
性感染症に関する特定感染症 予防指針に基づく対策の 推進 ...
298
― 5 ― 平成28(2016)年3月 厚生労働科学研究費補助金 新興・再興感染症及び予防接種政策推進研究事業 厚生労働科学研究費補助金 新興・再興感染症及び予防接種政策推進研究事業 性感染症に関する特定感染症 予防指針に基づく対策の 推進に関する研究 性感染症に関する特定感染症 予防指針に基づく対策の 推進に関する研究 (H27 - 新興行政 - 一般 - 001) 平成27年度 総括・分担研究報告書 研究代表者 荒 川 創 一
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 性感染症に関する特定感染症 予防指針に基づく対策の 推進 ...
― 5 ―
平成28(2016)年3月
厚生労働科学研究費補助金新興・再興感染症及び予防接種政策推進研究事業
厚生労働科学研究費補助金新興・再興感染症及び予防接種政策推進研究事業
性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究
性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究(H27 - 新興行政 - 一般 - 001)
平成27年度総括・分担研究報告書
研究代表者
荒 川 創 一

厚生労働科学研究費補助金新興・再興感染症及び予防接種政策推進研究事業
「性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究」研究班班員名簿
研究代表者 荒川 創一 神戸大学大学院医学研究科 地域社会医学健康科学講座 地域医療ネット
ワーク学分野 特命教授/泌尿器科/感染制御部長
研究分担者 砂川 富正 国立感染症研究所感染症疫学センター 第二室長
中瀨 克己 岡山大学医療教育統合開発センターGIMセンター部門 教授
小森 貴 日本医師会 常任理事
濵砂 良一 産業医科大学医学部泌尿器科 准教授
余田 敬子 東京女子医科大学東医療センター耳鼻咽喉科 准教授
三鴨 廣繁 愛知医科大学大学院医学研究科臨床感染症学 主任教授
川名 敬 東京大学大学院医学系研究科産婦人科学講座 准教授
白井 千香 神戸市保健福祉局 医務担当部長/大阪市立大学大学院医学研究科公衆衛生学
田中 一志 神戸大学大学院医学研究科外科系講座 腎泌尿器科学分野 特命教授
伊藤 晴夫 千葉大学 名誉教授
研究協力者 山岸 拓也 国立感染症研究所感染症疫学センター 主任研究官
有馬 雄三 国立感染症研究所感染症疫学センター 主任研究官
高橋 琢理 国立感染症研究所感染症疫学センター 研究員
加納 和彦 国立感染症研究所感染症疫学センター 研究員
石金 正裕 国立感染症研究所感染症疫学センター 実地疫学専門家養成コース 協力研究員金井 瑞恵 国立感染症研究所感染症疫学センター 実地疫学専門家養成コース 協力研究員加藤 博史 国立感染症研究所感染症疫学センター 実地疫学専門家養成コース 協力研究員安藤 美恵 国立感染症研究所感染症疫学センター 実地疫学専門家養成コース 協力研究員大西 真 国立感染症研究所細菌第一部 部長

谷畑 健生 神戸市東灘区保健福祉部 医務担当課長
五十嵐辰男 千葉大学フロンティア医工学センター 教授
出口 隆 岐阜大学医学部附属病院泌尿器科 教授
安田 満 岐阜大学医学部附属病院泌尿器科 講師
金山 博臣 徳島大学大学院医歯薬学研究部泌尿器科学分野 教授
高野つる代 横浜市旭区福祉保健センター センター長
川畑 拓也 大阪府立公衆衛生研究所感染症部ウイルス課 主任研究員
細井 舞子 大阪市保健所 係員
中谷 友樹 立命館大学文学部地理学教室 教授
尾本由美子 豊島区池袋保健所健康推進課 課長
樫原 摩紀 株式会社エスアールエル八王子ラボ感染免疫部感染症特殊検査課
金谷 泰宏 国立保健医療科学院健康危機管理研究部 部長
山岸 由佳 愛知医科大学病院感染症科 准教授
萩原 真生 愛知医科大学病院感染制御部
岩室 紳也 ヘルスプロモーション推進センター〔オフィスいわむろ〕 代表
種部 恭子 女性クリニックWe ! TOYAMA 院長/産婦人科
野々山未希子 自治医科大学看護学部 教授渡會 睦子 東京医療保健大学医療保健学部看護学科 准教授
秋元 義弘 岩手県立二戸病院 産婦人科長
武島 仁 龍ケ崎済生会病院 副院長/泌尿器科科長
渡部 享宏 NPO法人子宮頸がんを考える市民の会 事務局長
吉田 弘之 神戸大学医学部附属病院感染制御部

目 次
Ⅰ.総括研究報告書
性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究 ..........................7 荒川 創一
Ⅱ.分担研究報告書
1 .感染症発生動向調査から見たわが国の性感染症の動向、2015年 ......................................13 砂川 富正・他 2 .性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究 ......................45 ―センチネルサーベイランスの施行について― 谷畑 健生・他 3 .性感染症(STI)サーベイランスの評価と改善に関する研究 ...........................................77 中瀨 克己・他 4 .Mycoplasma genitalium検査法に関する研究 .....................................................................140 濵砂 良一 5 .口腔・咽頭梅毒および淋菌・クラミジアの咽頭感染に関する検討 ................................148 余田 敬子 6 .HPV関連子宮頸癌早期スクリーニングの啓発に関する研究 ..........................................159 三鴨 廣繁・他 7 .性感染症、特にHPVと子宮頸癌についての啓発に関する研究 ......................................164 川名 敬 8 .感染予防行動、早期受診促進のための性感染症啓発スライドについて ........................177 白井 千香・他
Ⅲ.研究成果の刊行に関する一覧表 .......................................................................................187
Ⅳ.研究成果の刊行物・別刷 ...................................................................................................191


Ⅰ.総括研究報告書


1.感染症発生動向調査から見たわが国の 性感染症の動向、2015年 発生動向調査から見た5類定点把握疾患の2015年の動向については、概ね例年並みであった。例年同様、男女共に、性器クラミジア感染症の報告数が最も多かった。また、淋菌感染症を除いて、男性と比べて女性症例の年齢分布の方が若かった。性器クラミジア感染症の定点当たり報告数は、概ね横ばいであった。性器ヘルペスウイルス感染症の定点当たり報告数は、男女ともに概ね横ばいであり、近年同様、女性の報告数が男性を若干上回った。尖圭コンジローマの定点当たり報告数は、男性報告数が女性を上回る傾向が続いており、男性においては微増した。淋菌感染症の定点当たり報告数は、女性と比べ男性の報告が例年通り多く、男女ともに低レベルであった。より適切な性感染症発生動向把握、若年者の人口減少を加味した指標、妊婦健診の結果を利用する仕組みづくり等がこれらの疾患の動向を監視していくことにおいて重要である。 梅毒は2011年以降急増しており、2015年は2,692例(男性1,930、女性762)で2000年以降最多であった。2015年の人口10万当たり報告数は全体で2.12、男性が3.13、女性が1.17
であり、男女とも増加が著しかった。
2.センチネルサーベイランスの結果について 調査年別性別感染症別に観察すると、2015年は男性に淋菌感染症が多く、女性に性器クラミジア感染症、性器ヘルペスが非常に多かった。性器クラミジアの感染が女性に極めて多く目立った。また2012年より梅毒、淋菌感染症、性器クラミジア感染症が増加した。調査年別性別年齢階級別感染症別に観察すると、各年とも男性では淋菌感染症及び性器クラミジア感染症とも20~24歳に多く、年次的に著増していた。同時に尖圭コンジローマも増加した。一方、女性での性器クラミジア感染症は15~29歳に非常に多く、年次ごとに増加している。全体に女性性器クラミジア感染症は男性に比べて極めて多かった。また男性は淋菌感染症、性器クラミジア、女性は性器クラミジア感染症、性器ヘルペスが全年齢階級で目立った。
3.性感染症(STI)サーベイランスの評価と改善に関する研究
わが国の性感染症(STI)に関するサーベイランスの改善を目的として本年度は以下の研究を行った。まず、性感染症に関する特定
― 7 ―
平成27年度厚生労働科学研究費補助金新興・再興感染症及び予防接種政策推進研究事業
性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究
【研究代表者】 荒川 創一 (神戸大学大学院医学研究科)
総括研究報告書

感染症予防指針に基づく対策の現状把握とその推進のために、 1 .「性感染症に関する特定感染症予防指針」への自治体の対応状況調査、 2 .地方自治体性感染症サーベイランス担当者向け情報還元を行った。また、国の行う感染症発生動向調査を補完する動向把握策等の検討として、 3 .検査結果サーベイランスの試行と検討、 4 .STI発生動向調査の報告情報の活用に関する検討を行った。 その結果、梅毒を含めた性感染症のアウトブレイクを15自治体が把握し対応していた。性感染症の報告は都市部に集中しており、病原体サーベイランスや詳細データの共有を圏域で進めると対策に有用と思われる。自治体別(都道府県、保健所別)の情報が活用できると、自治体や医療機関での対策の推進に有用である。自治体を越えた発生動向の活用が進まず、活用策が周知されていなかったり、一部で利用に制約があることが理由ではないかと考えられた。中央感染症情報センターに集約されている報告データの利用要望があり、利用可能な範囲や許可等の手順の明確化が望まれる。自治体の施策担当者の担当年限は短く経験や知見の蓄積が十分でないと思われる。梅毒の増加を踏まえると、多発していない自治体向けの基本的な調査介入手順等の提供が必要である。梅毒は近年急増し、伝播経路として異性間性的接触が増加している。MSMなどの個別施策層に加え、対象者の特性の把握に基づく対策が必要でありパートナー健診の有用性が高まると考えられる。梅毒報告事項に現在含まれていない患者居住地情報を加えることで、施策担当自治体が明確となり、自治体を越えた対策等の推進の基礎となる。
4.Mycoplasma genitalium検査法に関する研究
Mycoplasma genitalium検出のための2つの検出法について、基礎的、臨床的研究を行った。旭化成ファーマ社のマイコプラズマ抗原検出キット「リボテストRマイコプラズマ」を用いてM. genitalium検出のための基礎的研究を行った。17株のM. genitaliumを培養させた液体培地をそれぞれ段階希釈し、それぞれの希釈液を「リボテストRマイコプラズマ」に滴下した。また、希釈液中のM. genitaliumのDNAコピー数をreal-time法にて測定し、「リボテストRマイコプラズマ」法の検出限界を測定した。17株中16株が、その原液(希釈前)では「リボテストRマイコプラズマ」は陽性を示した。しかし、10倍希釈した液体では陽性を示さず、「リボテストRマイコプラズマ」の検出限界は4.6×105コピー/㎖と高く、臨床的には使用できない可能性が高い。
5.口腔・咽頭梅毒および淋菌・クラミジアの咽頭感染に関する検討
口腔・咽頭梅毒と淋菌・クラミジアの咽頭感染について、今後の調査や対策を考察する目的で、前者は当科で経験した症例の臨床的特徴について後ろ向きに検討し、後者は当科と研究協力施設において過去に実施した前向き研究の結果を比較検討した。 口腔・咽頭梅毒は、性器や皮膚に病変がなく口腔・咽頭の症状や病変が梅毒診断の契機になる場合が多かった。最近急激に患者数が増加している梅毒については、口腔・咽頭梅毒の特徴を含めた情報を発信すること、現行の梅毒発生届けに口腔咽頭梅毒の項目を追加することが望まれる。 特徴的な症状や所見に乏しい淋菌・クラミ
― 8 ―

ジアの咽頭感染については、性器と咽頭の同日検査が保険で認められること、現行の感染症発生動向調査(STD定点)の調査票の項目に「咽頭淋菌感染症」と「咽頭クラミジア感染症」を別項目として加えることが望まれる。
6.HPV関連子宮頸癌早期スクリーニングの啓発に関する研究
日本人健常女性240名におけるHPV(human papilloma virus)は、CSW(comercial sex worker)では、非CSWと比較して高率にHPV陽性であった(p<0.00001)。検討した対象全体ではHPV52型が最多で、次いで58型の順に多かった。non-CSWでは52型が多かったが、CSWでは53型が多いもののハイリスク型全体が万遍なく検出された。特に、
CSWでは、複数のハイリスク型が同時に検出される率が高かった(p<0.01)。ローリスク型HPVのみが検出された症例は陽性者全体の7.6%であった。日本人健常女性においても高リスク型のHPV感染(保ウイルス)率は高く、子宮がん検診では細胞診にHPVスクリーニング検査を併用することは臨床的意義が高いと考えられた。 AnyplexTM II HPV28 detection kitを用いて、スワブ検体と尿検体を用いて検出された
HPVジェノタイプの相同性を確認したところ、全体の感度は68.42%、特異度は99.87%であった。細胞診と尿検体の検査で低い相同性を示した遺伝子型HPVは単一もしくは複数の遺伝子型のHPVが同時に検出される場合でも検出率に影響はなかった。HPVスクリーニング検査において、尿検体は侵襲性が低い検査であるが、尿検体による検査では感度が十分とは言えず、スクリーニング法として使用するには注意する必要がある。
7.性感染症、特にHPVと子宮頸癌についての啓発に関する研究
尖圭コンジローマの有無を層別化し、女性の子宮頸部におけるHPVタイプの分布を解析し、さらに尖圭コンジローマ不顕性感染の実態把握を行った。 その結果、コンジローマの病変を認めない女性でも、コンジローマタイプの不顕性感染者が存在することが判明した。HPVタイピングで検出されていることから、ウイルスを排出していると考えられ、新たな罹患者の感染源になりうる。尖圭コンジローマの実態把握において、不顕性感染者の存在は無視できないと考えられた。
8.感染予防行動、早期受診促進のための性感染症啓発スライドについて
スライド作成にあたって、中高生向け(特に中学生)にわかるように以下の内容を盛り込むことを考慮した。① スライド一枚に示す情報は、できるだけ字数を少なくイラストや写真を活用する。
② 疾患については、無症状のもの、治るもの、生命の危険につながるものなどを説明する。
③ 性行動を分類し、性感染症がうつる行為とうつらない行為を明示する。
④ コンドームで予防できるものと必ずしもコンドームだけでは予防できないものを示す。
⑤ コンドームの使い方を詳しく説明する。例えば、Q&A形式で中学生が間違いや勘違いに気づくようにする。YouTubeに掲載されている動画を紹介する。
⑥ 性に関するリスクのうち若年での妊娠に関するものは、今回のスライドでは具体
― 9 ―

的な解説を除き、性感染症に焦点をあてる。⑦ HIVや性感染症にリスクのある状況は、性行動の相手との関係において、経済的優位、暴力、アルコール、薬物乱用などの問題が考えられることを例示し、コンドームを使えない関係性や、ドメスティックバイオレンスについても説明する。
⑧ 医療機関への受診を促し、早期に検査治療に結びつけるため、受診費用の概要を提示する。
⑨ 疾患の詳しい説明は、来年度以降の研究課題となる教師向けの資料に含める。
健康危機情報 2 .において、国・地方公共団体は性感染症対策の基本であるコンドームの使用を強く進めていく必要がある。一方で性感染症の感染源は明らかでないことも多いので,国民は安全な環境にあるとは言えない危機的状況にあると考えられる。
研究発表1.論文発表1 Shigemura K, Osawa K, Miura M, Tanaka K, Arakawa S, Shirakawa T, Fujisawa M:
Azithromycin resistance and its mechanism
in Neisseria gonorrhoeae strains in Hyogo,
Japan. Antimicrob Agents Chemother
59(5):2695-2699, 2015.
2 Hamasuna R, Yasuda M, Ishikawa K, Arakawa S, Fujisawa M, et al: The second
nationwide surveillance of the antimicro-
bial susceptibility of Neisseria gonorroeae
from male urethritis in Japan, 2012-2013.
J Infect Chemother 21, 340-345, 2015.
3 谷畑健生・秋元義弘・武島 仁・五十嵐
辰男・安田 満・種部恭子・金山博臣・荒川創一:平成25年7モデル県の性感染症診療医療機関全数調査推計有病率と国立率感染症研究所の定点報告推計有病率の比較~7県医療機関全数調査結果と定点調査報告結果の有病率はなぜ乖離したのか?.日本性感染症学会誌 26(1),109−116,2015.
4 荒川創一・井村裕夫(編):第4版 わかりやすい内科学 グラム陰性球菌感染症Ⅰ髄膜炎菌感染症 Ⅱ淋菌感染症.文光堂 394−395,2014.
2.学会発表1 荒川創一:性感染症を巡る最近の話題―様々な角度(排尿障害、……)から―.姫路皮膚科泌尿器科医会総会・講演会,2015.
2 荒川創一:再び増加している性感染症(STI)の現状とその対策.第6回東海
STI研究会,2015.3 Arakawa S: Prevention and Education of STIs. Asian UTI and STI Forum 2015
2015.
4 Arakawa S: Recent trend of STI incidence in Japan. 5th Korea _ Japan Workshop for Urogenital Infections _ Korea _ Japan Expert Meeting on Urological UTI _ 2015.
知的財産権の出願・登録状況1.特許取得 なし
2.実用新案登録 なし
3.その他 なし
― 10 ―

Ⅱ.分担研究報告書


― 13 ―
感染症発生動向調査から見たわが国の性感染症の動向、2015年
【研究分担者】 砂川 富正 (国立感染症研究所感染症情報センター)【研究協力者】 山岸 拓也 (国立感染症研究所感染症疫学センター) 砂川 富正 (同 上) 有馬 雄三 (同 上) 高橋 琢理 (同 上) 加納 和彦 (同 上) 石金 正裕 (同 上) 金井 瑞恵 (同 上) 加藤 博史 (同 上) 安藤 美恵 (同 上)
研究要旨
性感染症は近年国内での減少傾向が停滞、或は増加しており、その発生動向の把握と効果的な対策が重要である。対策の立案や評価に用いるための情報を提供するために、代表的な性感染症である性器クラミジア感染症、性器ヘルペスウイルス感染症、尖圭コンジローマ、淋菌感染症及び梅毒について、2000年以降の感染症発生動向調査の結果をまとめた。また、近年梅毒の報告が急増している為、梅毒の発生動向に注目した。 発生動向調査から見た5類定点把握疾患の2015年の動向については、概ね例年並みであった。例年同様、男女共に、性器クラミジア感染症の報告数が最も多かった。また、淋菌感染症を除いて、男性と比べて女性症例の年齢分布の方が若かった。性器クラミジア感染症の定点当たり報告数は、概ね横ばいであった。性器ヘルペスウイルス感染症の定点当たり報告数は、男女ともに概ね横ばいであり、近年同様、女性の報告数が男性を若干上回った。尖圭コンジローマの定点当たり報告数は、男性報告数が女性を上回る傾向が続いており、男性においては微増した。淋菌感染症の定点当たり報告数は、女性と比べ男性の報告が例年通り多く、男女ともに低レベルであった。より適切な性感染症発生動向把握、若年者の人口減少を加味した指標、妊婦健診の結果を利用する仕組みづくり等がこれらの疾患の動向を監視していくことにおいて重要である。 梅毒は2011年以降急増しており、2015年は2,692例(男性1,930、女性762)で2000年以降最多であった。2015年の人口10万当たり報告数は全体で2.12、男性が3.13、女性が1.17であり、男女とも増加が著しかった。2015年の病型別報告数は、無症候832例(31%)、早期顕症Ⅰ期788例(29%)、早期顕性Ⅱ期968例(36%)、晩期顕症91例(3%)、先天梅毒13例であり、2015年は男女ともに特に早期顕性が増加していた。性別は、男性では35~39

A.研究目的
近年国内では淋菌感染症、性器クラミジア感染症など、いわゆる性感染症が減少してきているといわれているが、疾患や年齢によっては増加に転じているものもあり1)梅毒等、顕著に増加しているものもある。これらの性感染症対策をしていくうえで、その発生状況の把握が重要である。 1999年4月に施行された「感染症の予防及び感染症の患者に対する医療に関する法律」(以下、感染症法)のもとで、性器クラミジア感染症、性器ヘルペスウイルス感染症(以下性器ヘルペス)、尖圭コンジローマ、淋菌感染症は5類定点把握疾患として、梅毒は5類全数把握疾患として、保健所を介して国に報告されることになった。定点把握4疾患は都道府県知事が定めた性感染症定点医療機関から毎月1回報告されている。性感染症定点医療機関は、産婦人科、産科、産婦人科、性感染症を組み合わせた診療科名の診療科、泌尿器科、皮膚科を標榜する医療機関が指定され
ており、その数は、保健所地域ごとに管内人口~7.5万人までは0(ゼロ)、管内人口7.5万人~では1+(人口−7.5万人)/13万人とされている。また、梅毒は診断した医師が診断から7日以内に報告することとされている。 性感染症対策の立案や評価に役立つ情報提供のために、感染症発生動向調査における性感染症定点把握4疾患(性器クラミジア感染症、性器ヘルペスウイルス、尖圭コンジローマ、淋菌感染症)及び梅毒の動向を調べることにした。近年梅毒の急増を認めている為、梅毒を中心とした発生動向調査から見た性感染症の動向について記述する。
B.研究方法
感染症発生動向調査の1987~2015年の定点把握4疾患と梅毒のデータ(2014年までのデータは感染症発生動向調査年報、2015年のデータは2016年2月10日現在の暫定報)と人口動態統計(毎年10月1日基準)を用いた。データは国立感染症研究所において感染症
― 14 ―
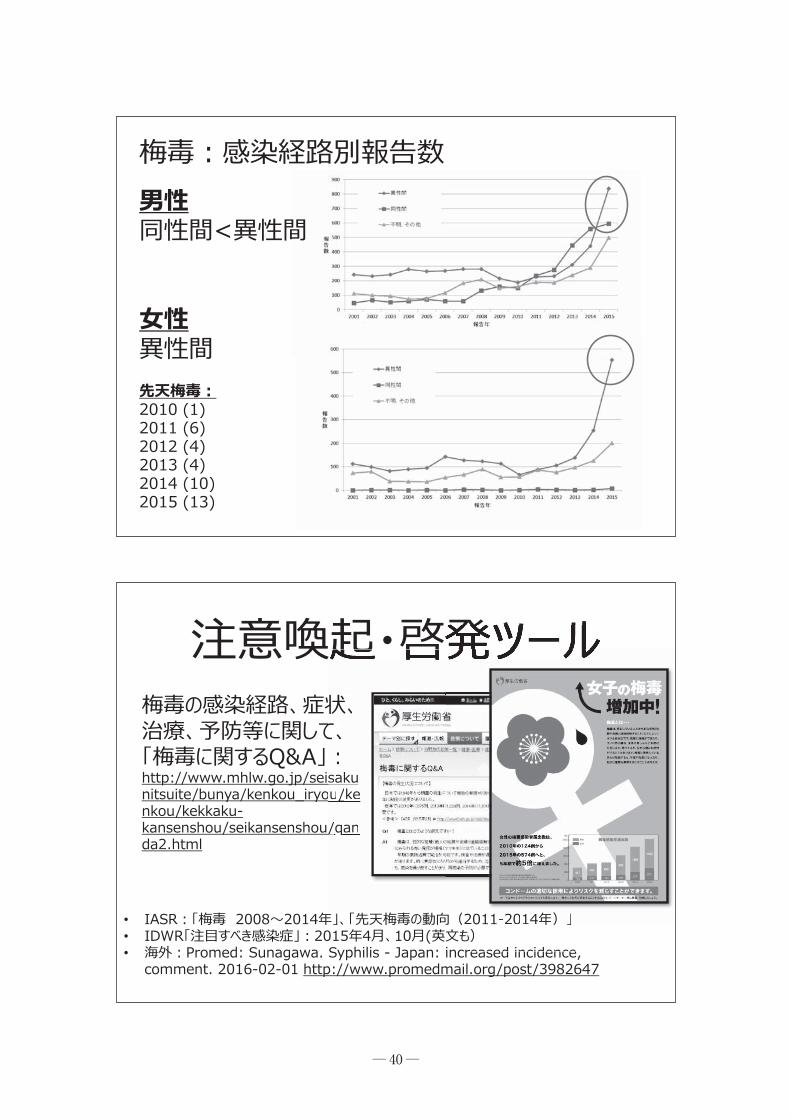
歳の報告が最も多かった。2014年に引き続き幅広い年齢で増加しており、特に20~40歳代の増加が目立った。女性は20~24歳の報告が最も多く、2014年の倍以上の報告数であった。感染経路は、男性では感染経路が報告されていた1,739例(全体の90%)でみると、1,722例(99%)が性的接触であり、内訳は同性間584例(性的接触による1,722例の中で34%)、異性間839例(同49%)、異性間/同性間12例(同1%)、性的接触の詳細不明287例(17%)であった。女性では感染経路が報告されていた667例(全体の88%)の中で664例(98%)が性的接触であり、内訳は異性間554例(性的接触による664例の中で83%)、同性間5例(同1%)、性的接触の詳細不明103例(同16%)であった。2011年以降の梅毒急増、異性間性的接触による男性と若年女性での増加は緊急事態である。医療従事者や行政担当者の間で危機感を共有するために、それら関係者に対して梅毒増加について周知を図ること、20~40歳代の男性と性交をする男性や20歳代女性というハイリスク集団に対して梅毒増加と予防法について情報提供を行う、あるいは患者のパートナーに検査を進めるなどの対策を、各関係者が行っていくことが急務である。

サーベイランスシステム(National Epidemio-logical Surveillance of Infectious Disease:
NESID)から抽出し、同所内で解析をおこなった。年齢群は5歳間隔とし、10歳未満や高齢者など、症例数が少ない年齢群は統合した。なお、NESIDデータは今後各自治体の届出修正により変更される可能性がある。
1.性感染症定点把握4疾患の動向 2000年以降の性感染症定点把握4疾患の感染症発生動向調査の結果をまとめた。定点当たり報告数の推移及び季節性、性別・年齢群別定点当たり報告数の推移、定点数の推移、都道府県別定点数を調べた。
2.梅毒の動向 報告数の推移、人口10万当たり報告数推移、年齢群別報告数推移、感染経路別報告数推移、年齢群別感染経路分布、都道府県別報告状況を調べた。感染経路では性的接触を含む複数の経路によるものを除いた。
倫理面への配慮 本研究で用いた感染症発生動向調査のデータには個人情報が含まれず、データ解析は国立感染症研究所内で行われ、倫理上の問題が発生する恐れはない。
C.結 果
1.性感染症定点把握4疾患の動向1)定点当たり報告数推移(図1,2) 発生動向調査から見た5類定点把握疾患の動向については、概ね例年並みであった。男女ともに、例年通り性感染症の中では性器クラミジア感染症の定点当たり報告数が最も多
かった。また、例年同様、性器クラミジア感染症の定点当たり報告数は、5月から10月の春~秋にかけて報告数が多い傾向が見られた。性器クラミジア感染症の定点当たり報告数は、男女ともに2003年に減少に転じ、2011年以降男性では概ね横ばい、女性では微減した。性器ヘルペスでは、男女ともに2009年を最小に、横ばいの状況であった。尖圭コンジローマは、近年女性は減少傾向だが、男性は2012以降微増した。淋菌感染症は、男女ともに2008年以降下がり止まった。
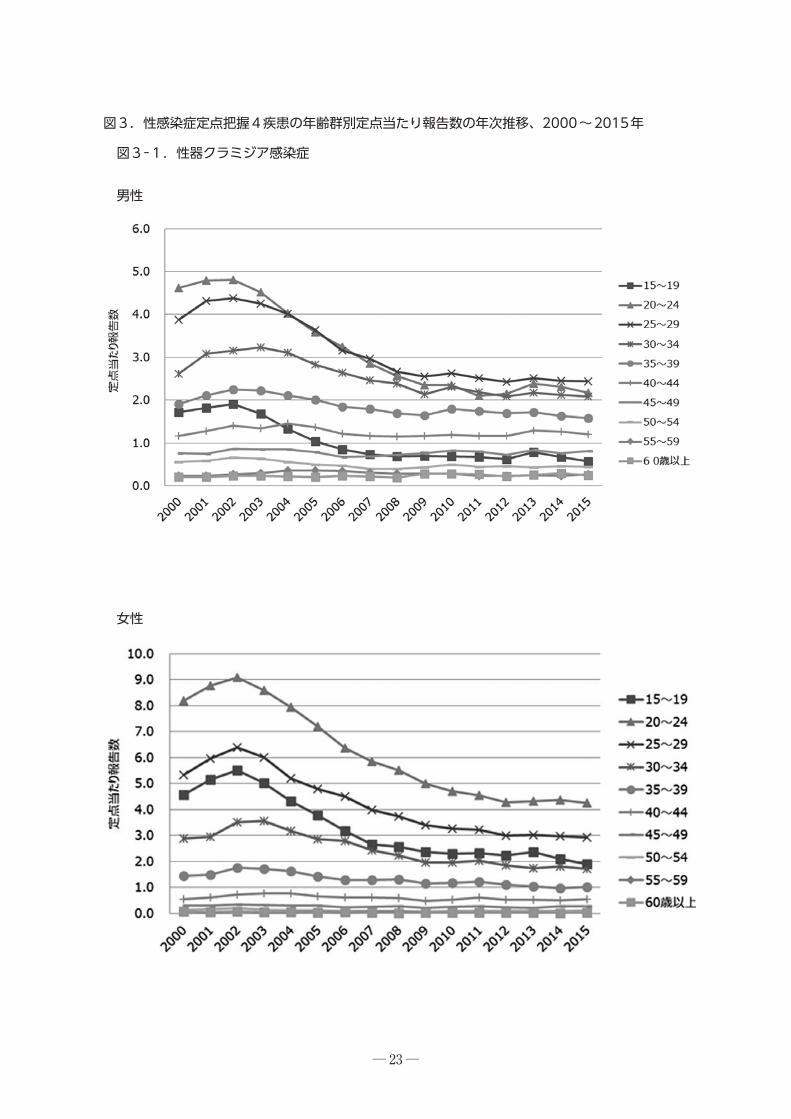
2)性別・年齢群別定点当たり報告数推移 (図2,3) 性器クラミジア感染症 2015年には、近年同様、男性と比べ女性の年齢分布の方が若く、男性は25~29歳、女性は20~24歳の報告が最も多かった。15~19歳では、男女共に2013年以降減少傾向であった。 性器ヘルペス 2015年には、例年と変わらず、男性と比べ女性の年齢分布の方が若く、男性は30代の報告が最も多いのに対して、女性は20代が多かった。また、定点当たり報告数は、女性の方が男性より多い傾向も近年と同様であった。 尖圭コンジローマ 2015年には、近年と同様に男性と比べ女性の年齢分布の方が若かった。男性は30~34歳の報告が最も多いのに対して、女性は20~24歳の報告が最も多かった。男性は近年多くの年齢群で微増しているが、女性は若干減少傾向である。15~19歳においては、男女共に2013年以降微減した。 淋菌感染症 2015年には、例年通り、男女ともに20代の報告が最も多かった。また、定点当たり報告
― 15 ―
数は、例年同様男性の方が高いが、近年男女ともに横ばい・微減に転じている。
3)性感染症定点医療機関数(図4,表1) 2015年性感染症定点医療機関数の12月平均は977(12月に報告された定点数も977)と過去よりも若干多く、その内訳は産婦人科(産科、婦人科、産婦人科の合計)477(49%)、泌尿器科404(41%)、皮膚科88(9%)、性病科8(1%)であった。2015年12月の定点医療機関数を都道府県別にみると、産婦人科系と泌尿器科との比率は岐阜県の3/9から岡山県の14/3まで幅広かった。
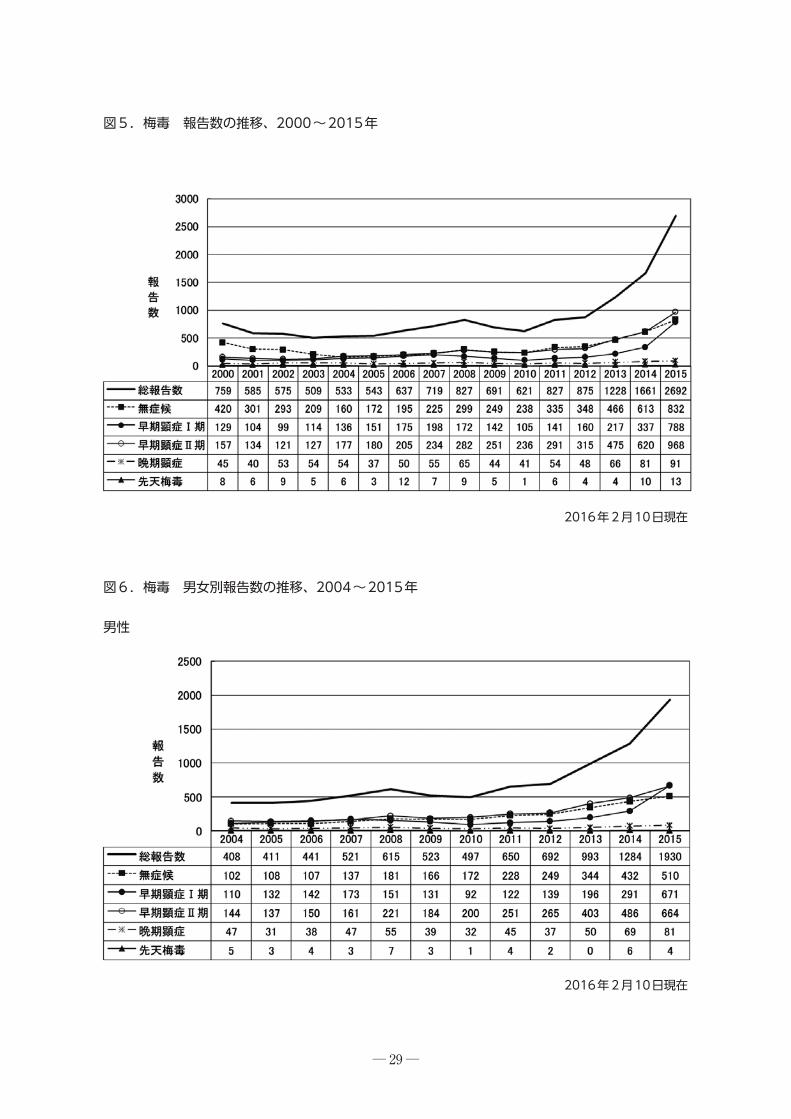
2.梅毒の動向1)報告数推移(図5,6) 梅毒の総報告数は、2000年以降減少していたが、2004年に増加に転じ、2009~2010年の減少を挟んで再び増加し、2015年は2,692例で2000年以降最も多かった。2011年以降の増加は男女ともに認められており、2015年は男性では1,930例、女性では762例で、どちらも2000年以降最も多かった。2015年の報告数で男女比(報告数の男性/女性)をみると、2.5であり、過去4.0前後で推移していたことを踏まえると、女性の割合が増加している[2011年(3.7)、2012年(3.8)2013年(4.2)、2014年(3.4)] 。 2015年の病型別報告数は、無症候832例(31%)、早期顕症Ⅰ期788例(29%)、早期顕性Ⅱ期968例(36%)、晩期顕症91例(3%)、先天梅毒13例であった。2015年は早期顕性Ⅰ、Ⅱ期の増加とともに、無症候の症例も増加が目立った。男女別にみると、男性では無症候510例(31%)、早期顕症Ⅰ期671例(35%)、早期顕性Ⅱ期664例(34%)、晩期顕症81例
(4%)であった。男性の早期顕症梅毒の報告が増加し、特に15歳~34歳代が2014年より多かった。女性では無症候322例(42%)、早期顕症Ⅰ期117例(15%)、早期顕性Ⅱ期304例(40%)、晩期顕症10例(1%)であった。女性の無症候症例は10代~50代の全ての年齢群で2014年よりも増加が見られたが、特に20~24歳代で約3倍(2014年:33例、2015年:89例)の増加がみられた。また、早期顕症梅毒も15歳~49歳代で増加しており、特に15歳~29歳代の増加が認められた。先天梅毒は2015年には男児4例、女児9例であった。
2)人口10万当たり報告数の推移(図7) 2015年の人口10万当たり報告数は全体で2.12、男性が3.13、女性が1.17であった。男女とも増加が著しかった。
3)年齢群別報告数の推移(図8) 男性は40~44歳の報告が最も多く、2015年は15~65歳の幅広い年齢で増加しており、特に30~40歳代の増加が目立った。女性は20~24歳の報告が最も多かった。また、2015年も2014年に引き続き15~34歳の年齢で増加しており、特に20代で2倍以上の増加があった。
4)感染経路(図9,10) 男性では2015年の1,930例の中で感染経路が報告されていた1739例(90%)でみると、1,722例(99%)が性的接触であり、内訳は同性間584例(性的接触による1,722例の中で34%)、異性間839例(同49%)、異性間/同性間12例(同1%)、性的接触の詳細不明287例(17%)であった。感染経路不明は194例(10%)であった。3例が複数の感染経路を報告していた。2011年以降、男性の同性間性的
― 16 ―

接触による感染が急増していたが、2015年は異性間性的接触による報告が増加した。 女性では2015年の感染経路が報告されていた677例(全体の88%)の中で664例(98%)が性的接触であり、内訳は異性間554例(性的接触による664例の中で83%)、同性間5例(同1%)、性的接触の詳細不明103例(同16%)であった。感染経路不明は85例(全体の11%)であった。また、複数の感染経路を報告したものはなかった。2011年以降、女性の異性間性的接触が急増していた。 年齢群別にみると、男性ではこれまで同性間性的接触による報告が異性間を上回っていたが2015年では異性間性的接触による感染が同性間性的接触を上回り、特に20歳代の増加が著しかった。女性では15歳~20歳代の異性間性的接触による感染が多かった。 なお、感染経路の報告には確定以外に推定が含まれていた。
5)都道府県別報告数(図11) 2015年の報告は東京都1055例、大阪府324例、神奈川県165例、愛知県122例などであった。2014年は東京都506例、大阪府240例、愛知県112例、神奈川県106例であった。2014年と比べ、東京都は2.1倍、大阪府では1.3倍、愛知県で1.1倍、神奈川県では1.6倍と、東京都の報告が大きく増加していた。
D.考 察
1.性感染症定点把握4疾患の動向 例年同様、淋菌感染症を除いて、性器クラミジア感染症、性器ヘルペス、尖圭コンジローマにおいては、女性症例の年齢分布の方が若かった。
性器クラミジア感染症は男女共に、依然として最も多く報告される性感染症であった。2009~2010年頃から減少が緩やかになり、概ね横ばいである。2013年には、10歳代後半~20歳代前半等での微増が認められたが、その後減少した。ただし、夏季にかけて報告数が多い傾向が例年通り見られる為、季節的な啓発も検討する事が考えられる。性器ヘルペス及び淋菌感染症は、男女とも横ばいの状況であった。性器ヘルペスは、女性の方が男性より多い傾向が続いており、淋菌感染症においては、男性の方が多い傾向が続いていた。尖圭コンジローマは、2012以降、男性が微増しているのに対して、女性では概ね微減している。2013年4月からヒトパピローマウイルスワクチンの定期接種化による4価ワクチン接種の影響は今後尖圭コンジローマの報告数に表れてくる可能性があり、特に若年者での動向を注意深く見ていく必要がある。その際は、若年者の人口減少を加味し、人口当たりの報告数でみていく必要がある。 報告数の増減を考えるとき、現行の感染症法のもとでの定点把握がどれだけ実態を反映しているかが重要である。2011年2月に「性感染症に関する特定感染症予防指針」が告示され、地方自治体での定点設定に各診療科の割合を反映させることや長期にわたって報告実績のない医療機関についての見直しなどが求められた。その結果、2012年から2013年にかけて、毎年10を超す都道府県で性感染症定点の変更が行われていた。今後も、地方自治体が地域で性感染症患者を多く診療している医師や医療機関を把握し、より良い定点設定、或はその他の情報も用いた発生動向把握等に向けて地域医療機関や医師会と協議していくことが期待される。
― 17 ―

感染症発生動向調査の結果を解釈する際には、いくつかの点に注意が必要である。まず、性器クラミジア感染症、淋菌感染症は無症候の症例が見逃されている可能性がある。両疾患とも咽頭感染が感染拡大の一つの原因とされているが、本調査では把握が出来ない。また、年齢群でみた定点当たり報告数の増減は各年齢群の人口構成を加味していないため、罹患率の評価は行えず、疾病負荷の概要の把握にのみ有用である。罹患率の推移を検討するためには、若年者人口の減少を加味し、若年者だけでの解析、あるいは年齢調整が必要である。また、定点当たり報告数は定点設定に大きく依存しているが、性感染症は居住地外のクリニックを受診することも多く、人口当たりで定められている定点は必ずしもその地域の住民の性感染症発生状況を反映していない。更に、定点当たり報告数の診療科別内訳は、都道府県によって大きく異なるので、都道府県別の比較等の解釈には制約が有る。 また、近年性感染症の郵送検査が普及してきており、その様な社会背景によって、検査・受診行動も影響を受けることが考えられる。よって、感染症発生動向調査の年次推移等の解釈については、注意が必要であり、その他の調査や情報と合わせて解釈するのが重要であると考えられる。
2.梅毒の動向 梅毒は2011年から男女ともに増加傾向であり、人口10万当たりの報告数をみると、2013年までは男性での増加、2014年からは女性の増加が著しく、その傾向は加速度的である。従来、感染経路として男性の同性間性的接触が多数を占めていたことから、男性と性交をする男性(Men who have sex with men: MSM)
の間で梅毒が流行していると推定されていたが、男女とも異性間性的接触の報告が急増しており、伝播の様相が変化している可能性がある。 病期では、男女とも早期顕性Ⅰ、Ⅱ期と無症候が増加していた。早期顕性症例の増加は真の梅毒罹患率の増加を反映している可能性がある。無症候症例の増加は検査件数の動きを反映している可能性があるが、検査数、陽性率の推移を把握していない為、発生動向調査では発見の契機が不明であり、原因は不明である。 年齢に関しては、男性では20歳代から40歳代が多く、女性では15歳から20歳代の増加が著しかった。米国でも2001年から梅毒が増加してきているが、流行の中心はMSMで、年齢は20歳代である2)。欧州3,4)と日本では30歳代男性での梅毒増加が目立ち、MSMの年齢分布あるいは自己申告の傾向が各地で異なる可能性がある。しかし、近年米国でも、女性と先天梅毒の増加を認めており5)、若い女性に増加がみられていることは緊急事態と捉えられる。 男性の梅毒は感染経路が報告されたもののうち、2015年は34%が同性間性的接触によるものであった。一方、異性間性的接触は約5割であった。2014年は同性間性的接触が約5割を占めており、異性間性的接触と同性間性的接触の報告数において逆転現象が生じている。異性間性的接触の動向を引き続き注意深く監視することが重要と考えられる。また、引き続きMSMにおける伝播への注意が欠かせないため、医療従事者や公衆衛生担当者は男性梅毒患者を見た時には、多くが男性と性交をする男性であることを意識し、丁寧なインタビューをもとに感染の可能性のあるパー
― 18 ―

トナーへの医療の提供を図っていく必要がある。 検査方法に関しては、これまで行われてきたRPRカードテスト、凝集法、ガラス板法に代わり、自動化法(自動分析器による測定)を用いた測定値を採用する医療機関が増えつつある。なお、ガラス板法、凝集法は検査キットの国内流通最終ロットの使用期限が2014年12月時点ですぎているため、信頼性に疑いが生じる。感染症発生動向調査では自動化法を用いた測定については、梅毒の正確な発生動向の把握のためには、多岐にわたる梅毒検査方法とその解釈を臨床医と行政担当者に適切に理解してもらうことが重要であり、届出基準の周知はその第一歩であると考えられた。 小児の先天梅毒は2015年には13例が報告された。先天梅毒の発生は、妊娠中の性感染対策の不備の表れとして重要である。男女とも異性間性的接触による伝播が報告され、また、女性の報告数が増加していることから、先天梅毒に対する注意は欠かせない。妊婦の未受診、妊娠中の感染の罹患率、適切な治療を受け、治療効果判定がされているか、など先天梅毒の疫学情報の把握を行い、適切な対策を行っていく必要がある。また、児の母親の妊娠前から妊娠中の梅毒感染・治療に関連する社会的背景についての情報も、先天梅毒の発生予防の為の対策立案に繋がる可能性もあり、検討すべきである。 梅毒の発生動向調査結果の解釈では過小評価の可能性を考える必要がある。梅毒は診断した全症例の届出が法律で義務付けられているが、このことは全ての医師に周知されていない可能性がある。 2011年以降の梅毒急増は緊急事態である。
医療従事者や行政担当者の間で危機感を共有するために、それら関係者に対して梅毒増加について周知を図ること、ハイリスク集団に対して梅毒増加と予防法について情報提供を行う、あるいは患者のパートナーに検査を進めるなどの対策を、各関係者が行っていくことが急務である。
E.健康危機情報
特になし
F.研究発表
1.論文発表 なし
2.学会発表1 有馬雄三:国内外の梅毒の疫学的状況.
日本性感染症学会第28回学術大会.日本エイズ学会動向シンポジウム「梅毒を見直す」.東京.2015年12月.
2 金井瑞恵・有馬雄三・島田智恵・松井珠乃・大石和徳:先天梅毒報告例の記述疫学―感染症発生動向調査(2011~2014年)より.日本性感染症学会第28回学術大会.東京.2015年12月.
G.知的所有権の所得状況
1.特許取得 なし
2.実用新案登録 なし
― 19 ―

参考文献
1 岡部信彦・山岸拓也・多田有希:感染症発生動向調査から見た我が国の性感染症の動向、2012年.性感染症に関する特定予防指針に基づく対策の推進に関する研究(研究代表者:荒川創一)平成24年度総括・分担研究報告書.29−55,2013.
2 2012 Sexually Transmitted Disease Sur-veillance. Centers for Disease Control and
Prevention. (www.cdc.gov/std/stats12/syphilis.htm, 閲覧2014年2月14日)
3 Savage EJ, Marsh K, Duffell S, et al. Rapid increase in gonorrhea and syphilis
diagnoses in England in 2011. Euro
Surveill. 2012;17(29):doi:pill:20224.
4 Bremer V, Marcus U, Hamouda O. Syphilis on the rise again in Germany-
results from surveillance data for 2011.
Euro Surveill. 2012;17(29):doi:pill:20222.
5 Bowen V, Su J, Torrone E, Kidd S, Weinstock H. Increase in incidence of
congenital syphilis _ United States, 2012-2014. MMWR Morb Mortal Wkly Rep.
2015 Nov 13;64(44):1241-5.
doi:10.15585/mmwr.mm6444a3.
― 20 ―

男性
女性
図1.性感染症定点把握4疾患の定点当たり報告数の月次推移、1987~2015年
2016年2月10日現在
― 21 ―

男性
女性
図2.性感染症定点把握4疾患の定点当たり報告数の年次推移、2000~2015年
― 22 ―
男性
女性
図3.性感染症定点把握4疾患の年齢群別定点当たり報告数の年次推移、2000~2015年
図3-1.性器クラミジア感染症
― 23 ―

図3-2.性器ヘルペスウイルス感染症
男性
女性
― 24 ―

― 25 ―
図3-3.尖圭コンジローマ
男性
女性

― 26 ―
図3-4.淋菌感染症
男性
女性

― 27 ―
図4.性感染症定点医療機関数の年次推移、1999~2015年
1999~2013年は各月に報告のあった定点数の平均(切り捨て)で、2015年は2015年12月に報告された定点数

― 28 ―
表1.診療科別・都道府県別STD定点数、2015年12月
2016年1月14日現在
総計性病科皮膚科泌尿器科産婦人科都道府県42121920北海道13175青森県15411岩手県1789宮城県1468秋田県1028山形県1587福島県223712茨城県17179栃木県2411112群馬県5632132埼玉県4391123千葉県5462028東京都59163319神奈川県15366新潟県10145富山県10154石川県532福井県927山梨県14248長野県15393岐阜県312920静岡県6563326愛知県17458三重県954滋賀県236413京都府664102626大阪府4612124兵庫県954奈良県8224和歌山県734鳥取県633島根県17314岡山県231157広島県12246山口県633徳島県1578香川県11362愛媛県633高知県3741320福岡県734佐賀県1046長崎県16106熊本県101135大分県131246宮崎県161105鹿児島県12138沖縄県977888404477総計
― 29 ―
図5.梅毒 報告数の推移、2000~2015年
2016年2月10日現在
図6.梅毒 男女別報告数の推移、2004~2015年
男性
2016年2月10日現在

― 30 ―
女性
図6(続き)
2016年2月10日現在の感染症発生動向調査と人口動態統計(毎年10月1日基準)を使用
2016年2月10日現在
図7.人口10万当たり報告数の推移、2001~2015年

― 31 ―
図8.梅毒の年齢群別報告数の推移、2006~2015年
男性
女性
2013年3月6日現在
2016年2月10日現在

― 32 ―
図9.梅毒の感染経路別報告数の推移、2006~2015年
2016年2月10日現在
男性
女性

― 33 ―
図10.梅毒の年齢群別感染経路分布、2015年
2016年2月10日現在

― 34 ―
図11.梅毒の都道府県別・年別報告数、2013~2015年 (n= 5581)
2016年2月10日現在
― 35 ―

― 36 ―
•••

― 37 ―

― 38 ―

― 39 ―
― 40 ―
•••

― 41 ―
•–
–––
•
–••

― 42 ―

― 43 ―

― 44 ―

A.研究目的
第一の目標として、平成24年から27年の荒川班から性感染症の多い県と少ない県で、性感染症がどう異なるのかを明らかにした。 第二の目標として、感染症法の改正に伴う性感染症予防指針の改定のための基礎データ
を提供する。国立感染症研究所疫学情報センターで集計されている全国定点報告は、その設計上、男女の比較、人口、性感染症同士の比較が出来ないように設計されている。われわれの本研究では、これらを比較可能とするため、人年法を使用し、男女、年齢、疾患ごとの直接比較が出来るようにした。
性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究―センチネルサーベイランスの施行について―
【研究協力者】 谷畑 健生 (神戸市東灘区保健福祉部・神戸市保健所)【研究代表者】 荒川 創一 (神戸大学大学院医学研究科)【研究協力者】 伊藤 晴夫 (千葉大学) 五十嵐辰男 (千葉大学フロンティア医工学センター) 三鴨 廣繁 (愛知医科大学大学院医学研究科) 安田 満 (岐阜大学医学部附属病院泌尿器科) 金山 博臣 (徳島大学大学院医歯薬学研究部泌尿器科学)
研究要旨
平成24~26年をベースとし、医療機関全数調査を行った。対象疾患は梅毒、淋菌感染症、性器クラミジア感染症、非淋菌非クラミジア感染症、性器ヘルペス、尖圭コンジローマを対象として実測値を人年法により安定化させ、男女比較などあらゆる比較を可能とした。 本年の研究は、前3年と異なり、前3年で性感染症の多かった千葉県・兵庫県と岐阜県・徳島県を比較した。 また医療機関が梅毒については病期別に観察した。また検査を行った検体についての陽性率を算出し、陽性率に県の差があるかどうか、即ち県の意思の能力についても検討を行った。 本研究の最も特徴とすることは、国の感染症動向調査:定点動向調査報告をトレンドだけではなく、いろいろな比較が出来る自由度の効く調査報告にするための基礎的な疫学研究である。性感染症定点動向調査は本研究に比べて感染者の推定値が低いことが明らかになったことから、定点の取り方について変更するべきであると考えられる。国は他の感染症と違えて新たな選定方法を考えるべき時期であると考えられる。 本研究は、感染症法の改正に伴う性感染症予防指針の改定のための基礎データを提供するものである。
― 45 ―

