
a comparison of a combination of physical exercise and placebo
138
1 A COMPARISON OF A COMBINATION OF PHYSICAL EXERCISE AND PLACEBO WITH PHYSICAL EXERCISE AND GINSENG IN THE TREATMENT OF ERECTILE DYSFUNCTION IN MARRIED MEN ATTENDING GENERAL OUT PATIENT CLINIC AND UROLOGY CLINIC, JOS UNIVERSITY TEACHING HOSPITAL, JOS BY DR BAKZAK ISAAC BULUS (MBBS, UNIJOS, JOS, 2006) A DISSERTATION SUBMITTED TO NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA (NPMCN) IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF FELLOWSHIP OF THE COLLEGE IN FAMILY MEDICINE (FMCFM) DEPARTMENT OF FAMILY MEDICINE, JOS UNIVERSITY TEACHING HOSPITAL JOS NIGERIA MAY, 2017
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of a comparison of a combination of physical exercise and placebo

1
A COMPARISON OF A COMBINATION OF PHYSICAL EXERCISE AND PLACEBO
WITH PHYSICAL EXERCISE AND GINSENG IN THE TREATMENT OF ERECTILE
DYSFUNCTION IN MARRIED MEN ATTENDING GENERAL OUT PATIENT CLINIC
AND UROLOGY CLINIC, JOS UNIVERSITY TEACHING HOSPITAL,
JOS
BY
DR BAKZAK ISAAC BULUS
(MBBS, UNIJOS, JOS, 2006)
A DISSERTATION SUBMITTED TO NATIONAL POSTGRADUATE MEDICAL
COLLEGE OF NIGERIA (NPMCN) IN PARTIAL FULFILMENT OF THE
REQUIREMENTS FOR THE AWARD OF FELLOWSHIP OF THE COLLEGE IN
FAMILY MEDICINE (FMCFM)
DEPARTMENT OF FAMILY MEDICINE,
JOS UNIVERSITY TEACHING HOSPITAL
JOS NIGERIA
MAY, 2017

2
DECLARATION
I hereby declare that this work is original and has not been submitted to any college for award of
fellowship or any university for award of degree. It has not been submitted elsewhere for journal
publication
___________________________________
DR. BAKZAK ISAAC BULUS
DATE _____________________________

3
CERTIFICATION
This research work was carried out by Dr Bakzak Isaac Bulus under our supervision. We also
supervised the writing of the dissertation.
SUPERVISORS:
1. Signature ________________ Date _____________________
Dr Lar N Nimkong (FMCGP)
Consultant family physician
Department of Family Medicine
Jos University Teaching Hospital, Jos Nigeria.
2. Signature ________________ Date ______________________
Dr Longmut Remen (FMCGP)
Consultant Family Physician
Department of Family Medicine
Jos University Teaching Hospital, Jos Nigeria.
HEAD OF DEPARTMENT
Signature __________________ Date ______________________
Dr Patricia Agaba (FWACP, FMCGP)
Consultant Family Physician and Head
Department of Family Medicine
Jos University Teaching Hospital,
Jos Nigeria.
4
DEDICATION
This book is dedicated to my God, my parents and my wife Nanbwet for the inspiration and
encouragement received in the course of this work.

5
ACKNOWLEDGEMENT
I want to acknowledge first and foremost my Lord and Saviour Jesus Christ for giving me the
strength and enablement to pursue this goal. It was because of his love, guidance and protection
that i was able to complete this work.
I am highly indebted to my supervisors Drs Lar and Longmut for guiding me through this part of
my training and their unending support.
I am also grateful to Drs Pitmang, Sule Joshua, Jonathan and professor Dakum for helping me
read through and make corrections in this book.
I want to thank all the consultants and residents of the departments of Family Medicine and
Urology of JUTH for their encouragement and support during this study. I have been encouraged
and blessed with the pleasure of working with each of you.
Thank you Drs Turshak and Abimuku for helping me in the analysis, Nenpalang, Maijida and
Madina Mohammed for helping me print this work.
I am also grateful to my support staff Mrs Chitau and Kyauta for their unrelenting love and
support that encouraged me to complete this work.
I am also grateful to my friends, staff of Sendi Hospital for helping me with stationaries,
encouragement and prayers that helped me to get to this day.
Finally, to my star and beacon of hope, my dear wife Nanbwet and my children Bwetsun,
Pandok and Africa for their unrelenting love, support and understanding through the period of
this research, thanks for the support

6
TABLE OF CONTENTS
Title page --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---- ----- i
Declaration --- --- --- --- --- --- --- --- --- --- --- --- --- -- ii
Dedication --- --- --- --- --- --- --- --- --- --- --- --- --- - ---- ----- iii
Acknowledgement --- --- --- --- --- --- --- --- --- --- --- ---- --- --- iv
Certification --- --- --- --- --- --- --- --- --- --- --- --- --- ---- ----- v
Table of contents --- --- --- --- --- --- --- --- --- --- --- --- ---- ------ vi-ix
List of figures --- --- --- --- --- --- --- --- --- --- --- --- -- ------- x
List of tables --- --- --- --- --- --- --- --- --- --- --- --- -- - ----- xi
List of abbreviations --- --- --- --- --- --- -- ---- ---- --- --- --- xii-xiv
Summary --- --- --- --- --- --- --- --- --- --- ---- --- --- --- ----- 1
CHAPTER ONE
1.1 Introduction - - - - - - - - 3
1.2 Statement of Problem - - - - - - - 9
1.3 Aim and Objectives of Study - - - - - - 10
1.4 Justification/ Relevance of the study to Family Medicine - - 10
CHAPTER TWO: Literature Review
2.1 Overview of erectile dysfunction - - - - - - 13
2.2 Epidemiology of erectile dysfunction - - - - - 16
2.3 Risk factor of erectile dysfunction - - - - 18

7
2.4 Anatomy and Pathophysiology of erectile dysfunction - - - 23
2.5 Classification of erectile dysfunction - - - - - 26
2.6 Assessment of patients with erectile dysfunction - - - - 28
2.7 Erectile dysfunction scores - - - - - 30
2.8 Severity of Erectile Dysfuntion - - - - - 33
2.9 Investigations of erectile dysfunction - - - - - 34
2.10 Treatment of Erectile Dysfunction - - - - 35
2.10.1 Pharmacological treatment - - - - - - - 36
2.10.2 Non pharmacological treatment - - - - - 37
2.10.3 Physical exercise- - - - - - - - - - - 39
2.10.3 Complementary and alternative medicine - - - - - - - 43
2.10.4.1Red Korean Ginseng - - - - - - - 46
2.10.4.2 Side Effects of Ginseng - - - - - - - - - 49
CHAPTER THREE: Methodology
3.1 Study area - - - - - - - - - 53
3.2 Study Population - - - - - - - - 54
3.3 Study period - - - - - - - - 54
3.4 Eligibility - - - - - - - - - 54

8
3.5 Sample size determination - - - - - - 55
3.6 Ethical consideration - - - - - - - 56
3.7 Instrument of data collection - - - - - - 56
3.8 Study designs - - - - - - - - 57
3.9 Statistical Analysis - - - - - - - 62
CHAPTER FOUR: Results
4.1 Baseline characteristics - - - - - - - 65
4.2 Medical characteristics - - - - - - - 67
4.3 Erectile dysfunction scores and side effects - - - - 74
CHAPTER FIVE: Discussion
5.1 Socio-demographic Characteristics - - - - - - - - - 81
5.2 Medical Characteristics - - - - - - - - - 81
5.3 Effectiveness of Ginseng on Erectile Dysfunction - - - - 84
5.4 Severity of Erectile Dysfunction - - - - - - 87
5.5 Ginseng Side Effects - - - - - - - 88
5.6 Relationship Between Clinical Characteristics and ED scores- - 89
5.7 Conclusion - - - - - - - - - 90
5.8 Recommendations - - - - - - - 90
9
5.9 Strength of the Study - - - - - - - 91
5.10 Limitations of the study - - - - - - - 91
5.11 Implication of the Study to Family Medicine - - - - 91
5.12 Suggestion for further studies - - - - - 92
REFERENCES - - - - - - - 93
LIST OFABBREVIATIONS/SYMBOLS
95% CI 95% confidence interval
% Percentage
/ Per
< Less than
≤ Less than or equal to
= Equal to
˃ Greater than
≥ Greater than or equal to
BMI Body Mass Index
CAM Complementary and alternative medicine
CBT Cognitive Behavioral Therapy
CDC Center for Disease Control and prevention
COX-2 Cyclo-Oxygenase enzyme 2
DSM-5 Diagnostic and Statistical manual Version 5
ED Erectile Dysfunction

10
ECG Electrocardiography
cGMP Cyclic Guanosine Monophosphate
ESR Erythrocyte Sedimentation Rate
g/dl gram(s) per deciliter
g/L grams(s) per litre
FBG Fasting Blood Glucose
FITT Frequency, Intensity, Type and Time
GABA Gaba Amino Butyric Acid
GAQ Global Assessment Questionaire
GOPD General Out-patient Department
GOPC General Out-patient Clinic
HA Hyaluronic Acid
HHR Heart Rate Researve
HRQoL Health Related Quality of Life
IIEF International Index of Erectile Function
JUTH Jos University Teaching Hospital
Kca Calcium Activated Potasium Channels
Kg Kilogram
MAOI Mono Amine Oxidase Inhibitors
MHR Maximum Heart Rate
Mm Millimeter (s)
M Meter (s)
MUSE Medicated Urethral System of Erections
No. Number
11
NPT Non-pharmacological Treatment
NICE National Institute for Health and Clinical Excellence
NSAIDs Non-Steroidal Anti-inflammatory Drugs
P P-value
PAIR Psychological And Interpersonal Relationship Scale
PCS Physical Component Summary
PHC Primary Health Care
PDE Phosphodiesterase Inhibitors
PTSD Post Traumatic Stress Disorders
QoL Quality of Life
RCTs Randomized Controlled Trials
RHR Resting Heart Rate
SEAR Self Esteem And Relationship
SEP Sexual Encounter Profile
SD Standard Deviation
SHBG Sex Hormone Binding Globuline
SF-36 Short Form-36
SPSS Statistical Package for Social Sciences
SSRI Selective Serotonine Receptor Inhibitors
T t-value
TCAs Tricyclic Antidepressants
US United States
VEGF Vascular Endothelial Growth Factor
WHO World Health Organization

12
WONCA World Organization of National Colleges, Academies,
and
Academic Associations of General Practioners /Family
Physicians
LIST OF FIGURES
Figure 2.1: The multi-factoral causes of erectile dysfunction --- --- --- --- ---23
Figure 2.2: Mechanism of erectile dysfunction --- --- --- --- --- --- --- --- --- 26
Figure 2.3: Algorithm for diagnosis and treatment of erectile dysfunction – 51
Figure 4.1: Study protocol --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 62
Figure 4.2: Complain on erectile dysfunction--- --- --- --- --- --- --- --- --- --- -67
Figure 4.3: Spouse presentation--- --- --- --- --- --- --- --- --- --- --- --- --- --- -68
Figure 4.4: Side effect of ginseng after treatment --- --- --- --- --- --- --- --- --79
Figure 4.5: Types of Side effect experience after treatment--- --- --- --- - -- 80
LIST OF TABLES
Table 2.1: classification of erectile dysfunction--- --- --- --- --- --- --- ---27
Table 4.1: Socio – demographic characteristics --- --- --- --- --- --- --- --- 65
Table 4.2 Medication used among the study participants --- --- --- --- --- 69
Table 4.3: Risk factors of erectile dysfunction --- --- --- --- --- --- --- --- 70
Table 4.4: Investigations results and examination findings--- --- --- --- - 72
Table 4.5: Erectile dysfunction scores at best line --- --- --- --- --- --- --- 74
Table 4.6: Erectile dysfunction scores post intervention --- --- --- --- --- 76
Table 4.7 Percentage difference in EF at baseline and post intervention—78
13
APPENDICES
1. JUTH ethical clearance I- - - - - - -- 107
2. Approval from National Postgraduate Medical College of Nigeria. I -- 108
3. Assessment of Synopsis of Desartation III - - - - - - 109
4. Consent form (English ) IV - - - - - - -- 110
5. Consent form (Hausa) V - - - - - - - --111
6. Study Questionnaires (English) VI - - - - - -- 112-114
7. Study questionnaires (Hausa) VII - - - - - - - -- 115-117
8. International index of erectile function questionnaire (English) VIII - --118
9. International index of erectile function questionnaire (Hausa) IX - - --- 119
10. Patient encounter form --- --- - - - - - - - - - - - - --120
11. IIEF Questionnaire - - - - - - - - - - - - 121-124
12. IIEF Q uestionaire - - - - - - - - - - - - ---125-127
13. Follow up Questionaire - - - - - - - - - - - -128
14
SUMMARY
BACKGROUND: Erectile dysfunction (ED) has been in existence for many years with majority
of those affected using complementary and alternative medicine for its treatment. Prevalence of
erective dysfunction has been on the increase due to increase in number of its risk factors such as
increase in number of the aging population, hypertension, diabetes, alcohol consumption and
cigarettes smoking.
ED has resulted to a lot of family problems such as marriage separation, family dysfunction and
even divorce, many of which the causes may not be known because of the difficulty in
expressing these problems. This study compared the effectiveness of exercise and ginseng with
exercise and placebo in the treatment of erectile dysfunction. The severity and pattern of ED
among the study population were determined with side effects of Ginseng.
METHOD: The study was a randomized controlled single blinded comparative study among
190 participants within the ages of 25 and 70 years who presented at GOPC and Urology clinic
of Jos University Teaching Hospital (JUTH). They were recruited consecutively as they came
into the clinic, the IIEF was applied and the patients were randomized using simple random
sampling method. Ninety five (95) participants each were randomly allocated into the control
and the intervention group using sealed opaque envelopes. The intervention group took 50mg of
ginseng extract daily plus exercise while the control group were on placebo daily plus physical
exercise for eight weeks. Ninety three from each group completed the study with two (2)
participants from each group lost to follow up.
RESULTS: The mean age of the subjects who participated in the study was 41.7 years .The
standard deviation was 55.6±12 years. The major risk factors of erectile dysfunction identified
15
among the participants were hypertension, alcohol consumption and medications for diabetes and
hypertension. The ED scores at baseline was 7(3.8%) in the intervention group compared to
10(5.4%) in the control group. After treatment 33(17.7%) of the participants in the intervention
group had mild ED compared to 16(8.6%) in the control group. The participants whose erectile
function became normal was 14(7.5%) in the intervention group compared to 2(1.1%) in the
control group after intervention. Majority 71(38.2%) of the participants in both groups had mild
to moderate ED. The proportion of the participants in the intervention groups who had mild side
effects was 34(5%). The commonest side effects were insomnia (50%), breast pain (25%) and
gum swelling (25%).
Conclusion: Ginseng showed significant improvement in erectile dysfunction with minimal side
effects in participants with mild (p=0.03) and moderate (p=0.04) ED. Majority of the
participants had mild to moderate ED. Therefore Ginseng may be integrated in management
protocol for erectile dysfunction which may in-turn reduce ED prevalence in Nigeria.
CHAPTER ONE

16
1.1 INTRODUCTION
Reproductive health is a state of complete physical, mental and social well-being and not merely
the absence of disease or infirmity in all matters relating to reproductive system, functions and
processes.1This implies that people are able to have a responsible satisfying and safer sex life and
also to have a capability to reproduce and the freedom to decide if, when and how to do so.1,2
Reproductive and sexual health problems account for 14% of global burden of ill health for men
between the ages of 35 and 70 years.2 Erectile dysfunction occurs in about 14% of men at 50
years, 17% at 60 years, and 47% at 75years and above.3 Transient and inadequate erection affect
as many as 50% of men between 40 and 50 years.3
Sex and reproduction have rights that are enshrined in many conventions, agreements, laws and
declarations which produce framework within which sexual and reproductive wellbeing can be
achieved.4
Sexual health is a state of physical, mental and social well-being in relation to sexuality and not
the mere absence of disease and infirmity.2 This requires positive and respectful approach to
sexuality and sexual relationship, as well as possibility of having pleasurable and safe sexual
experience free from coercion, discrimination and violence.3
Many of the patients that family physicians see have sexual problems, majority will not be
comfortable to ask questions about their sexual problems, while some will ask indirectly or
through humour or with great personal discomfort.5
Some patients have physical complaints that have psychological basis which can lead to sexual
problems.1Sexual functions and frequency of sexual intercourse have a tendency to decrease with
age while the prevalence of sexual dysfunction increases.6

17
Erectile dysfunction is a topic of considerable importance to men’s health.7 It is increasingly
being recognized as a comorbid condition in men with some diseases such as cardiovascular
diseases and diabetes mellitus.7
Erectile dysfunction is defined as the persistent inability to achieve or maintain an erection
adequate for satisfactory sexual intercourse for at least three months.8 It is a global problem
affecting all communities though not always talked about. It is the most common sexual
problems in men and affects about one third of men throughout their life time prompting them to
seek medical help they ordinarily would not have since it has been a serious problem and a focus
of attention by the general public in recent times.9,10
The burden of ED is as high as up to 30 million persons in the United State of America despite
the availability of effective oral medications for this condition. It is a form of sexual arousal
disorder which reportedly causes distress to both patients and their spouses.11 Erectile
dysfunction is usually underestimated in many under developed world including Nigeria.12,13
Data on erectile dysfunction in Nigeria is limited, but a study done in south west Nigeria found
that about 46.9% of patients between the ages of 20 and 70 years have erectile dysfunction.14 The
Prevalence showed that 28% of erectile dysfunction was found between the ages of 30 and 49
years, 40% between 40 and 69 years and 54% in those above 70 years.14 This shows that erectile
dysfunction increases with age and a menace to our society, causing negative impact on self-
esteem, relationships and quality of life.10 Erectile dysfunction affects about 100 million men
worldwide especially those with diabetes which also increases with age.15 In Saudi Arabia and
Amman, the incidence is 30% and 60% respectively.16Although about 10% of men within the
ages of 40 and 70 years have severe erectile dysfunction, only few of them seek medical
attention.17
18
Erectile dysfunction, called impotence in the past, is a very common condition and varies with
severity, some men have total inability to achieve erection, some have inconsistent ability to
achieve erection (moderate), while others can sustain only brief erection (mild).18
The severity of erectile dysfunction appeared to be stronger in younger men when adjusted to
only age as risk factors.18 The variation in severity of erectile dysfunction makes estimating its
frequency difficult, even though the frequency of nocturnal erections and intercourse decreases
whereas the prevalence of erectile dysfunction increases with age.6 Majority (60%) of the elderly
people have interest in maintaining their sexual function.19
Many men are reluctant to discuss erectile dysfunction with their doctors, thus the condition is
usually undiagnosed.2,19 Many family physicians see quite a number of sexual problems, many of
which are erectile dysfunction yet physicians are reluctant to address this problem largely due to
time constraints, feeling ill prepared, embarrassments, limited knowledge on the topic, cultural
and religious beliefs and that the topic is not relevant to the chief complaints.2 Majority of the
people with erectile dysfunction will not be able to talk about it due to cultural and religious
reasons therefore our response to it can affect them positively or negatively.2
The economic impact of erectile dysfunction can be classified into direct and indirect cost.10 The
direct cost includes physical evaluation, pharmacotherapy and diagnostic testing while indirect
cost include loss of time at work, lost productivity and effect on the partner, family and
coworkers.10
The first line management of erectile dysfunction involved risk factor reduction and oral
medications. Second line management include; Surgical management such as (i) Alprostidil:
This can be administered either intra-carvernosaly (better) or intra-urethral and titrated to an
adequate erectile response. (ii) Vacuum pump device. (iii) Penile prostheses-usually done with
the help of a urologist.10

19
Cognitive behavioral therapy (CBT) is another form of treatment aimed at improving
relationships with subsequent improvement in erectile dysfunction especially when there are no
obvious causes, then psychosocial factors should be explored.10 The potential clues to these
factors include; the ability to achieve normal erections and subsequently orgasm via
masturbation or sex with a different partner.20
Patients often use complementary and alternative medicine in the treatment of erectile
dysfunction aside orthodox medicines.21 Common methods include acupuncture, ginseng, maca,
yohimbin, Dihydroepiandrosterone, Arginine, Coleus, Damiana, Gingko and alpha lipoic acid
which is particularly suited for the treatment and prevention of diabetic complications including
erectile dysfunctions.21 Sex is a two way relationship, therefore erectile dysfunction affects both
the man and the woman depending on the behaviors and the reactions of the man to the
problem.21 These reactions may vary from negative attitudes, dissatisfaction with the problem,
taking no action or ignoring the problem which may end up with breakdown of the role of the
husband leading to family dysfunction.21
The full acknowledgement of the problem and good discussion of the problem is very vital in
seeking professional help.21Alternative treatment of this condition includes Korean Ginseng
which have been reported to improve erections.10
Ginseng is one of the eleven species of slow growing perennial plants with fleshy roots,
belonging to the genus panax of the family araliaceae.18,22 It is commonly found in cooler
climates such as northern hemisphere (North America and eastern Asia). Ginseng is typically
classified into two namely; (a) Asian ginseng: commonly found in Asia, it is further sub
classified into five types namely: Red ginseng which is usually unpeeled (harvested six years and
above), fresh ginseng (harvested less than four years old), white ginseng (harvested less than six

20
years old) – dried and peeled.21,22 Others are sun ginseng and wild ginseng. (b) American
ginseng (p. quinquefloius).21,22,23
Panax Ginseng is typically promoted for the treatment and protection of the following diseases;
anxiety, asthma, cancer, chronic fatigue syndrome, diabetes mellitus, depression, erectile
dysfunction, fever, fibromyalgia, headache, insomnia and stress.18,21 It is also used to slow down
ageing process, enhance memory, stimulate immune system and improved sports
performance.18,21
Most ginsengs are from roots and rarely from the leaf because the roots are more effective.23
Panax (all healing) Ginseng is available in different forms such as tinctures, liquid extracts,
powder and capsules.23
Ginseng appears to be non-toxic when used in both short and long term and reported side effects
are rare.23 Ginseng is used by many cultures as a remedy for erectile dysfunction,23 the reason for
this study therefore, proper identification and management of erectile dysfunction will
significantly improve their quality of life, the management of which has now moved into the
realm of primary care physician.23
Lifestyle is a way of life or style of living that reflects the attitude and values of a person or
group.24 This tends to affect our lives in about 53%, others are genetic, environmental and health
care.24 Physical activity is one of the seven dimensions of wellness, other dimensions of wellness
include occupational, intellectual, social, emotional, spiritual and environmental dimensions.24
Physical activity and sexology are part of the lifestyle practices relating to health, others are
smoking, nutrition, alcohol intake, stress/sleep, hygiene, health literacy, television over viewing
and spirituality.24 A planned, coordinated and regular physical activity is carried out to improve
one or more components of physical fitness.24

21
The human body is made to be physically active, therefore low physical activity leads to
sedentary lifestyle which results in a number of disease conditions including erectile dysfunction,
obesity, cardiovascular diseases and hypertension.25 This is because physical exercise in itself
improves aerobic capacity, muscular strength, metabolic function and coordination leading to
reduction in risk factors of ED.25
Other components of lifestyle that improves erectile dysfunction are diets especially
Mediterranean style of diet and reduced calorie intake which will lead to improved erectile
function, others are reduction or stoppage of alcohol consumption, cigarette smoking and weight
reduction.26 Therefore, good lifestyle maintenance are associated with maintenance of good
erectile function.27 But physical exercise is chosen because it can easily be adapted and
measured.
Regular physical activity is also found to be beneficial in the treatment of erectile dysfunction,
both in normal patients and patients with disease conditions such as cardiovascular diseases and
obesity.28
1.2 STATEMENT OF THE PROBLEM
Sexuality is a very important part of the total person, integral to health and general wellbeing. It
affects our ego, our sexual partners and the entire family either positively (through bonding) or
negatively.2 In our communities, it is usually difficult to get to the root cause of any family
problem caused by erectile problems because they are not usually talked about even in the face
of a serious family problem.2,3
22
The current prevalence of erectile dysfunction is reported as 25% and expected to rise with time.9
Majority of patients with erectile dysfunction seek help from traditional herbalist and
pharmaceutical stores for their problem, many of such drugs, the efficacies, safety and dosages
are not usually documented, The number of persons with ED consuming Ginsomin for the
treatment of ED in our community is increasing and more pharmaceutical companies are
advertising ginsomin for its treatment. Studies have also claimed the effectiveness of Ginsomin
in the treatment of ED. therefore, the family physician should be able to interact with patients in
a way that will make them feel comfortable and relaxed to talk about their sexual concerns. This
is in consideration of the limited health care facilities and poor services in Nigeria.12 The
problem is usually compounded by the few reports on prevalence and treatment pattern of
erectile dysfunction in our environment.12,29,30
The result of this research will provide information about the severity of erectile dysfunction in
our environment. It will also determine the effectiveness of commonly used Ginseng and its side
effects in the treatment of erectile dysfunction. This will help the Family Physician to better
equip himself with the knowledge and practice of sexual health. This will eventually lead to
more sexual satisfaction and build relationships amongst couples. It will eventually reduce the
rate of divorce, promiscuity and dysfunctional family tendencies in our society.1
1.3 AIM AND OBJECTIVES OF THE STUDY
1.3.1 THE AIM
To compare the effectiveness of a combination of physical exercise and ginseng with physical
exercise and placebo in the treatment of erectile dysfunction among married men attending
GOPD and Urology clinics in JUTH Jos, The finding of which may be used to advocate for the
use of Ginseng and life style modification in the management of erectile dysfunction.
1.3.2 SPECIFIC OBJECTIVES

23
a To compare erectile dysfunction scores between treatment and control groups at base line and
at eight weeks
b To determine the pattern of erectile dysfunction
c To determine the side effects of ginseng
1.4 JUSTIFICATION/RELEVANCE OF THE STUDY TO FAMILY MEDICINE
High prevalence of erectile dysfunction from literatures and the number of ED patients seen
daily in our clinics were becoming alarming in Jos. Erectile dysfunction is not always talked
about by both patients and physicians yet affects patient’s quality of life which had led to
emotional problems to the patients. Erectile dysfunction is a multi-factorial condition that results
from chronic diseases that requires long time follow up which is suitable in primary care.
Erectile dysfunction also affects the entire family resulting in patients withdrawing from their
spouses, to marital discords, family separation or dysfunction and even divorce.11,12 ED increases
with age and coupling with its negative effect on relationship, marriages and the entire family
and the psycho-social issues relating with it, therefore the family physician is in the best position
to manage these patients.
Family medicine is a medical specialty that encourages the use of cost effective and preventive
strategies in the management of erectile dysfunction. Physical exercise and ginseng are probably
one of the most cost effective modes of treatment of erectile dysfunction for now.
The family physician is a specialist who provides comprehensive, continuing and well-
coordinated care to patients irrespective of age, gender, and disease or disorder presented. He is
responsible in preventive health services (risk factors) and managing patients in a holistic
manner within the context of the family.
He is usually the first point of contact and the only physician who provides care from cradle to
grave. He manages both patient and the family which justifies this study. Quite a number of
24
patients seen by the family physicians daily are due to sexual (erectile) dysfunctions which when
corrected with the help of the spouse or the family will go a long way in stabilizing the family.
Many medical conditions such as diabetes, heart failure, hypertension and depression are its risk
factors, their long term management and follow up are commonly done by the primary care
physician.31 He understands that the patient’s knowledge of the disease and its issues are
important because he has interest in the patient’s health, happiness and satisfaction. The family
physician also enhance the patients sexual health, quality of life, self-esteem and relationship in
the family since he provides preventive, promotive, screening, test and treatment to these
patients.32 He is in a better position to manage patients with erectile dysfunction.
This study will significantly alleviate the distress associated with this condition for both patients
and their spouses, the result of which will provide information on the effectiveness of combining
physical exercise with ginseng.
The information gained will be helpful in providing care to all patients irrespective of their socio
economic status with reduction in side effects associated with phosphodiesterase inhibitors.
The study will contribute to family medicine specialty by educating the family physicians on the
scope, risk factors and management modalities of ED. It will also help the family physician
enquire on every encounter with adult men about their sexual life as most patients finds it
difficult to talk about it. This will stimulate the specialty in developing sex clinics and protocol
for the management of ED

25
CHAPTER TWO
2.0 LITERITURE REVIEW
2.1 OVERVIEW OF ERECTILE DYSFUNCTION
Erectile dysfunction is considered important to men’s health considering the vast co-
morbidity associated with it as they aged.7 It is the most common sexual problems in men
affecting about one third of men throughout their lifetime.9 Prompting them to seek medical
help they ordinarily would not have, this is because it is a serious problem and a focus of
attention by the general public in recent times.10
Erectile dysfunction is an important component of emotional and physical intimacy that men
and women experience throughout their life time, this is because adult desire love and they
enjoy sexual activity if the health status and personal circumstances allow them to experience
close relationships within marriage.33
In adulthood the commonest intimacy is the presence of
physical and sexual relationship when there is a partner.34
Erectile dysfunction is the persistent inability to achieve or maintain an erection adequate for
satisfactory sexual intercourse for a minimum of three months.8 This has been found to affect
the quality of life (QOL) of men significantly, hence it need to be address promptly.7 The
diagnostic and the statistical manual of mental disorders (DSM-5) classified erectile
dysfunction as belonging to sexual dysfunction disorders that is clinically a significant
inability to respond sexually or to experience sexual pleasure8. Sexual function involves
interaction between factors such as social, cultural, biological and psychological factors,
making the diagnosis of erectile dysfunction etiological difficulty.

