






Bahasa
Halaman
Hukum


I
UNIVERSIDAD REY JUAN CARLOS
FACULTAD DE CIENCIAS DE LA SALUD
TESIS DOCTORAL
Aspectos neurofisiológicos y biomecánicos de la región
cervical sobre el dolor cérvico-craneofacial:
Implicaciones del tratamiento y el diagnóstico
Departamento Bioquímica, Fisiología y Genética Molecular, Farmacología y
Nutrición, Anatomía y Embriología Humana e Histología Humana y Anatomía
Patológica
Roy La Touche Arbizu
MADRID, 2014

II

Facultad de Ciencias de la Salud Departamento de Bioquímica, Fisiología y Genética Molecular,
Farmacología y Nutrición, Anatomía y Embriología Humana e Histología Humana y Anatomía Patológica
III Avda. de Atenas s/n E 28922 Alcorcón Madrid España Tel. 34 91 4888855 Fax 34 91 4888831
Don Carlos Goicoechea García, Profesor Titular de Farmacología del Dpto. de
Bioquímica, Fisiología y Genética Molecular, Farmacología y Nutrición, Anatomía y
Embriología Humana e Histología Humana y Anatomía Patológica y D. Josué
Fernández Carnero, Profesor Colaborador del Dpto. de Fisioterapia, Terapia
Ocupacional, Rehabilitación y Medicina Física de la Universidad Rey Juan Carlos,
CERTIFICAN:
Que el Trabajo de investigación titulado “Aspectos neurofisiológicos y biomecánicos
de la región cervical sobre el dolor cérvico-craneofacial: Implicaciones del tratamiento
y el diagnóstico” ha sido realizado por Don. Roy La Touche Arbizu (D.N.I.: 50349803
C) bajo nuestra supervisión y dirección y cumple con los requisitos necesarios para
optar al grado de Doctor.
Y para que así conste a los efectos oportunos, firmamos el presente certificado en
Madrid, a 3 de Noviembre de 2014
Fdo. D. C. Goicoechea García Fdo. D. J. Fernández-Carnero

IV

V
A mis papás, Hilda y Melvin por su amor incondicional, esfuerzo constante y sacrificios
realizados durante toda la vida para que yo pudiera llegar hasta aquí, sin ellos este
proyecto no se hubiera podido realizar, gracias por ser mi ejemplo de vida y por las
enseñanzas en torno al esfuerzo, la perseverancia y la paciencia
A mis 5 hermanos y a todos mis sobrinos por estar ahí y comprender mi ausencia en
momentos importantes, a pesar de la distancia siempre están en mi mente y en mi
corazón

VI

VII
AGRADECIMIENTOS
Este proyecto al que he dedicado tiempo y esfuerzo, no se hubiera podido
concluir sin la inestimable ayuda y colaboración de muchas personas que han aportado
sus esfuerzos desinteresadamente en las investigaciones que conforman esta tesis, a
todos ellos quisiera expresarles mi más sincera gratitud.
En mi primer lugar quisiera agradecer a mis dos directores de tesis, el Dr. Carlos
Goicoechea García y el Dr. Josué Fernández Carnero por su ayuda y orientación durante
la elaboración de este trabajo.
Al Dr. Carlos Goicochea García quisiera agradecerle especialmente la
motivación que me ofreció para realizar la tesis una vez que terminé el Máster en
Estudio y Tratamiento del Dolor que él dirigía. Tanto el Dr. Carlos Goicochea como
Dra. Mª Isabel Martín Fontelles y todo su equipo han sido referentes para mí por su
dedicación, rigurosidad, humildad y vocación en la investigación del tratamiento del
dolor. Conocerles y que hayan sido mis profesores ha sido un privilegio que me ha
ayudado a orientar mi actividad investigadora y profesional. Siempre estaré agradecido
con ellos…
Al Dr. Josué Fernández Carnero tengo muchas cosas que agradecerle y algunas
van más allá de este mismo proyecto. Durante todos los años que he tardado en finalizar
este proyecto Josué siempre ha estado detrás de cada paso que di, aportando nuevas
ideas, motivándome y dedicando toda su capacidad y conocimiento en cada una de las
investigaciones. Para mí es un premio haberle conocido y poder establecer una
verdadera relación de amistad, tengo el orgullo de decir que además de conseguir
terminar la tesis he conseguido un gran amigo. Gracias al profesor, gracias al tutor y
sobre todo gracias al amigo que has sido durante estos años.

VIII
Haciendo una retrospectiva de lo que han sido estos años y el proceso para llegar
a conseguir este proyecto, tengo que reconocer que hay personas que han facilitado mi
adaptación a un país diferente al mío, pero el que considero un gran país del cual ya
formo parte, y en este sentido quiero agradecer especialmente al Dr. José Antonio
Martín Urrialde de la Universidad San Pablo CEU, quien me tendió una mano
desinteresadamente y me ayudó en todo momento para venir y estar en España y
conseguir finalmente este sueño. Muchas gracias por todo y más…
Hay varios profesores e investigadores de reconocido prestigio internacional que
han participado en algunas de las investigaciones de esta tesis, quiero agradecer su
colaboración al Dr. Mariano Rocabado Seaton de la Universidad Andrés Bello de Chile,
al Dr. Jeffrey Mannheimer de Columbia University de Estados Unidos de América, al
Dr. Harry Von Piekartz de la University of Applied Science Osnabruck de Alemania y
al Dr. Mark Bishop de la University of Florida de Estados Unidos de América.
Agradezco a mis compañeros y amigos del grupo de investigación Motion in
Brains de CSEU La Salle, los profesores Joaquín Pardo, Alfonso Gil, Ibai López de
Uralde y Héctor Beltrán por su colaboración en las últimas investigaciones de esta tesis.
Quiero agradecer a mi amigo el profesor Santiago Angulo Díaz-Parreño de la
Universidad San Pablo CEU por su ayuda y enseñanzas entorno al tratamiento y análisis
estadístico, su aporte a las investigaciones de esta tesis es incalculable. Muchas gracias
amigo por tu conocimiento, dedicación y amistad…
Si el título de doctor se pudiera compartir yo lo haría con mi pareja Alba París,
ella ha sido mi punto de apoyo en todo momento, ha entendido mi dedicación a la
investigación y ha estado implicada en todas los estudios que conforman esta tesis, su
aporte e implicación científica ha sido excepcional y sus palabras de motivación, su

IX
amor y cariño han sido suficientes para seguir adelante cuando se presentaron las
dificultades. Gracias mi vida por todo y porque cada día es único a tu lado…
A mis cinco hermanos, John, Vivian, Marco, Mayela y Dennis, y todos mis
sobrinos a los que amo mucho y añoro a diario, quiero dedicar esta tesis. Ellos han
sabido comprender mis muchas ausencias en momentos especiales en los que aunque
hubiera querido estar no me ha sido posible, sé que ellos se alegran de los éxitos que he
podido conseguir y yo me alegro de que sean mi familia del cual estoy muy orgulloso
de cada uno de ellos.
Finalmente quiero dedicar este proyecto a mis papás Hilda y Melvin que son
personas excepcionales, bondadosas, esforzadas a las cuales yo tengo una gran
admiración. Ambos con sus actos me han enseñado lecciones de vida impagables, son
pocas las palabras de gratitud que podría escribir en estas frases para expresar mi
profundo agradecimiento, todo y cada una de las cosas he podido conseguir se lo debo a
ellos.
Mi mamá lamentablemente no ha podido ver concluida esta fase profesional que
finalizo con esta tesis, a pesar de esto, en su memoria he querido darle este pequeño
homenaje que en su día le hice la promesa que lo finalizaría con el máximo esfuerzo.
Ella me apoyó en todo momento, sobre todo en los momentos difíciles y me arropó con
sus palabras de amor constantes. Gracias Mami te recuerdo todos los días y te voy a
querer siempre, esto es para ti…
A mi papá Melvin le debo muchas cosas, su vida es ejemplar y ha estado dedicada al
esfuerzo y trabajo por sus seis hijos, su vida es ejemplo de lucha diaria y en todo
momento, sea cual sea la adversidad. La honradez, la dignidad, la constancia y el
esfuerzo son principios que he podido aprender de mi papá, estos me han servido para
entender que el camino hacia un objetivo no siempre es fácil y que las metas no son lo
X
más importante sino el esfuerzo que dediques a ello. Gracias Papi por todo, te quiero
mucho y esto para ti…
En toda investigación clínica los pacientes son determinantes y sin duda alguna
lo más importante, quiero agradecer a todos los pacientes que amablemente accedieron
a participar en los estudios que conforman esta tesis, espero que el conocimiento que
hemos generado sirva de alguna manera para mejorar la atención que reciban o en
motivar a otros investigadores que continúen con estas líneas. Gracias a todos los
pacientes con dolor craneofacial, muchas gracias…

XI
ÍNDICE GENERAL
RESUMEN…………………………………………………………………………...XV
Lista de publicaciones originales………………………………………………...…XIX
Abreviaturas………………………………………………………………..…...…..XXI
1. INTRODUCCIÓN…………………………………………………………………..1
1.1 Aspectos Básicos del Dolor…………………………………………………....2
1.1.1 Proceso de sensibilización periférica………………………………….....4
1.1.2 Proceso de sensibilización central…………………………………….....6
1.2 Dolor Musculoesquelético Crónico…………………………………………...7
1.2.1 Epidemiología…………………………………………………………....7
1.3 Dolor Cervical Crónico………………………………………………………..8
1.3.1 Epidemiología…………………………………………………………..10
1.4 Dolor Craneofacial de Origen Musculoesquelético……………….………..12
1.4.1 Trastornos craneomandibulares………………………………………...12
1.4.2 Epidemiología…………………………………………………………..14
1.4.3 Epidemiología y comorbilidad entre trastornos craneomandibulares,
cefalea y dolor de cuello………………………………………………..16
1.5 Dolor Referido de la Región Cervical hacia la Región
Craneofacial…………………………………………………………………..18
1.6 Aspectos Anatomofuncionales de la Región Craneomandibular y la Región
Craneocervical………………………………………………………………..20
1.6.1 Modelos biomecánicos de la región craneomandibular/craneocervical..21
1.6.2 Estudios in-vivo de la relación craneomandibular/craneocervical……..23
1.6.3 Influencia de la región craneocervical sobre la dinámica mandibular…23
XII
1.6.4 Sinergias neuromusculares cervicales y masticatorias…………….……24
1.6.5 Cinemática y concomitancia craneocervical/craneomandibular………..27
1.7 Neurofisiología del Dolor Cérvico-craneofacial…………………………….28
1.7.1 Sistema sensorial trigeminal…………………………………………....29
1.7.2 Neuroanatomía de los segmentos cervicales superiores………………..35
1.7.3 Complejo trigeminocervical…………………………………………....37
1.7.4 Sensibilización del complejo trigeminocervical………………………..39
1.8 Modulación del Dolor en el Complejo Trigeminocervical…………………41
1.8.1 Influencia de las aplicaciones terapéuticas sobre el dolor craneofacial..43
2. JUSTIFICACIÓN DEL TRABAJO REALIZADO……………………………..47
3. OBJETIVOS……………………………………………………………….……….51
4. MATERIAL Y MÉTODOS……………………………………………………….57
4.1 Participantes……………………………………………………………….….60
4.2 Variables y Pruebas de Medición…………………………………………....62
4.2.1 Medidas de auto-registro…………………………………………….64
4.2.2 Instrumentos de medición…………………………………………...66
4.3 Resumen de los Procedimientos……………………………………………..70
4.4 Análisis Estadístico…………………………………………………………...72
5. RESULTADOS…………………………………………………………………….77
5.1 Estudio I…………………………………………………………………….....78
5.2 Estudio II……………………………………………………………………...87
5.3 Estudio III………………………………………………...………….……...114
5.4 Estudio IV…………………………………………………………………....123
5.5 Estudio V………………………………………………………………….…138
5.6 Estudio VI………………………………………………………………..…..182
XIII
5.7 Estudio VII……………………………………………………………..……192
6. DISCUSIÓN………………………………………………………………………205
6.1 Diferencias de Género en las Variables Somatosensoriales………….…...207
6.2 Postura Craneocervical, Dinámica Mandibular y
Dolor Craneocervical……………………………………………….………208
6.3 Influencia del Dolor y la Discapacidad Cervical sobre la Actividad
Sensoriomotora Trigeminal………………………………………………...209
6.4 Asociación entre la Discapacidad Cervical y la Discapacidad
Craneofacial/craneomandibular…………………………………………...213
6.5 Factores Bioconductuales Implicados en las Alteraciones Sensoomotoras
Trigeminales y la Discapacidad Craneofacial……………………………..213
6.6 Efecto del Tratamiento en la Región Cervical
sobre el Dolor Craneofacial…………………………………….…………..218
6.7 Implicaciones Científicas y Clínicas………………………………………..219
6.8 Limitaciones y Futuras Investigaciones…………………………………....222
7. CONCLUSIONES……………………………………………………………..…225
8. BIBLIOGRAFÍA………………………………………………………………....229

XIV

XV
RESUMEN
Introducción: El dolor craneofacial (DCF) de origen musculoesquelético, representa la
causa más común de DCF de origen no dental y puede afectar a la musculatura
masticatoria, la articulación temporomandibular y otras estructuras orofaciales. Entre
los diferentes tipos de DCF de origen musculoesquelético el más prevalente son los
denominados trastornos craneomandibulares (TCM) atribuidos o relacionados con el
dolor miofascial. Diversos estudios han descrito la presencia de comorbilidades entre la
cefalea, el dolor de cuello y los TCM, además se ha comprobado que el dolor de cuello
se asocia significativamente con los TCM y que la gravedad de estos se incrementa con
la gravedad del dolor de cuello. Evidencia científica reciente sugiere la existencia de
mecanismos neurofisiológicos trigeminocervicales implicados en las alteraciones
motoras craneomandibulares y en el DCF, a pesar de esto se necesitan más estudios
clínicos que aporten información más precisa en cuanto a la posible repercusión clínica
de características sensoriales y motoras cervicales que afectan a pacientes con DCF.
Objetivo general: Determinar la influencia biomecánica y neurofisiológica de la región
cervical sobre la discapacidad y el DCF, además se pretende identificar como
determinados factores bioconductuales influyen sobre la función craneomandibular, la
discapacidad y el DCF.
Métodos: Se realizaron 4 estudios transversales, un estudio de casos y controles, una
serie de casos y un ensayo clínico aleatorio controlado que incluyeron a pacientes con
dolor de cuello crónico mecánico, pacientes con TCM atribuido a dolor miofascial,
pacientes con dolor cérvico-craneofacial (DCCF) y pacientes con cefalea atribuida a
TCM. En tres de los estudios se realizaron comparaciones con sujetos asintomáticos.
En los estudios se evaluaron características sensoriales, motoras y factores psicológicos
implicados en el DCF mediante:

XVI
- Medidas de auto-registro psicológicas, de dolor y discapacidad (inventario de
dolor y discapacidad craneofacial, IDD-CF; índice de dolor de cuello, IDC;
inventario de depresión BECK, BDI; escala de catastrofismo ante el dolor, ECD;
escala tampa de kinesiofobia, TSK-11; Escala visual analógica del dolor, EVA;
escala visual analógica de la fatiga, EVAF).
- Mediciones de los umbrales de dolor a la presión (UDPs) en áreas trigeminales,
cervicales y extra-trigeminales mediante algometría digital.
- Medición de la máxima apertura interincisal (MAI) libre de dolor.
- Mediciones de la postura craneocervical.
En todos los estudios se realizó un análisis descriptivo e inferencial, y en algunos casos
se utilizaron análisis complementarios a los contrastes de significación como el tamaño
del efecto o el mínimo cambio detectable para determinar la relevancia clínica de los
resultados.
Resultados:
En la comparación de los resultados de los sujetos asintomáticos con respecto a los
pacientes se presentaron los siguientes hallazgos: 1) hay diferencias estadísticamente
significativas en la postura craneocervical en los pacientes con DCCF frente a los
sujetos asintomáticos, sin embargo estas diferencias son pequeñas; 2) Se identificó que
los pacientes con dolor de cuello crónico mecánico presentan hiperalgesia mecánica en
áreas trigeminales y cervicales pero no en otras áreas anatómicas a distancia; 3) Los
pacientes con cefalea atribuida a TCM con moderada discapacidad cervical presentaron
mayores niveles de dolor y fatiga masticatoria, y menores UDPS en áreas trigeminales y
cervicales y menor MAI libre de dolor. En las comparaciones intra-grupos se encontró
una fuerte correlación entre la discapacidad cervical y la discapacidad
craneofacial/craneomandibular en pacientes con TCM atribuido a dolor miofascial. Se

XVII
comprobó que distintas posturas craneocervicales inducidas experimentalmente
modifican la dinámica mandibular y alteran los UDPs de áreas trigeminales y
cervicales. Por otra parte, se identificó que el catastrofismo ante el dolor y la
kinesiofobia fueron predictores del estado funcional mandibular y de la discapacidad y
DCF. Finalmente, en los estudios en donde se realizó una intervención en pacientes con
TMC atribuido a dolor miofascial y en pacientes con DCCF se comprobó que el
ejercicio terapéutico en combinación de terapia manual o únicamente la aplicación de
terapia manual sobre la región cervical producen un efecto inmediato y a corto plazo en
la mejora MAI libre de dolor, una disminución de la intensidad de dolor y un aumento
de los UDPS en áreas trigeminales y cervicales.
Conclusiones:
Los resultados obtenidos en esta tesis sugieren la influencia de mecanismos
neurofisiológicos y biomecánicos de la región cervical sobre la función mandibular, las
alteraciones somatosensoriales en áreas trigeminales y sobre la discapacidad
craneofacial. Se ha demostrado que factores bioconductuales como el catastrofismo ante
el dolor y la kinesiofobia deben ser tomados en cuenta ya que son predictores de las
alteraciones funcionales craneomandibulares y el DCF. A nivel terapéutico se presentan
los primeros hallazgos sobre el efecto del tratamiento de fisioterapia específico sobre la
región cervical en la mejora de la dinámica mandibular y en la modulación del DCF.
Esta tesis aporta nuevos datos que pueden contribuir clínicamente al diagnóstico, la
valoración y el tratamiento de los TCM y el DCF.

XVIII

XIX
LISTA DE PUBLICACIONES ORIGINALES
Esta tesis está basada en las siguientes publicaciones originales que forman parte de una
línea de investigación que estudia los mecanismos neurofisiológicos, biomecánicos y
bioconductuales de la región cervical en pacientes con dolor craneofacial, las cuales se
presentan de forma completa en el apartado de resultados. En diferentes apartados del
texto se hace referencia a las publicaciones originales mediante números romanos:
I. La Touche R, París-Alemany A, von Piekartz H, Mannheimer JS,
Fernández-Carnero J, Rocabado M. The influence of cranio-cervical posture
on maximal mouth opening and pressure pain threshold in patients with
myofascial temporomandibular pain disorders. Clin J Pain. 2011
Jan;27(1):48-55
II. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A,
Angulo-Díaz-Parreño S, La Touche R. Reliability, Standard Error, and
Minimal Detectable Change of Two Tests for Craniocervical Posture
Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial Pain
Patients. (En revisión).
III. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-
Parreño S, Paris-Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain
sensitivity over the trigeminal region in patients with chronic mechanical
neck pain. J Pain. 2010 Mar;11(3):256-63
IV. La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-
Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero J.
Craniofacial pain and disability inventory (CF-PDI): development and

XX
psychometric validation of a new questionnaire. Pain Physician. 2014 Jan-
Feb;17(1):95-108.
V. La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-
Díaz-Parreño S, Fernández-Carnero J. The Influence of Neck Disability and
Pain Catastrophizing about Trigeminal Sensory-Motor System in Patients
with Headache Attributed to Temporomandibular Disorders. (En revision)
VI. La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K,
Angulo-Díaz-Parreño S, Paris-Alemany A, Cleland JA. The effects of
manual therapy and exercise directed at the cervical spine on pain and
pressure pain sensitivity in patients with myofascial temporomandibular
disorders. J Oral Rehabil. 2009 Sep;36(9):644-52.
VII. La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S,
Bishop MD, Lopéz-Valverde-Centeno A, von Piekartz H, Fernández-
Carnero J. Does mobilization of the upper cervical spine affect pain
sensitivity and autonomic nervous system function in patients with cervico-
craniofacial pain?: A randomized-controlled trial. Clin J Pain. 2013
Mar;29(3):205-15.

XXI
ABREVIATURAS
ATM Articulación temporomandibular
BDI Inventario de depresión Beck
CP Conductancia de la piel
CTC Complejo trigeminocervical
DCCF Dolor cérvico-craneofacial
DCF Dolor craneofacial
DMC Dolor musculoesquelético crónico
ECD Escala de catastrofismo ante el dolor
EMG Electromiografía
END Escala numérica del dolor
ETCM Ejercicio terapéutico de control motor
EVA Escala visual analógica del dolor
EVAF Escala visual analógica de fatiga
FC Frecuencia cardíaca
FR Frecuencia respiratoria
GC Grupo control
GE Grupo experimental
HIT-6 Cuestionario de impacto de la cefalea
IDC Índice de dolor cervical
IDD-CF Inventario de dolor y discapacidad craneofacial
MAI Máxima apertura interincisal
MC Migraña crónica
ME Migraña episódica
XXII
MIAD Modelo integrado de adaptación al dolor
NE Neuronas nociceptivas específicas
NMDA N-metil-D-aspartato
PMG Puntos gatillos miofasciales
RDA Neuronas de rango dinámico amplio
SDM Síndrome de dolor miofascial
STAI Cuestionario de ansiedad estado-rasgo
SVc Sub-núcleo trigeminal caudal
SVi Sub-núcleo trigeminal interpolar
SVo Sub-núcleo trigeminal oral
TC Temperatura cutánea.
TCM Trastornos craneomandibulares
TMO Terapia manual ortopédica
TSK-11 Escala de Tampa de Kinesiofobia
UDP Umbral de dolor a la presión
VPM Núcleo ventral posteromedial del tálamo

1
INTRODUCCIÓN

2
1. INTRODUCCIÓN
1.1 Aspectos Básicos del Dolor
En el modelo biomédico general, el dolor ha sido considerado como un síntoma
producido por un daño tisular, de manera que la experiencia de dolor se ha
simplificado a que, si no había daño no había dolor, si había daño tendría que
haber dolor y a mayor daño mayor dolor. El conocimiento sobre el dolor
evolucionó a partir de la compresión del procesamiento neurofisiológico del dolor
a nivel medular. Melzack y Wall (Melzack and Wall, 1965) tuvieron una
destacada labor en esta cuestión al proponer la teoría de la regulación del umbral
también conocida como la teoría de la puerta de entrada, básicamente esta teoría
explicaba el mecanismo en que el dolor estaba representado neuralmente en el asta
dorsal de la médula espinal, donde se podía facilitar o inhibir la puerta de entrada
de estímulos dolorosos hacia centros superiores. Esta teoría cobró mucha
importancia hace unas décadas a pesar de no poder explicar fisiológicamente la
situación del dolor crónico (Melzack, 1993), sin embargo lo que si permitió fue la
consideración de los factores psicológicos como parte integral del procesamiento
del dolor.
La teoría de regulación del umbral evolucionó hacia la teoría de la neuromatriz, en
esta se amplía el concepto del dolor integrando las influencias que puedan tener las
funciones cognitivas del cerebro, los sistemas de regulación del estrés y los
estímulos sensoriales (Melzack, 1999), además se expone que el dolor es una
experiencia multidimensional compuesta por la interacción de tres dimensiones:

3
- Dimensión sensorial-discriminativa: identifica, evalúa, valora y modifica
todos aquellos factores relacionados con la percepción sensorial del dolor
(intensidad, localización, cualidad, factores temporales y espaciales)
- Dimensión motivacional-afectiva: comporta el aspecto emocional del
dolor. En esta dimensión estarían implicadas estructuras troncoenfálicas y
límbicas.
- Dimensión cognitivo-evaluativa: analiza e interpreta el dolor en función de
la sensación y lo que puede ocurrir.
En la actualidad el dolor se mira desde la óptica del paradigma biopsicosocial, con
lo cual los factores fisiológicos, psicológicos y sociales son tomados en cuenta, así
lo muestra la descripción de dolor definida por la Asociación Internacional para el
Estudio del Dolor:
“Es una experiencia sensorial y emocional desagradable asociada a un daño
tisular real o potencial, o descrita en términos del daño” (Merskey and Bogduk,
1994).
Existen diversas clasificaciones del dolor basadas en el origen, la evolución, los
mecanismos fisiológicos y en la estructura anatómica implicada. Con frecuencia y
desde un punto de vista clínico el dolor musculoesquéletico se clasifica en agudo y
crónico, esta clasificación toma en cuenta la evolución del dolor desde el punto de
vista del tiempo y los aspectos neurofisiológicos relacionados con la génesis y el
mantenimiento.
El dolor agudo tiene un curso temporal relacionado con los procesos de reparación
(Chapman et al., 2011) y representa una señal de alarma disparada por los
sistemas protectores del organismo (Loeser and Treede, 2008). La ineficacia en el

4
tratamiento o en la recuperación del dolor agudo puede generar que este se
mantenga en el tiempo convirtiéndose en un dolor crónico y adquiriendo las
complicaciones que este presenta.
Se define el dolor crónico como “el que persiste más allá del tiempo normal de
reparación de los tejidos, que se supone en el dolor no maligno es de 3 meses…,
pero para fines de investigación se prefiere elegir un tiempo de 6 meses” (Merskey
y Bogduk, 1994). El tiempo (días, meses…) en el que se tiene dolor es el
parámetro más utilizado para definir la diferencia entre el dolor agudo y el dolor
crónico, esta clasificación tiene sus limitaciones teniendo en cuenta que el dolor
crónico presenta una naturaleza multifactorial (Turk and Rudy, 1988). En este
sentido Von Korff y Dunn (Von Korff and Dunn, 2008), han comprobado que un
modelo de clasificación de los pacientes basado en los niveles de discapacidad,
calidad vida, intensidad de dolor, síntomas depresivos y toma de medicamentos
tiene mayor valor predictivo que solo la clasificación basada en el tiempo de dolor
(Von Korff and Dunn, 2008).
1.1.1 Proceso de sensibilización periférica
Desde el punto de vista de la neurofisiología, el dolor agudo es considerado como
una respuesta sensorial de la activación del sistema nociceptivo a consecuencia de
un daño tisular que produce una respuesta inflamatoria que sensibiliza los
nociceptores periféricos (Loeser and Treede, 2008; Woolf, 2004); la
sensibilización se produce a consecuencia de la acción de mediadores químicos de
origen inflamatorio que se liberan en el área del daño tisular, tales como la
sustancia P y el péptido relacionado con el gen de la calcitonina que se liberan en
la periferia y se unen a otros mediadores como neutrófilos, mastocitos y basófilos;
esta unión produce a su vez la liberación de sustancias pro-inflamatorias

5
(citoquinas, bradiquinina, histamina) que favorecen la síntesis de la enzima
ciclooxigenasa-2 (COX-2) que conduce a la producción y secreción
de prostaglandinas (Woolf, 2004). Este mediador actúa como un sensibilizador
que altera la sensibilidad al dolor por el incremento de la capacidad de respuesta
de los nociceptores periféricos (Woolf, 2004).
La sensibilización periférica se define como un proceso en donde hay una
reducción del umbral y una amplificación de la capacidad de respuesta de los
nociceptores, que se produce cuando las terminales periféricas de las neuronas
sensoriales primarias de alto umbral están expuestos a mediadores de inflamación
en el tejido dañado (Chen et al., 1999; Guenther et al., 1999; Hucho and Levine,
2007).
Es un hecho más que contrastado que la sensibilización periférica contribuye a la
sensibilización del sistema nociceptivo y provoca dolor e hipersensibilidad en las
áreas en donde se produce inflamación (hiperalgesia primaria) (Latremoliere and
Woolf, 2009), este fenómeno representa una acción protectora del organismo con
el fin de evitar el uso de estructuras dañadas (Nijs et al., 2010). A la sensación
dolorosa que se extiende más allá del área de la lesión y abarca zonas no afectadas
por la lesión original, se la conoce como hiperalgesia secundaria, pero este no es
un proceso únicamente de carácter periférico, lleva implícitos mecanismos
centrales (Latremoliere and Woolf, 2009; Woolf, 2011).
El proceso de sensibilización periférica se asocia a una alteración en la
sensibilidad térmica, pero no se observa una alteración de la sensibilización
mecánica que parece ser una característica importante de la sensibilización central
(Latremoliere and Woolf, 2009; Woolf, 2004).
6
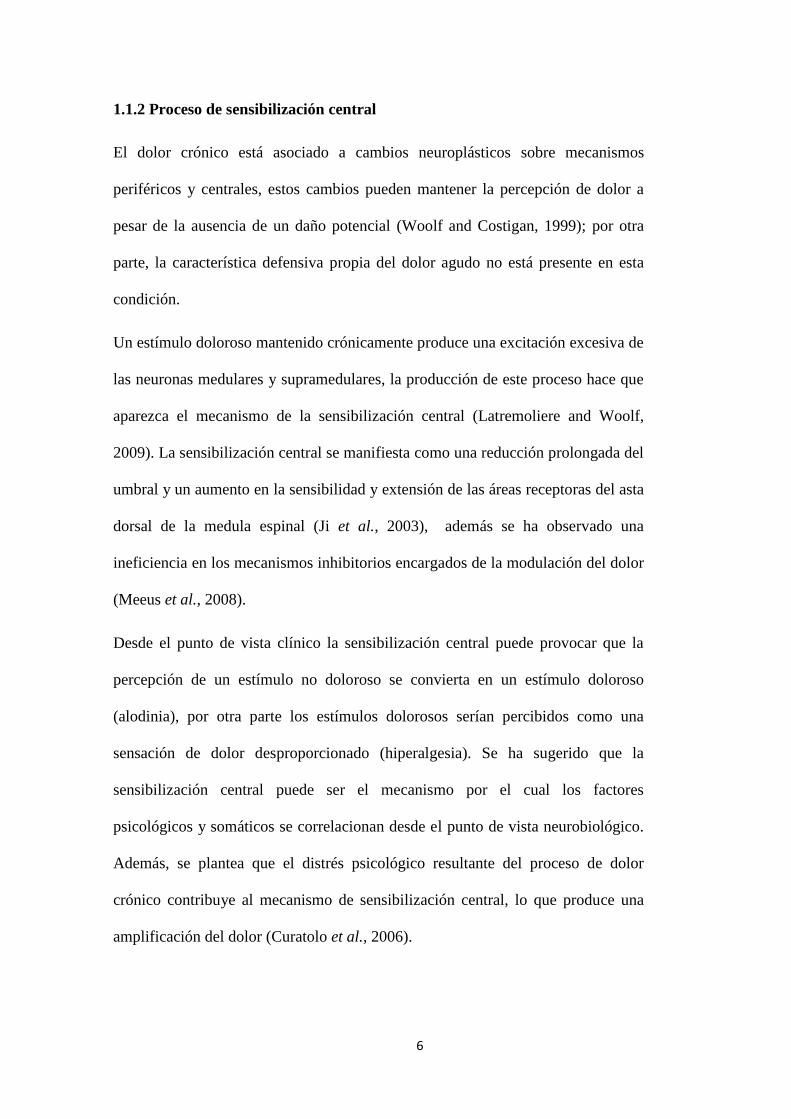
1.1.2 Proceso de sensibilización central
El dolor crónico está asociado a cambios neuroplásticos sobre mecanismos
periféricos y centrales, estos cambios pueden mantener la percepción de dolor a
pesar de la ausencia de un daño potencial (Woolf and Costigan, 1999); por otra
parte, la característica defensiva propia del dolor agudo no está presente en esta
condición.
Un estímulo doloroso mantenido crónicamente produce una excitación excesiva de
las neuronas medulares y supramedulares, la producción de este proceso hace que
aparezca el mecanismo de la sensibilización central (Latremoliere and Woolf,
2009). La sensibilización central se manifiesta como una reducción prolongada del
umbral y un aumento en la sensibilidad y extensión de las áreas receptoras del asta
dorsal de la medula espinal (Ji et al., 2003), además se ha observado una
ineficiencia en los mecanismos inhibitorios encargados de la modulación del dolor
(Meeus et al., 2008).
Desde el punto de vista clínico la sensibilización central puede provocar que la
percepción de un estímulo no doloroso se convierta en un estímulo doloroso
(alodinia), por otra parte los estímulos dolorosos serían percibidos como una
sensación de dolor desproporcionado (hiperalgesia). Se ha sugerido que la
sensibilización central puede ser el mecanismo por el cual los factores
psicológicos y somáticos se correlacionan desde el punto de vista neurobiológico.
Además, se plantea que el distrés psicológico resultante del proceso de dolor
crónico contribuye al mecanismo de sensibilización central, lo que produce una
amplificación del dolor (Curatolo et al., 2006).

