345519-eng.pdf - WHO | World Health Organization
34
PRESERWD FOR PROIECT LOGO/HEADING COUNTRYAIOTF: Tanzania Proiect Name: Ruvuma CDTI Focus Aporoval yearz 1997 Launching vear: 1998 Reportins Periodr From: January 2008 To: December 2008 (Month/Year) ( Mon!ryYeq) Proiectvearof thisreport: (circleone) I 2 3 4 5 6 7 8 9 (10) Date submitted: September 2009 NGDO oartner: Sight Savers International ANNUAL PROJECT TECHNICAL REPORT SUBMITTED TO TECHNICAL CONSULTATIVE COMMITTEE (TCC) DEADLINE SUBMISSION: To APOC Management by 31 Januarv for March TCC meeting To APOC Management by 31 Julv for September TCC meeting Hz Fo Tot frlhnabn ro -)in ORIGINAL : English I CoP C- 'To 56 H €sI ? i; Ju!t- 20t0 RECU LE APOC DIR H WHO/APOC, 24 November 2fi)4
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of 345519-eng.pdf - WHO | World Health Organization
PRESERWD FOR PROIECT LOGO/HEADING
COUNTRYAIOTF: Tanzania Proiect Name: Ruvuma CDTI Focus
Aporoval yearz 1997 Launching vear: 1998
Reportins Periodr From: January 2008 To: December 2008(Month/Year) ( Mon!ryYeq)
Proiectvearof thisreport: (circleone) I 2 3 4 5 6 7 8 9 (10)
Date submitted: September 2009 NGDO oartner: Sight Savers
International
ANNUAL PROJECT TECHNICAL REPORTSUBMITTED TO
TECHNICAL CONSULTATIVE COMMITTEE (TCC)
DEADLINE SUBMISSION:
To APOC Management by 31 Januarv for March TCC meeting
To APOC Management by 31 Julv for September TCC meeting
Hz
FoTot
frlhnabnro -)in
ORIGINAL : English
I
CoPC-'To56
H
€sI
? i; Ju!t- 20t0
RECU LE
APOC DIR
H
WHO/APOC, 24 November 2fi)4
(?^rU,*-,.\ oa{G
FRTCAN PROGRAMME FOR ONCHOCERCTASTS CONTROL (APOC)
AI\TIUAL PROJECT TECHNICAL REPORTTO
TECHNICAL CONSULTATIVE COMMITTEE (TCC)
EI{DORSEMENT
Please confirm you have read this report by signing in the appropriate space.
OFFICERS to sign the report:a
Regional Medical Officer Name: Dr. Daniel
Signature:
Malekela.
VDate: ..11kT.9y.f, Po..-tr-o
_*.r*aEclolltl MEDI€IL ofTlctR ntHUNnl
Country: Tanzania
National Coordinator Name: Dr
Signature:
Mwakyusa
Date:.......? tit u/.2orD
Kabole
Date: . .....A{.. J{*ui
This report has been prepared by Name : Dr. Ida M. Ngowi
Designation : Project Coordinator
Rre:tL}\t -JYy.i.+fl"
NGDO Representative Name: Dr,
Signature:
Signature:
Date
Io
{
Director,
ES SALAAM2513
-TCO
rv.4
2 WHO/APOC, 24 November 2004
Table of contents
ACROIYYMS............... .............* 5
DEFrNrrIONS......... .................* 6
FOLLOW UP ON TCC RECOMMENDATIONS .....* 7
EXECUTIVE SUMMARY............ ERREUR ! SIGNET NON DEFINI.
SECTION l: BACKGROUND INFORMATION ...-.-.8
1.1. GelreRAr-TNFoRMATIoNI .l.l Descriptton of the project (briefly) - Erreur ! Signet non d{ai
. Erreur ! Signet non diftnlI .l .2. Partnership1.2. PopuleuoN.......
SECTION 2: IMPLEMENTATION OF CDTI............ ERREUR ! SIGNET NON DEFINI.
2.1. Trr'clrNe oF ACTIVITIES ....
2.2. AovocecvEnnnun ! Srcxor NoN DEFTNI.
12
2.3. Mostt.zetroN, sENSITIZATIoN AND HEALTH EDUCATIoN oF ATRISK coMMt MTIES 13
2.4. ComnxnvnwoLVEMENT2.5. Cepecmv BUTLDTNG
l5........ t6
2.6. TRrerueNrs.. Ennnun ! StcxBr NoN DErtM.
2.6.1. Treatmentfigures ............. ...-Erreur ! Signet non d{uti2.6.2 What are the causes of absenteeism? .......... . Erreur ! Signet non d{url2.6.3 What are the reasons for refitsals? ............... . Erreur ! Signet non d{utl2.6.4 Brie/ly descrtbe all lcnown and verified serious adverse events (SAEr) thdheur ! Signet2.6.5. Trend of treatment achievementfrom CDTI project inception to the curuentyet2j
2.7 . ORoeRntc, sroRAGE AND DELIVERv oF IVERMECTIN 2526
27
2.9.1. Provide aflow chart of supervisionhterarchy. ......------27
2.9.2. What were the main issues identified during superviston? ........................--.--- 27
2.9.3. Was a supervision checklist used? -...-.------- 27
2.9.4. What were the outcomes at each level of CDTI implementation supervision? 27
2.9.5. Was feedback given to the person or groups supervised? ........................-...--- 27
2.9.6. How was thefeedbackused to improve the overall performance of the project?27
SECTION 3: SUPPORT TO CDTI....... ..*273.1. EqunueNr 27
29
29
3.4. ExpeNotruRE PER ACTIVITY ............ 3 I
SECTION 4: SUSTAINABILITY OF CDTI. ..........*31
4.1. INreRNnr,; INDEeENDENT rARTICIrAToRY MoNIToRINc; Eve1uerloN................- 3l4.1.1 Was Monitoring/evaluation carried out durtng the reporting period? (ttckuyof thefollowingwhich are appltcable)............ ........-.- 31
4.1.2. What were the recommendations? .................--.- 32
4.1.3. How have they been implemented? ............. .-.- i24.2. SusrnNnsILITy oF IRoJECTS: rLAN AND sET TARGETs (MANDAToRY AT.........-..-.32
....*.32
................... 9
................... t0
2.8. CouurrNlry sELF-MoNIToRING AND STAKEHoLDERS MpprrNlc...2.9 SuppnvtstoN
3.2. FrNeNcnl coNTRIBUTIoNS oF THE pARTNERS AND coMMUNITIES ...
J.J Orupn FoRMS oF coMMUNITY suPPoRT
Yn 3)................
3 WHO/APOC, 24 Novembcr 2fiM
4.2. t.4.2.2.4.2.34.2.4.4.2.5.
Planning at all relevant \eve\s.........Funds........Tr ansp o r t (r ep I ac e m e nt ond maint e nanc e) .....Other resources..To what extent has the plan been tmplemented.........
..........32
.......... 32
.......... 32
.......... 32
.......... 32
Traintng.......... ...- Erreur ! Signet non diJinl4.3.3. Jotnt supervision and monitortng with other programsErreur ! Signet non diJini-4.3.4. Release offunds for project activittes Erreur ! Signet non ddJinl4.3.5. Is CDTI included in the PHC budget? ..................... Erreur ! Signet non diJinl4.3.6. Describe other health programmes that are using the CDTI structure and howthis was achteved. What have been the achievements?........... Erueur ! Signet non diJinl4. j.7. Describe others issues considered in the integration of CDTI.Erueur ! Signet non difinl
4.4. OpenarroNAl RESEARCH........ 344.4.1. Summarize in not more than one half of a page the operattonal researchundertaken in the project area within the reporting period.4. 4. 2 . How were the results applied in the project? .. . .. .. . . .
SECTION 5: STRENGTHS, WEAKNESSES, CTIALLENGES, ANDoPPORTUNTTIES.... .................... 34
SECTION 6: UNIQUE FEATURES OF THE PROJECT/OTIIER MATTERS........... 34
4.3. INrecnarroN 324.3.1. Ivermecttn delivery mechanisms Erreur t Signet non ddlinl4.3.2.
... 34
... 34
4 WHO/APOC, 24 November 2004
Acronyms
APOC
ATO
ATrO
CBO
CDD
CDTI
CSM
LGAMOH
NGDO
NGO
NOTF
PHC
REMO
SAE
SHM
TCC
TOT
UNICEF
UTG
wHo
African Programme for Onchocerciasis Control
Annual Treatment Obj ective
Annual Training Objective
Community-Based Organization
Community-Directed Distributor
Community-Directed Treatment with lvermectin
Community S elf-Monitoring
Local Government Area
Ministry of Health
Non-Govemmental Development Organization
Non-Govemmental Organ ization
National Onchocerciasis Task Force
Primary health care
Rapid Epidemiological Mapping of Onchocerciasis
Severe adverse event
Stakeholders meeting
Technical Consultative Committee (APOC scientific advisory group)
Trainer of trainers
United Nations Children's Fund
Ultimate Treatment Goal
World Health Organization
5 WHO/APOC, 24 Novembcr 2004
Definitions
(vii)
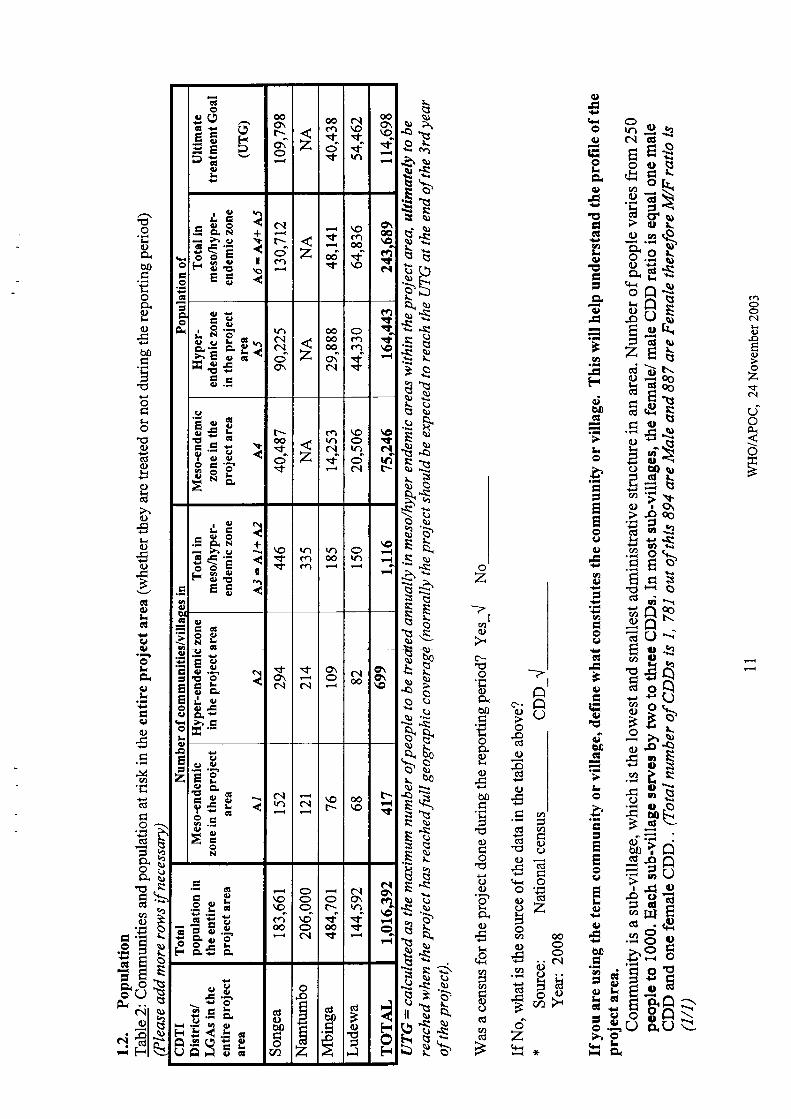
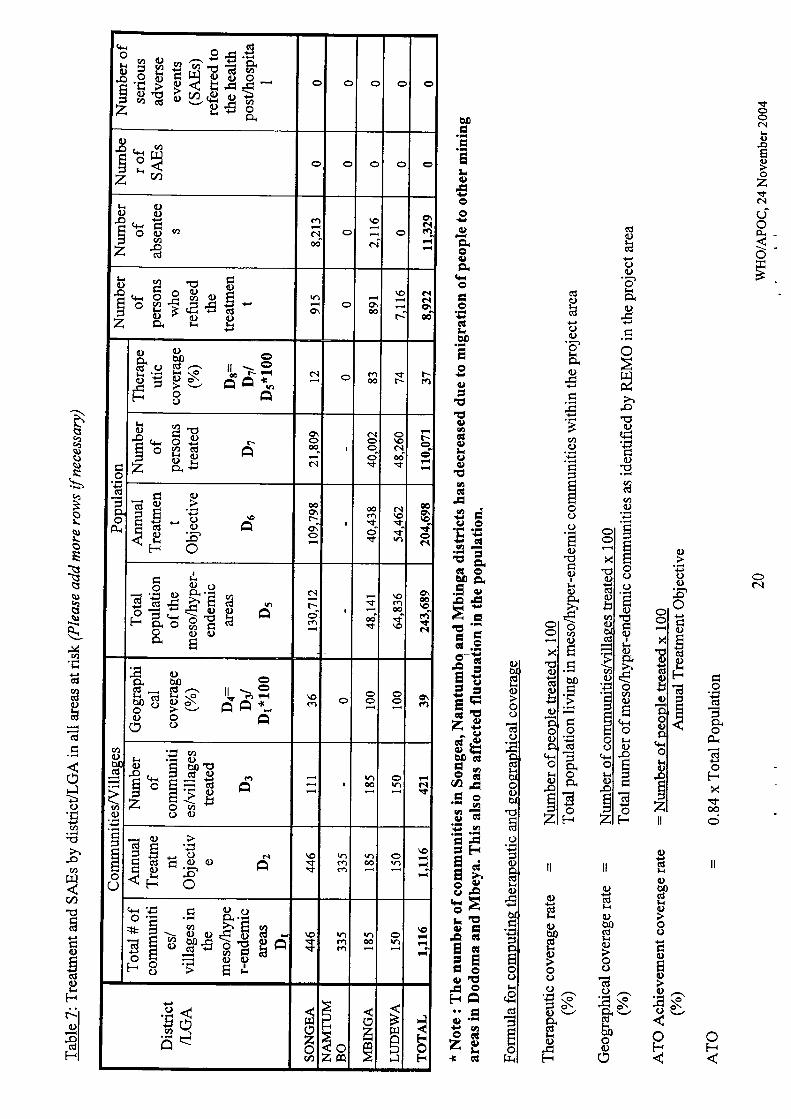
(i) Total population: the total population living in meso/hyper-endemiccommunities within the project area (based on REMO and census taking).
