Hypertensive Disorder in Pregnancy Untuk Kuliah
159
Hypertensive Disorders in Hypertensive Disorders in Pregnancy Pregnancy
-
Upload
trias-seorang-kapiten -
Category
Documents
-
view
220 -
download
0
Transcript of Hypertensive Disorder in Pregnancy Untuk Kuliah

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 1/159
Hypertensive Disorders inHypertensive Disorders in
PregnancyPregnancy

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 2/159
ScopeScope
Terminology and classificationTerminology and classification
Risk factorsRisk factors
EtiologyEtiology PathophysiologyPathophysiology
Prediction and preventionPrediction and prevention
ManagementManagement

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 3/159
IncidenceIncidence
33..77 % of pregnancies% of pregnancies
1616% of pregnancy% of pregnancy--related deathsrelated deaths
EclampsiaEclampsia 11 inin 20002000 deliveriesdeliveries

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 4/159
ClassificationClassification
by the working group of theby the working group of theNHBPEP (NHBPEP (20002000))
11. Gestational hypertension. Gestational hypertension
22. Chronic hypertension. Chronic hypertension
33. Preeclampsia. Preeclampsia
44. Eclampsia. Eclampsia55. Preeclampsia superimposed on chronic. Preeclampsia superimposed on chronic
hypertension (superimposed preeclampsia)hypertension (superimposed preeclampsia)
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 5/159
I. Gestational hypertensionI. Gestational hypertension
BP >=BP >= 140140//9090 mmHg for first time duringmmHg for first time during
pregnancypregnancy
No proteinuriaNo proteinuria BP returns to normal <BP returns to normal < 1212 wk postpartumwk postpartum
Final diagnosis made only postpartumFinal diagnosis made only postpartum
May have other signs & symptoms of May have other signs & symptoms of preeclampsia , eg. epigastric discomfort or preeclampsia , eg. epigastric discomfort or thrombocytopeniathrombocytopenia
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 6/159
II. Chronic hypertensionII. Chronic hypertension
BP >=BP >= 140140//9090 mmHg before pregnancy or mmHg before pregnancy or
diagnosed beforediagnosed before 2020 wk , not attributablewk , not attributable
to GTD or to GTD or Hypertension first diagnosed after Hypertension first diagnosed after 2020 wkwk
and persistent after and persistent after 1212 wk postpartumwk postpartum

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 7/159
Underlying causes of Underlying causes of Chronic HypertensionChronic Hypertension
Essential familial hypertensionEssential familial hypertension
ObesityObesity
Arterial abnormalities Arterial abnormalities
Endocrine disordersEndocrine disorders
GlomerulonephritisGlomerulonephritis
Renoprival hypertensionRenoprival hypertension
Connective tissue disease
Connective tissue disease
PCKDPCKD
ARF ARF

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 8/159
III. PreeclampsiaIII. Preeclampsia
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 9/159
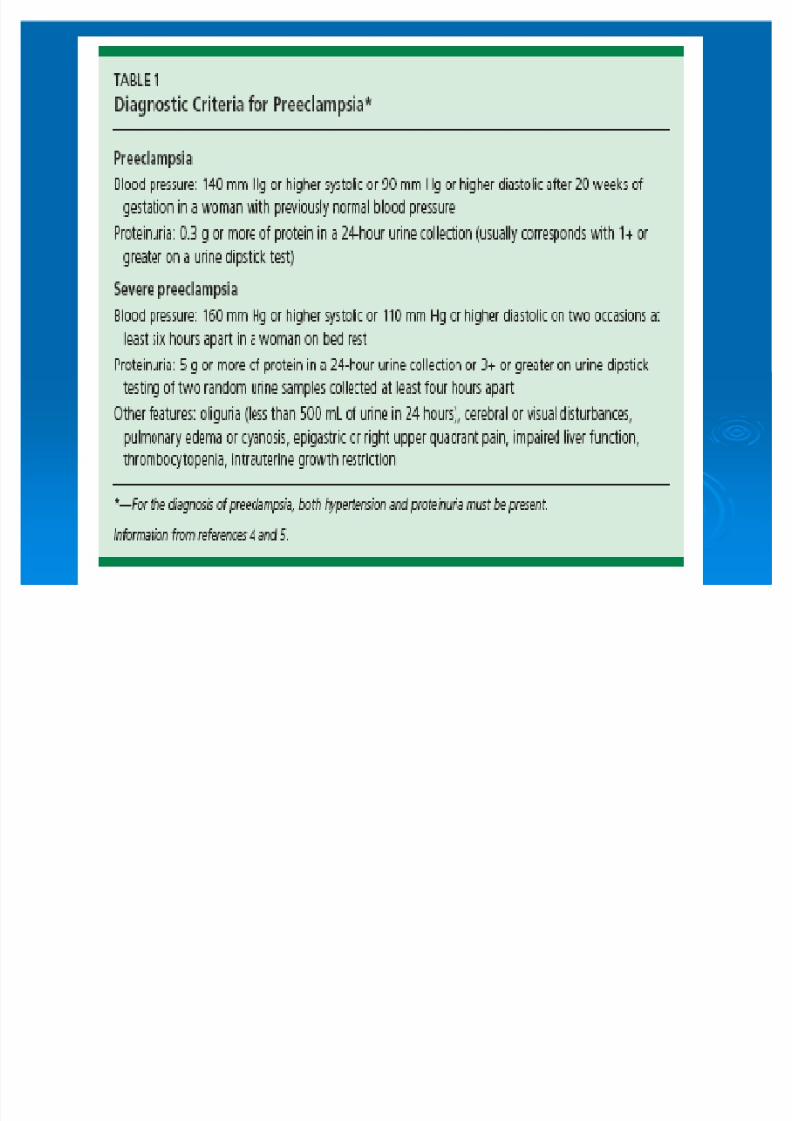
PreeclampsiaPreeclampsia
Mild preeclampsiaMild preeclampsia
BP >=BP >= 140140//9090 mmHg after mmHg after 2020 wk gestationwk gestation
Proteinuria >=Proteinuria >= 300300 mg/mg/2424hr or >=hr or >=11+ dipstick+ dipstick
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 10/159
Severe preeclampsiaSevere preeclampsia
Anyone who meets at least two of the Anyone who meets at least two of thefollowing signs:following signs:
BP >=BP >= 160160//110110 mmHgmmHg
ProteinuriaProteinuria 55 g/g/2424hr or >=hr or >= 22+ dipstick (persistent)+ dipstick (persistent)
Cr >Cr > 11..22 mg/dlmg/dl
Platelets <Platelets < 100100,,000000 /mm/mm33
Microangiopathic hemolysisMicroangiopathic hemolysis
Elevated ALT or ASTElevated ALT or AST
Persistent headache , visual disturbance ,Persistent headache , visual disturbance ,epigastric painepigastric pain
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 11/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 12/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 13/159
IV. EclampsiaIV. Eclampsia
Seizures that cannot be attributed to other Seizures that cannot be attributed to other causes in a woman with preeclampsiacauses in a woman with preeclampsia
Seizures are generalizedSeizures are generalized May appear before , during or after labor May appear before , during or after labor
1010% develop after % develop after 4848 hr postpartumhr postpartum
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 14/159
V. Superimposed preeclampsiaV. Superimposed preeclampsia
New onset proteinuria >=New onset proteinuria >= 300300mg/mg/2424 hr inhr in
hypertensive women but no proteinuriahypertensive women but no proteinuria
beforebefore 2020 wkwk
A sudden increase in proteinuria or BP or A sudden increase in proteinuria or BP or
platelet count <platelet count < 100100,,000000 in women within women withhypertension and proteinuria beforehypertension and proteinuria before 2020 wkwk

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 15/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 16/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 17/159
DiagnosisDiagnosis
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 18/159
Gestational HTGestational HT
Also called transient HT Also called transient HT
Final Dx : after delivery , by exclusionFinal Dx : after delivery , by exclusion
BP : resting BP , Korotkoff phase V isBP : resting BP , Korotkoff phase V is
used to defined diastolic pressureused to defined diastolic pressure
GHT may later develop preeclampsiaGHT may later develop preeclampsia
1010% of eclamptic seizures develop before% of eclamptic seizures develop before
overt proteinuria is identifiedovert proteinuria is identified
BP rise , increase both mother and fetusBP rise , increase both mother and fetusrisksrisks
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 19/159
PreeclampsiaPreeclampsia
Described as ³pregnancyDescribed as ³pregnancy--specificspecific
syndrome of reduced organ perfusionsyndrome of reduced organ perfusion
secondary to vasospasm and endothelialsecondary to vasospasm and endothelial
activation´activation´
Proteinuria & glomerular pathologyProteinuria & glomerular pathology
develop late in the course ,develop late in the course ,
pathophysiologic process begin as earlypathophysiologic process begin as earlyas implantationas implantation

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 20/159
PreeclampsiaPreeclampsia
Diastolic hypertension >=Diastolic hypertension >= 9595 , increase fetal, increase fetaldeath ratedeath rate 33 foldfold
Worsening proteinuria resulted in increasingWorsening proteinuria resulted in increasing
preterm deliverypreterm delivery Epigastric pain from hepatocellular necrosis ,Epigastric pain from hepatocellular necrosis ,
ischemia and edema that stretches Glissonischemia and edema that stretches Glissoncapsulecapsule
Thrombocytopenia from platelet activation &Thrombocytopenia from platelet activation &aggregation , microangiopathic hemolysisaggregation , microangiopathic hemolysisinduced by severe vasospasminduced by severe vasospasm

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 21/159
PreeclampsiaPreeclampsia
Hematuria , Hyperbilirubinemia : indicativeHematuria , Hyperbilirubinemia : indicative
of severe diseaseof severe disease
Cardiac dysfunction , pulm edema ,
Cardiac dysfunction , pulm edema ,obvious IUGR : indicative of severeobvious IUGR : indicative of severe
diseasedisease
Severity of preeclampsia assess by freq &Severity of preeclampsia assess by freq &intensity of abnormalitiesintensity of abnormalities

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 22/159
Risk factorsRisk factors for preeclampsiafor preeclampsia
NulliparousNulliparous
Advanced maternal age Advanced maternal age
Race and ethnicity (genetic predispositionRace and ethnicity (genetic predisposition& envoronmental factor)& envoronmental factor)
Multifetal gestationMultifetal gestation
ObesityObesity BMI >BMI > 3535 kg/mkg/m22

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 23/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 24/159
Superimposed preeclampsiaSuperimposed preeclampsia
11. Hypertension (>=. Hypertension (>=140140//9090) is documented) is documented
antecedent to pregnancyantecedent to pregnancy
22. Hypertension is detected before. Hypertension is detected before 2020 wk ,wk ,unless there is GTDunless there is GTD
33. Hypertension persists long after delivery. Hypertension persists long after delivery
Additional previous Hx or family Hx of HT Additional previous Hx or family Hx of HT
End organ damage : LVH , retinal changeEnd organ damage : LVH , retinal change
Risk abruption ,IU
GR , preterm & deathRisk abruption ,IU
GR , preterm & death
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 25/159
Etiology?Etiology?

