at_EBM-2.ppt
40
Evidence-Based Medicine, tuntutan baru dalam profesionalisme pengobatan seorang penderita Iwan Darmansjah Pusat Uji KLinik Obat, FKUI Dutch Foundation Seminar: Boerhaavse Kursus, FKUI 22-23 Apr.2002
-
Upload
fakrocev-charlie-gulo -
Category
Documents
-
view
9 -
download
5
Transcript of at_EBM-2.ppt

Evidence-Based Medicine, tuntutan baru dalam profesionalisme
pengobatan seorang penderita
Iwan DarmansjahPusat Uji KLinik Obat, FKUI
Dutch Foundation Seminar: Boerhaavse Kursus, FKUI 22-23 Apr.2002

Evidence Based Medicine (EBM)
• “Menggunakan segala pertimbangan bukti ilmiah (evidence) yang sahih yang diketahui hingga kini untuk menentukan pengobatan pada penderita yang sedang kita hadapi”.
• Merupakan penjabaran bukti ilmiah lebih lanjut setelah obat dipasarkan dan seiring dengan pengobatan rasional.

What is the level (L)of evidence ? (TGA)
• L1a. Randomized controlled trial (best evidence)• L1b. Meta-analysis (pros and cons)• L2. Retrospective analysis (case-control studies)• L2. Prospective follow-up (cohort studies)• Cross-sectional population (prevalence studies)• Previous reviews (position statements)• Clinical interventions (non-randomized)
• Safety data (important element !)A comprehensive evaluation of all data is the best approach!

How is LoE implemented in Recommendation Guidelines? (1)
• Levels of Evidence for Heart Failure:
– A. Data derived from multiple RCTs.– B. Data derived from a single randomized trial or
non-randomized studies.– C. Consensus opinion of experts was the primary
source of recommendation.
www.guidelines.gov/

How is LoE implemented in Recommendation Guidelines? (2)
• Strength of Recommendation:– Class I: Conditions for which there is evidence/general agreement
that a given procedure/therapy is useful and effective.
– Class II: Condition for which there is conflicting evidence or divergence of opinion about the usefulness /efficacy of performing the procedure /therapy.
» Class IIa: in favor of usefulness» Class IIb: usefulness is less well established
– Class III:Condition for which there is evidence/general agreement that a procedure/therapy is not useful/effective and may be harmful.
www.guidelines.gov/

How is LoE implemented in Recommendation Guidelines? (3)
• “The strength of evidence does not necessarily reflect the strength of recommendation. A treatment may be considered controversial although it has been evaluated in CTs; conversely, a strong recommendation may be based on years of clinical experience and be supported only by historical data or by no data at all”.
• Disini conflict of interest dari penilai dijaga ketat!!
www.guidelines.gov/

Drug Safety in increased focus around the world
• Increasing number of drug withdrawals because of harmful effects (recently: Prepulsid, Posicor, Hismanal, Rezulin, Lipobay, etc).
• Scientific report on epidemic proportions of serious ADRs in hospitalized patients.
(Lazarou, JAMA 1998)
• Medical mistakes (45.000 deaths/annually) and medication errors (28%) are reported, including under-utilization of proven drug therapies. (US Institute of Medicine, 2001)

Inhaled Steroids Can Cause Bone Loss in Young Asthmatic Women Effects of Inhaled Glucocorticoids on Bone Density in Premenopausal Women,
by Elliot Israel, M.D., Taruna R., Banerjee, M.P.H., Garrett M. Fitzmaurice, Sc.D., Tania V. Kotlov, M.S., Karen LaHive, M.D., and Meryl S. LeBoff, M.D.;
The New England Journal of Medicine, September 27, 2001.
Background
Here is the important background information that the authors give us:
-consensus reports recommend increased use of inhaled corticosteroids (also referred to as glucocorticoids) for patients with asthma,
-it is known that oral corticosteroids accelerate bone loss, and that fractures occur in 30 to 50% of patients on oral corticoids,
-it is not clear, however, whether inhaled corticosteroids accelerate bone loss.

ES obat kronis dapat diperkirakan dari parameter
Chronicity Index

CHRONICITY INDEX isa measure of chronic toxicity:
LD50 7Endrin : = = CI = 7
LD50 1(90 hari)
120Deksametason : = 1714 0.07

EBM sebenarnya merupakan cara yg biasa dilakukan dalam proses penilaian suatu obat baru yg akan dipasarkan.Disini malah diperlukan juga penilaian animal dan in-vitro studies.
Perbedaannya:* Penilaian obat pra-pemasaran mempertimbangkan seluruh masyarakat, * EBM menimbang untuk satu pasien.

