-a %. , l'gN-1 L.pJ8, - Sign in
241
.,'a.. : 'a- : E A + S : T E R N - MEDI liERR.X:N'E~ ' t'a.. : <- , . . . . . .-i.. : , ,'a.. : ,. e '.a- !' .. . J . 5 s.. : t : . I ~ , - a %. , l'gN-1 L.pJ8, . . . r' . ,.a- .%' .. . * - . ,, 1. . . .. : ,, 2 . - , .- - . , ,t .. t .- . .- .. .., ~ - , . . ' 0 , . .. ' 0 , . , i' ~ ., / ' a. : ., . . - : i' !' <. ' !' L. : . , -. .. . . .. , ,-.. : . ,'a- . i.' . . . . /> , . . ?i' _.' . ..' . . ,%- '- . , . t ?' .r. . - ., ' : I .', . t '; ... ' 8 . - _. . . , ,.t ' 0 $' i' . - .. .., ?.. a , ' .I . " . ..:. 3 .., ,.. i' ., , . ., ! i' ,. ..' \I- : . . . , .... . . . . .- . . i ALJLX~A'NMI~, #:(J$Y A . . ' . ? I:.. - / : - a , . . ' . I. 3. C . ,'a- 1 ' ) .,' .- ,,' : , . + t : ,' . . ., EEJRC. 3 ' . ) . r. + . C ., ' : ., . t &* . . .
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of -a %. , l'gN-1 L.pJ8, - Sign in
.,'a.. :
'a-
: E A + S : T E R N - M E D I l i E R R . X : N ' E ~ ~
' t'a.. : < - , . . . . . .-i.. : , ,'a.. :
,. e '.a- !' .. .
J . 5 s.. : t : . I ~ , - a %. , l ' g N - 1 L.pJ8, . . . r' . ,.a-
.%' .. . * - . ,, 1. . . .. : , ,
2 . - , .- - . , , t . . t
. - . .- .. .., ~ - , . . ' 0 , . .. ' 0
, . , i' ~ ., / 'a.. : ., . . - : i' !' <. ' !'
L. : . , -. .. . . .. , ,-.. : . ,'a- . i.' . . . . /> , . . ? i ' _.' . ..' . . ,%- '- . , .
t ?' .r. . - .,' : I .',
. t '; ... ' 8
. - _ . . . , , . t ' 0 $' i' . - .. .., ? . . a , ' .I .
" . . . : . 3 .., ,.. i' ., , . ., ! i' ,. ..'
\ I - : . .
. ,.... . . . . .- . . i ALJLX~A'NMI~, #:(J$Y A
. . ' .? I:.. - /:- a , . . ' . I .
3. C . ,'a- 1 ' )
.,' . - ,,' : , . + t : ,' . . ., EEJRC. 3 ' . ) . r. + . C .,' :
. , . t &* . . .
W O R L D H E A L T H O R G A N I Z A T I O N
R E G I O N A L O F F I C E
F O R
T H E E A S T E R N M E D I T E R R A N E A N
P R O P O S E D PROGRAMME BUDGET FOR THE BIENNIUM
1980 - 1981
A L E X A N D R I A , J U L Y 2978
The R e g i o n a l D i r e c t o r h a s t h e h o n o u r
t o p r e s e n t t o t h e R e g i o n 8 1 C o m m i t t e e t h e
programme b u d g e t p r o p o s a l s f o r t h e E a s t e r n
M e d i t e r r a n e a n R e g i o n f o r t h e 1980-1981
B i e n n i u m .
TABLE OF CONTENTS
EXPLWATKIRY NOTES
REGIONAL DIRECTOR'S PROGRAMME STATBMEHT
S-ES lum, TABLES:
Estimated Obligations by Source of Funds
Slsfmm-ry by Major P r a ~ / P m g r a ~ m d SmUFw 0.9 Flaas
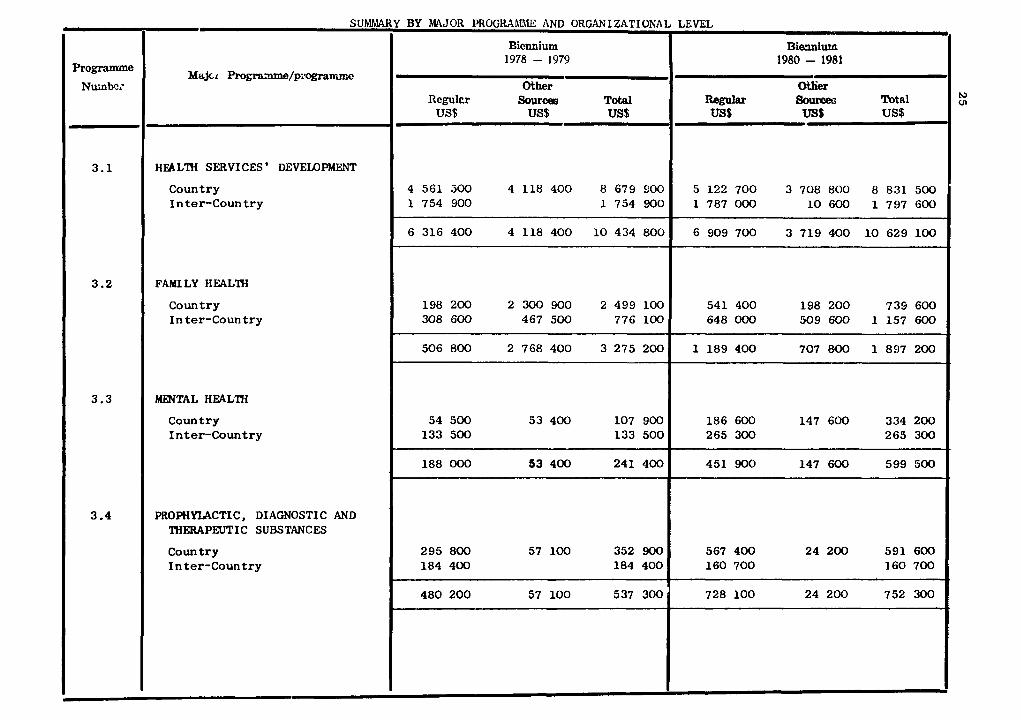
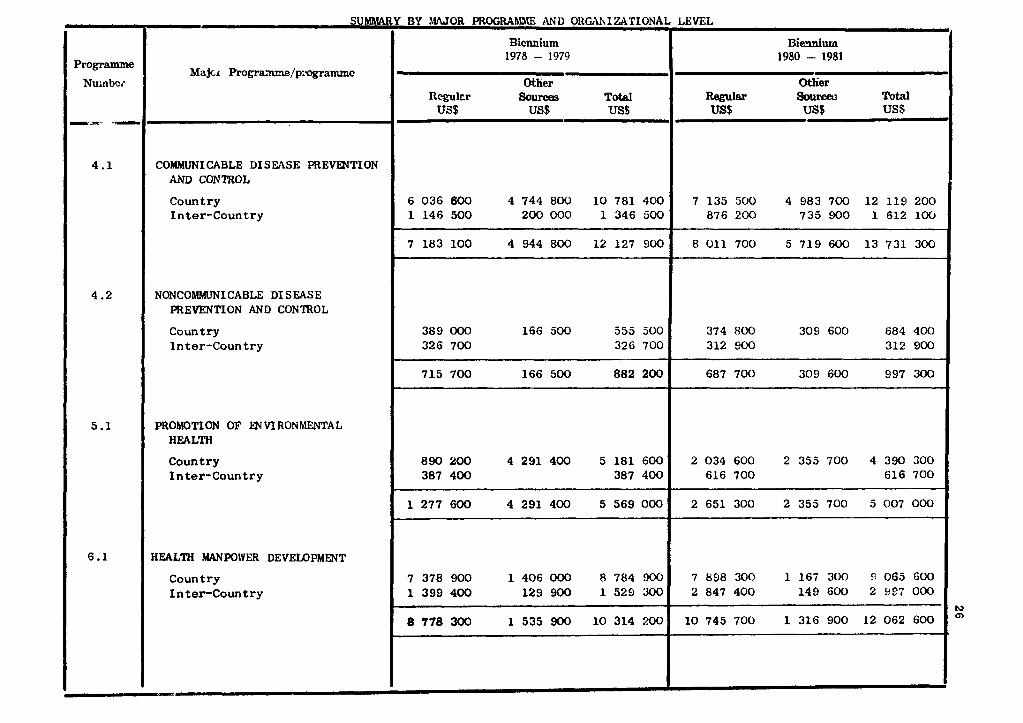
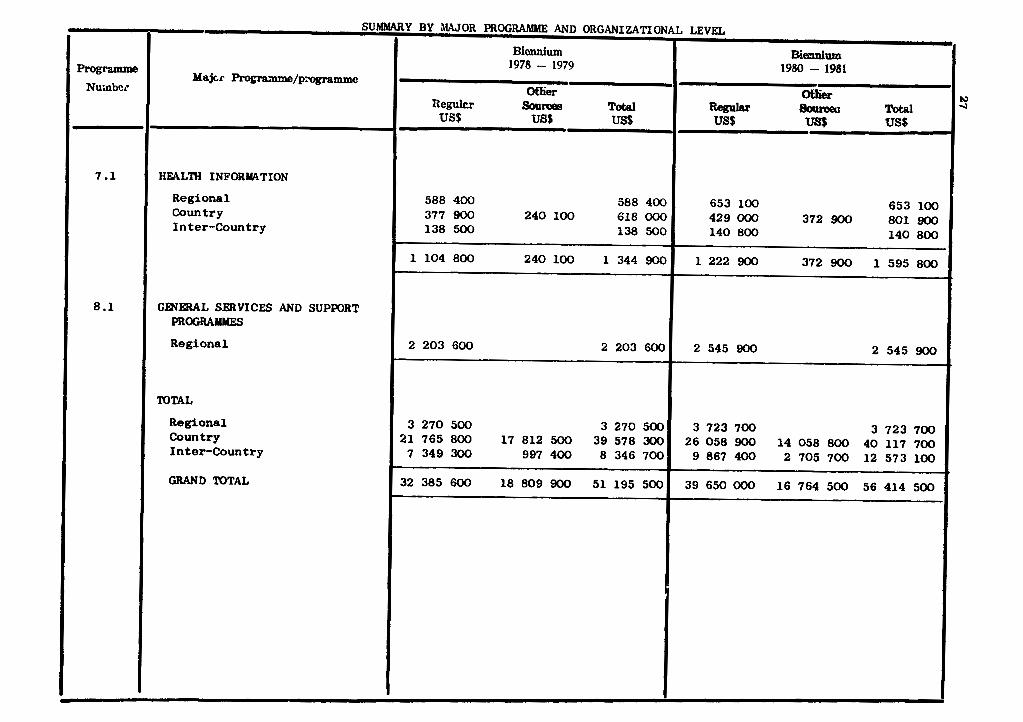
&rauy by Wsr 9rOg.m and 0ag.aismttomal-
Errtinwtes 1980-1981 by Appropriate Section w i t h
t e n t a t i v e project ions f o r 1982-,1983
MdJOR PROGRAMME AND PROGILAllME ANALYSES
1.3 Regional Committees
2 -1 Executive Uanagement
2.2 General Pmgramae Development and Masugmmrt
2.3 External Coordination f o r Health .end ~ c % & & + ~
Develeprent
RBSBB-M:~ Proleotion and Development
R e - 1 M ~ e c t o r 's Development Prggmamm
Health Services ' Development
Family Health
Mental Health
Prophylactic, Diagnostic and Therapeutic Suhstmmes
Col~aunicabXe Disease Prevent ion and Control
Noncommunicable Disease Prevention and Contml
Promotion of Environmental Health
Health M-er Development
liealth Information
8.1 General Services and Support Prograarrrss
Page
l NFORMATI ON ANNEXES
RF(;I~JNAI, OFFICE - NARRATIVE AND TABLE
C(XINTRY PROGRAMME STATEMENTS AND TABLES :
Summary o f s e r v i c e s and a s s i s t a n c e t o Governments
Afghanistan
Bahrain
Cyprus
Domoo ra t i c Yemen
D.11 bout i
E R Y P ~
I ran
1 raq
I s r a e l
Jordan
Kuwai t
Lebanon
Libyan Arab Jamahiri ya
Oman
Pakis tan
Qatar
Saudi Arabia
Somalia
Sudan
Syr ian Arab Republic
T u n i s i a
United Arab Emirates
Yemen Arab Republic
Regional Advi sers - Narrat ive
I nter-Country Programme
PROPOSED PROGWIME BUDGET
EASTERN MEDITERRWEiN REGION 1080/1981
E X P L A N A T O R Y N O T E S
Form of p re sen ta t ion
1. This Proposed Programme Budget Presenta t ion r e f l e c t s a depar ture from previous
procedure i n t h a t both progrdmme and budget f o r 1980-1981 cover two f u l l y in t eg ra t ed
years i n one biennium. This is In accordance wi th t h e World Health Assembly dec i s ion
t h a t " the programme budget of W H D s h a l l cover a two-year period beginning wi th t h e
biennium 1980-1981 and s h a l l be reviewed and approved by the Health Assembly on a two-
year b ~ s i s " (WHA30.20). The revised cs t imatcs fo r t h e yt.drs 1978 a d 1977 have a l s o
been combined i n t o onc s i n g l e blcmnlum for purpose of compdrison.
2. The Programme Budget f o r 1980-1981 has been developed, a s f a r a s poss ib l e , i n
accordance with the new approved procedures "emphasizing t h e need f o r c l o s e col labora-
t i o n between W H O and Member S t a t e s i n the development of well-defined country h e a l t h
programmes w i t h ln whl c:h individual p r o j e c t s dnd d c t i v i tles can subsequently be pl annod
i n de td l l dnd ~r\iplcmcntc?d i n r c l a t i o n t o o v e r ~ i l l p r o g r m e - o b j e c t i v e s In c l o s e r hclrmohy
wi th n a t i o n a l hea l th programmes processes(WHt~30.23). The new procedures t h e r e f o r e
r e s u l t i n t h e d e f e r r a l of d e t a i l e d p r o j e c t planning u n t i l c l o s e r t o t h e a c t u a l opera-
t i n g period, i n c l o s e r harmony wi th na t iona l h e a l t h programming processes.
3. The c l a s s i f l c a t r o n of programmes is based upon t h e S ix th General Programme of
Work covering the s p e c i f i c period 1978-1983. The progranrme c l a s s & f i c a t i o n s t r u c t u r e ,
however, r e f l e c t s some minor changes from t h a t applied t o previous programme budgets.
1978-1979 c ~ m p a r a t i v e budget da t a have been re-arranged t o accommodate t h e new c l a s s i -
f i c a t i o n s t r u c t u r e .
4. Country programme t a b l e s provide budgetary provis ions t o t h e programme l e v e l only
and no t , a s i n t h e p a s t , t o t h e p r o j e c t and project-component l eve l s . To compensate
p a r t i a l l y f o r l o s s of t he accustomed p ro jec t - l eve l d e t a i l , t h e a c t i v i t i e s r e l a t i n g t o
each programme have been described and a r e shown i n parentheses immediately below each
programme descr ip t ion .
In t h e Case, however, of Inter-Country prOgrmUES, some d e t a i l has been ret i t ined
and is r e f l e c t e d i n t h e tdbles .
5. An analytical statellent applyi- to the Region aa a whole forms a p u t of the
presentation for each major programe and its related subordinate programmes. These programe statements attempt to define clearly the objectives of each progr., to
assess past progress i n meeting these objectives and t o met forth the anticipated con-
tribution of the budget proposal towards achieving thm.
The programe proposals to be financed undsr the Regular Budget are b u d upoa 8
tentative alxocation of US $ 39 650 000 for the1980-1981 biennium period. This gigure represents an increase of US $ 7 265 000 or 22.4% over the 1978-1979 biennium, of which
US $ 2 857 500 or 8.8% represents growth i n real term8 and US $ 4 407 500 or 13 .6
the amount required t o offset the anticipated increase dbe to inflation. Stated in a
more f uiliar "per annum" context the budget proposals ref lec t an increase of 10.7%
per uurm of which 4.2% per annum represents growth i n real term8 while 6.5% per anzum
represtmts campansotion for inflation.
I t is worth noting that World Health Assembly resolution WHA.31.23 r e s ~ c t s a
m h i n real terms Sar the entire organization to 2% per annum for the 1980-1981 bion-
aim ofrer the preceding biennium. The higher r a t io of 4.2% per annum growth in real
teru for this Region, a8 referred t o above, is attributable t o the s h i f t i n resource8
from Headquarters, global and inter-regional ac t iv i t ies t o the repiom, in the s p i r i t of
resq&ut&m WHA39.48 which aims a t 60% of regular krdget resources being devoted to
tecbnioal oooperaticm and provision of servicer.
The table on page 28 provid68 a projection of the estimates into the 1982-1983
bi.nniam.
7. Other laurce8
Where ac t iv i t ies rra financed part ial ly o r completely from saarces other than Rogulu
madget the fund8 antioipated are ahom on table8 i n the 001- headed " O t h e r Sou~ces".
These other source8 of fund8 a m a8 follar8:
(a) United Natiaru D o v e l p m t P r o p r (DP)
The United Nation8 Dmvelopart P r o g r m (WDP), through i t 8 Governing Couaoil,
establishes oeiling8 on a five-year bruis for the ao8t of technical cooperation it i 8
abl. to provide for eaeh oountrp. I t is within th0.e .nwal ceilings, te~ed~'1ndioatitn
Pluming: Pigums" (IPF), that cauntriea can plrn and sub8qumtly request UWDP f-d
u.i8tulOe.
The proposed budget ref lects the availability of funds under th is category based
upon information available a t the time of its preparation. I t should be noted, hwever,
that there all be an increase i n funds from t h i s source as more information becores
available approaching the actual period of progrcrrme Implementation.
(b) United Nations Fund for Population Activities (FP)
The abbreviation "FP" shown i n the tables column headed " O t h e r Sources" indioates
those ac t iv i t ies part ial ly or completely financed by the United Nations Fund for Poplla-
tion Activities (UNFPA). A t this stage, UNFPA assistance is not known i n rosf ccues
beyond 1979 and therefore is not ful ly reflected i n the Proposed P r o g r m Budget for
1980-1981.
(c) Voluntary Fund for Health ProPlotion
Activities financed by voluntary contributions from M e m b e r States of the Region
f a l l und8r this category and are classified as follows:
"VA" - Assistance to the Least Developed Among Developing Countries.
"mu - Malaria
"VI" - Expanded Programme on Immunization
"M" - Miscellaneous Designated Contributions.
(d) Funds-in-Trust (ET)
Funds-inlPrust,indioated by the symbol "ET", represents those ac t iv i t ies requested
and paid for on a reimbursable basis by the cotmtriea aoncerned.
REGIONAL DIRECTOR'S PROGRANME STATEb1ENT
In accordance with the continuing evolution i n the ways i n which W H O collaborates
with its M e m b e r countries, there a re a number of s ignif icant changes i n the format
i n which the Proposed Programme Budget for 1980/81 is presented. T h i s represents a
logical next s t e p i n the continuum of our move, a s instructed by our Governing Bodies,
towards giving increasing emphasis on technical co-operation i n the r ea l sense, a s
opposed t o technical assistance.
I take pleasure i n proposing t o Member countries a programe which, developed i n
close consultation w i t h t h e m , sets out a series of ac t i v i t i e s , under the various
appropriation sections, which r e f l ec t the needs of the countries. The programmes
a re described i n a standard way, t he i r objectives being set out a s c lear ly a s possible,
followed by the steps which i t is proposed t o take i n order t o implement them i n col-
laboration with Member countries.
A s was done for the previous biennium, continuing attempts have been made t o i m -
prove the statement of objectives and to describe the nature of the proposed collabora-
t ion with and among countries i n a way which r e f l e c t s how the p r o g r a m has been re-
oriented t o increase relevance and benefit t o the countries of the Region.
* * * I t w i l l be noted that there a r e cer ta in themes running throughout the proposed
programme for the two years.
One of these is a c lear re f lec t ion of the greater involvement of the nationals of
our M e m b e r countries i n the carrying out of the proposed programmes, with a concomitant
diminution i n the expenditure upon WSUl s ta f f whether i n the Regional Office o r i n the
f ie ld .
There i s also, throughout the programre, an emphasis upon what might be cal led
a research and development approach, which r e f l e c t s the increasing respons ib i l i t i es
of the Regional Office i n a l l aspects of biomedical researuh and, i n ~ r t i c u l a r , the
need to approach the most v i t a l problems facing our Region i n such a way a s t o pro-
vide every possible co-operation with Member countries i n achieving the goal of health
for a l l by the year 2000.
I n t h i s connection i t w i l l immediately be noted tha t by f a r the highest proportion
of the budget i s devoted t o the development of comprehensive health services and the
key and closely related area of health manpower development. The largest s ingle
section of the budget, i n c lear response to the repeated guidance of our M e m b e r coun-
tries, goes t o health ranpower development, and the cab ined budget for health services
and manpower development taken together r ep resen t s 50% of t h e expenditure proposed.
A s WHO'S own systems o f programme development improve and become more responsive
t o the needs o f t he Member coun t r i e s , so i s i t t h e case t h a t t he Proposed Programme
Budget f o r t h i s p a r t i c u l a r biennium is c lose ly baaed on t h e o v e r a l l o b j e c t i v e s of t he
S i x t h General Progranme o f Work covering the period 1978/83, and t o t h e Medium-Term
Programmes which have been prepared i n s e l ec t ed sub jec t s .
* * * A s i s w e l l known, ou r Region has been inc reas ing ly cha rac t e r i aed i n r ecen t yea r s
by eve r more in t ima te and productive t echn ica l co l l abo ra t ion between ou r Nember
coun t r i e s , as wel l a s by the cont inuing generous support provided t o t h e less well-off
among them, by those economically more for tunate .
I t w i l l r e a d i l y be seen that by f a r t he highest propor t ion of tb budget is pro-
posed t o be devoted t o t h e needs o f t h e l e a s t well-off count r ies . Those f i v e
coun t r i e s i n our Region which are def ined by the United Nations as amongst t h e l e a s t
developed among developing coun t r i e s , account f o r no l e e s than 54 per c e n t o f t h e
expendi tures proposed i n c o m t r i e s .
Conversely i t w i l l be noted t h a t t h e moat a f f l u e n t among t h e c o u n t r i e s have aga in
w i l l i n g l y agreed t o reduce their demands upon t h e WHO budget i n t h e interests o f o t h e r
c o u n t r i e s and, a s i n t h e previous biennium, a t t e n t i o n $8 d r a m t o the generous volun-
t a r y con t r ibu t ions t o supplement the WHD programme which have been made by amueral
c o u n t r i e s inc luding Egypt, I r an , I r a q , Kuwait, Libya, Q a t a r , Saudi Arabia and United
Arab Emirates.
I n accordance wi th t h e d e f i n i t i o n s a r r ived a t by t h e World Health Assembly,
90.80 per cen t o f t h e t o t a l budget w i l l be devoted t o direct t echn ica l cooporat ion
wi th coun t r i e s , a f i gu re , i t w i l l be noted, which a l r eady exceeds the target o f 80 per
cen t e s t ab l i shed by the World Health Assembly Resolut ion WHA 29.48 t o be achieved by
1980 i n the world a s a whole.
I n this connection i t an11 be p a r t i c u l a r l y noted that expendi tures on such i t e m s
as pol icy organs, general programme development, management and co-ordination and
non-technical support programmes, which r ep resen t 9.40 pe r cen t o f t he t o t a l , cont inue
the long t r a d i t i o n o f t h i s Region o f providing s e r v i c e i n Nember c o u n t r i e s a t the
minimum overhead cos t .
A s i s w e l l known, WHD i n t h i s Region has always c a r r i e d o u t a l l o f its func t ions ,
whether advisory o r educational o r developmental, a t the l e a s t cos t to i t s Member
countr ies and this philosophy w i l l be maintained.
I n accordance wnth the recommendations of the Governing Bodies concerned, i t
w i l l be seen tha t specia l emphasis i s given t o the following subjects:
- The need not only t o increase the quant i ty and t o improve the qua l i ty of heal th
personnel, but a l s o t o increase the relevance of the t r a in ing of a l l hea l th
personnel t o the needs of the heal th services and t h e populations a s a whole;
- the need still t o make dramatic improvements i n the q u a l i t y of information upon
which heal th ac t ions a r e determined;
- the need to cont inueto explore, implement and evaluate e f f e c t i v e primary heal th
ca re services and t o t r a i n the manpower, a s well a s t o improve the s impl i f ied
technologies, which a r e appropriate for t h e m ;
- the need t o pay due a t t e n t i o n t o the overwhelming problems faced by the l a r g e s t
s ing le age group i n our population, chi ldren under the age of f i v e years;
- the need t o take, and the f e a s i b i l i t y of taking, urgent s t eps t o improve the
q u a l i t y of protection of the population, and i n p a r t i c u l a r the ch i ld population,
agains t those main d i seases f o r which we have, through immunization, a protect ive
mechanism readi 1 y a t hand ;
- the need, i n the l i g h t of the increas ingly rapid i n d u s t r i a l i z a t i o n of a l l M e m b e r
countries, t o promote and expand e f f o r t s p e c i f i c a l l y d i rec ted t o the hea l th of
working populations, t o the control of occupational hea l th r i s k s and t o the pro-
motion of the humanization of working condit ions;
- the need t o continue t o make pa r t i cu la r e f f o r t s t o control c e r t a i n d i seases whch ,
desp i t e a l l pas t e f f o r t s , a r e still espec ia l ly c h a r a c t e r i s t i c t o the countr ies of
the Region, notably the e n t e r i c in fec t ions , schistosomiasis , malaria, tuberculos is
and blindness;
- the need t o in tens i fy e f f o r t s i n a l l aspects of the promotion of environlnental
heal th , n t h specia l emphasis on opera t ional research, appropriate technology
t r a n s f e r and expanded t r a i n i n g e f f o r t s ;
- the need t o improve a number of very bas ic se rv ices on which e f f e c t i v e hea l th
se rv ices depend, such a s the laboratory se rv ices a s a whole, and the paramount
i s sue of the repa i r and maintenance of a l l forms of medical equipment.
For severa l years there has been continuing concern throughout the Region a s a
whole with the extent of ~ ~ m u n i c a t i o n and col laborat ion between those responsible
f o r the t r a i n i n g of the manpower needed for the heal th services and those responsible
f o r running the heal th se rv ices themselves.
Following the landmark Minis ter ia l Consultat&on on Health Services and Manpower
Development held i n Teheran i n 1978, with the pa r t i c ipa t ion a t the highest l eve l of
Ministers of Health and of Education, and of educational and heal th service leaders
from a l l over the Region, a p a r t i c u l a r l y strong e f f o r t w i l l be made, i n col laborat ion
with countr ies , s t e a d i l y t o improve upon the present s t a t e of a f f a i r s .
Likewise there w i l l be continuing e f f o r t s on the p a r t of the Organization i t s e l f
t o a s s i s t countr ies to improve the ex ten t t o which developments i n heal th a r e l inked
t o developments i n o ther sec to r s , notably i n agr icu l tu re , the economy, education and
comuni t y development.
Pa r t i cu la r p r i o r i t y w i l l be given t o the t r a in ing of teachers of a l l l e v e l s of
heal th personnel and the re w i l l be continuing emphasis a t the country l e v e l i n carry-
ing through the Regional Teacher Training Programe, with strong emphasis on eduua-
t iona l planning and technology, which has been i n operation i n the Region s ince 1972.
The Region has a long and honourable t r a d i t i o n i n medical education a s such.
I n recent years medical schools have expanded rapidly , and t h e i r output of doctors
has mul t ip l ied accordingly. Indeed i t can be argued, and is so argued by many
leaders i n the f i e l d , t h a t , a t l e a s t i n some countr ies , we a r e approaching sa tu ra t ion
point i n regard t o the numbers of doctors avai lable . A t the same time few people,
whether i n the profession i t s e l f , i n the Government a u t h o r i t i e s o r amongst the general
public, seem s a t i s f i e d with what those doctors do. A s elsewhere i n the world a
completely new look i s being taken a t medical education i n almost every country of
the Eastern Mediterranean Region, i n which WHO is proud to play i t s part . Many of
our a c t i v i t i e s i n medical education a s such w i l l be d i rec ted a t a continuous attempt
t o evaluate its product i n the l i g h t of the r e a l needs of the peoples' hea l th services.
A t the same t i m e , and r e f l e c t i n g the needs of a l l , and the experience i n recent
years of those who have experimented s o successful ly along such l i n e s , the re w i l l be
a much g rea te r e f f o r t than i n the pas t d i rec ted towards the planning, production and
e f fec t ive u t i l i z a t i o n of a l l o the r ca tegor ies of heal th workers.
I f the re a r e some who would question the point of view t h a t the Region i s reach-
ing near t o sa tu ra t ion point a s regards i t s production of doctors , o r a t any r a t e of
doctors a s present ly t ra ined, there a r e none who question the need t o t r a i n more, and
be t t e r , a l l i e d heal th workers of a l l kinds; a u x i l i a r i e s of a l l kinds; primary heal th
care workers t o meet the s p e c i f i c defined needs of the l a rge underserved population
of almost a l l countr ies , and heal th professionals o the r than doctors.
The heal th manpower stock of our countr ies i s i n danger of becoming not l e s s ,
but more, ou t of balance with need. Immense shorteges continue t o e x i s t among almost
a l l middle l e v e l and aux i l i a ry personnel, however the word "shortage" i s defined.
Cooperative ac t ion be t t e r t o def ine overa l l hea l th service needs, to f ind b e t t e r ways
of predic t ing manpower need and demand, t o design re levant t r a in ing programmes, t o
ca r ry ou t such programmes i n the most e f f e c t i v e and e f f i c i e n t way, and t o monitor
the use t o which t h e r e s u l t a n t manpower i s put, w i l l be high among the p r i o r i t i e s of
1980 and 1981.
Not l e a s t important among the heal th workers of the Region, t o whom specia l
a t t e n t i o n w i l l be devoted, a r e nursing personnel, denta l professionals and aux i l i a r i e s ,
and the manpower needed f o r the environmental hea l th services. Each of these groups
remains in shor t supply and in each the re is a need fo r much careful thought as to
the design of t r a i n i n g programmes. There has been, i n these areas , a s i n medicine
i t s e l f , too much emphasis over the years on supposedly high, yet largely i r r e levan t ,
s tandards of so-called academic excellence divorced from r e a l i t y . Given the deter-
mination of Member countr ies t o co r rec t t h i s s t a t e of a f f a i r s , W H D ' s programme is
ready t o provide co-operative help.
Renewed e f f o r t s w i l l be made, i n col laborat ion with those countr ies which have
rea l i zed the urgent need, t o develop organiced nat ional systems f o r continuing
education of hea l th personnel. I n a s imi lar connection col laborat ion w i l l be ex-
tended t o c e r t a i n countr ies of the Region, who, continuing t o be dependent t o a l a rge
extent on hea l th personnel imported from other countr ies , a r e i n s t i t u t i n g spec ia l
r eo r ien ta t ion programmes f o r such personnel.
A s reconmended by the Minis ter ia l Consultat ion on Health Services and Manpower
Development, the World Health Organization w i l l , i n p a r t i c u l a r , d i r e c t its e f f o r t s
i n these sub jec t s towards:
- Promotion of a c t i v i t i e s a t country a s w e l l a s Regional l e v e l t h a t enhance the
acceptance and implementation of an in tegra ted approach t o hea l th se rv ices and
manpower development.
- Collaboration with member countr ies i n conducting s t u d i e s on heal th needs and man-
power requirements, a s a bas i s f o r plans of ac t ion f o r an in tegra ted approach t o
hea l th services and manpower development. Such s t u d i e s may be i n the form of
country heal th programme exercises.
- Promotion and support of evaluat ive research on hea l th se rv ices and manpower
developanent, including research i n t o appropriate hea l th technologies, and d i s -
semination 02 information on the r e s u l t s of such research.
- Provision of information t o countr ies on a l t e r n a t i v e approaches to , and p rac t i ces
i n hea l th services and manpower development both within the Region and elsewhere.
- Emphasis, i n i t s t r a i n i n g progralmne, on the development of nat ional competencies
i n manpower planning and management, a s well a s i n the development of task-based
community-oriented cur r i cu la f o r the t r a in ing of a l l ca tegor ies of h e a l t h personneL
- Provision of technical advice, through appropriate consultancies, missions, work-
shops and task forbes, on s p e c i f i c a reas where co-ordination may be planned and
implemented.
- Continuous review of the progress made, a s well a s of the obs tac les t o progress.
A steady expansion of W H O ' S work i n occupational hea l th is proposed, and ex-
penditures i n t h i s programme area a r e proposed t o be doubled.
The funds avai lable , though small, w i l l be used i n a c a t a l y t i c fashion, i n co-
operation with o the r agencies concerned including IID, t o promote the expanding
e f f o r t s of Member countr ies themselves t o improve working condit ions, t o study needs
i n the subject , and t o formulate o r r ev i se standards and prepare guidel ines f o r pro-
t ec t ion aga ins t occupational hazards, including the improvement of occupational
hea l th l eg i s l a t ion . Provision i s made f o r ca re fu l ly designed fel lowships t o augment
the st i l l scarce heal th manpower spec ia l i z ing i n occupational heal th , with p a r t i c u l a r
emphasis on the t r a in ing of occupational hygienis ts and o the r middle-level personnel.
The huge proportion of nat ional heal th budgets which i s devoted t o the purchase
of drugs continues t o be a source of concern t o a l l M e m b e r s t a t e s and t o the Organiza-
t ion. Above a l l the re i s a need f o r improved r a t i o n a l i t y i n the use and production
of drugs of a l l kinds and i n a l l countries. This w i l l c a l l f o r continuing e f f o r t s
i n the t r a i n i n g of doctors and pharmacists and f o r subs tan t i a l programes of continu-
ing education and re-education of those whose ac t ions do i n f a c t determine both the
pa t t e rns and t h e cos t of prescribing. There is a continuing need, and provision w i l l
be made, f o r applied research i n t o the pa t t e rns of u t i l i z a t i o n of drugs, e s p e c i a l l y
by new categor ies of heal th workers i n t o whose hands expensive and powerful t o o l s a r e
being increasingly placed.
WHO w i l l co l laborate wi th Member countr ies i n the much needed strengthening of
regulatory a u t h o r i t i e s e spec ia l ly i n the f i e l d s of drug l icensing and inspection of
manufacture and d i s t r ibu t ion .
I n the p r o g r a m s r e l a t e d t o Disease Control i t w i l l be noted t h a t , desp i t e the
rapid advances made by and i n a majori ty of our M e m b e r countr ies , there is sti l l an
expressed need f o r subs tan t i a l WHO ac t iv i ty . There w i l l be continuing and expanding
emphasis on se lec ted aspec t s of communicable d i sease control . Three components of
this programe a r e of outstanding importance. I n budgetary terms the l a r g e s t item
i s fo r continuing a c t i v i t i e s d i rec ted towards the control of malaria and o the r
p a r a s i t i c diseases, of which those a f fec t ing the l a r g e s t populations a r e malaria
i t s e l f , and schistosomiasis.
Of equal importance, however, and with very promising po ten t i a l f o r fu tu re e f fec t -
iveness, a r e the proposed a c t i v i t i e s t o develop and improve the capacity of the
nat ional epidemiological services , with pa r t i cu la r regard t o t h e i r Capacity t o under-
take e f f e c t i v e survei l lance of communicable diseases.
A t t he same time, continuing the upsurge of a c t i v i t y t h a t has been notable s ince
1976,there w i l l be a s t rong d r ive , i n col laborat ion with the world-wide W H D Expanded
Progralme on Iarmunization, t o make immunization aga ins t d iphther ia , pe r tuss i s ,
tetanus, measles, pol iomyel i t i s and tuberculos is ,access ible t o more and more of the
chi ldren of the Region. A s i s well known the goal is t o make ths v i t a l and
e f f e c t i v e protect ion ava i l ab le t o every ch i ld by 1990. This i s one of the pro-
grammes i n which WHO is working i n c lose associa t ion with many d i f f e r e n t partners.
While the governmnts of t h e countr ies i n which the programme is a c t i v e a r e the most
e s s e n t i a l of these par tners , f o r without t h e m nothing can be achieved, w e look for-
ward t o continuing generous ass i s t ance from individual coun t r i e s t o the Voluntary
Fund f o r Health Promotion, a s w e l l a s t o continuing f r u i t f u l col laborat ion with
UNICEF and UNDP.
The Expanded Prograinme on Immunization provides r e a l i s t i c hope of r e l i e f ,
through the appl ica t ion of wel l - t r ied immunitation procedures t o vas t populations
h i t h e r t o deprived of them, from the s i x d iseases concerned, a s w e l l a s from a l l the
su f fe r ing and l o s s of l i f e they have represented over the h i s t o r y of mankind.
The e n t e r i c i n f e c t i o n s , i nc lud ing a l l forms of d ia r rhoea1 d i s e a s e , ranging from
cholera which causes s o much pub l i c anxie ty , but l i t t l e grave publ ic danger, t o t he
neglected d i a r rhoeas o f in fancy which q u i e t l y k i l l an es t imated th ree q u a r t e r s of
a mi l l i on ch i ld ren i n ou r Region every year , w i l l cont inue t o be a major focus o f
ou r work i n connnunicable d i s e a s e c o n t r o l and i n maternal and c h i l d hea l th . These
d i s e a s e s take a huge t o l l o f l i f e i n our Region. Thei r con t ro l depends t o a l a r g e
e x t e n t upon simple c l a s s i c pub l i c h e a l t h measures and the a v a i l a b i l i t y of r e l a t i v e l y
cheap and simple c u r a t i v e t o o l s , inc luding rehydra t ion ma te r i a l s .
I t i s a source of shame t h a t t h e d i a r rhoea l d i s e a s e s cont inue t o plague our
people a t a l l , and t h e i r c o n t r o l c a l l s f o r huge and gustained e f f o r t on tile p a r t o f
everyone involved i n pub l i c h e a l t h throughout the Region.
Within t h e programme a r e a of Family Heal th t h e r e w i l l be cont inuing emphasis, i n
an expanded form, on the important a c t i v i t i e s o f Maternal and Chl ld Heal th, N u t r i t i o n
and Heal th Education.
The pre-eminent importance of ch l ld ren under f i v e y e a r s o f age i n every count ry
of t h e Region i s inc reas ing ly w e l l recognized, a s i s t h e e x t e n t t o which l o s s of l i f e
among them, almost e n t i r e l y from d i s e a s e s whose prevent ion is understood, r e p r e s e n t s
perhaps t h e b igges t of a l l cha l l enges f ac ing ou r h e a l t h s e rv i ce s .
The i n t e r l o c k i n g e f f e c t s of uncont ro l led family s i z e , loadequate n u t r i t i o n and
i n f e c t i o u s d i s e a s e s , e s p e c i a l l y t h e e n t e r i c i n f e c t i o n s , i s very well underqtood.
Despi te cont inuing e f f o r t s over many years , t he propor t ion o f i l l n e s s and dea th
occu r r ing among i n f a n t s and ch i ld ren under f i v e cont inues t o be a dramat ic and t r a g i c
f e a t u r e of t h e g r e a t ma jo r i t y of our Member count r ies .
I n co l l abo ra t ion n t h UNICEF and UNFPA f u r t h e r e f f o r t s w i l l be maintained and
expanded, a doubling of Regular budget funds i n t h i s programme a rea i s proposed, and
s p e c i a l emphasis, c l o s e l y co-ordinated with t h e a c t i v i t i e s o f t h e Expanded Programme
on Immunization, w i l l be d i r e c t e d towards t h e r e s o l u t i o n of t he se problems.
There is still an urgent need f o r more e f f e c t i v e na t iona l food and n u t r i t i o n
p o l i c i e s , a s t h e r e i s f o r t r a i n e d personnel a t t h e p ro fe s s iona l and middle l e v e l s i n
n u t r i t i o n and i n h e a l t h educa t ion , and funds w i l l be made a v a i l a b l e f o r t r a i n i n g i n
t he se a r ea s .
The new and expanding r e sou rces of the WHO Global S p e c i a l Programme f o r Research-
and Tra in ing i n Tropica l Diseases w i l l be tapped, and merged wi th our own r eg iona l
programme, wherever t h e s i x d i s e a s e s malar ia , s ch l s to somias i s , f i l a r i a s i s ,
trypanosomiasi s, leishmaniasis and leprosy - with which i t is especia l ly , concerned
a r e of importance t o the Countries of the Eastern Mediterranean Region.
Should a l l forecas ts being made a t the time of wri t ing prove accurate, the years
1980 and 1981 should see t h e l a s t s tages of completion of the c e r t i f i c a t i o n of the
eradicat ion of smallpox from a l l countr ies of the Region.
I n so f a r a s the prevention and control of non-comunicable diseases i s con-
cerned, the highest emphasis w i l l be given t o e f f o r t s t o control chncer, t o improve
the capaci t ies of Member countr ies i n control l ing and handling the mounting t o l l
from the cardiovascular d iseases and t o measure the extent of mental disorder and t o
contain i ts spread and a i d i ts victims. I n the case of mental health, though the
programme remains a r e l a t i v e l y small one, the f a c t t h a t i t has doubled a s a per-
c e ~ t a g e of the proposed budget i s a recognition of the mounting importance being
attached t o t h i s all-pervading problem i n the countr ies of the Region. I t is a l s o
worthy of note t o r e a l i z e t h a t qu i t e a high proportion of the funds spent i n heel th
services development, and of those spent i n the promotion of t ra ining, do i n f a c t go
towards t h e preparation of men and measures t o deal with the non-communicable
diseases. The time is f a s t coming, of course, i f indeed i t is not upon us, when
the diseases of the more a f f l u e n t and advanced s o c i e t i e s become those of g rea tes t
s ignif ic iance i n our Region. There i s a tremendous need f o r improved quan t i f i ca t ion
of t h e i r prevalence and impact, and increasing e f f o r t s w i l l be made, through research
and otherwise, t o apply the basic pr inciples of epidemiology, the fundaaental science
of public health, t o the study of these diseases.
I n mental heal th work par t i cu la r ly , but i n many o ther f i e l d s a s w e l l , such a s
the study of heal th service needs and demands, and i n the development of up-to-date
guidance on t ra in ing programmes, the Organization expects t o be making more and more
use i n its own work, and t o see g rea t ly increased use made by M e m b e r countr ies , of
the h i the r to too much neglected contributions of the soc ia l and behavioural science8.
Biomedical Research, including applied research i n t o the effect iveness and
aoverage ~f heal th services, has now been a regional r espons ib i l i ty fo r three years;
and i n the coming biennium a c t i v i t i e s i n t h i s area a r e expected t o become even more
prominent. The Eastern Mediterranean Advisory C o m i t t e e on Biomedical Research
(EM ACMR) and its annual meetings, f o r which continuing provision is made, have become
cornerstones of our work. Emphatic p r i o r i t y has been l a i d d m regarding the over-
r id ing importance of applied research, and of support t o research a c t i v i t i e s re la ted
t o the disease problems of g rea tes t sever i ty i n the M e m b e r countries. There w i l l

be an expansion of t h e WHO Col labora t ing Cent res i n the Region, and of s p e c i f i c
agreements w i th s e l e c t e d c e n t r e s of exce l lence which a r e ca r ry ing ou t r e sea rch work
wi th in t he p r i o r i t i e s l a i d down by the EM ACMR. An i n t e r l o c k i n g s e r i e s of Advisory
Panels supplements t he work of t he EM ACMR i n f i e l d s such a s Canaer, Mental Heal th,
primary f iea l th- ta re and Nursing and, a s p a r t i c u l a r a r e a s of r e sea rch a c t i v i t y open
up, provis ion w i l l be made t o convene small S c i e n t i f i c Working Groups both t o adv i se
W I U on t h e best ways i n which i t can con t r ibu t e , and t o review s p e c i f i c r e sea rch
proposals .
An important new panel , set up i n 1978, is t h a t on Heal th Se rv i ce s and Manpower
Development,whose members w i l l be c a l l e d upon t o p lay an a c t i v e p a r t i n our programmes,
no t l e a s t i n Research i n t he se sub jec t s .
A s t h e o v e r a l l reg ional r e sea rch programme expands, s p e c i f i c r eques t s an11 be
made f o r Voluntary Funds t o supplement those made a v a i l a b l e i n t he Regular Budget,
and from the Regional D i r e c t o r ' s Development Programme.
The e f f e c t s o f environmental p o l l u t i o n on h e a l t h remain among the s e r i o u s pub l i c
h e a l t h problems of t he Region,and t h e i r con t ro l i s t h e cont inuing r e s p o n s i b i l i t y of
n a t i o n a l h e a l t h a u t h o r i t i e s and o f W H O , d e s p i t e t h e growth i n r ecen t yea r s of o t h e r
na t iona l and i n t e r n a t i o n a l agencies wi th environmental c o n t r o l func t ions . I n re-
sponse t o need i t is proposed t o provide a s i z e a b l e i nc rease i n t he propor t ion of
t he budget devoted t o t h e promotion of environmental h e a l t h i n the coming biennium,
These a c t i v i t i e s w i l l account f o r about 7% o f t h e t o t a l budget.
Basic s a n i t a r y measures, wi th s p e c i a l emphasis on the improvement o f food s a f e t y
and hygiene,are v i t a l i n an a r e a wi th the socio-economic and c l i m a t i c cond i t i ons o f
t h e Eas te rn Mediterranean Region. The bas i c problem of the provis ion of s a f e and
e f f e c t i v e exc re t a d i sposa l and t h e c o n t r o l of usage of f a e c a l l y contaminated waste
waters f o r food crop i r r i g a t i o n w i l l cont inue t o be tackled i n c o l l a b o r a t i o n wi th
na t iona l a u t h o r i t i e s . The p rov i s ion of a s a f e water supply i n adequate q u a n t i t i e s
w i l l a l s o be of high p r i o r i t y and i n t h i s WIQO w i l l cont inue t o work c l o s e l y w i th a l l
concerned.
A s i n o t h e r a c t i v i t i e s i t i s c l e a r t h a t progress i n environmental h e a l t h c o n t r o l
cont inues t o be hampered a t a l l l e v e l s , and i n almost a l l c o u n t r i e s , by an in -
s u f f i c i e n c y o f proper ly t r a i n e d manpower.
Within t h e environmental h e a l t h programme, a c t i v i t i e s t o promote t h e product ion
o f more, and more r e l e v a n t , manpower w i l l have p r i o r i t y . This w i l l c a l l e s p e c i a l l y
f o r the development of t r a i n i n g capac i t i e s f o r producing l a r g e numbers of middle
l eve l technical personnel t o complement and extend the e f f e c t i v e range of the pro-
fess ional l e v e l workers.
The protection and conservation of the f i n i t e supply of the world's water re-
sources i s of specia l importance i n the Eastern Mediterranean Region where f resh
water resources a r e generally l imi ted and the re is heavy dependence on the desaliniza-
t ion of marine waters. The W H D Global Environmental Monitoring system, i n collabora-
t ion with UNEP, which dea l s with both a i r pol lu t ion and water pol lu t ion,wi l l be
subs tan t i a l ly expanded i n the Region t o the point where i t is ant ic ipated t h a t a t
l e a s t 12 countr ies w i l l partake i n the network deal ing with the measurement of a i r
qua l i ty , and 11 countr ies w i l l have monitoring s t a t i o n s and/or col laborat ing
l abora to r i e s contributing t o the monitoring of water qual i ty . WHO w i l l he lp t o
f o s t e r the in ter regional col laborat ion required t o deal with marine pol lu t ion pro-
blems i n the Mediterranean.
A s a core contr ibut ion t o the i n t e n s i f i c a t i o n of e f f o r t s i n a l l aspects of
environmental health, the establishment of an Eastern Mediterranean Centre f o r Environ-
mental Health A c t i v i t i e s i s contemplated. Such a cen t re would address i t s e l f t o
research and t r a in ing , t o the i d e n t i f i c a t i o n and c l a s s i f i c a t i o n of environmental pro-
blems and t o the fu r the r development of a coordinated network of nat ional i n s t i t u t i o n s .
The World Health Organization i n t h i s Region has always enjoyed very f r i end ly
and f r u i t f u l col laborat ion with i ts s i s t e r United Nations Agencies and it is a n t i -
cipated t h a t these re la t ionsh ips w i l l become c lose r and more intimate. Amongst the
o the r agencies of the United Nations system which a r e most a c t i v e l y involved and
whose programne focus, l i k e W H D ' s , i s s t rongly upon the prcrmotion of heal th , UNDP
and UNICEF, UNFPA and UNEP a r e the most c ruc ia l .
There w i l l a l so be a continuation of f inanc ia l support from UNFPA and, i n those
a c t i v i t i e s i n which they a r e primarily concerned, wi th FAO, UNESCO, I m ' a n d the
Economic Commissions. An expansion is ant ic ipated i n the use of UN Volunteers i n
a va r ie ty of p ro jec t s , p a r t i c u l a r l y i n the l e a s t developed countries.
The continuing expanding involvement of the World Bank (IBRD) i n hea l th mat ters
w i l l be more and more c losely re la ted with W H D and i t i s an t i c ipa ted that W H D w i l l
continue t o a c t a s the executive agency for p ro jec t s financed by them i n the hea l th
area.
W H O ' S c o n s t i t u t i o n a l r o l e a s t he d i r e c t i n g and co-ordinat ing a u t h o r i t y on i n t e r -
na t iona l h e a l t h work i n t he world, has been inc reas ing ly r e a l i z e d i n r ecen t years
and, i n t he Eastern Mediterranean Region i n p a r t i c u l a r , t h i s type of work w i l l be
expanded and improved upon i n 1980/81. We welcome t h e way i n which those c o u n t r i e s
which a r e i n a p o s i t i o n t o provide b i l a t e r a l a i d t o t h e i r less f o r t u n a t e f r i e n d s ,
whether t he se be coun t r i e s w i th ln our Region o r from o u t s i d e , a r e i nc reas ing ly con-
s u l t i n g t h e Regional Of f i ce on t h e development of t h e i r own programmes. WHO has a
weal th of knowledge and understanding of t he h i s t o r y o f i n t e r n a t i o n a l h e a l t h develop-
ment throughout t he Middle Eas t . Our experience is r e a d i l y put a t t h e d i sposa l of
those who a r e newer t o t he f i e l d . We expect t o cont inue t o en joy cons t ruc t ive co-
o p e r a t i v e r e l a t i o n s h i p s w l t h t he I s lamic Development Bank and t h e Council o f Heal th
Min i s t e r s of t h e Arab League.
A s WHO'S po l i cy t o encourage the u t i l i z a t i o n of n a t i o n a l s t o work on W H O
a c t i v i t i e s i n t h e i r own c o u n t r i e s g a i n s momentum, i t i s a n t i c i p a t e d t h a t t h e r e w i l l
be a cont inuing t rend towards t h e provis ion o f funds t o enable governments and
educa t iona l i n s t i t u t i o n s t o undertake d i r e c t recru i tment of h e a l t h workers who might
no t o therwise be a v a i l a b l e t o them, but who a r e no t i n a d i r e c t employer/employee
r e l a t i o n s h i p wi th WHO i t s e l f .
No expansion i s a n t i c i p a t e d i n t h e number of Wm Programme Co-ordinators and
where no such pos t e x i s t s , s u i t a b l e arrangements m l l be made f o r co-ordinat ion of
W H O programme.
A s a l r eady mentioned i n connect ion wi th t h e Regional Research Programme, i n -
c r ea s ing use w i l l be made o f an interlocking s e r i e s of advisory panels , i n a v a r i e t y
of f i e l d s , drawn from t h e e x p e r t i s e which is s o r a p i d l y expanding among Member
count r ies .
The e x t e n t t o w h c h t h e s en io r h e a l t h o f f i c a l s of Member c o u n t r i e s a r e a c t i v e l y
involved i n pol icy p repa ra t ion and programme des ign is expected t o i n c r e a s e and the
work o f a committee s e t up f o r t h i s purpose by the Regional Committee a t i t s Twenty-
seventh s e s s ion I n 1977 w i l l become an inc reas ing ly important l i n k between our
Governing Body and t h e S e c r e t a r i a t . I n t he s p i r i t o f co-operat ion which has i n -
c r ea s ing ly cha rac t e r i zed the working relationship between WHO and the Member coun t r i e s
i n r ecen t yea r s , i t i s a n t i c i p a t e d t h a t t he re w i l l be more and more o p p o r t u n i t i e s f o r
exchange o f views and a c t i v e involvement of n a t i o n a l s a t every l eve l .
The World Health Organization has now been providing service t o the countr ies
of the Eastern Mediterranean Region over the pas t 29 years. I have reason t o believe
t h a t our Member countries take r e a l pr ide i n how we work together and i n what we have
achieved. Our Region i s one of extraordinary d ive r s i ty . Although its population is
not a l l that large , i t contains some of the r i c h e s t countr ies i n the world and some
of the poorest. I t i s i n many ways a cornerstone of the world, and i t has not been,
f o r many years, f r e e of the s t r i f e t h a t a t every point i n the h is tory of mankind has
characterized an area of constant and rapid change and d i v e r s i t y of r e l i g i o u s and
p o l i t i c a l bel iefs .
Not l e a s t among the sources of our g r a t i f i c a t i o n i n our work l i e s the f a c t that,
i n the face of every d i f f i c u l t y , WHO has remained a t the service of a l l , regardless
of p o l i t i c a l events, without in te r rup t ion s ince the inception of the Eastern Mediter-
ranean Regional Office i n 1949. I firmly believe t h a t our record w i l l be maintained.
I t is a source of continuing s a s t i s f a c t i o n t o observe the extent t o which heal th
concerns do i n f a c t override p o l i t i c a l consideration& and it w i l l be our continuing
e f f o r t t o ensure t h a t they do so more and more.
I submit t h i s Programme Budget for the years 1980/81 f o r the consideration of
Member countr ies , i n the knowledge t h a t i t has been b u i l t up i n the c l o s e s t collabora-
t ion and consultat ion with them, a s w e l l a s i n the confidence that, adapted and
adjusted a s needs may be, time passes, and circumstances change, i t w i l l play i ts
appropriate modest pa r t i n moving, with our Member countr ies , one s t e p f u r t h e r along
the road t o the defined goal which a l l countr ies of the world have set, of hea l th
f o r a l l by the year 2000.
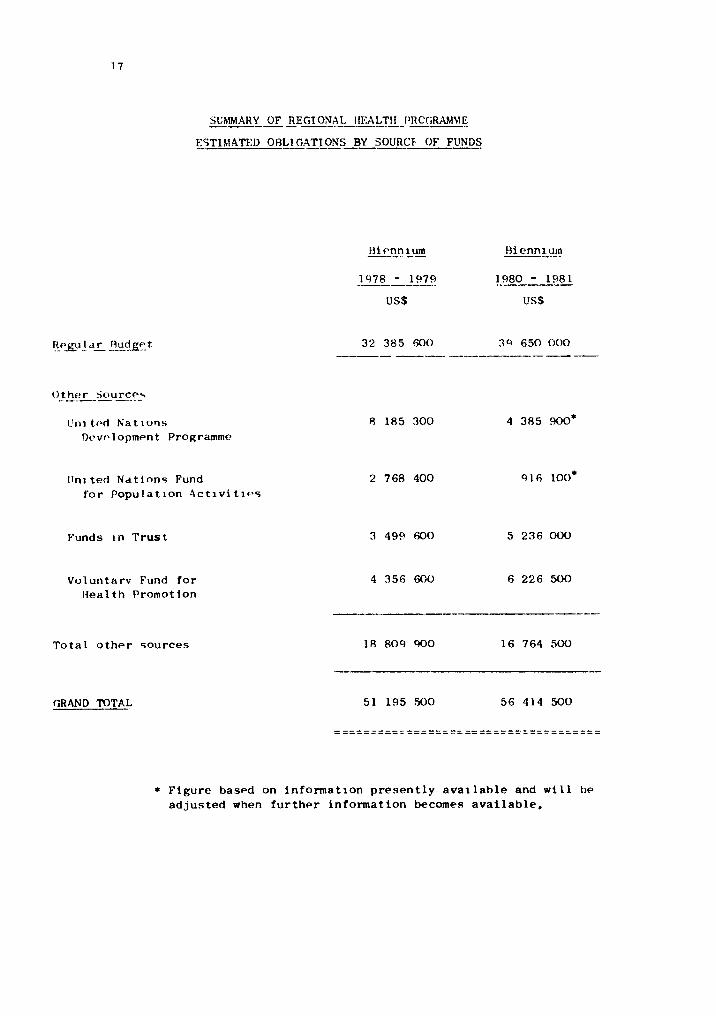
SUMMARY OF REGIONAL IIEALTH IJRCC~RAhlME --- -- ------ LSTIhlATED OALI GATIONS BY SOURCF OF FUNDS
V r r i tchd h'at~orls Dt~vc~lopment Programme
IJnl ted Nati nns Fund f o r Population A c t i v i t i e s
Funds In Trust
Voluntarv Fund f o r Health Promotion
Total o t h e r sources
GRAND TOTAL
Figure based on information p r e s e n t l y a v a ~ l a b l e and w i l l be adjus ted when fur ther information becomes a v a i l a b l e ,
Programme
Nuinbci
1.3
2.1
2.2
2.3
2.4
2.5
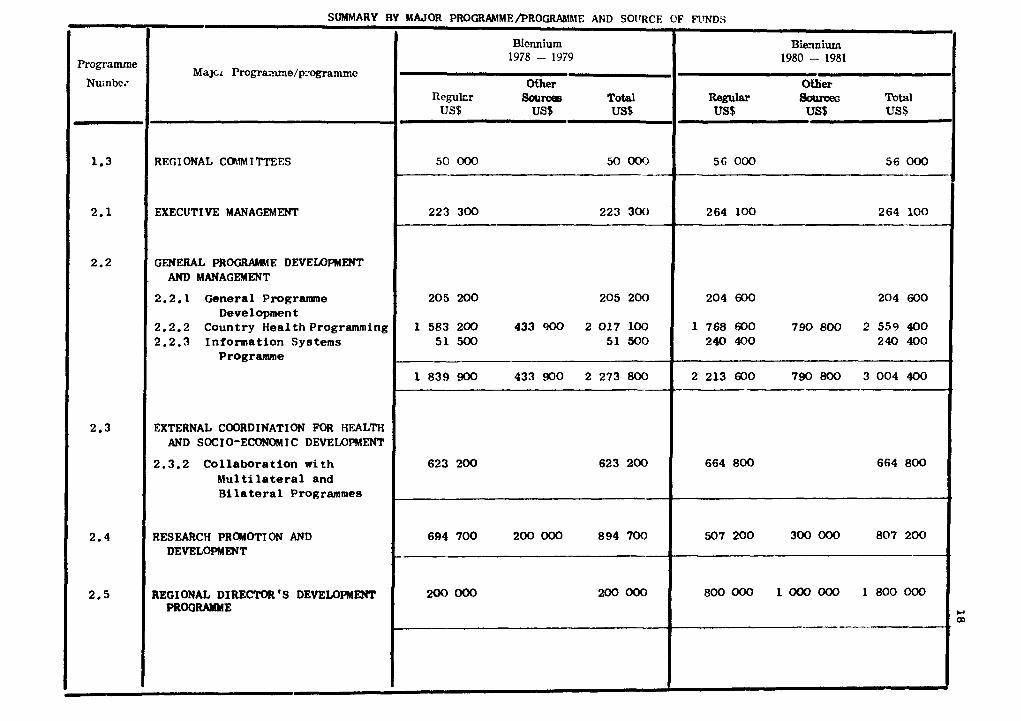
SUMMARY BY
Majcr Progmune/p:-0gram.c
REG1 ONAL COIW I TTEES
EXECUTIVE MANAGEMENT
GENERAL PROGRMtE DEVELOPMENT AND MANAGEMENT
2.2.1 General Programme Development
2.2.2 Country Healthprogramming 2.2.3 Information Systems
Programme
EXTERNAL COORDINATION FOR HEALTH AND SOCIO-ECONOMIC DEVELOPMENT
2.3.2 Collaboration with hlulti lateral and Bilateral Programmes
RESEARCH PROMOTION AND DEVELOPMENT
REGIONAL DIRECTOR 'S DEVElXlPMENT PROGRAMME
MAJOR PROCRAMME/PROGMfME AND SOIlRCE
Biennium 1978 - 1979
Ofher Reylcr Sources Total
US$ US$ US$
50 000 50 OOO - .
223 300 223 300
205 200 205 200
1 583 200 433 900 2 017 100 51 500 51 500
1 839 900 433 900 2 273 800
623 200 623 200
694 700 200 000 894 700
200 ooo 200 OOO
OF FTWDS
Biavliurn 1980 - 1981
W e r %war ao~mt?s Total US$ m US$
56 000 56 000
264 10 0 264 100
204 600 204 600
1 768 600 790800 2559400 240 400 240 400
2 213 600 790 800 3 004 400
664 800 664 800
507 200 300 000 807 200
800 000 1 000 000 1 800 000
1
P 01
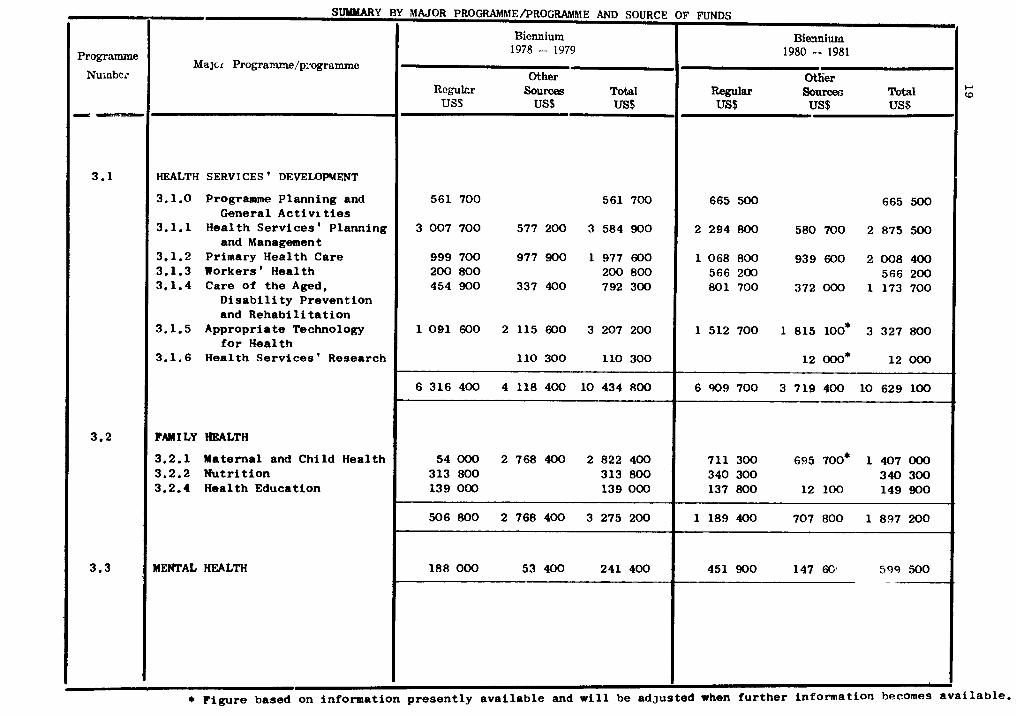
Programme
Nuinbcz
HEALTH SERVI CES * DEVELOPMENT
3.1.0 Programme P l a n n i n g and Genera l A c t i v i ties
3.1.1 H e a l t h S e r v i c e s 9 Planning and Management
3.1.2 Pr imary H e a l t h Care 3.1.3 Workers * H e a l t h 3.1.4 Care of t h e Aged,
D i s a b i l i t y P r e v e n t i o n and R e h a b i l i t a t i o n
3.1.5 A p p r o p r i a t e Technology f o r H e a l t h
3.1.6 H e a l t h S e r v i c e s ' Research
FAM I LY HEALTH
3.2.1 Mate rna l and C h i l d Hea l th 3.2.2 N u t r i t i o n 3.2.4 H e a l t h Educa t ion
MENTAL HEALTH
Y MAJOR PROGRAMMEDROGRAMME AND SOURCE OF FUNDS
Biennium I Biemim 1978 - 1979 1980 - 1981
1
* F i g u r e based on i n f o r m a t i o n p r e s e n t l y a v a i l a b l e and w i l l be a d j u s t e d when f u r t h e r i n f o r m a t i o n becomes a v a i l a b l e .
Other Rcylcr Sources Total US$ US$ US$
Otlier Regular Sourceri n t a l US$ US$ US$
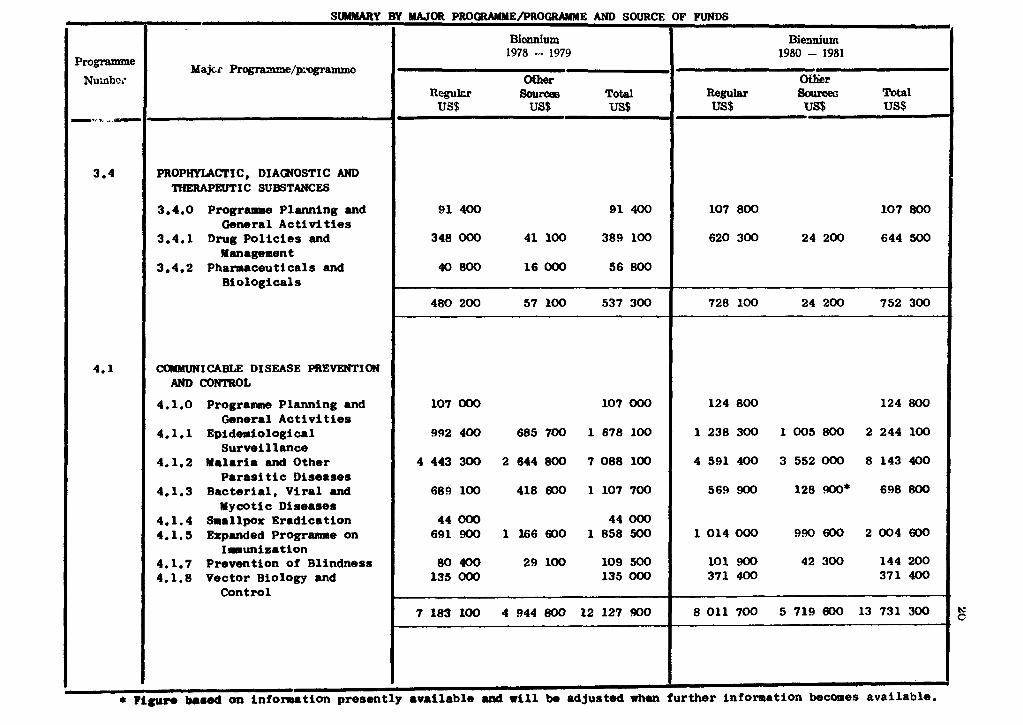
Programme I Majcr proSnmme/p:agramme Nuinb~~.
/ PROPHYLACTIC, DIA(NOST1C AND / TIfERAPEUTIC SUBSTANCES
1 3.4.0 P r o g r a m Planning end General Activities 1 3.4.1 Drug Pol ic ies end Management
3.4.2 Pharmaceuticals and , Biologicals
COMMUNICABLE DISEASE PREYENTION AND CONTROL
P r o g r a m Planning and General Act iv i t i es
Epidemiological Surveillance
Malaria end Other Parasi t i c Diseases
Bacterial , Viral end My cotic Diseases
Smallpox Eradication Expended Progrmm on
Imunisat ion Prevention of Blindness Vector Biology and
Control
* Figure bared on infomation presen
Y MAJOR PROCRAMME/PROGRAMME AND SOURCE OF FUNDS
Bicnnium Biemium 1978 - 1979 1980 - 1981
Ofher Oftier Rcy lrr Sourcaa Total Regular source^ Tots1 US$ us9 US$ US$ vsS US$
I
y available uni rill he adjusted rhon further information becaaes available.
Programme
Nu.nbci
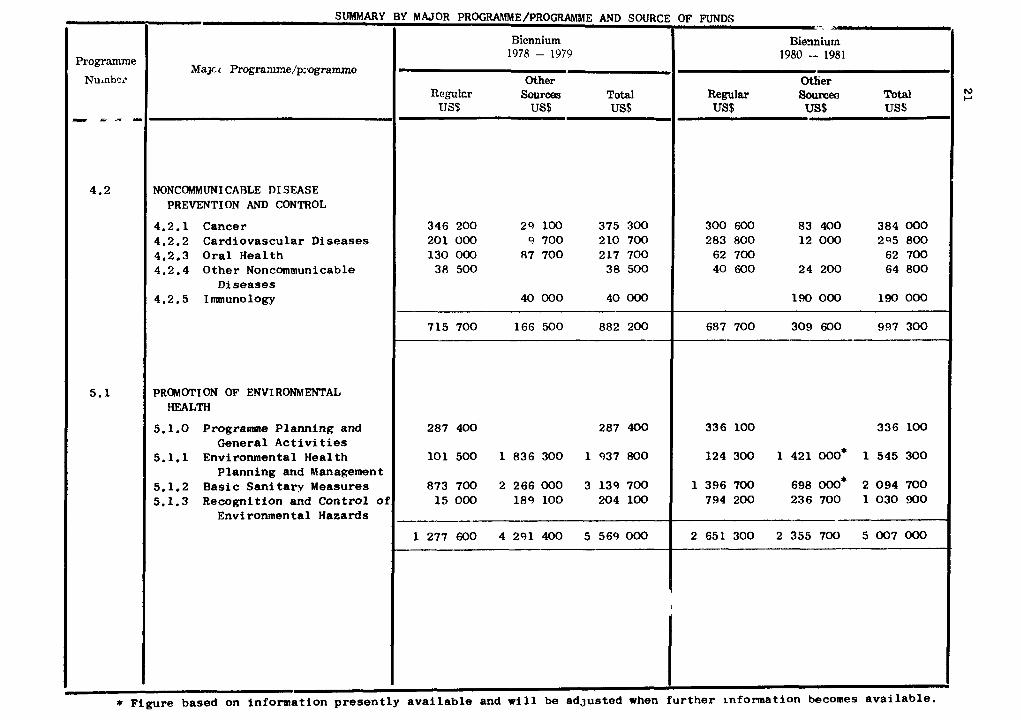
- SUMMARY
NONC~~UNI CABLE DI SEASE PREVENTION AND CONTROL
4.2.1 Cancer 4.2.2 C a r d i o v a s c u l a r Diseases 4.2.3 O r a l H e a l t h 4.2.4 O t h e r Noncommunicable
D i s e a s e s 4.2.5 Immunology
PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.0 Programme P l a ~ i n g and Genera l A c t i v i t i e s
5.1.1 Environmental H e a l t h P l a n n i n g and Management
5.1.2 B a s i c S a n i t a r v Measures 5.1.3 Recogni t ion and C o n t r o l of
Environmental Hazards
3Y MAJOR PROGRAMME/PROGRAMME AND SOURCE OF FUNDS . .
Other Otlier Rcgulcr Sources T w l hg~lu Soum?a Total I US$ US$ US$ US$ US$ US$
* F i g u r e based on i n f o r m a t i o n p r e s e n t l y a v a i l a b l e and w i l l be a d j u s t e d when f u r t h e r rn fonna t ion becomes a v a i l a b l e .
Programme
Nuiibc..
6.1
7.1
.
t
Pigum
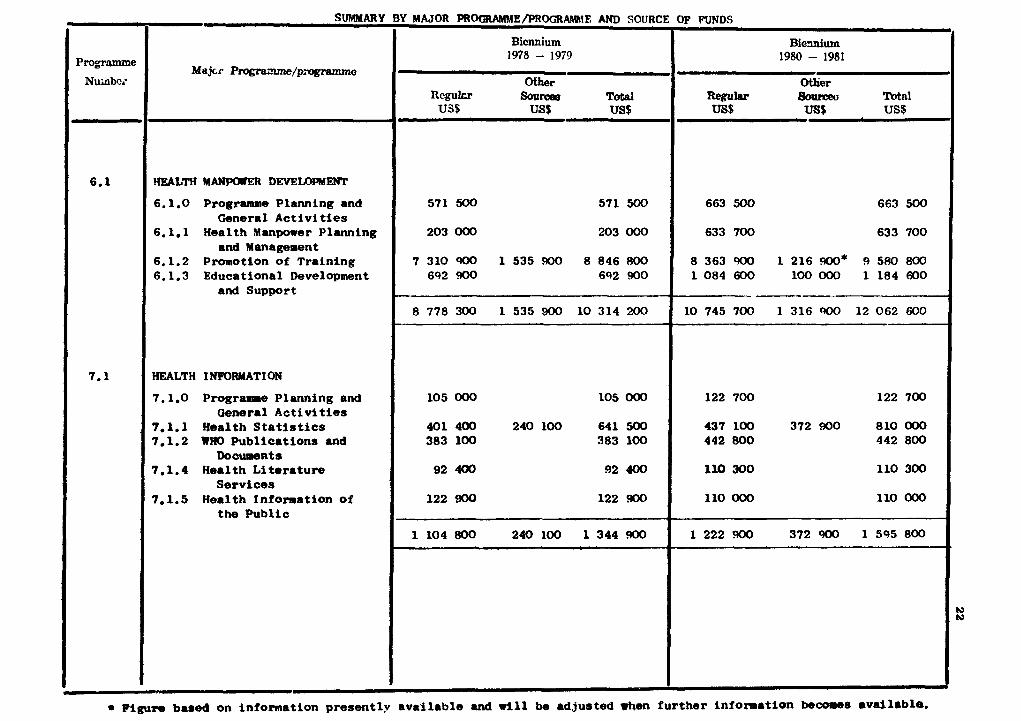
SUMMARY
Majcr. P m g r a z ~ / p . ~ m m c
HEALTH MANPOllER DEVEUIPMENT
6.1.0 Programme Planning and General A c t i v i t i e s
6.1.1 Health Manpower Planning and Management
6.1.2 Promotion of Tra in ing 6.1.3 Educational Development
and Support
HEALTH INFORMATION
7.1.0 Progranune Planning and General A c t i v i t i e s
7 . 1 Health S t a t i s t i c s 7.1.2 WHO Pub l i ca t ions and
Documents 7.1.4 Health L i t e r a t u r e
Se rv ices 7.1.5 Health f n f o n a t i o n of
the Pub l i c
based on information p resen t ly
BY MAJOR PROC;RAMME/PROGR~IE AND SOURCE
Biennium 1978 - 1979
Ofher R c y l c r Sou- Total US$ US$ US$
571 500 571 500
203 000 203 000
7 310 900 1 535 MI0 8 846 800 692 900 692 900
8 778 300 1 535 900 10 314 200
105 000 105 000
401 400 240 100 641 500 383 100 383 100
92 4CX) 92 400
122 900 122 900
1 1 0 4 800 240 100 1 344 900
a v a i l a b l e and rill be adjus ted .hen
OF FUNDS
Biemiurn 1980 - 1981
Otbier Regular souzceo T~tal US$ us$ US$
663 500 663 500
633 700 633 700
8 363 900 1 216 WO* 9 580 800 1 084 600 100000 1 1 8 4 600
10 745 700 1 316 900 12 062 600
122 700 122 700
437 100 372 900 810 000 442 800 442 800
110 300 110 300
110 000 110 000
1 222 900 372 900 1 595 800
f u r t h e r i n f o m a t i o n b~cole8 avai lable .
hl tu
h) 0
Programme
Nuinbci
--
8.1
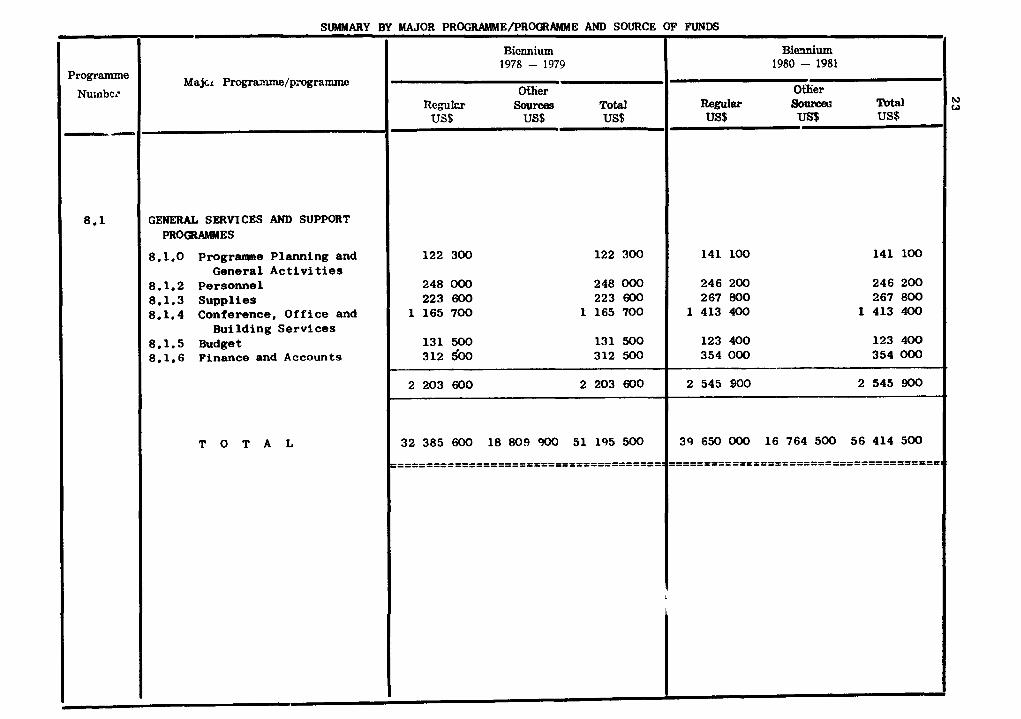
SUMMARY BY MAJOR PROGRAMME/PROGRAMME AND SOURCE OF FUNDS
T O T A L
2 203 600 2 203 600 2 545 900 2 545 900
I
32 385 600 18 809 900 51 195 500 39 650 000 16 764 500 56 414 500
.........................................
Bieanium 1980 - 1981
Oflier wi%lm Souroeu Total US$ us US$
Majci Progra2~e/p.-ogramnu?
Bionnium 1978 - 1979
Of lier Regukr Souram Total
US$ US$ US$
GENERAL SERVICES AND SUPPORT PROQtAMMES
8.1.0 Programne Planning and General A c t i v i t i e s
8.1.2 Pe r some 1 8.1.3 Suppl ies 8.1.4 Conference, O f f i c e and
Building Se rv ices 8.1.5 Budget 8.1.6 Finance and Accounts
122 300 122 300
248 000 248 000 223 600 223 600
1 165 700 1 165 700
131 500 131 500 312 $00 312 500
141 100 141 100
246 200 246 200 267 800 267 800
1 413 400 1 413 400
123 400 123 400 354 000 354 OoO
C
Progmmme Nuinbci
1 . 3
2.1
2 .2
2 .3
2.4
2.5
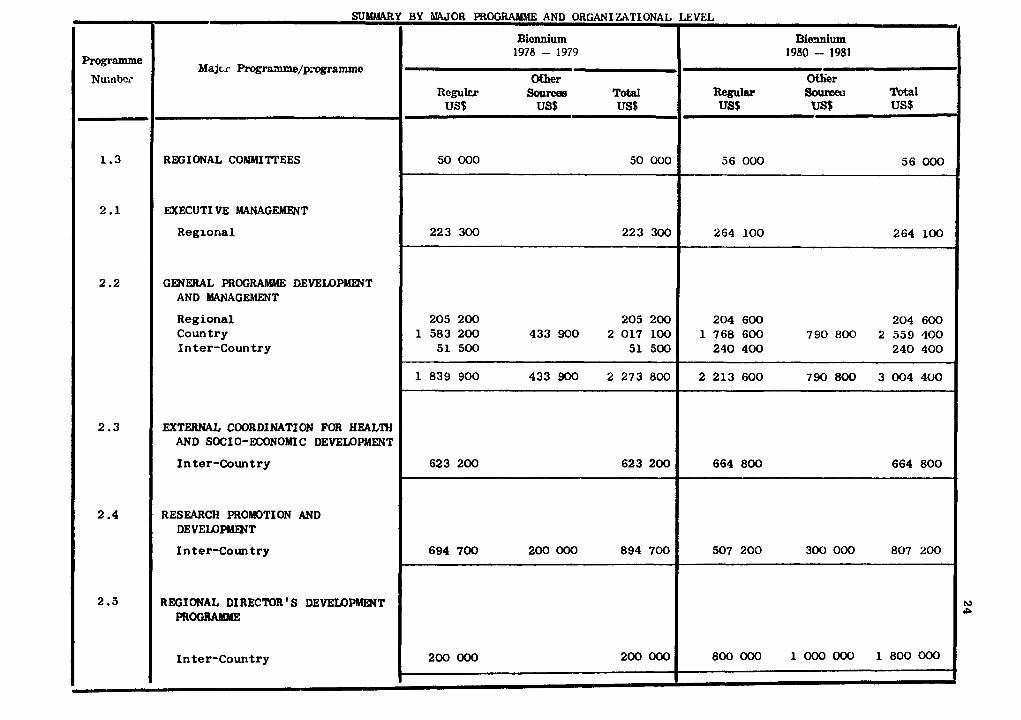
SUUMARY
Majcr P ~ r & 7 ~ / p i ~ ~ ~ e
RMiIONAL CONWZTEES
EXECUTI YE MANAGEWT
Regional
GENERAL PROGRAMME DEVELOPMENT AND MANAGEMENT
Regional Country Inter-Coun t r y
EXTERNAL COORDINATI ON FOR HEALTH AND SOCIO-ECONOMIC DEVELOPMENT
I n ter-Country
RESEARCH PROMOTION AND DEVELOF'MmT
I n t e r C o u n t r y
REGIONAL DIRECTOR'S DEVELOPMENT PROGRAMME
Inter-Country
IQ P
BY IWOR PROGRAMME AND ORGANIWTfONAL
Biennium 1978 - 1979
(Xfher Rey lcr Sources TOW US$ US$ US$
50 000 50 000
223 300 223 300
205 200 205 200 1 583 200 433 900 2 017 100
51 500 51 500
1 839 900 433 900 2 273 800
623 200 623 200
694 700 200 000 894 700
200 000 200 000
LEVEL
Bimium 1980 - 1981
Wlier m l a r Sounceu 'Dotal US$ vs$ US$
56 000 56 000
264 100 264 100 -
204 600 204 600 1 768 600 790 800 2 559 400
240 400 240 400
2 213 600 790 800 3 004 400
664 800 664 800
507 200 300 000 807 200
800 000 1 000 000 1 800 000
Programme Nuinbc~'
HEALTH SSERVICES' DEVELOPMENT
C o u n t r y I n t e r - C o u n t r y
FAMILY HEALTH
C o u n t r y I n t e r - C o u n t r y
MENTAL HEALTH
C o u n t r y I n t e r - C o u n t r y
PROPHYLACTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
C o u n t r y I n t e r - C o u n t r y
Y BY MAJOR PROGR;\hLr\lE AND ORGANIZATIONAL LEVEL
Bicnnium Bimium 1978 - 1979 1980 - 1981
COMMUNICABLE DISEZSE PREVJNTION 1 4.1 1 M m C O N r n O L
I Programme
1 Nu.nbci
_ 6 3-
I I c o u n t r y
Majc~ Programme/p;*ogrammc?
I n t e r - C o u n t r y
NONCOMhKlNI CABLE DI SEASE PREVENTION AND CONTROL
C o u n t r y I n t e r - C o u n t r y
PROMOTI ON OF ID VI RON MENTA L HEALTH
C o u n t r y I n t e r - C o u n t r y
HEALTH W P O W E R DEVELOPMENT
C o u n t r y I n t e r - C o u n t r y
Y BY W O R PROGRAMME AND ORGAhIZATIONAL LEVEL
Biennium 1978 - 1979
atlier R c y k r Sourcas Total
US$ US$ US$
B i d u m 1980 - 1981 I
Othier Regular So- Total US$ us$ US$
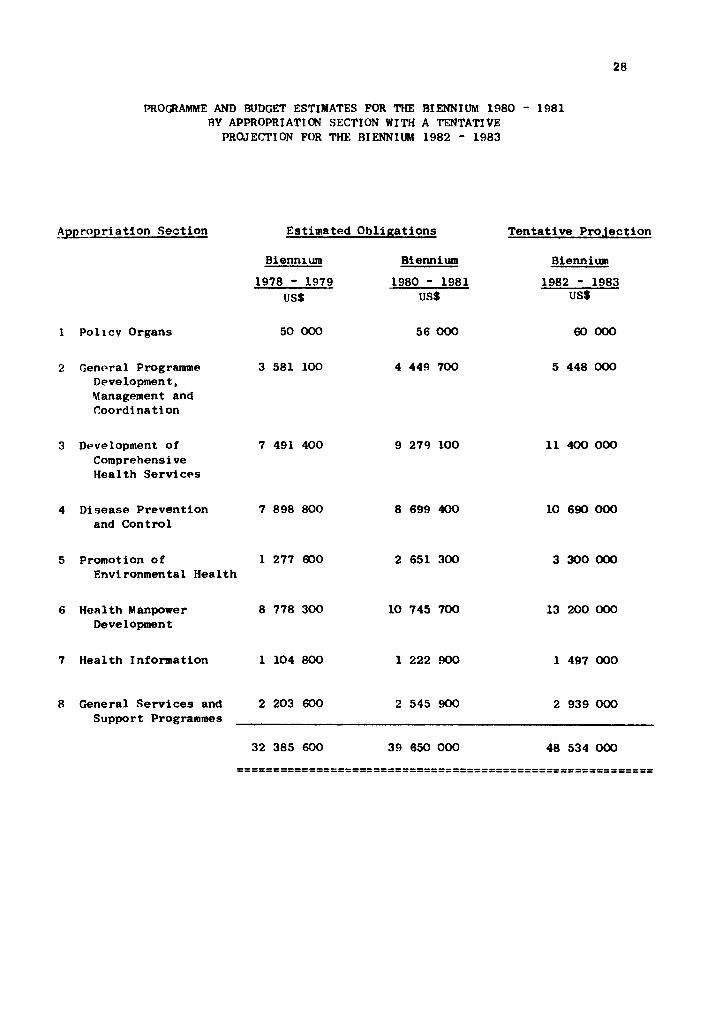
PRO(;RAMME AND BUDGET ESTIMATES FOR THE BIENNIUM 1980 - 1981 BY APPROPRIATION SECTION WITH A TENTATIVE
PROJECTION FOR THE BIENNIUM 1982 - 1983
A j ~ r o p r i a t i o n S e c t i o n Es t imated O b l i ~ a t i o n s T e n t a t i v e Pro. iect ion
Bienni urn B l e ~ i u m Biennium
1978 - 1979 1980 - 1981 1982 - 1983 US$ USS US$
1 P o l l c v Organs 50 000 56 000 60000
2 Fencra l Programme 3 581 100 4 449 700 Development , Management and Coord ina t ion
3 Development of 7 491 400 9 279 100 Comprehensive Hea l th S e r v i c e s
4 Disease Preven t ion 7 898 800 8 699 400 and C o n t r o l
5 Promation of 1 277 600 2 651 300 Envi ronmental H e a l t h
6 H e a l t h Manpower 8 778 300 10 745 700 Development
7 Hea l th In format ion 1 104 800 1 222 !300 1 497 000
8 General S e r v i c e s and 2 203 600 2 545 900 2 939 000 Support Programmes
Major Programme
REGIONAL COAllYlI TTEES 1.3 - The Regional Conunittee is a const i tu t ional organ of the Regional Organization.
Thus, i U s an inter-governmental organ corpssed of regweeentati*es.of t h e L ~ 8 8 ; p
S t a t e s (current ly 23 f u l l Members i n the Eastern Mediterranean Region). The Regional
Director i s ex-officio Secretary of the Regional Copnittee.
The Regional Committee is responsible for formulating po l ic ies governing matters
of exclusively regional character, and a l s o f o r supervising the a c t i v i t i e s of WHO i n
the Region. Through i ts annual meetings, the Regional Coltmaittee provides advice and
guidance t o the Regional Director on planning and implementation of the Rerrional Pro-
gramme. Further, it can tender advice through the Regional Director and the Director-
General t o the Organitation on in ternat ional hea l th matters which have wider than
regional significance.
The estimates provide f o r an annual meeting of Sub-cornittees A and B of the
Regional Colmnittee f o r the Eastern Mediterranean Region.
Major Programme
EXECUTf VE MANAGEMENT - --- -----
The Regional Director is the technical and administrative head of the Regional
Organization. In this capacity, he supervises the work of the WHD Secretar ia t i n
the Regional Office o r attached to country and interoountry programmes.
Within the overall policy of work, a s established by the World Health Assemblies,
and i n consultation with the Regional Conmittee, he is responsible for the execution
of the WHO programme i n h i s Region. I n t h i s connexion he establ ishes d i rec t contact
with the governments of the Region and consults the au thor i t i es e i ther d i rec t ly o r
through h i s s t a f f with regard t o the WH) a c t i v i t i e s i n t he i r respective countries.
He maintains contacts with appropriate professional groups i q the Region. H e a l so
co-ordinates health progrannnes assis ted by other international organizations within
the Regi~n.
The RegLonal Director formulates the Proposed Programe Budget for submission t o
the Regional Committee.
Major Programe
GEKERAL PROGRAMME DEVEUPlldWT AND MANAGEMENT
Objectives:
- t o col laborate with M e m b e r Countries i n the development of nat ional heal th plans
and programmes a s an i n t e g r a l pa r t of t h e i r overa l l socio-economic development systems
and through improved programme concepts t o enhance W H D ' s own c a p a b i l i t i e s t o respond
t o countr ies ' needs i n a coherent manner;
- t o col laborate i n the strengthening of countr ies ' c a p a b i l i t i e s f o r planning and
management of t h e i r heal th se rv ices through provision of necessary technical and
adminis t ra t ive support and l e g a l reforms wherever necessary;
- t o improve the u t i l i z a t i o n and e f f i c i ency of the ava i l ab le technical and f inanc ia l
resources of WHO, United Nations and o the r mul t i l a t e ra l and b i l a t e r a l agencies, f o r
heal th purposes through better coordination and mobil ization of these resources.
Co-operation with and among countr ies
During the l a s t t h i r t y years, almost a l l countr ies of the Region have developed
and improved organization f o r the planning, management and del ivery of hea l th services.
WHO has in general collaborated i n t h i s development with s p e c i f i c support t o planning,
management and technical aspects of t h e i r heal th se rv ices and t r a in ing of personnel.
A r eo r ien ta t ion of the heal th programes t o meet the pressing needs of the whole
population is required a s the present approaches t o planning, organization, f inancing
and management i n most of the countr ies a r e inadequate. Yoreover, there a r e many
gaps i n hea l th information i n technical development which would require f u r t h e r
support t o the countries. The proposed programoe envisages ass i s t ance t o various
a c t i v i t i e s planned under general programme development, country hea l th programming
and information systems development.
Programme
General Programme Development
Objectives:
- t o col laborate with M e m b e r S t a t e s i n providing by the year 2000 a l e v e l of hea l th
t h a t w i l l permit t h e i r populations t o lead a s o c i a l l y and economically productive
life;
- t o develop medium-term programmes covering three spans of two-year progralmne