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 26/159
EtiologyEtiology
Theory account for the observationTheory account for the observation
hypertensive disorder more likely to develophypertensive disorder more likely to develop
in :in :
11. exposed to chorionic villi for first time. exposed to chorionic villi for first time
22. exposed superabundance of chorionic villi. exposed superabundance of chorionic villi
(Twin ,mole)(Twin ,mole)
33. Preexisting vascular disease. Preexisting vascular disease44. Genetic predisposition. Genetic predisposition

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 27/159
EtiologyEtiology
11. Abnormal trophoblastic invasion of uterine. Abnormal trophoblastic invasion of uterine
vesselsvessels
22. Immunological intolerance between. Immunological intolerance between
maternal and fetoplacental tissuesmaternal and fetoplacental tissues
33. Maternal maladaptation to cardiovascular . Maternal maladaptation to cardiovascular
or inflammatory changes of normalor inflammatory changes of normal
pregnancy (vasculopathy)pregnancy (vasculopathy)44. Dietary deficiencies. Dietary deficiencies
55. Genetic influences. Genetic influences

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 28/159
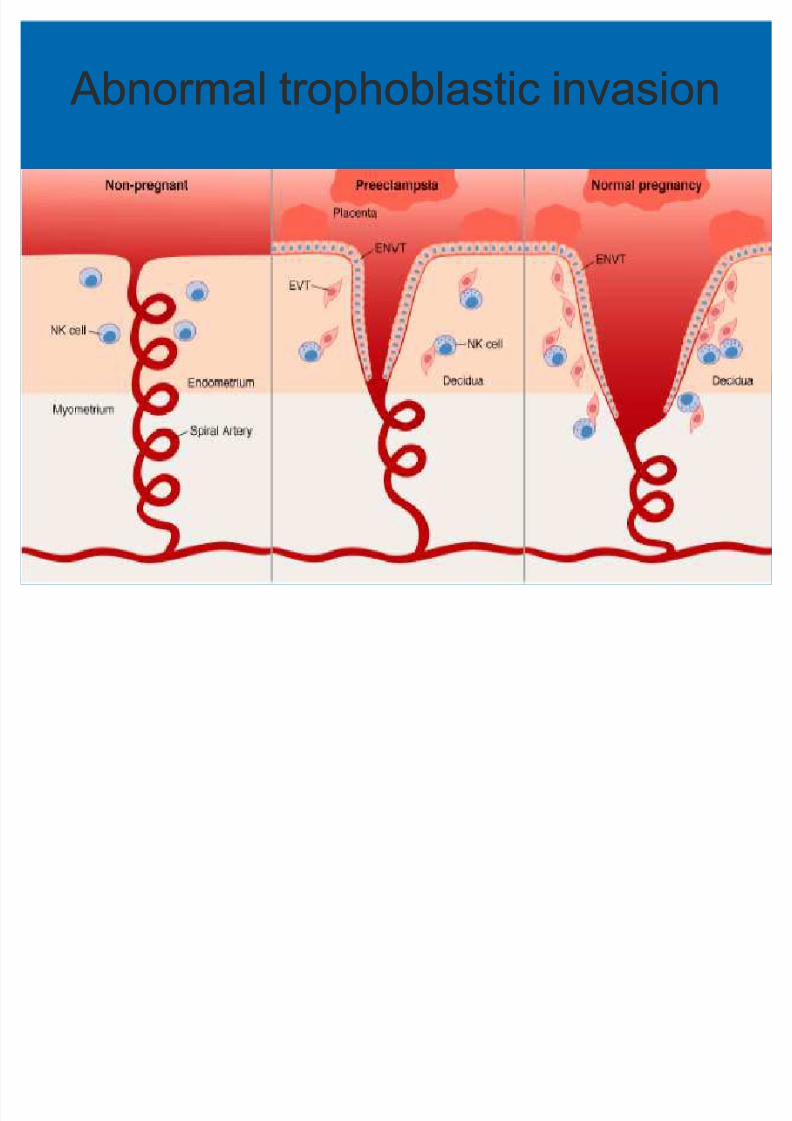
11. Abnormal trophoblastic invasion. Abnormal trophoblastic invasion
Normal implantation , uterine spiralNormal implantation , uterine spiral
arteries undergo extensive remodeling asarteries undergo extensive remodeling as
they are invaded by endovascular they are invaded by endovascular
trophoblaststrophoblasts
Incomplete invasion (decidual vessels ,Incomplete invasion (decidual vessels ,not myometrial vessels) : preeclampsianot myometrial vessels) : preeclampsia
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 29/159
Abnormal trophoblastic invasion Abnormal trophoblastic invasion

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 30/159
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 31/159
Atherosis : pathology Atherosis : pathology
Endothelial damageEndothelial damage
Insudation of plasma constituents into vesselInsudation of plasma constituents into vessel
wallswalls
Proliferation of myointimal cellsProliferation of myointimal cells
Medial necrosisMedial necrosis
Lipid accumulation in myointimal cells &Lipid accumulation in myointimal cells &
macrophagesmacrophages Aneurysmal dilatation Aneurysmal dilatation
Obstruction of spiral arterioleObstruction of spiral arteriole

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 32/159
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 33/159
22. Immunological factors. Immunological factors
Acute graft rejection Acute graft rejection
Impaired formation of blocking antibodiesImpaired formation of blocking antibodies
to placental antigenic sitesto placental antigenic sites Lack of effective immunization in firstLack of effective immunization in first
pregnanciespregnancies
Lower proportion of ThLower proportion of Th11 , Th, Th22 dominancedominance

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 34/159
22. Immunologic factors. Immunologic factors
Increased risk for first conception , newIncreased risk for first conception , newpartner , conception very shortly after partner , conception very shortly after beginning sexual relation (beginning sexual relation (55% if >% if > 1212mo)mo)
Any kind of previous pregnancy Any kind of previous pregnancy(completed , spontaneous miscarriage or (completed , spontaneous miscarriage or elective abortion) protective againstelective abortion) protective againstpreeclampsiapreeclampsia
Tolerate semiTolerate semi--allogenic graft throughallogenic graft throughfather¶s alloantigenfather¶s alloantigen
J. of Reprod Immunology J. of Reprod Immunology 20032003 ( (5959) : ) : 9393--100 100
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 35/159
22. Immunological factors. Immunological factors
ILIL1010 regulate s arterial pressure in earlyregulate s arterial pressure in earlyprimate pregnancyprimate pregnancy
ILIL--1010 & TNF& TNF : vasodilation of early: vasodilation of early
pregnancypregnancy
Anti Anti--human ILhuman IL--1010 MAb caused significantMAb caused significantincrease in MAPincrease in MAP
TNFTNF-- alone or combine with ILalone or combine with IL--1010 notnotalter MAPalter MAP
C ytokineC ytokine 2929 ( (2005 2005) ) 176 176--185 185

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 36/159
22. Immunological factors. Immunological factors
Serum from preeclamptic pt contains IgGSerum from preeclamptic pt contains IgGautoantibodyautoantibody
Reacts with ATReacts with AT11 receptor receptor
AT AT11--AA induce signaling in vascular cells AA induce signaling in vascular cellsand trophoblastsand trophoblasts
Including APIncluding AP--11 and NFand NF--kB activationkB activation
Results in tissue factor production ,Results in tissue factor production ,reactive oxygen species (ROS)generationreactive oxygen species (ROS)generation
Autoimmunity Reviews Autoimmunity Reviews 44 ((20052005) :) : 6161--6565
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 37/159
33. Vasculopathy & inflammatory. Vasculopathy & inflammatory
Placental factors released by ischemicPlacental factors released by ischemicchangeschanges
Decidua activated , release noxiousDecidua activated , release noxious
agents provoke endothelial cell injuryagents provoke endothelial cell injury
Endothelial cell dysfunctionEndothelial cell dysfunction
Cytokines : TNFCytokines : TNF , IL, IL

