A preliminary Quality Control (QC) for next generation sequencing (NGS) library evaluation turns out...
6
A preliminary Quality Control (QC) for next generation sequencing (NGS) library evaluation turns out to be a very useful tool for a rapid detection of BRCA1/2 deleterious mutations Paola Concolino a, ⁎, Alessandra Costella a , Angelo Minucci a , Giovanni Luca Scaglione a , Concetta Santonocito a , Vanda Salutari b , Giovanni Scambia b , Cecilia Zuppi a , Ettore Capoluongo a, ⁎ a Laboratory of Molecular Biology, Institute of Biochemistry and Clinical Biochemistry, Catholic University of Sacred Heart, Largo A. Gemelli 8, 00168 Rome, Italy b Department of Obstetrics and Gynecology, Catholic University of Sacred Heart, Largo A. Gemelli 8, 00168 Rome, Italy abstract article info Article history: Received 29 May 2014 Received in revised form 27 June 2014 Accepted 27 June 2014 Available online 5 July 2014 Keywords: BRCA1 BRCA2 Frameshift mutations NGS Breast cancer Background: Recent advances in next generation sequencing (NGS) technology have enabled comprehensive and accurate screening of the entire genomic region of BRCA1/2 genes and, to date, many studies report the effective- ness of these technologies. Here we show that Gene Scan (GS) labeling Quality Control (QC), performed before massive parallel pyrosequencing, coupled with Multiple Amplicon Quantification software (MAQ-S) analysis is a rapid and powerful tool in the detection of deleterious BRCA mutations carried by different patients. Methods: GS labeling QC assay was performed according to the manufacturers' instructions and MAQ-S software was employed for analysis results. Results: GS labeling QC was able to detect 14 different BRCA frameshift mutations in our patients. In addition, two novel BRCA mutations (c.1893_1894insTTAAGCCCACAAAT in BRCA1 gene and c.9413_9414insT in BRCA2 gene) were identified. Conclusion: We prove that a simple QC step may represent a valid and useful tool for a rapid detection of frame- shift mutations in BRCA genes. For this reason, we recommend using this approach before massive parallel sequencing. © 2014 Elsevier B.V. All rights reserved. 1. Introduction About 5–10% of all breast cancers are estimated to be heredi- tary; germline mutations in the tumor-suppressor genes BRCA1 (MIM#113705) and BRCA2 (MIM#600185) are found in a variable proportion of this group [1,2]. Family history of breast and ovarian can- cer, besides breast cancer bilaterality, early-onset breast cancer and eth- nicity constitute the basic criteria for identifying cases affected by BRCA1 or BRCA2 mutation. However, a negative family history does not exclude the presence of a germline mutation in these genes. In fact, in an unselected population of triple-negative breast cancer, the observed mutation rate was significantly higher than expected [3]. To date, BRCA testing for therapeutic purpose is a widely discussed topic due to the impact of PARP-1 inhibitor on BRCA-mutated or BRCA- ness ovarian cancer in women [4]. In fact, differences in outcome be- tween BRCA mutation carriers versus those with no mutations or with epigenetic or BRCA somatic mutations have been identified [4]. Most reported germline BRCA1/BRCA2 deleterious mutations are small deletions, small insertions, nonsense mutations and splice var- iants, as described at the Breast Cancer Information Core internet web site (BIC database) [5]. Recent advances in next generation se- quencing (NGS) technology have enabled comprehensive and accu- rate screening of the entire genomic region of BRCA1/2 genes and, to date, many studies report the validity of these technologies, highlighting advantages in terms of cost effectiveness and improved turnaround times [6–9]. We routinely perform BRCA genetic testing using the BRCA MASTR Dx assay (provided by Multiplicom) on the 454 TM GS Junior platform (Roche Diagnostics). According to our experience, this strategy, in com- bination with MLPA (multiplex ligation-dependent probe amplifica- tion) or MAQ (multiplex amplicon quantification) techniques for Locus Reference Genomic Sequence (LRGs) detection in BRCA genes, represents a valid and solid approach for breast cancer molecular diag- nostics [10]. The aim of this paper is to shed light on GS QC assay Clinica Chimica Acta 437 (2014) 72–77 Abbreviations: NGS, next generation sequencing; GS, Gene Scan; QC, Quality Control; MPS, massive parallel sequencing; MLPA, multiplex ligation-dependent probe amplifica- tion; MAQ, multiplex amplicon quantification. ⁎ Corresponding authors at: Laboratory of Clinical Molecular and Personalized Diagnostics, Department of Laboratory Medicine- Institute of Biochemistry and Clinical Biochemistry, Catholic University of Sacred Heart, Largo A. Gemelli 8, 00168 Rome, Italy. Tel.: +39 0630154250; fax: +39 0630156706. E-mail addresses: [email protected] (P. Concolino), [email protected] (E. Capoluongo). http://dx.doi.org/10.1016/j.cca.2014.06.026 0009-8981/© 2014 Elsevier B.V. All rights reserved. Contents lists available at ScienceDirect Clinica Chimica Acta journal homepage: www.elsevier.com/locate/clinchim
Transcript of A preliminary Quality Control (QC) for next generation sequencing (NGS) library evaluation turns out...

