A DESCRIPTIVE ANALYSIS OF PATIENT ENCOUNTER DATA FROM THE FLEET HOSPITAL 5 HUMANITARIAN RELIEF...
30
NAVAL HEALTH RESEARCH CENTER A DESCRIPTIVE ANALYSIS OF PATIENT ENCOUNTER DATA FROM THE FLEET HOSPITAL 5 HUMANITARIAN RELIEF MISSION IN HAITI E. D. Gauker K. Emens-Hesslink P. J. Konoske Report No. 98-38 DTIC QUALITY IKaEEGISD <3 Approved for public ttimaK djtribution miKmitort NAVAL HEALTH RESEARCH CENTER P O BOX 85122 SAN DIEGO, CA 92186-5122 BUREAU OF MEDICINE AND SURGERY (BUMED-26) WASHINGTON, DC 20372-5300
Transcript of A DESCRIPTIVE ANALYSIS OF PATIENT ENCOUNTER DATA FROM THE FLEET HOSPITAL 5 HUMANITARIAN RELIEF...
NAVAL HEALTH RESEARCH CENTER
A DESCRIPTIVE ANALYSIS OF PATIENT
ENCOUNTER DATA FROM THE FLEET HOSPITAL
5 HUMANITARIAN RELIEF MISSION IN HAITI
E. D. Gauker K. Emens-Hesslink
P. J. Konoske
Report No. 98-38
DTIC QUALITY IKaEEGISD <3 Approved for public ttimaK djtribution miKmitort
NAVAL HEALTH RESEARCH CENTER P O BOX 85122
SAN DIEGO, CA 92186-5122
BUREAU OF MEDICINE AND SURGERY (BUMED-26) WASHINGTON, DC 20372-5300

A Descriptive Analysis of Patient Encounter Data from the Fleet Hospital 5 Humanitarian Relief Mission in Haiti
Eleanor D. Gauker, M.A.* Kristee Emens-Hesslink, B.A.**
Paula J. Konoske, Ph. D.*
*Naval Health Research Center Medical Information Systems and Operational Research Department
P.O. Box 85122 San Diego, CA 92186-5122
**GEO Centers, Inc. 1801 Rockville Pike, Suite 405
Rockville, MD 20852-1633
Report No. 98-38, supported by the Office of Naval Research, Arlington, VA, Department of the Navy, under Work Unit No. 63706N M0095.005-6809. The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, or the US Government. Approved for public release; distribution is unlimited.
SUMMARY
Problem Military planners and logisticians determine medical requirements by projecting
the number of casualties that can be expected in a given combat scenario. Presently, the Deployable Medical Systems (DEPMEDS) program is used to project, assemble, and deploy the supplies, equipment, and personnel needed for a given combat mission. However, in recent years there has been a shift in US military strategy resulting in an increase in military operations other than war (MOOTW). Since this trend is likely to continue, it is important to update Department of Defense medical planning tools to account for MOOTW, such as humanitarian assistance, peacekeeping, and disaster relief.
Objective This report describes the patient demographics, type of medical encounter,
diagnoses, and medications provided by medical personnel of Fleet Hospital 5 (FH5) during a humanitarian assistance operation in Haiti. Results are presented for clinics, which provided humanitarian relief to Haitian civilians, and for the fleet hospital, which was a treatment facility for US and United Nations military personnel. These data can be used by medical planners to determine MOOTW requirements in the post-Cold War era.
Approach Patient encounter data, including type of medical encounter, diagnoses, and
medications prescribed, were collected for Haitian civilians who visited FH5 clinics and for military personnel who were treated at the fleet hospital. These data were encoded and entered into a database. The data were analyzed to provide descriptive information about the FH5 humanitarian relief mission in Haiti.
Results The database consists of 10,568 records, each representing one patient encounter.
The results are presented as descriptive frequencies and/or percentages. The 10,215 Haitian clinic patients were seen at 22 different sites between April 4 and August 5, 1997. Over three fifths (61.6%) were women, and children aged 1 to 10 years were the most frequent age category. Additionally, 353 US military and UN personnel were treated at the fleet hospital during the same period. Men represented 81% of patients, and those who were 21 to 50 years of age were seen most often. The most frequent type of patient encounter was a medical diagnosis based on the International Classification of Diseases, 9th Revision, Clinical Modification, representing 92.6% of clinic visits and 92.2% of fleet hospital visits. Infectious and parasitic diseases were diagnosed once in every four clinic visits. Injury cases were the most frequent (23.1%) at the fleet hospital.
Conclusion The resulting database, with the descriptive statistics that it generated, is a first
step toward fulfilling the Medical Readiness Strategic Plan-2004 objective of preparing for and maintaining readiness for MOOTW. Future areas of research for MOOTW medical planning should include the development of denominator data so that rates of occurrence for illnesses and injuries can be established for humanitarian relief as well as other MOOTW scenarios. Comparisons between different types of MOOTW also would provide useful information.
n
TABLE OF CONTENTS
LIST OF TABLES iv
INTRODUCTION 1
BACKGROUND 1
OBJECTIVE 2
METHOD 2
RESULTS AND DISCUSSION 3
DEMOGRAPHICS 3 Clinics for Haitian Civilians 3 Fleet Hospital for US Military and UN Personnel 4
DIAGNOSES 5 Clinics: Initial Visits 5 Clinics: Follow-up visits 7 Fleet Hospital: Initial Visits 9 Fleet Hospital: Follow-up Visits 10
PRESCRIPTIONS 11
CONCLUSION 15
ACKNOWLEDGEMENT 16
REFERENCES 17
APPENDICES
APPENDIX A Data Collection and Coding Forms APPENDIXE Medication Coding Chart
m
LIST OF TABLES
Table 1. Initial and Follow-up Encounters at Clinics and the Fleet Hospital 3 Table 2. Age and Sex of Patients in Visits to Clinics 3 Table 3. Age and Sex of Patients at the Fleet Hospital 4 Table 4. Military/Civilian Status of Patients at the Fleet Hospital 4 Table 5. Nationality and Military/Civilian Status of Patients at the Fleet Hospital ...5 Table 6. Number of Interventions (Diagnoses) per Visit at Clinics 5 Table 7. Initial Patient Encounters at Clinics: Type of Intervention 6 Table 8. ICD-9 Diagnoses for Initial Visits to Clinics 6 Table 9. Dental Diagnoses in Initial Clinic Encounters 7 Table 10. Preventive Med. (PM) in Initial Clinic Encounters 7 Table 11. Aftercare in Initial Clinic Encounters 7 Table 12. Number of Interventions per Follow-up Visit to Clinics 7 Table 13. Follow-up Patient Encounters at Clinics: Type of Intervention 8 Table 14. Breakdown of ICD-9 Diagnoses for Follow-up Visits to Clinics 8 Table 15. Breakdown of Aftercare Interventions for Follow-up Visits to Clinics 9 Table 16. Number of Interventions per Initial Visit at the Fleet Hospital 9 Table 17. Fleet Hospital Initial Visits: Type of Intervention 9 Table 18. Breakdown of Interventions for Fleet Hospital Initial Visits 10 Table 19. Number of Interventions per Fleet Hospital Follow-up Visit 10 Table 20. Intervention Frequencies for Fleet Hospital Follow-up Visits 11 Table 21. Classification of Medications 12 Table 22. Types and Frequency of Prescriptions at Clinics and the Fleet Hospital. 12 Table 23. Medications Prescribed for Interventions at Clinic Visits 13 Table 24. Medications Prescribed for Interventions at Fleet Hospital Visits 14
IV
A Descriptive Analysis Of Patient Encounter Data From The Fleet Hospital 5 Humanitarian Relief Mission In Haiti
INTRODUCTION
To determine supply, equipment, skill, and personnel requirements for military medical operations, planners and logisticians project types and occurrence rates of battle injuries and diseases likely to be encountered by US forces in a designated combat theater. In 1985 the joint services launched Deployable Medical Systems (DEPMEDS), a modular system designed to facilitate such medical resource planning. DEPMEDS projects medical requirements, then allocates sufficient supplies, equipment, and personnel to provide treatment to an anticipated array of casualties falling within 319 patient conditions.
Presently, these patient conditions describe medical conditions that would be seen during a combat scenario. In recent years, however, US defense policies have been modified. The Medical Readiness Strategic Plan-2004 (MRSP-2004) was initiated in 1998 as a response to changes in the global political situation. Since the late 1980s, there has been an increasing trend toward the use of US forces for military operations other than war (MOOTWs). MRSP-2004 has been implemented to define and clarify joint doctrine in regard to MOOTW, specifically addressing issues such as medical missions, roles, and functions. A new objective for the Military Health Services System, to "prepare for and maintain readiness for MOOTW," was added to the primary and secondary missions of supporting deployed US forces and providing beneficiary care. Recent years have seen US forces on peace enforcement missions in Bosnia, peacekeeping missions in Zagreb, noncombatant evacuation operations in Liberia, disaster relief in Rwanda, and humanitarian assistance in Somalia."
BACKGROUND
Haiti is an island republic in the West Indies with a population of approximately 6.7 million. Haitians have one TV for every 208 persons and one telephone for every 119 people. With a literacy rate of 53% and a per capita income of $400 per year, it is the poorest country, economically, in the Western Hemisphere. As of 1998, a Haitian man had a life expectancy of 47 years, while a woman could expect to live to the age of 51. There was one physician for every 10,041 persons, with 994 persons to fill each hospital bed, and the infant mortality rate was 102 per 1,000 live births.3
Fleet Hospital 5 (FH5) is a naval unit based at the Naval Hospital in Bremerton, Washington. In February, 1997 personnel assigned to FH5 arrived in Haiti to relieve Alpha Surgical Company, 2nd Medical Battalion, Camp Lejeune. This US military complement was tasked with providing humanitarian relief for the Haitian populace, and it operated separately from the United Nations (UN) peacekeeping force in Haiti. FH5 had the capability to provide internal medicine, family practice, general surgery, orthopedics, and dentistry care for the Haitian people. During their deployment, FH5
personnel fulfilled a dual role. First, they traveled from the slums of Port-au-Prince to the countryside, setting up clinics to deliver medical care to Haitian civilians. Second, they staffed the fleet hospital, located within the military compound known as Camp Kinzer, that was a medical treatment facility for US military personnel and UN forces.
OBJECTIVE
This report describes the patient demographics, type of medical encounter, diagnoses, and medications provided by medical personnel of Fleet Hospital 5 (FH5) during a humanitarian assistance operation in Haiti. Results are presented for clinics, which provided humanitarian relief to Haitian civilians, and for the fleet hospital, which was a treatment facility for US and United Nations military personnel. These data can be used by medical planners to determine MOOTW requirements in the post-Cold War era.
