j.1440-1843.2010.01738_FITRI.x
20
INVITED REVIEW SERIES: TUBERCULOSIS SERIES EDITORS: WING WAI YEW, GIOVANNI B. MIGLIORI AND CHRISTOPH LANGE Drug-resistant tuberculosis: Past, present, future CHEN-YUAN CHIANG, 1 ROSELLA CENTIS 2 AND GIOVANNI BATTISTA MIGLIORI 2 1 International Union Against Tuberculosis and Lung Disease, Paris, France, and 2 WHO Collaborating Centre for TB and Lung Diseases, Fondazione S. Maugeri, Care and Research Institute, Tradate, Italy ABSTRACT In a population of Mycobacterium tuberculosis, random chromosomal mutation that results in genetic resistance to anti-tuberculosis (TB) drugs occurs at a relatively low frequency. Anti-TB drugs impose selec- tion pressure so that mycobacterial mutants gradually outnumber susceptible bacilli and emerge as the domi- nant strains. Resistance to two or more anti-TB drugs represents cumulative results of sequential mutation. The fourth report on global anti-TB drug resistance provides the latest data on the extent of such problem in the world. The median prevalence of multi-drug- resistant TB (MDR-TB) in new TB cases was 1.6%, and in previously treated TB cases 11.7%. Of the half a million MDR-TB cases estimated to have emerged in 2006, 50% were in China and India. The optimal dura- tion of any given combination of anti-TB drugs for treatment of MDR- and extensively drug-resistant TB (XDR-TB) has not been defined in controlled clinical trials. Standardized treatment may be feasible for MDR-TB patients not previously treated with second- line drugs, but a different strategy needs to be applied in the treatment of MDR-TB patients who have received second-line drugs before. Unfortunately, the reliability of drug susceptibility testing of most second- line anti-TB drugs is still questionable. Drug-resistant TB is not necessarily less virulent. Findings from mod- elling exercise warned that if MDR-TB case detection and treatment rates increase to the World Health Organization target of 70%, without simultaneously increasing MDR-TB cure rates, XDR-TB prevalence could increase exponentially. Prevention of develop- ment of drug resistance must be accorded the top pri- ority in the era of MDR-/XDR-TB. Key words: extensively drug-resistant tuberculosis, human immunodeficiency virus, multi-drug-resistant tuberculosis, review, risk factor. INTRODUCTION Tuberculosis (TB) was thought to be incurable until the middle of the 20th century. Introduction of anti-TB drugs changed the fate of TB patients as dem- onstrated by Crofton in 1959 1 (Sir John Crofton died at the age of 97 on 3 November 2009). However, as Crofton stated, the greatest disaster that can happen to a patient with TB is that the organisms become resistant to two or more of the standard drugs, through selection of mycobacterial mutants that result from spontaneous chromosomal alterations. 1 Rifampicin (RMP)-containing short-course chemo- therapy remains efficacious in the treatment of iso- niazid (INH)-resistant TB 2 but its efficacy becomes substantially compromised in the treatment of multi- drug-resistant TB (MDR-TB), denoted by bacillary resistance to at least both INH and RMP. 3 MDR-TB is not incurable. A fluoroquinolone, if used properly alongside other second-line drugs, could cure the majority of MDR-TB patients; with a low risk of relapse in long-term follow up. 4 The term extensively drug-resistant TB (XDR-TB) appeared in the literature for the first time in March 2006, in a report jointly published by the US Centers for Disease Control and Prevention and the World Health Organization (WHO) to describe a severe form of disease, 5 presently defined as MDR-TB with additional bacillary resis- tance to any fluoroquinolone and at least one of three second-line injectable drugs: capreomycin, kanamy- cin and amikacin. 6,7 Although the definition of XDR-TB has been questioned, 8,9 a European study has demonstrated that the occurrence of XDR-TB, as The authors: Dr C.-Y.C. is Director of Department of Lung Health and NCDs, International Union Against Tuberculosis and Lung Disease, Paris, France. He organized and taught in several international and national training courses on clinical manage- ment of drug-resistant tuberculosis. He provided technical assis- tance on tuberculosis control in several developing countries in Africa and Asia. Professor G.B.M. is Director of the WHO Collabo- rating Center for TB and Lung Diseases at Fondazione S. Maugeri, Care and Research Institute, Tradate, Italy. He is pres- ently the head of the Respiratory Infection Assembly of the European Respiratory Society (ERS), being involved in research, technical assistance and training on TB and TB/HIV control at the global level. Dr R.C. is Health Economist in the same Institution. She is mainly involved in the research-related activities of the Centre. Correspondence: Giovanni Battista Migliori, WHO Collaborat- ing Centre for TB and Lung Diseases, Fondazione S. Maugeri, Care and Research Institute/TBNET Secretariat (TuBerculosis Network European Trialsgroup), via Roncaccio 16, 21049 Tradate, Italy. Email: [email protected] Received 11 November 2009; invited to revise 18 November 2009; revised 30 November 2009; accepted 1 December 2009. © 2010 The Authors Journal compilation © 2010 Asian Pacific Society of Respirology Respirology (2010) 15, 413–432 doi: 10.1111/j.1440-1843.2010.01738.x
-
Upload
divaa-oktavianita -
Category
Documents
-
view
6 -
download
1
description
journal
Transcript of j.1440-1843.2010.01738_FITRI.x
INVITED REVIEW SERIES: TUBERCULOSISSERIES EDITORS: WING WAI YEW, GIOVANNI B. MIGLIORI AND CHRISTOPH LANGE
Drug-resistant tuberculosis: Past, present, future
CHEN-YUAN CHIANG,1 ROSELLA CENTIS2 AND GIOVANNI BATTISTA MIGLIORI2
1International Union Against Tuberculosis and Lung Disease, Paris, France, and 2WHO Collaborating Centre forTB and Lung Diseases, Fondazione S. Maugeri, Care and Research Institute, Tradate, Italy
ABSTRACT
In a population of Mycobacterium tuberculosis,random chromosomal mutation that results in geneticresistance to anti-tuberculosis (TB) drugs occurs at arelatively low frequency. Anti-TB drugs impose selec-tion pressure so that mycobacterial mutants graduallyoutnumber susceptible bacilli and emerge as the domi-nant strains. Resistance to two or more anti-TB drugsrepresents cumulative results of sequential mutation.The fourth report on global anti-TB drug resistanceprovides the latest data on the extent of such problemin the world. The median prevalence of multi-drug-resistant TB (MDR-TB) in new TB cases was 1.6%, andin previously treated TB cases 11.7%. Of the half amillion MDR-TB cases estimated to have emerged in2006, 50% were in China and India. The optimal dura-tion of any given combination of anti-TB drugs fortreatment of MDR- and extensively drug-resistant TB(XDR-TB) has not been defined in controlled clinicaltrials. Standardized treatment may be feasible forMDR-TB patients not previously treated with second-line drugs, but a different strategy needs to be appliedin the treatment of MDR-TB patients who havereceived second-line drugs before. Unfortunately, thereliability of drug susceptibility testing of most second-line anti-TB drugs is still questionable. Drug-resistant
TB is not necessarily less virulent. Findings from mod-elling exercise warned that if MDR-TB case detectionand treatment rates increase to the World HealthOrganization target of 70%, without simultaneouslyincreasing MDR-TB cure rates, XDR-TB prevalencecould increase exponentially. Prevention of develop-ment of drug resistance must be accorded the top pri-ority in the era of MDR-/XDR-TB.
Key words: extensively drug-resistant tuberculosis,human immunodeficiency virus, multi-drug-resistanttuberculosis, review, risk factor.
INTRODUCTION
Tuberculosis (TB) was thought to be incurable untilthe middle of the 20th century. Introduction ofanti-TB drugs changed the fate of TB patients as dem-onstrated by Crofton in 19591 (Sir John Crofton died atthe age of 97 on 3 November 2009). However, asCrofton stated, the greatest disaster that can happento a patient with TB is that the organisms becomeresistant to two or more of the standard drugs,through selection of mycobacterial mutants thatresult from spontaneous chromosomal alterations.1
Rifampicin (RMP)-containing short-course chemo-therapy remains efficacious in the treatment of iso-niazid (INH)-resistant TB2 but its efficacy becomessubstantially compromised in the treatment of multi-drug-resistant TB (MDR-TB), denoted by bacillaryresistance to at least both INH and RMP.3 MDR-TB isnot incurable. A fluoroquinolone, if used properlyalongside other second-line drugs, could cure themajority of MDR-TB patients; with a low risk ofrelapse in long-term follow up.4 The term extensivelydrug-resistant TB (XDR-TB) appeared in the literaturefor the first time in March 2006, in a report jointlypublished by the US Centers for Disease Controland Prevention and the World Health Organization(WHO) to describe a severe form of disease,5 presentlydefined as MDR-TB with additional bacillary resis-tance to any fluoroquinolone and at least one of threesecond-line injectable drugs: capreomycin, kanamy-cin and amikacin.6,7 Although the definition ofXDR-TB has been questioned,8,9 a European study hasdemonstrated that the occurrence of XDR-TB, as
The authors: Dr C.-Y.C. is Director of Department of LungHealth and NCDs, International Union Against Tuberculosis andLung Disease, Paris, France. He organized and taught in severalinternational and national training courses on clinical manage-ment of drug-resistant tuberculosis. He provided technical assis-tance on tuberculosis control in several developing countries inAfrica and Asia. Professor G.B.M. is Director of the WHO Collabo-rating Center for TB and Lung Diseases at Fondazione S.Maugeri, Care and Research Institute, Tradate, Italy. He is pres-ently the head of the Respiratory Infection Assembly of theEuropean Respiratory Society (ERS), being involved in research,technical assistance and training on TB and TB/HIV control at theglobal level. Dr R.C. is Health Economist in the same Institution.She is mainly involved in the research-related activities of theCentre.
Correspondence: Giovanni Battista Migliori, WHO Collaborat-ing Centre for TB and Lung Diseases, Fondazione S. Maugeri,Care and Research Institute/TBNET Secretariat (TuBerculosisNetwork European Trialsgroup), via Roncaccio 16, 21049 Tradate,Italy. Email: [email protected]
Received 11 November 2009; invited to revise 18 November2009; revised 30 November 2009; accepted 1 December 2009.
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432doi: 10.1111/j.1440-1843.2010.01738.x

currently defined, has both a clinical value (predictingpoor outcome) and an operational significance (con-firming the loss of first-line drugs coupled with keysecond-line ones).10 Unfortunately, XDR-TB is not yetthe final product in the treatment of TB; amplificationof drug resistance is still likely to occur if we do notmanage XDR-TB properly. The questions are ‘willdrug-resistant mutants outnumber susceptibleorganisms and become the dominant bacilli in thefuture?’ and ‘could we avoid this from happening?’11–14
This paper will review mechanisms in and factorsassociated with the development of drug-resistant TB,epidemiology of drug-resistant TB, as well currentknowledge in the management of drug-resistant TB,and will elaborate on prospects of control of thedisease in the future.
METHODOLOGY
The present review was based on a Medline searchperformed using the key words TB, MDR-TB, XDR-TBcovering the period up to September 2009. In addi-tion, the Morbidity and Mortality Weekly Report of theUS Centers for Disease Control and Prevention wassearched from 1989 to the present for reports onMDR-TB and XDR-TB. The articles identified weredivided into the following sections: mechanisms inthe development of drug-resistant TB; anti-TB drugresistance in the world; epidemiology, risk factors,clinical presentation and outcome of drug resistantTB; design of an optimal drug regimen; HIV andMDR-/XDR-TB and prospects of the future, includingdisease prevention, improved diagnostic tools andnew drugs.
MECHANISM IN THE DEVELOPMENTOF DRUG-RESISTANT TUBERCULOSIS
In a population of Mycobacterium tuberculosis,random mutation that results in resistance toanti-TB drugs occurs at a relatively low frequency.15
Clinically significant drug resistance in TB candevelop during anti-TB treatment (acquired resis-tance). Anti-TB drugs impose selection pressure in apopulation of M. tuberculosis in which resistantmutants gradually outnumber susceptible bacilli andemerge as the dominant strains.16 Monotherapy ofTB resulting in emergence of resistance to the drugwas noted since 1940s when streptomycin (SM) wasused alone in the treatment of the disease.17,18 Para-aminosalicylic acid19 and subsequently INH wereincorporated into the drug regimen to prevent thedevelopment of SM resistance.20 Once resistantbacillary strains emerge during treatment, thesecould be transmitted in a community. Those who areso infected with drug-resistant strains may developdrug-resistant TB prior to treatment (primary resis-tance). The first national sampling survey of primarydrug resistance in Britain in 1955–1956 revealed theexistence of primary resistance to SM, Para-aminosalicylic acid and INH, which led to the estab-
lishment of triple drug therapy, as treatment ofpatients whose bacilli had primary resistance to asingle drug with a two-drug regimen was likelyequivalent monotherapy, especially in the presenceof a sizeable bacillary load (functional mono-therapy).20 No educated doctor will knowingly applya single drug to treat TB, but monotherapy of TB stilloccur. Fluoroquinolones are frequently used to treatacute lower respiratory tract infections but suchpatients so diagnosed may in fact have TB.21–23 Thistherapeutic practice causing delay in the diagnosisof TB and the emergence of fluoroquinolone-resistant TB is particularly dangerous in geographi-cal settings with a high prevalence of the disease.24,25
Treatment of latent TB infection is another practiceof potential monotherapy of TB if patients withactive disease are not identified.26 This may result inINH resistance.27 Furthermore, functional mono-therapy remains an important mechanism in thedevelopment of bacillary resistance in settings whereculture and drug susceptibility testing (DST) are notroutinely available.
Combination therapy in patients infected with sus-ceptible M. tuberculosis strains does not consistentlyprevent the emergence of drug resistance, especially ifpatients take medications irregularly. Mitchison pro-posed four basic mechanisms to explain how drugresistance emerges as a result of poor complianceduring TB treatment. These include (i) differentialbactericidal effects during initial killing; (ii) mono-therapy during sterilization of special populations;(iii) differential subinhibitory drug concentrationsduring regrowth; and (iv) differential bacterio-pausaleffects during regrowth.28 Among first-line anti-TBdrugs, INH has the strongest early bactericidal activ-ity and is most capable in preventing the emergenceof bacillary resistance to companion drugs,29 butusually is the first drug that becomes resistant when a6-month RMP-containing short-course regimen isapplied.30 Due to the long history of use of INH andSM in the treatment of TB and the microbiologicalcharacteristics of the drugs, resistance to INH or SM isthe most frequent bacillary resistance among newpatients in most settings.31 However, RMP monoresis-tance may emerge prior to INH resistance especiallyamong the HIV-infected.32,33 In addition to (func-tional) monotherapy and poor patient adherence,inadequate dosage and poor quality of drugs maylead to the emergence of drug resistance. To datethere has been no single genetic mutation identifiedresulting in resistance to two or more anti-TB drugs.34
The development of resistance in TB begins withmonoresistance, and subsequent resistance to addi-tional drugs may occur. Resistance to two or moreanti-TB drugs is the cumulative result of sequentialmutations.34
ANTI-TUBERCULOSIS DRUGRESISTANCE IN THE WORLD
In 1978, the committee on bacteriology and immu-nology of the International Union Against Tuberculo-sis and Lung Disease (IUATLD, The Union) decided
C-Y Chiang et al.414
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
that a documentation on the prevalence of drug resis-tance in TB was needed, which led to the publicationof ‘A world atlas of initial drug resistance’ in 1980.35
Another review on the worldwide situation of drug-resistant TB found it difficult to assess the situationbecause (i) there were few facilities for culture ofM. tuberculosis in developing countries; (ii) standard-ized laboratory methodologies were not followeduniformly; (iii) in many surveys, small or non-representative populations were sampled; and (iv) thedistinction between primary and acquired resistancewas not consistently made.36
In 1994, WHO and The Union launched the GlobalProject on Anti-tuberculosis Drug Resistance Surveil-lance. The project upheld three main principles: (i)the sample was representative of all TB cases in thesetting under evaluation; (ii) new patients wereclearly distinguished from those with previous treat-ment; and (iii) optimal laboratory performance wasassured and maintained through links with a TBsupranational reference laboratory.31,37–41 Subse-quently, in order to simplify drug resistance classifi-cation, that among new cases was defined as thepresence of resistant isolates of M. tuberculosis inpatients who denied having had any prior anti-TBtreatment (for as much as 1 month) and these casesmight result from the transmission of drug-resistantM. tuberculosis. Drug resistance among previouslytreated cases was defined as the presence of resistantisolates of M. tuberculosis in patients who had beentreated for TB for 1 month or more.
