







Bahasa
Halaman
Hukum


WOWERLÅSJBD
Sriestwh
C‡MvDAM‡Uf
2
Journal of the American College of Cardiology Vol. 45, No. 2, 2005© 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00P
Heart Failure
hat Resting Heart Rate Shouldne Aim For When Treating Patientsith Heart Failure With a Beta-Blocker?
xperiences From the Metoprolol Controlled Release/Extended Releaseandomized Intervention Trial in Chronic Heart Failure (MERIT-HF)ars Gullestad, MD, PHD,* John Wikstrand, MD, PHD,†‡ Prakash Deedwania, MD, FACC,§ke Hjalmarson, MD, PHD,� Kenneth Egstrup, MD, DMSCI, FESC,¶ Uri Elkayam, MD, PHD,#tephen Gottlieb, MD,** Andrew Rashkow, MD,†† Hans Wedel, PHD,‡‡ Georgina Bermann, PHD,‡ohn Kjekshus, MD, PHD§§, for the MERIT-HF Study Groupaerum and Olso, Norway; Göteborg and Mölndal, Sweden; Fresno and Los Angeles, California; Fyn Svendborg,enmark; Baltimore, Maryland; and Cooperstown, New York
OBJECTIVES The goal of this study was to explore the question: what resting heart rate (HR) should oneaim for when treating patients with heart failure with a beta-blocker?
BACKGROUND The interaction of pretreatment and achieved resting HR with the risk-reducing effect ofbeta-blocker treatment needs further evaluation.
METHODS Cardiovascular risk and risk reduction were analyzed in five subgroups defined by quintiles(Q) of pretreatment resting HR in the Metoprolol Controlled Release/Extended ReleaseRandomized Intervention Trial in Chronic Heart Failure (MERIT-HF).
RESULTS Mean baseline HR in the 5 Qs were 71, 76, 81, 87, and 98 beats/min; achieved HR 63, 66,68, 72, and 75 beats/min; and net change �8, �10, �11, �13, and �14 beats/min,respectively. Baseline HR was related to a number of baseline characteristics. Cardiovascularrisk was no different in Q1 toQ 4 (placebo groups) but increased in Q5 (HR above 90beats/min). No relationship was observed between the risk-reducing effect of metoprololcontrolled release/extended release (CR/XL) and baseline HR in the five Qs of baseline HR,or achieved HR, or change in HR during follow-up, respectively.
CONCLUSIONS Metoprolol CR/XL significantly reduced mortality and hospitalizations independent ofresting baseline HR, achieved HR, and change in HR. Achieved HR and change in HRduring follow-up were closely related to baseline HR; therefore, it was not possible to answerthe question posed. Instead, one has to apply a very simple rule: aim for the targetbeta-blocker dose used in clinical trials, and strive for the highest tolerated dose in all patientswith heart failure, regardless of baseline and achieved HR. (J Am Coll Cardiol 2005;45:
ublished by Elsevier Inc. doi:10.1016/j.jacc.2004.10.032
252–9) © 2005 by the American College of Cardiology Foundation
CttwFd1dafisrgH
M
S
everal studies have demonstrated an association betweenesting heart rate (HR) and long-term cardiovascular riskndependent of other major cardiovascular risk factors inpidemiologic studies (1–4) among patients with hyperten-ion (5) and after myocardial infarction (6–8). However,he interaction of pretreatment resting and achieved HRith the risk-reducing effect of beta-blocker treatment ineart failure needs further evaluation.
From the *Baerums Sykehus, Baerum, Norway; †Wallenberg Laboratory forardiovascular Research, Sahlgrenska University Hospital, Göteborg, Sweden;Clinical Science, AstraZeneca, Mölndal, Sweden; §Department of Veterans Affairsedical Center, Fresno, California; �Department of Cardiology, Sahlgrenska Uni-
ersity Hospital, Göteborg, Sweden; ¶Hospital Fyn Svendborg, Fyn Svendborg,enmark; #Keck School of Medicine, University of Southern California, Losngeles, California; **University of Maryland School of Medicine, Baltimore,aryland; ††Columbia University, Bassett Healthcare, Cooperstown, New York;
‡Nordic School of Public Health, Göteborg, Sweden; and §§Rikshospitalet,niversity of Oslo, Olso, Norway. The MERIT-HF study was supported by a grant
rom AstraZeneca.
rManuscript received May 19, 2004; revised manuscript received September 27,
004, accepted October 4, 2004.
The main aim of the present analysis of the Metoprololontrolled Release/Extended Release Randomized Interven-
ion Trial in Chronic Heart Failure (MERIT-HF) (9) was tory to answer the question: what resting HR should one aim forhen treating patients with heart failure with a beta-blocker?or this purpose, patients were divided into five subgroupsefined by quintiles (Q) of baseline resting HR. We report on:) baseline characteristics in the five HR subgroups; 2) risk foreath and hospitalizations in the five HR subgroups; 3)chieved HR and net change in HR during follow-up in theve metoprolol controlled release/extended release (CR/XL)ubgroups defined by Qs of baseline resting HR; and 4) relativeisk reduction with metoprolol CR/XL in the five HR sub-roups in relation to baseline HR, achieved HR, and change inR during follow-up.
ETHODS
tudy design. The MERIT-HF study was a prospective,
andomized, placebo-controlled clinical trial that random-
ifbHMBtNIwBrrlscrCmodoSvubtsTfTibraitCwb(ehmo
dtw
R
BcvfcfftlBHQbaaicnohmbpaQhpvlbRudidQtitf1d
iwshfv
253JACC Vol. 45, No. 2, 2005 Gullestad et al.January 18, 2005:252–9 Heart Rate and Risk in Chronic Heart Failure
zed 3,991 patients (9). The present subgroup analysisocuses on subgroups of patients arbitrarily defined by Qs ofaseline resting HR, giving a fair amount of events in eachR subgroup. The study design and main results ofERIT-HF study have been published previously (9).
