







Bahasa
Halaman
Hukum


Obesity Preventionobr_729 430..439
The effect of theory-based interventions on physicalactivity participation among overweight/obeseindividuals: a systematic review
A. Bélanger-Gravel1, G. Godin2, L.-A. Vézina-Im3, S. Amireault1 and P. Poirier4
1Department of Social and Preventive
Medicine, Division of Kinesiology, Laval
University, Quebec City, QC, Canada;2Canada Research Chair on Behaviour and
Health, Faculty of Nursing, Laval University,
Quebec City, QC, Canada; 3Faculty of
Nursing, Laval University, Quebec City, QC,
Canada; 4Department of cardiology, Centre
de recherche de l’Institut universitaire de
cardiologie et de pneumologie de Québec,
Hôpital Laval, Quebec City, QC, Canada
Received 12 November 2009; revised 21
December 2009; accepted 7 January 2010
Address for correspondence: A
Bélanger-Gravel, Canada Research Chair
on Behaviour and Health, FSI-Vandry,
Laval University, Quebec City, QC, G1V
0A6, Canada. E-mail:
SummaryLittle attention has been paid to the evaluation of the long-term impact oftheory-based interventions on physical activity participation among overweight/obese individuals after the interventions have ended. The primary aim of thissystematic review was to investigate the long-term effectiveness of theory-basedinterventions increasing physical activity and identify the most effective tech-niques for behaviour change among overweight/obese individuals. The secondaryaim was to investigate the effect of these interventions on theoretical variables.Eighteen studies were reviewed. Among these studies, three reported significantshort-term and two long-term effects of interventions on physical activity partici-pation. Most of the studies observed a significant short- or long-term effect of timeon this behaviour. Theoretical frameworks most often applied included the Behav-ioural Model and the Social Learning/Cognitive Theory. However, few of thestudies reported any impact on theoretical variables. The most prevalent tech-niques consisted of providing opportunities for social comparison and instructionas well as self-monitoring. Leading techniques differentiating the experimentalgroup from the control group included prompting practice and intentions forma-tion and barriers identification. Although the combination of these three tech-niques appears successful, the long-term impact of theory-based interventionsremains ambiguous.
Keywords: Obesity, physical activity, systematic review, theory-basedintervention.
obesity reviews (2011) 12, 430–439
Introduction
Both obesity and physical inactivity contribute to the devel-opment of several chronic diseases and generate importanthealthcare costs (1). Consequently, lifestyle interventionsfor weight loss and maintenance are an important publichealth priority (2,3). In recent decades, significant effortshave been invested in the development of more effectivebehavioural approaches to the treatment of obesity. Assuch, some systematic reviews and meta-analyses have been
published about the efficacy of interventions on weightloss (4,5). However, scant attention has been paid to theevaluation of the long-term effect of such interventions onphysical activity after the interruption of contact withparticipants (6,7). This observation is quite surprising,given that exercise represents one of the major componentsof behavioural treatment of obesity (8). In a systematicreview of this topic, mixed results about changes inphysical activity have been reported (9). Moreover,although individually adapted programmes or behaviour
obesity reviews doi: 10.1111/j.1467-789X.2010.00729.x
430 © 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

modification is effective in increasing physical activity onthe short term (10,11), the long-term effect of such pro-grammes is less conclusive (12).
The development of more effective interventions wouldbenefit from health behaviour theory research and, moreimportantly, from the identification of the psychologicalprocesses whereby these interventions have an impact onbehaviour (i.e. the ‘active ingredients’) (7,12–16). In theliterature, little attention has been paid to the identificationof the ‘active ingredients’ of theory-based interventions onphysical activity among overweight/obese adults using vali-dated taxonomy (9). Thus, the primary aim of this system-atic review was to investigate the long-term effectiveness oftheory-based interventions to increase physical activity par-ticipation among overweight/obese adults and identifypotential intervention components that might prove mosteffective. A secondary aim involved investigating the effectof these interventions on modifying key theoretical vari-ables (i.e. mediators).
Methods
Literature search
A literature search and data extraction were performedbetween April and October 2008. We searched for studiespublished in English in psycINFO, MEDLINE, EMBASE,CIHNAL, Sport Discuss, Cochrane library (CochraneCentral Trials Register) and PROQUEST dissertations &theses. The search strategy in MEDLINE involved (type ofbehavior) AND (targeted population) AND (intervention)AND adult (Table A1). The reference lists of all relevantarticles were checked manually and additional searches wereperformed for articles published by important authors in thefield of obesity treatment (e.g. Wing, Perri, Jeffery, etc.).
Inclusion and exclusion criteria
The mean age and body mass index was established asbeing between 18 and 64 years of age and 25.0 and39.9 kg m-2, respectively. Because the definition of obesityhas changed over time, the last criterion was adjusted forstudies that classified body weight according to other cri-teria such as the criterion developed by the MetropolitanLife Insurance Company (17).
Studies that included participants with known mentaldisorders, physical diseases or targeted specific populationswere excluded. However, studies that targeted overweight/obese adults with diabetes, glucose intolerance, impairedglucose tolerance, insulin resistance, hyperinsulinaemia,hypercholesterolaemia and hypertension were included.
Interventions based on one or several psychosocial theo-ries were considered. Because most of these theories weredeveloped in the late 1970s and thereafter, only studies
published after 1980 were included. Interventions thatused weight loss pharmacotherapy, herbal/natural prod-ucts, very-low-calorie diets, meal replacement or foodprovision were excluded. Studies reporting the effect ofstructured physical activity programmes or diets were alsoexcluded. Finally, studies that were included had to reportresults based on an objective (e.g. accelerometers andpedometers) or subjective (self-reported questionnaires)measure of participation in physical activity or an indicatorof participation (i.e. physical fitness), at baseline, post-intervention and at follow-up.
Randomized control trials as well as quasi-experimentaldesigns were included in the review, with the exceptionof studies adopting a one-group pre–post design. Thefollow-up period was defined as no contact with partici-pants for at least 3 weeks. All studies that maintained someform of contact, even at low intensity (or frequency) duringa maintenance phase, were not considered concurrent withour follow-up definition and were excluded if no additionalfollow-up was reported.
Data abstraction
Data were independently abstracted by two reviewers anddisagreements were resolved by consensus with a thirdreviewer. Where necessary, attempts were made to contactauthors by email for information on key missing dataelements.
Before analysing the data set, a number of decisions weretaken. First, several studies reported both on physical activ-ity behaviour and physical fitness levels. Because this studyconcerns observable behaviours, results for physical activ-ity instead of fitness were reported when information forthese two outcomes was available. In an attempt to stan-dardize outcome measures to the recommended amount ofphysical activity (i.e. 150 min/week of moderate physicalactivity) (18), only results on frequency or duration wereabstracted when several physical activity outcomes werereported in the same study. Second, the attrition rate atfollow-up was calculated only when the exact number ofparticipants was clearly reported. Third, the analysis ofbehaviour change techniques was based on a taxonomydeveloped by Abraham and Michie (19) (Table A2). Thisanalysis, as well as the analysis of the theoretical constructstargeted and assessed, was limited to intervention compo-nents explicitly related to physical activity. For more infor-mation on technical terms and expressions used in thepresent systematic review, please refer to Table S1.