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 38/159
33. Vasculopathy & inflammatory. Vasculopathy & inflammatory
Oxidative stress (ROS , free radical) self Oxidative stress (ROS , free radical) self--
propagating lipid peroxides formationpropagating lipid peroxides formation
Generate highly toxic radicals injureGenerate highly toxic radicals injureendothelial cellsendothelial cells
Modify NOModify NO22 productionproduction
Interfere PG balanceInterfere PG balance
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 39/159
33. Vasculopathy & inflammatory. Vasculopathy & inflammatory
Oxidative stress : produce lipidOxidative stress : produce lipid--ladenladen
macrophage foam cellsmacrophage foam cells
Activation of microvascular coagulation : Activation of microvascular coagulation :ThrombocytopeniaThrombocytopenia
Increased capillary permeability :Increased capillary permeability :proteinuria and edemaproteinuria and edema
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 40/159
44. Nutritional factors. Nutritional factors
Dietary taboos : meat , protein , purines ,Dietary taboos : meat , protein , purines ,
fat , dairy products , saltfat , dairy products , salt
Supplement of Zn ,C
a , Mg preventSupplement of Zn ,C
a , Mg preventpreeclampsia ?preeclampsia ?
Fruits & vegetables : antioxidantFruits & vegetables : antioxidant
Ascorbic acid intake < Ascorbic acid intake < 8585 mg/d ,mg/d ,predispose preeclmapsiapredispose preeclmapsia 22 foldfold
Obesity increase risk preeclampsiaObesity increase risk preeclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 41/159
55. Genetic factors. Genetic factors
Hereditary hypertension, preeclampsia ,Hereditary hypertension, preeclampsia ,
eclampsiaeclampsia
Polygenic inheritancePolygenic inheritance Asso with HLA Asso with HLA--DRDR44
Maternal Ab against fetal anti HLAMaternal Ab against fetal anti HLA--DR IgDR Ig
Heterozygous for angiotensinogen geneHeterozygous for angiotensinogen genevariant Tvariant T235235
Polymorphisms of genes for TNF , ILPolymorphisms of genes for TNF , IL 11 ,,
LymphotoxinLymphotoxin
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 42/159
Genetics of preeclampsiaGenetics of preeclampsia
Familial predispositionFamilial predisposition
AGT(encode angiotensinogen) & NOS AGT(encode angiotensinogen) & NOS 33
(encode nitric oxide synthestase) genes(encode nitric oxide synthestase) genesmutationmutation
C lin Genet C lin Genet 20032003 :: 6464 :: 96 96--103103
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 43/159
Is preeclampsia an infectiousIs preeclampsia an infectiousdisease?disease?
Analyze IgG Ab against HSV Analyze IgG Ab against HSV--22 , CMV ,, CMV ,
EBV , Toxoplasma gondii at first ANCEBV , Toxoplasma gondii at first ANC
Seronegative for HSV
Seronegative for HSV
--22,C
MV
, EBV
,C
MV
, EBV
increased risk preeclampsia (ORincreased risk preeclampsia (OR 11..77 ,,11..66,,
33..55))
Seronegative for Toxo not associated withSeronegative for Toxo not associated with
increase risk preeclampsia (ORincrease risk preeclampsia (OR 11..00))
Ac ta Obstet Gynec ol S c and Ac ta Obstet Gynec ol S c and 20012001 :: 80 80 :: 1036 1036--8 8
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 44/159
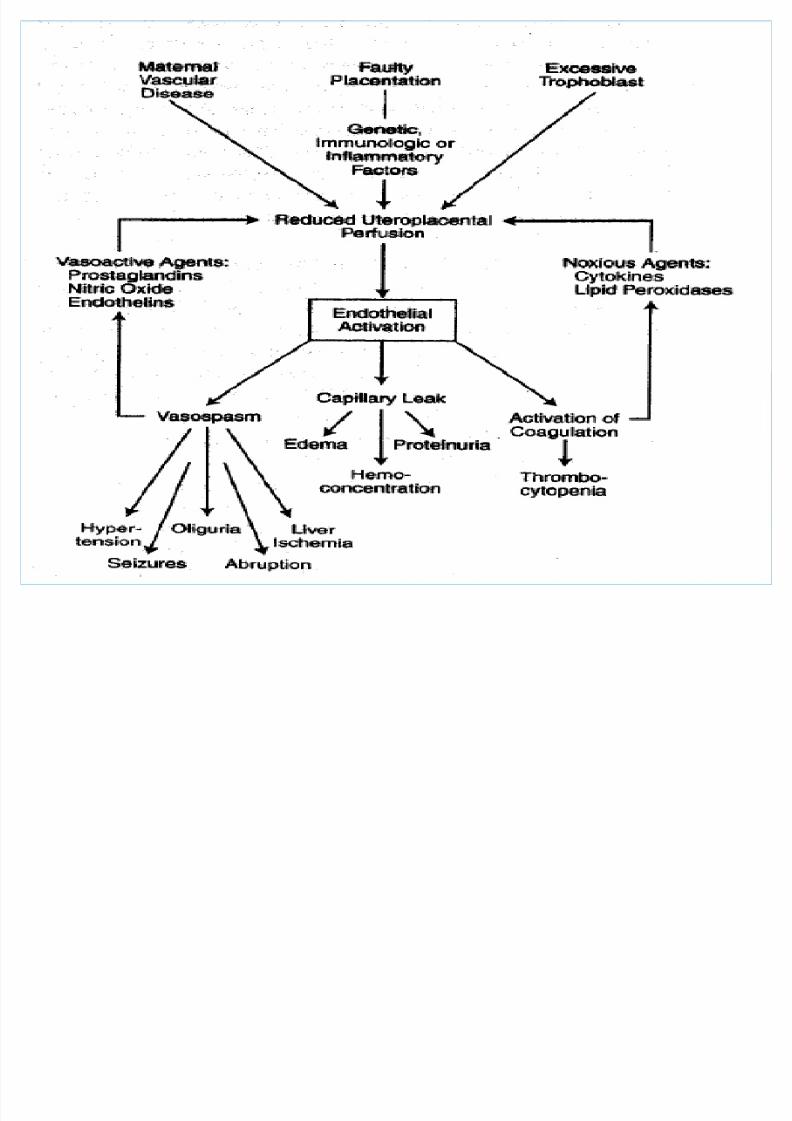
PathogenesisPathogenesis
VasospasmVasospasm
Endothelial cell activationEndothelial cell activation
Increased pressor resonsesIncreased pressor resonses
ProstaglandinsProstaglandins
Nitric oxideNitric oxide
EndothelinsEndothelins
Angiogenic factors (VEGF , PIGF) Angiogenic factors (VEGF , PIGF)

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 45/159
PathogenesisPathogenesis
Increased vascular reactivity toIncreased vascular reactivity to
vasopressor vasopressor
Decrease PGI
Decrease PGI22 production by endotheliumproduction by endothelium
Increase TxAIncrease TxA22 secretion by plateletsecretion by platelet
Increased NOIncreased NO22 synth by endotheliumsynth by endothelium
Decrease NODecrease NO22 syntheasesynthease
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 46/159
PathophysiologyPathophysiology
Endothelial damageEndothelial damage
Interstitial leakageInterstitial leakage
Platelet & fibrinogen depositPlatelet & fibrinogen deposit Increase subendothelial a. resistanceIncrease subendothelial a. resistance
Decreased blood flowDecreased blood flow
Ischemia necrosis , hemorrhageIschemia necrosis , hemorrhage Multiorgan involvementMultiorgan involvement

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 47/159
ComplicationsComplications

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 48/159
Cardiovascular systemCardiovascular system
Increase after loadIncrease after load
Preload diminishPreload diminish
Endothelial activation with extravasationEndothelial activation with extravasation Decreased cardiac outputDecreased cardiac output
Hemoconcentration from generalizedHemoconcentration from generalized
vasoconstriction and endothelialvasoconstriction and endothelialdysfynctiondysfynction
Decreased blood volumeDecreased blood volume
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 49/159
Blood and coagulationBlood and coagulation
Thrombocytopenia from platelet activation,Thrombocytopenia from platelet activation,
aggregation & consumptionaggregation & consumption
Increased platelets activating factor &Increased platelets activating factor &thrombopoietinthrombopoietin
Clotting factors decreaseClotting factors decrease
Erythrocytes rapid hemolysis (increaseErythrocytes rapid hemolysis (increaseLDH , schizocyte , MAHA)LDH , schizocyte , MAHA)

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 50/159
Volume homeostasisVolume homeostasis
Decrease plasma levels of renin , AT II ,Decrease plasma levels of renin , AT II ,
aldosteronealdosterone
DOC
increaseDOC
increase Vasopressin normal despite decreasedVasopressin normal despite decreased
plasma osmolalityplasma osmolality
ANP increased ANP increased
Extracellular fluid : edema : endothelialExtracellular fluid : edema : endothelialinjury , reduced oncotic pressureinjury , reduced oncotic pressure

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 51/159
KidneyKidney
RPF & GFR reducedRPF & GFR reduced
Uric acid elevatedUric acid elevated
Creatinine clearance reduced , oliguriaCreatinine clearance reduced , oliguria Diminished urinary Ca due to increasedDiminished urinary Ca due to increased
tubular reabsorptiontubular reabsorption
Urine sodium elevated
Urine sodium elevated
Urine osmolality , U:P Cr , FE Na :Urine osmolality , U:P Cr , FE Na :prerenal mechanismprerenal mechanism
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 52/159
KidneyKidney
Proteinuria : glomerulopathy : increasedProteinuria : glomerulopathy : increased
permeability : albumin , Hb , globulin ,permeability : albumin , Hb , globulin ,transferinstransferins
Anatomical changes : glomeruli enlarge , Anatomical changes : glomeruli enlarge ,
capillary loops dilated & contracted ,capillary loops dilated & contracted ,
endothelial cells swollen fibrils depositendothelial cells swollen fibrils deposit
(glomerular capillary endotheliosis)(glomerular capillary endotheliosis)
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 53/159
KidneyKidney
Renal tubular lesions : degenerativeRenal tubular lesions : degenerative
change , accumulation with castschange , accumulation with casts
ARF from ATN ARF from ATN Oliguria , azotemia induced byOliguria , azotemia induced by
hypovolemiahypovolemia
Preeclampsia with ARF occur in HELLPPreeclampsia with ARF occur in HELLP
syndrome ½ , placental abruptionsyndrome ½ , placental abruption 11//33
Rarely , irreversible renal cortical necrosisRarely , irreversible renal cortical necrosis