riefly, patients enrolled in the MERIT-HF study were 40o 80 years of age, with an ejection fraction �0.40 and inew York Heart Association (NYHA) functional class II to
V heart failure for at least three months before enrollment,ith an HR at or above 68 beats/min at the enrollment visit.aseline HR was taken as the mean of the two HRs
ecorded at the enrollment visit (start of a two-week placeboun-in) and the randomization visit, and may, therefore, beower than 68 beats/min. Patients were receiving optimumtandard therapy with diuretics and an angiotensin-onverting enzyme inhibitor. After the single-blind placeboun-in phase, patients were randomized to metoprololR/XL or placebo with starting doses of 12.5 mg (recom-ended for patients in NYHA functional class III and IV)
r 25 mg once daily. It was recommended to double theose every two weeks to a target dose of 200 mg once daily,r the highest tolerated dose (9).tatistical methods. Kruskal-Wallis test for continuousariables and Fisher exact test for categorical variables weresed when analyzing the relationship between a number ofaseline characteristics and resting baseline HR. The test ofreatment by HR interaction used the p value of the Waldtatistic of the interaction term in a Cox regression model.he risk defined as the number of events per patient year of
ollow-up (placebo group) was very similar in Q1 to Q4.herefore, in a secondary analysis, Q1 to Q4 were merged
nto one group when analyzing the difference in risketween Q1 to Q4 and Q5 utilizing Cox proportionalegression analysis, taking into account the following vari-bles: age; gender; ejection fraction; NYHA functional class;schemic etiology; history of myocardial infarction, hyper-ension, and diabetes mellitus; and systolic blood pressure.ox proportional regression analysis was also performedithin each Q to determine the risk-reducing effect ofeta-blocker treatment independent of baseline differencesadjusting for the following baseline variables: age; gender;jection fraction; NYHA functional class; ischemic etiology;istory of myocardial infarction, hypertension, and diabetesellitus; systolic blood pressure; and HR). When analyzing
Abbreviations and AcronymsCIBIS II � Cardiac Insufficiency Bisoprolol Study IICR/XL � controlled release/extended releaseHR � heart rateMERIT-HF � Metoprolol Controlled Release/Extended
Release Randomized Intervention Trialin Chronic Heart Failure
NYHA � New York Heart AssociationQ � quintile
utcome in relation to achieved HR and change in HR h
uring follow-up, respectively, outcome was analyzed fromhe date of the three-month visit to study closure. All dataere analyzed as intention to treat.
ESULTS
aseline HR as an independent risk factor for out-ome. In the placebo group, baseline HR as a continuousariable came out as a highly significant independent riskactor for all-cause mortality (p � 0.003; 217 deaths) forardiovascular mortality (p � 0.006; 203 deaths), and alsoor the number of patients hospitalized for worsening heartailure (p � 0.0001; 294 hospitalizations). No such statis-ically significant relationship was observed between base-ine HR and outcome in the beta-blocker group.
aseline characteristics by Qs of baseline HR. BaselineRs in the 5 Qs were: 71 beats/min in Q1, 76 beats/min in2, 81 beats/min in Q3, 87 beats/min in Q4, and 98
eats/min in Q5, respectively (Table 1). All patients in Q5 hadbaseline HR over 90 beats/min. Baseline HR was related tonumber of other baseline characteristics (Table 1). With
ncreasing HR, patients were more often in NYHA functionallass III and IV (52% in Q1 vs. 68% in Q5), more often hadon-ischemic etiology of heart failure (25% vs. 45%), a historyf diabetes (20% vs. 28%), atrial fibrillation (14% vs. 21%),igher diastolic blood pressure (76 vs. 80 mm Hg), and wereore often treated with diuretics (86% vs. 93%) and antidia-
etic drugs (10% vs. 16%). With increasing baseline HR, theroportion of women also increased (18% vs. 25%), there wasdecline in age (mean age 66.1 years in Q1 vs. 61.7 years in5), and also in ejection fraction (29% vs. 26%), fewer patients
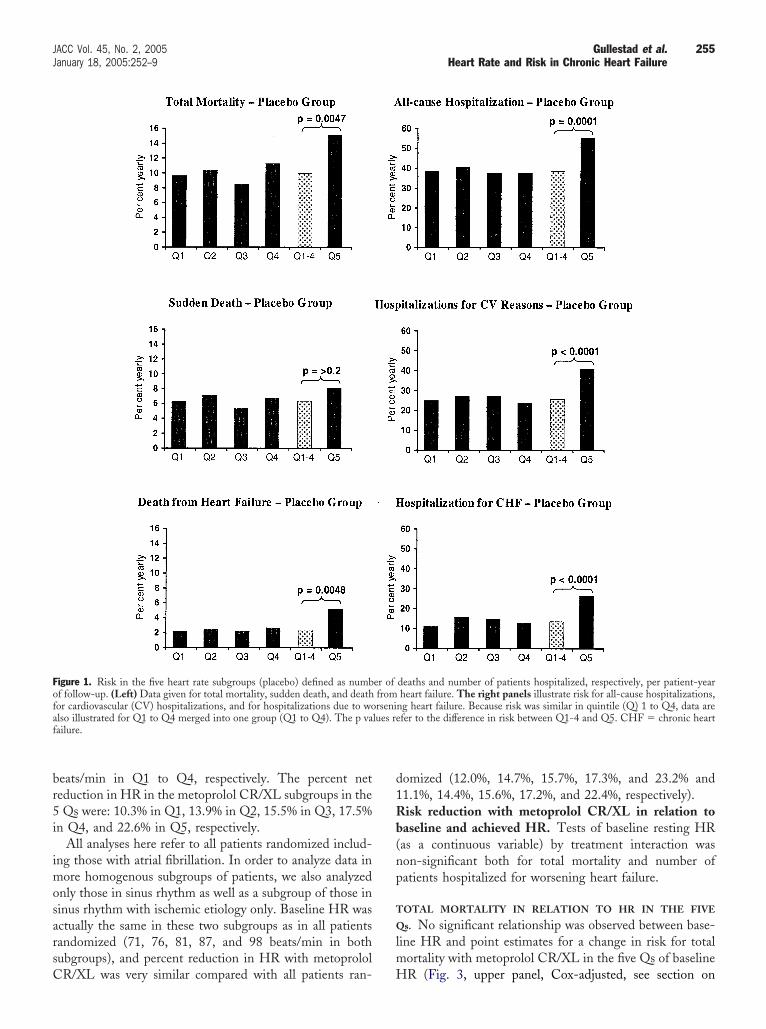
ad a history of myocardial infarction (60% vs. 36%), and feweratients were receiving aspirin (51% vs. 40%) and statins (30%s. 16%), respectively. Symptoms like peripheral edema, jugu-ar venous distension, and lung rales increased with increasingaseline HR (Table 1).isk in the placebo HR subgroups during follow-p. Figure 1 (left panel) is a bar diagram that illustrates riskefined as number of deaths per patient-years of follow-upn the five placebo HR subgroups. An inspection of theiagram reveals that the mortality risk was quite similar in1 to Q4. In the following analyses, Q1 to Q4 were,
herefore, merged into one group (Q1 to Q4). Relative riskn Q5 was significantly higher compared with Q1 to Q4 forotal mortality (1.51; 95% confidence interval 1.12 to 2.05);or deaths from heart failure (1.90; 95% confidence interval.09 to 3.33); but not for sudden death (1.27; 95% confi-ence interval 0.85 to 1.91).Similar data for the number of patients hospitalized are
llustrated in Figure 1 (right panel). Risk for hospitalizationsas very similar in Q1 to Q4. Relative risk in Q5 was
ignificantly higher compared with Q1 to Q4 for all-causeospitalizations (1.40; 95% confidence interval 1.18 to 1.68);or cardiovascular hospitalizations (1.55; 95% confidence inter-al 1.27 to 1.90); and also for hospitalization due to worsening
eart failure (1.78; 95% confidence interval 1.38 to 2.29).
