A cognitive blueprint of collaboration in context: Distributed cognition in the psychiatric...
11
A cognitive blueprint of collaboration in context: Distributed cognition in the psychiatric emergency department Trevor Cohen a, * , Brett Blatter b , Carlos Almeida b , Edward Shortliffe a , Vimla Patel a,c a Laboratory of Decision Making and Cognition, Department of Biomedical Informatics, Columbia University, 622 West 168th Street, Vanderbilt Clinic, 5th Floor, New York, NY 10032, USA b Psychiatric Emergency Department, Columbia University Medical Center, USA c Department of Psychiatry, New York State Psychiatric Institute, USA Received 30 June 2005; received in revised form 21 December 2005; accepted 17 March 2006 Artificial Intelligence in Medicine (2006) 37, 73—83 http://www.intl.elsevierhealth.com/journals/aiim KEYWORDS Distributed cognition; Model construction; Psychiatric emergencies collaboration Summary Objective: The complex cognitive processes that underlie human performance in ‘messy’ contexts such as critical care medicine suggest a need for a cognitive model with broad scope to support the understanding of error in such domains. The objective of this research is to characterize the cognition that underlies patient care in the domain of emergency psychiatry in order to enhance the understanding of error in this context. Methods and materials: The theoretical framework of distributed cognition has been used to study collaborative decision-making in a number of similarly complex envir- onments such as airline cockpits and air traffic control towers. These environments share certain characteristics with the critical care domain: the work is collaborative in nature, it is supported by artifacts that can be studied directly, and the consequences of error are dire. However, the nature of the work in this domain and the artifacts used to support it are unique. The application of the theoretical constructs of distributed cognition to this context is necessary in order to characterize the collective thinking that underlies critical care. Our research uses a combination of ethnographic and interview data to derive a distributed cognitive model of the psychiatric emergency department (PED), a high volume clinical unit dealing exclusively with the acute phases of psychiatric crises. The dynamics of workflow within the department are complex: several types of clinician collaborate by forming temporary multidisciplin- ary teams that attach to and manage particular patients. The component members of these teams change over time. * Corresponding author. Tel.: +1 212 342 1636; fax: +1 212 305 3302. E-mail address: [email protected] (T. Cohen). 0933-3657/$ — see front matter # 2006 Elsevier B.V. All rights reserved. doi:10.1016/j.artmed.2006.03.009
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of A cognitive blueprint of collaboration in context: Distributed cognition in the psychiatric...
A cognitive blueprint of collaboration in context:Distributed cognition in the psychiatricemergency department
Trevor Cohen a,*, Brett Blatter b, Carlos Almeida b,Edward Shortliffe a, Vimla Patel a,c
Artificial Intelligence in Medicine (2006) 37, 73—83
http://www.intl.elsevierhealth.com/journals/aiim
a Laboratory of Decision Making and Cognition, Department of Biomedical Informatics,Columbia University, 622 West 168th Street, Vanderbilt Clinic, 5th Floor, New York, NY 10032, USAb Psychiatric Emergency Department, Columbia University Medical Center, USAcDepartment of Psychiatry, New York State Psychiatric Institute, USA
Received 30 June 2005; received in revised form 21 December 2005; accepted 17 March 2006
KEYWORDSDistributed cognition;Model construction;Psychiatricemergenciescollaboration
Summary
Objective: The complex cognitive processes that underlie human performance in‘messy’ contexts such as critical care medicine suggest a need for a cognitive modelwith broad scope to support the understanding of error in such domains. The objectiveof this research is to characterize the cognition that underlies patient care in thedomain of emergency psychiatry in order to enhance the understanding of error in thiscontext.Methods and materials: The theoretical framework of distributed cognition has beenused to study collaborative decision-making in a number of similarly complex envir-onments such as airline cockpits and air traffic control towers. These environmentsshare certain characteristics with the critical care domain: thework is collaborative innature, it is supported by artifacts that can be studied directly, and the consequencesof error are dire. However, the nature of the work in this domain and the artifacts usedto support it are unique. The application of the theoretical constructs of distributedcognition to this context is necessary in order to characterize the collective thinkingthat underlies critical care. Our research uses a combination of ethnographic andinterview data to derive a distributed cognitive model of the psychiatric emergencydepartment (PED), a high volume clinical unit dealing exclusively with the acutephases of psychiatric crises. The dynamics of workflow within the department arecomplex: several types of clinician collaborate by forming temporary multidisciplin-ary teams that attach to and manage particular patients. The component members of
these teams change over time.* Corresponding author. Tel.: +1 212 342 1636; fax: +1 212 305 3302.E-mail address: [email protected] (T. Cohen).
0933-3657/$ — see front matter # 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.artmed.2006.03.009

74 T. Cohen et al.
Results: Using the theoretical framework of distributed cognition, we interpretedthe collected data to derive a cognitive model of the distribution of work andinformation flow in the PED. This modeling process has revealed several latent flawsin the system related to the underlying distribution of cognition across teams, time,space and artifacts.Conclusions: The characterization of this distribution has enhanced our understand-ing of the cognitive dynamics underlying error in this environment, and will serve toguide future research on error management in the ED and inform the development ofcontext-appropriate error-management systems.# 2006 Elsevier B.V. All rights reserved.
1. Introduction
Early work in artificial intelligence in medicine (AIM)concerned itself with the design of systems to per-form the complex diagnostic and therapeutic tasksof individual expert clinicians. However, the intelli-gence that supports critical care work cannot becaptured by focusing on the thought process of anyone individual, as this work is inherently collabora-tive. Rather than existing in the mind of any parti-cular individual, the cognition in critical caresettings can be characterized by its distributionacross the minds of members of the clinical teamand across physical media such as clinical notes [1].In a historical review of artificial intelligence inmedicine, Coiera suggests that in order for the fieldto be relevant to clinical medicine, it must adoptclinical medicine’s goals as its own [2]. The alter-native, an inward-looking approach in whichresearch is conducted in isolation from the concernsof related fields is characterized by Shortliffe as‘adolescent’ [3]. The recent Institute of Medicine(IOM) report [4] has drawn considerable attention tothe issue of error in medicine. This particular issuecannot be addressed without deep knowledge of theenvironment in which errors occur. Furthermore,designers of new technological artifacts to addresssuch issues must take into account the pre-existingdistributed cognitive structures that support theprocess of care. The design of systems that areclinically relevant requires an awareness of thereal-world distribution of cognitive work, as it isinto this environment that an artificial agent willneed to be integrated. Rather than isolated indivi-dual intelligence, it is the distribution of intelli-gence across team members and artifacts thatwill reveal opportunities for the design of contex-tually relevant technology. In summary, the rele-vance of AIM to the field of medicine requires thedevelopment of contextually relevant solutions toproblems that concern clinicians.