B.研究方法
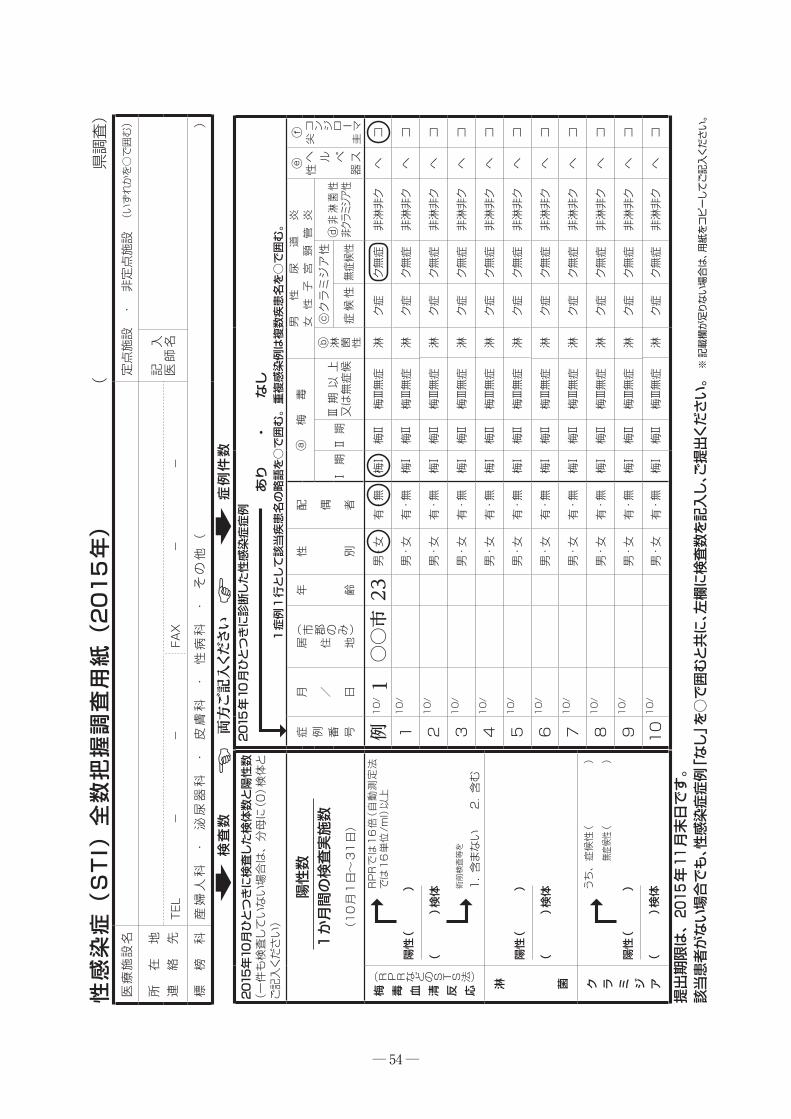
本研究は平成24年から27年の荒川班を基礎として、性感染症の多い千葉県・兵庫県、性感染症の少ない岐阜県・徳島県の4県を調査モデル県とした。 対象科は産婦人科(産科のみ、婦人科のみを含む)、泌尿器科(皮膚泌尿器科を含む)、皮膚科、性病科を標榜する全ての医療機関を対象とした。調査対象とした性感染症は梅毒(病期Ⅰ、病期Ⅱ、病期Ⅲ・無症候)、淋菌感染症、性器クラミジア感染症、非淋菌非クラミジア感染症、性器ヘルペス、尖圭コンジローマとした。 調査期間は平成27年10月1日から31日までとし、対象医療機関の医師自らが期間中に対象の5種性感染症と診断した全ての患者(氏名・住所等の個人が特定できる情報は収集しない)の受診日・性・年齢・また検査を行った場合、検査検体数、検体陽性数を記入することとした。そして診断した性感染症名を調査票に記録した。地区責任者(千葉大学・岐阜大学・神戸大学・徳島大学)は督促を2回
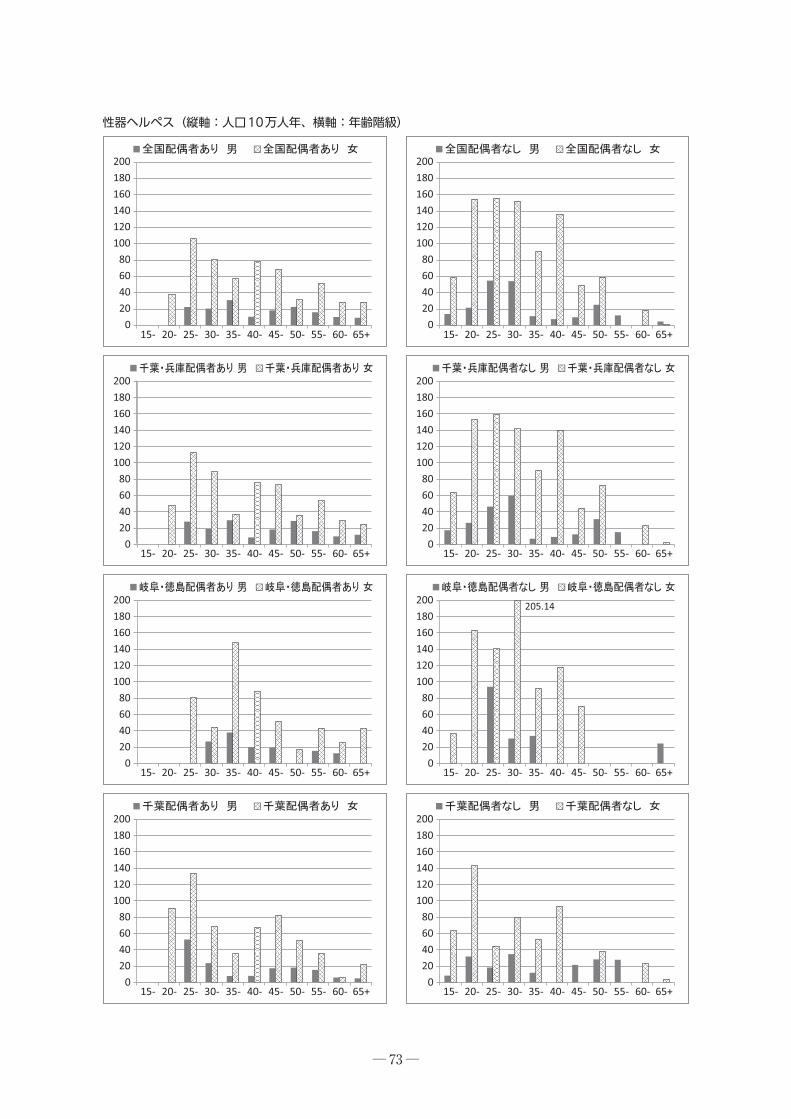
行い、回収率の向上を目指した。 医療機関への調査票の発送(9月初旬)及び回収は各県の共同研究者が行った。回収率は千葉県75.2%、岐阜県62.9%、兵庫県91.1%、徳島県100.0%、4県で80.0%であった。 調査票の回収及び督促は地区責任者が行い、調査票に記載された記録を電子データ化し、データクリーニングは委託先の中央調査社が行った。疫学解析は谷畑が行い、調査の安定化を図るため人年法・95%信頼区間を算出した。 95%区間はその区間で真の値が確率的にあることを示している。示されている推定値は、最も近い代表値を示していている。この推定値はこの区間の代表とされる値であり、計算に用いられる。グラフの縦軸は人年を使用している。本研究では観察期間を10月の1か月31日間の調査としており、1年356日に換算している。このことから縦軸は何人ではなく、何人年になる。この方法の方が、一日だけの調査よりも、年間の感染者数という真の実際受診値に近いため人年法を使用した。
データクリーニングについて(ア)診療科 無記入 → 入力せず(イ)定点施設/非定点施設 無記入 → 入力せず(ウ)感染症例有無 無記入 & 個別症例無記入 → 「なし」とする(エ)感染症例有無 無記入 & 個別症例記入あり → 「あり」とする(オ)感染症例有無 なしに○ & 個別症例記入あり → 「あり」に変更する(カ)女性に○ & 男性尿道炎欄に記入はERROR → 男性尿道炎欄に記入を削除(キ)男性尿道炎欄で 非淋非ク のように○がついている場合は、非淋菌・非クラミ
ジアの両方に「1」を入力
― 46 ―

C.研究結果
1 調査年別性別感染症別に観察すると、男性に淋菌感染症が多く、女性に性器クラミジア感染症・性器ヘルペスが非常に多かった。性器クラミジアの感染が女性に
極めて多く目立った。また2012年より梅毒、淋菌感染症、性器クラミジア感染症が増加した。
0
20406080
100120140
2012 2013 2014 2015
0
20406080
100120140
2012 2013 2014 2015
(男)(男) (女)(女)
0
50
100
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
150
200
250
300
0
50
100
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
150
200
250
300497.9
765.8
― 47 ―

2 また梅毒は、近年定点調査で増加しているとされているが、本研究においても著明に増加したと言えた。
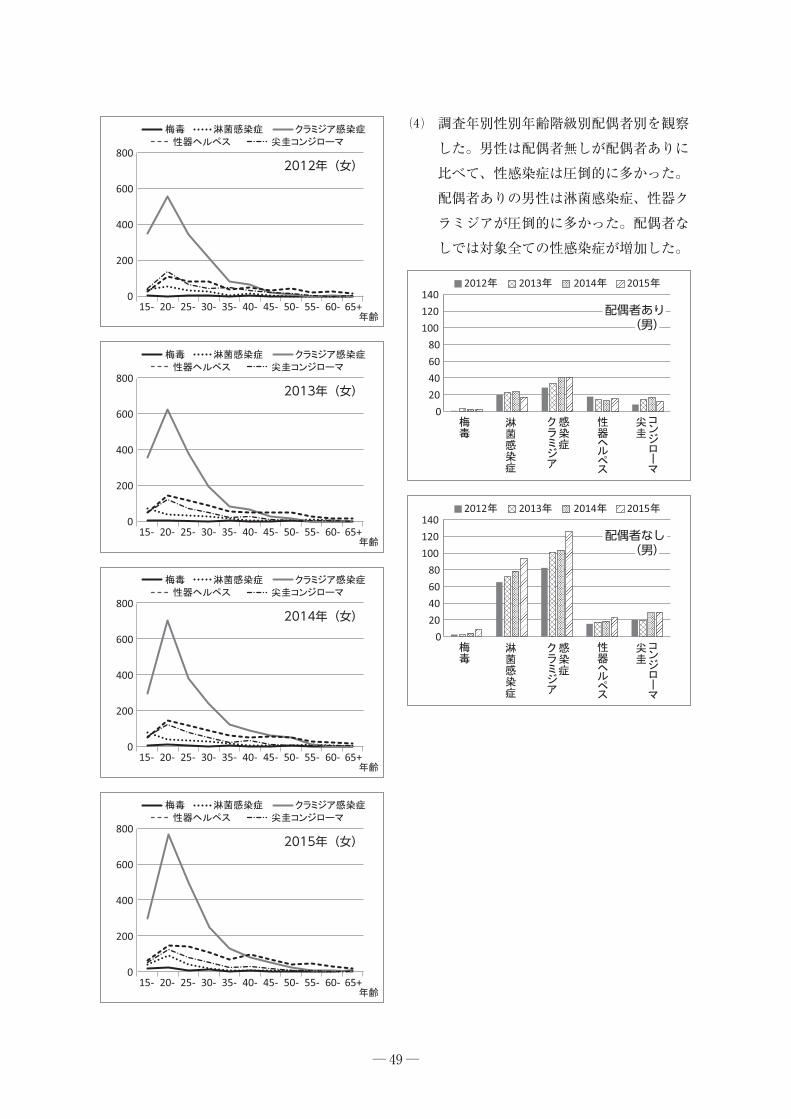
3 調査年別性別年齢階級別感染症別に観察すると、各年とも男性では淋菌感染症及び性器クラミジア感染症とも20~24歳に多く、年次的に著増していた。同時に尖圭コンジローマも増加した。一方、女性での性器クラミジア感染症は15~29歳に非常に多く、年次ごとに増加している。全体に女性性器クラミジア感染症は男性に比べて極めて多かった。また男性は淋菌感染症、性器クラミジア、女性は性器クラミジア感染症、性器ヘルペスが全年齢階級で目立った。
― 48 ―
2012 2013 2014 2015
2012 2013 2014 2015
梅毒(男)
0
1
2
3
4
5
梅毒(女)
0
1
2
3
4
5
2012年(男)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
2013年(男)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
2014年(男)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
2015年(男)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
― 49 ―
4 調査年別性別年齢階級別配偶者別を観察した。男性は配偶者無しが配偶者ありに比べて、性感染症は圧倒的に多かった。配偶者ありの男性は淋菌感染症、性器クラミジアが圧倒的に多かった。配偶者なしでは対象全ての性感染症が増加した。
2012年(女)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
200
400
600
800
0
200
400
600
800
0
200
400
600
800
0
200
400
600
800
2013年(女)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
2014年(女)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
2015年(女)
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
20406080
100120140
2012 2013 2014 2015
0
20406080
100120140
2012 2013 2014 2015
配偶者なし(男)
配偶者なし(男)
配偶者あり(男)
配偶者あり(男)

― 50 ―
女性は、配偶者ありに比べて配偶者無しの性感染症罹患率は、男性と同様に圧倒的に高かった。5種の疾患別に観察すると、性器クラミジアが他を圧倒している。また梅毒も増加した。
5 われわれは、2012~2014年までの前荒川班調査結果を検討したところ、千葉県と兵庫県は性感染症が多く、岐阜県と徳島県が少ないことを観察した。この傾向も今年度も続くことを仮説として、今年度は前3年間と本年度の調査を合わせて、性感染症のそれぞれの県の傾向と、多い県と少ない県の比較を行った。 梅毒は兵庫県・徳島県が0人であった年があることから比較は難しいが、梅毒は増加傾向にあった。
淋菌感染症は、仮説通りであった。千葉県・兵庫県が多かった。ただ兵庫県が突出していることも分かった。
0
50
100
150
2002012 2013 2014 2015
0
50
100
150
200
2012 2013 2014 2015
配偶者なし(女)
配偶者なし(女)
配偶者あり(女)
配偶者あり(女)
0
2
4
6
8
10
0
2
4
6
8
10
2012 2013 2014 2015
2012 2013 2014 2015
梅毒(女)梅毒(女)
梅毒(男)梅毒(男)
2012 2013 2014 2015
2012 2013 2014 2015
01020304050607080
01020304050607080
淋菌(女)淋菌(女)
淋菌(男)淋菌(男)

― 51 ―
淋菌は女性より男性が際立って多い感染症であるが、兵庫県男性が際立って多く、2014年に多くなったが、傾向として増加傾向にある。また千葉県と兵庫県は多く、岐阜県と徳島県が少ないことを観察した。 性器クラミジア感染症はこれまでの観察では千葉・兵庫県が多く、岐阜・徳島県で少ないとしていたが、性器クラミジアについては逆転していた。
次いで本研究と定点調査を比較した場合、定点は淋菌・性器クラミジア感染症で55歳代まで非常に低い値を示した。
D.研究考察
性感染症は決して少ない感染症とは言えない。男性は淋菌感染症が若い層で多く、女性は性器クラミジア感染症、性器ヘルペスが多いことがわかった。 また配偶者別には、どの感染症についても配偶者無しが配偶者ありよりも多いことが改めて追認できた。しかしながら「配偶者あり」であっても性感染症罹患者は現に存在しており、どうして感染したのかを、行動学的に調査する必要がある。感染源は「浮気相手」なのか、Commercial Sex Workerなのか、また性感染症に罹患した配偶者からなのか、現状では何ら情報は無い。この点にスポットを当てた研究が必要であり、性感染症予防指針に、性についての人の行動・行為を入れる必要が
2012 2013 2014 2015
2012 2013 2014 2015
020406080100120140160180
020406080100120140160180
性器クラミジア(女)
性器クラミジア(女)
性器クラミジア(男)
性器クラミジア(男)
0
50
100
15047
男性淋菌感染症について平成23年度47都道府県医療機関推定有病率と定点推定有病率の比較(10万人年対)
0100200300400500600700800
淋菌(男)淋菌(男)
20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
クラミジア(女)クラミジア(女)
20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
47
女性クラミジア感染症について平成23年度47都道府県医療機関推定有病率と定点推定有病率の比較(10万人年対)

あると考えられる。「配偶あり」の場合、配偶者に避妊目的以外でコンドームをつけることはないと考えられるため、個々にスポットを当てた指針の作成が必要と考えられる。 配偶者ありの場合「浮気」「Commercial Sex Worker」ともに家庭を壊すきっかけとなるので、人間行動学的アプローチによって、性感染症を減らす研究は必要であると考えられる。
女性の性器クラミジア感染症は他の感染症を圧倒するものがあり、これについても、感染源を明らかにしない限り、性器クラミジア感染症を減少させることは出来ない。男性の淋菌感染症も同様なことが言える。 これまでの研究の積み重ねで、本年度の研究において、これまで性感染症が多い県と少ない県を定義した。しかしながら、4年間の性感染症の増加トレンドは、われわれの想定を超えており、性感染症の多い県・少ない県は無くなった可能性はある。今後本研究班の活動によって追跡していきたい。
定点動向調査はあくまでもトレンドを追跡するのが目標であり、いろいろな比較ができないよう設計されている。一方本研究の特徴は男女比較、男女別の年齢層比較、同性での感染症罹患率の比較、異性での感染症罹患率の比較など、多様な比較が可能である。 また性感染症定点動向調査は本研究に比べて感染者の推定値が低いことが明らかになったことから、定点の取り方について変更するべきであると考えられる。
E.結 論
1 本研究は、国が行う感染症動向調査:定点調査に比べて感度が極めて良い。
2 性感染症は前研究班のころよりも増加した。
3 「配偶者あり」であっても、性感染症患者はおり、配偶者がありながら何故性感染症に罹患するかについて、人間行動学的に明らかにする必要が喫緊の課題である。
4 本研究は調査設計が定点調査設計と全く異なり、独立した研究である。このため定点調査の影響は受けない。
5 定点調査に比べて自由度が高いことから、解析結果を使って、男女別比較、性感染症間の比較を行うことが出来る。これらは定点調査では出来ないことである。性感染症は他の感染症とは異なり、大々的に医療機関に罹ることの出来ない物であることから、定点の選定においては十分な配慮が必要である。本研究から性感染症のあり方について、国は他の感染症と違えて新たな選定方法を考えるべき時期であると考えられる。
F.健康危機情報
国・地方公共団体は性感染症対策の基本であるコンドームの使用を強く進めていく必要がある。一方で性感染症の感染源は明らかでないことも多いので、国民は安全な環境にあるとは言えない危機的状況にあると考えられる。
― 52 ―

G.論文発表
谷畑健生・秋元義弘・武島 仁・五十嵐辰男・安田 満、種田恭子・金山博臣・荒川創一:平成25年7モデル県の性感染症診察医療機関全数調査推計有病率と国立感染症研究所の定点報告推計有病率の比較~7県医療医官全数調査結果と定点調査報告結果の有病率は何故乖離したのか? 日本性感染症学会誌.2015;26(1):109−116.
H.知的所有権の取得状況
1.特許取得 なし
2.実用新案登録 なし
3.そ の 他 なし
― 53 ―
2015年10月ひとつきに検査した検体数と陽性数
(一件も検査していない場合は、分母に(0)検体と
ご記入ください)
陽性数
1か月間の検査実施数
(10月1日~31日)
)法STSのどなRPR(
応反清血毒梅 菌淋 アジミラク
)年5102(
紙用
査調
握把
数全 )I
TS
( 症
染感
性
(
県調査)
医療施設名
定点施設
・非定点施設 (いずれかを○で囲む)
所在
地連
絡先
記入
医師名
TEL
-
-FAX
-
-
標榜
科産婦人科・泌尿器科・皮膚科・性病科・その他(
)
検査数
2015年10月ひとつきに診断した性感染症症例あり ・ なし
1症例1行として該当疾患名の略語を○で囲む。重複感染例は複数疾患名を○で囲む。
号番例症
日/月
)みの郡市(
地住居
齢年
別性
者偶配ⓐ
梅毒
男性
尿道
炎女性子宮頸管炎
ⓔⓕ
スペルヘ
器性
圭尖
Ⅰ期Ⅱ期Ⅲ期以上
又は無症候
ⓑ 性菌淋ⓒクラミジア性ⓓ非淋菌性
非クラミジア性
症候性無症候性
例10/ 1○○市23
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
110/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
210/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
310/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
410/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
510/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
610/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
710/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
810/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
910/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
1010/
男・女
有・無
梅Ⅰ梅Ⅱ
梅Ⅲ無症
淋ク症
ク無症
非淋非ク
ヘコ
RPRでは16倍(自動測定法
では16単位/ml)以上
陽性(
)
(
)検体
術前検査等を
1.含まない 2.含む
陽性(
)
(
)検体 うち、 症候性(
)
無症候性(
)
陽性(
)
(
)検体
提出期限は、2015年11月末日です。
該当患者がない場合でも、性感染症症例「なし」を○で囲むと共に、左欄に検査数を記入し、ご提出ください。※記載欄が足りない場合は、用紙をコピーしてご記入ください。
症例件数
両方ご記入ください
― 54 ―

182.05
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅 毒(縦軸:人口10万人年、横軸:年齢階級)
― 55 ―

15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅 毒(縦軸:人口10万人年、横軸:年齢階級)
― 56 ―

182.05
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅毒Ⅰ期(縦軸:人口10万人年、横軸:年齢階級)
― 57 ―

15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅 毒(縦軸:人口10万人対・人年、横軸:年齢)梅毒Ⅰ期(縦軸:人口10万人年、横軸:年齢階級)
― 58 ―

15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅毒Ⅱ期(縦軸:人口10万人年、横軸:年齢階級)
― 59 ―

15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅 毒(縦軸:人口10万人対・人年、横軸:年齢)梅毒Ⅱ期(縦軸:人口10万人年、横軸:年齢階級)
― 60 ―

15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅毒Ⅲ期以上・無症候(縦軸:人口10万人年、横軸:年齢階級)
― 61 ―

15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100
梅 毒(縦軸:人口10万人対・人年、横軸:年齢)梅毒Ⅲ期以上・無症候(縦軸:人口10万人年、横軸:年齢階級)
― 62 ―

0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
淋菌性尿道炎・頸管炎(縦軸:人口10万人年、横軸:年齢階級)
― 63 ―

0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
梅 毒(縦軸:人口10万人対・人年、横軸:年齢)淋菌性尿道炎・頸管炎(縦軸:人口10万人年、横軸:年齢階級)
― 64 ―

7874.871278.45
4912.521095.28
1536.58
19836.96
1965.82
0 0
1687.471092.32
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
クラミジア性尿道炎・頸管炎(縦軸:人口10万人年、横軸:年齢階級)
― 65 ―

18364.78
2392.19
7952.071098.53
3373.38
23624.60
1058.75
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
梅 毒(縦軸:人口10万人対・人年、横軸:年齢)クラミジア性尿道炎・頸管炎(縦軸:人口10万人年、横軸:年齢階級)
― 66 ―

1312.48
6612.32
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
クラミジア性尿道炎・頸管炎(症候性)(縦軸:人口10万人年、横軸:年齢階級)
― 67 ―

9182.39
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
梅 毒(縦軸:人口10万人対・人年、横軸:年齢)クラミジア性尿道炎・頸管炎(症候性)(縦軸:人口10万人年、横軸:年齢階級)
― 68 ―

6562.39
4912.52
1229.27
13224.64
1608.40
1687.471001.30
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
クラミジア性尿道炎・頸管炎(無症候性)(縦軸:人口10万人年、横軸:年齢階級)
― 69 ―

9182.391913.75
7952.07
3373.38
23624.60
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
0100200300400500600700800900
1000
クラミジア性尿道炎・頸管炎(無症候性)(縦軸:人口10万人年、横軸:年齢階級)
― 70 ―

656.24
818.75
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
非淋菌非クラミジア性尿道炎・頸管炎(縦軸:人口10万人年、横軸:年齢階級)
― 71 ―

312.49
1590.41
435.61 366.47
269.33
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
020406080
100120140160180200
0
20
40
60
80
100
120
140
160
180
非淋菌非クラミジア性尿道炎・頸管炎(縦軸:人口10万人年、横軸:年齢階級)
― 72 ―
205.14
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
性器ヘルペス(縦軸:人口10万人年、横軸:年齢階級)
― 73 ―

407.21
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+ 15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
020406080
100120140160180200
020406080
100120140160180200
020406080
100120140160180200
0
50
100
150
200
250
300
350
400
0
50
100
150
200
250
300
350
400
性器ヘルペス(縦軸:人口10万人年、横軸:年齢階級)
― 74 ―

656.24
818.75
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
尖圭コンジローマ(縦軸:人口10万人年、横軸:年齢階級)
― 75 ―

1590.41
325.77
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+0
50
100
150
200
250
300
15- 20- 25- 30- 35- 40- 45- 50- 55- 60- 65+
― 76 ―
尖圭コンジローマ(縦軸:人口10万人年、横軸:年齢階級)

Ⅰ. 「性感染症に関する特定感染症予防指針」への自治体の対応状況調査
A.研究目的
平成29(2018)年改訂が予想される「性感染症に関する特定感染症予防指針」(以降指針)への反映を目的に、自治体における性感染症(STD)発生動向調査の運営と活用の状況を平成24年度に改訂された点を中心に把握する。
B. 研究方法
サーベイランス活用を担う都道府県/保健所設置市のSTD対策担当者および地方感染症情報センター担当者を対象に2015年12月に電子メールあるいは郵送により質問紙を送付回収した。 2013(平成25)年12月にも同様の調査を行っており一部結果を比較した。
― 77 ―
性感染症(STI)サーベイランスの評価と改善に関する研究
【研究分担者】 中瀨 克己 (岡山大学医療教育統合開発センター)【研究協力者】 高野つる代 (横浜市旭区福祉保健センター) 川畑 拓也 (大阪府立公衆衛生研究所) 細井 舞子 (大阪市保健所) 中谷 友樹 (立命館大学) 尾本由美子 (豊島区池袋保健所) 砂川 富正 (国立感染症研究所) 有馬 雄三 (国立感染症研究所) 谷畑 健生 (神戸市保健所) 白井 千香 (神戸市保健所) 樫原 摩紀 (株式会社エスアールエル) 金谷 泰宏 (国立保健医療科学院)
研究要旨
わが国の性感染症(STI)に関するサーベイランスの改善を目的として本年度は以下の研究を行った。まず、性感染症に関する特定感染症予防指針に基づく対策の現状把握とその推進のためにⅠ.「性感染症に関する特定感染症予防指針」への自治体の対応状況調査、Ⅱ.地方自治体性感染症サーベイランス担当者向け情報還元を行った。また、国の行う感染症発生動向調査を補完する動向把握策等の検討として、Ⅲ.検査結果サーベイランスの試行と検討、Ⅳ.STI発生動向調査の報告情報の活用に関する検討を行った。

倫理面への配慮 本研究には、個人情報および人や動物への介入を行う内容は含まれていない。
C.研究結果及び D.考 察
調査結果概要およびこれを踏まえた考察を別添1、2に示す。
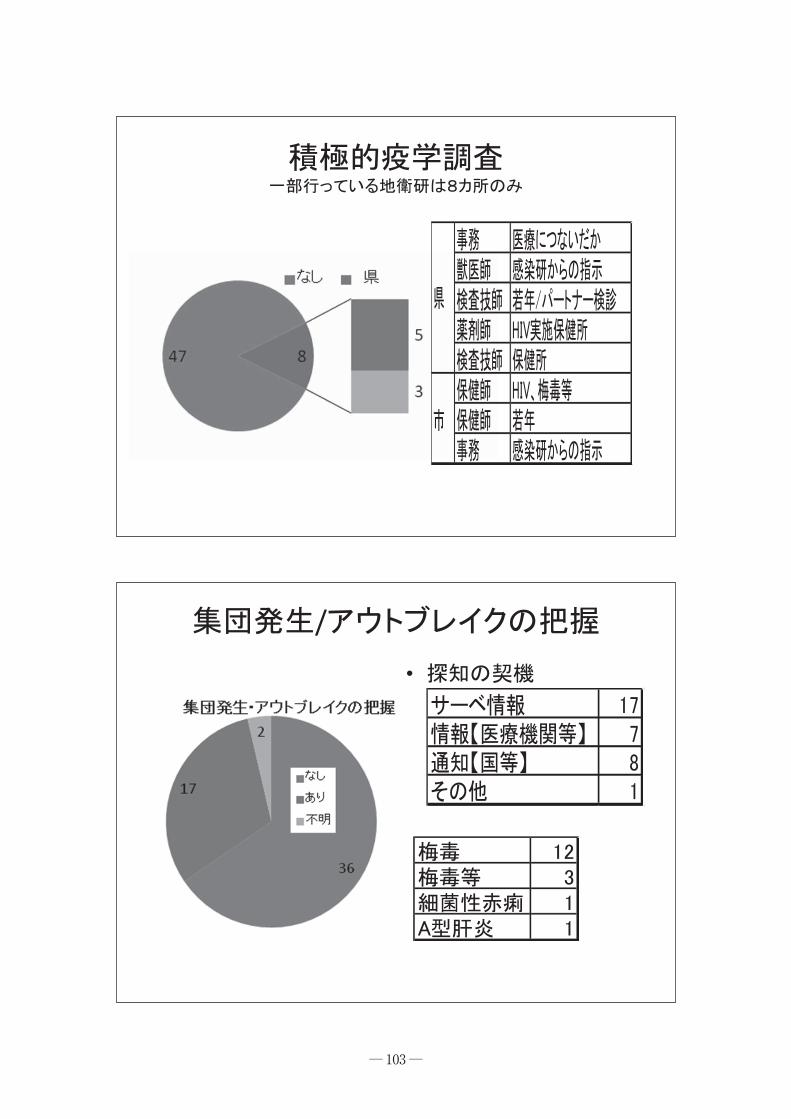
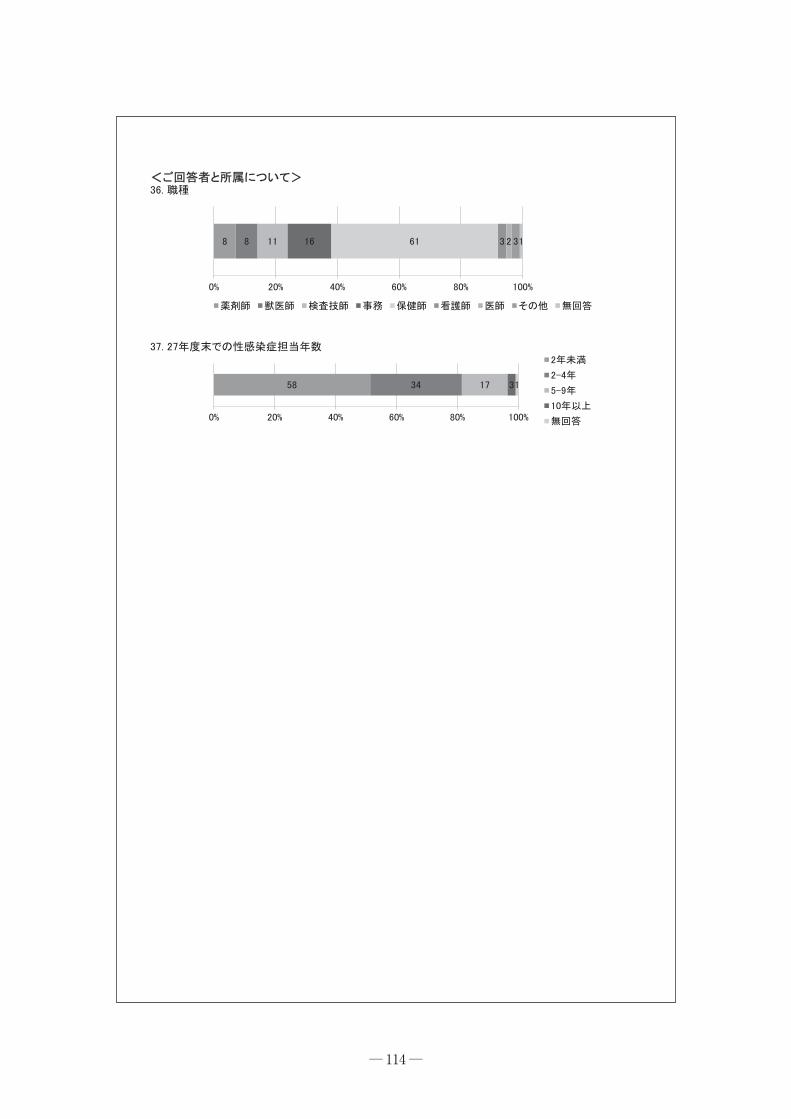
対策担当課における対応の要約・全国自治体のSTD対策担当者を対象に調査した結果、指針にある口腔を介した感染について把握体制を変更した自治体は少ない。一方で、全数調査など独自取り組みを行う自治体もある。・梅毒を中心に性感染症のアウトブレイクを15自治体で把握し、増加への対応や啓発が行われていた。・担当者の経験年数は短く、保健師等の背景を活かした関係機関や他自治体等との情報交換や的確な情報把握と効果的な還元のための体制の充実が期待される。
発生動向担当者における対応のまとめ・定期情報の発信は、殆どが行っているが・臨時情報の発信が、地衛研(地方感染症情報センター)でバラツキがあった。・若年女性層等、ターゲットに合わせた情報発信が課題。・関係機関との連携も課題。・性感染症罹患の指標として、性器ヘルペスは課題がある。・高度耐性淋菌に対する病原体定点等、疾患の流行に対応した新たな体制も必要か(その際は、都道府県一律ではなく、報告数の多い県等に限定するか)。
なお、この纏めは公衆衛生情報研究協議会にて報告した。 また、指針の変更内容に対応した、情報提供先やその内容、定点医療機関の変更、口腔を介した感染の把握(耳鼻科定点の設定)等への対応に加え、耐性淋菌などの病原体定点への考え方、性器ヘルペス動向把握の意義、自治体検査での未返却割合、パートナー健診、アウトブレイクの把握とその際の対応など調査結果の全体を別添3、4に示す。
Ⅱ. 地方自治体性感染症サーベイランス担当者向け情報還元
A.研究目的
我が国の安定的な性感染症サーベイランスである感染症発生動向調査の運営を地方で担う地方感染症情報センター職員および対策を担う自治体性感染症対策担当者への情報還元を行うことによって、指針に示す拠点としての保健所を始めとして都道府県等地域からの情報発信を強化するとともにその結果に基づく対策の推進を促す。
B.研究方法
地方感染症情報センター職員が集まる機会を捉えた情報還元を行うと伴に多様な媒体も活用して情報提供を図る。
倫理面への配慮 本研究には、個人情報および人や動物への介入を行う内容は含まれていない。
― 78 ―

C.研究結果及び D.考 察
多くの地方感染症情報センター職員が集まる地方衛生研究所全国協議会主催による公衆衛生情報研究協議会にて梅毒増加、自治体対応の現状、大阪市におけるサーベイランス活用手法の3演題を発表した。発表スライドを別添1、2、5に示す。 発表後の質疑や会場での質疑を踏まえ、
STIサーベイランスの更なる活用への動機付けや意義の理解に繋がったと推定される。参加者からの質問や意見等を別添11に示す。 アンケート結果と考察は調査対象とした全国自治体に対し、調査と同様にメールあるいは郵送により還元した。 全国の性感染症対策担当部門に配布され、見ることが多いと想定されるニューズレター「性の健康」に寄稿し、特定感染症予防指針への自治体対応の現状と考察を情報提供した。また、情報提供を目的としたホームページを運営し、過去の研究成果や発生動向調査ガイドラインなどを含め研究成果を還元した。(下図)
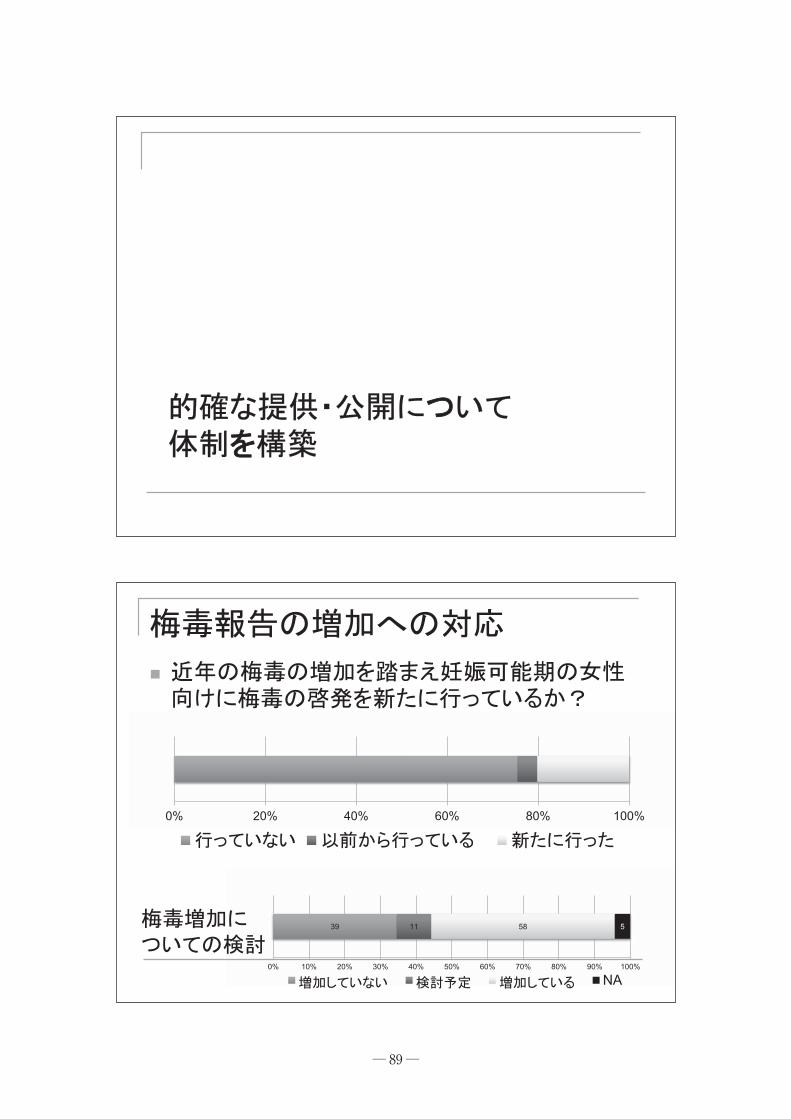
対策を担当する大阪市保健所感染症対策課における梅毒の発生動向を踏まえた対応報告では、以下を今後の課題としている。
1 .梅毒届出医療機関に対する積極的疫学調査
2 .男性とセックスする男性への広報に加え、女性への啓発
3 .梅毒検査結果陽性者のパートナー向け資材の作成
4 .他自治体と連携した普及啓発及び検査体制整備
研究Ⅰでの調査結果、Ⅳでの研究協力者間の協議等を踏まえると、以下のように考察された。 1 .届け出時の適切な内容確認や必要時の積
極的疫学調査が行われていることを自治体に周知する事が、対策の推進に有用と考えられる。今回も豊島区が用いている
Faxによる情報確認の様式を紹介した。 2 .HIV感染も含め、異性間性交渉による感染に関し改めて広い対象者に注意喚起する必要性が高い。
3 .先天梅毒のような稀だが重要な事例では積極的疫学調査により対象者の実情を把握する必要性が高い事の周知が必要である。増加しつつある新たな伝播への対応として、パートナーへの働きかけによる感染防止と合わせた伝播に関する情報把握(パートナー健診)を強化することで、対象者の実情に合わせた予防対策を行えることの自治体担当者への情報提供が有用と思われる。
4 .都市である大阪市では、梅毒報告の半数が市外での感染と報告されており、対策の基礎となる情報の共有が大阪市と近隣自治体で新たに個別に行われた。自治体間の発生動向情報共有が十分行われていない現状を踏まえ、①NESIDにおいて他自治体への公開範囲の設定で情報提供が
― 79 ―

可能な事をまず周知すると伴に、②事例の紹介や共有が進むような働きかけ③梅毒届け出における居住地情報の追加などにより情報の把握と共有の推進が必要と思われる。
Ⅲ. 検査結果サーベイランスの試行と検討
A.研究目的
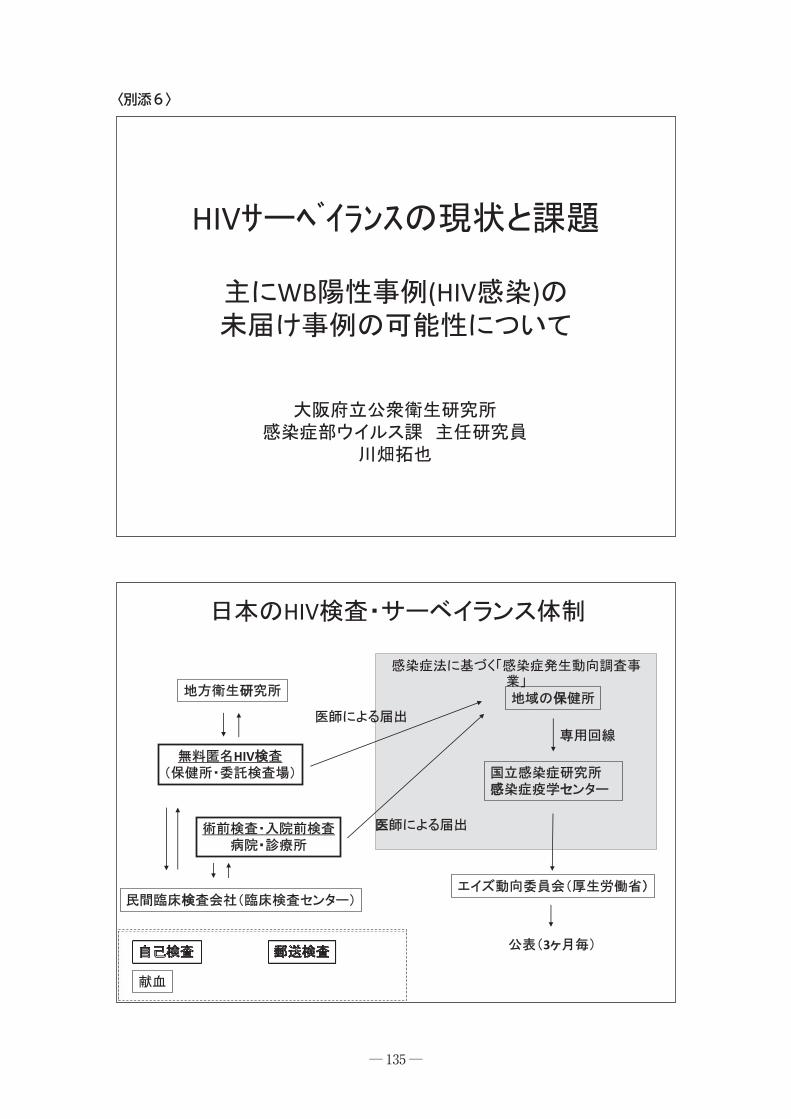
感染症サーベイランスにおける動向把握方法の一つとして、検査結果によるものがある。感染症発生動向調査を補完するサーベイランスとして検査結果サーベイランスの可能性を評価した。 WB法によるHIV抗体確認検査は通常HIV感染の診断目的で用いられ、基本的に一人の感染者には1回の陽性結果と考えられる。そのため、HIVのWB陽性件数はHIV感染症診断動向の指標となる。未届けが高い割合であれば、発生動向調査の結果との乖離がみられると考えられるので、HIV確認検査陽性数の意義を検討した。 また、HPVとHSVに関する委託検査の現状を問い合わせ、性感染症動向把握における活用の可能性を検討した。
B.研究方法
大規模検査受託会社と試薬メーカーで構成さるウイルス検査に関する連絡会(ウイルス検査技術連絡会)に2011年1月から2013年12月(検体提出時)に自施設で実施したWB法によるHIV抗体検査の集計値の提供を依頼した。また、研究目的等で同一人の重複検査が
行われる事があるので、重複の除外を依頼した。全国および大阪府における感染症発生動向調査結果の詳細と比較し、未届け事例の可能性について検討した。
倫理面への配慮 内容に個人情報は含まれず、各社内で提供に当たっての倫理等検討が行われた結果、3社から提供を受けた。 保健所WB陽性数は公表データを用い、2013年の近畿圏に関しては研究協力者が自治体に問い合わせて数値を得た。 HPV、HSVについては大規模委託会社1社の委託に関する現状を把握した。 上記のように本研究には、個人情報および人や動物への介入を行う内容は含まれていない。
C.研究結果及び D.考 察
WB法陽性数は2011年で約1500件であった。主要なHIVの届出元と確認検査は、①自施設でWB検査が出来ない医療機関における委託検査、②保健所による地方衛生研究での確認検査、③自医療機関内での確認検査、の3つであり、今回は③病院検査科における陽性数は把握できていない。 都道府県ごとの重複を考慮したWB法陽性数に保健所陽性分を加え、届出数とを比較した結果、14府県では両者の和が届け出数を上回った。診断されたHIV感染症例が届けられていない可能性が高い(別添6)。 HPVとHSVに関する大規模検査委託会社のコメントは以下のようであり、現在のところ、委託検査結果からHPV,HSVについて動向を把握するのは難しいと思われた。
― 80 ―

HPVは、女性の検診由来の検体が全てを占めており、男性由来の検体はない。
HSVは、依頼のある検査材料はほとんどが髄液で、その他は眼科由来、血液で泌尿器由来の検体はない。
E.結 論
HIV感染症診断例の報告の未届けは、かなりの数に上りそうであることが示唆された。今後は、病院内でのWB法陽性診断数を把握し正確な未届け事例の評価をする必要性が高い。 現在のところ、委託検査結果からHPV、
HSVについて動向を把握するのは難しいと思われた。
Ⅳ. STI発生動向調査の報告情報の活用に関する検討
A.研究目的
STIサーベイランスに関わる中央感染症情報センター、地方自治体担当者、検査受託機関、研究者が協議する事によって、より性感染症対策に資するサーベイランスの方策について検討する。
B.研究方法
本研究における自治体へのアンケート調査結果および他国におけるSTIサーベイランスの運用や活用の現状を踏まえ、研究協力者と協議した。
倫理面への配慮 本研究には、個人情報および人や動物への介入を行う内容は含まれていない。
C.研究結果及び D.考 察
指針では、引き続き「四.対象者の実情に応じた予防対策を講ずるに当たっては、年齢や性別等の対象者の実情に応じた配慮を行っていくことが重要である」としている。近年、梅毒伝播経路において異性間性的接触による感染が増加していること、連携を図るべきとされる後天性免疫不全症候群においても異性間性的接触による感染が増加していること、を踏まえ感染の実情の把握に基づく効果的な対策が重要と考えられる。罹患率の低い疾患対策としては、対象を特定しない啓発に加え、相手を特定した働きかけの有用性やこの際の情報把握が効果的とされ、パートナーへの働きかけが推奨されており1)、ヨーロッパ2)や米国の多くの州において梅毒等を対象に公的な働きかけがなされている1)。このようにパートナー健診が無症候期や自発的な受診が期待しにくい対象者への受診/加療の促進や実情の把握に有用と考えられることを踏まえ、我が国でも一層の推進が期待される。 また、現状では中央情報センターに集約された発生動向調査結果の公開手順が示されていない。諸外国では情報公開の範囲や手順が公開され、その活用がすすんでいる。 今回は保健所で入手可能なデータを用いて地理的情報を加味して分りやすい情報提供の例を示した。NESIDシステムの制約から保健所からは、近隣であっても他自治体の年齢階級別データを得る事ができない。このため、自治体をまたいだ都市圏や地域において、指針に
― 81 ―

示すような、性別年齢階級別の動向を踏まえて、対象者の特性にあった対策を行う事に制約がある。 結論に含まれる検討や今後の研究方向について、非常に有用な議論が行われた。今後の
STIサーベイランスの方向として、性感染症サーベイランスの目的の明確化が議論され、アウトブレイク対応としての梅毒サーベイランス、蔓延疾患(STD)対策としての定点疾患サーベイランスという、対策指向でサーベイランスの目的を区分するという考えかたが提示された。 検討結果は結論のように要約される。
E.結 論
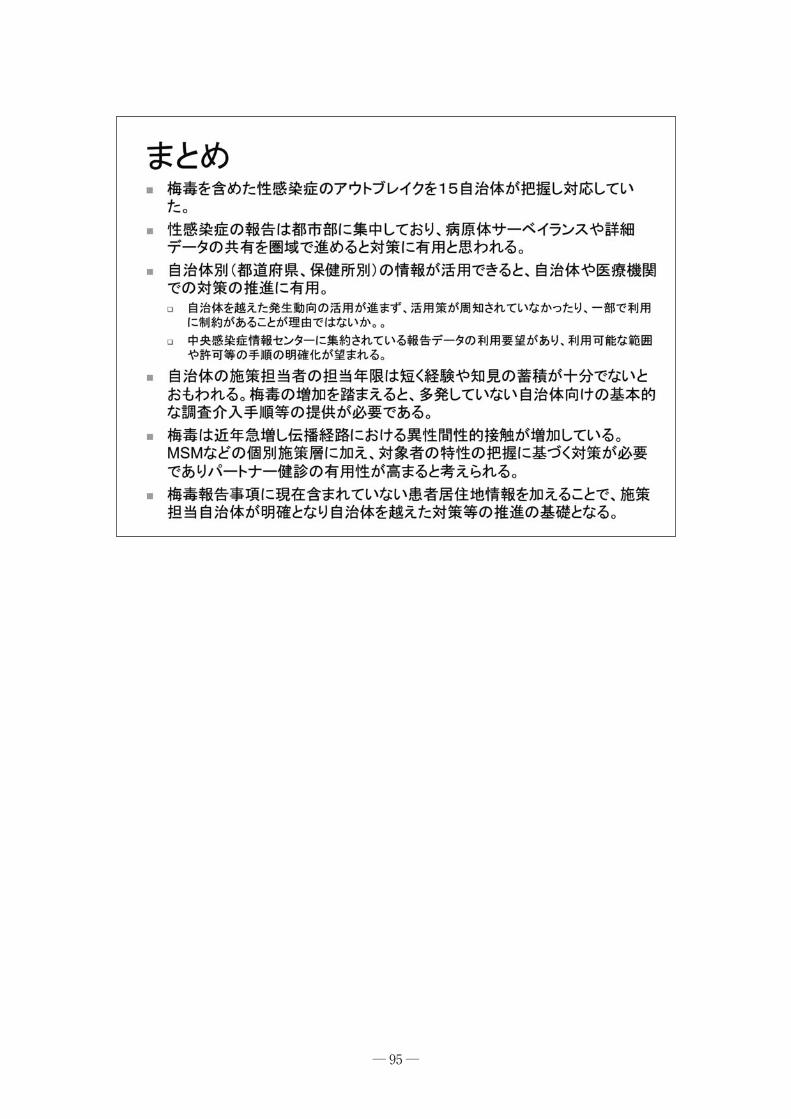
・梅毒を含めた性感染症のアウトブレイクを15自治体が把握し対応していた。・性感染症の報告は都市部に集中しており、病原体サーベイランスや詳細データの共有を圏域で進めると対策に有用と思われる。・自治体別(都道府県、保健所別)の情報が活用できると、自治体や医療機関での対策の推進に有用。 ・自治体を越えた発生動向の活用が進まず、活用策が周知されていなかったり、一部で利用に制約があることが理由ではないか。
・中央感染症情報センターに集約されている報告データの利用要望があり、利用可能な範囲や許可等の手順の明確化が望まれる。
・自治体の施策担当者の担当年限は短く経験や知見の蓄積が十分でないとおもわれる。梅毒の増加を踏まえると、多発していない
自治体向けの基本的な調査介入手順等の提供が必要である。・梅毒は近年急増し伝播経路における異性間性的接触が増加している。MSMなどの個別施策層に加え、対象者の特性の把握に基づく対策が必要でありパートナー健診の有用性が高まると考えられる。・梅毒報告事項に現在含まれていない患者居住地情報を加えることで、施策担当自治体が明確となり自治体を越えた対策等の推進の基礎となる。
参 考1 堀 成美:公立性感染症クリニックにお
ける接触者検診拡大の試み.平成25年度厚生労働科学研究費補助金(新型インフルエンザ等新興・再興感染症研究事業)「自然災害時を含めた感染症サーベイランスの強化・向上に関する研究」(研究代表者:松井珠乃)分担研究 STIサーベイランスの評価と改善.報告書.
2 CDC, Partner Services, Sexually Transmit-ted Diseases Treatment Guidelines 2015,
MMWR, June 5, Recommendations and
Reports / Vol. 64 / No. 3, pp. 8-9, 2015.
G.研究発表
1.論文発表1 中瀨克己:特定感染症予防指針の変更を踏まえた自治体における性感染症発生動向調査の活用.ニューズレター「性の健康」,Vol.15,No.1,1−3,2015.
2 白井千香・古林敬一・川畑拓也・吉田弘之・荒川創一:性感染クリニック及び産科における口腔内性感染症に関するアン
― 82 ―
ケートと検体検査の試み.日本性感染症学会誌,Vol.26,No.1,91−96,2015.
2.学会発表1 中瀨克己・中谷友樹・川畑拓也・中島一敏・神谷信行・杉下由行・高野つる代・尾本由美子・山内昭則・高橋裕明・樫原摩紀・山岸拓也・白井千香:Englandと比較した我が国の性感染症サーベイランスの特徴,日本性感染症学会,2015年12月6日,東京.
2 中谷友樹・安本晋也:地理情報システム(GIS)を用いた感染症流行の地理的視覚化・空間的モデリング.科学技術イノベーション政策のための科学研究開発プログラム(RISTEX)プログラムサロン(第7回)エビデンスに基づいた政策形成へ:医療における試み,政策研究大学院大学(GRIPS).(2016年2月22日)
3 川畑拓也:大阪府における梅毒とHIVの発生動向について.大阪STI研究会 第38回学術集会,大阪,2015年.
4 川畑拓也:HIV検査・サーベイランスの現状と課題.第8回近畿HIV FRONTIER研究会,大阪,2015年.
5 川畑拓也・中山周一・古林敬一・亀岡 博・安本亮二・志牟田健・石原朋子・大西 真:大阪府内で分離された淋菌株におけるアジスロマイシン感受性率の低下.第28回日本性感染症学会学術大会,東京,2015年.
6 川畑拓也・小島洋子・森 治代・柴田敏之・中山周一・大西 真:大阪地域における梅毒感染拡大阻止の取組み(2013−2015前半).第28回日本性感染症学会学術大会,東京,2015年.
7 細井舞子・松本健二・高野つる代・金谷泰宏・尾本由美子・川畑拓也・砂川富正・中瀨克己:大阪市における梅毒の発生動向と取り組み.第29回公衆衛生情報研究協議会研究会,東京,2016年.
8 高野つる代・中谷友樹・細井舞子・尾本由美子・川畑拓也・砂川富正・中瀨克己:地方感染症情報センターにおける
STIサーベイランスの運用の現状.第29回公衆衛生情報研究協議会研究会,東京,2016年.
9 中瀨克己・高野つる代・細井舞子・尾本由美子・川畑拓也・砂川富正・金谷泰宏:特定感染症予防指針の期待する性感染症発生動向の活用.第29回公衆衛生情報研究協議会研究会,東京,2016年.
H.知的財産権の出願・登録状況
1.特許取得 なし
2.実用新案登録 なし
3.そ の 他 なし
― 83 ―

― 84 ―
2016.1.29.
� H29(2018)
(STD)
�
STD 2015 12
� 2013(H25) 12
〈別添1〉

― 85 ―
�
35
1550
13
H24�
�
�
�

― 86 ―
32 48 38
0% 20% 40% 60% 80% 100%
NA
5

― 87 ―
2 5 74 10 5
0% 20% 40% 60% 80% 100%
NA
H2577
0% 20% 40% 60% 80% 100%
17
H
0301 H24 3 1�
�
�

― 88 ―
� H25
25
�
39
940
NA
98
15 3
1
24
� 10
― 89 ―
�
39 11 58 5
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
NA
0% 20% 40% 60% 80% 100%

― 90 ―
41% 46� 7, 8, 3,
7,4, 32
STD45% 51
14% 1612 A
STD
26
69
14
NA
4

― 91 ―
STD
58
34
17
30
10
20
30
40
50
60
70
64
16 11 8 8 2 20
10
20
30
40
50
60
70
� STD
�
�

― 92 ―
Tomoki Nakaya, MSc, PhDProfessor, Department of Geography,
Ritsumeikan University, JapanResearch seminar on “Analysing geographic informa�on
on STIs and sexual health”, HIV/STI Department, Public Health England
12 Feb 2014
Exploring spa�o-temporal trends
of HIV/STISyphilis in Japan
Exploring spa�o-temporal trends
of HIV/STISyphilis in Japan
Geographic reference of the surveillance data
HIV/AIDS• Reporting prefecture and
district: based on the location of reporting clinics/hospitals
• Living prefecture (from 2006)
Syphilis• Only reporting prefecture
and district
47 Prefectures552 Health Centre Districts in 2013
ctures CentreeDi tsstrict in2013

