







Bahasa
Halaman
Hukum


USE OF FEMINIST FAMILY THERAPY TO TREAT INTIMATE PARTNER
VIOLENCE IN SAME-SEX COUPLES
A Dissertation
Presented to
The Graduate Faculty of The University of Akron
In Partial Fulfillment
of the Requirements for the Degree
Doctor of Philosophy
Rachel Bell
August 2021

ii
USE OF FEMINIST FAMILY THERAPY TO TREAT INTIMATE PARTNER
VIOLENCE IN SAME-SEX COUPLES
Rachel Bell
Dissertation
Approved:
Advisor Dr. Heather Katafiasz Committee Member Dr. Rikki Patton Committee Member Dr. David Tefteller Committee Member Dr. Bernard Jesiolowski Committee Member Dr. Wondimu Ahmed
Accepted: Department Chair Dr. Varunee Faii Sangganjanavanich Acting Dean of the College Dr. Timothy M. McCarragher Interim Director of the Graduate School Dr. Marnie M. Saunders Date

iii
ABSTRACT
In the last 30 years, researchers have seen a steady increase in violence among
same-sex couples (Rolle et al., 2018). Current statistics show that same-sex couples
experience intimate partner violence (IPV) at a rate 25% higher than heterosexual couples
(National Coalition Against Domestic Violence [NCADV], 2019). In an effort to curb
the growing incidents of violence, mental health treatment providers have begun using
Feminist Family Therapy (FFT) to treat same-sex couples. The feminist approach is the
most widely recommended modality to treat IPV in all couples because it is believed to
address a core cause of violence (Bohall, et al., 2016): an imbalance of power; however,
it has faced criticism since it was originally designed to address unequal gender roles in
heterosexual couples. Questions have also been raised regarding the model’s
effectiveness because rates of violence continue to rise. Proponents of the model argue
that same-sex couples are less likely to seek out services when experiencing violence in
their relationship so the model’s effectiveness cannot be measured by these statistics. In
this study, a descriptive analysis and one-way ANOVA assess whether clinicians report
using FFT and whether criticisms of the approach influence its use. Analyses revealed
that the participants reported high levels of usage of the approach, although only 1.8%
identified it as their primary theoretical orientation. Results also showed that
participants’ level of agreement with the criticisms of FFT significantly influenced their
use of the approach.

iv
ACKNOWLEDGEMENTS
I have been a graduate student at the University of Akron for almost 10 years and
it goes without saying that this time has not been without its challenges. Throughout
those times, I have had the support of many around me and I do not believe I will ever
find the words to express the extent of my gratitude, but I will try. To Drs. Rebecca
Boyle and Karin Jordan, thank you for your challenges and your encouragement. To Dr.
Patton, thank you for your kindness and your authenticity. To Dr. Tefteller, I cannot
express enough gratitude for the ways in which you have supported me without hesitation
since we have met. It will never be forgotten. To Dr. J., I thank you for the validation
you provide every time we interact. I have cherished every conversation. To Dr. Ahmed,
thank you for your endless patience as I stumbled through my chapter four. To Dr. K.,
whom I have known almost my entire Akron career, thank you for all you have taught me
along the way. Thank you for not letting me give up on myself or this degree.
Additionally, I thank those that have been my support outside of school. To my mom,
thank you for listening to every part of my graduate education, even when you had no
idea what I was talking about. To James, thank you for never letting me give up. To my
college mentor, Dr. Frank Hamilton, who remains invested in my success to this day,
thank you for reminding me of my potential and for believing I can do anything. Finally,
I would like to dedicate this manuscript to my dad, who would have been too excited for
words to witness this accomplishment. I hope I have made him proud.

v
TABLE OF CONTENTS
LIST OF TABLES……………………………………………………………………….ix
LIST OF FIGURES……………………………………………………………………….x
CHAPTER
I. INTRODUCTION ……………………………………………………………………...1
Conceptual Framework……………………………………………………………2
Intimate Partner Violence………………………………...……………….2
Types of IPV………………………………………………………………3
Intimate Partner Violence Among Same-Sex Couples……………………5
Feminist Family Therapy and Intimate Partner Violence Among Same-Sex
Couples……………………………………………………………………7
Overview of Proposed Research…………………………………………...…….. 7
Research Goals.………………………………………………..…………. 7
Research Questions and Hypotheses……………………………………...9
Operational Definitions.……………………………………….………..... 9
Summary……………………………………………………………………..…..10
II. LITERATURE REVIEW……………………………………………………………. 12
Feminist Family Therapy………………………………………………………...12
Therapeutic Relationship………………………………………………...14
Gender……………………………………………………..……………..15
Egalitarian Relationships………………………………………………...15

vi
Empowerment……………………………………………………………16
Affirmation of the Less Powerful………………………………………..16
Power…………………………………………………………………….17
Interventions……………………………………………………………..17
Evolution of Feminist Family Therapy…………………………………..18
Clinical Use of Feminist Family Therapy………………………….…………….20
Criticisms of the FFT Approach ………...………………………………………21
Feminist Models for Treatment of IPV…………………………………………..24
The Duluth Model…………………………………….……………….....25
Criticisms of the Duluth Model………………………………………….27
The Integrative Feminist Model………………………………………....28
Criticisms of the Integrative Feminist Model……………………………29
Feminist Family Therapy to Treat IPV in Same-Sex Couples…………….…….30
Restatement of Research Questions and Hypotheses……………………………35
Summary…………………………………………………………………………35
III. RESEARCH METHODS……………………………………………………………36
Restatement of Research Goals………………………………………………….36
Restatement of Research Questions and Hypotheses…………………...……….37
Research Design…………………………………………………………………37
Participants………………………………………………………………………38
Criteria for Participation…………………………………………………38
Solicitation of Participants…………………………………………….…38
Incentives for Participation………………………………………………39

vii
Description of Sample……………………………………………………39
Sample Size………………………………………………………………40
Procedure…………………………………………………………...……...…….40
Data Analysis Method………………………………………………..…………..41
Measures…………………………………………………………………………41
Demographics Questionnaire………………………………………….…42
Feminist Family Therapist Behavior Checklist………………………….42
Adapting the Feminist Family Therapist Behavior Checklist……………43
Feminist Criticisms Questionnaire……………………………………….43
Summary…………………………………………………………………………43
IV. RESULTS………………………………………………………………………...…44
Restatement of Research Questions and Hypotheses…….……………………...44
Data Collection…………………………………………………………………..45
Demographic and Descriptive Statistics…………………………………………45
Recoding and Transforming of Variables………………………………………..49
Research Question One…………………………………………………………..50
Research Question Two………………………………………………………….51
Summary of Results……………………………………………………………...53
V. DISCUSSION………………………………………………………………………..55
Discussion of Overall Findings…………………………………………………..55
Demographics……………………………………………………………56
Research Question One…………………………………………………..56
Research Question Two………………………………………………….57

viii
Limitations of the Study…………………………………………………...……..58
Structure of the Study……………………………………………………58
Data Collection…………………………………………………………..59
Validity and Reliability of the Assessment Instruments…………………60
Clinical Implications……………………………………………………………..61
Future Research Implications……………………………………………………62
Summary…………………………………………………………………………64
REFERENCES…………………………………………………………………………..66
APPENDICES…………………………………………………………………………...75
APPENDIX A: INTEGRATIVE FEMINIST MODEL FOR INTIMATE
PARTNER VIOLENCE…………………………..…………………………….76
APPENDIX B: INFORMED CONSENT FORM……………………………….77
APPENDIX C: DEMOGRAPHICS QUESTIONNAIRE……………………….78
APPENDIX D: FEMINIST FAMILY THERAPY BEHAVIOR CHECKLIST...80
APPENDIX E: FEMINIST CRITCISMS QUESTIONNAIRE…………………82
APPENDIX F: GIFT CARD GIVEAWAY OPT-IN……………………………83
APPENDIX G: FFTBC SUBSCALES AND ITEMS…………………………...84
APPENDIX H: IRB APPROVAL……………………………...………………..87
ix
LIST OF TABLES
Table
4.1 Participants’ Demographic Information…………………………………………48
4.2 Criticism Groups Cutoff Scores………………………………………………….51
4.3 Participants’ Reported Usage of FFT and Subscales Based on Sum Score……...52
4.4 One-Way Analysis of Variance………………………………………………….53
4.5 Variables Significantly Influenced by Participants’ Level of Agreement with FFT
Criticisms………………………………………………………………………………...54

x
LIST OF FIGURES
Figure
2.1 Integrative Feminist Model for Intimate Partner Violence………………………76

1
CHAPTER ONE
INTRODUCTION TO THE USE OF FEMINIST FAMILY THERAPY TO TREAT
INTIMATE PARTNER VIOLENCE IN SAME-SEX COUPLES
In the last 30 years, researchers have seen a steady increase in violence among
same-sex couples (Rolle et al., 2018). Current statistics show that same-sex couples
experience intimate partner violence (IPV) at a rate 25% higher than heterosexual couples
(National Coalition Against Domestic Violence [NCADV], 2019). In an effort to curb
the growing incidents of violence, mental health treatment providers have begun using
Feminist Family Therapy (FFT) to treat same-sex couples. The feminist approach is the
most widely recommended modality to treat IPV in all couples because it is believed to
address a core cause of violence (Bohall, et al., 2016): an imbalance of power; however,
it has faced criticism due to the fact that it was originally designed to address unequal
gender roles in heterosexual couples. Questions have also been raised regarding the
model’s effectiveness because rates of violence continue to rise. Proponents of the model
argue that same-sex couples are less likely to seek out services when experiencing
violence in their relationship so the model’s effectiveness cannot be measured by these
statistics. The proposed study intends to gain clarity on some of these issues by
surveying clinicians who have or are currently treating IPV in same-sex couples to
determine three things: 1) whether they are using a feminist perspective, 2)

2
whether they agree with the criticisms of the model, and 3) whether these criticisms
appear to influence their use of the model.
This chapter provides an overview of the concepts involved in the proposed study,
a review of the proposed study’s research goals and research questions, and a total
chapter summary.
Conceptual Framework
The following section provides an overview of the main concepts of this study,
including IPV, prevalence of violence in same-sex couples, and the Feminist Family
Therapy model for treatment of IPV.
Intimate Partner Violence
For the purposes of this study, IPV is being defined as “Physical, sexual, or
psychological harm by a current or former partner or spouse. This type of violence can
occur among heterosexual or same-sex couples and does not require sexual intimacy”
(Center for Disease Control and Prevention [CDC], 2018, para. 1). The CDC has
identified IPV as a health epidemic having a broad range of significant consequences.
The most recent data from the CDC’s annual National Intimate Partner and Sexual
Violence Survey shows that nearly one in four women and one in seven men report have
experienced IPV in their lifetime (CDC, 2019).
In the United States, it is estimated that nearly 20 people per minute are
physically abused by a current or former intimate partner (NCADV, 2019). On a typical
day, domestic violence support hotlines receive over 20,000 calls from victims seeking
assistance (NCADV, 2019). In Ohio, support hotlines average more than 27 calls every
hour (NCADV, 2019). Research also indicates that one in six women and one in 14 men

3
report have experienced sexual violence in intimate relationships. Of those that have
experienced IPV, the CDC reports that 41% of women and 14% of men have sustained a
physical injury as a result of abuse in their relationships. Most shockingly, data from
U.S. crime reports show that 16% of murder victims are killed by a current or former
intimate partner, and that 40% of females killed die at the hand of a partner (CDC, 2019).
The CDC has declared the rising rates of IPV to be an epidemic with significant
physical and mental health risks (CDC, 2019). Additionally, the NCADV identified
economic consequences of IPV, reporting that victims of violence lose a total of eight
million days of paid work per year, and as many as 60% of victims lose their job due to
reasons tied to abuse (2019). As a result of these growing statistics, the CDC has
identified several health risks related to having endured IPV, including cardiovascular,
gastrointestinal, reproductive, musculoskeletal, and nervous system conditions (CDC,
2018). Additionally, there are obvious mental health implications, including increased
risk for depression, anxiety, and PTSD symptoms. These mental health symptoms have
already been found to be increasingly linked to physical health, such as impaired immune
responses, increased risk of substance abuse, and increased risk of stroke (CDC, 2018).
The evidence for the adverse effects of IPV is overwhelming and does not only influence
a victim’s mental health, but can have long-lasting consequences on physical health and
economic struggle.
Types of IPV
IPV, also sometimes referred to as domestic violence, is a broad term that
addresses several types of abusive behaviors towards a current or former romantic partner
(National Institute of Justice [NIJ], 2019). In the United States, these various types of

4
abusive behaviors have increased significantly and have been linked to several physical,
psychological, and economic concerns (NIJ, 2019). Contrary to popular belief, IPV does
not just involve physical and sexual violence towards a partner, but also includes
psychological aggression and stalking, both of which involve intimidation and coercion
of another person (CDC, 2019). There have been several different types of IPV identified
in research literature.
The following outlines the type of violence and provides their definitions.
Physical Violence. Most simply defined, physical violence “is when a person
hurts or tries to hurt a partner by hitting, kicking, or using another type of physical force”
(CDC, 2019, para. 1).
Sexual Violence. “Forcing or attempting to force a partner to take part in a sex
act, sexual touching, or a non-physical sexual event (e.g., sexting) when the partner does
not or cannot consent” (CDC, 2019, para. 2).
Stalking. “is a pattern of repeated, unwanted attention and contact by a partner
that causes fear or concern for one’s own safety or the safety of someone close to the
victim” (CDC, 2019, para. 3).
Psychological Aggression. Psychological aggression is defined as “the use of
verbal and non-verbal communication with the intent to harm another person mentally or
emotionally and/or exert control over another person” (CDC, 2019, para. 4).
Uni-Directional and Bi-Directional Violence. In addition to specific forms of
violence, there are also ways to describe which partner is abusive to the other. Uni-
directional and bi-directional violence, also referred to as uni-lateral and bi-lateral

5
violence, describes whether there is one abuser and one victim or whether both partners
engage in abusive behaviors (Madsen et al., 2012).
Intimate Partner Violence Among Same-Sex Couples
Despite this focus on heterosexual couples, IPV rates among same-sex couples
have been found to be significantly higher than that of heterosexual relationships
(National Coalition Against Domestic Violence [NCADV], 2019). According to the
NCADV, 43.8% of lesbian women and 26% of gay men have experienced rape, physical
violence, and/or stalking by an intimate partner in their lifetime (2019). These statistics
indicate a frequency of violence that is 10% higher than heterosexual couples, on
average. In addition to higher rates of violence, the NCADV found that gay and lesbian
victims of near-lethal domestic violence only called for the assistance of law enforcement
26% of the time and fewer than 5% of victims sought out orders of protection (2013).
It has also been documented that same-sex couples experiencing IPV face more
difficult outcomes compared to the heterosexual population (Rolle et al., 2018). While
reliable research organizations such as the CDC and the World Health Organization
(WHO) have found many substantiated health and economic consequences to
experiencing IPV, research suggests that same-sex partners experience these
consequences to an even greater degree (Rolle et al., 2018). This is attributed to the fact
that same-sex couples experience amplified adverse effects of IPV due to societal
oppression and the additional risk of judgment and discrimination associated with being a
sexual minority (Rolle et al., 2018).
Additionally, rates of bi-directional violence have also been found to be higher in
same-sex relationships, versus more common uni-directional violence in heterosexual