Drug resistance among previously treated casesmay not be a useful proxy of truly acquiredresistance as it contains a combination of threetypes of resistance (i) patients who have acquiredresistance during TB treatment; (ii) patients whohave been primarily infected with a resistantstrain and subsequently failed therapy; and (iii)patients who have been reinfected with a resistantstrain.41 Combined drug resistance was definedas the proportion of drug resistance in the popula-tion surveyed regardless of prior treatment, whichmay thus represent a better approximation of thelevel of drug resistance in the community. As the rateof drug resistance among new cases usually changesslowly, combined drug resistance has been proposedto be the best indicator of programme perfor-mance.42 Quality assurance programme for DST ofM. tuberculosis through supranational laboratorynetwork is essential. It was noted that the reliabilityof DST for RMP and INH was much better than thatof SM and ethambutol (EMB), and that regular pro-ficiency testing can significantly improve the qualityof DST43
Recently, the TuBerculosis Network European Tri-alsgroup studies have reported the epidemiologicaland clinical data for all culture-confirmed TB patients(n = 4583) diagnosed consecutively by the TB clinicalreference centres in Estonia (Tallin, Tartu), Germany(Borstel, Munich-Gauting, Grosshansdorf, Bad-Lippspringe), Italy (Sondalo, Milan, Rome) andRussian Federation (Archangels Oblast) between 1999and 2006 (Italy and Germany: 2003–2006; Estonia:2001–2004; Archangels Oblast: 1999–2001).10,44–47
EPIDEMIOLOGY OF DRUG-RESISTANTTUBERCULOSIS
The fourth report on global anti-TB drug resistance41,48
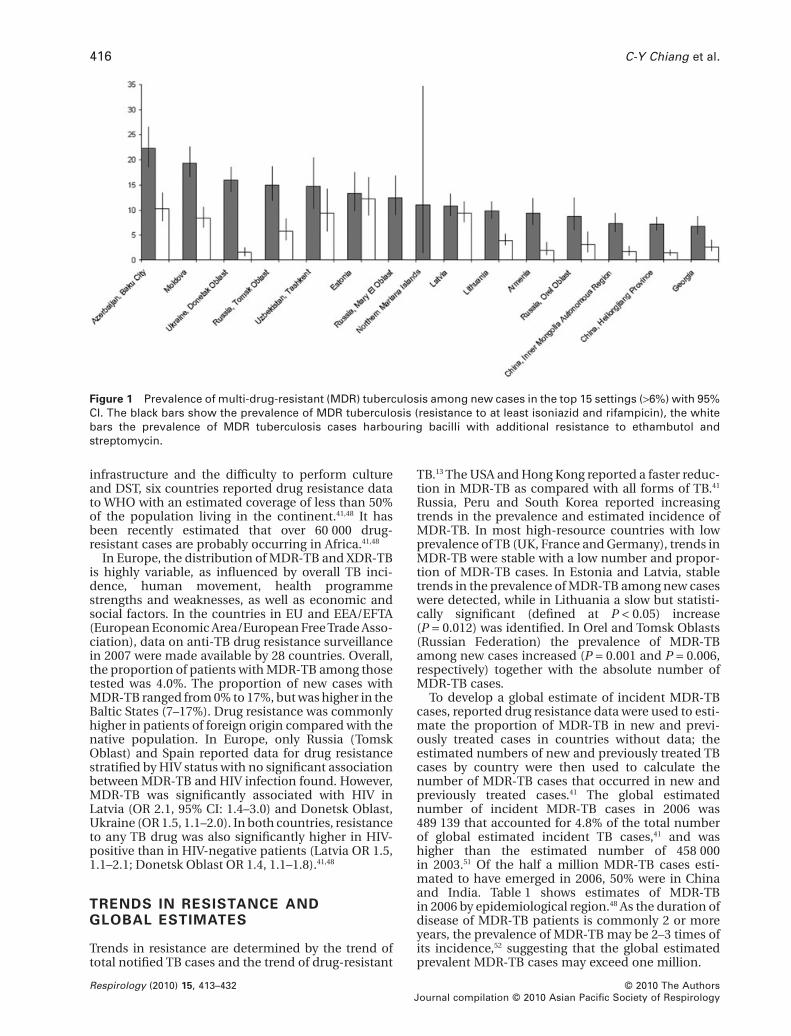
provides the latest data on the extent of drug-resistantTB between 2002 and 2007. This report includes datafor DST of 90 726 patients from 83 countries.48 Themedian prevalence of MDR-TB in new TB cases was1.6% (interquartile range 0.6–3.9), ranging from 0% ineight countries with low TB prevalence to 19.4% inMoldova and 22.3% in Baku, Azerbaijan.48 The preva-lence of MDR-TB in new TB cases was >6% in 15 set-tings, two of these settings were provinces in China, 12were in 10 countries of the former Soviet Union (FSU:Azerbaijan, Moldova, Ukraine, Russian Federation,Uzbekistan, Estonia, Latvia, Lithuania, Armenia andGeorgia).41 (Fig. 1).The median prevalence of MDR-TBin previously treated TB cases was 11.7% (interquartilerange 4.9–20.9).48 Six countries reported no patientswith MDR-TB, whereas 55.8% of retreatment cases inBaku (Azerbaijan) and 60% in Tashkent (Uzbekistan)had MDR-TB. Among the 17 settings reporting a preva-lence of MDR-TB > 25% in retreatment cases, ninewere in FSU countries.41 At least one country in all thesix WHO Regions reported a prevalence of at least 3%MDR- or XDR-TB cases among newly diagnosed TBcases.41
Seven countries and two special administrativeregions (Hong Kong and Macao, SAR, China) reporteddrug resistance data from the Western Pacific Region.MDR-TB among new cases ranged from less than1.0% in Hong Kong, SAR, Japan, New Zealand andSingapore, to 7.2% and 7.3% in Heilongjiang andInner Mongolia Autonomous Region of China.48 Theproportion of MDR-TB among previously treatedcases was 41.9% in Inner Mongolia AutonomousRegion and 30.4% in Heilongjiang,48 which impliesthat a very high successful rate and a low failure rateamong new and retreatment cases in these settingsmay be questionable.49
The proportion of non-MDR RMP resistance amongpreviously treated cases was substantial in severalsettings in China: 6.4% in Zhejiang Province, 5.7% inHeilongjiang Province 5.2% in Inner MongoliaAutonomous Region, 3.5% in Liaoning Province and3.0% in Henan Province.48 Because RMP resistanceunaccompanied by INH resistance is rare, especially inHIV-negative subjects, quality of laboratory testinghas been questioned. Possible factors are poor adher-ence and inadequate regimen, including the use ofrifapentine in health facilities where national guide-lines were not strictly followed. As rifapentine has along half-life,50 irregular treatment of rifapentine, INH,EMB and pyrazinamide (PZA) may impose the risk offunctional monotherapy of rifapentine resulting in theemergence of isolated rifamycin resistance. Thesefactors need to be investigated in China in settingswith a high proportion of non-MDR RMP resistance.
Six countries reported data from the South-EastAsia Region.41 The highest proportion of MDR-TBamong new cases was reported from Myanmar (4%)and among previously treated cases from Thailand(34.5%). Although data from Africa are in generalscanty, due to the overall weakness of the laboratory
MDR-TB overview 415
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
infrastructure and the difficulty to perform cultureand DST, six countries reported drug resistance datato WHO with an estimated coverage of less than 50%of the population living in the continent.41,48 It hasbeen recently estimated that over 60 000 drug-resistant cases are probably occurring in Africa.41,48
In Europe, the distribution of MDR-TB and XDR-TBis highly variable, as influenced by overall TB inci-dence, human movement, health programmestrengths and weaknesses, as well as economic andsocial factors. In the countries in EU and EEA/EFTA(European Economic Area/European Free Trade Asso-ciation), data on anti-TB drug resistance surveillancein 2007 were made available by 28 countries. Overall,the proportion of patients with MDR-TB among thosetested was 4.0%. The proportion of new cases withMDR-TB ranged from 0% to 17%, but was higher in theBaltic States (7–17%). Drug resistance was commonlyhigher in patients of foreign origin compared with thenative population. In Europe, only Russia (TomskOblast) and Spain reported data for drug resistancestratified by HIV status with no significant associationbetween MDR-TB and HIV infection found. However,MDR-TB was significantly associated with HIV inLatvia (OR 2.1, 95% CI: 1.4–3.0) and Donetsk Oblast,Ukraine (OR 1.5, 1.1–2.0). In both countries, resistanceto any TB drug was also significantly higher in HIV-positive than in HIV-negative patients (Latvia OR 1.5,1.1–2.1; Donetsk Oblast OR 1.4, 1.1–1.8).41,48
TRENDS IN RESISTANCE ANDGLOBAL ESTIMATES
Trends in resistance are determined by the trend oftotal notified TB cases and the trend of drug-resistant
TB.13 The USA and Hong Kong reported a faster reduc-tion in MDR-TB as compared with all forms of TB.41
Russia, Peru and South Korea reported increasingtrends in the prevalence and estimated incidence ofMDR-TB. In most high-resource countries with lowprevalence of TB (UK, France and Germany), trends inMDR-TB were stable with a low number and propor-tion of MDR-TB cases. In Estonia and Latvia, stabletrends in the prevalence of MDR-TB among new caseswere detected, while in Lithuania a slow but statisti-cally significant (defined at P < 0.05) increase(P = 0.012) was identified. In Orel and Tomsk Oblasts(Russian Federation) the prevalence of MDR-TBamong new cases increased (P = 0.001 and P = 0.006,respectively) together with the absolute number ofMDR-TB cases.
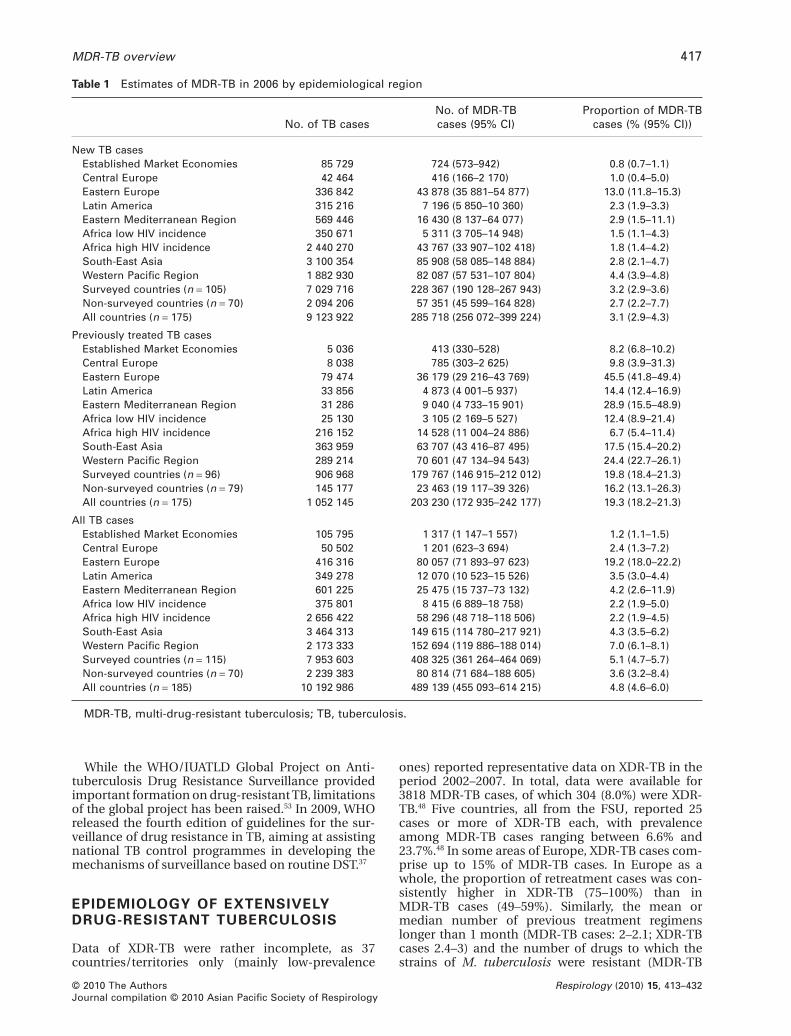
To develop a global estimate of incident MDR-TBcases, reported drug resistance data were used to esti-mate the proportion of MDR-TB in new and previ-ously treated cases in countries without data; theestimated numbers of new and previously treated TBcases by country were then used to calculate thenumber of MDR-TB cases that occurred in new andpreviously treated cases.41 The global estimatednumber of incident MDR-TB cases in 2006 was489 139 that accounted for 4.8% of the total numberof global estimated incident TB cases,41 and washigher than the estimated number of 458 000in 2003.51 Of the half a million MDR-TB cases esti-mated to have emerged in 2006, 50% were in Chinaand India. Table 1 shows estimates of MDR-TBin 2006 by epidemiological region.48 As the duration ofdisease of MDR-TB patients is commonly 2 or moreyears, the prevalence of MDR-TB may be 2–3 times ofits incidence,52 suggesting that the global estimatedprevalent MDR-TB cases may exceed one million.
Figure 1 Prevalence of multi-drug-resistant (MDR) tuberculosis among new cases in the top 15 settings (>6%) with 95%CI. The black bars show the prevalence of MDR tuberculosis (resistance to at least isoniazid and rifampicin), the whitebars the prevalence of MDR tuberculosis cases harbouring bacilli with additional resistance to ethambutol andstreptomycin.
C-Y Chiang et al.416
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
While the WHO/IUATLD Global Project on Anti-tuberculosis Drug Resistance Surveillance providedimportant formation on drug-resistant TB, limitationsof the global project has been raised.53 In 2009, WHOreleased the fourth edition of guidelines for the sur-veillance of drug resistance in TB, aiming at assistingnational TB control programmes in developing themechanisms of surveillance based on routine DST.37
EPIDEMIOLOGY OF EXTENSIVELYDRUG-RESISTANT TUBERCULOSIS
Data of XDR-TB were rather incomplete, as 37countries/territories only (mainly low-prevalence
ones) reported representative data on XDR-TB in theperiod 2002–2007. In total, data were available for3818 MDR-TB cases, of which 304 (8.0%) were XDR-TB.48 Five countries, all from the FSU, reported 25cases or more of XDR-TB each, with prevalenceamong MDR-TB cases ranging between 6.6% and23.7%.48 In some areas of Europe, XDR-TB cases com-prise up to 15% of MDR-TB cases. In Europe as awhole, the proportion of retreatment cases was con-sistently higher in XDR-TB (75–100%) than inMDR-TB cases (49–59%). Similarly, the mean ormedian number of previous treatment regimenslonger than 1 month (MDR-TB cases: 2–2.1; XDR-TBcases 2.4–3) and the number of drugs to which thestrains of M. tuberculosis were resistant (MDR-TB
Table 1 Estimates of MDR-TB in 2006 by epidemiological region
No. of TB casesNo. of MDR-TBcases (95% CI)
Proportion of MDR-TBcases (% (95% CI))
New TB casesEstablished Market Economies 85 729 724 (573–942) 0.8 (0.7–1.1)Central Europe 42 464 416 (166–2 170) 1.0 (0.4–5.0)Eastern Europe 336 842 43 878 (35 881–54 877) 13.0 (11.8–15.3)Latin America 315 216 7 196 (5 850–10 360) 2.3 (1.9–3.3)Eastern Mediterranean Region 569 446 16 430 (8 137–64 077) 2.9 (1.5–11.1)Africa low HIV incidence 350 671 5 311 (3 705–14 948) 1.5 (1.1–4.3)Africa high HIV incidence 2 440 270 43 767 (33 907–102 418) 1.8 (1.4–4.2)South-East Asia 3 100 354 85 908 (58 085–148 884) 2.8 (2.1–4.7)Western Pacific Region 1 882 930 82 087 (57 531–107 804) 4.4 (3.9–4.8)Surveyed countries (n = 105) 7 029 716 228 367 (190 128–267 943) 3.2 (2.9–3.6)Non-surveyed countries (n = 70) 2 094 206 57 351 (45 599–164 828) 2.7 (2.2–7.7)All countries (n = 175) 9 123 922 285 718 (256 072–399 224) 3.1 (2.9–4.3)
Previously treated TB casesEstablished Market Economies 5 036 413 (330–528) 8.2 (6.8–10.2)Central Europe 8 038 785 (303–2 625) 9.8 (3.9–31.3)Eastern Europe 79 474 36 179 (29 216–43 769) 45.5 (41.8–49.4)Latin America 33 856 4 873 (4 001–5 937) 14.4 (12.4–16.9)Eastern Mediterranean Region 31 286 9 040 (4 733–15 901) 28.9 (15.5–48.9)Africa low HIV incidence 25 130 3 105 (2 169–5 527) 12.4 (8.9–21.4)Africa high HIV incidence 216 152 14 528 (11 004–24 886) 6.7 (5.4–11.4)South-East Asia 363 959 63 707 (43 416–87 495) 17.5 (15.4–20.2)Western Pacific Region 289 214 70 601 (47 134–94 543) 24.4 (22.7–26.1)Surveyed countries (n = 96) 906 968 179 767 (146 915–212 012) 19.8 (18.4–21.3)Non-surveyed countries (n = 79) 145 177 23 463 (19 117–39 326) 16.2 (13.1–26.3)All countries (n = 175) 1 052 145 203 230 (172 935–242 177) 19.3 (18.2–21.3)
All TB casesEstablished Market Economies 105 795 1 317 (1 147–1 557) 1.2 (1.1–1.5)Central Europe 50 502 1 201 (623–3 694) 2.4 (1.3–7.2)Eastern Europe 416 316 80 057 (71 893–97 623) 19.2 (18.0–22.2)Latin America 349 278 12 070 (10 523–15 526) 3.5 (3.0–4.4)Eastern Mediterranean Region 601 225 25 475 (15 737–73 132) 4.2 (2.6–11.9)Africa low HIV incidence 375 801 8 415 (6 889–18 758) 2.2 (1.9–5.0)Africa high HIV incidence 2 656 422 58 296 (48 718–118 506) 2.2 (1.9–4.5)South-East Asia 3 464 313 149 615 (114 780–217 921) 4.3 (3.5–6.2)Western Pacific Region 2 173 333 152 694 (119 886–188 014) 7.0 (6.1–8.1)Surveyed countries (n = 115) 7 953 603 408 325 (361 264–464 069) 5.1 (4.7–5.7)Non-surveyed countries (n = 70) 2 239 383 80 814 (71 684–188 605) 3.6 (3.2–8.4)All countries (n = 185) 10 192 986 489 139 (455 093–614 215) 4.8 (4.6–6.0)
MDR-TB, multi-drug-resistant tuberculosis; TB, tuberculosis.
