Entrepreneurial Opportunity Emergence: Complex Simulation of Emergent Entrepreneurial Phenomenon
Upload
independentCategory
view
2download
0
Australian Journal of Public Administration • 63(2)16-30, June 2004© National Council of the Institute of Public Administration, Australia 2004. Published by Blackwell Publishing Limited
RESEARCH & EVALUATION
A comparative analysis of entrepreneurialapproaches within public healthcare organisations
Patricia A. Rowe Rosalie A. BoyceBusiness School Research FellowUniversity of Queensland School of Health and Rehabilitation SciencesBrisbane University of Queensland
Brisbane
Maree V. Boyle Kathleen O’ReillyDepartment of Management Business SchoolGriffith University University of QueenslandBrisbane Brisbane
This article examines the development of two distinct models of organising allied healthprofessionals within two public sector health service organisations in Australia. The firstcase illustrated a mode of organising that facilitated a culture that focused on assetprotection and whose external orientation was threat oriented because its disparatemultiple identities operated as a fractured, fragmented and competitive set of professiondisciplines. In this milieu, there was no evidence of entrepreneurial approaches beingused. In contrast, the second case study illustrated a mode of organising that facilitatedan entrepreneurial culture that focused on asset growth and an external orientation thatwas opportunity oriented because of the evolution of a strong superordinate allied healthidentity that operated as a single united health services stakeholder. This evolution wascoupled with the emergence of a corporate boardroom model of management that isconsonant with Savage et al. (1997) IDS/N model of management. Once this structure andstrategy were in place, corporate entrepreneurship became the modus operandi. Conse-quently, because the case study was a situation where corporate entrepreneurship existedin the public sector, it was possible to compare the factors that stimulate corporate entre-preneurship in Sadler’s (2000) study with factors that were observed in our study.
Health systems have experienced significantorganisational change in recent decades (Ham1997; Bigelow and Arndt 2000). The impetusfor this change has emerged from a number ofenvironmental triggers within the sector, suchas constrained budgetary environments,increased demand for health services andincreasing levels of professionalisation andspecialisation. There is also general agreementthat the New Public Management (NPM)policies of managerialism and marketisationhave had widespread influence on both publicand private health sector agencies inindustrialised Western countries (Hood 1995).In addition to institutional and sector-leveleffects, significant impacts from NPM policies
have also occurred at the workforce level. Thesechanges are reflected in the growing body ofwork looking at the shifting nature ofprofessional work (Ferlie et al. 1996; Broadbentet al. 1997; Leicht and Fennell 1997; Exworthyand Halford 1998; Malin 2000). Hood (1995)urged against the assumption of a universalistoutcome thesis for NPM, arguing that the effectsof NPM were dependent on the specificunderlying geopolitical arrangements of theimplementing nation-state. In this paper wepresent the findings from an Australiancomparative case study to add to the body ofinternational literature exploring the effects ofNPM reform agendas on professionals.
Rowe.p65 21/05/2004, 3:27 PM16

17
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
New Public Management:The Australian healthcare context
A raft of NPM-related policy changes withinAustralian industry has typically promoted theseparation of purchasers and providers,performance management systems, restructuringof public sector governance systems andappeals for more business-like practices inpublicly funded institutions (Hancock 1999;Harris 1999). Specific health sector strategiesinclude evidence-based medicine, populationcommissioning (pooling health funds andallocating funds to local communities tomanage priorities), casemix funding methodol-ogies and the restructuring of patients intoclients/consumers. These policy and financialdrivers have resulted in a wave of organisationrestructuring and new inter-agency relationships(Keating 2000; Leeder 2000; National HealthStrategy Unit 1991, 1993).
This changing policy environment hasencouraged some health services to explorealternative approaches to both establishedgovernance structures and internal modes oforganising. Within this context health profes-sions with a traditional focus on clinical carehave been forced to engage with issues relatedto the organisational domain of their practiceand service delivery. Similarly to other inter-national experiences reported in the literature,the Australian health professions, particularlymedicine and nursing, have responded to thechanging institutional context by reorganising.Typical patterns of reorganisation haveincluded the adoption of devolved clinical unitstructures, assuming clinical director roles andimplementing shared governance models(Degeling et al. 2001; Fournier 2000; Kitchener2000; Llewellyn 2001; Thorne 2002). In thisarticle we move beyond the focus on medicineand nursing to examine the experiences of otherhealthcare professions. This objective isaccomplished through a comparative study oftwo public sector health organisations subjectto identical government reform agendas.Reflecting the Australian research setting, theprofessions involved in the research arecollectively labelled as allied health profes-sions. There are 19 disciplines accepted as alliedhealth professions in Australia, ranging from thebetter-known disciplines of physiotherapy,occupational therapy, speech pathology,
psychology, pharmacy and dietetics to thesmaller disciplines of podiatry, orthotics andprosthetics (Boyce 1998). The Australian alliedhealth professions have many similarities withthe Professions Allied to Medicine (PAM)grouping in the United Kingdom. However,unlike the situation in parts of North America,recognition as an allied health professional inAustralia requires a university degree as theminimum entry-level qualification.
Professions in transition
Conducting research on health professions in acomplex organisational locale undergoingchange makes two important contributions toour understanding of the impact of potentialreforms on their internal modes of organising.First, hospitals are a data-rich multi-professionalinstitutional research setting capable ofrevealing insights into the complexity of aninteracting system of professions confrontingan active change agenda (Abbott 1988).Second, our deliberate focus on the allied healthprofessions as a distinct professional subculturereduces the medico-centric balance of existinganalyses in the health sector. In turn, thisapproach contributes towards a more compre-hensive understanding of the range ofprofessional responses that may be deployed inthe face of organisational and policy change.