budgetary cycles within the framework of the Organization's General Programme of Work
to meet the pr ior i ty needs of the countries i n the implementation of the i r plans;
- t o collaborate i n strengthening of countries' capacities for planning and manage-
ment of conprehensive national health services within the i r intersectoral endeavours
for socio-economic development,
- to foster a network of ins t i tu t iona l infrastructures and services able to cope,
through appropriate preventive and curative health, sanitary and social measures, with
the ident i f ied health needs of urban and rural communities;
- to develop a valid system of health progralrme evaluation, with a range of quanti-
t a t i ve and qual i ta t ive indicators, a s an integral component of health a ~ t i ~ i t i e s a t
a l l levels i n the Region;
- t o d i rec t and coordinate the a c t i v i t i e s of the technical un i t s of the Regional
Office;
- t o extend technical support t o the WHO Progall) CO-ordinators and f i e l d s t a f f
i n t he i r country and project ac t i v i t i e s , including the application of norms and stand-
ards for technical procedures and practices adopted by the Regional Office;
- t o provide consultative services i n various f i e ld s of health a t the request of
governments;
- t o maintain l i a i son with agencies interested i n health and related a c t i v i t i e s a s
w e l l a s those contributing funds for WHO-assisted projects.
Co-operation wlth and among countries
This p r o g r a covers the supervisory and co-ordinating s e rv ims provided by the
Director of P r o g r a m Nanagement and h i s immediate s t a f f i n planning, programming,
evaluation of the country and inter-country p r o g r a m s , and providing technical support
t o the countries on the instruct ion of the Regional Director.
I n the i r attempts t o reach the above objectives, a l l countries of the Region have
progressed during the l a s t three decades and many of them have developed national health
plans of various duration. The p8ce of progress has differed acmrding t o tkm ami l a -
b i l i t y of financial and manpower resources and some countries have a longer way than
others t o go t o provide adequate health services t o t he i r en t i r e population.
I n 1S80/81, W H ) rill continue t o cooperate with countries i n strengthening the i r
ccrp8city for planning and mnagelent of t he i r heal th progr-s.
The response t o coun t r i e s ' r eques t s w i l l be more f l e x i b l e and adapted t o s u i t s p e c i f i c
s i t u a t i o n s . Technical co l l abo ra t ion w i l l be provided through country and in t e rcoun t ry
s p e c i f i c p r o j e c t s o r programmes, t he W H O Programme Co-ordinators and Regional O f f i c e
s t a f f .
One o f the mechanisms through which W H O cooperates wi th coun t r i e s i n t h e i r en-
deavour t o provide a more comprehensive, coordinated and t echn ica l ly capable h e a l t h
s e rv i ce t o t h e e n t i r e population, i s medium-term programming. I t r ep resen t s , a t t h e
na t iona l and regional leve ls , t he t r a n s l a t i o n i n t o a c t i v i t i e s of the W H O General Pro-
gramme of Work concerning a s p e c i f i c period (now the S i x t h General Programme of Work
and period 1978-1983). S t a r t i n g from the a n a l y s i s of coun t r i e s ' needs and coun t r i e s*
priorities and ob jec t ives , medium-term programmes w i l l be formulated i n c l o s e consul-
t a t i o n and a s soc ia t ion wi th the na t iona l hea l th a u t h o r i t i e s ; thxs would al low WHO t o
respond more e f f e c t i v e l y t o t he needs o f t he coun t r i e s , through two-year programme
budget cyc le s , and t o make an eva lua t ion aimed a t programme improvement.
Exerc ises i n medium-term programming have been and a r e being c a r r i e d o u t i n the
a r e a s o f Health Manpower Development, Environmental Health, Comprehensive Health
Services. Other main a r e a s of the S i x t h General Programme o f Work w i l l be covered
dur ing the next biennium s t a r t i n g wi th Disease Prevention and Control .
The b a s i s o f the eva lua t ion o f h e a l t h programmes i s a comparison between planned
and a c t u a l achievements. To t h i s end, eva lua t ion must be continuous dur ing t h e i m -
plementation of a programme and, i n t h e d e f i n i t i o n of o b j e c t i v e s and formulat ion o f pro-
grammes, due regard must be paid t o t he measurabi l i ty cif r e s u l t s both from t h e quant i -
t a t i v e and q u a l i t a t i v e po in t s of view and, whenever poss ib l e , t a r g e t s must be de t e r -
mined i n s p e c i f i c terms. Recent and f u t u r e developments i n t he way WHO a s s i s t s and
w i l l a s s i s t coun t r i e s i n t h i s s e n s i t i v e a rea of h e a l t h programme development is re-
l evan t t o t h e Information Systems Programe (2.2.3)
Country Health Programming
Object ives:
- t o p a r t i c i p a t e , wi th planning bodies, m i n i s t r i e s o f h e a l t h and o the r related
m i n i s t r i e s o r organiza t ions , i n t h e promotion, review, adap ta t ion and improvement o f
i n t e r s e c t o r a l planning, progral~lming and management procedures and p r a c t i c e s f o r h e a l t h
s e rv i ces ;
- t o inc ream the productivity of heal th services systems by promoting technical ,
administrat ive and l ega l changes where necessary through s tud ies and research;
- t o ensure programme support by introducing advanced methods of assessment,
management, administrat ion and supervision i n the heal th services;
- t o improve the methods of formulation, implementation, monitoring and evaluation
of heal th programmes;
- t o plan fo r provision of heal th services su i t ed t o the needs of the communities,
a t an acceptable cost under prevai l ing socia l and economic conditions.
Co-operation with and among countr ies
Member S t a t e s have continued during the pas t biennium t o increase the capac i t i e s
of t h e i r hea l th services i n order t o r a i s e them t o a sa t i s fac to ry l eve l of ef fect ive-
ness and efficiency. WHO has helped them through various contributions i n t h e f i e l d
of planning/prograPning, a w n s t r a t i o n and management.
The country heal th programming approach t o heal th planning deserves specia l
a t tent ion. I t is a process designed t o iden t i fy p r i o r i t y heal th problems of prime
concern t o countries i n the context of t h e i r development plan and t o formulate appro-
p r i a t e programmes t o cope with them. I t r e s u l t s from a nat ional commitment and is
a national responsibi l i ty . I t i s an in te r sec to ra l continuous process through a cycle
of programmes formulation, implementation, evaluation and reprogramming. I t reqrures
the s e t t i n g o f a permanent mechanism within the National Health Planning system. WHO
helps in te res ted countr ies i n adapting this f lex ib le method t o nat ional s p e c i f i c con-
dit ions. A c r i t i c a l mass of national personnel, not only i n public heal th se rv ices
but a l s o i n other re la ted f i e l d s of socio-economic development, has t o be t ra ined a t
national l eve l , with the pa r t i c ipa t ion of W H O s t a f f a s necessary. The nat ional s t a f f
with knowledge and experience of the country hea l th programming process can, and w i l l ,
then, pa r t i c ipa te i n s imilar exercises i n other countr ies of the Region, thus concretely
contr ibut ing t o the e f f o r t towards technical cooperation among developing countries.
The country heal th programming approach has been used i n Afghanistan, Democratic
Yemen, I raq , Pakistan, Sudan and Yemen Arab Republic. Yore countr ies w i l l c e r t a i n l y
take benef i t of i t i n the coming years, and W H D w i l l contr ibute t o national e f f o r t s i n
t h i s respect by coming, on request , i n t o any point of en t ry of t h i s continuing, r o l l i n g
process. Courses and workshops w i l l a l s o be held, a s required, t o fu r the r the trans-
f e r of the country heal th programming process and methodology and to exchange experience
among the countr ies of the Region. The process i t s e l f and country experience of i t
w i l l be kept under review t o ensure i t s proper development, appl ica t ion and evaluation.
The programme includes the WHO programme coordination a t country.leve1. The
system of WHO Programme Co-ordinators ( W H D Representatives) countinues t o be an i m -
portant element i n the s t r u c t u r e and function of the Organization i n r e l a t i o n t o
technical col laborat ion a t the country level .
Among the main functions of the W H O Programme Co-ordinators a r e the following:
- t o e s t a b l i s h d i r e c t and continuous col laborat ion with the nat ional heal th
author1 t i e s ;
- t o col laborate with the Government i n the development of methods f o r country
hea l th programming, p ro jec t formulation and management;
- t o a s s i s t i n the assessment of country hea l th needs and resources and i n planning,
implementation and evaluation of nat ional heal th programmes;
- t o ensure e f f i c i e n t planning and del ivery of WHD's col laborat ion i n r e l a t i o n t o
these programmes;
- t o a s s i s t , a s may be appropriate, the Regional Off ice and Headquarters with i n t e r -
country and inter-regional p ro jec t s respect ively; and
- t o coordinate ac t ion and cooperate with country o f f i c e s o r representa t ives of
o the r organizations and agencies, p a r t i c u l a r l y those of the United Nations system.
I n 1980/81, W H D Programme Co-ordinators a r e foreseen i n Afghanistan, Democratic
Yemen, I r aq , Libya, Oman, Pakistan, Q a t a r , Saudi Arabia, Somalia, Sudan and Yemen.
Those i n I raq , Libya, Qa ta r and Saudi Arabia a r e expected t o be f u l l y financed by the
host Governments under funds-in-trust arrangements.
Programme
Informa t ion Systems Programme 2.2.3
Objectives:
- t o develop a heal th information system and t o disseminate re levant information
on Health S ta tus and Health Progrannne Development,
- t o develop a W H O information system f o r programme management, f o r the regional
and in te rna t iona l exchange of heal th and heal th r e la ted information;
- t o cooperate with countr ies of the Region i n the development of National Health
Information Systems providing re levant information on t h e i r hea l th s t a t u s , hea l th
se rv ices 9 .d development;
- t o ensure tha t WHO and the national heal th information systems be mutually
supportive and, whenever possible, compatible.
Co-operation with and among countr ies
Health progranvPe development, implementation and evaluation require r e l i a b l e
heal th information.
WHO is developing and w i l l continue t o develop during the next biennium an In-
formation System a t Country, Regional and Global l eve l s , the aim of which is not only
t o meet the need of the Organization f o r heal th information but to i n t e r a c t with the
National Health Information Services, i n order t o serve the Organi%ation's programmes
of technical collaboration with countr ies and the in te rna t iona l exchange of heal th
and health-related information.
I t w i l l a l s o promote the development o f , and d i r e c t support t o the national hea l th
information systems. I t w i l l cooperate with nat ional s t a f f on the f e a s i b i l i t y , design,
implementation and evaluation of the systems and w i l l 88sist i n the t ra in ing of
nat ionals i n systems development.
The memory component of the Information System i s bosed on the "prof i le concept"
a t each echelon of heal th a c t i v i t i e s (project , p r o g r a m , country ,regional programe,
global programme). The p r o f i l e provides information f o r s i t u a t i o n analys is , which
is se lec t ive and user-oriented a t nat ional and in te rna t iona l levels . I t is i n t e r -
linked with medium-term programming and country heal th programming (2.2.1 and 2.2.2).
Emphasis w i l l be given during the next biennium, i n c lose associa t ion with national
heal th a u t h o r i t i e s , t o the preparation of country progrrmne p r o f i l e s covering in-
formation on a l l national hea l th programnes, whether a s s i s t e d o r not by WHO and/or
o the r sources of technical cooperation.
The information system is useful i n heal th progranme evaluation (2.2.1). Pro-
g r a w e p r o f i l e s have an in tegrated element of evaluation which enables progralmes'
ef fect iveness and eff ic iency t o be determined. Conwlidated within country p rof i l e s ,
i t w i l l enable progress and d i f f i c u l t i e s i n countries ' hea l th p r o g r a m development
t o be ident i f ied .
Major Programme
EXTERNAL COORDINATION FOR HEALTH AND SOCIO-ECONOMIC DEWPMENT 2 3 - Programme
Collaboration with the United Nations System and other Organizations 2.3.1 - dbjectives:
- To a s s i s t i n the Organization's par t ic ipat ion i n the overall development pro-
gramme of the United Nations and i n par t icular t o promote a t the country level co-
ordinatxon with other organizations within the United Nations system especially with
UNICEF, FAO, WFP, UNESCO and the Region's Commissions;
- t o par t ic ipate i n the development of cooperative a c t i v i t i e s within the context
of the programmes of UNDP and the United Nations Capital Development Fund, and i n
Technical Co-operation among Developing Countries (TCDC).
Co-operation with and among countries
Close collaboration is maintained with UNDP, UNICEF, FAO, WFP, UNEP, UNFPA,
UNESCO and other Unxted Nations Agencxes a t country and Regional Office leve ls i n
order t o develop a coordinated development programe most suited t o countries' needs.
WHO provides technical support t o or a c t s a s Executing Agency for the other specia-
lirred agencies and UNDP. Jo in t projects have been in i t i a t ed with UNEP i n the con-
t r o l of pollution i n the Mediterranean and Red Seas, and i n countries of the Kuwait
Action Plan Region. Technical support is a l so provided t o UNICEF which has an ex-
tensive progranrme i n some countries of the Region i n maternal and chi ld health, -
primary health care, the Expanded Programme on Irmnuni%ation, nu t r i t ion and training.
The World Food Programe is ass i s t ing i n the development of large projects i n the
Region and technical support is provided t o the health aspects of these projects.
The development of family planning and population a c t i v i t i e s i n the context of
maternal and child health programmes is being undertaken i n collaboration with UNPPA
a t country and regional levels.
Close collaboration is maintained with UNDP. A t country level , consultations
between the UNDP Resident Representatives and WHO Programme Co-ordinators and/or with
the Regional Office ensures the best possible co-ordination of the United Nations
inputs t o serve the socio-economic development process i n member countries. For th i8
purpose jo in t programming between UM)P and W H D w i l l be encouraged and concerted with
the national planning and programming cycle.
s o f n t collaborative propammes w i l l continue t o serve the most deprived sectors
of t h sdmmunity, by means par t icular ly of the t ra ining of middle-/and lower-level
heal th workers, the provision of r u r a l water suppl ies and peripheral heal th services.
Special consideration i s given t o the i d e n t i f i c a t i o n of countries ' po ten t i a l f o r
WDC and the promotion of new and e x i s t i n g TCDC a c t i v i t i e s and programme.
Continuous e f f o r t s w i l l be made t o secure UNDP resources f o r the development of
regional heal th p ro jec t s t h a t benef i t a number of countr ies o r have a po ten t i a l multi-
p l i e r e f f e c t i n the form of stronger national i n s t i t u t i o n s o r new national programmes
i n p r i o r i t y hea l th areas.
Programme
Collaboration with Mul t i l a t e ra l and B i l a t e r a l Programmes
Objectives
To co-ordinate the regional programme with mul t i l a t e ra l development programmes,
funds and organizations within the United Nations system, and t o promote, enhance and
co-ordinate co-operation with m u l t i l a t e r a l and b i l a t e r a l sources of support f o r heal th
work i n the countr ies of the Region.
Co-operation with and among countr ies
A co-ordination u n i t has been set up i n the Regional Of f i ce a s an inter-country /
a c t i v i t y t o a c t a s a focal point f o r UNDP-assisted programes and p ro jec t s , a s s i s t i n g
the Regional Director i n guiding and co-ordinating heal th-re la ted a c t i v i t i e s executed
under the United Nations Development Programme. I n accordance wi th its cons t i tu t iona l
mandate, W H O a c t s a s the d i r e c t i n g and co-ordinating ah thor i ty of in te rna t iona l heal th ,
and an increas ing port ion of the functions of the technical advisory s t a f f of WHO is
di rected towards such co-ordination a c t i v i t i e s with the United Nations bodies, and
m u l t i l a t e r a l and b i l a t e r a l technical co-operation programmes. The co-ordinating u n i t
w i l l be s t a f fed , from 1980, by a senior adminis t ra t ive a s s i s t a n t and a secre tary .
This programme a l s o covers the technical d i r e c t i o n and support provided by WHO
t o the hea l th programme of the United Nations Rel ief and Works Agency f o r Pa les t ine
Refugees i n the Near East (UNRWA). I n accordance with an agreement reached between
W H O and UNRWA, which was f i r s t r a t i f i e d i n 1950, W H O provides the se rv ices of the
~ g e n c y ' s Director of Health and four o the r heal th s p e c i a l i s t s on a non-reimbursable
loan basis .
Countries' socio-economic development programmes a r e being supported by a number
of m u l t i l a t e r a l and b i l a t e r a l agencies including the World Bank, the Regional Develop-
ment Banks, the Islamic Development Bank, SIDA, DANIDA and USAID. Some Arab S t a t e s
such a s Saudi Arabia, Kuwait, UAE and Qatar are providing financial support through
WHO o r through special development funds such a s the Saudi Fund for Development, the
Abu Dhabi Fund for Arab Economic Development, and the Kuwait Fund for Economic Develop-
ment. WHO has collaborated with these Organieations i n Sector studies, f ea s ib i l i t y
studies, and ident i f icat ion of projects; and for some pro je t t s , WHO has been designtatbcl
a s Executing Agency. WHO is a l so collaborating with the sub-regional organizations
such a s the Council of Arab Ministers of Health and the Secretariat-General of Health
for Arab Countries of the Gulf Area.
These a c t i v i t i e s w i l l be further developed and strengthened during the next
Mennium.
Major Programme
RESEARCH PROKITION AND DEVELOPNIENT
- To promote t h e development of t h e c a p a b i l i t y i n Member coun t r i e s t o undertake
biomedical research i n a l l its aspec t s ;
- t o support research a c t i v i t i e s i n p r i o r i t y a r e a s e s p e c i a l l y i n the f i e l d o f
h e a l t h s e r v i c e s research, inc luding research i n h e a l t h manpower development;
- t o i n i t i a t e , conduct and co-ordinate co l l abora t ive r e sea rch work of r eg iona l
importance e s p e c i a l l y i n a r e a s which a r e not being adequately supported;
- t o promote the d i f f u s i o n o f new s c i e n t i f i c knowledge and r e sea rch methods i n t h e
coun t r i e s of t h e Region;
- t o co l l abora t e i n the app l i ca t ion o f r e sea rch f ind ings i n t he development o f com-
prehensive na t ional h e a l t h serv ices .
Co-opera t i o n wi th and among c o u n t r i e s
Even though promotion of research has always been a component o f t h e a c t i v i t i e s
of t he Region, i t has acquired a new dimension, i n t he l a s t three yea r s , i n pursuance
o f Assembly r e s o l u t i o n s WHA 27.61, WHA 28.70 and W H A 29.64. An a c t i v e Regional
Research programme has been b u l l t up and w i l l be continued and expanded.
The Eas tern Mediterranean Advisory Cormnittee on Medical Research (EM ACMR), con-
s t i t u t e d i n 1976, has s i n c e m e t annual ly and has i d e n t i f i e d the re sea rch p r i o r i t i e s
of t h e Region and recommended an o v e r a l l plan o f work. Provis ion is made f o r annual
meetings i n 1980 and 1981. I n accordance wi th t h e recomaendations of t h e Cormittee,
three teams of expe r t s v i s i t e d seven c o u n t r i e s t o survey t h e r e sea rch p o t e n t i a l i n the
Region. A d i r e c t o r y o f r e sea rch i n s t i t u t i o n s has been compiled wi th d e t a i l e d p r o f i l e s
of t h e most a c t i v e i n s t i t u t i o n s and i t w i l l be maintained on an up-dated basis.
S c i e n t i f i c working gmup meetings took place i n 1977 on Heal th Se rv ices Research
and on S o c i a l and Behavioural Sc iences i n Health Se rv ices and Heal th Manpower Develop-
ment. They provided a conceptual framework f o r t he r e sea rch and pointed t o t h e stra-
t e g i e s f o r s t rengtheniqg c a p a b i l i t y w i th in t h e Region f o r t hese r e sea rch a c t i v i t i e s .
WHO Col labora t ing Centres have been designated i n c e r t a i n c o u n t r i e s t o c a r r y o u t re-
sea rch i n s p e c i f i c f i e l d s of enquzry, and co l l abora t ion wi th these w i l l be continued
and expanded.

In the biennium 1980/81, W H D w i l l continue t o operate a research programme geared
t o the health needs of the Region, i n an e f f o r t t o prorote the continuing involvemant
and act ive participation of Nember c o u n t ~ i e s i n identifying the i r problems and managing
national research programmes.
The overriding p r i o r i t i e s of research i n health services and manpower development
la id down by the EM ACMR w i l l be respected and implemented, and the mechanisms set
down by the 1977 meeting of the coxmuittee regarding the award of Research Contracts,
Research Grants and Research Training Awards wall be followed. In addition t o health
services research, continuing collaboration i n selected pr ior i ty areas, including com-
municable disease research,and research i n a variety of aspects of pharmacology and
therapeutics, rill be extended.
Major Programme
REGIONAL DIRECTOR'S DEVELOPMENT PROGRAMME
This programme w i l l be used i n a s f l e x i b l e a manner a s possible t o promote and
support technical co-operation a c t i v i t i e s . Sums an11 be released a s and when
pa r t i cu la r technical co-operation programmes evolve and require funds t o launch and
support them o r t o a t t r a c t extrabudgetary recources.
Among the a c t i v i t i e s w b c h a r e l i k e l y t o benef i t from t h i s programme a r e co-
operation between the countr ies of the Region i n heal th research and development.
Likewise, i t w i l l be used, a s required, t o develop fu r the r a c t i v i t i e s i n such f i e l d s
a s educational technology, programmes re la ted t o primary heal th ca re and overa l l
heal th development, communicable d isease control , technical co-operation i n non-com-
municable d isease control , na t ional drug po l i c i es and management, basic san i t a ry
services and pre-investment planning. This programme w i l l a l s o be used t o meet some
of the needs i n emergency s i t u a t i o n s , thereby responding t o Regional C o w i t t e e recom-
mendations f o r the establishment of such an emergency fund. An amount of $ 800 000
has been t e n t a t i v e l y set as ide from the Regular Budget f o r the biennium 1980/81 f o r
the Regional Director ' s Development Progrannne.
Voluntary contr ibut ions a r e s o l i c i t e d from Member S t a t e s of the Region t o supple-
ment t h i s programme.
Major Programe
HEALTH SERVICES DEVELOPMENT
Objectives:
- t o promote the strengthening of countries' capaci t ies for the planniw anQ manage-
ment of comprehensive national health services ;
- t o promote the development of primary health care;
- t o promote workers' health;
- t o promote the development of standard health technologies;
- t o promote a more rat ional production, d i s t r ibu t ion and u t i l i t a t i o n of r f e ,
effect ive and economic prophylactic, diagnostic and therapeutic substances,
Co-operation with and among countries
In 1980/81, WHO w i l l continue t o cooperate v!ith countries t o strengthen the i r
capacity for the planning and management of t h e e eomprBhen'aive health serviaqa *<.the
various administrative levels , a s has been done i n previous years, notably, i n
Afghanistan, Democratic Yemen, I raq, Pakistan, Somalia, Sudan and the Yemen Arab
Republic.
Country health programming w i l l receive par t icular attention. WHO w i l l continue
to support national endeavours i n t h i s domain. Anotlrer area of collaborrtion wilJ
be medium-term programming (1928/83), an exercise which requires the closeat consulta-
t ion with countries. In addition, WHO w i l l a s s i s t whenever neoesa8ry i n the pro-
vision of emergency r e l i e f services t o meet the health needs of displaced persons,
a s requested.
The Regional Advisory Committee on Emergency Medical Services w i l l i n tens i fy i ts
e f f o r t s i n advising the Regional Director on ths development of these services i n the
countries interested. Collaboration i n the expansion of rehabi l i t a t ion services w i l l
a l so grow further.
The nature and scope of cooperation i n hospital services w i l l be guided to $0-
extent by the outcome of the study conducted by WHO i n 1976. P r io r i t y w i l l be
given t o t ra ining of non-medical hospital s ta f f .
Pr i lury health care w i l l oontinue t o receive p r io r i t y i n ths Context of technical
cooperation with and among, countries. This i s i n l i n e r i t h a Oe.olution (-5khZ.15)

adopted by the Regional Sub-committee A i n 1975 which "...INVITES Member S t a t e s to
continue t o cooperate i n exploring new ways of ensuring maximum coverage of t h e i r
populations by hea l th services..." Follow-up a c t i v i t i e s a r e under planning f o r the
period succeeding the 1978 Internat ional Conference on Primary Health Care (Alma Ata,
USSR) .
I n Appropriate Technology f o r Health, i t is envisaged tha t W H O col laborat ion w i l l
expand i n the biennium 1980/81 and w i l l involve designation of collaborating centres
i n the Region.
Under the same heading, (ATH), W H D w i l l support countr ies t o extend the scope of
t h e i r public heal th laboratory services t o the periphery. Co-operation w i l l a l s o
take place t o help countr ies t o design and improve nat ional l abora to r i e s f o r the
production and control of b iologicals , including vaccines.
The sub-programme i n Maintenance and Repair of Medical and Hospital Equipment is
expanding s teadi ly . I n 1980/81, WHO col laborat ion w i l l cover twelve countr ies and
w i l l include, i n addi t ion, support f o r two Regional Training Centres i n Cyprus and
I raq .
Many countr ies a r e expressing growing i n t e r e s t i n workers' health. W H O w i l l
co l laborate with Goverrunents and with o ther United Nations agencies ( e spec ia l ly L I B )
i n promoting the development of occupational heal th se rv ices with specia l emphasis on
t r a in ing of personnel including occupational hygienists .
Continuing support w i l l be given t o heal th se rv ices research geared pr imar i ly to
the tension of heal th coverage t o underserved communities.
Programme
Health Services Planning and Management
Objectives ;
- t o p a r t i c i p a t e with planning bodies and Minis t r ies of Health, i n the promotion,
review, adaptation and improvement of planning programming, and management procedures
and p rac t i ces f o r heal th services ;
- to increase the product iv i ty of hea l th se rv ices systems by promoting technical ,
adminis t ra t ive and l ega l changes where necessary, through s t u d i e s and research;
- t o extend the heal th i n f r a s t r u c t u r e , i n s t i t u t i o n s and se rv ices t o give access t o
hea l th care t o a s large a proportion a s possible of the population, urban and r u r a l ,
with pa r t i cu la r a t t en t ion t o the most remote and underprivileged people;
- t o provrde heal th se rv ices sui ted t o the needs of communities, a t an acceptable
c o s t under prevai l ing soc ia l and economic condrtions;
- t o give l o g i s t i c support t o hea l th programmes, with regard t o supplies, equipment,
pharmaceutical substances and t h e i r production, maintenance, etc. ;
- t o promote heal th information systems and disseminate the information on com-
prehensiue heal th services.
Co-operation with and among countr ies
Member S ta tes , with WHO co-operatron, have continued t o increase the capac i t i e s
of t h e i r heal th services and t h e i r ef fec t iveness and eff ic iency. WHO c o n t ~ ~ b u t i o n s
a r e i n planning/programming, administrat ion and management, hospi ta l and donucil iary
care se rv ices , primary heal th ca re , appropriate heal th technology, t r a in ing of a l l
ca tegor ies of personnel, and heal th information.
The country heal th programming approach t o heal th planning deserves spec ia l a t ten-
t ion. I t IS a process designed t o iden t r fy p r i o r i t y hea l th problems of prime concern
t o countr ies i n the context of t h e i r development plans and t o formulate appropriate
programmes t o implement them. I t r e s u l t s from a nat ional commitment and is a nat ional
r e spons ib r l i ty , I t is an in te r - sec to ra l contrnuous process through a cycle of pro-
gramme formulation, rmplementatron, evaluation and reprogramming. I t r equ i res the
s e t t i n g of a permanent mechanism within the National Health Planning system. WHO
col laborates with In te res ted countr ies i n adapting t h i s f l e x i b l e method t o s p e c i f i c
nat ional conditions, and i n t r a i n i n g a c r i t i c a l mass of nat ional personnel, not only
i n public heal th services but i n o the r r e l a ted f i e l d s of socio-econonlc development.
National s t a f f t ra ined and experienced i n country hea l th programming then, p a r t i c i p a t e
i n s rmilar exerc ises i n o the r countr ies of the Region, thus contr ibut ing concrete ly t o
Technical Cooperation among Developing Countries.
The country heal th programming approach, which i s being already used i n Afghanistan,
Democratic Yemen, I r aq , Pakistan, Sudan and the Yemen Arab Republic, w i l l be taken up
by more countr ies i n the new brennium,and W H D w i l l contr ibute , on request , t o nat ional
e f f o r t s a t various s t ages of t h i s continuous process.
Another mechanism through which WHO is prepared t o cooperate with countr ies i n
providing more comprehensive, coordinated and technical ly sound heal th services , is
medium-term programming. I t represents , a t the nat ional and regional l eve l s , the
translat.. -; i n t o a c t i v i t i e s of the WHO General Programme of Work concerning a Spec i f i c
Period (now the Sixth General Programe of Work fo r the period 1978-1983). S ta r t ing
from the analys is ~f countries ' needs, p r i o r i t i e s and object ives , medium-term pro-
grammes a r e formulated Ln c lose consul t a t ion and association wr th national heal th
au thor i t i e s ; t h i s allows WHO t o be t t e r respOnd t o the needs of countries, through
two-year prograarpe budgets, and to make an evalua$ion amed a t p r o g r a m improvement.
Exercises i n medium-term programing, wNch began with health manpoyer development,
environmental heal th , and comprehensive health services w i l l be extended during the
next biennium t o the other main a reas of the Sixth General Programme of Work.
Health progrfmme developlpent, implementation and evaluation require, f i r s t , r e l i a b l e
heal th information. W H O is developing and rill continue Qurlng the next bienniur an
information system a t regional and global l eve l s , the aim of which is not only t o
meet the need 99 WHO fo r heal th information but t o i n t e r a c t with and develop national
hea l th information services , I n order t o serve p r o g r a l e s o f technical w l l r b o r a t i o n
with countr ies and the in tornat ional exchange of heal th and health-related in f~rmat ion .
The memory component of the information system is based on the "prof i le oarrrrept" a t
each echelon of heal th a c t i v i t i e s . Emphasis w i l l be put by W H O i n tbe next biennium,
i n c lose associa t ion with national hea l th au thor i t i e s , on the preparation of country
p r o g r a m p r o f i l e s covering information on a l l national hea l th progranmer, whether
ass i s t ed o r not by WW) and/or o the r sources of technical cooperatAon,
Hoapi t a l Administration h .
Objectives:
To cooperate with the countr ies of t h e Region i n developing in tegrated and
e f f i c i e n t hospi ta l se rv ices by:
- improvement of hospi ta l service planning;
- in tegra t ion of horpit.1 re rv ices i n tbe hea l th a r e de l ive ry sp~ tem;
- applicatkon of mderq managerial methods and development of managerial @ k i l l s ;
- appl icat ion of -ern hospi ta l a rch i t ec tu re and design;
- procuring su i t ab le hospi ta l equippent; and
- trainAng of hospi ta l s t a f f
Co-operation with and among countr ies
A s countr ies of the Region spend a major p a r t of t h e i r heal th budgets on hospi ta l
services , these must be planned t o meet best medical care needs. I n pa r t i cu la r
tendency t o build specia l ized hosp i t a l s needs t o be curbed i n favour of general
hospi ta ls , which a r e considered bes t sui ted t o community needs, p a r t i c u l a r l y i n
developing countries. WHO cooperation is ava i l ab le i n hosp i t a l planning, i n stand-
a rd ia ing and procuring hospi ta l equipment, and i n r a i s i n g the q u a l i t y of hosp i t a l
management by the t ra in ing, p a r t i c u l a r l y of hosp i t a l administrators.
Consultant services w i l l be made ava i l ab le t o Djibouti t o study the hosp i t a l
services and advise on hosp i t a l planning and organization. Hospital equipment
needed t o improve the se rv ices w i l l be procured, and fellowships w i l l be ava i l ab le
e spec ia l ly f o r hospi ta l administrators.
I n Lebanon the organization of hospi ta l se rv ices w i l l be required. The necessary
equipment w i l l be provided a s w e l l a s fellowships i n hospi ta l management.
The Hospital Administration (UNDP) pro jec t i n Syr ia , s t a r t i n g i n 1978, w i l l
support the establishment of a hosp i t a l administrat ion u n i t i n the Ministry of Health,
the management of Al-Mojtahed Hospital i n Damascus; and the t r a i n i n g of hosp i t a l
personnel. I n addi t ion, WHO w i l l cooperate i n organizing and developing the capacity
of hosp i t a l s t o provide emergency medical care, including in tens ive care.
Emer~encv Medical Services
Objectives:
To a s s i s t the countr ies of the Region i n es tab l i sh ing e f f i c i e n t emergency medical
se rv ices a s in tegra l p a r t s of hea l th c a r e del ivery systems through co-operation in:
- making epidemiological s t u d i e s of the medical emergency condit ions, t o a s sess
the s i z e of the problem;
r planning and organizing emergency medical services ;
- standardizing equipment; and
- planning and Implementing t r a i n i n g p r o g r a m s f o r emergenay m ~ ~ I l a a l technia ians
(EMT's) and o the r personnel working i n these services .
Co-operation with and among countries
Cr i t i c a l medical and surgical conditions resul t ing from cardiovascular diseses,
t r a f f i c and industr ia l accidents, intoxication and other conditions a r e increasing
rapidly i n almost a l l countries of the Region. Nany pat ients d i e because health
care systems a r e not equipped to deal with t h e m eff ic ient ly . Medical technology nor
makes i t possible t o provide emergency care i n time i f properly trained personnel a r e
available.
In Jordan, WHO rill provide consultant advice on the organisation 02 emergency
medical services, fellowships t o t r a in nationals preferably instructors rho rill then
t r a i n more national s ta f f . Equipment wi l l a l so be provfided.
Cooperation w i l l eentinue with the Government of Tunisia i n developing erergencg
services, by the provision of consultants, equipment and fellowships.
A seminar on emergency lnedical services w i l l be held i n 1981.
Primary H e a l t h Care
Objectives:
Principal objective
to promote the development of primary health care
Detailed objective
t o p r m t e , within a comprehensive national heal th system appropriate t o the
conditions and needs of each country, the provision of prirrrry health care to the
whole population, ensuring tha t populations that a r e nor underserved, and high-risk
and vulnerable groups, a r e properly served.
Co-operation r i t h and among countries
A s outlined i n the Sixth General Program9 of Work, the t a rge ts sbould be t o
ensure that an adequate quantity and qua l i ty of health -re is made m i l a b l e to a11
members of a community o r a l l inhabitants of a country, as w e l l a s m a x i m coverage
of underserved populations and high-risk and vulnerable groups, by p r i r r y heal th care.
I t is hoped t h a t by 1981 addi t ional countr ies w i l l have adopted the primary hea l th ca re
approach a s nat ional policy, including possibly Afghanistan, Democratic Yemen, Pakistan
and the Libyan Arab Jamahiriya.
WH) w i l l co l laborate in :
- promotion of primary heal th ca re i n countr ies by means of regional and nat ional
seminars, and through dissemination of information;
- es tab l i sh ing p i l o t p ro jec t s fo r h i t h e r t o unserved communities, with the a c t i v e
pa r t i c ipa t ion of the communities involved;
- evaluation and research a c t i v i t i e s per ta in ing t o PHC developments;
- arranging v i s i t s by WH) s ta f f / consu l t an t s i n the s p i r i t of technical cooperation.
Educational programmes or iented t o primary heal th ca re w i l l be es tabl ished and/or
improved i n countr ies where primary hea l th care i s delivered by heal th professionals.
I n t h i s connection WHO'S r o l e w i l l include:
- col laborat ion i n t r a i n i n g na t iona l s i n methods of organizing continuing education;
and
- col laborat ion i n the organization of continuing and in-service educataon.
The t h r u s t of the Regional Off ice is thus t o promote nat ional ac t ion i n primary
hea l th ca re a s an expression of technical cooperation. The Organization w i l l a o i n t a i n
its c a t a l y t i c r o l e t o support the development of primary heal th ca re a t the country
level .
Programme
Workers' Health 3.1.3
Objectives:
t o promote the hea l th of working populations, t o con t ro l occupational hea l th
r i s k s , and t o p r o m t e the humanitation of work.
Co-operation with and among countr ies
A l m s t a l l countr ies i n the Region would be considered t o be i n a developing
s tage a s f a r a s workers* h e a l t h is concerned. Rapid urbanisation and i n d u s t r i a l i -
za t ion have given impetus t o the development of occupational hea l th se rv ices and have
st imulated Governments t o seek in te rna t iona l col laborat ion i n this important f i e l d .
T'he scopl of occupational hea l th se rv ices has widened and is aimed a t not only pre-
venting upational hazards but a l s o promoting workers' hea l th i n general. These
s e r v i c e s go beyond i n d u s t r i a l workers and embrace a l l ca t egor i e s of workers inc luding
of f ice-aorkers , a g r i c u l t u r a l workers and o thers . The bas i c problems of workers'
h e a l t h a r e somewhat s i m l a r i n t he var ious coun t r i e s of t he Region, but p r a c t i c a l
s o l u t i o n s may d i f f e r depending l a r g e l y on the development of genera l publ ic h e a l t h
s e r v i c e s i n each country.
A s ou t l ined i n the S i x t h General Programme of Work, W H O , i n co l l abo ra t ion with
ILO i n a r e a s of common i n t e r e s t , w i l l formulate o r r e v i s e s tandards and prepare guide-
l i n e s f o r p ro t ec t ion a g a i n s t occupational hazards and w i l l promote co-ordinat ion of
a c t i v i t i e s f o r s t rengthening t h e l e g a l , adminis t ra t ive and occupational framework t o
ensure h e a l t h and s a f e t y i n work places.
I t should be r eca l l ed t h a t a t t h e regional l e v e l , WHD has the mandate t o col labo-
r a t e with Member S t a t e s i n t he f u r t h e r development o f occupational h e a l t h s e rv i ces ,
a s expressed i n a number of Resolu t ions adopted by t h e Regional Committee i n 1950, 1966
and 1971. The Resolut ion (EM/RC21A/R,12) adopted by Sub-Committee A i n 1971 " ...... Requested the Regional Direc tor t o cont inue t o a s s i s t Governments i n co l l abora t ion
with o the r United Nations agencies concerned i n planning and developing t h e i r occupa-
t i o n a l hea l th a c t i v i t i e s wi th in the framework of publ ic h e a l t h s e r v i c e s , . . . . . . . . . " W H O w i l l co l l abo ra t e wi th coun t r i e s i n developing comprehensive occupational
h e a l t h programmes and s e r v i c e s t h a t a r e co-ordinated, and p re fe rab ly in t eg ra t ed wi th
the general publ ic h e a l t h serv ices .
WHO w i l l promote the development o f methods fo r t he e a r l y de t ec t ion of h e a l t h
impairment of workers; the c o l l e c t i o n and dissemination of information on s p e c i f i c
occupational h e a l t h problems and t h e i r so lu t ion , and on occupational hazards; and
w i l l coordina te and s t imu la t e research.
Col labora t ion i n the f i e l d of occupational h e a l t h w i l l continue t o expand. The
planned expenditure i n t he biennium 1980/81 amounts t o a sum of approximately $ 570 000
compared wi th about $ 200 000 expended i n the preceding biennium.
Programme
Care o f t h e Aged, D i s a b i l i t y Prevention and Rehab i l i t a t i on
Objec t ives :
To a s s i s t the coun t r i e s o f t h e Region i n e s t a b l i s h i n g and developing r e h a b i l i t a t i o n -- s e r v i c e s wi th spec ia l emphasis on prevention of d i s a b i l i t i e s through 'co-operation in :
assessment o f the d i s a b i l i t y problem;
- planning of su i t ab le rehab i l i t a t ion p r o g r a r e s ;
- in tegra t ion of the rehab i l i t a t ion p r o g r a m s i n the heal th eare hel ivery system;
- designing and Oquipping r e h b i l i t 8 t i o n aentrea; and
- pla&ng training;,progral~mes in the d i i f e r e n t aspects. o f rehabilitation;.
Co-operation with and among countr ies
Public demand i s increasing f o r the care of d i s a b i l i i i e s resu l t ing from war
i n j u r i e s , t r a f f i c and other accidents; and neurologioal, psychiatric, cardiovascular
and chest diseaseg. Countries a r e therefore es tab l i sh ing and developing rehab i l i t a -
t i o n services i n t h e i r hea l th care systems.
WHO w i l l continue its co-operation with the Governments of Afghanistan, Djibouti ,
Jordan, Lebanon, Saudi Arabia, Somalia, Sudan and Syria, i n the developrent of t h e i r
r ehab i l i t a t ion services, by the provision of consultant and advisory services , fellow-
ships, supplies and equipment, and by ass is tance with the recruitment of s t a f f a s
requested.
The Internat ional I n s t i t u t e of Rehabi l i ta t ion fo r the Developing Countries, an
I ran Government-UNDP project , is expected t o begin functioning i n 1980/81, and WHO
w i l l continue its col laborat ion with t h i s project .
Appropriate Technology f o r Health
Objectives:
General object ive
To col laborate with countr ies i n the development and adaptation of simple, low-
cos t and e f fec t ive technologies i n spec i f i c areas.
Spec i f i c object ive
To support, by means of appropriate technology f o r heal th , the e f f o r t s of the
countr ies of the Eastern Mediterranean Region t o develop t h e i r heal th services with
pa r t i cu la r reference t o primary heal th care.
Co-omration with and among countr ies
The following regional t a r g e t s f o r the period including the biennium were set by
a Working Group on Appropriate Technology fo r Health which m e t i n the Regional Office.
i n November 1977:
- The improvement and adapta t ion of e x i s i t i n g technologies and the development
of new technologies.
- The development of systems and p r a c t i c e s f o r e f f e c t i v e and wide a p p l i c a t i o ~ l of
appropr ia te techniques and methods.
- The establ ishment and development of management systems f o r the la rge-sca le
app l i ca t ion of e x i s t i n g and improved techniques.
The problem of d iar rhoea1 d i s e a s e s is i d e n t i f i e d a s one w h c h should r ece ive
major emphasis.
Following prel iminary surveys of needs and p r i o r i t i e s i n appropr ia te technology
f o r hea l th , WHO w i l l c o l l a b o r a t e i n :
- t h e formulation of p l ans f o r technological r e sea rch and developme~lt ( inc luding
con tac t s , f i nanc ia l support , e tc . . . ) ;
- incorpora t ing r ecen t techniques and methods i n the t r a i n i n g o f primary h e a l t h
workers and o t h e r h e a l t h c a r e personnel ;
- the dissemination of information;
- in -serv ice t r a i n i n g o f h e a l t h p r a c t i t i o n e r s i n o r d e r t o p r o m o t e t h e r e f i n e m e n t o f
technologies; and
- the i d e n t i f i c a t i o n of and support t o co l l abora t ing c e n t r e s i n ATH.
I n the s p i r i t of t echn ica l cooperat ion, WHO w i l l co l l abo ra t e t o set up a Regional
network of i n s t i t u t i o n s involved i n the app l i ca t ion of app ropr i a t e technology i n
support of primary h e a l t h care , s o t h a t coun t r i e s w i l l a cqu i r e a c a p a b i l i t y i n the
choice, adapta t ion and a p p l i c a t i o n of technology f o r heal th.
Radiat ion Technology
Object ives:
- To in t roduce the concept o f bas i c r ad io log ica l s e r v i c e s i n t h e coun t r i e s of the
Eas tern Mediterranean Region.
- t o s t rengthen departments of rad io therapy, nuclear medicine and r a d i a t i o n pro-
t e c t i o n i n t he coun t r i e s of t he Eas tern Mediterranean Region.
Co-operation with and among countr ies
I n t h i s f i e l d only two very small p ro jec t s a r e st i l l maintained %n the Programme
and Budget f o r the biennium 1980/81.
One d e a l s with the t r a i n i n g of radiographers i n Yemen Arab Republic and another
with the improvement of r ad ia t ion protect ion i n Saudi Arabia.
The concern of the Regional Off ice with the implementation of basic radiological
se rv ices and with the e f f i c i ency and eff icacy of r ad ia t ion medicine techniques,
although not expressed i n budgetary terms, w i l l be strengthened i n order t o prepare f o r
a more s u b s t a n a a l programme i n rad ia t ion technology f o r the 1982/83 biennium.
Maintenance and repa i r of medical and hospi ta l equipment
Objectives:
- To develop a network of workshops f o r the maintenance and repa i r of medical
equipment s t a r t i n g from the cen t ra l l e v e l and going towards the periphery;
- t o strengthen the Regional Training Centres f o r the Naintenance and Repair-of
Medical Equipment and t o d i v e r s i f y t h e i r t r a in ing a c t i v i t i e s .
Co-operation with and among countr ies
This programme i s growing continuously - twelve country and two inter-country
p ro jec t s being included i n the Progranrne Budget fo r the biennium 1980/81.
With the development of the two Regional Training Centres i n Cyprus and I r a q and
the co-operation with twelve countr ies of the Region i n developing a network of rork-
shops f o r maintenance and repair of medical and hosp i t a l equipment, it is expected t h a t
some of the needs of programmes such a s the Expanded Programme on Immunisation, Publ ic
-81th Laboratories, and Radiologic Techniques w i l l be covered.
The experience p i n e d i n maintaining and repa i r ing medical and hosp i t a l equipment
w i l l be used f o r the assessment of the type of equipment which is the most s u i t a b l e
f o r countr ies i n t h i s Region i n such terms a s s impl ic i ty of operation, technical per-
formances, r e l i a b i l i t y , a v a i l a b i l i t y of spare p a r t s , and cost .
Laboratory Technology
Objectives:
- To increase the scope of work of the public heal th laboratory services i n the
countr ies of the Region and expand to the periphery by organizing o r reorganizing
the services ;
- t o augment epidemiological surveil lance a c t i v i t i e s ;
- t o improve the qua l i ty and increase the quant i ty of vaccines and sera produced;
- to t r a i n personnel a t d i f f e r e n t l eve l s , t o man d i f f e r e n t d i sc ip l ines of laboratory
services;
- to r a i s e the technical performance of l abora to r i e s by the establishment of qual i ty-
control methodology j
- t o col laborate with countr ies i n the development and adaptation of simple low-
cos t technologies i n s p e c i f i c areas.
Co-operation with and among countr ies
Co-operation w i l l continue with almost every country i n the Region i n es tab l i sh -
ing o r modernizing t h e i r laboratory services. The general aim is the organization
o r reorganization of l abora to r i e s , increasing the quant i ty and improving the q u a l i t y
of vaccines and se ra products a s well a s of o ther b iologiaal material , and es tab l i sh -
ing departments t o apply the necessary methodology and bias-free controls. The
q u a l i t y of work and performance i n the laboratory an11 be emphasized and i n t e r n a l
mechanisms f o r the quali ty-control of more laboratory se rv lces w i l l be introduced.
Regional and national courses i n specia l laboratory techniques such a s have been
held throughout the Region i n recent years w i l l continue under t h i s programme a s the
need a r i ses .
I n the s p i r i t of TCDC, i t i s expected t h a t the donation of vaccines e.g. cholera,
TAB, r a b i e s and BCG, by some countr ies i n the Region t o o the r s w i l l continue.
P ro jec t s which have been successful ly completed i n Egypt and Sudan have increased
the capab i l i ty of the Region t o develop laboratory services.
The f i r s t phase of a four-year UNDP-financed project i n Tunisia has paved the way
f o r the development of four provincial l abora to r i e s during the biennium.
Co-operation w i l l continue a l s o i n developing Blood bank services and i n in t ro -
ducing the associated new techniques ~f p lasmphores is and application of component
therapy.
I n Lebanon a project document has been formulated f o r a lRJDP financed project
f o r the establishment of public hea l th laboratory services a t the cen t ra l public hea l th
laboratory i n Beirut and a t s i x provincial public heal th laboratories.
Progranane
Health Services Research
Objective :
To develop the capab i l i ty of Member Countries t o undertake operational research
with a view t o improving the design and management of t h e i r heal th services.
Co-opera t ion with and among countr ies
A S c i e n t i f i c Working Group on Health Services Research i n 1977, defined the
conceptual framework and the c h a r a c t e r i s t i c s of hea l th Services research. I t specif ied
c r i t e r i a f o r the designation of i n s t i t u t i o n s a s W H O Collaborating Centres f o r heal th
services research, a s w e l l a s the c r i t e r i a fo r the se lec t ion of research proposals f o r
WHO support. Also i t reviewed and approved research proposals which w i l l be imple-
mented during the period of the biennium.
The promotion of heal th services research w i l l continue, geared primarily t o
extending basic heal th services t o the a s yet unserved populations.
l a jo r Programme
FAMILY HEALTH
Objectives:
I n the context of the development programnes of the countr ies of the Region fo r
Comprehensive Health Services par t$cular ly f o r the populations l i v i n g i n r u r a l and
peripheral areas , and expecia l ly i n r e l a t i o n t o the vulnerrble groups of chi ldren and
women i n reproduotive l i f e , the main object ives of the family hea l th programe are:
- t o reduce morbidity and morta l i ty amongst in fan t s , chi ldren and mothers, and,
ul t imately, families and conmunities, from the c losely re la ted fac to r s of a l n u t r i t i o n ,
infect ion, unregulated f e r t i l i t y end lack of i n f o r m t i o n regarding health;
- t o develop and strengthen the family heal th component of heal th se rv ices part icu-
l a r l y a s p a r t of primary hea l th ca re and other developmental a c t i v i t i e s a f f e c t i n g the
l i v e s of famil ies and poople;
- t o promote a coordinated i n t e r s e c t o r a l approach t o improving the hea l th and
soc ia l welfare of the family a s a un i t ;
- to promote knowledge and appropriate technology f o r the p romt ion of human re-
production, the sound physioal growth and psychosoci+l development of the young, and
tho well-being of the family am a whole, through education, t r a i n i n g and research.
Co-operation with and among countriem
Between 42 and 50 per cent of the population i n countriem of the Region a r e under
the age of 15 years. Some 11 mil l ion chi ldren a r e born each year. An unacceptably
high proportion of t h 8 m d i e before reaching the age of f ive . Accompanyin@ t h i s
excessive morta l i ty is the high morbidity whlch represent8 much pain and almo mubmequont
permnent d i s a b i l i t y i n row ins tances t o the ch i ld and anguish t o the prentm. There
is a need t o i d e n t i f y mre c l e a r l y the problems and needm of the f a n i l y a s a whole i n
countr ies of the Region a s w e l l a s t o improve and re-orient hea l th ca re on the b a s i s
of the family a s a u n i t of care. Family heal th ca re u l t ima te ly depends upon the
education of family members about t h e i r remponsibil i ty f o r t h e i r own heal th care , and
of heal th workers who must see beyond the individual t o the family and the community.
I n giving p r i o r i t y t o a c t i v i t i e s i n maternal md c h i l d heal th , human reproduction,
n u t r i t i o n and heal th educzation, and working towards the development of canprehensive
hea l th services , hea l th manpower development and comunicable d isease con t ro l , WHO w i l l
co l laborate with governments in :
a ) improving the administrat ion and management of se rv ices f o r providing integra ted
maternal and chi ld heal th , n u t r i t i o n and f e r t i l i t y regula t ion ca re by:
- the development and adaptation of methods fo r improved del ivery of heal th ca re i n
the preconceptional, prenata l , na ta l and postnatal periods, i n infancy and i n child-
hood ;
- revised and appropriate t r a in ing f o r adminis t ra tors and senior teachers i n maternal
and chi ld heal th care , the t r a i n i n g of primary hea l th workers i n n u t r i t i o n and heal th
education, and the building and strengthening of nat ional c a p a b i l i t i e s f o r t r a i n i n g
i n specia l techniques fo r f e r t i l i t y management and maternity care;
- f e a s i b i l i t y t r i a l s on the del ivery of n u t r i t i o n and f e r t i l i t y r e g u l a t ~ a n service
a s an i n t e g r a l pa r t of primary heal th care ; and
- par t i c ipa t ion i n the WHO Expanded Programme on Immunization and i n spec ia l
ac t i v i t i e s f o r the improved management of diarrhoea1 d i seases i n c h l d r e n ;
b) improving information and technology development f o r family heal th in :
- the prevention and management of d isorders of pregnancy and c h i l d b i r t h e.g.
toxaemia of pregnancy;
- f e r t i l i t y regula t ion by means of s tud ies on the hea l th r a t iona le f o r family
planning; assessment, improvement and development of methods f o r f e r t i l i t y regula t ion;
epidemiological research on i n f e r t i l i t y ; and the strengthening of nat ional resources
f o r research i n human reproduction;
- the promotion o f , preparation f o r , establishment and protect ion of breast-feedings;
- the promotion of physical growth and psychosocial development of the young;
s t u d i e s on the epidemiology, prevention and soc ia l implications of low b i r t h weight;
improved ch i ld n u t r i t i o n i n the weaning and preschool periods;
- prevention and management of in fec t ions i n mothers and i n young chrldren;
c ) promoting the heal th o f the family a s a whole by the development of low-cost
educational methods f o r hea l th education of f ami l i e s i n family heal th ; and i n
d ) strengthening the i n t e r s e c t o r a l approach f o r improving the hea l th of the family
and cornunity a s a whole through support t o the development of food and n u t r i t i o n
p o l i c i e s , and assessment of the ex ten t and control of def ic iency diseases , i n collabora-
t i o n with FA0 and UNICEF.
Pronramme
Maternal and Child Health
O b ~ e c t i v e s :
The long- term ~ b j e ~ t l ~ t ? ~ of the programme are :
- t o a s s i s t governments i n t h e i r e f f o r t s t o reduce maternal, pe r ina ta l , i n fan t
and childhood mortal i ty and morbidity;
- to st imulate and f a c i l i t a t e the systematic and expanded appl ica t ion of preventive,
cura t ive and r e h a b i l i t a t i v e measures i n maternal and c N l d ca re through the provision
of heal th and other socia l services , i n order t o promote the optimum physical growth
and psychosocial development of the ch i ld , improve reproductive health, and enhance
the qua l i ty of human l i f e ;
- t o col laborate with countr ies i n the development and strengthening of nat ional
capac i t i e s f o r provision of maternal and ch i ld care, including family planning, a s
pa r t of heal th and re la ted soc ia l services.
The medium-term object ives are:
- t o col laborate with the countr ies i n MCH redevelopment programmes whlch aim a t
defining the problems, the resources, present coverage and p r i o r i t i e s , evaluat ing new
approaches, a s s i s t i n g with t r a in ing and f a c i l i t a t i n g expansion of improved MCH care;
- t o col laborate with the countr ies i n s p e c i f i c a reas of emphasis including ex-
pansion on immunization, the prevention and treatment of dehydration i n acute diarrhoea1
disease of e a r l y ahildhood, and the promotion of breast-feeding.
Co-operation with and among countr ies
The Organization w i l l continue t o col laborate with countr ies i n respect of
fu r the r development of t h e i r MCH se rv ices I n general . The B6ja project i n Tunisia
has been useful i n introducing a number of appropriate new techniques and methods.
I n Somalia the programme f o r the improvement and expansion of MCH se rv ices funded
by UNFPA with WHO a s Executing Agency is being implemented. Co-operation w i l l
continue with the Governments of Syr ia and I r a q and the United Nations Relief and
Works Agency f o r Pales t ine Refugees i n the Near East, i n the general development of
t h e i r MCH services.
The Technical Discussions on the Present S t a t e of Child Health i n the Region,
a t the Regional Committee i n 1978, and the i n t e r e s t aroused by the designation of 1979
a s In te rna t iona l Year of the Child, a r e l i k e l y t o r e s u l t i n increased a c t i v i t y t o
reduce morta l i ty and morbidity i n infancy and e a r l y childhood, during the biennium.
I n regard t o the second medium-term object ive , the r e s u l t s of o r a l rehydration
t r i a l s i n I r an and Egypt i n 1977-78 and i n Somalia i n 1978, w i l l be applied throughout
the Region during t h e biennium. Large q u a n t i t i e s of the WHO guidel ines on the pre-
vention and treatment of dehydration have been d i s t r i b u t e d i n English and i n Arabic.
Oral rehydration s a l t s a r e being produced i n Egypt and Syria. Research t o evaluate
various approaches towards popularising o r a l rehydration e a r l y i n the course of
d iar rhoeal a t t a c k s i n i n f a n t s and young chxldren has been approved a s high p r i o r i t y
by the Regional Advisory Cormnittee on Biomedical Research. The MCH and Nutr i t ion ex-
p e r t i s e i s pa r t of a new group formed a t the Regional Off ice t o a s s i s t the countr ies
t o formulate and implement programmes of control of e n t e r i c in fec t ions , one of whose
main t a r g e t s w i l l be subs tan t i a l reduction of the unbearably high morta l i ty and mor-
b i d i t y i n chi ldren under three years from acute d iar rhoeal diseases.
Programme
Nutr i t ion
Objectives:
- To a s s i s t the Governments i n reducing the incidence of a l l forms of malnutri t ion
and i n promoting b e t t e r n u t r i t i o n of a l l individuals;
- t o col laborate i n developing the heal th component of mul t isectora l food and
n u t r i t i o n p o l i c i e s and programmes;
- t o promote and f a c i l i t a t e the control of s p e c i f i c n u t r i t i o n a l def ic iencies ;
- t o promote the development of nu t r i t iona l - s t a tus survei l lance systems.
Co-operation with and among countr ies
The approaches taken by the countr ies i n col laborat ion with Wig) i n the period of
the S ix th General Programne of Work include assessment of t h e magnitude of n u t r i t i o n
problems; planning and implementing n u t r i t i o n progralaes i n the heal th se rv ices ;
opera t ional research t o i d e n t i f y and evaluate lost appropriate methods of resolving
n u t r i t i o n a l problems; t r a i n i n g i n n u t r i t i o n , with col laborat ion of FAO and UNICEF where
appropriate; and taking s t e p s towards the formulation of nat ional food and n u t r i t i o n
p o l i c i e s .
The experience gained i n national n u t r i t i o n surveys i n Tunisia and Egypt w i l l
be applied i n s imi lar surveys i n o ther countries. I n respect of Pales t ine refugees
an endeavour w i l l be made to construct a simple n u t r i t i o n a l survei l lance system based
on MCH records. Likewise the National Nutri t ion I n s t i t u t e of I r a n , with WHO consul-
t a n t ass is tance , has planned t o undertake a p i l o t n u t r i t ~ o n a l s t a t u s survol l lance
system based on the records of a primary heal th care programme north of Teheran.
S t i l l i n the a rea of assessment, but i n t h i s case i n respect of Vitamin A deficiency
and xerophthalmia, the preliminary appra i sa l s which a WHO consultant ophthalmologist
has carr ied out i n a number of c o r n t r i e s w i l l be repeated i n o ther countries; where
these appra i sa l s ind ica te the need, WHO w i l l a l s o col laborate i n nation-wide o r
province-wide Vitamin A-deficiency surveys t o provide baseline data f o r ac t ion pro-
grammes t o solve the problem.
The findings of operational research p ro jec t s t o evaluate home-made weaning foods,
i n the Sudan, and to f ind p rac t i ca l ways of including n u t r i t i o n i n primary heal th care ,
i n Somalia, w i l l influence programmes i n the biennium, a s w i l l t he outcome of t r i a l s
i n the Region on the appl ica t ion, a t v i l l age l e v e l , of o r a l rehydration f o r chi ldren
with diarrhoea1 diseases.
The Regional Food and Nutr i t ion Training project i n which W H O collaborated with
UNICEF, FA0 and UNESCO, and which ended i n 1978, w i l l be followed up by nat ional
t r a in ing programmes. Regional courses can still take place i n whatever sub jec t s the
need i s apparent. Collaboration between the agencies a t regional level w i l l be
maintained by the Inter-Agency Co-ordinating Committee on Food and Nutr i t ion which
held i t s f i r s t meeting i n April 1978.
In regard t o nat ional food and n u t r i t i o n policy, one of the d i f f i c u l t i e s facing
governments i s sometimes t h a t of iden t i fy ing the sources of re levant da ta , making some
in te rp re ta t ion of them, and iden t i fy ing the po ten t i a l resources within the government
min i s t r i e s and agencies a s a whole f o r formulating and implementing such a policy.
I n t h i s respect , j o i n t FAO/WHD/UNICEF missions such a s took place i n Somalia i n 1976
and the Sudan i n 1978 can be helpful , e spec ia l ly i f they can suggest some thoughts a l s o
on the machinery of formulation and implementation. Impl ic i t o r e x p l i c i t food policy
has exis ted i n almost every nat ion-s ta te s ince the e a r l i e s t recorded history. I n our
Region, the building-up of famine reserve stocks i n ancient Egypt i s a very widely
known example, I t remains t o be seen t o what extent i n any one s t a t e the mult i tude
of impl ic i t and e x p l i c i t food policy ac t ions can be r a t i o n a l i ~ e d and made mutually
supportive i n the shape of a formal food and n u t r i t i o n policy.

