







Bahasa
Halaman
Hukum


Copyright © Excerpta M
edica, Inc, 2
010
Not for Commercial
Distributio
n
Clinical Therapeutics/Volume 32, Number 12, 2010
November 2010 1987
Accepted for publication September 21, 2010.doi: 10.1016/j.clinthera.2010.11.0140149-2918/$ - see front matter
© 2010 Elsevier HS Journals, Inc. All rights reserved.
AbsTrACTBackground: Transdermal scopolamine (TDS) is a
potential long-acting prophylactic antiemetic initially developed to prevent motion sickness. TDS is a centrally acting anticholinergic agent that was approved in 2001 by the US Food and Drug Administration for the preven-tion of postoperative nausea and vomiting (PONV). Although TDS has been reported to be clinically efficacious in the prevention of PONV, several adverse events (AEs), such as sedation, dry mouth, blurred vision, central cho-linergic syndrome, and confusion (particularly in elder- ly patients with mild cognitive impairment), are potential concerns.
Objective: The aim of this study was to explore the efficacy and tolerability of TDS in the prevention of PONV in adults.
Methods: A systematic search of PubMed, EMBASE, and the Cochrane Library for randomized controlled trials in adults that compared the effects of TDS and placebo on postoperative nausea, vomiting, and PONV was conducted in March 2009, and an update was con-ducted in July 2010. Without any language restrictions, a search with the following terms was performed: post-operative, postoperative, postanesthe*, postanaesthe*, post-anesthe*, post-anaesthe*, anesthesia, anaesthesia, surgery, surgeries, surgical, nausea, vomiting, emesis, retching, scopolamine, and hyoscine. Identified studies were then hand-searched for further relevant literature.
Results: Data from 25 randomized controlled trials were analyzed (N = 3298). In the postanesthesia care
unit, TDS was associated with a significantly reduced risk for postoperative nausea compared with placebo (relative risk [RR] = 0.77; 95% CI, 0.61–0.98; P = 0.03). TDS was also associated with a significantly reduced risk for postoperative nausea (RR = 0.59; 95% CI, 0.48–0.73; P < 0.001), postoperative vomiting (RR = 0.68; 95% CI, 0.61–0.76; P < 0.001), and PONV (RR = 0.73; 95% CI, 0.60–0.88; P = 0.001) during the first 24 hours after the start of anesthesia. TDS appeared to be effective compared with placebo in the prevention of postoperative nausea when treatment was initiated the night before (early application) (RR = 0.56; 95% CI, 0.41–0.75; P < 0.001) or on the day of surgery (late application) (RR = 0.61; 95% CI, 0.47–0.79; P < 0.001). TDS was associated with a higher prevalence of visual disturbances at 24 to 48 hours compared with placebo (RR = 3.35; 95% CI, 1.78–6.32). Analyses of confusion and other AEs did not show a significant association with TDS.
Conclusions: In this systematic review and meta-analysis, TDS was associated with significant reductions in PONV with both early and late patch application during the first 24 hours after the start of anesthesia. TDS was associated with a higher prevalence of visual
Transdermal Scopolamine for the Prevention of Postoperative Nausea and Vomiting: A Systematic Review and Meta-Analysis
Christian C. Apfel, MD, PhD1; Kun Zhang, MD1,2; Elizabeth George1,3; Serena Shi, MD1,4; Leena Jalota, MD1; Cyrill Hornuss, MD1; Katherine E. Fero1; Felix Heidrich, MD1,5; Joseph V, Pergolizzi, MD6; Ozlem S. Cakmakkaya, MD7; and Peter Kranke, MD, PhD8
1Perioperative Clinical Research Core, Department of Anesthesia and Perioperative Care, University of California at San Francisco, San Francisco, California; 2Department of Cardiology and Angiology, Campus Mitte, Charité – University of Medicine Berlin, Berlin, Germany; 3Stanford University Medical School, Stanford, California; 4Department of Anesthesia, University of Southern California, Los Angeles, California; 5Department of Anaesthesia and Intensive Care, Charité – University of Medicine Berlin, Berlin, Germany; 6Department of Anesthesiology and Critical Care, The Johns Hopkins University, Baltimore, Maryland; 7Department of Anaesthesia, Cerrahpasa University Medical School, Istanbul, Turkey; and 8Department of Anaesthesia and Critical Care, University Hospitals of Würzburg, Würzburg, Germany

1988 Volume 32 Number 12
Clinical Therapeutics
and PONV.5 AEs such as dry mouth, visual disturbance, agitation, and sedation were reported. In the 7 years since the publication of that study, several new studies have been published, so that an up-to-date report of effect-size estimate and especially of the potential AEs is warranted.
The aim of this study was to explore the efficacy and tolerability of TDS in the prevention of PONV in adults.
MeThodsA systematic review and meta-analysis of the literature was conducted using randomized controlled trials that compared the effects of TDS and placebo in adults. To identify all of the available evidence, a search in 2009 of PubMed, EMBASE, and the Cochrane Library was conducted, without any language restrictions, using the terms postoperative, post-operative, postanesthe*, post- anaesthe*, post-anesthe*, post-anaesthe*, anesthesia, anaesthesia, surgery, surgeries, surgical, nausea, vomit-ing, emesis, retching, scopolamine, and hyoscine. In addition, references within the identified studies were hand-searched until no further new trials were identified. The last electronic search was performed in July 2010, and when possible weekly e-mail alerts for potentially relevant newly published studies were activated.
Two of the authors (K.Z. and F.H.) independently reviewed all full reports and abstracts that could pos-sibly meet the inclusion criteria, guided by the Cochrane Handbook for Systematic Reviews of Intervention.6 Dichotomous data (ie, presence or absence) on the prevalences of PN, PV, and PONV from arrival in the postanesthesia care unit (PACU), up to 48 hours after surgery; use of rescue treatment; and the prevalences of AEs over certain time periods were extracted by 3 of the authors independently (K.Z., L.J., and F.H.). If data were not present in the text or tables as numbers, the author or sponsor of the study was contacted, or the information was extracted from graphs if the scale al-lowed a sufficiently precise estimation. Inconsistency of the extracted data was discussed among the investi-gators and was clarified and accounted for.
Studies were excluded from the analysis if they were not placebo controlled or if they involved children. Studies in children were excluded for a number of reasons. TDS is contraindicated in children as its efficacy in children has yet to be established.7 Accordingly, a pediatric TDS patch is not available for use. The assess-ment of nausea is problematic as an end point in the
disturbances at 24 to 48 hours after surgery, but no other AEs, compared with placebo. (Clin Ther. 2010;32:1987–2002) © 2010 Elsevier HS Journals, Inc.
Key words: transdermal scopolamine patch, postop-erative nausea, postoperative vomiting, PONV, antiemetic, prophylaxis, systematic review, meta-analysis.
INTroduCTIoNPostoperative nausea and vomiting (PONV) occurs after 25% to 30% of surgeries and significantly contributes to patients’ discomfort, distress, and dissatisfaction.1,2 Prophylactic antiemetics are useful in patients at risk for PONV. Patients undergoing ambulatory or outpatient surgery are at a higher risk. Risk is estimated using a simplified risk score that incorporates the most signifi- cant predictors for PONV: patient- and anesthesia- related independent predictors (female sex, nonsmoking, history of motion sickness or PONV, and use of post-operative opioids). An increasing number of surgeries are performed on an outpatient basis and, once dis-charged, these patients might have limited access to health care and antiemetic treatment.3 Long-acting prophylactic antiemetics are crucial in the prevention of postdischarge nausea and vomiting in ambulatory patients.
Transdermal scopolamine (TDS) is a potential long-acting prophylactic antiemetic initially developed to prevent motion sickness. TDS is a centrally acting an-ticholinergic agent that was approved in 2001 by the US Food and Drug Administration for the prevention of PONV.4 This sustained-release transdermal patch provides activity at much lower quantities than other administration routes (initially ~140 µg, followed by ~5 µg/h for ~72 hours). This 72-hour duration may be particularly beneficial in outpatients. The TDS patch avoids the oral and intravenous routes of administration in the perioperative setting; thus, it can be applied by patients the night before surgery or by the anesthesiolo-gist before surgery.
Although TDS has been reported to be clinically ef-ficacious in the prevention of PONV, several adverse events (AEs), such as sedation, dry mouth, blurred vision, central cholinergic syndrome, and confusion (particularly in elderly patients with mild cognitive impairment), are potential concerns.5
A previously published systematic review and meta-analysis of TDS, which included 23 studies (N = 1963), reported significant reductions in the prevalences of postoperative nausea (PN), postoperative vomiting (PV),