6
relationships (NCADV, 2019). Due to the significant prevalence of violence in same-sex
relationships, it stands to reason that perhaps same-sex relationships are suffering as a
result of a societal power differential and the inability to maintain equality within the
relationship.
Despite the growing rates of IPV among same-sex couples, there is still relatively
little research in comparison with heterosexual couples. A 2015 literature review found
that studies focusing on same-sex couples made up only three percent of results, when
searching for literature focused on IPV (Rolle et al., 2018).
Several limitations have been identified to explain the lack of inclusive Lesbian,
Gay, Bisexual, Transgender, and Queer (LGBTQ) research on IPV. Most often, LGBTQ
participants are hesitant to self-identify due to fear of how the research may be used
(Baker et al., 2013, Clark et al., 2019). As will be discussed in chapter two, many
LGBTQ members avoid involvement with law enforcement, research initiatives, and
even mental health support, due to wanting to avoid unwanted attention and perpetuating
the stigma of LGBTQ violence in relationships (Baker et al., 2013; Clark et al., 2019).
Because researchers are aware of this fear, many large research surveys do not include
items that request participants to identify their sexual orientation, for fear of limiting or
biasing their results (Baker et al., 2013).
It has also been identified that it is sometimes difficult for participants to specify
their sexual orientation, as this concept is now considered to be more fluid than static
(Baker et al., 2013; Clark et al., 2019). Because orientation is not easily defined, it is
difficult for participants to identify themselves, and for researchers to provide appropriate
options on surveys, in order to allow participants to accurately self-identify. Again,

7
because orientation is not easily surmised, many large research initiatives have opted to
overlook this information altogether (Baker et al., 2013; Clark et al., 2019).
Feminist Family Therapy and Intimate Partner Violence Among Same-Sex Couples
Although there is relatively little treatment research in comparison with
heterosexual couples, the FFT model remains the most common recommendation for
treatment of IPV in same-sex couples (McPhail et al., 2007). The model has been largely
unadapted for use with same-sex couples, with the exception of some theoretical
literature and a handful of feminist models. Proponents of the feminist perspective point
to efforts to broaden its reach by including the concept of intersectionality, which
addresses not only gender oppression but also sexual, racial, and ethnic oppression when
treating IPV.
Overview of Proposed Research
This section introduces the specific research goals for this study and the research
questions that are being proposed. Operational definitions of key concepts are also
outlined.
Research Goals
The proposed study intends to determine whether clinicians who are actively
treating IPV in same-sex couples are utilizing FFT as a primary modality, as
recommended in the literature. Due to varying levels of training on couples therapy,
multicultural competence, and intersectionality, combined with the rising rates of IPV in
same-sex relationships, it is possible that clinicians are not utilizing the literature to guide
their approach to treat this important issue. This study aspires to determine the extent to
which clinicians are utilizing FFT as the most commonly suggested strategy to treat IPV

8
so that the frequency of violence in same-sex relationships can be decreased and treated
effectively.
As evident above, there is a significant dissonance between what is being
recommended for treatment of violence in same-sex relationships and criticisms of the
approach. The population for this study was narrowed to same-sex couples due to the
fluidity of sexual orientation, in general, making it difficult to research IPVs effects on
relationships for all members of the LGBTQ population. By focusing on a specific
portion of the LGBTQ community, this study can examine the effects of violence in
relationships among those who identify specifically as homosexual, as it is not yet clear
how to expand research to be inclusive of the entire spectrum of sexual orientation (Baker
et al., 2013; Clark et al., 2019). The proposed study attempts to explore the dissonance
by focusing on clinicians’ own perceptions of the approach and its criticisms, and
whether or not this impacts clinicians’ use of the approach. Since the rate of violence in
same-sex couples continues to rise, it is crucial that we investigate the effectiveness of
the recommended treatments and determine whether they are being used consistently or
not, in order to determine next steps in evaluating effective treatment options. Since the
feminist approach has been so heavily criticized within the mental health community, it is
a distinct possibility that these criticisms have influenced clinicians’ use of the theory.
The study intends to assess whether clinicians who have worked to treat violence in
same-sex relationships have used the feminist theory and whether they agree with its
criticisms.
In sum, due to the rising rates of IPV in same-sex relationships, this study aims to
assess whether clinicians are utilizing FFT; whether clinicians are confident in the
9
effectiveness of FFT; and whether their level of confidence is correlated with their
utilization of the approach to treat IPV in same-sex couples. This exploration is crucial
because the majority of literature written on treating IPV in same-sex couples suggests
that a feminist approach is the most effective methodology for this presenting issue.
However, the feminist perspective has also been under scrutiny for decades and often
elicits very strong and polarizing reactions.
Research Questions and Hypotheses
This study’s research questions are:
1) Are clinicians using Feminist Family Therapy principles to treat Intimate Partner
Violence in same-sex individual and couple clients?
Hypothesis 0: Clinicians are using Feminist Family Therapy thoroughly, as measured by
a response on the FFT checklist of either “Often,” or “Always”.
Hypothesis 1: Clinicians are not using Feminist Family Therapy thoroughly, as measured
by a response on the FFT checklist of either “Sometimes,” “Rarely,” or “Never”.
2) Is the use of Feminist Family Therapy being influenced by whether or not clinicians
agree with criticisms of the approach?
Hypothesis 0: The use of Feminist Family Therapy is not being influenced by clinicians’
agreement or disagreement with its criticisms.
Hypothesis 1: The use of Feminist Family Therapy is being influenced by clinicians’
agreement or disagreement with its criticisms.
Operational Definitions
Clinician: For the purposes of this study, “clinician” will refer to any mental-health
professional who is licensed to provide clinical therapy to clients diagnosed with any

10
disorder found in the Diagnostic and Statistical Manual V (American Psychiatric
Association, 2013). This may include licensed counselors, marriage and family
therapists, social workers, psychologists, and psychiatrists.
Feminist Family Therapy (FFT): A treatment model focused on challenging assumptions
regarding sex roles within all systems: family, society, and culture (Ault-Riche, 1986).
Gender: A human cultural status of feminine or masculine, differing from biological
status (Piercy et al., 1996).
Intimate Partner Violence (IPV): Physical, sexual, or psychological harm by a current or
former partner or spouse. This type of violence can occur among heterosexual or same-
sex couples and does not require sexual intimacy (Center for Disease Control and
Prevention, 2018).
Same-Sex Couple/Relationship: For the purposes of this study, a same-sex couple or
relationship is defined as two individuals of the same sex involved in an emotionally and
possibly physically intimate relationship.
Same-Sex Intimate Partner Violence (SSIPV): Intimate partner violence which occurs in
same-sex relationships (Rolle et al., 2018).
Power: Defined as "the capacity to gain whatever resources are necessary to remove
oneself from a condition of oppression, to guarantee one's ability to perform, and to affect
not only one's own circumstances, but also more general circumstances outside one's
intimate surroundings" (Goodrich, 1991, p. 10).
Summary
This chapter provides an overview of the focus of the proposed study. It presents
statistics demonstrating the prevalence of IPV in same-sex relationships, indicating our

11
need to ensure these couples are receiving evidence-based treatment. It also offers
foundational information on relevant concepts, such as FFT principles and treatment
guidelines suggested for same-sex couples.

12
CHAPTER II
LITERATURE REVIEW
This chapter provides an overview of the foundational concepts of this study and
the existing literature on them. Feminist Family Therapy (FFT) is outlined, including a
discussion of key concepts, the evolution of the theory, and a discussion of the clinical
applications of FFT. Finally, a thorough exploration of the recommended treatment
modalities for Intimate Partner Violence (IPV) in same-sex couples is provided. The
chapter concludes by highlighting the minimal literature in some of these areas, justifying
the need for studying clinicians’ frequency of use of the recommended treatments.
Feminist Family Therapy
Feminist Theory, created during the civil rights movement of the late 1960s and
early 1970s, originally focused on systemic issues born from gender inequality. From the
social movement, it was then integrated into approaches with therapy and involves
psychoeducation regarding systemic gender oppression and equalizing the power
differential between partners in couples' therapy (Thomas, 1977). As stated in an early
article on Feminist Therapy from 1977:
Coupled with the feminist humanism of such therapists is their feminist
consciousness and feminist framework, which are revealed in a particular
sensitivity to and understanding of the problems women bring to therapy,
the experience of being a woman, and the limitations that stereotypical sex

13
roles have historically placed on women and continue to place on their
achievement of self-actualization. (Thomas, 1977, p. 449)
Feminist Theory has broadened in the decades since its inception to include issues that
affect all oppressed groups, such as racial, cultural, ethnic, and sexual minorities. The
same principles for these various people groups apply, in that a feminist therapist would
seek to acknowledge the power differentials between the minority client and the
oppressor, whether that be the client’s partner or society as a whole.
Beginning in the 1980s, Feminist Theory began integrating feminist principles
into family therapy approaches. This integration manifested into six major tenets that
outline an FFT approach: 1) the therapist-client relationship is non-hierarchical and
invites open dialogue between clients and therapist; 2) gender is a primary focus in
therapy and is directly connected to a couple or family’s presenting concern(s); 3) the
therapist will encourage an egalitarian relationship, as unbalanced roles are considered
pathological from a feminist perspective; 4) empowerment is established as a formal
treatment goal, in order to ensure that both partners enjoy equal influence within the
relationship; 5) the therapist will avoid reinforcing traditional gender roles, which
feminist clinicians criticize in other family therapy models; and 6) the construct of power
is assessed, openly discussed in session, and made the focus of therapeutic interventions
(Vatcher & Bogo, 2001).
It should be emphasized that this framework is not considered a fully developed
systemic treatment model, but instead is a collection of principles that guide systemic
therapy approaches and prioritizes the empowerment of powerless clients (Goodrichet al.,
1988; Seligman & Reichenberg, 2010; Stith, 2006). FFT seeks to establish equality

14
throughout the many systems and subsystems involved in treatment. For example, the
therapist would take on an egalitarian role in treatment but also seek to reinforce equality
between partners, as well as address the greater societal oppression at play (Goodrich et
al.,1988; Seligman & Reichenberg, 2010; Stith, 2006).
In its infancy, FFT’s primary focus was to address traditional gender roles in
heterosexual couples and assess how these role assignments created an imbalance of
power in the relationship. Several analysis questions were developed in order to assess
for imbalances of power and the specific ways in which a couple’s gender roles were
linked to the couple’s presenting issues in therapy. These analysis questions assessed the
couple’s level of belief in gender stereotypes, how this affected the distribution of labor
in the household, how beliefs in stereotypes limited the solutions the couple would
entertain, how their belief in stereotypes influenced their expectations of their male or
female therapist, and how societal, social, and environmental pressures created or
exacerbated issues in their relationship (Goodrich et al., 1988; Seligman & Reichenberg,
2010, Stith, 2006).
Although FFT comes under criticism for not having thoroughly developed its
treatment model like many other established family therapy theories, it does abide by six
main tenets that guide feminist therapists: supportive therapeutic relationships; a focus on
addressing gender issues; egalitarian relationships; empowerment; affirming the less
powerful; and a focus on power dynamics (Goodrich, et al., 1988).
Therapeutic Relationship
The first tenet of FFT outlines the role of the therapist throughout treatment. A
feminist lens mandates that there be a non-hierarchical relationship between therapist and

15
client, allowing for open dialogue in sessions. This dynamic reinforces the overall goal
of feminist therapy, which is to empower clients and equalize power (Thomas, 1977). A
feminist therapist would accomplish this by establishing a relationship in which the
therapist is viewed as a supporter and collaborator. A feminist therapist may even refer
to their client as “the expert”, downplaying the assumption that the therapist knows best.
It has even been suggested that a feminist therapist use self-disclosure, in order to
normalize a client’s presenting issues (Goodrich et al., 1988)
Gender
The second tenet of FFT originally addressed differences in gender roles and how
this influences the client’s presenting problem(s). It asks that the feminist therapist view
the relationship between partners as egalitarian and focus on equalizing any imbalances
of power due to differing gender roles. A modern revision of this tenet also addresses the
concept of intersectionality, in order to broaden this focus to be more inclusive
(Crenshaw, 1989). The modern take also accounts for pressures minorities experience
within and outside of their relationship, as well as the unique pressures same-sex couples
face in trying to understand their roles in their relationship while navigating invalidating
societal pressure (McPhail et al., 2007). More will be discussed about this concept when
discussing the evolution of FFT.
Egalitarian Relationships
The third tenet of FFT emphasizes the importance of equality within relationships
as opposed to traditional roles in which one partner may wield more power than the other.
In traditional heterosexual gender roles, we often see that the “breadwinner” (usually the
male in heterosexual couples) has greater power, frequently having the final say in

16
decision-making, greater authority regarding finances, and less obligation in child rearing
and household duties. FFT seeks to equalize the power differential assigned to partners
in a relationship. Although each partner may play different roles within the relationship,
the overall goal is to ensure that each partner has equal influence, obligation, and regard
within and outside of the relationship (Thomas, 1977).
Empowerment
The fourth tenet of FFT involves the therapist aligning with and empowering
clients who experience a lesser degree of power and influence within their relationship,
similar to the concept of unbalancing in Structural Family Therapy (Seligman &
Reichenberg, 2010). A modernized revision of this tenet also addresses the
disempowerment same-sex couples may feel in their greater environment as the result of
identifying as a sexual minority (McPhail et al., 2007).
Affirmation of the Less Powerful
The fifth tenet of FFT originally focused on the empowerment of women, specifically,
and intended to address the power differential evident in many heterosexual relationships and in
greater society. FFT observes that the difference in power among genders stems from traditional
societal norms that saw men as the decision-makers, providers, and ultimate authority figures
within their family structures. While other family theories suggested that therapists take a
neutral role with their clients, FFT demands that clinicians assess client relationships for power
differentials and seek to create balance within them. While this approach began by addressing
gender inequality, it has broadened to acknowledge the power imbalances that exist for a
multitude of oppressed groups, including racial minority groups, the Lesbian, Gay, Bisexual,

