






Bahasa
Halaman
Hukum


2005;79:74-79 Ann Thorac SurgTore Eliasson, Clas Mannheimer and Christian Blomstrand
Paulin Andréll, Christer Jensen, Henrik Norrsell, Olof Ekre, Sven Ekholm, Ulf Norrsell, Complications After Coronary Artery Bypass Grafting
White Matter Disease in Magnetic Resonance Imaging Predicts Cerebral
http://ats.ctsnetjournals.org/cgi/content/full/79/1/74located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from

WICPOTCMS
nposdswc
eTimc
si0
Tgpptoi8arcsc9c
A
ASm
©P
CA
RD
IOV
AS
CU
LA
R
hite Matter Disease in Magnetic Resonancemaging Predicts Cerebral Complications Afteroronary Artery Bypass Grafting
aulin Andréll, MD, Christer Jensen, MD, Henrik Norrsell, MD, PhD,lof Ekre, MD, PhD, Sven Ekholm, MD, PhD, Ulf Norrsell, MD, PhD,ore Eliasson, MD, PhD, Clas Mannheimer, MD, PhD, andhristian Blomstrand, MD, PhDultidisciplinary Pain Center, Department of Radiology, and Institute of Clinical Neuroscience, Stroke Research Unit,
ahlgrenska University Hospital, Göteborg, Sweden
i0idwbg
ntpctact
Background. The aim of the present study was to assesseurologic and neuropsychologic complications in 104atients randomized to coronary artery bypass graftingr spinal cord stimulation. An additional objective of thetudy was to assess whether preoperative white matterisease might predict cerebral complications, as previoustudies have shown that there is a relationship betweenhite matter disease and neuropsychologic decline after
oronary artery bypass grafting.Methods. The patients were subjected to neurologic
xamination before and six months after intervention.he patients underwent a cerebral magnetic resonance
maging before intervention and the presence of whiteatter disease was related to development of cerebral
omplications.Results. More patients in the bypass group than in the
pinal cord stimulation group developed focal cerebralschemia (p < 0.05) and astheno-emotional disorder (p <
.001). More patients with white matter disease undergo-i[tTc
aipenwthttw[dac
ahlgrenska University Hospital/Östra, S-416 85 Göteborg, Sweden; e-ail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
ng bypass were affected by focal cerebral ischemia (p <.01) and astheno-emotional disorder (p < 0.001) after thentervention compared to patients with white matterisease undergoing spinal cord stimulation. In patientsith no white matter disease there were no differencesetween the bypass group and spinal cord stimulationroup with regard to cerebral complications.Conclusions. Patients undergoing bypass had more
eurologic and neuropsychologic complications than pa-ients undergoing spinal cord stimulation. Furthermore,atients with white matter disease were affected byerebral complications in a higher extent after bypasshan after spinal cord stimulation. Thus, preoperativessessment of white matter disease before undergoingoronary artery bypass grafting might predict the pa-ient’s risk of developing cerebral injury.
(Ann Thorac Surg 2005;79:74–80)
© 2005 by The Society of Thoracic Surgeonshere are several reports about neurologic and neuro-psychologic deficits after coronary artery bypass
rafting (CABG) [1–7]. Major neurologic complications inatients undergoing CABG occur in about 2% of theatients, although there have been reports of complica-
ion rates ranging from 1% to 5% [1, 3–5]. The percentagef patients suffering from neuropsychologic dysfunctions
s high at discharge, approximately 50% to 90% [2, 8]. Atweeks after surgery the prevalence falls to 36% and
fter six months to 24% [2, 6]. There have been severaleports of preoperative risk factors for cerebral compli-ations after CABG [1, 4, 5, 9, 10]. According to thesetudies, age is probably the strongest risk factor for focalerebral ischemia as well as for cognitive decline [4,–12]. Some of the main perioperative risk factors forerebral complications include an atherosclerotic ascend-
ccepted for publication June 25, 2004.
ddress reprint requests to Dr Andréll, Multidisciplinary Pain Center,
ng aorta, cardiopulmonary bypass time and emboli load1, 9, 10]. Other risk factors that have been discussed areemperature, arterial and cerebral perfusion pressure.he results regarding the impact of these factors onerebral complications are conflicting [9, 10].