November 2010 1989
C.C. Apfel et al.
0.001).36–38,47,49,50,61 TDS was associated with significant reductions in PN, PV, and PONV in the PACU but the effect in the 24- to 48-hour interval was nonsignificant (Table II and Figure 2).45,49,51,61 The overall RR for receiving rescue treatment was significantly decreased in the group that received TDS compared with placebo (RR = 0.68; 95% CI, 0.50–0.93; P < 0.05).‡
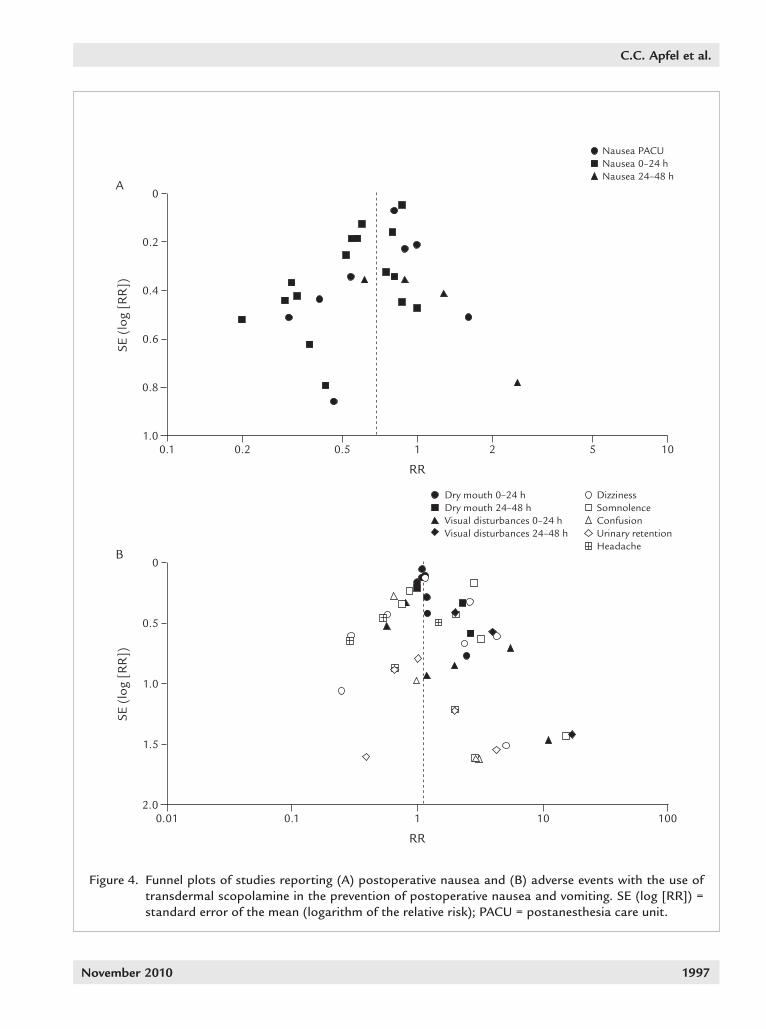
When the TDS patch was applied on the day/evening before surgery (early patch), the RR for PN within 24 hours was 0.56 (95% CI, 0.41–0.75; P < 0.001) (Figure 3).38,43,44,47,50,52,57,59 When the TDS patch was applied on the day of surgery (late patch), the RR for PN within 24 hours was 0.61 (95% CI, 0.47–0.79; P < 0.001) (Figure 3).§ Funnel plot analysis for nausea did not suggest publication bias (Figure 4).∥ The RR for vomiting within 24 hours after surgery after early TDS patch application was 0.56 (95% CI, 0.42–0.75; P < 0.001) (Figure 5).37,38,43,44,47,50,52,57,59 When the TDS patch was applied on the day of surgery (late patch), the RR for vomiting within 24 hours after surgery was 0.67 (95% CI, 0.53–0.86; P = 0.001) (Figure 5).39,41,49,56,60,61 A variety of AEs were reported, with dry mouth (18 patients) and visual disturbance (16) being the 2 most frequently reported AEs; others were dizziness (10), somnolence (7), confusion (5), skin irritation (5), urinary retention (5), and headache (4).
Eight studies reported the prevalence of dry mouth, and 7 reported the prevalences of visual disturbances in the 0- to 24-hour interval. Three studies reported each of these AEs in the 24- to 48-hour interval (Table III). Due to the heterogeneity of the reported time intervals, not all studies citing these AEs could be included for further analysis. In the first 24 hours after surgery, the RR for the prevalence of dry mouth in the TDS group was 1.09 (95% CI, 0.99–1.19; P = NS),36–38,49,57,59–61 with the RR increasing to 1.64 during the subsequent 24 hours (95% CI, 0.82–3.30; P = 0.16).38,49,57 The prevalence of visual disturbance was not significantly different between the scopolamine group and the control group during the first 24-hour postoperative period (RR = 1.43; 95% CI, 0.91–2.25).38,41,49,57,59–61 However, it was significantly more frequent in the TDS group during the 24- to 48-hour interval (RR = 3.35; 95% CI, 1.78–6.32; P < 0.001).38,49,57 On pooled analysis of available data for all other AEs, there was no statisti-
pediatric population, and to compare the efficacy of TDS for both nausea and vomiting it is important to have both outcomes from the same population.
PN was defined as an unpleasant sensation with awareness of the urge to vomit. PV was defined as suc-cessful or unsuccessful (retching) expulsion of gastric contents. PONV was defined as nausea, vomiting, or both. Rescue treatment was defined as any kind of ad-ditional intervention administered for the treatment of established PN, PV, or PONV. The use of rescue treat-ment varied across the studies, but because it is incon-sequential for the measured outcomes, rescue treatment was not further analyzed. AEs included any kind of associated adverse outcome that was reported.
Meta-analyses were conducted with Review Manager 5.0.14 (Cochrane Collaboration, Oxford, United King-dom), calculating relative risks (RRs) and corresponding 95% CIs using the fixed-effects model unless there was evidence for heterogeneity (based on χ2 test probability of <0.05). An RR <1 indicates a potentially beneficial effect, whereas an RR >1 indicates a potential AE for the application of TDS. P < 0.05 was considered statistically significant.
resulTsThe electronic search yielded 170 potentially useful articles, from which 52 relevant full-text reports of randomized controlled trials were identified. Twenty-eight of the retrieved studies were excluded for the following reasons: a different route of administration or a combination of drugs was applied (17 studies), the trial lacked a placebo control (4), the trial was conducted in children (4), and a post hoc design was used (3). The manual search of references provided one additional study to be incorporated. A total of 25 randomized controlled studies in 3298 patients were included in the analyses (Figure 18–35 and Table I36–60).
The risks for PN (RR = 0.59; 95% CI, 0.48–0.73; P < 0.001) (Figure 2)* and PV (RR = 0.68; 95% CI, 0.61–0.76; P < 0.001)† within the first 24 hours after surgery were significantly lower in patients who received TDS compared with placebo (Table II). Likewise, the RR for PONV during the first 24 hours was significantly lower in the scopolamine group compared with the placebo group (RR = 0.73; 95% CI, 0.60–0.88; P =
‡References 37, 39, 41, 44, 45, 47, 50, 52, 53, 55, 57, and 60.§ References 39, 41, 42, 44, 49, 55, 56, 60, and 61. References 38–41, 43, 45, 47–50, 52, and 55–59.
*References 36–39, 41–43, 47, 49, 50, 52, 54–57, and 59–61.† References 37–39, 41, 43, 47, 49, 50, 52, 54, 56, 57, and 59–61.

