11 years - Manmohan Cardiothoracic Vascular and Transplant ...
61
0 11 years of excellence in service Manmohan Cardiothoracic Vascular and Transplant Center Annual Report 2076
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of 11 years - Manmohan Cardiothoracic Vascular and Transplant ...

0
11 years of excellence in service
Manmohan
Cardiothoracic Vascular
and Transplant Center
Annual Report 2076

1
ÆdnfO{ 7'nf] dflg; xf]Og c;n dflg; eg]/ ;lDemP k'U5 .æ – dgdf]xg clwsf/L
Annual Report 2076 (2019/2020)
Published on: 15th Vaishakh 2077
Published by: Manmohan Cardiothoracic Vascular and Transplant Center (MCVTC)
Maharajgunj, Kathmandu

2
Contents Message from the Vice Chancellor………………………………………………………………………………………………………..1
Message from Rector .................................................................................................................................. 2
Message from Registrar .............................................................................................................................. 3
Message from the Dean, IOM ..................................................................................................................... 4
Message from Campus Chief ...................................................................................................................... 5
Editorial ....................................................................................................................................................... 6
Report of the Executive Director ................................................................................................................ 7
Annual report of department of Cardiology: 2076 ..................................................................................... 9
Annual report of department of CTVS: 2076 ............................................................................................ 16
Annual report of department of CTVA: 2076 ............................................................................................ 23
MCVTC – A financial review of 2076 ......................................................................................................... 29
Annual report of Nursing Administration: 2076 ....................................................................................... 32
The race against the virus: The anti-CoViD19 efforts at The Manmohan Centre ..................................... 35
A Novel approach for coronary Angiography and Angioplasty –Distal Transradial (DTR) Access from the
Anatomical Snuff Box ---A dream come true ............................................................................................ 38
COVID-19: A new worldwide challenge .................................................................................................... 41
One more patient centric effort of MCVTC: Online Appointment System ............................................... 44
Manmohan Center Cardiovascular Disease Prevention, Control and Treatment Outreach Program ..... 46
An Initiative of Developing Society of Cardiothoracic Vascular Nurses of Nepal (SCTVN) ....................... 50
ASD (atrial septal defect) device closure in MCVTC .................................................................................. 54

1
Message from Vice-Chancellor
It gives me great pleasure to extend my best wishes to the Manmohan Cardio-thoracic Vascular and Transplant Center on the 11th anniversary of its establishment. I would also like to take this opportunity to express my satisfaction at how the center has grown over this short period of time. It is heartening to see that the hospital has quickly become a center of excellent care in the field of Cardiac, Thoracic and Vascular medicine and surgery for the entire nation. In the past year, the center has distinguished itself both nationally and internationally by providing quality care to the prime minister of the country Rt. Honorable Mr. Khadga Prasad Sharma Oli on numerous occasions. This has no doubt helped elevate the level of trust and respect for the entire health services of Nepal amongst the common Nepalese population. I do firmly believe that the Manmohan Center deserves much commendation for this achievement. I am aware that the Manmohan center is still in the phase of continuous growth and improvement. The completion and functioning of the Annex building will add a lot to this capacity building. I would like to express and assure continued support from the University for further development and future quality improvement initiatives from the center. The last few months have been a difficult time for all of us given the ongoing COVID-19 worldwide pandemic. I appreciate and support the initiatives taken by the center towards fighting this disease in our community. While the ongoing pandemic will not allow us to collectively celebrate the anniversary as in the past, I would like to end by once again wishing a productive and successful year ahead for Manmohan Cardio-thoracic Vascular and Transplant Center, in terms of quality health services, quality medical education and research.
Prof. Dr. Dharma Kanta Banskota Vice Chancellor
Prof. Dr Dharma Kant Baskota Vice Chancellor
Tribhuvan University

2
Message from Rector
I am glad to know that Manmohan Cardiothoracic Vascular and Transplant Center (MCVTC) is going to continue its annual report even during the COVID19 crisis. Tribhuvan University is proud to have such a center-of-excellence that has served thousands of people from every corner of the country and has immense contribution to medical education especially on cardiac, thoracic and vascular specialty. It feels great to share that the Doctor of Medicine (DM) - Cardiology and Magister Chirurgie (MCh) – CTVS super-specialists trained in the Manmohan Center are serving in the leading health care institutions all over the country.
I believe the center will always be able to keep pace with the advances in the treatment of cardiac, thoracic and vascular specialties. Finally, I would like to express full support of the university and wish prosperous days ahead.
Prof. Shivalal Bhusal, PhD Rector
Prof. Dr Shivalal Bhusal Rector
Tribhuvan University

3
Message from Registrar
It gives me immense pleasure to write few words for the Annual report of Manmohan Cardiothoracic Vascular and Transplant Centre (MCVTC). It is one the centers of Tribhuvan University which has always made us proud, by its specialized service to the National dignitaries as well as to general public. It has become a popular hub for cardiology services in a short span of time.
Besides its service, it has been a center of par excellence in its academic program. It has been providing platform for education to MBBS, MD, MS, DM, MCh, Nursing, paramedic students. I would also like to congratulate for starting Bachelor in Perfusion for the first time in Nepal. I believe this center shall take a leading role in producing super specialized manpower for the nation in coming days too.
I also believe that its service expansion in the new annex building in near future will help to expand the horizon of services in its field. Finally, I would like to express my support on behalf of the University and take this opportunity to congratulate for their excellent service on their annual day.
Prof. Dr Peshal Dahal Registrar
Prof. Dr Peshal Dahal
Registrar Tribhuvan University

4
Message from the Dean, IOM
It gives me immense pleasure to write a few words for the "Annual Report 2076" of Manmohan Cardiothoracic Vascular and Transplant Center. The COVID19 pandemic has affected every aspect of our life. In this situation publishing a report has its own difficulties and I congratulate Manmohan Center for finding an option of publishing online version of annual report.
The center is well known for providing quality care and education from the vary inception. Discipline, work culture, involvement in national programs and international research activities are highly commendable. The extension program of the center will be a further milestone in its achievements to fulfill growing need of quality service affordable to people. I along with the staff of Dean's office wish to extend our best wishes to the entire family of Manmohan Cardiothoracic Vascular and Transplant Center on this important occasion. I hope people will get the desired services with dignity and respect. Students will maintain the highest academic excellence. Moreover, I also believe center will find safer ways to serve patient taking the corona concern. My Best Wishes are always with center. Prof. Dr. Jagadish Prasad Agarwal Dean, Institute of Medicine
Prof. Dr. Jagadish Prasad Agrawal
Dean, Institute of Medicine

5
Message from Campus Chief
It makes me proud to write down few words for annual report of Manmohan Cardiothoracic Vascular and Transplant Center. Manmohan Center is one of the pillars of Institute of Medicine and a great companion of the Maharajgunj Medical Campus. It has served great not only as a Tertiary Care Center but also as a teaching learning base for the various academic programs of the Campus. The Cardiac, Thoracic and Vascular service provided by the center is one of the best available in the country.
I appreciate the effort of the center to bring its annual report even in such a time of COVID19 crisis. I congratulate the Manmohan Center for all the achievements.
…………………… Prof. Dr. Pratap Narayan Prasad Campus Chief
Prof. Dr. Pratap Narayan Prasad Campus Chief
Maharajgunj Medical Campus
6
Editorial
Difficult times call for innovative measures! We are presently in the midst of a pandemic that threatens and binds the entirety of humanity. These are unprecedented times. Like countless other events and programs around the globe, the COVID-19 pandemic has forced us to with-hold/cancel the celebrations of the 11th Anniversary of Manmohan Cardio-thoracic Vascular and Transplant Centre. However, as a testament to the advantages of the technologies we now live with, we at the MCVTC have been able to work together while SOCIALLY DISTANCED to compile this, the 10th Annual report of the centre.
As is customary the report details the achievements of the past year and lists our aspirations for the coming one. However, what is different this time round is that the report also chronicles and describes the Centre’s attempts to be “COVID-wise” and also the arrangements made to be ready if and when a flow of COVID patients come our way. We would like to acknowledge the contributions of all the departments who helped us by providing us with their annual reports and also the individuals who provided us with articles. We hope our readers find this report a window into the work, achievements and challenges of the Manmohan Centre. Thank you. Dr Bibhusal Thapa Chief Editor
Dr Bibhusal Thapa
Jamuna Tamrakar Sayami
Dr Bibhush Shrestha
Dr Sanjeev Thapa
Prakash GC

7
Report of the Executive Director
Five years ago the country was shaken by earthquake one day before the scheduled 6th anniversary. We were compelled to cancel all celebratory programs. Instead, we spent all our energy in the treatment of earthquake victims. This time not only our country but the whole world is shaken by the unprecedented COVID-19 pandemic. The nation is under lockdown and, once again, we will not be able to celebrate our 11th anniversary. The pandemic has also forced us to postpone the planned inauguration of the new Annex of the Manmohan Centre scheduled during our anniversary. Like five years ago, we are spending all our Chi (energy) to fight the deadly invisible Corona virus.
Providing health care to all citizens has been the prime objective of the Centre. Our dedication to serve citizens at all levels reached it pinnacle when our nation’s Prime Minister was successfully treated and discharged earlier this year. The PM was admitted with an acute health condition. Long before the PM’s admission, the Centre’s good deed were recognized through decoration of highly prized honors, namely “Ujjwal Kirtimaya Rastradeep Dwitiya”, “Suprawal Janasewa Shree Tritiya” and “Prabal Janasewa Shree Chaturth”. I thank the government for this recognition of our Centre staff’s capabilities and their dedication.
Health and population ministry has remained generous for many years and this year the ministry provided us with an additional 524 million rupees for development. The amount was sufficient to complete construction and furnishing of the Annex of the Manmohan Centre to run high quality service. With the help of the ministry and other non-governmental organizations, we have been able to provide free service of almost 20 crore rupees to needy patients. For many years, our pharmacy has the sector in the country in providing affordable medicine to patients. The popularity of our pharmacy has led the institute to make a net profit of 7.33 crores rupees in the last financial year.
Prof. Dr. Uttam Krishna Shrestha Executive Director

