1- General Principles of GI Motility
42
Lecture Session General Principles of GI Motility Dr. Saif Ahmed MBBS , MD Assistant Professor Department of PHYSIOLOGY College of Medicine
Transcript of 1- General Principles of GI Motility

Lecture Session
General Principles of GI Motility
Dr. Saif Ahmed MBBS , MDAssistant Professor
Department of PHYSIOLOGYCollege of Medicine

Structural Organization of GIT

Control of the digestive system
• Movement of materials along the digestive tract is controlled by:– Neural mechanisms
•Intrinsic and Extrinsic– Hormonal mechanisms
•Enhance or inhibit smooth muscle contraction
– Local mechanisms •Coordinate response to changes in pH or chemical stimuli

Neural Control of the digestive system
• Myenteric nerve plexus ▪ Lies between circular and longitudinal
muscularis externa ▪ Controls peristalsis and segmentation
• Meissner’s nerve plexus ▪ Lies in submucosa ▪ Signals glands to secrete

Nerve Supply• The enteric nervous system is linked to the central nervous system via the autonomic
• The nerve plexuses in the mucosa, submucosa and muscularis propria are of three types:
– cholinergic parasympathetic (with muscarinic or nicotinic receptors)
– adrenergic sympathetic (with both α and β receptors)
– non-cholinergic non-adrenergic (NANC)•For NANC, the transmitters are thought to be either cyclic nucleotides and ATP or intestinal hormones (e.g. VIP) or nitric oxide

THE PHARYNX AND OESOPHAGUS

Deglutition• Movement of food from the mouth to the stomach is known as Deglutition (swallowing)
• Swallowing is facilitated by salivary and mucuos secretions.
• It occurs in 3 stages...Oral Phase
Pharyngeal Phase
Esophageal Phase
Voluntary
Involuntary

Nervous control of swallowing

Esophageal PhaseLower Esophageal Sphincter (LES)
• Anatomically indistinct, it is a “physiological” sphincter
• It is formed by the distal 4 cm of esophageal smooth muscle
• It normally remains constricted, relaxing only transiently to allow the passage of bolus into the stomach

Anti-reflux Mechanisms
• LES rapidly regains its normal tone (following relaxation to allow a bolus to enter the stomach) and thereby prevents reflux. It is capable of increasing tone in response to rises in intra-abdominal and intragastric pressures
• Forceful expulsion of food from stomach and/or intestine.
• Vomiting centre is Chemoreceptor Trigger Zone (CTZ) located in “area postrema” in medulla.
• Afferent impulses arise by irritation of GI mucosa, vestibular appartus and other organs to stimulate CTZ.
Vomiting/Emesis

GERD- Gastroesophageal Reflux Disease
• GERD May develop when anti-reflux mechanisms fail.
• This a condition in which the food or fluid content of the stomach regurgitates (backs up or refluxes) into the oesophagus.
• The regurgitated food or fluid usually contains acid and pepsin produced by the stomach and can inflame and damage the lining of the oesophagus leading to heartburn and oesophagitis.
• Acid is believed to be the most injurious component of the refluxed liquid and can lead to ulceration and stricture (narrowing) of oesophagus

Achalasia Cardia- a motility disorder of Oesophagus
• Achalasia cardia is a disease characterized by :– aperistalsis in the body of the esophagus – failure of relaxation of the lower esophageal sphincter on initiation of swallowing
• In the majority of cases the aetiology is unknown (idiopathic)
• Dysphagia- It means difficulty in swallowing. • It may occur due to disorder involving any of the stage of Deglutination

