






Bahasa
Halaman
Hukum


doi:10.1016/S0360-3016(03)01624-9
PHYSICS CONTRIBUTION
WEB-BASED SUBMISSION, ARCHIVE, AND REVIEW OF RADIOTHERAPYDATA FOR CLINICAL QUALITY ASSURANCE: A NEW PARADIGM
JATINDER R. PALTA, PH.D., VINCENT A. FROUHAR, PH.D., AND JAMES F. DEMPSEY, PH.D.
Department of Radiation Oncology, University of Florida College of Medicine, Gainesville, Florida
Purpose: To report on the implementation of a web-based system (the Resource Center for Emerging Technol-ogies [RCET] System) that provides immediate access to the patient radiotherapy planning and delivery data forclinical quality assurance (QA) by the experts.Methods and Materials: An infrastructure of comprehensive tools required for preparation, submission, auto-archiving, web-based review, and retrieval of diagnostic images, treatment planning images, and radiationtherapy objects has been developed. These tools represent approximately 1.1 million lines of computer codedevelopment in seven languages (V, C��, Visual Basic, Java, ASP, HTML, and SQL) and consist of a secureauto-anonymizing upload and auto-archiving patient database, a web-based secure object archiving networksystem, a web-based rapid review tool, a web-based upload/download tool, and a personal computer client dataapplication for data object preparation, visualization, and submission, named NetSys. The RCET system enablesusers to share radiotherapy data in a secure environment. This paradigm of electronic data exchange makesremote peer review very efficient and convenient.Results: The RCET system can help the radiation therapy community ensure consistent evaluation of itstherapies. It will encourage proactive QA. An example of proactive clinical QA would be to provide atlases oftarget and critical structure definitions, to serve as class solutions, as well as dose prescription, specification, andreporting examples for guidance to the radiation oncologists in the community. The web-based clinical qualityassurance is ideally suited for emerging technologies in radiation therapy that generate complex and voluminousmultimodality imaging and planning data.Conclusions: The RCET system enables users to share multimodality imaging data, radiation therapy planning,and delivery data on demand. Our design paradigm will allow rapid peer review of radiotherapy data througha simple personal computer–based web browser. © 2003 Elsevier Inc.
Radiotherapy data exchange, Clinical QA, Electronic review.
INTRODUCTION
The discipline of radiation therapy is reaching new pinna-cles with continued advancement in treatment planning,delivery, and treatment verification (1–3). Advances in im-aging have enhanced our ability to create a complete ana-tomic and functional 3D model of each patient that facili-tates the use of advanced technology radiation therapy (RT)delivery tools (4–10). These emerging technologies haveimpacted nearly all types of radiation delivery, including 3Dconformal radiation therapy (3D-CRT), intensity-modulatedradiation therapy (IMRT), stereotactic radiotherapy and ra-diosurgery, and image-guided brachytherapy. These newtechnologies can potentially impact significantly the futurepractice of radiation therapy, because they make it possibleto highly conform dose distributions to the target volumes
while sparing the surrounding critical structures, thus open-ing the doors for dose escalation and organ-sparing proto-cols (11, 12). However, these advances do not come withouta price and a risk. The price lies in the fact that theseemerging radiation therapy technologies utilize complexand voluminous multimodality imaging and planning data(13). The risk is that complex techniques can be misunder-stood and misapplied, possibly resulting in excess tumorrecurrences or excess complications that will negate thepotential benefits of these new technologies. Therefore, thetask of safely implementing these advances for patient treat-ments in clinics around the country will require innovativeand efficient methodologies of clinical quality assurance(QA). Furthermore, there is growing evidence that QA canactually improve outcomes for radiotherapy patients, a trend
Reprints are not available. Corresponding author: Jatinder R.Palta, Ph.D., Department of Radiation Oncology, University ofFlorida College of Medicine, Gainesville, FL. Tel: (352) 265-8217; Fax: (352) 265-8417; E-mail: [email protected]
Presented orally at the 44th Annual Meeting of the AmericanSociety for Therapeutic Radiology and Oncology, New Orleans,LA, Oct. 6–10, 2002.
Supported by Grant CA-81636 from the National Cancer Institute.The contents are solely the responsibility of the authors and
do not necessarily represent the official views of the NationalCancer Institute.
Received Mar 18, 2003, and in revised form Jul 15, 2003.Accepted for publication Jul 22, 2003.
Int. J. Radiation Oncology Biol. Phys., Vol. 57, No. 5, pp. 1427–1436, 2003Copyright © 2003 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/03/$–see front matter
1427

that we believe will be more evident in advanced technol-ogy-based RT (14, 15).
There is a great need for peer review, because the newadvanced technologies are initially implemented in radia-tion therapy clinics. The radiation dose distributions createdwith these techniques and the sharp dose gradients em-ployed in these novel therapies require a complete reeval-uation of the current paradigms to account for patient im-mobilization and definition of target volumes and criticalstructures, in addition to organ motion and deformation(16–18). These complexities challenge the conventionalwisdom previously accumulated by RT practitioners. Allthese issues extenuate the need for peer review for the safeimplementation of novel technologies. Compounding theseproblems further is that 3D-CRT and IMRT treatment plan-ning and delivery tools are now readily available in bothcommunity- and academic-based RT practices. The ad-vanced technology treatments are no longer limited to largepractices with significant resources. Therefore, it is veryimportant to provide resources to community- and academ-ic-based practices facilitating their access to peer review.We believe that this can be readily accomplished if thepatient data, such as clinical information, treatment plan-ning and diagnostic images, and radiotherapy plans fromthese facilities, are available via the web browser for remoteguidance and review.