Results
Characteristics of the interventions
The flow diagram of the bibliographic screen is presented inFig. 1. For the analysis, 23 studies describing 18 interven-
obesity reviews Physical activity and overweight/obese adults A. Bélanger-Gravel et al. 431
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

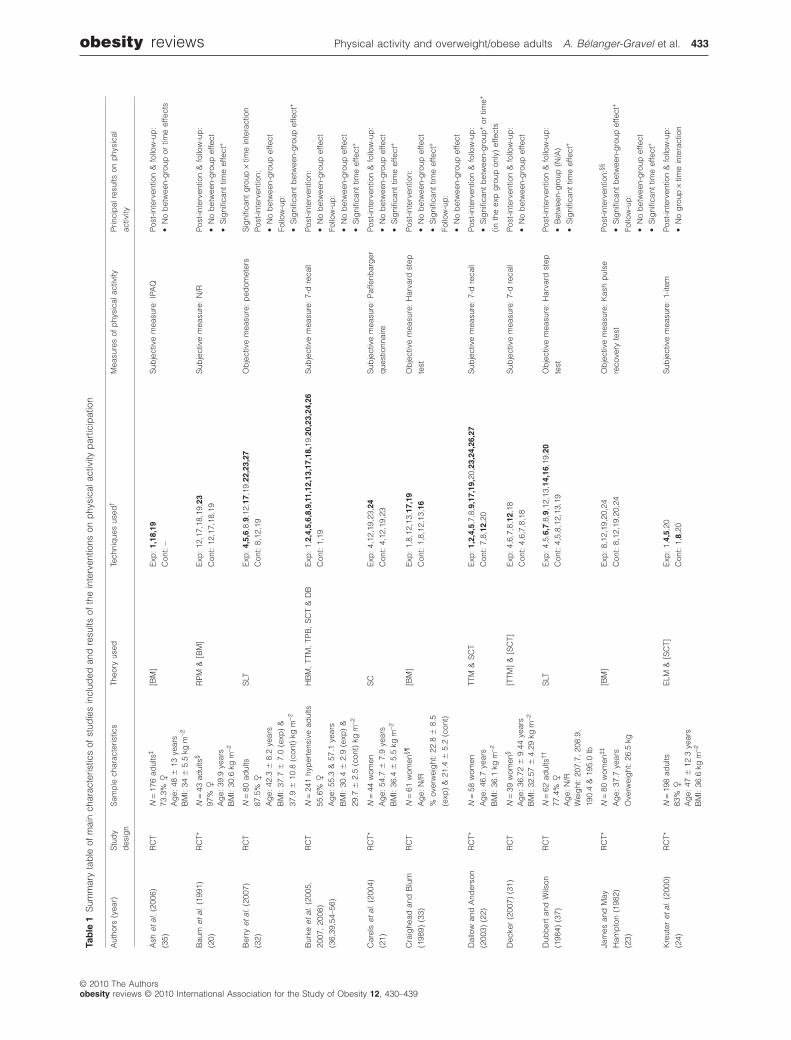
tions were included (see Table 1 for the summary of resultsand Tables S2 and S3 for more information on abstracteddata).
All studies included were described as randomizedcontrol trials but, for 11 studies (20–30), it was impos-sible to determine the randomization procedure used. Noquasi-experimental design met the inclusion criteria.Increasing physical activity was the primary purpose ofthree of the studies (22,29,31), whereas all other studieswere interested primarily in weight management(i.e. weight loss and/or post-weight-reduction weightmaintenance).
The duration of the studies, as well as the intensity andfrequency of contacts with the participants, varied sub-stantially across the studies. For most studies, thetreatment phase lasted 3 months (20,32,33) or less(23,24,26,31,34). The longest treatment phases were 6months (21,22,27,35) or more (28). For studies includinga maintenance phase (20,25,27,36), the duration variedbetween 3 and 12 months. Finally, for most of thestudies, the duration of the no-contact follow-up periodwas 6 months or more (20–23,25–28,30,33–37). Unfor-tunately, it was not possible to extract a clear picture ofthe intensity and frequency of contacts, given the variabil-ity of the studies.
Characteristics of the participants
The mean age and body mass index of the participantsvaried between 37.7 and 55.1 years and 29.7 and37.9 kg m-2, respectively. Participants in the studies weremostly female and highly educated Caucasian adults.African Americans were targeted in one study (34). Twostudies were conducted among individuals with type 2 dia-betes (29,30) and one targeted hypertensive (36) obeseparticipants. The number of participants varied between 24and 389 individuals at baseline, with an attrition rate atfollow-up varying between 6% and 46.3%. Only threestudies reported an attrition rate lower than 20% at 6- or12-month follow-up (26,28,30).
Characteristics of physical activity behaviour
For the most part, physical activity behaviour was subjec-tively (20–22,24,27,28,30,31,35,36) rather than objec-tively assessed (23,25,26,29,32–34,37). Subjective physicalactivity was usually assessed by means of self-reportedquestionnaires (21,22,24,27,30,31,35,36). The exact valid-ity and reliability values of the instruments used for evalu-ating subjective physical activity were rarely reported(22,28,35), although analysis of the cited references
Number of hits (n = 8172)
Studies retrieved for more detailed evaluation (n = 203)
Studies with usable information (n = 23), describing 18 interventions
Excluded studies (n = 340) Non-intervention evaluation studies (n = 41) Mean age ≥ 65 years (n = 4) Mean BMI < 25 or ≥ 40 kg m–2 (n = 16) Insufficient / no information about BMI or % overweight (n = 43) Physical and mental disorders / bariatric surgery (n = 10) Use of pharmacotherapy / supplementation / meal replacement/VLCD (n = 42) Test of different prescription of diets or physical activity (n = 60) One-group pre–post design (n = 65) No theoretical background (n = 59)
Excluded studies (n = 180) No no-contact follow-up (n = 59) No information on physical activity (n = 121)
Potentially relevant studiesidentified and screened for retrieval (n = 543)
Figure 1 The flow diagram of includedstudies. BMI, body mass index; VLCD, verylow calorie diet.
432 Physical activity and overweight/obese adults A. Bélanger-Gravel et al. obesity reviews
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439
Tab
le1
Sum
mar
yta
ble
ofm
ain
char
acte
ristic
sof
stud
ies
incl
uded
and
resu
ltsof
the
inte
rven
tions
onp
hysi
cala
ctiv
ityp
artic
ipat
ion
Aut
hors
(yea
r)S
tud
y
des
ign
Sam
ple
char
acte
ristic
sTh
eory
used
Tech
niq
ues
used
†M
easu
res
ofp
hysi
cala
ctiv
ityP
rinci
pal
resu
ltson
phy
sica
l
activ
ity
Ash
etal
.(2
006)
(35)
RC
TN
=17
6ad
ults
‡[B
M]
Exp
:1,
18,1
9
Con
t:–
Sub
ject
ive
mea
sure
:IP
AQ
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upor
time
effe
cts
73.3
%�
Ag
e:48
�13
year
sB
MI:
34�
5.5
kgm
-2
Bau
met
al.