17
Transgender and Queer (LGBTQ) community, those of lower socio-economic status, and those
who lack access to resources and education, such as urban and rural populations.
Power
Finally, the sixth tenet addresses the issue of power. Power is defined as "the
capacity to gain whatever resources are necessary to remove oneself from a condition of
oppression, to guarantee one's ability to perform, and to affect not only one's own
circumstances, but also more general circumstances outside one's intimate surroundings"
(Goodrich, 1991 p. 10). The primary goal of FFT is to first acknowledge differentials of
power in relationships, and then seek to create balance in relationships, in order to
equalize the distribution of power within those relationships (Thomas, 1977).
Interventions
The above tenets are accomplished in FFT through the use of three main
interventions: immediacy, self-disclosure, and psychoeducation (Ali & Naylor, 2013;
Allen, 2015). Immediacy is defined as a therapist “disclosing immediate feelings about
her- or himself in relation to the client or about the therapeutic situation” (APA, 2019,
para. 2) and is also how an FFT therapist would utilize self-disclosure. The intention of
this intervention is to promote insight for a client by reflecting either a therapist’s own
emotional response to a situation or behavior described by the client. Aptly named, this
skill is typically done as an immediate response in session (APA, 2019, para. 3).
Psychoeducation “refers to the process of providing education and information to
those seeking or receiving mental health services” (APA, 2019, para. 2). Therapists
utilize psychoeducation in a variety of ways, from providing clients information about
18
their diagnoses, how their brains and bodies process their emotions, and, specifically to
FFT, how a client’s presenting issues can be tied to societal norms and pressures.
It is encouraged for a feminist family therapist to consistently use immediacy and
psychoeducation to initiate conversations regarding apparent power imbalances in
relationships and the outside societal influences that may be adding pressure to a couple’s
dynamics. In fact, a feminist family therapist might align with the partner that appears to
have less power, in an effort to shift power dynamics and eventually equalize them. As
one study put it, to assume a neutral role as a therapist was to actually reinforce the
dysfunction occurring in the couple system (Siegenthaler & Boss, 1998).
As mentioned earlier, FFT therapists will often use self-disclosure in order to
ensure balance in the therapeutic relationship, normalize a client’s concerns, and to avoid
appearing as the expert. The FFT perspective believes that self-disclosure creates a
collaborative and safe environment, and one that does not reinforce a differential in
power dynamics between the therapist and the client (Black, 1991).
Evolution of Feminist Family Therapy
Although this approach centers on treating heterosexual couples in which partners
assume traditional gender roles, many of these concepts are still applicable to couples and
families today. In order to improve FFT’s relevance to modern family therapy treatment,
significant changes in its approach have been made. For instance, the introduction of
intersectionality into the feminist conceptual lens allowed the approach to broaden its
ability to apply to clients of varying backgrounds and experiences.
Intersectionality was originally introduced by Kimberlé Crenshaw in 1989, in her
published critique of feminist theory. Speaking specifically to her own experiences as a

19
black woman, Crenshaw (1989) argued that reducing a black woman’s identity to her
gender did not account for the layered experiences of a black woman and wrote that by
doing so, black women were being even more marginalized. She rightly argued that by
not acknowledging the complicated existence of those who are considered minorities on
multiple levels, the theory did not empower black women but instead continued to
oppress them by assuming that all women experience the same type of discrimination and
powerlessness (Crenshaw, 1989).
By introducing this concept of intersectionality, the feminist lens was able to
apply its principles of equality to a broad spectrum of couples with varying backgrounds
and identities (Crenshaw, 1989). No longer was the emphasis on gender, but it now
included the experience of being a minority in a variety of ways, by acknowledging race,
sexual orientation, and ethnicity. However, because this approach had its beginnings in
empowering women specifically, it is often misperceived as an approach for heterosexual
couples. Even the use of the root word “fem” can mislead clinicians and clients alike to
believe that the modern feminist approach is much narrower (Crenshaw, 1989).
For that reason, much of the literature regarding the clinical use of FFT focuses
specifically on gender and women’s issues. The majority of works published on FFT are
conceptual pieces that outline how to incorporate intersectionality into treatment with
heterosexual couples, how to integrate FFT with other systemic theories, and feminist
critiques of popular treatment models (Black, 1991; Blumer et al., 2013). The empirical
studies that have been conducted to show FFT’s effectiveness most often focus on female
survivors of physical and/or sexual abuse and the treatment of IPV in heterosexual
couples (Blumer et al., 2013).

20
Clinical Use of Feminist Family Therapy
FFT has been used in a variety of settings, often in conjunction with similarly
minded theoretical approaches, such as person-centered therapy, emotion-focused
therapy, and structural family therapy (Vatcher & Bogo, 2001). According to a 2015
literature review, the most common use of FFT is to address power imbalances in client
dynamics perpetuated by social inequality (Baugher & Gazmararian, 2015). This can
take several forms, including addressing multicultural issues, hierarchical imbalances
within a family system, and violence in relationships (Blumer, 2013; Chronister et al.,
2014).
As mentioned earlier, because FFT is not considered a standalone model for
family therapy, it is often utilized in conjunction with other models, particularly those
that emphasize a validating, egalitarian, and empowering therapeutic alliance with clients
(Enns, 1993; Hamel, 2010). Despite not being considered a comprehensive model, FFT
does emphasize issues overlooked by other models, such as the social context of the
client and their presenting issues, and the influence of society’s political climate on the
client.
A common tagline used in FFT is “the personal is political” (Brown, 2006;
McPhail et al. 2007). This has led to a significant feminist presence in areas of advocacy
for minorities, policy-making that addresses social justice issues, and involvement in the
court system (Greene & Bogo, 2002; McPhail et al., 2007; Staggs & Schewe, 2011).
This type of involvement is unlike the role encouraged by any other family therapy model
and assumes that a therapist’s role does not exist solely in the therapy room, but in every

21
aspect of society that influences our clients. In essence, a feminist family therapist’s role
is systemic in the purest sense by transcending the traditional expectation of a therapist.
Despite FFT’s long standing presence as a systemic approach, there is very little
evidence to demonstrate its effectiveness in empirical studies (Brown, 2006). There are a
handful of theories as to why FFT has not been studied rigorously, including suggestions
that it would be difficult to study since it is not a comprehensive model, that the
implementation of the theory varies too broadly to be operationalized, and that the
criticisms of FFT have biased researchers and clinicians against studying the model
(Brown, 2006). What is evidence-based about the approach, however, is the relationship
feminist therapists develop with their clients. Research endorses the value of a therapist
who is multiculturally competent and seeks to empower and support clients from an
egalitarian role (Brown, 2006). Many studies have validated that this type of therapeutic
alliance leads to better therapeutic outcomes for clients, including more frequent second-
order change, quicker resolution of presenting issues, and more frequent permanent
change (Macneil et al., 2009; Martin et al., 2000; Marziali et al., 1999).
Criticisms of the FFT Approach
Despite FFT being the most recommended approach for treatment of violence in
same-sex couples, the approach has been the focus of criticism. One such criticism is
that the underpinnings of feminism’s explanation of violence in relationships is rooted in
concepts only relevant to heterosexual relationships. Critics state that FFT assumes that a
power differential exists based on gender and does not take into account race,
socioeconomic status, income, or education. Critics dismiss the idea that patriarchal

22
dynamics can lead to violence in relationships, citing the increased rates of violence in
same-sex relationships where these dynamics arguably are not present.
The feminist community has been seen as resistant to acknowledging same-sex
violence, particularly among lesbian couples (Barnes, 2010; Rolle, 2018). While the
underlying theory regarding gender oppression seems to explain violence amongst male
same-sex couples, in that males are socialized to dominate their partners, same-sex
violence among women is more difficult to explain using these principles. In response,
feminist theory has argued that it has expanded its perspective to include concepts such as
intersectionality and oppression of sexual minorities (Brown, 2008).
Another common criticism of the feminist perspective is that it seems to focus
only on uni-directional violence, which is less common in same-sex relationships. By
definition, a uni-directional concept assumes that there is one abuser who holds the
majority of power in the relationship and that any violent behaviors from the abused
partner are in self-defense and not perpetuating violence in the relationship (Ali &
Naylor, 2013). In contrast, many studies have found that in heterosexual relationships,
women are just as likely be as violent as their male partners (Ali & Naylor, 2013).
Feminism is also criticized for its reliance on the criminal justice system in order
to respond to violence in relationships. Since one of the main tenets of feminism is to
become involved in the justice system and advocate for victims, feminists often support
criminal punishment as a consequence for violent behavior. Critics argue that this creates
a systemic issue in which the power of the abuser over their partner is simply replaced by
the power of the criminal justice system (Herzog, 2007). This creates a dependence on
external sources of control rather than empowering the victims to make decisions for

23
themselves. Additionally, involvement in the justice system sometimes results in
negative consequences for the victims of abuse, such as increased monitoring by law
enforcement and increased involvement in court proceedings.
Feminist approaches are also criticized due to the fragmented nature of the theory.
Feminism is divided into various approaches, including first, second, and third wave
feminism, neo-feminism, post-colonial feminism, and third world feminism. These
various denominations can, at times, contradict and even criticize one another, making it
difficult to present an easily defined understanding of what is meant by a “feminist
approach.” This division within the theory creates challenges for clinicians in
understanding how to implement the approach in treatment (Herzog, 2007).
Finally, criticism of the feminist approach comes due to the lack of empirical
evidence demonstrating its effectiveness. Much of what is written arguing for the use of
feminism is theoretical and very few empirical studies have been conducted. In a 2015
study on self-disclosure of IPV, researchers Sylaska and Edwards found that many
participants hesitated to identify as LGBTQ when sharing their experiences. The study
identified reasons for this hesitation, including participants not wanting to perpetuate
stereotypes of violence in same-sex relationships and concerns over how the data would
be used to generalize to the greater LGBTQ community (Sylaska & Edwards, 2015). The
study also noted that some of the largest studies on IPV in relationships did not ask
participants to identify their sexual orientation due to the possibility of decreasing
participation (Sylaska & Edwards, 2015).

24
Feminist Models for Treatment of IPV
Although there are no specific limitations on what populations FFT can be used
with, it is most frequently used with clients who can benefit from empowerment
(McPhail et al., 2007). For this reason, it is frequently used with survivors of abuse and
is often utilized in addressing IPV in relationships.
The minimal empirical data published on the use of FFT most frequently focuses
on addressing IPV; however, these treatments often require separating partners into
gender-specific groups (Karakurt et al., 2016; McPhail et al., 2007; Murray, 2009). More
specifically, heterosexual females in abusive relationships are often offered services and
support that are contingent on her leaving the relationship, thus limiting the data on how
effective feminist treatment for violence in relationships can be (Karakurt et al., 2016).
Additionally, the literature that does suggest using FFT to treat IPV is mostly conceptual
and does not offer tangible data to ascertain the effectiveness of the approach (Enns,
1993; McPhail et al., 2007). Although much of the literature is conceptual in nature,
there are a handful of studies that have offered structured feminist models for clinicians
to adopt in the treatment of IPV.
The Duluth Model, created in the 1980s, aims to take a communal approach to
addressing IPV. Informed by the principles of feminist theory, it works with victims and
perpetrators in a variety of environments, including the courts, detention centers, and
throughout their mental health treatment. In an attempt to address criticisms of FFT for
treatment of IPV, the Integrative Feminist Model was also developed in 2007 (McPhail et
al.). This model seeks to offer a feminist treatment modality for IPV that not only
incorporates the foundational tenets of feminism, but also has an increased emphasis on

25
multicultural competence and intersectionality, in order to broaden the relevance of
feminist treatment beyond just heterosexual dynamics. These models are outlined in the
following sections.
The Duluth Model
The most commonly used model to date for the treatment of IPV is the Duluth
Model. Developed by an organization called Domestic Abuse Intervention Programs
(DAIP), this model focuses on integrating feminist theory and sociocultural concepts, and
was created to treat court-ordered men convicted of domestic violence charges (Bohall et
al., 2016). IPV curriculums often include psychoeducation regarding gender oppression
and its link to relational violence. This approach is most often used in heterosexual
relationships, in which the power differential between a male batterer and a female victim
is most apparent.
The model seeks to intervene with both the victim and the perpetrator in the
various settings they may be involved in, including court proceedings, sentencing, and
treatment. Because it is rooted in the principles of feminist theory, the model seeks to
advocate for victims of abuse, while holding abusers accountable. Proponents of the
model say it has been successful in uniting agencies, such as 911 and the courts, by
offering psychoeducation and training that assist employees of these agencies in
recognizing various forms of abuse and familiarizing them with resources for victims and
perpetrators (DAIP, 2019).
Similar to the Feminist Therapy tenets, the Duluth Model outlines its values as
follows:

26
1. We listen to battered women: Our work involves active
engagement with women who have experienced violence so that
our efforts are guided by their realities and concerns.
2. We educate to promote liberation: An educational process of
dialogue and critical thinking is key to our efforts to assist women
in understanding and confronting the violence directed against
them, and to our efforts to challenge and support men who commit
to ending battering.
3. We advocate for institutional and social change: We examine the
practices and policies of social and governmental agencies that
intervene in the lives of battered women and address systemic
problems by engaging with institutional practitioners and leaders in
the development of creative and effective solutions.
4. We struggle against all forms of oppression. Women are not
defined by a single identity, but live in the intersection of their
race, gender, class, ethnicity, nationality, disability, age, religion
and sexual orientation. Our work must also challenge all systems
of oppression that create a climate of supremacy and intolerance
that facilitates violence and exploitation in women’s lives.
5. We promote non-violence and peace: Every step we take, every
interaction we have with others, is an opportunity to advance non-
violence, continually working toward and building a culture and a
future of peace. (DAIP, 2019, para. 1)

27
One of the most common tools of the Duluth Model is use of the Power and
Control Wheel. This tool visually illustrates ways in which men coerce and intimidate
their partners through emotional, physical, sexual, or economic abuse, and is used to
promote awareness of how the belief in gender inequality influences men’s likelihood of
responding violently to their partners. The wheel, along with an alternate “equality”
wheel and five other specialized versions, is available for free download on DAIPs
website. The Power and Control Wheel is available in fifteen languages, in addition to
English (DAIP, 2019), making it one of the most widely accessible free resources
addressing IPV to ever be available to the public.
In a 2014 study looking at the use of the Duluth Model, it was found that 63% of
men designated to participate in the Duluth treatment model agreed with the statement
that “women provoke IPV by using bad judgment or by provoking the man’s anger”
(Herman et al., 2014, p. 9). This same study also found that 45% of men believed that
“men have the natural right to be in charge of the relationship” (Herman et al., 2014, p.
9). Because these beliefs seem to be widely held by men convicted of IPV, it supports
the need to use a feminist perspective in their treatment. In post-test measures following
the use of the Duluth model, these beliefs were significantly reduced in participants
(Herman et al., 2014).
Criticisms of the Duluth Model
Despite its popularity, the Duluth model has come under scrutiny. The creators of
the model refer to themselves in the seminal publication as a “small group of activists in
the battered women’s movement” (Pence & Paymar, 1993, p. xiii). Critics take exception
to the fact that the model was not developed by trained clinicians and are concerned that

28
non-professionals, who cannot diagnose or clinically conceptualize participants, are
administering treatment to violent offenders. Critics call this use of treatment unethical
as it is being delivered by non-licensed individuals without specific clinical training.
The model was also criticized for being exclusive to a specific gender and a
limited number of races. The model was designed to be used with men who batter
women and has no protocol for addressing treatment with women who batter men, or
same-sex couples who experience partner violence (Pender, 2012). The model has also
only been used with Caucasian, African American, Native American, and Latino
populations.
Despite the issues with the model, it remains the most common form of treatment
for addressing IPV and had been shown to be effective (DAIP, 2019). Suggestions have
been made to overhaul the treatment approach, in order to include a broader spectrum of
violent offenders, a means of addressing bi-directional violence, and norming it to many
more sexual, racial, and ethnic groups. It has also been suggested that this and all other
treatments for IPV only be administered by licensed and qualified professionals in the
mental health field.
The Integrative Feminist Model
The Integrative Feminist Model (IFM) was developed as a means of modernizing
the feminist perspective by addressing common criticisms of a feminist approach
(McPhail et al., 2007). These criticisms challenge the use of a feminist perspective to
treat IPV by asserting that feminism is only designed to address uni-directional partner
violence in heterosexual couples and is limited in addressing a broader range of issues
that cause violence in relationships (McPhail et al., 2007).

