
A new theory of health promoting schools based on human functioning, school organisation and...
12
Social Science & Medicine 56 (2003) 1209–1220 A new theory of health promoting schools based on human functioning, school organisation and pedagogic practice Wolfgang A. Markham a, *, Paul Aveyard b a School of Education, University of Birmingham, Birmingham B15 2TT, UK b Department of Public Health and Epidemiology, University of Birmingham, Birmingham B15 2TT, UK Abstract This paper outlines a novel explanatory frame for understanding how schools may intervene in order to promote pupils’ health. The new theory is synthesised from an Aristotelian interpretation of human functioning and a theory of cultural transmission. In keeping with recent influential theoretical developments, it is proposed that health has its roots in human functioning. It follows from this concept that the promotion of pupils’ health is facilitated by the promotion of pupil functioning and the primary mechanisms through which schools promote pupil functioning and, hence, health, are through the influences of school organisation, curriculum development and pedagogic practice on pupil development. According to the new theory, good human functioning is dependent on the realisation of a number of identified essential human capacities and the meeting of identified fundamental human needs. Two essential capacities, the capacity for practical reasoning and the capacity for affiliation with other humans, plan and organise the other essential capacities. The realisation of these two capacities should, it is argued, be the primary focus of health promoting schools. Additionally, health promoting schools should ensure that fundamental human needs concerning non-useful pain and information about the body are met. A number of testable hypotheses are generated from the new theory. Comparisons with existing interpretations of health promoting schools indicate there are similarities in the actions schools should take to promote health. However, the new theory can, uniquely, be used to predict which pupils will enjoy the best health at school and in adulthood. Additionally, according to the new theory, schools do not need designated health education classes or teaching staff with specialist health education roles in order to be health promoting. It is concluded that the new theory may have a number of advantages over existing theories at both the policy and intervention levels. r 2002 Elsevier Science Ltd. All rights reserved. Keywords: School; Health promotion; Human functioning Introduction Recent influential theoretical developments in health promotion are underpinned by the notion that health has its roots in human functioning (Antonovsky, 1987; MacDonald, 1998; Marmot & Theorell, 1988; Seed- house, 1997). In this paper, we outline a new theory of health promoting schools, which draws on this notion, and is particularly relevant to adolescents. A funda- mental concept of this theory is that being autonomous and in a position to choose to function well and flourish is necessary to maximise health potential. It follows from this fundamental concept that the promotion of health is facilitated by the promotion of pupil function- ing and the primary mechanisms through which schools promote pupil functioning and, hence, health, are through the influences of school organisation, curricu- lum development and pedagogic practice on pupil development. When viewed from this perspective, schools do not need health education classes that focus on healthy lifestyle choices nor teaching staff with specialist health education roles in order to be health promoting. Although many aspects of our new theory *Corresponding author. Tel.: +44-121-414-7631; fax: +44- 121-414-4865. E-mail address: [email protected] (W.A. Markham). 0277-9536/03/$ - see front matter r 2002 Elsevier Science Ltd. All rights reserved. PII:S0277-9536(02)00120-X
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A new theory of health promoting schools based on human functioning, school organisation and...
Social Science & Medicine 56 (2003) 1209–1220
A new theory of health promoting schools based on humanfunctioning, school organisation and pedagogic practice
Wolfgang A. Markhama,*, Paul Aveyardb
aSchool of Education, University of Birmingham, Birmingham B15 2TT, UKbDepartment of Public Health and Epidemiology, University of Birmingham, Birmingham B15 2TT, UK
Abstract
This paper outlines a novel explanatory frame for understanding how schools may intervene in order to promote
pupils’ health. The new theory is synthesised from an Aristotelian interpretation of human functioning and a theory of
cultural transmission. In keeping with recent influential theoretical developments, it is proposed that health has its roots
in human functioning. It follows from this concept that the promotion of pupils’ health is facilitated by the promotion
of pupil functioning and the primary mechanisms through which schools promote pupil functioning and, hence, health,
are through the influences of school organisation, curriculum development and pedagogic practice on pupil
development. According to the new theory, good human functioning is dependent on the realisation of a number of
identified essential human capacities and the meeting of identified fundamental human needs. Two essential capacities,
the capacity for practical reasoning and the capacity for affiliation with other humans, plan and organise the other
essential capacities. The realisation of these two capacities should, it is argued, be the primary focus of health
promoting schools. Additionally, health promoting schools should ensure that fundamental human needs concerning
non-useful pain and information about the body are met. A number of testable hypotheses are generated from the new
theory. Comparisons with existing interpretations of health promoting schools indicate there are similarities in the
actions schools should take to promote health. However, the new theory can, uniquely, be used to predict which pupils
will enjoy the best health at school and in adulthood. Additionally, according to the new theory, schools do not need
designated health education classes or teaching staff with specialist health education roles in order to be health
promoting. It is concluded that the new theory may have a number of advantages over existing theories at both the
policy and intervention levels. r 2002 Elsevier Science Ltd. All rights reserved.
Keywords: School; Health promotion; Human functioning
Introduction
Recent influential theoretical developments in health
promotion are underpinned by the notion that health
has its roots in human functioning (Antonovsky, 1987;
MacDonald, 1998; Marmot & Theorell, 1988; Seed-
house, 1997). In this paper, we outline a new theory of
health promoting schools, which draws on this notion,
and is particularly relevant to adolescents. A funda-
mental concept of this theory is that being autonomous
and in a position to choose to function well and flourish
is necessary to maximise health potential. It follows
from this fundamental concept that the promotion of
health is facilitated by the promotion of pupil function-
ing and the primary mechanisms through which schools
promote pupil functioning and, hence, health, are
through the influences of school organisation, curricu-
lum development and pedagogic practice on pupil
development. When viewed from this perspective,
schools do not need health education classes that focus
on healthy lifestyle choices nor teaching staff with
specialist health education roles in order to be health
promoting. Although many aspects of our new theory
*Corresponding author. Tel.: +44-121-414-7631; fax: +44-
121-414-4865.
E-mail address: [email protected]
(W.A. Markham).
0277-9536/03/$ - see front matter r 2002 Elsevier Science Ltd. All rights reserved.
PII: S 0 2 7 7 - 9 5 3 6 ( 0 2 ) 0 0 1 2 0 - X

have been loosely discussed and practised under the
banner of health promoting schools, we believe our new
theory provides a rationale for why health promoting
schools should address certain issues and describes how
they should intervene. This rationale is grounded in
existing theoretical perspectives in education, health and
social functioning and, arguably, provides additional
insights into some key elements of the health promoting
school initiative. Our theory resonates with aspects of a
WHO definition of health promoting schools (WHO,
1998) and with the eco-holistic model of health
promoting schools developed by Parsons, Stears, &
Thomas (1996). It is also consistent with commentators’
views regarding the promotion of health within ‘settings’
(Baric, 1992, 1993) and the promotion of health and
community development (Labonte, 1998; Loeb, Mark-
ham, Naidoo, & Wills, 1998).
