
Bahan Kuliah Pakar Blok 9 Dewasa & Masa Tua
106
LABORATORY TEST & INTERPRETATION Department/Division of Clinical Pathology Zainoel Abidin Hospital-Medical Faculty University of Syiah Kuala Banda Aceh 2013 16 Desember 2014 Dr. Vivi Keumala Mutiawati, SpPK., MKes Blok 9: Dewasa & Masa Tua
-
Upload
ilham-ristananda -
Category
Documents
-
view
11 -
download
4
description
Bahan Kuliah Pakar Blok 9 Dewasa & Masa Tua
Transcript of Bahan Kuliah Pakar Blok 9 Dewasa & Masa Tua
LABORATORY TEST &
INTERPRETATION
Department/Division of Clinical Pathology Zainoel Abidin Hospital-Medical Faculty University of Syiah Kuala
Banda Aceh 2013
16 Desember 2014
Dr. Vivi Keumala Mutiawati, SpPK., MKes
Blok 9: Dewasa & Masa Tua

MEDICAL CHECK-UP/MCU
Persiapan Pemeriksaan Laboratorium untuk MCU:
1. Puasa selama 12 jam:
dimulai dari malam hari sebelum
pengambilan darah/sampling darah
2. Istirahat yang cukup:
dimulai ketika melaksanakan puasa
3. Tidak merokok
dimulai ketika melaksanakan puasa

MEDICAL CHECK-UP/MCU
Patient Preparation for Laboratory MCU 1. Fasting for 12 hours: Starting from one night before blood sample taken (stop eating after last night dinner at 8 pm) 2. Have enough rest and sleep: Starting same time with fasting 3. No smoking Starting same time with fasting
Laboratory MCU include:
1. Clinical Hematology
2. Clinical Chemistry
3. Urinalisis (Clinical Chemistry)
4. Clinical Immuno-serology
MEDICAL CHECK-UP/MCU
Laboratory MCU include:
1. Clinical Hematology
2. Clinical Chemistry
3. Urinalisis (Clinical Chemistry)
4. Clinical Immuno-serology
MEDICAL CHECK-UP/MCU

Clinical Hematology
Routine Blood Count
1. Hemoglobin/Hb
2. Hematocrit/Hct
3. Erythrocyte
4. Leucocyte
5. Thrombocyte
Complete Blood Count 1. Hemoglobin/Hb
2. Hematokrit/Hct
3. Erythrocyte
4. Leucocyte
5. Thrombocyte
6. Mean Corpuscular Volume/MCV
7. Mean Corpuscular
Hemoglobine/MCH
8. Mean Cospuscular
Hemoglobin Consentration/MCHC
9. Red Cell Distribution Width/RDW
10. Differential Counting/DC
MEDICAL CHECK-UP/MCU
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.
Complete Blood Count
1. Hemoglobin/Hb
2. Hematokrit/Hct
3. Erythrocyte
4. Leucocyte
5. Thrombocyte
6. Mean Corpuscular Volume/MCV
7. Mean Corpuscular
Hemoglobine/MCH
8. Mean Cospuscular
Hemoglobin Consentration/MCHC
9. Red Cell Distribution Width/RDW
10. Differential Counting/DC
MEDICAL CHECK-UP/MCU
Which one are RED BLOOD CELL
INDICES ???
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.

Complete Blood Count Main Function: Provide information about Size (MCV & RDW) Weight (MCH) Concentration (MCHC)
Investigating ANEMIA How to calculate: Necessary need the results of Erythrocyte Hematocrit Hemoglobin
MEDICAL CHECK-UP/MCU RED BLOOD CELL
INDICES
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.
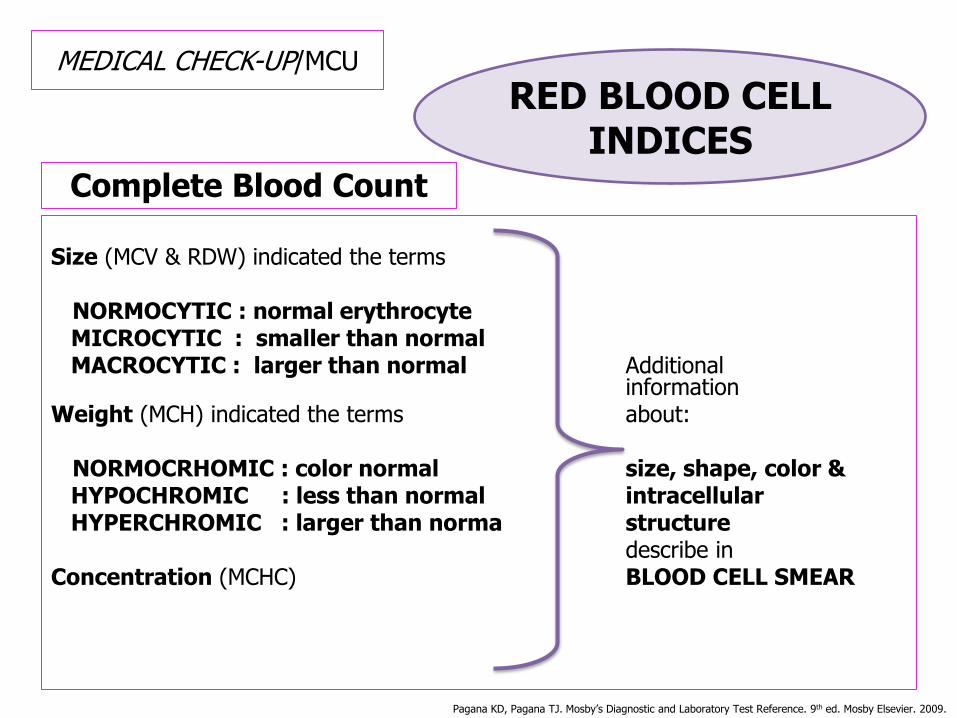
Complete Blood Count
Size (MCV & RDW) indicated the terms NORMOCYTIC : normal erythrocyte MICROCYTIC : smaller than normal MACROCYTIC : larger than normal Additional information Weight (MCH) indicated the terms about: NORMOCRHOMIC : color normal size, shape, color & HYPOCHROMIC : less than normal intracellular HYPERCHROMIC : larger than norma structure describe in Concentration (MCHC) BLOOD CELL SMEAR
MEDICAL CHECK-UP/MCU RED BLOOD CELL
INDICES
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.
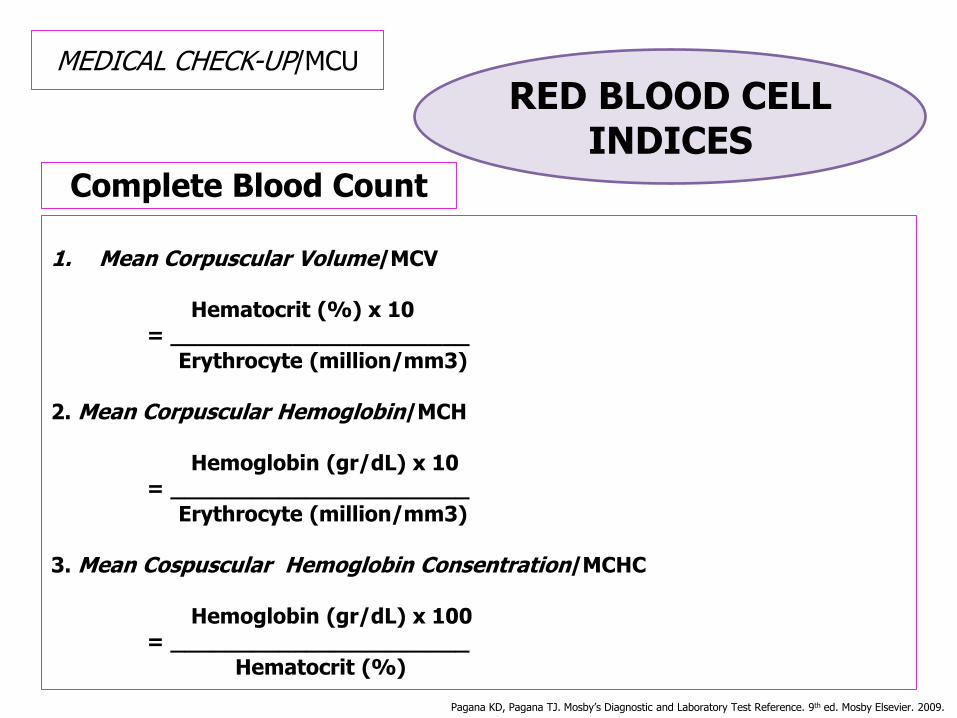
Complete Blood Count
1. Mean Corpuscular Volume/MCV Hematocrit (%) x 10 = ______________________ Erythrocyte (million/mm3) 2. Mean Corpuscular Hemoglobin/MCH Hemoglobin (gr/dL) x 10 = ______________________ Erythrocyte (million/mm3) 3. Mean Cospuscular Hemoglobin Consentration/MCHC Hemoglobin (gr/dL) x 100 = ______________________ Hematocrit (%)
MEDICAL CHECK-UP/MCU RED BLOOD CELL
INDICES
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.

Complete Blood Count
1. Mean Corpuscular Volume/MCV
Adult/Elderly/Child : 80-95 fL
Newborn : 96-108 fL
2. Mean Corpuscular Hemoglobine/MCH
Adult/Elderly/Child : 27-31 pg
Newborn : 32-34 pg
3. Mean Cospuscular Hemoglobin Consentration/MCHC
Adult/Elderly/Child : 32-36 gr/dL
Newborn : 32-33 gr/dL
MEDICAL CHECK-UP/MCU RED BLOOD CELL
INDICES
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.
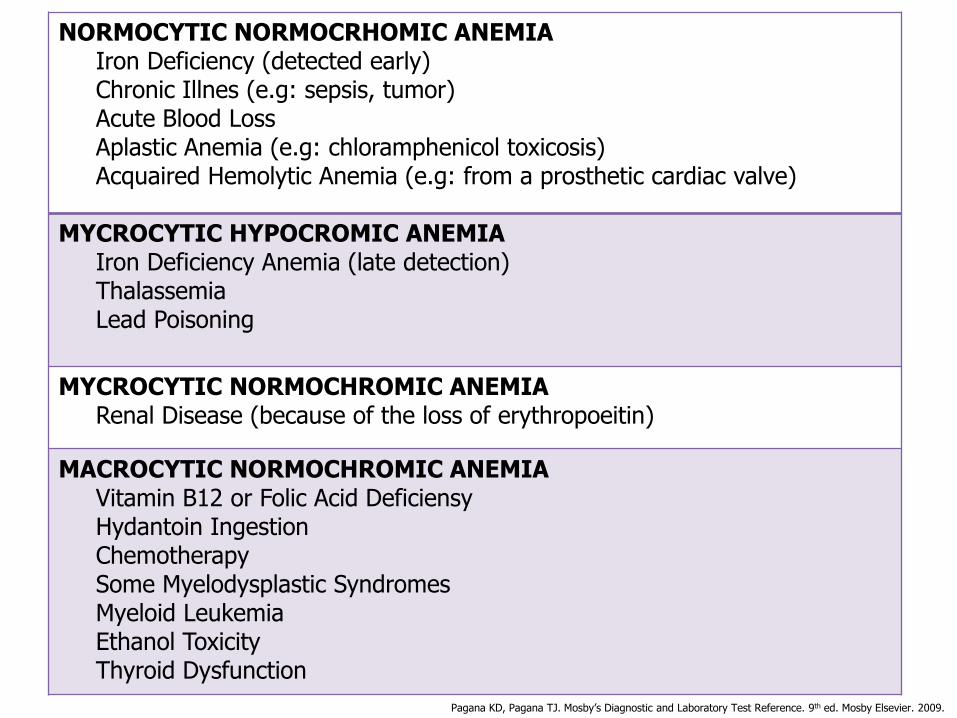
NORMOCYTIC NORMOCRHOMIC ANEMIA Iron Deficiency (detected early) Chronic Illnes (e.g: sepsis, tumor) Acute Blood Loss Aplastic Anemia (e.g: chloramphenicol toxicosis) Acquaired Hemolytic Anemia (e.g: from a prosthetic cardiac valve)
MYCROCYTIC HYPOCROMIC ANEMIA Iron Deficiency Anemia (late detection) Thalassemia Lead Poisoning
MYCROCYTIC NORMOCHROMIC ANEMIA Renal Disease (because of the loss of erythropoeitin)
MACROCYTIC NORMOCHROMIC ANEMIA Vitamin B12 or Folic Acid Deficiensy Hydantoin Ingestion Chemotherapy Some Myelodysplastic Syndromes Myeloid Leukemia Ethanol Toxicity Thyroid Dysfunction
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.
RED BLOOD CELL/RBC (ERYTHROCYTE)
Normal Erythrocytes • Colour : Red • Shape : Biconcave, with central area of pallor • Size : 6.7-7.7 µm (± 8 µm) • Nucleus : Anucleated cells • Consist : Haemoglobins (Hbs)
IMPORTANT CLINICALLY

RED BLOOD CELL/RBC (ERYTHROCYTE)
http://www.nature.com/leu/journal/v23/n5/images/leu200954f3.jpg
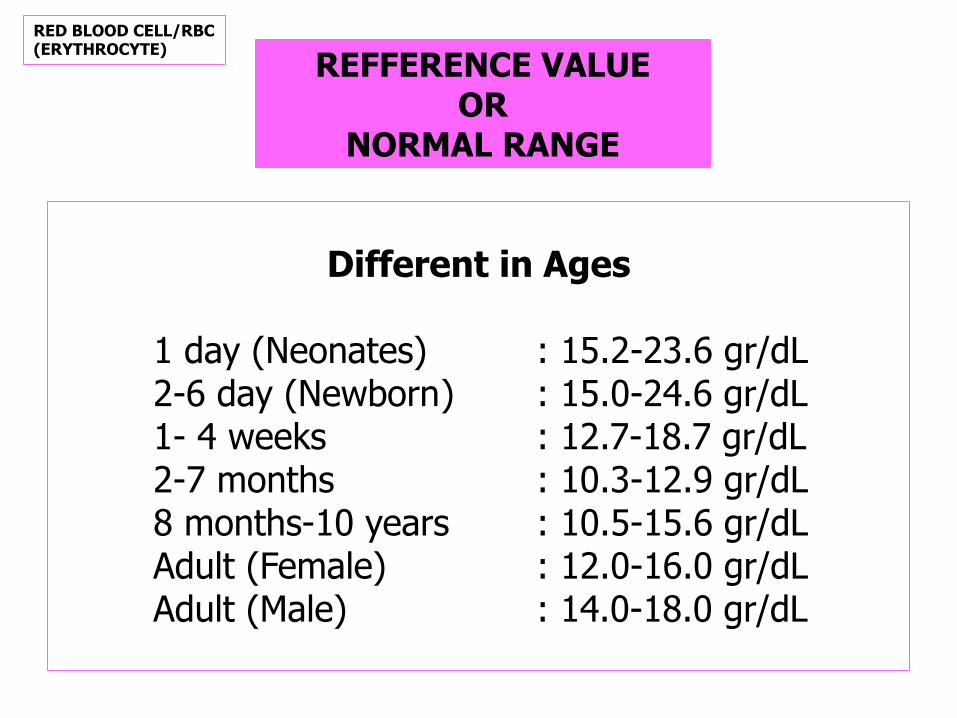
REFFERENCE VALUE OR
NORMAL RANGE
Different in Ages
1 day (Neonates) : 15.2-23.6 gr/dL 2-6 day (Newborn ) : 15.0-24.6 gr/dL 1- 4 weeks : 12.7-18.7 gr/dL 2-7 months : 10.3-12.9 gr/dL 8 months-10 years : 10.5-15.6 gr/dL Adult (Female) : 12.0-16.0 gr/dL Adult (Male) : 14.0-18.0 gr/dL
RED BLOOD CELL/RBC (ERYTHROCYTE)
METHODS
• Manual: Talquis
Sahli
• Analyzer:
Hemocytometer
Autoanalyzer (Flow Cytometry)
RED BLOOD CELL/RBC (ERYTHROCYTE)
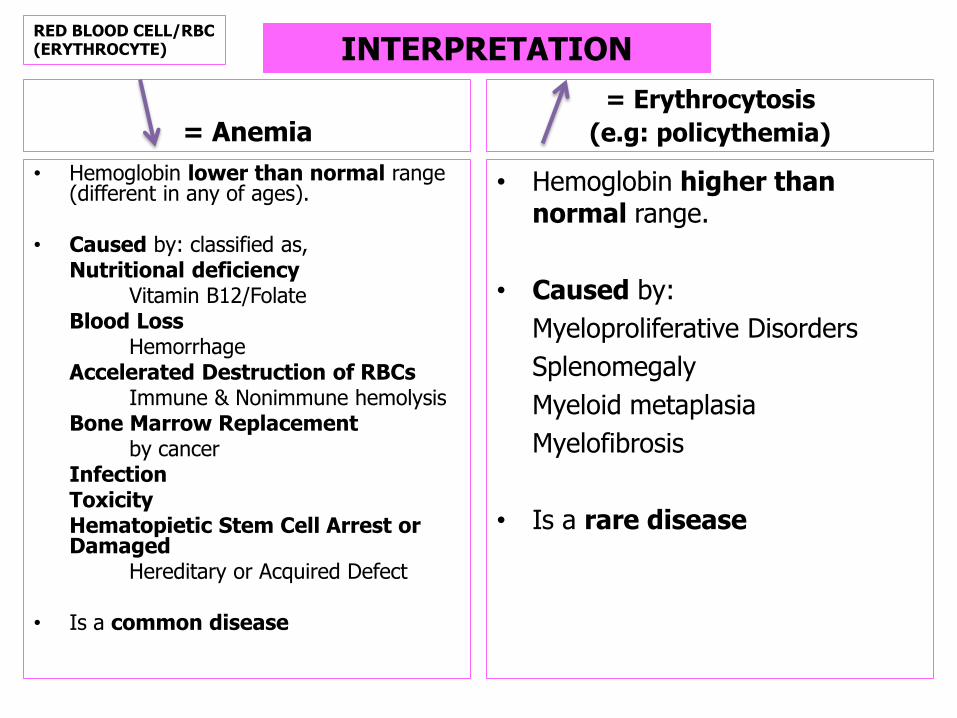
= Anemia
• Hemoglobin lower than normal range (different in any of ages).
• Caused by: classified as, Nutritional deficiency Vitamin B12/Folate Blood Loss Hemorrhage Accelerated Destruction of RBCs Immune & Nonimmune hemolysis Bone Marrow Replacement by cancer Infection Toxicity Hematopietic Stem Cell Arrest or
Damaged Hereditary or Acquired Defect • Is a common disease
= Erythrocytosis
(e.g: policythemia)
• Hemoglobin higher than normal range.
• Caused by:
Myeloproliferative Disorders
Splenomegaly
Myeloid metaplasia
Myelofibrosis
• Is a rare disease
INTERPRETATION RED BLOOD CELL/RBC (ERYTHROCYTE)

