textbook-mikrobiologi18.doc

of 29
Transcript of textbook-mikrobiologi18.doc
-
8/14/2019 textbook-mikrobiologi18.doc
1/29
BAB 18. PATOGENESIS
Patogenesis adalah mekanisme infeksi dan mekanisme perkembangan penyakit.
Infeksi adalah invasi inang oleh mikroba yang memperbanyak dan berasosiasi dengan
jaringan inang. Infeksi berbeda dengan penyakit. Kapasitas bakteri menyebabkan
penyakit tergantung pada patogenitasnya. Dengan kriteria ini, bakteri dikelompokan
menjadi 3, yaitu agen penyebab penyakit, patogen oportunistik, nonpatogen. Agen
penyebab penyakit adalah bakteri patogen yang menyebabkan suatu penyakit
(Salmonella spp.. Patogen oportunistik adalah bakteri yang berkemampuan sebagai
patogen ketika mekanisme pertahanan inang diperlemah (!ontoh E. coli menginfeksi
saluran urin ketika sistem pertahanan inang dikompromikan (diperlemah. "onpatogen
adalah bakteri yang tidak pernah menjadi patogen. "amun bakteri nonpatogen dapat
menjadi patogen karena kemampuan adaptasi terhadap efek mematikan terapi modern
seperti kemoterapi, imunoterapi, dan mekanisme resistensi. #akteri tanah Serratia
marcescensyang semula nonpatogen, berubah menjadi patogen yang menyebabkan
pneumonia, infeksi saluran urin, dan bakteremia pada inang terkompromi.
$irulensi adalah ukuran patogenitas organisme. %ingkat virulensi berbanding
lurus dengan kemampuan organisme menyebabkan penyakit. %ingkat virulensi
dipengaruhi oleh jumlah bakteri, jalur masuk ke tubuh inang, mekanisme pertahanan
inang, dan faktor virulensi bakteri. &e!ara eksperimental virulensi diukur dengan
menentukan jumlah bakteri yang menyebabkan kematian, sakit, atau lesi dalam 'aktu
yang ditentukan setelah introduksi.
KERENTANAN INANG
Kerentanan terhadap infeksi bakteri tergantung pada kondisi fisiologis dan
imunologis inang dan virulensi bakteri. Pertahanan inang terhadap infeksi bakteri adalah
mekanisme nonspesifik dan spesifik (antibodi. ekanisme nonspesifik dilakukan oleh
sel)sel neutrofil dan makrofag. Perkembangan imunitas spesifik seperti respons antibodi
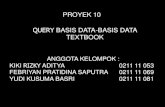
memerlukan 'aktu beberapa minggu (*ambar +.+. bakteri flora normal kulit dan
permukaan mukosa juga memberi perlindungan terhadap kolonisasi bakteri patogen.
Pada individu sehat, bakteri flora normal yang menembus ke tubuh dapat dimusnahkan
oleh mekanisme humoral dan seluler inang. -ontoh terbaik tentang kerentanan adalah
AID&, di mana limfosit helper -D/se!ara progresif berkurang +0+1 oleh virus
imunodefisiensi (2I$. ekanisme resistensi dipengaruhi oleh umur, defisiensi, dan
genetik. &istem pertahanan (baik spesifik maupun nonspesifik orang lanjut usia
-
8/14/2019 textbook-mikrobiologi18.doc
2/29
berkurang. &istem imun bayi belum berkembang, sehingga rentan terhadap infeksi
bakteri patogen. #eberapa individu memiliki kelainan genetik dalam sistem pertahanan.
Gambar 18.1espons serum antibodi terhadap Salmonella typhiiselama periodedemam tifoid.
esistensi inang dapat terkompromi oleh trauma dan penyakit lain yang diderita.
Individu menjadi rentan terhadap infeksi oleh berbagai bakteri jika kulit atau mukosa
melonggar atau rusak (terluka. Abnormalitas fungsi silia sel pernafasan mempermudah
infeksi Pseudomonas aeruginosa galur mukoid. Prosedur medis seperti kateterisasi dan
intubasi trakeal menyebabkan bakteri normal flora dapat masuk ke dalam tubuh melalui
plastik. 4leh karena itu, prosedur pengantian plastik kateter rutin dilakukan setiap
beberapa jam (56 jam untuk kateter intravena.
#anyak obat diproduksi dan dikembangkan untuk mengatasi infeksi bakteri.
Agen antimikroba efektif mela'an infeksi bakteri jika sistem imun dan fagosit inang turut
bekerja. "amun terdapat efek samping penggunaan antibiotik, yaitu kemampuan difusi
antibiotik ke organ nonsasaran (dapat mengganggu fungsi organ tersebut, kemampuan
bertahan bakteri terhadap dosis rendah (meningkatkan resistensi, dan kapasitas
beberapa organisme resisten terhadap multi)antibiotik.
DASAR GENETIK VIRULENSI
7aktor virulensi pada bakteri dapat dikode dari D"A kromosom, D"A
bakteriofag, plasmid, atau tranposon (%abel +.+. 7aktor virulensi Shigelladikode dari
-
8/14/2019 textbook-mikrobiologi18.doc
3/29
plasmid. 8nterotoksin 9%I dan 9%II E. coli dikode dari plasmid dan kromosom. %oksin
kolera Salmonella enterotoxin dan faktor invasi Yersiniadikode dari kromosom. "amun
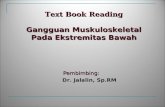
terdapat faktor vitulensi bakteri yang diperoleh dari bakteriofag (*ambar +.6 melalui
transduksi dan diikuti proses lisogeni. #akteriofag temperate sering berkontribusi
terhadap produksi faktor virulensi seperti toksin difteria (Corynebacterium diphtheriae,
toksin eritrogenik (Streptococcus pyogenes, toksin mirip)&higa (E. coli, dan toksin
botulinum tipe - dan D (Clostridium botulinum.
Tabel 18.1Dasar genetik faktor virulensi bakteri7aktor $irulensi #akteri Patogen Penghasil Dikode dari *en
8nterotoksin8nterotoksin, faktor invasi8nterotoksin, faktor invasi8nterotoksin, aerolisin8ksotoksin A
8nterotoksin #7aktor invasi7aktor invasi8nterotoksin 9%II7aktor invasi7aktor invasi, faktor kolini,
enterotoksin 9%I%oksin eksfoliatif%oksin anthraks%oksin difteria%oksin eritrogenik8nterotoksin mirip)&higa
%oksin botulinum - : D8nterotoksin &%A : &%#,akuisisi besi, hemolisin
Vibrio choleraeSalmonella typhimuriumShigell spp.