― 93 ―
Annual trends of reported syphilis cases (per popula�on) by prefecture, 2006-2013
2006 201330 per million
Okinawa
Tokyo
Miyagi
Osaka
Fukuoka
347521
622523 497
650 692
984
158 198 217 168 124 177 183 236
2006 2007 2008 2009 2010 2011 2012 2013
Men Women
Total number ofnewly reported cases
men
women
Cartogram of syphilis SIR (Bayesian es�mates),men, 2013
0.0 - 0
.5
0.6 - 1
.0
1.1 - 2
.0
2.1 - 4
.0
4.1 - 8
.0
8.1 - 1
6.0
16.1
+Area x height = volume(pop) x (risk) = (incidence)
Hyper-endemic districts
Shinjuku, TokyoRR = 67.9
Kita, OsakaRR = 43.2

― 94 ―
Comparison between sexes, syphilis SIR (Bayesian es�mates), 2013
men
women
0.0 - 0
.5
0.6 - 1
.0
1.1 - 2
.0
2.1 - 4
.0
4.1 - 8
.0
8.1 - 1
6.0
16.1
+
Sendai, Miyagi
Cartogram The areal size is proportional to the regional population size
Conclusion• In recent years, rapid increases in newly diagnosed syphilis cases
have been observed by the na�onal surveillance system in Japan.
• Mapping the surveillance data suggested the existence of areas with extremely high syphilis incidence rates in Japan, 2013.– Shinjuku in Tokyo and Kita & Chuo in Osaka: possibly sustained by
regional concentra�on of MSM popula�on and large agglomera�on of nightlife districts.
– Sendai in Miyagi: ‘rebuilding bubble’ effects on increased hetero sexual infec�on?
GIS-based disease mapping should be beneficial for enhancing the value of the surveillance data.
• Caveats: the following aspects need further a�en�ons– Regional differences in age and mode of infec�on– Repor�ng regions are not residen�al regions– Effects of late diagnosis and under-repor�ng
― 95 ―

― 96 ―
SIT
28 1 29
47 28 7555 ( 73
〈別添2〉

― 97 ―
•
•
7.57.5 ( 7.5 /13
•
E A

― 98 ―
STI• 95 53 / 2• 93 (51• 29 (16 )
10 /
36
15
13

― 99 ―
Web

― 100 ―
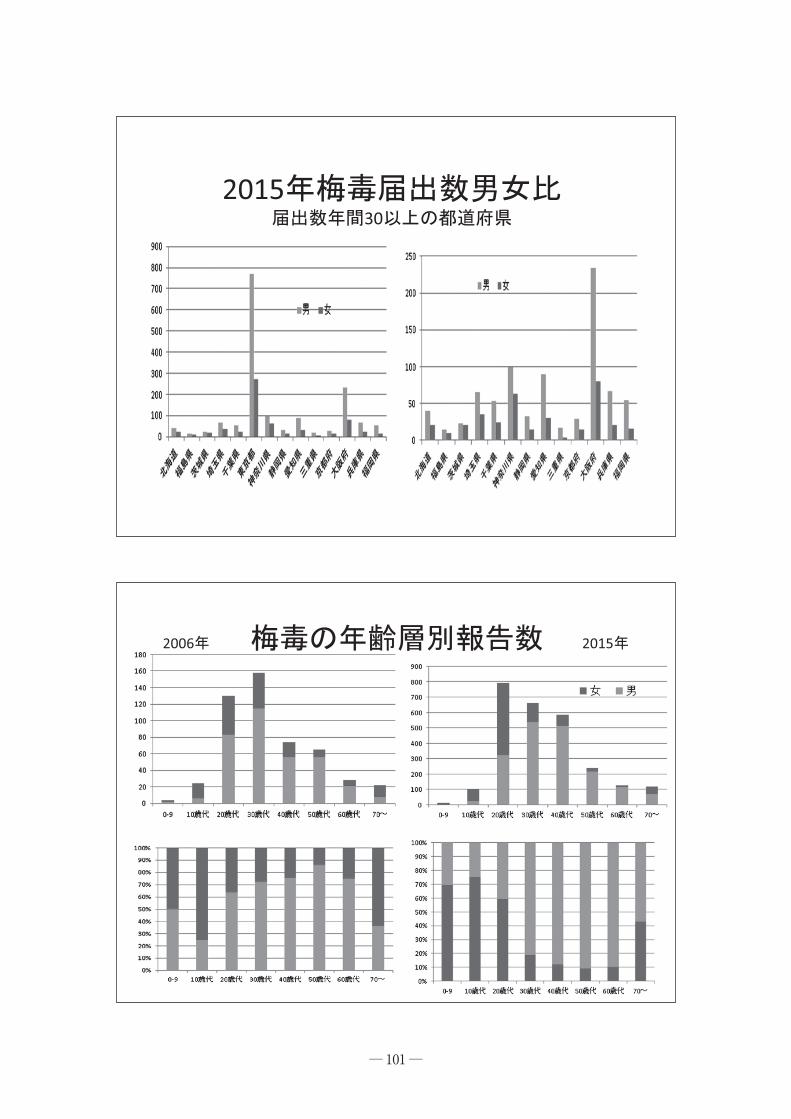
HIV 10 2015
10 10
― 101 ―
201530
2006 2015

― 102 ―
10 HIV 10
― 103 ―
/
•

― 104 ―
(2014
•

― 105 ―
h�p://idsc.nih.go.jp/iasr/31/362/kj3624.html

― 106 ―
•••
••
•

― 107 ―
〈別添3〉

― 108 ―

― 109 ―

― 110 ―

― 111 ―

― 112 ―

― 113 ―
― 114 ―

― 115 ―
, 38, 69%
, 14, 25%
, 3, 6%
, 0, 0%
53 2 0
0% 20% 40% 60% 80% 100%
36 1 15 3
0% 20% 40% 60% 80% 100%
10
1
16
12
11
3
3
1
12
9
12
2
4
1
12
9
0
1
0
0
0
0
0
0
0
0
0
0
1
0
0
0
1
1
8
7
0
1
1
0
5
5
0
1
1
0
5
5
18
6
7
2
12
1
4
0
7
2
14
1
4
0
7
2
3
1
3
5
3
1
1
0
4
2
2
1
1
0
4
2
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
14
4
2
2
12
5
4
0
3
0
10
5
4
0
3
0
7
40
18
26
15
42
40
52
22
35
14
43
38
52
22
35
2
1
1
1
2
2
2
2
2
2
3
2
2
2
2
2
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
HIV
HIV
HIV
HIV
HIV
HIV
Web
Web
Web
〈別添4〉

― 116 ―
42
22 1 6
33
0
10
20
30
40
50
42 32
2
32
15 2 6
0
10
20
30
40
50
14 13 4 2 2 1
0
5
10
15
Web
― 117 ―
11 10
0 2
14
0
5
10
15
14
6 1 1 2
0
5
10
15
NPO
2 3 3 7 2 1 37
0% 20% 40% 60% 80% 100%
24 0 1 10 20
0% 20% 40% 60% 80% 100%
5 15 32 3
0% 20% 40% 60% 80% 100%

― 118 ―
25 23 5 2
0% 20% 40% 60% 80% 100%
16 32 7 0
0% 20% 40% 60% 80% 100%
14 17
19 19
7 3
7 2
0
5
10
15
20
47 8 0
75% 80% 85% 90% 95% 100%

― 119 ―
7 5 4
1 5 4 3
0
5
10
9 6 2 38
0% 20% 40% 60% 80% 100%
17
4 2 3 5 2 0
5
10
15
20
36 2 17
0% 20% 40% 60% 80% 100%

― 120 ―
21
5 14
10 5
0
5
10
15
20
25
12 43
0% 20% 40% 60% 80% 100%
35 12 6 0 2
0% 20% 40% 60% 80% 100%
28 25 2
0% 20% 40% 60% 80% 100%
1 7 20
0% 20% 40% 60% 80% 100%

― 121 ―
1 17 5 28 0 4
0% 20% 40% 60% 80% 100%
28 17 0 3 1 6
0% 20% 40% 60% 80% 100%
26
6 6
13
2 6 0
5
10
15
20
25
30
19 3 32 1
0% 20% 40% 60% 80% 100%
4 9 1 4 36 1
0% 20% 40% 60% 80% 100%

― 122 ―
26
12 12 16 14
05
1015202530
22 32 1
0% 20% 40% 60% 80% 100%
9 11 1 1 32 1
0% 20% 40% 60% 80% 100%
7 17 30 1
0% 20% 40% 60% 80% 100%

― 123 ―
45 45 44
15 16
0
10
20
30
40
50
13 9 16 4 5 1 0 7
0% 20% 40% 60% 80% 100%
17 23 13 2
0% 20% 40% 60% 80% 100%
2
2-4
5-9
10

― 124 ―
2928 1 29
2
�
5
�
〈別添5〉

― 125 ―
�
�
3
4

― 126 ―
2010 2015
5
6

― 127 ―
39 54 65110
182 185
33
10
5
1467
0
50
100
150
200
250
300
2010 2011 2012 2013 2014 2015
1
7
8
92.9% 94.7% 86.7% 95.7% 92.9%73.4%
7.1% 5.3% 13.3% 4.3% 7.1%26.6%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
2010 2011 2012 2013 2014 2015

― 128 ―
9
36.1%52.9%
69.4% 67.3% 68.9%
39.1%
41.7%
35.3%21.0% 21.2% 24.9%
51.5%
0%
20%
40%
60%
80%
100%
2010 2011 2012 2013 2014 2015
2015
10

― 129 ―
11
N=252
12
36.6%
48.0%
8.7%
6.7%

― 130 ―
� n=185
13
� n=67
49.8%
33.5%
8.6%
8.1%
88.0%
9.0%
3.0%
N=252
14
, 29.0%
, 32.1%,
2.4%
, 36.5%

― 131 ―
� n=185
15
31.4%
33.5%3.2%
31.9%
� n=67
22.4%
28.4%
49.2%
N=252
16
53.2%
25.4%
7.9%
12.3%1.2%

― 132 ―
� n=185
17
� n=67
50.9%
29.2%
4.9%
14.0%1.0%
59.7%
14.9%
16.4%
7.5%1.5%
18

― 133 ―
2015
19
�
�
3�
�
�
20
�
�
�
HIV/�
�

― 134 ―
21
�
�
�
�
― 135 ―
HIV
WB (HIV )
HIV
HIV
3
〈別添6〉

― 136 ―
HIV (2013 )
HIV
3
136,400
5,205,819
73,86311 10 )
620 ( 21.1% )
2013 ( ) ( )
HIV
3
136,400(453)
5,205,819(63)
73,863(192 )86%:165 1,590 (HIV:1106,AIDS:484)
620 ( 21.1% )
6 4 ( 1,500 )
( )
( )

― 137 ―
HIVWB
2011 WB n=1181* n=1529
0
50
100
150
200
250
300
350
400
450
WB HIV + AIDS*
WB
HIV
( WB )
( WB )WB
HIV
W
HIV
WB

― 138 ―
HIV WBA
B2011 A =1556* n=1529
0
100
200
300
400
500
600
A WB ( + )B
A B
6
(2013)
12
45 46
236
13 2251
223
0
50
100
150
200
250

― 139 ―
• HIV
•
WB

― 140 ―
A.研究目的
わが国で保険適用となっているM. genitalium検出キットはなく、現在、数社から発売されている検出キットが臨床的に使用可能であるかどうか、検討している。旭化成ファーマ社のマイコプラズマ抗原検出キット「リボテストRマイコプラズマ」は、Mycoplasma pneu-moniaeの検出用に開発されたものであるが、
M. genitaliumと交差反応があり、初尿中の
M. genitaliumを検出できる可能性がある。本キットは約15分でM. pneumoniaeが検出可能であるため、M. genitaliumに応用できる場合、来院当日および治療後判定にも使用できる可能性がある。本研究では本キットの検出限界を測定し、臨床応用が可能かどうかの基礎試験を行った。
B.研究方法
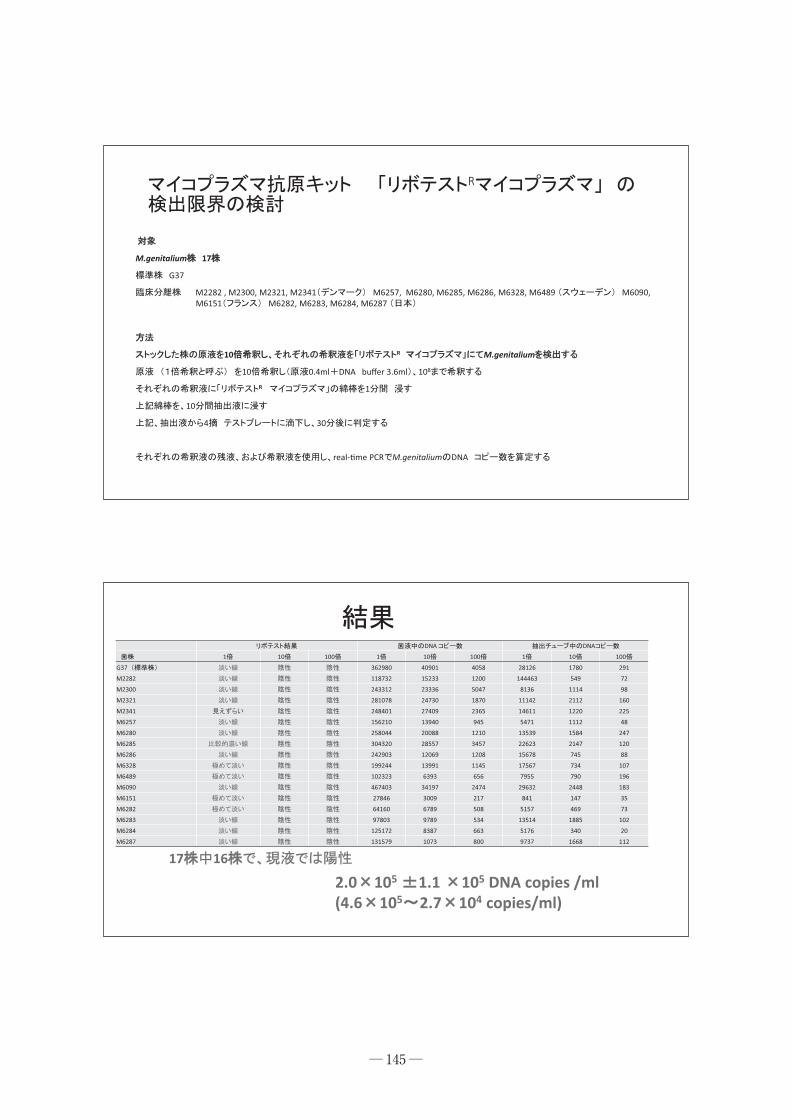
対象は産業医大学にて保存しているM. genitalium株 17株(標準株G37Tを含む)である。M. genitalium株はSP4マイコプラズマ培地(液体培地)で増殖、冷凍保存されている。保存株を再度、SP4マイコプラズマ培地にもどし増殖させ、その菌液をさらに本培地を段階希釈した。段階希釈したそれぞれの菌液を用いて、「リボテストRマイコプラズマ」を反応させた。さらに、希釈した菌液を
MgPa adhesion geneを標的とするreal-time PCR法にて、希釈菌液中のDNAコピー数を測定した。これにより本キットの検出限界(DNAコピー数)が推定できることとなる。 本研究は、保存したM. genitalium株を用いた。これらの株はすべて番号化され、ヒトの検体由来であること以外に、個人情報を有しないため、倫理に関する問題は生じない。
Mycoplasma genitalium検査法に関する研究
【研究分担者】 濵砂 良一 (産業医科大学医学部泌尿器科)
研究要旨
Mycoplasma genitalium検出のための2つの検出法について、基礎的、臨床的研究を行った。旭化成ファーマ社のマイコプラズマ抗原検出キット 「リボテストRマイコプラズマ」を用いてM. genitalium検出のための基礎的研究を行った。17株のM. genitaliumを培養させた液体培地をそれぞれ段階希釈し、それぞれの希釈液を「リボテストRマイコプラズマ」させた。また、希釈液中のM. genitaliumのDNAコピー数をreal-time法にて測定し、「リボテストRマイコプラズマ」法の検出限界を測定した。17株中16株が、その原液(希釈前)では「リボテストRマイコプラズマ」は陽性を示した。しかし、10倍希釈した液体では陽性を示さず、「リボテストRマイコプラズマ」の検出限界は4.6×105コピー/㎖と高く、臨床的には使用できない可能性が高い。

― 141 ―
C.研究結果
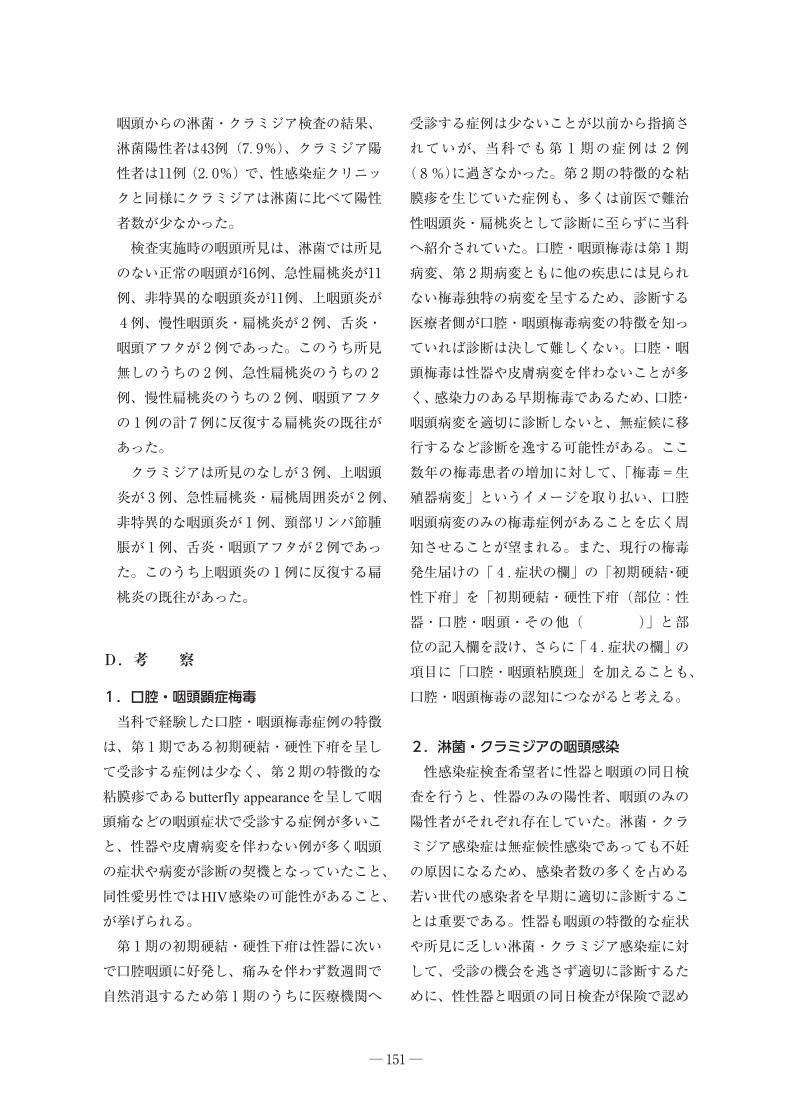
標準株以外に、当科で保存している臨床分離株16株、計17株を用いた。17株中、16株で、希釈する前の菌液で、「リボテストRマイコプラズマ」で陽性を示した。1株は判定不能であった。さらに10倍希釈をすると、すべての株の10倍希釈菌液で「リボテストRマイコプラズマ」は陰性を示し、M. genitaliumは検出できなかった。 「リボテストRマイコプラズマ」が陽性を示した菌液のDNAコピー数は2.0×105±1.1×105コピーであった(最大値4.6×105、最小値2.7×104コピー)であった。
D.考 察
北欧で検査の中心となっているMgPa adhesinを標的とするreal-time PCR法(検査室での検討)では、10コピー以上の検体を陽性としており、我々の研究室でもこの基準に従っている。これまで我々が検討したM. genitalium陽性初尿検体のDNAコピー数は、10~2.0×107コピーであり、大半は10~104コピーである。「リボテストRマイコプラズマ」では105コピー以上でないと陽性を示さないことがわかった。陽性となる検体は、臨床検体のごく一部であり、これまでの検出を考慮すると、大半の尿道炎症例ではM. genitaliumは陰性と判断されることになる。従って、本キットの臨床使用は極めて困難であると言わざるをえない。
E.結 論
旭化成ファーマ社のマイコプラズマ抗原検出キット「リボテストRマイコプラズマ」の
M. genitaliumの検出限界を測定した。測定限界は105DNAコピー前後であり、本キットの臨床応用は困難である。
G.研究発表
なし
H.知的財産権の出願・登録状況
1.特許取得 なし
2.実用新案登録 なし
3.そ の 他 なし

― 142 ―
MMycoplasma genitalium
27
M.genitalium
1) R
M.genitalium2) Seegene AnyplexR M.genitalium

R
• L7/L12• Mycoplasma pneumoniae• 15• Mycoplasma genitalium M.genitalium
M.genitalium:H26-174
M.pneumoniae PCR :57%, 91-92% 85% (
― 143 ―

M.genitalium→M.genitalium
― 144 ―
― 145 ―
R
M.genitalium 17
G37
M2282 , M2300, M2321, M2341 M6257, M6280, M6285, M6286, M6328, M6489 M6090, M6151 M6282, M6283, M6284, M6287
10 R M.genitalium
10 0.4ml DNA buffer 3.6ml 108
R 1
10
4 30
real-�me PCR M.genitalium DNA
DNA DNA
1 10 100 1 10 100 1 10 100
G37 362980 40901 4058 28126 1780 291
M2282 118732 15233 1200 144463 549 72
M2300 243312 23336 5047 8136 1114 98
M2321 281078 24730 1870 11142 2112 160
M2341 248401 27409 2365 14611 1220 225
M6257 156210 13940 945 5471 1112 48
M6280 258044 20088 1210 13539 1584 247
M6285 304320 28557 3457 22623 2147 120
M6286 242903 12069 1208 15678 745 88
M6328 199244 13991 1145 17567 734 107
M6489 102323 6393 656 7955 790 196
M6090 467403 34197 2474 29632 2448 183
M6151 27846 3009 217 841 147 35
M6282 64160 6789 508 5157 469 73
M6283 97803 9789 534 13514 1885 102
M6284 125172 8387 663 5176 340 20
M6287 131579 1073 800 9737 1668 112
17 16
2.0 105 1.1 105 DNA copies /ml(4.6 105 2.7 104 copies/ml)

― 146 ―
R M.genitalium105 copies/ml
M.genitalium 2 107
108copies/ml
real-�me PCR 10copies/mlR
R M.genitalium
AnyplexR M.genitalium
• Seegene AnyplexR M.genitalium17
50 copies/ml 10copies/ml
•
:H25-158

― 147 ―
Seegene vs MgPa PCR for M.genitalium
MgPaConcordance
Positive negative Total
Seegene
positive 27 1 28 Positive 96.4% (27/28)
negative 1 71 72 Negative 98.6% (71/72)
Total 28 72 100
AnyplexR MgPa real-�me PCR 96.4%98.6% AnyplexR
AnyplexR AllplexR PCRSeegene Anyplex
28

A.研究目的
性感染症のうち、患者数がこの数年で急増している梅毒と、従来から患者数が多いクラミジアトラコマティス(Chlamydia trachomatis;以下クラミジア)感染症と淋菌感染症は、口腔・咽頭に感染し病変を生じる場合があり、また口腔・咽頭が感染源ともなり得る。近年の性行動の多様化やオーラルセックスを提供する性風俗の増加を背景に、口腔・咽頭を介してこれらの性感染症に感染する人が増えている一方で、口腔・咽頭への具体的な対策は遅れているといわざるを得ない。口腔・咽頭梅毒と、淋菌・クラミジアの咽頭感染に対して、実際の感染者の特徴や臨床所見から、今後求められる対策について検討する。
B.研究方法
口腔・咽頭の顕症梅毒については、当科で経験した症例の臨床的特徴について後ろ向きに検討する。淋菌・クラミジアの咽頭感染については、当科と研究協力施設において過去に実施した前向き研究の結果を比較検討する。
1.口腔・咽頭顕症梅毒 1982年~2015年の間に当科で診断した口腔咽頭の顕症梅毒27例について、その臨床所見や特徴を提示する。
2.淋菌・クラミジアの咽頭感染 2005年~2015年の間に性感染症クリニックおよび耳鼻咽喉科施設で実施した淋菌・クラミジアの咽頭感染に関する前向き研究について、陽性者の結果を比較検討する。
― 148 ―
口腔・咽頭梅毒および淋菌・クラミジアの咽頭感染に関する検討
【研究分担者】 余田 敬子 (東京女子医科大学東医療センター耳鼻咽喉科)
研究要旨
口腔・咽頭梅毒と淋菌・クラミジアの咽頭感染について、今後の調査や対策を考察する目的に、前者は当科で経験した症例の臨床的特徴について後ろ向きに検討し、後者は当科と研究協力施設において過去に実施した前向き研究の結果を比較検討した。 口腔・咽頭梅毒は、性器や皮膚に病変がなく口腔・咽頭の症状や病変が梅毒診断の契機になる場合が多かった。最近急激に患者数が増加している梅毒については、口腔・咽頭梅毒の特徴を含めた情報を発信すること、現行の梅毒発生届けに口腔咽頭梅毒の項目を追加することが望まれる。 特徴的な症状や所見に乏しい淋菌・クラミジアの咽頭感染については、性器と咽頭の同日検査が保険で認められること、現行の感染症発生動向調査(STD定点)の調査票の項目に「咽頭淋菌感染症」と「咽頭クラミジア感染症」を別項目として加えることが望まれる。

1)性感染症クリニックにおける対象 神奈川県川崎市堀之内の性感染症(STI)クリニック1施設にて性感染症検査を希望して受診した人のうち、咽頭と性器から淋菌およびクラミジアの同日検査を受けた男女、2005年11月1日から2006年7月1日(期間a)の555人と、2008年9月1日から2009年1月16日(期間b)の250人。2)耳鼻咽喉科施設における対象 全国10箇所(表1)の耳鼻咽喉科施設において、口内炎、咽頭炎、扁桃炎、咽喉頭異常感などの患者、または咽頭の性感染症検査希望者のうち、同意の得られた18歳~65歳の男女、2010年11月18日から2012年3月6日(期間c)の182人と、2013年1月7日から2015年2月2日(期間d)の362人。
3)検査方法(表2) 咽頭スワブ、うがい液を検体とし、淋菌培養と核酸増幅検査のPCR法(olymerase chain reactionポリメラーゼ連鎖反応、アンプリコアSTD−1クラミジアトラコマティス)、
SDA法(strand displacement amplification、鎖置換増幅、BDプローブテックET CT/GC)、
TMA法(transcription-modiated amplification、転写介在増幅、アプティマコンボ2)、real time PCR(real time polymerase chain reaction、コバスR4800システムCT/NG)を用いて検出した。 ① 性感染症クリニック 期間a、bともに、同日に採取した咽頭スワブとうがい液を検体とし、淋菌は淋菌培養、SDA法、TMA法の3検査を、咽頭のクラミジア検査は核酸増幅法の
PCR法、SDA法、TMA法の3検査を実施し、いずれかの検査が2つ以上陽性だった人を陽性者と判定した。
性器の検査は、男性は初尿、女性は腟または子宮頸管スワブを検体として、淋菌・クラミジアともにSDA法で検出した
② 耳鼻咽喉科 期間cでは、上咽頭と咽頭からスワブを同日に採取し、SDA法を用いて淋菌とクラミジアの検出を行った。期間dでは、上咽頭および咽頭スワブとうがい液を同日に採取し、スワブはSDA法を用いて、うがい液はreal time PCR法を用いて淋菌とクラミジアの検出を行った。
4)倫理面での配慮 研究開始前に、研究内容および研究に関する事項について、本学倫理委員会にて承認(東京女子医科大学倫理委員会承認1350番および2030番)された説明文書を用いて口頭で説明を行い、文書にて研究参加の同意を得た。
C.研究結果
1.口腔・咽頭顕症梅毒症例1)男女比、年齢分布、年別患者数 男性15例、女性12例で、年齢分布は16~75歳、平均37.0歳で、男女とも各年齢層に幅広く分布していた(図1)。経時的変化として1997年以降男性例が多くなり、1999年と2000年に1例ずつHIV陽性の男性同性愛者が含まれていた。2001年からは症例が途絶えていたが、2013年から1例ずつではあるが毎年患者がみられている(図2)。2)主訴と口腔・咽頭所見(表3) 受診時の主訴は咽頭痛が最も多く15例(55%)、咽頭異常感が次いで多く6例(22%)であった。当科初診時の口腔咽頭所見としては、第2期病変である粘膜斑が口
― 149 ―

狭部粘膜、特に軟口蓋の後縁に沿って孤状に拡大して融合して蝶が羽を広げたような形を呈したbutterfly appearanceが最も多く13例(48%)、次いで粘膜斑が次いで多く10例(37%)、第1期病変である初期硬結・硬性下疳は2例(7%)であった。3)性器・皮膚病変の有無(表4) 性器病変を認めたのは6例(22%)、性器病変以外の皮膚病変を認めたのも6例(22%)であった。性器病変は扁平コンジローマが1例、他は詳細不明であるが性器病変に対して他院で精査・加療中が5例であった。皮膚病変は梅毒性乾癬が2例、梅毒性脱毛が2例、梅毒性丘疹が1例、梅毒性膿疱疹が1例で、うち1例は乾癬・脱毛・膿疱疹、扁平コンジローマを合併していた。4)病 期(表5) 第1期が2例、他はすべて第2期であった。第3~4期は認めなかった。5)感染経路(表5) 夫婦や交際相手など特定のパートナーからが最も多く9例(33%)、次いでソープランドなどの性風俗、水商売の女性からの感染が多かった。同性との性交渉で感染した例はいずれも1998年以降の男性例で、3例中2例はHIV感染を合併していた。
2.淋菌・クラミジアの咽頭感染1)男女別年齢分布 性感染症クリニックでの期間a・b、耳鼻咽喉科施設での期間c・dにおける被験者の男女別年齢分を図3に示す。性感染症クリニックと耳鼻咽喉科施設において、女性の年齢分布はほぼ同じであった。性感染症クリニックの男性被験者は耳鼻咽喉科に比べて20歳代が少ない傾向がみられた。
2)男女別咽頭陽性率(表5) 淋菌・クラミジアの咽頭陽性者それぞれの割合は、性感染症クリニックの期間aでは男性12.8%・2.6%、女性12.5%・8.7%、性感染症クリニックの期間bでは男性21.0%・2.5%、女 性15.4%・14.8%、耳鼻咽喉科施設の期間cでは男性8.7%・0%、女性7.9%・1.6%、性感染症クリニックの期間dでは男性7.9%・1.6%、女9.9%・4.1%であった。性感染症クリニックでも耳鼻咽喉科施設でも、a~d全ての検討において、陽性者の割合は淋菌の方がクラミジアを上回っており、そのうち性感染症クリニックでの男性では淋菌の咽頭陽性者がクラミジアの咽頭陽性より統計的に有意に多かった。3)咽頭・性器の同日検査の陽性者の割合 性感染症クリニックで実施した咽頭・性器の同日検査による陽性者の割合を図4、5に示す。 性器の陽性者の割合と咽頭の陽性者の割合を比較すると、男性のクラミジアにおいてのみ咽頭の陽性者の割合が性器の陽性者の割合に比べて統計的に有意に少なかった(Wilcocxon符号付順位検定)。男性の淋菌、女性の淋菌およびクラミジア検査では咽頭の陽性者の割合は性器の陽性者の割合に比べて少ないものの有意差はなく、さらに女性の淋菌においてはやはり有意差はないものの咽頭の陽性者の割合が性器の陽性者の割合を上回っていた。 また、淋菌もクラミジアも男女ともに性器が陰性で咽頭のみの陽性者が存在した。4)耳鼻咽喉科施設における淋菌・クラミジ ア陽性者の咽頭所見(表7) 耳鼻咽喉科施設の期間c・dの計544人の
― 150 ―
咽頭からの淋菌・クラミジア検査の結果、淋菌陽性者は43例(7.9%)、クラミジア陽性者は11例(2.0%)で、性感染症クリニックと同様にクラミジアは淋菌に比べて陽性者数が少なかった。 検査実施時の咽頭所見は、淋菌では所見のない正常の咽頭が16例、急性扁桃炎が11例、非特異的な咽頭炎が11例、上咽頭炎が4例、慢性咽頭炎・扁桃炎が2例、舌炎・咽頭アフタが2例であった。このうち所見無しのうちの2例、急性扁桃炎のうちの2例、慢性扁桃炎のうちの2例、咽頭アフタの1例の計7例に反復する扁桃炎の既往があった。 クラミジアは所見のなしが3例、上咽頭炎が3例、急性扁桃炎・扁桃周囲炎が2例、非特異的な咽頭炎が1例、頸部リンパ節腫脹が1例、舌炎・咽頭アフタが2例であった。このうち上咽頭炎の1例に反復する扁桃炎の既往があった。
D.考 察
1.口腔・咽頭顕症梅毒 当科で経験した口腔・咽頭梅毒症例の特徴は、第1期である初期硬結・硬性下疳を呈して受診する症例は少なく、第2期の特徴的な粘膜疹であるbutterfly appearanceを呈して咽頭痛などの咽頭症状で受診する症例が多いこと、性器や皮膚病変を伴わない例が多く咽頭の症状や病変が診断の契機となっていたこと、同性愛男性ではHIV感染の可能性があること、が挙げられる。 第1期の初期硬結・硬性下疳は性器に次いで口腔咽頭に好発し、痛みを伴わず数週間で自然消退するため第1期のうちに医療機関へ
受診する症例は少ないことが以前から指摘されていが、当科でも第1期の症例は2例(8%)に過ぎなかった。第2期の特徴的な粘膜疹を生じていた症例も、多くは前医で難治性咽頭炎・扁桃炎として診断に至らずに当科へ紹介されていた。口腔・咽頭梅毒は第1期病変、第2期病変ともに他の疾患には見られない梅毒独特の病変を呈するため、診断する医療者側が口腔・咽頭梅毒病変の特徴を知っていれば診断は決して難しくない。口腔・咽頭梅毒は性器や皮膚病変を伴わないことが多く、感染力のある早期梅毒であるため、口腔・咽頭病変を適切に診断しないと、無症候に移行するなど診断を逸する可能性がある。ここ数年の梅毒患者の増加に対して、「梅毒=生殖器病変」というイメージを取り払い、口腔咽頭病変のみの梅毒症例があることを広く周知させることが望まれる。また、現行の梅毒発生届けの「 4 .症状の欄」の「初期硬結・硬性下疳」を「初期硬結・硬性下疳(部位:性器・口腔・咽頭・その他( )」と部位の記入欄を設け、さらに「 4 .症状の欄」の項目に「口腔・咽頭粘膜斑」を加えることも、口腔・咽頭梅毒の認知につながると考える。
2.淋菌・クラミジアの咽頭感染 性感染症検査希望者に性器と咽頭の同日検査を行うと、性器のみの陽性者、咽頭のみの陽性者がそれぞれ存在していた。淋菌・クラミジア感染症は無症候性感染であっても不妊の原因になるため、感染者数の多くを占める若い世代の感染者を早期に適切に診断することは重要である。性器も咽頭の特徴的な症状や所見に乏しい淋菌・クラミジア感染症に対して、受診の機会を逃さず適切に診断するために、性性器と咽頭の同日検査が保険で認め
― 151 ―

られることが求められる。 また、耳鼻咽喉科施設においては性感染症と気づかず、咽頭炎や扁桃炎などの症状で耳鼻咽喉科を受診する人の中に淋菌やクラミジアの咽頭感染者が含まれていた。さらに淋菌・クラミジアの咽頭感染者のなかに反復性扁桃炎の既往を持つ人が含まれていたことは、淋菌・クラミジアが扁桃炎の診断で一般的に用いる細菌検査では検出できないために淋菌・クラミジアによる扁桃炎と気づかれずに、扁桃炎を繰り返している症例が含まれている可能性が示唆された。性的活動期を過ぎて扁桃炎を反復するようになった症例においては、淋菌・クラミジアの咽頭感染も除外診断に含めて対応するべきことを、耳鼻咽喉科の臨床現場に広く認知させることが必要と考えられた。
E.結 論
口腔・咽頭の顕症梅毒患者の多くは、性器や皮膚に病変がなく口腔・咽頭の症状や特徴的な病変が梅毒診断の契機になる場合が多い。そのような口腔・咽頭梅毒の特徴を広く周知すべく情報を発信するとともに、現行の梅毒発生届けに口腔咽頭梅毒の項目を追加することを提案する。 性器も咽頭も特徴的な症状や所見に乏しい淋菌・クラミジア感染症に対して、受診の機会を逃さず適切に診断するために性器と咽頭の同日検査が保険で認められること、淋菌・クラミジアについて現行の感染症発生動向調査(STD定点)の調査票の項目の「淋菌感染症」を「性器淋菌感染症」に改め(既にクラミジアは「性器クラミジア感染症」となっている)、「咽頭淋菌感染症」と「咽頭クラミジ
ア感染症」を別項目として加えることを提案する。
F.健康危険情報
なし
G.研究発表
1.論文発表1 余田敬子:口腔・咽頭に関連する性感染症 日本耳鼻咽喉科学会会報 118:841-853,2015.
2 余田敬子:診断・治療に必要な耳鼻咽喉科臨床検査 ―活用のpointとpitfall―咽喉頭炎の鑑別 MB ENT 179:156-164,2015.
3 余田敬子:口腔粘膜疾患 ―特徴と治療の要点― 性感染症を疑う口腔粘膜疾患の診療 MB ENT 178:62-72,2015.
2.学会発表 なし
H.知的所有権の取得状況
1.特許取得 なし
2.実用新案登録 なし
3.そのほか なし
― 152 ―

― 153 ―
A
B
C
D
E *
F *
G *
H #
I #
J #
2011 8 1
2010 11 18
# 2011 8 1
2
2005 112006 7
a
SDA TMA
SDA TMA
PCR SDA TMA
PCR SDA TMA
2008 92009 1
b
SDA TMA
SDA TMA
PCR SDA TMA
PCR SDA TMA2010 11
2012 2c
SDA
SDA
2013 12014 2
d
SDA
SDA
Real �me PCR

― 154 ―
1512 16 75 37.0
0
1
2
3
4
2

― 155 ―
3 27
%
15 55
6 22
3 11
2 7
1 4
%
bu�erfly appearance 13 48
10 37
2 7
1 4
1 4
%
6 22
19 70
2 8
%
5 19
22 81
4 27
2211

― 156 ―
%
9 33
5 19
3 11
3 11
4 15
3 11
%
1 2 8
2 23 92
5 27
01020304050
190 19 59 29.0172 57 28.0
d 362
01020304050
81 20 60 34.0169 18 57 29.0
b 250
01020304050
92 19 59 29.090 57 57 28.0
c 182
020406080
100120
272 18 69 37.0283 17 55 28.0
a 555
3

― 157 ―
6
2005 112006 7
a
272 12.8 % 2.6 %
283 12.5 % 8.7 %2008 92009 1
b
81 21.0 % 2.5 %
169 15.4 % 14.8 %2010 11
2012 2c
92 8.7 % 0 %
90 4.4 % 1.1 %
2013 12014 2
d
190 7.9 % 1.6 %
172 9.9 % 4.1 %
283
272
*P<0.001
*
*
4 a

― 158 ―
169
81
*P<0.001*
*
5 b
�
�
�

― 159 ―
A.研究目的
HPVの遺伝子型は100種類以上存在するが、癌化リスクが高い高リスク型群と低リスク型群に大別される。 HPVジェノタイプ判定検査は2011年に新規保険適用項目となっており、現在、クリニッチHPV(2011年より)、MEBGEN HPVキット(2013年より)が使用可能である。いずれも13タイプ(16,18,31,33,35,39,45,51,52,56,58,59,68型)の検出が可能である。
一方、IARC(International Agency for Re-search on Cancer, 国際がん研究機関)では、66型を含む14種をハイリスク型として提唱していることから、大手検査会社(SRL等)では上記13タイプに加えハイリスク型である66型を加えた14タイプの検出が可能としているが、16,18型以外は型別判定は実施されない。 そこで、健常女性におけるHPV検出状況およびHPV検出にあたって子宮勁管スワブ検体と比較して侵襲性が低い尿検体は使用可能かについて検討した。
HPV関連子宮頸癌早期スクリーニングの啓発に関する研究
【研究分担者】 三鴨 廣繁 (愛知医科大学大学院医学研究科)【研究協力者】 山岸 由佳 (愛知医科大学病院感染症科) 萩原 真生 (愛知医科大学病院感染制御部)
研究要旨
日本人健常女性240名におけるHPV(human papilloma virus)は、CSW(comercial sex worker)では、非CSWと比較して高率にHPV陽性であった(p<0.00001)。検討した症例全体ではHPV52型が最多で、次いで58型の順に多かった。non-CSWでは52型が多かったが、CSWでは53型が多いもののハイリスク型全体が万遍なく検出された。特に、CSWでは、複数のハイリスク型が同時に検出される率が高かった(p<0.01)。ローリスク型HPVのみが検出された症例は陽性者全体の7.6%であった。日本人健常女性においても高リスク型のHPV感染(保ウイルス)率は高く、子宮がん検診では細胞診にHPVスクリーニング検査を併用することは臨床的意義が高いと考えられた。 AnyplexTM II HPV28 detection kitを用いて、スワブ検体と尿検体を用いて検出された
HPVジェノタイプの相同性を確認したところ、全体の感度は68.42%、特異度は99.87%であった。細胞診と尿検体の検査で低い相同性を示した遺伝子型HPVは単一もしくは複数の遺伝子型のHPVが同時に検出される場合でも検出率に影響はなかった。HPVスクリーニング検査において、尿検体は侵襲性が低い検査であるが、尿検体による検査では感度が十分とは言えず、スクリーニング法として使用するには注意する必要がある。

― 160 ―
B.研究方法
研究1:健常女性におけるHPV検出状況 HPV高リスク型19種類、HPV低リスク型9種類の計28種類の型を検出できるSeegene社「AnyplexTM II HPV28 detection kit」を用い、既承認タイピングキットでは検出できない型も含めて日本人女性子宮頸部におけるHPV検出状況を検討した。
研究2:HPV検出に尿検体は使用可能か? HPVのスクリーニング検査の低侵襲化を目的として、スワブ検体の他に尿検体を用いた検査を行い、2種類の検体を用いた場合の結果の相同性を調査した。
倫理面への配慮 本研究は、愛知医科大学病院倫理委員会の承認を得て実施した(承認番号15-H044)。
C.研究結果
研究1:健常女性におけるHPV検出状況 健常女性240名(CSW 54名(23%)、非CSW 186名(77%))を対象とした。CSW群には妊婦は存在せず、非CSW群では妊婦は62名(33%)であった。 健常女性118名(49%)に何らかのHPVを検出した。HPV未検出例は120名(50%)、測定エラーが2名(1%)であった。 HPVが検出された118名におけるHPVの同時検出型について図1に示した。
HPV陽性118名の詳細なHPV血清型を図2に示した。
ハイリスク型HPVが検出された109例の複数菌検出例数を図3に示した。
HPVの検出状況をCSW群と非CSW群に分けて示した(図4)。
図1 HPVが検出された118名におけるHPVの同時検出型
図2 HPV陽性118名の詳細なHPV血清型
図3 ハイリスク型HPVが検出された109例の複数菌検出例数

― 161 ―
ハイリスク型HPV同時検出型数をCSW群と非CSW群にわけて表1に示した。
HPV検出118例の血清型別検出状況を図5に示した。
ローリスク型HPVの検出状況について表2に示した。
研究2:HPV検出に尿検体は使用可能か? スワブ検体と尿検体を用いて検出された HPVハイリスク型ジェノタイプの相同性を表3に示した。
スワブ検体と尿検体を用いて検出された
HPVローリスク型ジェノタイプの相同性を表4に示した。
p
p
図4 HPVの検出状況 CSW群と非CSW群の比較 56 58 59 68
* p
表2 ローリスク型HPVの検出状況
表4 スワブ検体と尿検体を用いて検出されたHPVローリスク型ジェノタイプの相同性
p p
表1 ハイリスク型HPV同時検出型数 CSW群と非CSW群の比較
図5 HPV検出118例の血清型別検出状況
High
High
High
High
High
High
High
High
High
High
High
High
High
High
High
High
High
High
High
0.317
1.000
0.046
0.317
0.157
0.083
0.046
NA
0.157
0.103
0.083
0.083
0.157
0.157
0.157
0.025
0.083
0.008
0.005
0.969
0.905
0.000
0.967
0.896
0.721
0.825
1.000
0.885
0.882
0.897
0.396
0.948
0.829
0.871
0.752
0.721
0.522
0.324
94.4
83.3
0.0
94.1
91.8
57.1
71.4
100.0
80.0
81.3
82.4
25.0
90.9
71.4
77.8
61.5
57.1
36.4
20.0
0.030
0.067
0.000
0.032
0.073
0.154
0.086
0.000
0.081
0.047
0.059
0.276
0.037
0.119
0.090
0.106
0.154
0.156
0.173
99.6
99.2
98.3
99.6
99.2
98.7
98.3
100.0
99.2
97.5
98.7
98.7
99.2
99.2
99.2
97.9
98.7
97.1
96.6
18
12
4
17
11
7
14
6
10
32
17
4
22
7
9
13
7
11
10
220
226
234
221
227
231
224
232
228
206
221
234
216
231
229
225
231
227
228
1
1
4
1
2
3
4
0
2
5
3
3
2
2
2
5
3
7
8
0
1
0
0
0
0
0
0
0
1
0
0
0
0
0
0
0
0
0
17
10
0
16
9
4
10
6
8
26
14
1
20
5
7
8
4
4
2
NP
NP
NA
NP
NP
ST
NP
PE
NP
NP
NP
PO
NP
NP
NP
ST
ST
PO
PO
16
18
26
31
33
35
39
45
51
52
53
56
58
59
66
68
69
73
82
No. of samples for each resultNo. of samples for each result
% agreement% agreementGenotypeGenotype RiskRisk -/--/- +/-+/- +/++/+-/+-/+Total no.Total no.posi�veposi�ve
% posi�ve% posi�veagreementagreement SDSD
Two-tailedTwo-tailedMacNemar’sMacNemar’s P
valuevalueInt.Int.K
Kappa dataKappa data
表3 スワブ検体と尿検体を用いて検出されたHPVハイリスク型ジェノタイプの相同性

― 162 ―
尿検体を用いた場合の感度と特異度(スワブ検体との比較)を表5に示した。
尿検体を用いて単一もしくは複数の遺伝子型のHPVが検出された場合の影響を表6に示した。
D.考 察
日本人健常女性240名におけるHPV(human papilloma virus)は、CSW(comercial sex worker)では、非CSWと比較して高率にHPV陽性であった(p<0.00001)。検討した症例全体ではHPV52型が最多で、次いで58型の順に多かった。non-CSWでは52型が多かったが、CSWでは53型が多いもののハイリス
ク型全体が万遍なく検出された。特に、CSWでは、複数のハイリスク型が同時に検出される率が高かった(p<0.01)。ローリスク型
HPVのみが検出された症例は陽性者全体の7.6%であった。日本人健常女性においても高リスク型のHPV感染(保ウイルス)率は高く、子宮がん検診では細胞診にHPVスクリーニング検査を併用することは臨床的意義が高いと考えられる。 AnyplexTM II HPV28 detection kitを用いて、スワブ検体と尿検体を用いて検出された
HPVジェノタイプの相同性を確認したところ、全体の感度は68.42%、特異度は99.87%であった。細胞診と尿検体の検査で低い相同性を示した遺伝子型HPVは単一もしくは複数の遺伝子型のHPVが同時に検出される場合でも検出率に影響はなかった。尿検体は侵襲性が低い検査であるが、尿検体を用い多場合、遺伝子検査であっても感度が十分とは言えず、スクリーニング法として使用するには注意する必要がある。
E.結 論
日本人健常女性においても高リスク型の
HPV感染(保ウイルス)率は高く、子宮がん検診では細胞診にHPVスクリーニング検査を併用することは臨床的意義が高いことが明らかになった。特に、CSW群では、HPV感染率は高く、高リスク群に対するHPVスクリーニングの意義はさらに高いものと推察された。 HPVスクリーニング遺伝子検査において尿検体は侵襲性が低い検査であるが、この方法による検査では感度が十分とは言えず、スクリーニング法として使用するには注意する必要がある。
0
2
0
0
2
1
0
1
0
0
0
1
5
1
2
0
1
1
High
High
High
High
High
Low
Low
Low
Low
3
3
4
3
7
2
4
9
5
0
9
8
3
0
5
3
5
1
1.000
1.000
0.385
0.182
0.067
0.500
1.000
1.000
1.000
26
39
68
73
82
42
43
54
70
No. of casesNo. of cases
*: Fisherの正確確率検定
Single infec�onSingle infec�on Mul�ple infec�onsMul�ple infec�ons
GenotypeGenotype RiskRisk DiscordantDiscordant ConcordantConcordant DiscordantDiscordant ConcordantConcordant p value* value*
表6 尿検体を用いて単一もしくは複数の遺伝子型のHPVが検出された場合の影響
表5 尿検体を用いた場合の感度と特異度 (スワブ検体との比較)

― 163 ―
G.研究発表
1.論文発表(本研究班で得られた成果のみ。海外も国内も含む。)
1 三鴨廣繁:淋菌感染症、今日の小児治療指針 第16版、pp. 382-383、医学書院、東京、2015.9.1.(書籍)
2 Mikamo H, Matsumizu M, Nakazuru Y, Nagashima M. Efficacy and safety of
metronidazole injection for the treatment
of infectious peritonitis, abdominal abscess
and pelvic inflammatory diseases in Japan.
J Infect Chemother. 21: 96-104, 2015.(原著論文)
3 Mikamo H, Matsumizu M, Nakazuru Y, Okayama A, Nagashima M. Efficacy and
safety of a single oral 150 mg dose of flucon-azole for the treatment of vulvovaginal
candidiasis in Japan. J Infect Chemother.
21(7): 520-526, 2015.(原著論文)4 山岸由佳・三鴨廣繁:梅毒、日本母性衛
生学会雑誌56(2):学6-学12,2015.(総説)
2.学会発表(本研究班で得られた成果のみ。海外も国内も含む。)
1 山岸由佳・和泉孝治・宮﨑成美・鈴木隆佳・末松寛之・西山直哉・小泉祐介・三鴨廣繁:「Anyplex II HPV28 Detection」キットの臨床現場での使用経験.日本性感染症学会第28回学術大会 O-17、2015.12.6、東京.
H.知的所有権の出願・登録状況
1.特許取得 該当なし
2.実用新案登録 該当なし
3.そ の 他 該当なし

― 164 ―
A.研究目的
尖圭コンジローマ(以下コンジローマ)の罹患者数は近年漸増傾向にある。女性の罹患年齢は20歳前後がピークであり、その後に妊娠・出産に与える影響が危惧される。HPV感染を予防するHPVワクチンが開発され、世界中で導入されている。尖圭コンジローマの主な原因となるHPV6/11型感染に対して、海外では4価HPVワクチンは高い予防効果が証明されている。国内においては、HPVワクチンの積極的勧奨が中止されており、現在に至っている。HPVワクチンの安全性が確認されるまで、HPVワクチンによるHPV6/11感染予防は実質的に期待できない。 一方、HPV6/11型の母子感染が起こると、感染した児は再発性呼吸器乳頭腫症(JORRP)のリスクにさらされる。JORRPはHPV6/11型によって引き起こされ、腫瘍が喉頭部や上気道で増大すると、嗄声や気道閉塞を生じうる。コンジローマ合併妊婦から出生した児のうち、145人あたり1人の割合でJORRPを発
症する。コンジローマ合併妊婦から出生した児は、コンジローマ罹患歴のない妊婦から出生した児と比較して、JORRPのリスクが231倍と言われている。JORRPのリスクとして、分娩時間や破水から出生までの時間の影響が示唆されている。一般的に、病変が小さい場合、コンジローマ合併妊娠において帝王切開を選択する適応はない。広範囲またはかなり大きな病変がある場合は、HPVの母子感染を完全に防ぐことはできないだろうが、帝王切開を推奨する相対的適応がある。 そこで、昨年度は、コンジローマ合併妊婦に焦点を絞り、その母体から出生する児への母子感染について検討することとした。妊娠中のコンジローマの疫学調査とその児における咽頭HPV検査を実施した。
本研究では、「尖圭コンジローマを有さないが、HPV6/11/42/44のコンジローマタイプのHPV-DNAが検出される」場合を「不顕性感染」と定義している。海外の先行研究では、コンジローマの不顕性感染者は、有病者
性感染症、特にHPVと子宮頸癌についての啓発に関する研究
【研究分担者】 川名 敬 (東京大学大学院医学系研究科産婦人科学講座)
研究要旨
尖圭コンジローマは日本における女性の第3番目の性感染症である。尖圭コンジローマは性器イボを形成する顕性感染とイボ形成を見ない不顕性感染があり、不顕性感染時に
HPVを排出していることが性行為感染による蔓延を助長している。また子宮頸癌の原因ウイルスであるハイリスクHPVの同時感染も大きな問題である。本研究では、尖圭コンジローマの有無を層別化し、女性の子宮頸部におけるHPVタイプの分布を解析し、さらに尖圭コンジローマ不顕性感染の実態把握を行った。