1990 Volume 32 Number 12
Clinical Therapeutics
cal difference between the TDS and control groups with respect to confusion, dizziness, headache, somnolence, or urinary retention (Table III). Funnel plot analysis for the AEs did not suggest publication bias (Figure 4).*
Articles retrieved from electronic search (N = 172)
Not relevant (n = 103)
Non-RCTs (n = 17)
Potentially relevant articles (n = 52)
Route of administration (n = 16)8–23
Combination of drugs (n = 1)24
No placebo control (n = 4)25–28
Children (n = 4)29–32
Post hoc analyses (n = 3)33–35
RCTs retrieved from electronic search (n = 24)36–47,49–60
Articles retrieved from manual search (n = 1)48
RCTs included in analysis (n = 25)36–60
Figure 1. Retrieved and analyzed studies. RCTs = randomized clinical trials.
dIsCussIoNThe findings from this study suggest that TDS was effective in reducing both PN and PV during the initial 24 hours after surgery in the studies analyzed. TDS was associated with a significantly increased prevalence of visual distur-bances at 24 to 48 hours compared with controls.
The RR reductions of PN, PV, and PONV with TDS use in this analysis were of a magnitude similar to those
*References 37, 39–41, 44, 45, 47, 50, 51, 53, 55–57, 59, and 61.

November 2010 1991
C.C. Apfel et al.
Tabl
e I.
Cha
ract
eris
tics
of t
he s
tudi
es in
clud
ed in
thi
s re
tros
pect
ive
met
a-an
alys
is o
f tra
nsde
rmal
sco
pola
min
e in
the
pre
vent
ion
of p
osto
pera
tive
na
usea
and
vom
itin
g.
Stud
yN
o. o
f Pa
tien
tsPa
rtic
ipan
ts: A
SA S
tatu
s*/
Type
of S
urge
ryIn
terv
enti
on(s
)Fi
ndin
gsC
omm
ent
Tolk
sdor
f et
al36
40M
inor
gyn
ecol
ogic
sur
gery
TD
S vs
pla
cebo
, m
orni
ng o
f sur
gery
Prev
alen
ce o
f vom
itin
g w
as
sign
ific
antl
y re
duce
d w
ith
TD
S–
Tolk
sdor
f et
al37
59A
ge >
50 y
, sur
gica
l or
gyne
colo
gic
surg
erie
s
1–6
h
TD
S or
pla
cebo
Pr
eval
ence
of P
ON
V w
as
sign
ific
antl
y re
duce
d w
ith
TD
S;
bett
er p
roph
ylax
is a
gain
st n
ause
a th
an v
omit
ing
–
Upp
ingt
on e
t al
3842
ASA
1–2
, age
18–
35 y
, m
ajor
gyn
ecol
ogic
sur
gery
TD
S or
pla
cebo
, ev
enin
g be
fore
sur
gery
Prev
alen
ce o
f PO
NV
in f
irst
24
h w
as r
educ
ed w
ith
TD
S –
Tig
erst
edt
et a
l3996
ASA
1–2
, sho
rt s
tay
surg
ery
TD
S vs
0.5
mL
drop
erid
ol v
s co
mbi
nati
on
No
diff
eren
ce in
the
pre
vale
nce
of
naus
ea o
r vo
mit
ing
betw
een
the
grou
ps
–
Jesp
erse
n et
al40
200
Am
bula
tory
gyn
ecol
ogic
su
rger
yT
DS
or p
lace
boN
o si
gnif
ican
t di
ffer
ence
was
fo
und
betw
een
TD
S an
d pl
aceb
o –
Kot
elko
et
al41
203
ASA
1–2
, age
18–
38 y
, el
ecti
ve c
esar
ean
sect
ion
TD
S or
pla
cebo
, in
the
preo
pera
tive
are
aPr
eval
ence
of P
ON
V in
2–1
0 h
w
as r
educ
ed w
ith
TD
SIn
trat
heca
l mor
phin
e fo
r po
stop
erat
ive
pain
Lope
r et
al42
32H
ealt
hy w
omen
un
derg
oing
maj
or
gyne
colo
gic
surg
ery
TD
S or
pla
cebo
just
be
fore
sur
gery
In p
atie
nts
rece
ivin
g ep
idur
al
mor
phin
e, p
osto
pera
tive
nau
sea
was
red
uced
wit
h T
DS
All
pati
ents
rec
eive
d ep
idur
al m
orph
ine
Wilk
inso
n et
al43
190
ASA
1–2
, age
16
–65
y,
min
or o
rtho
pedi
c or
pl
asti
c su
rger
y
TD
S or
pla
cebo
, 7–
12 h
bef
ore
surg
ery
Prev
alen
ce o
f nau
sea
and
the
num
ber
of v
omit
ing
epis
odes
du
ring
fir
st 2
4 h
afte
r su
rger
y w
ere
sign
ific
antl
y re
duce
d w
ith
TD
S
–
Bai
ley
et a
l44
138
ASA
1–2
, out
pati
ent
lapa
rosc
opic
sur
gery
T
DS
vs p
lace
bo; ≥
8 h
befo
re s
urge
ryPr
eval
ence
of n
ause
a, r
etch
ing,
an
d vo
mit
ing
and
need
for
res
cue
anti
emet
ic t
hera
py w
ere
sign
ific
antl
y re
duce
d w
ith
TD
S co
mpa
red
wit
h pl
aceb
o
– (con
tinu
ed)

