
A comparison of salivary substitutes versus a natural sialogogue (citric acid) in patients...
6
A comparison of salivary substitutes versus a natural sialogogue (citric acid) in patients complaining of dry mouth as an adverse drug reaction: a clinical, randomized controlled study Felice Femiano, MDM, PhD, a Rosario Rullo, MDMDr, a Federica di Spirito, DDSDr, a Alessandro Lanza, DDS, MScDr, a Vincenzo Maria Festa, DDS, MScDr, a and Nicola Cirillo, DDS, PhD, b Naples, Italy; and Bristol, United Kingdom SECOND UNIVERSITY OF MEDICINE AND SURGERY AND UNIVERSITY OF BRISTOL Objective. We aimed to compare the efficacy of saliva substitutes and citric acid long-term therapy for oral dryness relief and unstimulated salivary flow in patients reporting drug-induced xerostomia. Study design. Fifty-four patients reporting drug-induced xerostomia were randomly subdivided into 3 groups and respectively administered artificial saliva, 3% citric acid, or distilled water in mouthwash 4 times a day for 30 days. Patients underwent measurement of unstimulated whole saliva before and after they finished therapy and were asked to note in a daily diary any symptomatologic changes 15 minutes and 1 hour after each daily intake of test solution. Results. Fifteen minutes after solution intake, 12 patients (67%) belonging to the artificial saliva group, 9 (50%) from the citric acid group, and 2 (11%) from the water group reported significant symptomatologic improvement. One hour after solution intake, 7 patients (39%) from the artificial saliva group, 10 (56%) from the citric acid group, and 0 from the water group noted significant symptomatologic improvement. None of the drugs tested affected unstimulated whole saliva flow. Conclusions. Both artificial saliva and citric acid provided immediate relief from oral dryness. Citric acid also provided a longer-lasting feeling of oral moistness at 1 hour after use owing to its protracted activity on salivary gland function. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:e15-e20) The word “xerostomia” is derived from Greek. It comes from “xeros” (dry) and “stoma” (mouth), and is usually used to indicate the condition of not having enough saliva to keep the mouth moist. The term “xerostomia,” how- ever, may properly be used to describe the subjective sensation of dryness in the mouth reported by patients, whereas the more accurate term for measurable and ob- jectifiable changes in reduced salivary function is “sali- vary gland hypofunction” for a reduction in fluid output and “salivary gland dysfunction” for a more general al- teration in physiologic salivary gland function. 1-3 This semantic distinction is important, because a feel- ing of dry mouth is not always accompanied by an objec- tive decrease in the salivary flow. In fact, patients may occasionally report feelings of oral dryness, similar to a sticky or doughy sensation, without any objective clinical reduction being found. 4,5 This would indicate that other factors can influence the feeling of moistness in the mouth. Several short- and long-term conditions can dis- rupt salivary secretion, leading to hyposalivation. These include psychologic problems (stress and anxiety), auto- immune disease (Sjögren syndrome), and chemotherapy or radiotherapy of the head and neck. 6-9 The feeling of dry mouth is the most common oral adverse drug reaction in the oral cavity. In fact, a large number of medications, 500, list dry mouth as an adverse effect. Relatively few drugs, however, have been demonstrated to affect salivary function in controlled clinical studies. This apparent dis- parity may reflect the subjective sensation of oral dryness due to qualitative alterations of saliva rather than actual changes in the salivary flow rate. 10-12 The drugs most commonly reported to induce xerostomia are the tricyclic antidepressants, antipsychotics, benzodiazepines, atropin- ics, beta-blockers, antihistaminics, H 2 -receptor antago- nists, diuretics and angiotensin-converting enzyme inhib- itors, anti-HIV protease inhibitors, and omeprazole. 8,9 Dry mouth treatment requires an etiologic and/or symptomatic therapy. Etiologic therapy requires caus- ative recognition and management of conditions. In cases of drug-induced xerostomia, the intake of the drug causing the sensation of dryness should be inter- rupted and an alternative medication should be pre- a Department of Stomatology, Second University of Medicine and Surgery, Naples, Italy. b Department of Oral and Dental Science, University of Bristol, Bristol, UK. Received for publication Dec 25, 2010; returned for revision Jan 22, 2011; accepted for publication Jan 27, 2011. 1079-2104/$ - see front matter © 2011 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2011.01.039 e15
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of A comparison of salivary substitutes versus a natural sialogogue (citric acid) in patients...

