







Bahasa
Halaman
Hukum


“A Clinical Study On Effect Of Local
Application With Jyotishmati-Apamarga
Kshara Taila In The Management Of Shvitra
(Vitiligo) in children”
By
Nikhil D. Vhatkar
Dissertation Submitted to the
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, BANGALORE,
KARNATAKA
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATI
M.D. (Ayu.)
In
KAUMARABHRITYA
Under the guidance of
Dr. SHAILAJA.U M.D. (Ay.), Ph.D.,
H.O.D & PROFESSOR
DEPARTMENT OF POST GRADUATE STUDIES IN KAUMARABHRITYA
SDM COLLEGE OF AYURVEDA AND HOSPITAL
HASSAN - 573 201
2011

DEPARTMENT OF POST - GRADUATE
STUDIES IN KAUMARABHRITYA
SHRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL
HASSAN - 573 201
Certificate
This is to certify that the Dissertation entitled “A Clinical Study On
Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The
Management Of Shvitra (Vitiligo) in children” is the bonafide record of
research work conducted by “Nikhil D. Vhatkar” under my direct
supervision and guidance as a partial fulfillment for the award of the
degree of M.D. in Ayurveda - Kaumarabhritya.
The candidate has fulfilled all the requirements of ordinances laid
down in the prospectus of Rajiv Gandhi University of Health Sciences,
Bangalore, Karnataka for the award of Degree of Ayurveda Vachaspati
(MD Ayu.) in Kaumarabhritya.
I am fully satisfied with her work and recommend this
dissertation to be forwarded for adjudication.
Date: Guide & Supervisor Place: Hassan Dr. Shailaja U. H.O.D. & PROESSOR Dept. of P. G. Studies in Kaumarabhritya,
S D M College of Ayurveda & Hospital,
Hassan

DEPARTMENT OF POST - GRADUATE STUDIES IN
KAUAMARABHRITYA
SHRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL
HASSAN – 573 201
(Affiliated to R.G.U.H.S, Karnataka, Bangalore)
ENDORSEMENT BY THE HOD AND HEAD OF THE INSTITUTION
This is to certify that the Dissertation entitled “A Clinical Study On
Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The
Management Of Shvitra (Vitiligo) in children” is the bonafide record of research
work conducted by “Nikhil D. Vhatkar” under the guidance of Dr. Shailaja
U, Professor and H.O.D., Dept. of P. G. Studies In Kaumarabhritya, S D M
College of Ayurveda, Hassan.
Dr. Shailaja U. Dr. Prasanna N. Rao. Prof .& H.O.D. Principal
Dept. of P. G. Studies in Kaumarabhritya S D M College of Ayurveda,
S D M College of Ayurveda, Hassan Hassan
Prof. Gurdip Singh Director, Post Graduate Studies
S D M College of Ayurveda, Hassan
Date: Place: Hassan
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 64
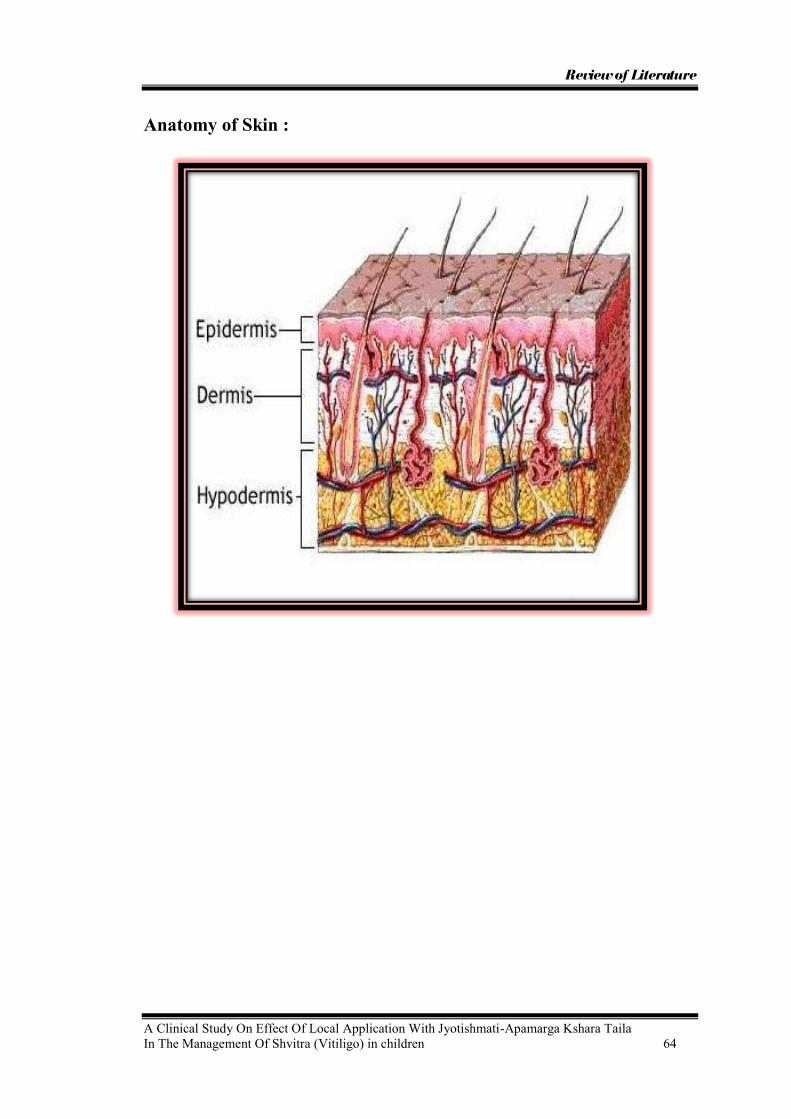
Anatomy of Skin :
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 85
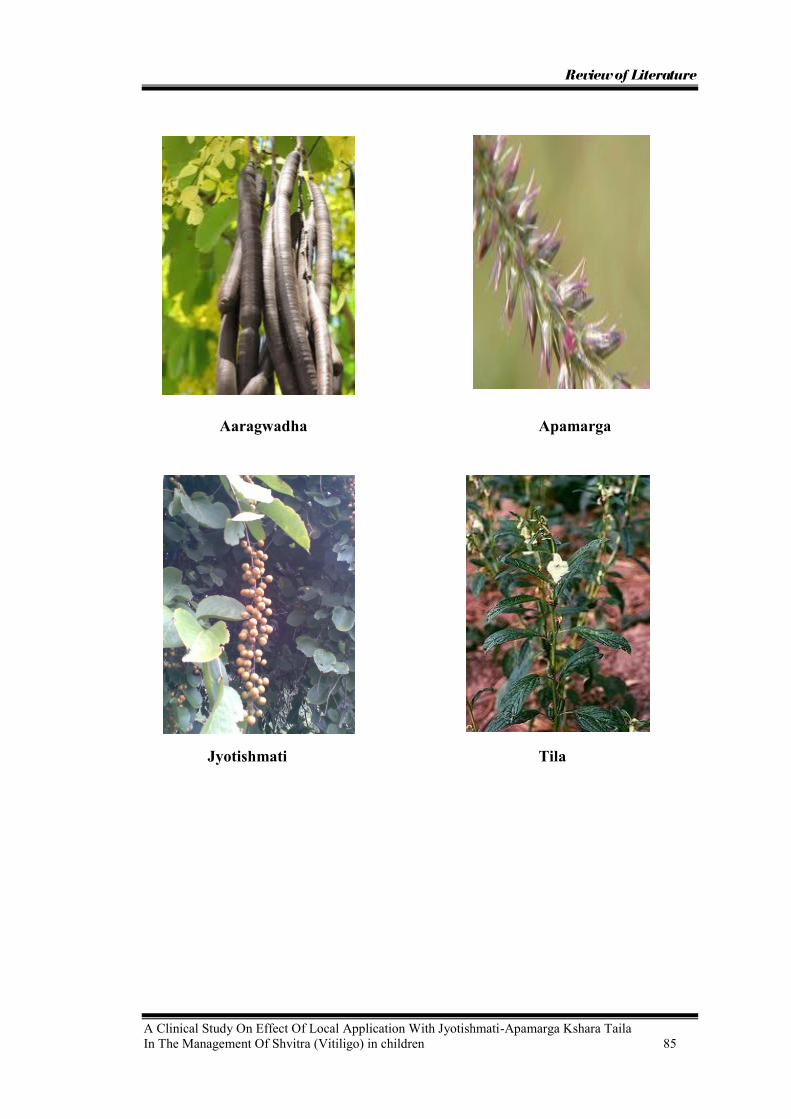
Aaragwadha Apamarga
Jyotishmati Tila
Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 97
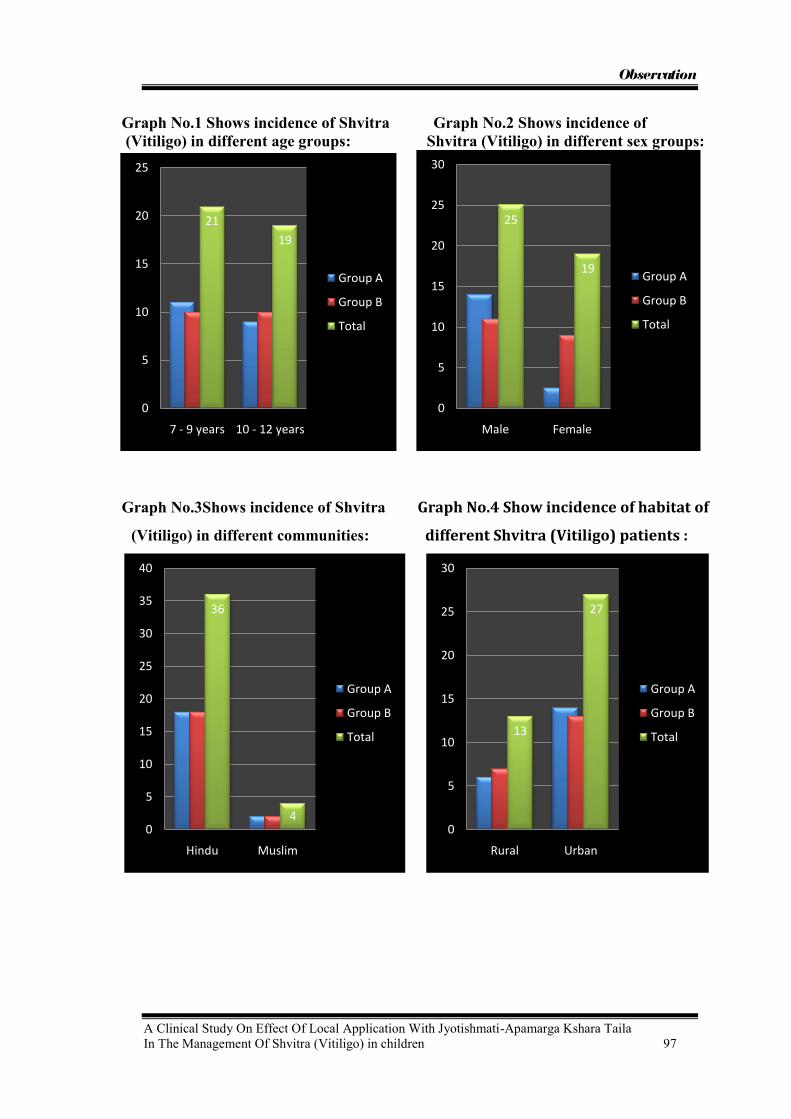
Graph No.1 Shows incidence of Shvitra Graph No.2 Shows incidence of (Vitiligo) in different age groups: Shvitra (Vitiligo) in different sex groups:
Graph No.3Shows incidence of Shvitra Graph No.4 Show incidence of habitat of
(Vitiligo) in different communities: different Shvitra (Vitiligo) patients :
21
19
0
5
10
15
20
25
7 - 9 years 10 - 12 years
Group A
Group B
Total
25
19
0
5
10
15
20
25
30
Male Female
Group A
Group B
Total
36
40
5
10
15
20
25
30
35
40
Hindu Muslim
Group A
Group B
Total 13
27
0
5
10
15
20
25
30
Rural Urban
Group A
Group B
Total

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 98
Graph No. 5 Show incidence of Shvitra Graph No.6 Shows incidence of shvitra
(Vitiligo) as per socio-economic status: as per food habits :
Graph No.7 Shows incidence of earlier Graph No. 8 Shows incidence of Deha
treatment history in the patients : Prakruthi in Shvitra patients :
of Shvitra:
3
15
22
0
5
10
15
20
25
Poor U M C L M C
Group A
Group B
Total
11
29
0
5
10
15
20
25
30
35
Group A
Group B
Total
16
24
0
5
10
15
20
25
30
Present Absent
Group A
Group B
Total
20
13
7
0
5
10
15
20
25
V.P. V.K. P.K.
Group A
Group B
Total

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 99
Graph No. 9 Shows incidence of dietic factors described to produce Shvitra
Graph No.10 Shows incidence of Viharaja Nidana in Shvitra patients
7
11
19
5
0
2
4
6
8
10
12
14
16
18
20
Virudhara onlyAti Mash, Mulaka, Dadhi, Amla sevana onlyBoth 1 & 2 None
Group A
Group B
Total
16
89
5
0
2
4
6
8
10
12
14
16
18
Intake of cold water after exposure to
sunlight
Cold water bath after expoxure to
sunlight
Both None
Group A
Group B
Total

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 100
Graph No. 11 Shows incidence of chronicity of Shvitra
Graph No.12 Shows incidence of number of mandalas (patches)
5
11
8
15
0
2
4
6
8
10
12
14
16
1-3 months 4-6 months 7-9 months 10-12 months
Group A
Group B
Total
17
7
15
10
2
4
6
8
10
12
14
16
18
1-5 mandalas 6-10 mandalas 11-20 mandalas Above 20
Group A
Group B
Total

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 101
Graph No.13 Shows incidence of distribution Graph No.14 Shows incidence of presence distribution of Mandalas of mandalas : of black spots in observed patch before
treatment
Graph No.15 Shows incidence of colour of Graph No.16 Shows incidence of number of patch in Shvitra (vitiligo) vegas after koshstashudi medicine given before treatment
:
12
28
0
5
10
15
20
25
30
Symmetrical Asymmetrical
Group A
Group B
Total
15
25
0
5
10
15
20
25
30
No spots 1-5 spots
Group A
Group B
Total
34
6
0
5
10
15
20
25
30
35
40
White Light pink
Group A
Group B
Total
1413 13
0
2
4
6
8
10
12
14
16
3 to 4 5 to 6 7 to 8
Group A
Group B
Total

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 102
Graph No. 17 Shows incidence of distribution of size of Mandalas :
4
18
12
6
0
2
4
6
8
10
12
14
16
18
20
< 5 square cm 6 -10 square cm 11 - 15 square cm 15 - 20 square cm
Group A
Group B
Total

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 113
Graph No. 18 Graph No.19 Showing improvement in Showing improvement in Appearance of Itching sensation Colour change in observed over observed Shvitra (Vitiligo) Shvitra (Vitiligo) patch : patch :
Graph No.20 Graph No.21 Showing improvement in Bleb Showing improvement in reduction in size formation in observed Shvitra of observed Shvitra (Vitiligo) patch: (Vitiligo) patch :
47.05
70.58
0
-12.5-20
-10
0
10
20
30
40
50
60
70
80
End of 1st month End of 2nd month
Group A Group B
41.37
65.51
0 1.78
0
10
20
30
40
50
60
70
End of 1st month End of 2nd month
GroupA Group B
10
30
0 00
5
10
15
20
25
30
35
End of 1st month End of 2nd month
Group A Group B
25
67.5
0 00
10
20
30
40
50
60
70
80
End of 1st month End of 2nd month
Group A Series 2

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 114
Graph No.22 Shows improvement in appearance of black spots in observed Shvitra (Vitiligo) patch :
Graph No. 23 Showing Over-all Percentage Improvement :
10
0
30
00
5
10
15
20
25
30
35
End of 1st month End of 2nd month
Group A Group B
70.5865.51
30
60.7167.5
-12.5
1.78 0 0 0
-20
-10
0
10
20
30
40
50
60
70
80
Appearance of Itching
sensation
Colour change Bleb formation No. of black spots
Size of observed
patch
Group A Group B

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 115
Study Group (Group A): Before treatment After treatment
Before treatment After treatment

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 116
Before treatment After treatment
Before treatment After treatment

RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
BANGALORE, KARNATAKA
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation / thesis entitled “A Clinical Study On
Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The
Management Of Shvitra (Vitiligo) in children” is a bonafide and genuine research
work carried out by me under the guidance of Dr. Shailaja. U, Professor and H.O.D.,
Dept. of P. G. Studies in Kaumarabhritya, S D M College of Ayurveda and Hospital,
Hassan.
Date: Signature of the candidate
Place: Hassan Nikhil D. Vhatkar

COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the rights to preserve, use and disseminate this
dissertation/ thesis in print or electronic format for academic/
research purpose.
Date: Signature of the candidate
Place: Hassan Nikhil D. Vhatkar
© Rajiv Gandhi University of Health Sciences, Karnataka

ACKNOWLEDGEMENT
My gratitude, which is the mother of all virtues and most capital of all duties,
has all there order and diligence to all those who graciously involved in this venture
of mine. There is much greatness of mind in acknowledging a good turn, as in doing
it.
I humbly, seek this opportunity to bow my head to the feet of almighty Lord
Ganesh, Lord Bhairavanatha and Lord Dhanwantari for showering their
blessings and empowering me to this eventful outcome without any impediments.
The truth dawns on me that, the language of words suffers very stringent
limitation to express my gratitude and indebt to the sacrifices of my most beloved
and respected parents Shri. Dhondiram Balavant Vhatkar and Sou. Malan
Dhondiram Vhatkar, who are the cause for me to take this noble profession and
shape me into what I am today,.
I pay my respectful salutations to his Holiness Poojya Sri Veerendra
Heggadeji, a founder father of SDMCA&H, Hassan and a fountainhead of
educational movements, for his divine blessings in disguise and who has been kind
enough to provide me an opportunity to render my service in this esteemed
institution. At this juncture, I am extremely grateful to Prof. S. Prabhakar, vice-
president and Dr. Yashovarma, secretary, S.D.M.E.S. Ujire.
The sacred blessings of national fame personality Poojya Professor Dr. C.
H. S. Sastry, whose insurmountable enthusiasm and best supervision made this
work materialized shape. I will be ever grateful for his invaluable guidance,
constructive suggestions, fatherly love and affection and thought provoking ideas in
every stage of my study.
My vocabulary falls short of suitable words to express my recondite sense of
indebtedness to my benevolent teacher Principal Prof. Prasanna.N.Rao, who has
been a guiding force and instrumental in all the proceedings of my life and stood as
an excellent encouraging stanchion in all strides in accomplishing this meticulous
effort.
The words are inadequate to express with profound reverence my heartiest
gratitude and indebtedness to my guide Dr. Shailaja U., H.O.D. SDMCA&H,

Hassan for his untiring help, close and constant attention with constructive and
valuable suggestions at every steps of this work.
It is beyond the reach of my language to inscribe the profound respect and
devotion towards affectionate Prof. Gurdip Singh for their constant support,
timely guidance and valuable suggestions to get this work done successfully.
I am thankful to Dept. of Dravyaguna, & Dept. Of Rasashashtra S.D.M
College of Ayurveda and Hospital, Hassan for providing me the drugs for my
research work.
I am thankful to our librarian Mr. Chandrasekhar, Mr. Krishnegowda,
Mr. Nagaraj & Digital Library in-charge Mr. Ravi Kumar & Mr. Dharma for their
great co-operation.
I express my gratitude and cordial thanks to my close friends Dr. Rahul,
Dr. Amol & Dr. Sheetal for providing support during my thesis work.
I should be very thankful to my well-wisher and loving friends Dr. Pankaj,
for supporting and praying for my success in my life.
I can’t forget my beloved seniors Dr. Abhijit, Dr. Shine, Dr. Purrushottam,
Dr. Raghamala, Dr. Veena, Dr. Arthi, Dr. Rahul, Dr. Prasad, Dr. Pravin,
Dr. Shwetha for their kind support. I am also specialy thankful to my juniors
Dr.Jyoti B., Dr.Pratibha Murthi, Dr.Niraja, Dr.Sahana, Dr.Saraswati, Dr.Basaveshwari and all who helped me knowingly and unknowingly.
I fail in my duty if I do not recall the support rendered by my friends.
I thank all my seniors, juniors and classmates for their timely suggestions
and help.
I thank my patients who exhibited high level of patience and subjected
themselves for cooperating with me in every stage of my clinical work and also
technical and non technical staff members of the department of Kaumarabhritya.
Last but not the least I extend my thanks to all those who have been directly
or indirectly associated with study at various levels but not mentioned in this thesis.
Dr. NIKHIL D. VHATKAR.

ABBREVIATIONS
Ri. Ve. : Rigveda
Ath. Ve : Atharvaveda
Ya. Ve : Yajurveda
Ma.Sm : Manu smrithi
Pa : Panini
A.K : Amarakosh
M. M. W : Monier Monier Williams
Ca.Sa.Su : Charaka Samhita Sutrasthana
Ca.Sa.Sha : Charaka Samhita Sharirasthana
Ca.Sa.Vi : Charaka Samhita Vimana
Ca.Sa.Chi : Charaka Samhita Chikitsa Sthana
Ca.Sa.Ka : Charaka Samhita Kalpasthana
Ca.Sa.Si : Charaka Samhita Siddisthana
Ca.Sa.Ni. : Charaka Samhita Nidanasthana
Su.Sa.Su : Sushruta Samhita Sutrasthana
Su. Sa.Sha : Sushruta Samhita Sharirasthana
Su. Sa. ni : Sushruta samhita nidanasthana
Su. Sa. chi : Sushruta samhita chikitsasthana
Su.Sa.Ut. : Sushruta Samhita Uttaratantra
A. sa. su : Astanga sangraha sutra sthana
A. sa. Sha : Astanga sangraha shareera sthana
A. sa. Ni : Astanga sangraha nidana sthana
A. sa. chi : Astanga sangraha chikitsa sthana
A.Hri.Su. : Astanga Hridaya Sutrasthana
A.Hri.Sha. : Astanga Hridaya Sharirasthana
A.Hri.ni. : Astanga Hridaya nidana sthana
A.Hri.chi. : Astanga Hridaya chikitsa sthana
Be.Sa.ni : Bhela Samhita nidanasthana
Be.Sa.Chi : Bhela Samhita Chikitsasthana
Ha.Sa : Harita Samhita
Ka.Sa.su : Kashyapa Samhita sutrasthana
Ka.Sa.Sha : Kashyapa Samhita Shareerasthana
Ka.Sa.Chi : Kashyapa Samhita Chikitsthana
Ka.Sa.ka : Kashyapa Samhita kalpasthana
Ka.Sa.Si : Kashyapa Samhita Siddisthana
Ka.Sa.khi : Kashyapa Samhita khilasthana
Y.R : Yoga Ratnakara
Sha.Pu. ka : Sharangadhara Samhita Purvakanda
Sha.ut. Ka : Sharangadhara Samhita uttarakhanda
Bhi.Rat : Bhashajya Ratnavali
Ma Ni : Madhava Nidana
Ga.Ni : Gada Nigraha
Bh. Pra : Bhava Prakasha
C.D : Chakra Dutta
T. B. A. D : Text book and Atlas of Dermatology
M : Mixed Diet
V : Vegetarian
U. M. C : Upper Middle Class
L. M. C : Lower Middle Class
V. P : Vata Pittaja
V. K : Vata Kaphaja
P.K : Pitta Kaphaja
B.T : Before treatment
A.T : After treatment
S.D. : Standard Deviation
S.E : Standard Error
G. S : Grading score
Sl.No : Serial Number
SYMBOLS
+ : Present
- : Absent
df : Degree of freedom
< : Lesser than
> : Greater than
% : Percentage
P : Probability
t : Test of significance
ABSTRACT
“A clinical study on effect of local application with Jyotishmati-Apamarga
Kshara Taila in the management of Shvitra (Vitiligo) in children.”
Background:
The Shvitra (Vitiligo) affects the estimated 1% of world population. The
disease may start at any age but usually seen in childhood at 10 years of age or in
second decade of life. Based on some dermatological out patient records it is roughly
estimated to be between 3 – 4% in India. Based on the symptoms, Shvitra can be
correlated with Vitiligo.
Objectives:
1. To evaluate the effect of local application with Jyotishmati-Apamarga Kshara
Taila in the management of Shvitra.
2. To observe the effect of local application with Tila Taila (control) in the
management of Shvitra.
3. To compare the effects of both the groups to ascertain the utility of local
application with Jyotishmati-Apamarga Kshara Taila in the management of
Shvitra.
Methods:
45 patients between the age group of 7 – 12 years attending the
Kaumarabhritya OPD and I P D of S.D.M College of Ayurveda and Hospital, Hassan
with diagnosis of Shvitra were taken up for the study after following the criteria laid
as above. Their age, sex, religion, socioeconomic status, food habits family history,
dehaprakruthi etc. were noted as given in master chart. Where there is more than one
patch of vitiligo in any patient only one patch was selected for the study. However
where improvement was found in that particular patch, patient was advised to treat
other patches also with the same drug. The size of the observed patch was
approximately measured in square centimeters by multiplying its breadth and length.

These 45 patients were divided randomly in to two groups.
1. Group A – Study group – containing 23 patients.
2. Group B – Placebo group – containing 22 patients.
Out of a total number of 45 patients taken for the study, five dropped out in
the middle and did not continue treatment. The left out 40 patients constituted of 20 in
study group and 20 in placebo group.
Complete history and clinical examination of all these patients was carried out
and recorded in a specially designed pro-forma by the Post-Graduate Department of
Kaumarabhritya of S.D.M. College of Ayurveda and Hospital Hassan. Their findings
are given in the enclosed master chart.
Result:
After two months of treatment statistically significantly result seen in study
group with respect to assessment criteria as follows:
1. Appearance of itching sensation over observed Shvitra (Vitiligo) patch with an
improvement of 70.58% (p >0.001)
2. Colour change in observed Shvitra (Vitiligo) patch with an improvement of 65.51%
(p >0.001)
3. Bleb formation on observed Shvitra (Vitiligo) patch with an improvement of 30%
(p 0.01)
4. Number of black spots appearing in observed Shvitra (Vitiligo) patch with an
improvement of 60.71% (p >0.001).
5. Decrease in size of Shvitra (Vitiligo) patch with an improvement of 67.50% (p
>0.001)
After two months of treatment statistically insignificantly results seen in placebo
group with respect to all assessment criteria’s.
Interpretation:
Apamarga Kshara produces irritation of depigmented skin over observed
Shvitra (Vitiligo) patches and may helps in removal of depigmented skin.
Apamarga has Rakta-Pitta Prasadanakara action and Jyotishmati has Pitta
Santpakara action. Hence they may be increase the activity of Bhrajaka Pitta leading
to formation of melanin pigments in Tvak (skin) resulting in normal Varna of the
patches.
Conclusion:
Jyotishmati-Apamarga Kshara Taila if continued for longer time for
treatment of Shvitra (Vitiligo) may give much better results.
(Key wards - Shvitra; Vitiligo; Apamarga, Jytishmati)

Table of Contents
Page No. 1. Introduction 1 - 3 2. Objectives 4 3. Review of Literature Ayurvedic Review 5 - 43 Modern Review 44 - 64 Drug Review 65 - 86
4. Methodology 87 - 90 5. Observations 91 - 102 Results 103 - 116
6. Discussion 117 - 124
7. Conclusion 125 8. Summary 126 - 127 9. References & Bibliography 128 - 132 10. Annexure 133 - 150

LIST OF TABLES
Sl. No Table name Page no.
Table 1 Showing varnothpathi based on combination of Pancha
mahabhuta according to different authors
9
Table 2 Showing layers of skin according to Charaka 9
Table 3 Showing layers of skin according to Sushruta 10
Table 4 Showing layers of skin according to Sharangadhara 10
Table 5 Showing nidanas of Shvitra according to different authors 21-23
Table 6 Showing lakshanas of Shvitra according to different
authors
26-27
Table 7 Showing sapeksha nidana of Shvitra 28
Table 8 Showing sadhyasadhyata of Shvitra 34
Table 9 Showing difference between Shvitra and Kustha 35
Table 10 Showing list of drugs used internally and externally in
Shvitra
38-40
Table 11 Showing pathyapathya of Shvitra 45-47
Table 12 Showing cells present in skin 48
Table 13 Showing Relation of hormones & skin 58
Table 14 Showing differential diagnosis of vitiligo 67
Table 15 Plants which are mixed to Mridu Kshara to make it
Madhyama Kshara
73
Table 16 Medicinal plants which are mixed to make Madhyama to
Tikshna Kshara
76
Table 17 Medicinal Plants useful for the preparations of Mridu
Kshara as prescribed in Shushruta Samhita
77
Table 18 The Physical characters of well prepared Teekshna Kshara 78
Table 19 The Physical properties of improperly prepared Kshara,
described by Sushruta as doshas of Kshara
79
Table 20 Incidence of Shvitra (Vitiligo) in different age groups 91
Table 21 Incidence of sex in Shvitra (Vitiligo) patient’s in different
groups
91
Table 22 Incidence of Shvitra (Vitiligo) in different communities 91
Table 23 Incidence of habitat in Shvitra ( Vitiligo) 92

Table 24 Incidence of socio-economic status 92
Table 25 Incidence of shvitra as per food habits 92
Table 26 Incidence of earlier treatment history in the patients of
Shvitra
93
Table 27 Incidence of Deha Prakruthi in Shvitra patients 93
Table 28 Incidence of Aharaja Nidanas described to produce
Shvitra
93
Table 29 Incidence of Viharaja Nidana in Shvitra patients 94
Table 30 Incidence of chronicity of Shvitra 94
Table 31 Incidence of number of mandalas (patches) 94
Table 32 Incidence of distribution of mandalas 95
Table 33 Incidence of presence of black spots in observed patch
before treatment
95
Table 34 Incidence of colour of patch in Shvitra (Vitiligo) before
treatment
95
Table 35 Incidence of size of Mandalas 96
Table 36 Incidence of number of Vegas after Koshstashudhi
medicine given
96
Table 37 Clinical improvement of signs after one month of
treatment in study group
103
Table 38 Clinical improvement of signs after two months of
treatment in study group
104
Table 39 Clinical improvement of signs after one month of
treatment in placebo group
105
Table 40 Clinical improvement of signs after two month of
treatment in placebo group
106
Table 41 Comparison of results of Appearance of Itching sensation
over observed Shvitra (Vitiligo) patch of group A and
group B at the end of first month
107
Table 42 Comparison of results of Appearance of Itching sensation
over observed Shvitra (Vitiligo) patch of group A and
group B at the end of second month
107
Table 43 Comparison of results of colour change in observed
Shvitra (Vitiligo) patch of group A and group B at the end
of first month
108
Table 44 Comparison of results of colour change in observed
Shvitra (Vitiligo) patch of group A and group B at the end
108

of second month
Table 45 Comparison of results of bleb formation on observed
Shvitra (Vitiligo) patch of group A and group B at the end
of first month
109
Table 46 Comparison of results of bleb formation on observed
Shvitra (Vitiligo) patch of group A and group B at the end
of second month
109
Table 47 Comparison of results of number of black spots in
observed patch of group A and group B at the end of first
month
110
Table 48 Comparison of results of number of black spots in
observed patch of group A and group B at the end of
second month
110
Table 49 Comparison of results of size of the observed patch of
group A and group B at the end of first month
111
Table 50 Comparison of results of size of the observed patch of
group A and group B at the end of second month
111
Table 51 Over-all Percentage Improvement 112

LIST OF GRAPHS
Sr.
No.
Graph Title Page
No.
1 Incidence of Shvitra (Vitiligo) in different age groups 97
2 Incidence of sex in Shvitra (Vitiligo) patient’s in different
groups
97
3 Incidence of Shvitra (Vitiligo) in different communities 97
4 Incidence of habitat in Shvitra ( Vitiligo) 97
5 Incidence of socio-economic status 98
6 Incidence of shvitra as per food habits 98
7 Incidence of earlier treatment history in the patients of Shvitra 98
8 Incidence of Deha Prakruthi in Shvitra patients 98
9 Incidence of Aharaja Nidanas described to produce Shvitra 99
10 Incidence of Viharaja Nidana in Shvitra patients 99
11 Incidence of chronicity of Shvitra 100
12 Incidence of number of mandalas (patches) 100
13 Incidence of distribution of mandalas 101
14 Incidence of presence of black spots in observed patch before
treatment
101
15 Incidence of colour of patch in Shvitra (Vitiligo) before
treatment
101
16 Incidence of size of Mandalas 101
17 Incidence of number of Vegas after Koshstashudhi medicine
given
102
18 Improvement in Itching sensation over observed Shvitra
(Vitiligo) patches in different groups
113

19 Improvement in colour change over observed Shvitra (Vitiligo)
patches in different groups
113
20 Improvement in bleb formation over observed Shvitra (Vitiligo)
patches in different groups
113
21 Improvement in reduction of size of observed Shvitra (Vitiligo)
patches in different groups
113
22 Improvement in appearance black spots over observed Shvitra
(Vitiligo) patches in different groups
114
23 Over-all percentage of improvement 114

INTRODUCTION

Introduction
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 1
INTRODUCTION
Since the beginning of the civilization the disease Shvitra is considered to be a
great social stigma and persons suffering from it could not command respectable
position in society. This disease does not cause any pain, ulcer or discomfort, but it
creates an inferiority complex in the person affected. Based on the symptoms, Shvitra
can be correlated with Vitiligo. The disease may start at any age but usually seen in
childhood at 10 years of age or in second decade of life. Based on some
dermatological out patient records it is roughly estimated to be between 3 – 4% in
India. The vitiligo affects the estimated 1% of world population.
“Some diseases do not take life, but they just ruin it.”
- Stephen Rothman.
Vitiligo is a common pigmentary disorder of great socio-medical importance.
It is defined as a circumscribed, acquired, idiopathic, progressive, hypomelanosis of
skin and hair, often familial and characterized by total absence of melanocytes
microscopically. This definition excludes post-inflammatory, chemically induced
depigmentation, those associated with melanoma, secondary to various dermatoses
and after burns.
Shvitra is considered as one of the varieties of Kusta in the Ayurvedic classics,
caused due to vitiation of Tridoshas and Dhatus like Rasa, Rakta, Mamsa and Meda.
Depending upon the duration of the disease and the involvement of Dhatus, the
disease becomes prognostically bad. While explaining Rakta Pradoshaja Vikara,
Shvitra is also mentioned.
According to modern science Vitiligo or Shvitra is a local hypo-
pigmentation of skin. Melanin is the most important pigment of skin formed from
phenylalanine & tyrosine under the influence of M.S.H. of anterior pituitary. Vitiligo
has an uncertain etiology for which autoimmune, self destructing, neural hypothesis
are suggested. In these hypothesis autoimmune hypothesis is mostly accepted & some
how the pigment could not be formed due to lack of certain enzymes in the tissues.