The two case study sites involved in thecurrent research are part of a 10-year program ofinvestigations into public sector health profes-sions undergoing organisational reform,including the effects of managerialism andmarketisation. These concepts were coined inthe 1984 White Paper, Budget Reform(McKenna 1996). This White Paper includedthe terms managerialism and marketisation thatall levels of government in Australia are stillendeavouring to internalise and implement. Theterm marketisation refers to the ability of publicand not-for-profit organisations to operatewithin a competitive ‘market’ environmentsimilar to that of the private sector. Marketisationprocesses such as purchaser–provider arrange-ments appropriated the language and practicesof the private sector buyer–seller relationships.Managerialism is a concept that is based on thebelief that the management of public sectorservices is primarily concerned with themanagement of scarce resources, or ‘doing more
Rowe.p65 21/05/2004, 3:27 PM17

18
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
with less’ (Yeatman 1991). The intent toimplement fundamental change in public sectoridentity is captured in terms such as privati-sation, contracting out, corporatisation and the‘contract state’.
The cases were selected for the specificresearch reported in this article because theywere the sites with the longest involvement inthe research program (approximately six yearsat 2000) and as such their ‘deep structure’ andhistorical context was well known to theresearchers. In addition, both sites also met thecriteria associated with different organisationalforms that are discussed in more detail below. Itis important to note that in the early 1990s whenthe sites initially became involved in theresearch program they were organised in alargely identical form. Each allied health depart-ment was managed by a member of theirprofession who reported to a corporate-levelmedical director within an overarching divisionof medicine. This organisational form was theuniversal structural configuration for alliedhealth professions in Australian public sectorhospitals until the early 1990s. For the purposesof our research program we have labelled thisorganising mode as a traditional model: theclassical medical model (Boyce 1991). Theclassical medical model of organising alliedhealth professions also serves the role of a refer-ence model against which emergent structuralforms can be interrogated.
Since the 1990s, when a wave of restructur-ing occurred in Australian public hospitals, twonew organising modes for the allied healthprofessions have emerged. Although there aresmall local variations in the implementation ofthe new approaches, as general types they canbe summarised as follows. First, there is thedivision of allied health in which individualprofessional departments are retained asmanagement units but with a move away frommedical management to form their own self-managing allied health division. The moststriking change is the establishment of a non-medical director of allied health role that hasmembership of the hospital executive. Second,there is the unit dispersement model, a closerelative of the patient-focused care approachpopularised internationally by managementconsulting firms. In a unit dispersementapproach the allied health profession depart-
ments are eliminated and the staff are assignedto, and managed by, medical clinical unitsaccording to their area of specialty practice.There may be some advisory leadership role fora senior member of the professions; however,this is not a managerial role.
The reduced dominance of the previouslyuniversal classical medical model was reportedin a recent national survey (Boyce 2001). Thesurvey was conducted on all Australian generalhospitals in the public sector with 100 or morebeds. A participation rate of 94 per cent wasachieved and data was collected on 107 hos-pitals. The results showed that by the year 2000the classical medical model accounted for 52per cent of the sites (n = 56). Divisions of alliedhealth were in situ at 35 per cent of locations (n= 37), but accounted for close to 45 per cent ofthe total beds in the survey (35,936), reflectingthe presence of the model at larger hospitals.The unit dispersement model was present at 6per cent of sites (n = 6). The remaining 7 percent of sites (n = 8) were distributed across threeother minor variants.
There are now several reports in theliterature describing the formation of divisionsof allied health and the organisationaldevelopment processes undertaken to achievesuccessfully functioning units (Astley 2000;Dawson 2001; Law and Boyce 2003; Wake-Dyster 2001). This small body of literature isbased on individual case study methodologyand is limited in scope to a structure and practiceperspective. In the current article we present datafrom a comparative case study approach to showhow a sustainable allied health subculture wasdeveloped in one setting, and the constraintsand difficulties encountered in trying toachieve a shift towards a similar allied healthidentity in another setting.
The evolution of an allied healthsubculture is not well understood. Evidence ofa shift in professional identity from one of ‘alliedto medicine’ to ‘allied to each other’ was a keyfinding in an analysis of a decade of reformswithin and between Australian allied healthprofessions (Boyce 2001). However, this workwas located at the health system level and notat the workplace level, which is the focus of thecurrent article. Using a comparative case studyapproach we are able to show that the form ofstructural organisation in the workplace
Rowe.p65 21/05/2004, 3:27 PM18

19
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
(division of allied health) is an important factorin building and sustaining a collective alliedhealth identity.
The other key difference in the two settingswas the use of entrepreneurial corporate meta-phors and processes as an inter-professionalregulatory management approach. A key ele-ment in the ability of allied health professionalsto operate in this novel corporate entrepreneurialmanner was the establishment of a single alliedhealth stakeholder entity underpinned by aunified identity. Appeals to public sector healthprofessionals to adopt behaviours more likethose in the private sector were not uncommonin the 1990s as part of NPM reforms (Aldridge1996; Boyce and Shepherd 2000). In this articlewe explore how public sector health profes-sionals operating in an environment favouringenterprising business-like conduct were able totranslate these appeals into a mode of organi-sing a multi-professional division.
The novelty of the corporate entrepreneur-ship approach in a public sector hospital’sprofessional workforce motivated our furtherstudy into investigating whether the factorsreported in the literature that stimulate corporateentrepreneurship in the private sector might alsooperate in a public health services organisation.
In order to understand the conditions thatstimulate corporate entrepreneurship in publicsector health service settings we reviewed theliterature to identify factors accepted as influen-tial. We were particularly interested in lookingat factors accepted as valid in the private sectorthat the literature suggested were not importantin the public sector and examining them in thecontext of our research setting, that is, the healthindustry. To accomplish this objective we drewon Sadler’s (2000) review of corporate entre-preneurship in the public sector as a primarysource. In the following section of the articlewe provide an overview of the literature oncorporate entrepreneurship and examine theconcept of professional identity more fullybefore describing the research method and casestudy sites in more detail.
Corporate entrepreneurship in thepublic sector
The private sector literature suggests that thereare numerous organisational factors thatfacilitate a tendency toward entrepreneurship
(Jennings 1994; Slevin and Covin 1990).Unlike the private sector entrepreneurshipliterature, there is little published material thataddresses those ‘structures, systems or cultures’that stimulate/constrain corporate entrepreneur-ship in the public sector (Sadler 2000). Anexception is a recently reported study, relevantto the current research, in which 24 such factorswere identified Sadler (2000). Sadler’s (2000)study of 322 publicly owned Australian urbanwater businesses found that 15 of these privatesector factors facilitate a tendency towardsentrepreneurship in the public sector.