The new theory is derived from the application of
Nussbaum’s ethical–political account of good human
functioning, outlined in her overview of Aristotelian
social democracy (Nussbaum, 1990), to Bernstein’s
influential theory of cultural transmission (Bernstein,
1975). In this theory, we extend Nussbaum’s account of
human functioning to understand why some individuals
are healthier than others. Nussbaum’s account of
human functioning is used because it has two important
advantages over other interpretations of good human
functioning. First, Nussbaum maintains that her con-
ception of good human functioning is both universal
and flexible. Second, her interpretation is detailed in
nature, although it does not include a detailed analysis
of how schools may be organised in order to promote
human functioning. In this new theory, we apply
Bernstein’s theory of cultural transmission to provide
insights into how schools influence pupils’ psychological
development and social behaviour because it has two
main advantages over other theories that attempt to
account for the same data. First, it relates macro-
institutional forms and constraints to micro-interac-
tional levels and processes. Second, it focuses on the
influences of school organisation, curriculum develop-
ment and pedagogic practice on pupil development,
which are the core activities of schools. Evidence in
support of Bernstein’s theoretical conception of how
individual schools influence pupil’s psychological devel-
opment and social behaviour is provided by Daniels,
Holst, Lunt, and Ulsoe-Johansen (1996). They used
Bernstein’s framework to show that pupils are aware of
the dominant approach to education, internalise the
schools’ expectations and value these in the same way
that the school does. However, Bernstein’s theory of
cultural transmission does not provide a universal
account of good human functioning. We propose,
therefore, a synthesis of the insights of Nussbaum and
Bernstein that builds upon each of these and is
explanatory in nature. From this theoretical position,
we produce a set of predictions on how different aspects
of the educational experience can be used to generate
health amongst pupils while at school and after they
have left and become adults. Health promotion in
schools when viewed from this perspective has the
potential to avoid becoming a bolt on extra. Finally, we
compare our interpretation of health promoting schools
with other commentator’s interpretations.
Nussbaum’s theory of human functioning (after
Nussbaum, 1990)
Through Nussbaum’s conception, we propose that,
irrespective of culture and situation, all humans have
fundamental human needs (Table 1) and inherent
capacities or potentialities (Table 2). The assuaging of
these fundamental needs and the realisation of these
essential human capacities is a pre-condition for
autonomy and for a person to be in a position to
choose to function well and flourish, which we believe is
a pre-requisite for health.
Drawing on Nussbaum (1990), it is acknowledged
that the list of essential capacities may not be exhaustive
and is open to revision. However, once the fundamental
human needs are met, a person who had sufficiently
realised all the capacities in this list (Table 2) would, we
propose, be in a position to be autonomous, and to
choose to function well. Such a person would also fulfil
his/her need to be human (Nussbaum, 1990). Two
capacities from Table 2 are, Nussbaum reasons, over-
arching and organise all others. The first of these focuses
Table 1
The fundamental human needs (after Nussbaum, 1990)
The need for a clean water supply, adequate food, warmth and shelter.
The need to address medical and human concerns that focus on years of life and to provide health care for the sick and/or injured.
The need to provide information about the body.
The need to facilitate the development of skills in order to be able to make appropriate choices concerning health related behaviours.
The need to have pleasurable experiences and opportunities for sexual satisfaction.
The need to be able to avoid unnecessary and non-useful pain.
The need to be able to move freely from place to place.
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–12201210
on practical reasoning i.e. to imagine, think and reason.
The second concerns affiliation i.e. to have concern for
other humans, to live for others, to have familial and
other interactions and attachments. Nussbaum argues
these two capacities are overarching because everything
a person does is planned and organised by her/his ability
to reason and is done with or to other humans.
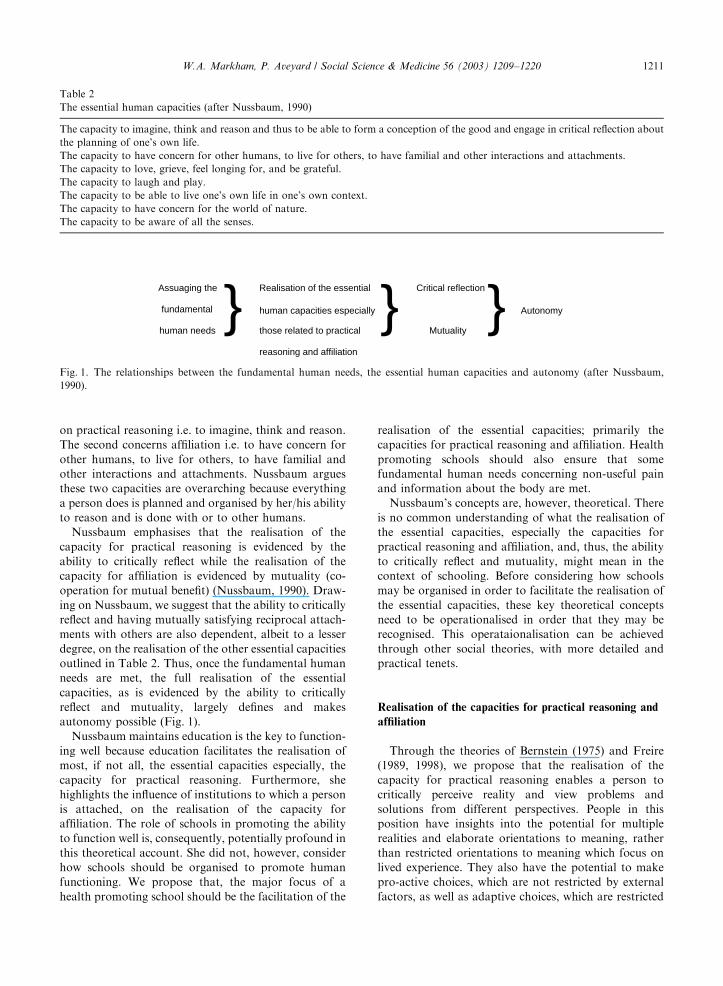
Nussbaum emphasises that the realisation of the
capacity for practical reasoning is evidenced by the
ability to critically reflect while the realisation of the
capacity for affiliation is evidenced by mutuality (co-
operation for mutual benefit) (Nussbaum, 1990). Draw-
ing on Nussbaum, we suggest that the ability to critically
reflect and having mutually satisfying reciprocal attach-
ments with others are also dependent, albeit to a lesser
degree, on the realisation of the other essential capacities
outlined in Table 2. Thus, once the fundamental human
needs are met, the full realisation of the essential
capacities, as is evidenced by the ability to critically
reflect and mutuality, largely defines and makes
autonomy possible (Fig. 1).
Nussbaum maintains education is the key to function-
ing well because education facilitates the realisation of
most, if not all, the essential capacities especially, the
capacity for practical reasoning. Furthermore, she
highlights the influence of institutions to which a person
is attached, on the realisation of the capacity for
affiliation. The role of schools in promoting the ability
to function well is, consequently, potentially profound in
this theoretical account. She did not, however, consider
how schools should be organised to promote human
functioning. We propose that, the major focus of a
health promoting school should be the facilitation of the
realisation of the essential capacities; primarily the
capacities for practical reasoning and affiliation. Health
promoting schools should also ensure that some
fundamental human needs concerning non-useful pain
and information about the body are met.