In this research we use the framework of distrib-uted cognition to characterize the cognition thatunderlies clinical care in the psychiatric emergencydepartment (PED), in order to reveal underlying
systemic mechanisms of medical error. Distributedcognitive research has revealed much about howthings work in complex collaborative settings [5,6].Recent research applying this framework to criticalcare settings has focused on the mediating role ofcognitive artifacts in supporting clinical care, andsuggested that the design of information technologyinterventions should take into account the effec-tiveness of pre-existing supportive artifacts [1].While we recognize the critical role of such artifactsin supporting clinical work, the specific aim of thisresearch is to identify features of the distributedcognitive system that may be conducive to error.This decision was motivated by a pressing need inthe medical community to understand and preventerror in the wake of the IOM report [4].
Reason defines error as the failure of a plannedsequence of mental or physical actions to achievethe intended outcome when this failure cannot beattributed to chance [7]. Most errors do not result inpatient injury [8]. However, errors represent thepreventable component of the causal pathway lead-ing to adverse events. An understanding of theunderlying mechanisms of error is essential if weare to design systems to protect patients from theseevents. Zhang et al. reveal the fundamental role ofcognition in the understanding of such mechanisms[9], proposing a theoretical framework that could beused to classify errors by constructing a taxonomywith explanatory and predictive power. This frame-work incorporates the role of cognition at each levelof the healthcare systems hierarchy, and is there-fore applicable to study of the systemic featuresunderlying medical error. Reason refers to ‘‘latentconditions’’ [7] to denote the potential for errorsthat exists within complex systems. For example,communication failures were found to contribute to91% of medical mishaps investigated by Sutcliffeet al. [10]. The study of error without an under-standing of the context in which it occurs is unlikelyto reveal the potentially remediable systemic fac-tors that lead to error. Much error research hasinvolved retrospective analysis of case reports[11—14]. However, this approach is vulnerable tobias (if a clinician involved with a particular case

Distributed cognition in the psychiatric emergency department 75
provides details missing from the case notes) andprecludes the study of error in evolution. Recentstudies have emphasized direct observation of theprocess of actual [15] and simulated [16] patientcare. The research presented here approaches thestudy of error in context prospectively, from acognitive science perspective. The advantage of thisapproach is that rather than attributing error toindividual clinicians, it focuses on latent systemicconditions that may lead to error. While individualerror is unlikely to be eradicated, the system itself isamenable to change. A deeper understanding of theweaknesses in this system will enable the design ofinterventions that address medical error at thesystemic level.
2. Theoretical framework
Distributed cognition is a theoretical frameworkdeveloped by Hutchins [5]. It has previously beenapplied to the study of cognitive systems underlyingtask performance on naval vessels [5] and in thecockpit [6]. It has also been proposed as a means toinform the design of relevant technology in emer-gency departments [17]. According to distributedcognition theory, cognitive process is not confined tothe thoughts of individuals, but rather is distributedacross individuals and artifacts such as clinicalnotes. This broader perspective allows for the studyof a range of representations and structures thatsupport cognitive processes. These may be internal,existing in an individual’s memory, external, pre-sent on physical media, or simultaneously distribu-ted across both, memory and a physical medium.These representations form part of a larger compu-tational system, with greater capacity than anyindividual component [5]. For example, the PEDmakes considerable use of a shared external repre-sentation in the form of a whiteboard1. This containsessential information such as patient demographicdetails, diagnoses, relevant symptoms, laboratorytests and disposition plan, as well as details ofbehavioral acuity such as violence or suicide risk.However, it is the combination of the succinctinformation on the whiteboard (external represen-tations) and details in the minds of various teammembers (internal representations) that drives thedecision-making process. The cognitive systemunderlying decision-making in a particular context
1 The PED contains two whiteboards which occupy the frontwall of the PED. They are readily accessible to all PED staff. Theycontain immediately accessible clinical summaries of allpatients, providing an overview of all patients assigned to thePED.
can be characterized by studying the representa-tions that support this decision process. The frame-work of distributed cognition is well suited to thestudy of error in complex clinical environments suchas the PED as it can characterize the cognitivesystem of groups of individuals, rather than simplysingle decision makers, in context.
Patel et al. describe the implications ofdistributedcognition for the design of intelligent systems thatare an integral part of the collaborative decision-makingprocess [18], drawing attention to theneed toconsider the cognitive, cultural and social frame-works into which systems are being deployed [19].From this perspective, an information system isdesigned to fit into the context of a functional cog-nitive system such as the PED. Characterization ofsuch a cognitive system can be used to inform thedesign of computer interventions that are contex-tually appropriate. Current research suggests thatcognitive modeling can support the design and inte-gration of appropriate technology. For example, Rothet al. use the phrase ‘cognitive engineering’ todescribe the design of systems to support cognitivedimensions of human performance [20]. Baxter et al.describe the use of cognitive task analysis to facil-itate the integration of an expert system into aneonatal intensive care unit [21]. Zhang and Normanpresent in-depth analyses of the supportive power ofeffective external representations at individual [22]and interpersonal [23] levels. Such analyses revealthe characteristics of effective external representa-tions, providing theoretical support for the construc-tion of appropriate interventions in the form of newartifacts. Rinkus et al. describe the integration ofdistributed cognitive and representational analysesinto the design phase of a knowledge-managementsystem for biomedical engineers in the Mission Con-trol Center at NASA Johnson Space Center [24].
Unlike previous research on distributed cognitionin critical care settings, the research described inthis manuscript uses this framework to revealmechanisms of error. The functional role of cogni-tive artifacts in supporting collaborative work hasbeen demonstrated in a number of studies in criticalcare [1]. However, the focus of this research is onthe characterization of aspects of this distributionthat may be dysfunctional. According to Reason [7],individualist approaches to error predominatewithin the medical mainstream. In our opinion,individual error cannot be eradicated. However,once revealed, latent flaws in the system can besupported by information technology interventions.By shifting focus in this way, we are moving thepurely descriptive to research that can supportrecommendations for contextually appropriateinterventions to address the issue of medical error.