We will focus on four of the factors unsup-ported or not tested in Sadler’s (2000) study.These unsupported or untested factors are: (1)consistent objectives; (2) few bureaucraticprocesses — little red tape; (3) decision-makingby staff with specialised training; and (4)innovative role model and mentors. In one ofthe case studies we report on, these fourentrepreneurship-stimulating factors workedhand in glove with the evolution of a singlestakeholder entity to promote corporateentrepreneurship.
The nature of stakeholderrelationships within allied health
The literature regarding stakeholders andmultiple identities provides some insights intohow the allied health professions in a publichealth services organisation positioned them-selves as a single stakeholder entity that adopteda corporate boardroom governance structure andculture. In the following sections we brieflyreview the literature on stakeholders andmultiple identities, showing how they apply inour contextual setting of health professions andthe public sector organisations they inhabit.
A broad definition of stakeholder, asapplied in this study, is any group or individualwho can affect or is affected by achievement ofthe organisation’s objectives (Freeman 1999).Kochan and Rubinstein (2000) cite fourconditions for stakeholder entities to emergewhich can be applied to our research setting.First, leadership values are open to the evolutionof a distinct allied health subculture in healthservices. Second, employees provide criticalknowledge assets to the organisation. Third,employees are affected by the fate of theorganisation and have a legitimate claim on‘property right’ for putting their assets at risk,
Rowe.p65 21/05/2004, 3:27 PM19

20
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
equivalent to the property rights granted tofinancial investors. And fourth, employees, as awould-be stakeholder of an organisation, amasssufficient power to challenge the privilegedposition that other investors and agents achievein the organisation.
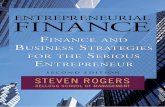
Most studies of stakeholder relationshipshave focused on a macro- or meso-level ofanalysis. In contrast, we explore stakeholderidentification and salience at the micro-levelof analysis. In particular, we focus on the stake-holder relationships within and between alliedhealth professions at two public sector healthservices organisations. At one of these organi-sations, the term ‘integrated delivery system/network’ (IDS/N) (Savage et al.1997) isintroduced as a way of describing an innovativegovernance structure and internal mode oforganising that was responsive to internal andexternal stakeholder needs. A key principle ofan IDS/N is the alignment of incentives toencourage cooperation rather than adversarialrelationships between a portfolio of healthcarestakeholders (Savage et al. 1997). Figure 1 is ahighly simplified stakeholder map from theperspective of an allied health IDS/N in theAustralian context.
It reflects some of the complexity ofstakeholder networks that can influence alliedhealth in both its day-to-day operations and atthe strategic planning level. For example, thedirection (positive or negative) and strength ofan allied health IDS/N’s relationship withspecific stakeholders can influence otherrelationships in the portfolio of healthcareindustry stakeholders. In the short term, thecomplex dynamics that result from the currentconfiguration of relationships the IDS/Ndevelops with these other healthcare stake-holders influences day-to-day operations. At astrategic level, configuration of relationshipsinfluences planning decisions. The outsideconcentric circle in Figure 1 lists major externalstakeholders. The hatched rectangular box thattranscends the IDS/N and the internal andexternal stakeholders represents the alliedhealth governing board of the IDS/N. The boardis ‘the glue that binds the IDS/N together’(Savage et al. 1997). One of the case studiesoutlined in this paper, through a corporateentrepreneurship strategy, successfully applieda corporate board governance structure to meetthe needs of all of its myriad stakeholders, even
Figure 1 Allied health stakeholders
INTERNAL STAKEHOLDERS
EXTERNAL STAKEHOLDERS
Hospital management
Patients
Competing medical practices
Other healthcare professionals
Medical practices
Employers
Competing integrated delivery systems/networks
Health plans
State and Federal governments
Professional/trade associations
Health industry organisationsAllied health professionals as individual healthcare givers
Local communities
Other healthcare providers: Home health, rehabilitation, etc.
Allied health disciplines
Functional allied health board consisting of
division head and heads of disciplines
Integrated delivery system/networkHospital committees
INTERNAL STAKEHOLDERS
EXTERNAL STAKEHOLDERS
Hospital management
Patients
Competing medical practices
Other healthcare professionals
Medical practices
Employers
Competing integrated delivery systems/networks
Health plans
State and Federal governments
Professional/trade associations
Health industry organisationsAllied health professionals as individual healthcare givers
Local communities
Other healthcare providers: Home health, rehabilitation, etc.
Allied health disciplines
Functional allied health board consisting of
division head and heads of disciplines
Integrated delivery system/networkHospital committees
Rowe.p65 21/05/2004, 3:27 PM20

21
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
though many of these stakeholders’ individualneeds conflicted or competed with each other.
Relationship between multipleprofession identities and allied healthidentity
Each of the two health services in this researchis a multiple identity organisation (Albert andWhetten 1985). For example, in relation to alliedhealth, there are different collectives, namelythe professions, which have unique sub-identities even if the allied health entity as awhole works hard to maintain a singular,common identity for its external constituencies.At best, management of multiple identities canresult in a significant competitive edge becauseit enhances response capacity through creativityand learning (Eccles et al. 1992; Nkomo andCox 1996; Fiol 1994). However, multipleidentities can also lead to organisationalinaction or vacillation (Pratt and Foreman 2000)or intraorganisational conflict (Golden-Biddleand Roa 1997; Pratt and Rafaeli 1997). Inaddition, they can cause ambivalence and thushave significant effects on the strategicmanagement of an organisation.
When a specific profession identity isstrong, it can be clearly articulated, it capturesthe imagination of organisational members andis robust in that as a profession it can independ-ently take action capable of accomplishingshort-term goals (Barney et al. 1998). If morethan one profession is high on all three charac-teristics, then conflict is likely. Conflictresolution is more likely if a strong superordinateidentity such as ‘allied health’ captures theimagination of the disparate profession identi-ties, is articulated in a way that encompassesthe subgroups and is also robust (Barney et al.1998).