29
In response, the IFM is made up of seven key concepts, or puzzle pieces, as
depicted in the model’s visual aid (Appendix A) indicating that the following foci overlap
with the original tenets of FFT and are systemic in nature: 1) the personal is political; 2)
acknowledging male victims and female perpetrators; 3) changing policies and
institutional responses; 4) exploring alternative interventions such as justice restoring
solutions; 5) increasing victim choice and voice by crafting personalized solutions; 6)
integrating additional explanatory models of violence causation; and 7) feminist analysis
of power differentials based on gender, class, race, national origin, disability, sexual
orientation, and age (McPhail et al., 2007).
These additions to the feminist perspective attempt to take into consideration the
concerns that some critics have had with the model, however, it is difficult to say whether
these new considerations have been effective in treatment due to such limited literature
being published as a follow up to this model’s introduction. It would be beneficial for
researchers and clinicians to continue exploring how effective these additions are in order
to continue the dialogue regarding best practices for treatment of this specific population.
Criticisms of the Integrative Feminist Model
While the IFM does not have any published responses or critiques, the creators of
the model offer their own suggestions for potential skepticism of the model from
clinicians (McPhail et al., 2007). The most obvious of these initial concerns is the fact
that the model is not evidence-based because it is a relatively new approach (McPhail et
al., 2007). The authors caution that, like any alternative treatment, client care and safety
must be considered. Should a clinician choose to implement the strategy outlined in their
article, close attention must be paid to effectiveness and ethics (McPhail et al., 2007).

30
The authors also point to Feminist purists who may be concerned that the
integration of intersectionality into the feminist perspective is deviating from the original
theory. In response, the authors welcome formal critiques of the IFM to be published, in
order to spur on professional dialogue. They also state that a singular feminist
perspective is not thorough enough to address the many layers of intersectionality that
exist in clients. Finally, they suggest that to have a feminist perspective on theoretical
development is to be progressive and adaptive to our culture (McPhail, 2007). By doing
this, feminist family therapists attend to the greatest call of feminism, which is meeting
the needs of clients otherwise marginalized by a social hierarchy (McPhail, 2007).
Feminist Family Therapy to Treat IPV in Same-Sex Couples
Although same-sex treatment of IPV using FFT is not as prevalent in the
literature, success with this approach has been documented with this population and
continues to be a common suggestion for treatment recommendations (George & Stith,
2014; Herzog, 2007; Hill et al., 2012). Proponents of the model say that the advantage of
using FFT with same-sex couples is that the principles of FFT address the core issues that
lead to violence in their relationships. For instance, studies show that same-sex couples
are less likely to seek assistance from mental health providers or law enforcement with
experiencing violence in their relationships (Martin-Storey, 2015). FFT addresses this in
several forms. First, FFT expects therapists to be informed about the context of their
clients and assumes that therapists would already be educated on this dynamic of silence
in same-sex couples (Barnes, 2010). Second, FFT is designed to empower clients to
assert and protect themselves, hopefully breaking the cycle of silence on violence
(Barnes, 2010).

31
Because a feminist approach was originally created specifically to empower
women, it continues to be used to focus on the treatment of heterosexual couples, even
today. A literature review revealed that IPV literature continues to center around
heterosexual couples and the gender differential in conceptualization and treatment of
IPV (Cannon & Buttell, 2015). It has been argued that clinicians and researchers alike
hold a heteronormative bias when exploring treatment options for IPV, as a significant
majority of the literature ignores same-sex couples.
One study identified several myths that heterosexuals hold about same-sex
relationships. The first is that violence in same-sex relationships is a conflict between
equals and assumes that each partner is physically similar and is received similarly in
society. In short, each partner in a same-sex relationship has the same number of
resources and that one does not hold any advantage or privilege over another (Brown,
2008). Another myth identified is that physical violence in a same-sex relationship could
be some form of sadomasochism. Again, this view of same-sex relationships reduces the
connection between partners to something sexual and does not acknowledge the
emotional connection between them, thereby invalidating the relationship and sending the
message that these partners do not experience the depth of emotion or validity of their
relationship to the extent that heterosexual couples do (Brown, 2008).
While these myths were found to be held by the general public, it is this
researcher’s opinion that it is certainly possible that clinicians may hold these biases to be
true, as well. For that reason, using FFT with same-sex couples may be counterintuitive
for some clinicians who assume that the power differential between genders or violent
behaviors between partners are non-issues. However, the societal pressure for same-sex

32
relationships can still manifest power differentials on many levels. There may be a
differential between the two partners for other reasons besides gender, such as income,
intelligence, career, and their individual roles at home and in their communities.
Surrounding the couple dynamics, both partners may feel less powerful in their greater
environment, in which heterosexual couples are still the vast majority of partnerships
considered “acceptable” by society and hold the sheer majority. Therefore, same-sex
relationships experience the dynamics that FFT was designed to address.
There is a clear relevancy to using FFT because of its ability to address unique
issues in same-sex relationships. A study looking at the treatment of violence in male
same-sex relationships revealed that clients report a very clear power differential when
describing their relationships (Kay & Jeffries, 2010). They reference language such as
“top” and “bottom” when describing themselves or their partners, and the role each of
them play. Clients also identified issues of inequality regarding income and reported that
the partner who earned more money had more power in the relationship. They spoke of
sometimes feeling as though the partner earning less money was forced into a more
traditional female role by the partner earning more money and were expected to
contribute to household chores to a greater degree.
A more recent study found that, despite societal progression in normalizing same-
sex relationships, sexual minorities continue to experience stigma, discrimination, and
resulting dissonance in their own identities (Martin-Storey, 2015). These stressors were
found to lead to increased abuse of substances, increased violence in same-sex
relationships, and more frequent aggressive behavior (Martin-Storey, 2015). In fact, the
group to experience the most violence in relationships was the group who identified as

33
“unsure” of their sexual preferences, indicating that perhaps the greater a person’s
deviation from the societal norm, the greater the stressors, resulting in more frequent
occurrences of violence.
This dissonance, coupled with conflict within a same-sex relationship, can result
in explosive reactions that can turn violent. It was also found that these dynamics are
surfacing very early on in the development of sexual minorities. Martin-Storey’s (2015)
study found that in a sample of 12,984 high school students, 16% of heterosexual females
and 6% of heterosexual males reported experiencing violence in their romantic
relationships. In contrast, 42% of lesbian females and 32% of gay males reported
violence in their relationships.
In a 2017 study that attempted to inventory societal stressors placed on same-sex
relationships, findings showed that the level of stigma consciousness for sexual
minorities contributed to increased violence in their relationships (Longobardi &
Badenes-Ribera). This validates the suggestion that because same-sex relationships are
more scrutinized in society, sexual minorities feel greater pressure and experience more
conflict within their relationships.
The research also demonstrates unique societal barriers to treatment faced by
those in same-sex relationships. An executive summary released from the Williams
Institute in November of 2015 found the following issues hindering access to treatment:
1) Legal definitions of domestic violence that exclude same-sex
couples
2) Dangers of “outing” oneself when seeking help and the risk of
rejection and isolation from family, friends, and society

34
3) The lack of, or survivors not knowing about, LGBT-specific or
LGBT-friendly assistance resources
4) Potential homophobia from staff of service providers or from non-
LGBT survivors of IPV and IPSA with whom they may interact
5) Low levels of confidence in the sensitivity and effectiveness of law
enforcement officials and courts for LGBT people. (Brown & Herman,
2015, p. 3)
This report also found that literature addressing treatment for same-sex couples
varied widely in the way its participants identified (Brown & Herman, 2015). Some
studies were conducted on self-identified lesbian or gay participants, while others were
included in such studies based on their behaviors, such as men who have sex with men
(MSM) (Baugher & Gazmararian, 2015; Ford et al., 2013). However, this degree of
variation in the participants studied makes it nearly impossible to develop accurate and
precise means of treatment that thoroughly address the above-mentioned barriers.
Research has already demonstrated that the level of identification as a gay or
lesbian, coupled with an individual’s level of stigma consciousness, is directly correlated
with violence in same-sex relationships (Lewis, et al., 2003; Lewis et al., 2014).
Therefore, to summarize all same-sex relationship research without regard to the level of
identity and stigma consciousness of each participant, creates a potentially inaccurate
guide in treating same-sex violence.

35
Restatement of Research Questions and Hypotheses
This study’s research questions are:
1) Are clinicians using Feminist Family Therapy principles to treat Intimate Partner
Violence in same-sex individual and couple clients?
Hypothesis 0: Clinicians are using Feminist Family Therapy thoroughly, as measured by
a response on the FFT checklist of either “Often,” or “Always”.
Hypothesis 1: Clinicians are not using Feminist Family Therapy thoroughly, as measured
by a response on the FFT checklist of either “Sometimes,” “Rarely,” or “Never”.
2) Is the use of the Feminist Family Therapy being influenced by whether or not
clinicians agree with criticisms of the approach?
Hypothesis 0: The use of Feminist Family Therapy is not being influenced by clinicians’
agreement or disagreement with its criticisms.
Hypothesis 1: The use of Feminist Family Therapy is being influenced by clinicians’
agreement or disagreement with its criticisms.
Summary
This chapter provided an overview of current literature relevant to this study by
outlining the major tenets of FFT, as well as FFT models that have been developed to
treat IPV. The chapter went on to explore how LGB individuals experience violence in
their relationships, as well as barriers to pursuing mental health treatment. The chapter
also provided an outline of criticisms of the FFT approach and reviewed the research
questions for this study.

36
.CHAPTER III
RESEARCH METHODS
This chapter focuses on the purpose of the research study as well as the statistical
methods utilized to conduct the study. This chapter will also outline the data collection
and data analysis methods utilized for this study.
Restatement of Research Goals
The proposed study intended to determine whether clinicians who are actively
treating Intimate Partner Violence (IPV) in same-sex couples are utilizing Feminist
Family Therapy (FFT) as a primary modality, as recommended in the literature. Due to
varying levels of training on couples therapy, multicultural competence, and
intersectionality, along with the rising rates of IPV in same-sex relationships, it is
possible that clinicians are not utilizing the literature to guide their approach to treat this
important issue. This study aspires to determine the extent to which clinicians are
utilizing FFT as the most commonly suggested strategy to treat IPV so that the frequency
of violence in same-sex relationships can be decreased and treated effectively.
As evident above, there is a significant dissonance between what is being
recommended for treatment of violence in same-sex relationships and criticisms of the
approach. The proposed study attempts to explore the dissonance by focusing on
clinicians’ own perceptions of the approach and its criticisms, and whether or not this
impacts clinicians’ use of the approach. Since the rate of violence in same-sex couples
continues to rise, it is crucial that we investigate the effectiveness of the recommended

37
treatments and determine whether they are being used consistently or not, in order to
determine next steps in evaluating effective treatment options. Since the feminist
approach has been so heavily criticized within the mental health community, it is a
distinct possibility that these criticisms have influenced clinicians’ use of the theory. The
study intended to assess whether or not clinicians who have worked to treat IPV in same-
sex relationships have used FFT and whether or not they agree with its criticisms.
Restatement of Research Questions and Hypotheses
This study’s research questions are:
1) Are clinicians using Feminist Family Therapy principles to treat Intimate Partner
Violence in same-sex individual and couple clients?
Hypothesis 0: Clinicians are using Feminist Family Therapy thoroughly, as measured by
a response on the FFT checklist of either “Often,” or “Always”.
Hypothesis 1: Clinicians are not using Feminist Family Therapy thoroughly, as measured
by a response on the FFT checklist of either “Sometimes,” “Rarely,” or “Never”.
2) Is the use of the Feminist Family Therapy being influenced by whether or not
clinicians agree with criticisms of the approach?
Hypothesis 0: The use of Feminist Family Therapy is not being influenced by clinicians’
agreement or disagreement with its criticisms.
Hypothesis 1: The use of Feminist Family Therapy is being influenced by clinicians’
agreement or disagreement with its criticisms.
Research Design
This was a quantitative exploratory study. The design format was chosen due to
the novel nature of these particular research questions, which do not have any precedent,

38
based on the literature review conducted. While this researcher has made a hypothesis
regarding the outcomes of the data collection, it is important to allow the flexibility
offered by an exploratory study in order to properly interpret the data and allow for
numerous possibilities. John Tukey, the lauded and influential mathematician and
statistician, wrote of the necessity of exploratory research, saying in part, “Neither
exploratory or confirmatory [research] is sufficient alone” (Tukey, 1980, p. 23).
Typically, a confirmatory study is based on exploratory research that has already
been completed (Tukey, 1980). These studies are founded on the discoveries of
exploratory research, however, when there has been no exploratory research done on a
topic, such as in the case of this study, an exploratory study is warranted.
Participants
Criteria for Participation. In order to participate in this study, the participants
had to be licensed as a mental health clinician, social worker, psychologist, or
psychiatrist, and have provided or were currently providing counseling services to at least
one individual or same-sex couple client that experienced intimate partner violence in
their relationship. Due to the advanced nature of the survey questions, participants with
trainee licenses were not permitted to complete the survey.
Solicitation of Participants. In order to attract participants, emails requesting
participation were sent to the counseling departments of the following schools:
Youngstown State University, The Ohio State University, Cleveland State University,
Kent State University, and the University of Akron. The survey was also be distributed
via the researcher’s personal social media accounts requesting participation from
qualified individuals, as well the following Facebook groups: Ohio MFT Network,

39
UAkron MFT Masters Alumni, Sex Positive Therapists Group, Counselor/Therapist
Networking/Consultation Group, and Ohio Social Workers.
Additionally, two mass emails to members of the Counselor, Social Worker, and
Marriage and Family Therapist Board of Ohio were sent requesting participation.
Colleagues at the Coleman Professional Service’s Akron location and OhioGuidestone’s
Lorain County location distributed the survey to qualified participants. Finally, a paid
advertisement was run nationally on Facebook and Instagram.
Incentives for Participation. In order to encourage participation, participants
were offered the opportunity to win one $100 Amazon gift card, which was determined
by a random drawing. Each participant was assigned a number and the winner was
chosen using Google’s random number generator. The participant was notified using the
email address they provided. Only participants who met the criteria of the study were
eligible to win. There were no other incentives offered, monetary or otherwise. The
form to opt into the giveaway can be found in Appendix F.
Description of Sample. The sample collected represented 29 out of 50 states,
although 81.3% of participants were located in the state of Ohio. Eighty-six point six
percent identified as female, 11.3% as male, 1.8% as non-binary, and 0.4% as gender
queer. Social workers made up the largest group of participants (37.7%), followed by
counselors (31%). MFTs made up 13.7%, and psychologists made up 1.8% of the
responses. Additionally, 15.8% of participants identified themselves as holding two or
more clinical licenses. When asked about their primary theoretical orientation,
participants reported a significant variety of approaches. The most common responses
were Cognitive Behavioral Therapy (23.9%) and Eclectic (26.3%). Only five participants