7
1.2 Dolor Musculoesquelético Crónico
Se considera dolor musculoesquelético crónico (DMC) cuando el dolor se
mantiene entre 3 y 6 meses (Walsh et al., 2008). El DMC se producen alteraciones
neurales, somáticas, cognitivas y conductuales (Walsh et al., 2008), que generan
una disminución de la calidad de vida del paciente y de su desempeño laboral.
El dolor musculoesquelético es descrito usualmente por los pacientes como una
sensación firme y de presión, de características difusas y que a menudo se
acompaña de hiperalgesia muscular profunda o alodinia (Graven-Nielsen, 2006),
este tipo de dolor puede manifestarse de forma localizada, regional y generalizado
(Graven-Nielsen and Arendt-Nielsen, 2010). El síndrome de dolor miofascial
(SDM), es un ejemplo de una condición de dolor regional muscular que se
caracteriza por la presencia de bandas tensas y dolor referido característico
causado por puntos gatillo miofasciales (PGM) (Simons, 1996).
La transición de dolor agudo musculoesquelético localizado a dolor crónico
generalizado está probablemente relacionada con la progresión de la
sensibilización periférica y central (Graven-Nielsen and Arendt-Nielsen, 2010). La
neurofisiología del DMC podría explicarse a través del proceso de sensibilización
central (Graven-Nielsen and Arendt-Nielsen, 2010).
1.2.1 Epidemiología
El dolor crónico es muy prevalente en la población general (Elliott et al., 1999) y
genera impacto negativo sobre la calidad de vida, el desempeño laboral y la
interacción psicosocial del paciente (Becker et al., 1997; Breivik et al., 2006).

8
El DMC se ha convertido en el principal motivo de consulta de dolor crónico en
atención primaria en la geografía española (Batlle-Gualda et al., 1998; Català et
al., 2002).
En una reciente revisión se ha descrito que la prevalencia del DMC se encuentra
entre el 13.5% y 47% de la población general y la del DMC generalizado varía
entre 11.4% y 24% (Cimmino et al., 2011).
En relación al SDM se ha sugerido que es el tipo de dolor más prevalente de entre
los de origen musculoesquelético (Simons, 1996), pero no hay datos precisos en
cuanto a la prevalencia de este en relación a la población general; a pesar de esto
en la actualidad clínica se tiene muy en cuenta al SDM, aún más conociendo que
en muchas investigaciones se ha demostrado que los PG son muy prevalentes en
diversos trastornos musculoesqueléticos como la cefalea tensional crónica
(Couppé et al., 2007), el dolor orofacial (Fernández-de-Las-Peñas et al., 2010), los
dolores relacionados con el raquis (Chen and Nizar, 2011), el dolor de hombro
(Bron et al., 2011) o la epicondilalgia lateral (Fernández-Carnero et al., 2007).
1.3 Dolor Cervical Crónico
La Neck Pain Task Force define el dolor cervical como un evento episódico a lo largo
de la vida que presenta una recuperación variable entre los diferentes episodios
(Guzman et al., 2009).
El dolor cervical frecuentemente denominado como no específico, de tejidos blandos o
dolor cervical mecánico se puede definir como aquel localizado en el territorio situado
entre la línea nucal superior y la línea de la espina de la escápula, en la parte posterior
del cuerpo, y en la parte anterior por encima del borde superior de la clavícula y el
esternón dejando fuera el contorno facial; con o sin irradiación a la cabeza, tronco y

9
miembros superiores (Guzman et al., 2009). Los signos de irradiación del dolor son
contemplados por esta definición, en relación con esto Bogduk (Bogduk, 2003) sugiere
que los signos de irradiación hacia la extremidad superior no deben asumirse como
parte del dolor cervical ya que estos son más propios del dolor cervical radicular y
fisiopatológicamente estas dos condiciones son muy distintas, además añade que la
confusión de estas dos entidades clínicas puede llevar a errores en el diagnóstico y
planteamientos de investigación y tratamiento poco adecuados (Bogduk, 2003).
Más acorde con la sugerencia de Bogduk (Bogduk, 2003) es la definición propuesta por
Merskey y Bogduk (Merskey and Bogduk, 1994), en esta, el dolor cervical se define
como el dolor que surge en una región limitada superiormente por la línea nucal
superior, lateralmente por los márgenes laterales del cuello, e inferiormente por una
línea imaginaria transversal a través de la apófisis espinosa T1.
El dolor cervical puede considerarse como un síntoma muy frecuente en la mayoría de
trastornos que afectan al cuadrante superior, aunque rara vez es síntoma de la presencia
de tumor, infección u otra afección grave (Bogduk, 2003). El dolor cervical puede
coexistir junto a otros trastornos musculoesqueléticos (Harris et al., 2006). Y puede
estar provocado o asociado a una patología local o una enfermedad sistémica tales como
lesiones de la piel, alteraciones de la laringe, tumores, infección, fracturas y
dislocaciones, traumatismos, mielopatías, artritis reumatoide u otras enfermedades
reumáticas (Haldeman et al., 2008).
El dolor cervical tiene una etiología multifactorial, con factores de riesgo no
modificables como la edad y el sexo (Hogg-Johnson et al., 2009). En estudios
realizados en población general relacionados con la edad, se ha observado que los
sujetos más jóvenes tienen mejor pronóstico de recuperación de la discapacidad cervical
(Hogg-Johnson et al., 2009). También se ha demostrado que otros trastornos
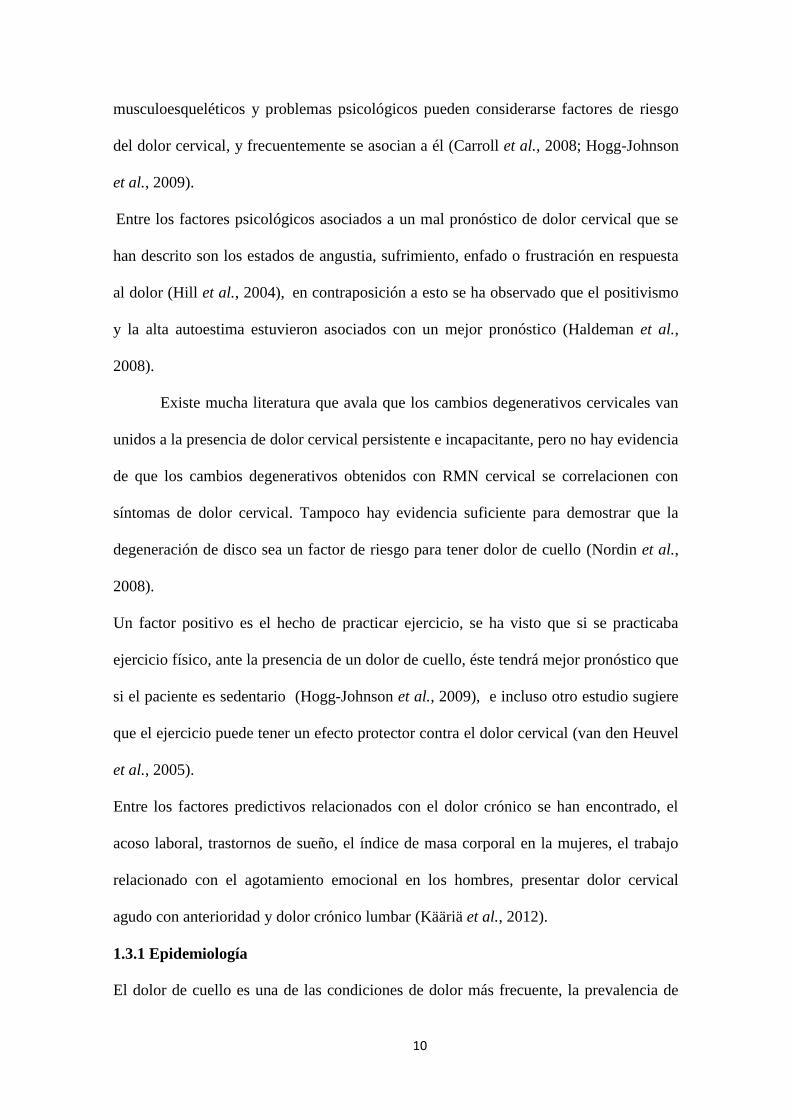
10
musculoesqueléticos y problemas psicológicos pueden considerarse factores de riesgo
del dolor cervical, y frecuentemente se asocian a él (Carroll et al., 2008; Hogg-Johnson
et al., 2009).
Entre los factores psicológicos asociados a un mal pronóstico de dolor cervical que se
han descrito son los estados de angustia, sufrimiento, enfado o frustración en respuesta
al dolor (Hill et al., 2004), en contraposición a esto se ha observado que el positivismo
y la alta autoestima estuvieron asociados con un mejor pronóstico (Haldeman et al.,
2008).
Existe mucha literatura que avala que los cambios degenerativos cervicales van
unidos a la presencia de dolor cervical persistente e incapacitante, pero no hay evidencia
de que los cambios degenerativos obtenidos con RMN cervical se correlacionen con
síntomas de dolor cervical. Tampoco hay evidencia suficiente para demostrar que la
degeneración de disco sea un factor de riesgo para tener dolor de cuello (Nordin et al.,
2008).
Un factor positivo es el hecho de practicar ejercicio, se ha visto que si se practicaba
ejercicio físico, ante la presencia de un dolor de cuello, éste tendrá mejor pronóstico que
si el paciente es sedentario (Hogg-Johnson et al., 2009), e incluso otro estudio sugiere
que el ejercicio puede tener un efecto protector contra el dolor cervical (van den Heuvel
et al., 2005).
Entre los factores predictivos relacionados con el dolor crónico se han encontrado, el
acoso laboral, trastornos de sueño, el índice de masa corporal en la mujeres, el trabajo
relacionado con el agotamiento emocional en los hombres, presentar dolor cervical
agudo con anterioridad y dolor crónico lumbar (Kääriä et al., 2012).
1.3.1 Epidemiología
El dolor de cuello es una de las condiciones de dolor más frecuente, la prevalencia de

11
dolor de cuello en la población general se ha estimado entre 10% y 15%, siendo más
común en mujeres que en hombres (Borghouts et al., 1999). En un reciente estudio de la
prevalencia de dolor en el cuello en la población española se ha estimado que indica un
19.5% anual entre los adultos españoles (Fernández-de-las-Peñas et al., 2011).
Un 70% aproximadamente de las personas, puede que experimenten un dolor cervical
en algún momento de sus vidas (Côté et al., 1998). En la población que sufre dolor
cervical se ha encontrado que a la hora de cualificarlo se representa en forma de
pirámide, en la que la base es conformada por un gran número de casos de dolor leve,
por encima pocos casos que consultan por su dolor y en la punta solo unos pocos casos
de dolor invalidante (Côté et al., 1998; Hogg-Johnson et al., 2009). Cote y cols.
encontraron que el 39.4 % de los individuos han tenido dolor cervical en los últimos 6
meses (Côté et al., 1998).
La literatura sugiere que entre el 50-80% de la población general que ha experimentado
dolor cervical, lo volverán a sufrir entre 1 -5 años más tarde y la mayor parte no se
recuperan totalmente del problema (Carroll et al., 2008). En general en la literatura se
dividen los grupos de edad en dos grandes grupos: jóvenes y mayores, siendo los de
peor pronóstico estos últimos. Hill y cols. (Hill et al., 2004) realizaron un estudio en el
que los sujetos se dividen en tres grupos de edades; se observó que en el grupo de edad
de entre 45-59 años, existe una tendencia 4 veces mayor a que el dolor cervical se
cronifique, recurra o sea continuo comparado con edades menores y mayores.
Más de 1/3 de los pacientes desarrollan síntomas crónicos que durarán más de 6 meses
(Côté et al., 2008). Entre un 15-32% de los individuos continúan experimentando
síntomas 5 años después del primer episodio de dolor de cuello (Enthoven et al., 2004;
Pernold et al., 2005). Después de 10 años, aproximadamente un 32% de los que
experimentan un primer episodio continuarán presentando síntomas moderados o

12
graves y un 79% mejoran del dolor pero no desaparece completamente (Gore et al.,
1987).
1.4 Dolor Craneofacial de Origen Musculoesquelético
El dolor craneofacial (DCF) es una denominación general que es utilizada para describir
la presencia de dolor en la cara, cabeza y estructuras asociadas, puede estar originado
por una variedad de condiciones, estructuras o etiologías (Armijo Olivo et al., 2006;
Kapur et al., 2003). El DCF se puede clasificar en neuropático, neurovascular y
musculoesquéletico (Benoliel et al., 2011). El DCF de origen musculoesquelético,
representa la causa más común de DCF de origen no dental y puede afectar la
musculatura masticatoria, la articulación temporomandibular (ATM) y estructuras
orofaciales (Okeson and de Leeuw, 2011). Los signos y síntomas más prevalentes que
se han observado en los pacientes con DCF son: dolor al abrir la boca, dolor a la
palpación muscular y dolor articular (Macfarlane et al., 2001), y por orden de
porcentaje, las áreas de expansión del dolor que se han descrito como más prevalentes
son: alrededor de los ojos, alrededor de la región temporal, en la zona anterior a la oreja
y en la ATM y alrededores de esta (Macfarlane, Blinkhorn, Davies, Kincey, et al.,
2002). Los factores psicológicos están muy presentes en el DCF y se han observado
múltiples comorbilidades con otras dolencias y patologías (Macfarlane et al., 2001).
El DCF de origen musculoesquelético según la Asociación Internacional para el Estudio
del Dolor se clasifica en cefalea tensional crónica, trastornos craneomandibulares
(TCM) dolorosos, TCM causados por artritis o artrosis, distonías y discinesias faciales y
traumatismos craneofaciales (Merskey and Bogduk, 1994).
1.4.1 Trastornos craneomandibulares
El término TCM se refiere a una serie de signos y síntomas que afectan a la musculatura
masticatoria, la ATM y estructuras asociadas o ambas (Okeson and de Leeuw, 2011;

13
Okeson, 1997), se considera un proceso patológico multifactorial causado posiblemente
por hiperactividad muscular o por parafunciones, lesiones traumáticas, influencias
hormonales y cambios a nivel articular (Liu and Steinkeler, 2013). Estos trastornos se
caracterizan por: (a) dolor orofacial y/o en la ATM o en los músculos masticatorios; (b)
alteraciones en el movimiento mandibular y/o limitación del rango de movimiento
mandibular; y (c) presencia de ruidos articulares durante la función mandibular (Liu
and Steinkeler, 2013; Okeson and de Leeuw, 2011).
Los factores psicosociales tienen un papel relevante en los TCM, en un reciente estudio
cohorte se identificó que el estrés, la afectividad negativa y las estrategias de
afrontamiento ante el dolor presentan una repercusión importante sobre los TMD
(Fillingim et al., 2011), por otra parte, Kindler y cols. (Kindler et al., 2012)
encontraron que los síntomas depresivos están más presentes en pacientes con TCM
articulares mientras la ansiedad estuvo más asociado con TCM de origen muscular.
Características psicológicas incluyendo la somatización, depresión y la ansiedad
relacionados con el género parecen tener un impacto significativo en la prevalencia de
TCM (Licini et al., n.d.). Evidencia reciente describe que las pacientes femeninas con
TCM presentan mayor percepción de intensidad del dolor y sensibilidad muscular a la
palpación que pacientes masculinos (Schmid-Schwap et al., 2013).
Existen diversos criterios diagnósticos para clasificar los TCM (Benoliel et al., 2011;
Schiffman et al., 2010), sin embargo la clasificación más utilizada en la actualidad son
los Criterios diagnósticos de investigación para TCM (en inglés, Research Diagnostic
Criteria for Temporomandibular Disorders; RDC/TMD) (Dworkin and LeResche, 1992;
Schiffman et al., 2010), estos criterios presentan una fiabilidad y validez contrastada
englobado en un protocolo sistematizado de valoración, diagnóstico y clasificación de
los subtipos más comunes de TCM (Look et al., 2010). Los Criterios diagnósticos de

14
investigación para TCM establecen la clasificación en dos grandes secciones definidos
en dos ejes: Eje I: Diagnóstico del dolor; y el Eje II Estatus psicosocial (Schiffman et
al., 2014). Es importante destacar que estos criterios han sido recientemente revisados y
el Eje I de diagnóstico ha sido dividido en dos grandes grupos de trastornos, TCM
relacionados con dolor y trastornos del disco y patología degenerativa de la ATM
(Tabla 1) (Schiffman et al., 2014).
Tabla 1. Clasificación diagnóstica de los trastornos craneomandibulares (Schiffman et
al., 2014).
Trastornos craneomandibulares
relacionados con dolor
Trastornos del disco y patología
degenerativa de la articulación
temporomandibular.
Mialgia Luxación del disco con reducción
Mialgia local Luxación del disco con reducción y con
bloqueos intermitentes
Dolor miofascial Luxación del disco sin reducción y con
limitación de la apertura
Dolor miofascial referido Luxación del disco sin reducción y sin
limitación de la apertura
Artralgia Trastornos degenerativos
Cefalea atribuida a trastornos
craneomandibulares
Subluxación
1.4.2 Epidemiología
El DCF es una dolencia muy prevalente en la población general en torno a un 17-26%
de los cuales el 11,7% llega a convertirse en condición crónica (Macfarlane, Blinkhorn,
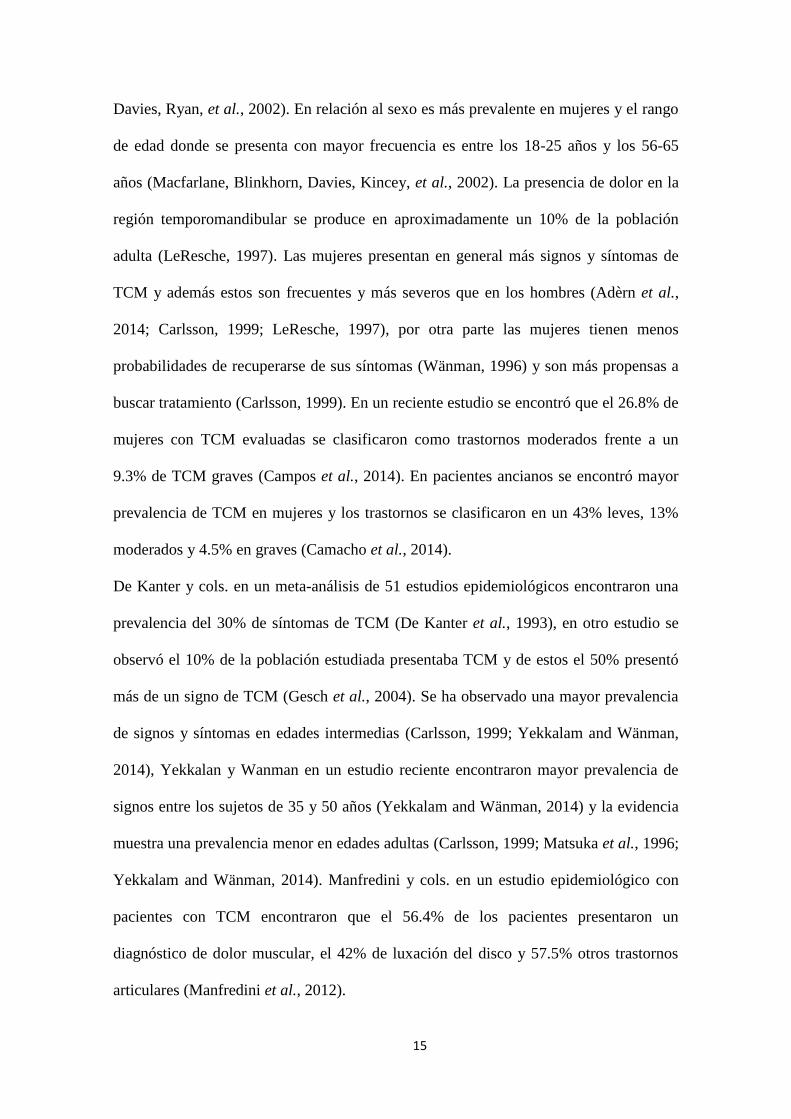
15
Davies, Ryan, et al., 2002). En relación al sexo es más prevalente en mujeres y el rango
de edad donde se presenta con mayor frecuencia es entre los 18-25 años y los 56-65
años (Macfarlane, Blinkhorn, Davies, Kincey, et al., 2002). La presencia de dolor en la
región temporomandibular se produce en aproximadamente un 10% de la población
adulta (LeResche, 1997). Las mujeres presentan en general más signos y síntomas de
TCM y además estos son frecuentes y más severos que en los hombres (Adèrn et al.,
2014; Carlsson, 1999; LeResche, 1997), por otra parte las mujeres tienen menos
probabilidades de recuperarse de sus síntomas (Wänman, 1996) y son más propensas a
buscar tratamiento (Carlsson, 1999). En un reciente estudio se encontró que el 26.8% de
mujeres con TCM evaluadas se clasificaron como trastornos moderados frente a un
9.3% de TCM graves (Campos et al., 2014). En pacientes ancianos se encontró mayor
prevalencia de TCM en mujeres y los trastornos se clasificaron en un 43% leves, 13%
moderados y 4.5% en graves (Camacho et al., 2014).
De Kanter y cols. en un meta-análisis de 51 estudios epidemiológicos encontraron una
prevalencia del 30% de síntomas de TCM (De Kanter et al., 1993), en otro estudio se
observó el 10% de la población estudiada presentaba TCM y de estos el 50% presentó
más de un signo de TCM (Gesch et al., 2004). Se ha observado una mayor prevalencia
de signos y síntomas en edades intermedias (Carlsson, 1999; Yekkalam and Wänman,
2014), Yekkalan y Wanman en un estudio reciente encontraron mayor prevalencia de
signos entre los sujetos de 35 y 50 años (Yekkalam and Wänman, 2014) y la evidencia
muestra una prevalencia menor en edades adultas (Carlsson, 1999; Matsuka et al., 1996;
Yekkalam and Wänman, 2014). Manfredini y cols. en un estudio epidemiológico con
pacientes con TCM encontraron que el 56.4% de los pacientes presentaron un
diagnóstico de dolor muscular, el 42% de luxación del disco y 57.5% otros trastornos
articulares (Manfredini et al., 2012).

16
En cuanto a la incidencia, Kamisaka y cols. realizaron un estudio longitudinal en un
espacio temporal de 4 años y encontraron una incidencia del 6% para el dolor en la
ATM y un 12.9% para ruidos articulares en la ATM, en esta misma investigación se
encontró en los sujetos menores de 40 años un mayor riesgo de presentar ruidos en
ATM y las mujeres presentaban un aumento en el riesgo de perpetuación de dolor en la
ATM (Kamisaka et al., 2000).
1.4.3 Epidemiología y comorbilidad entre trastornos craneomandibulares, cefalea
y dolor de cuello
Los TCM, las cefaleas y el dolor de cuello son trastornos muy relacionados (Sipilä et
al., 2002; Storm and Wänman, 2006; Wiesinger et al., 2007). Varios estudios han
informado que los signos y síntomas se superponen entre los pacientes con TCM,
cefaleas y dolor en el cuello respectivamente (Anderson et al., 2011; Rantala et al.,
2003), se ha demostrado que el dolor de cuello se asocia significativamente con los
TCM y que la gravedad de éstos se incrementa con la gravedad del dolor de cuello
(Ciancaglini et al., 1999; Nilsson et al., 2013; Wiesinger et al., 2009), adicionalmente,
se ha comprobado que los factores psicosociales a su vez están relacionados con la
presencia de cefalea, dolor de cuello y dolor orofacial (Rantala et al., 2003). Stuginski-
Barbosa investigaron recientemente los signos de TCM en pacientes con migraña
crónica (MC) y episódica (ME), en esta investigación se identificó que el 73% de los
pacientes con MC presentaron dolor a la palpación en la musculatura masticatoria, 63%
presentaron dolor a la palpación articular y 64% presentaron dolor a la palpación del
cuello (Stuginski-Barbosa et al., 2010), otras estudios similares, pero realizados en
pacientes adolecentes con cefalea han observado una alta comorbilidad con los TCM
dolorosos, además se encontró una asociación significativa con el dolor de cuello
(Nilsson et al., 2013), además en pacientes adolescentes con TCM, encontraron que los
17
pacientes que presentaban alteraciones musculares y alteraciones musculares y
articulares tuvieron mayores niveles de dolor mandibular y orofacial, cefalea, dolor de
cuello y dificultad para comer alimentos blandos (Karibe et al., 2010).
Se ha sugerido que los TCM, las cefaleas y el dolor de cuello pueden tener una base
fisiopatológica similar (Ashina et al., 2006; Marklund et al., 2010; Svensson, 2007), por
otra parte se ha identificado que la cefalea podría ser un factor de riesgo de sufrir dolor
de cuello (Leclerc et al., 1999).
Rantala y cols. describió que de entre 1339 sujetos evaluados la prevalencia de signos
relacionados con la ATM fue del 10%, el dolor orofacial fue del 7%, la cefalea del 15%
y el dolor de cuello el 39% (Rantala et al., 2003), por otra parte, Plesh y cols. mostró
que el 53% de los pacientes con TCM que presentaron dolor de cabeza severo, el 54%
tenía dolor de cuello (Plesh et al., 2011). Un estudio realizado con 487 mujeres Sami
encontró que un 17% de estas presentó dolor en la regiones mandibular y orofacial que
además lo asociaban a una limitación de su calidad de vida, y en este mismo estudio se
describe que la duración del dolor en la región mandibular, las molestias al realizar la
apertura, el dolor de cuello y un nivel educativo bajo estaban relacionados cuando los
síntomas de TCM influían en la vida cotidiana (Mienna and Wanman, 2012), en
relación con esto dato, Weber y cols. encontraron que el 88,24% de los pacientes con
TCM presentaron a su vez dolor cervical, en esta investigación se sugiere que esta
situación está generada principalmente por factores neurofisiológicos y no por factores
biomecánicos como la postura (Weber et al., 2012).
La prevalencia del latigazo cervical en pacientes con TCM ha sido estudiada en una
revisión sistemática reciente (Häggman-Henrikson et al., 2014), en esta se describe que
la prevalencia del latigazo cervical en pacientes con TCM varía entre 8,4% a un 70%,
este resultado se comparó con la población general sin TCM en donde la prevalencia de

18
latigazo cervical se encuentra entre 1,7% y 13%, además en esta revisión se señala que
los pacientes con TCM con antecedentes de haber sufrido un latigazo cervical presentan
más signos de alteración de la ATM como limitación de la apertura bucal, más dolor
articular, cefalea y síntomas de estrés. Los autores de esta revisión sugieren que el
latigazo cervical puede ser un iniciador y/o un factor agravante, así como una condición
comórbida con los TCM (Häggman-Henrikson et al., 2014)
1.5 Dolor Referido de la Región Cervical hacia la Región Craneofacial
Diversas estructuras de la región cervical pueden provocar dolor referido hacia la región
craneofacial, la literatura científica describe que las articulaciones cervicales, los
ligamentos y los músculos son estructuras relevantes a tener en cuenta en la
identificación de los patrones del dolor que pueden afectar al cráneo, la región
craneomandibular y la región orofacial. Son muchos los estudios que demuestran que
los PGM del trapecio, el esplenio, el esternocleidomastoideo y los músculos sub-
occipitales producen dolor referido hacia la región craneofacial en pacientes con TCM y
cefaleas (Alonso-Blanco et al., 2012; Fernández-de-Las-Peñas et al., 2006, 2010;
Fricton et al., 1985; Wright, 2000). Muchos de estos patrones de dolor referido
evocados por PGM fueron descritos por Simons y cols. (Simons et al., 1999) (Figura
1).