The Stomach

Structure• The stomach is divided into a small area immediately distal to the oesophagus (the cardia)– upper region (the fundus which lies under the left diaphragm)– mid-region or body, and – the antrum, which extends into the pyloric region
• Two sphincters: the gastro-oesophageal sphincter and the pyloric sphincter; the latter is largely made up of a thickening of the circular muscle layer
• The muscle wall of the stomach has three layers– outer longitudinal– inner circular– innermost oblique layer of smooth muscle
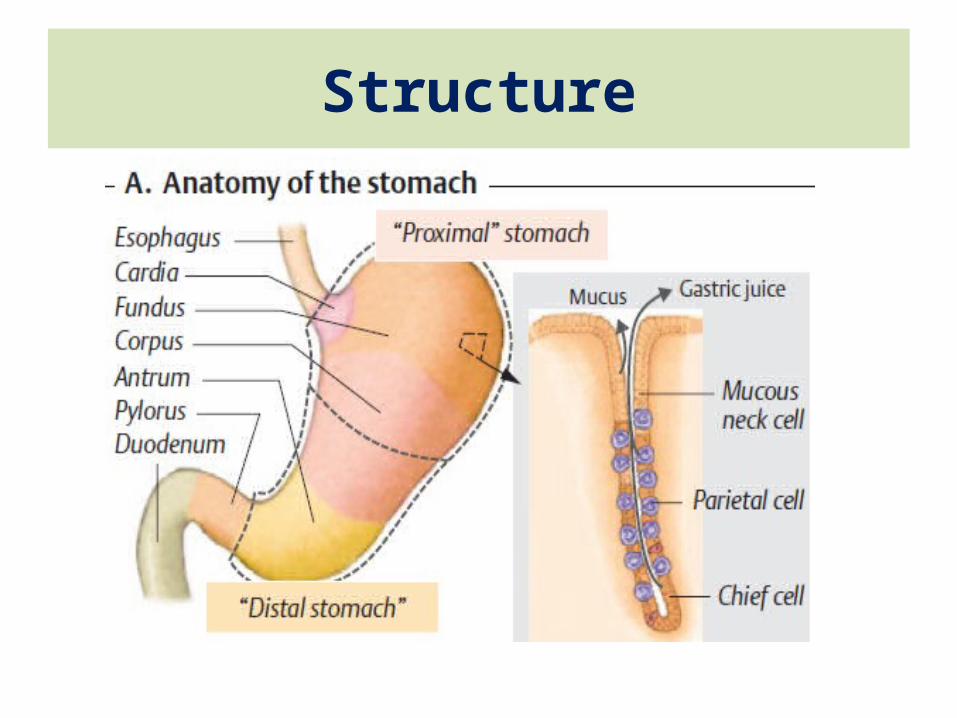
Structure

Motor functions of Stomach
• Storage of food until the food can be processed in the stomach, duodenum, and lower intestinal tract
• Mixing of this food with gastric secretions until it forms a semifluid mixture called chyme
• Slow emptying of the chyme from the stomach into the small intestine at a rate suitable for proper digestion and absorption by the small intestine

Basal Electrical
Rhythm
Peristalsis
Gastric Motility

Basic Electrical Rhythms [BER]• Cyclic Slow waves of depolarization in smooth muscle cells of Stomach
• Initiated by Pacemaker Cells (outer circular layer of smooth muscle in ‘Body’)
• BER Itself Rarely Cause Muscle Contraction
• Peristalsis of stomach occurs @ 3/min and is coordinated by BER.

• Stomach Musculature Relaxes Before and After Food Gets Into it
• Receptive Relaxation – occurs when food is still In Esophagus
• (Vagally Mediated and Gastrin-induced)
• Adaptive Relaxation – occurs when food is in Stomach
• (Local Nerve Plexus)

Gastric Emptying• Begins Near the Middle of the Body of the Stomach• Sweeps Towards Pylorus
• More Powerful Contractions in Pyloric Antrum• Peristalsis Near the Pylorus – Pyloric Sphincter Closes
• Only Small Amount of Liquid Chyme Squirts Through Sphincter
• Chyme Bounces Back – Mixing With Gastric Contents

The stomach& duodenum act
together as a PUMP
Pylorus pumps small amounts of
chyme (about 3 ml) into duodenum
Pylorus forces most of the chyme backwards
Peristaltic waves move towards pylorus
Peristalsis & mixing most vigorous close to pylorus

Gastric emptyingStimulated by • The vagus• Gastrin (hormone produced by the stomach)
Inhibited by • Sympathetic stimulation• Hormones SECRETIN, CHOLECYSTOKININ (CCK), GASTRIC INHIBITORY PEPTIDE (GIP)
• Fats, acid and hyperosmotic substances in the duodenum
• Fear and anxiety

Emptying time: Fat > protein > carbohydrates
Gastric Emptying
Fatty Meal

Prokinetic Agents• Drug which enhances gastrointestinal motility by increasing the frequency of contractions or making them stronger, but without disrupting their rhythm
• They are used to relieve gastrointestinal symptoms such as– abdominal discomfort, bloating, constipation, heart burn, nausea, and vomiting
– They are also used to treat a number of gastrointestinal disorders, including irritable bowel syndrome, gastritis, acid reflux disease, and functional dyspepsia

THE SMALL INTESTINE


Structure• The small intestine extends from the duodenum to the ileocaecal valve. It is approximately 6 m in length, the upper 40% - the jejunum; the remainder - the ileum.
• Its surface area is enormously increased by mucosal folds
• In addition, the mucosal folds, it has numerous finger-like projections called villi and the surface area is further increased by microvilli. Each villus consists of a core containing blood vessels, lacteals (lymphatics) and cells (e.g. plasma cells and lymphocytes), and is covered by epithelial columnar cells that are absorptive
• On its luminal side the epithelial cell has a brush border of microvilli that is covered by the glycocalyx
• The crypts of Lieberkühn open into the lumen, between the villi