1992 Volume 32 Number 12
Clinical Therapeutics
Stud
yN
o. o
f Pa
tien
tsPa
rtic
ipan
ts: A
SA S
tatu
s*/
Type
of S
urge
ryIn
terv
enti
on(s
)Fi
ndin
gsC
omm
ent
Kos
ki e
t al
4528
3Fe
mal
es r
equi
ring
gen
eral
an
esth
esia
TD
S pa
tch
or p
lace
bo
even
ing
befo
re s
urge
ryN
o si
gnif
ican
t ef
fect
on
PON
V w
ith
TD
S pa
tch
–
Sant
amar
ia e
t al
4624
ASA
1–2
, max
illof
acia
l su
rger
y T
DS
or p
lace
bo,
even
ing
befo
re s
urge
ryPr
eval
ence
of P
ON
V w
as
sign
ific
antl
y re
duce
d w
ith
scop
olam
ine
–
Stro
mbe
rg e
t al
4720
1A
SA 1
–3, g
ener
al p
last
ic
or o
rtho
pedi
c su
rger
yT
DS
or p
lace
bo, ≥
6 h
befo
re s
urge
ryPr
eval
ence
of v
omit
ing
epis
odes
w
as s
igni
fica
ntly
red
uced
wit
h T
DS
–
Bos
ek a
nd
Dow
ns48
60A
SA 1
–2, e
lect
ive
gyne
colo
gic
and
orth
oped
ic o
pera
tion
s
TD
S vs
sco
pola
min
e 0.
3 m
L IM
vs
com
bina
tion
Nei
ther
TD
S no
r IM
sco
pola
min
e ef
fect
ive
–
Sem
ple
et a
l4967
ASA
1–2
, abd
omin
al
hyst
erec
tom
yT
DS
or p
lace
bo, 2
h
befo
re s
urge
ryPr
eval
ence
of v
omit
ing
in t
he
reco
very
roo
m a
nd o
n th
e 3r
d po
stop
erat
ive
day
was
red
uced
w
ith
TD
S
–
Hon
kava
ara
et
al50
60A
SA 1
–2, m
iddl
e
ear
surg
ery
TD
S vs
pla
cebo
Prev
alen
ce o
f PO
NV
was
red
uced
w
ith
TD
S–
Rei
nhar
t et
al51
39A
SA 1
–2, 1
8–65
y, e
ar
surg
ery
TD
S or
pla
cebo
, 2 h
be
fore
sur
gery
Prev
alen
ce o
f nau
sea
and
vert
igo
afte
r di
scha
rge
was
red
uced
wit
h sc
opol
amin
e
–
Sohi
et
al52
125
Age
20
–60
y, e
lect
ive
lapa
rosc
opic
ch
olec
yste
ctom
y
TD
S or
pla
cebo
, ev
enin
g be
fore
sur
gery
No
sign
ific
ant
diff
eren
ce in
na
usea
or
freq
uenc
y of
em
esis
in
firs
t 24
h a
fter
sur
gery
–
Eber
hart
et
al53
304
Age
18–
76 y
, ele
ctiv
e su
rgic
al a
nd g
ynec
olog
ic
surg
ery
TD
S or
pla
cebo
, nig
ht
befo
re s
urge
ryPr
eval
ence
of P
ON
V w
ithi
n th
e fi
rst
48 h
ours
aft
er s
urge
ry w
ere
redu
ced
wit
h T
DS;
no
sign
ific
ant
effe
ct o
n po
stop
erat
ive
naus
ea
– (con
tinu
ed)
Tabl
e I (
cont
inue
d).

November 2010 1993
C.C. Apfel et al.
Stud
yN
o. o
f Pa
tien
tsPa
rtic
ipan
ts: A
SA S
tatu
s*/
Type
of S
urge
ryIn
terv
enti
on(s
)Fi
ndin
gsC
omm
ent
Hon
kava
ara54
56A
SA 1
–3, s
tape
do-
and
tym
pano
plas
ty u
nder
LA
TD
S vs
pla
cebo
pat
ch
day
befo
re t
he s
urge
ryPr
eval
ence
of P
ON
V re
duce
d w
ith
TD
S–
Jone
s et
al55
56A
SA 1
–2, p
atie
nts
rece
ivin
g ge
nera
l an
esth
esia
for
>1
h
TD
S or
pla
cebo
, 2 h
be
fore
sur
gery
Prev
alen
ce o
f PO
NV
and
anti
emet
ic r
equi
rem
ents
wer
e re
duce
d w
ith
TD
S
All
pati
ents
rec
eive
d pr
ophy
lact
ic
onda
nset
ron
Har
nett
et
al56
240
ASA
1, e
lect
ive
cesa
rean
de
liver
yT
DS
vs o
ndan
setr
on
4 m
g IV
vs
both
; at
tim
e of
cor
d cl
ampi
ng
Prev
alen
ce o
f PO
NV
at 6
–24
h w
as
redu
ced
wit
h T
DS
and
onda
nset
ron
Intr
athe
cal m
orph
ine
for
post
oper
ativ
e an
alge
sia
Eina
rsso
n et
al57
48G
ynec
olog
ic la
paro
scop
ic
surg
ery
TD
S or
pla
cebo
, nig
ht
befo
re s
urge
ryPr
eval
ence
s of
nau
sea
and
vom
itin
g in
fir
st 2
4 h
afte
r su
rger
y w
ere
redu
ced
wit
h T
DS
–
Gan
et
al58
620
ASA
1–3
, out
pati
ent
lapa
rosc
opic
or
brea
st
augm
enta
tion
sur
gery
TD
S or
pla
cebo
, 2 h
be
fore
sur
gery
Prev
alen
ce o
f PO
NV
was
red
uced
w
ith
TD
S an
d on
dans
etro
n co
mpa
red
wit
h on
dans
etro
n al
one
at 2
4 h
afte
r su
rger
y bu
t no
t at
48
h
Ond
anse
tron
4 m
g IV
be
fore
ane
sthe
sia
Laza
r et
al59
35A
ge 2
1–69
y, s
tape
s re
plac
emen
t su
rger
yT
DS
or p
lace
bo,
even
ing
befo
re s
urge
ry
Post
oper
ativ
e na
usea
but
not
vo
mit
ing
or d
izzi
ness
was
red
uced
w
ith
TD
S
–
Lee
et a
l6080
ASA
1–3
, age
20
–75
y,
elec
tive
, pri
mar
y, o
r re
visi
onar
y jo
int
surg
ery
Dex
amet
haso
ne 8
mg
vs d
exam
etha
sone
8
mg
plus
TD
S
PON
V m
ost
effe
ctiv
ely
redu
ced
wit
h de
xam
etha
sone
plu
s T
DS
All
pati
ents
rec
eive
d ep
idur
al P
CA
ASA
= A
mer
ican
Soc
iety
of
Ane
sthe
siol
ogis
ts;
TD
S =
tran
sder
mal
sco
pola
min
e; P
ON
V =
post
oper
ativ
e na
usea
and
vom
itin
g; I
M =
int
ram
uscu
lar;
LA
= l
ocal
an
esth
esia
; PC
A =
pat
ient
-con
trol
led
anal
gesi
a.*A
SA S
tatu
s 1
= no
rmal
, hea
lthy
; 2 =
mild
sys
tem
ic d
isea
se; 3
= s
ever
e sy
stem
ic d
isea
se.
Tabl
e I (
cont
inue
d).