Aeromonas hydrophylaPseudomonas aeruginosa
Staphylococcus aureusYersinia enterocoliticaYersinia pseudotuberculosisEscherichia coliShigella sppEscherichia coli
Staphylococcus aureusBacillus anthracisCorynebacterium diphtheriaeStreptococcus pyogenesEscherichia coli
Clostridium botulinumEscherichia coli
KromosomKromosomKromosomKromosomKromosom
KromosomKromosomKromosomKromosomPlasmidPlasmid
PlasmidPlasmid#akteriofag#akteriofag#akteriofag
#akteriofag%ransposon
-
8/14/2019 textbook-mikrobiologi18.doc
4/29
Gambar 18.2ekanisme bakteri memperoleh virulensi dari bakteriofag
MEKANISME PATOGENIK
Aktiita! I"#ek!i Bakteri
7aktor yang dihasilkan mikroba dan dapat membangkitkan penyakit disebut
faktor virulensi. -ontoh faktor virulensi adalah toksin (substansi yang menghambat
fagositosis dan dapat mengikat permukaan sel inang. Kebanyakan bakteri patogen
oportunistik mengembangkan faktor virulensi yang memungkinkan memperbanyak diri di
dalam inang tanpa terbunuh atau terbuang oleh sistem pertahanan inang. #anyak faktor
virulensi hanya diproduksi oleh mikroba galur virulen (enterotoksi diproduksi oleh E. coli
galur tertentu.
&e!ara praktis, bakteri dapat dikatakan sebagai obyek tunggal yang mampu
meyebabkan suatu penyakit (hanya beberapa jenis bakteri yang dapat menyebabkan
penyakit. &e!ara teleologis, tidak menguntungkan patogen membunuh inang. 2al ini
karena dengan kematian inang, maka patogen juga ikut mati. ikroba patogen
teradapatasi tinggi adalah yang dapat tumbuh dan menyebar dengan sedikit energi dan
sedikit kerusakan pada inang.
-
8/14/2019 textbook-mikrobiologi18.doc
5/29
Re!i!te"!i I"a"$
eskipun mudah rusak, kulit merupakan pembatas penting antara tubuh dengan
dunia luar. ;ntungnya, kebanyakan bakteri di lingkungan luar dapat diatasi dengan
sistem imun normal. "amun pasien dengan sistem imun rendah seperti pasien
kemoterapi kanker atau penderita AID& teran!am infeksi mikroba patogen oportunistik.
#agian terluar tubuh manusia dan men!egah masuknya benda asing adalah kulit
dan permukaan mukosa. #agian terluar kulit dan permukaan mukosa adalah lapisan sel)
sel epitel. &el epitel pipih berlapis kulit sangat sulit ditembus oleh mikroba. Pada
permukaan kulit berkembang bakteri flora normal dan dapat berkompetisi dengan
mikroba patogen. &el epitel mukosa berkembang dan membelah dengan !epat. 2anya
dalam 'aktu 3aringan rusak pada infeksi)infeksi
tersebut disebabkan oleh faktor toksis yang dilepaskan oleh limfosit, makrofag, dan
-
8/14/2019 textbook-mikrobiologi18.doc
6/29
neutrofil pada lokasi infeksi (*ambar +.3. kebanyakan respons inang sangat kuat,
sehingga jaringan inang rusak dan memungkinkan bakteri resisten memperbanyak diri.
Gambar 18.(ekanisme patogenesis termediasi respons inang
Pert)mb)*a" I"tra!el
&e!ara umum bakteri dapat masuk dan bertahan di dalam sel eukariota dapat
bertahan terhadap antibodi humoral, tetapi dapat dieliminasi hanya dengan respons
imun seluler. "amun bakteri ini harus memiliki mekanisme khusus untuk melindungi dari
efek en?im lisosim yang ada dalam sel inang. #erdasarkan pertumbuhan selama
patogenesis, bakteri patogen dapat dikelompokan menjadi 3, yaitu patogen intrasel
obligat, patogen fakultatif intrasel, dan patogen ekstrasel (*ambar +.. #akteri
patogen intrasel adalah bakteri patogen yang selalu tumbuh di dalam sel inang selama
proses patogenesis. #akteri patogen fakultatif intrasel adalah bakteri patogen tumbuh di
luar dan si dalam sel inang selama proses patogenesis. #akteri patogen ekstrasel
adalah bakteri patogen tumbuh di luar sel inang selama proses patogenesis.
-
8/14/2019 textbook-mikrobiologi18.doc
7/29
Gambar 18.+Pengelompokan bakteri patogen berdasarkan pertumbuhannya selamapatogenesis
R. ricketsii menghasilkan fosfolipase untuk melarutkan vesikel fagosit, sehingga
tidak pernah bertemu dengan lisosim. egionella pneumophila lebih memilih hidup di
dalam makrofag dan menghambat fusi lisosim dengan mekanisme yang belum
diketahui. Coxiella burnetiilebih menyukai lingkungan bernilai p2 asam di dalam granula
lisosomal. Salmonella dan !ycobacterium sangat resisten terhadap aktivitas sel
fagositosis.
#akteri yang tidak menginvasi sel inang, biasanya memperbanyak diri di fluida
tubuh yang kaya nutrisi. V. cholerae dan Bordetella pertussistidak pernah menembus
jarungan tubuh, tetapi hanya menempel di permukaan sel epitel dan menyekresi protein
toksin. E. coli dan P. aeruginosa bukan patogen invasif, tetapi mereka menyebar
dengan !epat ke berbagai jaringan ketika memperoleh akses. #akteri dapat dikatakan
patogen intrasel ketika dia di!erna oleh neutrofil dan makrofag, tetapi bakteri ini tidak
mempunyai kapasitas bertahan tumbuh di lingkungan intrasel.
,AKTOR ,AKTOR VIRULENSI
,akt%r K%l%"i!a!i &a" Perlekata"
-
8/14/2019 textbook-mikrobiologi18.doc
8/29
&el)sel epitel mukosa biasanya mengeluarkan mukus untuk membersihkan
permukaan mukosa se!ara teratur. &el)sel epitel mukosa hanya memerlukan 'aktu
jam untuk meregenerasi sel)sel yang rusak. ;ntuk menginfeksi, kebanyakan bakteri
harus melekatkan diri dan memperbanyak diri di permukaan mukosa sebelum mukus
dan silia sel epitel membuannya. ;ntuk itu, bakteri memiliki pili atau fimbria yang dapat
dipakai sebagai alat perlekatan ke permukaan mukosa. 7aktor kolonisasi juga
memerankan peranan penting dalam perlekatan bakteri ke permukaan mukosa.
#eberapa bakteri yang menghasilkan faktor kolonisasi adalah V. cholerae" E. coli"
Salmonella spp." #. gonorrheae" #. meningitidis" danStreptococcus pyogenes.