26
The following factors must be considered before the diagnosis of erectile dysfunction is made:
partner factors (health issues and sexual history of the partner), relationship factors (level of
sexual desire, communication problems or partner violence).35 Others are cultural or religions
factors (conflict with sexuality and sex inhibitions), medical factors (chronic medical conditions
and drug side effects) and individual factors such as (psychiatric conditions, sexual and
emotional abuse).35 Erectile dysfunction increases with age and a menace to our society causing
substantial impact that are negative on self-esteem, relationship and quality of life.10 This is
compounded by poverty and ignorance in the region suggesting that men with erectile
dysfunction may not have access to adequate care.11
In a study by Kubin et al in 2003 suggested that 5-20 of men have moderate to severe erectile
dysfunction and about 70 of these patients with erectile dysfunction are not treated.36 because
they rarely seek help10 or they find it difficult to talk about it due to cultural and religious
reasons.10,11,36 Therefore our responses to it can affect these patients either positively or
negatively.1 Erectile dysfunction is also seen to be common in people who are divorced or
separated than the married ones, this is because life events such as marriage separation and
divorce could be a possible cause of erectile dysfunction in them.11,13 These psychological causes
includes loss of self-esteem, low libido, pressure and frustration that may eventually leads to
depression.11,13 Erectile dysfunctions seems to be related to culture and environment since similar
cases of erectile dysfunction seen in primary health care clinics in developing countries are the
same compared to industrialized world.37
The impact created by erectile dysfunction could be devastating since sexual function is one of
the most important indices of quality of life.11 It could affect level of intimacy of these patients
27
such as emotions, social, sexual, recreational and intellectual intimacy with significant affection
of quality of life in these patients.11
These reactions may vary from negative attitudes, dissatisfaction with the problem or taking no
action by ignoring the problem which may end up with breakdown of the role of the husband
leading to family dysfunction.20The importance of sex is that it maintains good relationship and
this can persist even in old age, but can be disrupted by erectile dysfunction which gets worst
with advancing age.34 Normal changes occur in elderly group, therefore more time needed to
achieve a complete erection.34
2.2 EPIDEMIOLOGY OF ERECTILE DYSFUNCTION
ED is one of the most common problems in men worldwide.9 it ranges from partial decrease in
penile rigidity to complete erectile failure.9 The burden of erectile dysfunction is quite high as up
to 30 million of united State of Americans have erectile dysfunction.11It is estimated that world’s
population of erectile dysfunction patients will rise to 322 million by the year 2015.10 This is
usually underestimated in many developing countries because these patients rarely seek help due
to the stigma that is associated with it.10
Erectile dysfunction is about three times commoner in American diabetics compared to non-
diabetic men.38 A study done in Canada, USA and Europe found a prevalence of ED ranging
between 31.6% to 52% in men 40 years and above. in southeast Asia, it was between 36-51%,
18.8% in Iran and 63.2% in Japan.39 Similar study was done in Denmark Europe, 5.4% of men
reported reduction in their erectile function. Erectile dysfunction was 2% in men below 40 years
and about 18% in men between 55 and 88 years.40 Fugal Meyer also reported 29% of mild
erection dysfunction and 5% of severe erectile dysfunction.36
28
The prevalence of severe erectile dysfunction in South African diabetics was estimated at 50%
in patients 50 years and above with 95% of them having some forms of ED.41 There are a few
reports which documented erectile dysfunction in Nigeria. Total prevalence of 86.8% had some
forms of erectile dysfunction. About 2.4% of hypertensive patients had severe erectile
dysfunction while 10.4% had moderate erectile dysfunction.42
Another study in Nigeria showed that up to 46 of patients within the ages of 20 and 70 years
had erectile dysfunction, 28 of these patients are within the ages of 30 and 40 years, 40
between 40 and 69 years and 54 in those over 70 years.14 This shows that erectile dysfunction
increases with age and a menace to our society causing substantial impact that are negative on
self-esteem, relationship and quality of life.10 This is compounded by poverty and ignorance in
the region suggesting that men with erectile dysfunction may not have access to adequate care.11
In South Western Nigeria, the prevalence of 45.7% was found in patients who had some forms of
erectile dysfunction. Thirty four percent of these patients were below 40 years while 72% were
above 40 years.43 The participants who had hypertension, diabetes or both was 17.7% with
majority (60%) of the patients on traditional medication for treatment.43 Only 42.9% of the
patients were able to discuss their problems with their health personnel.43
The severity of erectile dysfunction from the Omisanjo study found 40% of the patients with
mild erectile dysfunction, 40% had mild to moderate erectile dysfunction, 10% had moderate
while another 10% had severe erectile dysfunction.43 The Massachusetts male aging study was a
community based survey of white non institutionalized married men, this study found that 25%
of men within ages of 40-70years had moderate degree of erectile dysfunction, and 10% of the
men had a completely absent erectile response.44
29
Erectile dysfunction is about 60 in married individuals and 45 in the unmarried suggesting it
increases with increased frequency of sexual intercourse. It is also commoner in educated men
than the uneducated because of their status and lifestyle which has a tendency to predispose them
to cardiovascular risk factors and erectile dysfunction.11 Nicolisi et al found an inverse
relationship between level of education and erectile dysfunction45
2.3 RISK FACTORS OF ERECTILE DYSFUNCTION
Common risk factors for developing erectile dysfunction include. (a) Age: This is common as
age advances.42 There are two reasons attributed to this,42 (i) older men are more likely to
develop chronic diseases such as hypertension and diabetes mellitus. These processes alone
cause vascular endothelial damage. (ii) Aging processes cause decrease compliance of tissues
including copora cavernosa. Prevalence studies in Nigeria showed erectile dysfunction is usually
related to age which can be a distressing or embarrassing part of andropause.14,42 About 60% of
these older men still expresses interest in maintaining their erection with ageing.34 Functional
decline may actually be the cause of erectile dysfunction in them when it is diagnosed.34
(b) Diabetes mellitus; Prevalence studies found that erectile dysfunction tends to develop 10 -15
years earlier in diabetic men, it is up to 55% in men between the ages 50 and 60 years who have
had diabetes for about 10 years. These are due to34 (i) Onset and greater severity of
atherosclerosis that narrow the arteries thereby reducing the delivery of blood to the penis. (ii)
Diabetic neuropathy occurs as a result of damage to both the sensory and autonomic nerves
supplying the penis as a result of high blood glucose level. (iii) Myopathy decreases the
compliance of the muscles in the copora cavernosa leading to inability of the penis to initiate and
or maintain erection. Erectile dysfunction is found in about 75 % of diabetic men over 60 years,
predisposing them to higher risk of developing coronary artery disease.34

30
(c) Hypertension and cardiovascular diseases: Studies have shown that those with essential
hypertension have been found to have (i) Low production of nitric oxide by the arteries of the
penises (ii) It accelerates the progression of atherosclerosis which contributes to erectile
dysfunction.18 Men with hypertension are likely to develop severe form of erectile dysfunction
(15%) and this will increase to (20%) if they also smoke.46 Hypertension, age and diabetes and
their drugs have been found to be the major risk factors for erectile dysfunction.11,47 It is seen to
be more severe in hypertensive patients on antihypertensive and about three times greater in
those on diabetic treatment thus making it difficult to differentiate the real cause.11 Olusegun et al
showed that erectile dysfunction is commoner in hypertensives, this is related to endothelial
damage found in hypertensives compared to non-hypertensives.48
(d) Smoking cigarettes: Smoking has been shown to aggravate atherosclerosis thereby increasing
the risk of developing erectile dysfunction.18 It is also seen to decrease nitric oxide synthetase
activity in the penis, this results in nicotine-induced vasoconstrictions of cavernous smooth
muscles, therefore people with erectile dysfunction are likely to be smokers than those who do
not smoke49
(e) Alcohol: A peer review article showed that alcohol consumption is related with erectile
dysfunction negatively. Its contribution is due to nerve damage that leads to testicular atrophy
resulting in decrease erectile function.18 The effect of alcohol on people’s erection largely
depends on the volume and duration of alcohol consumed. Omigbodun et al also showed that ED
occurs as a result of its central effects on the brain which include sedation, depression and loss of
libido. The study also showed that alcohol when taken in smaller quantity, it improves erectile
function.49 Consumption of 7% drinks or more per week increases the risk of erectile dysfunction
significantly while below 7% drinks per week may not affect erection.50 Alcohol is a central

31
nervous system depressant, therefore it increases sexual desire, but reduces sexual
performance.50 Alcohol is a known cause of ED and this is proportionate to the amount of
alcohol and duration consumed, about 33.3% of subjects with alcohol dependence complain of
ED.51 Alcohol in the form of palm wine, local gin and liquor are locally produced substances
with historical and traditional importance which are commonly used in celebrations can also lead
to erectile dysfunction51
(f) Substance abuse such as heroin, marijuana, cocaine and methamphetamines.18
(g) Drugs that have been found to cause erectile dysfunction are as a result of their side effects.10
these includes:
1. Analgesics e.g. opiates, anticholinergic e.g. TCA.
2. Anticonvulsants e.g. phenytoin, phenobarbital.
3. Antidepresants e.g. lithium, mono amine oxidase inhibitors (MAO), Selective serotonine
receptor inhibitors (SSR) I, Trycyclic antidepressants (TCA).
4. Antihistamines e.g. dimnehydranate, deplenhydramin, hydroxyzin (visteryl), Meclizine
(antivert), promethazine (phenergan).
5. Antihypertensives e.g. alpha blockers, B blocks, calcium channel blockers, clonidine (catapres),
methyldopa,( reserpine.)
6. Antiparkinsonian drugs e.g. bromocryptin (perlodel), levodopa, trihexyphenidil.
7. Cardiovascular agents e.g. digoxin, disopyamide (Norpace), gemfibrozil (lopid).
8. Cytotoxic agents e.g. methotrexate.
9. Diuretics e.g. spironolactone (aldactone), thiazides.
10. Hormones e.g. 5 alpha reductase inhibitors, corticosteroids, estrogens, leutinising hormones
releasing hormones agonist, progesterones.
32
(h)Psychogenic causes: psychological causes of erectile dysfunctions include stress, anxiety
disorders, prolong guilt, depression, widower’s syndrome, low self-esteem, post-traumatic stress
disorders and performance anxiety.10
The American Psychiatric Association have observed that depression is likely the commonest
cause of psychogenic erectile dysfunction with both cognitive and behavioral factors as
contributors to erectile dysfunction.35 Another common cause of Erectile dysfunction is
depression.35 Post traumatic stress disorders (PTSD) patients have a higher chance of developing
erectile dysfunction. Therefore, men who develop PTSDs should also be evaluated for erectile
dysfunction.35
(i) Low testosterone: Emily et al observed that testosterone is the primary sex hormone in men. It
is necessary for libido enhancement and maintenance of nitric oxide levels in the penis, thus,
hypogonadism results in both low sex drive and erectile dysfunction.18
Testosterone level in the body reduces with age while erectile dysfunction increases.52 This
occurred in about 45% of men 45 years and above.52 Prevalence studies on ED also showed that
low level of testosterone is associated with sexual dysfunction that includes low libido, poor
erection, reduced spontaneous erection, sexual activity, orgasmic or ejaculatory dysfunction.52,53
It is also responsible in moderating mood, cognition, vitality, muscle, bone and fat
compositions.53 The association between testosterone and erectile dysfunction is still unclear, but
about 35-40% of patients treated with testosterone replacement had significant improvement in
erectile function after six months of treatment similar to phosphodiesterase inhibitors type 5
(PDE-5.)53
(j) Nerve and spinal cord damage especially to the pelvis can cause erectile dysfunction.18 This
damage can be due to multiple sclerosis, trauma, surgical procedures such as pelvic and vertebral
33
cord compression, prostate surgeries and multiple sclerosis even though age and obesity are the
main risk factors.2,18 Others are pelvic irradiation, hyper-prolactinaemia and
hypercholesterolemia.
(k) Obesity: It is a state of chronic oxidative stress and inflammation. Obesity is associated with
increased oxidative stress which increase free radicals that results in deactivation of nitric oxide
within the vasculature with resultant reduction of erectile function.27,54
Prevalence studies showed that obesity is a significant cause of erectile dysfunction.10 Body mass
index (BMI) and lipid profile were found to be predictors of erectile dysfunction about 25 years
later.54 This is associated with higher level of pro-inflammatory cytokines and C-reactive cytokin
proteins that results in erectile dysfunction.55,56 and hypogonadism.34Weight loss may lead to
reduction in oxidative stress, therefore weight loss programs are seen to reduce erectile
dysfunction. Obesity has been positively related to endothelial dysfunction and increased
vascular inflammatory markers.55 A significant association between erectile dysfunction and
obesity due to the effect of inflammatory markers that contribute to vascular endothelial
damage.57 Elevated body fats and vascular response to l-arginine and cytokines exist with such
association resulting in reduction of nitric oxide activity in the vascular endothelium hence ED.57
(k) Chronic liver disease: Olusegun et al showed that erectile dysfunction is higher in caucasians
with chronic liver diseases, this is seen to have improved with liver transplant in cirrhotic
patients independent of alcohol aetiology.48 This occurs as a result of hormone problems such as
decrease in testosterone levels and reactions with other medications used in the treatment of
chronic liver disease.48 Therefore advance liver damage is associated with poor erectile
function.48
FIGURE 2.1 The multifactorial causes of erectile dysfunction.48

34
2.4 ANATOMY AND PATHOPHYSIOLOGY OF ERECTILE DYSFUNCTION
The main organ involved in sexual dysfunction is the penis.58 It is the male sex organ which
contains two chambers called the corpora cavernosa that runs the length of the upper side of the
penis while the corpus spongiosum lies ventral to the two cavernosa muscles.38 The corpus
cavernosa and the bulbo spongiosum originated from the pubic bones and join (terminated) at the
head of penis. The urethra which is the channel of urine and ejaculate runs along the underside of
the copora cavernosa to the tip of the penis.58 Arteries originates from internal pudendal artery
while veins drains blood from the superficial intermediate and deep veins to internal pudendal
veins.58 The corpora cavernosa is a spongy tissue consisting of smooth muscle and arteries.
Tunica albuginea is a membrane that surrounds the corpora cavernosa which drains blood out of
the penis to the internal pudendal veins58
The arterial supply of the penile skin originates from the left and right superficial external
pudendal arteries while the ventral part of the penis is from the arterial supply of deep structures
of the pelvis.59 The arterial supply to the penile muscles originates from the common penile
artery which is a branch of the internal pudedal artery.59 The common penile artery branches into
VASCULO GENIC
Arterial insufficiency
venous leak
Atherosclerosis
Arteriosclerosis
ENDOCRINOLOGIC
Hypogonadism
Psychogenic
ANATOMIC Peyronie’s Disease
NEUROLOGIC
Spinal cord injury
Peripheral neuropathy
Diabetes

35
the dorsal, bulbo urethral and cavernous arteries.59 The dorsal artery is responsible for the
engorgement of the glands during erection while the bulbo-urethral branch supplies the corpus
spongiosiom and the bulb of the penis. The carvenous branch supplies the corpus cavernosal
muscles which affects tumulscence and responsible for erection principally. It also supplies the
trabeculae erectile tissues and the sinusoids.59
The venous drainage originates from the venules of the sinusoids beneath the tunica albuginea,
these veins form the emissary veins of the penis.35 The primary nerve fibres to the penis
originated from the dorsal nerve of the penis which is a branch of the pudendal nerve. The
cavernous nerves of the penis serve both sympathetic and parasympathetic stimulus as part of the
autonomic nervous system. They enter the copora cavernosa and the corpus spongiosum through
the prostate to regulate blood flow in the penis during sexual stimulation.39 The pudendal nerve
also gives a branch (dorsal somatic nerves) which is responsible for penile sensation .35,59
Penile erection is a vascular event primarily which can be impaired in conditions that end with
endothelial dysfunction.13 Therefore physiological alteration related to hormonal changes
together with sedentary lifestyles have been implicated in erectile dysfunction.47
During intercourse, the penis must sustain an erection which is the state of rigidity induced in
erectile tissues of the penis as a result of engorgement of the tissues with blood in response to
sexual arousal or during sleep.60 This results from the combination of neurotransmitters and
vascular smooth muscles response largely due to impulse from the brain which stimulates the
flow of blood from arteries leading to engorgement of the penis.60
Erection occurs with specific sequence of events involving nerve impulse from the brain, spinal
column, muscles, penis, fibrous tissues, arteries and veins.61 The mechanism of erection begins
with sexual stimulation which can either be tactile or mental.61 Sexual stimulation generates

36
electrical impulses along the nerves going to the penis. This causes the nerves to release nitric
oxide which in turn increase the production of cyclic guanosine monophosphate (cGMP) in the
smooth muscle of the copora cavernosa. The cGMP causes the smooth muscle of the copora
cavernosa to relax and allow rapid flow into the penis.61
The incoming blood fills the corpora carvernosa making the penis to expand, the pressure from
the expanding penis compresses the veins in the tunica albugeneae helping to trap the blood in
the corpora carvernosa thereby sustaining the erection.61 Erection is reversed when cGMP levels
in the corpora cavernosa falls.62 This causes the smooth muscle of the corpora carvernosa to
contract stopping inflow of blood and opening veins that drain blood away from the penis.62 The
level of the cGMP in the corpora cavernosa falls because It is destroyed by an enzyme called
phosphodiesterase type 5 (PDE5).62
E n d o lle l ia l
c e l l a n d
n e u ro n e
P D E 5
5 G M T
(in a c tiv e )C G M P
C G M P -d e p e n d e n t
(p ro te in k in a s e )
G u s n ily l
c y la s e
G T P
P ro te in s
P h o s p h o p ro te in s
( in c lu d e s c a rtt p u m p s
R e d u c e c y to p la s m ic
c a tt
R e la x a tio n
- in c re a s e b lo o d flo w
- e re c tio n
S m o o th m u s c le s
N itr ic o x id e
F IG U R E 1
P D S 5 in h ib ito rs

37
Erectile dysfunction is commoner in older men because of hormonal changes which occur as a
result of changes in testicular size, hence a decline in sex hormones.63
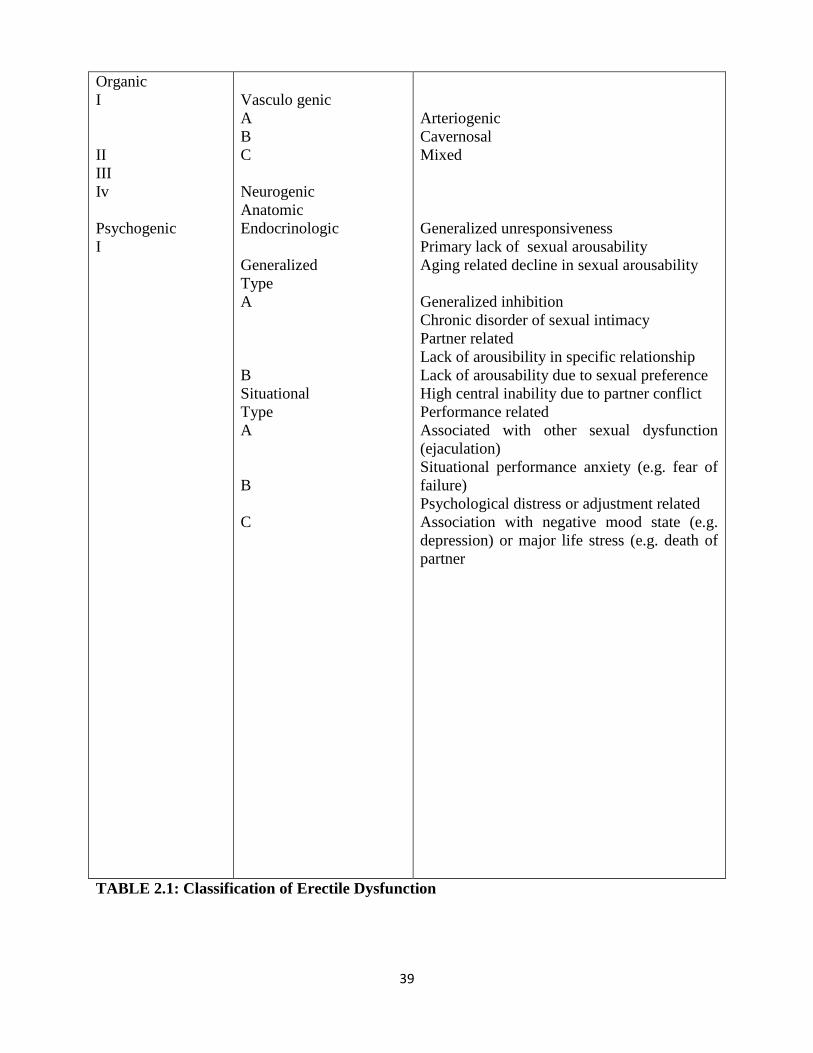
2.5 CLASSIFICATION OF ERECTILE DYSFUNCTION
The International Society of Impotence Research has adopted that erectile dysfunction is usually
multifactorial and classified primarily as organic or psychogenic.64 The organic component can
also be sub-classified to either vasculogenic, neurogenic, anatomic, endocrinologic or mixed.64
The psychogenic is further sub-divided to be either generalized which affects all situations,
stimulations and partners or situational which affect some partners situation or stimulations.64
The generalized psychogenic type is divided into type A which is generalized unresponsiveness
and type B which is generalized inhibition.64 The situational is subdivided into type A which is
partner related ,type B which is performance related and type C which is psychological distress
or adjustment related.35,64

38
Category Common disorders Pathopysiology
39
Organic
I
II
III
Iv
Psychogenic
I
Vasculo genic
A
B
C
Neurogenic
Anatomic
Endocrinologic
Generalized
Type
A
B
Situational
Type
A
B
C
Arteriogenic
Cavernosal
Mixed
Generalized unresponsiveness
1. Primary lack of sexual arousability
2. Aging related decline in sexual arousability
Generalized inhibition
1. Chronic disorder of sexual intimacy
Partner related
1. Lack of arousibility in specific relationship
2. Lack of arousability due to sexual preference
3. High central inability due to partner conflict
Performance related
1. Associated with other sexual dysfunction
(ejaculation)
2. Situational performance anxiety (e.g. fear of
failure)
Psychological distress or adjustment related
1. Association with negative mood state (e.g.
depression) or major life stress (e.g. death of
partner
TABLE 2.1: Classification of Erectile Dysfunction