Nussbaum’s concepts are, however, theoretical. There
is no common understanding of what the realisation of
the essential capacities, especially the capacities for
practical reasoning and affiliation, and, thus, the ability
to critically reflect and mutuality, might mean in the
context of schooling. Before considering how schools
may be organised in order to facilitate the realisation of
the essential capacities, these key theoretical concepts
need to be operationalised in order that they may be
recognised. This operataionalisation can be achieved
through other social theories, with more detailed and
practical tenets.
Realisation of the capacities for practical reasoning and
affiliation
Through the theories of Bernstein (1975) and Freire
(1989, 1998), we propose that the realisation of the
capacity for practical reasoning enables a person to
critically perceive reality and view problems and
solutions from different perspectives. People in this
position have insights into the potential for multiple
realities and elaborate orientations to meaning, rather
than restricted orientations to meaning which focus on
lived experience. They also have the potential to make
pro-active choices, which are not restricted by external
factors, as well as adaptive choices, which are restricted
Table 2
The essential human capacities (after Nussbaum, 1990)
The capacity to imagine, think and reason and thus to be able to form a conception of the good and engage in critical reflection about
the planning of one’s own life.
The capacity to have concern for other humans, to live for others, to have familial and other interactions and attachments.
The capacity to love, grieve, feel longing for, and be grateful.
The capacity to laugh and play.
The capacity to be able to live one’s own life in one’s own context.
The capacity to have concern for the world of nature.
The capacity to be aware of all the senses.
Assuaging the
fundamental
human needs }} Realisation of the essential
human capacities especially
those related to practical
reasoning and affiliation
} Critical reflection
Mutuality} Autonomy
Fig. 1. The relationships between the fundamental human needs, the essential human capacities and autonomy (after Nussbaum,
1990).
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–1220 1211

by external factors. Pro-active actions have the potential
to transform reality by changing the world in which a
person lives through invention, creation or recreation.
The potential to make pro-active choices is necessary if
the capacity for practical reasoning is to be fully
realised. This interpretation of the realisation of the
capacity for practical reasoning resonates with Piaget’s
views on the development of the capacity for formal
operational thinking (Ginsburg & Opper, 1979), that
was developed by Flavell (1985). People who have
sufficiently developed the capacity for formal opera-
tional thinking are able to reason in the abstract, can be
objective about their own subjective thoughts and are
aware that when seeking solutions to problems they
need to explore alternative possibilities that are not
solely based on lived experience. According to Piaget
(Ginsburg & Opper, 1979), and Flavell (1985), this is the
central cognitive ability commonly gained during
adolescence.
In the same way, through the theories of Bernstein
(1975), we propose that the realisation of the capacity
for affiliation depends on shared values and empathetic
understanding of others’ orientations to meaning.
People who have sufficiently realised the capacity for
affiliation would have mutually satisfying reciprocal
interactions and attachments with others and, conse-
quently, would experience a sense of belonging and feel
socially supported. They would also be in a position to
create a socially valued identity through, for example,
being involved in socially valued decision making. This,
in turn, promotes the development of characteristics
such as self-esteem. This statement recognises that
characteristics such as self-esteem are socially con-
structed, rather than solely derived from the individual.
This interpretation of the realisation of the capacity for
affiliation resonates with Erikson’s view that a key
developmental task during adolescence focuses on the
development of a well defined sense of identity which
involves defining social roles within different contexts
(Erikson, 1968). Cooper, Grotevant, and Condon (1983)
reported that developing a strong sense of identity is
most likely to occur when self assertion and freedom
(separateness) are encouraged within an atmosphere of
responsiveness to the needs of others and sensitivity and
respect for others (mutuality).
This analysis of Nussbaum’s account of human
functioning, therefore, describes what the full realisation
of the capacities for practical reasoning and affiliation
would, in our view, entail. This realisation largely
defines autonomy, makes possible the potential to
function well, and is a pre-requisite for maximising a
person’s health potential. A person in such a position is
able to make choices that are based on a fully developed
ability to critically reflect and fully developed mutual
affiliations. The world is understandable and can be
adapted to suit him/her further. People in this position
have mutually satisfying reciprocal interactions and
attachments and consequently experience a sense of
belonging and feel socially supported. They would
perceive that they had a socially valued identity and
would, consequently, have high self-esteem.
The focus of Nussbaum’s account of human function-
ing is how different forms of government may promote
or retard the realisation of the essential capacities. She
does not discuss in detail the type of educational
experience that would enable a person to realise the
essential capacities. Bernstein’s theory of cultural
transmission enables us to understand and predict how
educational experience may be operationalised to
promote the type of pupil–school interactions that
facilitate the realisation of the capacities for practical
reasoning and affiliation, and hence good human
functioning and health.
Bernstein’s theory of cultural transmission
Central to Bernstein’s theory of how schools are
involved in cultural transmission is the view that schools
relay two inter-related yet separate orders: the instruc-
tional order and the regulatory order. Pupils, according
to Bernstein, may be categorised according to their
responses to these orders. These insights are funda-
mental to our new interpretation of health promoting
schools and are consequently outlined.
The instructional order
Bernstein proposed that the instructional order is
concerned with the ability of pupils to contribute to
future production through work. The aims are to relay
knowledge and skills and to influence pupils’ orienta-
tions to meaning. What is understood as valued
knowledge and skills is shaped by the dominant culture.
Bernstein maintained that the aims of the instructional
order are driven by the knowledge and skill needs
of the state and, in particular, the knowledge and skills
needs of the economy and higher education institutions.
He reasoned that the predominant understanding of
knowledge in UK university settings is that each subject
has defined ways of thinking, knowledge and skills.
States of knowledge in each academic subject are gained
by increasingly deeper enquiry into the subject (Bern-
stein, 1996). He maintains that UK schools are
consequently forced to largely train their pupils to
develop the skills necessary for in depth enquiries and
pupils are generally encouraged to develop an ability to
think and reason predominantly within the context of
particular subjects.
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–12201212
The regulatory order
According to Bernstein, the regulatory order, on the
other hand, is concerned with the conduct, character,
and manner of pupils and focuses on the relaying of
values. The aims are to facilitate the attachment of the
pupils to the schools and the internalisation of the values
and beliefs of the school. Bernstein maintains this helps
to ensure that every pupil functions appropriately within
society while they are at school and after they have left.
The aims of the regulatory order are, he believes,
commonly driven by the set of values and beliefs that are
held outside the school by the ‘controlling classes’.
Bernstein described the controlling classes as that part of
the middle class who act as agents of cultural production
(Bernstein, 1975). However, not all sections and cultures
within society support the set of values and beliefs held
by the controlling classes (Bernstein, 1975).