19
Figura 1. Representación modificada de los patrones de dolor referido hacia la región craneofacial provocado por
PGM de músculos de la región cervical.
A nivel de las estructuras articulares de la región cervical, la investigación relacionada
con la infiltración de sustancias algógenas y estudios relacionados con el diagnóstico
estructural han identificado patrones o mapas de dolor referido hacia la región
craneofacial, específicamente Dreyfuss y cols. comprobaron en sujetos sanos que la
infiltración de sustancias algógenas sobre la articulación atlanto-occipital y la
articulación atlanto-axial lateral provocaban patrones de dolor referido sobre la región
cervical superior y la cabeza (Dreyfuss et al., 1994), también Dwyer y cols. con un
procedimiento similar en sujetos sanos identificaron que las articulaciones
zigoapofisarias C2-C3 provocan patrones de dolor referido hacia la región cervical y la
cabeza (Dwyer et al., 1990), estos patrones fueron confirmados con gran similitud en
pacientes (Aprill et al., 1990; Cooper et al., 2007). Se ha sugerido que el patrón de dolor
de las articulaciones zigoapofisarias C3-C4 ocasionalmente puede estar relacionado con

20
la cefalea cevicogénica (Cooper et al., 2007), sin embargo en el caso del disco
intervertebral C2-C3 sí se ha identificado como una fuente importante de dolor referido
hacia la cabeza en pacientes con cefalea cervicogénica (Schofferman et al., 2002)
(Figura 2).
Figura 2. Representación, según la evidencia científica de los patrones de dolor referido de estructuras articulares
cervicales hacia áreas craneocervicales (Aprill et al., 1990; Cooper et al., 2007; Dreyfuss et al., 1994; Dwyer et al.,
1990).
Destacar como hallazgo científico reciente, que Watson y Drummond encontraron
patrones de dolor referido hacia la cabeza muy similares al valorar la articulación
atlanto-occipital y las articulaciones zigoapofisarias C2-C3 en pacientes con migraña y
cefalea tensional (Watson and Drummond, 2012).
1.6 Aspectos Anatomofuncionales de la Región Craneomandibular y la Región
Craneocervical
La asociación entre la región craneomandibular y la región craneocervical ha sido
estudiada en las últimas décadas desde diversos paradigmas, incluyendo enfoques
anatómicos, biomecánicos, neurofisiológicos, y patofisiológicos (Armijo Olivo et al.,
2006), en este apartado se pretende hacer una descripción detallada de la evidencia
21
disponible relacionada con las posibles relaciones entre estas regiones tomando en
cuenta los enfoques anatómicos y biomecánicos desde la función normal.
1.6.1 Modelos biomecánicos de la relación cranemandibular/craneocervical
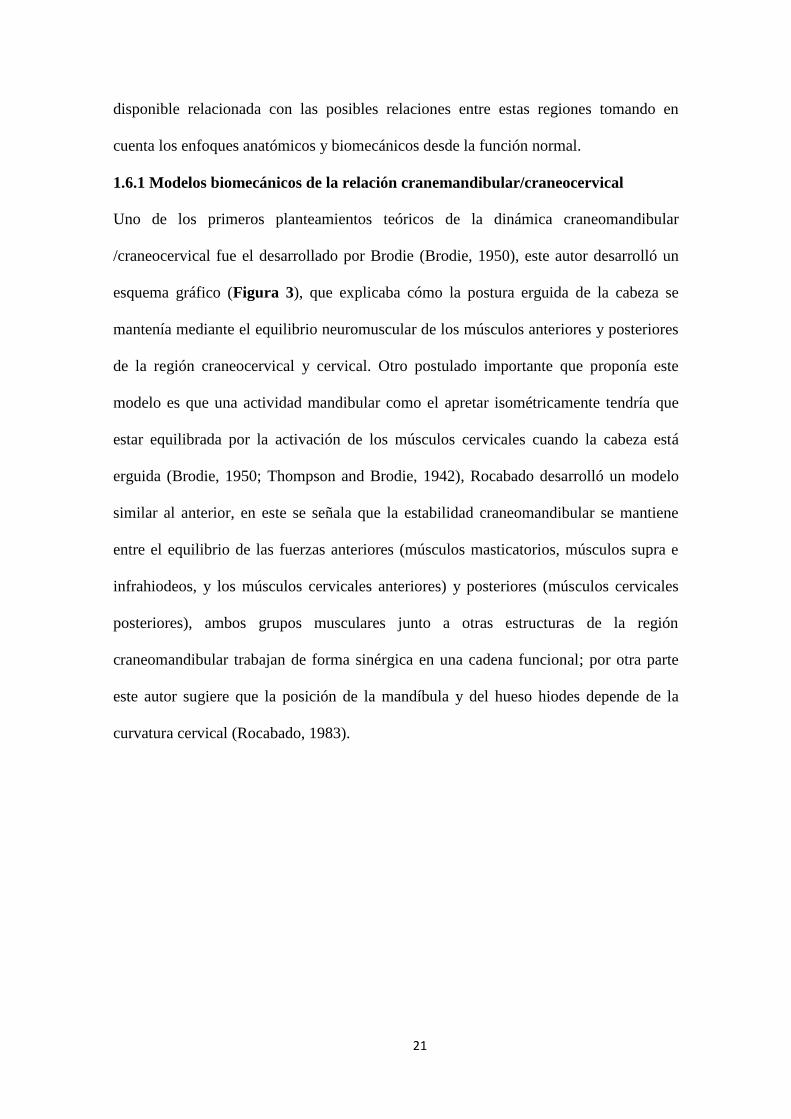
Uno de los primeros planteamientos teóricos de la dinámica craneomandibular
/craneocervical fue el desarrollado por Brodie (Brodie, 1950), este autor desarrolló un
esquema gráfico (Figura 3), que explicaba cómo la postura erguida de la cabeza se
mantenía mediante el equilibrio neuromuscular de los músculos anteriores y posteriores
de la región craneocervical y cervical. Otro postulado importante que proponía este
modelo es que una actividad mandibular como el apretar isométricamente tendría que
estar equilibrada por la activación de los músculos cervicales cuando la cabeza está
erguida (Brodie, 1950; Thompson and Brodie, 1942), Rocabado desarrolló un modelo
similar al anterior, en este se señala que la estabilidad craneomandibular se mantiene
entre el equilibrio de las fuerzas anteriores (músculos masticatorios, músculos supra e
infrahiodeos, y los músculos cervicales anteriores) y posteriores (músculos cervicales
posteriores), ambos grupos musculares junto a otras estructuras de la región
craneomandibular trabajan de forma sinérgica en una cadena funcional; por otra parte
este autor sugiere que la posición de la mandíbula y del hueso hiodes depende de la
curvatura cervical (Rocabado, 1983).

22
Figura 3. Esta figura representa el esquema diseñado por Brodie, para explicar el equilibrio mecánica neuromuscular
entre las regiones craneocervical y craneomandibular (Brodie, 1950; Thompson and Brodie, 1942).
Resultados de estudios basados en modelos matemáticos apoyan en gran medida las
tesis teóricas anteriormente descritas (Gillies et al., 1998; Suzuki et al., 2003), un
ejemplo de esto es el estudio de Suzuki y cols. en este se generó un sistema mecánico de
análisis dinámico del sistema estomatognático en condiciones de normalidad, se
observó como resultado principal que la actividad muscular de la región cervical influye
sobre la actividad mecánica de la mandíbula, además sugieren que los músculos
cervicales coordinan y resisten los cambios en la postura de la cabeza durante los
movimientos mandibulares (Suzuki et al., 2003). Otro de los modelos biomecánicos
relacionados con la dinámica mandibular, señala que el movimiento de extensión
craneocervical facilita la apertura mandibular y sugieren que esta situación se da para
lograr una mejor activación de los músculos que realizan la apertura y para generar una
posición más favorable para el movimiento (Koolstra and van Eijden, 2004).

23
1.6.2 Estudios in-vivo de la relación craneomandibular/craneocervical
La mayoría de estudios in-vivo en torno a las hipótesis de la relación
craneomandibular/craneocervical se han realizado con electromiografía (EMG), análisis
cinemático y estudios radiológicos; estas investigaciones se han diseñado con el
objetivo de comprobar la influencia mutua de ambas regiones en la dinámica articular
mandibular, en la estabilidad postural y en los aspectos funcionales más generales en los
que participa la ATM y las estructuras asociadas, como por ejemplo la deglución y la
masticación.
1.6.3 Influencia de la región craneocervical sobre la dinámica mandibular
En cuanto a la dinámica mandibular, Visscher y cols. demostraron pequeñas
variaciones en la posición del cóndilo mandibular según la postura craneocervical, sus
hallazgos mostraron que la distancia intra-articular en la ATM en el movimiento de
cierre es menor con retracción craneocervical y mayor con protrusión craneocervical
(Visscher et al., 2000), en relación con esto, Omure y cols. observaron que al inducir
experimentalmente la posición de protrusión craneocervical, el cóndilo mandibular se
posteriorizaba en comparación a la posición neutra (Ohmure et al., 2008), estos
hallazgos confirmarían las observaciones de Solow y Tallegren que en 1976 ya
describieron que el movimiento de extensión craneocervical se asocia a una retrusión
mandibular (Solow and Tallgren, 1976). Otro de los aspectos importantes que se han
investigado sobre la dinámica de la ATM es que la apertura mandibular se ve
directamente influenciada por la posición craneocervical, observándose un aumento de
la apertura mandibular en la posición de protracción craneocervical y una disminución
en la posición de retracción craneocervical cuando se comparan con la posición neutra
(Higbie et al., 1999). Un esquema de la relación de la postura craneocervical y la
dinámica intra-articular de la ATM es representada en la figura 4.

24
Figura 4. Este esquema representa el efecto de la postura de protracción craneocervical sobre la dinámica mandibular
y la musculatura masticatoria según la evidencia científica de estudios experimentales. La imagen A señala un
aumento de la actividad electromiográfica cuando se induce la postura de protracción craneocervical. La imagen B
representa una posteriorización del cóndilo mandibular asociado a la postura de protracción craneocervical.
1.6.4 Sinergias neuromusculares cervicales y masticatorias
La electromiografía ha sido uno de los instrumentos más utilizados para investigar las
acciones coordinadas, sinérgicas o asociadas entre la musculatura de la región
craneomandibular (musculatura masticatoria) y la musculatura del cuello. Diversos
estudios han comprobado la activación del músculo esternocleidomastoideo durante el
apretamiento (Clark et al., 1993; Davies, 1979; Hochberg et al., 1995; Rodríguez et al.,
2011; So et al., 2004; Venegas et al., 2009; Yoshida, 1988) (Figura 5) y el
rechinamiento dentario (Rodríguez et al., 2011; Venegas et al., 2009), en relación con
esto Clark y cols. describieron que para lograr un 5% de la contracción del
esternocleidomastoideo durante el apretamiento dentario se necesita una activación del
A
B

25
50% del músculo masetero (Clark et al., 1993), evidencia reciente demuestra que
durante la masticación se produce una acción concomitante entre los músculos masetero
y esternocleidomastoideo y el nivel activación de estos músculos se modula de acuerdo
a la demanda del elemento que se esté masticando (Häggman-Henrikson et al., 2013);
otras investigaciones realizadas con electromiografía profunda y superficial han
comprobado que durante diversas tareas de apretamiento dentario varios músculos de la
región cervical (esternocleidomastoideo, semiespinales del cuello y la cabeza,
multífidos cervical, elevador de la escápula, esplenio de la cabeza) son activados y este
reclutamiento se produce en torno al 2% y al 14% de la contracción voluntaria máxima
(Giannakopoulos, Hellmann, et al., 2013; Giannakopoulos, Schindler, et al., 2013;
Hellmann et al., 2012). Al contrario de la mayoría de los estudios que se han realizado
con la función de apretamiento dentario, Armijo-Olivo y Magee estudiaron la apertura
mandibular realizada contra resistencia, los resultados mostraron un aumento similar de
la actividad electromiográfica de los músculos masetero, temporal, esplenio de la
cabeza y de las fibras superiores del músculo trapecio. (Armijo-Olivo and Magee,
2007).
A B

26
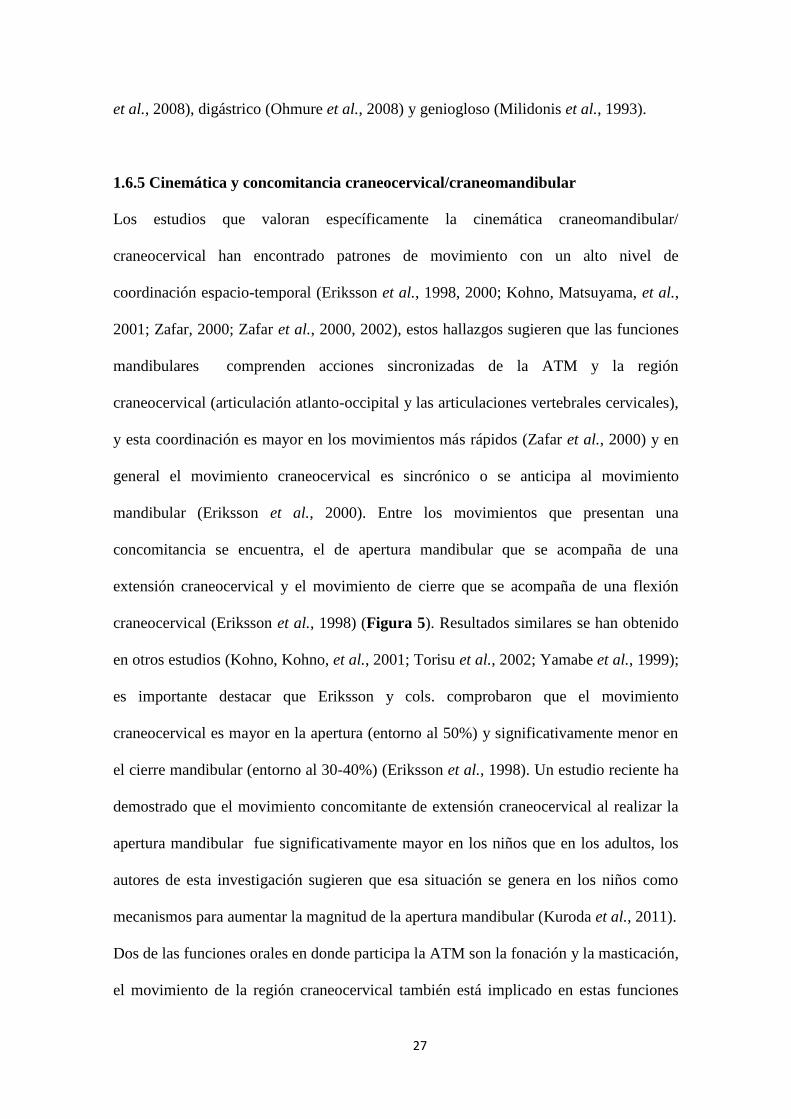
Figura 5. Esta figura representa un esquema diseñado según la evidencia científica que muestra que el apretamiento
dentario modifica la actividad electromiográfico de músculos cervicales (A). En la figura B se muestra una
concomitancia entre los movimientos craneocervicales y craneomandibulares (el movimiento de apertura bucal se
asocia un movimiento de extensión craneocervical y el movimiento de cierre al movimiento de flexión
craneocervical).
Un hallazgo importante a destacar es que se ha observado que en posiciones de reposo
mandibular se produce un descenso en la actividad electromiográfica de los músculos
trapecio y esternocleidomastoideo (Ceneviz et al., 2006), sin embargo parece ser que los
diferentes tipos de oclusión no influyen sobre la actividad eletromiográfica de la
musculatura del cuello (Ferrario et al., 2006). La figura 5 representa un esquema de la
elevación de la actividad electromiográfica de los músculos cervicales durante el
apretamiento dentario.
En cuanto a la influencia del movimiento craneocervical sobre la actividad
electromiográfica de la musculatura masticatoria, Funakoshi y cols. observaron que se
producía una gran activación del músculo temporal y una moderada activación del
músculo masetero al realizar una extensión craneocervical (Funakoshi et al., 1976), a
diferencia de este estudio, Ballenberger y cols. investigaron la influencia de los
movimientos de la región cervical superior (rotación, extensión, flexión e inclinación
lateral) y encontraron diferencias estadísticamente significativas sobre la actividad
electromiográfica del músculo masetero pero no sobre el músculo temporal, además en
este estudio se señala que la actividad electromiográfica se incrementa más en extensión
que la flexión craneocervical (Ballenberger et al., 2012), en relación con esto, Forsberg
y cols. determinaron que el incremento de actividad de masetero durante la extensión
craneocervical se produce entre 10º y los 20º (Forsberg et al., 1985). Estudios en donde
se ha inducido experimentalmente la posición de protracción craneocervical han
descrito un aumento de la actividad de los músculos masetero (McLean, 2005; Ohmure
27
et al., 2008), digástrico (Ohmure et al., 2008) y geniogloso (Milidonis et al., 1993).
1.6.5 Cinemática y concomitancia craneocervical/craneomandibular
Los estudios que valoran específicamente la cinemática craneomandibular/
craneocervical han encontrado patrones de movimiento con un alto nivel de
coordinación espacio-temporal (Eriksson et al., 1998, 2000; Kohno, Matsuyama, et al.,
2001; Zafar, 2000; Zafar et al., 2000, 2002), estos hallazgos sugieren que las funciones
mandibulares comprenden acciones sincronizadas de la ATM y la región
craneocervical (articulación atlanto-occipital y las articulaciones vertebrales cervicales),
y esta coordinación es mayor en los movimientos más rápidos (Zafar et al., 2000) y en
general el movimiento craneocervical es sincrónico o se anticipa al movimiento
mandibular (Eriksson et al., 2000). Entre los movimientos que presentan una
concomitancia se encuentra, el de apertura mandibular que se acompaña de una
extensión craneocervical y el movimiento de cierre que se acompaña de una flexión
craneocervical (Eriksson et al., 1998) (Figura 5). Resultados similares se han obtenido
en otros estudios (Kohno, Kohno, et al., 2001; Torisu et al., 2002; Yamabe et al., 1999);
es importante destacar que Eriksson y cols. comprobaron que el movimiento
craneocervical es mayor en la apertura (entorno al 50%) y significativamente menor en
el cierre mandibular (entorno al 30-40%) (Eriksson et al., 1998). Un estudio reciente ha
demostrado que el movimiento concomitante de extensión craneocervical al realizar la
apertura mandibular fue significativamente mayor en los niños que en los adultos, los
autores de esta investigación sugieren que esa situación se genera en los niños como
mecanismos para aumentar la magnitud de la apertura mandibular (Kuroda et al., 2011).
Dos de las funciones orales en donde participa la ATM son la fonación y la masticación,
el movimiento de la región craneocervical también está implicado en estas funciones
28
(Häggman-Henrikson and Eriksson, 2004; Miyaoka et al., 2004), específicamente se ha
demostrado que el movimiento de flexo-extensión craneocervical acompaña los ciclos
masticatorios, pero además de acuerdo a como sea el tamaño del bolo alimenticio que se
mastique, el movimiento de extensión craneocervical se ve modificado (Häggman-
Henrikson and Eriksson, 2004); en cuanto a la fonación se ha observado que diversas
tareas en donde se articulan palabras y se realiza apertura-cierre están asociada a
movimientos de la región craneocervical (Miyaoka et al., 2004).
En la actualidad contamos con evidencia científica muy abundante que demuestra las
relaciones anatomofuncionales entre la regiones craneomandibular y la craneocervical,
sin embargo esta información no es suficiente para demostrar los aspectos
neurofisiológicas implicados en ambas funciones; resultados de investigación básica en
conejos han descrito mecanismos neurales supramedulares implicadas en las acciones
rítmicas cervicales y craneomandibulares (Igarashi et al., 2000), otros autores han
teorizado que las acciones concomitantes son comandos pre-programados a nivel central
(Torisu et al., 2001; Zafar, 2000) y que las funciones vienen moduladas por
mecanismos sensoriomotores trigeminocervicales (Eriksson et al., 1998; Zafar, 2000).
El conocimiento entorno a la neurofisiología trigeminocervical puede ayudar a
comprender las situaciones comorbilidad del dolor de cuello y el DCF o las alteraciones
disfuncionales motoras craneocervicales/craneomandibulares; estos aspectos
neurofisiológicos se desarrollan en el siguiente apartado.
1.7 Neurofisiología del Dolor Cérvico-craneofacial
La base neurofisiológica del dolor referido de la región cervical hacia el área
craneofacial se puede explicar mediante un fenómeno anatómico y fisiológico de
convergencia de aferencias nociceptivas trigeminales y cervicales que confluyen en el
núcleo trigeminal espinal y en los segmentos cervicales superiores (Bartsch and

29
Goadsby, 2003a, 2003b; Bartsch, 2005; Piovesan et al., 2003), este centro de
procesamiento del dolor se ha denominado complejo trigeminocervical (CTC). Este
complejo es el responsable de transmitir información sensorial visceral e información
nociceptiva de la cabeza y la región orofacial hacia otros centros superiores como el
tálamo, el hipotálamo y la corteza somatosensorial primaria (Benjamin et al., 2004;
Malick and Burstein, 1998; Malick et al., 2000, 2001) (Figura 6) e inclusive tiene
conexiones neurales con áreas del diencéfalo y el tronco encefálico relacionadas con la
modulación del dolor (Akerman et al., 2011).
1.7.1 Sistema sensorial trigeminal
El sistema sensorial trigeminal lo conforman: a) el nervio trigémino (y sus tres
divisiones: oftálmica, V1; maxilar, V2; y mandibular, V3); b) el ganglio del trigémino
(Gasser); c) la raíces nerviosas trigeminales; y d) los componentes centrales
trigeminales del tronco encefálico (los núcleos trigeminales, los tractos trigeminales y
las vías tálamo-trigeminales) (Sessle, 2005b; Waite and Ashwell, 2004) (Figura 6). El
nervio trigémino es el más grande de los nervios craneales y es considerado un nervio
mixto ya que tiene una división sensorial y una motora (Majoie et al., 1995; Sanders,
2010), además es importante destacar que proporciona la inervación sensorial principal
de la cara, la cavidad oral y parte de cráneo (Majoie et al., 1995; Sessle, 2005a).

30
Figura 6. La imagen representa la organización neuroanatómica del sistema trigeminal desde la periferia hasta las
conexiones neurofisiológicas a nivel central. S1, corteza somatensorial primaria; VMP, núcleo ventral posteromedial
del tálamo; NTE, núcleo trigeminal espinal; GT ganglio trigeminal.
El ganglio de Gasser es una estructura fina, considerado como un análogo craneal de los
ganglios de la raíz dorsal en el sistema nervioso periférico, pero es significativamente
más grande anatómicamente (Dixon, 1963; Kerr, 1963; Moses, 1967). La mayoría de
los cuerpos celulares de aferencias primarias trigeminales procedentes de la tres
divisiones del nervio trigémino (V1, V2 y V3) residen en el ganglio de Gasser, en donde
se encuentran organizadas de manera somatotópica (Borsook et al., 2003; Byers and
Närhi, 1999; Jacquin et al., 1986; Leiser and Moxon, 2006), pero hay que tomar en
cuenta que los cuerpos celulares de algunas aferencias periodontales y de los husos
musculares residen en el núcleo mesencefálico (Capra and Dessem, 1992).
Las fibras aferentes primarias trigeminales terminan en los tejidos craneofaciales como
31
terminaciones nerviosas libres y funcionan como nociceptores, estos pueden activarse
con estímulos nocivos mecánicos, térmicos y químicos. Su activación puede resultar en
la excitación de fibras de pequeño diámetro y de conducción lenta (A-delta o C) (Sessle,
1999, 2005b, 2011; Takemura et al., 2006). Una serie de componentes neuroquímicos
(por ejemplo, la sustancia P, 5-HT, prostaglandinas, bradiquininas) están involucrados
en la activación de estas terminaciones periféricas por estimulación nociva o en su
sensibilización periférica; la sensibilidad de las terminaciones puede aumentar después
de una lesión leve, y esta sensibilización de las terminaciones nociceptivas es un
mecanismo periférico que ayuda a proteger los tejidos lesionados de repetidos agravios
(Sessle, 2000, 2005b, 2011).
La división V1 inerva la región nasal y peri-orbital (incluyendo la córnea y la
conjuntiva), la duramadre supratentorial, así como la frente y la parte superior de la
cabeza que se superpone con el dermatoma C2. La división V2 suministra inervación al
área cigomática, el labio superior, una parte de la cavidad nasal y oral (incluyendo los
dientes del maxilar y su periodonto asociado), y la división V3 inerva a las estructuras
extra e intra-orales restantes en el tercio inferior de la cara (incluyendo los dientes de la
mandíbula y su periodonto), el labio inferior, la piel de la mejilla, y dos tercios
anteriores de la lengua, el mentón, la ATM, además de la piel cubre la mandíbula y el
lado de la cabeza (parte de la región temporal) a excepción de el ángulo de la mandíbula
que es la parte del dermatoma C2 (Majoie et al., 1995; Sanders, 2010). Las fibras
eferentes motoras del V3 inervan los cuatro músculos de la masticación (masetero,
temporal y pterigoideo medial y lateral), el músculo milohiodeo, el fascículo anterior
del músculo digástrico, el músculo tensor del tímpano y el músculo tensor del velo
palatino (Kamel and Toland, 2001; Majoie et al., 1995). En la figura 7 se representan
gráficamente los dermatomas trigeminales (Figura 7).