40
Classification of erectile dysfunction is recommended by the nomenclature committee of the
International Society of Impotence Research as follows.64
The American Psychiatric association (DSM-5) classified erectile dysfunction based on the
duration of the disease as lifelong (disorder was present from first sexual experience), or
acquired (disorder occur after some period of normal sexual activity).35It can also be classified
based on its occurrence as generalized which occurred with all stimulations, partners or
situations or situational which occurred with either stimulations, partners involved or situations
of sexual activity.35,65 Lifelong erectile dysfunction is commonly seen in patients with
psychological factors while the acquired type is commonly seen in patients with biological
factors.35,65
Erectile dysfunction has a strong organic component, but can also be psychogenic in nature
especially in younger men who are less than 35 years.11 Psychogenic erectile dysfunction can be
found in about 10% of older men above 50 years.11
2.6 ASSESSMENT OF PATIENTS WITH ERECTILE DYSFUNCTION
The symptoms and signs of erectile dysfunction are difficult to get from patients because they
are not easily discussed like any other disease.66 Diagnosis of erectile dysfunction is usually
made from history and examination while investigations are usually done to determine its risk
factors.10 Sexual history should focus on erection adequacies, altered libido, quality and timing of
orgasms, volume and appearance of ejaculate, presence of sexually induced genital pains or
penile curvature (peyronies disease) and sexual functions.10
Patients usually present with inability to achieve and or maintain erection, poor sexual
satisfaction, symptoms and signs of risk factors and other psychological and psychiatric
41
manifestation.10 The guidance and counseling psychologist have adopted several methods that
can be used to identify patients with erectile dysfunction. These methods include.66
(a) Natural observation: This is done by observing the lifestyle of these individuals concerning
their sexual desires and the way they relate to opposite sex naturally.66 This can be a pointer to
erectile dysfunction.
(b) Case history: This involves taking a complete inquiry of the person sex life and his sexual
behavior. This is the commonest method of diagnosing erectile dysfunction in clinics.
(c) Surveys: This can be done through questionnaires or mails in obtaining ways in which they act
or think concerning erectile dysfunction, this is used to identify people with erectile dysfunction
in the communities.
(d) Correlation studies: This is usually done to make comparison between two categories ofpeople
to determine the level of their relationships. It measures between a person’s sexual desires and
his sexual performance.
(e) Experimental methods: This studies how animals and man behave in order to identify its cause
and effects. It identifies those suffering from erectile dysfunction and all kinds of abilities,
interests and achievements concerning erectile dysfunctions.
Sexual history: In assessing erectile dysfunction, the patient’s level of comfort must be first
assessed. This will avail the physician an opportunity to educate the patient on erectile
dysfunction and its treatment. If erectile dysfunction is suspected, history should be aimed at
determining the sexual response that is affected.65
The following questions should be asked when obtaining sexual history: Difficulty obtaining
erection, if erection is suitable for penetration, rigid erection that can be maintained until
completion of sexual intercourse, presence or absence of ejaculation and sexual satisfaction.65

42
This gives the clinician the avenue to make an objective opinion on relationship between the
patient and his sexual partner.65
2.7: ERECTILE DYSFUNCTION SCORES
The assessment of erectile function in most studies relies primarily on questionnaires which are
self reporting such as the international index of erectile function (IIEF).67 The erectile function
can generally be measured in three categories.67 (a) vascular capacity (neuro-physiological
testing (c) erectile capacity (penile dimensions of tumescence and rigidity). The vascular and
neuro-physiological studies usually diagnose the cause of erectile dysfunction.67 The erectile
function questionnaire measures solely the physiology aspect of erectile dysfunction and its
dimension.67
Other instruments that can be used to assess erectile function includes the Rigscan (commonly
used for nocturnal penile tumescence and rigidity measurements) and penile monitoring (audio
visual during sexual stimulation).67 The commonest instrument in most population studies is the
international index of erectile function which is a self reporting instrument that measures men’s
perception of erectile function with penile measurements that records anatomical changes.67 It is
commonly used because it is easier to use especially for large scale studies, but for smaller
studies, measurement of physiological changes of erectile function, penile measurement may
provide more clue.67
The IIEF has been validated in many languages and used all over the world.67 The limitation is
having sexual intercourse four weeks before assessment may give a wrong perception of his
erectile function.67 The international index of erectile function was introduced in 1997 for
assessment of erectile function.67 It is a brief, reliable and valid self-administered questionnaire
that contains five domains used in assessing erectile dysfunction and its severity.56 It is the gold
43
standard in the assessment, severity and treatment related responses in erectile dysfunction while
measuring the outcome measure in both groups before and after treatment.68
The IIEF questionnaire was developed to assist the clinician in evaluating patients with erectile
dysfunction. Other questionnaires that can be used includes, sexual encounter profile (SEP),
Global assessment Questionnaires (GAQ), Psychological and Interpersonal Relationship Scale
(PAIRS), Self-esteem and Relationship (SEAR).56 The investigation results should be discussed
with both the patient and his sexual partner. This discussion should involve the anatomy and
physiology of sexual response, activity and risk factors identified.68A score is usually awarded
before to measure severity and after to measure improvements. It has a total score that is usually
added up to a maximum of 25. The ratings are; 22-25 as no ED, 17-21 as mild ED, 12-16 as mild
to moderate ED, 8-11 as moderate ED and 5-7 as severe ED.68 This has been widely used in
many countries including Nigeria.68
The specific criteria used in the diagnosis of erectile dysfunction according to DSM-5 includes
one or more of the following: Marked difficulty obtaining erection prior to penetration, marked
difficulty in maintaining the erection until through the period of sexual activity and marked
decrease in rigidity of penis lasting for up to three months.35 These symptoms must cause stress
to both the individual or sexual partner.35 The limitation to using IIEF is its subjective nature and
it cannot be used in men who had sex four weeks before assessment as the score might have
changed over time.67 Interventions in erectile dysfunctions such as lifestyle changes, (diets and
exercise), drugs (phosphodiesterase inhibitors) and surgical interventions have led to significant
changes in IIEF.67 Ginseng has also been shown to improve IIEF in some studies such as.
44
Gaurang et al studied multi herbal supplements ( VxP) which is a polyherbal preparation used in
the treatment of erectile dysfunction, It contains ginseng and other vitamins. Only ginseng had
been proven to aid erectile function by improvement in IIEF scores in the VXP group.69
The study showed that VxP was well tolerated, the most common side effect was fever. It was
mild on the subjects with mild to moderate erectile dysfunction.69 It is an alternative to invasive
approaches with a good penile rigidity, penetration and maintenance of erection.69 There are little
evidences for the recommendation of natural supplements for enhancement of erectile
dysfunction, but there were positive effects of ginseng on erection , hence it can be
recommended as an aphrodisiac in the treatment of erectile dysfunction.70
Korean red ginseng is one of the most widely used herbal remedies.22 A meta-analysis of it
shows a significant effect with improvement in IIEF, a sub group analysis also shows its
beneficial effects on psychogenic erectile dysfunction.22 Erectile dysfunction including orgasmic
dysfunction, sexual desires, sexual satisfaction and overall satisfaction improved significantly
after 12 weeks of treatment with majority of the patients (90%) indicated interest in continuing
with the drug after the study.69
Thuryan et al showed that Red Ginseng is effective in the treatment of erectile dysfunction.71
Although, effort has been made to find the ideal treatment for erectile dysfunction, but this has
not been identified.72 A meta- analysis of seven Randomized control trials in South Korea
compared the therapeutic effect of ginseng and placebo, they found a significant effect in the
treatment of erectile dysfunction.73 A sub-group analysis of same also showed some beneficial
effect of Red Ginseng also in psychogenic erectile dysfunction.73 It is also an antioxidant and
plays a protective role with significant effects in rigidity, libido and patient satisfaction.72
45
Ginseng has both stimulation and inhibitory effect on the central nervous system and act
centrally in the process of erection through multiple mechanisms that have not been elucidated.72
2.8: SEVERITY OF ERECTILE DYSFUNCTION
Erectile dysfunction generally presents as mild, mild to moderate, moderate and severe forms.
The presentations differ with each study before or after ginseng treatment.44 The Massachusetts
study reported majority of subjects (25%) reported with mild to moderate erectile dysfunction.
This was followed by those who presented with mild erectile dysfunction, followed by those
with severe ED.44 Omisango study also showed higher population in patients with mild to
moderate erectile dysfunction.43 Idung et al study in Uyo Nigeria reported higher severity in the
mild ED.11 Panax Ginseng administration was found to reduce the severity of erectile
dysfunction in Gaurang69 et al and Peak studies74.
PHYSICAL EXAMINATION: Particular attention to risk factor, physical examination is an
important aspect of erectile dysfunction management which should assess for blood pressure and
heart rate, body habitus for central obesity, cardiovascular, neurological, genitourinary systems,
digital rectal examination, the testicles and the penis,75 examine the lips for evidence of prolong
cigarettes smoking.2,36 For the genitals, the following should be sought for: (a) characteristic of
the penis e.g. painful bending of the penis leading to peyronies disease, response of the penis to
touch (b) small testicles, lack of hair, Gynaecomastia pointing to hypogonadism. (c) Pedal artery
palpation for low blood flow which may be as a result of atherosclerosis.
There is no preferred first line diagnostic test for erectile dysfunction and routine screening is not
also recommended, but common investigations such as fasting blood glucose and urinalysis can
be done to identify risk factors of ED.10
46
It is necessary to include unsuspected signs such as small testes, prostate cancer, infections, and
penile plagues in the evaluation of erectile dysfunction.65
2.9 INVESTIGATIONS OF ERECTILE DYSFUNCTION
World health organization (WHO) recommend limited diagnosis test in erectile dysfunction
except in refractory case.10 Hence full blood count, urinalysis, blood glucose assay, prolactin
levels, sex hormones binding globulin, free testosterone and lipid profiles are usually the initial
investigations requested to ascertain the risk factors responsible.10 Other specialized diagnostic
testing not commonly done include (a) Neurological testing such as vibrometry, bulbo
cavernosus reflex latency, cavernosal electromyography. (b) Nocturnal penile tumescence and
rigidity assessment. (c) Psychiatric assessment (d) specialized endocrinologic testing such as
hypothalamic-pituitary- gonadal function test. (e) Magnetic resonance imaging of sella tursica
and computed tomography (f) Vascular diagnosis such as doppler ultrasound, penile pharmaco
cavernosography, penile arteriography and nuclear imaging even though doppler ultra-
sonography is not so useful in the diagnosis of erectile dysfunction.76
Diagnosis of erectile dysfunction is made in men who have repeated inability to achieve and or
maintain an erection for satisfactory sexual performance for at least three months.8 A good
communication between patient and doctor is important in establishing a diagnosis, assessing
severity and determining the cause.5
2.10 TREATMENT OF ERECTILE DYSFUNCTION
Considerable effort has been made to unravel the ideal treatment of identified erectile
dysfunction, but this has not been identified.69 Most of these patients do not take any form of

47
treatment for their illness which may be attributed to limited access to health care facility or they
are not bothered about milder forms of erectile dysfunction.77 Those who seek medical care,
majority of them (60%) resort to herbal medication, which is a prominent practice in our
localities.77
Treatment of erectile dysfunction is best when the sexual partners are involved in the
management.78 The first step in managing patients with erectile dysfunction is understanding the
patient’s problem. This helps in identifying the best treatment option for the patients.65
Treatment of erectile dysfunction is divided into:
2.10.1 Pharmacological treatment: Medication for treatment of erectile dysfunction such as
phosphodiesterase inhibitors type 5 are considered the most effective oral drug in the treatment
of erectile dysfunction.10 These includes: sildenafil, vardenafil and tadalafil. The
phosphodiesterase type 5 inhibitors are considered to be relatively similar in effectiveness, but
differences in dosing, onset of action and duration of therapeutic effect. There are no data
suggesting the superiority of one to the other.34 ( but most data suggest equal effectiveness, but
differ in dosing and onset of action, they are not effective in improving libido. 10 This oral
medication selectively inhibits the enzyme phosphodiesterese types 5 and has completely
changed the treatment of erectile dysfunction.79
Each of the three phosphodiesterase types and inhibitors has different pharmacokinetics and their
absorption is affected differently when co-administered with fatty meals. Their onset of action
are 11 minutes with sildenafil and 14 minutes with vardenafil and tadalafil.79 The most
significant difference in the three medications is their serum half life of 4 hours in sildenafil and
vardenafil, while that of tadalafil is 20 hours approximate. This is usually the reason for on
demand dosing for sildenafil and vardenafil while a daily dosing for tadalafil.79 PDE5 inhibitors
48
are generally well tolerated but the adverse effect include headache, facial flushing, dyspepsia,
rhinitis, abnormal vision, dizziness, syncope and rarely non arthritic anterior optic neuropathy.80
Other oral agents that were in use before the advent of PDE5 are Adrenergic receptor antagonist
(e.g phentolamin, yohimbine and delequamine), Dopamine receptor antagonist (e.g
apomorphine and bromocriptin), serotonergic receptor activators (e.g trazodone), xanthine
derivatives (e.g pentoxifyllin) and oxytocinergic receptor stimulators (e.g oxytocin) of which
some are still being reviewed.81 These act on the brain to facilitate or inhibit erection.81
Testosterone is better in primary than secondary hypogonadism. Side effects of testosterone
includes erythrocytosis, increased transaminases, exacerbation of untreated sleep apnea, benign
prostatic hyperplasia and increased risk of prostatic adenocarcinoma.34 It improves erectile
dysfunction and libido, but requires close monitoring of hemoglobin, serum transaminases and
should be considered first line.10
Testosterone replacement has been seen to improve libido, erectile function and overall
wellbeing.82 Testosterone can be administered as oral, injectable, dermal gel. A combination of
different routes of administration at the same time has been found to be more effective in
treatment of erectile dysfunction than single route, but the adverse effects of PDE5 should
considered especially in difficult to treat patients.83
Newer agents that are still undergoing trial for the treatment of erectile dysfunction include
dopamine and melanocortin receptor agents, second generation phosphodieterase inhibitors,
rhokinase inhibitors, soluble quanylate cyclases and maxi-k-channel activators.84
2.10.2: Non-Pharmacological Treatment: Non Pharmacological treatment of erectle
dysfunction includes:
49
(a) Improving life style which is aim at modifying risk factors of erectile dysfunction(ED).
Frequent exercise which help in reducing excess weight and sedentary lifestyle, controlling
hypertension and blood glucose, reduce alcohol consumption, cigarettes smoking and significant
risk factors of obesity thereby maintain good health.76
(b) Cognitive behavioral therapy (CBT) is a form of treatment specifically for psychogenic
erectile dysfunction which also improves relationship problems.10 Cognitive behavioral therapy
or psychogenic therapy such as sensate focus techniques is aimed at improving relationship
difficulties.10 It has equal effectiveness with alprostidyl injections and vacuum devices.10 Stress
management and sexual counseling are the most important part of treatment for patients with
sexual problems. It is usually done by sexual counselors, but the primary care physician, the
urologist and the gynecologist who commonly see these patients also serve in the capacity.
Ideally the patient’s partner should be involved in the counseling, and also discuss the mode of
treatment that is appropriate for him, stress management has been found to be beneficial in
treatment of erectile dysfunction.85
(c) Surgical management of erectile dysfunction includes (i) Intra cavernosal injection of
vasodilators: these are vasolidators that are injected into the corpus cavernosum to produce
erections e.g. Alprostidil which is synthetic prostaglandin (PGE1) and phentolamin which are
effective either as a single agent or when combined.78 They induced formation of nitric oxide
synthetase thereby inducing erections.80,86
Alprostidil is the commonest agent used in achieving rigid erections with enormous benefits.80,86
It is indicated in patients with healthy copora cavernosa and effective within or after 90 minutes
of injection.80,86
50
Intra urethral injection: Medicated urethral system for erections (MUSE) is a system that
involves injecting a vasodilator into the penile urethra to achieve or maintain an erection.65,87
prostaglandin E1 e.g Alprostidil is also commonly used and is effective in about 65% of the
patients. The limitation to this form of treatment are the cost of injection and inability to provide
rigid erection consistently.65,87
Newer agent that is still under study is the vascular endothelial growth factors (VEGF). It
increases nitric oxide which increases vascular blood flow.87 .Adverse effects include urethral
bleeding, dizziness dysuria, penile pain and hematoma.87
(d) Penal implant: This involves placement of a device inside the copora cavernosa with the sole
aim of achieving erection.97 It is effective in more than 90% of the patients that need it, but the
benefit and risk should be explained to the patient and their spouse88,89
Penile prosthesis is usually indicated in patients who did not respond to other forms of
management and in those who had penile reconstruction and those that went through radical
prostatectomy and cannot responding to PDE-5 inhibitors.88 Penile prosthesis are classified into
semi rigid and inflatable types both with similar disadvantages such as risk of infections,
consistent erection at all times, penile injuries etc. Patient reported better satisfaction with penile
implant compared to sildenafil and alprostidic (PGE1).89
(e) Vaccum devices are plastic devices that are placed over the penile skin and a partial pressure
is created to pump out air resulting in erections.89 A constricting band is later applied at the base
of the penis to sustain the erection already achieved. Erection is usually maintained until
constricting band is removed which should not be more than 30 minutes.89 These are non-
invasive and contraindicated in patients with sickle cell disease and patients on anticoagulants.
Penile prostheses are usually inserted with the help of urologist. These forms of management are
51
difficult with more adverse effects, thus, Ginseng will be preferred because of simplicity in
management with few side effects.77
Patients with erectile dysfunction should be educated on the benefits of physical exercise,
reduction of weight and to stop smoking so as to improve or restore erectile function in the
absence of co-morbidities.90 Good glycemic and blood pressure control is also important in
preventing or reducing erectile dysfunction.90
2.10.3: PHYSICAL EXERCISE
Physical inactivity affects erectile function negatively, therefore physical activity has a beneficial
effect on erectile function and has an additive effect when combined with diets especially
Mediterranean diets.91 This occurs due to decrease in metabolic disturbance of inflammatory
markers, insulin resistance, decrease visceral adipose tissue and improvement in vascular
function.92
Physical activity is beneficial in patients with heart diseases, stroke, hypertension, diabetes,
colorectal cancer, prostate disorders and arthritis.93 Studies done by Baccon et al found that men
who ran for an hour and a half or three hours of vigorous outdoor activity a week are found to be
20% less likely to develop erectile dysfunction than those who did not.93
The exercise that is required to reduce the risk of erectile dysfunction has no specification, but 30
minutes or an hour of physical activity in most days of the week has a good health benefit and
can be divided over the days.93
Physical exercise is not devoid of complications which occur as a result of quick movement
during exercise, these include muscle and joint problems, strains, tears or fractures, but too hard
exercise can lead to joint stiffness, tendon and ligament inflammations and sudden death.93
52
Physical activity is one of the seven dimension of wellness.25 It is defined as a planned, co-
ordinated and regular physical activity carried out to improved one or more component of
physical fitness.25 There is a shift from communicable disease to non-communicable disease
worldwide.85 One of the risk factors for non-communicable diseases is physical inactivity which
is now the fourth leading risk factor for global morbidity and mortality.103 Physical inactivity or
low activity contributed about 3.2 million death and 2.8% of disability-adjusted life years
globally in 2010.94
Olufemi et al observed that the prevalence of physical inactivity ranges between 31-61% in adult
Americans and 30.7% among Brazilians.95 Worldwide it is estimated that 31% of adults are
inactive and this level is rising and associated with major public health implication while
prevalence of inactivity in Nigeria and Ghana ranges between 25 and 57%.96,97 Physical activity
has been found to be beneficial to erectile dysfunction patients and obesity and might also be
protective against erectile dysfunction.27,107 This may even have reversal effect on the
development of erectile dysfunction regardless of the intensity and type of exercise done,50
Studies have shown that both interval and continues physical activity have been found to be
beneficial in erectile dysfunction27,98
An inverse relationship exists between physical exercise and biomarkers of inflammation in both
diabetes and cardiovascular disease and their complication which includes erectile dysfunction,
hence the role of exercise in the management of erectile dysfunction.99 Daily physical exercise is
divided into mild, moderate and high intensity based on the rating designed to keep the human
body active as follows ; (a) less than 5000 steps is considered sedentary (b) 5000-7499 steps in
low activity (c) 7500-9999 is somewhat active (d) 10000-12499 steps is active (e) greater than
12500 is highly active, the minimum any person can go to remain healthy is low activity.24

53
The relationship between physical exercise and erectile dysfunction is related to the biochemical,
hormonal and neural changes in the blood vessel walls, this results in blood vessel wall
relaxation with acute or long term exercise because of its local production of nitric oxide and
lactic acid, decrease nerve activity, changes in certain hormones and their receptors together with
the warming effect of exercise.109 As the exercise is increased or repeated, there is prolong effect
, thus regular or long term physical training can decrease basal concentration of inflammatory
markers.100
Exercise meant for improving physical fitness follows the FITT principle which states that
exercising a part of the body or system at intensity above that which it normally works leads to
an improved function of that part or system.26 Therefore prescribing physical exercise in order to
achieve these set goals are as follows; (a) moderate physical exercise done at least 30 minutes
over 5 days a week e.g. fast walking ( 3-4 miles/ hour), watering a garden, skipping, household
chores etc. (b) high intensity physical exercise i.e. 20 minutes for at least 3 times a week e.g.
jugging, running, cycling, farming, swimming and gymnastic based structured activities which
can be done either continuously or at an interval periods, both of which are beneficial in the
management of erectile dysfunction.99,100
An indirect way of assessing exercise intensity is the use of maximum heart rate (MHR), heart
rate reserve (HRR) and resting heart rate (RHR). Where the MHR=220- age in years. To assess
for heart rate reserve, HRR=MHR-RHR.87 An international physical activity questionnaire can
also be used to assess physical activity such as walking, moderate and vigorous intensity
exercise classified as low, moderate an high intensity.95
The five trans-theoretical model of change is used to assess readiness for exercise in humans.23
These are (a) pre contemplation: not considering or not ready to change (b) contemplation-
54
acknowledges the problem and considering taking an action within the next six months, (c)
preparation- planning to change the bad behavior within the coming next months (d) action-
actually carrying out the behavior (e) maintenance- continues to practice it for at least five years
(f) adoption/termination- has fully integrated the new behavior into his/her live.25
Factors or barriers limiting physical exercises in humans are; lack of enough time, not
enjoyable, not convenient, lack of self-motivation, unfavorable weather, ignorance of its benefits,
fear of being injured, no space for exercise, etc.25 Other forms of lifestyle that improve erectile
dysfunction are diets such as the Mediterranean style of diets and reduction in calorie intake
invariably leads to improvements in erectile dysfunction.26 Others are reduction or stoppage of
alcohol consumption, cigarettes smoking and weight reduction.57 Lifestyle changes that result in
weight reduction invariably improve erectile dysfunction in one third of obese patients under 55
years of age.57
Chevrolet-Meason et al postulated that spouses of patients are encouraged to be part of the
management because treatment of erectile dysfunction usually foster positive, realistic
expectations for couples and maintenance of drug use when partners are involved.28
2.10.4: COMPLEMENTARY AND ALTERNATIVE TREATMENT
Complementary and alternative medicines is defined as a group of various medical and health
care systems, practices and products that are not presently considered to be part of conventional
medicines.101 Complimentary interventions are health care approaches used in conjunction with
conventional interventions while alternative practices replace the conventional ones.101 They are
used all over the world and use varies from one country to the other.102 Commonly used
complementary and alternative practices all over the world are herbs, acupuncture, non- vitamins
and minerals, natural products and spirituality.101
55
In Africa and in India, about 38.5% of the population uses complementary and alternative
medicines with spirituality being the commonest,102 while in Saudi Arabia, about 80% of the
general population uses the product and traditional healing modalities for treatment.101 The
commonest aspect of complementary and alternative medicine are spirituality (49.4%) aloe- vera
(23.1%), forever living products (16.3%) and black stone(12.5%).101 It is commonly used by
people with low socio-economic status and low education, but reverse is the case in developed
countries.101
There are evidences to show that people use complementary and alternative medicine because of
the in- effectiveness of the conventional medicine or the adverse effects to them and also having
a holistic health approach and greater control of our health.103 Studies have shown that the
commonly used complementary and alternative medicine used all over the world is the biological
methods with Honey being the commonest, others are spirituality (49.4%) with faith and prayer
being the commonest and physical therapy (22.1%) with massage being the commonest in use
and black stone the most commonly used.101
Patient’s preference of complementary and alternative medicine compared to orthodox medicine
in our environment may be connected to social stigma, cultural perception on the etiology of the
disease and the perceived response to the indigenous herbs.9,11A study done by Ernest et al also
evaluated acupuncture, ginseng, meca and yohimbine for the treatment of erectile dysfunction,
insufficient evidence was found for meca and acupuncture, but positive conclusions were drawn
for ginseng and yohimbine.104
Other commonly used complementary and alternative medicines are Arginine, dihydro
epiandrosterone, coleus, Damina, Gingko and alpha lipoic acid which is particularly suited for
the treatment and prevention of diabetic complications including erectile dysfunction.105 Erectile

56
dysfunction with undiagnosed co-morbidities exist in about 6.8% of general population with
majority of them using complementary and alternative medicines for treatment.11
Herbal medications are usually the common choice therapy for self-care among individuals
taking more active roles in their health care.106 This has been promoted by mass media who have
enhanced widespread use of herbal medicine within the general population especially in
developing countries.106 According to WHO, Herbal medicines are medications prepared from
one or more herbs or plant parts (roots, stem, bark, seeds and or fruits).106,107
Herbs contain chemical compounds, vitamins, plant hormones and minerals which are essential
for plant growth and health in humans.107 Humans need the phyto-chemicals for metabolism and
healthy living which are naturally found in the plant.107 Herbal medicines are found to be better
than conventional medicines because they are natural and have minimal side effects, they are not
only used in the treatment of isolated symptoms, but also maintain general wellbeing.107 About
30-50% of adults in industrialized nations had used natural products in treating diseases and
prevention in one form or the other.107
Herbal medicine is a combination of fruits, vegetables, leaves etc used in the treatment of some
ailments.107 Men and their spouses are interested in using herbal and complementary medicines
in treating their ailments.107 The common herbal medications used in the treatment of erectile
dysfunctions include: red, white and fresh ginseng, ginko biloba, robus coreanus, schisandra
chinensis, epimedium koreanum, lepidum meyenii, male silkworm extract, artenisia capillaris
cuscuta chinensis and plant mixtures.107 The differences between herbal medicines and western
style medicines are that herbal medicines are mixture of all kinds of medicines, they act slowly,
they are natural while western medicines act fast, usually a single agent and artificial.107