Clinica Chimica Acta 437 (2014) 72–77
Contents lists available at ScienceDirect
Clinica Chimica Acta
j ourna l homepage: www.e lsev ie r .com/ locate /c l inch im
Apreliminary Quality Control (QC) for next generation sequencing (NGS)library evaluation turns out to be a very useful tool for a rapid detectionof BRCA1/2 deleterious mutations
Paola Concolino a,⁎, Alessandra Costella a, Angelo Minucci a, Giovanni Luca Scaglione a, Concetta Santonocito a,Vanda Salutari b, Giovanni Scambia b, Cecilia Zuppi a, Ettore Capoluongo a,⁎a Laboratory of Molecular Biology, Institute of Biochemistry and Clinical Biochemistry, Catholic University of Sacred Heart, Largo A. Gemelli 8, 00168 Rome, Italyb Department of Obstetrics and Gynecology, Catholic University of Sacred Heart, Largo A. Gemelli 8, 00168 Rome, Italy
Abbreviations: NGS, next generation sequencing; GS,MPS, massive parallel sequencing; MLPA, multiplex ligatition; MAQ, multiplex amplicon quantification.⁎ Corresponding authors at: Laboratory of Clinical
Diagnostics, Department of Laboratory Medicine- InstituBiochemistry, Catholic University of Sacred Heart, Largo ATel.: +39 0630154250; fax: +39 0630156706.
E-mail addresses: [email protected] (P. [email protected] (E. Capoluongo).
http://dx.doi.org/10.1016/j.cca.2014.06.0260009-8981/© 2014 Elsevier B.V. All rights reserved.
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 29 May 2014Received in revised form 27 June 2014Accepted 27 June 2014Available online 5 July 2014Keywords:BRCA1BRCA2Frameshift mutationsNGSBreast cancer
Background:Recent advances in next generation sequencing (NGS) technology have enabled comprehensive andaccurate screening of the entire genomic region of BRCA1/2 genes and, to date, many studies report the effective-ness of these technologies. Here we show that Gene Scan (GS) labeling Quality Control (QC), performed beforemassive parallel pyrosequencing, coupled with Multiple Amplicon Quantification software (MAQ-S) analysis isa rapid and powerful tool in the detection of deleterious BRCAmutations carried by different patients.Methods:GS labeling QC assay was performed according to the manufacturers' instructions andMAQ-S softwarewas employed for analysis results.Results: GS labeling QCwas able to detect 14 different BRCA frameshiftmutations in our patients. In addition, twonovel BRCAmutations (c.1893_1894insTTAAGCCCACAAAT in BRCA1 gene and c.9413_9414insT in BRCA2 gene)were identified.Conclusion:We prove that a simple QC step may represent a valid and useful tool for a rapid detection of frame-
shift mutations in BRCA genes. For this reason, we recommend using this approach before massive parallelsequencing.© 2014 Elsevier B.V. All rights reserved.