The categorisation of pupils according to their responses
to the instructional and regulatory orders
Understanding Bernstein’s categorisation of pupils is
facilitated by Bronfenbrenner’s insights into the socio-
ecological influences on human development (Bronfen-
brenner, 1989). Drawing on Bronfenbrenner (1989) and
Bernstein (1975), we propose that each pupil’s response
to the instructional and regulatory orders of the school,
and consequent involvement with the school, depends
on several factors. These include the family and socio-
cultural origins of the pupil, the pupil’s friendship
groups, the pupil’s perceived or expected future occupa-
tion, the pupil’s hopes and interests and the pupil’s view
of the purpose of the institution. Each school’s culture,
hopes, and expectations can also modify pupil involve-
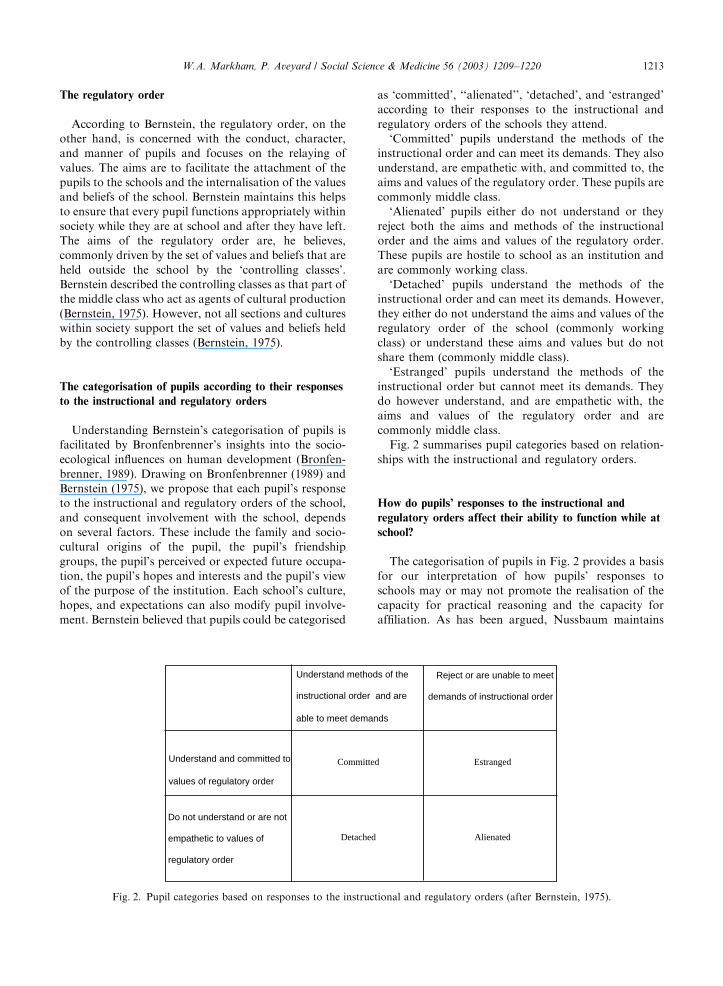
ment. Bernstein believed that pupils could be categorised
as ‘committed’, ‘‘alienated’’, ‘detached’, and ‘estranged’
according to their responses to the instructional and
regulatory orders of the schools they attend.
‘Committed’ pupils understand the methods of the
instructional order and can meet its demands. They also
understand, are empathetic with, and committed to, the
aims and values of the regulatory order. These pupils are
commonly middle class.
‘Alienated’ pupils either do not understand or they
reject both the aims and methods of the instructional
order and the aims and values of the regulatory order.
These pupils are hostile to school as an institution and
are commonly working class.
‘Detached’ pupils understand the methods of the
instructional order and can meet its demands. However,
they either do not understand the aims and values of the
regulatory order of the school (commonly working
class) or understand these aims and values but do not
share them (commonly middle class).
‘Estranged’ pupils understand the methods of the
instructional order but cannot meet its demands. They
do however understand, and are empathetic with, the
aims and values of the regulatory order and are
commonly middle class.
Fig. 2 summarises pupil categories based on relation-
ships with the instructional and regulatory orders.
How do pupils’ responses to the instructional and
regulatory orders affect their ability to function while at
school?
The categorisation of pupils in Fig. 2 provides a basis
for our interpretation of how pupils’ responses to
schools may or may not promote the realisation of the
capacity for practical reasoning and the capacity for
affiliation. As has been argued, Nussbaum maintains
Understand methods of the
instructional order and are
able to meet demands
Reject or are unable to meet
demands of instructional order
Understand and committed to
values of regulatory order
Committed Estranged
Do not understand or are not
empathetic to values of
regulatory order
Detached Alienated
Fig. 2. Pupil categories based on responses to the instructional and regulatory orders (after Bernstein, 1975).
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–1220 1213

these two capacities are overarching and plan and
organise the others. They also, we propose, have the
greatest influence on a person’s health.
The aims of the instructional order, according to our
theoretical frame, are to relay knowledge and skills and
to influence pupils’ orientations to meaning, which will
influence the realisation of the capacity for practical
reasoning. When the pupil is ‘committed’ or ‘detached’,
the school has the greatest potential to facilitate the
realisation of the capacity for practical reasoning
through mastery of the learning opportunities provided
by the school. As previously outlined, Bernstein main-
tains, that these opportunities are commonly driven by
the needs of the state, the economy, and higher
education. When the pupil is ‘estranged’ or ‘alienated’,
we suggest that the potential for the school to facilitate
the realisation of this capacity is greatly reduced because
these pupils cannot engage as effectively with the
learning environment.
We also reason that the aims of the regulatory order,
which are to influence pupil’s values, will influence the
realisation of the capacity for affiliation. We propose
that when pupils are ‘committed’, the school is
supportive of, and supported by, the values of their
families and other social aspects of the pupils’ lives. The
realisation of the capacity for affiliation is, we argue,
dependent on shared values and orientations to mean-
ing. Thus, schools will promote the realisation of this
capacity when pupils are ‘committed’. This will facilitate
the creation of a socially valued identity and promote
the development of characteristics such as self-esteem.
‘Committed’ pupils are also likely to feel socially
supported, experience a sense of belonging and feel that
the cultures and institutions to which they are affiliated
are consistent and stable. ‘Alienated’ and ‘detached’
pupils are not empathetic with the values of the school.
We reason that the lack of shared values will hinder the
realisation of the capacity for affiliation amongst
‘alienated’ and ‘detached’ pupils. This will make it
difficult for these pupils to fulfil their need to create a
socially valued identity and hence develop character-
istics such as self-esteem and a sense of belonging. The
inconsistency and possible conflict between the values of
the school and those of the communities to which these
pupils are affiliated is likely to result in ‘alienated’ or
‘detached’ pupils experiencing cultural instability. ‘Alie-
nated’ and ‘detached’ pupils must develop relationships
with people who share their values in order to realise the
capacity for affiliation and, thus, create a socially valued
identity and meet their needs to feel a sense of belonging
and feel socially supported. They will, commonly,
consequently adopt the values of particular youth
culture(s) and/or remain loyal to the values of their
family, culture or local community. Bernstein main-
tained that ‘estranged’ pupils are empathetic to the
school’s regulatory order. However, their failure to meet
the demands of the instructional order is likely to
result in reduced opportunities to affiliate with a peer
group that shares their values. This is because most
pupils who share their values can, and do, meet the
demands of the instructional order and will, as a
consequence, often be in different classes. School for
‘estranged’ pupils’ is not consistent with other social
aspects of their lives. We propose that school is a
potentially damaging experience for ‘estranged’ pupils
because it could hinder the realisation of the capacity for
affiliation and, thus, the fulfilment of the needs of
‘estranged’ pupils to create a socially valued identity and
feel a sense of belonging. This is likely to affect their self-
esteem.