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 54/159
Liver Liver
Periportal hemorrhage in liver peripheryPeriportal hemorrhage in liver periphery
Elevated transaminaseElevated transaminase
HELLP syndromeHELLP syndrome Bleeding cause hepatic rupture(mortalityBleeding cause hepatic rupture(mortality
3030%) , subcapsular hematoma%) , subcapsular hematoma
Conservative treatment
Conservative treatment
Recombinant factor VIIaRecombinant factor VIIa
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 55/159
HELLP syndromeHELLP syndrome
No strict definitionNo strict definition
IncidenceIncidence 2020% of severe preeclampsia or % of severe preeclampsia or
eclampsiaeclampsia
Factors contributing to death : includeFactors contributing to death : include
stroke , coagulopathy , ARDS , ARF ,stroke , coagulopathy , ARDS , ARF ,
sepsissepsis
Insufficient evidence : adjunctive steroidInsufficient evidence : adjunctive steroid
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 56/159
BrainBrain
Headache & visual symptoms associatedHeadache & visual symptoms associated
with eclampsiawith eclampsia
Two cerebral pathology relatedTwo cerebral pathology related
11. gross hemorrhage due to ruptured a.. gross hemorrhage due to ruptured a.
caused by severe HTcaused by severe HT
22. more widespread , edema hyperemia ,. more widespread , edema hyperemia ,ischemia , thrombosis & hemorrhageischemia , thrombosis & hemorrhage caused by preeclampsiacaused by preeclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 57/159
NeuroimagingNeuroimaging
CT : hypodense area in cortex ,CT : hypodense area in cortex ,
correspond to petechial hemorrhage andcorrespond to petechial hemorrhage and
infarctionsinfarctions
Remarkable changes in area of Remarkable changes in area of distribution of posterior cerebral a.distribution of posterior cerebral a.
MRI : hyperperfusion due to vasogenicMRI : hyperperfusion due to vasogenic
edemaedema
Eclampsia :Eclampsia : 2525% were area of infarction% were area of infarction
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 58/159
Cerebral blood flowCerebral blood flow
Transcranial doppler ultrasonographyTranscranial doppler ultrasonography
Preeclampsia : increase perfusionPreeclampsia : increase perfusionpressure , counter by increasepressure , counter by increase
cerebrovascular resistance(net no change)cerebrovascular resistance(net no change) Eclampsia : loss of autoregulation ,Eclampsia : loss of autoregulation ,
hyperperfusion similar to hypertensivehyperperfusion similar to hypertensive
encephalopathyencephalopathy Eclampsia caused by transient loss of Eclampsia caused by transient loss of
cerebrovascular autoregulationcerebrovascular autoregulation

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 59/159
BlindnessBlindness
Visual disturbance common in SPEVisual disturbance common in SPE
It follows eclampsia in >It follows eclampsia in >1010%%
Develop uptoDevelop upto 11 wk or more after deliverywk or more after delivery
Called ³Amaurosis´Called ³Amaurosis´
Extensive ocipital lobe vasogenic edemaExtensive ocipital lobe vasogenic edema
Resolve completely in all caseResolve completely in all case
Rare cerebral infarct or retinal a. ischemiaRare cerebral infarct or retinal a. ischemia
Retinal detach : resolve withinRetinal detach : resolve within 11 wkwk

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 60/159
Cerebral edemaCerebral edema
Widespread vasogenic edemaWidespread vasogenic edema
S&S : Lethargy , confusion , blurred vision,S&S : Lethargy , confusion , blurred vision,
comacoma
Waxed & wanedWaxed & waned
Rx : Manitol , DexamethasoneRx : Manitol , Dexamethasone

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 61/159
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 62/159
Uteroplacental perfusionUteroplacental perfusion
Compromised uteroplacental perfusionCompromised uteroplacental perfusion
from vasospasmfrom vasospasm
Mean diameter of myometrial spiralMean diameter of myometrial spiral
arterioles decreasearterioles decrease
Doppler flow velocity of uterine arteryDoppler flow velocity of uterine artery
RingRing--like : higher in peripheral than inlike : higher in peripheral than in
central vesselscentral vessels
Preeclampsia was higher resistancePreeclampsia was higher resistance
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 63/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 64/159
Can we predict preeclampsia?
Can we predict preeclampsia?

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 65/159
PredictionPrediction
Biological , biochemical & biophysicalBiological , biochemical & biophysicalmarkersmarkers
To identify markers of To identify markers of
faulty placentationfaulty placentation
reduced placental perfusion ,reduced placental perfusion ,
endothelial cell activation & dysfunction ,endothelial cell activation & dysfunction ,
activation of coagulationactivation of coagulation
HOW?
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 66/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 67/159
Uric acidUric acid
Decreased renal urate excretion inDecreased renal urate excretion in
preeclampsiapreeclampsia
Serum uric acid exceedingSerum uric acid exceeding 55..99 atat 2424 wkwk
(PPV (PPV 3333%)%)
Not useful in differentiating GHT fromNot useful in differentiating GHT frompreeclampsiapreeclampsia
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 68/159
FibronectinFibronectin
Endothelial cell activationEndothelial cell activation
Low sensitivityLow sensitivity 6969%%
Positive predictive vaulesPositive predictive vaules 1212%% Higher levels byHigher levels by 1212 wks (PPV wks (PPV 2929% NPV % NPV
9898%)%)
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 69/159
Coagulation activationCoagulation activation
Thrombocytopenia and plateletThrombocytopenia and platelet
dysfunctiondysfunction
Increased destruction cause plateletIncreased destruction cause platelet
volumes increase (younger platelet)volumes increase (younger platelet)
Preeclampsia : PAIPreeclampsia : PAI--11 increase increasedincrease increased
relative to PAIrelative to PAI--22 because of endothelialbecause of endothelial
cell dysfunctioncell dysfunction

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 70/159
CytokinesCytokines
Released by vascular endothelium &Released by vascular endothelium &
leukocytes , and macrophages &leukocytes , and macrophages &
lymphocytes at decidualymphocytes at decidua
Interleukin , TNFInterleukin , TNF , CRP : inflammatory, CRP : inflammatory
responseresponse
Possibly predictive preeclampsiaPossibly predictive preeclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 71/159
Fetal DNAFetal DNA
Fetal DNA in maternal serumFetal DNA in maternal serum
At the time endothelial activation , fetal At the time endothelial activation , fetal
cells released into maternal circulationcells released into maternal circulation
Elevations after Elevations after 2828 wk indicate impendingwk indicate impendingdiseasedisease

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 72/159
Placental peptidesPlacental peptides
CorticotropinCorticotropin--releasing hormone , hCG ,releasing hormone , hCG , Activin A , inhibin A Activin A , inhibin A
Variably elevated depend on duration &Variably elevated depend on duration &
severity of preeclampsiaseverity of preeclampsia Overlap with normal pregnancyOverlap with normal pregnancy
VEGF and PIGF : regulate placentalVEGF and PIGF : regulate placental
development , both antagonized by sFltdevelopment , both antagonized by sFlt11 Excessive sFltExcessive sFlt11 , PIGF in, PIGF in 11stst trimester :trimester :
high riskhigh risk
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 73/159
hCGhCG
hCG in second trimester , >hCG in second trimester , > 22..00 MoMMoM
SensitivitySensitivity 2323..77%%
SpecificitySpecificity 8989..44%% Relative riskRelative risk 22..5454
Positive predictive valuePositive predictive value 99..55%%
Negative predictive valueNegative predictive value 9696..66%%
E ndoc rine Reviews , A pril E ndoc rine Reviews , A pril2002 2002 :: 2323 :: 230 230--257 257

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 74/159
Inhibin A and Activin AInhibin A and Activin A
Activin A : control trophoblast Activin A : control trophoblastdifferentiation in first trimester : high indifferentiation in first trimester : high inpreeclampsiapreeclampsia
Inhibin AInhibin A 1515--1919 wk , >wk , > 22..00 MoMMoM SensitivitySensitivity 4848..66%%
SpecificitySpecificity 2323..66%%
Activin A more sensitive than inhibin A at Activin A more sensitive than inhibin A at2121--2525 wkwk
E ndoc rine Reviews , A pril E ndoc rine Reviews , A pril2002 2002 :: 2323 :: 230 230--257 257
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 75/159
VasoactiveVasoactive
Decrease active renin , AT I & I ,Decrease active renin , AT I & I ,
aldosterone , activity of ACE inaldosterone , activity of ACE in 33rdrd trimtrim
AT II infused test : positive at less than AT II infused test : positive at less than 1010
ng/kgng/kg
Ratio inactive urinary kallikrein /urineRatio inactive urinary kallikrein /urine
creatinine atcreatinine at 1616--2020 wk : lower wk : lower 55 fold in whofold in who
developed preeclampsiadeveloped preeclampsia E ndoc rine Reviews , A pril E ndoc rine Reviews , A pril2002 2002 :: 2323 :: 230 230--257 257
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 76/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 77/159
Can we prevent preeclampsia?Can we prevent preeclampsia?
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 78/159
PreventionPrevention
Salt restriction : ineffectiveSalt restriction : ineffective
Inappropriate diuretic therapyInappropriate diuretic therapy
Low dietary calcium increased risk GHTLow dietary calcium increased risk GHT
Fish oil capsules : modify abnormal PGFish oil capsules : modify abnormal PGbalance : ineffectivebalance : ineffective
Low dose aspirin (Low dose aspirin (6060mg) : ineffectivemg) : ineffective
Antioxidants : vitamin C & E : reduced Antioxidants : vitamin C & E : reducedendothelial cell activation , reduction inendothelial cell activation , reduction inpreeclampsiapreeclampsia
L ilk i t k & i k fL ilk i t k & i k f
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 79/159
Low milk intake & risk of Low milk intake & risk of preeclampsiapreeclampsia
Case control studyCase control study
Mean milk intake per day in preeclampsiaMean milk intake per day in preeclampsia
< control group< control group
Drinking more thanDrinking more than 55 glasses per day hasglasses per day has
evident protective effect of developingevident protective effect of developing
preeclampsia (odd ratiopreeclampsia (odd ratio 00..11))
E ur J of Obs & Gyn & Repro BioE ur J of Obs & Gyn & Repro Bio 105 105 ( (2002 2002) ) 1111--1414
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 80/159
Calcium supplementCalcium supplement
Reduction in high BP (RRReduction in high BP (RR 00..5858))
The effect greater among women at highThe effect greater among women at highrisk of developing HT and those with lowrisk of developing HT and those with low
baseline dietary calcium (RRbaseline dietary calcium (RR 00..4747 && 00..3838)) Reduction risk of preeclampsia (RRReduction risk of preeclampsia (RR 00..3535))
The effect greatest in women at high riskThe effect greatest in women at high risk
of developing HT and those with lowof developing HT and those with lowbaseline dietary calcium (RRbaseline dietary calcium (RR 00..2222 && 00..2929)) The C oc hrane database of systemati c reviewsThe C oc hrane database of systemati c reviews 2002 2002
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 81/159
Aspirin Aspirin
Significant benefit in reducingSignificant benefit in reducing
preeclampsia (odds ratiopreeclampsia (odds ratio 00..5555))
Baseline risk of preeclampsia in womenBaseline risk of preeclampsia in women
with abnormal uterine a doppler waswith abnormal uterine a doppler was 1616%%
Obs & Gyn Nov Obs & Gyn Nov 20012001 :: 92 92 :: 861861--6 6

