 9 (50) 2 (4) o0.001Duration of first CR o1 year or primary refractory disease 10 (56) 33 (72) NSTime from diagnosis to BMT, months, median (range) 41 (10–123) 20 (8–128) 0.02
Time from diagnosis to BMT 0.03X36 months 9 (50) 10 (22)o36 months 9 (50) 36 (78)
Time from last therapy to BMT, months, median (range) 2.6 (0.8–15) 1.5 (0.3–39) NS
Conditioning regimen o0.001VCB 0 (0) 28 (61)TtCp 12 (67) 10 (22)Other 6 (33) 8 (17)
Conditioning regimen NSTBI-containing 4 (22) 4 (9)Non-TBI-containing 14 (78) 42 (91)
NS¼not significant: P40.1; CR¼ complete response; KPS¼Karnofsky performance status; NE¼not evaluated; BM¼ bone marrow; PB¼ peripheralblood; VCB¼Etoposide+cyclophosphamide (Cy)+BCNU (carmustine); TtCp¼ thiotepa+carboplatin; Other¼Thiotepa+total body irradiation (TBI),or Busulfan+Cy or Etoposide+Cy+TBI.
PreBMT prognostic factors in HDT Hahn et al
559
Bone Marrow Transplantation

studies; only three additional events occurred between 3and 4 years post-transplantation. The prognostic model ofEFS at 2 years used a Cox proportional hazards model withforward stepwise selection conditional on the likelihoodratio with Po0.1 to enter and P40.05 to remove eachfactor from the model.53
Complete response was defined as complete disappear-ance of all known disease with the exception of persistentscan abnormalities of unknown significance for X4 weeks;partial response was defined as X50% reduction in thegreatest diameter of all sites of known disease and no newsites of disease development. Patients who achieved acomplete or partial response to salvage therapy werecategorized as chemotherapy-sensitive, those who under-went BMT directly without salvage therapy and those whoreceived salvage therapy but were not evaluated for diseaseresponse were categorized as not evaluated (NE), all otherswere defined as having chemotherapy-resistant disease.Disease progression post-transplantation was defined as (1)evidence of relapse in patients with a documented completeresponse after BMT, (2) evidence of new areas of diseasepost-BMT, (3) evidence of tumor growth in areas ofpersistent disease post-BMT or (4) death due to disease.For the validation of the MSKCC model, the prognostic
factors evaluated were B symptoms at the time of initiationof last salvage chemotherapy before BMT, extranodalinvolvement (defined as involvement of a noncontiguousextranodal site, including bone marrow, or direct extensionto an adjacent organ from a nodal mass) at the time of lastsalvage chemotherapy before BMT, and CR duration p1year or primary refractory disease. For the four patientswho did not receive salvage chemotherapy for their mostrecent relapse before BMT, we collected the prognosticfactors at the time of last disease relapse pre-BMT.
Results
Patient characteristics
Pretransplant patient demographics and disease character-istics of the 64 patients (46 auto BMT, 18 allo BMT)treated for relapsed or refractory HD are summarized inTable 1. A significantly higher proportion of allo BMTpatients had B symptoms at the time of salvage chemother-
apy, more chemotherapy-resistant disease at the time oftransplant, X3 standard chemotherapy regimens beforetransplant, received a prior transplant and received bonemarrow as the source of stem cells than auto BMT patients.There was also a significantly longer time from diagnosis ofHD to BMT in the allo BMT group.
Engraftment
The median times to absolute neutrophil count (ANC)X500/mm3 and plateletsX20 000/mm3 were similar in boththe auto and allo BMT groups (Table 2). Two auto BMTpatients died before neutrophil recovery on days þ 14 andþ 26. Six auto BMT patients died before platelet recoveryon days þ 14 to 1384 (median 236 days); two auto BMTpatients never dropped platelet counts below 20 000/mm3.One auto BMT patient has not yet achieved plateletrecovery on day þ 572. Three allo BMT patients diedbefore achieving neutrophil recovery on days 0 to þ 4. Inall, 11 allo BMT patients died before achieving plateletrecovery on days þ 0 to 215 (median 59 days).
Toxicity and causes of death
In the allo BMT group, 10 patients (56%) developed acuteGVHD, five (29%) developed chronic GVHD, four ofwhom were previously diagnosed with acute GVHD. Therewere 14 early transplant-related deaths within the first 100days following BMT; five (11%) in the auto BMT groupand eight (44%) in the allo BMT (P¼ 0.006). Treatment-related mortality (TRM) in the allo BMT group wasattributable to RRT (n¼ 5), acute GVHD (n¼ 2) andinfection (n¼ 1). TRM in the auto BMT group was due toRRT (n¼ 3) and infection (n¼ 2). Overall, 28 patients(62%) died within the follow-up period (13 auto vs 15 allo).Causes of death for the auto BMT group were underlyingdisease (n¼ 8), RRT (n¼ 3) and infection (n¼ 2), and forthe allo BMT group were RRT (n¼ 5), infection (n¼ 4),GVHD (n¼ 3) and underlying disease (n¼ 3).