76 T. Cohen et al.
The research presented here aims to characterizethe cognitive mechanisms underlying error in thePED. Ethnographic and interview methods are usedto derive amodel of the distribution of cognition thatunderlies the functioning of the PED. Prospectiveerror-related data, as they are collected, can thenbe interpreted in light of this model, in order toreveal the relationship between each error and thebroader cognitive context in which the error wasidentified. This is analogous to the analysis ofrecorded ‘black box’ data in the airline industry:without an understanding of the function of thevarious components of the aircraft, these data aremeaningless. Furthermore, in the same way thatairline pilots may lack the technical knowledge tounderstand these data, the depth of understandingrequired to determine the underlying mechanisms oferror in the PED cannot be obtained by simply askingclinicians how the fault might have happened. Theresearchers have to infer this information from pro-spective data such as verbal recordings. A cognitiveblueprint of PED information flow and decision-mak-ing must be established beforehand.
3. Domain description
The psychiatric emergency department is a uniquecritical care environment. It is mandated to provideacute-phase psychiatric care, with license to holdpatients for observation and acute management forup to 72 h. It differs from other psychiatric contexts:patients present in crisis, and limited information isavailable at the outset to guide management. Man-agement emphasis is on assessment, stabilizationand disposition. At times, acute-phase managementcan preclude admission to a psychiatric hospital. Italso differs substantially from other critical carecontexts: patients are cared for by multidisciplinaryteams that address a broad range of psychosocialissues in addition to the patient’s immediate clinicalproblem. Patients are often unable to communicateinformation that is sufficiently detailed or reliableto support clinical decision-making. Consequently,clinicians are reliant on historical information fromother sources. While certain categories of adversedrug events in psychiatry have been studied, there islittle published research on the nature of error inpsychiatry [25]. This may be a consequence of thedifficulty involved in linking adverse events in psy-chiatry to human error. As most psychiatric diag-noses cannot presently be confirmed by laboratorytests, diagnostic errors are difficult to demonstratedefinitively–—as are therapeutic errors based on aparticular diagnosis. It is readily apparent that someof the adverse events occurring in this domain are
unique. For example, patients may kill or injurethemselves or others while admitted to the PED.Alternatively a patient might have to return foracute care shortly after being discharged. In thisinstance it is difficult to determine whether this wasdue to human error or chance, as the patient isvulnerable to many other influences while out of thehospital. We consider these adverse events aspotentially indicative of error. The purpose of thispaper is to illustrate the characterization of thedistribution of cognitive work to enhance the under-standing of error within this context.
The primary tasks in the PED are acute-phasediagnosis and management followed by dispositionplanning. Patientsmay be observed for a period of upto 72 h, against their will if necessary. This observa-tion period allows for acute-phase managementwhich may obviate the need for inpatient admission,as well as giving clinicians time to seek the necessaryinformation to support clinical decision-making.Eventually, a decision must be taken to either admitto an inpatient unit or discharge with a suitabledisposition plan. Several disparate sources of infor-mation must be integrated in order to support thisdecision. As thepatient is oftenunable or unwilling toprovide historical information that is sufficient andreliable enough to support sound clinical decision-making, parallel history from relatives and othercaregivers must be collected. While in the PED,short-term management is initiated to stabilize thepatient: this may include medication, supportivetherapy and family sessions. Prior to discharge, anacceptable disposition/referral plan must beinitiated. If the patient is to be admitted, a bedmustbe found at an inpatient unit. Acceptance to this unitmust then be arranged. Factors determiningwhetheror not a patient is accepted at other units are oftenbeyond the control of the referring clinician. Choos-ing to revoke the civil liberties of patients to facil-itate admission against their will, but for their ownsafety, is a significant clinical decision. It requires thegathering of substantial supportive collateral history,confrontation of the patient and meetings with thepatient’s family or clinicians.
4. Methods
We used approximately two months of ethnographicobservation and semi-structured interviews togather the data for this study. While the theoreticalframeworks that inform ethnography differ in thecontext of cognitive studies, the essential metho-dology is consistent with that employed in socio-logical and observational studies [26]. Approval fordata collection was provided by the institutional IRB
Distributed cognition in the psychiatric emergency department 77
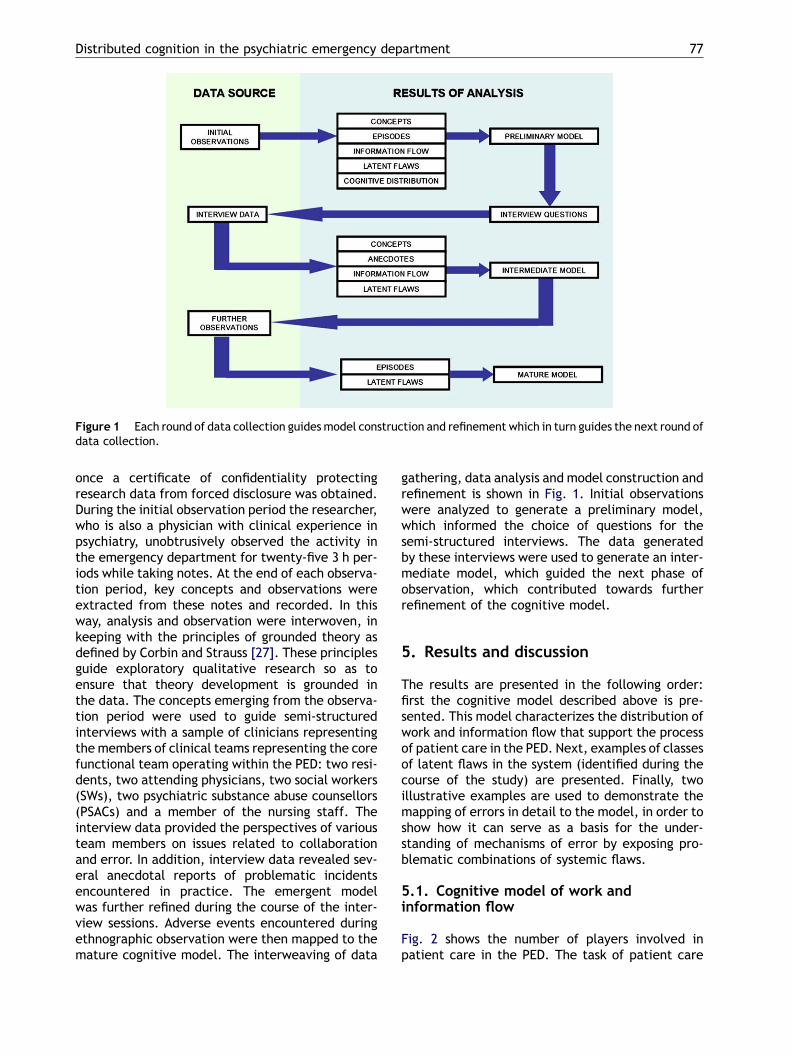
Figure 1 Each round of data collection guides model construction and refinement which in turn guides the next round ofdata collection.