A comparison of salivary substitutes versus a natural sialogogue(citric acid) in patients complaining of dry mouth as anadverse drug reaction: a clinical, randomized controlledstudyFelice Femiano, MDM, PhD,a Rosario Rullo, MDMDr,a Federica di Spirito, DDSDr,a
Alessandro Lanza, DDS, MScDr,a Vincenzo Maria Festa, DDS, MScDr,a andNicola Cirillo, DDS, PhD,b Naples, Italy; and Bristol, United KingdomSECOND UNIVERSITY OF MEDICINE AND SURGERY AND UNIVERSITY OF BRISTOL
Objective. We aimed to compare the efficacy of saliva substitutes and citric acid long-term therapy for oral drynessrelief and unstimulated salivary flow in patients reporting drug-induced xerostomia.Study design. Fifty-four patients reporting drug-induced xerostomia were randomly subdivided into 3 groups andrespectively administered artificial saliva, 3% citric acid, or distilled water in mouthwash 4 times a day for 30 days.Patients underwent measurement of unstimulated whole saliva before and after they finished therapy and were askedto note in a daily diary any symptomatologic changes 15 minutes and 1 hour after each daily intake of test solution.Results. Fifteen minutes after solution intake, 12 patients (67%) belonging to the artificial saliva group, 9 (50%) fromthe citric acid group, and 2 (11%) from the water group reported significant symptomatologic improvement. One hourafter solution intake, 7 patients (39%) from the artificial saliva group, 10 (56%) from the citric acid group, and 0 fromthe water group noted significant symptomatologic improvement. None of the drugs tested affected unstimulatedwhole saliva flow.Conclusions. Both artificial saliva and citric acid provided immediate relief from oral dryness. Citric acid alsoprovided a longer-lasting feeling of oral moistness at 1 hour after use owing to its protracted activity on salivary gland
function. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:e15-e20)The word “xerostomia” is derived from Greek. It comesfrom “xeros” (dry) and “stoma” (mouth), and is usuallyused to indicate the condition of not having enough salivato keep the mouth moist. The term “xerostomia,” how-ever, may properly be used to describe the subjectivesensation of dryness in the mouth reported by patients,whereas the more accurate term for measurable and ob-jectifiable changes in reduced salivary function is “sali-vary gland hypofunction” for a reduction in fluid outputand “salivary gland dysfunction” for a more general al-teration in physiologic salivary gland function.1-3
This semantic distinction is important, because a feel-ing of dry mouth is not always accompanied by an objec-tive decrease in the salivary flow. In fact, patients mayoccasionally report feelings of oral dryness, similar to asticky or doughy sensation, without any objective clinicalreduction being found.4,5 This would indicate that other
aDepartment of Stomatology, Second University of Medicine andSurgery, Naples, Italy.bDepartment of Oral and Dental Science, University of Bristol, Bristol, UK.Received for publication Dec 25, 2010; returned for revision Jan 22,2011; accepted for publication Jan 27, 2011.1079-2104/$ - see front matter© 2011 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2011.01.039factors can influence the feeling of moistness in themouth. Several short- and long-term conditions can dis-rupt salivary secretion, leading to hyposalivation. Theseinclude psychologic problems (stress and anxiety), auto-immune disease (Sjögren syndrome), and chemotherapyor radiotherapy of the head and neck.6-9 The feeling of drymouth is the most common oral adverse drug reaction inthe oral cavity. In fact, a large number of medications,�500, list dry mouth as an adverse effect. Relatively fewdrugs, however, have been demonstrated to affect salivaryfunction in controlled clinical studies. This apparent dis-parity may reflect the subjective sensation of oral drynessdue to qualitative alterations of saliva rather than actualchanges in the salivary flow rate.10-12 The drugs mostcommonly reported to induce xerostomia are the tricyclicantidepressants, antipsychotics, benzodiazepines, atropin-ics, beta-blockers, antihistaminics, H2-receptor antago-nists, diuretics and angiotensin-converting enzyme inhib-itors, anti-HIV protease inhibitors, and omeprazole.8,9
Dry mouth treatment requires an etiologic and/orsymptomatic therapy. Etiologic therapy requires caus-ative recognition and management of conditions. Incases of drug-induced xerostomia, the intake of thedrug causing the sensation of dryness should be inter-
rupted and an alternative medication should be pre-e15

OOOOEe16 Femiano et al. July 2011
scribed; when that is not possible, the dose should bereduced.13,14 Alternatively, a symptomatic pharmaco-logic treatment of xerostomia, based on saliva sub-stitutes (artificial saliva) in mouthwashes or in gelformulations (containing carboxymethyl cellulose orhydroxyethyl cellulose), oral moisturizers in sprays orgels (xylitol, maltitol, sorbitol, mannitol, aspartame,acesulfame K), and sialogogues (pharmacologic sali-vary production stimulants) should be considered.15