(iD Eligible population: calculated as84Yo of the total population in meso/hyper-endemic communities in the project area.
(iii) Annual Treatment Objective: (ATO): the estimated number of persons livingin meso/tryper-endemic areas that a CDTI project intends to heat withivermectin in a given year.
(iv) Ultimate Treatment Goal (UTG): calculated as the maximum number of peopleto be treated annually in meso/tryper endemic areas within the project area"
ultimately to be reached when the project has reached full geographiccoverage (normally the project should be expected to reach the UTG at the end
of the 3'd year of the project).
(v) Therapeutic coverage: number of people treated in a given year over the totalpopulation (this should be expressed as a percentage).
(ui) Geographical coveraee: number of communities treated in a given year overthe total number of mesoftryper-endemic communities as identified by REMOin the project area (this should be expressed as a percentage).
Intesration: delivering additional health interventions (i.e. vitamin Asupplements, albendazole for LF, screening for cataract, etc.) through CDTI(using the same systems, training, supervision and personnel) in order tomaximise cost-effectiveness and empower corlnrunities to solve more of theirhealth problems. This does not include activities or interventions carried outby community distributors outiide of CDTI.
(viii) Sustainabilitv: CDTI activities in an area are sustainable when they continue tofunction effectively for the foreseeable future, with high treaftnent coverage,integrated into the available healthcare service, with strong communityownership, using resources mobilised by the comrnunity and the government.
(ix) Community self-monitoring (CSM): The process by which the community isempowered to oversee and monitor the performance of CDTI (or anycommunity-based health intervention prograrnme), with a view to ensuring thatthe programme is being executed in the way intended. It encourages thecommunity to take full responsibility of ivermectin distribution and makeappropriate modifications when necessary.
6 WHO/APOC, 24 November 2004
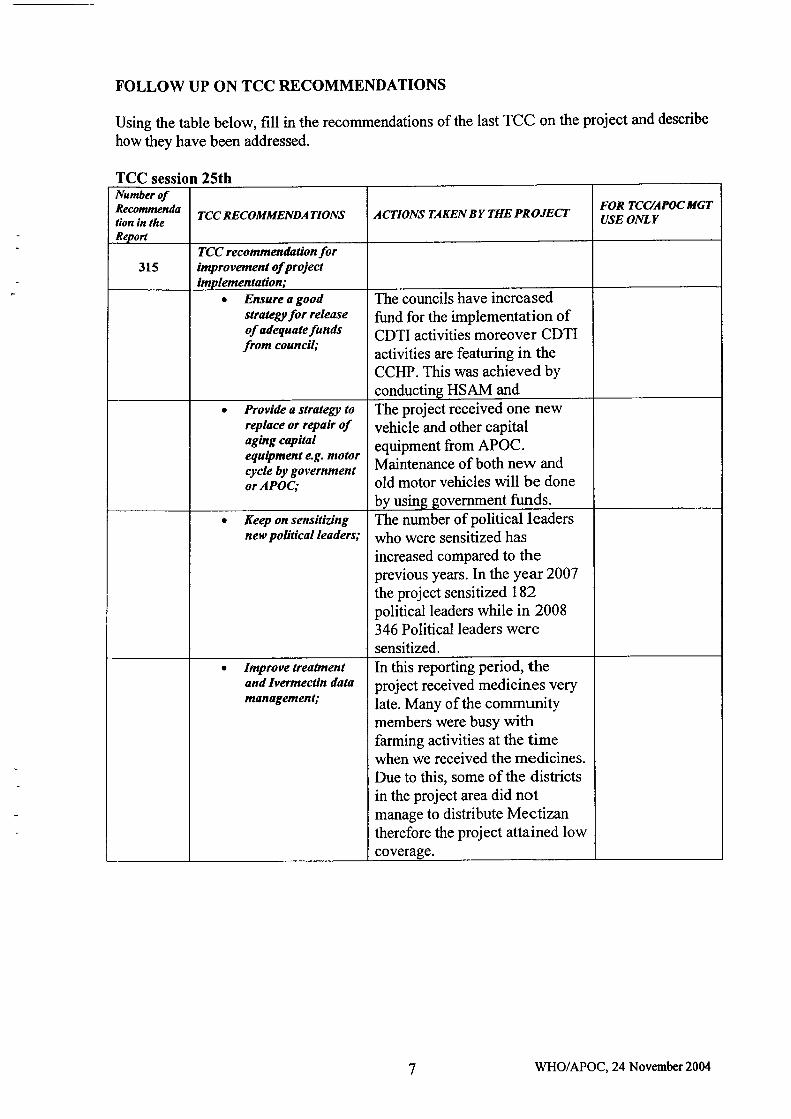
FOLLOW UP ON TCC RECOMMENDATIONS
Using the table below, fill in the recommendations of the last TCC on the project and describe
how they have been addressed.
TCC session 25th
7
Numbcr ofRecommcndation ln theReport
TCC RECOMMENDATIONS ACTIONS TAKEN BY THE PROJECTFORTCAAPOCITGTUSE ONLY
315TCC recommeadationforimprovement of projectimplementalion;
a Ensure a goodstrategt for releaseofadequalefundsfrom council;
The councils have increasedfund for the implementation ofCDTI activities moreover CDTIactivities are featuring in theCCHP. This was achieved byconducting HSAM and
a Provide s stralegt toreplace or repair ofaging capilalequipment eg. motorcycle by governmentor APOC;
The project received one newvehicle and other capitalequipment from APOC.Maintenance of both new and
old motor vehicles will be done
by using government funds.a Keep on sensitiTing
new political leaders;The number of political leaderswho were sensitized has
increased compared to theprevious years. In the year 2007
the project sensitized 182political leaders while in 2008346 Political leaders weresensitized.
a Improve treatmenland lvermectin datam&nagemenl;
In this reporting period, theproject received medicines verylate. Many of the communitymembers were busy withfarming activities at the timewhen we received the medicines.Due to this, some of the districtsin the project area did notmanage to distribute Mectizantherefore the project attained lowcoverage.
WHO/APOC, 24 November 20M
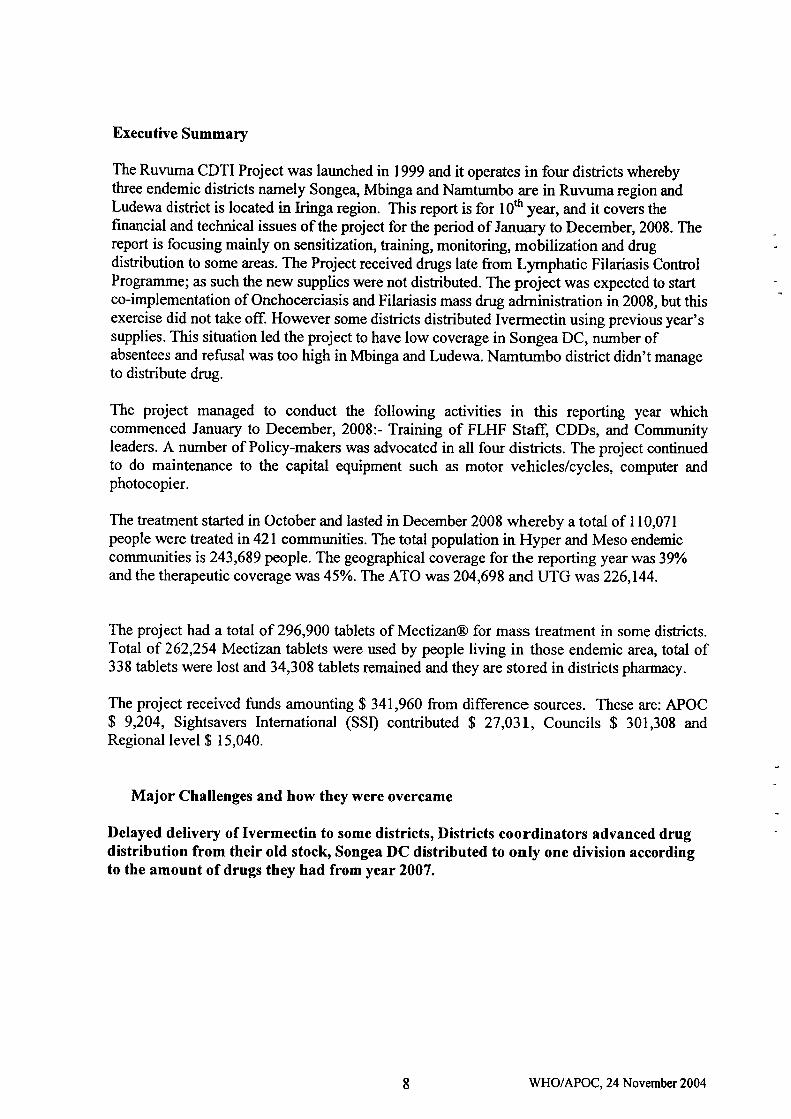
Executive Summary
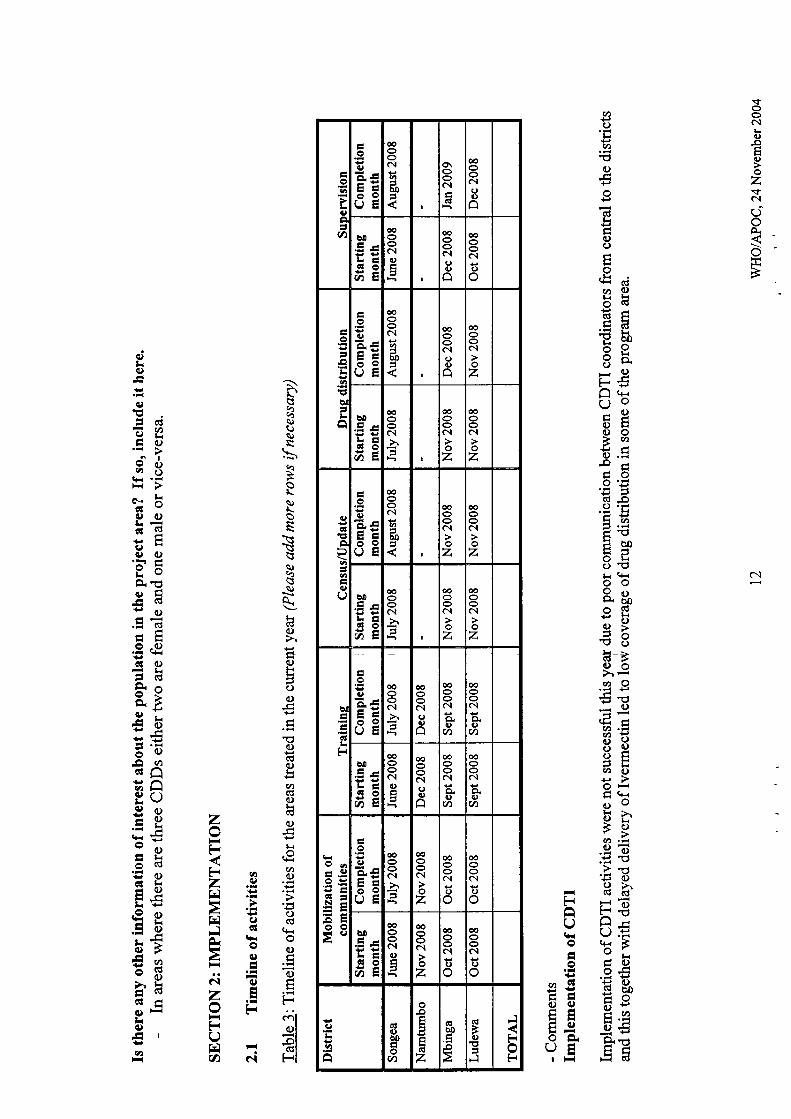
The Ruvuma CDTI Project was launched in 1999 and it operates in four districts wherebythree endemic districts namely Songea, Mbinga and Namtumbo are in Ruvuma region andLudewa district is located in Iringa region. This report is for 10ft year, and it covers thefinancial and technical issues of the project for the period of January to December, 2008. Thereport is focusing mainly on sensitization, training, monitoring, mobilization and drugdistribution to some areas. The Project received drugs late from Lymphatic Filariasis ControlProgramrne; as such the new supplies were not distributed. The project was expected to startco-implernentation of Onchocerciasis and Filariasis mass drug adrninistration in 2008, but thisexercise did not take off. However some districts distributed Ivermectin using previous year'ssupplies. This situation led the project to have low coverage in Songea DC, number ofabsentees and refrrsal was too high in Mbinga and Ludewa. Namtumbo district didn't manageto distribute drug.
The project managed to conduct the following activities in this reporting year whichcommenced January to December, 2008:- Training of FLHF Staff, CDDs, and Communityleaders. A number of Policy-makers was advocated in all four districts. The project continuedto do maintenance to the capital equipment such as motor vehicles/cycles, computer andphotocopier.