Programme
Special Programme o f Research, Development and Research Training i n 3.2.3 Human Reproduction
Objectives:
- To improve the hea l th of mothers and children and ul t imate ly of famil ies and
comunities, through reduction of hea l th r i s k s i n human reproduction, encouragement
of responsible parenthood, and promotion of growth and development of children and
youths;
- t o col laborate with countr ies on t h e i r request , i n improving maternal and ch i ld
heal th services , with specia l a t t e n t i o n t o prenatal care , midwifery services both
i n s t i t u t i o n a l and donucil iary, postnatal care of mothers, care of i n f a n t s and chi ldren,
and f e r t i l i t y regula t ion including treatment of i n f e r t i l i t y ;
- t o col laborate i n the development and improvement of o b s t e t r i c , gynaecological
and paed ia t r i c services i n r e l a t e d i n s t i t u t i o n s , and i n the t r a in ing of required
categor ies and numbers of hea l th personnel fo r these services ;
- t o help t o c l a r i f y the re la t ionsh ips between heal th , human reproduction, popula-
t i o n dynamics and family plannang;
- t o undertake, support and guide appropriate research i n human reproduction.
Co-operation with and amonP countr ies
A c t i v i t i e s under t h i s programme a r e c losely r e l a t e d t o those described under the
NCH programme, but with added emphasis on maternity care and midwifery services , and
re la ted research i n human reproduction. Family planning a c t i v i t i e s a r e o r i en ted t o
hea l th object ives , 1.e. primarily r e l a t e d t o the hea l th of mothers, chi ldren and
families. Moreover, the problems of s u b - f e r t i l i t y and i n f e r t i l i t y , deserve equal
a t t e n t i o n with those of high f e r t i l i t y .
Programmes and p ro jec t s of in tegra ted MCH and family planning a c t i v i t i e s with
hea l th ob jec t ives have been es tabl ished i n col laborat ion with UNFPA i n Afghanistan,
Democratic Yemen, Jordan, Somalia, Sudan, Syria and Yemen. The main purpose of these
p ro jec t s is t o improve the q u a l i t y and coverage of MCH care se rv ices , through w e l l -
planned expansion of the i n f r a s t r u c t u r e of urban and r u r a l MCH Centres. Such improve-
ment depends, apa r t from physical f a c i l i t i e s on e f f e c t i v e t r a i n i n g and s t a f f i n g pa t t e rns ;
on good co-ordination with, and support to , primary heal th care; and on s imi la r
e f f e c t i v e co-ordination with and support from specia l ized medical cen t res and maternity
hosp i t a l s ,
During the biennium (1980-81),an inter-country project on socia l and preventive
o b s t e t r i c s w i l l begin under the WHO regular budget, I t i s intended t o supplement
and strengthen tho a c t i v i t i e s already carr ied out under a UNFPA-supported inter-country
project i n Family liealth, and t o give specia l a t t e n t i o n t o problems of pe r ina ta l and
maternal morta l i ty , low birth-weight and cervical cancer, Other s ign i f i can t heal th
problems re la ted t o o b s t e t r i c s and midwifery, e.g. abort ions, breast-feeding, f e r t i l i t y /
i n f e r t i l i t y w i l l a l s o be looked in to . The matter of t r a in ing and u t i l i z a t i o n of
t r a d i t i o n a l b i r t h a t tendants , and su i t ab le involvement and pa r t i c ipa t ion of the com-
munity i n this regard, w i l l continue t o be emphasized through meetings, courses and
exchange of v r s i t s among s imi lar and in te res ted countr ies of the Region.
The needs of in te res ted countr ies i n research i n human reproduction a r e being
responded t o through coordination from WHO Headquarters and the Regional Off ice ,
through technical advisory ass i s t ance (Tunisia) , establishment of Collaborating Centres
of C l in ica l Research (Egypt, Pakistan and possibly I r a n ) and pa r t i c ipa t ion of se lec ted
nat ionals i n specia l ised meetings and f i e l d s tudies . These a c t i v i t i e s w i l l be
strengthened i n accordance with needs and accomplishments.
Programme
Health Education
Objectives:
- To col laborate with member s t a t e s i n the development of s u i t a b l e heal th education
programmes and a c t i v i t i e s , with main emphasis being l a i d on individual and community
involvement i n the ac t ion programmes;
- t o a s s i s t the general publ ic , both urban and r u r a l , i n t h e i r understanding o f ,
and s e l f-education i n , heal th matters, s o tha t they may assume more respons ib i l i ty
i n the promotion of individual , family and community health;
- t o encourage the expansion of hea l th education a s an important and e s s e n t i a l
component of ex i s t ing and developing heal th se rv ices i n member s t a t es .
- to help in tegra te heal th education i n t o the overa l l heal th and welfare services.
Co-operation with and among countr ies
Guidance on the promotion of hea l th education has been derived from the Regional
Sub-committee A Resolution (No.EM/RC27A/R.B) of 1977, which s t a t e s i n t e r a l i a t h a t ,
"programmes i n primary heal th ca re w i l l not be successful without adequate heal th
education based on the needs and wants of the communities", and t h a t Member S t a t e s
should "strengthen t h e i r hea l th education services ... "; and from Regional meetings
on Health Education Aspects of Family Health, i n 1977; on the Expanded Programme on
Immunization, i n 1977; and on Primary Health Care, i n 1978.
During the b i e ~ i u m (1980-81) WHO w i l l promote hea l th education a c t i v i t i e s i n sup-
por t of primary heal th care ; family heal th , with Special a t t e n t i o n t o maternal and ch i ld
heal th , immunization and n u t r i t i o n ; and the control of diarrhoea1 diseases p a r t i c u l a r l y
among children. I n addi t ion, specif i c programmes t o improve midwifery services , e.g.
t r a i n i n g and use of t r a d i t i o n a l b i r t h a t tendants , w i l l be promoted. Research and
f i e l d s t u d i e s a r e needed on socio-cul tura l pa t t e rns and the "needs and wants of the
communities", and it i s proposed t o carry out a t l e a s t one f i e l d study i n a s u i t a b l e
country during the biennium, More such s tud ies w i l l be promoted. Such s t u d i e s and
research could be carr ied out i n f i e l d t r a in ing a reas of heal th personnel t r a i n i n g
i n s t i t u t i o n s .
WH) w i l l continue t o col laborate with a l l countr ies of the Region, on request ,
i n the promotion of heal th education.
Major Programme
MENTAL HEALTH
Objectives :
- to promote mental health ac t i v i t i e s through bet ter planning and a more effect ive
organizational framework6
- to prevent o r reduce mental and neurological morbidity and i ts consequences;
- t o strengthen mental health services, improve the quality of care and provide
training f a c i l i t i e s for the development of manpower resources ;
- t o increase awareness of the mental health implications of socio-economic changes
and establ ish preventive measures,;
- to promote national p i l o t projects for the developept of bet ter preventive,
therapeutio and rehabi l i ta t ion measures i n drug dependence;
Cooporation with and among countries :
The t ! r n s t of the programme w i l l be directed into the following major areas a t
Regional and country levels:
A. REGIONAL
(a ) Planning, organization and management in mental health care
The important targets t o be achieved are:
- developent of competent national administrative bodies for proper planning and
e f fec t ive prograaming;
- integration of mental health care with the general health system and co-ordination
of a c t i v i t i e s with related social services;
- developent of relevant psychiatric f a c i l i t i e s more responsive t o ooplpp~nity needs
with due emphasis on extension of services to the periphery;
- up-dating mental health regulatiomand laws;
- development of an appropriate model for mental heplth information systems.
(b) Developpent of mental health workers and promotion of psychiatric t ra ining
programmes
Along with the promotion of psychiatric t ra ining i n general, special emphasis w i l l
be given to the developent of psychiatric nurse teachers i n the Region, This is
considered a major ac t iv i ty for strenthening the mental health t ra ining programme for
general health workers as well as for psychiatric personnel.
Other camponensof the proposed programme w i l l focus on mental health t ra ining i n
schools of public health and on the promotion of postgraduate s tudies i n psychological
medicine.
(c) Programme ac t iv i t i e s for dealing with specif ic problems o r issues:
- prevention and treatment of drug dependence and alcoholism;
- promotion of child psycho-soc~al development and mental health care;
- c a r e o f long-termpsychiatricpatients,
B. COUNTRY
Development of country mental health programme
- i n i t i a t i o n of mental health programmes i n cer ta in countries where no such a c t i v i t i e s
have been previously available, as i n Yemen Arab Republic ;
- supporting exis t ing rudimentaiy programmes, as i n Afghanistan, Somalia and Sudan
(Southern Region) ;
- i n i t i a t i n g t ra ining and promoting the developnent of professional mental health
workers ;
- collaborating with national au thor i t i es t o move mental health care from hosptial-
based services t o community-oriented f a c i l i t i e s , e.g. the Libya project.;
- developent of rura l psychiatry - new models a r e under way i n Sudan and Egypt;

Major Programme
PROPHYLICTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES 3.4 - Objectives :
- t o provide ass is tance i n the establishment and promotion of pharmaceutical
production and drug-supply se rv ices ;
- t o formulate in te rna t iona l spec i f i ca t ions f o r t h e qua l i ty of drugs, guidelines f o r
good manufacturing pract ices , and in te rna t iona l non-proprietary names fo r pharmaceut-
i c a l substances ;
- t o promote the exchange of information by nat ional regulatory au thor i t i e s on the
s c i e n t i f i c evaluation of drugs f o r sa fe ty and eff icacy, on drug r e g i s t r a t i o n and on
data t h a t form the bas is fo r decisions t o withdraw drugs from the market ;
- t o promote the monitoring of drug utilization and assessment of ef f icacy i n
medical pract ice , and the assessment of drug requirements with spec ia l reference t o
primary heal th ca re and r u r a l areas , and thereby give guidance on the se lec t ion of
e s s e n t i a l d rugs ;
- t o a s s i s t member countr ies i n the development of capab i l i ty t o formulate and
implement r e a l i s t i c drug p o l i c i e s ;
Cooperation with and among countr ies
For e f f e c t i v e and economic prophylaxis and therapy of d iseases an appropriate
supply of drugs is required. Governments have requested t h e col laborat ion of W H O i n
the establishment and fu r the r development of t h e i r drug supply and control organiza-
t ions f o r the period 1980/81 a s i n previous years.
A s e f f i c i e n t heal th ca re se rv ice r e l i e s on the cor rec t choice and use of drugs,
W H O has been requested t o strengthen nat ional e f f o r t s t o improve t h e r a t i o n a l i t y of
drug u t i l i z a t i o n .
I n countr ies where it is intended t o extend the heal th services , heal th planning
must include a r e l i a b l e fo recas t of the kinds and cos t of drugs t o be supplied t o
newly es tabl ished heal th care services , especia l ly i n t h e r u r a l and prlmary hea l th
ca re area. The WHO publ ica t ion "The Select ion of Essent ia l Drugs" (Technical r epor t
series 615, 1977), provides a valuable reference.
Drug u t i l i z a t i o n s tud ies can contr ibute necessary data and should be included
i n planned programmes. In c a n t r i e s where ecoi~omic conditrons permit medical ca re
free of charge for everyone rho needs it, priority is allocated to improvements of the
existing services and strengthening of their efficiency. In such countries, the drug
utilization study is one of several tools to approach optimal drug therapy. Precise
information on e.g. irrational prescribing, abuse of drugs or insufficient information
to patients on the use of drugs, provides the basis for corrective action. This
Wm activity requires the interdisciplinary collaboration of technical units respon-
sible for prophylactic and therapeutic substances, developaent of health manpower and
primary health care; it has opened a new area of operational research. The import-
ance of keeping drug costs as low as is consistent with reliability is self-evident.
The application of a realistic purchasing policy particularly in the case of imported
drugs presents some substantial difficulties. In this respect evidence of manufac-
turers* standards of operations provides a better safeguard than a c e r t i f i c ~ ~ ~ of
analysis relating to an individual batch or consignment.
The importance of these two factors is underlined by the fact that pvrchase of
drugs consumes about 15 to 20 percent of total health budgets, and that miscalculations
in drug supply and utilization threaten the functioning of otherwise well-planned
projects at the root. Drug utilization studies are under way in two countries:
Democratic Yemen and Sudan, in an endeavour to assess drug needs in the oontext bf
primary health care.
Wm will continue to collaborate by providing fellowships for the training of
various professional categories of personnel; organizing regional seminars and train-
Ing courses on subjects relating to drug regulation and surveillance; providing
consultants to advise on and train in drug procurement control, utilization and
surveillance; supplying information on drug specifications and warning of any adverse
reactions to drugs in use; and supplying materials and equipment for quality control.
Drug policies and management
Objectives :
- to collaborate with Member States in the development and improvement of national
services responsible for drug legislation and administration ;
- to strengthen the potential of Member States to secure m adequate supply of
the most suitable and useful drugs at reasonable cost to the public and private sectors
of health services ;
- to assist in the asressnent~of countries* needs for ph'annaceutical products in
the light national health goals ;
Cooperation with and among countries
For effective planning and management of pharmaceutical services, government
agencies must be adequately staffed with specialists in the relevant branches of
medicine (0.g. clinical pharmacology) and pharmacy (e.g. pharmaceutics, biopharmacy).
Sons, countries have sent nationals abroad for specialized training; others plan to do
so. Consultants advise on structural improvements of drug administrative services.
They facilitate modernizing of drug legislation and the updating of National Formularies.
Evaluation of drugs for efficacy, safety, economy and their compliance with the health
needs of the country, is promoted by WHO'S drug information services, and by training
of professionals. Continuingoomparisonof drug demands with substantiated drug require-
ments has been and will continue to be organized at the national and intercountry levels
in collaboration with WHO. Countries participating in these activities are Democratic
Yemen, Egypt, Iran, Iraq, Libyan Arab Jamahiria, Pakistan, Sudan and Tunisia.
WHO will continue to collaborate by providing consultants, advisory services and
fellowships, and arranging for the exchange of ideas and experience by means of group
meetings and consultations .
Phannaceutioals & Biologicals 3.4.2 - Objective :
To collaborate with Member States in the development and improvement of drug
production, standardisation, storage, distribution and in all aspects of control of
quality of drugs produced in Member Countries and/or wving in international commerce.
Cooperation with and among countries
The quality of pharmaceutical preparation is ensured by proper product developnent
including stability studies, establishment of a product specification, observance of
a code of good practice3 and quality control in manufacture, and, finally, by storage
under appropriate conditions during all stages of the distribution chain. Government
regulatory organizations contribute to the assurance of quality by inspection of
facilities and operations in all stages of production and distribution and by planned
sampling programmes for the laboratory testing of drugs. They may also give technical
guidance regarding quality assurance, and publicise matters such as the WHO code of
Good Manufacturing Practices. Collaboration in this field involves assistance in the
establishment or upgrading of pharmaceutical inspection services and quality control
laboratories especially by training personnel. This collaboration will continue during
1980/81. Special emphasis w i l l be placed on effect ive inspection of pharmaceutical plan
and operations for adherence t o good manufacturing practices, t h i s being potent ia l ly
the most economically beneficial aspect of the work of a regulatory authority.
I t is recognized that there is a need for substant ia l quant i t ies of standard
reference substances for use i n governmental and commercial quality-control laboratories
of the Region. I t is intended therefore t o explore the poss ib i l i ty of developing
the potential of one o r more national laboratories t o prepare, ca l ib ra te and d i s t r i bu t e
standard reference materials. The aim would be tha t such laboratories would be
designated by WHO as suppliers of Regional Reference Standards.
WHO w i l l continue t o collaborate by the provision of long- and short-term consul-
tants , advisory services, fellowships, reference literature, standard reference materials
and equipment necessary for WHO-supported projects.
Major Programme
00MMUNICABLE DISEASE PREVmION AND CONTROL 4.1 - O b j e ~ t i ~ o S :
- t o strengthen national and international epidemiological surveillance of commun-
icable diseases of major public health importance;
- t o collaborate with countries i n evolving programmes for the control of commun-
icable diseases, in particular: malaria, schistosomiasis, f i l a r i a l infections, trypano-
somiasis, communicable diseases of the respiratorygstem, tuberculosis, en te r ic
infections, leprosy, sexually transmitted diseases, zoonoses and other communicable
diseases of major public health importance; and t o provide prompt and effect ive
assistance i n emergencies;
- t o complete and maintain smallpox eradication i n the Region;
- t o expand the use of immunization, through the health services, i n the control
of those diseases for which effect ive inmunizing agents and methods ex is t ;
- t o promote research on e f fec t ive and economical measures for the prevention and
control of the communicable diseases i n close association and aollaboration with the
Global Promamme for Reseach and Training i n Tropical Diseases.
Cooperation with and among countries
Communicable diseases continue t o be one of the most important health problems
i n the Region i n s p i t e of the considerable change which has occurred in patterns of
morbidity and mortality and the progress achieved i n t he i r ~0ntN3l . The problems posed by these diseases c a l l fo r a f lex ib le approach and theiwiaptation
of preventive and control measures t o national circumstances and poss ib i l i t i es .
WHO is continuing collaboration with governments i n the control and eradication
of specif ic communicabl3 diseases through organized campaigns, manpower training,
fellowships, supplies and equipment. Special a t tent ion w i l l be given t o strengthening
surveillance reporting and recording systems. The main thrusts w i l l be through the
Expanded Programme on Immunization (EPI), the control of vector-borne and water-
associated diseases, the prevention of blindness and the programme for diarrhoea1 d i s -
eases including cholera. Appropriate measures for the maintenance of smallpox eradica-
t ion w i l l be continued.
Contributions to the Voluntary Fund for Health Promotion, for EPI, have been
made by Saudi Arabia, Kuwait, Iran and the United Arab Ehirates; and W H ) with UNICEF
is collaborating with national EPI projects throughout the Region, and i n an inter-
regional UNDP-supported project concerned with vaccine production, quality control,
c o l d chains for presgrvation of vaccine and logis t ic support.
The regional plan for the control of diarrhoea1 diseases and the prevention of
cholera,fomulated by the Regional Meeting on Cholera and Diarrhoea1 Mseases,will be
pursued during the biennium with WH) collaboration.
The "border" meetings w i l l be continued to enhanoe necessary oooperation among
neighbouring countries i n malaria eradication and control.
Similar "border" meetings involving Syria, Jordan, Lebanon and possibl- *&ey
are thought advisable for schistosomiasis control. In th i s respect also, provision
w i l l be made a t the pre-planning stages of new irr igat ion schemes and water develop-
ment peojects to minimize the i r potential health hasards.
The plan of action prepared by the Cor~lnittee t o study the prevention of blindness
i n the Region established by the Regional Sub-Committee "A" w i l l be follarnd Qlting the
biennium.
Prograume
Programme planning and general ac t iv i t ies
Objective:
TO prepare a medium-term programe for conmanicable disease control.
Cooperation with and among countries
The W H 3 Collaborative Medium-Term Prograring Working Group, including Headquarters
and Regional Office participants, is scheduled to m e e t during the f i r s t w . d r of October
1978 (tentatively in E3HRO), to prepare for the draring-up of regional mediur-ten
p r o g r a e s on w-icable diseases.
I t is therefore anticipated that, following t h i s meeting, a medium-term program8
on unmunicable diseases prevention and control i n the Region for 1978/83 w i l l be
formulated.
Consultations with Governments i n the Region wi l l take place for th i s purpose
as necessary.
Programme
Epidemiological surveillance
Objectives:
- t o a s s i s t countries i n planning and develop&ng national epidemiological service& and
coordinate regional ~ ~ r ~ e i l l a n ~ e of comunicable diseabar;
- t o a s s i s t i n studying development, implementation and evaluation of cop.uniqable
disease control prograamer including @valur$ion of Imunization prograaraes;
- t o promote and a s s i s t with Seminars, conferences, technical meetings and t ra ining
courses i n the broad f i e ld of epidemiology and other more spec i f ic f ie lds ;
Cooperation with and among countries
The epidemiological services have not developed equally i n the oountriee of the
Region and there a re considerable gaps i n knowledge of geographical dis t r ibut ion of
most communicable diseases, of populations a t r isk, of what degree of p r ior i ty cummun-
icable diseases should receive among health problems, and on the f ea s ib i l i t y of control.
Epidemics of new diseases have occurred with considerable loss of l i f e . In the
absence of adequate epidemiological services and laboratories, assistance is provided
a t government request for emergenay services and/or the ident i f icat ion of aet iological
agents. Mssernination of information is also undertaken.
To achieve the objectives of t h i s programe, oountries must es tabl ish oontral
epidemiological intell igence un i t s supported by a network of no t i f ica t ion agents
reaching the most remote areas. Such surveillance mechanlsns ex i s t i n many oountries
of the Region as part of former mass campaigns, but a re not fu l l y uti l ized. Simple
screening mechanisns su i tab le for use by primary health care workers can be of great
value i n defining t h e geographical dis t r ibut ion of disease and for ear ly warning of
impending epidemics.
W K ) w i l l oontinue its collaboration with the countries of the Region in establish-
ing ep idg~io logioa l services end t ra ining epidemiologists and other s ta f f by providihg
consultants and advisory services and supplies and equiprent when nmeesary.
Governments are nor w e l l aware of the importance of inter-wuntry ooordiaation, in
part icular i n the control of qlrarantinable dieeases. The oorron policy rhioh emerged
from meetings held during the 1977 Session of the Regional Cornittee and of the Arab
League, concerning measures t o prevent the importation and spread of cholera i n the
Region, w i l l be pursued with WHO collaboration during the biennium, as w i l l the
regional plan for en te r ic diseases control formulated by a technical group of experts
from countries of the Region.
Similar inter-country coordination w i l l be promoted i n respect of R i f t Valley
Fever and brucellosis as well as other areas of epidemiological studies.
Programme
Malaria and other pa ra s i t i c diseases
Objectives:
- t o collaborate with Governments i n assessing malaria s i tua t ions and programmes
and i n the planning of anti-malaria programmes as par t of overal l health plans;
- t o cooperate with Governments towards the eradxcation of malaria when t h i s
is feasible, o r reduction of i ts incidence where i t is not feasible i n the near
future; t o a s s i s t countries i n the development of their basic health services, to
enable them t o es tabl ish anti-malaria operations a t peripheral level and eventually
undertake sat isfactory vigilance against the re-introduction of malaria;
- t o conduct epidemiological surveys of other paras i t i c diseases, par t icular ly
schistosomiasis, for determination of t h e i r nature, character is t ics and geographical
dis t r ibut ion;
- t o collaborate with countries i n evolving programmes for the control of other
paras i t i c diseases, par t icular ly schistosomiasis, with the ult imate aim of eradicating
them ;
- t o develop control a c t i v i t i e s for preventing the spread of schistosomiasis and for
t reat ing and curing infected cases;
- t o promote t ra ining of natxonal manpower;
- t o develop health education for the information of the public;
- t o apply environmental measures t o avoid introduction of diseases i n i r r iga ted
areas ;
- to etrengthen programme coordination and cooperation amongst neighbouring countries.
Cooperation with and among countries
Assessment of malaria s i tuat ions and programmes carried out with national o f f icers
show tha t , i n Spite of set-backs and administrative and technical d i f f i cu l t i e s , most
countries have been able t o maintain t he i r achievements by means of a f lexible approach,
aimed a t a t ta ining predetermined targets . WHD w i l l maintain i ts cooperation with
countries i n t h i s approach. In cer ta in countries,however, a serious s i tuat ion ex is t s
and the Regional Office is providing a l l possible administrative support and technical
cooperation t o improve it. Training of national s ta f f receives the highest p r ior i ty
and technical self-rel iance has been s teadi ly increasing in the Region.
The integration of malaria a c t i v i t i e s into the general health services w i l l be
stimulated whenever practicable by promoting the trend towards a multi-purpose
u t i l i z a t i on of malaria personnel for the control of communicable diseases other than
malaria, and a more consistent participation of the general health services i n the
control of communicable diseases.
Cooperation among neighbouring countries w i l l be continued as signified by
border meetings and by the continued assistance offered by the r icher countries t o
others.
Of par t icular importance is the plan for a medium-term coordinated malaria
programme i n the Arabia Peninsula.
In schistosomiasis, collaboration with countries of the Region is focussed on:
- undertaking studies (epidemiological and malacological) to assess the public
health importance of schistosomiasis control;
- organizing programes for the control of schistosomiasis;
- the follow-up of schistosomiasis programmes and the i r progress;
- the evaluation of control programmes.
The importance of national administrative support and self-rel iance for the
implementation of schistosomiasis control programmes cannot be over-eolphasized. In
view of the success achieved i n Bulinus control by the use of the molluscicide
niclosamide, under re la t ive ly economical conditions, i t w i l l be suf f ic ien t i n the future
t o maintain the vigilance of breeding s i t e s a t its present level and to react t o any
re-infestation of waters by Bulinus, and to obtain the expected r e su l t s through system-
a t i c treatment of infected persons.

The t h r u s t of the programme w i l l be d i rec ted pa r t ly towards malntaxning and
strengthening the pos i t ive r e s u l t s so f a r achieved i n some countries, and p a r t l y a s
i n Jordan where no Bulinus nor Biomphalariasnaiis could be traced, towards ensuring
the permanent absence of these vectors from the country by the survei l lance of water
bodies, and the search f o r human cases and t h e i r treatment.
The improvement of san i t a ry standards, pa r t i cu la r ly s a f e water supplies and the
provision of su i t ab le l a t r i n e s a s well a s heal th education, w i l l be promoted i n
schistosomiasis control programmes; spec ia l emphasis w i l l be given t o protect ive en-
gineering measures i n i r r i g a t i o n schemes.
The col laborat ion of WHO i n schistosomiasis control p ro jec t s I n Somalia, Syr ia ,
the Yemen Arab Republic, Democratic Yemen, Jordan, Sudan and Tunlsia w i l l be extended
t o o ther countr ies during the next biennium.
A s a r e s u l t of the development of nat ional manpower and exper t i se , the tendency
t o provide countries more and more with consultant services , suppl ies and equipment,
and fellowships, r a the r than longrterm exper ts , w i l l be continued.
Apart from d i r e c t involvement WHO w i l l follow closely the development of na t iona l
programmes and w i l l co l laborate a s required. I n t h i s respect , schistosomiasis con t ro l
a c t i v i t i e s i n Egypt, where t h e d lsease is considered the most important public heal th
problem and where the nature of its l r r i g a t i o n system (from basin t o perennial) , together
with the high r a t e of ~ n f e c t i o n , provide f o r various aspects of schistosomiasis research,
s tud ies and control .
I n Upper Egypt, where a s a r e s u l t of the Aswan Dam, l a rge areas were converted
from basin t o perennial i r r i g a t i o n , the prevalence of S. haematobium in fec t ion is
s t a t e d t o have increased i n some such a reas from 5 per cent t o 33 per cent wi th in two
years a f t e r conversion. Moreover, S. haematobium occurs very commonly among t h e
Lake Nasser fishermen(approximate1y 60 per cent). The na t iona l control programme
a t Lake Nasser is l inked with t h e I R UNDP/WHD Project i n Research on the Epidemiology
and Methodology of Control of Schistosomiasis i n Man-Made Lakes (Ghana and Egypt),
where t h e main a c t i v i t i e s a r e concentrated i n Accra around Lake Volta . I t is expected t h a t
the activi*eson the Egyptian s ide of the project , which have so f a r been l imited,
w i l l be developed during the biennium. Other national a c t i v i t i e s of importance a re
undertaken a t the National Research Centre, Dokki, Cairo; the Bilharzia Research
I n s t i t u t e , Faculty of Medicine, Cairo University; and the I n s t i t u t e of Research fo r
Tropical Medicine, Cairo, i n addit ion t o t ropioal medical departments i n a number
of un ivers i t i ee i n Egypt.
In I raq, s tudies and controJ a c t i v i t i e s a r e being undertaken a t the I n s t i t u t e
of Endemic DiSeaSeS, which cover communicable and p a r a s i t i c diseases including schisto-
somiasis; and, i n I ran, important s tudies covering a l l aspects of schistosomiasis
prevention and control a re being undertaken a t the Bi lharzias is Research and Control
Project a t Dezful, Khuzestan as well a$ a t the I n s t i t u t e of Public Health Research
i n Teheran.
Cutaneous leishmaniasis is present i n most countries of the Region. Recent
s tudies i n Afghanistan and Saudi Arabia showed t h a t cutaneous leishmaniasis follows
a focal pa t t e rn of d i s t r ibu t ion i n both countries. I t was suggested t h a t , i n view
of the resources avai lable t o t h e i r malaria control services , cutaneous l e i s b a n i a s i s
control should be entrusted t o the already established network of those services
i n these two countries; however, a cen t ra l u n i t responsible f o r cutaneous l e i s b a n i a s i s
control should be es tabl ished as pa r t of the cen t ra l malaria organization, t o be
responsible f o r t r a in ing of s t a f f i n case-finding and treatment. W I D collaboration
w i l l continue a s required i n t h i s f ie ld . WW> collaboration with the Government of
I raq w i l l be maintained a l so i n respect of the control of v i sce ra l leishmaniasis
(Kala-azar 1.
The problem of Tryponosomiasls i n the Region is l i m i t e d t o Southern Sudan where
i t is a po ten t i a l ba r r i e r t o socio-economic development. A review of the s i t u a t i o n
by a consultant , following an increase i n the number of regis tered cases i n the
Yambio area, and deta i led epidemiological s tud ies t o demonstrate t h e existence of an
ac t ive focus has been followed by control measures using t h e l o c a l resources. W K )
w i l l continue t o col laborate as required i n these measures and i n t h e t r a in ing of
loca l mioroscopists.
A bilateral agreement has been signed between the Governments of Sudan and Belgium
for the setting up and implementation of a programme for survey, treatment and control
of human trypanosomiasxs. WHO will continue collaboration in this field as required.
Programme
Cholera and enteric infectims 4.1.3 - Objectives:
- to establish a system of notification, reporting, storage,retrieval and analysis
of information on cholera and enteric infections at national and regional levels;
- to disseminate knowledge on the most appropriate techniques of epidemiological
surveillance, laboratory testing, treatment of infections and rehydration;
- to provide emergency assistance in case of epidemics.
Cooperation with and among countries
The control of enteric infections depends on knowledge of the environmental factors
responsible for the completion of the cycle of transmission. The chain can be inter-
rupted through the progressive long-term provision of safe water supplies, appropriate
sewage disposal and health education of the public . As a first step towards thislong-
term~target , W H D will cooperate in the establishment of adequate surveillance,.mechan-
isms, the introduction of suitable methods of treatment, in particular, rehydration,
the development of laboratory diagnostic services and epidemic control measures. The
regional plan formulated by a regional group of experts to achieve the short-term objec-
tives provides for oral rehydration to reduce mortality from gastroenteritis particular-
ly among the youngest age groups, and at the most remote village level, as well as
the rapid notification of all forms of gastroenteritis. It provides also for contin-
uous surveillance of food, water and sewage, for the early detection of enteropathogens,
and the prevention of food and water-borne infections.
W H D collaboration in the biennium will be by means of advisory services on a
short and long-term basis (epidemiologists), the training of staff in epidemiology
and laboratory techniques and research, and material support to establish and implemt
oral rehydration. Inter-country coordination of activities is expected to be further
enhanced. Agreenlent is being sopght from all countries concerned on a common policy
for international travel and trade.
Tuberculosis
Objectives:
The long-term object ive is t o reduce the d isease by u t i l i z i n g modern control
techniques, inexpensive and adapted t o the loca l and f inancia l p o s s i b i l i t i e s , u n t i l a
s t age of t o t a l eradication is reached.
The medium-term object ives a r e prevention of the d isease through BCG vaccination;
ea r ly diagnosis; ambulatory treatment with the most e f f e c t i v e and inexpensive drugs;
establishment of a r e t r i e v a l system f o r de fau l t e r s ; education of the population; w n t r o l programmes against bovine tuberculosis where necessary; t ra in ing of personnel
f o r the in tegra t ion of tuberculos is w n t r o l i n t o the basic heal th services , and the
organization of r e f resher courses, seminars and workshops a t cen t ra l and provincial
levels .
Cooperation with and among countr ies
Tuberculosis i s a major public heal th problem i n the Region. There a r e nat ional
tuberculosis control programmes i n a l l countries of the Region, with var iable degrees
of success.
The t h r u s t of the WHO col laborat ive programme is on the in tegra t ion of tuberculos is
w n t r o l a c t i v i t i e s i n t o the general heal th servzces. Importance is given t o the
t r a i n i n g of nat ional heal th workers so t h a t they can play an e f f e c t i v e r o l e i n integra-
t ion.
The inclus ion of BCG vaccination i n the Expanded Programme on Illmunization is
expected t o play a major p a r t i n protect ing the population agains t tuberculosis once
the EPI bui lds up momentum i n an increasing number of countries.
In t h i s connection W H 3 w i l l continue t o cooperate i n procuring BCG vaccine f o r
countr ies with mass BCr,-itaccination campaigns. Pa r t i cu la r a t t e n t i o n w i l l be d i rec ted
a t qua l i ty control of BCG vaccine, i n accordance with the guidelines which have been
s e t ou t t o meet the requirements f o r dr ied BCO vaccine i n t h e context of the WH)-
sponsored in te rna t iona l qua l i ty control system.
I t is expected t h a t , a s government support of control measures inareases , t h e
problems such a s breakdown i n drug provision systems, lack of e f f e c t i v e supervision
and weakness of r u r a l heal th laboratory f a c i l i t i e s , w i l l be c l e a r l y i d e n t i f i e d and
solved by the countries. The improved coverage of r u r a l communities by hea l th se rv ices

which is expected during the biennium should be a major factor in establishing
comprehensive national tuberculosis control programmes.
WHO collaboration through long-term projects with the Governments of Afghanistan,
Democratic Yemen, Libya, Pakistan, Somalia and Yemen Arab Republic, by mg- of
technical expertise to support the national programmes, fellowships, supplies and
equipment will continue as necessary.
The marked decline in incidence among children in Libya is expected to be
maintained.
WI13 collaboration will continue in Pakistan where expansion of the pmgraPPlPe
to more districts will be continued; and,in Oman, where the outcome of a review
of the tuberculosis control programme carried out by a consultant in 1977 will be
followed through during the biennium.
Leprosy
Objectives:
The long-term objective is to prevent and control leprosy, using the recognized,
effective and economically suitable methods so that the disease is brought gradually
under control and ceases to be a medical, social and economical problem.
The medium-term objectives are the collection and analysis of epidemiolog!loal
data in various areas through surveys, the training of personnel, the development
of health education, the integration of control methods in basic health services, and
the development of a rehabilitation system for leprosy patients.
Cooperation with and among countries
Although the number of leprosy cases is not known and cannot be estinated with
great precision, it is thought that there are at least 178 601 cases in the Eastern
Mediterranean Region.
The prob2em is very limited in Bahrain, Cyprus, Israel, Jordan, Lebanon, Libya,
Syria, Tunisia and the United Arab Bairates. It is of public health importance in
Democratic Yemen, Egypt, Iraq, Saudi Arabia and Yemen Arab Republic where cases number
between a few hundred and 10 000 to 20 000; and in Iran, Pakistan, Somalia and Sudan
where there is a relatively higher endemicity in some parts of their territories.
Despite the efforts of governments and the cooperation of private international
institutiqns, the problem has not been substantially reduced during the lastBn years.
The approaches t o meet the objectives are based on the collection of epidemiological
data, case-finding focussed on school children and other high-risk groups, and t rea t -
ment systems adjusted t o local s i tuat ions. Also recommended are the demonstration and
u t i l i z a t i on of simple methods t o combat d i s ab i l i t i e s , the development of health educa-
t ion programmes, the gradual integration of ac t i v i t i e s in to the basic health services,
the granting of fellowships t o key s t a f f for training abroad, and the organization of
short seminars and workshops t o inform and t ra in health workers.
Direct WHD cooperation by means of supplies and equipment t o the leprosy control
projects i n Pakistan and Sudan, w i l l be followed up by the assignment of a W H D lepro-
l og i s t to the new leprosy control centre a t Wau i n Sudan. The German Leprosy Relief
Association, which has collaborated extensively with the Government i n the construction
of the Wail centre, w i l l finance the provision of the leprologist .
Bi la te ra l assistanoe t o the leprosy programme i n general has been p r~v ided by the
Sasakawa Memorial Health Foundation of Japan, which has granted $ 17 000 to WHO fo r
the provision of advisory services and fellowships.
Veterinary public health
Objectives:
- t o promote the development of and coordinate veterinary services a t the appropriate
minis ter ia l levels as w e l l a s the regional level for those aspects relevant t o the
protection of human health;
- t o develop a system of surveillance and control of zoonoses including food-borne
infections ;
- t o stimulate exchange of knowledge and information and promote inter-country
coordination.
Cooperation with and among countries
The health problems connected with zoonoses i n the Region a re as yet t o be
thoroughly investigated and there is a growing awareness of such problems. A s the need
for regional centres for dissemination of information has become obvious some countries
have agreed to t he i r establishment. National epidemiological services are not yet
developed t o a p o i n t which could ensure tha t zoonoses problems a re fu l ly evaluated.
Furthermore, collaboration among veterinary services and health services leaves much
row for improvement.
Some zoonoses have assumed epidemic proportions before the health services could
be made aware of it. Coordination of e f fo r t s a t country and inter-country levels is
the main need.
The main emphasis of WHO collaboration w i l l be on the improveanent and dissemina-
t ion of knowledge on zoonoses and the para l le l and coordinated expansion of e p i m i o -
logical surveillance i n human and animal health services.
This w i l l be achieved through the establishment of regional and inter-regional
centres for the collection and dissemination of information and training of medical
and veterinary s t a f f .
The Inter-Regional Zoonoses Centre i n Athens for the countries of the Mediterran-
ean area (supported by UNDP) is expected to be operational by 1979 and the possibi l i ty
has been raised of the establishment of similar centres for the Arab countries of the
Gulf area.
A technical meeting on brucellosis for 1979 i n collaboration with W H O Headquarters
and the FAO/WHO Centre i n Berlin for Research and Training i n Veterinary Public Health
is expected t o indicate a sound approach to the control of the disease.
An inventory of regional wsources i n the veterinary public health f i e l d is also
being undertaken as a s tep towards greater xnvolvement of the available technical
expertise and f a c i l i t i e s i n a regional programme.
Surveillance measures to monitor and prevent the spread of R i f t Valley Fever
w i l l be maintained i n accordance with the recolmnendations of a seminar on the subject
i n Egypt i n 1978.
Smallpox eradication
Objectives:
- t o complete cer t i f ica t ion of eradication of smallpox from a l l countries of the
Region ;
- t o maintain an ef f eat ive surveillance system;
- t o vaccinate where appropriate and according to circumstances;
- t o consolidate r-esults achieved and par t ic ipate i n the col lect ion and prompt
exchange of information.
Cooperation with and among w u n t r i e s
With the apparent in terrupt ion of transmission of the disease on a global basis,
a c t i v i t i e s a r e now directed towards c e r t i f i c a t i o n and au thor i t a t ive endorsement of
eradication.
I f no new case of sanllpox is detected, a l l countries of the Region w i l l have been
c e r t i f i e d before the beginning of the biennium. I n t h i s case, surveil lance w i l l con-
t inue as pa r t of the overa l l survei l lance of communicable diseases.
Programme
Expanded programme on Immunization
Objectives:
The long-term objectives are:
- t o make immunization agains t diphtheria, pe r tuss i s , tetanus, measles, poliomyeli t is
and tuberculosis accessible t o every chi ld i n the Region by 1990, and as a consequence
t o reduce morbidity and morta l i ty from these diseases.
- t o reduce morbidity and morta l i ty s imilar ly f o r o ther se lected diseases of public
heal th importance f o r which s a f e and e f fec t ive vaccines become available.
- t o f a c i l i t a t e regional se l f - re l i ance , pa r t i cu la r ly i n mat ters of vaccine production
and qual i ty control.
Cooperation with and among countries
The considerable upsurge of a c t i v i t y tha t hasoccur red in t h i s programme r e f l e c t s
the considerable degree of cooperation which e x i s t s between w u n t r i e s f o the Region.
Saudi Arabia, Kuwait, I r an and t h e United Arab Rnirates contributed through t h e WH)
Voluntary Fund fo r Health Promotion t o finance expanded immunization programmes i n
countries with low per cap i ta GNF. Much support a l so comes from UNICEF which is i n
e f f e c t WHO'S steady partner i n t h i s programme. Inter-country cooperation (TCDC) i n
vaccine production and qual i ty control takes the form of a UNDP supported project i n
whkch I ran, Egypt, Tunisia, Jordan, I raq and Pakistan a r e a l l par t ic ipants .
With WHO and o f ten UNICEF collaboration the Governments have formulated Plans of
Operations and/or Plans of Action fo r Expanded Programmes on Imuniza t ion i n Afghanistan,
Democratic Yemen, Egypt, Pakistan, Somalia, the Sudan, Syr ia and the Yemen Arab
Republic. I n most oases the supplies and equipment specif ied i n these plans have been
delivered and operations have begun. WHO collaboration has taken the form of assignment
of s t a f f i n most of those countries, consultant services and planning missions by
Regional Off i ce or W m / m s t a f f .
Training which began with a Regional Seminar i n December 1977 for the Programme
Directors, National Operations Officers and WH3 country s t a f f assigned t o EP1,is
being continued by intensive national courses i n EPI management (Pakistan i n September
1978 and probably Egypt for early 1979) and w i l l continue t o be supported by WHD i n
1980/81.
The great tasks which remain i n EPI to be undertaken during the bienniumaretomove
from p i lo t phases t o country-wide implementation where applicable; t o sustain momentum
and inter-country and WH3 collaboration a f t e r the periods covered by the present
plans(most1y f ive years); and to develop information systems as the essent ia l tool of
management they must be. In addition, research i n appropriate technology i n respect
of cold chain and other operational aspects such as sa fe and speedy injections,and
research i n public motivation is planned and have t o be developed. Finally, many
lessons are to b& learned and applied from the experiences of t h i s Programme i n its
f i r s t few years.
Programme
Special programme for research and training i n t ropical diseases 4.1.6 - Objective :
This programme aims a t promoting and assis t ing the developnent and coordination
of biomedical research in the Region, par t icular ly i n major paras i t i c diseases.
Cooperation with and among countries
The Regional Office w i l l collaborate closely with governments and WH) Headquarters
within the overal l global programme of Research and Training i n Tropical Diseases.
An adviser t o be assigned a t the Regional Office for the General WH3 Research Prograrmne,
w i l l a lso coordinate with governments and WHO Headquarters, prograrmnes for Research
and Training i n Tropical Diseases within the context of overal l biomedical researah
i n the Region.
The Eastern Mediterranean Advisory Connni t tee on Bionedical Research, a t its th i rd
meeting which took place i n Alexandria i n March 1978, showed par t icular i n t e r e s t i n
the Research and Training i n Tropical Diseases Programme, and r-dedthatthe Region-
a l Ofdbe continue the iden t i f ica t ionof research in s t i t u t i ons available fo r project8 i
in the field. It also emphasized the importance of strengthening Research Institutions,
particularly by the training of research workers in TDR, in harmony with the global
programme.
Budgetary provision is available for fellowships to research workers in the Region
in the field of Tropical Diseases. The Government of Iran has paedged a special
contribution of US $ 500 000 for the Progrannne for Research and Training in Tropical
Diseases in the Eastern Mediterranean Region, for the specific purpose of establishing
a Regional Centre, for Research and Training in Tropical Diseases with the suggestion
that the site of this centre be in Iran in view of the availability of technical and
financial capacities and resources in the country.
Programme
Prevention of Blindness - 4.1.7
Objectives:
- to strengthen and expand the ophthalmological services, in particular towards the
more peripheral rural areas, for the early treatment of blindness producing affections,
such as trachoma, ~nchocerciasis, cataract and glauwma.
- to support mass preventive measures aiming at reducing the incidence, particularly
among young age groups, of trachoma and xerophthalmia.
Cooperation with and among countries
The Eastern Mediterranean Regional Committee (Sub-Committee A) has established a
Committee to study Prevention of Blindness in the Region, wmposed of the Ministers of
Health of Kuwait, Saudi Arabia, Bahrain, Egypt and Iran, the Regional Dir-tor and a
representative of the International Agency for the Prevention of Blindness. At its
request, WHO convened a meeting of experts to draw up a plan of action for the prevention
of blindness in the Region and to study the feasibility of a proposal to establish a
regional ophthalmological centre for training and research. WHO will continue its
collaborative role in implementing the plan during the biennium. The group is expected
to continue to meet regularly to follow up and evaluate the implementation of the plan.
Wm, in collaborataon with the Regional Countries, envisages strengthening of some of the already existing centres for control, treatment and research on eye diseases and is
also studying the creation of one or more Regional Centres for prevention of blindness.
The main emphasis i s being placed on the expansion of services t o populations
l iv ing i n the most remote areas, where lack of curative ophthalmologiaal services and
consequent delays i n treatment lead t o blindness. The second, equally important, thrust
is towards mass chemoprophylaxis and chemotherapy of trachoma, and Vitamin A t o prevent
xerophthalmia, where conditions permit reasonable benefit against the kosts .invglved.
Onchocerciasis, which is a problem i n Sudan and the Yemen Arab Republic, iswrecoqlplex, and appropriate control methodolo&es have not yet been devised. The main emphasis
a t present is on the use of drugs, intermittently and a t reduced non-toxYc dosages, t o
reduce microfilaraemxa and the r i s k of blindness. No large-scale operations are encou-
raged against the vector, un t i l r e l i ab l e methodologies have been developed by the ad hoc study xn West Africa. -
The programme provides for consultant services for country projects, i n par t icular
i n trachoma control and onchocerciasis, and for evaluation. There is provision also
fo r essen t ia l supplies and equipment within the l i m x t s of available resources, and for
t ra ining through fellowships.
Programme
Vector biology and control
Objectives:
To cooperate m t h the countries of the Regxon towards:
- the assessment of vector-borne diseases and programmes;
- the planning of vector control i n vector-borne diseases as par t of an overal l
health plan;
- the establishment, within the exis t ing resources, of f lex ib le and dynamic programmes
adapted t o diversified biological, ecological and chemical vector control, taking in to
consideration the socio-economic s i tua t ions ;
- the promotion within each country of intra-sector ia l and inter-sector ia l cooperation
so tha t exis t ing resources can be u t i l i z ed i n the most economical and e f f i c i en t ways;
- the promotion of control and prevention of vector-borne diseases i n the water re-
sources developulent projects through engineering methods;
- the promotion of sa fe use of pest ic ides and provision of regulatory measures for
t h i s purpose;
- the ts aining of nationals; and
- the cprrying out of applied research.
Cooperation with and among countries
The p r i o r l t y of prevention and control of vector-borne diseases is f u l l y recognized
among the communicable diseases and heal th problems i n the Region.
The most important vector-borne diseases i n the Region a r e malarxa, schistosomiasis,
leishmaniasis, trypanosomiasis, f i l a r i a s i s , onchocerciasis, some of the arbovirus
diseases and plague foc i ( s i l v a t i c ) . Vector control is one of the major components
of campaigns f o r prevention and control of these diseases.
Vector control measures (including control of intermediate hos t s and rodents
reservoirs of the diseases) a r e applied for:
- malarxa (mosquito control ) I n f i f t e e n countries of t h e Region;
- schistosomiasis ( sna i l control ) In s i x countries;
- leishmaniasis (sand f l y control ) i n two countries; and
- rodent borne diseases (rodent control ) i n SIX countries.
The Regional Office w i l l continue t o provide administrat ive and technical wopera-
t i o n i n the promotion of the s a f e use of pesticldes.
.d te rna t ive methods of vector control a re being introduced i n order t o reduce t h e
t o t a l re l iance on chemical control . Biological control of vectors, and environmental
managenent, especia l ly i n water resources developnent projects , w i l l be speoia l ly
promoted . Training of nat ional s t a f f w i l l continue t o receive high p r i o r i t y , m order t o
promote technical se l f - re l iance. A plan f o r establishing a Regional Training and Re-
search Centre i n I raq is being formulated.
Applled research on different aspects oP vector control w i l l continue i n coopera-
t i o n with the countries of the Region. Thls research includes t e s t s of new insec t i c ides
and spraying equipnent and experiments on biological control of vectors of malaria,
u t i l i z i n g larvivorous f xsh.
A t a Seminar on t h e Prevention and Control of Vector-Borne Diseases i n Water
Resources Development Projects , i n Ilexandria and Khartoum m 1978, s c i e n t i s t s and
heal th workers formulated plans for control . Including measures against the spread of
schistosomiasis vectors, which w i l l pursued during the biennium. A s a follow-up of
t h i s Seminar, a project is already being envisaged for the control of water-associated
diseases i n Sudan (Jezi ra and Rahat I r r i g a t i o n Areas) with collaboration of UNEP
and b i l a t e r a l agencies. ii preliminary Plan of Operation fo r t h i s project is under
negotiat ion with the Government of Sudan. The programme, which is scheduled t o cover
a period of ten years, has for i t s objectives the improvement of i r r i g a t i o n i n the
agr icu l tu ra l and economic areas of Sudan and the control of some of the water-borne
diseases of t h e area such as malaria and schistosomiasis.
Inter-agency cooperation and coordination, with FhO, UNDP and DANIDA vector control
d l 1 be continued.
Major Programme
NON-COWUUNICABLE D l SEASE PRGVENTION AND CONTROL
Principal objoc t i v e
- to prevent and cont r o l non-communicable diseases.
Detailed object ives .%.
- to promote cancer prevention and control , including coordinated cancer research;
- t a promote the prevention asd control of d iseases of the cardiovascular system;
- t o promote and develop programmes f o r the control of o the r non-communicable
d iseases of public heal th importance, a i t h due regard f o r the c r i t e r i a f o r determining
p r i o r i t i e s ;
- t o promote the development of p o l i c i e s and programes f o r o r a l health.
Co-operation with pnd among countr ies
Reorientat ion of the cancer programme has been taking place with increas ing zea l ,
i n col laborat ion with the Governments of the Region. I n t h s context , cancer is be-
coming incrcas ingly recognized a s an important public hea l th problem. W H O technical
co-operation i s expected t o reach a peak i n 19W/lll through consultant se rv ices , fellow-
sh ips and suppl ies and equipment. Meetings w i l l be organized t o exchange s c i e n t i f i c
information. Cancer r e g i s t r a t i o n and cancer epidemiology w i l l head the list of prio-
r i t y a reas f o r collaboratioq.
Of cardiovascular d isease , rheumatic heart d isease , hypertension and ischaemic
hea r t d isease a r e among the common causes of morbidity and morta l i ty i n the coun t r i e s
of the Regian. W H D w i l l continue i t s co-operation with countr ies i n epidem&ological
s t u d i e s and i n improving the standard and qua l i ty of care , including in tens ive care.
I t ~s expected t h a t col laborat ion with countr ies i n e s t a b l i s h n g and developing
o r a l heal th se rv ices w i l l grow fur ther . A major object of co-operation w l r l be to
determine the magnitude of the problem of dental i l l - h e a l t h espec ia l ly den ta l caries.
Training of denta l a u x i l i a r i e s w i l l a l s o receive spec ia l a t t e n t i o n e.g. i n Sudan.
WHO w i l l increase its support f o r the fu r the r development of immunology se rv ices
and f a c i l i t i e s by organizing courses, fos te r ing research, sponsoring s c i e n t i f i c
meetings and awarding $ellowships.
I n human genet ics , dissemination of i n f o r m t i o n , promotion of research, and
technical guidance on request , w i l l be m j o r f a c e t s f o r WW co-operatioa with coyntries.
Programme
Cancer
Objectives:
- To continue the implementation of the Regional Cancer Programme;
- t o strengthen cancer a c t i v i t i e s a t country l e v e l , iden t i fy ing the principa4 causes
hindering cancer detect ion, diagnosis, treatment, r e h a b i l i t a t i o n and prevention and
f inding adequate solut ions;
- t o co-operate with countr ies i n improving t r a i n i n g of medical personnel and the
heal th education of the public i n the f i e l d of cancer;
- t o promote cg-operation within the Region and a t in te rna t iona l l eve l i n cancer
epidemiology, cancer detect ion, diagnosis and treatment, increas ing the r o l e of Regional
Reference Centres f o r various cancer sites and of the Regional Advisory Panel i n t h i s
d i rec t ion.
Co-operation with and among countr ies
Continuing the e f f o r t s i n cancer control , nine country pro jec t s and -*en i n t e r -
country p ro jec t s a r e included i n the Programme Budget f o r 1980/81.
I r a q , Kuwait and Sudan have undertaken t o S t a r t a p i l o t p ro jec t on strengthening
cancer a c t i v i t i e s a t country level . The major f a e t o r s which a r e hindering canoer de-
t ec t ion , diagnosis, treatment and prevention have been reviewed i n the three countr ies ,
and recommendations h v e been made f o r improving the s i tua t ion . These a r e t o be fo l -
lowed up and a l t e r n a t i v e opt ions w i l l be promoted i n order t o obta in a r e a l improvement
of the s i tuat ion. The pro jec t could then be extended t o o ther countries.
A new country p ro jec t i n cancer is s t a r t i n g i n Saudi- Arabia.
The courses on cancer epidemiology and on cancer r e g i s t r y w i l l be repeated, and a
Seminar aimed a t improving undergradute and postgraduate teaching i n cancer is a l s o
planned.
Programme
Cardiovascular Diseases
Objec t ives :
- To a s s i s t i n making epidemiological s t u d i e s t o a s s e s s t he card iovascular d i s ease
problem i n c o u n t r i e s of t h e Region,
- t o he lp i n c o n t r o l l i n g these d i s e a s e s by developing medical s e r v i c e s and p a r t i -
c u l a r l y emergency medical s e rv i ce s ,
- t o t r a i n c l i n i c a l and pub l i c h e a l t h workers i n card iovascular d i s ease con t ro l .
Co-operation wi th and among c o u n t r i e s
Cardiovascular d l s ea scs , mainly rheumatic hea r t d i s e a s e , hypertension and
ischaemic hea r t d i s ease , a r e among t h e common causes o f morbidi ty and m o r t a l i t y i n
t h e Region.
WHO a c t i v i t i e s i n t h i s a r e a w i l l d ea l with:
- t h e prevent ive a s p e c t , which w i l l focus on epidemrological s t u d i e s t o assess the
card iovascular d i s ease problem, and
- the c u r a t i v e a s p e c t , i n which WHO w i l l promote h igher s t anda rds of c a r e of cardio-
vascular d$seases, w i th t h e focus mainly on i n t e n s i v e c a r e s e r v i c e s , i nc lud ing coronary
care .
WHO w i l l cont inue i t s co-operat ion with Egypt t o develop and expand i t s i n t e n s i v e
c a r e s e r v i c e s inc luding coronary c a r e u n i t s i n u n i v e r s i t y h o s p i t a l s by suppor t t o
t r a i n i n g and i n t he es tab l i shment of f a c i l i t i e s . Advisory s e r v i c e s , equipment and
supp l i e s , and fe l lowships w i l l be provided.
To he lp f u r t h e r improve Lebanon's c a p a b i l i t i e s i n c o n t r o l l i n g card iovascular
d i s e a s e s WHO w i l l provxdo s u p p l i e s and equipment, and consu l t an t s e r v i c e s t o eva lua t e
and adv i se on the count ry ' s programmes.
A Regional Seminar on Epidemiological S t u d i e s i n Cardiovascular Diseases w i l l be
he ld t o p lan s c i e n t i f i c s t u d i e s a s a b a s i s f o r prevent ive measures i n c o n t r o l l i n g
card iovascular d i s eases .
Programme
O r a l Health
Object ives:
To a s s i s t the coun t r i e s of t he Region i n e s t ab l i shzng and developing o r a l h e a l t h
s e rv i ces , both preventive and cu ra t ive , through:
- co-operation i n undertaking epidemiological s t u d i e s t o i d e n t i f y o r a l d i s e a s e and
a s s e s s the e x t e n t of the o r a l h e a l t h problem;
- promotion o f prevent ive s e r v i c e s f o r o r a l and den ta l d i seases ;
- promotion of water f l u o r i d a t i o n , and co-operation i n such p ro jec t s ; acd
- t r a i n i n g of o r a l h e a l t h personnel.
Co-operation wi th and among c o u n t r i e s
Dental c a r i e s , e s p e c i a l l y among school ch i ld ren , is an important and inc reas ing
o r a l h e a l t h problem i n the Region. I t s ex ten t has t o be determined and o r a l h e a l t h
s e rv i ces , p a r t i c u l a r l y preventive measures, have t o be developed.
Co-operation i n o r a l h e a l t h w i l l continue. I n I r a q the preventive o r a l h e a l t h
s e r v i c e s w i l l be evaluated wi th the he lp of consul tan ts . I n t h e Sudan t h e training
of o r a l a s s i s t a n t s w i l l r ece ive p r i o r i t y . Other c o u n t r i e s a r e l i k e l y t o r eques t 00-
opera t ion and support f o r t h e i r o r a l h e a l t h serv ices .
A s p a r t of t he Regional Ora l Health Programme, WHO w i l l hold a Seminar on Ora l
Health i n 1980, t o review the o r a l h e a l t h s t a t u s i n the c o u n t r i e s of t he Region and
exchange i d e a s on the subjec t .
Programme
0 t h e r Non-Conmunicable Diseases
Genet ics
Object ives:
- To c o l l e c t , ana lyse and d isseminate information on human gene t i c s ;
- to promote research on s p e c i f i c f a c t o r s t h a t may cause i n h e r i t e d d i seases , through
changes i n t he s t r u c t u r e o f genes, i n t he mechanism o f t h e i r a c t i o n , o r i n t h e com-
pos i t i on o f t h e i r products , and through changes i n chromosome s t r u c t u r e and mechanisms;
- t o provide t echn ica l guidance and advice on human g e n e t i c s t o na t iona l p rog rames
concernec' with the s tudy o f t h e pub l i c h e a l t h imp l i ca t ions o f i n h e r i t e d d i seases ; and
- t o co l l abo ra t e wi th d r f f e r e n t c e n t r e s f o r the development of r e sea rch i n t h e i r
s p e c i f i c f i e l d s of competence.
Co-operation wi th and among c o u n t r i e s
Two g e n e t i c counse l l ing p r o j e c t s have been planned: one, i n Egypt, due t o s t a r t
i n 1978 and the o t h e r i n Cyprus, o r i g i n a l l y planned f o r 1975 bu t , owing t o t h e pre-
v a i l i n g s i t u a t i o n a t the t i m e , kep t i n abeyance.
A course on l abo ra to ry diagnosis i n haematology dea l ing mainly wkth anaemiasis
and haemoglobinopathies he ld i n Thailand i n 1978 was a t tended by p a r t i c i p a n t s from
Sudan, Pakis tan , I r aq and Egypt.
A course is proposed on haemoglobinopathies and o t h e r r e l a t e d d i s o r d e r s i n 1980
and another on cy togene t i c s and katyotyping i n 1981.
Programme
Immunology
Objec t ives :
Long-term o b j e c t i v e s
- t o f o s t e r the development o f immunology on a l l i ts a s p e c t s i n developing c o u n t r i e s ,
e s p e c i a l l y resoarch i n t o t he immunology of d i s e a s e s posing pub l i c h e a l t h problems,
w i th s p e c i a l emphasis on t r a i n i n g conducted m those c o u n t r i e s , i n order t o speed t h e
development o f t h e i r own e x p e r t i s e ;
- t o encourage t h e i n t roduc t ion of e s t a b l i s h e d immunology techniques i n t o p a t i e n t
c a r e , and t o s t anda rd i ze r eagen t s and methodology;
- t o develop and i d e n t i f y new knowledge on immunology wi th p o t e n t i a l a p p l i c a t i o n t o
d i s e a s e s of pub l i c hea l t h importance;
- t o co-ord ina te r e sea rch on a l l branches o f immunology;
- t o s tandard ize t h e nomenclature of immunological terms.
Medium and short- term o b j e c t i v e s
- Organizat ion of courses ;
- t o support r e sea rch i n t h e immunopathology and immunology;
- t o pub l i sh r e p o r t s on s u b j e c t s o f publ ic h e a l t h importance.
Co-operation with and among countries
Courses are being proposed, for 1980, on immunological methods ( t o promote re-
search i n immunology), and on the immunopathology of sohistosoma and f i l a r i a s i s , and,
for 1981, on the immunology o f v ira l and r icketts ia1 diseases, and on immunogenetics
including its practical and theoretical aspects.
w o r Programme
PROMOTION OF ENYI RONMENTAL HEALTH
Programme
l$nvironnental Health Planning and Management
- To provide tuchnacal con$ultation i q the development o f both p e g i ~ n a l and national
envaronincntal heal t b a c t i v l t i e s ,
- t o promote and develop environmental heal th policqes, panagement and financing
of services , ins ta tu t ions and programmes;
- t o encourage ac t ivc and aystcmatlc parcicigataon of the hea l th sector i n the for-
mulation and exeoution of socio-economic devslopment plans;
- t o promote the development of innovative and apprspr ia te technology f o r environ-
mental control that wall be within the f inancra l c a p a b i l i t i e s of the area; and,
- to a s s i s t i n planning, project formul t a t ion , management and evaluation of t r a in -
ang programmes fo r various ca tegor ies of envrronnwntsl heal th workers an the w n t e x t
of need and avai lable resources.
CQ-oneration with an6 among c o u n t r i ,
Baseline data on environmental heal th needs and ava i l ab le reseurces for a t t ack ing
both e x i s t i n g and emerging environmental problems w i l l bq? marntained on a current Pas i s
i n col laborat ion with nat ional a u t h o r i t i e s i n order to a s s $ s t planr)&n&, as tab l i sh ing
act ion p r i o r i t i e s , allowing f o r evaluation of r e s u l t s and providing the input necessary
fo r e f f e c t i v e qccisionwmaking.
Moro comprohensive data r e l a t i n g to spec1 f ac problems w i l l be provided a s needed
by consul tants on survey missions t o a ssess s i t u a t i o n s $or fens ibJe means of ac t ion
wrthin current ly gvailable resot+rces. Emphasas w i l l be ggven t o the development of ln-
novative and appropraate tachnoLogy through operational rssvarch focused on regional
and national problems. Wide dissemination of such dcvelopmcnts i s r e q u i s i t e to pro-
gramme ~mplemuqtntion.
Jntensaf ica t lon gf e f f o r t s to a s s i s t the Menrbar S t n t a s i n dcqling with those severe
bas ic cnvirorunttntal heal th problems yet remaining a s wel4 a s t o f a c i l i t a t e the a t t ack
s n emerging and cQmplex now environmental problcms r e s u l t i n g from population growth,
rapid &ndus t r i a l i za t ion , the trend toward urbanazat~on and also Current socio-econvmrc
devgloplncnts,can best be promoted by the establishment o i an Eagtern Mediterranean
Centre far Enviroru~ental A c t i v i t i e s (CENA) . This Centre w i l l address i t s e l f rn tens i vely
t o developing e f f e c t i v e means of deal ing with environmental and ecological prablegls,
t~ environmental research, t o strenthening national and regional environmental pro-
gra-s, t o developing a comprehensive and in tegra ted educational and t r a in ing capa-
b i l i t y , t o e s tab l i sh ing a co-orbinated network of nat ional i n s t i t u t i o n s working &-
l e c t i v e l y on environmental problems and t o providing f o r Wady technology and iqforma-
t ion t r ans fe r .
The r e l a t i v e p r i o r i t i e s assignable t o e n v r r ~ m e n t a l heal th problems may vary from
country t o country depending upon l o c a l s i t u a t i o n s and largely influenced by s t ages
of development, lndust r ia lxzat ion and urbanization. Inadequacy of basic sanatary
measures still remains a major concern i n much of the Region so t h a t emphasis i s still
being given t o provision of sa fe water supply and e f f e c t i v e excre ta d i s p o s A , Food
san i t a t ion problems a l s o reaain a s a high p r i o r i t y i t e m .
Prevention of environmental pol lu t ion is more economical than correct ive measure$.
For this reason a s w e l E a s f o r the public heal th benef i t s t o be gained, e f f o r t s t o
encourage e a r l y a t t e n t i o n t o newly'emerging problems a r e being made. Since such a c t i -
v i t i e s cannot be e f fec t ive ly undertaken without a properly organized in f ras t ruc tu fe ,
equal a t t e n t i o n must be given t o strengthening environmental heal th se rv ices and in-
s t i t u t i o n s . Training must therefore be provided i f the qua l i f i ed manper needed t o
s t a f f these services i s t o be avai lable . An a rea o i g rea t need i s i n t h e development
of t r a in ing c a p a b i l i t i e s f o r producing large numbers of middle-level technician per-
sonnel who can complement and extend the e f f e c t i v e range of highly t ra ined profess ional
personnel .
Basic Sani tarv Measures
Objectives:
- To promote and col laborate i n nat ional planning of se rv ices and i n i n s t i t u t i o n -
building fo? the provision and survei l lance of drinking-water suppl ies and wastes d i s -
posal ;
- t o a s s i sk c a u n t r i e i I n the formulation and implewntat ion of comuni ty water supply,
mate disp~sal and r u r a l scmitat ion p ro jec t s , and t o col laborate with nat ional and
multi-national agsncies concerned with a view t o mobiliasing nat ional and/or in terne-
t iorml rebources fo r the impleimentation of these projects ;
- to provide technical cooperative se rv ices t o supple-nt the technical c a p 8 M l i t y
of ~ t i m L eater supply and s a n i t a t i o n agencies a s and when required.
Co-operation wi th and among coun t r i e s
WHO i s co l l abo ra t ing wlth coun t r i e s i n ca r ry ing o u t assessment of t he water supply
and sanitation situation, i n improving d a t a collection precedures, and i n formulat ing
long-, medium- and short- term water supply and s a n i t a t i o n programnes. h a t e r supply
and s a n i t a t i o n agencies a r c being strengthened through t r a i n i n g of na t i o n a l personnel
and the provis ion of technica l s e r v i c e s t o supplement na t iona l s t a f f and t o adv i se on
improved o rgan iza t iona l , admin i s t r a t i ve and managerial procedures. Programmes f o r
su rve i l l ance of drinking water q u a l i t y and waste d i sposa l networks a r e being e s t ab l i shed .
The Organization co-operates a l s o i n preparing pre-investment p r o j e c t s , i n car ry-
i n g ou t master p lan and f e a s i b l l l t y s t u d i e s , and i n ob t a in ing f inanc ing from b i l a t e r a l
and i n t e r n a t i o n a l sources.
Consultancy se rv i ce s a r e provided In spec i a l i zed a r e a s a s requi red and t o i n t e r -
p r e t new developments of environmental concern a s w e l l a s f o r t h e prepara t ion o f
po l icy recommendations.
Subsequent t o t h e dec i s ion of the United Nations Water Conference t o dcs lgna t e
1981-1990 a s tho I n t e r n a t i o n a l Drinking Water Supply and S a n i t a t i o n Decade, cons ide rab l e
e f f o r t i s being made t o c o l l a b o r a t e wi th Member governments i n t he preparacion f o r t h e
Decade. Ons a c t i o n has been t h e rdpid assessment of water supply and s a n i t a t i o n
programmes and of t h e e x t e n t t o which these might be u se fu l ly expanded t o meet t h e
o b ~ e c t i v e s recommended by the Unlted Nations Water Conference, i.e., water and s a n i t a t i o n
f o r a l l by 1990. With W X I c o l l b o r a t i o n , t h i s e x e r c i s e was c a r r i e d o u t i n about ten
c o u n t r i e s of t he Region.
The development of na t iona l p l ans f o r water supply and s a n i t a t i o n is being given
p r i o r i t y i n c o u n t r i e s of t he Region and thc p r o j e c t s under way i n t he se f i e l d s w i l l be
continued. Consultant s e r v i c e s a r e being made a v a i l a b l e t o Somalia f o r t h e e s t a b l i s h -
ment of a water q u a l i t y su rve i l l ance programme.
The management and d i sposa l of s o l i d wastes a r e becoming a problem i n s eve ra l
c o u n t r i e s of t he Region. Counsultancy s e r v i c e s w i l l cont inue t o bo provided a t the
r eques t of governments.
Technical advice i s being provided t o s eve ra l Count r ies of t he Reglon on s p e c i f i c
problems such as the high concent ra t ion of n i t r a t e s i n water , p o t e n t i a l carcrnogenic
ch lo r ina t ed o rgan ic s An d r ink ing water a s a r e s u l t of water c h l o r i n a t i o n , excess ive
f l u o r i d e s i n water and de f luo r ida t ion . Technical information on s t a b i l r z a t i o n ponds
has been disseminated to a l l Member s t a t e s of the Region and t h e i r use f o r the t r e a t -
ment of waste water promoted.
Programme
Recognition and Control of Environmental Hazards
Objectives:
- To promote the development and implementation of progralqmes fo r the e a r l y de-
t ec t ion and control of pol lu t ion i n the environment (chemical, physical and b io log ica l ) ;
- t o evaluate the e f f e c t s of environmental f a c t o r s on heal th ;
- t o promote and co-ordinate re levant research; and t o f o s t e r the p rac t i ca l ap-
p l i ca t ion of research findings; and,
- t o promote environmental san i t a t ion , e spec ia l ly a s r e la ted t o urban and r u r a l
development and primary heal th ca re , t h a t contr ibutes t o the prevention of communicable
disease.
Co-operatson with and among countr ies
Increased a c t i v i t i e s aimed a t developing sus ta inable c a p a b r l i t i e s i n the a reas
of pol lu t ion monitoring and control i n a i r , water and s o i l a r e planned f o r the biennium.
These w i l l involve environmental impact assessments i n order t o determine the magnitude
of the problem and t o p r i o r i t i z e a c t i o n programmes, Development of basic p o l i c i e s ,
c r i t e r i a and standards, regula t ions and l e g i s l a t i o n w i l l be needed, S ta f f a c t i v i t i e s
supplemented by consultant surveys, assessments and recommendations ar r ived a t through
ac t ive co-ordination with nat ional input of needs and c a p a b i l i t i e s w i l l be a c t i v e l y
pursued. Workshops, seminars, t r a i n i n g courses and academic placements w i l l be used
t o produce a steady supply of the r e q u i s i t e specia l ized personnel a t a l l l e v e l s of
operation within the nat ional in f ras t ruc tu re ,
The WHO Global Environmental Monitoring System has been expanding i t s operations
by increas ing ex i s t ing monitoring cen t res and ac t ive ly promoting the c rea t iop of new
networks, The major t h r u s t of t h i s programme i n concept is t o i n t e g r a t e and i n t e r -
d i g i t a t e a l l data- measuring l e v e l s of toxic mater ia ls i n various media leading t o
degradation of the environment.
The bas ic aims of these programmes a r e f i r s t l y t o assl ist Member s t a t e s i n develop-
ing anr$/or strengthening nat ional c a p a b i l i t i e s i n manpowed and i n r t i t u t i o n s f o r i m -
plementing programmes i n these f i e lds . Secondly, they become p a r t of a g l ~ b a l network
which feeds data concerning pol lu t ion to a centra l computer f a c i l i t y f o r ana lys i s ,
s torage and r e t r i e v a l . Such baseline data on a global bas i s w i l l allow f o r demonstra-
t ion of pol lu t lonal l eve l s and trends a s an a id t o the dsci$$on-meking processes in-
volved an a t t a i n i n g improvement of environmental condit ionsr
For the measurcmnt of a i r q u a l i t y , four countr ies i n the Region - Egypt, I r a n ,
I r a q and Pakistah - have been added t o the network which already included I s r a e l .
A c t i v i t i e s a r c under 'way t o add seven additronal countr ies t o the network a t t h e i r
governments' request. These a r e Kuwait, Lebanon, Libyan Arab Jamahiriya, Saudi Arabia,
Sudan, Syria and Tunisla.
For the protection and conservation of the f l n i t e supply of the world's water re-
sources, @ global monitoring programme fo r water qua l i ty i s being established. I n
the Eastern Mediterranean Region t h i s assumes an important place since the Region's
fresh-water reqources a re generally q u i t e l imited and many must depend upon desalina-
t i o n of marine waters fo r potable, domestic, i n d u s t r i a l and a$r icu l tu ra l supplies.
Establishment of monitoring citations and se lec t ion of colXaborcting l abora to r i e s is
underway ,$n eleven countr ies - Egypt, I r an , I r aq , I s r a e l , Kuwait, Libyan Arab
Jamahiriya, Pakistan, Sauda Arabia, Sudan, Syria and Tunisla.
Inter-regional, programmes dealing wlth marine pol lu t ion problems i n the Mediter- 1
ranean have addressed the problem of inventoryang land-based sources ~f po l lu tan t s
and t h a t of mQnitoring the qua l i ty of coas ta l r ec rea t iona l and seafood growing waters,
s ince Mediterranean tourism has a great economic impact on the Region. A c t i v i t i e s
a r e cantinrung. i n Cyprus, Eqypt, I s r a e l , Lebanon, Libyan Arab Ja~ahiriya, Gyr- and
Tunisia, Designation of col laborat ing l abora to r i e s and comencemeqt of sampling
which has begun i n $$ypt, I s r a e l and Lebanon, w i l l be extended t o o ther countries.
Two o the r closed sea programmes a r e being developed f o r rapid implementation
a l o ~ g l i n e s s imi lar to those developed i n the Mediterranean Action Plan* The f i r s t
involves the following e igh t countries: Bahrain, I r an , I r a q , Kuwa~t, Oman, Q a t a r ,
Saudi Arabia and the Ungted Arab Emirates. An extensive programme with contr ibutory
funding has beqn approved f o r t h i s a c t i v i t y f o r the area of the Kuwait Action Plan
Region (KGPR). A l a rge por t ion of the planned programme i s involved with human hea l th
e f f e c t s 04 pol iu t ional burdens while the remainder dea l s with marine ecological e f f e c t s
l a rge ly i n f l u e n ~ e d by o i l contamination. The second involves e igh t c ~ u n t r i e s of t k
Region bordering the Red Sea qnd the Gulf of Aden. These &re Demcratkc Yemen,
Djabouti, Egypt, Jordan, Saudi Arabia, Somalia, Sudan qnd Yemen Arab Republic. This
programme w i l l a l s o be developed around two major components: human hea l th e f f e c t s
and marine ecological concerns. Since the Red Sea/Gulf of Aden L$ l inked with the
Mediterranean through the Suez Canal, in tegra t ion of f indings on both ends of the Canal
w i l l provide valuable data.
A c t i v i t i e s i n b iological monitoring for determination of t o t a l b?dy l e v e l s and
heal th e f f e c t s of toxic mater ia ls contaminating more than one medium, such a s lead,
mercury, cadmium and chlorinated hydrocarbons, a r e commencing i n a n e f f o r t t o a s sess
t o t a l heal th impact a s a guide t o more re levant standards and c r i t e r i a f o r auch sub-
s tances i n a l l meidia i n which they occur. I n i t i a l e f f o r t s a r e under way i n I r a n and
I s r a e l on this programme with o ther countr ies t o be added l a t e r .
Promotion of Food Safe ty
Objectives:
- To promote the deQelopmnt of programmes t o ensure food s a f e t y and to supply in-
formation f o r planning and implementation;
- t o promote reduction i n human i l l n e s s and economic losses caused by microbial ,
chemical and physical contamination of food products; and
- t o a s s i s t i n e s tab l i sh ing c r i t e r i a and standards f o r tood handling, production
and preservation t h a t w i l l ensure the protection of the consumer.
Co-operation with and among countr ies
The improvement of food sa fe ty and hygiene is of utmost codcefn i n a Regron where
the t o l l among chi ldren under f i v e from acute diarrhoea1 disease s t f l k dons t i tu tes
a grave public heal th problem. Repeated outbreaks of cholera have been t raced t'o
f aeca l ly contaminated foodstuffs r a t h e r than t o water supplies.
S ta f f e f f o r t s i n collaboration with nat ional input w i l l be i n t e n s i f i e d on a l l re-
levant f r o n t s t o ameliorate this pr~blem. Additional input from consul tants tb corn-.
plement and expand these e f f o r t s w i l l be obtained. I n s t i t u t i o n strengthening bbtki a s
t o manpower t ra ined f o r meeting the problems and a s t o laboratory c & p a b l l i t i e s f o r per-
forming the necessary sampling and t e s t r n g wall be emphasized,
Public education campaigns w i l l be encouraged and a s s i s t e d an order t o provide
bas ic personal hygiene and sa fe ty i n food-handling i n the home. Such e f f o r t s can be
focused a s an i n t e g r a l pa r t of primary heal th care a c t i v i t i e s . he bas ic problems of
provision of s a f e and e f f e c t i v e excre ta disposal a s well a$ control of usage of f aeca l ly
contaminated waste waters fo r food crop i r r i g a t i o n w i l l continue t o be emphasized a s
w i l l the ready a v a i l a b i l i t y of adequate supplies of water f o r domestic use.
Collaboration continues with nat ional governments and with in te rna t iona l organizo-
t i o n s such a s FA0 a s well a s with the Arab Organization fo r Standardization and hletro-
logy (ASMO) on mutual i n t e r e s t s i n improving food control and hygiene a c t i v i t i e s .
Collaborating laborator ies f o r food sa fe ty programmes have been designated i n Egypt
and I r a n with o the r s t o be added gradually.
Training e f f o r t s on an in te rna t iona l bas is a s well a s strengthening t r a i n i n g
c a p a b i l i t i e s f o r food control and inspectional a c t i v i t i e s have resu l t ed i n adding t o
the manpowor pool fo r these programmes. Such i n s t i t u t e s have been a s s i s t e d i n
Democratic Yemen, Jordan, Libyan Arab Jamahiriya, Pakistan, Saudi Arabia, Tunisia and
Yemen Arab Republic.
The Organization i s co-operating with various countr ies i n strengthening food
san i t a t ion services , and i n programes t o e s t a b l i s h a s u i t a b l e and e f f e c t i v e in f ras -
t ruc tu re fo r implementing municipal, provincial and nat ional s t r a t eg ies .
Major Programme
Programme
Programme planning and general ac t i v i t i e s 6.1.0
Objectives:
Within the context of the Sixth General Programme of Work, and the Medium Tern
Progranune on Health Manpower Development for the period 1978-1983 approved by the
Regional Committee a t its Twenty-Seventh Session i n October 1977, the broad objectives
w i l l be:
(a) t o promote the development of appropriate health personnel t o meet the needs of
en t i r e populations;
(b) t o promote the development and application of relevant processes for basic and
continuing education.
Cooperation with and among countries
A s i n previous years the programme area of Health Manpower Development is the
largest s ingle component i n the Programme Budget. I t should also be noted tha t , as i n
the past, i n addition t o the substant ia l a c t i v i t i e s and expenditure under t h i s specif ic
heading very substantial t ra ining e f fo r t s are a lso proposed within a l l other programme
areas.
The high pr ior i ty devoted t o the Health Manpower Development Programme by the
Member Countries of t he Region continues t o be a source of g ra t i f ica t ion ; the Organiza-
t ion w i l l continue t o play an act ive ro le as regards the t ra ining of a l l categories of
health manpower and the sensi t izat ion of governments t o the need for the reorientation
of t ra ining programmes to meet health services needs. Indeed, the overriding considera-
t ion which w i l l govern the programme i n 1980-81 w i l l be the need not only t o increase
the numbers and improve the qual i ty of health personnel but a lso t o make t h e i r t ra ining
more relevant t o the needs of populations. Accordingly, a research and development
approach t o health services and manpower development w i l l be increasingly emphasized.
The prograrmne w i l l continue t o be characterized by constant exchange of views and
consultation with Mmber countries. I t w i l l be based on the perspective t ha t health