Research design
The findings reported in this article are part of a10-year research program investigating thehealth professions and public sector reformssuch as organisational restructuring, manager-ialism and marketisation. Over the life of theprogram, 100 semi-structured interviews havebeen conducted with senior allied health,medical, nursing and general management staff.
Nine case studies (two longitudinal) based inmetropolitan, rural and remote locations havealso been undertaken (Boyce 2001).
The case study sites for the current investi-gation, Provincial Health Services and CoastalHealth Services, have participated in severaldata collection phases over this 10-year researchperiod.
In this paper we are drawing on interviewswith 13 allied health profession managers fromthe two study sites. A semi-structured interviewprotocol was developed following theprocedural guidelines recommended by Yin(1994). The protocol was based on a proposi-tional model of allied health organisationalsubculture developed from Boyce (1996).Questions focused on the following topics:intra-profession stability; resource environ-ment; profession interests; critical mass ofparticipants; level of organisational support forallied health; medical management environ-ment; structural support; leadership; emergenceof allied health associations; support ofprofession associations and unions; identity;and ambiguity.
Each interview was tape recorded,transcribed and returned to each interviewee forclarifying amendments. The corrected trans-cripts were then coded using the qualitative dataanalysis package NUD*IST NVivo to aidanalysis of coded data through indexing themesand illustrative extracts. Qualitative datamanagement and analysis techniques recom-mended by Miles and Huberman (1994) wereutilised throughout the research to achieveconceptual grouping around the themes of anindividualistic, threat-oriented, arbitrationmodel of management in the stakeholder-oriented case environment at Coastal HealthServices and a collective, opportunity-oriented,boardroom model of management in the IDS/N-oriented case environment at ProvincialHealth Services.
Coastal Health Services
Coastal Health Services have approximately500 registered beds providing acute and tertiaryhealthcare services. The allied health profes-sionals were organised at the macro-level withina classical medical model with each disciplinestructured as a profession hierarchy managed
Rowe.p65 21/05/2004, 3:27 PM21

22
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
by a member of the profession reporting to acorporate-level medical executive position.The profession managers were accountable forthe management of financial and humanresources and were accountable to an executive-level medical manager. This medical managerrepresented the interests of all allied healthprofessionals and the medical profession on top-level management committees. The servicedelivery approach involved each allied healthprofession independently allocating profes-sionals from their discipline to geographicallyseparate areas of the health services organisationwhere they provided services to various medicalclinical units. The professionals were not,however, managed by those medical clinicalunits.
Coastal Health Services had an allied healthsubculture with competing visions and anarbitration-type model of management. Lessthan one-third of the profession managers hadpostgraduate business degrees. Intervieweesidentified with both an allied health identityand a profession identity. However, theyidentified more strongly with their professionidentity. Allied health professionals wereextremely individualist. As a result, manage-
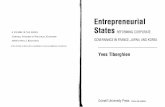
ment perceived the allied health professions asindividualist, competitive and non-influentialstakeholders in the health services organisationrather than as a united and influential super-ordinate allied health stakeholder entity. Therewas no single allied health representative withlegitimate leadership over the multiple profes-sion disciplines. Divisive work practices andcompeting visions were frequently describedin interviews. Further, there was much evidenceof attempted dispute resolution and arbitrationbetween threat-oriented, individual stake-holders over limited resources. The externalorientation of these stakeholders was bothindividualistic and threat oriented. Forexample, individual allied health professionalsfrequently breached formal governancestructures in their own self-interests to secureresources and/or jobs, as indicated by thebroken arrows in Figure 2.
In summary, the way in which CoastalHealth Services organised its internal environ-ment was underpinned by an emphasis on assetprotection by individual profession managerswho perceived themselves as individual stake-holders with scant influence, competing forrapidly shrinking assets.
Figure 2 Organisational structures at Coastal Health Services
Unbroken arrows represent formal (espoused) governance structuresBroken arrows represent informal (observed) governance structures
CEO
Health services deputy CEO/ chief operations officer
Medical division
Clinical unit
Allied health discipline
head
Allied health discipline
head
Allied health discipline
head
Allied health discipline
head
Discipline staff
member
Discipline staff
member
Discipline staff
member
Discipline staff
member
Rowe.p65 21/05/2004, 3:27 PM22

23
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
Provincial Health Services
The Provincial Health Services is a 280-bedfacility providing acute healthcare services toa rural district in Australia. Like the precedingcase study, it is considered to be one of the top10 hospitals in its state based on activity andexpenditure. In addition to the provision ofdirect acute care, the Provincial Health Servicesprovide specialist consultative services to somesmaller health services in surrounding districts.
In the late 1980s, allied health professionalsin this health services’ district were organisedtraditionally as a classical medical model. Eachprofession had its own department with a seniorclinician providing management expertise aswell as managing a full clinical caseload. Thesenior clinician of each profession would reportdirectly to a corporate-level medical director.The chief executive officer at the time wasreported to have expressed concern that the‘paramedical professions’ were ‘out of control’and needed ‘stronger’ management. As a resultthe traditional classical organisational modelwas restructured in 1992. The new structure wasa division of allied health, under the leadershipof a director of allied health. The director was amember of the health services executivemanagement team. This position gave alliedhealth professionals their own voice at the mostsenior levels for the first time. All intervieweesin this case had postgraduate business qualifi-cations at the time of this study. The director ofallied health held both professional qualifi-cations and a postgraduate qualification inbusiness. The director successfully encouragedall discipline managers to pursue postgraduatebusiness qualifications by the time of this study.A further restructuring within the division ofallied health occurred in 1997. This internalrestructuring, which was instigated directly bythe allied health professionals, involved theformation of several allied health resourceteams. The teams brought a variety of profes-sions together including physiotherapist, socialworkers, occupational therapists, speechpathologists, psychologists, dieticians andpodiatrists. Decisions about which allied healthprofessionals to allocate to a specific client weremade at an executive level by the director ofallied health and his or her management team.The restructure also involved the physicalreloca-tion of all discipline managers into a
single, open-plan workspace. This new work-space was designed to maximise interpersonalcontact and to enhance knowledge creation/utilisation (Nonaka and Takeuchi 1995;Nonaka and Konno 1998).