57
Common herbal treatments used in erectile dysfunction are ginseng and yohimbine, but
yohimbine has serious side effects compared to gingering, these side effect includes headaches,
insomnia, gastric upset and constipation.18,71 Others are bradycardia, hypoglycaemia,
nervousness, diarrhea, high blood pressure, palpitation and high estrogenic effect.18,108
Ginseng in one of the complementary and alternative drugs used in the treatment of erectile
dysfunction.104 There are evidences to show that the use of herbal medication is not strange
especially in African society as about 80% of Africans and 27 million South Africans used
traditional herbs.109,110 but general use of herbs in Nigeria is not well documented.111
Ezeoma et al observed that the reasons several people use herbs for treatment of erectile
dysfunction are that they are natural and safe.112 Others are for economic reasons, high cost of
health care, poor access to conventional medicines, protracted health issues, religion, traditional
or cultured beliefs as well as dissatisfaction with the efficacy of conventional medications and
the perception that it is much more efficacious than orthodox medicines.113,114 Panax Ginseng is
an important medicinal herb that is widely cultivated in Korea, China and Japan.115 It has been
used for over 200 years in oriental countries and use is rapidly increasing in western countries.115
2.10.4.1: RED KOREAN GINSENG
Korean ginseng also known as panax ginseng is one of the most widely used herbal remedies in
the world and commonly in Asia.116 It is usually steamed before it is dried and ready for use.116 It
is long been used and seen to be effective in the treatment of psychological erectile
dysfunction.116 Panax ginseng had been in use for decades for the treatment of erectile
dysfunctions and other ailments such as nausea, diabetes mellitus.72 A Randomized Controlled
Trial found that Ginseng is effective at the dose of 1000mg when taken over twelve weeks.72
Kim et al study found that Panax Ginseng does not affect the level of cholesterol or prolactin,
58
therefore it is an alternative to invasive procedures for treating erectile dysfunctions. The study
also found that the effect of Korean red ginseng on erectile dysfunction is dose dependent.117 The
higher the dose of ginseng the higher the levels of nitric oxide in corpus cavernosum.117 It all
inhibits penile fibrosis and can be used to improve erectile function in patients with erectile
dysfunction.117 Ginseng is broadly classified into two i.e. Asian and American Ginseng which
are both made up of similar chemicals such as Ginsenosides.118,119 This is considered the active
ingredient in Ginseng. Others are saponins, glycans polysaccharides fractions, peptides, maltol,
vitamin B, flavonoids and volatile oils.118,119 There are more than 30 sub types of ginsenosides
that have been identified and more attempt are being made to increase its production because of
its increased use.119 Ginseng is a perineal plant that grows slowly and has a long production
cycle of 4-6 years, it is a snarled roots that looks like arms and legs.119
The different types of ginsenosides extract exist in the form of Rg1, Rb1,Rb2, and Rb0 depending
on their polarity which is usually graded A-Z. Ginsenoside Rg1 has been found to be more
effective in treatment of sexual dysfunctions.91 The effect of ginsenocides are induction and
activation of large conductance (KCa) channels in human copora carvenosal smooth muscle
relaxation by hyper-polararizing the smooth muscle membrane via the KCa channels which is
one of the mechanism of action of ginsenocides.91
Korean ginseng is commonly used in Korea to treat erectile dysfunction because it relaxes the
penile smooth muscle by ultimately increasing nitric oxide – cyclic guanosin monophosphate
pathway (cGMP) leading to increased erectile and endothelial functions.73 Korean red ginseng is
a mixture of lytium babarium, cuscuta chinese, rubus coreanus, miqi torilis Japanica fruits,
Schisandra fruit concentrate.73
59
Ginsenoside is found in all parts of the ginseng plant that is leaves, roots, barks and berries, but
the roots and the berries produce more ginsenoside of up to 4-6 times more than other parts of
the plants.120 The berries also have anti glycaemic and anti-obesity effects in mice.120 Panex
ginseng also improves glucose metabolism and immune response, maintains vitality and body
restoration in humans.121 Red Korean ginseng derived from the roots of ginseng plant has
stimulating effects on corpus spongiosum smooth muscle, therefore it is being promoted for the
treatment of erectile dysfunction.122 A randomized Controlled Trial observed that drug
interaction with panax ginseng includes theophylline and other asthmatic drugs, metabolism of
monoamine oxidase inhibitors such as phenelzine, tranylcypromine, isocabaxazid and
antipsychotics.18,123
Ginseng is usually available as tincture, liquid extract, powders and capsules.124 Studies have
found out that Ginseng preparation that has been used and found to be more effective in the
treatment of erectile dysfunction are in the form of root that are chewed or taken in the form of
tea as short term for six months and 100 mg to 600 mg capsule daily in divided dose.61,123 Even
though optimal dose of ginseng is unknown but when taken for a long time at high dose can lead
to a phenomenon called ginseng abuse syndrome. This occurs when ginseng is used for a long
period of time presenting with increased blood pressure, nervousness, insomnia, diarrhea and
skin eruptions.124 It is usually non toxic when used for a short time.124
It has also been postulated that uptake of gamma aminobutyric acid (GABA),glutamate,
dopamine, nor-adrenaline and serotonine in rats brains synaptosomes sin a concentration
dependent fashion which competes with the agonist of GABA receptor.72 Studies has also shown
a marked improvement in erectile performance in person including sexual satisfaction after
treatment with Red korean ginseng including moderate to severe forms after taking 900mg three

60
times a day.7,8,.72 An animal study also using red korean ginseng has been shown to significantly
relax the pre-contracted penile corpus cavernosum smooth muscle in rabbits9,10 Ginseng has
been used by many cultures as a remedy for erectile dysfunction. There is a significant
relationship between erectile dysfunction and weight, triglycerides and diabetes, but no
difference between testosterone fractions and sex hormone binding globulin (SHBG) levels.125
There is also a positive correlation between diabetes and hypertension with severity of erectile
dysfunction.125 Ginseng was used to restore and enhance normal wellbeing of the body, the effect
of which acts on the central nervous system, cardiovascular system and metabolism.125 Korean
ginseng is also effective in the treatment of orgasmic disorders and sexual desires.74 There exists
a significant relationship between weight, triglycerides and diabetes mellitus.119,125 There is also
a positive correlation between diabetes mellitus, hypertension and severity of erectile
dysfunction.125
Erectile dysfunction is a medical condition where patients patronize Complementary and
alternative medicine (CAM) heavily since most cannot express their problems to the physician,
2.10.4.2 SIDE EFFECTS OF GINSENG
Panax ginseng has been in used and its among the top 10 selling herbal supplements in the
United State as an adaptogen.126 There has been some few reports of side effects in human
studies. Panax ginseng is also considered a very safe and well tolerated drugs in animal studies
with a few reports of toxicity.126
Nam et al study, a randomized controlled double blinded study done in healthy volunteers
showed mild adverse events after using 1gram and 2grams of Ginseng.126 These adverse events
included dyspepsia, insomnia, hot flushes, constipation, low energy, dizziness and nausea which
were similarly seen in the placebo group.126 There was no significant difference between in

61
adverse events between the placebo and the ginseng group. The study conducted in subjects with
mild ED.126 Similar study conducted by Hyong et al, also a Randomized Controlled study
showed 1% side effect with one participant withdrawing from the study because of the side
effect. (systemic rash and pruritus) after using 1gram of ginseng within seven days of the
study.127
A systematic review of forty four selected studies on safety analysis of panax Ginseng, sixteen
of the studies reported minimal side effects while 23 studies did not report on side effects.128
Panax Ginseng used as a mono preparation in the study showed a safe profile with no significant
difference between Red Korean Ginseng and placebo.128 The side effects recorded were similar
to Nam. Aksam and Thuryan et al found that the optimum dose of red ginseng in the treatment of
erectile dysfunction is not known, but had been found to improve sexual dysfunction which had
been used at different dosages such as 100mg, 500mg and1000mg125,126. Same studies also
showed that the safety profile of red ginseng reported no adverse drug reaction but effective in
the treatment of erectile dysfunction.125,126 Many patients with erectile dysfunction use herbal
medication in addition to conventional medicines.129 Common side effects of ginseng by Fakeye
et al are sleeping problems. Other side effects not commonly seen are menstrual problems in
women, increased blood pressure, tachycardia, headaches, dizziness, diarrhea, skin rash and
gastric upset.129
Ginseng rarely interacts with some conventional medications such as blood thinners, monoamine
oxide inhibitors (MAO), immune system suppressants and insulin for treatment of diabetes
mellitus and the side effect was reported to be mild .129,69 De Adraede and Thuryan et al
reviewed the safety profile of red ginseng. They reported no evidence of adverse drug reaction
with normal dose of red ginseng.71,72
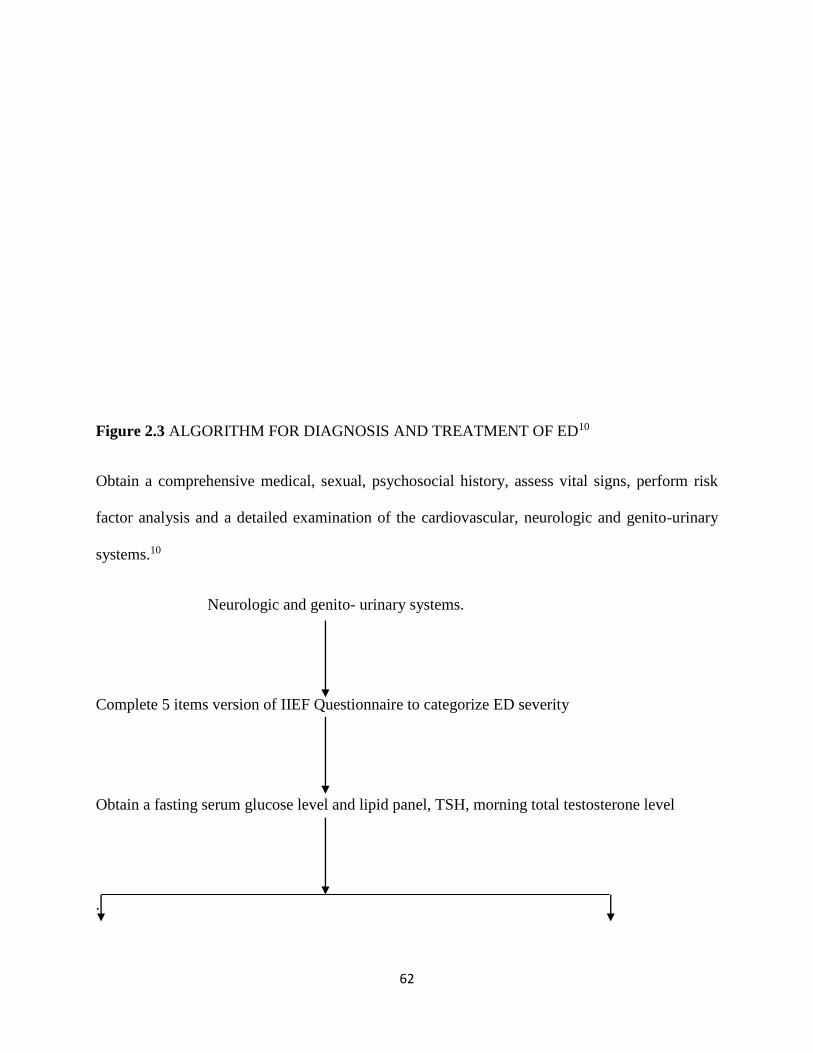
62
Figure 2.3 ALGORITHM FOR DIAGNOSIS AND TREATMENT OF ED10
Obtain a comprehensive medical, sexual, psychosocial history, assess vital signs, perform risk
factor analysis and a detailed examination of the cardiovascular, neurologic and genito-urinary
systems.10
Neurologic and genito- urinary systems.
Complete 5 items version of IIEF Questionnaire to categorize ED severity
Obtain a fasting serum glucose level and lipid panel, TSH, morning total testosterone level
.

63
Definable medical etiology Non definable medical etiology
1. Maximize treatment of coronary artery disease 1. Screening for psychological
2. Diabetes Mellitus causes e.g. anxiety, Depression
Guilt, sexual abuse, marital
2. Referred for behavioral
Therapy
3. Hormones disorder e.g.hypogonadism 3. Removal of negative
Hypothyroidism,psychosocial factors thoughts
4. Hypercholesteronamia
5. Hypertension
6. Metabolic syndrome
7. Neurologic conditions e.g. Alzheimer’s
disease, multiple sclerosis
8. Obesity
9. Vascular disease
10.
FIRST LINE THERAPY
1. Lifestyle and pharmacotherapy modification
(a) Oral therapy with phosphodiesterases inhibitors type 5 (ensure patients is not taking nitrates).
(b) Testosterone supplementation if patients has clinical hypogonadism
SECOND LINE THERAPY
64
Intraurethral and intracavernosalalprostidyl or
Vacuum pump devices
Referral to the urologist for further evaluation
CHAPTER THREE
3.0 METHODOLOGY
3.1 STUDY AREA
The study was carried out in Jos, the Plateau State Capital. Plateau State is located in the North
central zone of Nigeria bounded by Bauchi in the North while Bauchi and Taraba states are in
the north and East respectively, to the South by Nassarawa State while to the West by parts of
Nassarawa and Kaduna States. It is located on latitude 90 55 N and longitude 8053 E at an altitude
of about 1300m (about 4100 ft) above sea level.130
Its landscape is mostly treeless in the North and comprises features like hills and captivating rock
formations ranging from bare rocks, artificial hillocks and deep ponds which emanated from
years of mining. It has a dry season between November and March and a rainy season between
April and October. It covers an area of 7800 sq/km.130
The temperature on the Plateau is generally about 40C lower than that on the coast and annual
rainfall of about 1300mm is considerably higher than the surrounding lowland.

65
The State has an estimated population of over 3.1 million130 as at 2006 census which majority are
farmers, civil servants and traders. The capital city of the State is Jos, comprising of Jos North,
Jos South and part of Jos East. It is a cosmopolitan city where various tribes are represented.
The estimated population of Jos North is 429,300 while that of Jos South is 306,716.91 (2006
census). Plateau State has fairly well distributed health facilities with two teaching hospitals
(JUTH) and Bingham University Teaching hospital), General hospitals and over 500 Primary
health care (PHC) distributed over 17 local government councils130.
Jos University Teaching Hospital is the first and the largest teaching hospital in the whole of
North central Nigeria. It is located in Lamingo (new site).The hospital is a 525 bed hospital that
provides primary, secondary, tertiary health care to people of Plateau State and other adjourning
States.
The General Outpatient Clinic (GOPC) is the first point of contact for all patients including
patients with erectile dysfunction. Many of the patients are managed and followed up in the
GOPC while those who need specialist care are referred to the specialist in the various
departments of the hospital. Both Urology clinic and GOPC are located in the permanent site in
Lamingo.
3.2 STUDY POPULATION
The study population comprises all male patients with ED within the ages of 25 and 70 years
presenting at GOPC and urology clinic in Jos University Teaching Hospital with erectile
dysfunction. An average of 60 (15 Patients per week and 3 patients per clinic day) patients with
erectile dysfunctions are usually seen in GOPC and 30 (8 patients per clinic visit) patients per
month usually seen in Urology clinic.
3.3 STUDY PERIOD
The study was carried out between November 2014 and March 2015 – four months.

66
3.4 ELIGIBILITY
3.4.1 Inclusion Criteria
(1) Married men between the ages of 25 and 70 years who presented with erectile dysfunction for
at least three months (2) Participants who are were willing to participate in the study.(3) Subjects
who were not on Ginseng and other medications for ED and had the ability to come for
stipulated follow up.
3.4.2 Exclusion Criteria (1) Participants who were too ill to participate in the study (2)
participants who had significant cardiovascular diseases such as myocardial infarction, cardiac
failure and stroke because they may not be stable for regular follow up appointment. (3)
Asthmatics and patients on theophylline were also excluded because of rare adverse reactions
associated with ginseng (4) Patients on antipsychotics for instance, phenelzine, tranylcypromine
and isocarbaxazide due to drug interactions with Ginseng.
3.5 SAMPLE SIZE DETERMINATION
The sample size is determined by the following formula.131
N = 2P(1-P) (za + zb)2 where P = PA +PBD D= PB – PA
D2 2
Where N = Sample size (sample size in one study arm i.e group A or B)
PA = proportion of those in group A who have 50% improvement in erectile function using
11EF after 8 weeks of placebo and exercise from Assumption
PB = Proportion of those group B who will have at least 75% of improvement in erectile
function using 11EF after 8 weeks of treatment with Ginseng and exercise i.e. 25%
improvements
D = PB – PA = Smallest clinically significant difference to be detected = 75% - 50%
D = 25% = 0.25

67
P = PA + PB = 50% + 75% = 125% = 63% P=0.63
2 2
The alpha error of 5% = 9 = P value = 0.05, 95% confidence interval (Cl) and power of 80% (B
error = 20%)
Za = value of alpha error = 1.96
Zb = value of B error = 0.842
The sample size is therefore calculated
2x 0.63 (1 – 0.63) (1.96 +0. 842)2
(0.25)2
= 1.26 (0.37) (7.851204)
0.0625
= 3.6602313/0.04= 91.5
= 92 in each arm
This gives a minimum sample size of 184 for both the control and intervention groups for the
study.
Providing for a 10% attrition rate 10100⁄ × 184 = 18.4.
This will give rise to a maximum sample size of 101 on each group giving a total of 202
participants.
3.6 ETHICAL CONSIDERATION
Ethical clearance was obtained from the ethical committee of Jos University Teaching Hospital.
The aims, objectives and benefits were explained to the patients. Confidentiality was ascertained
throughout the study and written consent from each patient was obtained prior to recruitment.
They were told they could opt out of the study any time they wished with no consequences or
penalty.

68
3.7 INSTRUMENTS OF DATA COLLECTION
(i) Consent form written both in English and Hausa
(ii) Questionnaire: International Index of Erectile Function (IIEF) which is validated for the
diagnosis and classification of erectile dysfunction. It was scored before and after the study. The
scores are 22-25 (Normal erectile function), 17-21 (Mild ED), 12-16 (Mild to moderate ED), 8-
11 (Moderate ED), and 5-7 (Severe ED).
(iii) Standard bathroom weighing scale (Hamson) for weight measurement of the participants,
Calibrated from 0 to 120kg and adjusted to zero before each participant weight was measured.
The weight was measured by removing shoes and other heavy objects and standing straight on
the weighing scale.
(iv) Wall-mounted stadiometer was used to measure height of the participants (SECA cooperation.
Maryland USA). The participant stood straight while backing the stediometer. The height was
measured by moving the reader to the head . The readings ranged between 5.5- 78.75 in (14-
200cm) with graduation of 0.125 in 0.1cm
(v) Calculator (TAKSUN TS 568) for calculation of BMI, Sample Size and Statistics. A scientific
calculator with a rigid dual cover and scientific buttons with model size of 101x60x11MM.
(vi) Mercury sphygmomanometer (AccosonDecamet – Essex Cm19, 96p) for blood pressure
measurement. A table top sphygmomanometer containing a bulb, a cuff, tubbing, metal case and
a meter with a mercury measurement ranging from 0 to 220mmH. The cuff was tight to mid
portion of the left arm and inflated to 30mmHg above palpable systolic pressure. The bulb was
released gradually while listening with the stethoscope for systolic and diastolic blood pressures.
(vii) Stethoscope (Littman’s) for blood pressure measurement. It contains the ear piece, head set, the
bell and the diaphragm to complement sphygmomanometer in blood pressure measurement.

69
(viii) Urinalysis strips for urinalysis. It’s a plastic diagnostic chemical reagent strips containing URS-
K for detection of ketones, URS-3 for glucose, protein and ph, and URS-10 for glucose,
billirubin and blood. The urinalysis strip was immersed inside the urine and compares the colour
change with a standared colour chart.
(ix) Glucometer for blood glucose measurement (life scan one touch ultra easy-made in Switzerland).
It has a meter for the readings, tests strips, sterile lancets and a carrying case. It has a storing
capacity of up to 300 test result with dates and time. The tip of the thumb was cleaned and
pricked. The blood was collected on the test strip and the blood glucose read through the meter.
3.8 STUDY DESIGNS
The study was a randomized controlled single blinded comparative study where clients were
randomly allocated through simple random sampling after obtaining informed consent from the
subjects.
3.8.1 SAMPLING METHOD The participants were recruited consecutively as they come into
the clinic and selected at random by picking sealed envelopes randomly containing letter A and
B allocated into control and intervention groups respectively (Each participant had equal chance
of being selected). Sixty (60) patients per month are usually seen in GOPC (from records) ie 180
over three months and thirty (30) patients seen in Urology clinic per month ie 90 patients over
three months. The ratio of patients to be seen in GOPC and Urology making up the sample size
is 180:90 making a total of 270 in three months.
3.8.2: HYPOTHESIS The study was set to test the hypothesis that physical exercise and
Ginseng will reduce the severity and prevalence of erectile dysfunction in Jos.
HO The study was set to test the hypothesis that physical exercise and Ginseng is not effective in
the treatment and reduction of ED severity.
H1 Physical exercise and Ginseng is effective in the treatment and reduction of ED severity

70
3.9 STUDY PROTOCOL
Married men within the ages of 25 and 70 years who attended either GOPC or urology clinic in
JUTH with erectile dysfunction. Subjects who had persistent inability to achieve or maintain
erection for satisfactory sexual intercourse for about three months and who met the inclusion
criteria and consented for the study were recruited. One hundred and sixty two (162) participants
were recruited from GOPC over four months (two patients per day within five clinic days in a
week) and twenty eight (28) were recruited from Urology clinic (Two patients per day within
one clinic day per day) making a total of 190 participants. The duration of the study was
extended by one month because the minimum number of patients seen in the two clinics could
not meet up the minimum sample size in three months (due to security reasons) therefore, the
total number expected in three months was not feasible. Direct interview during history taking
was done by the investigator and also referral from colleagues as notices were placed in all the
consulting rooms to refer all patients who complained of poor erection. They were counseled on
the aim of the study and its implication on the management of erectile dysfunction and randomly
allocated equally to control and treatment groups. The consent form and the international index
of erectile function (IIEF) forms were completed by the interviewer. The nurse assistant in
GOPC arrange the patients after referral from colleagues before calling the researcher for the
interview on Uroiogy clinic days. The IIEF Questionnaires were interviewer administered with
the help of two nursing assistants. Full explanation and information concerning the research
processes was given to the participants. The IIEF questionnaire was used to diagnose and
measure the severity of erectile dysfunction.
The socio-demographic questionnaire included socio demographic data (including phone
numbers of subjects and or their spouses), history of sicknesses, medical and social histories
(hypertension, diabetes mellitus, heart disease, alcohol, cigarettes smoking, substance abuse and

71
drugs they were presently on) (1) exercise monitoring and drug adherence form (2) spouse
presentation form and ED severity (3) drug side effects forms. Results of physical examinations
as weight, height, blood pressure (120-139/80-89mmHg was considered normal), BMI (18-
24.9kg/m2 as normal), and the genitals (presence of both testes in the scrotum, firm and equal
sizes),laboratory results (urinalysis with absence of protein and glucose in urine), FBG (blood
glucose less than 7.1mmol/l as normal) lipid profile (with T chol 200mg/dl and below was
considered normal, LDL 70mg/dl, HDL of 60mg/dl and below was considered normal, and
triglycerides 150-200mg/dl, ECG (with normal rate, rhythm and heart size) and testicular
ultrasound results with testicular volume 12-28cm3 as normal). The IIEF was used to measure
outcome in both groups A and B before interventions. Scores were awarded for each subject
which classified erectile dysfunction into no erectile dysfunction rated from 22-25, mild ED from
17-21, mild to moderate ED from 12-16, moderate ED from 8-11 and severe ED from 5-7.
One hundred and ninety subjects who met the inclusion criteria were recruited for the study.
These subjects were randomly assigned into two study arms using letters A and B written on a
separate sealed opaque envelopes by the researcher in equal numbers of the total of 190
envelops. Ninety five (95) subjects were allocated to group A (control group) while ninety five
(95) were allocated to group B (treatment group) after obtaining informed consent from both
groups. Twenty (20) sealed envelopes from group A and 20 sealed envelopes from group B were
selected and mixed together. The first 40 subjects picked the envelopes at random until the first
40 got exhausted before another set of 40 was made available. This continued until the total 190
envelopes were picked. The envelopes were opened only at the time of allocation. The study arm
B was subjected to treatment using 50mg daily of Ginseng from Mega life sciences in addition to
physical exercise (at least brisk walking 30 minutes daily for at least five days per week), while
the control group A received placebo daily with physical exercise (at least brisk walking 30
72
minutes daily for at least five days per week). Reload multivitamin was used as placebo because
it contained Vit A, C, D3, E, K, B1, B2, B3, B6, B12, Biotin, Pentatonic acid, Ca2 iodine, Zn,
Mg, Chromium and was not a common drug for easy identification by the subjects. These
vitamins were also present in Ginsomin except ginseng. Both study arms were counseled on the
need for physical exercise (brisk walking 30 minutes daily for at least five days) a week while a
self administered physical activity questionnaire was completed each day of exercise (simply
ticking day and duration of exercise) and submitted at next visit for adherence assessment.
They were encouraged to come with their spouses because treatment of erectile dysfunction
usually fosters positive, realistic expectations for couples and maintenance of drug use when
partners are involved.28 Their role was to help their husbands in terms of adherence to
medication and physical exercise.
Both study arms were followed up in two weekly intervals (monitored on the follow up
questionnaire) of a total of five follow up visits (where lab results were reviewed in first follow
up visit, adherence to medication by reviewing the adherence form, exercise and follow up were
assessed at second to fourth visits while IIEF questionnaires were completed in the fifth follow
up visit). Four participants were lost to follow up with two participants losing follow up at six
weeks in the control group while two lost to follow up at the first two weeks in the intervention
group. One participant travelled for a holiday in the intervention group while other participants
who lost to follow up gave no reason. The subjects were contacted through phone calls about a
week to each follow up visit as a reminder.
At the end of the study, 186 participants completed the study and the data was analysed. The
international index of erectile function (IIEF) questionnaire was administered and completed by
the assistants using a separate questionnaire from the one used at recruitment. This was used to
assess the ED scores and the side effects between the two groups.