Survival
A total of 24 patients (38%) were alive and in CR at thetime of analysis at a median follow-up for survivingpatients of 51.7 months. Of those, two (11%) were in theallo BMT and 22 (48%) were in the auto BMT group. Allsurvival parameters, except PFS, were significantly superior
Table 2 Transplant outcomes
Allo BMT (n¼ 18) Auto BMT (n¼ 46) P
Time to ANC X500/mm3, days, median (range) 11 (8–33) (n¼ 14) 11 (9–61) (n¼ 44) NSTime to platelets X20 000/mm3, days, median (range) 22 (14–41) (n¼ 7) 15 (9–60) (n¼ 37) NS
Survival100-day, n (%) 10 (56) 40 (87) 0.0061-year, n (%) 6 (33) 37 (80) o0.001Median EFS, months 3 36 0.001Median PFS, months NYR (21+) NYR (36+) NSMedian OS, months 3 NYR (48+) o0.001
Allo¼ allogeneic; Auto¼ autologous; ANC¼ absolute neutrophil count; NS¼ not significant: P40.1; EFS¼ event-free survival; PFS¼progression-freesurvival; NYR¼ not yet reached; OS¼ overall survival.
PreBMT prognostic factors in HDT Hahn et al
560
Bone Marrow Transplantation
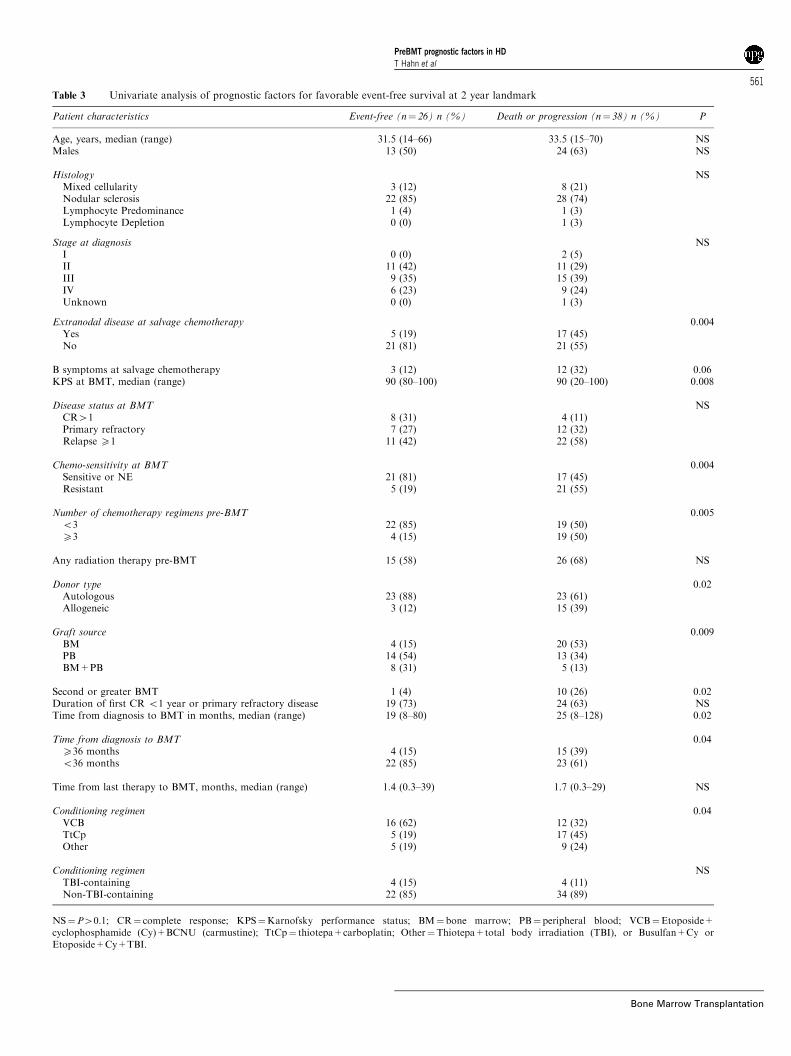
Table 3 Univariate analysis of prognostic factors for favorable event-free survival at 2 year landmark
Patient characteristics Event-free (n¼ 26) n (%) Death or progression (n¼ 38) n (%) P
Age, years, median (range) 31.5 (14–66) 33.5 (15–70) NSMales 13 (50) 24 (63) NS
Histology NSMixed cellularity 3 (12) 8 (21)Nodular sclerosis 22 (85) 28 (74)Lymphocyte Predominance 1 (4) 1 (3)Lymphocyte Depletion 0 (0) 1 (3)
Stage at diagnosis NSI 0 (0) 2 (5)II 11 (42) 11 (29)III 9 (35) 15 (39)IV 6 (23) 9 (24)Unknown 0 (0) 1 (3)
Extranodal disease at salvage chemotherapy 0.004Yes 5 (19) 17 (45)No 21 (81) 21 (55)
B symptoms at salvage chemotherapy 3 (12) 12 (32) 0.06KPS at BMT, median (range) 90 (80–100) 90 (20–100) 0.008
Disease status at BMT NSCR41 8 (31) 4 (11)Primary refractory 7 (27) 12 (32)Relapse X1 11 (42) 22 (58)
Chemo-sensitivity at BMT 0.004Sensitive or NE 21 (81) 17 (45)Resistant 5 (19) 21 (55)
Number of chemotherapy regimens pre-BMT 0.005o3 22 (85) 19 (50)X3 4 (15) 19 (50)
Any radiation therapy pre-BMT 15 (58) 26 (68) NS
Donor type 0.02Autologous 23 (88) 23 (61)Allogeneic 3 (12) 15 (39)
Graft source 0.009BM 4 (15) 20 (53)PB 14 (54) 13 (34)BM+PB 8 (31) 5 (13)
Second or greater BMT 1 (4) 10 (26) 0.02Duration of first CR o1 year or primary refractory disease 19 (73) 24 (63) NSTime from diagnosis to BMT in months, median (range) 19 (8–80) 25 (8–128) 0.02
Time from diagnosis to BMT 0.04X36 months 4 (15) 15 (39)o36 months 22 (85) 23 (61)
Time from last therapy to BMT, months, median (range) 1.4 (0.3–39) 1.7 (0.3–29) NS
Conditioning regimen 0.04VCB 16 (62) 12 (32)TtCp 5 (19) 17 (45)Other 5 (19) 9 (24)
Conditioning regimen NSTBI-containing 4 (15) 4 (11)Non-TBI-containing 22 (85) 34 (89)
NS¼P40.1; CR¼ complete response; KPS¼Karnofsky performance status; BM¼bone marrow; PB¼peripheral blood; VCB¼Etoposide+cyclophosphamide (Cy)+BCNU (carmustine); TtCp¼ thiotepa+carboplatin; Other¼Thiotepa+total body irradiation (TBI), or Busulfan+Cy orEtoposide+Cy+TBI.