METHOD
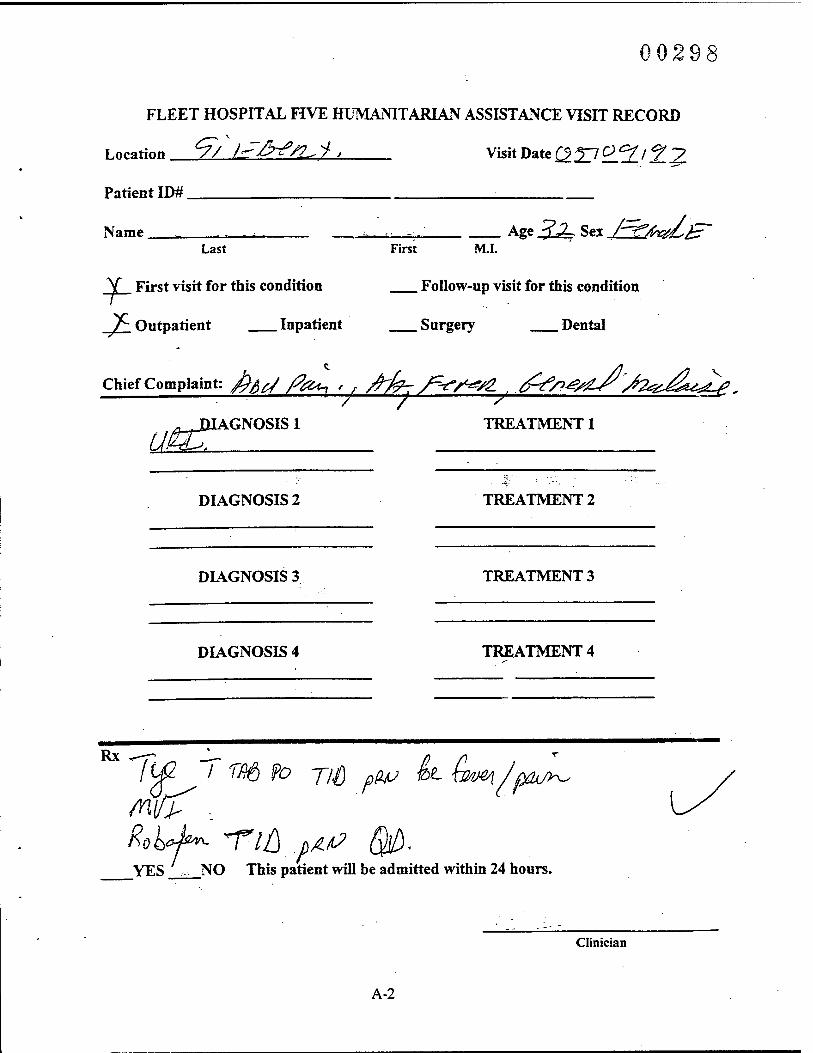
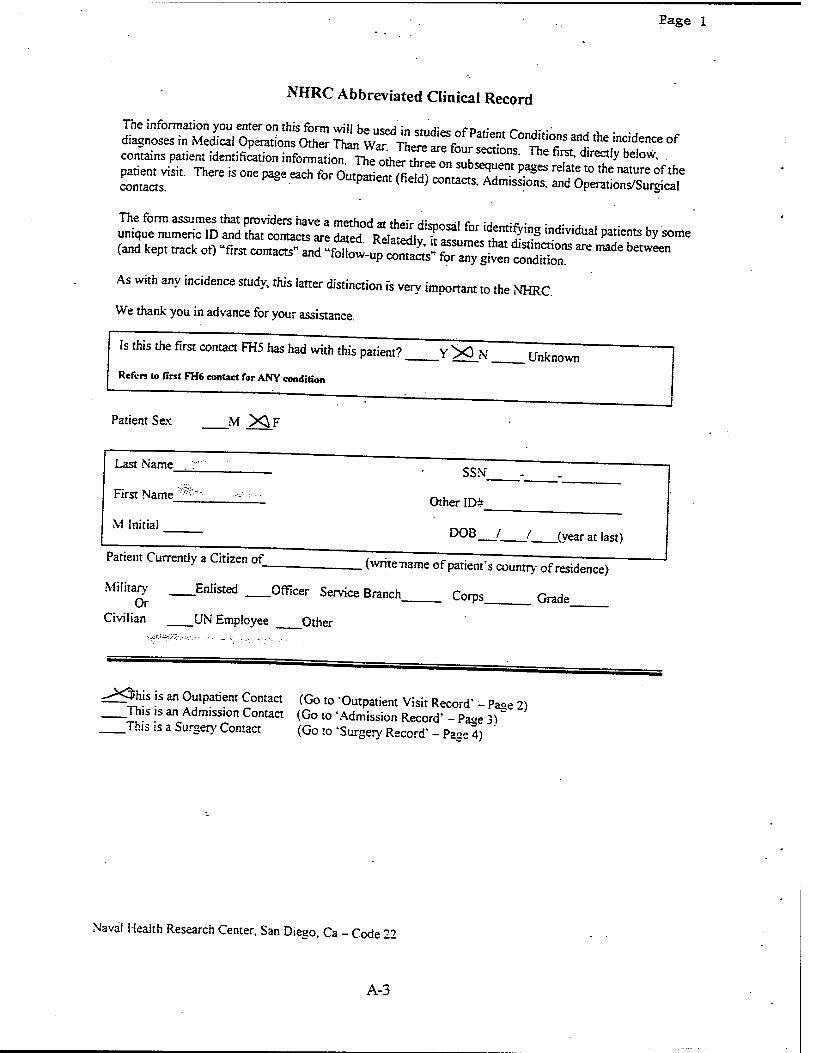
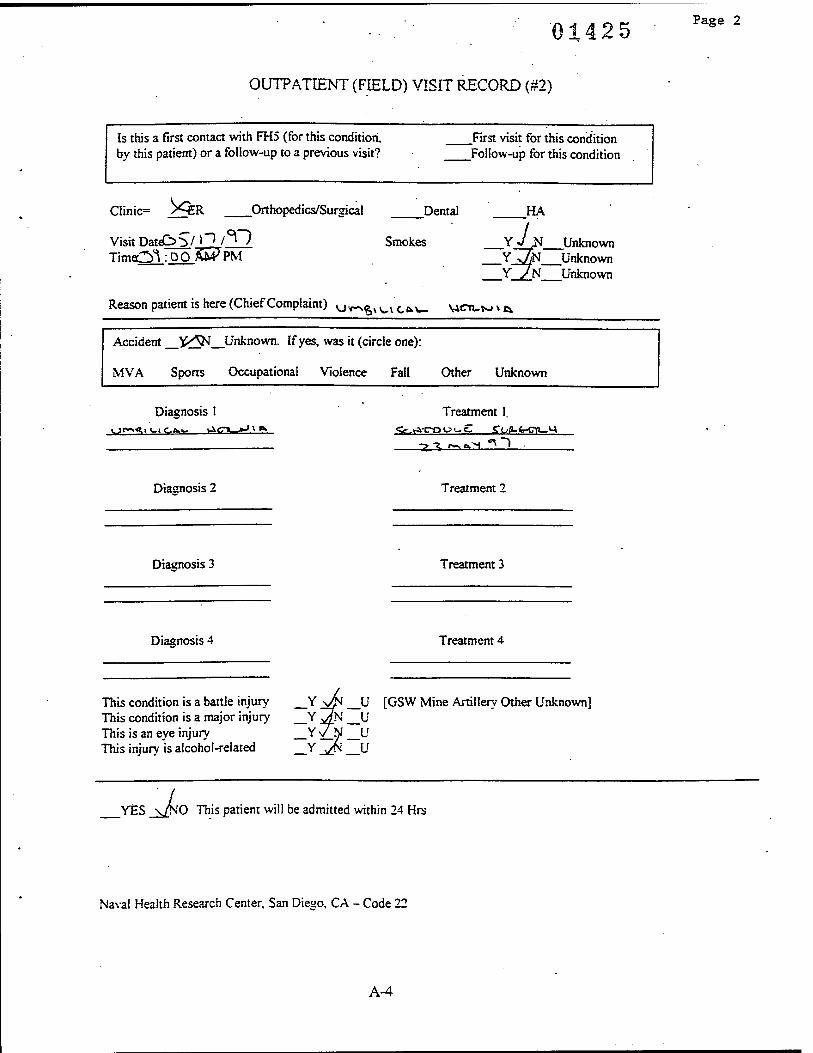
Medical personnel assigned to FH5 completed a Humanitarian Assistance Visit Record form for each patient seen in a clinic visit. The Visit Record format was free text, with spaces provided to record data. Demographic information included name, age, and sex. The type of visit, either first or follow-up, was recorded, along with patient status, defined as outpatient, inpatient, surgery, or dental. The form provided space for up to four diagnoses and their treatments. Space also was provided to record prescriptions. The Naval Health Research Center (NHRC) Abbreviated Clinical Record was completed for each patient encounter at the fleet hospital. In addition to demographic information, the patient's military status and nationality were recorded. Data describing the cause of injury were recorded where applicable. Examples of completed Humanitarian Assistance Visit Record and NHRC Abbreviated Clinical Record forms are shown in Appendix A.
The record forms, sorted by date and clinic site, were forwarded and converted into an electronic database. Inspection of the data sheets indicated that the free-text format was unsuitable for data entry. Illegibility, blank spaces, and inconsistency in medical terminology were some of the reasons why the raw data could not be transcribed directly. To standardize the data, a coding sheet (as seen in Appendix A) was developed to record the place and date of the patient encounter, the patient's age and sex, visit type, military or civilian status, nationality, up to four diagnoses using International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) terminology4, medical procedures performed, applications used, medications prescribed, and referrals made. Identifying data such as patient name and identification number were not transcribed, although coding sheets were numbered for purposes of data verification. Encoded data were then entered into an Excel™ database.
Using Excel™ computer software, the database was sorted into clinic visits, where the local population was treated, and fleet hospital visits, where US military or UN personnel were treated. These two categories were further classified into initial or follow- up visits, and frequencies were tabulated for demographics, diagnoses, and medications prescribed. A cross-tabulation of diagnosis by medication also was performed.
RESULTS AND DISCUSSION
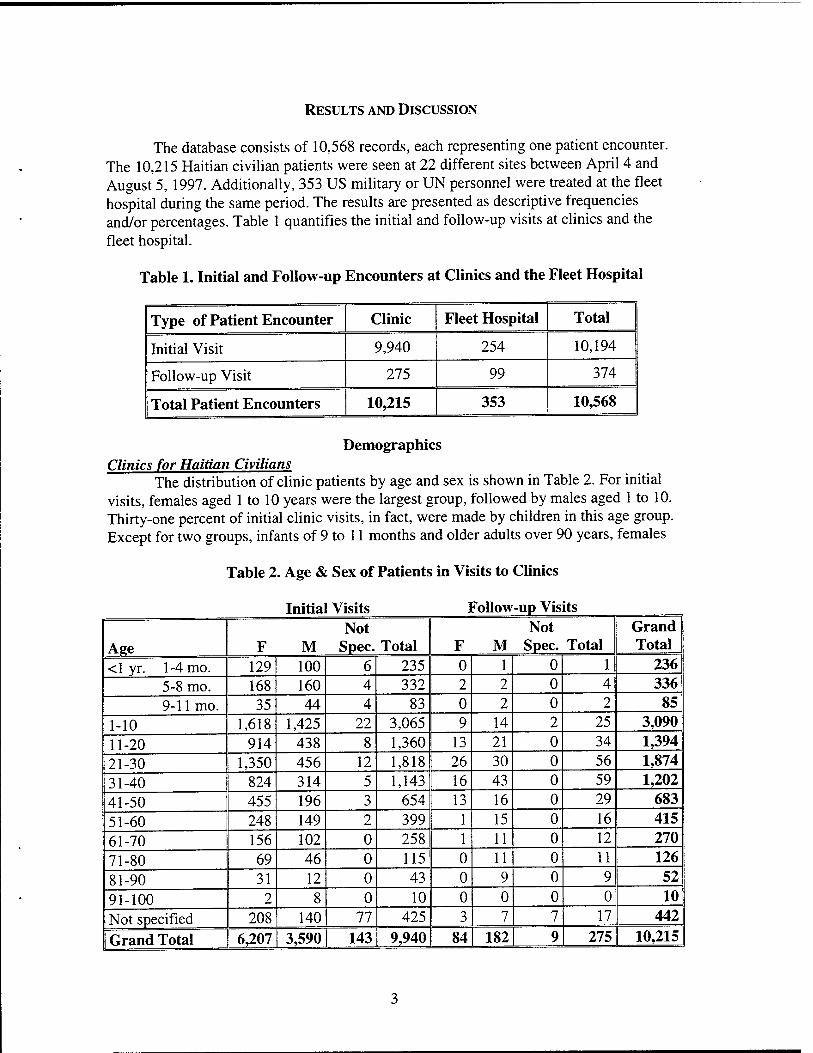
The database consists of 10,568 records, each representing one patient encounter. The 10,215 Haitian civilian patients were seen at 22 different sites between April 4 and August 5, 1997. Additionally, 353 US military or UN personnel were treated at the fleet hospital during the same period. The results are presented as descriptive frequencies and/or percentages. Table 1 quantifies the initial and follow-up visits at clinics and the fleet hospital.