8
This year Institute of Medicine has added a new 4-year-course of Perfusion Technology and we have been able to enroll 3 candidates. This course has added new dimension for the first time in the country. Two candidates have been awarded DM in cardiology and are providing high end services in different parts of the country. Prof Dr Bhagawan Koirala has been appointed as Chairman of Nepal Medical Council by the government of Nepal. Manmohan Center family congratulates him on this important appointment and wishes him success in extending the council’s image further. Last year we provided services to 74,000 individuals from our outpatient clinic. Fifteen hundred sixty four of these patients got cath lab services whereas 2288 were provided cardiac, thoracic and vascular surgeries. For benefit of patients we have launched online ticketing for all clients with hassle free services. I would like to take this opportunity to thank each and every member of Manmohan Center whose tireless dedicated work helped us achieve such success. I would also like to thank all others who have been supportive in our endeavor to serve those in need.
Prof Dr Uttam Krishna Shrestha Executive Director

9
Annual report of department of Cardiology: 2076
Introduction Department of Cardiology is one of the departments under the umbrella of Maharajgunj Medical Campus, Institute of Medicine, Tribhuvan University. Previously this department was under department of internal medicine as a cardiac unit. Later on Department of Cardiology was established on 2066/10/21 and was shifted to Manmohan cardiothoracic vascular and transplant center (MCVTC). After establishment of the cardiac department, it is running academic activities of MBBS, MD and DM program. By 2076, 14 DM cardiology students have already passed out. Seventh batch of DM residents passed out this year. Seven of them are working as a faculty in this center, while others are providing quality cardiology services at other centers. Besides these, the department is planning to expand advanced invasive and noninvasive procedures in the years to come. The department is mainly concentrated to develop excellent faculties, to provide best super specialist training, to do excellent research and provide quality service to the patients. Faculties The department is run by three professors - Prof Arun Sayami, Prof S C Jha and Prof Ratna Mani Gajurel. Dr Chadra Mani Poudyal was promoted to Associate professor this year. There are three units in the department of cardiology. With the motto to provide best quality services and training comparable to international level, the department is promoting all the faculties at
Prof. Dr Arun Sayami
Head
Department of Cardiology

10
their individual level. The faculties working in cardiology department are:
Prof Arun Sayami MBBS, MD
Cardiology. Head of Department, Chief Unit III/Unit I
Prof Sunil Chandra Jha MBBS, MD, Chief Unit II
Prof Ratna Mani Gajurel MD, DM Cardiology, fellowship in interventional cardiology (NHC, Singapore), fellowship in paediatrics and grown up congenital heart diseases (Milan/Italy).
Associate Prof Chandra Mani Poudel, MD, DM Cardiology, fellowship in interventional cardiology
Asst Prof Subarna Mani Acharya Asst Prof Hemant Shrestha, MD, DM
Cardiology Asst Prof Surya Devkota , MD, DM
cardiology Asst Prof Sanjeev Thapa ,MD, DM
cardiology Asst Prof Raja Ram Khanal ,MD, DM
cardiology Asst Prof Smriti Shakya,MD, DM
cardiology
Services Service provided to the people by the department is increasing each year. The number of patients visiting in OPD, emergency department and in patients has significantly increased this year. Since we have multiple specialties within the premises of teaching hospital, patients from different parts of Nepal as well as other national cardiac center are being referred to our center. There are now total 79 beds functioning in the hospital including 15 CCU beds and a new CATH LAB has been installed last year. Besides, we are planning to extend
our services in our new six-storied building in near future.
MCVTC is providing advance cardiac services to the people. Coronary angiography and percutaneous coronary interventions were started from 2069 Shrawan. We are also doing ASD device closure, PTMC, CRT and PVBD. We have started using FFR this year. IVUS and rota ablation will be started in this coming year in our cath lab and will provide newer services to the people. Our hospital is getting popular day by day. This may be the evidence that our hospital was chosen by the honorable Prime Minister K.P. Sharma Oli for his treatment. He was admitted in our center several times and was discharged in good health. It was a proud moment for the treating team and the MCVTC family. Services provided by the cardiology department in the year 2076: Non Invasive lab in numbers Echocardiogram (TTE/TEE) 13794/84
Dobutamine stress echo 29
Tread Mill Test (TMT) 884
Holter 677
ABP 433
INVASIVE Procedures in numbers
Coronary angiography 916
Coronary angioplasty (Elective/Primary) 391/137
Permanent Pacemaker implantation 77
Temporary Pacemaker implantation 29
Pulse generator replacement 5
Right and left heart catheterization 35
Pericardiocentesis 23
PTMC 57
ASD device closure 24

11
What do we do?
We provide the region’s most comprehensive cardiovascular evaluation and consultation along with a full suite of state of art cardiac testing. We evaluate and treat heart problems such as coronary artery disease, high blood pressure, high cholesterol and heart valve problems. We are one of the few comprehensive pulmonary hypertension treatment and evaluation centers in the country. We also specialize in the evaluation of preventive cardiology, exercise physiology and nutrition to improve and reduce cardiovascular risk.
Academic Activities
The department is very concerned regarding teaching and learning activities not only for the students and residents but also for the faculties. Faculties are involved in teaching and learning activities of the followings: DM Cardiology Residents MD (Internal Medicine) Residents MD (Internal Medicine) Residents
from TU affiliated medical colleges MDGP Residents DM Critical care residents MBBS students BAMS students B Sc Pharmacy students House officers Training of ICU/CCU staffs
Following is the academic activities of the department:
Every Sunday : Journal/Topic presentation by MD Residents
Every Tuesday : Topic/Journal presentation by 2nd/1st year DM Residents
Every Thursday : Case Presentation by 3rd year DM Residents
First Wednesday of the month : Faculty presentation
Second Wednesday of every month : Mortality presentation by 1st year DM Residents
Presentations by invited foreign specialist and academicians
Theory class of MBBS Program : Faculties/DM Residents
Bedside Clinical teaching for MBBS : Faculties
DM Program
DM Cardiology Program was started from 2067 Ashwin. Earlier there used to be two DM residents enrolled per year but now three DM Residents are enrolled each year. With the aim of advanced exposure in cardiology, DM residents are sent to MEDANTA, India for cardiology training for 1 months. Another achievement this year was our seventh batch of DM residents successfully passed out this year. They are:
Dr Avisesh Shakya Dr Ravi Sahi
DM Residents:
Dr Parash Koirala 3rd year Dr Shovit Thapa 3rd year Dr Surya Pathak 3rd year Dr Manju Sharma 2nd year Dr Suman Adhikari 2nd year Dr Vijay Yadav 2nd year
Research Research is also the core of department’s attention. Promotion of this field is also department’s main concern. Every DM resident is involved in at least three research activities during the residency period. The number of research activities is increasing in the department of cardiology.

12
Our Center is a part of an ongoing trial INVICTUS, a trial of Rivaroxaban in Rheumatic Mitral stenosis with Atrial fibrillation. Publications Total of 5 articles has been published in the year 2076 among which 3 were published in the national journals and 2 in the international journal. The articles that were published are as follows:
1. Study of etiological profile, clinical profile and short term outcome of patients presenting with pericardial effusion in a tertiary care center, Nepal: World journal of cardiovascular disease: Raja Ram Khanal, Ratna Mani Gajurel, Ravi Sahi, Hemant Shrestha, Chandra Mani Poudel, Surya Devkota, Sanjeev Thapa, Smriti Shakya.
2. Clinical characteristics, risk factor and
angiographic profile of acuter coronary syndrome patients in a tertiary care centre of Nepal: Nepalese Heart Journal(NHJ): Abhishesh Shakya, Sunil Chandra Jha, Ratna Mani Gajurel, Chandra Mani Poudel, Ravi Sahi, Hemant Shrestha, Surya Devkota, Sanjeev Thapa
3. Study of clinical profile and indications of Permanent Pacemaker Insertion in Nepali population presenting to tertiary care centre in Nepal: Nepalese Heart Journal(NHJ): Shovit Thapa, Ratna Mani Gajurel, Chandra Mani Poudel, Hemant Shrestha, Sanjeev Thapa, Surya Devkota, Parash Koirala, Surya Pathak
4. Study of clinical profile and outcomes
of Percutaneous Coronary Intervention in ST Elevation Myocardial Infraction: Nepalese Heart
Journal(NHJ): Parash Koirala, Ratna Mani Gajurel, Chandra Mani Poudel, Hemant Shrestha, Surya Devkota, Sanjeev Thapa, Shovit Thapa, Surya Pathak
5. Case report: Atrial myxoma with cerebellar signs. BMC: Dr. Chandra Mani Poudel
Rewards and achievements Dr. Ratna mani Gajurel was invited as a faculty for “SINGAPORE LIVE 2020, and presented “Nightmare in cath lab: management of dislodged stent” from 16th to 17th January 2020”. His Paper ”Comparison of conventional transradial access Vs distal trans radial access in the anatomical snuffbox for coronary angiography and angioplasty” was awarded best of the best scientific paper among 380 abstracts accepted at SCAI 2019( The Society of cardiovascular angiography and interventions) Los Vegas. He was there to present this as a poster presentation. He also joined as a faculty and presented on “Cardiology services in Nepal” in SIMONCN held on March 2020 at Birgunj and moderated different sessions as well as evaluated free papers. He was also the chairman of scientific committee for XVII International Congress of Management of Cardiovascular Disease held on November 2019. Dr Ratna Mani Gajurel got promoted to Professor of Internal Medicine (Cardiology) this year. Besides, Prof Gajurel has been nominated for The Jana Sewa Shree award by the President of Nepal on last Constitution day for his untiring effort and contribution in the field on Cardiology in Nepal.