PreBMT prognostic factors in HDT Hahn et al
561
Bone Marrow Transplantation
in the auto BMT group (see Table 2). The median PFS hasnot yet been reached in either group.The 2-year landmark univariate analysis yielded several
factors at BMT that were associated with shorter EFS(Table 3). The multivariate analysis of prognostic factorsfound chemotherapy-resistant disease at BMT, KPSo90 atBMT, and X3 chemotherapy regimens prior to BMT asstatistically significant indicators of disease progression ordeath (inferior EFS) at 2 years post-BMT (Table 4). Donorrelation (auto vs allo), stem cell type (BM vs PB vsPBþBM), second BMT (yes vs no) and conditioningregimen (VCB vs TtCp vs other) were not prognostic forEFS. Extranodal disease at the time of salvage chemo-therapy was significant in the univariate analysis; however,it was not included as a factor in the multivariate analysis,since we aimed to develop a predictive model based on pre-transplant characteristics. Two sensitivity analyses wereperformed on the multivariate model. Extranodal disease atthe time of salvage chemotherapy was considered as afactor in the multivariate analysis; however, it failed toreach statistical significance as an independent predictor.The multivariate analysis was also repeated, while restrictedto patients receiving their first BMT (second BMT patientswere excluded), yielding the same predictive factors withsimilar relative risks.
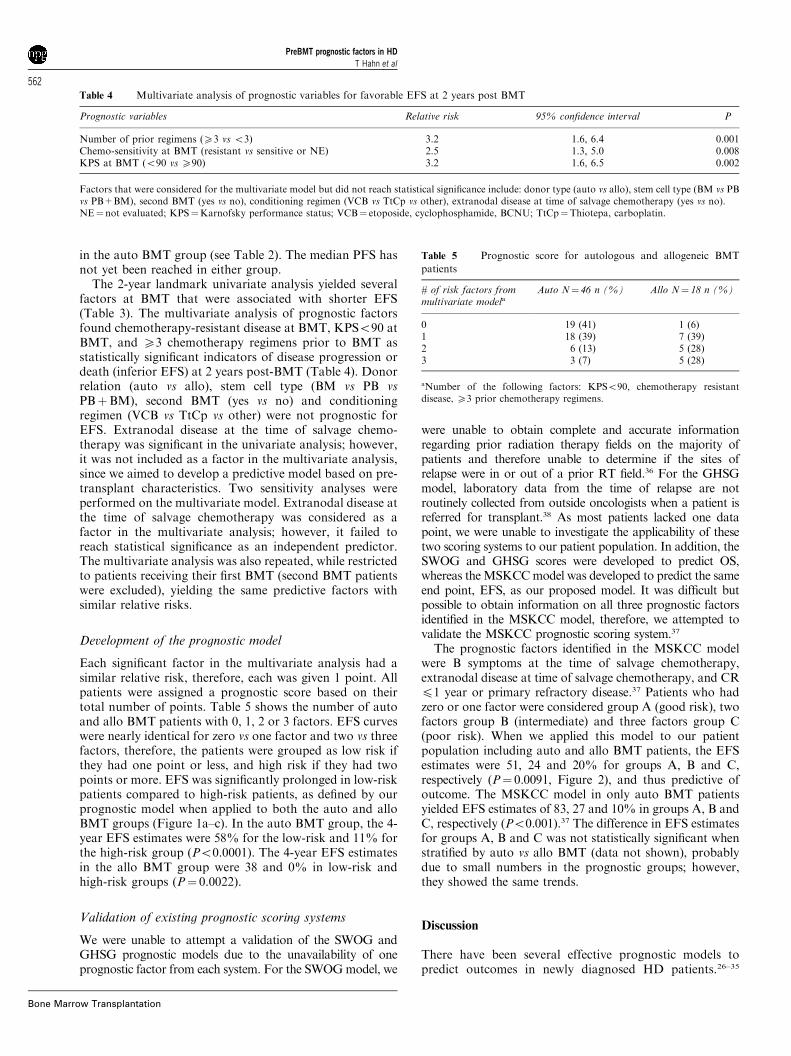
Development of the prognostic model
Each significant factor in the multivariate analysis had asimilar relative risk, therefore, each was given 1 point. Allpatients were assigned a prognostic score based on theirtotal number of points. Table 5 shows the number of autoand allo BMT patients with 0, 1, 2 or 3 factors. EFS curveswere nearly identical for zero vs one factor and two vs threefactors, therefore, the patients were grouped as low risk ifthey had one point or less, and high risk if they had twopoints or more. EFS was significantly prolonged in low-riskpatients compared to high-risk patients, as defined by ourprognostic model when applied to both the auto and alloBMT groups (Figure 1a–c). In the auto BMT group, the 4-year EFS estimates were 58% for the low-risk and 11% forthe high-risk group (Po0.0001). The 4-year EFS estimatesin the allo BMT group were 38 and 0% in low-risk andhigh-risk groups (P¼ 0.0022).