1. Introduction
About 5–10% of all breast cancers are estimated to be heredi-tary; germline mutations in the tumor-suppressor genes BRCA1(MIM#113705) and BRCA2 (MIM#600185) are found in a variableproportion of this group [1,2]. Family history of breast and ovarian can-cer, besides breast cancer bilaterality, early-onset breast cancer and eth-nicity constitute the basic criteria for identifying cases affected byBRCA1 or BRCA2 mutation. However, a negative family history doesnot exclude the presence of a germline mutation in these genes. Infact, in an unselected population of triple-negative breast cancer, theobserved mutation rate was significantly higher than expected [3].
Gene Scan; QC, Quality Control;on-dependent probe amplifica-
Molecular and Personalizedte of Biochemistry and Clinical. Gemelli 8, 00168 Rome, Italy.
olino),
To date, BRCA testing for therapeutic purpose is a widely discussedtopic due to the impact of PARP-1 inhibitor on BRCA-mutated or BRCA-ness ovarian cancer in women [4]. In fact, differences in outcome be-tween BRCA mutation carriers versus those with no mutations or withepigenetic or BRCA somatic mutations have been identified [4].
Most reported germline BRCA1/BRCA2 deleterious mutations aresmall deletions, small insertions, nonsense mutations and splice var-iants, as described at the Breast Cancer Information Core internetweb site (BIC database) [5]. Recent advances in next generation se-quencing (NGS) technology have enabled comprehensive and accu-rate screening of the entire genomic region of BRCA1/2 genes and,to date, many studies report the validity of these technologies,highlighting advantages in terms of cost effectiveness and improvedturnaround times [6–9].
We routinely perform BRCA genetic testing using the BRCA MASTRDx assay (provided by Multiplicom) on the 454TM GS Junior platform(Roche Diagnostics). According to our experience, this strategy, in com-bination with MLPA (multiplex ligation-dependent probe amplifica-tion) or MAQ (multiplex amplicon quantification) techniques forLocus Reference Genomic Sequence (LRGs) detection in BRCA genes,represents a valid and solid approach for breast cancer molecular diag-nostics [10]. The aim of this paper is to shed light on GS QC assay

Table 1BRCA1/2 mutations detected by GS labeling QC assay.
Gene Exon Codon HGVS genomic (h19) HGVS cDNA Predicted effect HGVS protein
BRCA2 10 413 g.32906853delT c.1238_1238delT Stop 429 p.Leu413Hisfs10 437 g.32906924_32906927delAAAG c.1309_1312delAAAG Stop 459 p.Lys437_Asp438?fs11 1248 g.32912236_32912239delTGAG c.3744_3747delTGAG Stop 1257 p.Ser1248_Glu1249?fs11 1428 g.32912776_32912777insT c.4284_4285insT Stop 1437 p.Phe1428_Gln1429?fs11 2156 g.32914960_32914961delTC c.6468_6469delTC Stop 2174 p.Ser2156_Gln2157SerIlefs19 2825 g.32944681delC c.8474_8474delC Stop 2862 p.Ala2825Aspfs25 3138 g.32968982_32968983insT c.9413_9414insT Stop 3149 p.Leu3138_Phe3139?fs
BRCA1 11 802 g.41245142_41245143delCA c.2405_2406delTG Stop 808 p.Val802Glufs11 1252 g.41243789_41243792delAGAC c.3756_3759delGTCT Stop 1262 p.Leu1252_Ser1253?fs11 327 g.41246566_41246567delAT c.981_982delAT Stop 328 p.Thr327_Cys328ThrTerfs11 631 g.41247478_41247479
insTTAAGCCCACAAATc.1893_1894insTTAAGCCCACAAAT
Stop 636 p.Pro634Glufs
16 1571 g.41223215_41223219delAGAGA c.4712_4716delTCTCT Stop 1571 p.Phe1571_Ser1572?fs17 1688 g.41219635_41219637delAAC c.5062_5064delGTT del Val p.Val1688delVal20 1755 g.41209082_41209083insG c.5263_5264insC Stop 1829 p.Ser1755?fs
Variants are reported according to the Human Genome Variation Society (HGVS).