DHf(medotisQ0“tw
D
Ccw
ac
bd(sCwpAptbbb1w8
T
HHAFCHWBNNLS
HHHAM
SDSS
*ss ind
n
254 Gullestad et al. JACC Vol. 45, No. 2, 2005Heart Rate and Risk in Chronic Heart Failure January 18, 2005:252–9
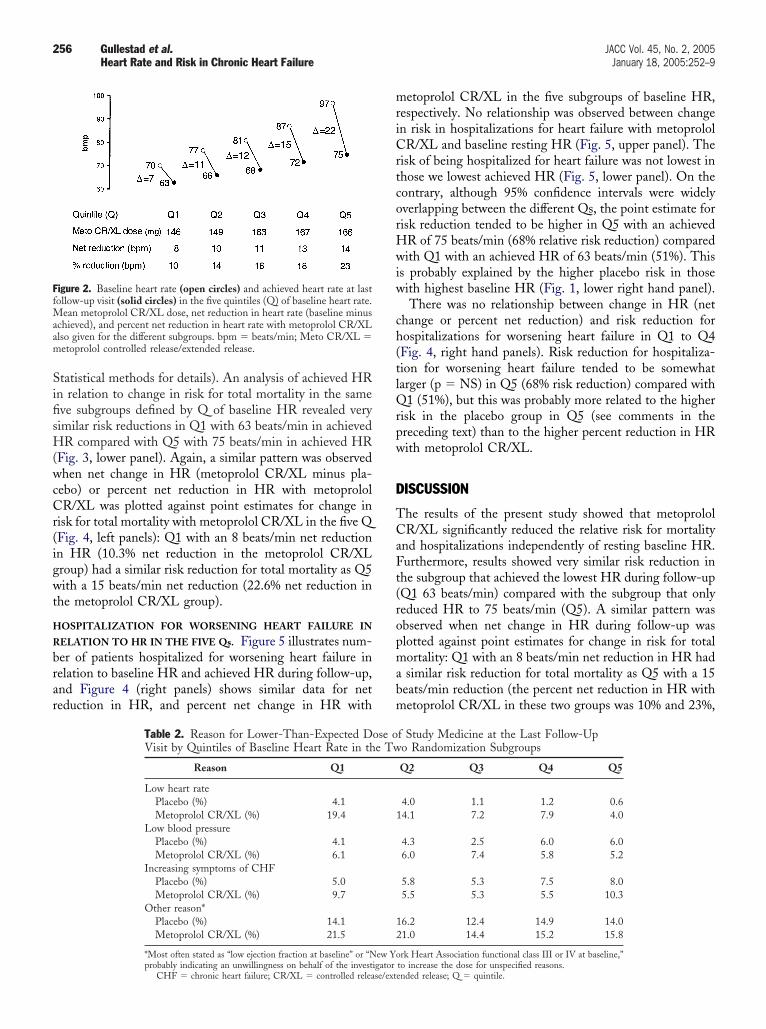
ose of study medicine in the five Qs of baselineR. The mean dose of metoprolol CR/XL at last
ollow-up visit in the 5 Qs of baseline HR were: 146 mgQ1), 149 mg (Q2), 163 mg (Q3), 167 mg (Q4), and 166g (Q5), respectively (Fig. 2). Over 80% of the patients in
ach Q reached at least 100 mg of metoprolol CR/XL onceaily, and 54% in Q1 reached the target dose of 200 mgnce daily compared with 69% in Q5. The reasons for lowerhan target dose in the beta-blocker group (as stated by thenvestigator) in the 5 Qs are given in Table 2; low HR wastated as the reason for 19.4% in Q1 compared with 4.0% in5 (corresponding figures in the placebo group 4.1% vs.
.6%, respectively). The reasons “low blood pressure” andincreasing symptoms of chronic heart failure” occurred inhe relatively similar proportion in the five different Qs, andere no different from placebo (Table 2).