Relative Erythrocytosis
• The red cell mass is absence,
but the Hematocrit is elevated
• Caused by:
Dehydration
Hypertensive
Obese
Heavy smoking
Extreme Alcohol Consumption
Diuretic Therapy
Absolute Erythrocytosis
• The red cell mass is elevated
• Caused by:
Compensatory Increase in erythropoietin in response to tissue hypoxia
Those resulting from an inappropriate or pathologic secretion of erythropoietin
Those resulting from defective oxygen transport
INTERPRETATION RED BLOOD CELL/RBC (ERYTHROCYTE)

MORPHOLOGY OF
RBC
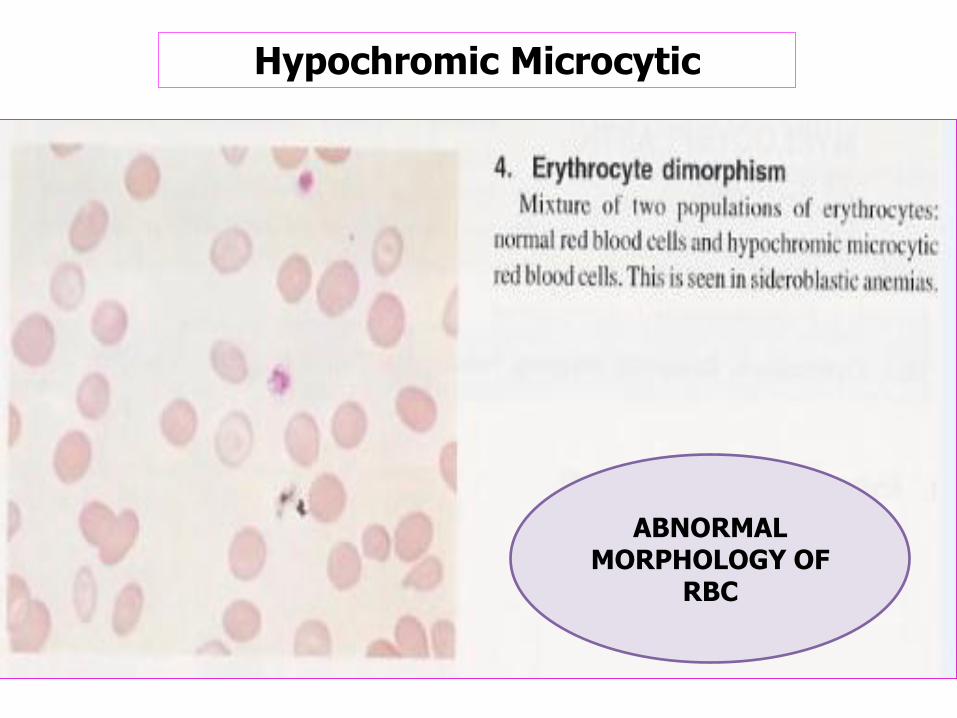
ABNORMAL MORPHOLOGY OF
RBC
Hypochromic Microcytic
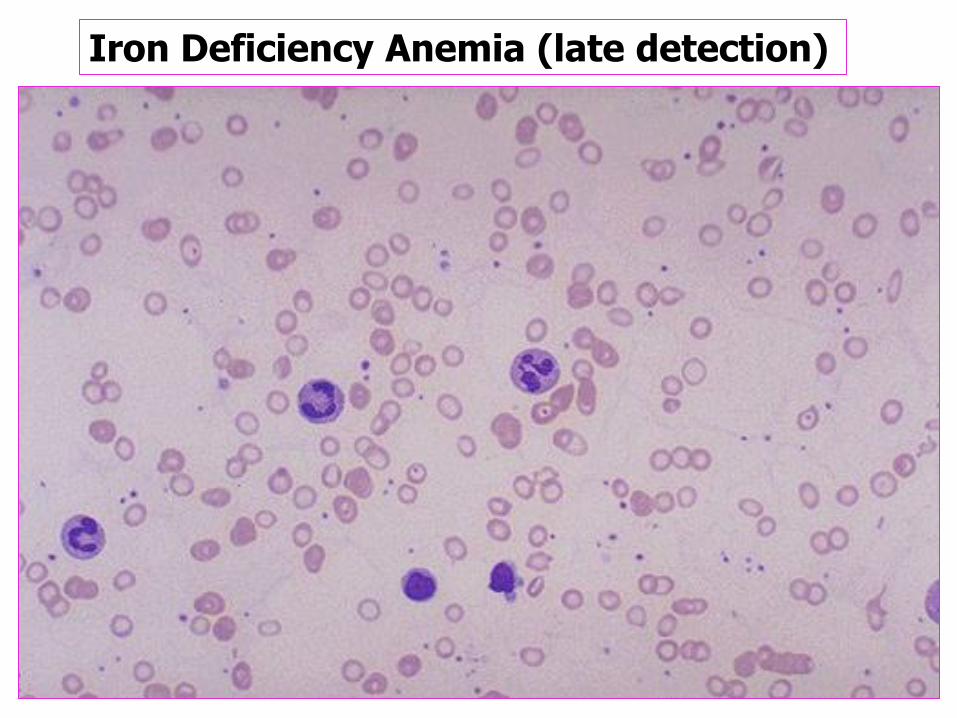
Iron Deficiency Anemia (late detection)

ANEMIA DEFISIENSI FE (berat)
Pencil cell
Tear drops
Mikrosit
RETICULOCYTE (= polychromatic erythrocyte)
One type of NORMOBLASTIC SERIES, Just seen in bone marrow (unusually seen in pheripheral) Morphologic findings, known as: NORMOBLAST Contain : Ribonucleic Acid/RNA Size : 8-10 µm Ratio of Cytoplasm: No nucleus Granules : No granules
RETICULOCYTE
1. Reticulocyte Count
• Also call as: Reticulocyte Index
• Manual
• Reagen
Bryliant Crecil Blue/BCB
• Refference Value
Newborn: 2.5-6.0%
Adult : 0.5-2.0%
2. Absolute Reticulocyte
• Calculation:
% Retic x RBC
• Refference Value
24.000-84.000/µL
METHODS
= Reticulositosis
1. Bleeding
2. Hemolytic Anemias
3. Hemoglobinopathy
4. Sickle Cell Anemias
5. Enzyme Deficiency (Erythrocyte)
6. Malaria
Interpretation
RETICULOCYTE

WHITE BLOOD CELL/WBC (LEUCOCYTE)
1. Granulocyte:
young cell: Blast, Promyelocyte,
Myelocyte, Metamyelocyte,
Band
old cell: Neutrophil, Eosinophil,
Basophil
2. Lymphocyte
3. Monocyte
METHODS
• Manual: Counting Chamber
• Analyzer:
Hemocytometer
Autoanalyzer (Flow Cytometry)
WHITE BLOOD CELL/WBC (LEUCOCYTE)
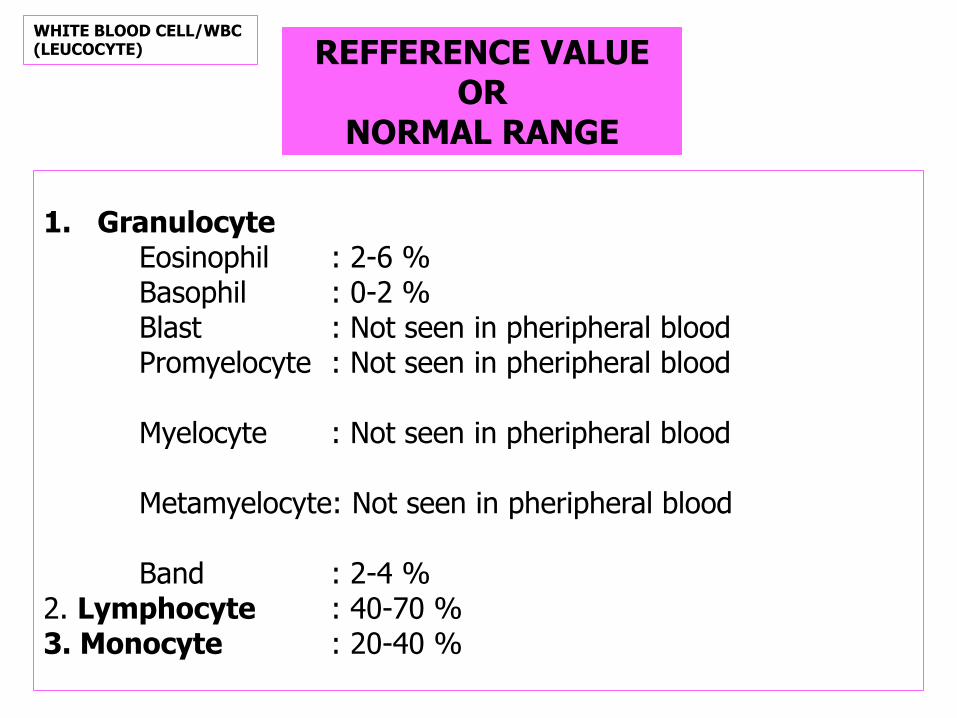
REFFERENCE VALUE OR
NORMAL RANGE
1. Granulocyte Eosinophil : 2-6 % Basophil : 0-2 % Blast : Not seen in pheripheral blood Promyelocyte : Not seen in pheripheral blood Myelocyte : Not seen in pheripheral blood Metamyelocyte: Not seen in pheripheral blood Band : 2-4 % 2. Lymphocyte : 40-70 % 3. Monocyte : 20-40 %
WHITE BLOOD CELL/WBC (LEUCOCYTE)
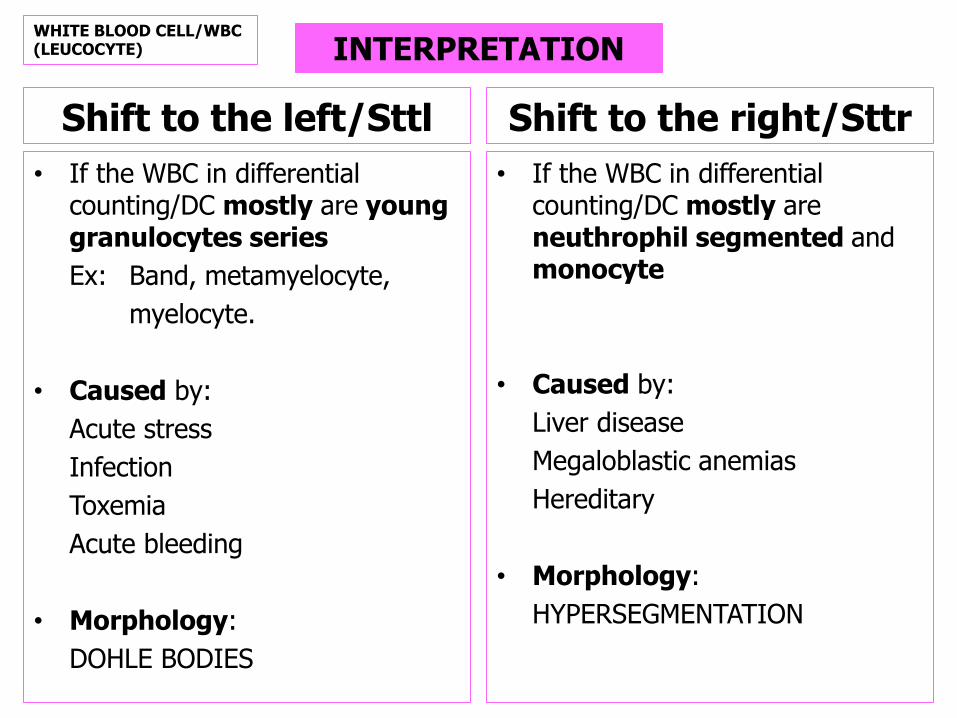
Shift to the left/Sttl
• If the WBC in differential counting/DC mostly are young granulocytes series
Ex: Band, metamyelocyte,
myelocyte.
• Caused by:
Acute stress
Infection
Toxemia
Acute bleeding
• Morphology:
DOHLE BODIES
Shift to the right/Sttr
• If the WBC in differential counting/DC mostly are neuthrophil segmented and monocyte
• Caused by:
Liver disease
Megaloblastic anemias
Hereditary
• Morphology:
HYPERSEGMENTATION
INTERPRETATION WHITE BLOOD CELL/WBC (LEUCOCYTE)
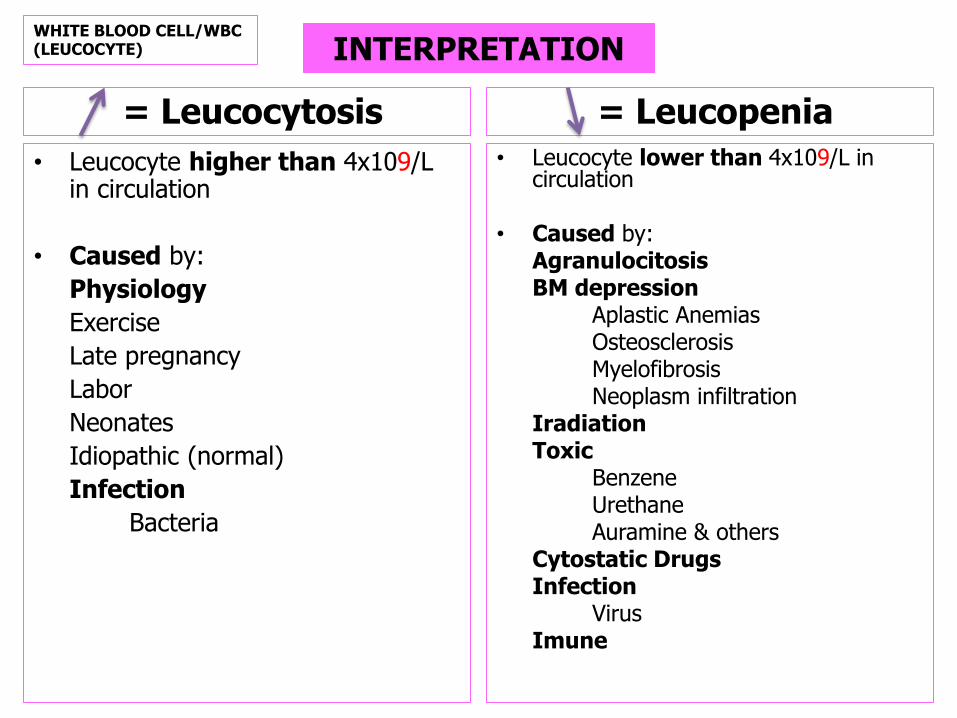
= Leucocytosis
• Leucocyte higher than 4x109/L in circulation
• Caused by:
Physiology
Exercise
Late pregnancy
Labor
Neonates
Idiopathic (normal)
Infection
Bacteria
= Leucopenia • Leucocyte lower than 4x109/L in
circulation • Caused by: Agranulocitosis BM depression Aplastic Anemias Osteosclerosis Myelofibrosis Neoplasm infiltration Iradiation Toxic Benzene Urethane Auramine & others Cytostatic Drugs Infection Virus Imune
INTERPRETATION WHITE BLOOD CELL/WBC (LEUCOCYTE)
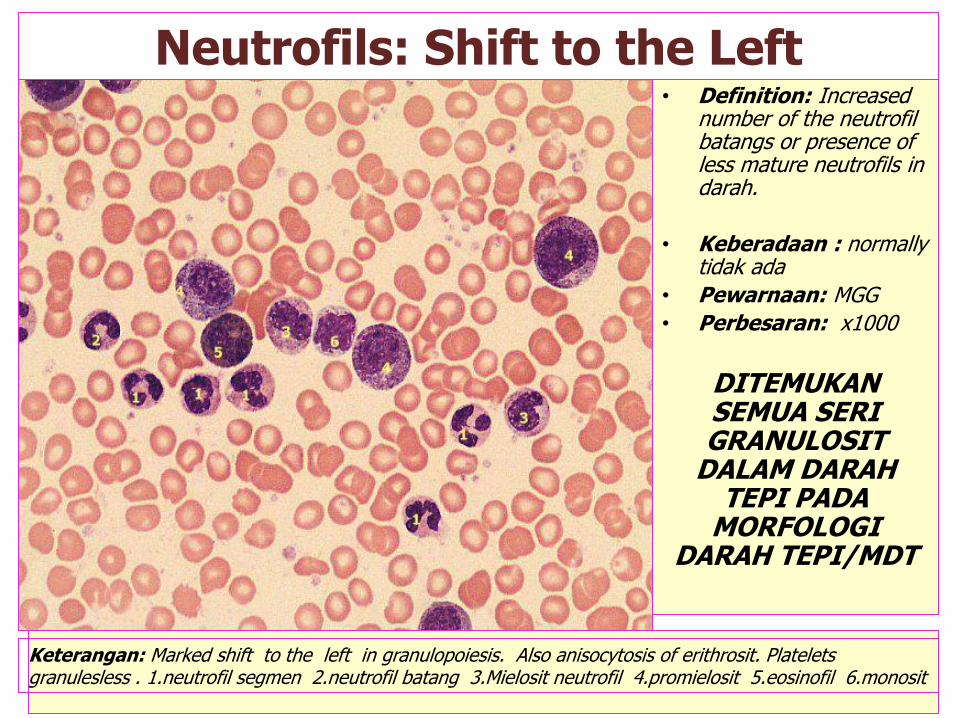
Neutrofils: Shift to the Left • Definition: Increased
number of the neutrofil batangs or presence of less mature neutrofils in darah.
• Keberadaan : normally tidak ada
• Pewarnaan: MGG
• Perbesaran: x1000
DITEMUKAN SEMUA SERI GRANULOSIT
DALAM DARAH TEPI PADA
MORFOLOGI DARAH TEPI/MDT
Keterangan: Marked shift to the left in granulopoiesis. Also anisocytosis of erithrosit. Platelets granulesless . 1.neutrofil segmen 2.neutrofil batang 3.Mielosit neutrofil 4.promielosit 5.eosinofil 6.monosit