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 82/159
Aspirin in historical risk Aspirin in historical risk
Hx risk : Hx preclampsia ,CHT , DM , renalHx risk : Hx preclampsia ,CHT , DM , renaldisease , FH of preeclampsiadisease , FH of preeclampsia
Significant benefit in reducing perinatalSignificant benefit in reducing perinatal
death (ORdeath (OR 00..7979) & preeclampsia (OR) & preeclampsia (OR00..8686))
Reduction in rates of spontaneous pretermReduction in rates of spontaneous pretermbirth (ORbirth (OR 00..8686))
Increase of mean birth weightIncrease of mean birth weight
No increase risk of placental abruptionNo increase risk of placental abruption Obs & Gyn ,JunObs & Gyn ,Jun 20032003 :: 101101 :: 13191319--32 32

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 83/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 84/159
Antiplatelet prevent preeclampsia Antiplatelet prevent preeclampsia
For high risk (previous SPE , DM , CHT ,For high risk (previous SPE , DM , CHT ,renal dis , autoimmune disease) :renal dis , autoimmune disease) : 2727%%reduction in risk of preeclampsiareduction in risk of preeclampsia
For mod risk (first preg , mild rise BP noFor mod risk (first preg , mild rise BP noproteinuria , abnormal uterine a doppler,proteinuria , abnormal uterine a doppler,positive roll over test , multiple preg , FHpositive roll over test , multiple preg , FHSPE , teenage) :SPE , teenage) : 1515% reduction% reduction
Started before implantation & trophoblastStarted before implantation & trophoblastinvasion ,crucial time beforeinvasion ,crucial time before 1616 or or 1212 wkwk
The C oc hrane Database of Systemati c ReviewsThe C oc hrane Database of Systemati c Reviews 20032003
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 85/159
Vitamin E supplementVitamin E supplement
Either at high risk of preeclampsia or withEither at high risk of preeclampsia or withestablished preeclampsiaestablished preeclampsia
No difference in risk of stillbirth , neonatalNo difference in risk of stillbirth , neonatal
death , perinatal death , preterm birth ,death , perinatal death , preterm birth ,IUGR & birthweightIUGR & birthweight
Decrease risk of developing clinicalDecrease risk of developing clinicalpreeclampsia (RRpreeclampsia (RR 00..4444) using fixed) using fixed--effecteffectmodels (no diff using randommodels (no diff using random--effectseffectsmodels)models)
The C oc hrane Database of systemati c ReviewsThe C oc hrane Database of systemati c Reviews 2005 2005

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 86/159
Vitamin E supplementVitamin E supplement
Dosage : above recommended dietaryDosage : above recommended dietaryintake of intake of 77 mg of alphamg of alpha--TE (dailyTE (daily 400400 iu or iu or 800800 iu)iu)
GA : no difference in risk of stillbirth ,GA : no difference in risk of stillbirth ,preterm birth ,IUGR & preeclampsiapreterm birth ,IUGR & preeclampsiabetween before tobetween before to 2020 wk and both beforewk and both before& after & after 2020 wkwk
No difference sideNo difference side--effect (acne , transienteffect (acne , transientweakness, skin rash)weakness, skin rash)
The C oc hrane Database of systemati c ReviewsThe C oc hrane Database of systemati c Reviews 2005 2005
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 87/159
Vitamin C supplementVitamin C supplement
No difference in risk of stillbirth , perinatalNo difference in risk of stillbirth , perinataldeath, IUGR , birthweightdeath, IUGR , birthweight
Increase risk of preterm birth (RRIncrease risk of preterm birth (RR 11..3838))
Heterogeneity : Decreased preeclampsiaHeterogeneity : Decreased preeclampsia(RR(RR 00..4747))
Dosage : above RDI of Dosage : above RDI of 6060 mg (mg (500500 ,,
10001000mg)mg) GA : no difference before & after GA : no difference before & after 2020 wkwk
The C oc hrane Database of Systemati c ReviewsThe C oc hrane Database of Systemati c Reviews 2005 2005

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 88/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 89/159
Dietary saltDietary salt
Reduce dietary salt intake vs continue aReduce dietary salt intake vs continue a
normal dietnormal diet
No effect in preeclampsia (RRNo effect in preeclampsia (RR 11..1111))
Insuffient evidence for reliable conclusionsInsuffient evidence for reliable conclusionsabout effect of advice to reduce diet saltabout effect of advice to reduce diet salt
The C oc hrane Database of Systemati c reviewsThe C oc hrane Database of Systemati c reviews 2005 2005
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 90/159
Folic acid supplementFolic acid supplement
Reduction in risk of preeclampsia inReduction in risk of preeclampsia in
supplemented groups (supplemented groups ( 200200 ug &ug & 55 mg/d)mg/d)
In low serum folate pregnancy & womenIn low serum folate pregnancy & women
with Hx preeclampsiawith Hx preeclampsia
Odd ratios of preeclampsia no diff Odd ratios of preeclampsia no diff
between receive folicbetween receive folic 200200 ug VSug VS 55 mg/dmg/d
((00..4646 VSVS 00..5959))
P ed & P erinatal E pid P ed & P erinatal E pid 2005 2005:: 1919 :: 112 112--124124
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 91/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 92/159
ManagementManagement

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 93/159
ManagementManagement
Early prenatal detectionEarly prenatal detection
Antepartum hospital management Antepartum hospital management
Termination of pregnancyTermination of pregnancy Antihypertensive drug therapy Antihypertensive drug therapy
Delayed delivery with SPEDelayed delivery with SPE

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 94/159
11. Early prenatal detection. Early prenatal detection
Early preeclampsia without overt HT :Early preeclampsia without overt HT :
increased surveillanceincreased surveillance
NewNew--onset diastolic BPonset diastolic BP 8181--8989 mmHg or mmHg or
sudden abnormal wt gain (>sudden abnormal wt gain (> 22 lb/wk duringlb/wk during
33rdrd trimester)trimester)
OPD surveillance unless overt HT ,OPD surveillance unless overt HT ,
proteinuria , visual disturbances or proteinuria , visual disturbances or epigastric discomfortepigastric discomfort

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 95/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 96/159
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 97/159
22 A t t tA t t t
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 98/159
22. Antepartum management. Antepartum management
Admit if new onset HT , esp persistent or Admit if new onset HT , esp persistent or
worsening HT or develop proteinuriaworsening HT or develop proteinuria
Detail examine : headache , visualDetail examine : headache , visual
disturbances , epigastric pain , weight gaindisturbances , epigastric pain , weight gain
Proteinuria at least everyProteinuria at least every 22 dd
BP qBP q 44 hr , except midnight & morninghr , except midnight & morning
Creatinine , hematocrit , platelets , liver Creatinine , hematocrit , platelets , liver
enzymes.enzymes.
A t t tA t t t

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 99/159
Antepartum management Antepartum management
Evaluate fetal size , AFEvaluate fetal size , AF
Reduced physical activityReduced physical activity
Sedative not prescribedSedative not prescribed
Ample, not excess, protein & calories diet Ample, not excess, protein & calories diet
Sodium & fluid intake not limit or forcedSodium & fluid intake not limit or forced
Further Mg depend on : severity ,Further Mg depend on : severity ,Gestational Age , condition of cervixGestational Age , condition of cervix

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 100/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 101/159
PreeclampsiaPreeclampsia--Initial EvaluationInitial EvaluationPreeclampsiaPreeclampsia--Initial EvaluationInitial Evaluation
Serial blood pressure measurementsSerial blood pressure measurements
Urine protein excretionUrine protein excretion
Fetal monitoringFetal monitoring
Tests to rule out HELLP and other Tests to rule out HELLP and other
complications: Hematocrit, platelets, uriccomplications: Hematocrit, platelets, uric
acid, alanine aminotransferase (ALT),acid, alanine aminotransferase (ALT),
aspartate aminotransferase (AST), lacticaspartate aminotransferase (AST), lacticdehydrogenase (LDH)dehydrogenase (LDH)
Chronic HypertensionChronic Hypertension --
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 102/159
Chronic HypertensionChronic Hypertension
ManagementManagement
Generally, deliver at term, unlessGenerally, deliver at term, unless
superimposed preeclampsia, HELLPsuperimposed preeclampsia, HELLP
syndromesyndrome
Avoid ACE inhibitors (renal failure, Avoid ACE inhibitors (renal failure,
oligohydramnios, pulmonary hypoplasia,oligohydramnios, pulmonary hypoplasia,
IUGR) and atenolol (IUGR)IUGR) and atenolol (IUGR)
P l iP l i M tM tP l iP l i M tM t

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 103/159
PreeclampsiaPreeclampsia--ManagementManagementPreeclampsiaPreeclampsia--ManagementManagement
Seizure prophylaxisSeizure prophylaxis
Blood pressure controlBlood pressure control
DeliveryDelivery
P l iP l i T PT PP l iP l i T PT P
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 104/159
PreeclampsiaPreeclampsia--Term PregnancyTerm PregnancyPreeclampsiaPreeclampsia--Term PregnancyTerm Pregnancy
Delivery is a shortDelivery is a short--term goalterm goal
Induction of labor is appropriate after Induction of labor is appropriate after
maternalmaternal--fetal observation/stabilizationfetal observation/stabilization
Cesarean reserved for standard obstetricCesarean reserved for standard obstetric
indicationsindications
Cesarean may be recommended in casesCesarean may be recommended in cases
of severe preeclampsia where delivery isof severe preeclampsia where delivery isremoteremote
PreeclampsiaPreeclampsia--PretermPretermPreeclampsiaPreeclampsia--PretermPreterm