manpower development is only one factor, a lbe i t a key one, i n developing health services
t o meet the needs of en t i re populations.
Tho Eastern llediterranean Region was one of the f i r s t t o support Medium-Term
PrograPmneforIIealth hlanpower Development, and, i n the programme developed for tine period
up t o 1983, ovory e f fo r t has been made to s t a t e objectives as clear ly as possible so
tha t the programme can be monitored, evaluated and ~0nt inuously adjusted as required.
There w i l l be a steadily increasing thrust t o take collaboration with Member
Countries beyond consultation and exchange of views, which have long characterized the
way of working, t o the development of programmes i n which national personnel w i l l be
more and more fu l ly involved i n planning and execution.
The ~ rgan iza t ion ' s collaboration with Member Countries does not moan collaboration
w i t h health authori t ies alone, but a lso with those governmental agencies whioh have the
responsibili ty for the training of health personnel, frequently the Ministries of
Education, and invariably the national planning authorit ies.
A s has long been recognized, and i n recent years expl ioi t ly s ta ted, the balance of
t h e health manpower stock of the Region needs correction as muah as do actual shortages;
par t icular emphagis w i l l accordingly be la id on correction of the imbalance which exists.
~ h r s w i l l include e f fo r t s t o increase the stock of well-trained in temedla te and auxiliary
personnel, while a t the same t i m e the thrust of recent years towards improving education
and t ra ining a t the profession41 and primary health care levels w i l l be continued.
he programme i n 1960-81 w ~ l l continue t o r e f l ec t the reoomme~dations of the 1978
Ministerial Consultation on Health Services and Manpower Development.
The programme has three components:
- health manpower planning and management;
- promotion of training;
- educational development and Support.
While major a c t i v i t i e s and a high proportion of the regular budget wl l l continue to
ae mostly devoted t o the d i rec t promotion of t raming, there w i l l a lso be an increased
e f fo r t t o promote heagth manpower planning and reforms i n the management of health man-
power. These a re areas whLM are i n great need of development i n most Member Countries.
I t 1s i n these areas a l s o t h a t there w i l l be a pa r t i cu la r th rus t towards improving
the capacity to predic t manpower needs.
Under Educationcrl 1)evelopment a d Support, high p r i o r i t y w i l l be given t o meeting
the needs of the Region f o r heal th learning mater ia ls , a s w e l l a s t o increasing the
capacity of countries f o r e f f e c t i v e educational planning. These represent an e s s e n t i a l
underpinning of. the whole heal th manpower development movement.
P r o g r m e
Health manpower planning and management 6.1.1
Objectives:
- to promote the concept of in tegra ted health services and manpower development
(HSIJID) and its acceptance by Member Countries, and provide information on a l t e r n a t i v e
approaches to the establishment of permanent mechanisms f o r its implementation ;
- t o promote and col laborate with in te res ted Member Countries i n the development
of s u i t a b l e permanent HShlD mechanlsmS,adapted t o the requirements of- ihdividual
countries, and evaluate t h e i r impact on the pa t t e rn of heal th profeSsiona1 t r a i n i n g i n
r e l a t i o n t o the health services needs; and
- t o promote nat ional capac i t i e s f o r , and opera t ional research i n , pldnning, manage-
ment and evaluation of heal th services and manpower development.
Cooperation with a d among countr ies
The programme 1s formulated t o ensure dialogue among a l l s e c t o r s concerned i n
HSMD within countr ies , and t o involve nat ional groups i n s tud ies on coordination
between heal th services and educational systems. Countries must have expressed i n t e r e s t
i n and a commitment t o developing HSMD mechanisms and operat ional research i n HSMD.
Guidelines on heal th manpower planning w i l l have been t e s t e d i n a t l e a s t one country,
on the bas i s of which they w i l l be revised and d i s t r ibu ted t o a l l countries. hietho-
dologies f o r manpower s tud ies w i l l have been developed i n severa l countr ies and t h e i r
impact on the qua l i ty of country heal th programming w i l l be assessed. The t r a i n i n g
of nat ionals i n country heal th programming w i l l be continued. A s e r i e s of regional
and na t iona l workshops on management and planning of hea l th se rv ices w i l l ensure t h i t
a s countr ies become increasingly s e l f - r e l i a n t i n these f i e l d s t h e i r experiences w i l l be
made ava i l ab le t o the Region a s a whole. Guidelines f o r the planning and implementation
of continuing education f o r heal th personnel, including primary ca re workers, w i l l be
t e s t e d i n .it ledst one country i n 1980; rn inter-country workshop on t h e i r use w i l l be
he ld l r l 1981, and the ~ o l l ~ r b o r ' r t i n g country w i l l b e supported i n dcvcloping continuin;:
cducdtzon yrogr~unmes. Fellow.si~ips w i l l be provided f o r nationcrl coordan.ltors of
continuing educatio.: progrunmos.
ObjCCtlVeS:
- t o promote,in coll.lbordtion with governments, t h e planned tr.i ining of h e a l t h
personnel , a t all l e v e l s , requi red f o r t h e hea l th s e r v i c e s with s p e c i a l omph.isis on
middle-level and primdry hed l th workers;
- t o promote, i n coun t r i e s of t he Region, the planned development of bas i c programmes
f o r t r a i n i n g the numbers md ca tcgor i c s of requi red h e a l t h personnel , a s determined
through country hea l th p r o g r m l n g o r o t h e r hea l th manpower s t i d i e s ;
- t o promote dnd c o l l a l ~ o r d t e with governments i n tho deveLopment of po:;tgrcrduate,
post-basic and continuing educ,ltlon programmes f o r a11 ca t egor i e s of h e a l t h personnel ,
a t n a t i o n a l m d regzondl l eve l s .
Cooperation w i t l l and among c ~ u n t r l e s
Increas ing emphasis w i l l be given t o c o l l ~ t b o r ~ t i o n wi th Member Countries i n t h e
development of educat ional i n s t i t u t i o n s f o r in termedia te , a u x i l i a r y and primary c u e
workers; and i n the development of t , ~ s k and cor,u:luni t y o r i e n t e d mul t ip ro fe s s iona l t r a i n -
rng p r o g r m e s f o r a l l cd t egor i e s of hedltll pCrSOnncl and s p e a i f i c a l l y f o r d e n t a l and
environmental h e a l t h workers.
,is p a r t of t h e e f f o r t t o improve t h c q u ~ l l t y and use ol: tho Itcgional ur rec tory of
Education a d Trdining Programmc?s f o r Health Personnel, WtIO w l l l utrclertake, i n c o l l ~ b o r a -
t i o n with Member Count r ics , a s tudy on t h e utilization of tho 'D l rcc to ry , whlch w i l l s e rve
a s J. basas f o r i ts revis ion . The c o l l e c t i o n of information on inn6v.itive educat ional
programmes w i k l be continued .is wel l a s t he promotion of information exchange on such
progrvmaes among Mcmbcr Countr ies .
Col labora t ion w l l l continue wi th Member Countr ies i n t h e planning and development o f
new h e a l t h t r a i n i n g i n s t i t u t i o n s rnd i n promoting the reform o f e x i s t i n g ones, f o r a l l
c a t e g o r i e s of h e a l t h p r s o n n c l . I n add i t i on t o fe l lowships , workshops and t ra in ing-cbus-
s e s t o promote i n s t i t u t i o n a l development, WHO w i l l c o l l a b o r a t e i n f i e l d - t e s t i n g case-
s t u d i e s on non-tradit ional types of t r a in ing programmes f o r heal th professionals and
a u x i l i a r i e s , and prepare guidelines on a l t e r n a t i v e approaches t o strengthening dnd
innovating the t r a in ing of health personnel.
The fellowship progrnmme, which COntinu~s t o receive the strong support of a l l
countries, w i l l continue a s a key core ac t iv i ty . I t s procedures are more e f fec t ive ly
s t r e m l i n e d each year, and i t focusses more and more in tens ively on e f fec t ive e d u ~ ~ l t i o n -
experiences fo r the fellows. Intlmdte day-to-day collaboration with Member Coantries
w i l l be maintained a t its present high l eve l ; provision i s made f o r the usual biennldl
meeting of nat lonal fellowships o f f i c e r s which has been dn important f ea tu re i n ensuring
the ef fect iveness of the Programme f o r severa l years past . There w i l l be wnt inu ing
e f f o r t s t o define more e f fec t ive ly the educational object ives of individual fellowships
and t o monitor and evaluate the ef fect iveness of the programme,
Nursing t r a in ing and services have not advanced i n the Region at the same r a t e
a s medical educatron and some other professional t r a in ing activities, and the whole
question of nursing, including the r o l e of the nurse i n the heal th team, requires
much more a t t en t ion than has been given i n the past.
Based on a review of the ex i s t ing pat terns of nursing ca re i n the Region, specidl
e f f o r t s w i l l be made i n col laborat ion with Member Covntsies, t o develop t r a in ing areas
t o demonstrate s a f e and e f f e c t i v e nursing care. Support w i l l a l s o be given t o the
development of job descr ip t ions and procedure manuals t o guide the t r a i n i n g and p rac t i ce
of middle-level nurses. WHO w i l l promote the use of nursing personnel i n the t r a i n i n g
and supervision of t r a d i t i o n a l b i r t h at tendants and o the r t r a d i t i o n a l heal th workers
with pa r t i cu la r reference t o primary heal th care.
k survey of pa t t e rns of nursing ca re i n countr ies of the Region w i l l be conducted
with the aim of ident i fy ing methods f o r improving and con t ro l l ing the qua l i ty of
nursing care. This w i l l be a col laborat ive a c t i v i t y between nursing and o the r heal th
personnel and w i l l concentrate initially on a c t i v i t i e s i n hospi ta l , but the f indings
and methods of control w i l l have equal relevance f o r community care.
The pressing need f ~ r teachers of midwifery continues t o be met i n severa l ways,
including the WIfOAJY+IICEF-supported Regional Midwifery Teacher Training Programme;
thks programme i s being expanded t o support new developments i n midwifery cars.
The Organization.wil1 continue i t s collaboration with Member Countries i n the devel-
opment of sound t ra in lng programmes f o r o ther categories of auxi l iary and primary heal th
workers . I n postgraduate medical education WHO w i l l col laborate with medical schools i n
defining the object ives of t h e l r programmes In r e l a t i o n t o heal th ca re needs, and pre-
paring competency-based task-oriented cur r i cu la t o meet them.
Continuing education of doctors and of o ther heal th profess ionals w i l l be fu r the r
promoted and e f f o r t s w i l l be made t o encourage Member Countries t o develop systematically
nat ional programmes of continuing education. Where a subs tan t i a l proportion of hea l th
manpower is sti l l imported from o ther countries, pa r t i cu la r e f f o r t s w i l l be di rected
towards continuing education programmes, re-or ienta t ion courses, and other mechanisms
t o ensure t h a t the imported professional manpower has a t r u e understanding of t h e needs
of the country fo r which they a r e working.
I n postgraduate education i n public heal th , the Organization w i l l continue to col la-
borate i n reforming educational programmes t o meet the needs of heal th se rv ices and
communities, and w i l l promote t r a in ing t n heal th services research. A meeting o f
Directors of Schools of Public Health i n Africa and Asia is due t o be held i n t h e African
Region i n 1981 and the pa r t i c ipa t ion of d i rec to rs of schools of public heal th and heads
of departments providing postgraduate t r a in ing i n public heal th , from the Eastern
Mediterranean Region, w i l l be supported a s i n t h e past.
Programme
Educational development and support
Objectives:
- t o e s t a b l i s h a regional network f o r t h e t r a in ing of teachers and educational l eaders
i n educational planning;
- t o promote the systematic design of educational programmes, a s f a r a s poss ible
problem-oriented and competency-based; and t o ensure the a v a i l a b i l i t y of na t iona l
s t a f f s k i l l e d i n educational process and management;
- t o e s t a b l i s h t h e evaluation of educational programmes arld i n s t i t u t i o n s as a means
of increasing t h e i r impact, and t o assess t h e i r relevance t o systematically defined
hea l th needs;
- t o ensure that properly designed and tested teaching/ leming materials are pro-
duced, and t o support research into communication problems;
- t o collaborate With Member S ta tes i n establishing and developing a regxonal l ibsary
system comprxsing a network of regional and sub-regional l ib ra r ies , w i t h inter- l ibrary
cooperation.
Cooperation with and among countrxes
This programme deals with educational planning and technology i n the health sciences;
health learning materials; and health l i t e r a t u r e services, resources and personnel.
I t represents a fundamental infrastructure upon which the e f fec t ive promotion of t ra in?
ing programmes themselves can be developed.
Main thrusts and p r io r i t i e s i n educational planning and technology continue t o be
i n the systematic trqining of teachers of health personnel. Par t icular a t tent ion rill
be given to teachers of middle-level, auxiliary and primary health care personnel. The
needs of ins t i tu t ions and minis t r ies w i l l be ref lected i n workshops and spec i f ic fellow-
ships i n overal l educational planning, curricuhm developleqt, inst ruct ional methods
and materials, evaluation of students and of educational prograrmpes, and educational
managemen t . Close collaboration w i l l continue with the WK) Regional Teacher Trauling Centre,
Department of Medical Education, Faculty of Medicine, Pahlavi University, Shiraz, Iran,
whose a c t i v i t i e s w i l l be expanded and reoriented increasingly towards teacher t ra ining
a c t i v i t i e s for health personnel other than physicians. The centres which have been
established under the leadership of the Regional Teacher Training Centre i n other coun-
t r i e s of the Region w i l l assume increasing responsibili ty for t ra ining fellows of t h e i r
own and other countries.
Support w a l l be provided on request t o the developnent of t ra inipg technology for
community health workers and the t ra ining of natronal s t a f f i n the methodology.
Act ivi t ies w i l l foaus on re la t ing education and t ra ining programmes t o health needs
and the tasks of health personnel.
Main ezfor ts w i l l focus f i r s t l y on completing the surveys of countries of the Region
begun i n 1977, which form the basis of future action. The surveys w i l l be carr ied out
a s f a r as poss ible by-joint teams of na t iona l and Wm-recruited s t a f r ; and secondly
on the o s t d o l ~ s ~ l m e n t w d development of nat ional panels of ;ruthors/contributors who
can design, prcydre ~ i l l t l t e s t basic heal th learning mater ia ls t o meet l o c a l needs. WHO
w i l l co l laborate w i tn p ~ t r t l c i p . t l n g countr ies and UNICEF i n planning a sy2tem t o produce
health-learning mater ia ls and uls t r i . , i l to thcm t o o the r countries. An in ter im programme
evaluation working group w i l l convened.
The WHD regional medlcal l i b r a r y system es tabl ished i n 1978 whereby the Pahlnvi
Medical Library of the Imperlal Medical Library of I r a was designated a s a Wm Regional
Medical Library w i l l be fu r the r developed and i ts services expanded i n l i n e with the
recommendatlolls of a meetlng of col laborat ing countr ies i n 1979. I t is ant ic ipated t h a t
In th ree o r four countr ies appropriate l l n k s w i l l be es tabl ished t o the MEDLINE terminal
i n Teheran.
The t r a i n i n g of a l l l e v e l s of heal th sciences l i b r a r i a n s w i l l be supported, with
spec ia l a t t e n t i o n t o a s s i s t a n t and aux i l i a ry l eve l s , based on t h e 1977 regional workshop
and using the t r a in ing manual issued i n 1978.
Continuing education on heal th sciences l ib ra r i ansh ip w i l l be promoted by the develop-
ment of guidel ines , the establishment of new programmes and t h e support of e x i s t i n g pro-
grammes.
Guidelines w i l l be developed f o r bas ic source lists f o r heal th professions l i b r a r i e s
o the r than medical, using an adapted model of t h e 1977 medical bas ic sciences list.
Major Programme
HEALTH INFORnL'rTION
Progr m e
Health s t a t i s t i c s
Objectives:
( a ) t o col laborate with Member S t a t e s i n the development, improvement and adequate
r eor ien ta t ion of t h e i r heal th information systems m d services , a s an i n t e g r a l com-
ponent of t h e i r general heal th services , with a view to:
- the i d e n t i f i c a t i o n , provision and proper use of t h e information necessary f o r
the e f f i c i e n t planning and management of heal th services ;
- the establishment and promotion of mechanisms t o ensure the permanent flow of
such infonaatzon i n t o the decision-making process;
- the development of manpower resources f o r the management of such hea l th information
services and f o r the u t i l i z a t i o n of information;
- the establishment of c e n t r a l heal th s t a t i s t i c a l u n i t s and the gradual and pro-
gress ive development of sub-national u n i t s as and when t ra ined heal th s t a t i s t i c a l
personnel become available.
(b) t o advise on education and t r a i n i n g f o r various ca tegor ies of heal th s t a t i s -
t i c a l personnel;
( c ) t o c o l l e c t , analyse and promote the exchange and disseminataon of heal th and
heal th-re la ted information, from Member S t a t e s and other sources, and t o serve a s
a foca l point f o r on-request feedback of such information t o Member Countries a s
well a s t o o t h e r u n i t s i n the Regional Off ice o r i n WHO/Headquarters;
(d) t o provide support se rv ices t o o the r programmes i n the Region as regards both
information and s t a t i s t i c a l methodology i n the s t ages of design, co l l ec t ion ,ana lys i s
and/or in te rp re ta t ion of datd;
(e) t o promote the use of t h e In te rna t iona l C lass l f i cd t ion of Diseases, s o t h a t
s t a t i s t i c s emanating from a va r i e ty of sources can be compared with reasonable
confidence.
( f ) t o col laborate i n the development of the W H O Information System.

Cooperation with and among countr ies
Ef f i c i en t nat ional heal th information se rv ices and systems, capable of making
avai lable timely, medningful and up-to-date information, a r e rqcognized a s pre-requis i te
t o sound plgnning, ddministrntion, management and cvaludtion of heal th seyvaces. A s many
hlember S t a t e s have poorly developed and poorly s t a f f e d hea l th s t a t i s t i c a l services ,
they can carry ou t only i so la ted s t a t i s t i c a l a c t i v i t i e s , producing data f o r non-specified
c l i e n t s , without focussing on the s p e c i f i c requirements of decision-makers i n t h e heal th
administrat ion. k few countr ies , on the o ther hmd, t r y t 6 adopt heal th*informat ion
systems of devcloped countr ies , without adpating them t o l o c a l circumstances. hiore
important is t h a t , i n e i t h e r case, whatever s t a t i s t i c s a r e being produced a r e not being
properly u t i l i z e d .
Technical cooperati011 with Member Countries i n the development, improvement and
reor ien ta t ion of hegrlth s t a t i s t i c d l system r e t a i n s a h i g h , p r i o r i t y i n WHO'S programme.
Such coopcr,ctlon is achieved e i t h e r through country p ro jec t s spec i f j ca lay (or with compo-
nenls ln heal th s t d t i s t i c s , o r through intercountry p ro jec t s and the se rv ices of the
Regional Adviser. I n a l l cases , c lose r cooperation with JIcmber S t a t e s i n promoting a
d i r e c t l i n k between the users and producers of infonnatipn is peomoted, thus permitt ing
i d e n t i f i c a t i o n of information needs and of the gaps between exzs t lng and required in-
formation, and seeking appropriate remedies. Collaboratron with natxonal institutions
is being promoted, through establishing col laborat ing centres , and through con t rac t s
f o r technical services , to deal with development of appropriate methods and procedures
of common i n t e r e s t t o Member Sta tes . Supplies and equipment w i l l be provided when
necessary f o r the development of nat ional heal th information services. Trazning
a c t i v i t i e s form m e s s e n t i a l component of the p r o g r m e , through provision of fellow-
sh ips , col laborat ion i n na t iona l teaching and t r a i n i n g a c t i v i t i e s , o r pa r t i c ipa t ion i n
regional seminars and workshops.
Requests from Member S t a t e s f o r hea l th s t a t i s t i c c l l information i n s p e c i f i c f i e l d s
a r e frequently received. hloreover, W H O i t s e l f , so ds t o be ab le t o plan and execute
e f f i c i e n t l y i t s programme o i col labordt ion with hlember S t a t e s , necds re levant informa-
t ion. Therefore, the co l l ec t ion and disscminatlon of information from and t o countr ies ,
In a meaningful and useful mmncr, r cqu i rcs concerted e i f o r t by the Organization and
countries.
Programme
WHO publications and documents
This programme provides budgetary provision f o r the issuance of WHO publications,
whether of a technical nature o r otherwise, including the RegiOnol Office t r ans la t ion
s t a f f and services , a s well as the se rv ices of the Reports Off ice a t the Regional
o f f i ce .
Programme
Health l i t e r a t u r e se rv ices
The Regional Off ice Library is included under t h i s programme the purpose of which
is t o provide a referelice and d~cumentation se rv ice on medical and public hea l th sub-
j e c t s t o W H D s t a f f i n the Regional Off ice and i n the f i e l d , and on raquemt, t o o the r
persons and i n s t i t u t i o n s .
The programme al$o eovers technicdl cooperation with Member S t a t e s I n developing
nat ional heal th l i b r a r y se rv ices and promoting regional l i b r a r y services.
Programme
Health information o i the public
The Regional In fomat ion Off ice is included under t h i s prograarme the purpose 00
which is t o help the creat ion of an informed opinion on public heal th mat ters and t o
e n l i s t publ ic suppQrt f o r heal th ac t ion, pa r t i cu la r ly i n relrrqion t o WH3-supported
Major Programme
GENER.& SERVICES AND SUPPORT PROGRMhIES
his major programme provides the f u l l range of non- tochn~cal support se rv ices to
the o the r programmes, i n the Regional Off ice and the f i e l d . Assistance is given
t o the technical u n i t s i n the planning and development of regional programmes. The
programme a l s o contributes t o the elaboration of regional policy on the administrat ive
aspects oi p r o g r m e plannlng and execution.
The major prograqune is divided i n t o t h e following programmes:
Programme
Planning and general a c t i v i t i e s 8.1.0 - This programme comprises the Of f i ce of the Director, Support Programme, who is the
p r inc ipa l ddviser t o the Regional Director on a l l adminis t ra t ive , f inanc ia l , budgetary
and l e g a l matters clnd d i r e c t s the adminis t ra t ive se rv ices provided t o the Regional
Off ice shown i n the support programmes l i s t e d below.
Personnel 8.1.2
This programme covers the a c t i v i t i e s of the personnel u n i t with its respons ib i l i ty
f o r personnel recruitment and assignment, post c l a s s i f r c a t i o n and sa la ry systems, per-
formance appraisa l system, s t a f f r u l e s and personnel procedures/policies, s t a f f r e l a t i o n s ,
personnel records and f i l e s and s t a f f t r a in ing and development.
Supplies 8.1.3
This progrcunme covers the medical supply u n i t which is responsible f o r the procure-
ment of suppl ies and equipment f o r the opera t ing programmes and f o r purchases f o r
Member Countries.
Progrcuame
Conference, Off ice and Building Services
This programme covers the conference and general services , conference arrangements
and records, buildlng management, p r in t ing services , adminis t ra t ive suppl ies and equip-
'ment, communications and mai l , t ranspor ta t ion, inventory records and common services.
Programme
Budget 8.1.5 - This programme covers the budget unit wath its responslbll ity for budget devel-
opment and executipn.
Programme
Finance arid accounts 8 .1 .6 7
This programme csvers the f inancial servkces of the Regional OPfipe w i t h their
responsibil ity f ~ r implomenti~g financial and auqountlog pQlic ies , rules and procedures
as w e l l 4s dlsburolng and reporting On the funds of the Orgmxzation.
INM3RMATION ANNEXES
REGIONAL OFF1 CE
Personnel : A s i n the previous biennium every e f fo r t has been made t o hold Regional
Office expenditure a t a minimum level. In accordance with t h i s policy the following
professional posts have been eliminitated and replaced by posts of the general service
category resul t ing i n a saving of U S $ 64 500 for the 1980-1981 biennium.
Deletions:
2.2.1 GiNERAL PROGRAMME DEVEWPMENT - The post of Administrative Officer (Pl) has beem
deleted, effecltive 1980, substituted by a general service category post a t the
QM level.
7.1.5 HEALTH INFORMATION OF THE PUBLIC - The post of Information Officer(P4) has been
deleted,effective 1981, and replaced by a general service category post a t the M level.
Taking in to consideration the above changes, posts a t the Regional Office dl1
be as follows for the 1980-1981 biennium:
2.1 EXECUTIVE MANAGEMDTC - (Office of the Regional Director )- The Regional Director
(UG), an administrative of f icer (P2) and an administrative assis tant (IM8).
2.2.1 GBNERAL PROGRAMME DEVEIDFWEWT - The Director, Programe Management (D2), an
administrative assis tant (RAX), a junior administrative ass i s tan t (W), a secretary
(M6) and a clerk-stenographer(a5);
7.2.1 Wf13 PUBLICATIONS AND DOCUMENTS - (Reports and Documents and Translation)- a reports
of f icer (P3), a secretary (M6), two clerks (At51 and a clerk typist(B14), three trans-
l a to r s (two P4 and one P3), two clerks (m6) and one clerk-stenographer (m5);
7.1.4 HEALTH LITERATURE SERVICES - a l ib rar ian (W), an assis tant l ibrarian(=?),
and a l ibrary olerk (M4);
7.1.5 HEALTH INFORMATION OF THE PUBLIC - an information of f icer (P4) to be abolished
i n 1981 and replaced by an administrative assistant(E1Qo and a secretary (g16);
8.1 GmERAL SERVICES AND SUPPORT PROGRAMMES
8.1.0 Programme Planning and General Act ivi t ies - the Director, Support Progra8me(Dl),
a junior administrative ass i s tan t (W7) and a clerk-stenographer ( a 5 ) ;
8.1.2 Personnel - a personnel of f icer (P4), an administrative a s s i s t a n t ( M ) , a j ~ n i 0 r
administrative assis tant(m7), a secretary (M6), a nurse clerk(m6) and four clerk-
stenographers (M5 ) ;
8.1.3 Supplies - two supply officers(0ne P3 and one P l ) , an administrative ass i s tan t
(mix), two clerk-stenographers (EMS), two clerks (EV5), three clerk t v p i s t s (F.4);
8.1.4 CONFERENCE, OFFICE AND BUILDING SERVICES
Conference Services - a conference of f icer (P2) and a clerk-stenographer(W5);
General Services Unit - a general services officer(P41, a regis t ry ass i s tan t
(Ehd8), a general services ass i s tan t (M), two t rave l c lerks (one Qb7 and one m5) ,
four regis t ry clerks (one EN6 , two W5 and one EM4), two general services c le rks
(one EM6 and one m5), a clerk-stenographer (m5),a telephonist (W5), two clerk
typ is t s (W4) and one clerk (W3).
Liaison of f ice i n Cairo - one administrative o f f i ce r (Pl)
8.1.5 Budget - an administrative ass i s tan t (=), a junior administrative ass i s tan t
(m), a budget ass i s tan t (EM6), a budget acwunt c lerk (EY6), a budget c l e r k ( a 6 ) and
a c lerk typ is t (Rd4) ;
8.1.6 Finance and Accounts - a budget and f ~ n a n c e o f f i ce r (P4), a finance officer(P3),
an administrative ass i s tan t (QdX), a cashier (EM8), three a s s i s t an t accountants(one EM8
and two =6), a secretary (M6), an accounts clerk(m5), an acwunts/budget clerk(gl5)
and a clerk-stenographer (M5);
To summarise, provision is made i n 1980 for the post of the Regional Director,
sixteen posts i n the professional category and sixty-five posts i n the general services
category; i n 1981 for the post of the Regional Director, f i f t e en posts i n the profession-
a l category and sixty-six posts i n the general services category.
In addition, provision of US $ 180 000 is made t o w v e r twenty-two custodial
s t a f f and US $ 73 000 t o cover the cost of temporary s t a f f fo r the biennium.
Provision has been made for duty t ravel amounting to US $ 45 200 in 1980 and
US $ 50 700 i n 1981 t o enable the Regional Director and his senior of f icers t o v i s i t
countries of the Region t o consult with governments on questions of policy and programe
support, t o discuss the development and execution of' projects with health administrations
and f i e ld s t a f f , t o attend o f f i c i a l meetings, to co l lec t public infomation material ,
t o maintain press and radio contacts and to v i s i t Headquarters fo r discussion of policy
and other matters.
The common services provisions amount to US$ 320 000 i n 1980 and US $ 350 000
i n 1981 while library books and materials provisions are estimated a t US $ 19 000 and
US $ 20 900 md public information material and supplies provisions are US $ 8 000
and US $ 8 500.
In t o t a l , Regional Off ice costs w i l l amount t o US $ 3 667 700 for the biennium.

Regular Budget
REGliONAL 0mCE
2.1 EXECUTIVE MANAGEMENT
Off ice o f t h e Regional D i r e c t o r
2.2 GENERAL PROCRAMME DEVEMlWENT AND MANAGEMENT
2.2.1 General Programme Deve lopmen t
O f f i c e of t h e D i r e c t o r , Programme Management
7 . 1 ' HW LTH I NM.)RMATI ON
7.1.2 WHO P u b l i c a t i o n s and Documentat i o n s
Repor t s and Documents T r a n s l a t i o n
7. I . 4 r i ea l th L i t e r a t u r e S e r v i c e s
L i b r a r y Books and m a t e r i a l
7.1.5 H e a l t h In format ion of t h e P u b l i c
P u b l i c i n f o r m a t i o n S u p p l i e s and m a t e r i a l s
Bienluum 1978
-/Man Ye.- 1978 1979 - -
3 3 - _--
5 5 - --
5 5 6 6 --
11 11 - --
3 3
-- 3 3 --
2 2
-- 2 2 -- - .
- 1979 Biennium
1978 - 1979 US$
223 300 --I_
205 200 .-----
LOR 700 274 400
383 100
49 600 32 ROO ,
82 400
107 300 1 5 600 -
122 900
W l a r Budget
1980 -
1980 1981 - - -
3 3 --
5 5 --
5 5 -- 6 6
11 11 --
3 3 --
3 3 - - -
2 2
-- 2 2 - - .
Biennium 1981
Btenn~um 1980 - 1981 u s
264 100
204 600
123 700 319 100
442 800
60 400 3 9 900
100 300
93 500 1 6 500
110 000
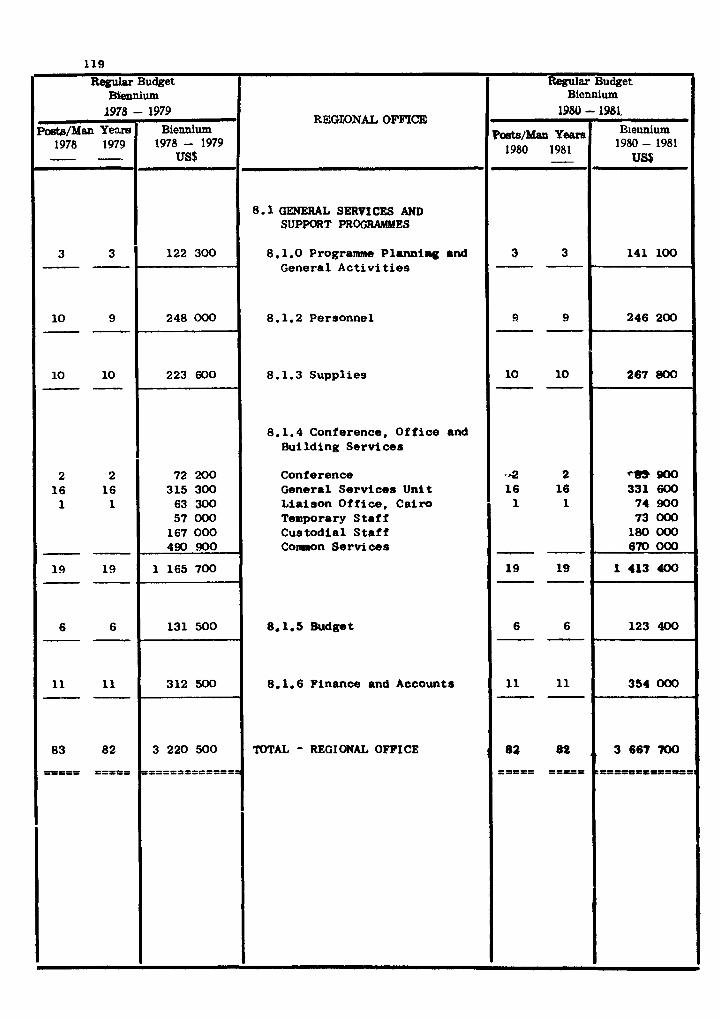
Regular Budget
REGXONAL OFFICB)
8.1 GENERAL SERVICES AND SUPPORT PROGRAMMES
8.1.0 Programme P l u m i n g and General A c t i v i t i e s
8.1.2 Personnel
8.1.3 Suppl ies
8.1.4 Conference, Of f i ce and Building Services
Conference General Serv ices Unit Lia ison Off ice , Cai ro Temporary S t a f f Cus todia l S t a f f C o m n Se rv ices
8.1.5 Budget
8.1.6 Finance and Accounts
TOTAL - REGIONAL OFFICE !
B i d u m 1978 -
-/Man Yeam 1978 1979 - 7
3 3 --
10 9 - - .
10 10 --
2 2 16 16 1 1
-- 19 19 --
6 6 --
11 11 --
83 82
=PI== ==PI==
1
1979 Biennium
1978 - 1979 US$
122 300
248 000
223 600
72 200 315 300
63 300 57 000
167 000 490 !mO
1 165 700
131 500
312 500
3 220 500
P====f==s====
Reguler Budget
1980 - 5.
1980 1981 -
3 3 - - ,
9 9 - - v
10 10 P - 8
-42 2 1 6 16 1 1
- - . 19 19 --
6 6 --
11 11 - - .
82 02
=PP3= PI===
Biennium 1981,
Blennium 1980 - 1981
USE
141 100
246 200
267 800
*€m 900 331 600
74 900 73 000
180 000 670 000
1 413 400
123 400
354 000
, 3667 'WlO
C = I P = U E = l l f PDII

COUNTRY PROc,RM E STATEMENTS
AND T A B l d S
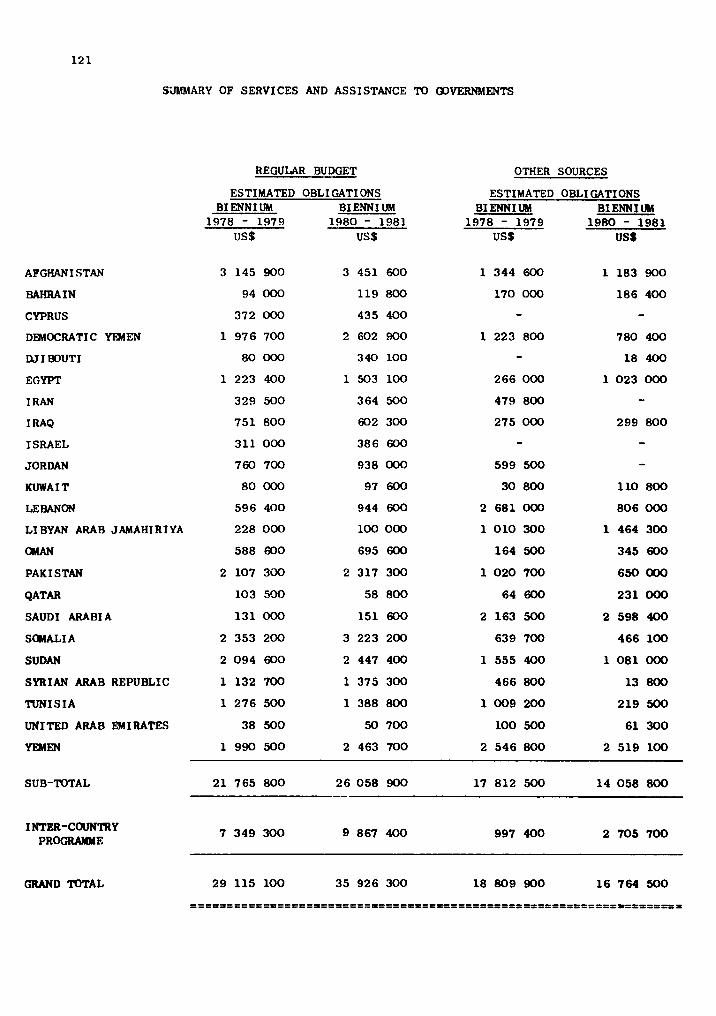
StlMMARY OF SERVICES AND ASSISTANCE TO GOVERNMENTS
REGULAR BUDGET
ESTIMATED OBLIGATIONS
OTHER SOURCES
ESTIMATED OBLI CATIONS BI ENNI UM BI ENN I UM BIENNIUM BIENNIUM
1978 - 1979 1980 - 1981 1978 - 1979 1980 - 1981 us S us s US$ US$
AFGHANI STAN 3 145 900 3 451 600 1 344 600 1 183 900
BAHRAIN 94 000 119 800 170 000 186 400
CYPRUS 372 000 435 400 - - DEMOCRAT1 C YIMEN 1 976 700 2 602 900 1 223 800 780 400
WI BOUT1 80 000 340 100 - 18 400
EGYPT 1 223 400 1 503 100 266 000 1 023 000
I RAN 329 500 364 500 479 800 - 1 RAQ 751 800 602 300 275 000 299 800
ISRAEL 311 000 386 600 - - JORDAN 760 700 938 000 599 500 - KUWA I T 80 000 97 600 30 800 110 800
LEBANON 596 400 944 600 2 681 000 806 000
LI BYAN ARAB JAMAHI RI YA 228 000 100 000 1 010 300 1 464 300
OMAN 588 600 695 600 164 500 345 600
PAK I STAN 2 107 3~10 2 317 300 1 020 700 650 000
QATAR 103 590 58 800 64 600 231 000
SAUDI ARABIA 131 000 151 600 2 163 500 2 598 400
SOMALI A 2 353 200 3 223 200 639 700 466 100
SUDAN 2 094 600 2 447 400 1 555 400 1 081 000
SYRIAN ARAB REPUBLIC 1 132 700 1 375 300 466 800 13 800
TUNISIA 1 276 500 1 388 800 1009 200 219 500
UNITED ARAB EMIRATES 38 500 50 700 100 500 61 300
YEMEN 1 990 500 2 463 700 2 546 800 2 519 100
SUB-TOTAL 21 765 800 26 058 900 17 812 500 14 058 800
INTER-COUNTRY PROGRAMME
GRAND TOTAL
C O W R Y PROGRAYYE STATENF3lT
AFGHANISTAN
NATIONAL HEALTH DEVELOPMENT STRATEGY
The national health strategy has been expressed through the Afghan Seven-Year
Health Programme, AH 1355-61 (1976-1982) dram up in the context ~f the first Republican
Social and Economic Developrsnt Plan.
Tbe ~overmnt's health objectives fall under three main headings:(.) to build up
health infrastructure, i.e. health facilities and installations, health manpower and
water resources; (b) to control specific diseases and groups of diseases by appropriate
health technologies; (c) to establish and develop central support systems for health,
with special reference to administration and management of health services, supplies
and distribution of pharmaceuticals, diagnostic and therapeutic services.
Ten major programmes have been dram up to fulfil these objectives, dealing respect-
ively with hospitals, basic health services (including priury health care),environmntal
health, health manpower development, malaria and leishmaniasis, tuberculosis and leprosy,
imunioation, drugs and biologicals, technical support services, administration and
planning.
Country health progrcring began in AH 1355, (1976) and the first annual revision
of the National Health Programme, within the seven-year perspective, took place late in
AH 1356 (1977). This seven-year Health Prograne, includes the sector-specific provis-
ions (mainly for construction of health installations, training units 8nd wawr supplies)
of tho seven-year Social and Economic Development Plan, but in addition outlirw8 the
operational programmes and development81 efforts in each of the major component8 of the
national health services.
The oollaboratign of external agencies is being increasingly brought into line with . the priority provisions of the progrmw. WHO collaboration is expected to cover only
selected aspects of the seven-year Health Programme.
TBCHNICAL COOPERATION PROGRAMMES FOR HEALTH
Health planning, progr..~ina and project formulation
The preparation of tho Afghan National Health Progr- ud the seven-year Health
Progrlrre led to a recognition th8t(a) planning ud progr8uing require a continuous or
cyclic process based on-the monitoring of results ud pe r f o ~ n c e in the light of
123
changing circumstances, and(b1 development projects o r service improvements have a
much b e t t e r chance of success and of a t t r a c t i n g external support when properly formulated.
Therefore one important aspect of technical cooperation with WHO w i l l cons i s t of
j o i n t programming of a c t i v i t i e s leading t o programme budgeting; programme evaluation,
and e laborat ion of f e a s i b i l i t y analyses and a c t i v i t y formulation a s a bas is f o r both
nat ional ac t ion and external support.
Health services and primary heal th care development
There is 8 major e f f o r t t o extend the heal th services network. The key e l e e n t is
the all-purpose basic heal th centre a t d i s t r i c t level , and thus the major t h r u s t is i n
t h e d i rec t ion of commissioning more such centres, but a t t e n t i o n is a l s o being paid t o
extensions of services t o bring them closer t o the sca t t e red r u r a l communities, and t o
the strengthening of more specia l ized r e f e r r a l centres.
Several external sources a r e col laborat ing with the Government i n t h i s domain.
WHO col laborat ion i s required only f o r two s p e c i f i c components:
- strengthening of comprehensive community services espec ia l ly a t the r u r a l periphery
and with emphasis on reaching women and children. WHO w i l l support the t r a i n i n g
and supervision of community heal th workers i n both regular and extension services
espec ia l ly f o r family heal th care. There is a need a l s o t o develop aspects of
personal and community care which h i t h e r t o have had a low pr io r i ty , but which c a l l
f o r more a t t e n t i o n as the pa t t e rn of i l l - h e a l t h changes. WHO w i l l co l laborate i n
such e f f o r t s - e.g. i n building up a mental heal th component of the general hea l th
services.
- strengthening of support systems required f o r the proper functioning of heal th
services. While i n some respects the Government benef i ts from col laborat ion with
o ther sources, WHO is expected t o contr ibute technical ly by arranging f o r add i t iona l
t r a in ing and by the piovision of supplies and equipment.
Drug pol ic ies and managpment
The Government proposes t o deal systematically with i s sues re la ted t o drugs,
vaccines and re la ted therapeut ic o r prophylactic agents. The Government has inv i t ed
WHO par t i c ipa t ion i n es tab l i sh ing a drug qual i ty-control capabi l i ty . This implies a
comprehensive policy on drugs and biologicals . The expanded programme w j l l cover a l l
aspects of t h i s comprehensive policy f o r drugs and pharmaceuticals, with s p e c i a l emphasis
on formulation (based on sound and f e a s i b l e p r inc ip les ) and its application. Sound
manufacturing and processing practices and quality-control of local and imported prsducts
required for the control of common conditions will be promoted. Another component will
be tho study and large-scale application of herbs and plants traditionally employed in
folk medicine.
Communicable disease prevention and control
Control programmes for specific diseases will be intensified by technologies of
mass application, Special field forces engaged in specific disease control activities
will broaden and diversify the scope of their work, and serve to link more effectively
the community and its health workers with the network services installations.
Malaria control will show a progressive shift to more cost-effective methods, and
more insistence on community rusponsibility in reduction of vector breeding etc, Never-
theless, as malaria will continue to be associated with surface water its ultimate
control will depend largely on change in irrigation practices. Control of other vector-
borne diseases, notably leishmaniasis, is already being associated with malaria control.
The extended immunization programme is expected to have become established as a
permanent component of community health services.
In the case of tuberculosis and leprosy, special control measures will largely be
absorbed by regular services; only selected control and referral functions will be
carried out by specialist units.
Until safe water supplies and excreta disposal can be universally ensured, diarrhoea1
disease control will largely depend on prompt treatment and prevention of severe dehydra-
tion. There will be a major expansion in the production and use of oral rehydration
mixtures through health services and extension workers.
WHO participation will promote mastery of appropriate technology and a shift towards
full national responsibility and control.
Promotion of environmental health
Recognizing that judicious exploitatton of water resources lies at the very root of
general development in this country, and also represents the most important single factor
in reducing disease, both the Government and external agencies are spurring the develop-
ment of water supplies for domestic use. The next few years will see a marked increase
in WHO participation in this domain mainly by making available a study and design group
to analyse the feasibility of, and design, large-scale schemes calculated to provide
considerable numbers of r u r a l inhabi tants with water suppl ies with low maintenance cos ts .
Management of water resources w i l l assume an increasingly important r o l e i n the
control of malaria and of po l lu t ion from sources o ther than animal excreta. A t the same
time, WHO w i l l be associated with nat ional e f f o r t s t o overcome other s a n i t a t i o n problems,
including the d isposal of wastes and excreta, not only by engineering methods, but a l s o
and espec ia l ly by behavioural approaches.
Health manpower development
The Government is keenly aware of the d e s i r a b i l i t y of proceeding f u r t h e r and f a s t e r
with "double integration" i n t h i s domain - i.e. of t r a i n i n g d i f f e r e n t members of the
heal th team together, and of bringing t r a in ing and continuing education more c losely i n t o
l i n e with service needs.
WHO col laborat ion has been ca l l ed f o r i n order t o cover some of the c r i t i c a l gaps
caused by the rapid extension and expansion of hea l th services : f u l l advantage w i l l be
taken of the provisions of the regional medium-terra programme f o r heal th manpower develop-
ment including pa r t i cu la r ly those elements deal ing with a more object ive appraisa l of
se rv ice requirements a s a bas is f o r both manpower and educational planning, development
of teaching a i d s and learning mater ia ls , curriculum revis ion and teacher t ra in ing. W h i l e
t r a d i t i o n a l domains, such a s continuing o r advanced education abroad, w i l l a l s o remain an
important p a r t of WHO'S contr ibut ion, the new t rend i n manpower development is expected
t o r e s u l t i n WHO collaborating, not with separa te i n s t i t u t i o n s , b u t by deploying its
resources a s t o make them ava i l ab le t o a l l groups and schools concerned with education,
t r a i n i n g and management of manpower.
RoaLth i n f o n u t i o n
The Government has r ecen t ly made a s izeable input towards strengthening of t h e i r
hea l th information services. These se rv ices were reorganimd, and a t r a ined un ive rs i ty
graduate was appointed t o head the service. In col laborat ion with WHO, an ad hoc survey
f o r i n f a n t and e a r l y childhood morta l i ty has been ca r r i ed out i n Greater Kabul a rea and
the repor t , containing very useful r e s u l t s , has now come out.
WHO col laborat ion w i l l continue towards f u r t h e r strengthening of the heal th inform-
a t i o n services , and extension of the ad hoc survey t o o the r p a r t s of the country, par t -
i c u l a r l y r u r a l areas.
WHO col laborat ion w i l l a l s o continue towards making ava i l ab le necessary medical
l i t e r a t u r e t o the medical schools and other teaching i n s t i t u t i o n s .