Pupils’ responses to the instructional and regulatory
orders, we propose, will also influence the continued
realisation of the capacities for practical reasoning and
affiliation, and thus, the potential to function well and
be healthy after the pupils have left school. This is
because the responses of pupils to the instructional and
regulatory orders will, we believe, affect what each pupil
is able to do and be as an adult.
How do pupils’ responses to the instructional and
regulatory orders affect their ability to function and
their health after they have left school?
‘Committed’ pupils have the best chance of function-
ing well and maximising their health potential as adults.
They are more likely, than other pupils, to enter higher
education, take up positions with high social status and
receive high income. Higher education will facilitate the
continued realisation of the capacity for practical
reasoning through the learning opportunities provided
within this context. Holding relatively high social status
positions is likely to increase the potential to be involved
in socially valued decision making outside of the
contexts of friends and family, which will facilitate the
realisation of the capacity for affiliation. A good income
is likely to provide adults with the time, space, and
opportunity to fully realise a number of essential
capacities including the capacity for affiliation and the
capacity to live life in one’s own context. Thus,
potentially, ‘committed’ pupils are more likely to
function well and enjoy better health after they have
left school as well as when they are at school.
Based on the same principles, we maintain that
‘alienated’ pupils are least likely to enter higher
education and hold positions of high social status.
They, therefore, need to find other avenues to facilitate
the realisation of the capacity for practical reasoning
and the capacity for affiliation. In addition, they are also
less likely to have a sufficient income. Insufficient funds
may force people to focus on their fundamental needs
such as the need for food, warmth and shelter at the
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–12201214

expense of fully realising some capacities such as the
capacity for affiliation.
‘Detached’ pupils have the potential to access higher
education, hold high social status positions and access
sufficient income. We suggest, however, that their values
may continue to differ from those of the controlling
classes when they reach adulthood. If this happens, they
are likely to look to their affiliations with alternative
cultures or family and community to promote the
continued realisation of the essential capacity to laugh
and play and the essential capacity to love, grieve, feel
longing for and gratitude. This will emphasise their non-
acceptance of the values of the controlling classes and
possible exclusion from groups of people, such as work
colleagues, who hold these values, which, in turn,
hinders the realisation of the capacity for affiliation.
Alternatively, detached pupils may choose to accept the
values of the controlling classes and reject the values of
their family and/or communities when they become
adults. The resulting conflict between their own values
and those of the people with whom they grew up will
also hinder the realisation of the capacity for affiliation.
To function well and maximise health potential, adults
in either of these situations would have to develop the
ability to understand, manage, and resolve the resulting
conflicts. This would require them to grasp the concept
of multiple realities. Alternatively, detached pupils who,
as adults, continue to reject the values of the controlling
classes, could aim to hold positions of high social status
that are not based on the values of the controlling
classes. Such positions have the potential to enable these
adults to become involved in socially valued decision
making outside the contexts of friends and family and to
work with people who are empathetic with their values.
We believe that the likelihood of ‘estranged’ pupils
taking up positions that have high social status and
accessing sufficient income is greater than that of
‘alienated’ pupils. This is because they are frequently
better connected, and understand, and are empathetic
with, the language and the necessary conduct, manner
and behaviour that is required. However, their ability to
function well as adults will depend on finding means,
commonly other than higher education, to facilitate the
realisation of the capacity for practical reasoning.
Sufficient realisation of this capacity would enable them
to understand, manage, and resolve conflicts when they
were school pupils. These conflicts arise because of an
understanding of the aims of the instructional order but
an inability to meet its demands and because of a wish to
be a valued member of a social group and the potential
exclusion from this group.
Bernstein acknowledges that schools are not homo-
geneous. Thus, a pupil’s response to the instructional
and regulatory orders will vary according to the school
he/she attends. For example, a pupil who is ‘detached’ in
one school could be ‘committed’ to another school
where the aims and values of the regulatory order are
different. Schools, therefore, have the potential to
intervene in order to promote the commitment of pupils
to the school’s instructional and regulatory orders and
offset the potential disadvantages of pupils susceptible
to becoming ‘alienated’, ‘detached’ and ‘estranged’.
How can schools promote pupil functioning and maximise
the health potential of all its pupils?
Drawing on Bernstein, the key to the potential of
schools for intervening in order to promote pupil
functioning lies in the classification and framing of the
school. Classification and framing focus on school
organisation, curriculum development and pedagogic
practice. The classification and framing of a school,
consequently, determines the school’s influence on the
learning and social experiences of pupils. Through these
arguments, we propose that the classification and
framing of individual schools will greatly influence the
realisation of the capacities for practical reasoning and
affiliation amongst pupils. Schools, we suggest, could
adopt appropriate forms of school organisation, curri-
culum development and pedagogic practice to facilitate
all pupils’ ability to function well and, therefore,
promote health. This proposal forms the basis for our
concept of health promoting schools.
How might the classification be organised in order to
promote pupil functioning?
Classification refers to the boundaries between the
school and the outside world and boundaries within the
school that occur between teachers and pupils, between
pupils and between subjects. Classification encompasses
school organisation and some aspects of curriculum
development. When the boundaries between the school
and the outside world and the boundaries within schools
are strong and well insulated the school is ‘strongly
classified’. The strength of these boundaries is the key
factor that we believe determines the relationships
between classification and health through pupil func-
tioning. However, the influences of the strength of the
various boundaries on pupil functioning and, therefore
pupil health, will, we propose, vary according to the
boundary in question.
Boundaries between the school and the outside world
According to Bernstein, strong boundaries between
school and the outside world prevent parents, the local
community, and outside agencies from being involved in
decision making within the school. These strong
boundaries ensure that the regulatory order is not
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–1220 1215

tainted by external influences and remains true to the
values and beliefs of the school, commonly those of the
controlling classes. The wider community may not share
the values of the school. In these situations, weakening
the boundaries between the school and the wider
community results in the convergence of the values,
beliefs, and interests of the school and the wider
community (Bernstein, 1975). The resulting regulatory
order would be based on more general principles rather
than being commonly directly attributable to the values
of the controlling classes. We propose that weakening
the classification by reducing boundaries between
schools and communities would promote the realisation
of the capacity for affiliation amongst more pupils. This
is because a larger proportion of pupils, particularly
those susceptible to being ‘alienated’ or ‘detached’,
would share school values as these would be based on
general principles and would, consequently, be more
likely to feel at ease with the school.