73
3.10 STATISTICAL ANALYSIS
Excel spread sheet and Statistical Package for Social Sciences (SPSS version 20) were used for
statistical analyses. The data was tested with One-sample Kolmogrorov-Smirnov test and the
Levenne test for equality of variances to satisfy the assumption of test model. Parametric tests
were used on variables that were normally distributed, while equivalent non-parametric tests
were used on variables that were not normally distributed.
Student T-Test was used to analysed any differences between the control and intervention group
in relation to age structure, educational level and the used of medication. Similarly, Student T-
test was used to analysed erectile dysfunction score and severity in the control and the
intervention groups. To compare the statistical difference in side effects of Gingseng
(intervention), Mann-Whitney-U test was carried out.
CHAPTER FOUR

74
4.0 RESULTS
4.1 Subject Flow through the Study
About one hundred and ninety (190) patients who met the inclusion criteria participated in the
study. This comprises of one hundred and sixty two (85.1%) subjects from the GOPC and twenty
eight (14.9%) subjects from the urology clinic. A total of four subjects were lost to follow up,
two from the intervention group and two from the control group. A total of one hundred and
eighty six subjects (97.9%) who completed the study were analyzed. The analysis was done
based on the number of subjects that completed the study. The study protocol through the study
is illustrated in figure 4.1
There were no subjects that were followed up to the end of the study that abandoned the study
and no subject crossed over the group.
Fig 4.1: STUDY PROTOCOL
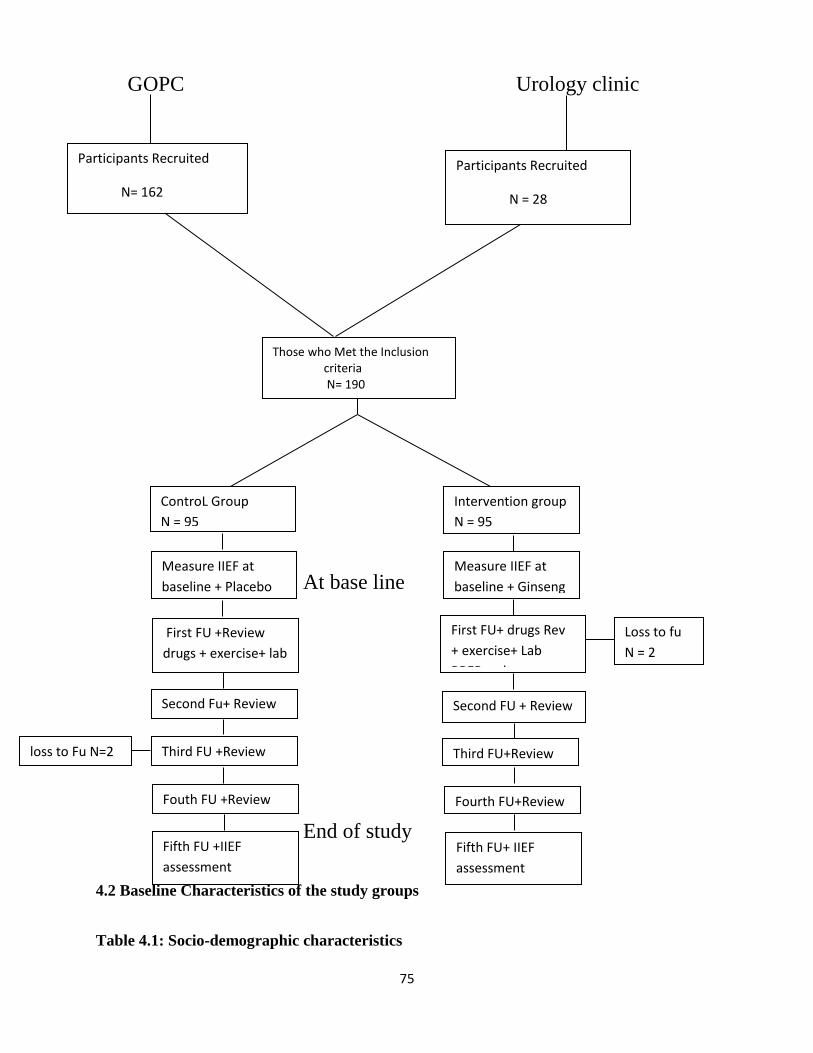
75
GOPC Urology clinic
At base line
End of study
4.2 Baseline Characteristics of the study groups
Table 4.1: Socio-demographic characteristics
Participants Recruited
N= 162
Participants Recruited
N = 28
Those who Met the Inclusion criteria N= 190
ControL Group
N = 95
Intervention group
N = 95
Measure IIEF at
baseline + Placebo
First FU +Review
drugs + exercise+ lab
re adhirateform
Second Fu+ Review
Third FU +Review loss to Fu N=2
Fouth FU +Review
Fifth FU +IIEF
assessment
N = 93
Measure IIEF at
baseline + Ginseng
First FU+ drugs Rev
+ exercise+ Lab
RREResults
Second FU + Review
Third FU+Review
Loss to fu
N = 2
Fourth FU+Review
Fifth FU+ IIEF
assessment
N = 93
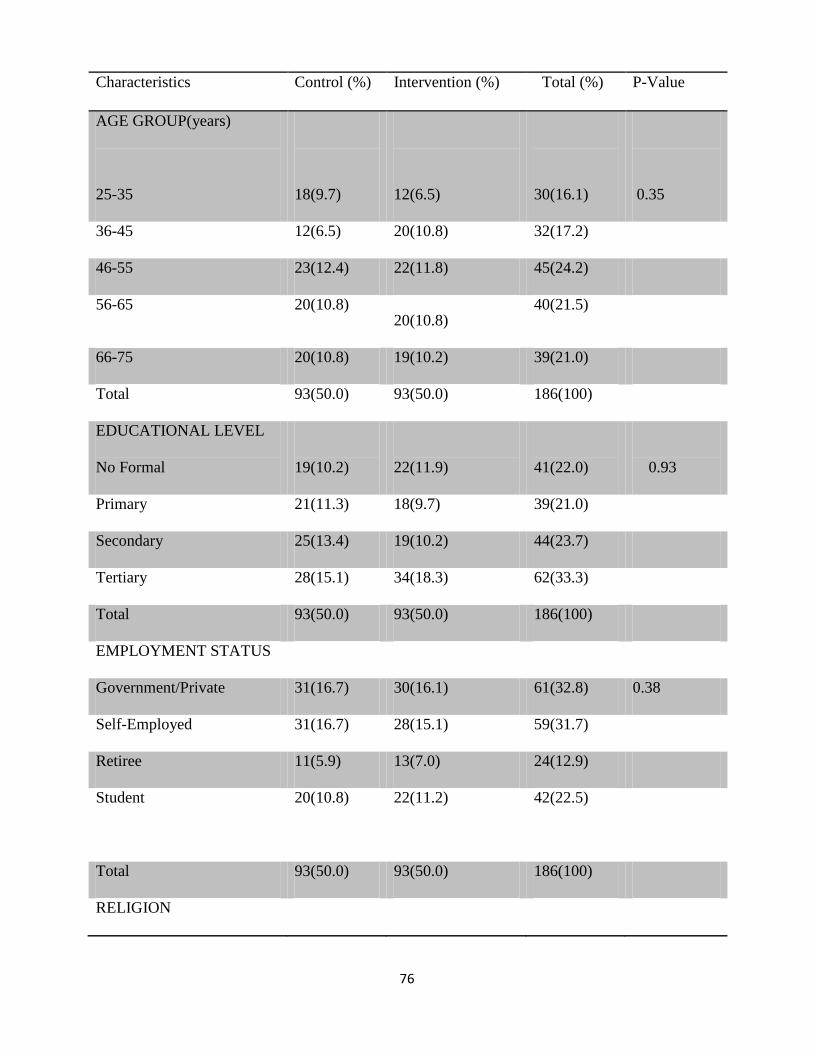
76
Characteristics Control (%) Intervention (%) Total (%) P-Value
AGE GROUP(years)
25-35
18(9.7)
12(6.5)
30(16.1)
0.35
36-45 12(6.5) 20(10.8) 32(17.2)
46-55 23(12.4) 22(11.8) 45(24.2)
56-65 20(10.8) 20(10.8)
40(21.5)
66-75 20(10.8) 19(10.2) 39(21.0)
Total 93(50.0) 93(50.0) 186(100)
EDUCATIONAL LEVEL
No Formal
19(10.2)
22(11.9)
41(22.0)
0.93
Primary 21(11.3) 18(9.7) 39(21.0)
Secondary 25(13.4) 19(10.2) 44(23.7)
Tertiary 28(15.1) 34(18.3) 62(33.3)
Total 93(50.0) 93(50.0) 186(100)
EMPLOYMENT STATUS
Government/Private 31(16.7) 30(16.1) 61(32.8) 0.38
Self-Employed 31(16.7) 28(15.1) 59(31.7)
Retiree 11(5.9) 13(7.0) 24(12.9)
Student
20(10.8) 22(11.2) 42(22.5)
Total 93(50.0) 93(50.0) 186(100)
RELIGION

77
Christianity 64(34.4) 60(32.3) 124(66.7) 0.98
Islam 29(15.6) 33(17.7) 62(13.3)
Traditional 0(0) 0(0) 0(0)
Total 93(50.0) 93(50.0) 186(100)
A total of 186 patients were analyzed. The mean age with standard deviation of the study
population (N = 186) was 41.7±25years. The age ranged range in this study was from 25-70
years. There was no significant difference in age distribution between the intervention and
control group (t=0.097, p=0.35)
The educational level of the 186 participants is shown in table 4.1. Forty-one (22.0%) of the
participants had no formal education, 39(21.0%) had primary education, 44(23.7%) had
secondary education and 62 (33.3%) had tertiary education. The employment status of the
participants indicated 61(32.8%) were government or privately employed, 59(31.7%) were self
employed, 24(12.9) were retirees, and 42(22.5%) were students,.
Among the 186 participants in this study, 124 (66.7%) were Christians, 62 (13.2%) were
Muslims. The overall table 4.1 showed that randomization was effective as there was no
significant difference in the baseline socio- demographic characteristics.

78
4.3 Medical Characteristic of the study Group
Fig 4.2 primary complain of erectile dysfunction
Participants who presented to the clinic with primary complaint of erectile dysfunction were:
29.0% while subjects who came with a different complaint were 71.0%
0
10
20
30
40
50
60
70
80
Self Presentation Physician Motivated
Res
po
nd
ents
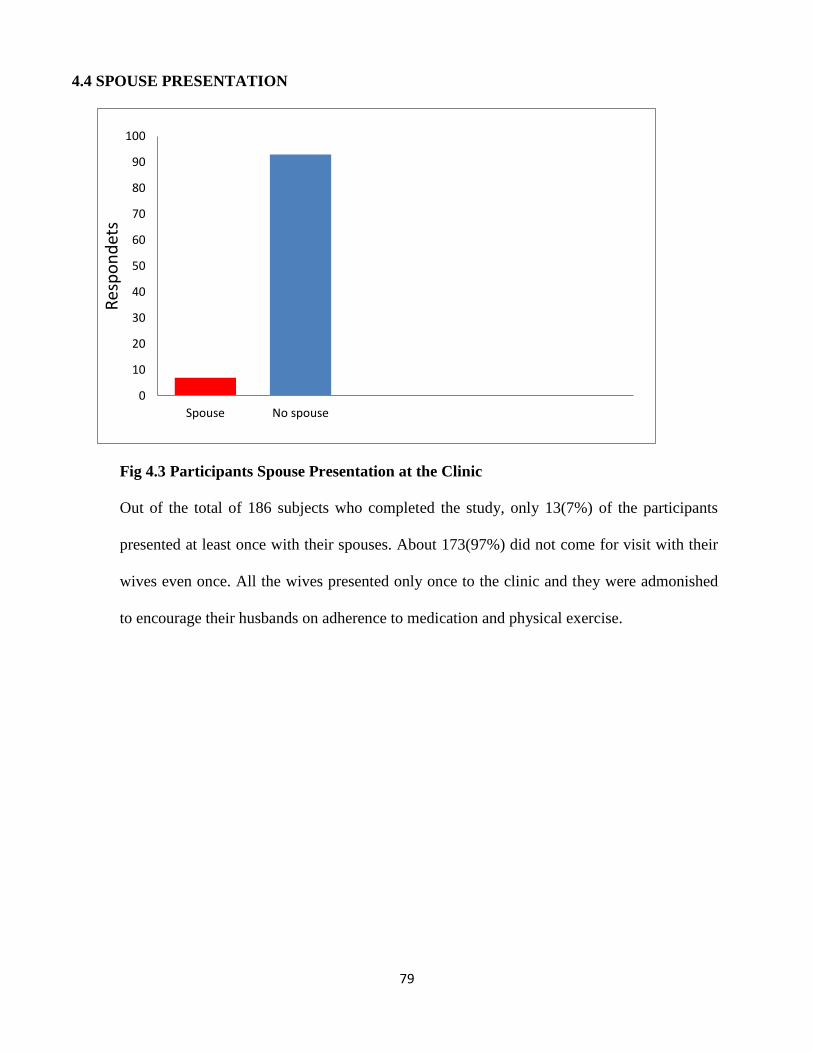
79
4.4 SPOUSE PRESENTATION
Fig 4.3 Participants Spouse Presentation at the Clinic
Out of the total of 186 subjects who completed the study, only 13(7%) of the participants
presented at least once with their spouses. About 173(97%) did not come for visit with their
wives even once. All the wives presented only once to the clinic and they were admonished
to encourage their husbands on adherence to medication and physical exercise.
0
10
20
30
40
50
60
70
80
90
100
Spouse No spouse
Res
po
nd
ets
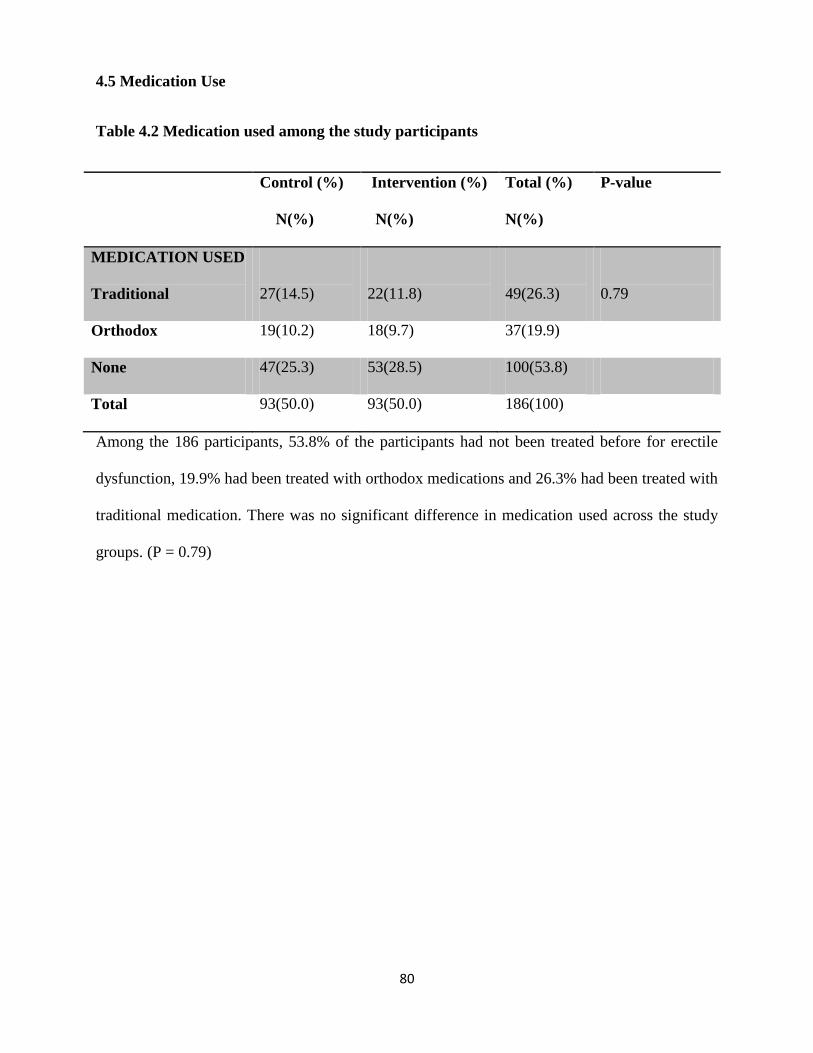
80
4.5 Medication Use
Table 4.2 Medication used among the study participants
Control (%)
N(%)
Intervention (%)
N(%)
Total (%)
N(%)
P-value
MEDICATION USED
Traditional
27(14.5)
22(11.8)
49(26.3)
0.79
Orthodox 19(10.2) 18(9.7) 37(19.9)
None 47(25.3) 53(28.5) 100(53.8)
Total 93(50.0) 93(50.0) 186(100)
Among the 186 participants, 53.8% of the participants had not been treated before for erectile
dysfunction, 19.9% had been treated with orthodox medications and 26.3% had been treated with
traditional medication. There was no significant difference in medication used across the study
groups. (P = 0.79)
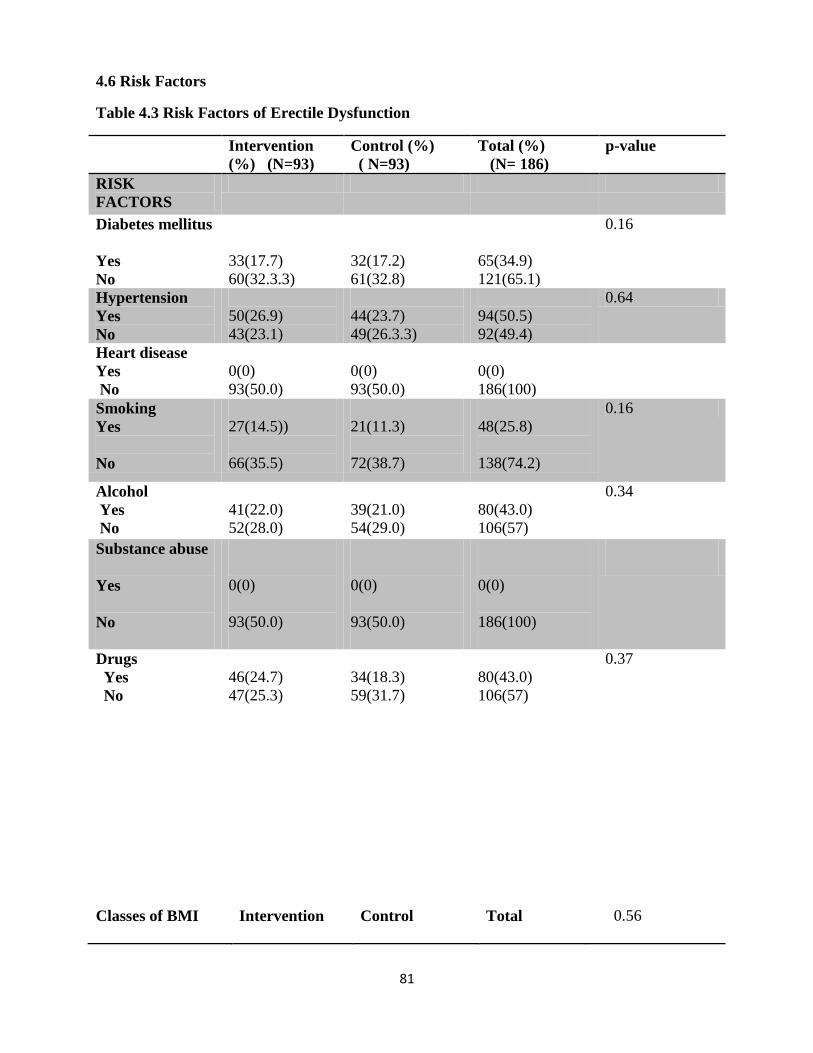
81
4.6 Risk Factors
Table 4.3 Risk Factors of Erectile Dysfunction
Intervention
(%) (N=93)
Control (%)
( N=93)
Total (%)
(N= 186)
p-value
RISK
FACTORS
Diabetes mellitus
Yes
No
33(17.7)
60(32.3.3)
32(17.2)
61(32.8)
65(34.9)
121(65.1)
0.16
Hypertension
Yes
No
50(26.9)
43(23.1)
44(23.7)
49(26.3.3)
94(50.5)
92(49.4)
0.64
Heart disease
Yes
No
0(0)
93(50.0)
0(0)
93(50.0)
0(0)
186(100)
Smoking
Yes
No
27(14.5))
66(35.5)
21(11.3)
72(38.7)
48(25.8)
138(74.2)
0.16
Alcohol
Yes
No
41(22.0)
52(28.0)
39(21.0)
54(29.0)
80(43.0)
106(57)
0.34
Substance abuse
Yes
No
0(0)
93(50.0)
0(0)
93(50.0)
0(0)
186(100)
Drugs
Yes
No
46(24.7)
47(25.3)
34(18.3)
59(31.7)
80(43.0)
106(57)
0.37
Classes of BMI Intervention Control Total 0.56
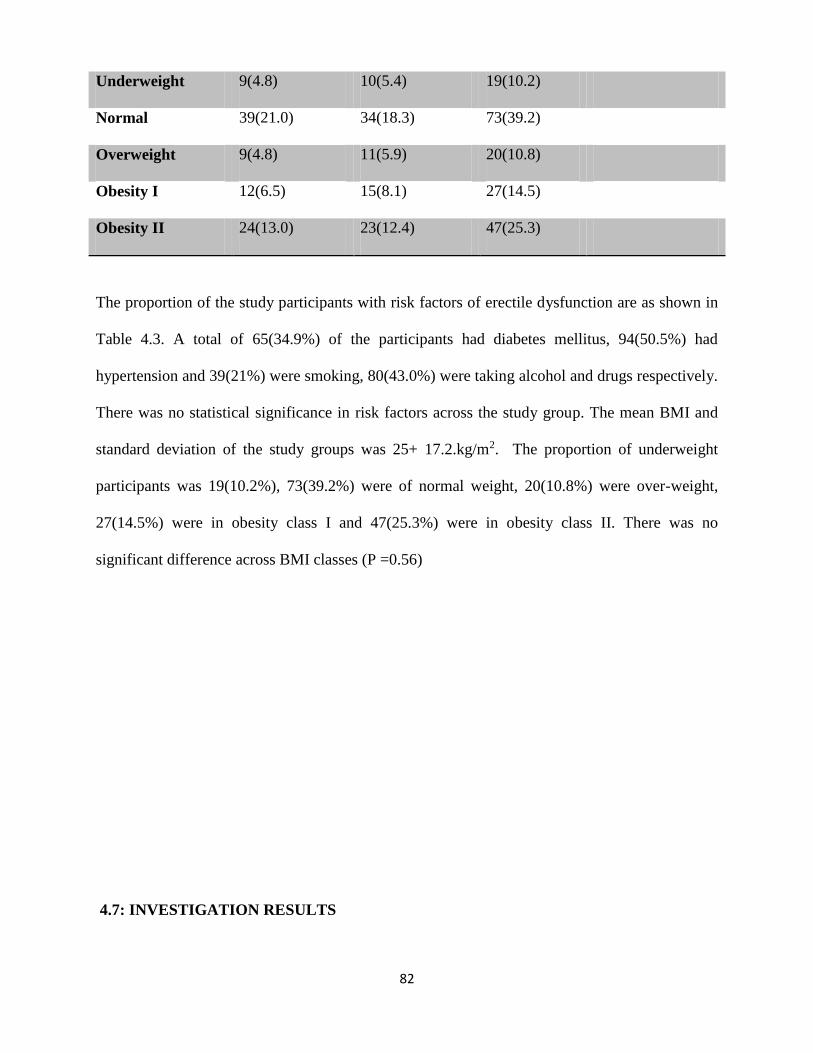
82
The proportion of the study participants with risk factors of erectile dysfunction are as shown in
Table 4.3. A total of 65(34.9%) of the participants had diabetes mellitus, 94(50.5%) had
hypertension and 39(21%) were smoking, 80(43.0%) were taking alcohol and drugs respectively.
There was no statistical significance in risk factors across the study group. The mean BMI and
standard deviation of the study groups was 25+ 17.2.kg/m2. The proportion of underweight
participants was 19(10.2%), 73(39.2%) were of normal weight, 20(10.8%) were over-weight,
27(14.5%) were in obesity class I and 47(25.3%) were in obesity class II. There was no
significant difference across BMI classes (P =0.56)
4.7: INVESTIGATION RESULTS
Underweight 9(4.8) 10(5.4) 19(10.2)
Normal 39(21.0) 34(18.3) 73(39.2)
Overweight 9(4.8) 11(5.9) 20(10.8)
Obesity I 12(6.5) 15(8.1) 27(14.5)
Obesity II 24(13.0) 23(12.4) 47(25.3)

83
Table 4.4: General
Investigation Results
Intervention Control Total P-value
FBG
Normal 80 (43) 75 (40) 155 (83.3) 0.003
Abnormal 13 (7.0) 18 (9.7) 31 (16.7)
Urinalysis 0.001
Normal 89 (47.8) 88 (47.3) 177 (95.2)
Protein 2 (1.01) 3 (1.6) 5 (2.7)
Glucose 2 (1.01) 2 (1.01) 4(2.2)
Lipid Profile
Normal 93 (50) 93(50) 186 (100) -
Abnormal 0 (0) 0 (0) 0(0)
ECG 0.001
Normal 90(48.4) 91(48.9) 181 (97.3)
Cardiomegally 3(1.6) 2(1.01) 5(2.7)
Testicular Ultra Sound
Normal 92(49.5) 93(50) 185(99.5) 0.001
Single Testes 1(0.5) 0(0) 1(0.5)
Genital Examination 0.001
Normal 92(49.5) 93(50) 185(99.5)
Single Testes 1(0.5) 0(0) 1(0.5)
Among the 186 participants that completed the study, 155(83.3%) had their fasting blood
glucose within the normal range while 31(16.7%) had high blood glucose results at baseline. For
urinalysis, 177(95.2%) had normal result while 5(2.7%) had protein and 4(2.2%) had glucose in
84
urine. All the participants had normal lipid profile. About 181(97.3%) of the participants had
normal ECG results while 5(2.7%) had cardiomegaly. On testicular ultrasound results and
examination findings, 185(99.5%) had normal results while only 1(0.5%) had one testis. There
was a significant difference between participants who had normal results and those with
abnormal results in both the control and intervention groups at baseline.

85
4.8: Erectile Dysfunction Scores of the Participant Before and after the Study
Table 4.5 : Erectile dysfunction Scores at baseline
Intervention
(%) (N=93)
Control
(%)
(N=93)
Difference
(%)
Total (%)
(N=186)
p-value
ED Scores
Mild (17-21)
7(3.8) 10(5.4) 3(1.6) 17(9.1) 0.11
Mild to
moderate(12-
16)
33(17.7) 38(20.4) 5(2.7) 71(38.2) 0.08
Moderate (8-
11)
30(16.1) 26(14.0) 4(2.1) 56(30.1) 0.07
Severe (1-7)
23(12.4) 19(10.2) 4(2.2) 42(22.6) 0.06
Total
93(50%) 93(50%) 186 (100%)
The above table indicated that at baseline the proportion of the participants with mild ED was
7(3.8%) in the intervention group compared to 10(5.4%) in the control group (p=0.11),
33(17.7%) with the mild to moderate ED in the intervention group compared to 38(20.4%) in the
control group (p=0.08), 30(16.1) in the intervention compared to 26 (14.0) in the control groups
had moderate ED (p=0.07) and 23(12.4%) in the intervention compared to 19(10.2%) in the
intervention groups had severe ED (p=0.06). There was no significant difference in erectile
dysfunction scores between the control and intervention groups in each of the domains at
baseline.