13
Dr. Chandra Mani Poudel presented on “Pharmacoinvasive therapy in STEMI” on Cardiovascular conference held on December 2019 at Dhaka, Bangladesh. He also presented on “ Management of Acute coronary syndrome” at ANEMECON at Pokhara on February 2020 and “Management of Late STEMI” on 1st Symposium on the management of ST Elevation Myocardial Infarction in Nepal by Cardiac society of Nepal held on March 2020. Dr. Poudel, was also promoted to Associate Professor of Cardiology this year. Dr. Paras Koirala, 3rd yr DM Resident stood first place in “Torrent Young Scholar Award” among the DM cardiology residents of Nepal held on March 2020. We are truly fortunate to have such incredibly gifted and dedicated doctors working in our midst, walking our hallways and representing us throughout the country and across the globe. This is a prestigious achievement. International conference attended
a. Dr. Chandra Mani Poudel and Dr. Surya Devkota attended a conference “Asia AICT PCR” held on July 2019 at Singapore.
b. Dr. Ratna Mani Gajurel, Dr. Hemant Shreshta and Dr. Surya Devkota attended an ESC (European Society of cardiology) conference held on Aug 2019 at Paris.
c. Dr. Sanjeev Thapa and Dr. Raja Ram Khanal attended conference on “Perspectives in Cardiology 2019” conducted by Emirates Cardiac Society at Abu Dhabi on September 2019.
Training
Dr. Sanjeev Thapa underwent one month Interventional Cardiology training at Fuwai Yunnan
Cardiovascular Hospital at Kunming, China from 26th December 2019 to 23rd January 2020.
Camps: As every year, this year also cardiology camp was held at different places inside and outside the valley mainly at Dhankuta, Pokhara, Gorkha and Nala. Faculties and residents from the department of cardiology also participated in the same. Future Plan: Cardiology is ever evolving subject. Newer development and advances in cardiology are ongoing every day. The department is trying its best to deliver the new and advanced services to the general population. To overcome the new and upcoming challenges, the department is planning to extend the quality services
Long Term
In the long run, considering the need of society and technical advancement, following fields will be established one after another: Cardiac CT Electrophysiology and catheter ablation Hybrid Cath lab Nuclear cardiac imaging Optical coherence tomography (OCT) TAVR(Trans catheter aortic valve
replacement) Ventricular assist device and cardiac
transplant Research regarding prevalence of
hypertension/CAD/RHD in Nepal.
Challenges and Change Management With respect to advances in cardiovascular care and treatment technology, most of

14
today’s conversations center on how they impact and improve patient care, treatment costs and outcomes. Patients after all stand at the center of everything we do in healthcare. Many technological solutions are emerging to help cardiac care providers to help their way through a health care environment that is increasingly competitive and challenging. One of the main objectives of the department is to provide excellent services and maximum level of care to the general population. The cost of different devices used are very high such that most of the common people cannot afford it. Though the government is trying to help such group, it is not sufficient. Lack of fund for research is another challenging issue. The key lies in effective change management with respect to both people and technology. With respect to the goal of creating a single and easily accessible patient record that includes data and image, there is no shortage of technology in today’s world but the challenge is to separate the truly valuable and necessary tools.
Conclusion The department of cardiology within its ten years of establishment is able to provide one of the best levels of services to increasing number of patients. It is providing one of the best and up to date academic activities to students and residents. Seven batches of DM residents have successfully passed out and are giving specialist cardiology services both inside and outside the valley. Our further plan is to produce more specialized manpower to serve different parts of Nepal. Still a lot has to be done in the field of research. The department of cardiology is guided by very active and dedicated faculty members and hardworking DM Residents and is trying to provide the best level of care in the country and excellent level of cardiology training in Asia. The cardiovascular community needs to better manage several components that play a role in transition of care scenario. Besides focusing on physicians practice it is important to focus on other parties like insurance to be involved on patients care. The partnership with physician executives and insurance companies will be important when designing more efficient programs for patients, physicians and hospitals.

15

16
Annual report of department of CTVS: 2076
As I compose this, the 10th Annual Report of the Department of Cardio-Thoracic Vascular Surgery, I cannot help marvel at how the department and the hospital has grown in the last eleven years since its establishment. It gives me a sense of satisfaction and that of collective accomplishment to see how we have developed and diversified our services in the fields of Cardiac, Thoracic and Vascular surgery. As we strengthen in numbers and capability, I can say with pride that we have proven in more than one occasion in the past year to be one of the premier services of our kind in the whole country. In the past year, Dr. Ranjan Sapkota and Dr. Anil Bhattarai have been promoted to Associate Professor. On behalf of the department I would like to take the lead in congratulating them both for their hard earned and well deserved advancements. I am of the opinion that it has added significantly to the department’s strengths and will be crucial in diversification, responsibility dispersal and succession planning in the department. With the ever-evolving nature of the science of medicine, it is imperative that we continue to learn and apply new techniques and technologies in the service of our patients. I am very happy to announce that in the last year we have been able to induct several such initiatives. The Endobronchial Ultrasound and Transbronchial aspiration services was initiated to improve lung cancer staging and also aid the diagnosis of mediastinal lymphadenopathy via
Prof. Dr Bhagawan Koirala
Head
Department of CTVS

17
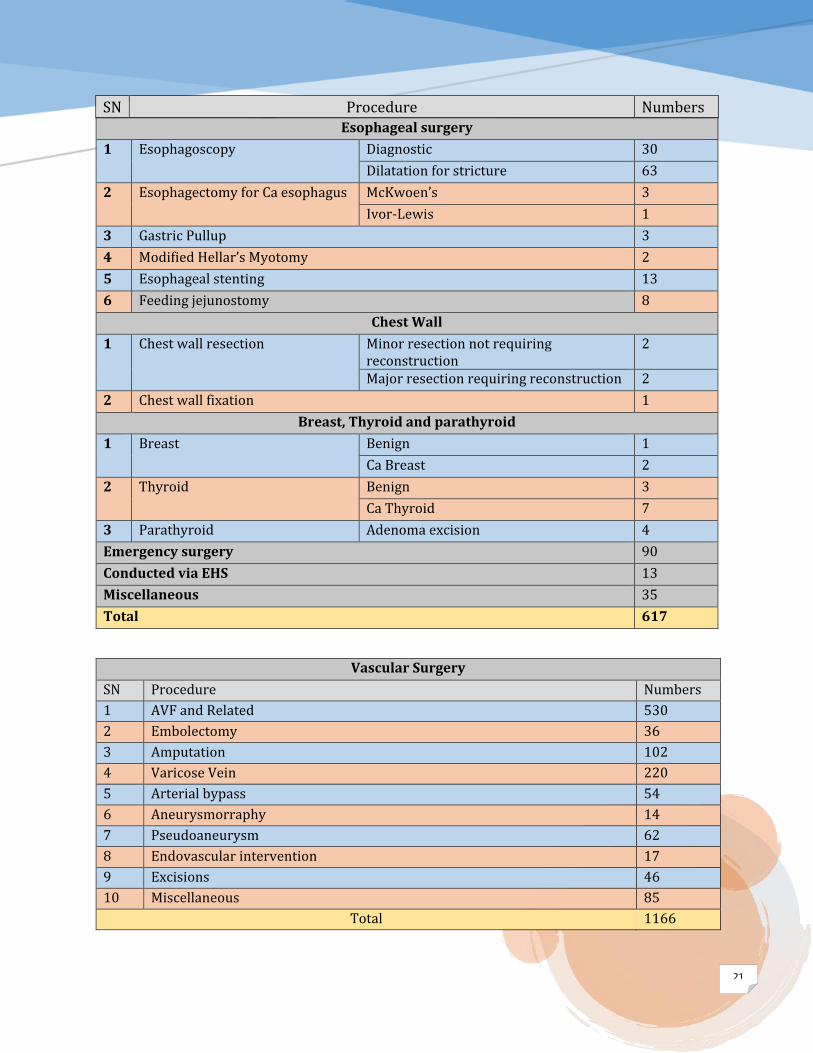
minimally invasive technology. In the space of 8 months, 16 such procedures have been completed. Dr. Diego Gonzalez-Rivas, a renowned proponent of the uniportal VATS technique was instrumental in the initiation of this procedure in the centre. This is a testament to the international collaboration conducted via the department. The case load of the department has only continually increased in the past years and the year past was no exception. In 2076, we conducted 502 Cardiac, 617 Thoracic and 1166 vascular procedures. This represents a 28.8% rise on the numbers of 2075 (2285 Vs 1773). However, it has not been only the numbers but also the repertoire of our operative loads that has increased. Two hundred and forty-seven of these cases were done on an emergency basis. A hundred and twenty-four patients accessed surgery via the extended hospital service. A summary of our workload in the three units of the department is presented in table 1. As in the past, the department has been active in conducting outreach programs in the form of health camps in various parts of the country. We have in the past year extended our services to patients from different remote regions and underprivileged communities. I am also happy to note that our surgeons have also been involved in conducting workshops in MCVTC and in different institutes around the country. Academic activities have always been an important aspect of the day to day running of the department. In the past year, there has been significant output in term of research papers, conference presentations, teaching –learning activities etc. from our faculty. Listed below are some notable additions.
1) Cardiac Surgery unit: I, myself coauthored several scientific
papers in the past year
Relationship between Serum Total Testosterone and Coronary Artery Disease in Men.
Mean dietary salt intake in Nepal: A population survey with 24-hour urine collections
Designing and implementing an integrated non-communicable disease primary care intervention in rural Nepal
Dr Anil Bhattarai: Participated in minimally invasive
cardiac surgery work shop in Apollo hospital Bengaluru India, 12-13 August 2019
Presented a paper " hundred plus minimally access cardiac surgery: troubleshooting" in 4th annual meeting of society of minimally invasive cardiovascular and thoracic surgeons of India (SMICTSI), Mumbai, India, 12-15 Sept. 2019
Panelist in XVII international congress on management of cardiovascular disease, organized by Cardiac society of Nepal, Kathmandu, Nepal, 21-23 Nov 2019
Participated in Heart Transplantation workshop in M. S. Ramaiah Institute Bengaluru, India, 18-19 January 2020
Dr. Ravi Baral
Houston aortic symposium March 2019

18
Indian association of cardio thoracic surgery - Ahmedabad India February 2020
Workshop of Ozaki aortic valve repair procedure - AAIMS, New Delhi- March 2020
2) Thoracic Surgery unit
Sapkota R, Thapa B, Sayami P.
Esophageal 'pyocele': thoracoscopic management. J Surg Case Rep. 2019 Sep 27; 2019(9):rjz250. doi: 10.1093/jscr/rjz250. eCollection 2019 Sep.
Dr. Bibhusal Thapa Invited speaker at National
Conference of Society of Surgeons of Nepal and presented on “Thoracic Surgery at MCVTC – Challenges and Future Avenues” in November 2019
Invited speaker at conference of the SAARC federation of Oncologists and spoke on “Lung Cancer: A Surgeon’s Perspective” in December 2019
Organised through the Thoracic Society of Nepal with active participation of Dr. Bibhusal Thapa and Dr. Ranjan Sapkota: CME on “Management of Tracheo-
esophageal fistula” on 18th November 2019 featuring prominent national and international speakers including Prof. John D Mitchell.
CME on “Lung cancer management in Nepal” on 1st December 2019 featuring prominent national and
international speakers including Dr. Diego Gonzalez – Rivas.
3) Vascular Surgery unit Shrestha KR. Early post-operative
outcome and complications of Arterio-venous fistu;la creation under regional anaesthaesia. Journal of Institute of medicine. 41(3), 39-43,2019
Shrestha KR, Gurung D, Shrestha UK. Brachio-basilic fistula at Manmohan Centre: A retrospective review. 41(1), 31-37,2019
Conducted through the Vascular Society of Nepal: 8th Vascular Surgery workshop
16th March 2019, Dhulikhel 9th Vascular Surgery workshop in
Lumbini Organised International Vascular
Surgery Conference of the Vascular Society of Nepal in Dhulikhel
Prof. Uttam Krishna Shrestha Attended 4th EVL in New Delhi –
Feb 13-15
Dr. Kajan Shrestha Attended Asian society of vascular
surgery conference in Bali. Attended a Vascutek meeting and
Terumo factory visit, Glasgow 2nd to 16th November
Attended 4th EVL in New Delhi – Feb 13-15
Our Mch residents have also had the opportunity to participate and present and participate in national and international conferences as detailed below:
a) Dr. Nikesh Bhandari (Mch-3rd year)