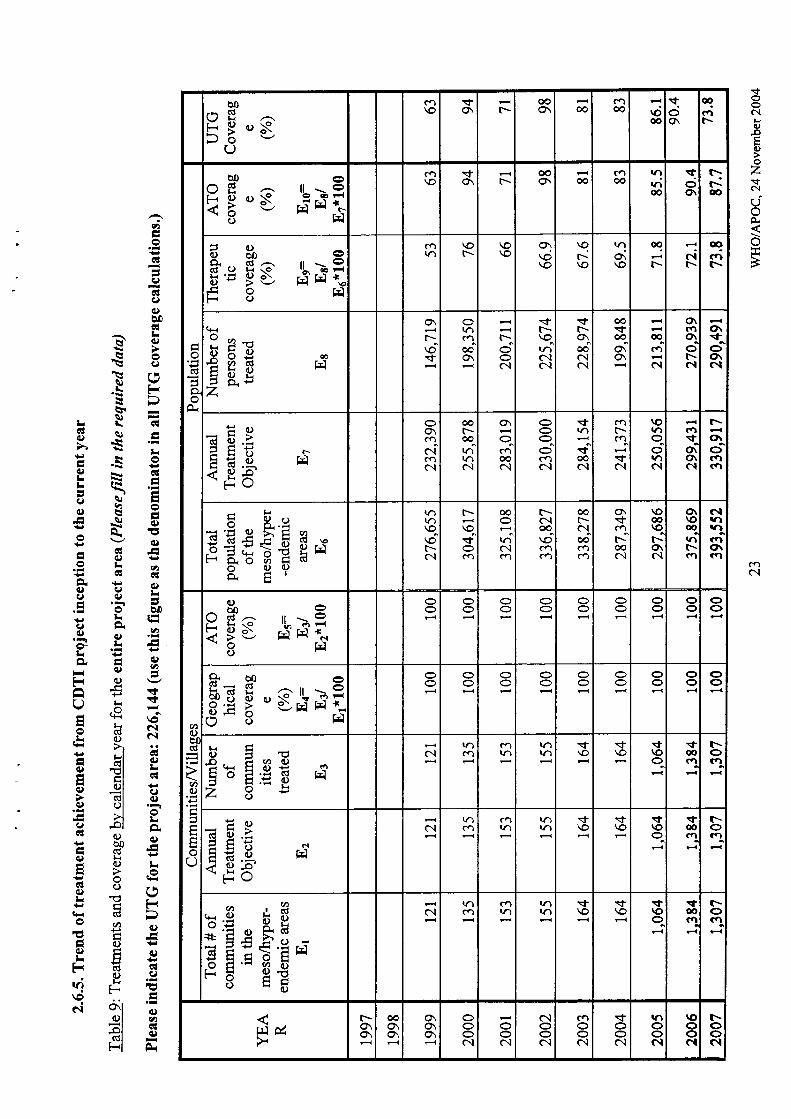
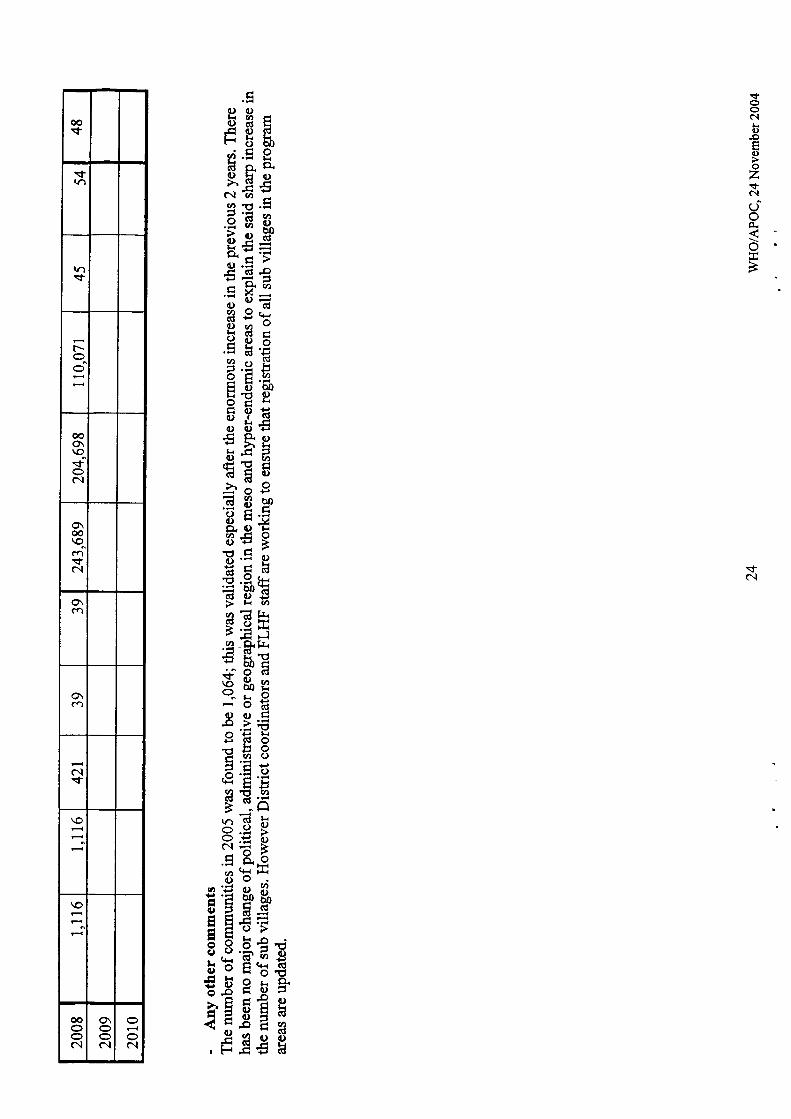
The treatrnent started in October and lasted in December 2008 whereby a total of 110,071people were treatedin42l communities. The total population in Hyper and Meso endemiccommunities is 243,689 people. The geographical coverage for the reporting year was3gYoand the therapeutic coverage was 45o/o. The ATO was204,698 and UTG was 226,144.
The project had a total of 296,900 tablets of Mectizan@ for mass treatment in some dishicts.Total of 262,254 Mectizan tablets were used by people living in those endemic are4 total of338 tablets were lost and 34,308 tablets remained and they are stored in districts pharmacy.
The project received funds amounting $ 341,960 from difference sources. These are: APOC$ 9,204, Sightsavers lnternationd (SSD contributed $ 27,031, Councils $ 301,308 andRegional level $ 15,040.
Major Challenges and how they were overcame
Delayed delivery of Ivermectin to some districts, Districts coordinators advanced drugdistribution from their old stock, Songea DC distributed to only one division accordingto the amount of drugs they had from year 2007.
8 WHO/APOC, 24 November 2004
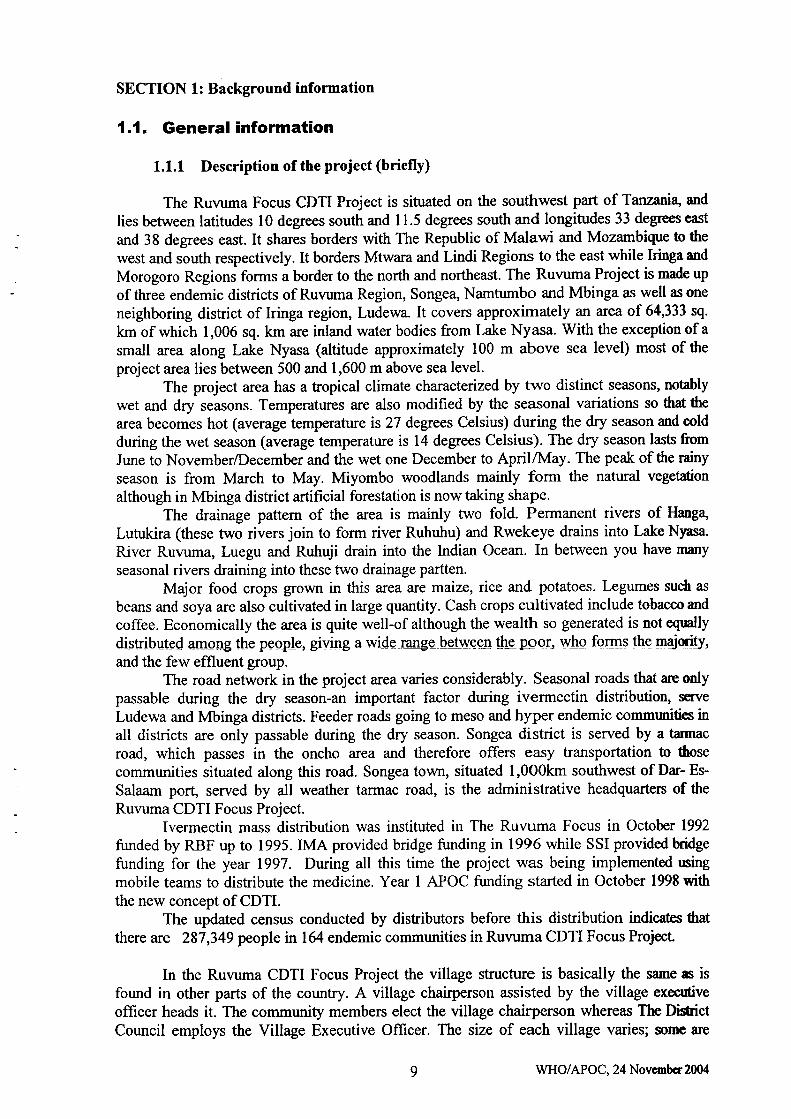
SECTION l: Background information
1.1, General information
1.1.1 Description of the project (briefly)
The Ruvuma Focus CDTI Project is situated on the southwest part of Tanzani4 and
lies between latitudes 10 degrees south and 11.5 degrees south and longitudes 33 degrees cast
and 38 degrees east. It shares borders with The Republic of Malawi and Mozambique to the
west and south respectively. It borders Mtwara and Lindi Regions to the east while kinga and
Morogoro Regions forms a border to the north and northeast. The Ruvuma Project is made up
of three endemic districts of Ruvuma Region, Songea, Namtumbo and Mbinga as well as one
neighboring district of Iringa region, Ludewa. It covers approximately an area of 64,333 sq.
km of which 1,006 sq. km are inland water bodies from Lake Nyasa. With the exception of a
small area along Lake Nyasa (altitude approximately 100 m above sea level) most of the
project area lies between 500 and 1,600 m above sea level.The project area has a tropical climate characterized by two distinct seasons, notably
wet and dry seasons. Temperatures are also modified by the seasonal variations so that the
area becornes hot (average temperature is 27 degrees Celsius) during the dry season and cold
during the wet season (average temperature is 14 degrees Celsius). The dry season lasts from
June to NovemberlDecember and the wet one December to April/Trrtay. The peak of the rainy
season is from March to May. Miyombo woodlands mainly form the natural vegetation
although in Mbinga district artihcial forestation is now taking shape'The drainage pattem of the area is mainly two fold. Permanent rivers of Hanga,
Lutukira (these two rivers join to form river Ruhuhu) and Rwekeye drains into Lake Nyasa.
River Ruvuma, Luegu and Ruhuji drain into the Indian Ocean. In between you have many
seasonal rivers draining into these two drainage partten.
Major food crops grown in this area are maize, rice and potatoes. Legumes such as
beans and soya are also cultivated in large quantity. Cash crops cultivated include tobacco mdcoffee. Economically the area is quite well-of although the wealth so generated is not equally
distributsd among the people, giving a wi-dc rcnge bet\ryeen the por, whq fqms the pgipr-rry,
and the few effluent group.The road network in the project area varies considerably. Seasonal roads that are only
passable during the dry season-an important factor during ivermectin distribution, scrve
Ludewa and Mbinga districts. Feeder roads going to meso and hyper endemic commrmities inall districts are only passable during the dry season. Songea district is served by a tarmac
road, which passes in the oncho area and therefore offers easy transportation to those
communities situated along this road. Songea town, situated l,0o0km southwest of Dar- Es-
Salaam port, served by all weather tarmac road, is the administrative headquarters of the
Ruvuma CDTI Focus Project.Ivermectin mass distribution was instituted in The Ruvuma Focus in October 1992
funded by RBF up to 1995. tMA provided bridge funding in 1996 while SSI provided tridgefunding for the year 1997. During all this time the project was being implemented rsingmobile teams to distribute the medicine. Year 1 APOC funding started in October 1998 wittrthe new concept of CDTI.
The updated census conducted by distributors before this distribution indicales thatthere are 287,349 people in 164 endemic communities in Ruvuma CDTI Focus Project
In the Ruvuma CDTI Focus Project the village structure is basically the same s is
found in other parts of the country. A village chairperson assisted by the village execrfive
offrcer heads it. The community members elect the village chairperson whereas The DiCrictCouncil employs the Village Executive Officer. The size of each village varies; sonrc are
9 WHO/APOC, 24 Novcmbcr 2004
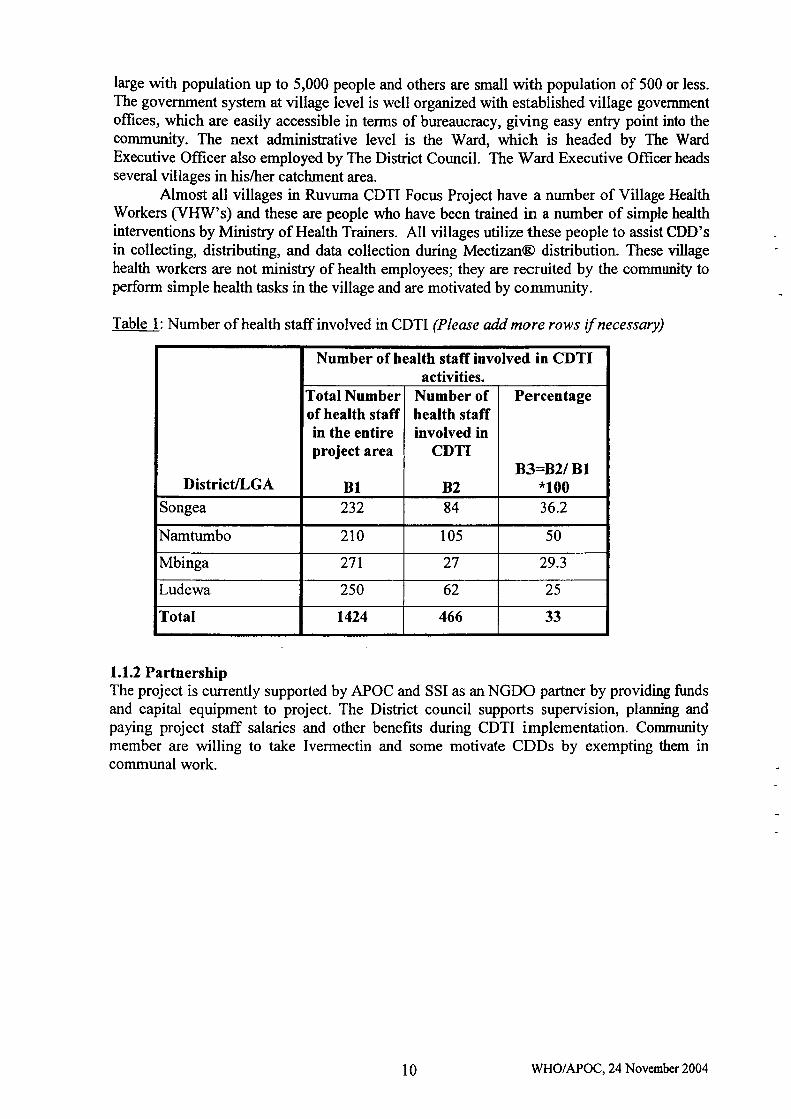
large with population up to 5,000 people and others are small with population of 500 or less.The government system at village level is well organized with established village governmentoffices, which are easily accessible in terms of bureaucracy, giving easy entry point into tlrecommunity. The next administrative level is the Ward, which is headed by The WardExecutive Offrcer also employed by The Distict Council. The rfr/ard Executive Officer headsseveral villages in his/trer catchment area.