EOSINOPHIL
Normal Eosinophil Size : 12-17 µm Colour : Pale Blue Ratio of Cytoplasmic: High Granules : Many, large & Rounded, Reddish- Orange Nucleus : Usually two segments Main Function : Effector cells for antibody-dependent damage to metazoal parasites Regulate immediate-type hypersensitivity reactions (inactivate histamine and heparin and proteases)
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008

INTERPRETATION
= EOSINOPHILIA • Eosinophilia is defined as an
absolute eosinophil count above 0.4x109/L
• Caused by: Allergic Reaction (Ex: Asthma, Hay Fever, Drug Sensitivity) Parasitic Infection Hypersensitivity Reaction (Ex: Looeffler Syndrome) Skin Disease (Ex: Dermatitis Herpetiformis) Tropical Eosinophilia Malignant Myeloproliferative Disorders Certain Infection (Ex: Scarlet Fever)
= EOSINOPENIA
• Eosinopenia is defined as an absolute eosinophil count below 0.4x109/L
• Caused by:
Thymoma
Hypogammaglobulinemia
Rare Inherited Forms
Autoimmune Disorders with
Antieosinophilia Antibodies
Unknown Causes
EOSINOPHIL
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008

NORMAL MORPHOLOG OF EOSINOPHILS

Mature Eosinofils in Periferal darah • Ukuran sel: 15 - 25 m
• Bentuk sel: oval atau bulat
• Warna sitoplasma: pale, covered by granules
• Granularitas: abundant eosinofilik (orange-red)
• Bentuk inti: lobulated, semicircular
• Tipe kromatin: condensed
• Ratio inti/sitoplasma: low or veri low
• Nukleolus: not visible
• Keberadaan:
• darah: 2 - 4 %
• sumsum tulang: < 2 %
• Pewarnaan: MGG
• Perbesaran: x 1000
Keterangan: Single eosinofil leucosit with bi-lobulated nucleus. Also anisocytosis of erithrosit and ovalosit. Normal platelets.

BASOPHIL
Normal Basophil Size : 10-14 µm Colour : - Ratio of Cytoplasmic: High Granules : Several, large & rounded, dark purplis-black Nucleus : Usually two segments, granules overlie nucleus Main Function: • Mediate immediate-type hypersensitivity (IgE-coated basophilia react with spesific antigen and release histamine and leukotrines). • Modulate inflammatory response by releasing heparin and
protease.
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008
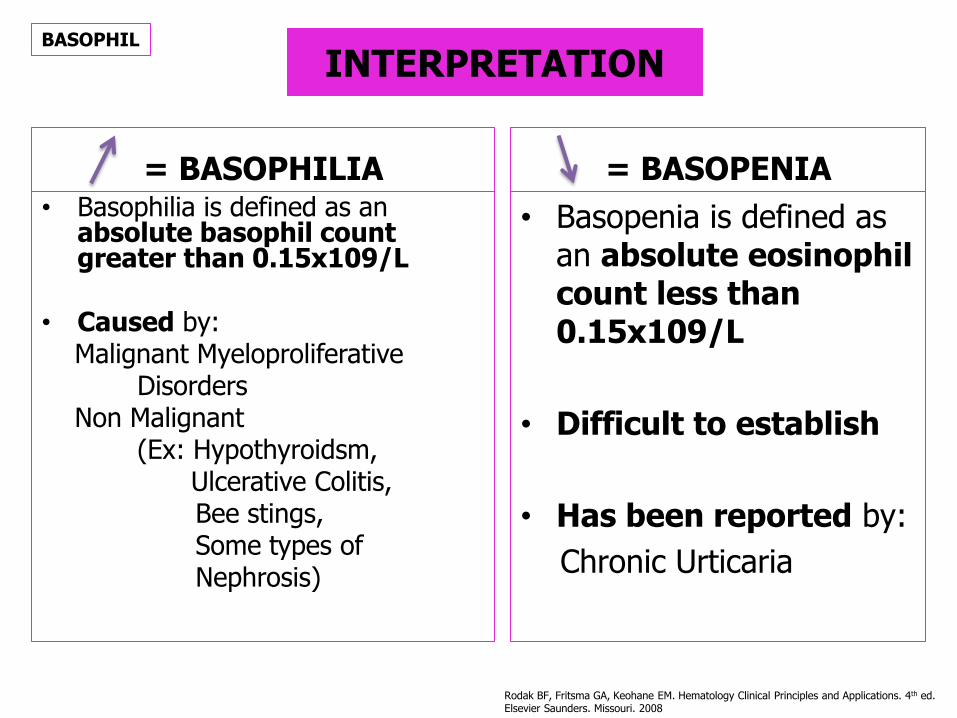
INTERPRETATION
= BASOPHILIA • Basophilia is defined as an
absolute basophil count greater than 0.15x109/L
• Caused by: Malignant Myeloproliferative Disorders Non Malignant (Ex: Hypothyroidsm, Ulcerative Colitis, Bee stings, Some types of Nephrosis)
= BASOPENIA
• Basopenia is defined as an absolute eosinophil count less than 0.15x109/L
• Difficult to establish
• Has been reported by:
Chronic Urticaria
BASOPHIL
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008
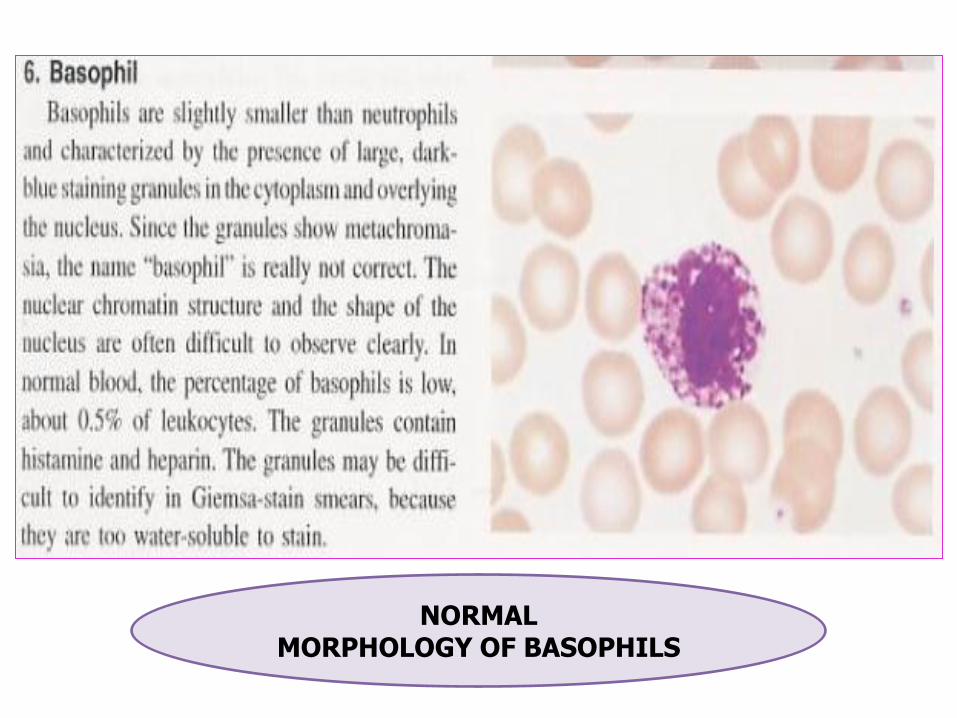
NORMAL MORPHOLOGY OF BASOPHILS
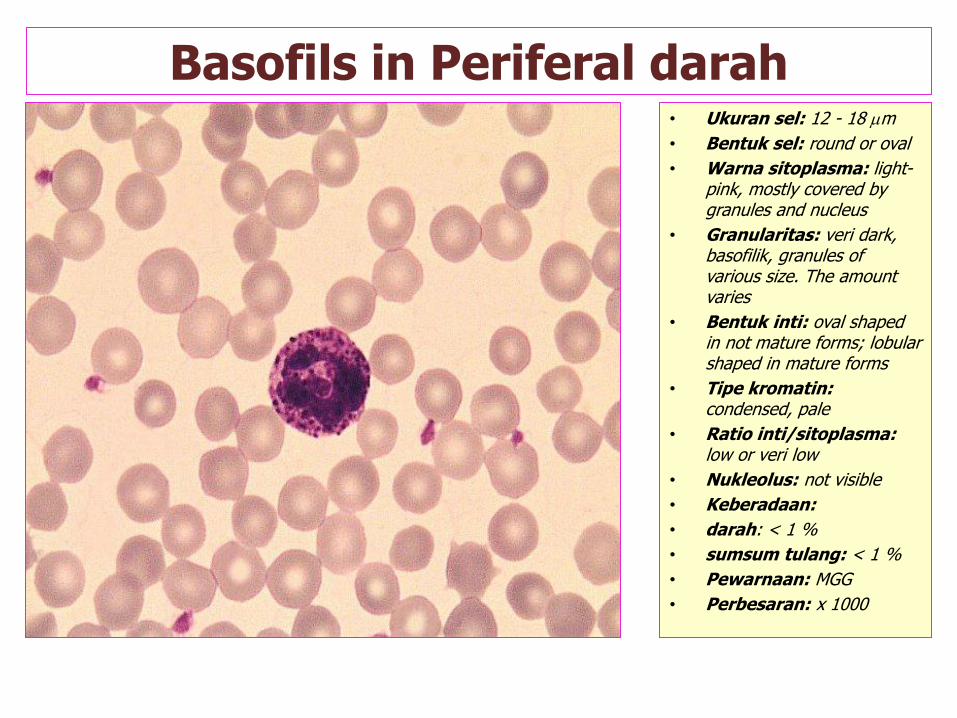
Basofils in Periferal darah • Ukuran sel: 12 - 18 m
• Bentuk sel: round or oval
• Warna sitoplasma: light-pink, mostly covered by granules and nucleus
• Granularitas: veri dark, basofilik, granules of various size. The amount varies
• Bentuk inti: oval shaped in not mature forms; lobular shaped in mature forms
• Tipe kromatin: condensed, pale
• Ratio inti/sitoplasma: low or veri low
• Nukleolus: not visible
• Keberadaan:
• darah: < 1 %
• sumsum tulang: < 1 %
• Pewarnaan: MGG
• Perbesaran: x 1000
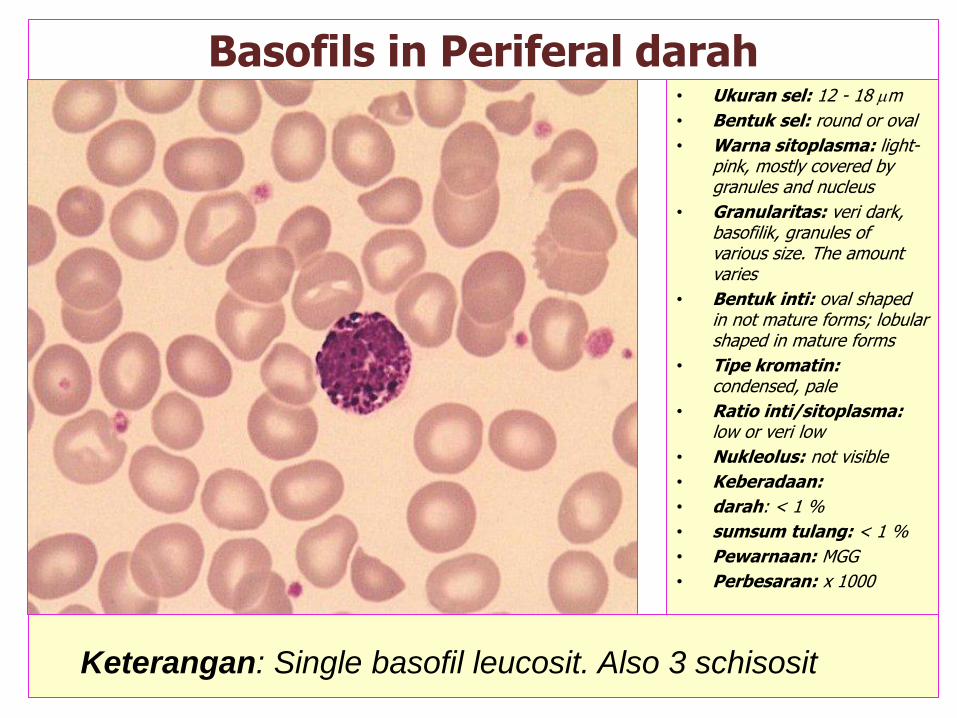
Basofils in Periferal darah • Ukuran sel: 12 - 18 m
• Bentuk sel: round or oval
• Warna sitoplasma: light-pink, mostly covered by granules and nucleus
• Granularitas: veri dark, basofilik, granules of various size. The amount varies
• Bentuk inti: oval shaped in not mature forms; lobular shaped in mature forms
• Tipe kromatin: condensed, pale
• Ratio inti/sitoplasma: low or veri low
• Nukleolus: not visible
• Keberadaan:
• darah: < 1 %
• sumsum tulang: < 1 %
• Pewarnaan: MGG
• Perbesaran: x 1000
Keterangan: Single basofil leucosit. Also 3 schisosit

NEUTROPHIL SEGMENTED
Normal Neutrophil
In the blood are distributed between a marginated granulocyte pool.
When cell counts are determined on samples of periphera venous blood, only the circulating granulocytes are being studied.
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008

NEUTROPHIL SEGMENTED
Normal Neutrophil
Size : 9-15 µm
Colour : Slightly pink
Ratio of Cytoplasmic:
High
Granules : Numerous, very fine, faint purple
Nucleus : Usually two to five segments
Main Function :
Chemotaxis, Phagocytosis, Killing
of Phagocytososed Bacteria
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008

INTERPRETATION
= NEUTROPHILIA
• Is defined as an absolute neutrophil count above 8.7x109/L.
• Caused by: Physiologyc (Ex: Sternous exercise) Acute Infections Inflammation (Ex: Burns, After Surgery, Myocardial Infarction) Intoxication (Ex: Uremia, Diabetic Acidosis, Poisoning, Insect Envenomation) Acute Hemorrhage or Hemolysis Response to Fast-Growing Tumors Malignant Myeloproliferative Disorders Certain Medications (Ex: Steroids)
= NEUTROPENIA
• Is defined as an absolute neutrophil count below 2.0x109/L.
• Caused by: Overwhelming Infection Hemodialysis Physical Agents/Drugs (Ex: Chemotherapy, Radiation, Chloramphenicol, any agent causing Aplasia) Decreased or Ineffective Production (Ex: Megaloblastic Anemia) Splenic Sequestratio Autoimmune Disorders Debilitated States (ex: Alcoholism) Hereditary Disorders (Ex: Cyclic Neutropenia)
NEUTROPHIL SEGMENTED
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008

= Neutrophilia
• Netrophil segmented higher than >70% counted in differential counting/DC.
• Caused by: Infection, after fagocitation
process Organ Injury Crush Injury Neoplasm Burn Intoxication (Ex: Co, Pb) Metabolic Disorder Eclampsia Acute Gout Diabetes (Ketosis) Cushing Syndrome Leukemias Granulocytic Policytemia Vera Myelosis (erythremic)
= Neutropenia
• Netrophil segmented lower than >70% counted in differential counting/DC.
• Caused by: Famial Idiophatic Chediac Higashi Syndrome Hypersplenism Anafilactic Syock Chirosis Hepatis PNH Tirotoxicosis Drugs Analgetic antipiretic (Ex: Amydopirine, Metampiron) Antityroid (Ex: Thiouracyl, methylthiouracyl) Antihistamine (Ex: Promethazine, Chlorpheniramine) Tranquilizer (Ex: Chlorpromazine,Meprobamate, Imipramine) Antibiotic (Ex: Ristocetin, Tethracycline, Salicyl- azo sulfa pyridien, Strepthomycine) Anticoagulant (Ex: Dicoumarol) Antituberculosis (Ex: INH, PAS) Antimalaria (Ex: Primaquine) Diuretic (Ex; Thiazide) Others (Ex: Metronidazole)
INTERPRETATION WHITE BLOOD CELL/WBC (LEUCOCYTE)