40
(1.8%) indicated that they utilized FFT as their primary approach. Being that there was
such a wide variety of responses, the rest were categorized as “All Others” which made
up almost half of the responses (49.8%).
Sample Size. A power analysis using a hypothesized medium effect size and an alpha
level of p < .05 revealed that a total of 252 participants were necessary to accurately
assess the above hypotheses (Cohen, 1992). Upon completion of data collection, a
sample size of 284 was collected.
Procedure
Participants were asked to complete an online survey based in Qualtrics, which
presented them with an informed consent form (Appendix B), a demographic
questionnaire to ensure they met eligibility criteria (Appendix C), the Feminist Family
Therapist Behavior Checklist (Appendix D), and a Feminist Criticism Questionnaire
(Appendix E). Once data collection was complete, a descriptive analysis was used to
determine demographics of the participants such as gender identification, type of
licensure, years practicing, and what theoretical orientation is used as the participant’s
primary approach.
Responses to the FFTBC were summed to calculate a total raw score. FFTBC
subscale scores were also summed to calculate a raw score for each scale. Responses to
the FCQ were recoded to reflect any responses of Always or Often to be calculated as a 1,
and all other responses to be calculated as 0. A one-way between-subjects ANOVA was
conducted to compare participants’ responses to the FCQ to those on their FFTBC. This
allowed the researcher to determine whether clinicians use of FFT is being influenced by

41
the criticisms of the approach. Cut-off scores were determined (as detailed in the next
chapter) in order to sort participants into one of three conditions of their FCQ score.
Data Analysis Method
This study involved conducting a descriptive analysis to determine the
demographics of the participants, and a one-way between-subjects ANOVA, which
compared participants on their use of FFT, based on their level of agreement with the
FFT criticisms. To address research question one, reported frequency of FFT behaviors
was assessed to determine how frequently FFT and its specific interventions were used to
treat same-sex couples experiencing IPV.
To address research question two, a one-way between-subjects ANOVA assessed
how clinicians differed from one another on the FFTBC when taken with their level of
agreement of the criticisms. The use of the ANOVA is based on the need to divide
participants’ responses on the FCQ into one of three conditions: low agreement, medium
agreement/undecided, and high agreement. Chapter four discusses cut-off scores that
were developed to determine how to sort participants into one of the three mentioned
groups.
Measures
In order to collect data from participants, three instruments were used: a
demographic questionnaire; with permission from the author, an adapted version of the
38-item Feminist Family Therapist Behavior Checklist (Chaney & Piercy, 1988); and a
Feminist Criticisms Questionnaire, created by this researcher, using criticisms of
Feminist Family Therapy, as noted in relevant literature, that were summarized into one-
sentence statements to assess participants’ agreement with those statements.

42
Demographics Questionnaire
Modeled after the demographic questionnaire included in the FFTBC, this survey
included questions that participants responded to in order to determine their eligibility for
the study and provide data for the descriptive analysis. A copy of this questionnaire can
be found in Appendix B.
Feminist Family Therapist Behavior Checklist
The Feminist Family Therapist Behavior Checklist (FFTBC) was developed by
Drs. Chaney and Piercy in 1988. The checklist is the only one of its kind and was
developed in order to measure the FFT behaviors of clinicians in their work with clients.
It is designed as a self-report instrument and contains 38 items which measure the
following subscales: Sex-Role Analysis, Shifts Balance of Power Between Male and
Female Clients, Therapist Empowers Female Clients, Skills Training, and Therapist
Minimizes Hierarchy Between Therapist and Clients.
The original checklist items were developed from a Delphi questionnaire
administered to 40 experienced feminist family therapists and subsequently normed on 60
family therapists, 33 of whom identified as female and 27 of whom identified as male.
The mean age of the participants was 35 and mean years of experience conducting
therapy was 4.4 years. 54 of the participants identified as White, three identified as
Black, two identified as Hispanic, and one identified as Asian. Test-Retest Reliability
was calculated using Kappa to account for chance and equaling a 92.5% rate of
agreement between time one administration and time two administration. A copy of this
questionnaire with revised items can be found in Appendix C.

43
Adapting the Feminist Family Therapist Behavior Checklist
Due to the heteronormative nature of the original scale, permission from Dr.
Piercy to alter the checklist items was obtained via email. Dr. Piercy noted that the first
author of the original instrument, Dr. Chaney, had passed away and only his permission
was necessary. The items were altered minimally in order to include wording that was
relevant to same-sex couples. Additionally, the names of the original subscales have
been minimally revised to reflect more inclusive language. The revised subscale names
are: Sex-Role Analysis, Shifts Balance of Power Between Dominant and Non-Dominant
Clients, Therapist Empowers Both Clients, Skill Training, and Therapist Minimizes
Hierarchy Between Therapist and Clients.
Feminist Criticism Questionnaire
This instrument consisted of six statements, each of which summarized a specific
and documented criticism of the feminist perspective. Responses to this questionnaire
were on a five-point Likert scale: Strongly Agree, Agree, Undecided, Disagree, and
Strongly Disagree. A copy of this questionnaire can be found in Appendix D.
Summary
This chapter provided an overview of the methods of this study, including the desired
sample demographics, utilization of incentives for participation, the statistical analysis
used to address the research questions, and an overview of the instruments used in the
study. It also discussed the revising of the FFTBC instrument to eliminate hetero-
normative language.. Finally, it discussed the formatting of the individual questionnaires
and provided a description of the Likert scale questions. The actual survey
questionnaires are included in the Appendices.

44
CHAPTER IV
RESULTS
The purpose of this study was to examine the use of Feminist Family Therapy
(FFT) by clinicians who work with same sex couples and whether the use of it is
influenced by their level of agreement with the common criticisms of the FFT approach.
This chapter outlines the details of data collection, data cleaning, and then is followed by
a detailed summary of the descriptive statistics of the study variables. Finally, the results
of the one-way between-subjects ANOVA are shared.
Restatement of Research Questions and Hypotheses
This study’s research questions are:
1) Are clinicians using Feminist Family Therapy principles to treat Intimate Partner
Violence in same-sex individual and couple clients?
Hypothesis 0: Clinicians are using Feminist Family Therapy thoroughly, as measured by
a response on the FFTBC of either “Often,” or “Always”.
Hypothesis 1: Clinicians are not using Feminist Family Therapy thoroughly, as measured
by a response on the FFTBC of either “Sometimes,” “Rarely,” or “Never”.
2) Is the use of the Feminist Family Therapy being influenced by whether or not
clinicians agree with criticisms of the approach?
Hypothesis 0: The use of Feminist Family Therapy is not being influenced by clinicians’
agreement or disagreement with its criticisms.

45
Hypothesis 1: The use of Feminist Family Therapy is being influenced by clinicians’
agreement or disagreement with its criticisms.
Data Collection
Data was collected via Qualtrics over the course of six months, from December
2019 to May 2020. To minimize the potential for incomplete data, incomplete surveys
were not saved to the data set. Additionally, participants who did not meet the eligibility
criteria were routed out of the survey and were not given a chance to continue. Due to
this structure, very little data cleaning was necessary. With the focus of this study being
on same-sex couples, the survey attracted significant negative attention when advertised
on Facebook. Some individuals were able to submit erroneous and/or homophobic
responses. For this reason, data was checked for erroneous responses and removed from
the set. These responses were clearly identifiable due to these participants being unable
to appropriately answer very field-specific questions, such as “What is your primary
theoretical orientation?” Once the data set reached the appropriate sample size,
advertisements were stopped, and the survey closed. The data were then exported to
SPSS for analysis.
Demographics and Descriptive Statistics
There were a total of 284 participants in this study. In order to qualify for the
study, each participant had to be a licensed mental health clinician with full licensure in
their state of practice. Participants represented 29 out of 50 states, with Ohio making up
81.3% of total responses. The majority (86.6%) identified as female, 11.3% as male,
1.8% identified as non-binary, and 0.4% identified as gender queer. Social workers made
up the largest group of participants (37.7%), followed by counselors (31%). MFTs made

46
up 13.7%, and psychologists made up 1.8% of responses. Additionally, 15.8% of
participants identified themselves as holding two or more clinical licenses.
When asked about their primary theoretical orientation, participants reported a
significant variety of approaches. The most common responses were Cognitive
Behavioral Therapy (23.9%) and Eclectic (26.3%). Only five participants (1.8%)
indicated that they utilized FFT as their primary approach. Being that there was such a
wide variety of responses, the rest were categorized as “All Others,” which made up
almost half of the responses (49.8%).
Regarding the ages of their clientele, clinicians were given the option to select any
age groups that applied. Thirty-nine point four percent of the participants reported seeing
children ages 0 to 12, while 56.7% reported seeing adolescents ages 13 to 17. 81.3%
reported seeing adult individuals ages 18 and over, and 46.5% reported seeing adult
couples. Forty-one point five percent reported seeing families, and 4.9% identified the
age demographic of their clients as “Other”.
Since this study focused on same-sex couples who are experiencing intimate
partner violence, the questionnaire went on to ask participants to identify the percentage
of clients that they believe are experiencing violence in their romantic relationships.
Over half the participants (55.3%) reported that 0-25% of their clientele experience
violence. Twenty-seven point eight percent of responses reported up to half of their
clients experienced violence, 12.7% reported that up to 75% of their clients experience
violence, and 4.2% reported that up to 100% of their clients experience violence.
The majority of participants (78.5%) reported that up to 25% of their caseload
identifies as gay or lesbian, 15.5% reported up to 50% of their caseload identifies as gay

47
or lesbian, 4.9% reported that up to 75% of their clients identify as gay or lesbian, and
1.1% of participants report that up to 100% of their clients identify as gay or lesbian.
Finally, when asked to identify their primary employment setting, a third of
participants (31.3%) reported working at a non-profit outpatient setting. Another third
(30.6%) reported working at a private practice outpatient setting. Eleven percent reported
either an inpatient setting and/or a partial hospitalization setting. Four point nine percent
reported working in an Intensive Outpatient Program and 9.9% reported their
employment setting as “other”. The demographics are reported by category in the table
below.
Table 4.1
Participants’ Demographic Information
Category Frequency (n) Percent (%)
Gender Identity
Male 32 11.3 Female 246 86.6 Non-Binary 5 1.8 Gender Queer 1 .4
License
MFT 39 13.7 Counseling 88 31 Social Work 107 37.7 Psychologist 5 1.8 2 or more licenses 45 15.8
Years Licensed
0-2 80 28.2 3-5 101 35.6 6-8 33 11.6 9+ 70 24.6

48
Primary Theory
CBT 68 23.9 Eclectic 75 26.3 Feminist 5 1.8 All Others 141 49.8
Client Populations
Children 0-12 112 39.4 Adolescents 13-17 161 56.7 Adult Individuals 231 81.3 Adult Couples 132 46.5 Families 118 41.5 Other Groups 14 4.9
Employment Setting
Outpatient - Nonprofit
31.3
Outpatient - Private Practice
30.6
Inpatient/Hospital
8.5
IOP
4.9 PHP
2.5
Other
9.9
Estimated % on caseload that are experiencing violence in relationships
0-25%
55.30%
26-50%
27.80% 51-75%
12.70%
76-100%
4.20%

49
Recoding and Transforming of Variables
Several steps were taken in order to recode and transform variables measured in
the survey. First, as indicated in the seminal FFTBC article, each participant’s responses
to the FFTBC were summed to determine their overall score, creating a new variable
referred to as FFT Practice. Although this variable provided us with the total score on the
FFTBC, the original authors of the instrument never provided cutoff scores to interpret
whether the score indicated a low or high level of usage of the approach. Each item on
the FFTBC was a Likert scale question from one to five, with one being “Often” and five
being “Never.” As proposed, the analysis separated participants’ responses into two
groups: Responses that were marked as “Always” or “Often” were recoded as 1, and
responses marked as “Sometimes,” “Rarely,” or “Never” were recoded as 0. This
effectively separated participants into two groups: those that were thoroughly utilizing
the FFT approach and those who were not.
Second, items corresponding to each of the five subscales of the FFTBC were
recoded so that individual subscale scores could be assessed. This was done by
identifying the items of each subscale on the questionnaire and sorting the responses into
the following newly created variables: Role Analysis, Shifts Balance, Therapist
Empowers, Skills Training, and Therapist Minimizes Hierarchy. Table one (Appendix
Estimated % on caseload that identify as gay/lesbian
0-25%
78.50%
26-50%
15.50% 51-75%
4.90%
76-100% 1.10%