Regular Budget
A F G I W I STAN
.
Plajor programme/programme
2.2 GENERAL PROGKAF*IME DEVEMWENT AND \!ANACEMENT
2.2.2 Country Health Programming (WHO Programme Coordinator)
3.1 HEALTH SERVICES ' DEVELOPMENT
3.1.1 Health Services' Planning and Management (School of Radiography; Maintenance and repair of medical equipment; Hospital administration)
3.1.2 Primary Health Care (Development of basic health services)
3.1.4 Care of the Aged, Disability Prevention and Rehabilitation (Rehabilitation services)
3.1.5 Appropriate Technology for Health ( Institute of Pathology, Kabul; Health laboratory services)
3.2 FA,,! I LY HEALTH
3.2.1 bfaternal and Child Health (Family health services development)
3.2.4 Health Education (Health education)
Estimated - Biennium
1978 - 1979 US$
174 300
252 800
183000
93 100
Y
Obligations
Biennium 1980 - 1981
US$
200 300
56 300
213CjO
5.1 200
101 000
15 900
Source
of
FP
Othcr Sourcee
Estimated
Biennium 1978- 1979
US$
189 600
Obligations
Blennium 1980-1981
US$
28 000
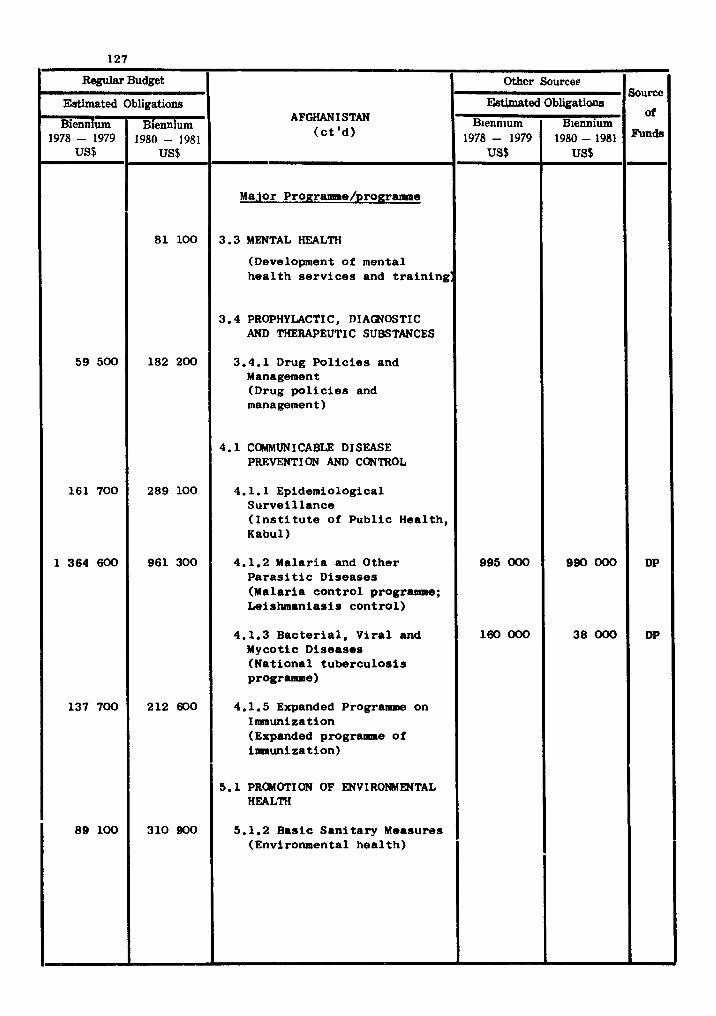
Regular Budget
Estimated Obligations
Bienn urn Blenn urn 1978 - 1979 1980 - 1981 .F
AFGHAN I STAN ( c t ' d )
Major Prouraume/programae
3.3 MENTAL HEALTH
(Development of mental h e a l t h s e r v i c e s and t r a i n i n g :
3.4 PROPHYLACTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
3.4.1 Drug P o l i c i e s and Management (Drug p o l i c i e s and management)
4.1 COMMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.1 Epidemiological S u r v e i l l a n c e ( I n s t i t u t e of P u b l i c Hea l th , Kabul)
4.1.2 Malar ia and O the r P a r a s i t i c Diseases (Ma la r i a c o n t r o l prograame; Le ishmanias i s c o n t r o l )
4.1.3 B a c t e r i a l , Viral and Mycotic Diseases (Na t i ona l t u b e r c u l o s i s programme)
4.1.5 Expanded Programme on Ilmnuni z a t i o n (Expanded pMgramIe o f immunization)
5.1 PR(MOTION OF ENVIRONMENTAL HEALTH
5.1.2 Bas i c S a n i t a r y Measures (Environmental h e a l t h )
59 500
1 6 1 7 0 0
1 364 600
137 700
89 100
8 1 100
182 200
2 8 9 1 0 0
961 300
212 600
310 900
J
Sourcc
ai
DP
DP
Other Sources
Estimated
Blenn~um 1978 - 1979
US$
995 000
160 000
Obliiationa
Biennium 1980 - 1981 US$
990 000
38000
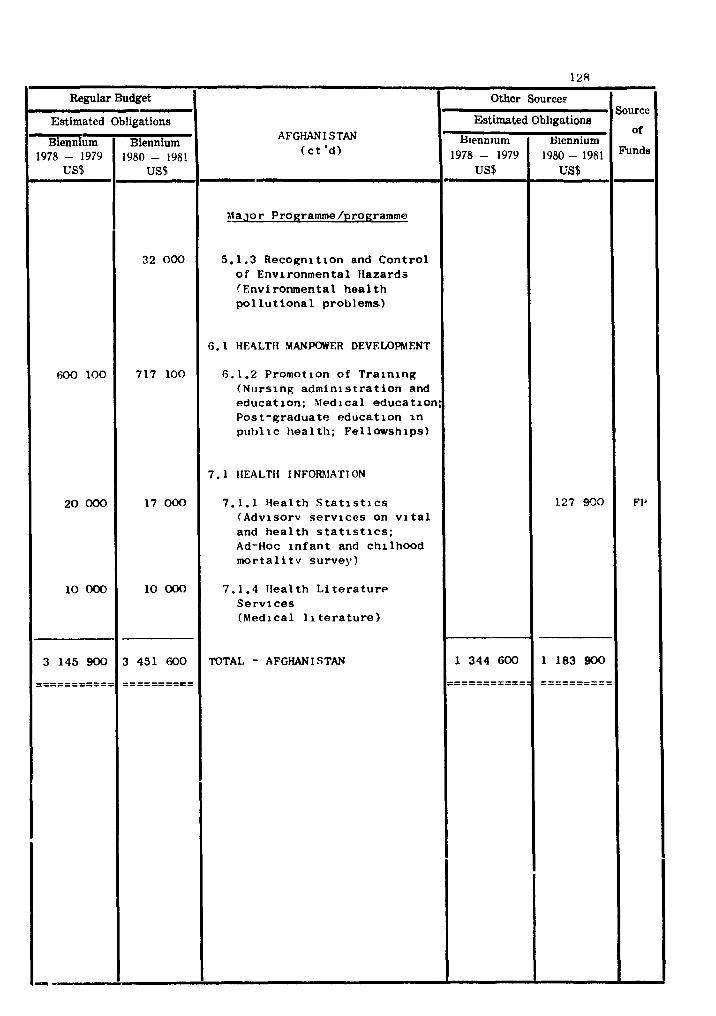
COUNTRY PROGRAMME STATmENT
BAHRAIN
NATIONAL HEALTH DEVEWPMENT STRATW
Health services have developed i n the context of long-term health plan fo r the per-
iod 1969-1986, and under which appreciable progress has been made i n the control of ccnn-
municable diseases and i n making health services readily accessible t o the en t i r e popula-
tion. Major thrusts now are towards providing high-quality family primary care through
a network of recently constructed health centres, and developing environmental health
and workers' health services t o deal with the problems associated w ~ t h the very rapid
economic and industr ia l development of the muntry and the associated inf lux of immigrPrt
workers.
Bahrain sti l l depends t o some extent on expatr ia te professional s t a f f fo r its
services ; W H ) w i l l collaborate par t icular ly i n the pr ior i ty area of health man-
power development, which has implications for Bahrain and a l so neighbouring s ta tes , i n
the control of environmental pollution problems, the develoment of workers' health
services, and i n organizing the health information system.
TECHNICAL COOPERATIm PBOGWMMES FaR HEALTH
Health services development - Workers' health (occupational health)
In addition t o the petroleum refinery, during the l a s t ten years,ship-repairing
yards, an aluminium smelter and a large number of small indus t r ia l concerns have been
developed, and the Government is concerned about the protection of the health of the
workers. WH) w i l l continue t o collaborate i n developing the occupational heal th laws,
the introduction of occupation health services, the establishment of regular health
screening and services for expatr ia te workers par t icular ly i n respect of theUtroduot ion
of communicable diseases, and developing t ra ining programmes on occupational health for
phsysicians and nurses employed i n health services, and for inspectors and hygienists.
Promotion of environmental heal th
High pr ior i ty is being given t o the development of a modem sewage system i n
Manama, where 43% of the t o t a l population lives. A plan has been d ram up by a firm
of sub-contractors and WH3 has collaborated i n its review and evaluation.
Bahrain is actively involved i n the plans fo r Qontrol of environmental pollution
and of the de le te r ious ez fec t s of coas ta l polLution within the countries of the Gulf
area. W H O w i l l co l iaborate i n the deve lopen t of wa$te d isposal and other environ-
mental heal th programmes. In addi t ion, ass is tance w i l l be provided together with UNEP
i n the regronal coas ta l pol lu t ion control programes fo r the protect ion and d e v e l o p e n t
of the marine environment and coas ta l areas.
Health manpowor deve lopen t - Nat$onals a r e being t ra ined abroad and a t home t o man the services ; meanwhile
t ~ l e r o a r e t raaning progrE)mmes t o o r i e n t expe t r i a t e s t o the hea l th problems of the
country. WHO has oollaboreted i n the development of the College of Health Sciences
and the School of Nursing and i n o t h r r t r a in ing a c t i v t i e s f o r various ca tegor ies
of technicians, and w i l l cont%nue t o provide technical support f o r continued education
of the heal th professional s t a f f i n the country.
Health information
With tho growth of heal th se rv ices the need f o r heal th information f o r the manage-
ment and monitoring of hea l th se rv ices has been recognized.
WHO w i l l continue t o w l l a b o r a t e i n technical guidance and t r a in ing of personnel
f o r medical records and heal th s t a t i s t i c s .
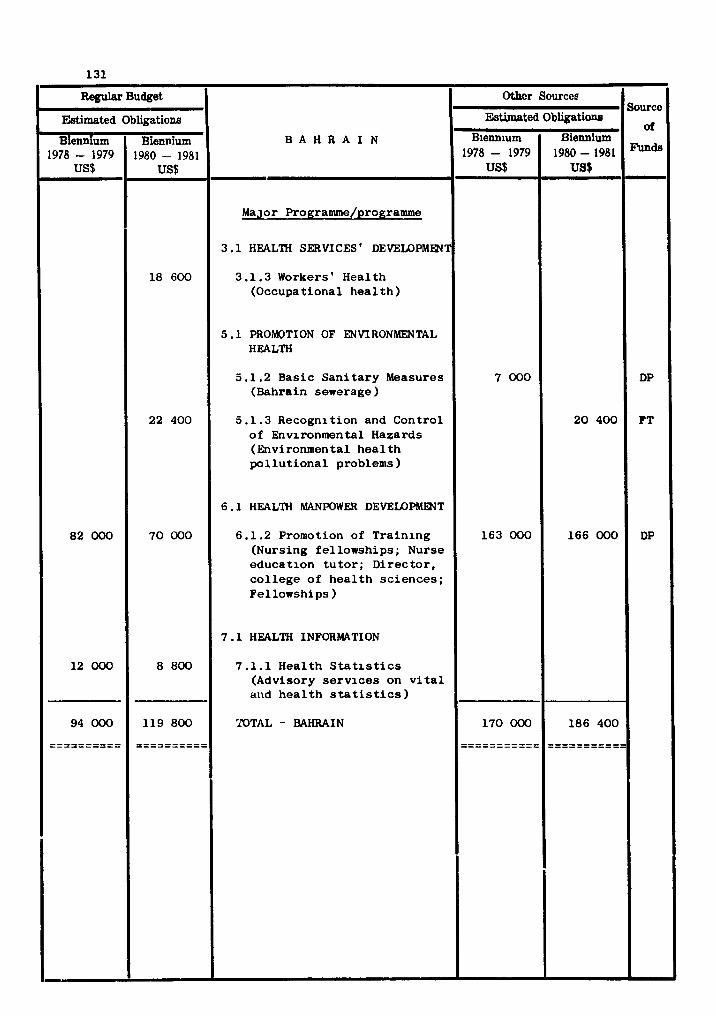
COUNTRY PROGRAMm STATEMENT
CYPRUS
NATIONAL HEALTH DEVELOPMENT STRATEGY
The long-term objective of the Government is t o a t t a i n a high standard of health
services so a s t o offer the best possible medical care and at tent ion to a l l c i t i zens
and t o implement an effect ive programme of preventive medicine and hygiene.
I t ig proposed t o increase the number and improve the qual i ty of health manpower,
t o expand hospi ta l services, t o improve the health information system, and t o move
towards a national health service.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
Health services development
The Government is determined t o make health care f a c i l i t i e s available and access-
i b l e t o the population a t large with pat icular a t tent ion t o rura l communities. In this
context the health centres and hospital networks a re being expanded and the qual i ty of
t he i r services improved. Attention is a l so being given t o expansion of laboratories
and strengthening of medical rehabi l i t a t ion services through the e~tabl ishment of add-
i t i ona l physiotherapy centres.
WHO w i l l continue t o collaborate closely with the Government i n the development of
the Regional Centre fo r the t ra ining of p e r s o m l i n the mainteWmnae and repair of medical
equipment. The Centre received i ts f i r s t group of t ra inees i n 1978.
WHO w i l l continue a s necessary i ts cooperation with UNHCR i n ass i s t ing the health
au thor i t i es i n the northern and southern sectors t o meet the health needs of the
population . WHO w i l l collaborate also, i n the organization and delivery of health care, care
of the Aged, and hospital administration, the fur ther development of basic heal th
services, medical rehabi l i ta t ion, and maintenance and repair of medical equipment, i n
r e l i e f and rehabi l i t a t ion a c t i v i t i e s and i n the promotion of Publich Health Laboratories.
Disease Prevention and control
There are no quarantinable diseases in Cyprus, and most infectious diseases are
under control. However, echinococcosis is of some concern and a recently initiated
control programme will be continued. Among the non-coauuunicable diseases there is an
increase in cardiovascular diseases, diabetes and cancer. Road accidents constitute
the leading cause of death in the age group 15 - 49 years.
Thalassaemia is a major problem; about 14 per cent of the population carry the
trait, and one child in 200 is reportedly born with the disease. Possible control
measures will be explored.
WHO will assist the Government in the field of non-communicable diseases as
required.
Promotion of environmental health
The Government intends to establish and maintain the best possible environmental
control manures and facilities, taking also into account the needs of displaced persons.
Surveillance will be continued to maintain the status of malaria eradication.
WHO will cooperate by providing consultant services in environmental health.
Emphasis will be on problems of Mediterranean pollution and solid wastes disposal.
Health manpower development
The health manpower situation is improving steadily. The WHO fellowship programme
will continue to be used for the improvement of the manpower situation.
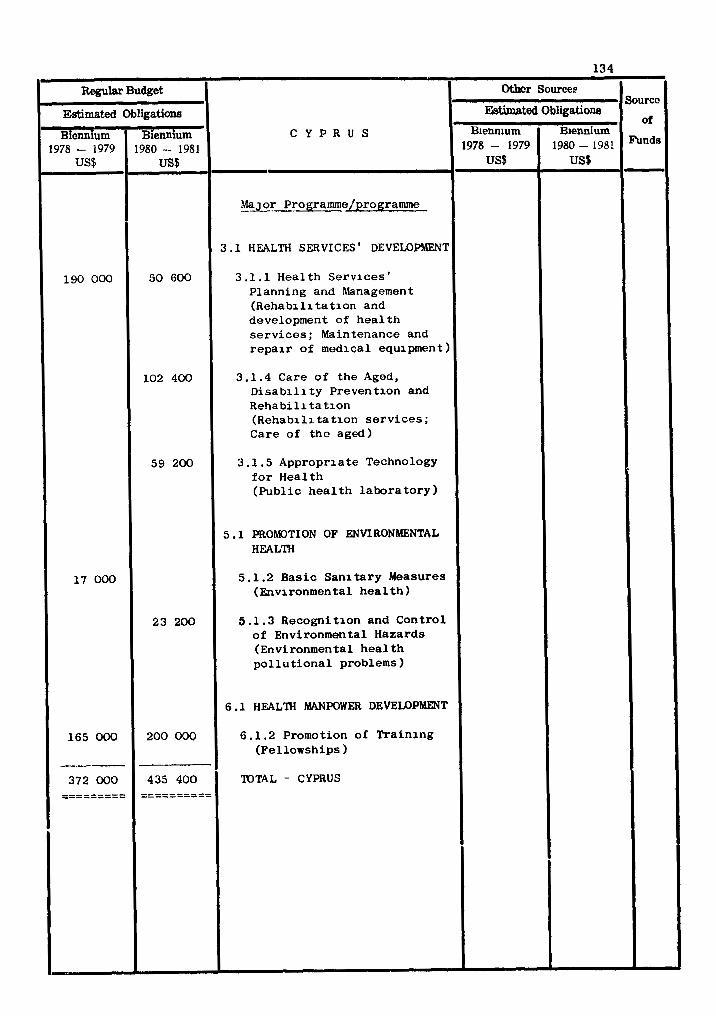
COUNTRY PROGRAMME STATEMENT
DEHOCRATI C YEMEN
NATIONAL HEALTH DEVELOPMENT STRATEGY
The cu r ren t na t iona l h e a l t h development s t r a t e g y is formulated wi th in t h e con-
t e x t o f t h e Five-Year Development Plan f o r 1979-1983 and programed i n a country
h e a l t h programming e x e r c i s e c a r r i e d o u t i n 1978 i n co l l abora t ion wi th WHO. The
major programme a r e a s i d e n t i f i e d a s p r i o r i t i e s a r e communicable d i sease c o n t r o l , i n -
c luding malar ia , schis tosomias is , t ube rcu los i s , com~lunicable eye d i s e a s e s and collPon
childhood i n f e c t i o n s ; primary h e a l t h care ; maternal and c h i l d h e a l t h and family
planning; t h e provis ion o f p o l y c l i n i c s i n urban a reas ; h e a l t h adminis t ra t ion; and
h e a l t h manpower development.
TECHNICAL CO-OPERATION P R O G W S lWR HEALTH
Health s e r v i c e s development
The Government p l ans t o e s t a b l i s h p o l y c l i n i c s i n c i t i e s f o r f i r s t - p o i n t con tac t
wi th the h e a l t h s e r v i c e s and wi th r e f e r r a l f a c i l i t i e s f o r s p e c i a l i s t serv ices . The
h e a l t h information s e r v i c e , n a t i o n a l h e a l t h l abo ra to ry s e r v i c e , the pharmaceutical
s e r v i c e s and the s e r v i c e f o r t h e maintenance and repair o f medlcal equipment w i l l be
f u r t h e r developed wi th WHO co l l abora t ion .
I n o rde r t o implement t h e r a p i d l y expanding h e a l t h s e r v i c e s t he Government
proposes t o s t rengthen t h e c e n t r a l h e a l t h admin i s t r a t ion and t o set up s t r o n g de-
c e n t r a l i z e d admin i s t r a t ive u n i t s i n governorates, provinces and d i a t r i a t s .
Primary h e a l t h c a r e
This programme i s a major component of t he h e a l t h c a r e system. I t is designed
t o ensure increased coverage o f t h e r u r a l populat ion through a network o f primary
h e a l t h c a r e u n i t s a t v i l l a g e l e v e l , s t a f f e d by workers s e l e c t e d by the community and
t r a i n e d l o c a l l y . Community p a r t i c i p a t i o n is s t r e s s e d a t a l l l e v e l s o f supervis ion ,
implementation, motivat ion and evalua t ion .
Some p r i o r i t y con t ro l programmes i n communicable d i s e a s e s and ma lnu t r i t i on a s
w e l l as a s p e c t s of maternal and c h i l d h e a l t h a r e incorpora ted i n t he primary h e a l t h
c a r e programme.
The a s p e c t s of t h e programme on which WHO co-operation is l i k e l y t o focus a r e
i ts t r a i n i n g component and t h e t r a n s f e r o f t he information and experience gained i n
s i m i l a r p rog rames elsewhere.
Family hea l th
A comprehensive approach t o Family heal th is to be developed so a s t o include
elements of maternal and ch i ld heal th , the expanded programme on immunization, the
control of diarrhoea1 d i seases of children, and nu t r i t ion . WHO w i l l co l laborate
p a r t i c u l a r l y i n regard t o the t r a in ing of manpower f o r ch i ld heal th services , and
the supervision of the MCH component of primary heal th care.
Disease prevention and control
Malaria, tuberculos is , comunicable eye diseases and schzstosomiasis a r e major
hea l th problems t o the control of which the Government has assigned high p r i o r i t y
and s p e c i f i c t a r g e t s f o r the end of the 1979-1983 Development Plan. W H D w i l l be
associated with these control progralunes a s well a s with the Expanded Programe on
Immunization which aims a t 80% coverage of e l i g i b l e age-groups of children, and 80%
coverage of pregnant women with te tanus toxoid. With regard t o sohistosomiasis, a
study is t o be made of i ts epidemiological, malacological and environmental aspects
before designing a control programme. Epidemiological se rv ices an11 be fu r the r
strengthened.
Promotion of environmental hea l th
The Government i s sys temat ica l ly developing cornunity water supply systems as a
high p r i o r i t y i n environmental heal th ; waste d isposal and food hygiene a r e a l s o
given p r io r i ty . Community pa r t i c ipa t ion is being fos tered i n the improvement of
environmental conditions. W H D col laborat ion w i l l continue i n the form of s t a f f ,
dissemination of information, co-operation i n f e a s i b i l i t y s t u d i e s and i n the mobiliza-
t i o n of addi t ional investment and extra-budgetary resources,
Health manpower development
This programme i s incorporated i n the a c t i v i t i e s of a l l the o the r programmes.
The manpower requirements and t r a i n i n g fo r the p r i o r i t y heal th programmes necess i ta te
the expansion and extension of the t r a in ing f a c i l i t i e s a t the c a p i t a l and the o the r
governorates. Though nat ional c a p a b i l i t i e s have a l ready been g r e a t l y enhanced,
in te rna t iona l co-operation i n providing teaching s t a f f w i l l be required t o meet the
addi t ional demand f o r t r a ined hea l th manpower. W H D w i l l co l laborate i n the pre-
para t ion of teachers and the development of i n s t i t u t i o n s and cur r i cu la t o meet the
increased manpower needs.
Health information
A c e n t r a l heal th s t a t i s t i c a l u n i t has been i n exis tence fo r some years. A
number of nat ional s t a f f have been t ra ined, and professional expa t r i a t e s have been
jo ining i n the service through b i l a t e r a l and in te rna t iona l arrangements. There i s
sti l l need t o fu r the r strengthen the heal th s t a t i s t i c a l services , pa r t iou la r ly i n
the provinces, and t o t r a i n nat ional heal th s t a t i o t i c a l personnel. WHD col laborat ion
w i l l continue through advisory se rv ices i n t h i s area.
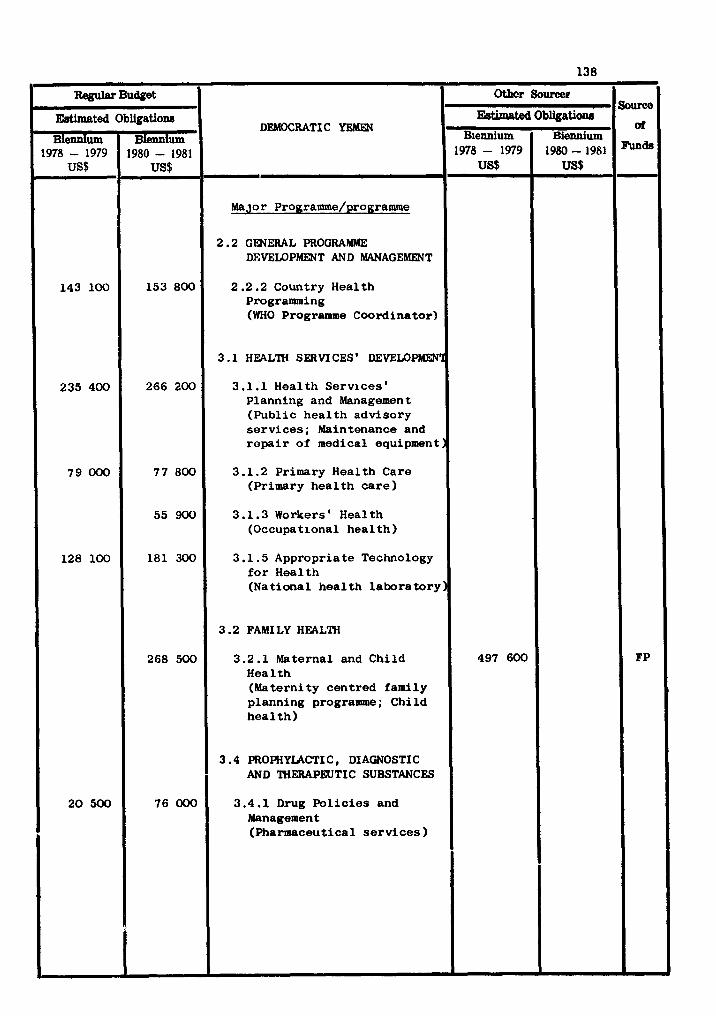
DEMOCRATIC YEMEN
Major Programme/programme
2.2 GENERAL PROGRAMME DEVELOPMENT AND WAGEMENT
2.2.2 Country Health Programming (WHO Programme Coordinator)
3.1 HEALTH SERVICES' DEVELOPMPI'I
3.1.1 Health Services' Planning and Management (Public heal th advisory services ; Maintenance and repa i r of medical equipment)
3.1.2 Primary Health Care (Primary heal th ca re )
3.1.3 Workers' Health (Occupational heal th )
3.1.5 Appropriate Technology f o r Health (National heal th laboratory:
3.2 FAMI LY HEALTH
3.2.1 Maternal and Child Hea 1 t h (Maternity centred family planning programme; Child hea l th )
3.4 PROPHYLACTIC , DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
3.4.1 Drug Pol ic ies and Management (Pharmaceutical services )
Regsrr Budpet Soun?e
aZ
FP
Othcr S o m e
EBtimated
Biennium 1978 - 1979
US$
143 100
235 400
79 000
128 100
20 500
Estimated Biennium
1978- 1979 US$
497 600
Obligation8
Biennium 1980 - 1981
US$
153 800
266 200
77 800
55 900
181 300
268 500
76 000
. Obligation8
Biennium 1980-1981
US$
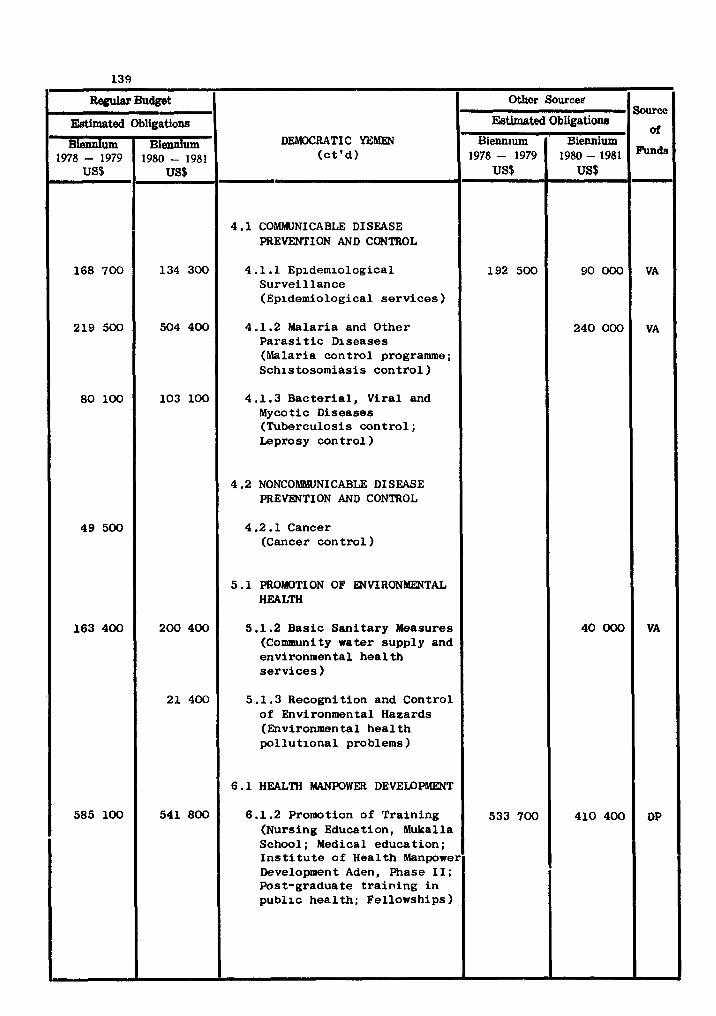
DEMOCRATIC YEMEN ( c t ' d )
4.1 COMMUNICABLE DISEASE F'REVENTION AND CONTROL
4 .1.1 Epidemiological Survei l lance (Epidemiological s e r v i c e s )
4.1.2 hlalaria and Other P a r a s i t i c Diseases (Malaria control programme; Schistosomiasis contro l )
4.1.3 Bacter ia l , Viral and Mycotic Diseases (Tuberculosis con t ro l ; Leprosy control 1
4.2 NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
4.2.1 Cancer (Cancer control )
5 .1 PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.2 Basic Sani tary Measures (Community water supply and environmental hea l th se rv ices 1
5.1.3 Recognition and Control of Environmental Hazards (Environmental hea l th po l lu t iona l problems)
6.1 HEALTH MANPOWER DEVELOPMENT
6.1.2 Promotion of Training (Nursing Education, Mukalla School; Medical education; I n s t i t u t e of Health Manpower Development Aden, Phase I I ; Post-gradua t e t r a i n i n g i n publ ic hea l th ; Fellowships )
m Budget Source
of
finds
VA
VA
VA
DP
Othcr Sourcee
Estimated
Biennium 1978 - 1979
US$
168 700
219 500
80 100
49 500
163 400
585 100
EBtimated Biem~um
1978- 1979 US$
192 500
533 700
Obligations
Biennium 1980 - 1981
US$
134 300
504 400
103 100
200 400
21 400
541 800
Obligations
' Biennium 1980-1981 US$
90 000
240 000
40 000
410 400
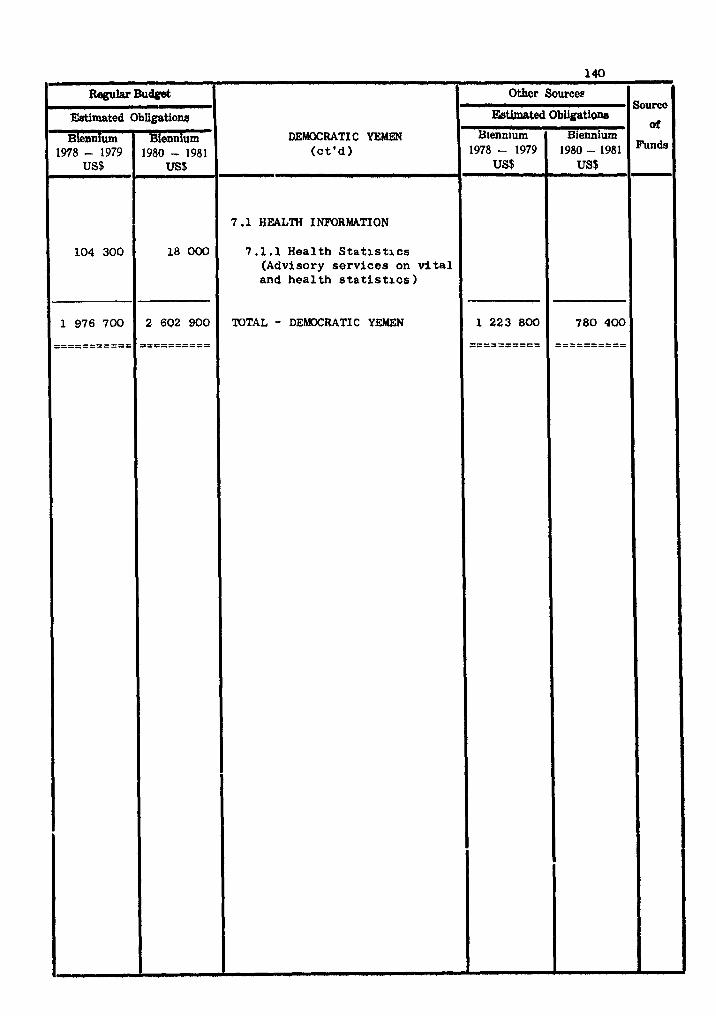
DJIBOUTI
INTRODUCTION
Djibouti gained its independence oilly recently i n June 1977,, and joined WHO member-
ship i n March 1978. I t is a small country, with a surface area of 22 000 sq. km, but
with population estimates widely varying between 110 000 and 350 000. Three quarters
of the population l i v e i n the capi ta l c i t y (DjiboutP) and the four provincial capitals3
the remainder l i v e i n rura l areas, mostly nomads.
TECHNICAL COOPERATION PROORAWYeS FOR HEALTH
Health services dsveloa~lent
Communicable diseases const i tute major problem. The diseases most frequently
not i f ied i n 1975 were: influensa, tuberculosis and sexually-transmitted diaeaae$,but
such diseases a s whooping cough, neasles, mumps and infectious hepa t i t i s a re very comon.
Administratively, the country is divided into four provinces. There were ( i n 1975) one
general hospital with 822 beds, and 10 medical centres with about 200 bed.. Out-patient
f a c i l i t i e s , prenatal and chi ld health centres, s ~ h o o l health uni ts and dental health
un i t s provide additional services.
WHO w i l l collaborate i n the reorganisation and development of health services a t
various levels. Hospital services development and rehabi l i t a t ion services a r e add-
i t i o n a l venues fo r collaboration.
Communicable disease prevention and control
Malaria does not seem t o be endemic i n Djibouti, but l imited outbreaks a r i s e i n
vulnerable areas due t o the introduction both of A. nambiae and gamatocyte oarriers
along the roads followed by nomadic population. Thus 191 cases w e n , reported during
1973-76 (with 96 cases i n 1975 alone); similar outbreaks occurred e a r l i e r during 1963-65.
WHO collaboration w i l l be i n i t i a l l y directed towards assessment of the present
s i tua t ion and developing m t i o n a l aapabi l i t ies .
Promotion of environmental health
The Oovernmnt is appreciative of the need fo r the development of its environmental
health progrulmae.Thoughthe oountry is occasionally confronted with floods and droughts,
the ahronic problems a re those of environmental pollution.
Apart from Djibouti (c i ty) , no dis infect ion is carr ied out i n public water supplies
i n urban and ru ra l areas. Water supply is mostly through bore holes, unprotected shallow
dug w e l l s or surface sources. Sewerage systems are ra ther limited, end so l id wastes
disposal i s uncontrolled, offer ing breeding grounds for f l i e s and rodents. Red Sea
pollution is a l so a problem.
WHO rill continue ~0118b0t8tion i n these areas, with q strqng element of 0 r g - e
t i on and a t ra ining progrolanns of nationals.
Health manwwer development
Djibouti relie@ mainly on expatr ia tes fo r health personnel. In 1975, of the 52
physicians, 6 dent i s t s and 6 pharmacists, 141 p r o f e 8 8 i o ~ l nurser and r idr iver , 102
ass i s tan t nurses and 193 nursing auxi l iar ies , dental, phuuceu t ioa l , laboratory and
radAology teehnlcirnr, the majority were expatriates. Changes i n ava i lab i l i ty a f t e r
independence is qui te l ikely. WHO collaboration rill be through providing advisory
mrvices i n health manpower developlent .ad i n t ra ining rurtional personnel.
Health information
The ava i lab i l i ty of timely, re l iable , reuringful and up-to-date i n f o r u t i o n is
recognised a s a prerequisite t o sound planning, adr inir t ra t ion, management and evaluation
of health services. WHO w i l l collaborate towards the es t ab l i8bon t of a nation8Z health
information system and t ra ining nation81 s ta f f .
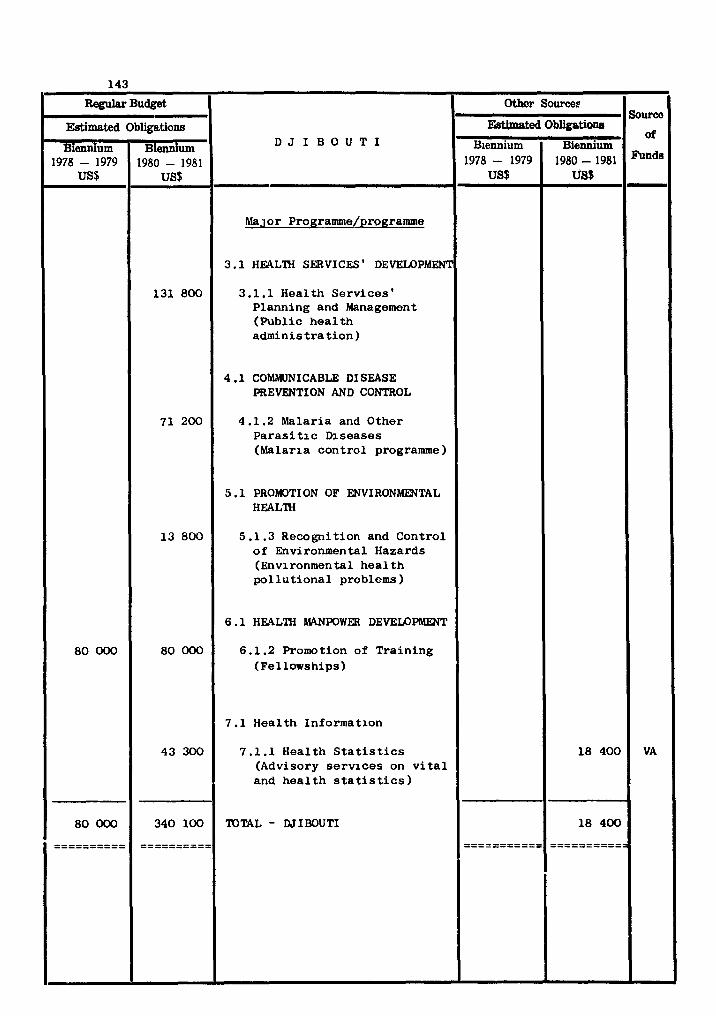
COUNTRY PROGRAMME STATEMENT
EGYPT
NATIONAL HEALTH DEVELOPMENT STRATEGY
The Fourth Five-Year National Development Plan, 1978-1982, incorporates a strategy
of decentralization based on autonomous regional development areas. It provides for
preventive health services, primary health care, curative and specialized health services
and the production of all required pharmaceuticals and vaccines. There is emphasis on
people's participation in the planning and administration of the services, delegation of
authority, strengthening the central planning machinery in the Ministry of Health,
raising the quality of care, continuing education of a11 health personnel, co-ordinating
medical education and research with health services, the control of environmental
pollution, developing information services to support planning and evaluati.?, and
health-services research particularly in health economics and information.
There is considerable bilateral and multilateral technical cooperation and WHO
collaboration is available for the various components of the Governments' programe.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
Health services development
Egypt has a well developed network of rural and urban health facilities and services.
A referral system is being developed through urban policlinics designed to serve 100 000
to 200 000 inhabitants. District and general hospitals with specialized units are being
upgraded.
One of the problems in the management of these facilities is the maintenance and
repair of medical equipment, and WHO is collaborating in the training of technicians for
this purpose.
As a result of the increase in population, traffic and industrial development, a
serious problem of environmental pollution has arisen. In the rural areas the luge
quantities of fertilizers and pesticides being used to promote agricultural production
are contaminating the environment and soil to an unknown extent. The Government has
established an environmental and occupational health centre to study chemioal and
bacteriological contami~tion of air, water and food and to conduct toxicological
studies; to study fresh and canned food with a view to determine the effects w the8 of
heavy letals, additives, preservatives, pesticides and bacteria; to determine quantities
of heavy metals in drinking water; to examine and determine the effects of contaminants
and chemicals on the health of the working population in industries; and to find
possible solutions to the problems studied.
WHO and UNEP are aollaborating in the ertablishment of the centre in developing
a system for early identification of health problems associated with pollution and the
general environment of work, and in developing guidetines and criteria adapted to
~ 0 n d i t i 0 ~ in egypt.
, Shigella and Salmonella infections are major cases of gastro-enteritis particularly
in children. WHO is collaborating in studies for identification and typing of SNgella
and Salmone3la.
In order to develop a comprehonsive immunization progrsume, the Government intends
to produce DPT as well as BCG vaacines for the Expanded Programe in I~munination and
to achieve self-sufficiency in vaccine production. WHO and UNDP are aollaborating in
this development and in quality control procedures.
A large phrrrmaceutical industry h8s grown and is being further exp8nded to achieve
self-sufficiency in ph8~ceutical products. WHO is collaborating in developing drug
policies, in improving pharmaceutical production practises, and ph8rm8eeutical quality
control, through the provision of consultants, fellowships and supplies and equiprent.
Disease rev en ti on and control
The Oovernaent plans to set up a surveillanae system for the rapid diagnosis and
early notifimtion of unusual corunicable disease. which soretires appear as sudden
epidemias ud to establish oo~rdination uongat veterinary 8nd publia health authorities
at administrative and teahniaal levels. WHO will collaborate through the provision of
consultants, supplies and equipwmt.
Anti-ularia aotivities are plumed and executed as p8rt of the general health
activities through the malaria control service of the Yinistry of Health and Malaria
Control Units distributed all over tho aountry. The risk of amlaria is now restriated
to limited areas. WHO collaboration will continue through limited provision for supplies
and by cooperating in teahniaal aspects of the progr-, including the training of
mtiomlr.
The Government h8s embarked upon 8n extensive progrusre of developing further the
intensive care, emergency services and other specialized units already available in
larger hospital., in collaboration with WHO , USAID, and bilateral agencies. WHO will
cooperate particularly in the establishment of national training centres.
An increasing number of genetic health problems, especially haemo-globinopathies
and neural disorders, are being recognized, and studies are being undertaken with WHO
collaboration to assess their extent and to provide a basis for establishing genetic
counselling services.
The large textile and sugar industries are responsible for respiratory diseases
from cotton and bagasse dust. WHO will collaborate in developing programmes for the
control of such allergic diseases and in strengthening the institutions responsible for
these programmes.
Promotion of environmental health
Egypt is participating in the inter-regional programme for the control of pollution
in the Mediterranean. A complete inventory has been made of land-based sources of
pollutants and a programme has been established to monitor pollution in recreational
waters and shell-fish beds. A collaborating centre has been designated and laboratory
analyses are being made.
The air-pollution monitoring system established in Cairo is being expanded and
extended to the provinces.
Solid waste collection and disposal systems are being strengthened.
WHO is collaborating through the provision of consultants, fellowships, supplies
and equipment to programmes for air quality, water quality, the monitoring and control
of pollution in the Mediterranean and Red Seas, and solid wastes disposal.
Health manpower development
The programme of health personnel training continues to be an active one involving
large numbers of trainees in various categories. In the case of health personnel
trained under the Ministry of Education e.g. physicians, dentists, pharmacists,
professional nurses, this has called for greater collaboration with the Ministry of
Health in the utilization of health care facilities other than University hospitals for
training purposes.
In medical education, as a result of the emphasis given in previous years to train-
ing teachers in educational planning and technology, the programme has reached a stage
where those responsible are re-examining the relevance of training to health-service
requirements and are aware of the need for changes in ways of organizing curricula,
instructional methods and m8terial8, and evaluation. Accordingly, more emphasis is
being given to the support of new medical or health-sciences education units/departmnts
or centres.
In addition to the staff of medical schools, training in educational planning
and technology has included teachers in nursing, public health, dentistry and Ministry
of Health staff. Those in nursing are mainly teachers from W Hi~har.bstitutes--d.
Nursing, and they are expected to play an important role in improving nursing education
programmes in their om institutions as well as in other nursing institutions in the
country.
As the Seaoaduy Nurm Technia81 Sahools Programs which are nor graduating large
nurbers,became established, emphasis rill be given to post-bsic nursing and midwifery
education.
Progress is being made also in training and utilizing traditional birth attendants
within YCH progr-8.
The Centre for Educational Technology in Health Sciences, Cairo, whoso major funa-
Uonis develomnt of learning MterialS, is gradually overcoming the difficulties of its
earlier stages of development and a significant increase in its activities is 8nticip.t.d.
WHO will eontinru to collaborate in developing the above training activities in the
different institutes.
Health information
Iaforrut%on is rvquind for pla~ing, unageoent and monitoring of health, social
w l f a n and enviromntal health progr...es. The Authority for Yobiliution and
8t.ti.tics is responsible for tho collection and processing of national statistics. The
Ninistry of Health collocts and pr-sses information on disoasea, serviaes, and other
factor. related to the managememt of health services. In addition, the Institute of
Statistical Studies and Research, Cairo, and the High Institute of Public Health,
Alexandria, h a m progrrno. for training, teaching and research in health statistics.
WHO is continuing its collaboration with a11 these organitations and institutions,
partiaularly in developing data-processing capabilities at various administrative and
or#8niqational levels and the training of personnel.
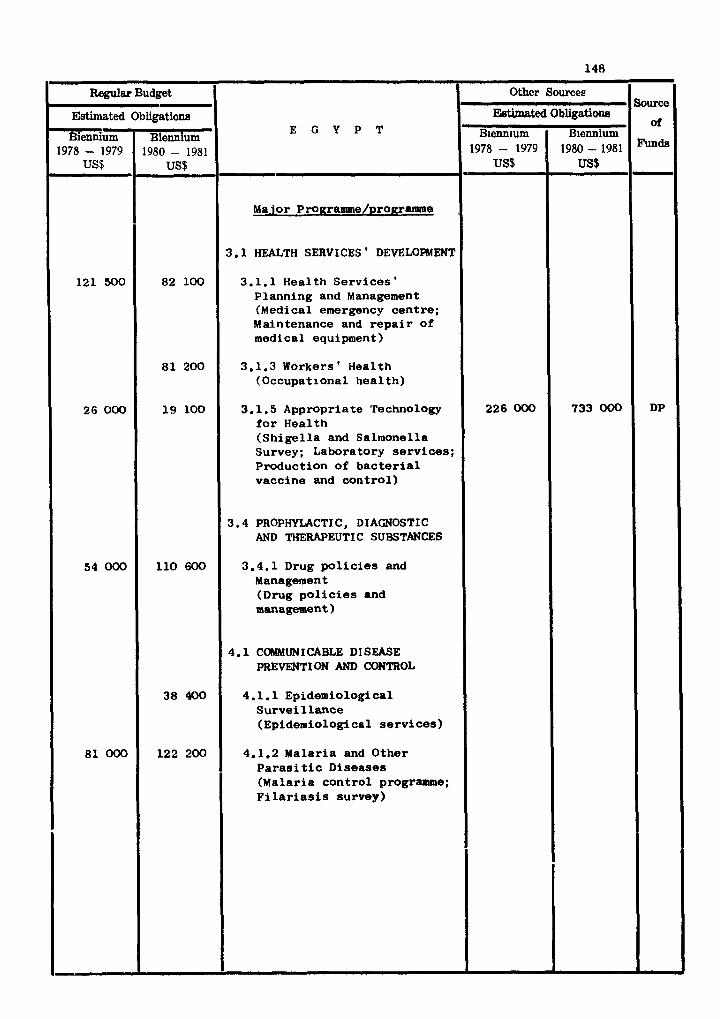
E G Y P T
~- Ma.ior Programme/progr~~lle
3.1 HEALTH SERVICES ' DEVELOPMENT
3.1.1 Health Serv ices ' Planning and Management (Medical emergency cent re ; Maintenance and r e p a i r Of
medical equipment)
3.1.3 Workers ' Health (Occupational hea l th )
3.1.5 Appropriate Technology f o r Health (Sh ige l l a and Salmonella Survey; Laboratory se rv i ces ; Production of b a c t e r i a l vaccine and con t ro l )
3.4 PROPHYLACTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
3.4.1 Drug p o l i c i e s and Management (Drug p o l i c i e s and management)
4.1 COMMUNICABLE DISEASE PREVENTION AND COElTROL
4.1.1 Epidemiological Su rve i l l ance (Epidemiological s e rv i ces )
4.1.2 Malaria and Other P a r a s i t i c Diseases (Malaria con t ro l programme; F i l a r i a s i s survey)
Regular Budget , ,/-
Estimated Obligations
~iennium Biennlum USI- 1978 - 1979 1980 - 1981
Sourcc
of
Funds
DP
Other Sources
121 500
26 000
5 4 0 0 0
81 000
&timated
B~enn~um 1978- 1979
US$
226 OOO
82 100
81 200
19 100
1 1 0 6 0 0
38 400
122 200
Obligations
B~ennium 1980-1981 US$
733 000
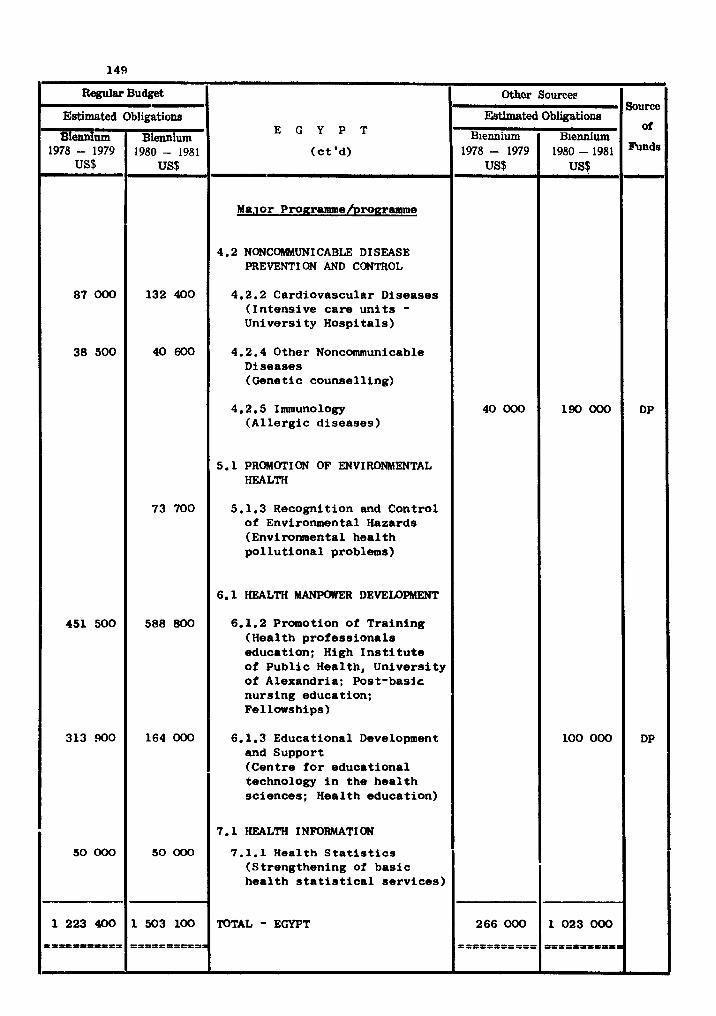
Regular Budget
E G Y P T
(ct 'd)
Ma.lor Pro~ramme/pro~rararne
4.2 NONCOWUNICABLE DISEASE PREVENT1 ON AND CONTROL
4.2.2 Cardiovascular Diseases (Intensive care units - University Hospitals)
4.2.4 Other Noncommunicable Diseases (Genetic counselling)
4.2.5 Immunology (Allergic diseases)
5.1 PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.3 Recognition and Control of Environmental Hazards (Environmental health pollutional problems)
6.1 HEALTH MANPWER DEVEUlPMENT
6.1.2 Promotion of Training (Health professionals education; High Institute of Public Health, University of Alexandria; Post-basic nursing educatton; Fellowships)
6.1.3 Educational Development and Support (Centre for educational technology in the health sciences; Health education)
7.1 HEALTH INFORMATI ON
7.1.1 Health S t a t i s t i c s (Strengthening of basic health statistical services)
TOTAL - EGYPT
Estimated
T u m 1978 - 1979
US$
87 000
38 500
451 500
313900
50 000
1 223 400
l l l D P U P I t L l
- Obligations
Biennium 1980 - 1981
US$
132 400
40 600
73 700
588 800
164000
50 000
1 503 100
I P I P I D S P I P I
Source
or
DP
DP
Othcr Souree~
Egtimated B~ennium
1978 - 1979 US$
40000
266 000
P t l e = l P P f P 0
Obligatione
Biennium 1980 - 1981
uss
190 000
100 000
1 023 000
PPt lP IPPDI3
COUNTRY PROGRAMLlE STATElYIENT
I RAN - NATIONAL HEALTH DEVEMPMENI' STRATEGY
In the past decade Iran has experienced an extremely fast economic growth and has
had one of the most rapidly rising Gross National Products in the world.
This economic growth has been accompanied by many social changes, not least in the
field of public health and welfare. The rapid development of an integrated approach to
health and welfare, with decentralization on a regional basis, has taken place in close
conjunction with a wide variety of other social reforms including land reform, workers
profit sharing schemes, the establishment of an educational corps and a health corps,
compulsory social security, nutritional programmes and a wide range of preventive
medicine activities.
The current national health development strategy was formulated in the context of
the Sixth National Development Plan (1978-19831, which envisages a substantial increase
in annual per capita expenditure on health.
Particular efforts are being taken by the Government in the field of health man-
power development, where the authorities are taking steps to ensure that all training
programmes for health workers are as closely as possible integrated with those for
the development of health services.
High priority is given to the establishment of health and welfare networks, and
the development of primary health care.
Primary health care is seen in a broad context which encompasses the prevention
and control of communicable diseases, including ipp~unisation, maternal and child health,
and the promotion of environmental health.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
Primary health care
The development of frontline health care delivery and the promotion of the concept
of health services development as an integral part of overall comnunity develop~ent has
received Government approbation as a result of the outcome of research and developlent
projects in primary health care in various regions of the country. WHO will continue
to be associated with the primary health care programw mainly in relation to its
periodic evaluation and to making its experience available to other countries in the
Region, including a s a spec i f i c f e a t ~ r e the co l lec t ion and t rans fe r of information on
appropriate technology f o r health. Research i n heal th services development is a part-
i c u l a r concern of the Government, and WHO w i l l col laborate c losely i n t h i s respect.
Disease prevention and control
The heal th author i t ieg propose t o exploi t the opportunity which I ran presents f o r
c e r t a i n aspects of cancer epidemiology and control ; WHO w i l l cooperate i n this a c t i v i t y
by providing consultant services and t rans fe r r ing information on epidemiological find-
gngs t o other countries.
The Government is concerned a l s o t o formulate new drug p o l i c i e s and t o introduce
e f fec t ive management of the preparation, d i s t r i b u t i o n and use of drugs.
Promotion of environwntal heal th
The main t h r u s t of WHO collaboration i n t h i s respect w i l l be i n r e l a t i o n t o the
monitoring and control of a i r and water qual i ty , t o marine pol lu t ion control i n the
Kuwait Action Plan Region (Urn), and t o environmental improvement projects.
Health manpower development
WHO'S r o l e w i l l be t o col laborate with the Government a s required i n c a t a l y t i c
a c t i v i t i e s , based t o the extent possible on a research and d e v e l o p e n t approach, t o
fu r the r the Government's expressed in ten t ion of c rea t ing an e f f e c t i v e in tegrated hea l th
service and manpower development programme.
Specif ic input w i l l be made, a s requested, t o a number of experimental i n s t i t u t i o n s
including Bu A l i Sina University, Hamadan, the University of Retaiyeh, West Azerbaidjua
and Fassa University i n Fars Province a s w e l l a s o the r i n s t i t u t i o n s where new approaches
t o t r a in ing a r e being developed.
Continuing c lose col laborat ion i n a l l aspects of educational planning and
technology, under the overa l l leadership of the Department of Medical Education Pahlavi
University, Shiraz (WHO Regional Teacher Training Centre) i s anticipated.
Continuing col laborat ion i n i n s t i t u t i o n a l development with the School of Public
Health, I n s t i t u t e of Public Health Research, University of Teheran, w i l l be extended.
There rill be continuing col laborat ion with t r a in ing programmes i n c e r t a i n s p e c i f i c
f i e l d s including nursing and medical l ibrar ianship .
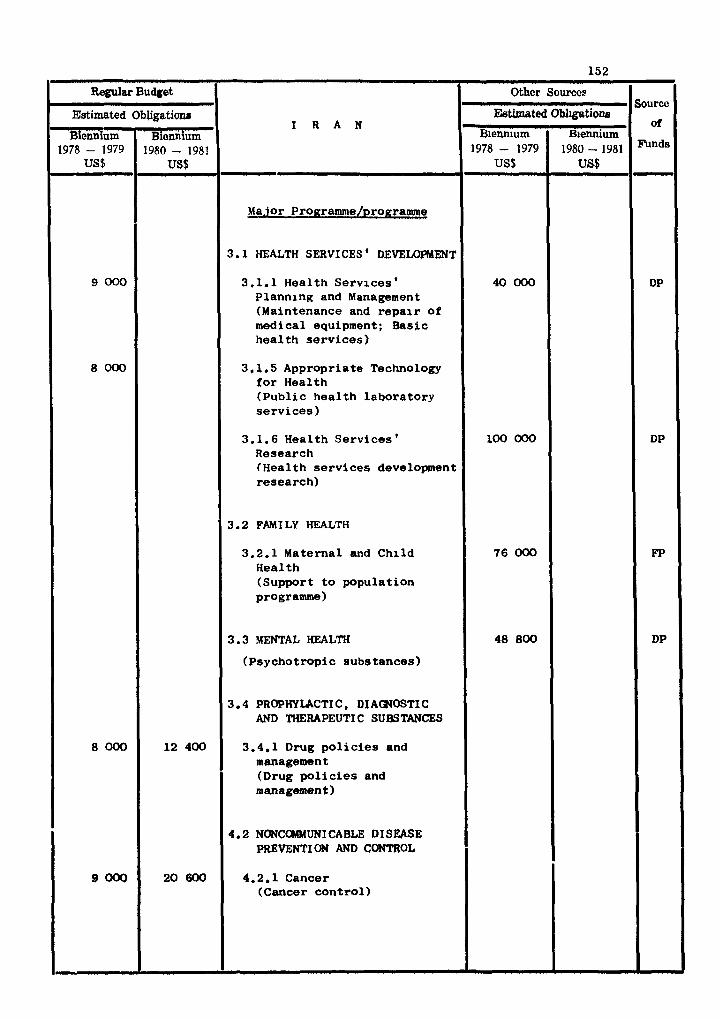
Wcr Sourcee Sourcc
Estimated Obl~gatione I R A N of
Biennium Biennium 1978 - 1979 1980 - 1981 - US$ US$
3.1 HEALTH SERVICES* DEVELOPMENT
3.1.1 Health Services' 40 000 DP Planning and Management (Maintenance and repair of medical equipment; Basic health services)
3.1.5 Appropriate Technology for Health (Public health laboratory services)
3.1.6 Health Services ' 100 000 DP Research (Health services development research)
3.2 FAM I LY HEALTH
3.2.1 Maternal and Child 76 000 FP Health (Support to population programme)
3.3 MENTAL HEALTH 48 800 DP
(Psychotropic subetances)
3.4 PROPHYLACTIC , DI AWOSTI C AND THERAPEUTIC SUBSTANCES
3.4.1 Drug policies and management (Drug policies and management )
4.2 NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
4.2.1 Cancer (Cancer control)
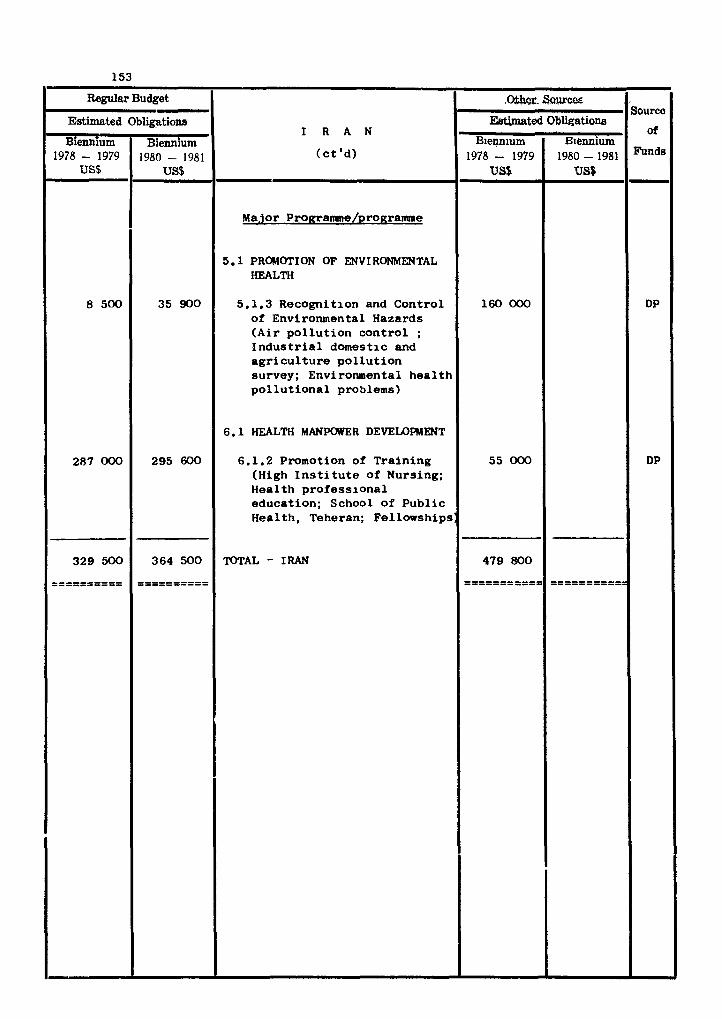
Regular Budget
I R A N
( c t 'd)
Major Pro~rarmne/pro~ramme
5.1 PROMOTION OF ENVIRONMENTAL HEALTH
5.1.3 Recogni t ion and C o n t r o l of Environmental Hazards ( A i r p o l l u t i o n c o n t r o l ; I n d u s t r i a l domest ic and a g r i c u l t u r e p o l l u t i o n survey ; Environmental h e a l t h p o l l u t i o n a l problems)
6.1 HEALTH MANPOWER DEVELOPMENT
6.1.2 Promotion of T r a i n i n g (High I n s t i t u t e o f Nursing; Hea l th p r o f e s s i o n a l e d u c a t i o n ; School o f P u b l i c Hea l th , Teheran; Fel lowships:
TOTAL - IRAN
Estimated
Biennium 1978 - 1979
US$
8 500
287 000
329 500
---------- ----------
7
Obligations
Biennium 1980 - 1981
US$
35 900
295 600
364 500
---------- ----------
Source
of
Funds
DP
DP
,Ww- &urm Estimated
B~ennium 1978- 1979
US$
160 000
55 000
479 800
----------- -----------
Obligations
Biennium 198Q-1981
US$
----------- -----------
COUNTRY PROGRAMME STATEMWT
lKig - NATJONAL HEALTH DEVEIPPMENT STRATEGY
The main emphasis is on fur ther well-balanced development of health manpowerinolud-
ing the rec t i f ica t ion of the imbalance between the various categories and the improve-
ment of the geographical distributzon of health workers; the gradual extension of
aomprehensive rura l health services as well as of the health insurance scrheme aiming
a t t o t a l population coverage; increased e f f o r t s towards the preventron and control
of diseases, with pr ior i ty on communicable diseases, inuluding bet ter immunization
coverages, and an overal l improvement of environmental conditions.
The complet$on of a detai led national health plan for the period 1976/1980, was
postponed due t o delay i n completing the overall National Developsnt Plan for the
same period.
The National pevelopent Plan for the period 1981/1985 is under preparation and
there are etudies i n progress towards abng-term plan t o the year 2 000.
Country health programming was carried out i n 1978.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
Comprehensive health services
The provision of aomprehensive health services t o the ru ra l population by 1980will
continue through an expansion of s t a f f i ng gf the main health centre*, sub-centres and
mobile rura l health unrts. Village-level s ta t ions, below sub-centres, a r e being
expanded.
Improvement of medical care implies increasing the r a t i o of 2.0 beds per 1 0 0 0
inhabitants i n 1977 t o 2.3 i n 1980.
MCH services are being expanded so tha t the number of centres w i l l have increased
from 100 i n 1975 to LBO i n 1980.
The National Nutrit ion I n s t i t u t e w i l l be strengthened and attempts w i l l be made
t o integrate the national nu t r i t ion policy i n to the general health services.
Continuous emphasis w i l l be l s i d on health education.
A Regional Training Centre i n Maintenanae and Repair of Medical Equipment estab- l ished i n 1978 w i l l recerve continuing support.
Hospital services administration is being adapted and modernized in consonance
with new developments.
The Directorate of Public Health Laboratory Services aims at co-ordinating the
laboratories, improving training and standardizing equipment and methodology.
More personnel will be trained for the National Rehabilitation Institute.
There will be an increased use of locally produced drugs, and WHO will collaborate
in advising on drug policies and management.
Within the entire context of comprehensive health services, technical cooperation
with WHO will be centered around the Regional Training Centre for Maintenance and
Repair of Medical Equipment and hospital services administration. As and when required,
in the other specified areas, WHO collaboration is available in respect of information
transfer, consultant services, co-ordination functions and fellowships.
Communicable disease prevention and control
The main trends and objectives will be to promote epidemiological surveillance,
the expanded immunization programme with its gradual integration into the general health
services, strengthening of the staffing pattern, modernization of equipment, and to
support administrative decisions, payment of financial incentives to health workers,
as well as the purchase of modern equipment and additional transport. It is estimated
that the transmission of malaria may be controlled by the end of 1980. The Endemic
Diseases Institute in Baghdad will be strengthened A Malaria Training Research Centre
is being established in Baghdad to train malaria personnel from the Arab Countries.
The Ministry of Health wishes to continue technical cooperation with WHO in
epidemiological surveillance, aiming at further assessment of communicable diseases,
training of the national staff and in obtaining advice for future planning.
The Malaria Eradication Programme may require technical co-operation on a rather
broad basis through 1gCf2,
On a lesser scale, technical cooperation will continue in visceral leishmaniasis
control as well as in communicable diseases control and prevention of visual impairment.
&le disease reve en ti on and - - control
A new National Cancer Institute will be constructed and the National Cancer
Register will extend beyond the boundaries of Baghdad city.
The national oral health survey is expected to be completed by the end of 1980.
Other non-communicable diseases will receive due attention through the Institutes
concerned.
Technical co-operation with WHO, through consultants, fellowships and inforution
transfer, will continue in cancer control and preventive oral health services.
Promotion of environmental health
The Directorate-General of Humon Environment was established in 1975, under the
Ministry of Health. It now includes also the Directorate of Occupational Health, At
the national level, plans and activities related to the human environment as a whole
are coordinated through the Supreme Council of Human Environment in which 18 ministries
are represented. Coordination of matters related to environmental health will contin-
through the Council and that will include applied research, air pollution monitoring
and control, food safety and occupational health, among other subjects.
Technical cooperation with WHO, UNDP and ILO will continue in building the required
infrastructure for large environmental programmes, including occupational health.
Health manpower develomnt
The health problems of the country are rather well defined. The required tasks of
health workers are being elaborated by a study on job descriptions. In order to keep
pace with the growth of the health services and the increasing population, three n e w
medical colleges were established: A1 Nustansariyah, in Baghdad, (1975) at Sulaiun-
iyah in 1977; and at Kufa (Kerbala Province) in 1978.
The national authorities are fully aware of the amfavourable ratio between medical
and other health personnel. Increasing attention must be given to training the "medium
level" and auxiliary personnel, if the desired balance is to be attained.
Technical co-operation with WHO will continue in medical and nursing education
through consultantships, provision of teaching and training aids, meetings, workshops,
exohange of visiting professors and fellowships.
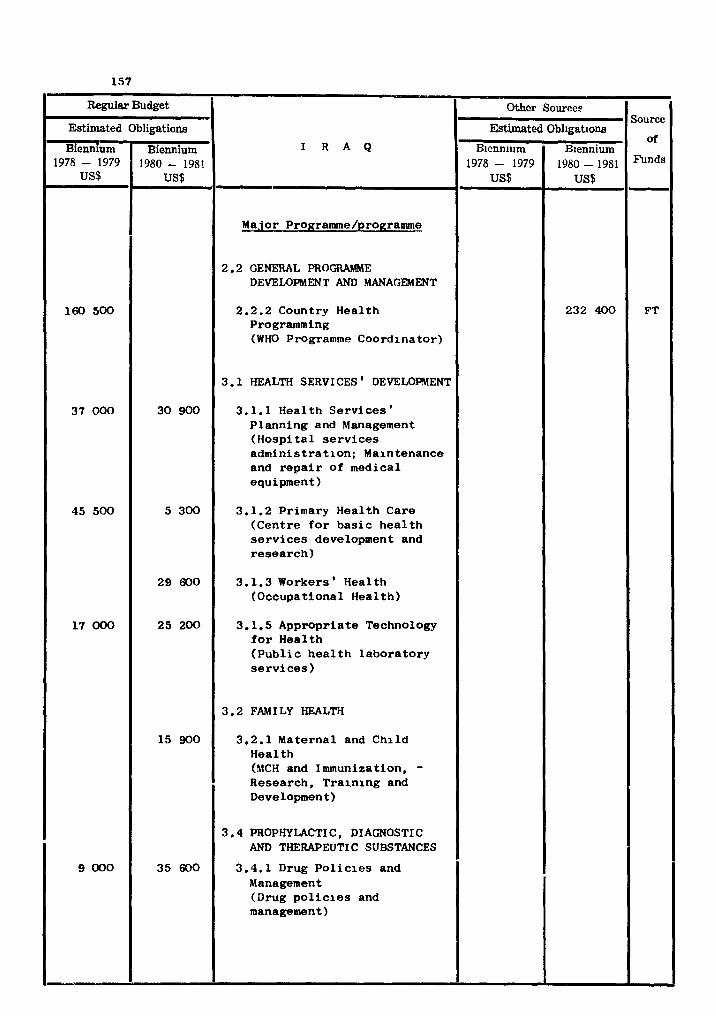
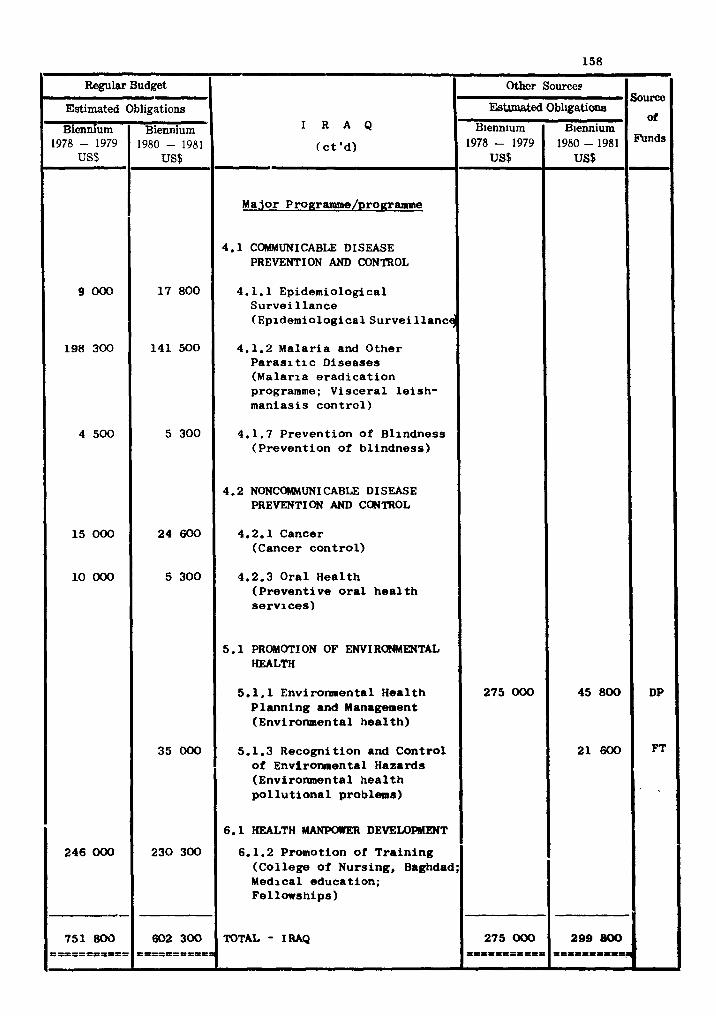
Regular Budget
Estimated Obligations
Biennium ' Biennium
us$ F 1978 - 1979 1980 - 1981
Other Sourcee Sourec
Ebtmated Obl~gatione I R A Q
of B~ennlum Biennium
9 000
198 300
4 500
15 000
10 000
246 000
- 751 800
P I I P = P I I I P P -
(ct 'd) - Major Progranune/prograrmne
4.1 COMMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.1 Epidemiological Surveillance (~pidemiological~urveillanc~
4.1.2 Malaria and Other Paras1 tic Diseases (Malaria eradication programme; Visceral leish- maniasis control)
4.1.7 Prevention of Blindness (Prevention of blindness)
4.2 NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
4.2.1 Cancer (Cancer control)
4.2.3 Oral Health (Preventive oral health services)
5.1 PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.1 Environmental Health Planning and Management (Environmental health)
5.1.3 Recognition and Control of Environmental Hazards (Environmental health pollutional problems)
6.1 HEALTH MANPOIlER DEVELORnENT
6.1.2 Promotion of Training (College of Nursing, Baghdad; Medical education; Fellowships)
TOTAL - IRAQ
17 800
141 500
5 300
24 600
5 300
35 000
230 300
602 300 PI==P=tt l=a
1978 - 1979 US$
275 000
275 000
1980-1981 US$
45800
21 600
299 &00
DP
FT
, I
COUNTRY PROGRAMME STATEMENT
ISRAEL - NATIONAL HEALTH DEVELOPMENT STRATEGY
I t i s the policy of the Government of I s rae l to make high-quality primary medical
care available t o the en t i r e population withln the framework of a national health in-
surance system, and with ready interact ion between the primary, secondary and t e r t i a ry
aare sectors. The integration of curative and preventive services is seen a high prior-
i t y i n order t o avoid overlapping and t o f a c i l i t a t e continuity i n health care. Anumber
of groups, based on the exis t ing health insurance system, Ministry of Health services
and medical schools, have been developing different approaches t o the implementation of
t h i s policy, and much empirical knowledge has been gained about the feas ib i l i ty , c o s t ,
advantages and disadvantages of d i f fe ren t approaches. There i a a growing movement to
establ ish family medicine as the focus of primary medical care, which aims a t wmprehens-
i ve and continuing care for the family unit .
Disease patterns i n I s r ae l a re mainly those of industr ia l ized soc ie t ies and in-
areasing at tent ion is being given therefore t o the control of non-comunicable diseases
and of environmantal hazards associated w i t h industry and urbanization.
TECIHI CAL COOPERATION PROGRAMMES FOR HEALTH
Non-communxcable disease prevention and control
WHO collaboration, i n the form of fellowships and conaultants, w i l l focus mainly
on cancer control, which is the object of a very act ive voluntary organization conaerned
par t icular ly with prevention and ear ly detection.
Promotion of environmental heal th
WW collaboration i n environmental health w i l l r e l a t e mainly t o the monitoring
and oantrol of a i r and r r t % r quality, t o marine pollution i n the Mediterranean and Red
Seas, and t o environmental improvement.
Health manpower development
Continuing collaboration w i l l be extended i n the carefully designed W H D Fellow-
ships programme which is constructively used by the Government and Universities, p r e
dominantly for short periods of t ra ining abroad for potent ia l ly key individuals i n
selected f ie lds .
Collaboration will be specifically targeted upon nursing education, and upon s u p
port and continuing evaluation and monitoring of the programmes of the Centre for Health
Sciences of the Ben Gurion University of the Negev. A t the latter University and other
universities having health professional schools, particular mphaais will be laid on the
training of key teachers and on training in appropriate aspects of community medicine.
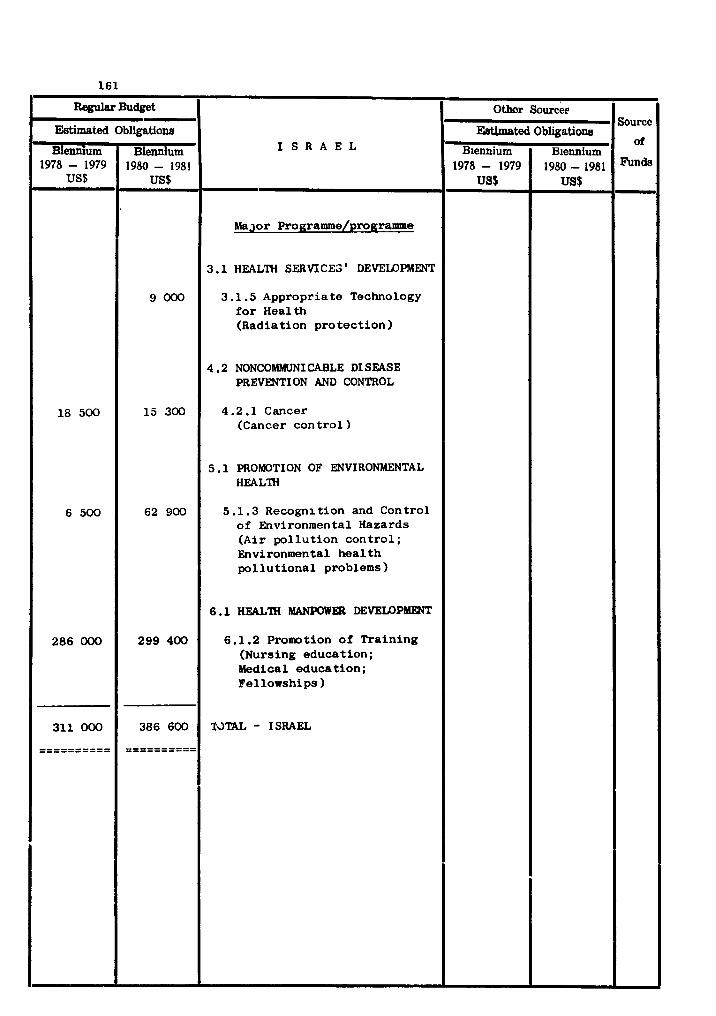
w@= Budget
I S R A E L
~a j o r Prog~amme/programme
3.1 HEALTH SERVICEB' DEVELOPMENT
3 .l. 5 Appropriate Technology f o r Health (Radiation p ro t ec t ion )
4.2 NONCOMNRMICABLE DI SEASE PREVENTION AND CONTROL
4.2.1 Cancer (Cancer con t ro l
5 .1 PROMOTION OF ENVIRONMENTAL HEALTH
5.1.3 Recognl t i on and Control of Environmental Hazards (Air po l lu t ion con t ro l ; Environmental h e a l t h p o l l u t i o n a l problems)
6.1 HEALTH W W E R DEVELOPMENT
6.1.2 Promotion o f Tra in ing (Nursing education; Medical educat ion; Fellowships )
WTAL - ISRAEL
Estimated
Biennium 1978 - 1979
US$
18 500
6 500
286 000
311 000
==========
Obligations
Biennium 1980 - 1981
US$
9000
15 300
62 900
299 400
386 600
==========
Source
' d
Othor Sources
-ted
Biennium 1978- 1979
US$
Obligations
Biennium 1980-1981 US$
COUNTRY PROGRAlldh(E STATEMENT
JORDAN
NATIONAL HEALTH DEVELOPMENT STRATEGY
Medium-term socio-economic development plans are periodically prepared by the
Jordan Development Board and resources a re allocated fo r the development of the health
sector, i n addition t o provisions for health a c t i v i t i e s i n other sectoral p r o g r m s .
The principal health service problems are: the poor d i s t r ibu t ion and variable
qual i ty of health services i n rura l and desert areas; a shortage of professional and
auxi l iary health manpower; overlapping of curative services and limited coordination
between the public and private sectors; inadequate control of drugs; need fo r mre
modern methods of managing health ins t i tu t ions , and lack of proper educjtron of the
public i n the best way t o u t i l i z e medical services.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
Health services development
A s par t of the development plan, the Yinistry of Health w i l l be strengthened,
and improved administrative practices introduced. A comprehensive long-term plan fo r
the development of the health services w i l l be developed. Health leg is la t ion rill be
up-dated t o define the respons ib i l i t i es and coordinating ro l e of the Ministry of Health,
and s t a t i s t i c a l and information services w x l l be improved. Attention w i l l k given to
the administration and management of hospital services and t o co-ordinating t h n with
other health services. The health insurance scheme wi l l be fur ther developed. Part-
icu la r a t ten t ion w i l l be given t o improving the maternal and chi ld health serviaes.
WHO w i l l continue t o collaborate with the Government i n various aspects of public
health, i n primary health care a s a pr ior i ty , i n esfabl ishing a network of workshops
f o r the maintenance and repair of medical equipment, i n medical rehabi l i ta t ion, and i n
the emergency medical services, and i n public heal th laboratory services Par t icular ly
i n the improvement of the Vaccine Ins t i tu te , and the establ ishrent of an adequcrte
v i rus section.
Family health/maternal and chi ld health
I t is envisaged that the collaboration of internat ional agencies with the Govern-
ment wi l l continue i n maternal and chi ld h e a l t h / f u i l y health.
Communicable disease prevention and control
The importation of malaria from neighbouring countries continues to be a threat
to the eradication programe. WHO cooperation is directed towards technical support
and a minimum amount of supplies as required, the coordination of activities between
Jordan and neighbouring countries through the promotion of malaria border meetings,
and fellowships.
A national programme is being developed as part of inter-country plan for the
control of enteric infections. WHO will provide consultant services, fellowships,
local training of staff, supplies and equipment.
Promotion of environmental health
WHO will collaborate by providing consultant services for problems of Red Sea
pollution, strengthening of environmental control programmes, and solid wastes disposal.
Fellowships will be awarded for developing manpower capabilities for the monitoring and
control of marine environment pollution and for environmental health pollution problems.
Health manpower development
In health manpower development, WHO will continue to promote the training of
national teachers for medical and nursing education, the further strengthening of the
Faculty of Medicine and Pharmacy of the University of Amman, the strengthening of nurs-
ing services and the development of professional and auxiliary nursing education pro-
grammes. Preparation of graduate nurses as midwives has been receiving considerable
attention.
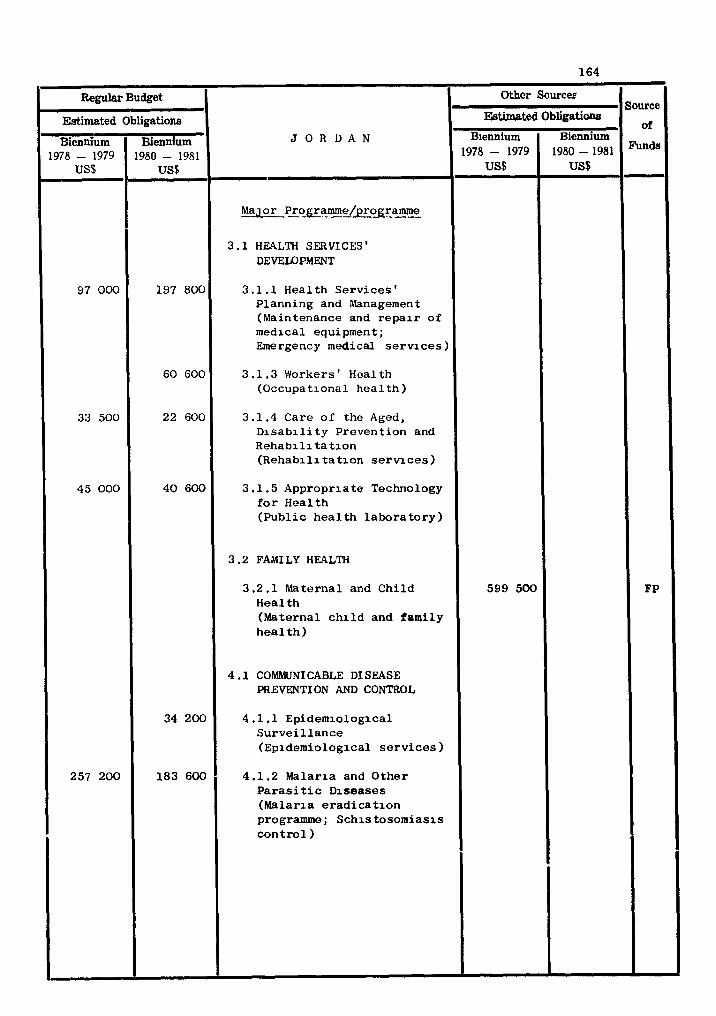
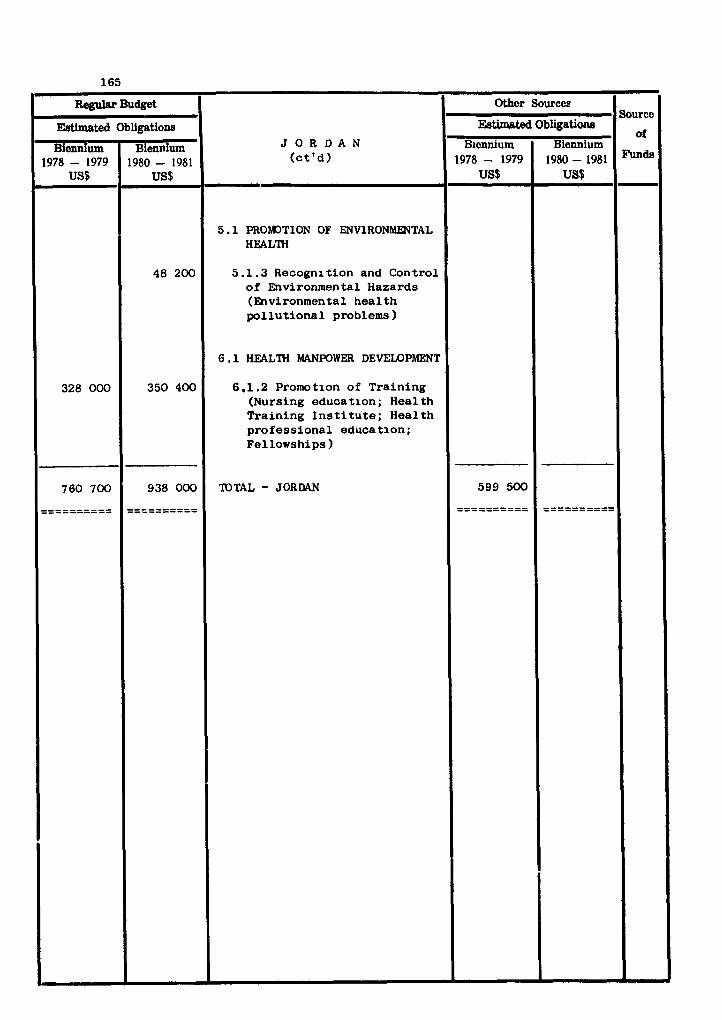
COUNTRY PROGRAMME STATEMENT
KUWAIT
NATIONAL HEALTH DEVEU)PhlENT STRATEGY
The Health services i n Kuwait have developed a t a f a s t pace during the l a s t three
decades. In 1974 there were 11 hospi ta ls with 3 500 beds; ten polyclinics and 34
cl inics . The budget i n 1977 was US$ 184 million (K.D. 54 million). The per capi ta
health expenditure being US$ 167 (K.D. 49 per annum). The t o t a l number of s t a f f em-
ployed by the Ministry of Health is between 16 to 17 000 which is increasing by more
than 15% per year. There a re fur ther plans t o expand the services during the next few
years and i n 1976 a medical college s ta r ted functioning.
The Government is committed t o the welfare of the people and therefore it is con-
cerned about the effectiveness and efficiency of health services and is anxious t o i m -
prove it so that Kuwait should develop one of the best health care systems i n the world.
Availabili ty of financial resources has not been the l imit ing factor. However, the
health services depend upon expatr ia te manpower and expertise which is being drawn from
other friendly countries. There is a great variation i n the qual i ty of professional
and middle level personnel.- The Government has made a great e f f o r t t o bring the health
care as near t o people i n t he i r homes as posssible, with the r e su l t tha t Kuwait has a
re la t ive ly greater level of coverage by medical care than other countries i n the Region.
I t is expected tha t i n the next few years, a l l homes w i l l be within ten minutes' driving
distance from a f i r s t quality hospistal.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
Health services planning and management
In view of these developments and plans, the Government is concerned about defini-
t ion of agreed goals, objectives and pr ior i t i es . Wm and other organizations have
collaborated i n developing the capacities for planning and strengthening of the planning
process.
WID would continue to collaborate i n strengthening the planning process, develop-
ment of t ra ining of personnel, improvement of management and reorganization of health
structure, development of information systems, aol lect ion and re t re iva l of data.
Non-communicable disease prevention and control
Cancer (Comprehensive programme a t community leve l )
Cancer ac t i v i t i e s i n Kuwait s ta r ted i n the late '60s with the new Radiotherapy . ... Department a t A 1 Sabah Hospital. In 1971 a Cancer Registry was organized which pro-
vides information on cancer dis t r ibut ion by site, age, sex and population arlgin.
Cancer c l i n i c s have been introduced during the l a s t few years and preventive measures
i n terms of decreasing population exposure t o environmental carcinogens i n the occupa-
t ional area are being gradually undertaken.
W m would collaborate i n developing a Comprehensive National Cancer Programme which
is envisaged t o strengthen ear ly detection, public and professional education, improved
follow-up, rehabi l i ta t ion and primary prevention addressed t o the general population
(control of smoking, eating, chewing and other habi ts re la ted with carcinogenesis).
Promotion of environmental health
Recognition and control of environmental hazards (Environmental health pollution
problems)
Kuwait,on account of its geographical s i tua t ion and climate,depends on desalination
of water. The 0x1 industry has created a number of environmental health problems and
therefore the Government is concerned about the pollution of the environment. Kuwait
is also signatory t o the convention for the control of environmental pollution and the
deleterious e f fec t s of the ooastal developent within the Gulf. WH) would collaborate
with the Government and UNEP i n the developent of manpower capabi l i t i es i n a i r qual i ty
control, marine pollution problems of the Gulf and environmental improvement a c t i v i t i e s
i n the country.
Health manpower developent
Promotion of t ra in ina (Fellowships)
Manpower development is especially important for health services i n view of t h e i r
labour intensive nature. Importation of expatriates is only a temporary solution.
Eventually nationals would have to be trained for the various professional and middle
level positions. WH) would collaborate i n the t ra ining of national teachers, re-
or ientat ion of expatr ia te s t a f f t o prepare them t o meet the needs of the country and t o
t r a i n and reorient the nursing s t a f f through establishment of new nursing teaching pro-
g r m e s and in-service training.
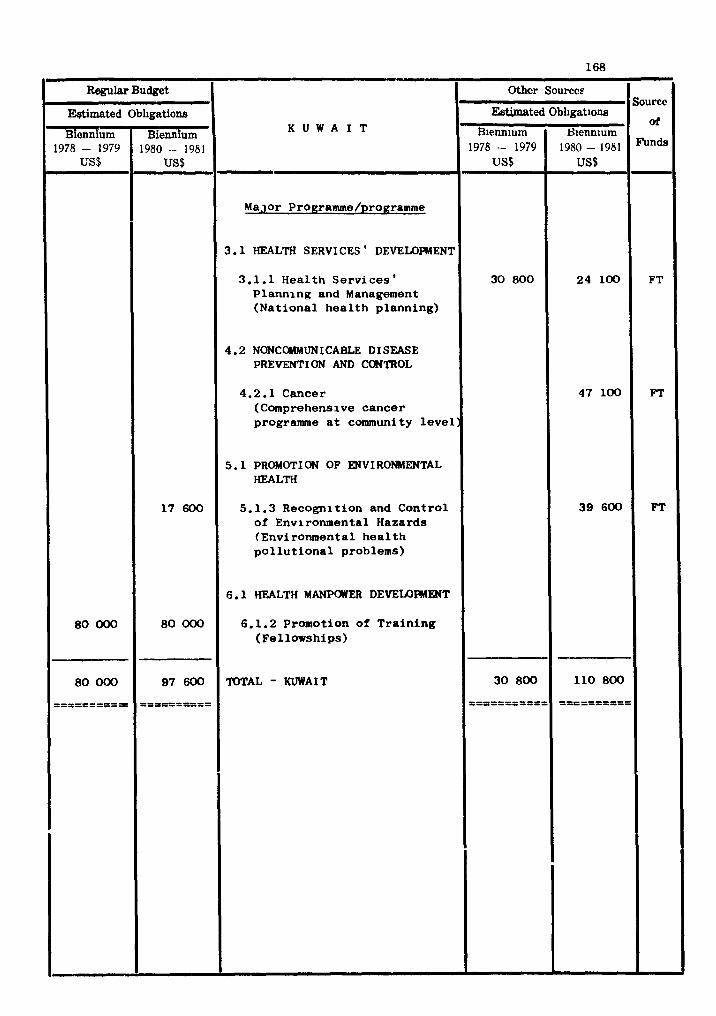
Regular Budget - Mimated Obligations
K U W A I T
-
Othcr Sourccs
Estimated Blennium
1978 - 1979 US$
30 800
30 800
======I====
- - -
Major Progrannne/pro~ramme
3.1 HEALTH SERVICES ' DEVELOFMENT
3.1.1 Hea l th S e r v i c e s 1 P l a n n i n g and Management ( N a t i o n a l h e a l t h p lann ing)
4.2 NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
4.2.1 Cancer (Comprehensive c a n c e r programme a t community l eve l :
5 .1 PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.3 Recogni t ion and C o n t r o l of Environmental Hazards (Environmental h e a l t h p o l l u t i o n a l problems)
6.1 HEALTH MANPOWER DEVELOEWMT
6.1.2 Promotion of T r a i n i n g (Fe l lowships )
TOTAL - KUWAIT
80 000
80 000
==========
1 7 600
80 000
97 600
53====2===
Source Obligatione
S~ennium 1980 - 1981 US$
24 100
4 7 1 0 0
3 9 600
110 800
==E===3===
- - -
or
-
FT
FT
FT
-- -
COUNTRY P R O C ~ STATEWT
LEBANON
NATIONAL HEALTH DEVEYAPMENT STRATEGY
The events of 1975 and 1976 have deeply disturbed the nat ional heal th planning
machinery, a s i n the o the r nat ional sectors , and the re was delay i n developing the
subaequest Five-Year Health Plan, taking i n t o account the changed manpower and heal th
se rv ices parameters.
However, the broad object ives of the Government a r e to:
- reorganize and strengthen the Ministry of Health, and i n pa r t i cu la r , t o e s t a b l i s h
a hea l th planning u n i t a s well a s t o revive and expand the c e n t r a l hea l th o t a t i s -
t i c a l u n i t ;
- reorganize the basic hea l th se rv ices and improve the hosp i t a l se rv ices administra-
t ion;
- s t e p up t r a in ing of personnel and gear the t r a in ing towards nat ional hea l th require-
ments;
- continue prevention and control of communicable d iseases and explore deeper the
epidemiology of the main non-communicable d iseases ; and
- implement a national environmental heal th programme with emphasis on water supply,
sewerage and disposal of s o l i d wastes.
TECHNICAL CO-OPERATION PRO- mR HEALTH
Health 8ervice development
A t the cen t ra l l eve l , a study group has made recomendations on the reorganisa-
t i o n and strengthening of the Ministry of Health. A nat ional heal th planning group
has been established.
Primary heal th care is del ivered through r u r a l and peri-urban dispensaries. Of
more than 300 dispensar ies a small proportion f a l l s under the j u r i s d i c t i o n of the
Ministry of Health; by and l a rge dispensar ies a r e or iented towards cura t ive medicine.
A ser ious reshaping of bas ic heal th se rv ices i s a f e l t need with a view t o improving
the overa l l coordination between the Ministry of Health, various groups and non-
governmental national agencies, t o design a proper s t a f f i n g pa t t e rn and a geographical
d i s t r i b u t i o n of bas ic u n i t s which w i l l ensure f a i r population coverage.
Of 143 hospi ta ls , 20 belong t o the Government and contain 1400 of the t o t a l of
11 370 beds. Logis t ics problems a r e recognized and the Government intends t o ex-
plore the def ic iencies i n the administrat ion of t h e i r hospi ta l services.
Maternal and chi ld heal th a r e beingstrengthened a s ex i s t ing f a c i l i t i e s , both
governmental and pr ivate , a r e inadequate t o meet growing demands.
Epidemiological s tud ies of mental i l l n e s s e s t o provide a bas is a r e required f o r
the improvement of the national mental heal th services i n accordance with recognized
in ternat ional standards.
The Government project fo r the advancement of pharmaceutical administrat ion i n
the Ministry of Health, includrng l eg i s la t ion , regulation, qua l i ty con t re l and drug
procurement and storage a s w e l l a s the establishment of drug information services
has been revived and w i l l continue i n 1980-1981.
Along with th strengthening of the Central Public Health Laboratory i n Beirut ,
plans a r e under way t o s e t up public heal th l abora to r ies i n the provinces and thus
t o develop a national public hea l th laboratory service. This w i l l back up the con-
t r o l of the major, pa r t i cu la r ly the communicable diseases and the reduction of en-
vironmental hazards.
WE?,) w i l l be ac t ive ly involved, i n a l l these a c t i v i t i e s , through 1980-1981.
Disease prevention and control
The higher ranking communicable diseases a r e typhoid and paratyphoid fevers,
r e sp i ra to ry tuberculosis, schistosomiasis, v i r a l hepatitis and poliomyelitis. The
extent of p a r a s i t i c d iseases i s not known. I n absolute f igures i t can be s t a t e d
t h a t the global problem of comunicable diseases does not represent a cause of major
public hea l th concern. However, s t r i c t epidemiological vigilanoe w i l l be maintained
and an expanded immunization programme i s being implemented. The n o t i f i c a t i o n
system is being revived.
I n 1980/1981 WHO w i l l continue t o col laborate c lose ly i n the f i e l d of epidemio-
log ica l surveil lance.
b n g the non-comunicalbe diseases, the Government w i l l g ive more emphasis t o
the epidemiology and control of cancer and the cardiovascular diseases. These a r e
the two spec i f i c f i e l d 6 i n wMch WHO w i l l be ac t ive ly involved i n 1980/1981.
Prolaotion o f environmental hea l th
The major th rus t w i l l be towards the provision of s a f e water, d isposal of used
and r a i n waters, co l l ec t ion and disposal of s o l i d wastes, prevention of coas ta l water
pol lu t ion and control of o the r environmental hazards. A s the e n t i r e undertaking is
complex, expensive and time-consuming, the Government is counting on ipnu t s freni
various sources i n support of the nat ional e f f o r t .
I n 1980/1981 WHO w i l l be c lose ly col laborat ing i n the National Waste Management
Plan.
Health manpower development
Both the r a t i o s and the geographical d i s t r i b u t i o n of personnel need improvement,
and f o r t h i s , heal th manpower planning and management require strengthening. The
current Five-Year National Plan, provides the bas i s f o r the e f f o r t i n t h i s d i rec t ion.
I n medical education the main tasks w i l l be t o evaluate the undergraduate curriculum
i n r e l a t i o n t o the hea l th needs of the country and t o review coordination between
t r a in ing i n s t i t u t i o n s . The redevelopment of the Government Nursing School w i l l
continue and its curriculum w i l l be revised.
I n 1980/1981, W H O w i l l co l laborate i n the above described process.
Health information
The revival and strengthening of Health S t a t i s t i c s se rv ices w i l l continue. The
Ministry of Health is f u l l y aware that data co l l ec t ion , processing and ana lys i s a r e
the beckbone of planning, implementation and evaluation. The major a r e a s t h a t w i l l
receive c lose a t t e n t i o n a re :
- the establishment of a c e n t r a l s t a t i s t i c a l department a t the Ministry of Health,
and
- the establishment of recording and repor t ing a t a l l l e v e l s including the t r a i n i n g
of personnel.
W I I ) i n 1980/1981 w i l l co l laborate c losely i n the a c t i v i t i e s enumerated.
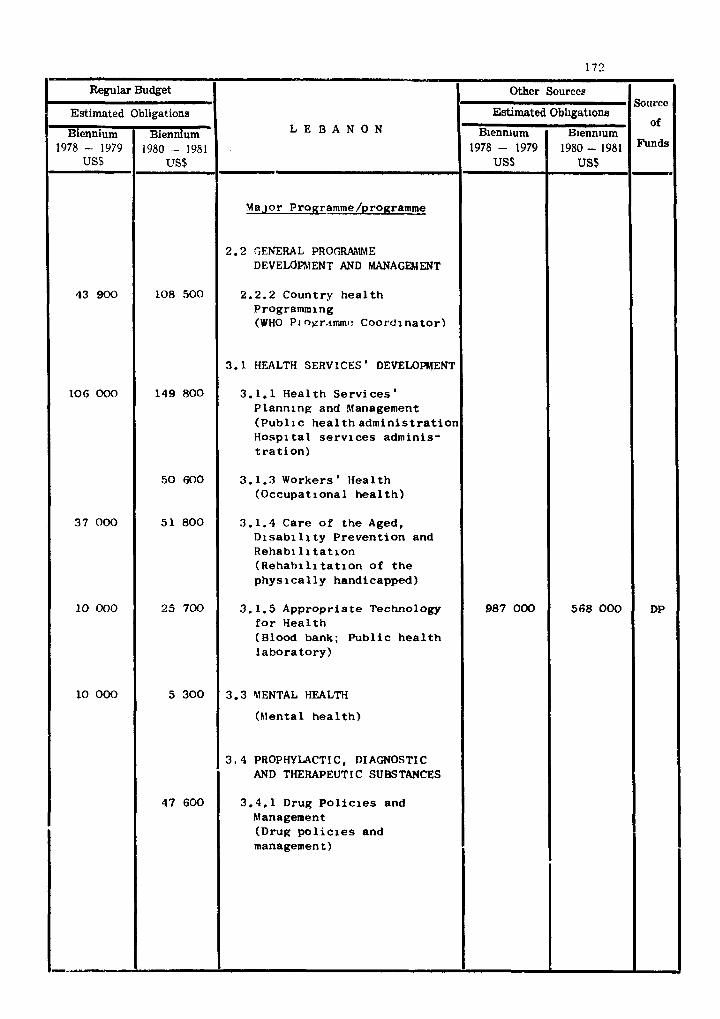
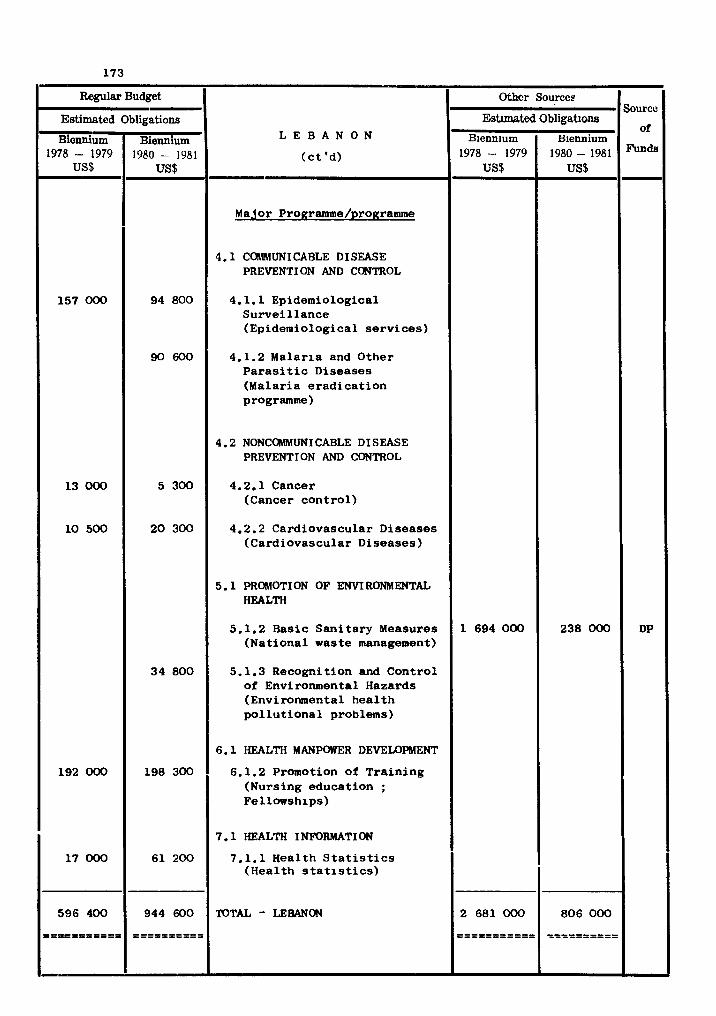
COUNTRY PROGRAMME STATEMENT
LIBYAN ARAB JAMAH1 RI YA
NATIONAL HEALTH DEVELOPMENT STRATEGY
Provision of curative and preventive health services on an integrated and decen-
t ra l ized basis, f ree of charge t o a l l c i t izens, has been the essence of the national
health policy since 1969. The main objectives s e t for th t o implement t h i s policy a re
(a) eradication of endemic and epidemic diseases, (b) expansion and decentralization
of health f a c i l i t i e s and services, (c) t ra ining of health personnel of a l l categories,
and (d) a t ta ining eventual self-sufficiency i n the production of cer ta in therapeutic
substances.
The above objectives a re amply ref lected i n the s t ra teg ies adopted for health
development ac t i v i t i e s tha t are integrated into the current five-year (1976-80)
National Development Plan,
The Jamahiriya has made rapid s t r i de s i n developing i ts health services. Overall
phys lc lhea l th f a c i l i t i e s (such as hospitals, polyclinics, health centres) have been
nearly doubled, the budgetary resources have been t r ip led and the health s t a f f of variom
categories has increased fourfold.
The f i e l d s t o which the Government has given pr ior i ty and i n which WHO technical
collaboration is anticipated i n 1980-81, are (a ) health manpower development, (b) prim-
ary health care, (c ) health administration and management, (d) ra t ional production
and dis t r ibut ion of pharmaceuticals, and (e ) promotion of applied research on health
problems of importance t o developing countries.
TECHNICAL COOPERATION PROGRAMMES FOR HElZLTH
Prmary health care and health services development
The decentralization of health services received a strong impetus with the creation
of health directorates (Murakbat E l Saha) for each municipality. New hospi ta ls and
health un i t s have extended coverage t o previously under-served communities. The crea-
t ion of peoples' Health C o m m i t t e s , an element of the new po l i t i c a l s t ructure , has
f a c i l i t a t e d increased community participation i n health services. The Government,
with the collaboration of WHD, has made an evaluation of the mpact of basic health
services with a view to further strengthening them, par t icular ly front-l ine health care.
WH) w i l l continue, i n 1980-81, i ts cooperation with the Government i n the evaluation
of its programmes of immunization, disease control, health education, water supplies
and sani ta t ion, a l l of which a re components of community development. W H D technical
collaboration is also planned to strengthen supportive services such as nationalhealth
information systems, and health administration and management.
Disease prevention and control
The control programmes for tuberculosis and trachoma have been highly successful.
The compulsory immunization programme though requiring further improvements, has
brought about a declining prevalence of some infectious diseases. The Government . while recognizing the need t o continue these e f for t s , proposes t o organize control
programmes for other health problems, including non-communicable diseases. I t is
planned accordingly to enlarge the present endemic diseases un i t in to an endemic and
non-communicable disease unit . WH) w i l l work closely with t h i s uni t and i n 1980-81
w i l l be involved i n periodical evaluation of the prograrmmes with a view to the i r
integration into basic health services, and i n the development of epidemiological
s tudies and preventive measures against problems such as rheumatic and other cardio-
vascular diseases, diabetes, cancer, v i ra l diseases, bi lharziasis , cutaneous leishma-
n ias i s and especially rodent plague which is posing a threat t o communities i n sca t t -
ered areas. The country w i l l take advantage of the Organizatim's programmes of
technical cooperation i n the qual i ty control and production of drugs and biologicals
locally o r regionally and of support t o national seminars for the dissemination of
drug information and the concept of essent ia l drugs t o ra t ional ize drug use and
expenditures incurred on them. WH) w i l l continue t o collaborate i n t h e reorganization
of mental health services and the development of preventive ophthalmological sorvices.
Promotion of environmental health
Considerable investments are being channelled through the Secretar ia ts of
Municipalities and Housing for the provision of sa fe water and sani ta t ion programmes.
The Secretar ia t of Health continues t o s e t up standards, promulgate necessary legis la-
t ion and generally coordinate ac t i v i t i e s i n t h i s f ie ld . Systems of water supply and
sewage disposal are constantly being upgraded to meet the needs of growlng c i t i e s and
towns. Increasing at tent ion is being given to t h e disposal of industr ia l wastes,
and coastal water monitoring and pollution control. Other environmental hazards
including t r a f f i c accidents have been a source of concern and the Government proposes
to invest igate these problems with a view t o organizing programmes of prevention.
WHO w i l l continue to collaQorate i n these e f f o r t s through i n f ~ r m a t i o n t r ans fe r , provi-
s ion of appropriate technology, study and survei l lance of environmental heal th problems,
t r a in ing of personnel and promotion of san i t a ry measures with emphasis on the needs
o l r u r a l areas.
:leal t h manpower development
The T;ovornment is giving t h i s a c ~ i v i t y high p r io r i ty . The t o t a l heal th s t a f f
increased fourfold between 1971 and 1978. While the immediate s t a f f i n g needs of
a l l heal th establishments a r e being met by d i r e c t recruitment o r on the bas is of b i l a t -
e r a l technical cooperation w i t h f r iendly countries, utmost ihrportance is being given
t o the development of nat ional manpower i n a l l hcal th f i e l d s . The new schools fo r
a s s i s t a n t nurses a r e t o be strengthened s t ead i ly and new t ra in ing programmes a r e being
i n i t i a t e d . WHO w i l l continue t o col laborate with nat ional medical and heal th t r a in ing
i n s t i t u t i o n s i n curriculum development, evaluation of t r a i n i n g programmes, introduction
of modern teaching techniques, and provision of teachers, teaching a ids and l i t e r a t u r e .
Special a t t en t ion w i l l be given through the fellowships programme to the t r a in ing of
personnel i n p r i o r i t y areas such a s primary heal th care, heal th administrat ion and
management,and heal th se rv ices research.
Health information
Advisory services to review the health s t a t i s t i c a l a c t i v i t i e s were provided i n
1976, and a plan f o r t h e i r strengthening followed. A na t iona l is presently following
postgraduate s tud ies t o head on re tu rn the heal th s t a t i s t i c a l services , and a number
of nat ionals a r e being t r a ined a s middle l eve l personnel. WHO col laborat ion w i l l
continue t o fu r the r develop the heal th s t a t i s t i c a l i n f r a s t r u c t u r e and expansion of
a c t i v i t i e s .
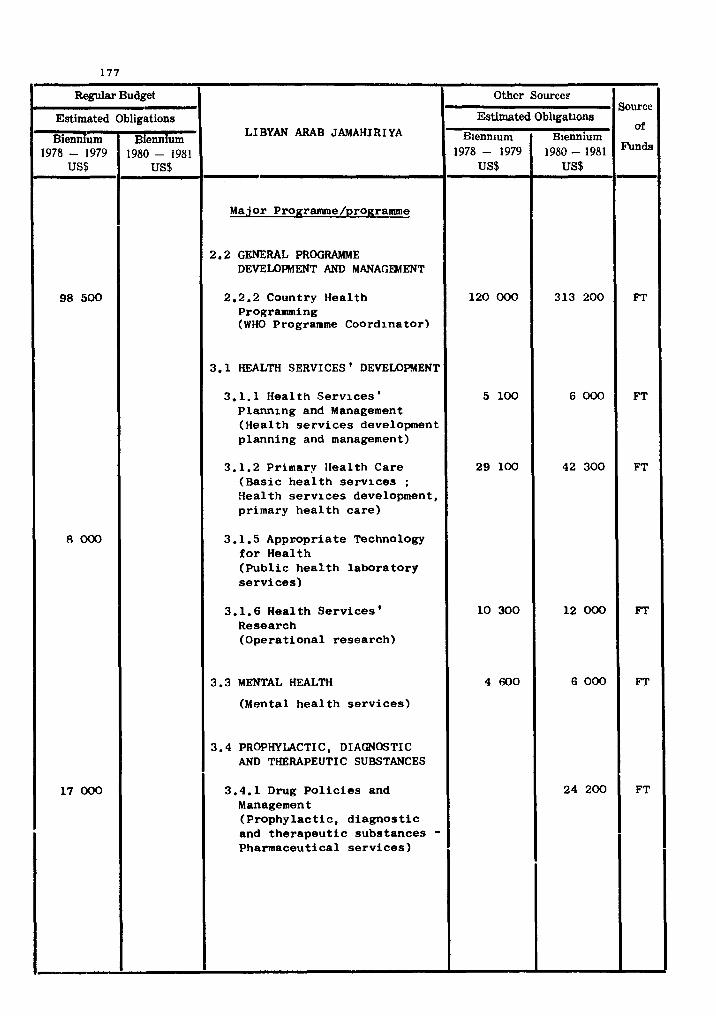
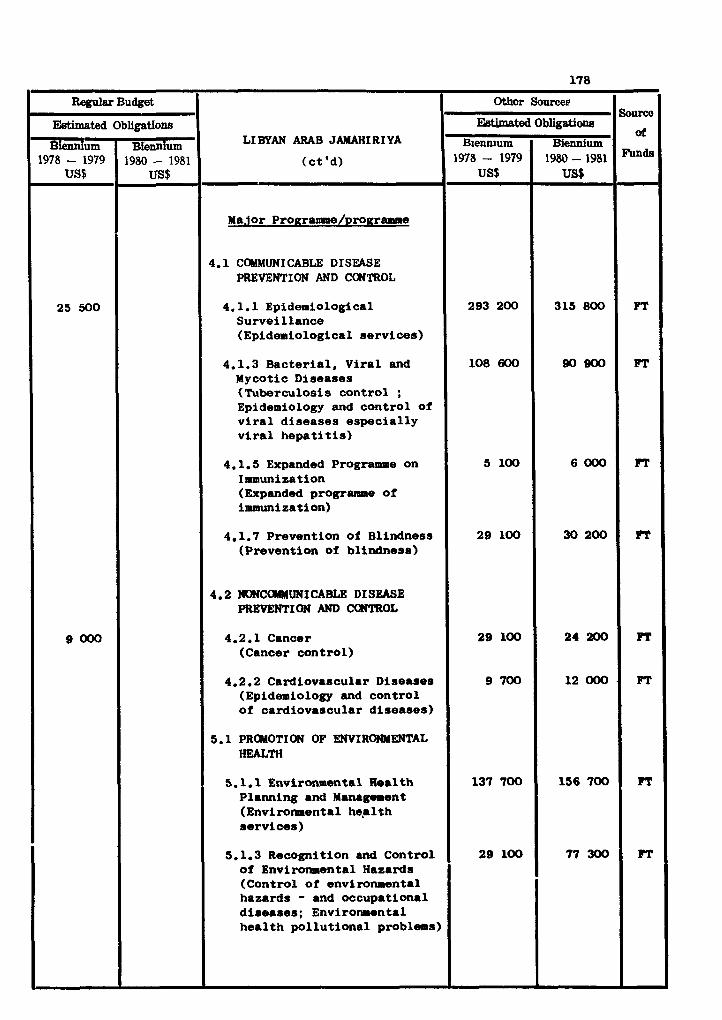
Regular Burnt
LI BYAN ARAB JAMAHIRI YA
(ct 'd) - Major Proaramme/~ro~ramme
4.1 CmMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.1 Epidemiological Surveillance (Epidemiological services)
4.1.3 Bacterial, Viral and Mycotic Diseases (Tuberculosis control ; Epidemiology and control of viral diseases especially viral hepatitis)
4.1.5 Expanded Programme on Immunization (Expanded programme of immunization)
4.1.7 Prevention of Blindness (Prevention of blindness)
4.2 NONCOMMUNICABLE DI S W E PREYENTION AND CWTROL
4.2.1 Cancer (Cancer control)
4.2.2 Cardiovascular Diseases (Epidemiology and control of cardiovascular diseases)
5.1 PROMOTION OF ENVIROMaENTAL HEALTH
5.1.1 Environmental H.alth Planning and Management (Environnental heplth services)
5.1.3 Recognition and Control of Envirornmental Hazards (Control of environmental hazards - and occupational diseases; Environmental health pollutional problems)
EWmated
1978 - 1979 US$
25 500
9000
- Obligatio118
1980 - 1981 US$
Sourco
or
PT
FT
FT
FT
FT
FT
FT
FT
Othcr Sourcee
EWmated Biennium
1978 - 1979 US$
293 200
108 600
5 100
29 100
29 100
9 700
137 700
29 100
Obligatiw
Biennium 1980 - 1981 US$
315 800
SOB00
6000
30 200
24200
12000.
156 700
77 300
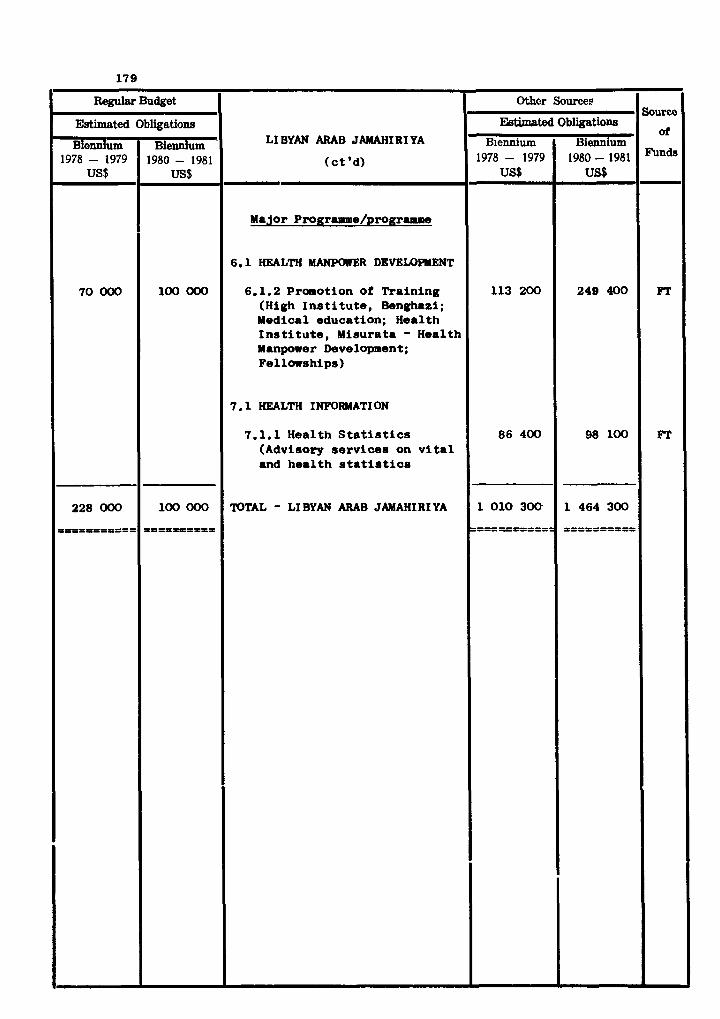
Regular Budget
Estimated
Biennium 1978 - 1979
US$
70 000
228 OOO
O=PPPI=P=IP
Sourco
of
Funds
FT
FT
LIBYAN ARAB JAMAHIRIYA
( c t 'd)
Ma lor Programme/programm
6.1 HEALTH MANPOslER DEVELOPHENT
6.1.2 Proaot ion of Tra in ing (High I n s t i t u t e , Benghazi; Medical education; Health I n s t i t u t e , Misurata - Health Manpower Development; Fellowships)
7.1 HEALTH INFORMATI ON
7.1.1 Health S t a t i s t i c s (Advisory s e r v i c e s on v i t a l and h e a l t h statistics
TOTAL - LIBYAN ARAB JAMAHIRIYA
Obligations
Biennium ' 1980 - 1981
US$
100 000
100 000
I P = P h t = = D
Othcr Sources
EWawted Biennium
1978 - 1979 US$
113 200
86 400
1 010 300
=====a======
Obligatians
Biennium 1980 - 1981 US$
249 400
98 100
1 464 300
P I = I = I P P P I