19
Attended the first International Vascular Surgery Conference of the Vascular Society of Nepal and presented papers titled Comparative observational
study of chronic venous insufficiency treatment: open Vs RFA Vs EVLA at MCVTC
Extra cranial Carotid artery pseudoaneurysm: MCVTC experience
b) Dr. Krishna Bashyal (Mch 2nd year) Attended conference of American
college of Cardiology Attended workshop on basic
surgical skills in Vascular surgery Attended the first International
Vascular Surgery Conference of the Vascular Society of Nepal and presented a paper titled “Carotid body tumours- retrospective review at a Tertiary level university hospital”
c) Dr. Prasiddha Kandel Attended the first International
Vascular Surgery Conference of the Vascular Society of Nepal and presented a paper titled “ Hybrid
TEVAR, a novel approach to thoracic aortic aneurysm”
The last year has been no doubt a year of significant challenges. Not the least by the onset of and continued worry imposed by the COVID-19 pandemic that has swept the world. It has forced us to change how we live and work. Also, it has forced a review of our healthcare priorities and goals; to rethink and re-structure our working environments. It is not hidden to anyone that these changes have been hard to come to terms with. However, as head, I am proud of how our department has contributed in the hospital’s effort to be prepared for this pandemic. As we look ahead towards the coming year, we hope we will have these difficult times behind us very soon. We look forward to exciting new developments within the hospital and the department. The construction of two brand new theatres including a hybrid theatre facility at the annex building will significantly enhance our ability to provide world-class service to our patients. Advent of new technologies like endobronchial laser in the department will hopefully be another highlight of the coming year.
Table 1: List of procedures done in the department in 2076
SN Type of Operation Number of procedures done
Cardiac Surgery
1 Coronary Surgery 105
2 Valve Surgery 153
3 Congenital 144
4 Aortic 13
5 Miscellaneous 87
Total 502

20
Thoracic Surgery
Lung Procedures
SN Procedure Numbers
1 Flexible Bronchoscopy 65
2 Rigid Bronchoscopy 9
3 VATS bullectomy 29
4 Pulmonary resections
Pneumonectomy Post-Tb 4
Lung Cancer 2
Lobectomy Bronchiectasis/aspergilloma 54
Lung Cancer 11
Segmentectomy Aspergilloma 6
Lung Cancer 1
5 Hydatid Cyst Enucleation 17
Mediastinum
1 Mediastinoscopy 8
2 EBUS 16
3 Mediastinal mass excision (other than thymus)
Excision via sternotomy/thoracotomy 4
Via VATS 11
4 Thymectomy
Myasthenia only 2
Thymoma 6
Thymomatous myasthenia 7
Diaphragm
1 Congenital diaphragmatic hernia 2
2 Ruptured diaphragm repair 4
Pleura
1 Pleural biopsy 14
2 Deloculation/decortication Via VATS 51
Via thoracotomy 10
Trachea and bronchi (airway)
1 Tracheal resection and anastomosis
Post-intubation stenosis 2
Tracheal tumour 1
2 Tracheo-esophageal fistula Tracheal stent 2
3 Tracheal T-tube placement 2
21
SN Procedure Numbers Esophageal surgery
1 Esophagoscopy Diagnostic 30
Dilatation for stricture 63
2 Esophagectomy for Ca esophagus McKwoen’s 3
Ivor-Lewis 1
3 Gastric Pullup 3
4 Modified Hellar’s Myotomy 2
5 Esophageal stenting 13
6 Feeding jejunostomy 8
Chest Wall
1 Chest wall resection Minor resection not requiring reconstruction
2
Major resection requiring reconstruction 2
2 Chest wall fixation 1
Breast, Thyroid and parathyroid
1 Breast Benign 1
Ca Breast 2
2 Thyroid Benign 3
Ca Thyroid 7
3 Parathyroid Adenoma excision 4
Emergency surgery 90
Conducted via EHS 13
Miscellaneous 35
Total 617
Vascular Surgery
SN Procedure Numbers
1 AVF and Related 530
2 Embolectomy 36
3 Amputation 102
4 Varicose Vein 220
5 Arterial bypass 54
6 Aneurysmorraphy 14
7 Pseudoaneurysm 62
8 Endovascular intervention 17
9 Excisions 46
10 Miscellaneous 85
Total 1166

22

23
Annual report of department of CTVA: 2076
Department of Cardiothoracic and Vascular Anesthesiology (CTVA) was upgraded from Cardiothoracic and Vascular Anesthesia unit and was established on 20th Asar 2074 (4th July 2017). Cardiothoracic and Vascular anesthesia Unit was established on 26th Falgun 2068 (9th March 2012) and consistently provided specialized anesthesia services for patients with cardiac, thoracic and vascular problems in and out of operation theater. CTVA department has following faculties as team members
1. Professor Dr Bishwas Pradhan Professor, Head of the Department
2. Dr Madindra Basnet Assistant Professor
3. Dr Bibhush Shrestha Assistant Professor
4. Dr Shailendra Sigdel Assistant Professor
5. Dr Priska Bastola Assistant Professor
6. Dr Arjun Gurung Assistant Professor
Dr Dipesh Man Singh joined the department as Senior Resident. While Dr Bidur Dhungel, Dr Pramee Bajracharya and Dr Tenzing Lobsel worked as part time consultants. The department has 2 to 3 anesthesiology residents posted from Maharajgunj Medical campus as well as from other affiliated colleges of Tribhuvan University and Kathmandu University for cardiothoracic and vascular anesthesia training. Six
Prof. Dr Bishwas Pradhan
Head
Department of CTVA

24
Medical officers are also allocated to the department.
Current Residents: 1. Dr. Sajina Silwal (MMC) 2. Dr. Sachana KC Sharma (Lumbini
medical college, Palpa)
Medical officers:
1. Dr Himanshu Karna 2. Dr Rashmi Tamang 3. Dr Binam Raj Sharma 4. Dr Samana Gairhe 5. Dr Sneh Rana 6. Dr Shriya Shrestha
Total number of residents and medical officers trained in the year 2076 were 35 (21 residents and 14 medical officers). The following services are being provided by the department.
1. Providing regular consultation for pre anesthetic evaluation.
2. Conducting anesthesia services for a. Cardiac surgeries b. Thoracic surgeries c. Vascular surgeries d. Other high risk surgeries
3. Providing anesthesia service outside Operation Theater in Cardiac Catheterisation-lab.
4. Providing 24hour critical care services in Intensive Care Units
5. Providing critical care specialized services in CCU.
6. Providing resuscitation and post resuscitation care in ICUs and CCU.
7. Conducting academic activities for DM critical care residents, post graduate MD Anesthesiology residents and bachelor level medical students of Maharajgunj Medical Campus (MMC),
Institute of Medicine (IOM), Tribhuvan University (TU)
8. Providing cardio-pulmonary resuscitation (CPR) training for residents, medical officers, nursing staffs and other non-medical staffs.
9. Conducting teaching/learning activities of cardiothoracic and vascular anesthesia for anesthesiology residents of Maharajgunj Medical College, IOM as well as other medical colleges affiliated with Tribhuvan University and Kathmandu University.
10. Representing Department of CTVA in various seminars, workshops and conferences.
State of Art technologies used by the department for management of patients are:
Anesthesia work station with facilities of Sevoflurane vaporizer
Bispectral Index Score (BIS) Monitoring
Transesophageal Echocardiography
Continuous Cardiac Output monitoring
Intra-aortic Balloon Pump ECMO (Extra Corporeal Membrane
Oxygenation) Continuous Renal Replacement
Therapy (CRRT) Thromboelastography (TEG) Ultrasound guided vascular access
and regional blocks Cerebral oximetry/ NIRS CONOX Autologous Blood Transfusion
system

25
A brief statistics of the functioning of the department in the 12 months of 2076 BS is presented below
Total Number of cases: 1625 surgeries + 69 Cath. lab cases

26
Procedures
Central venous lines: 707
Arterial lines: 744
Double Lumen Tubes: 153
Epidural Catheter : 34
Future plans The department aims to achieve excellence in clinical, academic and research activities. The main aim of the department is to provide evidence based high standard per-operative and postoperative care to the most complicated cardiothoracic and vascular surgeries. Some of the short and long term goals of the department are
To provide anaesthesia services to advanced services like hybrid surgeries, robotic surgeries, lung/heart transplants in future
To increase the number of faculties to operate at full clinical and academic potential.
To train and facilitate faculties for super specialization in cardiothoracic vascular anesthesia and critical care.
To establish this department as centre of excellence and academic focal point for postgraduate training center in cardiothoracic vascular anaesthesia and critical care of MMC, IOM, TU
To develop and maintain bilateral relations with international institutes for expertise and knowledge sharing
Department of CTVA is thankful to the administration of MCVTC for its support, and expects a constructive approach and unconditional support in future for
expansion of clinical services, academic activities and research.
Academic participations:
1. Professor Dr. Bishwas Pradhan (HOD)
Conferences: a. Faculty/Organizing Committee
Member, 1st International Transplant Conference, 20, 21 April 2020, Kathmandu, Nepal
b. Participant, Best of American College of Cardiology (ACC) Cardiovascular Medicine, 7 May 2020, Kathmandu, Nepal
c. Faculty/Speaker – “Perioperative myocardial protection”; 52nd Annual conference of Indian Society of Anaesthesiologists (ISA), Gujarat state branch and 15th annual conference of ISA, West Zone, India,11, 12, 13 October 2019
d. Faculty/Speaker– “Anesthesiology clinical researches in Nepal – “39th Annual Meeting of the Japanese Society for Clinical Anesthesia (JSCA 2019) Karuizawa, Japan, 7, 9 November 2019.
e. Faculty- 23rd National Conference of the Indian Association of Cardiovascular and Thoracic Anaesthesiologists (IACTACON) 7 - 9 February 2020, Goa, India
f. Instructor/Coordinator– Advanced Cardiac Life Support Training, 26, 27 September 2019, Maharajgunj Medical Campus,