1994 Volume 32 Number 12
Clinical Therapeutics
Scopolamine Placebo
Subgroup/Study Events Total Events TotalWeight,
%Risk Ratio M-H,
Random (95% CI)Risk Ratio M-H,
Random (95% CI)
2.1.1 Nausea PACUTigerstedt et al39 8 32 5 32 5.0 1.60 (0.59–4.37)Jespersen et al40 2 102 4 95 2.0 0.47 (0.09–2.48)Kotelko et al41 26 102 29 101 16.9 0.89 (0.56–1.40)Koski et al45 32 127 33 130 18.4 0.99 (0.65–1.51)Bosek and Downs48 7 20 13 20 9.6 0.54 (0.27–1.06)Semple et al49 6 37 12 30 6.7 0.41 (0.17–0.95)Honkavaara et al50 4 30 13 30 5.1 0.31 (0.11–0.84)Gan et al58 149 304 183 304 36.4 0.81 (0.70–0.94)Subtotal – 754 – 742 100.1* 0.77 (0.60–0.97)Total events 234 – 292 – – –Heterogeneity: τ2 = 0.04; χ2 = 10.77; df = 7 (P = 0.15); I2 = 35%Test for overall effect: z = 2.18 (P = 0.03)
2.1.2 Nausea 0–24 hUppington et al38 6 19 6 19 3.6 1.00 (0.39–2.55)Tigerstedt et al39 20 32 25 32 10.2 0.80 (0.58–1.11)Kotelko et al41 43 102 71 101 11.2 0.60 (0.46–0.78)Loper et al42 3 16 15 16 3.1 0.20 (0.07–0.56)Wilkinson et al43 27 95 49 95 9.4 0.55 (0.38–0.80)Stromberg et al47 8 59 9 58 3.9 0.87 (0.36–2.11)Semple et al49 11 37 11 30 5.5 0.81 (0.41–1.61)Honkavaara et al50 3 30 8 30 2.4 0.38 (0.11–1.28)Sohi et al52 11 43 16 47 5.9 0.75 (0.39–1.43)Honkavaara54 2 27 5 29 1.6 0.43 (0.09–2.03)Jones et al55 11 28 21 28 7.5 0.52 (0.32–0.87)Harnett et al56 25 80 44 81 9.3 0.58 (0.39–0.84)Einarsson et al57 5 24 15 24 4.2 0.33 (0.14–0.77)Lazar et al59 4 16 16 19 4.0 0.30 (0.12–0.71)Lee et al60 7 40 22 40 5.1 0.32 (0.15–0.66)Gan et al61 193 304 222 304 13.1 0.87 (0.78–0.97)Subtotal – 952 – 953 100.0 0.59 (0.48–0.73)Total events 379 – 555 – – –
Heterogeneity: τ2 = 0.08; χ2 = 42.20; df = 15 (P < 0.001); I2 = 64%Test for overall effect: z = 4.99 (P < 0.001)
2.1.3 Nausea 24–48 hUppington et al38 8 19 9 19 32.8 0.89 (0.44–1.81)Semple et al49 11 37 7 30 26.0 1.27 (0.56–2.88)Jones et al55 8 28 13 28 32.9 0.62 (0.30–1.25)Einarsson et al57 5 24 2 24 8.3 2.50 (0.54–11.65)Subtotal – 108 – 101 100.0 0.94 (0.60–1.49)Total events 32 – 31 – – –Heterogeneity: τ2 = 0.03; χ2 = 3.53; df = 3 (P = 0.32); I2 = 15%Test for overall effect: z = 0.25 (P = 0.80)
Favors scopolamine
Favors placebo
0.1 0.2 0.5 1 2 5 10
Figure 2. Efficacy of transdermal scopolamine in the prevention of postoperative nausea at various time intervals. M-H = Mantel-Haenszel test; PACU = postanesthesia care unit. *Percentages do not total 100 due to rounding.

November 2010 1995
C.C. Apfel et al.
significantly increased prevalence of visual disturbance at 24 to 48 hours, which typically resolves gradually on removal of the patch.57,65 For this reason, if the TDS patch is prescribed, patients should be instructed before its application to remove the patch should AEs occur and they should be informed about the gradual resolu-tion of AEs.
The delayed observation of visual disturbance may be due to a variety of reasons. This AE may be masked by the sedation during the recovery from anesthesia in the early postoperative period. Plasma scopolamine concentrations may not peak until 24 hours after patch application, therefore leading to a delayed onset of AEs.7 Pharmacokinetic distribution effects of TDS may result in delayed AEs.
Despite the updated analysis, statistical power for some other AEs (eg, dry mouth, dizziness, somnolence) was insufficient to suggest that their prevalences were increased with TDS use.
with the use of other antiemetic drugs (eg, ondansetron, droperidol, dexamethasone) as reported in a large study in >5000 patients.62
Consistent with the findings from the previously published systematic review,5 this analysis showed that TDS had antiemetic properties in the early postoperative period (ie, PACU) as well as during the first 24 post- operative hours.5 However, there was no statistically significant benefit for the intervention during the late postoperative period (24–48 hours after surgery). This might be related to the limited number of studies, as the point estimates for PV and PONV with RRs of 0.53 (95% CI, 0.28–1.00) and 0.80 (95% CI, 0.56–1.13) are encouraging. In addition, the TDS patch was associ-ated with comparable RR reductions of both PN and PV, which is in line with findings from previously pub-lished studies on ondansetron and droperidol.63,64
On analysis of AEs, there were no significant findings during the first 24 hours after patch application, but a
Table II. Efficacy of transdermal scopolamine in the prevention of postoperative nausea (PN), postoperative vomiting (PV), or both (PONV).a
Outcome/ Time Interval
No. of Studies
Active/ Inactive Patients RR (95% CI) P
PN PACUb 8 754/742 0.77 (0.61–0.98) 0.03 0–24 hc 16 952/953 0.59 (0.48–0.73) <0.001 24–48 hd 4 108/101 0.94 (0.60–1.49) 0.80
PV PACUe 11 1004/996 0.75 (0.64–0.87) <0.001 0–24 hf 15 939/938 0.68 (0.61–0.76) <0.001 24–48 hg 6 333/329 0.53 (0.28–1.00) 0.05
PONV PACUh 4 484/480 0.84 (0.73–0.96) 0.009 0–24 hi 7 499/490 0.73 (0.60–0.88) 0.001 24–48 hj 3 84/77 0.80 (0.56–1.13) 0.20a Data are relative risk (RR) (95% CI) of PN, PV, and PONV in the postanesthesia care unit (PACU) and at 0–24 and 24–48 hours after surgery.
bReferences39–41, 45, 48, 50, and 58.c References 38, 39, 41–45, 47, 50, 52, and 54–60.dReferences 38, 45, 55, and 57.e References 39–41, 45, 48–50, 53, 56, 58, and 60. f References 37–39, 41, 43, 47, 49, 50, 52, 54, and 56–60.g References 38, 43, 49, 53, 55, and 57. h References 45, 49, 51, and 58.i References 36–38 and 47–50. j References 38, 49, and 55.

1996 Volume 32 Number 12
Clinical Therapeutics
in clinical practice. In general, the extent of antiemetic prophylaxis should be based on the baseline risk of the patient. In high-risk patients, no single antiemetic in-tervention is known to effectively prevent PONV. There-fore, a multimodal approach combining different classes of antiemetics may be necessary.66,67 In addition, even with multimodal prophylaxis, a patient may develop PONV in the postoperative period or at home, so there remains a need for a reliable rescue antiemetic. On-dansetron is frequently used for the prevention of PONV and as a rescue treatment once PONV occurs. However, in a large randomized controlled trial, ondansetron was
Postoperative confusion has remained an important concern and was one of the reasons for this update. However, with an RR of 0.73, the data do not support the hypothesis that scopolamine increases the risk for postoperative confusion. This prevalent notion that postoperative confusion is associated with TDS use may be the result of the general attribution of confusion to anticholinergics. In addition, it is known that elderly patients may be more susceptible to anticholinergic effects such as confusion.
Based on its efficacy and its moderate AE profile, TDS may be a good option for the prevention of PONV
Scopolamine Placebo
Subgroup/Study Events Total Events TotalWeight,
%Risk Ratio M-H,
Random (95% CI)Risk Ratio M-H,
Random (95% CI)
3.2.1 Early patch applicationUppington et al38 6 19 6 19 3.7 1.00 (0.39–2.55)Wilkinson et al43 27 95 49 95 9.6 0.55 (0.38–0.80)Stromberg et al47 8 59 9 58 4.0 0.87 (0.36–2.11)Honkavaara et al50 3 30 8 30 2.4 0.38 (0.11–1.28)Sohi et al52 11 43 16 47 6.0 0.75 (0.39–1.43)Einarsson et al57 5 24 15 24 4.3 0.33 (0.14–0.77)Lazar et al59 4 16 16 19 4.1 0.30 (0.12–0.71)Subtotal – 286 – 292 34.1 0.56 (0.41–0.75)Total events 64 – 119 – – –Heterogeneity: τ2 = 0.03; χ2 = 7.18; df = 6 (P = 0.30); I2 = 16%Test for overall effect: z = 3.82 (P < 0.001)
3.2.2 Late patch applicationTigerstedt et al39 20 32 25 32 10.3 0.80 (0.58–1.11)Kotelko et al41 43 102 71 101 11.3 0.60 (0.46–0.78)Loper et al42 3 16 15 16 3.2 0.20 (0.07–0.56)Semple et al49 11 37 11 30 5.6 0.81 (0.41–1.61)Jones et al55 11 28 21 28 7.6 0.52 (0.32–0.87)Harnett et al56 25 80 44 81 9.4 0.58 (0.39–0.84)Lee et al60 7 40 22 40 5.2 0.32 (0.15–0.66)Gan et al61 193 304 222 304 13.2 0.87 (0.78–0.97)Subtotal – 639 – 632 65.8 0.61 (0.47–0.79)Total events 313 – 431 – – –Heterogeneity: τ2 = 0.08; χ2 = 27.35; df = 7 (P < 0.001); I2 = 74%Test for overall effect: z = 3.73 (P < 0.001)
Total – 925 – 924 99.9* 0.59 (0.48–0.73)Total events 377 – 550 – – –Heterogeneity: τ2 = 0.08; χ2 = 41.56; df = 14 (P < 0.001); I2 = 66%Test for overall effect: z = 4.88 (P < 0.001)
Favors scopolamine
Favors placebo
Figure 3. Effects of early and late transdermal scopolamine patch application on nausea in the first 24 hours after surgery. M-H = Mantel-Haenszel Test. *Percentages do not total 100 due to rounding.
0.1 0.2 0.5 1 2 5 10
November 2010 1997
C.C. Apfel et al.
Nausea PACUNausea 0–24 hNausea 24–48 h
0.8
0.4
1.0
SE (
log
[RR
])
5210.50.20.1
A
10
0
0.6
0.2
Dry mouth 0–24 hDry mouth 24–48 hVisual disturbances 0–24 hVisual disturbances 24–48 h
DizzinessSomnolenceConfusionUrinary retentionHeadache
1.0
2.0
SE (
log
[RR
])
101
RR
RR
0.10.01
B
100
0
1.5
0.5
Figure 4. Funnel plots of studies reporting (A) postoperative nausea and (B) adverse events with the use of transdermal scopolamine in the prevention of postoperative nausea and vomiting. SE (log [RR]) = standard error of the mean (logarithm of the relative risk); PACU = postanesthesia care unit.