(199
1)
(20)
RC
T*N
=43
adul
ts§
RP
M&
[BM
]E
xp:
12,1
7,18
,19,
23
Con
t:12
,17,
18,1
9
Sub
ject
ive
mea
sure
:N
/RP
ost-
inte
rven
tion
&fo
llow
-up
:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+
97%
�
Ag
e:39
.9ye
ars
BM
I:30
.6kg
m-2
Ber
ryet
al.
(200
7)
(32)
RC
TN
=80
adul
tsS
LTE
xp:
4,5,
6,8,
9,12
,17,
19,2
2,23
,27
Con
t:8,
12,1
9
Ob
ject
ive
mea
sure
:p
edom
eter
sS
igni
fican
tg
roup
¥tim
ein
tera
ctio
n
Pos
t-in
terv
entio
n:
•N
ob
etw
een-
gro
upef
fect
Follo
w-u
p:
•S
igni
fican
tb
etw
een-
gro
upef
fect
+
87.5
%�
Ag
e:42
.3�
8.2
year
sB
MI:
37.7
�7.
0(e
xp)
&
37.9
�10
.8(c
ont)
kgm
-2
Bur
keet
al.
(200
5,
2007
,20
08)
(36,
39,5
4–56
)
RC
TN
=24
1hy
per
tens
ive
adul
tsH
BM
,TT
M,
TPB
,S
CT
&D
BE
xp:
1,2,
4,5,
6,8,
9,11
,12,
13,1
7,18
,19,
20,2
3,24
,26
Con
t:1,
19
Sub
ject
ive
mea
sure
:7-
dre
call
Pos
t-in
terv
entio
n:
•N
ob
etw
een-
gro
upef
fect
Follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+
55.6
%�
Ag
e:55
.3&
57.1
year
sB
MI:
30.4
�2.
9(e
xp)
&
29.7
�2.
5(c
ont)
kgm
-2
Car
els
etal
.(2
004)
(21)
RC
T*N
=44
wom
enS
CE
xp:
4,12
,19,
23,2
4
Con
t:4,
12,1
9,23
Sub
ject
ive
mea
sure
:P
affe
nbar
ger
que
stio
nnai
re
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+A
ge:
54.7
�7.
9ye
ars
BM
I:36
.4�
5.5
kgm
-2
Cra
ighe
adan
dB
lum
(198
9)(3
3)
RC
TN
=61
wom
en§¶
Ag
e:N
/R
%ov
erw
eig
ht:
22.8
�8.
5
(exp
)&
21.4
�5.
2(c
ont)
[BM
]E
xp:
1,8,
12,1
3,17
,19
Con
t:1,
8,12
,13,
16
Ob
ject
ive
mea
sure
:H
arva
rdst
ep
test
Pos
t-in
terv
entio
n:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+
Follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
Dal
low
and
And
erso
n
(200
3)(2
2)
RC
T*N
=58
wom
enTT
M&
SC
TE
xp:
1,2,
4,5,
7,8,
9,17
,19,
20,2
3,24
,26,
27
Con
t:7,
8,12
,20
Sub
ject
ive
mea
sure
:7-
dre
call
Pos
t-in
terv
entio
n&
follo
w-u
p:
•S
igni
fican
tb
etw
een-
gro
up+
ortim
e+
(inth
eex
pg
roup
only
)ef
fect
s
Ag
e:46
.7ye
ars
BM
I:36
.1kg
m-2
Dec
ker
(200
7)(3
1)R
CT
N=
39w
omen
§[T
TM]
&[S
CT]
Exp
:4,
6,7,
8,12
,18
Con
t:4,
6,7,
8,18
Sub
ject
ive
mea
sure
:7-
dre
call
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
Ag
e:36
.72
�9.
44ye
ars
BM
I:32
.57
�4.
29kg
m-2
Dub
ber
tan
dW
ilson
(198
4)(3
7)
RC
TN
=62
adul
ts††
SLT
Exp
:4,
5,6,
7,8,
9,12
,13,
14,1
6,19
,20
Con
t:4,
5,8,
12,1
3,19
Ob
ject
ive
mea
sure
:H
arva
rdst
ep
test
Pos
t-in
terv
entio
n&
follo
w-u
p:
•B
etw
een-
gro
up(N
/A)
•S
igni
fican
ttim
eef
fect
+
77.4
%�
Ag
e:N
/RW
eig
ht:
207.
7,20
8.9,
190.
4&
195.
0lb
Jam
esan
dM
ay
Ham
pto
n(1
982)
(23)
RC
T*N
=80
wom
en‡‡
Ag
e:37
.7ye
ars
Ove
rwei
ght
:26
.5kg
[BM
]E
xp:
8,12
,19,
20,2
4
Con
t:8,
12,1
9,20
,24
Ob
ject
ive
mea
sure
:K
ash
pul
se
reco
very
test
Pos
t-in
terv
entio
n:§§
•S
igni
fican
tb
etw
een-
gro
upef
fect
+
Follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+
Kre
uter
etal
.(2
000)
(24)
RC
T*N
=19
8ad
ults
ELM
&[S
CT]
Exp
:1,
4,5,
20
Con
t:1,
8,20
Sub
ject
ive
mea
sure
:1-
item
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
og
roup
¥tim
ein
tera
ctio
n83
%�
Ag
e:47
�12
.3ye
ars
BM
I:36
.6kg
m-2
obesity reviews Physical activity and overweight/obese adults A. Bélanger-Gravel et al. 433
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

Tab
le1
Con
tinue
d
Aut
hors
(yea
r)S
tud
y
des
ign
Sam
ple
char
acte
ristic
sTh
eory
used
Tech
niq
ues
used
†M
easu
res
ofp
hysi
cala
ctiv
ityP
rinci
pal
resu
ltson
phy
sica
lact
ivity
Leer
mak
ers
etal
.
(199
9)(2
5)
RC
T*N
=67
adul
ts[R
PM
]E
xp:
8,12
,14,
17,1
9,23
Con
t:5,
8,12
,19
Ob
ject
ive
mea
sure
:
acce
lero
met
er
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upor
time
effe
cts
80%
�
Ag
e:50
.8�
11.1
year
sB
MI:
30.8
�4.
5kg
m-2
Mat
hieu
(200
5)(3
4)R
CT
N=
389
Afr
ican
Am
eric
an
wom
en
SLT
Exp
:1,
8,19
,20
Con
t:19
Ob
ject
ive
mea
sure
:on
e-m
ile
run/
wal
kte
st
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+A
ge:
45ye
ars
BM
I:30
.16
kgm
-2
Rap
opor
tet
al.