Small-artery disease is often a manifestation of gener-lized arteriosclerosis that leads to subcortical brainschemia (white matter disease [WMD]), and a slowlyrogressive decline in cognitive function [13, 14]. Isch-mic WMD is visible on T2-weighted magnetic reso-ance images as signal hyperintensities in the brain’shite matter. Post-mortem examinations have shown
hat the grade of magnetic resonance imaging (MRI)yperintensities corresponds to the severity of ischemic
issue damage. There are several reports about the rela-ion between MRI hyperintensities in the brain’s deephite matter and neuropsychologic decline after CABG
15–19]. Magnetic resonance image hyperintensities ineep white matter are present in 47.5% of neurologicallysymptomatic subjects (31 to 84 years) [20]. These signal
hanges progress over time, but the progression seems0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.06.085
by on June 2, 2013 als.org

nc
sohawab
1nembhwt
plctW
P
STlapTcfwsbonfcgBp
CBiegtatf(oe
td“eaesdd3iictntprBrl
MMmwNc70
WTm
T
C
GMA
PPHDHCP
PCPR
Ag
75Ann Thorac Surg ANDRÉLL ET AL2005;79:74–80 MRI PREDICTS CEREBRAL COMPLICATIONS
CA
RD
IOV
AS
CU
LA
R
ot to be associated with a corresponding decline inognitive function [21, 22].
Fazekas’ rating scale [18] has been developed as aimple method for classification of the hyperintensitiesn MRI to reflect the severity of the WMD. The MRIyperintensities are rated as punctate, early confluent,nd confluent lesions [19]. The Fazekas’ rating scale is aell-known and validated method for grading WMD, butdisadvantage of the scale is that it does not differentiateetween the causes of the lesions [19, 23, 24].Spinal cord stimulation (SCS) has been used since the
980s for treatment of angina pectoris [25]. The antiangi-al effect has been found to be secondary to an antiisch-mic effect, which in turn seems to be due to reducedyocardial oxygen consumption [26]. The treatment has
een proven to be safe and favorable long-term resultsave been demonstrated [27, 28]. Spinal cord stimulation,hich is a less invasive form of procedure, served as a
herapeutic alternative to CABG in the present study.The aim of the present study was to assess and com-
are cerebral complications after CABG with those fol-owing SCS. Furthermore, the study assessed whethererebral complications after CABG and SCS, respec-ively, can be predicted preoperatively by the presence of
MD on MRI according to the Fazekas’ rating scale.
atients and Methods
tudy Patientshe present study is a follow-up of the Electrical Stimu-
ation versus coronary artery Bypass surgery in severengina pectoris (ESBY) study, which was a randomized,rospective, open comparison of CABG and SCS [28].he inclusion criteria were severe angina pectoris due tooronary artery disease, no anticipated prognostic benefitrom CABG and increased surgical risk. The patientsere all acceptable for CABG on a strict indication of
ymptom relief. Within six months after intervention,oth groups experienced adequate symptom relief, with-ut any differences between the groups [28]. There wereo health-related differences between the groups, except
or current smoking, renal disease, and presence oflinically significant carotid artery stenosis (ie, stenosis ofreater than or equal to 70% of the vessel diameter).aseline health characteristics for the ESBY patients areresented in Table 1 [28].
erebral Complicationsefore primary intervention and six months post-
ntervention, the patients had a thorough neurologicxamination by one and the same experienced neurolo-ist. Focal cerebral ischemia was defined as stroke and/orransient ischemic attacks (TIA). The diagnoses of strokend TIA were classified according to prevalent defini-ions [29]. The neurologic examination included searchor symptoms indicative of astheno-emotional disorderAED); enhanced psychic fatigability, diminished powerf concentration, amnesic problems, irritability, and
motional instability [30–33]. Furthermore, the symp- 1ats.ctsnetjournDownloaded from
oms must not be secondary to a depressed mood disor-er. Each symptom was judged separately and graded asnot existing in pathological extent” or “existent in mod-rately to severe extent.” If all symptoms were present in“moderately to severe extent,” the patient was consid-
red to have AED. Astheno-emotional disorder has manyimilarities to the microvascular frontal-subcortical syn-rome of aging and the dysexecutive syndrome, but theiagnosis does not include motor control impairment [14,0]. The AED diagnosis is validated and has a highnterrater reliability [32, 33]. Astheno-emotional disordermplies a significant impairment for the patient thatauses pronounced suffering [30]. The patients wereested preoperatively and postoperatively by a licensedeuropsychologist, with a battery of 14 neuropsychologic
ests encompassing attention, memory functions, andsychomotor performance. The tests included a simpleeaction time test and Trail-Making Test, parts A and[34]. All deaths related to cerebrovascular disease were
ecorded in the period from inclusion up to five yearsater.