1998 Volume 32 Number 12
Clinical Therapeutics
interval may be due to the limited statistical power of only 4, 6, and 3 trials eligible for a pooled analysis of TDS in the prevention of PN, PV, and PONV, respectively, in the 24- to 48-hour interval. Given the long duration of action of scopolamine, one might predict the antiemetic potential to last well into the 24- to 48-hour interval. Future studies of the effects of TDS during the 24- to 48-hour interval may be particularly beneficial in the future.
The timing of the patch application—the night before surgery (early) versus before surgery in the hospital (late)—is also of interest to clinicians. When the TDS patch was applied early, the RRs for PN and for PV
not reported to be effective as a rescue treatment if it was unsuccessfully applied as a part of a prophylactic strategy.68 Thus, TDS may be used for prophylaxis, sparing ondansetron as a rescue treatment.
In theory, due to its simple and long-lasting mode of application, TDS may be particularly useful for the preven-tion of postdischarge nausea and vomiting; that is, for the prevention of symptoms when patients have already left the hospital and have no immediate access to health care. However, this analysis did not find a statistically significant effect of TDS during the 24- to 48-hour interval. The un-expected nonsignificant effect of scopolamine during this
Scopolamine Placebo
Subgroup/Study Events Total Events TotalWeight,
%Risk Ratio M-H,
Random (95% CI)Risk Ratio M-H,
Random (95% CI)
3.5.1 Early patch applicationTolksdorf et al37 0 30 7 29 0.5 0.06 (0.00–1.08)Uppington et al38 8 19 13 19 6.6 0.62 (0.33–1.13)Wilkinson et al43 24 95 36 95 9.8 0.67 (0.43–1.03)Stromberg et al47 6 59 15 58 3.9 0.39 (0.16–0.94)Honkavaara et al50 6 30 16 30 4.6 0.38 (0.17–0.83)Sohi et al52 17 43 24 47 9.1 0.77 (0.49–1.23)Einarsson et al57 2 24 9 24 1.7 0.22 (0.05–0.92)Lazar et al59 4 16 9 19 3.3 0.53 (0.20–1.40)Subtotal – 316 – 321 39.5 0.56 (0.42–0.75)Total events 67 – 129 – – –Heterogeneity: τ2 = 0.03; χ2 = 8.51; df = 7 (P = 0.29); I2 = 18%Test for overall effect: z = 3.99 (P < 0.001)
3.5.2 Late patch applicationTigerstedt et al39 13 32 19 32 8.3 0.68 (0.41–1.14)Kotelko et al41 33 102 53 101 12.2 0.62 (0.44–0.86)Semple et al49 13 37 14 30 7.0 0.75 (0.42–1.35)Harnett et al56 32 81 48 81 12.5 0.67 (0.48–0.92)Lee et al60 4 40 20 40 3.2 0.20 (0.08–0.53)Gan et al61 158 304 186 304 17.5 0.85 (0.74–0.98)Subtotal – 596 – 588 60.7 0.67 (0.53–0.86)Total events 253 – 340 – – –Heterogeneity: τ2 = 0.05; χ2 = 12.31; df = 5 (P = 0.03); I2 = 59%Test for overall effect: z = 3.20 (P = 0.001)
Total – 912 – 909 100.2* 0.62 (0.51–0.75)Total events 320 – 469 – – –Heterogeneity: τ2 = 0.05; χ2 = 25.41; df = 13 (P = 0.02); I2 = 49%Test for overall effect: z = 4.83 (P < 0.001)
Favors scopolamine
Favors placebo
Figure 5. Effects of early and late transdermal scopolamine application on postoperative vomiting in the first 24 hours after surgery. M-H = Mantel-Haenszel test. *Percentages do not total 100 due to rounding.
0.2 0.5 1 2 5

November 2010 1999
C.C. Apfel et al.
no other conflicts of interest with regard to the content of this article.
refereNCes 1. Kovac AL. Prevention and treatment of postoperative
nausea and vomiting. Drugs. 2000;59:213–243. 2. Watcha MF, White PF. Postoperative nausea and vomit-
ing. Its etiology, treatment, and prevention. Anesthesiology. 1992;77:162–184.
3. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Report. 2009: 1–25.
4. Clissold SP, Heel RC. Transdermal hyoscine (scopol-amine). A preliminary review of its pharmacodynamic properties and therapeutic efficacy. Drugs. 1985;29:189– 207.
5. Kranke P, Morin AM, Roewer N, et al. The efficacy and safety of transdermal scopolamine for the prevention of postoperative nausea and vomiting: A quantitative sys-tematic review. Anesth Analg. 2002;95:133–143.
were 0.56 and 0.54, respectively, and when the patch was applied later, the corresponding RRs were 0.61 and 0.74. Although in registration trials TDS was applied the day before surgery, the subanalyses suggest that both times of application are efficacious for the preven-tion of PONV.
CoNClusIoNsIn this systematic review and meta-analysis, the use of TDS was associated with efficacy in the prevention of both PN and PV in the first 24 hours after surgery. TDS was associated with an increased prevalence of visual disturbances at 24 to 48 hours compared with controls. TDS was not associated with a significantly increased risk for postoperative confusion or other AEs.
ACkNowledgMeNTsDr. Pergolizzi has received consultant’s fees from Baxter Healthcare. The authors have indicated that they have
Table III. Adverse events with transdermal scopolamine.a
OutcomeNo. of Studies
Active/ Inactive Patients
Relative Risk (95% CI) P
Dry mouth 0–24 hb 8 494/491 1.09 (0.99–1.19) 0.08 24–48 hc 3 80/73 1.64 (0.82–3.30) 0.16
Visual disturbance 0–24 hd 7 546/543 1.43 (0.91–2.25) 0.12 24–48 he 3 80/73 3.35 (1.78–6.32) <0.001
Dizziness (overall)f 8 744/736 1.24 (0.68–2.25) 0.48
Somnolence (overall)g 7 345/335 1.74 (0.89–3.40) 0.11
Confusion (overall)h 4 629/632 0.73 (0.43–1.24) 0.24
Urinary retention (overall)i 5 606/601 1.05 (0.41–2.72) 0.91
Headache (overall)j 5 558/545 0.71 (0.38–1.35) 0.30a Dry mouth and visual disturbances were reported more consistently than the other adverse events and thus listed separately if reported for the 0–24-hour and 24–48-hour intervals. All other adverse events were summarized for the analysis and indicated as overall.
bReferences 36–38, 49, and 57–60.c References 38, 49, and 57. dReferences 38, 41, 49, and 57–60.e References 38, 49, and 57.f References 37, 40, 44, 45, 50, 51, 56, and 58.g References 39, 40, 44, 50, 56, 57, and 59.h References 41, 47, 53, and 58.i References 40, 47, 53, 58, and 59.j References 40, 44, 47, 55, and 58.