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 105/159
PreeclampsiaPreeclampsia PretermPreterm
PregnancyPregnancy
PreeclampsiaPreeclampsia PretermPreterm
PregnancyPregnancy Mild preeclampsiaMild preeclampsia -- expectantexpectant
management is acceptable under certainmanagement is acceptable under certain
conditionsconditions
Close maternalClose maternal--fetal surveillancefetal surveillance
Ability to intervene either if conditions Ability to intervene either if conditions
worsen or if acceptable gestational ageworsen or if acceptable gestational age
reachedreached InIn--hospital vs. home care?hospital vs. home care?
PreeclampsiaPreeclampsia--PretermPretermPreeclampsiaPreeclampsia--PretermPreterm
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 106/159
PreeclampsiaPreeclampsia PretermPreterm
PregnancyPregnancy
PreeclampsiaPreeclampsia PretermPreterm
PregnancyPregnancy Severe preeclampsiaSevere preeclampsia -- controversialcontroversial
Delivery for poor maternal condition isDelivery for poor maternal condition is
likely to be necessary over the short termlikely to be necessary over the short term
Sibai has advocated expectantSibai has advocated expectant
management for selected patients tomanagement for selected patients to
attempt to reduce perinatal morbidity andattempt to reduce perinatal morbidity and
mortality due to prematuritymortality due to prematurity
PreeclampsiaPreeclampsia--PretermPreterm
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 107/159
PreeclampsiaPreeclampsia PretermPreterm
PregnancyPregnancy Expectant management of severeExpectant management of severe
preeclampsia at preterm gestational age:preeclampsia at preterm gestational age:
HospitalizationHospitalization
Magnesium sulfate for seizure prophylaxis, atMagnesium sulfate for seizure prophylaxis, atleast during initial observation periodleast during initial observation period
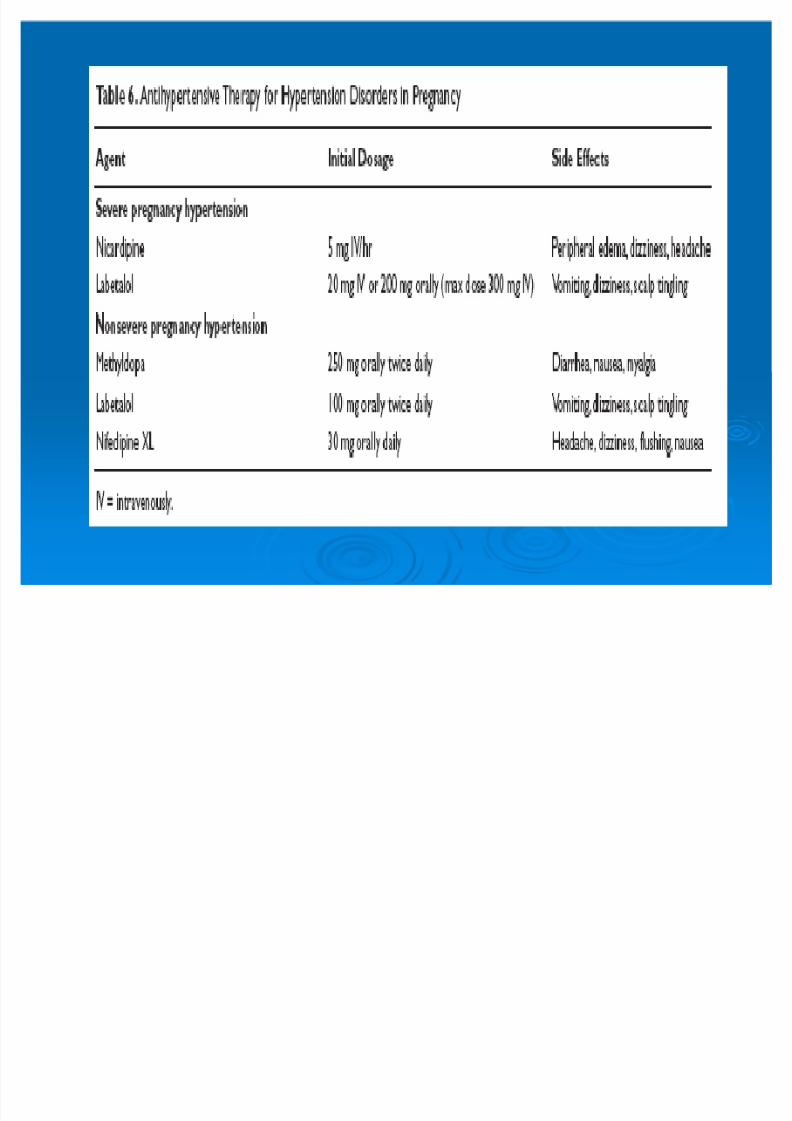
Blood pressure control to range of Blood pressure control to range of 140140--
155155//9090--105105 (labetalol or nifedipine)(labetalol or nifedipine) Daily assessment of maternalDaily assessment of maternal--fetal conditionfetal condition
PreeclampsiaPreeclampsia--PretermPreterm
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 108/159
PreeclampsiaPreeclampsia PretermPreterm
PregnancyPregnancy 2424--3434 weeksweeks ± ± corticosteroids for fetalcorticosteroids for fetal
lung maturationlung maturation
2424--3232 weeksweeks ± ± ongoing daily surveillance if ongoing daily surveillance if
stablestable 3333--3434 weeksweeks ± ± deliver after deliver after 4848 hourshours
Deliver for HELLP syndrome, severeDeliver for HELLP syndrome, severe
headache, uncontrolled hypertension,headache, uncontrolled hypertension,eclampsiaeclampsia
33 Termination of pregnancyTermination of pregnancy
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 109/159
33. Termination of pregnancy. Termination of pregnancy
Delivery is the cure for preeclampsiaDelivery is the cure for preeclampsia
Headache , visual disturbances or Headache , visual disturbances or
epigastric pain : indicative convulsionsepigastric pain : indicative convulsions
(imminent eclampsia)(imminent eclampsia)
Oliguria : ominous signOliguria : ominous sign
SPE : objectives to forestall convulsions ,SPE : objectives to forestall convulsions ,
prevent intracranial hemorrhage , &prevent intracranial hemorrhage , &serious vital organ damageserious vital organ damage
Termination of pregnancyTermination of pregnancy
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 110/159
Termination of pregnancyTermination of pregnancy
Preterm : conservative justified in mildPreterm : conservative justified in mild
preeclampsia, closed observation andpreeclampsia, closed observation and
monitoring to complicationsmonitoring to complications
severe preeclampsia : prompt deliverysevere preeclampsia : prompt delivery
vaginal deliveryvaginal delivery
cc--section if indicatedsection if indicated
Induction of labor not harmful to infants ,Induction of labor not harmful to infants ,but unsuccessfulbut unsuccessful 3535%%

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 111/159
44 Antihypertensive drugAntihypertensive drug

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 112/159
44. Antihypertensive drug. Antihypertensive drug
To prolong pregnancy , or modify perinatalTo prolong pregnancy , or modify perinatal
outcomesoutcomes
Labetolol :Labetolol :
lower mean BP,lower mean BP,
no difference : mean pregnancy prolongation ,no difference : mean pregnancy prolongation ,
birthweight , c/s ratebirthweight , c/s rate
IUGRIUGR 22 foldfold
Antihypertensive drugAntihypertensive drug
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 113/159
Antihypertensive drug Antihypertensive drug
RCT :RCT : blocker (Labetolol) , calciumblocker (Labetolol) , calcium
channel blockers (Nifedipine , Isradipine)channel blockers (Nifedipine , Isradipine)
no benefitno benefit
MetaMeta--analysis : treatment inducedanalysis : treatment induceddecrease maternal BP , may adverselydecrease maternal BP , may adversely
affect fetal growthaffect fetal growth
Prophylactic atenolol decrease incidenceProphylactic atenolol decrease incidencepreeclampsiapreeclampsia
Antihypertensive drugAntihypertensive drug

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 114/159
Antihypertensive drug Antihypertensive drug
ACE Inhibitor should avoid in ACE Inhibitor should avoid in 22ndnd && 33rdrd
trimester trimester
Complication : oligohydram , IUGR , bonyComplication : oligohydram , IUGR , bony
malformations , limb contractures ,malformations , limb contractures ,persistent PDA , pulm hypoplasia , RDS ,persistent PDA , pulm hypoplasia , RDS ,prolonged neonatal hypotension , neonatalprolonged neonatal hypotension , neonataldeathdeath
Early preg taken ACE Inhb : discontinuedEarly preg taken ACE Inhb : discontinuedas soon as possibleas soon as possible

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 115/159
NicardipineNicardipine
Nicardipine startNicardipine start 33 mg/hr ,titrate , maxmg/hr ,titrate , max 33--99mg/hr mg/hr
Target DBP <Target DBP < 100100 or <or < 9090 in HELLPin HELLP
syndrome ptsyndrome pt Median time to obtained targetMedian time to obtained target 2323 minmin
Delivery postponedDelivery postponed 44..77 daysdays
Potential use for second line drug whenPotential use for second line drug whenother antiHT drugs failedother antiHT drugs failed J. of hypertension : Dec J. of hypertension : Dec 2005 2005 :: 2323 :: 23192319--20 20