Which kind of symptomatic pharmacologic therapy(saliva substitutes, oral moisturizers, or sialogogues) touse essentially depends on the efficiency of the salivarygland parenchyma. Therefore, sialogogue prescriptionis justified only if functioning salivary tissue is avail-able, whereas moisturizing agents are to be adminis-tered, exclusively, in cases of compromised and unre-sponsive salivary gland parenchyma (e.g., severe casesof Sjogren syndrome).14
Sialogogue drugs, whether natural or artificial, stim-ulate the salivary glands by targeting the autonomicnervous system pathways. Citric acid, a natural sia-logogue that stimulates the taste buds through parasym-pathetic efferent pathways, and pilocarpine, bethanecol,and cevimeline, which act directly on specific musca-rinic cholinergic receptors within the salivary glandparenchyma, all stimulate abundant saliva secretion.Muscarinic agonists can be responsible for several sys-temic side effects, such as sweating, upset stomach,runny nose, flushes, chills, dizziness, weakness, fre-quent urination, and perspiration, and are, therefore,suitable only in the treatment of severe xerostomia (i.e.,Sjögren syndrome and other serious diseases, chemo-therapy, radiation treatment, etc.). In contrast, onlylocal but preventable side effects have been reported forcitric acid in mouthwash (e.g., erosion of tooth enamel),which makes it potentially safer than treatment withmuscarinic agonist drugs.12,16-24
The aim of the present study was to compare theefficacy of saliva substitutes that do not contain citricacid with that of a solution of 3% citric acid on thefeeling of dry mouth and on unstimulated saliva flowrates in patients taking drugs with documented negativeinfluence on salivary flow rate.
MATERIAL AND METHODSStudy design
For this trial, a group of physicians (group A) re-cruited patients, and different physicians (group B)evaluated the therapy and study outcomes.
A total of 78 patients complaining of a sensation ofdry mouth were clinically evaluated and asked to ab-stain from smoking, eating, and drinking for 1 hourbefore the measurement of their salivary flow. Un-
stimulated whole saliva (UWS) was collected for 5minutes by means of the spitting method, and stimu-lated whole saliva (SWS) was collected for 1 minuteafter using the paraffin stimulation technique for 5minutes. The whole saliva flow rate is expressed inmL/min. UWS flow �0.1 mL/min was considered sal-ivary hypofunction. Values �0.1 and �0.25 mL/minwere defined as slight dysfunction, and values �0.25mL/min were interpreted as a normal resting flow rate.SWS flow �0.7 mL/min indicated normal activity ofthe salivary glands. All patients were also asked toprovide a subjective assessment of their feeling ofdryness using 2 ranking scales (RS), both based on ascale of 0 to 4 points: one for the daily frequency of oraldryness (RS-A), rated as “never” (0), “hardly ever”(1),’“occasionally” (2), “fairly often” (3), and “veryoften” (4); and the other for the perceived intensity ofthe dry mouth sensation (RS-B), rated as being “ab-sent” (0), “slight” (1), “moderate” (2), “rather severe”(3), and of “maximum discomfort” (4). These valuesrepresented the patients’ baseline conditions.
Eligibility criteriaPatients satisfying the following criteria were con-
sidered to be suitable for the study:
1. They had experienced feelings of dry mouth for �7days with UWS values �0.1 and � 0.25 mL/min.
2. For �1 week before the start of the study they hadbeen taking a minimum of 2 drugs with documentedinduction of salivary gland hypofunction (e.g., anx-iolytics, anorexiants, antiasthmatics, anticholin-ergics, antidepressants, antiemetics, antihistamines,antihypertensives, antiparkinsonians, antipsychot-ics, decongestants, diuretics, and sedatives) and con-tinued taking them for the duration of the study(specialized consultation did not authorize anychange of drugs or modification of dose).
3. They complained of dry mouth with an RS score �3for both frequency (mode A) and intensity (mode B).
Patients were excluded if:
1. They had a history of systemic diseases explaining thediminished salivary flow (i.e., Sjogren syndrome, dia-betes mellitus, infection of the salivary glands, cancerpatients irradiated for head and neck cancer, anteced-ents of maxillofacial surgery with total or partial re-moval of major salivary glands, etc.).
2. Their SWS was �.7 mL/min, thus excluding pa-tients with potentially undiagnosed systemic diseasethat might influence salivary flow rates.
3. They complained of dry mouth with a normal sali-vary flow rate (UWS with values �.25 mL/min).
On the basis of these criteria, 24 patients were ex-
cluded from the study.