Validation of existing prognostic scoring systems
We were unable to attempt a validation of the SWOG andGHSG prognostic models due to the unavailability of oneprognostic factor from each system. For the SWOGmodel, we
were unable to obtain complete and accurate informationregarding prior radiation therapy fields on the majority ofpatients and therefore unable to determine if the sites ofrelapse were in or out of a prior RT field.36 For the GHSGmodel, laboratory data from the time of relapse are notroutinely collected from outside oncologists when a patient isreferred for transplant.38 As most patients lacked one datapoint, we were unable to investigate the applicability of thesetwo scoring systems to our patient population. In addition, theSWOG and GHSG scores were developed to predict OS,whereas theMSKCCmodel was developed to predict the sameend point, EFS, as our proposed model. It was difficult butpossible to obtain information on all three prognostic factorsidentified in the MSKCC model, therefore, we attempted tovalidate the MSKCC prognostic scoring system.37
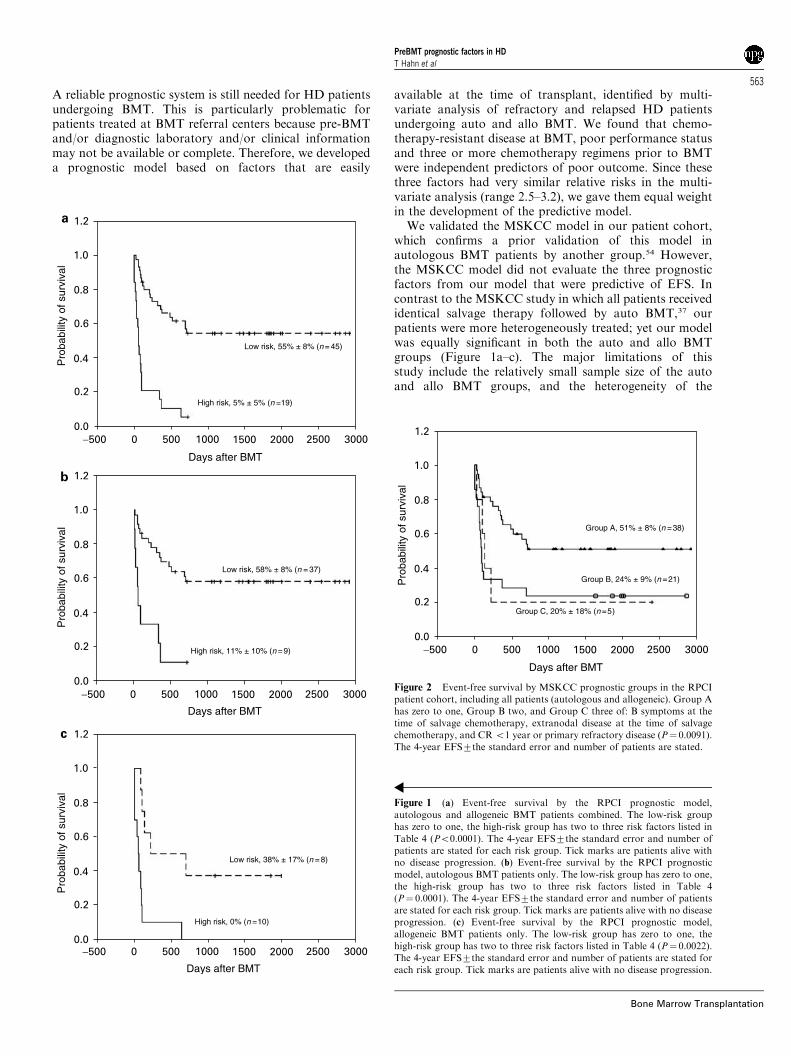
The prognostic factors identified in the MSKCC modelwere B symptoms at the time of salvage chemotherapy,extranodal disease at time of salvage chemotherapy, and CRp1 year or primary refractory disease.37 Patients who hadzero or one factor were considered group A (good risk), twofactors group B (intermediate) and three factors group C(poor risk). When we applied this model to our patientpopulation including auto and allo BMT patients, the EFSestimates were 51, 24 and 20% for groups A, B and C,respectively (P¼ 0.0091, Figure 2), and thus predictive ofoutcome. The MSKCC model in only auto BMT patientsyielded EFS estimates of 83, 27 and 10% in groups A, B andC, respectively (Po0.001).37 The difference in EFS estimatesfor groups A, B and C was not statistically significant whenstratified by auto vs allo BMT (data not shown), probablydue to small numbers in the prognostic groups; however,they showed the same trends.