ISCONTINUATION. Although discontinuation of metoprololR/XL tended to be slightly higher than on placebo in Q1 (52
ases on placebo and 69 on metoprolol CR/XL; p � NS), it
able 1. Baseline Clinical Characteristics in the Five Heart Rate
Q1(n � 802)
Q2(n � 772)
eart rate (mean, beats/min) 70.6 � 2.3 76.0 � 1.3eart rate (range, beats/min) 58.0–73.3 73.7–78.5ge (yrs) 66.1 � 9.1 64.8 � 9.4emales (%) 18 22aucasian (%) 95 94eight (cm) 172 � 8.8 172 � 8.7eight (kg) 79.7 � 15.2 80.9 � 16.3
MI (kg/m2) 26.8 � 4.1 27.3 � 4.7YHA functional class II/III/IV (%) 49/50/2 42/54/3onischemic etiology (%) 25.4 30.2V ejection fraction (%) 29 � 7 28 � 7moking habitsNever 26.2 25.1Daily 12.1 15.3istory of diabetes (%) 19.5 24.7istory of hypertension (%) 42.8 41.3istory of MI (%) 59.6 52.6trial fibrillation (%) 13.5 15.3edications (%)Diuretics 86.3 89.9ACE inhibitors 88.0 88.2AII blocker 8.0 7.3Digitalis 60.0 59.7Aspirin 50.9 48.3Statin 29.8 26.2Oral antidiabetic 9.6 11.8
ystolic BP (mm Hg) 129 � 16 130 � 17iastolic BP (mm Hg) 76 � 8.8 78 � 8.6
-creatinine (�mol/l) 109 � 31 106 � 31ymptoms (%)Peripheral edema 13.5 12.0Jugular venous distension 10.1 11.4Lung rales 7.7 11.4
See Statistical methods section.ACE � angiotensin-converting enzyme; AII � angiontensin II; BMI � body ma
ot analyzed, NYHA � New York Heart Association; Q � quintile.
as lower on metoprolol CR/XL compared with placebo Q
mong those with the highest baseline HR (Q5): 89 versus 51ases (0.59; 95% confidence interval 0.42 to 0.83; p � 0.003).
In the first Q, eight patients stopped treatment because ofradycardia in the metoprolol CR/XL group; correspondingata in the other Qs were five patients (Q2), two patientsQ3), and one patient (Q4). None of the patients in Q5topped treatment because of bradycardia in the metoprololR/XL group. Corresponding data in the placebo groupere two patients (Q1), no patient (Q2 to Q4), and threeatients (Q5), respectively.chieved HR in the five Qs of baseline HR. Figure 2resents baseline HR, achieved HR, and change in HR athe last follow-up visit in the five Qs defined by Q ofaseline HR. Achieved HR at the last follow-up visit was 63eats/min in Q1, 66 in Q2, 68 in Q3, 72 in Q4, and 75eats/min in Q5. Heart rates in the 5 Qs were reduced by 7,1, 12, 15, and 22 beats/min, respectively. However, HRas also reduced in the placebo group, especially in Q5 withbeats/min leading to a net reduction of 14 beats/min in
roups
Q3(n � 833)
Q4(n � 770)
Q5(n � 814)
Interaction WithHeart Rate*
p Value
80.9 � 1.5 86.8 � 2.0 98.1 � 7.2 NA78.7–83.3 83.5–90.3 90.7–141.7 NA
63.0 � 9.8 63.2 � 9.7 61.7 � 9.8 � 0.000122 25 26 � 0.0194 94 94 NS
172 � 8.8 171 � 8.6 171 � 8.7 NS81.1 � 16.0 80.7 � 16.4 80.9 � 16.8 NS27.3 � 4.5 27.4 � 4.9 27.5 � 5.1 NS
42/55/4 41/55/4 32/63/5 � 0.000132.9 39.9 45.0 � 0.0001
28 � 7 28 � 7 26 � 7 � 0.0001NS
25.2 27.9 25.114.6 14.0 16.325.2 25.7 28.3 � 0.00144.9 47.4 42.5 NS52.2 40.5 36.2 � 0.000113.6 16.5 20.8 � 0.001
89.6 92.7 93.4 � 0.000190.5 90.8 88.3 NS6.6 5.6 7.7 NS
62.8 65.7 70.4 � 0.000148.1 41.9 39.6 � 0.000124.1 20.3 16.1 � 0.000114.0 15.1 15.8 � 0.001
130 � 17 132 � 17 128 � 18 NS78 � 9.2 80 � 8.8 80 � 9.9 � 0.0001
107 � 39 106 � 30 106 � 33 � 0.05
14.9 15.6 18.9 � 0.0112.7 13.8 20.5 � 0.000111.0 12.3 13.0 � 0.01
ex; BP � blood pressure; LV � left ventricular; MI � myocardial infarction; NA �
Subg
5, which should be compared with 8, 10, 11, and 13
br5i
imosarsC
d1Rb(np
T
Q
lm
Fofaf
255JACC Vol. 45, No. 2, 2005 Gullestad et al.January 18, 2005:252–9 Heart Rate and Risk in Chronic Heart Failure
eats/min in Q1 to Q4, respectively. The percent neteduction in HR in the metoprolol CR/XL subgroups in theQs were: 10.3% in Q1, 13.9% in Q2, 15.5% in Q3, 17.5%
n Q4, and 22.6% in Q5, respectively.All analyses here refer to all patients randomized includ-
ng those with atrial fibrillation. In order to analyze data inore homogenous subgroups of patients, we also analyzed
nly those in sinus rhythm as well as a subgroup of those ininus rhythm with ischemic etiology only. Baseline HR wasctually the same in these two subgroups as in all patientsandomized (71, 76, 81, 87, and 98 beats/min in bothubgroups), and percent reduction in HR with metoprolol
igure 1. Risk in the five heart rate subgroups (placebo) defined as numbf follow-up. (Left) Data given for total mortality, sudden death, and deathor cardiovascular (CV) hospitalizations, and for hospitalizations due to wolso illustrated for Q1 to Q4 merged into one group (Q1 to Q4). The p vaailure.
R/XL was very similar compared with all patients ran- H
omized (12.0%, 14.7%, 15.7%, 17.3%, and 23.2% and1.1%, 14.4%, 15.6%, 17.2%, and 22.4%, respectively).isk reduction with metoprolol CR/XL in relation to
aseline and achieved HR. Tests of baseline resting HRas a continuous variable) by treatment interaction wason-significant both for total mortality and number ofatients hospitalized for worsening heart failure.