In 1999, the Radiation Research Program, part of the CancerTreatment and Diagnosis division of the National Cancer In-stitute (NCI) of the National Institutes of Health, issued arequest for funding proposals. In response, we proposed thedevelopment of the Resource Center for Emerging Technolo-gies (RCET) at the University of Florida, to develop anddisseminate advanced medical informatics resources, facilitat-ing quality assurance for the conduct of NCI-sponsored clinicaltrials. Current experience with remote review of electronicimaging data and radiation therapy objects is limited. The onlyrecent initiatives are a few NCI-sponsored clinical protocolsunder the auspices of the Radiation Therapy Oncology Group(RTOG) and the exchange of radiotherapy data as part of anelectronic patient referral system in Switzerland (19, 20). Inboth, nonanonymized patient data are submitted to a centraldata archive by means of either recording media (tape or CD)or unsecured file transfers via the standard file transfer protocol(FTP). The local staff processes these data and presents themto local experts. The patient data transmission via unsecuredFTP may become difficult, because recent federal guidelinesregarding patient confidentiality prohibit such data transfer.According to the new regulations, protecting the confidential-ity of medical information is extremely important. New federalregulations [45 CFR 46.111(a)(7)] and multiple high-profilepublications have recently focused attention on the need toincrease attention to confidentiality issues (21). The federalregulations make it clear that any type of information from aperson’s medical record must be treated as “private” from theregulatory standpoint [45 CFR 46.102(f)(2)]. The Health In-surance Portability and Accountability Act now requires for-mal documentation of confidentiality procedures that limit
access to information from a medical record (22). Any projectattempting to transmit oncology records between institutionsand to a wide range of technical and medical groups for reviewand consultation will be required to establish procedures pro-tecting patient confidentiality to the maximum degree. TheRCET system is designed to be compliant with the HealthInsurance Portability and Accountability Act requirements, asdiscussed in the description of the system.
Electronic review of clinical data is only one aspect ofclinical trial QA with advanced emerging technologies.Uniform methodologies for dose prescription, specifica-tion, reporting, and evaluation are very important (23,24). Another important consideration in 3D-CRT andIMRT is the consistent definition of target volumes andorgans at risk (25). To address these issues, proactive QAcan be provided through computer aided or automatedQA tools. These tools can help the radiation therapycommunity ensure consistent evaluation of its therapies.An example of proactive QA would be to provide atlasesof target and critical structure definitions, to serve asclass solutions, as well as dose prescription, specifica-tion, and reporting examples for guidance to the radiationoncologists in the community. The goal of high-preci-sion, high-dose radiation therapy is to improve tumorcontrol and decrease treatment morbidity; it is importantto clearly define target volumes based on knowledge ofthe patterns of disease spread, so all local and regionalareas are treated with adequate doses. With emergingtechnologies, the clinical experience of treating variouscancers using what is now termed “wide-area treatments”must be carefully reviewed before dramatic changes aremade in the target volume definitions for highly confor-mal techniques.
The implementation of a web-based system providingimmediate access to the patient radiotherapy planning anddelivery data for clinical QA by the experts is discussedherein. The patient data for the advanced technology radi-ation therapy techniques can be quite voluminous. In par-ticular, the clinical QA of an IMRT plan and delivery mayrequire comprehensive review of multiple image sets ofmultiple modalities and 3D treatment plans that includeprecise 3D anatomic structure sets and large dose matrices.A typical patient data set includes 50–400 MB of imagedata, 1–50 MB of plan data, and extensive informationregarding patient history, diagnosis, treatment, and out-come. We will describe how the system developed at theUniversity of Florida enables users to share multimodalityimaging data, radiation therapy planning and delivery data,and conventional database objects in a distributed environ-ment (26). Our aim has been to design and implement asystem that functionally analyzes, stores, and visualizes thedata on demand. In addition, the system allows the users toenter the information at any site and to share and analyze itremotely. Our design paradigm will allow rapid review ofradiotherapy data through a simple personal computer (PC)-based web browser. This makes it easier for even the most
1428 I. J. Radiation Oncology ● Biology ● Physics Volume 57, Number 5, 2003

remote facilities to participate in peer review of their ad-vanced technology radiation therapy.
MATERIALS AND METHODS
Resource Center for Emerging TechnologiesThe impetus for this project has been the University of
Florida development of a resource center to facilitate theconduct of NCI-sponsored advanced technology RT clinicaltrials. The RCET was established at the University of Flor-ida in 1999, through an NCI-funded grant to provide thetechnical resources for the clinical cooperative groups. TheRCET provides a collection of services for investigators tointeract with clinical data. The technology developed at theRCET enables users to share multimodality imaging data,RT planning and delivery data, and conventional databaseobjects in a distributed environment (26). Therefore, itenables clinical trial groups to design and implement moreadvanced and comprehensive clinical protocols. For exam-ple, a clinical group can design a protocol that includesmultimodality electronic imaging and planning data fromdifferent phases of treatment. For the design of the RCETsystem, we recognized that it is neither efficient nor cost-effective to bring together radiation oncologists, radiolo-gists, and other professionals to a single location to evaluatestudy cases. We were also acutely aware that patient datasecurity and confidentiality must be enforced throughout thereview process. Envisioned was an environment where re-mote collaboration on clinical data review and protocoldesign could occur. In this environment, the desire for theability to edit the clinical data while preserving the originaldata submission was also recognized. The value of a cen-tralized repository of electronic patient data stored in arelational database for retrospective analysis was also ac-knowledged. Finally, the rapid pace of technology develop-ment in radiation oncology prompted us to consider theproliferation of electronic patient data and focus on theautomation of data submission to conserve personnel re-sources.
With these considerations, the RCET system was de-signed to meet the following criteria:
1. Reviewers can review data anywhere they have access toa PC and a fast internet connection.
2. Submitted clinical data must be made immediately avail-able for review.
3. All types of imaging and RT data are accepted, archived,and disseminated.
4. Patient confidentiality is maintained throughout the pro-cess.
5. Multiple users with secure access to the RCET databasefor collaborative review of case images and RT objectsare provided.