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 116/159
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 117/159
55. Delayed delivery with. Delayed delivery with
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 118/159
y yy ySuperimposed Pre Eclampsia (SPE)Superimposed Pre Eclampsia (SPE)
SPE remote from termSPE remote from term
Conservative or expectant management inConservative or expectant management in
selected groupselected group SibaiSibai 19851985 : SPE: SPE 1818--2727 wk : perinatalwk : perinatal
mortalitymortality 8787% , no mothers died , placental% , no mothers died , placentalabruption eclampsia , consumptiveabruption eclampsia , consumptivecoagulopathy , RF , encephalopathy ,coagulopathy , RF , encephalopathy ,intracerebral hemorrhage , rupturedintracerebral hemorrhage , rupturedhepatic hematomahepatic hematoma
Delayed delivery with SPEDelayed delivery with SPE
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 119/159
Delayed delivery with SPEDelayed delivery with SPE
SibaiSibai 19941994 : SPE: SPE 2828--3232 wk (excludewk (excludeHELLP) : prolonged mean of HELLP) : prolonged mean of 1515..44 d :d :sustainedsustained 44% placental abruption% placental abruption
Abramovici Abramovici 19991999 :: better neonatal outcomes in SPE ,better neonatal outcomes in SPE ,
IUGR not relate to severity of disease ,IUGR not relate to severity of disease ,
IUGR affected survival infants ,IUGR affected survival infants ,
median elapsed timemedian elapsed time 00 ,, 11 ,, 22 days in HELLP ,days in HELLP ,partial , & SPEpartial , & SPE
Delayed delivery with SPEDelayed delivery with SPE

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 120/159
Delayed delivery with SPEDelayed delivery with SPE
VigilVigil 20032003 : bed rest , MgSO: bed rest , MgSO4 484 48 hr , bolushr , bolus
antihypertensive drug , volume expansion,antihypertensive drug , volume expansion,
& Dexa& Dexa
Indications for delivery : uncontrollable BP,Indications for delivery : uncontrollable BP,fetal distress , placental abruption , renalfetal distress , placental abruption , renal
failure, HELLP synd , persistent symptomfailure, HELLP synd , persistent symptom
Average pregnancy prolong Average pregnancy prolong 88dd No maternal deaths,No maternal deaths, 66 stillbirth ,stillbirth , 1111
placental abruption ,placental abruption , 2828 IUGRIUGR
Intervention VS ExpectantIntervention VS Expectant

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 121/159
Intervention VS ExpectantIntervention VS Expectant
Insufficient data for reliable conclusions onInsufficient data for reliable conclusions on
maternal outcomematernal outcome
For baby : insufficient reliable conclusionsFor baby : insufficient reliable conclusions
on stillbirth or death after delivery (RRon stillbirth or death after delivery (RR11..5050))
More RDS (RRMore RDS (RR 22..33) , NEC (RR) , NEC (RR55..55))
Less likely to SGA (RRLess likely to SGA (RR 00..3636))
The C oc hrane Database of Systemati c ReviewsThe C oc hrane Database of Systemati c Reviews 2002 2002
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 122/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 123/159

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 124/159
EclampsiaEclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 125/159
EclampsiaEclampsia
Appear before, during or after labor Appear before, during or after labor
Most common in last trimester Most common in last trimester
Shift in incidence toward postpartumShift in incidence toward postpartum
Usually begin in facial twitch , entire bodyUsually begin in facial twitch , entire body
rigid , generalized muscle contraction , jawrigid , generalized muscle contraction , jawopen & close violentlyopen & close violently
Diaphragm fixed , resp halted , then longDiaphragm fixed , resp halted , then longdeep stertorous inhalationdeep stertorous inhalation

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 126/159
EclampsiaEclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 127/159
EclampsiaEclampsia
Duration of coma variableDuration of coma variable
Hypercarbia , lactic acidemia , fetal bradyHypercarbia , lactic acidemia , fetal bradycardiacardia
High fever High fever ProteinuriaProteinuria
Diminished urine output , hemoglobinuriaDiminished urine output , hemoglobinuria
Pronounced edemaPronounced edema Proteinuria & edema disappear withinProteinuria & edema disappear within 11 wkwk
BP return within a few days toBP return within a few days to 22 wk PPwk PP
EclampsiaEclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 128/159
EclampsiaEclampsia
Pulmonary edema from aspirationPulmonary edema from aspiration
pneumonitis or heart failurepneumonitis or heart failure
Death from massive cerebral hemorrhageDeath from massive cerebral hemorrhage
Hemiplegia from sublethal hemorrhageHemiplegia from sublethal hemorrhage
Blindness from retinal detachment or Blindness from retinal detachment or
occipital lobe ischemia & edemaoccipital lobe ischemia & edema
Persistent coma due to uncal herniationPersistent coma due to uncal herniation
Rarely eclampsia followed by psychosisRarely eclampsia followed by psychosis
EclampsiaEclampsia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 129/159
EclampsiaEclampsia
Differential diagnosis : epilepsy ,Differential diagnosis : epilepsy ,
encephalitis , meningitis , cerebral tumor ,encephalitis , meningitis , cerebral tumor ,
cysticercosis , ruptured cerebral aneurysmcysticercosis , ruptured cerebral aneurysm
Prognosis always seriousPrognosis always serious
66% of Maternal death relate to eclampsia% of Maternal death relate to eclampsia
Among PIH patient , maternal death Among PIH patient , maternal death 1616%%
TreatmentTreatment

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 130/159
TreatmentTreatment
11. control of convulsions using IV MgSO. control of convulsions using IV MgSO44
22. Intermittent IV or oral of antihypertensive. Intermittent IV or oral of antihypertensive
drug to lower Diastolic BP <drug to lower Diastolic BP <100100
33. Avoidance of diuretics , limit IV fluid. Avoidance of diuretics , limit IV fluid
adminstration , avoid hyperosmotic agentsadminstration , avoid hyperosmotic agents
44. Delivery. Delivery
Continuous IV regimenContinuous IV regimen
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 131/159
Continuous IV regimenContinuous IV regimen
44--66 gm MgSOgm MgSO44 dilute indilute in 100100 ml fluid , adminml fluid , admin
over over 1515--2020 minmin
BeginBegin 22 g/hr ing/hr in 100100 ml IV maintenanceml IV maintenance
Measure Mg level atMeasure Mg level at 44--66 hr , adjust levelhr , adjust level
betweenbetween 44--77 mEq/LmEq/L
MgSOMgSO44 discontinueddiscontinued 2424 hr after deliveryhr after delivery
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 132/159
MgSOMgSO44

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 133/159
Effective anticonvulsant without producingEffective anticonvulsant without producingCNS depression in either mother or infantCNS depression in either mother or infant
Not given to treat HTNot given to treat HT
Exert specific on cerebral cortexExert specific on cerebral cortex
1010--1515% after MgSO% after MgSO44 : subsequent: subsequentconvulsionconvulsion
Sodium amobarbital & thiopental , if Sodium amobarbital & thiopental , if
excessive agitate in postconvulsion stateexcessive agitate in postconvulsion state In Eclampsia , admin for In Eclampsia , admin for 2424 hr after onsethr after onset
of convulsionof convulsion
M SOM SO44
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 134/159
MgSOMgSO44
Almost totally cleared by renal excretion Almost totally cleared by renal excretion
Monitor urine output , DTR , RRMonitor urine output , DTR , RR
Maintained levelMaintained level 44--77 mEq/LmEq/L
IM & IV regimen , no significant differenceIM & IV regimen , no significant differenceMg levelMg level
MgMg 1010 mEq/L : patellar reflex disappear mEq/L : patellar reflex disappear
>> 1010 mEq/L : respiratory depressionmEq/L : respiratory depression >> 1212 mEq/L : respiratory paralysis & arrestmEq/L : respiratory paralysis & arrest
Cr >Cr >11..33 : half dose MgSO: half dose MgSO44
MgSOMgSO44
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 135/159
MgSOMgSO44
Acute cardiovascular effect Acute cardiovascular effect
Decrease MAPDecrease MAP
Increase COIncrease CO 1313%%
Decrease SVRDecrease SVR
Transient nausea & flushingTransient nausea & flushing
Persist for onlyPersist for only 1515 minmin
MgSOMgSO44

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 136/159
Uterine effectsUterine effects
Depress myometrial contractilityDepress myometrial contractility
Inh calcium entry to myometrial cellInh calcium entry to myometrial cell
Dose dependent : at leastDose dependent : at least 88--1010 mEq/LmEq/L
No uterine effect , when given for No uterine effect , when given for
prophylaxis eclampsia (oxytocinprophylaxis eclampsia (oxytocin
stimulation of labor , admit to deliverystimulation of labor , admit to deliveryintervals , route of delivery)intervals , route of delivery)
MgSOMgSO44

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 137/159
gg
Fetal effectsFetal effects
Promptly cross placentaPromptly cross placenta
Neonatal depression occurs only if severeNeonatal depression occurs only if severe
hypermagnesemia at deliveryhypermagnesemia at delivery Dec rease in beat Dec rease in beat--toto--beat variability beat variability
Possible protective effect against cerebral palsyPossible protective effect against cerebral palsy
in VLBW infantsin VLBW infants
Substantial gross motor dysfunction reducedSubstantial gross motor dysfunction reduced
No serious harmful effectsNo serious harmful effects
Compared with anticonvulsantsCompared with anticonvulsants
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 138/159
Compared with anticonvulsantsCompared with anticonvulsants
MgSOMgSO44 reduce recurrent szreduce recurrent sz 5050%%
compared to diazepam , reduce maternalcompared to diazepam , reduce maternal
& perinatal morbidity (not sig)& perinatal morbidity (not sig)
Maternal mortality reduced compared toMaternal mortality reduced compared tophenytoin (not sig) , less neonatalphenytoin (not sig) , less neonatal
intubation & NICU admissionintubation & NICU admission
Prevent eclamptic sz superior to phenytoinPrevent eclamptic sz superior to phenytoin Lower risk placental abruptionLower risk placental abruption
MgSOMgSO44 & other anticonvulsant& other anticonvulsant