agnetic Resonance Imagingagnetic resonance imaging examination before treat-ent was planned for all the patients. All examinationsere performed on a 0.5 T magnet (Philips GyroscanT5, Eindhoven, the Netherlands). The protocol in-
luded a double spin-echo sequence. Slice thickness wasmm in axial projection and the in-plane pixel size was
.9 � 0.9 mm.
hite Matter Diseaseo grade lesion load of MRI hyperintensities in the whiteatter of the brain, Fazekas’ rating scale was used [18,
able 1. Baseline Characteristics in the ESBY Study
haracteristicCABG
(n � 51)SCS
(n � 53)
ender: male/female, n 42/9 41/12ean age (range), years 68.7 (40–81) 72.2 (42–82)nginaclass 3, n 48 50class 4, n 3 3
revious CABG, n 11 14revious myocardial infarction, n 34 36ypertension, n 19 23iabetes, n 13 14yperlipidemia, n 10 8urrent smoking, n 10 2reexisting cerebrovasculardisease, n
11 13
reexisting AED, n 14 15arotid artery stenosis �70%, n 6 16eripheral vascular disease, n 14 13enal disease, n 6 12
ED � astheno-emotional disorder; CABG � coronary artery bypassrafting; SCS � spinal cord stimulation.
9]. The presence and grade of WMD according to
by on June 2, 2013 als.org

Fbbwb
miaetoiafipmT
CArpive
STsscoctamaca
aintiaown
DDfHa
SDnartUt(Eta
R
TfEpc
C�(9cviwdenrtcr1Mier
d
TA“
M
APBLM
Cid
76 ANDRÉLL ET AL Ann Thorac SurgMRI PREDICTS CEREBRAL COMPLICATIONS 2005;79:74–80
CA
RD
IOV
AS
CU
LA
R
azekas’ rating scale were assessed before interventiony the one and the same neuroradiologist, who waslinded to the treatment allocation. White matter diseaseas defined as punctate foci of MRI hyperintensities,eginning confluence of foci, and large confluent areas.The MRI changes according to Fazekas’ rating scaleight be due to “pure” WMD, but also to cerebral
nfarctions or to unspecific periventricular changesround the posterior horns, a common finding in thelderly [35]. Thus, in order to be able to relate pure WMDo cerebral complications, one and the same neuroradi-logist scrutinized the white matter changes to exclude
solated periventricular areas around the posterior hornsnd focal solitary infarctions. In this manner a “modi-ed” Fazekas’ rating scale was used to evaluate theatients. Presence of WMD according to the ordinary andodified Fazekas’ rating scale at baseline is presented in
able 2.
arotid Diseasell patients were examined with duplex Doppler sonog-
aphy before the intervention in order to establish anyresence and extent of carotid disease. Clinically signif-
cant carotid stenosis was judged to be present if flowelocities corresponded to a stenosis of greater than orqual to 70% of the lumen of the vessel.
urgeryhe CABG operations were performed as open-hearturgery with extracorporeal circulation according to thetandard clinical practice during the study period. Theardiopulmonary bypass circuit included a membranexygenator and a nonpulsatile flow during bypass, typi-ally 2.4 L/m2 of body surface area per minute (reducedo 2.0 L/m2 per minute during hypothermia). The meanrterial pressure was maintained in the range of 50 to 70m Hg. Hypothermia (28 to 32°C) and cardioplegia were
pplied. The duration of extracorporeal circulation, aortaross-clamping, surgery, and anesthesia were monitorednd related to development of cerebral complications.
able 2. Presence of WMD; ie, MRI Hyperintensities,ccording to the Original Fazekas’ Rating Scale and theModified” Fazekas’ Rating Scale Before Intervention
RI Hyperintensities
OriginalFazekas’
Rating Scale
ModifiedFazekas’
Rating Scale
CABG(n)
SCS(n)
CABG(n)
SCS(n)
bsence 13 12 16 15unctate foci 17 23 18 25eginning confluence of foci 12 14 10 10arge confluent areas 3 2 1 1RI not performed 6 2 6 2
ABG � coronary artery bypass grafting; MRI � magnetic resonancemaging; SCS � spinal cord stimulation; WMD � white matterisease.