27
Institute of Medicine, Kathmandu, Nepal
g. Coordinator/Instructor– Multiple Basic Life Support Trainings in Community, Nepal
Publications/Research: a. Comparison of Sevoflurane and
Isoflurane for Myocardial Protection during Coronary Artery Bypass Surgery in a Tertiary Care Center in Nepal. Priska Bastola, Bishwas Pradhan, Madindra Basnet. Journal of Institute of Medicine 2019 A prospective observational study. Sigdel Shailendra; Ozaki Akihiko; Basnet Madindra; Kobashi Yurie; Pradhan Bishwas; Higuchi Asaka; Uprety Anup, Medicine, February 2020, 99(9) : e19302
b. Ongoing research – Analgesia in
VATS surgery: The role of continuous extrapleural analgesia for postoperative pain control.
c. Ongoing research - “Attenuating effects of lignocaine on hemodynamic response to laryngoscopy and intubation with etomidate induction for CABG surgery”
2. Assistant Prof. Dr Madindra Basnet a. Comparison of Sevoflurane and
Isoflurane for Myocardial Protection during Coronary Artery Bypass Surgery in a Tertiary Care Center in Nepal. Priska Bastola, Bishwas Pradhan,
Madindra Basnet. Journal of Institute of Medicine 2019
b. Anxiety evaluation in Nepalese adult patients awaiting cardiac surgery:A prospective observational study. Sigdel Shailendra; Ozaki Akihiko; Basnet Madindra; Kobashi Yurie; Pradhan Bishwas; Higuchi Asaka; Uprety Anup, Medicine, February 2020, 99(9) : e19302.
c. Ongoing research - “Attenuating effects of lignocaine on hemodynamic response to laryngoscopy and intubation with etomidate induction for CABG surgery”
3. Assistant Prof. Dr. Bibhush Shrestha a. Attended 23rd National
Conference of the Indian Association of Cardiovascular and Thoracic Anaesthesiologists (IACTACON) 7 - 9 February, 2020, Goa, India
4. Assistant Prof. Dr Shailendra Sigdel
Conferences
a. Attended 13th SAARC- AA held in Lahore, Pakistan as a World Federation of Society of Anesthesiologists (WFSA) Scholar.
Research
a. Anxiety evaluation in Nepalese adult patients awaiting cardiac surgery: prospective observational study. Sigdel Shailendra; Ozaki Akihiko;

28
Basnet Madindra; Kobashi Yurie; Pradhan Bishwas; Higuchi Asaka; Uprety Anup, Medicine, February 2020, 99(9) : e19302.
b. Effect of low dose bupivacaine
and fentanyl during elective cesarean section under spinal anesthesia. Journal of Anesthesia and Clinical research, 2019
5. Assistant Prof. Dr Priska Bastola
Conferences
a. Speaker - CURRENT, Institute of Medicine, Maharajgunj, Kathmandu, on 'Practicing Enhanced recovery ERAS in cardiac surgery: Anaesthetists Role', 14th Dec, 2019.
b. Speaker - CEEA Refresher course
at Kathmandu medical college and teaching hospital, Kathmandu,
Nepal on' Anaesthesia for Transplanted Patients' on 21st Dec 201 9
Research Comparison of Sevoflurane and Isoflurane for Myocardial Protection during Coronary Artery Bypass Surgery in a Tertiary Care Center in Nepal. Priska Bastola, Bishwas Pradhan, Madindra Basnet. Journal of Institute of Medicine 2019
a. Ongoing research – Analgesia in VATS surgery: The role of continuous extrapleural analgesia for postoperative pain control.
6. Assistant Prof. Dr Arjun Gurung
a. Attended PGA73 Postgraduate Assembly in Anesthesiology held in New York , USA from December 13-17 as an International Scholar

29
MCVTC – A financial review of 2076
Completing 11th year of excellence in
service is actually a proud moment. This
is a milestone the center has achieved.
However, looking back, form the point of
financial management, the last year
presented to us series of struggles.
The Center is now established as one of
the best tertiary care center of the nation
within this decade. In some specialties it
is the only centre providing the services
in the whole nation. Undoubtedly, some
of the credit for the recognition the
hospital has garnered, the quality and
variety of services we have been able to
provide and the skills and amenities we
have accumulated has to go to the
effective financial management at the
centre. This despite having to cope with
these harsh times.
The financial management has always
been tough for this institution. Actually,
we have had the long standing problem
of inadequate permanent human
resource since our inception. This means
that we have to rely largely on temporary
contract staff which drains a large
portion of our internal revenue. At the
same time, we have to keep pace with the
recent advancement of patient care and
treatment that also needs huge resources.
We at The Manmohan Center believe
that fiscal discipline and transparency
are the means to overcome the challenges
Tanka Prasad Dhungana
Chief,
Account section

30
of financial management. So, prioritizing
the needs without interrupting the pace
of service and quality is what we are
following here. Being a public nonprofit
institution, we just cannot rely solely on
the internal revenue generation.
Therefore, we require a regular
government budget. The budgetary
sources of the Center, as usual, are: a) the
revenue we generate, b) annual budget
from our mother institution TU, and c)
budget allocated from Ministry of Health
and Population (MOHP), Government of
Nepal. It is not easy to be in the priority
list of ministry because of their own
limitations. However, they have
extended a continuous support
throughout the years. We are grateful to
the Ministry of Health for their support.
The Annex building is the result of the
trust the Ministry of Health has shown to
us. Budget form TU is basically the
remuneration of permanent staff only.
The revenue we generate is basically
used for salary, unexpected huge repair
and maintenance cost, purchase of
essential medical logistics, and other day
to day running costs.
Running cost constitutes a major portion
of our total expenditure. Arrangement of
medical utilities, lab reagents and
consumables require a huge sum.
Transportation cost, electricity and
communication cost are some other
elements of expenditure. Despite our
constant effort to minimize operation
cost, it requires a significant sum of our
annual budget.
Following is the budgetary status of the
last five years.
5 YEARS INCOME & EXPENDITURE OF MCVTC 2072/073 2073/074 2074/075 2075/076
2076/077 (up to 10 months)
EXPENSES
Capital Expenditure
96,063,996.07
80,150,207.00
131,607,558.76
196,179,407.00 78,200,723.00
General Expenditure
197,138,529.45
266,734,939.96
291,701,182.16
318,775,227.00 284,181,619.00
INCOME
MOHP 60,000,000.00
90,000,000.00
255,000,000.00
334,000,000.00 501,060,000.00
TU/Revenue
115,762,832.42
173,435,628.24
233,407,807.49
259,702,015.00 197,629,304.00
Covid -19 has caused huge disruptions
around the world. We have not remained
untroubled. Because of COVID -19 we
have lost around NRS 65.00 million in
this fiscal year. The major challenge we
are going to face in this and coming
Fiscal Year is to manage budget for the
service extension in the Annex building.
The estimated sum required for the full-
fledged service extension is NRS 324

31
million in next fiscal year. We hope to get
a major portion from Ministry of Health
in the coming Fiscal Year.
We have maintained the legacy of
financial discipline since its inception.
We have cleared audit on regular
interval of fiscal year. Financial audit for
the F.Y.2075/076 has been completed we
presently await the audit report.
Overcoming problems and challenges,
Manmohan Center is continuously
serving the nation since its inception and
will certainly serve in the days ahead.
With co-operation of Tribhuvan
University, Nepal government and
everyone involved in the centre,
Manmohan Center will definitely
perform better in the years ahead to
serve the nation.

32
Annual report of Nursing Administration: 2076
Manmohan center is one of the highly respected places that specializes in tertiary care for cardiac thoracic & vascular patients. The center is located within the Tribhuvan University Teaching hospital complex and has played a massive role in cardiothoracic and vascular study. There are currently 161 nurses being employed who’ve been working day and night around the clock to provide quality service to the public. All of our team from junior to senior level are responsible, qualified and have equal sense of duty towards their profession. Likewise, we deploy nursing officer morning and evening every day to ensure active supervision and increase & improve the quality care. Along with the services we’ve provided with the help of above-mentioned colleagues, we’ve also been equally active in health camps and community service. We’ve conducted various training programs for quality service in the field of cardiac, thoracic and vascular care. We are proud to be a part of the International Congress on Management of Cardiovascular Disease which was held on November 21st to 23rd, which was a grand success and a step forward towards knowledge sharing in management of cardiovascular disease. Similarly, On November 14th 2019, we were able to organize a Nursing Conference based on Improving Perioperative Quality with the help of Jayanti Trust. The event was a grand success and focused on quality care as a primary topic, where we got the
Bindeshwori Gurung
Chief
Nursing Administration

33
chance to get insights on Medical team which was based on the US. We are proud to announce that we’ll be opening a new annex building this year which will have 41 beds, hybrid modular OT, modular OT 1, ICU, Suit cabin and so on. We would also like to mention our no-
stop procedures during lockdown that includes around the clock 12 hours duty shift without any hindrance to the patients even during these difficult circumstances. There will be no decrease in the quality of our care and we will be working hard to make sure it happens.
Our existing nursing team comprises of Total Nurses being employed 161 Staff Nurses 151 Nursing officers 7 Deputy Nursing controller 1 Nursing administrator 1 Nursing Administration Chief 1 Excluding 11 nursing staff who’re currently in study leave for higher nursing education. Nursing department honorable mentions Nursing Administration Chief Bindeswori Gurung Nursing Administrator Jamuna Shyami Tamrakar (CPD unit coordinator) Deputy Nursing Controller Bimala Neupane (Incharge of General ward D &
supervisor of Cardiology department) Nursing Officer Til Kumari Basnet Khatri (Cath-lab Incharge) Nursing Officer Pramila Shakya (OPD/NICL incharge) Nursing Officer Durga Thapaliya Dhungana (OT incharge) Nursing Officer Purnalaxmi Shrestha (CCU I, II incharge) Nursing Officer Uma Khanal (CTVS, ICU I&II incharge) Nursing Officer Kamala Saki Shrestha (Emergency Incharge) Nursing Officer Sarita Manandhar (General Ward A, B, C Incharge)