EBM in terms of Benefit-Risk Ratio
• The seriousness of the problem to be treated• The efficacy of the drug you intend to use• The seriousness and frequency of possible
adverse effects• The efficacy of other drugs which might be
used instead• The safety of other drugs which might be
used instead.

Bagaimana dokter bisa mengerti EBM ?
• Evidence perlu diterapkan pada penderita dg segala penyakit/komplikasi-nya.
• Evidence berubah menurut perkem- bangan ilmu.
• Perlu CME model baru untuk men-sosialisasikan pengetahuan baru ini.
• Forum seminar biasa tidak lagi adekuat.• Pengobatan profesional membutuhkan
paradigma baru dalam CME.

The Knowledge Filter(H.H. Bauer, 1995)
Primary literature
How much is incorrect?
Correction of errors
Much of it is correct
(adapted)

Untuk menunjang EBM, FDA telah melakukan perubahan label indikasi obat sewaktu ijin pemasaran melalui
undang-undang.
Misalnya: Indikasi antibiotik yang luas, seperti untuk
“upper respiratory tract infection”, terdiri dari banyak lokasi yang kuman
penyebab maupun antibiotiknya berbeda.

Respiratory Tract Infections(FDA “Points to Consider” doc.)
• The terms of URTI and LRTI are being refined by more specific infections:
5. Community-acquired pneumonia (CAP) 6. Nosocomial pneumonia 7. Acute bacterial exacerbations of chronic bronchitis 8. Secondary bacterial infections of acute bronchitis 9. Acute otitis media10. Acute sinusitis11. Streptococcal pharyngitis (More indications may follow in response to industry’s marketing
application of claims)

Community acquired pneumonia (1):(FDA “Points to Consider” doc.)
Differentiation of CAP acc. to Label Claim:
• Atypical pneumonia• Viral peumonia• Acute bacterial pneumonia• Aspiration pneumonia• Ventilator-associated pneumonia• Pneumonia in an immuno-compromised
and/or neutropenic host.

Community acquired pneumonia (2):(FDA “Points to Consider” doc.)
Differentiation made for bacterial pneumonia:
• Pediatric patients:– no sputum for culture– infants (3-24 mo) higher baseline value for fever– WBC count >15.000 usually assoc. with severe
infection.– Radiographic findings different, etc
• Geriatric patients: ……………..

Susceptibility of S.pneumoniae to commonly used ABs, stratified by susceptibility to penicillin
Susceptibility to indicated agent,
per penicillin MIC categoryAgent
Amoxicillin ……..
Doxycycline
Ery, Clari, Azi-
Clindamycin
TMP-SMZ …….
Cefuroxime
Cefotaxime
Levo, Grepa, Trova-
Imipenem
Vancomycin …..
< 0.1 µg/mL 0.1-1.0 µg/mL > 2 µg/mL
+++ +++ +
+++ + +/-
+++ + +/-
+++ ++ +
++ _ _
+++ + _
+++ +++ +
+++ +++ +++
+++ +++ _
+++ +++ +++
+++ : > 90%
++ : > 75%
+ : > 50%
+/- : > 40%
- : < 40%

Bagaimana dg penisilin G untuk CAP tanpa penyulit?
• Intravenous crystalline Pen G, 3 - 5 juta Unit, setiap 3 jam menghasilkan Cmax rata-rata
+ 20 – 45 µg/ml*, yaitu 10 – 22 kali > MIC S. pneumoniae yg resisten, tapi tidak disebut dalam informasi tabel tadi.
• Rasio Cmax / MIC yang besar merupakan faktor daya bunuh kuman (conc.dependant) yg ampuh.
• CAP tanpa penyulit juga dianjurkan diobati di rumah untuk menghindari nosocomial infection.
*(Kucers & Bennett, 4th ed. 1987, pg 23)

Bagaimana interpretasi hasil Lab yg tidak pas?
• Nilai Widal yg dipakai untuk diagnosis tifus.• SGPT yg merupakan surrogate endpoint.• Hasil antibiogram yg mengikutsertakan AB yg
tidak semestinya: – gentamicin (tidak pas) untuk kuman tifus,– tidak mengikutsertakan AB terpilih seperti
flukloksasilin, dikloksasilin atau penisilin G untuk Staph. aureus atau stretokokkus, tapi menyertakan berbagai sefalosporin,... dsb.