once a certificate of confidentiality protectingresearch data from forced disclosure was obtained.During the initial observation period the researcher,who is also a physician with clinical experience inpsychiatry, unobtrusively observed the activity inthe emergency department for twenty-five 3 h per-iods while taking notes. At the end of each observa-tion period, key concepts and observations wereextracted from these notes and recorded. In thisway, analysis and observation were interwoven, inkeeping with the principles of grounded theory asdefined by Corbin and Strauss [27]. These principlesguide exploratory qualitative research so as toensure that theory development is grounded inthe data. The concepts emerging from the observa-tion period were used to guide semi-structuredinterviews with a sample of clinicians representingthe members of clinical teams representing the corefunctional team operating within the PED: two resi-dents, two attending physicians, two social workers(SWs), two psychiatric substance abuse counsellors(PSACs) and a member of the nursing staff. Theinterview data provided the perspectives of variousteam members on issues related to collaborationand error. In addition, interview data revealed sev-eral anecdotal reports of problematic incidentsencountered in practice. The emergent modelwas further refined during the course of the inter-view sessions. Adverse events encountered duringethnographic observation were then mapped to themature cognitive model. The interweaving of data
gathering, data analysis and model construction andrefinement is shown in Fig. 1. Initial observationswere analyzed to generate a preliminary model,which informed the choice of questions for thesemi-structured interviews. The data generatedby these interviews were used to generate an inter-mediate model, which guided the next phase ofobservation, which contributed towards furtherrefinement of the cognitive model.
5. Results and discussion
The results are presented in the following order:first the cognitive model described above is pre-sented. This model characterizes the distribution ofwork and information flow that support the processof patient care in the PED. Next, examples of classesof latent flaws in the system (identified during thecourse of the study) are presented. Finally, twoillustrative examples are used to demonstrate themapping of errors in detail to the model, in order toshow how it can serve as a basis for the under-standing of mechanisms of error by exposing pro-blematic combinations of systemic flaws.
5.1. Cognitive model of work andinformation flow
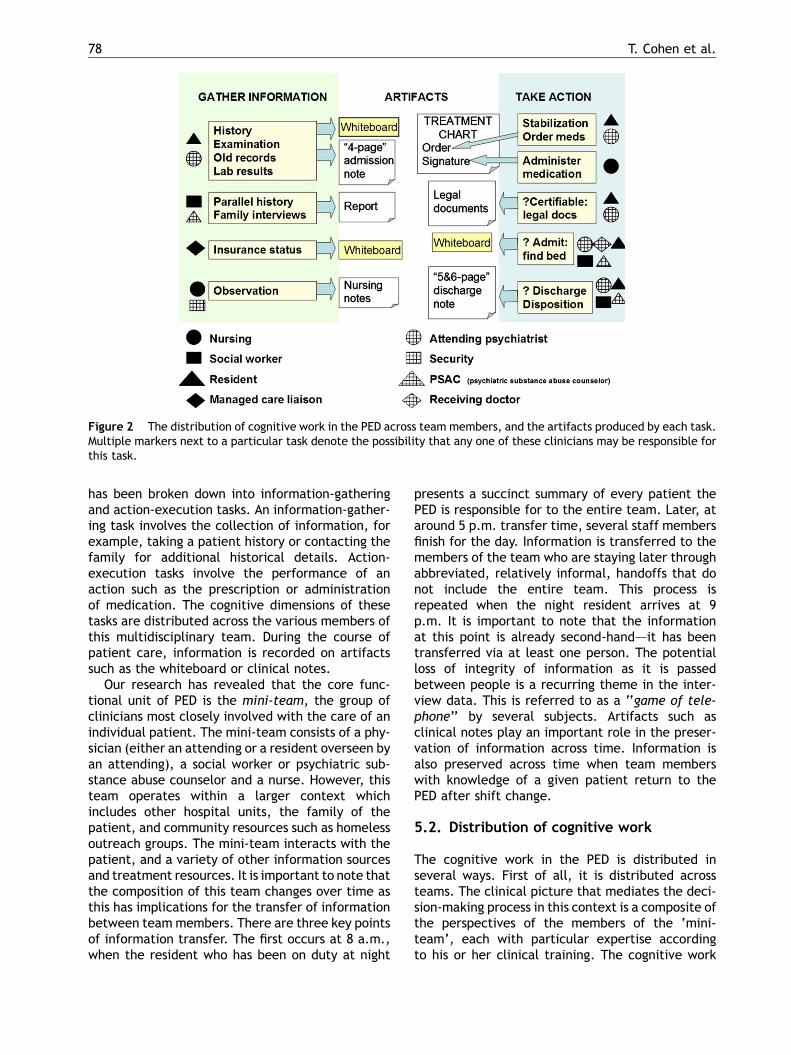
Fig. 2 shows the number of players involved inpatient care in the PED. The task of patient care
78 T. Cohen et al.
Figure 2 The distribution of cognitive work in the PED across team members, and the artifacts produced by each task.Multiple markers next to a particular task denote the possibility that any one of these clinicians may be responsible forthis task.
has been broken down into information-gatheringand action-execution tasks. An information-gather-ing task involves the collection of information, forexample, taking a patient history or contacting thefamily for additional historical details. Action-execution tasks involve the performance of anaction such as the prescription or administrationof medication. The cognitive dimensions of thesetasks are distributed across the various members ofthis multidisciplinary team. During the course ofpatient care, information is recorded on artifactssuch as the whiteboard or clinical notes.
Our research has revealed that the core func-tional unit of PED is the mini-team, the group ofclinicians most closely involved with the care of anindividual patient. The mini-team consists of a phy-sician (either an attending or a resident overseen byan attending), a social worker or psychiatric sub-stance abuse counselor and a nurse. However, thisteam operates within a larger context whichincludes other hospital units, the family of thepatient, and community resources such as homelessoutreach groups. The mini-team interacts with thepatient, and a variety of other information sourcesand treatment resources. It is important to note thatthe composition of this team changes over time asthis has implications for the transfer of informationbetween team members. There are three key pointsof information transfer. The first occurs at 8 a.m.,when the resident who has been on duty at night
presents a succinct summary of every patient thePED is responsible for to the entire team. Later, ataround 5 p.m. transfer time, several staff membersfinish for the day. Information is transferred to themembers of the team who are staying later throughabbreviated, relatively informal, handoffs that donot include the entire team. This process isrepeated when the night resident arrives at 9p.m. It is important to note that the informationat this point is already second-hand–—it has beentransferred via at least one person. The potentialloss of integrity of information as it is passedbetween people is a recurring theme in the inter-view data. This is referred to as a ‘‘game of tele-phone’’ by several subjects. Artifacts such asclinical notes play an important role in the preser-vation of information across time. Information isalso preserved across time when team memberswith knowledge of a given patient return to thePED after shift change.