MDR-TB overview 417
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
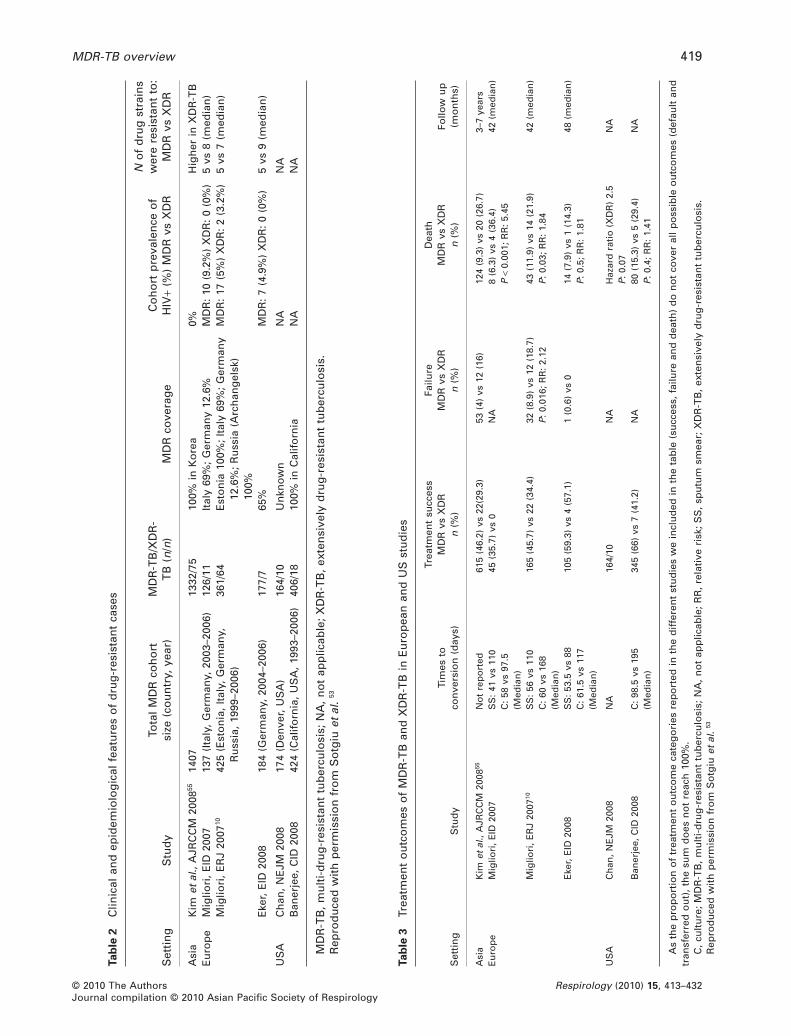
cases: 4–5.3; XDR-TB cases 5–6) were higher in XDR-than in MDR-TB cases (Table 2).54
While the majority of the countries in the westernworld have equipped their surveillance to monitorMDR-TB, the situation remains challenging for XDR-TB. In Europe, for example, the first evidence thatsurveillance systems were unable to provide timelyinformation on the occurrence of XDR-TB cases wasrepresented by the media storm following publica-tion56 of the first study reporting poor outcomes forXDR-TB cases (XDR-TB cases having a relative risk ofdeath 5.5 times higher than MDR-TB cases) (Table 3).
The surveillance system was unable to detect thesecases simply because the entire set of XDR-TB defin-ing drugs was not systematically tested. This problemhas been underlined in the majority of the studiesinvestigating or commenting on XDR-TB54,59 andby official documents. DST of aminoglycosides,polypeptides and fluoroquinolones has been shownto have relatively good reliability and reproducibility.Recommended systematic approach to implementa-tion of DST under routine programmatic conditions isto test resistance to INH and RMP as step 1, to EMB,SM and PZA as step 2 and to amikacin, kanamycin,capreomycin and ofloxacin (or fluoroquinolone ofchoice in treatment strategy) as step 3. In settingswhere XDR is a concern, steps 1 and 3 may be mergedin order to enable the rapid identification of XDR-TBpatients.60
In order to provide timely detection of incidentXDR-TB cases the following conditions need to bemet: (i) adequate technical capacity to test all isolatedMDR strains for all XDR-defining drugs by quality-assured laboratories; (ii) policy in force ensuringreferral of all strains from culture/first-line DST labo-ratories to second-line DST referral laboratories; (iii)links between the notification system and the refer-ence laboratories established to ensure that second-line DST results are available; and (iv) availability,within the surveillance system, of the appropriatefields necessary to record the information on theXDR-defining drugs on which DST is performed inreference laboratories. Interim approach is to test atleast RMP and fluoroquinolone(s) as a proxy monitor-ing of fluoroquinolone-resistant MDR-TB.
Furthermore, surveillance systems should beequipped to report treatment outcomes for at least24 months following treatment initiation to capturethe outcomes of MDR- and XDR-TB cases.
Although the different countries of Europe aretaking action to improve their surveillance systems,most of the information presently available onXDR-TB is based on ‘ad hoc’ designed studies.54,59
RISK FACTORS ASSOCIATED WITHDRUG-RESISTANT TUBERCULOSIS
It has been consistently shown that drug-resistant TBis associated with previous TB treatment, and that theprevalence of drug resistance among previouslytreated TB cases was much higher than that amongnew TB cases.31,40,41,61,62 Previously treated TB casesconsist of relapse, treatment after default, treatment
after failure (and chronic cases in some settings); theproportion of drug-resistant TB among these patientsvaried considerably in different settings dependingon the prevalence of primary resistance, the regimenused for the treatment of TB, the quality of TB servicesand the risk of reinfection of TB. Although the preva-lence of primary resistance is one of the determinantsaffecting the prevalence of drug resistance amongpreviously treated cases, in general, the reported pro-portion of MDR-TB among previously treated cases incountries applying an 8-month regimen with RMP forthe initial 2 months for new patients was less thanthat in countries using a 6-month RMP-containingregimen throughout. The proportion of MDR-TBamong relapse, treatment after default and treatmentafter failure in Benin where the regimen for new TBpatients was composed of a 2-month intensive phase(four drugs, SM-RMP-INH-PZA) followed by a6-month continuation phase (T-INH (T, thiaceta-zone) was 4%, 12% and 22%, respectively,61 and that inTaiwan where the regimen for new TB patients wascomposed of the same 2-month intensive phase(INH-EMB-RMP-PZA) followed by a 4-month con-tinuation phase with three drugs (INH-EMB-RMP)was 13%, 19% and 67%, respectively.63 In Peru wherethe regimen for new TB patients was that recom-mended by WHO (2 months with four drugs, INH-RMP-EMB-PZA followed by 4 months with two drugs,INH-RMP), the reported proportion of MDR-TBamong treatment after failure was very high (88%64
and 94%65).There are three sets of determinants that influence
the proportion of drug-resistant TB among all cases ina population-based study. First, the size of the sub-population infected with susceptible strains and theprobability of developing TB among those infectedwith susceptible strains. Second, the size of the sub-population infected with drug-resistant strains andthe probability of developing TB among thoseinfected with resistant strains. Third, factors associ-ated with the emergence of drug-resistant strainduring treatment among TB patients initially infectedwith susceptible strains and that with the amplifica-tion of drug resistance among those initially infectedwith resistant strains.14 The first two sets of risk factorsare influenced by the risk of infection as well as theimmunity of the infected subpopulation in contain-ing the infection, while the third set is largely associ-ated with the interaction between the bacillarypopulation and the treatment regimen (type and doseof drugs, quality of drugs, scheduling of drugs andadherence). As drug resistance among new casesimplies transmission and that among previouslytreated cases is a combination of emergence of addi-tional resistance during treatment, reinfection byresistant strains and primary resistance that was notidentified in the beginning of treatment,52 factorsassociated with drug resistance in incidence-basedsurveillance study is best investigated by stratificationof new and previously treated cases. A study fromHong Kong reported that non-permanent residents(OR 6.85, 95% CI: 1.38–34.09), frequent travel (OR2.48, 95% CI: 1.07–5.74) and younger age were foundto be independent predictors of MDR-TB in
C-Y Chiang et al.418
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
Tab
le2
Clin
ical
and
epid
emio
log
ical
feat
ure
so
fd
rug
-res
ista
nt
case
s
Set
tin
gS
tud
yTo
tal
MD
Rco
ho
rtsi
ze(c
ou
ntr
y,ye
ar)
MD
R-T
B/X
DR
-T
B(n
/n)
MD
Rco
vera
ge
Co
ho
rtp
reva
len
ceo
fH
IV+
(%)
MD
Rvs
XD
R
No
fd
rug
stra
ins
wer
ere
sist
ant
to:
MD
Rvs
XD
R
Asi
aK
imet
al.,
AJR
CC
M20
0855
1407
1332
/75
100%
inK
ore
a0%
Hig
her
inX
DR
-TB
Eu
rop
eM
iglio
ri,
EID
2007
137
(Ita
ly,
Ger
man
y,20
03–2
006)
126/
11It
aly
69%
;G
erm
any
12.6
%M
DR
:10
(9.2
%)
XD
R:
0(0
%)
5vs
8(m
edia
n)
Mig
liori
,E
RJ
2007
1042
5(E
sto
nia
,It
aly,
Ger
man
y,R
uss
ia,
1999
–200
6)36
1/64
Est
on
ia10
0%;
Ital
y69
%;
Ger
man
y12
.6%
;R
uss
ia(A
rch
ang
elsk
)10
0%
MD
R:
17(5
%)
XD
R:
2(3
.2%
)5
vs7
(med
ian
)
Eke
r,E
ID20
0818
4(G
erm
any,
2004
–200
6)17
7/7
65%
MD
R:
7(4
.9%
)X
DR
:0
(0%
)5
vs9
(med
ian
)
US
AC
han
,N
EJM
2008
174
(Den
ver,
US
A)
164/
10U
nkn
ow
nN
AN
AB
aner
jee,
CID
2008
424
(Cal
ifo
rnia
,U
SA
,19
93–2
006)
406/
1810
0%in
Cal
ifo
rnia
NA
NA
MD
R-T
B,
mu
lti-
dru
g-r
esis
tan
ttu
ber
culo
sis;
NA
,n
ot
app
licab
le;
XD
R-T
B,
exte
nsi
vely
dru
g-r
esis
tan
ttu
ber
culo
sis.
Rep
rod
uce
dw
ith
per
mis
sio
nfr
om
So
tgiu
etal
.53
Tab
le3
Trea
tmen
to
utc
om
eso
fM
DR
-TB
and
XD
R-T
Bin
Eu
rop
ean
and
US
stu
die
s
Set
tin
gS
tud
yTi
mes
toco
nve
rsio
n(d
ays)
Trea
tmen
tsu
cces
sFa
ilure
Dea
thFo
llow
up
(mo
nth
s)M
DR
vsX
DR
MD
Rvs
XD
RM
DR
vsX
DR
n(%
)n
(%)
n(%
)
Asi
aK
imet
al.,
AJR
CC
M20
0855
No
tre
po
rted
615
(46.
2)vs
22(2
9.3)
53(4
)vs
12(1
6)12
4(9
.3)
vs20
(26.
7)3–
7ye
ars
Eu
rop
eM
iglio
ri,
EID
2007
SS
:41
vs11
045
(35.
7)vs
0N
A8
(6.3
)vs
4(3
6.4)
P<
0.00
1;R
R:
5.45
42(m
edia
n)
C:
58vs
97.5
(Med
ian
)M
iglio
ri,
ER
J20
0710
SS
:56
vs11
016
5(4
5.7)
vs22
(34.
4)32
(8.9
)vs
12(1
8.7)
P:
0.01
6;R
R:
2.12
43(1
1.9)
vs14
(21.
9)P
:0.
03;
RR
:1.
8442
(med
ian
)C
:60
vs16
8(M
edia
n)
Eke
r,E
ID20
08S
S:
53.5
vs88
105
(59.
3)vs
4(5
7.1)
1(0
.6)
vs0
14(7
.9)
vs1
(14.
3)P
:0.
5;R
R:
1.81
48(m
edia
n)
C:
61.5
vs11
7(M
edia
n)
US
AC
han
,N
EJM
2008
NA
164/
10N
AH
azar
dra
tio
(XD
R)
2.5
P:
0.07
NA
Ban
erje
e,C
ID20
08C
:98
.5vs
195
345
(66)
vs7
(41.
2)N
A80
(15.
3)vs
5(2
9.4)
P:
0.4;
RR
:1.
41N
A(M
edia
n)
As
the
pro
po
rtio
no
ftr
eatm
ent
ou
tco
me
cate
go
ries
rep
ort
edin
the
dif
fere
nt
stu
die
sw
ein
clu
ded
inth
eta
ble
(su
cces
s,fa
ilure
and
dea
th)
do
no
tco
ver
allp
oss
ible
ou
tco
mes
(def
ault
and
tran
sfer
red
ou
t),
the
sum
do
esn
ot
reac
h10
0%.
C,
cult
ure
;M
DR
-TB
,m
ult
i-d
rug
-res
ista
nt
tub
ercu
losi
s;N
A,
no
tap
plic
able
;R
R,
rela
tive
risk
;S
S,
spu
tum
smea
r;X
DR
-TB
,ex
ten
sive
lyd
rug
-res
ista
nt
tub
ercu
losi
s.R
epro
du
ced
wit
hp
erm
issi
on
fro
mS
otg
iuet
al.
53
MDR-TB overview 419
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
previously treated patients.66 Most published studieson risk factors associated with drug-resistant TB didnot separately assess factors associated with drugresistance among new cases and that among previ-ously treated cases.
Espinal and colleagues reported that in previouslytreated patients, the probability of any resistance isover fourfold higher, and that of MDR-TB over10-fold higher, than for untreated patients.62 Severalstudies confirmed the relationship between MDR-TBand prior exposure to anti-TB drugs, and a recentstudy has reported that XDR-TB is associated withprevious TB treatment even more strongly thanMDR-TB.67–70 The duration of previous treatmentplays a key role in the generation of extremely resis-tant strains, clearly demonstrated by the higher pro-portion of retreated cases among MDR-TB andXDR-TB patients (49–98% and 45–100%, respectively,in different studies) versus the percentage amongnon-MDR-TB patients.54,69 Previous anti-TB treat-ment increased the chance of MDR fivefold (OR5.41) and MDR-TB occurred significantly more likelyin people aged 25–44 (OR 2.5) and 45–64 years (OR1.9). Alcohol abuse (OR 1.6) was also an independentrisk factor for MDR-TB due to its impact on TB treat-ment adherence.69 Among the patients less than25 years of age, female gender (OR 7.8) and place ofbirth outside the host country (in data from Estonia),mainly in individuals coming from the FSU (OR79.7), were strongly associated with MDR-TB.
