






Bahasa
Halaman
Hukum

Penile Cancer
The Role of Magnetic Resonance Imaging in theLocal Staging of Penile Cancer
Oliver Kayes, Suks Minhas, Clare Allen, Chris Hare, Alex Freeman, David Ralph *
St Peter’s Hospital and The Institute of Urology, London, UK
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 9
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Article info
Article history:Accepted November 3, 2006Published online ahead ofprint on November 13, 2006
Keywords:MRIPenile cancerStaging
Abstract
Objectives: To assess the accuracy of magnetic resonance imaging (MRI)as a local staging technique in penile cancer and its role in selectingpatients for conservative surgical management.Methods: Fifty-five men diagnosed with invasive penile carcinoma onbiopsy were locally staged with the use of MRI. Prostaglandin E1 (alpros-tadil) was injected into the corpora to induce an artificial erection.Radiologic staging was compared against final histopathologic stage ofthe tumour. Sensitivity, specificity, and kappa agreement values werecalculated for each tumour stage. Additionally, corpora cavernosa invol-vement was reviewed in 20 consecutive cases and suitability for con-servative surgery assessed.Results: A good correlation between radiologic and histologic stagingwas achieved with an overall kappa value of 0.75 ( p < 0.001). Stage-specific sensitivities and specificities were calculated: T1 (85%; 83%),T2 (75%; 89%), and T3 (88%; 98%). MRI accurately predicted corporacavernosa invasion in all cases of pathologically proven disease. Thesepatients were selected to undergo partial penectomy. There were nocomplications using this imaging technique.Conclusions: This study demonstrates that penile MRI is highly accuratein the local staging of penile cancer. Associated improvements in surgi-cal planning allow the provision of conservative surgical treatments overmore radical procedures.# 2006 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. St Peter’s Hospital, 235, Euston Road, London NW1 2BU,United Kingdom.E-mail address: [email protected] (D. Ralph).