Fig. 1.Detection of the c.9413_9414insTmutation in BRCA2 exon 25. Panel A shows thewild type profile of the plex B. The arrow indicates thewild type peak (402 bp) relative to amplicon2 of BRCA2 exon 25. Panel B shows themutated profile of plex B in the patient carrying the novel frameshift mutation. The arrow indicates the peak relative to themutated allele (403 bp).Sanger sequencing, chromatogram in the panel C, confirmed the presence of the c.9413_9414insT mutation in this patient.
73P. Concolino et al. / Clinica Chimica Acta 437 (2014) 72–77

74 P. Concolino et al. / Clinica Chimica Acta 437 (2014) 72–77
robustness, efficacy and rapidity, when performed just before massiveparallel sequencing in the BRCA genetic testing pipeline.
2. Methods
The quality and quantity of the DNA samples are critical for the per-formance and success of the procedures that follow. According to ourexperience, the use of commercial columns may represent thehighest-quality method for DNA blood extraction in order to obtain agood amount of pure and intact nucleic acid. Therefore, genomic DNAwas isolated from peripheral blood samples using High Pure PCR Tem-plate Preparation Kits (Roche Diagnostic, USA) eluted in 100 μl ofElution Buffer (Roche Diagnostic, USA), quantified by spectrophotome-ter at 260 nm and stored at −20 °C until use. Only DNA that meet therequirements (OD260/280 ratio ≥ 1.7, concentration ≥ 15 ng/μl, andno degradation signals visible on agarose gel) were used in the study.
The BRCA MASTR Dx (Multiplicom, MR-2012.040) assay for theidentification of BRCA1 and BRCA2 mutations was performed
Fig. 2.Detection of the c.4284_4285insTmutation in BRCA2 exon 11. Panel A shows thewild typ10 of BRCA2 exon 11. Panel B shows the mutated profile of plex A in the patient carrying the fSanger sequencing, chromatogram in the panel C, confirmed the presence of the c.4284_4285i
following the manufacturers' instructions provided by Multiplicom(www.multiplicom.com). Differently, GS QC assay (Multiplicom,MR-2012.040) was fulfilled as follows: briefly, 1.5 μl of each plexwas mixed with 13 μl of GS-labeling PCR Mix and 0.075 μl of TaqDNA Polymerase. The following PCR profile was performed: 10 minto 98 °C, 5 cycles consisting of 30 s to 95 °C, 30 s to 65 °C and 30 s to68 °C, and a final step at 72 °C for 10 min. Successively, 10 μl of Hi-DiTM Formamide and 0.3 μl of GS600 size standard were mixed with0.6 μl of each GS labeling PCR-product for fragment analysis. MAQ-Ssoftware (www.multiplicom.com) was employed for analysis resultsusing provided Assay Description file (.enc) and GS Reference Pat-tern. The Universal PCR amplification was valid if the analysis pat-tern was consistent with the GS Reference Pattern provided byMultiplicom (www.multiplicom.com).
Finally, in order to allow a rapid detection of small insertion/deletionmutations in the coding homopolymer stretches, the homopolymerassay (HP BRCA) (Multiplicom, MP-0110.050) was used according toprovided instructions (www.multiplicom.com).
e profile of the plexA. The arrow indicates thewild type peak (447 bp) relative to ampliconrameshift mutation. The arrow indicates the peak relative to the mutated allele (448 bp).nsT mutation in this patient.
75P. Concolino et al. / Clinica Chimica Acta 437 (2014) 72–77
3. Results
Table 1 shows mutations that were identified using this QC ap-proach. Fig. 1B shows the fragment analysis of a patient carrying anovel mutation (c.9413_9414insT) in BRCA2 exon 25. The BRCA2 exon25 wild type amplicon (plex B) consists of a single peak at 402 bp(Fig.1A). Meanwhile, a second peak at 403 bp is detectable representingthe mutated allele in Fig. 1B. This single nucleotide insertion at 3138codon introduces a stop codon after 11 amino acids.
Fig. 2B shows the fragment analysis of a patient carrying thec.4284_4285insT mutation in BRCA2 exon 11. The wild type ampliconconsists of a single peak at 447 bp within the plex A (Fig. 2A). Mean-while, it is possible to note a second pick at 448 bp representing themu-tated allele in Fig. 2B. In this case a targeted sequencing of the specificBRCA2 exon 11 region revealed the frameshift mutation (Fig.2C).