34

35
The race against the virus:
The anti-CoViD19 efforts at The Manmohan Centre
Ranjan Sapkota with Bibhush Shrestha, Chandramani Poudel, Bindeshwari Gurung, Sarita Manandhar and Prakash GC
The world today is engaged in a
comprehensive combat against an
invisible army called the SARS-CoV-2
which has proven to be highly contagious
and alarmingly fatal. The public health
systems and health infrastructures around
the world are facing unprecedented
challenges; one of the worst since the last
world war. The healthcare institutions and
the healthcare workers are faced with
having to fight it as front liners;
sandwiched between an unwavering call-
of-duty and ever-evident constraints of
treatment, supplies, plan and
preparedness.
The Manmohan Centre is no exception;
and the hospital is engaged in various
ways and in different stages after the
World Health Organization declared the
CoViD-19 a global pandemic on 11th
March, 2020, and warned Nepal against a
‘high risk’ she faces. Although the first case
was reported on 24th January, it would be
only on 23rd of March that the second case
was reported. The ensuing 2 months, as it
would seem in retrospect, could have been
spent on a war-speed preparation against
the growing threat. But it was only after
March 24th, when the government
declared a nationwide lock-down that the
sensitization and preparations visibly took
off. In keeping with this, The Manmohan
Centre also entered a phase of
Dr Ranjan Sapkota
Associate Professor, CTVS
Dr Bibhush Shrestha
Assistant Professor, CTVA

36
preparation, actions and some historic
decisions.
Public Service
On 23rd March, The hospital launched the
first-ever virtual OPD Platform- The
Manmohan Centre Online OPD wherein
our patients would post their problems
directed to concerned doctors, along with
pictures and past records. The doctors
would respond as soon as possible,
typically within 24 hours. This was
received well in the public, and the effort
was replicated in the neighboring and
other hospitals nationwide. A number of
patients still continue to seek service
through the platform. As Nepal Medical
Council called for a cut-down in elective
surgeries and elective procedures,
massive public education and information
campaign was launched, all the while
making sure the patients already admitted
or in Kathmandu at the time were duly
served. A number of public notices and
flexes were put up to advise patients and
visitors about the precautions, masks,
hand-sanitization and social distancing.
Emergency services were offered as usual,
and a number of cardiac, thoracic and
vascular procedures and operations
continue to be done amidst the lock-down.
Sixteen major (majority thoracic) and 51
minor (majority vascular) operations
were done during lockdown until the 15th
of Vaishakh. During the same period, 34
patients have been ‘seen’ in the Online
OPD, 50 in the hospital outpatients, and
555 in the ER; with a total of 129
admissions. Radiology, Lab, Pharmacy and
in-patient services, including ICU and CCU
have been regular.
Health Care Workers (HCW)
In the framework of the pandemic and
lock-down, everybody potentially
involved in patient care, including not only
doctors and nurses, but also
radiographers, pharmacists, lab
personnel, patient-attendants and even
the security staff and drivers have been
considered ‘HCWs’. With great efforts and
support from the administration,
measures to limit HCW exposure have
been put in place. Regular physical
meetings are replaced by participatory
online meetings twice a day. Inventory
appraisals are put in place. Mandatory
digital attendance is replaced with that on
paper. The staffs were rostered in a
participatory, restrictive and sharing
manner, helping each other limit the
other’s exposure. Regular supply of
surgical masks and hospital attire was
ensured. Clinical Protocols in keeping with
WHO, MoHP and NMC were formulated so
as to suit specific patients and practice at
the Centre; and circulated widely among
staff. Faculties, residents and medical
officers from all the 3 departments have
been participating in the clinical activities
at the Isolation facility at the Ganeshman
Building in the premises. The Centre is
represented in the TUTH CoViD-19
Committee as Advisor, in keeping with the
aim of the ‘whole TUTH premises fighting
as a family’. A protected code blue concept
has been in place. All the staffs have
followed mutual teaching/learning and
have showed a heightened sense of mutual
respect and coordination in this fight
against the common enemy.

37
Thinking different: going noble against
the novel virus
Necessity is the mother of invention, they
say. In a span of mere 3 weeks, a number
of smart moves have been taken.
Hundreds of litres of hand-sanitizers have
been made out of locally available
ingredients as per standard
recommendations. Hundreds of protective
face-shields have been designed and
prepared in the hospital. Locally furnished
protective intubation head-boxes have
been adopted into our practice. A number
of video-laryngoscopes have been devised
in the Centre itself, utilizing locally
available protocol and accessories. An
Ultraviolet Germicidal Irradiation (UVGI)
unit has been designed, validated and put
in practice for limited reprocessing of the
N95 masks, face-shields and the goggles.
As per international recommendations,
the existing Ethylene Oxide (EtO) facility
has been exploited to resterilise the
coverall gowns. A number of water-
resistant coverall gowns designed and
devised in the community, have been
adopted for use.
Supply chain
The inventory appraisal early-on helped
identify the gaps in supply chain. Surgical
masks, N95 masks, protective goggles and
PPEs have been procured from national
and international markets. EtO cartridges
and papers have been stocked for ongoing
use. Drugs and disposables have been
stocked.
The way forward
Preparations to partially ‘open up’
services are under way. But the fight is far
from over. While ensuring the
international and national guidelines and
policies are followed, we also have to start
catering to the needs of a vast number of
‘other’ patients, too. Dealing with the
pandemic-situation and serving the
routine C-T-V patients are two entirely
different, and often contradictory,
domains of care. It is a formidable
challenge for the Centre to be able to strike
a perfect balance between the two: all the
while protecting patients’ health as well
the HCWs’! The situation is still fluid at
best, and the trends still baffling (the
national toll standing at 49 as of this
publication). Understandably, the fight in
the future will demand a disciplined-yet-
dynamic and firm-yet-flexible efforts
based on mutual support, care and service
to humanity.
Together we can, and we WILL!

38
A Novel approach for coronary Angiography and
Angioplasty –Distal Transradial (DTR) Access from the
Anatomical Snuff Box ---A dream come true
Coronary angiogram and interventions are commonly performed via the femoral route. Transradial coronary catheterization is presently the popular & therefore default technique due to less vascular access site complications. Distal transradial (the anatomical snuff box access) has advantages over standard proximal access for patients and operators. Radial artery preservation could be another relevant issue in patients requiring multiple radial artery procedures, future use for coronary bypass surgery and construction of Arterio-Venous fistula in chronic kidney disease.
1. Anatomical Snuff Box
Prof. Dr. Ratna Mani Gajurel
Interventional Cardiologist

39
2. Steps in DTR
3. Hemostasis in DTR after the Procedure
DTR access technique is very new, very much safe, effective, easy, and comfortable and relatively free from major complications for coronary angiography and interventions compared to Conventional Trans-Radial access and femoral access. It merits consideration regarding proper patient selection, preparation, operator’s experiences and equipment for successful transradial catheterization. Till date we have done a total of 400 plus patients’ coronary angiogram or angioplasty through DTR access from July 2018 in our Cath Lab, Department of Cardiology, Manmohan centre. As this is
the very new technique and very sparse data is available on safety and procedural success, our work has been recognized by the international community also. During our initial study period we made an article on our initial experiences and it was accepted and published in World Journal of Cardiovascular Disease. This was the milestone for all of us and also the proud moment for MCVTC also because our initial work was published in International forum in December 2018. Then we continued doing the procedure through same route in suitable patient and made a paper of 320 cases with titled “Comparison of Conventional Transradial Access versus Distal Transradial Access in the

40
Anatomical Snuffbox for Coronary
Angiography and Angioplasty”. This paper was accepted by SCAI (Society of coronary angiography and Intervention) for the conference held on 2019, May 19-22, Las Vegas, Nevada, USA. SCAI is the world’s largest forum for coronary Intervention. The SCAI conference scientific committee 2019 also awarded our paper among the “Best of the Best” scientific paper out of 380 abstract accepted. This was the day our dream
came true, actually we tried to shoot for the moon but happened to land over one of the bright star. This was really a big achievement we received from international community for the work done in our centre. Thanks to my team, the Professors, Faculties, residents, Cath lab nurses, radiographers, hospital administration and other directly and indirectly involved persons to get this breakthrough international achievement of Manmohan centre.

41
COVID-19: A new worldwide challenge
An outbreak of COVID-19 infection that arose in December 2019 in Wuhan, Hubei province of China is deemed to have spread from Huanan Seafood market and has been affecting the lives worldwide as a pandemic like a nightmare. It is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) which is a single positive-stranded, enveloped RNA virus that can infect many animal species and humans. Its manifestation ranges from mild symptoms like sore throat to severe pneumonia like any other corona viruses that had outbreaks in the past such as SARS (severe acute respiratory syndrome) in 2002 and MERS (Middle East respiratory syndrome) in 2012. SARS and MERS had significantly higher case fatality rates than COVID-19 however unlike them; COVID-19 is highly transmissible through airborne droplets that spread more easily among people leading to larger case numbers.
Dr. Smriti Shakya
Clinical Lecturer, Cardiology

42
COVID-19 is well known for its cardinal symptoms of fever, cough and shortness of breath however the clinical factors that lead to fatality are older age, underlying medical conditions including diabetes mellitus, cardiovascular diseases like Coronary Artery Disease (CAD), hypertension and immunocompromised conditions. Apart from its primary effect on the respiratory system, it also contributes to cardiovascular damage. Covid-19 may either induce new cardiac pathologies and/or exacerbate underlying cardiovascular diseases. The virus invades cells through binding of its S-spike protein to the angiotensin-converting enzyme 2 (ACE2) receptor which is a membrane-bound aminopeptidase highly expressed in the heart and lungs and has a vital role in the cardiovascular and immune systems. The cardiac injury may occur as a result of direct viral invasion into myocardial cells or cytokine storm induced by the virus itself i.e. mobilization of a storm of immune cells which releases molecules called cytokines into the bloodstream with the intent to eradicate the virus, which when excessive may have toxic effects on the myocardium and thus weaken it, which is further assisted by respiratory dysfunction and hypoxemia. However in some conditions like immunocompromised states and diabetes mellitus, body’s ability to fight against the
virus becomes ineffective, thus flaring up the infection. Hence SARS-CoV-2 infection may lead to acute myocarditis, heart failure, arrhythmias and cardiac arrest. This was shown by a study done in Wuhan where 5 out of the first 41 patients diagnosed with COVID-19 had myocardial injury.
Furthermore, among those with COVID-19, there is a higher prevalence of preexisting cardiovascular disease and such patients are at higher risk of morbidity and mortality as they are more likely to develop severe symptoms. According to data released by the National Health Commission of China, 35% of patients with SARS-CoV-2 infection had a history of hypertension and 17% had a history of CAD. Furthermore, data show that patients aged >60 years with COVID-19 had more systemic symptoms and more severe pneumonia than patients aged ≤60 years. Therefore the underlying cardiovascular disease can aggravate SARS-CoV-2 infection as well as predispose to cardiac injury. Most of the cardiac manifestations usually overlap with the respiratory symptoms so it may be difficult to demarcate at the