1. Introduction
Penile malignancy is a rare tumour, comprising0.4–0.6% of all cancers in the United Kingdom [1].There is varied geographical incidence, with some
0302-2838/$ – see back matter # 2006 European Association of Urology. Publis
areas of South America, Africa, and India reportingrates as high as 20% of all male cancers [2].Squamous cell carcinoma (SCC) is the predominantmalignant process, accounting for 95% of cases [3].The primary tumour is located in the glans in 48% of
hed by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2006.11.014
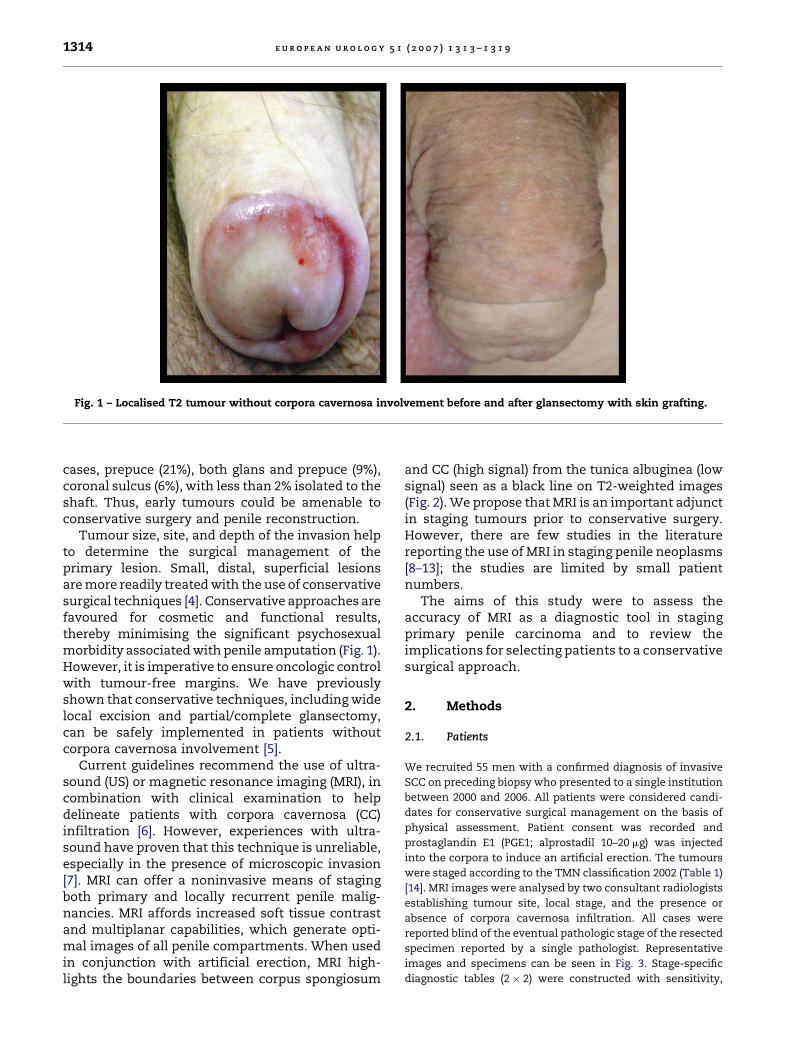
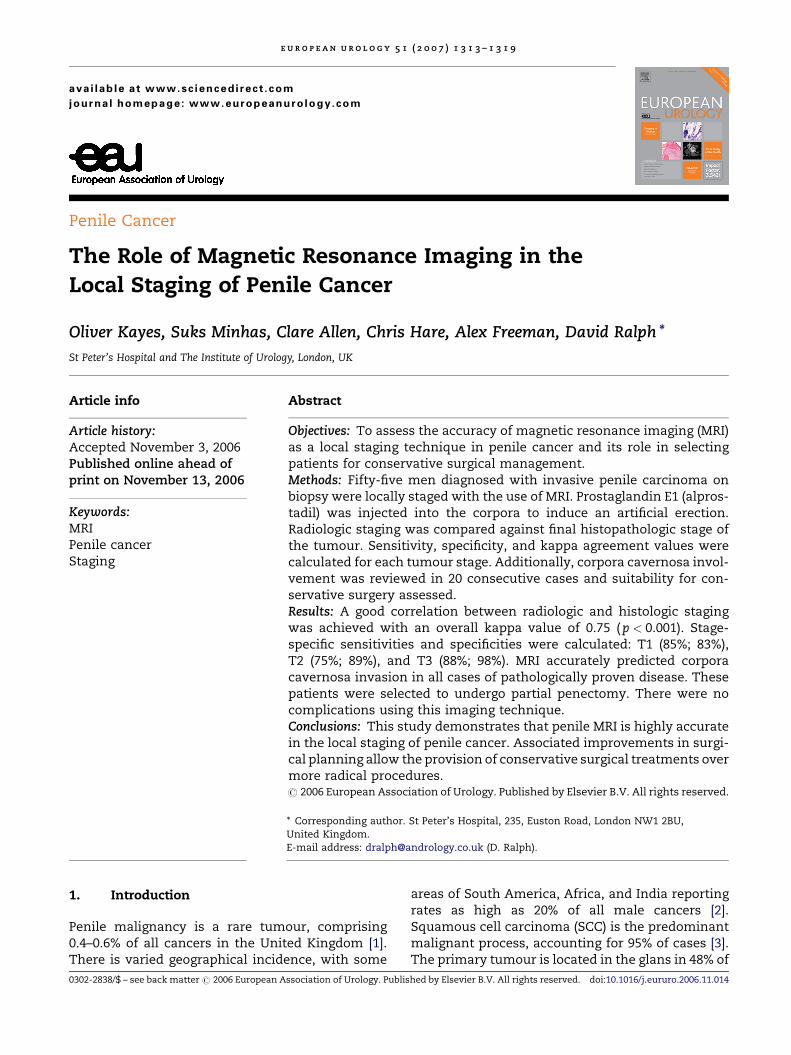
Fig. 1 – Localised T2 tumour without corpora cavernosa involvement before and after glansectomy with skin grafting.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 91314
cases, prepuce (21%), both glans and prepuce (9%),coronal sulcus (6%), with less than 2% isolated to theshaft. Thus, early tumours could be amenable toconservative surgery and penile reconstruction.
Tumour size, site, and depth of the invasion helpto determine the surgical management of theprimary lesion. Small, distal, superficial lesionsare more readily treated with the use of conservativesurgical techniques [4]. Conservative approaches arefavoured for cosmetic and functional results,thereby minimising the significant psychosexualmorbidity associated with penile amputation (Fig. 1).However, it is imperative to ensure oncologic controlwith tumour-free margins. We have previouslyshown that conservative techniques, including widelocal excision and partial/complete glansectomy,can be safely implemented in patients withoutcorpora cavernosa involvement [5].