ABNORMAL
NORMAL MORPHOLOGY OF
NEUTROPHILS
LYMPHOCYTES
Normal Lymphocytes
Peripheral blood:
65-80% are T cells
10-30% are B cells
2-10% are non-T & non-B cells
Function:
Involved in immune responses and production of haemopoietic growth factors
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008
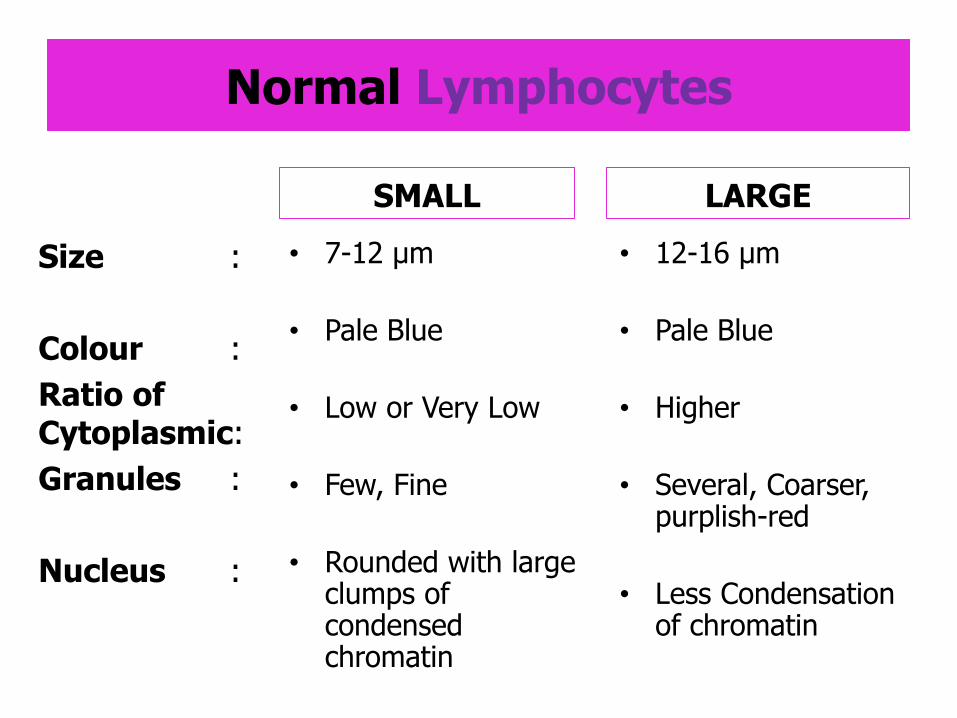
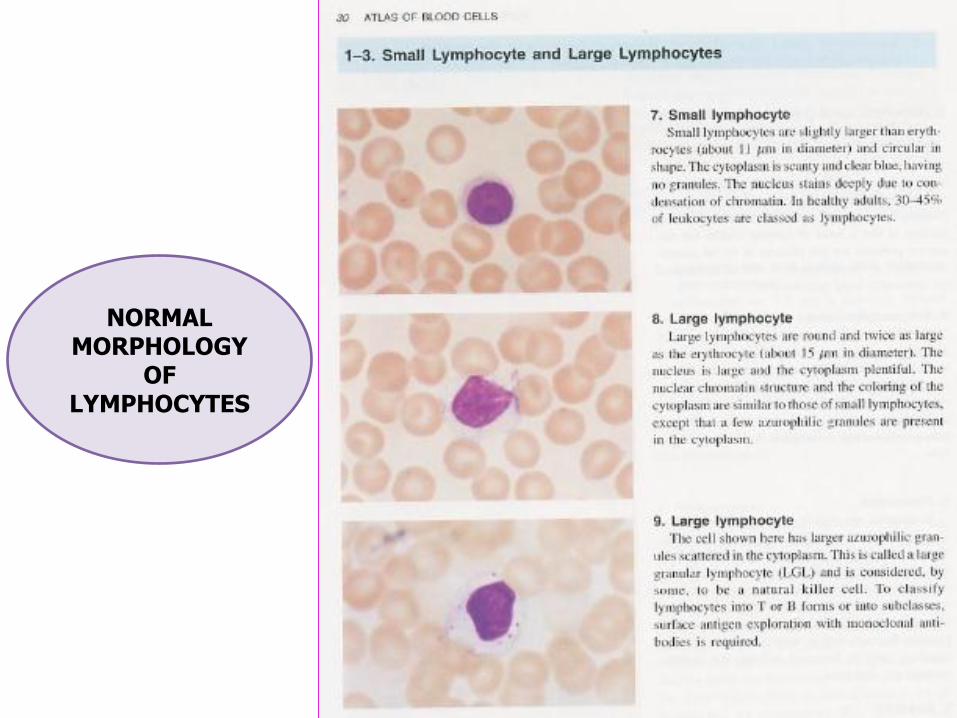
Normal Lymphocytes
SMALL
Size :
Colour :
Ratio of Cytoplasmic:
Granules :
Nucleus :
• 12-16 µm
• Pale Blue
• Higher
• Several, Coarser, purplish-red
• Less Condensation of chromatin
• 7-12 µm
• Pale Blue
• Low or Very Low
• Few, Fine
• Rounded with large clumps of condensed chromatin
LARGE
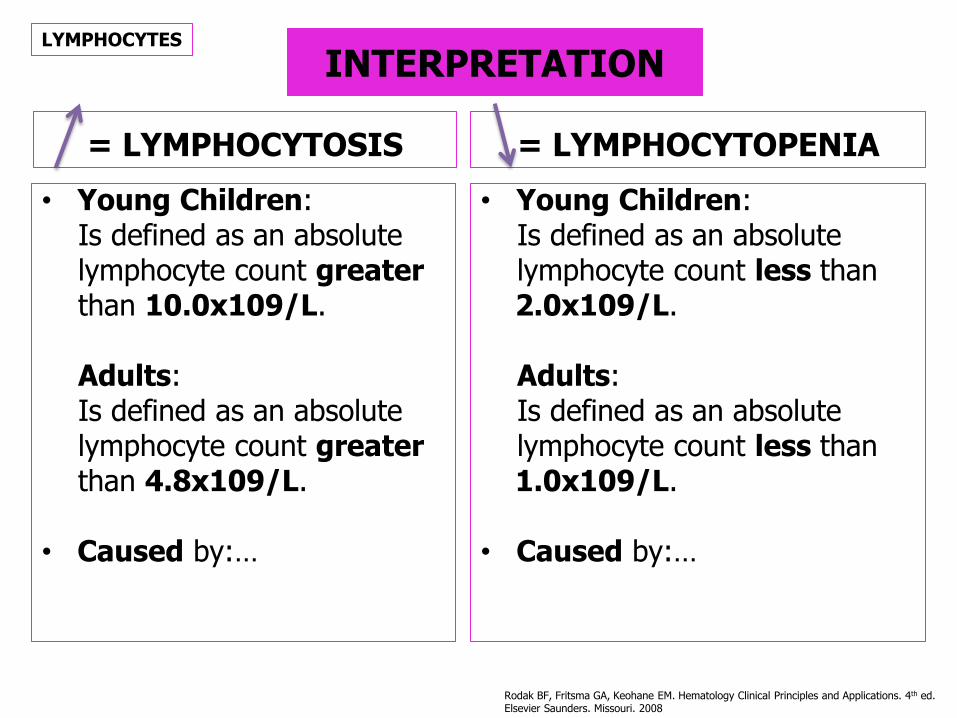
INTERPRETATION
= LYMPHOCYTOSIS
• Young Children: Is defined as an absolute lymphocyte count greater than 10.0x109/L. Adults: Is defined as an absolute lymphocyte count greater than 4.8x109/L.
• Caused by:…
= LYMPHOCYTOPENIA
• Young Children: Is defined as an absolute lymphocyte count less than 2.0x109/L. Adults: Is defined as an absolute lymphocyte count less than 1.0x109/L.
• Caused by:…
LYMPHOCYTES
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008
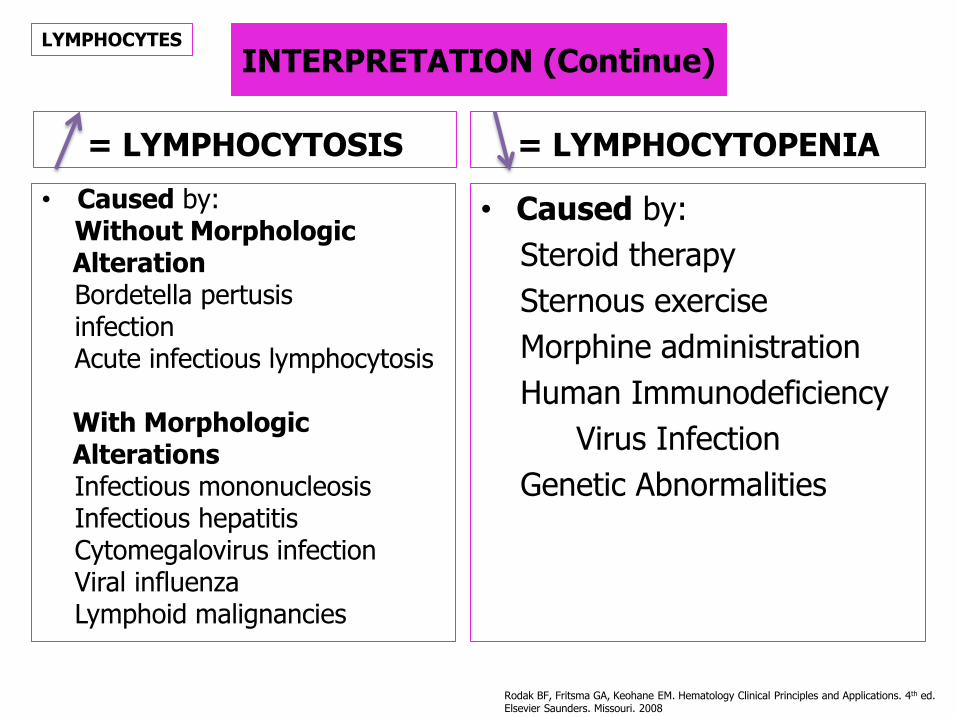
INTERPRETATION (Continue)
= LYMPHOCYTOSIS
• Caused by: Without Morphologic Alteration Bordetella pertusis infection Acute infectious lymphocytosis With Morphologic Alterations Infectious mononucleosis Infectious hepatitis Cytomegalovirus infection Viral influenza Lymphoid malignancies
= LYMPHOCYTOPENIA
• Caused by:
Steroid therapy
Sternous exercise
Morphine administration
Human Immunodeficiency
Virus Infection
Genetic Abnormalities
LYMPHOCYTES
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008
NORMAL MORPHOLOGY
OF LYMPHOCYTES
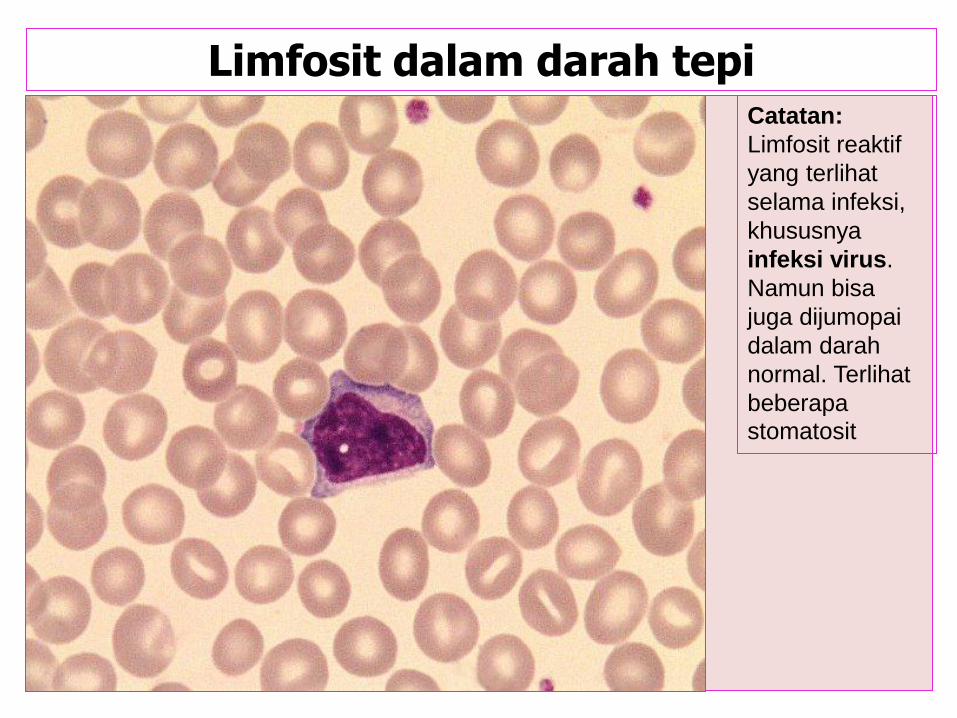
Limfosit dalam darah tepi Catatan:
Limfosit reaktif
yang terlihat
selama infeksi,
khususnya
infeksi virus.
Namun bisa
juga dijumopai
dalam darah
normal. Terlihat
beberapa
stomatosit

MONOCYTES Normal Monocytes Size : 15-30 Colour : Pale, Greyish Blue, Cytoplasmic vacuole may be seen Ratio of Cytoplasmic: Moderately High to High Granules : Variabel number, fine, purplish-red (unussual) Nucleus : Various shapes (rounded, C or U shape, lobulated), skin-like or lacy chromatin Main Function : The precursor of tissue macrophage. Phagositosis of microorganisms and cells coated with antibody. Chemotaxis, Phagocytosis, Killing of some microorganisms, Antigen presentation (dendritic cells/antigen presenting cell), Release of Interleukin (IL) -1 and Tumor Necrozing Factor/TNF which stimulate bone marrow stromal to produce GM-CSF, G-CFS, M-CFS and IL-6
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008

= Monocytosis
• Is defined as an absolute monocyte count above 1.1x109/L.
• Caused by: Bacterial Infection (Ex: Tbc, subacute bacterial endocarditis, syphillis) Recovery from Acute Infection Protozoal & Rickettsial Infection (Ex: malaria, typhus) Certain Carcinomas Granulomatous Disease Collagen Vascular Disease (Ex: SLE) Malignancies of Monocyte Cell Line
= Monocytopenia
• Is defined as an absolute monocyte count below 0.4x109/L.
• Caused by:
Overwhelming Infections in Immunocompromised
Patients
Hemodialysis
Epstein-Barr Virus Infection
Steroid Therapy
INTERPRETATION WHITE BLOOD CELL/WBC (LEUCOCYTE)

INTERPRETATION
= MONOCYTOSIS
• Is defined as an absolute monocyte count greater than 1.1x109/L. • Caused by: Bacterial Infections (Ex: Tuberculosis, Subacute Bacterial Endocarditis, Syphillis) Recovery from Acute Infection Protozoal & Rickettsial Infection (Ex: Malaria, Thypus) Certain Carcinomas Granulomatous Diseases Collagen Vascular Disease (Ex: SLE) Malignancies of monocytes cell line
= MONOCYTOPENIA
• Is defined as an absolute
monocyte count less
than 0.4x109/L.
• Caused by:
Overwhelming Infections in
Immunocompromised -
Patients
Hemodialysis
Epstein-Barr Virus Infection
Steroid Therapy
MONOCYTES
Rodak BF, Fritsma GA, Keohane EM. Hematology Clinical Principles and Applications. 4th ed. Elsevier Saunders. Missouri. 2008
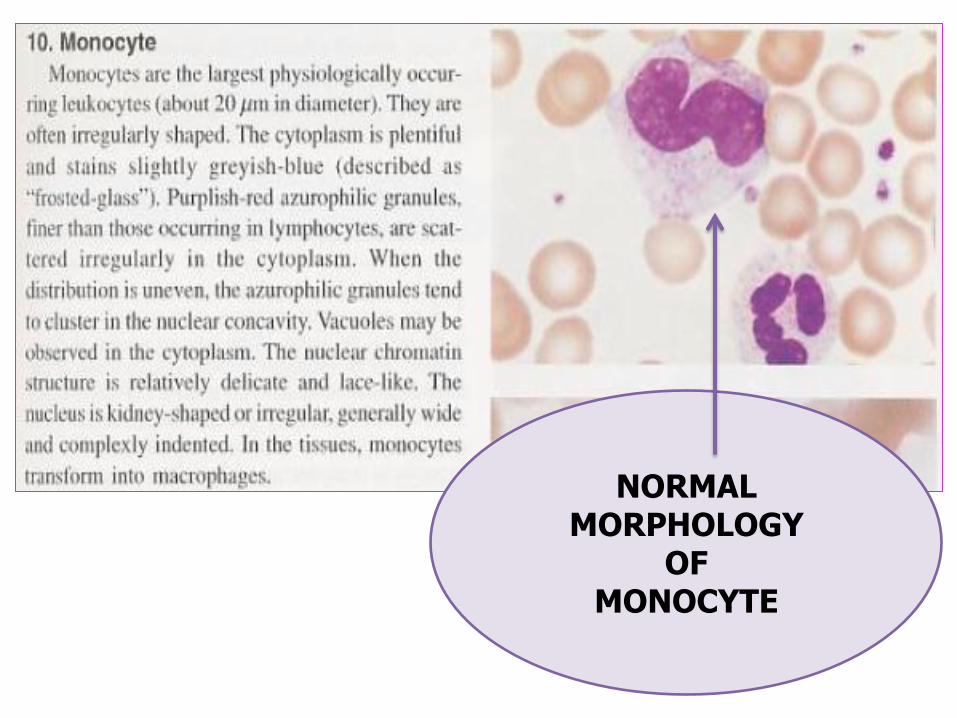
NORMAL MORPHOLOGY
OF MONOCYTE
PLATELETS / TROMBOCYTE
Size : 2-4 µm
Colour : Pale blue
Granules : Fine Azurophillic
Nucleus : Anucleated
Main Function:
Adhere to subendothelial connective tissue, Participate in Blood Clotting (Hemostasis & Thrombosis)
METHODS
• Manual: Counting Chamber
• Analyzer:
Hemocytometer
Autoanalyzer (Flow Cytometry)
PLATELETS (TROMBOCYTE)
REFFERENCE VALUE OR
NORMAL RANGE
150.000-450.000 U/L