(200
0)
(26)
RC
T*N
=84
wom
en
Ag
e:47
.5ye
ars
BM
I:35
.4kg
m-2
BM
Exp
:1,
4,6,
7,8,
12,1
9,24
,25
Con
t:1,
4,6,
12,1
3,19
Ob
ject
ive
mea
sure
:Te
chum
seh
step
test
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
og
roup
¥tim
ein
tera
ctio
n
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+
Rie
be
etal
.(2
003,
2005
)(2
7,57
)
RC
T*N
=19
0ad
ults
¶¶
TTM
&R
PM
Exp
:2,
6,7,
8,12
,13,
14,1
7,19
,20,
23
Con
t:1,
2,6,
7,8,
12,1
3,14
,17
,19,
20,2
3
Sub
ject
ive
mea
sure
:3-
item
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+
78%
�
Ag
e:50
.2�
9.2
year
sB
MI:
32.5
�3.
8kg
m-2
§
Sb
rocc
oet
al.
(199
9)
(28)
RC
T*N
=24
wom
enD
T&
BM
Exp
:8,
12,1
9
Con
t:8,
12,1
9
Sub
ject
ive
mea
sure
:d
aily
exer
cise
log
s
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
og
roup
¥tim
ein
tera
ctio
n
•N
ob
etw
een-
gro
upor
time
effe
cts
Ag
e:18
–55
year
sB
MI:
32.8
2�
3.20
(exp
)&
32.5
�3.
6(c
ont)
kgm
-2
Tud
or-L
ocke
etal
.
(200
4)(2
9)
RC
T*N
=60
adul
tsw
ithty
pe
2
dia
bet
es
SC
TE
xp:
4,5,
7,12
,13,
15,1
6,17
,18,
19,2
0,23
Con
t:–
Ob
ject
ive
mea
sure
:p
edom
eter
sP
ost-
inte
rven
tion:
•S
igni
fican
tb
etw
een-
gro
up+
&tim
e
effe
cts+
(inth
eex
pg
roup
only
)
Follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
45%
�
Ag
e:52
.7�
5.2
year
sB
MI:
33.9
�5.
6kg
m-2
Win
get
al.
(198
5)
(30)
RC
T*N
=53
adul
tsw
ithty
pe
2
dia
bet
es
BM
Exp
:1,
7,8,
9,13
,17,
19,2
0
Con
t:1,
19
Sub
ject
ive
mea
sure
:P
affe
nbar
ger
que
stio
nnai
re
Pos
t-in
terv
entio
n&
follo
w-u
p:
•N
ob
etw
een-
gro
upef
fect
•S
igni
fican
ttim
eef
fect
+62
.3%
�
Ag
e:55
.1�
1.0
year
sW
eig
ht:
96.4
�2.
3kg
[]:
Theo
ryex
trap
olat
edb
yau
thor
s.Th
ed
irect
ion
ofch
ang
esin
phy
sica
lact
ivity
:+:
Res
ults
favo
ured
the
exp
erim
enta
lgro
up(b
etw
een-
gro
upef
fect
)or
the
leve
lof
phy
sica
lact
ivity
incr
ease
d(t
ime
effe
ct).
*The
rand
omiz
atio
np
roce
dur
ew
asno
tsp
ecifi
ed.
† Diff
eren
cing
tech
niq
ues
are
pre
sent
edin
bol
dch
arac
ter.
‡ For
the
pre
sent
syst
emat
icre
view
,on
lyth
ech
arac
teris
tics
and
resu
ltsof
the
FBI
and
BO
gro
ups
wer
ere
por
ted
.§ B
asel
ine
char
acte
ristic
sof
the
com
ple
ters
.¶Fo
rth
ep
rese
ntsy
stem
atic
revi
ew,
only
the
char
acte
ristic
san
dre
sults
ofth
esu
per
vise
dex
erci
sean
dm
inim
alco
ntac
tg
roup
sw
ere
rep
orte
d.
††Fo
rth
ep
rese
ntsy
stem
atic
revi
ew,
coup
leg
roup
sw
ere
cons
ider
edas
one
gro
up,
asw
ella
sth
eg
roup
sof
ind
ivid
uals
.‡‡
For
the
pre
sent
syst
emat
icre
view
,on
lyth
ech
arac
teris
tics
and
resu
ltsof
the
HD
and
PD
gro
ups
wer
ere
por
ted
.N
ote
that
ano
-con
tact
cont
rolg
roup
was
initi
ally
form
ed,
but
par
ticip
ants
inth
isg
roup
rece
ived
the
HD
cond
ition
bef
ore
follo
w-u
pas
sess
men
t.§§
At
pos
t-in
terv
entio
n,ex
per
imen
talg
roup
sar
eco
mp
ared
with
the
no-c
onta
ctg
roup
.A
tfo
llow
-up
,on
lyth
eH
Dan
dP
Dco
nditi
ons
wer
eco
mp
ared
giv
enth
ecr
oss-
over
des
ign
ofth
est
udy.
¶¶C
omp
lete
rsof
the
initi
alw
eig
htm
anag
emen
tp
rog
ram
me
only
.B
M,
Beh
avio
ural
Mod
el;
BM
I,b
ody
mas
sin
dex
;B
O,
boo
klet
only
;C
ont,
cont
rolg
roup
;D
B,
Dec
isio
nalB
alan
ce;
DT,
dec
isio
nth
eory
;E
LM,
Ela
bor
atio
nLi
kelih
ood
Mod
el;
Exp
,ex
per
imen
talg
roup
;FB
I,Fa
tB
oote
rsIn
corp
orat
ed;
HB
M,
Hea
lthB
elie
fM
odel
;H
D,
hig
hly
dire
ctiv
e;IP
AQ
,In
tern
atio
nalP
hysi
calA
ctiv
ityQ
uest
ionn
aire
;N
/A,
not
app
licab
le;
N/R
,no
tre
por
ted
;P
D,
par
tially
dire
cted
;R
CT,
rand
omiz
edco
ntro
ltria
l;R
PM
,R
elap
seP
reve
ntio
nM
odel
;S
C,
Sel
f-C
ontro
lTh
eory
;S
CT,
Soc
ialC
ogni
tive
Theo
ry;
SLT
,S
ocia
lLea
rnin
gTh
eory
;TP
B,
Theo
ryof
Pla
nned
Beh
avio
ur;
TTM
,Tr
anst
heor
etic
alM
odel
.
434 Physical activity and overweight/obese adults A. Bélanger-Gravel et al. obesity reviews
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

revealed that almost all questionnaires used were adequate,except for three studies in which the instruments used werenot validated (20,24,27).
Measurements of objective physical activity wereobtained by means of pedometers (29,32), accelerometers(25) or physical fitness indicators (23,26,33,34,37). Threestudies specified that the tool was valid or reliable(25,29,34). For physical fitness, however, there was nomention of the reliability and validity of almost all of thetests used (23,26,33,37).
Results of interventions on physical activity
One study reported results for an intention-to-treat analysisat follow-up (36). Two additional authors mentioned thatthey used this statistical approach (27,35), but provided noinformation on the management of missing data; likewise,the number of participants included in the analysis waseither missing or inexact.
Overall, three studies reported significant between-groupeffects at post-intervention (including treatment and main-tenance phases) on physical activity behaviour (22,23,29);one of these studies reported a sustained and significantbetween-group effect at follow-up (22). Another studyreported a significant between-group effect at follow-upwithout significant results at post-intervention (32).Twelve of the 18 studies reported a significant effectof time at post-intervention and/or at follow-up (20–23,26,27,29,30,33,34,36,37). Given the observed variabil-ity between the studies for almost all methodologicalparameters, no meta-analysis of the results was performed.