2000 Volume 32 Number 12
Clinical Therapeutics
26. Schuh R, Tolksdorf W, Hucke H. Transdermal scopolamine or dro-peridol in the prevention of post- operative nausea and vomiting in cholecystectomy patients [in Ger-man]. Anasth Intensivther Notfallmed. 1987;22:261–266.
27. Thune A, Appelgren L, Haglind E. Prevention of postoperative nausea and vomiting after laparoscopic cholecystectomy. A prospective ran-domized study of metoclopramide and transdermal hyoscine. Eur J Surg. 1995;161:265–268.
28. White PF, Tang J, Song D, et al. Transdermal scopolamine: An alter-native to ondansetron and droperi-dol for the prevention of postopera-tive and postdischarge emetic symp- toms. Anesth Analg. 2007;104:92–96.
29. Doyle E, Byers G, McNicol LR, Mor-ton NS. Prevention of postoperative nausea and vomiting with trans- dermal hyoscine in children using patient-controlled analgesia. Br J Anaesth. 1994;72:72–76.
30. Honkavaara P, Saarnivaara L, Klem-ola UM. Effect of transdermal hyo-scine on nausea and vomiting after surgical correction of prominent ears under general anaesthesia. Br J Anaesth. 1995;74:647–650.
31. Horimoto Y, Naide M. Transdermal scopolamine patches reduce post-operative emesis in pediatric pa-tients undergoing strabismus sur-gery. Can J Anaesth. 1990;37(4 Pt 2): S94.
32. Horimoto Y, Tomie H, Hanzawa K, Nishida Y. Scopolamine patch re-duces postoperative emesis in pae-diatric patients following strabis-mus surgery. Can J Anaesth. 1991;38 (4 Pt 1):441–444.
33. Honkavaara P, Pyykkö I. Surgeon’s experience as a factor for emetic sequelae after middle ear surgery. Acta Anaesthesiol Scand. 1998;42: 1033–1037.
34. Honkavaara P, Pyykkö I. Effects of at-ropine and scopolamine on bradycar-dia and emetic symptoms in otoplasty. Laryngoscope. 1999;109:108–112.
patient sedation in minor oral surgery. Acta Anaesthesiol Scand. 1985; 29:674–678.
17. Michaloudis D, O’Keeffe N, O’Sullivan K, Healy TE. Postoperative nausea and vomiting: A comparison of anti-emetic drugs used alone or in com-bination. J R Soc Med. 1993;86:137– 138.
18. Moscovici R, Prego G, Schwartz M, Steinfeld O. Epidural scopolamine administration in preventing nau-sea after epidural morphine. J Clin Anesth. 1995;7:474–476.
19. Paymaster NJ. Evaluation of anxio- lytic and amnesic effects of intra- muscular lorazepam as a pre-operative medication. Curr Med Res Opin. 1976; 4:388–394.
20. Raeder JC, Breivik H. Premedication with midazolam in out-patient gen-eral anaesthesia. A comparison with morphine-scopolamine and placebo. Acta Anaesthesiol Scand. 1987;31: 509–514.
21. Raeder JC, van der Linden J, Breivik H. Premedication for day-case sur-gery: Double-blind comparison of ketobemidone + dimethylaminodi-phenylbuten (A-29) and morphine + scopolamine. Acta Anaesthesiol Scand. 1986;30:502–506.
22. Sear JW, Alexander JI. Comparison of buprenorphine-hyoscine and papaveretum-hyoscine as premedi-cants for gynaecological surgery. Br J Anaesth. 1983;55:319–324.
23. Simpson KH, Dearden MJ, Ellis FR, Jack TM. Premedication with slow release morphine (MST) and adju-vants. Br J Anaesth. 1988;60:825–830.
24. Tarkkila P, Törn K, Tuominen M, Lindgren L. Premedication with promethazine and transdermal sco-polamine reduces the incidence of nausea and vomiting after intrathe-cal morphine. Acta Anaesthesiol Scand. 1995;39:983–986.
25. Harris SN, Sevarino FB, Sinatra RS, et al. Nausea prophylaxis using trans-dermal scopolamine in the setting of patient-controlled analgesia. Obstet Gynecol. 1991;78:673–677.
6. Higgins JP, Green S. Cochrane Hand-book for Systematic Reviews of Interven-tions Version 5.0.2. Hoboken, NJ: Wiley-Blackwell; 2009.
7. Transderm Scop [package Insert]. Parsippany, NJ: Novartis Consumer Health, Inc; 2006.
8. Bradford TH, Robertson K, Nor-man PF, Meeks GR. Reduction of pain and nausea after laparoscopic sterilization with bupivacaine, meto-clopramide, scopolamine, ketoro-lac, and gastric suctioning. Obstet Gynecol. 1995;85(5 Pt 1):687–691.
9. Clarke RS, Dundee JW, Carson IW, et al. Clinical studies of induction agents. XL. Althesin with various pre- medicants. Br J Anaesth. 1972;44: 845–848.
10. Clarke RS, Dundee JW, Love WJ. Studies of drugs given before anaes-thesia. 8. Morphine 10 mg alone and with atropine or hyoscine. Br J An-aesth. 1965;37:772–778.
11. Davies DR, Doughty A. Premedica-tion of children with papaveretum-hyoscine. The effect of varying dosage schemes. Br J Anaesth. 1967;39:638– 644.
12. Davies DR, Doughty AG. Premedi- cation in children. A trial of intra-muscular droperidol, droperidol-phenoperidine, papaveretum-hyoscine and normal saline. Br J Anaesth. 1971;43:65–75.
13. Guldbrand P, Mellström A. Rectal versus intramuscular morphine-scopolamine as premedication in children. Acta Anaesthesiol Scand. 1995;39:224–227.
14. Kamath B, Curran J, Hawkey C, et al. Anaesthesia, movement and emesis. Br J Anaesth. 1990;64:728–730.
15. Larsson S, Hägerdal M, Lundberg D. Premedication with intramuscular dixyrazine: (Esucos). A controlled double-blind comparison with morphine-scopolamine and place-bo. Acta Anaesthesiol Scand. 1988;32: 131–134.
16. Lundgren S. Comparison of rectal di-azepam and subcutaneous morphine-scopolamine administration for out-