Current guidelines recommend the use of ultra-sound (US) or magnetic resonance imaging (MRI), incombination with clinical examination to helpdelineate patients with corpora cavernosa (CC)infiltration [6]. However, experiences with ultra-sound have proven that this technique is unreliable,especially in the presence of microscopic invasion[7]. MRI can offer a noninvasive means of stagingboth primary and locally recurrent penile malig-nancies. MRI affords increased soft tissue contrastand multiplanar capabilities, which generate opti-mal images of all penile compartments. When usedin conjunction with artificial erection, MRI high-lights the boundaries between corpus spongiosum
and CC (high signal) from the tunica albuginea (lowsignal) seen as a black line on T2-weighted images(Fig. 2). We propose that MRI is an important adjunctin staging tumours prior to conservative surgery.However, there are few studies in the literaturereporting the use of MRI in staging penile neoplasms[8–13]; the studies are limited by small patientnumbers.
The aims of this study were to assess theaccuracy of MRI as a diagnostic tool in stagingprimary penile carcinoma and to review theimplications for selecting patients to a conservativesurgical approach.
2. Methods
2.1. Patients
We recruited 55 men with a confirmed diagnosis of invasive
SCC on preceding biopsy who presented to a single institution
between 2000 and 2006. All patients were considered candi-
dates for conservative surgical management on the basis of
physical assessment. Patient consent was recorded and
prostaglandin E1 (PGE1; alprostadil 10–20 mg) was injected
into the corpora to induce an artificial erection. The tumours
were staged according to the TMN classification 2002 (Table 1)
[14]. MRI images were analysed by two consultant radiologists
establishing tumour site, local stage, and the presence or
absence of corpora cavernosa infiltration. All cases were
reported blind of the eventual pathologic stage of the resected
specimen reported by a single pathologist. Representative
images and specimens can be seen in Fig. 3. Stage-specific
diagnostic tables (2 � 2) were constructed with sensitivity,
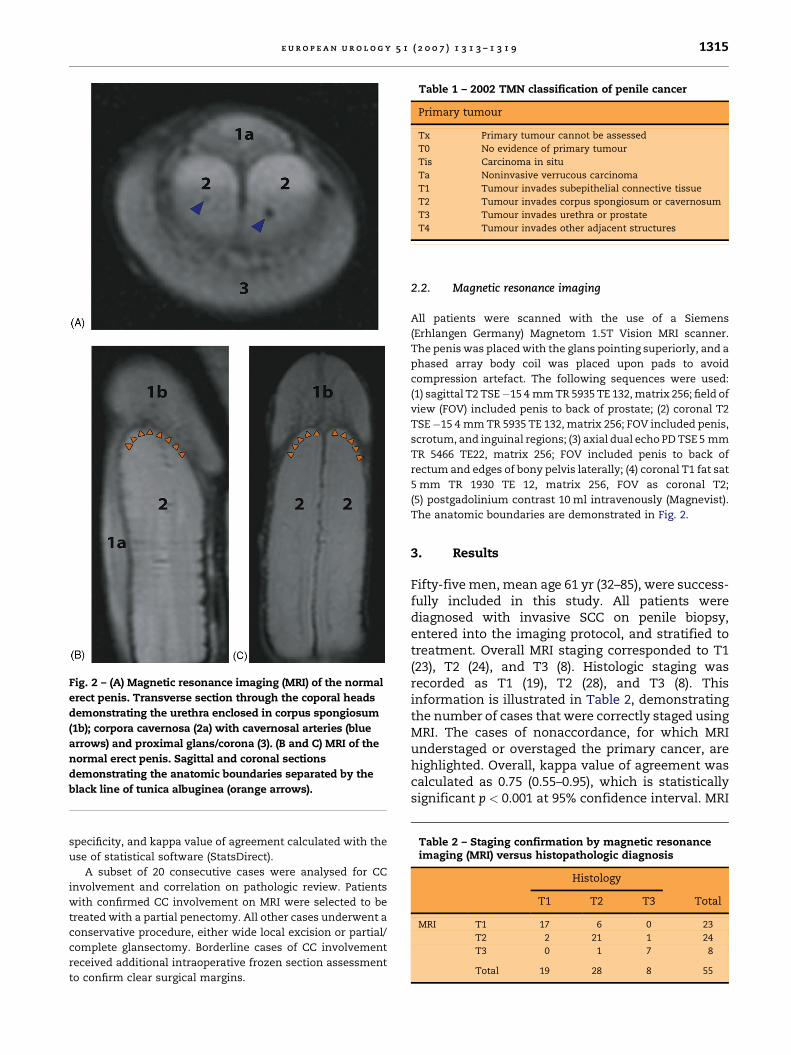
Fig. 2 – (A) Magnetic resonance imaging (MRI) of the normal
erect penis. Transverse section through the coporal heads
demonstrating the urethra enclosed in corpus spongiosum
(1b); corpora cavernosa (2a) with cavernosal arteries (blue
arrows) and proximal glans/corona (3). (B and C) MRI of the
normal erect penis. Sagittal and coronal sections
demonstrating the anatomic boundaries separated by the
black line of tunica albuginea (orange arrows).