6. Data objects must be editable, and the database mustsupport data authoring and versioning (DAV) control.
7. Data mining of the RCET database is available for re-searchers.
8. The system must be largely automated as advances in RToccur, so the required personnel resources do not grow inproportion to the increase in patient-related data.
With this design criterion in mind, the RCET system wasdeveloped. Our system consists of a worldwide web-baseddata management system, digital imaging and communica-tions in medicine (DICOM) format, compliant picture ar-chiving computerized system (PACS), DICOM-RT–com-pliant data object server, and web-based rapid reviewsystem. It provides facilities for archiving, sharing, anddistributing electronic data. The institutions can send patientdata, including textual information, image sets, and treat-ment planning information, using an easily accessible webbrowser interface to a central database. Web technologyallows users to easily enter and access case information in aunified database system. Once a patient is registered, thereis an extensive set of data that must be received, archived,categorized, analyzed, and disseminated by the RCET cen-tralized database. The principal design criterion is the im-plementation of a system that functionally analyzes, stores,and presents the data on demand. In addition, the systemmust allow the users to enter the patient information at anysite and analyze it remotely on demand via a web browser,such as Microsoft Internet Explorer. The RCET systemconsists of three central tools that meet the following goals:a centralized auto-archiving database; a web-based secureobject archiving network system (SOANS); and a suite ofuser-friendly client applications for clinical data prepara-tion, submission, and review. A diagram of the flow of datausing the RCET system is shown in Fig. 1.
In the first step, clinical data flow from treatment plan-ning systems and/or imaging devices to a PC client softwarenamed NetSys, which can receive datasets in standard elec-tronic image, DICOM, DICOM-RT, and RTOG formats.Users load and visualize the datasets using the NetSyssoftware, which includes clinical images and RT parame-ters. NetSys is designed to have similar functionality as aclinical treatment planning review workstation; i.e., planparameters and values calculated by a treatment planningsystem cannot be changed, and only the presentation ofthese values can be modified. In the second step, the userinputs a unique case identifier, after which all informationabout the patient is replaced with this identifier, and the dataare anonymized. Then NetSys compresses and encrypts thedataset before uploading to the RCET web server. Becauseof logistic limitations, some users may wish to submitdatasets without using NetSys as a means of preprocessing.In such situations, there is a web-based secure data upload/download tool. This mechanism anonymizes, encrypts, anduploads the case datasets to the RCET server. In the thirdstep, the uploaded data are automatically archived and reg-istered with the database. If the case is new, an “electronicfolder” is created. If the case already exists, the new data aresimply appended to the existing case electronic folder. Atthis time, all case data are registered in the RCET databaseand are made available for web-based rapid review. The
1429A new paradigm for review of radiotherapy data ● J. R. PALTA et al.
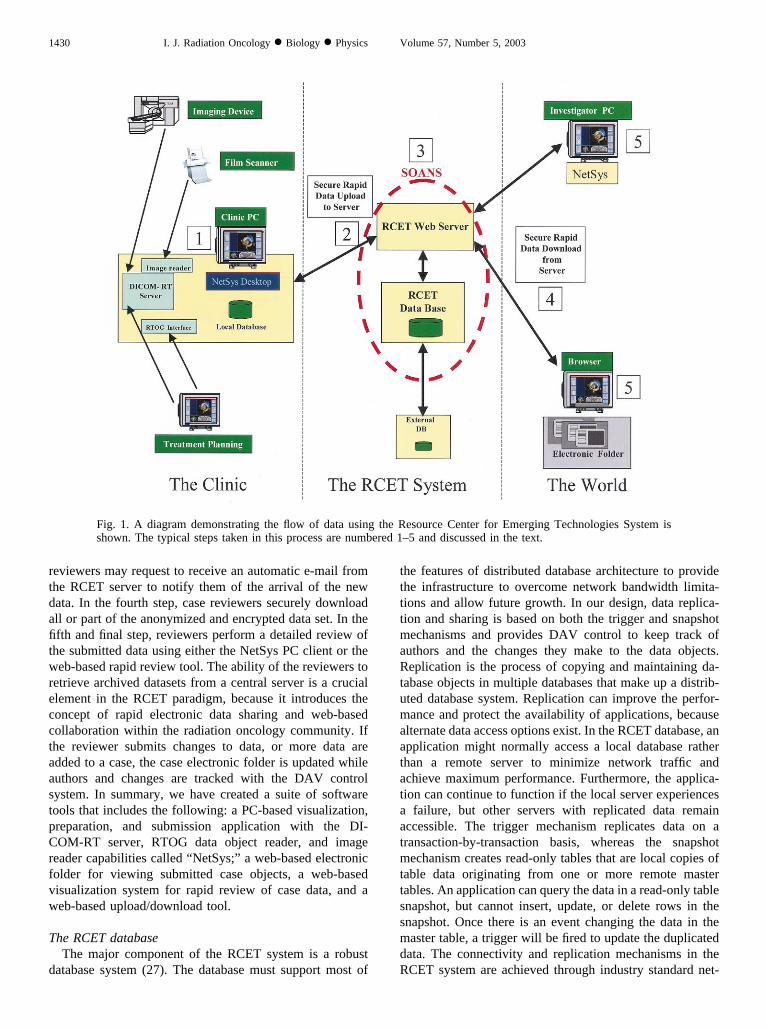
reviewers may request to receive an automatic e-mail fromthe RCET server to notify them of the arrival of the newdata. In the fourth step, case reviewers securely downloadall or part of the anonymized and encrypted data set. In thefifth and final step, reviewers perform a detailed review ofthe submitted data using either the NetSys PC client or theweb-based rapid review tool. The ability of the reviewers toretrieve archived datasets from a central server is a crucialelement in the RCET paradigm, because it introduces theconcept of rapid electronic data sharing and web-basedcollaboration within the radiation oncology community. Ifthe reviewer submits changes to data, or more data areadded to a case, the case electronic folder is updated whileauthors and changes are tracked with the DAV controlsystem. In summary, we have created a suite of softwaretools that includes the following: a PC-based visualization,preparation, and submission application with the DI-COM-RT server, RTOG data object reader, and imagereader capabilities called “NetSys;” a web-based electronicfolder for viewing submitted case objects, a web-basedvisualization system for rapid review of case data, and aweb-based upload/download tool.