Table 1. Initial and Follow-up Encounters at Clinics and the Fleet Hospital
Type of Patient Encounter Clinic Fleet Hospital Total
Initial Visit 9,940 254 10,194
Follow-up Visit 275 99 374
Total Patient Encounters 10,215 353 10,568
Demographics Clinics for Haitian Civilians
The distribution of clinic patients by age and sex is shown in Table 2. For initial visits, females aged 1 to 10 years were the largest group, followed by males aged 1 to 10. Thirty-one percent of initial clinic visits, in fact, were made by children in this age group. Except for two groups, infants of 9 to 11 months and older adults over 90 years, females
Table 2. Age & Sex of Patients in Visits to Clinics
Initial Visits Follow -up Visits
Age F M Not
Spec. Total F M Not
Spec. Total Grand Total
<1 yr. 1-4 mo. 129 100 6 235 0 1 0 1 236 5-8 mo. 168 160 4 332 2 2 0 4 336 9-11 mo. 35 44 4 83 0 2 0 2 85
1-10 1,618 1,425 22 3,065 9 14 2 25 3,090
11-20 914 438 8 1,360 13 21 0 34 1,394
21-30 1,350 456 12 1,818 26 30 0 56 1,874 31-40 824 314 5 1,143 16 43 0 59 1,202
41-50 455 196 3 654 13 16 0 29 683 51-60 248 149 2 399 1 15 0 16 415 61-70 156 102 0 258 1 11 0 12 270 71-80 69 46 0 115 0 11 0 11 126
81-90 31 12 0 43 0 9 0 9 52
91-100 2 8 0 10 0 0 0 0 10 Not specified 208 140 77 425 3 7 7 17 442
Grand Total 6,207 3,590 143 9,940 84 182 9 275 10,215
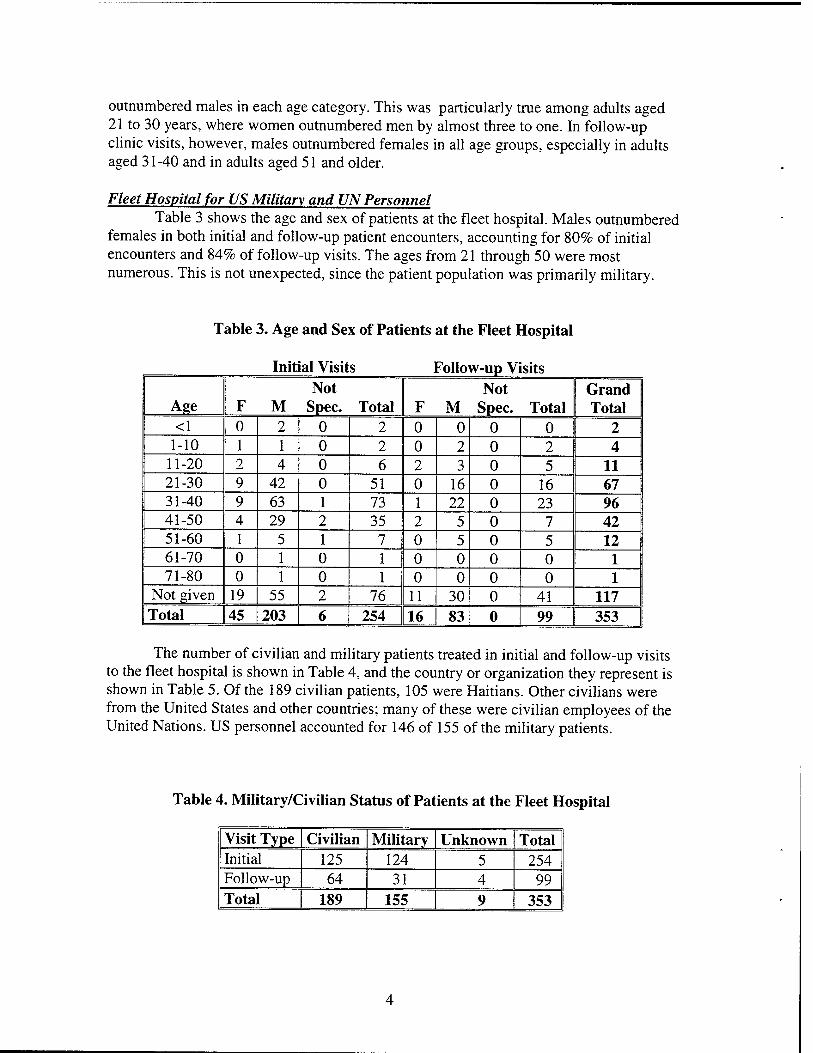
outnumbered males in each age category. This was particularly true among adults aged 21 to 30 years, where women outnumbered men by almost three to one. In follow-up clinic visits, however, males outnumbered females in all age groups, especially in adults aged 31-40 and in adults aged 51 and older.
Fleet Hospital for US Military and UN Personnel Table 3 shows the age and sex of patients at the fleet hospital. Males outnumbered
females in both initial and follow-up patient encounters, accounting for 80% of initial encounters and 84% of follow-up visits. The ages from 21 through 50 were most numerous. This is not unexpected, since the patient population was primarily military.
Table 3. Age and Sex of Patients at the Fleet Hospital
Initial Visits ] ?ollow-up Visits
Age F M Not
Spec. Total F Not
M Spec. Total Grand Total
<1 0 2 0 2 0 0 0 0 2 1-10 1 1 0 2 0 2 0 2 4
11-20 2 4 0 6 2 3 0 5 11 21-30 9 42 0 51 0 16 0 16 67 31-40 9 63 1 73 1 22 0 23 96 41-50 4 29 2 35 2 5 0 7 42 51-60 1 5 1 7 0 5 0 5 12 61-70 0 1 0 1 0 0 0 0 1 71-80 0 1 0 1 0 0 0 0 1
Not given 19 55 2 76 11 30 0 41 117 Total 45 203 6 254 16 83 0 99 353
The number of civilian and military patients treated in initial and follow-up visits to the fleet hospital is shown in Table 4, and the country or organization they represent is shown in Table 5. Of the 189 civilian patients, 105 were Haitians. Other civilians were from the United States and other countries; many of these were civilian employees of the United Nations. US personnel accounted for 146 of 155 of the military patients.
Table 4. Military/Civilian Status of Patients at the Fleet Hospital
Visit Type Civilian Military Unknown Total Initial 125 124 5 254 Follow-up 64 31 4 99 Total 189 155 9 353
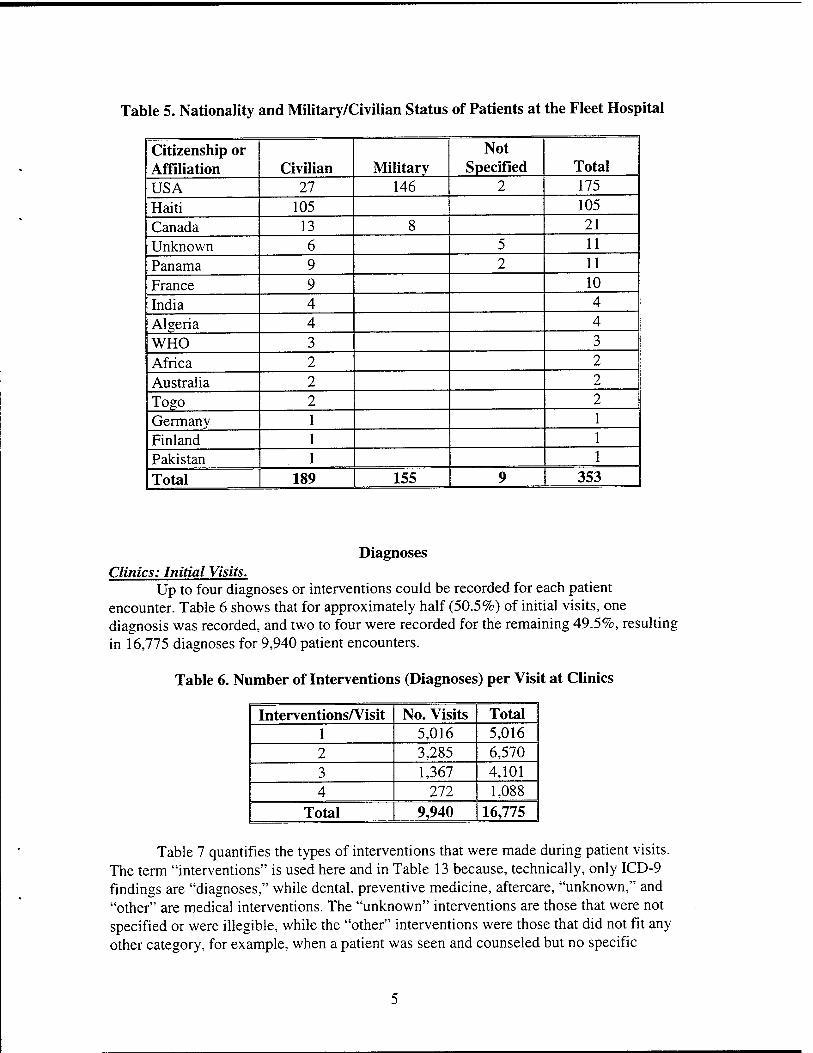
Table 5. Nationality and Military/Civilian Status of Patients at the Fleet Hospital
Citizenship or Affiliation Civilian Military
Not Specified Total
USA 27 146 2 175 Haiti 105 105 Canada 13 8 21 Unknown 6 5 11 Panama 9 2 11 France 9 10 India 4 4 Algeria 4 4 WHO 3 3 Africa 2 2 Australia 2 2 Togo 2 2 Germany 1 1 Finland 1 1
1 Pakistan 1 1
1 Total 189 155 9 353
Diagnoses Clinics: Initial Visits.
Up to four diagnoses or interventions could be recorded for each patient encounter. Table 6 shows that for approximately half (50.5%) of initial visits, one diagnosis was recorded, and two to four were recorded for the remaining 49.5%, resulting in 16,775 diagnoses for 9,940 patient encounters.