= Thrombocitosis
• Thrombocyte in circulation higher than refference value (>450.000).
• Caused by: Iron Deficiency Anemia Hyposplenism Postsplenectomy Malignancy Collagen Vascular Disease Inflamatory Bowel Disease Infection Hemolysis Hemorrhage Idiopatic Mielofibrosis Essential Thrombocytosis Chronic Myelocitic Leucemia Idiopathic Sideroblastic Anemia Myelodysplasia Post operation Rebound ( stop alcohol, post correction
from Vitamin B12 deficiency/Folate) Policythemia vera
= Thrombocitopenia
• Thrombocyte in circulation lower than refference value (<150.000).
• Caused by:
Lower Production ec:
BMP damage
Aplasia Drugs/Toxin
Hepatitis Carcinoma
Congenital Defect
Fanconi’s anemia TAR Syndrome
Rubella May-Hegglin Syndrome
Wiskott Aldrich Dominant Autosomal
Ineffective Production
B12/Folate Deficiency
Distribution ec:
Splenomegaly
Liver disease Myelofibrosis
Higher Destruction ec:
Non Imune
DIC HUS
TTP HELLP Syndrome
Imune
SLE Limphoproliferative Disease
AIDS ITP
INTERPRETATION PLATELETS
(TROMBOCYTE)
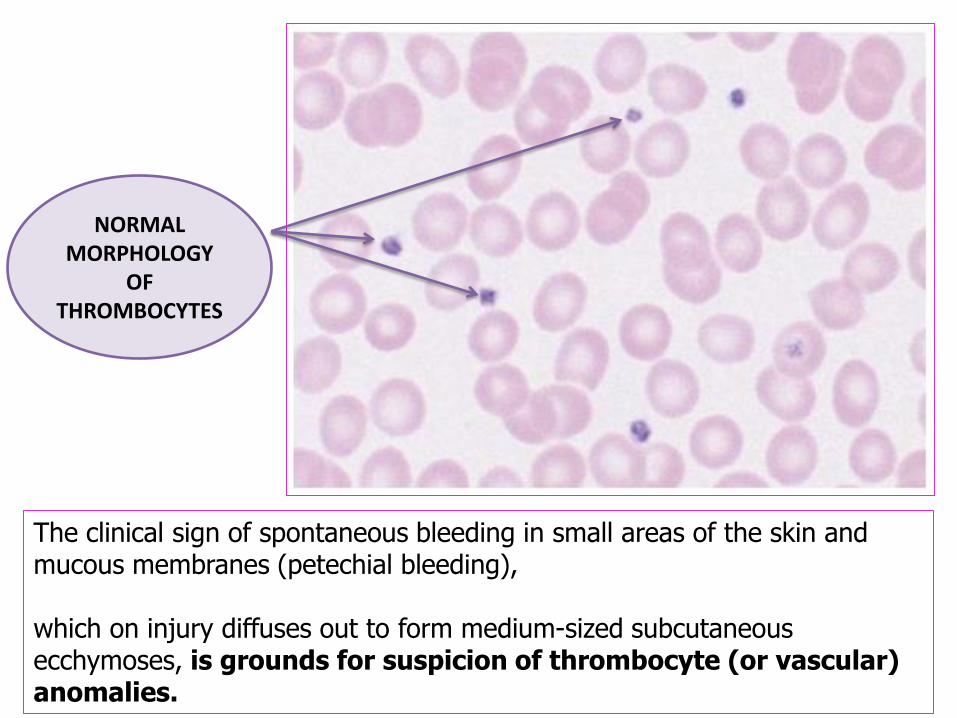
The clinical sign of spontaneous bleeding in small areas of the skin and mucous membranes (petechial bleeding), which on injury diffuses out to form medium-sized subcutaneous ecchymoses, is grounds for suspicion of thrombocyte (or vascular) anomalies.
NORMAL MORPHOLOGY
OF THROMBOCYTES
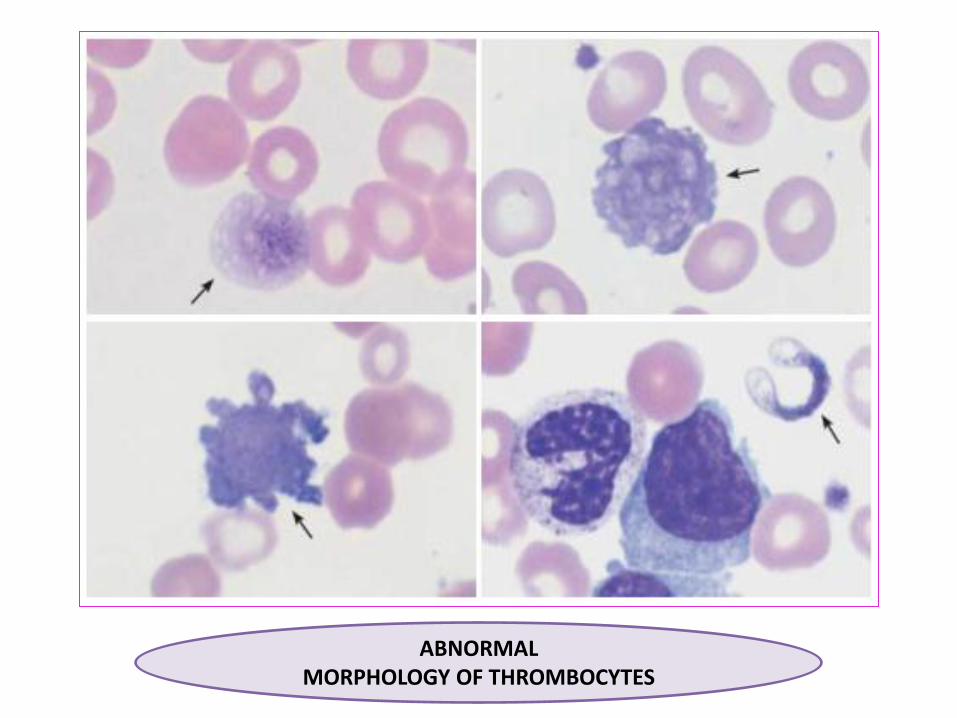
ABNORMAL MORPHOLOGY OF THROMBOCYTES
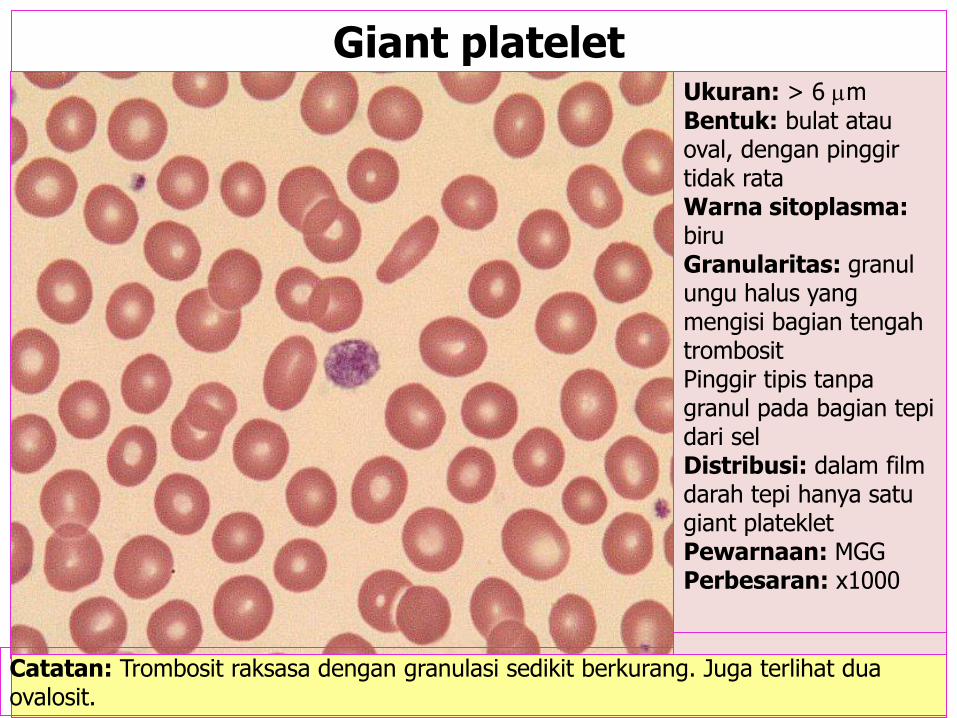
Catatan: Trombosit raksasa dengan granulasi sedikit berkurang. Juga terlihat dua ovalosit.
Giant platelet Ukuran: > 6 m Bentuk: bulat atau oval, dengan pinggir tidak rata Warna sitoplasma: biru Granularitas: granul ungu halus yang mengisi bagian tengah trombosit Pinggir tipis tanpa granul pada bagian tepi dari sel Distribusi: dalam film darah tepi hanya satu giant plateklet Pewarnaan: MGG Perbesaran: x1000

INFLAMATION MARKERS
Erythrocyte Sedimentation Rate/ESR
C-Reactive Protein/CRP
Serum Amiloid A/SAA
Procalcitonin/PCT
Known as
Acute Phase Reactan
Erythrocyte Sedimentation Rate/ESR Laju Endapan Darah/LED
Principle of examination,
have 3 phase:
1. Rouleaux phase
2. Sedimentation phase
3. Consolidation phase
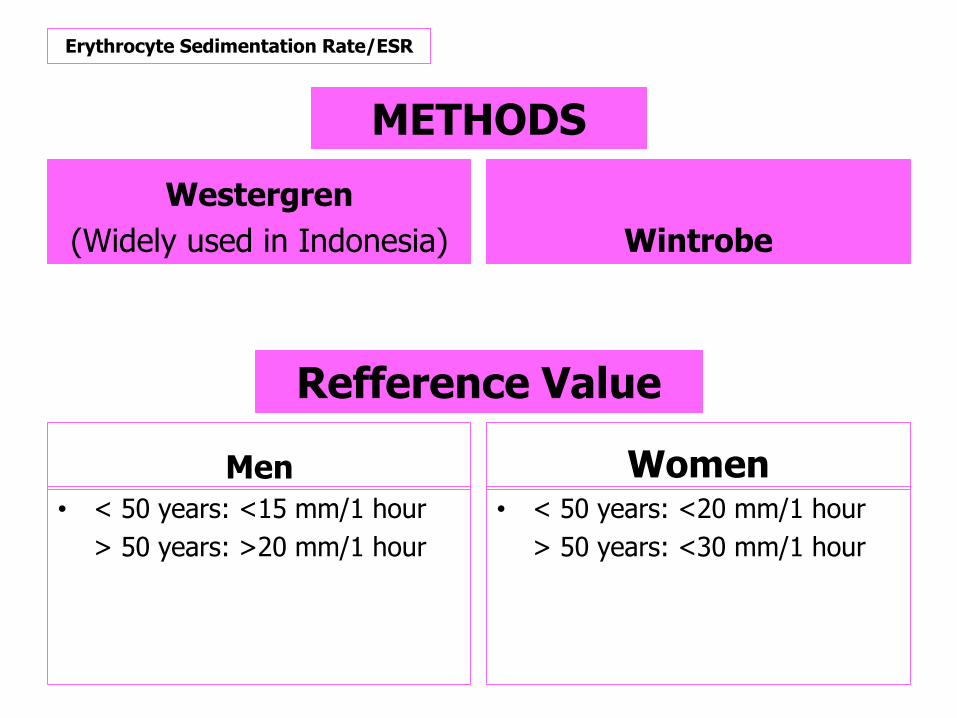
Men
• < 50 years: <15 mm/1 hour
> 50 years: >20 mm/1 hour
Women • < 50 years: <20 mm/1 hour
> 50 years: <30 mm/1 hour
Refference Value
Erythrocyte Sedimentation Rate/ESR
METHODS
Westergren
(Widely used in Indonesia) Wintrobe

Erythrocyte Sedimentation Rate/ESR
Advantage
• Cheap
• Simply
• Usually:
monitoring therapy
(ex: Tuberculosis)
Disadvantage
• Time Consuming
• As screening test
METHODS

= ESR Higher
• Injury • Inflamation • Pregnancy • Acute Inflamatory Disease: Local Systemic • Chronic Disease Ex: Rheumatoid Arthritis • Dysproteinemia Ex: Multiple Myeloma • Solid Tumor • Collagen Disease Ex: SLE • Macroglobulinemia Ex: Waldenstrom Syndrome • Nefritis, Nefrosis • Tuberculosis • Carcinoma
= ESR Lower
• Polyglobulin
Ex: Polycythemia
Interpretation
Erythrocyte Sedimentation Rate/ESR

Clinical Chemistry

SERUM GLUTAMIC OXALOACETIC TRANSAMINASE/SGOT = ASPARTATE AMINOTRANSFERASE/AST
Production: Cleared from the blood in a few days Become elevated 8 hours after cell injury Peak at 24-36 hours Return to normal in 3-7 days Main Function: Is used in the evaluation of patients with suspected hepatocellular disease. Very High Concentrations Highly metabolic tissue: Heart muscle Liver cells Skeletal muscle cells Lesser degree Kidneys Pancreas Red Blood Cells/RBCs Release by: When disease or injury affects the of the tissues, the lyse. If the cellular injury is chronic, levels will be persistently elevated.
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
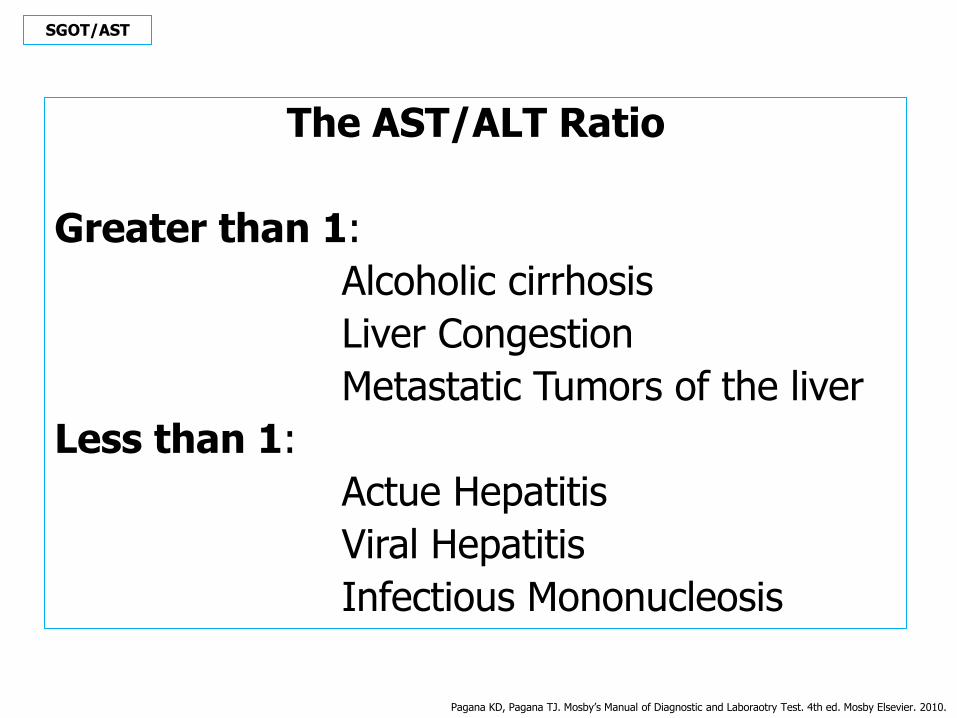
The AST/ALT Ratio
Greater than 1:
Alcoholic cirrhosis
Liver Congestion
Metastatic Tumors of the liver
Less than 1:
Actue Hepatitis
Viral Hepatitis
Infectious Mononucleosis
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
SGOT/AST