Introduction
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 2
Shvitra (Vitiligo) is characterized by milky white macules on skin.
Modern medicine has developed many treatment modalities still a large group of
people fail to get the achieved results and is refractory to treatment. In spite of
advanced modern technology and medicine the treatment of Vitiligo is not
satisfactory.
We get the reference of Shvitra right from Vedic literature, where the principle
line of treatment is mentioned as Sramsana and the use of Lepa after Sramsana.
According to Ayurveda “Shvetha Bhavchwitra” that is Shveta Bhavata is called
Shvitra. In spite of the use of various preparations by modern doctors, the cure rate in
Shvitra is considerably low & the incidence of such cases appears to be on the
increase. Lot of work was done on the use of Bakuchi, yet with poor results.
Shvitra is a disease where Bhrajaka Pitta present in Tvak is involved, Virechana
is considered as the best line of treatment if Pitta is involved, classics also mentioned
Sramsana as a line of treatment for Shvitra. Aragvadha phala majja has Sramsana
guna and is also indicated for Virechana in Bala since it is Mrudu; so Aragvadha
phala majja Kashaya was selected as a Koshtashudhikara dravya in the present study.
A number of yogas are mentioned for the purpose of external application after
Shodhana by many classics for Shvitra. Yogaratnakara and Vangasen Samhitha have
mentioned the use of Jyotishmati-Apamarga Taila for the treatment of Shvitra.
Apamarga has Rakta-Pitta Prasadanakara action and Jyotishmati has
Pitta Santpakara action. Hence they may be increase the activity of Bhrajaka Pitta
leading to formation of melanin pigments in Tvak (skin) resulting in normal Varna of
the patches..
By considering the nature of the disease, chronicity and its impact on
the psychological aspect of the children and Gunas of Aushadhi which may be very
helpful in treatment of Shvitra, present dessertion “the clinical study on the role of
local application with Jyotishmati-Apamarga Kshara Taila in the management of
Shvitra (Vitiligo)” is taken up.
Introduction
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 3
The entire study has been presented under various headings as follows :
The first part review of literature provides various literary factors of Shvitra as
available in authentic Ayurvedic and modern texts. This chapter also includes details
of Shvitra Chikitsa along with pharmacodynamics, properties, chemical composition
of the drugs, which were taken for the study.
The next part clinical study includes materials and methods as well as clinical
observations recorded in Shvitra patients along with statistical analysis of
observations.
The third important part discussion enlightens the observations from
the present study and other reported studies and research works.
The last part summery and conclusions provides in a nutshell, the entire study
including conclusions derived out of it.
Finally the thesis has been concluded with bibliography, references and an
appendix.

OBJECTIVES

Objectives
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 4
OBJECTIVES
Shvitra (Vitiligo) is considered as a great social stigma as it creates an
inferiority complex in the person affected, though it does not cause any pain, ulcer or
discomfort. Shvitra may start at any age but usually seen in childhood at 10 years of
age or in second decade of life. The children getting Shvitra becomes unable to
mingle with other children in the society and the social stigma continues to exist.
The incidence of the disease is alarming. Based on some dermatological out
patient records it is roughly estimated to be between 3 - 4% in India
We get the reference of Shvitra right from Vedic literature, where they have told
many Lepas for Shvitra. Ayurvedic Samhitas mentioned about the need of Shodhana
in Shvitra and described the use of many Lepas for Shvitra. Hence there is a
necessarity to explore the indigenous source for the treatment. So, A clinical study on
effect of local application with Jyotishmati-Apamarga Kshara Taila in the
management of Shvitra (Vitiligo) was taken up with the following objectives.
Objectives of the study:
1. To evaluate the effect of local application with Jyotishmati-Apamarga
Kshara Taila in the management of Shvitra.
2. To observe the effect of local application with Tila Taila (control) in the
management of Shvitra.
3. To compare the effects of both the groups to ascertain the utility of local
application with Jyotishmati-Apamarga Kshara Taila in the management of
Shvitra.

REVIEW OF
LITERATURE

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 5
Historical review
It is the past that has created the present. Knowing the history of the disease gives us
the knowledge regarding the origin of the disease, presentation of the disease during
those days and our ancestor‟s knowledge about them.
Vedic period (2500 BC – 1000 BC)
In Rig Veda a story is narrated where Shveta Kusta is mentioned. Ghosha daughter of
Kakshivat suffered from Sheta Kusta so did not get married. For this she prayed the
Ashwinis when her age has advanced. The Ashwinis cured her from Shveta Kusta and
restored her youth and beauty, and she got married12. In Rig Veda, the word Kilasa is
used for the white spots found over the body of the deer, which has resemblance with
the disease Shvitra13.In Atharvaveda the term Kilasa is used when prayers are offered
to the drugs to cure diseases like Kilasa and Khalitya. In Koushika sutra of
Atharvaveda Rama, Krishna, Asikni and Rajani are the herbs described as a remedy
for the diseases Kilasa and Khalitya. The fourth drug appreciated in the maintenance
of colour is Rajani or turmeric14 In Yajurveda there is a reference mentioning that
Chandra or moon was affected by the disease kilasa15 In Manu-smrithi there is a
reference stating that persons suffering from Shvitra and their progeny are
disqualified for marriage16. Sama veada probably has no reference of Shvitra.
Reference of Shvitra is also found in Panini vyakarana sutra17
Samhita kala (1000 BC – 100 AD)
Acharya Caraka describes Shvitra in Kusta chikitsa adhyaya of chikitsa
sthana after explaining other types of Kusta. Special emphasis is given to the Nidanas
of Shvitra in this book18
Acharya Susrutha mentioned Shvitra in Kusta Nidana of Nidana sthana where the
difference between Kusta and Kilasa, types of Shvitra and its Sadhyasadhyata is
explained19. The treatment of the disease is mentioned in Chikitsa sthana20. In
Dalhana commentary of Nidanasthana Bhoja‟s opinion on types of Shvitra is
mentioned21.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 6
In Kashyapa samhita scattered references regarding disease Shvitra are available. In
Sutrasthana while classifying the diseases Shvitra is said to be three types22. In
Shareerasthana it is mentioned that the disease Shvitra is caused due to vitiation of
Tvakgata udaka23. In Chikitsastahana definition of Shvitra is mentioned and
enumerated as five types24. In Kalpasthana it is mentioned that the person suffering
from Shvitra should not take Ikshu rasa25. Lashuna and Gandhasarpi are indicated in
Shvitra26. In Siddhisthana Virechana and Niruha Basthi are indicated for Shvitra27.
In Bhela Samhita Lakshanas of Shvitra are mentioned in Chikitsasthana28.
In Harita Samhita Pandura Kusta Chikitsa is mentioned, which is similar to Shvitra
Chikitsa29.
Sangraha kala (800 AD – 1700 AD)
In Astanga Sangraha the Nidana, Lakshana, Bheda and Sadhyasadhayta of Shvitra are
mentioned30. In Chikitsasthana a separate chapter is dedicated for Shvitra Chikitsa31.
In Astanga Hridaya similar references like Astanga Sangraha are available32.
Madhava Nidana described the difference between Kusta and Kilasa, its type‟s
Lakshanas and Sadhyasadhayata as well33.
In Sharangadhara Samhita Shvitra types34 and many yogas are described for its
treatment.35
Bhavaprakasha mentioned a combined opinion of Charaka and Sushruta by explaining
Dhatugata and Doshaja shvitra. He explained Sadhyasadhyata and treatment of
Shvitra36.
Yogaratnakara explained Samanya Lakshana, Sadhyasadhyata and Chikitsa37.
Bhaishajya Ratnavali described many yogas for the management of Shvitra38.
Gada Nigraha explained the types, Lakshanas, Sadhyasadhyata and Chikitsa of
Shvitra39.
Chakradautta mentioned many yogas for Shvitra under Kusta Chikitsa40.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 7
Review of previous research works-
1. Ojha D. – Studies on etiology, pathology and management of vitiligo.
1973, B H U, Varanasi. (Ph. D.)
2. Mishra S. – Clinical trial of some indigenous drug on Shvitra. 1986,
Gopabandhu Ayurveda Mahavidyalaya, Bhubaneshwar.
3. Sharma M, Avalgujadi gutica in Shvitra (Bahya prayoga) and datri kadira
kwatha (Abhyantara), 1989, National Institute of Ayurveda, Jaipur.
4. Burman S, Therapeutic effect of tuttadi Lepa in Shvitra. 1994,
Gopabandhu Ayurveda Mahavidyalaya, Puri.
5. Prabhakar S. – A clinical study on the effect of Somarajyadi choorna
(internally) and Somarajyadi Lepa (externally) in Shvitra. 1996, Dr. B. K.
R. R. Govt. Ayurveda college, Vijayawada.
6. Venkataiah G. – Organotherapy (Krishna karma) in the management of
Shvitra. 1996, Dr. B. K. R. R. Govt. Ayurveda college, Vijayawada.
7. Sarda C. L. – A clinical study on management of Shvitra w. s. r. to
Caraka‟s “Yat Cha Anyat Kushthanghnam, Shvitram eva tat Shastam
Khadirodaka Samyuktam.”. 1996, Gujarath Ayurveda University,
Jamnagar. (Ph. D.)
8. Sharada M. K. - A Clinical Study on the Management of Shvitra (Vitiligo)
With Special Reference to Lepa. 2003, S. D. M. College of Ayurveda and
Hospital, Hassan.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 8
Ayurvedic Review
Before proceeding to study Vikruthi one should know the Prakrutha form 41. There
fore it is necessary to look in to the Prakrutha rachana and Kriya of Tvacha, because it
is the seat where the disease Shvitra manifests.
Tvacha is derived from “Tvach-Samvarne” Dhatu meaning the covering of the body42.
Skin formation:
Sushtura described the formation of Tvacha in the developing foetus. He says that
after fertilization of ovum Tvacha develops just like a cream on the surface of milk.43
Charaka and Astanga sangraha kara opine Tvak as a matruja angavayava.44
Vagbhata described the formation of Tvacha due to Paka of Rakta Dhatu by its
Dhatvagni in the foetus. After Paka, it dries up, to form Tvacha, just like the
deposition of cream over the surface of boiled milk45.Tvak is mentioned as a Vayuvya
Anga by all the authors.
Varnotpattikarana in garbha:
The complexion does not depend only on karma but it depends on the Tejo
mahabhuta. Different complexions arise on the basis of association of Tejomahabhuta
with other mahabhutas46.
Astanga Sangrahakara mentioned causes of Varnotpatti as follows,
1. The garbha attains shukla Varna if shukra has the colour of ghrutha manda.
The garbha attains gouravarna if shukra is of taila Varna and garbha attains
Krishna Varna if shukra is like madhu.
2. The colour of garbha depends on ahara taken by garbhini. The garbha attains
gouravarna if she consumes madhuradravyas and by udaka vihara. The garbha
attains krishnavarna if she consumes vidahi padarthas and if she consumes the
combination of madhura and vidahi padartha garbha attains shyama Varna.
3. Varna depends on desha, kala and anuvrutti (mode of living) 47.
4. Hareetha explained varnotpathi on the basis of doshas48.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 9
Table 1: Varnothpatthi based on combination of Pancha Mahabhutas
Varna C.S / A.S S.S H.S
Gaura Teja + Jala +
Akasha
Teja + Jala Pitta
Krishna Teja + Pruthvi +
Vayu
Teja + Pruthvi Vata + Raktha
Shyama All mahabhutas in
equal proportion
-- Vata + Kapha and
Raktha + Kapha
Gaurashyama -- Teja + Jala +
Akasha
--
Krishnashyama -- Teja + Pruthvi +
akasha
--
Pingala -- -- Pitta + Raktha
Tvak is made out of all mahabhutas with the predominace of Vata.49
Layers of the skin:
a) Charaka described six layers of skin but while elaborating these layers he has
named only two layers the rest four layers have been described in terms of the
diseases50.
Table 2: Layers of the skin according to Charaka
No. Layers Diseases
1 Udakadhara -
2 Asrugdhara -
3 Third Layer Sidhma, Kilasa
4 Fourth Layer Dadru, Kushtha
5 Fifth Layer Alaji, Vidradhi
6 Sixth Layer Arunshi
b) Sushruta has described seven layers of skin along with the specific names. He has
also mentioned the thickness of each layer along with the diseases, which are prone to
that layer51.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 10
Table 3: Layers of the skin according to Sushruta
Name Thickness Diseases Avabhasini 1/18 of the Vrihi Sidhma, Padmakantaka Lohita 1/16 of the Vrihi Tilakalaka, Nyachcha, Vyanga Shweta 1/12 of the Vrihi Charmadala, Ajagallika,
Mashaka Tamra 1/8 of the Vrihi Kilasa & Kushtha Vedini 1/5 of the Vrihi Kushtha & Visarpa Rohini 1 Vrihi Granthi, Arbuda, Galaganda,
Apachi, Shleepada Mamsadhara 2 Vrihi Bhagandhara, Vidradhi, Arsha
c) Vagbhatta has described seven layers of skin similar to Sushruta. He has not
given any description. Commentator Arunadatta and Hemadri have named
them according to Sushrtua52.
d) Sharangdhara has also mentioned seven layers of skin along with the probable
onset of diseases. The names of first six layers are same as Sushruta but
seventh layer is named as “Sthula” which is the site of Vidradhi53.
Table 4: Layers of skin according to Sharangadhara
Name Diseases
Avabhasini Sidhma
Lohita Tilakalaka
Shweta Charmadala
Tamra Kilasa & Shvitra
Vedini All types of Kushtha
Rohini Granthi,Galaganda, Apachi
Sthula (2 vreehi) Vidradhi
Dr. Ghanekar has written commentary on Sushruta Sharira Sthana. He has
correlated the layers of skin mentioned by Sushruta with the latest anatomy of skin as
under54
.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 11
Ancient Term Modern Term Types of skin
1) Avabhasini Stratum Corneum
2) Lohita Stratum Lucidum Epidermis
3) Shweta Stratum Granulosum
4) Tamra Malpighian layer
5) Vedini Papillary Layer
6) Rohini Reticular Layer Dermis
7) Mamsadhara Subcutaneous tissue and
Muscular layer
Relation of doshas with Tvacha
Vata:
Among the five types of Vata PranaVata is the one, which controls all the Indriyas.
Udana Vata maintains the varna55.
Pitta:
Pitta situated in Tvak is called bhrajaka Pitta and does Tvak bhrajana56. Arunadutta
comments as the Pitta located in the skin is designated as Bhrajakagni and is
responsible for digestion and absorption of the substances used for Abhyanga,
Parisheka, Avagaha and Lepa. The Bhrajaka Pitta located in Tvak manifests the
colour in Avabhasini layer57.
Relation of Tvak with Dhatus
The mobile water (interstitial fluid) in the body is 10 Anjalis and the Udakadhara
layer helps in evaporation of such fluid to maintain body temperature58. Among the
Sapthadhatusaras the first Sara explained is Tvak sara59.
Nirukti
The term Shvitra is derived from the root shvith – which means shveta varna
(white colour). When the suffix rik is added to the root shvith, by the rule, letter ka is
deleted resulting in, formation of the word Shvitra.
Paribhasha:
Shvirta has been defined in different ways, but all definitions carry the same meaning.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 12
Shvetate iti shvitram – Shvitra is a disease of white patches.
Shveta bhava micchanthi Shvitram – disease characterized by white colour60.
Shvetate anena iti shevta kustam – Kusta characterized by white colour61.
Paryaya:
1. Shvitra – Shvetate iti Shvitra – which is characterized by white colour.
2. Kilasa – Kila Varna yasyati kshiyathi vikruti karothi yat - gives vikruta varna.
3. Shveta kusta – Shvetate anena iti Shveta kustam62– Characterized by shveta
varna.
4. Charuna – Reddish brown color of the morning, i.e. Dawn.
5. Daruna – Difficult to treat
Shvitra Nidan (Etiology of Shvitra)
Clinical significance of a disease is based on its etiological factors which a physician
can conform by proper interrogation about the diet, regimen and exact reason of
onset.
Except Caraka, no other Acharya has given specific etiology for Shvitra. He
considered Shvitra under Kustha roga prakarna, Acharya Sushruta has stated that
Kilasa is a type of Kustha64. Vriddha Vagbhata and Vagbhata described that the
etiology of Shvitra is similar to Kustha65.
As per Ayurvedic principle of treatment, avoiding the etiology is the way of
treatment, so if the treatment of Kustha and Shvitra is similar, the etiology of both
should be similar66. Based on the this statements one can take the etiology of Kustha
as etiology of Shvitra, which can be divided into following types -
Fig No 1 : Classification as per Nidana
SHVITRA NIDAN
Abhyantara Kulaja Nidan Bahaya Nidan
Nija Beeja Bhagavyava Dushti Agantuja
1. Aharaja
2. Viharaja
3. Vaidyakruta Vranaja Agnidagdha
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 13
4. Pragnyaparadha
5. Manasika
6. Nidanarthakara
I. Abhyantara Nidana
(a) Aharaja Nidana
Viruddha Ahara
Achary Caraka has mentioned the important role of diet especially Viruddhahara in
the cause of Shvitra. He mentioned the disease Shvitra along with other diseases
owing to intake of Viruddhahara67.
Defination of Viruddhahara
1. Substances which are contrary to Dehadhatus are considered as Viruddha
(antagonistic). This antagonism may be interms of guna, samyoga, samskara,
desha, kala, matra etc or by Swabhava68.
2. The entire (drug or) diet, which excites the dosha but fails to get eliminated from
the body, becomes harmful69.
According to Acharya Sushruta whatever food one could take if antagonistic to the
body, vitiates Vata etc doshas but it does not get eliminated or remove doshas from
body like Vamana or Virechana are considered as viruddha70.
Vagbhata described that viruddhahara at times may cause instantaneous death like
Visha (Poison), or may cause slow poisoning like Garavisha71.
Vruddha Vagbhata emphasizes about the character of viruddha substance, that the
substance which vitiates doshas but does not get eliminated from the body, with its
antagonistic nature to deha dhatus and will stay in the body72.
Brihatreayi has described viruddhaharas, e.g. taking fish with milk together is
incompatible, because both are madhura rasa, madhur vipaka, abhishyandi (obstructer
for channels). But both have viruddha virya i.e. milk – shita and fish – ushna, due to
opposite viryas, it vitiates blood and due to being abhishyandi, creates obstruction in
channels. Hence one should not take any fish along with milk particularly chilichima.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 14
Factors responsible for Dietetic incompatibility
Acharya Craka has given eighteen factors responsible for dietetic
incompatibility. Those are drugs and diets which are at variance with –
1.Desh
2.Kala
3.Agni
4.Matra
5.Satmya
6.Dosha
7.Samskara
8.Veerya
9. Kostha
10. Avastha
11. Kram
12. Parihar
13. Upachar
14. pak
15. Samyog
16. Hridya
17. Sampat
18. Vidhi
all are un-whole-some.73
These are illustrated below –
1. Desh viruddha – In take of ruksh and tikshna substances in jangal desh, snigdh
and sheetal substances in anupa desha etc.
2. Kala viruddha – In take of sheetal and ruksha substances in cold climates (winter),
katu and ushna substances in hot climate (summer).
3. Agni viruddha – In take of guru ahara when the Agni is manda and in take of
laghu ahara when Agni is tikshna. Similarly intake of food at variance with
vishama and Sama Agni.
4. Matra viruddha – Intake of honey and ghee in equal quantities.
5. Satmya viruddha – Intake of madhura rasa and shita virya substances by a person
who is satmya to katurasa and ushna virya.
6. Dosha viruddha – Utilization of aushadha, ahara and vihara having similar
qualities with doshas but at variance with the satmya of individual.
7. Samskara viruddha – Aushadha and ahara when prepared in a particular way
produce poisonous effect for example meat of peacock roasted with castor stick.
8. Virya viruddha – Intake of substances having shita virya in combination with
those of ushna virya.
9. Koshtha viruddha - Administration of mild purgative in a small dose for a person
of krura koshtha and administration of strong purgatives in large doses for a
person having mrudu koshtha is koshtha viruddha.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 15
10. Avastha viruddha – Intake of Vata aggravating food by a person after exhaustion,
sexual act and physical exercise or intake of Kapha aggravating substances by a
person with sedentary (alasi) habits.
11. Krama viruddha – If a person used to take food before evacuation of his bowel
and bladder or without appetite or after feeling of excessive hunger.
12. Parihar viruddha – Intake of ushna substances after taking the meat of sukara.
13. Upchara viruddha – Intake of sheetal aushadha ahara and drava after drinking of
ghee etc. snigdha substances.
14. Paka viruddha – Preparation of food etc with a bad or rotten fuel and
undercooking, overcooking or burning during the process of preparation.
15. Samyoga viruddha – Intake of sour substances with milk. Milk is a madhura rasa
and shita virya substance; where as sour substances have amla rasa and ushna
virya. So both are mutually contradictory in their nature.
16. Hridya viruddha – Taking of unpleasant substances. There is a great role of mind
in the digestion of food, because agni may be normal but without equilibrium state
of mind digestion gets hampered. So one should take food which is pleasant to the
mind.74
17. Sampad viruddha – Intake of substances which are not matured, over matured or
putrefied.
18. Vidhi viruddha – One should eat in lonely place not in open (public) place.
These eighteen types are viruddhas taught by acharya Caraka. By these above
viruddhas Agni is disturbed. If Agni is disturbed pachana karma is disturbed.
Causes for antagonism
Dietetic substances are antagonistic to the deha dhahus by the incompatiblity
of their rasa, guna, virya, vipak and prabhav or by samskara, matra, desh, kala,
samyoga and parihara etc. or by swabhava. It means whole-some substances also
become unwhole-some because of the above reasons.75

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 16
Mithyahara
Acharya Caraka has emphasized on the method of taking diet by giving eight
factors. These are called Astavidhaahara Visheshayatanani. If one has taken food
against these eight factors then it is called mithyahara or Mithyayoga of food76.
Eight factors determining the utility of food
The eight factors which determine the utility or otherwise of various types of food are
1. Prakrithi (nature of the food articles)
2. Karana (Method of their processing)
3. Samyoga (Combination)
4. Rasi (Quantity)
5. Desh (Habitat)
6. Kala (time i.e. stage of the disease)
7. Upayoga samstha (rules governlng the intake of food)
8. Upayokta (whole-some ness to the individual who intakes it) 77.
If the person has taken diet contravening the above said eight factors then the
digestion of the food is not proper, then the metabolism (formation of dhatus) is also
disturbed. This leads to improper supplement of deha dhatus. In the whole some diet
person should avoid Samasan, Adhyasan, Amatrasan and Vishamasan.
Samasan – Pathya and apathya dravya taking together is called samasan.
Adhyasan - In take of food before the previous food is digested.
Vishamasan – Untimely diet or irregular diet78.
Amatraasan - It is of two types –
Diet taken in low quantity than normal amount.
Diet taken in high quantity than normal amount79.
If the diet is taken in less quantity it causes Vibandh, Avairshya, Anayushya,
Anaujasya, destructs Tvaksar and causes Vata rogas80.
If food is taken in excess quantity all the three doshas are vitiated and cause visuchika
and alasaka81.
By taking Viruddha Ahara and mithyaahara the Agni is disturbed. If the
Jatharagni is disturbed which is the seat of pachana karma (digestion) other agnis
Ranjakagni, Bhrajakagni, Alochakagni, Bhutagnis and Dhatwagnis are not nourished.
So they fail to do their prakrita karya.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 17
The name of pachaka Pitta itself is Agni. So by the sevana of Viruddha and
mithya aharas, this Agni will be disturbed along with other agnis or pitas which are
under the control of pachaka Pitta will be disturbed. So due to disturbance of Ranjaka
Pitta, Bhrajaka Pitta and Alochak Pitta and their function of pigmentation is also
disturbed giving the disease Shvitra.
(b) Viharaja Nidana
Vihara means physical exercise of person which causes strain to Indriyas. It is
of two types.
Viruddhavihara Mithya vihar
(i) Viruddha Vihara
It means doing opposing types of work at the same time or one after other
without any time gap e.g. - person who once gets exhausted with exercise, heat or
sunlight, using the cold water for drinking or for bathing or cold air with air cooler is
Viruddha Vihara.
Skin is the very important and largest sense organ which is affected more by
these Viruddha Viharas and getting damaged. This damage may leads to Shvitra.
(ii) Mithya Viharaja Nidan
One should do labour according to the strength of his body. If the labour
exceeds the body strength then it is called Mithya Vihara81. By this Mithya Vihara
vitiation of Doshas occur leading to the disease Shvitra.
For example -
Night awaking (Ratri Jagarana).
Day sleep (Diva Swapna).
Exercise or sexual act after vomiting.
(c) Vaidya Krita Nidana - ( Iatrogenic)
These are the Nidanas produced due to the fault of doctor. In Ayurvedic treatment,
Panchakarma therapy is having an important place. While doing these procedures, if
the doctor does not have proper knowledge of it, he may commit mistakes. e.g. In the
procedure of vomiting, if the vomiting is not proper then there will be aggregation of
Kapha or if the vomiting is excessive then the aggravation of Pitta occurs. In the same
way other faulty procedures of Panchakarma may cause Shvitra.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 18
(d) Pragyaparadhajanya Nidan
Following are some examples of "Pragnya-paradha” which may cause Shvitra.
Untruthfulness of speech
Ingratitude
Bleshphemy against the
God
Not respecting elderly
people and teachers
Sinful actions
Evil acts of past lives
Disgrace to teachers
Stealing others things
Not giving, offerings like
homa, bali etc to God
(e) Manasika Nidan (Psychological Causes)
Psychological factors like tension, fear and anger are responsible for Psychic
diseases. Not only psychic diseases, these causes also lead to diseases of body
channels by vitiating Vata, Pitta or Kapha. These are termed as psychosomatic
illnesses. The Psychological factors increase the raja and tama qualities, which in turn
vitiates the Vata, Pitta and Kapha Doshas giving rise to various diseases. In the case
of Shvitra these causes are, e.g. –
Homicide of Brahmanas (Brahman vadh)
Homicide of Ladies (Stree vadh)
Homicide of Sajjan (Sajjan vadh) etc.
(f) Nidanarthakara Nidan
If a disease becomes the causative factor of another disease then it is called
Nidanarthakara Nidana. e.g. - Improper treatment of Vrana leads to Shvitra.
II. Kulaja Nidan
This can be taken as Beeja-Bhagavayava Dushti, i.e. chromosomal and genetic
factors. The word Beeja means seed i.e. fertilized ovum, sperm Beejabhaga means
chromosome, which is derived from Bhaga, i.e. part of Beeja. The word Beeja
Bhagavayava means 'gene' which is Avayava i.e. part of Beejabhaga i.e. chromosome
Beejabhaga i.e. chromosomes constitute the parts of ovum and sperm and are
responsible for the hereditary characters. A defective chromosome or a part of
chromosome i.e. gene is responsible for Abnormalities of sex organs and defects in a
particular organ. Members of certain families are inherently predisposed to develop
certain diseases82.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 19
Health as well as disease is primarily determined by quality of the genes. A
person with all the genes of good quality leads a healthy and vigorous life of hundred
years, provided he gets good food, pure air, and clean water and follows dietatis of his
conscience. Genes play an important role in the causation of all natural diseases.
III. Bahya Nidana
These are the Nidanas by which there is no Sanchaya of Doshas. Immediately
by exposure itself they are producing the disease. It is also called Agantuja. It is
divided in to two types Vranaja and Agnidagdhaja. Because of external trauma if
Shvitra is produced then it can be considered as Vranaja and if the Shvitra is produced
by burn; then these two causes can be considered under Bahya Nidana.
Table 5: Nidanas of Shvitra
S. N.
Nidanas C.S
S.S
A.S
A.H
B.P
Y.R
M.N
B.S
H.S
G.N
Aharaja nidana 1 Amlathi sevana + - - - + + + - - + 2 Ati drava ahara + - - - + + + - - + 3 Ati snigdha ahara + - - - + + + - - + 4 Ati guru ahara + - - - + + + - - + 5 Ajeerna + + - - + + + + - + 6 Adhyashana + - - - + + + + - + 7 Ahitashana + - - - + + + + - + 8 Asathmya ahara - + - - - - - - - - 9 Ati dadhi sevana + - - - + + + - - + 10 Chilichima + milk + - - - - - - - - - 11 Haviprashana - - - - - - - - + - 12 Pippali + kakamachi +
lakucha with dadhi + sarpi
- - - - - - - + - -
13 Garmyanupoudaka + haritha shaka
- - - - - - - + - -
14 Madhu + mamsa after ushnaahara sevana
- - - - - - - + - -
15 Ushna ahara after madhu and madhaya sevana
- - - - - - - + - -
16 Gramya oudaka anupa mamsa with milk
- + - - - - - - - -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 20
17 Ati masha mulaka pistanna tila Kshara and guda sevana
+ - - - + + + - - +
18 Ati Madhya amla sevana after intake of ksheera
- - - - - - - + - -
19 Ati madhu phanita matsya lakucha mulaka kakamachi sevana during ajeerna
+ - - - - - - - - -
20 In take of yavaka and chanaka with ksheera
+ - - - - - - - - -
21 Ati dadhi takra kola kulatha masha athasi and kusumba snehasevana
+ - - - - - - - - -
22 Intake of mathsya+mamsa+ksheera + nimbuka
- - - - - - - + - -
23 Lavanathi sevana + - - - + + + - - + 24 Mithyahara - + + + - - - - - - 25 Mathsyathi sevana + - - - + + + - - + 26 Ati navanna sevana + - - - + + + - - + 27 Papodaka sevana - - - - - - - - + - 28 Viruddhahara + + + + + + + + - + 29 Vidagdhahara + - - - - - - + - - 30 Vidahi ahara + - - - - - - + - - Viharaja nidana 1 Ativyayama
atisantapa after atibhukta
+ - - - + + + - - +
2 Ati maithuna + - - - - - - - - - 3 Ati vyayama + - - - - - - - - - 4 Bhaya + - - - - - - - - - 5 Chardhi nigraha + + - - + + + - - + 6 Divaswapna + - - - + + + - - + 7 Gramyadharma after
intake of vidagdha ahara
- - - - - - - + - -
8 Chardhi nigraha after intake of mithya samsarga ahara
- - - - - - - + - -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 21
9 Intake of sheeta and ushna padartha with out difference
+ - - - - - - - -
10 Mithya vihara - + + + - - - - - - 11 Parishrama + - - - - - - - - - 12 Rathri jagarana - - - - - - - - + - 13 Sheetambu sevana
after atapa sevana + + - - - - - + - -
14 Sheetambu snana or sevana after long walk
- - - - - - - + - -
15 Tevra dhoopa sevana + - - - - - - - - - 16 Vegavarodha + + - - + + + - - + 17 Vyayama during
ajeerna + - - - + + + - - +
Anya nidana 1 Anyasthi apaharana - + + + - - - - - - 2 Bhramhana, sthree,
sajjna vadha - + + + - - - - - -
3 Gohathya - - - - - - - - + - 4 Poorvakrutha karma - - + + - - - - - - 5 Sadhu ninda and
vadha - - + + - - - - - -
6 Vipra and guru garshana
+ - - - + + + - - +
Chikitsa sambandhi nidana 1 Vidahi vidagdha
aharaasevana with out shodhana
+ - - - - - - + - -
2 Vyayama and gramya dharma after snehapana and Vamana
- + - - - - - - - -
3 Intake of santharpana and apatharpana with out differentiating
+ - - - - - - - - -
4 Panchakarma apachara
+ - - - + + + - - -
5 Ati snehapana + - - - - - - - - - Vishista nidana 1 Papa karma + - - - - - - - - - 2 Krithagna bhava + - - - - - - - - - 3 Poorva kritha karma + - - - - - - - - -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 22
4 Guru gharshana + - - - - - - - - - 5 Viruddhahara + - - - - - - - - -
Purva Rupa (Prodromal Features)
In Ayurveda, Acharyas have not given any specific prodromal features of
Shvitra. But Acharya Sushruta, Vagbhata, Bhel and Kashyap have been stated that
Shvitra is produced like Kushta, so Purvarupa are also similar to Kushta.
Most of the Acharyas included Shvitra in Kushta Rogadhikara. Hence they
considered the Purvarupa of Kushta as Purvarupa of Shvitra83. But in general these
Purvarupas of Kushta are not seen in Shvitra. However few features seem to be
similar with prodromal features of Shvitra.
Rupa (Clinical Features)
Exposure to etiological factors causes vitiation of Doshas (Sanchaya and
Prakopa).Vata, Pitta and Kapha after vitiation of these Doshas while circulating
(Prasara) in the body, where-ever they get Khavaigunya (Khavaigunya or Srotodushti)
is stated to produce Srotorodha (occlusion or obstruction) of the Srotas. There, these
Doshas are retained and interact with Dushyas of the affected region. This
phenomenon is called Doshadushya Sammurchana, which is called Vyadhi84.
Indistinct symptoms present in the Purvarupa stage when manifested clearly
and show the features or symptoms indicating specific disease (Vyadhi) are Rupa85.
These clinical manifestations give us an important clue to the diagnosis; the
stage of the disease, differential diagnosis, prognosis and treatment of disease.
Cardinal feature of Shvitra is development of depigmented patches on the
skin.
Lakshanas
The Lakshanas of Shvitra mentioned in the classics can be classified under two
catogaries.
Samanya Lakshanas Vishishta Lakshanas
Shvitra word itself means Shvetha Varna of Tvacha, it is the cardinal feature
of the disease. Acharyas while mentioning the difference between Shvitra and Kusta
mentioned Shvitra as aparisravi86. Yogarathnakara mentioned Pandura Varna, Sasrava