43
outset. However few patients may present with chest pain and palpitation. Apart from the most common manifestation of myocarditis which may be focal or global myocardial inflammation, necrosis eventually leading to ventricular dysfunction, COVID-19 has also impact on the conduction system. In a study, about 16.7% of people had arrhythmia, with an increase to 44.4% of those admitted to the ICU. The most likely pathologic arrhythmias include atrial fibrillation, atrial flutter, and monomorphic or polymorphic VT. The ventricular arrhythmia may be attributed to hypoxia-mediated, worsening of coronary perfusion, direct tissue damage, hyperacute systemic inflammatory response, effects of QTc interval prolonging medications or electrolyte disturbance like hypokalemia as a result of interaction of SARS-CoV2 with the Renin Angiotensin system. Bradyarrhythmias, including sinus pauses or high-grade heart block, have not typically been seen. However, a hospital admitted case was reported from Iran who had transient complete heart block which could be drug induced or disease per se. A recent case has been reported from England of a COVID-19 patient complicated with myopericarditis causing life-threatening cardiac tamponade requiring pericardiocentesis. Newly diagnosed cardiomyopathy or acute exacerbation of chronic heart failure has been experienced. Cardiogenic shock has
also been observed and the use of ECMO has been emphasized in the studies. Incoming data from China and Europe suggest that COVID-19 may be associated with a hypercoagulable state and increased risk for venous thrombo-embolism leading to pulmonary embolism. In one of the studies done in New York City hospitals which included COVID-19 infection and ST segment elevation in ECG, revealed the higher prevalence of non-obstructive disease and its consequence to a poor prognosis, however there were fewer cases of coronary obstructive disease. Hence it further concluded that myocardial injury in Covid-19 could be due to plaque rupture, cytokine storm, hypoxic injury, coronary spasm, microthrombi, or direct endothelial or vascular injury. The acute coronary syndrome with obstructive disease could be due to the systemic inflammation and catecholamine surge that precipitated acute plaque rupture. Therefore, in the present scenario it is imperative to contain the burgeoning spread of SARS-CoV-2 infection where even the asymptomatic or presymptomatic (average of 5-6 days may be upto 14 days before symptoms appear) people may be attributable to the transmission of infection in up to 40 to 50% of cases. In addition to that, the identification and management of the cardiac involvement in such cases is a major challenge.

44
One more patient centric effort of MCVTC: Online
Appointment System
All of us would have had the experience of
waiting a couple of hours in a queue in
hospitals just to secure an appointment with a
doctor. Things might be a little different in
private clinics or hospitals, but long queues in
front of registration desks are commonplace
in most renowned public hospitals of this
country. Almost all of us would have hated the
experience but would had to tolerate it up till
now for the lack of a better option.
Manmohan Centre is a busy hospital where we
serve 250 clients per day on an average. It is
therefore natural that long troublesome
queues have been a concern for the
administration at MCVTC which always strives
to make our services patient friendly. The
hospital administration has been in search of
ways to make the experience of coming for a
doctor’s appointment at our hospital as stress
less and hassle free as possible. In this
endeavor, the Information Technology
department of the center, led by Dr. Ranjan
Sapkota came up with an idea of launching an
appointment application that seamlessly
routes our clients to their doctor of choice. The
Manmohan Appointment Application is now
available in Google play store.
In this technologically advanced age, one could
be forgiven for thinking that this is no “big
deal”. A lot of us who live in the major cities are
abreast with developments in Information
Technology (IT) and use it in our daily lives.
However, at the MCVTC, we have had to put in
a lot of thought and ideas before initiating the
online registration system!!
Prakash GC
Head Assistant, Administration

45
WHY??? You may ask!
The answer lies in the spectrum of the people
we serve. We served 73952 visits from all 77
districts of Nepal in the last year. A large
proportion of our patients come from rural
and often remote areas of our country. It goes
without saying that a large proportion of our
clientele cannot be expected to have optimum
access to the internet and/or the basic skills to
use online service. This was the cause of
significant anxiety and doubt regarding the
effectiveness of online appointment system in
our scenario. But, as connectivity and literacy
in the country continues to improve, we are
very optimistic that the online appointment
system will replace the queue in front of the
registration counter in the days to come.
Prof Dr Jagdish Prasad Agrawal, the Dean of
Institute of Medicine (IOM), launched our
online appointment system amidst our clients
on 26 Jan 2020. Since then, only 300 clients
have used this facility. Yet, we are very
optimistic that fifty percent of our clients will
come through online appointment with in a
year.
Here we would like to assure that it's simple.
It's easy. In just 7 clicks patients are able to
choose desired service and doctor and can get
a paid and confirmed appointment.
Alternatively, any e-sewa agencies, now
available in nearly every stationery, can help
get our appointment.
It is worth your attention and a little effort to
know about our online appointment service
that can save your couple of golden hours of
the early morning that can save you from
hateful waiting time in a queue.

46
Manmohan Center Cardiovascular Disease Prevention,
Control and Treatment Outreach Program
Background
Cardiovascular disease is the leading cause of morbidity and mortality in the world. It is a major public health problem in developed as well as developing countries. Any age group of the population may suffer from this disease. In Nepal children suffer more from congenital heart diseases, young people suffer from rheumatic heart disease and middle age and older age group mainly suffer from hypertension and coronary artery disease. Most of the cardiovascular diseases are not curable but can be controlled if proper measure is carried out on time. The cardiovascular services are not accessible to every individual and not affordable to every person. Out of pocket expenses are relatively high to get this service. So to provide specialty services to the large group of population at a time in their own home town or in their district with free of cost; every year Manmohan center organizes cardiovascular disease screening Camp with the coordination of different organizations, institutions and local partners. If diseases are diagnosed in the screening camp or needed further investigation we refer them to our center for further management. As being a chronic disease, it affects individual, family and the whole population and also alters the social and economic balance of the society. The financial crisis occurs due to the large expenses in daily medication and in another way the productivity of the individual decreases due to the disease in the body. So timely preventive advice, diagnosis and treatment services in local
Kalanath Thapaliya
Head Technical Assistant
(Medical)

47
level by consultant doctors are very useful but it is not accessible and feasible in regular basis in our context. This service is only possible by screening health camp until equitable distribution of human resources and infrastructure in a decentralized ways.
To fulfill this specialty services gaps in different parts of Nepal, in last year Manmohan center has carried out eight cardiovascular disease screening camp.
Date District Total patients examined
Total ECG Total Echo
2076/01/01 Jhapa 410 198 152 2076/02/11 Nuwakot 288 175 110
2076/7/22-24 Dhanakuta 3747 1531 569 2076/7/30 Kaski 582 233 216 2076/8/2 Gorkha 847 342 205
2076/9/26 Kavrepalanchok 197 89 54 2076/10/4 Kathmandu 351 139 92
2076/10/11 Kathmandu 162 92 38 Total 6584 2799 1436
Direct financial benefit to the people from Camp according to current hospital rate
SN Characteristics Unit cost Total unit Total cost (RS) 1 OPD check up 50 6584 3,29,200 2 ECG 170 2799 4,75,830 3 Echo 1100 1436 15,79,600 Total 23,84,630 In the screening camp, total 6584 suspected patients of cardiovascular diseases were examined. From ECG, Echocardiography and clinical examination different disease condition were identified. This information is very important for planner, policy maker and
different stakeholder for prevention, control and treatment of cardiovascular disease. Total 141 patients were referred to our center for further surgical or Cath lab procedure. The below table shows the identified disease condition from screening camp.

48
Case Total number Case Total number Hypertension 1521 Coronary Artery
Disease 55
Diabetes 121 TGA 4 Rheumatic Heart Disease
102 PCI done 14
ASD 25 DCM 619 VSD 23 PSVT 13 ASD+ VSD 3 Complex CHD 5 Operated Case 90 Other heart disease 31
What could be done to reach to unreached group and limit the disease process? To provide services in the community level for the prevention, control and treatment of cardiovascular disease following program could be carried out.
1. Cardiothoracic and vascular disease related health camp: At least one regular cardiothoracic and vascular health camp covering all the geographical region in every month in different district.
2. Public awareness related
orientation program: In the district where the health camp is organized there should be parallel orientation program to the school teacher, social volunteers and political representative about high blood pressure, hyperlipidaemia, rheumatic heart disease, heart attack, cancer, diabetes and COPD. In this orientation program the information of different non communicable disease, its impact in the population and measures of
prevention and control could be provided by consultant doctors.
3. Heart disease related school health program: The interaction program should be organized to impart the knowledge to the student about heart disease and the way to keep the healthy heart. School health club could be formulated and different reading material should be provided. Health and behavior related quiz competition, speech, assay writing, debate can be carried out for prevention and control of heart disease. The student of school health club should be trained for blood pressure measurement.
4. Those patients who need special
cardiac services should be made available by making coordination with the different hospital in the rural area. For that referred OPD and inpatient services can be started.
5. To measure the output and impact of
the program data collection and research activities need to be carried out together.