During the SCS implantation the patient was awake �
ats.ctsnetjournDownloaded from
nd local anesthesia was used. The epidural space wasdentified at the midthoracic level, using a Touhyeedle. Through this an electrode was introduced to
he level of Th1-Th2 during roentgenogram monitor-ng. Using test stimulation the electrode position wasdjusted until the paresthesia covered the distributionf the angina. The electrode was fixed and an extensionire was tunneled to below the costal arch and con-ected to a pulse generator [28].
ata Collectionata on causes of death were obtained from the Center
or Epidemiology at the Swedish National Board ofealth and Welfare. Data concerning cerebral morbidity
nd surgical variables were collected from patient charts.
tatistical Analysisue to the small number of patients and few events,onparametric tests were used. Categorical data werenalyzed using �2 tests and Fisher’s exact test; relativeisk and 95% confidence intervals (CI) are quoted. Con-inuous variables were analyzed with the Mann-Whitney-test. All data analysis was performed using the Statis-
ical Package for Social Sciences (SPSS 11.0.0) softwareSPSS Inc, Chicago, IL) on an intention-to-treat basis. Thethics Committee of the Göteborg University approved
he study. Written informed consent was obtained fromll patients.
esults
here were five crossovers during the study period, tworom the SCS group and three from the CABG group [36].ight patients did not undergo any MRI due to theresence of claustrophobia, implanted devices, earlyrossover, or study termination.
During six months of follow-up eleven patients in theABG group developed focal cerebral ischemia (stroke, n
11) compared with four patients in the SCS groupstroke, n � 3; TIA, n � 1) (p � 0.05, relative risk 2.9, CI5% 1.0 to 8.4). In the SCS group there were no events oferebral ischemia in connection with the primary inter-ention, whereas nine of the eleven patients with focalschemia in the CABG group were affected in connectionith the primary intervention (p � 0.05). No patienteveloped more than one event of focal cerebral isch-mia. There was no significant difference between theeuropsychologic consequences for the two groups withegard to formal tests. Nevertheless, more CABG pa-ients developed AED after intervention; 14 patientsompared with one patient in the SCS group (p � 0.001,elative risk 14.5, CI 95% 2.0 to 106.6). On average, these4 patients had slower reaction times and worse Trail-aking Test results than the other subjects. The mortal-
ty data for the ESBY patients have been presentedlsewhere [27, 28, 36]. The groups did not differ withegard to 5 year cerebrovascular mortality.
Patients with preoperative WMD undergoing CABGeveloped focal cerebral ischemia (p � 0.01) and AED (p
0.001) after the intervention to a higher extent than
by on June 2, 2013 als.org

pWc
poWmlt(SawcCai
roctcame
C
Tcf
ocpbhcaTricioCcaSttcp
dptts
otf[h
TD
FA
E
A ss graW
TD
FA
E
AW
77Ann Thorac Surg ANDRÉLL ET AL2005;79:74–80 MRI PREDICTS CEREBRAL COMPLICATIONS
CA
RD
IOV
AS
CU
LA
R
atients with WMD undergoing SCS. In patients with noMD, there were no significant differences in cerebral
omplications between the groups (Table 3).According to the modified Fazekas’ rating scale, six
atients who were judged to have WMD according to theriginal Fazekas’ rating scale did not have any pureMD. Sixteen patients had less WMD according to theodified Fazekas’ rating scale (Table 2). Nevertheless, a
arger number of CABG patients with WMD, accordingo the modified Fazekas’ rating scale, had focal ischemiap � 0.05) and AED (p � 0.01) after the intervention thanCS patients with WMD. In patients with no WMD,ccording to the modified Fazekas’ rating scale, thereere no differences with regard to development of focal
erebral ischemia between the groups. However, moreABG patients, with and without WMD, developed AEDfter the intervention compared with patients undergo-ng SCS (p � 0.05) (Table 4).