― 165 ―
の約3倍との報告がある。母子感染という観点からは、不顕性感染者でも妊娠すると免疫制御能が落ちるために顕性(コンジローマを発症)になる。そのため、若年女性における不顕性感染者の把握は重要であった。 本年度は、女性における子宮頸部の不顕性感染の実態を把握することを目的とした。
B.研究方法
1.患者背景 2010年~2015年に当科でHPVタイピングを実施した子宮頸部擦過細胞464検体について、尖圭コンジローマの有無を分けて、HPVタイプの分布を検討した。本研究に関しては東京大学医学部研究倫理委員会の承認を得ている。HPV検査は一般診療の中で実施されている。
2.ウイルス学的検討 外来受診の女性患者464例で、尖圭コンジローマの有無を視診によって確認した。STDクリニックを受診した患者も一部に含まれる。子宮頸部擦過細胞を採取し、その一部でHPV検査を行った。
3.HPVタイピング HPVタイピングを行うために、児の咽頭スワブからthe DNeasy Blood Mini Kit (Qiagen, Crawley, UK)を用いてDNAを抽出した。
HPVタイピングはPGMY-CHUV法により行った。本法は HPV6,11,16,18,26,31,33,34,35,39,40,42,43,44,45,51,52,53,54,55,56,57,58,59,66,68,69,70が検出できる方法である。全例でHLA遺伝子が陽性であることを確認しており、ス
ワブ中の擦過細胞が採取されていることを確認している。
(倫理面への配慮) 本研究にあたっては、厚生労働省の「ヒトゲノム解析研究に関する共通指針」に則り、東京大学医学部の医学部研究倫理審査委員会の承認を得て研究を実施した。また、提供試料、個人情報をコード化したうえで厳格に管理・保存した。HPV検査は一般的な検査として一般診療で実施されている検査であるが、本研究では研究費によってin houseで検査を行っている。
C.研究結果
1.HPV感染率について 視診によって、411例は尖圭コンジローマ無し(CA-群)、53例は尖圭コンジローマ(CA+群)に分けた。HPV陽性者は、CA-群では72.3%に対して、CA+群は96.2%であり、
CA+群ではHPV感染者が多かった。本検体は医療機関に受診している集団であり、一般的なHPV陽性率よりも明らかに高かった。本調査の対象患者は、このような特殊性があることを加味しておく必要がある。CA+群でHPV陰性が2例いたが、これは外陰コンジローマ患者で、子宮頸部にはHPVが検出されなかった症例である。
2.重複感染率について 複数のHPVタイプが検出されるHPVの重複感染率は、CA+群では約50%、CA-群では26.5%であり、CA+群では倍の重複感染者がいることが判明した。特に4タイプ以上の
HPV多重感染者は、CA+群で12.7%に対し
― 166 ―
て、CA-群では3.8%であり、尖圭コンジローマ患者では、HPV感染・増殖が盛んに起こっていることが窺われる。
3.ハイリスクHPV感染について 子宮頸癌の関連するハイリスクHPVとは、
HPV16,18,31,33,35,39,45,51,52,56,58,66,68のことを指す。CA-群における
HPVタイプののべ検出数は、477タイプ(重複感染含)であり、そのうち264タイプ(55.3%)がハイリスクタイプであった。一方、CA+群では、103タイプのうち32タイプ(31.0%)がハイリスクタイプであった。CA+群では、コンジローマタイプが多くなるために、相対的にハイリスクタイプの割合は少なかった。
4.コンジローマタイプの不顕性感染率 このような集団におけるコンジローマタイプ(HPV6/11/42/44)の感染率を検討した。
CA-群411例のうち、HPV6が48例(11.6%)、
HPV11が13例(3.2%)、HPV42/44が7例(1.6%)であった。少なくとも約15%の女性が、コンジローマを発症していないにも関わらずHPV6/11の不顕性感染となっていることが判明した。 一方、CA+群53例のうち、3例のみコンジローマタイプが検出されなかったが、これは外陰コンジローマのみで子宮頸部への感染はなかったためと考えられた。
D.考 察
本検討では、検討対象患者に医療機関受診と言うバイアスがかかっているため、HPV感染率等のデータは先行研究と一致しない。国内の既報では、子宮頸部細胞診正常女性(健
常成人女性)のHPV陽性率は約10%である。本研究のCA-群の73%というHPV陽性率は特殊な集団と考えるべきである。本検討では子宮頸部細胞診は全例には試行されていないために、細胞診異常の女性も含まれている。細胞診の軽度異常(LSIL)の場合は、国内では79.4%のHPV陽性率であることから、これに近い集団であったと考えられる。細胞診異常者が多く含まれることが示唆された。 重複感染率の検討では、CA+群では、ハイリスクHPVを含む複数のHPVタイプに感染していることから、CA-群に比して、子宮頸癌のリスクは高まると予想される。 CA-群において、約半数がハイリスクタイプであったことは、この集団においてハイリスクHPVが蔓延していることを示している。国内からの既報では、子宮頸部細胞診正常女性のうち、約10%にハイリスクHPVが検出されると言われる。またHPVワクチンの国内臨床試験の基礎データでは、約30%の健常女性でHPV16/18抗体が陽性になっている。これと比べ、本検討では、CA-群のうち71検体(約15%)がHPV16/18であった。細胞診の正常・異常を考慮しない健常女性という集団においては、本検討対象のCA-群は、一般集団に近い可能性がある。 そのCA-群において、HPV6/11の不顕性感染が51例(約15%)にみられたことは特記すべきことである。以前の我々の研究(厚労省小野寺班)では、子宮頸部細胞診異常を認める女性のうち、不顕性感染率は約4~6%であったことを考えると、今回の検討では明らかに高い不顕性感染率であった。その原因として、コンジローマの既往患者(治療後の患者等)も含まれている可能性が考えられた。サンプリング施設が限定されているため、本

― 167 ―
研究の結果がすぐに国内の実態を反映しているとは言えなかったが、少なくとも本研究の結果に示されたような地域があることは言えるだろう。
E.結 論
HPVタイピングをベースとした疫学調査を行った。コンジローマの病変を認めない女性でも、コンジローマタイプの不顕性感染者が存在する。HPVタイピングで検出されていることから、ウイルスを排出していると考えられ、新たな罹患者の感染源になりうる。尖圭コンジローマの実態把握において、不顕性感染者の存在は無視できないと考えられた。
G.研究発表
1.論文発表1 Matsumoto K, Maeda H, Oki A, Takatsuka N, Yasugi T, Furuta R, Hirata R, Mitsuhashi
A, Kawana K, Fujii T, Iwata T, Hirai Y,
Yokoyama M, Yaegashi N, Watanabe Y,
Nagai Y, Yoshikawa H, Human leukocyte
antigen class II DRB1*1302 allele protects
against cervical cancer: at which step of
multistage carcinogenesis?, Cancer Sci,
doi: 10.1111/cas.12760, 2015.
2 Seiki T, Nagasaka K, Kranjec C, Kawana K, Maeda D, Taguchi A, Wada-Hiraike O,
Oda K, Nakagawa S, Yano T, Fukayama
M, Banks L, Osuga Y, Fujii T, HPV-16
E6 impairs the subcellular distribution
and levels of expression of protein
phosphatase 1γ in cervical malignancy,
BMC Cancer, 15; 230, 2015.
2.学会発表1 川名 敬:今どうなっているか、HPVワクチン HPVワクチン普及のためになすべきことは? 第28回日本性感染症学会、教育講演、平成27年12月5日、神戸.
2 川名 敬:HPV予防ワクチンの光と影~接種の必要性と有害事象の可能性~、中央区医師会学術講演会、平成27年7月22日、東京.
H.知的財産権の出願・登録状況
1.特許取得 特になし
2.実用新案登録 特になし
3.そ の 他 特になし

― 168 ―
�
�

― 169 ―

― 170 ―
�
�
�
�
�

― 171 ―
2
6
5 5
4
3
4
1
0
1
2
3
4
5
6
7
0 5 10 15 20 25 30 35
�
�

― 172 ―
�
�
�
�
(zur Hausen, H. Nat Rev Cancer, 2002)

― 173 ―

― 174 ―
6 11 16 18 2631 33 35 39 4244 45 51 52 5354 55 56 58 5966 68 69 70 7382 83 84 unknown negative

― 175 ―
CA(-) CA(+)
�

― 176 ―
�
�
�
�
�
�
�

― 177 ―
A.研究目的
若年者の健康課題である性感染症について、『性感染症に関する特定感染症予防指針』には「若年層に対しては、性感染症から自分の身体を守るための情報について、適切な人材の協力を得て、正確な情報提供を適切な媒体を用いて行い、広く理解を得ることが重要」と示されている。若年者の感染予防行動を促し、感染を疑ったら医療機関に早期に適切に受診できるよう、特に中高生向けの情報提供の方法を探る。
B.研究方法
思春期における10代の若者を対象とした性感染症予防啓発スライド(PDF)を提供し、信頼できるサイト(厚生労働省健康局結核感染症課のホームページ)から情報発信する。スライド作成の資料収集等については、2012年に日本性感染症学会と日本思春期学会が共編したスライド集「思春期の性の健康-性感染症から身を守るために」の活用状況1)からその見直しを踏まえ、研究協力者で議論を行い資料を収集し、実践的研究として新たなスライド集を研究協力者の共同制作とした。
倫理面への配慮 個人情報を扱わないため特になし。
感染予防行動、早期受診促進のための性感染症啓発スライドについて
【研究分担者】 白井 千香 (神戸市保健福祉局)【研究協力者】 岩室 紳也 (ヘルスプロモーション推進センター
〔オフィスいわむろ〕) 種部 恭子 (女性クリニックWe ! TOYAMA) 野々山未希子(自治医科大学看護学部) 渡會 睦子 (東京医療保健大学医療保健学部)
研究要旨
性感染症に関する特定感染症予防指針に示されている、若年層への情報提供について、性感染症の知識のみならず性感染症の予防を支援する環境づくりが必要であることから、予防行動や早期受診を促す情報提供を目的に、予防啓発資料をスライドで作成した。学校では指導要領に沿って保健体育の教科書を使い、性感染症予防教育の授業がなされるべきだが、それを補い、中高生が自己学習できるスライドを厚生労働省のホームページから健康局結核感染症課のサイトに掲載可能とし、実際の普及を試みる。

― 178 ―
C.研究結果
スライド作成にあたって、中高生向け(特に中学生)にわかるように以下の内容を盛り込むことを考慮した。・スライド一枚に示す情報は、できるだけ字数を少なくイラストや写真を活用する。・疾患については、無症状のもの、治るもの、生命の危険につながるものなどを説明する。・性行動を分類し、性感染症がうつる行為とうつらない行為を明示する。・コンドームで予防できるものと必ずしもコンドームだけでは予防できないものを示す。・コンドームの使い方を詳しく説明する。例えば、Q&A形式で中学生が間違いや勘違いに気づくようにする。YouTubeに掲載されている動画を紹介する。・性に関するリスクのうち若年での妊娠に関するものは、今回のスライドでは具体的な解説を除き、性感染症に焦点をあてる。・HIVや性感染症にリスクのある状況は、性行動の相手との関係において、経済的優位、暴力、アルコール、薬物乱用などの問題が考えられることを例示し、コンドームを使えない関係性や、ドメスティックバイオレンスについても説明する。・医療機関への受診を促し、早期に検査治療に結びつけるため、受診費用の概要を提示する。・疾患の詳しい説明は、来年度以降の研究課題となる教師向けの資料に含める。
D.考 察
スライド作成にあたり、議論した点のひとつは、若年者向けにどの程度の知識を提供す
るか、であった。学校では指導要領に沿って保健体育の教科書を使い、性感染症予防教育の授業が可能である。教科書や副読本にも性感染症に関する知識の記述は丁寧で、高校生向けにはコンドームの使い方なども写真付きで詳細に書かれている。ただし、それらの授業の学習をさらに補うため、特に中高生がこのスライドを一人で見ても、性感染症予防について的確な情報を得られるようなスライド作成を意図した。 教科書とは違い、身近な自分自身のための情報提供を行うには、医学的な正確性より、伝える情報が簡潔でわかりやすいものであることを優先した。疾患の詳細や一般的治療、統計などは、講演会などで保健医療の専門家から説明を得ながら理解することはできるかもしれないが、自分自身の問題としてとらえるための情報とはなりにくい。 ただし、それぞれのスライドの補足説明やさらに詳細を知りたい者は、インターネットやスマートフォンから情報を得るであろう。その検索の際に「性感染症」のうわさやガセネタにはつながらないよう、日本性感染症学会の診療ガイドラインをホームページ上で会員外にもオープンに閲覧可能にしておくことは参考になると考える。 若年者向けとして作成したスライドが実際どのような対象者に活用されるか、閲覧頻度はどの程度か、啓発スライドの影響力などを推測して、評価することを今後検討したい。 診療の場では医療従事者、学校では教育関係者が中高生の性の相談などにかかわる際に、大人から若年者に伝える情報も重要であるので、来年度はそれらの指導者向けにスライド集を作成することを計画する。

― 179 ―
E.結 論
作成したスライドが性感染症予防の一助となるよう、閲覧をオープンにして、実際に若年者(中高生)に情報が届いているか、今後、スライドの周知や普及活用状況を評価し、さらなる改善を続ける。
G.研究発表
1.論文発表 なし
2.学会発表 参考資料として 1 性感染症予防における啓発教育用資料の
活用について 白井千香・荒川創一.日本性感染症学会第28回学術大会(一般演題)(東京)
H.知的財産権の出願・登録状況
なし

― 180 ―
�
�
� 3-4� 5-7� 8-9� 10-15� 16-17� 18-22� 23� 24-31� 32-36
37-39� 40-44� 45-46

― 181 ―

― 182 ―
�
�

― 183 ―

― 184 ―
Safer Sex
�
�
�

― 185 ―
�
�
�
�
�


Ⅲ.研究成果の刊行に関する一覧表


― 189 ―
研究成果の刊行に関する一覧表
〈雑 誌〉
出版年ページ巻 号発 表 誌 名論文タイトル名発表者氏名
20152695−269959(5)Antimicrob Agents Chemother
Azithromycin resistance and its mechanism in Neisseria gonorrhoeae strains in Hyogo, Japan
Shigemura K, Osawa K, Miura M, Tanaka K, Arakawa S, Shirakawa T, Fujisawa M
2015340−34521J Infect Chemother
The second nationwide surveillance of the antimicrobial susceptibility of Neisseria gonorroeae from male urethritis in Japan, 2012-2013
Hamasuna R, Yasuda M, Ishikawa K, Arakawa S, Fujisawa M, et al.
2015109−11626(1)日本性感染症学会誌
平成25年7モデル県の性感染症診療医療機関全数調査推計有病率と国立率感染症研究所の定点報告推計有病率の比較~7県医療機関全数調査結果と定点調査報告結果の有病率はなぜ乖離したのか?
谷畑 健生,秋元 義弘,武島 仁,五十嵐辰男,安田 満,種部 恭子,金山 博臣,荒川 創一
20151−3Vol.15 No.1
ニューズレター「性の健康」
特定感染症予防指針の変更を踏まえた自治体における性感染症発生動向調査の活用
中瀨 克己
201591−9626(1)日本性感染症学会誌
性感染クリニック及び産科における口腔内性感染症に関するアンケートと検体検査の試み
白井 千香,古林 敬一,川畑 拓也,吉田 弘之,荒川 創一
2015841−853118日本耳鼻咽喉科学会会報
口腔・咽頭に関連する性感染症余田 敬子
201562−72178MB ENT
口腔粘膜疾患―特徴と治療の要点―性感染症を疑う口腔粘膜疾患の診療
余田 敬子
2015156−164179MB ENT
診断・治療に必要な耳鼻咽喉科臨床検査 ―活用のpointとpitfall―咽喉頭炎の鑑別
余田 敬子
― 190 ―
出版年ページ巻 号発 表 誌 名論文タイトル名発表者氏名
201596−10421J Infect Chemother
Efficacy and safety of metronidazole injection for the treatment of infectious peritonitis, abdominal abscess and pelvic inflam-matory diseases in Japan.
Mikamo H,Matsumizu M, Nakazuru Y, Nagashima M
2015520−52621J Infect Chemother
Efficacy and safety of a single oral 150 mg dose of fluconazole for the treatment of vulvovaginal candidiasis in Japan.
Mikamo H, Matsumizu M, Nakazuru Y, Okayama A, Nagashima M.
2015学6−学1256(2)日本母性衛生学会雑誌梅毒山岸 由佳,
三鴨 廣繁
20151448106Cancer Sci, doi: 10.1111/cas.12760
Human leukocyte antigen class II DRB1*1302 allele protects against cervical cancer: at which step of multistage carcinogenesis?
Matsumoto K, Maeda H, Oki A, Takatsuka N, Yasugi T, Furuta R, Hirata R, Mitsuhashi A, Kawana K, Fujii T, Iwata T, Hirai Y, Yokoyama M, Yaegashi N, Watanabe Y, Nagai Y, Yoshikawa H
201523015BMC Cancer
HPV-16 E6 impairs the subcellular distribution and levels of expression of protein phosphatase 1γ in cervical malignancy
Seiki T, Nagasaka K,Kranjec C, Kawana K, Maeda D, Taguchi A, Wada-Hiraike O, Oda K, Nakagawa S, Yano T, Fukayama M, Banks L, Osuga Y,Fujii T
〈書 籍〉
ページ出版年出版地出版社名書 籍 名書籍全体の編集者名論文タイトル名著者氏名
394−3952014文光堂わかりやすい内科学第4版
井村 裕夫
グラム陰性球菌感染症Ⅰ髄膜炎菌感染症Ⅱ淋菌感染症
荒川 創一
382−3832015東京医学書院今日の小児治療指針第16版
淋菌感染症三鴨 廣繁
Ⅳ.研究成果の刊行物・別刷


― 193 ―
Azithromycin Resistance and Its Mechanism in Neisseria gonorrhoeaeStrains in Hyogo, Japan
Katsumi Shigemura,a,b Kayo Osawa,b,c Makiko Miura,c,d Kazushi Tanaka,a Soichi Arakawa,a,b Toshiro Shirakawa,a,c,e Masato Fujisawaa
Division of Urology, Department of Organ Therapeutics, Faculty of Medicine, Kobe University Graduate School of Medicine, Kobe, Japana; Department of Infection Control
and Prevention, Kobe University Hospital, Kobe, Japanb; Division of Infectious Diseases, Department of International Health, Kobe University Graduate School of Health
Science, Kobe, Japanc; Department of Medical Technology, Kobe Tokiwa University, Kobe, Japand; Center for Infectious Diseases, Kobe University Graduate School of
Medicine, Kobe, Japane
Therapeutic options are limited for Neisseria gonorrhoeae infection, especially for oral drugs. The purpose of this study was toinvestigate the susceptibility of N. gonorrhoeae to oral azithromycin (AZM) and the correlation between AZM resistance-relatedgene mutations and MIC. We examined the AZM MICs of clinical strains of N. gonorrhoeae, sequenced the peptidyltransferaseloop in domain V of 23S rRNA, and investigated the statistical correlation between AZM MIC and the presence and number ofthe mutations. Among 59 N. gonorrhoeae strains, our statistical data showed that a deletion mutation was seen significantlymore often in the higher-MIC group (0.5 �g/ml or higher) (35/37; 94.6%) than in the lower-MIC group (0.25 �g/ml or less) (4/22; 18.2%) (P < 0.0001). However, a mutation of codon 40 (Ala¡Asp) in the¡ mtrR gene (helix-turn-helix) was seen significantlymore often in the lower-MIC group (12/22; 54.5%) (P < 0.0001). In N. gonorrhoeae multiantigen sequence typing (NG-MAST)analyses, ST4777 was representative of the lower-MIC group and ST1407, ST6798, and ST6800 were representative of the higher-MIC group. NG-MAST type 1407 was detected as the most prevalent type in AZM-resistant or -intermediate strains, as previ-ously described. In conclusion, a deletion mutation in the mtrR promoter region may be a significant indicator for higher MIC(0.5 �g/ml or higher). ST4777 was often seen in the lower-MIC group, and ST1407, ST6798, and ST6800 were characteristic ofthe higher-MIC group. Further research with a greater number of strains would help elucidate the mechanism of AZM resistancein N. gonorrhoeae infection.
Neisseria gonorrhoeae infection is often seen in male urethritisand female cervicitis, and its diagnosis has historically led to
prompt initiation of treatments with a single antibiotic (1, 2). Inthe 1990s in most Asian countries, fluoroquinolones (FQs) wereoften used for this infection, partly because FQs have higher con-centrations in the urinary tract. FQs showed good initial outcomesfor this infection, but the results were not enduring. This may bepartly due to the trend for single use of FQs for this infection, withno guidelines to recommend other choices (3–9).
In addition to the FQs, cephalosporins such as cefixime werealso recommended as oral antibiotics until these drugs showeddecreased activity against N. gonorrhoeae (10). They are no longera recommended choice for this infection (11–13). Oral antibioticsfor outpatient treatment would be highly desirable for this kind ofinfection. Azithromycin (AZM) is an oral antibiotic with medicalinsurance approval for use against chlamydia infections (14), andthere are many reports of good activity against N. gonorrhoeaeinfection (15). Other reports suggest that N. gonorrhoeae infectionis less susceptible to AZM and that AZM-resistant strains haveemerged (5). We investigated the AZM susceptibilities of N. gon-orrhoeae strains and the correlation between mutations of macro-lide resistance-related genes and the AZM MICs of clinically iso-lated strains of N. gonorrhoeae.
Three mechanisms of resistance to AZM are known: overex-pression of the efflux pump, mutation in the peptidyltransferaseloop in domain V of 23S rRNA, and modification of the ribosomaltarget by methylase. Macrolides such as AZM and erythromycin(EM) bind to 4 alleles of the 23S rRNA component of the 50Ssubunit of the bacterial ribosome and restrain protein synthesis byinhibiting the elongation of peptide chains (16).
Overexpression of the MtrCDE pump is due to either the lack
of repressor MtrR protein, which occurs by a single-base-pair de-letion or TT insertion in the promoter region, or missense muta-tions in the mtrR coding region (17). Modification of the ribo-somal target by methylase or mutations reduces the affinity of themacrolide antibiotics for ribosomes (18). Since the use of antimi-crobial agents for treatment of gonococcal infections is different ineach country, the trend of drug resistance in gonococci is likelydifferent geographically (19). Hence, epidemiological investiga-tions should be done in each country. Previous studies have re-ported a high use of N. gonorrhoeae multiantigen sequence typing(NG-MAST), which is based on limited DNA sequence analyses oftwo highly polymorphic loci, porB and tbpB, in sequence type (ST)1407 N. gonorrhoeae, which is multidrug resistant and appears tobe disseminated basically worldwide (20). The selection andspread of AZM resistance are driven by inappropriate treatment ofpatients with suboptimal doses of AZM for gonococcal infection.N. gonorrhoeae maintains its genetic resistance determinants evenafter the removal of antibiotic selection pressure.
Received 16 September 2014 Returned for modification 9 December 2014
Accepted 14 February 2015
Accepted manuscript posted online 23 February 2015
Citation Shigemura K, Osawa K, Miura M, Tanaka K, Arakawa S, Shirakawa T,
Fujisawa M. 2015. Azithromycin resistance and its mechanism in Neisseriagonorrhoeae strains in Hyogo, Japan. Antimicrob Agents Chemother
59:2695–2699. doi:10.1128/AAC.04320-14.
Address correspondence to Katsumi Shigemura, [email protected].
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
doi:10.1128/AAC.04320-14
May 2015 Volume 59 Number 5 aac.asm.org 2695Antimicrobial Agents and Chemotherapy
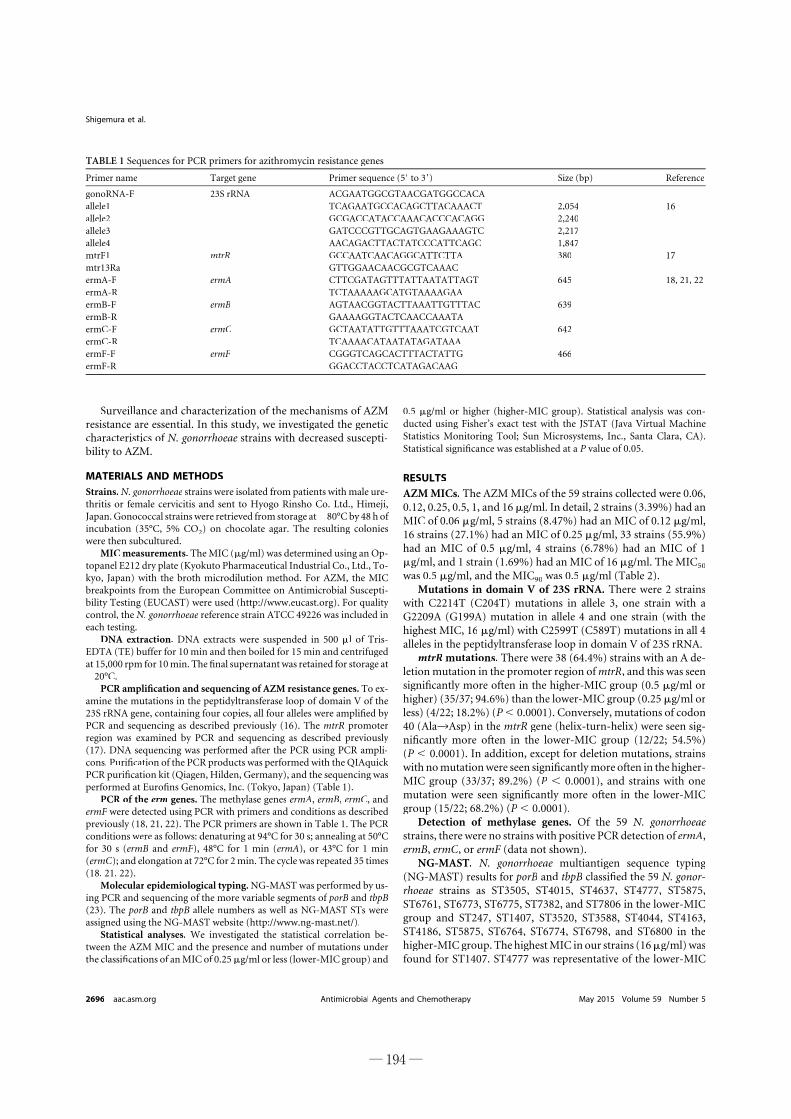
Surveillance and characterization of the mechanisms of AZMresistance are essential. In this study, we investigated the geneticcharacteristics of N. gonorrhoeae strains with decreased suscepti-bility to AZM.
MATERIALS AND METHODSStrains. N. gonorrhoeae strains were isolated from patients with male ure-thritis or female cervicitis and sent to Hyogo Rinsho Co. Ltd., Himeji,Japan. Gonococcal strains were retrieved from storage at �80°C by 48 h ofincubation (35°C, 5% CO2) on chocolate agar. The resulting colonieswere then subcultured.
MIC measurements. The MIC (�g/ml) was determined using an Op-topanel E212 dry plate (Kyokuto Pharmaceutical Industrial Co., Ltd., To-kyo, Japan) with the broth microdilution method. For AZM, the MICbreakpoints from the European Committee on Antimicrobial Suscepti-bility Testing (EUCAST) were used (http://www.eucast.org). For qualitycontrol, the N. gonorrhoeae reference strain ATCC 49226 was included ineach testing.
DNA extraction. DNA extracts were suspended in 500 �l of Tris-EDTA (TE) buffer for 10 min and then boiled for 15 min and centrifugedat 15,000 rpm for 10 min. The final supernatant was retained for storage at�20°C.
PCR amplification and sequencing of AZM resistance genes. To ex-amine the mutations in the peptidyltransferase loop of domain V of the23S rRNA gene, containing four copies, all four alleles were amplified byPCR and sequencing as described previously (16). The mtrR promoterregion was examined by PCR and sequencing as described previously(17). DNA sequencing was performed after the PCR using PCR ampli-cons. Purification of the PCR products was performed with the QIAquickPCR purification kit (Qiagen, Hilden, Germany), and the sequencing wasperformed at Eurofins Genomics, Inc. (Tokyo, Japan) (Table 1).
PCR of the erm genes. The methylase genes ermA, ermB, ermC, andermF were detected using PCR with primers and conditions as describedpreviously (18, 21, 22). The PCR primers are shown in Table 1. The PCRconditions were as follows: denaturing at 94°C for 30 s; annealing at 50°Cfor 30 s (ermB and ermF), 48°C for 1 min (ermA), or 43°C for 1 min(ermC); and elongation at 72°C for 2 min. The cycle was repeated 35 times(18, 21, 22).
Molecular epidemiological typing. NG-MAST was performed by us-ing PCR and sequencing of the more variable segments of porB and tbpB(23). The porB and tbpB allele numbers as well as NG-MAST STs wereassigned using the NG-MAST website (http://www.ng-mast.net/).
Statistical analyses. We investigated the statistical correlation be-tween the AZM MIC and the presence and number of mutations underthe classifications of an MIC of 0.25 �g/ml or less (lower-MIC group) and
0.5 �g/ml or higher (higher-MIC group). Statistical analysis was con-ducted using Fisher’s exact test with the JSTAT (Java Virtual MachineStatistics Monitoring Tool; Sun Microsystems, Inc., Santa Clara, CA).Statistical significance was established at a P value of 0.05.
RESULTSAZM MICs. The AZM MICs of the 59 strains collected were 0.06,0.12, 0.25, 0.5, 1, and 16 �g/ml. In detail, 2 strains (3.39%) had anMIC of 0.06 �g/ml, 5 strains (8.47%) had an MIC of 0.12 �g/ml,16 strains (27.1%) had an MIC of 0.25 �g/ml, 33 strains (55.9%)had an MIC of 0.5 �g/ml, 4 strains (6.78%) had an MIC of 1�g/ml, and 1 strain (1.69%) had an MIC of 16 �g/ml. The MIC50
was 0.5 �g/ml, and the MIC90 was 0.5 �g/ml (Table 2).Mutations in domain V of 23S rRNA. There were 2 strains
with C2214T (C204T) mutations in allele 3, one strain with aG2209A (G199A) mutation in allele 4 and one strain (with thehighest MIC, 16 �g/ml) with C2599T (C589T) mutations in all 4alleles in the peptidyltransferase loop in domain V of 23S rRNA.
mtrR mutations. There were 38 (64.4%) strains with an A de-letion mutation in the promoter region of mtrR, and this was seensignificantly more often in the higher-MIC group (0.5 �g/ml orhigher) (35/37; 94.6%) than the lower-MIC group (0.25 �g/ml orless) (4/22; 18.2%) (P � 0.0001). Conversely, mutations of codon40 (Ala¡Asp) in the¡ mtrR gene (helix-turn-helix) were seen sig-nificantly more often in the lower-MIC group (12/22; 54.5%)(P � 0.0001). In addition, except for deletion mutations, strainswith no mutation were seen significantly more often in the higher-MIC group (33/37; 89.2%) (P � 0.0001), and strains with onemutation were seen significantly more often in the lower-MICgroup (15/22; 68.2%) (P � 0.0001).
Detection of methylase genes. Of the 59 N. gonorrhoeaestrains, there were no strains with positive PCR detection of ermA,ermB, ermC, or ermF (data not shown).
NG-MAST. N. gonorrhoeae multiantigen sequence typing(NG-MAST) results for porB and tbpB classified the 59 N. gonor-rhoeae strains as ST3505, ST4015, ST4637, ST4777, ST5875,ST6761, ST6773, ST6775, ST7382, and ST7806 in the lower-MICgroup and ST247, ST1407, ST3520, ST3588, ST4044, ST4163,ST4186, ST5875, ST6764, ST6774, ST6798, and ST6800 in thehigher-MIC group. The highest MIC in our strains (16 �g/ml) wasfound for ST1407. ST4777 was representative of the lower-MIC
TABLE 1 Sequences for PCR primers for azithromycin resistance genes
Primer name Target gene Primer sequence (5= to 3=) Size (bp) Reference
gonoRNA-F 23S rRNA ACGAATGGCGTAACGATGGCCACAallele1 TCAGAATGCCACAGCTTACAAACT 2,054 16allele2 GCGACCATACCAAACACCCACAGG 2,240allele3 GATCCCGTTGCAGTGAAGAAAGTC 2,217allele4 AACAGACTTACTATCCCATTCAGC 1,847mtrF1 mtrR GCCAATCAACAGGCATTCTTA 380 17mtr13Ra GTTGGAACAACGCGTCAAACermA-F ermA CTTCGATAGTTTATTAATATTAGT 645 18, 21, 22ermA-R TCTAAAAAGCATGTAAAAGAAermB-F ermB AGTAACGGTACTTAAATTGTTTAC 639ermB-R GAAAAGGTACTCAACCAAATAermC-F ermC GCTAATATTGTTTAAATCGTCAAT 642ermC-R TCAAAACATAATATAGATAAAermF-F ermF CGGGTCAGCACTTTACTATTG 466ermF-R GGACCTACCTCATAGACAAG
Shigemura et al.
2696 aac.asm.org May 2015 Volume 59 Number 5Antimicrobial Agents and Chemotherapy
― 194 ―

― 195 ―
group, and ST1407, ST6798, and ST6800 were representative ofthe higher-MIC group (Table 2).
DISCUSSION
The mechanism of resistance for the AZM-resistant N. gonor-rhoeae phenotype is currently unknown in detail. AZM and othermacrolides exert a bacteriostatic effect by interacting directly withthe central loop of domain V, the site of peptide bond formation,thereby inhibiting protein synthesis. Alteration in 23S rRNA isreported to contribute to low-level resistance. A 23S rRNA muta-tion (C2611T) has been proposed to contribute to the low-levelresistance observed in two Canadian gonococcal strains (24). Ch-isholm et al. showed that very-high-level resistance to AZM (MIC,256 �g/ml) occurs in N. gonorrhoeae as a result of a single pointmutation in the peptidyltransferase region of domain V of the 23SrRNA gene (24). Our study included a high-level AZM-resistantstrain (MIC, 16 �g/ml) with C2599T mutations in all the alleles(alleles 1 to 4) tested. This suggests that gonococcal strains fromJapan may have more mutations, even in strains with lower MICs,than those from other countries, such as the United Kingdom.
We observed that all AZM-resistant strains contained severalmutated alleles and that highly resistant strains had at least 3 mu-tations, while sensitive and moderately resistant isolates had amaximum of one mutated allele. Mutation of A2059G in highlyresistant gonococci and C2611T mutations in the 23S rRNAs ofmoderately resistant gonococci were reported previously (16).Our study found strains with mutations in one allele even instrains with low MICs (0.25 to 0.50 �g/ml), indicating that evengonococci with comparatively lower MICs harbor mutations.
Another mechanism of AZM resistance, the efflux pump, is
well known to contribute to macrolide resistance. This pump ex-cretes antibiotics, resulting in insufficient intracellular accumula-tion. The MtrCDE efflux pump regulated by the MtrR repressorprotein is a representative efflux pump system. mtrR mutations inthe gene itself or in its promoter region have been reported inlow-level macrolide-resistant gonococcal strains (25, 26) becauseof decreased MtrR expression and upregulation of the MtrCDEefflux pump. Clinical isolates or laboratory-derived mutants thatdisplay resistance to hydrophobic agents frequently contain loss-of-function mutations in the mtrR coding sequence or a single-base-pair deletion in a 13-bp inverted repeat within the mtrR pro-moter (27–29).
The mtrR mutations in the clinical isolates described abovewere identical to those reported for other strains of gonococci thatexpress resistance to multiple hydrophobic compounds (30, 31).The combined genetic and molecular results obtained in this in-vestigation implicate the mtrCDE-encoded efflux pump as amechanism by which gonococci can express decreased suscepti-bility to AZM. Through known mutations (27) that abrogatetranscription of the gene (mtrR) that encodes a transcriptionalrepressor of mtrCDE or loss-of-function mutations in the repres-sor-encoding gene, gonococci can overproduce the MtrCDE ef-flux pump to increase their capacity to export hydrophobicagents. Our data showed that a deletion mutation in the promoterregion of mtrR was seen significantly more often in the higher-MIC group (0.5 �g/ml or higher) compared with the lower-MICgroup (0.25 �g/ml or less) (P � 0.0001), and conversely, a muta-tion of codon 40 (Ala¡Asp) in the¡ mtrR gene (helix-turn-helix)was seen significantly more often in the lower-MIC group (P �
TABLE 2 MICs, mutations, and NG-MAST results for the N. gonorrhoeae strains
AZMMIC
No. ofstrains
% ofstrains
Mutationsa
NG-MAST type(s) (no. of strains)
mtrR promoterregion
mtrR gene
Helix-turn-helixCodon 29(silentmutation)
Codon 30(silentmutation)
Adeletion
C¡Tmutation
Codon 39(Ala¡Thr)
Codon 40(Ala¡Asp)¡
Codon 45(Gly¡Asp)¡
16 1 100 � ST1407 (1)1 4 100 � ST6798 (3), ST1407 (1)
0.5 28 88 � ST1407 (5), ST6800 (5), ST6798 (2),ST4044 (2), ST3588 (2), ST247(1), ST3520 (1), ST4163 (1),ST4186 (1), ST5875 (1), ST6764(1), ST6774 (1), nontypeable (9)
2 6 � �1 3 � � � �1 3 �
0.25 8 50 � ST4777 (2), ST6761 (2), ST6775 (2),ST4015 (1), ST4637 (1), ST5875(1), ST7382 (1), ST7806 (1),nontypeable (5)
3 19 � � � �2 13 ND ND ND ND ND ND ND1 6 �1 6 �1b 6
0.125 4 100 � ST4777 (1), ST6773 (1),nontypeable (2)
0.06 2 100 � � ST3505 (1), nontypeable (1)
Total 59a �, mutation present; ND, not determined.b 100-bp insertion and mutation.
AZM Resistance and Its Mechanism in N. gonorrhoeae
May 2015 Volume 59 Number 5 aac.asm.org 2697Antimicrobial Agents and Chemotherapy

― 196 ―
0.0001). These findings contribute to the current understandingof the mechanism of AZM resistance in N. gonorrhoeae. However,the methylase genes were not detected in our tested N. gonorrhoeaestrains, indicating that our AZM-resistant strains did not have thesame mechanisms of macrolide resistance as seen in the study byRoberts et al. (18). The trend of AZM resistance has not yet be-come widespread, and thus we need to continue surveillance ofgonococcal sensitivity to AZM but also continue with mechanisticstudies.
As an epidemiological study tool, the NG-MAST method (32–36) is based on limited DNA sequence analyses of two highly poly-morphic loci, porB and tbpB (23). There is public Internet accessfor sequence submission and assignment of sequence types, eitherfor porB or tbpB or for the assignment of STs using a combinationof these two loci (23). Our study clearly showed that STs could beusefully classified according to high-level and low-level AZMMICs. To our knowledge, there is no report of NG-MAST STs andAZM MICs. We identified ST1407 as a highly ASM-resistantstrain (MIC, 16 �g/ml) in Japan, suggesting that future epidemi-ological studies are needed for detecting the spread of this gono-coccal antibiotic-resistant phenotype in order to prevent a repeti-tion of the failure that resulted from continuous use ofquinolones, producing a high prevalence of quinolone-resistantgonococci.
This study has some limitations. First, the number of testedgonococcal strains may not be enough for definitive conclusions.Second, additional mechanistic investigation may be necessary forfurther understanding of gonococcal AZM resistance. These lim-itations should be overcome by our future studies.
In conclusion, a deletion mutation of the mtrR promoter re-gion is a possible mechanism of AZM resistance and may be asignificant indicator for higher MICs (0.5 �g/ml or higher) in N.gonorrhoeae infection. ST4777 was often seen in the lower-MICgroup and ST1407, ST6798, and ST6800 in the higher-MIC group,and this correlation with MIC was statistically significant. Furthermechanistic studies are needed, including the use of a greaternumber of strains.
ACKNOWLEDGMENTS
We thank Masahiro Miyata for data analysis and Miki Fujiwara and Hi-royuki Yoshida for gonococcal samples.
We declare that we have no conflicts of interest.
REFERENCES1. Edwards JL, Apicella MA. 2004. The molecular mechanisms used by
Neisseria gonorrhoeae to initiate infection differ between men and women.Clin Microbiol Rev 17:965–981. http://dx.doi.org/10.1128/CMR.17.4.965-981.2004.
2. Ndowa F, Lusti-Narasimhan M. 2012. The threat of untreatable gonor-rhoea: implications and consequences for reproductive and sexual mor-bidity. Reprod Health Matters 20:76 – 82. http://dx.doi.org/10.1016/S0968-8080(12)40653-X.
3. Centers for Disease Control and Prevention. 1993. 1993 sexually trans-mitted diseases treatment guidelines. MMWR Recommend Rep42(RR14):1102.
4. Centers for Disease Control and Prevention. 2007. Update to CDC’ssexually transmitted diseases treatment guidelines, 2006: fluoroquinolo-nes no longer recommended for treatment of gonococcal infections.MMWR Morb Mortal Wkly Rep 56:332–336.
5. Chisholm SA, Dave J, Ison CA. 2010. High-level azithromycin resistanceoccurs in Neisseria gonorrhoeae as a result of a single point mutation in the23S rRNA genes. Antimicrob Agents Chemother 54:3812–3816. http://dx.doi.org/10.1128/AAC.00309-10.
6. Dalhoff A. 2012. Global fluoroquinolone resistance epidemiology andimplictions for clinical use. Interdiscip Perspect Infect Dis 2012:976273.http://dx.doi.org/10.1155/2012/976273.
7. Dan M. 2004. The use of fluoroquinolones in gonorrhoea: the increasingproblem of resistance. Expert Opin Pharmacother 5:829 – 854. http://dx.doi.org/10.1517/14656566.5.4.829.
8. Roddy RE, Handsfield HH, Hook EW, III. 1986. Comparative trial ofsingle-dose ciprofloxacin and ampicillin plus probenecid for treatment ofgonococcal urethritis in men. Antimicrob Agents Chemother 30:267–269.http://dx.doi.org/10.1128/AAC.30.2.267.
9. Zhang T, Zhou X, Chen Y, Gu W, Zhang T, Jiang Q. 2009. Fluoro-quinolone resistance and mutation patterns in gyrA and parC genes inNeisseria gonorrhoeae isolates from Shanghai, China. J HuazhongUniv Sci Technolog Med Sci 29:29 –34. http://dx.doi.org/10.1007/s11596-009-0106-4.
10. Barry PM, Klausner JD. 2009. The use of cephalosporins for gonorrhea:the impending problem of resistance. Expert Opin Pharmacother 10:555–577. http://dx.doi.org/10.1517/14656560902731993.
11. Kojima M, Masuda K, Yada Y, Hayase Y, Muratani T, Matsumoto T. 2008.Single-dose treatment of male patients with gonococcal urethritis using 2gspectinomycin: microbiological and clinical evaluations. Int J AntimicrobAgents 32:50–54. http://dx.doi.org/10.1016/j.ijantimicag.2008.02.023.
12. Osaka K, Takakura T, Narukawa K, Takahata M, Endo K, Kiyota H,Onodera S. 2008. Analysis of amino acid sequences of penicillin-bindingprotein 2 in clinical isolates of Neisseria gonorrhoeae with reduced suscep-tibility to cefixime and ceftriaxone. J Infect Chemother 14:195–203. http://dx.doi.org/10.1007/s10156-008-0610-7.
13. Yokoi S, Deguchi T, Ozawa T, Yasuda M, Ito S, Kubota Y, Tamaki M,Maeda S. 2007. Threat to cefixime treatment for gonorrhea. Emerg InfectDis 13:1275–1277. http://dx.doi.org/10.3201/eid1308.060948.
14. Delpech V, Martin IM, Hughes G, Nichols T, James L, Ison CA,Gonococcal Resistance to Antimicrobials Surveillance ProgrammeSteering Group. 2009. Epidemiology and clinical presentation of gonor-rhoea in England and Wales: findings from the Gonococcal Resistance toAntimicrobials Surveillance Programme 2001-2006. Sex Transm Infect85:317–321. http://dx.doi.org/10.1136/sti.2008.034843.
15. Yasuda M, Ito S, Kido A, Hamano K, Uchijima YY, Uwatoko N,Kusuyama H, Watanabe A, Miyamura RR, Miyata K, Deguchi T. 2014.A single 2 g oral dose of extended-release azithromycin for treatment ofgonococcal urethritis. J Antimicrob Chemother 69:3116 –3118. http://dx.doi.org/10.1093/jac/dku221.
16. Ng LK, Martin I, Liu GG, Bryden L. 2002. Mutation in 23S rRNAassociated with macrolide resistance in Neisseiria gonorrhoeae. AntimicrobAgents Chemother 46:3020 –3025. http://dx.doi.org/10.1128/AAC.46.9.3020-3025.2002.
17. Cousin SL, Jr, Whittington WL, Roberts MC. 2003. Acquired macrolideresistance genes and the 1 bp deletion in the mtrR promoter in Neisseriagonorrhoeae. J Antimicrob Chemother 51:131–133. http://dx.doi.org/10.1093/jac/dkg040.
18. Roberts MC, Chung WO, Roe D, Xia M, Marquez C, Borthagaray G,Whittington WL, Holmes KK. 1999. Erythromycin-resistant Neisseriagonorrhoeae and oral commensal Neisseria spp. carry known rRNA meth-ylase genes. Antimicrob Agents Chemother 43:1367–1372.
19. National Institute of Infectious Diseases. 2015. http://www.nih.go.jp/niid/ja/diseases/ta/typhi/392-encyclopedia/527-gonorrhea.html.
20. Unemo M, Nicholas RA. 2012. Emergence of multidrug-resistant, exten-sively drug-resistant and untreatable gonorrhea. Future Microbiol7:1401–1422. http://dx.doi.org/10.2217/fmb.12.117.
21. Chung WO, Werckenthin C, Schwarz S, Roberts MC. 1999. Hostrange of the ermF rRNA methylase gene in bacteria of human andanimal origin. J Antimicrob Chemother 43:5–14. http://dx.doi.org/10.1093/jac/43.1.5.
22. Sutcliffe J, Grebe T, Tait-Kamradt A, Wondrack L. 1996. Detection oferythromycin-resistant determinants by PCR. Antimicrob Agents Che-mother 40:2562–2566.
23. Martin I, Ison C, Aanensen D, Fenton K, Spratt B. 2004. Rapid se-quence-based identification of gonococcal transmission clusters in a largemetropolitan area. J Infect Dis 189:1497–1505. http://dx.doi.org/10.1086/383047.
24. Chisholm SA, Neal TJ, Alawattegama AB, Birley HD, Howe RA, IsonCA. 2009. 2009 Emergence of high-level azithromycin resistance in Neis-seria gonorrhoeae in England and Wales. J Antimicrob Chemother 64:353–358. http://dx.doi.org/10.1093/jac/dkp188.
Shigemura et al.
2698 aac.asm.org May 2015 Volume 59 Number 5Antimicrobial Agents and Chemotherapy

― 197 ―
25. Barthélémy P, Autissier D, Gerbaud G, Courvalin P. 1984. Enzymatichydrolysis of erythromycin by a strain of Escherichia coli: a new mecha-nism of resistance. J Antibiot 37:1692–1696. http://dx.doi.org/10.7164/antibiotics.37.1692.
26. Le Goffic F, Capmau ML, Abbe J, Cerceau C, Dublanchet A, Duval J.1977. Plasmid-mediated pristinamycin resistance: PH1A, a pristinamycin1A hydrolase. Ann Inst Pasteur (Paris) 128:471– 474.
27. Hagman KE, Lucas CE, Balthazar JT, Snyder L, Nilles M, Judd RC,Shafer WM. 1997. The MtrD protein of Neisseria gonorrhoeae is a memberof the resistance/nodulation/division protein family constituting part ofan efflux system. Microbiology 131:2117–2125.
28. Pan W, Spratt BG. 1994. Regulation of the permeability of the gonococcalcell envelope by the mtr system. Mol Microbiol 11:769 –775. http://dx.doi.org/10.1111/j.1365-2958.1994.tb00354.x.
29. Shafer WM, Balthazar JT, Hagman KE, Morse SA. 1995. Missensemutations that alter the DNA-binding domain of the MtrR proteinoccur frequently in rectal isolates of Neisseria gonorrhoeae that are resis-tant to faecal lipids. Microbiology 141:907–911. http://dx.doi.org/10.1099/13500872-141-4-907.
30. Hagman KE, Shafer W. 1995. Transcriptional control of the mtr effluxsystem of Neisseria gonorrhoeae. J Bacteriol 177:4162– 4165.
31. Slaney L, Chubb H, Ronald A, Brunham R. 1990. In-vitro activity ofazithromycin, erythromycin, ciprofloxacin and norfloxacin against Neis-seria gonorrhoeae, Haemophilus ducreyi, and Chlamydia trachomatis.
J Antimicrob Chemother 25(Suppl A):1–5. http://dx.doi.org/10.1093/jac/25.suppl_A.1.
32. Bilek N, Martin I, Bell G, Kinghorn G, Ison C, Spratt B. 2007. Concor-dance between Neisseria gonorrhoeae genotypes recovered from knownsexual contacts. J Clin Microbiol 45:3564 –3567. http://dx.doi.org/10.1128/JCM.01453-07.
33. Lundbäck D, Fredlund H, Berglund T, Wretlind B, Unemo M. 2006.Molecular epidemiology of Neisseria gonorrhoeae—identification of the firsteepresumed Swedish transmission chain of an azithromycin-resistant strain.APMIS 114:67–71. http://dx.doi.org/10.1111/j.1600-0463.2006.apm_332.x.
34. Olsen B, Hadad R, Fredlund H, Unemo M. 2008. The Neisseria gonor-rhoeae population in Sweden during 2005—phenotypes, genotypesand antibiotic resistance. APMIS 116:181–189. http://dx.doi.org/10.1111/j.1600-0463.2008.00895.x.
35. Unemo M, Sjöstrand A, Akhras M, Gharizadeh B, Lindbäck E, Pour-mand N, Wretlind B, Fredlund H. 2007. Molecular characterization ofNeisseria gonorrhoeae identifies transmission and resistance of one cipro-floxacin-resistant strain. APMIS 115:231–241. http://dx.doi.org/10.1111/j.1600-0463.2007.apm_487.x.
36. Unemo M, Vorobieva V, Firsova N, Ababkova T, Leniv I, Haldorsen B,Fredlund H, Skogen V. 2007. Neisseria gonorrhoeae population in Arkhan-gelsk, Russia: phenotypic and genotypic heterogeneity. Clin MicrobiolInfect 13:873– 878. http://dx.doi.org/10.1111/j.1469-0691.2007.01764.x.
AZM Resistance and Its Mechanism in N. gonorrhoeae
May 2015 Volume 59 Number 5 aac.asm.org 2699Antimicrobial Agents and Chemotherapy

― 198 ―
Surveillance
The second nationwide surveillance of the antimicrobial susceptibilityof Neisseria gonorrhoeae from male urethritis in Japan, 2012e2013
Ryoichi Hamasuna a, c, *, Mitsuru Yasuda a, d, Kiyohito Ishikawa a, e, Shinya Uehara a, f,Hiroshi Hayami a, g, Satoshi Takahashi a, h, Tetsuro Matsumoto a, c, Shingo Yamamoto a, i,Shinichi Minamitani a, Akira Watanabe b, Satoshi Iwata b, Mitsuo Kaku b, Junichi Kadota b,Keisuke Sunakawa b, Junko Sato b, Hideaki Hanaki j, Taiji Tsukamoto h, Hiroshi Kiyota k,Shin Egawa l, Kazushi Tanaka m, Soichi Arakawa m, Masato Fujisawa m, Hiromi Kumon f,Kanao Kobayashi n, Akio Matsubara n, Seiji Naito o, Kentaro Kuroiwa o, Hideo Hirayama p,Harunori Narita q, Takahide Hosobe r, Shin Ito s, Kenji Ito t, Shuichi Kawai u,Masayasu Ito v, Hirofumi Chokyu w, Masaru Matsumura x, Masaru Yoshioka y,Satoshi Uno z, Koichi Monden aa, Kazuo Takayama ab, Shinichi Kaji ac,Motoshi Kawahara ad, Toru Sumii ae, Hitoshi Kadena af, Takamasa Yamaguchi ag,Shinichi Maeda ah, Shohei Nishi ai, Hirofumi Nishimura aj, Takeshi Shirane ak,Mutsumasa Yoh al, Kikuo Akiyama am, Toshio Imai an, Motonori Kano ao
a The Urogenital Sub-committee and the Surveillance Committee of Japanese Society of Chemotherapy (JSC), The Japanese Association for InfectiousDiseases (JAID) and The Japanese Society for Clinical Microbiology (JSCM), Tokyo, Japanb The Surveillance Committee of JSC, JAID and JSCM, Tokyo, Japanc Department of Urology, University of Occupational and Environmental Health, Kitakyushu, Japand Department of Urology, Gifu University Hospital, Gifu, Japane Department of Urology, School of Medicine, Fujita Health University, Toyoake, Japanf Department of Urology, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama, Japang Blood Purification Center, Kagoshima University Hospital, Kagoshima, Japanh Department of Urology, Sapporo Medical University School of Medicine, Sapporo, Japani Department of Urology, Hyogo College of Medicine, Nishinomiya, Japanj Research Center for Anti-infectious Drugs, Kitasato Institute for Life Sciences, Kitasato University, Tokyo, Japank Department of Urology, The Jikei University Katsushika Medical Center, Tokyo, Japanl Department of Urology, The Jikei University School of Medicine, Tokyo, Japanm Division of Urology, Kobe University Graduate School of Medicine, Kobe, Japann Department of Urology, Institute of Biomedical & Health Sciences Hiroshima University, Hiroshima, Japano Department of Urology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japanp Hirayama Urology Clinic, Kumamoto, Japanq Narita Clinic, Nagoya, Japanr Hosobe Clinic, Tokyo, Japans iClinic, Sendai, Japant Ito Urology Clinic, Kitakyushu, Japanu Kawai Urology Clinic, Kitakyushu, Japanv Gifu Urological Clinic, Gifu, Japanw Chokyu Tenma Clinic, Himeji, Japanx Matsumura Urology Clinic, Kato, Japany Yoshioka Urology Clinic, Nishinomiya, Japanz Hirajima Clinic, Okayama, Japanaa Araki Urological Clinic, Kurashiki, Japanab Department of Urology, Takayama Hospital, Chikushino, Japanac Kaji Clinic, Fukuoka, Japanad Kawahara Urology Clinic, Kagoshima, Japanae Sumii Clinic, Hiroshima, Japanaf Kadena Urological Clinic, Hiroshima, Japan
* Corresponding author. Department of Urology, University of Occupational and Environmental Health Japan, 1-1 Iseigaoka, Yahatanishi-ku, Kitakyuhsu, 807-8555, Japan.Tel.: þ81 93 692 7446; fax: þ81 93 603 8724.
E-mail address: [email protected] (R. Hamasuna).
Contents lists available at ScienceDirect
Journal of Infection and Chemotherapy
journal homepage: http: / /www.elsevier .com/locate/ j ic
http://dx.doi.org/10.1016/j.jiac.2015.01.0101341-321X/© 2015, Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
J Infect Chemother 21 (2015) 340e345