50
H) displays the five subscales of the FFTBC and the specific questionnaire items that
correspond with each of them.
Third, participants’ responses to the FCQ were averaged to calculate each
participant’s total mean score. This was done in an attempt to identify and utilize cutoff
scores to sort participants’ FCQ scores into a new variable referred to as Criticism Group
with the following three conditions: High Agreement, Medium Agreement/Undecided,
and Low Agreement. The cutoff scores for the Criticism Group conditions can be seen in
the table below.
Table 4.2
Criticism Groups Cutoff Scores
Mean Criticism Score Criticism Groups N Percentage (%) 1-2.99 High Agreement 126 44.40% 3-3.99 Med Agreement 60 21.10%
4-5 Low Agreement 98 34.50% Note. Responses were on a Likert scale from 1 to 5, with 1 being Strongly Agree and 5 being Strongly Disagree
Research Question One
Participants were compared on their scores on the FFTBC to determine their level
of usage of the FFT approach, as well as their level of usage of each subscale technique.
Descriptive results indicated that 63% of participants were utilizing FFT thoroughly,
according to their overall FFTBC score (M = 24.07, SD = 9.97). Role Analysis was
shown to be thoroughly utilized by 63% of participants (M = 5.66, SD = 2.38); Shifts
Balance was thoroughly utilized by 60% of participants (M = 7.24, SD = 3.82); Therapist
Empowers was utilized thoroughly by 66% of participants (M = 3.30, SD = 0.93); Skills
training was utilized thoroughly by 66% of participants (M = 4.64, SD = 2.04); and
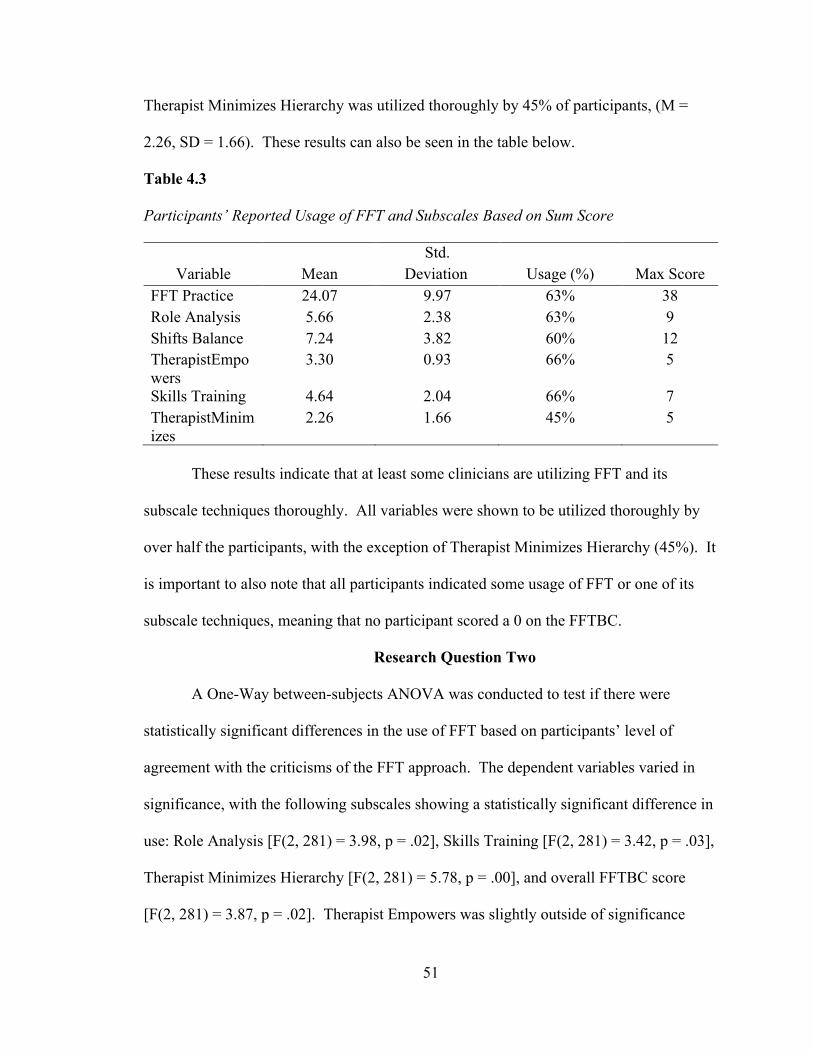
51
Therapist Minimizes Hierarchy was utilized thoroughly by 45% of participants, (M =
2.26, SD = 1.66). These results can also be seen in the table below.
Table 4.3
Participants’ Reported Usage of FFT and Subscales Based on Sum Score
Std. Variable Mean Deviation Usage (%) Max Score
FFT Practice 24.07 9.97 63% 38 Role Analysis 5.66 2.38 63% 9 Shifts Balance 7.24 3.82 60% 12 TherapistEmpowers
3.30 0.93 66% 5
Skills Training 4.64 2.04 66% 7 TherapistMinimizes
2.26 1.66 45% 5
These results indicate that at least some clinicians are utilizing FFT and its
subscale techniques thoroughly. All variables were shown to be utilized thoroughly by
over half the participants, with the exception of Therapist Minimizes Hierarchy (45%). It
is important to also note that all participants indicated some usage of FFT or one of its
subscale techniques, meaning that no participant scored a 0 on the FFTBC.
Research Question Two
A One-Way between-subjects ANOVA was conducted to test if there were
statistically significant differences in the use of FFT based on participants’ level of
agreement with the criticisms of the FFT approach. The dependent variables varied in
significance, with the following subscales showing a statistically significant difference in
use: Role Analysis [F(2, 281) = 3.98, p = .02], Skills Training [F(2, 281) = 3.42, p = .03],
Therapist Minimizes Hierarchy [F(2, 281) = 5.78, p = .00], and overall FFTBC score
[F(2, 281) = 3.87, p = .02]. Therapist Empowers was slightly outside of significance

52
[F(2, 281) = 2.89, p = .06], and Therapist Shifts Balance was not statistically significant
[F(2, 281) = 1.85, p = .16].
Table 4.4
One-Way Analysis of Variance
Levene’s Test for Equality of Variances indicated that the assumption of
normality for the dependent variables were met. An inspection of the boxplot determined
there to be no outliers in the data set. The skewness was found to be within acceptable
range however the kurtosis was outside acceptable range at -1.498.
Due to the exploratory nature of this study, the Bonferoni correction post hoc was
chosen in order to minimize Type I Error (Ludbrook, 1998). Post hoc comparisons
indicated significant differences in the use of the majority of the dependent variables,
when taken with participants’ level of agreement with FFT criticisms. However,
Therapist Empowers and Therapist Shifts Balance did not significantly differ based on
participants’ level of agreement.
When looking at overall FFTBC scores, we see a statistically significant
difference in use of FFT between those with low agreement (M = 22.25), SD = 10.17)
and those with high agreement (M = 25.67, SD = 9.74). There were significant
differences in the use of Role Analysis between those with low agreement (M = 2.35, SD
Dependent Variable
Sum of Squares df
Mean Square F Sig.
FFT Practice 753.434 2 376.72 3.87 .02 Role Analysis 5.015 2 2.51 3.98 .02 Shifts Balance 2.748 2 1.37 1.85 .16 TherapistEmpowers 2.688 2 1.34 2.89 .06 Skills_Training 4.830 2 2.42 3.42 .03 TherapistMinimizes 9.038 2 4.52 5.78 .00

53
= 0.86) with FFT criticisms and those with high agreement (M = 2.07, SD = .69)
Significant differences in use of Skills Training between those with low agreement (M =
2.42, SD = .89) and those with high agreement (M = 2.14, SD = .79); Significant
differences in use of Therapist Minimizes Hierarchy between those with low agreement
(M = 2.90, SD = .94) and those with medium agreement (M.= 2.51, SD = .87), and also
between those with low agreement and those with high agreement (M = 2.56, SD = .81).
Table 4.5 Variables Significantly Influenced by Participants’ Level of Agreement with FFT Criticisms Variable Crit
Group Crit
Group Mean
Difference Std.
Error Sig.
FFT Practice
Low Agreement
High Agreement
-3.420 1.329 .03
Role Analysis
Low Agreement
High Agreement
.281 0.107 .03
Skills Training
Low Agreement
High Agreement
.277 0.113 .05
Therapist Minimizes
Low Agreement
Med Agreement
.390 0.139 .02
High Agreement
.337 0.119 .02
Summary of Results
Results indicated that FFT is being used thoroughly by at least some clinicians.
Specifically, over half of participants utilized FFT and its specific techniques thoroughly,
with the exception of the use of Therapist Minimizes Hierarchy (45%). A one-way
between-subjects ANOVA indicated that use of four of the six dependent variables were
significantly based on participants’ level of agreement with the criticisms of FFT. The
results indicate that the higher participants’ level of agreement with the criticisms of FFT,

54
the less likely they were to thoroughly utilize FFT in their clinical work with lesbian and
gay clients experiencing intimate partner violence. These findings are consistent with the
alternative hypothesis for research question two.

55
CHAPTER V
Discussion
The goal of this research was to explore whether Feminist Family Therapy (FFT)
is being utilized as commonly as it is recommended in literature for treatment of violence
in relationships. A secondary goal for this study was to determine whether there was a
clear indication that a clinicians’ agreement or disagreement with the common criticisms
of FFT seemed to influence whether a clinician utilized feminist techniques. This study
attempted to explore some novel questions not addressed in the existing literature. The
data revealed several interesting trends and created implications for future clinical
application and research. These findings are summarized and discussed in this chapter. A
critique of the methodology and limitations of the study are also explored.
Discussion of Overall Findings
Demographics
The demographics revealed interesting data regarding the sample of this study.
Although the majority of participants reported being licensed in Ohio, the demographic
statistics regarding reported intimate partner violence and mental healthcare utilization
reflect national trends that are reported in well-known and credible studies (SAMSHA,
2019). This means that, although the majority of the participants provided experiences
based on their clinical work in Ohio, it accurately parallels what is reported in national
studies.

56
Further, the percentage of estimated gay and lesbian clients on participants’
caseloads was extremely low, as is the estimated percentage of clients reporting violence
in their relationships. This also accurately parallels the rates of mental health utilization
by gay and lesbian individuals, as well as those that experience violence in their
relationships (SAMHSA, 2019). Despite these low numbers, almost half the participants
(45%) indicated that at least a quarter of their LGB clients experience intimate partner
violence, which can potentially translate to countless affected victims.
The demographic data also revealed that only 5% of participants identified FFT as
their primary theoretical orientation. This result was surprising, considering the majority
of participants indicated using FFT techniques in some capacity on the FFTBC.
However, the data also indicates that almost half of the participants (49.8%) identified
themselves as utilizing a wide variety of approaches, while the other half of participants
(50.2%) reported utilizing CBT or “Eclectic” as their primary theory. The next section
will discuss this disparity in greater detail.
Research Question One
This study’s first research question regarding whether FFT is being utilized by
clinicians to treat intimate partner violence in same-sex couples revealed that despite
whether clinicians self-reported that they utilize the approach, results indicated that over
half of the participants (63%) use the FFT approach and its specific techniques
thoroughly, with the exception of minimizing power imbalances (45%). There was a
noticeable contrast between the use of the FFT approach when compared to clinicians’
self-reported primary theoretical orientation. Although 63% were found to be utilizing

57
FFT thoroughly, only 1.8% of participants reported FFT as their primary theoretical
orientation.
These results do not provide a clear explanation of why this contrast occurred;
however, it could be explained by the apparent overlap of FFT techniques with the
mental health field’s prioritizing of intersectionality and cultural competency as best
practices (Gutierrez, 2018). In recent years, mental health clinicians have increased their
focus on cultural competency, which more recently includes competency in working with
sexual minorities (Springer et al., 2021). This trend reflects the goal of the FFT approach
but according to the data, clinicians may not be associating FFT with these priorities.
Recent studies have suggested integrating FFT with many modern theoretical
approaches. Popular clinical models such as Emotion-Focused Therapy (Coppola, 2019),
Narrative Family Therapy (Crumb, 2018), and Structural Family Therapy (Levittt, et al.,
2019) have all been the focus of publications looking to integrate FFT principles in order
to ensure these models are inclusive and can treat a diverse number of clients and
presenting issues. These recent publications indicate that the use of FFT is still seen as
relevant and important. In fact, the integration of FFT into popular clinical models may
make the common criticism that it is not a well-developed treatment model on its own a
moot point.
Research Question Two
This study’s second research question explored whether a participant’s agreement
with the criticisms of FFT would influence their use of the approach. The data analysis
revealed that there were some statistically significant differences in the use of FFT and
some of its techniques, based on a participant’s level of agreement. When looking at

58
overall use of the FFT approach, there was a statistically significant difference between
those who held high agreement with FFT’s criticisms and those who held low agreement.
Those with high agreement utilized the approach less frequently than those with low
agreement. This was also the case for participants’ use of role analysis assessment,
feminist skills training, and minimizing role imbalance within a couple. This means that
the higher the level of agreement of the FFT criticisms, the less frequently the above-
mentioned techniques were used, as well as the overall approach. Interestingly,
minimizing role imbalance showed a statistically significant difference in usage between
low and high agreement groups, and low and medium agreement groups.
Limitations of the Study
Due to the novel nature of this study, several limitations became apparent. These
limitations are regarding the structure of the study, data collection, and the instruments
used. They are discussed in detail below.
Structure of the Study
While reviewing the data and analyses, several limitations regarding the structure
of the study were apparent. The first limitation was in the sampling method chosen for
the study. Convenience and snowball sampling did not provide a wide variety of
participants, with the majority of participants (81.3%) responding from Ohio. In order to
be able to better generalize the results to the greater population, all states should be
represented and in correspondence with each state’s population.
Second, the focus of this study may have been too narrow. Assessing FFT and
gay and lesbian clients specifically may be too specific considering there is much
conversation about overall intersectionality and fluidity of sexuality and gender, when

59
looking at current literature (Ramos et al., 2021). Although FFT does include the concept
of intersectionality, it may not be a well-known fact among clinicians. This could be
especially true considering only 1.8% of participants identified FFT as their primary
theoretical orientation, yet 63% of participants were utilizing FFT thoroughly, according
to their FFTBC scores. Additionally, some participants indicated that they were not
familiar with FFT, even though all participants indicated using FFT in some capacity.
Data Collection
The quantitative nature of the survey likely limited responses from participants
and did not allow them to discuss nuances and factors that may not have been taken into
consideration during this study. The survey also did not provide an operational definition
of feminism and FFT to the participants. There were a handful of participants that
indicated they did not know the meaning of those terms.
There were also multiple purposeful attempts to distort data with falsified
responses. In order to advertise the survey, a Facebook ad was taken out during the initial
months of data collection. The ad attracted homophobic and politically extreme
responses. Some of these individuals also attempted to complete the survey with
incomplete, false, and/or nonsensical responses. Although these individuals intended on
interfering with data collection, it was clear from their responses which data sets needed
to be removed. This is likely due to the highly specialized nature of the questions on the
survey, which individuals who are not clinical professionals would have difficulty
answering. For example, when participants were asked to write in their response for their
primary theoretical orientation, irrelevant or vulgar responses were provided.

60
Although not widely researched, this phenomenon has received attention from
scholars. Research has identified issues with data collection when large entities and
organization attempt to skew results, referred to as “political interference” (Prewitt,
2010). However, in recent years, there has been a closer exploration of small-scale
interference by small groups of individuals. In 2017, Fish and Russell published on their
experiences with what they referred to as “mischievous responders”. Fronek and Briggs
(2018) proposed an actual term and operational definition to identify and describe this
phenomenon. They refer to it as “political interference by fake participants” defined as
“political motivation (agency and power struggles) whether personal or organizational, is
not driven by financial or other rewards, and involves active, covert deception with the
purpose of negatively impacting on the viability of research or to manipulate the
findings” (p. 3). Although the focus on political motives is relevant, it may be necessary
to expand these terms to include phobic motivations for interference.
Validity and Reliability of the Assessment Instruments
The FFTBC is not a well-developed instrument. Revisions of the wording of each
item were necessary in order to make the checklist relevant to same-sex couples and to
remove heterosexual-specific language. Also, no cutoff scores for the subscales of the
checklist were provided, so it was necessary to use best judgement and consultation to
determine cutoff scores that were reasonable.
The FCQ, which was designed by this researcher, may also deliver questionable
results. The FCQ was created because no other instrument that measured the level of
agreement of common criticisms of FFT existed. A factor analysis on the items of this

61
questionnaire was also not done, which would have provided more insight into whether
the items were accurately measuring participants’ level of agreement.
Finally, some demographic questions, such as the percentage of clients who
identify as gay or lesbian on a participants’ caseload, and the percentage of clients
experiencing violence in their relationships, relied on an estimate from participants. The
implication, of course, is that the data received from participants may not reflect accurate
trends that are generalizable to the greater population of clinicians.
Clinical Implications
Based on the data, FFT and its techniques, in some form, do appear to be widely
used by clinicians. However, it seems as though clinicians are not associating the
techniques they use with the FFT approach. Perhaps it may be more productive to ensure
all theoretical models include concepts like intersectionality, social justice, cultural and
social competency, and a trauma-informed perspective (Coppola, 2019; Gutierrez, 2018;
Crumb, 2018; Levitt et al., 2019). Due to the continual increase in violence in same-sex
relationships, clinicians may need to pay special attention to the effectiveness of their
treatment approaches (SAMSHA, 2019).
The results of the ANOVA demonstrated a clear connection between the thorough
use of the FFT approach and a clinician’s level of agreement with the criticisms.
However, because all participants indicated they use the techniques on some level, it may
be important to explore what the next steps for FFT should be. Since the inclusion of
intersectionality and cultural competence is now generally expected, regardless of the
model a clinician uses, it is worth considering how FFT can be integrated into models
that lack attention to diversity. It is also important to consider that if the criticisms of the

62
approach are influential enough to affect a clinician’s use of it, this may render the
approach irrelevant in its current form. Some critics of the approach have even suggested
a “rebranding” of FFT, which would include a name change, moving away from using
the word “feminism,” in order to be more inclusive of all oppressed and minority groups
(Evans & Bussey-Chamberlin, 2021).
Regardless of what direction FFT must move in, it is clear that there needs to be
more education among clinicians regarding the source of the techniques the majority of
participants report utilizing at such a high level. As discussed in the next section, there
appears to be a need for research to demonstrate that clinicians are scoring high on the
FFTBC yet are not attributing these techniques to FFT. This could mean moving forward
with the idea to integrate FFT into popular clinical models, which has been a topic of
research in recent years.
Future Research Implications
For future research, it would be much needed to assess the validity and reliability
of the reworded items on the FFTBC. Running a factor analysis would give a much
clearer idea of whether these items are appropriately measuring their intended subscales.
It would also be important to develop an appropriately assessed FCQ to ensure validity.
Although there is not necessarily a debate about what common criticisms of FFT exist in
the literature, ensuring that items are clearly written and easy to understand would be
meaningful for gathering accurate data. This would also allow us to see whether one item
per criticism, as it is written in the current FCQ, is sufficient for measuring agreement or
disagreement. Additionally, developing statistically sound cutoff scores for each
instrument would be imperative.