Discussion
There have been several effective prognostic models topredict outcomes in newly diagnosed HD patients.26–35
Table 4 Multivariate analysis of prognostic variables for favorable EFS at 2 years post BMT
Prognostic variables Relative risk 95% confidence interval P
Number of prior regimens (X3 vs o3) 3.2 1.6, 6.4 0.001Chemo-sensitivity at BMT (resistant vs sensitive or NE) 2.5 1.3, 5.0 0.008KPS at BMT (o90 vs X90) 3.2 1.6, 6.5 0.002
Factors that were considered for the multivariate model but did not reach statistical significance include: donor type (auto vs allo), stem cell type (BM vs PBvs PB+BM), second BMT (yes vs no), conditioning regimen (VCB vs TtCp vs other), extranodal disease at time of salvage chemotherapy (yes vs no).NE¼ not evaluated; KPS¼Karnofsky performance status; VCB¼ etoposide, cyclophosphamide, BCNU; TtCp¼Thiotepa, carboplatin.
Table 5 Prognostic score for autologous and allogeneic BMT
patients
# of risk factors frommultivariate modela
Auto N¼ 46 n (%) Allo N¼ 18 n (%)
0 19 (41) 1 (6)1 18 (39) 7 (39)2 6 (13) 5 (28)3 3 (7) 5 (28)
aNumber of the following factors: KPSo90, chemotherapy resistantdisease, X3 prior chemotherapy regimens.
PreBMT prognostic factors in HDT Hahn et al
562
Bone Marrow Transplantation
A reliable prognostic system is still needed for HD patientsundergoing BMT. This is particularly problematic forpatients treated at BMT referral centers because pre-BMTand/or diagnostic laboratory and/or clinical informationmay not be available or complete. Therefore, we developeda prognostic model based on factors that are easily
available at the time of transplant, identified by multi-variate analysis of refractory and relapsed HD patientsundergoing auto and allo BMT. We found that chemo-therapy-resistant disease at BMT, poor performance statusand three or more chemotherapy regimens prior to BMTwere independent predictors of poor outcome. Since thesethree factors had very similar relative risks in the multi-variate analysis (range 2.5–3.2), we gave them equal weightin the development of the predictive model.We validated the MSKCC model in our patient cohort,
which confirms a prior validation of this model inautologous BMT patients by another group.54 However,the MSKCC model did not evaluate the three prognosticfactors from our model that were predictive of EFS. Incontrast to the MSKCC study in which all patients receivedidentical salvage therapy followed by auto BMT,37 ourpatients were more heterogeneously treated; yet our modelwas equally significant in both the auto and allo BMTgroups (Figure 1a–c). The major limitations of thisstudy include the relatively small sample size of the autoand allo BMT groups, and the heterogeneity of the
Pro
babi
lity
of s
urvi
val
Pro
babi
lity
of s
urvi
val
Pro
babi
lity
of s
urvi
val
High risk, 5% ± 5% (n =19)
Low risk, 55% ± 8% (n= 45)
Low risk, 58% ± 8% (n = 37)
High risk, 11% ± 10% (n =9)
Low risk, 38% ± 17% (n = 8)
High risk, 0% (n =10)
Days after BMT
−500 5000 1000 1500 2000 2500 3000
−500 5000 1000 1500 2000 2500 3000
−500 5000 1000 1500 2000 2500 3000
1.2
1.0
0.8
0.6
0.4
0.2
0.0
1.2
1.0
0.8
0.6
0.4
0.2
0.0
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Days after BMT
Days after BMT
a
b
c
Figure 1 (a) Event-free survival by the RPCI prognostic model,autologous and allogeneic BMT patients combined. The low-risk grouphas zero to one, the high-risk group has two to three risk factors listed inTable 4 (Po0.0001). The 4-year EFS7the standard error and number ofpatients are stated for each risk group. Tick marks are patients alive withno disease progression. (b) Event-free survival by the RPCI prognosticmodel, autologous BMT patients only. The low-risk group has zero to one,the high-risk group has two to three risk factors listed in Table 4(P¼ 0.0001). The 4-year EFS7the standard error and number of patientsare stated for each risk group. Tick marks are patients alive with no diseaseprogression. (c) Event-free survival by the RPCI prognostic model,allogeneic BMT patients only. The low-risk group has zero to one, thehigh-risk group has two to three risk factors listed in Table 4 (P¼ 0.0022).The 4-year EFS7the standard error and number of patients are stated foreach risk group. Tick marks are patients alive with no disease progression.
Group A, 51% ± 8% (n =38)
Group C, 20% ± 18% (n=5)
Group B, 24% ± 9% (n =21)Pro
babi
lity
of s
urvi
val
−500 5000 1000 1500 2000 2500 3000
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Days after BMT
Figure 2 Event-free survival by MSKCC prognostic groups in the RPCIpatient cohort, including all patients (autologous and allogeneic). Group Ahas zero to one, Group B two, and Group C three of: B symptoms at thetime of salvage chemotherapy, extranodal disease at the time of salvagechemotherapy, and CRo1 year or primary refractory disease (P¼ 0.0091).The 4-year EFS7the standard error and number of patients are stated.