Immigration, mainly from high MDR-TB prevalencecountries, could increase the risk of being infected by aresistant strain not only among foreign-born peoplebut also native individuals.69,71 MDR-TB may affectyoung adults, which may result in increased rates ofTBtransmission to their children. Moreover, HIV-infectedchildren are at increased risk of TB and there is strongevidence that TB is more common in children living inhouseholds affected by TB. On the other hand, living inurban area resulted in significantly less likelihood ofhaving MDR-TB (OR 0.2).70
The independent variables associated with XDR-TBwere previous anti-TB treatment (OR 4.0) and home-lessness (OR 3.4); homeless people, living in poorconditions and malnourished, usually have reducedaccess to health-care assistance, prolonging theperiod of infectiousness and, consequently, increas-ing the risk of mycobacterial transmission amongtheir close contacts.
Another important issue, frequently described byseveral authors, is the high rate of defaulting fromtreatment and treatment failure among socially dis-advantaged patients, including alcohol abusers andhomeless people.69,72,73
Unfortunately poverty and inadequate access todrugs continue to play a role in the development ofdrug resistance through several mechanisms includ-ing, among others, access to poor-quality drugs ortruncated treatment courses.
Previous reports have described the associationbetween MDR-TB and HIV infection, and a Europeanmeta-analysis well described the higher risk (OR 3.5)of developing active MDR-TB disease.67,70 However, arecent systematic review has reported no clear asso-
ciation between MDR-TB and HIV infection acrosstime and geographic locations and that assessmentby geographical region or study period did not revealnoticeable patterns.74 High TB prevalence in prisonsand transmission of resistant strains related to over-crowding and inability to isolate resistant patients hasbeen well documented in Russia (relative risk forMDR-TB is 1.9).73,75
CLINICAL PRESENTATION ANDTREATMENT OF MDR- AND XDR-TB
The initial clinical presentation of patients with drug-resistant TB in most cases does not differ from that ofpatients with TB due to pan-susceptible strains of M.tuberculosis.76 In fact, clinical presentation of patientswith MDR- and XDR-TB may be quite variable (Fig. 2).However, extrapulmonary involvement54 and progres-sive disease in patients with a previous history ofanti-TB treatment may be more frequently expected.
Data from a large retrospective cohort (>5550patients) have provided evidence that standard short-course chemotherapy, based on first-line drugs, wasinadequate to treat patients with MDR-TB.3 A studyfrom Russia demonstrated a high relapse rate (27.8%)of MDR-TB cases declared ‘successfully’ cured withstandard short-course chemotherapy regimens (WHOcategory 1, e.g. 2 months with four drugs, INH-RMP-EMB-PZA followed by 4 months with two drugs, INH-RMP; and WHO category 2, e.g. 2 months with fivedrugs, INH-RMP-EMB-PZA-SM plus 1 months withfour drugs INH-RMP-EMB-PZA followed by continua-tion phase of 5 months with three drugs, INH-RMP-EMB) within a median time of 8 months (2.46recurrences were observed in 100 person-months).58 A6-year follow-up study from Taiwan found thatpatients treated with quinolone-containing second-line regimen were significantly less likely to relapsethan those treated with first-line drugs. (hazard ratio
Figure 2 Mycobacterium tuberculosis drug resistancecannot be identified by radiographical imaging.
C-Y Chiang et al.420
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
0.16, 95% CI: 0.03–0.81).4 Clearly, the category 2retreatment regimen 2(INH-EMB-RMP-PZA-SM)/1(INH-EMB-RMP-PZA)/5(INH-EMB-RMP) recom-mended by WHO is not adequate for settings with ahigh proportion of MDR-TB patients among failure ofcategory 1 regimen.57,64,77 Treating MDR-TB patientsusing category 2 regimen runs the risk of amplificationof resistance as well.78 As M. tuberculosis drug resis-tance increases, it has become more obvious that theclinical outcome is mostly dependent on the degree ofM. tuberculosis drug resistance, availability of second-and third-line drugs and adherence to the therapy.
The treatment of patients with MDR-TB andXDR-TB relies on drugs that are less potent, need tobe administered for a much longer time and aresubstantially more toxic than those used to treat TBcaused by drug-susceptible strains (Table 4). In con-trast, the cost of a second-line drug regimen is muchhigher: up to thousands of dollars compared with thecost of about $US 20 per patient for the standard6-month short-course, first-line chemotherapyregimen (WHO category 1).
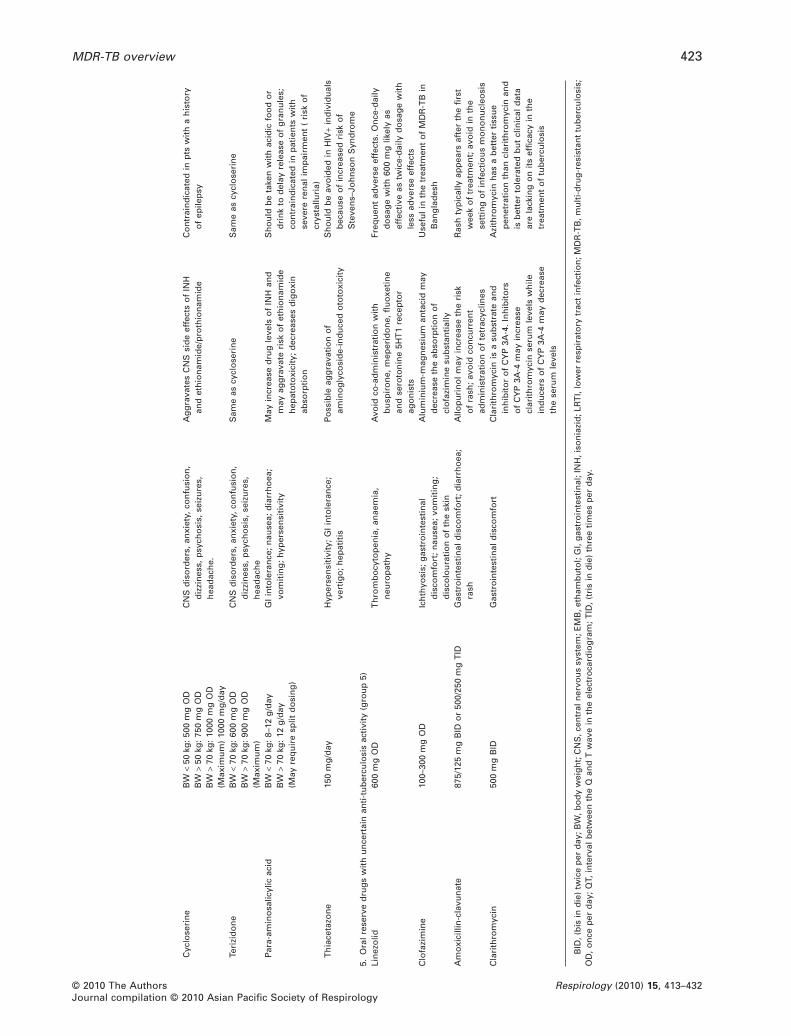
The optimal duration of any given combination ofanti-TB drugs for treatment of MDR- and XDR-TB hasnot been defined in controlled clinical trials.80 In addi-tion, the role of single drugs or drug combinations ineffective MDR-TB and XDR-TB treatment is difficultto investigate in double-blinded, placebo-controlled,prospective clinical trials due to ethical consider-ations and cost. Especially the effectiveness oftreatment with third-line anti-TB drugs (amoxicillin-clavulanate, clarithromycin, clofazimine and lin-ezolid: called Group 5 drugs in the WHO guidelines,Table 4) is difficult to ascertain. Recently, long-termtreatment of patients with MDR- and XDR-TB withlinezolid at a regular dosage of 600 mg bd was shownto incur severe toxicity with little additional benefit inclinical outcome in a large retrospective cohortstudy.81 This recent study performed in four Europeancountries on 85 patients treated with linezolid dem-onstrated that the toxicity was lower when the 600 mgonce-daily scheme was used: 54.4% patients treatedwith 600 mg bd experienced adverse events versus14.3% in the group treated with the lower dosage.81 Itwas concluded that the drug should be prescribed tothe most severe patients only, for example, those inwhich resistance to >7 drugs has been identified.Reducing the dosage of linezolid to 300 mg per day82
in the treatment of MDR-TB has also been reportedbut emergence of linezolid resistance can be a causefor concern. Meropenem-clavulanate, which hasrecently been reported to be potentially promisingwill need to be further investigated before it can berecommended for clinical use.83
OUTCOME OF EXTENSIVELYDRUG-RESISTANT ANDMULTI-DRUG-RESISTANTTUBERCULOSIS
There have been several publications reportingoutcome of MDR-TB treated with second-line drugs
but methods used to assess outcome varied. Someresearchers focused on efficacy of treatment andreported only those who had adequate adherenceto treatment and sufficient follow-up data. Thisapproach may overestimate the proportion ofpatients with a successful outcome.84–86 Othersreported outcome of the whole cohort of patientswithout excluding any cases from outcome analy-sis.87,88 Laserson and colleagues proposed standard-ized definitions for outcome of MDR-TB treatment,which have enabled international comparison ofoutcome of MDR-TB treatment89 but the definition oftreatment failure still allows for different interpreta-tions.90 Nevertheless, it is clear that defaulting is oneof the major challenges in the treatment of MDR-TB.
Risk factors for adverse treatment outcome inpatients with MDR-TB and XDR-TB have beenrecently reviewed in detail.54,91 They include delayedtreatment initiation, prior treatment with anti-TBdrugs, previously treated with second-line drugs,prior exposure to fluoroquinolones, resistance tofluoroquinolones or to capreomycin, low BMI,HIV seropositivity and other immunosuppressiveconditions.
Treatment outcome of MDR-TB patients fromresource-limited settings reported cure rates of60–75%.92 The proportion of MDR-TB patients whowere successfully treated ranged from 77% amongnew cases to 69% among previously treated patients.A recent report has confirmed that XDR-TB hadhigher probability of death, longer hospitalization,longer treatment duration and delayed microbiologi-cal conversion when compared with MDR-TB at TBreference centres in Italy and Germany.44
Earlier observations from the Tugela Ferry outbreakin the Republic of South Africa that XDR-TB isuntreatable have not been confirmed in other areas ofthe world where HIV was not a big problem.93 A recentsystematic review on MDR-TB and XDR-TB, includingstudies from North and South America, Europe andKorea,55 has shown that XDR-TB can be successfullytreated in more than 50% of patients (Table 3).However, treatment duration is significantly longerand outcomes are in general poorer than for non-XDR-TB patients. A very recent study presented at theEuropean Respiratory Society (ERS, Vienna, 12–16September 2009) has demonstrated on a large cohortof XDR-TB patients from South Africa (n = 220, 43%being HIV-seropositive) that the success rate was nothigher than 50%, similar in HIV-positive and HIVnegative individuals, but still significantly lower inHIV-positive patients not treated with anti-retroviraltherapy.94
SURGICAL RESECTION ASAN ADJUNCT
Surgical resection of infected lung tissue has beenreported to be a useful strategy in the treatment ofMDR- and XDR-TB. While some studies reported thatsurgery was associated with a better outcome,55,84
others found no additional benefit of surgery in thetreatment of MDR-TB.95 The contribution of surgical
MDR-TB overview 421
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
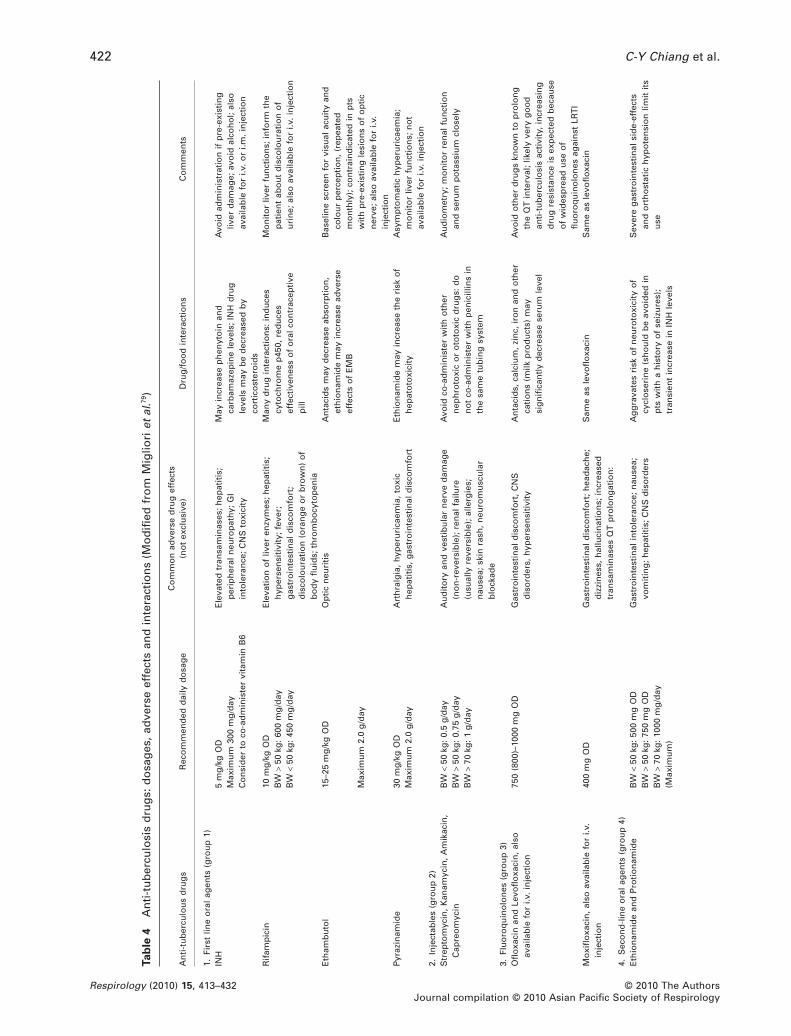
Tab
le4
An
ti-t
ub
ercu
losi
sd
rug
s:d
osa
ges
,ad
vers
eef
fect
san
din
tera
ctio
ns
(Mo
difi
edfr
om
Mig
liori
etal
.79)
An
ti-t
ub
ercu
lou
sd
rug
sR
eco
mm
end
edd
aily
do
sag
eC
om
mo
nad
vers
ed
rug
effe
cts
(no
tex
clu
sive
)D
rug
/fo
od
inte
ract
ion
sC
om
men
ts
1.Fi
rst
line
ora
lag
ents
(gro
up
1)IN
H5
mg
/kg
OD
Ele
vate
dtr
ansa
min
ases
;h
epat
itis
;p
erip
her
aln
euro
pat
hy;
GI
into
lera
nce
;C
NS
toxi
city
May
incr
ease
ph
enyt
oin
and
carb
amaz
epin
ele
vels
;IN
Hd
rug
leve
lsm
ayb
ed
ecre
ased
by
cort
ico
ster
oid
s
Avo
idad
min
istr
atio
nif
pre
-exi
stin
gliv
erd
amag
e;av
oid
alco
ho
l;al
soav
aila
ble
for
i.v.
or
i.m.
inje
ctio
nM
axim
um
300
mg
/day
Co
nsi
der
toco
-ad
min
iste
rvi
tam
inB
6
Rif
amp
icin
10m
g/k
gO
DE
leva
tio
no
fliv
eren
zym
es;
hep
atit
is;
hyp
erse
nsi
tivi
ty;
feve
r;g
astr
oin
test
inal
dis
com
fort
;d
isco
lou
rati
on
(ora
ng
eo
rb
row
n)
of
bo
dy
flu
ids;
thro
mb
ocy
top
enia
Man
yd
rug
inte
ract
ion
s:in
du
ces
cyto
chro
me
p45
0,re
du
ces
effe
ctiv
enes
so
fo
ral
con
trac
epti
vep
ill
Mo
nit
or
liver
fun
ctio
ns;
info
rmth
ep
atie
nt
abo
ut
dis
colo
ura
tio
no
fu
rin
e;al
soav
aila
ble
for
i.v.
inje
ctio
nB
W>
50kg
:60
0m
g/d
ayB
W<
50kg
:45
0m
g/d
ay
Eth
amb
uto
l15
–25
mg
/kg
OD
Op
tic
neu
riti
sA
nta
cid
sm
ayd
ecre
ase
abso
rpti
on
,et
hio
nam
ide
may
incr
ease
adve
rse
effe
cts
of
EM
B
Bas
elin
esc
reen
for
visu
alac
uit
yan
dco
lou
rp
erce
pti
on
,(r
epea
ted
mo
nth
ly);
con
trai
nd
icat
edin
pts
wit
hp
re-e
xist
ing
lesi
on
so
fo
pti
cn
erve
;al
soav
aila
ble
for
i.v.
inje
ctio
n
Max
imu
m2.