Almost all villages in Ruvuma CDTI Focus Project have a number of Village HealthWorkers (VHW's) and these are people who have been ftained in a number of simple healthinterventions by Ministry of Health Trainers. All villages utilize these people to assist CDD'sin collecting, distributing, and data collection during Mectizan@ distribution. These villagehealth workers are not ministry of health employees; they are recruited by the community toperform simple health tasks in the village and are motivated by community.
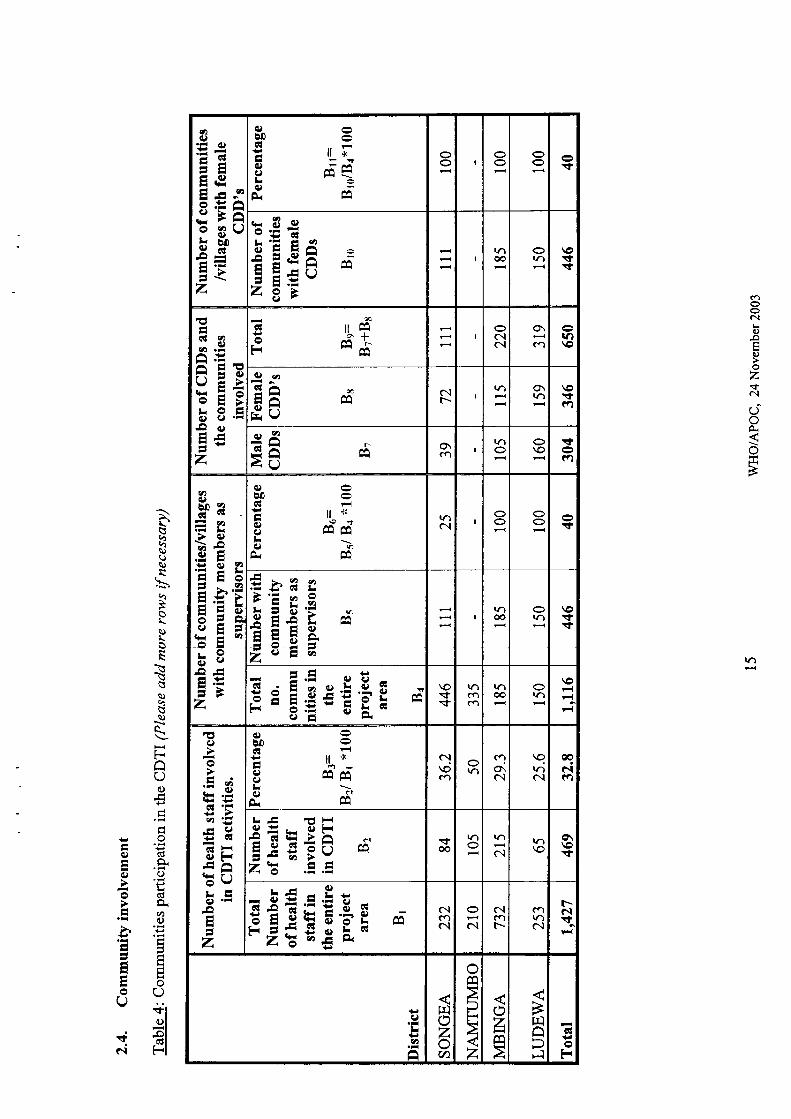
Table l: Number of health staffinvolved in CDTI (Please add more rows if necessary)
Districtl[.GA
Number of health staffinvolved in CDTIactivities.
Total Numberof health staffin the entireproject area
BI
Number ofhealth staffinvolved in
CDTI
B2
Percentage
B3=B2lBl*100
Songea 232 84 36.2
Namtumbo 210 105 50
Mbinga 271 27 29.3
Ludewa 250 62 25
Total 1424 466 33
1.1.2 PartnershipThe project is currently supported by APOC and SSI as an NGDO partner by providing fundsand capital equipment to project. The District council supports supervision, planning andpaying project staff salaries and other benefits during CDTI implementation. Communitymember are willing to take lvermectin and some motivate CDDs by exempting them incommunal work.
10 WHO/APOC, 24 November 2004
tlooc.l
o,oE()oz$c.l
rioP{
o
Q)E
! Rt*E E 5Ea ,H F:I s;sE 1g dq)4.lu\
E fl37T E.E*
s ;et= E qr\i zE$E HtH
# FES5 E EE.E E* ta @'ivtr c)io\= >96E E 7*; E ETt .gEo'8 E qS: EH OE cd d*.
E E8RI Eo*.'E H 8.3E EE(o cd ot-l
E x EFct -= >rI
E, €;E't .=isLr a l)to toNE EgE
E 3.sn
E ;$tI xstP .E'.9 t'E ,i E eEIEEiA-e.86 EU\>ogE
€ooN
clo
-7
Ac-. Oguo-o(do.oct
o
trv)cl v)dx'o5(D-
363ijEi(+{ O
E2oV)Q)
t^e.Hc-E -o'> v)
dzH*
oz
IU)o
c...ooLro&o0
.EEo&olro)
.Eb0tr.E
'13o)tro'oIoo'aL<a(.)
l.i€U',U'
oodU)cd
Lsq)o>..a \'OL
tsEk-NO'.S +rsiS\'-rq)BSbrRHirJtrs)p€!l "sEQ
sPis"2 tius\()Bq).s*sq)$q)\"4S \-.$NbB*t.ts's\oQa)ai o'N\.s3Xrr
N}SFB6\.so)v-H s)
rysr$"o6oQ*(ls).i
BE,B.I\oO' s)lbop=S\:st(JSB.sP}{?)s$Nt$u"S q)
", 9'rsIss"li * 4.:.{$uf s $r ts\stst\ S,h5 Pb
V1q)u\)
aa
=oLq)\o
tsq)b1Bq)
Eoko&oodLoqotiq)
h0cL{totrts<o.oo)d(l)L{
c)L{cd
o)
lro
o3d()LGI
()q)
olra6)fr
Eq)
o-(tr
JZrn
t-{
(d
ioCd
=aoa€trGIa)(l)
E.Ecttrq-QO L,,0r ..NI
ol
"i El- F-<l
(Jt<D
cgog(JCY.=oajE
-G q)
@o\\o\o z
ooCA+ot
c\l\o*.fra
ooo\\otf,
+€$
\oca@.+\o
o\€\o.?atN
!n
+\Tb
rE-(u0.= o.NdE.-e\ C
€ E€
C\I
F*Oca z
?at-1-$\o
=6fd.No'C.g h 8"1ffE€ ="
(, .=
|r)o.l6Ioo\
zoo@@oic.l
oc.lCA
tt
o
o6!
go0r
s+ Hriso E'=gsx
r-@s^o.t z
colalc.l$
\oOraOC.l
\otclrar-
T+
I
.or:trr()O.= a,Na E.-+a\ Ei r3
\os$rncftc.l
rr)€ orat
\o
oEqlocNLpdEa)b.gEO6o.lqr(l)E>rtr
x.+o\c\I
.tol
o\o (\€ o\o\\o
Ooblcl
q(l)
E
o(,oLopE
z()
.9.9EE616
E tsr:6q.=
9,zt oN
ol\at c.t \or- oo\o
t-!C
;Foo=.-Lw9.- -
-r e:{6 t rD.aE 89 E'tsai5a
\o\ocooo
Ooo^\ooN
oc-+€$
c.lo\'rI\f,+
GIo\ro\oe
E.E-e Pfr.E a
>< .a ot otFts{-!aEf 3E H
G,(,)bI)
oo
ooAa+)
clz
((,b0H
o
dBoE)Fl
Fl
Hot'r
sooGILq)-oEq)
oz.tc..l
C,oO.\o*{B
U)IoL.Iv)\,o-qo6l.€tr(l)aEoG;o9)l.Ho(gEgtrEEFo=oEEtr8O ,+.uo-oiitrrDO,V'6.E-Oaiocd -Oo;F2{E.9HEFooti5or<c)Ek({-<oo&8,ose9€8HB(l)o>\-.2eE!-qGcv) .ia6P9E5tr5trt/,)q,+r)oHd+{oobhFg(r1 .i.95.E TJ.EBQ>\(gdF'dE:().H!iBEC)os+r c)sqo6sd(n6tQrt
.EE
c.l
F.iaQ(toEo
ssirEoq)EE(l€)OQOEI l-'l
-:.tBV)V)q)aa)
S4
oLq)Lo
NBq)qvq)
ELr(dq)>.EI(l)
EooI
tr€(l)
Cd(l)Lr
v,dot<Gt(l)
r<
€ano
ocl(+io(l)tr(l)
F..irol
.ol(BI
FI
4)q)
IG
ocE(u
Et''(
N
zo-FFrzfrlbtzHFIF{HaNzo-t<(JH0
e,Lo
ordAGIE2trc)
fBtboq)GtqEEoo
A.UotrE(!eo).= Gl
o .c)
6l c)AclQ^qEoiJgr,t=c)!o.!o.h a-)q) r\
g8.=HtE=o
6")trl{oGl5 c.)
Ebtr.cL. +)€sr.=9bEoEhE6l .t(|) )-{L(l)ElIA
-
oo
()c
(n
o(uE*Etroo9E
@ooc.lq
bo
o\ooo.ldc,
@oo(\lo()o
E!c-LEclo(DE
6ooolIt)E
I
€ooo{ooo
€oo(\.l
oo
o
Eq
!E,I
o
ooA.s=eEtrooUE
ooooo.laabI)
I
€oc.looa
€ooo{
oz
60
LEqto(DE
€ooC\l
a
€ooc.l
oz
@ooc\l
oz
(1)
clEqa0q
oo
.9()eEOOUE
€ooc..l
obn
€ooc..t
oz
@ooc.l
oz
bD
LE60AE
€ooc.l>.
=
@
ootoz
6ooc.l
oz
BI
6t
tr
oa)ZE=eooUE
ooooc.l>.
00ooo{ooo
€ooc.l
Erua
€ooc.l
rru
c/)
o0c-l-EGIOCNE
ooooc\totr
€ooC\looa
coooolo.ruV)
@ooa.t
ac)a
O6
.9.:aiEs=EEooE"
oc)7E=+jEtroOUE
ooooc.l
=
€ooC\l
oz
6ooc.loo
@ooc.loo
b0
LEctoAE
€ooo.l(l)
a
€oocloz
€oootoo
€oooe.loo
o
oa
c,!)o0trou)
opEEEdz
G,0t)t.o
G,
B[)EF.l
FI
Fotr
I
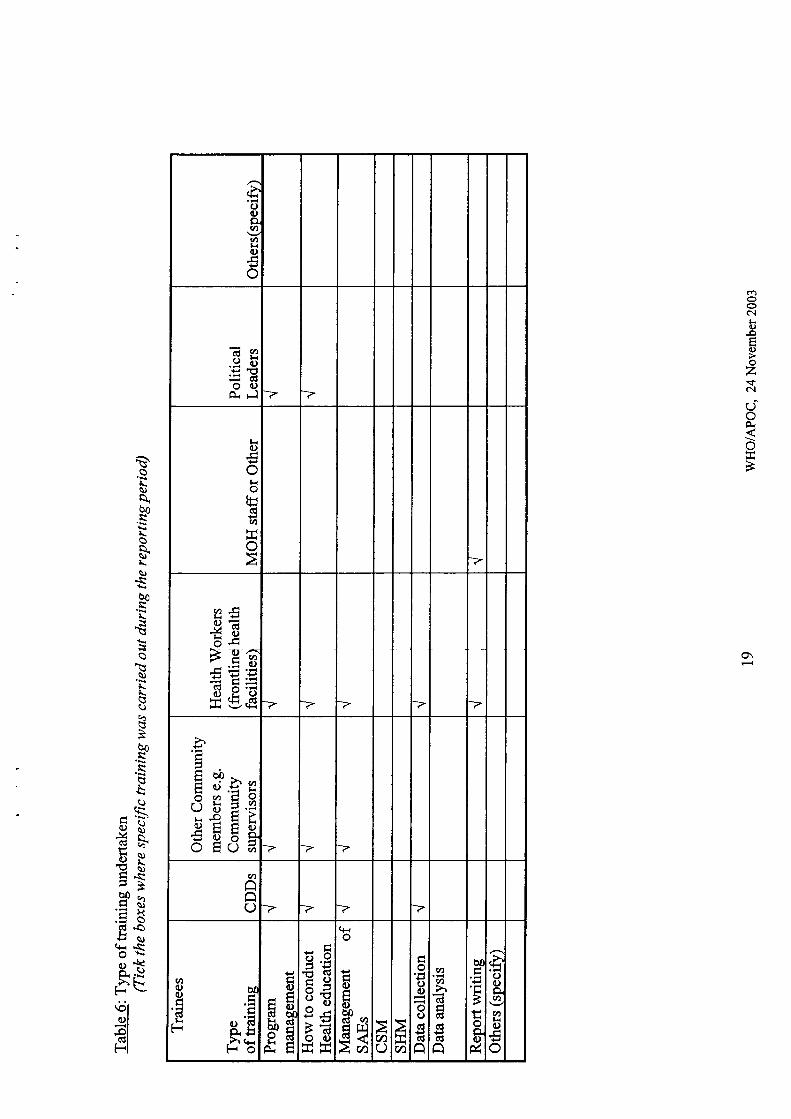
2.2. Advocacy
The reason for mobilization and sensitization:District level:-
-Induction of new district leadership to Onchocerciasis prograrnme.Ward and village level:-
-lnduction of new ward leaders to Onchocerciasis progmmme and increased
uptake of drugs by the community.
Problems encounteredFunds allocated were not enough to carter for the plarured activities.