32
Figura 7. Representación gráfica de los dermatomas trigeminales y cervicales.
El nervio trigémino tiene cuatro núcleos centrales en el tronco encefálico (un núcleo
motor y 3 sensoriales): a) el núcleo mesencefálico trigeminal, que media la
propiocepción; b) el núcleo sensitivo principal, que media la sensación táctil
(principalmente tacto epicrítico y en menor medida tacto protopático); c) el núcleo
motor que proporciona inervación motora: y d) el núcleo espinal trigeminal, que media
el dolor, la sensibilidad térmica y táctil (Majoie et al., 1995; Sessle, 2000) (Figura 8).
El núcleo espinal trigeminal consiste en la división de tres sub-núcleos: a) oral (SVo);
b) interpolar (SVi); y c) caudal (SVc) (Sessle, 1999, 2000, 2005b, 2011). Los sub-
núcleos SVo y SVi se asocian con la transmisión de la percepción táctil; por otra parte,
están implicados principalmente en mecanismos nociceptivos orofaciales relacionados
especialmente con el dolor intra-oral y peri-oral (Dallel et al., 1988, 1990; Raboisson et
al., 1995). Los núcleos trigeminales se representan en la figura 8.
33
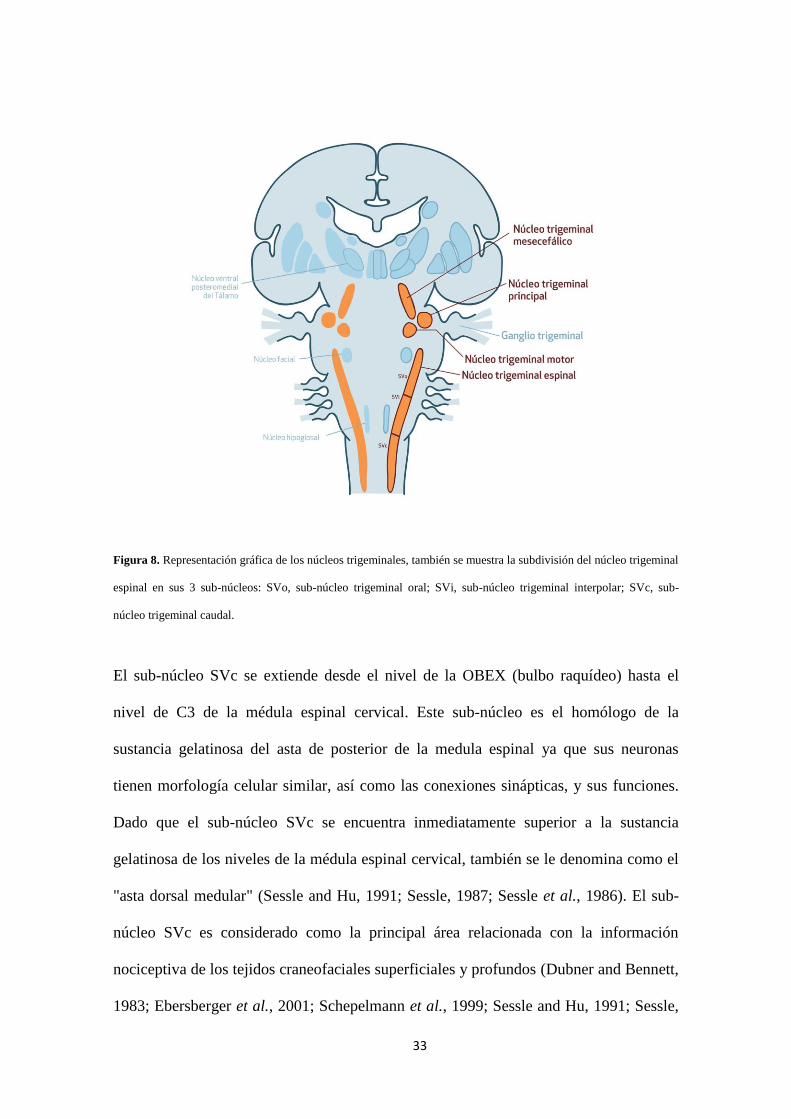
Figura 8. Representación gráfica de los núcleos trigeminales, también se muestra la subdivisión del núcleo trigeminal
espinal en sus 3 sub-núcleos: SVo, sub-núcleo trigeminal oral; SVi, sub-núcleo trigeminal interpolar; SVc, sub-
núcleo trigeminal caudal.
El sub-núcleo SVc se extiende desde el nivel de la OBEX (bulbo raquídeo) hasta el
nivel de C3 de la médula espinal cervical. Este sub-núcleo es el homólogo de la
sustancia gelatinosa del asta de posterior de la medula espinal ya que sus neuronas
tienen morfología celular similar, así como las conexiones sinápticas, y sus funciones.
Dado que el sub-núcleo SVc se encuentra inmediatamente superior a la sustancia
gelatinosa de los niveles de la médula espinal cervical, también se le denomina como el
"asta dorsal medular" (Sessle and Hu, 1991; Sessle, 1987; Sessle et al., 1986). El sub-
núcleo SVc es considerado como la principal área relacionada con la información
nociceptiva de los tejidos craneofaciales superficiales y profundos (Dubner and Bennett,
1983; Ebersberger et al., 2001; Schepelmann et al., 1999; Sessle and Hu, 1991; Sessle,
34
1987, 2005b).
En las láminas superficiales y profundas del SVc predominan dos tipos de neuronas
nociceptivas (neuronas nociceptivas específicas [NE] y neuronas de rango dinámico
amplio [RDA]), estas neuronas trasmiten información aferente nociceptiva hacia centros
superiores (núcleo ventral posteromedial del tálamo [VPM]) (Sessle, 1987, 2000,
2005a, 2011). Las neuronas NE sólo responden a estímulos nocivos (por ejemplo,
pellizcar, estímulos térmicos nocivos) aplicados a un campo receptivo craneofacial
localizado y reciben impulsos aferentes de fibras de diámetro pequeño (fibras A delta
y/o C); las neuronas RDA son excitadas por estímulos no nocivos (por ejemplo
estímulos táctiles), así como por estímulos nocivos, y pueden recibir impulsos aferentes
de fibras de gran diámetro (fibras A) y de pequeño diámetro (fibras C) (Sessle, 1999).
La mayoría de neuronas NE y RDA, también pueden ser excitadas por otros tipos de
entradas aferentes periféricas de diversas regiones como las meninges, tejido vascular,
los dientes, la ATM o en los músculos masticatorios (Burstein et al., 1998; Dostrovsky
et al., 1991; Sessle, 1996, 1999, 2000). Los extensos patrones convergentes de entradas
aferentes que son característicos de la ATM o de la duramadre son activados por
neuronas NE y RDA en el SVc, este fenómeno podría explicar la mala localización del
dolor profundo, así como la difusión del dolor referido que es condición típica de
dolencias que implican la ATM y la musculatura asociada (Sessle, 1999, 2011).
Las neuronas trigeminales somatosensoriales del tronco encefálico proyectan a otras
estructuras de esta misma región anatómica como la formación reticular y los núcleos
motores de otros nervios craneales; estas conexiones proporcionan respuestas
autonómicas y motoras ante estímulos craneofaciales (Sessle, 1987, 1996, 1999).
Específicamente las neuronas del SVc proyectan hacia el núcleo VPM del tálamo a
través de una vía multisináptica denominada tracto lemnisco trigeminal dorsal (tracto

35
trigeminotalámico dorsal) (Dougherty and Willis, 1992; Dougherty et al., 1992; Sessle,
1999; Sherman et al., 1997) (Figura 9). Las neuronas nociceptivas del núcleo VPM
tienen conexiones con la corteza somatosensorial (Sherman et al., 1997), representando
la dimensión sensorial-discriminativa del dolor. También se ha observado otras
conexiones como por ejemplo con la corteza cingulada anterior, situando a estos
circuitos neurales como parte de la dimensión afectivo-emocional del dolor (Sessle and
Hu, 1991; Sessle, 1999).
Figura 9. Representación gráfica del tracto trigeminotalámico dorsal. GT, ganglio trigeminal; NTE, núcleo
trigeminal espinal; SVc; sub-núcleo trigeminal caudal; VPM, Núcleo ventral posteromedial del tálamo; S1, corteza
somatosensorial primaria.
1.7.2 Neuroanatomía de los segmentos cervicales superiores
La médula espinal cervical superior incluye los segmentos espinales C1 y C2 en donde
emergen periféricamente los tres primeros nervios cervicales que se distribuyen en un
ramo dorsal, un ramo ventral y los nervios sinovertebrales (Alix and Bates, 1999;
36
Bogduk, 1981), estos nervios inervan a nivel motor y sensitivo diversas estructuras de la
parte posterior de la cabeza y el cuello (Bogduk, 2001) que pueden generar dolor
referido hacia la cabeza y la región orofacial (Johnston et al., 2013). El nervio C1
presenta un ganglio de la raíz dorsal ectópico, se ha observado que en algunos casos
(20%) este nervio carece de raíz dorsal y en estos casos las células ganglionares se
pueden encontrar entre las raíces del nervio espinal accesorio (Ouaknine and Nathan,
1973). Este nervio carece de distribución sensitiva cutánea, sin embargo a través de su
rama dorsal inerva sensitivamente a nivel profundo los músculos cortos del triángulo
suboccipital (Bogduk, 1982), su ramo ventral pasa por detrás y debajo de articulación
atlanto-occipital a la que suministra inervación (Bogduk, 2001)
El nervio C2 da inervación sensitiva a las articulaciones atlantoaxoideas laterales y
mediales; la duramadre de la fosa craneal posterior y de la médula espinal superior; y la
arteria carótida y vertebral. La rama ventral de este nervio inerva los músculos
paravertebrales, el músculo esternocleidomastoideo y el trapecio y la rama dorsal los
músculos semiespinales de la cabeza y el músculo esplenio de la cabeza. El nervio
sinovertebral de C2 se une a los de C1 y C3 para suministrar inervación a los
ligamentos transversal, alar y a la membrana tectoria (Bogduk, 2001). La rama ventral
de C3 se une al plexo cervical e inerva los músculos paravertebrales. La rama medial
del ramo dorsal de C3 inerva el músculo semiespinoso cervical y el músculo multifidus
y además inerva las articulaciones cigapofisiarias de C2-C3. El nervio sinovertebral de
C3 inerva el disco intervertebral C2-3 en su cara posterior (Bogduk, 2001; Bogduk et
al., 1988).
A nivel cutáneo la inervación sensitiva de la región craneocervical la suministran los
nervios occipital menor, occipital mayor y el nervio auricular mayor (Poletti, 1991; Shin
et al., 2007), estos tres nervios sensitivos más la zona cutánea que inervan conformarían

37
los dermatomas de la región craneocervical, estos dermatomas (C2, C3) tienen una
representación que incluye la parte posterior del cráneo (cuero cabelludo), el ángulo de
mandíbula, la región sub-occipital, la parte posterior de la oreja y la garganta (Poletti,
1991). Es importante destacar que la mayor distribución cutánea del nervio C2 está
representada por el nervio occipital mayor (Poletti, 1991).
1.7.3 Complejo trigeminocervical
El CTC es una unidad anatómica-funcional que forman las astas dorsales de los dos
segmentos superiores de la médula cervical y el SVc del núcleo espinal trigeminal
(Becker, 2010; Hoskin et al., 1999; Hu et al., 2005; Piovesan et al., 2003). Estudios
anatómicos en animales han encontrado que el CTC se extiende hasta el segmento
cervical C2-C3 (Goadsby and Hoskin, 1997; Kaube et al., 1993; Strassman et al., 1994).
En el CTC se produce una convergencia de neuronas nociceptivas de segundo orden que
reciben aferencias nociceptivas primarias trigeminales y de los tres primeros nervios
cervicales (Bartsch and Goadsby, 2003b; Bartsch, 2005; Bogduk, 2001; Goadsby et al.,
2008; Hu et al., 1995, 2005; Piovesan et al., 2003) (Figura 10). Evidencia científica de
estudios básicos en animales ha demostrado este fenómeno de convergencia (Bartsch
and Goadsby, 2002, 2003a; Hu et al., 1993; Sessle et al., 1986; Yu et al., 1995), y
también se tiene evidencia de este mecanismo en seres humanos (Busch et al., 2006;
Piovesan et al., 2001).

38
Figura 10. Representación gráfica del complejo trigeminocervical (CTC).
El CTC puede ser sensibilizado por aferencias nociceptivas primarias provenientes del
músculo masetero y de la ATM (Cairns et al., 2001, 2002; Nishimori et al., 1986;
Shigenaga et al., 1988), además se ha descrito que las aferencias primarias nociceptivas
provenientes de la piel y de los músculos cervicales son capaces de excitar neuronas del
CTC (Bartsch and Goadsby, 2003a; Le Doaré et al., 2006; Sessle et al., 1986), sin
embargo parece ser que la principal contribución aferente cervical hacia este complejo
neural está mediada por la raíz de C2, representada periféricamente por el nervio
occipital mayor (Bartsch, 2005), en relación con esto, Goadsby y cols. demostraron que
la activación de las fibras aferentes del nervio occipital mayor aumentan la actividad
metabólica de neuronas del CTC (Goadsby et al., 1997), por otra parte, Le Doare y cols.
observaron que los receptores N-metil-D-aspartato (NMDA) glutamatérgicos están

39
implicados en estas sinapsis (Le Doaré et al., 2006), varios estudios han demostrado que
los receptores NMDA son importantes en el desarrollo de la sensibilización central del
SVc (Chiang et al., 1998; Yu et al., 1996), así como los receptores de la neuroquinina y
purinérgicos (Dubner and Ren, 2004). Recientemente se ha comprobado en modelo
animal, que la lesión sobre un nervio espinal superior provoca alodinia mecánica y la
hiperalgesia térmica en la piel de la cara, los resultados de esta investigación también
sugieren que la fosforilación de la kinasa de regulación extracelular en el SVc y en las
neuronas de C1-C2 y la activación de las células astrogliales están involucradas en el
dolor orofacial extraterritorial producido después de una lesión (Kobayashi et al., 2011).
Xie describe que en la sensibilización central trigeminal las células gliales tienen una
importante implicación incluyendo la interacción con los receptores NMDA
glutamatérgicos y purinérgicos (Xie, 2008).
1.7.4 Sensibilización central del complejo trigeminocervical
Neurofisiológicamente la recepción de entradas de aferencias nociceptivas en el sistema
nervioso central forma parte de la sensibilización central que es un proceso fundamental
en el desarrollo y mantenimiento del dolor referido y el dolor crónico (Arendt-Nielsen
et al., 2000; Salter, 2004). En la sensibilización central trigeminal se produce una
expansión de los campos receptivos profundos y cutáneos neuronales, y además se han
observado otros cambios en las propiedades de las neuronas del trigeminales y en las
vías nociceptivas medulares (Bereiter et al., 2005; Chiang et al., 1998, 2005; Lam et al.,
2009; Salter, 2004; Vernon et al., 2009), específicamente se ha demostrado que la
aplicación experimental de una “sopa inflamatoria” en la duramadre puede inducir una
sensibilización central de las neuronas trigeminales nociceptivas de segundo orden en el
SVc, generando una mayor capacidad de respuesta a la estimulación cutánea de la
región facial y en la duramadre (Burstein et al., 1998), en relación con este hallazgo,

40
Bartsch y Goadsby encontraron que la estimulación del nervio occipital mayor podía
causar una sensibilización central con un aumento de la excitabilidad de la entrada de la
duramadre (Bartsch and Goadsby, 2002), además, se ha observado que la activación de
los nociceptores meníngeos por mediadores pro-inflamatorios sensibilizan a las
neuronas de primer orden en el ganglio trigeminal (Strassman et al., 1996) y las
neuronas de segundo orden trigeminovasculares en el CTC (Burstein et al., 1998).
En el proceso de sensibilización central se producen salidas eferentes que involucran
conexiones entre motoneuronas y aferencias nociceptivas neuronales que su vez generan
respuestas motoras (Bartsch, 2005; Sessle, 2002). Evidencia científica basada en
estudios realizados con modelos animales han demostrado que la estimulación química
nociceptiva de estructuras profundas paravertebrales musculares de la región cervical
evocan efectos reflejos, incluyendo un aumento de la actividad electromiográfica en los
músculos masticatorios y cervicales ipsilaterales (Hu et al., 1993, 1996; Shin et al.,
2005) y alteraciones en los reflejos de apertura mandibular (Makowska et al., 2005).
Similares resultados se han observado en la estimulación nociceptiva de las meninges
posteriores de la rata (Hu et al., 1995). Por otra parte, se ha demostrado que la inyección
de bradiquinina en el músculo masetero en conejos provoca un aumento de la actividad
fusimotora de los husos musculares paravertebrales de la región cervical, estos
hallazgos sugieren que existe una potente conexión refleja entre el sistema trigeminal y
el sistema neuromuscular cervical (Hellström et al., 2000, 2002), resultados similares se
han descrito en estudios realizados en sujetos sanos, en donde se observó que un dolor
provocado experimentalmente en el músculo masetero provoca un aumento de la
actividad electromiográfica en los músculos esternocleidomastoideo y el esplenio del
cuello (Svensson et al., 2004), además de un aumento del reflejo de estiramiento de
estos músculos (Wang et al., 2004); otra de las manifestaciones motoras a nivel

41
mandibular que se han observado es la limitación momentánea de la apertura
mandibular después de provocar un dolor experimental en el músculo trapecio mediante
la infiltración de suero salino hipertónico (Komiyama et al., 2005). Un hallazgo
importante observado recientemente es que al provocar un dolor experimental sobre el
músculo masetero se produce una alteración del control motor de las acciones
integradas de la región craneocervical y craneomandibular al realizar los movimientos
de apertura y cierre (Wiesinger et al., 2013).
La sensibilización central del CTC se manifiesta clínicamente con un aumento de las
áreas de expansión del dolor en territorios trigeminales y cervicales, una mala
localización del dolor, hiperalgesia, alodinia mecánica (Katsarava et al., 2002; Kaube et
al., 2002; Sessle, 1999, 2002, 2011) y una disfunción de la activación del sistema
inhibitorio descendente (King et al., 2009; Maixner et al., 1998; Sarlani et al., 2004)
1.8 Modulación del Dolor en el Complejo Trigeminocervical
La recepción de los estímulos nociceptivos por las neuronas de segundo orden del CTC
está modulada por proyecciones inhibitorias descendentes de estructuras del tronco
encefálico, el diencéfalo y la corteza somatosensorial (Akerman et al., 2011; Bartsch
and Goadsby, 2003b; Sessle, 1999, 2000), se ha demostrado que la manipulación de las
neuronas ventrolaterales de la sustancia gris periacueductal (Bartsch, Knight, et al.,
2004; Knight and Goadsby, 2001; Knight et al., 2002), el núcleo magno del rafe
(Edelmayer et al., 2009) y el bulbo rostroventral (Lambert et al., 2008) pueden modular
la actividad nociceptiva evocada en el CTC, evidencia previa ha demostrado que la
estimulación de estas áreas produce un importante efecto inhibitorio anti-nociceptivo
(Fields et al., 1991) (Figura 11), sin embargo es importante destacar que la activación
del bulbo rostroventral también puede facilitar la hiperalgesia, el dolor neuropático y el
dolor crónico (Porreca et al., 2002; Ren and Dubner, 2002; Sugiyo et al., 2005; Venegas

42
et al., 2009). Otros estudios en donde se ha estimulado químicamente la región posterior
del hipotálamo han demostrado que esta región también influye en la modulación
nociceptiva del CTC (Bartsch et al., 2005; Bartsch, Levy, et al., 2004).
Figura 11. Representación gráfica del sistema inhibitorio descendente y las estructuras implicadas en la modulación
de la actividad nociceptiva. SVc, sub-núcleo trigeminal cervical; NTE, núcleo trigeminal espinal; BRV, bulbo
rostroventral; vlPAG; área ventrolateral de la sustancia gris periacueductal; HT, hipotálamo; S1, corteza
somatosensorial primaria.
En el proceso de activación del sistema inhibitorio descendente se producen diversos
mecanismos que incluyen la participación de los receptores opioides y de
neurotransmisores como el GABA y la serotonina (5-HT) (Sessle, 1999, 2002). El SVc
recibe proyecciones serotoninérgicas y encefalinérgicas del núcleo magno del rafe
(Beitz, 1982; Beitz et al., 1987) que tienen una actuación en la modulación del dolor
(Mason and Fields, 1989). Por otra parte, se ha demostrado que en la médula espinal y
en el SVc el principal neurotransmisor que actúa en la actividad eferente inhibitoria en
43
el bulbo rostroventral es la 5-HT (Beitz, 1982; Clatworthy et al., 1988; Fields et al.,
1991), en relación con esto, Okamato y cols. comprobaron en un modelo animal de
dolor inflamatorio persistente de la ATM que los receptores 5-HT3 en el CTC están
involucrados en los circuitos inhibitorios serotoninérgicos centrales que modulan la
actividad nociceptiva profunda y superficial (Okamoto et al., 2005).
Acciones terapéuticas relacionadas con los cambios del comportamiento, intervenciones
farmacológicas y otros tratamientos que actúan a nivel estructural, influyen sobre
mecanismos tronco encefálicos relacionados con la modulación descendente del dolor
craniofacial (Sessle, 2002).
1.8.1 Influencia de las aplicaciones terapéuticas sobre el dolor craneofacial
A partir de los resultados de estudios experimentales sobre mecanismos
neurofisiológicos implicados en la modulación de dolor en el CTC, muchos
investigadores han planteado estrategias terapéuticas para influir sobre estructuras de la
región cervical y a su vez modular el dolor de cabeza y orofacial. Las intervenciones
sobre el nervio occipital han sido de las más utilizadas en las últimas décadas, son
varios los estudios que se sugieren que la neuro-estimulación periférica del nervio
occipital es efectiva en la disminución del dolor orofacial y la cefalea en un porcentaje
importante de los pacientes en los que se aplica este tratamiento (Jasper and Hayek,
2008; Lee and Huh, 2013; Saper et al., 2011; Serra and Marchioretto, 2012; Silberstein
et al., 2012; Slavin et al., 2006). Siguiendo con las intervenciones sobre el nervio
occipital, hay que destacar que Leroux y Ducros en una recientemente revisión de
ensayos clínicos y series de casos, describen que la infiltración mediante cortico-
esteroides con o sin adición de anestésicos locales sobre el nervio occipital en pacientes
con cefalea en racimos produce efectos inmediatos en la disminución de la frecuencia
de los ataques, sin embargo varios estudios describen que el dolor local tras la

44
intervención es un efecto secundario muy común pero no considerado grave (Leroux
and Ducros, 2013), en otra revisión narrativa se sugiere que la infiltración del nervio
occipital mayor presenta efectos positivos sobre los pacientes con migraña pero se
señala que estos datos se interpreten con precaución ya que se han extraído de estudios
con pobres diseños metodológicos (Ashkenazi and Levin, 2007). Posterior a esta
revisión, se publicaron dos ensayos clínicos aleatorizados en donde se pretendía
comprobar el efecto de una infiltración del nervio occipital mayor y de puntos gatillo de
músculos paravertebrales y del trapecio utilizando anestésicos locales con y sin cortico-
esteroides en pacientes con migraña, los resultados de ambas investigaciones
demostraron la efectividad de ambas intervenciones en la reducción del dolor de cuello
y el dolor de cabeza pero no hubo diferencia en la comparación de los dos tratamientos
(Ashkenazi et al., 2008; Saracco et al., 2010). Evidencia científica proveniente de
estudios de series de casos retrospectivos describen que la infiltración intramuscular de
bupivacaina en la musculatura paravertebral reduce el dolor en pacientes adultos
(Mellick and Mellick, 2003, 2008; Mellick et al., 2006) y en niños (Mellick and
Pleasant, 2010) que presentan dolor orofacial y/o cefalea.
La evidencia sobre la administración de bupivacaina intratecal en la región cervical para
dolores refractarios cervicales, de cabeza y orofaciales es limitada, sin embargo las
series de casos publicadas describen una eficacia en la analgesia producida y una
disminución de la utilización de fármacos opiáceos (Appelgren et al., 1996; Lundborg
et al., 2009) por otra parte, los efectos adversos descritos fueron pocos y la mayoría de
los casos transitorios (Lundborg et al., 2009).
Intervenciones específicas de fisioterapia aplicadas al tratamiento de la región cervical
para modular el dolor en pacientes con cefalea han sido muy investigadas en las últimas
dos décadas, específicamente se debe destacar que un gran número de ensayos clínicos

45
muestran que la terapia manual, el ejercicio terapéutico o la combinación de ambas
enfocadas a tratar estructuras musculoesqueléticas de la región cervical han demostrado
efectividad en las disminución de la intensidad y la frecuencia del dolor en pacientes
con cefalea tensional y cefalea cervicogénica (Castien et al., 2011, 2012, 2013; Espí-
López and Gómez-Conesa, 2014; Espí-López et al., 2014; van Ettekoven and Lucas,
2006; Hall et al., 2007; Mongini et al., 2012; Ylinen et al., 2010).

46
47
JUSTIFICACIÓN

48
2. JUSTIFICACIÓN DEL TRABAJO REALIZADO
La región orofacial y el cráneo, que a su vez incluyen estructuras orales y dentales
representan una de las zonas anatómicas más complejas del organismo, esta situación
conlleva a una difícil compresión de los mecanismos fisiopatológicos de los trastornos
que afectan a la región craneofacial como por ejemplo los TCM, las cefaleas y el dolor
orofacial (Fricton, 2014). La comprensión de la clínica, la patogénesis y el tratamiento
es esencial para ayudar a los pacientes que presentan estos problemas (Graff-Radford,
2007).
Es manifiesto que en la últimas décadas se ha incrementado de manera exponencial la
investigación en torno al DCF, estos estudios en su mayoría se han enfocado en estudiar
los mecanismos biológicos periféricos y centrales relacionados con la transmisión y
modulación nociceptiva, así como los sistemas de clasificación del paciente y los
factores psicosociales implicados (Hargreaves, 2011), los resultados de algunas
investigaciones en esta línea sugieren, que áreas extra-trigeminales como la región
cervical parecen tener un papel relevante en la fisiopatología de las cefaleas y el dolor
orofacial (Graff-Radford, 2012), a pesar de esto, consideramos que aún es necesario
contar con más estudios que apoyen los hallazgos demostrados y que además terminen
de identificar con mayor exactitud las implicaciones biomecánicas y neurofisiológicas
de la región cervical sobre el DCF, por otra parte, creemos que es importante aclarar
cómo estos datos se pueden utilizar para el diagnóstico clínico y el planteamiento
terapéutico de fisioterapia. En los últimos años el tratamiento de fisioterapia ha
adquirido un estatus importante en el tratamiento de los TCM y el DCF (Aggarwal and
Keluskar, 2012), sin embargo no contamos con evidencia científica suficiente que
demuestre la relevancia o el papel del tratamiento de fisioterapia sobre la región cervical
en los pacientes con TCM, este es uno de los motivos centrales que justifica esta tesis

49
doctoral y que nos lleva a plantear diversos objetivos entorno a esta cuestión.
La evidencia científica contemporánea nos ha llevado a la reflexión sobre las
limitaciones que presentan los estudios y los abordajes clínicos basados en modelos
mecanicistas o que toman en cuenta únicamente la dimensión sensorial-discriminativa
del DCF (Reid and Greene, 2013), en una parte de esta tesis hemos intentado contestar
interrogantes desde un punto de vista más integral utilizando un enfoque bioconductual
en el que planteamos las posibles interacciones entre el dolor y la discapacidad
craneofacial, con variables motoras, de discapacidad cervical y variables psicológicas.
El enfoque bioconductual para el tratamiento, el diagnóstico y la valoración del DCF
reconoce la importancia de los factores psicosociales, como antecedentes de dolor, los
estados emocionales en curso, el estatus cognitivo, las creencias de salud, y las
habilidades de afrontamiento, que interactúan con las alteraciones fisiológicas en la
determinación de la experiencia del dolor para los pacientes (Carlson, 2008; Shephard et
al., 2014).

50

51
OBJETIVOS

52
3. OBJETIVOS
El objetivo general de esta investigación es determinar la influencia biomecánica y
neurofisiológica de la región cervical sobre el dolor y la discapacidad craneofacial
crónica. Además se pretende identificar como determinados factores bioconductuales
influyen sobre la función craneomandibular, la discapacidad y el dolor craneofacial.
A continuación se detallan los objetivos específicos:
1- Evaluar la influencia de la postura craneocervical sobre la discapacidad
craneofacial, la dinámica mandibular y el umbral de dolor a la presión,
además se pretende analizar las diferencias de postura craneocervical entre
sujetos asintomáticos y pacientes con dolor cérvico-craneofacial (DCCF)
crónico.
Este objetivo se ha abordado en las publicaciones originales I y II:
I. La Touche R, París-Alemany A, von Piekartz H, Mannheimer JS,
Fernández-Carnero J, Rocabado M. The influence of cranio-cervical posture
on maximal mouth opening and pressure pain threshold in patients with
myofascial temporomandibular pain disorders. Clin J Pain. 2011
Jan;27(1):48-55
II. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A,
Angulo-Díaz-Parreño S, La Touche R. Reliability, Standard Error, and
Minimal Detectable Change of Two Tests for Craniocervical Posture

53
Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial Pain
Patients. 2014 (En revisión).
2- Determinar la influencia del dolor y la discapacidad cervical sobre la función
sensoriomotora trigeminal.
Este objetivo se ha abordado en las publicaciones originales III y V:
III. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-
Parreño S, Paris-Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain
sensitivity over the trigeminal region in patients with chronic mechanical
neck pain. J Pain. 2010 Mar;11(3):256-63
V. La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-
Díaz-Parreño S, Fernández-Carnero J. The Influence of Neck Disability and
Pain Catastrophizing about Trigeminal Sensory-Motor System in Patients
with Headache Attributed to Temporomandibular Disorders. 2014 (En
revision)
3- Estudiar la asociación entre la discapacidad craneofacial y la discapacidad
cervical en pacientes con trastornos craneomandibulares, cefaleas y dolor
craneofacial crónico.
Este objetivo se ha abordado en las publicaciones originales II y IV:
II. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A,
Angulo-Díaz-Parreño S, La Touche R. Reliability, Standard Error, and

54
Minimal Detectable Change of Two Tests for Craniocervical Posture
Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial Pain
Patients. 2014 (En revisión).
IV. La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A,
Angulo-Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero
J. Craniofacial pain and disability inventory (CF-PDI): development and
psychometric validation of a new questionnaire. Pain Physician. 2014 Jan-
Feb;17(1):95-108.
4- Analizar la asociación de factores psicológicos como la depresión, el miedo
al movimiento y el catastrofismo ante el dolor con variable motoras, de dolor
y discapacidad cervical y craneofacial.
Este objetivo se ha abordado en las publicaciones originales III, IV y V:
III. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-
Parreño S, Paris-Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain
sensitivity over the trigeminal region in patients with chronic mechanical
neck pain. J Pain. 2010 Mar;11(3):256-63
IV. La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A,
Angulo-Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero
J. Craniofacial pain and disability inventory (CF-PDI): development and
psychometric validation of a new questionnaire. Pain Physician. 2014 Jan-
Feb;17(1):95-108.
V. La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-
Díaz-Parreño S, Fernández-Carnero J. The Influence of Neck Disability and
Pain Catastrophizing about Trigeminal Sensory-Motor System in Patients

55
with Headache Attributed to Temporomandibular Disorders. 2014 (En
revision)
5- Determinar el efecto del tratamiento de fisioterapia aplicado en la región
cervical sobre la función mandibular y el dolor craneofacial.
Este objetivo se ha abordado en las publicaciones originales VI y VII:
VI. La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J,
Escalante K, Angulo-Díaz-Parreño S, Paris-Alemany A, Cleland JA. The
effects of manual therapy and exercise directed at the cervical spine on pain
and pressure pain sensitivity in patients with myofascial temporomandibular
disorders. J Oral Rehabil. 2009 Sep;36(9):644-52.
VII. La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S,
Bishop MD, Lopéz-Valverde-Centeno A, von Piekartz H, Fernández-
Carnero J. Does mobilization of the upper cervical spine affect pain
sensitivity and autonomic nervous system function in patients with cervico-
craniofacial pain?: A randomized-controlled trial. Clin J Pain. 2013
Mar;29(3):205-15.