Table 2 – Staging confirmation by magnetic resonanceimaging (MRI) versus histopathologic diagnosis
Histology
T1 T2 T3 Total
MRI T1 17 6 0 23
T2 2 21 1 24
T3 0 1 7 8
Total 19 28 8 55
Table 1 – 2002 TMN classification of penile cancer
Primary tumour
Tx Primary tumour cannot be assessed
T0 No evidence of primary tumour
Tis Carcinoma in situ
Ta Noninvasive verrucous carcinoma
T1 Tumour invades subepithelial connective tissue
T2 Tumour invades corpus spongiosum or cavernosum
T3 Tumour invades urethra or prostate
T4 Tumour invades other adjacent structures
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 9 1315
specificity, and kappa value of agreement calculated with the
use of statistical software (StatsDirect).
A subset of 20 consecutive cases were analysed for CC
involvement and correlation on pathologic review. Patients
with confirmed CC involvement on MRI were selected to be
treated with a partial penectomy. All other cases underwent a
conservative procedure, either wide local excision or partial/
complete glansectomy. Borderline cases of CC involvement
received additional intraoperative frozen section assessment
to confirm clear surgical margins.
2.2. Magnetic resonance imaging
All patients were scanned with the use of a Siemens
(Erhlangen Germany) Magnetom 1.5T Vision MRI scanner.
The penis was placed with the glans pointing superiorly, and a
phased array body coil was placed upon pads to avoid
compression artefact. The following sequences were used:
(1) sagittal T2 TSE�15 4 mm TR 5935 TE 132, matrix 256; field of
view (FOV) included penis to back of prostate; (2) coronal T2
TSE�15 4 mm TR 5935 TE 132, matrix 256; FOV included penis,
scrotum, and inguinal regions; (3) axial dual echo PD TSE 5 mm
TR 5466 TE22, matrix 256; FOV included penis to back of
rectum and edges of bony pelvis laterally; (4) coronal T1 fat sat
5 mm TR 1930 TE 12, matrix 256, FOV as coronal T2;
(5) postgadolinium contrast 10 ml intravenously (Magnevist).
The anatomic boundaries are demonstrated in Fig. 2.
3. Results