Pili dan 7imbria
Pili adalah apendages yang keluar dari dalam sel. &truktur pili berongga,
sehingga memudahkan sintesis pili. Pili adalah polimer protein yang disintesis dari dasar
ke ujung. Protein ujung pili mampu mengenali reseptornya pada sel inang, sehingga
memungkinkan perlekatan pada sel inang. eaksi perlekatan antara pili dan reseptornya
sangat kuat dan sangat sulit dipisahkan. &etelah kontak dengan sel inang pili berdifusi
dengan membran sel inang, sehingga pili menyediakan jembatan atau kanal bagi
eksport material toksis bakteri patogen ke sitoplasma sel inang. &intesis pili diregulasi
oleh lingkungan, sehingga pili hanya disintesis dalam kondisi tertentu. Kebanyakan pili
adalah antigen kuat, sehingga mudah dikenali oleh imunitas humoral dan seluler.
"amun beberapa populasi bakteri patogen dapat mengubah struktur protein ujung pili
(melalui mutasi, sehingga tidak mudah dikenali sistem pertahanan inang.
7imbria lebih langsing daripada pili. 7imbria juga menyediakan mekanisme
perlekatan pada sel inang. "amun struktur fimbria kompak dan tidak berongga,
sehingga tidak memfasilitasi eksport berbagai faktor virulenke ke sel inang.
Kapsula dan &truktur Permukaan 9ain
#akteri memiliki beberapa struktur untuk dapat bertahan dalam inang. Kapsula
telah diketahui sejak lama sebagai faktor pelindung bakteri dari pertahanan inang.
#akteri berkapsula lebih virulen dan resisten terhadap fagositosis dan pertahanan
intrasel daripada bakteri tanpa kapsula. 4rganisme penyebab bakteremia(Pseudomonas menghasilkan komponen yang disebut serum resistant. Komposisi dan
struktur serum resistantmirip dengan komposisi kapsula. Salmonella typhii dan
beberapa organisme penyebab paratifoid memiliki antigen permukaan, yaitu antigen Vi.
Antigen Vi dapat meningkatkan virulensi bakteri. Antigen Vi terdiri atas polimer
galaktosamin dan asam uronat. Antigen Vimampu bertahan terhadap antibodi inang.
-
8/14/2019 textbook-mikrobiologi18.doc
9/29
#eberapa bakteri dan parasit mampu bertahan dan memperbanyak diri di dalam
sel fagositosis. !ycobacterium tuberculosis mampu bertahan dan memperbanyak diri
karena struktur permukaan selnya tahan terhadap aktivitas lisosomal sel inang. Parasit
$oxoplasma gondii mampu menghambat fusi lisosom dan vakuola fagositosis.
&edangkan mekanisme bertahan dan memperbanyak diri egionella pneumophila"
Brucella abortus" danisteria monocytogenesdi dalam sel fagositosis belum diketahu
dengan jelas.
&intesis kapsula memerlukan energi dan karbon tinggi. #akteri mampu
meregulasi sintesis kapsula, sehingga memungkinkan merekan menyintesis kapsula
dalam keadaan tertentu (menguntungkan. #akteri mempunyai mekasime yang dapay
mendeteksi inang dan dengan !epat mengekspresikan gen pengkode faktor virulensi
termasuk kapsula. #akteri patogen tidak menghasilkan kapsula jika dikultur dalam
laboratorium. ekanisme kapsula dalam virulensi bakteri patogen adalah men!egah
fagositosis sel inang, memfasilitasi kolonisasi di sel inang, memberikan struktur unik
yang mampu @menyembunyikan dirinya dari sistem imun inang, dan memungkinkan
perlekatan bersama membentuk biofilm yang tidak mudah dihan!urkan oleh sistem
pertahanan inang.
,akt%r I"a!i
&etelah melekat di permukaan mukosa, bakteri harus mampu menembus lapisan
mukosa, sehingga dapat tersebar ke seluruh jaringan tubuh inang. #akteri patogen
obligat intrasel seperti Rickettsiadan Chlamydiaspe!ies dan bakteri patogen fakultatif
intrasel menghasilkan faktor)faktor yang memfasilitasi invasi. 7aktor invasi Shigella
dikode dari plasmid +1 megadalton. ekanisme invasi Rickettsiadan Chlamydia
spe!ies belum diketahu dengan jelas.
E"&%t%k!i"
8ndotoksi terdiri atas komponen lipopolisakarida toksis membran luar bakteri
gram negatif. 8ndotoksin berefek serius terhadap sel inang bahkan letal. Istilah
endotoksi diintroduksi oleh Pfeiffer pada tahun +B3 untuk membedakan substansi
toksis yang dikeluarkan setelah sel bakteri mengalami lisis dari substansi toksis(eksotoksin.
&truktur endotoksin adalah kompleks lipid dan polisakarida. &truktur molekul
endotoksin Salmonella spp. Dan E. coli telah diketahui se!ara detail. eskipun semua
molekul endotoksin mirip se!ara struktur kimia'i dan aktivitas biologis, tetapi terdapat
keragaman di antara mereka. Kompleks molekul endotoksin dapat dibagi menjadi 3
-
8/14/2019 textbook-mikrobiologi18.doc
10/29
bagian (*ambar +.C mulai terluar, yaitu rantai oligosakarida atau disebut rantai
antigen)4, polisakarida coreyang merupakan tulang punggu molekul, dan lipid A yang
biasanya terdiri atas disakarida glukosamin yang melekat pada asam lemak dan fosfat.
>ika bagian polisakarida diganti dengan polisakarida lain, maka toksisitas endotoksin
masih terjaga. "amun jika bagian lipid A diganti dengan lipid lain, maka toksisitas
endotoksin melemah. 4leh karena itu bagian toksis endotoksin adalah lipid A. Peran
polisakarida adalah sebagai agen pelarut lipid A dan se!ara laboratorium posisakarida
dapat diganti dengan protein pemba'a seperti bovins erum albumin. Anggota famili
8nteroba!teria!eae memiliki beragam panjang rantai antigen)4. &ementara itu, #.
gonorrhoeae" #. meningitidis" danB. Pertussistidak memiliki rantai antigen)4.
Gambar 18.-&truktur endotoksin dari bakteri gram negatif
Aktivitas #iologis 8ndotoksin
8fek biologis endotoksin telah dipelajari se!ara mendalam. 8fek biologis
endotoksin bervariasi, yaitu leukopenia, leukositosis, depresi tekanan darah, aktivasi
keping darah, nekrosis sumsum tulang, hipotermia dan toksisitas letal (pada tikus, dan
induksi sintesis prostaglandin. "amun terdapat efek dari endotoksin yang
menguntungkan inang, yaitu efek mitogenik limfosit # (dapat meningkatkan resistensi
terhadap infeksi virus dan bakteri, induksi sintesis )interferon oleh limfosit %(dapat
mengaktifkan makrofag dan sel)sel pembunuh dan mengaktifkan penolakan terhadap
sel tumor, aktivasi komplemen, induksi nonspesifik resistensi infeksi, aktivasi makrofag,
induksi sintesis faktor nekrosis tumor, dan induksi toleransi endotoksin.