Theoretical framework and psychosocial variables
The traditional Behavioural Model used in clinical psychol-ogy (i.e. behaviour therapy) and the Social Learning/Cognitive Theory were the two theories most often applied(83%). They were used alone (23,26,29,30,32–35,37) or incombination with other theories (20,22,24,28,31,36). Nolong-term between-group effect on physical activity wasobserved in any of the interventions based on the Behav-ioural Model (20,23,26,28,30,33,35), whereas a significanteffect of time was observed in five studies (71%). On theother hand, the two studies that had reported significantbetween-group effects at follow-up were partially (22) orexclusively (32) based on the Social Learning/CognitiveTheory.
Others theories used included the TranstheoreticalModel (22,27,31,36), Relapse Prevention Model(20,25,27), Self-Control Theory (21), Elaboration Likeli-hood Model (24), Decision Theory (28) and the HealthBelief Model, Decisional Balance and Theory of PlannedBehaviour (36). Some of these theories were used alone(21,25), but most were applied in combination with other
theories. Among the four studies based on the Transtheo-retical Model, only one reported a between-group differ-ence at follow-up (22). However, this latter study was alsobased on the Social Learning/Cognitive Theory. As it wasobserved for the Behavioural Model, the majority of thestudies based on the Transtheoretical Model (75%)reported a significant effect over time. None of the studiesbased on the Relapse Prevention Model reported significantbetween-group effects at follow-up, although they observedsignificant effects over time (66%).
Eight of the theory-based interventions clearly specifiedwhich theoretical variables were targeted to change physi-cal activity (21,22,24,27,29,31,34,36). Among these,self-efficacy was the predominant variable targeted(22,24,27,29,31,34,36), as most of the studies were basedon Social Learning/Cognitive Theory. Two studies based onthis model did not explicitly target self-efficacy (32,37). Inone study, self-control was targeted according to the Self-Control Theory (21). In the same way, both stages andprocesses of change were targeted in almost all interven-tions partially or exclusively based on the TranstheoreticalModel (22,27,31). Any of the studies based on the Behav-ioural Model specified the mechanisms of behaviouralchange. The psychometric qualities of the constructs werereported (or retrieved in cited reference) as adequate in fivestudies (22,27,31,34,35), but this information was notalways retrievable (21,24,31,36).
Two studies reported significant between-group effectson some theoretical variables at post-intervention (22,36).For instance, in the intervention by Burke et al. (36),between-group effects were reported for perceived barriers,self-efficacy (this effect was observed in post-treatment, butwas not sustained after the maintenance phase) and somecoping mechanisms. In the intervention by Dallow andAnderson (22), between-group effects were observed forsome processes of change, but not for self-efficacy. Thiseffect was not sustained at follow-up.
Two studies reported significant group effects on sometheoretical variables at follow-up, but there was no consis-tency in the results obtained. In the study by Ash et al. (35),general self-efficacy was higher in the experimental groupthan in the control group, whereas no significant groupeffect was observed for this variable in the study by Kreuteret al. (24). In this latter study, some between-group effectswere observed for several levels of thought, personal con-nection, self-assessment and intention.
Theoretical techniques used
Providing opportunities for social comparison was thetechnique most often used in the experimental groups (20–23,25–30,32–37). Significant effects of time were observedin 75% of the studies using this technique (20–23,26,27,29,30,33,34,36,37), and a between-group effect
obesity reviews Physical activity and overweight/obese adults A. Bélanger-Gravel et al. 435
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

at follow-up was observed in the two studies that reportedsignificant effects of their treatment on physical activity(22,32). The other main techniques used in the experimen-tal groups were providing instructions (22,23,25–28,30–34,36,37) and self-monitoring (20,21,23,25–29,31–33,36,37). Significant time effects were observed in six ofthe studies (67%) using the combination of these threetechniques (23,26,27,33,36,37). Two studies reported sig-nificant short-term (23) and long-term (32) effects of thetreatment. Finally, among all techniques listed by Abrahamand Michie (19), providing information on others’approval, setting specific goals and identification as a rolemodel were not used in any of the included studies.
Notwithstanding the above observations, the techniquesthat distinguished or characterized the experimentalgroups from the control groups were promptingpractice (22,25,29,30,32,33,36), barrier identification(22,24,25,29,32,36) and prompting intention formation(22,24,29,32,36,37). All of the studies that reported sig-nificant between-group effects on physical activity atpost-intervention (22,29) and follow-up (22,32) used acombination of these three techniques, except for the studyby James and May Hampton (23).
The number of theoretical techniques used varied sub-stantially across studies, although the interventions referredto the same theoretical background. For instance, betweenfour and twelve techniques were used for interventionsbased exclusively on the Social Learning/Cognitive theory(32,34,37). Moreover, for these interventions based exclu-sively on the Social Learning/Cognitive Theory, there wasno consistency in the techniques used that could character-ize the differences between the experimental groups and thecontrol groups. This was also observed for studies exclu-sively based on the Behavioural Model in which betweenthree and nine techniques were used in the experimentalgroups (23,26,30,33,35).
Discussion
Findings of the present systematic review indicate that themost frequently observed pattern of results was a signifi-cant improvement in the level of physical activity overtime, suggesting that all participants increased their levelof physical activity regardless of the assignment group. Inaddition, it was observed that the long-term effectiveness oftheory-based interventions to increase the level of physicalactivity among overweight/obese is weakly supportedbecause very few studies observed a superior effect of theirexperimental conditions (22,32). Overall, the informationin the literature adds little to our understanding of howinterventions succeed or fail to change physical activityamong this population.
These findings are somewhat surprising, given that theuse of theoretical frameworks should increase the likeli-
hood of developing more effective interventions (13–15). Ina recent meta-analysis (38), strong support was providedfor several behaviour change theories in the context of HIVprevention. In the present context, however, it must beacknowledged that almost all interventions were driven byproblem-solving rather than theory-testing. Thus, the theo-retical processes underlying behaviour change were seldomexplicitly described and no mediation test was carried outin most of the studies.
This apparent lack of concern for theoretical issues limitsthe possibility of developing evidence-based interventionsfor overweight/obese individuals to increase physical activ-ity. According to our systematic review, appropriate media-tion analysis was performed only by Burke et al. (39). Theiranalysis revealed that the short-term effect of the Activity,Diet and Blood Pressure Trial (ADAPT) programme wasmediated by self-efficacy. Their results compared favourablywith a previous review in which self-efficacy was the mostsupported mediator of interventions aimed at increasingphysical activity among adults (40) and could provide someempirical support for Bandura’s Social Cognitive Theory.