0g
/day
Pyr
azin
amid
e30
mg
/kg
OD
Art
hra
lgia
,h
yper
uri
caem
ia,
toxi
ch
epat
itis
,g
astr
oin
test
inal
dis
com
fort
Eth
ion
amid
em
ayin
crea
seth
eri
sko
fh
epat
oto
xici
tyA
sym
pto
mat
ich
yper
uri
caem
ia;
mo
nit
or
liver
fun
ctio
ns;
no
tav
aila
ble
for
i.v.
inje
ctio
nM
axim
um
2.0
g/d
ay
2.In
ject
able
s(g
rou
p2)
Str
epto
myc
in,
Kan
amyc
in,
Am
ikac
in,
Cap
reo
myc
inB
W<
50kg
:0.
5g
/day
Au
dit
ory
and
vest
ibu
lar
ner
ved
amag
e(n
on
-rev
ersi
ble
);re
nal
failu
re(u
sual
lyre
vers
ible
);al
lerg
ies;
nau
sea;
skin
rash
,n
euro
mu
scu
lar
blo
ckad
e
Avo
idco
-ad
min
iste
rw
ith
oth
ern
eph
roto
xic
or
oto
toxi
cd
rug
s:d
on
ot
co-a
dm
inis
ter
wit
hp
enic
illin
sin
the
sam
etu
bin
gsy
stem
Au
dio
met
ry;
mo
nit
or
ren
alfu
nct
ion
and
seru
mp
ota
ssiu
mcl
ose
lyB
W>
50kg
:0.
75g
/day
BW
>70
kg:
1g
/day
3.Fl
uo
roq
uin
olo
nes
(gro
up
3)O
flo
xaci
nan
dLe
vofl
oxa
cin
,al
soav
aila
ble
for
i.v.
inje
ctio
n75
0(8
00)–
1000
mg
OD
Gas
tro
inte
stin
ald
isco
mfo
rt,
CN
Sd
iso
rder
s,h
yper
sen
siti
vity
An
taci
ds,
calc
ium
,zi
nc,
iro
nan
do
ther
cati
on
s(m
ilkp
rod
uct
s)m
aysi
gn
ifica
ntl
yd
ecre
ase
seru
mle
vel
Avo
ido
ther
dru
gs
kno
wn
top
rolo
ng
the
QT
inte
rval
;lik
ely
very
go
od
anti
-tu
ber
culo
sis
acti
vity
,in
crea
sin
gd
rug
resi
stan
ceis
exp
ecte
db
ecau
seo
fw
ides
pre
adu
seo
ffl
uo
roq
uin
olo
nes
agai
nst
LRT
IM
oxi
flo
xaci
n,
also
avai
lab
lefo
ri.v
.in
ject
ion
400
mg
OD
Gas
tro
inte
stin
ald
isco
mfo
rt;
hea
dac
he;
diz
zin
ess,
hal
luci
nat
ion
s;in
crea
sed
tran
sam
inas
esQ
Tp
rolo
ng
atio
n:
Sam
eas
levo
flo
xaci
nS
ame
asle
vofl
oxa
cin
4.S
eco
nd
-lin
eo
ral
agen
ts(g
rou
p4)
Eth
ion
amid
ean
dP
roti
on
amid
eB
W<
50kg
:50
0m
gO
DG
astr
oin
test
inal
into
lera
nce
;n
ause
a;vo
mit
ing
;h
epat
itis
;C
NS
dis
ord
ers
Ag
gra
vate
sri
sko
fn
euro
toxi
city
of
cycl
ose
rin
e(s
ho
uld
be
avo
ided
inp
tsw
ith
ah
isto
ryo
fse
izu
res)
;tr
ansi
ent
incr
ease
inIN
Hle
vels
Sev
ere
gas
tro
inte
stin
alsi
de-
effe
cts
and
ort
ho
stat
ich
ypo
ten
sio
nlim
itit
su
seB
W>
50kg
:75
0m
gO
DB
W>
70kg
:10
00m
g/d
ay(M
axim
um
)
C-Y Chiang et al.422
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
Cyc
lose
rin
eB
W<
50kg
:50
0m
gO
DC
NS
dis
ord
ers,
anxi
ety,
con
fusi
on
,d
izzi
nes
s,p
sych
osi
s,se
izu
res,
hea
dac
he.
Ag
gra
vate
sC
NS
sid
eef
fect
so
fIN
Han
det
hio
nam
ide/
pro
thio
nam
ide
Co
ntr
ain
dic
ated
inp
tsw
ith
ah
isto
ryo
fep
ilep
syB
W>
50kg
:75
0m
gO
DB
W>
70kg
:10
00m
gO
D(M
axim
um
)10
00m
g/d
ayTe
rizi
do
ne
BW
<70
kg:
600
mg
OD
CN
Sd
iso
rder
s,an
xiet
y,co
nfu
sio
n,
diz
zin
ess,
psy
cho
sis,
seiz
ure
s,h
ead
ach
e
Sam
eas
cycl
ose
rin
eS
ame
ascy
clo
seri
ne
BW
>70
kg:
900
mg
OD
(Max
imu
m)
Par
a-am
ino
salic
ylic
acid
BW
<70
kg:
8–12
g/d
ayG
Iin
tole
ran
ce;
nau
sea;
dia
rrh
oea
;vo
mit
ing
;h
yper
sen
siti
vity
May
incr
ease
dru
gle
vels
of
INH
and
may
agg
rava
teri
sko
fet
hio
nam
ide
hep
ato
toxi
city
;d
ecre
ases
dig
oxi
nab
sorp
tio
n
Sh
ou
ldb
eta
ken
wit
hac
idic
foo
do
rd
rin
kto
del
ayre
leas
eo
fg
ran
ule
s;co
ntr
ain
dic
ated
inp
atie
nts
wit
hse
vere
ren
alim
pai
rmen
t(
risk
of
crys
tallu
ria)
BW
>70
kg:
12g
/day
(May
req
uir
esp
litd
osi
ng
)
Th
iace
tazo
ne
150
mg
/day
Hyp
erse
nsi
tivi
ty;
GI
into
lera
nce
;ve
rtig
o;
hep
atit
isP
oss
ible
agg
rava
tio
no
fam
ino
gly
cosi
de-
ind
uce
do
toto
xici
tyS
ho
uld
be
avo
ided
inH
IV+
ind
ivid
ual
sb
ecau
seo
fin
crea
sed
risk
of
Ste
ven
s–Jo
hn
son
Syn
dro
me
5.O
ral
rese
rve
dru
gs
wit
hu
nce
rtai
nan
ti-t
ub
ercu
losi
sac
tivi
ty(g
rou
p5)
Lin
ezo
lid60
0m
gO
DT
hro
mb
ocy
top
enia
,an
aem
ia,
neu
rop
ath
yA
void
co-a
dm
inis
trat
ion
wit
hb
usp
iro
ne,
mep
erid
on
e,fl
uo
xeti
ne
and
sero
ton
ine
5HT
1re
cep
tor
ago
nis
ts
Freq
uen
tad
vers
eef
fect
s.O
nce
-dai
lyd
osa
ge
wit
h60
0m
glik
ely
asef
fect
ive
astw
ice-
dai
lyd
osa
ge
wit
hle
ssad
vers
eef
fect
sC
lofa
zim
ine
100–
300
mg
OD
Ich
thyo
sis;
gas
tro
inte
stin
ald
isco
mfo
rt;
nau
sea;
vom
itin
g;
dis
colo
ura
tio
no
fth
esk
in
Alu
min
ium
-mag
nes
ium
anta
cid
may
dec
reas
eth
eab
sorp
tio
no
fcl
ofa
zim
ine
sub
stan
tial
ly
Use
ful
inth
etr
eatm
ent
of
MD
R-T
Bin
Ban
gla
des
h
Am
oxi
cilli
n-c
lavu
nat
e87
5/12
5m
gB
IDo
r50
0/25
0m
gT
IDG
astr
oin
test
inal
dis
com
fort
;d
iarr
ho
ea;
rash
Allo
pu
rin
ol
may
incr
ease
the
risk
of
rash
;av
oid
con
curr
ent
adm
inis
trat
ion
of
tetr
acyc
lines
Ras
hty
pic
ally
app
ears
afte
rth
efi
rst
wee
ko
ftr
eatm
ent;
avo
idin
the
sett
ing
of
infe
ctio
us
mo
no
nu
cleo
sis
Cla
rith
rom
ycin
500
mg
BID
Gas
tro
inte
stin
ald
isco
mfo
rtC
lari
thro
myc
inis
asu
bst
rate
and
inh
ibit
or
of
CY
P3A
-4.
Inh
ibit
ors
of
CY
P3A
-4m
ayin
crea
secl
arit
hro
myc
inse
rum
leve
lsw
hile
ind
uce
rso
fC
YP
3A-4
may
dec
reas
eth
ese
rum
leve
ls
Azi
thro
myc
inh
asa
bet
ter
tiss
ue
pen
etra
tio
nth
ancl
arit
hro
myc
inan
dis
bet
ter
tole
rate
db
ut
clin
ical
dat
aar
ela
ckin
go
nit
sef
fica
cyin
the
trea
tmen
to
ftu
ber
culo
sis
BID
,(b
isin
die
)tw
ice
per
day
;BW
,bo
dy
wei
gh
t;C
NS
,cen
tral
ner
vou
ssy
stem
;EM
B,e
tham
bu
tol;
GI,
gas
tro
inte
stin
al;I
NH
,iso
nia
zid
;LR
TI,
low
erre
spir
ato
rytr
act
infe
ctio
n;M
DR
-TB
,mu
lti-
dru
g-r
esis
tan
ttu
ber
culo
sis;
OD
,o
nce
per
day
;Q
T,in
terv
alb
etw
een
the
Qan
dT
wav
ein
the
elec
tro
card
iog
ram
;T
ID,
(tri
sin
die
)th
ree
tim
esp
erd
ay.
MDR-TB overview 423
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432

intervention is most impressive among patientswith persistent positive sputum under medicaltreatment.96–98 Surgical intervention is indicated forsevere drug resistance with a high probability of treat-ment failure with medical therapy alone,96,99 but thetiming of surgical intervention is not yet well defined.Furthermore, whether it is feasible to perform surgeryalso depends on the following two factors: (i) local-ized disease with good chances for complete or nearlycomplete resection and adequate expected postop-erative lung function; and (ii) sufficient activity ofanti-TB drugs to ensure post-surgery stump healing.99
Effective anti-TB treatment offered for at least3 months prior to the surgical intervention to reducebacillary load is recommended.99 Surgical interven-tions complementing individualized chemotherapyregimens guided by DST have led to treatmentsuccess rates in selected MDR-TB patients of >90% ina number of studies, but success rates in patientswith XDR-TB are lower. A study from Ekaterinburg(Russian Federation) evaluated the outcomes of 214culture-confirmed patients with cavitary pulmonaryTB (79.9% of them being MDR): 109 underwent arti-ficial pneumothorax and 105 were treated with che-motherapy only. Among new cases, those who hadartificial pneumothorax had a higher proportion ofsputum smear conversion than controls (100% vs70.9%; P < 0.01). Similarly, among retreament cases,the proportion of smear conversion was, respectively,81% among cases with pneumothorax versus 40%among controls (P < 0.01). The time to conversionwas also faster in group than in control cases.100
Further studies are necessary to evaluate the role ofartificial pneumothorax in treating XDR-TB patients.
DESIGNING AN OPTIMALDRUG REGIMEN
Recommendations for the management of patientswith MDR- and XDR-TB have recently beenreviewed.101A method of grouping anti-TB drugsbased on potency, experience of use and drug classcan be used to design an empirical regimen for thetreatment of MDR-TB cases (Table 4).101 The generalprinciples for designing a regimen are reported inTable 5. Treatment outcomes are optimized if patientswith MDR- or XDR-TB receive timely and adequateempirical therapy including multiple drugs withwhich the patient has not been treated before.
To treat the majority of patients with a minimum offour effective drugs is recommended, but it may benecessary to use five or more drugs to manageMDR-TB patients who have previously been treatedwith second-line drugs. As summarized in Table 5, aninjectable agent and a fluoroquinolone form the coreof the preferred regimen.101
The latest WHO guidelines propose three differenttreatment strategies for individuals known/suspectedto harbour MDR strains of M. tuberculosis.101 Depend-ing on specific country conditions, treatment proto-cols may recommend a standardized treatmentregimen for all MDR-TB patients (e.g. in countrieswhere DST is not widely available and second-line
drugs have not yet been widely used), or may alterna-tively recommend individualized treatment based onindividual DST results. If standardized combinationsof second-line drugs are chosen, representativenational drug resistance surveillance data for specifictreatment categories are needed. However, it is essen-tial to note that standardized treatment is not appli-cable in MDR-TB patients who have been treated withsecond-line drugs. These patients need to bemanaged by individualized approach taking intoaccount individual history of previous anti-TBtherapy and DST results. Unfortunately, the reliabilityof DST of most second-line anti-TB drugs is question-able, with the exception of fluoroquinolones andthe injectables.102,103 Studies have shown substantialmisclassification of probably susceptible and prob-ably resistant strains in the DST of second-line drugs.Therefore, current WHO policy guidance on DST doesnot recommend routine assessment of second-linedrugs.101 Relevant laboratory capacity is necessary ifindividualized treatment is applied, as DST onsecond-line drugs (fluoroquinolone and injectableagents) must be performed.60
Although the individual patient’s treatment dura-tion should be guided by sputum smear and cultureconversion, in general an injectable agent should becontinued for at least the first 6 months of treatment.The entire treatment should be no less than18 months after culture conversion.101 Extension to24 months may be indicated in patients defined as‘chronic cases’ with extensive pulmonary damage. Ofnote is that these recommendations heavily relied onexperts’ experience. It has been reported that a sub-stantial proportion of patients who were treated witha well-designed fluoroquinolone-containing regimenmight be cured after 12 months of therapy.104,105 There-fore, the number of drugs required, optimal durationof injectable drug use and total duration of treatmentrequired for the treatment of MDR merit further sys-tematic evaluation.80 Furthermore, the fourth genera-tion fluoroquinolones have both excellent bactercidaland sterilzing activities and their potential contribu-tion in the treatment of MDR-TB has not yet beenfully investigated. Initial evidence is emerging that ashorter duration of treatment of MDR-TB patientswho have never been previously treated with second-line drugs is feasible if a fourth generation fluoroqui-nolone is used.106 In clinical practice, the treatmentwith second- and third-line anti-TB chemotherapy inMDR- and XDR-TB is frequently influenced by theoccurrence of adverse drug events.