COUNTRY PROGRAlYME STATBdSJT
o x NATIONAL HEALTH DEVEU)PIIIFNT STRATEGY
The f i r s t Five-Year Developent Plan was formulated for the period 1976-80 by the
Developent Council, the interminis ter ial body responsible for national sooie-io
developent planning.
One of the resolutions of the Council defines a s a primary target of the plan: " t o narrow the gap i n the standards of l iving i n different regions with special
emphasis on the l ea s t developed regions".
Other resolutions deal specif ical ly w i t h the hgalth f ie ld: "to impro*r rmtr i t ional
and public health conditions" and "providing for sc ien t i fc studies i n relat ion to water
resources and ways of preserving and increasing its supply".
The capi ta l expenditure component of the health developlent budget fo r the biennium
1980-81 remains, a s for previous years, a t approximately 18 million dol lars per year.
Recurrent expenditure which for 1978 was 33 million dollars, is expected to inoreaae i n
l i n e with the expansion of health services.
Country health programming is tentatively scheduled fo r 1979.
The stage of developolent of the country, where foma l education has begun only very
recently, obliges the health sector t o rely heavily on the services of expatr ia te s ta f f .
However, as more nationals with basic education became available fo r training, the pro-
portion of Omani personnel in the health services w i l l inereme rapidly.
W H ) cooperation has s ignif icant ly expanded over recent years and the Organization's
services a r e being well u t i l i zed by the Government.
TECHJICAL COOPERATICN PROGRAMhlES FOR HEALTH
General programne develoment, management and co-ordination
The WK) Programme Coordinator w i l l continue to part ic ipate i n the developnent of
country health programming i n the context of the national 8ooio-economic developeet
plans, and w i l l ensure a t country level, --ordination with the United Nations p r o g r m s
related t o the health field.
Development of wmprehensive health services
The development of an integrated approach to the delivery of health care remains a'"
major pre-occupation of the Ministry of Health. Against a background of division and
and separate ac t i v i t i e s of the curative and preventive departments, the advocated
policy of the Government for the future is an integrated approach to comprehensive
health care for the en t i r e population. This w i l l require a change i n the orientation
and qual i ty of s ta f f which w i l l be pursued progressively i n the coming years.
Physical health f a c i l i t i e s a re expected t o be suf f ic ien t i n the biennium to
provide adequate coverage to the population. To achieve the objective of affording
comprehensive health care t o the en t i r e population, additional s ta f f w i l l have t o be
recruited, and others w i l l have t o be replaced o r re-trained.
Pr ior i ty w i l l be accorded, i n the context of an integrated approach to health care
delivery, t o an accelerated development of maternal and chi ld health services so tha t
they can be available t o the en t i r e rura l population by the end of the biennium.
Simultaneously, studies on the nu t r i t iona l s ta tus of the young w i l l lead to the
development of a national nu t r i t ion policy.
To promote the achievement of the proposed goals, the recently established na-
t ional health. education committee w i l l be concerned with the strengthening of the
Health Education Section.
The s ignif icant improvement which has taken place i n the health s t a t i s t i c a l system
w i l l be reinforced.
WHO cooperation is expected i n the planning and implementation of this policy.
Disease prevention and control
Malaria const i tutes a major problem. During the biennium, the Malaria Control
Programme w i l l cover the e n t i r e national t e r r i to ry , on the basis of the par t ic ipat ion
of a l l the health services and the communities themselves.
WK) w i l l continue t o afford technical co-operation par t icular ly i n the f i e ld s of
t ra ining personnel and planning. UNDP rill remain a par t ic ipant i n t h i s programme.
The Ikpanded Programmeon I~ll~unizationlaunchedon a country-wide basis a t the end
of 1977, w i l l continue to be implemented by the bait health services on a t o t a l
coverage basis.
The programme on the prevention of blindness w i l l be strengthened with progressive
expansion to a l l vulnerable segments of the population and wi l l include vector control
and hygiene measures besides drug administration.
The o ra l health programme w i l l be developed to include pre-school children besides
those already attending school.
WH3 w i l l par t ic ipate i n a l l these programmes through the provision of wnsul tant-
ships, t ra ining and basic supplies and equipment.
Promotion of environmental health
The inadequacy of sa fe water supply and S a n i t a t i ~ n systems account predominantly
for causes of diseases and deaths, par t icular ly with infants and children of ru ra l
communities.
Responding t o the appeal of the populations involved and i n concomitance w i t h the
launchingo-fthe International Drinking Water and Sanitation Deoades, the Government w i l l
endeavour t o provide t o the ru ra l population water supply f a c i l i t i e s based on simple
and r e l i ab l e systems. The Government w i l l concurrently s t r i v e t o improve human wastes
disposal systems in a l l areas.
W H ) w i l l be requested t o par t ic ipa te fu l ly i n these undertakings by providing
technical operational personnel and co-operating i n the t ra in ing of s ta f f and education
of the communities.
Health manpower development
While the need for a large number of expatr ia te medical and para-medical personnel
t o s t a f f the health services w i l l continue, with the increasing ava i lab i l i ty of educated
nationals t ra ining programmes i n the various health f i e l d s will be of paramount impor-
tance. The overall training programme w i l l have t o be oriented to provide qualified
s t a f f t o carry out functions according to t he new pol ic ies of the Government. Physical
f a c i l i t i e s allowing the conduot of national multidisciplinary health training programmes
basis w i l l have been provided before t h e s t a r t of the biennium.
Health information
The Government is keen about strengthening the health s t a t i s t i c a l services,
being fu l ly aware tha t proper health data are the backbone of planning,im@lea~entation
and evaluation of health services.
WH) contributed i n the assessment of needs and i n preparing a plan fo r developent
of the health s t a t i s t i c a l services.
WH: 111 continue collaboration through provision of advisory services and t ra in ing
of natic---a1 s t a f f .
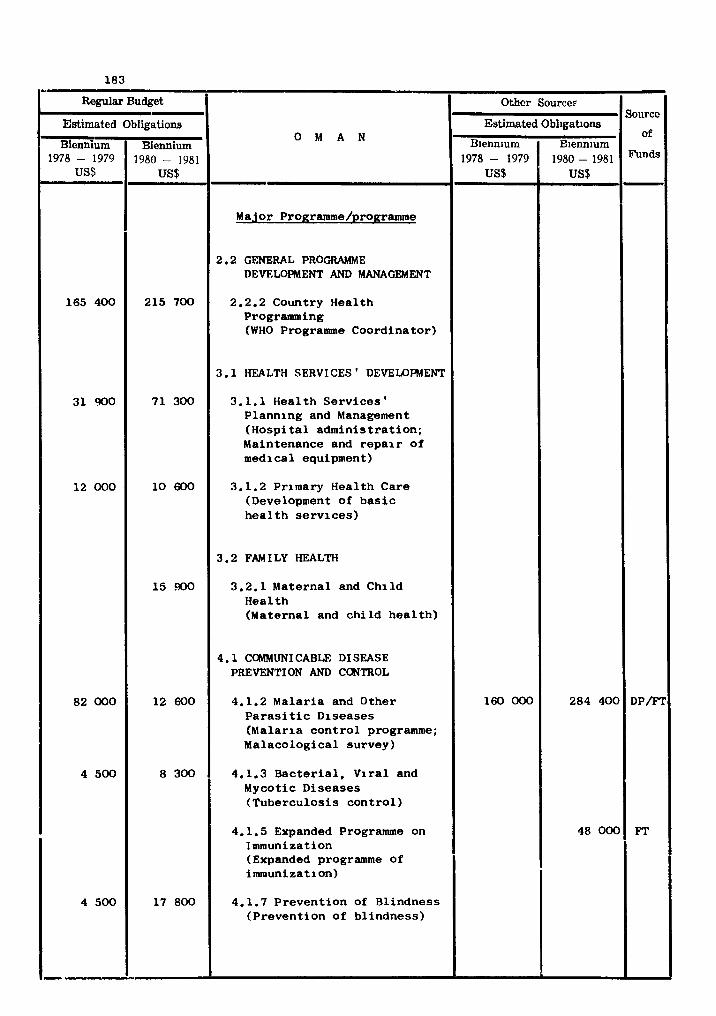
Regular Budget
O M A N
Major Pro~ramme/pro~ramme
2.2 GENERAL PROGRAMME DEVELOFWENT AND MANAGEMENT
2.2.2 Country Hea l th Programming (WHO Programme Coord ina tor )
3.1 HEALTH SERVICES ' DEVELOPMENT
3.1.1 Hea l th S e r v i c e s ' P lann ing and Management ( H o s p i t a l a d m i n i s t r a t i o n ; Maintenance and r e p a i r o f medica l equipment)
3.1.2 Primary Hea l th Care (Development of b a s i c h e a l t h s e r v i c e s )
3.2 FAM I LY HEALTH
3.2.1 Mate rna l and C h i l d H e a l t h (Maternal and c h i l d h e a l t h )
4.1 COMMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.2 M a l a r i a and Other P a r a s i t i c Diseases (Mala r ia c o n t r o l programme; Malaco log ica l su rvey)
4.1.3 B a c t e r i a l , V i r a l and Mycotic D i s e a s e s ( T u b e r c u l o s i s c o n t r o l )
4.1.5 Expanded Programme on Immunization (Expanded programme of i m u n i z a t i o n )
4.1.7 P r e v e n t i o n of Bl indness ( P r e v e n t i o n of b l i n d n e s s )
Estimated - Biennium
1978 - 1979 US$
165 400
3 1 900
12 000
82 000
4 500
4 500
Obligations
Biennium 1980 - 1981
US$
215 700
7 1 300
10 600
1 5 XI0
12 600
8 300
17 800
Othcr Source?
Estimated
Biennium 1978- 1979
US$
160 000
Obligations
Biennium 1980-1981
US$
284 40(
48 00(
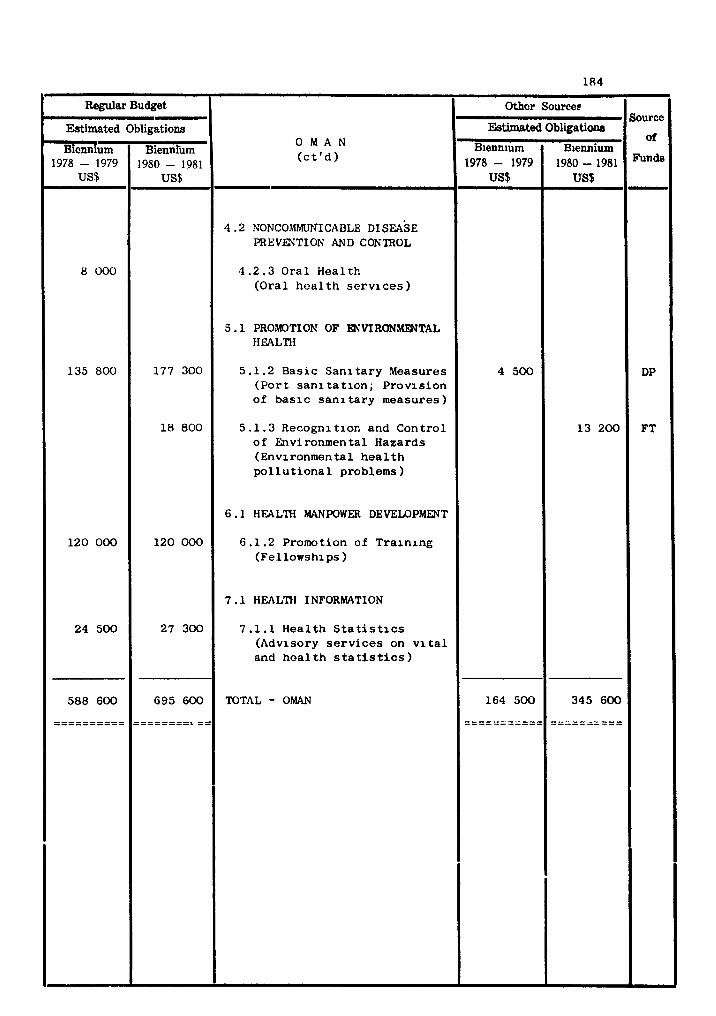
Regular Budget
O M A N ( c t ' d )
4 .2 NONCOMMUE~I CABLE DISEASE PREVENTION AND CONTROL
4 . 2 . 3 O r a l H e a l t h (Ora l h e a l t h s e r v i c e s )
5 .1 PROMOTION OF ENVIRONWTAL HEALTH
5.1.2 Bas ic S a n i t a r y Measures ( P o r t s a n i t a t i o n ; P r o v i s i o n of b a s i c s a n i t a r y measures )
5 . 1 . 3 Recogni t ion and Cont ro l o f Environmental Hazards (Environmental h e a l t h p o l l u t i o n a l problems)
6 .1 HEALTH MANPOWER DEVELOPMENT
6.1.2 Promotion of T r a i n i n g (Fe l lowships )
7 .1 HEALTH INFORMATION
7 .1 .1 H e a l t h Statistics (Advisory s e r v i c e s on v i t a l and h e a l t h s t a t i s t i c s )
TOTAL - OMAN
Estimated
Biennium 1978 - 1979
US$
8 000
135 800
120 000
24 500
588 600
---------- ----------
- Obligations
Bienniium 1980 - 1981
US$
177 300
18 800
120 000
27 300
695 600
-------- --------L ==
Source
of
DP
FT
Othor source^
Estimated
Blennlum 1978 - 1979
US$
4 500
164 500
- - - - - - - - - - - -----------
Obligations
Biennium 1980 - 1981 US$
1 3 200
345 600
- - - - - - - - - - ----------
COUNTRY PROGRAMME STATEMENT
PAKI STAN
NATIONAL HEALTH DEVELOPMENT STRATEGY
The na t iona l h e a l t h development s t r a t e g y has been formulated wi th in the frame-
work of t he hea l th pol icy promulgated i n 1976 and programmed i n a country h e a l t h
programing exerc ise . The h e a l t h p lan a i m s a t a coverage of 50% of the populat ion
wi th bas i c hea l th c a r e by 1981.
The p r inc ipa l pol icy o b j e c t i v e s o f the p lan are t o move from a predominantly
medical s e rv i ce t o a t h r e e - t i e r system manned by phys ic ians , h e a l t h a u x i l i a r i e s and
community h e a l t h workers, wi th a major expansion o f bas i c h e a l t h s e r v i c e s i n r u r a l
a r eas ; t o progress ive ly i n t e g r a t e s p e c i a l h e a l t h and hea l th - r e l a t ed programmes wi th
the bas i c h e a l t h s e rv i ces ; and t o s h f t the emphasis from c u r a t i v e t o prevent ive
measures. Targets have been set f o r populat ion coverage by h e a l t h s e rv i ces , f o r
malaria con t ro l , f o r thecont ro l o f communicable d i s e a s e s o f ch i ldren , and f o r environ-
mental h e a l t h serv ices .
The preventive programme, i n which community h e a l t h workers w i l l be a c t i v e , w i l l
be implemented through the Expanded Programme on Immunization and the improvement o f
environmental s an i ta t ion .
TECHNICAL COOPERATION PROGRAMMES FOR HEALH
Health s e r v i c e s development
The provision o f f ron t - l i ne h e a l t h c a r e t o remote and underaerved communities,
which has been a f e a t u r e of h e a l t h s e r v i c e s development i n Pakis tan f o r s e v e r a l years,
w i l l be extended and r e in fo rced wi th emphasis on community p r t i c i p a t i o n and o v e r a l l
c o m u n i t y development. The na t iona l h e a l t h p lan provides f o r t h e continued develop-
ment of basic h e a l t h r a r v i c e s p a r t i c u l a r l y i n r u r a l a r eas . WHD w i l l co l l abo ra t e by
providing s t a f f and advisory s e r v i c e s f o r t he improvement o f family h e a l t h and w i l l
a l s o g ive s p e c i a l a t t e n t i o n t o t h e development of c o m u n i t y h e a l t h workers.
WHD w i l l a l s o cooperate i n t h e development o f t he na t iona l h e a l t h l abo ra to ry
s e r v i c e , i n workers' h e a l t h and i n r e in fo rc ing the h e a l t h educat ion programme.
A l a r g e pharmaceutical i ndus t ry has grown i n the country and WHD is co l l abora t -
i n g i n developing drug p o l i c i e s and q u a l i t y c o n t r o l o f pharmaceuticals.
Disease p reven t ion and c o n t r o l
There is a n o v e r a l l f a l l i n t h e i n c i d e n c e o f m a l a r i a and t h e c o n t r o l programme
is being g r a d u a l l y i n t e g r a t e d w i t h t h e c o n t r o l o f connnunicable d i s e a s e s i n g e n e r a l .
W H O c o l l a u o r a t i o n w i l l c o n t i n u e i n t h e form o f c o n s u l t a n t s e r v i c e s , t h e ass ignment
of n a t i o n a l s t a f f , f e l l o w s h i p s , and s u p p l i e s and equipment.
W H O w i l l be a s s o c i a t e d s u b s t a n t i a l l y through t h e Expanded Programme on Immun-
i z a t i o n w i t h t h e c o n t r o l o f t h e communicable d i s e a s e s o f c h i l d r e n .
A comprehensive cancer c o n t r o l programme i s be ing developed - a cancer r e g i s t r y
was e s t a b l i s h e d i n 1978 and W H O c o l l a b o r a t i o n i n t h i s f i e l d w i l l con t inue .
Promotion o f environmental h e a l t h
The a r e a s i n which WHO c o l l a b o r a t i o n w i l l c o n t i n u e i n 1980-1981 a r e t h e p lann ing
and managment o f environmental h e a l t h s e r v i c e s , wa te r supp ly systems and t h e c o n t r o l
o f environmental hazards .
Hea l th manpower development
The c r u c i a l r o l e o f h e a l t h manpower development f o r t h e promotion o f h e a l t h
s e r v i c e s i s mani fes ted by t h e p r i o r i t y r o l e accorded t o i t by t h e n a t i o n a l a u t h o r i -
ties. The implementation o f t h e new t h r e e - t i e r system o f h e a l t h s e r v i c e s depends
on a s u b s t a n t i a l i n c r e a s e i n t h e amount and q u a l i t y o f t r a i n i n g programmes f o r h e a l t h
a u x i l i a r i e s and pr imary h e a l t h c a r e workers , w h i l e a t t h e same t i m e a n o r i e n t a t i o n
o f p r o f e s s i o n a l e d u c a t i o n towards community s e r v i c e s must be emphasized. T h i s c a l l s
f o r much more communication between t h e h e a l t h - s e r v i c e and e d u c a t i o n sys tems a s w e l l
a s f o r t h e a v a i l a b i l i t y o f s k i l l e d e d u c a t i o n a l a d m i n i s t r a t o r s and t e a c h e r s . WHO is
c o n t i n u i n g i ts c o l l a b o r a t i o n , i n t h e c o n t e x t o f t h e medium-term programme i n h e a l t h
manpower development, i n v a r i o u s a s p e c t s of h e a l t h s e r v i c e s and manpower development.
H e a l t h i n f o r m a t i o n
The problem is n o t s o much t h e u n a v a i l a b i l i t y o f t r a i n e d h e a l t h s t a t i s t i c a l
pe rsonne l . Ra ther t h e r e i s need f o r s t r e n g t h e n i n g of t h e p r o v i n c i a l h e a l t h s t a -
t ist ical s e r v i c e s , and an o v e r a l l r e o r g a n i z a t i o n o f t h e n a t i o n a l h e a l t h s t a t i s t i c a l
s e r v i c e s t o e n s u r e t h e a v a i l a b i l i t y o f t ime1 y, r e l i a b l e and u s a b l e i n f o r m a t i o n , and
t h e f r e e f low o f t h a t i n f o r m a t i o n between t h e p r o v i n c i a l and c e n t r a l l e v e l s . W H O
c o l l a b o r a t i o n w i l l c o n t i n u e i n t h i s a r e a .
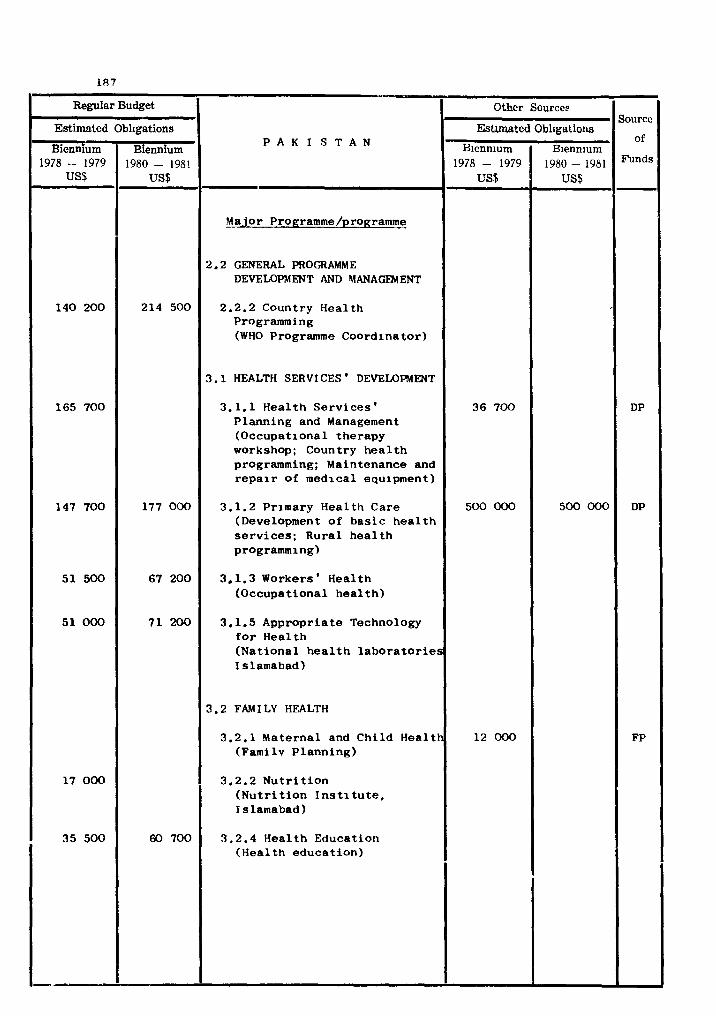
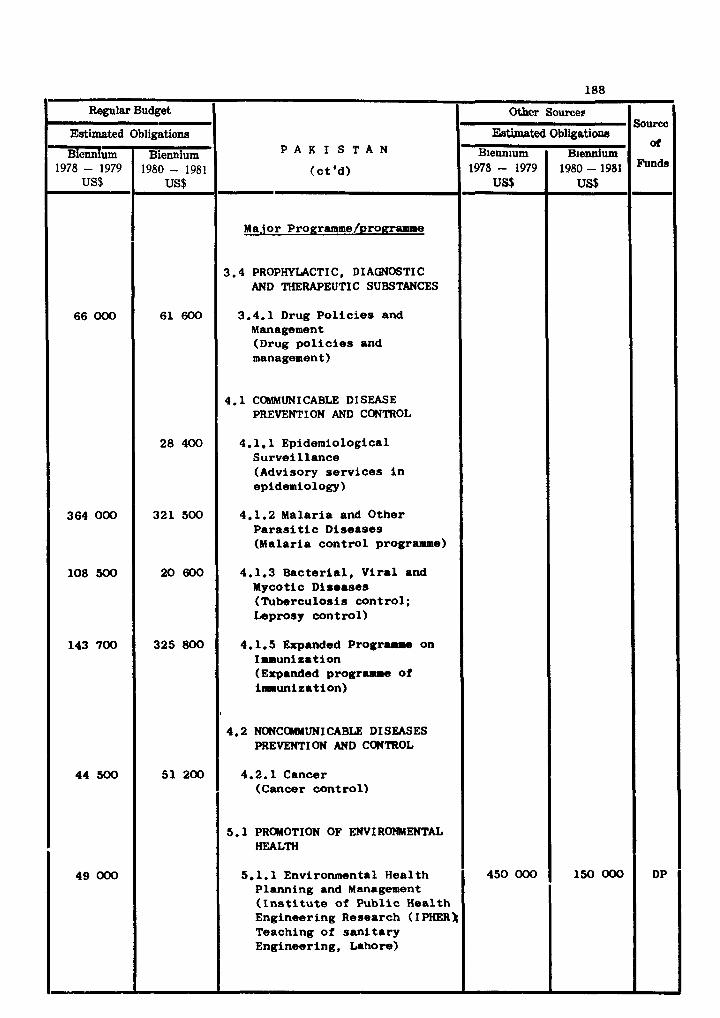
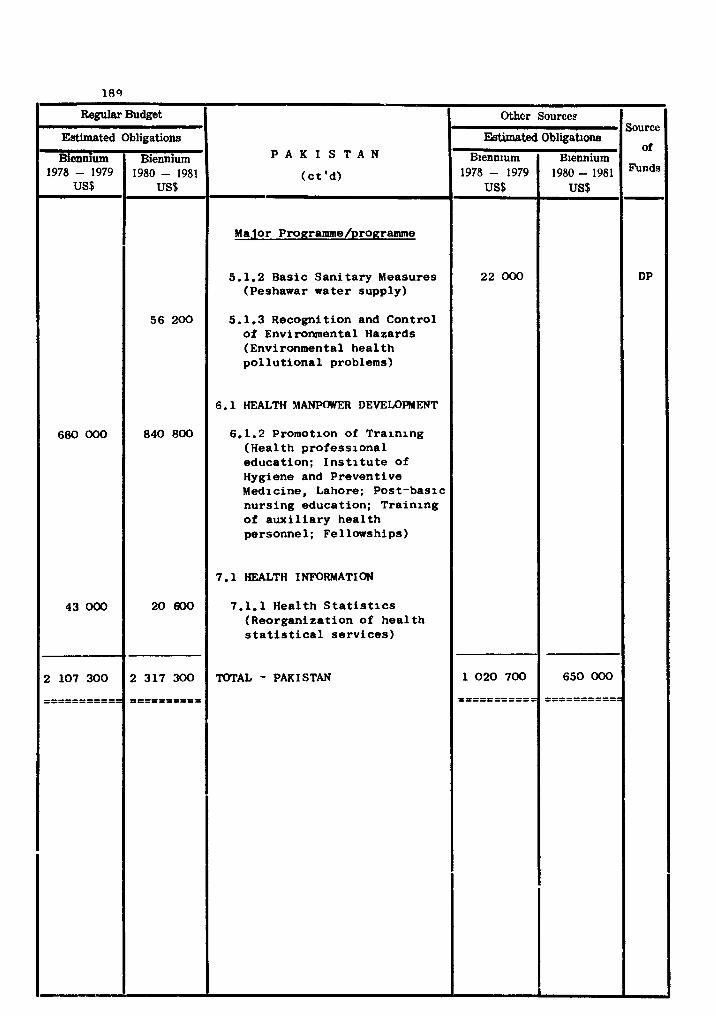
Regular Budget
P A K I S T A N
(ct 'dl - Major Prouramme/programme
5.1.2 Basic Sanitary Measures (Peshawar water supply)
5.1.3 Recognition and Control of Environmental Hazards (Environmental health pollutional problems)
6.1 HEALTH MANPOWER DEVEmRHENT
6.1.2 Promotion of Training (Health professional education; Institute of Hygiene and Preventive Medicine, Lahore; Post-basic nursing education; Training of auxiliary health personne 1; Fellowships)
7.1 HEALTH I NFORMATI ON
7.1.1 Health Statistics (Reorganization of health statistical services)
TOTAL - PAKISTAN
Estimated
Biennium 1978 - 1979
us9
680 000
43 000
2 107 300
----------- -----------
Obligations
Biennium 1980 - 1981
US$
56 200
840 800
20 600
2 317 300
---------- ----------
Sourcc
of
-
DP
Other Sources
Estimated
Blenn~um 1978 - 1979
US$
22 000
1 020 700
----------- -----------
Obligations
Blennium 1980 - 1981 US$
650 000
----------- -----------