A second finding of this systematic review was that mostof the interventions failed to modify the theoretical media-tors of change under experimental conditions when com-pared with the control group. This apparent lack ofsupport for theories could be attributed to the failure toexperimentally manipulate the theoretical constructs.Indeed, in many studies, several techniques related to thetheoretical framework were used in both experimental andcontrol conditions. For instance, self-monitoring, a tech-nique usually associated with behavioural treatmentprogrammes, and providing opportunities for socialcomparison, a fundamental technique of the SocialLearning/Cognitive Theory, were used in all groups. More-over, when looking at the techniques that can distinguishcharacteristics of experimental groups and control groups,no similarity was observed between studies based on thesame theoretical model. This lack of coherence suggeststhat there are some problems with the correct operational-ization of theoretical frameworks. Consequently, no clearconclusion could be drawn regarding the most effectivetheories or components, as well as the most effective com-bination of these to promote a long-term physical activitypattern among overweight/obese individuals. Notwith-standing the above conclusion, our results suggest that itcould be interesting, in future studies, to investigate theeffect of combining techniques such as prompting practice,barrier identification and prompting intention formation.According to Michie et al. (41), these latter three tech-niques could be used to enhance beliefs about capabilities,motivation and goals.
Interestingly, little attention has been paid to the litera-ture on the determinants of physical activity and the impor-tant contribution of theories such as the Theory of Planned
436 Physical activity and overweight/obese adults A. Bélanger-Gravel et al. obesity reviews
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

Behaviour (42). Recently, this theory was suggested as oneof the most appropriate theories to guide the developmentof interventions aimed at weight management (43).According to this theory, intention is the proximal deter-minant of behaviour. Perceived behavioural control, or per-ceived ease or difficulty associated with the performance ofthe behaviour, is also viewed as a determinant of behaviouralong with intention. Meta-analyses of the predictive valueof this theory have reported that both intention and per-ceived control are significant determinants of physicalactivity among adults, with intention responsible for mostof the explained variance (21–27%) (44,45). Among obeseadults, intention has also been identified as the most impor-tant determinant of physical activity (46).
Finally, given that these interventions were quite inten-sive and involved multiple assessments of participants’physiological and/or behavioural characteristics, it cannotbe excluded that mere-measurement effects interfered withthe effect of interventions (47). Mere-measurement refersto the reactivity of measures on participants’ future behav-iour; some individuals change their behaviour followingexamination of information obtained from measurement.In previous investigations, it was observed that the mea-surement of physical fitness or the completion of a psycho-social questionnaire has a significant impact on futurebehaviour (48–50).
A number of limitations should be noted. First, only alimited number of studies met the inclusion criteria. It wouldappear that most of the effort deployed by such interven-tions concerned the evaluation of short-term effects onweight loss. Also, most of the studies included were con-ducted among well-educated and healthy participants,involved a greater proportion of women and reported highattrition rates. Second, this systematic review was onlydescriptive, as too much variability was observed in thestudies included. This limited the possibility of reportingaccurate pooled effect sizes. Likewise, the small number ofstudies included limited the possibility of resorting to moresophisticated meta-analysis techniques. Third, it is notewor-thy that the taxonomy used to identify techniques of behav-iour change was probably not exhaustive. Indeed, Michieet al. (41) recently published another taxonomy in whichmore techniques are listed. It may be possible that sometechniques used in the studies included were not listed in thepresent review. Also, given that the description of the inter-vention was frequently incomplete or unclear, other tech-niques could have been missed. However, this was a firstattempt to apply this new taxonomy to a systematic reviewamong overweight/obese individuals. Finally, most of thestudies relied on subjective physical activity assessments toevaluate the impact of their interventions. Consequently,between-group effects might have been overshadowedbecause of the lack of power of self-report instruments todetect small effect size.
Recommendations for future studies
Based on this systematic review, a few recommendationscould be made. First, more evaluation studies of long-termeffect of interventions (i.e. after all the intervention con-tacts ceased) are needed to gain better insight into thelong-term efficacy of modifying physical activity. Second, toincrease the likelihood of developing more effective inter-ventions, researchers should isolate targeted theoreticalconstructs and, more importantly, techniques in theirexperimental conditions to evaluate the specific contribu-tion of these variables. In the same way, they should payparticular attention to carefully selecting and describing thetheoretical techniques adopted to change key theoreticalconstructs. Presently, taxonomies developed by Abrahamand Michie (19) and Michie et al. (41) could help research-ers select the most appropriate techniques. Also, targetedtheoretical variables should be assessed in order to performmediation analysis (51). Finally, researchers should try totest the effectiveness of alternative social cognitive modelshaving good predictive validity such as the Theory ofPlanned Behaviour (42) and the Self-Determination Theory(52). Likewise, strategies such as implementation intentionsdeserve more attention, considering their estimated largeeffect size in changing health-related behaviours (53).
Conflict of Interest Statement
No conflict of interest was declared.
Acknowledgement
The first author is supported by a grant from the CanadianInstitute of Health Research
References
1. Katzmarzyk PT, Janssen I. The economic costs associated withphysical inactivity and obesity in Canada: an update. Can J ApplPhysiol 2004; 29: 90–115.2. Lau DC, Douketis JD, Morrison KM, Hramiak IM, SharmaAM, Ur E. The obesity Canada clinical practice guidelines expertpanel. 2006 Canadian clinical practice guidelines on the manage-ment and prevention of obesity in adults and children. CMAJ2006; 176: 1–117.3. NHLBI Obesity Education Initiative Expert Panel. The practi-cal guide to the identification, evaluation and treatment of over-weight and obesity in adults. NIH, NHLBI, NAASO; 2000.4. Shaw K, O’Rourke P, Del Mar C, Kenardy J. Psychologicalinterventions for overweight or obesity. Cochrane Database SystRev 2005; 2: CD003818.5. Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, StearnsSC, Smith WC, Jung RT, Campbell MK, Grant AM. Systematicreview of the long-term effects and economic consequences oftreatments for obesity and implications for health improvement.Health Technol Assess 2004; 8: 1–182.