-
8/14/2019 textbook-mikrobiologi18.doc
11/29
Penelitian terakhir terfokus pada eksploitasi efek positif endotoksin khususnya
dalam perkembangan menstimulasi respons imun. enghidrolisis gugus fosfat atau
deasilasi satu atau beberapa asam lemak dari lipid A dapat menurunkan toksisitas lipid
A. %oleransi terhadap endotoksin dapat dihasilkan dengan mengintroduksi lebih dulu
endotoksin dosis rendah atau mengintroduksi lipid A nontoksis sebelum endotoksin
dosis tinggi.
Deteksi 8ndotoksin
8ndotoksin adalah bagian dari membran luar sel bakteri patogen. 4leh karena itu
meskipun bakteri tersebut mati, tetapi endotoksin masih tetap aktif. 2al ini karena
endotoksin tahan panas, sehingga tidak mudah rusak oleh aktivitas sterilisasi.
8ndotoksin dalam larutan medis dapat dihilangkan dengan filtrasi dengan ion exchange
resin.
Keberadaan endotoksin dari perlalatan dan larutan medis dapat dideteksi denga
metode uji pirogenitas kelin!i atau uji 9imulus lysate. ;ji pirogenitas kelin!i berdasarkan
sensitivitas kelin!i terhadap endotoksin. ;ji ini sangat mudah, yaitu mengintroduksi
!airan yang diduga mengandung endotoksin ke dalam kelin!i melalui vena telinga. &uhu
rektum kelin!i dimonitor setiap saat. >ika suhu rektum meningkat, maka !airan tersebut
mengandung endotoksin.
;ji 9imulus lysate merupakan uji deteksi endotoksin yang umum dan lebih murah
dibandingkan uji pirogentitas kelin!i. ;ji ini berdasarkan kemampuan endotoksin
menginduksi lysate gelationsel amoebosit imulus polyphemus (ketam kaki kuda. ;ji
ini sederhana dan sangat sensitif (mendeteksi sampai + ng0ml. Perangkat uji telah
tersedia se!ara komersial.
Ek!%t%k!i"
8ksotoksin berbeda dengan endotoksin. 8ksotoksin adalah protein toksis yang
dilepaskan oleh bakteri patogen. &ebagian besar eksotoksin dengan berat molekul tinggi
tidak tahan panas, tetapi eksotoksin dengan berat molekul rendah tahan panas.
8ksotoksin dapat diproduksi oleh bakteri gram positif dan baktri gram negatif. Aksi
eksotoksin terhadap sel inang biasanya terlokalisir dan khusus pada sel dan lokasitertentu. 2al ini karena setiap eksotoksin memiliki masing)masing reseptor pada sel
inang, misalnya toksin tetanus hanya berefek pada internuncial neuron. Kebanyakan
eksotoksin dapat dikenali oleh antibodi.
8ksotoksin dapat dikelompokan menjadi beberapa kelompok berdasarkan efek
eksotoksin terhadap sel inang, seperti neurotoksin, sitotoksin, dan enterotoksin. -ontoh
-
8/14/2019 textbook-mikrobiologi18.doc
12/29
nerotoksin adalah toksin botulinum ayng dihasilkan Clostridium botulinum. -ontoh
sitotoksin adalah toksin dipteria yang dihasilkan Corynebacterium diphtheriae.
Si&er%#%r
#aik he'an dan mikroba memerlukan besi dalam pertumbuhan dan
metabolisme. 2e'an memiliki mekanisme menahan besi dalam jaringan sehingga
membatasi pertumbuhan bakteri patogen. eskipun darah kaya akan besi, tetapi sangat
sedikit dijumpai besi bebas di dalam darah. &ebagian besar besi telah diambil oleh
hemoglobin dari eritrosit dan transferin dari plasma darah. #akteri mampu menghasilkan
reseptor untuk protein penangkap besi, sehingga menghambat penagkapan besi oleh
sel inang. Dengan demikian jumlah besi bebas untuk pertumbuhan bakteri meningkat.
#akteri lain memperoleh besi bebas dengan mengekstraksi besi dari sel inang
dan menyintesis protein penagkap besi. &iderofor adalah substansi yang dihasilkan
bakteri, untuk menangkap besi baik dari inang maupun dari lingkungan (*ambar +.
-
8/14/2019 textbook-mikrobiologi18.doc
13/29
PATOGENESIS Bacillus anthracis
Bacillus anthracis adalah bakteri batang gram positif pembentuk endospora
fakultatif anaerob. &pora B. anthracis terletak di tengah sel dan tetap berada di dalam
sel vegetatif. B. anthracis merupakan bakteri tanah dan dapat diisolasi dari he'an dan
manusia terinfeksi.
Ma"i#e!ta!i I"#ek!i
%erdapat 3 bentuk penyakit yang ditimbulkan B. anthracis, yaitu anthra
kutaneus, anthra gastrointestinal, dan anthra inhalasi. Ketiga penyakit menunjukkan
rute masuk dan infeksi B. anthracis. Anthra kutaneus merupakan penyakit akibat infeksi
B. anthracis melalui luka minor kulit dan dapat menyebabkan ne!rosti! ul!er. Anthra
gastrointestinal merupakan penyakit akibat infeksi B. anthracis melalui saluran
pen!ernaan dan menyebabkan ne!roti! ul!er di saluran pen!ernaan dan sistem
limfatikus. Anthra inhalasi merupakan penyakit akibat infeksi B. anthracis melalui
saluran pernafasan dan menembus jaringan paru. *ejala anthra inhalasi mirip dengan
influen?a dan penyakit akibat virus lainnya, yaitu demam tinggi dan sakit di dada. &emua
penyakit anthra ini bersifat letal jika tanpa pera'atan memadai.
Meka"i!me Pat%$e"e!i!
B. anthracis memiliki 6 properti dasar virulensi, yaitu pembentukan kapsula dan
produksi toksin anthra. Kapsula B. anthracis adalah polimer asam amino glutamat.
*alur patogen B. anthracis memiliki karakter koloni sebagai berikut, koloni basah,
mukoid, kenampakan halus. *alur nonpatogen B. anthracis mempunyai koloni kasar
(tetap menghasilkan kapsula. Kapsulamelindungi B. anthracis dari berbagai respons
imunologi inang, seperti serum, lisin, fagositosis. *en pengkode kapsula terdapat pada
plasmid. &e!ara laboratorium, gen pengkode kapsula dapat diekspresikan dengan
menumbuhkan B. anthracis pada media berisi serum dan kadar -46atmosfir CE.