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 23
and Kandu as Samanya Lakshana of Shvitra, most probably it refers to Vranaja
Shvitra87.
Acharya Charaka explained Daruna, Charuna and Shvitra as three names of
kilasa and are caused by Tridoshas. Colour of the skin varies when Doshas are
situated at different Dhathus. These are –
o When doshas are situated in Raktha dhatu – Raktha Varna
o When doshas are situated in Mamsa dhathu - Thamra Varna
o When doshas are situated in Medo dhathu – Shweta Varna88
In this context dhatu gatatwa of Shvitra up to Meda dhathu is explained.
Acharya Bhela mentioned the precence of Shali shuka prathikasha loma,
shukla lohitha Anyonya mandala as samanya lakshana89.
Vishista Lakshanas90:
Acharya Charaka did not mention the Doshaja classification of Shvitra.
Astanga hridaya, Bhavaprakasha, Madhavanidana, Gadanigraha, followed the opinion
mentioned in Astanga sangraha, which is as follows.
Vathaja Shvita
Pittaja Shvitra
Kapahaja Shvitra
Vathaja Shvitra
Aruna Varna Mandala -Ishat Lohitha Varna as commented by Bhava Prakash
Parushatha-roughness
Paridhwamsi-powder like material on scratching the patch
Rookshatha-roughness, Dhathu involved is Raktha Dhathu
Pittaja Shvitra
Padmapatra Varna –colour of lotus leaves (dull white as seen in dorsal aspect)
Daha-burning sensation in the lesion
Roma Vidhwamsatha-distruction of hair at the site
Dhathu involved is Mamsa Dhathu
Kaphaja Shvitra
Shvetha Varna –white colour of the leasion
Snigdhatha -unctousness
Bahala -thick
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 24
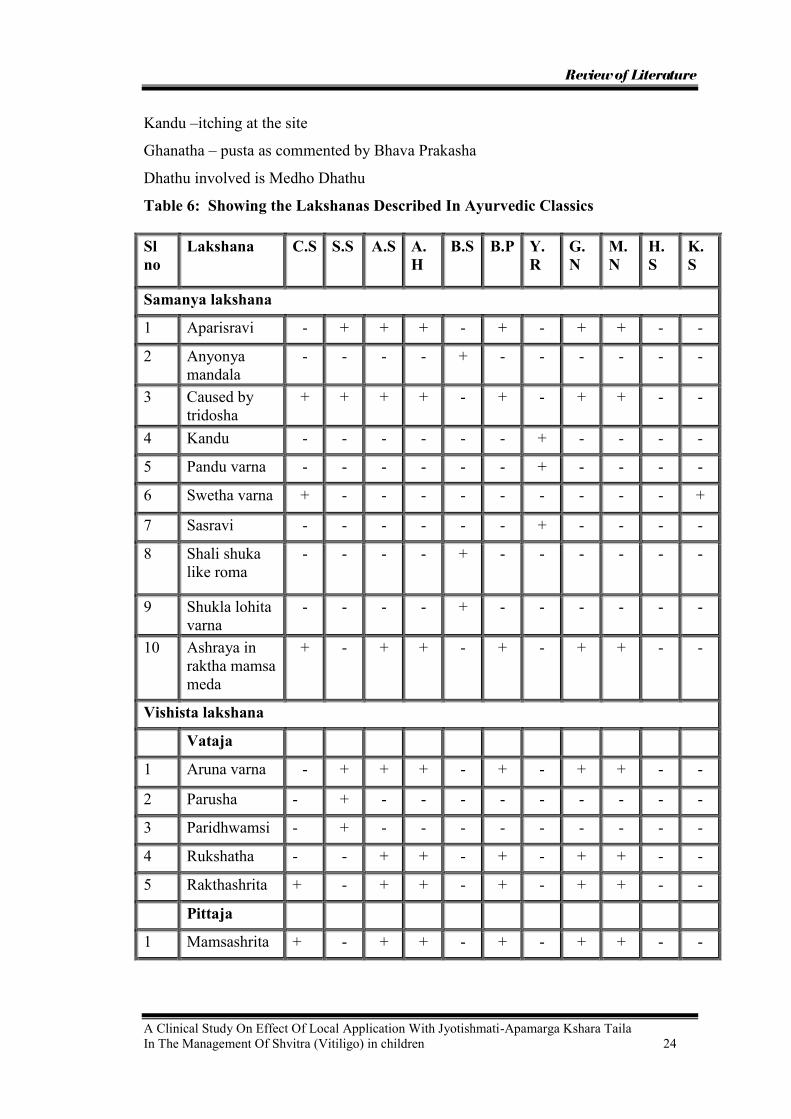
Kandu –itching at the site
Ghanatha – pusta as commented by Bhava Prakasha
Dhathu involved is Medho Dhathu
Table 6: Showing the Lakshanas Described In Ayurvedic Classics
Sl no
Lakshana C.S S.S A.S A.H
B.S B.P Y.R
G.N
M.N
H.S
K.S
Samanya lakshana
1 Aparisravi - + + + - + - + + - -
2 Anyonya mandala
- - - - + - - - - - -
3 Caused by tridosha
+ + + + - + - + + - -
4 Kandu - - - - - - + - - - -
5 Pandu varna - - - - - - + - - - -
6 Swetha varna + - - - - - - - - - +
7 Sasravi - - - - - - + - - - -
8 Shali shuka like roma
- - - - + - - - - - -
9 Shukla lohita varna
- - - - + - - - - - -
10 Ashraya in raktha mamsa meda
+ - + + - + - + + - -
Vishista lakshana
Vataja
1 Aruna varna - + + + - + - + + - -
2 Parusha - + - - - - - - - - -
3 Paridhwamsi - + - - - - - - - - -
4 Rukshatha - - + + - + - + + - -
5 Rakthashrita + - + + - + - + + - -
Pittaja
1 Mamsashrita + - + + - + - + + - -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 25
2 Padmapatra prakasha
- + + + - + - + + - -
3 Paridaha - + + + - + - + + - -
4 Romavidhwamsi
- - + + - + - + + - -
5 Raktha/ tamra Varna
- - + + - + - + + - -
Kaphaja 1 Bahala - + - - - - - - - - -
2 Guru - - + + - + - + + - -
3 Ghana - - + + - + - + + - -
4 Kandu - + + + - + - + + - -
5 Medashrita + - + + - + - + + - -
6 Snigdha - + - - - - - - - - -
7 Shweta varna - + + + - + - + + - -
Sapeksha Nidana
It is essential to rule out other possible diseases, which are having similar
symptoms. The cardinal feature of Shvitra i.e, Tvacha Shwetata and Aparisravi are
not present together in any of the disorders mentioned in the classics. Sidhma, which
is one of the Mahakusta, simulates Shvitra. Differentiating features between these two
are as shown in the table no.7. 91
Table 7: Sapeksha nidana of Shvitra
Sl no Distinguishing features
Shvitra Sidhma
1. Dosha Tridoshaja Kapha – Vataja 2. Dhatu Rakta – mamsa –
meda Sapta dhatu
3. Poorvaroopa -- Present 4. Color sweta Sweta, tamra, alabu pushpavat 5. Thickness tanu or thin Tanu or thin 6. Itching -- Present 7. Roopa
Aparisravi or no change on scratching
Rajo ghrustam vimunchati or powder like material on scratching
8. Area of lesion Occurs anywhere Most common in upper part of the body

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 26
Bheda: Bheda is a part of Sankhya Samprapti.
Classification according to etiology 92
1. Doshaja
a. Atmaja – caused by Vata, Pitta or Rakta and Kapha
b. Paraja – caused by Paragatra Sparsha.
2. Vranaja – caused by Vrana
According to Dosha93
1.Vataja Raktashrita 2.Pittaja Mamsashrita 3.Kaphaja Medashrita
According to Ashraya94
1. Raktashrita 2.Mamsashrita 3. Medashrita
According to prognosis95
1. Sadhya 2. Asadhya

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 27
SAMPRAPTI
The manner in which the Doshas are vitiated and traversing throughout the body and
produce the symptom is termed as Samprapti96.
Ayurveda describes in detail the various stages of evolution of diseases. Such as –
(1) Chaya i.e. accumulation of Doshas because of action of etiological factors
(2) Prakopa i.e. further increase in the Doshas,
(3) Prasara i. e. dissemination of Doshas which correspond to the stage of septicemia,
or toxemia.
(4) Sthana Sanshraya i.e. localisation of Dosha in a particular tissue or organ
(5) Vyakta i.e. manifestation of disease because of derangement of functions of the
organ involved.
(6) Bheda i.e. further differentiation into the sub-type of the disease.
Caraka has given etiology and clinical features. But he doesn't give any
description about pathogenesis (Samprapti). He has mentioned Kilasa as Tridoshaja,
Dwidoshaja and Ekdoshaja. Both Shvitra and Kushta are Tridoshaja.
Acharya Sushruta interpreted Shvitra as a type of Kushta. According to him,
by Nidan Sevana Vata is vitiated and associated with vitiated Pitta and Kapha, spreads
in those Siras, which are going in Tiryak Marga and their Sthana Sansraya occurs on
the skin (Tvak, Rakta, Mamsa and Lasika). These vitiated Doshas enter in the skin, if
not treated in proper way, they gradually enter the Rakta and Mamsa etc. Dhatus,
vitiate them and produce Kushta (Shvitra) 97.
Kilasa is a type of Kushta, and is limited to only skin98. Pathogenesis
explained by the Harita for Kilasa is very much specific, because no other text has
given such type of pathogenesis. According to him, major Dosha Pitta contaminated
with Rakta is carried by vitiated Dosha, Vata and gets lodged in Tvak. By his opinion
Pitta carried by Vata, when contaminates Rakta produces Pandura Varna in skin99.
This Pandura Varna of Tvak is known by the name of Shvitra or Pandura
Kushta. But other Acharyas opine that the vitiated Rakta; Mamsa and Medodhatu as
responsible for Shvitra.
Acharya Bhela says that by Nidana sevana, Kapha Dosha when gets excited
and lodges in Tvak, Rakta and Mamsa, produces Kushta (Shvitra) 100. Acharya Bhela

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 28
described Shveta Kushta along with Kshudra Kushtas. Hence we can consider the
pathogenesis of Shvitra similar to Kustha.
According to Chakrapanidatta, commentator of Charaka samhita by the Nidan
sevana (Ahara Vyatyas) Vitiation of Tridoshas take place. This vitiation leads to the
Shaithilya of Tvak, Lasika, and Rakta and Mamsa Dhatus which means that there is
production of Ama 101. Vihara Vyatas and Vegarodhatmak Nidana leads to the 'Kha'
Vaigunya of Varnotpadak avayav of Tvacha which is Bahya Nivesa Sthana of Rasa
and Raktavaha Srotas. Because of this 'kha' vaigunya dosha dushya Sammurchana
takes place in the Shithila, Tvak, Lasika, Rakta or Mamsa. In this Dosha Dushya
Sarnrnurchana, by the association of one, two or three Doshas with one, two or three
Dhatus depending on the Papakarma of the person (which will give Shighratva,
Chiratva, Tanutva and Ghantva) Asankhyey Kushta, or Kshudra Kushta or Maha-
Kushta or Shvitra Kushta is produced. Hence this is the common Samprapti for all
type of Kushta Rogas but depending on the type and amount of Nidana Sevana the
type of Kushta produced gets changed102.
Fig. No. 2 Schematic representation of Samprapti
Abhyanthara nidana sevana Vitiation of Dosha Agni mandya Formation of Ama
Dusta dosha sanchara in tiryag gata Siras
Vrana Stanika Brajaka Pitta Kshaya Shvitra

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 29
Acharya Vagbhata, Sodhaa, Bhavamishra, Yogratnakara and Madavkara
described Shvitra as Tridoshaja Vyadhi and interpreted Shvitra as a type of Kushta.
Hence the pathogenesis of Kushta can be accepted as pathogenesis of Shvitra.
According to them vitiated Doshas vitiates Tvak, Rakta, Mamsa and Lasika, produce
Kushta (Shvitra) 103.
Kashyapacharya has given the description of Shvitra in this way. 'Udaka
present in the skin is 10 Anja1is. By this Udaka only Rakta and Sharir Dhatus are
nourished. If this Udaka gets vitiated then Dadru, Kandu, Vicharchika, Kilasa and
other skin diseases occur104.
Acharya Sarangadhara has counted Shvitra in Kushta Roga. According to him
Shvitra is of three types Vataj, Pittaj and Kaphaja105.
Based on the scientific analysis of metrical texts pathogenesis of Shvitra is
clarified in this way. Excitation of Tridoshas leads to Agni Vaishamya which results
in increased Vata, this Vata enforces Pitta and Kapha into Bahyarogamarga by
Tiryaggami Siras. During this period Tridoshas vitiate the skin and attain Sthana
Sansraya in Tvak. By the obstruction or Sanga where the excited Dosha gets
lodged in the Tvak, there it vitiates Rakta, Mamsa and Medo Dhatus gradually
producing Vataja Shvitra of Aruna varna, Pittaja Shvitra of Tamra varna, or Kaphaja
Shvitra of Shveta varna. If these Doshas get lodged in deeper Dhatus from skin then
Shvitra becomes incurable.
If a pregnant lady takes excessive Sleshmala food then the fetus develops
Shvitra. This means that dietetic indulgence made by mother during pregnancy also
causes Shvitra in the baby. This indicates the association of Sleshma in the
pathogenesis of Shvitra106. In the formation of varna (Skin colour) Udana Vayu also
takes part. Hence vitiation of Vayu causes Varna vikruti107.
Illustration of Participants of Pathogenesis
1. Dosha - Vata - Samana, Apana, Udana.
Pitta - Pachak, Bhrajak, Ranjak and Alochak
Kapha - Avalambak
2. Dushya - Ras, Rakta, Mamsa and Meda.
3. Srotas - Rasavaha.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 30
4. Srotodushti - Sanga.
5. Adhisthan - Udbhavasthan - Amashaya samutha
Vyadhi-vyaktasthan - twacha.
6. Vyadhi Swarup- Chirakari.
Sadhyasadyata - Ayurvedic Concept
Shvitra being a Papatmaja Vyadhi is Kruchchra Sadhya. Shvitra responds to
treatment in those who practice Dana – Dharma along with the treatment; thereby
they get rid of their Papatmaja Vyadhi by getting rid of their Pap.
Sadhya Shvitra
The two Scholars have given the description of the region affected, where in
the hairs are not of 'Raktavarna', the region being small in size and not very close to
each other, not too white and of recent origin, the central portion of which is elevated
and is not caused by burns is curable108.
Asadhya Shvitra
The form where in the lesions extend and become confluent are situated very
close to each other so they can not be differentiated from one another or are multiple,
covered with red hair and of more than a year‟s duration are incurable. Especially
where in the lesions have invaded the palmer and the planter surfaces, the anal area,
the genitals the lips and cicatrix due to burns though of recent origin are incurable109.
The Shvitra situated in Medo Dhatu is relatively most difficult to treat than that in
Mamsa and Rakta.
If the depigmented patches coalesced and the palmer plantar aspects of hands,
legs, lips and a genital organ are associated with this disease, and if the hairs on this
Shvitra affected area become white, then that Shvitra is incurable110.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 31
Table 8: Sadhyasadhyata of Shvitra
Sl no
Lakshana C.S S.S A.S A.H B.P M.N Y.R G.N
Sadhya lakshana 1 Araktha loma + - - - - - - - 2 Thanu + - - - - - - - 3 Pandu + - - - - - - - 4 Natichirottitam + - - - - - - - 5 Madhya vaksha chochunam + - - - - - - - 6 Ashukla loma - - + + + + - + 7 Abahalam - - + + + + - + 8 Nava / avarshati krantha - - + + + + - + 9 Agni dagdha - - + + + + + + 10 Mitha asamsrusta / paraspara
animilitha - - + + + + - +
Asadhya lakshana 1 Sambadha mandala - + - - - - - - 2 Raktha roma + + - - - - - - 3 Agni dagdha - + - - - - - - 4 Paraspara abhinna + - - - - - - - 5 Bahu + - - - - - - - 6 Varsha ganotpanna + - - - - - - - 7 Anthe jatham - + - - - - - - 8 Present in guhya pani thala
osta - - + + + + - +
Differences between Shvitra and Kushta
The differences mentioned in samhitas are as follows –
Tvak Dosha is the name given to Kushta where as Shvitra pertains to the skin.
Hence it is also included in Kushta rogadhikara111.
The vitiated Doshas and Dushyas if untreated for a long time undergo
Swedata, Kledata and Kodhata. By this Sukshma Krimi (Microscopic organisms) will
be produced, in those areas and this Krimi will eat or erode gradually hair, skin,
ligaments, arteries and cartilages. Because of this the condition is called Kushta. And
the Shvitra Kushta which is pertaining to skin is separated from Kushta (leprosy) and
is called Bahya Kushta112.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 32
Table 9: Showing the Differences
Sr. No. Shvitra Kustha 1. It is pertaining to skin only
and is called Bahya Kushta Kushta occurs in Rakta, mansa meda etc. internal dhatus.
2. No Secretions obtained from Shvitra affected area.
Secretions obtained by the death of internal dhatus in Kushta.
3. Shvitra is not an infectious disease and produced· due destruction of to the melanocytes, by this absence of melanin leads to depigmentation. This pigment gives colour to the skin and protects body from external atmosphere.
Kushta is produced by varied micro-organisms.
4. In the Shvitra affected area sense of touch is normal.
But in Kushta loss of sensation of affected area will be observed.
5. It is not a infections disease. Hence patient of Shvitra need not be kept away from Society.
Kushta is an infections disease. Hence Isolation of patients of the Kustha is necessary.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 33
CHIKITSA
Shvitra is a Bhibhatsya Vyadhi when compared to Kusta and the disease soon
becomes Asadhya if not treated. So the treatment should be started as early as
possible similar to putting off the fire of a burning house113.
Chikitsa can be mainly divided in to three types‟ Daivavyapashraya, Yukthi
vyapashraya and Satvavajaya114.
Aushadha prayoga can be mainly done in two forms
1) Anthahparimarjana where Aushadha and ahara dravya are given internally.
2) Bahi parimarjana where Aushadha dravya are used externally in the form of
abhyanga, Lepa, sweda, parisheka and unmardana115.
Aushadha given acts in two forms
1) Shodhana where vitiated Doshas are removed out of the body through Urdhwa and
Adho marga116.
2) Shamana where Doshas are brought in to normalacy with out expelling them out117.
Shvitra is a disease in which Yukthivyapashrya Chikitsa in the form of Shodhana and
Shamana is administered. Both Bahya and Abhyanthara prayoga of Oushadha Dravya
is done. Daivavyapashraya Chikitsa is also mentioned in the context of kusta
Line of treatment of Shvitra
The treatment of Shvitra should begin with a Vishesha Shodhana that is by
Vamanadi kriya118 followed by administration of Malayu rasa with Guda for the
purpose of Sramsana. The person whose Shareera is made Snigdha by Snehapana
should be anointed with Taila and exposed to sunlight as per his Bala. If the person
feels thirsty due to Virechana Peya should be given to him119.
The drug Malayu Rasa given for the purpose of Sramsana is commented as
Bakuchi Kwatha by Arunadutta120and Kakodumbarika by Chakrapani121.
Yogarathnakara indicates the intake of Khadirodka and Anna after Vamana,
Virechana and Raktha Mokshana, and then Malayu rasa with Guda should be given
after which the person has to take Manda and Yavagu as pathya122.
Certain Kwathas are told by different authors, which have to be given before the
patient is exposed to sunlight.
1) Bakuchi Kwatha with Guda acts as Sramsaka and also patient is exposed to sun
light after consuming it123.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 34
2) Kakodumbara + Vibhitaki kwatha with Bakuchi kalka124.
3) Acharya Charaka mentioned exposure to sunlight after Sramsana, for three days125.
4) Bakuchi choorna given bhavana with Gomoothra should be consumed with
Kwatha of Kakodumbara + Madanaphala + Karanja + Vibhitaki during pratha kala126.
5) Vibhitaki and Kakodumbara kwatha with Bakuchi choorna should be administered
for two to three days127.
Blebs which develop due to exposure to sunlight should be opened by a thorn
after which Shamana Aushadhis are given internally and externally. Gadanigraha
specifies the intake of Takra without salt after the blebs are opened128.
Savarneekarana is one among the sixty upakramas mentioned by Sushrutha to
bring back the normal colour of the skin at the site of a healing wound.
Savarneekarana includes Krishna karma and pandu karma. Krishna karma can be used
in treatment of Vranaja Shvitra129.
Daivavyapashraya Chikitsa130
After Vamana, Virechana, Raktha Mokshana and Virookshana Sakthu is given
as Pathya. After all these procedures shvitra gets cured if papa of the patient gets
reduced131. As Papakarma is a Vishista Nidana of Shvitra, Daivavyapashraya chikitsa
has a greater role in reducing it.
With all the Yukthi vyapshraya chikitsa the patient has to follow –
1. Vratha –that is surya aradhana
2. Dharma –controlling the ninditha chitha vrithi
3. Yama –controlling the indriyas
4. Seva –doing the seva of dana and thyaga sheela purusha
5. Dwija seva and guru pooja
6. Performing pooja of shiva, shivasutha that is ganesha, tara ana surya
7. Roupyadana or giving silver as alms, helps in curing Shvitra

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 35
Table 10: List of drugs used internally and externally
Sl no
Name of the yoga C.S S.S A.H A.S B.P Y.R B.R G.N C.D
Virechana dravyas 1 Patola muladi kwatha - - + - - - - - - 2 Manibhadra yoga - - + - - - - - - 3 Malayu rasa + guda + - + + - - - + - Shamanoushadhis - Kwatha 1 Malayu + asana+
priyangu + shatapushpa + - + - - - - + -
2 Badrodumbaradi yoga - + - - - - - + - 3 Dhatriyadi kwatha - + - - - - - + + 4 Khadiradi kashaya + - - - - + - - - 5 Vibhitaki Tvak +
malayu mula + bakuchi churna
- - - - + - - - -
6 Bakuchi + amalaki + khadira
- - - - + - + - -
7 Dhatri khadira kwatha - - - - - - + - - 8 Vibhitakyadi kwatha - - - - - - + - - 9 Manjistadi mahakashaya - - - - - - + - - 10 Gomutradi yoga - + - - - - - - - Churna 1 Musthadi churna + - + - - - - - - 2 Pancha nimba churna - - - - - - + + + 3 Khadirasaradi churna - - - - - - - + - Avaleha 1 Bhallataka avaleha - - - - - + - - - 2 Panchanimbavaleha - - - - + - - - - 3 Mahabhallataka guda - - - - - - + - - 4 Mahabhallataka avaleha - - - - + - - - - Asava - Arista 1 Madhvasava + - - - - - - - 2 Kanaka bindwarista + - - - - - - - - 3 Gomutrasava - - + - - - - - - Vati 1 Swambu guggulu - - - - + - - - - 2 Swetari rasa - - - - - - + - - 3 Triphala gutika - - - - - + - - - 4 Shashilekha vati - - - - - + - - -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 36
5 Vijayeshwara rasa - - - - - + - - - Ghrutha 1 Thiktaka ghrutha - - + - - - - - - 2 Mahathiktaka ghrutha - - + - - - - - - 3 Mahavajraka ghrutha - - + - - - - - - 4 Avarthaki ghrutha - - + - - - - + - 5 Somaraji ghrutha - - - - + - - - - Bahya oushadhi – taila 1 Mahavajraka taila - - + - - - - - - 2 Aragvadhadhy taila - - - - - - - - + 3 Swalpa marichadhya taila - - - - + - - - + 4 Visha taila - - - - - + + - + 5 Kusta rakshasa taila - - - - - - + - - 6 Marichadya taila - - - - - + + - - 7 Kandarpasara taila - - - - - - + - - 8 Jyothishmathi taila - - - - - + - - - 9 Laghu vishagarbha taila - - - - - - - + - Ghrutha 1 Mahaneela ghrutha - + - - - - - - - Lepas 1 Shiki Pitta Lepa + - + - - - - - - 2 Krishna sarpodbhava
masi + aksha taila - + + - - - - - -
3 Savarnakara Lepa - - + - - - - - - 4 Gajalinda kshara +
bakuchi - + + - - - + - +
5 Bhallatakadi Lepa - - + - - - - + + 6 Burnt skin of elephant +
taila - + + - - - + - +
7 Puti keeta + aragvadhakshara
- + + - - - + - -
8 Kukkuta pureesha yoga - + - - - - - - - 9 Avalgujadi varthi - + - - - - - - - 10 Thuttadi Lepa - + - - - - - - - 11 Shvitranashana Lepa - - + - - - - - - 12 Marichadi Lepa - - + - - - - + - 13 Bhallataka Lepa - - + - - - - - - 14 Aragvadha shatchurna
pradeha - - - - - - - + +
15 Puthikadi Lepa - - - - - - - + +

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 37
16 Avalguja beejadi Lepa - - - - - - - - + 17 Shweta jayanthi mula
kalka - - - - - - + - +
18 Shiladi Lepa + - - - - + - - - 19 Triphaladi Lepa - - - - - + - - - 20 Ayorajadi Lepa - - - - - + - - - 21 Kadalikshara + kharasthi
bhasma + goraktha + - - - - - - - -
22 Malathi koraka Kshara+ hasthi mada
+ - - - - - - - -
23 Neelotpala + kusta +saindhava + gaja mutra
+ - - - - - - - -
24 Mulaka beeja + avalguja + gomutra
+ - - - - - - - -
25 Kakodumbara + avalguja + chitraka + gomutra
+ - - - - - - - -
26 Bakuchi beejadi Lepa + - - - - - - - - 27 Bakuchi + haratala +
manashila + gunja + chitraka
- - - - + - + - -
28 Neelaparajitha mula Lepa - - - - + - - - - 29 Manashila + apamarga
bhasma - - - - - - + - -
30 Gandhaka + chitraka + pippali + haratala + haritaki
- - - - - - + - -
31 Gruhadhumadi Lepa - - - - - - - + - 32 Sudarshana mulayoga - - - - - - - + - 33 BakuchyadiLepa - - - - - - - + -
TREATMENT PRINCIPLES & CONCEPT OF SHODHANA IN CHILDREN
The Vata Pitta Kapha and Asrik in Baala are similar to that of an adult but
lesser in quantities. So the physician according to his intelligence should use Alpa
anna pana and Oushadha in children because the dose of the drug and diet mainly
depends on Agni, Bala and Vaya of the person132.
Excessive Shodhana and Rakta Mokshana is contraindicated in Baala.
Medicines which are Snigdha, Mrudu and which do not produce Daha should be
given orally or in the form of Lepa133.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 38
Vamanadi kriya is contraindicated for Mrudu and Paratanthra Bala. Seeing the
ability of Vak and Chesta in the bala alpa mathra oushadhi should be given134.
Commenting on this Chakrapani mentioned that baalas are of two types‟ Swatantra
and Paratantra. If the child is Paratantra, Vamanadi kriyas are contraindicated and in
Swatantra baala Vamanadi kriya can be performed, but it should be Mrudu in
nature135.
Shodhana Oushadhis on basis of Ksheerada Ksheeraannada and Annada
classification of Vaya is mentioned136.
By observing all these opinions, it is clear that therapies like Vamana and
Vrechana should not be Teekshna when adopted in children instead should be given
mildly considering the age of the child.
CONCEPT OF VIRECHANA
Virechana is one amoung the five types of shodhana where Doshas are
removed from Adhomarga and is considered as the best Pittahara Chikitsa137.
Types of Virechana
Sharangadhara explained four types of Virechana138
1) Anulomana – Dravyas that do the paka of mala and breaks it and removes it
through adhomarga eg Harithaki
2) Sramsana- Dravyas which remove the mala stuck in the kosta without causing paka
of mala. Eg Aragwadha
3) Rechana – Dravyas which remove the mala by making it Drava irrespective of its
pakwa or apakwatha is called rechana eg Trivrit
4) Bhedhana- Dravyas which breaks the pinditha and badha mala and removes it
through adho marga eg-katuki
Among the four types of Virechana, sramsana is indicated in shwithra.
VIRECHANA IN CHILDREN
Adopting the treatment principles mentioned for Bala, Mrudu Virechana could
be administered in Swatantra bala.
Aragwadha can be given for Virechana especially for Sukumara and Bala, as it
is Mrudu and does not produce any complications139, 12 different yogas have been
explained in Aragwadhakalpadhyaya especially for children140.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 39
Aragwadha is explained as Sramsaka, Kosta PittaKaphahara and Kosta shudhikara141.
Acharyas mentioned Aragwadha Phalamajja with Ksheera for Virechana in baala142.
CONCEPT OF LEPA
Lepa means the one, which is used for anointing.
Different authors mentioned different types of Lepas.
Types of Lepa according to sushrutha143
1. PraLepa – It is applied in a thin and cold form and may be applied where pidana
karma is not necessary. Used in the cases of raktha and Pitta pradhana shotha.
2. Pradeha – It is thick or thin warm or cold based on doshic involvement and it
should not be allowed to dry completely. It is used in Vata and sleshma
pradhana shotha.
3. ALepa -It has the quality of both praLepa and pradeha
4. Lepa used for wound is called kalka or nirudha Lepa
Types of Lepa according to Astanga sangraha144
Astanga sangrahakara told pradeha is sheetha, thanu and used in raktha Pitta vikara.
He mentioned 10 types of Lepa based on its action.
1) Snaihika Lepa – This is ment for Vata dosha & is prepared with snigdha dravya.
2) Nirvapana Lepa – This is ment for Pitta dosha and used in Pittaja & vishaja
shotha, Agni & ksharadagdha wounds. Sheeta veerya dravyas are used.
3) Prasadhana Lepa – It has raktha prasadana property.
4) Sthambhana Lepa – In addition to the property of nirvapana Lepa it has
raktastambhaka property.
5) Vilayana Lepa – It is used in shelshmaja & medajashotha.
6) Pachana Lepa – It does the pachana of apakva shotha.
7) Pidana Lepa – Rooksha, picchalia dravyas are used, useful in sookshama vrana.
8) Shodhana Lepa – It is indicated in ashudda vrana. Shodhana dravyas are used.
9) Ropana dravya – Used for Ropana of shuddha vrana.
10) Savarnakara Lepa – Helps in attaining normal skin colour.
Types of Lepa according to Charaka) 145
1) Shodhana –It is Tvak shudhikara
2) Ropana praLepa –It is used to bind the torn skin