5.2. Distribution of cognitive work
The cognitive work in the PED is distributed inseveral ways. First of all, it is distributed acrossteams. The clinical picture that mediates the deci-sion-making process in this context is a composite ofthe perspectives of the members of the ‘mini-team’, each with particular expertise accordingto his or her clinical training. The cognitive work
Distributed cognition in the psychiatric emergency department 79
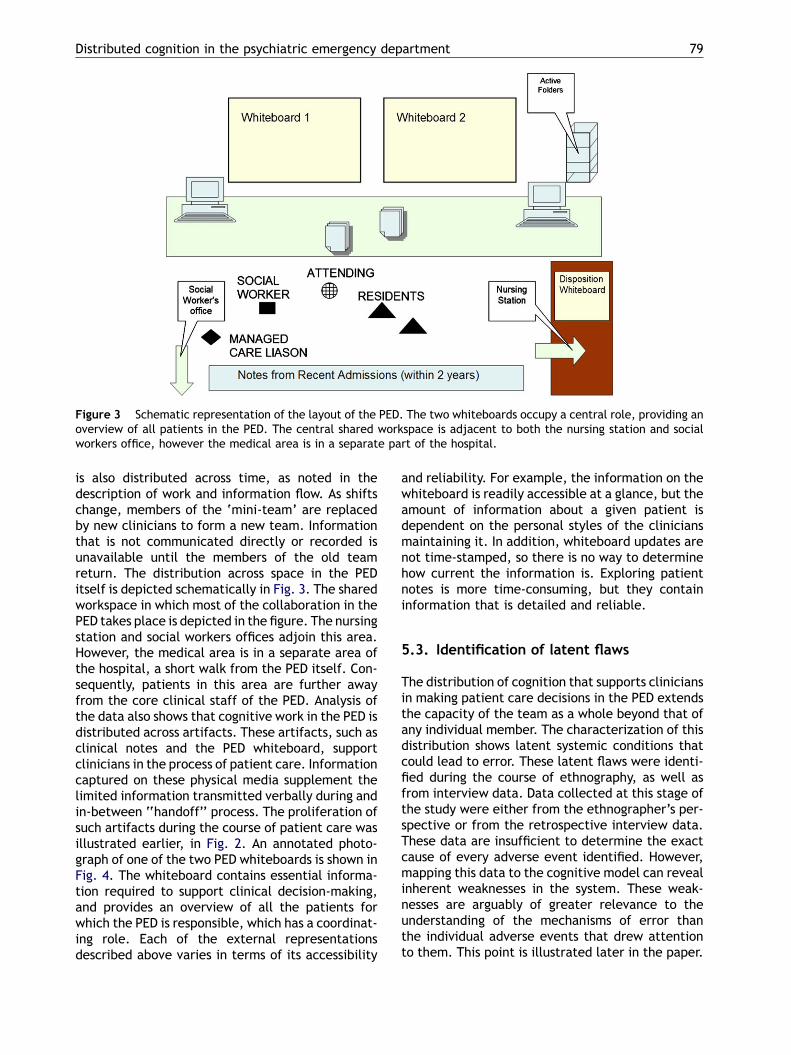
Figure 3 Schematic representation of the layout of the PED. The two whiteboards occupy a central role, providing anoverview of all patients in the PED. The central shared workspace is adjacent to both the nursing station and socialworkers office, however the medical area is in a separate part of the hospital.
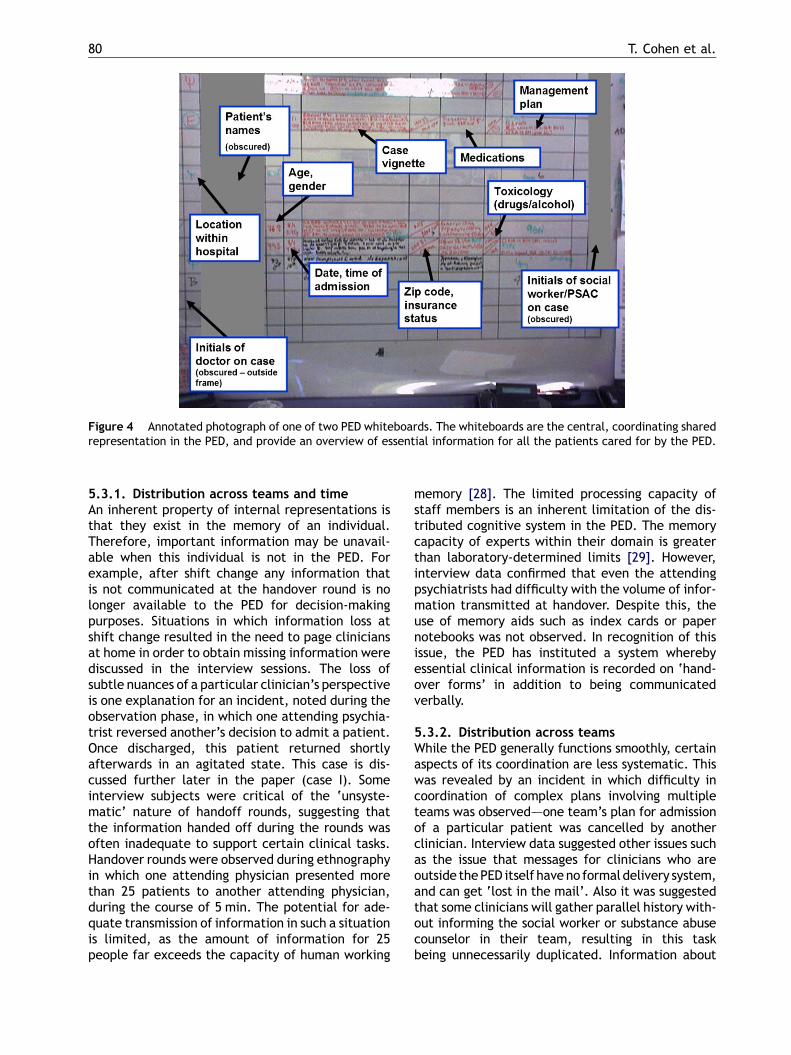
is also distributed across time, as noted in thedescription of work and information flow. As shiftschange, members of the ‘mini-team’ are replacedby new clinicians to form a new team. Informationthat is not communicated directly or recorded isunavailable until the members of the old teamreturn. The distribution across space in the PEDitself is depicted schematically in Fig. 3. The sharedworkspace in which most of the collaboration in thePED takes place is depicted in the figure. The nursingstation and social workers offices adjoin this area.However, the medical area is in a separate area ofthe hospital, a short walk from the PED itself. Con-sequently, patients in this area are further awayfrom the core clinical staff of the PED. Analysis ofthe data also shows that cognitive work in the PED isdistributed across artifacts. These artifacts, such asclinical notes and the PED whiteboard, supportclinicians in the process of patient care. Informationcaptured on these physical media supplement thelimited information transmitted verbally during andin-between ‘‘handoff’’ process. The proliferation ofsuch artifacts during the course of patient care wasillustrated earlier, in Fig. 2. An annotated photo-graph of one of the two PED whiteboards is shown inFig. 4. The whiteboard contains essential informa-tion required to support clinical decision-making,and provides an overview of all the patients forwhich the PED is responsible, which has a coordinat-ing role. Each of the external representationsdescribed above varies in terms of its accessibility
and reliability. For example, the information on thewhiteboard is readily accessible at a glance, but theamount of information about a given patient isdependent on the personal styles of the cliniciansmaintaining it. In addition, whiteboard updates arenot time-stamped, so there is no way to determinehow current the information is. Exploring patientnotes is more time-consuming, but they containinformation that is detailed and reliable.