PreBMT prognostic factors in HDT Hahn et al
563
Bone Marrow Transplantation

treatment regimens within each donor group. Therefore, itis important to further validate both models in largerpatient populations treated at other institutions. The RPCImodel may be more rapidly tested using data fromregistries such as the International Bone Marrow Trans-plant Registry or the Autologous Blood and MarrowTransplant Registry because reported patient factors areassessed at the time of BMT rather than at the time ofsalvage chemotherapy. In order to validate the MKSCCmodel using Registry data, additional requests for datawould be required from all Registry sites, whereas theRPCI model could be validated using Registry data with nofurther data collection.We acknowledge that the allo BMT group was biased
due to a higher rate of poor prognostic features comparedto the auto BMT group. These unfavorable factors had asignificant confounding effect on the EFS and OS rates andany potential benefits of allo BMT have been offset by thepoor disease characteristics of these patients. However,donor type (auto vs allo) was not significant in themultivariate analysis, probably because the poor prognosticfeatures of the allo patients exhibited a stronger effect onoutcome than their type of BMT. Therefore, a risk-adaptedapproach derived from our model can be applied to thesepatients with poor prognostic features. Nonmyeloablativeallo BMT following less intensive conditioning regimenshas been shown to offer sustained clinical responses withless RRT and lower peri-transplant mortality ratescompared to standard myeloablative conditioning regi-mens.55–58 High-risk patients should be considered fornovel salvage therapies prior to nonmyeloablative alloBMT or other alternative therapies (ie, auto BMT followedby a nonmyeloablative allo BMT), since a myeloablativeallo BMT has unacceptably high toxicity and an auto BMTalone is ineffective in controlling disease in these poorprognosis patients.The results of this study support previous reports
favoring the use of auto BMT in refractory and relapsedHD patients with good prognostic features. We could notdemonstrate a beneficial role for myeloablative allo BMT inthis patient population which had poor survival outcomesdue to severe post-transplant complications. The RPCIprognostic model predicting shorter EFS in patients withchemotherapy-resistant disease, poor performance status,and three or more chemotherapy regimens prior to BMTwill require validation with larger patient numbers.
Acknowledgements
We thank Dr James Kepner, Chair of Biostatistics, Roswell ParkCancer Institute, for reviewing and commenting on the manu-script, the clinical services, data managers and transplant co-ordinators for help with data collection, and Ms DorothyMacchio for editorial assistance.
References
1 Aisenberg AC. Problems in Hodgkin’s disease management.Blood 1999; 93: 761–779.
2 Fung HC, Nademanee AP. Approach to Hodgkin’s lymphomain the new millenium. Hematol Oncol 2002; 20: 1–15.
3 Longo DL, Duffey PL, Young RC et al. Conventional-dosesalvage combination chemotherapy in patients relapsing withHodgkin’s disease after combination chemotherapy: The lowprobability of cure. J Clin Oncol 1992; 10: 210–218.
4 Bonfante V, Santoro A, Viviani S et al. Outcome of patientswith Hodgkin’s disease failing after primary MOPP-ABVD.J Clin Oncol 1997; 15: 528–534.
5 Rapoport AP, Rowe JM, Kouides PA et al. One hundredautotransplants for relapsed or refractory Hodgkin’s diseaseand lymphoma: value of pretransplant disease status forpredicting outcome. J Clin Oncol 1993; 11: 2351–2361.
6 Bierman PJ, Bagin RG, Jagannath S et al. High-dosechemotherapy followed by autologous hematopoietic rescuein Hodgkin’s disease: long-term follow-up in 128 patients. AnnOncol 1993; 4: 767–773.
7 Nademanee A, O’Donnell MR, Snyder DS et al. High-dosechemotherapy with or without total body irradiation followedby autologous bone marrow and/or peripheral blood stem celltransplantation for patients with relapsed and refractoryHodgkin’s disease: results in 85 patients with analysis ofprognostic factors. Blood 1995; 85: 1381–1390.
8 Horning SJ, Chao NJ, Negrin RS et al. High-dose therapy andautologous hematopoietic progenitor cell transplantation forrecurrent or refractory Hodgkin’s disease: analysis of theStanford University results and prognostic indices. Blood 1997;89: 801–813.
9 Sweetenham JW, Taghipour G, Milligan D et al. High-dosetherapy and autologous stem cell rescue for patients withHodgkin’s disease in first relapse after chemotherapy: resultsfrom the EBMT. Bone Marrow Transplant 1997; 20: 745–752.
10 Lazarus HM, Rowlings RA, Zhang M-J et al. Autotransplantsfor Hodgkin’s disease in patients never achieving remission:a report from the autologous blood and marrow transplantregistry. J Clin Oncol 1999; 17: 534–545.
11 Lazarus HM, Loberiza FR, Zhang M-J et al. Autotransplantsfor Hodgkin’s disease in first relapse or second remission: areport from the autologous blood and marrow transplantregistry (ABMTR). Bone Marrow Transplant 2001; 27:387–396.
12 Sureda A, Arranz R, Iriondo A et al. Autologous stem celltransplantation for Hodgkin’s disease: results and prognosticfactors in 494 patients from the Grupo Espanol de Linfomas/transplante autologo de medula osea Spanish cooperativegroup. J Clin Oncol 2001; 19: 1395–1404.
13 Linch DC, Winfield D, Goldstone AH et al. Dose intensifica-tion with autologous bone-marrow transplantation in relapsedand resistant Hodgkin’s disease: results of a BNLI randomisedtrial. Lancet 1993; 341: 1051–1054.
14 Andre M, Henry-Amar M, Pico J-L et al. Comparison of high-dose therapy and autologous stem cell transplantation withconventional therapy for Hodgkin’s disease induction failure:a case control study. J Clin Oncol 1999; 17: 222–229.
15 Anselmo AP, Meloni G, Cavalieri E et al. Conventionalsalvage chemotherapy vs high-dose therapy with autograftingfor recurrent or refractory Hodgkin’s disease patients. AnnHematol 2000; 79: 79–82.