COUNTRY PROGRAYYE STATEMENT
NATIONAL HEALTH DEVELOPME?iT STRATEGY
The nat ional heal th development s t r a t egy is formulated i n a nat ional hea l th plan
prepared by the Government i n 1978 with the col laborat ion of W H D and other i n t e r -
national and mul t i l a t e ra l agencies.
The p r i o r i t i e s spec i f i ed i n the plan a r e ( a ) primary hea l th care , (b) hea l th
manpower development, ( c ) the upgrading of hosp i t a l s and c l i n i c s , (d ) the commission-
ing of a new 660-bed general hosp i t a l , ( e l the in t roduct ion of new medical spec ia l i -
ties t o reduce t r ave l l ing abroad f o r treatment, ( f ) the upgrading and strengthening
of preventive heal th se rv ices by the creat ion of specia l ized u n i t s and an increased
a l loca t ion of resources.
The plan envisages the strengthening of t h e organizat ional and managerial s t r U C -
t u r e of the Ministry of Health and of the adminis t ra t ive i n f r a s t r u c t u r e i n general ,
a s well a s the reinforcement of technical cadres.
TECHNICAL CO-OPERATION PROGRAMMES FOR HEALTH
Primary heal th ca re
The Government is committed t o a primary care system based on hea l th c e n t r e s
and in tegra ted with the hosp i t a l se rv ices t o meet the needs of the whole population.
The service depends on e x p a t r i a t e s t a f f .
Health se rv ices development and disease control
The new organization of the Ministry of Health has provided f o r a wide range of new
a c t i v i t i e s i n the Department of Preventive Medicine, including p a r t i c u l a r l y hea l th
education, v i t a l and hea l th s t a t i s t i c s , and i n d u s t r i a l health.
WHO w i l l co l laborate i n the heal th education programme and i n aspects of com-
municable d isease control , p a r t i c u l a r l y the immunization of chi ldren, por t heal th ,
and food and water control .
Promotion of environmental hea l th
I n view of t h e rapid i n d u s t r i a l i z a t i o n of the country the Government is concerned
with problems of environmental pol lu t ion. WHD w i l l co l l abora te i n t h i s r e spec t by
t h e provision of consul tants and fellowships.

Health manpower development
Health manpower of a l l ca tegor ies is almost exclusively foreign and is l i k e l y t o
remain so f o r some time. E f f o r t s a r e being made t o a t t r a c t nat ionals t o the hea l th
professions and to be t ra ined a t the Health Training I n s t i t u t e of the country.
WHO is collaborating i n the promotion of nat ional t r a in ing programmes by i ts
associa t ion with the Health Training I n s t i t u t e and the provision of fellowships.
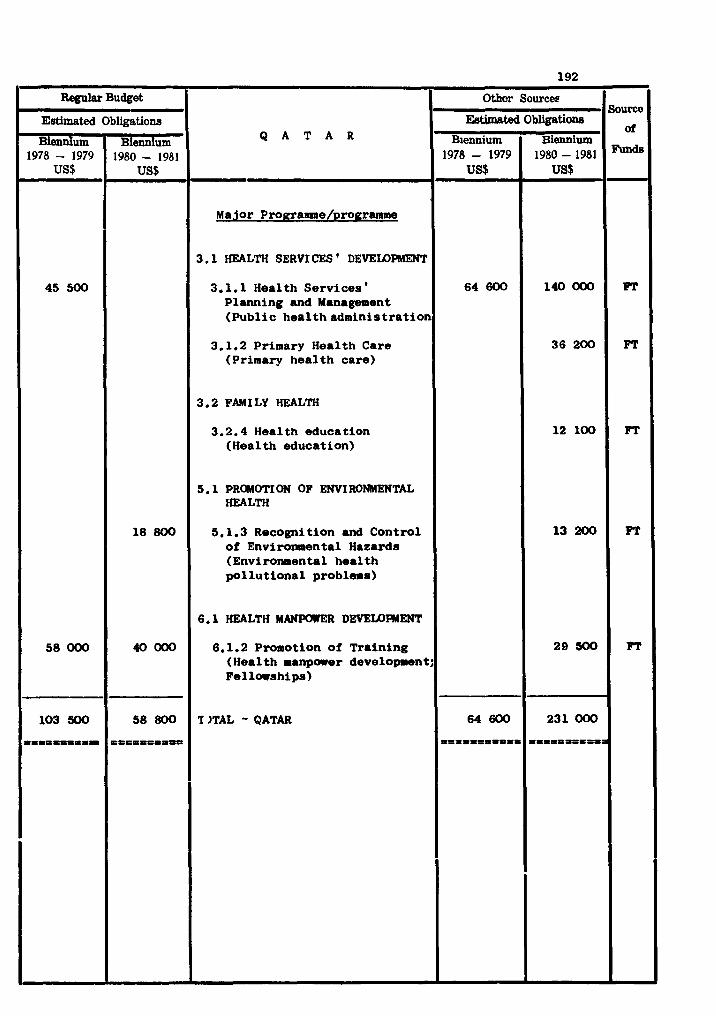
Regular Budget
Q A T A R
- Major Pro~.rame/programme
3.1 HEALTH SERVI CES ' DEVELOPMENT
3.1.1 Health Services ' Planning and Management (Publ ic heal thadminis t ra t ion
3.1.2 Primary Health Care (Primary hea l th care)
3.2 FAM I LY HEALTH
3.2.4 Health education (Health education)
5.1 PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.3 Recognition and Control of Enviror~sental Hazards (Environmental heal th po l lu t iona l problems)
6.1 HEALTH MANKMF.R DEVELDIMENT
6.1.2 Promotion of Training (Health manpower d e v e l o m n t ; Fel larships)
'I JTAL - QATAR
Estimated
Biennium 1978 - 1979
US$
45 500
58 000
103 500
I=PP=P=PDI
Obligations
Biennium 1980 - 1981
US$
18 800
40000
58 800
===I==*=-
Sourcc
oi
Funds
PF
PT
PF
FT
FT
Other Sourcee
%timated
Biennium 1978 - 1979
us$
64 600
64 600
--- - - - l l t t = t t P
Obligations
Biennium 1980-1981 US$
140000
3 6 2 0 0
12 100
13 200
29 300
231 000
P P I I P P I I I I l
COUNTRY PROORAMaE STATEWT
SAUDI ARABIA
NATIONAL HEALTH DEVELOPMENT STRATEGY
me national wealth of Saudi Arabia is being applied to socio-economic develop-
ment of which health i s considered an integral par t . During the National Develop-
ment Plan period ending i n 1980 high pr ior i ty has been given t o comprehensive health
services. The National Development Plan's objectives i n the heal th sector were to :
a ) provide and develop a chain of integrated heal th un i t s fo r delivery of com-
prehensive health care t o a l l segments of the population;
b) control communicable disease;
C) reduce infant mortali ty from 152 to 110 per thousand;
d) increase t o t a l hospital beds from 1.1 : 1000 t o 2.5 : 1000 of tho population ;
e ) develop and strengthen the administrative in f ras t ruc ture with a v ie r t o
regionalitation and decentralization;
f ) develop an adequate health information system; and
g) develop health manpower to meet the c r i t i c a l shortages i n s ta f f ing of heal th
services.
Country health progrpmming has not been undertaken. Several min is t r ies besides
the Ministry of Health provide heal th inputs t o the National Development Plan and
thus make i t d i f f i c u l t t o ident i fy agreed indicators of social relevance f o r eva-
luat ing health programmes.
The Ministry of Health's development programme ta rge ts a r e a s follows:
a ) development of integrated, comprehensive heal th care delivery system both
a t the periphery and i n urban areas;
b) balanced development of health manpower responsive t o the country's needs;
c ) a t tent ion to basic sani tary and environmental health measures ( in co-ordina-
t ion with the Ministry of Municipal and Rural Affairs) ;
d) control of communicable diseases and development of e f fec t ive categorical
programmes with a view to t h e i r ult imate integrat ion i n the overa l l heal th
services; and
e ) promo tion of intercoun t r y coordination i n the health f ie ld .
The o b j e c t i v e s and t a r g e t s conform broadly wi th WHD programme o b j e c t i v e s and
c l a s s i f i c a t i o n contained i n t h e S i x t h General Programme o f Work f o r 1978-83.
The Minis t ry o f Health has a l s o begun t o r eo rgan i t e , r eg iona l i ze and decen t r a l i ze
t h e serv ices . The t r a i n l n g Of n a t i o n a l s is being cons tant ly expanded i n o rde r to
s t a f f t h e developing h e a l t h s e rv i ces . A s t a r t has been made on coordina t ing h i t h e r t o
independent h e a l t h a c t i v i t i e s . National coordina t ing bodies and t echn ica l cornmitees
a t supervisory and execut ive l e v e l s have been e s t ab l i shed f o r environmental h e a l t h and
h e a l t h manpower d e v e l o p e n t . A High Health Advisory Board is being c o n s i d ~ r e d f o r t h e
o v e r a l l coordina t ion of h e a l t h pol icy and implementation.
TECHNICAL COOPERATION PROGRAMMES FOR HEALTH
WH3 t echn ica l cooperat ion w i l l cont inue while t h e Government w i l l assume most
f i n a n c i a l commitments i n accordance wi th present agreements.
Development o f comprehensive h e a l t h s e r v i c e s
The t rend towards i n t e g r a t e d , comprehensive h e a l t h care i s growing wi th t h e w m -
p l e t i o n o f t h e i n i t i a l h o s p i t a l bui ld ing programme; i n t e g r a t e d pe r iphe ra l h e a l t h u n i t s
wi th a well-defined r e f e r r a l system a r e being provided. Most new urban developments
have new h o s p i t a l s ; t h e emphasis i s now on consol ida t ing e x i s t i n g f a c i l i t i e s r a t h e r
than on the cons t ruc t ion of more new f a c i l i t i e s . The primary h e a l t h c a r e concept is
ga in ing ground and a p i l o t p r o j e c t is contemplated. The need f o r comprehensive
country h e a l t h programing is a l s o apprec ia ted .
WHO w i l l w n t i n u e i t s cooperat ion i n t h e promotion, planning and implementation
of i n t e g r a t e d h e a l t h s e rv i ces , i n t h e eva lua t ion o f c u r r e n t p lan r e s u l t s and i n f u t u r e
h e a l t h planning e s p e c i a l l y i n respect of hea l th economics and h e a l t h information.
Communicable d i s e a s e prevention and con t ro l
A h e a l t h informat o? system is t o be developed. The primary h e a l t h care pro-
gramme w i l l provide a b a s i s f o r d a t a co l l ec t ion . The Government i s l ay ing Spec ia l
emphasis on t h e Expanded Programme on Immunization. The malar ia c o n t r o l programme
is being strengthened by a d d i t i o n a l malaria u n l t s f o r a r e a s h i t h e r t o unserved; i n t e r -
country coordinat ion of malaria c o n t r o l i n t he e n t i r e Arabian peninsula i s being
a c t i v e l y pursued. Schis tosomias is con t ro l is rece iv ing i n c r e a s i n g a t t e n t i o n because
of t h e hazards r e s u l t i n g from a g r i c u l t u r a l and water development p ro j ec t s .
WHO w i l l continue its cooperat ion when requi red , f o r d i sease prevention and
con t ro l gene ra l ly and f o r t h e Haj period i n p a r t i c u l a r ; and a s requested by the
Government w i l l co l l abo ra t e i n implementing and eva lua t ing a permanent expanded
immunization programme.
Advisory se rv l ces f o r t h e Malaria Control Programme w i l l continue i n o rde r t o
s t rengthen the country 's own malar ia con t ro l measures and t o assist i n coordina t ion
wi th neighbouring count r ies .
Non-communicable d i sease prevention and con t ro l
The Government proposes t o set up con t ro l programmes f o r cancer , card iovascular ,
mental and i n d u s t r i a l d i s e a s e s a s soc ia t ed wi th urbaniza t ion and i n d u s t r i a l i z a t i o n .
WHO w i l l be a s soc ia t ed wi th these programmes a s required.
Promotion of environmental h e a l t h
The numerous development programmes, r u r a l and urban, t h e cons t ruc t ion o f new
townships, i n d u s t r i a l i z a t i o n and changing demographic p a t t e r n s have added t o the
complexit ies of environmental h e a l t h problems. The Minis t ry o f Municipal and Rural
A f f a i r s has a major r e s p o n s i b i l i t y i n t h i s f i e l d , p a r t i c u l a r l y f o r s a n i t a t i o n , water
s u p p l i e s and building. UNDP and W m a r e co l l abora t ing mainly i n providing consul-
t a n t s f o r pre-investment and f e a s i b i l i t y s t u d i e s o f var ious pro jec ts .
Health manpower development
The High Connnittee f o r Health Manpower Development and i ts subordina te t e c h m c a l
committee (wi th r ep resen ta t ion a t app ropr i a t e l e v e l s from M i n i s t r i e s o f Health, Higher
Education, Planning and Finance) has ind ica t ed i t s commitment t o a balanced and rea-
l i s t ic development o f h e a l t h manpower through an i n t e g r a t e d mechanism f o r h e a l t h
s e r v i c e s and manpower development. A r eappra i sa l o f t h e o v e r a l l t r a i n i n g programmes,
i d e n t i f i c a t i o n of p r - o r i t i e s and r e s t r u c t u r i n g of c u r r i c u l a t o make them responsive
t o needs and requirements of t he h e a l t h s e rv i ces , was begun i n 1978 i n accordance wi th
the o b j e c t i v e s of the Regional Medium Term Programme on Health Manpower Development.
WHO co l l abora t ion w i l l be mainly i n manpower planning and management and the
implementation of balanced, coordinated, t r a i n i n g programmes.
WHO fe l lowships w i l l be u t i l i z e d main1 y t o develop f u r t h e r teacher t r a i n i n g
p o t e n t i a l .
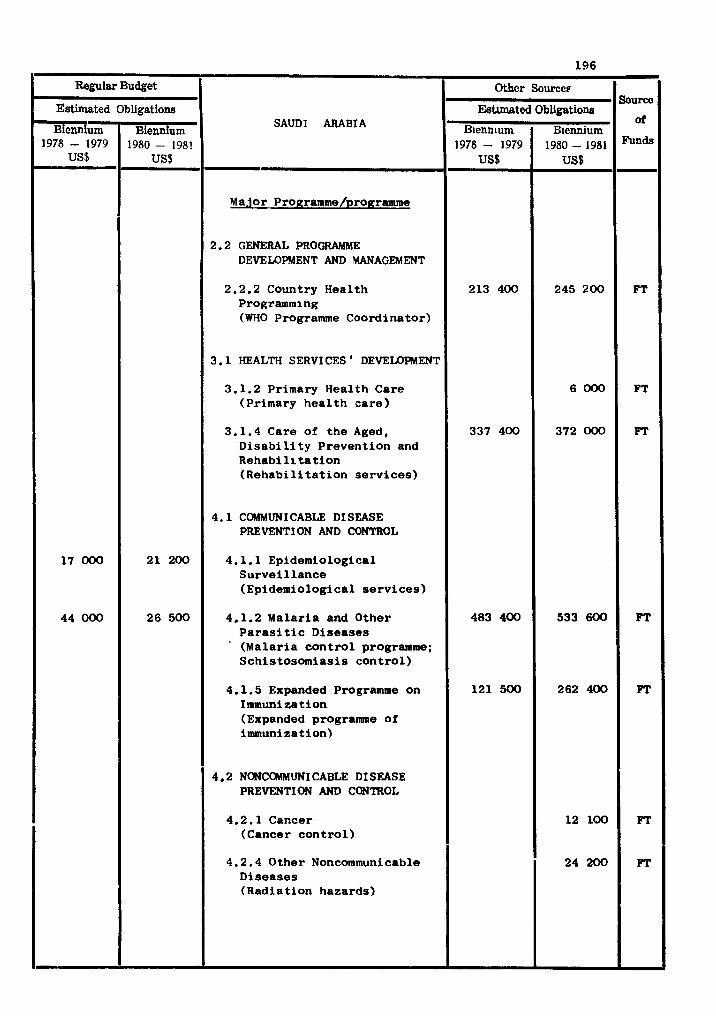
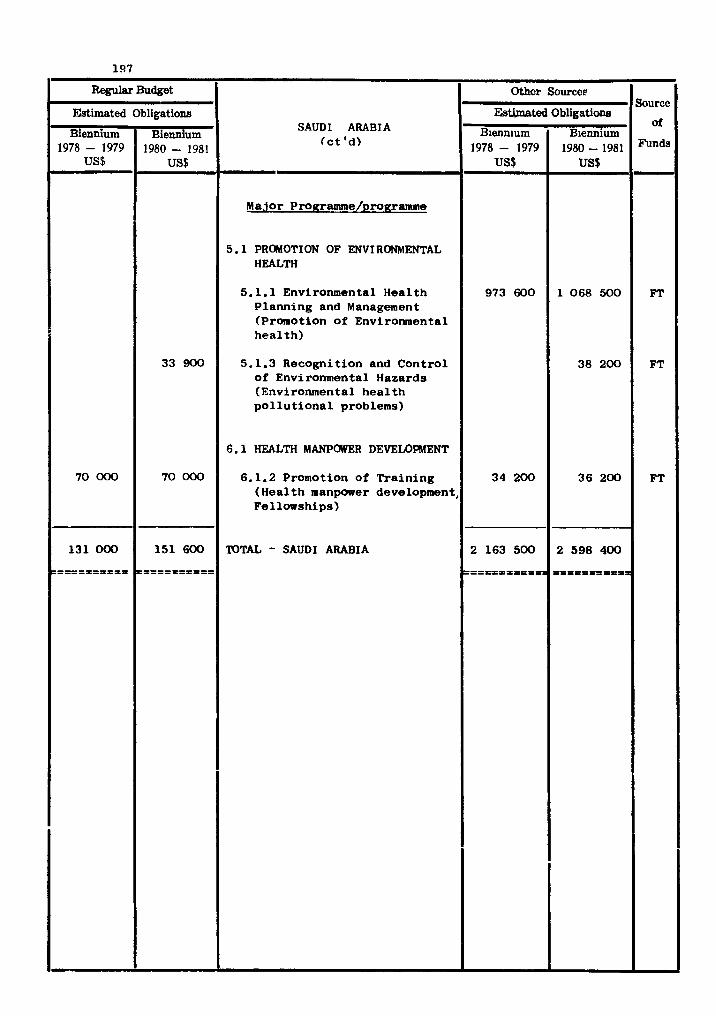
Regular Budget
Estimated
Biennium 1978- 1979
US$
70 000
131 000
---------- ----------
Other Sources Source
Btimated Obligationa SAUDI ARABIA of
Biennium Biennium
I
Obligations
Biennium 1980- 1981
US$
33 900
70 000
151 600
----------- -----------
(ct 'd)
Major Programme/~roffranune
5.1 PROMOTION OF ENVIRONMENTAL HEALTH
5.1.1 Environmental Health Planning and Management (Promotion of Environmental health)
5.1.3 Recognition and Control of Environmental Hazards (Environmental health pollutional problems)
6.1 HEALTH MANPOWER DEVELOPMENT
6.1.2 Promotion of Training ( Health manpower development, Fellowships)
VITAL - SAUDI ARABIA
1978- 1979
973 600
34 200
2 163 500
----------- -----------a
1980-1981
1 068 500
38 200
36 200
2 598 400
------- -------==PI
FT
FT
FT
COUNTRY PROGRAMME STATWWT
SOMALIA
NATIONAL HEALTH DEVEWPMENT STRATEGY
The current national health developent strategy is based on a Government policy
of increasing as rapidly as possible the health manpower stock of the country and re-
forming the administration of health services, i n order t o deal more effectively with
the problem of communicable diseases as pr ior i ty , and to develop environmental health
services and primary health care. Systematic health planning, including health nhn-
power planning, began i n 1978 and WHO has cooperated i n country health programing.
I t is o f f i c i a l policy t o cu l t iva te i n the people an awareness of the burden of
preventable disease and of measures t o reduce it. Similarly, other government
authori t ies are being oriented t o the need to develop community preventive services
a s well as hospital f a c i l i t i e s . '
TECHNICAL CWPEIWTIW PROGRAMMES FOR HEALTH
Health services developent
Primary health care is the major focus of collaboration with WHO i n the area and
the programme w i l l be reinforced by the Government's e f f o r t t o a t t a i n self-sufficiency
i n the production of drugs, i n i ts measures to control drug production and use, and i n
the developent of a r e f e r r a l system which w i l l make the best use of the other levels of
the health services inoluding the growing spec ia l i s t services. Mental health services
w i l l a lso be developed.
I n the area of Family Health, MCH services a re t o be developed both i n coverage and
quality. The f i r s t phase of the programme would cover Mogadishu and the Shibe l l i Region
where technical advisory services as well as material assistance i n the building and
improvement of physical f a c i l i t i e s w i l l be provided. In nu t r i t ion , WID w i l l collaborate
i n t ra ining and providing advisory services par t icular ly for the assessment of nu t r i t ion
s t a tu s of vulnerable groups.
A oentre for the repair and maintenance of medical equipuent w i l l continue t o re-
ceive the support of WHO and the public health laboratory services w i l l be fur ther
developed. An e f f o r t is being made to develop rehabi l i t a t ion services.
Disease prevention and control
The main emphasls w i l l be on developing epidemiological services and on the con-
trol of schlstosomiasrs whrch is widespread i n the two major r iver basins of the coun-
try. Trachoma w i l l continue t o reoeive attention. W H O w i l l collaborate i n these
a c t i v i t i e s as well as i n the Expanded Programme on Immunization against the leading
communicable diseases of childhood. WHO w i l l also collaborate In s t a r t i ng a pro-
gramme for the prevention of Blindness.
Promotxon of environmental health
While there has been some progress in providing a s a f e water supply and sani ta t ion
services there is need for much development i n these f ie lds . Unfavourable environ-
mental aonditlons a re s t i l l among the leading causes of diseases i n the country. WHO
w i l l contlnue its collaboration i n these f i e ld s by the provision of s ta f f and consul-
t an ts and a t Government request w i l l provide pre-investment services for basic
sanitary measures and the mobilization of additional investments from the internat ional
and b i l a t e r a l agencies.
Health manpower development
The intake of t ra inee intermediate and auxiliary health workers has increased
almost fourfold i n recent years and t ra ining f a c i l i t i e s a re being expanded accordingly.
The need to strengthen the t ra ining of publlc health s t a f f is par t icular ly realized.
Nursing t ra ining is being raised t o degree level i n order t o a t t r a c t good qual i ty
entrants. Speaial a t tent ion is being glven to the t ra ining of laboratory and X-ray
technicians, sani tar ians and pharmacists. The production of physicians is being
increased so that , with a redis t r ibut ion of exis t ing physicians, each d i s t r i c t w i l l
have a t l e a s t one physician. Opportunities fo r contlnuing in-service education are
being increased. An attempt is being made to make health careers more a t t r ac t i ve
professionally and f-.nancially.
WHO technical cooperation i n health manpower development w i l l be mainly i n
developing the educational capabilities of teachers and ins t i tu t ions , and, through the
fellowshlp programme, i n ra i s ing the level of health services administration.
Health information
The Government 1s eager t o strengthen i ts health s t a t i s t i c a l services. They a re
i n great need of timely, re l iab le , meaningful and up-to-date information for the sound
planning, adminxstration, management and evaluation of the health services.
W W w i l l continue its collaboratron for the development of national health s t a t l s -
t i c a l services and t ra inlng of national s t a f f .
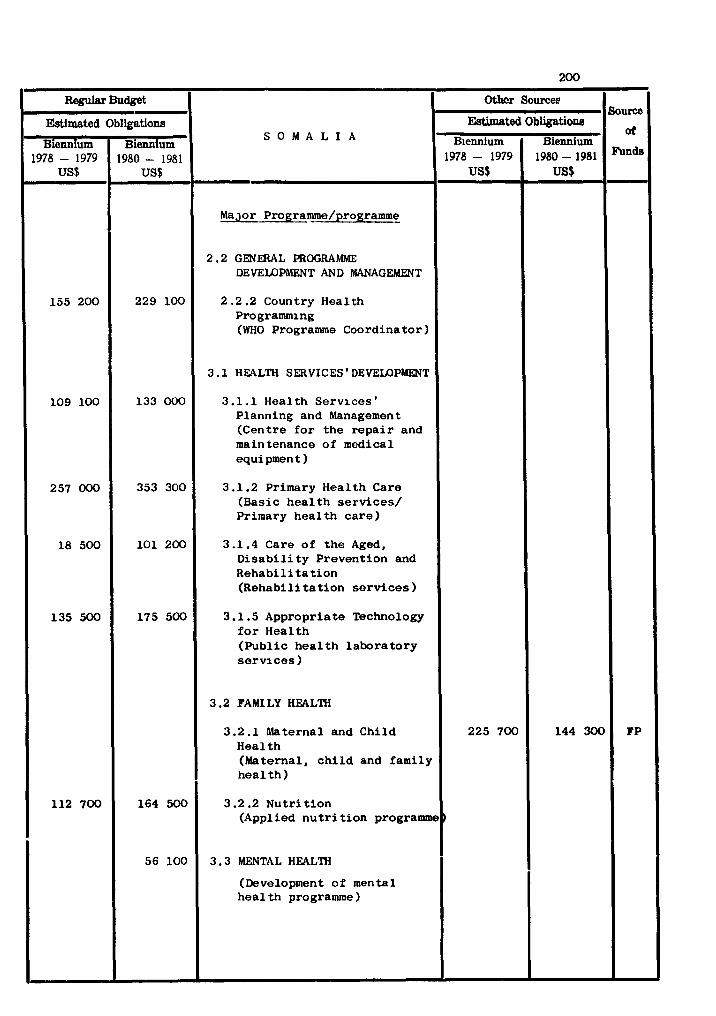
Budget
S O M A L I A
Major Programme/programme_
2.2 GENE3AL PROGRAMME DEVEUIPMFNT AND MANAGEMENT
2.2.2 Country Health Programming (WHO Programme Coordinator)
3.1 HEALTH SERVICES ' DEVELOPMENT
3.1.1 Health Serv ices ' Planning and Management (Centre f o r t he r e p a i r and maintenance of medical equipment )
3.1.2 Primary Health Care (Basic h e a l t h s e rv i ces / Primary h e a l t h c a r e )
3.1 .4 Care of t he Aged, D i s a b i l i t y Prevention and Rehab i l i t a t i on (Rehab i l i t a t i on s e r v i c e s )
3.1.5 Appropriate Technology f o r Health (Publ ic h e a l t h labora tory s e r v i c e s )
3.2 FAMILY HEALTH
3.2.1 Maternal and Child Health (Maternal, c h i l d and family h e a l t h )
3.2.2 Nu t r i t i on (Applied n u t r i t i o n programme
3.3 MENTAL HEALTH
(Development of mental hea l t h programme 1
Estimated
Biennium 1978 - 1979
US$
155 200
109 100
257 000
18 500
135 500
112 700
Obligations
Biennium 1980 - 1981
US$
229 100
133 000
353 300
101 200
175 500
164 500
56 100
Soum
of
FP
Othcr Sowee
Estimated Blennium
1978 - 1979 US$
225 700
)
Obligation6
Biennium 1980 - 1981 US$
144 300
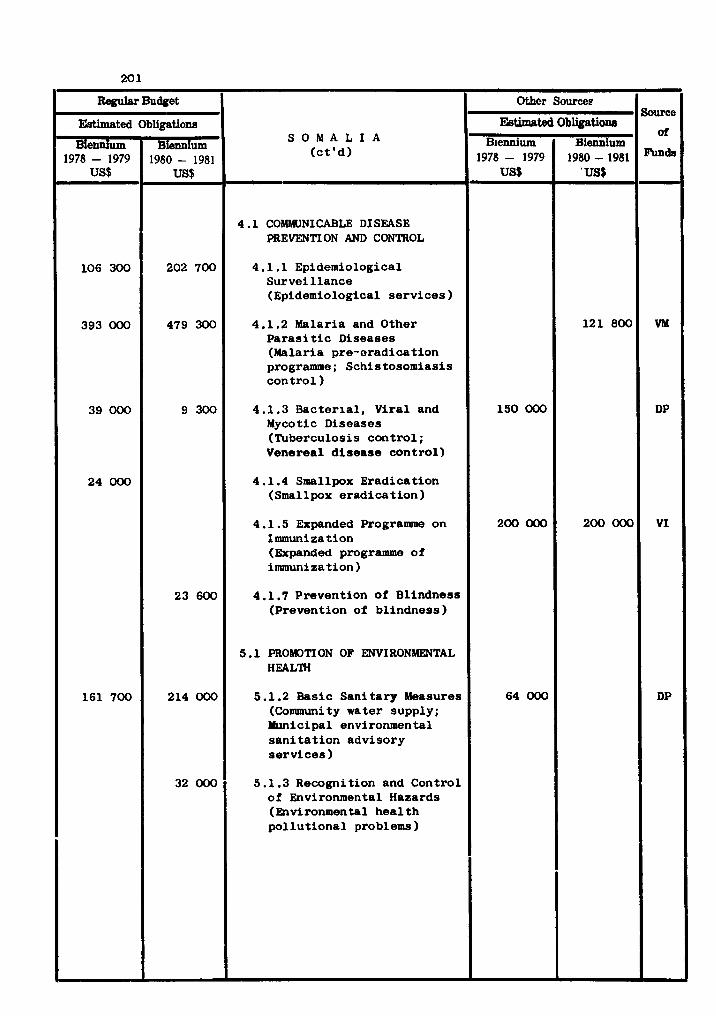
Regulrrr Budget
S O M A L I A (ct'd) -
4.1 COMMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.1 Epidemiological Surveillance (Epidemiological services)
4.1.2 Malaria and Other Parasitic Diseases (Malaria pre-eradication programme; Schistosomiasis control )
4.1.3 Bacterial, Viral and Mycotic Diseases (Tuberculosis control; Venereal disease control)
4.1.4 Smallpox Eradication (Smallpox eradication)
4.1 .5 Expanded Programme on Immunization (Expanded programme of immunization 1
4.1.7 Prevention of Blindness (Prevention of blindness)
5.1 PROMOTION OF ENVIRONMENTAL HEALTH
5.1.2 Basic Sanitary Measures (Community water supply; Municipal environmental sanitation advisory services)
5.1.3 Recognition and Control of Environmental Hazards (Environmental health pollutional problems)
Estimated
Btennium 1978 - 1979
US$
106 300
393 000
39 000
24 000
161 700
Obligations
B i d u m 1980 - 1981
202 700
479 300
9 300
23 600
214 000
32 000
&wco
oi
VM
DP
VI
DP
Other Sources
Ebtbted B~ennium
1978 - 1979 US$
150 000
200 000
64 000
Obligations
Biennium 1980 - 1981
' US$
121 800
200 000
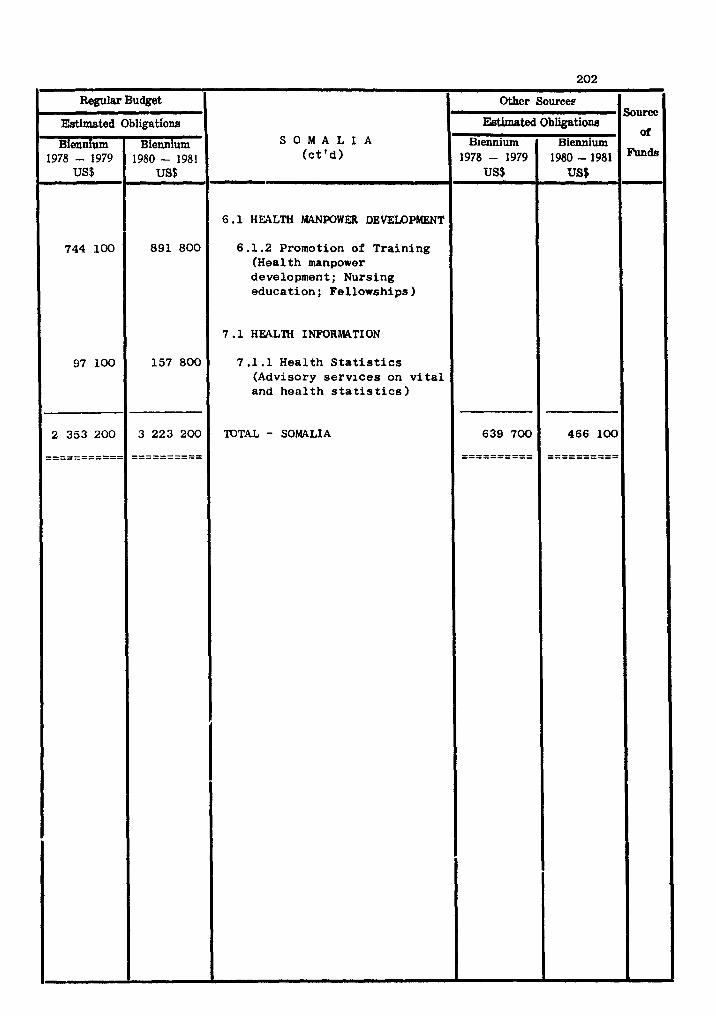
WWW
S O M A L I A ( e t ' d ) -
6 . 1 HEALTH AQINWWFJI' DEVELOPMENT
6 . 1 . 2 Promotion of Training (Health manpower development; Nursing education: Fe l lowships )
7 .1 HEAL2H INFORMATION
7 . 1 . 1 Health S t a t i s t i c s (Advisory s e r v i c e s on v i t a l and h e a l t h s t a t i s t i c s )
TOTAL - SOMALIA
Estimated
Biennium 1978 - 1979
US$
744 100
97 100
2 353 200 ----------- -----------
Obligations
Biennium 1980 - 1981
US$
891 800
157 800
3 223 200
----------
Source
or
,-
Othcr Source~
Estimated Biennium
1978 - 1979 US$
639 700
---------- ----------
Obliationa
Biennium 1980-1981 US$
466 100
---------- ----------
COUNTRY PROGRANME STATENENT
SUDAN - NATIONAL HEALTH DEVEJIOPMEN'I' STRATEGY
The phased programme f o r ac t ion f o r socio-economic development formulated by the
Sudanese S o c i a l i s t Union prescribed t h e following p r i o r i t i e s f o r the heal th sector :
( a ) preventive and w c i a l medicine espec ia l ly i n the control of environmental hea l th
problems, maternal and ch i ld health, and school heal th ; (b) strengthening of r u r a l
heal th care f a c i l i t i e s t o ensure complete coverage and f a i r d i s t r i b u t i o n of bas ic
heal th care t o the e n t i r e population; ( c ) t r a i n i n g f o r 811 l e v e l s of professional ,
technical and aux i l i a ry hea l th manpower; (d) consolidation of ex i s t ing cura t ive
heal th care f a c i l i t i e s t o provide better services f o r the population and allow f o r
some expansion of f a d l i t i e s i n the less developed areas ; and (e) d i r e c t pedical re-
search on heal th problems according t o t h e i r p r i o r i t i e s .
A National Health Programme f o r 1977/78-1983/84 was formulated i n 1974 a s a pa r t
of the socio-economic plan and was approved by the Cabinet a s well a s the Sudanese
S o c i a l i s t Union i n Yay 1975. I t covers Sudan's e igh t main heal th problems, some of
which a r e i n t e r s e c t o r a l - e.g., man-made malaria and the provision of primary hea l th
ca re t o r u r a l and nomadic populations. These e igh t problems a r e given p r i o r i t y f o r
the a l loca t ion of f inanc ia l resources.
Some of the main programme a reas - nationwide malaria; man-made malaria; primary
hea l th care ; schisfosomiasis control i n i r r i g a t e d areas ; sa fe water supply; environ-
mental heal th ; food supply (mainly m i l l e t ) i n c e r t a i n regions; and onchocerciasis - have been considered a s hea l th development programmes, o the r s a s i n t e r s e c t o r a l develop-
ment programmes. Primary heal th ca re covers not only the heal th se rv ices per se , but
a l s o g a s t r o e n t e r i t i s i n chi ldren, immuniration, tuberculosis , publ ic hea l th information,
and hygiene. A s regarxis communicable diseases, such a s man-made malaria and schis to-
somiasis, the heal th f a c t o r s have been considered together with the economic and socio-
p o l i t i c a l fac tors . This app l i e s a l s o t o onchocerciasis, which i s causing considerable
economic l o s s due t o blindness, mainly i n the Southern Region but a l s o i n c e r t a i n parts
of the Northern provinces.
TECHNICAL COOPERATION PROGRAhWES FOR HEALTH
Primary hea l th ca re
Of the e i g h t programmes comprising the Sudanese nat ional hea l th programme, primary
heal th ca re has been singled out a s the most important f i e l d f o r governmental ac t ion
during the development plan period July 1977 - June 1984. The main objective of the
primary health care programme may be summed up as maximum coverage of the rura l and
nomadic populations by 1984. The programme w i l l require the t ra ining of approxxmately
4 000 persons. This w i l l necessi ta te the construction and equipment of community t ra in?
ing centres attached to rura l dispensaries so tha t trainees may learn i n an environment
similar t o tha t i n which they w i l l subsequently work. Specially modified t ra ining
schemes a re t o be evolved for nomadic community health workers. W H D w i l l be actively
involved i n 1980-81 i n the development of basic health' uni ts , and w i l l cooperate i n
innnunization programmes, malaria control, family health, health education, nu t r i t ion
and rural water supplies. The national health authori t ies w i l l be engaged i n technical
cooperation w i t h a number of countries i n the Region, with WHD providing consultant and
coordination functions.
Disease prevention and control
Communicable endemo-epidemic diseases are highly prevalent i n the Sudan and a f fec t
par t icular ly the child population. In general,,diseases resul t ing from poor environ-
mental sani ta t ion const i tute the bulk of the health problems with which the Sudanese
Government has t o deal. Furthermore. some of the economic progress which has been
accomplished during the l a s t decade i n agriculture developent has aggravated cer ta in
disease problems, such as malaria and schiotosomiasis; t h i s r e su l t s i n a decrease of
the expected economic output of the projects. A project is being planned by the
Government i n collaboration with WHD for the prevention and control of vector-borne
diseases associated with water. The project which is long-tern is being planned with
the anticipated collaboration of other United Nations Agencies such as UNEP and FA0
as w e l l a s b i l a t e r a l contributors. WflD w i l l be associated during 1980-81 with malaria
control, expanded immunization against measles and other leading communicable diseases
of childhood, the control of onchocerciasis, t r ypanomias i s , leishmaniasis and leprosy.
WflD w i l l a lso collabo-ate i n a comprehensive cancer programme a t co~munity level.
Promotion of environmental health
The demand for sa fe water supply and proper sewage disposal system is increasing.
As a resu l t , an overal l control of water and envimmumtal pollution is of the utmost
importance. Industr ia l waste is an added problem w i t h n w l y created industr ies i n big
c i t i e s where water supply is a l so inadequate. The extensive agricul tural and industr ia l
developent plans launched by the Government w i l l involve employment of a large number
of workers who w i l l be exposed t o occupational hazards, both from the environment i n
which they work .and from the endemic diseases t o which they might be e x p o d .
Personnel trained i n sanitary engineering and occupational health w i l l be required
t o meet the situation. WH3 w i l l provide supplies and equipment, and fellowships, t o
support the environmental health programme.
Health manpower development
To m e e t the objectives of the national health plan, the Government is making
intensive e f f fo r t s i n the t ra ining and u t i l i z a t i on of intermediate and auxiliary
health cadres. There a re nineteen training programmes for professional and sub-
professional categories, and s i x postgraduate courses fo r various special is ts .
special is tsand ins t i tu t ions i n the Sudan a re being u t i l i z ed by HM3 for t ra ining
of auxiliary p e r s o ~ e l from neighbouring countries i n the Region.
WH3 w i l l continue t o collaborate i n health manpower developnent by providing
consultants i n medical and dental education to the Faculty of Medicine a t Khartoum
and Wad Medani as well as advisers i n nursing and sani ta t ion and fellowhsips;
supplies and equipment.
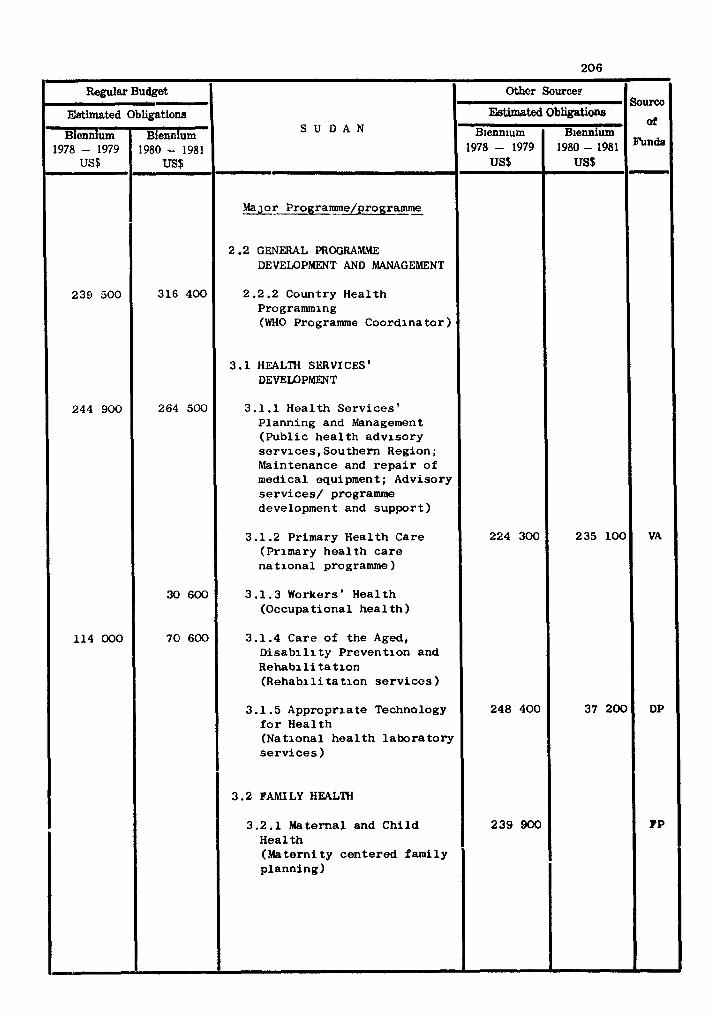
Regular Budget
Estimated
Biennium 1978 - 1979
US$
239 500
244 900
114 000
Other Sources Source
Ekkimated Obligktione S U D A N
of Blenn~urn B~ennium
' -
Obligations
Biennium 1980 - 1981
US$
316 400
264 500
30 600
70 600
MaJor Programme/programmn
2 .2 GENERAL PROGRAMME DEVELOPMENT AND MANAGEMENT
2.2.2 Country Health Programming (WHO Programme Coordinator)
3.1 HEALTH SERVICES ' DEVELOPMEXT
3.1.1 Health Serv ices ' Planning and Management (Publ ic h e a l t h advisory se rv i ces , Southern Region; Maintenance and r e p a i r of medical equipment ; Advisory se rv i ces / programme development and suppor t )
3.1.2 Primary Health Care (Primary h e a l t h c a r e na t iona l programme )
3.1.3 Workers' Health (Occupational h e a l t h )
3.1.4 Care of the Aged, D i s a b i l i t y Prevention and Rehab i l i t a t i on (Rehab1 li t a t i on s e r v i c e s )
3.1.5 Appropriate Technology f o r Health (National h e a l t h l abo ra to ry s e r v i c e s )
3.2 FAMI LY HEALTH
3.2.1 Maternal and Chi ld Health (Materni ty centered family planning)
1978- 1979
224 300
248 400
239 900
1980-1981
2 3 5 1 0 0
37 200
Funds
VA
DP
FP
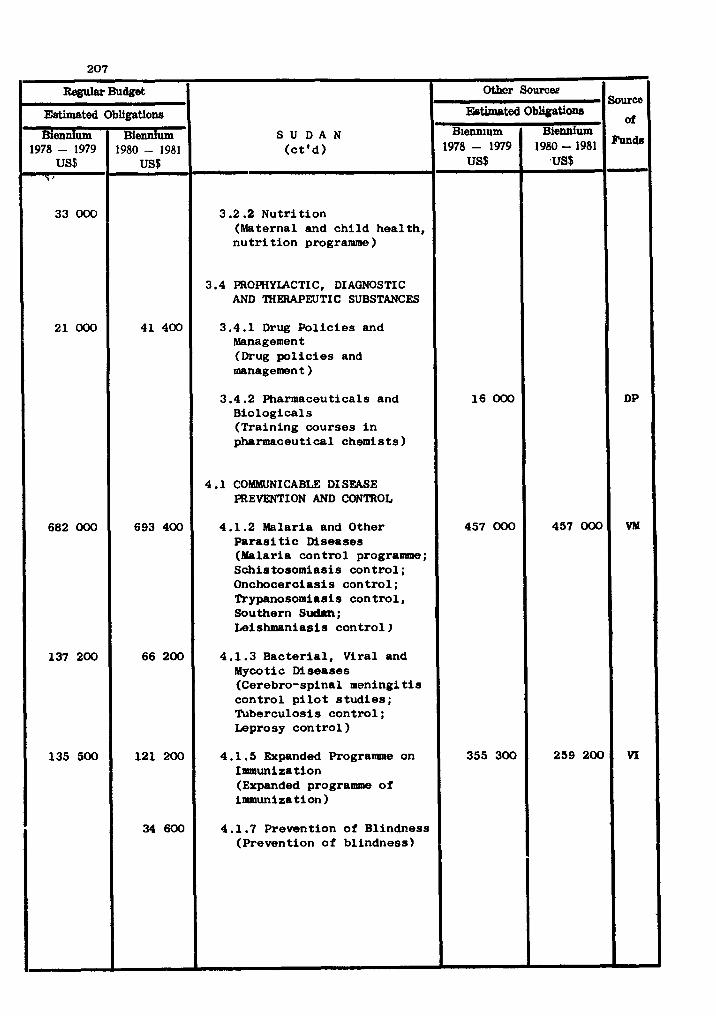
Source
oi
fin&
DP
VM
V I
S U D A N ( c t ' d )
3.2.2 Nu t r i t i on (Maternal and c h i l d hea l th , n u t r i t i o n programme)
3.4 PROPHYLACTIC , DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
3.4.1 Drug P o l i c i e s and Management (Drug p o l i c i e s and management )
3.4.2 Pharmaceuticals and Biologica ls (Training courses i n pharmaceutical chemists)
4 .1 COMMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.2 Malaria and Other P a r a s i t i c Diseases (Malaria con t ro l programme; Schistosomiasis con t ro l ; Onchocerciasis con t ro l ; Trypanosomiasis con t ro l , Southern Sudan; Leishmaniasis con t ro l )
4.1.3 Bac te r i a l , Viral and ~ y c o t i c Diseases (Cerebro-spinal meningi t i s con t ro l p i l o t s t u d i e s ; Tuberculosis con t ro l ; Leprosy con t ro l )
4.1.5 Expanded Programme on Inrmuniza t i o n (Expanded programme o f immunization)
4.1.7 Prevention of Blindness (Prevention of bl indness)
Other Sourcee Regular Budget
E&bated Biennium
1978 - 1979 US$
16 000
457 000
355 300
EWmated
Biennium 1978 - 1979
US$ 'i '
33 000
21 000
682 000
137 200
135 500
Obligstiwe Biennium
1980-1981 ,US$
457 000
259 200
- Obligations
Biennium 1980 - 1981
US$
41 400
693 400
66 200
121 200
34 600
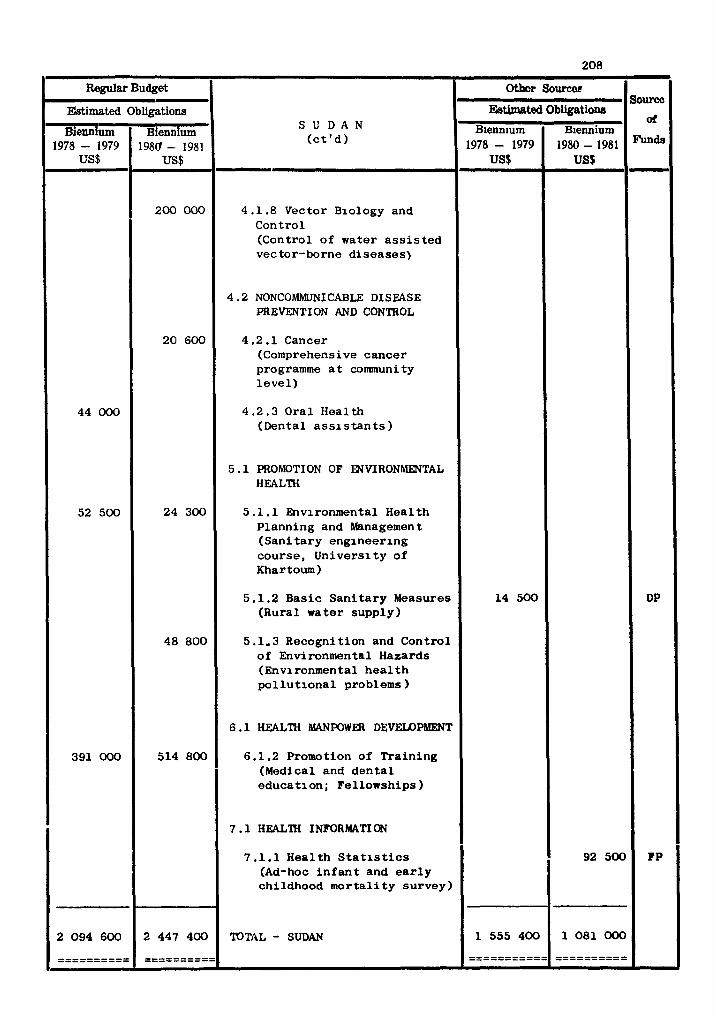
Regular Budget
S U D A N ( c t ' d )
4.1.8 Vector Biology and Control (Control of water a s s i s t e d vector-borne d iseases)
4 .2 NONCOMMUNICABLE DISEASE PREVENT1 ON AND CONTROL
4.2.1 Cancer (Comprehensive cancer programme a t community l e v e l )
4.2.3 Ora l Health (Dental a s s i s t a n t s )
5 .1 PROMOTION OF WVIRONMENTAL HEALTH
5.1.1 Environmental Heal th Planning and Management (San i t a ry engineer ing course, Univers i ty of Khartoum)
5.1.2 Basic S a n i t a r y Measures (Rural water supply)
5.1-3 Recognition and Control of Environmental Hazards (Environmental h e a l t h p o l l u t i o n a l problems)
6 . 1 HEALTH MANWWER DEVELOPMENT
6.1.2 Promotion of Tra in ing (Medical and d e n t a l educa t ion; Fel lowships)
7 .1 HEALTH INFORMATI ON
7.1.1 Heal th S t a t i s t i c s (Ad-hoc i n f a n t and e a r l y childhood m o r t a l i t y survey)
TOTAL - SUDAN
Estimated
Biennium 1978 - 1979
US$
44 000
52 500
391 000
2 094 600
---------- ----------
Obligations
Biennium 1980 - 1981
US$
200 000
20 600
24 300
48 800
514 800
2 447 400
---------- ----------
Source
of
DP
FP
Othor Sources
Eotimated B~enn~um
1978 - 1979 US$
14 500
1 555 400
----------- -----------
Obligatione
B~ennium 1980 - 1981 US$
92 500
1 081 000
----------
00-Y PROGRAIIQIE STAT-
SYRIAN ARAB REHlBLIC
NATIONAL HEALTH DEVEZIDPIYIMT STRATEXY
The Government had drawn up an out l ine of planned development targets fo r the per-
iod 1971/1985. The health sector of the fourth Five-Year Plan prepared by the Planning
Office of the Ministry of Health foresees.coverage of the entkro population w i t h a f u l l
range of preventive and curative health services.
The Ministry intends to concentrate on the development of basic health services i n
two o r three provinces each year, with the ultimate objective of providing an acceptable
standard of health serviae for the e n t i r e population. The Health Plan a a l l s fo r the
establishment of 47 n w health centres, the construction of f i ve n.r provinoial hospitals,
increasing the to t a l number of beds t o 10 118, upgrading of exis t ing provincial and
d i s t r i c t hospitals, and i n i t i a t i o n of a country-wide health education.campaign.
TEW1CA.L COOPERATION PMG- POR HEALTH
Health serviaes dovelopent
The Fourth Fivo-Year Plan aims a t coverage of the e n t i r e population with preventive
and curative health servioee. W H l w i l l continue to aollaborate with the Government i n
a t ta in ing t h i s goal, Support w i l l be given for the further development of hospi ta l
administration serviaes and for the strengthening of emergency medical care, including
intensive care. Likewise, WHD w i l l continue its cooperation with the Government i n the
expansion of medical rehabi l i ta t ion services t o dewlop a network of rehabi l i t a t ion
f a c i l i t i e s i n the country.
Public health laboratory services w i l l be expanded t o cover more population i n the
provinces as well as i n &he peri@ery, and VH) w i l l collaborate i n achieving this goal.
Maternal and chi ld health/fanily health m H
The f i r s t phase of the MCWFH projeat, funded by UNPPA, came t o an end i n 1978/79;
the seaond phase which w i l l oontinue through 1981, is e x p e a t d to see the extension of
integrated YCH and family planning services t o a l l usban areas. WH) w i l l continueto.
aollaborate i n this plan.
Disease prevention and control
The programme of surveillance of communicable diseases w i l l be concerned mainly
with en te r ic infections, zoonoses and food-borne infections but w i l l include also the
evaluation of the immunization programme and the expansion of surveillance a t prlmary
level.
WHO collaboration w i l l be focussed on control of en te r ic infections, including the
prevention of introduction of cholera and the diffusion of the pract ice of o r a l rehydra-
tion.
Programme expansion of schistosomiasis control w i l l continue. More bordermeetings
w i l l take place between Syria, Jordan, Lebanon and possibly Turkey.
The number of discovered indigenous cases of malaria has been s teadi ly increasing
due mainly t o operational and administrative d i f f i cu l t i e s . WHO w i l l continue to co-
operate i n assessing the progress of the programme and i n the planning of ac tzv i t ies
adapted t o the divers i f ied epidemiological and socio-economic s i tua t ions of the various
provinces. Provisions for supplies, fellowships and d i r ec t par t ic ipat ion i n t ra ining
of national s ta f f are a lso par t of WHO support t o the Government's effor ts .
Promotion of environmental health
WHO w i l l provide consultant services i n programes for a i r quality, water quality,
marine pollution, environmental improvement and food sanitation. Fellorrshipa w i l l
a lso be provided t o develop manpower capabi l i t i es i n a i r qual i ty control, water qual i ty
rutvei l lance and food sanitation. In addition, l imited amountrdsuppl ies and equip-
ment relevant to needs w i l l be provided.
Health manpower develop~ent
In medical and dental education WHO collaboration w i l l continue i n the fur ther
development and imprcvement of the qual i ty of teachers and ins t ruc tors i n medicine and
dentistry. Speaial a t tent ion w i l l be given to the promotion of postgraduate medical
education and the development of the dental school.
There a r e eleven nursing schools i n the country preparing nurses and midwives.
Their major needs are t o develop curricula re la ted t o job descriptions, and t o improve
teaching through t ra ining i n education methods. WH3 w i l l continue to help i n preparing
qual i f ied faculty members by provision of fellowships and through strengthening f i e l d
t ra ining areas.
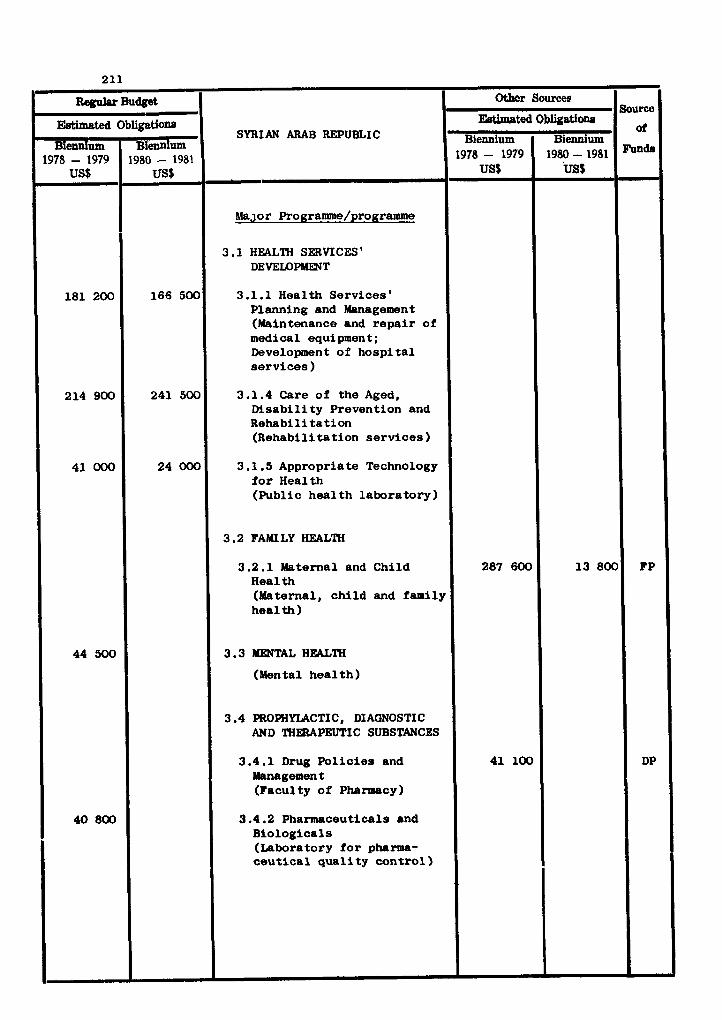
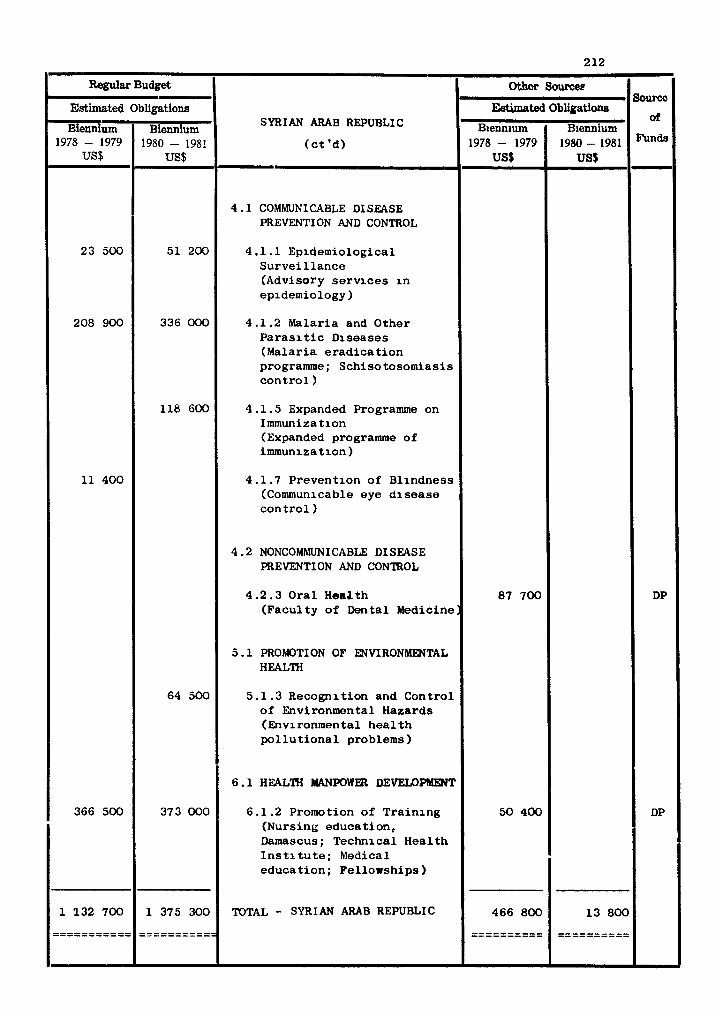
Regular Budget
SYRIAN ARAB REPUBLIC
( c t 'd)
4 . 1 COMMUNICABLE DISEASE PREVENTION AND CONTROL
4.1.1 Epidemiological S u r v e i l l a n c e (Advisory s e r v i c e s i n epidemiology)
4 .1 .2 Malar ia and Other P a r a s i t i c Diseases (Malar ia e r a d i c a t i o n programme; Schiso tosomias i s c o n t r o l )
4.1 .5 Expanded Programme on Immunization (Expanded programme of immunization)
4 .1 .7 Prevent ion of Bl indness (Communicable eye d i s e a s e c o n t r o l )
4.2 NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
4 .2 .3 Ora l Heaath (Facul ty o f Dental Medicine ]
5 .1 PROhIOTI ON OF ENVIRONMENTAL HEALTH
5.1.3 Recogni t ion and Cont ro l of Environmental Hazards (Environmental h e a l t h p o l l u t i o n a l problems )
6 . 1 HEAL'lW MANPOWER DEVEU)PMENT
6.1.2 Promo t i o n of T ra in ing (Nursing educa t ion , Damascus; Technical Hea l t h I n s t i t u t e ; Medical educa t i on ; Fe l lowships )
TOTAL - SYRIAN ARAB REPUBLIC
Estimated
Biennium 1978 - 1979
US$
23 500
208 900
11 400
366 500
1 132 700
----------- -----------
- Obligations
Biennium 1980 - 1981
US$
51 200
336 000
118 600
64 500
373 000
1 375 300
----------- -----------
Source
of
Funds
DP
DP
Othor Sources
&timated
B~ennium 1978 - 1979
US$
87 700
50 400
466 800
----- ---- - ----------
Obliiatione
Biemium 1980 - 1981
US$
1 3 800
---------- ----------