Boundaries between teachers and pupils
Pupils are prevented from being involved in organisa-
tional decision making when there are strong boundaries
between teachers and pupils (Bernstein, 1975). Increas-
ing pupil involvement in the school’s decision making
processes through, for example, staff/student councils,
can weaken these boundaries and, we propose, promote
greater insights of both pupils and staff into each other’s
realities and, thus, greater insights into the potential for
multiple realities. This would facilitate the realisation of
the capacity for practical reasoning, especially amongst
pupils susceptible to being ‘alienated’ or ‘estranged’.
Increasing pupil involvement could also promote a
greater understanding of each other’s values, which, in
turn, would facilitate the realisation of the capacity for
affiliation, especially amongst pupils who are susceptible
to being ‘alienated’ or ‘detached’.
Boundaries between pupils
Strong boundaries between pupils based on celebrated
hierarchies, such as year groups, facilitate division and
subordination (Bernstein, 1975). Bernstein (1975) main-
tained that these boundaries could be weakened through
greater communication, shared tasks, and greater co-
operation. We propose that weakening the boundaries
between pupils facilitates the development of insights
into the potential for multiple realities and, hence, the
realisation of the capacity for practical reasoning.
Boundaries between subjects
Strong boundaries between subjects occurs when each
subject is considered to be separate and to have defined
and different ways of thinking, knowledge, and skills
(Bernstein, 1996). Bernstein reasoned that when bound-
aries between subjects are strong, an ‘education in depth’
approach is adopted and learners are expected to
develop their educational identities through the acquisi-
tion of states of knowledge in individual subjects.
‘Education in breadth’, on the other hand, occurs when
the insulation between subjects is breached (Bernstein,
1996). The introduction of cross-curricular themes that
subordinate subjects breaches the boundaries between
subjects. For example, natural selection as a cross-
curricular theme could be viewed from both biological
and sociological perspectives. Bernstein (1996) empha-
sised the difference between cross-curricular themes and
a focused curriculum. A focused curriculum occurs
when the same topic is addressed in different subject
lessons which have defined and separate ways of
thinking, for example studies on smoking in mathe-
matics and biology lessons. This tends to reinforce
pupils’ understanding that each subject has distinct ways
of thinking and separate states of knowledge. Education
in breadth, in contrast, encourages pupils to develop an
understanding of ways of knowing and an under-
standing of how knowledge is socially constructed. It
also encourages pupils to view knowledge as a range of
equally valid and sometimes conflicting realities. We
believe that such an approach is more likely than
education in depth to facilitate the development of
insights into the potential for multiple realities at an
earlier developmental stage and, therefore, the realisa-
tion of the capacity for practical reasoning for all pupils
at an earlier age. Bernstein reasoned that when an
education in depth approach is adopted, most people
have to study to university level and beyond before they
sufficiently grasp the concept that knowledge is socially
constructed, or may never do so.
How might the framing be organised in order to promote
pupil functioning?
Framing refers to communication and encompasses
pedagogic practice and additional aspects of curriculum
development. As with classification, the strength of the
framing is the key factor that we believe determines the
relationships between framing and health through pupil
functioning. Different methods for weakening the
framing will, we propose, favourably influence pupil
functioning and, therefore, pupil health.
Teaching that is primarily didactic and teacher led is
strongly framed. Weakening framing by increasing pupil
input to the management of her/his own learning, and
therefore, increasing pupil input into curriculum devel-
opment can be achieved by increasing pupil choice
regarding the selection, pacing, and sequencing of
classroom activities (Bernstein, 1996). We reason that
this develops pupils’ understanding of how to manage
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–12201216

challenges and mobilise resources to cope and, thus,
facilitates the realisation of the capacity for practical
reasoning.
Increasing the contribution of pupils’ own knowledge
and skills to the learning process may also weaken the
framing (Bernstein, 1996). We propose that this can be
achieved through the introduction of pupil-centred
techniques, such as discussion groups, brainstorms,
mind maps, and role-plays. These generic tools for
‘learning how to learn’ can be used in a wide range of
situations. Their use encourages pupils to develop self-
reflective skills and to identify and understand the
origins of their own and their classmates’ orientations to
meaning, values, interests, and expectations. This facil-
itates understanding of multiple realities and, thus, the
realisation of the capacity for practical reasoning. This
type of pupil input may also promote increased under-
standing of a range of orientations to meaning and
values and, thus, has the potential to reduce the threat of
values that are not shared which would facilitate the
realisation of the capacity for affiliation.
Conclusion of how schools may promote that realisation of
the capacity for practical reasoning and the capacity for
affiliation
We have argued that weakly classified schools
promote pupils’ capacity for practical reasoning by
weakening boundaries between teachers and pupils,
boundaries between pupils, and boundaries between
subjects. Weakly classified schools also facilitate the
realisation of the capacity for affiliation, especially
amongst pupils, who in other schools would be ‘alienated’
or ‘detached’, by weakening the boundaries between
school and the outside world, boundaries between
teachers and pupils and boundaries between pupils.
Similarly, weakly framed schools facilitate the realisa-
tion of the capacity for practical reasoning by providing
students with more responsibility for their own learning
and increasing pupil input into curriculum development.
They also promote the realisation of both the capacity
for practical reasoning and the capacity for affiliation
through the greater use of pupil centred techniques and
generic tools for leaning how to learn.
A new interpretation of a health promoting school
As we have argued, health has its roots in human
functioning. The realisation of the essential capacities,
particularly practical reasoning and affiliation, are
necessary to function well. A health promoting school
then would primarily aim to promote health by
facilitating the realisation of the capacities for practical
reasoning and affiliation and, thus, pupil development
and pupils’ ability to function well. Bernstein’s insights
into school organisation, curriculum development and
pedagogic practice facilitate an understanding of how
schools may influence the realisation of these essential
capacities. We propose that health promoting schools
would be both weakly classified and weakly framed. The
resulting school organisation, curriculum development
and pedagogic practice would promote pupils’ critical
reflection, sense of belonging, sense of being socially
supported, and self-esteem and this, in turn, would
promote pupils’ health. According to our interpretation
of health promoting schools, such schools would also
aim to encourage pupils to become ‘committed’ to the
school by promoting cultural congruence between the
school and the wider community. This approach, we
believe, has the greatest potential to offer social support,
consistency and cultural stability, especially for pupils
who are susceptible to being ‘alienated’, ‘detached’ or
‘estranged’. Antonovsky (1987) also highlights the
influence of ‘generalised resistance resources’ including
social support, consistency and cultural stability on the
promotion of health. From an educational perspective,
health promoting schools would adopt an education in
breadth approach which facilitates greater pupil input to
the management of their own learning and greater use of
pupils’ knowledge and skills. By greater pupil input, we
do not, however, mean peer led education, such as has
been observed in some smoking and sexual health
interventions (Bloor et al., 1999; Mellanby, Phelps,
Crichton, & Tripp, 1995; Mellanby, Newcombe, Rees, &
Tripp, 2001). Adolescents involved in interventions such
as these, are often selected on the basis of popularity or
perceived maturity and, as highlighted by Milburn
(1995), primed to deliver adult messages. In practice,
we suggest two major aims of health promoting schools
would be to increase partnerships between the schools
and parents and to increase community involvement in
the decision making processes of the school. Achieve-
ment of these aims would be facilitated by inter-sectoral
collaboration between the school and statutory and non-
statutory agencies that have close working relationships
with the community. Another major practical aim of
health promoting schools would be to encourage wider
pupil involvement with each other and with the decision
making processes of the school. This aim is consistent
with the views of Jensen, Schnack, & Simovska (2000)
regarding the importance of ‘action competence’. How-
ever, as they maintain, token pupil representation
without interventions that facilitate the development of
pupil confidence and pupil skills is unlikely to encourage
pupils to take responsibility for generating change
though the conversion of their own ideas into action
plans and positive outcomes (Jensen et al., 2000).