Under the new model, the internalconfiguration of the division of allied healthinvolved a complex matrix arrangement. It main-tained traditional professional hierarchies foreach discipline but introduced a new dimensionby simultaneously integrating these hierarchieswith the allied health resource team servicedelivery structure. This structure is shown inFigure 3. The service delivery team structuremirrored the organisational structure of themedical clinical units in this health servicesorganisation. In the Australian context,organising allied health professionals in thisform of internal matrix has been classified as anintegrated decentralisation model (Boyce2001). The underlying organising principles ofthe internal matrix structure address many ofthe concerns raised by Anderson and McDaniel(2001) about the need for complex adaptivesystems in managing the health professionalworkforce. An integrated decentralisationstructure for allied health professions had afacilitating role in developing new inter-disciplinary work practices at Provincial HealthServices that were considered ‘best practice’examples by other organisations.
The restructured division of allied healthis loosely and informally run as a ‘corporateentity’. Discipline managers take on a role asboard members and the director of allied healthis chairman of the board. This model ensuresthat each allied health manager is accountableto his or her peers and that the division of alliedhealth takes responsibility for all its businessprocesses and internal and external relation-ships. According to the then director of alliedhealth, this arrangement is beneficial for seniormanagement of the organisation as well.
I think senior management wants there tobe an allied health identity... They are verykeen to have an allied health point of contactso that they’re not dealing with competingdemands from five different professions, butthat allied health works as an entity and putsits priorities as an entity.
The staff from within the division of alliedhealth provides a wide range of services to the
Rowe.p65 21/05/2004, 3:27 PM23

24
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
health services as a whole, the community anda range of outreach and visiting services acrossthe rural district it serves. Within the newcorporatised and brokerage model, the divisionwas able to negotiate service agreements with anumber of other government and non-government agencies. The agreements were withthe Department of Education, privatephysiotherapy service providers and thedivision of general practice. Also at this time, alarge number of research, services and develop-ment grants were attracted to the organisationthrough the division of allied health. Betweenthe years 1993 and 1999 $5.2 million inservice, research and development grants hadbeen obtained by the division of allied health,most recently an $80,000 grant from thewomen’s health policy unit. In addition staffwithin allied health were encouraged to ‘worksmarter together’, dividing the labour across andbetween profession disciplines in the mostefficient manner. One senior allied healthprofessional commented on her flexibility todivide the labour:
…like [name] is the word person, I’m thenumber person, we’re meant to be managersand do monthly reports for our two teams.We’ve decided that I’ll do all the figures forall of them and she will do all the word stufffor all of them.
Strategically, the superordinate allied healthentity is influential when negotiating serviceagreements with these other stakeholders.Analysis of institutional documents and inter-view data shows that the division of alliedhealth’s decision to move toward an integrateddecentralisation model based on an internalmatrix of profession hierarchies and teams wasdeveloped to overcome a number of functionalbarriers to the efficient provision of scarce alliedhealth services to purchasers and consumers.Profession leaders had a dual role of managingtheir respective disciplines and also providedfunctional leadership across the whole divisionof allied health. Five functional areas includedtwo roles as managers of allied health resourceteams and one each for research and develop-ment, information management/technology andprofessional development/standards. At anoperational level, the mix of both professionhierarchies and multidisciplinary teams (theintegrated management model) minimised
internal competition and maximised externalopportunity for extra funding in negotiatingwith the hospital.
The model, as enumerated in divisionalplanning documents and espoused byinterviewees, is based on a number of principles.First, allied health professional resources mustbe closely linked to budget holder priorities forservice, which in turn are linked to both majorcorporate policy direction and communities’health needs. Second, allied health professionaldisciplines’ individual developmental needsand processes are strengthened. Third, alliedhealth professional services are increasinglypatient and team focused. Fourth, allied healthprofessional clinical services are price competi-tive, giving the very best value for money.
Overlying these principles were a numberof internal and external ‘drivers’ of change,emphasising the need to work smarter. Consider-able resources were being spent in supportingcommunication and information flow to sixdifferent profession-specific managers.Previously, repetitive and routine managementtasks were replicated by all five profession-specific managers. The time spent in the dutiesof filing, developing reports, in-serviceeducation and generic procedural skills wasincreasing. This was considered a major wasteof high-level and expensive managers’ time,while other important but not as pressing issuessuch as research and development were beinggiven less than optimal time during work hours.The introduction of an automated networkedinformation system designed to support andintegrate allied health professional practice anddata collection allowed for a major reductionin managing information by paper and providedmany opportunities for efficiency.
With major changes across the organisation,the division of allied health was also beingincreasingly requested to become involved inprojects and organisational priorities outsidethe traditional scope of practice. Some of these‘projects’ included hospital informationmanagement systems development, humanresource management reforms, workplace healthand safety reforms and institutional accredit-ation. The following extract reflects thisdevelopment at Provincial Health Services:
We [allied health] form alliances withwhoever or whatever systems are required
Rowe.p65 21/05/2004, 3:28 PM24

25
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
in order to fulfil whatever it is we want todo… it’s very much a systems approach, theidea being that we are part of like a multi-plicity of systems and depending on whatneeds to be achieved, we ally ourselves withthat part of the system (doc1, 3–7).
The emergence of entrepreneurialapproaches to organising
The combination of governance system,structure and culture at Provincial HealthServices is atypical of traditional health servicesorganisations. The integrated decentralisationmodel on which Provincial Health Services’allied health division is based is a new approachin Australia. A recent national study of govern-ance structures in the acute-care public hospitalsector showed that the model had beenimplemented in fewer than 10 of the 107 sitessurveyed (Boyce 2001). However, those sitesthat had committed to the model were largehospitals with leadership status in terms ofinnovative practice approaches.