― 199 ―
ag Yamaguchi Dermatology and Urology Clinic, Munakata, Japanah Department of Urology, Toyota Memorial Hospital, Toyota, Japanai Nishi Urology and Dermatology Clinic, Kitakyushu, Japanaj Nishimura Urology Clinic, Kitakyushu, Japanak Shirane Urology Clinic, Aki-gun, Japanal Yoh Urology and Dermatology Clinic, Inazawa, Japanam Akiyama Urology Clinic, Nishinomiya, Japanan Imai Urology Clinic, Akashi, Japanao Department of Urology, Kano Hospital, Kasuya-gun, Japan
a r t i c l e i n f o
Article history:Received 15 October 2014Received in revised form15 January 2015Accepted 20 January 2015Available online 31 January 2015
Keywords:Neisseria gonorrhoeaeNationwide surveillanceAntimicrobial susceptibilitiesJapan20122013
a b s t r a c t
Worldwide, the most important concern in the treatment of sexually transmitted infections is the in-crease in antimicrobial resistant Neisseria gonorrhoeae strains including resistance to cephalosporins,penicillins, fluoroquinolones or macrolides. To investigate the trends of antimicrobial susceptibilityamong N. gonorrhoeae strains isolated from male patients with urethritis, a Japanese surveillancecommittee conducted the second nationwide surveillance study. Urethral discharge was collected frommale patients with urethritis at 26 medical facilities from March 2012 to January 2013. Of the 151specimens, 103 N. gonorrhoeae strains were tested for susceptibility to 20 antimicrobial agents. None ofthe strains was resistant to ceftriaxone, but the minimum inhibitory concentration (MIC) 90% of ceftri-axone increased to 0.125 mg/ml, and 11 (10.7%) strains were considered less susceptible with an MIC of0.125 mg/ml. There were 11 strains resistant to cefixime, and the MICs of these strains were 0.5 mg/ml. Thedistributions of the MICs of fluoroquinolones, such as ciprofloxacin, levofloxacin and tosufloxacin, werebimodal. Sitafloxacin, a fluoroquinolone, showed strong activity against all strains, including strainsresistant to other three fluoroquinolones, such as ciprofloxacin, levofloxacin and tosufloxacin. The azi-thromycin MICs in 2 strains were 1 mg/ml.
© 2015, Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases.Published by Elsevier Ltd. All rights reserved.
1. Introduction
The antimicrobial resistance of Neisseria gonorrhoeae strainsagainst penicillins, tetracyclines, fluoroquinolones, cephalosporinsand macrolides is increasing worldwide. Surveillance of the anti-microbial susceptibilities of N. gonorrhoeae provides importantinformation for treating gonococcal infections. We have reportedthe antimicrobial susceptibilities of N. gonorrhoeae strains, whichwere collected at 2009e2010, in the first national surveillancestudy in Japan [1]. In summary, the rate of less susceptible strains toceftriaxone was 8.4%; the susceptibility rate to cefixime accordingto the criteria of the Clinical and Laboratory Standards Institutes(CLSI) [2] was 98.8%; the minimum inhibitory concentrations(MICs) of fluoroquinolones, such as ciprofloxacin, showed abimodal distribution and resistance rates were 78.3%; sitafloxacnshowed low MICs of �0.5 mg/ml against ciprofloxacin-resistantstrains; the proportion of strains with azithromycin MICs of morethan 0.5 mg/ml was 3.6%.
After a ceftriaxone-resistant N. gonorrhoeae strain was discov-ered in a pharyngeal specimen of a female commercial sex workerin Kyoto, Japan [3], other ceftriaxone-resistant N. gonorrhoeaestrains were discovered in France [4] and Spain [5], but not other-wise in Japan [1,6].
Since 2009, a 2-g azithromycin dose has been accepted by Jap-anese national insurance for the treatment of both gonococcal andchlamydial urethritis. High-level azithromycin-resistant strainshave emerged in many sites worldwide [7e10], and a relationshipbetween the use of azithromycin and an increase in the azi-thromycinMIC has been described [11]. The Japanese Association ofSexually Transmitted Infections [12] has not recommended the useof azithromycin for treating gonococcal infections. However, somephysicians prefer to use azithromycin to treat gonococcal in-fections, and we anticipate the emergence of high-level azi-thromycin-resistant strains of N. gonorrhoeae in Japan.
In this report, the antimicrobial susceptibility patterns ofN. gonorrhoeae strains collected from 2012 to 2013 are compared tothe patterns from 2009 to 2010 [1]. This national surveillance wasconducted by the surveillance committee of three Japanese soci-eties including the Japanese Association of Infectious Diseases, theJapanese Society of Chemotherapy and the Japanese Society ofClinical Microbiology. The committee has previously performedand published other surveillance studies regarding the antimicro-bial susceptibilities of pathogens causing respiratory infections,urinary tract infections, urethritis and surgical site infections. Thepresent surveillance study was the second study performed onN. gonorrhoeae strains collected from male patients with gono-coccal urethritis.
2. Materials and methods
2.1. Patients and participating facilities
The targets were male patients older than 16 years with ure-thral discharge and symptoms of urethritis, such as pain uponmicturition, urethral pain or urethral discomfort. Included patientswere diagnosed with gonococcal urethritis by a clinician. Theperiod of specimen collection was between March 2012 andJanuary 2013. The 38 participating facilities included departmentsof urology in hospitals and private clinics that specialized inurology or urology and dermatology in Japan. The clinicians whoparticipated in this study explained the purpose of the study to thepatients orally or through written documents and obtained thewritten consent of each patient. This study was approved by theethical committee of each facility. The facilities that did not havean ethical committee submitted this study to the ethical com-mittee of the specific non-profit organization CREC net, Kita-kyushu, Japan, which approved it.
R. Hamasuna et al. / J Infect Chemother 21 (2015) 340e345 341

― 200 ―
2.2. Specimens and patient information
The discharge from the urethral meatus was collected with asterilized cotton swab, placed in transport agar (SEEDSWAB gNo2,Eiken Chemical Co. Ltd., Tokyo, Japan) and sent at room tempera-ture to the Infection Scientific Control Research Center, The KitasatoInstitution, Tokyo, Japan. Only one specimen was collected fromeach patient. The patient's information, including age, diagnosisand the properties of the discharge were reported for each sample.
2.3. Isolation of N. gonorrhoeae strains and antimicrobialsusceptibility testing
The bacterial isolation and antimicrobial susceptibility testingwere performed in the Infection Scientific Control Research Center,The Kitasato Institution, Tokyo, Japan. For each specimen,N. gonorrhoeae strain isolation and identification was attempted.
The antimicrobial susceptibility testing was performed accord-ing to the CLSI Document M100-S22 [2], and the minimum inhib-itory concentrations (MICs) were determined by the agar dilutionmethod. Supplemented 1% GC agar (1.1 g L-cysteine, 0.03 g guanineHCL, 3 mg thiamine HCL,13mg para-aminobenzoic acid, 0.01 g B12,0.1 g cocarboxylase, 0.25 g nicotinamide adenine dinucleotide, 1 gadenine, 10 g L-glutamine, 100 g glucose, and 0.02 g ferric nitrateper liter) was used for determining the MICs. When the MIC ofcarbapenems or clavulanic acid was measured, cysteine was notincluded in the agar. The range of concentrations for testingincluded 12 two-fold serial dilutions (128e0.063 mg/ml) of anti-microbials, but the starting concentration fluctuated depending onthe particular type of antimicrobial used. The inoculum wasadjusted to a 0.5 MacFarland standard by the direct adjustmentmethod. The N. gonorrhoeae strains were cultured at 36 ± 1 �C in 5%CO2 atmosphere overnight. N. gonorrhoeae ATCC 49226 was used asthe standard control.
The MICs of the following 20 antimicrobial agents weremeasured: penicillin G, ampicillin, amoxicillin, clavulanic acid-amoxicillin, cefpodoxime, cefdinir, cefixime, cefditoren, ceftriax-one, cefodizime, flomoxef, aztreonam, meropenem, spectinomycin,ciprofloxacin, levofloxacin, tosufloxacin, sitafloxacin, minocyclineand azithromycin. The susceptibility or resistance of the isolate toeach antibiotic was determined according to CLSI Document M100-S22 [2].The antimicrobial susceptibility data in this surveillancewere compared with those in the first surveillance.
b-lactamase activity in the N. gonorrhoeae isolates was detectedby the nitrocefin method (Cefinase Disk™; BD BBL™). TheN. gonorrhoeae strains that were resistant to penicillin G (MIC:�2 mg/ml) and in which b-lactamase activity was detected weredetermined to be penicillinase-producing N. gonorrhoeae (PPNG).Among b-lactamase-non-producing strains, strains that wereresistant to penicillin G (MIC: �2 mg/ml) were determined to bechromosomally mediated resistant N. gonorrhoeae (CMRNG).
The threshold MICs for antimicrobial resistance are assumedaccording to the following criteria: �2 mg/ml of penicillin G, �2 mg/ml of minocycline, �1 mg/ml of cefpodoxime, �1 mg/ml of cipro-floxacin or �0.5 mg/ml of azithromycin. The phenotypes ofN. gonorrhoeae strains were classified by their resistance to anti-microbial agents.
3. Results
3.1. Number of specimens and isolated strains
Of the 152 specimens from 26 medical facilities, one wasomitted because the patient's agewas 14 years. Themedian agewas32 years (range: 18e65), and 39.7% and 33.8% of specimens were
collected from patients in their 20s and 30s, respectively. Theurethral discharge was described as purulent for 139 specimensand serous for 11. Of the 151 specimens from 151 patients, 103strains could be cultured and identified as N. gonorrhoeae. From the139 purulent specimens, 100 strains (71.9%) were isolated. Of these103 strains, 36, 21, 16, 14, 9 and 7 strains were collected from theKyushu, Chugoku, Kinki, Chubu, Tohoku and Tokyo areas,respectively.
3.2. Antimicrobial susceptibilities
Antimicrobial susceptibility testing was performed on all 103isolated strains (Table 1). Nonewas susceptible to penicillin G (MIC:�0.06). Only two strains (1.9%) were determined to be PPNG, andthe MICs of penicillin G to these strains were 2 and 32 mg/ml. TheMIC of clavulanic acid-amoxicillin MIC to PPNG strains was 0.5 mg/ml. Among b-lactamase-non-producing strains, 21 strains (20.8%)had higher MICs to penicillin G (MIC �2 mg/ml, range: 2e4 mg/ml)and were determined to be CMRNG. The MIC90 of four kinds ofpenicillins including penicillin G, ampicillin, amoxicillin andamoxicillin-clavulanic acid for b-lactamase-non-producing strainswas 2 mg/ml.
The MICs of minocycline for two PPNG strains were also higher(8 and 16 mg/ml). The MIC range for minocycline in the b-lacta-mase-non-producing strains was �0.06e32 mg/ml and 3 strains(2.9%) were resistant to minocycline. (MIC: 16 or 32 mg/ml).
The susceptibility rates of all the strains to oral cephalospo-rins such as cefixime and cefpodoxime were 89.3% and 59.2%according to CLSI criteria [2], respectively. The susceptibility ofcefixime evidently decreased compared to the strains collectedin the first surveillance study. The MICs of the parenteral ceph-alosporins ceftriaxone and cefodizime were relatively low. Thehigh-level ceftriaxone-resistant strains, such as Ohnishi's report[3], were not found in the surveillance. The MIC90 of ceftriaxoneincreased from �0.06 mg/ml in the first surveillance study to0.125 mg/ml in this study. All 11 strains with a ceftriaxone MIC of0.125 mg/ml had cefixime MICs of 0.25 or 0.5 mg/ml. However, 3strains with cexifime MIC of 0.5 mg/ml had a ceftriaxone MIC of�0.06 mg/ml.
The MIC distribution for fluoroquinolones, such as ciprofloxa-cin, levofloxacin and tosufloxacin, showed bimodal. The MICs ofthese three antimicrobials for the 21 susceptible strains were�0.06 mg/ml. The MIC of sitafloxacin was lower than that of theother fluoroquinolones. Strains with ciprofloxacin MICs of�0.06 mg/ml had also sitafloxacin MIC of�0.06 mg/ml. Strains withciprofloxacin MICs between 0.5 and 32 mg/ml showed sitafloxacinMIC of �0.06, 0.125 or 0.25 mg/ml. Only one strains with sita-floxacin MIC of 0.5 mg/ml and ciprofloxacin MIC of 64 mg/ml wasnewly identified.
Strains with resistance to spectinomycin were not identified inthis study. No high-level azithromycin resistant strains were found,but two strains had an MIC of 1 mg/ml.
3.3. Phenotypes of antimicrobial resistance among N. gonorrhoeaestrains
Table 2 shows the antimicrobial resistance phenotypes of thestrains. Among the isolated strains, 83 (80.6%) met resistancecriteria to one or more tested antimicrobials and 34 were resistantto a single antimicrobial (ciprofloxacin: 33 azithromycin 1). Forty-nine strains (47.5%) showed resistance to more than two types ofantimicrobials such as penicillins, cephalosporins, tetracyclines,fluoroquinolones and macrolides.
R. Hamasuna et al. / J Infect Chemother 21 (2015) 340e345342

― 201 ―
4. Discussion
The guideline of the Japanese Association of Sexually Trans-mitted Infections recommends that gonococcal urethritis andcervicitis be treated with 1 g of ceftriaxone in a single intravenousdose, 1 g of cefodizime in a single intravenous dose and 2 g ofspectinomycin in a single intramuscular dose [12]. This recom-mendation did not change during the first and second surveillancestudies. The second surveillance study revealed that the patientdemographics and clinical features of the urethral discharges werethe same as in the first study, although the antimicrobial suscep-tibility data were different.
The prevalence of PPNG decreased compared to the firstsurveillance data. Previous to 2009, the prevalence of PPNG inJapan had been approximately 1% [13]. However, the prevalencewas 7.2% in the first surveillance study. The second surveillancedata showed the prevalence of PPNG to be 0.2%, which is a returnto historic levels. We are not able to explain why the prevalencewas higher in 2009e2010. One explanation is that patients whowere infected in foreign countries were included in the firststudy. Penicillins are not available for the treatment of gonococcalinfections in Japan. No strain was sensitive to penicillin G inthis study. In addition, penicillin with a b-lactamase inhibitor
cannot be recommended to treat gonococcal urethritis, becausethe MICs of amoxicillin are relatively higher and the MICof clavulanic acid-amoxicillin was not low for PPNG strains(0.5 mg/ml).
The most serious problem for the treatment of gonococcal in-fections worldwide is the increase in cephalosporin-resistantstrains. We did not find further evidence of high-level ceftriax-one-resistant strains in Japan. However, ceftriaxone-resistantstrains were reported from France and Spain [4,5] and there arereports of ceftriaxone treatment failure in patients withN. gonorrhoeae strains isolated from the pharynx [14e17]. Inparticular, Swedish case-report described a N. gonorrhoeae strainwith a ceftriaxone MIC of 0.25 mg/ml that was detected from thepharynx of a male patient after treatment with 250 mg and 500 mgof ceftriaxone; this patient was most likely infected through un-protected oral sexwith a female partner in Japan [14]. This indicatesthat some women in Japan have N. gonorrhoeae strains with a highceftriaxone MIC, but these strains were not found in any surveil-lance. Indeed, the MIC90 of ceftriaxone increased from �0.06 mg/mlin the first surveillance study to 0.125 mg/ml in this study. Thestrains with a ceftriaxone MIC of 0.125 mg/ml, those are termed as“less susceptible strains,” increased. In addition, the strains sensi-tive to cefixime with an MIC �0.06 mg/ml, which Deguchi recom-mended as the breakpoint MIC of cefixime in Japan [18], decreasedfrom 55.4% to 40.8%. These resistance or those less susceptibility inN. gonorrhoeae to cephalosporins are closely related to the mosaicstructure of penA gene which codes for PBP2 [4,5,19,20]. Our dataare evidence that this type of resistance has been spreading inJapan.
The MICs of fluoroquinolones did not differ between the firstand second surveillance studies. The fluoroquinolone-resistantrates of strains have shown nearly the same level as in Tanaka'sreports [21]. This likely means that physicians treating gonococcalinfections are complying with the guidelines of the Japanese Soci-ety of Sexually Transmitted Infections. The activity of sitafloxacinremains stable in two our surveillances. As described previously [1],sitafloxacin has activity against ciprofloxacin-resistantN. gonorrhoeae strains. Sitafloxacin can be one of treatment op-tions for untreatable N. gonorrhoeae strains. However, one strainswith sitafloxacin MIC of 0.5 mg/ml was found and further obser-vation or clinical study would be necessary.
Table 1Antimicrobial MIC distribution for 103 N. gonorrhoeae strains.
Antibacterial agent MIC (mg/ml)
�0.06 0.125 0.25 0.5 1 2 4 8 16 32 64 128 �256 MIC50 MIC90
Penicillin G 6 24 17 33 20 2 1 1 2Ampicillin 8 14 11 29 33 7 1 1 2Amoxicillin 21 8 20 52 1 1 2 2Clavulanic acid-amoxicillin 1 21 10 25 46 1 2Cefpodoxime 38 3 5 15 23 17 2 0.5 2Cefdinir 41 2 25 35 0.5 1Cefixime 42 8 42 11 0.25 0.5Cefditoren 52 24 22 5 �0.06 0.25Ceftriaxone 92 11 �0.06 0.125Cefodizime 79 21 3 �0.06 0.125Flomoxef 3 20 8 22 41 9 1 2Aztreonam 10 15 14 2 1 1 38 22 4 8Meropenem 68 35 �0.06 0.125Spectinomycin 3 95 5 16 16Ciprofloxacin 21 1 1 13 18 36 12 1 8 32Levofloxacin 21 1 1 6 26 38 10 4 8Tosufloxacin 21 3 4 31 14 19 11 2 16Sitafloxacin 38 32 32 1 0.125 0.25Minocycline 2 29 26 40 1 1 3 1 0.25 0.5Azithromycin 15 44 39 3 2 0.125 0.25
Table 2The phenotypes of antimicrobial resistance among N. gonorrhoeae strains.
Antimicrobials Numbers
Penicillin G Minocycline Cefpodoxime Ciprofloxacin Azithromycin
R 33R 1
R R 1R R 1
R R 22R R 3
R R 1R R R 17R R R 1R R R R 3
R: Resistance to antimicrobial agents that was determined by the criteria below.MICs of�2 mg/ml of penicillin G,�2 mg/ml of minocycline,�1 mg/ml of cefpodoxime,�1 mg/ml of ciprofloxacin or �0.5 mg/ml of azithromycin.
R. Hamasuna et al. / J Infect Chemother 21 (2015) 340e345 343

― 202 ―
In both the first and second surveillance study, high-levelresistant strains to azithromycin were not found. The main mech-anism for azithromycin-resistance in N. gonorrhoeae is mutations ofthe macrolide target, 23S rRNA as A2059G or C2611T mutations[7e10,20]. N. gonorrhoeae has four 23S rRNA alleles and the resis-tance to azithromycin depends on the numbers of alleles withmutations [20]. Unemo described that the azithromycin MIC in-crease to 4,096 mg/ml in strains with A2059G mutations in three orfour alleles, but the MICs of strains with the mutation in one alleleare not changed as wild-type strains [10]. Through this theory, atleast two strains (1.9%) with an azithromycin MIC of 1 mg/ml havemutations in more than 2 alleles of the 23S rRNA. In other Japanesesurveillance data, 3.6% (7/193) of strains in the Kyoto and Osakaareas or 6.6% (8/122) of strains in the Tokyo area were resistant toazithromycin (>0.5 mg/ml) [6,22]. In the Tokyo area, higher-resistant strains were found (one and two strains with MIC 16and 8 mg/ml, respectively). Yasuda et al. showed clinical study usingazithromycin 2g in Japan and strains with MIC 2 or 4 mg/ml ofazithromycin remained after the treatment [23]. Among strainswith MIC 1 or 0.5 mg/ml eradication rates were 58% (7/12) and 97%(31/32), respectively. Even if azithromycin 2g is used, a high dose ofazithromycin could covered only strains with MIC �0.5 mg/ml andwe wonder that azithromycin-resistance would increase.
Table 2 shows the numbers of strains according to the antimi-crobial resistant phenotype. Among 103 strains, 20 were classifiedas “not resistant” to all antimicrobials. These strains were 20 of 21the strains with ciprofloxacin MIC�0.06 mg/ml (another one had anazithromycin MIC of 0.5 mg/ml). Regarding N. gonorrhoeae strains inJapan, the susceptibility for fluoroquinolone, which are lessfrequently used now is important. According to Tapsall's criteria formulti-drug resistant N. gonorrhoeae (MDR-NG) [24], 42 strains(40.1%) met the criteria of MDR-NG. In 2009e2010, 39.8% of thestrains were classified as MDR-NG, which was quite similar to theproportion in 2011e2012.
The next Japanese antimicrobial surveillance initiative forN. gonorrhoeae is planned for 2016. The increase in cephalosporin-resistance is more prominent worldwide. Dual therapies, such asceftriaxone plus azithromycin or ceftriaxone and effective quino-lones are recommended and being used worldwide. The recom-mendation of Japanese Association of Sexually TransmittedInfections for treating gonococcal infections has remained thesame. The purpose of the next surveillance study is to evaluate theappropriateness of the present recommendation for the treatmentof gonococcal infection and to determine whether the recom-mendation should be modified.
Conflicts of interest
Mitsuru Yasuda has received donation from Astellas Pharma Inc.Akira Watanabe has received speaker's honorarium fromMSD K.K.,Glaxo SmithKline K.K., Shionogi & Co., Ltd., Daiichi Sankyo Co., Ltd.,Taisho Toyama Pharmaceutical Co., Ltd. and Pfizer Japan Inc.; grantsupport from Kyorin Pharmaceutical Co., Ltd., Shionogi & Co., Ltd.
Taisho Pharmaceutical Co., Ltd., Toyama Chemical Co., Ltd.,Daiichi Sankyo Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd.,Taiho Pharmaceutical Co., Ltd. and Meiji Seika Pharma Co., Ltd.Satoshi Iwata has received speaker's honorarium from AstellasPharma Inc., Pfizer Japan Inc., Taisho Toyama Pharmaceutical Co.,Ltd., MSD K.K., Meiji Seika Pharma Co., Ltd., Daiichi Sankyo Co., Ltd.and Japan Vaccine Co., Ltd., donation from Taisho Toyama Phar-maceutical Co., Ltd. and supported, in part, by a fund from NikonCorporation. Mitsuo Kaku has received speaker's honorarium fromTaisho Toyama Pharmaceutical Co., Ltd., Shionogi & Co., Ltd., PfizerJapan Inc. and Sumitomo Dainippon Pharma Co., Ltd. and donationfrom Astellas Pharma Inc. Junichi Kadota has received speaker's
honorarium from Taisho Toyama Pharmaceutical Co., Ltd., PfizerJapan Inc., MSD K.K., Kyorin Pharmaceutical Co., Ltd., Daiichi SankyoCo., Ltd., Glaxo SmithKline K.K., payments for a manuscript draftingand editing from Nankodo Co., Ltd. and donation from AstellasPharma Inc. Keisuke Sunakawa has received speaker's honorariumfrom Taisho Toyama Pharmaceutical Co., Ltd., Toyama Chemical Co.,Ltd. and Meiji Seika Pharma Co., Ltd. Hideaki Hanaki is a member ofa laboratory endowed chair from Kohjin Bio Co., Ltd. Taiji Tsuka-moto has received speaker's honorarium from Astellas Pharma Inc.,and payments for a manuscript drafting and editing from RichHillMedical Inc. Shin Egawa has received donation from Takeda Phar-maceutical Co., Ltd., Astellas Pharma Inc., Asahi Kasei Corp. andEuro Meditech Co., Ltd. Soichi Arakawa has received speaker'shonorarium from Taisho Toyama Pharmaceutical Co., Ltd.
References
[1] Hamasuna R, Yasuda M, Ishikawa K, Uehara S, Takahashi S, Hayami H, et al.Nationwide surveillance of the antimicrobial susceptibility of Neisseria gon-orrhoeae from male urethritis in Japan. J Infect Chemother 2013;19:571e8.
[2] Clinical and Laboratory Standards Institute. Performance standards for anti-microbial susceptibility testing : twenty-second informational supplementM100-S22. PA, USA: CLSI; 2012.
[3] Ohnishi M, Saika T, Hoshina S, Iwasaku K, Nakayama S, Watanabe H, et al.Ceftriaxone-resistant Neisseria gonorrhoeae, Japan. Emerg Infect Dis 2011;17:148e9.
[4] Unemo M, Golparian D, Nicholas R, Ohnishi M, Gallay A, Sednaoui P. High-level cefixime- and ceftriaxone-resistant Neisseria gonorrhoeae in France:novel penA mosaic allele in a successful international clone causes treatmentfailure. Antimicrob Agents Chemother 2012;56:1273e80.
[5] Camara J, Serra J, Ayats J, Bastida T, Carnicer-Pont D, Andreu A, et al. Molecularcharacterization of two high-level ceftriaxone-resistant Neisseria gonorrhoeaeisolates detected in Catalonia, Spain. J Antimicrob Chemother 2012;67:1858e60.
[6] Shimuta K, Unemo M, Nakayama S, Morita-Ishihara T, Dorin M, Kawahata T,et al. Antimicrobial resistance and molecular typing of Neisseria gonorrhoeaeisolates in Kyoto and Osaka, Japan, 2010 to 2012: intensified surveillance afteridentification of the first strain (H041) with high-level ceftriaxone resistance.Antimicrob Agents Chemother 2013;57:5225e32.
[7] Chisholm SA, Dave J, Ison CA. High-level azithromycin resistance occurs inNeisseria gonorrhoeae as a result of a single point mutation in the 23S rRNAgenes. Antimicrob Agents Chemother 2010;54:3812e6.
[8] Galarza PG, Abad R, Canigia LF, Buscemi L, Pagano I, Oviedo C, et al. Newmutation in 23S rRNA gene associated with high level of azithromycinresistance in Neisseria gonorrhoeae. Antimicrob Agents Chemother 2010;54:1652e3.
[9] Katz AR, Komeya AY, Soge OO, Kiaha MI, Lee MV, Wasserman GM, et al.Neisseria gonorrhoeae with high-level resistance to azithromycin: case reportof the first isolate identified in the United States. Clin Infect Dis 2012;54:841e3.
[10] Unemo M, Golparian D, Hellmark B. First three Neisseria gonorrhoeae isolateswith high-level resistance to azithromycin in Sweden: a threat to currentlyavailable dual-antimicrobial regimens for treatment of gonorrhea? Anti-microb Agents Chemother 2014;58:624e5.
[11] Palmer HM, Young H, Winter A, Dave J. Emergence and spread ofazithromycin-resistant Neisseria gonorrhoeae in Scotland. J Antimicrob Che-mother 2008;62:490e4.
[12] Japanese Society of Sexually Transmitted Infection. Gonococcal infection.Sexually transmitted infections, diagnosis and treatment guidelines 2011 (inJapanese) Jpn J Sex Transm Dis 2011;22:52e9.
[13] Surveillance of antibiotic resistance in Neisseria gonorrhoeae in the WHOwestern pacific and south east Asian regions, 2009. Commun Dis Intell2011;35:2e7.
[14] Unemo M, Golparian D, Hestner A. Ceftriaxone treatment failure of pharyn-geal gonorrhoea verified by international recommendations, Sweden, July2010. Euro Surveill 2011;16.
[15] Unemo M, Golparian D, Potocnik M, Jeverica S. Treatment failure of pharyn-geal gonorrhoea with internationally recommended first-line ceftriaxoneverified in Slovenia, September 2011. Euro Surveill 2012;17.
[16] YC M, Stevens K, Tideman R, Zaia A, Tomita T, Fairley CK, et al. Failure of 500mg of ceftriaxone to eradicate pharyngeal gonorrhoea, Australia. J AntimicrobChemother 2013;68:1445e7.
[17] Read PJ, Limnios EA, McNulty A, Whiley D, Lahra MM. One confirmed and onesuspected case of pharyngeal gonorrhoea treatment failure following 500 mgceftriaxone in Sydney, Australia. Sex Health 2013;10:460e2.
[18] Deguchi T, Yasuda M, Yokoi S, Ishida K, Ito M, Ishihara S, et al. Treatment ofuncomplicated gonococcal urethritis by double-dosing of 200 mg cefixime ata 6-h interval. J Infect Chemother 2003;9:35e9.
[19] Ohnishi M, Golparian D, Shimuta K, Saika T, Hoshina S, Iwasaku K, et al. IsNeisseria gonorrhoeae initiating a future era of untreatable gonorrhea?:
R. Hamasuna et al. / J Infect Chemother 21 (2015) 340e345344

― 203 ―
detailed characterization of the first strain with high-level resistance to cef-triaxone. Antimicrob Agents Chemother 2011;55:3538e45.
[20] Unemo M, Shafer WM. Antimicrobial resistance in Neisseria gonorrhoeae inthe 21st century: past, evolution, and future. Clin Microbiol Rev 2014;27:587e613.
[21] Tanaka M, Nakayama H, Notomi T, Irie S, Tsunoda Y, Okadome A, et al.Antimicrobial resistance of Neisseria gonorrhoeae in Japan, 1993-2002:continuous increasing of ciprofloxacin-resistant isolates. Int J AntimicrobAgents 2004;1:S15e22.
[22] Takayama Y, Nakayama S, Shimuta K, Morita-Ishihara T, Ohnishi M. Charac-terization of azithromycin-resistant Neisseria gonorrhoeae isolated in Tokyoin 2005e2011. J Infect Chemother 2014;20:339e41.
[23] Yasuda M, Ito S, Kido A, Hamano K, Uchijima Y, Uwatoko N, et al. A single 2 goral dose of extended-release azithromycin for treatment of gonococcalurethritis. J Antimicrob Chemother 2015;69:3116e8.
[24] Tapsall JW, Ndowa F, Lewis DA, Unemo M. Meeting the public health chal-lenge of multidrug- and extensively drug-resistant Neisseria gonorrhoeae.Expert Rev Anti Infect Ther 2009;7:821e34.
R. Hamasuna et al. / J Infect Chemother 21 (2015) 340e345 345
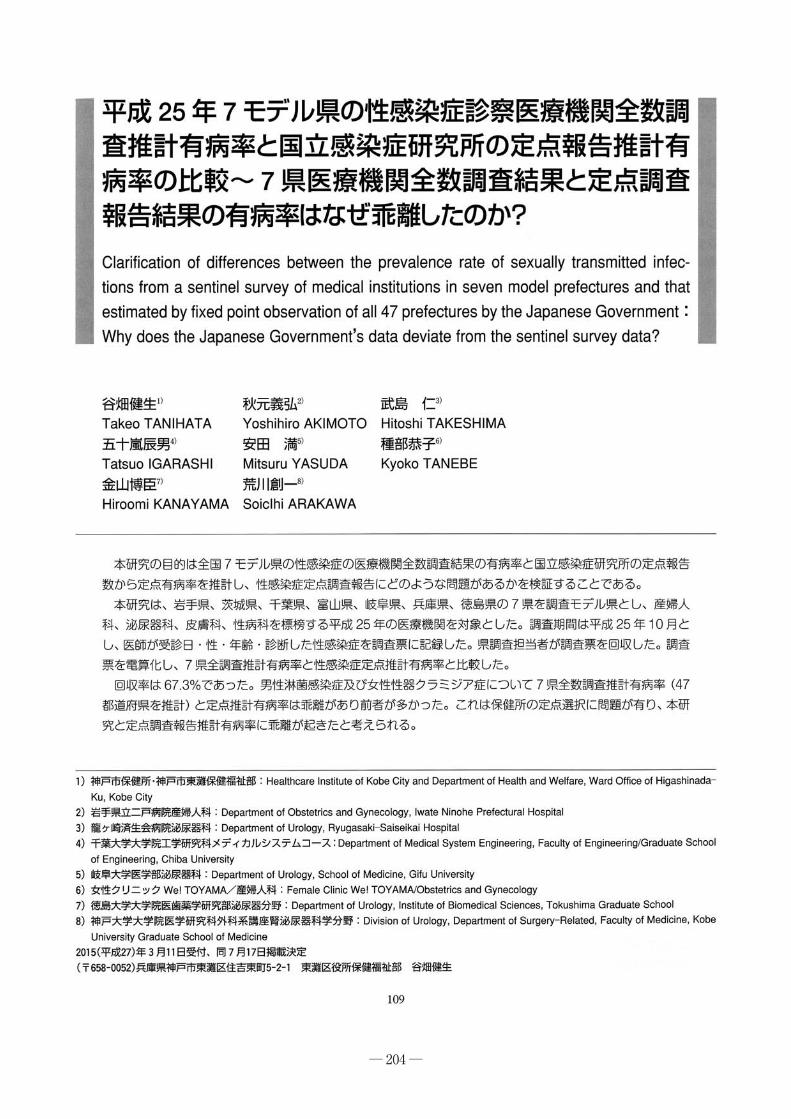
― 204 ―

― 205 ―

― 206 ―

― 207 ―

― 208 ―

― 209 ―

― 210 ―

― 211 ―

― 212 ―

― 213 ―

― 214 ―

― 215 ―

― 216 ―
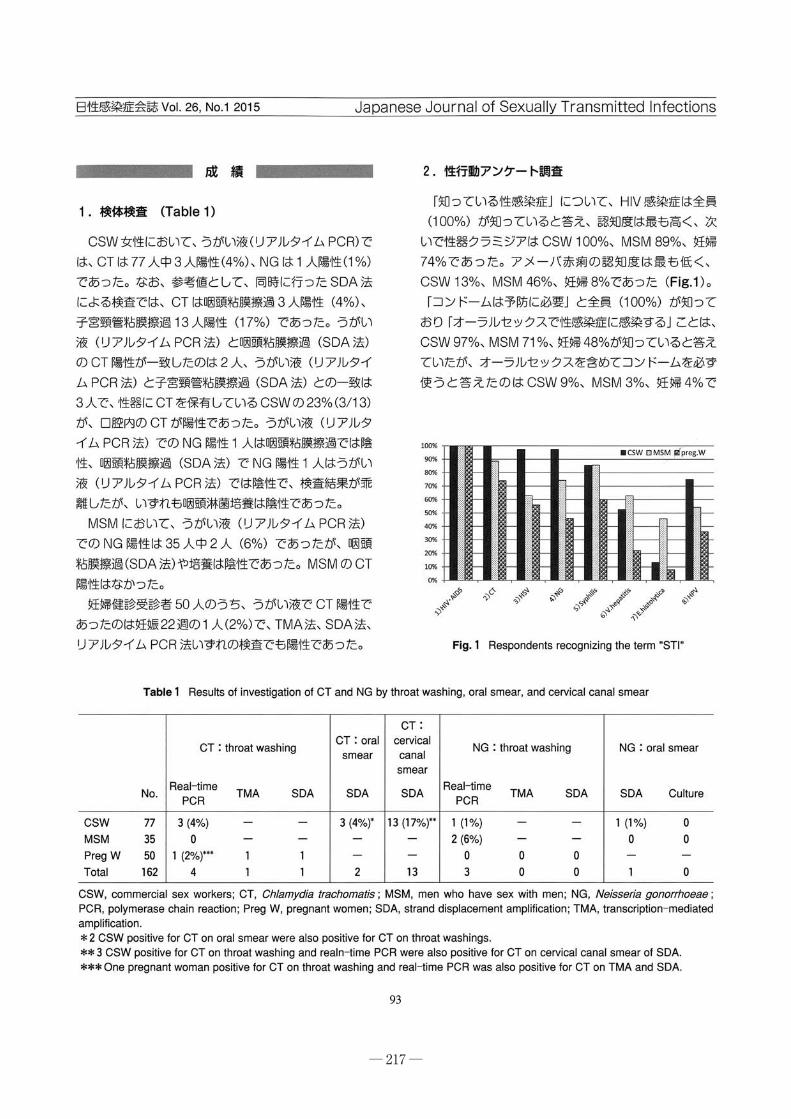
― 217 ―

― 218 ―

― 219 ―

― 220 ―

― 221 ―
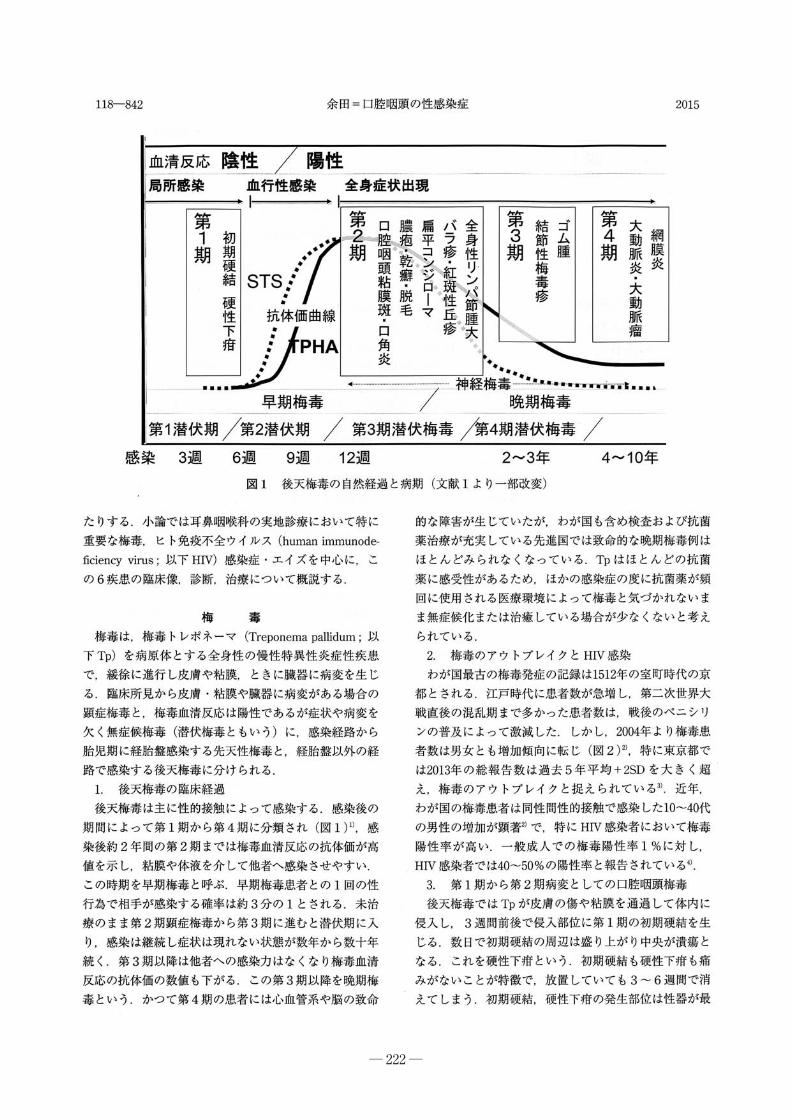
― 222 ―

― 223 ―

― 224 ―
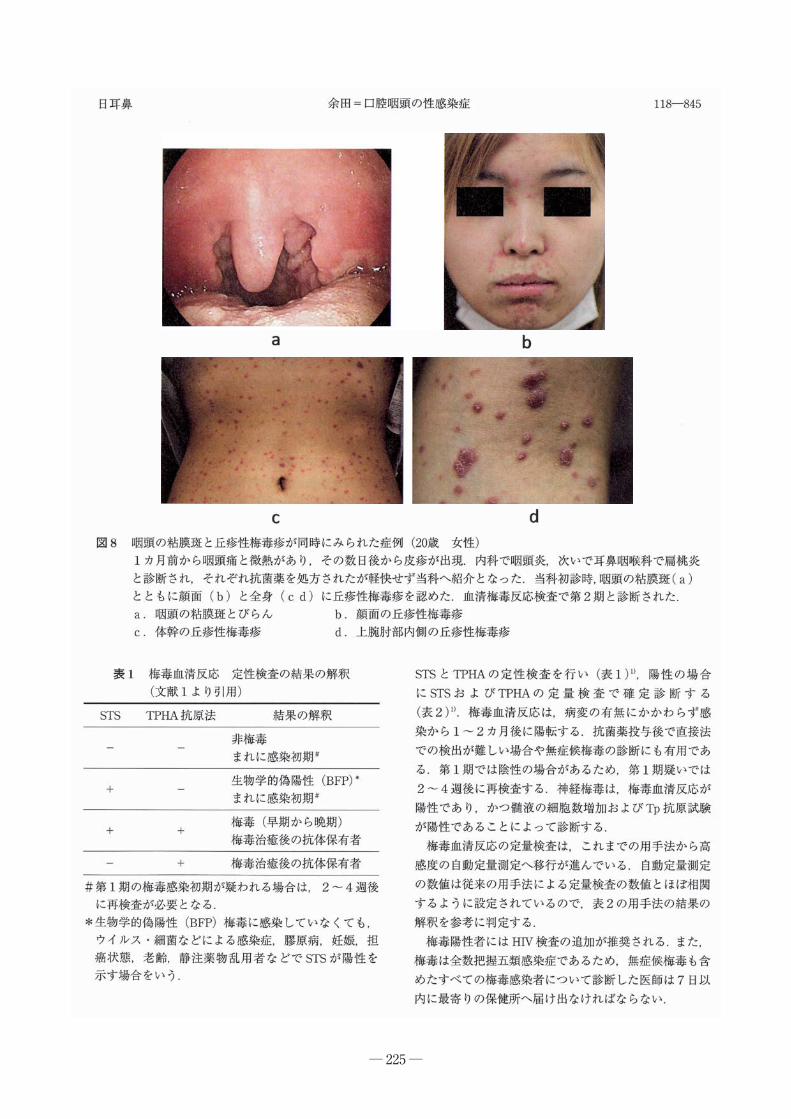
― 225 ―

― 226 ―

― 227 ―

― 228 ―

― 229 ―

― 230 ―
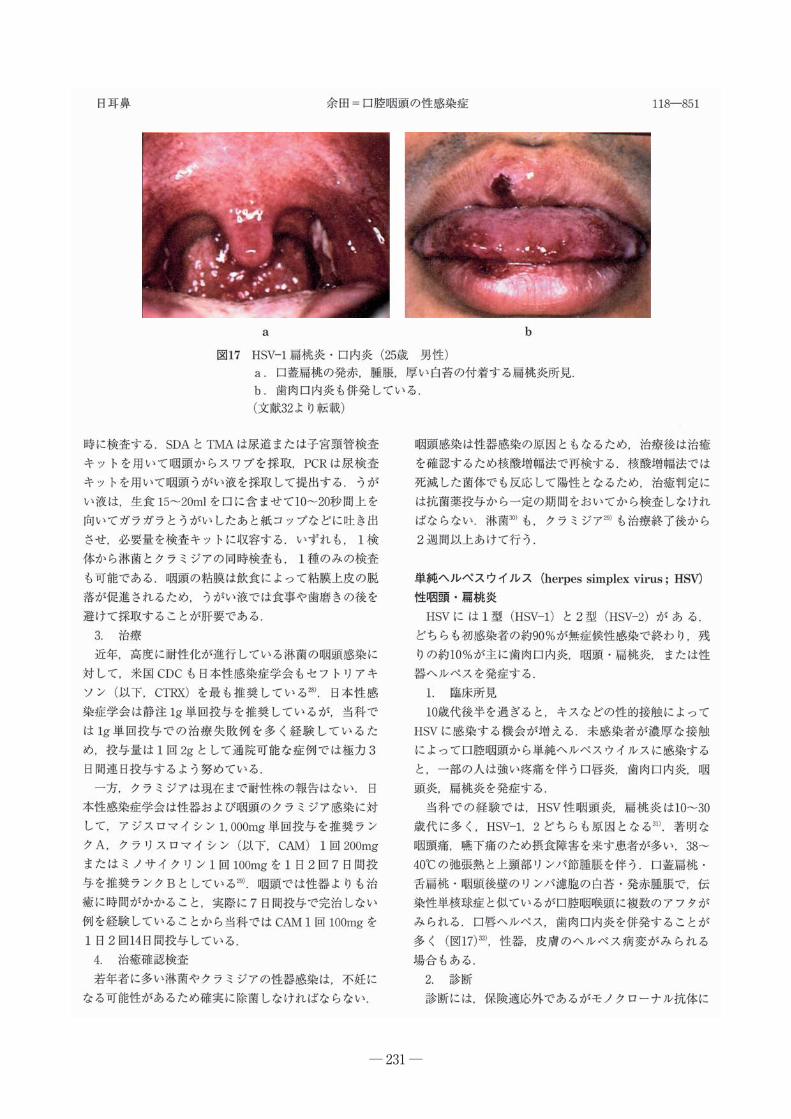
― 231 ―

― 232 ―
― 233 ―

― 234 ―
Abstract
Key words

― 235 ―

― 236 ―

― 237 ―

― 238 ―
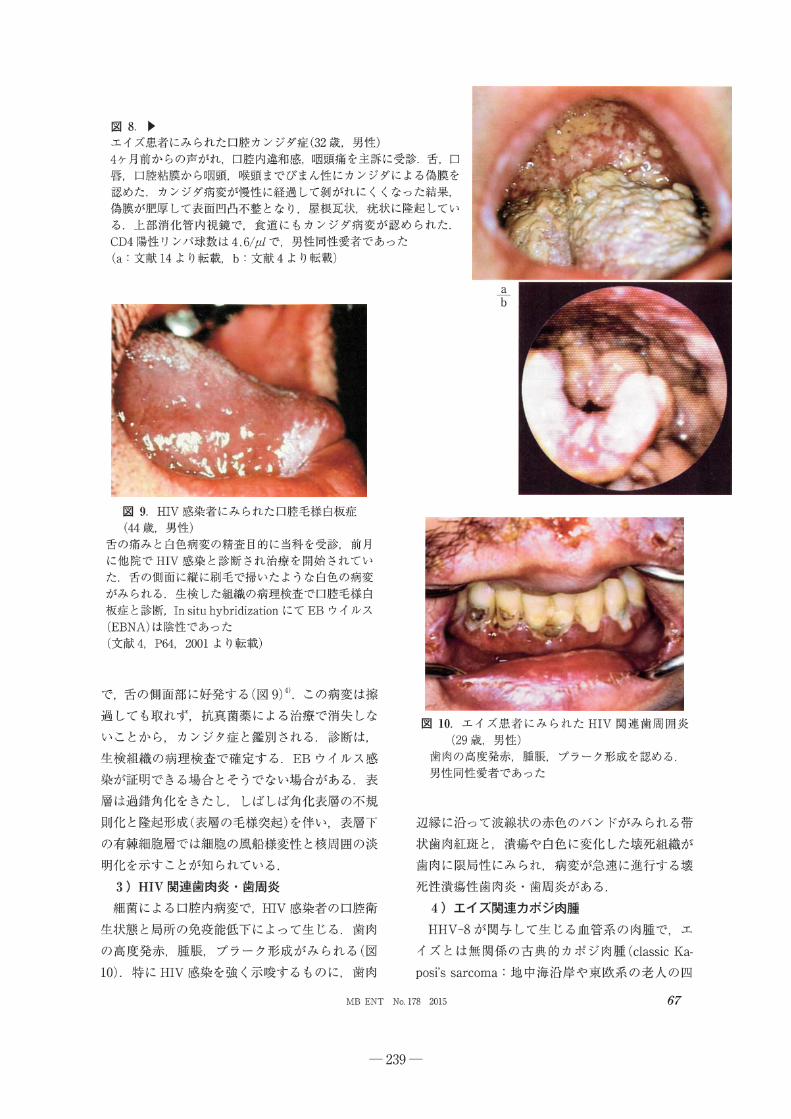
― 239 ―

― 240 ―

― 241 ―

― 242 ―

― 243 ―
Summary
Summary
Summary

― 244 ―
Summary

― 245 ―
Abstract

― 246 ―

― 247 ―

― 248 ―

― 249 ―

― 250 ―

― 251 ―

― 252 ―

― 253 ―
Summary
Summary
Summary
Summary
Summary

― 254 ―
Original article
Efficacy and safety of metronidazole injection for the treatment ofinfectious peritonitis, abdominal abscess and pelvic inflammatorydiseases in Japan
Hiroshige Mikamo a, Miyako Matsumizu b, *, Yoshiomi Nakazuru c,Masahito Nagashima a, b
a Department of Clinical Infectious Diseases, Aichi Medical University Graduate School of Medicine, Aichi, Japanb Clinical Research, Development Japan, Pfizer Japan Inc., Tokyo, Japanc Clinical Statistics, Development Japan, Pfizer Japan Inc., Tokyo, Japan
a r t i c l e i n f o
Article history:Received 18 June 2014Received in revised form6 October 2014Accepted 7 October 2014Available online 28 November 2014
Keywords:MetronidazoleCeftriaxoneInfectious peritonitisAbdominal abscessPelvic inflammatory diseasesMetronidazole/ceftriaxone combinationtherapy
a b s t r a c t
Although metronidazole (MNZ) has been used worldwide for more than 4 decades as a standard therapyfor trichomoniasis, anaerobic and amebic infections, resistance to MNZ is still low. MNZ is available asoral, intravenous, and vaginal formulations, but the intravenous formulation of MNZ has not beenapproved in Japan. We conducted a phase 3 study to evaluate the efficacy and safety of intravenous MNZcombined with ceftriaxone (CTRX) in Japanese subjects with infectious peritonitis, abdominal abscess orpelvic inflammatory diseases (PIDs) to obtain regulatory approval. A combination of MNZ/CTRX at dosesof 500 mg 3 or 4 times a day/1 or 2 g twice a day was administered intravenously to a total of 38hospitalized subjects. MNZ/CTRX was well tolerated and exhibited excellent clinical and bacteriologicalefficacy with clinical efficacy rates of 100% (20/20) in infectious peritonitis or abdominal abscess subjectsand 90.0% (9/10) in PID subjects, and the eradication rates in infectious peritonitis or abdominal abscesssubjects and PID subjects were 100% (16/16) and 100% (4/4), respectively, at the test of cure. MNZ/CTRXwas effective in 1 subject in whom a metallo-b-lactamase-producing Bacteroides fragilis strain (MIC ofMNZ, 2 mg/ml) was identified. The most common treatment-related adverse event was diarrhea (23.7%),followed by nausea (5.3%). No new safety signals were identified. MNZ/CTRX demonstrated excellentefficacy and was well tolerated in Japanese infectious peritonitis, abdominal abscess and PID subjects.This treatment regimen can be useful for anaerobic infections.
Clinical registration number: NCT01473836.© 2014, Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases.
Published by Elsevier Ltd. All rights reserved.
1. Introduction
Metronidazole (MNZ) is a nitroimidazole antimicrobial agentwith a potent anti-anaerobic, amebicidal, and antiprotozoal activ-ity. Intravenous (IV) MNZ (MNZ-IV) has been used worldwide formore than 30 years as the standard therapy for the treatment oftrichomoniasis, anaerobic and amebic infections [1e5]. Harrison'sPrinciples of Internal Medicine and the Sanford Guide to Antimi-crobial Therapy recommend the use of MNZ-IV for the treatment ofinfections involving commonly encountered anaerobic gram-negative rods [6] and anaerobic infections [7] respectively. The
guideline of the Infectious Diseases Society of America (IDSA) forthe Diagnosis and Management of Complicated Intra-abdominalInfection in Adults and Children, the 2010 Sexually transmitteddisease treatment guidelines of the Centers for Disease Control andPrevention (CDC), and the IDSA practice guidelines for the diag-nosis and management of skin and soft-tissue infections [8e10]also recommended the use of MNZ for various infections.
MNZ-IV has not been developed in Japan. Antimicrobial agentspresently used for the treatment of anaerobic infections in Japanare penicillins, b-lactam/b-lactamase inhibitor combination drugs,and some cephalosporins, carbapenams, and clindamycin. How-ever, the emergence of resistance to penicillins, cephalosporins andclindamycin among clinically isolated pathogenic anaerobes hasraised great concern [11e13]. In recent years, a high prevalence ofresistance to clindamycin has been observed among the Bacteroides
* Corresponding author. Clinical Research, Development Japan, Pfizer Japan Inc.,3-22-7 Yoyogi, Shibuya-ku, Tokyo 151-8589, Japan. Tel.: þ81 3 5309 7010; fax: þ813 5309 9060.
E-mail address: [email protected] (M. Matsumizu).
Contents lists available at ScienceDirect
Journal of Infection and Chemotherapy
journal homepage: http: / /www.elsevier .com/locate/ j ic
http://dx.doi.org/10.1016/j.jiac.2014.10.0051341-321X/© 2014, Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
J Infect Chemother 21 (2015) 96e104