HIV AND EXTENSIVELYDRUG-RESISTANT/MULTI-DRUG-RESISTANTTUBERCULOSIS
HIV may not consistently be a risk factor of MDR-/XDR-TB, depending on the population investigated.However, outbreaks of TB and MDR-/XDR-TB havebeen repeatedly reported from different settings.107
This highlights the essential role of infection control
C-Y Chiang et al.424
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432

to prevent the spread of MDR-/XDR-TB in health-carefacilities and congregate settings as well as withinhouseholds.108 While modern ventilation systemmight be useful to reduce the risk of transmission inhealth-care facilities, natural ventilation for the pre-vention of airborne transmission should not beunderestimated.109 Health-care workers should beeducated to be aware of the risk of transmission of TBin health-care facilities and should take actions toprevent TB transmission accordingly. Infectioncontrol begins with risk assessment and an infectioncontrol plan, which needs to be rigorously imple-mented and carefully monitored.110 Administrativepolicies focusing on identification and isolation/separation of infectious TB patients, together withenvironment control and proper personal protectionconstitute the three pillars of infection control.111 Toprevent the spread of MDR-/XDR-TB in health-carefacilities, a high index of suspicion enabling efficientidentification of suspect of MDR-/XDR-TB is
required.112 Among the high risk groups of MDR-TB,failure of retreatment regimen and contact ofMDR-TB may have the highest probability of MDR-TBand deserve special attention. Rapid testing of resis-tance to RMP might be particularly useful in the con-firmation of MDR-TB. Challenges in the treatmentof MDR-TB among the HIV-infected include highnumber of drugs per day and overlap or additive ofadverse reactions. Furthermore, studies to evaluatedrug–drug interactions between second-line anti-TBdrugs and antiretroviral drugs are lacking.113
THE PRESENT AND FUTUREPERSPECTIVE OF DRUG-RESISTANTTUBERCULOSIS CONTROL
It has been observed that drug-resistant mutant wasless virulent as compared with the susceptible origi-nal strain114 and that acquisition of drug resistance in
Table 5 General principles for designing an empirical regimen to treat MDR-TB (Reproduced with permission from‘Guidelines for the programmatic management of drug-resistant tuberculosis’ WHO/HTM/TB/2006.361. and from itsupdated version101)
Basic principles Comments
1. Use at least fourdrugs of knowneffectiveness orhighly likely to beeffective
Effectiveness is supported by a number of factors (likely to be effective if more of factors arepresent):A. No previous history of treatment failure with the drugB. No resistance by DSTC. No close contact with patients whose isolates are resistant to the drugD. No common use of the drug in the area.Five to seven drugs may be needed especially in patients previously treated with MDR-TBdepending on the level of uncertainty
2. Do not use drugs withhigh risk of crossresistance
A. Rifamycins (rifampicin, rifabutin, rifapentine, rifalazil): have high level of cross resistanceB. Fluoroquinolones: variable cross resistance; in vitro data show that Moxifloxacin may
remain susceptible in ofloxacin-resistant strains (clinical significance of the phenomenonstill not fully evaluated)
C. Aminoglycosides and polypeptides: variable cross resistance among capreomycin,kanamycin and amikacin; cross resistance of amikacin with kanamycin and capreomycinusually
3. Eliminate drugs likelyto be not safe for thepatient
A. Avoid drugs that patients have known severe allergy or difficult-to-manage intoleranceB. Monitor closely in patients with renal failure, deafness, hepatitis, depression and/or
psychosisC. Do not use drugs with unknown or questionable quality
4. Include drugs fromgroup 1–5 in ahierarchical order,based on potency
A. Use any group 1 (oral first-line) drugs that are likely to be effective (see section 1 of thistable)
B. Use an effective injectable aminoglycoside or polypeptide (group 2 drugs)C. Use a fluoroquinolone (group 3)D. Use the remaining group 4 drugs to make a regimen consisting of at least four effective
drugsE. Use group 5 drugs as needed to design a regimen with at least four effective drugs
5. Be prepared toprevent, monitor andmanage adverseeffects for each of thedrugs selected
A. Ensure laboratory services for haematology, biochemistry, serology and audiometry areavailable
B. Establish a clinical and laboratory baseline before starting the regimenC. Initiate treatment gradually for a difficult-to-tolerate drug, and split daily doses of Eto/Pto,
Cs and PASD. Ensure ancillary drugs are available to manage adverse effectsE. Organize intake supervision for all doses
MDR-TB, multi-drug-resistant tuberculosis; DST, drug susceptibility testing.
MDR-TB overview 425
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
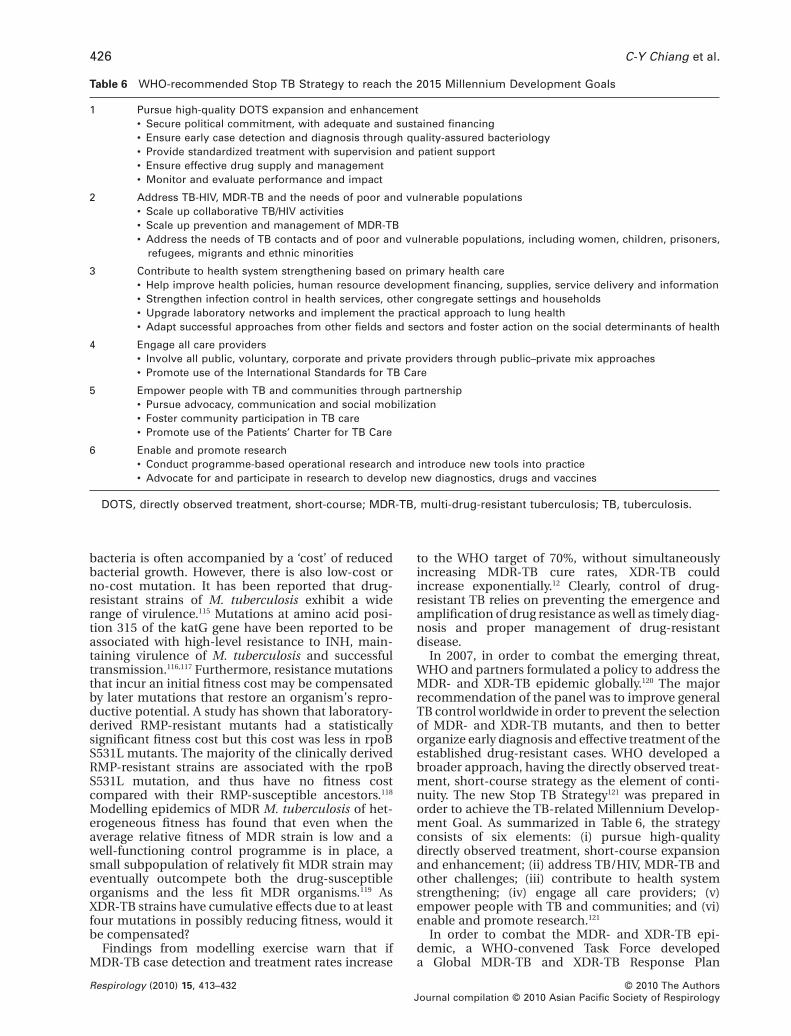
bacteria is often accompanied by a ‘cost’ of reducedbacterial growth. However, there is also low-cost orno-cost mutation. It has been reported that drug-resistant strains of M. tuberculosis exhibit a widerange of virulence.115 Mutations at amino acid posi-tion 315 of the katG gene have been reported to beassociated with high-level resistance to INH, main-taining virulence of M. tuberculosis and successfultransmission.116,117 Furthermore, resistance mutationsthat incur an initial fitness cost may be compensatedby later mutations that restore an organism’s repro-ductive potential. A study has shown that laboratory-derived RMP-resistant mutants had a statisticallysignificant fitness cost but this cost was less in rpoBS531L mutants. The majority of the clinically derivedRMP-resistant strains are associated with the rpoBS531L mutation, and thus have no fitness costcompared with their RMP-susceptible ancestors.118
Modelling epidemics of MDR M. tuberculosis of het-erogeneous fitness has found that even when theaverage relative fitness of MDR strain is low and awell-functioning control programme is in place, asmall subpopulation of relatively fit MDR strain mayeventually outcompete both the drug-susceptibleorganisms and the less fit MDR organisms.119 AsXDR-TB strains have cumulative effects due to at leastfour mutations in possibly reducing fitness, would itbe compensated?
Findings from modelling exercise warn that ifMDR-TB case detection and treatment rates increase
to the WHO target of 70%, without simultaneouslyincreasing MDR-TB cure rates, XDR-TB couldincrease exponentially.12 Clearly, control of drug-resistant TB relies on preventing the emergence andamplification of drug resistance as well as timely diag-nosis and proper management of drug-resistantdisease.
In 2007, in order to combat the emerging threat,WHO and partners formulated a policy to address theMDR- and XDR-TB epidemic globally.120 The majorrecommendation of the panel was to improve generalTB control worldwide in order to prevent the selectionof MDR- and XDR-TB mutants, and then to betterorganize early diagnosis and effective treatment of theestablished drug-resistant cases. WHO developed abroader approach, having the directly observed treat-ment, short-course strategy as the element of conti-nuity. The new Stop TB Strategy121 was prepared inorder to achieve the TB-related Millennium Develop-ment Goal. As summarized in Table 6, the strategyconsists of six elements: (i) pursue high-qualitydirectly observed treatment, short-course expansionand enhancement; (ii) address TB/HIV, MDR-TB andother challenges; (iii) contribute to health systemstrengthening; (iv) engage all care providers; (v)empower people with TB and communities; and (vi)enable and promote research.121
In order to combat the MDR- and XDR-TB epi-demic, a WHO-convened Task Force developeda Global MDR-TB and XDR-TB Response Plan
Table 6 WHO-recommended Stop TB Strategy to reach the 2015 Millennium Development Goals
1 Pursue high-quality DOTS expansion and enhancement• Secure political commitment, with adequate and sustained financing• Ensure early case detection and diagnosis through quality-assured bacteriology• Provide standardized treatment with supervision and patient support• Ensure effective drug supply and management• Monitor and evaluate performance and impact
2 Address TB-HIV, MDR-TB and the needs of poor and vulnerable populations• Scale up collaborative TB/HIV activities• Scale up prevention and management of MDR-TB• Address the needs of TB contacts and of poor and vulnerable populations, including women, children, prisoners,
refugees, migrants and ethnic minorities
3 Contribute to health system strengthening based on primary health care• Help improve health policies, human resource development financing, supplies, service delivery and information• Strengthen infection control in health services, other congregate settings and households• Upgrade laboratory networks and implement the practical approach to lung health• Adapt successful approaches from other fields and sectors and foster action on the social determinants of health
4 Engage all care providers• Involve all public, voluntary, corporate and private providers through public–private mix approaches• Promote use of the International Standards for TB Care
5 Empower people with TB and communities through partnership• Pursue advocacy, communication and social mobilization• Foster community participation in TB care• Promote use of the Patients’ Charter for TB Care
6 Enable and promote research• Conduct programme-based operational research and introduce new tools into practice• Advocate for and participate in research to develop new diagnostics, drugs and vaccines
DOTS, directly observed treatment, short-course; MDR-TB, multi-drug-resistant tuberculosis; TB, tuberculosis.
C-Y Chiang et al.426
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432

(2007–2008)122 and in April 2009 a governmental con-ference was organized in China to develop the BeijingCall for Action,123 committing the 27 high MDR-TBburden countries to a specific set of actions for MDR-and XDR-TB containment and prevention.
Seven additional recommendations124 were devel-oped to prevent and control XDR-TB, including:1 Preventing XDR-TB through basic strengthening TBand HIV control. The new Stop TB Strategy and theGlobal Plan to Stop TB are the key reference docu-ments to guide these priority interventions.2 Improving management of individuals suspectedto be affected by XDR-TB through accelerated accessto laboratory facilities with rapid DST test for RMPand INH resistance and DST for MDR cases andimproved detection of cases suspecting of harbouringMDR strains both in high and low HIV prevalencesettings.3 Strengthening management of XDR-TB and treat-ment design in both HIV-negative and positive indi-viduals, through adequate use of second-line drugsand patient-centred approaches to ensure supportand supervision.4 Standardizing the definition of XDR-TB.5 Increasing health-care worker infection controland protection mainly (but not exclusively) in highHIV prevalence settings.6 Implementing immediate XDR-TB surveillanceactivities through the existing network of suprana-tional reference laboratories and national referencelaboratories.7 Initiating advocacy, communication and socialmobilization activities to inform and raise awarenessabout TB and XDR-TB.
Within the framework of these recommendations,United States Agency for International Development,in collaboration with WHO and other partners, hasdeveloped a tool (the MDR-/XDR-TB Assessment andMonitoring Tool) to be used for preparing national orsubnational plans for MDR-/XDR-TB prevention andcontrol; providing baseline information and monitor-ing progress; providing data and analysis to prepareGreen Light Committee and Global Fund to FightAIDS, Tuberculosis and Malaria applications; provid-ing information to guide requests for external techni-cal assistance; providing information to guide donorinvestment in MDR-/XDR-TB interventions.
Research priorities to improve MDR- and XDR-TBprevention and control can be identified at all levels,including basic, applied and operational research.125
As the main focus of this review is on MDR-TBcontrol, we will specifically address the new diagnos-tics and new drugs issues, leaving out the newvaccines.
RATIONALE FORMULTI-DRUG-RESISTANTTUBERCULOSIS RESEARCHPRIORITIES: PREVENTION FIRSTOF ALL
The history of TB treatment has observed sequentialdevelopment of resistance to key anti-TB drugs over
the decades, from SM resistance, to INH resistance,RMP resistance, then fluoroquinolone resistance. Infact, we probably are losing fluoroquinolone rapidly.Fluoroquinolone-resistant TB emerges efficiently asexplained in the earlier part of this review. XDR-TBis the result of sequential mutations cumulativelyleading to combined resistance to INH, RMP, fluoro-quinolone(s) and second-line injectable agent(s). Theorder of mutation could vary widely, and may rarelybegin with fluoroquinolone resistance. The increasedprevalence of fluoroquinolone resistance in M. tuber-culosis creates a fertile ground for the emergenceof fluoroquinolone-resistant MDR-TB and XDR-TB.Unfortunately, international recommendations andnational policies on protecting fluoroquinolone arenot yet in place.126 Clearly, this deficiency needs to beaddressed quickly. Furthermore, prevention of selec-tion of new MDR requires sound application of theWHO Stop TB Strategy, acting on the different com-ponents of the treatment delivery process chain:from uninterrupted supply of quality drugs topatient-centred support.
IMPROVED DIAGNOSTIC TOOLS
Rifampicin resistance has been proposed as molecu-lar marker for MDR-TB. Detecting RMP resistance as ascreening strategy in the diagnosis of MDR-TB needsto be tested in settings with a low risk of non-MDRRMP resistance.
In contrast to the ‘ex novo’ development of drugresistance, the transmission of MDR- and XDR-strainsof M. tuberculosis is becoming an increasing problemin settings where the prevalence of TB and MDR-TB ishigh and that of HIV is increasing (e.g. FSU countries).It is necessary to efficiently interrupt the MDR- andXDR-TB ongoing transmission through early diagno-sis and effective treatment. Several options of rapidtesting of anti-TB drug resistance are available,127
including DNA sequencing,34 solid-phase hybridiza-tion techniques,128,129 microarrays,130 real-time PCRtechniques,131 microscopic observation drug suscep-tibility assay,132 slide DST,133 phage-based assays,134
colorimetric methods (the MTT and resazurin asredox indicators)135 and nitrate reductase assay.136
National TB control programmes need to take cost,sustainability, turnaround time, reliability and acces-sibility into consideration in selecting rapid testing.Furthermore, the new GenoType Mycobacterium TBdrug resistance second-line (MTBDRsl) assay (HainLifescience, Nehren, Germany) provides a potentialnew tool for the detection of XDR strains of M. tuber-culosis within 1–2 days directly in clinical specimen,137
which could be particularly useful in settings with ahigh risk of XDR-TB.
Diagnosis of latent TB infection specifically causedby drug-resistant strains is currently not possible. Yet,early diagnosis and exact identification of drug resis-tance during M. tuberculosis latency could have a sub-stantial impact on TB control. The early diagnosis ofdrug resistance in M. tuberculosis infection should bea priority target of future research activities.
MDR-TB overview 427
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432

NEW DRUGS
For more than 40 years, not a single new drug hasbeen developed and licensed for the treatmentagainst TB. Under these circumstances and underconstant evolutionary pressure of the same anti-TBdrugs, it was only a matter of time before drug resis-tance of M. tuberculosis emerged as a seriousproblem. The emergence of MDR- and XDR-TB hasspurred interest in the development of new drugs.Recently, the first report of a phase 2 clinical trial ofTMC207 for the treatment of MDR-TB has been pub-lished.106 Adding TMC207 to standard therapy forMDR-TB reduced the time to conversion to a negativesputum culture, as compared with placebo (hazardratio 11.8; 95% CI: 2.3–61.3). TMC207, a first-in-classdiarylquinoline, has a unique mechanism of actiontargeting the c subunit of adenosine triphosphatesynthase138 and exhibits a long half-life. TMC207 plusrifapentine plus PZA given once weekly was moreactive than the current standard regimen of RMP plusINH plus PZA given five times per week in murine TB,suggesting that it has the potential to be used todevelop a fully intermittent once-weekly regimen.139
PA-824140 is a novel nitroimidazo-oxazine, inhibitsmycolic acid and protein biosynthesis and kills non-replicating M. tuberculosis as well.141 PA-824 enhancesbactericidal activity of RMP and/or PZA in a murinemodel of TB.142 The combination of PA-824, moxi-floxacin and PZA cured mice more rapidly than thefirst-line regimen of RMP, INH and PZA in a murinemodel of TB, implying the potential to shorten theduration of TB treatment.143 Other imidazo-oxazole,diamine and pyrrole compounds are being investi-gated in clinical phase 1 or 2 drug trials as well, yetnone of the compounds will have passed phase 3 to beavailable before the year 2011 (Table 7). Randomizedclinical trials are now urgently needed to develop newregimens for improved treatment outcomes ofpatients with MDR- and XDR-TB. The development ofnew potent drugs with a low toxicity profile, allowingfor shorter and more effective treatment against TB,and the exploration regarding the role of possibleadjunctive therapies, such as vitamin D supplemen-
tation,144 and the use of existing compounds withnovel anti-mycobacterial mechanisms, such as thior-idazine145 likely constitute a priorities.