Discussion of these case studies draws onthe work of Sadler (2000) and others to helpexplain how and why one allied health service
successfully developed entrepreneurial modesof organising in contrast to the other which didnot. Our key focus here is to discuss how corpo-rate entrepreneurial approaches emerged withina public sector context. The manner in whichProvincial Health Services organised its internalenvironment was underpinned by an emphasison asset growth by the director of allied healthand his team of discipline managers. Theyperceived themselves as an IDS/N in the busi-ness of allied health services delivery. Roleswere formalised within a corporate boardmanagement model. The external orientationof allied health was a single collective stake-holder entity that was opportunity oriented.
We will now discuss both case studies inrelation to the nature of Sadler’s (2000) fourfactors which are purported to be the majorfacilitators of corporate entrepreneurial activitywithin a public sector context.
Figure 3 Organisational structures at Provincial Health Services
Diminished bureaucratic processes
One of the key facilitators of entrepreneurialapproaches at Provincial Health Services wasthe development of a singular superordinateallied health identity, which had the effect ofminimising red tape. In turn, this assisted
Head, allied health division
(Chair)
Hospital executive
Discipline head/functional manager
Discipline head/functional manager
Discipline head/functional manager
Discipline head/functional manager
Other stakeholders
Discipline head/functional manager
Allied health professional
Internal matrix structure
IDS/N
Rowe.p65 21/05/2004, 3:28 PM25

26
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
Coastal Health Services because of agreed inter-professional protocols to reduce tension. Therewas also a more stable resource environment atProvincial Health Services because theirorganisational model styled on entrepreneurialgovernance permitted the professions to collect-ively focus on asset growth as part of proactivelyseeking alternative sources of revenue bothwithin the organisation and externally. Incontrast, at Coastal Health Services the alliedhealth professions focused on asset protectionand defending threats to their discipline’sresource base.
The steadying influences of intra-profes-sion stability and a stable resource environmentactively managed by the board was one of themajor reasons for a more harmonious workplaceclimate. Thus, this environment was moreconducive to staff training, professionaldevelopment and mentoring than the CoastalHealth Services work environment, where manyof the professions seemed fractured and frag-mented and the resource environment wasmarkedly less stable despite both host healthservices operating in an identical public sectorenvironment.
In contrast, Coastal Health Services had anallied health subculture with competing visionsand an arbitration-type model of management.Allied health professions were extremelyindividualist focusing on defining and defend-ing their unique, distinct discipline-basedidentity. As a result, individual non-influentialstakeholders prevailed rather than a unitedallied health stakeholder entity. There was nosingle allied health representative with legiti-mate leadership over the professions. Thefollowing interview extract from Coastal HealthServices succinctly articulates this situation:
So much energy just goes into survival. Youknow, what the hell are we arguing about?There’s no way you want to go out and hurtanybody else, any more than anyone else,[but] it’s like family turning against family.I just can’t get away from the feeling that,for me personally that is so unproductive(doc 3,63).
Decision-making efficacy and quality
Provincial Health Services was characterised bya high level of postgraduate business qualifica-tions among discipline managers/board
Provincial Health Services in developing astrong sense of shared vision of the direction,mission and philosophy of the service. Acorporate model of management was employedto achieve their shared objectives. The manage-ment team consisted of discipline leaders andthe director of the allied health division, thelatter taking a leading director’s role at alliedhealth business meetings. Relationships at thismanagement level appeared to be based moreon trust and reciprocity than on explicit notionsof power and legitimacy. The following extractof an interview with the then director of theallied health division captures the spirit of themanagement team’s approach to decision-making.
Everybody has an equal say … I like tomanage by consensus … at times we haveto play the board room rules so the overallmajority win … once outside of this[meeting] we will become allied healthprofessionals … we will not show dissentoutside this room (doc 6,10).
Externally, this approach resulted in alliedhealth being perceived as an organised, single,united influential stakeholder (Mitchell et al.1997).
Consistent objectives
A key long-term objective within ProvincialHealth Services was the achievement andsustenance of a stable resource environment.This developed through the evolution of botha mode of organising that focused internally onasset growth, and an external orientation thatwas opportunity oriented. This consistentobjective guided allied health in their evolu-tion as a single collective stakeholder entitythat facilitated consistent objectives throughan IDS/N governance structure.
Innovative role model and mentors
Our study of Provincial Health Servicessuggested that the leadership values of thedirector of allied health coupled with a stableresource environment had implications fortraining, professional development andmentoring. On the one hand, at Provincial HealthServices, the mode of organising resulted in ahigher level of intra-profession stability than at
Rowe.p65 21/05/2004, 3:28 PM26

27
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
members in addition to their clinico-professionqualifications. While all such staff at ProvincialHealth Services possessed management quali-fications or were enrolled in a formal program,only one of the equivalent positions at CoastalHealth Services had management qualifications.It was an explicit policy of the division of alliedhealth at Provincial Health Services that seniorhealth professionals gain formal managerialqualifications. This policy reflected the culturalvalue that was placed on such expertise andexplains in part the willingness of staff to engagewith managerialist reforms. As a result of theirdistinctive approach to management and con-sensus, they developed and actively supportedformal protocols that contributed to theeffectiveness of management-related decision-making within allied health. Significantexamples of the quality of the decision-makinginclude the development of skills and expertisethat resulted in the evolution of an IDS/Ngovernance structure, the introduction of aninternal matrix structure and the introductionof sophisticated automated systems.
Comparative findings regarding the fourfactors that stimulate corporate entrepreneur-ship are summarised in Table1.
Implications for governance in thenew public sector
The implications of the structures within whichallied health is organised are salient in thesetwo cases. Allied health demonstrated atProvincial Health Services that it is possible toevolve a strong superordinate identity withinthe integrated decentralisation model. As aresult, they were able to achieve high status asan influential stakeholder in their organisation.In contrast, with a classical medical model atCoastal Health Services, the tyranny of compet-ing visions and a low-trust environment meantthat allied health was constrained in its abilityto gain influence and garner resources.