OTAL MORTALITY IN RELATION TO HR IN THE FIVE
s. No significant relationship was observed between base-ine HR and point estimates for a change in risk for total
ortality with metoprolol CR/XL in the five Qs of baseline
deaths and number of patients hospitalized, respectively, per patient-yearheart failure. The right panels illustrate risk for all-cause hospitalizations,
ng heart failure. Because risk was similar in quintile (Q) 1 to Q4, data arefer to the difference in risk between Q1-4 and Q5. CHF � chronic heart
er offromrseni
lues re
R (Fig. 3, upper panel, Cox-adjusted, see section on
SifisH(wcCr(igwt
H
R
brar
mriCrtcorHwiw
ch(tlQrpw
D
TCaFt(ropmabm
FfMaam
256 Gullestad et al. JACC Vol. 45, No. 2, 2005Heart Rate and Risk in Chronic Heart Failure January 18, 2005:252–9
tatistical methods for details). An analysis of achieved HRn relation to change in risk for total mortality in the sameve subgroups defined by Q of baseline HR revealed veryimilar risk reductions in Q1 with 63 beats/min in achievedR compared with Q5 with 75 beats/min in achieved HR
Fig. 3, lower panel). Again, a similar pattern was observedhen net change in HR (metoprolol CR/XL minus pla-
ebo) or percent net reduction in HR with metoprololR/XL was plotted against point estimates for change in
isk for total mortality with metoprolol CR/XL in the five QFig. 4, left panels): Q1 with an 8 beats/min net reductionn HR (10.3% net reduction in the metoprolol CR/XLroup) had a similar risk reduction for total mortality as Q5ith a 15 beats/min net reduction (22.6% net reduction in
he metoprolol CR/XL group).
OSPITALIZATION FOR WORSENING HEART FAILURE IN
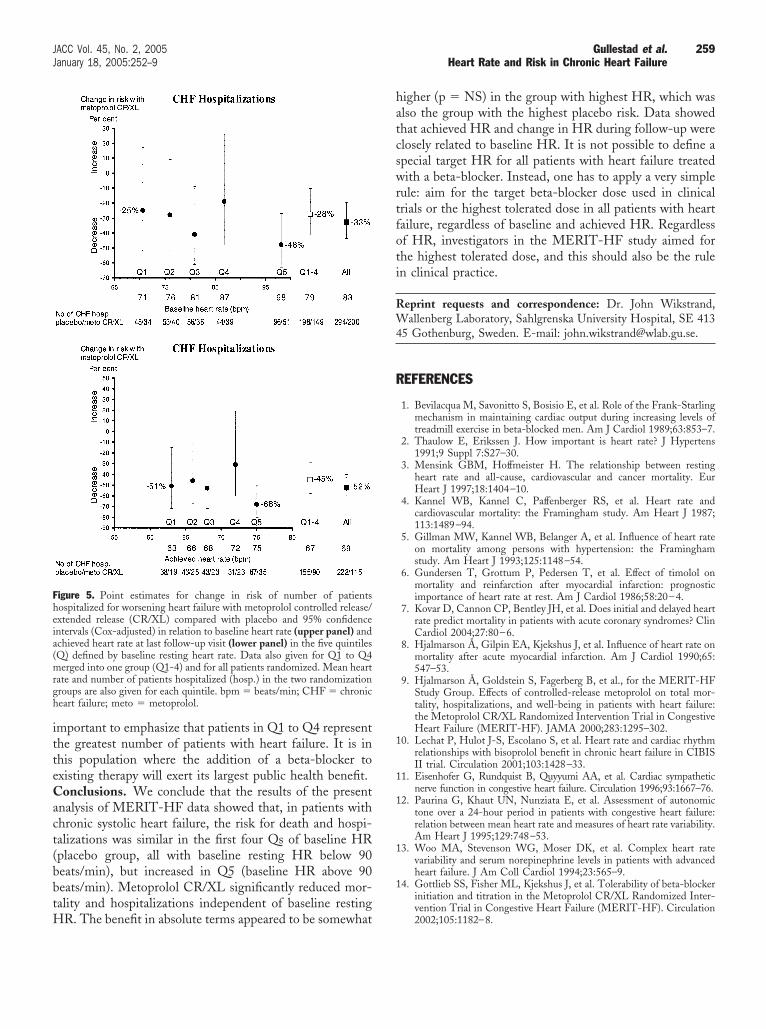
ELATION TO HR IN THE FIVE Qs. Figure 5 illustrates num-er of patients hospitalized for worsening heart failure inelation to baseline HR and achieved HR during follow-up,nd Figure 4 (right panels) shows similar data for neteduction in HR, and percent net change in HR with
igure 2. Baseline heart rate (open circles) and achieved heart rate at lastollow-up visit (solid circles) in the five quintiles (Q) of baseline heart rate.
ean metoprolol CR/XL dose, net reduction in heart rate (baseline minuschieved), and percent net reduction in heart rate with metoprolol CR/XLlso given for the different subgroups. bpm � beats/min; Meto CR/XL �etoprolol controlled release/extended release.
Table 2. Reason for Lower-Than-Expected DVisit by Quintiles of Baseline Heart Rate in th
Reason Q1
Low heart ratePlacebo (%) 4.1Metoprolol CR/XL (%) 19.4
Low blood pressurePlacebo (%) 4.1Metoprolol CR/XL (%) 6.1
Increasing symptoms of CHFPlacebo (%) 5.0Metoprolol CR/XL (%) 9.7
Other reason*Placebo (%) 14.1Metoprolol CR/XL (%) 21.5
*Most often stated as “low ejection fraction at baseline” or “N
probably indicating an unwillingness on behalf of the investigatorCHF � chronic heart failure; CR/XL � controlled release/ext
etoprolol CR/XL in the five subgroups of baseline HR,espectively. No relationship was observed between changen risk in hospitalizations for heart failure with metoprololR/XL and baseline resting HR (Fig. 5, upper panel). The
isk of being hospitalized for heart failure was not lowest inhose we lowest achieved HR (Fig. 5, lower panel). On theontrary, although 95% confidence intervals were widelyverlapping between the different Qs, the point estimate forisk reduction tended to be higher in Q5 with an achieved
R of 75 beats/min (68% relative risk reduction) comparedith Q1 with an achieved HR of 63 beats/min (51%). This
s probably explained by the higher placebo risk in thoseith highest baseline HR (Fig. 1, lower right hand panel).There was no relationship between change in HR (net
hange or percent net reduction) and risk reduction forospitalizations for worsening heart failure in Q1 to Q4Fig. 4, right hand panels). Risk reduction for hospitaliza-ion for worsening heart failure tended to be somewhatarger (p � NS) in Q5 (68% risk reduction) compared with
1 (51%), but this was probably more related to the higherisk in the placebo group in Q5 (see comments in thereceding text) than to the higher percent reduction in HRith metoprolol CR/XL.