Table 6. Number of Interventions (Diagnoses) per Visit at Clinics
Interventions/Visit No. Visits Total 1 5,016 5,016 2 3,285 6,570 3 1,367 4,101 4 272 1,088
Total 9,940 16,775
Table 7 quantifies the types of interventions that were made during patient visits. The term "interventions" is used here and in Table 13 because, technically, only ICD-9 findings are "diagnoses," while dental, preventive medicine, aftercare, "unknown," and "other" are medical interventions. The "unknown" interventions are those that were not specified or were illegible, while the "other" interventions were those that did not fit any other category, for example, when a patient was seen and counseled but no specific
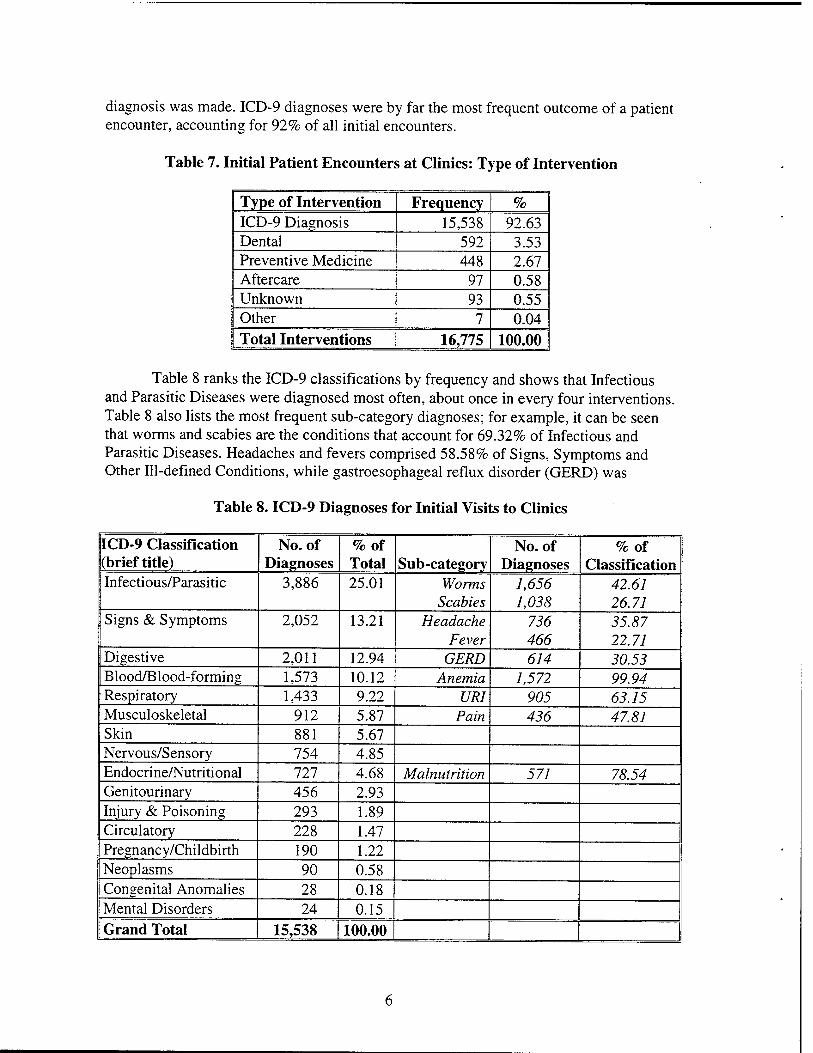
diagnosis was made. ICD-9 diagnoses were by far the most frequent outcome of a patient encounter, accounting for 92% of all initial encounters.
Table 7. Initial Patient Encounters at Clinics: Type of Intervention
Type of Intervention Frequency %
ICD-9 Diagnosis 15,538 92.63 Dental 592 3.53 Preventive Medicine 448 2.67 Aftercare 97 0.58 Unknown 93 0.55 Other 7 0.04 Total Interventions 16,775 100.00
Table 8 ranks the ICD-9 classifications by frequency and shows that Infectious and Parasitic Diseases were diagnosed most often, about once in every four interventions. Table 8 also lists the most frequent sub-category diagnoses; for example, it can be seen that worms and scabies are the conditions that account for 69.32% of Infectious and Parasitic Diseases. Headaches and fevers comprised 58.58% of Signs, Symptoms and Other Ill-defined Conditions, while gastroesophageal reflux disorder (GERD) was
Table 8. ICD-9 Diagnoses for Initial Visits to Clinics
ICD-9 Classification (brief title)
No. of Diagnoses
%of Total Sub-category
No. of Diagnoses
%of Classification
Infectious/Parasitic 3,886 25.01 Worms Scabies
1,656 1,038
42.61 26.71
Signs & Symptoms 2,052 13.21 Headache Fever
736 466
35.87 22.71
Digestive 2,011 12.94 GERD 614 30.53 Blood/Blood-forming 1,573 10.12 Anemia 1,572 99.94 Respiratory 1,433 9.22 URI 905 63.15 Musculoskeletal 912 5.87 Pain 436 47.81 Skin 881 5.67 Nervous/Sensory 754 4.85 Endocrine/Nutritional 727 4.68 Malnutrition 571 78.54 Genitourinary 456 2.93 Injury & Poisoning 293 1.89 Circulatory 228 1.47 Pregnancy/Childbirth 190 1.22 Neoplasms 90 0.58 Congenital Anomalies 28 0.18 Mental Disorders 24 0.15 Grand Total 15,538 100.00
diagnosed in 30.53% of Diseases of the Digestive System classification. Another notable sub-category diagnosis was anemia, which accounted for all but one Disease of the Blood and Blood-forming Organs. URI was the most commonly-diagnosed Disease of the Respiratory System, with 63.15% of diagnoses in that classification, and, under Diseases of the Musculoskeletal System, non-specific pain was diagnosed in nearly half the cases. Malnutrition was diagnosed frequently as a sub-category (n = 571) and accounted for 78.54% of Endocrine, Nutritional and Metabolic Diseases and Immune Disorders even though that major classification represented only 4.68% of the total number of diagnoses.
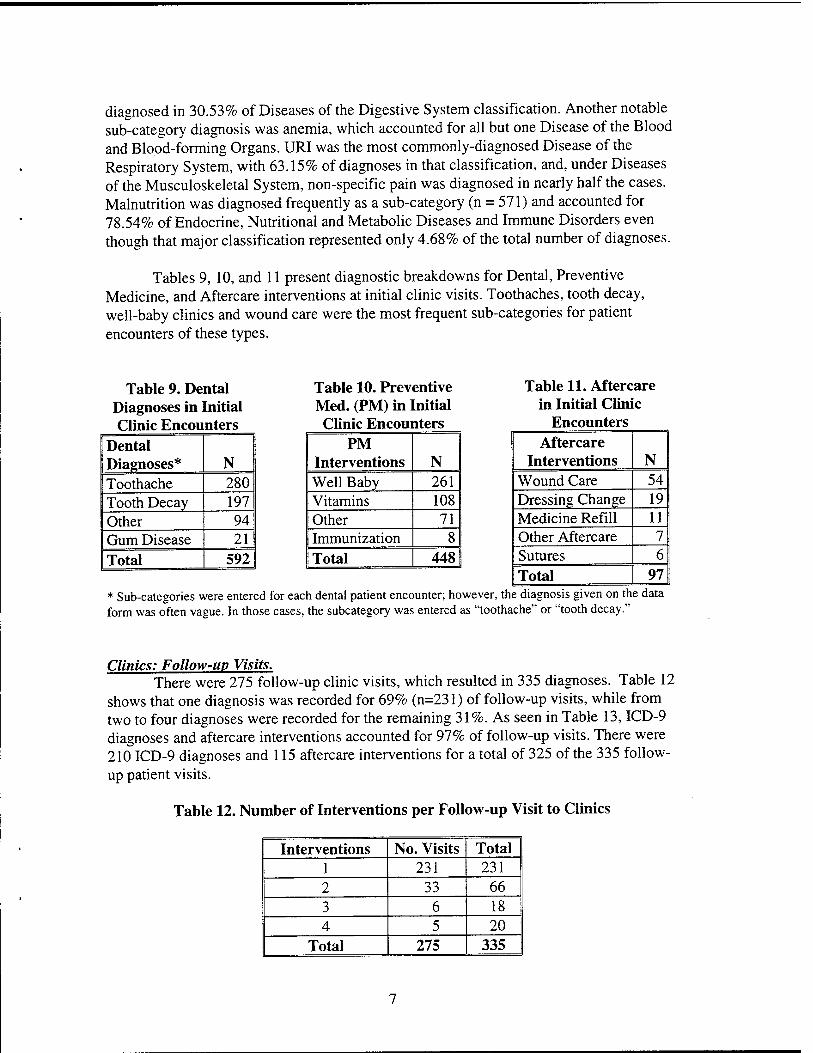
Tables 9, 10, and 11 present diagnostic breakdowns for Dental, Preventive Medicine, and Aftercare interventions at initial clinic visits. Toothaches, tooth decay, well-baby clinics and wound care were the most frequent sub-categories for patient encounters of these types.
Table 9. Dental Diagnoses in Initial Clinic Encounters
Dental Diagnoses* N Toothache 280 Tooth Decay 197 Other 94 Gum Disease 21 Total 592
Table 10. Preventive Med. (PM) in Initial Clinic Encounters
PM Interventions N Well Baby 261 Vitamins 108 Other 71 Immunization 8 Total 448
Table 11. Aftercare in Initial Clinic
Encounters Aftercare
Interventions N Wound Care 54 Dressing Change 19 Medicine Refill 11 Other Aftercare 7 Sutures 6 Total 97
* Sub-categories were entered for each dental patient encounter; however, the diagnosis given on the data form was often vague. In those cases, the subcategory was entered as "toothache" or "tooth decay."
Clinics: Follow-up Visits. There were 275 follow-up clinic visits, which resulted in 335 diagnoses. Table 12
shows that one diagnosis was recorded for 69% (n=231) of follow-up visits, while from two to four diagnoses were recorded for the remaining 31%. As seen in Table 13, ICD-9 diagnoses and aftercare interventions accounted for 97% of follow-up visits. There were 210 ICD-9 diagnoses and 115 aftercare interventions for a total of 325 of the 335 follow- up patient visits.
Table 12. Number of Interventions per Follow-up Visit to Clinics
Interventions No. Visits Total 1 231 231 2 33 66 3 6 18 4 5 20
Total 275 335
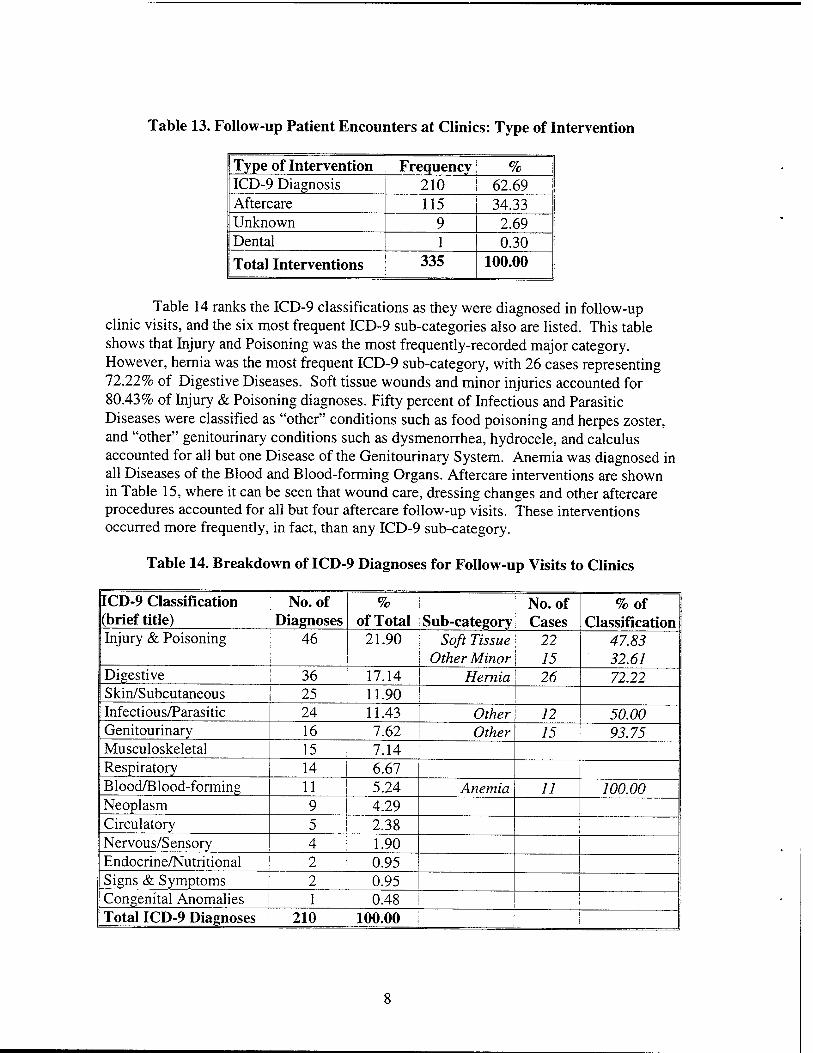
Table 13. Follow-up Patient Encounters at Clinics: Type of Intervention
Type of Intervention Frequency; % ICD-9 Diagnosis 210 1 62.69 Aftercare 115 34.33 Unknown 9 2.69 Dental 1 0.30 Total Interventions 335 100.00
Table 14 ranks the ICD-9 classifications as they were diagnosed in follow-up clinic visits, and the six most frequent ICD-9 sub-categories also are listed. This table shows that Injury and Poisoning was the most frequently-recorded major category. However, hernia was the most frequent ICD-9 sub-category, with 26 cases representing 72.22% of Digestive Diseases. Soft tissue wounds and minor injuries accounted for 80.43% of Injury & Poisoning diagnoses. Fifty percent of Infectious and Parasitic Diseases were classified as "other" conditions such as food poisoning and herpes zoster, and "other" genitourinary conditions such as dysmenorrhea, hydrocele, and calculus accounted for all but one Disease of the Genitourinary System. Anemia was diagnosed in all Diseases of the Blood and Blood-forming Organs. Aftercare interventions are shown in Table 15, where it can be seen that wound care, dressing changes and other aftercare procedures accounted for all but four aftercare follow-up visits. These interventions occurred more frequently, in fact, than any ICD-9 sub-category.