OOOOEVolume 112, Number 1 Femiano et al. e17
Study population, protocol, and outcomemeasures
Fifty-four patients were considered to be suitable forour study (32 women and 22 men; aged 51-78 years,mean 66 years). Each of the patients signed an in-formed consent form, and the procedures of this studywere in accordance with institutional and national eth-ical standards on human experimentation and the Hel-sinki Declaration of 1975 as revised in 2000. Possiblecarious lesions or dental erosions for all enrolled pa-tients were corrected before beginning the study.
Using random number–generator computer soft-ware, another operator (not a doctor) divided the pa-tients into 3 groups of 18 subjects each according togender, age, and drug types. Before the groups wererandomly divided, a number was assigned to each ther-apeutic protocol as prearranged for the 3 patient groups.This sequence of numbers was known only to investi-gator A, who administered the drugs for each group.Investigator A provided patients with mouthwash inidentical white containers, marked with numbers 1, 2,and 3, respectively, for the artificial saliva group (group1: 10 women and 8 men; mean age 68 years), the citricacid group (group 2: 11 women and 7 men; mean age65 years), and the distilled water group (group 3: 11women and 7 men; mean age 66 years).
All patients were given identical instructions, i.e., tokeep 5 mL of the administered solution in the mouth for30 seconds, 4 times daily for 30 days, 1 hour aftereating meals and brushing teeth. The patients in group1 received a salivary substitute (containing water, hy-droxypropyl cellulose, sorbitol, dipotassium chloride,sodium chloride, magnesium chloride, calcium chlo-ride, and potassium phosphate) with a neutral pH (�7)and were marked as the artificial saliva group. Thepatients in group 2 received a solution of citric acid (3%in essential water) with pH of �3.5 and were marked asthe citric acid group. The patients in group 3 receiveddistilled water with a pH of 7 and were marked as thewater group. All patients were instructed to note in adiary their sensations about the efficacy of the therapythey had undergone; this was to be done 4 times a dayfor 30 days, both 15 minutes and 1 hour after the 4 dailydrug intakes (giving a total of 8 daily records), using anRS-C based on a scale of 0 to 3 points for any changeof baseline symptomatology related to sensations of drymouth, defined as “worsening” (0), “unchanged” (1),“slight improvement” (2), and “significant improve-ment of dry mouth and feeling of oral moisture” (3). Allpatients were also encouraged to note in the diary anyother sensations they felt after intake of liquid test.
At the end of the study (30 days), all patients wereevaluated by investigator B, who was blinded to the form
of therapy given to each group, and UWS was measured1 hour after the last dose of therapy. Investigator B alsoreceived all patients’ daily diaries and calculated 2 nu-meric values per subject per day, representing the meanvalue of the 4 daily RS-C scores recorded by the patients15 minutes and 1 hour after the treatment.
The highest daily RS-C score for every liquid treat-ment (both 15 minutes and 1 hour after treatment) wascalculated, obtaining only 1 score value from the meanof 4 daily administrations and assigning, for 30 days, apossible total score of 90 corresponding with oral com-fort. A total score �70 was considered to be a signif-icant symptomatologic improvement of oral dryness, atotal score �40 but �70 a slight symptomatologicimprovement, a score �20 but �40 an unchanged orunmodified symptomatology, and a total score �20 asymptomatologic deterioration. At the end of the study,all patients received a dental examination of the softand hard tissues to determine any potential adverseeffects from the study therapy.
Statistical analysisThe data were analyzed using the 2-way analysis of
variance test by GraphPad Software to gain an under-standing of the efficacy of the solutions.
RESULTSThe medicaments used for our study were well toler-
ated, and no patient noted serious adverse effects in theirdiaries. The final dental examination of all patients did notreveal any soft or hard tissue lesions. Patients’ compliancewas optimal, and all 54 patients completed the study.
Table I reports the daily mean of RS-C scores of all thepatients, after 15 minutes and after 1 hour, and theirdistribution in relationship to the total score of 30 days’therapy.