Motility of Small Intestine
• The contractile patterns of the small intestinal muscular layers are primarily determined by integrated neural circuits within the gut wall - the enteric nervous system
• The CNS and gut hormones also have a modulatory role on motility.
• The interstitial cells of Cajal lie within the smooth muscle. These mesenchymal cells appear to govern rhythmic contractions
• During fasting, a distally migrating sequence of motor events termed the migrating motor complexes (MMC) occurs in a cyclical fashion

Migrating Motor Complexes (MMC)
• MMC is motor activity in smooth muscle of GIT, migrating to distal ileum and increases during fasting
• Each MMC cycle consists of 3 phases: – period of motor quiescence (phase I)– period of irregular contractile activity (phase II)– a short (5-10 min) burst of regular phasic contractions (phase III)
• Each MMC cycle lasts for approximately 90 -120 minutes and is completely inhibited by meals.
• The role of the MMC -- strong phase III contractions propel secretions, residual food and desquamated cells towards the colon, acting as an 'intestinal housekeeper'

Motility of Small Intestine
• After a meal, the MMC pattern is disrupted and replaced by irregular contractions. This seemingly chaotic-fed pattern lasts typically for 2-5 hours, depending on the size and nutrient content of the meal
• The irregular contractions of the fed pattern have a mixing function, moving intraluminal contents to and fro, aiding the digestive process
• Segmentation and Peristaltic Movements

Segmentation• Mixing movements• Ring-like contractions at regular intervals(Contraction of circular muscles)
• Moves the chyme to & fro, increasing its exposure to mucosal surface for absorption
• No propulsion

Peristalsis• Propulsive movements that propels the intestinal contents (chyme) toward the large intestine.
• Occurs at any part of small intestine, most frequent in duodenum then slows down in jejunum & ileum
• Peristalsis at Proximal intestine >>> faster than terminal intestine
• Peristaltic movements are weak, and continues unidirectionally towards the anus. This is called Law of Gut.
• Net movement of chyme ~ 1 cm/min
• 3-5 hours journey from pylorus to ileocecal valve


Gastroileal reflex Gastroileal reflex ▪ When the food leaves the stomach , it triggers relaxation of ileocecal valve.
o This is vagally mediated reflex.
▪ This allows chyme to pass from small intestine into large intestine

The Large Intestine

Movements of the Colon• The proximal half of the colon is concerned principally with absorption, and the distal half with storage.
• Because intense colon wall movements are not required for these functions, the movements of the colon are normally very sluggish
• The movements are similar to those of the small intestine and can be divided once again into– mixing movements- segmentation– propulsive movements-peristalsis.

Presence of Faeces in RECTUMStretch Receptors in the wall gets stimulated (Afferent fibres of Pelvic nerve)
Series of peristaltic contractions of rectum moving towards anus (SHORT REFLEX LOOP)
Desire to DEFAECATE, a coordinated reflex (S2, S3, S4) empties Descending colon, Sigmoid colon into Rectum (LONG REFLEX LOOP)
Contraction of Ant Abdominal muscles
Tonic relaxation of Internal Anal sphincters But External
Anal sphincter remains closedRelaxation of Puborectal
sling
Actual release of faeces requires a conscious effort to relax EXTERNAL SPHINCTER
by Pudendal nerve
Defecation Reflex

Defecation Reflex

Gastrocolic Reflex• Both segmentation and peristaltic movements occur frequently following meals.
• The distention of stomach by food initiates contraction in rectum and desire to defecate, called as Gastrocolic Reflex.
• This is comman in children and may be due to action of gastrin on the colon.

Constipation• 'Constipation' is a very common symptom, particularly in women and the elderly.
• A consensus definition used in research (The Rome II criteria) defines constipation as having two or more of the following for at least 12 weeks: – infrequent passage of stools (< 3/week)– straining > 25% of time– passage of hard stools– incomplete evacuation and sensation of anorectal blockage
• According to these definitions 'constipation' affects more than 1 in 5 of the population

Megacolon• The term 'megacolon' is used to describe, congenital and acquired conditions in which the colon is dilated.
• In many instances it is secondary to chronic constipation and Chagas' disease.
• All young patients with megacolon should have Hirschsprung's disease excluded
Hirschsprung's diseaseIt presents in the first years of life, an aganglionic segment of the rectum (megarectum) gives rise to constipation and subacute obstruction .
A preliminary rectal biopsy is performed and stained with special stains for ganglion cells in the submucosal plexus