― 255 ―
fragilis group and non-fragilis Bacteroides spp., which are the mostcommon anaerobes isolated from intra-abdominal infections, aswell as Prevotella spp., a causative pathogen of aspiration pneu-monia [14,15]. Decreased susceptibility and the emergence ofresistance to carbapenems among the B. fragilis group and non-fragilis Bacteroides spp. have also been reported [16].
Although MNZ has been used as a therapeutic drug for in-fections for longer than 45 years, the rate of resistance to MNZamong anaerobes is still generally low. Therefore, MNZ is stillsuccessfully used for the treatment of anaerobic infections causedby Bacteroides spp., Fusobacterium spp., and Clostridium spp [17].
Infectious anaerobic diseases often result in a serious conditionand treatment with appropriate antimicrobials is crucial, becausepatients are highly compromised when the primary disease is se-vere. It is desirable that MNZ-IV would also be available in Japan forthe treatment of severe infectious diseases in hospitalized patientswho cannot take oral medication.
We planned this phase 3 study to evaluate the efficacy andsafety of MNZ-IV administered at a dose of 500 mg 3 times a day(TID), or 4 times a day (QID) in severe cases, to Japanese adult pa-tients with infectious peritonitis, abdominal abscess or PID incombination with IV ceftriaxone (CTRX).
2. Subjects and methods
This study was conducted in accordance with the InternationalConference on Harmonisation of Good Clinical Practice Guidelines,the principle of the Declaration of Helsinki, and all applicable lawsand regulations at 15 medical centers nationwide in Japan betweenNovember 2011 and October 2012. The protocol was reviewed andapproved by the Institutional Review Boards of all participatingstudy sites. All subjects provided written informed consent beforeenrollment.
2.1. Study design
This multicenter, non-randomized, unblinded, non-comparativephase 3 study was designed to investigate the safety and efficacyprofile of MNZ-IV in Japanese subjects with infectious peritonitis,abdominal abscess or PID in combinationwith CTRX. A Data ReviewCommittee (DRC) was organized as an independent organization toperform objective and unified efficacy evaluation based on theclinical condition and diagnostic imaging findings. All subjectsreceived 500 mg MNZ administered by intravenous infusion over20 min TID (or QID in subjects with refractory or severe infection)for 3e14 days in general. At the investigator's discretion, theduration of treatment could be prolonged for up to 21 daysdepending on the subject's condition. All subjects received CTRX asa combination drug for the same period as MNZ-IV. CTRX, a 3rd-generation cephalosporin with broad-spectrum activity againstaerobic bacteria is widely used in Japan and its efficacy and safetyprofiles are well established. Overseas textbooks and guidelinesrecommend MNZ combined with agents that have antibiotic ac-tivity against aerobic pathogens, and for infectious peritonitis orabdominal abscess subjects, the target of this study, MNZ combinedwith 3rd generation cephalosporin antibacterial drugs, becauseinfections caused by anaerobic pathogens, the target diseases ofthis study, are often mixed infections including aerobic pathogens,and MNZ is not effective against them. Since CTRX can be given tosubjects once a day, it is considered useful in terms of decreasingthe burden on subjects. We therefore decided to use CTRX as thecombined drug. MNZ-IV was studied based on the following: (1)The safety and efficacy of MNZ-IV has been demonstrated; and (2)the development of MNZ-IV was requested by the committee on“Unapproved Drugs and Indications with Unmet Medical Needs”
under the Ministry of Health, Labour, andWelfare of Japan, becauseit is an unapproved drug with high medical needs. As a result of aconsultation with the Pharmaceutical and Medical Devices Agencyof Japan, the target number of subjects who meet the eligibilitycriteria and receive the test drugs was set at 30, provided that wecould enroll at least 7 subjects in whom bacterial transition couldbe evaluated with more than 80% probability, since the detectionrate of causative pathogens was assumed to be approximately 30%.
2.2. Eligibility criteria
Male and female subjects (for pelvic infections, subjects had tobe female) aged 16 years or older who had been diagnosed ashaving infectious peritonitis, abdominal abscess or PID, requiredhospitalization, and initial IV antibacterial therapy were eligible.
The diagnostic criteria for infectious peritonitis or abdominalabscess included: confirmed infectious peritonitis or abdominalabscess based on the presence of symptoms and signs of an in-flammatory response (fever, increased white blood cell [WBC]count, CRP elevation), imaging findings, and the abdominal signsand symptoms (lower abdominal pain, lower abdominal tender-ness, upper abdominal pain, upper abdominal tenderness,abdominal rebound, abdominal guarding, nausea, vomiting,decreased appetite, abdominal distension, diarrhea, constipation,drainage, or abscess), and meeting either of the following criteria:1) planned (or performed within the previous 24 h) drainage ofinfective sites; and 2) for postoperative infectious peritonitis orabdominal abscess, confirmed gastrointestinal tract secretion orpurulent discharge from an indwelling drain.
The diagnostic criteria for PID and related diseases (endome-tritis, myometritis, adnexitis, salpingitis, oophoritis, parametritis,pelvic peritonitis, pelvic abscess, Douglas' abscess, perihepatitis,and perihepatic abscess) included: (1) one of the following symp-toms should be observed: 1) lower abdominal pain or lowerabdominal tenderness; 2) uterus/uterine adnexa pain or uterus/uterine adnexa tenderness; and 3) hypochondrial pain or hypo-chondrial tenderness; (2) negative for Chlamydia trachomatis; (3)once the above criteria are satisfied, one of the following 6 condi-tions should be observed: 1) fever �37 �C (axillary); 2) WBCcount > upper limit of normal range; 3) CRP > upper limit of normalrange; 4) purulent discharge or pus observed by culdocentesis orlaparoscopy; 5) pelvic abscess confirmed by ultrasonography; and6) positive for Neisseria gonorrhoeae.
Exclusion criteria included the following: subjects who hadundergone surgery for perforation of the digestive tract within 12 h,or who had undergone surgery for perforation of gastroduodenalulcers within 24 h; subjects with suspected or confirmed simpleappendicitis, necrotizing pancreatitis, infectious mononucleosis,non-infectious peritonitis, or non-infectious endometriosis; sub-jects who did not undergo appropriate drainage; subjects expectedto be cured only by the surgical procedures (e.g., drainage) withoutantimicrobial treatment; subjects who had open abdominal cavitydrainage; subjects with hypersensitivity to, intolerance of oranother contraindication to MNZ or CTRX or other cephem antibi-otics; subjects with alcohol abuse; subjects with severe renaldysfunction; subjects with hepatic dysfunction; subjects with se-vere underlying disease or other complications; subjects whorequired additional systemic antibiotics; subjects who had receivedtreatment with systemic antibiotics within 7 days before the study;subjects who had already received MNZ for the disease; subjectswhose causative pathogens were insusceptible to MNZ; and preg-nant or lactating women.
The following concomitant medications were prohibited up tothe test of cure (TOC) assessment: systemic antibiotics (oral, in-jection); human immunoglobulin; colony-stimulating factor;
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104 97

― 256 ―
corticosteroids; continuous use of analgesic antipyretics; otherinvestigational drugs ormedical devices; and anti-malignant tumoragents.
2.3. Clinical and radiologic assessments
The primary efficacy endpoint was the clinical responseassessed by the DRC at the end of treatment (EOT) and TOC (1 weekafter EOT). Clinical efficacy was mainly assessed based on theevaluation of clinical signs and symptoms, body temperature, WBCcount, CRP, and diagnostic radiographic imaging findings. Theclinical responsewas evaluated as “effective (cured or improved)” ifall of the following criteria were met: (1) resolution (cure) orimprovement of all inflammatory and abdominal findings, and/orimaging abnormalities that were observed at the start of the study,at the assessment time point, and (2) treatment with other anti-biotics was not required during the study or after the assessmenttime point. The clinical response was evaluated as “ineffective” ifeither of the following criteria were met: (1) the requirements for“effective” assessment were not satisfied; or (2) the treatmentfailed and other systemic antibiotic therapy was applied to treat thetarget disease. The clinical response was evaluated as “indetermi-nate” if clinical efficacy assessmentwas difficult due tomissing dataor other reasons.
2.4. Bacteriological assessment
The secondary efficacy endpoint was the bacteriologicalresponse assessed by the DRC on Day 4, EOT, and TOC. At thebaseline visit, all subjects provided clinical specimens (infectionsites), which were sent to a central laboratory for culture and theisolated pathogens were tested for susceptibility according to theprocedures of the Clinical and Laboratory Standards Institute atbaseline, Day 4, EOT, and TOC. The specimens from PID subjects(intrauterine materials, puncture fluid from Douglas' pouch, or apurulent discharge) were also submitted for detection ofC. trachomatis, N. gonorrhoeae, or Mycoplasma genitalium,M. hominis using antigen tests at baseline, EOT, and TOC.
The bacteriological responsewas assessed as “eradication” if theoriginal pathogen was not identified in the specimens; “presumederadication” if evaluable specimens were not obtained from a focusof infection; “colonization” if an organism was isolated from asubject who had no signs or symptoms of infection; “persistence” ifthe original pathogen remained in the specimens; “presumedpersistence” if a culture was difficult or was not done in subjectswho were judged to be clinical failures and persistence of theoriginal pathogen was presumed; “replacement bacterium” if theoriginal pathogens were eradicated by treatment but other newpathogens had appeared in the same specimen with symptoms orfindings of infection; “superinfection” if a pathogen other than theoriginal pathogens was isolated from a specimen taken while thesubject was on therapy and who had signs and symptoms ofinfection; “recurrence” if the original pathogen was isolated from aspecimen culture taken after the TOC visit; and “indeterminate” if aspecimen was not assessed according to the above-mentionedcriteria for various reasons.
2.5. Safety assessment
Safety data were obtained from the findings of clinical signs/symptoms, physical examinations, vital signs, and laboratory dataup to TOC. The causality and severity of the adverse events wereevaluated by the investigators (or sub-investigators), based on theMedDRA terminology.
2.6. Statistical analysis
Efficacy analyses were mainly conducted on the Clinical PerProtocol Set (CPPS) and the Bacteriologic Per Protocol Set (BPPS).The CPPS consisted of all subjects in the Full Analysis Set (FAS) whohad no significant protocol violations and who underwent theprescribed evaluations during the observation period as specified inthe protocol. The BPPS consisted of all subjects in the CPPS inwhomcausative pathogens were identified by culture and antigen tests atbaseline.
The primary endpoint was the clinical efficacy assessed by theDRC at EOT and TOC. As the primary analysis of the primaryendpoint, the efficacy rate and its 95% confidence interval (CI) werecalculated at the TOC in the CPPS. The efficacy rate and its 95% CIwere also calculated for infectious peritonitis or abdominal abscessand for PID.
For analysis of the bacteriological response, the secondaryendpoint, assessed by the DRC, the eradication rate and its 95% CIwere calculated for the BPPS.
Safety analysis was performed in the “Safety Analysis Set,” thepopulation of subjects who received at least 1 dose of the studydrug.
3. Results
3.1. Subject disposition
A total of 38 subjects were enrolled at 15 medical centers inJapan and all of them received the study medication. Of these, 6subjects (15.8%) discontinued the study (Table 1). Among the totalof 38 subjects, 23 were diagnosed as having infectious peritonitis orabdominal abscess and 13 with PID. Two subjects were judged tohave a disease not included in this study; 1 subject was diagnosedas having lumbar disc herniation by the investigator after enroll-ment and the other as having suspected PID (non-infectious dis-ease) by the DRC. Since 3 of the 23 infectious peritonitis orabdominal abscess subjects in the FAS were excluded because theyhad received prohibited concomitant medications (2 subjects) orlacked theminimum 3 days of dosing (1 subject), the CPPS included20 subjects with infectious peritonitis or abdominal abscess. The
Table 1Subject disposition and analysis set.
Total Diagnosis
Infectiousperitonitis orabdominalabscess
PID
SubjectEnrolled and treated 38a 23 13Completed 32b(84.2) 22 (95.7) 9 (69.2)Discontinued 6 (15.8) 1 (4.3) 4 (30.8)Deviation of inclusion criteria 1c (2.6) 0 0Insufficient efficacy 1 (2.6) 0 1 (7.7)Adverse event 4 (10.5) 1 (4.3) 3 (23.1)Not related to the study drug 3 (7.9) 0 3 (23.1)Related to the study drug 1 (2.6) 1 (4.3) 0
Values represent the number (%) of subjects.PID: pelvic inflammatory disease.
a Thirty-eight subjects included 2 subjects who were judged by the Data ReviewCommittee to have a disease not included in the study and who did not have in-fectious peritonitis, abdominal abscess or PID.
b One subject was diagnosed as having suspected PID (non-infectious disease) bythe DRC and did not have infectious peritonitis, abdominal abscess or PID.
c The subject was diagnosed as having lumbar disc herniation by the investigatorafter enrollment and did not have infectious peritonitis, abdominal abscess or PID.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e10498

― 257 ―
BPPS included 17 subjects with infectious peritonitis or abdominalabscess in whom baseline causative pathogens were identified byculture. Since 3 of the 13 PID subjects in the FAS were excludedbecause they met the exclusion criteria (2 subjects) or lacked theminimum 3 days of dosing (1 subject), the CPPS included 10 sub-jects with PID. The BPPS included 4 subjects with PID in whom thebaseline causative pathogens were identified by culture.
The baseline demographic characteristics of the subjects aresummarized in Table 2.
The details of the diagnoses in the CPPS are shown in Table 3.Eleven of 20 infectious peritonitis or abdominal abscess subjectshad both abdominal abscess and infectious peritonitis. Among 10PID subjects, 5 subjects had an abscess.
The average duration of treatment with MNZ-IV was 5.8 days(range: 3e9 days) for infectious peritonitis or abdominal abscesssubjects and 8.3 days (range: 5e14 days) for PID subjects in theCPPS. Most subjects received 500 mg of MNZ-IV TID. Only 2 sub-jects in the CPPS (1 subject with both infectious peritonitis andabdominal abscess and 1 subject with PID) received MNZ-IV QID.
At baseline, 29 causative pathogens were identified in 21 sub-jects (70.0%) in the CPPS (Table 4). Among infectious peritonitis orabdominal abscess subjects, 9 subjects had mixed infections withanaerobic and aerobic pathogens, 3 subjects had anaerobic in-fections, and 5 subjects had aerobic infections. For PID subjects, 2subjects had mixed infections with anaerobic and aerobic patho-gens and 2 subjects had aerobic infections. The major causativeanaerobic pathogens identified at baseline were B. fragilis (5strains), Parvimonas micra and Bacteroides thetaiotaomicron (2strains each) in the CPPS.
3.2. Efficacy results
For the clinical response assessed by the DRC in the CPPS (pri-mary endpoint), the overall efficacy rate was 96.7% (95% CI: 82.8%e99.9%) at TOC (primary analysis) and 96.6% (95% CI: 82.2%e99.9%)at EOT (secondary analysis) (Table 5). The efficacy rate was 100% inthe subjects with infectious peritonitis or abdominal abscess and90.0% in the subjects with PID, both at TOC and EOT. The therapyfailed only in 1 subject with PID (pelvic peritonitis).
For the clinical response by causative pathogen assessed by theDRC in the BPPS, the efficacy rate was 100% for all pathogens at EOTand TOC.
For the bacteriological response in the BPPS overall assessed bythe DRC, the eradication rate was 100% on Day 4, EOT and TOC(Table 6). The eradication rates were also 100% in all subjects withinfectious peritonitis or abdominal abscess and PID on Day 4, EOTand TOC (Table 6). TheMICs ofMNZ against the identified anaerobicpathogens ranged from �0.06 to >128 mg/ml (Tables 7 and 8).
Among the 8 subjects with infectious peritonitis or abdominalabscess who had 10 strains of anaerobic pathogens with resistanceto other antimicrobials than MNZ and CTRX, the clinical responsewas assessed as cured or improved, except for 1 subject who wasjudged as indeterminate at EOT, and the bacteriological responsewas assessed as eradication or presumed eradication except in 2subjects who were judged as colonization and indeterminate (1subject each) (Table 9).
3.3. Safety results
Among 38 subjects, 14 subjects (36.8%) experienced treatment-related adverse events during the entire treatment period. Themost common treatment-related adverse event was diarrhea (9subjects), followed by nausea (2 subjects), and vomiting andabdominal pain upper (1 subject each). The majority of adverse
Table 2Demographic characteristics.
Group FAS CPPS BPPS
Infectious peritonitis or abdominal abscessNumber of subjects 23 20 17SexMale 14 12 11Female 9 8 6
Age (years)16 � 44 6 (26.1) 6 (30.0) 4 (23.5)45 � 64 8 (34.8) 8 (40.0) 8 (47.1)65 � 74 5 (21.7) 4 (20.0) 4 (23.5)75 � 79 4 (17.4) 2 (10.0) 1 (5.9)Mean ± SD 55.5 ± 16.3 52.7 ± 15.6 53.6 ± 13.7Range 25 � 78 25 � 78 25e75
Weight (kg)�45 kg 2 (8.7) 2 (10.0) 1 (5.9)>45 kg 21 (91.3) 18 (90.0) 16 (94.1)Mean ± SD 64 ± 14.3 64.4 ± 14.8 65.6 ± 14.9Range 44.0e108.5 44.0e108.5 45.0e108.5
PIDNumber of subjects 13 10 4SexFemale 13 10 4
Age (years)16e19 1 (7.7) 1 (10.0) 020e29 1 (7.7) 0 030e39 5 (38.5) 4 (40.0) 2 (50.0)�40 6 (46.2) 5 (50.0) 2 (50.0)Mean ± SD 39.4 ± 12.8 41.3 ± 13.2 39.0 ± 1.8Range 19 � 67 19 � 67 37 � 41
Weight (kg)�45 kg 2 (15.4) 2 (20.0) 0>45 kg 11 (84.6) 8 (80.0) 4 (100)Mean ± SD 55.1 ± 13.2 54.5 ± 14.5 63.1 ± 19.3Range 40.0e90.5 40.0e90.5 45.3e90.5
FAS: full analysis set; CPPS: clinical per protocol set; BPPS: bacteriologic per protocolset; PID: pelvic inflammatory disease.
Table 3Details of diagnosis in the CPPS.
Diagnosis Infection site N ¼ 30
Infectious peritonitis orabdominal abscess
20
Abdominal abscess Appendix, peritoneal cavity,mesentery, sigmoid colon,perihepatic area, ascending colon
6
Abdominal abscess,infectious peritonitis
Appendix, peritoneal cavity,peritoneum, douglas' pouch, smallintestine, colon, stomach, others
11
Infectious peritonitis Peritoneum, small intestine,sigmoid colon, appendix
3
PID 10Douglas abscess, pelvicperitonitis, tubo-ovarianabscess
Douglas' pouch, pelvic peritoneum,bilateral uterine, adnexia
1
Adnexal abscess, adnexitis,pelvic peritonitis
Right adnexia, pelvic peritoneum 1
Adnexal abscess, pelvicperitonitis
Left adnexia, pelvic peritoneum 1
Adnexitis, endometritis,pelvic peritonitis
Left adnexia, uterus, pelvicperitoneum
1
Adnexitis, intrauterineinfection, pelvic peritonitis
Right adnexia, uterus, pelvicperitoneum
1
Adnexitis, pelvic peritonitis Right adnexia, pelvic peritoneum 1Pelvic peritonitis Pelvic peritoneum 2Adnexitis, right adnexalabscess
Right adnexia 1
Right ovarian abscess Right ovary 1
Values represent the number of subjects.CPPS: clinical per protocol set; N: number of subjects evaluated; PID: pelvic in-flammatory disease.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104 99

― 258 ―
events occurred within 6 days after starting the treatment, and wasmild to moderate in severity. There were no treatment-relatedadverse events associated with intravenous injection.
One subject discontinued the study because of treatment-related adverse events (atrial fibrillation and sinus tachycardia),
which occurred after extubation following ileocecal resection sur-gery on Day 2. These adverse events were mild and moderate inseverity and resolved after discontinuation of the studymedication.
There were no deaths or treatment-related serious adverseevents reported during the entire period.
4. Discussion
Overall, MNZ-IV combined with CTRX exhibited excellent clin-ical and bacteriological efficacy for the treatment of infectiousperitonitis, abdominal abscess and PID in Japanese subjects.
It is noted that MNZ-IV/CTRX was also effective in 1 subject whohad sepsis complicated by infectious peritonitis, indicating theeffectiveness of this dosing regimen in the treatment of patientswith severe complications of sepsis [18,19].
The combination therapy failed only in 1 subject with PID(pelvic peritonitis) who received MNZ-IV/CTRX for 8 days.Although the spontaneous abdominal pain and tenderness, and thespontaneous pain of the uterus and its appendages improved,tenderness of the uterus and its appendages remained, and a highWBC count (12,600/mm3) and CRP (8.5 mg/dl) as well as aggrava-tion on computerized tomography and ultrasonic imaging wereobserved at EOT, the subject discontinued the study. This subjectrecovered after administration of piperacillin, minocyline, andazithromycin. Since involvement of atypical microorganisms wasnot confirmed and no baseline causative pathogenswere identified,the clinical efficacy in this subject at EOT and TOC was assessed asineffective.
MNZ is known to have high antimicrobial activity against an-aerobes, including those identified in this study [5]. The MICs ofMNZ for most anaerobic pathogens identified in this study rangedfrom �0.06 to 2 mg/ml, which may be associated with the highefficacy for infectious peritonitis, abdominal abscess and PID.
Since MNZ has in vitro activity against most anaerobes includingPeptostreptococcus spp., Porphyromonas spp., Eubacterium spp.,Veillonella spp., and Clostridium tetanii, which were not identified inthis study [5,20,21], MNZ-IV may be effective to treat infectionscaused by these anaerobes. However, it is noted that MNZ is notactive in vitro against Actinomyces spp. or Propionibacterium acnes[22,23].
MNZ-IV/CTRX was also effective for mixed infections withanaerobic and aerobic pathogens, which may result due to theantibacterial activity of MNZ on anaerobes and the antibacterialactivity of CTRX on aerobes. When it is suspected that patients havemixed infections with anaerobic and aerobic pathogens, it isdesirable to use MNZ combined with an antibiotic drug that hasantibacterial activity on aerobes as recommended by many thera-peutic guidelines.
For the treatment of anaerobic infections, the long-term use ofantianaerobic agents including b-lactam/b-lactamase-inhibitor
Table 4Number of subjects in the CPPS classified by identified pathogen.
Infectious peritonitis or abdominal abscessTotal number of subjects 20Total number of subjects in whom pathogens were identified 17
(85.0)Number of subjects in whom a single pathogen was identified 5
(25.0)Bacteroides fragilis 2Staphylococcus epidermidis* 1Escherichia coli 2
Number of subjects in whom multiple pathogens were identified 12(60.0)
2 pathogens identifiedParvimonas micra þ Escherichia coli 1Bacteroides thetaiotaomicron þ Escherichia coli 1Bacteroides vulgatus þ Escherichia coli 1Enterococcus avium þ Escherichia coli 1Escherichia coli þ Morganella morganii 1
3 pathogens identifiedBacteroides fragilis þ Streptococcus anginosus þ Escherichia coli 1Bacteroides fragilis þ Streptococcus constellatus þ Escherichia coli 1Bacteroides fragilis þ Enterococcus avium þ Klebsiella pneumoniae 1
4 or more pathogens identifiedEggerthella lenta þ Bacteroides xylanisolvens þ Escherichia coli þKlebsiella oxytoca
1
Parvimonas micra þ Bacteroides salyersiae þ Bacteroidesthetaiotaomicron þ Fusobacterium nucleatum þ Escherichia coli
1
Clostridium sp. þ Bacteroides ovatus þ Fusobacteriumnecrophorum þ Streptococcus constellatus þ Escherichia coli
1
Streptococcus agalactiae þ Streptococcus constellatus þStreptococcus oralis þ Klebsiella pneumoniae þ Proteusmirabilis þ Edwardsiella tarda
1
PIDTotal number of subjects 10Total number of subjects in whom pathogens were identified 4
(40.0)Number of subjects in whom a single pathogen was identified 0
Number of subjects in whom multiple pathogens were identified 4(40.0)
2 pathogens identifiedFusobacterium nucleatum þ Streptococcus agalactiae 1Staphylococus haemolyticus þ Streptococus group G 1Streptococcus agalactiae þ Citrobacter koseri 1
4 pathogens identifiedGemella morbillorum þ Prevotella intermedia þ Streptococcusconstellatus þ Streptococcus sanguis
1
Values represent the number (%) of subjects.Underlined pathogens are anaerobic bacteria.*: mutating into obligatory anaerobe.CPPS: clinical per protocol set; PID: pelvic inflammatory disease.
Table 5Clinical response assessed by the Data Review Committee (CPPS).
Diagnosis Visit N Clinical response Efficacy ratea (%) 95% CI
Cure (%) Improved (%) Ineffective (%) Ind (%)
Overall EOT 30 4 (13.3) 24 (80.0) 1 (3.3) 1 (3.3) 96.6 (82.2e99.9)TOC 30 25 (83.3) 4 (13.3) 1 (3.3) 0 96.7 (82.8e99.9)
Infectious peritonitis or abdominal abscess EOT 20 1 (5.0) 18 (90.0) 0 1 (5.0) 100 (82.4e100.0)TOC 20 19 (95.0) 1 (5.0) 0 0 100 (83.2e100)
PID EOT 10 3 (30.0) 6 (60.0) 1 (10.0) 0 90.0 (55.5e99.7)TOC 10 6 (60.0) 3 (30.0) 1 (10.0) 0 90.0 (55.5e99.7)
Values represent the number (%) of subjects.CPPS: clinical per protocol set; N: number of subjects evaluated; Ind: indeterminate; CI: confidence interval; EOT: end of treatment; TOC: test of cure; PID, pelvic inflammatorydisease.
a Efficacy rate ¼ effective (cure þ improved)/(N � Ind) � 100.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104100

― 259 ―
Table 6Bacteriological response assessed by the Data Review Committee in the BPPS.
Diagnosis Visit n Bacteriological response Eradicationratea (%)
95% CI
Era P Era Col Per P per Mic Sup Rec Ind
Overall Day 4 13 11 (84.6) 2 (15.4) 0 0 0 0 0 0 0 100 75.3e100EOT 21 12 (57.1) 6 (28.6) 2 (9.5) 0 0 0 0 0 1 (4.8) 100 83.2e100TOC 21 4 (19.0) 17 (81.0) 0 0 0 0 0 0 0 100 83.9e100
Infectious peritonitis or abdominal abscess Day 4 9 7 (77.8) 2 (22.2) 0 0 0 0 0 0 0 100 66.4e100EOT 17 8 (47.1) 6 (35.3) 2 (11.8) 0 0 0 0 0 1 (5.9) 100 79.4e100TOC 17 0 17 (100) 0 0 0 0 0 0 0 100 80.5e100
PID Day 4 4 4 (100) 0 0 0 0 0 0 0 0 100 39.8e100EOT 4 4 (100) 0 0 0 0 0 0 0 0 100 39.8e100TOC 4 4 (100) 0 0 0 0 0 0 0 0 100 39.8e100
Values represent the number (%) of subjects.BPPS: bacteriologic per protocol set; n: number of subjects in whom infections were identified; Era: eradication; P Era: presumed eradication; Col: colonization; Per:persistence; P Per: presumed persistence; Mic: microbial substitution; Sup: superinfection; Rec: recurrence of infection; Ind: indeterminate; CI: confidence interval; EOT: endof treatment; TOC: test of cure; PID: pelvic inflammatory disease.
a Eradication rate ¼ (Era þ P Era þ Col)/(n � Ind) � 100.
Table 7Clinical response by MIC for anaerobic pathogens assessed by the Data Review Committee in the BPPS.
Pathogen MICa Visit n Clinical response Eradication rateb (%)
(mg/ml) Cure Improved Ineffective Ind
Infectious peritonitis or abdominal abscessEggerthella lenta 1/128 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Parvimonas micra 0.5/�0.06 EOT 2 0 2 (100) 0 0 100
TOC 2 2 (100) 0 0 0 100Clostridium spp. �0.06/1 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Bacteroides fragilis 1/>128 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 1002/4 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 1002/16 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 1002/32 EOT 1 0 1 (100) 0 0 100
TOC 1 0 1 (100) 0 0 1002/64 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Bacteroides salyersiae 1/32 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Bacteroides thetaiotaomicron 0.25/128 EOT 1 0 0 0 1 (100) e
TOC 1 1 (100) 0 0 0 1002/64 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Bacteroides vulgatus 0.25/>128 EOT 1 1 (100) 0 0 0 100
TOC 1 1 (100) 0 0 0 100Bacteroides xylanisolvens 1/32 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Bacteroides ovatus 2/>128 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Fusobacterium nucleatum �0.06/0.5 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Fusobacterium necrophorum NA EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100PIDGemella morbillorum >128/0.5 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Prevotella intermedia 0.5/�0.06 EOT 1 0 1 (100) 0 0 100
TOC 1 1 (100) 0 0 0 100Fusobacterium nucleatum �0.06/1 EOT 1 0 1 (100) 0 0 100
TOC 1 0 1 (100) 0 0 100
Values represent the number (%) of subjects.BPPS: bacteriologic per protocol set; n: number of subjects in whom pathogens were identified; Ind: indeterminate; EOT: end of treatment; TOC: test of cure; NA: notapplicable; PID: pelvic inflammatory disease.
a MIC of MNZ/MIC of CTRX.b Eradication rate ¼ (Cure þ Improved)/(n � Ind) � 100.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104 101

― 260 ―
combination, carbapenams, moxifloxacin, garenoxacin, and sita-floxacin resulted in the emergence of resistant pathogens and anincreased risk for Clostridium difficile infection. Increased resistancerates to clindamycin, which is used as an alternative antianaerobicagent, have also been reported among anaerobic pathogens[11e13,16]. Therefore, MNZ-IV/CTRX can be useful to treat anaer-obic infections as an antimicrobial therapy that prevents theemergence of drug-resistant strains.
MNZ-IV/CTRX was effective in 1 subject with both infectiousperitonitis and abdominal abscess inwhom ametallo-b-lactamase-producing B. fragilis strain (MIC of MNZ, 2 mg/ml) was identified.Since MNZ shows in vitro antimicrobial activity against metallo-b-
lactamase-producing carbapenem-resistant strains [24], MNZ mayprovide a useful option for the treatment of infectious diseaseinvolving metallo-b-lactamase-producing anaerobic pathogens.
The emergence rate ofMNZ-resistant anaerobes is generally low,but a slight decrease in susceptibility to MNZ among anaerobesincluding Bacteroides spp. has been reported [24,25]. The appro-priate use of MNZ is important for the treatment of anaerobic in-fections to prevent the emergence of MNZ-resistant anaerobes. It isthus desirable to not only administer MNZ, but also various anti-microbial classes equally for anaerobic infections to prevent theexcessive use of MNZ. Since clinicians frequently choose clindamy-cin for anaerobic infections, resistance to clindamycin is a growing
Table 8Bacteriological response by MIC for anaerobic pathogens assessed by the Data Review Committee in the BPPS.
Pathogen MICa
(mg/ml)Visit n Bacteriological response Eradication rateb (%)
Era P Era Col Per P Per Rec Ind
Infectious peritonitis or abdominal abscessEggerthella lenta 1/128 EOT 1 1 (100) 0 0 0 0 0 0 100
TOC 1 0 1 (100) 0 0 0 0 0 100Parvimonas micra 0.5/�0.06 Day 4 1 0 1 (100) 0 0 0 0 0 100
EOT 2 1 (50.0) 1 (50.0) 0 0 0 0 0 100TOC 2 0 2 (100) 0 0 0 0 0 100
Clostridium spp. �0.06/1 EOT 1 0 0 0 0 0 0 1 (100) e
TOC 1 0 1 (100) 0 0 0 0 0 100Bacteroides fragilis 1/>128 Day 4 1 1 (100) 0 0 0 0 0 0 100
EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
2/4 EOT 1 0 1 (100) 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
2/16 Day 4 1 1 (100) 0 0 0 0 0 0 100EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
2/32 EOT 1 0 0 1 (100) 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
2/64 Day 4 1 1 (100) 0 0 0 0 0 0 100EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
Bacteroides salyersiae 1/32 Day 4 1 0 1 (100) 0 0 0 0 0 100EOT 1 0 1 (100) 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
Bacteroides thetaiotaomicron 0.25/128 EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
2/64 Day 4 1 0 1 (100) 0 0 0 0 0 100EOT 1 0 1 (100) 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
Bacteroides vulgatus 0.25/>128 Day 4 1 0 1 (100) 0 0 0 0 0 100EOT 1 0 1 (100) 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
Bacteroides xylanisolvens 1/32 EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
Bacteroides ovatus 2/>128 EOT 1 0 0 0 0 0 0 1 (100) e
TOC 1 0 1 (100) 0 0 0 0 0 100Fusobacterium nucleatum �0.06/0.5 Day 4 1 0 1 (100) 0 0 0 0 0 100
EOT 1 0 1 (100) 0 0 0 0 0 100TOC 1 0 1 (100) 0 0 0 0 0 100
Fusobacterium necrophorum NA EOT 1 0 0 0 0 0 0 1 (100) e
TOC 1 0 1 (100) 0 0 0 0 0 100PIDGemella morbillorum >128/0.5 Day 4 1 1 (100) 0 0 0 0 0 0 100
EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 1 (100) 0 0 0 0 0 0 100
Prevotella intermedia 0.5/�0.06 Day 4 1 1 (100) 0 0 0 0 0 0 100EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 1 (100) 0 0 0 0 0 0 100
Fusobacterium nucleatum �0.06/1 Day 4 1 1 (100) 0 0 0 0 0 0 100EOT 1 1 (100) 0 0 0 0 0 0 100TOC 1 1 (100) 0 0 0 0 0 0 100
Values represent the number (%) of subjects.BPPS: bacteriologic per protocol set; n: number of subjects in whom pathogens were identified; Era: eradication; P Era: presumed eradication; Col: colonization; Per:persistence; P Per: presumed persistence; Rec: recurrence of infection; Ind: indeterminate; EOT: end of treatment; TOC: test of cure; NA: not applicable; PID: pelvic in-flammatory disease.
a MIC of MNZ/MIC of CTRX.b Eradication rate ¼ (Era þ P Era þ Col)/(n � Ind) � 100.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104102

― 261 ―
issue in the treatment of anaerobic infections. Similarly, theremightbe a possibility that the excessive use of MNZ for anaerobic in-fections may result in an increase in MNZ resistant anaerobes.
In this study, MNZ-IV in combination with CTRX was welltolerated, and demonstrated excellent clinical and bacteriolog-ical efficacy in the treatment of hospitalized Japanese subjectswith infectious peritonitis, abdominal abscess or PID. These re-sults indicate that MNZ-IV/CTRX therapy can be a reasonableoption for the empirical treatment of anaerobic infectious dis-eases involving antibiotic-resistant organisms in clinicalpractice.
The use of MNZ is recommended for the treatment of thevarious anaerobic infections referred to in textbooks and guide-lines [7e10,26e31]. However, there has been little information onthe efficacy and safety of MNZ-IV in Japanese patients with otheranaerobic infections than infectious peritonitis, abdominal ab-scess, or PID. Therefore, some clinical research will be needed forfurther evaluation of the efficacy and safety of MNZ-IV in Japanesepatients.
Conflict of interest
H. Mikamo has received a consultant fee and a fee for partici-pation in the Committee from Pfizer Japan Inc. M. Matsumizu, Y.Nakazuru, and M. Nagashima are employees of Pfizer Japan Inc.
Acknowledgments
Wewish to thank the investigators who have contributed to thisclinical study. This study was sponsored by Pfizer Japan Inc.
References
[1] Cosar C, Julou L. The activity of 1-(2-hydroxyethyl)-2-methyl-5-nitro-imidazole (R. P. 8823) against experimental Trichomonas vaginalis infections.Ann Inst Pasteur 1959;96:238e41 [in French].
[2] Freeman CD, Klutman NE, Lamp KC, Metronidazole. A therapeutic review andupdate. Drugs 1997;54:679e708.
[3] Samuelson J. Why metronidazole is active against both bacteria and parasites.Antimicrob Agents Chemother 1999;43:1533e41.
[4] Goldman P, Koch RL, Yeung TC, Chrystal EJ, Beaulieu BB Jr, McLafferty MA, et al.Comparing the reduction of nitroimidazoles in bacteria andmammalian tissuesand relating it to biological activity. Biochem Pharmacol 1986;35:43e51.
[5] Tran CM, Tanaka K, Yamagishi Y, Goto T, Mikamo H, Watanabe K. In vitroantimicrobial activity of razupenem (SMP-601, PTZ601) against anaerobicbacteria. Antimicrob Agents Chemother 2011;55:2398e402.
[6] Kasper DL, Cohen-Poradosu R. Part 8 infectious diseases, chapter 164 in-fections due to mixed anaerobic organisms. In: Longo D, Fauci A, Kasper D,Hauser S, Jameson J, Loscalzo J, editors. Harrison's principles of internalmedicine. 18th ed. The McGraw-Hill Companies, Inc; 2011.
[7] Gilbert DN, Moellering RC, Eliopoulos GM, Chambers HF, Saag MS, editors. TheSanford guide to antimicrobial therapy 2013. 43rd ed. Antimicrobial Therapy,Inc; 2013.
[8] Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJC, Baron EJ, et al.Diagnosis and management of complicated intra-abdominal infection inadults and children: guidelines by the Surgical Infection Society and the In-fectious Diseases Society of America. Clin Infect Dis 2010;50:133e64.
Table 9Anaerobic pathogens with resistance to antimicrobials other than MNZ and CTRX, MICs, and clinical and bacteriological responses to the pathogens when MNZ-IV combiniedwith CTRX was administered.
Subject ID Anaerobic pathogen MIC of MNZ(mg/ml)
MIC of CTRX(mg/ml)
MIC of other drugs(mg/ml)
Clinical response Bacteriological response
1 Bacteroides xylanisolvens 1 32 Clindamycin: >128 EOT: ImprovedTOC: Cure
EOT: EraTOC: P EraCefepime: 128
Cefozopran: >64Eggerthella lenta 1 128 Clindamycin: 0.12
Cefepime: 128Cefozopran: 32Sulbactam/Cefoperazone: 64
2 Bacteroides vulgatus 0.25 >128 Clindamycin: >128 EOT: CureTOC: Cure
Day 4: P EraEOT: P EraTOC: P Era
Cefepime: >128Cefozopran: >64Penicillin G: >128Ampicillin: >128Piperacillin: 128
3 Bacteroides thetaiotaomicron 2 64 Cefepime: >128 EOT: ImprovedTOC: Cure
Day 4: P EraEOT: P EraTOC: P Era
Cefozopran: >64Bacteroides salyersiae 1 32 Cefepime: 64
Cefozopran: >644 Bacteroides ovatus 2 >128 Cefepime: >128 EOT: Improved
TOC: CureEOT: IndTOC: P EraCefozopran: >64
Penicillin G: >128Ampicillin: >128Piperacillin: >128
5 Bacteroides thetaiotaomicron 0.25 128 Cefepime: >128 EOT: Ind EOT: EraTOC: P EraCefozopran: >64 TOC: Cure
6 Bacteroides fragilis 2 32 Cefepime: 64 EOT: ImprovedTOC: Improved
EOT: ColTOC: P EraCefozopran: 64
Penicillin G: 647 Bacteroides fragilis 1 >128 Cefepime: >128 EOT: Improved
TOC: CureDay 4: EraEOT: EraTOC: P Era
Cefozopran: >64Penicillin G: >128Ampicillin: >128Piperacillin: 128
8 Bacteroides fragilis 2 64 Cefepime: 128 EOT: ImprovedTOC: Cure
Day 4: EraEOT: EraTOC: P Era
Cefozopran: >64Penicillin G: >128Ampicillin: >128Piperacillin: >128
MNZ: metronidazole; CTRX: ceftriaxone; IV: intravenous; EOT: end of treatment; TOC: test of cure; Era: eradication; P Era: presumed eradication; Col: colonization; Ind:indeterminate.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104 103

― 262 ―
[9] Centers for Disease Control and Prevention. Sexually transmitted diseasestreatment guidelines. 2010. http://www.cdc.gov/mmwr/pdf/rr/rr5912.pdf.
[10] Stevens DL, Bisno AL, Chambers HF, Everett ED, Dellinger P, Goldstein EJC,et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis 2005;41:1373e406.
[11] Tran CM, Tanaka K, Watanabe K. PCR-based detection of resistance genes inanaerobic bacteria isolated from intra-abdominal infections. J Infect Chemo-ther 2013;19:279e90.
[12] Takesue Y, Watanabe A, Hanaki H, Kusachi S, Matsumoto T, Iwamoto A, et al.Nationwide surveillance of antimicrobial susceptibility patterns of pathogensisolated from surgical site infections (SSI) in Japan. J Infect Chemother2012;18:816e26.
[13] Falagas ME, Siakavellas E. Bacteroides, Prevotella, and Porphyromonas species: areview of antibiotic resistance and therapeutic options. Int J AntimicrobAgents 2000;15:1e9.
[14] Veloo AC, Seme K, Raangs E, Rurenga P, Singadji Z, Wekema-Mulder G, et al.Antibiotic susceptibility profiles of oral pathogens. Int J Antimicrob Agents2012;40:450e4.
[15] Sobottka I, Wegscheider K, Balzer L, B€oger RH, Hallier O, Giersdorf I, et al.Microbiological analysis of a prospective, randomized, double-blind trialcomparing moxifloxacin and clindamycin in the treatment ofodontogenic infiltrates and abscesses. Antimicrob Agents Chemother2012;56:2565e9.
[16] Yoshida I, Yamaguchi T, Kudo R, Fuji R, Takahashi C, Oota R, et al. Antimi-crobial susceptibility of clinical isolates of aerobic gram-positive cocci andanaerobic bacteria in 2008. Jpn J Antibiot 2012;65:49e72 [in Japanese].
[17] L€ofmark S, Edlund C, Nord CE. Metronidazole is still the drug of choice fortreatment of anaerobic infections. Clin Infect Dis 2010;50:S16e23.
[18] Smith JA, Skidmore AG, Forward AD, Clarke AM, Sutherland E. Prospective,randomized, double-blind comparison of metronidazole and tobramycin withclindamycin and tobramycin in the treatment of intra-abdominal sepsis. AnnSurg 1980;192:213e20.
[19] Mehtar S, Dewar EP, Leaper DJ, Taylor EW. A multi-centre study to comparemeropenem and cefotaxime and metronidazole in the treatment of hospi-talized patients with serious infections. J Antimicrob Chemother 1997;39:631e8.
[20] Finegold SM, John SS, Vu AW, Li CM, Molitoris D, Song Y, et al. In vitro activityof ramoplanin and comparator drugs against anaerobic intestinal bacteriafrom the perspective of potential utility in pathology involving bowel flora.Anaerobe 2004;10:205e11.
[21] Campbell JI, Lam TM, Huynh TL, To SD, Tran TT, Nguyen VM, et al. Microbi-ologic characterization and antimicrobial susceptibility of Clostridium tetani
isolated from wounds of patients with clinically diagnosed tetanus. Am J TropMed Hyg 2009;80:827e31.
[22] LeCorn DW, Vertucci FJ, Rojas MF, Progulske-Fox A, B�elanger M. In vitro ac-tivity of amoxicillin, clindamycin, doxycycline, metronidazole, and moxi-floxacin against oral actinomyces. J Endod 2007;33:557e60.
[23] Olsson J, Davidsson S, Unemo M, M€olling P, Andersson SO, Andr�en O, et al.Antibiotic susceptibility in prostate-derived Propionibacterium acnes isolates.APMIS 2012;120:778e85.
[24] Trevi~no M, Areses P, Pe~nalver MD, Cortizo S, Pardo S, del Molino ML, et al.Susceptibility trends of Bacteroides fragilis group and characterisation ofcarbapenemase-producing strains by automated REP-PCR and MALDI TOF.Anaerobe 2012;18:37e43.
[25] S�oki J, Eitel Z, Urb�an E, Nagy E, ESCMID Study Group on Anaerobic Infections.Molecular analysis of the carbapenem and metronidazole resistance mecha-nisms of Bacteroides strains reported in a Europe-wide antibiotic resistancesurvey. Int J Antimicrob Agents 2013;41:122e5.
[26] Japanese Society of Chemotherapy Committee on guidelines for treatment ofanaerobic infections; Japanese Association for Anaerobic Infection Research.Chapter 2-6-1. Anaerobic infections (individual fields): female genital in-fections. In: guidelines for diagnosis and treatment of anaerobic infections.J Infect Chemother 2011;17:92e8.
[27] Marrazzo JM, Holmes KK. Part 8 infectious diseases, chapter 130 sexuallytransmitted infections: overview and clinical approach. In: Longo D, Fauci A,Kasper D, Hauser S, Jameson J, Loscalzo J, editors. Harrison's principles ofinternal medicine. 18th ed. The McGraw-Hill Companies, Inc; 2011.
[28] Baron MJ, Kasper DL. Part 8 infectious diseases, chapter 127 intraabdominalinfections and abscesses. In: Longo D, Fauci A, Kasper D, Hauser S, Jameson J,Loscalzo J, editors. Harrison's principles of internal medicine. 18th ed. TheMcGraw-Hill Companies, Inc; 2011.
[29] Gomi H, Solomkin JS, Takada T, Strasberg SM, Pitt HA, Yoshida M, et al. TG13antimicrobial therapy for acute cholangitis and cholecystitis. J HepatobiliaryPancreat Sci 2013;20:60e70.
[30] Japanese Society of Chemotherapy Committee on guidelines for treatment ofanaerobic infections; Japanese Association for Anaerobic Infection Research.Chapter 2e3. Anaerobic infections (individual fields): central nervous systeminfections (brain abscess, subdural abscess, epidural abscess and bacterialmeningitis). In: guidelines for diagnosis and treatment of anaerobic infections.J Infect Chemother 2011;17:50e5.
[31] Barlam TF, Kasper DL. Part 8 infectious diseases, chapter 121 approach to theacutely Ill infected febrile patient. In: Longo D, Fauci A, Kasper D, Hauser S,Jameson J, Loscalzo J, editors. Harrison's principles of internal medicine. 18thed. The McGraw-Hill Companies, Inc; 2011.
H. Mikamo et al. / J Infect Chemother 21 (2015) 96e104104

― 263 ―
Original article
Efficacy and safety of a single oral 150 mg dose of fluconazole for thetreatment of vulvovaginal candidiasis in Japan
Hiroshige Mikamo a, Miyako Matsumizu b, *, Yoshiomi Nakazuru c, Akifumi Okayama c,Masahito Nagashima a, b
a Department of Clinical Infectious Diseases, Aichi Medical University Graduate School of Medicine, Aichi, Japanb Clinical Research, Development Japan, Pfizer Japan Inc., Tokyo, Japanc Clinical Statistics, Development Japan, Pfizer Japan Inc., Tokyo, Japan
a r t i c l e i n f o
Article history:Received 15 December 2014Received in revised form19 March 2015Accepted 22 March 2015Available online 30 March 2015
Keywords:FluconazoleSingle oral doseVulvovaginal candidiasisCandidal vulvovaginitis
a b s t r a c t
Vulvovaginal candidiasis is the second most common cause of vaginal infections following bacterialvaginosis. For the treatment of vulvovaginal candidiasis, antifungal agents are used either as topical(vaginal tablets and cream) or oral formulations. A single oral 150 mg dose of fluconazole has beenrecommended as the standard therapy for uncomplicated, acute vulvovaginal candidiasis in globalguidelines; however, in Japan oral fluconazole therapy has not been approved. We conducted a phase 3study to evaluate the efficacy and safety of a single oral 150 mg dose of fluconazole in Japanese subjectswith vulvovaginal candidiasis for regulatory submission. A total of 157 subjects received a single oral150 mg dose of fluconazole. Candida species (104 strains) were identified by fungal culture from 102subjects at baseline, including Candida albicans (100 strains). The efficacy rate for the therapeuticoutcome (assessed based on a comprehensive evaluation of the clinical and mycological efficacy in eachsubject) was 74.7% (74/99) on Day 28 in the modified Intent-To-Treat (m-ITT) population. Concerning theclinical and mycological efficacy on Day 28 in the m-ITT population, the cure, cure or improvement, anderadication rates were 81.6%, 95.9%, and 85.9%, respectively. The most common treatment-relatedadverse events were diarrhea and nausea (1.9% for each). No clinically significant safety issues werereported. A single oral 150 mg dose of fluconazole demonstrated excellent therapeutic efficacy and waswell tolerated in Japanese subjects with vulvovaginal candidiasis.Clinical registration number: NCT01806623.
© 2015, Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases.Published by Elsevier Ltd. All rights reserved.
1. Introduction
Vulvovaginal candidiasis is an infection of the vulva and/or va-gina caused by Candida species. Vulvovaginal candidiasis is thesecond most common cause of vaginal infections after bacterialvaginosis, and is often diagnosed at primary care clinics for ob-stetrics and gynecology [1e3].
The most common causative pathogen of vulvovaginal candi-diasis is Candida albicans, followed by Candida glabrata, which arepart of the indigenous flora of the gastrointestinal tract and skin
[1e3]. A positive vaginal culture for Candida species is found inapproximately 15% of non-pregnant adolescent women, and 30% ofpregnant women in Japan, but most women only have Candidaspecies in the vagina and are asymptomatic, but are not diagnosedas having candidiasis, and do not require treatment. Treatment isrequired by approximately 35% of non-pregnant women withvaginal Candida species, and 15e30% of pregnant women withvaginal Candida species [1]. The infection caused by Candida affects70e75% of women at least once during their lives, and is mostcommon in young women of childbearing age [1e3].
For the treatment of vulvovaginal candidiasis, antifungal agents,either as topical (vaginal tablets and cream) or oral formulations,are used. In European countries and the United States (US), for thetreatment of uncomplicated vaginal candidiasis, a single oral150 mg dose of fluconazole is recommended by the 2010 Sexually
* Corresponding author. Clinical Research, Development Japan, Pfizer Japan Inc.,3-22-7 Yoyogi, Shibuya-ku, Tokyo 151-8589, Japan. Tel.: þ81 3 5309 7010; fax: þ813 5309 9060. .
E-mail address: [email protected] (M. Matsumizu).
Contents lists available at ScienceDirect
Journal of Infection and Chemotherapy
journal homepage: http: / /www.elsevier .com/locate/ j ic
http://dx.doi.org/10.1016/j.jiac.2015.03.0111341-321X/© 2015, Japanese Society of Chemotherapy and The Japanese Association for Infectious Diseases. Published by Elsevier Ltd. All rights reserved.
J Infect Chemother 21 (2015) 520e526