Table 14. Breakdown of ICD-9 Diagnoses for Follow-up Visits to Clinics
ICD-9 Classification (brief title)
No. of Diagnoses
% of Total Sub-category
No. of Cases
%of Classification
Injury & Poisoning 46 21.90 Soft Tissue Other Minor
22 15
47.83 32.61
Digestive 36 17.14 Hernia 26 72.22 Skin/Subcutaneous 25 11.90 Infectious/Parasitic 24 11.43 Other 12 50.00 Genitourinary 16 7.62 Other 15 93.75 Musculoskeletal 15 7.14 Respiratory 14 6.67 Blood/Blood-forming 11 5.24 Anemia 11 100.00 Neoplasm 9 4.29 Circulatory 5 2.38 Nervous/Sensory 4 1.90 Endocrine/Nutritional 2 0.95 Signs & Symptoms 2 0.95 Congenital Anomalies 1 0.48 Total ICD-9 Diagnoses 210 100.00 j
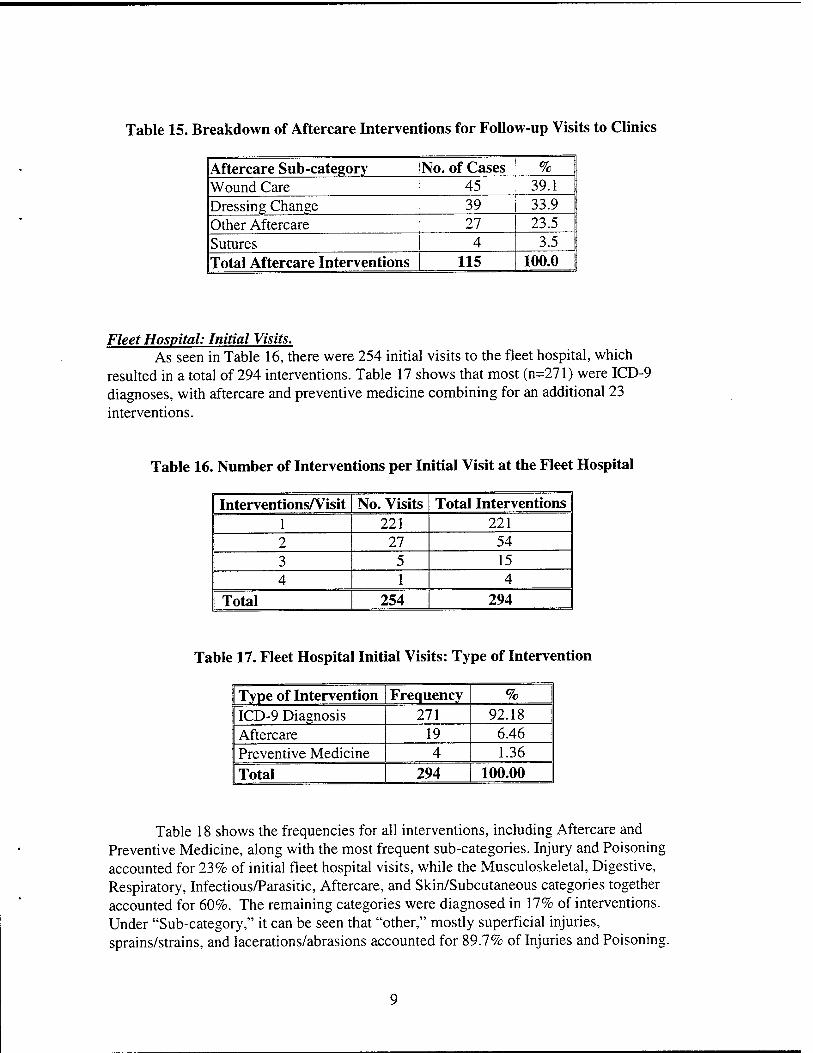
Table 15. Breakdown of Aftercare Interventions for Follow-up Visits to Clinics
Aftercare Sub-category No. of Cases %
Wound Care 45 39.1 Dressing Change 39 33.9 Other Aftercare 27 23.5 Sutures 4 3.5 Total Aftercare Interventions 115 100.0
Fleet Hospital: Initial Visits. As seen in Table 16, there were 254 initial visits to the fleet hospital, which
resulted in a total of 294 interventions. Table 17 shows that most (n=271) were ICD-9 diagnoses, with aftercare and preventive medicine combining for an additional 23 interventions.
Table 16. Number of Interventions per Initial Visit at the Fleet Hospital
Interventions/Visit No. Visits Total Interventions 1 221 221 2 27 54 3 5 15 4 1 4
I Total 254 294
Table 17. Fleet Hospital Initial Visits: Type of Intervention
Type of Intervention Frequency %
ICD-9 Diagnosis 271 92.18 Aftercare 19 6.46 Preventive Medicine 4 1.36 Total 294 100.00
Table 18 shows the frequencies for all interventions, including Aftercare and Preventive Medicine, along with the most frequent sub-categories. Injury and Poisoning accounted for 23% of initial fleet hospital visits, while the Musculoskeletal, Digestive, Respiratory, Infectious/Parasitic, Aftercare, and Skin/Subcutaneous categories together accounted for 60%. The remaining categories were diagnosed in 17% of interventions. Under "Sub-category," it can be seen that "other," mostly superficial injuries, sprains/strains, and lacerations/abrasions accounted for 89.7% of Injuries and Poisoning.
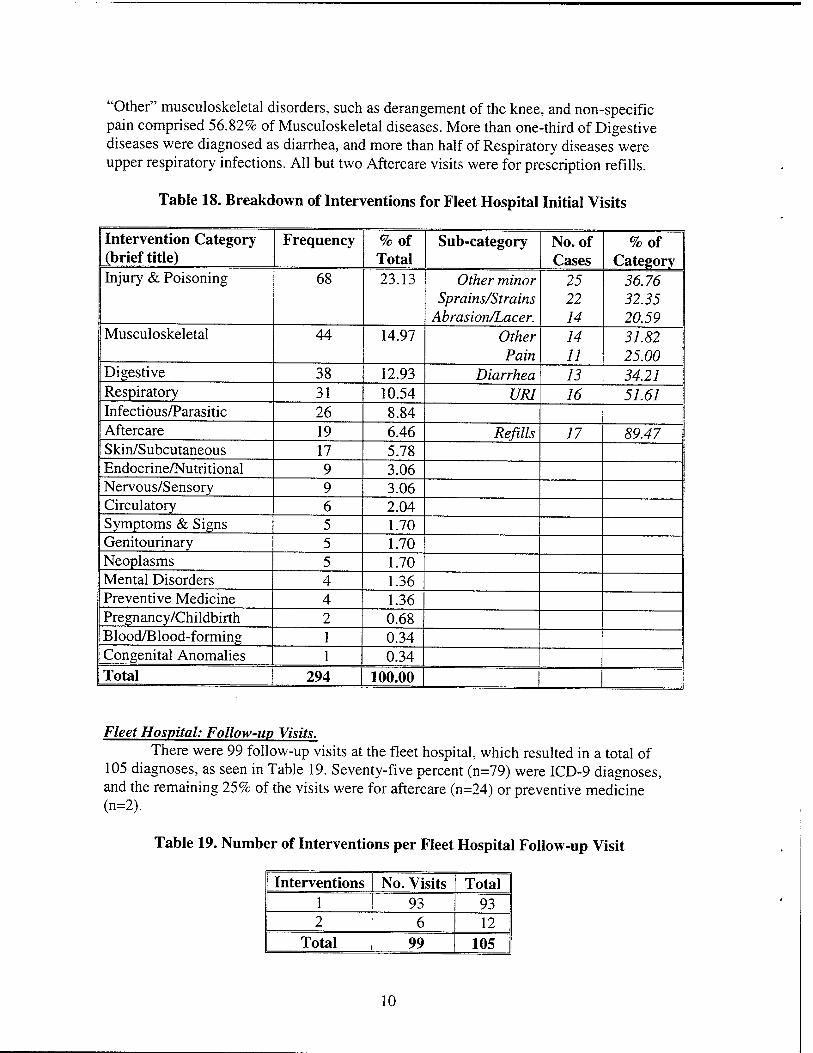
"Other" musculoskeletal disorders, such as derangement of the knee, and non-specific pain comprised 56.82% of Musculoskeletal diseases. More than one-third of Digestive diseases were diagnosed as diarrhea, and more than half of Respiratory diseases were upper respiratory infections. All but two Aftercare visits were for prescription refills.
Table 18. Breakdown of Interventions for Fleet Hospital Initial Visits
Intervention Category (brief title)
Frequency %of Total
Sub-category No. of Cases
%of Category
Injury & Poisoning 68 23.13 Other minor Sprains/Strains
Abrasion/Lacer.
25 22 14
36.76' 32.35 20.59
Musculoskeletal 44 14.97 Other Pain
14 11
31.82 25.00
Digestive 38 12.93 Diarrhea 13 34.21 Respiratory 31 10.54 URI 16 51.61 Infectious/Parasitic 26 8.84 Aftercare 19 6.46 Refills 17 89.47 Skin/Subcutaneous 17 5.78 Endocrine/Nutritional 9 3.06 Nervous/Sensory 9 3.06 Circulatory 6 2.04 Symptoms & Signs 5 1.70 Genitourinary 5 1.70 Neoplasms 5 1.70 Mental Disorders 4 1.36 Preventive Medicine 4 1.36 Pregnancy/Childbirth 2 0.68 Blood/Blood-forming 1 0.34 Congenital Anomalies 1 0.34 Total 294 100.00
Fleet Hospital: Follow-up Visits. There were 99 follow-up visits at the fleet hospital, which resulted in a total of
105 diagnoses, as seen in Table 19. Seventy-five percent (n=79) were ICD-9 diagnoses, and the remaining 25% of the visits were for aftercare (n=24) or preventive medicine (n=2).