%oksin anthra B. anthracis baru dikenal sejak tahun +BC. %oksin anthra B.
anthracisterdiri atas 3 komponen yaitu faktor letal, faktor edema, dan antigen protektif.
7aktor letal adalah en?im kinase yang mampu merusak fungsi sel. akrofag merupakan
target toksin anthra. 7aktor edema adalah en?im yang memiliki aktivitas adenilatsiklase (menghasilkan AP dari A%P, sehingga menurunkan kadar A%P yang berguna
untuk mrnyuplai energi untuk fagositosis. Antigen protektif tidak memiliki efek toksis,
melainkan untuk perlekatan dengan sel sasaran, sehingga ke)6 faktor lainnya dapat
dieksport ke sel inang.
Dia$"%!i! &a" Perlak)a"
-
8/14/2019 textbook-mikrobiologi18.doc
14/29
Identifikasi B. anthracis!ukup sulit, karena B. anthracis mirip dengan anggota
Bacillus lainnya. etode umum untuk mengidentifikasi B. anthracis adalah dengan uji
biokimia'i (%abel +.6. &ejumlah uji lainnya diperlukan untuk mengkonfirmasi hasil
identifikasi. ;ji biokimia'i memerlukan 'aktu jam. 4leh karena itu diperlukan uji yang
!epat mengidentifikasi B. anthracis. ;ji !epat (rapid test berdasarkan reaksi antara
antibodi dengan toksin atau kapsula telah tersedia dan mampu memberi informasi
hanya dalam beberapa jam. ;ji terbaru berdasarkan reaksi rantai polimerase
(polymerase chain reaction yang mampu mendeteksi urutan D"A spesifik pengkode
faktor virulensi dan hanya memerlukan 'aktu +C menit.
%abel +.6 Karakteristik Bacillus spe!iesKarakteristik B. anthracis B. cereus dan
B. thuringiensisKebutuhan akan thiamin
2emolisis pada sheep blood agarKapsula polipeptida glutamil9isis oleh gama)fagotilitasPertumbuhan pada chloralhydrate agar
Aransemen rantai ujung ke ujung sel
/
)//))/
/
)//))/
Perlakuan pada penderita anthra dengan antibiotik. B. anthracis sensitif
terhadap berbagai antibiotik, khususnya penisilin. >ika sebelum infeksi B. anthracis
sedang dilakukan perlakuan antibiotik, maka perlakuan antibiotik memiliki efek ke!il.
$aksin anthra untuk he'an telah tersedia sejak Pasteur memformulasikan vaksin
anthra pertama kali. Konsentrasi rendah toksin dapat menstimulasi sistem antibodi
inang.
PEN/AKIT STREPTOKOKUS
Infeksi bakteri Streptococcus menghasilkan penyakit serius pada manusia. #aktri
patogen penting Streptococcus adalah S. pneumoniae dan S. pyrogenes. Streptococcus
merupakan kelompok organisme heterogen yang se!ara normal berasosiasi dengan
organisme tingkat tinggi. #eberapa galur merupakan bakteri patogen dan yang lainnya
merupakan bakteri flora normal manusia. Streptococcus adalah bakteri kokus gram
positif dan membelah dalam satu model arah (one plane di%ision . &etelah membelah,
sel1selnya saling berasosiasi menghasilkan struktur rantai. S. pneumoniae dan S.
pyrogenestidak memiliki en?im katalase. Streptococcus mampu memfermentasi
berbagai sumber karbon, tetapi lebih menyukai gula sebagai sember karbon. Pada
-
8/14/2019 textbook-mikrobiologi18.doc
15/29
media padat, Streptococcus menghasilkan koloni halus. Pada media blood agar,
terdapat karakteristik berbeda pada beberapa jenis Streptococcus.
Ma"i#e!ta!i I"#ek!i
S. pyrogenes merupakan bakteri penginfeksi saluran pernafasan, kulit, dan aliran
darah. Infeksi kulit dapat mengakibatkan impetigo, selulitis, ne!roti! fas!itis, dan
myositis. Penyakit saluran pernafasan, yaitu faringitis akut dan pneumonia. eskipun
jarang, S. pyrogenes mampu menyebar sampai aliran darah dan mengakibatkan
bakteremia dan sepsis dan dalam beberapa kesempatan menghasilkan toxic shock
syndromeyang bersifat letal. espons imunologis terhadap S. pyrogenes pada otot
jantung menyebabkan demam rematik dan ini mungkin terjadi sekitar 3E dari kasus
faringitis. Pera'atan intensif terhadap S. pyrogenesdapat men!egah perkembangan
demam rematik.
S. pneumoniaemerupakan penyebab utama infeksi saluran ernafasan pada
orang de'asa. S. pneumoniae dapat berubah menjadi karier (tidak memun!ulkan
simptom, sehinga tertransfer ke orng lain melalui udara. S. pneumoniaemenginfeksi
telinga, sinus, dan mata. Pasien dengan infeksi bakteri ini sering terlihat adanya
peradangan.
Meka"i!me Pat%$e"e!i!
S. pyrogenes
%erdapat 6 tahap perlekatan S. pyrogenes terhadap sel inang. Pertama, bakteri
melekat pada permukaan sel inang menggunakan asam lipotekoat dinding sel. &etelah
perlekatan pertama ini, diikuti perlekatan (ikatan protein pada ujung fimbria dengan
fibronektin dan menghasilkan perlekatan kuat.
&etelah melekat, S. pyrogenes menyekresi berbagai en?im untuk invasi sampai
ke jaringan dalam. 8n?im hialuronidase mendegradasi asam hialuronat yang ada di
antara 6 sel inang. 8n?im streptokinase merusak fibrin inang. #eberapa en?im
streptodornase mendegradasi D"A dan "A. Kumpulan en?im ini juga membantu S.
pyrogenes dalam menghindari dan mela'an sistem imun inang. S. pyrogenes
menghasilkan kapsula yang terbuat dari asam hialuronat (berasal dari sel inang.Kapsula berperan dalam menghindari fagositosis. 8n?im streptolisin dan "ADase
mampu membunuh leukosit. 8n?im protease -Ca menghan!urkan protein kompleman
-Ca inang yang merupakan kemoatraktan untuk fagosit.
-
8/14/2019 textbook-mikrobiologi18.doc
16/29
#eberapa galur S. pyrogenesmenyekresi eksotoksin pirogenik yang
menginduksi demam. #eberapa galur S. pyrogenes yang menghasilkan infeksi serius
dan merusak kulit, juga menghasilkan toksin pirogenik.