16 Yuen AR, Rosenberg SA, Hoppe RT et al. Comparisonbetween conventional salvage therapy and high-dose therapywith autografting for recurrent or refractory Hodgkin’sdisease. Blood 1997; 89: 814–822.
17 Moskowitz CH, Kewalramani T, Nimer SD et al. Effectivenessof high dose chemoradiotherapy and autologous stem celltransplantation for patients with biopsy-proven primaryrefractory Hodgkin’s disease. Br J Haematol 2004; 124:645–652.
PreBMT prognostic factors in HDT Hahn et al
564
Bone Marrow Transplantation
18 Phillips GL, Reece DE, Barnett MJ et al. Allogeneic marrowtransplantation for refractory Hodgkin’s disease. J Clin Oncol1989; 7: 1039–1045.
19 Gajewski JL, Phillips GL, Sobocinski KA et al. Bone marrowtransplants from HLA-identical siblings in advanced Hodg-kin’s disease. J Clin Oncol 1996; 14: 572–578.
20 Milpied N, Fielding AK, Pearce RM et al. Allogeneic bonemarrow transplant is not better than autologous transplant forpatients with relapsed Hodgkin’s disease. J Clin Oncol 1996;14: 1291–1296.
21 Jones RJ, Piantadosi S, Mann RB et al. High-dose cytotoxictherapy and bone marrow transplantation for relapsedHodgkin’s disease. J Clin Oncol 1990; 8: 527–537.
22 Jones RJ, Ambinder RF, Piantadosi S et al. Evidence of agraft-versus-lymphoma effect associated with allogeneic bonemarrow transplantation. Blood 1991; 77: 649–653.
23 Anderson JE, Litzow MR, Appelbaum FR et al. Allogeneic,syngeneic, and autologous marrow transplantation for Hodg-kin’s disease: the 21-year Seattle experience. J Clin Oncol 1993;11: 2342–2350.
24 Akpek G, Ambinder RF, Piantadosi S et al. Long-term resultsof blood and marrow transplantation for Hodgkin’s lym-phoma. J Clin Oncol 2001; 19: 4314–4321.
25 Nachbaur D, Oberaigner W, Fritsch E et al. Allogeneic orautologous stem cell transplantation (SCT) for relapsed andrefractory Hodgkin’s disease and non-Hodgkin’s lymphoma:a single center experience. Eur J Haematol 2001; 66: 43–49.
26 Gobbi PG, Zinzani PL, Broglia C et al. Comparison ofprognostic models in patients with advanced Hodgkin disease.Promising results from integration of the best three systems.Cancer 2001; 91: 1467–1478.
27 Gobbi PG, Cavalli C, Federico M et al. Hodgkin’sdisease prognosis: a directly predictive equation. Lancet 1988;1: 675–679.
28 Wagstaff J, Gregory WM, Swindell R et al. Prognostic factorsfor survival in Stage III B and IV Hodgkin’s disease: amultivariate analysis comparing two specialist treatmentcentres. Br J Cancer 1988; 58: 487–492.
29 Straus DJ, Gaynor JJ, Myers J et al. Prognostic factors among185 adults with newly diagnosed advanced Hodgkin’s diseasetreated with alternating potentially noncross-resistantchemotherapy and intermediate-dose radiation therapy. J ClinOncol 1990; 7: 1173–1186.
30 Carella AM, Carlier P, Congiu A et al. Autologous bonemarrow transplantation as adjuvant treatment for high-riskHodgkin’s disease in first complete remission after MOPP/ABVD protocol. Bone Marrow Transplant 1991; 8: 99–103.
31 Proctor SJ, Taylor P, Donnan P, et al, with the members of theScotland and Newcastle Lymphoma Group (SNLG) TherapyWorking Party. A numerical prognostic index for clinical usein identification of poor-risk patients with Hodgkin’s disease atdiagnosis. Eur J Cancer 1991; 27: 624–629.
32 Gobbi PG, Comelli M, Grignani GE et al. Estimate ofexpected survival at diagnosis in Hodgkin’s disease: a means ofweighting prognostic factors and a tool for treatment choiceand clinical research. A report from the InternationalDatabase on Hodgkin’s Disease (IDHD). Haematologica 1994;79: 241–255.
33 Lee SM, Radford JA, Ryder WDJ et al. Prognostic factors fordisease progression in advanced Hodgkin’s disease: an analysisof patients aged under 60 years showing no progression in thefirst 6 months after starting primary chemotherapy. Br JCancer 1997; 75: 110–115.
34 Ferme C, Bastion Y, Brice P et al. Prognosis of patients withadvanced Hodgkin’s disease. Evaluation of four prognosticmodels using 344 patients included in the Group d’Etudes desLymphomes de l’Adulte Study. Cancer 1997; 80: 1124–1133.
35 Hasenclever D, Diehl V, for the International PrognosticFactors Project on Advanced Hodgkin’s Disease. A prognosticscore to predict tumor control in advanced Hodgkin’s disease.N Engl J Med 1998; 339: 1506–1514.
36 Stiff PJ, Unger JM, Forman SJ et al. The value of augmentedpreparative regimens combined with an autologous bonemarrow transplant for the management of relapsed orrefractory Hodgkin disease: A Southwest Oncology Groupphase II trial. Biol Blood Marrow Transplant 2003; 9: 529–539.