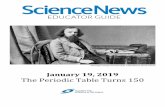
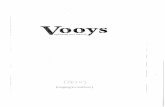
Fig. 3. Detection of the c.1893_1894insTTAAGCCCACAAATmutation in BRCA1 exon 11. Panel Arelative to amplicon 9 of BRCA1 exon 11. Panel B shows the mutated profile of plex D in the pamutated allele (497 bp). Sanger sequencing, chromatogram in the panel C, confirmed the pres
The GS labeling QC step was also able to detect a second novelBRCA1 mutation, the p.Pro634Glufs, due to a 14 bp insertion(c.1893_1894insTTAAGCCCACAAAT) in exon 11 determining a stopcodon at 636 amino acid. Fig. 3A shows the wild type profile of theplex Dwhere the wild type pick has a size of 483 bp. Themutated alleleappears in Fig. 3B as an additional peak of 497 bp, while the wild typepick at 483 bp shows half- height. Direct sequencing confirmed theframeshift mutation (Fig.3C). Finally, the c.1893_1894insTTAAGCCCACAAAT mutation was also clearly detected by the HP assay (Fig. 4).
4. Discussion
The BRCA MASTR Dx (Multiplicom) is a molecular diagnostic assayable to identifymutations in the entire BRCA1 and BRCA2 coding regionsin individuals with increased risk for breast, ovarian and/or BRCA-
shows the wild type profile of the plex D. The arrow indicates the wild type peak (483 bp)tient carrying the novel frameshift mutation. The arrow indicates the peak relative to theence of the c.1893_1894insTTAAGCCCACAAAT mutation in this patient.

Fig. 4. BRCA HP assay, fragment analysis profile. Panel A shows the wild type profile of the plex A relative to BRCA HP assay. The arrow indicates the wild type peak (202 bp) relative to aspecific BRCA1 exon 11 region. Panel B shows themutatedprofile of plexA in thepatient carrying the novel c.1893_1894insTTAAGCCCACAAATmutation.Arrows indicate thepeaks relativeto the wild type (202 bp) and mutated allele (216 bp).
76 P. Concolino et al. / Clinica Chimica Acta 437 (2014) 72–77
related cancers. In the first step, all coding regions of BRCA1 and BRCA2are amplified in five separate multiplex PCR amplification reactions(Plex 1–5; 93 amplicons) per individual, using a hot-start DNApolymer-ase. In the second step, a second round of Universal PCR is performedenabling tagging of the amplicons with specific MIDs and adaptors re-quired for sequencing using MPS (massive parallel sequencing) instru-ments. At this point, a QC of multiplex PCR by agarose gel is stronglyrecommended. In fact, successful amplification is detected as a clearlyvisible but dispersed band that ranges between 250 and 500 bp. Howev-er, an alternative amplicon control step, by PCR fluorescent labeling andfragment analysis (GS labeling QC), is offered. The quality of the multi-plex PCR can be reviewed in detail based on the pattern of the ampliconsof a given plex for the specific BRCAMASTRDx. The required chromato-grams can be obtained using a capillary sequencer with Gene Scan (GS)module. In the BRCAMASTR Dx protocol, the GS labeling QC step is rec-ommended, but not mandatory, and, at the best of our knowledge, veryfew users perform this procedure. However, according to our experi-ence, we can affirm that this check represents a very useful tool sinceit allows the rapid detection of deleterious frameshift (ins/del) muta-tions in BRCA genes. In fact, fragment analysis is able to discriminateall BRCA amplicons basing on their length. For this reason, comparingpatient's pattern with the BRCA GS Reference Pattern, it is possible toidentify a suspected peak representing a specific amplicon (exon) carry-ing a mutation (Figs. 1–3). In order to identify and confirm thisframeshift mutation, the detected amplicon (exon) can be directlysequenced by Sanger method avoiding the use of massive parallelpyrosequencing.
Last year, we analyzed 56 unrelated individuals, affected by breastand/or ovarian cancer, and this approach allowed us to identify 14 dif-ferent BRCA frameshift mutations (Table 1) representing 65% of all mu-tations detected in our patients. No false positive or false negative
results were obtained in independent repetitive experiments showingthe good reproducibility of this method.