The RCET databaseThe major component of the RCET system is a robust
database system (27). The database must support most of
the features of distributed database architecture to providethe infrastructure to overcome network bandwidth limita-tions and allow future growth. In our design, data replica-tion and sharing is based on both the trigger and snapshotmechanisms and provides DAV control to keep track ofauthors and the changes they make to the data objects.Replication is the process of copying and maintaining da-tabase objects in multiple databases that make up a distrib-uted database system. Replication can improve the perfor-mance and protect the availability of applications, becausealternate data access options exist. In the RCET database, anapplication might normally access a local database ratherthan a remote server to minimize network traffic andachieve maximum performance. Furthermore, the applica-tion can continue to function if the local server experiencesa failure, but other servers with replicated data remainaccessible. The trigger mechanism replicates data on atransaction-by-transaction basis, whereas the snapshotmechanism creates read-only tables that are local copies oftable data originating from one or more remote mastertables. An application can query the data in a read-only tablesnapshot, but cannot insert, update, or delete rows in thesnapshot. Once there is an event changing the data in themaster table, a trigger will be fired to update the duplicateddata. The connectivity and replication mechanisms in theRCET system are achieved through industry standard net-
Fig. 1. A diagram demonstrating the flow of data using the Resource Center for Emerging Technologies System isshown. The typical steps taken in this process are numbered 1–5 and discussed in the text.
1430 I. J. Radiation Oncology ● Biology ● Physics Volume 57, Number 5, 2003

work-based database connectivity interfaces. In our situa-tion, the distributable objects are primarily DICOM-RTobjects in the form of DICOM files. Highly reliable com-munication between databases is essential, and connectivityrequirements with multiple databases allowing subsets ofarchived objects to be shared with other patient databasesare a major design issue. The RCET system’s native data-base is the Microsoft SQL server (28) with interconnectivitysupport for external ORACLE, Sybase, and IBM DB2 da-tabases. Information uploaded by users must be sharedamong databases on a real-time basis. To maintain theintegrity and security of a centralized database, distributedconnectivity between databases must be dynamic and basedon the master-slave paradigm. In such an environment, themaster database, the primary repository for data, maintainsa set of records and tables. Differential changes to recordsare transmitted to slave databases. It is neither practical nornecessary to copy a whole set of records and tables to theslave database. In summary, our database has been designedto maximize performance, allow rapid multi-user internetaccess, provide DAV control, and interface with existingdatabases.
The RCET web-based SOANSPACS have been available for the last decade. These
systems have been based on a well-defined informationexchange protocol (DICOM). Naturally, the question aroseas to why one cannot deploy a commercially availablePACS to achieve the RCET goals. Conventional PACSwere designed around centralized databases that communi-cate only within a local area network (LAN) for security andfirewall reasons. The communication protocol used byPACS workstations is the DICOM messaging protocol,which is not secure and does not support encryption securitymechanisms. The DICOM standard was designed for radi-ology departments where strong support for a universaldatabase is not of primary importance. At the time of ourdevelopment, there were no commercial PACS that sup-ported DICOM-RT or the American Association of Physi-cists in Medicine (AAPM)/RTOG data exchange format fortreatment plans. We conceived and developed a SOANS toact as a wide area network (WAN) server for RT images anddata objects—analogous to a PACS working with diagnos-tic images within a LAN (Note that a highly secure networkwithin a clinic is considered an example of a LAN, whereasthe internet at large is considered a WAN) (29). We imple-mented this completely new system based on C�� object-oriented code. We distinguished the SOANS from thePACS in that the SOANS deals with any data object en-countered in RT, supports a secure encrypted security mech-anism, and is available across a WAN.
In summary, the SOANS provides the following func-tions:
1. Imports AAPM/RTOG data objects from the major 3Dtreatment planning systems,
2. Imports DICOM-RT objects from the major 3D treat-ment planning systems,
3. Supports a high level of conformance to the DICOMstandard,
4. Supports multiple industry standard databases,5. Supports bidirectional network transport mechanisms
across a WAN, and6. Supports patient confidentiality via data anonymization
and encryption security mechanisms.