S. pneumoniae
ekanisme patogenesis S. pneumoniae belum diketaui dengan jelas. eskipun
demikian kapsula S. pneumoniae berperan dalam resistensi fagositosis dan
memfasilitasi penyebaran bakteri ini. Protein lain sebagai faktor virulensi adalah
pneumolisis dan permease, tetapi mekanisme keduanya tidak jelas.
Dia$"%!i! &a" Perlak)a"
Diagnosis Streptococcus tergantung pada teknik kultur dari jaringan tubuh. S.
pyrogenes se!ara normal dikonfirmasi dengan hemolisis pada media blood agar, bakteri
gram positif rantai kokus (S. pneumoniae bakteri gram positif rantai lan!et, sensitif
ba!itra!in dan opto!hin.
S. pyrogenes biasanya diperlakukan dengan penisilin dan bakteri ini tidak
mampu mengembangkan resistensi terhadap antibiotik. $aksin berbagai serotipe protein
sedang dikembangkan. S. pneumoniae diperlakukan dengan antibiotik penisilin, tetapi
bakteri ini mengembangkan resistensi terhadap antiobiotik. Pada bakteri resisten
penisilin, antibitik !efrriaone dan !efotaime sangat efektif. $aksin polisakarida dengan
lebih dari 63 serotipe sedang dikembangkan. $aksin untuk S. pneumoniae biasanya
efektif terhadap orang de'asa, tetapi tidak efektif untuk anak)anak.
Viral Pathogenesis
Samuel Baron, Michael Fons & Thomas Albrecht
General ConceptsPat*%$e"e!i!
Pathogenesis is the process by which an infection leads to disease. Pathogenic
mechanisms of viral disease include (1) implantation of virus at the portal of entry, (2)local replication, (3) spread to target organs (disease sites), and (4) spread to sites of
shedding of virus into the environment. actors that affect pathogenic mechanisms are (1)
-
8/14/2019 textbook-mikrobiologi18.doc
17/29
accessibility of virus to tissue, (2) cell susceptibility to virus multiplication, and (3) virus
susceptibility to host defenses. !atural selection favors the dominance of low"virulence
virus strains.
0ell)lar Pat*%$e"e!i!
#irect cell damage and death from viral infection may result from (1) diversion of the
cell$s energy, (2) shutoff of cell macromolecular synthesis, (3) competition of viral
m%!& for cellular ribosomes, (4) competition of viral promoters and transcriptionalenhancers for cellular transcriptional factors such as %!& polymerases, and inhibition of
the interferon defense mechanisms. 'ndirect cell damage can result from integration of
the viral genome, induction of mutations in the host genome, inflammation, and the hostimmune response.
Ti!!)e Tr%'i!m
iral affinity for specific body tissues (tropism) is determined by (1) cell receptors forvirus, (2) cell transcription factors that recognie viral promoters and enhancerse*uences, (3) ability of the cell to support virus replication, (4) physical barriers, (+)
local temperature, p, and o-ygen tension enymes and non"specific factors in body
secretions, and () digestive enymes and bile in the gastrointestinal tract that mayinactivate some viruses.
Im'la"tati%" at t*e P%rtal %# E"tr
irions implant onto living cells mainly via the respiratory, gastrointestinal, s/in"
penetrating, and genital routes although other routes can be used. 0he final outcome of
infection may be determined by the dose and location of the virus as well as its infectivityand virulence.
L%al Re'liati%" a"& L%al S'rea&
ost virus types spread among cells e-tracellularly, but some may also spreadintracellularly. stablishment of local infection may lead to localied disease and
localied shedding of virus.
Di!!emi"ati%" #r%m t*e P%rtal %# E"tr
iremic 0he most common route of systemic spread from the portal of entry is thecirculation, which the virus reaches via the lymphatics. irus may enter the target organs
from the capillaries by (1) multiplying in endothelial cells or fi-ed macrophages, (2)
diffusing through gaps, and (3) being carried in a migrating leu/ocyte.
!eural #issemination via nerves usually occurs with rabies virus and sometimes withherpesvirus and poliovirus infections.
-
8/14/2019 textbook-mikrobiologi18.doc
18/29
I")bati%" Peri%&
0he incubation period is the time between e-posure to virus and onset of disease. #uring
this usually asymptomatic period, implantation, local multiplication, and spread (fordisseminated infections) occur.
M)lti'liati%" i" Tar$et Or$a"!
#epending on the balance between virus and host defenses, virus multiplication in the
target organ may be sufficient to cause disease and death.
S*e&&i"$ %# Vir)!
<hough the respiratory tract, alimentary tract, urogenital tract and blood are the most
fre*uent sites of shedding, diverse viruses may be shed at virtually every site.
0%"$e"ital I"#eti%"!
'nfection of the fetus as a target organ is special because the virus must traverse
additional physical barriers, the early fetal immune and interferon defense systems may
be immature, transfer of the maternal defenses are partially bloc/ed by the placenta, thedeveloping first"trimester fetal organs are vulnerable to infection, and hormonal changes
are ta/ing place.
!T"#$%CT#!
Pathogenesis is the process by which virus infection leads to disease. Pathogenic
mechanisms include implantation of the virus at a body site (the portal of entry),replication at that site, and then spread to and multiplication within sites (target organs)
where disease or shedding of virus into the environment occurs. ost viral infections are
subclinical, suggesting that body defenses against viruses arrest most infections beforedisease symptoms become manifest. 5nowledge of subclinical infections comes from
serologic studies showing that sieable portions of the population have specific
antibodies to viruses even though the individuals have no history of disease. 0heseinapparent infections have great epidemiologic importance they constitute ma6or sources
for dissemination of virus through the population, and they confer immunity (see 7h. 48).
any factors affect pathogenic mechanisms. &n early determinant is the e-tent to which
body tissues and organs are accessible to the virus. &ccessibility is influenced by physicalbarriers (such as mucus and tissue barriers), by the distance to be traversed within the
body, and by natural defense mechanisms. 'f the virus reaches an organ, infection occurs
only if cells capable of supporting virus replication are present. 7ellular susceptibilityre*uires a cell surface attachment site (receptor) for the virions and also an intracellular
environment that permits virus replication and release. ven if virus initiates infection in
a susceptible organ, replication of sufficient virus to cause disease may be prevented by
host defenses (see 7hs. 49 and +:).
-
8/14/2019 textbook-mikrobiologi18.doc
19/29
;ther factors that determine whether infection and disease occur are the many virulence
characteristics of the infecting virus. 0o cause disease, the infecting virus must be able to
overcome the inhibitory effects of physical barriers, distance, host defenses, and differingcellular susceptibilities to infection. 0he inhibitory effects are genetically controlled and
therefore may vary among individuals and races. irulence characteristics enable the
virus to initiate infection, spread in the body, and replicate to large enough numbers toimpair the target organ. 0hese factors include the ability to replicate under certain
circumstances during inflammation, during the febrile response, in migratory cells, and in
the presence of natural body inhibitors and interferon. -tremely virulent strains oftenoccur within virus populations. ;ccasionally, these strains become dominant as a result
of unusual selective pressures (see 7h. 48). 0he viral proteins and genes responsible for
specific virulence functions are only 6ust beginning to be identified.
ortunately for the survival of humans and animals (and hence for the infecting virus),most natural selective pressures favor the dominance of less virulent strains. they cause only inapparent infections and yet are able to replicate sufficiently to induce
immunity.