= SGOT/AST
Increased Levels
• Liver Disease • Hepatits • Hepatic Chirrhosis • Drug-Induced Liver
Injury • Hepatic Metastasis • Hepatic Necrosis (Initial State Only) • Hepatic Surgery • Infectious
Mononucleosis with Hepatitis
• Hepatic Infiltrative (e.g: Tumor) • Skeletal Muscle
Disease • Skeletal Muscle
Trauma
= SGOT/AST
Increased Levels
(Cont...)
• Recent Non Cardiac Surgery
• Multiple Traumas
• Severe, Deep Burns
• Progressive Muscular Dystrophy
• Recent Convulsions
• Heat Stroke
• Primary Muscle Disease
• Other Disease
Acute Hemolytic Anemia
Acute Pancreatitis
INTERPRETATION SGOT/AST
= SGOT/AST
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Decreased Levels
• Acute Renal Disease
• Beriberi
• Diabetec Ketoacidosis
• Pregnancy
• Chronic Renal Dialysis
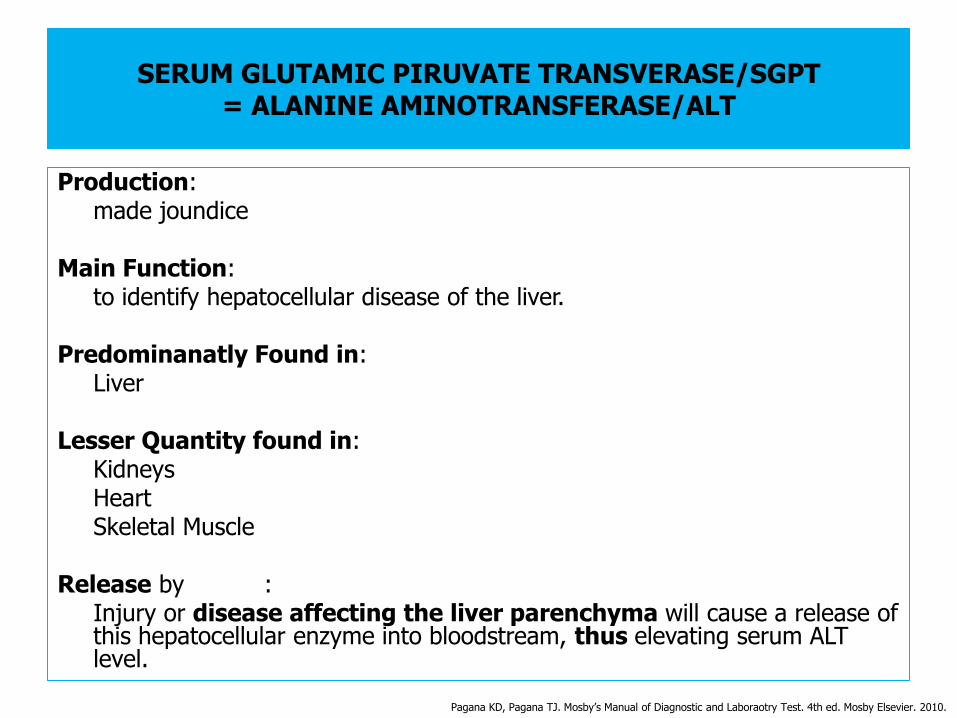
SERUM GLUTAMIC PIRUVATE TRANSVERASE/SGPT = ALANINE AMINOTRANSFERASE/ALT
Production: made joundice Main Function: to identify hepatocellular disease of the liver. Predominanatly Found in: Liver Lesser Quantity found in: Kidneys Heart Skeletal Muscle Release by : Injury or disease affecting the liver parenchyma will cause a release of
this hepatocellular enzyme into bloodstream, thus elevating serum ALT level.
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
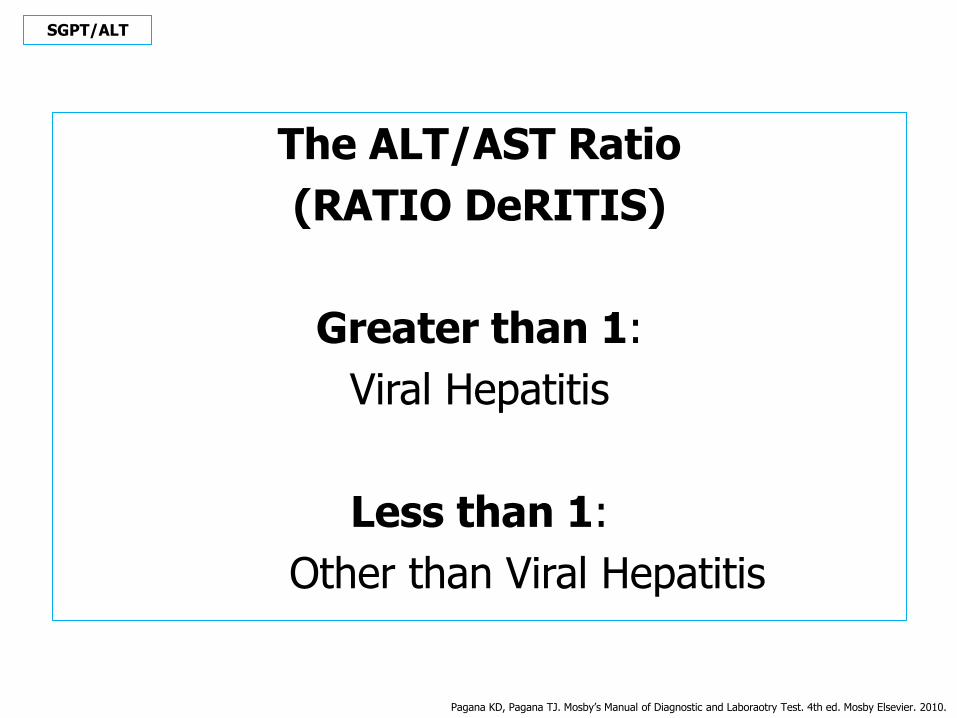
The ALT/AST Ratio
(RATIO DeRITIS)
Greater than 1:
Viral Hepatitis
Less than 1:
Other than Viral Hepatitis
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
SGPT/ALT

REFFERENCE VALUE OR
NORMAL RANGE
Elderly : may be slightly higher than adults values Adult/Child : 4-36 international unit/L at 37ºC Infant : may be twice as high as adults values
SGOT/AST-SGPT/ALT
Manual : Spectrophotometer
Analyzer : Autoanalyzer (Flow Cytometry)
METHODS
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.

= SGPT/ALT
Mildly
Increased Levels
• Myositis
• Pancreatis
• Myocardial Infarction
• Shock
= SGPT/ALT
Moderately
Increased Levels
• Cirrhosis
• Cholestasis
• Hepatic Tumor
• Hepatotoxic Drugs
• Obstructive Jaundice
• Severe Burns
• Trauma to Striated Muscle
INTERPRETATION SGPT/ALT
= SGPT/ALT
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Significantly
Increased Levels
• Hepatitis
• Hepatic Necrosis
• Hepatic Ischemia

UREA & BLOOD UREA NITROGEN/BUN CREATININE
UREA : direct from serum BUN : indirect from serum (calculation)
Production: Protein (exogenous/dietary or endogenous/tissue)
(Liver)
(metabolism & digestion)
(breakdown)
Amino Acid
(catabolized)
Ammonia
(deposited)
Blood
(transport)
Kidneys
(excretion)
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
RENAL FUNCTION STUDIES
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
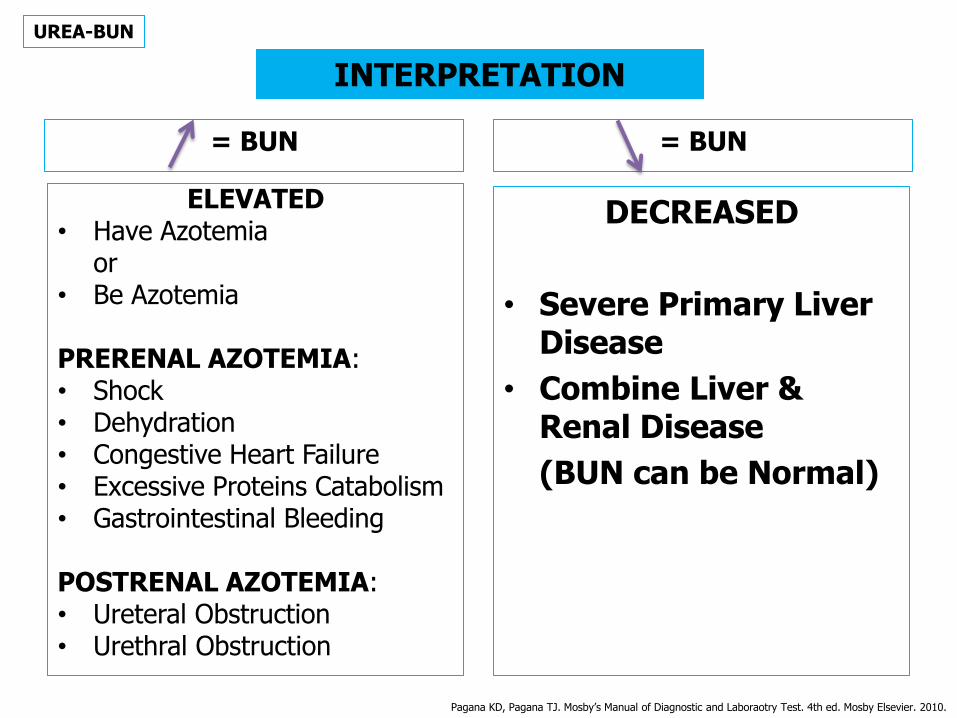
ELEVATED • Have Azotemia or • Be Azotemia PRERENAL AZOTEMIA: • Shock • Dehydration • Congestive Heart Failure • Excessive Proteins Catabolism • Gastrointestinal Bleeding POSTRENAL AZOTEMIA: • Ureteral Obstruction • Urethral Obstruction
UREA-BUN
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
= BUN = BUN
DECREASED
• Severe Primary Liver Disease
• Combine Liver & Renal Disease
(BUN can be Normal)
INTERPRETATION

METHODS
Manual : Spectrophotometer
Analyzer : Autoanalyzer (Flow Cytometry)
UREA-BUN
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
REFFERENCE VALUE OR NORMAL RANGE (depend on the methods)
Adult : 6-20 mg/dL
Newborn : 3-25 mg/dL
Adult >60 years : 8-23 mg/dL
(Elderly)
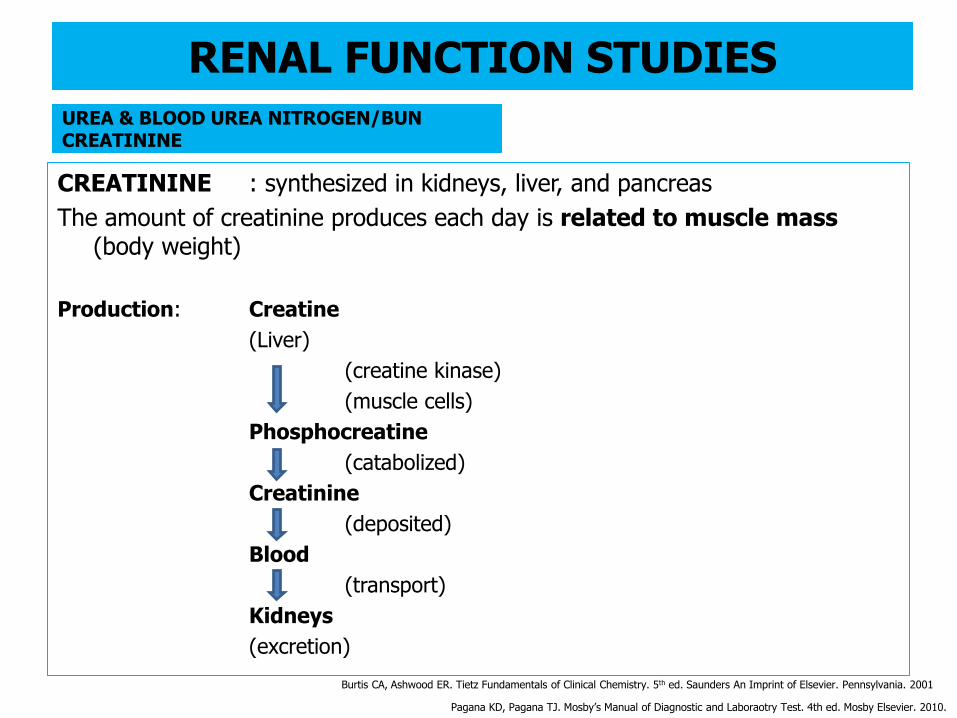
UREA & BLOOD UREA NITROGEN/BUN CREATININE
CREATININE : synthesized in kidneys, liver, and pancreas
The amount of creatinine produces each day is related to muscle mass (body weight)
Production: Creatine
(Liver)
(creatine kinase)
(muscle cells)
Phosphocreatine
(catabolized)
Creatinine
(deposited)
Blood
(transport)
Kidneys
(excretion)
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
RENAL FUNCTION STUDIES
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
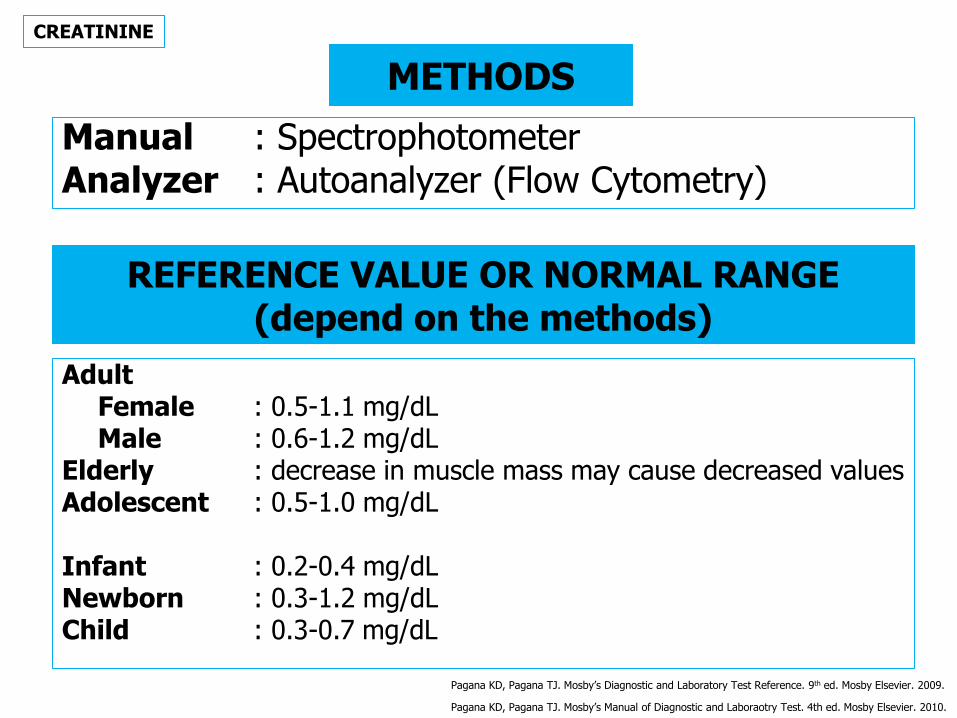
METHODS
Manual : Spectrophotometer Analyzer : Autoanalyzer (Flow Cytometry)
CREATININE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
REFERENCE VALUE OR NORMAL RANGE (depend on the methods)
Adult Female : 0.5-1.1 mg/dL Male : 0.6-1.2 mg/dL Elderly : decrease in muscle mass may cause decreased values Adolescent : 0.5-1.0 mg/dL Infant : 0.2-0.4 mg/dL Newborn : 0.3-1.2 mg/dL Child : 0.3-0.7 mg/dL
Pagana KD, Pagana TJ. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. Mosby Elsevier. 2009.

= CREATININE
ELEVATED (suggest chronicity of the disease)
• Dehydration • Glomerulonephritis • Pyelonephritis • Acute Tubular Necrosis • Urinary Obstruction • Diabetic Nephrophaty • Rhabdomyolysis • Acromegaly • Gigantism
SLIGHTLY ELEVATED • After meals (specially large
quantities of meat) • Diurnals variations (at 7 am-peak
at 7 pm)
= CREATININE
DECREASED
• Debilitation
• Decreased Muscle Mass
(e.g: muscular dysthropy,
myasthenia gravis)
INTERPRETATION CREATININE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001