Import capability for the RTOG data objects is veryimportant, because most 3D treatment planning systemsalready support the RTOG data transfer format. To mini-mize the development cycle, we wrote a data format con-verter. This converter translates AAPM/RTOG data objectsinto DICOM-RT–compatible objects. After the conversion,the new objects are processed as any other DICOM-RTobjects. We have successfully imported AAPM/RTOG dataobjects from all commercial treatment planning systems thatsupport this format. AAPM/RTOG data objects’ conversionto DICOM-RT objects allows data transfer from systemsnot yet supporting DICOM-RT export and provides back-ward compatibility (e.g. an existing AAPM/RTOG formatobject database could be converted to DICOM-RT format).We have also demonstrated the ability to import DI-COM-RT objects from the commercial treatment planningsystems that support this new format at the present time. Itis our goal to continue developing our DICOM-RT con-formance and maintain the most inclusive implementationpossible. In addition to implementing the DICOM standard,we had to impose an external structure to the existingDICOM-RT objects suitable to the structure of our database,because DICOM-RT does not concern itself with processmanagement. To maintain patient confidentiality, all pa-tient-related information is removed from the data objectsbefore they are transported to the central database. Thisprocess is called anonymizing; after the anonymization pro-cess we refer to “cases” in deference to patients, to empha-size their anonymity. All objects relating to a case areindividually compressed, encrypted, transported, and regis-tered with the database. The data transport protocols em-ployed throughout are the hypertext transfer protocol(HTTP) and the secure HTTP (S-HTTP). Transport securityis provided by the secure socket layer and pretty-good-privacy encryption schemes (30). We refer to this entiresystem of archiving tools as a SOANS. It is designed toprovide independent software clients the flexibility to accessdata objects. In addition, access security, DAV control, anddatabase interconnectivity are provided independently foreach SOANS component through the RCET database. Themain advantage of such a design is that multiple users canaccess the same data simultaneously and independentlywhile integrity and version control of the components arepreserved. In summary, the SOANS is a data object serverthat deals with all objects encountered in RT, and supportsa secure encrypted security mechanism and is availableacross a WAN.
1431A new paradigm for review of radiotherapy data ● J. R. PALTA et al.

The RCET suite of PC- and web-based applicationsThe RCET software suite interacts with the SOANS to
submit and retrieve data objects from the RCET databaseand includes the following: a PC-based visualization, prep-aration, and submission application with the DICOM-RTserver, RTOG data object reader, and image reader capa-bilities called “NetSys”; a web-based electronic folder forviewing submitted case objects; a web-based visualizationsystem for rapid review of case data; and a web-basedupload/download tool. NetSys assists users in collecting,visualizing, and submitting clinical data objects to theRCET database. It allows the user to assign a specific caseidentification number and anonymize the data before theyare transmitted. It converts all data into a homogeneousDICOM-RT format that is compatible with the SOANS.The client software is currently designed for reading, ana-lyzing, and submitting DICOM images (CT, magnetic res-onance, and ultrasound), digital images (secondary capture),scanned films, and AAPM/RTOG data exchange output.Although NetSys provides DICOM-RT server capabilitiesallowing data submission, visualizing DICOM-RT objectspresently requires intervention from the RCET staff. NetSysconverts all data to DICOM-RT objects, which become thefundamental data objects for exchanging, modifying, andstoring 3D treatment planning information. To support theexisting hard copy-based data submission, a high-resolutionelectronic image processing module is provided, which con-verts electronic images to secondary capture DICOM ob-jects. The NetSys software automatically creates an elec-tronic folder of submitted data that consists of textualinformation, multiple image sets, and treatment planninginformation for each case study by communicating throughthe SOANS. NetSys compresses and then encrypts all datafor transmission to the RCET site. The encryption key is arandomly generated, unique identification key. For bettersecurity, data files are not decrypted when stored in thedatabase. Decryption is possible only with the unique keyfor that particular data file. Decryption keys for data files arestored in a binary format file within the database and are notaccessible by users. Users can also download data sets fromthe RCET site using the NetSys software. First, users haveto log in to the system by providing their user name andpassword. Access to cases is based on the privilege levelassigned to the user. Exchange of user information (e.g.,user name and password) is performed using a secure pri-vate-public-key cryptography method. After a user logs in,he can see only cases based on his access level. After theuser selects data objects to download, encrypted data filesare transferred to the user’s computer. Finally, the keyneeded for decryption is sent to the NetSys client through asecure socket layer.
We realized that some users would not have the resourcesto support the NetSys application and make use of the rapidreview tool. Therefore, we developed an easy and efficientweb-based upload/download application allowing for thedirect transfer of secure anonymized case data. Selectingdata for upload with this tool launches a process that ano-
nymizes all DICOM and RTOG data objects before transfer(similar to the features in NetSys). This method of datasubmission requires little effort on the part of the user, butdoes not allow for immediate use of the rapid review tool.With this form of data submission, the RCET staff wouldhave to prepare the data for web-based review.
After data submission, the case electronic folder is im-mediately available for review on the RCET web site withpassword access. It is accessible using a common webbrowser (Microsoft Internet Explorer). Figure 2 shows anelectronic folder for a typical clinical case. The electronicfolder organizes the data objects for each case and continuesto be updated by the database as more data are received onsubsequent submissions. The data objects can include thefollowing: diagnostic CT, magnetic resonance, ultrasound,and nuclear medicine images; pathology slides; port films,radiographs, and digitally reconstructed radiographs; iso-dose distributions; and dose–volume histographs. This pro-cess is completely automated and requires no human inter-vention from the RCET staff. Hyperlinks in the electronicfolder allow reviewers to immediately access submittedcases for a rapid review using a web-based visualizationsystem. The RCET web site is divided into secure andunsecured sections. Access to secure sections is based on awell-defined hierarchical scheme of privilege levels. Forexample, a designated principal reviewer for an institutionwill have access to all cases submitted by that particularinstitution, whereas an individual can access only cases theyhave submitted. The data communication between the clientsoftware (a browser application or NetSys) and the RCETserver is secure and robust. Because we use the HTTP andS-HTTP throughout our system design, we can easily over-come issues regarding firewalls and network access limita-tions for end users.
When the electronic folder is being used, a session vari-able is created to maintain the identity of the user. Only abrowser session that has created this session variable canaccess the pages for that user. Access to the database and theexchange of variable values and data between a session andthe server are verified based on the session value createdafter login. As soon as the user session terminates, therelated session variable is deleted. For better security, theexchange of variables between the browser and the server isperformed via session variables. Thus, values are hiddenfrom the users and transmitted to the server through theS-HTTP communication. There are no presorted data,scripts, or user information in hypertext markup language(HTML) format on the web server. All pages transmitted bythe web server are dynamically created from the activeserver pages (ASP) scripts.