Suggestion to improve advocacyo Adequate funds should be allocated and released in time.o Advocacy should be done just before mass drug administration.o Timing of mass drug distribution should take into account availability of
community members (during off season)
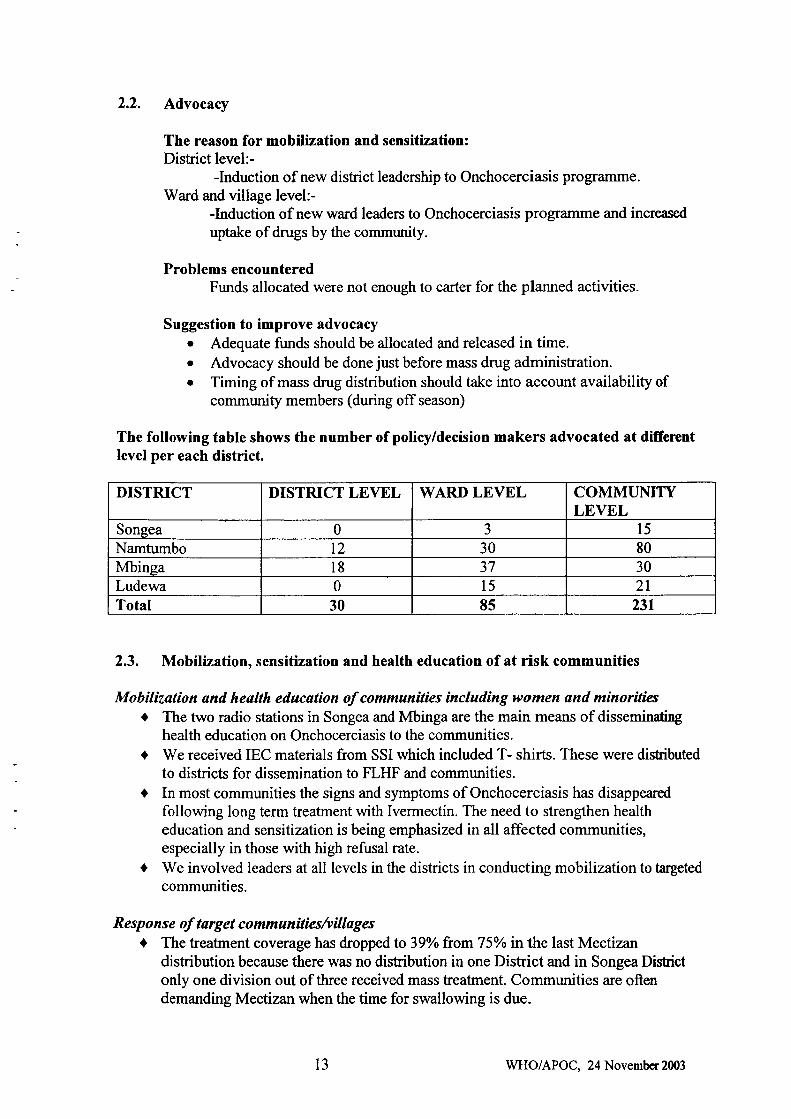
The following table shows the number of policy/decision makers advocated at differentlevel per each district.
2.3. Mobilization, sensitization and health education of at risk communities
Mobilization and health education of communities including women and minoriticst The two radio stations in Songea and Mbinga are the main means of disseminating
health education on Onchocerciasis to the communities.. We received IEC materials from SSI which included T- shirts. These were dishibuted
to districts for dissemination to FLHF and communities.o In most communities the signs and symptoms of Onchocerciasis has disappeared
following long term treatment with Ivermectin. The need to strengthen healtheducation and sensitization is being emphasized in all affected communities,especially in those with high refusal rate.
a We involved leaders at all levels in the districts in conducting mobilization to targeted
communities.
Resp o ns e of target co mmunitiesh illagesa The treafrnent coverage has droppedto 39yo fromTlo/o in the last Mectizan
distribution because there was no distribution in one Dishict and in Songea Distictonly one division out of three received mass teatment. Communities are oftendemanding Mectizan when the time for swallowing is due.
DISTRICT DISTRICT LEYEL WARD LEVEL COMMT]MTYLEVEL
Songea 0 J 15
Namtumbo t2 30 80
Mbinga 18 37 30
Ludewa 0 15 2tTotal 30 85 231
t3 WHO/APOC, 24 Novembcr2003
Accomplishments of the project in this year are-o The project conducted CDTI activities based on funds provided by Councils, APOC
and NGDO partner (SSD.t Community ownership of the Programme is still maintained arnongst community
members by selecting their own CDDs and giving them motivation and incentives.The village leaders are supervisors of the CDDs activities at sub-village level.
a CDDs are willing to distribute Mectizan@ to their appropriate sub-villages. In alldistricts targeted, training of CDD'S was done according to plan.
Suggestion of way to improve mobilizafion and sensitization of target communities -a Mobilization and sensitization meetings should be conduct every year prior to
Mectizan@ distribution cycle starts.o Health education should be done continuous to remind the community their
responsibility.o To strengthen Community self Monitoring and Stakeholders meetings in all affected
communities
t4 WHO/APOC, 24 November 2004
ah(l)5-9'=6
=EEEAttllo.tsa.l ieo 89b10-aJiEEz
ll *Ft
=ca
(l)b0GI
q)g)Lo9{
oo Ioo oo et
E.g*
I EEEz a'i
lat@
orat
\o=!+
E6l z)
o)Ots
i^ EEirrgv l.zlH
='OcE>Lotrq) 9'-EqrEtz
rr 6da
doH
Oc..lc..l
o\c-t
ia\o
€ca
Q)0GIA
ERt=volt'- I
lal o\tat
\E)!+(a
r*{\=r l-laQ
o\ca
lato o\o =era
ah0)oo26l tt
=?>q)8E+.o?)trEo5-aE .g.FE=&oE5*Iboll l.o6c)s,.g 1tr.: 1
--l--lZI
ll ''r.9t
EA CQ
taFA
€)a0cltrq)q)lroe{
ra,c..t
oo oO !+
bd'rET EEE9ox5rr)Ao)
E!tro&E
z
Irr,oo rr)
\or+t
!tcI e Ec;tttL'v.-gi 9Ex
\o.f,.<r
tncoca
lat@
orar
\o
Eq)
o
,1 i6l'-o'E€Hut<E,^OvLtrc) 'xEE
z
ll 'x
taFQal
ca
ou0Gtr6)ILq)
P.{
cl\oco
Otrl(.1o\o.l
9tr)c.l
€Nro
al
r.E EF
{EriF=E;;vzz .E.E
s@
\.lo rat
ailr)\o
o\\ot
s;EEItsolcnc.l
Oc!
c.lcar-
ca\.|N
r-Ntc
q)
treh
a
rrl()zoa
omaP
z
oztr
tsraaDFl
6c
oH
caooo.lr().ooozs
c.l
doOr
so
TA
oBU)
:?()q)
S%>oLq)L
NB!)4q)
5Fo()o
+.Oo(\,EA,ooo(dE v-).-O
Lt=- ,-jEEEOso
tta:l
Hl+*lci I-:l
I
I
2.5. Capacity buitdingThere has been no change of staffat the project and district levels. Few transfers wereeffected at FLHF level but all those transferred to other areas were replaced by trainedpersonnel in implementing CDTI.
- Describe the adequacy of available knowledgeable manpower at all levets.As stated above, the staffat all levels in the project has remained stable for the last four years.We had no shortage of staffin the last distribution.
Where frequent transfers of trained staff occur, state what the project is doing, orintends to do, to remedy the situation.
We have extended taining of FLHF staff to include other competent health worker at thislevel in order to decrease the work load of the FLHF in charge or when helshe is transferred
l6 WI{O/APOC, 24 November 2003
ao
u-r(a
ia\o
c.tooNr<Q)pEooz.+N
doO.
o*{>
F
(JE'uFd
*.$'o< U
ofrH
6loltt-N,-l(J
U
ool
oro
oo.fI
oo(\l
oo
o
o
o
o
o o
ool
cfi
oc{
t\ {
\o
olg oE
q)
R
o
o
o
o
o
o
o o
EI0zoa
oo
P
z
€(l)dc,tsan
ooU(r{oE(u
..oE
z
an()()
(dF<
9{o(nl-.(.)
.=q(tll-Ebkf<()'.-! v
oq{ok(.)otr=z
a)oa.L{otr8B-( .E=adGlr<()--H!Hr& (+i+.Sov,l-ro
-otr
z
€o)tr(!lr
!+i(+icl9v,U'Iot<v)
o(rrok(l)pdHz U
ol.{F
oFloLIv,
o
.Li+{oil
Boz
iEUU
oLt'r
dl9r,OUI'ltUUUE, E,ln \o'OU
ot<F
Eca-o (Jtsr ll +--r'sf, C.lQC)O
>\Lrc!v)lr)OoG)
(t<
C')
BoL{(l)l<oA!.d(d
otncdo
ortro(d
c)troO.E
FoUqioU)(.)
C)
trC)HflEo
PGI
ao(ddLF
a;o
-o(dF
U
!+ooc\lr<()5E(.)oz$(..lOoo"\oA
\o
E€)Eq)
o)
Ee)
s
|,acaca
oo
c.l
ON
oo
ti)
o(Jq)
"o
€os14
q)Ls)
B
q)Lt4q)
,\e.B
o
o
q)
q)\oL
\i"a(J
Bo
t3
ts+.si
.q)R*
({)t-N
ratol
ooeaco
I6ro6
c.l
o.l
o
O
O
rn
ot
c.l o ra
oo
o
c)
6)
Ae
s
Oca
\oN
$
\t
o
.+
.+r-
t*.t
r-ct
oca N
(\T(t
tr€)Eq)
o&I
s
\o|f)
@
.+
$
o
o
6
.+
t
€ O a
ozm
rJ]o*l
FI
HoH
tr6)Aq)
c)
EI
s
oo
,ho(ugv,v)lr(u
o
drl.95EEo(l)O< Fl -7 -7
ko-cot<oHctu)
lJ<oa
0&LrPsl?*c)6.(F E6€EEE€E 7 -7 7
>.
Etr bb-E dREi e'E I\-/ o ='5uS E f8EEtsO EO d 7
ah
ooO -7 7 7
bI)dc
otdAJJ-h <rrHO
U)oq)trEF
(u
dugl (l)cl b0FoE9EO{tr
EEE3s#9-c}Eoc)
q<o
ItroEob0d")
ETaa aL)
*<a
tro€oooodcln
V)
V)hclccl(0
GI
a
bntr
'.=L.
BLoac)&
,i'o0)gv)
V'koIo
c.tooc.lL(.)-oEooz$c.l
t,oO.
o+i>
o\
So\q)a.bo
Lo$Lq)
b0
\\a\a)LLB()
Fil
bos
B,\U\\
ox**ES,ES
ooIAqi'=}<d"oEs)qr -S,'.\ct1;EF\-riiro-rl
.ol(!tFI
.tooat(),oE(.)oz
lrfc.l()oO.
orJ<
>
u0.EtrELq)Eoo
.9qo(l)a
+ro
oGIL.sEo(l)
rdE(uac()L(.)(u
.1,t)6
gEi.9 .9L+j+. Gl
6toAO Q..= e)EEl.l e2aEr6l .=
E5 9JEE EIEE 9IE; 8lzX Elsg flboa e{lo i:ld-E s.1 a 9d
8? El.i ,t El.i.- IdE ol,tr ElE-: dlE} Elua ril
=> tjlI.o gq()E .=l.a ct.lil
EE Eltrii otoE ol-E EI..E olc)'- Elt,)=loct Elz? 5l+ 6l fr{l
oc\
HoCd
)aoA(d
oFXrf,€O
(.)
ooFa?Hl o)xl E
EIEH;el 2olH8liol
tsl
;l-olEIJIzlI
(B(l)LrdE(.)'a
EaH9€Poo.='aLr \./
E.ErP&.Eh.dP.E€,.9tt) :1:.9E
.=(DEEEHE v'tooo'E.9 o,'EE OI E(,) -l B
E #I Hb El.e* .EI E: E]Et) ell (D6'j) (gl -rE Et B..H >t bbo .91<F EI H; EIEo Hl o'E ol r.cr, ol o)E tslEO lrl !q gl trE 'trIEE 3I EF Zt?
x!o)((lq)L+Jgo1oG)
cq<1otr-. I
(t)l-olEIatzt
oF
o(Blr6)bn(dkooodC)
Eo
.9a€5oF
il
o)dLi(l)b0dL{(u
o()GI9a-(xO. <iclbooo
q)(dLrobo(dLi(l)
oo.9^9rO5o\(I)vp.dtsrq)
F
! -,.^^s€'E{E$E$EE-g_E 8E oetsE
a
o o o o o
t:tzu)o o o o c
b8EtE,,avlz€
c.l
o{€o
\o
c\lo
o\CI(a
be!F
E=af68E-ino\ a o\
@
\o
r..