ISCUSSION
he results of the present study showed that metoprololR/XL significantly reduced the relative risk for mortality
nd hospitalizations independently of resting baseline HR.urthermore, results showed very similar risk reduction in
he subgroup that achieved the lowest HR during follow-upQ1 63 beats/min) compared with the subgroup that onlyeduced HR to 75 beats/min (Q5). A similar pattern wasbserved when net change in HR during follow-up waslotted against point estimates for change in risk for totalortality: Q1 with an 8 beats/min net reduction in HR hadsimilar risk reduction for total mortality as Q5 with a 15eats/min reduction (the percent net reduction in HR withetoprolol CR/XL in these two groups was 10% and 23%,
f Study Medicine at the Last Follow-Upo Randomization Subgroups
Q2 Q3 Q4 Q5
4.0 1.1 1.2 0.64.1 7.2 7.9 4.0
4.3 2.5 6.0 6.06.0 7.4 5.8 5.2
5.8 5.3 7.5 8.05.5 5.3 5.5 10.3
6.2 12.4 14.9 14.01.0 14.4 15.2 15.8
rk Heart Association functional class III or IV at baseline,”
ose oe Tw
1
12
ew Yo
to increase the dose for unspecified reasons.ended release; Q � quintile.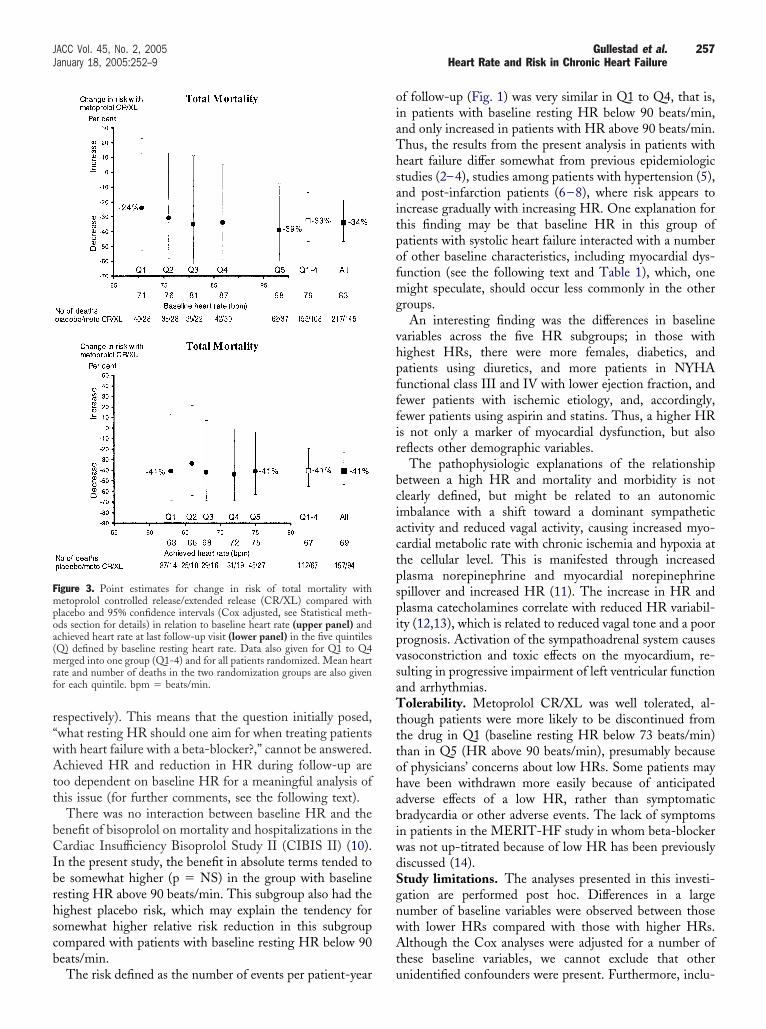
r“wAtt
bCIbrhscb
oiaThsaitpofmg
vhpfffir
bciactpspipvsaTtttohabiwdSgnwAt
Fmpoa(mrf
257JACC Vol. 45, No. 2, 2005 Gullestad et al.January 18, 2005:252–9 Heart Rate and Risk in Chronic Heart Failure
espectively). This means that the question initially posed,what resting HR should one aim for when treating patientsith heart failure with a beta-blocker?,” cannot be answered.chieved HR and reduction in HR during follow-up are
oo dependent on baseline HR for a meaningful analysis ofhis issue (for further comments, see the following text).
There was no interaction between baseline HR and theenefit of bisoprolol on mortality and hospitalizations in theardiac Insufficiency Bisoprolol Study II (CIBIS II) (10).
n the present study, the benefit in absolute terms tended toe somewhat higher (p � NS) in the group with baselineesting HR above 90 beats/min. This subgroup also had theighest placebo risk, which may explain the tendency foromewhat higher relative risk reduction in this subgroupompared with patients with baseline resting HR below 90eats/min.
igure 3. Point estimates for change in risk of total mortality withetoprolol controlled release/extended release (CR/XL) compared with
lacebo and 95% confidence intervals (Cox adjusted, see Statistical meth-ds section for details) in relation to baseline heart rate (upper panel) andchieved heart rate at last follow-up visit (lower panel) in the five quintilesQ) defined by baseline resting heart rate. Data also given for Q1 to Q4erged into one group (Q1-4) and for all patients randomized. Mean heart
ate and number of deaths in the two randomization groups are also givenor each quintile. bpm � beats/min.