After 15 minutes both salivary substitutes and 3%citric acid induce early relief from dryness in themouth
Figure 1 shows that after 15 minutes the mean RS-Cscore was highest in the artificial saliva group: 67.8(tertile range 69.3-80.7). A slightly lower mean RS-Cscore, 61.7 (tertile range 49.7-78.7), was observed forthe citric acid group, and the water group demonstratedthe lowest RS-C score, with a mean of 34.9 (tertilerange 26.7-36.7). Collectively, these data show a sig-nificant relief of oral dryness with the reappearance ofa feeling of oral moisture by both salivary substitutes(artificial saliva group vs. water group: P � .0001) andthe 3% citric acid solution (citric acid group vs. watergroup: P � .0001) at 15 minutes after the intake. Nosignificant difference was found between the artificialsaliva and the citric acid groups for overlapping effi-
cacy in oral dryness (P � .1320) (Table I).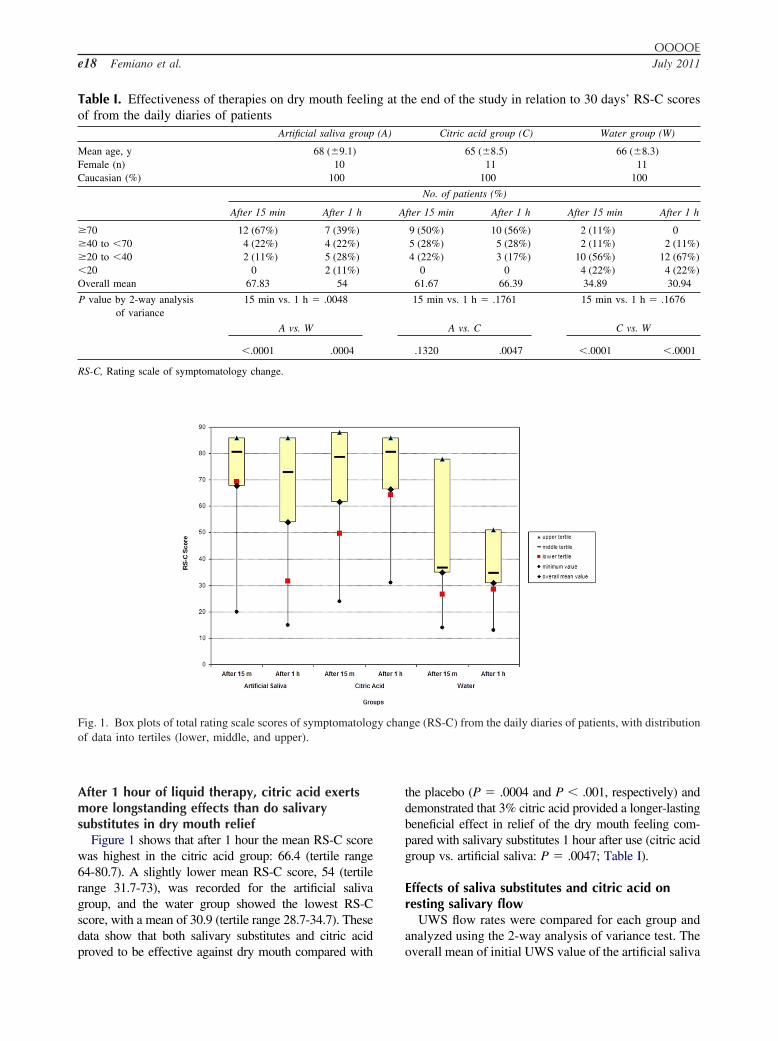
OOOOEe18 Femiano et al. July 2011
After 1 hour of liquid therapy, citric acid exertsmore longstanding effects than do salivarysubstitutes in dry mouth relief
Figure 1 shows that after 1 hour the mean RS-C scorewas highest in the citric acid group: 66.4 (tertile range64-80.7). A slightly lower mean RS-C score, 54 (tertilerange 31.7-73), was recorded for the artificial salivagroup, and the water group showed the lowest RS-Cscore, with a mean of 30.9 (tertile range 28.7-34.7). Thesedata show that both salivary substitutes and citric acid
Table I. Effectiveness of therapies on dry mouth feelinof from the daily diaries of patients
Artificial saliva group
Mean age, y 68 (�9.1)Female (n) 10Caucasian (%) 100
After 15 min After 1 h
�70 12 (67%) 7 (39%)�40 to �70 4 (22%) 4 (22%)�20 to �40 2 (11%) 5 (28%)�20 0 2 (11%)Overall mean 67.83 54
P value by 2-way analysisof variance
15 min vs. 1 h � .0048
A vs. W
�.0001 .0004
RS-C, Rating scale of symptomatology change.
Fig. 1. Box plots of total rating scale scores of symptomatologof data into tertiles (lower, middle, and upper).
proved to be effective against dry mouth compared with
the placebo (P � .0004 and P � .001, respectively) anddemonstrated that 3% citric acid provided a longer-lastingbeneficial effect in relief of the dry mouth feeling com-pared with salivary substitutes 1 hour after use (citric acidgroup vs. artificial saliva: P � .0047; Table I).