63
The focus of a study such as this may also be too specific. The study did not
expand beyond assessing clinicians’ work with same-sex couples. Although, same-sex
couples have been a significant focus in literature, discussions are trending more towards
the fluidity of sexuality, possibly creating the need for an operationalized definition of
sexuality that is both broad enough to be inclusive of all types of clients, while also being
specific enough to study and quantify.
Having more demographic data would add important details of participants’
context to our understanding. It may be possible to focus on pulling more specific and
accurate data about demographic information from organizations such as clinics,
hospitals, and practices, instead of relying on clinicians’ estimated description of their
clientele.
This study would also likely garner more information if it was conducted as a
qualitative project. There are an incredible number of nuances that influence the way a
clinician may address minority clients who experience violence in their relationships.
Hearing from a small number of qualitative participants regarding these nuances and
influences would add significant context to the data received in this study. Qualitative
interviews may also shed light on influential concepts not considered in this study. One
such topic may be clinicians’ perspectives on whether FFT remains a relevant treatment
approach in mental health. Interviewing a small group of clinicians would also make it
possible to better confirm that each participant was actively seeing LGBTQ clients
experiencing violence in their relationships, versus relying on their self-report and
estimates.

64
Finally, it may be very necessary to assess clinicians’ fear of addressing violence
in relationships as a possible treatment barrier. Although clinicians typically have good
intentions for treating their clients to the best of their ability, it is also well known that
there are certain topics that arise which clinicians may struggle with acknowledging
(Olszowy, 2020). Violence in relationships, especially among minority clients, may not
be as frequently addressed as is needed. This possible barrier could be investigated during
a qualitative interview, as mentioned above.
Summary
This chapter included a discussion of the results following the collection of
demographic data and a one-way between-subjects ANOVA. It also explored
implications for both clinicians and future research, while providing an in-depth analysis
of possible limitations. The overall goal of this study was to determine the level of usage
of FFT as a treatment for violence in same-sex relationships. Further, it examined how
the level of agreement with common criticisms of FFT may or may not influence a
clinician’s use of the approach.
The study revealed that FFT and its techniques seem to be utilized within
participants’ clinical practice, however, it was rarely identified as a primary theoretical
orientation. In contrast, other approaches such as CBT and identifying as eclectic were
more common. The data also revealed that a clinician’s level of agreement of FFT
criticisms was influential on whether participants used the approach thoroughly. These
results provide a foundation for further exploration of treatment barriers for minorities
experiencing violence, as well as the consideration that FFT may be seen as irrelevant
within the mental health field.

65
The most urgent aspect of this study is to draw more attention to statistical trends
indicating that violence among sexual minorities continues to rise and likely coincides
with the low rate of mental health services utilization. To conclude, this researcher holds
two hopes. First, that we can continue to explore what we can do for our clients and our
communities to ensure each individual’s emotional and physical safety. Secondly, that we
can all look forward to there being effective treatment solutions to this significant cultural
issue in the future.

66
REFERENCES
(n.d.). American Psychological Association. Retrieved from https://www.apa.org/
(n.d.). National Institute of Justice. Retrieved from https://www.nij.gov/Pages/welcome.aspx
Ali, P. A., & Naylor, P. B. (2013). Intimate partner violence: A narrative review of the
feminist, social and ecological explanations for its causation. Aggression and Violent
Behavior, 18(6), 611–619.doi:10.1016/j.avb.2013.07.009
Ault-Riche, M. (1986). A feminist critique of five schools of family therapy. PsycEXTRA
Dataset. doi:10.1037/e437082004-001
Barnes, R. (2010). Suffering in a silent vacuum: Woman-to-woman partner abuse as a
challenge to the lesbian feminist vision. Feminism & Psychology, 21(2), 233–
239.doi:10.1177/0959353510370183
Baugher, A. R., & Gazmararian, J. A. (2015). Masculine gender role stress and violence: A
literature review and future directions. Aggression and Violent Behavior, 24, 107–
112.doi:10.1016/j.avb.2015.04.002
Black, L., & Piercy, F. P. (1991). A feminist family therapy scale. Journal of Marital and
Family Therapy, 17(2), 111–120. doi:10.1111/j.1752-0606.1991.tb00874.x
Blumer, M. L. C., Papaj, A. K., & Erolin, K. S. (2013). Feminist family therapy for treating
female survivors of childhood sexual abuse. Journal of Feminist Family Therapy,
25(2), 65–79.doi:10.1080/08952833.2013.777871

67
Bohall, G., Bautista, M.-J., & Musson, S. (2016). Intimate partner iolence and the Duluth
Model: An examination of the model and recommendations for future research and
practice. Journal of Family Violence, 31(8), 1029–1033. doi:10.1007/s10896-016-
9888-x
Brown, C. (2008). Gender-Role implications on same-sex intimate partner abuse. Journal of
Family Violence, 23(6), 457–462.doi:10.1007/s10896-008-9172-9
Brown, M. J., Serovich, J. M., & Kimberly, J. A. (2016). Depressive symptoms, substance use
and partner violence victimization associated with HIV disclosure among men who
have sex with men. AIDS and Behavior, 20(1), 184–192.doi:10.1007/s10461-015-
1122-y
Brown, T., & Herman, J. (2015) Intimate partner violence and sexual abuse among LGBT
people: A review of existing research. The Williams Institute. Los Angeles, CA.
Cannon, C. (2015). Illusion of inclusion: The failure of the gender paradigm to account for
intimate partner violence in LGBT relationships. Partner Abuse, 6(1), 65-77.
doi:10.1891/1946-6560.6.1.65
Centers for Disease Control and Prevention. (n.d.). Retrieved August 2, 2019, from
https://www.cdc.gov/
Chaney, S. E., & Piercy, F. P. (1988). A feminist family therapist behavior checklist. The
American Journal of Family Therapy, 16(4), 305-
318.doi:10.1080/01926188808250736
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159.

68
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A black feminist
critique of antidiscrimination doctrine, feminist theory, and antiracist politics. Feminist
Legal Theory, 57-80. doi:10.4324/9780429500480-5
Coppola, J., (2019). An integrated EFT-Contextual approach for couples therapy: Suggested
model and ideas for practice. Journal of Family Therapy 42(4), 588-612.
https://doi.org/10.1111/1467-6427.12282
Diagnostic and statistical manual of mental disorders: DSM-5. (2017). Arlington, VA:
American Psychiatric Association.
Enns, C. Z. (1993). Twenty years of feminist counseling and therapy. The Counseling
Psychologist, 21(1), 3–87.doi:10.1177/0011000093211001
Evans, E. & Bussey-Chamberlain, P. (2021). The problems with feminist nostalgia:
Intersectionality and white popular feminism. European Journal of Women’s Studies,
ISSN 1350-5068 [Article] (Forthcoming)
Fish, J. & Russell, S. (2018). Have mischievous responders misidentified sexual minority
youth disparities in the National Longitudinal Study of Adolescent to Adult Health?
Archives of Sexual Behavior, 47, 1053-1067. https://doi.org/10.1007/s10508-017-0993-
6
Ford, C. L., Slavin, T., Hilton, K. L., & Holt, S. L. (2012). Intimate partner violence
prevention services and resources in Los Angeles. Health Promotion Practice, 14(6),
841–849.doi:10.1177/1524839912467645
Fronek, P., & Briggs, L. (2018). Faking participant identity: Vested interests and purposeful
interference. Research Ethics, 14(2), 1–5. https://doi.org/10.1177/1747016117740177

69
George, J., & Stith, S. M. (2014). An updated feminist view of intimate partner violence.
Family Process, 53(2), 179–193.doi:10.1111/famp.12073
Goodrich, T. J. (1988). Feminist family therapy: A casebook. New York: W.W. Norton &
Company.
Goodrich, T. J. (1991). Women, power, and family therapy. Journal of Feminist Family
Therapy, 3(1-2), 5-37. doi:10.1300/j086v03n01_02
Greene, K., & Bogo, M. (2002). The different faces of intimate violence: Implications for
assessment and treatment. Journal of Marital and Family Therapy, 28(4), 455–
466. doi:10.1111/j.1752-0606.2002.tb00370.x
Hamel, J. (2010). Do we want to be politically correct, or do we want to reduce partner
violence in our communities? Partner Abuse, 1(1), 82-91. doi:10.1891/1946-
6560.1.1.82
Herman, K., Rotunda, R., Williamson, G., & Vodanovich, S. (2014). Outcomes from a Duluth
Model batterer intervention program at completion and long term follow-up. Journal of
Offender Rehabilitation, 53(1), 1–18.doi:10.1080/10509674.2013.861316
Herzog, S. (2007). An empirical test of feminist theory and research. Feminist Criminology,
2(3), 223–244.doi:10.1177/1557085107301836
Hill, N. A., Woodson, K. M., Ferguson, A. D., & Parks, C. W. (2012). Intimate partner abuse
among African American lesbians: Prevalence, risk factors, theory, and resilience.
Journal of Family Violence, 27(5), 401–413. doi:10.1007/s10896-012-9439-z
(n.d.). Domestic Abuse Intervention Programs. Retrieved August 2, 2019, from
https://www.theduluthmodel.org/

70
Home. (n.d.). World Health Organization. Retrieved August 2, 2019, from
https://www.who.int/
http://dx.doi.org/10.1037/0033-2909.112.1.155
Karakurt, G., Whiting, K., van Esch, C., Bolen, S. D., & Calabrese, J. R. (2016). Couples
therapy for intimate partner violence: A systematic review and meta-analysis. Journal
of Marital and Family Therapy, 42(4), 567–583.doi:10.1111/jmft.12178
Kay, M., & Jeffries, S. (2010). Homophobia, heteronormativism and hegemonic masculinity:
Male same-sex intimate violence from the perspective of Brisbane service providers.
Psychiatry, Psychology and Law, 17(3), 412–423.doi:10.1080/13218710903566953
Leong, F. T. (2014). APA handbook of multicultural psychology. Washington, DC: American
Psychological Association.
Lewis, R. J., Derlega, V. J., Griffin, J. L., & Krowinski, A. C. (2003). Stressors for gay men
and lesbians: Life stress, gay-related stress, stigma consciousness, and depressive
symptoms. Journal of Social and Clinical Psychology, 22(6), 716–
729.doi:10.1521/jscp.22.6.716.22932
Lewis, R. J., Milletich, R. J., Derlega, V. J., & Padilla, M. A. (2014). Sexual minority stressors
and psychological aggression in lesbian women’s intimate relationships. Psychology of
Women Quarterly, 38(4), 535–550.doi:10.1177/0361684313517866
Levitt, H., Whelton, W., & Iwakabe, S. (2019). Integrating feminist-multicultural perspectives
into emotion-focused therapy. Clinical handbook of emotion-focused therapy, 425–444.
American Psychological Association. https://doi.org/10.1037/0000112-019 Longobardi, C., & Badenes-Ribera, L. (2017). Intimate partner violence in same-sex
relationships and the role of sexual minority stressors: A systematic review of the past

71
10 Years. Journal of Child and Family Studies, 26(8), 2039–2049.doi:10.1007/s10826-
017-0734-4
Ludbrook, J. (1998). Multiple comparison procedures updated. Clinical and Experiemental
Pharmacology and Physiology, 25, 1032-1037.
Macneil, C. A., Hasty, M. K., Evans, M., Redlich, C., & Berk, M. (2009). The therapeutic
alliance: Is it necessary or sufficient to engender positive outcomes? Neuropsychiatry,
21(02), 95–98. doi:10.1111/j.1601-5215.2009.00372.x
Madsen, C. A., Stith, S. M., Thomsen, C. J., & Mccollum, E. E. (2012). Violent Couples
Seeking Therapy: Bilateral and Unilateral Violence. Partner Abuse, 3(1), 43-58.
doi:10.1891/1946-6560.3.1.43
Martin-Storey, A. (2014). Prevalence of dating violence among sexual minority youth:
Variation across gender, sexual minority identity and gender of sexual partners.
Journal of Youth and Adolescence, 44(1), 211–224. doi:10.1007/s10964-013-0089-0
Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance with
outcome and other variables: A meta-analytic review. Journal of Consulting and
Clinical Psychology, 68(3), 438–450.doi:10.1037/0022-006x.68.3.438
Marziali, E., Munroe-Blum, H., & McCleary, L. (1999). The effects of the therapeutic alliance
on the outcomes of individual and group psychotherapy with Borderline Personality
Disorder. Psychotherapy Research, 9(4), 424–
436.doi:10.1080/10503309912331332841
Mcphail, B. A., Busch, N. B., Kulkarni, S., & Rice, G. (2007). An integrative feminist model.
Violence Against Women, 13(8), 817-841. doi:10.1177/1077801207302039