5.3. Identification of latent flaws
The distribution of cognition that supports cliniciansin making patient care decisions in the PED extendsthe capacity of the team as a whole beyond that ofany individual member. The characterization of thisdistribution shows latent systemic conditions thatcould lead to error. These latent flaws were identi-fied during the course of ethnography, as well asfrom interview data. Data collected at this stage ofthe study were either from the ethnographer’s per-spective or from the retrospective interview data.These data are insufficient to determine the exactcause of every adverse event identified. However,mapping this data to the cognitive model can revealinherent weaknesses in the system. These weak-nesses are arguably of greater relevance to theunderstanding of the mechanisms of error thanthe individual adverse events that drew attentionto them. This point is illustrated later in the paper.
80 T. Cohen et al.
Figure 4 Annotated photograph of one of two PED whiteboards. The whiteboards are the central, coordinating sharedrepresentation in the PED, and provide an overview of essential information for all the patients cared for by the PED.
5.3.1. Distribution across teams and timeAn inherent property of internal representations isthat they exist in the memory of an individual.Therefore, important information may be unavail-able when this individual is not in the PED. Forexample, after shift change any information thatis not communicated at the handover round is nolonger available to the PED for decision-makingpurposes. Situations in which information loss atshift change resulted in the need to page cliniciansat home in order to obtain missing information werediscussed in the interview sessions. The loss ofsubtle nuances of a particular clinician’s perspectiveis one explanation for an incident, noted during theobservation phase, in which one attending psychia-trist reversed another’s decision to admit a patient.Once discharged, this patient returned shortlyafterwards in an agitated state. This case is dis-cussed further later in the paper (case I). Someinterview subjects were critical of the ‘unsyste-matic’ nature of handoff rounds, suggesting thatthe information handed off during the rounds wasoften inadequate to support certain clinical tasks.Handover rounds were observed during ethnographyin which one attending physician presented morethan 25 patients to another attending physician,during the course of 5 min. The potential for ade-quate transmission of information in such a situationis limited, as the amount of information for 25people far exceeds the capacity of human working
memory [28]. The limited processing capacity ofstaff members is an inherent limitation of the dis-tributed cognitive system in the PED. The memorycapacity of experts within their domain is greaterthan laboratory-determined limits [29]. However,interview data confirmed that even the attendingpsychiatrists had difficulty with the volume of infor-mation transmitted at handover. Despite this, theuse of memory aids such as index cards or papernotebooks was not observed. In recognition of thisissue, the PED has instituted a system wherebyessential clinical information is recorded on ‘hand-over forms’ in addition to being communicatedverbally.
5.3.2. Distribution across teamsWhile the PED generally functions smoothly, certainaspects of its coordination are less systematic. Thiswas revealed by an incident in which difficulty incoordination of complex plans involving multipleteams was observed–—one team’s plan for admissionof a particular patient was cancelled by anotherclinician. Interview data suggested other issues suchas the issue that messages for clinicians who areoutside thePED itself have no formaldelivery system,and can get ‘lost in the mail’. Also it was suggestedthat some clinicians will gather parallel history with-out informing the social worker or substance abusecounselor in their team, resulting in this taskbeing unnecessarily duplicated. Information about

Distributed cognition in the psychiatric emergency department 81
prescribed treatment on occasion was not commu-nicated between team members. In one incidentnoted during the observation period, a patient wasdiscovered tohave receivednomedicationduring thenight, despite this medication having been pre-scribed. The doctor on duty was not informed of thiserror until morning. Analysis of the Interview datasuggests that more experienced clinicians have a‘check-and-balance’ approach to written orders,supplementing them with verbal instructions so asto ensure that a two-way channel of communicationexists.
5.3.3. Distribution across spaceThe management of psychiatric patients in the gen-eral medical area of the ED appears to be anothersource of potential error. Biddinger et al. suggestthat the process of medical clearance (in whichpatients are medically evaluated prior to admissionto a psychiatric unit) is inherently problematic [30].On several occasions, patients were referred fromthe medical emergency department as ‘medicallyclear’ however medical problems were discoveredonce they were in the PED. For example, a patientwith gangrenous fingers (and a severe lice infesta-tion) was medically cleared and a patient with anambulance form documenting symptoms suggestiveof a stroke was ‘medically cleared’ without a docu-mented neurological examination. Observed inci-dents described in the interviews included apatient with undetected Lupus Cerebritis (a seriousneurological complication of the autoimmune dis-ease, Systemic Lupus Erythematosis) and a patientwith severe metabolic instability due to anorexiabeing ‘medically cleared’.