Effects of saliva substitutes and citric acid onresting salivary flow
UWS flow rates were compared for each group andanalyzed using the 2-way analysis of variance test. The
he end of the study in relation to 30 days’ RS-C scores
Citric acid group (C) Water group (W)
65 (�8.5) 66 (�8.3)11 11
100 100
No. of patients (%)
fter 15 min After 1 h After 15 min After 1 h
9 (50%) 10 (56%) 2 (11%) 05 (28%) 5 (28%) 2 (11%) 2 (11%)4 (22%) 3 (17%) 10 (56%) 12 (67%)
0 0 4 (22%) 4 (22%)61.67 66.39 34.89 30.94
15 min vs. 1 h � .1761 15 min vs. 1 h � .1676
A vs. C C vs. W
.1320 .0047 �.0001 �.0001
ge (RS-C) from the daily diaries of patients, with distribution
g at t
(A)
A
y chan
overall mean of initial UWS value of the artificial saliva

OOOOEVolume 112, Number 1 Femiano et al. e19
group (0.14 mL/min) was compared with the finalUWS value (0.18 mL/min), showing P � .1100. Theoverall mean of initial UWS value of the citric acidgroup (0.15 mL/min) was compared with final UWSvalue (0.16 mL/min), showing P � .1355. The overallmean of initial UWS value of the water group (0.14mL/min) was compared with final UWS value (0.15mL/min), showing P � .5425. These results indicate, aspredicted, that neither the 3% citric acid nor the salivasubstitutes affect the UWS flow rate.
DISCUSSIONA recent clinical study conducted by Eliasson et al.
(2009)26 showed a strong association between minor pal-atal and labial salivary gland secretion rates and subjectiveoral dryness. A decrease in the salivary film retained on,and moistening, the oral surfaces appears to be an essen-tial element in oral discomfort in this context, and itsreduction is related to a worsening of the feeling of dry-ness.15,25,26 This could explain the current conflicting re-ports, often leading to mistaking a dry mouth feeling forhyposalivation due to a hypofunctioning salivary gland,validating the hypothesis that the sensation of moisteningin the mouth is not so much related to the quantity ofliquid within the mouth but rather to the moistness of theoral mucosal surfaces.27-36
We examined the efficacy of salivary substitutesversus 3% citric acid in patients complaining of oraldryness for slight salivary gland hypofunction (UWSvalues �0.1 and �0.25 mL/min) that was drug inducedwithout alteration in SWS (i.e., �0.7 mL/min). In thistrial, participants with more severe salivary gland hy-pofunction (UWS values �0.1 mL/min) and with SWS�0.7 mL/min, who may have prejudiced the sialogogueefficacy of citric acid, were excluded. Our findingsshow that both salivary substitutes and citric acid in-duce an immediate and significant symptomatologicimprovement in the feeling of dry mouth 15 minutesafter solution use (Fig. 1; Table I). This finding is inaccordance with data presented by Silvestre et al.(2009),32 who administered artificial saliva as a spray to37 patients complaining of dry mouth, 20 of whomshowed an almost immediate improvement after appli-cation. Moreover, we found that the use of 3% citricacid provides a prolonged and significant symptomat-ologic improvement 1 hour after its intake (10 patients(56%) with score �70) compared with the use of arti-ficial saliva (7 patients (39%) with a score �70; P �.0047). This longer-lasting efficacy of 3% citric couldbe the consequence of the stimulation of both major andminor salivary glands and an increase in the rate ofwhole salivary flow and the formation of salivary film
upon the oral mucosa.UWS represented a second parameter evaluated afterthe intake of the solutions. Comparison of the initial UWSflow rate values (collected for each group before the startof treatment) and the final UWS flow rate values (col-lected for each group 1 hour after the last tested drugtreatment) showed no significant difference in any group.These overlapping initial and final UWS flow rate values,reflecting the inefficacy of the tested liquids on UWSenhancement, were predictable for water and artificialsaliva, and for patients in the citric acid group the ineffi-cacy could be related to the negative influence of xeros-tomia-inducing drugs themselves on the salivary glandparenchyma, which did not permit sufficient gland acti-vation. Interestingly, drug-induced xerostomia is mainlyreported by elderly patients on polypharmacy therapy,with a reduction of the baseline resting salivary flow ratebut not of the stimulated saliva secretion (i.e., food orsalivary flow rate testing with citric acid stimulation).15,37
Drug-induced xerostomia therapy requires replacement orat least a reduced dosage of the responsible drug. If this isnot possible, symptomatic treatment based on salivaryproduction stimulants (sialogogues) or moisturizingagents (saliva substitutes) are recommended. Becausecholinergic sialogogues are potentially responsible formuscarinic adverse drug reactions, they are used selec-tively for advanced salivary gland hypofunction. Incontrast, natural sialogogues, such as 3% citric acid, arepreferred in less advanced cases or as supplementaltherapy because of their minor side effects.