There were no differences between the groups withegard to cerebral complications related to the presencef clinically significant carotid stenosis. Development oferebral complications after intervention was not relatedo the duration of extracorporal circulation, aorta cross-lamping, surgery or anesthesia, or to age. Presence orbsence of WMD according to the original or to theodified Fazekas’ rating scale was not related to age
ither.
omment
he patients of the ESBY study had a higher cerebrovas-ular morbidity in terms of stroke and TIA than reportedrom other studies [1, 3–5, 37]. This may be expected since
able 3. Relation Between Presence of WMD According to thevelopment of Cerebral Complications up to Six Months Aft
Patients With WMD (n � 71)
VariableCABG
(n � 32)SCS
(n � 39) p Value
ocal cerebral ischemia 9 2 �0.01ED 10 0 �0.001 N
ight patients did not undergo any MRI (Table 2).
ED � astheno-emotional disorder; CABG � coronary artery bypaMD � white matter disease.
able 4. Relation Between Presence of WMD According to thevelopment of Cerebral Complications up to Six Months Aft
Patients With WMD (n � 66)
VariableCABG
(n � 29)SCS
(n � 37) p Value
ocal cerebral ischemia 8 2 �0.05ED 8 0 �0.01 N
ight patients did not undergo any MRI (Table 2).
ED � astheno-emotional disorder; CABG � coronary artery bypass graMD � white matter disease.
ats.ctsnetjournDownloaded from
ne of the inclusion criteria was high surgical risk due toerebrovascular and other concomitant diseases. Theatients also had a high frequency (74%) of WMD ataseline, which may also be expected since the patientsad extensive coronary artery disease [38]. Presence ofognitive dysfunction, described as AED, six monthsfter CABG did not differ from other studies [2, 6, 37].here were no differences between the groups withegard to performance on neuropsychologic tests, whichs in line with results from previous studies [39]. Aonsiderable number of the CABG patients (n � 7) diedn connection with the primary intervention and in ninef the eleven patients with focal cerebral ischemia in theABG group; the event was related to the surgery [28]. In
ontrast, SCS has no known cerebral complication risksnd is implanted during local anesthesia [27, 28]. In theCS group none of the cerebral incidents were related to
he primary intervention, although one event was relatedo CABG. In the ESBY material there were no majoromplications related to the implantation, only minorerioperative complications [36].In the present study, age was not associated with either
evelopment of cerebral complications, or with a greaterresence of WMD. This might be due to selection bias;
he patients may have similar risk of cerebral complica-ions and similar extent of WMD, despite age differences,ince they all were considered to be high-risk patients.
Some investigators have suggested that neurologicutcome is related to the duration of the procedure sincehe duration of surgery may be prolonged by severalactors that may themselves contribute to cerebral injury1, 9]. However, in the present study all patients had aigh risk of perioperative complications, which may
ginal Fazekas’ Rating Scale Before Intervention andtervention
Patients Without WMD (n � 25)
ive Risk% CI)
CABG(n � 13)
SCS(n � 12) p Value
Relative Risk(95% CI)
.3–23.6) 2 1 1.0 1.8 (0.2–17.8)pplicable 4 0 0.10 Not applicable
fting; CI � confidence interval; SCS � spinal cord stimulation;
odified” Fazekas’ Rating Scale Before Intervention andtervention
Patients Without WMD (n � 30)
ive Risk% CI)
CABG(n � 16)
SCS(n � 14) p Value
Relative Risk(95% CI)
.2–22.2) 3 1 0.60 2.7 (0.3–22.5)pplicable 6 0 �0.05 Not applicable
e Orier In
Relat(95
5.5 (1ot a
e “Mer In
Relat(95
5.1 (1ot a
fting; CI � confidence interval; SCS � spinal cord stimulation;
by on June 2, 2013 als.org

eo
wwcpFsitWicciwadSWbstobrt
in
STdks
CWswtScCtpFpttp
WpitNR
R
Fc(lrtt
78 ANDRÉLL ET AL Ann Thorac SurgMRI PREDICTS CEREBRAL COMPLICATIONS 2005;79:74–80
CA
RD
IOV
AS
CU
LA
R
xplain the minor impact of the surgery-related variablesn cerebral and other events.A novel finding in the present study is that patientsith increased surgical risk of cerebral complicationsith WMD, in addition to other known risk factors for
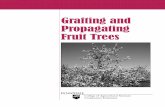
erebrovascular lesions, developed more cerebral com-lications in connection with CABG than with SCS.urthermore, the results imply that the Fazekas’ ratingcale may be too crude to grade WMD, as cerebralnfarctions and periventricular changes around the pos-erior horn will contribute to the assessment (Fig 1).