One danger of this process is that medical carewill be delayed while patients are transferred backto the medical area. Another problem is thatpatients will not be re-evaluated medically oncethey have been labeled as ‘clear’. One clinicianinterviewed suggested that the primary cause ofthe failure of general medical staff to detect med-ical conditions in psychiatric patients is not negli-gence or a dismissive attitude towards psychiatricpatients on the part of the medical department, butrather that psychiatric patients generally are unableto express their medical complaints clearly. It wasalso further recognized that the clinicians and con-ditions in the general medical area are poorly suitedto the specific needs of psychiatric patients. Com-munication failures between the mini-team andother units of the hospital were observed whereseveral patients were sent to the PED without areceiving doctor being informed in advance. This isin violation of protocol, as referred patients shouldbe accepted by the PED before transfer occurs.
5.3.4. Distribution across artifactsAn external representation may be intentionallyprivate (such as a note on a piece of paper as apersonal reminder). However, the strength of thewhiteboard as a resource is that the information onit is shared. This is only advantageous if it can bereadily interpreted by relevant members of theclinical team, which was not always the case. Exam-ples include indecipherable handwriting, and theuse of abbreviations without consensual meaningsuch as ‘am’ for Amitryptiline (an antidepressantmedication) or the initials of a resident unknown tothe nursing staff. Another example of this problemwhich resulted in a medication error is discussed, inmore detail later in the paper in the context ofcase II. In addition, the degree of detail on patientinformation written on the whiteboard varies fromclinician to clinician, as does the regularity withwhich it is updated. There is no way to determinehow recently it was last updated.
5.4. Use of cognitive model to interpretadverse events: illustrative examples
5.4.1. Case#1In this incident it was noted during the observationperiod that two mini-teams disagreed in theirassessment of a given patient over a 24-h period.The first team considered the patient to be poten-tially suicidal and recommended that the patientshould not be discharged. However, the second teamre-evaluated the patient, and decided to dischargehim. Each team evaluated the same patient differ-ently with different outcomes. The first attendingpsychiatrist’s goal of admitting the patient to aninpatient unit was not realized by the psychiatrist onthe second team and the patient was discharged.The patient returned later in an agitated state.While this is not an ideal outcome, it is not neces-sarily evidence of an error. These data were delib-erately gathered unobtrusively without disruptingthe process of care. Consequently, we did not ‘digdeeper’ to try to determine the exact cause of thisincident. Mapping the incident to the model revealsseveral plausible possible causes. The first is simplythat the patient’s state improved in-betweenassessments, or that the clinical judgment of thetwo attending psychiatrists differed. However, italso possible that certain nuances of the firstattending psychiatrist’s evaluation were not trans-mitted through the information pathways mappedby our cognitive model. This would require thecombination of at least two of the latent flaws wehave identified: the private nature of internal repre-sentations and the limited information transferoccurring during handover rounds. During interview

82 T. Cohen et al.
sessions several clinicians expressed doubts aboutthe adequacy and reliability of information trans-mitted in the relatively informal evening handoffs,particularly once the information is no longer beingrelated by a clinician directly involved with a parti-cular patient. The support provided by externalrepresentations may also have been inadequate.The whiteboard provides immediately accessibleinformation, however the level of detail recordedis insufficient to convey the subtleties underlying agiven management decision. While these may berecorded in the patient record, interview data sug-gested that the degree to which personal impres-sions are recorded is a matter of individual style (asopposed to essential facts which are generallyrecorded). While we cannot conclude with certaintywhich one of these mechanisms was responsible inthis instance, mapping this adverse event to ourmodel has revealed several combinations of sys-temic flaws that constitute mechanisms of error.
5.4.2. Case#2A retrospective description of this incident wasrecorded during ward rounds, the morning after itoccurred. This incident was noted during the finalobservation period, after the construction of ourmodel. A patient was assessed by an attendingpsychiatrist in the PED. One of this patients treat-ments was the anti-epileptic drug, Lamictal.According to the explanation suggested on the wardround, this psychiatrist allegedly misinterpreted awritten note of the dose ‘‘Lamictal 200 mg b.i.d.’’as ‘‘Lamictal 1200 mg b.i.d.’’. Further inquiry sug-gested that this note may have been written on thewhiteboard, although we were unable to determinethis with certainty. Another clinician who was veryfamiliar with this patient was present in the PEDearlier in the evening, but was not contacted forclarification by the attending psychiatrist. The psy-chiatrist then prescribed the dose of 1200 mg, whichis six times higher than the patient’s actual dose andthree times higher than the top of the usual refer-ence range for Lamictal. The nurse on duty receivedthe order, and requested this dose from pharmacy asLamictal is not commonly used in the PED. Pharmacyprovided the medication without warning aboutthe unusually high dose. The dose was administered.Once this was detected, the patient was transferredto the medical ER where oral charcoal was adminis-tered. Fortunately, the patient suffered no perma-nent ill effects. While it is tempting to attribute thisevent to a combination of individual errors, it is thefeatures of the system that contribute to this errorthat are amenable to intervention. The latent flawsthat appear responsible are related to the dis-tribution of cognition across teams and artifacts.
The potential for misinterpretation of handwritingwas identified as a weakness of the handwrittenartifacts used, and is supported by both observationand recorded shadowing data. The clinician who wasfamiliar with this patient was not consulted. Thisclinician’s perspective was not immediately avail-able once shift change had occurred. The loss ofinformation at shift change is a feature of thedistribution of cognition across teams and time thatwe have described earlier in this manuscript. Thesystemic components of this error that relate to ourarea of study in the PED were predicted by ourcognitive model. Additional systemic factors, suchas the reason no alert was provided by the phar-macy, are beyond the scope of this study.
6. Future work
There are a number of limitations with our study, allof which we plan to address in our subsequent work.The interview data describing specific events arepredominantly retrospective and as such are sub-ject to individual bias. The ethnographic data weregathered with an emphasis on unobtrusive observa-tion so as not to interfere with the process of care.As such there has been little opportunity to ‘drilldown’ on what appear to be potential or actualadverse events. Observations provide limitedinsight into the thoughts of clinicians during theprocess of care. Our future work will focus on thecollection of real-time, prospective recorded dataof clinician interactions, allowing us to observe theevolution of adverse events. These data will beinterpreted in the light of the cognitive model wehave described in this paper. In addition, capturingreal-time clinical discourse will facilitate a deeperanalysis of the collaborative decision-making pro-cess. The characterization of the informationresources required at each stage of clinical workwill drive the development of technological inter-ventions that shift the distribution of cognitivework so as to support the latent flaws we haveidentified. Our future work will include the designand evaluation of such interventions.