November 2010 2001
C.C. Apfel et al.
gynecologic patients [in German]. Anaesthesist. 1996;45:259–267.
54. Honkavaara P. Effect of transder-mal hyoscine on nausea and vomit-ing during and after middle ear surgery under local anaesthesia. Br J Anaesth. 1996;76:49–53.
55. Jones S, Strobl R, Crosby D, et al. The effect of transdermal scopol-amine on the incidence and severity of postoperative nausea and vomit-ing in a group of high-risk patients given prophylactic intravenous on-dansetron. AANA J. 2006;74:127– 132.
56. Harnett MJ, O’Rourke N, Walsh M, et al. Transdermal scopolamine for prevention of intrathecal morphine-induced nausea and vomiting after cesarean delivery. Anesth Analg. 2007; 105:764–769.
57. Einarsson JI, Audbergsson BO, Thorsteinsson A. Scopolamine for prevention of postoperative nausea in gynecologic laparoscopy, a ran-domized trial. J Minim Invasive Gyne-col. 2008;15:26–31.
58. Gan TJ, Sinha AC, Kovac AL, et al, for the TDS Study Group. A ran-domized, double-blind, multicenter trial comparing transdermal sco-polamine plus ondansetron to on-dansetron alone for the prevention of postoperative nausea and vomit-ing in the outpatient setting. Anesth Analg. 2009;108:1498–1504.
59. Lazar RH, Alperin KM, Hughes GB, et al. Efficacy of transdermal sco-polamine as an antinauseant for stapes operation. Surg Forum. 1984; 35:558–561.
60. Lee HK, Lee JH, Chon SS, et al. The effect of transdermal scopolamine plus intravenous dexamethasone for the prevention of postoperative nausea and vomiting in patients with epidural PCA after major or-thopedic surgery. Korean J Anesthesiol. 2010;58:50–55.
61. Gan TJ, Kovac LA, Sinha AC, et al. Comparison of transdermal scopol-amine patch and ondansetron to ondansetron for prevention of PONV. Anesthesiology. 2007;107:(A1020).
44. Bailey PL, Streisand JB, Pace NL, et al. Transdermal scopolamine re-duces nausea and vomiting after outpatient laparoscopy. Anesthesiol-ogy. 1990;72:977–980.
45. Koski EM, Mattila MA, Knapik D, et al. Double blind comparison of transdermal hyoscine and placebo for the prevention of postoperative nausea. Br J Anaesth. 1990;64:16–20.
46. Santamaria LB, Fodale V, Man-dolfino T, et al. Transdermal sco-polamine reduces nausea, vomiting and sialorrhea in the postoperative period in teeth and mouth surgery [in Italian]. Minerva Anestesiol. 1991;57:686–687.
47. Stromberg BV, Reines DH, Ackerly J. Transderm scopolamine for the control of perioperative nausea. Am Surg. 1991;57:712–715.
48. Bosek V, Downs JB. Nausea and vomiting after alfentanil anesthesia: Effect of transdermal scopolamine. Anesthesiol Rev. 1992;19:19–22.
49. Semple P, Madej TH, Wheatley RG, et al. Transdermal hyoscine with patient-controlled analgesia. Anaes-thesia. 1992;47:399–401.
50. Honkavaara P, Saarnivaara L, Klem-ola UM. Prevention of nausea and vomiting with transdermal hyoscine in adults after middle ear surgery during general anaesthesia. Br J Anaesth. 1994;73:763–766.
51. Reinhart DJ, Klein KW, Schroff E. Transdermal scopolamine for the reduction of postoperative nausea in outpatient ear surgery: A double-blind, randomized study. Anesth Analg. 1994;79:281–284.
52. Sohi HS, Heipel J, Inman KJ, et al. Preoperative transdermal scopol-amine does not reduce the level of nausea and frequency of vomiting after laparoscopic cholecystectomy. Can J Surg. 1994;37:307–312.
53. Eberhart LH, Holzrichter P, Roscher R. Transdermal scopolamine for prevention of postoperative nausea and vomiting. No clinically relevant result in spite of reduced postopera-tive vomiting in general surgical and
35. Honkavaara P, Pyykkö I, Rutanen EM. Increased incidence of retching and vomiting during periovulatory phase after middle ear surgery. Can J Anaesth. 1996;43:1108–1114.
36. Tolksdorf W, Meisel R, Müller P, Bender HJ. Transdermal scopolamine (TTS-scopolamine) for the preven-tion of postoperative nausea and vomiting [in German]. Anaesthesist. 1985;34:656–662.
37. Tolksdorf W, Baumann S, Heine C, Hettenbach A. Effects and side ef-fects of transdermal scopolamine for premedication in general anes-thesia in elderly patients [in German]. Anasth Intensivther Notfallmed. 1986; 21:301–306.
38. Uppington J, Dunnet J, Blogg CE. Transdermal hyoscine and postop-erative nausea and vomiting. Anaes-thesia. 1986;41:16–20.
39. Tigerstedt I, Salmela L, Aromaa U. Double-blind comparison of trans-dermal scopolamine, droperidol and placebo against postoperative nausea and vomiting. Acta Anaesthe-siol Scand. 1988;32:454–457.
40. Jespersen TW, Koch J, Anker-Møller E, et al. Transdermal scopolamine to prevent postoperative nausea and vomiting after uterine curettage and termination of pregnancy. A double-blind clinically controlled study with placebo [in Danish]. Ugeskr Laeger. 1989;151:1246–1248.
41. Kotelko DM, Rottman RL, Wright WC, et al. Transdermal scopolamine decreases nausea and vomiting fol-lowing cesarean section in patients receiving epidural morphine. Anes-thesiology. 1989;71:675–678.
42. Loper KA, Ready LB, Dorman BH. Prophylactic transdermal scopol-amine patches reduce nausea in post- operative patients receiving epidural morphine. Anesth Analg. 1989;68: 144–146.
43. Wilkinson AR, Frampton CM, Glover PW, Davis FM. Preoperative transder-mal hyoscine for the prevention of postoperative nausea and vomiting. Anaesth Intens Care. 1989;17:285– 289.

2002 Volume 32 Number 12
Clinical Therapeutics
62. Apfel CC, Korttila K, Abdalla M, et al, for the IMPACT Investigators. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;350:2441–2451.
63. Apfel CC, Cakmakkaya OS, Frings G, et al. Droperidol has comparable clinical efficacy against both nausea and vomiting. Br J Anaesth. 2009; 103:359–363.
64. Jokela RM, Cakmakkaya OS, Dan-zeisen O, et al. Ondansetron has similar clinical efficacy against both nausea and vomiting. Anaesthesia. 2009;64:147–151.
65. Firth AY, Walker K. Visual side- effects from transdermal scopol-amine (hyoscine). Dev Med Child Neurol. 2006;48:137–138.
66. Apfel CC, Läärä E, Koivuranta M, et al. A simplified risk score for pre-dicting postoperative nausea and vomiting: Conclusions from cross-validations between two centers. Anesthesiology. 1999;91:693–700.
67. Gan TJ, Meyer TA, Apfel CC, et al, for the Society for Ambulatory Anesthesia. Society for Ambulatory Anesthesia guidelines for the man-agement of postoperative nausea and vomiting. Anesth Analg. 2007;105: 1615–1628.
68. Kovac AL, O’Connor TA, Pearman MH, et al. Efficacy of repeat intra-venous dosing of ondansetron in controlling postoperative nausea and vomiting: A randomized, double-blind, placebo-controlled multicenter trial. J Clin Anesth. 1999;11:453–459.
Address correspondence to: Christian C. Apfel, MD, PhD, Perioperative Clinical Research Core, Department of Anesthesia and Perioperative Care, University of California at San Francisco, 1600 Divisadero Street, San Francisco, CA 94115. E-mail: [email protected] or [email protected]
Top Related
Copyright © 2022 FDOKUMEN