56

57
MATERIAL Y MÉTODOS
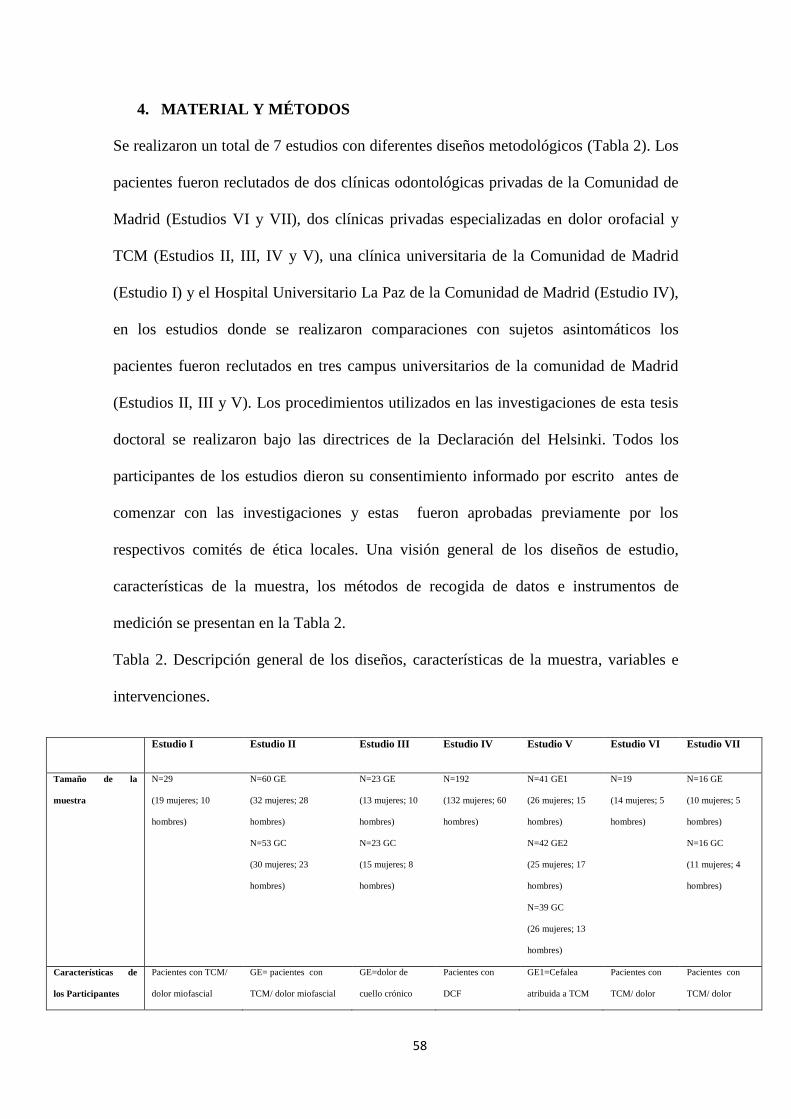
58
4. MATERIAL Y MÉTODOS
Se realizaron un total de 7 estudios con diferentes diseños metodológicos (Tabla 2). Los
pacientes fueron reclutados de dos clínicas odontológicas privadas de la Comunidad de
Madrid (Estudios VI y VII), dos clínicas privadas especializadas en dolor orofacial y
TCM (Estudios II, III, IV y V), una clínica universitaria de la Comunidad de Madrid
(Estudio I) y el Hospital Universitario La Paz de la Comunidad de Madrid (Estudio IV),
en los estudios donde se realizaron comparaciones con sujetos asintomáticos los
pacientes fueron reclutados en tres campus universitarios de la comunidad de Madrid
(Estudios II, III y V). Los procedimientos utilizados en las investigaciones de esta tesis
doctoral se realizaron bajo las directrices de la Declaración del Helsinki. Todos los
participantes de los estudios dieron su consentimiento informado por escrito antes de
comenzar con las investigaciones y estas fueron aprobadas previamente por los
respectivos comités de ética locales. Una visión general de los diseños de estudio,
características de la muestra, los métodos de recogida de datos e instrumentos de
medición se presentan en la Tabla 2.
Tabla 2. Descripción general de los diseños, características de la muestra, variables e
intervenciones.
Estudio I Estudio II Estudio III Estudio IV Estudio V Estudio VI Estudio VII
Tamaño de la
muestra
N=29
(19 mujeres; 10
hombres)
N=60 GE
(32 mujeres; 28
hombres)
N=53 GC
(30 mujeres; 23
hombres)
N=23 GE
(13 mujeres; 10
hombres)
N=23 GC
(15 mujeres; 8
hombres)
N=192
(132 mujeres; 60
hombres)
N=41 GE1
(26 mujeres; 15
hombres)
N=42 GE2
(25 mujeres; 17
hombres)
N=39 GC
(26 mujeres; 13
hombres)
N=19
(14 mujeres; 5
hombres)
N=16 GE
(10 mujeres; 5
hombres)
N=16 GC
(11 mujeres; 4
hombres)
Características de
los Participantes
Pacientes con TCM/
dolor miofascial
GE= pacientes con
TCM/ dolor miofascial
GE=dolor de
cuello crónico
Pacientes con
DCF
GE1=Cefalea
atribuida a TCM
Pacientes con
TCM/ dolor
Pacientes con
TCM/ dolor
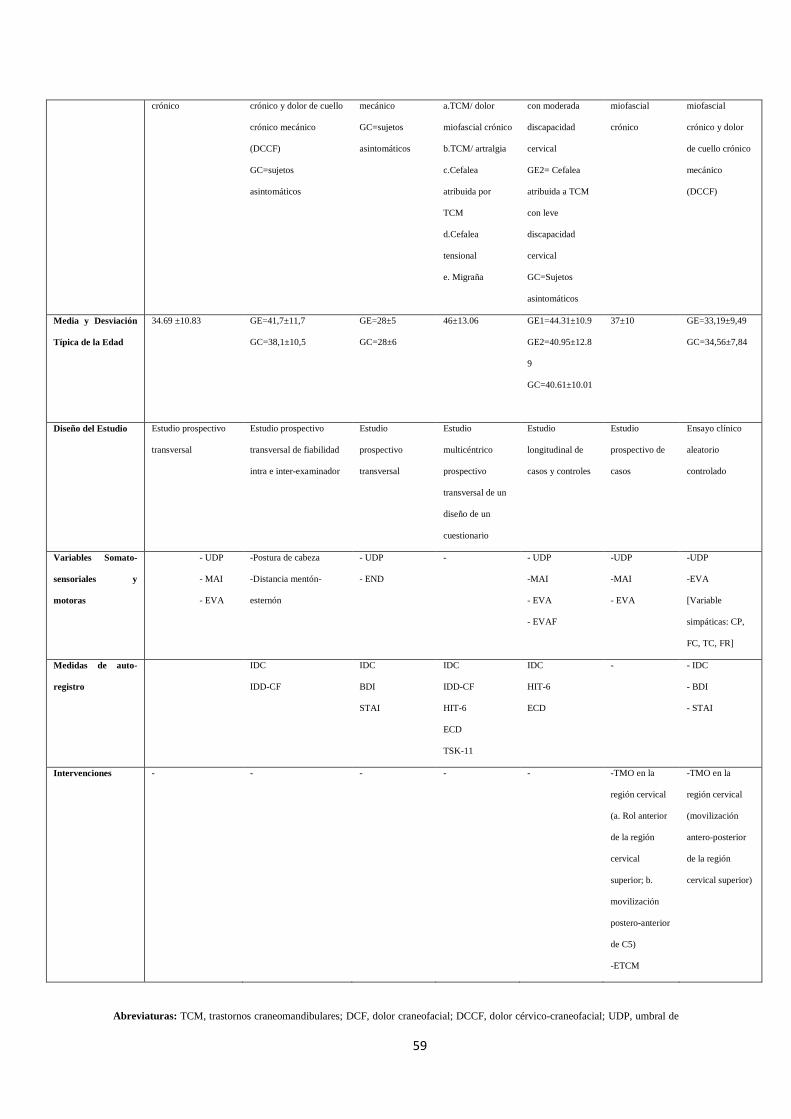
59
crónico crónico y dolor de cuello
crónico mecánico
(DCCF)
GC=sujetos
asintomáticos
mecánico
GC=sujetos
asintomáticos
a.TCM/ dolor
miofascial crónico
b.TCM/ artralgia
c.Cefalea
atribuida por
TCM
d.Cefalea
tensional
e. Migraña
con moderada
discapacidad
cervical
GE2= Cefalea
atribuida a TCM
con leve
discapacidad
cervical
GC=Sujetos
asintomáticos
miofascial
crónico
miofascial
crónico y dolor
de cuello crónico
mecánico
(DCCF)
Media y Desviación
Típica de la Edad
34.69 ±10.83 GE=41,7±11,7
GC=38,1±10,5
GE=28±5
GC=28±6
46±13.06 GE1=44.31±10.9
GE2=40.95±12.8
9
GC=40.61±10.01
37±10 GE=33,19±9,49
GC=34,56±7,84
Diseño del Estudio Estudio prospectivo
transversal
Estudio prospectivo
transversal de fiabilidad
intra e inter-examinador
Estudio
prospectivo
transversal
Estudio
multicéntrico
prospectivo
transversal de un
diseño de un
cuestionario
Estudio
longitudinal de
casos y controles
Estudio
prospectivo de
casos
Ensayo clínico
aleatorio
controlado
Variables Somato-
sensoriales y
motoras
- UDP
- MAI
- EVA
-Postura de cabeza
-Distancia mentón-
esternón
- UDP
- END
- - UDP
-MAI
- EVA
- EVAF
-UDP
-MAI
- EVA
-UDP
-EVA
[Variable
simpáticas: CP,
FC, TC, FR]
Medidas de auto-
registro
IDC
IDD-CF
IDC
BDI
STAI
IDC
IDD-CF
HIT-6
ECD
TSK-11
IDC
HIT-6
ECD
- - IDC
- BDI
- STAI
Intervenciones - - - - - -TMO en la
región cervical
(a. Rol anterior
de la región
cervical
superior; b.
movilización
postero-anterior
de C5)
-ETCM
-TMO en la
región cervical
(movilización
antero-posterior
de la región
cervical superior)
Abreviaturas: TCM, trastornos craneomandibulares; DCF, dolor craneofacial; DCCF, dolor cérvico-craneofacial; UDP, umbral de

60
dolor a la presión; MAI, máxima apertura interincisal; EVA, escala visual analógica del dolor; END, escala numérica del dolor; GE,
grupo experimental; GC, grupo control; IDC, índice de dolor cervical; IDD-CF, inventario de dolor y discapacidad craneofacial;
BDI, inventario de depresión Beck; STAI, cuestionario de ansiedad estado-rasgo; HIT-6, cuestionario de impacto de la cefalea;
ECD; escala de catastrofismo ante el dolor; TSK-11, escala de Tampa de Kinesiofobia; EVAF, escala visual analógica de fatiga;
TMO, terapia manual ortopédica; ETCM, ejercicio terapéutico de control motor; CP, conductancia de la piel; FC, frecuencia
cardíaca; FR, frecuencia respiratoria; TC, temperatura cutánea.
4.1 Participantes
La muestra de los estudios I y VI estuvo conformada por pacientes que presentaban
TCM atribuido a dolor miofascial, esta denominación se extrae de los Criterios
diagnósticos de investigación para TCM (Dworkin and LeResche, 1992; Schiffman et
al., 2010), aunque es importante mencionar que además se establecieron otros criterios
de inclusión que se exponen a continuación: a) diagnóstico primario de dolor miofascial
de acuerdo a los Criterios diagnósticos de investigación para TCM; (Dworkin and
LeResche, 1992; Schiffman et al., 2010); b) dolor bilateral en los músculos masetero y
temporal; c) duración del dolor mayor a 6 meses; d) intensidad del dolor mayor a 30mm
según la escala visual analógica (EVA); y e) presencia de PGM en la musculatura
masticatoria. Los criterios de exclusión adoptados en estos estudios fueron los
siguientes: a) TCM atribuidos a disfunciones articulares o enfermedades degenerativos
de acuerdo a los Criterios diagnósticos de investigación para TCM (Dworkin and
LeResche, 1992; Schiffman et al., 2010); b) lesiones traumáticas como fracturas o
latigazo cervical; c) enfermedades sistémicas reumatológicas como fibromialgia y
artritis; c; dolor neuropático; y d) concomitancia con cefaleas primarias.
El estudio III contó con una muestra de pacientes con dolor de cuello crónico mecánico
inespecífico. Conceptualmente esta dolencia se define como una afectación que presenta
signos y síntomas de disfunción muscular como empeoramiento de dolor con el
mantenimiento de la postura, limitación del rango del movimiento y dolor a la palpación
de la musculatura cervical. Además los pacientes incluidos en este estudio tenían que

61
tener el dolor en un periodo superior a 6 meses. Los criterios de exclusión adoptados en
este estudio fueron los siguientes: a) dolor de cuello unilateral; b) enfermedades
reumáticas; c) latigazo cervical; d) cirugías previas de la región cervical; e) diagnóstico
de radiculopatía cervical; f) diagnóstico de TCM.
La muestra del estudio IV estuvo representada por pacientes con distintos tipos de DCF
como los siguientes, cefalea tensional, migraña, cefalea atribuida a TCM, artralgia y
dolor miofascial. Los criterios de inclusión fueron los siguientes: a) pacientes mayores
de 18 años; b) diagnóstico de dolor facial o cefalea de acuerdo a los criterios de la
Clasificación Internacional de las Cefaleas (IHS, 2013); c) diagnóstico de TCM de
acuerdo a los Criterios diagnósticos de investigación para TCM; (Dworkin and
LeResche, 1992; Schiffman et al., 2010); d) presencia de los síntomas dolorosos de más
de 6 meses; y e) buena compresión del idioma español. Los criterios de exclusión
adoptados en este estudio fueron los siguientes: a) dificultad en la compresión del
idioma español; b) deterioro cognitivo; y trastornos psiquiátricos.
El estudio V fue conformado por pacientes con cefalea atribuida a TCM de acuerdo a
los criterios de la Clasificación Internacional de las Cefaleas (IHS, 2013) y los criterios
clínicos y de investigación para TCM (Schiffman et al., 2014), además se incluyeron
los siguientes criterios de inclusión: a) presencia de dolor superior a 6 meses; b) dolor
en mandíbula, zona temporal, cara y cuello en reposo o en movimiento; c) ser mayor de
18 años; y d) discapacidad de cuello cuantificado de acuerdo al índice de discapacidad
cervical (IDC) (Andrade Ortega et al., 2010), por otra parte se debe mencionar que en
este estudio los pacientes se subdividieron de acuerdo a los niveles de discapacidad
cervical según el IDC (discapacidad leve y moderada) (Andrade Ortega et al., 2010).
Los criterios de exclusión adoptados en estos estudios fueron los siguientes: a) TCM
atribuidos a disfunciones articulares o enfermedades degenerativos de acuerdo los

62
Criterios diagnósticos de investigación para TCM (Dworkin and LeResche, 1992;
Schiffman et al., 2010); b) lesiones traumáticas como fracturas o latigazo cervical; c)
enfermedades sistémicas reumatológicas como fibromialgia y artritis; c; dolor
neuropático; d) concomitancia con cefaleas primarias; e) dolor de cuello unilateral; f)
procedimientos quirúrgicos previos en la región cervical; y g) radiculopatía cervical.
Los estudios II y VII contaron con una muestra de pacientes con DCCF crónico, estos
pacientes integran clínicamente una comorbilidad entre el dolor de cuello crónico
mecánico inespecífico (descrito en estudio III) y TCM atribuido a dolor miofascial
(descrito en los estudios I y VI). Definimos DCCF como un dolor de origen muscular
que presenta mecanismos disfuncionales como limitación del movimiento, movimientos
in-coordinados y debilidad y falta de resistencia en el cuello y la mandíbula, estos
síntomas pueden exacerbarse con posturas mantenidas generando dolor en la región
cervical y craneofacial. Los criterios de exclusión adoptados en estos estudios fueron los
mismos que en los estudios I, III y VI.
También es importante destacar que en los estudios II, III y V se realizaron
comparaciones con participantes asintomáticos.
4.2 Variables y Pruebas de Medición
En todos los estudios se registraron diversos tipos de variables sociodemográficas como
la edad, peso, altura, sexo y la duración de los síntomas, además en el estudio V se
cuantifico el nivel de estudios y el estado laboral. A parte de las variables
sociodemográficas en los estudios también se evaluaron variables somatosensoriales,
motoras y psicológicas mediante la utilización de diversos instrumentos y otras
herramientas de auto-registro especializadas. En la tabla 3 se presenta un resumen de la
variables e instrumentos de medición utilizadas en cada estudio.
Tabla 3. Variables e instrumentos utilizados en los estudios.

63
Variables Medidas Estudios
I II III IV V VI VII
Intensidad del dolor
a. Escala visual
analógica del dolor
b. Escala numérica de
dolor
X-a X-b X-a X-a X-a
Máxima apertura interincisal a. Escala therabite
b. Escala CMD
c.
X-a X-b X-a
Umbral de dolor a la presión Algométro
X X X X X
Postura craneocervical a. Distancia mentón
esternón medido con
un calibre digital.
b. Postura de cabeza
medido con CROM
X-ab
Percepción de fatiga Escala visual analógica de fatiga
X
Discapacidad cervical Índice de discapacidad cervical
X X X X X
Discapacidad craneofacial y
función mandibular
Inventario de dolor y
discapacidad craneofacial
X X
Síntomas depresivos Inventario de depresión Beck
X
Estado de ansiedad Cuestionario de ansiedad
estado/rasgo
X X
Miedo al movimiento Escala Tampa de Kinesiofobia
X
Catastrofismo ante el dolor Escala de catastrofismo ante el
dolor
X X
Impacto de la cefalea en la
vida diaria
Cuestionario de impacto de la
cefalea HIT-6
X X

64
4.2.1 Medidas de auto-registro
Catastrofismo ante el Dolor
Se utilizó la versión española de la escala de catastrofismo ante el dolor (ECD) para
evaluar el nivel de catastrofismo (García Campayo et al., 2008). La ECD está
compuesta por 13 ítems, cada ítem puntúa del 0 al 4. El rango de puntuación total se
encuentra de 0 a 52, donde puntuaciones mayores indican mayor nivel de catastrofismo.
Este instrumento presentó la misma estructura factorial original presentando tres
factores (rumiación, magnificación y desesperanza), así como unas adecuadas
propiedades psicométricas (García Campayo et al., 2008).
Miedo al Movimiento
La versión en español de la escala Tampa de kinesiofobia (TSK-11) mide el miedo al
dolor y al movimiento (Gómez-Pérez et al., 2011). La TSK-11 contiene 11 ítems en su
versión española, tras el análisis factorial se eliminaron algunos ítems de la versión
original que fueron psicométricamente pobres (Gómez-Pérez et al., 2011; Kori et al.,
1990). La puntuación total del TSK-11 se encuentra entre 11 – 44 puntos y cada ítem
presenta una escala likert que puntúa del 1 al 4 (1 = totalmente en desacuerdo, 4 =
totalmente de acuerdo). Puntuaciones más altas indican mayor miedo al movimiento y
al dolor. El TSK-11 tiene dos sub-escalas: evitación de actividad y daño, además esta
escala ha demostrado aceptables propiedades psicométricas (Gómez-Pérez et al., 2011).
Intensidad del Dolor
La intensidad del dolor se midió con la escala visual analógica del dolor (EVA). La
EVA consiste en una línea de 100 mm, en el que el lado izquierdo representa "ningún
dolor" y el lado derecho "el peor dolor imaginable". Los pacientes colocan una marca
donde se sentían que representan la intensidad del dolor. Se ha comprobado que este
instrumento tiene una buena fiabilidad (Bijur et al., 2001).

65
En la medición de la intensidad del dolor también se utilizó la escala numérica del dolor
(END), esta escala presenta 11 puntos posibles representados en números del 0 (sin
dolor) al 10 (máximo dolor). Se ha demostrado que END presenta una buena fiabilidad
y validez en pacientes crónicos (Jensen and McFarland, 1993; Jensen et al., 1999).
Percepción de Fatiga
La escala visual analógica de fatiga (EVAF) se utilizó para cuantificar la fatiga
percibida. La EVAF consiste en una línea vertical de 100 mm en la que la parte inferior
representa "ninguna fatiga" (0 mm), y la parte superior representa la "fatiga máxima"
(100 mm). El investigador registra el resultado en mm. Se ha comprobado que este
instrumento tiene una buena fiabilidad (Tseng et al., 2010).
Discapacidad Cervical
La versión española del índice de discapacidad cervical (IDC) es instrumento utilizado
para evaluar la discapacidad percibida en relación a la dolencia en el cuello (Andrade
Ortega et al., 2010; Vernon and Mior, 1991). Este cuestionario consta de 10 ítems, con
6 posibles respuestas que representa 6 niveles de capacidad funcional, que van desde 0
(sin discapacidad) a 5 (discapacidad total) puntos. Las puntuaciones más altas indican
mayor discapacidad percibida. El IDC ha demostrado propiedades psicométricas
aceptables (Andrade Ortega et al., 2010).
Impacto de la Cefalea en la Vida Diaria
La versión española del HIT-6 (Bjorner et al., 2003; Gandek et al., 2003) consiste en un
cuestionario de seis ítems que evalúa la gravedad y el impacto del dolor de cabeza en la
vida del paciente. Los resultados de HIT-6 están estratificados en cuatro clases basadas
en el grado de impacto: poco o ningún impacto (HIT-6 puntuación de: 36-49), impacto
moderado (HIT-6 puntuación de: 50-55), impacto sustancial (HIT-6 puntuación de: 56-
59), y el impacto severo (HIT-6 puntuación de: 60-78) (Bjorner et al., 2003). El HIT-6

66
ha demostrado propiedades psicométricas aceptables (Martin et al., 2004).
Síntomas de Ansiedad
La versión española del cuestionario de ansiedad estado-rasgo (STAI) es una medida de
auto-informe de 40 ítems, diseñado para evaluar los síntomas de la ansiedad (Spielberg
and Lushene, 1982). Consta de 2 escalas independientes, una escala de ansiedad estado
y una escala de ansiedad rasgo, con 20 puntos cada uno, lo que resulta en una
puntuación entre 20 y 80. Superiores puntuaciones indican un mayor nivel de ansiedad.
Las escalas de estado y rasgo evalúan la ansiedad como un estado emocional actual y
como un rasgo de la personalidad, respectivamente. El STAI ha demostrado
propiedades psicométricas aceptables en su versión en español (Spielberg and Lushene,
1982).
Síntomas Depresivos
Los síntomas depresivos se evaluaron con el Inventario de Depresión Beck (BDI-II),
este instrumento de auto-registro evalúa síntomas afectivos, cognitivos y somáticos de
depresión. Se ha comprobado en estudios con población general y clínica que el BDI-II
presenta adecuadas propiedades psicométricas (Penley et al., 2003; Wiebe and Penley,
2005)
4.2.2 Instrumentos de medición
Máxima Apertura Interincisal
La máxima apertura interincisal (MAI) es la capacidad de abrir la boca tan amplio
como se pueda sin dolor. Esta distancia se mide en milímetros entre el incisivo superior
y el incisivo inferior. La MAI se midió con la escala TheraBite (Model CPT 95851;
Atos Medical AB; Sweden) y con la escala craneomandibular (Escala CMD. Patente.
No. ES 1075174 U, INDCRAN: 2011. INDCRAN, Madrid, Spain) (Figura 12). El
procedimiento para medir la MAI ha demostrado una buena fiabilidad inter-evaluador

67
(ICC = 0,95 - 0,96) (Beltran-Alacreu et al., 2014).
Figura 12. Medición de máxima apertura interincisal con la escala CMD.
Umbral de Dolor a la Presión
Un algómetro digital (FDX 25, Wagner Instruments, Greenwich, CT, EE.UU.),
compuesto por un cabezal de goma (1 cm2) unido a un manómetro, se utilizó para medir
UDPs (Figura 13). La presión ejercida se mide en kilogramos (kg); por lo tanto, los
UDPs se expresaron en kg /cm2. El protocolo utilizado fue una secuencia de 3
mediciones, con un intervalo de 30 segundos entre cada una de las mediciones. Un
promedio de las 3 mediciones se calculó para obtener un único valor para cada uno de
los puntos medidos en cada una de las evaluaciones. Los UDPs se evaluaron en varios
puntos de la región craneofacial y craneomandibular (Figura 14). El dispositivo se
aplica perpendicular a la piel. Se pidió a los pacientes que levantasen la mano en el
momento en que la presión comenzara a cambiar a una sensación de dolor, y en ese
momento el evaluador dejó de aplicar presión. La presión aplicada en la prueba se
aumentó gradualmente a una velocidad de aproximadamente 1 kg/s. Este procedimiento
de algometría tiene alta fiabilidad intra-evaluador (ICC = 0,94 a 0,97) para la medición

68
de los UDPs (Walton et al., 2011).
Figura 13. Medición del umbral de dolor a la presión con el algómetro digital.
Figura 14. Puntos de áreas trigeminales y cervicales en donde se midieron los umbrales de dolor a la presión en los
diferentes estudios.
Postura Craneocervical
Utilizamos el dispositivo CROM para medir la postura de cabeza (PC). Este dispositivo

69
tiene tres partes: a) una estructura plástica con forma de gafas; b) tres inclinómetros,
uno para cada plano de movimiento; y c) un brazo plástico para medir la de cabeza
hacia adelante y un localizador de vértebra (Figura 15). La medición de la PC está
graduada en el instrumento en 0,5 cm, que indican la distancia horizontal entre el puente
de la nariz y el localizador de vértebras. El localizador de vértebras tiene un nivel de
burbuja en la parte superior para ayudar a la colocación exacta. Los inclinómetros no se
utilizaron debido a los movimientos del cuello no se evaluaron.
Figura 15. Medición de la postura craneocervical
Para medir la distancia mentón-esternón (DME) se utilizó un calibre digital. El
dispositivo está hecho de plástico con una pantalla LCD de 5 dígitos y se puede medir
en pulgadas o en milímetros (mm) con un rango de 0,01 mm a 150 mm.
El evaluador explica en primer lugar que la medición se llevará a cabo mientras está

70
acostado en una camilla. En este momento, el evaluador mostró los calibradores
digitales al tema y dijo: "Usted sentirá que el instrumento contactará con su esternón y
en la barbilla; en ese momento no se debe mover”. Una vez en su lugar, la medición fue
tomada de la escotadura yugular del esternón a la protuberancia de la barbilla (Figura
16). La medida fue tomada en dos ocasiones.
Figura 16. Medición de la distancia mentón-esternón.
4.3 Resumen de los Procedimientos
Estudio I
Se registraron inicialmente las variables sociodemográficas y la intensidad del dolor y
después se procedió a medir los UDPs y la MAI en tres posturas craneocervicales
inducidas experimentalmente (posición neutra craneocervical, retracción craneocervical
y protracción craneocervical)
Estudio II
Se seleccionaron a los pacientes y los sujetos asintomáticos del grupo control, después
se registraron las variables sociodemográficas y las medidas de auto-registro (IDC y
IDD-CF) y finalmente se realizaron las mediciones de la postura craneocervical.

71
Estudio III
Se registraron las variables sociodemográficas y las medidas de auto-registro y después
se procedió a realizar mediciones del UDP en los puntos trigeminales.
Estudio IV
Se seleccionaron a los pacientes y después se procedió a registrar las variables
sociodemográficas y una batería de medidas de auto-registro de variables psicológicas,
dolor y discapacidad.
Estudio V
Una vez seleccionados los pacientes y el grupo control se procedió al registro de
variables sociodemográficas y las medidas de auto-registro, después de esa fase se
realizó el test masticatorio de provocación durante 6 minutos en donde se evaluó la
fatiga y la intensidad del dolor. Al finalizar el test masticatorio de provocación se
procedió a realizar las mediciones de la MAI y los UDPs.
Estudio VI
Se realizó un tratamiento sobre los pacientes seleccionados durante 10 sesiones, este
tratamiento estaba enfocado a la región cervical y específicamente se utilizó un
protocolo de estabilización cervical y un tratamiento de terapia manual sobre la región
cervical, además se realizaron mediciones de variables somatosensoriales y motoras
pre-intervención, post-intervención y tres meses después.
Estudio VII
Se seleccionaron un grupo de pacientes que se subdividen aleatoriamente en dos grupos,
un grupo recibe un tratamiento placebo y el otro un tratamiento manual sobre la región
cervical superior. Se realizaron mediciones de variables somatosensoriales y del sistema
nervioso simpático pre-intervención y post-intervención.

72
4.4 Análisis Estadístico
En el análisis de datos se ha utilizado estadística descriptiva para mostrar los datos de
las variables continuas que se presentan como media ± desviación típica (DT), intervalo
de confianza del 95% (IC) y frecuencia relativa (porcentaje). Prueba de Chi-cuadrado,
se utilizó para comparar las diferencian entre las variables categóricas (nominales). Se
realizo la prueba de Kolmogorov Smirnov para comprobar la normalidad.
Se utilizó la t de Student para la comparar las variables continuas entre los dos grupos.
Cuando las comparaciones se realizaron con más de dos grupos o se intentó analizar la
interacción con otras variables se aplicó una ANOVA de una, dos o tres vías según
procediese, seguido de un test post hoc de Bonferroni para analizar las comparaciones
múltiples. En uno de los estudios se realizó un análisis con una ANCOVA de dos vías
para identificar múltiples interacciones entre variables.
Se calculó el tamaño del efecto (d de Cohen) para las variables principales estudiadas.
De acuerdo con el método de Cohen, la magnitud del efecto fue considerado como
pequeño (0,20 a 0,49), medio (0,50 a 0,79), y grande (0,8) (Cohen, 1988).
La estructura factorial se analizó mediante un análisis factorial exploratorio (es decir,
análisis de componentes principales, ACP) con la rotación Oblimin. El número de
factores para la extracción se basa en el criterio de valor propio de Kaiser (valor propio
≥1) y la evaluación del gráfico de sedimentación (Ferguson and Cox, 1993). La calidad
de los modelos de análisis factorial se evaluó mediante la prueba de Bartlett para la
esfericidad y la prueba de Kaiser-Meyer-Olkin (KMO). Prueba de Bartlett es una
medida de la probabilidad de que la matriz de correlación inicial es una matriz de
identidad y debe ser <0,05 (Bartlett, 1954). La prueba de KMO mide el grado de
multicolinealidad y varía entre 0 y 1 (debe ser mayor que 0,50-0,60) (Kaiser, 1974).
El efecto suelo-techo se midieron mediante el cálculo del porcentaje de pacientes que

73
indican los puntajes mínimos y máximos posibles en los cuestionarios. El efecto suelo-
techo se considera que está presente si más del 15% de los encuestados logró el mayor o
menor puntuación total posible (Terwee et al., 2007).
La fiabilidad intra e inter-evaluador se analizo mediante coeficiente de correlación intra-
clase (CCI). Niveles de fiabilidad se definieron en base a la siguiente clasificación:
buena fiabilidad: ICC ≥ 0,75; fiabilidad moderada: ICC ≥ 0,50 y <0,75; y escasa
fiabilidad: ICC <0,50 (Portney LG, 2009).
El error de medición se expresa como un error estándar de medición (EEM), que se
calcula como 𝐷𝑇 × √1 − 𝐶𝐶𝐼, donde DT es la de los valores de todos los participantes,
y el CCI es el coeficiente de fiabilidad (Weir, 2005). El error de medición es el error
sistemático y aleatorio de la puntuación de un paciente que no es atribuible a los
cambios reales en el constructo a medir (Mokkink et al., 2010). Capacidad de respuesta
se evaluó utilizando el mínimo cambio detectable (MCD). MCD expresa el cambio
mínimo necesario para identificar el 90% de confianza de que el cambio observado
entre las dos medidas refleja un cambio real y no un error de medición (Haley and
Fragala-Pinkham, 2006). Se calcula como 𝐸𝐸𝑀 × √2 × 1,96 (Haley and Fragala-
Pinkham, 2006).
La asociación entre las variables se determinó mediante el coeficiente de correlación de
Pearson. Un coeficiente de correlación de Pearson mayor que 0,60 indica una fuerte
correlación, un valor entre 0,30 y 0,60 indica una correlación moderada, y uno por
debajo de 0,30 indica una correlación baja o muy baja (Hinkle et al., 1988). También se
utilizó en uno de los estudios el coeficiente de correlación de Spearman.
Se realizó un análisis de regresión lineal múltiple para estimar la fuerza de las
asociaciones entre los resultados variables primarias (variables criterio) con las
secundarias (variables predictoras). Se calcularon los factores de inflación de varianza

74
(FIV) para determinar si existían problemas de multicolinealidad en cualquiera de los
modelos analizados.
La fuerza de asociación se examinó utilizando los coeficientes de regresión (β), los
valores de P y r2 ajustado. Coeficientes beta estandarizados fueron reportados para cada
variable de predicción incluida en los modelos finales reducidas para permitir una
comparación directa entre las variables predictoras en el modelo de regresión y la
variable criterio que se está estudiando. Para el análisis de regresión, se utilizó la regla
de 10 casos por variable con el fin de obtener estimaciones razonablemente estables de
coeficientes de regresión (Peduzzi et al., 1996).
En la tabla 4 se presenta un resumen de los test estadísticos utilizados en cada uno de
los estudios.
El programa estadístico para Ciencias Sociales (SPSS 21, SPSS Inc., Chicago, IL
EE.UU.) se utilizó para el análisis estadístico. El nivel de significación para todas las
pruebas se estableció a un nivel de P <0,05.