Clinicians should be aware that long-term use of 3%citric acid in mouthwash can cause oral adverse effects,i.e., dental hypersensibility and erosion, due to the demin-eralization of dental hard tissues from salivary pH reduc-tion (3.5-3.0). However, when an acid enters the mouth,whether from an intrinsic or extrinsic source, salivary flowrate normally increases, along with the pH and buffercapacity. Within minutes, the acid is neutralized andcleared from the oral cavity and the pH returns to normal.In the presence of xerostomia the oral intake of citric acid,when not counteracted, can lower salivary pH. Our re-search found no dental erosion among patients in the citricacid group at the final appointment, which may be relatedto both the short time of contact with citric acid in themouth (30 seconds) and insufficient study time (30 days).The use of citric acid in mouthwash for long periodsrequires continuous dental monitoring and some essentialbehavioral recommendations, such as restricting the timeof contact with the tooth surface, not brushing teeth for atleast 1 hour after taking the citric acid, limiting or elimi-nating other substances responsible for dental erosionfrom the diet (i.e., spicy or acidic foods, soft drinks,alcoholic beverages, fizzy mineral water, fruit juice, etc.),and rinsing with a mouthwash of sodium bicarbonate in
water to raise the oral pH. Additionally, we recommend
OOOOEe20 Femiano et al. July 2011
the use of calcium phosphates and fluorides to promotedental remineralization to counteract citric acid dentalerosion.38 On the basis of the results of our study, forpatients complaining of drug-induced xerostomia withpreservation of responsive salivary gland parenchyma, werecommend a long-term therapy using a mouthwash con-taining both a salivary substitute and citric acid in solutionfor combined immediate and long-lasting relief, in addi-tion to the use of a remineralizing products and consistentperiodic dental monitoring.
REFERENCES1. Nederfors T. Xerostomia and hyposalivation. Adv Dent Res
2000;14:48-56.2. Gonsalves WC, Wrightson AS, Henry RG. Common oral con-
ditions in older persons. Am Fam Physician 2008;78:845-52.3. Eveson JW. Xerostomia. Periodontol 2000 2008;48:85-91.4. Gallardo JM. Xerostomia: etiology, diagnosis and treatment. Rev
Med Inst Mex Seguro Soc 2008;46:109-16.5. Turner MD, Ship JA. Dry mouth and its effects on the oral health
of elderly people. J Am Dent Assoc 2008;139:252-3.6. Mouly S, Salom M, Tillet Y, Coudert AC, Oberli F, Preshaw
PM, et al. Management of xerostomia in older patients: a ran-domised controlled trial evaluating the efficacy of a new orallubricant solution. Drugs Aging 2007;24:957-65.
7. Sreebny LM, Schwartz SS. A reference guide to drugs and drymouth. Gerodontology 1997;14:33-47.
8. Moore PA, Guggenheimer J. Medication-induced hyposaliva-tion: etiology, diagnosis, and treatment. Compend Contin EducDent 2008;29:50-5.
9. Femiano F, Lanza A, Buonaiuto C, Gombos F, Rullo R, Festa V,et al. Oral manifestations of adverse drug reactions: guidelines. JEur Acad Dermatol Venereol 2008;22:681-91.
10. Ben-Aryeh H, Miron D, Berdicevsky I, Szargel R, Gutman D.Xerostomia in the elderly: prevalence, diagnosis, complicationsand treatment. Gerodontology 1985;4:77-82.
11. Thomson WM. Issues in the epidemiological investigation of drymouth. Gerodontology 2005;22:65-76.
12. Scully C. Drug effects on salivary glands: dry mouth. Oral Dis2003;9:165-76.
13. Fox PC. Xerostomia: recognition and management. Dent Assist2008;77:44-8.
14. Gil-Montoya JA, Guardia-López I, González-Moles MA. Eval-uation of the clinical efficacy of a mouthwash and oral gelcontaining the antimicrobial proteins lactoperoxidase, lysozymeand lactoferrin in elderly patients with dry mouth—a pilot study.Gerodontology 2008;25:3-9.