We acknowledge that strongly classified and strongly
framed schools may have very ‘committed’ pupils
especially when such schools select pupils, for example
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–1220 1217

by academic attainment. Schools that operate a strict
selection process are, almost by definition, fully sup-
ported by pupils’ families who share the values of the
schools and are often supported by the wider commu-
nity as well. Pupils at these schools will feel socially
supported, a sense of belonging and experience cultural
stability. They will, therefore, probably have enhanced
self-esteem and be likely to be functioning relatively
well. Furthermore, these pupils will often have greater
opportunities to function well as adults. However, even
in these usually advantaged circumstances, weakening
the classification and the framing would, we believe,
further promote pupil functioning by facilitating greater
understanding of multiple realities and, thus, elaborate
orientations to meaning. This, we surmise, would
facilitate even greater realisation of the capacity for
practical reasoning.
According to our theory, health promoting schools
would also ensure that some fundamental human needs
are met concerning non-useful pain and information
about the body (Table 1). Anti-bullying initiatives are
required to prevent non-useful pain. Pupils who feel that
their personal security is continuously under threat may
take time off school, which could hinder the realisation
of the capacities for practical reasoning and affiliation.
We propose that anti-bullying interventions would have
the greatest potential to promote health when they are
based on the principles of weakening the classification
and weakening the framing highlighted above. In
practice this would involve pupils in the choice of the
focus of the intervention and in all stages of the
planning, implementation and evaluation of the initia-
tive. We also acknowledge that health promoting
schools should provide information about the body.
However, the provision of this information should also
be based on the principles of weakening the classification
and weakening the framing that we highlight. Thus,
information about the body should be a cross-curricular
theme rather than provided solely within the contexts of
health education and biology lessons. The use of
‘learning how to learn’ techniques should also be
employed in order that pupils come to understand their
own values and expectations regarding the body.
Hypotheses generated from the new interpretation of
health promoting schools
The key issue regarding theoretical frames is whether
they have explanatory power in addition to being able to
describe. The validity of our new theory of health
promoting schools could be investigated through the
testing of the following examples of hypotheses that
have been inductively derived from the theory.
First, while attending school, ‘committed’ pupils
would enjoy better psychological health outcomes
than pupils who are ‘alienated’, ‘detached’ or ‘es-
tranged’.
Second, ‘committed’ pupils would also enjoy more
favourable psychological well being, psychological ill-
ness outcomes and physical health outcomes in adult life
than ‘alienated’, ‘detached’ and ‘estranged’ pupils.
Third, a greater proportion of pupils would enjoy
favourable psychological well-being outcomes in weakly
classified and weakly framed schools than in strongly
classified and strongly framed schools when both types
of schools have equivalent pupil populations. Equiva-
lence would be based on socio-cultural origins of the
pupils.
Fourth, schools that meet the following criteria would
promote pupil health and well-being. First, they would
actively promote the involvement of the local commu-
nity and pupils in the decision making processes of the
school. Second, they would have a teacher with a
designated responsibility for ensuring that cross-curri-
cular themes were taught in each school year and across
pupil attainment levels. Third, they would actively
promote the involvement of pupils in the development
of the curriculum. Fourth, they would actively promote
the use of learning ‘how to learn’ skills. This criterion
could be met, for example, by encouraging teachers to
adopt the principles and practice of the University of the
First Age initiative (Burgess, 2000).
Comparisons with other interpretations of health
promoting schools
As indicated in the introduction, our interpretation of
health promoting schools resonates with the eco-holistic
model of health promoting schools developed by
Parsons et al. (1996). Both models highlight the need
for increased community and pupil involvement with the
decision making processes of the school and focus on the
formal curriculum. Our views are also supported by
relevant WHO documentation. For example the WHO
European Office definition of health promoting schools
indicates that in order to promote health, schools should
focus on their management structures, internal and
external relationships and teaching and learning (WHO,
1998). While Tones (1996), drawing on the Ottawa
Charter, maintains that the best defence against disease
and premature death is the empowerment of people. Our
interpretation is also consistent with Baric (1992, 1993)
who reasoned that in order to be health promoting,
organisations such as schools should focus on their
organisational systems and peoples’ interactions within
the organisation.
There are, however, differences between our inter-
pretation of health promoting schools and other
commentators’ interpretations. First, we focus on pupils
and their families rather than adults working in the
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–12201218

schools. Second, unlike the WHO which asserts that
there is a two-way relationship between health and
education our model states that education facilitates the
ability to function well and this ability is the basis of
good health. Third, unlike other related theories, the
new theory has the potential to offer insights into the
relationships between school experience and adults’
health and to predict which pupils will enjoy the best
health while they are at school and after they leave
school. Fourth, we reason that there is no requirement
for the allocation of specialist health education and
health promotion roles to teaching staff or a require-
ment for inter-sectoral collaboration with outside
agencies with a specialist remit for health, unless that
is, these agencies can help facilitate community involve-
ment with the school. Fifth, we believe that cross-
curricular themes should be encouraged whenever
possible and should not focus solely on topics that fall
under the traditional health education remit such as
information about the body. For example, Denman,
Moon, Parsons, and Stears (2002) describe a health
promoting school that had thematic weeks on topics
such as communication skills and good manners. Sixth,
according to our interpretation, schools do not need a
formal health education curriculum that aims to prevent
individuals from adopting behaviours that increase their
chances of developing chronic disease in adulthood in
order to be health promoting. However, when English
schools do have designated health education lessons,
they should capitalise on the non-mandatory nature of
the health education curriculum. Currently, such lessons
often focus on healthy lifestyle choices and the devel-
opment of individual skills, such as assertiveness, to
resist social pressure to make unhealthy lifestyle choices.
We believe health education classes should instead,
focus on the development of the skills necessary for
collective action. This, we reason, would facilitate the
realisation of the capacity for affiliation. Disenfran-
chised pupils or adults who become disenfranchised
after leaving school could perhaps use these skills to
break the seemingly unbreakable links between social
disadvantage and psychological well being, psychologi-
cal illness and physical health.
Conclusion
This paper proposes that the application of our
analysis of Nussbaum’s Aristotelian interpretation of
human functioning to Bernstein’s theory of cultural
transmission outlines a potentially helpful explanatory
frame for understanding schools as health promoting
organisations. This outline indicates how school orga-
nisation, curriculum development and pedagogic prac-
tice may be advantageously implemented to promote
pupil health by facilitating the realisation of the
capacities for practical reasoning and affiliation and
thus, pupil development and pupil functioning. Our
notion that health promoting schools are weakly
classified and weakly framed (Bernstein, 1975) is explicit
about the underpinning values and theoretical base.