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 40
3) Kanthikara Lepa –It is used in vrana shaithilyatha and has prasadana property
4) Mardavakara Lepa – It is used in saruja Katina sthbdha and nisravya vrana
5) Savarnakara Lepa –It is used for enhancing the colour and complexion
6) Varnakara Lepa – It helps in bringing back the prakrutha Varna of twacha
7) Romasanjanana Lepa – It is used for the reproduction of the destroyed roma.
8) Tvak karshnya karaka Lepa – It produces krishnathwa of Tvak at applied site.
General rules to be followed during application of Lepa
1) PraLepa should be applied uniformly & thickness should be 1/3rd of an anguli.
2) Before applying the Lepa, the previous Lepa, which is dried, should be removed.
If not it increases the doshas.
3) Lepa should be removed with out washing it in water.
4) Lepa used once should not be used again by making it wet.
5) After applying Lepa nothing should be covered over it
6) Fresh Lepa should not be applied over the dried Lepa.
7) The Lepa should not be too thin because it dries up before it reaches the moola
stana & reduses the dosha146.
8) The thickness of the Lepa should be equal to the wet skin of a buffalo147.
9) A Lepa should be applied in opposite direction of romakoopa, and then it enters
the roomakoopa & reaches the swedavaha Srotas & Siramukha.
10) Lepas should not be completely dried except where pidanakarma is necessary. If
dried it produces pain148.
11) Lepa should not be applied during night time because during night, the ushnata of
shareera goes out through roomakoopa; if Lepa is applied the ushanatha is
retained inside, which vitiates the doshas149.
12) Lepa prepared in the previous day should not be used.
13) Lepa prepared should not be kept for long time since it looses its veerya150.
General uses of Lepa151
It is used in the case of avidagdha shopha
1) It does twacha shuddi & also purifies mamsa & raktha
2) It reduces daha, toda & kandu.
3) It can be applied in diseases of marmasthana & guhya sthana, where it does the
shudhi & shamana of the diseases.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 41
Amount of sneha, which is to be used in aLepa152
1) Pittaja shopha - 1/6th part
2) Vataja - 1/4th part
3) Kaphaja - 1/8th part
Pathyapathya
Pathya is hita for patha i.e Srotas and priya for mana, that which is ahita and
apriya for patha and mana respectively is apathya153.
One who follows pathya ahara vihara with shraddha, takes vishista oushadhi and
does punya karma gets rid of kusta quickly154.
Hence following the pathyas mentioned, and avoiding apathya will help in
preventing the further aggravation of the disease. Since Shvitra is mentioned as a
kusta bheda the pathyapathya of the disease kusta can be taken for Shvitra also. The
pathyapathya of Shvitra is enlisted below.
Table 11: Pathyapathya of Shvitra155
Sl no
Pathyapathya C.S S.S A.S A.H Y.R G.N B.R C.D
Pathya 1 Laghu anna + - - - - - + - 2 Thiktashaka + - + + - + + + 3 Bhallataka + - + + - + + - 4 Thriphala + nimba + - - - - - + - 5 Anna + ghruta + - - - - - - - 6 Purana dhanya + - - - - - + + 7 Jangala mamsa + - + + - + + + 8 Mudga + - + + - + + + 9 Patola + - + + - + + - 10 Shali - - + + - + + + 11 Yava - - + + - + + + 12 Godhuma - - + + - + + - 13 Priyangu - - + + - + - - 14 Masura - - + + - + - - 15 Tuvari - - + + - + - - 16 Khadira - - + + - + + - 17 Rakthashodaka oushada siddha
Madhya - - + + - + - -
18 Bakuchiyukta annapana - - + + - + - -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 42
19 Adhaki - - - - - - + - 20 Makshika - - - - - - + - 21 Ashada masa Phala - - - - - - + - 22 Brihathi phala - - - - - - + - 23 Kakamachi - - - - - - + - 24 Lashuna - - - - - - + - 25 Punarnava - - - - - - + - 26 Meshashrungi - - - - - - + - 27 Chakramardha - - - - - - + - 28 Pakwathala - - - - - - + - 29 Chitraka - - - - - - + - 30 Jathiphala - - - - - - + - 31 Nagakesara - - - - - - + - 32 Kumkuma - - - - - - + - 33 Purana ghruta - - - - - - + - 34 Koshataki - - - - - - + - 35 Karanja - - - - - - + - 36 Tila taila - - - - - - + - 37 Sarshapa taila - - - - - - + - 38 Nimba taila - - - - - - + - 39 Ingudi taila - - - - - - + - 40 Sarala taila - - - - - - + - 41 Devadaru taila - - - - - - + - 42 Shimshipa taila - - - - - - + - 43 Agaru taila - - - - - - + - 44 Gomutra - - - - - - + - 45 Karamutra - - - - - - + - 46 Ustra mutra - - - - - - + - 47 Ashwa mutra - - - - - - + - 48 Aja mutra - - - - - - + - 49 Kasturi - - - - - - + - 50 Gandhaka - - - - - - + - V1haraja pathya 1 Cutting of kesha and nakha - + - - - + - - 2 Vishrama - - - - - - - Apathya 1 Guruahara + - - - - - - - 2 Amlaahara + - + + + + + - 3 Payas + - + + + + + -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 43
4 Dadhi + - + + + + + - 5 Anupa mamsa + - + + + + + - 6 Matsya + - - - - - - - 7 Guda + - + + + + + - 8 Tila + - + + + + + - 9 Ushna ahara - - + + + + - - 10 Lavana - - + + + + - - 11 Masha - - + + + + + - 12 Mamsa - + - - - + - + 13 Sura - + - - - + + + 14 Virudha pana - - - - - - + - 15 Viruda ashana - - - - - - + - 16 Dravanna - - - - - - + - 17 Guruanna - - - - - - + - 18 Navanna - - - - - - + - 19 Vidahi anna - - - - - - + - 20 Vistambi anna - - - - - - + - 21 Mulaka - - - - - - + - 22 Udaka of sahyadri and vindhya - - - - - - + - 23 Vishamashana - - - - - - + - Apathya vihara 1 Stree sanga - + - - - + - + 2 Papakarma - - - - - - + - 3 Kruthaghna bhava - - - - - - + - 4 Guruninda - - - - - - + - 5 Gurugarshana - - - - - - + - 6 Ati nidra - - - - - - + - 7 Chandramshutapa - - - - - - + - 8 Atisweda - - - - - - + - 9 Vegavarodha - - - - - - + - 10 Vyayama - - - - - - + -

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 44
Modern View
Skin is the largest organ in the body, having a surface area of 1.8 m2 and
making up about 16% of body weight.
Anatomy
The skin consists of two parts. The outer one is epidermis, which is thinner
and composed of epithelium, and inner subcutaneous layer, which is thicker and
contains connective tissue is called Dermis. The dermis is also called the superficial
fascia or hypodermis, which consists of areolar and adipose tissue. The subcutaneous
layer, in turn, attaches itself to underlying tissues and organs.
Epidermis:
Thickness of epidermis ranges from 0.04 mm (eyelids) to 0.16 mm (palms / soles). It
undergo continuous turnover of the layers, and requires 28 days for keratinocytes to
move from stratum basale to stratum corneum, 52 days for epithelial cycling.
Cells present in Skin:
Cells Origin Functions
Keratinocytes Ectodermal, move
upward from
stratum basale to
stratum corneum
Synthesize tonofilaments which is
precursor of keratin. Keratinocytes mature
to form cornified cells (loss of nucleus).
Melanocytes
(Ratio of
keratinocytes to
melanocytes is 4:1
to 10:1)
Neural crest These dendritic cells containing
melanosomes secrete melanin. Imparts
colour and gives protection against UV
light.
Langerhan‟s cells Mesenchymal Dendritic cells with intra-cytoplasmic
granules.
Role in immune reaction of delayed
hypersensitivity
Merkel‟s cells Neural crest Dendritic cells with intra-cytoplasmic
granules. Function as slow adopting touch
receptor.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 45
The names of the five layers, from the most superficial to the deepest are as
follows:
Stratum corneum:
This is the most superficial layer, which consists of 25 to 30 rows of flat, dead
cells completely filled with keratin. These cells are continuously shed and replaced by
cells from deeper strata. The stratum corneum serves as an effective barrier against
light and heat waves, bacteria, and many chemicals.
Stratum Lucidum:
Normally, this layer is limited to thick skin of the palms and soles. It consists
of three to five rows of clear, flat, dead cells that contain droplets of an intermediate
substance that is formed from Keratomyelin and is eventually transformed to Keratin.
Stratum granulosum:
Stratum granulosum consists of about three to five rows of flattened cells that
develop darkly staining granules of a substance called Keratomyelin. This compound
is the precursor of keratin. Keratin forms a barrier that protects deeper layers from
injury and microbial invasion and makes the skin waterproof.
Stratum spinosum or Malpighian layer:
This prickle cell layers lies upon the basal layer and has 8 to 10 rows of
polyhydral cells that fit close together. This layer involves most of the pathological
conditions of the skin.
Stratum basalis or Germinativum:
This layer forms the lowest, most sensitive, single row of columnar cells,
which is capable of continued cell division. As these cells multiply, they push up
towards the surface and become part of the upper layers. The stratum basalis also
contains tactile (Merkel) discs that are sensitive to touch.
Dermis:
Dermis contains two layers. The outer portion of the dermis, which is about
one fifth of the thickness of the total layer, is named the papillary region. The deeper
portion of the dermis which consists of dense irregular connective tissue containing
interlacing bundles of collagen and coarse elastic fibers is called reticular region. The
dermis chiefly consists of white fibrous tissue, elastic fibers and non-striped muscles
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 46
and contains blood vessels, nerves, hair, sweat glands and sebaceous glands and nerve
corpuscles.
The reticular region is attached with underlying organs, such as bone and
muscle, by the subcutaneous layer, also called the hypodermis or superficial fascia.
Sebaceous glands:
They are scattered all over the skin in association with the hair follicles. They
are absent in hairless portion of the body like palms of the hands, soles and side of the
feet.
These lipid-producing glands are out growth of hair follicles except
Meibomian glands (eyelids), buccal mucosa of vermilion border of lip (Fordyce spot),
prepuce (Tyson glands), and female breast areola (Montgomerry tubercles).
Outermost single layer of geminative cells mature into innermost lipid rich
cells, which on disintegration produce sebum, which is secreted by the sebaceous
duct.
Sweat glands: These are of two types,
These are of two types,
Eccrine glands – They are the ordinary small sized sweat glands, which are
distributed all over the skin except on the beds of nails, margins of lips and the glans
penis.
Apocraine glands – They occur in the axillae, areola and nipples of breasts,
umbilicus, around the anus and genitalia. They are specialized sweat glands.
Hair:
Hair is found on almost every part of the body surface except on the palms and
the soles, the dorsal surface of the terminal phalanges, the inner surface of the labia,
the inner surface of the prepuce and the glans penis.
Melanocytes:
Melanocytes can be found in nearly every tissue. But they are most common
in superficial epidermis, hair follicals, dermis, eye, around blood vessels, peripheral
nerves and the sympathetic chain. In the basal layer of the human epidermis, there are
about two billion melanocytes distributed through out the body. A reduction in the
number of melanocytes occurs in the skin with advancing age.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 47
Biochemistry of Melanin:
Melanin is a complex polymer synthesized from tyrosine and have two forms,
1. Eumelanin – It is more common and gives a brown-black colour. It is a high
molecular weight polymer of complex structure formed by oxidative
polymerization.
2. Phaeomelanin – It is less common and produces yellow or red colour. It is
synthesized from dopaquinone and cysteine.
Most common and natural melanins are mixtures of Eumelanin and
Phaeomelanin. Melanins act as energy sink and free-radical scavengers, and absorb
the energy of UV radiation.
Structure of melanocytes:
Melanocytes form a network of dendritic cells in the basal layer of epidermis.
They are also found in the external hair root sheaths and in the bulbs of the hair
follicles. It is these scretory melanocytes, which behave as unicellular glands
producing melanosomes, which are transferred to the surrounding epidermal
keratinocytes. The transfer of melanosomes involves the insertion of tip of the
dendrite of the melanocytes that becomes embedded in the cytoplasm of
keratinocytes.
The end becomes pinched off and a package of melanosomes is transferred to
keratinocyte that acts as a phagocyte. The melanosomes are packed according to size,
the larger ones as single units and the smaller ones as complexes of two or more.
Melanocytes are distinguishable from the keratinocytes by their lack of desmosomes,
tonofibrils and by a more lucent cytoplasm. The characteristic feature of this cell is
the presence of special cytoplasmic organelles, the melanosomes on which melanin is
formed by the action of the enzyme tyrocinase. The developing melanosomes show
varying degrees of electron density, the more fully melanized being very dense.
Melanocyte function
Melanocytes are located in the basal layer. In this location, they produce the
pigment melanin in elongated, membrane-bound organelles known as melanosomes.
Melanin is packaged into granules which are moved down dendritic processes and
transferred by phagocytosis to adjacent keratinocytes. In the inner layers of the
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 48
epidermis, melanin granules form a protective cap over the outer part of keratinocyte
nuclei.
In the stratum corneum, melanin granules are uniformly distributed to form a
UV-absorbing blanket which reduces the amount of radiation penetrating the skin.
Four stages of melanosomal antagony are recognized.
1. Stage one is a membrane bounded spherical vesicle may show tyrocinase activity.
According to classical theory, tyrocinase is produced on membrane bound ribosome
and transferred via the endoplasmic reticulum to the golgi apparatus where it
accumulates in vesicles that are derived from the golgi bodies.
2. In stage two melanosomes are oval in shape and show numerous melanofilaments
with and without cross – linking.
3. In stage three the internal structure of melanosomes is partially obscured by the
deposition of melanin.
4. In stage four, the mature melanosome appear electron dense.
Keratinization:
In the process of Keratinization, cells newly formed in the basal layers
undergo a developmental process as they are pushed to the surface. As the cells
relocate, they accumulate keratin. At the same time the cytoplasm, nucleus, and other
organelles disappear, and the cells die. Eventually, the keratinized cells are
desquamated and are replaced by underlying cells that, in turn become keratinized.
Kinetic studies show that, on average the dividing basal cells replicate every
200 to 400 hrs. The resultant differentiating cells take about 14 days to reach the
stratum corneum and a further 14 days to be shed. The cell turnover time is
considerably shortened in Keratinization e.g. Psoriasis.
Pigmentation of the skin:
Pigments, melanin, carotene and hemoglobin – give skin a wide variety of
colors. Melanin is located mostly in the epidermis; carotene is mostly in the stratum
corneum and dermis; and hemoglobin is in red blood cells within capillaries in the
dermis. Color of the human skin is derived from a variety of chemical and physical
properties associated with the structure. Normal skin color is dependent on
hemoglobin, (oxygenated / reduced state) carotinoids and melanin pigment. Five
pigments are known to influence the skin color. They are,

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 49
1. Melanin is a pigment which is found more in stratum malpighi. Melanin contributes
color and quality to skin and protects the organism from the ultraviolet rays. It is in
the form of granules, which vary from light brown to black in color. Melanin is
formed from the amino acid tyrosine by the action of the enzyme tryosinase and
copper protein complex. Hence it is clear that copper ions are essential for normal
pigmentation of skin.
2. Melanoid is supposed to be a degradation product of melanin and is diffusesd
through out the epidermis. Melanoid has a different absorption band of visisble light.
3. Carotene is yellow orange pigment in lipid rich areas like stratum corneum,
subcutaneous fat etc. this adds yellow color to the skin of women than in men.
4. Oxy-hemoglobin imparts reddish hue to the skin color and it is evident in areas
where there is rich arterial supply like face, neck, palm, soles and nipples.
5. Reduced hemoglobin contributes bluish or purple character to skin color and is
more evident in lower areas of the trunk.
Two types of melanin pigmentation occur in man. The first constructive skin
color, that is the amount of melanin pigmentation, which is genetically determined in
the absence of sun exposure and other influences. The other facultative or inducible
skins color or tan which results from sun exposure.
Variation in the thickness of the skin may modify the skin color. Subjects with
thin epidermis have a reddish color complexion and with a thicker epidermis look
yellowish. Thicker epidermis is less transparent than the thin one. As the transparent
stratum corneum scatters light slightly, the deeper layer appears blue.
The skin remains light colored when the pigment appears in the center of the
melanopores and dark when it is dispersed to their periphery.
Three different mechanisms may be involved in the control of color change.
Firstly, the pigment cell may act as an independent effect or respond directly to the
stimulus of light. There is evidence that this can occur in some fish and amphibians
and the tanning of human skin both immediate and delayed can be considered as an
analogous process. Secondly, the movement of pigment with the melanophore may be
under the nervous control. Thirdly the activity of pigment cells or melanocytes may
be under hormonal influence. Pitutary hormone causes expansion of melanophores or
promotes the formation of melanin in epidermal melanocytes.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 50
Bruno – Bloch is the person who elucidated the mode of melanin formation.
According to him melanin is formed from tyrosine through the intermediatory stage of
dioxyphenyl – alanine (dopa). Melanocytes contain enzymes, which convert tyrosine
in to melanin.
Tyrosine Tyrocinase DOPA Dopa oxidase Melanin
Scientist like Fitz patric have extensively studied the ultra structure of
melanocyte and melanin formation. From the golgi body of the cell arises a vacuole
like premelanozome, which incorporates zinc and becomes a melanosome. This later
becomes heavy and loses tyrocinase activity to be formed in to melanin granule.
Melani formation is physiologically under the control of M S H of the pitutary gland.
The sun, UV rays, X – rays etc. stimulate melanin formation, while ascorbic acid
tends to reduce it.
Blood supply of skin:
There are two horizontal and parallel systems of plexuses, which supply the
skin. The plexus or network of blood vessels exists between the dermis and the
subcutaneous tissue. Its exact position can never be accurately described. Each
arteriole supplies an area of skin and each venous plexus is associated with it drains
the same area.
Nerve supply:
The nerve supply of the skin is very complicated, and the pathways for the
mediation of sensations through various nerves are very much under debate. The
varied sensations arising from skin are derived from a diverse population of cutaneous
nerve endings or receptors, thus tactile, temperature and pain sensations each of which
are sub served by different groups of receptors.
Functions of the skin:
The skin is a metabolically active organ with vital functions including the
protection and homeostasis of the body. It has many functions, the most
important of which is as a barrier to protect the body from noxious external
factors and to keep the internal system intact.
[a] Regulation of body temperature:
Via heat loss Sweat evaporation - Eccrine sweat gland.
Vasomotor regulation - Vasculature

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 51
Via heat conservation Body hair, Insulation provided by body fat.
[b] Protection:
The skin is considered under the Integumentary system. It provides a physical
barrier that protects the underlying tissues from physical abrasion, bacterial
invasion, dehydration, and UV radiation.
Water loss - Stratum corneum
Water gain - Stratum corneum
Toxic substance penetration - Stratum corneum
Microbial attack - Stratum corneum
Mechanical injury - Stratum corneum + dermis
[c] Sensation:
The skin contains abundant nerve endings and receptors that detect stimuli
related to temperatures, touch, pressure and pain.
[d] Immunity:
Sweat of the epidermal cells (Langerhan‟s cells) has important components of
the skin immune system, which tends off foreign invaders.
[e] Excretion:
Sweat is the vehicle for loss of a small quantity of ions and several organic
compounds along with removal of heat and some part of water.
[f] Blood reservoir:
The dermis is a house of extensive networks of blood vessels that carry 8 –
10% of the total blood flow in a resting adult. In moderate exercise this flow
increases, and helps to dissipate the heat from the body. While during the
exercise skin‟s blood vessels constrict so this allows more blood to circulate
through contracting muscles.
[g] Synthesis of Vitamin – D:
Synthesis of vitamin D begins with activation of a precursor molecule in the
skin by ultraviolet rays in the sunlight. Enzymes in the liver kidneys then modify
this molecule and produces calciferol, the most active form of vitamin D.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 52
Table No. 13 Hormones and the Skin:
No. Hormone Site of production Effect
1. Vitamin D In dermis from precursors though action of UV radiation.
Important for absorption of calcium and calcification
2. Corticosteroids Adrenal cortex -Receptor on several cells in both epidermis and dermis -Produce vasoconstriction -Reduce mitosis by basal cells -Anti-inflammatory effect on leucocytes
3. MSH and ACTH
Pituitary gland Stimulate melanogenesis
4. Estrogens Adrenal cortex and Ovaries
Stimulate melanogenesis
5. Epidermal Growth Factor
Skin -Receptors found on -Keratinocytes, hair, follicles, sebaceous gland & sweat gland duct cells
6. Cytokines and eicosanoids
Cell membrane On immune function, inflammation and cell proliferation
The skin is the site of production of one hormone i.e. vitamin D, but it is often
a target organ for other hormones and is frequently affected in endocrine diseases.
Vitiligo:
The origin of the term vitiligo is obscure like the disease itself. Some believe
that it is from the Latin word vitellus – means vale that is pale pink flesh of a calf,
while others tell that it‟s from the word vitium – means blemish (pale).
Synonyms:
1. Vitiligo – Depigmented or Hypopigmented patches that result from absence or
reduction of melanocytes due to unknown cause.
2. Leukoderma – Term is applied for depigmented patches of known cause like
burns, contact with chemicals like phenols or following an inflammatory skin
disease.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 53
Etiology of vitiligo:
Vitiligo is a multifactorial malady. Influence of genetic predisposition varies
from 10 – 35 % and in cases of positive family history 1 – 2 family members are
affected.
1. Nutritional causes – defect in copper, protein and vitamins in diet. Prolonged
consumption of diet poor in proteins. Digestive upsets amoebiasis, helminthes,
chronic diarrhea and dysentery
2. Endocrine causes – Association of the disease vitiligo is seen with
thyrotoxicosis and diabetes. Among endocrine factors anterior pituitary is
possibly the most important. Intermediate lobe of pituitary secretes
melanocyte-stimulating hormone, which further stimulates melanin formation
and dispersal.
3. Trophoneurosis and autoimmune imbalance – it includes emotional stress and
strain.
4. Infections and toxic products – Enteric fever, Ill health, Focal sepsis.
5. Chemical causes - Drugs and chemicals like quinines, guana furacin,
amylphenol, chlorthiazide, broad-spectrum antibiotics, beta-blockers and
chloroquin. Chemicals are known to inhibit melanogenisis enzymatic actions
and several chain biochemical reactions. They also cause inter ference with
nutrition of the tissues.
6. Misscellaneous factors - contact with rubber and ferric cyanide induce vitiligo,
pressure, trauma, tight wearing of sarees and dhotis can precipitate vitiligo
lesion.
7. Industrial chemicals and dyes containing water and foods may cause vitiligo.
But not proved.
8. Severe trauma like burns can destroy pigment cells resulting in vitiligo.
9. Vitiligo has assumed epidemic proportions in several parts of India especially
in Gujarat and Rajasthan.
10. Vitiligo is usually associated with following disorders

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 54
a. Pernicious anemia
b. Addison‟s disease
c. Graves disease
d. Hyperthyroidism
e. Hypothyroidism
f. Thyroiditis
g. Hyper Parathyroidism
h. Diabetes mellitus
i. Rheumatic disorders
j. Malignant melanoma and
internal malignancy
k. Gastritis
l. Gastric carcinoma
m. IgA deficiency
n. Myasthenia gravis
o. Suppression of the thymus
p. Sezary „s syndrome
q. Ulcerative colitis
r. Thymoma
s. Acquired hyper-gamma
globulinaemia
t. Auto immune hemolytic anemia
u. Vogt – koyanagi – harada
syndrome
v. Mucocutaneous candidiasis
w. Biliary cirrhosis
x. Downs syndrome
y. AIDS
Clinical features of vitiligo:
Clinical profile
About 1-2% of general population suffers from vitiligo. Both sexes are equally
affected. Family history is present only in about 25% cases. The disease commonly
begins at second to 4th decade of life.
Clinical features
A typical lesion is a well-defined de pigmented (milky white) macule, often
showing a variable number of depigmented hair and no change in skin texture. In
many cases the margin is hyper pigmented and in some may be inflammatory. Some
times a depigmented area surrounded by a comparatively hypopigmented zone is seen
to separate from normal skin by a thin hyper pigmented rim.
The number, size, shape and location of individual macules vary widely.
Frequently the intial macule occurs on exposed areas (such as dorsal surface of hand,
elbow, feet, legs, knees, neck and face), body folds (such as axilla, groin, and
submammary region in woman), lips and genitals. When the lesion occurs bilaterally
distribution is generally more or less symmetrical. The lesions get enlarged as if the
normally pigmented surrounding skin assumes a concave shape at the border.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 55
Common sites of vitiligo lesions include extensor bony surfaces such as peri orbital
region, sites of ankle, knees, elbows and peri orificial areas. The peri tibial region is
the most commonly affected site in India.
Achromotrichia is a common feature of vitiligo lesions on hairy parts. The number of
such hairs varies and it is rare to find all the hairs white uniformly over a macule.
Some cases show localized vitiligenious macule with a variable degree of eczematous
reaction resembling chemical leucoderma, but new lesions may develop elsewhere.
Koebner‟s phenomenon is often observed in vitiligo vulgaris. Minor trauma, such as a
scratch mark, laceration or stiches on the skin, results in development of a
corresponding linear depigmented macule, within 2 – 4 weeks.
Types of vitiligo
1. Vitiligo vulgaris / Nondermatomal vitiligo:
In this form of vitiligo widespread and symmetrical patches involving
extremities and trunk are found. Common sites include skin of forearm, palms,
soles, elbows, knee, lips, eyelids, upper trunk, genitals, axilla and groins. The
other types of vitiligo vulgaris are
a. Acro-orificial - it involves acral area like fingers, toes, palms, soles and
periorificial areas like lips, perioral, peri ocular and glans penis.
b. Vitiligo universalis – Total or near total affection of the whole body will be
present
c. Lip tip subtype – here lesions are restricted to the lips and the distal part of
fingers and toes.
d. Some time static lesions distributed at distant sites are seen.
2. Vitiligo pseudosegmentalis / Viltiligo Zosteri formis / Dermatomal /
Segmental
Here patches are limited to the region of one or two nerve segments.
Vitiligo focalis where patches are seen over one region of the body is a sub type of
dermatomal type or it may be a variant of non-dermatomal type.
In few cases both typical dermatomal lesions and vitiligo vulgaris like scattered
lesions are seen.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 56
Types based on prognosis
1. Active progressive stage (V1) – New lesions developing, increasing in size
and border ill defined.
2. Quiescent / Stable (V2) – Lesions are stationary in size and have well defined
hyper-pigmented border with no development of new lesions.
3. Improving (V3) – The size of the lesion decreases with well defined border
and signs of spontaneous repigmentation is seen. No new lesions develop.
Involvement of other pigment epithelium:
Various ocular abnormalities chiefly involving retinal pigment layers have
been noted among many vitiligo patients. In retina two pigment layers that is the inner
pigment epithelium adjacent to neuro retina and outer choroids show evidence of
destruction of pigment cells giving the retina a tigroid appearance. Following
destruction of the choroids there may be reactive proliferation of glial cells resulting
in yellowish discoloration of retina. In some patients of vitiligo rapidly progressive
chorio retinitis markedly impairs the visual activity. Dilution of retinal pigment due to
healed choriod retinitis may be detected.
Associated skin disorders:
It includes canitis, alopecia areata, atopic eczema, psoriasis, scleroderma,
Lichen planus, and Lichen simplex, halonaevus and icthiosis vulgaris. The
significance of this association is not well understood it appears to be more than
coincidental.
Course of the disease:
It is unpredictable and uncertain, most often shows slow progression. Lesion
in psedo segmental type remains static for an indefinite period after a certain degree
of regional extention. Vitiligo vulgaris lesions develop on different areas in
succession with varying rapidity. In some extension of individual lesions and
development of new lesions at different sites take place in episodic bouts.
Many lesions remain static for an indefinite period or show some degree of
spontaneous regression with development of pigment spots, others may show
repigmentations of some lesions, extension of others and appearance of new lesions at
other sites simultaneously. Some times the lesions disappear but may again reappear.
Residual depigmentation may be left behind after repigmentation of a large macule.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 57
EXAMINATION OF SKIN
Examination of skin plays a very important role in the diagnosis of switra.
Examination is carried out as follows.
Darshana pareeksha:
By inspection following factors are to be noted.
1. Distribution and arrangement of patch – Areas where the patch is located is
noted and whether the patch is generalized or localized, whether the patches
are symmetrical or asymmetrical and the exact location of the patches whether
it is present over exposed area scalp region, hand, extensor or flexor aspect
etc. are noted.
2. Morphology of the patch
– By naked eye examination also morphology can be explained. If the patch is
an early primary lesion the help of magnifying glass is needed.
– Shape and size: These factors are noted, as the shape of the patch is oval or
irregular or rectangular and size of the individual patch.
– Color: It is a very important factor whether the patch is pure white,
erythamatous or pinkish. In ayurvedic view, the color of the patch depends
upon doshic involvement and is noted as aruna varna, tamra varna, swetha
varna.
– Margins: Margin of the patch is inspected to know whether it is hyper
pigmented or inflamed.
Sparshana pareeksha:
This pareeksha is carried out to know the rooksha, snigdha etc. qualities of the
patch, that is to say the extent of the patch, temperature of the patch and to see any
elevation in the patch. Tests to know about the sensation of the patch are very
important which are as follows.
i. Pin and needle prick test: This test is done to know the deep and
superficial pain sensation.
ii. Hot and Cold touch test: This is to test the hot and cold sensation in
the patch.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 58
Special investigations:
Wood’s lamp examination:
Diagnosis of vitiligo is made by inspection with wood‟s lamp. Ultra violet
light of 356 nm wavelength is obtained by passing the beam through a wood‟s filter
composed of nickel, vitiligo patch appears milky white.
Skin biopsy:
Skin biopsy will show absence of melanocytes and melanin in the affected
area.
Differential diagnosis of vitiligo:
Most patients presenting with the complaint are worried about the diagnosis of
leprosy and vitiligo, hence sypmpethetic attention and careful assessment of this
complaint are essential. The diseases considered for differential diagnosis are
- Vitiligo
- Albinism
- Naevus depigmentosus
- Leprosy
- Petiriasis versicolor

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 59
Table No. 14 Differential diagnosis of vitiligo
Sl.
No
Distinguishing
features
Albinism Navus
depigmentosus
Vitiligo Leprosy Pitiriasis versicolor
1 Age Congenital Congenital Acquired Acquired Acquired
2 Distribution Complete/ partial Unilateral Any area Any area Trunk, neck and face
3. Course Stationary Stationary Progressive Progressive Progressive, worse in monsoon and
summer when sweating occur.
4. Hyper pigmentory
border
- - Present Inflammatory -
5. Heredo – familial Hereditary Non hereditary - - -
6. Other features Hairs and eyes may be
affected
- Hairs may be
affected
Anesthesia,
thickened nerves
Furfuraceous scaling, pin head
macules and large patches of
microscopic examination

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 60
Pathology of vitiligo:
In vitiligo there is a marked absence of melanocytes and melanin in epidermis. Exact
pathogenesis is not fully elucidated, but some theories are explained.
1. Immune hypothesis:
Primarily there may be some kind of biochemical trauma to melanocytes
resulting in release of some antigenic substances and subsequent auto
immunization. Alternatively there may be certain immune cells directed against
certain antigenic components of autologuse melanocytes. The circumstantial
evidence for this hypothesis is frequent association of vitiligo with many
autoimmune disorders.
2. Neural hypothesis:
This hypothesis theorizes that destruction of melanocytes occur as a
consequence of liberation of some unusual neurochemical mediator or due to
gross alteration in ratio of normal neurotransmitter substances in the lesion. Study
of electron microscopy shows abnormality of terminal portion of peripheral
nerves.
3. Auto toxic, self destructive or Free radical hypothesis:
The recent hypothesis tells that an intermediate metabolite of melanin
synthesis cause destruction of melanocytes or the normal process of melanosome
destruction proceeds unabated to cause melanocyte death. This theory is based on
an experimental study on cutaneous de-pigmentation by chemical compounds that
have selective lethal effect on functional melanocytes.
4. Melanocytes growth factor reduction hypothesis:
It has been proposed that de-pigmentation in vitiligo might be due to
reduced local and circulating levels of growth factor which is necessary for the
normal proliferation and maintenance of Melanocytes i.e. M.S.H.
Prognosis of vitiligo:
The prognosis is unpredictable and unsatisfactory. There is no indicator of a good
prognosis. Following are the factors, which lead to poor prognosis.
1. Lesion on the resistant sites such as bony prominences, non-fleshy areas, non-
hairy areas and mucosal areas. They comprise the sides of the ankles, front of