UREA & BLOOD UREA NITROGEN/BUN CREATININE
The Most Important ‘Renal Clearance’ as an Indicator
GLOMERULAR FILTRATION RATE/GFR (Calculation)
The rate in millimeters per minute that substances, such as urea and creatinine, are filtered through the kidney’s glomeruli; a measure of the number of functioning nephrons.
The formula as follow:
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
RENAL FUNCTION STUDIES
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
UREA & BLOOD UREA NITROGEN/BUN CREATININE
The Most Important ‘Renal Clearance’ as an Indicator
CREATININE CLEARANCE (Calculation)
The volume (V) of
The urine measured (mL)
Urine flow rate is calculated (mL/min)
Creatinine is measured in mg/dL or mmol/L in
Both of th urine (urine/U and serum/S)
The formula as follow:
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
RENAL FUNCTION STUDIES
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
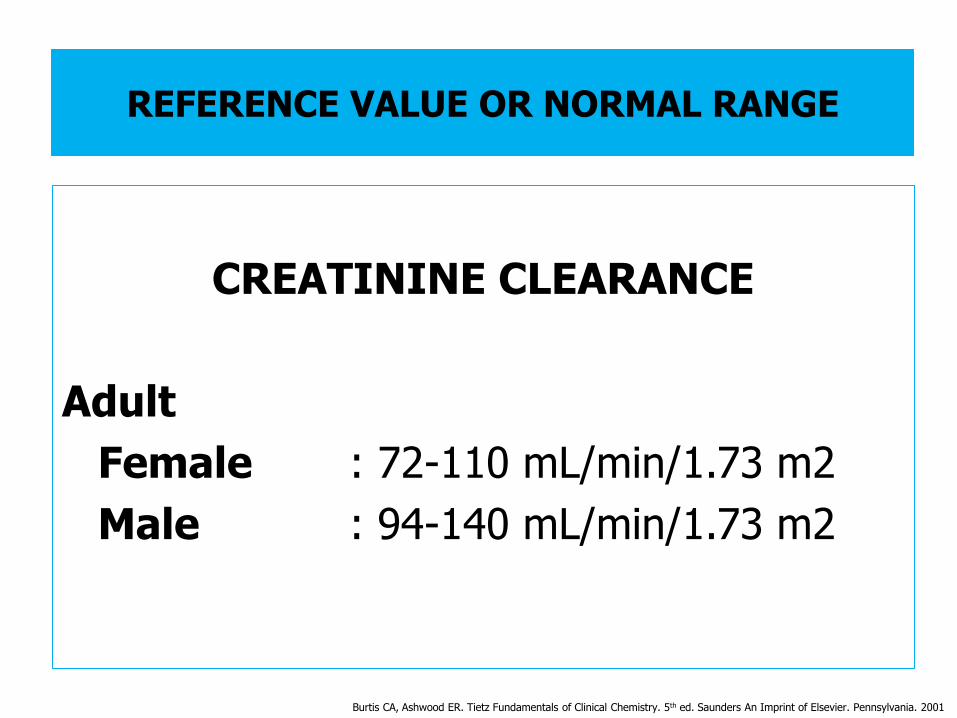
REFERENCE VALUE OR NORMAL RANGE
CREATININE CLEARANCE
Adult
Female : 72-110 mL/min/1.73 m2
Male : 94-140 mL/min/1.73 m2
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
URIC ACID/UA
URIC ACID: Nitrogenous Compound Large Degree Excreted by: Kidney Small Degree Excreted by: Intestinal Tract Production: Dietary Nucleic Acid (Purine Catabolism) Uric Acid Directly
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
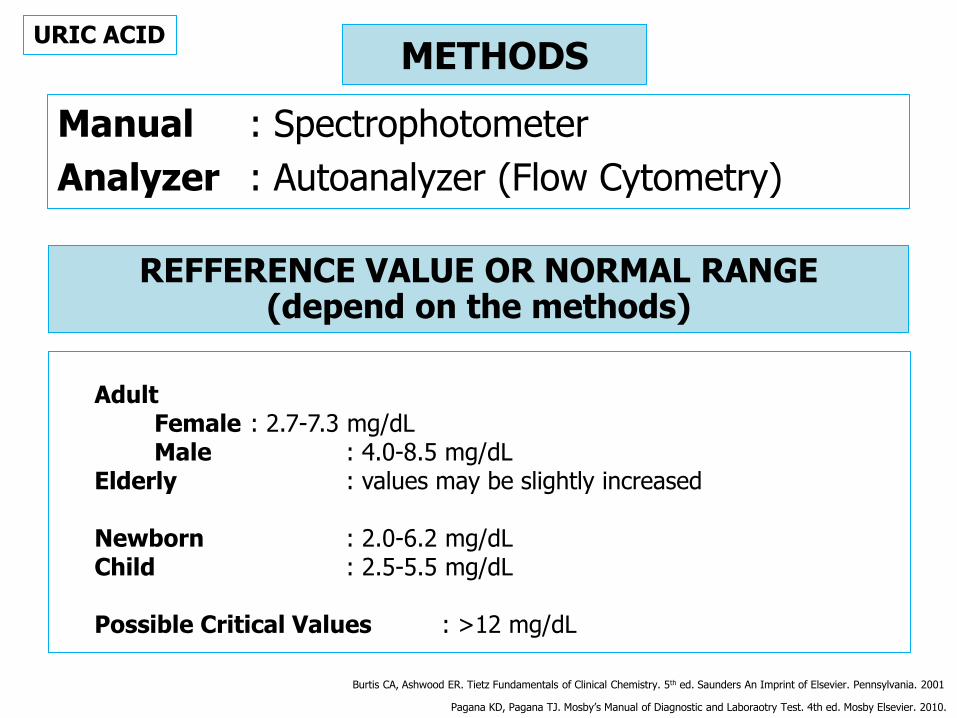
METHODS
Manual : Spectrophotometer
Analyzer : Autoanalyzer (Flow Cytometry)
URIC ACID
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
REFFERENCE VALUE OR NORMAL RANGE (depend on the methods)
Adult Female : 2.7-7.3 mg/dL Male : 4.0-8.5 mg/dL Elderly : values may be slightly increased Newborn : 2.0-6.2 mg/dL Child : 2.5-5.5 mg/dL Possible Critical Values : >12 mg/dL
Burtis CA, Ashwood ER. Tietz Fundamentals of Clinical Chemistry. 5th ed. Saunders An Imprint of Elsevier. Pennsylvania. 2001
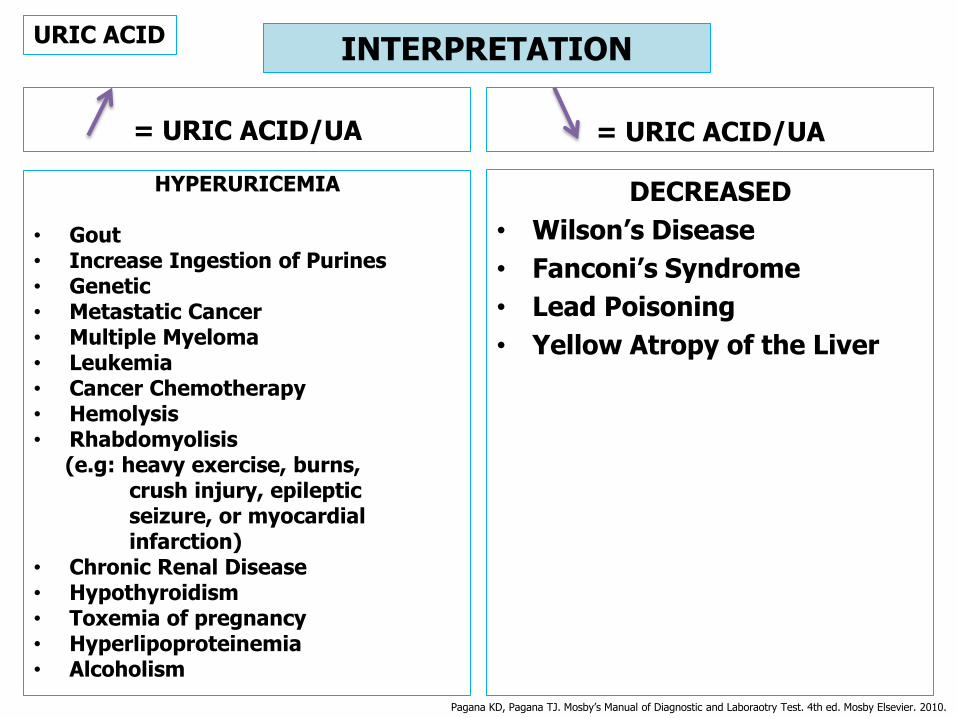
= URIC ACID/UA
HYPERURICEMIA
• Gout • Increase Ingestion of Purines • Genetic • Metastatic Cancer • Multiple Myeloma • Leukemia • Cancer Chemotherapy • Hemolysis • Rhabdomyolisis (e.g: heavy exercise, burns, crush injury, epileptic seizure, or myocardial infarction) • Chronic Renal Disease • Hypothyroidism • Toxemia of pregnancy • Hyperlipoproteinemia • Alcoholism
= URIC ACID/UA
DECREASED
• Wilson’s Disease
• Fanconi’s Syndrome
• Lead Poisoning
• Yellow Atropy of the Liver
INTERPRETATION URIC ACID
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
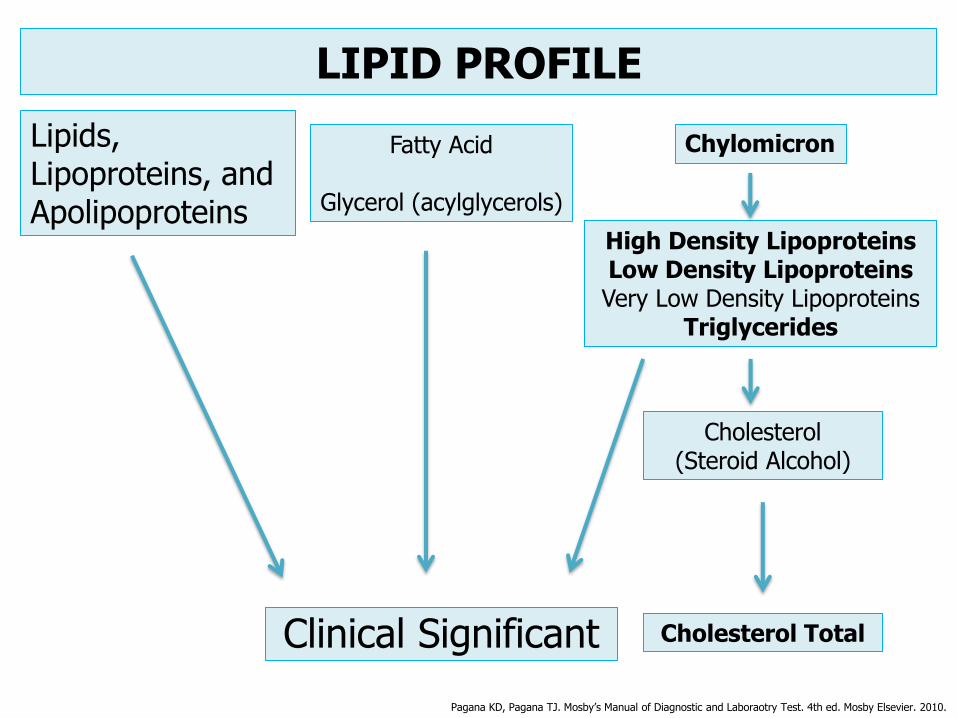
LIPID PROFILE
Clinical Significant
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Lipids, Lipoproteins, and Apolipoproteins
High Density Lipoproteins Low Density Lipoproteins Very Low Density Lipoproteins
Triglycerides
Fatty Acid
Glycerol (acylglycerols)
Cholesterol (Steroid Alcohol)
Cholesterol Total
Chylomicron

REMEMBER !!!
The purpose of cholesterol testing is:
To identify patients at risk for ATERIOSCLEROTIC
LIPID PROFILE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Required the for production of:
steroids, sex hormones, bile acid, and
cellular membranes
Main Function
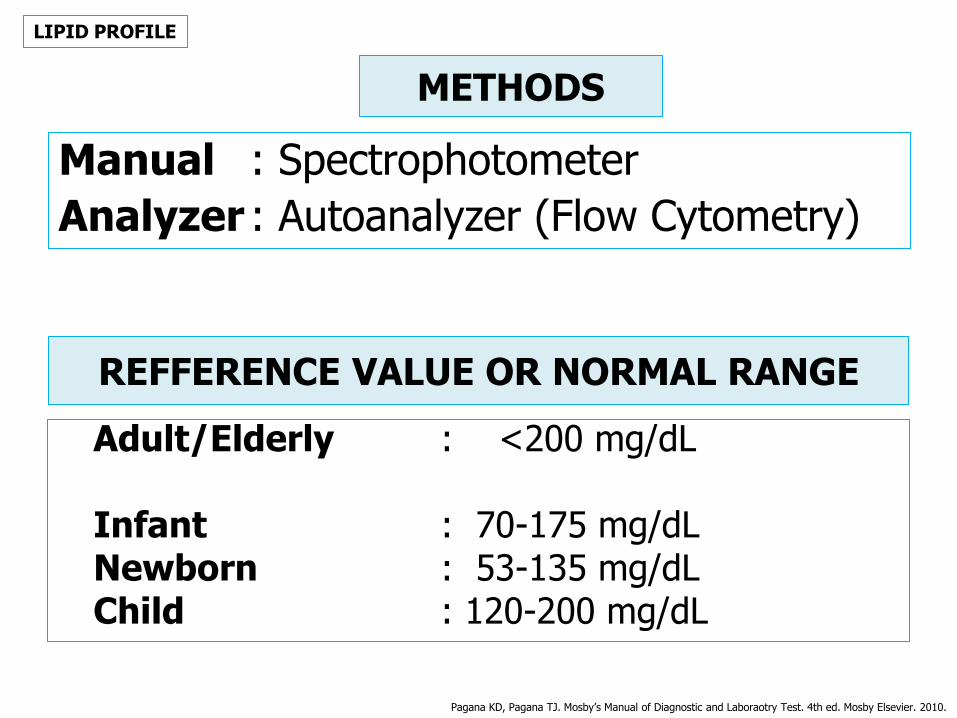
REFFERENCE VALUE OR NORMAL RANGE
Adult/Elderly : <200 mg/dL Infant : 70-175 mg/dL Newborn : 53-135 mg/dL Child : 120-200 mg/dL
LIPID PROFILE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Manual : Spectrophotometer
Analyzer : Autoanalyzer (Flow Cytometry)
METHODS

= Hyperlipidemia
INCREASED LEVELS
• Hypercholesterolemia • Hyperlipidemia • Hypothyroidism • Uncontroled Diabetes Mellitus • Nephrotic Syndrome • Pregnancy • High-cholesterol Diet • Xanthomatosis • Hypertension • Myocardial Infarction • Atherosclerosis • Biliary Cirrhosis • Stress • Nephrosis
= Hypolipidemia
DECREASED LEVEL
• Malabsorption
• Malnutrition
• Hyperthyroidism
• Cholesterol-lowering medication
• Pernicious Anemia
• Sepsis
• Stress
• Liver Disease
• Acute Myocardial Infarction
INTERPRETATION LIPID PROFILE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.

=
INCREASED LEVELS
• Hypercholesterolemia • Hyperlipidemia • Hypothyroidism • Uncontroled Diabetes Mellitus • Nephrotic Syndrome • Pregnancy • High-cholesterol Diet • Xanthomatosis • Hypertension • Myocardial Infarction • Atherosclerosis • Biliary Cirrhosis • Stress • Nephrosis
=
DECREASED LEVEL
• Malabsorption
• Malnutrition
• Hyperthyroidism
• Cholesterol-lowering medication
• Pernicious Anemia
• Sepsis
• Stress
• Liver Disease
• Acute Myocardial Infarction
INTERPRETATION LIPID PROFILE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.