CONCLUSIONS
The global epidemic of MDR-TB (estimated half amillion new cases and 150 000 deaths annually) has acase–fatality ratio of 30 per 100 affected individuals,and XDR-TB (estimated 50 000 cases and 30 000deaths) of 60 per 100 affected cases. This means thatevery day there are about 400 deaths related toMDR-TB and 80 related to XDR-TB. The situation canget even worse if proper action is not taken efficientlyat global and local levels. The main challenges are thefollowing79:1 Human resource development for the diagnosisand management of MDR- and XDR-TB is urgentlyneeded, especially in China, India and other countrieswith a high burden of MDR-TB.2 The capacity of laboratory needs to be strength-ened and a laboratory network established for thedetection of resistance to RMP and INH, as well asresistance to fluoroquinolone(s) and second-lineinjectables drug(s) in settings with a high risk of XDR-TB. The utility of rapid testing of resistance needs tobe pilot tested in resource limited setting as early aspossible.3 Although a high proportion of MDR-TB patientscan be cured, treatment of MDR-TB remains difficultand expensive. Strategies to reduce proportiondefaulted and to increase the proportion cured in thetreatment of MDR-TB need to be investigated rapidly.4 The prevalence of MDR-TB is related to poor TBcontrol,49 and the emergence and spread of XDR-TB isdue to the improper regulation and use of second-lineanti-TB drugs. Prevention of drug resistance throughadherence to proper standards of care and control isimperative and a top priority for all TB control efforts.
REFERENCES
1 Crofton J. Chemotherapy of pulmonary tuberculosis. BMJ 1959;1: 1610–14.
Table 7 Examples of new anti-tuberculosis drugs under clinical development (Reproduced with permission from:http://www.stoptb.org/wg/new_drugs/assets/documents/2008GlobalTBDrugsPipelineFOR%20_WEBSITE_Oct%2021°Corrected.pdf)
Advanced preclinical evaluation Phase 1 Phase 2
TB Oxazolidinone PNU-100480 Diamine SQ-109 Diarylquinoline TMC207Pfizer Pfizer TibotecTBK-613—Quinolone Pyrrole LL3858 Rifapentine TBTC-29TB Alliance, various CROs Lupin Pharmaceuticals Sanofi Pasteur, TBTC, CDC
Nitro-dihydro-imidazooxazole OPC-67683Otsuka PharmaceuticalsNitroimidazole-oxazine PA-824TB Alliance
Drugs, like Moxifloxacin and Linezolid, which are already licensed for other indications and used in the treatmentagainst multi-drug-resistant tuberculosis and extensively drug-resistant tuberculosis, are in clinical evaluation.
TB, tuberculosis.
C-Y Chiang et al.428
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
2 Bai K-J, Yu M-C, Chiang C-Y et al. Short-course chemotherapyfor isoniazid-resistant pulmonary tuberculosis. J. Formos. Med.Assoc. 1998; 97: 278–82.
3 Espinal MA, Kim SJ, Suarez PG et al. Standard short-course che-motherapy for drug-resistant tuberculosis. Treatment out-comes in 6 countries. JAMA 2000; 283: 2537–45.
4 Chiang C-Y, Enarson DA, Yu M-C et al. Outcome of pulmonarymultidrug-resistant tuberculosis: a 6-yr follow-up study. Eur.Respir. J. 2006; 28: 980–5.
5 Centers for Disease Control and Prevention. Emergence ofMycobacterium tuberculosis with extensive resistance tosecond-line drugs—worldwide, 2000-2004. MMWR Morb.Mortal. Wkly. Rep. 2006; 55: 301–5.
6 Holtz TH, Cegielski JP. Origin of the term XDR-TB. Eur. Respir. J.2007; 30: 396.
7 Migliori GB, Loddenkemper R, Blasi F et al. 125 years afterRobert Koch’s discovery of the tubercle bacillus: the newXDR-TB threat. Is ‘science’ enough to tackle the epidemic? Eur.Respir. J. 2007; 29: 423–7.
8 Caminero JA. Extensively drug-resistant tuberculosis: is its defi-nition correct? Eur. Respir. J. 2008; 32: 1413–15.
9 Chiang C-Y. Outcome of extensively drug-resistant tuberculo-sis. Int. J. Tuberc. Lung Dis. 2009; 13: 794.
10 Migliori GB, Besozzi G, Girardi E et al. Clinical and operationalvalue of the extensively drug-resistant tuberculosis definition.Eur. Respir. J. 2007; 30: 623–6.
11 Dye C, Espinal MA. Will tuberculosis become resistant to allantibiotics? Proc. R. Soc. Lond., B, Biol. Sci. 2001; 268: 45–52.
12 Blower S, Supervie V. Predicting the future of XDR tuberculosis.(Reflection and reaction). Lancet Infect. Dis. 2007; 7: 443.
13 Dye C. Doomsday postponed? Preventing and reversing epi-demics of drug-resistant tuberculosis. Nat. Rev. 2009; 7: 81–7.
14 Cohen T, Dye C, Colijin C et al. Mathematical models of theepidemiology and control of drug-resistant TB. Expert Rev.Respir. Med. 2009; 3: 67–79.
15 David HL. Probability distribution of drug-resistant mutants inunselected populations of Mycobacterium tuberculosis. Appl.Microbiol. 1970; 20: 810–14.
16 Mitchison DA. Problems of drug resistance. Br. Med. Bull. 1954;10: 115–24.
17 Crofton J, Mitchison DA. Streptomycin resistance in pulmonarytuberculosis. BMJ 1948; 2: 1009–15.
18 British Medical Research Council. Streptomycin treatment ofpulmonary tuberculosis. A Medical Research Council investiga-tion. BMJ 1948; 2: 769–83.
19 Fox W, Sutherland I. A five-year assessment of patients in acontrolled trial of streptomycin, para-aminosalicylic acid, andstreptomycin plus para-aminosalicylic acid, in pulmonarytuberculosis. Report to the Tuberculosis Chemotherapy TrialsCommittee of the Medical Research Council. Q. J. Med. New Ser.1956; 25: 221–43.
20 Fox W, Ellard GA, Mitchison DA. Studies on the treatment oftuberculosis undertaken by the British Medical ResearchCouncil Tuberculosis Units, 1946–1986, with relevant subse-quent publications. Int. J. Tuberc. Lung Dis. 1999; 3 (Suppl. 2):S231–79.
21 Devasia RA, Blackman A, Gebretsadik T et al. Fluoroquinoloneresistance in Mycobacterium tuberculosis. The effect of durationand timing of fluoroquinolone exposure. Am. J. Respir. Crit. CareMed. 2009; 180: 365–70.
22 Wang JY, Hsueh PR, Jan IS et al. Empirical treatment with afluoroquinolone delays the treatment for tuberculosis and isassociated with a poor prognosis in endemic areas. Thorax2006; 61: 903–8.
23 Long R, Chong H, Hoeppner V et al. Empirical treatment ofcommunity-acquired pneumonia and the development offluoroquinolone-resistant tuberculosis. Clin. Infect. Dis. 2009;48: 1354–60.
24 Grimaldo ER, Tupasi TE, Rivera AB et al. Increased resistance tociprofloxacin and ofloxacin in multidrug-resistant Mycobacte-
rium tuberculosis isolates from patients seen at a tertiary hos-pital in the Philippines. Int. J. Tuberc. Lung Dis. 2001; 5: 546–50.
25 Agrawal D, Udwadia ZF, Rodriguez C et al. Increasing incidenceof fluoroquinolone-resistant Mycobacterium tuberculosis inMumbai, India. Int. J. Tuberc. Lung Dis. 2009; 13: 79–83.
26 Ait-Khaled N, Alarcon E, Bissell K et al. Isoniazid preventivetherapy for people living with HIV: public health challenges andimplementation issues. Int. J. Tuberc. Lung Dis. 2009; 13: 927–35.
27 Cattamanchi A, Dantes RB, Metcalfe JZ et al. Clinical character-istics and treatment outcomes of patients with isoniazid-monoresistant tuberculosis. Clin. Infect. Dis. 2009; 48: 179–85.
28 Mitchison DA. How drug resistance emerges as a result of poorcompliance during short course chemotherapy of tuberculosis.Int. J. Tuberc. Lung Dis. 1998; 2: 10–15.
29 Mitchison DA. The action of antituberculosis drugs in short-course chemotherapy. Tubercle 1985; 66: 219–25.
30 Yoshiyama T, Yanai H, Rhiengtong D et al. Development ofacquired drug resistance in recurrent tuberculosis patients withvarious previous treatment outcomes. Int. J. Tuberc. Lung Dis.2004; 8: 31–8.
31 World Health Organization. The WHO/IUATLD global projecton anti-tuberculosis drug resistance surveillance. Anti-tuberculosis drug resistance in the world. Report No. 3. WorldHealth Organization Document 2004; WHO/CDS/TB/2004.343:1–129.
32 Lutfey M, Della-Latta P, Kapur V et al. Independent origin ofmono-rifampin-resistant Mycobacterium tuberculosis inpatients with AIDS. Am. J. Respir. Crit. Care Med. 1996; 153:837–40.
33 Ridzon R, Whitney CG, McKenna MT et al. Risk factors forrifampin mono-resistant tuberculosis. Am. J. Respir. Crit. CareMed. 1998; 157: 1881–4.
34 Zhang Y, Yew WW. Mechanisms of drug resistance in Mycobac-terium tuberculosis. Int. J. Tuberc. Lung Dis. 2009; 13: 1320–30.
35 Kleeberg HH, Boshoff MS. A World Atlas of Initial Drug Resis-tance. Prepared for the Scientific Committee on Bacteriologyand Immunology of the International Union Against Tubercu-losis. Tuberculosis Research Institute of the South AfricanMedical Research Council, Pretoria, 1980; 1–23.
36 Cohn DL, Bustreo F, Raviglione MC. Drug-resistant tuberculo-sis: review of the worldwide situation and the WHO/IUATLDglobal surveillance project. Clin. Infect. Dis. 1997; 24 (Suppl. 1):S121–30.
37 World Health Organization. Guidelines for surveillance of drugresistance in tuberculosis. World Health Organization Docu-ment 1994; WHO/TB/94.178:1–24.
38 World Health Organization. Guidelines for the surveillance ofdrug resistance in tuberculosis. Fourth edition. World HealthOrganization Document 2009; WHO/HTM/TB/2009.442.
39 World Health Organization. Anti-tuberculosis drug resistancein the world. The WHO/IUATLD global project on anti-tuberculosis drug resistance surveillance. World Health Organi-zation Document 1997; WHO/TB/97.229:1–227.
40 World Health Organization. The WHO/IUATLD global projecton anti-tuberculosis drug resistance surveillance. Anti-tuberculosis drug resistance in the world. Report No.2—prevalence and trends. World Health Organization Docu-ment 2000; WHO/CDC/TB/2000.278:1–253.
41 World Health Organization. The WHO/IUATLD global projecton anti-tuberculosis drug resistance surveillance. Anti-tuberculosis drug resistance in the world. Report No. 4. WorldHealth Organization Document 2008; WHO/HTM/TB/2008.394:1–120.
42 Van Deun A, Salim AH, Daru P et al. Drug resistance monitor-ing: combined rates may be the best indicator of programmeperformance. Int. J. Tuberc. Lung Dis. 2004; 8: 23–30.
43 Laszlo A, Rahman M, Espinal M et al. Quality assurance pro-gramme for drug susceptibility testing of Mycobacterium
MDR-TB overview 429
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
tuberculosis in the WHO/IUATLD Supranational ReferenceLaboratory Network: five rounds of proficiency testing, 1994–1998. Int. J. Tuberc. Lung Dis. 2002; 6: 748–56.
44 Migliori GB, Lange C, Centi R et al. Resistance to second-lineinjectables and treatment outcomes in multidrug-resistant andextensively drug-resistant tuberculosis cases. Eur. Respir. J.2008; 31: 1155–9.
45 Migliori GB, Lange C, Girardi E et al. Extensively drug-resistanttuberculosis is worse than multidrug-resistant tuberculosis: dif-ferent methodology and settings, same results. Clin. Infect. Dis.2008; 46: 958–9.
46 Migliori GB, Lange C, Girardi E et al. Fluoroquinolones: are theyessential to treat multidrug-resistant tuberculosis? Eur. Respir. J.2008; 31: 904–10.
47 Migliori GB, Sotgiu G, D’Arcy Richardson M et al. Consensusnot yet reached on key drugs for extensively drug-resistanttuberculosis treatment. Clin. Infect. Dis. 2009; 49: 315–16.
48 Wright A, Zignol M, Van Deun A et al. Epidemiology of antitu-berculosis drug resistance 2002–07: an updated analysis of theGlobal Project on Anti-Tuberculosis Drug Resistance Surveil-lance. Lancet 2009; 373: 1861–73.
49 World Health Organization. Global tuberculosis control: sur-veillance, planning, financing. WHO Report 2009. World HealthOrganization Document 2009; WHO/HTM/TM/2009.411:1–303.
50 Vernon A, Burman W, Benator D et al. Acquired rifamycinmonoresistance in patients with HIV-related tuberculosistreated with once-weekly rifapentine and isoniazid. Lancet1999; 353: 1843–7.
51 Zignol M, Hosseini MS, Wright A et al. Global incidence ofmultidrug-resistant tuberculosis. J. Infect. Dis. 2006; 194: 479–85.
52 Blower SM, Chou T. Modeling the emergence if the ‘hot zones’:tuberculosis and the amplification dynamics of drug resistance.Nat. Med. 2004; 10: 1111–16.
53 Cohen T, Coljin C, Wright A et al. Challenges in estimating thetotal burden of drug-resistant tuberculosis. Am. J. Respir. Crit.Care Med. 2008; 177: 1302–6.
54 Sotgiu G, Ferrara G, Matteelli A et al. Epidemiology and clinicalmanagement of XDR-TB: a systematic review by TBNET. Eur.Respir. J. 2009; 33: 871–81.
55 Kim DH, Kim HJ, Park SK et al. Treatment outcomes and long-term survival in patients with extensively drug-resistant tuber-culosis. Am. J. Respir. Crit. Care Med. 2008; 178: 1075–82.
56 Migliori GB, Cirillo DM, Spanevello A et al. Ripped from theheadlines: how can we harness communications to control TB?Eur. Respir. J. 2007; 30: 194–8.
57 Quy HTW, Lan NTN, Borgdorff MW et al. Drug resistanceamong failure and relapse cases of tuberculosis: is the standardre-treatment regimen adequate? Int. J. Tuberc. Lung Dis. 2003; 7:631–6.
58 Migliori GB, Espinal M, Danilova ID et al. Frequency of recur-rence among MDR-TB cases ‘successfully’ treated with standar-dised short-course chemotherapy. Int. J. Tuberc. Lung Dis. 2002;6: 858–64.
59 Migliori GB, D’Arcy Richardson M, Lange C. Of blind men andelephants: making sense of extensively drug-resistant tubercu-losis. Am. J. Respir. Crit. Care Med. 2008; 178: 1000–1.
60 World Health Organization. Policy guidance on drug-susceptibility testing (DST) of second-line antituberculosisdrugs. World Health Organization Document 2008; WHO/HTM/TB/2008.392:1–20.
61 Trebucq A, Anagonou S, Gninafon M et al. Prevalence ofprimary and acquired resistance of Mycobacterium tuberculo-sis to antituberculosis drugs in Benin after 12 years ofshort-course chemotherapy. Int. J. Tuberc. Lung Dis. 1999; 3:466–70.
62 Espinal MA, Laserson K, Camacho M et al. Determinants ofdrug-resistant tuberculosis: analysis of 11 countries. Int. J.Tuberc. Lung Dis. 2001; 5: 887–93.
63 Chiang CY, Hsu CJ, Huang RM et al. Antituberculosis drug resis-tance among retreatment tuberculosis patients in a referralcenter in Taipei. J. Formos. Med. Assoc. 2004; 103: 411–15.
64 Saravia JC, Appleton SC, Rich ML et al. Retreatment strategieswhen first-line tuberculosis therapy fails. Int. J. Tuberc. LungDis. 2005; 9: 421–9.
65 Becerra MC, Freeman J, Bayona J et al. Using treatment failureunder effective directly observed short-course chemotherapyprograms to identify persons with multidrug-resistant tubercu-losis. Int. J. Tuberc. Lung Dis. 2000; 4: 108–14.
66 Law WS, Yew WW, Chiu Leung C et al. Risk factors formultidrug-resistant tuberculosis in Hong Kong. Int. J. Tuberc.Lung Dis. 2008; 12: 1065–70.
67 Faustini A, Hall AJ, Perucci CA. Risk factors for multidrug resis-tant tuberculosis in Europe: a systematic review. Thorax 2006;61: 158–63.
68 Frieden TR, Sterling T, Pablos-Mendez A et al. The emergenceof drug-resistant tuberculosis in New York City. N. Engl. J. Med.1993; 328: 521–6.
69 Kliiman K, Altraja A. Predictors of poor treatment outcome inmulti- and extensively drug-resistant pulmonary TB. Eur.Respir. J. 2009; 33: 1085–94.