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 61
the wrists, back of the elbows, dorsum of feet and hands (specially the
knuckles), palms, soles, nipples, areola, lips and genitals.
2. The greater the percentage of associated white hair, the worse the prognosis.
3. Persistent friction or itching on the affected areas.
4. Emotional liability and psychic turmoil of the patients.
5. If it is associated with systemic ailments.
6. If herido – familial background is present.
7. Old age.
8. Iatrogenic factors, including injudicious administration of topical or systemic
medicines, particularly photo chemotherapeutic agents.
Management of vitiligo:
In the absence of clear understanding of etiopathogenesis there is no ideal
treatment.
Principles of treatment are as follows
V1 stage – Correct the cause and give nutritional supportive therapy
V2 stage – Give specific treatment of vitiligo orally and topically.
V3 stage – If no further improvement with V2 treatment, adopt surgical treatment.
Treatment of vitiligo can be mainly divided under
1. General aspects
2. Specific
3. Surgical
4. Cosmetic Camouflaging
5. Bleaching
General:
Explanation of the nature of the disease, its unpredictable course, prognosis
and reassurance is given to the patient. Educating the patient regarding the good
general health and balanced nutritious diet enriched with adequate good quality
protein specially the phenylalanine and tyrosine, vitamins B complex and E and
minerals such as copper, zinc and iron.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 62
Patients are instructed to avoid physical, chemical and emotional trauma as far
as possible and also avoidance of soap, detergents containing phenolic compounds
and rubber goods.
Specific:
It can be given orally and topically.
Systemic:
Ammeimajus (meladinine-p), Psoraliacorylifolia (seeds), Psoralin, Meosoralin
or Macsoralin one tablet contains 10 mg active substance ammidin and Ammodin and
the daily dose is 10 – 20 mg. It should be followed by expoture to sun 2 hours later.
To achieve this, it is preferable to take the dose early in the morning.
Side effects:
A sense of heat in the body, nervousness and some times hypertension,
giddiness and an allergic eczematous reaction is seen. If the side effects are mild the
drug can be continued in small doses.
Local:
Local ammimajus or psoralin ointment, Croton oil babchi (Psoralia cardifolia),
or bergamot oil locally.all these have photosensetizing action. They produce erythema
and at times blisters, which are more common in those, who have not taken systemic
psoralins previously. When this occurs further application should be stopped and
soothing lotion or cream should be prescribed. Later it it can be used in a diluted form
and less frequently.
A cream containing 10% para amino benzoic acid is applied to the normal skin
surrounding the vitiligo patches; particularly the face, before the paint is used or
irradiation is given. This helps to avoid disfiguring hyper pigmentation of the border
areas.
Treatment using a combination psoralin derivities or any other
photosensitizing agent orally or topically, followed by irradiation with long wave ultra
violet light (320 - 400 wavelength) constitutes photo chemotherapy, the predominant
modality of treatment for vitiligo. Photosensitization induced by the psoralin group of
drugs in conjunction with long wave UV rays irradiation from an artificial source is

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 63
called PUVA therapy, when sun exposure is utilized as a source of UVA it is called
PUVASOL therapy
Corticosteroids: With the current inclination of viewing vitiligo as auto immune
disorder a number of corticosteroid preparations in different forms and routes (topical,
intralesional and oral) have been used in last 3 decades with encouraging results.
Surgical treatment: it includes
Thin thiersch grafting – Thin split thickness grafts are performed in cases
with long standing quiescent lesions, ranging from 6 – 100 cm2 in area.
Epidermal grafting – Normally pigmented epidermis is separated from the
dermis of the donor site by suction blistering of the skin at a negetive pressure
of 200 mm of Hg.
Mini grafting – implanting small punch grafts 3 – 4 mm apart with in minute
beds perforated in the depigmented recipient area forms mini grafting. It has
been noted that pigment cells proliferate and migrate from the mini grafts in to
adjacent achromic skin.
Transplantation of vitro cultured epidermis-bearing melanocytes.
Cosmetic camouflaging:
Suitable cosmetic preparations like silver nitrate or potassium permanganate
solutions in variable strengths help the patient by mashing the achromic macules.
Bleaching:
In extensive vitiligo with scattered pigmented islands of skin and with out any
hope of recovery, removal of the remaining pigment to give the skin a uniformly
white appearance may be cosmetically desirable.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 65
DRUG REVIEW
Ayurveda considers Oushadha as one of the four essential
components for maintaining health. The drug which is rich in pharmacological
activities, which could be made into various forms of medicaments, having specific
therapeutic action and available in plenty are praised by the legendaries of science.
Ample of references are available in the classics regarding the wonders a good drug
can produce as well as the ill effects an improper drug can create. The combinations
of medicines described in the textbooks of Ayurveda are the products of thorough
analysis and clinical trials. Many of them indicated in the context of various disorders
are able to work both in the curative as well as preventive perspective.
The drugs that were used in the study are -
1) Aragwadha phalamajja
2) Apamarga Kshara
3) Jyotishmati Taila
4) Tila Taila
Aragwadha
Botonical name: Cassia fistula
Family: Caesalpinioideae
Kula: Shimbikula
Gana: Kustaghna, Kandughna,
Tikthaskanda, Virechana (Charaka)
Aragwadhadi, Shyamai, Sleshmasamshamana,
Adhobhagahara (Sushrutha)
Aragavdhadhi, Shyamadi (Vaghbata)
Rasa: Madhura and Tikta
Guna: Mrudu, Guru, Snigdha
Veerya: Sheeta
Vipaka: Madhura
Doshaghnata: Kapha Pittahara
Karma: Sramsana

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 66
Chemical composition:
Seeds: Sugar, Glactomannan.
Flowers: Fistuline, Leucopelargonidin, Tetramen
and Haempherol.
Pods: Fistulic acid.
Bark and heart wood: Barbaloin, Fistucalidin and recine.
Leaves: Rhein, Sennosoids A and B.
The aqueous extract of the fruit pulp has significant purgative action.
Purgation action is maximum in 6 – 9 hours and lasts for 24 hours as per research.
Useful parts: Phalamajja, Roots, Leaves, Flowers, Bark, Seeds.
Dosage:
Phalamajja: 5 –10 grams
For Virechana – 10 – 20 grams
Moola Twak Kwatha: 50 – 100 ml
Mode of action:
The recommended dose in the present study was Aragvadha Phalamajja
Kashaya prepared with 20 grams of Aragvadha phalamajja. By the presence of Prithvi
and Aap mahabhootha in Aragwadha the doshas will be made to pass through the
Guda. Vata, Mala, Pitta, Udaka and Kapha are excreted by Sramsana respectively.
Aragwadha contains gluten a glycoside, which produces the purgative action.
Apamarga
Botanical name : Achyranthes aspera Linn.
Family : Amaranthaceae
Kula : Apamarga kula .
Gana : Shirovirechana, Krimighna, Vamanopaga [ Charaka],
Arkadi [Suhshruta]
Rasa : Katu, Tikta
Guna : Laghu, Ruksha, Tikshana
Veerya : Ushana
Vipaka : Katu
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 67
Doshaghanta : Kapha – Vata shamaka
Kapha – Pitta samshodhaka
Karma : Deepana-pachana, Krimighna, Rocana, Sangrahi,
Pittasaraka, Pittasamshodhaka
Chemical Compositions :
The plant ( whole herb ) and seeds contain alkaline
substance specially potash
Synonyms:-
Dhamargava, Mayuraka, Pratyak parni, Pratyak puspha , Keeshavalli,
Kinihi, Kharamanjari, Adhahasalya , Durgraha Shikari, Mayurashikhi , Aghata.
Kannada Name:- Uttarane.
English Name:- Choff tree [ prickly chaff flower ]
Hindi Name:- [ Chichidi] , Chirhita, Chirachita, Chichrha.
Bengali Name :- Apang.
Telugu Name:- Apamargam.
Punjabi Name :- Puthakanda
Marathi Name :- Aghada
Classical categorization :-
Charaka- Sirovirecanopaga, Krimighna, Vamanopaga
Sushruta- Arkadi Vagbhata- Arkadi
Botanical Description:-
Annual or perennial herbs , 30-90 cm tall, often with a woody base
stms simple or branched from the base, often tinged with reddish, purple, ribbed,
visceral pubescent. Obtusrly 4 amgled , leaves varieable, ovate – elliptic or obovate –
rounded plant is very variable in habit. Degree of hairness, size & shape of leaves &
length of spikes flowers greenish white, numerous, in axillary or terminal spiks , seeds
subcylidrical, truncate at the apx. Round at the base, reddish brown.throughout India ,
plant is found as a waste places roadsides, hedgs, gardens, fields or farms.
Part used:- whole plant [ panchanga]
Pharmacodynamics:- [Ayuvedic]
Rasa:- Katu, Tikta..
Guna:- Laghu, ruksha, Teekshna.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 68
Veerya:- Ushna.
Vipaka:- Katu.
Doshaghnata:- Kaphavatashamaka, Kaphapitthasamshoshaka.
Rogaghnata:-
Netraroga, Vrana, Vrishchikadashana, Sarpadansha, Karsnashoola,
Pama,
Aruchi, Chardi, Agnimandhya, Udararoga, Shoda,Adhmana, Arsha, Pittashmari,
Krimi, Hridroga, Raktavikara, Pandu, Gandamala, Amavata, Shosha, kasa shwasa &
in charma rogas.
Doses:-
Juices: - 10-20 ml
Root powder: - 3/ 6 gm.
Seeds: - 3gms
Kshara: [water soluble extract of ash] – ½-2gm.
CHEMICAL CONSTITUTES:-
Ecdysene, ecdysterone, inokosterone, oleanolic acid and glycoside from
roots, Saponin A & B from seeds along with hentriacontane, two new Saponin C& D
and oleanolic acid based Saponins from fruit alkaloids achyranthine and betaine from
the whole plant are reported.
MODE OF ACTION : -
Apamarga has Katu-Tikta Rasa, Katu Vipaka, Ushna Virya and Rakta-
Pitta Prasadanakara action. So it may help in proper functioning of Bhrajaka Pitta.
KSHARA KARMA:-
Historical review:
Prevedic & Vedic period: - No relevant references are available.
Samhita Period: -
Various references of Ksharas are found in the Samhitas with detailed
description about the preparation and usage of the same, both internally and externally
in various diseases.
Sushruta says that Kshara is superior to Shastra and other Anushastras
because of its unique functions like Chedana [excision] and Bhedana [incision]
karmas, relieving the derangement of tridoshas etc.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 69
According to Vagbhata, Kshara is a very good substitute for surgical
operations and they do the function of Chedana and Bhedana in the delicate areas and
diseases where the Shastras can be used with difficulty or in those diseases where
Shastra karma is not possible.
Kshara may be used in very difficult cases very liberally. Charaka has
dealt in detail about the internal uses of Kshara than its external uses. In Bhela
samhita, we find the usage of kshara internally as well as externally, particularly in
arsho chikista where he describes about the application of pratisaraneeya kshara after
surgical excision of arshas.
In Kashyapa samhita, Dwivraneeya chikitsadhyaya, author describes
about the applicaton of ksharasutra in the disease “arakeelika”. In Madhavanidana,
Sharangadara Samitha, Yogaratnakara and other literatures of Ayurveda, likewise
description about Kshara is found.
MODREN PERIOD:
Kshara is being used extensively n therapeutics and as well as in clinical
studies in the management of diseases like Arshas, Bhagandara , Vrana, Charmakeela,
Kadara etc. In morden medicine, alkalies and caustics which can be considered as
kshara are being used both internally and externally in various diseases. The
application of caustic chemicals to the tissues can be used to the advantage to treat
certain lesions.
VYUTPATTI
The word “Kshara” is derived from the root “Kshar” which means “to
melt away” or “to perish away”. The morden equivalent term for kshara is alkali or
caustic. The term „alkali‟ is derived from an Arabic word “aquili” which means
“substance derived from the ash”. The word caustic is derived from the Greek word
“Kaushitcos” which means “to burn”.
According to Monnier Williams Dictionary, Kshara: melt away,
perishable. In Amarkosa, Kshara has been used in the sense of “Kacha”; it may also
mean „Chapala‟ Rasa. “Kacha” is derived from the root meaning to fasten or to shine.
Kshara also means “ash”.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 70
NIRUKTI
Kshara is defined as that which moves or melts. Acarya Sushuta has
defined Kshara as- Tatra ksharanad kshananadva kshara : means which cleans the
excessive morbid doshas and which destroys the skin or tissues.[Dalhana teeka :
ksharanad twangmamsadi chalanat shatanat ] Kshanana means to make ksheena or to
destroy by reducing.
Charaka defines Kshara as the one which, because of its corrosives nature,
scrapes away the abnormal tissues form its locations and drags it down after
dissolving.
Many more authors have given similar definition for Kshara.
Paryayas of Kshara:-
1. Kaach 2. Bhasma 3. Guda 4. Dhatu dravaka 5. Sarja kshara
6. Dhusara 7. Lavana 8. Modini 9. Soubhagyam 10. Tankanam
IMPORTANCE OF KSHARA:-
Kshara is an alkaline substance obtained by processing the ash of drugs.
They are considered as Anushastras because of various actions like Chedana, Bhedana
etc., even in the absence of shastras. Kshara has been deemed to be superior to
shastras & anushastras because of its actions as said above i.e., Chedana, Lekhana and
alleviation of tridoshas and also being used for specific functions. Kshara is that
which cuts off tvak , mamsadi, putrified tissues and removes the vitiated doshas.
Ksharanat – means by producing injury in skin, muscle etc. Kshara derived from the
drug possesses various properties like – it is Sarva rasayukta, Katu, Lavana rasa
pradhana etc. Due to Teekshna & Ushna guna, it has many functions such as Dahana,
Pachana, Vidarana and Vilayana, and also does Shodhana & Ropana karma. By the
action & it rest the purified issued by carrying it down disintegrating the vitiated
twak, manasadi tissues. Ksharas serves the purpose even in the shastras & where
shastra chikitsa is contraindicated & fit to be used in places where sharp instrument
can be used with difficulty such as nasa arsha &arbudha , where treatment with sharp
instrument does not succeed & in diseases by ati prakupita doshas. Anushastras are
bamboo, quartz , kacha , kuruvinda, leeches , agni, nail, leaves of gojihva ,
sphephalika & shaka, sprints, hairs & Anguli. Apamarga & Chitraka plant kshara was
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 71
prepared acc. to the procedure mentioned in the classics by our acharyas. The
principle behind the preparation of kshara was based as pr the need of the study
required for clinical trial.
Classification of Kshara :-
1. On the basis of administration :-
a) Pratisaraneeya Kshara – External application.
b) Paneeya Kshara – Internal application.
Acarya Vagbhata opines the same by considering them as
a) Bhaya Parimarjaneeya.
b) Antah parimarjneeya.
2. On the basis of Concentration:-
a) Mrudu Kshara.
b) Madhyama Kshara.
c) Teekshna Kshara.
3. On the basis of Origin:-
a) Vanaspatijanya – Herbal.
b) Pranijanya – Animal.
c) Khanijajanya – Mineral.
4. According to season of preparation:-
a) Uttama – prepared in Greeshma Ritu ( Summer )
b) Madhyama – prepared in Sharad Ritu ( Winter )
c) Adhama – prepared in Varsha Ritu (Rainy )
5. The Paneeya Kshara is also further classified on the basis of Kshara Varga:-
a) Kshara Dwaya.
b) Kshara Traya.
c) Kshara Panchaka .
d) Kshara Ashtaka.
Pratisaraneeya Kshara :-
The tem Parteesarana is used to denote healing or dressing the edges of
a wound or an instrument used for anointing a wound.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 72
Classical Method of Preparation of Pratisraneeya Kshara:-
Acharya Shushruta has dedicated the whole of 11th chapter of Sutra
Sthana to describe Kshara. After review in all the classical texts, Sushruta‟s maneuver
seems to be ideal regarding the preparation of Pratisaraneeya Kshara.
The physician who prepares the Kshara should have a clean bath in the
morning of Sharad Ritu in an auspicious day. He fasts that day & goes up the hills &
looks for such plants which are middle aged and free from insects. The panchangas of
such plants are collected, dried up & made into small pieces. Then these are burnt
with limestone. While burning, the dispersed parts of the plants are kept with the help
of tilnala. When the ash cools down it should be mixed well with six times of water or
cow‟s urine , then filtered twenty one times in a big vessel through a piece of cloth.
The residual portion is thrown away and the filtrate ( Ksharodaka) should be kept on
mandagni and continuously stirred well until it turns reddish brown and attains
picchilata or get reduced to 1/3 rd . If this is heated till powder form, Mrudukshara is
obtained. If not then, from the ksharodaka eight palas has to be taken and mixed with
Shankanabhi, Shukti and Kata sharkara, each in eight palas, to make Prativapa. In the
meantime, heating should be continued and prativapa should be mixed. Care should
be taken that it is not too liquid nor too dried up. The solution thus obtained is known
as Madhyama Kshara. Madhyama Kshara should be heated up again by adding some
medicinal plants such as danti, chitraka etc., with this a thick solution is obtained
which is known as Tikshna Kshara. If Tikshna Kshara loses its potency then it should
be mixed new kshara and heated again to maintain sufficient concentration.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 73
Table No. 15: Plants which are mixed to Mridu Kshara to make it Madhyama
Kshara:-
Sl. No. Sanskrit Name Source
1 Bhasma Sarkara Secreted drops from plant edges
during burning became solid form.
2 Kata Sharkara or Sudha
Sarkara
Unburnt , semi burnt pieces of
limestone (CaO )
3 Shukti Animal product
4 Sankha Nabhi Animal product (CaCo3)
Table No.16: Medicinal plants which are mixed to make Madhyama to Tikshna
Kshara:-
Sl.
No.
Sanskrit Name Latin Name Family
1 Danti Baliospemummontanum
Muell
Euphorbiaceae
2 Dravanti Crotontiglium Euphorbiaceae
3 Chitraka Plumbagozeylanica Linn Plumbaginaceae
4 Langali Gloriosasuperba Liliaceae
5 Hingu Ferulanorthax Bioss. Apiaceae
6 Vacha Acoruscalamus Linn. Araceae
7 Shukti Mytilusmargarferns Pearl ( Oyster)
8 Pravala Coralliumrubrum Animal product( CaCo3)
9 Bida lavana Navasada Mineral product ( NH4Cl)
10 Sauvarchala
Lavana
Rock Salt Mineral product (NaCl)
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 74
DANTI: -
Latin name:- Baliospemummontanum Muell.
Family:- Euphorbiaceae.
Rasa:- Katu.
Guna:- Guru, Teekhsna.
Veerya:- Ushna.
Vipaka:- Katu.
Doshagnata:- Kaphapitahara.
Karma:- Deepana, Shothakara, Vedana Shamaka.
DRAVANTI:-
Latin name :- Crotontiglium .
Family:- Euphorbiaceae.
Rasa:- Katu.
Guna:- Guru, Ruksha, Teekhsna.
Veerya:- Ushna.
Vipaka:- Katu.
Doshagnata:- Kaphapitahara.
Karma:- Deepana, Shothakara, Vedana Shamaka.
CHITRAKA:-
Latin name:- Plumbagozeylanica Linn.
Family:- Plumbaginaceaea.
Rasa:- Katu.
Guna:- Laghu, Ruksha, Teekhsna.
Veerya:- Ushna. Vipaka:- Katu.
Doshagnata:- Kaphavata shamaka, pittvardhaka..
Karma:-Lekhana, Deepana, Pachana.
LANGALI:-
Latin name:- Gloriosasuperba.
Family:- Liliaceae.

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 75
Rasa:- Katu,Tikta.
Guna:- Laghu, Teekhsna.
Veerya:- Ushna.
Vipaka:- Katu.
Doshagnata:- Kaphavata shamaka.
Karma:- Deepana, Balya, Rakta, Shodhaka.
HINGU:-
Latin name:- Ferulanorthax Bioss.
Family:- Umbellliferae.
Rasa:- Katu .
Guna:- Laghu, Snigdha , Teekhsna.
Veerya:- Ushna.
Vipaka:- Katu.
Doshagnata:- Kaphavata shamaka, pitta vardhaka.
Karma:- Deepana, Vedana sthapana, pachana.
VACHA:-
Latin name:- Acoruscalamus Linn.
Family:- Araceae.
Rasa:- Katu, Tikta.
Guna:- Guru, Teekhsna.
Veerya:- Ushna.
Vipaka:- Katu.
Doshagnata:- Kaphavata shamaka, pitta hara.
Karma:- Shotahara, vedana shamaka, arshoghna.
SHUKTI (Pearl Oyster):-
Latin name:- Mytilusmargarferns
Rasa:- Madhura.
Guna:- Kshareeya.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 76
Veerya:-Sheeta.
Vipaka:- Mdhura
Doshagnata:- Raktapitta nashaka.
Karma:- Deepana, Shulahara, Udara roga nashaka.
PRAVALA (Coral, Calcium Carbonate, CaCo3):-
Latin name :- Coralliumrubrum
Rasa:- Kshareeya.
Guna:- Sheeta.
Veerya:-Sheeta.
Vipaka:- Mdhura
Doshagnata:- kaphavatanashaka, raktapitta shamaka.
Karma:- Deepana, pachana, Balya.
SOUVARCHALA LAVANA:-
Latin name:- Unaqua Sodium Chloride.
Rasa:- Lavana.
Guna:- Teekshna.
Veerya:-Ushna.
Vipaka:- Madhura.
Doshagnata:- Kaphavata shamaka.
Karma:- Agnideepaka, Virechaka.
VIDA LAVANA: -
Mineral product ( NH4Cl)
Rasa:- Lavana.
Guna:- Kshara, Teekshna.
Veerya:-Ushna.
Vipaka:- Madhura.
Doshagnata:- Kapha shamaka, Vatahara.
Karma:-Vatanulmana, Deepana, Vibandha hara..

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 77
Table No.17: Medicinal Plants useful for the preparations of Mridu Kshara as
prescribed in Shushruta Samhita:-
Sl. No. Sanskrit Name Latin Name Family
1 Apamarga Achyranthus aspera Linn Amaranthaceae
2 Kutaja Holarrhena antidysentrica Apocynaceae
3 Paribhandra Erythrina indica Lamk Fabacesea
4 Asva Karna Dipterocarpus turbinatus gaertn.f. Dipterocarpaceae
5 Vibhitaki Terminalia bellerica Roxb. Combrataceae
6 Aragvadha Cassia fistula Linn Caesalpinoidea
7 Tilvaka Seasamum indicum DC Pedalianceae
8 Arka Calotropis gigantean(l.) Dryand Asclepiadaceae
9 Snuhi Euphorbia neriifolia Linn Euphorbiaecae
10 Palasha Butea monosperma (Lam.) Kuntz. Fabaceae
11 Nakramala Pongamia pinnata (Linn.) Merr. Fabaceae
12 Vrisa Adhathoda vasica Nees Acanthaceae
Properties of Kshara:-
Rasa:- Katu.
Virya:- Ushna.
Varna:- Shukla.
Guna:- Sowmya, Tikshna, Agneya.
Doshagna:- Tridoshagna.
Karma:-
Dahana, Pachana, Darana, Vilayana, Shodhana, Ropana, Sthambak ,
Lekhana.
Prepared Kshara, being a composite of many drugs alleviates the three
doshas. Being white in colour it is plain. In spite of placidity, its actions like
cauterizing, digesting and splitting is carried out as it is made of drugs having the
property of pungent, hot, sharp, digestive and suppurative. When used, it is cleansing,
heating, absorbant and scarping. When used internally, it destroys Krimi, Amadosha,
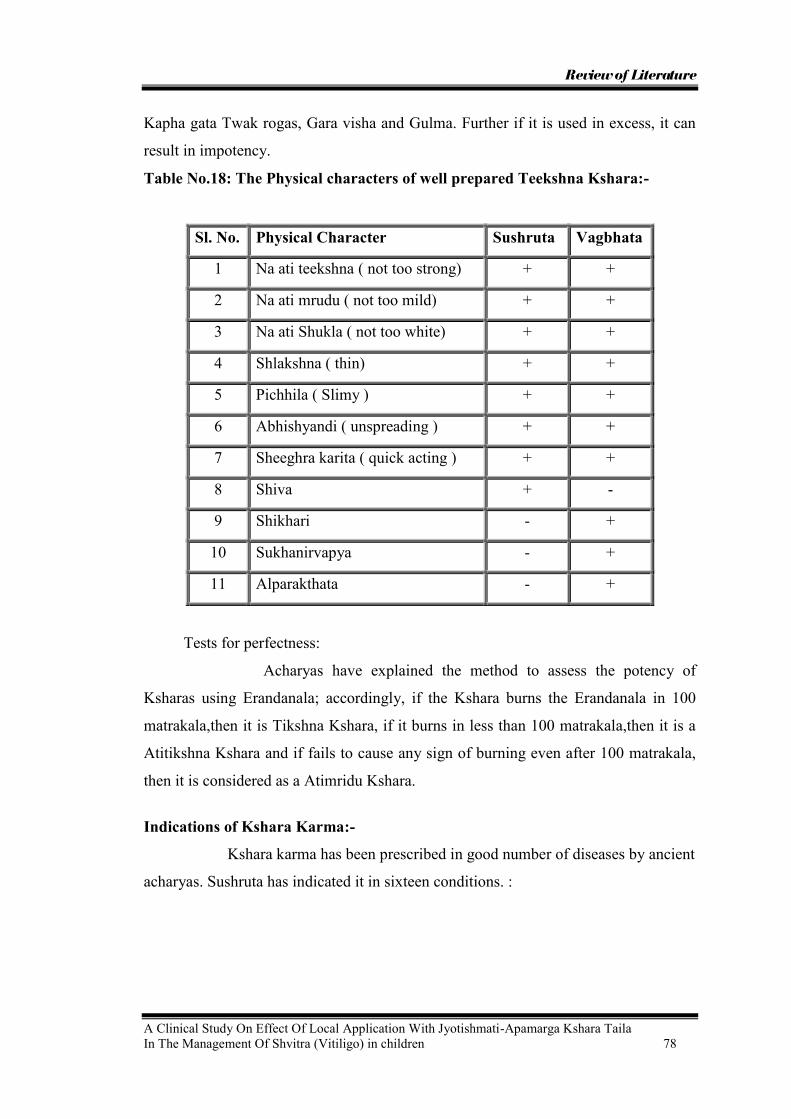
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 78
Kapha gata Twak rogas, Gara visha and Gulma. Further if it is used in excess, it can
result in impotency.
Table No.18: The Physical characters of well prepared Teekshna Kshara:-
Sl. No. Physical Character Sushruta Vagbhata
1 Na ati teekshna ( not too strong) + +
2 Na ati mrudu ( not too mild) + +
3 Na ati Shukla ( not too white) + +
4 Shlakshna ( thin) + +
5 Pichhila ( Slimy ) + +
6 Abhishyandi ( unspreading ) + +
7 Sheeghra karita ( quick acting ) + +
8 Shiva + -
9 Shikhari - +
10 Sukhanirvapya - +
11 Alparakthata - +
Tests for perfectness:
Acharyas have explained the method to assess the potency of
Ksharas using Erandanala; accordingly, if the Kshara burns the Erandanala in 100
matrakala,then it is Tikshna Kshara, if it burns in less than 100 matrakala,then it is a
Atitikshna Kshara and if fails to cause any sign of burning even after 100 matrakala,
then it is considered as a Atimridu Kshara.
Indications of Kshara Karma:-
Kshara karma has been prescribed in good number of diseases by ancient
acharyas. Sushruta has indicated it in sixteen conditions. :
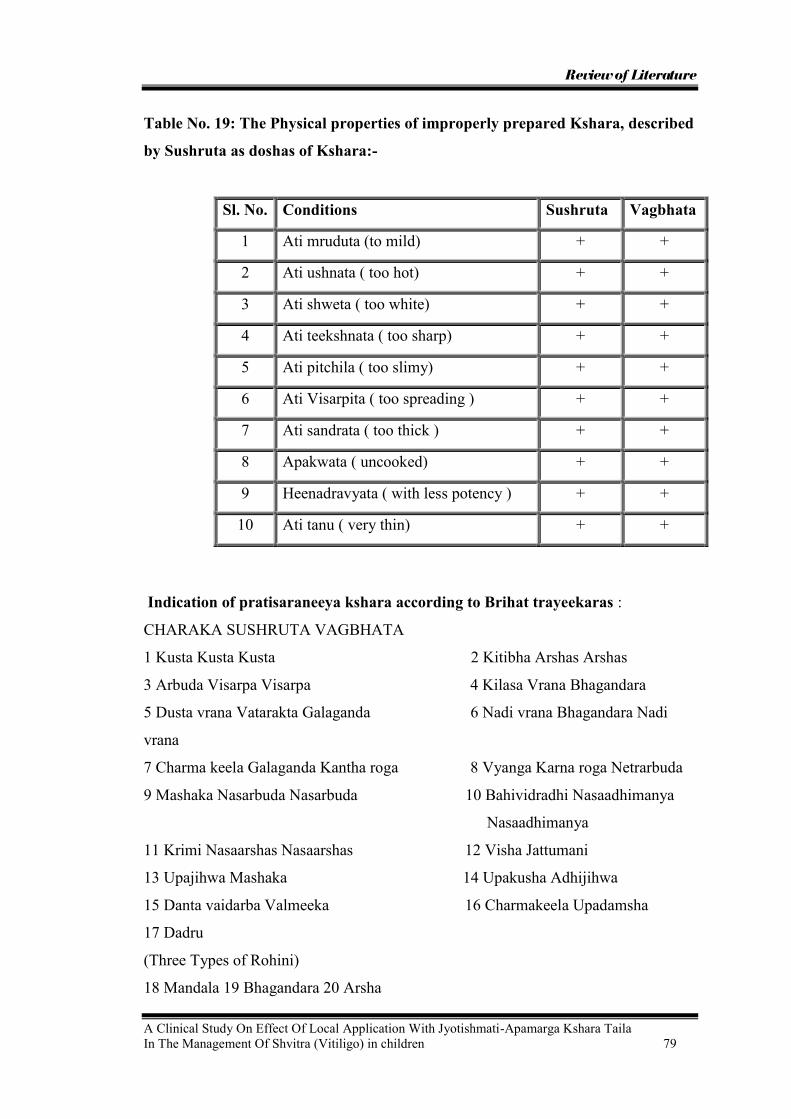
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 79
Table No. 19: The Physical properties of improperly prepared Kshara, described
by Sushruta as doshas of Kshara:-
Sl. No. Conditions Sushruta Vagbhata
1 Ati mruduta (to mild) + +
2 Ati ushnata ( too hot) + +
3 Ati shweta ( too white) + +
4 Ati teekshnata ( too sharp) + +
5 Ati pitchila ( too slimy) + +
6 Ati Visarpita ( too spreading ) + +
7 Ati sandrata ( too thick ) + +
8 Apakwata ( uncooked) + +
9 Heenadravyata ( with less potency ) + +
10 Ati tanu ( very thin) + +
Indication of pratisaraneeya kshara according to Brihat trayeekaras :
CHARAKA SUSHRUTA VAGBHATA
1 Kusta Kusta Kusta 2 Kitibha Arshas Arshas
3 Arbuda Visarpa Visarpa 4 Kilasa Vrana Bhagandara
5 Dusta vrana Vatarakta Galaganda 6 Nadi vrana Bhagandara Nadi
vrana
7 Charma keela Galaganda Kantha roga 8 Vyanga Karna roga Netrarbuda
9 Mashaka Nasarbuda Nasarbuda 10 Bahividradhi Nasaadhimanya
Nasaadhimanya
11 Krimi Nasaarshas Nasaarshas 12 Visha Jattumani
13 Upajihwa Mashaka 14 Upakusha Adhijihwa
15 Danta vaidarba Valmeeka 16 Charmakeela Upadamsha
17 Dadru
(Three Types of Rohini)
18 Mandala 19 Bhagandara 20 Arsha

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 80
Containdications of Kshara Karma :-
Before the application of Kshara it is necessary to observe the fitness
of the patient, contraindications of Kshara can be classified into following groups:-
According to diseases –
Jwara, Hrudroga, Shiraroga, Panduroga, Arochacaka,
Sarvangashopha, Raktajagulma, Udararoga are contraindicated in general.
According to physical & mental state of the patient –
Children, Phobic people , Aged, Menstruating women , Pregnant women
, Physical weak persons.
According to sites –
Arteries, Joints, Vital parts, Cartilages, Veins, Ligaments, Throat,
Umbilicus, Penis, Insufficient musculature, Nail bed, Testis, all parts of the eye
expect eye lid.
According to seasons –
summer, autumn and cloudy weather are contraindicated. The above
contraindications are applicable for both Paneeya & Pratisaraneeya Kshara.
Apart from these, few anatomical sites and some diseases may also be
fit for contraindications of Pratisaraneeya Kshara. Excessive use of Kshara leads to
Pumsatva Upagatha. Charaka said Kshara helps in digestion but excessive use of it
causes impairment of vision. Vagbhata described that due to Katurarsa , Kshara is
injurious to Hridaya, Kasa, Chakshu, Ojus and Shukra. Further Shushruta has
observed that Kshara may be ineffective in Kshara sadyavyadhi also if it is
complicated by edema, pain in the bones , aversion for food, pain in precardial region
and joints . However, external application of Apamaraga Kshara is indicated in
children, weak persons and Decrepit.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 81
UNSUITABLE SITES FOR KSHARA KARMA :-
Khhara should not be appliend on marma, sira, snayu, asthisandhi,
tarunasthi, sevani, dhamani , gala, nabhi, nakhantara pradesha, mushka, shepha srota,
alpamamsa pradesha and netra (except in vartma rogas).
CAUTION WHILE USING KSHARA :-
When the Kshara is applied by a less intelligent person, it acts like a
poison, fire, sharp instrument, lightning and thunder and causes death.
SIGNS OF SAMYAK DAGDHA LAKSHANAS:-
When the kshara has been properly applied, the disease gets relieved,
the patient feels comfortable and cessation of discharge occurs.
SIGNS OF HEENA DAGDA LAKSHANAS:-
When the kshara application is inadequate, features of pain, irritation,
heaviness and aggravation of disease occur.
SIGNS OF ATIDAGDHA LAKSHANAS:
When there is excessive application of Kshara, there is burning
sensation, inflammation, reddish discolouration, discharge, body ache, fatigue, thirst,
fainting or even death.
Chemical Composition of Kshara:-
Prof. A.R. Vasudeva Murthy, describes the chemical composition of
Kshara in his Indian tradition of Chemistry & Chemical technology , as follows:
The wood ashes contain Potassium & Sodium Carbonate ( K2CO3&
Na2CO3 ). Limestone & sea shells contain Calcium carbonate ( CaCO3) . On heating
strongly carbonate decomposes into calcium oxide ( CaO ) , quick lime and carbon
dioxide ( CO2) escapes into the air. Calcium oxide reacts with water vigorously and
with Potassium / Sodium carbonate gives rise to Calcium carbonate which comes
down as precipitate . Alkali hydroxide (KOH) remains in the solution which may be
concentrated in terms of the following equations
CaCo3 → CaO + CO2↑
1. CaO + H2O→Ca (OH) 2
2. K2CO3 + Ca( OH)2→2KOH + CaCO3