15. Zunt S. Evaluation of the dry mouth patient. Alpha Omegan2007;100:203-9.
16. Aframian DJ, Helcer M, Livni D, Robinson SD, Markitziu A,Nadler C. Pilocarpine treatment in a mixed cohort of xerostomicpatients. Oral Dis 2007;13:88-92.
17. Wolff A, Zuk-Paz L, Kaplan I. Major salivary gland outputdiffers between users and nonusers of specific medication cate-gories. Gerodontology 2008;25:210-6.
18. Oh DJ, Lee JY, Kim YK, Kho HS. Effects of carboxymethyl-cellulose (CMC)–based artificial saliva in patients with xerosto-mia. Int J Oral Maxillofac Surg 2008;37:1027-31.
19. Curro FA. Gum chewing as an adjunct to use of medications.
J Am Dent Assoc 2008;139.20. Gravenmade EJ, Vissink A, Panders AK, Vermey A. Artificialsaliva in the management of patients suffering from xerostomia.Gerodontology 1984;3:243-50.
21. Ship JA, McCutcheon JA, Spivakovsky S, Kerr AR. Safety andeffectiveness of topical dry mouth products containing olive oil,betaine, and xylitol in reducing xerostomia for polypharmacy-induced dry mouth. J Oral Rehabil 2007;34:724-32.
22. Peker I, Alkurt MT, Usalan G. Clinical evaluation of medicationson oral and dental health. Int Dent J 2008;58:218-22.
23. Márton K, Madléna M, Bánóczy J, Varga G, Fejérdy P, SreebnyLM, et al. Unstimulated whole saliva flow rate in relation to siccasymptoms in Hungary. Oral Dis 2008;14:472-7.
24. Kaplan I, Zuk-Paz L, Wolff A. Association between salivaryflow rates, oral symptoms, and oral mucosal status. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2008;106:235-41.
25. Wick JY. Xerostomia: causes and treatment. Consult Pharmazie2007;22:985-92.
26. Eliasson L, Birkhed D, Carlén A. Feeling of dry mouth inrelation to whole and minor gland saliva secretion rate. Arch OralBiol 2009;54:263-7.
27. Hedner E, Birkhed D, Hedner J, Ekström J, Helander HF. Stim-ulation of minor salivary glands by intraoral treatment with thecholinesterase inhibitor physostigmine in man. Eur J Oral Sci2001;109:371-4.
28. Carlson GW. The salivary glands. Embryology, anatomy, andsurgical applications. Surg Clin North Am 2000;80:261-73.
29. Gerdin EW, Einarson S, Jonsson M, Aronsson K, Johansson I.Impact of dry mouth conditions on oral health–related quality oflife in older people. Gerodontology 2005;22:219-26.
30. Nagy K, Urban E, Fazekas O, Thurzo L, Nagy E. Controlledstudy of lactoperoxidase gel on oral flora and saliva in irradiatedpatients with oral cancer. J Craniofac Surg 2007;18:1157-64.
31. Turner M, Jahangiri L, Ship JA. Hyposalivation, xerostomia andthe complete denture: a systematic review. J Am Dent Assoc2008;139:146-50.
32. Silvestre FJ, Minguez MP, Suñe-Negre JM. Clinical evaluationof a new artificial saliva in spray form for patients with drymouth. Med Oral Patol Oral Cir Bucal 2009;14:8-11.
33. Longman LP, McCracken CF, Higham SM, Field EA. Theclinical assessment of oral dryness is a significant predictor ofsalivary gland hypofunction. Oral Dis 2000;6:366-70.
34. Suh KI, Lee JY, Chung JW, Kim YK, Kho HS. Relationshipbetween salivary flow rate and clinical symptoms and behavioursin patients with dry mouth. J Oral Rehabil 2007;34:739-44.
35. Thelin WR, Brennan MT, Lockhart PB, Singh ML, Fox PC,Papas AS, et al. The oral mucosa as a therapeutic target forxerostomia. Oral Dis 2008;7:683-89.
36. Mese H, Matsuo R. Salivary secretion, taste and hyposalivation.J Oral Rehabil 2007;34:711-23.
37. Durán V, Domínguez P, Morales I, López RO. Kinetic assess-ment of salivary secretory response to citric acid. Differenceswith pilocarpine. Rev Med Chil 1998;126:1330-7.
38. Meyer-Lueckel H, Tschoppe P, Kielbassa AM. Linseed basedsaliva substitutes and their effect on mineral dissolution of pre-demineralized bovine dentin in vitro. J Dent 2006;34:751-6.
Reprint requests:Dr. Felice FemianoVia Francesco Girardi 2S. Antimo (NA) 80029Italy
[email protected]



