0he occurrence of spontaneous or induced mutations in viral genetic material may alter
the pathogenesis of the induced disease, e.g. '. 0hese mutations can be of particularimportance with the development of drug resistant strains of virus.
#isease does not always follow successful virus replication in the target organ. #isease
occurs only if the virus replicates sufficiently to damage essential cells directly, to causethe release of to-ic substances from infected tissues, to damage cellular genes or to
damage organ function indirectly as a result of the host immune response to the presence
of virus antigens.
&s a group, viruses use all conceivable portals of entry, mechanisms of spread, targetorgans, and sites of e-cretion. 0his abundance of possibilities is not surprising
considering the astronomic numbers of viruses and their variants (see 7h. 43).
0ell)lar Pat*%$e"e!i!
#irect cell damage and death may result from disruption of cellular macromolecularsynthesis by the infecting virus. &lso, viruses cannot synthesie their genetic and
structural components, and so they rely almost e-clusively on the host cell for these
functions. 0heir parasitic replication therefore robs the host cell of energy andmacromolecular components, severely impairing the host$s ability to function and often
resulting in cell death and disease.
-
8/14/2019 textbook-mikrobiologi18.doc
20/29
Pathogenesis at the cellular level can be viewed as a process that occurs in progressive
stages leading to cellular disease. &s noted above, an essential aspect of viral
pathogenesis at the cellular level is the competition between the synthetic needs of thevirus and those of the host cell. ?ince viruses must use the cell$s machinery to synthesie
their own nucleic acids and proteins, they have evolved various mechanisms to subvert
the cell$s normal functions to those re*uired for production of viral macromolecules andeventually viral progeny. 0he function of some of the viral genetic elements associated
with virulence may be related to providing conditions in which the synthetic needs of the
virus compete effectively for a limited supply of cellular macromolecule components andsynthetic machinery, such as ribosomes.
#amage of cells by replicating virus and damage by the immune response are considered
further in 7hapters 44 and +:, respectively.
Ti!!)e Tr%'i!m
ost viruses have an affinity for specific tissues> that is, they display tissue specificity ortropism. 0his specificity is determined by selective susceptibility of cells, physical
barriers, local temperature and p, and host defenses. any e-amples of viral tissue
tropism are /nown. Polioviruses selectively infect and destroy certain nerve cells, whichhave a higher concentration of surface receptors for polioviruses than do virus"resistant
cells. %hinoviruses multiply e-clusively in the upper respiratory tract because they are
adapted to multiply best at low temperature and p and high o-ygen tension.nteroviruses can multiply in the intestine, partly because they resist inactivation by
digestive enymes, bile, and acid.
0he cell receptors for some viruses have been identified. %abies virus uses the
acetylcholine receptor present on neurons as a receptor, and hepatitis < virus binds topolymeried albumin receptors found on liver cells. ?imilarly, pstein"
-
8/14/2019 textbook-mikrobiologi18.doc
21/29
Se3)e"e %# Vir)! S'rea& i" t*e 4%!t
Implantation at Portal of Entry
iruses are carried to the body by all possible routes (air, food, bites, and any
contaminated ob6ect). ?imilarly, all possible sites of implantation (all body surfaces andinternal sites reached by mechanical penetration) may be used. 0he fre*uency of
implantation is greatest where virus contacts living cells directly (in the respiratory tract,
in the alimentary tract, in the genital tract, and subcutaneously). Aith some viruses,implantation in the fetus may occur at the time of fertiliation through infected germ
cells, as well as later in gestation via the placenta, or at birth.
ven at the earliest stage of pathogenesis (implantation), certain variables may influence
the final outcome of the infection. or e-ample, the dose, infectivity, and virulence ofvirus implanted and the location of implantation may determine whether the infection
will be inapparent (subclinical) or will cause mild, severe, or lethal disease.
Local Replication and Local Spread
?uccessful implantation may be followed by local replication and local spread of virus(ig. 4+"1). irus that replicates within the initially infected cell may spread to ad6acent
cells e-tracellularly or intracellularly. -tracellular spread occurs by release of virus into
the e-tracellular fluid and subse*uent infection of the ad6acent cell. 'ntracellular spread
occurs by fusion of infected cells with ad6acent, uninfected cells or by way ofcytoplasmic bridges between cells. ost viruses spread e-tracellularly, but herpesviruses,
paramy-oviruses, and po-viruses may spread through both intracellular and e-tra cellular
routes. 'ntracellular spread provides virus with a partially protected environment because
the antibody defense does not penetrate cell membranes.
-
8/14/2019 textbook-mikrobiologi18.doc
22/29
FIGURE 45- Vir!s spread d!ring locali"ed infection#!umbers indicate se*uence of
events.
?pread to cells beyond ad6acent cells may occur through the li*uid spaces within the localsite (e.g., lymphatics) or by diffusion through surface fluids such as the mucous layer of
the respiratory tract. &lso, infected migratory cells such as lymphocytes and macrophages
may spread the virus within local tissue.
stablishment of infection at the portal of entry may be followed by continued local virusmultiplication, leading to localied virus shedding and localied disease. 'n this way,
local sites of implantation also are target organs and sites of shedding in many infections
(0able 4+"1). %espiratory tract infections that fall into this category include influena, thecommon cold, and parainfluena virus infections. &limentary tract infections caused by
several gastroenteritis viruses (e.g., rotaviruses and picornaviruses) also may fall into this
category. =ocalied s/in infections of this type include warts, cowpo-, and molluscumcontagiosum. =ocalied infections may spread over body surfaces to infect distant
surfaces. &n e-ample of this is the picornavirus epidemic con6unctivitis shown in igure4+"2> in the absence of viremia, virus spreads directly from the eye (site of implantation)
to the pharyn- and intestine. ;ther viruses may spread internally to distant target organsand sites of e-cretion (disseminated infection). & third category of viruses may cause
both local and disseminated disease, as in herpes simple- and measles.
-
8/14/2019 textbook-mikrobiologi18.doc
23/29
FIGURE 45-$ Spread of picorna%ir!s o%er &ody s!rfaces from eye to pharyn' and
intestine d!ring nat!ral infection. =ocal neutraliing antibody activity is shown.