hen pure WMD was estimated according to the mod-fied Fazekas’ rating scale, the results regarding theonnection between WMD and the development of focalerebral ischemia were consistent compared to the orig-nal Fazekas’ rating scale (Tables 3 and 4). However,hen pure WMD was related to the development of AED
fter surgery, the CABG patients with and without WMDeveloped more cases of AED than the patients in theCS group (Tables 3 and 4). In summary, the presence ofMD seems to indicate an increased risk of focal cere-
ral ischemia after CABG, independent of the ratingcale used to assess the MRI hyperintensities. Regardinghe impact of WMD on the development of AED, theriginal Fazekas’ rating scale indicates that WMD mighte of importance, but according to the modified Fazekas’ating scale the results indicate that it is the CABG per se
ig 1. According to the original Fazekas’ rating scale this patient isonsidered to have confluent lesions of magnetic resonance imagingMRI) hyperintensities. The MRI hyperintensities are, however, to aarge degree due to a nonspecific periventricular change around theight posterior horn, which cannot be regarded as “pure” white mat-er disease. The remaining MRI hyperintensities are rated as punc-ate according to the “modified” Fazekas’ rating scale.
hat increases the risk of developing AED. However, the
ats.ctsnetjournDownloaded from
nterpretations should be cautious due to the smallumber of patients.
tudy Limitationshe ESBY study was not blinded because the two proce-ures differ significantly; ie, the treatment allocation wasnown by the patient and the surgeon. Furthermore, thetudy included a limited number of patients.
onclusionshite matter disease may be a previously unobserved
urgical risk factor for cerebral complications. Patientsith preoperative WMD developed cerebral complica-
ions to a higher extent following CABG than followingCS. Thus, presence of WMD might indicate an in-reased risk of cerebral complications for a patient afterABG. It may be valuable to perform a MRI and assess
he extent of WMD before CABG and avoid surgery inatients with WMD to prevent cerebral complications.urther studies are needed to evaluate the predictiveotential of WMD. The present study further supports
he results from the ESBY study; that SCS might be aherapeutic alternative in patients with severe anginaectoris and surgical risk factors.
e thank our medical statistician, Martin Gellerstedt, for expertrofessional advice and for careful and precise guidance regard-
ng the interpretation of the results. The study was supported byhe Faculty of Medicine, University of Göteborg, the Swedishational Heart-Lung Foundation, and the Swedish Medicalesearch Council.
eferences
1. McKhann GM, Goldsborough MA, Borowicz LM, Jr, et al.Predictors of stroke risk in coronary artery bypass patients.Ann Thorac Surg 1997;63:516–21.
2. Newman MF, Kirchner JL, Phillips-Bute B, et al. Longitudi-nal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med 2001;344:395–402.
3. Bucerius J, Gummert JF, Borger MA, et al. Stroke aftercardiac surgery: a risk factor analysis of 16,184 consecutiveadult patients. Ann Thorac Surg 2003;75:472–8.
4. Roach GW, Kanchuger M, Mangano CM, et al. Adversecerebral outcomes after coronary bypass surgery. Multi-center study of perioperative ischemia research group andthe ischemia research and education foundation investiga-tors. N Engl J Med 1996;335:1857–63.
5. Svedjeholm R, Hakanson E, Szabo Z, Vanky F. Neurologicalinjury after surgery for ischemic heart disease: risk factors,outcome and role of metabolic interventions. Eur J Cardio-thorac Surg 2001;19:611–8.
6. Smith PL, Treasure T, Newman SP, et al. Cerebral conse-quences of cardiopulmonary bypass. Lancet 1986;1:823–5.
7. Toner I, Taylor KM, Newman S, Smith PL. Cerebral func-tional changes following cardiac surgery: neuropsychologi-cal and EEG assessment. Eur J Cardiothorac Surg 1998;13:13–20.
8. Shaw PJ, Bates D, Cartlidge NE, et al. Neurologic andneuropsychological morbidity following major surgery:comparison of coronary artery bypass and peripheral vascu-lar surgery. Stroke 1987;18:700–7.