COUNTRY P R O G ~ STATEMENT
TUNISIA
NATIONAL HEALTH DEVELOPMENT STRATEGY
The main heal th problems of Tunisia are:
- communicable diseases, of which the most important a r e i n t e 8 t i n a l infect ions
due t o inadequate san i t a t ion , p a r a s i t i c diseases, rabies ;
- chronic diseases, especia l ly anaemia and haemglobinopathy, lymphoma of the
diges t ive t r a c t , cancer of the u te r ine cervix and cavi ty , and of the breas t ;
- malnutri t ion, e spec ia l ly i n r u r a l areas;
- a r a t e of in fan t morta l i ty which reaches 120 per thousand i n r u r a l areas ; and
- inadequate health-care coverage of the r u r a l population.
The current national hea l th s t ra tegy is incorporated i n a National Health
Development Plan. Major goals of the Government a r e the improvement of r u r a l hea l th
ca re coverage, the control of comunicable diseases and canaer, the prevention of
environmental pollution, and the development of heal th planning capab i l i t i e s .
A p r i o r i t y programme a rea i n which WHO has a major input is hea l th manpower
development.
TECHNICAL COOPERATION PROGRALlldES H)R HEALTH
Health services development
A considerable extension of bas ic heal th services is proposed, which envisages
the construction of heal th service u n i t s d i s t r ibu ted throughout the country u n t i l
a11 c o m u n i t i e s have ready access t o primary hea l th a a r e d i rec ted toward8 the manage-
ment and control of prevalent diseaaes. WHD col laborat ion w i l l be mainly by means
of advisory services re la ted t o hea l th planning and management, the development of
medical emergenay services , and the expansion of the public heal th laboratory service
including radia t ion pr\jtuction. A 8 well , WHD w i l l cooperate i n developing a
national heal th information system.
Disease prevention and control
The programme f o r the eradicat ion of malaria and the control of sohisto.oria8is
which have been very sucaessful w i l l be pursued, and WHD w i l l continue col laborat ion
as necessary u n t i l both diseases have disappeard. Of the chronic d imases , cancer
receives much a t t en t ion , and WHD collaboration with the National Cancer I n s t i t u t e ,
Tunis, which i s a W H D Regional Reference Centre, w i l l continue.
Promotion of environmental heal th
The Government is pursuing a long-term progralame f o r construction of sewerage
systems and treatment p lants , and the maintenance of the q u a l i t y of drinking water.
The "Organisation Nationale de 1 'Assainissement" is responsible f o r the planning,
execution and operation of waste management projects . WHO collaboration w i l l con-
t inue by means of consultant services and fellowships.
Health manpower development
A high proportion of W H ) ' s co l laborat ive e f f o r t w i l l be devoted t o the correct ion
of continuxng severe shortages i n c e r t a i n ca teaor ies of Health Manpower p a r t i c u l a r l y
a t the middle and lower l eve l s , and specia l e f f o r t s w i l l be devoted t o the t r a in ing
of teachers of a l l categories. There w i l l be continuing col laborat ion i n the ex-
tens ive medical education project with a l l th ree medical f a c u l t i e s a t the Uruvers i t les
of Tunis, Sousse, and Sfax, i n accordance with a five-year plan fo r development with
pa r t i cu la r emphasis on teacher t r a in ing and re-or ienta t ion of the curriculum towards
the preparation of doctors who w i l l serve the heal th needs of the Tunisian community.
I n col laborat ion with UNDP there w i l l be continuing e f f o r t s t o promote the work
of a nat ional centre f o r the development of heal th personnel teachers. I n the
s p e c i f i c case of t h e Medical Faculty of the Universi ty of Tunis, a nat ional cen t re fo r
teacher t r a i n i n g i n medicine i t s e l f is envisaged. I n the area of educational develop-
ment and support, s p e c i f i c emphasis w i l l continue t o be given t o the development of a
nat ional biomedical information system, strengthening o f hea l th service l i b r a r i e s ,
and i n i t i a l s t eps towards the creat ion of a nat ional documentation centre.
The general fel lowship a l l o c a t i o n f o r Tunisia rill increas ingly be used t o com-
plement these a c t i v i t i e s and w i l l be s p e c i f i c a l l y related t o the o ther co l l abora t ive
programes of W H O , with a diminishing emphasis on the use of WZr) fellowships f o r
c l i n i c a l t r a i n i n g cP physicians.
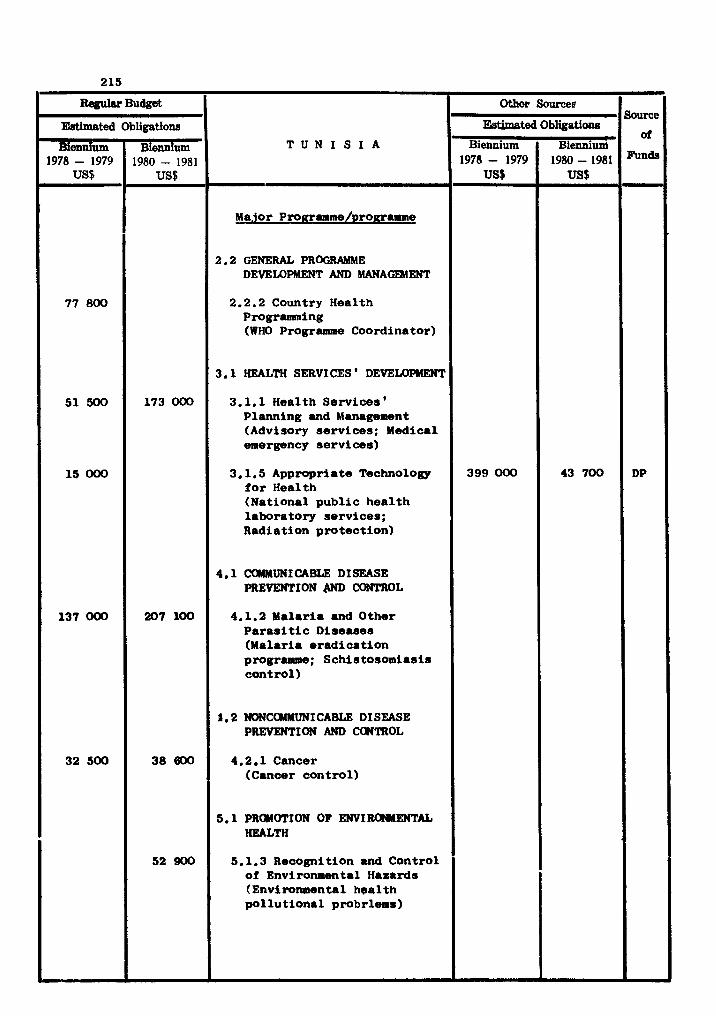
mWU Budget
T U N I S I A
- Major ProRramme/~roRramme
2.2 GENERAL PROORAMME DEVELOPMENT AND MANAGEMENT
2.2.2 Country Health Programming (WHO Programme Coordinator)
3.1 HEALTH SERVICES ' DEVEU)PMMST
3.1.1 Health Services ' Planning and Management (Advisory services; Medical emergency services)
3.1.5 Appropriate Technology for Health (National public health laboratory services; Radiation protection)
4.1 COMMUNICABLE DISEASE PREVENTION m CONTROL
4.1.2 Malaria and Other Parasitic Diseases (Malaria eradication programme; Schistosomiasis control)
P. 2 NONCaMMUNI CABLE DISEASE PREVENTION AND CWTROL
4.2.1 Cancer (Cancer control)
5.1 PROMWION OF ENVIRUWENTAL HEALTH
5.1.3 Recognition and Control of Environmental Hazards (Environmental health pollutional probrlems)
Estimated
B i d um 1978 - 1979
US6
77 800
51 !JOo
15 000
137 000
32 500
Obligations
Biennium 1980 - 1981
US$
173 000
207 100
38 600
52 900
Source
of
DP
Ckhcr Sources
Ebtbted
Biennium 1978- 1979
US$
399 000
Obligatione
Bienniunl 1980-1981 US$
43 700
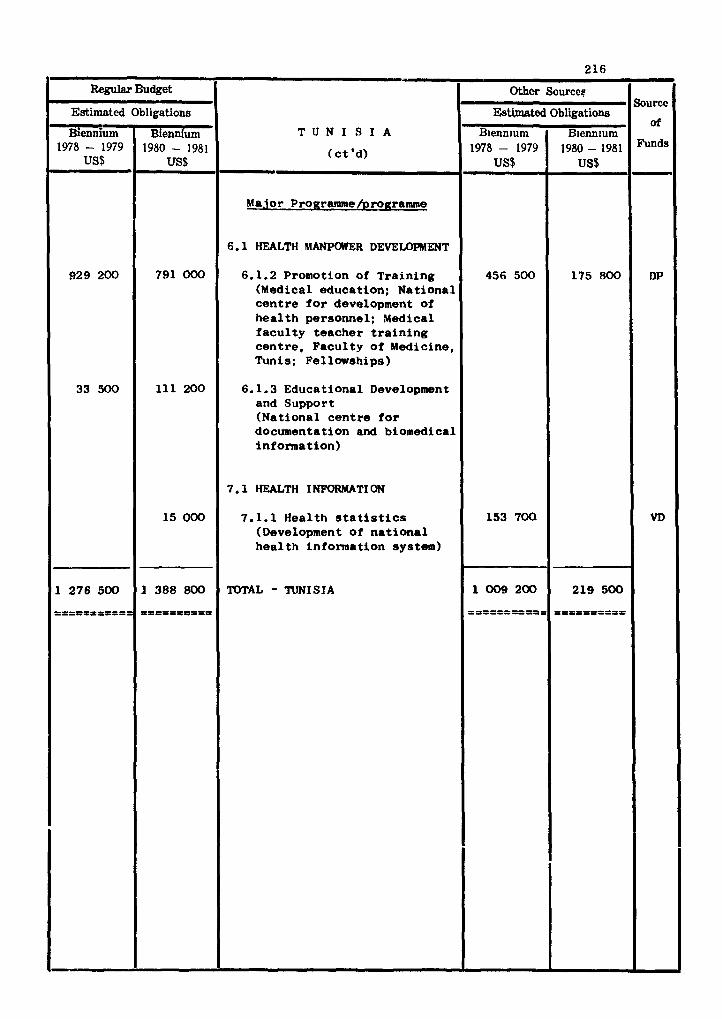
COUNTRY PRDCZUMW STATmPNT
UNITED ARAB =RATES
WATIWAL HEALTH D E V W m STRATEGY
The fledera1 f in is try of health of the United Arab m i r a t e s is responsible for
providing health services t o the seven federated emirates. Provision of health
f a c i l i t i e s during the l a s t ten years has greatly increased. A t present 2 423 beds i n
twenty-five hospitals and eigthy-three general and specialired clinioa a re avallable
i n the country. In addition, about twenty-four hospitals and cl inica are under eon-
atmotion which wi l l provide about 4 000 more hosptial beds for treatment.
The health services a re expanding a t a very f a s t paoe and therefore the quality
of services being provided varies from one emirate t o another. In addition, a number
of other government departments and organizations a re providing health servfces.
The Ministry of Health was established i n 1972 and its administrative s t ructure
and process a re st i l l being developed. The budget of the Ministry of Health i n 1978
was 818 million dirhams (approximately US $ 212 500 000).
TECIWICAL COOPHZATION PROORAMlldES FOR IBALTH
Health services developont
WR3 is collaborating w i t h the Federal Government i n restructuring the administration
and the organization of health services w i t h a v ie r to improve the planning, propmming
and u t i l i s a t i an of the available resources and the quality of services being provided.
The recorendations of WID mission consisting of a pharmacist, public health adminimtra-
tor, and management oonsultant, which vis i ted the country i n 1978, w i l l be taken into
-count-in the WID Technical Cooperation Programme for the biennium.
Disease prevention and control
The Malaria Control Progr-e, i n progress i n the Bnirates,will be continued and
its coordination with the programmes of the neighbouring Arab Sta tes w i l l be promoted . Prowtion of environmental health
Because of the rapid Urbanization and industr ia l izat ion i n the country, partioular-
l y the growth of the o i l industry,the probleu of environmental hazards and pollution
of the s o i l a r e assuming greater importance.
Tne Fede ra t i on is a l s o s l gnd to ry t o t h e convention f o r t h e c o n t r o l of environmental
pollution m d t h e d e l c t c r i o u s e r f e c t s of t h e c o a s t a l deve lopnen t (Kuw~i t ..ction P lan 3e-
gioi l ) . \,I30 ! w i l l c o l l a ' J c rd t e w i th t h e Government and CXCP i n t h e development o f manpower
c a p a b i l i t i e s and i n t h e implementation of programmes f o r a l r q u a l i t y c o n t r o l , marine
p o l l u t i o n c o n t r o l and enviroxunental xmprovement a c t r v i t i e s i n t h e vclrlous c o u n t r i e s
involved.
The Government depends l < l r g e l y upon e x p a t r i a t e p r o f e s s i o n a l s , middle- level m d
a u x i l l d r y personne l f o r i ts h e a l t h s e r v i c e s . E f f o r t s a r e being made t o t r a r n n a t i o n a l s
t o assume p r o l e s s l o n a l r e s p o n s i b i l i t ~ e s f o r running ti-re s e r v i c e s a s we l l ds t o give
r e o r i e n t a t i o n courses f o r t h e expatriate p r o f e s s i o n a l s and middle - leve l workers t o
meet t h e requirements of h e d l t h s e r v i c e s of t h e country.
Heal th in format ion
S t a t i s t i c s a r e be ing c o l l e c t e d i n va r i ous h o s p i t a l s and h e a l t h o rgan i za t i ons .
There is a need t o c o l l a t e and coordinate i n f o r . ~ d t i o n . \VIO w r l l c o l l d b o r a t e i n
s t r e n g t h e n i n g t h e h e a l t h i n f o r n a t i o n i n f r a s t r u c t u r e o f t h e h l rn i s t ry of Hedlth.
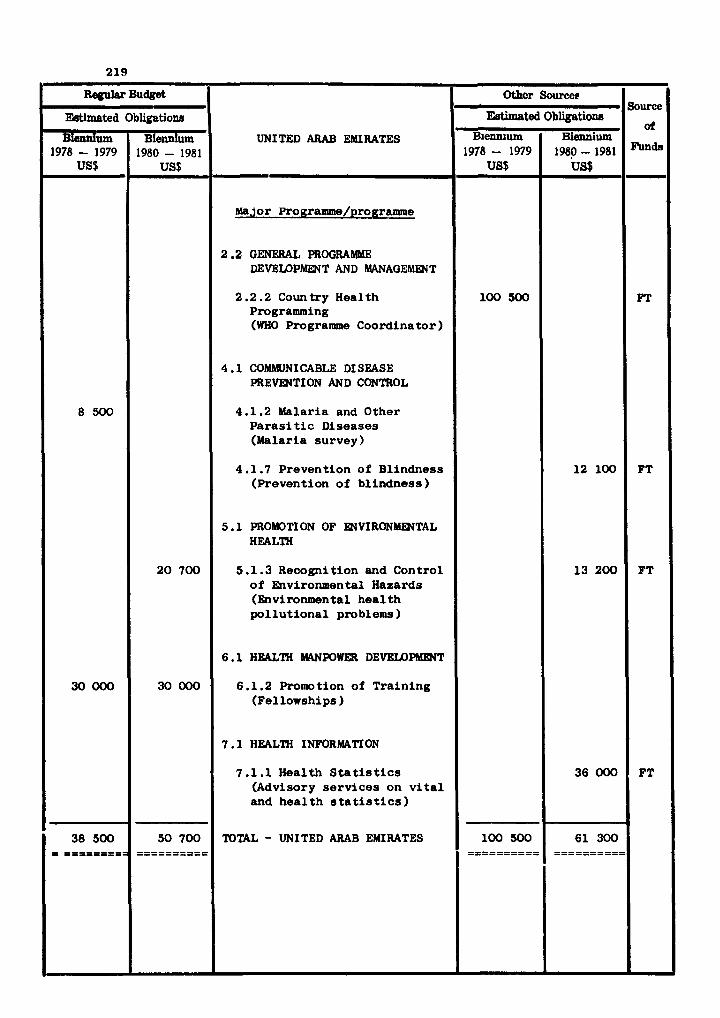
Regular Budget
UNITED ARAB EMIRATES
major Programme/programme
2.2 GENERAL PROGRAMME DEVELOPMENT AND MANAGEMPlT
2.2.2 Country Health Programming (WHO Programme Coordinator)
4 .1 COMMUNICABLE DI SEASE PREVENTION AND CONTROL
4.1.2 Malaria and Other Paras i t i c Diseases (Malaria survey)
4.1.7 Prevention of Blindness (Prevention of b l indness)
5.1 PROMOTION OF WVIRONlYENTAL HEALTH
5 .l. 3 Recognition and Control o f Environmental Hazards (Environmental hea l th p o l l u t i o n a l problems
6 .1 HEALTH MANPOWER DEVELDPMENT
6.1.2 Promo t i o n of Tra in ing (Fellowships )
7 .1 HEALTH INFORMATION
7.1.1 Health S t a t i s tics (Advisory s e r v i c e s on v i t a l and h e a l t h s t a t i s t i c s )
TOTAL - UNITED ARAB EMIRATES
Estimated
Biennium 1978 - 1979
US$ L
8 5 0 0
30000
38 500 = ========a
Obligations
Biennium 1980 - 1981
US$
20 700
30 000
50 700 ==========
Othor Sourceg
EWmated
B~enn~um 1978- 1979
US$
100 500
Source Obligations
Biennium 1980-1981
US$
12 100
13 200
36 000
61 300
or
FT
FT
FT
FT
COUNTRY PROGRAMME STATEMENT
YEMEN ARAB REPUBLIC
NATIONAL HEALTH DEVEWFWENT STRATEGY
The Five-Year National Socio-economic Development Plan covers the period 1976/77-
1980/81, and inc ludes a plan f o r t he h e a l t h s ec to r . About YR 420 mi l l i on has been
provided f o r hea l th . P r i o r i t y a r e a s inc lude development of bas i c h e a l t h s e rv i ces /
primary h e a l t h ca re ; s t rengthening of h e a l t h admin i s t r a t ion ; s trengthening of
h o s p i t a l s e rv i ces : h e a l t h manpower development; con t ro l of communicable d i s e a s e s
e s p e c i a l l y tuberculos is , malar ia and ur inary schis tosomias is ; and hea l th educat ion.
TECHNICAL CO-OPERATION PROGRAMMES BUR HEALTH
Health s e r v i c e s development
The country h e a l t h programming exe rc i se c a r r i e d o u t i n t he context of t h e h e a l t h
p lan f o r 1976/77-1980/81 provides f o r a primary h e a l t h c a r e programe (PHC) which is
t o be developed along wi th b a s i c h e a l t h s e r v i c e s (BHS). I t i s envisaged t h a t the
BHS/PHC programme w i l l see the es tab l i shment by 1981 o f a network of h e a l t h c e n t r e s
and sub-centres together wi th nea r ly 300 primary h e a l t h care un i t s . Voluntary
o rgan iza t ions w i l l continue t o support maternal and c h i l d h e a l t h , immunization and
mobile c l i n i c serv ices .
The development o f b a s i c h e a l t h s e r v i c e s and primary h e a l t h c a r e w i l l be re-
inforced by cont inuing o rgan iza t iona l development a t t h e Minis t ry of Health where,
p a r t i c u l a r l y , t he epidemiology, h e a l t h s t a t i s t i c s and h e a l t h educat ion s e c t i o n s w i l l
be strengthened. Technical support w i l l be provided by t h e s t rengthening of the
pub l i c h e a l t h l abo ra to ry s e r v i c e and t h e p r o j e c t f o r t h e maintenance and repair o f
medical equipment a s w e l l as development of mental h e a l t h serv ices . I n a l l o f t hese
a c t i v i t i e s WHO w i l l c o l l a b o r a t e by making a v a i l a b l e advisory se rv i ces , fe l lowships ,
s u p p l i e s and equipment.
Conmiunicable d i s e a s e prevention and con t ro l
The major t h r u s t s of communicable d i s e a s e con t ro l -11 cont inue t o be i n r e l a t i o n
t o ~ n a l a r i a , t ube rcu los i s , s ch i s to somias i s and d iar rhoea1 d iseases . WHO w i l l cont inue
i t s co l l abora t ion i n these f i e l d s , and w i l l p l ay a 8 a j o r r o l e i n t he expanded pro-
gramme on i m u n i x a t i o n and i n the f u r t h e r s t rengthening o f epidemiological s e rv i ces .

Promotion of environmental health
The Government assigns high p r io r i t y to thm provision of a u f e water supply, and
there ha8 been considerable progress i n a o n s t r u c t i ~ rrter aupply s y s t e u i n Samoa
and weid . a s w e l l a s i n sore rural areas. WiKl rill continua t o collaborate i n
developing environmental health 8ervice8 and water supply and -werage s y s t e u ; and
as executing agency for UNDP, i n strengthening the Rural Water Supply Departnent of
the Ministry of Public Health.
The inarea& r a t e of development of health urpower t o net the needs of t b ~
Governmmntos pr ior i ty health program86 is to be maintained through 1981. A oonsider-
able proportion of the required manpower is expected t o be trained by 1981. The
implementation of the p r i n r y hoalth atre p r o g r a m rill call for special a t ten t ion
to the t ra ining of front-l ine workers.
WHD rill aontinue i n its ro l e of executing agenoy for the UNDP-fimnoed Health
Manpower I n s t i t u t e project i n Suraoa, and rill co-owrate a1.o i n nursing education
and the t ra ining of primary health care workers. Fellowships rill continue t o be a
n j o r component of WHD collaboration i n health manpower developlent.
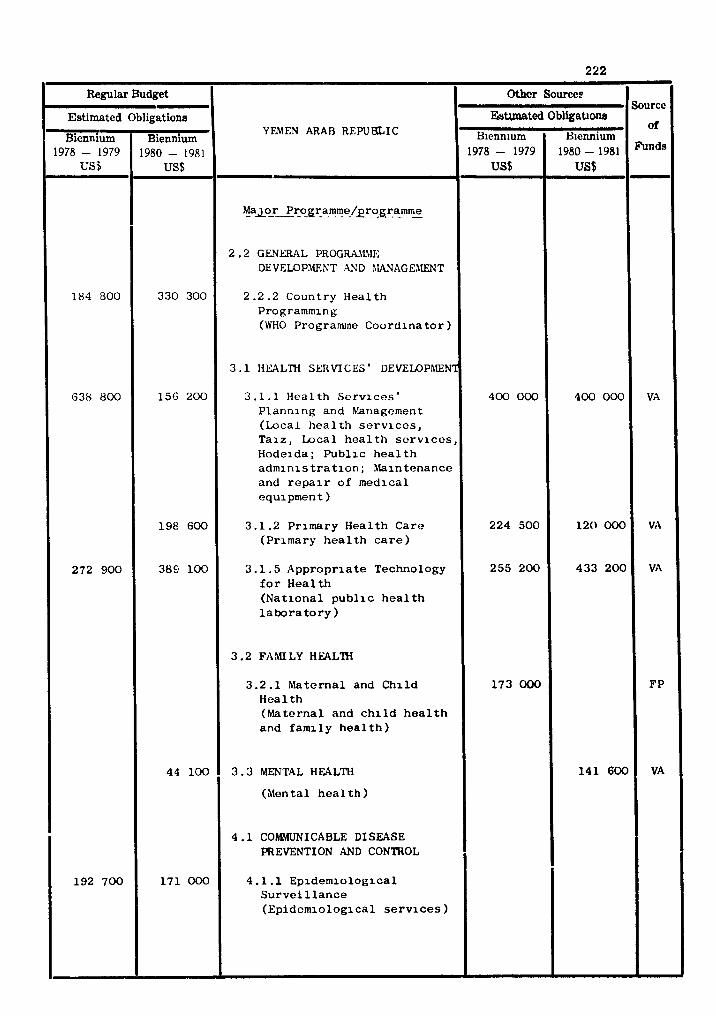
Regular Budget - Estimated Obligations
Biennium Biennium 1978 - 1979 1980 - 1981 F
YEMEN ARAB REPU5LIC
- !a~~rPr_o_gra_"1m_e_/~r?gr_a_m.me
2 . 2 G E N r n L PRoGWhZ!lE DEVELOPMEKT AID hWAGE1lENT
2 . 2 . 2 Coun t ry H e a l t h Programming (WHO Programme C o o r d i n a t o r )
3 . 1 HEALM SERVICES ' DEVEMPhlENT
3 . 1 . 1 H e a l t h S e r v i c e s ' P l a n n l n g and hlarlagement (Loca l h e a l t h s e r v i c e s , T a l z , Loca l h e a l t h s e r v i c e s , Hode ida ; P u b l i c h e a l t h a d m l n i s t r a t i o n ; hla in tenance and r e p a i r o f m e d i c a l e q u i p m e n t )
3 .1 .2 P r imary H e a l t h C a r e (P r imary h e a l t h c a r e )
3 . l . 5 A p p r o p r i a t e Technology f o r H e a l t h ( N a t i o n a l p u b l i c h e a l t h l a b o r a t o r y )
3 . 2 FAMILY HUL'IH
3 . 2 . 1 M a t e r n a l and C h i l d H e a l t h ( M a t e r n a l and c h i l d h e a l t h and f a m i l y h e a l t h )
3 . 3 MENTAL HEALTH
(Menta l h e a l t h )
4 .1 COhMJNICABLE DISEASE PREVENTION AND CONTROL
4 . 1 . 1 E p i d e m i o l o g i c a l S u r v e i l l a n c e ( E p i d e m i o l o g i c a l s e r v i c e s )
184 300
638 800
272 900
192 700
330 300
156 200
198 600
389 100
44 1 0 0
171 000
Sourcc
of
VA
VA
VA
FP
VA
Other source^
Estrmated
B~enn~um 1978- 1979
US$
400 000
224 500
255 200
1 7 3 000
Obligatlom
H~ennium 1980-1981 US$
400 000
1 2 0 000
4 3 3 2 0 0
1 4 1 6 0 0
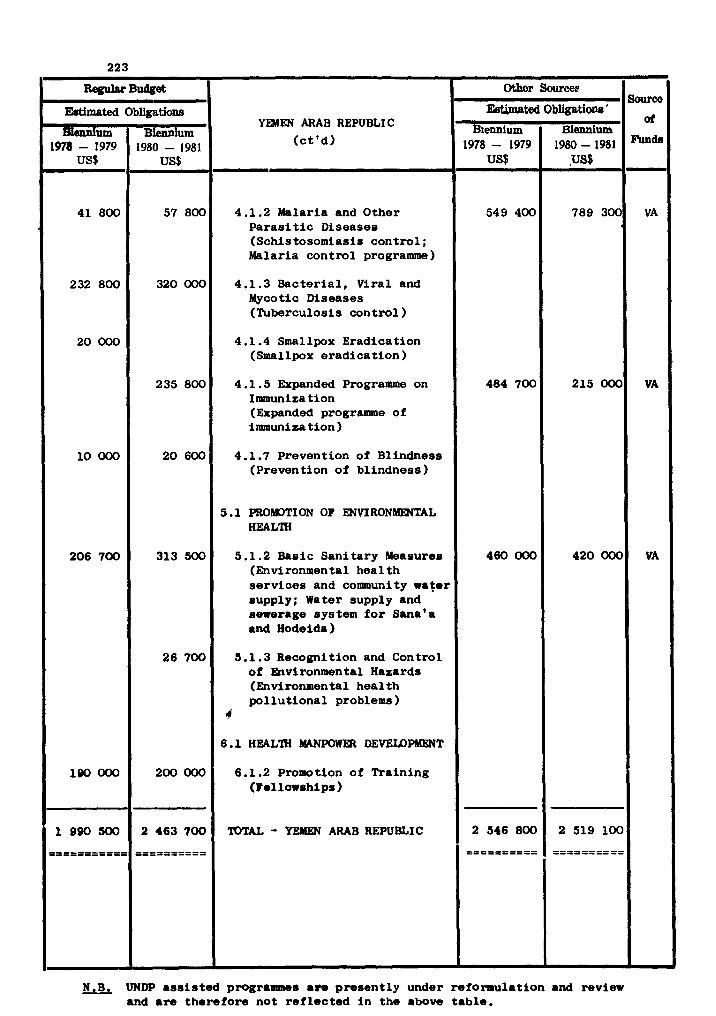
YEMEN ARAB REPUBLIC
(c t ' d )
4.1.2 Malaria and Other P a r a s i t i c Diseaseo (Schistosomiasir control ; Malaria control programme)
4.1.3 Bacter ia l , Viral and Mycotic Diseases (Rtberculosis control )
4.1.4 Smallpox Eradication (Smallpox eradicat ion )
4.1.5 Expanded Programme on Immunization (Expanded programme of immunization )
4.1.7 Prevention of Blindness (Prevention of blindness )
5.1 PROMOTION OF ENVIRONMENTAL HEALTH
5.1.2 & s i c Sanitary Measures (Environmental heal t h se rv ices and community r a t e l supply; Water supply and sewerage system f o r Sana'a and Hodeida)
5.1.3 Recognition and Control of Environmental Haoards (Environmental heal th po l lu t iona l problems )
4
6.1.2 Promo t ion of Training (Fellowahips )
TOTAL - YEMEN ARAB REPUBLIC
Othor Sourcee b Source
EWuted Obligatione ' or
Biennium Biennium 1978- 1979 1980-1981
549 400 789 300 VA
484 700 215 000 VA
460 000 420 000 VA
2 546 800 2 519 100
=====x==== ====a=====
N.B. UNDP ass i s t ed programmes a m present ly under reformulation and review and a r e therefore not r e f l ec ted i n the above table .
REGIONAL ADVISERS
'personnel : Provision is made under the Regular Budget f o r 26 posts i n the profession-
a l category and 35 posts i n the general services Category during t h e biennium, Under
UNFPA , provision is a l so made f o r one post i n the professional category and one i n
the general services category.
The following addit ions and o f f s e t t i n g dele t ions of posts a r e re f l ec ted i n the
proposed Programme Budget:
(1) One MCH Adviser (P4) and one Clerk-Stenographer (m5) have been added t o Maternal
and Child Health (3.2.1), whlle one Health Education Adviser (P4) and one Clerk-
Stenographer (Rd5) have been deleted from Health Education (3.2.4).
( 2 ) One Health Economies Adviser(P4) and one Clerk-Stenographer (lB15) have been added
t o Health Services Development, i n Programme Planning and General Ac t iv i t es (3. l o o ) ,
while one Adviser (P4) and one Clerk-Stenographer (EM5)have been deleted from Cardio-
vascular Diseases. (4.2.2).
(3) The post of Public Iiealth Administrator (P5) under t h e Programme "Collaboration w i t h
m u l t i l a t e r a l and b i l a t e r a l programme" (2.3.2) has been deleted and replaced by an
Administrative Assistant (EXiX) post.
The establishment of Regional Advisers fo r t h e 1980-1981 biennium is a s follows:
2.3.2 Collaboration with m u l t i l a t e r a l and b i l a t e r a l programme - one, administrat ive
a s s i s t a n t (EW() and one clerk-stenographer (mfXIG).
3.1 HEALTH SERVICES DEVELOPMENT
3.1.0 Programme Ranning and General Act ivi t ies (two Dl) th ree P5 and one P4 a s froln
1981; two m7 and one addltronal W S a s f r o m 1981,
3.1.3 Workers' Health - (one P4, one 3325).
3.1.5 Appropriate Bchnology f o r Health - (two PJ and two Rd5).
3.2 FAMILY HEALTH
3.2.1 Maternal and Child Health - (two P4 and two Rd5 of which one professional and
one general services post financed from UNFPA).
3.2.2 Nutr i t ion - (one P5 and one M5)
3.3 MENTAL HEALTH - (one P5 and one m16).
3.4.0 Prophylactic, Diagnostic and Therapeutic Substances - programme planning and
general ac t iv i t i e s (one P4).
4.1 COSlQmMICABLE DISEASE PREVENTION AND CONTROL
4.1.0 Programme Planning and General Act ivi t ies - (one D l and one M7).
4.1.1 Epidemiological Surveillance - (one P5 and one m5).
4.1.2 Malaria and Other Paras i t ic Diseases - (one P5, one P4 and two M5).
4.1.8 Vector Biology and Control - (one P4 and one m5).
4.2 NON-COMMUNICABLE bISEASE -ION AND CUNTROL
4.2.2 Cardiovascular Disease - (one P4 and one EN15 i n 1980 ohly).
5.1 PROWION OF WIRONMENTAL HEALTH
5.1.0 Programme Planning and General Act ivi t ies - (three P5 and two m5).
6.1 HEALTH MANPOWER DEVEXDPIIIENT
6.1.0 P r o g r m e Planning and General Act ivi t ies t one D l , one P5 and t w o P4, one
IWC, one m, two M7, one EY6, s i x EM5 and two QL4).
7 • HEALTH 1WK)RMATION
7.1.0 Programe Planning and General Act ivi t ies - (one P5 and one g15).
Estimated obligations for Regional Advisers under the Regular Bugdet of US $
3 368 900includeprovision for duty t ravel of US $ 250 700 t o enable Regional Adviaera
t o advise f i e l d s t a f f , to a s s i s t i n the planning, implementation and evaluation of f i e l d
projects and to consult health authori t ies i n the countries of the Region.
Estimated obligations fo r UNFPA Regional Advisers of US $ 121 000 include provision
for duty t ravel of US $ 9 200.
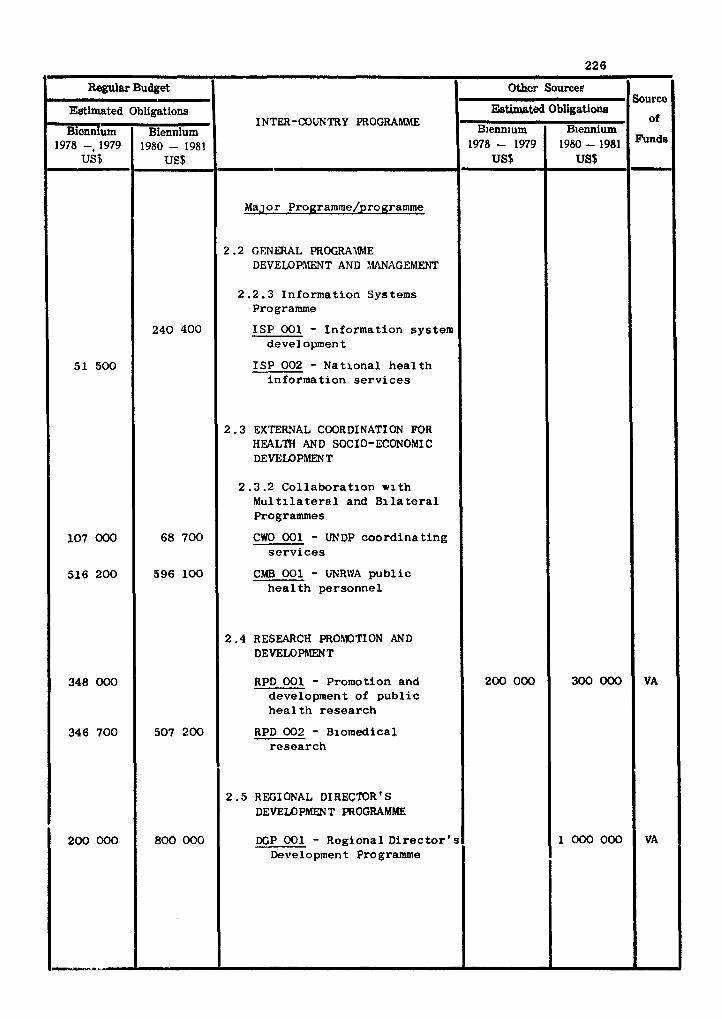
Regular Budget
INTER-COUNTRY PROGRAMME
Major Programme/programme
2 .2 GENERAL PROGRAIlhiE DEVELOPMENT AND MANAGEMENT
2.2.3 In format ion Systems Pro gramme
ISP 001 - In format ion system development
ISP 002 - Nat iona l h e a l t h in format ion s e r v i c e s
2 . 3 EXTERNAL COORDINATION FOR HEALTH AND SOCIO-ECONOMI C DEVELOPMENT
2.3.2 C o l l a b o r a t i o n w i t h M u l t i l a t e r a l and B i l a t e r a l Programmes
CWO 001 - UNDP c o o r d i n a t i n g s e r v i c e s
CMB 001 - UNR\VA p u b l i c h e a l t h personne l
2 .4 RESEARCH PROMOTION AND DEVELOPMENT
RPD 001 - Promotion and development of p u b l i c h e a l t h r e s e a r c h
RPD 002 - Biomedical r e s e a r c h
2 .5 REGIONAL DIRECTOR ' s DEVELOPMEN T PROGRAMME
DCP 001 - Regional D i r e c t o r ' s Development Programme
Estimated
Biennium 1978 -, 1979
US8
51 500
107 OOO
516 200
348 000
346 700
200 000
-- -
- Obligations
Biennium 1980 - 1981
US$
240 400
68 700
596 100
507 200
800 000
Sourco
of
Funds
VA
VA
Othcr Sources
Estimated Bienn~um
1978 - 1979 US$
200 000
Obligations
Biennium 1980 - 1981 US$
300 000
1000 000
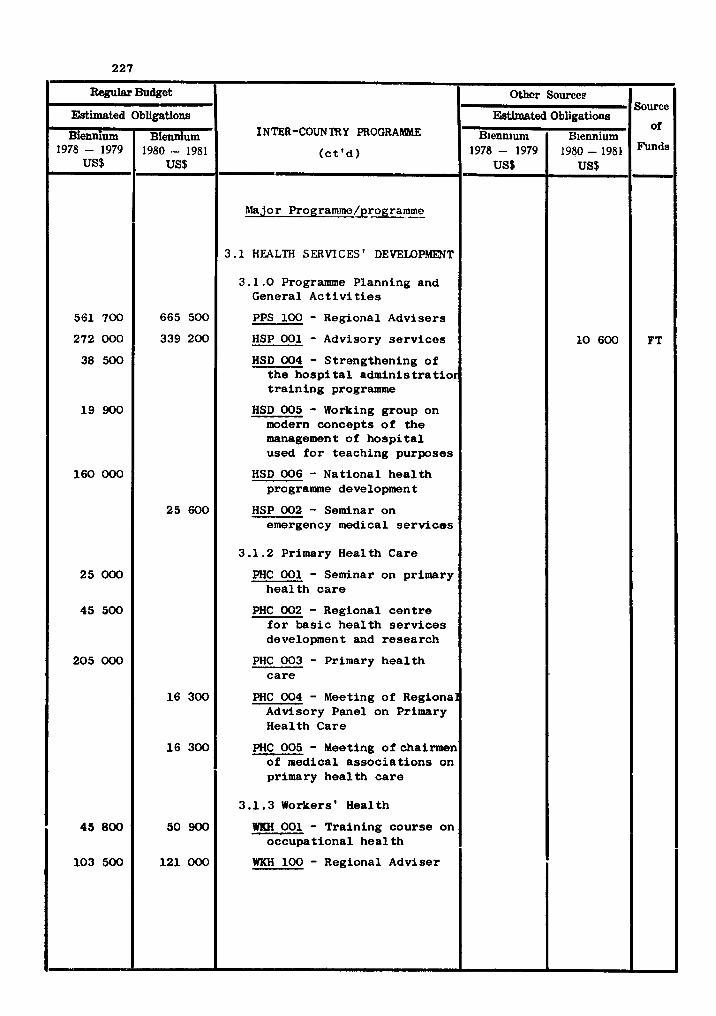
Regular Budget
Estimated Obligations
Biennium Biennium 1978 - 1979 1980 - 1981 1
INTER-COUNTRY PROGRAMME
( c t ' d ) - Major Programme/programme
3.1 HEALTH SERVICES ' DEVEMPMENT
3 .1 .0 Programme Planning and General A c t i v i t i e s
PPS 100 - Regional Advisers
HSP 001 - Advisory s e r v i c e s
HSD 004 - Strengthening of t h e h o s p i t a l adminis t r a t i o r t r a i n i n g programme
HSD 005 - Working group on modern concepts o f the management of h o s p i t a l used f o r teaching purposes
HSD 006 - National h e a l t h programme development
HSP 002 - Seminar on emergency medical s e r v i c e s
3.1.2 Primary Health Care
PHC 001 - Seminar on primary h e a l t h c a r e
PHC 002 - Regional c e n t r e f o r bas i c h e a l t h s e r v i c e s development atad research
PHC 003 - Primary h e a l t h c a r e
PHC 004 - Meeting of Regiona: Advisory Panel on Primary Health Care
PHC 005 - Meeting of chairmen of medical a s soc ia t ions on primary hea l th c a r e
3.1.3 Workers ' Health
WKH 001 - Training course on occupational h e a l t h
WKH 100 - Regional Adviser
561 700
272 000
38 500
1 9 900
160 000
25 000
45 500
205 000
45 800
103 500
665 500
339 200
25 600
16 300
16 300
50 900
121 000
Sourcc
ai
Funds
FT
Othor Sourcee
Ebtbated
Biennium 1978- 1979
US$
Obligations
Biennium 1940-1981
US$
10 600
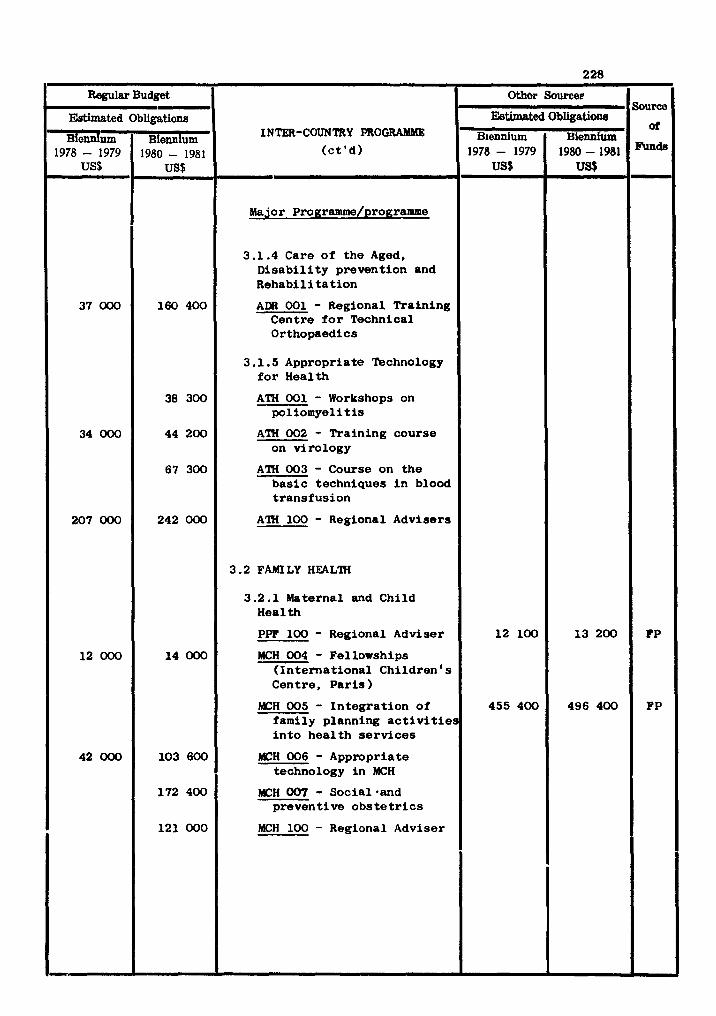
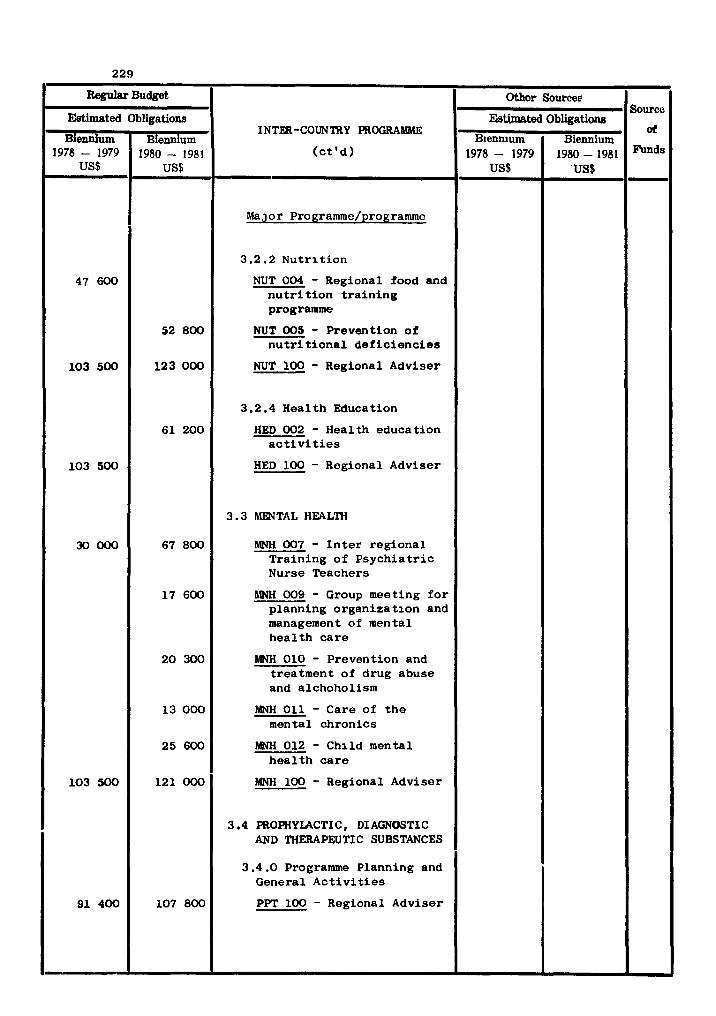
m Budget
INTER-COUNTRY P R O G R A W
( c t ' d ) ~- Major Programme/programme
3.2.2 Nu t r i t i on
NUT 004 - Regional food and n u t r i t i o n t r a i n i n g programme
NUT 005 - Prevention of n u t r i t i o n a l d e f i c i e n c i e s
NUT 100 - Regional Adviser
3.2.4 Health Education
HED 002 - Health educat ion a c t i v i t i e s
HED 100 - Regional Adviser
3.3 WTAL HEALTH
MNH 007 - I n t e r reg ional Training of Psych ia t r i c Nurse Teachers
MNH 009 - Group meeting f o r planning organiza t ion and management of mental h e a l t h c a r e
MNH 010 - Prevention and treatment of drug abuse and alchoholism
MNH 011 - Care of t h e mental chronics
MNH 012 - Child mental h e a l t h c a r e
MNH 100 - Regional Adviser
3.4 PROPHYLACTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
3.4.0 Programme Planning and General A c t i v i t i e s
PPT 100 - Regional Adviser
Estimated
Biennium 1978 - 1979
US$
47 600
103 500
103 500
30000
103 500
91 400
Obligations
Biennium 1980 - 1981
US$
52 800
123 000
61 200
67 800
17 600
20 300
13 000
25 600
121 000
107 800
Source
at
Other Sources
Estimated B~ennium
1978- 1979 US$
Obligations
Biennium 1980-1981
'US$
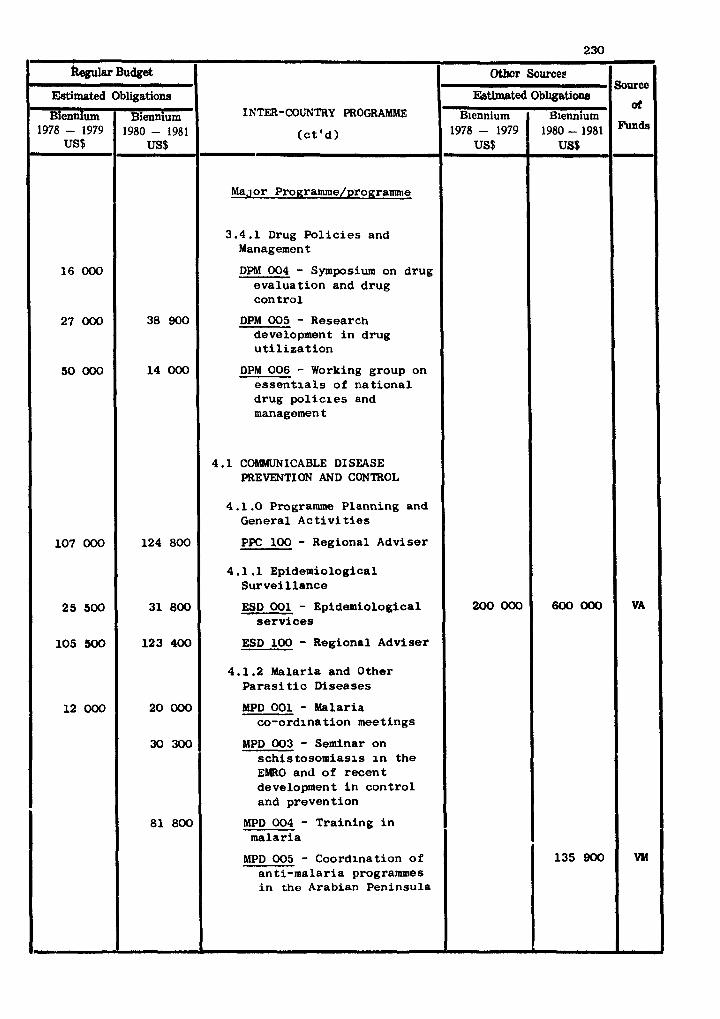
k l a r Budget
INTER-COUNTRY PROGRAMME
( c t ' d )
,-
Major Programme/programme
3.4.1 Drug P o l i c i e s and Management
DPM 004 - Symposium on drug evalua t ion and drug con t ro l
DPM 005 - Research development i n drug u t i l i z a t i o n
DPM 006 - Working group on e s s e n t i a l s of n a t i o n a l drug p o l i c l e s and management
4 .1 COMMUNICABLE DISEASE PREVENT1 ON AND CONTROL
4.1.0 Programme Planning and General A c t i v i t i e s
PPC 100 - Regional Adviser
4.1.1 Epidemiological Su rve i l l ance
ESD 001 - Epidemiological s e r v i c e s
ESD 100 - Regional Adviser
4.1.2 Malaria and Other P a r a s i t i c Diseases
MPD 001 - Malaria co-ordinat ion meetings
MPD 003 - Seminar on s c h i s tosomiasis i n t h e EMRO and of r ecen t development i n con t ro l and prevention
MPD 004 - Training i n malar ia
MPD 005 - Coordination o f an t i -malar ia programmes i n the Arabian Peninsula
Estimated
Bicndum 1978 - 1979
US$
16 000
27 000
50 000
107 000
25 500
105 300
12 000
Obligations
Biennium 1980 - 1981
US$
38 900
14 000
124 800
31 800
123 400
20 000
30 300
81 800
Sourca
d
VA
WI
Othcr Sources
Estimated
Blennium 1978 - 1979
US$
200 000
Obl~gatione
'Biennium 1980 - 1981 US$
600 000
135 900
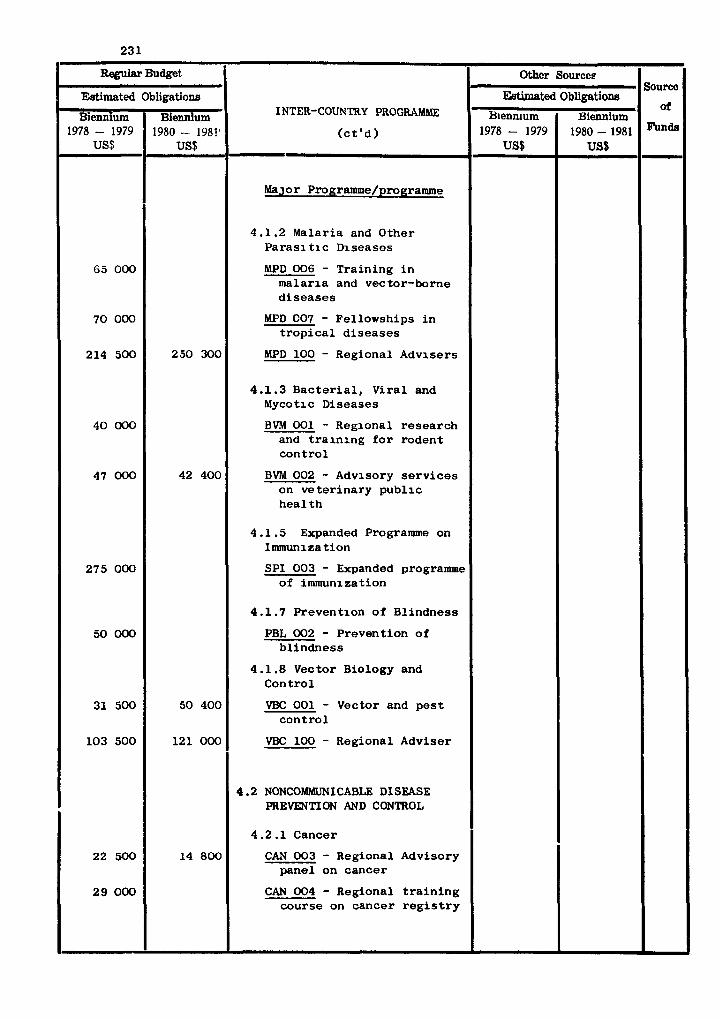
war Budget
INTER-COUNTRY PROGRAMNIE
( c t ' d )
% J O ~ Pm~ramme/programme
4.1.2 Malar ia and Other Paras1 t i c Diseases
MPD 006 - Tra in ing i n ma l a r i a and vector-borne d i s e a s e s
MPD C07 - Fellowships i n t r o p i c a l d i s e a s e s
MPD 100 - Regional Advisers
4 .1 .3 B a c t e r i a l , V i r a l and Mycotic Diseases
BV?d 001 - Regional r e s ea r ch and t r a i n i n g f o r rodent c o n t r o l
BVM 002 - Advisory s e r v i c e s on v e t e r i n a r y p u b l i c h e a l t h
4 .1 .5 Expanded Programme on Immunization
SPI 003 - Expanded programme of immunization
4.1.7 Prevent ion of Bl indness
PBL 002 - Prevent ion of b l i ndnes s
4 .1 .8 Vector Biology and Cont ro l
VBC 001 - Vector and p e s t c o n t r o l
VBC 100 - Regional Adviser
4.2 NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
4 .2 .1 Cancer
CAN 003 - Regional Advisory pane l on cancer
CAN 004 - Regional t r a i n i n g course on cancer r e g i s t r y
Mimated
Biennium 1978 - 1979
US$
65 000
70 000
214 500
40 000
47 000
275 000
50 000
31 500
103 500
22 500
29 000
Obligations
Biennium 1980 - 1981'
US$
250 300
42 400
50 400
121 000
14 800
Source
of
Othcr Sources
Estimated Biennium
1978 - 1979 US$
Obligations
Biennium 1980 - 1981
US$
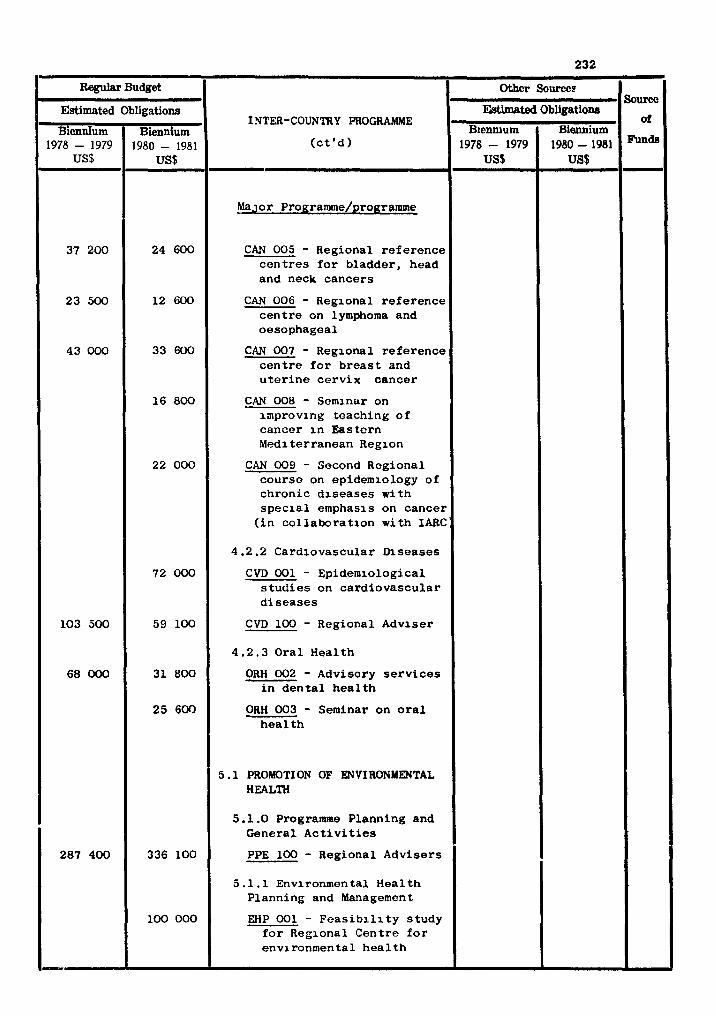
Regular Budget
INTER-COUNTRY PROGRAMME
( c t ' d ) - Major Programme/programme
CAN 005 - Regional re ference con tres f o r bladder, head and neck cancers
CAN 006 - Regional re ference c e n t r e on lymphoma and oesophageal
CAN 007 - Regional re ference c e n t r e f o r b reas t and u t e r i n e ce rv ix cancer
CAN 008 - Seminar on improving teaching o f cancer i n Eastern Mediterranean Region
CAN 009 - Second Regional course on epidemiology of chronic d i seases with s p e c i a l emphasis on cancer
( i n co l l abora t ion wi th IARC:
4.2.2 Cardiovascular Diseases
C M 001 - Epidemiological s t u d i e s on card iovascular d i seases
CVD 100 - Regional Adviser
4 .2 .3 Oral Health
ORH 002 - Advisory s e r v i c e s i n d e n t a l h e a l t h
ORH 003 - Seminar on o r a l h e a l t h
5 .1 PROMOTI ON OF ENVIRONMENTAL HEALTH
5.1.0 Programme Planning and General A c t i v i t i e s
PPE 100 - Regional Advisers
5.1.1 Environmental Heal th Planning and Management
EHP 001 - F e a s i b i l i t y s tudy f o r Regional Centre f o r environmental h e a l t h
Estimated
Biennium 1978 - 1979
US$
37 200
23 500
43 000
103 500
68 000
287 400
II
- Obligations
Biennium 1980 - 1981
US$
24 600
12 600
33 600
16 800
22 000
72 OW
59 100
31 800
25 600
336 100
100 000
Sourco
of
Othcr Sourcee
EWmated
B~ennium 1978 - 1979
US$
Obligations
Biennium 1980 - 1981 US$
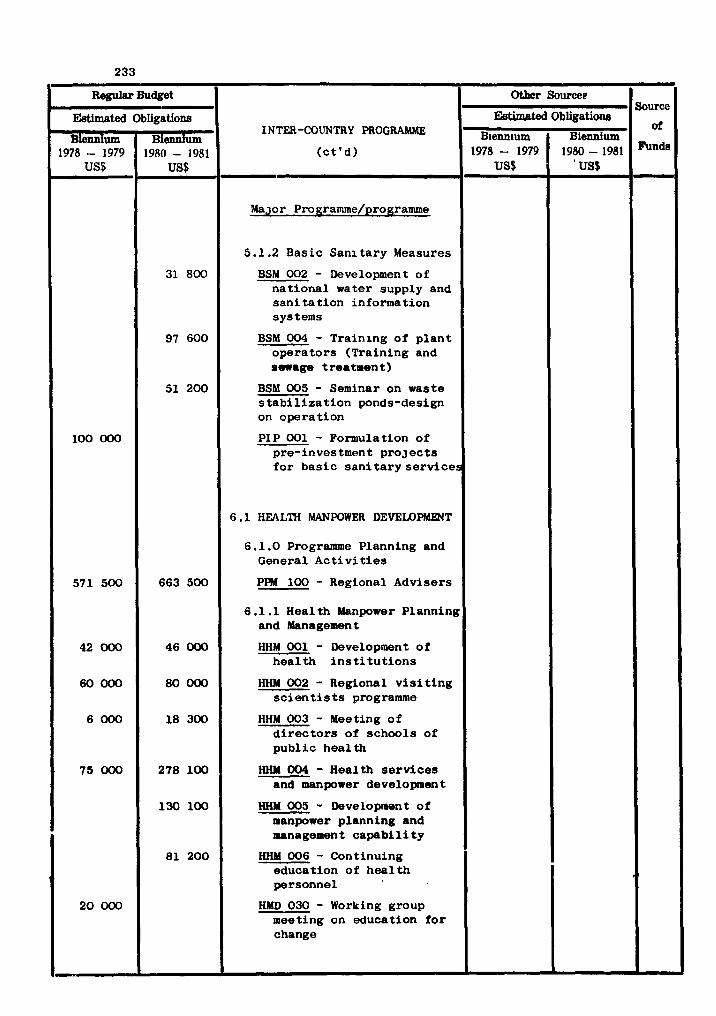
Regular Budget
INTER-COUNTRY PROGRAMNlE
( c t ' d )
Major Programme/programme
5.1.2 Bas ic San i t a ry Measures
BSM 002 - Development of na t iona l water supply and s a n i t a t i o n information systems
BSM 004 - Training of p l a n t ope ra to r s (Training and s w a g e treatment 1
BSM 005 - Seminar on waste s t a b i l i z a t i o n ponds-design on opera t ion
PIP 001 - Formulation of pre-investment p r o j e c t s f o r b a s i c s a n i t a r y s e r v i c e s
6 .1 HEALTH MANPOWER DEVEMPMENT
6.1.0 Programme Planning and General A c t i v i t i e s
PPM 100 - Regional Advisers
6.1 .1 Health Manpower Planning and Management
HHM 001 - Development of h e a l t h i n s ti t u t i o n s
HHM 002 - Regional v i s i t i n g s c i e n t i s t s programme
HHM 003 - Meeting o f d i r e c t o r s of schools of pub1 i c hea l th
H W 004 - Health s e r v i c e s and manpower development
HHM 005 - Development of manpower planning and management capabi 1 i t y
HHM 006 - Continuing education of hea l t h personnel
HMD 030 - Working group meeting on education f o r change
Estimated
Biennium 1978 - 1979
US$
100 000
571 500
42 000
60 000
6000
75 000
20 000
- Obligations
Biennium 1980 - 1981
US$
31 800
97 600
51 200
663 500
46 000
80 000
18 300
278 100
130 100
81 200
Soum of
0-r Sourceg
EMmated B~enn~um
1978 - 1979 US$
Obligations
Biennium 1980 - 1981
' US$
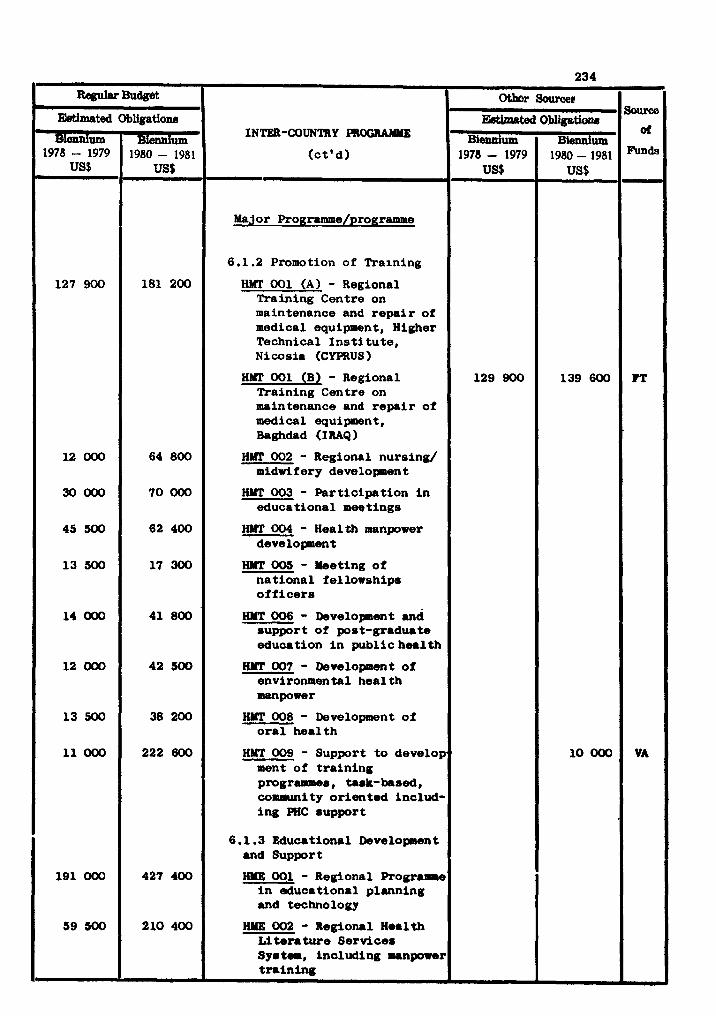
234
INTER-COUNTRY PROGUIWE
Major Programme/programme
6.1.2 Promotion of Training
HMT 001 (A) - Regional Training Centre on maintenance and r e p a i r of medical equipment, Higher Technical I n s t i t u t e , Nicosia (CYPRUS)
H#r 001 (B) - Regional Training Centre on maintenance and r e p a i r of medical equipment, Baghdad (IRAQ )
002 - Regional nursing/ midri f e ry developen t
HNT 003 - Part ic ipat ion i n educational meetings
HYT 004 - Health manpower deve lopnent
HMT 005 - Meeting of nat ional f ellowships o f f i c e r s
HMT 006 - Developnent and support of post-graduate educeition i n public himlth
HYT 007 - Development of environmental heal th
W T 008 - Development of o r a l hea l th
HMT 009 - Support t o develop ment of t r a in ing progrrraaes , task-based, coa~runity or iented includ- ing PHC support
6.1.3 Educational Development and Support
HUE 001 - Regional Programhe i n d u c a t i o n a l planning and techno logy
- Regional Health ture Services
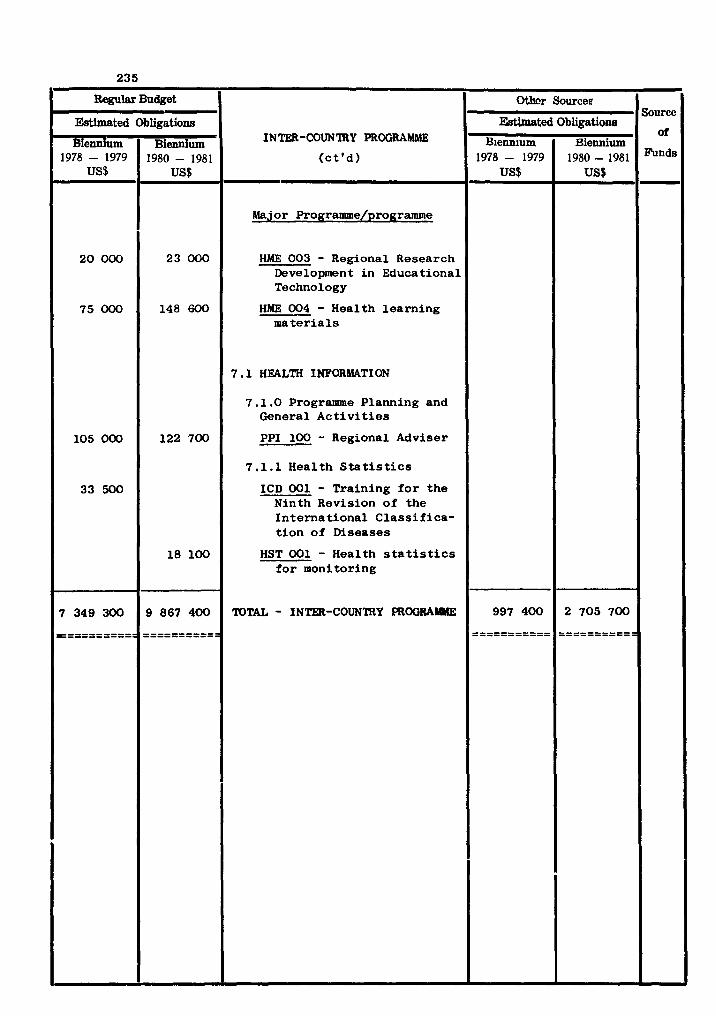
Regular Budget
Estimated
Biennium 1978 - 1979
US$
20 000
75 000
105 000
33 500
7 349 300
===========
Othcr Source9 Sourcc
Ektbated Obligatione INTER-COUN'IRY PROGRAMblE
- Obligations
Biennium 1980 - 1981
US$
23 000
148 600
122 700
18 100
9 867 400
===========
( c t ' d )
.-
Major Programme/programme
HME 003 - Regional Research Development i n Educational Technology
HME 004 - Health l ea rn ing m a t e r i a l s
7 .1 HEALTH INFORMATION
7.1.0 Programme Planning and General A c t i v i t i e s
PPI 100 - Regional Adviser
7 .l. 1 Heal th S t a t i s t i c s
ICD 001 - Train ing f o r t h e Ninth Revision o f t he I n t e r n a t i o n a l C l a s s i f i ca - t i o n o f Diseases
HST 001 - Health s t a t i s t i c s f o r monitoring
TOTAL - INTER-COUNTRY PROGRAMME 997 400
----------- ----------- 2 705 700
----------- -----------