CIclo\€
oGI
tooA{
oll -OEATa
R$&-o $abE 0xd))>vtrgc.t o co
@tr- F-
?a
t-.ab Po€,* 5IE " [E
o\o@
c.l
c.loqo.+
o\oc\6t
h-
o
\oa
tr(l)
E€*Eig F-F O
€o\t-o\o
oocft-to.t
c.t\oatao\\o!coN
rno
drl5 g<->
E € E S'e s€EEET Ha H'
c.l
\o(fI
I$€$
\oc.l€t\o
o\€\o(fltcl
U,ob,0CI
6)o)P
c
EoC)
orL>=dn**a
-C c)o. u0d- (daLr 'i li -obO ;'\ () o\o - >:-'0)oo()
\oc.t o oo oo q\
(fl
a
'!=! u,t{ .i C)q)trbot,P, 5 (rt o
E=E=Eoo
ta€ ora) clrc
alacrtr."=EEr["<F 6
\o\tr+r.)ttc.)
rat€ o \o
ts.E .E &.s
E E.$_E* H.\ostt
inrntt
raoo
oia)
\o
.9<sqo\
E]ozoa om
Fez
ozB
FrqI5
Fl
t<oF
-:.IrtJ4s)aa)
SVa1o\a)Lo\Esq)g4
ctq)
5&U'L<
clU'd()L.d
(!I
tr
oF.l
o'trt/)
tx-o.t)rrl
atcrd
()E(do)kFr-fol
-ol(dlFI
ilil
I
$oootlH(1;)
.oE(l)oz
r<fc\UoO.
o
o.l
tsoa(uLroPov)cd()oz
xo-o(l)
Jio(l)U)(d(l)
O.rookoabI)trtso&o)t<a/)
bI)trLJ€slOItro)
ooU')l-ioE(!v)toLroU)
q<oo)v)dootrv)Cd
Poo'akqo€oq)(BoH
B,cgBE- r-r
=.o(L)Heo-(ta-9PL)V).P HEJJ o€q)-u)E A8
Gl lrY ()Et o.o- >c,E 8.9@ ll)rtR AEH EIE .EE.
i 8Efr, €gA or+i.o Eea9H Eh'F{ li C)
A TdEYldr<(J 0-t(,)c!E .otr€ p.Etr .q!9!?6aO.ias f;T#a S{:' E HEH € 9,
HU ESgS E=Eg € HES ots= ;8EE E.E-d.q E EooE I o.E=.2 o .-8 E BHEE 9;:EH ;gEtr €q)
A?6
EO .E€,E'B ft Eq-t t r.E,+r.-(l)tr d 'dP
EF €EEE :€9 E EEAE EE
(l)+rdan
F.dH'd
.6s "'$3 s\s ss'Bo tt.blQ'i N$EE*S uq)
s !BEgEE {ts $ssE \Fi
E :t.E '$sB\t$ *I\ IS
H EiI Er-:Qq)\ u'Qq '=\
s rss[Ei Es* s;.S' .s
='5 \Ss E!tr PsOo$0,)s' ,all
'!. \.i Npq., St
E$!* b;t"
€ t$S sooI sa-B$\ sas s\iel Sq)S EEB SN
$\)altt SSIt FrS
,ll Jl. Htr x's,t b\
oF(dC)L(d
oC)'aL{q(l)
I
E5a,CBoLr(doEo'otroIli
C)aoq)(l)
tr.oo)€dc)tr
o9oqoC)aqroko
,otr
d
EoF
'o(u(l)
o(B
F
s
il
-7
tOo6lL(l)oEC)
oz*o.t
qtoO{
orf<
>
c.lc.l
q)
S\a)
\--o'\q)ssBLa)
V)*
.\i.,sv;q)(Jq)
S%io\q)Lo
tBa)
Uq)
s€oL{oO.boqLoO.q)L.o
a0
l<
rd.oC)t<k
oooGI
-qan
rq
aV'
(l)
0)oV)LrId(n
otr(uu,
(+ioooatdO#r6)l
-oldtFI
Esao7 tsJ256:<.E E X
h0 PoBe '=tr-
dP (Ei5Gr.o'a
B trEEaEE,,
U)v)otrh0ol-{a(+i
o
(L)
trooto
Lr,-* Eo.x EU)* U)
d30o)u:9F4gE?*1 oo.9 -c 6q,) i i==
E€EEE H
tro-db'B H e.o)'= q=
E*;E z3PHt s
EfE o
v)
oo.>\
V) zdaO)*1y H(l)=o)HFa*Q #E Ho
N
8s E*+<o(I)
loc*'5oLH
-oxoa(l)ho
4v)*
brO
E x "s(J
ro\o so\ tr-@o\ oo
c-loo 6€
aoo\
oqGIr-
troCd
tpo
Or
ell -Oe @FldH *.-
rd
h0OE -.r t "5o
ca\o.f,o\ t--
ooo\ @ca@
r,r)r.l@
aoo\
t\d@
o*\o
rdaa
=o(uboO. tda
Hg gEFOFo
calrl\ot--
\o\o q\o\o
9r-\o,..!o\\o
oq
t.rc.it-
oq(?It\
6frl
(H
E eu+(lldEbE.= P.9z
o\t--\o$
Ora)c-looo\
t--ooc.l
st--\o"ratctlC\
$F'q@NN
@$@oio\
@cft
C{
o\raqor-c{
CAt^oo\(\l
t-r{
tsar6d q.=zE6E E.gI< g*'
t< L,
Oo\dIc.lcac.l
@F-oo^ra)lr)N
o\Ocnooc..l
OOocac..l
$la)
{ooN
cor-.crl.f,c.l
\orao^oir|ol
c"l$o\o\c{
t\CAoGI(fl
I E-.g
EEg€€ uuts ir,i5 6 tr (gooqP.Er
rr)lat\o\otr-N
tr-\o^sOcA
ooO,riC.lca
F.c.t@\dcocfl
ootrrc\@coco
o\tdIr-.coc'l
\o@\o^c-o\o.l
o\\[email protected]\(ft
(\lratr.rGI((a
U'ob!(d
tv,o€
dEoU
o*al
H&n
q)
9Satl Oo\< B-()
OOOO OO OO oO Oo oo oo oo
B_P P
gg t"8,58i.Oo oO Oo oo o
Ooo oo oo oo
rdt= EEfizg5
c.ltr)co
carr)
rnral
t\o .t\o $\oo
$q)(a
t-oGi
clfEl
ts o.l
od (t).=2E6EE.9< 9*'FU
Nlr)ca
c.Irnra)ra)
$\o.t\o sf\oo
\t@CA
t--o(.I
tsE IEt Et$:nE E
- HE
N\ncn
caral
Llla)
.f\o
-+\o $\o
o-t@ra
t-oGi
rI] &r-o\o\
00o\o\
o\o\o\
oOoc.l
ooc{
C\ooC\
coooo.l
$ooN
rnooc.l
\ooool
t-oo(\l
$ooc.lLoFEooz.+e.t
doA{<o*rB
cf)N
-chL
€s-.9clI(l)a0€€r.!
NA\ rrt$YLF{
!{t-S.qr-
LL6I
+.=A.SE9\clL\A!R,.=6y.Hoti=it€; \-/ q)
ctEr6)+.€heBtec)o=.= o' bo+.llE!,1 Lri o.;9'=:-.-9aHglrrv=FgvattUH=t.ts\i=B6tiUNrlr xe .l GtE€I H
E TI E.llAEHEH 'ol tr'{i, b0
=EEI-(Ulr+a
^ l-rE:9+rdF
!dP; E.Etrot9trq)txsf-'( Ei cl
": 8€Xdr :(l)l oh
EI -EFI Fr
$ooc\t
o!EIt)
oz*C..t
doo<
o
\f,c.l
.Eo(l)l< U, .1.(l)(6tr:tC)(gHbhei.E IE o.ag.E3c{%:aq<-Y
EE$#€;'- &6
BieEEE.HGIE9oE
EE-E.g HE€ *eb& e
EEgEPHc) -!o- o -riqr'n Oo'+r >
EEI*FE>'-1(/,,
EEE.g g.I!E ix'o- boc-f o c,
Q 9oe
=5€{E€E!doeg8E:E.E9{ li li
Lg
g 8"fi!E b5:E 6
fEE
EE $$H=k^o P ot.d;i g":$€.8 e E F?E EE H
lfiEE H
€s
t+tr)
rr|st
r-.Oo
@o\qsOol
o\oo\o^c-t$c\l
o\co
o\c-t
c.lsf,
\o
\o
€ooc{
o\oON
ooc!
2.7. Ordering, storage and delivery of Ivermectin
Mectizan@ ordered/applied for by - @lease tick the appropriate answer)
MOH{ WHO I]NICEF NGDO
Other (please speciff):
Mectizan@ delivered by - @lease tick the appropriate answer)
MOH ./ WHO N UNICEF tr NGDOtr
Other (please speciff)
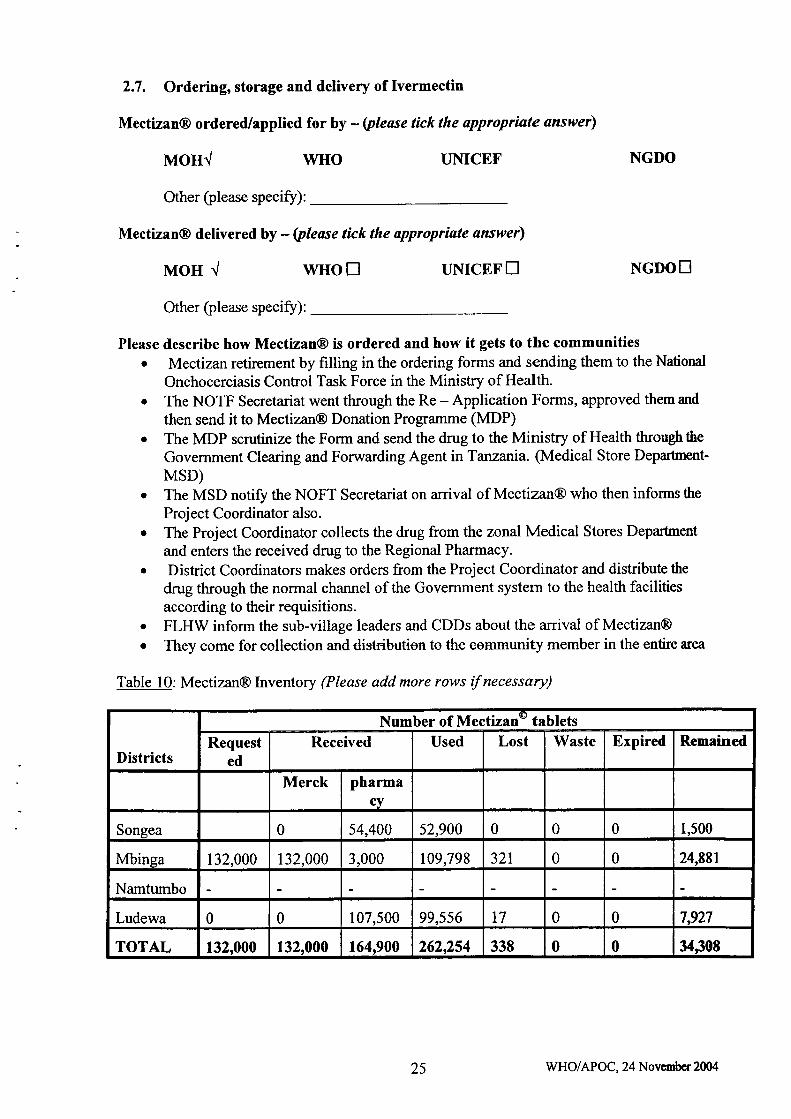
Please describe how Mectizan@ is ordered and how it gets to the communitieso Mectizan retirement by filling in the ordering forms and sending them to the National
Onchocerciasis Control Task Force in the Ministry of Health.o The NOTF Secretariat went through the Re - Application Forms, approved themand
then send it to Mectizan@ Donation Programme (t!DP). The MDP scrutinize the Form and send the drug to the Ministry of Health throughthe
Government Clearing and Forwarding Agent in Tanzania. (Medical Store Departuent-MSD)
. The MSD notiff the NOFT Secretariat on arrival of Mectizzur@ who then informs the
Proj ect Coordinator also.. The Project Coordinator collects the drug from the zonal. Medical Stores Departuent
and enters the received drug to the Regional Pharmacy.o Dishict Coordinators makes orders from the Project Coordinator and distribute the
drug through the normal channel of the Govemment systern to the health facilitiesaccording to their requisitions.
. FLHW inform the sub-village leaders and CDDs about the arrival of Mectizan@
. They come for collection and distribution to the eommunity member in the entire area
Table l0: Mectizan@ Inventory (Please add more rows if necessary)
Districts
Number of Mectizan@ tabletsRequest
edReceived Used Lost Waste Expired Remained
Merck pharmacy
Songea 0 54,400 52,900 0 0 0 1,500
Mbinga 132,000 132,000 3,000 109,798 321 0 0 24,881
Namturnbo
Ludewa 0 0 107,500 99,556 t7 0 0 7,927
TOTAL 132,000 132,000 164,900 2622s4 338 0 0 34J08
25 WHO/APOC, 24 Novcmbcr 2fiX
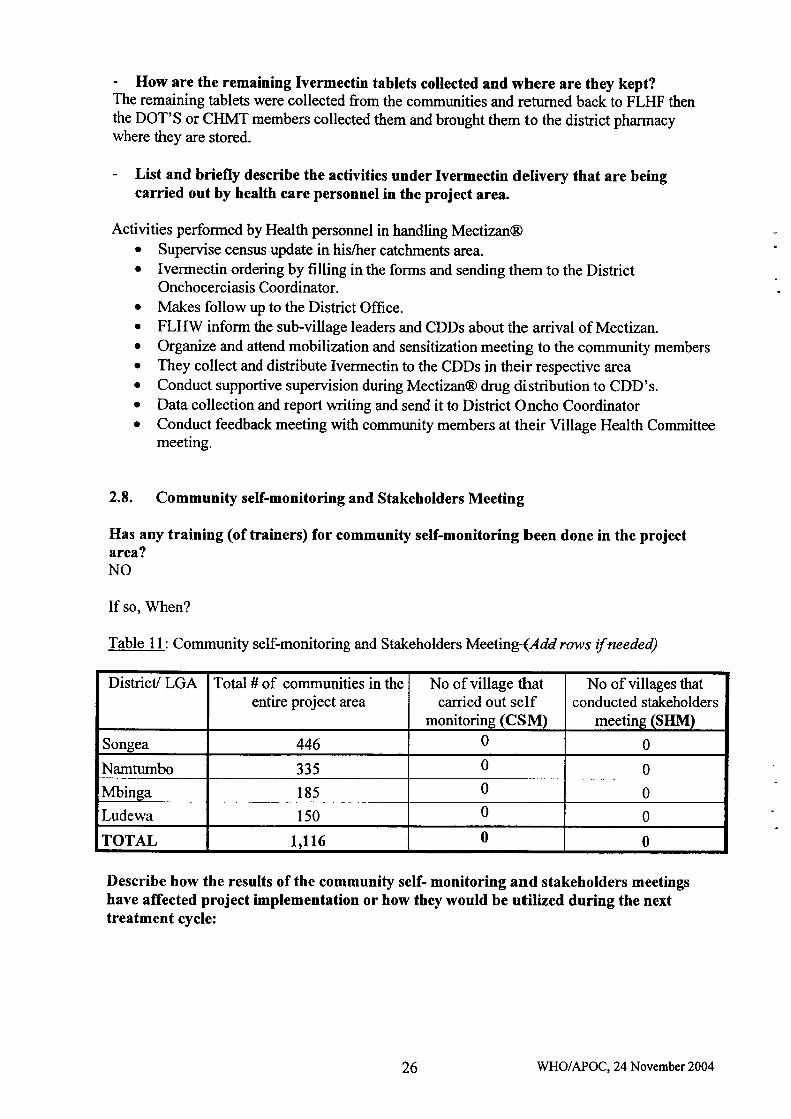
- How are the remaining Ivermectin tablets collected and where are they kept?The remaining tablets were collected from the communities and returned back to FLHF thenthe DOT'S or CHMT members collected them and brought them to the district pharmacywhere they are stored.