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 82
Drug Analysis :-
Apamarga Kshara :-
Description :- Fine powder , dull white in colour.
Odour :- Faint.
Taste :- saline.
Identification:- An aqueous solution yields reaction characteristic of Sodium and
Potassium.
Water soluble matter - 96-98 %
Water insoluble – 1.02%
Moisture content – 8.1%
Water insoluble organic matter (carbonaceous) – nil
PH – 12.2
Potassium content – 27.45%w/w
Sodium content – 20.83%w/w
Jyotishmati
Latin Name : Celastrus panniculatus
Family : Celastraceae
English Name : Black oil tree, climbing staff tree.
Hindi : Malkangani, Malkai, Malkamni.
Kannada : Gouri Kayi.
Synonyms-
The word synonym is the word identical or word denoting the same thing.
1. Jyotishmati- Jyoti = Bright, shining, Mati = Intelligence. In which the Jyoti
resides or that which brightens intelligence is Jyotishmati.
2. Peeta Taila - The seeds of Jyotishmati yields oil which is yellowish in color.
3. Kaakandaki- Fruit resembles the egg of crow.
4. Kanguni- It is Agnidepaka, Budhivardhaka and gives Sukha to body.
5. Vega- Spread very fast or it induces enthusiasm.
6. Others are Malkangi, Medhya, Pooti Taila, Swarna Lata etc.
Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 83
Distribution:
It is found in sub-Himalaya tracts and up to 6000 ft in central India and
province in India, It has spread from Jheleem to Assam and in eastern Bengal, Bihar
and Burma.
It is also seen in hilly parts of Bombay, South Gujarat and in Madras presidency.
Commonly occurs in all parts of Karnataka.
Habit:
A large deciduous climber with stem up to 23 cm diameter and 18 m height,
some times twining dexterously but more often rambling. Twigs fairly smooth,
reddish brown, densely covered with small elongate whitish lenticels. Bark pale
brown, rough with hallow cracks, exfoliating in small soft scales.Stem - 7.5- 10 mm
not fibrous, pink finely streaked with red or reddish brown, the juice turning blue on
the blade of a knife.Leaves - 6.3 - 10 by 3.8 - 7.5 cm, broadly elliptic obviate,
abruptly short- acuminate, crenate- serrate, rather coraicaous, glabrous, lateral nerves
arching. Petiole-7.5to15 mm long. Flowers - 3.8 mm diameter, in terminal drooping,
panicle 5- 20 cm long.Capsules - 1to 1.3 cm diameter, depressed- globose, 3- lobed,
bright- yellow, 3 - 6 seeds. Seeds completely enclosed in an orange - red aril.
Chemical Constituents
Seeds yield brownish oil (52.2%) with unpleasant taste. Oil contain
coloring matter, fat contains formic acid, acetic acid, benzoic acid. Fleshy aril yields
fat. Alkaloid celastrine, panicalatine.
Rasapanchaka
Rasa : Katu, Tikta
Guna : Tikshna, Snigdha, sara
Virya : Ushna
Vipaka : Katu
Dosa Karma : Snigda Ushana passify Vata and Kayu,Tikta and Ushana
passify Kapha .
Prabhava : Medhya

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 84
Samsathanika Karma –
On Nadi Samsthana Medhya, due to Ushana Guna improves grasping
power. And on Pachana Samsthan it does Deepana due to its Katu, Tikta and Ushana
Guna,Vata Anulomana due to its Snigdha,Ushana Guna.
Prayojyanga : Beeja and Beeja Taila.
Matra : Beeja = 1to 2 gm.
Beeja Taila = 5 to 15 drops
MODE OF ACTION :
Jyotishmati has Katu-Tikta Rasa, Katu Vipaka, Ati-Ushna Virya and
Pitta Santpakara action. Thereby it may enhance the proper formation of Bhrajaka
Pitta in Tvak.
Method of oil extraction
The fresh seeds of Jyotishmati are taken and dried in sun light. All the
impurities is taken out and then subjected for oil extraction. Method used for the oil
extraction is by crushing the seeds in an electric fitted crusher.
Tila
Botanical name : Sesamum indicum
Family : Pedaliaceae
Kula : Tilakula
Rasa : Madhura, Kashaya, Tikta, Katu
Guna : Guru, Snigdha
Virya : Ushna
Vipaka : Madhura
Doshaghnata : Vatashamaka, Kapha-pittaprakopi
Chemical Composition :
Seed Oil The tila seeds (Sesame seeds) contain many vitamins like thiamine,
niacin, riboflavin, nicotinic acid, pantothenic, folic and ascorbic acids, choline,
inositol, pyridoxine, vitamin A, and tocopherol. Sugars present are glucose, sucrose,
galactose, planteose and raffinose. The fatty acids in the seeds are myristic, palmitic,
stearic, arachidic, oleic, linoelic, hexadecenoic and linoceric acids. Sesamin isolated
from seed oil and three stereoisomeric forms of sesamin, viz. sesamin, asarinin and
epiasarinin

Review of Literature
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 86
METHOD OF PREPARATION OF THE DRUG COMPOUND:
The Jyotishmati-Apamarg Kshara Taila was prepared by General Method
of preparation of Kharapaka Taila as per Sharangdhar Samhitha.
Contents of Jyotishmati-Apamarg Kshara Taila were as follow:
1) 1 part - Apamarga Kshara used as Kalka.
2) 4 part - Jyotishmati Taila.
3) 16 part - Apamarga Kshara Jala.
Process of Talia Siddhi :
Apamarga Kshara was taken as Kalka and Apamarga Kshara Jala was taken
as Drava dravya and mixed together in Sneha patra. Jyotishmati taila was then added
as Sneha. Then this mixture boiled on Mandagni and stirred continuously upto
appearance of Kharapaka Lashanas.This procedure seven times done.
Lakshanas of Taila Siddhi :
1) A small quantity of Kalka taken out at the end of boiling and rolled in
between the fingers, if it assumes a varthi ( wick – like shape )
2) Kalka does not produces crackling sound if thrown on fire
3) Appearence of Phena ( froth, bubbles ) at the terminal stages of sneha paka
respectively
Lakshanas of Kharapaka :
1) The Kalka does not yield any sneha and is hard rough due to excess of heating

MATERIALS AND METHODS
Materials & Methods
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 87
Materials and Methods
Objectives of the study
The present study named, “A clinical study on effect of local application
with Jyotishmati Apamarga Kshara Taila in the management of Shvirta
(Vitiligo) in children” was carried out with following objectives -
4. To evaluate the effect of local application with Jyotishmati-Apamarga Kshara
Taila in the management of Shvitra.
5. To observe the effect of local application with Tila Taila (control) in the
management of Shvitra.
6. To compare the effects of both the groups to ascertain the utility of local
application with Jyotishmati-Apamarga Kshara Taila in the management of
Shvitra.
Materials for the study
(A) Source of data:
40 patients of Shvitra attending the Kaumarabhritya O.P.D. and I.P.D. of
S.D.M.C.A. Hospital, Hassan and Chikkmagalore will be selected for the study.
(B) Methods of collection of data :
The diagnosed cases of Shvitra will be selected for the study based on the
Diagnostic criteria and Inclusion criteria as mentioned.
1) Diagnostic criteria :
1. Lakshanas of Shvitra as mentioned in Ayurvedic classics.
2. Borders of patches hyperpigmented and well defined.
3. Sensation is normal.
4. Absence of scaling, crusting
2) Inclusion criteria :
1. Patients with Sadhya Lakshana of Shvitra.
2. Patients in the age group of 7 to 12 years.
3. Patches up to 1 year old.
4. Size of patches less than 5cm × 5cm.

Materials & Methods
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 88
3) Exclusion criteria :
1. White anesthetic spots which are characteristic of leprosy.
2. Patients below 7 year and above 12 years.
3. Vitiligo patches complicated by eczema.
4. Patches arising on the finger tips, near nail bed, on the lips, over mucosal
layer and in genital area.
(B) Drug Materials taken for the study :-
1. Aragvadha Phala Majja Kashaya
2. Jyotishmati-Apamarga Kshara Taila
3. Tila Taila
Method of study
45 patients between the age group of 7 – 12 years attending the
Kaumarabhritya OPD and I P D of S.D.M College of Ayurveda and Hospital, Hassan
with diagnosis of Shvitra were taken up for the study after following the criteria laid
as above. Their age, sex, religion, socioeconomic status, food habits family history,
dehaprakruthi etc. were noted as given in master chart. Where there is more than one
patch of vitiligo in any patient only one patch was selected for the study. However
where improvement was found in that particular patch, patient was advised to treat
other patches also with the same drug. The size of the observed patch was
approximately measured in square centimetres by multiplying its breadth and length.
These 45 patients were divided randomly in to two groups.
1. Group A – Study group – containing 23 patients.
2. Group B – Placebo group – containing 22 patients.
Out of a total number of 45 patients taken for the study, five dropped out in
the middle and did not continue treatment. The left out 40 patients constituted of 20 in
study group and 20 in placebo group.
Complete history and clinical examination of all these patients was carried out
and recorded in a specially designed pro-forma by the Post-Graduate Department of
Kaumarabhritya of S.D.M. College of Ayurveda and Hospital Hassan. Their findings
are given in the enclosed master chart.
All these patients were screened with following routine investigations.

Materials & Methods
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 89
Laboratory investigations
Blood:
Hemoglobin estimation,
Total leukocyte count,
Differential WBC count,
Erythrocyte sedimentation rate.
Mode of administration of drug:
All patients of both the groups were administered the drugs as follows –
1. All patients of both the groups will be administered Aragvadha Phala Majja
20 grams with warm milk after Abhyanga and Svedana, in the morning on
empty stomach.
2. Local application of Jyotishmati-Apamarg Kshara Taila and Tila Taila to
study and control groups respectively followed by sunexposure 30 minutes,
twice daily for the period of 2 months.
Duration of the treatment:
Patients of both the groups (study and control) will be advised to apply
the drugs given to them daily twice followed by sunexposure for 30 minutes, for the
period of two months.
Criteria for assessment:
Patients of both the groups were examined initially, at the end of one month
and at the end of two months for changes in the patches if any.
The criteria for assessment included,
1. Appearance of itching sensation over observed Shvitra (vitiligo) patches.
2. Alteration in the colour of observed Shvitra (vitiligo) patches.
3. Bleb formation on observed Shvitra (vitiligo) patches.
4. Number of black dots appearing in the observed Shvitra (vitiligo) patches.
5. Change in the size of observed Shvitra (vitiligo) patches.

Materials & Methods
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 90
The criteria kept for grading to observe any improvement is as following.
1. Appearance of itching sensation over observed Shvitra (vitiligo) patches.
a. If no Itching sensation over observed 1
b. If Itching sensation over observed 0
2. Colour change in the observed Shvitra (vitiligo) patches.
a. No change in colour (White) 3
b. Light pink 2
c. Dark pink 1
d. Normal skin colour 0
3. Bleb formation on observed Shvitra (vitiligo) patches.
a. If no bleb formation 1
b. If bleb formation 0
4. Number of black spots in observed Shvitra (vitiligo) patch
a. If no black spots appear 2
b. If less than three spots appear 1
c. If three or more spots appear 0
5. Size of the observed Shvitra (Vitiligo) patch
a. If size remains same or increases 2
b. 10% reduction in size 1
c. If more than 10% reduction 0
Follow up:
Follow up study will be done after completion of course of the treatment
for a period of 1 month in every fortnight to ascertain whether relief provided by the
drug is sustained.
OBSERVATIONS
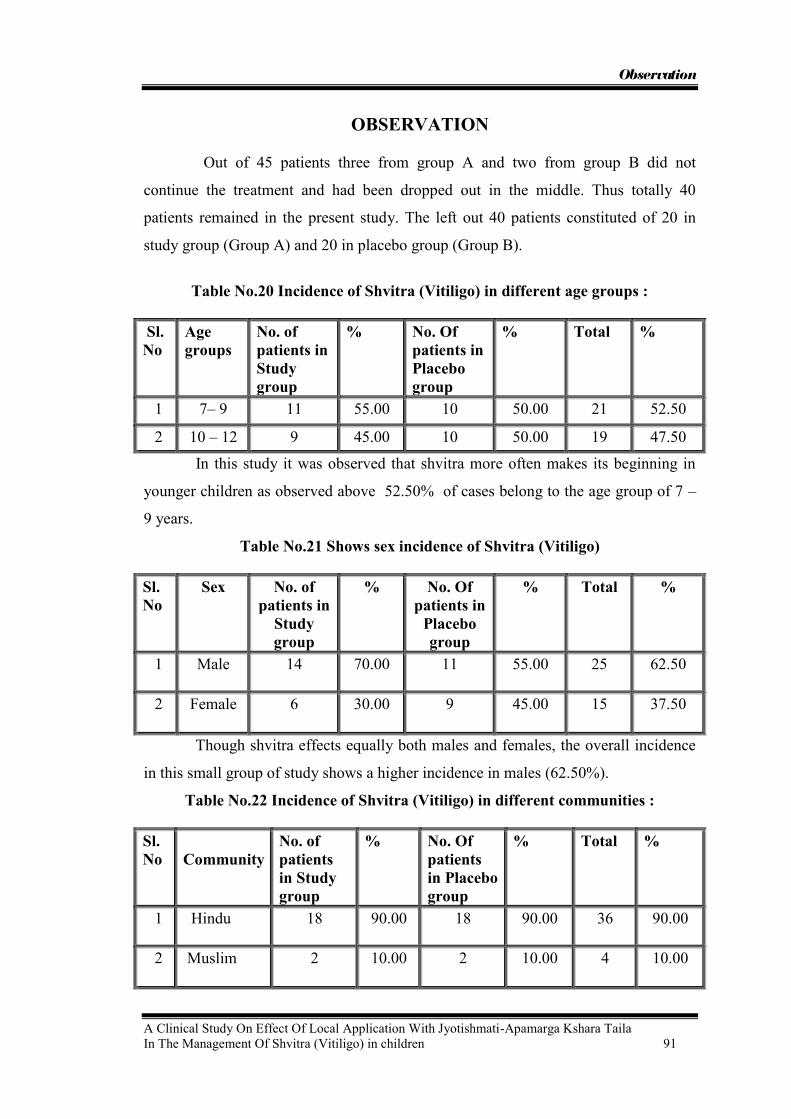
Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 91
OBSERVATION
Out of 45 patients three from group A and two from group B did not
continue the treatment and had been dropped out in the middle. Thus totally 40
patients remained in the present study. The left out 40 patients constituted of 20 in
study group (Group A) and 20 in placebo group (Group B).
Table No.20 Incidence of Shvitra (Vitiligo) in different age groups :
Sl. No
Age groups
No. of patients in Study group
% No. Of patients in Placebo group
% Total %
1 7– 9 11 55.00 10 50.00 21 52.50
2 10 – 12 9 45.00 10 50.00 19 47.50
In this study it was observed that shvitra more often makes its beginning in
younger children as observed above 52.50% of cases belong to the age group of 7 –
9 years.
Table No.21 Shows sex incidence of Shvitra (Vitiligo)
Sl. No
Sex No. of patients in
Study group
% No. Of patients in
Placebo group
% Total %
1 Male 14 70.00 11 55.00 25 62.50
2 Female 6 30.00 9 45.00 15 37.50
Though shvitra effects equally both males and females, the overall incidence
in this small group of study shows a higher incidence in males (62.50%).
Table No.22 Incidence of Shvitra (Vitiligo) in different communities : Sl. No
Community
No. of patients in Study group
% No. Of patients in Placebo group
% Total %
1 Hindu 18 90.00 18 90.00 36 90.00
2 Muslim 2 10.00 2 10.00 4 10.00

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 92
The present study with the few patients (40) of Shvitra showed a higher
incidence of Shvitra in Hindus. 90.00% of the cases in the present study belonged to
Hindu community while only 10.00% of cases were from Muslim community. None
were christian.
Table No.23 Show incidence of habitat :
Sl. No
Habitat No. of patients in
Study group
% No. Of patients in
Placebo group
% Total %
1 Rural 6 30.00 7 35.00 13 32.50
2 Urban 14 70.00 13 65.00 27 67.50
Habitat incidence of Shvitra patients in the present study shows that majority
of patient‟s i.e. 67.50% were from urban locality and only 32.50% of patients were
from rural area.
Table No. 24 Show incidence of socio-economic status :
Sl. No
Socio economic
status
Study group
% Placebo group
% Total %
1 Poor 2 10.00 1 05.00 3 07.50
2 U M C 7 35.00 8 40.00 15 37.50
3 L M C 11 55.00 11 55.00 22 55.00
In the present study Shvitra (Vitiligo) appears to arise more in Lower middle
class (55.00%), than in Poor class (7.50%) and in Upper middle class (37.50%).
Table No. 25 Shows incidence of shvitra as per food habits :
Sl. No
Food Habit Study group
% Placebo group
% Total %
1 Vegetarian 6 30.00 5 25.00 11 27.50
2 Non vegetarians (mixed diet)
14
70.00
15
75.00
29
72.50
The incidence of food habit in the present study showed that majority of
patients of Shvitra was non-vegetarians (mixed diet) (i.e.72.50%) when compared to
vegetarians in whom the incidence is 27.50%.

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 93
Table No.26 Shows incidence of earlier treatment history in the patients of Shvitra :
Sl. No
Treatment history
Study group
% Placebo group
% Total %
1 Present 9 45.00 7 35.00 16 40.00
2 Absent 11 55.00 13 65.00 24 60.00
It is observed that 24 out of 40 patients (60.00%) came direct to SDM Hospital
for treatment of Shvitra without going anywhere; where as 16 patients (40.00%) had
given history of having taken treatment earlier without any success.
Table No.27 Shows incidence of Deha Prakruthi in Shvitra patients :
The Deha Prakruthi was assessed as per the chart followed in Shareerakriya
department of S.D.M. College of Ayurveda, Hassan.
Sl. No
Prakruthi Study group
% Placebo group
% Total %
1 Vata-Pitta 9 45.00 11 55.00 20 50.00
2 Vata-Kapha 7 35.00 6 30.00 13 32.50
3 Pitta-Kapha 4 20.00 3 15.00 7 17.50
The incidence of Deha Prakruthi in the present study showed that
majority of patients suffering from Shvitra were of Vata Pitta Prakruthi i.e. 50.00%
when compared to Vata Kapha and Pitta Kapha Deha Prakruthi which was 32.50%
and 17.50% respectively.
Table No. 28 Shows incidence of Aharaja Nidanas described to produce Shvitra :
Sl. No
Nidana described in ayurvedic texts
Study group
% Placebo group
% Total %
1 Virudhahara only 4 20.00 3 15.00 7 17.50
2 Ati Masha, Mulaka, Dadhi, Amla sevana
only
6 30.00 5 25.00 11 27.50
3 Both 1 & 2 9 45.00 10 50.00 19 47.50
4 None 1 05.00 2 10.00 3 07.50

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 94
Incidence of Aharaja Nidana in the patients showed that 47.50% of patients
are found consuming Viruddhahara and Ati Masha, Mulaka, Dadhi and Amla
padarthas as a routine in their diet
Table No.29 Shows incidence of Viharaja Nidana in Shvitra patients
Sl. No.
Nidana described in ayurvedic texts
Study group
% Placebo group
% Total %
1 Intake of cold water after exposure to sunlight
9 45.00 7 35.00 16 40.00
2 Cold water bath after exposure to sunlight
4 20.00 4 20.00 8 20.00
3 Both 4 20.00 5 25.00 9 22.50
4 None 3 15.00 4 20.00 7 17.50
It is observed from the above chart that Shvitra is found more
(40.00%) among those using cold water after sun exposure and those who are not
accustomed to do so.
Table No. 30 Shows incidence of chronicity of Shvitra
Sl. No
Chronicity (In months)
Study group
% Placebo group
% Total %
1 1 – 3 2 10.00 3 15.00 5 25.00 2 4 – 6 5 25.00 6 30.00 11 27.50 3 7 – 9 6 30.00 2 10.00 8 20.00 4 10 – 12 7 35.00 9 45.00 15 37.50
The incidence of chronicity 0f Shvitra in the present study showed that in
majority of patients the disease was 10 – 12 months old (37.50%)
Table No.31 Shows incidence of number of mandalas (patches)
Sl. No
No. of patches (mandalas)
Study group
% Placebo group
% Total %
1 1 – 5 9 45.00 8 40.00 17 42.50
2 6 – 10 1 05.00 6 30.00 7 17.50
3 11 – 20 9 45.00 6 30.00 15 37.50
4 Above 20 1 05.00 0 00.00 1 02.50

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 95
In the present study 42.50% of patients (17) had less than 5
mandalas of Shvitra while in 37.50% of patients it was between 11-20 madalas, in
17.50% of patients it was between 6-10 mandalas and only 02.50% of patients more
than 20 mandalas were found.
Table No.32 Shows incidence of distribution of mandalas
Sl. No
Distribution Study group
% Placebo group
% Total %
1 Symmetrical 5 25.00 7 35.00 12 30.00
2 Asymmetrical 15 75.00 13 65.00 28 70.00
In the present study 70.00% of patients of Shvitra showed assymetrical
distribution of Mandalas while 30.00% of patients of Shvitra showed symmetrical
distribution of Mandalas.
Table No.33 Shows incidence of presence of black spots in observed patch before
treatment
Sr.No Black spots Study group
% Placebo group
% Total %
1 No spots 8 40.00 7 35.00 15 37.50
2 1- 5 12 60.00 13 65.00 25 62.50
Before treatment 37.50% of patients did not show any black spots in the
observed patch. 62.50% of patients showed 1 – 5 black spots in the observed patch.
Table No. 34 Shows incidence of colour of patch in Shvitra (Vitiligo) before
treatment : Sl. No
Colour Study group
% Placebo group
% Total %
1 White 18 90.00 16 80.00 34 85.00
2 Light pink 2 10.00 4 20.00 6 15.00
Incidence of colour of the Shvitra patch in the present study showed that in
majority of patients i.e. in 85.00% (34) the lesion was of white colour and only in
15.00% of patients the colour of the lesion was of light pink.

Observation
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 96
Table No.35 Shows incidence of size of Mandalas :
In present study the size of Shvitra (VItiligo) patch measured in
square cm for convenience of comparison between before treatment and after
treatment size of Shvitra (Vitiligo) patch.
Sl. No
Size of Shvitra patch taken for study( in square cm)
Study group
% Placebo group
% Total %
1 < 5 2 10.00 2 10.00 4 10.00
2 6 – 10 8 40.00 10 50.00 18 45.00
3 11 – 15 8 40.00 4 20.00 12 30.00
4 15 – 20 2 10.00 4 20.00 6 15.00
In the present study in majority of patient‟s i.e. 45.00 % (18) the
patches were of in between 6 -10 sq.cm. and in 30.00% of patients patches were of in
between 11 – 15 sq. cm.In 15.00% and 10.00% of patients patches were of in between
15 – 20 sq. cm. and < 5 sq. cm. respectively.
Table No. 36 Shows incidence of number of Vegas after Koshstashudhi medicine
given:
Sl. No
Number of Vegas
Study group
% Placebo group
% Total %
1 3 - 4 6 30.00 8 40.00 14 35.00
2 5 - 6 8 40.00 5 25.00 13 32.50
3 7 - 8 6 30.00 7 35.00 13 32.50
In present study incidence of 3-4 Vegas after Koshstashudhi seen in
35.00% of Shvitra (Vitiligo) patients & 5-6 & 7-8 Vegas after Koshstashudhi seen in
32.50% of shvitra (Vitiligo) patients.

RESULTS

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 103
Results of improvement in Shvitra (Vitiligo) based on the criteria of assessment:
Group A ( Study Group ): Table No.37 Showing clinical improvement of signs after one month of treatment
Signs seen in observed shvitra (Vitiligo) patch
Mean (G.S) Mean difference
% of improvement
S.D S. E. t - value
P – value
Inference
BT AT
Appearance of Itching sensation
0.85 0.45 0.4 47.05 0.50 0.11 3.55 >0.01 Significant
Colour change 2.9 1.7 1.2 41.37 0.41 0.09 13.07 >0.001 Highly significant
Bleb formation 1 0.9 0.1 10.00 0.30 0.06 1.45 <0.05 Not significant
No. of black spots
1.4 0.75 0.65 46.42 0.48 0.10 5.94 >0.001 Highly significant
Size of observed patch
2 1.5 0.5 25 0.51 0.11 4.35 >0.001 Highly significant
The effect of the study drug provides highly significant result in colour
change, no. of black spots and size of observed Shvitra (Vitiligo) patch with p values
at >0.001 and significant result in appearance of itching sensation over Shvitra
(Vitiligo) patch with p values at >0.01 at the end of first month of treatment.
However, it gives insignificant results on the clinical criteria i.e. bleb formation on
Shvitra (Vitiligo) patch with P value < 0.05.

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 104
Group A ( Study Group ): Table No. 38 Showing clinical improvement of signs after two months of treatment :
Signs seen in observed shvitra (Vitiligo) patch
Mean (G.S) Mean difference
% of improvement
S.D S. E. t - value
P – value (df-12)
Inference
BT AT
Appearance of Itching sensation
0.85 0.25 0.6 70.58 0.50 0.11 5.33 >0.001 Highly significant
Colour change
2.9 1 1.9 65.51 0.30 0.06 27.60 >0.001 Highly significant
Bleb formation
1 0.7 0.3 30.00 0.47 0.10 2.85 0.01 Significant
No. of black spots
1.4 0.55 0.85 60.71 0.58 0.13 6.47 >0.001 Highly significant
Size of observed patch
2 0.65 1.35 67.50 0.48 0.10 12.33 >0.001 Highly significant
The effect of the study drug provides highly significant result in appearance of
itching sensation, colour change, no. of black spots and size of observed Shvitra
(Vitiligo) patch with p values at >0.001 at the end of second month of treatment.
However, it gives significant results on the clinical criteria i.e. No. of black spot
observed in Shvitra (Vitiligo) patch with P value 0.01.

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 105
Group B ( Placebo Group ): Table No. 39 Showing clinical improvement of signs after one month of treatment :
Signs seen in observed shvitra (Vitiligo) patch
Mean (G.S) Mean difference
% of improvement
S.D S. E. t - value
P – value (df-12)
Inference
BT AT
Appearance of Itching sensation
0.8 0.8 0 0 0 0 0 <0.05 Not significant
Colour change
2.8 2.8 0 0 0 0 0 <0.05 Not significant
Bleb formation
1 1 0 0 0 0 0 <0.05 Not significant
No. of black spots
1.3 1.3 0 0 0 0 0 <0.05 Not significant
Size of observed patch
2 2 0 0 0 0 0 <0.05 Not significant
The effect of the placebo drug provides insignificant result in all clinical
criteria‟s i.e. appearance of itching sensation, colour change, bleb formation, no. of
black spots and size of observed Shvitra (Vitiligo) patch with p values at <0.05 at the
end of first month of treatment.

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 106
Group B ( Placebo Group ): Table No. 40 Showing clinical improvement of signs after two month of treatment :
Signs seen in observed shvitra (Vitiligo) patch
Mean (G.S) Mean difference
% of improvement
S.D S. E. t - value
P – value
Inference
BT AT
Appearance of Itching sensation
0.8 0.9 - 0.1 - 12.5 0.30 0.06 1.45 <0.05 Not significant
Colour change
2.8 2.75 0.05 1.78 0.22 0.05 1 <0.05 Not significant
Bleb formation
1 1 0 0 0 0 0 <0.05 Not significant
No. of black spots
1.3 1.3 0 0 0 0 0 <0.05 Not significant
Size 2 2 0 0 0 0 0 <0.05 Not significant
The effect of the placebo drug provides insignificant result in all clinical
criteria‟s i.e. appearance of itching sensation, colour change, bleb formation, no. of
black spots and size of observed Shvitra (Vitiligo) patch with p values at <0.05 at the
end of second month of treatment.
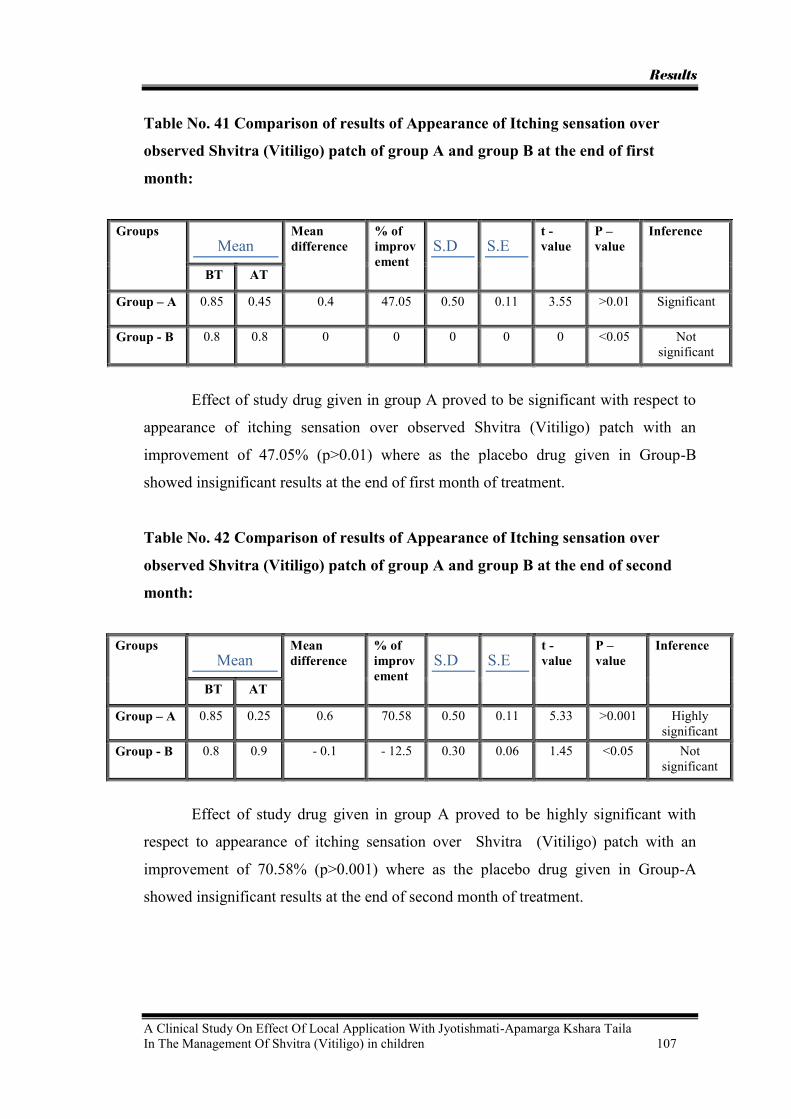
Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 107
Table No. 41 Comparison of results of Appearance of Itching sensation over
observed Shvitra (Vitiligo) patch of group A and group B at the end of first
month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 0.85 0.45 0.4 47.05 0.50 0.11 3.55 >0.01 Significant
Group - B 0.8 0.8 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be significant with respect to
appearance of itching sensation over observed Shvitra (Vitiligo) patch with an
improvement of 47.05% (p>0.01) where as the placebo drug given in Group-B
showed insignificant results at the end of first month of treatment.
Table No. 42 Comparison of results of Appearance of Itching sensation over
observed Shvitra (Vitiligo) patch of group A and group B at the end of second
month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 0.85 0.25 0.6 70.58 0.50 0.11 5.33 >0.001 Highly significant
Group - B 0.8 0.9 - 0.1 - 12.5 0.30 0.06 1.45 <0.05 Not significant
Effect of study drug given in group A proved to be highly significant with
respect to appearance of itching sensation over Shvitra (Vitiligo) patch with an
improvement of 70.58% (p>0.001) where as the placebo drug given in Group-A
showed insignificant results at the end of second month of treatment.