72
Murray, S. (2009). Somewhere safe to call home: Violence against women during
homelessness. Melbourne: RMIT University.
NCADV: National Coalition Against Domestic Violence. (n.d.). Retrieved August 2, 2019,
from https://ncadv.org/
Olszowy, L., Jaffe, P., Dawson, M., Straatman, A., Saxton, M. (2020). Voices from the
frontline: Child protection workers’ perspectives on barriers to assessing risk in
domestic violence cases. Children and Youth Services Review,16, 105208.
https://doi.org/10.1016/j.childyouth.2020.105208.
Pence, E., & Paymar, M. (1993). Education groups for men who batter: The Duluth model.
New York: Springer.
Pender, R. L. (2012). ASGW best practice guidelines: An evaluation of the Duluth Model. The
Journal for Specialists in Group Work, 37(3), 218
231.doi:10.1080/01933922.2011.632813
Piercy, F. P., Sprenkle, D. H., & Wetchler, J. L. (1996). Family therapy sourcebook. New
York: Guilford Press.
Prewitt, K. (2010). What is political interference in federal statistics? The ANNALS of the
American Academy of Political and Social Science, 631(1), 225–238.
https://doi.org/10.1177/0002716210373737
Ramos, S., Lardier, D., Jr, Opara, I., Turpin, R., Boyd, D., Gutierrez, J., Jr, Williams, C.,
Nelson, L., & Kershaw, T. (2021). Intersectional effects of sexual orientation
concealment, internalized homophobia, and gender expression on sexual identity and
HIV risk among sexual minority men of color: A path analysis. The Journal of the

73
Association of Nurses in AIDS Care : JANAC, 32(4), 495–511.
https://doi.org/10.1097/JNC.0000000000000274
Rollè, L., Giardina, G., Caldarera, A. M., Gerino, E., & Brustia, P. (2018). When intimate
partner violence meets same sex couples: A review of same sex intimate partner
violence. Frontiers in Psychology, 10. doi:10.3389/fpsyg.2019.01706
Seligman, L., & Reichenberg, L. W. (2010). Theories of counseling and psychotherapy:
Systems, strategies, and skills. Upper Saddle River: Pearson.
Siegenthaler, A. L., & Boss, P. (1998). Contemporary Family Therapy, 20(3), 333–
340.doi:10.1023/a:1022468913378
Staggs, S. L., & Schewe, P. A. (n.d.). Primary prevention of domestic violence. Violence
against women and children, Vol 2: Navigating Solutions., 237-257.
doi:10.1037/12308-012
Stith, S., Pruitt, I., Dees, J., Fronce, M., Green, N., Som, A., & Linkh, D. (2006).
Implementing community-based prevention programming: A review of the literature.
The Journal of Primary Prevention, 27(6), 599-617. doi:10.1007/s10935-006-0062-8
Substance Abuse and Mental Health Services Administration. (2019). 2019 National
survey on drug use and health: Lesbian, gay, and bisexual (LGB) adults. Retrieved
August 2, 2019 from https://www.samhsa.gov/data/report/2019-nsduh-lesbian-gay-
bisexual-lgb-adults.
Springer, P., Bischoff, R., Taylor, N., Neuhaus, V., & Leow, C. (2021). Competency-based
training in the supervision of relational telemental supervision. Journal of Marital and
Family Therapy, 47(2), 375-391. https://doi.org/10.1111/jmft.12513

74
Thomas, S. (1977). Theory and practice in feminist therapy. Social Work, 447-454.
doi:10.1093/sw/22.6.447
Tukey, J. W. (1980). We Need Both Exploratory and Confirmatory. The American Statistician,
34(1), 23–25.doi:10.1080/00031305.1980.10482706
Vatcher, C., & Bogo, M. (2007). The Feminist/Emotionally-Focused Therapy practice model:
An integrated approach For couple therapy. Journal of Marital and Family Therapy,
27(1), 69-83. doi:10.1111/j.1752-0606.2001.tb01140.x

75
APPENDICES

76
APPENDIX A
INTEGRATIVE FEMINIST MODEL FOR INTIMATE PARTNER VIOLENCE
Figure 1. Integrative Feminist model for intimate partner violence

77
APPENDIX B
INFORMED CONSENT FORM
You are invited to participate in a research project being conducted by Rachel Bell, a doctoral student in the School of Counseling at The University of Akron. The purpose of this research is to determine how licensed clinicians feel about feminist family therapy techniques and how often they are being utilized with a specific population. While there are no tangible benefits for the participants of this study, your participation will assist in the collection and analysis of data to address an important issue in the mental health field. If you decide to participate, you will be asked to complete an anonymous web-based survey. The survey should take no more than 30 minutes and I hope to recruit 252 participants. The survey will not collect any identifiable information, and no one will be able to connect your responses to you. Your anonymity is further protected by not asking you to sign and return a consent form. Your completion of the survey will serve as your consent. Please print this introduction for future reference. At the end of the survey, you will be given an opportunity to opt-in to an Amazon gift card giveaway, as an incentive for participating in the survey and you will be asked to provide your email address as a means of contacting you. One winner will be chosen at random and will be sent a $100 Amazon gift card electronically via the email address you provide. Please note that your email address will be kept separate from your survey responses and will not be used for anything other than contacting you, should you win a gift card. If you have any questions about this study, you may email me at [email protected], or my advisor, Dr. Heather Katafiasz, at [email protected]. This project has been reviewed and approved by The University of Akron Institutional Review Board. If you have any questions about your rights as a research participant, you may call the IRB at (330) 972-7666. Please click on the link below to access the survey. Thank you. By pressing the “continue” button, I hereby consent to participate in this research project.

78
APPENDIX C
DEMOGRAPHIC QUESTIONNAIRE
1. Are you a licensed clinician (this does not include trainee licenses)? a. Yes b. No
2. Type of Clinician/License (please write out full title of license): a. Text box
3. What state do you practice in? a. Drop down menu of states
4. Years You’ve held Your Current License: a. Text box
5. Your gender identity: a. Male b. Female c. Non-Binary d. Other. Please Specify: (Text box)
6. What client populations do you typically see (select all that apply)? a. Children (Ages 0 to 12) b. Adolescents (Ages 13 to 17) c. Adult individuals (Ages 18 and up) d. Adult couples (Ages 18 and up) e. Families f. Other. Please specify: (Text box)
7. What are your areas of specialty? a. (Text box)
8. What percentage of your adult clients do you estimate experience violence in their relationships?
a. 0%-25% b. 26%-50% c. 51%-75% d. 76%-100%
9. Have you or are you currently treating either an adult gay/lesbian individual client or a same-sex adult couple who has experienced violence in their relationship?
a. Yes b. No
10. What is/was your employment setting when seeing the client(s) referenced in question 9 (Check all that apply)?
a. Outpatient at Non-Profit Agency

79
b. Outpatient at Private Practice c. Inpatient/Hospital d. Partial Hospitalization Program e. Intensive Outpatient f. Other. Please specify: (Text box) g. I answered “no” to question 8
11. What percentage of your clients identify as either gay or lesbian (Please estimate)?
a. 0% to 25% b. 26% to 50% c. 51% to 75% d. 76% to 100%
12. What is your primary theoretical orientation? a. Text box
13. Do you regularly integrate feminist family therapy techniques into your practice of counseling/therapy?
a. Always b. Often c. Sometimes d. Rarely e. Never

80
APPENDIX D
FEMINIST FAMILY THERAPY BEHAVIOR CHECKLIST
Please answer how frequently you use each skill in your clinical work using the following
scale:
1-Always 2-Often 3-Sometimes 4-Rarely 5-Never
1. Encourage couples to develop more egalitarian relationships. 2. Negotiate a more equal distribution of parenting and/or household tasks. 3. Encourage clients to become more aware of their own needs and make those
needs a priority. 4. Encourage clients to better identify and express their feelings in their relationship. 5. Educate couples about aspects of social inequality that have been oppressive and
hurtful. 6. Reframe and challenge the clients’ definitions of the problem to include the
impact of social inequality. 7. If there is a partner with less power, support that partner in asserting their
decision-making power. 8. Raise issues of social inequality whether or not the couple brings them up. 9. Teach couples about the concept of social privilege. 10. If there is a dominant partner, hold that partner equally responsible for change in
their relationship. 11. If there is a partner with less power, support that partner in continuing to assert
themselves in their couple relationship. 12. If there is a dominant partner, encourage that partner to be more nurturing and
better meet the emotional needs of their partner. 13. Address derogatory comments towards each other and self-deprecating comments
related to their own social inequality when they are expressed by clients. 14. Reframe and challenge the clients’ definition of the problem(s) to include the
impact of social inequality. 15. Ask if control and manipulation is occurring or has occurred in their couple
relationship. 16. Ask if emotional violence is occurring or has occurred in their couple
relationship. 17. Ask if sexual violence is occurring or has occurred in their couple relationship. 18. Ask if physical violence is occurring or has occurred in their couple relationship. 19. Raise and explore issues of social inequality that disadvantages either partner
regardless of presenting issue.

81
20. Clearly communicate through my words and actions my opposition to controlling, violent, and abusive behaviors.
21. Assess for and attend to issues of safety when violence and control are present in relationships.
22. Clearly communicate through my words and actions my opposition to any behaviors by either partner that are intended to control or subtly control their partner’s actions, times, choices, and relationships with others.
23. Promote relationships characterized by mutuality, reciprocity, interdependence, and a balance between intimacy and autonomy.
24. Encourage a shared knowledge of financial information and shared financial decision-making power.
25. Encourage a mutual, consensual sexual relationship based on intimacy. 26. Encourage partners to grant equal value to each other’s activities, work, life goals,
opinions, hopes, and dreams. 27. Explore the ways that social inequality has influenced both partners’ identities. 28. If there is a dominant partner, explore with that partner potential ways they may
be misusing power in their relationship with their partner. 29. If there is a dominant partner, encourage that partner to grant greater value to their
partner’s activities, work, career, life goals, hopes, and dreams than their own in an effort to offset social inequalities.
30. If there is a dominant partner, encourage that partner to explore potential ways they may be misusing power in their sexual relationship.
31. Challenge couples to develop equal levels of power in their relationship. 32. If there is a dominant partner, hold that partner more responsible for change when
there is a power imbalance in their relationship. 33. If there is a dominant partner, challenge that partner to accept their partner’s
decision-making power. 34. Raise and explore issues of social privilege with clients regardless of the
presenting issue. 35. Explore ways that social inequality has influenced both partners’ identities. 36. If there is a dominant partner, challenge that partner to give up power in order to
establish more equal levels of power in their relationship. 37. If there is a dominant partner, hold that partner more responsible for the change
than their partner. 38. If there is a dominant partner, encourage that partner to grant equal value to their
partner’s activities, work, career, life goals, hopes, and dream

82
APPENDIX E
FEMINIST CRITICISMS QUESTIONNAIRE
Please rate your level of agreement with the following statements regarding Feminism and Feminist Family Therapy using: 1-Strongly Agree 2-Somewhat Agree 3-Undecided 4-Somewhat Disagree 5-Strongly
Disagree
1. Feminism assumes that a power differential exists based only on gender and
does not take into account other aspects of social inequality such as race, sexual orientation, socioeconomic status, income, or education.
2. The feminist community has been resistant to acknowledge the issue of same-sex violence.
3. The feminist perspective focuses only on uni-directional violence. 4. Feminism is too reliant on the criminal justice system in order to respond to
violence in relationships, giving the power to the courts and not empowering the victims.
5. Feminist Family Therapy is not a comprehensive treatment model and is too fragmented to be considered a standalone approach.
6. Feminist Family Therapy lacks empirical evidence demonstrating its effectiveness in treating intimate partner violence in same-sex couple

83
APPENDIX F
GIFT CARD GIVEAWAY OPT-IN
Please enter your email address if you wish to be entered into the gift card giveaway.
Please note that your email address will be kept separate from your questionnaire
responses and will not be used for anything other than contacting you, should you win a
gift card.
1. Text Box for Email

84
APPENDIX G
FFTBC SUBSCALES AND ITEMS
FFTBC Subscales and Items
FFTBC Subscale FFTBC Item
Subscale 1: Role Analysis
6. Reframes and challenge the client's definition of the problem to include the impact of social inequality
14. Reframe and challenge the clients’ definition of the problem(s) to include the impact of social inequality.
15. Ask if control and manipulation is occurring or has occurred in their couple relationship.
16. Ask if emotional violence is occurring or has occurred in their couple relationship.
17. Ask if sexual violence is occurring or has occurred in their couple relationship.
18. Ask if physical violence is occurring or has occurred in their couple relationship.
19. Raise and explore issues of social inequality that disadvantages either partner regardless of presenting issue.
20. Clearly communicate through my words and actions my opposition to controlling, violent, and abusive behaviors.
21. Assess for and attend to issues of safety when violence and control are present in relationships.
Subscale 2: Shifts Balance
2. Negotiate a more equal distribution of parenting and/or household tasks.
10. If there is a dominant partner, hold that partner equally responsible for change in their relationship.
12. If there is a dominant partner, encourage that partner to be more nurturing and better meet the emotional needs of their partner.
22. Clearly communicate through my words and actions my opposition to any behaviors by either partner that are intended to
85
control or subtly control their partner’s actions, times, choices, and relationships with others.
28. If there is a dominant partner, explore with that partner potential ways they may be misusing power in their relationship with their partner.
29. If there is a dominant partner, encourage that partner to grant greater value to their partner’s activities, work, career, life goals, hopes, and dreams than their own in an effort to offset social inequalities.
30. If there is a dominant partner, encourage that partner to explore potential ways they may be misusing power in their sexual relationship.
32. If there is a dominant partner, hold that partner more responsible for change when there is a power imbalance in their relationship.
33. If there is a dominant partner, challenge that partner to accept their partner’s decision making power.
36. If there is a dominant partner, challenge that partner to give up power in order to establish more equal levels of power in their relationship.
37. If there is a dominant partner, hold that partner more responsible for the change than their partner.
38. If there is a dominant partner, encourage that partner to grant equal value to their partner’s activities, work, career, life goals, hopes, and dreams.
Subscale 3: Therapist Empowers 1. Encourage couples to develop more egalitarian relationships.
3. Encourage clients to become more aware of their own needs and make those needs a priority.
4. Encourage clients to better identify and express their feelings in their relationship.
7. If there is a partner with less power, support that partner in asserting their decision-making power.
11. If there is a partner with less power, support that partner in continuing to assert themselves in their couple relationship.
Subscale 4: Skills Training
5. Educate couples about aspects of social inequality that have been oppressive and hurtful.
9. Educate couples about the concept of social privilege.

86
13. Address derogatory comments towards each other and self-deprecating comments related to their own social inequality when they are expressed by clients.
24. Encourage a shared knowledge of financial information and shared financial decision-making power.
25. Encourage a mutual, consensual sexual relationship based on intimacy.
26. Encourage partners to grant equal value to each other’s activities, work, life goals, opinions, hopes, and dreams.
31. Challenge couples to develop equal levels of power in their relationship.
Subscale 5: Minimizes Hierarchy
8. Raise issues of social inequality whether or not the couple brings them up.
23. Promote relationships characterized by mutuality, reciprocity, interdependence, and a balance between intimacy and autonomy.
27. Explore the ways that social inequality has influenced both partners’ identities.
34. Raise and explore issues of social privilege with clients regardless of the presenting issue.
35. Explore ways that social inequality has influenced both partners' identities.

87
APPENDIX H
IRB APPROVAL
Top Related
Copyright © 2022 FDOKUMEN