70 Casal M, Vaquero M, Rinder H et al. A case-control study formultidrug-resistant tuberculosis: risk factors in four Europeancountries. Microb. Drug Resist. 2005; 11: 62–7.
71 Clark CM, Li J, Driver CR et al. Risk factors for drug-resistanttuberculosis among non-US-born persons in New York City. Int.J. Tuberc. Lung Dis. 2005; 9: 964–9.
72 Jakubowiak WM, Bogorodskaya EM, Borisov ES et al. Riskfactors associated with default among new pulmonary TBpatients and social support in six Russian regions. Int. J. Tuberc.Lung Dis. 2007; 11: 46–53.
73 Ruddy M, Balababanova Y, Graham C et al. Rates of drug resis-tance and risk factor analysis in cilvilian and prison patientswith tuberculosis in Samara Region, Russia. Thorax 2005; 60:130–5.
74 Suchindran S, Brouwer ES, Van Rie A. Is HIV infection a riskfactor for multi-drug resistant tuberculosis? A systematicreview. PLoS ONE 2009; 4 (5): e5561; doi:10.1371/journal.pone.0005561.
75 Coker R, McKee M, Atun R et al. Risk factors for pulmonarytuberculosis in Russia: case-control study. BMJ 2006; 332: 85–7.
76 Balabanova Y, Ruddy M, Hubb J et al. Multidrug-resistanttuberculosis in Russia: clinical characteristics, analysis ofsecond-line drug resistance and development of standardizedtherapy. Eur. J. Clin. Microbiol. Infect. Dis. 2005; 24: 136–9.
77 Espinal MA. Time to abandon the standard retreatmentregimen with first-line drugs for failures of standard treatment.Int. J. Tuberc. Lung Dis. 2003; 7: 607–8.
78 Caminero JA. Likelihood of generating MDR-TB and XDR-TBunder adequate National Tuberculosis Programme implemen-tation. Int. J. Tuberc. Lung Dis. 2008; 12: 869–77.
79 Migliori GB, Richardson MDA, Sotgiu G et al. MDR—andXDR-TB in the West: Europe and USA: epidemiology, surveil-lance and control. Clin. Chest Med. 2009; 30: 637–65.
80 Caminero JA. Treatment of multidrug-resistant tuberculosis:evidence and controversies. Int. J. Tuberc. Lung Dis. 2006; 10:829–37.
81 Migliori GB, Eker B, Richardson MD et al. A retrospectve TBNETassessment of linezolid safety, tolerability and efficacy inmultidrug-resistant tuberculosis. Eur. Respir. J. 2009; 34: 387–93.
82 Koh WJ, Kwon OJ, Gwak H et al. J. Antimicrob. Chemother. 2009;64: 388–91.
83 Hugonnet JE, Tremblay LW, Boshoff HIE. Meropenem-clavulanate is effective against extensively drug-resistant Myco-bacterium tuberculosis. Science 2009; 323: 1215–18.
84 Chan ED, Laurel V, Strand MJ et al. Treatment and outcomeanalysis of 205 patients with multidrug-resistant tuberculosis.Am. J. Respir. Crit. Care Med. 2004; 169: 1103–9.
C-Y Chiang et al.430
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
85 Goble M, Iseman MD, Madsen LA et al. Treatment of 171patients with pulmonary tuberculosis resistant to isoniazid andrifampin. N. Engl. J. Med. 1993; 328: 527–32.
86 Park SK, Kim CT, Song SD. Outcome of chemotherapy in 107patients with pulmonary tuberculosis resistant to isoniazid andrifampicin. Int. J. Tuberc. Lung Dis. 1998; 2: 877–84.
87 Flament-Saillour M, Robert J, Jarlier V et al. Outcome of multi-drug-resistant tuberculosis in France. A nationwide case-control study. Am. J. Respir. Crit. Care Med. 1999; 160: 587–93.
88 Kim HJ, Hong YP, Kim SJ et al. Ambulatory treatment ofmultidrug-resistant pulmonary tuberculosis patients at a chestclinic. Int. J. Tuberc. Lung Dis. 2001; 5: 1129–36.
89 Laserson KF, Thorpe LE, Leimane V et al. Speaking the samelanguage: treatment outcome definitions for multidrug-resistant tuberculosis. Int. J. Tuberc. Lung Dis. 2005; 9: 640–5.
90 Chiang C-Y, Caminero JA, Enarson DA. Reporting onmultidrug-resistant tuberculosis: a proposed definition for thetreatment outcome ‘failed’. Int. J. Tuberc. Lung Dis. 2009; 13:548–50.
91 Orenstein EW, Basu S, Shah NS et al. Treatment outcomeamong patients with multidrug-resistant tuberculosis: system-atic review and meta-analysis. Lancet Infect. Dis. 2009; 9: 153–61.
92 Nathanson E, Lambregts van Weezenbeek C, Rich ML et al.Multidrug-resistant tuberculosis management in resource-limited settings. Emerg Infect. Dis. 2006; 12: 1389–97.
93 Gandhi NR, Moll A, Sturm AW et al. Extensively drug-resistanttuberculosis as a cause of death in patients co-infected withtuberculosis in a rural area of South Africa. Lancet 2006; 368:1575–80.
94 Shean K, Badri M, Page-Shipp L et al. South African patientswith extensively drug-resistant tuberculosis have poor out-comes regardless of HIV status. Eur. Respir. J. 2009; 34 (Suppl.53): Abstract N 5068.
95 Torun T, Tahaoglu K, Ozmen I et al. The role of surgery andfluoroquinolones in the treatment of multidrug-reistant tuber-culosis. Int. J. Tuberc. Lung Dis. 2007; 11: 979–85.
96 Chiang C-Y, Yu M-C, Bai K-J et al. Pulmonary resection in thetreatment of patients with pulmonary multidrug-resistanttuberculosis in Taiwan. Int. J. Tuberc. Lung Dis. 2001; 5: 272–7.
97 Somocurcio JG, Sotomayor A, Shin S et al. Surgery for patientswith drug-resistant tuberculosis: report of 121 cases receivingcommunity-based treatment in Lima, Peru. Thorax 2007; 62:416–21.
98 Dravniece G, Cain KP, Holtz TH et al. Adjunctive resectionallung surgery for extensively drug-resistant tuberculosis. Eur.Respir. J. 2009; 34: 180–3.
99 Iseman MD, Madsen L, Goble M et al. Surgical intervention inthe treatment of pulmonary disease caused by drug-resistantMycobacterium tuberculosis. Am. Rev. Respir. Dis. 1990; 141:623–5.
100 Motus IY, Skorniakov SN, Sokolov VA et al. Reviving an old idea:can artificial pneumothorax play a role in the modern manage-ment of tuberculosis? Int. J. Tuberc. Lung Dis. 2006; 10: 571–7.
101 World Health Organization. Guidelines for the programmaticmanagement of drug-resistant tuberculosis. Emergency update2008. World Health Organization Document 2008; WHO/HTM/TB/2008.402:1–247.
102 Kim SJ. Drug-susceptibility testing in tuberculosis: methodsand reliability of results. Eur. Respir. J. 2005; 25: 564–9.
103 Kim SJ, Espinal MA, Abe C et al. Is second-line anti-tuberculosisdrug susceptibility testing reliable? (Correspondence). Int. J.Tuberc. Lung Dis. 2004; 8: 1157–8.
104 Yew WW, Chan CK, Chau CH et al. Outcomes of patients withmultidrug-resistant pulmonary tuberculosis treated withofloxacin/levofloxacin-containing regimens. Chest 2000; 117:744–51.
105 Perez-Guzman C, Vargaz MH, Martinez-Rossier LA et al. Resultsof a 12-month regimen for drug-resistant pulmonary tubercu-losis. Int. J. Tuberc. Lung Dis. 2002; 6: 1102–9.
106 Diacon AH, Pym A, Grobusch M et al. The diarylquinolineTMC207 for multidrug-resistant tuberculosis. N. Engl. J. Med.2009; 360: 2397–405.
107 Wells CD, Cegielski JP, Nelson LJ et al. HIV infection andmultidrug-resistant tuberculosis—the perfect storm. J. Infect.Dis. 2007; 196 (Suppl.): S86–107.
108 World Health Organization. WHO policy on TB infectioncontrol in health-care facilities, congregate settings and house-holds. World Health Organization Document 2009; WHO/HTM/TB/2009.419:1–40.
109 Escombe AR, Oeser CC, Gilman RH et al. Natural ventilation forthe prevention of airborne contagion. PLoS Med. 2007; 4: e68;doi:10.1371/journal.pmed.0040068.
110 Harries AD, Hargreaves NJ, Gausi F et al. Preventing tuberculo-sis among health workers in Malawi. Bull. World Health Organ.2002; 80: 526–31.
111 World Health Organization. Guidelines for the prevention oftuberculosis in health care facilities in resource-limited set-tings. World Health Organization Document 1999; WHO/CDC/TB/99.269:1–51.
112 Chiang C-Y, Enarson DA, Fujiwara PI et al. Strategies ofextensively drug-resistant TB risk management for healthworkers and other care givers. Expert Rev. Respir. Med. 2008; 2:47–54.
113 Coyne KM, Pozniak AL, Lamorde M et al. Pharmacology ofsceond-line antituberculosis drugs and potential for interac-tions with antiretroviral agents. AIDS 2009; 23: 437–46.
114 Middlebrook G, Cohn ML. Some observations on the pathoge-nicity of isoniazid-resistant variants of tubercle bacilli. Science1953; 118: 297–9.
115 Ordway DJ, Sonnenberg MG, Donahue SA et al. Drug-resistantstrains of Mycobacterium tuberculosis exhibit a range of viru-lence for mice. Infect. Immun. 1995; 63: 741–3.
116 van Soolingen D, de Haas PEW, van Doorn HR et al. Mutationsat amino acid position 315 of the katG gene are associated withhigh-level resistance to isoniazid, other drug resistance, andsuccessful transmission of Mycobacterium tuberculosis in TheNetherlands. J. Infect. Dis. 2000; 182: 1788–90.
117 Ano H, Matsumoto T, Suetake T et al. Relationship between theisoniazid-resistant mutation katGS315T and the prevalence ofMDR-/XDR-TB in Osaka, Japan. Int. J. Tuberc. Lung Dis. 2008;12: 1300–5.
118 Gagneux S, Davis Long C, Small PM et al. The competitive costof antibiotic resistance in Mycobacterium tuberculosis. Science2006; 312: 1944–6.
119 Cohen T, Murray M. Modeling epidemics of multidrug-resistantM. tuberculosis of heterogenous fitness. Nat. Med. 2004; 10:1117–21.
120 World Health Organization. Control of XDR-TB—Update onprogress since the Global XDR-TB Task Force Meeting, 9–10October 2006. [Accessed 12 February 2010.] Available athttp://www.who.int/tb/challenges/xdr/globaltaskforce_update_feb07.pdf
121 World Health Organization, Stop TB Partnership. The Stop TBStrategy. World Health Organization Document 2006; WHO/HTM/2006.37:1–20.
122 World Health Organization. The global MDR-TB & XDR-TBresponse plan 2007–2008. World Health Organization Docu-ment 2007; WHO/HTM/STB/2007.387:1–51.
123 The global tuberculosis control and patient care. The Beijing“call for action” on tuberculosis control and patient care:together addressing the global M/XDR-TB epidemic. [Accessed12 February 2010.] Available from URL: http://www.who.int/tb_beijingmeeting/media/en_call_for_action.pdf
124 Matteelli A, Migliori GB, Cirillo D et al. Multidrug-resistant andextensively drug-resistant Mycobacterium tuberculosis: epide-miology and control. Expert Rev. Anti Infect. Ther. 2007; 5 (5):857–71.
125 Cobelens FGJ, Heldal E, Kimerling ME et al. Scaling upprogrammatic managment of drug-resistant tuberculosis: a
MDR-TB overview 431
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432
prioritized research agenda. PLoS Med. 2008; 5 (7): e150;doi:10.1371/journal.pmed.0050150.
126 Chiang C-Y. State of the art series on drug-resistant tuberculo-sis: it’s time to protect fluoroquinolones [Editorial]. Int. J.Tuberc. Lung Dis. 2009; 13: 1319.
127 Palomino JC. Newer diagnostics for tuberculosis and multi-drugresistant tuberculosis. Curr. Opin. Pulm. Med. 2006; 12: 172–8.
128 Barnard M, Albert H, Coetzee G et al. Rapid molecular screen-ing for multidrug-resistant tuberculosis in a high-volumepublic health laboratory in South Africa. Am. J. Respir. Crit. CareMed. 2008; 177: 787–92.
129 Evans J, Stead MC, Nicol MP et al. Rapid genotypic assays toidentify drug-resistant Mycobacterium tuberculosis in SouthAfrica. J. Antimicrob. Chemother. 2009; 63: 11–16.
130 Nolte FS, Metchock B, McGowan JE et al. Direct detection ofMycobacterium tuberculosis in sputum by polymerase chainreaction and DNA hybridization. J. Clin. Microbiol. 1993; 31:1777–82.
131 Lin SYG, Probert W, Lo M et al. Rapid detection of isoniazid andrifampin resistance mutations in Mycobacterium tuberculosiscomplex from cultures or smear-positive sputa by use ofmolecular beacons. J. Clin. Microbiol. 2004; 42: 4204–8.
132 Caviedes L, Lee TS, Gilman RH et al. Rapid, efficient detectionand drug susceptibility testing of Mycobacterium tuberculosis insputum by microscopic observation of broth cultures. J. Clin.Microbiol. 2000; 38: 1203–8.
133 Hamid Salim A, Aung KJM, Hossain MA et al. Early and rapidmicroscopy-based diagnosis of true treatment failure andMDR-TB. Int. J. Tuberc. Lung Dis. 2006; 10: 1248–54.
134 Pai M, Kalantri S, Pascopella L et al. Bacteriophage-basedassays for the rapid detection of rifampicin resistance in Myco-bacterium tuberculosis: a meta-analysis. J. Infect. 2005; 51: 175–87.
135 Martin A, Portaels F, Palomino JC. Colorimetric redox-indicatormethods for the rapid detection of multidrug resistance inMycobacterium tuberculosis: a systematic review and meta-analysis. J. Antimicrob. Chemother. 2007; 59: 175–83.
136 Martin A, Cubillos-Ruiz A, Von Groll A et al. Nitrate reductaseassay for the rapid detection of pyrazinamide resistance inMycobacterium tuberculosis using nicotinamide. J. Antimicrob.Chemother. 2008; 61: 123–7.
137 Hillemann D, Ruesch-Gerdes S, Richter E. Feasibility of theGenoType MTBDRsl assay for fluoroquinolone, amikacin-capreomycin, and ethambutol resistance testing of Mycobacte-rium tuberculosis strains and clinical specimens. J. Clin.Microbiol. 2009; 47: 1767–72.
138 Global Alliance for TB Drug Development. Handbook of anti-tuberculosis agents. TMC-207. Tuberculosis 2008; 88: 168–9.
139 Veziris N, Ibrahim M, Lounis N et al. A once-weekly R207910-containing regimen exceeds activity of the standard dailyregimen in murine tuberculosis. Am. J. Respir. Crit. Care Med.2009; 179: 75–9.
140 Global Alliance for TB Drug Development. Handbook of anti-tuberculosis agents. PA-824. Tuberculosis 2008; 88: 134–6.
141 Singh R, Manjunatha U, Boshoff HIM et al. PA-824 kills nonrep-licating Mycobacterium tuberculosis by intracellular NO release.Science 2008; 322: 1392–5.
142 Tasneen R, Tyagi S, Williams K et al. Enhanced bactericidalactivity of rifampin and/or pyrazinamide when combined withPA-824 in a murine model of tuberculosis. Antimicrob. AgentsChemother. 2008; 52: 3664–8.
143 Nuermberger E, Tyagi S, Tasneen R et al. Powerful and steriliz-ing activity of a regimen containing PA-824, moxifloxacin, andpyrazinamide in a murine model of tuberculosis. Antimicrob.Agents Chemother. 2008; 52: 1522–4.
144 Wilkinson RJ, Lange C. Vitamin D and tuberculosis. New lighton a potent biologic therapy? Am. J. Respir. Crit. Care Med. 2009;179: 740–2.
145 Abbate E, Vescovo M, Natiello M et al. Tuberculosis extensa-mente resistente (XDR-TB) en Argentina: aspectos destacables,epidemiologicos, bacteriologicos, terapeuticos y evolutivos.Rev. Argent. Med. Respir. 2007; 7: 19–25.
C-Y Chiang et al.432
© 2010 The AuthorsJournal compilation © 2010 Asian Pacific Society of Respirology
Respirology (2010) 15, 413–432