9. Gardner TJ, Horneffer PJ, Manolio TA, et al. Stroke following
coronary artery bypass grafting: a ten-year study. AnnThorac Surg 1985;40:574–81.by on June 2, 2013 als.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
I
Asahcspslmw
79Ann Thorac Surg ANDRÉLL ET AL2005;79:74–80 MRI PREDICTS CEREBRAL COMPLICATIONS
©P
CA
RD
IOV
AS
CU
LA
R
0. Newman MF, Croughwell ND, Blumenthal JA, et al. Predic-tors of cognitive decline after cardiac operation. Ann ThoracSurg 1995;59:1326–30.
1. Tuman KJ, McCarthy RJ, Najafi H, Ivankovich AD. Differen-tial effects of advanced age on neurologic and cardiac risks ofcoronary artery operations. J Thorac Cardiovasc Surg 1992;104:1510–7.
2. He GW, Acuff TE, Ryan WH, He YH, Mack MJ. Influence ofold age, gender, and internal mammary artery grafting onoperative mortality and morbidity in coronary artery bypassgrafting. Am J Geriatr Cardiol 1996;5:22–35.
3. Chui H. Dementia due to subcortical ischemic vasculardisease. Clin Cornerstone 2001;3:40–51.
4. Pugh KG, Lipsitz LA. The microvascular frontal-subcorticalsyndrome of aging. Neurobiol Aging 2002;23:421–31.
5. Goto T, Baba T, Honma K, et al. Magnetic resonance imagingfindings and postoperative neurologic dysfunction in elderlypatients undergoing coronary artery bypass grafting. AnnThorac Surg 2001;72:137–42.
6. Restrepo L, Wityk RJ, Grega MA, et al. Diffusion- andperfusion-weighted magnetic resonance imaging of thebrain before and after coronary artery bypass grafting sur-gery. Stroke 2002;33:2909–15.
7. Fazekas F, Kleinert R, Offenbacher H, et al. The morphologiccorrelate of incidental punctate white matter hyperintensi-ties on MR images. AJNR Am J Neuroradiol 1991;12:915–21.
8. Fazekas F, Chawluk JB, Alavi A, Hurtig HI, Zimmerman RA.MR signal abnormalities at 1.5 T in Alzheimer’s dementiaand normal aging. AJR Am J Roentgenol 1987;149:351–6.
9. Fazekas F, Kleinert R, Offenbacher H, et al. Pathologiccorrelates of incidental MRI white matter signal hyperinten-sities. Neurology 1993;43:1683–9.
0. Schmidt R, Fazekas F, Kleinert G, et al. Magnetic resonanceimaging signal hyperintensities in the deep and subcorticalwhite matter. A comparative study between stroke patientsand normal volunteers. Arch Neurol 1992;49:825–7.
1. Schmidt R, Schmidt H, Kapeller P, et al. The natural courseof MRI white matter hyperintensities. J Neurol Sci 2002;203–204:253–7.
2. Bronge L, Wahlund LO. Prognostic significance of whitematter changes in a memory clinic population. PsychiatryRes 2003;122:199–206.
3. Scheltens P, Erkinjunti T, Leys D, et al. White matterchanges on CT and MRI: an overview of visual rating scales.European task force on age-related white matter changes.Eur Neurol 1998;39:80–9.
4. Kapeller P, Barber R, Vermeulen RJ, et al. Visual rating ofage-related white matter changes on magnetic resonanceimaging: scale comparison, interrater agreement, and corre-lations with quantitative measurements. Stroke 2003;34:
441–5.The prevalence of preoperative magnetic resonance
igpwC
toappn
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
5. Mannheimer C, Augustinsson LE, Carlsson CA, Manhem K,Wilhelmsson C. Epidural spinal electrical stimulation insevere angina pectoris. Br Heart J 1988;59:56–61.
6. Mannheimer C, Eliasson T, Andersson B, et al. Effects ofspinal cord stimulation in angina pectoris induced by pacingand possible mechanisms of action. BMJ 1993;307:477–80.
7. Ekre O, Eliasson T, Norrsell H, Wahrborg P, Mannheimer C.Long-term effects of spinal cord stimulation and coronaryartery bypass grafting on quality of life and survival in theESBY study. Eur Heart J 2002;23:1938–45.