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 108
Table No. 43 Comparison of results of colour change in observed Shvitra
(Vitiligo) patch of group A and group B at the end of first month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 2.9 1.7 1.2 41.37 0.41 0.09 13.07 >0.001 Highly significant
Group - B 2.8 2.8 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be highly significant with
respect to colour change in observed Shvitra (Vitiligo) patch with an improvement of
41.37% (p>0.001) where as the placebo drug given in group B showed insignificant
results at the end of first month of treatment.
Table No. 44 Comparison of results of colour change in observed Shvitra
(Vitiligo) patch of group A and group B at the end of second month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 2.9 1 1.9 65.51 0.30 0.06 27.60 >0.001 Highly significant
Group - B 2.8 2.75 0.05 1.78 0.22 0.05 1 <0.05 Not significant
Effect of study drug given in group A proved to be highly significant with
respect to colour change in observed Shvitra (Vitiligo) patch with an improvement of
65.51% (p>0.001) where as the placebo drug given in group B showed insignificant
results at the end of second month of treatment.
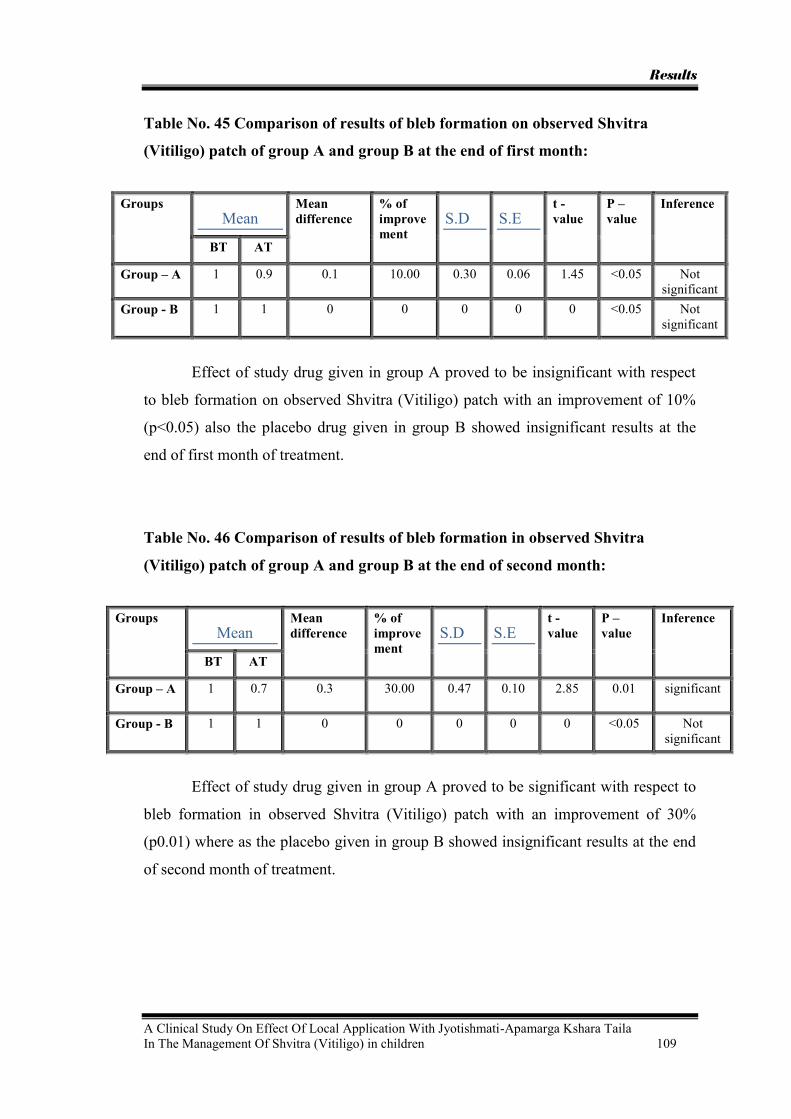
Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 109
Table No. 45 Comparison of results of bleb formation on observed Shvitra
(Vitiligo) patch of group A and group B at the end of first month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 1 0.9 0.1 10.00 0.30 0.06 1.45 <0.05 Not significant
Group - B 1 1 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be insignificant with respect
to bleb formation on observed Shvitra (Vitiligo) patch with an improvement of 10%
(p<0.05) also the placebo drug given in group B showed insignificant results at the
end of first month of treatment.
Table No. 46 Comparison of results of bleb formation in observed Shvitra
(Vitiligo) patch of group A and group B at the end of second month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 1 0.7 0.3 30.00 0.47 0.10 2.85 0.01 significant
Group - B 1 1 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be significant with respect to
bleb formation in observed Shvitra (Vitiligo) patch with an improvement of 30%
(p0.01) where as the placebo given in group B showed insignificant results at the end
of second month of treatment.
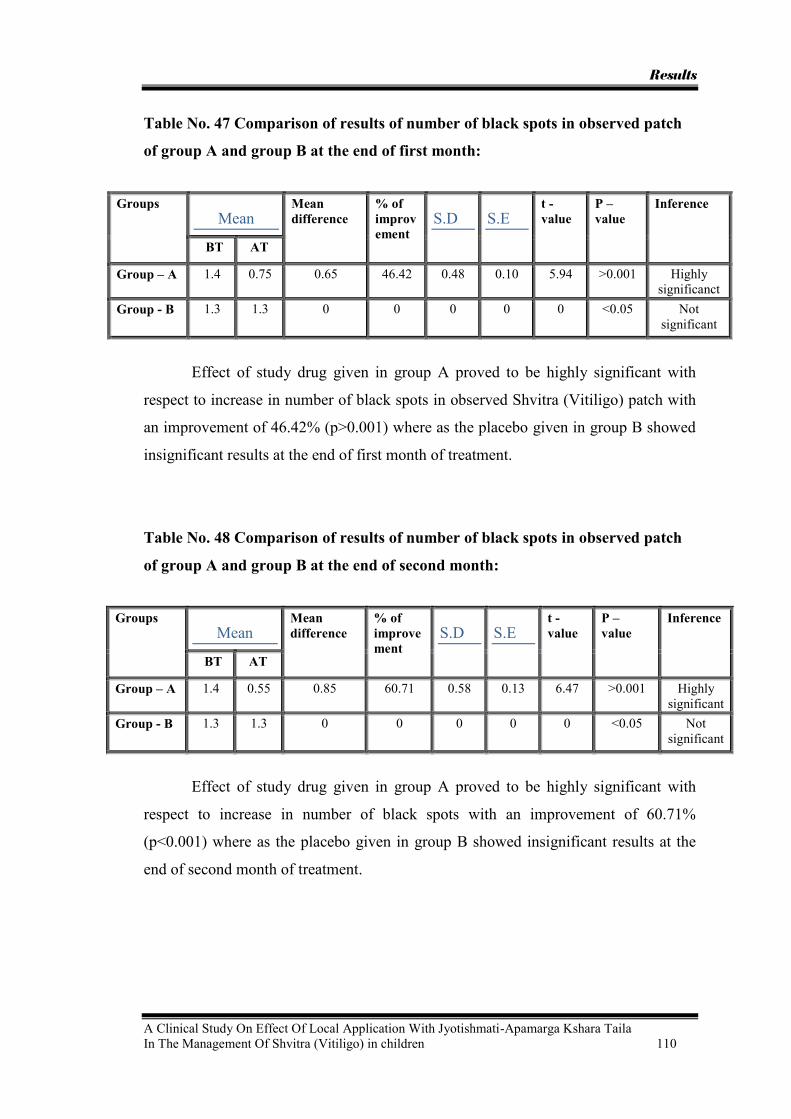
Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 110
Table No. 47 Comparison of results of number of black spots in observed patch
of group A and group B at the end of first month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 1.4 0.75 0.65 46.42 0.48 0.10 5.94 >0.001 Highly significanct
Group - B 1.3 1.3 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be highly significant with
respect to increase in number of black spots in observed Shvitra (Vitiligo) patch with
an improvement of 46.42% (p>0.001) where as the placebo given in group B showed
insignificant results at the end of first month of treatment.
Table No. 48 Comparison of results of number of black spots in observed patch
of group A and group B at the end of second month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 1.4 0.55 0.85 60.71 0.58 0.13 6.47 >0.001 Highly significant
Group - B 1.3 1.3 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be highly significant with
respect to increase in number of black spots with an improvement of 60.71%
(p<0.001) where as the placebo given in group B showed insignificant results at the
end of second month of treatment.

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 111
Table No. 49 Comparison of results of size of the observed patch of group A and
group B at the end of first month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 2 1.5 0.5 25 0.51 0.11 4.35 >0.001 Highly significant
Group - B 2 2 0 0 0 0 0 <0.05 Not significant
Effect of study drug proved to be highly significant with respect to increase in
size of Shvitra (Vitiligo) patch with an improvement of 25% (p>0.001) where as the
placebo given in group B showed insignificant results at the end of first month of
treatment.
Table No.50 Comparison of results of size of the observed patch of group A and
group B at the end of second month:
Groups Mean
Mean difference
% of improvement
S.D S.E t - value
P – value
Inference
BT AT
Group – A 2 0.65 1.35 67.50 0.48 0.10 12.33 >0.001 Highly significant
Group - B 2 2 0 0 0 0 0 <0.05 Not significant
Effect of study drug given in group A proved to be highly significant with
respect to increase in size of Shvitra (Vitiligo) with an improvement of 67.50%
(p>0.001) where as the placebo given in group B showed insignificant results at the
end of second month of treatment.

Results
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 112
Table No. 51 Showing Over-all Percentage Improvement:
Sr. No. Signs seen in observed shvitra (Vitiligo) patch
Group A Group B
1. Appearance of Itching sensation
70.58 % - 12.5%
2. Colour change 65.51% 1.78% 3. Bleb formation 30.00% 0% 4. No. of black spots 60.71% 0% 5. Size of observed patch 67.50% 0%

DISCUSSION

Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 117
DISCUSSION The colour of the skin plays a very important role in the society especially in
India. Shvitra is a depigmentary disorder of the skin. This disease does not cause any
pain or ulcer but it creates an inferiority complex in the affected child.
We get the references of Shvitra right from Vedic literature where the
principal line of treatment is mentioned as Sramsana and many Lepas are mentioned
for application after Sramsana.
Shvitra is a disease where Bhrajaka Pitta present in Tvak is involved,
Virechana is considered as the best line of treatment if Pitta is involved.
Aragvadha phalamajja is mentioned as a Sramsana dravya and is harmless and
conveniently used in children. Hence Aragvadha phalamajja was selected for the
purpose of Koshtashudhi.
A number of Yogas are mentioned for the purpose of external application after
Shodhana by many classics for Shvitra. Yogaratnakara and Vangasen Samhitha have
mentioned the use of Jyotishmati-Apamarga Taila for the treatment of Shvitra.
Apamarga has Rakta-Pitta Prasadanakara action and Jyotishmati has Pitta
Santpakara action. Hence they may be increase the activity of Bhrajaka Pitta leading
to formation of melanin pigments in Tvak (skin) resulting in normal Varna of the
patches..
So far as this study is concerned group A patients were given Koshtashudhi
with Aragvadha phalamajja followed by application of study drug i.e. Jyotishmati-
Apamarga Kshara Taila on the Shvitra (Vitiligo) patches daily twice followed by sun
exposure for 30 minutes and group B patients were given Koshtashudhi with
Aragvadha phalamajja followed by application of placebo drug i.e. Tila taila daily
twice on the Shvitra (Vitiligo) patches followed by sun exposure for 30 mintues.
Discussion on incidence and results:
The present study was planned in two groups, aimed to manage Shvitra with
Aragvada phalamajja given for Koshtashudhi in both the groups. After Koshtashudhi
study drug is used for application in group A, and placebo drug was advised to be
applied in group B. This was continued for two months with a follow up for 1 month.

Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 118
The discussion on the incidence is as follows,
Age incidences:
This study shows that 52.50% of patients are between 7-9 years. Where as
worldwide study in the particular research gives the prevalence of vitiligo at the age
of 10 years of life in children or between 2nd to 4th decades of life.
Sex incidence:
Both male and female children are described to be affected equally, where as
in this study the incidence of Shvitra is found 62.50% in female patients. As Shvitra
(Vitiligo) causes social stigma so for cosmetic purpose female patients were coming
more in number as compared to male for the treatment of same.
Incidence of Shvitra (Vitiligo) in different communities:
In present study 90.00% of children belonged to Hindu community and the
Muslims were found to be 10.00%, this may be because of predominance of Hindu
residents in this area. None were Christian.
Incidence of habitat
In the present study 67.50% of patients were hailing from urban area and
32.50% of patients were from rural area. This may be because of increased awareness
for treatment in urban residents compared to rural people.
Incidence of socio economic status
In present study Shvitra (Vitiligo) appears to arise more in Lower middle
class (55.00%), than in Poor class (7.50%) and in Upper middle class (37.50%).
The number of Shvitra (Vtiligo) patients was more in lower middle class as our
SDM hospital set up more convenient for them.
Incidence of immunization
Present study showed 100%of patients immunized because of maximum
health awareness. However the immunization status of a child appears not to play any
role in the genesis or incidence of the disease.
Incidence of food habits:
The incidence of food habit in the present study showed that majority of
patients of Shvitra was non-vegetarians (mixed diet) (i.e.72.50%) when
compared to vegetarians in whom the incidence is 27.50%. This may due to
Virudha ahara sevana was more in non-vegetarians such as fish & milk etc.

Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 119
Incidence of family history
All the modern text books mentioned a hereditary prevalence of about 25%
but in the present study 100% were showing negative family history and no one
showed positive family history of Shvitra. But this does not deny the significance of
family history, since the present study consists only of a small group.
Incidence of treatment history
In present study it is observed that 24 out of 40 patients (60.00%) came direct
to SDM Hospital for treatment of Shvitra without going anywhere; whereas 16
patients (40.00%) had given history of having taken treatment earlier without any
success.
Incidence of Deha Prakruti
The incidence of Deha Prakruthi in the present study showed that majority
of patients suffering from Shvitra were of Vata Pitta Prakruthi i.e. 50.00% when
compared to Vata Kapha and Pitta Kapha Deha Prakruthi which was 32.50% and
17.50% respectively.
Incidence of Aharaja Nidanas
In present study incidence of Aharaja Nidana in the patients showed that
47.50% of patients are found consuming Viruddhahara and Ati Masha, Mulaka, Dadhi
and Amla padarthas as a routine in their diet. The prevalence of these Nidanas were
found to be more since these food items are consumed in the daily food in this
locality, but it appears when these items are consumed excessively it may predispose
to Shvitra. Dr. Chavali in his Ph.D. thesis considered that Viruddha substances do not
get digested to body components but remain as foreign substances in circulation
invoking immunological reactions. Thus Viruddahara by invoking such
immunological reaction could produce Shvitra, if it could be considered as a disorder
of autoimmunity.
Incidence of Viharaja Nidanas:
The incidence of Viharaja Nidana in the present study showed that 40.00%
patients were using cold water after sun exposure, 20.00% patients were using Cold
water bath after exposure to sunlight and 22.50% patients were using both Viharaja
Nidanas. Only 17.50 % patients were not found with any of Viharaja Nidanas.

Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 120
Incidence of chronicity
The incidence of chronicity of Shvitra in the present study showed that in
majority of patients the disease was 10 – 12 months old (37.50%) followed by 4 – 6
months old in 27.50%. In very few patients chronicity was seen less than 4 months as
patients coming for treatment after unsatisfactory result of modern medicine.
Incidence of number of mandalas
In present study 42.50% of patients (17) had less than 5 mandalas of Shvitra
while in 37.50% of patients it was between 11-20 madalas, in 17.50% of patients it
was between 6-10 mandalas and only 02.50% of patients more than 20 mandalas
were found.
Incidence of distribution of mandalas
In present study 70.00% of patients of Shvitra showed assymetrical
distribution of Mandalas while 30.00% of patients of Shvitra showed symmetrical
distribution of Mandalas.
Incidence of size of Mandalas :
In the present study in majority of patient‟s i.e. 45.00 % (18) the patches were
of in between 6 -10 sq.cm. and in 30.00% of patients patches were of in between 11 –
15 sq. cm.
In 15.00% and 10.00% of patients patches were of in between 15 – 20 sq. cm.
and < 5 sq. cm. respectively.
Incidence of black spots in the observed patch
In the present study there were 37.50% of patients did not show any black
spots in the observed patch. 62.50% of patients showed 1 – 5 black spots in the
observed Shvitra (Vitiligo) patch because before including them in study they were
taking another treatment for the Shvitra (Vitiliogo) which was stoped 1week before
starting the study.
Incidence in colour changes of observed patches
Incidence of colour of the Shvitra patch in the present study showed that in
majority of patients i.e. in 85.00% (34) the lesion was of white colour and only in
15.00% of patients the colour of the lesion was of light pink.
Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 121
Incidence of number of Vegas after Koshstashudhi :
In present study incidence of 3-4 Vegas after Koshstashudhi seen in 35.00% of
Shvitra (Vitiligo) patients & 5-6 & 7-8 Vegas after Koshstashudhi seen in 32.50% of
shvitra (Vitiligo) patients.
In present study all patients under gone Koshstshudhi with Aaragwadha
phalamajja, as Aaragwadha known for Sramasana, all patients shown Avara Lashanas
of Koshstashudhi.
Discussion on effect of study drug on different assessment criteria:
1. Appearance of itching sensation over observed Shvitra (vitiligo) patches:
Effect of study drug given in group A proved to be significant with
respect to appearance of itching sensation over observed Shvitra (Vitiligo) patch with
an improvement of 47.05% (p>0.01) after one month and 70.58% (p>0.001) after two
months of treatment.
`In present study after local application of study drug over Shvitra
(Vitilgo) patches appearance of itching sensation was markedly noticed as study drug
contains Apamarga Kshara which is having Ksharana property. So study drug causes
irritation of depigmented skin over Shvitra (Vitiligo) patches hence appearance of
itching sensation over observed Shvitra (Vitiligo) patches were seen.
2. Alteration in the colour of observed Shvitra (Vitiligo) patches:
Effect of study drug given in group A proved to be highly significant with
respect to colour change in observed Shvitra (Vitiligo) patch with an improvement of
41.37% (p>0.001) after one month and 65.51% (p>0.001) after two months of
treatment.
In present study alteration in the colour of observed Shvitra (Vitilgo) patches
after local application of study drug was moderately seen as Apamarga is known for
Rakta-Pitta Prasadhanakar and Jyotishmati is known for Pitta Santapakara action.
After the local application of study drug may be the proper action of Bhrajaka Pitta
took place so that alteration in the colour of Shvitra (Vitilgo) patches was
moderately observed. Therefore for getting good results the duration of application of
study drug should be increased.

Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 122
3. Bleb formation on observed Shvitra (vitiligo) patches:
Effect of study drug given in group A proved to be insignificant with respect
to bleb formation on observed Shvitra (Vitiligo) patch with an improvement of 10%
(p<0.05) after one month and proved to be significant with an improvement of 30% (p
0.01) after two months of treatment.
In the present study bleb formation on observed Shvitra (Vitilgo) patches was
seen in few patients only after local application of study drug. As study drug contains
Apamarga Kshara which has Tikshana Guna, Ushana Virya and Ksharana property.
Due to Teekshna & Ushna guna, it has many functions such as Dahana, Pachana,
Vidarana and Vilayana, and also does Shodhana. Thus the Apamarga Kshra does
irritation of depigmentated skin leading to Visphota (bleb) formation due to Pitta
Prakopa.
4. Number of black spots appearing in the observed Shvitra (vitiligo) patches:
Effect of study drug given in group A proved to be highly significant with
respect to increase in number of black spots in observed Shvitra (Vitiligo) patch with
an improvement of 46.42% (p>0.001) after one month and 60.71% (p<0.001) after
two months of treatment.
In the present study after the local application of study drug the number of
black spots appearing in the observed Shvitra (Vitiligo) patches was moderately seen.
As Apamarga has Katu; Tikta Rasa, Laghu; Ruksha; Tikshana Guna, Ushana Virya,
Katu Vipaka and Rakta-Pitta Prasadanakara action and Jyotishmati has Katu, Tikta
Rasa; Tikshna, Snigdha, sara Guna; Ushna Virya,Katu Vipaka and Pitta-Santpakara
action. Hence there may be increase in the activity of Bhrajaka Pitta leading to
formation of melanin pigments in Tvak (skin) resulting in appearance of black spots.
Therefore for getting good results the duration of local application of study
drug should be increased.
5. Change in the size of observed Shvitra (vitiligo) patches:
Effect of study drug proved to be highly significant with respect to decrease in
size of Shvitra (Vitiligo) patch with an improvement of 25% (p>0.001) after one
month and 67.50% (p>0.001) after two months of treatment.
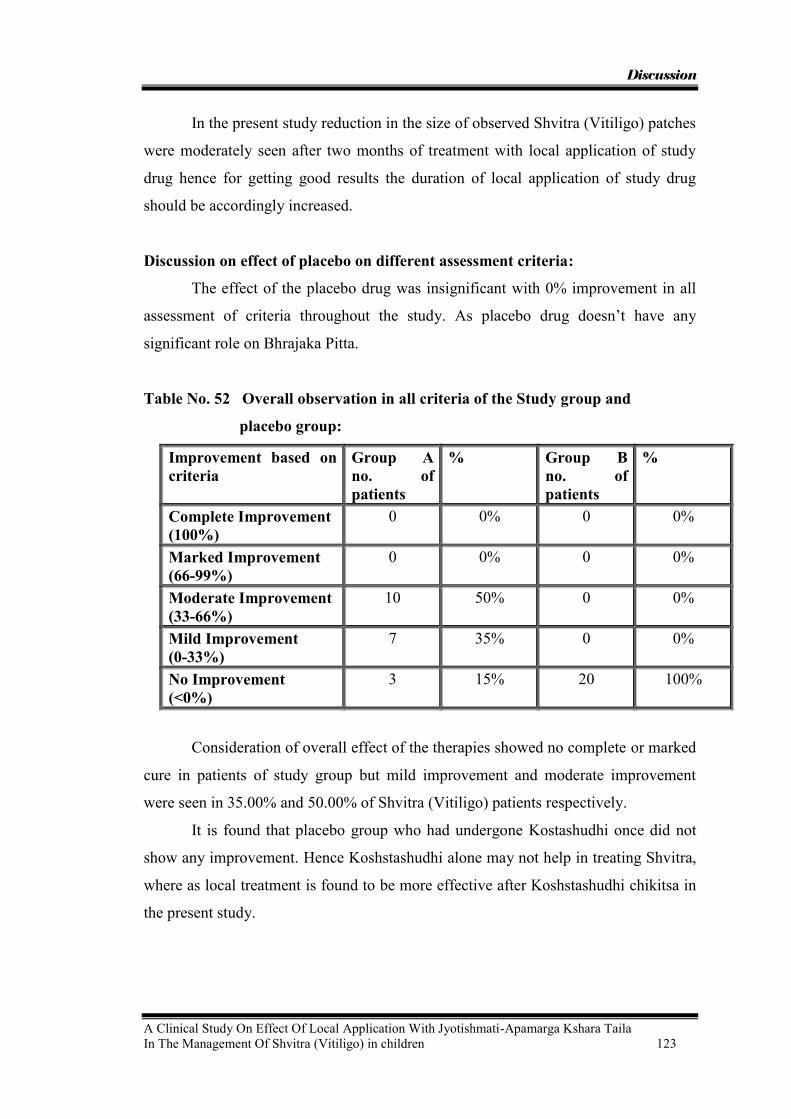
Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 123
In the present study reduction in the size of observed Shvitra (Vitiligo) patches
were moderately seen after two months of treatment with local application of study
drug hence for getting good results the duration of local application of study drug
should be accordingly increased.
Discussion on effect of placebo on different assessment criteria:
The effect of the placebo drug was insignificant with 0% improvement in all
assessment of criteria throughout the study. As placebo drug doesn‟t have any
significant role on Bhrajaka Pitta.
Table No. 52 Overall observation in all criteria of the Study group and
placebo group:
Improvement based on criteria
Group A no. of patients
% Group B no. of patients
%
Complete Improvement (100%)
0 0% 0 0%
Marked Improvement (66-99%)
0 0% 0 0%
Moderate Improvement (33-66%)
10 50% 0 0%
Mild Improvement (0-33%)
7 35% 0 0%
No Improvement (<0%)
3 15% 20 100%
Consideration of overall effect of the therapies showed no complete or marked
cure in patients of study group but mild improvement and moderate improvement
were seen in 35.00% and 50.00% of Shvitra (Vitiligo) patients respectively.
It is found that placebo group who had undergone Kostashudhi once did not
show any improvement. Hence Koshstashudhi alone may not help in treating Shvitra,
where as local treatment is found to be more effective after Koshstashudhi chikitsa in
the present study.

Discussion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 124
General observations
During the course of the study it has been observed that one patient of study
group developed Vispota and the improvement was fast in that patient.
During re-pigmentation two processes were observed, first pattern was re-
pigmentation from the periphery to centre, which showed delayed reduction of size.
Second pattern was where the mandalas developed pigmented spots in between, later
configured the normal skin colour by aggregation.
The pigmentation process was quick in small mandalas when compared to
bigger ones. Mandalas having white hair (four cases) did not respond quickly to the
treatment. In the patients who followed the advised Pathya, relief was found earlier. In
modern medicine also tyrosine rich diet is advised for Shvitra (Vitiligo) patients.
Even after the course of the study no patient showed increase in signs and no
recurrence was seen in study group patients Discussion on study drug ( Jyotishmati-Apamarga Kshara Taila) :
Yogaratnakara and Vangasen Samhitha have mentioned the use of
Jyotishmati-Apamarga Kshara Taila for the treatment of Shvitra.
Kshara has been deemed to be superior to Shastras & Anushastras because of
its actions as said above i.e., Chedana, Lekhana and alleviation of Tridoshas and also
being used for specific functions. Kshara is that which does Lekhana of Tvak ,
Mamsadi and removes the vitiated Doshas. Ksharanat – means which produces skin
injury.
As Apamarga Kshara has Teekshna & Ushna guna, it has many functions such
as Dahana, Pachana, Vidarana and Vilayana, and Shodhana. Due to these properties
Apamarga Kshara produces irritation of depigmented skin over observed Shvitra
(Vitiligo) patches and may helps in removal of depigmented skin and will encourage
formation of normal skin with better pigmentation.
Apamarga has Katu, Tikta Rasa,Laghu, Ruksha, Tikshana Guna, Ushana
Virya, Katu Vipaka, Rakta-Pitta Prasadanakara action and Jyotishmati has Katu, Tikta
Rasa; Tikshna, Snigdha, Sara Guna; Ushna Virya,Katu Vipaka, Pitta-Santpakara
action. Hence they may be increase the activity of Bhrajaka Pitta which leads to
stimulation of melanin pigments in Tvak (skin) resulting in normal Varna of the
patches.

CONCLUSION

Conclusion
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 125
CONCLUSION
The conclusion derived from the present study is as follows
1. Though no Poorvaroopa lakshanas are described in Ayurveda, one case of Shvitra
gave prodromal symptom of itching at the place where patch was developed later.
This could be due to Viruddha ahara alone invoking auto-immunological response
but it was also seen that after application of study drug over Shvitra (Vitiligo)
patch, Itching sensation was noticed as improving sign.
2. The Lakshnas of Doshaja Shvitra, as mentioned in classics were not found in the
patients taken for the study.
3. Early improvement is seen if Visphota is developed on application of study drug.
4. Improvement is earlier if re-pigmentation starts with pigmented spots which later
configured to normal skin color; when compared to repigmentation, which occurs
from periphery to center.
5. The pigmentation process is earlier in small patches when compared to bigger
one.
6. Patches having white hairs responded late to treatment.
7. The patches over the outer border of palm and sole respond quickly to treatment.
8. The improvement could be earlier if tyrosine rich diet is given to the patients.
9. Placebo group who had undergone Koshtashudhi once did not show any
improvement; hence, Koshstashudhi alone may not help in treating Shvitra.
However, it needs a further study to find as to wether repeated Koshstashudhi
helps in Shvitra or not.
10. Local treatment is found to be more effective after Koshstashudhi chikitsa in the
present study. It is possible that local application even without Koshstashudhi may
help in treating the Shvitra; however, this also needs further study.
11. The same drug compound if continued for longer time may give much better
results.
SUMMARY
Summary
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 126
SUMMARY
The dissertation starts with the conceptual part of the subject taken for the study both
from modern and Ayurvedic concepts.
The study was carried out on 23 patients of Shvitra in whom lepa of study
drug was applied locally daily twice followed by sun exposure for 30 minutes for two
months after subjecting the patients for Koshstashudhi karma. A similar treatment
was given with local placebo application in 22 patients exactly the same way as in the
study group. But 3 patients and 2 patients dropped out off study from study and
placebo groups respectively.
Both Ayurvedic and modern concepts in historical aspects of Shvitra, anatomy
and physiology of skin, Nirukti, Paribhasha, Paryaya, Nidana, Bheda with Roopa,
examination of skin and differential diagnosis, Samprapthi, Sadhyasadhyata, Chikitsa
of Shvitra, treatment principle in children and Pathyapathya of all these aspects are
dealt in detail. The conceptual study ends with drug review in which details of
description of each drug taken for the study was given.
Clinical study forms the second part of the dissertation.
A comparative study was undertaken to evaluate the effect of local application
of the trial drug on Shvitra in study group. After Koshtashudhi, local application was
applied daily twice followed by sunexposure for 30 minutes for two months. Similarly
a placebo was applied locally after Koshtashudhi in placebo group. The study drug
consisted of Apamarga Kshara & Jyotishmati Taila.
The criteria for assessment of the results taken were -
1. Appearance of itching sensation over observed Shvitra (vitiligo) patches.
2. Alteration in the colour of observed Shvitra (vitiligo) patches.
3. Bleb formation on observed Shvitra (vitiligo) patches.
4. Number of black dots appearing in the observed Shvitra (vitiligo) patches.
5. Change in the size of observed Shvitra (vitiligo) patches.
Improvement was further studied by giving grading score to the above criteria.
After two months of treatment statistically significantly result seen in study
group with respect to assessment criteria as follows:
Summary
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 127
1. Appearance of itching sensation over observed Shvitra (Vitiligo) patch with an
improvement of 70.58% (p >0.001)
2. Colour change in observed Shvitra (Vitiligo) patch with an improvement of 65.51%
(p >0.001)
3. Bleb formation on observed Shvitra (Vitiligo) patch with an improvement of 30%
(p 0.01)
4. Number of black spots appearing in observed Shvitra (Vitiligo) patch with an
improvement of 60.71% (p >0.001).
5. Decrease in size of Shvitra (Vitiligo) patch with an improvement of 67.50% (p
>0.001)
After two months of treatment statistically insignificantly results seen in
placebo group with respect to all assessment criteria‟s.
Jyotishmati-Apamarga Kshara Taila if continued for longer time for
treatment of Shvitra (Vitiligo) may give much better results.