Fifty-five men, mean age 61 yr (32–85), were success-fully included in this study. All patients werediagnosed with invasive SCC on penile biopsy,entered into the imaging protocol, and stratified totreatment. Overall MRI staging corresponded to T1(23), T2 (24), and T3 (8). Histologic staging wasrecorded as T1 (19), T2 (28), and T3 (8). Thisinformation is illustrated in Table 2, demonstratingthe number of cases that were correctly staged usingMRI. The cases of nonaccordance, for which MRIunderstaged or overstaged the primary cancer, arehighlighted. Overall, kappa value of agreement wascalculated as 0.75 (0.55–0.95), which is statisticallysignificant p < 0.001 at 95% confidence interval. MRI
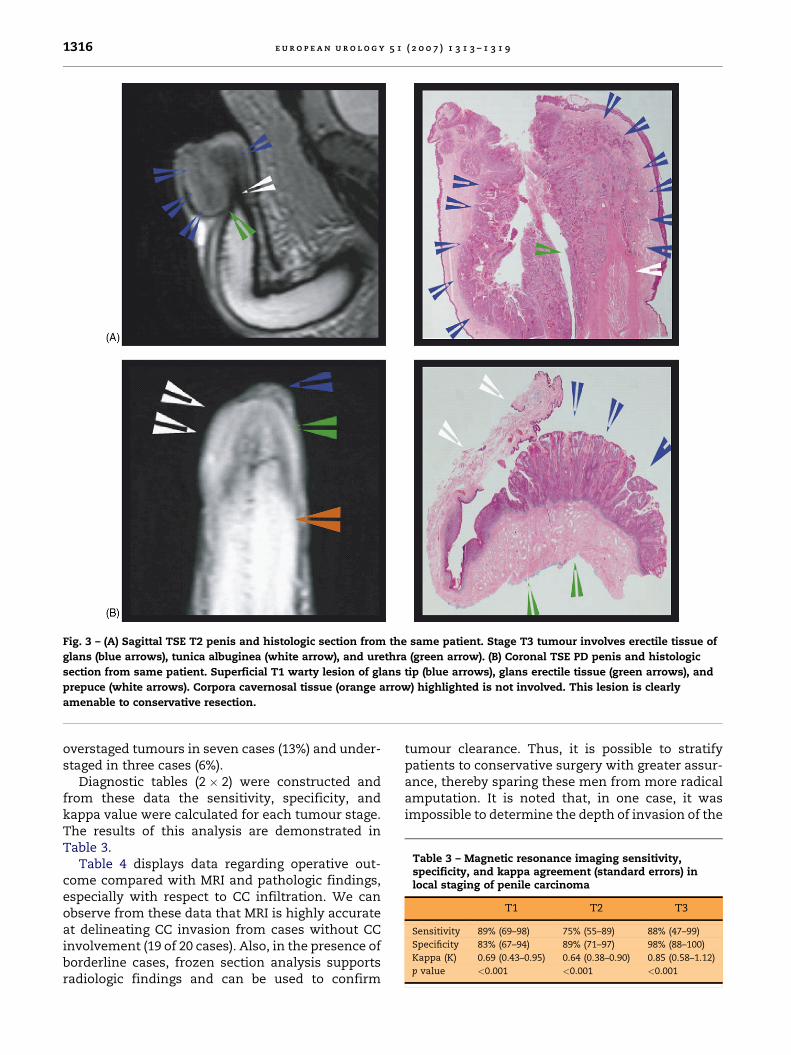
Fig. 3 – (A) Sagittal TSE T2 penis and histologic section from the same patient. Stage T3 tumour involves erectile tissue of
glans (blue arrows), tunica albuginea (white arrow), and urethra (green arrow). (B) Coronal TSE PD penis and histologic
section from same patient. Superficial T1 warty lesion of glans tip (blue arrows), glans erectile tissue (green arrows), and
prepuce (white arrows). Corpora cavernosal tissue (orange arrow) highlighted is not involved. This lesion is clearly
amenable to conservative resection.
Table 3 – Magnetic resonance imaging sensitivity,specificity, and kappa agreement (standard errors) inlocal staging of penile carcinoma
T1 T2 T3
Sensitivity 89% (69–98) 75% (55–89) 88% (47–99)
Specificity 83% (67–94) 89% (71–97) 98% (88–100)
Kappa (K) 0.69 (0.43–0.95) 0.64 (0.38–0.90) 0.85 (0.58–1.12)
p value <0.001 <0.001 <0.001
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 91316
overstaged tumours in seven cases (13%) and under-staged in three cases (6%).
Diagnostic tables (2 � 2) were constructed andfrom these data the sensitivity, specificity, andkappa value were calculated for each tumour stage.The results of this analysis are demonstrated inTable 3.
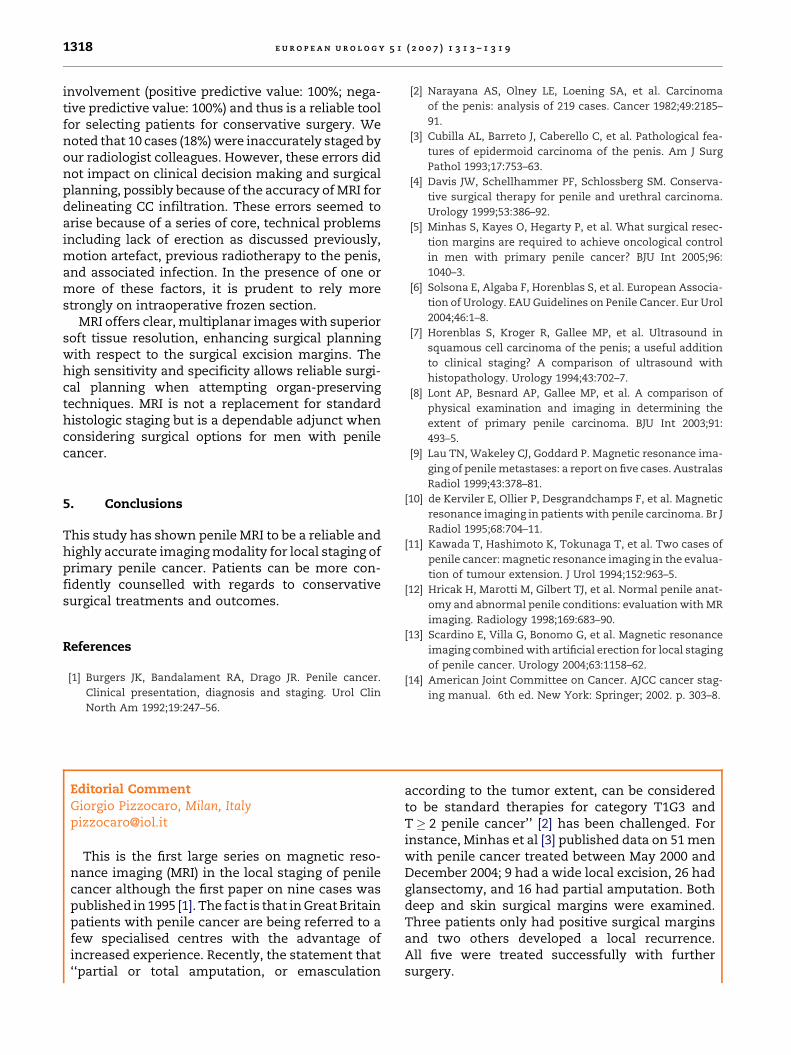