75
Tabla 4. En esta tabla se puede observar las pruebas estadísticas utilizadas en cada uno
de los estudios.
Pruebas estadísticas Estudios
I II III IV V VI VII
- Análisis descriptivo X X X X X X X
- Pruebas de normalidad (test de Kolmogorov Smirnov) X X X X X X X
- t de student X X X
- ANOVA X X X X X
- ANCOVA X
- Calculo del tamaño del efecto (d) X X
- Análisis factorial exploratorio X
- Efecto suelo-techo X
- Coeficiente de correlación intra-clase X X X
- Error estándar de medición X X X X
- Mínimo cambio detectable X X
- Coeficiente de correlación de Pearson X X X
- Coeficiente de correlación de Spearman X
- Análisis de regresión lineal múltiple X X

76
77
RESULTADOS

78
5. RESULTADOS
5.1 Estudio I
La Touche R, París-Alemany A, von Piekartz H, Mannheimer JS, Fernández-Carnero J,
Rocabado M. The influence of cranio-cervical posture on maximal mouth opening and
pressure pain threshold in patients with myofascial temporomandibular pain disorders. Clin
J Pain. 2011 Jan;27(1):48-55.
Objetivo del estudio
El objetivo de este estudio fue evaluar la influencia de la postura craneocervical sobre la
MAI y el UDP en pacientes TCM atribuidos a dolor miofascial.
Resultados
Las comparaciones indicaron diferencias significativas en los UDPs de los 3 puntos
musculares con inervación trigeminal [masetero (M1 y M2) y temporal anterior (T1)] entre
las 3 posturas de cabeza [M1 (F = 117.78, p <0,001), M2 (F = 129.04, p <0,001), y T1 (F =
195,44, p <0,001)]. También hubo diferencias significativas en la MAI medidas en las 3
posturas de cabeza (F = 208.06, p <0,001). La fiabilidad intra-evaluador en base a pruebas
realizadas día a día fue buena, presentando un coeficiente de correlación intra-clase en los
rangos de 0,89-0,94 y 0,92 hasta 0,94 para UDP y la MAI, respectivamente, entre las
diferentes posturas craneocervicales.
Conclusiones
Los resultados de este estudio muestran que la inducción experimental de diferentes
posturas craneocervicales influye en los valores de la MAI y los UDPS de la ATM y
músculos de la masticación que reciben inervación motora y sensitiva por el nervio
trigémino. Nuestros resultados proporcionan información que respalda la relación
biomecánica entre la región craneocervical y la dinámica de la ATM, así como las
modificaciones en el procesamiento nociceptivo trigeminal en diferentes posturas
craneocervicale.

The Influence of Cranio-cervical Posture on Maximal MouthOpening and Pressure Pain Threshold in Patients With
Myofascial Temporomandibular Pain Disorders
Roy La Touche, PT, MSc,*w z Alba Parıs-Alemany, PT, MSc,w Harry von Piekartz, PT, PhD,yJeffrey S. Mannheimer, PT, PhD, CCTT,J Josue Fernandez-Carnero, PT, PhD,w z
and Mariano Rocabado, PT, DPT#
Objective: The aim of this study was to assess the influence ofcranio-cervical posture on the maximal mouth opening (MMO)and pressure pain threshold (PPT) in patients with myofascialtemporomandibular pain disorders.
Materials and Methods: A total of 29 patients (19 females and 10males) with myofascial temporomandibular pain disorders, aged19 to 59 years participated in the study (mean years±SD;34.69±10.83 y). MMO and the PPT (on the right side) of patientsin neutral, retracted, and forward head postures were measured. A1-way repeated measures analysis of variance followed by 3 pair-wise comparisons were used to determine differences.
Results: Comparisons indicated significant differences in PPT at 3points within the trigeminal innervated musculature [masseter (M1and M2) and anterior temporalis (T1)] among the 3 head postures[M1 (F=117.78; P<0.001), M2 (F=129.04; P<0.001), and T1(F=195.44; P<0.001)]. There were also significant differencesin MMO among the 3 head postures (F=208.06; P<0.001). Theintrarater reliability on a given day-to-day basis was good with theinterclass correlation coefficient ranging from 0.89 to 0.94 and 0.92to 0.94 for PPT and MMO, respectively, among the different headpostures.
Conclusions: The results of this study shows that the experimentalinduction of different cranio-cervical postures influences the MMOand PPT values of the temporomandibular joint and musclesof mastication that receive motor and sensory innervation by thetrigeminal nerve. Our results provide data that supports thebiomechanical relationship between the cranio-cervical region andthe dynamics of the temporomandibular joint, as well as trigeminalnociceptive processing in different cranio-cervical postures.
Key Words: temporomandibular disorders, myofascial pain, posture,
cervical spine, orofacial pain
(Clin J Pain 2011;27:48–55)
Pain in the masticatory muscles and arthralgia of thetemporomandibular joints are some of the features of
the term temporomandibular disorders (TMD) that havebeen categorized into 3 major groups by the ResearchDiagnostic Criteria (RDC) that is most commonly used toclassify symptomatology of TMD.1,2 Myofascial pain, discdisplacements, and arthralgia/osteoarthrosis constitute thisdiagnostic grouping. TMD of myofascial origin is categor-ized by episodic pain with periods of exacerbation andremission.3 Nevertheless, some patients may suffer persis-tent pain, and their prognosis is determined by psycho-metric evaluation (Axis II of the RDC/TMD). Myofascialpain is frequently associated with the presence of triggerpoints (TrPs) and the discomfort is considered to representa taut and painful disturbance of muscle and fascia that canbe local or referred with tenderness and pressure uponpalpation.4,5
It is well known that cervical spine tissues can referpain to the head and orofacial region.6,7 Comorbidity ofTMD and cervical spine disorders is quite common andconsists of a composite of functional limitation, pain,tender points, and hyperalgesia indigenous to the upperquarter.8 Some authors believe that neuronal plasticity,local interactions, and general predisposing musculoskeletalfactors might be behind this coexistence, but the relation-ship between the orofacial and cervical region is stronglyrooted by dense neuromusculoskeletal and neurophysiolo-gic connections.8,9 The trigeminal brainstem sensorynuclear complex located within the suboccipital spine,represents the prime neurophysiologic region where theconvergence of sensory information from the first 3 cervicalspinal nerves converge with trigeminal afferents, whereassome fibers descend to lower segmental levels.10–15 There-fore ascending cervicogenic and descending trigeminalreferral is mediated through the trigeminal brainstemsensory nuclear complex.15,16 The convergence of differenttypes of afferent and efferent neurotransmission on thetrigeminal nucleus together with the good evidence forneuronal plasticity that is known to occur in chronic painstates17–19 may account for the concomitant pain anddysfunction of the cervical, temporomandibular joints, andmasticatory system because of changes in head posture.17,20
Forward positioning of the head may contribute toor occur concomitantly with TMD,21,22 cervicogenic head-ache,23 and tension-type headache.24 Some authors supportthe connection between TMD and head posture,20–22,25
whereas others do not.26,27 The mechanism whereby headposture might be related to craniofacial signs and symptomsis unclear. The neuroplastic changes associated withCopyright r 2010 by Lippincott Williams & Wilkins
Received for publication April 7, 2010; revised June 9, 2010; acceptedJune 14, 2010.
From the *School of Health Science, Department of Physical Therapy;wGroup for Musculoskeletal Pain and Motor Control ClinicalResearch; zOrofacial Pain Unit of the Policlınica Universitaria,Universidad Europea de Madrid, Villaviciosa de Odon; zDepart-ment of Physical Therapy, Occupational Therapy, Rehabilitationand Physical Medicine, Universidad Rey Juan Carlos, Alcorcon,Madrid, Spain; yFaculty of Business, Management and SocialScience, University of Applied Science Osnabruck, Osnabruck,Germany; JProgram in Physical Therapy, Columbia University,New York, NY; and #Faculty of Rehabilitation Science, UniversidadAndres Bello, Santiago, Chile.
Reprints: Roy La Touche, PT, MSc, Facultad de Ciencias de la Salud/Departamento de Fisioterapia, Universidad Europea de Madrid,C/Tajo s/n, 28670 Villaviciosa de Odon, Madrid, Espana (e-mail:[email protected]).
ORIGINAL ARTICLE
48 | www.clinicalpain.com Clin J Pain � Volume 27, Number 1, January 2011

convergent afferent inputs mentioned above might play aconsiderable role. Further, it is noteworthy that changes inhead posture can alter the position of the mandible28,29 andthe activity of the masticatory muscles.30 Higbie et al31
demonstrated increased mouth opening in a forward headposition as compared with the neutral or retracted headposition, in healthy individuals. Furthermore, postural anddeep cervical flexor training as well as cervical manualtherapy have been shown to improve TMD signs andsymptoms.21,32,33
Although Visscher et al27 did obtain a wide rangeof head postures in both patients with craniomandibulardysfunction and healthy ones, their results data did notsupport the suggestion that craniomandibular dysfunctionis related to abnormal head posture, even in the presence ofcervical spine dysfunction. On the basis of their findings,Olivo et al34 found that the association between head andcervical posture with intra-articular or muscular TMD isnot clear.
Given the conflict in the literature as to whether thereis an association between head posture might be relatedto craniofacial signs and symptoms; the aim of this study isto assess the influence of cranio-cervical posture on themaximal mouth opening (MMO) and pressure pain thresh-old (PPT) of the trigeminal region in patients withmyofascial TMD pain.
MATERIALS AND METHODS
PatientsTMD patients were recruited from November 2008 to
March 2009 and were referred from 3 private dental clinicsin Madrid, Spain. Patients were selected if they met all ofthe following criteria: (1) a primary diagnosis of myofascialpain as defined by the Axis I, category Ia and Ib (ie,myofascial pain with or without limited opening), of theRDC/TMD,2 (2) bilateral pain involving the masseter andtemporalis, (3) a duration of pain of at least 6 months, (4) apain intensity corresponding to a weekly average of at least30mm on a 100mm visual analog scale, and (5) a presenceof bilateral TrPs in both the masseter and temporalismuscles diagnosed following the criteria described bySimons et al.35 TrPs were diagnosed according to thefollowing criteria: (1) presence of a palpable taut band inskeletal muscle, (2) presence of a hypersensitive tender spotwithin the taut band, (3) local twitch response elicited bythe snapping palpation of the taut band, and (4) reproduc-tion of referred pain in response to TrP compression. Thesecriteria have shown good interrater reliability (k) rangingfrom 0.84 to 0.88.36
All patients included in the study were examined byan experienced TMD specialist, with more than 4 years ofclinical practice, from the University Center of ClinicalResearch of the Cranial-Cervical-Mandibular System,Faculty of Medicine, San Pablo CEU University.
Patients were excluded if they presented any signs,symptoms, or history of the following diseases: (1) intra-articular disc displacement, ostheoarthrosis, or arthritis ofthe temporomandibular joint (TMJ), according to cate-gories II and III of the RDC/TMD2; (2) history of trauma-tic injuries (eg, contusion, fracture, and whiplash injury);(3) systemic diseases: (fibromyalgia, systemic lupus erythe-matosus, and psoriatic arthritis); (4) neurologic disorders(eg, trigeminal neuralgia); (5) concomitant diagnosis ofany primary headache (tension type or migraine); and
(6) current or recent therapy for the disorder within theprevious 2 months.
Each participant received a thorough explanationabout the content and purpose of the treatment beforesigning an informed consent relative to the procedures. Allprocedures were approved by the local ethics committee inaccordance with the Helsinki Declaration.
Experimental ProceduresEach patient with myofascial TMD pain were
subjected to a protocol for assessing maximum activeopening and PPT in 3 different cranio-cervical postures asfollows and illustrated in Figure 1:
Neutral head posture (NHP) defined as the positionassumed when the individual was told to sit and maintaintheir head in a vertical position. This position was furtherconfirmed as neutral if the tragus of the ear and acromionwere bisected by a plumb line.Forward head posture (FHP) defined as anteriortranslation of the head with or without lower cervicalflexion. It is claimed that the FHP is associated with anincrease in upper-cervical extension.37,38
Retracted head posture (RHP) defined as posteriortranslation of the head over the trunk associated withupper cranio-cervical flexion and extension of the low-to-mid cervical spine.39
All measurements were conducted by 2 physiothera-pists who had experience in research evaluations, one incharge of placing the patient in the measurement positionand the other responsible for the recording of MMOand PPT. All patients underwent 3 measurements of eachvariable in the 3 head positions on 3 different days. Awashout period of 24 hours was incorporated between eachmeasurement day.
A software program was used to obtain blockedrandomization of the size to arrange the order of measure-ment (GraphPad Software, Inc, CA). An average of 15minutes per patient was required to perform the random-ized measurements of MMO and PPT in NHP, FHP, andRHP. Every patient maintained their head in each positionfor 5 seconds during these measurements.
Establishment of the Measurement PositionsA plumb line hanging from the ceiling and a cervical
range of motion (CROM) device (Performance AttainmentAssociates, 958 Lydia DR, Roseville, MN) was usedto determine each patients’ cranio-cervical postures. TheCROM instrument measured the degree of FHP or RHPand the active cervical range of movement. The CROMinstrument uses a clear plastic eyeglass-like frame with 2dial-angle meters, a head arm that includes a vertebrallocator and bubble leveller (Fig. 2). The head arm wasplaced in the frame of the CROM horizontally to the head.The base of the vertebral locator was placed on the C-7spinous process so that the bubble leveller was centeredwithin the 2 vertical lines on the dial with the examinerstanding to the left of the patient to read the sagittal planemeter (Fig. 2). When the sagittal plane meter read zero andwith the head arm horizontal (parallel to the floor), theintersection of the head arm and vertebral locator wasrecorded as the head posture measurement in centimeters.Excellent reliability has been showed for the measurementof FHP using the CROM instrument [intrarater reliability
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 49

(interclass correlation coefficient, ICC=0.93) and interraterreliability (ICC=0.83)].40
Cranio-cervical postures were measured in the sittingposition attained by instructing the patient to sit in acomfortable upright position with the thoracic spine incontact with the back of the chair. The feet were positionedflat on the floor with knees and hips at 90 degrees and armsresting freely alongside.
Forward and retruded head postures were achieved byinitial placement into the NHP using the plumb line asexplained earlier. Movement into a FHP was performedwith the CROM after verbal instruction to position thehead forward in a horizontal plane allowing the tragus to bealigned to a target plumb line placed 8 cm anterior to thebase plumb line. Each patient was instructed to continuallymaintain their eyes at the same horizontal level while being
told to “slide your jaw and head forward until the examinertells you to stop” upon reaching the target plum line (Fig. 1).
Movement into a RHP was also performed with theCROM by instruction to position the head posteriorly ina horizontal plane allowing the tragus to be aligned to thetarget plumb line placed 4 cm posterior to the base plumbline. Each patient was instructed to continually maintaintheir eyes at the same horizontal level while being told to“slide your jaw and head backward until the examiner tellsyou to stop” upon reaching the target plum line (Fig. 1).
Measurement of MMOThe MMO was measured with a TheraBite range of
motion scale (Model CPT 95851; Atos Medical AB;Sweden) (Fig. 2). The patients were told to: “Open yourmouth as wide as possible without causing pain or
FIGURE 1. Measurement of maximum mouth opening with TheraBite, controlling the head position with the CROM device and plumline: A, retracted head posture. B, Forward head position. Measurement of pressure pain thresholds at masseter and temporalis muscleswith a mechanical algometer, controlling head position with CROM device: C, forward head position. D, Neutral head position. CROMindicates cervical range of motion.
FIGURE 2. Description and representation of measurement devices: TheraBite scale (A); CROM device: plastic eyeglass-like frame with 2dial-angle meters (B), head arm (C), and vertebral locator and bubble leveller (D).
La Touche et al Clin J Pain � Volume 27, Number 1, January 2011
50 | www.clinicalpain.com r 2010 Lippincott Williams & Wilkins
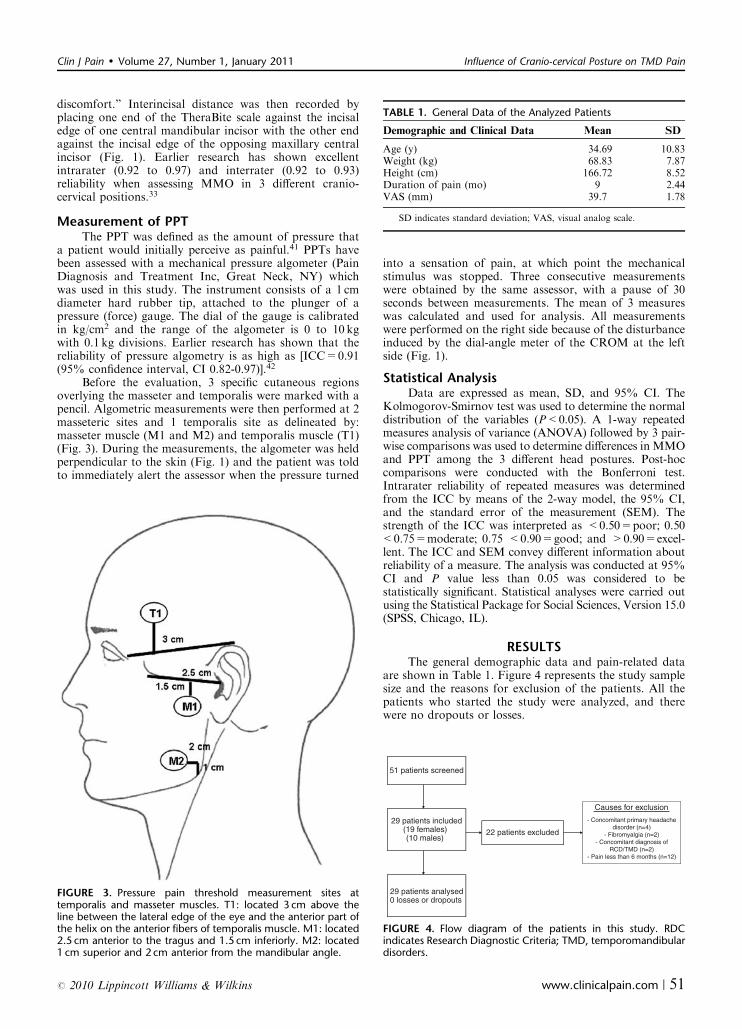
discomfort.” Interincisal distance was then recorded byplacing one end of the TheraBite scale against the incisaledge of one central mandibular incisor with the other endagainst the incisal edge of the opposing maxillary centralincisor (Fig. 1). Earlier research has shown excellentintrarater (0.92 to 0.97) and interrater (0.92 to 0.93)reliability when assessing MMO in 3 different cranio-cervical positions.33
Measurement of PPTThe PPT was defined as the amount of pressure that
a patient would initially perceive as painful.41 PPTs havebeen assessed with a mechanical pressure algometer (PainDiagnosis and Treatment Inc, Great Neck, NY) whichwas used in this study. The instrument consists of a 1 cmdiameter hard rubber tip, attached to the plunger of apressure (force) gauge. The dial of the gauge is calibratedin kg/cm2 and the range of the algometer is 0 to 10 kgwith 0.1 kg divisions. Earlier research has shown that thereliability of pressure algometry is as high as [ICC=0.91(95% confidence interval, CI 0.82-0.97)].42
Before the evaluation, 3 specific cutaneous regionsoverlying the masseter and temporalis were marked with apencil. Algometric measurements were then performed at 2masseteric sites and 1 temporalis site as delineated by:masseter muscle (M1 and M2) and temporalis muscle (T1)(Fig. 3). During the measurements, the algometer was heldperpendicular to the skin (Fig. 1) and the patient was toldto immediately alert the assessor when the pressure turned
into a sensation of pain, at which point the mechanicalstimulus was stopped. Three consecutive measurementswere obtained by the same assessor, with a pause of 30seconds between measurements. The mean of 3 measureswas calculated and used for analysis. All measurementswere performed on the right side because of the disturbanceinduced by the dial-angle meter of the CROM at the leftside (Fig. 1).
Statistical AnalysisData are expressed as mean, SD, and 95% CI. The
Kolmogorov-Smirnov test was used to determine the normaldistribution of the variables (P<0.05). A 1-way repeatedmeasures analysis of variance (ANOVA) followed by 3 pair-wise comparisons was used to determine differences in MMOand PPT among the 3 different head postures. Post-hoccomparisons were conducted with the Bonferroni test.Intrarater reliability of repeated measures was determinedfrom the ICC by means of the 2-way model, the 95% CI,and the standard error of the measurement (SEM). Thestrength of the ICC was interpreted as <0.50=poor; 0.50<0.75=moderate; 0.75 <0.90=good; and >0.90=excel-lent. The ICC and SEM convey different information aboutreliability of a measure. The analysis was conducted at 95%CI and P value less than 0.05 was considered to bestatistically significant. Statistical analyses were carried outusing the Statistical Package for Social Sciences, Version 15.0(SPSS, Chicago, IL).
RESULTSThe general demographic data and pain-related data
are shown in Table 1. Figure 4 represents the study samplesize and the reasons for exclusion of the patients. All thepatients who started the study were analyzed, and therewere no dropouts or losses.
FIGURE 3. Pressure pain threshold measurement sites attemporalis and masseter muscles. T1: located 3 cm above theline between the lateral edge of the eye and the anterior part ofthe helix on the anterior fibers of temporalis muscle. M1: located2.5 cm anterior to the tragus and 1.5 cm inferiorly. M2: located1 cm superior and 2 cm anterior from the mandibular angle.
TABLE 1. General Data of the Analyzed Patients
Demographic and Clinical Data Mean SD
Age (y) 34.69 10.83Weight (kg) 68.83 7.87Height (cm) 166.72 8.52Duration of pain (mo) 9 2.44VAS (mm) 39.7 1.78
SD indicates standard deviation; VAS, visual analog scale.
51 patients screened
Causes for exclusion
29 patients included(19 females)(10 males)
22 patients excluded
29 patients analysed0 losses or dropouts
FIGURE 4. Flow diagram of the patients in this study. RDCindicates Research Diagnostic Criteria; TMD, temporomandibulardisorders.
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 51
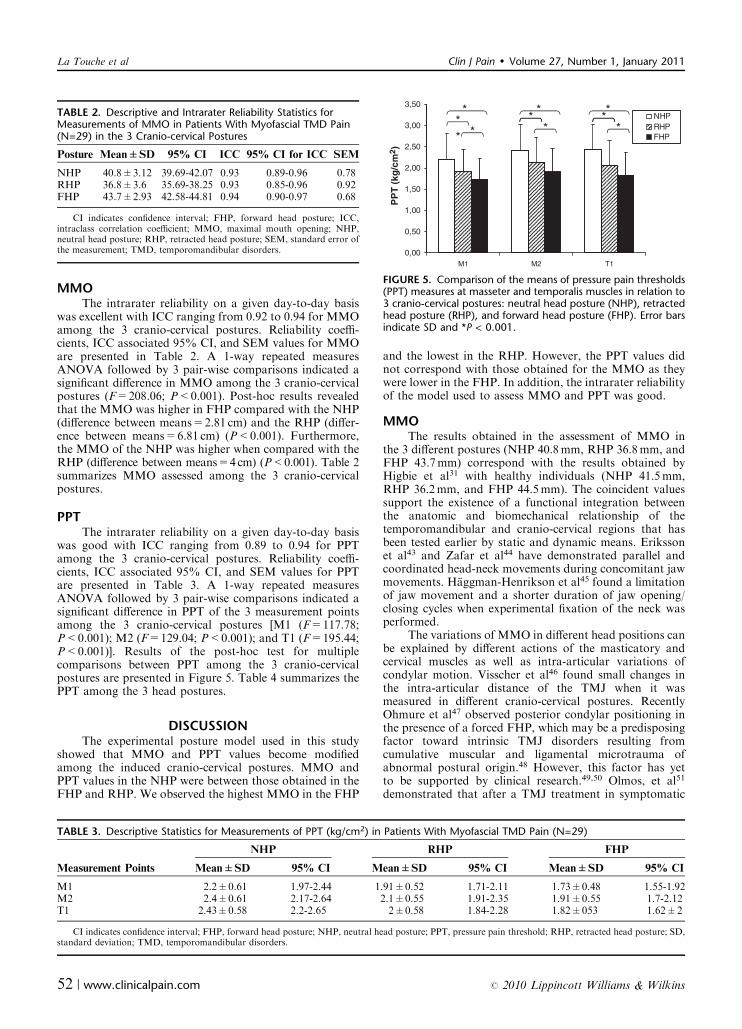
MMOThe intrarater reliability on a given day-to-day basis
was excellent with ICC ranging from 0.92 to 0.94 for MMOamong the 3 cranio-cervical postures. Reliability coeffi-cients, ICC associated 95% CI, and SEM values for MMOare presented in Table 2. A 1-way repeated measuresANOVA followed by 3 pair-wise comparisons indicated asignificant difference in MMO among the 3 cranio-cervicalpostures (F=208.06; P<0.001). Post-hoc results revealedthat the MMO was higher in FHP compared with the NHP(difference between means=2.81 cm) and the RHP (differ-ence between means=6.81 cm) (P<0.001). Furthermore,the MMO of the NHP was higher when compared with theRHP (difference between means=4cm) (P<0.001). Table 2summarizes MMO assessed among the 3 cranio-cervicalpostures.
PPTThe intrarater reliability on a given day-to-day basis
was good with ICC ranging from 0.89 to 0.94 for PPTamong the 3 cranio-cervical postures. Reliability coeffi-cients, ICC associated 95% CI, and SEM values for PPTare presented in Table 3. A 1-way repeated measuresANOVA followed by 3 pair-wise comparisons indicated asignificant difference in PPT of the 3 measurement pointsamong the 3 cranio-cervical postures [M1 (F=117.78;P<0.001); M2 (F=129.04; P<0.001); and T1 (F=195.44;P<0.001)]. Results of the post-hoc test for multiplecomparisons between PPT among the 3 cranio-cervicalpostures are presented in Figure 5. Table 4 summarizes thePPT among the 3 head postures.
DISCUSSIONThe experimental posture model used in this study
showed that MMO and PPT values become modifiedamong the induced cranio-cervical postures. MMO andPPT values in the NHP were between those obtained in theFHP and RHP. We observed the highest MMO in the FHP
and the lowest in the RHP. However, the PPT values didnot correspond with those obtained for the MMO as theywere lower in the FHP. In addition, the intrarater reliabilityof the model used to assess MMO and PPT was good.
MMOThe results obtained in the assessment of MMO in
the 3 different postures (NHP 40.8mm, RHP 36.8mm, andFHP 43.7mm) correspond with the results obtained byHigbie et al31 with healthy individuals (NHP 41.5mm,RHP 36.2mm, and FHP 44.5mm). The coincident valuessupport the existence of a functional integration betweenthe anatomic and biomechanical relationship of thetemporomandibular and cranio-cervical regions that hasbeen tested earlier by static and dynamic means. Erikssonet al43 and Zafar et al44 have demonstrated parallel andcoordinated head-neck movements during concomitant jawmovements. Haggman-Henrikson et al45 found a limitationof jaw movement and a shorter duration of jaw opening/closing cycles when experimental fixation of the neck wasperformed.
The variations of MMO in different head positions canbe explained by different actions of the masticatory andcervical muscles as well as intra-articular variations ofcondylar motion. Visscher et al46 found small changes inthe intra-articular distance of the TMJ when it wasmeasured in different cranio-cervical postures. RecentlyOhmure et al47 observed posterior condylar positioning inthe presence of a forced FHP, which may be a predisposingfactor toward intrinsic TMJ disorders resulting fromcumulative muscular and ligamental microtrauma ofabnormal postural origin.48 However, this factor has yetto be supported by clinical research.49,50 Olmos, et al51
demonstrated that after a TMJ treatment in symptomatic
TABLE 2. Descriptive and Intrarater Reliability Statistics forMeasurements of MMO in Patients With Myofascial TMD Pain(N=29) in the 3 Cranio-cervical Postures
Posture Mean±SD 95% CI ICC 95% CI for ICC SEM
NHP 40.8±3.12 39.69-42.07 0.93 0.89-0.96 0.78RHP 36.8±3.6 35.69-38.25 0.93 0.85-0.96 0.92FHP 43.7±2.93 42.58-44.81 0.94 0.90-0.97 0.68
CI indicates confidence interval; FHP, forward head posture; ICC,intraclass correlation coefficient; MMO, maximal mouth opening; NHP,neutral head posture; RHP, retracted head posture; SEM, standard error ofthe measurement; TMD, temporomandibular disorders.
TABLE 3. Descriptive Statistics for Measurements of PPT (kg/cm2) in Patients With Myofascial TMD Pain (N=29)
NHP RHP FHP
Measurement Points Mean±SD 95% CI Mean±SD 95% CI Mean±SD 95% CI
M1 2.2±0.61 1.97-2.44 1.91±0.52 1.71-2.11 1.73±0.48 1.55-1.92M2 2.4±0.61 2.17-2.64 2.1±0.55 1.91-2.35 1.91±0.55 1.7-2.12T1 2.43±0.58 2.2-2.65 2±0.58 1.84-2.28 1.82±053 1.62±2
CI indicates confidence interval; FHP, forward head posture; NHP, neutral head posture; PPT, pressure pain threshold; RHP, retracted head posture; SD,standard deviation; TMD, temporomandibular disorders.
3,50
NHP* * ** *
*2,50
3,00 RHPFHP
** * *
1,00
1,50
2,00
PP
T (
kg/c
m2 )
0,00
0,50
T1M1 M2
FIGURE 5. Comparison of the means of pressure pain thresholds(PPT) measures at masseter and temporalis muscles in relation to3 cranio-cervical postures: neutral head posture (NHP), retractedhead posture (RHP), and forward head posture (FHP). Error barsindicate SD and *P < 0.001.
La Touche et al Clin J Pain � Volume 27, Number 1, January 2011
52 | www.clinicalpain.com r 2010 Lippincott Williams & Wilkins