REFERENCES

References
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 128
REFERANCES
1. T. B. A. D-pp 518, 519 Vol – 1
2. A Hand Book of Vitiligo and Colour Atlas PP 6
3. Su. Sa. ni – 5/17
4. Ca. sa. Chi – 7/174
5. Ca. sa. su – 28/12
6. T. B. A. D-pp 518.Vol – 1
7. Ca. sa. Chi – 7/162
8. Ba. pra. Vol. 1 – pp 68/ 149 -150
9. Rajamartanda 8/8 (Dravyaguna Vijanyan by Dr. Pande)
10. Prof. Sastry C.H.S. in the department of pediatrics in S.D.M college of ayurveda hassan,
suggested use of Sweta Aparajita moola with Ewe‟s milk locally in cases of vitiligo and this
was tried successfully in few cases (personal communication).
11. C. Chi. 7/167
12. Ri. Ve. Mandala 1, suktha 117, shloka 7, vol. 1
13. Ri. Ve. Mandala 5, suktha 53, shloka 1, vol. 2
14. Ath. Ve – Hym 23/ 1 khanda 1
15. Ya. Ve – 30/21
16. Ma. Sm – 3/7
17. Pa. – 5/2/120
18. Ca. sa. Chi – 7
19. Su. sa. ni – 5
20. Su. sa. Chi – 9
21. Su. sa. ni – 5 (Dalhana)
22. Ka. sa. su – 27/51
23. Ka. sa. sha – 4/33
24. Ka. sa. Chi – 9/2
25. Ka. sa. Ka – 7/106.2
26. Ka. sa. Ka – 2/98
27. Ka. sa. si – 7/5, 14
28. Be. sa. Chi – 6/28
29. Ha. Sa – 39/39
30. A. sa. ni – 14/39 – 43
31. A. sa. Chi – 22
32. A. hri. Ni – 14, A. hri. Chi – 20
33. Ma. Ni – 49
34. Sha. Pu. K – 7/90
35. Sha. Ut. K – 11/40 – 44
36. Ba. pra. Ma. K -54
References
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 129
37. Y. R – Kustanidana chikitsa prakarana
38. Bai. Rat – 54
39. Ga. Ni – 36, Vol. 2
40. C. D – 50
41. Ca. sa. Chi. 15/4- Chakrapani
42. Ca. sa. sha – 7/16
43. Su. sa. sha – 4/4
44. A. sa. Sha. 5/14
45. Ca. sa. sha – 4/12, A. sa. sha – 5/10, A. hri. Sha – 3/3, Ka. Sa. sha – ¾
46. Su. sa. sha – 2/35, Ca. sa. sha – 8/15
47. A. sa. Sha. 1/65
48. Ha. sa. Sha– 1/31 – 33
49. A. sa. Sha. 5/17
50. Ca. sa. Sha. 7/4
51. Su. sa. Sha. 4/4
52. A. hri. Sha. 3/8- Arunadutta
53. Sha. Pu. K. 5/19-22
54. Su. sa. Sha. 4/4 - Ghanekar
55. A. hri. Su. 12/4
56. A. hri. Su. 12/14
57. A.hri. Su. 12/14 - Arunadutta
58. Ca. sa. Sha. 7/15
59. Ca. sa. Vi. 8/103
60. Ka. sa. Chi. 9/2
61. Amarakosha
62. Amarakosha
63. Ca. sa. Chi. 7/173
64. Su. sa. Ni. 5/17
65. A. hri. Ni.14/37
66. Su. sa. U 1
67. Ca. sa. Su. 26/102,103
68. Ca. sa. Su. 26/81
69. Ca. sa. Su. 26/85
70. Su. sa. Su. 20/20
71. A. hri. Su. 7/29
72. A. S. Su. 9/25
73. Ca. sa. Su. 26/86-87
74. Ma. Ni. 6/8
75. A. sa. Su. 9/26

References
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 130
76. Ca. sa. Vi. 9/21
77. Ca. sa. Vi. 9/21
78. A. sa. Su. 10/34
79. A. sa. Su. 10/34
80. A. sa. Su. 11/11
81. A. sa. Su. 11/12
82. C. S. Sha.4/30
83. Su. sa. Ni 5/4, Bh. S. 6/16-17, Ka. S. Khi. 1
84. Ma. Ni.
85. Va. Ni. 1
86. Su.Sa.Ni.5/17,A.hri.Ni.14/37–39,Ba.pra.Mad.54/45-46,Ma.Ni.49/38-39,
Ga.Ni 36/38
87. Y. R – Kustanidana chikitsa prakarana – 26
88. Ca. sa. Chi – 7/173
89. Be. sa. Chi – 6/28
90. Su. sa. ni – 5/17, A. hri. Ni – 14/38, Ba. pra. Mad – 54/45 - 46, Ma. Ni – 49/38
- 39, Ga. Ni – 36/39 – 40, A. sa. ni – 15/40
91. Ca. sa. Chi – 7/152
92. Su. sa. Ni. 5/17- Daihana, Ba. Pra. Mad. 54/46
93. Su.sa.Ni.5/17, A.sa.Ni.15/40, Ba.Pra.Mad.54/46,Ma.Ni.49/37-39,
Ga.Ni.36/38-40
94. Ca. sa. Chi – 7/174
95. Ca. sa. Chi – 7/175 – 176, Su. Sa. ni – 5/17, A. hri. Ni – 15/42 – 43, A. hri. Ni – 14/40, Ma. Ni
– 49/40 – 41, Y. R – Kustanidana chikitsa prakarana – 27, Ba. pra. Mad – 54/47 – 48, Be. sa.
Chi – 4/ 34, Ga. Ni – 36/41–42
96. Ma. Ni. 1
97. Su. sa. Ni. 5/3
98. Su. sa. Ni. 5/17
99. H. S. 50
100. Bhel. Ni.5/5-6
101. Ca. Chakrapani
102. Ca. Chakrapani
103. A. hri. Chi. 14/2-3
104. Kasyapa S. Sharira
105. Sha. sa. 7/90
106. A. hri. Sha. 1/48
107. A. hri. Su. 12/5
108. Ca. sa. Chi. 7/176, A. S. Ni.14/40
109. A. S. Ni.14/43, Ca.sa. Chi. 7/175

References
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 131
110. Su. Ni. 5/17
111. Su. Ni. 5/17
112. A. hri. Ni. 14/4-6
113. A. hri. Chi. 20/11, Ga. Ni. 36/227
114. Ca. sa. Su. 11/54
115. Ca. sa. Su. 11/55
116. Sha. Pu. K. 4/8
117. Sha. Pu. K. 4/2
118. Ca. sa. Chi. 7/162- Chakrapani
119. Ca. sa. Chi. 7/162-163, A. hri. Chi. 20/2-3, Ga. Ni. 36/228
120. A. hri. Chi 20/2
121. Ca. sa. Chi. 7/163
122. Y.R.- Kusthanidana chikitsa prakarana- 202
123. A.hri. Chi.20/2
124. A.hri. Chi.20/2, Ga. Ni. 36/232
125. Ca. sa. Chi. 7/164
126. Ga.Ni- 36/233-234
127. Ga.Ni- 36/236-239
128. Ca. sa, C hi. 7/164-165, A. hri. Chi. 20/5, Ga.Ni- 36/230
129. Su. sa. Chi. 1/90-93
130. A.hri. Chi.19/98, Ga. Ni. 36/226
131. Ca. sa. Chi. 7/172
132. Ka. Sa. Khi. 3/117 – 118, Ca. sa. Chi.30/282, A. hri. Ut.2/30, Ma. Ni.68/16
133. Ka. sa. Su. 27/66
134. Ca. sa. Chi. 30/283-284
135. Ca. sa. Chi. 30/283-Chakrapani
136. A. hri. Ut. 2/31-33
137. Ca. sa. Ka. 1/4 –Chakrapani
138. Sha. Pu. K. 4/3-6
139. Ca. sa. Ka. 8/5
140. Ca. sa. Ka. 8
141. Ba. Pra. Haritkyadi varga 1/149-150
142. Ka. sa. Khi. 7/61
143. Su. sa. Su. 18/6-7
144. A. sa. Ut. 30/89
145. Ca. sa. Chi. 25/110-118
146. Ca. sa. Chi. 21/98-105
147. Su. sa. Su. 18/12
148. Su. sa. Su. 18/4-5

References
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 132
149. Ba. Pra. Pu. 6/104, Su. sa. Su. 18/13
150. Su. sa. Su. 18/15-16
151. Su. sa. Su. 18/8-10
152. Su. sa. Su. 18/11
153. Ca. sa. Su. 25/45
154. Su. sa. Ni. 5/31
155. Ca. sa. Chi – 7/82 – 83, Su. Sa. chi – 9/72, A. sa. chi – 21/26, A. hri. Chi.19/25–27, Y. R.–
Kustanidana chikitsa prakarana – 220, Ga.Ni. 36/45–47, Bai.Rat. 54/372–381, C. D – 50/167
156. http://www.medicinalplantskr.org/SOURCES_OF_INFORMATION_ON_M_1.HTM
157. http://www.bergeriesurlelac.ca/bergerie_analyse_lait_en.html
BIBLIOGRAPHY

Bibliography
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 133
BIBLIOGRAPHY
1. Agnivesha - Charakasamhita with Ayurveda Dipika commentary of
charkapani. Chaukhambha surabharathi prakashana, Varanasi, reprint
2000 Pp-179, 666, 339, 318, 337, 278, 132, 217, 151, 196, 77-78, 645,
596, 564, 21, 450-459, 342.
2. Amarasimha- amarakosha by haragovindha Shasthri, chokamba Sanskrit
series office Varanasi 5th edition 1984.
3. Atharva Veda – by Devichand.M.A.,MunshiramManoram publications
New Delhi 1997 P-18.
4. Bhavamishra- Bhavaprakasha edited with the vidhyothini hindi
commentary, published by choukamba Sanskrit sanstan, 7th edition 2000,
vol-1 P-68, vol 2- Pp- 518, 532-541.
5. Bhela- b-Bhela samhitha text with English translation commentary and
critical notes by Dr. K.H.Krishnamurthy, publishe by choukamba vishwa
barathi oriental publishers Varanasi, 1st edition – 2000, Pp: 330, 327 –
328, 150.
6. Chakrapanidutta – Chakradutt (Sanskrit text with English translation) a
treatise on principles and practices of ayurvedic medicine. Edited and
translated by P V Sharma, Chaukamba publishers, Varanasi, 2nd edition –
1998, Pp – 389 - 409.
7. Gerard J Tortora – Principles of anatomy and physiology, Harper Collins
publishers, 8th edition – 1996, Pp: 124 – 129.
8. Govind Dasa – Bhaishajyarathnavali vidhyodhini hindi vyakya vimarsha
by Kaviraj Sri Ambikadutta Shastri, Chaukhambha Sanskrit Sansthan,
Varanasi, 15th edition – 2002, Pp: 618 – 640.
9. Gray‟s - Anotomy, Churchill Living stone, Newyork, Reprint – 2000,
Pp: 376 – 417.
10. Hareetha - Hareetha samhita translated by Ravidutta, Venkateshwara
mudralaya, Mumbai, Pp: 412, 420 – 421, 505 - 506.

Bibliography
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 134
11. Harrison‟s – Principle of internal medicine, Mac Grawhill Medical
publishing division, New york, 15th edition – 2001, Pp: 320 – 321.
12. Harsh Mohan textbook of pathology, Published by Jaypee brother‟s
publications, New Delhi. 4th edition - 2002, p. – 30.
13. J S Pasricha – Illustrated text book of Dermatology, Jaypee brothers,
New Delhi, 1st edition – 1996, P: 101.
14. L K Bhutani – Colour atlas of Dermatology, Interprint, New Delhi, 4th
edition – 1993, Pp: 147 – 149, 278.
15. Madhavakara - Madava nidana with madhukosha sanskrit commentory –
by Sri Vijaya rakshita and srikantadutta with Vidhyodhini hindi
comentary and notes by sudarshana shastry, Published by Chaukhambha
Sanskrit Sansthan, Varanasi, 27th edition 1998.Pp: 153 – 154, 164 – 167.
16. Manu smrithi – With Manoratha Mukthavali commentary of Kulluka
Bhatta by Haragovinda Shastri, Choukambha Sanskrit sansthan,
Varanasi, 6th Edition – 1999, P: 100.
17. Nelson, Textbook of pediatrics, published by W B Sundrs Company,
Pennsylvania, 14th edition - 1992, p. 1638.
18. P N Bhel – Practice of dermatology, C B S Publishers and distributors,
New Delhi, 9th Edition, reprint – 2004, Pp: 304 – 310.
19. Rigveda samhita – Sanskrit text, English translation and notes according
to the translation of H H Wilson, Parimal publications, 1st edition – 1997,
P: 294, Vol2-P: 212
20. Raja Radhakantha deva – Shabdha kalpa dhruma, Chaukamba sanskrit
series office, Varanasi, 3rd Edition – 1967. Vol. 5
21. Sastry C H S (Chavlis) – Principles and practice of peadiatrics in
Ayurveda, 1946, Ph D Thesis.
22. Sharangadharacharya - Sharangadhara Samhita with Adamalla‟s Dipika
and Kashirams gudartha dipika, Chaukhambha Orientalia, Varanasi, 5th
edition 2002, P: 115, Pp: 49, 98, 359.
23. Sir Monier Monier Williams – A Sanskrit – English Dictionary, Mothilal
banarasi das publishers, Delhi, Reprint – 1997.

Bibliography
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 135
24. Sushruta - Sushurtasamhita with Nibandha Sangraha Commentary of Sri
Dalhanacharya and Nyayachandrika panjika of Sri Gayadasacharya on
Nidanasthana. Chaukhambha Orientalia, Varanasi, 7th edition 2002.Pp:
355, 213, 348, 597, 514, 85, 86, 282 – 289, 442 – 448.
25. S.K. Punshi- A Hand Book of Vitiligo and Colour Atlas by Jaypee
Brothers, New Delhi 2000 Pp. 6
26. Tripaty K D, Essential of medical pharmacology, Published by Jaypee
brother‟s publications, New Delhi, 4th edition - 1999, p. 855
27. Vagbhata - Astanga Hridya with Sarvanga Sundara commentary of
arunadutta and Ayurveda rasayana of Hemadri. Chaukambha
Surabharathi prakashan, Varanasi, Reprint 2002. Pp: 385 – 386, 193 –
194, 524 – 529, 711 – 722, 79, 783, 370.
28. Valia R G, textbook and atlas of dermatology, published by Bhalani
publishing, Bombay, 1st edition – 1994, pp. 518 – 532.
29. Vaidhya shodala- Gadanigraha with vidhyothini hindi commentry by
indradevTripati choukamba sanskrit series office Varanasi 1st edition
1969 vol 2 – 758, 766 – 767, 770 – 810.
30. Vriddha Jivaka – Kashyapa Samhita, textbook with English translation
and commentary by Prof. P. V. Tewari, Published by Chaukhambha
Vishwabharati Oriental Publishers, 1st edition, 1996 Pp-117, 132, 71,
198, 335, 395, 307, 310, 483, 467, 519, 74.
31. Vrudda Vagbhata - Astanga Sangraha with hindi commentry by Kaviraj
Atridev Gupta, Krishana das Academy, Varanasi, Reprint 1993,Vol 2:
120 - 123, Pp: Vol 1: 398 – 399, 298 – 299, 270.
32. Yajurveda Samhita – Raviprakash Arya, Parimal Publications, Delhi, 2nd
edition 1999, P: 419.
33. Yogarathnakara - Vaidhya Prabha hindi commentory by Indradev tripaty
and Dr.dayashankar tripaty. Krishnadas Academy, Varanasi, 1st edition,
1998 Pp- 642, 644, 646 - 664.
ANNEXURE

Annexure
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 136
POST GRADUATE DEPARTMENT OF KAUMARABHRITHYA
S.D.M. COLLAGE OF AYURVEDA & HOSPITAL
HASSAN (KARNATAKA)
PROFORMA FOR CLNICAL STUDY
A CLINICAL STUDY ON EFFECT OF LOCAL APPLICATION WITH
APAMARGA KSHARA YUKTA JYOTISHMATI TAILA IN THE
MANAGEMENT OF SHVITRA (VITILIGO) IN CHILDREN.
Name: Serial No:
Age: yrs Sex: M / F OPD / IPD No:
Religion: H / M / C / others D.O.S.T:
Occupation: D.O.C.T:
Socio-economic Status:
Address:
Phone No :
Roga pareeksha :
Pradhaan vedana :
Aruna varna mandala
Paridhwamsi ( powder like material on starching )
Padmapatra varna
Daha
Roma vidhwamsatha ( distruction of hair at the site )
Shvetha varna
Kandu
Spread in body
Number of lesions
Nature of lesions
Rogi pareeksha
A) Prakruthitha
Kula pareeksha/vrittantha
Jatha poorvika vrithantha
Annexure
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 137
Jathottara pareeksha
Status of prana/ conciousness
Samskriti achieved/ Samskaras performed
Anya viruddhabhi samskriti
Prakruthi Satva
Agni bala Ahara intake
Sathmya Kosta
Dehabala Samhanana
Bhara Pramana
Sara Danta
Vikruthi
Dosha vichara
Assesment of vata, pitta and kapha
Nadi Drika
Mutra Akruthi
Mala Raktha bara
Jihwa Tapa krama
Shabdha Swasana
Sparsha Samata/ Niramata
Dushya pareeksha
Sambaddha stroto pareeksha
Sthanika pareeksha/ Local examination of selected lesion for study :
Laboratory investigation
Blood: B.T. A.T.
Hb%:
T.C.:
Urine:
Koshtha Shuddhi with Argvadha Kashaya :
No. of vegas:

Annexure
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 138
Local application
Drug :
Placebo :
EFFECT OF LOCAL APPLICATION WITH
Sl no
Assessment criteria Before treatment
End of 1 st month
End of 2 nd month
Follow Up
1 Appearance of itching sensation over
observed Shvitra (Vitiligo) patch.
2 Alteration in the colour of observed
Shvitra (Vitiligo) patch.
3 Bleb formation on observed Shvitra
(vitiligo) patch.
4 Number of black dots appearing in the
observed Shvitra (vitiligo) patch.
5 Change in the size of observed Shvitra
(vitiligo) patch.
Signature of student Signature of Guide

Annexure
A Clinical Study On Effect Of Local Application With Jyotishmati-Apamarga Kshara Taila In The Management Of Shvitra (Vitiligo) in children 139
The criteria kept for grading to observe any improvement is as following:
1. Appearance of itching sensation over observed Shvitra (vitiligo) patches.
a. If no Itching sensation over observed 1
b. If Itching sensation over observed 0
2. Colour change in the observed Shvitra (vitiligo) patches.
e. No change in colour (White) 3
f. Light pink 2
g. Dark pink 1
h. Normal skin colour 0
3. Bleb formation on observed Shvitra (vitiligo) patches.
a. If no bleb formation 1
b. If bleb formation 0
4. Number of black spots in observed Shvitra (vitiligo) patch
d. If no black spots appear 2
e. If less than three spots appear 1
f. If three or more spots appear 0
5. Size of the observed Shvitra (Vitiligo) patch
d. If size remains same or increases 2
e. 10% reduction in size 1
f. If more than 10% reduction 0

STUDY GROUP (GROUP - A)
*(A- Vruddahara, B- Masha,mulaka,dadhi,amla, C-Intake of cold items after hot exposure,
V-P – Vata-Pitta Prakruti, V-K – Pitta-Kapha Prakruti, P-K – Pitta-Kapha Prakruti.)
Sr. No.
Name
OPD no.
Age in yrs
Sex
Religion
Prakruthi
Place
Socio economic status
Diet
Family history
Nidana
A B C
1. Spoorthi 3830 9 F Hindu K-P Rural U.M.C Veg. -ve _ + _
2. Shashidhara 3866 11 M Hindu K-P Urban U.M.C Mix. -ve + _ +
3. Mohammed
Sameer
3519 11 M Muslim V-P Urban U.M.C Mix. -ve + _ +
4. Namratha 3364 11 F Hindu V-P Urban L.M.C Veg. -ve _ + _
5. Karthik S. 3583 8 F Hindu P-V Urban U.M.C Mix. -ve _ _ +
6. Muskan 3370 8 F Hindu P-V Rural L.M.C Veg. -ve _ _ _
7. Sneha 3873 10 F Hindu P-V Rural L.M.C Mix. -ve _ + _
8. Harshavardhana 3261 8 M Hindu V-P Urban U.M.C Mix. -ve _ _ +
9. Kunal 3892 12 M Hindu P-V Urban L.M.C Veg. -ve _ _ +
10. Rabiya Khan 3897 11 F Muslim P-V Urban U.M.C Mix. -ve + _ _
11. Prasad 3899 6 M Hindu P-V Urban L.M.C Mix. -ve _ _ _
12. Yash S. 3830 8 M Hindu P-V Urban L.M.C Mix. -ve _ _ _
13. Santosh 3868 11 M Hindu V-P Urban L.M.C Mix. -ve _ + +
14. Chidankumar 3739 8 M Hindu V-P Rural Poor Mix. -ve _ _ _
15. Shashank 3301 6 M Hindu P-V Urban L.M.C Veg. -ve _ _ _
16. Akshay 3806 12 M Hindu P-V Urban L.M.C Mix. -ve + _ +
17. Dore swammy 3927 8 M Hindu P-V Rural Poor Mix. -ve _ + +
18. Harsh 3932 7 M Hindu P-V Urban U.M.C Veg. -ve _ _ _
19. Sumanth 2357 12 M Hindu P-V Rural L.M.C Mix. -ve _ _ +
20. Chethan 3946 9 M Hindu P-V Urban L.M.C Mix. -ve _ + _
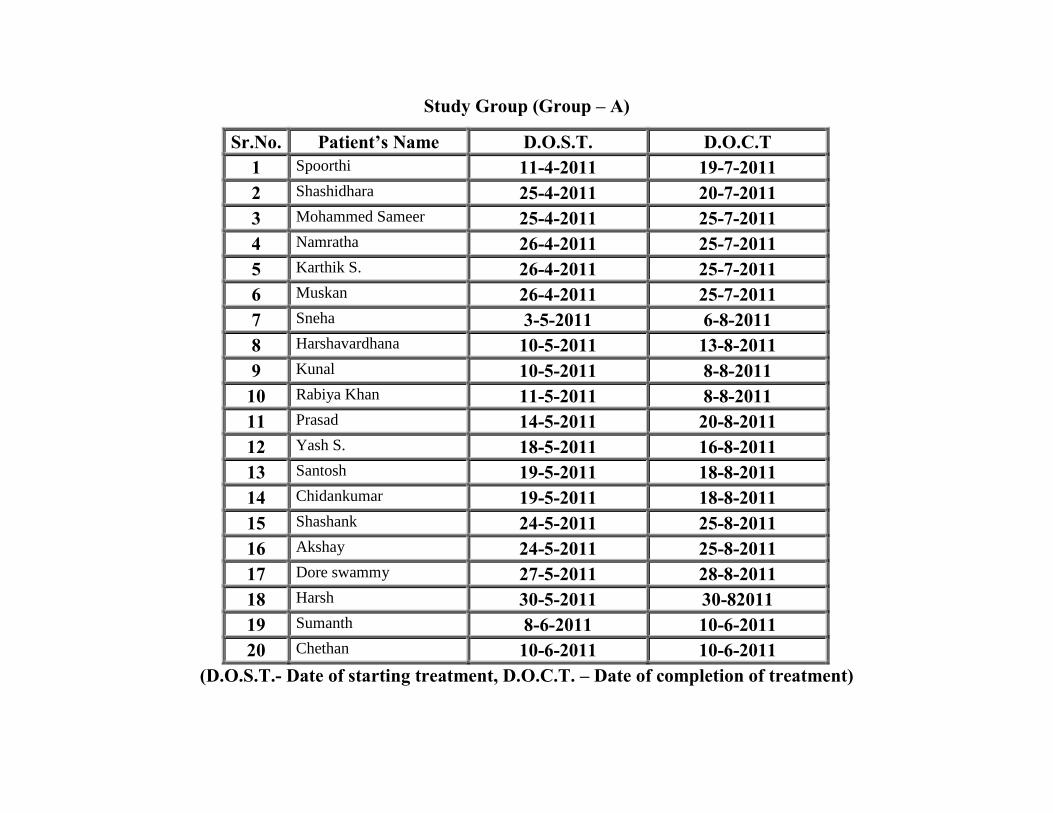
Study Group (Group – A)
Sr.No. Patient’s Name D.O.S.T. D.O.C.T 1 Spoorthi 11-4-2011 19-7-2011 2 Shashidhara 25-4-2011 20-7-2011 3 Mohammed Sameer 25-4-2011 25-7-2011 4 Namratha 26-4-2011 25-7-2011 5 Karthik S. 26-4-2011 25-7-2011 6 Muskan 26-4-2011 25-7-2011 7 Sneha 3-5-2011 6-8-2011 8 Harshavardhana 10-5-2011 13-8-2011 9 Kunal 10-5-2011 8-8-2011
10 Rabiya Khan 11-5-2011 8-8-2011 11 Prasad 14-5-2011 20-8-2011 12 Yash S. 18-5-2011 16-8-2011 13 Santosh 19-5-2011 18-8-2011 14 Chidankumar 19-5-2011 18-8-2011 15 Shashank 24-5-2011 25-8-2011 16 Akshay 24-5-2011 25-8-2011 17 Dore swammy 27-5-2011 28-8-2011 18 Harsh 30-5-2011 30-82011 19 Sumanth 8-6-2011 10-6-2011 20 Chethan 10-6-2011 10-6-2011
(D.O.S.T.- Date of starting treatment, D.O.C.T. – Date of completion of treatment)

Study Group (Group - A)
Sl. No.
Appearance of Itching sensation over observed Shvitra (Vitiligo) patch
Colour change in observed Shvitra (Vitiligo) patch
Bleb formation in observed Shvitra (Vitiligo) patch
No. of black spots in observed Shvitra (Vitiligo) patch
Size of observed Shvitra (Vitiligo) patch
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
1. 1 1 0 1 3 2 1 2 1 1 1 1 2 1 1 1 2 2 1 2
2. 1 0 0 0 3 1 1 1 1 1 0 1 1 0 0 0 2 1 0 0
3. 0 0 0 0 3 2 1 1 1 0 0 1 1 0 0 0 2 1 0 0
4. 1 1 0 0 3 2 1 1 1 1 1 1 1 0 0 0 2 1 0 0
5. 1 0 0 1 3 2 1 2 1 1 1 1 2 1 1 1 2 2 1 1
6. 0 0 0 0 2 1 1 1 1 1 1 1 2 1 0 0 2 2 1 1
7. 1 1 1 1 3 2 1 2 1 1 1 1 1 1 1 1 2 2 1 1
8. 0 0 0 0 3 2 1 2 1 1 0 1 1 1 0 0 2 1 1 1
9. 1 0 0 1 3 1 1 1 1 1 0 1 2 1 0 0 2 1 0 0
10. 1 0 0 1 2 1 1 1 1 0 0 1 1 1 1 1 2 1 0 1
11. 1 1 1 1 3 1 1 1 1 1 1 1 1 1 1 1 2 2 1 1
12. 1 1 0 1 3 2 1 2 1 1 1 1 2 2 1 1 2 2 1 1
13. 1 1 0 1 3 2 1 2 1 1 1 1 1 1 1 1 2 1 0 1
14. 1 0 0 0 3 2 1 1 1 1 0 1 1 0 0 0 2 1 0 0
15. 1 0 0 0 3 1 1 1 1 1 1 1 2 1 1 1 2 1 1 1
16. 1 1 1 1 3 2 1 2 1 1 1 1 1 0 0 0 2 2 1 1
17. 1 1 1 1 3 2 1 1 1 1 1 1 2 1 1 1 2 2 1 1
18. 1 1 1 1 3 2 1 2 1 1 1 1 2 1 1 1 2 2 1 1
19. 1 0 0 0 3 2 1 1 1 1 1 1 1 0 0 0 2 1 1 1
20. 1 0 0 1 3 2 1 2 1 1 1 1 1 1 1 1 2 2 1 2
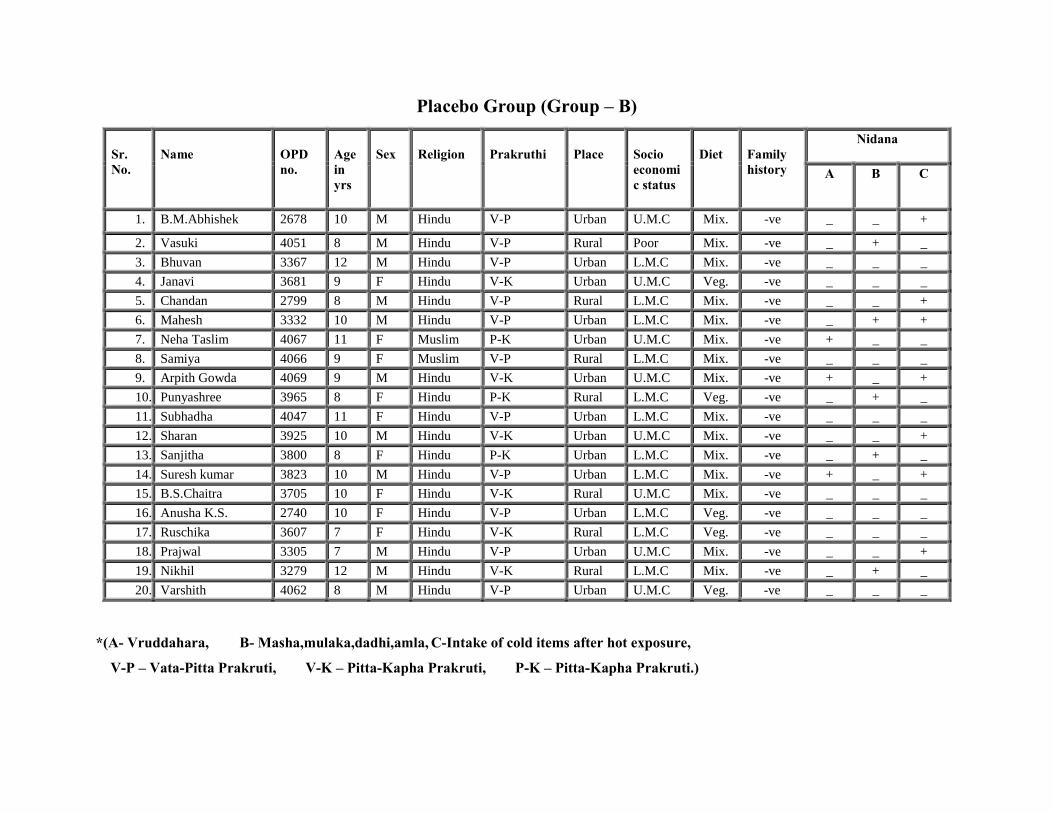
Placebo Group (Group – B)
Sr. No.
Name
OPD no.
Age in yrs
Sex
Religion
Prakruthi
Place
Socio economic status
Diet
Family history
Nidana
A B C
1. B.M.Abhishek 2678 10 M Hindu V-P Urban U.M.C Mix. -ve _ _ +
2. Vasuki 4051 8 M Hindu V-P Rural Poor Mix. -ve _ + _
3. Bhuvan 3367 12 M Hindu V-P Urban L.M.C Mix. -ve _ _ _
4. Janavi 3681 9 F Hindu V-K Urban U.M.C Veg. -ve _ _ _
5. Chandan 2799 8 M Hindu V-P Rural L.M.C Mix. -ve _ _ +
6. Mahesh 3332 10 M Hindu V-P Urban L.M.C Mix. -ve _ + +
7. Neha Taslim 4067 11 F Muslim P-K Urban U.M.C Mix. -ve + _ _
8. Samiya 4066 9 F Muslim V-P Rural L.M.C Mix. -ve _ _ _
9. Arpith Gowda 4069 9 M Hindu V-K Urban U.M.C Mix. -ve + _ +
10. Punyashree 3965 8 F Hindu P-K Rural L.M.C Veg. -ve _ + _
11. Subhadha 4047 11 F Hindu V-P Urban L.M.C Mix. -ve _ _ _
12. Sharan 3925 10 M Hindu V-K Urban U.M.C Mix. -ve _ _ +
13. Sanjitha 3800 8 F Hindu P-K Urban L.M.C Mix. -ve _ + _
14. Suresh kumar 3823 10 M Hindu V-P Urban L.M.C Mix. -ve + _ +
15. B.S.Chaitra 3705 10 F Hindu V-K Rural U.M.C Mix. -ve _ _ _
16. Anusha K.S. 2740 10 F Hindu V-P Urban L.M.C Veg. -ve _ _ _
17. Ruschika 3607 7 F Hindu V-K Rural L.M.C Veg. -ve _ _ _
18. Prajwal 3305 7 M Hindu V-P Urban U.M.C Mix. -ve _ _ +
19. Nikhil 3279 12 M Hindu V-K Rural L.M.C Mix. -ve _ + _
20. Varshith 4062 8 M Hindu V-P Urban U.M.C Veg. -ve _ _ _
*(A- Vruddahara, B- Masha,mulaka,dadhi,amla, C-Intake of cold items after hot exposure,
V-P – Vata-Pitta Prakruti, V-K – Pitta-Kapha Prakruti, P-K – Pitta-Kapha Prakruti.)

Placebo Group (Group – B)
Sr.No. Patient’s Name D.O.S.T. D.O.C.T 1 B.M.Abhishek 14-4-2011 19-7-2011 2 Vasuki 14-4-2011 17-7-2011 3 Bhuvan 23-4-2011 26-7-2011 4 Janavi 23-4-2011 26-7-2011 5 Chandan 23-4-2011 26-7-2011 6 Mahesh 24-4-2011 26-7-2011 7 Neha Taslim 25-4-2011 25-7-2011 8 Samiya 25-4-2011 25-7-2011 9 Arpith Gowda 25-4-2011 25-7-2011 10 Punyashree 25-4-2011 25-7-2011 11 Subhadha 25-4-2011 25-7-2011 12 Sharan 25-4-2011 25-7-2011 13 Sanjitha 25-4-2011 25-7-2011 14 Suresh kumar 25-4-2011 25-7-2011 15 B.S.Chaitra 25-4-2011 25-7-2011 16 Anusha K.S. 25-4-2011 11-8-2011 17 Ruschika 25-4-2011 20-8-2011 18 Prajwal 25-4-2011 16-8-2011 19 Nikhil 25-4-2011 18-8-2011 20 Varshith 25-4-2011 27-8-2011
(D.O.S.T.- Date of starting treatment, D.O.C.T. – Date of completion of treatment)

Placebo Group (Group - B)
Sl. No.
Appearance of Itching sensation over observed Shvitra (Vitiligo) patch
Colour change in observed Shvitra (Vitiligo) patch
Bleb formation in observed Shvitra (Vitiligo) patch
No. of black spots in observed Shvitra (Vitiligo) patch
Size of observed Shvitra (Vitiligo) patch
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
BT End of 1st mo.
End of 2nd mo.
Follow up End of 3rd mo.
1. 0 0 1 1 3 3 3 3 1 1 1 1 2 2 2 2 2 2 2 2
2. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
3. 1 1 1 1 2 2 1 2 1 1 1 1 2 2 2 2 2 2 2 2
4. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
5. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
6. 1 1 1 1 3 3 3 3 1 1 1 1 2 2 2 2 2 2 2 2
7. 1 1 1 1 3 3 3 3 1 1 1 1 2 2 2 2 2 2 2 2
8. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
9. 1 1 1 1 2 2 2 2 1 1 1 1 1 1 1 1 2 2 2 2
10. 0 0 0 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
11. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
12. 0 0 0 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
13. 1 1 1 1 3 3 3 3 1 1 1 1 2 2 2 2 2 2 2 2
14. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
15. 1 1 1 1 2 2 2 2 1 1 1 1 1 1 1 1 2 2 2 2
16. 1 1 1 1 3 3 3 3 1 1 1 1 1 1 1 1 2 2 2 2
17. 1 1 1 1 3 3 3 3 1 1 1 1 0 0 0 1 2 2 2 2
18. 1 1 1 1 3 3 3 3 1 1 1 1 2 2 2 2 2 2 2 2
19. 1 1 1 1 2 2 2 2 1 1 1 1 1 1 1 1 2 2 2 2
20. 0 0 1 1 3 3 3 3 1 1 1 1 2 2 2 2 2 2 2 2
Top Related
Copyright © 2022 FDOKUMEN