(&dapted from =angford P, ?tanton B@,
-
8/14/2019 textbook-mikrobiologi18.doc
24/29
through the blood after an initial period of replication at the portal of entry (the
alimentary and respiratory tracts), where the infection often causes no significant
symptoms or signs of illness because the virus /ills cells that are e-pendable and easilyreplaced. irus progeny diffuse through the afferent lymphatics to the lymphoid tissue
and then through the efferent lymphatics to infect cells in close contact with the
bloodstream (e.g., endothelial cells, especially those of the lymphoreticular organs). 0hisinitial spread may result in a brief primary viremia. ?ubse*uent release of virus directly
into the bloodstream induces a secondary viremia, which usually lasts several days and
puts the virus in contact with the capillary system of all body tissues. irus may enter thetarget organ from the capillaries by replicating within a capillary endothelial cell or fi-ed
macrophage and then being released on the target organ side of the capillary. irus may
also diffuse through small gaps in the capillary endothelium or penetrate the capillary
wall through an infected, migrating leu/ocyte. 0he virus may then replicate and spreadwithin the target organ or site of e-cretion by the same mechanisms as for local
dissemination at the portal of entry. #isease occurs if the virus replicates in a sufficient
number of essential cells and destroys them. or e-ample, in poliomyelitis the central
nervous system is the target organ, whereas the alimentary tract is both the portal of entryand the site of shedding. 'n some situations, the target organ and site of shedding may be
the same.
(issemination in *er%es
#issemination through the nerves is less common than bloodstream dissemination, but is
the means of spread in a number of important diseases (ig. 4+"4). 0his mechanism
occurs in rabies virus, herpesvirus, and, occasionally, poliomyelitis virus infections. ore-ample, rabies virus implanted by a bite from a rabid animal replicates subcutaneously
and within muscular tissue to reach nerve endings. vidence indicates that the virus
spreads centrally in the neurites (a-ons and dendrites) and perineural cells, where virus isshielded from antibody. 0his nerve route leads rabies virus to the central nervous system,where disease originates. %abies virus then spreads centrifugally through the nerves to
reach the salivary glands, the site of shedding. 0able 4+"2 shows other e-amples of nerve
spread.
-
8/14/2019 textbook-mikrobiologi18.doc
25/29
FIGURE 45-+ Vir!s spread thro!gh &loodstream d!ring a generali"ed infection .
!umbers indicate se*uence of events.
Inc!&ation Period
#uring most virus infections, no signs or symptoms of disease occur through the stage ofvirus dissemination. 0hus, the incubation period (the time between e-posure to virus and
onset of disease) e-tends from the time of implantation through the phase of
dissemination, ending when virus replication in the target organs causes disease.;ccasionally, mild fever and malaise occur during viremia, but they often are transient
and have little diagnostic value.
0he incubation period tends to be brief (1 to 3 days) in infections in which virus travels
only a short distance to reach the target organ (i.e., in infections in which disease is due tovirus replication at the portal of entry). 7onversely, incubation periods in generalied
infections are longer because of the stepwise fashion by which the virus moves through
the body before reaching the target organs. ;ther factors also may influence theincubation period. Beneralied infections produced by togaviruses may have an
une-pectedly short incubation period because of direct intravascular in6ection (insect
bite) of a rapidly multiplying virus. 0he mechanisms governing the long incubationperiod (months to years) of persistent infections are poorly understood. 0he persistently
infected cell is often not lysed, or lysis is delayed. 'n addition, disease may result from a
late immune reaction to viral antigen (e.g., arenaviruses in rodents), from un/nown
-
8/14/2019 textbook-mikrobiologi18.doc
26/29
mechanisms in slow viral infections during which no immune response has been detected
(as in the scrapie"/uru group), or mutation in the host genetic material resulting in
cellular transformation and cancer.
FIGURE 45-4 Vir!s spread thro!gh ner%es d!ring a generali"ed infection . !umbers
indicate se*uence of events.
M)lti'liati%" i" Tar$et Or$a"!
irus replication in the target organ resembles replication at other body sites e-cept that
(1) the target organ in systemic infections is usually reached late during the stepwiseprogression of virus through the body, and (2) clinical disease originates there. &t each
step of virus progression through the body, the local recovery mechanisms (local body
defenses, including interferon, local inflammation, and local immunity) are activated.0hus, when the target organ is infected, the previously infected sites may have reached
various stages of recovery. igure 4+"2 illustrates this staging of infection and recovery in
different tissues during a spreading surface infection. 7irculating interferon and immuneresponses probably account for the termination of viremia, but these responses may betoo late to prevent seeding of virus into the target organ and into sites of shedding.
!evertheless, these systemic defenses can diffuse in various degrees into target organs
and thereby help retard virus replication and disease.
#epending on the balance between virus and host defenses (see 7hs. 49 and +:), virusmultiplication in the target organ may be sufficient to produce dysfunction manifested by
-
8/14/2019 textbook-mikrobiologi18.doc
27/29
disease or death. &dditional constitutional disease such as fever and malaise may result
from diffusion of to-ic products of virus replication and cell necrosis, as well as from
release of lympho/ines and other inflammatory mediators. %elease of leu/otriene 74during respiratory infection may cause bronchospasm. iral antigens also may participate
in immune reactions, leading to disease manifestations. 'n addition, impairment of
leu/ocytes and immunosuppression by some viruses may cause secondary bacterialinfection.
S*e&&i"$ %# Vir)!
-
8/14/2019 textbook-mikrobiologi18.doc
28/29
0%"$e"ital I"#eti%"!
'nfection of the fetus is a special case of infection in a target organ. 0he factors that
determine whether a target organ is infected also apply to the fetus, but the fetus presents
additional variables. 0he immune and interferon systems of the very young fetus areimmature. 0his immaturity, coupled with the partial placental barrier to transfer of
maternal immunity and interferon, deprive the very young fetus of important defense
mechanisms. ¬her variable is the high vulnerability to disruption of the rapidly
developing fetal organs, especially during the first trimester of pregnancy. urthermore,
susceptibility to virus replication may be modulated by the undifferentiated state of thefetal cells and by hormonal changes during pregnancy. <hough virus multiplication in
the fetus may lead to congenital anomalies or fetal death, the mother may have only amild or inapparent infection.
0o cause congenital anomalies, virus must reach the fetus and multiply in it, thereby
causing maldeveloped organs. Benerally, virus reaches the fetus during maternal viremia
by infecting or passing through the placenta to the fetal circulation and then to fetal target
-
8/14/2019 textbook-mikrobiologi18.doc
29/29
organs. ?ufficient virus multiplication may disrupt development of fetal organs,
especially during their rapid development (the first trimester of pregnancy). <hough
many viruses occasionally cause congenital anomalies, cytomegalovirus and rubella virusare the most common offenders. irus shedding by the congenitally infected newborn
infant may occur as a result of persistence of the virus infection at sites of shedding.