8. Mannheimer C, Eliasson T, Augustinsson LE, et al. Elec-trical stimulation versus coronary artery bypass surgery insevere angina pectoris: the ESBY study. Circulation 1998;97:1157– 63.
9. Recommendations on stroke prevention, diagnosis, andtherapy. Report of the WHO task force on stroke and othercerebrovascular disorders. Stroke 1989;20:1407–31.
0. Lindqvist G, Malmgren H. Organic mental disorders ashypothetical pathogenetic processes. Acta Psychiatr ScandSuppl 1993;373:5–17.
1. Carlsson GE, Moller A, Blomstrand C. Consequences of mildstroke in persons �75 years—a 1-year follow-up. Cerebro-vasc Dis 2003;16:383–8.
2. Rodholm M, Starmark JE, Svensson E, Von Essen C. As-theno-emotional disorder after aneurysmal SAH: reliability,symptomatology and relation to outcome. Acta NeurolScand 2001;103:379–85.
3. Rodholm M, Hellstrom P, Bilting M, Starmark JE. Diagnosticclassification of organic psychiatric disorders after aneurys-mal subarachnoid hemorrhage: a comparison between ICD-10, DSM-IV and the Lindqvist & Malmgren classificationsystem. Acta Psychiatr Scand 2003;108:222–31.
4. Spreen O, Strauss E. A compendium of neuropsychologicaltests: administration, norms and commentary. New York,NY: Oxford University Press; 1991:1–442.
5. Meguro K, Yamaguchi T, Hishinuma T, et al. Periventricularhyperintensity on magnetic resonance imaging correlatedwith brain ageing and atrophy. Neuroradiology 1993;35:125–9.
6. Andrell P, Ekre O, Eliasson T, et al. Cost-effectiveness ofspinal cord stimulation versus coronary artery bypass graft-ing in patients with severe angina pectoris. Long-term re-sults from the ESBY study. Cardiology 2003;99:20–4.
7. Shaw PJ, Bates D, Cartlidge NE, et al. Early neurologicalcomplications of coronary artery bypass surgery. Br Med J(Clin Res Ed) 1985;291:1384–7.
8. Schmidt R, Fazekas F, Offenbacher H, et al. Brain magneticresonance imaging in coronary artery bypass grafts: a pre-and postoperative assessment. Neurology 1993;43:775–8.
9. Newman S, Klinger L, Venn G, et al. Subjective reports ofcognition in relation to assessed cognitive performancefollowing coronary artery bypass surgery. J Psychosom Res
1989;33:227–33.NVITED COMMENTARY
ndréll and colleagues document an important relation-hip between preoperative magnetic resonance imagingbnormalities and risk of adverse neurologic outcomes inigh-risk patients randomized to either conventionaloronary artery bypass surgery (CABG) or spinal cordtimulation. A principal finding from their study is thatatients who undergo CABG are more likely than thepinal cord stimulation patients to have adverse neuro-ogic outcomes, regardless of whether or not they have
agnetic resonance imaging evidence of preoperativehite matter disease (WMD).
maging abnormalities was high in both of the studyroups; in fact, substantially higher than in the onlyrevious large scale study by Goto and colleagues [1]ho found that approximately 50% of their candidates forABG had WMD.Within the group of CABG patients, a similar propor-
ion of postoperative neurocognitive impairment wasbserved in both groups (with and without WMD). Usingmodified scale for quantifying the degree of WMD thatlaces less emphasis on periventricular lesions, 8 of 29atients (28%) with WMD and 6 of 16 (38%) without had
eurocognitive impairment develop. None of the pa-0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.08.075
by on June 2, 2013 als.org

2005;79:74-79 Ann Thorac SurgTore Eliasson, Clas Mannheimer and Christian Blomstrand
Paulin Andréll, Christer Jensen, Henrik Norrsell, Olof Ekre, Sven Ekholm, Ulf Norrsell, Complications After Coronary Artery Bypass Grafting
White Matter Disease in Magnetic Resonance Imaging Predicts Cerebral
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/79/1/74including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/79/1/74#BIBL
This article cites 37 articles, 20 of which you can access for free at:
Citations http://ats.ctsnetjournals.org/cgi/content/full/79/1/74#otherarticles
This article has been cited by 3 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/coronary_disease Coronary disease
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
Top Related
Copyright © 2022 FDOKUMEN