Table 19. Number of Interventions per Fleet Hospital Follow-up Visit
Interventions No. Visits Total 1 93 93 2 6 12
Total 99 105
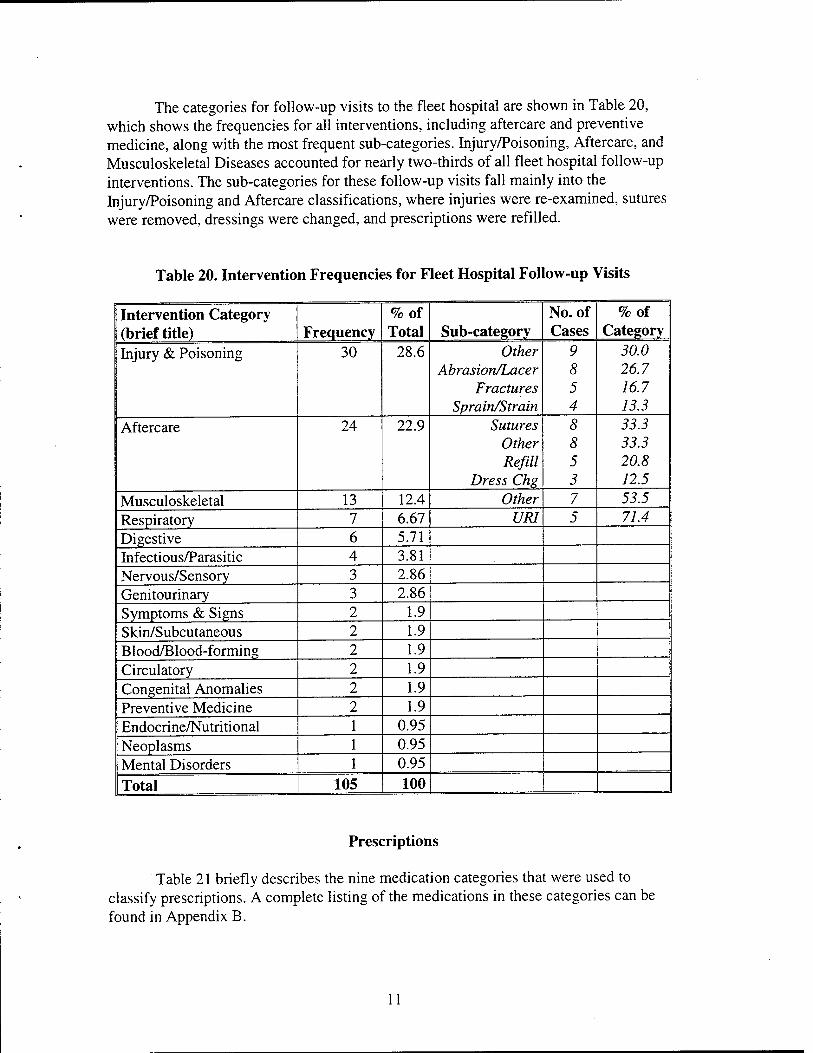
The categories for follow-up visits to the fleet hospital are shown in Table 20, which shows the frequencies for all interventions, including aftercare and preventive medicine, along with the most frequent sub-categories. Injury/Poisoning, Aftercare, and Musculoskeletal Diseases accounted for nearly two-thirds of all fleet hospital follow-up interventions. The sub-categories for these follow-up visits fall mainly into the Injury/Poisoning and Aftercare classifications, where injuries were re-examined, sutures were removed, dressings were changed, and prescriptions were refilled.
Table 20. Intervention Frequencies for Fleet Hospital Follow-up Visits
Intervention Category (brief title) Frequency
%of Total Sub-category
No. of Cases
%of Category
Injury & Poisoning 30 28.6 Other Abrasion/Lacer
Fractures Sprain/Strain
9 8 5 4
30.0 26.7 16.7 13.3
Aftercare 24 22.9 Sutures Other Refill
Dress Chg
8 8 5 3
33.3 33.3 20.8 12.5
Musculoskeletal 13 12.4 Other 7 53.5 Respiratory 7 6.67 URI 5 71.4 Digestive 6 5.71 Infectious/Parasitic 4 3.81 Nervous/Sensory 3 2.86 Genitourinary 3 2.86 Symptoms & Signs 2 1.9 Skin/Subcutaneous 2 1.9 Blood/Blood-forming 2 1.9 Circulatory 2 1.9 Congenital Anomalies 2 1.9 Preventive Medicine 2 1.9 Endocrine/Nutritional 1 0.95 Neoplasms 1 0.95 Mental Disorders 1 0.95
Total 105 100
Prescriptions
Table 21 briefly describes the nine medication categories that were used to classify prescriptions. A complete listing of the medications in these categories can be found in Appendix B.
11
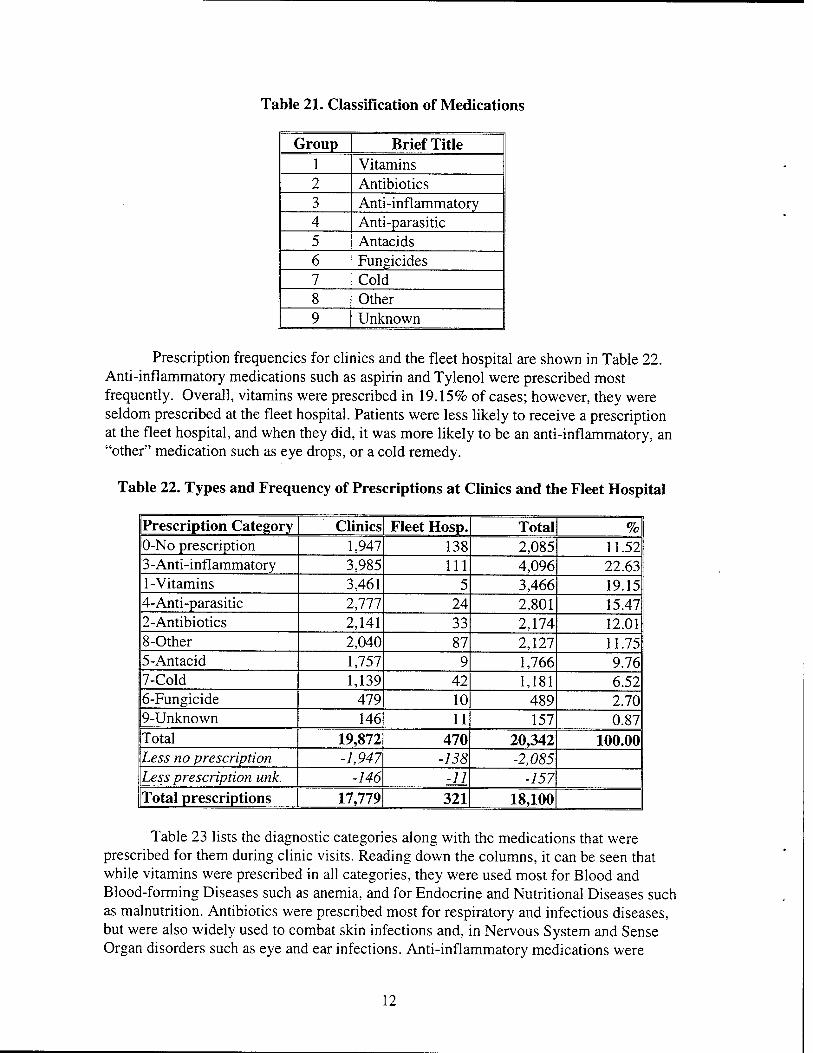
Table 21. Classification of Medications
Group Brief Title 1 Vitamins 2 Antibiotics 3 Anti-inflammatory 4 Anti-parasitic 5 Antacids 6 Fungicides 7 Cold 8 Other 9 Unknown
Prescription frequencies for clinics and the fleet hospital are shown in Table 22. Anti-inflammatory medications such as aspirin and Tylenol were prescribed most frequently. Overall, vitamins were prescribed in 19.15% of cases; however, they were seldom prescribed at the fleet hospital. Patients were less likely to receive a prescription at the fleet hospital, and when they did, it was more likely to be an anti-inflammatory, an "other" medication such as eye drops, or a cold remedy.
Table 22. Types and Frequency of Prescriptions at Clinics and the Fleet Hospital
Prescription Category Clinics Fleet Hosp. Total % 0-No prescription 1,947 138 2,085 11.52 3-Anti-inflammatory 3,985 111 4,096 22.63 1-Vitamins 3,461 5 3,466 19.15 4-Anti-parasitic 2,777 24 2,801 15.47 2-Antibiotics 2,141 33 2,174 12.01 8-Other 2,040 87 2,127 11.75 5-Antacid 1,757 9 1,766 9.76 7-Cold 1,139 42 1,181 6.52 6-Fungicide 479 10 489 2.70 9-Unknown 146 11 157 0.87 Total 19,872 470 20,342 100.00 Less no prescription -1,947 -138 -2,085 Less prescription unk. -146 -11 -157 Total prescriptions 17,779 321 18,100
Table 23 lists the diagnostic categories along with the medications that were prescribed for them during clinic visits. Reading down the columns, it can be seen that while vitamins were prescribed in all categories, they were used most for Blood and Blood-forming Diseases such as anemia, and for Endocrine and Nutritional Diseases such as malnutrition. Antibiotics were prescribed most for respiratory and infectious diseases, but were also widely used to combat skin infections and, in Nervous System and Sense Organ disorders such as eye and ear infections. Anti-inflammatory medications were
12

prescribed most frequently for Symptoms, Signs, and Hi-defined Conditions such as fever of unknown origin and headaches. Anti-parasitic medications were prescribed most for Infectious and Parasitic Diseases, and in fact worms and parasites were the most frequent sub-category of this ICD-9 category. Antacids were used to alleviate Diseases of the Digestive System such as GERD and indigestion. Fungicides were prescribed most often for Infectious and Parasitic Diseases, particularly for scabies. Cold and allergy medications were prescribed to fight Diseases of the Respiratory System such as upper respiratory infections, and also for Symptoms, Signs, and Hi-defined Conditions such as coughs. "Other" medications were prescribed frequently in several ICD-9 categories. There was an outbreak of herpes zoster, an Infectious and Parasitic Disease, which was typically treated with acyclovir. Calamine and betadine were often prescribed for skin discomfort caused by rashes or secondary effects of scabies. The frequent "other" medications prescribed for Diseases of the Nervous System and Sense Organs were over- the-counter eyedrops or eardrops.