RESULTS
Current status of the RCET systemAs described previously, we have developed a system
consisting of three central tools: a centralized auto-archiv-ing database, a web-based SOANS, and a suite of user-
1432 I. J. Radiation Oncology ● Biology ● Physics Volume 57, Number 5, 2003
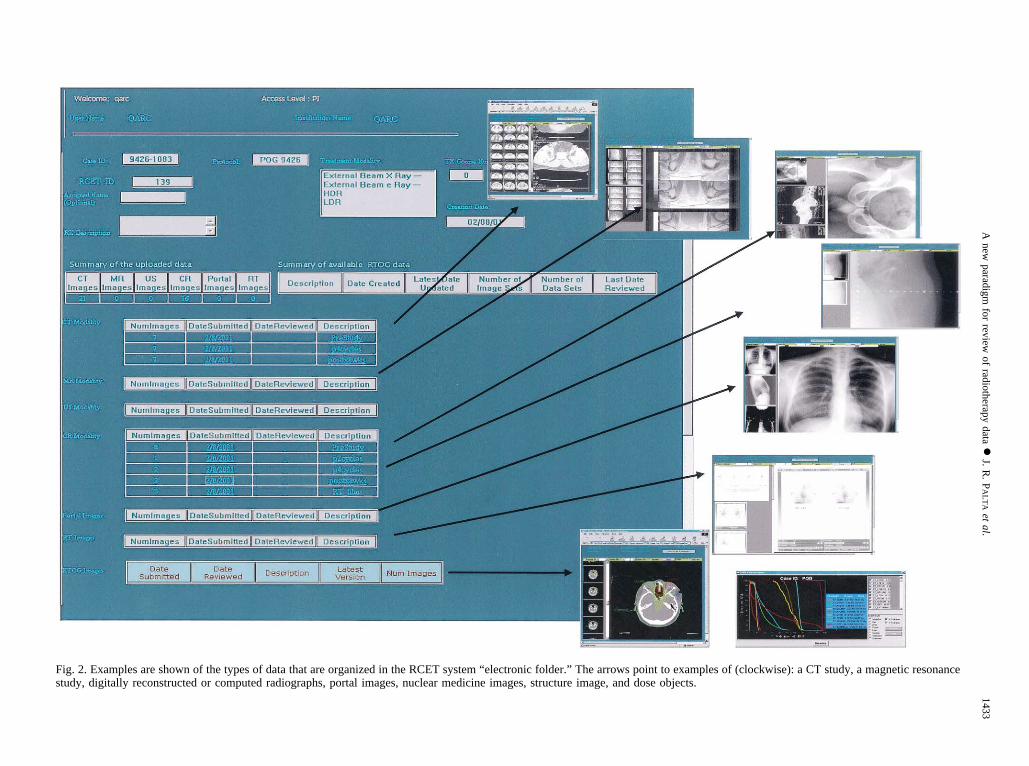
Fig. 2. Examples are shown of the types of data that are organized in the RCET system “electronic folder.” The arrows point to examples of (clockwise): a CT study, a magnetic resonancestudy, digitally reconstructed or computed radiographs, portal images, nuclear medicine images, structure image, and dose objects.
1433A
newparadigm
forreview
ofradiotherapy
data●
J.R
.P
AL
TA
etal.
friendly client applications for clinical data preparation,submission, and review. After completing 2 years of devel-opment and extensive in-house validation, we began seek-ing institutions to test the RCET system connectivity. Ourinitial system field testing began by testing the connectivityof the system at a few academic institutions. These testsrevealed several programming issues (“bugs”) and unex-pected hardware-related problems with our PC application,NetSys. We repaired the applications and revised our min-imum requirements for running the NetSys software. Afterthis period, we found the NetSys software to be robust aslong as the institutions complied with the minimum hard-ware requirements (http://rcetsystem.org). To date, 56 insti-tutions have established connectivity to the RCET systemand have uploaded test data to the RCET database using theNetSys software tools. Test data include diagnostic imagesand RT objects from several commercial treatment plan-ning systems. We are able to import RTOG data objectsfrom all commercial treatment planning systems support-ing this format. Most treatment planning system vendorsare now moving toward the implementation of the DI-COM-RT specification, but the progress is very slow.Moreover, the conformance statements of vendors are notconsistent for all data types. We have made goodprogress in importing DICOM-RT objects from the com-mercial treatment planning systems that support this newformat. However, it should be noted that any user of theRCET system could upload case data to the RCET serverusing our web-based secure upload/download tool. How-ever, our intent is to have each user send the data usingPC-based tools that can be readily downloaded from theRCET web site.
Web-based clinical QA using the RCET systemAs we were designing a system in which clinical inves-
tigators could receive, share, and analyze voluminous mul-timodality clinical data, it quickly became apparent thatsuch a system would be ideally suited for a distributedclinical QA environment. It is envisioned that the advancedtechnology RT will be available even at facilities that do nothave adequate infrastructure to support it locally. For ex-ample, most academic RT departments have satellite facil-ities that are often staffed at the minimum acceptable level.Such facilities can take advantage of the RCET system toremotely monitor and peer review the quality of patienttreatments. Peers at the home institution, using the webbrowser, can immediately review an electronic folder cre-ated at the remote facility. They can provide a more rigorousand in-depth review by downloading the raw data to theirlocal PC and using the NetSys software tools to reviewthem. One of the biggest challenges of conformal radiother-apy is the accurate definition of the target volumes andcritical structures. This is one area in which the peer reviewis critically important. The ability to annotate data allowsthe remote facilities to pass on messages to the peer review-ers, while the ability to resegment the data allows peers to
edit data remotely, if necessary. This obviates the need tohave experts travel to the satellite facilities more frequently.