BLOOD GLUCOSE
• Product: Carbohydrates Metabolism Diets (e.g: grains, legumes) (breakdown) Glycogen (Body stores) (Adipose tissue, Liver, Muscle) Exceed Calorie Intake • Hormon: Insulin Glucagon
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
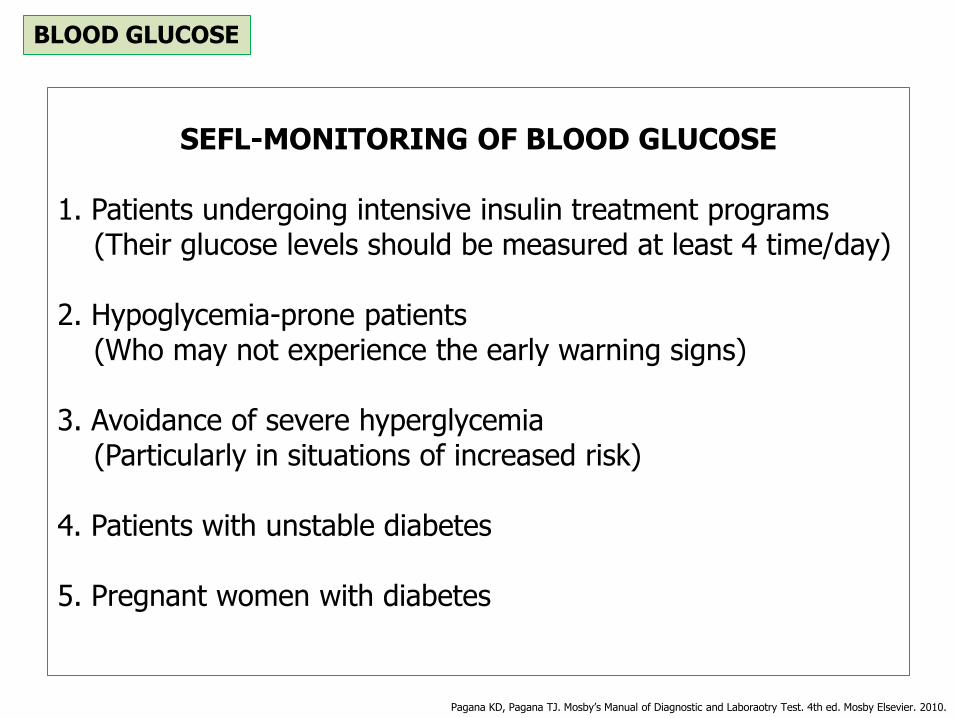
SEFL-MONITORING OF BLOOD GLUCOSE
1. Patients undergoing intensive insulin treatment programs (Their glucose levels should be measured at least 4 time/day) 2. Hypoglycemia-prone patients (Who may not experience the early warning signs) 3. Avoidance of severe hyperglycemia (Particularly in situations of increased risk) 4. Patients with unstable diabetes 5. Pregnant women with diabetes
BLOOD GLUCOSE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
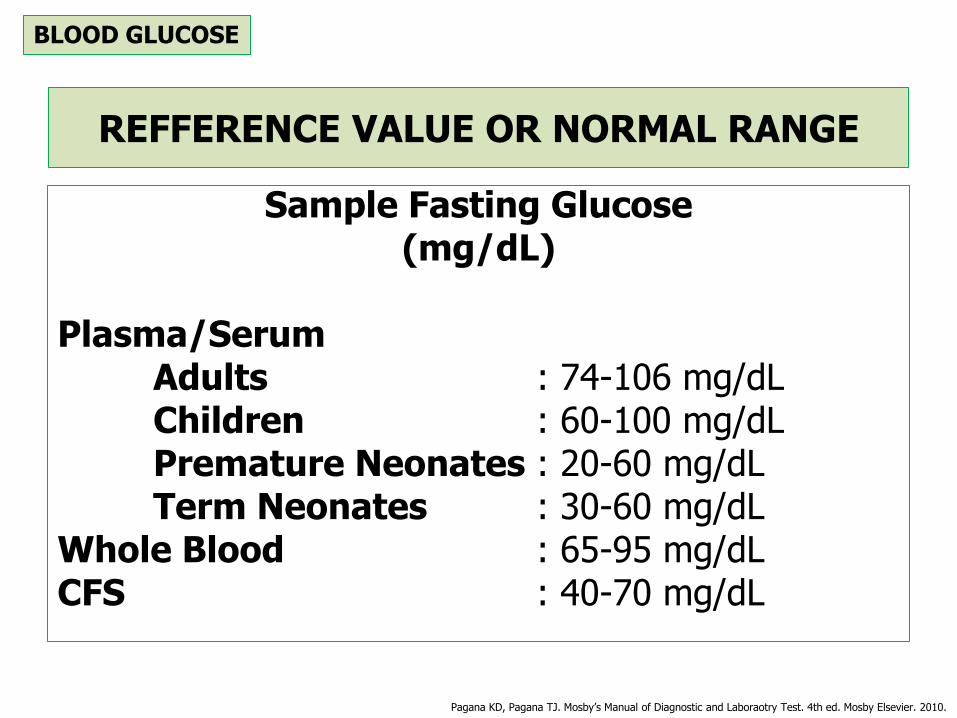
REFFERENCE VALUE OR NORMAL RANGE
Sample Fasting Glucose (mg/dL)
Plasma/Serum Adults : 74-106 mg/dL Children : 60-100 mg/dL Premature Neonates : 20-60 mg/dL Term Neonates : 30-60 mg/dL Whole Blood : 65-95 mg/dL CFS : 40-70 mg/dL
BLOOD GLUCOSE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
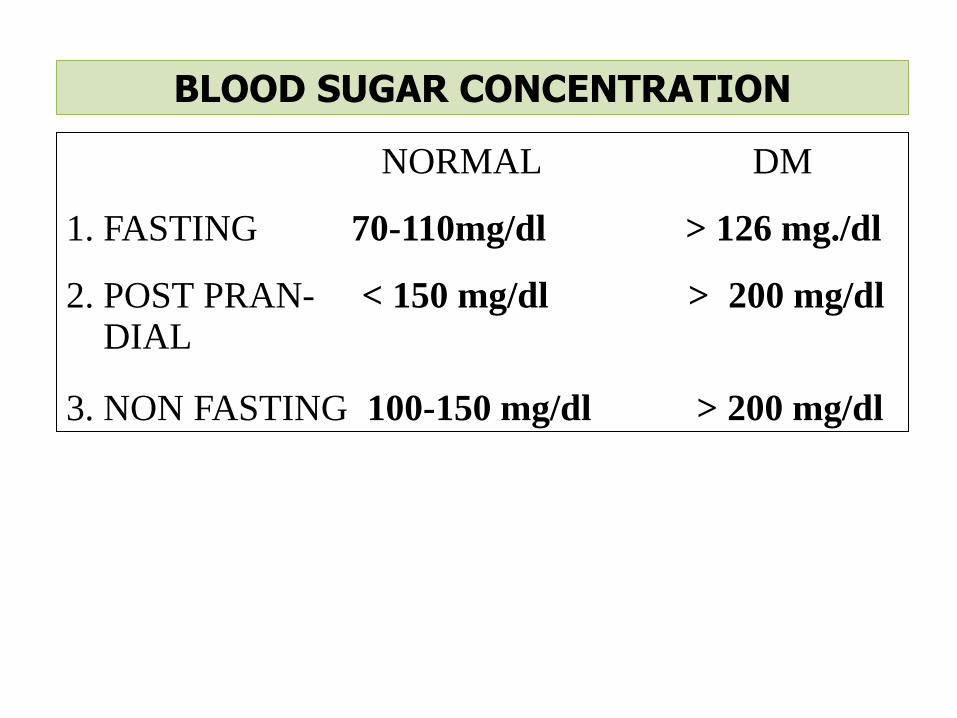
NORMAL DM
1. FASTING 70-110mg/dl > 126 mg./dl
2. POST PRAN- < 150 mg/dl > 200 mg/dl DIAL 3. NON FASTING 100-150 mg/dl > 200 mg/dl
BLOOD SUGAR CONCENTRATION
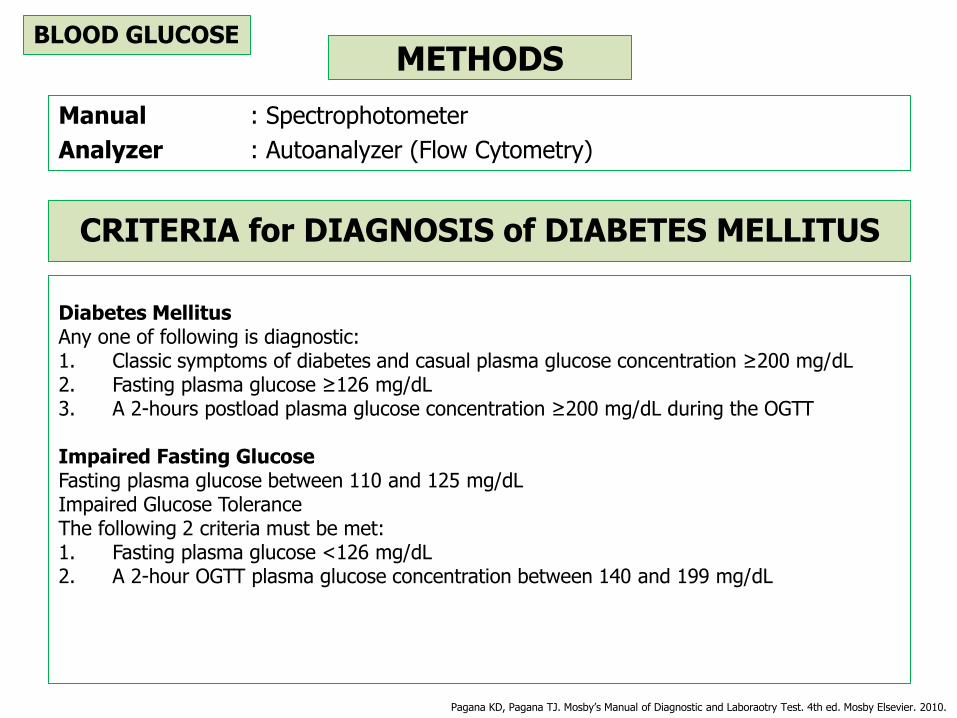
METHODS
Manual : Spectrophotometer
Analyzer : Autoanalyzer (Flow Cytometry)
BLOOD GLUCOSE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.
Diabetes Mellitus Any one of following is diagnostic: 1. Classic symptoms of diabetes and casual plasma glucose concentration ≥200 mg/dL 2. Fasting plasma glucose ≥126 mg/dL 3. A 2-hours postload plasma glucose concentration ≥200 mg/dL during the OGTT
Impaired Fasting Glucose Fasting plasma glucose between 110 and 125 mg/dL Impaired Glucose Tolerance The following 2 criteria must be met: 1. Fasting plasma glucose <126 mg/dL 2. A 2-hour OGTT plasma glucose concentration between 140 and 199 mg/dL
CRITERIA for DIAGNOSIS of DIABETES MELLITUS
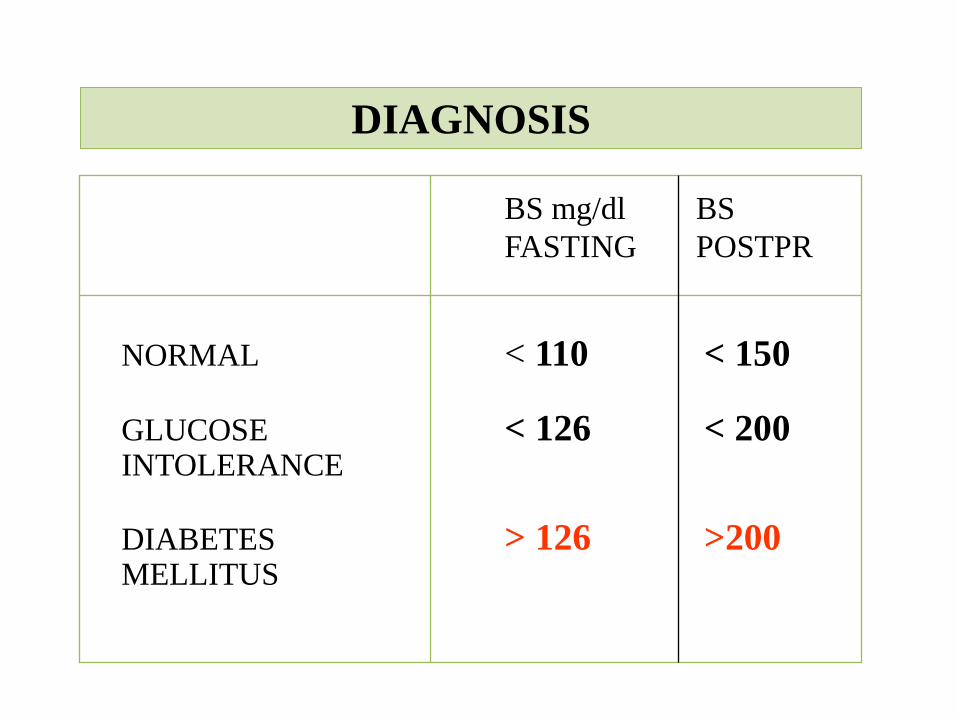
BS mg/dl BS
FASTING POSTPR
NORMAL < 110 < 150
GLUCOSE < 126 < 200 INTOLERANCE
DIABETES > 126 >200 MELLITUS
DIAGNOSIS
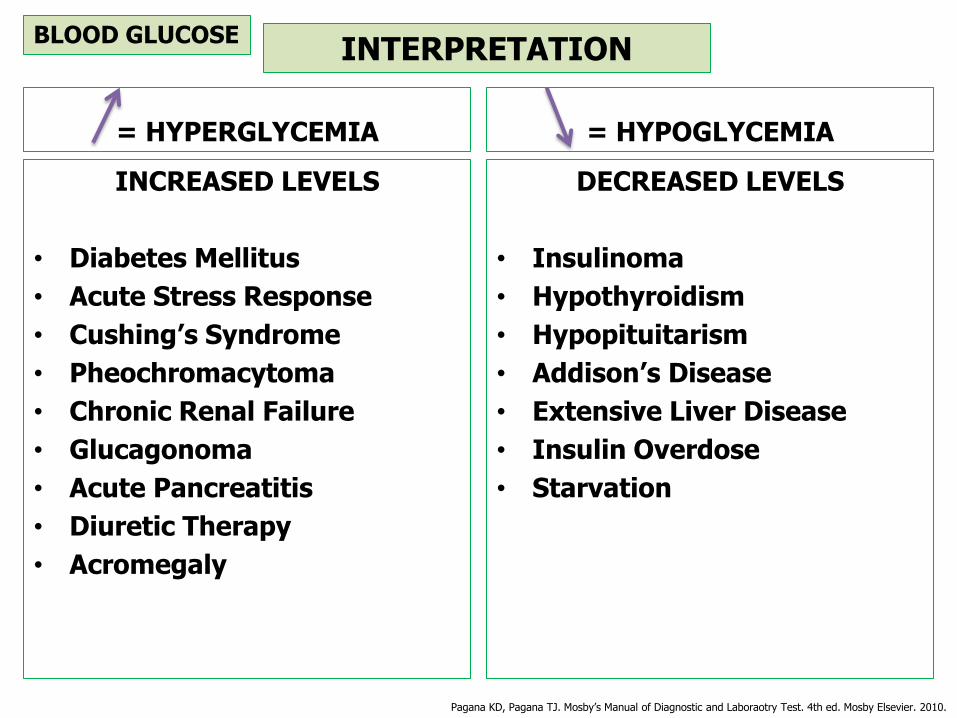
= HYPERGLYCEMIA
INCREASED LEVELS
• Diabetes Mellitus
• Acute Stress Response
• Cushing’s Syndrome
• Pheochromacytoma
• Chronic Renal Failure
• Glucagonoma
• Acute Pancreatitis
• Diuretic Therapy
• Acromegaly
= HYPOGLYCEMIA
DECREASED LEVELS
• Insulinoma
• Hypothyroidism
• Hypopituitarism
• Addison’s Disease
• Extensive Liver Disease
• Insulin Overdose
• Starvation
INTERPRETATION BLOOD GLUCOSE
Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboraotry Test. 4th ed. Mosby Elsevier. 2010.

METHODS
• Manual:
• Analyzer:
Specrophotometer
Autoanalyzer (Flow Cytometry)
CARDIAC MARKER
CARDIAC MARKER

Christenson RH, Azzazy HME. Biomarkers of Myocardial Necrosis, Past, Present and Future. In: Cardivascular Markers Pathophysiology and Disease Management. Humana Press Inc. New Jersey. 2006.
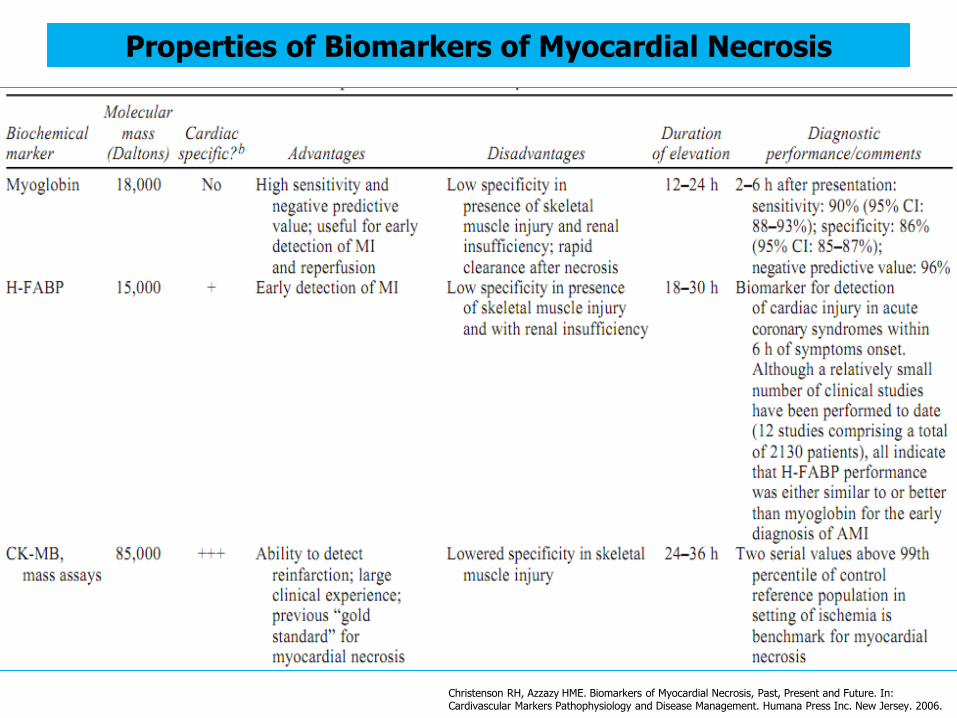
Properties of Biomarkers of Myocardial Necrosis
Christenson RH, Azzazy HME. Biomarkers of Myocardial Necrosis, Past, Present and Future. In: Cardivascular Markers Pathophysiology and Disease Management. Humana Press Inc. New Jersey. 2006.
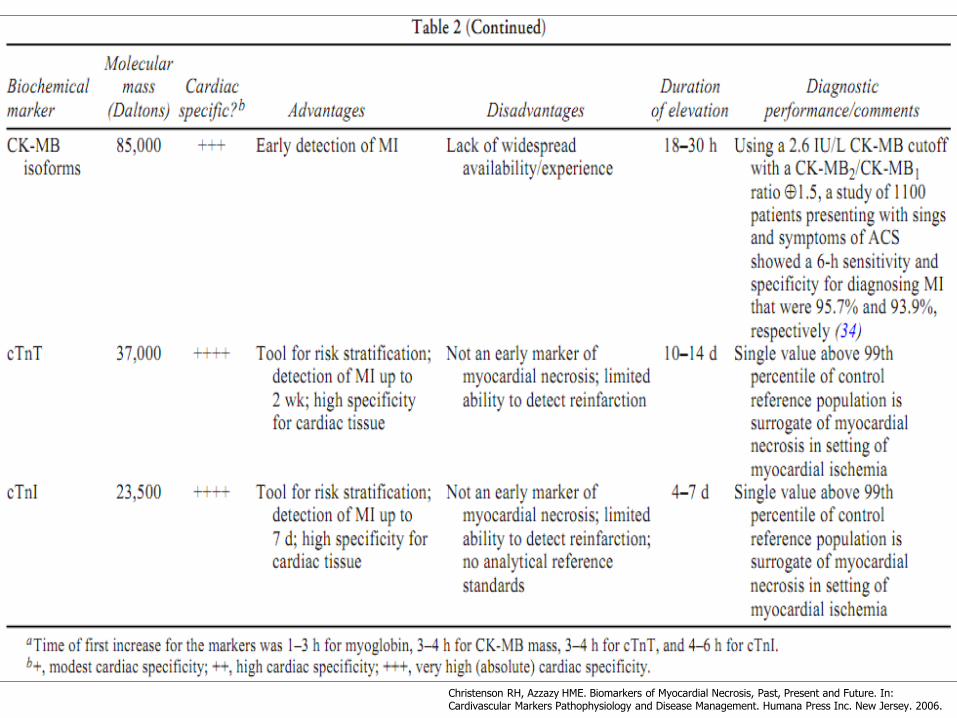
Christenson RH, Azzazy HME. Biomarkers of Myocardial Necrosis, Past, Present and Future. In: Cardivascular Markers Pathophysiology and Disease Management. Humana Press Inc. New Jersey. 2006.

FORM PERMINTAAN PEMERIKSAAN
LABORATORIUM DI
RSUDZA BANDA ACEH
MANUAL

THANK YOU




