List and briefly describe the activities under Ivermectin delivery that are beingcarried out by health care personnel in the project area.
Activities performed by Health personnel in handling Mectizan@. Supervise census update in his/trer catchments area.o Ivermectin ordering by filling in the forms and sending them to the District
Onchocerciasis Coordinator.o Makes follow up to the District Office.o FLHW inform the sub-village leaders and CDDs about the arrival of Mectizan.o Orgaruze and attend mobilization and sensitization meeting to the community members. They collect and distribute Ivermectin to the CDDs in their respective areao Conduct supportive supervision during Mectizan@ drug distribution to CDD's.o Data collection and report writing and send it to District Oncho Coordinatoro Conduct feedback meeting with community members at their Village Health Committee
meeting.
2.8, Community self-monitoring and Stakeholders Meeting
Has any training (of trainers) for community self-monitoring been done in the projectarea?NO
If so, When?
Table 11: Community self-monitoring and Stakeholders Meeting (Add rows if needed)
Describe how the results of the community self- monitoring and stakeholders meetingshave affected project implementation or how they would be utilized during the nexttreatment cycle:
District/ LGA Total # of communities in theentire project area
No of village thatcarried out self
monitoring (CSM)
No of villages thatconducted stakeholders
meeting (SIilVt)
Songea 446 0 0
Namtumbo 335 0 0
Mbinga 185 0 0
Ludewa 150 0 0
TOTAL 1,116 0 0
26 WHO/APOC, 24 November 2004
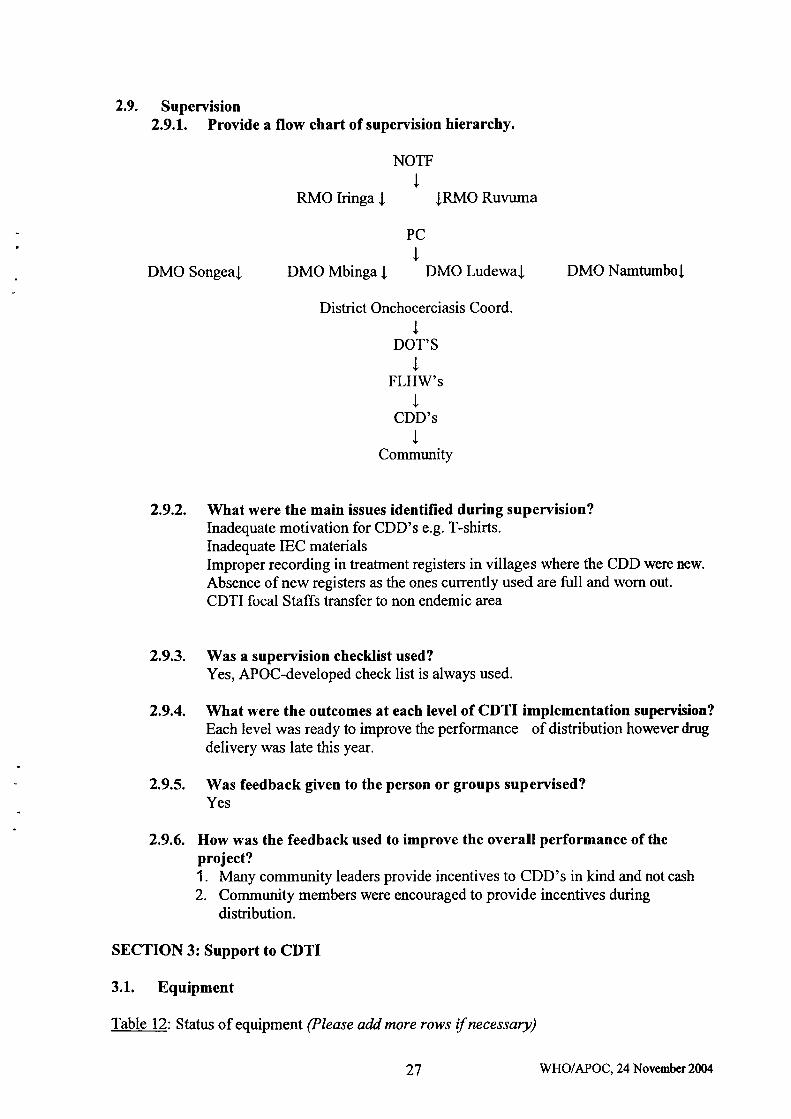
2.9. Supervision2.9.1, Provide a flow chart of supervision hierarchy.
NOTF
IRMO Iringa I IRMO Ruvuma
PC
T
DMO Songeaf DMO Mbinga I DMO Ludewa| DMO Namtumbol
District Onchocerciasis Coord.
tDOT'S
JFLHW's
tCDD's
tCommunity
2.9.2. What were the main issues identified during supervision?Inadequate motivation for CDD's e.g. T-shirts.Inadequate IEC materialsImproper recording in treatrnent registers in villages where the CDD were new,
Absence of new registers as the ones currently used are full and worn out.
CDTI focal Staffs transfer to non endemic area
2.9.3. Was a supervision checklist used?Yes, APOC-developed check list is always used.
2.9.4. What were the outcomes at each level of CDTI implementation supervision?Each level was ready to improve the performance of distribution however drugdelivery was late this year.
2.9.5. Was feedback given to the person or groups supervised?Yes
2.9.6. How was the feedback used to improve the overall performance of theproject?1. Many community leaders provide incentives to CDD's in kind and not cash
2. Community members were encouraged to provide incentives duringdistribution.
SECTION 3: Support to CDTI
3.1. Equipment
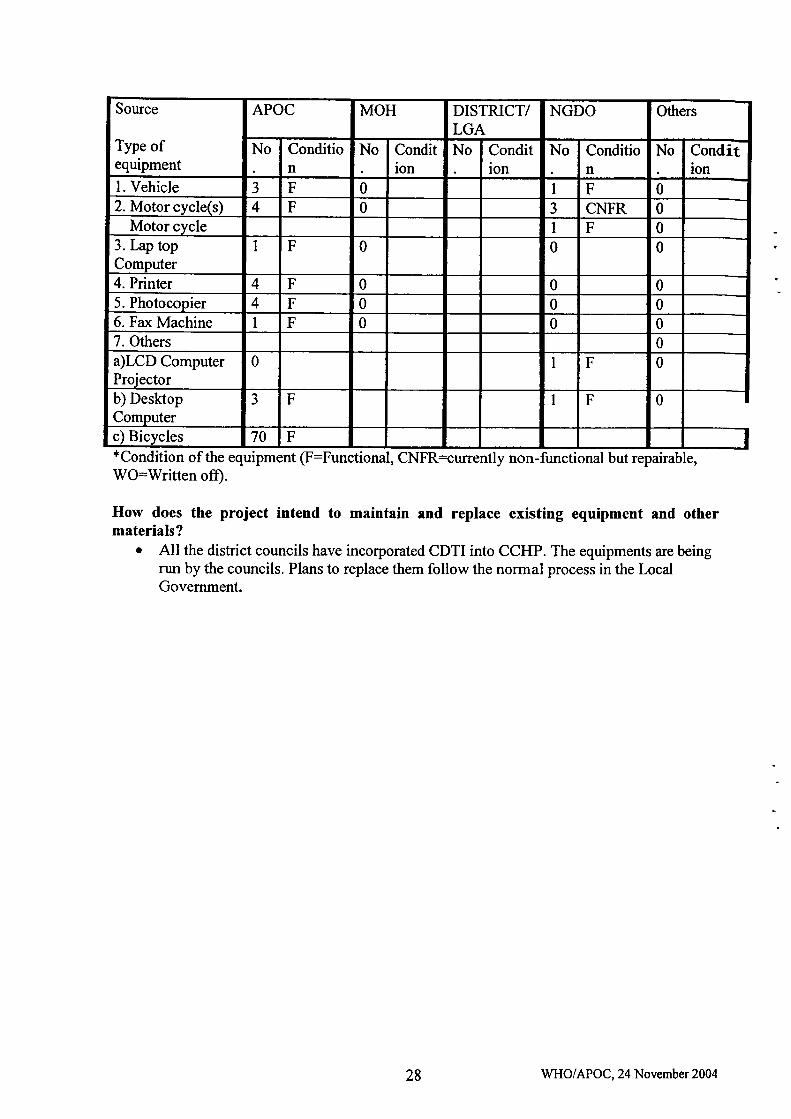
Table 12: Status of equipment (Please add more rows if necessary)
27 WHO/APOC,24 November2(M
Source
Type ofequipment
APOC MOH DISTRICT/LGA
NGDO Others
No Condition
No Condition
No Condition
No Condition
No Condition
l. Vehicle 3 F 0 I F 02. Motor cycle(s) 4 F 0 3 CNFR 0
Motor cycle I F 03. tap topComputer
I F 0 0 0
4. Printer 4 F 0 0 05. Photocopier 4 F 0 0 06. Fax Machine 1 F 0 0 07. Others 0
a)LCD ComputerProjector
0 I F 0
b) DesktopComputer
3 F F 0
c) Bicycles 70 F*Condition of the equipment (F:Functional, CNFR=urrently non-functional but repairable,Wo:Written off).
How does the project intend to maintain and replace existing equipment and othermaterials?
o All the district councils have incorporated CDTI into CCHP. The equipments are beingrun by the councils. Plans to replace them follow the normal process in the LocalGovemment.
28 WHO/APOC, 24 November 2004
I
\tooc\lLq)&Eru
oz$c.l()oO.so>
o\C\
dt)-c3hdooqln()o)l)
{od
(+<
otroGt9coEoO.Eth()-oGItrlu#ad
-(!Iot)'atr&()&ov,tcdmtr1,
oLAl.€trlt)
Et)utclcGI
agHGIadv)trgtrddoogo;tHo=E()FE.e5-c)(do.g€Hc:i, o()GEg#E
uEoEEoI
Ho
E
r-i.9L(dc)v,+).t)
6.9E)gU
U)6)trL=nro.te6t '=o=
e9o(l)}EEE-E _8aA ;iE'EAu)(i<P
t€TbLC).,9 5rltro:ic)tr!g90u) lr6laoolib5A9n
i>(dta) -qHe,
:(d-o a.)'e6Li L.Iii E6)trE.Eo'uL(l)c)X,glcd
U'Ldo8>..- o).EoEF
=EEaEdE-gcl q:.a) thL l-ro)oFE!(dGlo-a-'oE
rH -OOv)
?.EO +.1.-=
Lt!troO-e)(g-t()cEd'6Etr.=6l f!
tug,l
6l 'xl?d tjl
oosSS(?)Lcl(D
-q
essF
O\fola)
oooc.l
Oc.t
c.tOr-c..l
!tr
J1tr
$Oc*o\
(a6laclrara
-G'6a(d F-.\(.) g?Et$li)'c0
$Orat
o\
\oOca
c.tOc--o.l
.dtrJ
$O\sc.l
to\€^NF-?a
RSSsollr6t(D
3-to *aF.l 9q castebe(F
Olrlqo\+
o\qolatc.lO
Oc\lqca
q\olatt-r$
N6o\to\\o
U)d€r) o ^;83<rrD
(1 =lJbcaF
O\oqo\.+
OOdIc.lc\I
Oc.IcaCI
v?
@o\r-
vl(a€€(.lo\
-\oSSe!LGIq)
3:,o HaF.l !q caste6eF
o\o\?a
rA
oOo^€
(t)c.l+cA(ac\l
oo\€\Nia
s@'6adF1OUiE53'co
o\o\co
ca
c.lF=cA
Oa-)
co$
Nr-rt^ia\o
Lo
&IitroQ
+6E{J?Es4'5,t, .E6B\E{ l.rztu
ol-loU)
go
U'kotrts(B&oa(,z
q1L(l)Eo c, !