We decided to pilot the RCET paradigm of web-basedclinical quality assurance for our weekly new patient dis-position conference. The 3D treatment planning data fromthe ADAC Pinnacle3 (Phillips Medical Systems, Andover,MA) for each new patient were uploaded to the RCET webserver using the NetSys software tools. All pertinent imag-ing study data were also loaded at the same time. Theelectronic folder for each patient is automatically populatedwith the submitted data. The clinical residents can accessthese data using a web browser for case presentations.Current applications have included presentation of imagingstudies, interactive assessment of the treatment plans, andpeer review of the port films. The faculty at our remotefacilities in Gainesville and Jacksonville have the sameaccess for review and comments. The clinical faculty havenow used the web-based review facility between ShandsHospital in Gainesville and Shands Hospital in Jacksonvillefor interactive discussion of patient data and treatmentplans. The web-based review is currently a mechanism toprovide feedback to the treating radiation oncologists. Asthe system evolves, a more formalized review process willbe put in place. The advantage of this new paradigm of peerreview is that our radiation oncologists do not have to relyon the bandwidth of the WAN for the interactive sessions.It is the opinion of the clinical faculty that the RCETparadigm of web-based clinical quality assurance has thepotential to enhance the peer review process. This is evenmore attractive for the clinical faculty working at outreachfacilities, because they feel that they are truly participatingin the peer review of patient disposition. In practical appli-cations, our experience has shown that the bandwidth of theinternet connection limits the transmission rate of data; i.e.,the performance of the RCET system is not limiting. Forexample, for a T1 (196 KB/s) rated connection, with theeffective transfer rate of �120 KB/s, the total time of thedownload of a complete data set (approximately 200 MB)will take approximately 11 min (including the compressionfactor of �2.5).
DISCUSSION
The discipline of RT is developing rapidly with continuedadvancement in treatment planning, delivery, and treatmentverification. New technologies have impacted nearly alltypes of radiation delivery (3D-CRT, IMRT, stereotacticradiotherapy and radiosurgery, and image-guided brachy-therapy). These technologies are very pervasive and can befound to a large degree at every scale of practice from thesmallest community clinics to the largest medical centers.Appropriate selection and safe use of advanced technologiesrequire great vigilance. There is always a risk that complexRT techniques can be misunderstood and misapplied, re-sulting in excess tumor recurrences or excess complicationsthat negate the potential benefits of these new technologies.Therefore, the onus is on the clinical practitioner to establish
1434 I. J. Radiation Oncology ● Biology ● Physics Volume 57, Number 5, 2003

strict quality assurance procedures to assure patient safety.More importantly, clinical practitioners need to understandthat higher level of complexity results in the need forexpanded peer review. The web-based clinical quality as-surance is ideally suited for emerging technologies in RTgenerating complex and voluminous multimodality imagingand planning data. The current RCET system represents asignificant amount of software development and consists ofthree primary components: (1) a secure auto-anonymizingupload and auto-archiving patient database, (2) a web-basedSOANS, and (3) a suite of software applications. Each ofthese components represents a significant development initself; together, the components provide an infrastructurethat is optimal for remote reviews and safe implementationof new techniques.
In this work, our goal has been to establish a proof-of-principle for a completely new paradigm in clinical qualityassurance of RT data. The system is still in its infancy, andwe have plans to implement several enhancements to thesystem that will make it more suitable for web-based qualityassurance. We believe that these enhancements will allowreviewers to perform more extensive and effective QAwhile allowing users to prepare and submit clinical datamore efficiently. These tools will provide users the ability toannotate data, resegment planning structures, recalculatedose–volume information, and perform multimodality im-age registration. The ability to annotate data allows remotefacility users and reviewers to exchange patient-specificinformation, while the ability to resegment the data allowsreviewers to provide immediate feedback on target volumethat is inadequately defined.
Proactive QA tools will allow dissemination of newknowledge via example cases. Providing example cases
to serve as atlases of target and critical structure defini-tions, as well as dose prescription, specification, andreporting examples for guidance to remote facilities, willimprove the delivery of safe and appropriate RT. Web-based resources can be provided that clearly and unam-biguously describe the treatment planning parameters,i.e., target volumes, critical structures, dose specifica-tions, and dose reporting. On-line atlases will assist userswith clear definitions and graphic presentations of sampletarget volumes and critical structures for each diseasesite. Users will be able to query the database to select theappropriate atlas of data corresponding to a specific dis-ease site and tumor histology, etc. The ability to performmultimodality image registration will allow reviewers toperform QA tests on targets and structures defined viaimage fusion.
The RCET system was developed to support the ad-vanced technology clinical trial initiative of the NCI. For thefirst 3 years, we focused our efforts mainly on the develop-ment of an infrastructure of comprehensive tools requiredfor preparation, submission, auto-archiving, web-based re-view, and retrieval of diagnostic images, treatment planningimages, and RT objects. These tools represent approxi-mately 1.1 million lines of computer code development inseven languages (V, C��, Visual Basic, Java, ASP,HTML, and SQL) and consist of a secure auto-anonymizingupload and auto-archiving patient database, a web-basedSOANS, a web-based rapid review tool, a web-based up-load/download tool, and a PC client data application for dataobject preparation, visualization, and submission namedNetSys. These tools, while fulfilling the NCI mandate forclinical cooperative groups, are ideally suited for remotequality assurance in RT.
REFERENCES
1. Webb S. Intensity modulated radiation therapy. Philadelphia:Institute of Physics Publishing; 2001. p. 1–34.
2. Webb S. The physics of three-dimensional radiation therapy:Conformal radiotherapy, radiosurgery and treatment planning.Philadelphia: Institute of Physics Publishing; 1993. p. 1–55.