86
The severity of erectile dysfunction at baseline (Table 4.5) showed majority of the participants
had mild to moderate ED 71(38.2%), 33(17.7%) were in the intervention group and 38(20.4) in
the control groups. Thirty (16.1%) in the intervention group and 26(14.0) in the control groups in
the moderate domain and 23(12.4%) and 19(10.2.7%) in the intervention and control groups in
the severe domain respectively.
Table 4.6: Erectile Dysfunction Scores post intervention
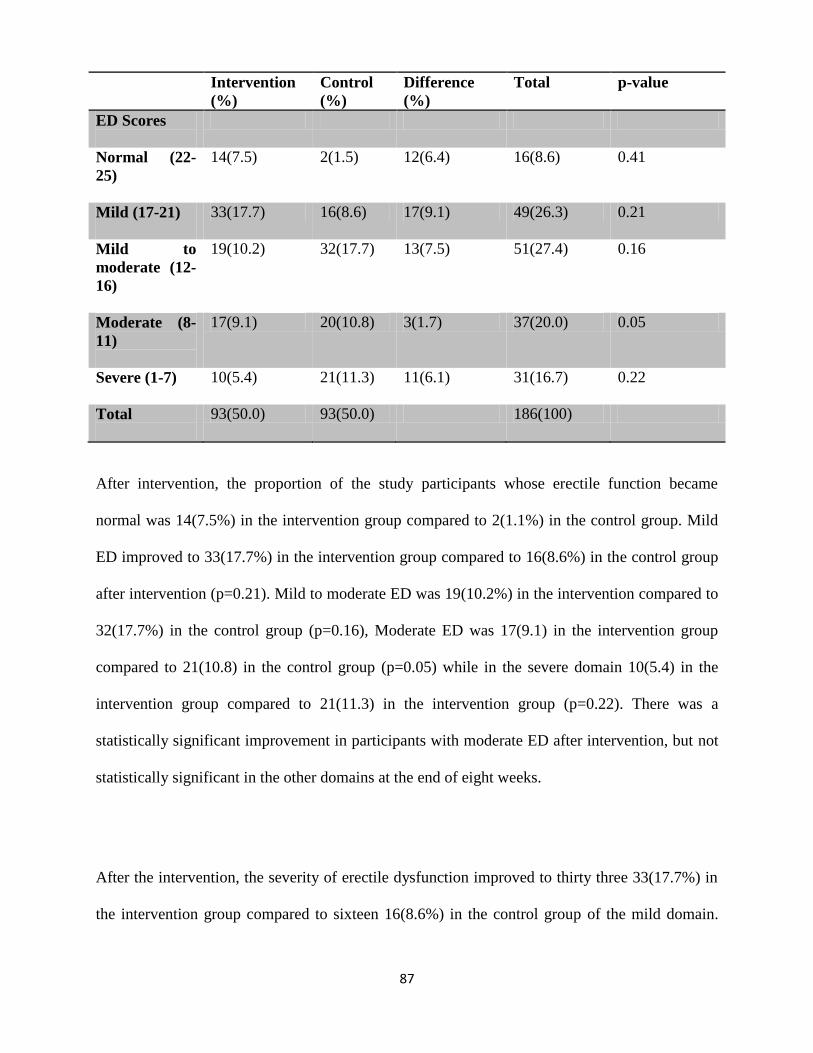
87
Intervention
(%)
Control
(%)
Difference
(%)
Total p-value
ED Scores
Normal (22-
25)
14(7.5) 2(1.5) 12(6.4) 16(8.6) 0.41
Mild (17-21)
33(17.7) 16(8.6) 17(9.1) 49(26.3) 0.21
Mild to
moderate (12-
16)
19(10.2) 32(17.7) 13(7.5) 51(27.4) 0.16
Moderate (8-
11)
17(9.1) 20(10.8) 3(1.7) 37(20.0) 0.05
Severe (1-7)
10(5.4) 21(11.3) 11(6.1) 31(16.7) 0.22
Total
93(50.0) 93(50.0) 186(100)
After intervention, the proportion of the study participants whose erectile function became
normal was 14(7.5%) in the intervention group compared to 2(1.1%) in the control group. Mild
ED improved to 33(17.7%) in the intervention group compared to 16(8.6%) in the control group
after intervention (p=0.21). Mild to moderate ED was 19(10.2%) in the intervention compared to
32(17.7%) in the control group (p=0.16), Moderate ED was 17(9.1) in the intervention group
compared to 21(10.8) in the control group (p=0.05) while in the severe domain 10(5.4) in the
intervention group compared to 21(11.3) in the intervention group (p=0.22). There was a
statistically significant improvement in participants with moderate ED after intervention, but not
statistically significant in the other domains at the end of eight weeks.
After the intervention, the severity of erectile dysfunction improved to thirty three 33(17.7%) in
the intervention group compared to sixteen 16(8.6%) in the control group of the mild domain.

88
Fourteen participants 14(7.5%) had no ED compared to two 2(1.1%) in the control group.
Nineteen 19 (10.2%) in the intervention group compared to thirty two 32(17.7%) in the control
group of the mild to moderate dormain. In the moderate dormain, 17 (9.1%) in the intervention
group compared to 20(10.8) in the control group. In the severe dormain 10 (5.4%) was in the
intervention group compared to 21(11.3%) in the control groups.
Table 4.7 Percentage difference in erectile function between baseline and post intervention
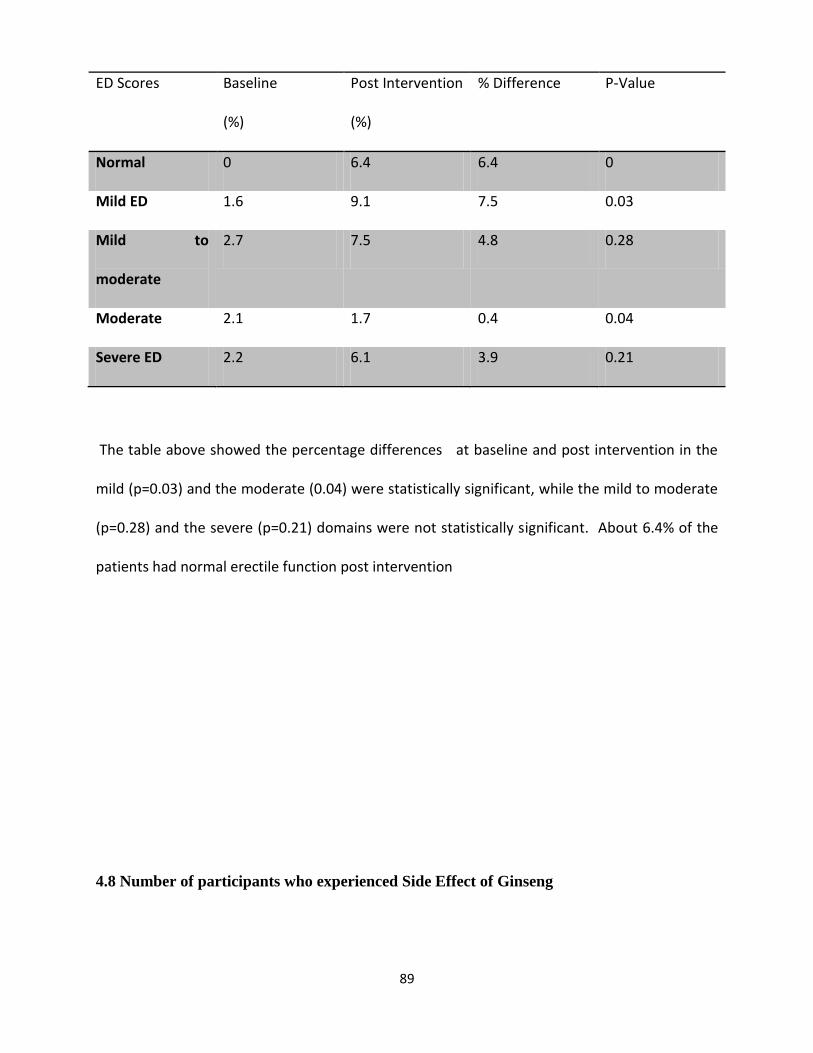
89
ED Scores Baseline
(%)
Post Intervention
(%)
% Difference P-Value
Normal 0 6.4 6.4 0
Mild ED 1.6 9.1 7.5 0.03
Mild to
moderate
2.7 7.5 4.8 0.28
Moderate 2.1 1.7 0.4 0.04
Severe ED 2.2 6.1 3.9 0.21
The table above showed the percentage differences at baseline and post intervention in the
mild (p=0.03) and the moderate (0.04) were statistically significant, while the mild to moderate
(p=0.28) and the severe (p=0.21) domains were not statistically significant. About 6.4% of the
patients had normal erectile function post intervention
4.8 Number of participants who experienced Side Effect of Ginseng

90
Fig 4.4: Side effect of Ginseng after Treatment
Figure 4.4 above showed the side effects of Ginseng after treatment, four participants (4%) out
of 95 (96%) experienced side effects of the drug.
Fig 4.5 Types of Side effects experienced after treatment with Ginseng
0
20
40
60
80
100
120
Side Effects No Side Effects
Res
po
nd
ents
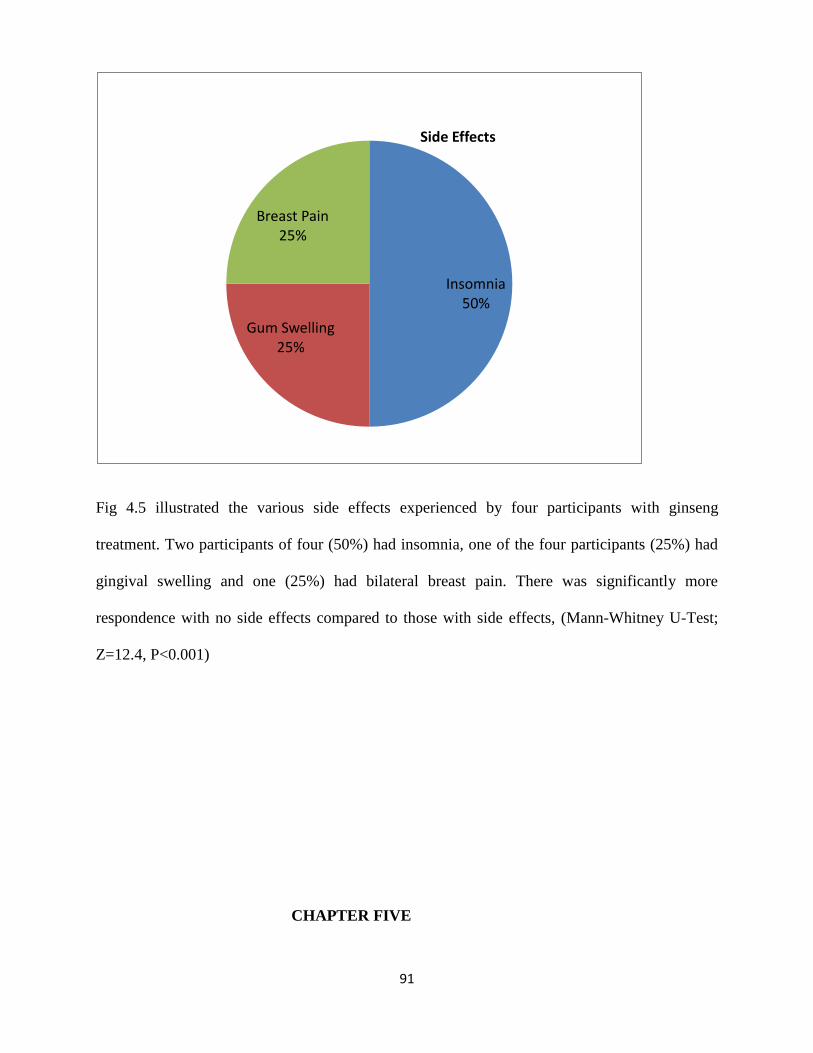
91
Fig 4.5 illustrated the various side effects experienced by four participants with ginseng
treatment. Two participants of four (50%) had insomnia, one of the four participants (25%) had
gingival swelling and one (25%) had bilateral breast pain. There was significantly more
respondence with no side effects compared to those with side effects, (Mann-Whitney U-Test;
Z=12.4, P<0.001)
CHAPTER FIVE
Insomnia50%
Gum Swelling25%
Breast Pain25%
Side Effects

92
5.0. DISCUSSION
5.1 SOCIO DEMOGRAPHIC CHARACTERISTICS
This study was made up of 186 males within the ages of 25 and 70 years. The mean age of the
participant’s was 41.7+25years. The mean age was higher than the mean age (38.8) reported in
Omisanjo study.43 This may be attributed to the wider age range (21-70 years) compared to this
study (25-70 years). This study reported higher proportion of 43(23.1%) participants with
erectile dysfunction within the ages of 46-55 years. The study showed an increase in erectile
dysfunction among participants aged 45-55 and above as shown in table 1.This is comparable to
Oladiji et al’s study in subjects within the ages of 20 and 70 years in Nigeria14 and Cheng et al
within the ages of 26 and 70years.50 These studies are similar in the age ranges of the
participants. However, this study was in contrast to the Massachusetts male aging study in
Tanzania which was carried out in subjects within the ages of 40 and 70 years.44 These studies
demonstrated a consistent increase in erectile dysfunction with age. This could be attributed to
increase in chronic diseases and decrease in compliance of copora cavernosa as they get older.42
This study demonstrated that majority (80%) of participants had formal education. Thirty eight
38(20.4%) had primary level of education, 47(25.3%) had secondary level of education and
64(34.4% ) had tertiary level of education. This showed that erectile dysfunction is higher in men
with higher level of education. Idung etal11 in Uyo, Nigeria reported a similar finding that 99%
of the subjects had at least primary school education and 1% had no formal education.11 45 This
was attributed to the lifestyle associated with higher social class which exposes them to risk
factors of erectile dysfunction such as obesity.11,45 This study was in contrast to a study done by
Nicolisi et al in 2003 which reported that erectile dysfunction is inversely related to higher level
of education.45 He reported (14.0%) of erectile dysfunction among those that completed high

93
school and 9.4% in degree holders. This relationship is attributed to poverty and less access to
medical care.45
Majority (53.8%) of the participants did not seek for help or were treated for erectile dysfunction
in the past. The proportion of participants who used orthodox medication in the past six weeks
was 19.9% while 26.3% had used traditional medication for treatment of ED. Okoli et al77 had
similar finding with 73% of the participants not taking any form of treatment while 60% of the
participants that were treated resorted to herbal medications. This was attributed to limited access
to health care, the culture, and religion of the participants especially in patient with ED38,77,.
Among the 186 subjects who completed the study, majority (93%) came with their wives, while
only 7% came with their wives at least once at either initial visit or as part of follow up. Chevret
et al found that involving their partners in the treatment foster positive, realistic expectation and
also positive drug adherence in the patients.
The study showed 67(36%) of the participants were employed by the government or private
organizations, sixty five (34.9%) were self employed , twenty nine (16.6%) were retirees, twenty
five (13.4%) were students. There was no statistically significant difference (p=0.3) between the
control and the intervention regarding employment status. Idung et al11 study was not in
agreement with his study. He demonstrated that 21.8% of the respondents with ED were
unemployed and 79.2% were employed. Both studies were done in Nigeria but differences may
be attributed to larger sample size and longer duration of study in the Idung study.11 On the
religious domain, The study showed that Christians were 32.3% in the control group and 34.4%
in the intervention group while 17.2% and 16.1% in the control and intervention groups were
Muslims respectively. There was no significant difference across religion in the control and
intervention group
94
5.2 MDDICAL CHARACTERISTICS
This study showed that hypertension (50.5%), DM (34.9%), alcohol and other drugs (43%) are
the commonest risk factors of erectile dysfunction. This study was similar to a study reported by
Chukwunonso in south west Nigeria.42 He reported that hypertension was 16.6% in the study
popoulation.42 Similar studies conducted by Lawrence7 and Idung11 reported that hypertension
was 70% and 92% respectively in their study population. These studies were comparable because
they were done within the same geographical location and in the same age groups.
However, Lawrence7 reported diabetes was 72% in the study population whereas Idung11
reported 7.3% as second commonest risk factors for erectile dysfunction. This study showed that
alcohol (43.0%) and other drugs (43.0%) were next commonest risk factors while DM (34.9%)
was third commonest risk factor.
This study was in contrast with a study done by Fung et al in 2004 which showed that heart
disease was the commonest risk factor for erectile dysfunction.51 Heart disease was reported in
5.8% of the study population. The study also showed that hypertension and higher fasting blood
glucose were not related to erectile dysfunction51. This finding may be attributed to age of the
participants (average72 years) and the study was carried out in patient with heart diseases.
Alcohol was reported in 43% of the study population in this study. This may be attributed to the
high level of alcohol consumption in this environment as alcohol is commonly seen as part of
marriage rites49. Cheng et al in Hong Kong also found negative effects of alcohol (39.1%) on ED
(P<0.007),
The body mass index (BMI) of the participants ranged between 17.5kg/m2 (underweight) to 39.9
9kg/m2 (obesity type II). The mean BMI of the participants at baseline was 25.36±17.5kgm2.
This is significantly lower than Cheng report with mean BMI of 36.6kg/m2. This is sufficient in

95
the fact that Cheng50 study was done in obesed patients. About 39.3% of the study participants
were within normal weight. This study demonstrated that majority of the participants did not
complain to their physicians about their erectile dysfunction similar to Omisanjo study who
demonstrated that majority (57.1%) of patients with erectile dysfunction cannot comfortably
complain or ask questions about their sexual problems.
The laboratory results at baseline showed majority of the participants had normal results with
only few having abnormal results. Five participants had cardiomegaly on ECG and five had
protein in urine all of which were hypertensive patients. The four participants who had glucose in
urine were all diabetic patients while one participant had one absent testis on the right on
examination was confirmed by testicular ultrasound scan. All the participants had normal lipid
profile results. There was a significant difference between participants with normal results and
those with abnormal results in both control and intervention groups.
5.3: EFFECTIVENESS OF GINSENG ON ERECTILE DYSFUNCTION
The present study found an increase in IIEF scores in the intervention group of the mild domain
from 3.8% to 17.7% compared to 5.4% to 8.6% in the control groups. This showed a statistically
significant improvement of red Korean Ginseng in the moderate domain (p=0.05) after
intervention, the mild domain was (p=0.21), mild to moderate domain (p=0.16), and severe
(p=0.22). The proportion of participants whose ED improved to normal erectile function was
encouraging in the intervention groups 7.5% compared to 1.5% in the control group which
suggest that red Korean Ginseng is superior to placebo.
The percentage difference in erectile function at baseline and post intervention (table 4.7)
showed mild ED (p= 0.03) and moderate ED (p=0.04) were statistically significant while the
mild to moderate ED (p=0.28) and severe ED (p=0.21) were not statistically significant. A study

96
done by Jang et al also showed that red ginseng had a significant effect (P<0.00001) on
improvement of erectile function compared to placebo (P=0.96).22 A sub group analysis of the
study also found a significant improvement in psychogenic erectile dysfunction (P=0.001).22
however, the Jang study was a meta analysis that utilizes six RCTs using 600mg, 900mg and
1000mg three times a day as adopted doses for the studies as compared to 50mg of Ginseng daily
for this study. De Andrade et al in their study also found a significant effect (p<0.0001) after
using 1000mg of red ginseng three times a day in the intervention group compared to p>0.05 in
the control group, but the sample size was low (60) and the comparison was between mild with
mild to moderate compared to all the domains of ED in this study.
Peak used a ginseng extract from a tissue red mountain ginseng plant, he also found a significant
improvement in IIEF from 29.78 to 13.14 in the treatment group compared to 39.86 to 15.29 in
the placebo group.84 The improvement in IIEF which was similar to this study showed a
significant improvement in organic function and sexual desire in those subjects.
This study is also similar to Gaurang study who used a poly herbal preparation that contains
ginseng (VXP) as the only ingredient known to improve erectile dysfunction.69 The VXP group
had a significant improvement (P<0.0001) in erectile function with the IIEF improved from
16.08 to 25.08 in the treatment group compared to 15.86 to 16.47 improvement in the placebo
group (P=0.61). The percentage improvement in erectile function with ginseng in this study was
statistically significant only in the mild ED (P=0.03) and moderate ED (p=0.04). This may be
attributed to the lower dose and frequency of ginseng extract (50mg daily) used in the study as
compared to higher dose and frequency (600mg, 900mg and 1000mg three times a day)72 in Jang
studies where all the domains had statistically significant improvement. It may also be attributed
to the duration of study (8 weeks) compared to (12 weeks) in de Andrade and Jang study.22
97
This study showed an increase in IIEF domain scores in eight weeks. However, this study was
conducted in all erectile dysfunction domain (mild, mild to moderate, moderate and severe)
whereas Guarang et al study demonstrated only in patients who had mild to moderate erectile
dysfunction only. This showed that this study had a wider scope of ED assessment compared to
Gaurang study Similarly, De Andrade study demonstrated significant improvement in ginseng
group (P<0.001).72 in patients with mild and mild to moderate ED only. This study showed
significant improvement in the mild ED (p=0.03) and moderate ED (p=0.04) while Kubin etal,36
showed improvement in erectile function (17%) in patients with moderate to severe erectile
dysfunction compared to mild erectile dysfunction and moderate ED. This may also be attributed
to the higher dosages of red Korean ginseng used in these studies.36
Overall, this study in comparison to reports of previous studies indicated that ginseng may be
used in the treatment of mild and moderate erectile dysfunction.
5.4 SEVERITY OF ERECTILE DYSFUNCTION
Significantly, this study showed a total of 71 (38.2%) of the participants with erectile
dysfunction had the mild to moderate form at baseline. This was followed by 56 (30.1%)
participants in the moderate domain, 42(22.6%) in the severe domain and 17(9.1%) in the mild
domain. The control group had more participants with mild to moderate ED while the
intervention had more of the moderate and the severe type before the study. This result support
the findings of Massachusetts study44 which demonstrated that majority (25%) of the participants
98
had mild to moderate erectile dysfunction, 17% had mild ED while 10% had severe ED44 similar
to a study done by Omisanjo also demonstrated higher population with mild to moderate erectile
dysfunction.43 This study showed a significantly lower population with severe ED after the study
in the intervention group. This finding is comparable to Gaurang et al study which IIEF
improved from 16.08 to 25.08 and peak et al study which improved from 29.78-13.14 who also
demonstrated a decrease in population of erectile dysfunction after intervention. This study
showed higher proportion of subjects with mild to moderate erectile dysfunction before (38.2%)
and after (27.4%) the study. however the proportion of subjects with mild to moderate and
moderate ED was lower in the treatment groups (10.2%) compared to the control groups (17.7%)
after the study.
The findings in this study highlighted the severity of erectile dysfunction in the mild to moderate
group. A contrasting reported by Idung etal in Uyo Nigeria reported higher severity (16%) in the
mild domain compared to (8.6%) in the mild to moderate at baseline. Both studies were hospital
based but the differences may be attributed to larger sample size (400 men) and study design
(cross sectional) as compared to this study.
5.5 GINSENG SIDE EFFECTS
This study demonstrated minimal side effects (4.3%) of ginseng across the treatment group
compared to 95.7% without side effects after treatment. The minimal side effects in this study
correspond to De Andrade study (0%) which showed no side effects after 12 weeks of ginseng
treatment in a randomized controlled trial.72 This is expected as ginseng is a natural product
(CAM) commonly seen with minimal or no side effects. There was no adverse reaction recorded
in the study which was similar to De Andrade study.72 The side effects recorded in this study
included poor sleep, gum swelling and bilateral breast pain. However, Young et al in a
99
systematic review of 44 selected Randomized Controlled Studies of the safety profile of ginseng
over 12 weeks.128 They found only 16 studies (36%) reported minimal side effects of Ginseng.
The side effects were similar to this study and there was no significant difference (p=378) in side
effects between the treatment and the placebo group.128
This study was Similar to Hyong et al study in patients with chronic fatique syndrome.127 They
assessed side effects of ginseng in two groups (1g and 2g) and recorded 1% side effects of
Ginseng in each group similar to this study. Their similarities were their study designs, results
and the age of the participants (20-65 years), but the difference is their shorter duration of study
(4 weeks) compared to this study.
In contrast to this study, Nam-Hum et al assessed the safety profile of red ginseng in two groups
of participants using 500mg and 1000mg of ginseng which was matched with placebo.126 They
found higher side effects in all the groups compared to this study. The placebo group recorded
31.6% side effects, 33.9% in the 500mg group and 29.8% in the 1000mg group but there was no
statistical difference (p=0.895) in side effects between the placebo and the treatment group. The
side effects may be attributed to the higher doses of ginseng used in their study compared to this
study, The similarities in the two studies was their sample size (170) but difference was their
duration of treatment (4weeks).
5.6 RELATIONSHIP BETWEEN CLINICAL CHARACTERISTICS AND ERECTILE
DYSFUNCTION SCORES
This study demonstrated a positive relationship between risk factors such as age diabetes
mellitus, alcohol and educational level with erectile dysfunction. Nicolisi did not find any
positive relationship between level of education and erectile dysfunction.45

100
The researcher could not find anything relating age and level of education with erectile
dysfunction scores. A number of studies have found a relationship between increased risk factors
with decrease in erectile function scores.59,72 which is an inverse relationship.
The improvement in erectile dysfunction in this study was lower after using 50mg of ginseng
compared to Jang and De Andrade study that used 1000mg for the study. The results of these
studies corresponds to the finding of De Andrade et al that erectile dysfunction may improve
with increase in dose of ginseng.72 This may suggests that increasing the dosage may improve
scores in mild to moderate and severe erectile dysfunction since improvement in erectile function
is better in studies that used higher dosages of ginseng as seen in Jang study.
There was a U-shaped relationship between BMI and ED in this study. The highest proportion of
participants (39.2%) with ED were with normal BMI followed by obesity type II (25.3%) and I
(14.5%). The lowest ED was found in participants who were underweight (10.2%) or overweight
(10.8%). This relationship is similar to Cheng et al studies which showed similar characteristics,
but Cheng;s study was a cross sectional study.
5.7 CONCLUSION
The purpose of the study was to determine the effects of ginseng and its side effects in the
treatment of unselected erectile dysfunction in JUTH. In line with the first objectives, the study
found some clinical improvement in patients with mild and moderate erectile dysfunction in
groups on ginseng compared to the groups on placebo which were statistically significant. The
pattern of erectile dysfunction showed more patients had mild to moderate ED among the study
population. The severity of erectile dysfunction was markedly reduced in the treatment groups
after the intervention. The side effects of Ginseng were minimal on patients with erectile
101
dysfunction. These side effects include breast pain, gum selling and insomnia which all resolved
within two weeks of treatment.
5.8 RECOMMENDATION
The results of this study showed significant improvement in mild and moderate erectile
dysfunction, (1) Red Korean ginseng should be included in the routine care of patients with mild
and moderate erectile dysfunction. With the minimal side effects (2%) encountered in the
treatment of erectile dysfunction with Ginseng which were observed to be mild, Ginseng is
considered to be safe in the treatment of mild erectile dysfunction.
(2) Family Physicians should be on a watch for patients with ED as majority of the patients have
mild to moderate erectile dysfunction with majority of the patients within the ages of 46-55
years. (3) It is recommended that sexual histories should be included in routine patient encounter
as majority of them may not complain to the physicians of their condition.
(4) A multi-disciplinary approach should also be adopted as Family Physicians, Psychiatrist,
health counselors, psychologist, dieticians, endocrinologist and nurses who are interested in this
discipline in order to significantly reduce the prevalence of erectile dysfunction in Nigeria.
5.9 STRENGTH OF THE STUDY.
The strength of the study was that it was interventional study, where the subjects were
randomized into two groups. The researcher was of the same sex with the subjects thereby
increasing their comfort ability in discussing their problems. There was a good communication
between the researcher and the subjects as researcher understood both English and Hausa spoken
by the subjects. The questionnaires were both in English and Hausa. There was also a good
support between the researcher and his colleagues in GOPC and urology clinic.
102
5.10: LIMITATIONS OF THE STUDY.
Most of the work done on erectile dysfunction in Nigeria and other African countries were not
interventional studies but little observational studies on this topic. This could explain limited
information on this topic from this part of the world. Culture and religion was also a barrier as
some patients found it difficult expressing their concerns. Cost of drugs especially ginseng was a
problem for this study. security was a great concern to patients coming from afar as it was at the
peak of insurgency in Northern Nigeria.
5.11: IMPLICATIONS OF THE STUDY TO FAMILY PHYSICIANS
Family physicians render comprehensive care to all ages, sex and disease at a primary level. He
is the first doctor to be seen, hence he must be equipped in managing all kinds of diseases. The
study is important to family medicine because it demonstrated the effectiveness of ginseng in the
management of erectile dysfunction. The result showed erectile dysfunction is common in our
environment with majority of the patient seen in GOPC of the Jos University Teaching Hospital.
This study further highlighted the risk factors and treatment modalities associated with this
disease. Family physicians should acquire knowledge and skills in managing erectile dysfunction
and sexual problems in general.
5.12: SUGGESTION FOR FURTHER STUDIES
To the best of knowledge, there are no available interventional studies done in this subject in
Nigeria therefore, more interventional studies are required. Further studies with higher dosages
of ginseng with longer duration is required in order to draw more conclusive evidence in the use
of ginseng in management of erectile dysfunction. Robust sponsorship is recommended for
studies in order to encourage larger studies. Sex clinic should be opened in GOPC with adequate

103
privacy considering the larger number of patients with erectile dysfunction drawn from these
studies.
REFERENCE
1. United Nations. Sexual and reproductive health/UNFPA.2015 (Accessed on April 15, 2015).
Available from http.unfpa.org.sexual-reproductive health.html
2. Ojomo F. Sexual Problems Amongst Married Women in the Reproductive Age Group Seeking
Medical Care in Jos, Nigeria. FWACFM Dissertation. West African College of Physicians. 2005;
1-9: 59–62
3. World Health Organization (WHO).Sexual and Reproductive Health. 2015 (Accessed on May
12, 2015). Available from http:www.who.int.reproductivehealthhtml
4. Baryamutuma R, Baingana F. Sexual, Reproductive Health Needs and Rights of Young people
with Perinataly Acquired HIV in Uganda. Afri Health Sci 2011; 2: 211 – 18.