Testing the generated hypotheses would ground the
theory in an evidence base and may potentially lead to
improved understanding of the relationships between
the postulated key concepts and health. This, in turn,
could lead to improvements in the planning, implemen-
tation, and evaluation of future health promoting school
initiatives. Research validation is required before our
suggested approach is accepted. However, the great
benefit of this theory is that it does offer a range of
testable hypotheses. In addition, it has three potential
advantages at the policy and intervention levels. First, a
greater proportion of the teacher workforce could
potentially be informed about our theory and the
postulated health benefits of schools which is likely to
positively impact on policy implementation. This is
possible because Bernstein and Nussbaum are already
extremely influential in the field of education. The only
additional requirement would be to highlight the
relevance of their insights to health. Thus, our theory
is more likely than existing theories to be incorporated
into the mainstream teacher training/education sylla-
buses of higher education institutions and into in-service
training and continuing professional development train-
ing syllabuses in higher education institutions. Cur-
rently, existing theories of health promoting schools
tend to be disseminated primarily to trainee teachers and
teachers with a special interest in health promotion.
Second, the UK health promoting schools initiative is
heavily influenced by government policy that primarily
equates health with healthy lifestyles. However, a central
plank of the current UK government policy focuses on
reducing social exclusion. The new theory could draw on
the social exclusion aspect of government policy and,
potentially influence the direction and purpose of the
health promoting school initiative in the UK. Perhaps
the greatest drawback to the adoption of the new theory
is the predominant belief, particularly in UK univer-
sities, that education in depth is preferable to education
in breadth. However, the continuing popularity of
courses such as gender studies and media studies indicates
that this view may not be as entrenched as it once was.
Third, our theoretically based approach provides a basis
for understanding why some health promoting school
interventions seem to have been successful and others,
perhaps with a different emphasis, appear to have failed.
Acknowledgements
We are very grateful to Rita Jordan for her
encouragement and willingness to debate the contents
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–1220 1219

of this paper. We would also like to thank Alison
Bullock, Vickie Firmstone and Harry Daniels.
References
Antonovsky, A. (1987). Unravelling the mystery of health. San
Francisco: Jossey-Bass.
Baric, L. (1992). Promoting health—new approaches and
developments. Journal of the Institute of Health Education,
30, 6–16.
Baric, L. (1993). The ‘settings approach’—implications for
policy and strategy. Journal of the Institute of Health
Education, 31, 17–24.
Bernstein, B. (1975). Class, codes and control, Vol. 3: Towards a
theory of educational transmission. London: Routledge.
Bernstein, B. (1996). Pedagogy, symbolic control and identity.
London: Taylor & Francis.
Bloor, M., Frankland, J., Langdon, N. P., Robinson, M.,
Allerston, S., Catherine, A., Cooper, L., Gibbs, L., Gibbs,
N., Hamilton-Kirkwood, L., Jones, E., Smith, R. W., &
Spragg, B. (1999). A controlled evaluation of an intensive,
peer-led, schools-based, anti-smoking programme. Health
Education Journal, 58, 17–25.
Bronfenbrenner, U. (1989). Ecological systems theory. Annals
of Child Development, 6, 187–249.
Burgess, S. (2000). The University of the First Age extended
learning centres: A model of study support for the new
millennium. Educational Review, 52, 229–237.
Cooper, C. R., Grotevant, H. D., & Condon, S. M. (1983).
Individuality and connectedness in the family as a context
for adolescent identity formation and role-taking skill. In H.
D. Grotevant, & C. R. Cooper (Eds.), Adolescent develop-
ment in the family (pp. 43–60). San Francisco: Jossey-Bass.
Daniels, H., Holst, J., Lunt, I., & Ulsoe-Johansen, L. (1996). A
comparative study of the relation between different models
of pedagogic practice and constructs of deviance. Oxford
Review of Education, 22, 63–77.
Denman, S., Moon, A., Parsons, C., & Stears, D. (2002). The
health promoting school: Policy, research and practice.
London: Routledge Falmer.
Erikson, E. H. (1968). Identity: Youth and crisis. New York:
Norton.
Flavell, J. H. (1985). Cognitive development (2nd ed). Engle-
wood Cliffs, NJ: Prentice-Hall.
Freire, P. (1989). Pedagogy of the oppressed. Trowbridge: Sheed
and Ward.
Freire, P. (1998). Education for critical consciousness. Con-
tinuum: New York.
Ginsburg, H. P., & Opper, S. (1979). Piaget’s theory of
intellectual development (2nd ed). Englewood Cliffs, NJ:
Prentice- Hall.
Jensen, B.B., Schnack, K., & Simovska, V. (2000). Critical
Environmental and Health Education: Research issues and
challenges. Publication No.46. Copenhagen: The Danish
University of Education.
Labonte, R. (1998). A community development approach to
health promotion. Edinburgh: Health Education Board for
Scotland.
Loeb, D., Markham, W., Naidoo, J., & Wills, J. (1998). Mental
health promotion. In J. Naidoo, & J. Wills (Eds.), Practising
health promotion: dilemmas and challenges (pp. 254–276).
London: Bailliere and Tindall.
MacDonald, T. H. (1998). Rethinking health promotion: A
global approach. Routledge: London.
Marmot, M. G., & Theorell, T. (1988). Social class and
cardiovascular health: The contribution of work. Interna-
tional Journal of Health Services, 18, 659–674.
Mellanby, A. R., Newcombe, R. G., Rees, J., & Tripp, J. H.
(2001). A comparative study of peer-led and adult-led
school sex education. Health Education Research, 16,
481–492.
Mellanby, A. R., Phelps, F. A., Crichton, N. J., & Tripp, J. H.
(1995). School sex education: An experimental programme
with educational and medical benefit. British Medical
Journal, 311, 414–417.
Milburn, K. (1995). Critical review of peer education with
young people with special reference to sexual health. Health
Education Research, 10, 407–420.
Nussbaum, M. C. (1990). Aristotelian social democracy. In R.
B. Douglas, G. M. Mara, & H. Richardson (Eds.),
Liberalism and the good (pp. 203–251). London: Routledge.
Parsons, C., Stears, D., & Thomas, C. (1996). The health
promoting school in Europe: Conceptualising and evaluat-
ing the change. Health Education Journal, 55, 311–321.
Seedhouse, D. (1997). Health promotion: Philosophy, prejudice
and practice. Chichester: Wiley.
Tones, K. (1996). The health promoting school: Some reflec-
tions on evaluation (editorial). Health Education Research,
11, i–vii.
World Health Organisation (1998). The health promoting
school—an investment in education, health and democracy.
(Report of the first conference of the European Network of
Health Promoting Schools, Thessaloniki -Halkidiki, Greece
1–5 May 1997). Copenhagen: WHO.
W.A. Markham, P. Aveyard / Social Science & Medicine 56 (2003) 1209–12201220




