Table 4 displays data regarding operative out-come compared with MRI and pathologic findings,especially with respect to CC infiltration. We canobserve from these data that MRI is highly accurateat delineating CC invasion from cases without CCinvolvement (19 of 20 cases). Also, in the presence ofborderline cases, frozen section analysis supportsradiologic findings and can be used to confirm
tumour clearance. Thus, it is possible to stratifypatients to conservative surgery with greater assur-ance, thereby sparing these men from more radicalamputation. It is noted that, in one case, it wasimpossible to determine the depth of invasion of the
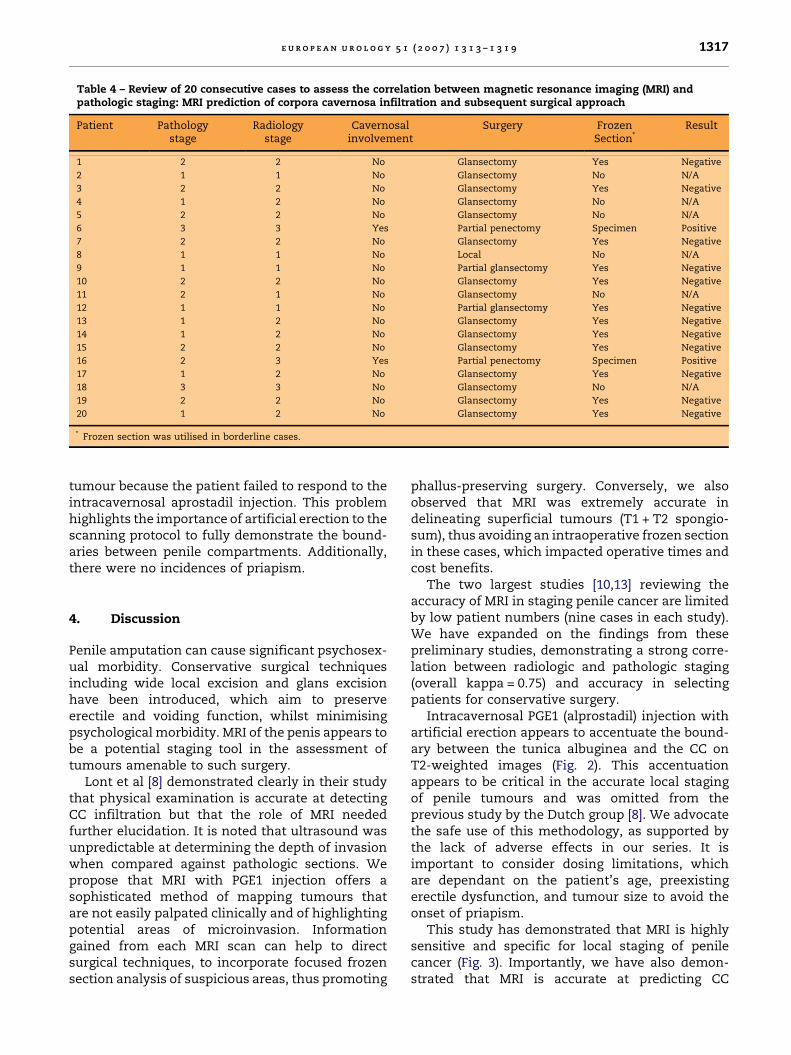
Table 4 – Review of 20 consecutive cases to assess the correlation between magnetic resonance imaging (MRI) andpathologic staging: MRI prediction of corpora cavernosa infiltration and subsequent surgical approach
Patient Pathologystage
Radiologystage
Cavernosalinvolvement
Surgery FrozenSection*
Result
1 2 2 No Glansectomy Yes Negative
2 1 1 No Glansectomy No N/A
3 2 2 No Glansectomy Yes Negative
4 1 2 No Glansectomy No N/A
5 2 2 No Glansectomy No N/A
6 3 3 Yes Partial penectomy Specimen Positive
7 2 2 No Glansectomy Yes Negative
8 1 1 No Local No N/A
9 1 1 No Partial glansectomy Yes Negative
10 2 2 No Glansectomy Yes Negative
11 2 1 No Glansectomy No N/A
12 1 1 No Partial glansectomy Yes Negative
13 1 2 No Glansectomy Yes Negative
14 1 2 No Glansectomy Yes Negative
15 2 2 No Glansectomy Yes Negative
16 2 3 Yes Partial penectomy Specimen Positive
17 1 2 No Glansectomy Yes Negative
18 3 3 No Glansectomy No N/A
19 2 2 No Glansectomy Yes Negative
20 1 2 No Glansectomy Yes Negative
* Frozen section was utilised in borderline cases.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 9 1317
tumour because the patient failed to respond to theintracavernosal aprostadil injection. This problemhighlights the importance of artificial erection to thescanning protocol to fully demonstrate the bound-aries between penile compartments. Additionally,there were no incidences of priapism.