patients there seemed to be an increase in the retrodiscalspace and decrease in the distance between the shoulder andexternal auditory meatus. Therefore, an improved condylefossa relationship was apparent as the resting condylarposition became more anterior in conjunction with areduction of the FHP.
Recent evidence and the results of this study support theexistence of a relationship between the biomechanical actionof the cranio-cervical region and jaw movements, but ourresults do not show the degree of clinical implication that thedifferent postures have specific to intrinsic TMJ disorders.
PPTOur findings show that PPT values modify depending
upon the head posture in which they are measured. Thisvariability could be because of increased excitability ofthe trigeminal muscular nociceptors induced by differentcranio-cervical postures within which the PPT was mea-sured. In relation to orofacial nociception, an interactionbetween somatosensory processing and sensory-motorfunction is supported by our data.52
The results of our research cannot determine thereason by which the PPT decreases in the RHP and FHP ascompared with the NHP values. However, if our datais added to the findings of others it may lead to thedevelopment of different theories that offer additionalexplanations. We suggest that the PPT variations may bebecause of experimental biomechanical modifications ofmuscle and soft tissue that were produced when the patientstried to hold the FHP and the RHP, which generatedaugmented electromyography (EMG) activity and masti-catory reflexes. Modification of the activity produced ateach of the aforementioned postures could be causing PPTalteration. Furthermore, increased jaw-reflex activity maybe triggered by enhanced fusimotor drive, thereby elevatingmuscle spindle discharge resulting in reflex facilitation.Elevated fusimotor drive may in turn lead to increased TMJstiffness and pain. Earlier research has supported thepremise that experimental pain can augment masticatoryreflex activity.53–56
A recent study has shown that masseteric EMGactivity increases in the presence of a forced FHP.48 Inaddition, EMG changes in the suprahyoid muscles havebeen observed in experimentally induced FHP.57 However,in direct contrast, earlier studies have found increasedmasticatory EMG activity in head extension,58 which isa component of the RHP. Johansson and Sojka59 haveproposed a model to explain the spread of muscle painbased on the g-motoneuron system in which muscle stiffnessand pain are increased by enhanced activity of primarymuscle spindle afferents. This hypothesis may explain someof the results of this study, however, such thoughts are only
theoretical reflections and future research needs to provewhether postural changes truly alter the nociceptive trigem-inal mechanism.
Study LimitationsThe results of this study must be taken with caution
because the objective measurements were performed inan experimentally forced posture and not a natural one. Itwould also be interesting to determine in future researchwhether the PPT is modified with different natural posturesand whether postural alterations may affect or may be anaggravating factor in the development of orofacial pain. Itis also important to state that our participant sample onlyincluded patients with myofascial TMD. Therefore, it isimperative that future research apply the same method-ology with healthy individuals and other cohorts of TMDto determine whether the results can be replicated.
Clinical ImplicationsThe anatomic and physiological interaction between
the cranio-cervical and temporomandibular regions asshowed in this research supports the concept of a functionaltrigeminocervical coupling during jaw activities that influ-ences the inherent modifications that we observed in MMOand PPT. This factor must be taken into account duringpatient evaluation to control for variations in measurement.
The methodology that we used can result in a morestructured assessment of the MMO and PPT in neutralposition, within which we observed that average values wereobtained with excellent intrarater reliability. Postural treat-ment has already been shown to be useful for reducing TMDmyofascial pain and improving MMO.33,60 We have demon-strated experimentally that pain thresholds at the trigeminalarea can be modified only by changing the cranio-cervicalposture. As PPT values diminish in FHP and RHP, it wouldbe useful to consider new therapeutic strategies to improvethe cranio-cervical posture toward a NHP and futureresearch should determine whether postural treatments canhelp to modulate pain in myofascial TMD patients.
CONCLUSIONSThe results of this study shows that the experimental
induction of different cranio-cervical postures influencesthe MMO and PPT values of masticatory and joint func-tion of the temporomandibular complex. Our observationssupport the concept of a biomechanical relationship andinteraction within the trigeminocervical complex as well asinherent nociceptive processing in different cranio-cervicalpostures. Why or how postural modifications influence thePPT and MMO values are issues that are beyond the scopeof this study.
TABLE 4. Intrarater Reliability Statistics for Measurements of PPT in Patients With Myofascial TMD Pain (N=29) in the 3 Cranio-cervicalPostures
NHP RHP FHP
Measurement Points ICC 95% CI for ICC SEM ICC 95% CI for ICC SEM ICC 95% CI for ICC SEM
M1 0.93 0.87-0.96 0.16 0.9 0.82-0.94 0.16 0.93 0.87-0.96 0.12M2 0.91 0.84-0.95 0.18 0.92 0.86-0.96 0.16 0.92 0.87-0.96 0.15T1 0.89 0.82-0.94 0.19 0.94 0.89-0.97 0.14 0.92 0.86-0.96 0.13
CI indicates confidence interval; FHP, forward head posture; ICC, intraclass correlation coefficient; NHP, neutral head posture; PPT, pressure painthreshold; RHP, retracted head posture; SD, standard deviation; SEM, standard error of the measurement; TMD, temporomandibular disorders.
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 53

ACKNOWLEDGMENT
The authors thank Dr Greg Murray (Professor ofDentistry, Jaw Function and Orofacial Pain Research Unit,Faculty of Dentistry, University of Sydney, Australia) for hishelpful contribution in this article.
REFERENCES
1. Okeson JP. Management of Temporomandibular Disorders andOcclusion. 6 th ed. St. Louis: Mosby; 2007:300.
2. Dworkin SF, LeResche L. Research diagnostic criteria fortemporomandibular disorders: review, criteria, examinations andspecifications, critique. J Craniomandib Disord. 1992;6:301–355.
3. Dworkin SF, Huggins KH, Wilson L, et al. A randomizedclinical trial using research diagnostic criteria for temporoman-dibular disorders-axis II to target clinic cases for a tailored self-care TMD treatment program. J Orofac Pain. 2002;16:48–63.
4. Mense S, Simons DG. Muscle Pain: Understanding Its Nature,Diagnosis, and Treatment. Philadelphia: Lippincott Williams &Wilkins; 2001:253–259.
5. Shindler HJ, Svensson P. Myofascial temporomandibulardisorder pain. In: Turp JC, Sommer C, Hugger A. Pathophy-siology and Management. Basel: Karger; 2007:91–123.
6. Sessle BJ, Hu JW, Amano M, et al. Convergence of cutaneous,tooth pulp, visceral, neck and muscle afferents onto nociceptiveand non-nociceptive neurons in trigeminal subnucleus caudalis(medullary dorsal horn) and its implications for referred pain.Pain. 1986;27:219–235.
7. Bogduk N. The neck and headaches. Neurol Clin. 2004;22:151–171.
8. De Laat A, Meuleman H, Stevens A, et al. Correlation betweencervical spine and temporomandibular disorders. Clin OralInvestig. 1998;2:54–57.
9. De Laat A. Reflexes elicitable in jaw muscles and their roleduring jaw function and dysfunction: a review of the literature.Part II. Central connections of orofacial afferents. Cranio.1987;5:246–253.
10. Bogduk N. The anatomical basis for cervicogenic headache.J Manipulative Physiol Ther. 1992;15:67–70.
11. Kerr FW. Structural relation of the trigeminal spinal tract toupper cervical roots and the solitary nucleus in the cat. ExpNeurol. 1961;4:134–148.
12. Marfurt CF. The central projections of trigeminal primaryafferent neurons in the cat as determined by the tranganglionictransport of horseradish peroxidase. J Comp Neurol. 1981;203:785–798.
13. Jacquin MF, Rhoades RW, Enfiejian HL, et al. Organisationand morphology of masticatory neurons in the rat: a retro-grade HRP study. J Comp Neurol. 1983;218:139–156.
14. Bogduk N. Cervical causes of headache and dizziness. In:Grieve G, ed. Modern Manual Therapy. Edinburgh (UK):Churchill Livingstone; 1994:317–331.
15. Hu JW, Sun KQ, Vernon H, et al. Craniofacial inputs to uppercervical dorsal horn: implications for somatosensory informa-tion processing. Brain Res. 2005;1044:93–106.
16. Michler RP, Bovim G, Sjaastad O. Disorders in the lowercervical spine. A cause of unilateral headache? A case report.Headache. 1991;31:550–551.
17. Coderre TJ, Katz J, Vaccarino AL, et al. Contribution ofcentral neuroplasticity to pathological pain: review of clinicaland experimental evidence. Pain. 1993;52:259–285.
18. Latremoliere A, Woolf CJ. Central sensitization: a generator ofpain hypersensitivity by central neural plasticity. J Pain. 2009;10:895–926.
19. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: amaladaptive response of the nervous system to damage. AnnuRev Neurosci. 2009;32:1–32.
20. Huggare JA, Raustia AM. Head posture and cervicovertebraland craniofacial morphology in patients with craniomandibu-lar dysfunction. Cranio. 1992;10:173–177.
21. Mannheimer JS. Prevention and restoration of abnormalupper quarter posture. In: Gelb H, Gelb M, eds. PosturalConsiderations in the Diagnosis and Treatment of Cranio-Cervical-Mandibular and Related Chronic Pain Disorders.London: Mosby-Wolfe; 1994:277–323.
22. Gonzalez HE, Manns A. Forward head posture: its structuraland functional influence on the stomatognathic system,a conceptual study. Cranio. 1996;14:71–80.
23. Watson DH, Trott PH. Cervical headache: an investigation ofnatural head posture and upper cervical flexor muscleperformance. Cephalagia. 1993;13:272–284.
24. Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML,et al. Trigger points in the suboccipital muscles and forwardhead posture in tension-type headache. Headache. 2006;46:454–460.
25. Nicolakis P, Nicolakis M, Piehslinger E, et al. Relationshipbetween craniomandibular disorders and poor posture. Cranio.2000;18:106–112.
26. Darlow LA, Pesco J, Greenberg MS. The relationship ofposture to myofascial pain dysfunction syndrome. J Am DentAssoc. 1987;114:73–75.
27. Visscher CM, De Boer W, Lobbezoo F, et al. Is there arelationship between head posture and craniomandibular pain?J Oral Rehabil. 2002;29:1030–1036.
28. Darling DW, Kraus S, Glasheen-Wray MB. Relationship ofhead posture and the rest position of the mandible. J ProsthetDent. 1984;52:111–115.
29. Goldstein DF, Kraus SL, Williams WB, et al. Influence ofcervical posture on mandibular movement. J Prosthet Dent.1984;52:421–426.
30. Forsberg CM, Hellsing E, Linder-Aronson S, et al.EMG activity in neck and masticatory muscles in relation toextension and flexion of the head. Eur J Orthod. 1985;7:177–184.
31. Higbie E, Seidel-Cobb D, Taylor LF, et al. Effect of headposition on vertical mandibular opening. J Orthop Sports PhysTher. 1999;29:127–130.
32. La Touche R, Fernandez-de-las-Penas C, Fernandez-CarneroJ, et al. The effects of manual therapy and exercise directed atthe cervical spine on pain and pressure pain sensitivity inpatients with myofascial temporomandibular disorders. J OralRehabil. 2009;36:644–652.
33. Wright EF, Domenech MA, Fischer JR Jr. Usefulness ofposture training for patients with temporomandibular dis-orders. J Am Dent Assoc. 2000;131:202–210.
34. Olivo SA, Bravo J, Magee DJ, et al. The association betweenhead and cervical posture and temporomandibular disorders:a systematic review. J Orofac Pain. 2006;20:9–23.
35. Simons DG, Travell J, Simons LS. Myofascial Pain andDysfunction: The Trigger Point Manual. 2nd ed. Vol. 1.Baltimore: Williams & Wilkins; 1999:11–28.
36. Gerwin RD, Shanon S, Hong CZ, et al. Interrater reliabilityin myofascial trigger point examination. Pain. 1997;69:65–73.
37. Hanten WP, Lucio RM, Russell JL, et al. Assessment of totalhead excursion and resting head posture. Arch Phys MedRehabil. 1991;71:877–880.
38. Enwemeka CS, Bonet IM, Ingle JA, et al. Postural correctionin persons with neck pain. II. Integrated electromyography ofthe upper trapezius in three simulated neck positions. J OrthopSports Phys Ther. 1986;8:240–242.
39. Lentell G, Kruse M, Chock B, et al. Dimensions of the cervicalneural foramina in resting and retracted positions usingmagnetic resonance imaging. J Orthop Sports Phys Ther. 2002;32:380–390.
40. Garrett TR, Youdas JW, Madson TJ. Reliability of measuringforward head posture in a clinical setting. J Orthop Sports PhysTher. 1993;17:155–160.
41. Svensson P, Arendt-Nielsen L, Nielsen H, et al. Effect ofchronic and experimental jaw muscle pain on pressure painthresholds and stimulus response curves. J Orofac Pain.1995;9:347–356.
La Touche et al Clin J Pain � Volume 27, Number 1, January 2011
54 | www.clinicalpain.com r 2010 Lippincott Williams & Wilkins

42. Chesterson LS, Sim J, Wright CC, et al. Inter-rater reliabilityof algometry in measuring pressure pain thresholds in healthyhumans, using multiple raters. Clin J Pain. 2007;23:760–766.
43. Eriksson PO, Zafar H, Nordh E. Concomitant mandibular andhead-neck movements during jaw opening-closing in man.J Oral Rehabil. 1998;25:859–870.
44. Zafar H, Nordh E, Eriksson PO. Temporal coordinationbetween mandibular and head-neck movements during jawopening-closing tasks in man. Arch Oral Biol. 2000;45:675–682.
45. Haggman-Henrikson B, Nordh E, Zafar H, et al. Headimmobilization can impair jaw function. J Dent Res. 2006;85:1001–1005.
46. Visscher CM, Huddleston Slater JJ, Lobbezoo F, et al.Kinematics of the human mandible for different head postures.J Oral Rehabil. 2000;27:299–305.
47. Ohmure H,Miyawaki S, Nagata J, et al. Influence of forward headposture on condylar position. J Oral Rehabil. 2008;35:795–800.
48. Rocabado M. Arthrokinematics of the temporomandibularjoint. Dent Clin North Am. 1983;27:573–594.
49. Hackney J, Bade D, Clawson A. Relationship between forwardhead posture and diagnosed internal derangement of thetemporomandibular joint. J Orofac Pain. 1993;7:386–390.
50. MunhozWC, Marques AP, de Siqueira JT. Evaluation of bodyposture in individuals with internal temporomandibular jointderangement. Cranio. 2005;23:269–277.
51. Olmos SR, Kritz-Silverstein D, Halligan W, et al. The effect ofcondyle fossa relationships on head posture. Cranio. 2005;23:48–52.
52. Sessle BJ. Mechanisms of oral somatosensory and motorfunctions and their clinical correlates. J Oral Rehabil. 2006;33:243–261.
53. Svensson P, Macaluso GM, De Laat A, et al. Effects of localand remote muscle pain on human jaw reflexes evoked by faststretches at different clenching levels. Exp Brain Res.2001;139:495–502.
54. Wang K, Svensson P, Arendt-Nielsen L. Effect of tonic musclepain on short-latency jaw-stretch reflexes in humans. Pain.2000;88:189–197.
55. Wang K, Arendt-Nielsen L, Svensson P. Excitatory actions ofexperimental muscle pain on early and late components ofhuman jaw stretch reflexes. Arch Oral Biol. 2001;46:433–442.
56. Wang K, Arendt-Nielsen L, Svensson P. Capsaicin-inducedmuscle pain alters the excitability of the human jawstretchreflex. J Dent Res. 2002;81:650–654.
57. Milidonis MK, Kraus SL, Segal RL, et al. Genioglossi muscleactivity in response to changes in anterior/neutral headposture. Am J Orthod Dentofacial Orthop. 1993;103:39–44.
58. Funakoshi M, Fujita N, Takehana S. Relations betweenocclusal interference and jaw muscle activities in response tochanges in head position. J Dent Res. 1976;55:684–690.
59. Johansson H, Sojka P. Pathophysiological mechanisms in-volved in genesis and spread of muscular tension in occupa-tional muscle pain. Med Hypotheses. 1991;135:196–203.
60. Komiyama O, Kawara M, Arai M, et al. Posture correction aspart of behavioural therapy in treatment of myofascial painwith limited opening. J Oral Rehabil. 1999;26:428–435.
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 55

87
5.2 Estudio II
López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A, Angulo-Díaz-Parreño S,
La Touche R. Reliability, Standard Error, and Minimal Detectable Change of Two Tests for
Craniocervical Posture Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial
Pain Patients. (En revisión).
Objetivo del Estudio
Nuestro objetivo fue examinar la fiabilidad de dos mediciones para evaluar la postura
craneocervical (PC y DME). Además, se evaluó una posible asociación entre las variables
registradas. Como objetivo final, tenemos la intención de evaluar si existen diferencias en la
postura craneocervical entre sujetos asintomáticos y pacientes con dolor cérvico- craneofacial.
Resultados
La fiabilidad intra-evaluador de la medición de PC fue alta para los sujetos asintomáticos y
pacientes DCCF (CCI = 0,93 y 0,81, respectivamente) y para DME (rango CCI entre 0,78-0,99).
La fiabilidad intra-evaluador se mantuvo alta cuando se evaluó 9 días más tarde. Los resultados
de fiabilidad inter-evaluador fue alta para la PC (rango CCI entre 0,94 a 0,96) y fue justa para la
DME (rango CCI entre 0,78 a 0,79). El EEM de PC fue de 0,41 hasta 0,75 cm, mientras que el
MCD fue 0,96 a 1,74 cm. El SEM para la DME fue 1,61 a 7,06 mm, mientras que el MCD fue
3,76 a 16,47 mm. Se observó una correlación positiva moderada en ambos grupos entre HP y
SCD (sujetos asintomáticos, r = 0,447; pacientes con DCCF, r = 0,52). Análisis realizado con
una t de student mostró diferencias estadísticamente significativas entre los grupos para las
medidas de la postura craneocervical, pero estas diferencias eran muy pequeñas. Se encontró
una correlación positiva fuerte entre la discapacidad cervical y la craneofacial.
Conclusiones
Las mediciones para evaluar la postura craneocervical son fiables cuando se realizan por uno o
por dos evaluadores en sujetos asintomáticos o pacientes con DCCF.

1
Reliability, Standard Error, and Minimal Detectable Change of Two Tests for
Craniocervical Posture Assessment in Asymptomatic Subjects and Chronic
Neck/craniofacial Pain Patients
Ibai López-de-Uralde-Villanueva, PT, MSc1-4
, Hector Beltran-Alacreu, PT, MSc 2,3
,
Alba Paris-Alemany, PT, MSc1-4
, Santiago Angulo-Díaz-Parreño, MSc2,3,5
, Roy La
Touche, PT, MSc1-4
,
1. Department of Physiotherapy, Faculty of Health Science, The Center for
Advanced Studies University La Salle, Universidad Autónoma de Madrid,
Aravaca, Madrid, Spain.
2. Research Group on Movement and Behavioral Science and Study of Pain, The
Center for Advanced Studies University La Salle, Universidad Autónoma de
Madrid.
3. Institute of Neuroscience and Craniofacial Pain (INDCRAN), Madrid, Spain
4. Hospital La Paz Institute for Health Research, IdiPAZ. Madrid, Spain.
Madrid, Spain
5. Faculty of Medicine, Universidad San Pablo CEU, Madrid, Spain
Address for reprint requests / Corresponding author:
Roy La Touche
Facultad de Ciencias de la Salud
Centro Superior de Estudios Universitarios La Salle.
Calle la Salle, 10
28023 Madrid
SPAIN
Telephone number: + 34 91 7401980 (EXT.256)
Fax number:
Email address: [email protected]
The study protocol was approved by the local ethics committee of the Center for
Advanced Studies University La Salle, Madrid (Spain).

2
Reliability, Standard Error, and Minimal Detectable Change of Two Tests for
Craniocervical Posture Assessment in Asymptomatic Subjects and Chronic
Neck/craniofacial Pain Patients
ABSTRACT
PURPOSE:
Is recommended to quantifying the craniocervical posture as part of the assessment of
patients with neck and craniofacial pain to facilitate diagnosis and determine
treatment strategies. There is insufficient research regarding the intra-rater and inter-
rater reliability of craniocervical posture measurement using a CROM device and a
Digital Calliper.
OBJETIVE:
Determine the intra-rater and inter-rater reliability of two craniocervical posture
measurements on asymptomatic subjects and chronic neck/craniofacial pain (chronic
cervico-craniofacial pain, CCFP).
METHODS:
Two-groups repeated measures for inter- and intra-rater reliability study. 53
asymptomatic adult subjects and 60 CCFP patients who volunteered for the study.
Two raters measured head posture (HP) and the sternomental distance (SMD) using
the CROM device and Digital Calliper respectively.
RESULTS:
Intra-rater reliability of the HP measurement was high for asymptomatic subjects and
CCFP patients (Intraclass Correlation Coefficients (ICC)=0.93 and 0.81 respectively)
and for SMD (ICC range between 0.78-0.99), the intra-rater reliability remained high

3
when evaluated 9 days later. Inter-rater reliability was high for HP (ICC range
between 0.94-0.96) and fair for SMD (ICC range between 0.78-0.79). The HP
standard error of measurement (SEM) was 0.41–0.75cm while the minimal detectable
change (MDC) was 0.96–1.74cm. The SMD SEM was 1.61-7.06mm while the MDC
was 3.76-16.47mm. A moderate positive correlation for both groups was observed
between HP and SCD (asymptomatic subjects, r=0.447; CCFP patients, r=0.52).
Analysis with an independent t-test showed statistically significant differences
between groups for measures of craniocervical posture, but these differences were
very small. No statistically significant correlations between the HP and SMD with the
disabilities variables. Neck disability is strong positively correlated with the
craniofacial disability (r=0.79, p<0.001, n=60).
CONCLUSION:
The CROM device and Digital Calliper were reliable means of measuring HP and
SMD when performed by two or one raters in asymptomatic subjects and CCFP
patients.
KEYWORDS:
Reliability, Posture, Reproducibility of Results, Rehabilitation, Measurement, Neck
Pain, Temporomandibular disorders
INTRODUCTION
The optimal position of the head is the one in which the cranium is not inclined,
retracted, rotated, or extended. This position minimizes the muscle forces needed to
compensate the tendency of the head to tilt forward.[1] Currently, many professions
(office workers, clerks, carriers, etc.) require workers to spend much of their work day
sitting. In this situation one may adopt an excessive forward head posture (FHP).[2]

4
This head posture (HP) may occur due to a front translation of the head, a flexion of
the lower cervical spine, or both, and is also associated with an increase in extension
of the upper cervical spine.[3] It has been suggested that FHP increases the
compressive forces of the cervical zygapophyseal joint and those in the rear of the
vertebrae,[4] causing changes in the length and strength of the connective tissue
leading to stretching of the anterior neck structures and shortening of the posterior
neck muscles, all leading to pain.[5]
It is recommended that HP is quantified as part of the examination of patients with
neck pain to facilitate the diagnosis and determine treatment strategies. In addition, it
is very important to monitor a patient’s progress.[5] This growing interest around the
importance of the HP by researchers and clinicians is due to the belief that FHP is
associated with the development and persistence of certain disorders, such as cervical
headaches and migraines,[6] myofascial pain syndrome,[7] and woman with
craniofacial pain.[8] Regarding the association between the FHP and pain, there are
numerous studies with conflicting results: some showed differences in the HP of
patients with neck pain versus asymptomatic subjects,[9] while others do not.[10]
Attempts have been made to quantify FHP in many ways, both objectively and
subjectively. Subjective methods are described by some authors,[11] while objective
methods use photographs (to measure the tragus-C7-horizontal angle),[12]
radiographic images,[13] or the Cervical Range of Motion instrument (CROM),[14]
among others.
The CROM was designed to measure cervical range of motion but it can also measure
protraction and retraction of the head.[14] In the trial conducted by Garret et al.[14],
HP was measured in a sitting position with the CROM. The authors found high intra-
5
examiner reliability (ICC=0.93) while inter-examiner reliability was good
(ICC=0.83).
Another measurement that may be of interest is the sternomental distance (SMD). We
hypothesize a direct association between the SMD and the HP. We found only two
studies that evaluated the SMD, but they did not association it with HP.[15, 16]
There is little evidence concerning the reliability of intra-examiner and inter-examiner
measurement of HP using the CROM, therefore our purpose was to examine this
reliability and of using a Digital Calliper to measure the SMD. In addition, we
assessed a possible association between the variables recorded by these instruments
and as ultimate objective, we intend to assess whether there are differences in
craniocervical posture between asymptomatic subjects and patients with chronic
cervico-craniofacial pain (CCFP).
METHODS
Study design
We employed two-group repeated measures for intra- and inter-rater reliability
design. This study was planned and conducted in accordance with the Guidelines for
Reporting Reliability and Agreement Studies (GRRAS).[17]
Sample size
Sample size was calculated using the method described by Walter et al.[18]. This
method is recommended for estimating of sample size based on the Intraclass
Correlation Coefficient (ICC). The minimally acceptable ICC value (ρ1 = 0.7) versus
an alternative ICC reflecting the expected value (ρ1 = 0.8) was chosen. To obtain a
power of 80% (β = 0.2) and significance level of 5%, we determined that a sample of
at least 53 healthy subjects was required for intra-rater and inter-rater reliability (two
sets of 2 measurements were performed each day for two days). In addition, under the

6
same conditions, we determined that a sample of at least 57 symptomatic subjects was
required for intra-rater reliability (1 set of 2 measurements were performed each day
for three days). To estimate sample size we used the Power Analysis & Sample Size
Software (PASS 12).
Subjects
Two convenience samples of asymptomatic subjects were obtained from our
university campus and the local community through flyers, posters, and social media.
To participate in this study, the asymptomatic subjects were required to be between
18 and 65 years of age and must not have experienced: (1) neck or face pain during
data collection, or (2) a history of neck or face pain in the prior six months.
The second convenience sample of symptomatic subjects consisted in chronic
cervico-craniofacial pain patients. The sample was recruited two private clinics
specialized in spine, craniofacial pain and temporomandibular disorders (TMD)
(Madrid, Spain). A diagnosis of CCFP of muscular origin was the first inclusion
criterion. We defined CCFP of muscular origin as the presence of mechanical signs of
dysfunction and muscular pain (e.g. limited movement, uncoordinated movement,
weakness and lack of endurance in the neck and jaw) that were exacerbated by
maintained postures and movement, generating pain at the cervical and craniofacial
regions [19]. The specific inclusion criteria were: a) signs of disability and pain in the
orofacial and craniomandibular region, according to the Craniofacial pain and
disability inventory (CF-PDI) [20]; b) a primary diagnosis of myofascial pain
following Axis 1 (myofascial pain) of the Research Diagnostic Criteria for
Temporomandibular Disorders[21]; c) ≥ 6 months with the presence of the pain; d) ≥
5 points on the Neck Disability Index (NDI)[22]; f) bilateral pain of the temporal,
masseter, suboccipital and trapezius muscles. Patients were excluded if they had any

7
"red flags,"[23] a rheumatologic disease, any type of cancer, cervical radiculopathy,
myelopathy, a history of cervical surgery or whiplash trauma. The study was
conducted in accordance with the Declaration of Helsinki and was approved by the
local ethics committee. Prior to their participation, subjects gave written informed
consent.
Evaluators
The assessments were made by two physical therapists with more than three years of
clinical experience using the CROM to measure range of movement (ROM) and head
posture (HP) in clinical practice. Both therapists received a 120-minute training
session on how to use the Digital Calliper and how to measure the SMD.
Instrumentation
In this study we used the CROM equipped to measure the HP. The device used was
the CROM 3. It has the appearance of eyeglasses and is made from a lightweight
plastic with three inclinometers, one for each plane of motion. It is adjusted using a
hook-and-loop strap. The part of the device used to measure HP includes the forward
head arm and the vertebra locator. The forward head arm is equipped with a ruler
marked in 0.5 cm units, indicating the horizontal distance between the bridge of the
nose and the vertebra locator. The vertebra locator has a leveler bubble on top to
assist with accurate positioning. In this study the inclinometers were not used because
neck movements were not evaluated.
The digital calliper was used to quantify the SMD. The device is made of plastic with
a 5-digit LCD display, and can measure in inches or millimeters (mm) and with a
range of 0.01 mm to 150 mm. It also includes a ruler provided with a nonius, for
accurate measurement of lengths or angles. The one used for measuring length
comprised of a rule divided into equal parts on which a nonius slides such that n-1

8
divisions of the rule are divided into n equal parts of the nonius. It has two tips for
controlling internal and external measurements. The digital calliper is used for direct
measurement. Also, it is a fast and accurate instrument.
Procedures
The assessments were made between May and June of 2012 in our university
laboratory for asymptomatic subjects and between July and September of 2014 for
symptomatic subjects. Each healthy subject visited the laboratory on two different
occasions separated by a space of 48 hours. On the first day, rater A performed the
first assessment followed by rater B. On the second day, rater B performed the first
assessment followed by rater A. Moreover, each symptomatic subject visited the
laboratory on three different occasions separated by a space of 48 hours (between trial
1 and trial 2) and 9 days (between trial 2 and trial 3). In symptomatic subjects, the
assessment always was performed by the same rater. In both samples of subjects, each
rater used a data collection sheet on which to record the measurements. Before the
assessments, subjects removed eyeglasses, caps, and any jewelry. The measurements
in this study were taken twice, and the order in which they were performed was as
follows:
1. Head Posture
To quantify HP, the subjects were told to stay in the starting position: sitting in a chair
with a back rest, feet flat on the floor, and arms hanging alongside the body. The
evaluator placed the CROM on the subject’s head like a pair of eyeglasses and
adjusted it with the strap. The evaluator then located the spinous process of C7 and
placed the vertebra locator on it, adjusting the pressure until the subject indicated that
the pressure of the device was felt. Once the subject felt the pressure over C7, the

9
evaluator stated, “From this moment you should not move”. This was performed as a
means for the subject to become familiar with the test.
Then the subject was asked to stand up and then sit back into the starting position.
The evaluator standing to the left side of the subject, found the spinous process of C7
and placed the vertebra locator such that it formed a 90° angle with the head arm of
the CROM with the bubble indicating the instrument was level (Figure 1. A). This
measurement was made twice, and between the first and the second measurements the
subjects were asked to stand up and sit back into the starting position again,
whereupon the evaluator completed the procedure.
2. Sternomental Distance
The evaluator first explained to the subject that the measurement would take place
while lying on a couch. Also at this time the evaluator showed the Digital Calliper to
the subject and said: “You will notice contact on your sternum and on your chin; at
the moment you notice that you should not move.” When the subject understood the
statement and gave the evaluator permission to proceed, the subject was asked to lie
in a supine position on the couch, looking at the ceiling. When the subject was in
position the evaluator gave the instruction: “Don’t move your head.” Once in place,
the measurement was taken from the jugular notch of the sternum to the chin
protuberance (Figure 1. B). The measurement was taken twice between the subject
was instructed to roll to a right lateral position and then return to the supine position.
DATA ANALYSIS
Data were analysed with the SPSS statistical package (SPSS v.20.0; SPSS, Inc,
Chicago, IL). The Kolmogorov-Smirnov test was used to analyze the normal
distribution of the variables (P>0.05).