37 Moskowitz CH, Nimer SD, Zelenetz AD et al. A 2-stepcomprehensive high-dose chemoradiotherapy second-line pro-gram for relapsed and refractory Hodgkin disease: analysis byintent to treat and development of a prognostic model. Blood2001; 97: 616–623.
38 Josting A, Franklin J, May M et al. New Prognostic Scorebased on treatment outcomes of patients with relapsedHodgkin’s lymphoma registered in the database of the GermanHodgkin’s Lymphoma Study Group. J Clin Oncol 2002; 20:221–230.
39 Alidina A, Lawrence D, Ford LA et al. Thiotepa-associatedcardiomyopathy during blood or marrow transplantation:association with the female sex and cardiac risk factors. BiolBlood Marrow Transplant 1999; 5: 322–327.
40 Tutschka PJ, Copelan EA, Klein JP. Bone marrow transplan-tation for leukemia following a new busulfan and cyclopho-sphamide regimen. Blood 1987; 70: 1382–1388.
41 Brown RA, Wolff SN, Fay JW et al. High-dose etoposide,cyclophosphamide, and total body irradiation with allogeneicbone marrow transplantation for patients with acute myeloidleukemia in first untreated relapse: a study by the NorthAmerican Marrow Transplant Group. Blood 1995; 85:1391–1395.
42 Giralt S, Estey E, Albitar M et al. Engraftment of allogeneichematopoietic progenitor cells with purine analog-containingchemotherapy: harnessing graft-versus-leukemia withoutmyeloablative therapy. Blood 1997; 89: 4531–4536.
43 Alam AR, Younis T, Hahn T et al. High dose therapy andautologous hematopoietic stem cell transplantation(autoHSCT) with an intensive VCB conditioning regimen forrelapsed and refractory Hodgkin’s disease. Blood 2002; 100:863a (abstr. 3404).
44 Santos GW, Tutschka PJ, Brookmeyer R. Marrow transplan-tation for acute nonlymphocytic leukemia after treatment withbusulfan and cyclophosphamide. N Engl J Med 1983; 309:1347–1353.
45 Bearman SI, Appelbaum FR, Buckner CD et al. Regimen-related toxicity in patients undergoing bone marrow trans-plantation. J Clin Oncol 1988; 6: 1562–1568.
46 Nash RA, Pepe MS, Storb R et al. Acute graft-vs-host disease:analysis of risk factors after allogeneic marrow transplantationand prophylaxis with cyclosporine and methotrexate. Blood1992; 80: 1838–1845.
47 Chao NJ, Schmidt GM, Niland JC et al. Cyclosporine,methotrexate and prednisone compared with cyclosporineand prednisone for prophylaxis of acute graft-vs-host disease.N Engl J Med 1993; 329: 1225–1229.
48 Shepherd JD, Shore TB, Reece DE et al. Cyclosporine andmethylprednisolone for prophylaxis of acute graft-versus-hostdisease. Bone Marrow Transplant 1988; 3: 553–557.
49 Alam AR, Baer MR, Bernstein S et al. Phase II clinical trial ofOKT3 for acute graft-vs-host disease (GVHD) prophylaxis inallogeneic bone marrow transplantation (alloBMT). Blood1997; 90: 102a (abstr.).
50 Glucksberg H, Storb R, Fefer A et al. Clinical manifestationsof graft-versus-host disease in human recipients of marrowfrom HL-A matched sibling donors. Transplantation 1974; 18:295–304.
PreBMT prognostic factors in HDT Hahn et al
565
Bone Marrow Transplantation

51 Przepiorka D, Weisdorf D, Martin P et al. 1994 Consensusconference on acute GVHD grading. Bone Marrow Transplant1995; 15: 825–828.
52 Kaplan EL, Meier P. Nonparametric estimation for incom-plete observations. J Am Stat Assoc 1958; 53: 457–481.
53 Cox DR, Oakes D. Analysis of Survival Data. Chapman andHall: New York, 1984.
54 Qazilbash MH, Devetten MP, Abraham J et al. High-dosetherapy and autologous stem cell transplantation in relapsedand refractory Hodgkin’s disease: outcome based on aprognostic model. Acta Haematol 2003; 110: 173–178.
55 Carella AM, Cavaliere M, Lerma E et al. Autograftingfollowed by nonmyeloablative immunosuppressive chemo-therapy and allogeneic peripheral blood hematopoietic stem cell
transplantation as treatment of resistant Hodgkin’s disease andnon-Hodgkin’s lymphoma. J Clin Oncol 2000; 18: 3918–3924.
56 Anderlini P, Giralt S, Andersson B et al. Allogeneic stem celltransplantation with fludarabine-based, less intensive condi-tioning regimens as adoptive immunotherapy in advancedHodgkin’s disease. Bone Marrow Transplant 2000; 26: 615–620.
57 Branson K, Chopra R, Kottaridis PD et al. Role ofnonmyeloablative allogeneic stem cell transplantation afterfailure of autologous transplantation in patients with lympho-proliferative malignancies. J Clin Oncol 2002; 20: 4022–4031.
58 Cooney JP, Stiff PJ, Toor AA, Parthasarathy M. BEAMallogeneic transplantation for patients with Hodgkin’s diseasewho relapse after autologous transplantation is safe andeffective. Biol Blood Marrow Transplant 2003; 9: 177–182.
PreBMT prognostic factors in HDT Hahn et al
566
Bone Marrow Transplantation
Copyright © 2022 FDOKUMEN




