In addition, we report two novel BRCA mutations: c.1893_1894insTTAAGCCCACAAAT and c.9413_9414insT in exon 11 of BRCA1gene and in exon 25 of BRCA2 gene, respectively. The first mutationwas identified in an Italianwoman affected by breast andovarian cancerat the age of 31 and 47 years, respectively,while the lattermutationwasdetected within an Italian family with multiple members affected bybreast and ovarian cancer.
One of the 454 pyrosequencing technology limitations is differenti-ating between stretches of identical bases (homopolymers). For thisreason Multiplicom has developed a homopolymer assay (HP BRCA)for BRCA MASTR™ allowing a rapid detection of small insertion/deletion mutations in the coding homopolymer stretches. The HPassay is a multiplex PCR based test that amplifies fragments containingthe homopolymer stretches of interest. The obtained fluorescently la-beled fragments need to be analyzed on a fragment analyzer with theGene Scan module resulting in Gene Scan profiles. Detailed analysis ofthese profiles will show changes in length of the amplified fragmentscontaining homopolymer stretch(es). Based on our experience, we canaffirm that the HP assay may be replaced by the GS labeling QC stepwith significant reduction in costs. In fact, here we assess that thec.1893_1894insTTAAGCCCACAAAT mutation is clearly detected byboth HP BRCA assay (Fig. 4) and GS labeling QC (Fig. 3). However,since the HP BRCA assay analyzes a predefined limited number ofBRCA regions, in our workflow we applied GS labeling QC to obtain acomplete coverage of all BRCAMASTR amplicons.
In conclusion, herewe clearly show that the simple QC stepmay rep-resent a valid and useful tool for a rapid detection of frameshift muta-tions in BRCA genes. For this reason, we recommend the use of thisapproach before massive parallel sequencing since it determines a

77P. Concolino et al. / Clinica Chimica Acta 437 (2014) 72–77
reduction in costs and in timing, along with an improvement of qualityof NGS pipeline.
References
[1] Miki Y, Swensen J, Shattuck-EidensD, et al. A strong candidate for thebreast andovar-ian cancer susceptibility gene BRCA1. Science (New York, NY) 1994;5182:66–71.
[2] Wooster R, Bignell G, Lancaster J, et al. Identification of the breast cancer susceptibil-ity gene BRCA2. Nature 1995;378:789–92.
[3] Hartman AR, Kaldate RR, Sailer LM, et al. Prevalence of BRCA mutations in an unse-lected population of triple-negative breast cancer. Cancer 2012;118:2787–95.
[4] Muggia F, Safra T. 'BRCAness' and its implications for platinum action in gynecologiccancer. Anticancer Res 2014;34(2):551–6.
[5] BIC Database. http://research.nhgri.nih.gov/bic/.
[6] Feliubadaló L, Lopez-Doriga A, Castellsagué E, et al. Next-generation sequencingmeets genetic diagnostics: development of a comprehensive workflow for the anal-ysis of BRCA1 and BRCA2 genes. Eur J Hum Genet 2013;21:864–70.
[7] Michils G, Hollants S, Dehaspe L, et al. Molecular analysis of the breast cancer genesBRCA1 and BRCA2 using amplicon-based massive parallel pyrosequencing. J MolDiagn 2012;14:623–30.
[8] Hernan I, Borràs E, de Sousa Dias M, et al. Detection of genomic variations in BRCA1and BRCA2 genes by long-range PCR and next-generation sequencing. J Mol Diagn2012;14:286–93.
[9] Vaca-Paniagua F, Alvarez-Gomez RM, Fragoso-Ontiveros V, et al. Full-exon pyrose-quencing screening of BRCA germline mutations in Mexican women with inheritedbreast and ovarian cancer. PLoS One 2012;7:e37432.
[10] Concolino P, Mello E, Minucci A, et al. Advanced tools for BRCA1/2 mutationalscreening: comparison between two methods for large genomic rearrangements(LGRs) detection. Clin Chem Lab Med 2014;52:1119–27.