The risk defined as the number of events per patient-year u
f follow-up (Fig. 1) was very similar in Q1 to Q4, that is,n patients with baseline resting HR below 90 beats/min,nd only increased in patients with HR above 90 beats/min.hus, the results from the present analysis in patients witheart failure differ somewhat from previous epidemiologictudies (2–4), studies among patients with hypertension (5),nd post-infarction patients (6–8), where risk appears toncrease gradually with increasing HR. One explanation forhis finding may be that baseline HR in this group ofatients with systolic heart failure interacted with a numberf other baseline characteristics, including myocardial dys-unction (see the following text and Table 1), which, oneight speculate, should occur less commonly in the other
roups.An interesting finding was the differences in baseline
ariables across the five HR subgroups; in those withighest HRs, there were more females, diabetics, andatients using diuretics, and more patients in NYHAunctional class III and IV with lower ejection fraction, andewer patients with ischemic etiology, and, accordingly,ewer patients using aspirin and statins. Thus, a higher HRs not only a marker of myocardial dysfunction, but alsoeflects other demographic variables.
The pathophysiologic explanations of the relationshipetween a high HR and mortality and morbidity is notlearly defined, but might be related to an autonomicmbalance with a shift toward a dominant sympatheticctivity and reduced vagal activity, causing increased myo-ardial metabolic rate with chronic ischemia and hypoxia athe cellular level. This is manifested through increasedlasma norepinephrine and myocardial norepinephrinepillover and increased HR (11). The increase in HR andlasma catecholamines correlate with reduced HR variabil-ty (12,13), which is related to reduced vagal tone and a poorrognosis. Activation of the sympathoadrenal system causesasoconstriction and toxic effects on the myocardium, re-ulting in progressive impairment of left ventricular functionnd arrhythmias.olerability. Metoprolol CR/XL was well tolerated, al-
hough patients were more likely to be discontinued fromhe drug in Q1 (baseline resting HR below 73 beats/min)han in Q5 (HR above 90 beats/min), presumably becausef physicians’ concerns about low HRs. Some patients mayave been withdrawn more easily because of anticipateddverse effects of a low HR, rather than symptomaticradycardia or other adverse events. The lack of symptomsn patients in the MERIT-HF study in whom beta-blockeras not up-titrated because of low HR has been previouslyiscussed (14).tudy limitations. The analyses presented in this investi-ation are performed post hoc. Differences in a largeumber of baseline variables were observed between thoseith lower HRs compared with those with higher HRs.lthough the Cox analyses were adjusted for a number of
hese baseline variables, we cannot exclude that other
nidentified confounders were present. Furthermore, inclu-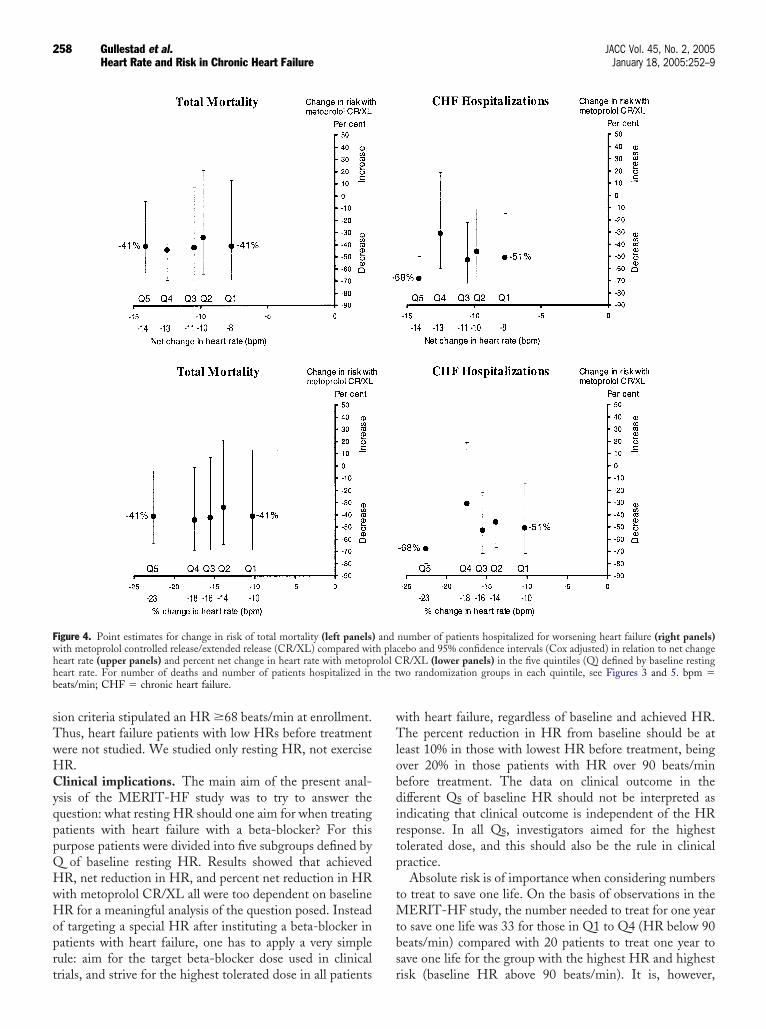
sTwHCyqppQHwHoprt
wTlobdirtp
tMtbs
Fwhh the tb
258 Gullestad et al. JACC Vol. 45, No. 2, 2005Heart Rate and Risk in Chronic Heart Failure January 18, 2005:252–9
ion criteria stipulated an HR �68 beats/min at enrollment.hus, heart failure patients with low HRs before treatmentere not studied. We studied only resting HR, not exerciseR.linical implications. The main aim of the present anal-
sis of the MERIT-HF study was to try to answer theuestion: what resting HR should one aim for when treatingatients with heart failure with a beta-blocker? For thisurpose patients were divided into five subgroups defined by
of baseline resting HR. Results showed that achievedR, net reduction in HR, and percent net reduction in HRith metoprolol CR/XL all were too dependent on baselineR for a meaningful analysis of the question posed. Instead
f targeting a special HR after instituting a beta-blocker inatients with heart failure, one has to apply a very simpleule: aim for the target beta-blocker dose used in clinical
igure 4. Point estimates for change in risk of total mortality (left panels)ith metoprolol controlled release/extended release (CR/XL) compared witeart rate (upper panels) and percent net change in heart rate with metopreart rate. For number of deaths and number of patients hospitalized ineats/min; CHF � chronic heart failure.