4. Discussion
Penile amputation can cause significant psychosex-ual morbidity. Conservative surgical techniquesincluding wide local excision and glans excisionhave been introduced, which aim to preserveerectile and voiding function, whilst minimisingpsychological morbidity. MRI of the penis appears tobe a potential staging tool in the assessment oftumours amenable to such surgery.
Lont et al [8] demonstrated clearly in their studythat physical examination is accurate at detectingCC infiltration but that the role of MRI neededfurther elucidation. It is noted that ultrasound wasunpredictable at determining the depth of invasionwhen compared against pathologic sections. Wepropose that MRI with PGE1 injection offers asophisticated method of mapping tumours thatare not easily palpated clinically and of highlightingpotential areas of microinvasion. Informationgained from each MRI scan can help to directsurgical techniques, to incorporate focused frozensection analysis of suspicious areas, thus promoting
phallus-preserving surgery. Conversely, we alsoobserved that MRI was extremely accurate indelineating superficial tumours (T1 + T2 spongio-sum), thus avoiding an intraoperative frozen sectionin these cases, which impacted operative times andcost benefits.
The two largest studies [10,13] reviewing theaccuracy of MRI in staging penile cancer are limitedby low patient numbers (nine cases in each study).We have expanded on the findings from thesepreliminary studies, demonstrating a strong corre-lation between radiologic and pathologic staging(overall kappa = 0.75) and accuracy in selectingpatients for conservative surgery.
Intracavernosal PGE1 (alprostadil) injection withartificial erection appears to accentuate the bound-ary between the tunica albuginea and the CC onT2-weighted images (Fig. 2). This accentuationappears to be critical in the accurate local stagingof penile tumours and was omitted from theprevious study by the Dutch group [8]. We advocatethe safe use of this methodology, as supported bythe lack of adverse effects in our series. It isimportant to consider dosing limitations, whichare dependant on the patient’s age, preexistingerectile dysfunction, and tumour size to avoid theonset of priapism.
This study has demonstrated that MRI is highlysensitive and specific for local staging of penilecancer (Fig. 3). Importantly, we have also demon-strated that MRI is accurate at predicting CC
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 91318
involvement (positive predictive value: 100%; nega-tive predictive value: 100%) and thus is a reliable toolfor selecting patients for conservative surgery. Wenoted that 10 cases (18%) were inaccurately staged byour radiologist colleagues. However, these errors didnot impact on clinical decision making and surgicalplanning, possibly because of the accuracy of MRI fordelineating CC infiltration. These errors seemed toarise because of a series of core, technical problemsincluding lack of erection as discussed previously,motion artefact, previous radiotherapy to the penis,and associated infection. In the presence of one ormore of these factors, it is prudent to rely morestrongly on intraoperative frozen section.
MRI offers clear, multiplanar images with superiorsoft tissue resolution, enhancing surgical planningwith respect to the surgical excision margins. Thehigh sensitivity and specificity allows reliable surgi-cal planning when attempting organ-preservingtechniques. MRI is not a replacement for standardhistologic staging but is a dependable adjunct whenconsidering surgical options for men with penilecancer.
5. Conclusions
This study has shown penile MRI to be a reliable andhighly accurate imaging modality for local staging ofprimary penile cancer. Patients can be more con-fidently counselled with regards to conservativesurgical treatments and outcomes.
References
[1] Burgers JK, Bandalament RA, Drago JR. Penile cancer.
Clinical presentation, diagnosis and staging. Urol Clin
North Am 1992;19:247–56.