104
5. Theobold I, Sally E. Strengthening the Research to Policy and Practice Interface Exploring
Strategies Used by Research Organizations Working on Sexual and Reproductive Health and
HIV/AIDS, Health Research Policy and Systems 2011; 9 (1):12.
6. Araugo AB, Mohr BA, Mohr BA, Mckinlay JB. Changes in Sexual Function in Middle Aged
and Older Men: Longitudinal Data from the Massachusetts Male Aging Study. J AM Geriatric
Soc. 2004; 9: 1502- 9.
7. Lawrence AA, Olubunmi Z, Olapade O, Modupe M L, Emeto TO, Prevalence and Correlates of
Erectile Dysfunction Among Primary Care Clinic Attendees in Nigeria. Global Health Sci
2012; 4(4):17.
8. Ronald W, Lewis MD, Kersten S ,Fugl M, Bosch R, Axel R.et al. Epidemiology /Risk Factors of
Sexual Dysfunction. Journal of Sexual Medicine 2004; 1(1): 36-9.
9. Ariba AJ, Oladapo OT, Iyaniwura CA. Dada OA. Management of Erectile Dysfunction,
Perception and Practice of Nigerian Primary Care Clinicians. South African Family Practice
2007; 49(9):16-29.
10. Joel JH. Management of Erectile dysfunction. American Family Physician 2010; 81(3): 305-12.
11. Idung AU, Abasiubong F, Ukott A, Udoh SB, Unadike BC Prevalence and Risk Factors of
Erectile Dysfunction in Niger Delta Region Nigeria. Afri Health Sci 2012; 12(2): 160 -5
12. Olarinoye JK, Kuranga SA, Katibi IA, Adeniran OS, Jimoh AA, Sanye EO. Prevalence and
Determinants of Erectile Dysfunction among People with Type 2 Diabetes in Ilorin, Nigeria. The
Nigerian Postgraduate Medical Journal 2006; 13(4):291-6.
13. Quek FK, Sallam AA, Chai Heng NG, Chua CB. Prevalence of Sexual Problems and its
Association with Social, Phychological and Physical Factors Among men in Malaysian
Population, Cross Sectional Study SEJournal of Sexual Medicine 2008;5(1): 70-6.

105
14. OladijiF. Kayode O, Parakoy DB, Influence of Socio-demographic Characteristics on Prevalence
of Erectile Dysfunction in Nigeria. Int J Impot Res 2013; 25: 18-23.
15. Thieti T, Adjaye a, FousekaV. Erectile Dysfunction. Clinical Diabetes 2005; 23:105-13.
16. Khatibi FA, Jarrah NS, Shegem NS, Bateiha A, Abu-Ali RM, Adj louni K. Sexual Dysfunction
Among Jordanian Men with Diabetes. Saudi Medical Journal 2006; 27(3):351-6.
17. Yousef AA. Erectile Dysfunction among Diabetic Patients in Saudi Arabia. Journal of
Community Medicine 2007; 14(1):19-23.
18. Emily B, Joshy G, walter PA, Leonard K, Peters M, Korde RJ, et al. Erectile Dysfunction
Severity as a Risk Marker for Cardiovascular Disease, Hospitalization and all Cause Motility.
Open Access Peer Review Article 2013; 10:101– 7.
19. Sandro LV, Rosita C, Enzo V, Rosario D, Aldo EC. Physical Activity and Erectile Dysfunction
in Middle Aged Men. Journal of Andrology 2012; 33(2):154-61.
20. Giti O, Saeideh Z, Fazlollah A, Mahger A. Transition stages in Adjustment of wives with their
husbands with erectile dysfunction. Iran Red Creascent Med J 2014;16(3):16594
21. Edzard E. Panax Ginseng. An Overview of Clinical Evidence. J Ginseng Res 2010; 34(4): 259-
63.
22. Jang DJ, Lee MS, Shin BC. Lee YC, Ernst E Red Ginseng for treating Erectile Dysfunction. A
Systematic Review Br. J. Clin Pharmacol 2008; 66 (4):444-50.
23. Hoeger WK, Hoeger WK. Behaviour Modification in Lifetime Physical Fitness and Wellness.
Belmonth: Thompson Wadsworth 2009;10:34-60.
24. Philip EM, Capel J, Jonas S. Getting Started as a Regular Exercise In Jonas S and Philip EM
(Ed). EMS, exercise in medicine. A clinicians guide to exercise prescription. Lipincot –Williams
and Wilkins: Philadelphia. 2009; 86-98.

106
25. Hoeger WK, Hoeger SA. Introduction to Physical Fitness and Wellness. 6th edition Wadsworth:
Belmonth 2005;6: 1-22.
26. Sport Fitness Advisor. The FITT Principle of Training. Available at http:// www.sport-fitness
Advisor.com/ fit principle.html. Accessed 19th January 2014.
27. Sikiru L, Agbanusi EC, Richard CN. Effects of Aerobic Exercise in the Management of Erectile
Dysfunction. Ethiop J Health Sci 2011; 21(3): 195-201
28. Chevret – MeassonM, Lavallee E, Troy S, Arnould B Improvement in Quality of Sexual Life in
Female Partners of Men With Erectile Dysfunction Treatment with Sildenafil Citrate. J sex med
2009; 6:225.
29. Masaku E .Erectile Dysfunction in Sample of Patients attending a psychiatric out-patient Clinic.
International Journal of Impotence Research. 2009; 21:235-9.
30. Okeahalam BN. Erectile Dysfunction in Nigerian Hypertensive. African Journal of Medical
Sciences.2007; 36:221-4.
31. Truls Q, Kimberly SH, Yarnal MP, Katrina MK, Kathryn IP, Gradison M. Is there time for
Management of Patients with Chronic Diseases in Primary Care? Annals of Fam Med 2005;
3(3): 2009-14.
32. Richard S, Kevin C. How a Primary Care Clinicians Approaches Erectile Dysfunction. Current
Clinical Urology.2006; 8:77-104.
33. Babaei AR, Safarinejad MR, Kolahi AA. Penile Revascularization for Erectile Dysfunction. A
Systematic Review and Meta Analysis of Effectiveness and Complications. Urol J 2009; 6(1): 1-
7.
34. Camacho ME, Reyes-Ortiz CA. Sexual dysfunction in the Elderly: Age or Disease? Int J Impot
Research.2005;17:52-56
107
35. American psychiatric association diagnostic and statistical manual of mental disorders. Fifth
edition, Arlington VA: American psychiatric Association; 2013; 426-9.
36. Kubin M. Wagner G, Fugl-Mayer AR, Epidemiology of Erectile Dysfunction. Int J Impot Res
2003; 15(1):63-71.
37. Khalaf IM, Levinson IP. Erectile Dysfunction in the Africa/Middle East Regions. Epidemiology
and Experience with Sildenafil Citrate (viagraR). Institutional Journal of Impot Research 2003;
15(1). 51-2
38. Reuben KM, Janeth L, Muhsin A, Bejamin AK. Prevalence of erectile dysfunction and
associated factors among diabetic men attending diabetic clinic at Muhimbili National Hospital
in Dar-es-salam, Tanzania. Pan African Medical Journal 2014;17-:227
39. Peera B, meta P, sarachais. Prevalence of erectile dysfunction among treated hypertensive in
Thailand. J Med association Thai 2006; 89(5): 528-36
40. Campbell MM, stein DJ. Sexual dysfunction. A systematic review of South African research. SA
Med J 2014; 104(6): 440-513.
41. Kempt T, Reeder P. The prevalence and association of erectile dysfunction in South African
male diabetic urban population. Journal of endocrinology, metabolism and diabetes of South
Africa 2015; 20(3): 134-9.
42. Chukwunonso ECC, Kingsley CE, Chinemerem EO. Erectile Dysfunction and Hypertension
Among Adult Males in Umudike, Nigeria: A Study of Prevalence and Relationships. Asian
Journal of Scientific Research 2015; 8(3):315-323.
43. Omisanjo O, Faboya O, Babatunde A, Taiwo A, Ikuerowo S. Aleetan O.Prevalence and
Treatment Pattern of Erectile Dysfunction Amongst Men in South Western Nigeria. Internet
Journal of Sexual Medicine 2014;3(1).38-62

108
44. Jonathan L. Impotence and its Medical and Psychological Correlates, Massachusetts Male Aging
Study. Br J Diabetes and Vascular Diseases 2002; 2:278.
45. Nicolisi A, Glasser DB, Moreira ED, Villa M. Prevalence of Erectile Dysfunction and
Associated Factors among men without Concomitant Disease. A population Study. Int J Impot
Research 2003; 15(4): 253-57.
46. Garko SB, Ogunsina MO, Danbauchi SS. Sexual Dysfunction in Hypertensive Patients.
Implications for Therapy. Ann Afri Med 2005; 4(2): 46-51.
47. Billups KI, Bank AJ, Padma-Nathan H, Katz S, William R. Erectile Dysfunction as a Marker of
Cardiovascular Disease: Results of Minority health institude expert advisory Panel. J sex Med.
2005;2(1) :40-52
48. Olusegun A, Denis AN, Ernest OJ, Oluwasegun I. Assessment of the Sexual Function of Males
with Chronic Liver Disease in South Western Nigeria. Annals of African Med 2014: 13(2): 81-6
49. Omigbodun OO, Babalola O. Psychosocial Dynamics of Psychoactive Substance Mis-use among
Nigerian Adolesents. Annals of African Medicine 2004;3(3):111-5
50. Cheng JYW, Ng EML, Ko JSN,Chen RYL. Physical Activity and Erectile Dysfunction: A Meta-
analysis of Population Based Studies. 2007;19: 245-52
51. Fung MM, Beltencout R, Barret C E. Heart Disease Risk Factors Predict Erectile Dysfunction
25years later: The Rancho Bernardo Study. J AM Cardio 2004;43:1405-11
52. Mulligan T, Frick MF, Zuraw QC, Stemhagen A, Mcwhirter C. Prevalence of Hypogonadism in
Males Aged at least 45 years: the HIM study. Int J clin pract 2006;60(7):762-9.
53. Guay AT. Testosterone and Erectile Physiology- Aging Male 2006;9(4):201-6.
54. Esposito K, Giugliano D. Obesity the Metabolic Syndrome and Sexual Dysfunction. Int J Impot
Research 2005;17(5):391-98

109
55. Giugliano F, Maiorrino MI, Bellastella G, Autorino R, De Sio M, Giugliano D et al. Adherence
to Mediterranean Diet and Erectile Dysfunction in Men with Type 2 Diabetes. J Sex Med. 2010;
7(5):1911-17.
56. James EF, Culley CC. Phosphodiesterase Type 5 Inhibitors as a Treatment for Erectile
Dysfunction: Current Information and New Horizons. Arab Journal of Urology. 2013; 11(3):222-
9.
57. Espositor K, Guiglano F, Dipalo G. Effect of Lifetime changes on Erectile Dysfunction in
Obesed Men, JAMA;2004291(24):2978-84
58. Kerin TM. Erectile Dysfunction, New Engl J Med 2007; 357:2472-81
59. Jordan GH, Mc Cammon KA. Surgery of the Penis and Urethra. In Wein AJ, Kavoussi LR,
Novick AC, Partin AW, Peters CP, ed. Cambell’s Urology, 10th ed. Philadelphia PA: Elsevier
Sounders; 2012.
60. Umeh CS. Erectile Dysfunction. Proceeding of the West African College of Physicians (WACP),
Revision Course, 2012, May 15. Ibadan Nigeria.
61. Andersson KE. Mechanism of Penile Erection and Basis of Pharmacological Treatment of
Erectile Dysfunction. Int. pharmacol Journals 2011; 63(4):813-28.
62. Robert CD, Tom FL. Physiology of Penile Erection and Pathophysiology of Erectile
Dysfunction. Urol Clin North AM 2005;32(4):379.
63. Piores OM, Jimeno CA, Acampado LT. Erectile Dysfunction Among Diabetic Men at UP-OGH
Out- Patient Department: Prevalence and Risk Factors. Phil J Internet Medicine 2004; 42:197-
202
64. Benjamin DS.The First Organic Psychogenic Destruction and Related Problems in the
Classification of Erectile Dysfunction. Int J impot Res 2003; 15:72-8.

110
65. Chou PS, Chou WP, Chen MC, Lai CL, Yeh KC,Wen YC et al. Newly Diagnosed Erectile
dysfunction and Risk of Depression. A population Based five year follow up study in Taiwan. J
Sex Med 2015;12(3):804-12.
66. Nnamdi JO, Ifeoma EO. Counseling Against Sexual Dysfunction in Nigerian Men. Ansu Journal
of Integrated Knowledge 2014;3(1)2315-5857
67. Yang CC, Michael PP, David FP. Comparison of the International Index of Erectile Function,
Domain Scores and Nuctural Penile Tumescence and Rigidity Measurement. Does One Predict
the other? Bju Int 2006; 98 (1): 105 – 9.
68. Unadike BC, Eregie A, Ohwovoriole AE. Prevalence and Types of Sexual Dysfunctions Among
Males with Diabetes in Nigeria. African Journal of Diabetes Medicine 2008;18-20.
69. Gaurang RS, Manoj kumar VC, Suresh BP, Shrikant VP, Vilas PS, Navneet AS. Evaluation of a
multi herb supplements for Erectile Dysfunction: A randomized double blind placebo controlled
study. BMC complementary and alternative med 2012:12:155
70. Shanloul R. Natural Aphrodisiac: J Sex Med 2010;7:39-49.
71. Thuryan P, Gopala-Krishanan G. Erectile Dysfunction. Clin Evid. 2006; 15(57):1227-51.
72. De Andrade E, De Mesquita AA, Claro JA, de Andrade PM, Ortiz V, Paranhos M et al. Study of
the Efficacy of Korean Red Ginseng in the Treatment of erectile dysfunction. Asian J Androl
2007;9(2): 241-44.
73. Sung HH, Chae MR, So I, Jeon JH, Park JK, Lee SW. Effects of Ginsenocids on Large
Conductance K(ca) Channels on Human Corporal Smooth Muscle Cells. Int J Impot Res 2011;
23(5):193-9
74. Peak ky, Park JK, Youn NY. Effects of Tissue Cultured Mountain Ginseng (Panax Ginseng CA
Meyer) Extracts on Male Patients with ED. Asian J androl 2009;11:356-61.
111
75. Erectile Dysfunction Guidelines Panel. The Management of Erectile Dysfunction. An Update
Baltimore, MD. American Urology Association, Education And Research2005.http://www.ngc.
gov/summary.aspx?doc1d=10018&.jnbr=00532&string=erectile+AND+dysfunction.
Assessed August 13 2015
76. Bocchio M, Scarpeli P, Necozoiner OS, Pelticcione F,Spartera C, Francavilla F et al. Penile
Duplex Pharmaco Ultrasonography of Cavernous Arteries in Men with Erectile Dysfunction and
Generalized Atherosclerosis. International Journal of Andrology. 2006; 29(4): 496-501
77. Okoli RI, Aigbo O. Ohaju O, Mensah JK. Medicinal Herbs Use for Managing Common
Ailments Among Esan People of Edo State,Nigeria. Pakistan Journal OF Nutri 2007; 6:490-496
78. Rosen RC, Jackson G, Kostis JB. Erectile dysfunction and cardiac Disease: Recommendation of
the Second Princeton Conference. Curr Urol Rep 2006;7(6):490-6.
79. Jenny HY, Lawrence SB, Penile Embryology and Anatomy. Science world Journal.
2010;10:1174-1179
80. Montague DK, Jarow JP, Broderick GA lue TF, Imochowski RR, Henton JP et al. The
Management of Erectile Dysfunction, an AUA update.2005 J. Urol;174(1): 230-9.
81. Anderson KE, Mechanism of Penile Erection and Basis for Pharmacological Treatment of
Erectile Dysfunction. Pharmacological Reviews 2011; 63(4):811-59.
82. Corona G, Isidori AM, Buvat J, Aversa A, Rastrelli G, Hackett G et al. Testosterone
Supplementation and Sexual Function: A Meta Analysis Study. J Sex Med 2014;11(6):1577-92.
83. Aversa A, Francomano D, Lenzi A. Does Testosterone Supplementation Increase PDE5-
inhibitors Responses in Difficult to Treat Erectile Dysfunction Patients? Expert opin
Pharmacotherapy 2015;16(5):625-8
84. Peak ky, Park JK, Youn NY. Effects of Tissue Cultured Mountain Ginseng (Panax Ginseng CA
Meyer) Extracts on Male Patients with ED. Asian J androl 2009;11:356-61.

112
85. Kalaizidou I, Venetikou MS, Konstadinidis K, Artemiadis AK, Chrousos G, Darviri C. Stress
Management and Erectile Dysfunction. A Pilot Comparative Study. Andrologia 2014; 46(6)698-
702
86. Lin CS, Ho HC, Chen KC, Lin G, Nunes L, Lue TF. Intra Cavernosal Injection of Vascular
Endotheleal Growth Factor Induces Nitric Oxide Synthatase 150 Forms. BJU Int
2002;89(9):955-60.
87. Williams G, Abbou CC, Amar ET, Desvaux P, Flam TA, Lycklama A et al. Efficacy and Safety
of Transurethral Alprostidil Therapy in Men with Erectile Dysfunction. The MUSE Study
Group. Br J urol 1998;81(6):889-94.
88. Burchardt M, Burchardt T. Anastasiadis AG, Buttyan R, De la ta A, ShabsighA et al. Application
of Angiogenic Growth Factors for Therapy of Erectile Dysfunction: Protein and DNA Transfer
of VEGF 65 Into the Penis. J Urology 2005;66(3):665-70.
89. Mulhall JP, Ahmed A, Branch J, Parker M. Sereal Assessment of Efficacy and Satisfaction
Profile Following Penile Prosthesis Surgery. J urology 2003;169(4):1429-33.
90. Glina S, Sharlip ID, Hellstrom WS. Modifying Risk Factors to Prevent and Treat Erectile
Dysfunction. J Sex Med 2013;10(1):115-9.
91. Aksam AY,Joanne EN, Farid S Yousef A, Dany-Jan y, Yousef ED. Is There a Relationship
Between the Severity of Erectile Dysfunction and Comorbidity Profile in Men with Late Onset
Hypoganadism. Arab Journal of Urology 2015;13(3):162-8.
92. La Vignera S, Condorelli R, Vicari E, D’Agata R, CalogEro AE. Physical Activity and Erectile
Dysfunction in Middle Aged Men. J Androl 2012;33(2):154-61.
93. Bacon CG, Mittleman MA, Kawachi I, Giovannucci E, Giovannucci E, Glasser DB, Rimmo E B.
A Prospective Study of Risk Factors for Erectile Dysfunction. J of Urology 2006;176:217-21.

113
94. Lim SS, Vos J, Flaxman AD, Daei G, Shibuya K, Adair-Rohani KG et al. A Comparative Risk
Assessment of Burden of Disease and Injury Attributable to 67 Risk Factors and Risk Factor
Clusters in 21 Regions, Miao-2010 in systematic analysis for the global burden of disease study
2010. Lancet 2012;380:2224-2260
95. Olufemi OO, Olatunde O, Kolawole SO, Akolade OI. Physical Activity Among Type II
Diabetic Adults in Nigerians. Annals of African Medicine 2014;13(4):189-194.
96. Hallal PC, Anderson LB, Bull FC, Guthold R, Haskel W, Ekelund U .Global Physical Activity
Levels: Surveillance Progress, Pitfalls and Prospects. Lancet 2012;380: 247-257.
97. Abubakari AR, Bhopal RS. Systematic Review on the Prevalence of Diabetes, Overweight/
Obesity and Physical inactivity in Ghanaians and Nigerians. Public Health 2008;122:173-182
98. Maio G, Saraed S, Marchiori A. Physical Activity and PDES Inhibitory in the Treatment of
Erectile Dysfunction. Result of a Randomized Controlled study. J Sex Med 2010;7(6): 2201-08
99. Kullo JJ, Khaleghi M, Hensrud DD. Markers of Inflamation are Inversely Associated With VO2
Max in Symptomatic Men. Journal of Applied Physiology 2007;102:1374-79.
100. Lamina S, Okoye CG, Dagogo TT. Therapeutic Effect of an Interval exchange Training Program
in the Management of Erectile Dysfunction in Hypertensive Patients. Journal of Clinical
Hypertension 2009;11(3):125-129.
101. Jane –lovena EO, Okoronkwo IL, Ogowonaya NP. Complementary and alternative medIcine use
among adults in Enugu Nigeria. BMC complementary and alternative med 2011;11:19
102. Singh V, Raidoo DM, Harries CS. The prevalence pattern of usage and peoples attitude towards
complementary and alternative medicine among the CAM Indian community in Chartsworred,
South Africa. Biomed central, Complementary and Alternatuve medicine 2004;4:3.
103. Humpel N, Jones SC. Gaining insight into the what, why and where of complementary and
alternative medicine use by cancer patients and survivors. Euro J cancer care 2006;15(4):362-8.