― 264 ―
transmitted disease treatment guidelines of the CDC [3] and theSanford Guide to Antimicrobial Therapy 2014 [4].
In Japan, oral therapy with antifungal triazoles such as flucon-azole has not been approved for vulvovaginal candidiasis, andtopical therapies such as vaginal tablets and cream has been clin-ically used. In accordance with the Diagnosis and TreatmentGuidelines for Sexually Transmitted Diseases 2011 in Japan, 100 mgof either clotrimazole, miconazole, isoconazole or oxiconazole isrecommended as a daily treatment with vaginal tablets or pessaryfor uncomplicated acute vulvovaginal candidiasis, which in prin-ciple requires daily hospital visits and a vaginal douche prior toadministration. For patients who cannot visit the hospital daily,vaginal administration of a weekly dose of 600 mg isoconazole oroxiconazole is recommended after vaginal douche [1]. However, itis difficult for patients to administer vaginal tablets or a pessary,which is painful, by themselves, and therefore it often results inincompliance due to the burden of treatment [5e7].
Fluconazole, a triazole antifungal agent, has clinically beenwidely used with the indication for deep mycosis as an oral drug(capsules) and injection in Japan since it was launched in 1989. Asfor the treatment of vulvovaginal candidiasis, a single oral 150 mgdose of fluconazole, if implemented in Japan, would be of clinicalsignificance as a new and satisfactory treatment option providingbetter dose compliance than topical therapies.
The aim of this study was to investigate the efficacy and safetyprofile of a single oral 150 mg dose of fluconazole for the treatmentof Japanese subjects with vulvovaginal candidiasis for regulatorysubmission.
2. Subjects and methods
This study was conducted in accordance with the InternationalConference on Harmonisation of Good Clinical Practice Guidelines,the principle of the Declaration of Helsinki, and all applicable lawsand regulations at 10 medical centers nationwide in Japan betweenMarch 2013 and November 2013. The protocol was approved by theInstitutional Review Boards of all participating study sites. Allsubjects provided written informed consent before enrollment. Thestudy was conducted in accordance with advice from the Phar-maceuticals and Medical Devices Agency (PMDA) after the appro-priateness of the study design, endpoints, analysis set, inclusioncriteria, and so on were discussed with the PMDA.
2.1. Study design
This multicenter, open-label, non-comparative phase 3 studywas designed to evaluate the efficacy and safety of a single oral150 mg dose of fluconazole in Japanese subjects with vulvovaginalcandidiasis. The target number of subjects was 99 who were in themodified Intent-To-Treat (m-ITT) population and whose thera-peutic outcomes on Day 28 would be evaluated as effective orineffective. All the subjects took 3 fluconazole 50mg capsules orallyonly once on the first day of the treatment. The efficacy and safetywere evaluated up to Day 28.
2.2. Eligibility criteria
Female Japanese subjects aged 18 years or older (<80 years inprinciple), who had clinical signs and symptoms of vulvovaginalcandidiasis with a total symptom severity scores of 4 or higher, andwere positive for Candida by fungal culture were eligible. Clinicalsigns and symptoms were evaluated as follows: (A) symptomseverity scores: 0 ¼ no symptoms, 1 ¼ mild, 2 ¼ moderate, and3 ¼ severe, for vulvovaginal itching, vulvovaginal burning sensa-tion, excoriation of the vulva, vaginal discharge, vulva edema,
redness of the vulva, and vaginal redness; and (B) property ofvaginal content scores: 0 ¼ normal, 1 ¼mucoid, 2 ¼ paste-like, and3 ¼ cottage cheese-like, cheese-like or granular.
Exclusion criteria included the following: a history of hyper-sensitivity to fluconazole; diabetes; severe renal dysfunction; liverdisorder; heart disease or electrolyte abnormality; pregnancy orlactation; serious underlying diseases or complications; possibleaccompanying trichomonas vaginitis or bacterial vaginosis, vagi-nitis caused by Chlamydia or Gonococcus, or herpes simplex;chronic vulvovaginal candidiasis; vaginal pH � 5.0; the previoususe of systemic antifungals within 4 weeks before starting thestudy medication, or the previous use of local (vulval or intra-vaginal) antifungals within 2 weeks before starting the studymedication; not willing to avoid sexual relations up to 28 days afterthe dosing; menstruation at enrollment, or next menstruation ex-pected to start within 1 week after the study medication; diagnosisof being immunocompromised.
The following concomitant medications and therapy were pro-hibited up to Day 28: antifungals, antimicrobials, and antiallergicdrugs (oral, injection, topical [vulval or intravaginal] drugs); humanimmunoglobulin; colony stimulating factor; corticosteroids;vaginal douching after the study medication; and other investiga-tional drugs or medical devices. The use of antimicrobials wasallowed for subjects who turned out to have accompanying tri-chomonas vaginitis, bacterial vaginosis, vaginitis caused by Chla-mydia or Gonococcus or herpes simplex after enrollment.
2.3. Assessments
The primary endpoints included therapeutic outcomes deter-mined by investigators on Days 7, 14, 28, and at discontinuation.Primary evaluation was therapeutic outcome on Day 28.
Therapeutic outcomewas assessed based on the comprehensiveevaluation of clinical and mycological efficacy of each subject ac-cording to the criteria shown in Table 1.
2.3.1. Clinical efficacyClinical efficacy was assessed based on the evaluation of clinical
signs and symptoms (vulvovaginal itching, vulvovaginal burningsensation, excoriation of the vulva, vaginal discharge, vulval edema,redness of the vulva, vaginal redness, property of vaginal content).Clinical efficacy was judged as “cured” or “improved” if the clinicalsymptoms at the start of treatment had resolved or improved at theassessment time point; “ineffective” if neither the criteria for“cured” nor “improved”weremet, or the treatment failed and otherantifungals were administered for the treatment of vulvovaginalcandidiasis; “indeterminate” if efficacy assessment was difficult ornot determined because of missing data or failure to conduct thetest, or other antifungals were administered for the treatment ofother infections than vulvovaginal candidiasis.
2.3.2. Mycological efficacyThe causative pathogen was identified by vaginal discharge
culture before the study medication on Day 1 and on Days 7, 14 and
Table 1Criteria for determining the therapeutic outcomes.
Clinical efficacy Mycological efficacy
Eradication Persistent Indeterminate
Cure Effective Ineffective IndeterminateImprovement Ineffective Ineffective IndeterminateIneffective Ineffective Ineffective IneffectiveIndeterminate Indeterminate Ineffective Indeterminate
H. Mikamo et al. / J Infect Chemother 21 (2015) 520e526 521
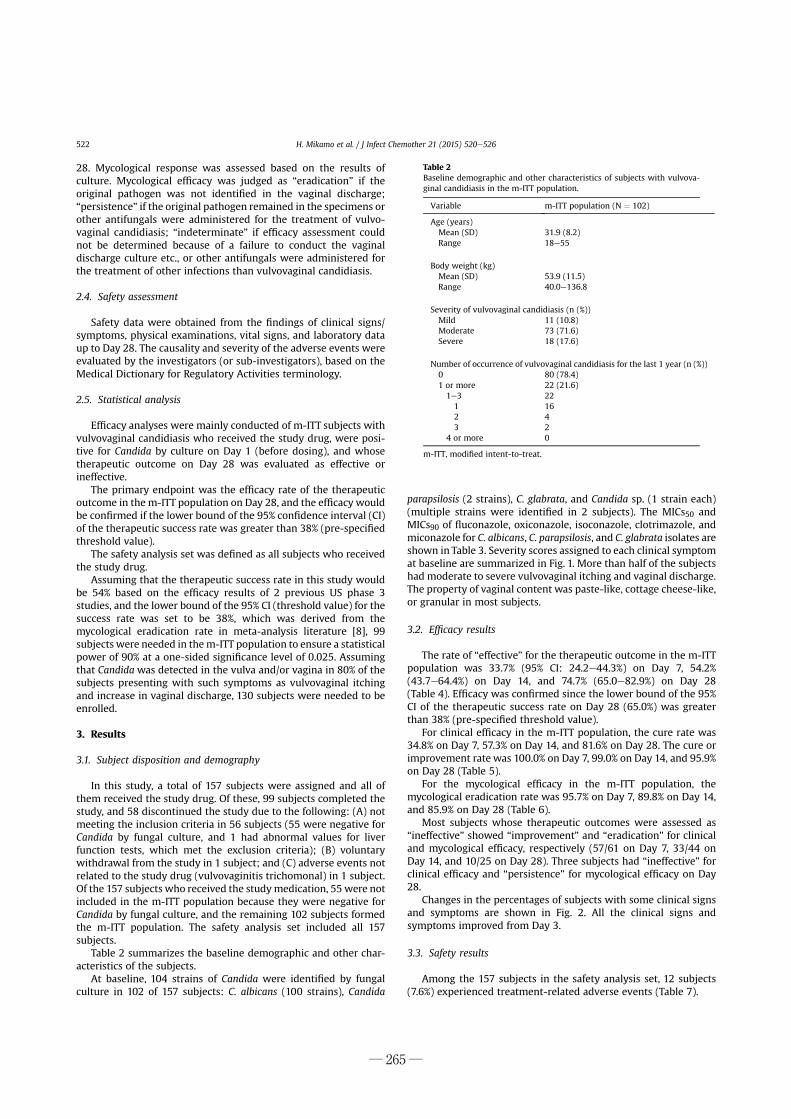
― 265 ―
28. Mycological response was assessed based on the results ofculture. Mycological efficacy was judged as “eradication” if theoriginal pathogen was not identified in the vaginal discharge;“persistence” if the original pathogen remained in the specimens orother antifungals were administered for the treatment of vulvo-vaginal candidiasis; “indeterminate” if efficacy assessment couldnot be determined because of a failure to conduct the vaginaldischarge culture etc., or other antifungals were administered forthe treatment of other infections than vulvovaginal candidiasis.
2.4. Safety assessment
Safety data were obtained from the findings of clinical signs/symptoms, physical examinations, vital signs, and laboratory dataup to Day 28. The causality and severity of the adverse events wereevaluated by the investigators (or sub-investigators), based on theMedical Dictionary for Regulatory Activities terminology.
2.5. Statistical analysis
Efficacy analyses were mainly conducted of m-ITT subjects withvulvovaginal candidiasis who received the study drug, were posi-tive for Candida by culture on Day 1 (before dosing), and whosetherapeutic outcome on Day 28 was evaluated as effective orineffective.
The primary endpoint was the efficacy rate of the therapeuticoutcome in the m-ITT population on Day 28, and the efficacy wouldbe confirmed if the lower bound of the 95% confidence interval (CI)of the therapeutic success rate was greater than 38% (pre-specifiedthreshold value).
The safety analysis set was defined as all subjects who receivedthe study drug.
Assuming that the therapeutic success rate in this study wouldbe 54% based on the efficacy results of 2 previous US phase 3studies, and the lower bound of the 95% CI (threshold value) for thesuccess rate was set to be 38%, which was derived from themycological eradication rate in meta-analysis literature [8], 99subjects were needed in them-ITT population to ensure a statisticalpower of 90% at a one-sided significance level of 0.025. Assumingthat Candida was detected in the vulva and/or vagina in 80% of thesubjects presenting with such symptoms as vulvovaginal itchingand increase in vaginal discharge, 130 subjects were needed to beenrolled.
3. Results
3.1. Subject disposition and demography
In this study, a total of 157 subjects were assigned and all ofthem received the study drug. Of these, 99 subjects completed thestudy, and 58 discontinued the study due to the following: (A) notmeeting the inclusion criteria in 56 subjects (55 were negative forCandida by fungal culture, and 1 had abnormal values for liverfunction tests, which met the exclusion criteria); (B) voluntarywithdrawal from the study in 1 subject; and (C) adverse events notrelated to the study drug (vulvovaginitis trichomonal) in 1 subject.Of the 157 subjects who received the studymedication, 55 were notincluded in the m-ITT population because they were negative forCandida by fungal culture, and the remaining 102 subjects formedthe m-ITT population. The safety analysis set included all 157subjects.
Table 2 summarizes the baseline demographic and other char-acteristics of the subjects.
At baseline, 104 strains of Candida were identified by fungalculture in 102 of 157 subjects: C. albicans (100 strains), Candida
parapsilosis (2 strains), C. glabrata, and Candida sp. (1 strain each)(multiple strains were identified in 2 subjects). The MICs50 andMICs90 of fluconazole, oxiconazole, isoconazole, clotrimazole, andmiconazole for C. albicans, C. parapsilosis, and C. glabrata isolates areshown in Table 3. Severity scores assigned to each clinical symptomat baseline are summarized in Fig. 1. More than half of the subjectshad moderate to severe vulvovaginal itching and vaginal discharge.The property of vaginal content was paste-like, cottage cheese-like,or granular in most subjects.
3.2. Efficacy results
The rate of “effective” for the therapeutic outcome in the m-ITTpopulation was 33.7% (95% CI: 24.2e44.3%) on Day 7, 54.2%(43.7e64.4%) on Day 14, and 74.7% (65.0e82.9%) on Day 28(Table 4). Efficacy was confirmed since the lower bound of the 95%CI of the therapeutic success rate on Day 28 (65.0%) was greaterthan 38% (pre-specified threshold value).
For clinical efficacy in the m-ITT population, the cure rate was34.8% on Day 7, 57.3% on Day 14, and 81.6% on Day 28. The cure orimprovement rate was 100.0% on Day 7, 99.0% on Day 14, and 95.9%on Day 28 (Table 5).
For the mycological efficacy in the m-ITT population, themycological eradication rate was 95.7% on Day 7, 89.8% on Day 14,and 85.9% on Day 28 (Table 6).
Most subjects whose therapeutic outcomes were assessed as“ineffective” showed “improvement” and “eradication” for clinicaland mycological efficacy, respectively (57/61 on Day 7, 33/44 onDay 14, and 10/25 on Day 28). Three subjects had “ineffective” forclinical efficacy and “persistence” for mycological efficacy on Day28.
Changes in the percentages of subjects with some clinical signsand symptoms are shown in Fig. 2. All the clinical signs andsymptoms improved from Day 3.
3.3. Safety results
Among the 157 subjects in the safety analysis set, 12 subjects(7.6%) experienced treatment-related adverse events (Table 7).
Table 2Baseline demographic and other characteristics of subjects with vulvova-ginal candidiasis in the m-ITT population.
Variable m-ITT population (N ¼ 102)
Age (years)Mean (SD) 31.9 (8.2)Range 18e55
Body weight (kg)Mean (SD) 53.9 (11.5)Range 40.0e136.8
Severity of vulvovaginal candidiasis (n (%))Mild 11 (10.8)Moderate 73 (71.6)Severe 18 (17.6)
Number of occurrence of vulvovaginal candidiasis for the last 1 year (n (%))0 80 (78.4)1 or more 22 (21.6)1e3 221 162 43 2
4 or more 0
m-ITT, modified intent-to-treat.
H. Mikamo et al. / J Infect Chemother 21 (2015) 520e526522

― 266 ―
The most common treatment-related adverse events werediarrhea and nausea (1.9% each). All adverse events were mild ormoderate in severity, and no deaths, serious adverse events, ordiscontinuations due to treatment-related adverse event werereported.
4. Discussion
Overall, in this non-comparative phase 3 study, a single oral150 mg dose of fluconazole was effective for the treatment of Jap-anese subjects with vulvovaginal candidiasis.
The efficacy rate for the therapeutic outcome on Day 28 in them-ITT population in this study was comparable to the clinical ef-ficacy rates of a single oral 150 mg dose of fluconazole (80% atshort-term assessment [Days 5e15] and 76% at long-term assess-ment [Days 30e60]) reported in previous clinical trials in Japanesesubjects with vulvovaginal candidiasis [9,10]. The mycological ef-ficacy on Day 28 in the present study was higher than 76% (short-term assessment) and 70% (long-term assessment) in previousJapanese studies. The difference in mycological efficacy betweenthe current and previous studies may partly be due to the differ-ence in the assessment time (Day 28 versus Days 5e15 or 30e60).
Table 3MICs of fluconazole, oxiconazole, isoconazole, clotrimazole, and miconazole for C. albicans, C. parapsilosis and C. glabrata isolates.
C. albicans (N ¼ 100) C. parapsilosis (N ¼ 2) C. glabrata (N ¼ 1)
Range MIC50 MIC90 Range MIC50 MIC90 Range MIC50 MIC90
Fluconazole 0.12e4 0.25 0.25 1e1 e e 8e8 e e
Oxiconazole 0.06e0.25 0.06 0.06 0.25e0.5 e e 0.06e0.06 e e
Isoconazole 0.06e0.25 0.06 0.06 0.5e0.5 e e 0.5e0.5 e e
Clotrimazole 0.06e0.06 0.06 0.06 0.06e0.06 e e 0.5e0.5 e e
Miconazole 0.06e1 0.06 0.06 0.5e0.5 e e 0.5e0.5 e e
Fig. 1. Percentage graphs of severity scores of clinical signs and symptoms at baseline in the m-ITT population. Clinical signs and symptoms: A ¼ vulvovaginal itching,B ¼ vulvovaginal burning sensation, C ¼ vaginal discharge, D ¼ excoriation, E ¼ vulval edema, F ¼ redness of vulva, G ¼ vaginal redness, and H ¼ Property of vaginal content. Scores:0 ¼ normal, 1 ¼ mild, 2 ¼ moderate, and 3 ¼ severe in A to G; and 0 ¼ normal, 1 ¼ mucoid, 2 ¼ paste-like, and 3 ¼ cottage cheese-like, cheese-like or granular in H.
Table 4Therapeutic outcome in the m-ITT population.
Assessment time point N Therapeutic outcome
Effectiven (%)
Ineffectiven (%)
Indeterminaten (%)
Efficacy ratea
(%) 95% CI (%)
Day 7 95 31 (32.6) 61 (64.2) 3 (3.2) 33.7 24.2e44.3Day 14 100 52 (52.0) 44 (44.0) 4 (4.0) 54.2 43.7e64.4Day 28 102 74 (72.5) 25 (24.5) 3 (2.9) 74.7 65.0e82.9
m-ITT, modified intent-to-treat; CI, confidence interval.a Efficacy rate (%) ¼ (number of subjects considered effective/[number of evaluated subjects � number of subjects considered indeterminate]) � 100.
H. Mikamo et al. / J Infect Chemother 21 (2015) 520e526 523

― 267 ―
Similarly, in 2 global clinical studies of a single oral 150 mg dose offluconazole, the clinical efficacy rates (97 and 94%, respectively) atthe short-term follow-up visit (Day 7 and Days 5e16, respectively)remained at a high level (87 and 84%, respectively) at the long-termfollow-up visit (Day 21 and Days 26e50, respectively), while themycological efficacy rates were lower at the long-term follow-upvisit (76 and 59%, respectively) than those at the short-term follow-up visit (97 and 81%, respectively) [11,12]. This may reflect that theindigenous flora of the vagina that was affected once by a single oraldose of fluconazole returned to normal after administration [5]. Inother words, mycological assessment at the long-term follow-upvisit detected Candida as normal vaginal flora.
Mizuno et al. conducted 2 clinical studies of vaginal tablets[13,14]. They reported the cure rates and improvement rates at 3
weeks after the treatment were respectively 61.5% and 92.3% for 1-day treatment with oxiconazole, 72.8% and 95.7% for 6-day treat-ment with oxiconazole, 63.3% and 90.8% for 1-day treatment withisoconazole, and 73.9% and 95.7% for 6-day treatment with clotri-mazole. Mikamo et al. also reported the clinical efficacy of clotri-mazole was 58% on Days 30e60 [9,10]. Although the evaluationmethods and timing in these studies were different from those inour study, the results of our study were generally consistent withthose of these studies.
A single oral 150 mg dose of fluconazole is an easy-to-managedosing regimen and has many advantages. Research based on in-terviews with prescription doctors in the UK revealed that 27% ofpatients complaint of pain and difficulties with insertion of vaginaltablets and pessary, and 62% of prescription doctors also think there
Table 5Clinical efficacy in the m-ITT population.
Assessment time point N Clinical efficacy
Curen (%)
Improvementn (%)
Ineffectiven (%)
Indeterminaten (%)
Cure ratea Cure or improvement rateb
% 95% CI (%) % 95% CI (%)
Day 7 99 32 (32.3) 60 (60.6) 0 7 (7.1) 34.8 25.1e45.4 100.0 96.1e100.0Day 14 101 55 (54.5) 40 (39.6) 1 (1.0) 5 (5.0) 57.3 46.8e67.3 99.0 94.3e100.0Day 28 102 80 (78.4) 14 (13.7) 4 (3.9) 4 (3.9) 81.6 72.5e88.7 95.9 89.9e98.9
m-ITT, modified intent-to-treat; CI ¼ confidence interval.a Cure rate (%) ¼ (number of subjects considered cure/[number of evaluated subjects � number of subjects considered indeterminate]) � 100.b Cure or improvement rate (%) ¼ (number of subjects considered cure or improvement/[number of evaluated subjects � number of subjects considered
indeterminate]) � 100.
Table 6Mycological efficacy in the m-ITT population.
Assessment time point N Mycological efficacy
Eradicationn (%)
Persistencen (%)
Indeterminaten (%)
Eradication ratea
(%) 95% CI (%)
Day 7 95 90 (94.7) 4 (4.2) 1 (1.1) 95.7 89.5e98.8Day 14 100 88 (88.0) 10 (10.0) 2 (2.0) 89.8 82.0e95.0Day 28 102 85 (83.3) 14 (13.7) 3 (2.9) 85.9 77.4e92.0
m-ITT, modified intent-to-treat; CI ¼ confidence interval.a Eradication rate (%) ¼ (number of subjects considered eradication/[number of evaluated subjects � number of subjects considered indeterminate]) � 100.
Fig. 2. Changes in the percentages of subjects with clinical signs and symptoms. Percentage ¼ (number of subjects with clinical signs and symptoms/[N � NA]) � 100. NA, numberof subjects whose data were not available due to menstruation.
H. Mikamo et al. / J Infect Chemother 21 (2015) 520e526524

― 268 ―
is a problemwith leakage of vaginal cream [6]. There are also somereports stating easy-to-administer oral therapies are preferred totopical vaginal therapies among patients [5,7]. In this study, vul-vovaginal redness, irritation, tingling, itching, and pain were notreported as adverse events, suggesting that a single oral 150 mgdose of fluconazole had little adverse effect on the vulva and vaginaand the daily life of subjects compared with topical therapies, andthus provides the improved quality of life and satisfaction of pa-tients besides resolving the difficulties with topical drugadministration.
Symptoms of vulvovaginal candidiasis often develop beforemenstruation [15]. It is difficult to apply topical vaginal therapiesbefore and duringmenstruation, when a sufficient effect of treatmentcannot be expectedbecause of leakage and reduction indrug contentscaused by menstrual bleeding. Single oral administration of flucona-zole can be used regardless of the menstrual status of patients.
It is known that 6-day topical vaginal therapies show problemsof early discontinuation of treatment for the reason of disappear-ance of symptoms and accidental dislodgement of inserted vaginaltablets that are not in place, leading to reduce compliance. With asingle oral dose of fluconazole, there is no concern about suchproblems.
A single oral 150 mg dose of fluconazole can be prescribed atclinics of internal medicine as well as obstetrics and gynecology,raising concern that some clinicians may make a diagnosis of vul-vovaginal candidiasis based on the patient's complaints withoutconfirming the vulvovaginal findings, and prescribe the drug,resulting in delayed proper treatment of similar diseases such asvaginal trichomoniasis and bacterial vaginosis. To prevent inap-propriate use, clinicians should make a definite diagnosis of thedisease giving the utmost care before prescribing the drug.
In this study, 4 subjects had complications of genital infectioncaused by other pathogens than Candida (1 with Trichomonasvulvovaginitis, 3 with chlamydial cervicitis) at baseline. Thesecomplications were found in the microbiological tests conducted atbaseline after a single oral 150 mg dose of fluconazole on Day 1. Asubject with trichomonas vulvovaginitis received tinidazole and 3subjects with chlamydial cervicitis received azithromycin. Theinvestigator considered that it was possible to assess the efficacy offluconazole in these 4 subjects. For these 4 subjects, the clinicalefficacy was assessed as either “cure” or “improvement,” and themycological efficacy was assessed as either “eradication” or“persistence.” For 3 of the 4 subjects, the therapeutic outcomeswere assessed as “ineffective.” These findings suggest that a singleoral 150 mg dose of fluconazole in combination with other anti-microbial agents is effective for the treatment of vulvovaginalcandidiasis complicated with genital infection caused by otherpathogens than Candida.
A subject had complications of diabetes mellitus in this study.Although the subject was considered to have had them beforeenrollment, the investigator considered that it was possible toassess the efficacy of fluconazole in the subject because the dura-tion of diabetes mellitus was short, and the subject was considerednot to be immunocompromised. The therapeutic outcome of thesubject was assessed as “effective.” There were few studiesreporting the efficacy of a single oral dose of fluconazole in subjectscomplicated with diabetes mellitus [16,17]. As diabetes mellitus is arisk factor for vulvovaginal candidiasis, the efficacy in these sub-jects has to be studied further.
In this study, the most commonly identified pathogen wasC. albicans (100/104 strains), and all isolates were highly susceptibleto fluconazole judging from the fluconazole breakpoints forC. albicans in the criteria of Clinical and Laboratory StandardsInstitute (CLSI) (susceptible � 2 mg/ml, susceptible-dosedependent ¼ 4 mg/ml, resistant � 8 mg/ml) [18], and the criteriaof the European Committee on Antimicrobial Susceptibility Testing(EUCAST) (susceptible � 2 mg/ml, resistant � 4 mg/ml) [19]. In thisstudy, C. glabrata was identified in a subject whose therapeuticoutcome was assessed as “effective” at all assessment time points.This C. glabrata isolate (MIC of fluconazole was 8 mg/ml) was notclassified into the category of resistant based on the fluconazolebreakpoints for C. glabrata (susceptible-dose dependent�32 mg/ml,resistant � 64 mg/ml [CLSI criteria]; susceptible � 0.002 mg/ml,resistant > 32 mg/ml [EUCAST criteria]). C. glabrata, the secondmostcommonpathogen of vulvovaginal candidiasis following C. albicans,is however reported to be resistant to fluconazole [20,21]. If flu-conazole is not effective, other topical drugs should be used instead.
The most common treatment-related adverse events occurringin 1% or more of the subjects were only gastrointestinal-relatedevents (diarrhea and nausea), and there were no significantsafety issues in this study. However, fluconazole, even given as asingle oral dose, has more potential to produce side effects such asgastrointestinal disorders and other systemic events comparedwith topical vaginal therapies, and subjects treated with flucona-zole should be monitored carefully. Since fluconazole inhibits CYP2C9 and 3A4, caution should be exercisedwhen a single oral dose offluconazole is applied in combination with other drugs to preventpotential drug interactions.
There are 3 limitations to this study that should be consideredwhen these findings are interpreted. First, this was not a controlledstudy. Second, there were not sufficient other pathogens thanC. albicans to assess their efficacy. Although further investigation,such as a large comparative study, accordingly needs to be per-formed to confirm our study results, the methods of this study withsufficient clinical efficacy will be useful for the treatment of pa-tients with vulvovaginal candidiasis in Japan. Third, this was aclinical study led by the sponsor and the possibility of conflicts ofinterest between the authors and the sponsor could not be ruledout.
In conclusion, the results of this study demonstrated that asingle oral 150 mg dose of fluconazole was effective for the treat-ment of vulvovaginal candidiasis in Japanese subjects, and no sig-nificant safety issues were reported. A single oral 150 mg dose offluconazole is recommended for the treatment of vulvovaginalcandidiasis in global guidelines. Therefore, a single oral 150 mgdose of fluconazole will be positioned as one of the first-linetreatment options for vulvovaginal candidiasis in Japan.
Conflict of interest
H. Mikamo has received a consultant fee and a fee for partici-pation in the Committee from Pfizer Japan Inc. M. Matsumizu, Y.
Table 7Treatment-related adverse events in the safety analysis set.
Preferred terma Safety analysis set (N ¼ 157)
Treatment-related adverse eventn (%)
Palpitations 1 (0.6)Abdominal distension 1 (0.6)Diarrhea 3 (1.9)Nausea 3 (1.9)Pyrexia 1 (0.6)Cystitis 1 (0.6)Genital herpes 1 (0.6)Hepatic enzyme increased 1 (0.6)Genital hemorrhage 1 (0.6)Urticaria 1 (0.6)
a Medical Dictionary for Regulatory Activities Terminology version 16.1.
H. Mikamo et al. / J Infect Chemother 21 (2015) 520e526 525

― 269 ―
Nakazuru, A. Okayama, and M. Nagashima are employees of PfizerJapan Inc.
Acknowledgments
Wewish to thank the investigators who have contributed to thisclinical study. This study was sponsored by Pfizer Japan Inc.
References
[1] Japanese Society for Sexually Transmitted Infections. Diagnosis and treatmentguidelines for sexually transmitted diseases 2011 in Japan. Jpn J Sex TransmInfect 2011;22:87e91 [in Japanese].
[2] Sobel JD. Vulvovaginal candidosis. Lancet 2007;369:1961e71.[3] Workowski KA, Berman S, Centers for Disease Control and Prevention (CDC).
Sexually transmitted diseases treatment guidelines, 2010. MMWR RecommRep 2010;59:1e110.
[4] Gilbert DN, Moellering RC, Eliopoulos GM, Chambers HF, Saag MS, editors. TheSanford guide to antimicrobial therapy 2014. 44th ed. Antimicrobial Therapy,Inc.; 2014.
[5] Pitsouni E, Iavazzo C, Falagas ME. Itraconazole vs fluconazole for the treatmentof uncomplicated acute vaginal and vulvovaginal candidiasis in nonpregnantwomen: a metaanalysis of randomized controlled trials. Am J Obstet Gynecol2008;198:153e60.
[6] Tooley P. Preferences in the treatment of vaginal candidosis. Practitioner1989;233:668e9.
[7] A comparison of single-dose oral fluconazole with 3-day intravaginal clotri-mazole in the treatment of vaginal candidiasis. Report of an internationalmulticentre trial. Br J Obstet Gynaecol 1989;96:226e32.
[8] Nurbhai M, Grimshaw J, Watson M, Bond C, Mollison J, Ludbrook A. Oralversus intra-vaginal imidazole and triazole anti-fungal treatment of uncom-plicated vulvovaginal candidiasis (thrush). Cochrane Database Syst Rev 2007.Art. No.: CD002845, http://dx.doi.org/10.1002/14651858.CD002845.pub2.
[9] Mikamo H, Izumi K, Ito K, Tamaya T. Comparative study of the effectiveness oforal fluconazole and intravaginal clotrimazole in the treatment of vaginalcandidiasis. Infect Dis Obstet Gynecol 1995;3:7e11.
[10] Mikamo H, Kawazoe K, Sato Y, Hayasaki Y, Tamaya T. Comparative study onthe effectiveness of antifungal agents in different regimens against vaginalcandidiasis. Chemotherapy 1998;44:364e8.
[11] De Punzio C, Garutti P, Mollica G, Nappi C, Piccoli R, Genazzani AR. Fluconazole150 mg single dose versus itraconazole 200 mg per day for 3 days in thetreatment of acute vaginal candidiasis: a double-blind randomized study. EurJ Obstet Gynecol Reprod Biol 2003;106:193e7.
[12] Rees T, Phillips R. Multicenter comparison of one-day oral therapy with flu-conazole or itraconazole in vaginal candidiasis. Int J Gynecol Obstet 1992;37:33e8.
[13] Mizuno S, Hashimoto M, Shimoya Y, Sagae S, Yajima A, Hamazaki Y, et al.A double-blind comparative study of the efficacy of one-day administration ofoxiconazole tablets for the treatment of vulvovaginal candidiasis. WorldObstet Gynecol (Sanfujinkanosekai) 1989;41:633e45 [in Japanese].
[14] Mizuno S, Hashimoto M, Shimoya Y, Sagae S, Yajima A, Hamazaki Y, et al.A double-blind comparative study of the efficacy of six-day administration ofoxiconazole tablets for the treatment of vulvovaginal candidiasis. WorldObstet Gynecol (Sanfujinkanosekai) 1989;41:713e25 [in Japanese].
[15] Eckert LO, Hawes SE, Stevens CE, Koutsky LA, Eschenbach DA, Holmes KK.Vulvovaginal candidiasis: clinical manifestations, risk factors, managementalgorithm. Obstet Gynecol 1998;92:757e65.
[16] Gunther LS, Martins HP, Gimenes F, Abreu AL, Consolaro ME, Svidzinski TI.Prevalence of Candida albicans and non-albicans isolates from vaginal secre-tions: comparative evaluation of colonization, vaginal candidiasis and recur-rent vaginal candidiasis in diabetic and non-diabetic women. Sao Paulo Med J2014;132:116e20.
[17] Goswami D, Goswami R, Banerjee U, Dadhwal V, Miglani S, Lattif AA, et al.Pattern of Candida species isolated from patients with diabetes mellitus andvulvovaginal candidiasis and their response to single dose oral fluconazoletherapy. J Infect 2006;52:111e7.
[18] Clinical and Laboratory Standards Institute. Reference method for brothdilution antifungal susceptibility testing of yeasts. Fourth Inf Suppl 2012;32:1e28.
[19] European Committee on Antimicrobial Susceptibility Testing. Antifungalagents breakpoint tables for interpretation of MICs. http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Antifungal_breakpoints_v_6.1.pdf; 2013.
[20] Kobayashi T, Muratani T. Drug susceptibilities of yeast-like fungi isolated fromvaginal discharge (proceedings). Jpn J Sex Transm Infect 2012;23:64 [inJapanese].
[21] Mikamo S, Yamagishi Y. Trichomoniasis and genital candidiasis. Rin-shofujinkasanka 2013;67:52e7 [in Japanese].
H. Mikamo et al. / J Infect Chemother 21 (2015) 520e526526

― 270 ―
梅毒
愛知医科大学病院感染症科愛知医科大学病院感染制御部 山岸 由佳 三鴨 廣繁

― 271 ―

― 272 ―

― 273 ―

― 274 ―

― 275 ―
― 276 ―

― 277 ―
Human leukocyte antigen class II DRB1*1302 alleleprotects against cervical cancer: At which step ofmultistage carcinogenesis?Koji Matsumoto,1 Hiroo Maeda,2 Akinori Oki,1 Naoyoshi Takatsuka,3 Toshiharu Yasugi,4 Reiko Furuta,5
Ranko Hirata,2 Akira Mitsuhashi,6 Kei Kawana,4 Takuma Fujii,7 Takashi Iwata,7 Yasuo Hirai,8
Masatoshi Yokoyama,9 Nobuo Yaegashi,10 Yoh Watanabe,11 Yutaka Nagai,12 Hiroyuki Yoshikawa1 and for theJapan HPV and Cervical Cancer (JHACC) Study Group
1Department of Obstetrics and Gynecology, University of Tsukuba, Tsukuba; 2Department of Transfusion Medicine and Cell Therapy, Saitama MedicalCenter, Saitama Medical University, Saitama; 3Department of Health Economics, Gifu University Graduate School of Medicine, Gifu; 4Department ofObstetrics and Gynecology, University of Tokyo, Tokyo; 5Department of Pathology, Cancer Institute, Japanese Foundation of Cancer Research, Tokyo;6Department of Reproductive Medicine, Graduate School of Medicine, Chiba University, Chiba; 7Department of Obstetrics and Gynecology, Keio UniversitySchool of Medicine, Tokyo; 8Departments of Gynecology and Cytopathology, Cancer Institute Hospital, Japanese Foundation of Cancer Research, Tokyo;9Department of Obstetrics and Gynecology, Faculty of Medicine, Saga University, Saga; 10Department of Obstetrics and Gynecology, Tohoku UniversitySchool of Medicine, Sendai; 11Department of Obstetrics and Gynecology, Kinki University School of Medicine, Osaka; 12Department of Obstetrics andGynecology, Faculty of Medicine, University of the Ryukyus, Okinawa, Japan
Key words
cervical cancer, cervical intraepithelial neoplasia, humanleukocyte antigen, human papillomavirus, low-gradesquamous intraepithelial lesion
Correspondence
Koji Matsumoto, Department of Obstetrics and Gynecol-ogy, Faculty of Medicine, University of Tsukuba, Tsukuba305-8575, Japan.Tel: +81 29 853 3073; Fax: +81 29 853 3072;E-mail: [email protected]
Funding InformationThis work was supported by Ministry of Education,Science, Sports and Culture of Japan (grant nos. 12218102and 25462585).
Received May 7, 2015; Revised July 22, 2015; AcceptedJuly 29, 2015
Cancer Sci 106 (2015) 1448–1454
doi: 10.1111/cas.12760
We investigated the role of human leukocyte antigen (HLA) class II alleles in mul-
tistage cervical carcinogenesis. Cross-sectional analysis for HLA association with
cervical cancer included 1253 Japanese women: normal cytology (NL, n = 341),
cervical intraepithelial neoplasia grade 1 (CIN1, n = 505), CIN grade 2 or 3 (CIN2
⁄ 3, n = 96), or invasive cervical cancer (ICC, n = 311). The HLA class II allele fre-
quencies were compared by Fisher’s exact test or the v2-test. The Bonferroni
adjustment corrected for multiple comparisons. Among the study subjects, 454
women with low-grade squamous intraepithelial lesion cytology were prospec-
tively monitored by cytology and colposcopy every 3–4 months to analyze cumu-
lative risk of CIN3 within the next 10 years in relation to HLA class II alleles. HLA
class II DRB1*1302 allele frequency was similar between women with NL (11.7%)
and CIN1 (11.9%), but significantly decreased to 5.2% for CIN2 ⁄ 3 and 5.8% for
ICC (P = 0.0003). Correction for multiple testing did not change this finding. In
women with low-grade squamous intraepithelial lesion cytology, the cumulative
risk of CIN3 diagnosed within 10 years was significantly reduced among
DRB1*1302-positive women (3.2% vs. 23.7%, P = 0.03). In conclusion, the two dif-
ferent types of analysis in this single study showed the protective effect of the
DRB1*1302 allele against progression from CIN1 to CIN2 ⁄ 3.
C ervical cancer is the third most common cancer in womenworldwide, with approximately 530 000 women develop-
ing the disease every year. (1) Virtually all cases of cervicalcancer are caused by persistent infection with carcinogenicHPVs, specifically, HPV types 16, 18, 31, 33, 35, 39, 45, 51,52, 56, 58, 59, and 68.(2) However, although carcinogenicHPV infection is common among young women of reproduc-tive age, only a small subset of infected women develop cervi-cal cancer, implying the involvement of additional riskfactors.(3) Environmental factors such as smoking, parity, andOC use have been suggested as relevant to cervical carcino-genesis in numerous case–control studies.(4)
Genetic linkage with cervical cancer has also beenimplied.(5) There is a priori biological plausibility supportingHLA involvement in the development of HPV-related can-cer.(6) HLA molecules are responsible for the presentation ofviral antigens to the host immune system, thus playing a cen-tral role in immune recognition and subsequent clearance of
virus-infected cells. Therefore, genetic variations in HLAregions may influence the efficiency of HPV antigen presenta-tion and condition the immune responsiveness to HPV infec-tions.(7)
It is known that rabbit MHC class II genes are associatedwith malignant conversion of cottontail rabbit papillomavirus-induced tumors.(8) To date, epidemiological studies have sug-gested that HLA class II DRB1*1501 and DQB1*03 may beassociated with an increased risk of cervical cancer, whereasDRB1*13 may protect against cervical carcinogenesis.(7)
However, results from these studies have not been entirelyconsistent. In addition, very little is known about the step atwhich HLA class II alleles may play a central role in multi-step cervical cancer pathogenesis from HPV infection to can-cer development because most HLA data on cervical cancerare based on case–control studies comparing HLA class IIallele frequencies between cancer patients and healthy con-trols. There are few prospective studies addressing HLA
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1448–1454 © 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.This is an open access article under the terms of the Creative CommonsAttribution-NonCommercial-NoDerivs License, which permits use and distributionin any medium, provided the original work is properly cited, the use is non-commercial and no modifications or adaptations are made.

association with the development of cervical cancer andprecancer.In the present study, we analyzed HLA class II data from
1253 women with normal cytology, cervical precursor lesions,or invasive cervical cancer by using a cross-sectional studydesign. To reduce the risk of chance findings, putative linksbetween cervical cancer and specific HLA class II alleles werealso examined in a prospective cohort study of 454 womenwith low-grade cervical lesions. By using cross-sectional andprospective study designs, we investigated the protective effectof the HLA class II DRB1*1302 allele against progression tocervical precancer.
Materials and Methods
Study design. Our study subjects consisted of 1253 Japanesewomen (341 with NL, 505 with CIN1, 86 with CIN2, 10 withCIN3, and 311 with ICC) who visited 10 hospitals for cervicalcancer screening, treatment of cervical diseases, or other rea-sons between April 1998 and March 2011. These women wereincluded in the cross-sectional HLA class II analysis. Non-Ja-panese women were excluded from the present study based onself-reported ethnicity. At enrolment, blood samples were col-lected for HLA genotyping. Histological specimens werestained with H&E and reviewed by two pathologists (R. F.[author] and Tomoyuki Kitagawa [Department of Pathology,Cancer Institute Hospital, Japanese Foundation of CancerResearch, Tokyo, Japan]).Of the study subjects included in the cross-sectional analysis,
591 women with CIN1 or CIN2 were followed at 3–4-monthintervals and received cytology and colposcopic examinationsat each visit. Of these, 454 women with evident LSIL cytologyat baseline were included in the prospective analysis. Thisprospective cohort study has been described elsewhere.(9)
Briefly, baseline cytology was reviewed by two cytopathologists(Y. H. [author] and Masafumi Tsuzuku [Department ofCytopathology, Cancer Institute Hospital, Japanese Foundationof Cancer Research]). At the time of study entry, cervical HPVDNA was determined by PCR-based methodology. In addition,information about smoking, contraceptive and reproductivehistory, and sexual behavior was also obtained from a self-administered questionnaire. During follow-up, a cervical biopsywas carried out only when Pap smears and colposcopic findingswere suggestive of progression to CIN3 or worse.For women whose condition was regarded as progressing,
based on cytology and histology examinations carried out inthe participating hospitals, the two cytopathologists and twopathologists reviewed all cytological and histological speci-mens collected for diagnosis of disease progression. In theprospective study, the primary endpoint was histological CIN3lesions or worse diagnosed after rigorous pathological review.Occasionally a few difficult cases were adjudicated by jointreview with consideration of cytology as well as histology. Weused the primary endpoint of CIN3 or worse because CIN3 isa more certain, rigorous histological diagnosis of precancerthan CIN2.(3)
Women entered the study voluntarily only after giving theirsigned informed consent. The study protocol was approved bythe ethical and research review boards of the participatinginstitutions.
Genotyping of HLA class II. Blood leukocytes were used forHLA genotyping. Total cellular DNA was extracted from thesespecimens and amplified by PCR using locus-specific primers.All samples were initially typed at the HLA-DRB1 and DQB1
loci using a commercially available reverse sequence-specificoligonucleotide probe typing kit (Dynal RELI SSO; DynalBiotech, Oslo, Norway). For subtyping, group-specific amplifi-cations were carried out as previously described.(10) DRB1 andDQB1 alleles were identified by SSCP and RFLP using thePCR products. Laboratory staff who carried out the HLA classII typing were blinded to the clinical data collected from thestudy subjects.
Genotyping of HPV. We detected HPV DNA in cervical sam-ples by PCR-based methodology as described previously.(11) Inbrief, HPV DNA was amplified by PCR using consensus pri-mers (L1C1 ⁄ L1C2 + L1C2M) for the HPV L1 region. TheHPV types were identified by RFLP that has been shown toidentify at least 26 types of genital HPVs.(12) Laboratory staffwho carried out HPV genotyping were blinded to the clinicaldata collected from the study subjects.
Statistical analysis. In the cross-sectional study, HLA class IIallele frequencies were compared by Fisher’s exact test or thev2-test. When an expected cell value in the 2 9 2 tables was<5, Fisher’s exact test was used. We also analyzed the datausing the Bonferroni adjustment, a conventional method ofcorrecting for multiple comparisons.In the prospective cohort study, time to event was measured
from the date of the index visit (i.e., the first instance of anabnormal cytology result) to the date of the visit at whichcytological transition to CIN3 was first detected. Womenwhose lesions did not progress to CIN3 were censored at theirlast recorded return visit dates. The cumulative probability ofprogression to CIN3 was estimated using the Kaplan–Meiermethod and compared with a log–rank test, and the Coxregression model was used for statistical adjustments. Patientage, CIN grade, at the time of entry, HPV risk category(HPV16 ⁄18 ⁄31 ⁄33 ⁄35 ⁄45 ⁄52 ⁄58, other carcinogenic types, orcarcinogenic HPV negative), smoking status, parity, OC use,number of lifetime sexual partners, and age at first sexualintercourse were included in the multivariate model for adjust-ments. As the results did not differ among the 10 hospitals, thestudy sites were not included in the multivariate models.All analyses were carried out using the STATA 9 (StataCorp
LP, College Station, TX, USA) statistics package. Two-sidedP-values were calculated throughout and considered to be sig-nificant at <0.05.
Results
Cross-sectional analysis. The distribution of HLA-DRB1 andHLA-DQB1 alleles in 1253 Japanese women with normalcytology or cervical diseases is shown in Table 1. To examinethe step at which HLA class II alleles may contribute to cervi-cal carcinogenesis, the HLA data were compared among fourgroups: NL (n = 341), CIN1 (n = 505), CIN2 ⁄3 (n = 96), andICC (n = 311).We could not find any association between HLA class II
alleles and development of CIN1, because HLA class II allelefrequencies were very similar between women with NL andCIN1 (Table 1). DRB1*0901 frequency was significantlydecreased among women with CIN2 or worse (CIN2+) com-pared with women with NL or CIN1 (<CIN2) (15.0% vs.26.2%; P = 0.0003; Pc = 0.007). In addition, DRB1*1302 fre-quency was also significantly lower among women withCIN2 + (5.9% vs. 11.2%, P = 0.0003, Pc = 0.007). Althoughthe number of women with CIN2 ⁄3 was small (n = 96),DRB1*0901 frequency was significantly decreased in womenwith ICC compared with women with CIN2 ⁄ 3 (14.5% vs.
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1449 © 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.
Original Articlewww.wileyonlinelibrary.com/journal/cas Matsumoto et al.
― 278 ―

28.1%; P = 0.003). DRB1*1302 frequency was similarbetween women with ICC and CIN2 ⁄3 (5.8% vs. 5.2%;P = 0.99).DQB1*0604 frequency was also significantly decreased
among women with CIN2+ compared to those with <CIN2(5.2% vs. 11.6%; P = 0.0001; Pc = 0.001).In the cross-sectional analysis, we could not detect any sig-
nificant associations between other HLA class II alleles anddevelopment of CIN2 + (Table 1). The DRB1*0401,DRB1*1502, and DQB1*0601 allele frequencies were signifi-cantly associated with an increased risk of CIN2 + (P = 0.03,P = 0.02, and P = 0.01, respectively), but these associationslost significance after correction for multiple comparison.
Although DRB1*1501 and DQB1*03 alleles have been sug-gested as relevant to an increased risk of cervical cancer inprevious HLA studies,(7) the frequencies of these alleles weresimilar between women with <CIN2 and CIN2 + (P = 0.99and P = 0.95, respectively). Another analysis comparing HLAallele frequencies between women with and without ICC didnot change the findings (data not shown).
Prospective analysis. The clinical outcomes of 454 womenwith LSIL cytology were monitored by cytologic and colpo-scopic testing at intervals of 3–4 months. Table 2 shows thecharacteristics of the study subjects included in the prospectiveanalysis. At baseline, 407 women had biopsy-proven CIN1 and47 had biopsy results of CIN2. The mean age of the study sub-
Table 1. Correlation between human leukocyte antigen class II carrier frequencies and cervical diseases in Japanese women (n = 1253) at the
commencement of the study
NL CIN1 CIN2 ⁄ 3 ICCRelative risk of CIN2 or
worse†Correction for
multiple comparison
n = 341 % n = 505 % n = 96 % n = 311 % OR (95% CI) P-value Corrected P-value‡
DRB1*
0101 30 9 57 11 8 8 33 11 0.98 (0.66–1.45) 0.91
0401 9 3 5 1 3 3 12 4 2.27 (1.09–4.76) 0.03 0.72
0403 25 7 27 5 8 8 18 6 1.04 (0.64–1.69) 0.87
0405 91 27 107 21 18 19 68 22 0.87 (0.66–1.17) 0.37
0406 17 5 25 5 4 4 10 3 0.68 (0.37–1.26) 0.21
0407 5 1 6 1 0 0 1 0 0.19 (0.02–1.45) 0.12
0410 16 5 32 6 4 4 18 6 0.95 (0.57–1.60) 0.85
0701 4 1 3 1 2 2 5 2 2.10 (0.73–6.02) 0.17
0802 28 8 44 9 9 9 24 8 0.95 (0.62–1.49) 0.81
0803 45 13 92 18 16 17 48 15 0.97 (0.70–1.33) 0.83
0901 90 26 136 27 27 28 45 14 0.59 (0.44–0.79) 0.0003§ 0.007
1001 3 1 10 2 1 1 5 2 0.96 (0.36–2.54) 0.93
1101 18 5 26 5 6 6 14 5 0.94 (0.54–1.62) 0.83
1201 22 6 22 4 4 4 17 5 0.99 (0.58–1.69) 0.98
1202 9 3 13 3 1 1 4 1 0.47 (0.18–1.24) 0.15
1301 2 1 5 1 3 3 1 0 1.19 (0.35–4.09) 0.75
1302 40 12 60 12 5 5 18 6 0.44 (0.28–0.71) 0.0003§ 0.007
1401 33 10 36 7 9 9 22 7 0.92 (0.60–1.44) 0.74
1403 12 4 18 4 4 4 10 3 0.97 (0.51–1.85) 0.92
1405 11 3 18 4 7 7 14 5 1.52 (0.86–2.72) 0.15
1406 10 3 16 3 3 3 11 4 1.12 (0.58–2.18) 0.73
1501 46 13 84 17 18 19 48 15 1.07 (0.77–1.47) 0.70
1502 76 22 115 23 25 26 91 29 1.37 (1.04–1.79) 0.02 0.48
1602 5 1 7 1 2 2 1 0 0.52 (0.14–1.84) 0.41
DQB1*
0202 2 1 2 0 1 1 3 1 2.09 (0.51–8.40) 0.28
03 203 60 282 56 58 60 176 57 1.01 (0.79–1.28) 0.96
0301 77 23 94 19 21 22 56 18 0.92 (0.68–1.24) 0.59
0302 60 18 86 17 15 16 50 16 0.91 (0.66–1.25) 0.57
03032 96 28 138 27 31 32 86 28 1.06 (0.81–1.37) 0.69
0401 89 26 105 21 18 19 66 21 0.87 (0.65–1.17) 0.35
0402 29 9 55 11 10 10 29 9 0.96 (0.64–1.43) 0.85
0501 33 10 66 13 9 9 37 12 0.96 (0.66–1.39) 0.84
0502 24 7 24 5 6 6 14 5 0.86 (0.52–1.47) 0.58
05031 26 8 41 8 8 8 29 9 1.16 (0.76–1.77) 0.48
0601 110 32 189 37 40 42 134 43 1.37 (1.07–1.74) 0.01 0.24
0602 42 12 80 16 17 18 46 15 1.09 (0.78–1.51) 0.62
0603 2 1 5 1 3 3 1 0 1.19 (0.35–4.09) 0.78
0604 39 11 59 12 5 5 16 5 0.41 (0.26–0.68) 0.0001§ 0.001
†Relative risks of cervical intraepithelial neoplasia grade 2 ⁄ 3 (CIN2 ⁄ 3) ⁄ invasive cervical cancer (ICC) were analyzed in comparison with <CIN2(normal cytology or CIN1, n = 846). ‡P-values were calculated by Bonferroni adjustment to correct for multiple comparison. §Bold letters indicatestatistical significance. CI, confidence interval; NL, normal cytology; OR, odds ratio.
© 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1450
Original ArticleHLA class II alleles and risk of cervical cancer in Japan www.wileyonlinelibrary.com/journal/cas
― 279 ―

― 280 ―
jects was 35.9 years (range, 19–54 years). In the current study,we updated the previous cohort data and extended the meanfollow-up period from 39.0 months (range, 6.8–84.9 months)to 62.7 months (range, 6.8–155.9 months). By updating thedata, the number of women diagnosed as progressing to CIN3over the period of follow-up increased from 39 to 61.Unlike the cross-sectional analysis results, DRB1*0901 was
not associated with progression to CIN3 in the prospective
analysis (P = 0.88; Fig. 1a). Adjustment for age, CIN grade atthe time of entry, HPV risk category, parity, smoking status,OC use, number of lifetime sexual partners, and age at firstsexual intercourse did not change this finding (P = 0.71;Table 3).The risk of progression to CIN3 was significantly reduced
among DRB1*1302-positive women (P = 0.03, log–rank test;Fig. 1b), which was consistent with the cross-sectional analysisresults. This protective effect of DRB1*1302 against progres-sion to CIN3 remained statistically significant, even afteradjustment for possible risk factors of cervical cancer (adjustedP = 0.04; Table 3). Distributions of baseline characteristicsamong the DRB1*1302-positive and DRB1*1302-negativewomen are presented in Table 2. Because of the poor repro-ducibility of cervical histologic interpretations,(13,14) someCIN3 lesions may have been classified incorrectly as CIN2 atbaseline. Therefore, we also analyzed the follow-up data forCIN1 and CIN2 separately. In women with CIN1 histology(n = 407), the cumulative risk of CIN3 diagnosed within10 years was lower among DRB1*1302-positive women (3.5%vs. 17.6%; P = 0.09). In women with CIN2 histology(n = 47), progression to CIN3 did not occur in DRB1*1302-positive women (cumulative probability of histological CIN3diagnosis within 10 years, 0.0% vs. 48.9%; P = 0.28).Although these associations did not reach statistical signifi-cance due to limitations imposed by the small sample size,similar patterns were observed in separate analyses for CIN1and CIN2.We analyzed the protective effect of DRB1*1302 allele in
relation to HPV type-specific risk category. AmongDRB1*1302-positive women, only one case positive forHPV33 progressed to CIN3. Therefore, in women positive forHPV16, 18, 31, 33, 35, 45, 52, or 58, the cumulative risk ofCIN3 diagnosed within 10 years was 5.9% for those who wereDRB1*1302-positive and 39.6% for those who wereDRB1*1302-negative (P = 0.04, log–rank test). In women pos-itive for HPV39, 51, 56, 59, or 68, the CIN3 risk within10 years was 0.0% for those who were DRB1*1302-positiveand 9.6% for those who were DRB1*1302-negative (P = 0.29,log–rank test). In women negative for high-risk HPVs, theCIN3 risk was 0.0% for DRB1*1302-positives and 1.9% forDRB1*1302-negatives (P = 0.78).The DQB1*0604 allele was closely linked to the
DRB1*1302 allele, indicating a strong correlation (r2 = 0.96).As the DRB1*1302 and DQB1*0604 alleles were in linkagedisequilibrium, similar findings were observed for theDRB1*1302 and DQB1*0604 alleles (Table 3). Therefore,only DRB1*1302 data are shown in Fig. 1.We could not find any significant association between other
HLA class II alleles and progression to CIN3. Data are onlyshown on two representative HLA class II alleles (DRB1*1501and DQB1*03) that have been reported to be a risk factor forcervical cancer in previous HLA studies.(7) In the presentstudy, these alleles did not affect the risk of progression toCIN3 within the next 10 years (Fig. 1c,d). Adjustment for pos-sible cervical cancer risk factors did not change these findings(Table 3).
Discussion
By using cross-sectional and prospective study designs, weindicated the protective effect of the DRB1*1302 allele againstprogression to cervical cancer and precancer. The consistentresults obtained by two different analyses appear to provide
Table 2. Characteristics of Japanese women with low-grade
squamous intraepithelial lesion cytology (n = 454) included in
prospective analysis
All study
subjects
(n = 454),
n (%)
DRB1*1302 status
P-valuePositive
(n = 47),
n (%)
Negative
(n = 407),
n (%)
Age, years
18–29 86 (18.9) 7 (14.9) 79 (19.4) 0.13
30–39 217 (47.8) 18 (38.3) 199 (48.9)
40+ 151 (33.3) 22 (46.8) 129 (31.7)
Histology at entry
CIN grade 1 389 (85.7) 44 (94) 345 (85) 0.10
CIN grade 2 65 (14.3) 3 (6) 62 (15)
HPV genotypes
HPV16, 18, 31, 33,
35, 45, 52, 58
201 (44.3) 19 (40.4) 182 (44.7) 0.49
HPV39, 51, 56, 59, 68 110 (24.2) 17 (36.2) 93 (22.9)
Low-risk types
or negative
67 (14.8) 4 (8.5) 63 (15.5)
Undetermined 32 (7.0) 5 (10.6) 27 (6.6)
Multiple infection 38 (8.4) 2 (4.2) 36 (8.8)
Parity
0 151 (33.3) 15 (31.9) 136 (30.4) 0.50
1–2 243 (53.5) 28 (59.6) 215 (52.8)
3+ 60 (13.2) 4 (8.5) 56 (13.8)
Use of oral contraceptives
Yes 39 (8.6) 3 (6.7) 36 (8.8) 0.49
No 378 (90.6) 42 (93.3) 336 (82.6)
Unknown 37 (8.1) 4 (8.5) 33 (8.1)
Smoking
Never smokers 209 (46.0) 15 (31.9) 185 (45.5) 0.89
Smokers 210 (46.3) 30 (63.8) 189 (46.4)
Current smokers 151 (33.3) 24 (51.1) 136 (33.4)
Former smokers 59 (13.0) 6 (12.8) 53 (14.2)
Unknown 35 (7.8) 2 (4.3) 33 (8.1)
Number of lifetime sexual partners
1 68 (15.0) 6 (12.8) 62 (15.2) 0.84
2–3 115 (25.3) 13 (27.7) 102 (25.1)
4 235 (51.8) 26 (55.3) 209 (51.4)
Unknown 36 (7.9) 2 (4.3) 34 (8.4)
Age at first sexual intercourse, years
≤20 150 (33.0) 16 (34.0) 134 (32.9) 0.72
21–23 176 (38.8) 17 (36.2) 159 (39.1)
≥24 93 (20.5) 12 (25.5) 81 (19.9)
Unknown 35 (7.7) 2 (4.3) 33 (8.1)
CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus.
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1451 © 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.
Original Articlewww.wileyonlinelibrary.com/journal/cas Matsumoto et al.