Lalu, bagaimana dg evidence pengobatan empirik yg tidak ada uji klinik formal, tetapi sangat berguna?
• Varisella: cukup mandi teratur, tidak perlu AB rutin
• Parotitis epidemika: cukup permen karet.• Dikloksasilin atau flukloksasilin untuk staph.
resisten, juga penisilin prokain tidak dipakai lagi.• Probenesid (dosis kecil) telah dilupakan untk
gout, walaupun 65% merupakan masalah ekskresi asam urat (alopurinol di-indikasikan untk masalah pembentukan urat {35%}).

Case: Yn. 18 yrs with Grand Mal for 14 years since 4 yrs old.
• 2-4 convulsions a day with coma now and then, but now controlled. Evidence?
• Anticonvulsant blood levels were: daily dose blood l. norm. rangenorm. range (mcg/ml)
- Dilantin 400 mg 1.57 /10-20/ - Luminal 200 mg 30.19 /15-40/- Carb’zepine 200 mg 1.97 /4-10/

Masalah terbesar ialah bahwa “evidence”dapat diartikan berbeda-bedamenurut setiap orangatau profesi.
•FDA•Industri•Dokter•Spesialis•Farmasis•Herbalis•Naturo- patis•Awamdsb.

Number Needed to Treat (NNT)sebagai petunjuk statistik & klinis EBM
• RCT, karena keterbatasannya sendiri, kadang-kadang tidak memberi petunjuk jelas akan manfaat suatu pengobatan untk penderita yg akan diobati (EBM).
• NNT mungkin dapat memberi pegangan yg lebih mudah diartikan dalam keputusan memberi (obat) atau tidak.
• NNT= “the number of patients who must be treated for a given period to prevent a clinical outcome (e.g. stroke)”.
• NNT= 100/absolute risk reduction.• Absolute risk reduction (stroke) = Stroke Pla (20%) - Stroke Aktif (12%) = 0.20 - 0.12 = 0.08.

NNT untuk mengobati hipertensi mencegah stroke
Stroke in 5 yrs Control group
Active group
Hypertension
Mod. hypertension (diast. < 115 mm Hg)
Event rate (P)
Tot. N patients
Mild hypertension (diast. < 110 mm Hg)
Event rate (P)
Tot. N patients
0.20 0.12 0.40 0.08 13
16 778 16 898
0. 015 0.009 0.40 0.006 167
15 165 15 238
RRR Absolute RR NNT
(PC - PA)/PC PC - PA 1/(PC - PA)
(BMJ 1995;310:452-4)

LIPID study: 9014 pats, 6.1 yrs follow-up, secondary prevention of fatal & non-fatal
myocardial infarction by pravastatin
Placebo PravastatinCHD death &MI non-fatal
15.9% 12.3%
RR (relative risk) 0.76 (0.68-0.85)
Absolute riskreduction
3.6%
Relative reduction 24%
Number Needed to Treat: Diperlukan mengobati 28 orang dgn pravastatin selama 6 tahun untuk mencegah 1 event (koroner)

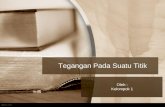
What is the status of clopidogrel ?

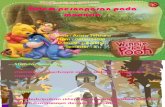
Clopidogrel in addition to aspirin in unstable angina (source of Figure: Chris Cates , from internet) original article: NEJM 2001;345(7):494-502)

Slide sebelumnya sangat jelas menggambarkan risiko kematian, MI, atau stroke bila pakai aspirin saja atau ditambah dg clopidogrel.Data ini sebelumnya dilaporkan dalam berbagai media kedokteran dengan mengatakan RRR (relative risk reduction) adalah 20%. Tanpa memperhitungkan absolute risk angka ini tidak cukup jelas artinya dan seolah-olah besar.Namun dg analisis NNT, terlihat secara visual (Visual Rx) jelas sekali, karena 20% tadi berarti perbedaan antara 11,4% (11 dari 100 orang) kematian dalam group aspirin saja (active plasebo) vs 9.3% (9 orang) dalam group clopidogrel.Dengan lain kata: bila kita mengobati 100 orang dg clopidogrel dan aspirin selama 9 bulan, akan mencegah 2 kematian, MI, atau stroke.NNT = 48: karena dalam praktek kita tidak bisa mengetahui 2 pasien yg mana yg akan tertolong, semua 100 pasien harus diobati dg clopidogrel.
Data ini ialah untuk unstable angina. In practice: dipakai untuk kasus lain dengan indikasi yg berbeda. Apakah ini evidence -based atau ‘extended evidence’?