114
104. Tamler R, Mechanick JI. Dietary supplements and nentroceuticals in the management of
andrologcologic disorder. Endocrinol metab clin north AM 2007;36(2): 533-52.
105. Ernst E, Posadzki P, Lee MS. Complementary and Alternative Medicine (CAM) for Sexual
Dysfunction and Erectile Dysfunction in Older Men and Women: an Over view of Systematic
Reviews. Maturitas. 2011;70(1):37-41.
106. Hurdaq C, Ozkara A, Citci S, Uyaney I, Damirci C. The Effects of Alpha Lipoic Acid on Nitric
oxide Synthetase Dispersion in Penile Function in Steptozotocin induced Diabetic Rats.
International Journal of Tissue Reaction 2005;27(3)145-150.
107. Oshikoya KA, Senbanjo IO, Njokanma OF, Soipe A, Use of Complemetary ans Alternatine
medicine for Children with Chronic Health Condition in Lagos, Nigeria. BMC CAM.2008; 8:66.
108. Yucel S, Baskin LS. Identification of Communicating Branches Among the Dorsal, Perineal and
Cavernous Nerves of the Penis. J urol 2003;170(1):153-8.
109. David k, Traci P. Panax Ginseng AM FAM Physican.2003; 15. 68(8): 1539-42.
110. Afolayan AJ, Sunmonu TO. In vivo Studies on Anti Diabetic Patients use in South Africa Herbal
Med. J Clin Biochem Nutri 2010;47:98-106.
111. Folodun A. Herbal Medicine African Distribution, Standardization and Prospects. Research
Journal of Phyto Chemistry 2010;4:154-61
112. Ezeome ER, Anarado AN. Use of complementary and alternative medicine by Cancer Patients
at University of Nigeria Teaching Hospital Enugu, Nigeria. BMC CAM 2007;7:28.
113. Constable S, Ham A, Pir Mohammed M. Herbal Medicine and Acute Medical Emergency
Admissions to Hospital. Br J Clin Pharmacol 2007; 63:247-8.
114. King AR, Flint SR, Russett FS, Generali JA, Gruer DW. Evaluation and Implications of Natural
Product use in Pre-operative Patients. A Retrospective Review. BMC Complementary and
Alternative Medicine 2009;9:38
115
115. Collins D, Oakey S, Ramakrishnan V. Peri-operative Use of Herbal Complementary and Over
the Counter Medicine in Plastic Surgery Patients. Eplasty 2011;11:e27
116. Jane DJ, Leem S, Shim BC, LeeYC, Einst E. Red Ginseng For Treating Erectile Dysfunction; A
Systematic Review Br J Clin Pharmacol 2008;66(4)444-50
117. Kim SD, Kim JY, Huh JS, Kim SY, Sohn DW. Improvement of Erectile Function by Korean
Red Ginseng (panax ginseng) in Male Rat Model of Metabolic Syndrome. Asian J Androl
2013;15:395-99
118. Collins D, Oakey S, Ramakrishnan V. Peri-operative Use of Herbal Complementary and Over
the Counter Medicine in Plastic Surgery Patients. Eplasty 2011;11:e27
119. Shim M, Lee YJ. Ginseng as a Complementary and Alternative Medicine for Post-Menopausal
Symptoms. J Ginseng Res. 2009; 33:89-92.
120. Kim HS,Woo SH, Jo S, Hahne J, Youn NY, Lee HL, Double Blind Placebo Controlled Multi
Center Study for the Therapeutic Effect of Mountain Panax Ginseng: A Mayer Extracts in men
with erectile dysfunction: a preliminary report.Korean J Androl. 2006; 24(2): 84-8
121. Dey L, Xie JT, Wang A, Wu J, Maleckar SA, Yuan CS. Anti hyperglycemic Effects on Ginseng.
Comparison Between Root and Berry Phyto-medicine 2003;10(6-7):600-5.
122. Ker WL, Alice STW. Ginseng and Male Reproductive Function Asia J Androl 2013; 3 (3)
E26391
123. Yucel S, Baskin LS. Identification of Communicating Branches Among the Dorsal, Perineal and
Cavernous Nerves of the Penis. J urol 2003;170(1):153-8.
124. Ham WS, Kim WT, Lee JS, Ju HJ, Kang SJ. Efficacy and Safety of Red Ginseng Extract Powder
in Patients with Erectile Dysfunction: Multi Center, Randomized, Double-Blind, Placebo-
controlled study). Korean J Urol 2009; 50:159-64.
116
125. Aksam AY,Joanne EN, Farid S Yousef A, Dany-Jan y, Yousef ED. Is There a Relationship
Between the Severity of Erectile Dysfunction and Comorbidity Profile in Men with Late Onset
Hypoganadism. Arab Journal of Urology 2015;13(3):162-8.
126. Nam – HL, Ray S, Hyeong GK, Jung HC, Chang GS. Safety Profile of Panax Ginseng Root
Extracts. A Randomized Controlled Trial in Healthy Korean Volunteers. J CAM Alt Med 2012;
18(11): 1061 – 69.
127. Hyong GK, Jung HC, Sa RY, Jin SL, Jong MH, Yo CA et al. Adverse Effects of Panax Ginseng.
CA Meyer. A Randomized Controlled Double Blinded Trial PLOS one 2013; 8 (4): 61271.
128. Young SK, Jung YW, Chang KH, Moo C. Safety Analysis of Panax Ginseng in a Randomized
Controlled Trial. A Systematic Review. Medicines 2015; 2: 106 – 26.
129. Fakeye TO, Tijani A, Adebisi O. A Survey on Use of Herbs among Patient Attending
Secondarylevel of Health Care Facilities in South Western Nigeria. J Herb Pharmacotherapy
2007;7(3-4): 213-27.
130. Plateau State Government Website [web page].[ Accessed on: September 10,2015].Available
from www.plateau State gorvnment.org/visit.htm.
131. Charab J, Biswas T. How to calculate sample size for different study designs in medical research.
Indian J psychol Med.2013; 35(2):121-6
APPENDIX I
JOS UNIVERSITY TEACHING HOSPITAL
JOS, NIGERIA
117
Phone: 073-450226-9 Cables & Telegram: JUTH
e-mail: [email protected] P.M.2076
JUTH/DCS/ADM/127/XIX/5865
Dr. Bakzak Isaac Bulus,
Department of Family Medicine,
Jos University Teaching Hospital,
Jos-Nigeria.
RE: ETHICAL CLEARANCE/APPROVAL
I am directed to refer to your application dated 2nd December, 2013 on the research proposal
teed:
“A Comprison of a Combination of Physical Exercise and Placebo with Physical Exercise
and Ginseng in the Treatment of Erectile Dysfunction in Adult Black Men” and your
appearance before the Ethical Committee on 6th December, 2013.
Following recommendation from the Institutional Health Research Ethical Committee, I am to
inform you that Management has given approval for you to proceed on your research topic as
indicated.
You are however required to obtain a separate approval for use of patients and facilities from the
department(s) you intend to use for your research.
The Principal Investigator is required to send a progress report to the Ethical Committee at the
ration of three (3) months after ethical clearance to enable the Committee carry its oversight
function.
Submission of final research work should be made to the Institutional Health Research Ethical
committee through the Secretary in Room 2 Administration Department, please.
On behalf of the Management of this Hospital, I wish you a successful research outing.
20m January, 2014.
Ref: ………………………………… Date:………….…………….………

118
119
120
APPENDIX IV
CONSENT FORM (ENGLISH)
I Dr. Bakzak Isaac Bulus a senior registrar of the Department of Family Medicine Jos
University Teaching Hospital, Jos.
I want to carry out a proposal on the topic A comparison of a combination of physical
exercise and placebo with physical exercise and Ginseng in the treatment of erectile
dysfunction in adult married men in Jos University Teaching Hospital, Jos.
To compare the effectiveness of the combination of physical exercise and ginseng and
comparing it with the effectiveness of physical exercise alone in the treatment of erectile
dysfunction amongst married men attending GODP and urology clinic in JUTH Jos.
This study will involve asking you question to fill in my questionnaire. It will also
involve physical examination and laboratory samples for various investigations related to
the study. you are free to participate in this study but if you decide not to, this study will
in no way affect the outcome of your treatment. All information filled in the
questionnaire will be kept strictly confidential and your identity will not be disclosed.
If you accept to participate in the study, kindly sign in the space below.
I, (initials) …………………………………….have asked questions regarding this
research and have been satisfactorily answered. I therefore wish to participate in the
research.
Thank you.
Signature of the Patient or Parent or Guardian/Date ………………………………….
Signature of witness/Date ……………………………………………………………..
Signature of investigator/Date …………………………………………………………
121
APPENDIX V
CONSENT FORM (HAUSA)
Ni Likita Isaac Bulus,Bakzak, ni likita ne a bangare na Family Medicine a Jos University
Teaching Hospital Jos
Ina son in hada magunguna kashi biyu saboda in gan wane magani da ya fi aiki a kan tashiwan
gaban maza. Ina so in hada mwosa jiki da wadansu magunguna guda biyu in gani ko wacece tafi
aiki a kan karfin tashiwan gaban na miji a JUTH na JOS.
Wannan gwajin zata kumshi cikan wadansu tagarda, a duba jikin ku gaba daya da kuma wadansu
gwaje gwaje a duba lafiyan ku. Zaka iya ka shiga cikin gwajin, amma in baka so ba, ba bu tilas a
ciki, kuma ba zata hana kula da kai ba. Duk abinda muka yi da kai ba mai ji ko ya sani.
In ka yarda, sai ka sa hanu a nan.
Ni ___________, na yi tambayoyi kuma an bani amsa da ta gamshe ni. Na kuma yarda in shiga
cikin gwajin.
Na gode.
Sa hanu da ranan sa hanu______________________________
Sa hanu shaida da ranar sa hanu____________________________
Sa hanun mai gwajin_____________________________
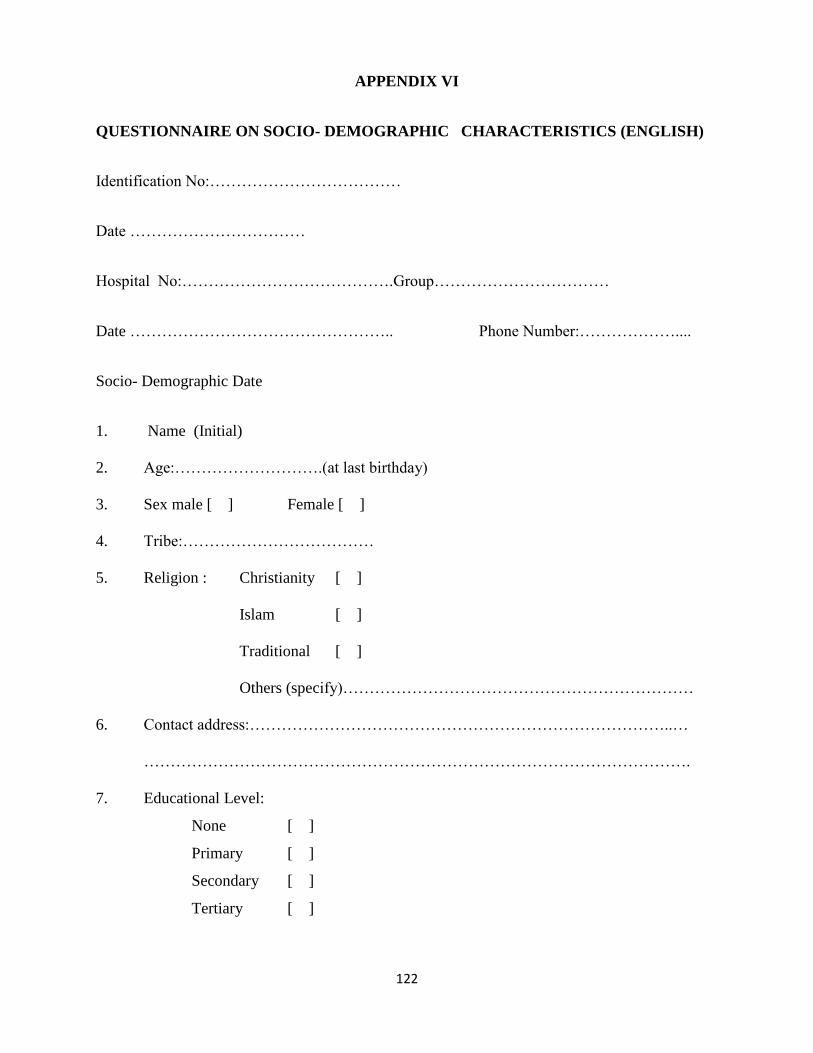
122
APPENDIX VI
QUESTIONNAIRE ON SOCIO- DEMOGRAPHIC CHARACTERISTICS (ENGLISH)
Identification No:………………………………
Date ……………………………
Hospital No:………………………………….Group……………………………
Date ………………………………………….. Phone Number:………………....
Socio- Demographic Date
1. Name (Initial)
2. Age:……………………….(at last birthday)
3. Sex male [ ] Female [ ]
4. Tribe:………………………………
5. Religion : Christianity [ ]
Islam [ ]
Traditional [ ]
Others (specify)…………………………………………………………
6. Contact address:……………………………………………………………………..…
………………………………………………………………………………………….
7. Educational Level:
None [ ]
Primary [ ]
Secondary [ ]
Tertiary [ ]
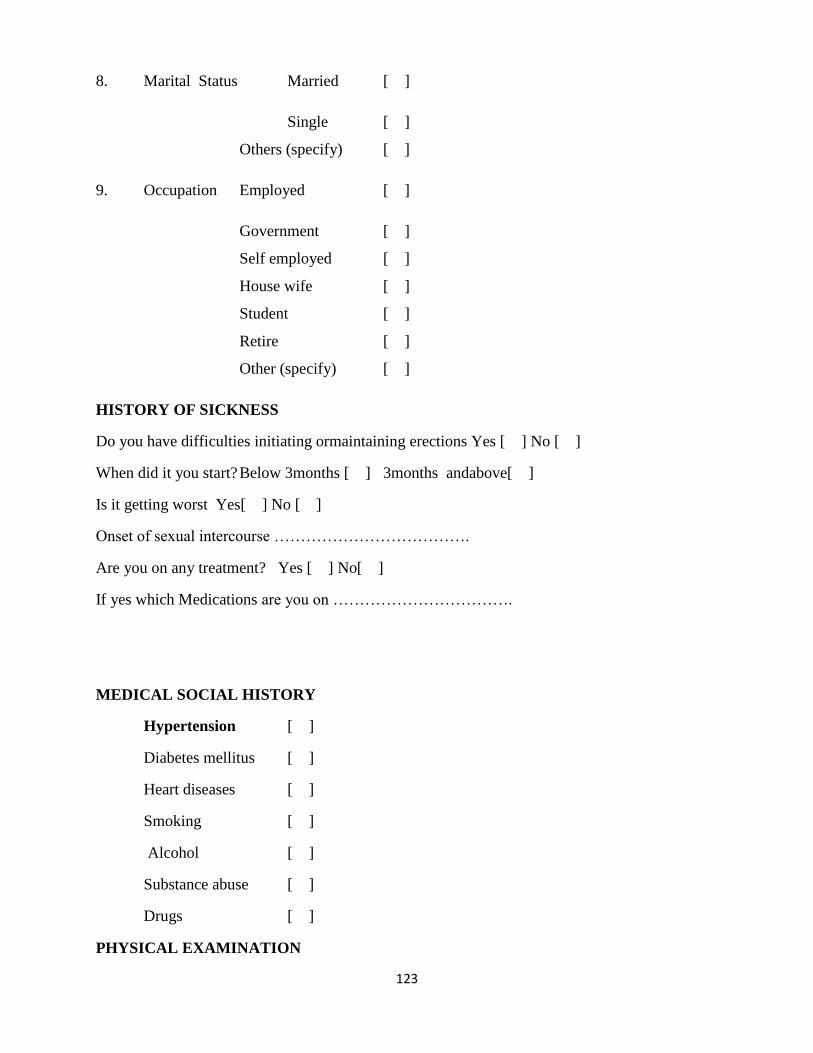
123
8. Marital Status Married [ ]
Single [ ]
Others (specify) [ ]
9. Occupation Employed [ ]
Government [ ]
Self employed [ ]
House wife [ ]
Student [ ]
Retire [ ]
Other (specify) [ ]
HISTORY OF SICKNESS
Do you have difficulties initiating ormaintaining erections Yes [ ] No [ ]
When did it you start? Below 3months [ ] 3months andabove[ ]
Is it getting worst Yes[ ] No [ ]
Onset of sexual intercourse ……………………………….
Are you on any treatment? Yes [ ] No[ ]
If yes which Medications are you on …………………………….
MEDICAL SOCIAL HISTORY
Hypertension [ ]
Diabetes mellitus [ ]
Heart diseases [ ]
Smoking [ ]
Alcohol [ ]
Substance abuse [ ]
Drugs [ ]
PHYSICAL EXAMINATION

124
a Weight…………………………
b Height ……………………………
c. Blood pressure………………….
d. Body Mass index (BMI)…………………
e. Genitals………………………………….
LABORATORY TEST RESULTS (baseline and fourth month)
a. Urinalysis……………………………..
b. Fasting blood glucose………………….
c. Lipid profile…………………………...
d. ECG…………………………………..
e. Testicular USS………………………...
APPENDIX VII
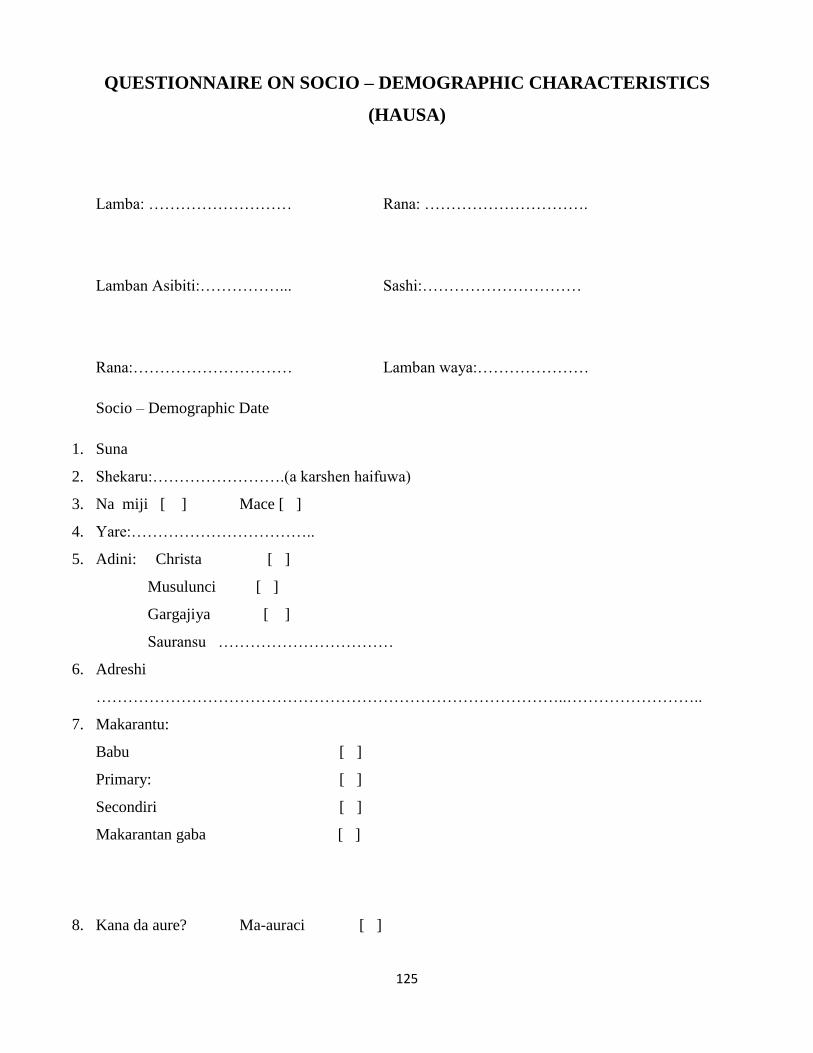
125
QUESTIONNAIRE ON SOCIO – DEMOGRAPHIC CHARACTERISTICS
(HAUSA)
Lamba: ……………………… Rana: ………………………….
Lamban Asibiti:……………... Sashi:…………………………
Rana:………………………… Lamban waya:…………………
Socio – Demographic Date
1. Suna
2. Shekaru:…………………….(a karshen haifuwa)
3. Na miji [ ] Mace [ ]
4. Yare:……………………………..
5. Adini: Christa [ ]
Musulunci [ ]
Gargajiya [ ]
Sauransu ……………………………
6. Adreshi
……………………………………………………………………………..……………………..
7. Makarantu:
Babu [ ]
Primary: [ ]
Secondiri [ ]
Makarantan gaba [ ]
8. Kana da aure? Ma-auraci [ ]

126
Ba aure [ ]
Sauran [ ]
9. Sana’ a:
Aikin Gobnati [ ]
Aikin Kanka [ ]
mace mai zaman aure [ ]
Dan makaranta [ ]
Mai ritaya [ ]
Da sauran su [ ]
TARIHIN CHIWO
Akwai damuwan tashiwan gaban ka? akwai [ ] babu [ ]
Yaushe ya fara? Kasa da wata uku [ ] sama da wata uku [ ]
Yana karuwa? Ai [ ] a’a [ ]
Yaushe ne ka soma jima’i……………………………...
Kana kan magani? …………………………………….
In haka ne, wace magani……………………………….
TARIHIN JIKI
Akwai hawan jinni? [ ]
Akwai ciwon shuga? [ ]
Akwai ciwon zuciya? [ ]
Kana shan taba? [ ]
Kana shan kwaya? [ ]

127
Sauran magunguna fa [ ]
GWAJIN JIKI GABA DAYA
a. Nauyi ka………………………………………..
b. Tsayi ka ………………………………………..
c. Hawan jinni …………………………………
d. Tsayi da nauyi (BMI)…………………….
e. Gaban ka ……………………………………..
GWAJE GWAJE (na fari da karshe)
a. Gwajin fisari ……………………………………….
b. Gwajin shuga ………………………………………..
c. Gwajin kitse ………………………………………..
d. Gwajin aikin zuciya ………………………………..
e. Gwaji (duban gwaiwa)……………………………..
APPENDIX VIII

128
EXERCISE PRESCRIPTION AND ADHERENCE
TO MEDICATION FORM DAYS EXERCISE DRUGS SIGNATURE DAYS EXERCISE DRUGS SIGNATURE
Day1 Day1
Day2 Day2
Day3 Day3
Day4 Day4
Day5 Day5
Day6 Day6
Day7 Day7
Day8 Day8
Day9 Day9
Day10 Day10
Day11 Day11
Day12 Day12
Day13 Day13
Day14 Day14
Day15 Day15
Day16 Day16
Day17 Day17
Day18 Day18
Day19 Day19
Day20 Day20
Day21 Day21
Day22 Day22
Day23 Day23
Day24 Day24
Day25 Day25
Day26 Day26
Day27 Day27
Day28 Day28
Day29 Day29
Day30 Day30
Day31 Day31
MEDICATION SIDE EFFECTS……………………………………………..
APPENDIX IX
FILE NO: SPOUSE PRESENTATION QUESTIONNAIRE
129
NAME AGE GROUP SPOUSE NAME
DATE VISIT YES NO
SPOUSE TEL________________________
APPENDIX X
PATIENT ENCOUNTER FORM

130
Name, Age, Group, File no.
Primary complain Yes No
Secondary complain Yes No
131
APPENDIX XI
IIEF QUESTIONNAIRE (ENGLISH)
Hospital No………………………..
Date of Birth………………………… Age……………
Address…………………………………………………..
Tel. No……………………………………………………
The International Index of Erectile Function (IIEF-5) Questionnaire for Health Care
Providers
IIEF-5 scoring:
The IIEF-5 score is the sum of the ordinal responses to the 5 items.
22-25: No erectile dysfunction
17-21: Mild erectile dysfunction
12-16: Mild to moderate erectile dysfunction
8-11: Moderate erectile dysfunction
5-7: Severe erectile dysfunction
The international index of erectile function IIEF (Gold standard in the assessment of severity and
treatment related responses in erectile dysfunction) will be used to measure outcome in both
groups before and after treatment. A score will be awarded before (to measure severity) and after
(to measure improvement) in erectile dysfunction.

132
It is a veritable tool because of its wide adoption, strong psychometric properties, highly
sensitive and specific, highly predictive of patient’s ability to achieve satisfactory intercourse
and focus mainly on erectile dysfunction.
Its limitations are that, it focuses only on current sexual functioning, no information on partner
relationship or sexual functioning, it does not identify the course of erectile dysfunction.
The IIEF – 5 Questionnaires (SHIM)

133
Please encircle the response that best describes you for the following five questions:
Over the past 6 months:
1. How do you rate Very low Low Moderate High Very high
your confidence
that you could get
and keep an erection? 1 2 3 4 5
2. When you had Almost never A few Sometimes Most times Almost Always
Erections with or never times or always
sexual stimulation,
how often were your
erections hard enough (much less (about (much
for penetration? than half half the more than
the time) time) half the time)
1 2 3 4 5
3. During sexual Almost never A few Sometimes Most Almost always
Intercourses, how or never times times or always
Often were you (much less (about half (much
Able to maintain than half the time) more than
Your erection after time) half the
You had penetrated time)
Your partner?
1 2 3 4 5

134
4. During sexual Extremely Very Difficult Slightly Not difficult
Intercourses, how difficult difficult difficult
difficult was it to
maintain your
erection to completion
of intercourse?
1 2 3 4 5
5. When you Almost never A few Sometimes Most times Almost always
attempted or never times or always
sexual intercourse
how often was it (much less (about half (much more
satisfactory for than half the time) than half
you? the time) the time)
1 2 3 4 5
Total Score: ________________________
1-7: Severed ED 8-11: Moderate ED 12-16: Mild-Moderate ED 17-21: Mild ED 22-25:
No ED
APPENDIX XII
IIEF QUESTIONNAIRE (HAUSA)
Lamban Asibiti: ……………………………
Ranan Haifuwa:…………………………. Shekaru:…………………

135
Adereshi: …………………………………………………………..
Lamban Waya:………………………………….
The international index of Erectile function (IIEF - 5) questionnaire for Health Care
Provides
IIEF-5 scoring:
The IIEF-5 score is the ordinal responses to the 5 items
22-25: No erectile dysfunction
17-21: Mild erectile dysfunction
12-16: Mild to moderate erectile dysfunction
8-11: Moderate erectile dysfunction
5-7: Severe erectile dysfunction
The international index of erectile function IIEF (Gold standard in the assessment of severity and
treatment related responses in erectile dysfunction) will be used to measure outcome in both
groups before and after treatment. A score will be awarded before (to measure severity) and after
(to measure improvement) in erectile dysfunction.
The IIEF – 5 Questionnaires (SHIM)
Ka zana amsa da ta dace da kai a cikin tamboyi nan guda biyar.
Ka zana amsa da ta dace da kai a cikin tamboyoyi nan guda biyar.
A CIKIN WATA SHIDA DA TA WUCE:
1. Ya ya kake babu karfi ko kadan.. babu karfi.. dadan karfi kadan.. da karfi..da karfi sosai
ganin karfin
tashiwar gaban
ka har ka riketa? 1 2 3 4 5
2. In gabarka ta tashi babu ko kadan dan kadan lokaci kada lokaci son da dama kowace
bayan ka ji ka hadu daba ta kai rabin kamar rahin data fi rahin lokaci
dana mace son nawa lokaci ba. lokaci lokaci
yak e karfi da zai shege

136
2 In gabarka ta tashi Babu ko kadan Dan kadan Kadan lokaci Son da dama kowace
bayan ka ji ka yi jima’i, lokaci da ba ta kamar rabin data fi rabin lokaci
yaya karfin kai rabin lokaci lokace
da zai shige lokaci ba
ta
1 2 3 4 5
3. A lokacin jima’i babu ko dan kadan Kaman son kowane
son nawa kake kadan lokacin da rabin da dama lokaci
iya rike tashin bai kai rabin lokaci da ya fi
gabanka bayan ba rabin
ka shiga matarka? Lokaci
1 2 3 4 5
4. A lokacin jima’i da wuya sosai da wuya dawuya da wuya kadan babu wuya
Ya ya wahalar sosai sosai
rike gabanka a
cikin matarka
har ka gama?
1 2 3 4 5
126
5. In kayi jima’i babu ko wata rana wani yawan cin kowace
da matarka, kadan da ba ta lokaci lokaci da lokaci
kana jin dadin kai rabin kamar ta fi rabin
har ta ishe ka? lokacin ba rabin lokaci
lokaci
1 2 3 4 5

137
Total score; _________________________________1 –7 Severed ED 8- 11: Moderate ED 12-
16: Mild- Moderate ED 17- 21: Mild ED 22- 25: No ED

138
Appendix XIII
FOLLOW UP QUESTIONAIRE
Physical Finding
Laboratory Finding Drugs
First Follow Up
Second Follow Up
Third Follow Up
Fourth Follow Up
Fifth Follow Up
IIEF




