The implications of different structures forother health services are also clear. LikeProvincial Health Services, they too must learnto be more flexible in the ways they ‘do business’with the allied health community. One exampleof this flexibility was the inclusion of alliedhealth middle managers on decision-makinghealth services-wide committees where theirmanagement expertise was highly valued andcontributed to more systemic decision-making.Another example is the flexibility that
Table 1 Comparison of factors stimulating corporate entrepreneurship inthe private sector with Sadler (2000) and the health services case studies
Private sectorcorporate Provincial Coastal Healthentrepreneurship Health Services Services Nature of Provincialstimulating factors Sadler (2000) case study case study Health Services’ support
Leadership values of theof allied health and stableresource environmentconducive to staff training,
Innovative role Not professional developmentmodel and mentors Not tested Supported supported and mentoring
Few bureaucraticprocesses — little Not Single superordinatered tape Not supported Supported supported identity, minimised red tape
Decision-making Each discipline manager/by staff with board member had post-specialised Not graduate businesstraining Not supported Supported supported qualifications
Single collective stakeholderentity facilitated consistent
Consistant Not objectives through IDS/Nobjectives Not supported Supported supported governance structure
Rowe.p65 21/05/2004, 3:28 PM27

28
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
Provincial Health Services displayed inencouraging the development of partnershipsbetween allied health and external fundingsources drawn from both government and non-government agencies. These are just twoexamples of the positive outcomes that resultedfrom the evolution of a strong allied healthprofession community operating within an IDS/N mode of organising.
This study adds to a growing body ofliterature that looks at systemic ways of dealingwith the influence of marketisation, managerial-ism and NPM upon health services within theAustralian context and elsewhere (Keating2000; Harris 1999). The impact of these changeshas led allied health services to review andtransform both their clinical and administrativepractice (Boyce 2001). However, differenthealth professions and the organisations theyinhabit have responded to these changes indisparate ways. It is not surprising then to findthat allied health will develop a variety ofapproaches to organising in response to bothinternal and environmental pressure to engagein organisational transformation.
While Australia is yet to move to a managedcare environment, budgetary pressure for inter-disciplinary teams to operate more efficientlyis strong (Schofield and Amodeo 1999). Giventhat allied health already work within aninterdisciplinary framework, the pressure toensure increased efficient and effective outputthroughout will grow substantially (Boyce1998). This means that allied health professionswill need to look for more innovative ways oforganising internal management structures aswell as service delivery approaches.
Future trends for organising healthservices
It needs to be recognised that the uniquehistories of these cases and the attitudes ofleaders within these health services may havefacilitated or constrained the development ofdisparate approaches to organising alliedhealth. Therefore, these case studies must beconsidered in light of this context. These twocases are not meant to be representative in thesense of being generalisable to the widerpopulation of sites. Rather, they are critical casesthat reflect the organising principles andentrepreneurial possibilities and limitations of
each of the discrete models from which they aredrawn.
Future trends within allied health indicatethat there will be significant pressure placedupon health services worldwide to further alignprofessional education with healthcarepriorities. New forms of organising healthservices in general and allied health in particularwill have a direct impact on this alignment.Future research will need to consider theimplications of these changes and the impactthis may have upon the status of allied healthwithin the broader healthcare system. Thisincludes the effect of stakeholders, salience andidentification within allied health and thechallenges this creates when working within adecentralised structure.
Conclusion
In conclusion, the transformation of healthservices in Australia and elsewhere is character-ised by the introduction of new forms oforganising. This trend has been exacerbated bya healthcare environment that is fraught withenvironmental uncertainty and turbulence.Individual health services are constantly facedwith trying to integrate professional groupingsand structures that have traditionally been incompetition with each other. In order to be moreresponsive to both internal and externalstakeholders, stakeholders within the healthcareenvironment need to develop structures andways of organising that maximise entrepreneur-ship, innovation and both human and systemicresources.
References
Abbott, A 1988 The System of Professions: An Essayon the Division of Expert Labor, University ofChicago Press, Chicago.
Albert, S & DA Whetten 1985 ‘Organisationalidentity’, in BM Staw & LL Cummings edsResearch on Organisational Behavior, JAI Press,Greenwich, CT.
Aldridge, M 1996 ‘Dragged to market: Being aprofession in the postmodern world’, BritishJournal of Social Work, 26:177–94.
Anderson, RE & RR McDaniel Jr 2001 ‘Managinghealth care organisations: Where professionalismmeets complexity science’, Health CareManagement Review, 25(1): 83–92.
Rowe.p65 21/05/2004, 3:28 PM28

29
© National Council of the Institute of Public Administration, Australia 2004
Entrepreneurial approaches within public healthcare organisations
Astley, J 2000 ‘Transforming allied health’, AustralianHealth Review, 23(4):160–9.
Barney, JB, S Bunderson, P Foreman, LT Gustafson,AS Huff, LL Martins, RK Reger, Y Sarason, Y &JL Stimpert 1998 ‘What does identity imply forstrategy?’, in SA Whetten & PC Godfrey edsIdentity in Organisations: Building Theory throughConversation, Sage, Thousand Oaks, CA.
Bigelow, B & M Arndt 2000 ‘The more things change,the more they stay the same’, Health CareManagement Review, 25(1):65–72.
Boyce, RA 1991 ‘Hospital restructuring — theimplications for allied health professions’,Australian Health Review, 14(2):147–54.
Boyce, RA 1996 ‘The organisation of allied healthprofessions in Australian general hospitals’,Unpublished PhD Thesis, Queensland Universityof Technology, Brisbane.
Boyce, RA 1998 ‘The allied health professions’, in MClinton & D Scheiwe eds Management in theAustralian Health Care Industry, 2nd edn,Longman, Melbourne.
Boyce, RA 2001 ‘Organisational governance in alliedhealth services: a decade of change’, AustralianHealth Review, 24(1):22–36.
Boyce, RA & N Shepherd 2000 ‘Entrepreneurship asa dimension of professional culture’, Proceedingsof the Annual Conference of the AustralianSociological Association, Adelaide, 6–8 December.
Broadbent, JM Dietrich et al. eds 1997 The End of theProfessions? The Restructuring of ProfessionalWork, London, Routledge.
Dawson, D 2001 ‘Carving and identity for alliedhealth’, Australian Health Review, 24(4):119–27.