EBM menjembatani Ilmu Kedokteran dan Hukum ?
• EBM mulai dibutuhkan juga oleh seorang hakim menentukan apakah suatu pengobatan tertentu sudah benar dalam persidangan. Diperlukan “ilmu” (evidence) di belakang pertimbangan suatu testimoni seorang saksi ahli. (JAMA Vol. 283 No.21, June 2000)
• Juga, EBM menentukan harga saham pabrik obat, yang disebarkan mass media ekonomi.

• Namun, masih akan dijumpai berbagai kendala, karena ilmu pengobatan dan EBM sendiri tidak sesederhana itu.

New Pediatric Studieswill change current State of the Art
• Pediatric studies are rare, although FDA had recommended since 1962.
• There will be more pediatric clinical trials in the future to support claim.
• FDA Modernization Act (FDAMA 1993) and the Pediatric Exclusivity Right Act (1998) will make the above an incentive for the industry to do pediatric clinical trials.

FDA’s Approved Drugs underPediatric Exclusivity Rights Act (1998)
(36/37 active moieties)
AbacavirAmmon. lactateAzelastineBisoprololBuspironeCalcitriolCromolynDidanosineEnalapril
GlaxoWestwod-SquibbAsta MedicaWyeth AyerstBMSAbbottPharmacia-UpjohnBMSMerck
KetorolacLamivudineLoratadineLovastatinMetforminMidazolamNabumetoneOmeprazoleOxaprozin
AllerganGlaxoSchering Corp.MerckBMSRocheSmithKlineAstra ZenecaGlaxo
EtodolacFamotidineFelodipineFluoxetineFlufoxamineGabapentinIbuprofenInsulin glargineisotretinoin
Wyeth-AyerstMerckAstra ZenecaLillySolvayParke-Davis2 companiesAventisRoche
PemiroplastPropofolRanitidineRemifentanilRibavirin/Intron ASevofluraneSotalolStavudineTramadol
SantenZenecaGlaxoAbbottSchering Corp.AbbottBerlexBMSJohnson
(FDA data: Sept. 2001)

EBM is challenged by the very presence of neutraceuticals
• While orthodox medicine is requiring stricter use of drugs by scientific evidence, unrestricted availability of alternative methods and medicines are worldwide - most without even any evidence of efficacy and safety - at a price that surpass “new pharmaceuticals”.

(1) Sepuluh Pedoman Pengobatan Rasional :
1. Timbanglah manfaat-risiko dgn memperhitungkan prinsip “Primum non nocere”.
2. Gunakanlah pertama-tama obat yg paling “established”, dan kenalilah obat pilihan ini untuk setiap indikasi.
3. Gunakanlah obat pilihan yg anda ketahui paling baik efeknya.
4. Batasilah pemberian jenis obat seminimal mungkin5. Sesuaikanlah dosis obat untuk setiap penderita.

(2) Sepuluh Pedoman Pengobatan Rasional :
6. Gunakanlah dosis efektif terkecil.7. Pilihlah cara pemberian obat yg paling aman,
tanpa mengurangi efektivitas.
8. Jangan memilih preparat terbaru, karena barunya.
9. Janganlah ketinggalan menggunakan obat baru yang (lebih) baik.
10. Cocokkanlah kebenaran data promosi pabrik obat.
(Darmansjah, 1979)

EBM is perhaps not always applicable for many reasons:
• Some times we cannot treat just the numbers.• Other times we cannot use statistics to treat a specific patient.• Large outcome studies includes patients with uncontrollable
variables.• Controlled clinical trials are not always flawless.• Pediatric CTs have not been required until 1998, although
compulsory for adults since 1962.• Dose-finding studies are rare, not the least in pediatrics. • Ultimately: ask 3 specialists and you will get 2-3 different
answers. Equipoise of opinions should perhaps be set at around 70 : 30, or more.

Conclusion• Proper drug use should be promoted nationally. • Education on drugs and EBM must take a
different approach (not education by coercive, pharmaceutical marketing needs).
• The cause of irrationalism is linked with a perpetuating error in a larger (health) system.
• Health and DrugUsePolicy must be established. • If the Health Department is failing, universities
and the profession should - morally - take initiative.