rials, and strive for the highest tolerated dose in all patients r
ith heart failure, regardless of baseline and achieved HR.he percent reduction in HR from baseline should be at
east 10% in those with lowest HR before treatment, beingver 20% in those patients with HR over 90 beats/minefore treatment. The data on clinical outcome in theifferent Qs of baseline HR should not be interpreted asndicating that clinical outcome is independent of the HResponse. In all Qs, investigators aimed for the highestolerated dose, and this should also be the rule in clinicalractice.Absolute risk is of importance when considering numbers
o treat to save one life. On the basis of observations in theERIT-HF study, the number needed to treat for one year
o save one life was 33 for those in Q1 to Q4 (HR below 90eats/min) compared with 20 patients to treat one year toave one life for the group with the highest HR and highest
number of patients hospitalized for worsening heart failure (right panels)cebo and 95% confidence intervals (Cox adjusted) in relation to net change
R/XL (lower panels) in the five quintiles (Q) defined by baseline restingwo randomization groups in each quintile, see Figures 3 and 5. bpm �
andh plaolol C
isk (baseline HR above 90 beats/min). It is, however,
itteCact(bbtH
hatcswrtfoti
RW4
R
1
1
1
1
1
Fheia(mrgh
259JACC Vol. 45, No. 2, 2005 Gullestad et al.January 18, 2005:252–9 Heart Rate and Risk in Chronic Heart Failure
mportant to emphasize that patients in Q1 to Q4 representhe greatest number of patients with heart failure. It is inhis population where the addition of a beta-blocker toxisting therapy will exert its largest public health benefit.onclusions. We conclude that the results of the present
nalysis of MERIT-HF data showed that, in patients withhronic systolic heart failure, the risk for death and hospi-alizations was similar in the first four Qs of baseline HRplacebo group, all with baseline resting HR below 90eats/min), but increased in Q5 (baseline HR above 90eats/min). Metoprolol CR/XL significantly reduced mor-ality and hospitalizations independent of baseline resting
igure 5. Point estimates for change in risk of number of patientsospitalized for worsening heart failure with metoprolol controlled release/xtended release (CR/XL) compared with placebo and 95% confidencentervals (Cox-adjusted) in relation to baseline heart rate (upper panel) andchieved heart rate at last follow-up visit (lower panel) in the five quintilesQ) defined by baseline resting heart rate. Data also given for Q1 to Q4erged into one group (Q1-4) and for all patients randomized. Mean heart
ate and number of patients hospitalized (hosp.) in the two randomizationroups are also given for each quintile. bpm � beats/min; CHF � chroniceart failure; meto � metoprolol.
R. The benefit in absolute terms appeared to be somewhat
igher (p � NS) in the group with highest HR, which waslso the group with the highest placebo risk. Data showedhat achieved HR and change in HR during follow-up werelosely related to baseline HR. It is not possible to define apecial target HR for all patients with heart failure treatedith a beta-blocker. Instead, one has to apply a very simple
ule: aim for the target beta-blocker dose used in clinicalrials or the highest tolerated dose in all patients with heartailure, regardless of baseline and achieved HR. Regardlessf HR, investigators in the MERIT-HF study aimed forhe highest tolerated dose, and this should also be the rulen clinical practice.
eprint requests and correspondence: Dr. John Wikstrand,allenberg Laboratory, Sahlgrenska University Hospital, SE 413
5 Gothenburg, Sweden. E-mail: [email protected].
EFERENCES
1. Bevilacqua M, Savonitto S, Bosisio E, et al. Role of the Frank-Starlingmechanism in maintaining cardiac output during increasing levels oftreadmill exercise in beta-blocked men. Am J Cardiol 1989;63:853–7.
2. Thaulow E, Erikssen J. How important is heart rate? J Hypertens1991;9 Suppl 7:S27–30.
3. Mensink GBM, Hoffmeister H. The relationship between restingheart rate and all-cause, cardiovascular and cancer mortality. EurHeart J 1997;18:1404–10.
4. Kannel WB, Kannel C, Paffenberger RS, et al. Heart rate andcardiovascular mortality: the Framingham study. Am Heart J 1987;113:1489–94.
5. Gillman MW, Kannel WB, Belanger A, et al. Influence of heart rateon mortality among persons with hypertension: the Framinghamstudy. Am Heart J 1993;125:1148–54.
6. Gundersen T, Grottum P, Pedersen T, et al. Effect of timolol onmortality and reinfarction after myocardial infarction: prognosticimportance of heart rate at rest. Am J Cardiol 1986;58:20–4.
7. Kovar D, Cannon CP, Bentley JH, et al. Does initial and delayed heartrate predict mortality in patients with acute coronary syndromes? ClinCardiol 2004;27:80–6.
8. Hjalmarson Å, Gilpin EA, Kjekshus J, et al. Influence of heart rate onmortality after acute myocardial infarction. Am J Cardiol 1990;65:547–53.
9. Hjalmarson Å, Goldstein S, Fagerberg B, et al., for the MERIT-HFStudy Group. Effects of controlled-release metoprolol on total mor-tality, hospitalizations, and well-being in patients with heart failure:the Metoprolol CR/XL Randomized Intervention Trial in CongestiveHeart Failure (MERIT-HF). JAMA 2000;283:1295–302.
0. Lechat P, Hulot J-S, Escolano S, et al. Heart rate and cardiac rhythmrelationships with bisoprolol benefit in chronic heart failure in CIBISII trial. Circulation 2001;103:1428–33.
1. Eisenhofer G, Rundquist B, Quyyumi AA, et al. Cardiac sympatheticnerve function in congestive heart failure. Circulation 1996;93:1667–76.
2. Paurina G, Khaut UN, Nunziata E, et al. Assessment of autonomictone over a 24-hour period in patients with congestive heart failure:relation between mean heart rate and measures of heart rate variability.Am Heart J 1995;129:748–53.
3. Woo MA, Stevenson WG, Moser DK, et al. Complex heart ratevariability and serum norepinephrine levels in patients with advancedheart failure. J Am Coll Cardiol 1994;23:565–9.
4. Gottlieb SS, Fisher ML, Kjekshus J, et al. Tolerability of beta-blockerinitiation and titration in the Metoprolol CR/XL Randomized Inter-
vention Trial in Congestive Heart Failure (MERIT-HF). Circulation2002;105:1182–8.Top Related
Copyright © 2022 FDOKUMEN