Editorial CommentGiorgio Pizzocaro, Milan, [email protected]
This is the first large series on magnetic reso-nance imaging (MRI) in the local staging of penilecancer although the first paper on nine cases waspublished in 1995 [1]. The fact is that in Great Britainpatients with penile cancer are being referred to afew specialised centres with the advantage ofincreased experience. Recently, the statement that‘‘partial or total amputation, or emasculation
[2] Narayana AS, Olney LE, Loening SA, et al. Carcinoma
of the penis: analysis of 219 cases. Cancer 1982;49:2185–
91.
[3] Cubilla AL, Barreto J, Caberello C, et al. Pathological fea-
tures of epidermoid carcinoma of the penis. Am J Surg
Pathol 1993;17:753–63.
[4] Davis JW, Schellhammer PF, Schlossberg SM. Conserva-
tive surgical therapy for penile and urethral carcinoma.
Urology 1999;53:386–92.
[5] Minhas S, Kayes O, Hegarty P, et al. What surgical resec-
tion margins are required to achieve oncological control
in men with primary penile cancer? BJU Int 2005;96:
1040–3.
[6] Solsona E, Algaba F, Horenblas S, et al. European Associa-
tion of Urology. EAU Guidelines on Penile Cancer. Eur Urol
2004;46:1–8.
[7] Horenblas S, Kroger R, Gallee MP, et al. Ultrasound in
squamous cell carcinoma of the penis; a useful addition
to clinical staging? A comparison of ultrasound with
histopathology. Urology 1994;43:702–7.
[8] Lont AP, Besnard AP, Gallee MP, et al. A comparison of
physical examination and imaging in determining the
extent of primary penile carcinoma. BJU Int 2003;91:
493–5.
[9] Lau TN, Wakeley CJ, Goddard P. Magnetic resonance ima-
ging of penile metastases: a report on five cases. Australas
Radiol 1999;43:378–81.
[10] de Kerviler E, Ollier P, Desgrandchamps F, et al. Magnetic
resonance imaging in patients with penile carcinoma. Br J
Radiol 1995;68:704–11.
[11] Kawada T, Hashimoto K, Tokunaga T, et al. Two cases of
penile cancer: magnetic resonance imaging in the evalua-
tion of tumour extension. J Urol 1994;152:963–5.
[12] Hricak H, Marotti M, Gilbert TJ, et al. Normal penile anat-
omy and abnormal penile conditions: evaluation with MR
imaging. Radiology 1998;169:683–90.
[13] Scardino E, Villa G, Bonomo G, et al. Magnetic resonance
imaging combined with artificial erection for local staging
of penile cancer. Urology 2004;63:1158–62.
[14] American Joint Committee on Cancer. AJCC cancer stag-
ing manual. 6th ed. New York: Springer; 2002. p. 303–8.
according to the tumor extent, can be consideredto be standard therapies for category T1G3 andT � 2 penile cancer’’ [2] has been challenged. Forinstance, Minhas et al [3] published data on 51 menwith penile cancer treated between May 2000 andDecember 2004; 9 had a wide local excision, 26 hadglansectomy, and 16 had partial amputation. Bothdeep and skin surgical margins were examined.Three patients only had positive surgical marginsand two others developed a local recurrence.All five were treated successfully with furthersurgery.

Finally, Romero et al [4] interviewed 18 patients(median age, 52 yr) who had undergone partialpenectomy; the medium penile length after surgerywas 4 cm in the flaccid state. Ten patients reportedpostoperative erectile function that could allowintercourse, but the main reason for not resumingsexual activity was the feeling of shame and onlysix continued sexual activity.
We need both good preoperative imaging and acareful examination of surgical margins to performradical and less aggressive surgery for cathegory T1and T2 squamous cell carcinoma of the glans penis.MRI with injection of prostaglandin E1 can be ofhelp in predicting corpora cavernosa invasion inmost cases.
References
[1] de Kerviler E, Ollier P, Desgrandchamps F, et al. Magnetic
resonance imaging in patients with penile carcinoma. Br J
Radiol 1995;68:704–11.
[2] Solsona E, Algaba F, Horenblas S, Pizzocaro G, Windahl T.
European Association of Urology. EAU guidelines on
penile cancer. Eur Urol 2004;46:1–8.
[3] Minhas S, Kayes O, Hegarty P, Kumar P, Freeman A, Ralph
D. What surgical resection margins are required to
achieve oncological control in men with primary penile
cancer? BJU Int 2005;96:1040–3.
[4] Romero FR, Pereira Dos Santos R, Romero K, et al. Sexual
function after partial penectomy for penile cancer.
Urology 2005;66:1292–5.
e u r o p e a n u r o l o g y 5 1 ( 2 0 0 7 ) 1 3 1 3 – 1 3 1 9 1319
Top Related
Copyright © 2022 FDOKUMEN