Table 23. Medications Prescribed for Interventions at Clinic Visits
ICD-9 or Other Diagnostic Category
in S
E « -** >
VI
'•3 #o IS '-5 C < A
nti-
in
flam
mat
Ant
i-
para
siti
c V)
"3 a *-* s <
VI <u 2 "5 "3D s s "© u O
Grand Total
Infectious /Parasitic 278 371 253 2651 15 370 62 487 4,487 Respiratory 81 470 611 23 8 2 795 158 2,148 Symptoms & Signs 193 62 1243 17 239 2 211 130 2,097 Digestive 147 108 107 56 1465 4 7 153 2,047 Blood/Blood-forming 1566 1 40 3 6 0 0 16 1,632 Skin/Subcutaneous 35 330 59 10 2 50 32 450 968 Musculoskeletal 48 7 852 0 4 0 3 20 934
Nervous/Sensory 41 336 78 3 0 2 20 270 750 Endocrine/Nutritional 554 4 13 4 2 0 0 115 692
Genitourinary 29 267 95 5 1 46 0 27 470
Dental 31 20 390 0 0 0 0 9 450
Injury & Poisoning 15 92 82 0 0 Q 7 70 266 Preventive Medicine 220 1 16 0 5 0 0 5 247 Pregnancy/Childbirth 163 5 10 0 7 0 0 6 191 Circulatory 19 3 60 0 0 0 0 97 179 Unknown 14 11 10 4 1 2 1 11 54
Neoplasms 10 13 26 0 0 0 0 3 52
Aftercare 4 37 23 1 1 1 1 7 75 Mental Disorders 3 0 16 0 1 0 0 1 21
Other 4 2 0 0 0 0 0 4 10
Congenital Anomalies 6 1 1 0 0 0 0 1 9
Grand Total 3,461 2,141 3,985 2,777 1,757 479 1,139 2,040 17,779
13
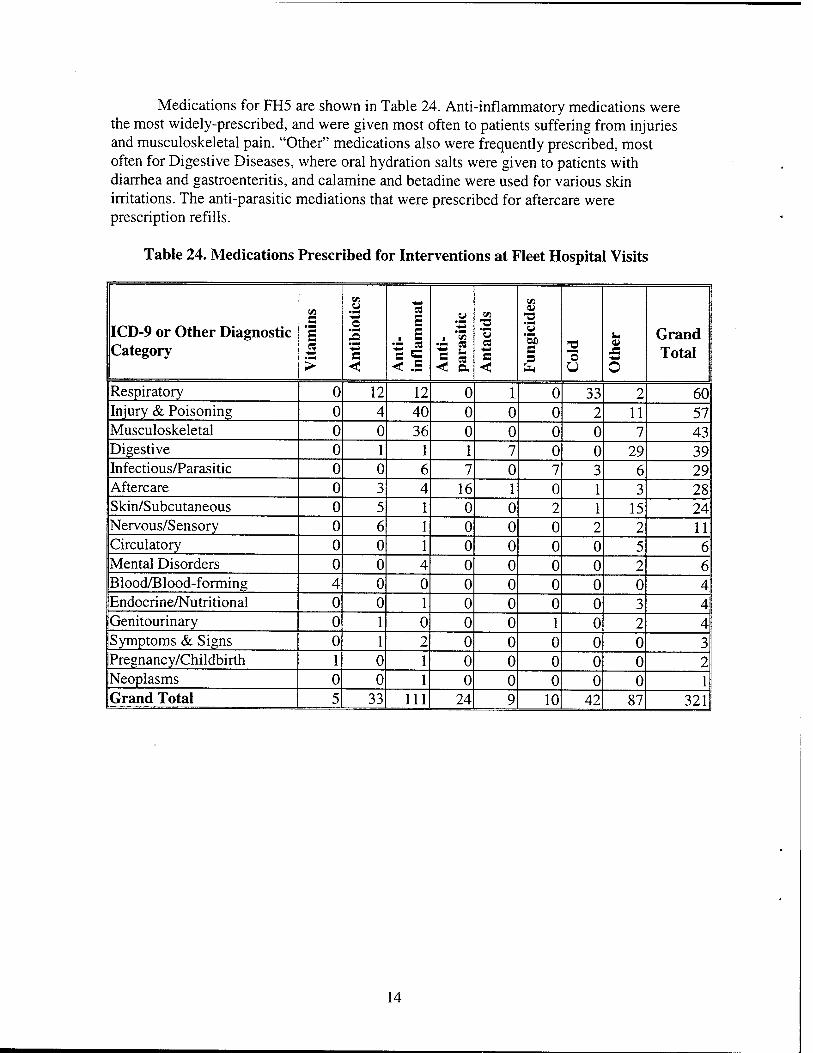
Medications for FH5 are shown in Table 24. Anti-inflammatory medications were the most widely-prescribed, and were given most often to patients suffering from injuries and musculoskeletal pain. "Other" medications also were frequently prescribed, most often for Digestive Diseases, where oral hydration salts were given to patients with diarrhea and gastroenteritis, and calamine and betadine were used for various skin irritations. The anti-parasitic mediations that were prescribed for aftercare were prescription refills.
Table 24. Medications Prescribed for Interventions at Fleet Hospital Visits
ICD-9 or Other Diagnostic Category
X C
1 *-* >
X
'S #© 15 'S s < A
nti-
in
flam
mat
Ant
i-
para
siti
c X
"3 es C <
X
2 "3 "53D c s "© u o
Grand Total
Respiratory 0 12 12 0 1 0 33 2 60 Injury & Poisoning 0 4 40 0 0 0 2 11 57 Musculoskeletal 0 0 36 0 0 0 0 7 43 Digestive 0 1 1 1 7 0 0 29 39 Infectious/Parasitic 0 0 6 7 0 7 3 6 29 Aftercare 0 3 4 16 1 0 1 3 28 Skin/Subcutaneous 0 5 1 0 0 2 1 15 24 Nervous/Sensory 0 6 1 0 0 0 2 2 11 Circulatory 0 0 1 0 0 0 0 5 6 Mental Disorders 0 0 4 0 0 0 0 2 6 Blood/Blood-forming 4 0 0 0 0 0 0 0 4 Endocrine/Nutritional 0 0 1 0 0 0 0 3 4 Genitourinary 0 1 0 0 0 1 0 2 4 (Symptoms & Signs 0 1 2 0 0 0 0 0 3 Pregnancy/Childbirth 1 0 1 0 0 0 0 0 2 Neoplasms 0 0 1 0 0 0 0 0 1 Grand Total 5 33 111 24 9 10 42 87 321
14
CONCLUSION
Medical planning is a complex process. To determine supply, equipment, skill, training, and personnel requirements for military medical operations, planners and logisticians project types and occurrence rates of injuries and illnesses likely to be encountered in a given scenario. One such scenario is the deployment of FH5 to Haiti on a humanitarian relief mission. Through the efforts of FH5 personnel to document every patient encounter during their deployment, a complete and extensive data set, including demographics, illness and injury frequencies, and the medications needed to treat them, has been collected. The resulting database, and the descriptive statistics that it generated, is a first step toward fulfilling the MRSP-2004 objective of preparing for and maintaining readiness for MOOTW.
Future areas of research for MOOTW medical planning should include the development of denominator data so that rates of occurrence for illnesses and injuries can be established for humanitarian relief as well as for other MOOTW scenarios. Comparisons between different types of MOOTW also will provide useful information. Specifically, baseline estimates of clinical capability requirements could be established for those parameters common to many scenarios, and variations might be defined for areas that are unique to particular types of MOOTW. For example, this study found that, in a humanitarian relief MOOTW, a large portion of the population are civilian children with diseases such as worms and scabies, and that anemia is prevalent among both children and adults. In contrast, previous studies of a peacekeeping MOOTW found that the field hospital in Zagreb, Croatia, served a mostly adult, military population who were treated most often for injuries, both combat and non-combat related, and for respiratory disorders.5'6
In a military deployment, there are four levels, or echelons, of medical care, ranging from Echelon I, battlefield care, to Echelon IV, definitive care. Echelon V provides convalescent care in the continental United States. The DEPMEDS model determines Echelon III and IV requirements,1 and NHRC has developed a compatible model for Echelons I and II.7 Both of these models link a patient condition to a list of medical tasks required to treat the condition at a given echelon. The supplies, skills, and time required to perform each task can be quantified, and a supply stream can be generated. Since MOOTW is a relatively recent trend that is likely to continue, it is important to account for patient conditions, as well as patient populations, that might differ from those of standard combat scenarios now found in military medical planning models.
Providing efficient and effective medical care, first, for the US military and second, for the target populations, is the goal of planners for MOOTW. Systematic research to determine baseline MOOTW requirements, as well as the unique medical requirements for humanitarian relief, peacekeeping, and disaster relief efforts will provide the data needed to achieve that goal. Further research will enable planners to use the data to establish an updated list of patient conditions, which are the basis for planning models such as DEPMEDS and the NHRC model.
15
ACKNOWLEDGEMENT
The authors recognize and appreciate the efforts of personnel assigned to Fleet Hospital 5 to document every patient encounter during their Haiti deployment. The result of this endeavor is a complete and accurate database. In particular, the assistance of CAPT Dana Covey and LCDR Nancy Moya, who shared their firsthand information about the mission and provided guidance for this study, has been invaluable.
16
REFERENCES
1. Burke M. Deployable medical systems begin to reach field, US Med. October 1987; 23:3.
2. US Department of Defense. Medical Readiness Strategic Plan 2004. Washington, DC: DoD; August 1998.
3. Famighetti R, ed. The World Almanac Book of Facts 1998. Mahway, N.J: K-m Reference Corporation; 1997.
4. International Classification of Diseases, 9th Revision, Clinical Modification. 5 ed. Salt Lake City, Utah: Medicode Publications; 1996.
5. Reed RJ, Martino J, Pugh WM. The field hospital at Zagreb: a database for military medical resource planning in operations other than war. Mil Med. 1998; 163:413-419.
6. Gauker ED, Reed RJ. Medical diagnoses in operations other than war (OOTW): relationship to DEPMEDS patient conditions. San Diego, CA: Naval Health Research Center, 1997; Report No. 97-27.
7. Galarneau MR, Mahoney KJ, Konoske PJ, Emens-Hesslink KE. Development of a model for predicting medical supply requirements at the forward echelons of care: preliminary findings for echelon ii laboratory and x-ray ancillaries. San Diego, CA: Naval Health Research Center, 1997; Report No. 97-3.
17
APPENDIX A
Data Collection and Coding Forms
A-l
00298
FLEET HOSPITAL FIVE HUMANITARIAN ASSISTANCE VISIT RECORD
Location *7/ I^/^/2^i > Visit Date [22J ¥2.'2.2
Patient ID#
Name - - - - -■ ■-■.: Age ?JL. Sex jb€./fat£,£T Last First M.I.
V First visit for this condition Follow-up visit for this condition
)_ Outpatient Inpatient Surgery Dental
Chief Complaint: farf /^ , /^-/V/^^ , {£fr?^J' AZ&J%z<>Jl#,
-.DIAGNOSIS 1 TREATMENT 1
DIAGNOSIS 2
DIAGNOSIS 3
DIAGNOSIS 4
TREATMENT 2
TREATMENT 3
TREATMENT 4
Rx
MVP -
YES ,., NO This patient will be admitted within 24 hours.
Clinician
A-2
Bage 1
NHRC Abbreviated Clinical Record
The information you enter on this form will be ii-wrl ;n ct,,^;« „fB,.- . r~ _.- •• diagnoses in Medical Operations Other Cw?Cl?lh ^? wT ^ *" inddence °f
contains patient identification h^n^Z^^^^f ^ "f *«** bei°W' patient visit. There is one page each tor OutoaLTrfiTZTrl ^T ^ "^t0 the nature of the
contacts. outpatient (field) contacts. Admissions, and Operations/Surgical
(-d kept track oO«first^^^
As with any incidence study, this latter distinction is very important to the NHRC
We thank you in advance for your assistance.
some
Is this the first contact FH5 has had with this patient? Y>0 N
Refer» to first FH6 contact for ANY condition
Patient Sex _M X^F
Unknown
Last Name
First Name ^
M Initial
Patient Currentiy a Citizen of
Enlisted
SSN
Other ID*_
DOB _(year at last)
Military Or
Civilian
_ (write-name of patient's country of residence)
Officer Service Branch Corps Grade
_UN Employee Other
^h.s is an Outpatient Contact (Go to 'Outpatient Visit Record" - Paae 2) This is an Admission Contact (Go to * Admission Record' - Pa«e 3)" This is a Surgery Coma« (Go to 'Surgery Record' - Pa"e 4) '
Naval Health Research Center, San Diego, Ca - Code 22
A-3
01425 Page 2
OUTPATIENT (FIELD) VISIT RECORD (#2)
Is this a first contact with FH5 (for this condition, by this patient) or a follow-up to a previous visit?
_First visit for this condition Follow-up for this condition
CIinic= y* R _Orthopedics/Surgical Dental HA
Visit DateCbS/^/Q TimeOV-ÜOta?PM
Smokes J: Y -J N Unknown Y >JN Unknown Y JH Unknown
Reason patient is here (Chief Complaint) \j <*>§•> ^v c*\- UCn_io \ a
Accident YX^ Unknown. If yes, was it (circle one):
MVA Sports Occupational Violence Fall Other Unknown
Diagnosis 1
Diagnosis 2
Diagnosis 3
Diagnosis 4
This condition is a battle injury This condition is a major injury This is an eye injury This injury is alcohol-related
Treatment 1.