U)o.Ed
EEoO
tdt\U)
EF(-)oOi
Fl
F<oFr
$oo(\tLq)
-oE()ozs
c..t
()oAso
Oco
eEfll!ic HIr-.ra).r!=qrEt38ts'a hop
=.9 3ElHE:383er-. d dJO'5 d
E FE:{ E.r O'5
-E B IEE*E3E E. -U
8E C E.-E
EE E6E o.9AH o) q r\E E*rv
SEEE;t E.EH.9 O H
.EE H*.lL\/u)+r
EE8 EO UU E
$AE8,oa
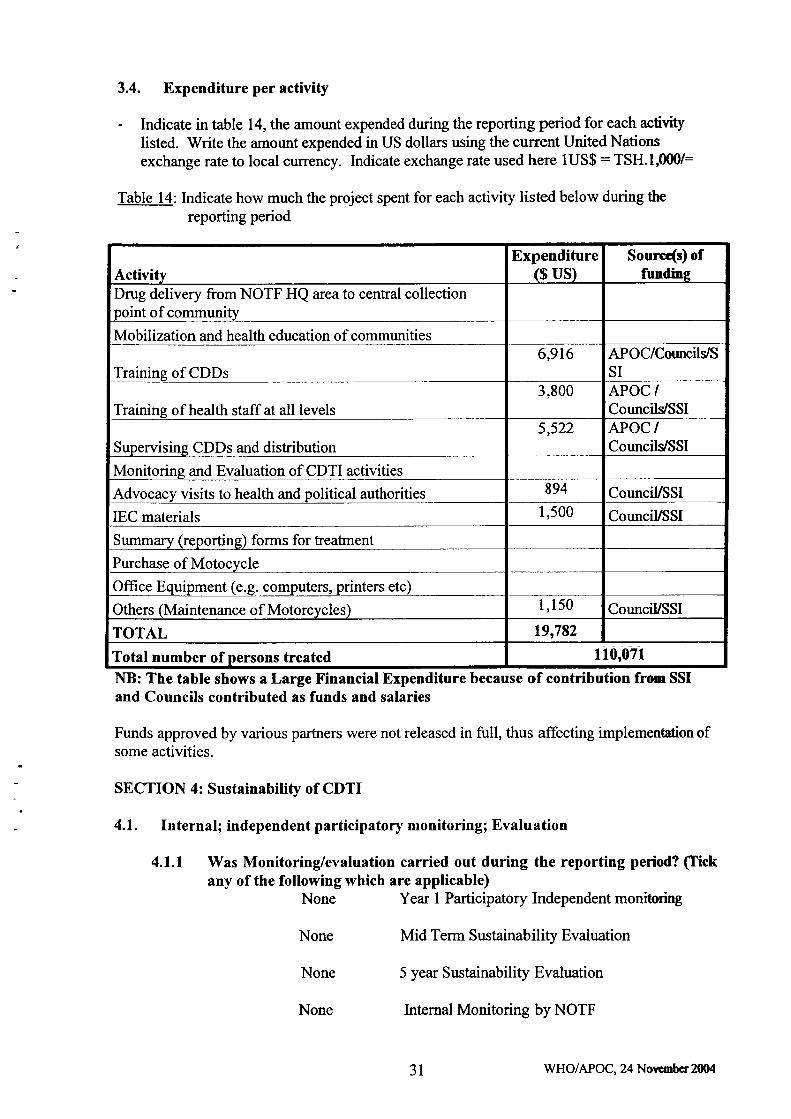
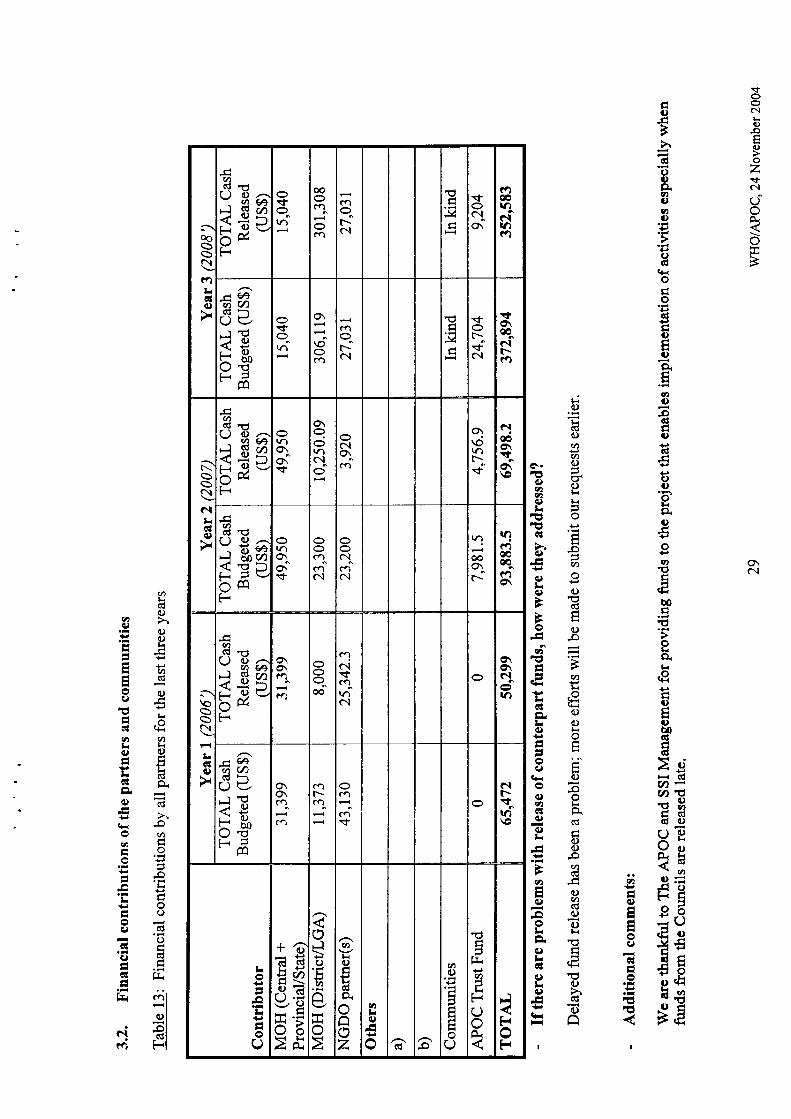
3.4. Expenditure per activity
- Indicate in table 14, the amount expended during the reporting period for each activitylisted. Write the amount expended in US dollars using the current United Nationsexchange rate to local currency. Indicate exchange rate used here lUS$ : TSH.I,000/:
Table 14: Indicate how much the project spent for each activity listed below during the
reporting period
I\B: The table shows a Large Financial Expenditure because of contribution from SSIand Councils contributed as funds and salaries
Funds approved by various partners were not released in full, thus affecting implementation ofsome activities.
SECTION 4: Sustainability of CDTI
4.L. Internall independent participatory monitoring; Evaluation
4.1.1 Was Monitoring/evaluation carried out during the reporting period? (tickany of the following which are applicable)
None Year I Participatory Independent monitoring
None Mid Tenn Sustainability Evaluation
None 5 year Sustainability Evaluation
None Internal Monitoring by NOTF
ActivityExpenditure
($ us)Sourrds) of
fundingDrug delivery from NOTF HQ area to central collectionpoint of community
Mobilization and health education of communities
Training of CDDs6,916 APOC/CotmcilstS
SI
Training of health staff at all levels3,800 APOC /
Councils/SSI
Supervising CDDs and distribution5,522 APOC /
CouncilJSSI
Monitoring and Evaluation of CDTI activities
Advocacy visits to health and political authorities
IEC materials
894 CounciUSSI1,500 CounciUSSI
Summary (reporting) forms for treatrnent
Purchase of Motocycle
Office Equipment (e.g. computers, printers etc)
Others (Maintenance of Motorcycles) I , I 50 CounciVSSI
TOTAL 19,782
Total number of persons treated 110,071
31 WHO/APOC, 24 Nowmbcr 2fl)4
NoneNone
Other Evaluation by other parhrersYear I Participatory Independent monitoring
4.1,2. What were the recommendations? NONE
4.1,3. How have they been implemented? NONE
4-2. sustainability of projects: plan and set targets (mandatory atYr3)
Was the project evaluated during the reporting period? NO
Was a sustainability plan written? NO
What arrangements have been made to sustain CDTI after APOC funding ceases interms of cash?
4.2.1. Planning at all relevant levels
4.2.2. FundsDistrict Councils are ready to take over the programme. Budget for the implementation ofCDTI activities are incorporated into CCHPs. The district council has started releasingfunds for the implementation of CDTI activities. The Local Government Authority hassupported CDTI activities in this reporting year.
4.2.3 Transport(replacement and maintenance)The equipments are being run by the councils. Plans to replace them follow the normalprocess in the Local Governmenl Maintenance of motor vehicle will be done by usingGovernment funds.
4.2,4. Other resourcesGradual incorporation of CDTI activities into CCHP and the project has a prominentparfirer who has assured to continue to provide support to the project.
4.2.5. To what extent has the plan been implementedIn this year the implementation of CDTI activities in the places whereby activities havebeen implemented had been executed according to the sustainability plans which weredeveloped after the project evaluation.
4.3. Integration
Outline the extent of integration of CDTI into the PHC structure and the plans for completeintegration:
CDTI activities are executed under the directive of RMO/DMO who is the in charge of allmatters pertaining to Health and therefore all plans to implernent CDTI activities passes inhislher office then are tabled in RHMT/CHMT. The District Onchocerciasis Coordinator is
32 WHO/APOC, 24 Novcmber 2004
t
a co-opted member of this team at district level and always they conduct routine
supervision as a team. All districts have included CDTI in the CCHP budget'
CDTI structure is being applied in many projects in our Region. Intemational Trachoma
Initiative is using the same structure in Tunduru, Songea and Namtumbo Districts inlmplementing the SAFE Strategy. The Neglected Tropical Disease Program has been
planned to take off in 2008. Essentiatly this Programme is going to be linked with CDTI inits execution and the same CDDs are going to be involved in irnplementing thisProgramme. The structure is not identical but has many components similar to CDTI. The
Mectizan@ drug is transported through the existing PHC structure during supervision and
monitoring.
4.3.1 Ivermectin delivery mechanismlvermectin is delivered using Government structures, CHMT rnember delivers Mectizan
tables to FLHF those are within the Onchocerciasis endemic area together with other
essential drugs/drug kit and vaccines. The FLHF in charge and hisftrer subordinates are
responsible to all medical drugs and equipment brought to thern from DMO's officeincluding Mectizan drug. The CDD come to the FLHF to collect Mectizan ready to
distribute to the community members. The same CDD are also responsible on distibuteMectizan and Albendazole for Lymphatic Filariasis Elimination.
4.3.2 TrainingThere were only few new CDDs and FLHFs so training and re-training for CDTI and LFwere conduct at the same time.
4.3.3 Joint superision and monitoring with other programsSupervision and Monitoring of CDTI activities are integrated within system. Therefore at
Region and District level supervision is done by joint team using the developed checklist.
The team includes medical staffand program staff. At regional level the team sometimes
includes other regional leaders.
4.3.4 Release of funds for project activitiesFunds are released through normal channel according to budget line item and everyresponsible part plays its role. The responsible part in our budget is APOC, Council and
Governrnent.
4.3.5Is CDTI included in the PHC budget?Yes
4.3.6 Describe other health programmes that are using the CDTI structure and howthis was achieved. What have been the achievements?Other prograrnme that is using CDTI structure is Lymphatic Filariasis EliminationProgramme, TASAF and National Trachoma Control Program
r Achievements are:o Cost and time effectiveo Many people are served within short timeo Increasesustainability
4.3.7 Other issues considered in the integration of CDTI. Drug used is the sarne to both Programmes - Mectizan addition is just only
Albendazoleo Communities served are the same therefore it is easy to conduct HSAM
33 WHO/APOC, 24 November 2004
I
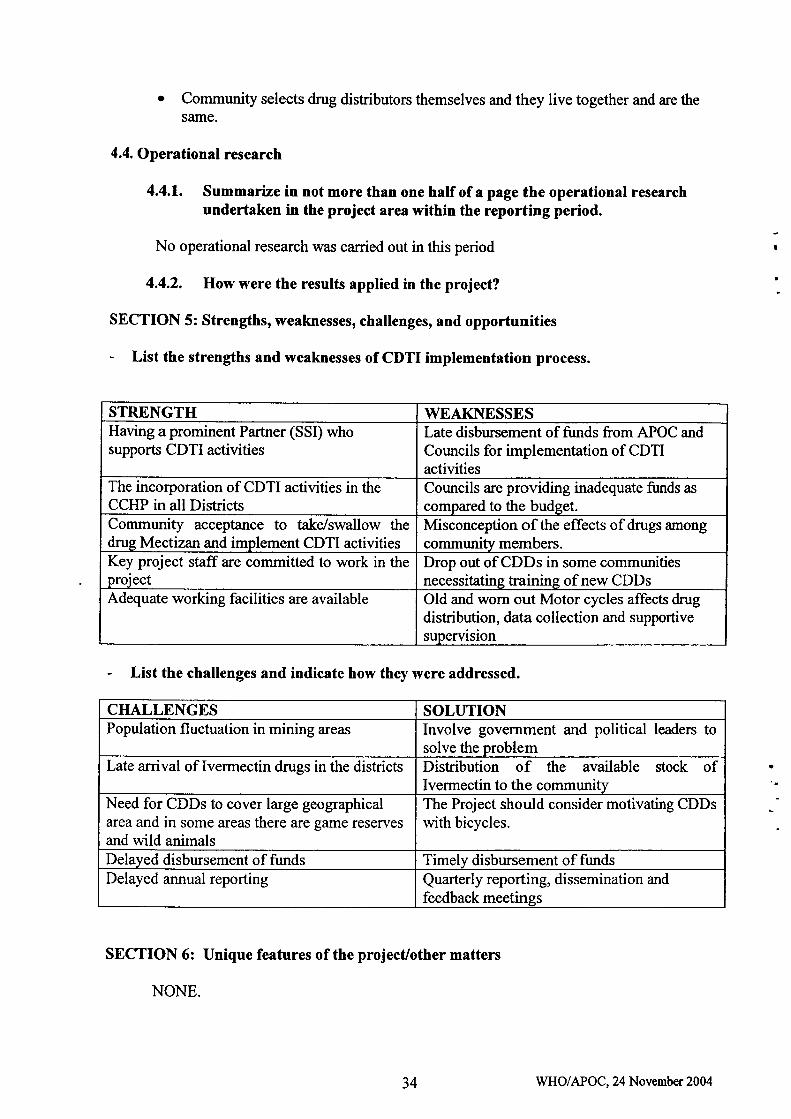
Community selects drug distributors themselves and they live together and are thesame.
4.4. Operational research
4.4.1. Summarize in not more than one half of a page the operational researchundertaken in the project area within the reporting period.
No operational research was carried out in this period
4.4.2, How were the results applied in the project?
SECTION 5: Strengths, weaknesses, challenges, and opportunities
- List the strengths and weaknesses of CDTI implementation process.
List the challenges and indicate how they were addressed.
SECTION 6: Unique features of the project/other matters
NONE.
I
STRENGTH WEAKNESSESHaving aprominent Partner (SSI) whosupports CDTI activities
Late disbursernent of funds from APOC andCouncils for implementation of CDTIactivities
The incorporation of CDTI activities in theCCHP in all Districts
Councils are providing inadequate funds as
compared to the budget.Community acceptance to take/swallow thedrug Mectizan and implement CDTI activities
Misconception of the effects of drugs amongcommunity members.
Key project staff are committed to work in theproject
Drop out of CDDs in some communitiesnecessitating training of new CDDs
Adequate working facilities are available Old and wom out Motor cycles affects drugdistribution, data collection and supportivesupervision
CHALLENGES SOLUTIONPopulation fluctuation in mining areas Involve government and political leaders to
solve the problemLate arrival of lvermectin drugs in the districts Distribution of the available stock of
Ivermectin to the communityNeed for CDDs to cover large geographicalarea and in some areas there are game reservesand wild animals
The Project should consider motivating CDDswith bicycles.
Delayed disbursement of funds Timely disbursement of fundsDelayed annual reporting Quarterly reporting, dissemination and
feedback meetings
34 WHO/APOC, 24 November 2004
O
a