7. Conclusion
The research we have presented addresses an issueof importance to today’s clinicians, the problem ofhow to manage medical error. We have incorporatedtheoretical constructs drawn from the frameworkof distributed cognitive theory into a data-drivencognitive model of the PED, in order to enhanceour understanding of error within this environment.
Distributed cognition in the psychiatric emergency department 83
This model provides a blueprint of the informationflow supporting clinical decision-making in thisenvironment. Several inherent weaknesses of thecognitive system of the PED were revealed duringthe process of model construction. These are iden-tified as latent flaws and have implications for theunderstanding of error in other environments, asmany features of the underlying distribution ofhuman cognition in the PED are similar in othercritical care environments. It has been argued thatcharacterization of the distributed cognitive pro-cesses underlying medical decision-making is essen-tial to the design of appropriate technology tosupport cognitive work in complex critical careenvironments [17]. An understanding of the compo-nents and limitations of the cognitive system atwork allows for the ecologically sensitive designof information resources that enhance the naturalflow of information in their environment–—by sup-porting existing weak points and providing relevantinformation where and when it is needed. Likewise,the design of systems to manage error in suchenvironments requires an understanding of the dis-tributed cognitive processes by which these errorsoccur.
Acknowledgements
This research was supported by a grant from theNational Library of Medicine (R01 LM07894) to VimlaPatel. We thank the clinicians who generously gavetheir time for our study.
References
[1] Xiao Y. Artifacts and collaborative work in healthcare:methodological, theoretical and technological implicationsof the tangible. JBMI 2005;38:26—33.
[2] Coiera E. Artificial intelligence in medicine: the challengesahead. JAMIA 1996;3(6):363—6.
[3] Shortliffe, Edward H. The adolescence of AI in medicine: willthe field come of age in the ’90s? Artif Intell Med 1993;5(2):93—106.
[4] Institute of Medicine, Committee on Quality of Health Carein America. In: Kohn LT, Corrigan JM, Donaldson MS, editors.To Err is Human Building a Safer Health System. Washington,DC: National Academy Press; 2000.
[5] Hutchins E. Cognition in the wild. Cambridge, Massachu-setts: MIT Press; 1995.
[6] Hutchins E. How a cockpit remembers its speed. Cogn Sci1995;19:265—88.
[7] Reason J. Human error. Cambridge UK: Cambridge UniversityPress; 1992.
[8] Leape L. Error in medicine. JAMA 1994;272:1851—7.[9] Zhang J, Patel VL, Johnson TR, Shortliffe EH. A cognitive
taxonomy of medical errors. J Biomed Inform 2004;37(3):193—204.
[10] Sutcliffe K, Lewton E, Rosenthal M. Communication failures:an insidious contributor to medical mishaps. Acad Med2004;79(2):186—94.
[11] Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR,Lawthers AG, et al. Incidence of adverse events and negli-gence in hospitalized patients. Results of the Harvard Med-ical Practice Study. NEJM 1991;324:370—6.
[12] Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR,Barnes BA, et al. The nature of adverse events in hospita-lized patients. Results of the Harvard Medical Practice StudyII. NEJM 1991;324:377—84.
[13] Wilson R, Harrison BT, Gibberd RW, Hamilton J. An analysis ofthe causes of adverse events from the Quality in AustralianHealth Care Study. Med J Aust 1999;170:411—5.
[14] Grasso B, Genest R, Jordan CW, Bates D. Use of chart andrecord reviews to detect medication errors in a state psy-chiatric hospital. Psychiatr Serv 2003;54:677—81.
[15] Taxis K, Barber N. Causes of intravenous medication errors:an ethnographic study. Qual Saf Health Care 2003;12:343—7.
[16] Koren G, Jarvis AD, Kozar E, Seto W, Verjee Z, Parshuram C,et al. Prospective observational study on the incidence ofmedication errors during simulated resuscitation in a pedia-tric emergency department. BMJ 2004;329:1321.
[17] Nemeth C, O’connor M, Cook R, Wears R, Perry S. Craftinginformation technology solutions, not experiments, for theemergency department. Acad Emerg Med 2004;11:1114—7.
[18] Patel VL, Kaufman DR, Arocha JF. Steering through themurky waters of a scientific conflict: situated and sym-bolic models of clinical cognition. Artif Intell Med 1995;7:413—38.
[19] Patel VL. Editorial: individual to collaborative cognition: aparadigm shift? Artif Intell Med 1998;12(2):93—6.
[20] Roth EM, Patterson ES, Mumaw RJ. Cognitive engineering:issues in user-centered system design. In: Marciniak JJ,editor. Encyclopedia of Software Engineering. 2nd ed., NewYork: Wiley-Interscience, John Wiley & Sons; 2002. p. 163—79.
[21] Baxter G, Monk F, Tan K, Dear P, Newell S. Using cognitivetask analysis to facilitate the integration of decision supportsystems into the neonatal intensive care unit. Artif IntellMed 2005;35:243—57.
[22] Zhang J, Norman DA. Representations in distributed cogni-tive tasks. Cogn Sci 1994;18:87—122.
[23] Zhang J. A distributed representation approach to groupproblem solving. J Am Soc Inf Sci 1996;49(9):801—9.
[24] Rinkus S, Walji M, Johnson-Throop K, Malin J, Turley J, SmithJ, et al. Human centered design of a distributed knowledge-management system. J Biomed Inform 2005;38:4—17.
[25] Grasso BC, Rothschild JM, Genest R, Bates DW. What do weknow about medication errors in inpatient psychiatry? JtCommun J Qual Saf 2003;29(8):391—400.
[26] Ball LJ, Ormerod TC. Putting ethnography to work: the casefor a cognitive ethnography of design. Int J Hum-ComputStud 2000;53:147—68.
[27] Corbin J, Strauss A. Grounded theory research: procedures,canons, and evaluative criteria. Qual Sociol 1990;13(1):3—21.
[28] Miller G. The magical number seven, plus or minus two:some limits on our capacity for processing information.Psychol Rev 1956;63:81—97.
[29] Ericsson A, Kintsch W. Long term working memory. PsycholRev 1995;102(2):211—45.
[30] Biddinger PD, Isselbacher EM, Fan D, Shepard JA. Caserecords of the Massachusetts General Hospital. Weekly clin-icopathological exercises. Case 5-2005. A 53-year-old manwith depression and sudden shortness of breath. N Engl JMed 2005;352(7):709—16.