obesity reviews Physical activity and overweight/obese adults A. Bélanger-Gravel et al. 437
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439

6. Dishman RK. Increasing and maintaining exercise and physicalactivity. Behav Ther 1991; 22: 345–378.7. Marcus BH, Williams DM, Dubbert PM, Sallis JF, King AC,Yancey AK, Franklin BA, Buchner D, Daniels SR, Claytor RP.Physical activity intervention studies: what we know and what weneed to know: a scientific statement from the American HeartAssociation Council on Nutrition, Physical Activity, and Metabo-lism (Subcommittee on Physical Activity); Council on Cardiovas-cular Disease in the Young; and the Interdisciplinary WorkingGroup on Quality of Care and Outcomes Research. Circulation2006; 114: 2739–2752.8. Wing RR. Behavioral approaches to the treatment of obesity.In: Bray GA, Bouchard C (eds). Handbook of Obesity. MarcelDekker, Inc: New York, 2004, 147–167.9. Hardeman W, Griffin S, Johnston M, Kinmonth AL, WarehamNJ. Interventions to prevent weight gain: a systematic review ofpsychological models and behaviour change methods. Int J ObesRelat Metab Disord 2000; 24: 131–143.10. Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH,Powell KE, Stone EJ, Rajab MW, Corso P. The effectiveness ofinterventions to increase physical activity. A systematic review. AmJ Prev Med 2002; 22: 73–107.11. Dishman RK, Buckworth J. Increasing physical activity: aquantitative synthesis. Med Sci Sports Exerc 1996; 28: 706–719.12. Buckworth J, Dishman RK. Exercise adherence. In: Tenen-baum G, Eklund RC (eds). Handbook of Sport Psychology. JohnWiley & Sons Inc.: Hoboken, NJ, 2007, pp. 509–536.13. Michie S, Abraham C. Interventions to change health behav-iours: evidence-based or evidence-inspired? Psychol Health 2004;19: 29–49.14. Bartholomew LK, Parcel GS, Kok G, Gottlieb NH. PlanningHealth Promotion Programs: An Intervention Mapping Approach.John Wiley & Sons, Inc: San Francisc, CA, 2006.15. Norman P, Conner M. Predicting and changing health behav-iour: future directions. In: Conner M, Norman P (eds). PredictingHealth Behaviour, 2nd edn. Open University Press: Maidenhead,2005, 324–371.16. Baranowski T, Cerin E, Baranowski J. Steps in the design, de-velopment and formative evaluation of obesity prevention-relatedbehavior change trials. Int J Behav Nutr Phys Act 2009; 6: 6.17. Metropolitan Life Insurance Company. New weight standardsfor men and women. Stat Bull 1959; 40: 1–5.18. American College of Sport Medicine. Acsm’s ResourceManual for Guidelines for Exercise Testing and Prescription, 6thedn. Lippincott Williams & Wilkins: Baltimore, MD, 2010.19. Abraham C, Michie S. A taxonomy of behavior change tech-niques used in interventions. Health Psychol 2008; 27: 379–387.20. Baum JG, Clark HB, Sandler J. Preventing relapse in obesitythrough posttreatment maintenance systems: comparing the rela-tive efficacy of two levels of therapist support. J Behav Med 1991;14: 287–302.21. Carels RA, Darby LA, Cacciapaglia HM, Douglass OM.Reducing cardiovascular risk factors in postmenopausal womenthrough a lifestyle change intervention. J Womens Health(Larchmt) 2004; 13: 412–426.22. Dallow CB, Anderson J. Using self-efficacy and a transtheo-retical model to develop a physical activity intervention for obesewomen. Am J Health Promot 2003; 17: 373–381.23. James JE, May Hampton BA. The relative efficacy of directiveand nondirective treatment in behavioral weight control. BehavTher 1982; 13: 463–475.24. Kreuter MW, Oswald DL, Bull FC, Clark EM. Are tailoredhealth education materials always more effective than non-tailoredmaterials? Health Educ Res 2000; 15: 305–315.
25. Leermakers EA, Perri MG, Shigaki CL, Fuller PR. Effects ofexercise-focused versus weight-focused maintenance programs onthe management of obesity. Addict Behav 1999; 24: 219–227.26. Rapoport L, Clark M, Wardle J. Evaluation of a modifiedcognitive-behavioural programme for weight management. Int JObes Relat Metab Disord 2000; 24: 1726–1737.27. Riebe D, Blissmer B, Greene G, Caldwell M, Ruggiero L,Stillwell KM, Nigg CR. Long-term maintenance of exercise andhealthy eating behaviors in overweight adults. Prev Med 2005; 40:769–778.28. Sbrocco T, Nedegaard RC, Stone JM, Lewis EL. Behavioralchoice treatment promotes continuing weight loss: preliminaryresults of a cognitive-behavioral decision-based treatment forobesity. J Consult Clin Psychol 1999; 67: 260–266.29. Tudor-Locke C, Bell RC, Myers AM, Harris SB, EcclestoneNA, Lauzon N, Rodger NW. Controlled outcome evaluation ofthe First Step Program: a daily physical activity intervention forindividuals with type II diabetes. Int J Obes Relat Metab Disord2004; 28: 113–119.30. Wing RR, Epstein LH, Nowalk MP, Koeske R, Hagg S. Behav-ior change, weight loss, and physiological improvements in type IIdiabetic patients. J Consult Clin Psychol 1985; 53: 111–122.31. Decker EB. Physician Interventions Combined with aPedometer-Driven Walking Program to Increase Physical Activity[M.S.]. Utah State University: Logan, UT, 2007.32. Berry D, Savoye M, Melkus G, Grey M. An intervention formultiethnic obese parents and overweight children. Appl Nurs Res2007; 20: 63–71.33. Craighead LW, Blum MD. Supervised exercise in behavioraltreatment for moderate obesity. Behav Ther 1989; 20: 49–59.34. Mathieu CL. Self-concept and weight loss maintenance amongAfrican American women [Ph.D.]