-£-l ^-.ix^ "O
Treatment 2
Treatment 3
Treatment 4
_Y ^F _U [GSW Mine Artillery Other Unknown] _Y 2N _U _Y7N_U
YES \jNO This patient will be admitted within 24 Hrs
Naval Health Research Center, San Diego, CA - Code 22
A^
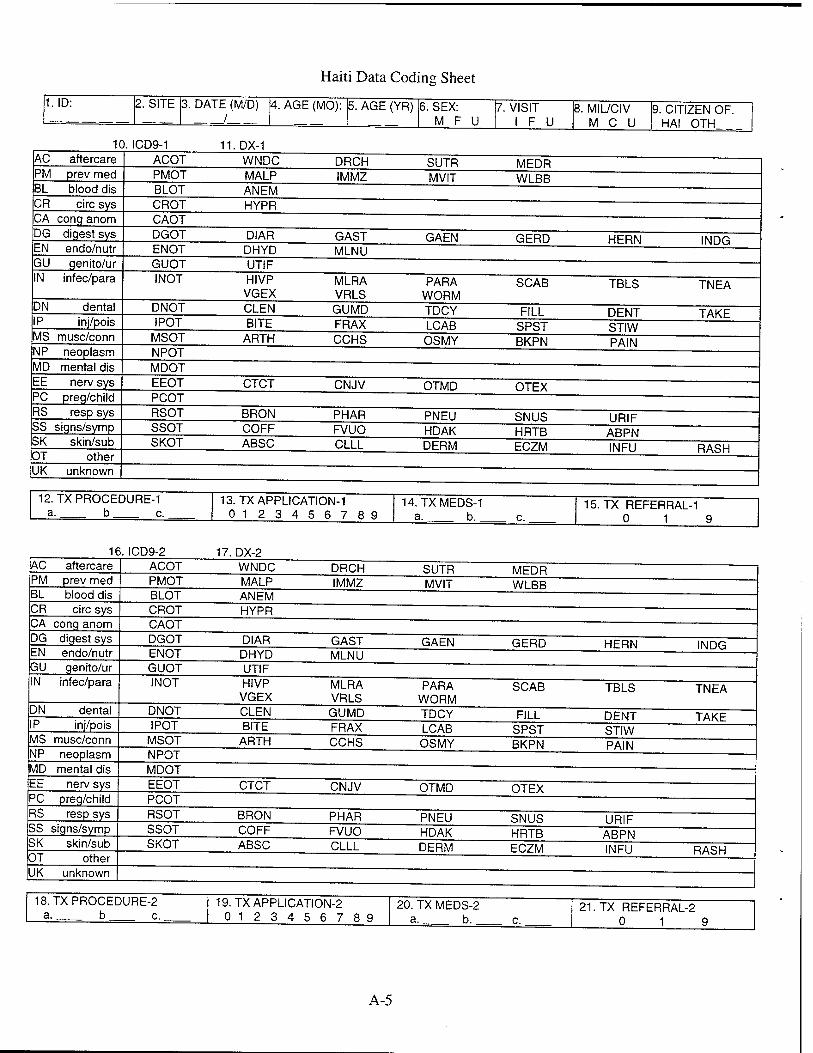
Haiti Data Coding Sheet
1. ID:
AC aftercare PM prev med
DN IP
2. SITE 3. DATE (M/D)
10. ICD9-1
BL blood dis CR circ sys CA cong anom DG digest sys EN endo/nutr GU genito/ur IN infec/para
dental inj/pois
MS muse/conn NP neoplasm MD mental dis EE nerv sys PC preg/child RS resp sys SS signs/symp SK skin/sub OT other UK unknown
ACOT PMOT BLOT CROT CAOT DGOT ENOT GUOT INOT
DNOT I POT
MSOT NPOT MDOT EEOT PCOT RSOT SSOT SKOT
12. TX PROCEDURE-1 a. b c.
/ 4. AGE (MO):
11. DX-1 WNDC MALP AN EM HYPR
DIAR DHYD UTIF HIVP VGEX CLEN BITE
ARTH
CTCT
BRON COFF ABSC
5. AGE (YR)
DRCH IMMZ
GAST MLNU
MLRA VRLS GUMD FRAX CCHS
CNJV
PHAR FVUO CLLL
13.TXAPPLICATION-1 0 12 3 4 5 6 7 8 9
6. SEX: M F
SUTR MVIT
GAEN
PARA WORM TDCY LCAB OSMY
OTMD
PNEU HDAK DERM
7. VISIT i F U
14. TXMEDS-1 a. b.
MEDR WLBB
GERD
SCAB
FILL SPST BKPN
OTEX
SNUS HRTB ECZM
8. MIL/CIV M C U
9. CITIZEN OF. HAI OTH
HERN INDG
TBLS TNEA
DENT TAKE STIW PAIN
URIF ABPN INFU RASH
c.. 15. TX REFERRAL-1 0 1 9
16. ICD9-2 AC aftercare PM prev med
CR circ sys CA cong anom DG digest sys EN endo/nutr GU genito/ur IN infec/para
BL blood dis
DN dental IP inj/pois MS muse/conn NP neoplasm MD mental dis EE nerv sys PC preg/child RS resp sys SS signs/symp SK skin/sub OT other UK unknown
17. DX-2 ACOT PMOT BLOT CROT CAOT DGOT ENOT GUOT INOT
DNOT I POT
MSOT NPOT MDOT EEOT PCOT RSOT SSOT SKOT
18.TXPROCEDURE-2 a. b c.
WNDC MALP ANEM HYPR
DIAR DHYD UTIF HIVP VGEX CLEN BITE
ARTH
CTCT
BRON COFF ABSC
DRCH IMMZ
GAST MLNU
MLRA VRLS GUMD FRAX CCHS
CNJV
PHAR FVUO CLLL
19. TX APPLICATION-2 0 12 3 4 5 6 7 8 9
SUTR MVIT
GAEN
PARA WORM TDCY LCAB OSMY
OTMD
PNEU HDAK DERM
MEDR WLBB
GERD
SCAB
FILL SPST BKPN
OTEX
SNUS HRTB ECZM
20. TX MEDS-2 a. b.
HERN INDG
TBLS TNEA
DENT TAKE STIW PAIN
URIF ABPN INFU RASH
21. TX REFERRAL-2 0 1 9
A-5

APPENDIX B
Medication Coding Chart
B-l

t/I s
*s « cj
i-
(5
DC
■5 o U
8 C
old/
Cou
gh/
Alle
rgy
-5 a c
CQ
a
P p
pa
o o CO a u U
a o. «
£ 5
3 •4—J
15 c oi
X
s c p o
c*
7 A
ntif
unga
ls
c C3 O 3
Q
'p
o u c >> Ü
c
o o
c 4—»
es
O o >1
o N
z
c 4—»
z
£ C3 Ü
u 4—>
o o 2
Tri
amci
nolo
ne
Ace
toni
de
6 A
ntac
ids
T3
"x <
u c
£
U
c C3
-a
&
■4—»
£
CNS
5 A
ntip
aras
itic
s/
Ant
imal
aria
ls
P J5 .3 U
P 5 P U
I
£ c3 P U X
5 1 c
o N C3
-o c <D
X) O
o N C3
'E o X
c (X
C
D OH
CÜ
X o £
>
4 O
ther
'> _o o o <
c
<U
CQ
c 'E
U
c c
— 5
X o £ o
c5 ■D
■4—»
3 o o Ora
l H
ydra
tion
Salts
■4—*
s
">^ jr a o
-a o
0-,
3 P
ain/
Fev
er
< 00 <
"5. <
p
§< JO
3
"5 o ■a c
c
C3
Ü P 5
•o c
U
"p 5 u o
c
P &
z
o c
>>
3 p_ 3
-a Q < 00
Z
2 A
ntib
ioti
cs
x o E <
3
"x o E <
D U 3 <
*-*—4
c £
<
E -4—»
o
CQ
c "x
CQ
C
X
CH
U Cep
hazo
lin
Sodi
um
Cef
tria
xone
So
dium
c
X
o 5
c
>^ E p
.3 O
£
a
"5 £
3
Ü
3
>
a o o
6
X o
3 <D
OH,
3
'o 'E D-
c IE D o O
DC
X
E 5
N
1 V
itam
ins
&
Min
eral
s
"c
y
CQ 5
P
c OX)
i
c £
•4—>
>
-4—4
ü Cu
"p
">
o CU
c3 -4—4
E p
CQ
REPORT DOCUMENTATION PAGE Form Approved
OMB No. 07044188
Public reporting burden for this collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to Washington Headquarters Services, Directorate for Information Operations and Reports, 1215 Jefferson Davis Highway, Suite 1204, Arlington, VA 22202-4302, and to the Office of Management and Budget, Paperwork Reduction Project (0704-0188),
Washington, DC 20503.
1. AGENCY USE ONLY {Leave blank} 2. REPORT DATE
9Nov1998 4. TITLE AND SUBTITLE A Descriptive Analysis of Patient Encounter Data from the Fleet Hospital 5 Humanitarian Relief Mission in Haiti
6. AUTHOR(S) Eleanor D. Gauker, Kristee Emens-Hesslink, and Paula J. Konoske
7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES)
Naval Health Research Center P.O. Box 85122 San Diego, CA 92186-5122
8. SPONSORING/MONITORING AGENCY NAME(S) AND ADDRESS(ES)
Office of Naval Research 800 North Quincy St. Arlington, VA 22217-5660
3. REPORT TYPE AND DATE COVERED Interim Jan-Nov 1998 5. FUNDING NUMBERS
Program Element: 63706N
Work Unit Number: M0095.005-6809
8. PERFORMING ORGANIZATION NUMBER
Report No. 98-38
10. SPONSORING/MONITORING AGENCY REPORT NUMBER
11. SUPPLEMENTARY NOTES
12a. DISTRIBUTION/AVAILABILITY STATEMENT
Approved for public release; distribution is unlimited.
12b. DISTRIBUTION CODE
12. ABSTRACT (Maximum 200 words)
Military planners determine medical requirements by projecting the number of casualties expected in a combat scenario. A recent shift in US military policy has resulted in an increase in military operations other than war (MOOTW); therefore, it is important to update military medical planning tools to account for MOOTW such as humanitarian assistance, peacekeeping, and disaster relief. This report describes the patient demographics, type of medical encounter, diagnoses, and medications provided by medical personnel of Fleet Hospital 5 (FH5) in community clinics that provided humanitarian relief to Haitian civilians, and at the FH5 treatment facility, where US and United Nations military personnel were treated during a humanitarian relief operation in Haiti. These data formed a database consisting of 10,568 records, each representing one patient encounter. The 10,215 clinic patients were seen at 22 sites between April 4 and August 5, 1997. Almost two-thirds (61.6%) were women, and children aged 1 to 10 years comprised the largest age category. Additionally, 353 patients were treated at FH5 during the same period. A majority of patients (81%) were men; those aged 21 to 50 years were seen most often. Medical diagnoses were the most frequent type of patient encounter, representing 92.6% of clinic visits and 92.2% of FH5 visits. Infectious and parasitic diseases were diagnosed in one of every four clinic visits. At FH5, injury and poisoning diagnoses were the most frequent (23.1%). 13. SUBJECT TERMS
Military Operations Other Than War, medical planning, humanitarian relief, diagnoses, patient condition
17. SECURITY CLASSIFICA- TION OF REPORT
Unclassified
18. SECURITY CLASSIFICATION OF THIS PAGE
Unclassified
14. NUMBER OF PAGES
26 16. PRICE CODE
19. SECURITY CLASSIFICATION OF ABSTRACT
Unclassified
20. LIMITATION OF ABSTRACT
Unlimited
NSN 7540-01-280-5500 Standard Form 298 (Rev. 2-89)
Prescribed by ANSI Std. Z39-18
298-102