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 139/159
gSOgSO & ot e a t co u sa t& ot e a t co u sa t
Compared with placeboCompared with placebo
Reduce risk eclampsia (RRReduce risk eclampsia (RR 00..4141))
Reduce risk of dying (RRReduce risk of dying (RR 00..5656))
More Side effect (flushing) (More Side effect (flushing) (2424% VS% VS 55%)%) Reduce risk placental abruption (RRReduce risk placental abruption (RR 00..6464))
55% Increase risk c/s% Increase risk c/s
No difference in stillbirth or neonatal deathNo difference in stillbirth or neonatal death(RR(RR 11..0404))
The C oc hrane Database of Systemati c ReviewsThe C oc hrane Database of Systemati c Reviews 20032003
MgSOMgSO44 & other anticonvulsant& other anticonvulsant

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 140/159
gg
Compared to phenytoinCompared to phenytoin
Better Reduce risk of eclampsia (RRBetter Reduce risk of eclampsia (RR 00..0505))
Increase risk c/s (RRIncrease risk c/s (RR 11..2121))
Compared to diazepamCompared to diazepam
Too small for any reliable conclusionsToo small for any reliable conclusions
The C oc hrane Database of Systemati c ReviewsThe C oc hrane Database of Systemati c Reviews 20032003

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 141/159
MgSOMgSO44
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 142/159
MgSOMgSO44
Sz rate in preeclampsia , no szSz rate in preeclampsia , no sz
prophylaxisprophylaxis 33..99%% reduced toreduced to 11..55%%
Mild preeclampsia , estimated risk withoutMild preeclampsia , estimated risk without
prophylaxisprophylaxis 11 inin 100100 , & not asso with, & not asso withsevere maternal morbiditysevere maternal morbidity
Do not given sz prophylaxis in Mild PEDo not given sz prophylaxis in Mild PE
Antihypertensive Antihypertensive

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 143/159
ypyp
Hydralazine suggested if persistentHydralazine suggested if persistent
systolic >systolic > 160160 , or diastolic >, or diastolic > 105105 mmHgmmHg
(NHBPEP(NHBPEP20002000))
55--1010 mg doses atmg doses at 1515--2020 min inervalsmin inervals
Satisfactory response ante or intrapartum :Satisfactory response ante or intrapartum :
diastolicdiastolic 9090--100100
Seldom another antihypertensive neededSeldom another antihypertensive needed FHR deceleration when BP fell toFHR deceleration when BP fell to 110110//8080
Antihypertensives Antihypertensives

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 144/159
ypyp
Labetolol : IV Labetolol : IV 11& nonselective& nonselective --blocker blocker
Lower BP more rapidly , associatedLower BP more rapidly , associated
tachycardiatachycardia
NHBPEP(NHBPEP(20002000) : recommends) : recommends 2020 mg IV mg IV
bolus , if not effective withinbolus , if not effective within 1010 min ,min ,
followed byfollowed by 4040 mg , thenmg , then 8080 mg qmg q 1010 minmin
but not exceedbut not exceed 220220 mg total dose per mg total dose per episode treatedepisode treated
Antihypertensives Antihypertensives
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 145/159
ypyp
NifedipineNifedipine 1010 mg Oral , repeated inmg Oral , repeated in 3030 minmin
, if necessary (NHBPEP, if necessary (NHBPEP 20002000))
Fewer dose required to achieve BP controlFewer dose required to achieve BP control
without increased adverse effectswithout increased adverse effects
Sublingual : potent & rapid :Sublingual : potent & rapid :
cerebrovascular ischemia , MI , conductioncerebrovascular ischemia , MI , conduction
disturbance , deathdisturbance , death Not superior to other hypertensivesNot superior to other hypertensives
Antihypertensives Antihypertensives
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 146/159
ypyp
Verapamil IV Verapamil IV 55--1010 mg/hr mg/hr
Nimodipine IV & oralNimodipine IV & oral
Ketanserin IV (selectiveKetanserin IV (selective 55--HT blocker)HT blocker)
Nitroprusside not recommend unless noNitroprusside not recommend unless no
response , continuous IV , startresponse , continuous IV , start 00..2525
ug/kg/min , increase toug/kg/min , increase to 55 ug/kg/min , fetalug/kg/min , fetal
cyanide toxicity may occur after cyanide toxicity may occur after 44 hr hr
Persistent postpartum HTPersistent postpartum HT
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 147/159
p pp p
HydralazineHydralazine 1010--2525 mg IM qmg IM q 44--66 hr hr
If HT persists or recur : oral labetolol or If HT persists or recur : oral labetolol or
thiazide diuretic are giventhiazide diuretic are given
Two mechanisms :Two mechanisms :
11. Underlying chronic hypertension ,. Underlying chronic hypertension ,
22. Mobilization of edema fluid. Mobilization of edema fluid
Persistent postpartum HTPersistent postpartum HT

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 148/159
p pp p
Atypical syndrome in which SPE Atypical syndrome in which SPE--
eclampsia persists despite deliveryeclampsia persists despite delivery
Single or multiple plasma exchangeSingle or multiple plasma exchange
Plasma exchange performed inPlasma exchange performed in
postpartum women with HELLP syndromepostpartum women with HELLP syndrome
Very few women : persistent HypertensionVery few women : persistent Hypertension
, thrombocytopenia and renal dysfunction, thrombocytopenia and renal dysfunctiondue to thrombotic microangiopathydue to thrombotic microangiopathy
Diuretics & hyperosmotic agentsDiuretics & hyperosmotic agents
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 149/159
yp gyp g
Diuretics : deplete intravascular volume ,Diuretics : deplete intravascular volume ,
compromise placental perfusion , limitedcompromise placental perfusion , limited
used to pulmonary edemaused to pulmonary edema
Hyperosmotic agents : leaks of agentsHyperosmotic agents : leaks of agentsthrough capillaries into lungs & brainthrough capillaries into lungs & brainpromote accumulation of edemapromote accumulation of edema
Fluid therapyFluid therapy

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 150/159
pypy
Lactate Ringers Solution , rateLactate Ringers Solution , rate 6060 ml toml to
125125 ml/hr ml/hr
Unless unusual fluid loss : N/V , diarrhea ,Unless unusual fluid loss : N/V , diarrhea ,
excessive blood lossexcessive blood loss
Oliguria : maternal blood volumeOliguria : maternal blood volume
constricted, admin IV fluid more vigorouslyconstricted, admin IV fluid more vigorously
Women with eclampsia already hasWomen with eclampsia already hasexcessive extracelular fluidexcessive extracelular fluid
Plasma volume expander Plasma volume expander
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 151/159
Plasma volume expansion for treatment of Plasma volume expansion for treatment of
preeclampsiapreeclampsia
Compared colloid with no plasma volumeCompared colloid with no plasma volume
expansionexpansion
Insufficient evidence for any reliable effectInsufficient evidence for any reliable effect
The C oc hrane Database of Systemati c ReviewsThe C oc hrane Database of Systemati c Reviews 19991999
Pulmonary edemaPulmonary edema
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 152/159
Most often do so postpartumMost often do so postpartum
Aspiration should be exclude Aspiration should be exclude
Majority have cardiac failureMajority have cardiac failure
Decrease plasma oncotic pressure , increaseDecrease plasma oncotic pressure , increaseextravascular oncotic pressure , increaseextravascular oncotic pressure , increase
capillary permeability , hemoconcentration ,capillary permeability , hemoconcentration ,
reduced CVP , PCWPreduced CVP , PCWP
Excessive colloid & cyrstalloid cause pulmExcessive colloid & cyrstalloid cause pulmedemaedema
Invasive monitoringInvasive monitoring
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 153/159
Use of pulmonary artery catheterizationUse of pulmonary artery catheterization
Reserved for women with severe cardiacReserved for women with severe cardiac
disease , renal disease , refractorydisease , renal disease , refractory
hypertension , oliguria , pulmonary edemahypertension , oliguria , pulmonary edema
Pulmonary edema by more than onePulmonary edema by more than one
mechanismmechanism
If questionable pulmonary edema :If questionable pulmonary edema :furosemide IV , hydralazine IVfurosemide IV , hydralazine IV
DeliveryDelivery

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 154/159
After eclamptic sz , labor often ensues After eclamptic sz , labor often ensues
spontaneously or can be inducedspontaneously or can be induced
successfully even in remote from termsuccessfully even in remote from term
Because lack of normal pregnancyBecause lack of normal pregnancyhypervolemia , so less tolerant of bloodhypervolemia , so less tolerant of bloodloss at deliveryloss at delivery
Analgesia & anesthesia Analgesia & anesthesia

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 155/159
In the past , SAB , EB were avoidIn the past , SAB , EB were avoid
GA caused by tracheal intubation, suddenGA caused by tracheal intubation, sudden
HT ,pulm edema , intracranial hgeHT ,pulm edema , intracranial hge
Epidural preferred : no serious maternal or Epidural preferred : no serious maternal or fetal complication , lower MAP , Cardiacfetal complication , lower MAP , Cardiacoutput not falloutput not fall
LongLong--term consequenceterm consequence

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 156/159
More prone to hypertensive complicationsMore prone to hypertensive complicationsin future pregnanciesin future pregnancies
Earlier diagnosed , greater recurrenceEarlier diagnosed , greater recurrence
Diagnose beforeDiagnose before 3030 wk , recur wk , recur 4040%% Recurrence rate for women withRecurrence rate for women with 11 episodeepisode
of HELLPof HELLP 55%%
Subsequent preeclampsia , high incidenceSubsequent preeclampsia , high incidenceof preterm , IUGR , placental abruption ,of preterm , IUGR , placental abruption ,c/s deliveryc/s delivery
LongLong--term consequenceterm consequence

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 157/159
Multiparous develop preeclampsia ,Multiparous develop preeclampsia ,
increased risk recur in subsequentincreased risk recur in subsequent
pregnancy compared with nulliparaspregnancy compared with nulliparas
EarlyEarly--onset SPE may have underlyingonset SPE may have underlyingthrombophilias, complicate subsequentthrombophilias, complicate subsequent
pregnanciespregnancies
Preeclampsia not cause chronicPreeclampsia not cause chronichypertensionhypertension

8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 158/159
8/3/2019 Hypertensive Disorder in Pregnancy Untuk Kuliah
http://slidepdf.com/reader/full/hypertensive-disorder-in-pregnancy-untuk-kuliah 159/159
Thank you for your attentionThank you for your attention