― 281 ―
stronger evidence for the protective effect of the DRB1*1302allele. In addition, negative associations between the DRB1*13alleles and cervical cancer have been consistently reported incase–control studies.(7) In a small prospective study of Frenchwomen with CIN1 (n = 86), a relationship between theDRB1*13 alleles and cytological regression was observed.(15)
These observations also support the protective effect of theDRB1*13 alleles. However, some studies have reported a pro-tective effect of DRB1*1301,(16,17) and other studies have sug-gested that DRB1*1302 decreases the risk of cervicalcancer.(18,19) In the present study, we confirmed only the pro-tective effect of the DRB1*1302 allele because theDRB1*1301 allele is rarely detected in Japanese populations.Cervical cancer arises by way of several carcinogenic steps:
HPV acquisition, HPV persistence (development of low-gradecervical precursor lesion), progression of a persisting infectionto cervical precancer, and invasion through the basement mem-brane of the epithelium.(3,20) In multistage cervical carcinogen-esis, however, the step at which DRB1*13 alleles exert theirprotective effect is not fully understood. Two prospective stud-ies of HPV infections have shown that DRB1*13 alleles donot play a protective role against the acquisition and persis-tence of viral infections.(21,22) This is consistent with our find-ing that the DRB1*1302 frequency was similar betweenwomen with NL (12%) and CIN1 (11%). In the present study,
the DRB1*1302 frequency significantly decreased to 5.2% forCIN2 ⁄3 and 5.8% for ICC. In the prospective analysis ofwomen with cytological LSIL and histological CIN1 ⁄2, thecumulative probability of CIN3 diagnosed within the next10 years was significantly low among DRB1*1302-positivewomen. These observations suggest that the DRB1*1302 allelemay act protectively against progression from CIN1 to CIN2⁄3. Several studies have reported the poor reproducibility ofCIN grading, even among well-trained observers.(13,14) In par-ticular, CIN2 is an equivocal diagnosis of precancer (a heterol-ogous borderline category between CIN1 and CIN3).(3)
Therefore, it may be difficult to strictly determine whether theDRB1*1302 allele protects against progression from CIN1 toCIN2, or from CIN2 to CIN3. The protective effect of theDRB1*1302 allele against progression to cervical precancersuggests that DRB1*13 alleles could contribute to theimmunological recognition of viral antigens such as the E7protein, which is increasingly expressed during progression tocervical precancer.(23,24) However, very little is known aboutthe binding of DRB1*13 molecules to HPV-related antigens.As the DRB1*1302 and DQB1*0604 alleles were in linkage
disequilibrium, very similar findings were observed for theDRB1*1302 and DQB1*0604 alleles in both cross-sectionaland prospective analyses. Although the protective effect ofDRB1*13 alleles is the most consistent HLA finding in
(a)
(b)
(c)
(d)
Fig. 1. Cumulative risks of cervical intraepithelial neoplasia grade 3 within 10 years in relation to human leukocyte antigen class II polymor-phisms. A Kaplan–Meier plot was used to estimate the cumulative 10-year probabilities of progression to cervical intraepithelial neoplasia grade3 among women with low-grade squamous intraepithelial lesion cytology for selected human leukocyte antigen class II alleles: DRB1*0901 (a),DRB1*1302 (b), DRB1*1501 (c), and DQB1*03 alleles (d). P-values were calculated using the log–rank test.
© 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1452
Original ArticleHLA class II alleles and risk of cervical cancer in Japan www.wileyonlinelibrary.com/journal/cas

― 282 ―
published reports, the question is still open as to whetherDRB1*1302 alone, DQB1*0604 alone, or both are associatedwith reduced risk of cervical diseases, or whether other MHCcomplex genes in linkage disequilibrium with these alleles aremore important. To evaluate the independent effect of theDRB1*1302 and DQB1*0604 alleles, larger studies will berequired.The cross-sectional analysis suggested that the DRB1*0901
allele may act protectively against cervical cancer pathogene-sis. A meta-analysis also reported the protective effect ofDRB1*0901 against invasive cervical squamous cell carcinomain Caucasian populations.(25) Interestingly, this allele was notassociated with progression to CIN3 in the prospective analy-sis, suggesting that the DRB1*0901 allele could exert a protec-tive effect on progression from CIN2 ⁄3 to ICC. TheDRB1*0901 allele frequency was significantly lower in womenwith ICC than in those with CIN2 ⁄3. Alternatively or addition-ally, the discrepancy may be explained by the HPV type-speci-fic effect of the DRB1*0901 allele. When the analysis wasconfined to HPV16-positive women with LSIL cytology, thecumulative probability of progression to CIN3 was loweramong DRB1*0901-positive women compared withDRB1*0901-negative women (data not shown), but this effectwas not statistically significant (P = 0.12) due to limitationsimposed by the small sample size.We could not find any significant association between
DRB1*1501 or DQB1*03 and risk of developing CIN2 ⁄3 orICC. Effects of the DRB1*1501 and DQB1*03 alleles havenot been found in prospective cohort studies so far,(15,21,22)
and the results from case–control studies have not beenentirely consistent.(7,16–19,25–27) Although several groups havesuggested a significant association of DRB1*1501 orDQB1*0602 (or the corresponding haplotype DRB1*1501-DQB1*0602) with HPV16-positive cervical cancer,(17,26,27) an
increased risk of progression to CIN3 was not observed foreither the DRB1*1501 or DQB1*0602 allele, even amongHPV16-positive women in the present study (data not shown).The inconsistent results regarding the DRB1*1501 andDQB1*0602 alleles may be explained by two studies suggest-ing that cancer risks associated with these alleles may varyaccording to HPV16 E6 variations.(27,28)
One may speculate that HLA class II DRB1*13 testing,alone or in combination with genotype-specific HPV testing,for women with low-grade cervical abnormalities might beuseful for identifying populations at decreased risk of diseaseprogression. Interestingly, the protective effect of theDRB1*1302 allele appears to be non-specific to the HPVgenotype. However, HLA class II testing may not be recom-mended in clinical practice because only 10–20% of womenamong various ethnic populations have the DRB1*13 alleles.(7)
In addition, DRB1*13 does not prevent all cervical cancer;some women with cervical cancer are positive for DRB1*13.The present study had several limitations. First, possible
misclassification of CIN lesions may have affected the results.Recently, p16INK4a immunohistochemistry has been shown toincrease the sensitivity and specificity of CIN2–3 detection incervical biopsies.(29) Although two pathologists reviewed allhistological specimens, the histological diagnosis of cervicalspecimens was obtained by H&E examination alone. Second,the present study may have missed several HLA associationswith cervical diseases due to limitations imposed by the smallsample size. Although this is the first large-scale study onHLA association with cervical cancer in Japan, larger studieswill be required to further evaluate the risk of cervical cancerand precancer in relation to HLA polymorphism. Finally, thepresent study did not clarify the mechanism by which theDRB1*1302 allele protects against cervical precancer. Toaddress this, immunological studies on the binding of
Table 3. Effect of selected human leukocyte antigen (HLA) class II alleles on progression to cervical intraepithelial neoplasia grade 3 in
Japanese women with low-grade squamous intraepithelial lesion (n=454)
HLA class
II allelesn
Person-
monthsEvents
10-year progression
rate (95% CI)
Log–rank testAdjusted analysis†
P-value Hazard ratio (95% CI) P-value
DRB1*0901
Positive 118 7274.9 15 22.5 (11.9–38.6) 0.88 1.15 (0.53–2.33) 0.71
Negative 336 20 715.1 43 21.4 (15.2–29.4) 1.00
DRB1*1302
Positive 47 2916.7 1 3.2 (0.5–20.8) 0.03 0.13 (0.02–0.94) 0.04
Negative 407 25 073.3 57 23.7 (17.6–31.5) 1.00
DRB1*1501
Positive 82 5163.5 13 21.3 (12.3–35.5) 0.43 1.12 (0.56–2.425 0.76
Negative 372 22 826.5 45 21.8 (15.5–30.1) 1.00
DQB1*03
Positive 244 14 438.9 32 23.5 (15.3–35.0) 0.62 1.26 (0.72–2.20) 0.41
Negative 210 13 551.1 26 19.8 (13.1–29.2) 1.00
DQB1*0604
Positive 46 2879.6 1 3.2 (0.5–20.8) 0.03 0.13 (0.02–0.95) 0.04
Negative 408 25 110.4 57 23.7 (17.6–31.4) 1.00
†Cox regression model was used for statistical adjustments. Patient age, histological grade at the time of entry, human papillomavirus (HPV) riskcategory (HPV16 ⁄ 18 ⁄ 31 ⁄ 33 ⁄ 35 ⁄ 45 ⁄ 52 ⁄ 58, other carcinogenic types, or carcinogenic HPV negative), smoking status, parity, use of oral contracep-tives, number of lifetime sexual partners, and age at first sexual intercourse were included in the multivariate model for adjustments. CI, confi-dence interval.
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1453 © 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.
Original Articlewww.wileyonlinelibrary.com/journal/cas Matsumoto et al.

― 283 ―
DRB1*13 molecules to HPV-related antigens will be required.Analyses of other genes in the MHC complex found in linkagedisequilibrium with the DRB1*13 alleles may also give insightto this protective effect.In conclusion, our results confirmed the protective effects of
DRB1*1302 through two different types of analysis in a singlestudy. Our data also suggested that the DRB1*1302 allele mayfunction protectively against progression from CIN1 to CIN2⁄3. However, the mechanism underlying the protective effectof DRB1*1302 allele is not fully understood. To enhance ourbiological understanding of this effect, identification of specificviral epitopes presented by the DRB1*1302 allele will beneeded.
Acknowledgments
The authors thank Dr. Tadahito Kanda (Center for Pathogen Genomics,National Institute of Infectious Diseases, Tokyo, Japan) for his com-ments on the study design, Dr. Tomoyuki Kitagawa (Department ofPathology, Cancer Institute Hospital, Japanese Foundation of CancerResearch, Tokyo, Japan) for his histological review, Mr. Masafumi
Tsuzuku (Department of Cytopathology, Cancer Institute Hospital,Japanese Foundation of Cancer Research) for his cytological review,many other researchers who facilitated this study, and all the womenwho participated in the study. This work was supported by a grantfrom the Ministry of Education, Science, Sports and Culture of Japan(grant nos. 12218102 and 25462585).
Disclosure Statement
The authors have no conflict of interest.
Abbreviations
CIN1–3 cervical intraepithelial neoplasia grade 1–3HLA human leukocyte antigenICC invasive cervical cancerHPV human papillomavirusLSIL low-grade squamous intraepithelial lesionNL normal cytologyOC oral contraceptivePc P corrected by the Bonferroni method
References
1 Ferlay J, Shin HR, Bray F et al. Estimates of worldwide burden of cancer in2008: GLOBOCAN 2008. Int J Cancer 2008; 127: 2893–917.
2 Bouvard V, Baan R, Straif K et al. WHO International Agency for Researchon Cancer Monograph Working Group. A review of human carcinogens–PartB: biological agents. Lancet Oncol 2009; 10: 321–2.
3 Schiffman M, Castle PE, Jeronimo J, Rodriguez AC, Wacholder S. Humanpapillomavirus and cervical cancer. Lancet 2007; 370: 890–907.
4 Castellsagu�e X, Mu~noz N. Chapter 3: cofactors in human papillomavirus car-cinogenesis–role of parity, oral contraceptives, and tobacco smoking. J NatlCancer Inst Monogr 2003; 31: 20–8.
5 Magnusson PK, Spar�en P, Gyllensten UB. Genetic link to cervical tumours.Nature 1999; 400: 29–30.
6 Breitburd F, Ramoz N, Salmon J, Orth G. HLA control in the progression ofhuman papillomavirus infections. Semin Cancer Biol 1996; 7: 359–71.
7 Hildesheim A, Wang SS. Host and viral genetics and risk of cervical cancer:a review. Virus Res 2002; 89: 229–40.
8 Han R, Breitburd F, Marche PN, Orth G. Linkage of regression and malig-nant conversion of rabbit viral papillomas to MHC class II genes. Nature1992; 356: 66–8.
9 Matsumoto K, Maeda H, Oki A, et al. for Japan HPV And Cervical Cancer(JHACC) Study Group. HLA class II DRB1*1302 allele protects against pro-gression to cervical intraepithelial neoplasia grade 3: a multicenter prospec-tive cohort study. Int J Gynecol Cancer 2012; 22: 471–8.
10 Konno Y, Numaga J, Tsuchiya N et al. HLA-B27 subtypes and HLA classII alleles in Japanese patients with anterior uveitis. Invest Ophthalmol VisSci 1999; 40: 1838–44.
11 Yoshikawa H, Kawana T, Kitagawa K et al. Detection and typing of multi-ple genital human papillomaviruses by DNA amplification with consensusprimers. Jpn J Cancer Res 1991; 82: 524–31.
12 Nagano H, Yoshikawa H, Kawana T et al. Association of multiple humanpapillomavirus types with vulvar neoplasias. J Obstet Gynaecol Res 1996;22: 1–8.
13 Stoler MH, Schiffman M; Atypical Squamous Cells of Undetermined Signifi-cance-Low-grade Squamous Intraepithelial Lesion Triage Study (ALTS)Group. Interobserver reproducibility of cervical cytologic and histologicinterpretations: realistic estimates from the ASCUS-LSIL Triage Study.JAMA 2001; 285: 1500–5.
14 Carreon JD, Sherman ME, Guill�en D et al. CIN2 is a much less reproducibleand less valid diagnosis than CIN3: results from a histological review ofpopulation-based cervical samples. Int J Gynecol Pathol 2007; 26: 441–6.
15 Sastre-Garau X, Cartier I, Jourdan-Da Silva N et al. Regression of low-gradecervical intraepithelial neoplasia in patients with HLA-DRB1*13 genotype.Obstet Gynecol 2004; 104: 751–5.
16 Wang SS, Wheeler CM, Hildesheim A et al. Human leukocyte antigen classI and II alleles and risk of cervical neoplasia: results from a population-based study in Costa Rica. J Infect Dis 2001; 184: 1310–14.
17 Beskow AH, Josefsson AM, Gyllensten UB. HLA class II alleles associatedwith infection by HPV16 in cervical cancer in situ. Int J Cancer 2001; 93:817–22.
18 Maciag PC, Schlecht NF, Souza PS et al. Major histocompatibility complexclass II polymorphisms and risk of cervical cancer and human papillo-mavirus infection in Brazilian women. Cancer Epidemiol Biomarkers Prev2000; 9: 1183–91.
19 Madeleine MM, Johnson LG, Smith AG et al. Comprehensive analysis ofHLA-A, HLA-B, HLA-C, HLA-DRB1, and HLA-DQB1 loci and squamouscell cervical cancer risk. Cancer Res 2008; 68: 3532–9.
20 Scarinci IC, Garcia FA, Kobetz E et al. Cervical cancer prevention: newtools and old barriers. Cancer 2010; 116: 2531–42.
21 Maciag PC, Schlecht NF, Souza PS et al. Polymorphisms of the humanleukocyte antigen DRB1 and DQB1 genes and the natural history of humanpapillomavirus infection. J Infect Dis 2002; 186: 164–72.
22 Mahmud SM, Robinson K, Richardson H et al. HLA polymorphisms andcervical human Papillomavirus infection in a cohort of Montreal Universitystudents. J Infect Dis 2007; 196: 82–90.
23 Nakagawa S, Yoshikawa H, Yasugi T et al. Ubiquitous presence of E6 andE7 transcripts in human papillomavirus-positive cervical carcinomas regard-less of its type. J Med Virol 2000; 62: 251–8.
24 Coquillard G, Palao B, Patterson BK. Quantification of intracellular HPVE6 ⁄ E7 mRNA expression increases the specificity and positive predictivevalue of cervical cancer screening compared to HPV DNA. Gynecol Oncol2011; 120: 89–93.
25 Yang YC, Chang TY, Lee YJ et al. HLA-DRB1 alleles and cervical squa-mous cell carcinoma: experimental study and meta-analysis. Hum Immunol2006; 67: 331–40.
26 Apple RJ, Erlich HA, Klitz W et al. HLA DR-DQ associations with cervicalcarcinoma show papillomavirus-type specificity. Nat Genet 1994; 6: 157–62.
27 Cuzick J, Terry G, Ho L et al. Association between high-risk HPV types,HLA DRB1* and DQB1* alleles and cervical cancer in British women. Br JCancer 2000; 82: 1348–55.
28 Matsumoto K, Yasugi T, Nakagawa S et al. Human papillomavirus type 16E6 variants and HLA class II alleles among Japanese women with cervicalcancer. Int J Cancer 2003; 106: 919–22.
29 Darragh TM, Colgan TJ, Cox JT et al. Members of LAST Project WorkGroups. The lower anogenital squamous terminology standardization Projectfor HPV-Associated Lesions: background and consensus recommenda-tions from the College of American Pathologists and the American Societyfor Colposcopy and Cervical Pathology. Arch Pathol Lab Med 2012; 136:1266–97.
© 2015 The Authors. Cancer Science published by Wiley Publishing Asia Pty Ltdon behalf of Japanese Cancer Association.
Cancer Sci | October 2015 | vol. 106 | no. 10 | 1454
Original ArticleHLA class II alleles and risk of cervical cancer in Japan www.wileyonlinelibrary.com/journal/cas

― 284 ―
RESEARCH ARTICLE Open Access
HPV-16 impairs the subcellular distribution andlevels of expression of protein phosphatase 1γ incervical malignancyTakayuki Seiki1, Kazunori Nagasaka1*, Christian Kranjec2, Kei Kawana1, Daichi Maeda3, Hiroe Nakamura1,Ayumi Taguchi1, Yoko Matsumoto1, Takahide Arimoto1, Osamu Wada-Hiraike1, Katsutoshi Oda1,Shunsuke Nakagawa4, Tetsu Yano5, Masashi Fukayama3, Lawrence Banks2, Yutaka Osuga1 and Tomoyuki Fujii1
Abstract
Background: The high risk Human Papillomavirus (HPV) E6 oncoproteins play an essential role in the developmentof cervical malignancy. Important cellular targets of E6 include p53 and the PDZ domain containing substrates suchas hScrib and Dlg. We recently showed that hScrib activity was mediated in part through recruitment of proteinphosphatase 1γ (PP1γ).Methods: Expression patterns of hScrib and PP1γ were assessed by immunohistochemistry of HPV-16 positivecervical intraepithelial neoplasm (CIN), classified as CIN1 (n = 4), CIN2 (n = 8), CIN3 (n = 8), cervical carcinoma tissues(n = 11), and HPV-negative cervical tissues (n = 8), as well as by subfractionation assay of the HPV-16 positive cervicalcancer cell lines, CaSki and SiHa. To explore the effects of the HPV-16 oncoproteins, we have performed siRNAknockdown of E6/E7 expression, and monitored the effects on the expression patterns of hScrib and PP1γ.Results: We show that PP1γ levels in HPV-16 positive tumour cells are reduced in an E6/E7 dependent manner.Residual PP1γ in these cells is found mostly in the cytoplasm as opposed to the nucleus where it is predominantlyfound in normal cells. We have found a striking concordance with redistribution in the pattern of expression (9/11;81.8%) and loss of PP1γ expression in HPV-16 positive cervical tumours (2/11; 18.2%). Furthermore, this loss of PP1γexpression and redistribution in the pattern of expression occurs progressively as the lesions develop (8/8; 100%).
Conclusion: Together, these results suggest that PP1γ may be a novel target of the HPV-16 oncoproteins andindicate that it might be a potential novel biomarker for HPV-16 induced malignancy.
Keywords: Cervical cancer, Immunohistochemistry, hScrib, Protein phosphatase 1, Proteasome degradation, Humanpapillomavirus 16
BackgroundHuman Papillomaviruses (HPVs) are the aetiologicalagents of cervical cancer [1]. This is caused by infectionwith the high risk subset of HPV types, of which HPV-16 is the most important, being responsible for over 60%of global cervical cancer cases [2]. Cancer-causing HPVsencode two oncoproteins, E6 and E7, whose continued ex-pression and activity is essential for maintaining the malig-nant phenotype, many years after the initial immortalising
events [3,4]. Both viral oncoproteins function by perturb-ing the normal activity of a variety of different cellularcontrol mechanisms. HPV E7 promotes cell cycle progres-sion, in part through its association with members of thepocket protein family of tumour suppressors [5], whilstHPV E6 counteracts the pro-apoptotic effects of E7through targeting the p53 tumour suppressor [6]. In bothcases, the viral oncoproteins make efficient use of the cel-lular ubiquitin-proteasome machinery, with E7 targetingpRb through the cullin 2 ubiquitin ligase complex [7],whilst E6 uses the E6AP ubiquitin ligase to target p53 [8].The effects of E6 and E7 are therefore cooperative, andthis is reflected both in tissue culture systems, where they
* Correspondence: [email protected] of Obstetrics and Gynecology, Faculty of Medicine, TheUniversity of Tokyo, Tokyo 113-8655, JapanFull list of author information is available at the end of the article
© 2015 Seiki et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Seiki et al. BMC Cancer (2015) 15:230 DOI 10.1186/s12885-015-1141-0

― 285 ―
cooperate in the immortalisation of primary keratinocytes[9-11], and in animal models of tumourigenesis, wherethey cooperate in the induction of tumours in the skinand cervix [12,13].Whilst targeting the pRb and p53 pathways is obvi-
ously very important for cervical tumourigenesis, it isalso clear that E6 and E7 have a large number of otheractivities, many of which are also important for tumourdevelopment. In the case of high risk HPV E6 oncopro-teins, an intriguing class of targets that appear to be im-portant for HPV E6 induced malignancy are the PDZ(PSD/Dlg/ZO) domain containing substrates [14,15].These are bound by E6 via a short stretch of amino acidswithin the extreme carboxy terminal region of the E6oncoprotein. Most importantly, this PDZ binding motif(PBM) is only found in the high risk HPV E6 oncopro-teins and is absent from the benign HPV E6 proteins[16,17]. Through this PBM, E6 can interact with a largenumber of cellular PDZ domain containing proteins,many of which are subject to E6-induced proteasomaldegradation and E6-induced redistribution [16,18-21].One of the most important of these targets is the cellulartumour suppressor hScrib. In Drosophila Scrib was ori-ginally identified as a potential tumour suppressor [22],and more recent studies in mammalian tissues also indi-cate tumour suppressive potential for hScrib. Loss ofScrib cooperates with c-Myc in the development ofmammary carcinogenesis and Scrib also downregulatesERK signaling, with hScrib deregulation correlating withpoor cancer prognosis [23-27]. In cervical tumourigen-esis, hScrib patterns of expression are also perturbed aslesions develop, with hScrib being completely absent inmany late stage tumours [28]. We recently found thathScrib could interact with PP1γ [29] a protein phosphat-ase that plays a critical role in controlling chromatinorganization and also has an important role in the DNAdamage response pathway [30,31] This suggested thatPP1γ expression patterns in cervical tumourigenesismight likewise be perturbed. Therefore we initiated aseries of studies to investigate the pattern of PP1γ ex-pression in HPV16 positive cervical tumours and derivedcell lines. We show that PP1γ is indeed subject to astriking alteration in both its levels of expression and lo-calisation, both as lesions develop, and in the tumourderived cell lines. However this altered pattern of ex-pression is independent of hScrib, is due directly to E6/E7 expression, and highlights PP1γ as potential novelbiomarker of HPV induced neoplasia.
MethodsCell lines and cultureHPV positive cervical cancer cell lines, CaSki, SiHa andHeLa plus HPV negative C33A (cervical cancer derived)and HaCaT (human keratinocytes) cells were cultured in
Dulbecco’s modified Eagle’s medium (DMEM) supple-mented with 10% fetal bovine serum at 37°C in a hu-midified incubator with 5% CO2 [32]. The effect ofproteasome inhibitor was determined 24 hours post-transfection after 3 hours of treatment with 10 μMMG132 (Calbiochem).For plasmid transfection, 293 cells were transfected
using TransIT-293 transfection reagent (Mirus Bio) andHaCaT cells were transfected using Lipofectamine 2000(Invitrogen), according to the manufacturer’s instruc-tions, with pcDNA-HPV-16 E6. A plasmid expressing β-galactosidase was included in each transfection andpcDNA was used to equalize the input DNA.
AntibodiesThe following commercial antibodies were used at thedilution indicated: anti-hScrib goat polyclonal antibody(Santa Cruz WB 1:1000, IHC 1:100), anti-PP1γ goatpolyclonal antibody (Santa Cruz WB 1:1000), anti-PP1Gamma/PPP1CC Antibody LS-B4960 IHC-plus (tm)rabbit polyclonal antibody (Lifespan bioscience, Inc. IHC1:200), anti-PP1γ sheep polyclonal antibody (Abcam,WB 1:1000), anti-actin monoclonal antibody (Sigma,WB 1:5000), mouse monoclonal anti-p53 (DO-1) (SantaCruz WB 1:500), anti-p84 mouse monoclonal antibody(Abcam, WB 1:1000), anti-E-Cadherin rabbit polyclonalantibody (Santa Cruz WB 1:500), anti-α-tubulin mousemonoclonal antibody (Abcam, WB 1:1000), mouse mono-clonal anti-vimentin antibody (Santa Cruz WB 1:500).
siRNA transfectionThe HPV-positive cervical cancer cells were seeded on6 cm dishes and transfected using Lipofectamine 2000(Invitrogen) with control siRNA against Luciferase (siLuc),or siRNA against HPV-16 and 18 E6 sequences (Dharma-con) described previously by Kranjec C et al., 2011.72 hours post-transfection cells were harvested and totalcell extracts or cell fractionated extracts were then ana-lysed by western blotting. Alexa 568 labeled negative con-trol siRNA (Qiagen) was used to measure transfectionefficiency. The transfection efficiency was determined tobe over 70% for each cell line.
Subcellular fractionation assaysDifferential extraction of the cells to obtain cytoplasmic,membrane, cytoskeleton, and nuclear fractions was per-formed using the Calbiochem Proteo Extract Fraction-ation Kit according to the manufacturer’s instructions.To inhibit phosphatase activity during the preparation ofcell lysates, phosphatase inhibitors (1 mM Na3VO4,1 mM β-Glycerophosphate, 2.5 mM Sodium Pyrophos-phate, 1 mM Sodium Fluoride) were also included.
Seiki et al. BMC Cancer (2015) 15:230 Page 2 of 9

― 286 ―
Western blottingTotal cellular extracts were prepared by directly lysingcells from dishes in SDS lysis buffer. Alternatively cellswere lysed in either E1A buffer (25 mM HEPES pH 7.0,0.1% NP-40, 150 mM NaCl, plus protease inhibitorcocktail; Calbiochem) or RIPA buffer (50 mM Tris HClpH 7.4, 1% NP-40, 150 mM NaCl, 1 mM EDTA, plusprotease inhibitor cocktail; Calbiochem). For westernblotting, 0.45 μm nitrocellulose membrane (Schleicher
and Schuell) was used and membranes were blockedfor 1 hour at 37°C in 10% milk/PBS followed by incuba-tion with the appropriate primary antibody diluted in10% milk/0.5% Tween 20 for 1 hour. After severalwashings with PBS 0.5% Tween 20, HRP-conjugatedsecondary antibodies (DAKO) in 10% milk/0.5% Tween20 were incubated for 1 hour. Blots were developed usingAmersham ECL reagents according to the manufacturer'sinstructions.
PP1hScrib
HPV16 SCC
patternA
patternB
HPV (-)
PP1hScrib
PP1hScrib
HPV negative normal cervix
HPV 16 type positive SCC cervical cancer
PP1 PP1
A
B
Figure 1 Immunohistochemical analysis of the expression and localisation of hScrib and PP1γ in advanced squamous cervical carcinomas.(A) Paraffin embedded excised tissues were immunostained with anti-hScrib or anti-PP1γ as indicated, and counterstained with haematoxylin. For theantibodies, immunostaining was performed according to standard techniques using an autostainer (BenchMark XT; Ventana Medical Systems, Inc.,Tucson, AZ, USA). Representative experiments for a section of cervical epitheliums from normal cervix and advanced squamous cervical carcinomas(×200 original magnification). (B) High resolution microscopic images (scale bars: 20 μm) for a section of cervical epitheliums from normal cervix andHPV-16 positive advanced squamous cervical carcinomas.
Seiki et al. BMC Cancer (2015) 15:230 Page 3 of 9

― 287 ―
ImmunohistochemistryAll tissue samples were fixed in formalin and embeddedin paraffin (obtained from patients under InstitutionalReview Board approval through the University of TokyoHospital). For all antibodies, immunostaining was per-formed according to standard techniques using an auto-stainer (BenchMark XT; Ventana Medical Systems, Inc.,Tucson, AZ, USA). Immunoreactivity was interpretedbased on the negative control, which was incubatedwithout the primary antibody. Detection of hScrib ex-pression was evaluated based on the existence of baso-lateral membrane staining as described previously [28].For PP1γ, the expression was evaluated by nuclear stain-ing. The immunostaining patterns of each sample wereevaluated independently and blindly by pathologists spe-cializing in gynaecological pathology, and cytology.
PCR-based HPV DNA testingDNA was extracted from cervical smear samples by usingthe QIAGEN® DNeasy® Blood & Tissue Kits. PCR-basedHPV DNA testing was performed using the PGMY-CHUV assay. Briefly, standard PCR was conducted usingthe PGMY09/11 L1 consensus primer sets and HLA-dQprimer sets. Reverse blotting hybridization was subse-quently performed as described previously [33].
ResultsDistribution patterns of hScrib and PP1γ in HPV-16positive cervical intraepithelial neoplasm (CIN) andcervical carcinoma tissuesPrevious studies had highlighted hScrib as a potentialbiomarker for HPV-16 induced malignancy [19,28,34].We reasoned that if PP1γ was also regulated directly byhScrib, this should be similarly affected in HPV-16 in-duced malignancy. In order to investigate this we per-formed IHC analysis of hScrib and PP1γ expression inHPV-16 positive cervical tumours and control cervix.The results obtained are shown in Figure 1 and Table 1.In normal tissue hScrib is found primarily at cell-celljunctions, with high levels of expression as the cellsbegin to differentiate. However, hScrib distribution is al-tered significantly in all the HPV-16 positive tumours,with significant redistribution in the pattern of expres-sion in 5/11 tumours and a complete loss of expressionin 6/11 tumours. These results are largely in agreementwith previous studies [28,35]. In the case of PP1γ, thisdisplays a largely nuclear pattern of expression and thisis present throughout the differentiating epithelium inthe normal cervical tissue. In contrast, in the cervical tu-mours there is a complete loss of expression of PP1γ in2/11 cases, with a striking redistribution in the patternof expression in the remaining 9 samples, where therewas a shift from a nuclear localisation to a cytoplasmicpattern of expression.
We were then interested in investigating whether per-turbation in the pattern of PP1γ expression was an earlyor late event during HPV-induced neoplastic progres-sion. To do this we repeated the PP1γ IHC analysis onlesions exhibiting different grades of CIN. The lesionswere classified as CIN1 (n = 4), CIN2 (n = 8), CIN3 (n = 8).As shown in Figure 2, there is a marked loss in nuclearPP1γ expression, which is already apparent in CIN2, andthis is more evident in the CIN3 lesion, where there arealso much lower levels of PP1γ expression. Interestingly,PP1γ positive cells were distributed only in the lower thirdof the epithelial layer in CIN1 cases (4/4) and 8/8 of pa-tients with CIN3 had PP1γ positive cells distributed inthe lower, middle, and upper third of the epithelium(Figure 2B). In the case of hScrib, there is a similar per-turbation in the pattern of expression as the lesions de-velop, but similar to what has been reported previously,there is a tendency in some lower grade lesions to findhighly overexpressed hScrib in regions of the epithelium.These results indicate that hScrib and PP1γ, whilst
both being perturbed during the progression to malig-nancy, are altered in a manner that is not interdepend-ent, suggesting that PP1γ might be an independentmarker for cervical tumour development. Indeed, thepattern and expression levels of PP1γ declined with analmost linear relationship from normal tissue, throughincreasing grades of CIN lesion, to invasive cancer.
Analysis of PP1γ expression in HPV-16-positive cellsIn order to determine whether perturbation of PP1γ ex-pression was a direct result of HPV-16 oncoproteinfunction, we proceeded to examine the pattern of PP1γexpression in cell lines derived from HPV-16 positivecervical tumours. To do this we analysed the pattern ofPP1γ expression in HPV-16 positive CaSki and SiHa
Table 1 Immunostaining patterns for hScrib and PP1γ inclinical samples of human uterine cervix
hScrib
Normal 16-positive
Membrane 8 0
Cytoplasm 0 5
Nuclear 0 0
No expression 0 6
Total 8 11
PP1y
HPV negative 16-positive
Membrane 0 0
Cytoplasm 0 9
Nuclear 8 0
No expression 0 2
Total 8 11
Seiki et al. BMC Cancer (2015) 15:230 Page 4 of 9

― 288 ―
cells, and compared this with HPV negative HaCaT cells.To determine whether any alterations might be HPV-specific, we also transfected the cells with siRNA E6/E7and siLuc as a control. After 72 hours the cells were har-vested and cells fractionated into cytosolic, membrane,nuclear and cytoskeletal pools, such that the pattern ofPP1γ subcellular distribution could be monitored. Thepattern of PP1γ expression was then ascertained bywestern blotting and the results obtained are shown inFigure 3. PP1γ is found predominantly within the nu-cleus in HaCaT cells (Figure 3A), whilst in the HPV-16
positive cells it is found weakly re-localised both in nu-clear and cytoplasmic locations. However when E6/E7expression is ablated there is a dramatic redistributionin the pattern of PP1γ expression, with much higherlevels being found within the nuclear fraction of the cells(Figure 3B). In contrast, we found no difference in PP1γtranscript levels after siRNA E6/E7 treatment in HPV-16positive cells (data not shown).These results suggest that loss of nuclear PP1γ expres-
sion in HPV positive tumour cells is a direct result ofthe expression of the HPV E6/E7 oncoproteins.
Normal HPV16 positive CIN2-3
CIN2CIN3
Normal HPV16 positive CIN2-3
CIN2CIN3
PP1
hScrib hScrib
PP1
A
B CIN3CIN1
Figure 2 Immunohistochemical analysis of the expression and localisation of hScrib and PP1γ in various stages of cervical intraepithelialneoplasms. (A) Paraffin embedded excised tissues were immunostained with anti-hScrib or anti-PP1γ as indicated, and counterstained withhaematoxylin. For the antibodies, immunostaining was performed according to standard techniques using an autostainer (BenchMark XT; VentanaMedical Systems, Inc., Tucson, AZ, USA). Representative experiments for a section of cervical epitheliums from normal cervix (left) and cervicalintraepithelial neoplasms (CIN) grade 2 and 3 (right) (×200 original magnification). (B) High resolution microscopic images (scale bars: 20 μm) for asection of cervical epithelia from CIN grade 1 and 3.
Seiki et al. BMC Cancer (2015) 15:230 Page 5 of 9

― 289 ―
PP1γ is subject to degradation in HPV-16 positive cellsInterestingly, the fractionation studies indicate thatwhilst there is a significant increase in nuclear PP1γ inthe absence of E6/E7, there is not a significant loss ofcytoplasmic PP1γ, suggesting that some of the loss ofnuclear expression may be due to proteasome mediateddegradation. Therefore we were first interested in deter-mining whether E6/E7 expression could affect the totallevels of PP1γ expression. To do this we analysed thelevels of PP1γ expression in total cell extracts from
CaSki and SiHa cells previously transfected with siRNAE6/E7 or siLuc as a control. After 72 hours the cellswere extracted and the levels of PP1γ expression moni-tored by western blotting. The results in Figure 4A showthat loss of E6/E7 expression induces a marked increasein the total levels of PP1γ expression in HPV-16 positivecells, in a manner similar to that seen for restoration ofp53 levels, which served as a positive control for efficientablation of E6/E7 expression. We also monitored the ef-ficiency of E6/E7 knockdown by RT-PCR and found that
CaSkisi luciferase siE6/E7
F1 F2 F3 F4 F1 F2 F3 F4
hScrib
alfa-tubulin
p84
Vimentin
F1: cytosol F2: membrane&organ F3: nucleus F4: cytoskeleton
p53
B
E-Cadherin
SiHa
alfa-tubulin
F1: cytosol F2: membrane&organ F3: nucleus F4: cytoskeleton
hScrib
p84
Vimentin
E-Cadherin
hScrib
PP1
p84
Vimentin
alfa-tubulin
E-Cadherin
F1 F2 F3 F4
HaCaTA
F1: cytosol F2: membrane&organ F3: nucleus F4: cytoskeleton
si luciferase siE6/E7
F1 F2 F3 F4 F1 F2 F3 F4
PP1
PP1
Figure 3 PP1γ is mislocalised in HPV-16 positive tumour cells. (A) HaCaT cells, and (B) siE6/E7or siluciferase control transfected CaSki andSiHa cells were fractioned into cytoplasmic (F1), membrane (F2), nuclear (F3), and cytoskeleton (F4) pools and hScrib and PP1γ were detected bywestern blotting. α-tubulin was a loading control for the cytoplasmic fraction, E-Cadherin was a loading control for the membrane fraction, p84was a loading control for the nuclear fraction, and Vimentin was a loading control for the cytoskeleton fraction.
Seiki et al. BMC Cancer (2015) 15:230 Page 6 of 9

― 290 ―
E6/E7 transcripts were reduced by around 60% followingsiRNA transfection (data not shown). In contrast to thechange in PP1γ protein levels, we found no difference inPP1γ transcript levels after siRNA E6/E7 treatment inHPV-16 positive cells. Furthermore, to determine whetherthe cell type or E6 expression contributed to the alter-ations in PP1γ expression levels, we compared the abilityof E6 to direct the degradation of PP1γ in 293 and HaCaTcells. First 293 cells were transfected with increasing
amounts of HPV-16 E6, as indicated in Figure 4B.Then, we performed the same analysis using HaCaTcells (Figure 4C). The results demonstrated that overex-pression of HPV-16 E6 results in a decrease in the levelof PP1γ expression. In order to determine whether theloss of PP1γ expression was proteasome-mediated HPV-positive SiHa, CaSki and HeLa cells, and HPV-negativeC33A and HaCaT cells were grown in the presence of theproteasome inhibitor, MG132 for 3 hours, after which the
A
B
PP1
Actin
Si: si luciferase siE6/E7
CaSKi
p53
hScrib
Si: si luciferase siE6/E7
SiHa
- + - + - + - + - + MG132
SiHa CaSki HaCaT
p53
Actin
D
hScrib
PP1
Lac Z
pcDNA16E64μg
16E68μg
16E610μg
hScrib
PP1
pcDNA16E65μg
C
C33A HeLa
PP1
Figure 4 PP1γ levels are downregulated in HPV16 positive cells by HPV E6/E7 oncogenes. (A) HPV-16 positive CaSki and SiHa cells weretransfected with siRNAE6/E7 or siLuc as control. Total cell extracts were then made after 72 hours, and hScrib, PP1γ, p53 and Actin were detectedby western blotting. (B) 293 cells were transfected with 4, 8, 10 μg of HPV-16 E6 expression plasmid, and hScrib and PP1γ were analysed byWestern blotting. The middle panel shows the LacZ transfection efficiency and loading control. (C) HaCaT cells were transfected with 5 μg ofHPV-16 E6 expression plasmid, and hScrib and PP1γ were analysed by Western blotting. Tubulin was detected as control. (D) CaSki, SiHa, HeLa,C33A and HaCaT cells were incubated in the presence of either 10 μM MG132 or solvent before harvesting and analysed by western blotting.Actin was used as a loading control.
Seiki et al. BMC Cancer (2015) 15:230 Page 7 of 9

― 291 ―
cells were harvested and the levels of PP1γ expressionascertained by western blotting. As can be seen fromFigure 4D, there are minimal changes in the levels of PP1γexpression following proteasome inhibition, regardless ofthe presence or absence of HPV DNA sequences, whilstthere is efficient rescue of p53 following proteasome in-hibition in HPV positive cells. These results indicate thatthe effects of E6 upon PP1γ patterns of expression aremost likely proteasome independent.
DiscussionPP1 is a major serine/threonine protein phosphatase,normally regulating the phosphorylation status of a largenumber of important cellular regulatory proteins [36-39].Important activities include the regulation of chromosomestructure during mitosis and also following DNA damage,through de-phosphorylation of histones [30,40], and thecontrol of centrosome disjunction through antagonism ofNek2A kinase activity [41].In this study we have identified PP1γ as a potential new
biomarker of HPV-16 induced malignancy. Using HPV-16positive cervical tumour derived cell lines, IHC analysis ofHPV-16 positive cervical tumours and CIN lesions, wepresent compelling evidence that PP1γ expression pat-terns are perturbed as a result of infection with HPV-16.We originally considered that the PP1γ/hScrib com-
plex might be a general target for HPV-16 E6, based onour previous studies showing complex formation be-tween hScrib and PP1γ. However, analysis of the expres-sion patterns of PP1γ and hScrib in cervical tissuesindicate that this is not the case. Most importantly how-ever, this highlights PP1γ as an independent target ofthe HPV-16 oncoproteins. In the normal cervix, PP1γ isexpressed throughout the differentiating cervical epithe-lium, with a predominantly nuclear pattern of expres-sion, which is consistent with previous studies [42]. Toour surprise, we found that in all the HPV-16 positivecervical tumours analysed, this nuclear localisation ofPP1γ was undetectable. Low levels of PP1γ can still befound within the cytoplasm of many cells within the ma-jority of the cervical tumours that we analysed, althoughin 2/11 cases all PP1γ expression appeared to be lost.Similarly, perturbation in the pattern of PP1γ expressionis apparent in CIN2 lesions, and this becomes moremarked as the lesions progress to CIN3, suggesting thatperturbation in the pattern of PP1γ expression is anearly event in the development of cervical malignancy.In order to understand whether these effects on PP1γ
expression patterns were a direct consequence of E6/E7activity, we then focused our attention on cells derivedfrom HPV-16 positive cervical tumours. Again we foundstriking parallels with the IHC data, with very little PP1γexpression in the nucleus of HPV-16 positive CaSki orSiHa cells. In contrast, readily detectable nuclear PP1γ
was observed in HaCaT cells. Most strikingly, siRNA ab-lation of E6/E7 expression resulted in a dramatic rescueof PP1γ expression within the nucleus of the HPV-16positive cells, which appeared very similar to the effectsseen upon the pattern of p53 expression. In contrast top53 however, the alteration in the levels and pattern ofPP1γ expression by E6 does not appear to involve theproteasome in cells derived from cervical tumours. Ob-viously further studies will be required to elucidate theprecise mechanisms by which HPV-16 targets PP1γ.
ConclusionsCurrently we have no information as to whether theHPV-16 E6/E7 oncoproteins can modulate any of thesephosphorylation events in a PP1γ dependent manner, itis nonetheless intriguing that all of these pathways areperturbed to some extent in cells containing the HPV-16oncoproteins. Future studies will investigate these as-pects further, but it is tempting to speculate that target-ing of the nuclear forms of PP1γ might contributedirectly towards the generation of genome instability,chromatin remodeling and tumour progression. The cel-lular redistribution of PP1γ seems to have an importantrole in the development of centrosome abnormalitiesand chromosomal instability at early stages of cervicalcarcinogenesis. Taken together this study highlights thepotential value of PP1γ as a novel biomarker for HPV-induced cervical neoplasia.
Competing interestsAll the authors declare no competing interests.
Authors' contributionsTS performed the experiments and wrote the manuscript. KN (correspondingauthor) and LB supervised the experiments and wrote the manuscript. TS,KN, CK, KK, DM, HK-N, AT, YM, TA, OH-W, KO, SN, TY, MF, LB, YO, and TFcontributed reagents, materials, experimental techniques, and data analysis.KN, DM, MF contributed pathological evaluation. All authors read andapproved the final manuscript.
AcknowledgementThe authors are grateful to Kei Sakuma (Department of Pathology, GraduateSchool of Medicine, The University of Tokyo) for technical support on thepreparation of IHC staining. Additionally, we thank Michihiro Tanikawa, YuichiroMiyamoto, Kenbun Sone, Yuriko Uehara, Yuji Ikeda, Aki Miyasaka, Takahiro Koso,Tomoko Kashiyama, Tomohiko Fukuda, Kanako Inaba, Satoko Kojima, andKensuke Tomio for their support and assistance. We also gratefullyacknowledge the particular assistance of all members in Lawrence Banks's lab,and valuable comments on the manuscript from Miranda Thomas and DavidPim. This work was supported by a Grant-in-Aid for Scientific Research (K.N.)from the Ministry of Education, Science and Culture, Japan, and in part by aresearch grant from the Associazione Italiana per la Ricerca sul Cancro (L.B).
Author details1Department of Obstetrics and Gynecology, Faculty of Medicine, TheUniversity of Tokyo, Tokyo 113-8655, Japan. 2International Centre for GeneticEngineering and Biotechnology, Area Science Park, Padriciano-99, I-34012Trieste, Italy. 3Department of Pathology, Graduate School of Medicine, TheUniversity of Tokyo, Tokyo 113-8655, Japan. 4Department of Obstetrics andGynecology, Graduate School of Medicine, Teikyo University, Tokyo 173-8605,Japan. 5Department of Obstetrics and Gynecology, National Center for GlobalHealth and Medicine, Tokyo 162-8655, Japan.
Seiki et al. BMC Cancer (2015) 15:230 Page 8 of 9

― 292 ―
Received: 31 May 2014 Accepted: 27 February 2015
References1. Zur HH. Papillomaviruses and cancer: from basic studies to clinical
application. Nat Rev Cancer. 2002;2:342–50.2. Bouvard V, Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, et al. WHO
international agency for research on cancer monograph working group. Areview of human carcinogens–part B: biological agents. Lancet Oncol.2009;10:321–2.
3. Butz K, Ristriani T, Hengstermann A, Denk C, Scheffner M, Hoppe-Seyler F.siRNA targeting of the viral E6 oncogene efficiently kills humanpapillomavirus-positive cancer cells. Oncogene. 2003;22:5938–45.
4. Yoshinouchi M. In vitro and in vivo growth suppression of humanpapillomavirus 16-positive cervical cancer cells by e6 siRNA. Mol Ther.2003;8:762–8.
5. McLaughlin-Drubin ME, Meyers J, Munger K. Cancer associated humanpapillomaviruses. Curr Opin Virol. 2012;2:459–66.
6. Mantovani F, Banks L. The human papillomavirus E6 protein and itscontribution to malignant progression. Oncogene. 2001;20:7874–87.
7. Huh K, Zhou X, Hayakawa H, Cho J-Y, Libermann TA, Jin J, et al. Humanpapillomavirus type 16 E7 oncoprotein associates with the cullin 2 ubiquitinligase complex, which contributes to degradation of the retinoblastomatumor suppressor. J Virol. 2007;81:9737–47.
8. Scheffner M, Huibregtse JM, Vierstra RD, Howley PM. The HPV-16 E6 andE6-AP complex functions as a ubiquitin-protein ligase in the ubiquitinationof p53. Cell. 1993;75:495–505.
9. Schlegel R, Phelps WC, Zhang YL, Barbosa M. Quantitative keratinocyteassay detects two biological activities of human papillomavirus DNA andidentifies viral types associated with cervical carcinoma. EMBO J.1988;7:3181–7.
10. Barbosa MS, Schlegel R. The E6 and E7 genes of HPV-18 are sufficient forinducing two-stage in vitro transformation of human keratinocytes. Oncogene1989:1529-32.
11. Munger K, Phelps WC, Bubb V, Howley PM. The E6 and E7 genes of thehuman papillomavirus type 16 together Are necessary and sufficient fortransformation of primary human keratinocytes. J Virol. 1989;63:4417–21.
12. Song S, Liem A, Miller JA, Lambert PF. Human papillomavirus types 16 E6and E7 contribute differently to carcinogenesis. Virology. 2000;267:141–50.
13. Shai A, Nguyen ML, Wagstaff J, Jiang Y-H, Lambert PF. HPV16 E6 confersp53-dependent and p53-independent phenotypes in the epidermis of micedeficient for E6AP. Oncogene. 2007;26:3321–8.
14. Thomas M, Narayan N, Pim D, Tomaić V, Massimi P, Nagasaka K, et al.Human papillomaviruses, cervical cancer and cell polarity. Oncogene.2008;27:7018–30.
15. Pim D, Banks L. Interaction of viral oncoproteins with cellular targetmolecules: infection with high-risk vs low-risk human papillomaviruses.APMIS. 2010;118:471–93.
16. Kiyono T, Kiyono T, Hiraiwa A, Fujita M, Hayashi Y, Akiyama T, et al. Bindingof high-risk human papillomavirus E6 oncoproteins to the humanhomologue of the Drosophila discs large tumor suppressor protein. ProcNatl Acad Sci U S A. 1997;94:11612–6.
17. Lee SS, Weiss RS, Javier RT. Binding of human virus oncoproteins to hDlg/SAP97, a mammalian homolog of the Drosophila discs large tumorsuppressor protein. Proc Natl Acad Sci U S A. 1997;94:6670–5.
18. Gardiol D, Kühne C, Glaunsinger B, Lee SS, Javier R, Banks L. Oncogenichuman papillomavirus E6 proteins target the discs large tumour suppressorfor proteasome-mediated degradation. Oncogene. 1999;18:5487–96.
19. Nakagawa S, Huibregtse JM. Human scribble (Vartul) is targeted forubiquitin-mediated degradation by the high-risk papillomavirus E6 proteinsand the E6AP ubiquitin-protein ligase. Mol Cell Biol. 2000;20:8244–53.
20. Glaunsinger BA, Lee SS, Thomas M, Banks L, Javier R. Interactions of thePDZ-protein MAGI-1 with adenovirus E4-ORF1 and high-risk papillomavirusE6 oncoproteins. Oncogene. 2000;19:5270–80.
21. Kranjec C, Banks L. A systematic analysis of human papillomavirus (HPV) E6PDZ substrates identifies MAGI-1 as a major target of HPV type 16 (HPV-16)and HPV-18 whose loss accompanies disruption of tight junctions. J Virol.2011;85:1757–64.
22. Bilder D, Li M, Perrimon N. Cooperative regulation of cell polarity andgrowth by Drosophila tumor suppressors. Science. 2000;289:113–6.
23. Zhan L. Deregulation of scribble promotes mammary tumorigenesis andreveals a role for cell polarity in carcinoma. Cell. 2008;135:865–78.
24. Dow LE. Loss of human Scribble cooperates with H-Ras to promote cellinvasion through deregulation of MAPK signalling. Oncogene.2008;27:5988–6001.
25. Nagasaka K, Pim D, Massimi P, Thomas M, Tomaić V, Subbaiah VK, et al. Thecell polarity regulator hScrib controls ERK activation through a KIM site-dependent interaction. Oncogene. 2010;29:5311–21.
26. Pearson HB, Perez-mancera PA, Dow LE, Ryan A, Tennstedt P, Bogani D, et al.SCRIB expression is deregulated in human prostate cancer, and its deficiencyin mice promotes prostate neoplasia. J Clin Invest. 2011;121:4257–67.
27. Elsum I a, Yates LL, Pearson HB, Phesse TJ, Long F, O’Donoghue R, Ernst M,Cullinane C, Humbert PO. Scrib heterozygosity predisposes to lung cancerand cooperates with KRas hyperactivation to accelerate lung cancerprogression in vivo. Oncogene 2013;:1–11.
28. Nakagawa S, Yano T, Nakagawa K, Takizawa S, Suzuki Y, Yasugi T, et al.Analysis of the expression and localisation of a LAP protein, human scribble,in the normal and neoplastic epithelium of uterine cervix. Br J Cancer.2004;90:194–9.
29. Nagasaka K, Seiki T, Yamashita A, Massimi P, Subbaiah VK, Thomas M, et al.A novel interaction between hScrib and PP1γ downregulates ERK signalingand suppresses oncogene-induced cell transformation. PLoS One.2013;8:e53752.
30. Shimada M, Haruta M, Niida H, Sawamoto K, Nakanishi M. Proteinphosphatase 1γ is responsible for dephosphorylation of histone H3 at Thr11 after DNA damage. EMBO Rep. 2010;11:883–9.
31. Trinkle-mulcahy L, Andrews PD, Wickramasinghe S, Sleeman J, Prescott A,Lam YW, et al. Time-lapse imaging reveals dynamic relocalization of PP1γthroughout the mammalian cell cycle. Mol Biol Cell. 2003;14:107–17.
32. Boukamp P, Petrussevska RT, Breitkreutz D, Hornung J, Markham A, FusenigNE. Normal keratinization in a spontaneously immortalized aneuploidhuman keratinocyte cell line. J Cell Biol. 1988;106:761–71.
33. Gravitt PE, Peyton CL, Alessi TQ, Wheeler CM, Hildesheim A, Schiffman MH,et al. Improved amplification of genital human papillomaviruses. J ClinMicrobiol. 2000;38:357–61.
34. Thomas M, Massimi P, Navarro C, Borg J, Banks L. The hScrib/Dlg apico-basal control complex is differentially targeted by HPV-16 and HPV-18 E6proteins. Oncogene. 2005;24:6222–30.
35. Gardiol D, Zacchi A, Petrera F, Stanta G, Banks L. Human discs large andscrib are localized at the same regions in colon mucosa and changes intheir expression patterns are correlated with loss of tissue architectureduring malignant progression. Int J Cancer. 2006;119:1285–90.
36. Bollen M. Combinatorial control of protein phosphatase-1. Trends BiochemSci. 2001;26:426–31.
37. Cohen PTW. Protein phosphatase 1 – targeted in many directions. J Cell Sci.2002;115:241–56.
38. Margolis SS, Walsh S, Weiser DC, Yoshida M, Shenolikar S, Kornbluth S. PP1control of M phase entry exerted through 14-3-3-regulated Cdc25dephosphorylation. EMBO J. 2003;22:5734–45.
39. Wu JQ, Guo JY, Tang W, Yang CS, Freel CD, Chen C, et al. PP1-mediateddephosphorylation of phosphoproteins at mitotic exit is controlled byinhibitor-1 and PP1 phosphorylation. Nat Cell Biol. 2009;11:644–51.
40. Vagnarelli P, Ribeiro S, Sennels L, Sanchez-Pulido L, de Lima AF, Verheyen T,et al. Repo-Man coordinates chromosomal reorganization with nuclearenvelope reassembly during mitotic exit. Dev Cell. 2011;21:328–42.
41. Mardin BR, Agircan FG, Lange C, Schiebel E. Plk1 controls the Nek2A-PP1γantagonism in centrosome disjunction. Curr Biol. 2011;21:1145–51.
42. Andreassen PR, Lacroix FB, Villa-Moruzzi E, Margolis RL. Differential subcellularlocalization of protein phosphatase-1 alpha, gamma1, and delta isoformsduring both interphase and mitosis in mammalian cells. J Cell Biol.1998;141:1207–15.
Seiki et al. BMC Cancer (2015) 15:230 Page 9 of 9
― 293 ―

― 294 ―
― 295 ―
― 296 ―

厚生労働科学研究費補助金新興・再興感染症及び予防接種政策推進研究事業
性感染症に関する特定感染症予防指針に基づく対策の推進に関する研究(H27-新興行政-一般-001)平成27年度 総括・分担研究報告書
2016年3月31日発行
研究代表者 荒 川 創 一
連絡先 神戸大学医学部附属病院 感染制御部 〒650-0017 神戸市中央区楠町7-5-2 TEL. 078-382-5531(直通) FAX. 078-382-6611
本報告書が掲載された論文及び図表には著作権が発生しておりますので利用にあたりご留意ください。






![第七章电磁感应.ppt [兼容模式]](https://static.fdokumen.com/doc/165x107/633fcab8e45d77ee070533bb/ppt-.jpg)