. United States – California:University of California, Los Angeles; 2005.35. Ash S, Reeves M, Bauer J, Dover T, Vivanti A, Leong C,Sullivan TO, Capra S. A randomised control trial comparing lif-estyle groups, individual counselling and written information inthe management of weight and health outcomes over 12 months.Int J Obes (Lond) 2006; 30: 1557–1564.36. Burke V, Mansour J, Beilin LJ, Mori TA. Long-term follow-upof participants in a health promotion program for treated hyper-tensives (ADAPT). Nutr Metab Cardiovasc Dis 2008; 18: 198–206.37. Dubbert PM, Wilson GT. Goal-setting and spouse involve-ment in the treatment of obesity. Behav Res Ther 1984; 22: 227–242.38. Albarracin D, Gillette JC, Earl AN, Glasman LR, DurantiniMR, Ho MH. A test of major assumptions about behavior change:a comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic.Psychol Bull 2005; 131: 856–897.39. Burke V, Beilin LJ, Cutt HE, Mansour J, Mori TA. Modera-tors and mediators of behaviour change in a lifestyle program fortreated hypertensives: a randomized controlled trial (ADAPT).Health Educ Res 2008; 23: 583–591.40. Lewis BA, Marcus BH, Pate RR, Dunn AL. Psychosocialmediators of physical activity behavior among adults and children.Am J Prev Med 2002; 23: 26–35.41. Michie S, Johnston M, Francis J, Hardeman W, Eccles M.From theory to intervention: mapping theoretically derived behav-ioural determinants to behaviour change techniques. Appl PsycholInt Rev 2008; 57: 660–680.42. Ajzen I. The theory of planned behavior. Organ Behav HumDecis Process 1991; 50: 179–211.43. Baranowski T, Cullen KW, Nicklas T, Thompson D, Bara-nowski J. Are current health behavioral change models helpful in
438 Physical activity and overweight/obese adults A. Bélanger-Gravel et al. obesity reviews
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439
guiding prevention of weight gain efforts? Obes Res 2003; 11(Suppl.): 23S–43S.44. Hagger MS, Chatzisarantis NLD, Biddle SJH. A meta-analyticreview of the theories of reasoned action and planned behavior inphysical activity: predictive validity and the contribution of addi-tional variables. J Sport Exerc Psychol 2002; 24: 3–32.45. Hausenblas HA, Carron AV. Application of the theories ofreasoned action and planned behavior to exercise behavior: ameta-analysis. J Sport Exerc Psychol 1997; 19: 36–51.46. Godin G, Amireault S, Belanger-Gravel A, Vohl MC, PerusseL. Prediction of leisure-time physical activity among obese indi-viduals. Obesity (Silver Spring) 2009; 17: 706–712.47. Fitzsimons GJ, Williams P. Asking questions can changechoice behavior: does it do so automatically or effortfully? J ExpPsychol Appl 2000; 6: 195–206.48. van Sluijs EM, van Poppel MN, Twisk JW, van Mechelen W.Physical activity measurements affected participants’ behavior in arandomized controlled trial. J Clin Epidemiol 2006; 59: 404–411.49. Williams P, Block LG, Fitzsimons GJ. Simply asking questionsabout health behaviors increases both healthy and unhealthybehaviors. Soc Infl 2006; 1: 117–127.50. Godin G, Sheeran P, Conner M, Germain M. Asking ques-tions changes behavior: mere measurement effects on frequency ofblood donation. Health Psychol 2008; 27: 179–184.51. MacKinnon D. Introduction to Statistical Mediation Analysis.Taylor & Francis Group, LLC: New York, 2008.52. Ryan RM, Deci EL. Self-determination theory and the facili-tation of intrinsic motivation, social development, and well-being.Am Psychol 2000; 55: 68–78.53. Gollwitzer PM, Sheeran P. Implementation intentions andgoal achievement: a meta-analysis of effects and processes. In:Mark PZ (ed.). Advances in Experimental Social Psychology.Academic Press: Waterloo, ON, 2006, 69–119.54. Burke V, Beilin LJ, Cutt HE, Mansour J, Williams A, MoriTA. A lifestyle program for treated hypertensives improved health-related behaviors and cardiovascular risk factors, a randomizedcontrolled trial. J Clin Epidemiol 2007; 60: 133–141.55. Burke V, Beilin LJ, Cutt HE, Mansour J, Wilson A, Mori TA.Effects of a lifestyle programme on ambulatory blood pressure anddrug dosage in treated hypertensive patients: a randomized con-trolled trial. J Hypertens 2005; 23: 1241–1249.56. Burke V, Mansour J, Mori TA, Beilin LJ, Cutt HE, Wilson A.Changes in cognitive measures associated with a lifestyle programfor treated hypertensives: a randomized controlled trial (ADAPT).Health Educ Res 2008; 23: 202–217.57. Riebe D, Greene GW, Ruggiero L, Stillwell KM, Blissmer B,Nigg CR, Caldwell M. Evaluation of a healthy-lifestyle approachto weight management. Prev Med 2003; 36: 45–54.
Supporting Information
Additional Supporting Information may be found in theonline version of this article:
Table S1. Glossary of technical terms and expressions usedin the systematic review.Table S2. Characteristics of the studies included andprincipal results of the interventions on physical activityparticipation.Table S3. Theoretical characteristics of the studies includedand principal results of the intervention on theoreticalvariables.
Please note: Wiley-Blackwell is not responsible for thecontent or functionality of any supporting materials sup-plied by the authors. Any queries (other than missing mate-rial) should be directed to the corresponding author for thearticle.
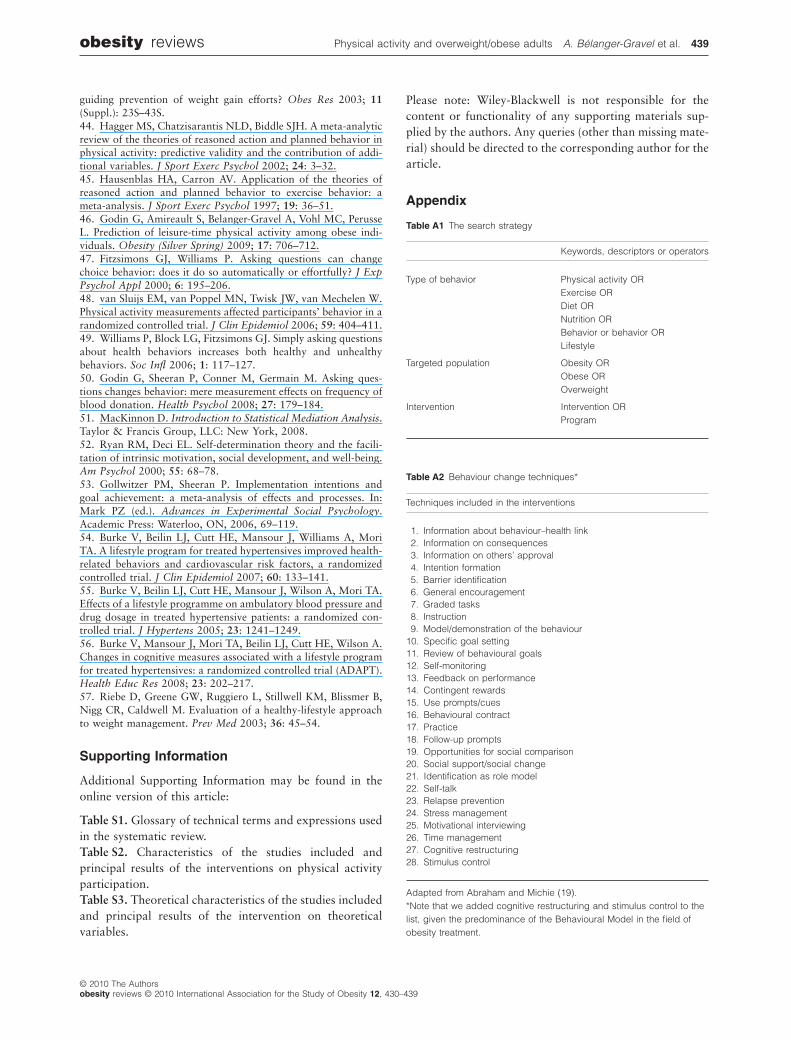
Appendix
Table A1 The search strategy
Keywords, descriptors or operators
Type of behavior Physical activity ORExercise ORDiet ORNutrition ORBehavior or behavior ORLifestyle
Targeted population Obesity ORObese OROverweight
Intervention Intervention ORProgram
Table A2 Behaviour change techniques*
Techniques included in the interventions
1. Information about behaviour–health link2. Information on consequences3. Information on others’ approval4. Intention formation5. Barrier identification6. General encouragement7. Graded tasks8. Instruction9. Model/demonstration of the behaviour
10. Specific goal setting11. Review of behavioural goals12. Self-monitoring13. Feedback on performance14. Contingent rewards15. Use prompts/cues16. Behavioural contract17. Practice18. Follow-up prompts19. Opportunities for social comparison20. Social support/social change21. Identification as role model22. Self-talk23. Relapse prevention24. Stress management25. Motivational interviewing26. Time management27. Cognitive restructuring28. Stimulus control
Adapted from Abraham and Michie (19).*Note that we added cognitive restructuring and stimulus control to thelist, given the predominance of the Behavioural Model in the field ofobesity treatment.
obesity reviews Physical activity and overweight/obese adults A. Bélanger-Gravel et al. 439
© 2010 The Authorsobesity reviews © 2010 International Association for the Study of Obesity 12, 430–439
Top Related
Copyright © 2022 FDOKUMEN