Degeling, P, J Kennedy & M Hill 2001 ‘Mediating thecultural boundaries between medicine, nursing andmanagement — the central challenge in hospitalreform’, Health Services Management Research,14:36–48.
Eccles, RG, N Nohria & JD Berkley 1992 Beyond theHype. Rediscovering the Essence of Management,Harvard Business School Press, Boston.
Exworthy, M & S Halford 1998 Professionals and theNew Managerialism in the Public Ssector, OpenUniversity Press, Buckingham.
Ferlie, E, A Pettigrew, L Ashburner & L Fitzgerald1996 The New Public Management in Action,Oxford University Press, Oxford.
Fiol, CM 1994 ‘Consensus, diversity, and learning inorganisations’, Organisation Science, 5:21–50.
Fournier, V 2000 ‘Boundary work and (un)making ofthe professions’, in N Malin ed. Professionalism,Boundaries and the Workplace, London,Routledge.
Freeman, RE 1999 ‘Divergent stakeholder theory’,Academy of Management Review, 233–6.
Golden-Biddle, K & H Rao 1997 ‘Breaches in theboardroom: Organisational identity and conflict
of commitment in a non-profit organisation’,Organisation Science, 8:593–611.
Ham, C 1997 Health Care Reform: Learning fromInternational Experience, Open University Press,Buckingham, Philadelphia.
Hancock, L 1999 Health policy in the market state,Allen & Unwin, Sydney.
Harris, P 1999 ‘Changing patterns of governance:Developments in Australian public hospitals anduniversities’, Policy Studies, 20(4):255–72.
Hood, C 1995 ‘The new public management in the1980s: Variations on a theme’, Accounting,Organisations and Society, 20(2/3):93–109.
Jennings, DF 1994 Multiple Perspectives of Entre-preneurship, South Western Publishing, Ohio.
Keating, M 2000 ‘Lessons from the market place forhealth and human services’, Australian EconomicReview, 33(2):198–204.
Kitchener, M 2000 ‘The “bureaucratisation” ofprofessional roles: The case of clinical directors inUK hospitals’, Organisation, 7(1):129–54.
Kochan, TA & SA Rubinstein 2000 ‘Toward astakeholder theory of the firm: The Saturnpartnership’, Organisation Science, 11(4):367–86.
Law, D & RA Boyce 2003 ‘Beyond organisationaldesign: Moving from structure to serviceenhancement’, Australian Health Review,26(1):161–71.
Leeder, S 2000 ‘A comprehensive health policy forAustralia — challenge or oxymoron?’, Journal ofAustralian Political Economy, 45:123–34.
Leicht, KT & ML Fennell 1997 ‘The changingorganisational context of professional work’,Annual Review of Sociology, 23:215–31.
Llewellyn, S 2001 ‘“Two-way windows”: Cliniciansas medical managers’, Organisation Studies,22(4):593–623.
McKenna, H 1996 ‘Ethical dilemmas in anentrepreneurial public service’, in J Wanna, JForster & P Graham eds EntrepreneurialManagement in the Public Sector, Macmillan,Melbourne.
Malin, N 2000 Professionalism, Boundaries and theWorkplace, Routledge, London.
Miles, MB & AM Huberman 1994 Qualitative DataAnalysis, 2nd edn, Sage, London.
Mitchell, RK, BR Agle & DJ Wood 1997 ‘Toward atheory of stakeholder identification and salience:Defining the principle of who and what reallycounts’, Academy of Management Review,22(4):853–86.
National Health Strategy Unit 1991 Hospital Servicesin Australia — Access and Financing, NationalHealth Strategy Unit, Melbourne.
National Health Strategy Unit 1993 Health that Works:Reform and Best Practice in the Australian HealthIndustry, National Health Strategy Unit,Melbourne.
Rowe.p65 21/05/2004, 3:28 PM29

30
© National Council of the Institute of Public Administration, Australia 2004
Rowe, Boyce, Boyle and O’Reilly
Nkomo, SM & T Cox 1996 ‘Diverse identities inorganisations’, in SR Clegg, C Hardy & WR Nordeds Handbook of Organisation Studies, Sage,Thousand Oaks, CA.
Nonaka, I & H Takeuchi 1995 The KnowledgeCreating Company: How Japanese CompaniesCreate the Dynamics of Innovation, OxfordUniversity Press, New York.
Nonaka, I & N Konno 1998 ‘The concept of “Ba”:Building a foundation for knowledge creation,’California Management Review, 40(3):40–54.
Pratt, MG & PO Foreman 2000 ‘Classifyingmanagerial responses to multiple organisationalidentities’, Academy of Management Review,25(1):18–42.
Pratt, MG & A Rafaeli 1997 ‘Organisational dress asa symbol of multi-layered social identities’,Academy of Management Journal, 40:862–98.
Sadler, RJ 2000 ‘Corporate entrepreneurship in thepublic sector: The dance of the chameleon’, AJPA,9(2):25–43.
Savage, GT, RL Taylor, TM Rotarius & JA Buesseler1997 ‘Governance of integrated delivery systems/
networks: A stakeholder approach’, Health CareManagement Review, 22(1):7–20.
Schofield, RF & M Amodeo 1999 ‘Interdisciplinaryteams in health care and human services settings:are they effective?’, Health and Social Work,24(3):210–19.
Slevin, DP & JG Covin 1990 ‘Juggling entrepreneurialstyle and organisational structure: How to get youract together’, Sloan Management Review,Winter:43–53.
Thorne, ML 2002 ‘Colonising the new world of NHSmanagement: The shifting power of professionals’,Health Services Management Research, 15:14–26.
Wake-Dyster, W 2001 ‘Designing teams that work’,Australian Health Review, 24(4):34–41.
Yeatman, A 1991 ‘Postmodernity and revisioning thepolitical’, Social Analysis No. 30, December,Special Issue Postmodern Critical Theorising, AYeatman ed., pp. 116–130.
Yin, RK 1994 Case Study Research Design andMethods, 2nd edn, Sage, Newbury Park.
Rowe.p65 21/05/2004, 3:28 PM30
Copyright © 2022 FDOKUMEN