49

50
An Initiative of Developing
Society of Cardiothoracic Vascular Nurses of Nepal
(SCTVN)
Introduction
Introduction The cardiothoracic vascular diseases are in increasing trend in Nepal. According to Nepal country profile 20181, WHO estimates cardiovascular diseases remains 30% among 66% of all deaths due to non-communicable disease (NCDs). Nearly one third of the population has hypertension2 and 15 % has diabetes3. Chronic obstructive pulmonary diseases (43%) are the most common NCDs among outpatients followed by cardiovascular disease (40%), diabetes mellitus (12 %) and cancer (5%) 4. To cater required health care services to this population is one of the national targets of government of Nepal. Man Mohan Cardiothoracic Vascular Centre (MCVTC) is paving the way in providing super specialized cardiothoracic vascular care to the patients as highest referral centre of the country. The centre is running Cardiothoracic Vascular Intensive Nursing Training (CTVIN) for the provision of competent nursing staffs with specialized knowledge and skill with clinical experience. These nurses have vital role in detecting different life threatening conditions and take prompt actions to save the lives of patients for 24 hours, is the
RN Jamuna Tamrakar Sayami
Nursing Administrator, MCVTC

51
main features of this training. Thus CTVIN has become an accepted areas of specialized clinical nursing and considered as expanded role of nurses and documented the evidence demonstrating nursing effectiveness in saving lives and improving the quality and productivity of the lives that were saved.
Rationale
The nurses working in the Man Mohan Cardiac Centre felt a need to establish a professional organization in the field of cardiothoracic and vascular nursing for the advancement, development and recognition of this specialty nursing in the light of evolving many other specialized nursing organization in the country such as Critical care nursing association of Nepal, Society of Emergency Nursing, Paediatric Nursing Association and Midsol etc. So the Society of Cardiothoracic Vascular Nurses of Nepal is being proposed to be established in the country with the following objectives.
Objectives
1. To establish an independent society of cardiothoracic vascular specialty nursing professionals in Nepal as non-profit organization.
2. To develop and advance the cardiothoracic vascular nursing specialty in the country to deliver quality services.
3. To unite and get recognition as cardiothoracic vascular nurses and secure welfare of its members with mutual understanding and trust.
4. To support the patients and family in critical need with technical and financial means through fund generation.
5. To support nurses in this field by necessary counselling and financial means.
6. To network and build relationship with other national and international organization of relevance for learning and sharing experiences.
7. To create environment for conduct of education, training, research in the field of cardiothoracic vascular nursing for the human resource development I this field...
8. To organize seminar, conference and workshops for enhancement and update in this specialty.
9. To conduct public awareness and education programs in cardiothoracic and vascular health problems for prevention, treatment and rehabilitation.
10. To advocate for cardiothoracic vascular nursing specialty course development in advance level at master’s level to run in the country through appropriate institutions.
Membership criteria
1. Nepali citizen 2. Registered in Nepal Nursing Council 3. Nurses working in the
cardiothoracic vascular specialty at least for one year after completion of PCl/ Bsc Nursing /BN/PBN/ BNS etc.
4. Nurses trained for three months or more in the cardiothoracic vascular specialty
5. Nurse with PBN, BNS, and BSC degree with at least three months clinical experience in the cardiothoracic vascular nursing.

52
Membership type and fees
1. General member – annual entry with Rupees 1000 fee. 2. Life member – once for all time with Rupees 5000 fee. 3. Honorary member – distinguished personalities in the country no fee. 4. Founder member - working members who are involved in the inception period of this organization development. 5. Advisory member – Expert from the nursing and co professionals.
The office
The office of the SCTVN will be run in the office of chief nursing officer of the Man Mohan Cardio-thoracic Vascular and Transplant Centre, Maharajgunj, Kathmandu temporarily till a permanent location is decided. Executive Board The executive board consisted of eleven
members.
1. President: RN. Jamuna Tamrakar Sayami, Nursing Administrator, MCVTC, IOMTU.
2. Vice President: RN Til Kumari Basnet, Nursing Officer Cath Lab, MCVTC, IOMTU.
3. General Secretary: RN. Bimala Neupane, Deputi Nursing Officer, MCVTC, IOMTU.
4. Treasurer: RN. Bindeswori Gurung, Chief nursing officer, MCVTC, IOMTU.
5. Secretary: RN. Durga Thapaliya, Nursing Officer OT, MCVTC, IOMTU.
6. Member: RN.Tulaja KC, Lectuter,Maharajgunj Nursing Campus, IOMTU.
7. Member: RN. Jayanti Rai, Nursing Officer TUTH, IOM. .
8. Member: RN. Anita Dewan, Nursing Director, SGNHC
9. Member: RN. Sujata Pasachhen, Nursing Officer Cath Lab, Dhulikhel Hospital, KU.
10. Member: RN. Dilpana Maskye, Grande International Hospital,
11. Member: RN. Sheela Subedi, Nursing Officer, CTVS, Bir Hospital.
Activities of the SCTVN
This organization will act as an independent society of cardiothoracic vascular specialty nursing professionals in Nepal as non-profit organization to attain its objectives as per the regulation of Nepal government.
1. Obtain necessary equipment’s and utilities such as computers, telephone, fax and other office stationaries to function with daily activities.
2. Functions as pure professional organization for common platform for exchange of ideas, knowledge and the cardiothoracic vascular nurses of the country to deliver quality services.
3. Unite to get recognition as cardiothoracic vascular nurses and secure welfare of its members with mutual understanding and trust.
4. Support the patients and family in critical need of financial help and technical care through fund generation.
5. Support nurses in this field by necessary counselling and financial means.
6. Build relationship through networking with other national and international organization of relevance for resource

53
mobilization and sharing experiences.
7. Create environment for development of teaching learning materials resources such as procedure manuals, skill learning guide, feature films and audio video films, standard protocols and course books of cardiothoracic vascular nursing.
8. Conduct education and training, in the field of cardiothoracic vascular nursing for the knowledge and skill development and production of expert human resource.
9. Organize seminar, conference and workshops for update and enhancement of cardiothoracic vascular nurse’s credibility and scope of practice in the country.
10. Conduct public awareness campaign, education programs, and exhibitions, Mass media interaction show about the cardiothoracic and vascular health problems for prevention, treatment and rehabilitation.
11. Advocate for cardiothoracic vascular nursing specialty course development and run in the country in advance level at master’s level through appropriate institutions.
12. Conduct relevant research in the cardiothoracic vascular health problems and nursing services and develop good clinical practice standards as well as centre of excellence.

54
ASD (atrial septal defect) device closure in MCVTC
ASD device closure was introduced in Manmohan cath lab in the year 2073B.S. This is a modern state of art technique where the congenital defect is closed with minimal invasive procedure with or without general anesthesia. The team involved in this procedure includes;
Interventional cardiologist Anesthesiologists Nurses Radiology staffs Ward Helpers
An atrial septal defect (ASD) is a hole in the wall (septum) between the two upper chambers of the heart, the right and left atria. This defect allows oxygen-rich blood to leak into the oxygen-poor blood chambers in the heart. The exact cause is unknown; however a combination of genes and other risk factors, such as the exposure of mother to various environmental factors during pregnancy are also thought to be the likely cause of this problem.
RN Shasmita Maskey
Staff Nurse, Cathlab

55
The sign and symptoms depend upon the size of the defect and a very small one may not cause any symptoms or problems, however those having a big defect may present with following sign and symptoms;
Shortness of breath, especially on exertion
Fatigue Swelling of legs, feet or abdomen Heart palpitations or skipped beats Stroke Heart murmur, a whooshing sound
that can be heard through a stethoscope
Poor appetite, poor growth Lung problems and infections, such
as pneumonia
There are two approaches for the treatment of ASD.
1. Surgical management: Open heart surgery is required for patients with ostium primum and sinus venous ASD and is recommended in early childhood. Smaller defects are closed with sutures, whereas large defects require patches made of synthetic material or pericardium.
2. Non-surgical management/ASD Device Closure: this is commonly performed for ostium secondum ASDs with adequate rim and devisable size ( <40 mm).
In the cardiac catheterization lab an alternative to surgical closure of atrial septal defect (ASD) is performed with the use of specially made devices to close the ASD. These devices are implanted using special delivery system. This is considered
to be less invasive method than open heart surgery.
During this procedure, the catheter is introduced commonly through the right femoral vein to reach the right atrium via inferior venacava. The device looks like a short tube with two discs (circles) on either end. The device is introduced through specially made delivery system and once in place it is inflated to occlude the defect and the adjacent discs supports the device in place from either side.
The commonest device used in our institution is the Amplatzer Septal Occluder.

56
Amplatzer Septal Occluder ASD device under fluoroscopy
Procedure: ASD device closure
Advantages of device closure
Minimally invasive procedure with no need of cardiopulmonary bypass and large chest incision. Decreased hospital stay and less painful compared to surgical ASD closure.
Contraindications
Severe pulmonary hypertension Eisenmenger syndrome Net right to left shunt Defects larger than 41 mm in
diameter Absent or insufficient rim of tissue
around the defect
Complications
Device embolization Erosion of the cardiac structures
from the device Atrial arrhythmias Atrioventricular block (AV block) Persistent atrial aneurysm Thromboembolism Pericardial effusion and
tamponade
Nursing management:
Before the procedure Assessment of vital signs, baseline
investigations Maintain NPO status for at least 6
hours prior to the procedure. Removal of any jewelries and
artificial dentures Part preparation includes shaving of
both groins IV access is established Prophylactic antibiotics to be given
as prescribed Pre procedure medications (tab.
Ecospirin 300mg and Clopidogrel 300mg) to be given as prescribed.
Patient counseling and ensuring that the informed consent has been obtained.
During the procedure Patient positioning and attaching the patient to hemodynamic monitor As a circulatory nurse preparing all
the equipments required for the procedure including emergency trolley, defibrillator, fluids and infusion devices.
Preparing drugs required for general anesthesia and assisting with intubation and mechanical ventilation. As a scrub nurse assisting the
cardiologist throughout the procedure.
After the procedure
Prepare for reversal from General anesthesia.
Reorienting the patient and transfer of the patient to CCU.
Assessing the vital signs as per hospital guidelines.

57
Neurovascular observation- Continue observations as per clinical guideline
Assess puncture site every 30 minutes for 4 hours then hourly until ambulation
Ensure head of bed is no higher than 30 degree for duration of bed rest.
Dressing is to be removed prior to discharge.
Provide post procedure medications including antiplatelet and antibiotic as prescribed.
We stared ASD device closure from 2073 BS. So far we have successfully closed 70 cases and one patient underwent open heart surgery for device dislodgement.
References:
Moscucci, m. (2014). Grossman and baim's cardiac catheterization angiography and intervention. New Delhi: Wolters Kluwer (India pvt.ltd).
Sayami, P. A. (2015). Cardiology & Critical Care. Kathmandu: Sopan Press Pvt. Ltd.
58