3. Webb S. The physics of conformal radiotherapy: Advances intechnology. Philadelphia: Institute of Physics Publishing;1997. p. 1–30.
4. Chao KSC, Bosch WR, Mutic S, et al. A novel approach toovercome hypoxic tumor resistance: Cu-ATSM-guided inten-sity-modulated radiation therapy. Int J Radiat Oncol Biol Phys2001;49(4):1171–1182.
5. Jaffray DA, Drake DG, Moreau M, Martinez AA, Wong JW.A radiographic and tomographic imaging system integratedinto a medical linear accelerator for localization of bone andsoft-tissue targets. Int J Radiat Oncol Biol Phys 1999;45(3):773–789.
6. Christensen GE, Carlson B, Chao KSC, et al. Image-baseddose planning of intracavitary brachytherapy: Registration ofserial-imaging studies using deformable anatomic templates.Int J Radiat Oncol Biol Phys 2001;51(1):227–243.
7. Vicini FA, Jaffray DA, Horwitz EM, et al. Implementation of3D-virtual brachytherapy in the management of breast cancer:A description of a new method of interstitial brachytherapy.Int J Radiat Oncol Biol Phys 1998;40(3):629–635.
8. Rosenman J. Incorporating functional imaging informationinto radiation treatment. Semin Radiat Oncol 2001;11(1):83–92.
9. Ling CC, Humm J, Larson S, et al. Towards multidimensionalradiotherapy (MD-CRT): Biological imaging and biologicalconformality. Int J Radiat Oncol Biol Phys 2000;47(3):551–560.
10. Liu WC, Schulder M, Narra V, et al. Functional magneticresonance imaging aided radiation treatment planning. MedPhys 2000;27(7):1563–1572.
11. Chao KSC, Deasy JO, Markman J, et al. A prospective studyof salivary function sparing in patients with head-and-neckcancers receiving intensity-modulated or three-dimensionalradiation therapy: Initial results. Int J Radiat Oncol Biol Phys2001;49(4):907–916.
12. Zelefsky MJ, Fuks Z, Hunt M, et al. High dose radiationdelivered by intensity modulated conformal radiotherapy im-proves the outcome of localized prostate cancer. J Urol 2001;166(3):876–881.
13. Chen GTY, Pelizzari CA. Medical imaging in radiotherapy.In: Palta JR, Mackie TR, editors. Teletherapy: Present andfuture. Madison, WI: Advanced Medical Publishing; 1996. p.37–62.
14. Duhmke E, Franklin J, Pfreundschuh M, et al. Low-doseradiation is sufficient for the noninvolved extended-field treat-
1435A new paradigm for review of radiotherapy data ● J. R. PALTA et al.
ment in favorable early-stage Hodgkin’s disease: Long-termresults of a randomized trial of radiotherapy alone. J ClinOncol 2001;19(11):2905–2914.
15. Miralbell R, der Weid N, Bieri S, et al. Pediatric medulloblas-toma: Results of the Swiss Pediatric Oncology Group. IntJ Pediat Hemat Oncol 1999;6(4):275–281.
16. Yan D, Jaffray DA, Wong JW. A model to accumulate frac-tionated dose in a deforming organ. Int J Radiat Oncol BiolPhys 1999;44(3):665–675.
17. Langen KM, Jones DTL. Organ motion and its management.Int J Radiat Oncol Biol Phys 2001;50(1):265–278.
18. Padhani AR, Khoo VS, Suckling J, et al. Evaluating the effectof rectal distension and rectal movement on prostate glandposition using cine MRI. Int J Radiat Oncol Biol Phys 1999;44(3):525–533.
19. Lomax A, Grossmann M, Cozzi L, et al. The exchange ofradiotherapy data as part of an electronic patient-referralsystem. Int J Radiat Oncol Biol Phys 2000;47(5):1449–1456.
20. Purdy JA, Harms WB, Michalski J, Bosch WR. Initial expe-rience with quality assurance of multi-institutional 3D radio-therapy clinical trials. A brief report. Strahlenther Onkol 1998;174(Suppl. 2):40–42.
21. Hodge JG, Gostin LO, Jacobson PD. Legal issues concerningelectronic health information privacy, quality, and liability.JAMA 1999;282(15):1466–1471.
22. Gostin LO. National health information privacy: Regulationsunder the Health Insurance Portability and Accountability Act.JAMA 2001;285(23):3015–3021.
23. Prescribing, recording and reporting photon beam therapy.ICRU Report 50. 1993. International Commission on Radia-tion Units and Measurements.
24. Prescribing, Recording and Reporting Photon Beam Therapy(Supplement to ICRU Report 50). ICRU Report 62. 1999.International Commission on Radiation Units and Measure-ments.
25. Leunens G, Menten J, Weltens C, et al. Quality assessment ofmedical decision-making in radiation oncology—variability intarget volume delineation for brain tumors. Radiother Oncol1993;29(2):169–175.
26. McCarty B, Cassady-Dorion L. JAVA distributed objects: Theauthoritative solution. Indianapolis: SAMS; 1999. p. 1–56.
27. Frouhar V, Palta J, Li Z. Implementation of a distributedbrowser-based database system for radiotherapy QA centers.Med Phys 2000;27(6):1401 (abstract).
28. Vieira R. Professional SQL Server 7 programming. Chicago:Wrox Press Inc.; 1999.
29. Frouhar V, Palta J. An internet-based real-time RT PACS forsharing DICOM-RT objects: Implementations for QA centers.Med Phys 2002;28(6):1216 (abstract).
30. Shapiro J, Boyce J. Windows 2000 server bible. New York:IDG Books World Wide; 2000.
1436 I. J. Radiation Oncology ● Biology ● Physics Volume 57, Number 5, 2003
Copyright © 2022 FDOKUMEN