10
The intra-rater and inter-rater reliability was evaluated using the Intraclass Correlation
Coefficient (ICC). Reliability levels were defined based on the following
classification: good reliability, ICC ≥ 0.75; moderate reliability, ICC ≥ 0.50 and
<0.75; and poor reliability, <0.50 [24].
Bland-Altman analysis were performed by calculating the mean difference between
two measurements and the standard deviation (SD) of the difference.[25] A 95% of
the differences is expected to be less than two SDs. The closer the mean difference
was to 0 and the smaller the SD of this difference, the better was the agreement.[25]
The Bland–Altman analysis was used to compare the values of HP and SMD obtained
by the two raters separately. Similarly, comparisons were made to confirm the
reproducibility by analyzing the measurements values obtained on two trials. Bland-
Altman analysis was performed using MedCalc for Windows, version 12.5.0.0
(MedCalc Software, Mariakerke, Belgium).
Measurement error is expressed as a standard error of measurement (SEM), which is
calculated as , where SD is the SD of values from all participants and
ICC is the reliability coefficient.[26] Measurement error is the systematic and random
error of a patient’s score that is not attributable to true changes in the construct to be
measured.[27]
Responsiveness was assessed using the Minimal Detectable Change (MDC). The
MDC90 expresses the minimal change required to be 90% confident that the observed
change between the two measures reflects real change and not measurement error.[28]
It is calculated as .[28]
The Pearson correlation coefficient was used to analyze the association between HP
and SMD in the two samples of subjects, also used to analyze the correlations
between the variables of disability with the data HP and SMD in patients with CCFP.

11
A Pearson correlation coefficient greater then 0.60 indicated a strong correlation,
between 0.30 and 0.60 indicated a moderate correlation, and below 0.30 indicated a
low or very low correlation.[29]
Finally, the independent t-test was used for the analysis of HP and SMD variables
(using the mean of the trial 1 and 2), comparing the collection data for the two
samples.
RESULTS
The asymptomatic subjects sample consisted of 53 participants, 30 of whom were
women; the subjects were between 18 and 53 years of age (mean=38.1, SD=10.5
years). The symptomatic subjects sample consisted of 60 CCFP patients, 32 of whom
were women; the subjects were between 19 and 61 years of age (mean=41.7, SD=11.7
years). No statistically significant differences between the general characteristics of
both groups are presented. The group of symptomatic subjects presented a mean of
14.78 ±4.04 of neck disability and 16.30±7.11 of craniofacial disability. All variables
were normally distributed according to the Kolmogorov-Smirnov test (P>0.05). No
subjects were excluded from the study based on the inclusion and exclusion criteria.
Asymptomatic subjects
The ICC value for intra-rater reliability of single measures separated by a space of 48
hours was 0.93 for HP and ranged from 0.95 to 0.99 for SMD. Descriptive statistics,
ICCs and associated 95% CIs, SEMs and MDC90 between each evaluator´s trials are
presented in Table 1.
ICC values for interrater reliability of single measures ranged from 0.78 to 0.79 for
SMD and from 0.94 to 0.96 for HP. Descriptive statistics, ICCs and associated 95%
CIs, SEMs, and MDC90 between each rater´s trials are presented in Table 1.

12
The Bland-Almand analysis for the intra-rater and inter-rater performances are shown
for assessement of HP and SMD in Table 2. The mean differences in all Bland-
Almand analysis were close to zero, suggesting that appropriate intra-rater and inter-
rater reliability. Inter-rater performances of SMD at the 95% confidence intervals
showed large variability, would indicate error and suggesting that SMD assessment is
reliable but not precise (Table 2).
The scatter diagram (Figure 2. A) shows a moderate positive correlation between HP
and the SMD (r=0.44, p=0.001, n=53).
Chronic cervico-craniofacial pain patients
The ICC value for intra-rater reliability of single measures separated by a space of 48
hours was 0.88 for HP and 0.79 for SMD. When the singles measures were separated
by a space of 9 days, the ICC value for intra-rater reliability was 0.81 for HP and 0.76
for SMD. Descriptive statistics, ICCs and associated 95% CIs, SEMs and MDC90
between trials are presented in Table 3.
The Bland-Almand analysis for the intra-rater performances are shown for
assessement of HP and SMD in Table 4. The mean differences in all Bland-Almand
analysis were close to zero, suggesting that appropriate intra-rater and inter-rater
reliability. Inter-rater performances of SMD at the 95% confidence intervals showed
large variability, would indicate error and suggesting that SMD assessment is reliable
but not precise. (Table 4).
The scatter diagram (Figure 2. B) shows a moderate positive correlation between HP
and the SMD (r=0.56, p<0.001, n=60). No statistically significant correlations
between the HP and SMD with the disabilities variables. Neck disability is strong
positively correlated with the craniofacial disability (r=0.79, p<0.001, n=60).

13
Asymptomatic subjects versus chronic cervico-craniofacial pain patients
The independent t-test for comparison between the asymptomatic and symptomatic
samples, using the mean of the trial 1 and 2 (separated by 48 hours), found
statistically significant differences for HP and SMD (p<0.05). Descriptive statistics,
mean differences and associated 95% CIs between the two samples are presented in
Table 5.
DISCUSSION
The evaluation of HP is a variable to consider evaluating in clinical practice due to its
influence on the pathophysiology of the cervical region.[4, 30] Our results show
strong intra- and inter-rater reliability when measuring HP with the CROM device. As
for the examination of the SMD, results obtained with the Digital Calliper reflected
strong reliability.
Recently, several studies have measured HP using different methods and
instruments,[1, 11–13] but disadvantages were low reliability,[11, 31] high cost, and
difficulty in transporting the equipment.[13, 32, 33] Furthermore, where a
radiological diagnosis was used, the risk of radiation exposure to the subject must be
considered.
In the literature we found only one study in which the intra- and inter-rater
reliabilities were evaluated in measuring HP using CROM; results showed a good
intra and inter-rater reliability.[14] If we compare this data with our own, we find
strong intra-rater reliability in both investigations, while our inter-rater reliability was
superior to that obtained by Garrett et al.[14] for asymptomatic subjects but not for
CCFP patients. Both investigations followed a rigorous standardized protocol using
similar samples. An important aspect to note is that the time did not influence the

14
intra-rater reliability and the results were very similar at 48 hours and 9 days later. It
has been suggested that a range of 2 to 14 days is generally acceptable for analyzing
test reliability.[34]
As we mentioned, the SMD measured by the Digital Calliper showed high intra-rater
reliability where it showed acceptable inter-rater reliability. Again, we find only one
article that mentions the SMD, but that investigation was designed to generate a
prediction rule for the degree of difficulty when performing a laryngoscopy.[15, 16]
The SMD measurement used in a study by Al Ramadhani et al.[15], was of 142.8
(SD=1.50), whereas we found SMD to be between 107.5 and 113.57 of our study.
This difference could be explained by the fact that their measurement protocol was
performed measuring the cervical extension. It is also worth mentioning that the
measure was performed using a ruler with an accuracy of 5 mm rather than a Digital
Calliper with a resolution of 0.01 mm. We feel this fact supports a contention that our
investigation is more rigorous and reliable.
We found the intra-rater MDC of HP varied from 1.27 cm to 1.74 cm but that the
inter-rater MDC was between 0.96 cm and 1.30 cm. We also found that the intra-rater
MDC of the SMD was between 3.76 mm and 14.55 mm while the inter-rater MDC
was between 16.13 mm and 16.47 mm. Is considered MDC the smallest quantity
above the SEM, although it should not be assumed that this change has reached the
threshold of clinically significant improvement.[35]
With regard to the comparison of the means of the 2 measurements of the
craniocervical posture, the results show that there are statistically significant
differences between both groups, with higher measures in the group of CCFP,
however you have to take into account that the differences are very small and exceed
slightly the MDC in the HP measurement (mean difference -1.27 cm), nor for the
15
SMD (mean difference -5.01 mm), other studies have found similar results to ours,
finding very small differences between measurements of craniocervical posture in
asymptomatic subjects versus symptomatic subjects with neck pain [30] and
TMD.[36] We did not find association between measurements of craniocervical
posture and disability variables, this result is supported by recent evidence [36, 37],
being this issue controversial.[38] We have found a strong correlation between neck
disability and craniofacial disability (r=0.79), other studies have also found similar
results to our findings. [20, 36]
Furthermore, the Pearson correlation coefficient between HP and the SMD is 0.447
for asymptomatic subject and 0.56 for symptomatic subjects, suggesting a moderate
correlation. We believe this is the first study to determine this association; we found
that the previous studies measuring the SMD do not correlate it to HP. Thus, we can
assume that there is a relationship between HP in the sitting position and SMD in
supine position in healthy subjects.
Limitations
This study has several limitations that must be discussed. We agree with Garret et
al.[14] that a limitation exists in the head arm of the CROM in that it is marked in
increments of 0.5 cm, making it hard to determine a measurement when the indicator
is between two marks. We believe that the reliability and data collection could be
improved if the head arm was marked in mm. Lastly, we calculated the MDC but not
the minimal clinically relevant change (MCRC), which we believe is of special
interest in clinical practice. We must remember that the MDC is not the same as the
MCRC, which is the grade of clinically significant improvement and is normally
associated with an external criteria that indicates when that change has occurred.[35]
We have not calculated the MCRC, so we do not know the grade of clinically

16
significant improvement. Future randomized controlled trials should identify
interventions that influence the HP and SMD, this could help assess the performance
of this test when subjected to clinical interventions and also with those results could
calculate the MCRC.
CONCLUSIONS
The CROM and the Digital Calliper are reliable instruments for measuring HP and the
SMD in healthy subjects and CCFP patients. Furthermore, there is a moderate
correlation between HP and the SMD and strong correlation between neck disability
and craniofacial disability. We did not find association between measurements of
craniocervical posture and disability variables. We also believe further studies should
consider the MCRC and the influence of longer periods between examinations on the
measures.

17
REFERENCES
1. Silva AG, Johnson MI (2012) Does forward head posture affect postural control in
human healthy volunteers? Gait Posture. doi: 10.1016/j.gaitpost.2012.11.014
2. Seghers J, Jochem A, Spaepen A (2003) Posture, muscle activity and muscle
fatigue in prolonged VDT work at different screen height settings. Ergonomics
46:714–30. doi: 10.1080/0014013031000090107
3. Enwemeka CS, Bonet IM, Ingle JA, et al. (1986) Postural Correction in Persons
with Neck Pain (II. Integrated Electromyography of the Upper Trapezius in
Three Simulated Neck Positions). J Orthop Sports Phys Ther 8:240–2.
4. Bonney RA, Corlett EN (2002) Head posture and loading of the cervical spine.
Appl Ergon 33:415–7.
5. Cheung Lau HM, Wing Chiu TT, Lam T-H (2009) Clinical measurement of
craniovertebral angle by electronic head posture instrument: a test of reliability
and validity. Man Ther 14:363–8. doi: 10.1016/j.math.2008.05.004
6. Fernández-de-Las-Peñas C, Cuadrado ML, Pareja JA (2006) Myofascial trigger
points, neck mobility and forward head posture in unilateral migraine.
Cephalalgia 26:1061–70. doi: 10.1111/j.1468-2982.2006.01162.x
7. Cimbiz A, Beydemir F, Manisaligil U (2006) Evaluation of Trigger Points in
Young Subjects. J Musculoskelet Pain 14:27–35.
8. Braun BL (1991) Postural differences between asymptomatic men and women and
craniofacial pain patients. Arch Phys Med Rehabil 72:653–6.
9. Haughie LJ, Fiebert IM, Roach KE (1995) Relationship of forward head posture
and the cervical backward bending to neck pain. J Man Manip Ther 3:91–7.
10. Hanten WP, Olson SL, Russell JL, et al. (2000) Total head excursion and resting
head posture: normal and patient comparisons. Arch Phys Med Rehabil 81:62–6.
11. Silva AG, Punt TD, Johnson MI (2010) Reliability and validity of head posture
assessment by observation and a four-category scale. Man Ther 15:490–5. doi:
10.1016/j.math.2010.05.002
12. Horton SJ, Johnson GM, Skinner MA (2010) Changes in head and neck posture
using an office chair with and without lumbar roll support. Spine (Phila Pa 1976)
35:E542–8. doi: 10.1097/BRS.0b013e3181cb8f82
13. Gadotti IC, Magee D (2013) Assessment of intrasubject reliability of radiographic
craniocervical posture of asymptomatic female subjects. J Manipulative Physiol
Ther 36:27–32. doi: 10.1016/j.jmpt.2012.12.009

18
14. Garrett TR, Youdas JW, Madson TJ (1993) Reliability of measuring forward head
posture in a clinical setting. J Orthop Sports Phys Ther 17:155–60.
15. Al Ramadhani S, Mohamed LA, Rocke DA, Gouws E (1996) Sternomental
distance as the sole predictor of difficult laryngoscopy in obstetric anaesthesia.
Br J Anaesth 77:312–6.
16. Khan ZH, Mohammadi M, Rasouli MR, et al. (2009) The diagnostic value of the
upper lip bite test combined with sternomental distance, thyromental distance,
and interincisor distance for prediction of easy laryngoscopy and intubation: a
prospective study. Anesth Analg 109:822–4. doi:
10.1213/ane.0b013e3181af7f0d
17. Kottner J, Audige L, Brorson S, et al. (2011) Guidelines for Reporting Reliability
and Agreement Studies (GRRAS) were proposed. Int J Nurs Stud 48:661–71.
doi: 10.1016/j.ijnurstu.2011.01.016
18. Walter SD, Eliasziw M, Donner A (1998) Sample size and optimal designs for
reliability studies. Stat Med 17:101–10.
19. La Touche R, París-Alemany A, Mannheimer JS, et al. (2013) Does mobilization
of the upper cervical spine affect pain sensitivity and autonomic nervous system
function in patients with cervico-craniofacial pain?: A randomized-controlled
trial. Clin J Pain 29:205–15. doi: 10.1097/AJP.0b013e318250f3cd
20. La Touche R, Pardo-Montero J, Gil-Martínez A, et al. (2014) Craniofacial pain
and disability inventory (CF-PDI): development and psychometric validation of
a new questionnaire. Pain Physician 17:95–108.
21. Dworkin SF, LeResche L (1992) Research diagnostic criteria for
temporomandibular disorders: review, criteria, examinations and specifications,
critique. J Craniomandib Disord 6:301–55.
22. Andrade Ortega JA, Delgado Martínez AD, Almécija Ruiz R (2010) Validation of
the Spanish version of the Neck Disability Index. Spine (Phila Pa 1976)
35:E114–8. doi: 10.1097/BRS.0b013e3181afea5d
23. Greenhalgh S, Selfe J (2009) A qualitative investigation of Red Flags for serious
spinal pathology. Physiotherapy 95:224–7. doi: 10.1016/j.physio.2009.04.006
24. Portney LG WM. (2009) Foundations of Clinical Research; Applications to
Practice. New Jersey
25. Bland JM, Altman DG (1986) Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet 1:307–10.
26. Weir JP (2005) Quantifying test-retest reliability using the intraclass correlation
coefficient and the SEM. J Strength Cond Res 19:231–40. doi: 10.1519/15184.1

19
27. Mokkink LB, Terwee CB, Patrick DL, et al. (2010) The COSMIN study reached
international consensus on taxonomy, terminology, and definitions of
measurement properties for health-related patient-reported outcomes. J Clin
Epidemiol 63:737–45. doi: 10.1016/j.jclinepi.2010.02.006
28. Haley SM, Fragala-Pinkham MA (2006) Interpreting change scores of tests and
measures used in physical therapy. Phys Ther 86:735–43.
29. Hinkle D, Jurs S, Wiersma W (1988) Applied statistics for the behavioral
sciences, 2nd ed. Houghton Mifflin, Boston
30. Silva AG, Punt TD, Sharples P, et al. (2009) Head posture and neck pain of
chronic nontraumatic origin: a comparison between patients and pain-free
persons. Arch Phys Med Rehabil 90:669–74. doi: 10.1016/j.apmr.2008.10.018
31. Juul-Kristensen B, Hansson GA, Fallentin N, et al. (2001) Assessment of work
postures and movements using a video-based observation method and direct
technical measurements. Appl Ergon 32:517–24.
32. Harrison DE, Haas JW, Cailliet R, et al. (2005) Concurrent validity of flexicurve
instrument measurements: sagittal skin contour of the cervical spine compared
with lateral cervical radiographic measurements. J Manipulative Physiol Ther
28:597–603. doi: 10.1016/j.jmpt.2005.08.012
33. Van Niekerk S-M, Louw Q, Vaughan C, et al. (2008) Photographic measurement
of upper-body sitting posture of high school students: a reliability and validity
study. BMC Musculoskelet Disord 9:113. doi: 10.1186/1471-2474-9-113
34. Streiner DL, Norman GR (1989) Health Measurement Scales: a Guide to Their
Development and Use. Oxford Oxford Univ. Press
35. Fletcher JP, Bandy WD (2008) Intrarater reliability of CROM measurement of
cervical spine active range of motion in persons with and without neck pain. J
Orthop Sports Phys Ther 38:640–5. doi: 10.2519/jospt.2008.2680
36. Armijo-Olivo S, Rappoport K, Fuentes J, et al. (2011) Head and cervical posture
in patients with temporomandibular disorders. J Orofac Pain 25:199–209.
37. Cheung CH, Shum ST, Tang SF, et al. (2010) The correlation between
craniovertebral angle, backpack weights, and disability due to neck pain in
adolescents. J Back Musculoskelet Rehabil 23:129–36. doi: 10.3233/BMR-2010-
0259
38. Lau KT, Cheung KY, Chan KB, et al. (2010) Relationships between sagittal
postures of thoracic and cervical spine, presence of neck pain, neck pain severity
and disability. Man Ther 15:457–62. doi: 10.1016/j.math.2010.03.009

20
FIGURES AND LEGENDS
Figure 1. A) Placement of CROM with the head arm for the measure of Head Posture
with the vertebra locator. B) Evaluator taking measure from the jugular notch of the
sternum to the chin protuberance to quantitative the Sternomental Distance.

21
Figure 2. Scatter Diagram showing correlation between Head Posture and the
Sternomental Distance. A) Scatter diagram for asymptomatic subjects (n=53); B)
scatter diagram for chronic cervico-craniofacial pain patients (n=60).

22
Table 1. Intra-rater and Inter-rater reliability and descriptive statistics for
measurements in asymptomatic subjects.
Abbreviations: CI, confidence interval; ICC 3,1, intraclass correlation coefficient,
model 3,1; HP, head posture; MDC90, minimal detectable change at the 90%
confidence level; SMD, sternomental distance; SD, standard deviation; SEM,
standard error of the measurement.
Rater A Rater B
Trial 1
(Mean
± SD)
Trial 2
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90 Trial 1
(Mean
± SD)
Trial 2
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90
HP (cm) 18.97 ±
2.47
19.07
± 2.19
0.93 0.88 –
0.96
0.60 1.40 18.77
± 2.35
18.96
± 2.19
0.93 0.89 –
0.96
0.55 1.30
SMD
(mm)
108.50
± 16.55
109.03
±
16.14
0.99
0.98 –
0.99
1.61 3.76 105.07
±
14.55
107.54
±
14.21
0.95 0.85 –
0.97
2.75 6.42
Trial 1
Trial 2
Rater A
(Mean
± SD)
Rater
B
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90 Rater
A
(Mean
± SD)
Rater
B
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90
HP (cm) 18.97 ±
2.47
18.77
± 2.35
0.94 0.90 –
0.96
0.56 1.30 19.07
± 2.19
18.96
± 2.19
0.96 0.93 –
0.98
0.41 0.96
SMD
(mm)
108.50
± 16.55
105.07
±
14.55
0.78 0.63 –
0.87
7.06 16.47 109.03
±
16.14
107.54
±
14.21
0.79 0.66 –
0.87
6.91 16.13

23
Table 2. Statistical metrics from Bland-Altman analysis of the intra-rater and inter-
rater measurements in asymptomatic subjects.
Intra-rater
Rater A Rater B
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
HP (cm) -0.10 ± 0.85 -0.34 to 0.15 -1.76 to 1.57 -0.19 ± 0.79 -0.41 to 0.04 -1.73 to 1.36
SMD (mm) -0.53 ± 2.28 -1.18 to 0.12 -4.99 to 3.94 -2.47 ± 3.89 -3.58 to -1.37 -10.10 to 5.16
Inter-rater
Trial 1 Trial 2
HP (cm)
0.19 ± 0.79 -0.03 to 0.42 -1.35 to 1.74 0.10 ± 0.59 -0.06 to 0.27 -1.05 to 1.25
SMD (mm) 3.43 ± 9.99 0.59 to 6.27 -16.14 to 23 1.49 ± 9.78 -1.29 to 4.26 -17.68 to 20.65
Abbreviations: CI, confidence interval; HP, head posture; LOA, limits of agreement;
SMD, sternomental distance; SD, standard deviation.

24
Table 3. Intra-rater reliability and descriptive statistics for measurements in chronic
cervico-craniofacial pain patients.
Abbreviations: CI, confidence interval; ICC 3,1, intraclass correlation coefficient,
model 3,1; HP, head posture; MDC90, minimal detectable change at the 90%
confidence level; SMD, sternomental distance; SD, standard deviation; SEM,
standard error of the measurement.
Rater A
Trial 1
(Mean
± SD)
Trial 2
(Mean
± SD)
Trial 3
(Mean
± SD)
48 hours between trials
(Trial 1-Trial 2)
9 days between trials
(Trial 2-Trial 3)
ICC
3,1
95% CI
for ICC
SEM MDC90 ICC
3,1
95% CI
for ICC
SEM MDC90
HP (cm) 20.40 ±
1.50
20.23
± 1.58
20.03 ±
1.84
0.88 0.80 –
0.92
0.54 1.27 0.81 0.70 –
0.88
0.75 1.74
SMD
(mm)
111.53
± 12.41
113.57
±
11.83
112.73
± 13.78
0.79
0.67 –
0.87
5.60 13.07 0.76 0.63 –
0.85
6.24 14.55

25
Table 4. Statistical metrics from Bland-Altman analysis of the intra-rater
measurements in chronic cervico-craniofacial pain patients.
Intra-rater
48 hours (Trial 1 – Trial 2) 9 days (Trial 2 – Trial 3)
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
HP (cm) 0.17 ± 0.77 -0.03 to 0.37 -1.34 to 1.67 0.21 ± 1.06 -0.06 to 0.48 -1.86 to 2.28
SMD (mm) -2.03 ± 7.92 -4.08 to 0.01 -17.56 to 13.49 0.83 ± 8.82 -1.45 to 3.11 -16.46 to 18.12
Abbreviations: CI, confidence interval; HP, head posture; LOA, limits of agreement;
SMD, sternomental distance; SD, standard deviation.
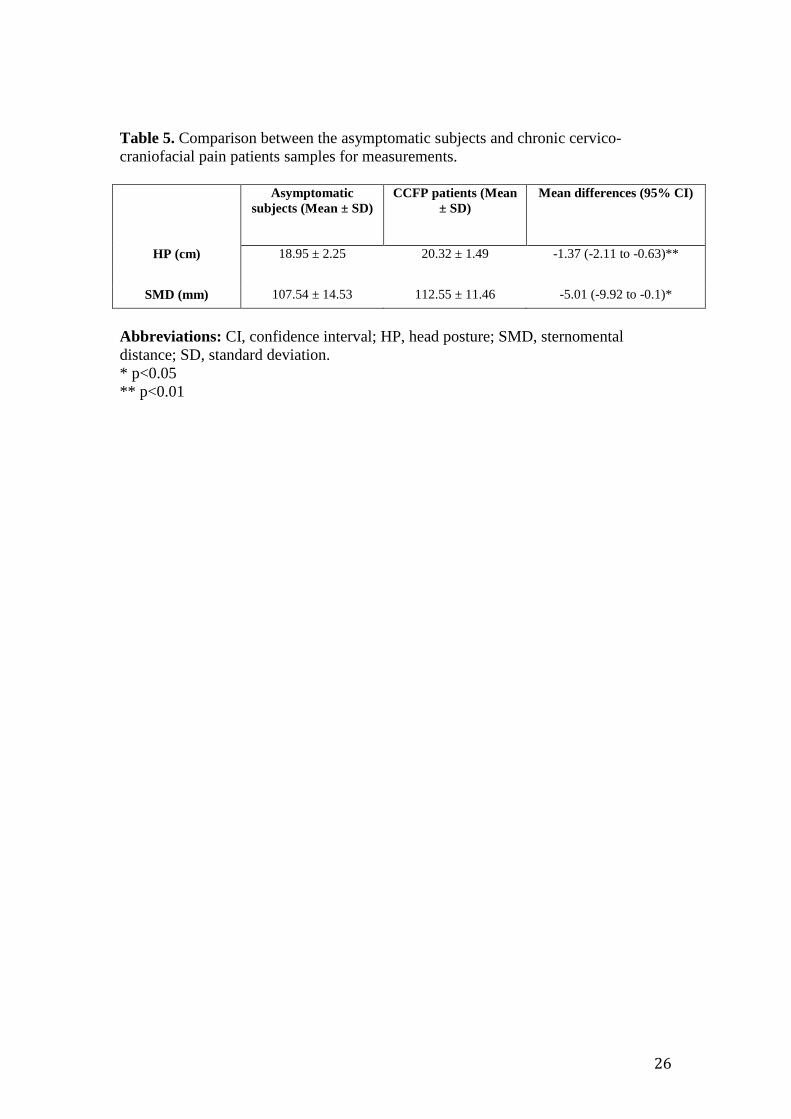
26
Table 5. Comparison between the asymptomatic subjects and chronic cervico-
craniofacial pain patients samples for measurements.
Asymptomatic
subjects (Mean ± SD)
CCFP patients (Mean
± SD)
Mean differences (95% CI)
HP (cm) 18.95 ± 2.25 20.32 ± 1.49 -1.37 (-2.11 to -0.63)**
SMD (mm) 107.54 ± 14.53 112.55 ± 11.46 -5.01 (-9.92 to -0.1)*
Abbreviations: CI, confidence interval; HP, head posture; SMD, sternomental
distance; SD, standard deviation.
* p<0.05
** p<0.01

114
5.3 Estudio III
La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-Parreño S, Paris-
Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain sensitivity over the trigeminal region
in patients with chronic mechanical neck pain. J Pain. 2010 Mar;11(3):256-63
Objetivos del estudio
El objetivo del presente estudio fue investigar la sensibilización del trigémino en pacientes con
dolor de cuello crónico mecánico, además se observaron la interacción de los resultados con
variables psicológicos, como la depresión y la ansiedad.
Resultado
Los resultados mostraron que los niveles de UDPS son significativamente menores
bilateralmente sobre los puntos musculares del masetero, temporal, los del trapecio superior, y
también los puntos medidos en las articulaciones cigapofisiarias de C5-C6 (P <0,001), pero no
sobre los puntos del músculo tibial anterior (P = 0,4) en pacientes con dolor de cuello crónico
mecánico, en comparación con los controles. La magnitud de la disminución de los UDPs fue
mayor en la región cervical, en comparación con la región del trigeminal (P <0,01). Los UDPs
en los músculos maseteros se correlacionaron negativamente tanto a la duración de los síntomas
de dolor y la intensidad del dolor (P <0,001). Además se encontraron correlaciones positivas
entre la intensidad de dolor con la discapacidad de cuello y los síntomas depresivos.
Conclusiones
Nuestros resultados revelaron la presencia de hiperalgesia mecánica en la región trigeminal en
pacientes con dolor de cuello crónico mecánico, lo que sugiere la difusión de la sensibilización a
la región del trigémino en esta población de pacientes. Los resultados de este estudio sugieren
que existe la presencia de un proceso de sensibilización del NCT en esta población. Este
hallazgo tiene implicaciones para el desarrollo de estrategias de gestión.
The Journal of Pain, Vol 11, No 3 (March), 2010: pp 256-263Available online at www.sciencedirect.com
Bilateral Mechanical-Pain Sensitivity Over the Trigeminal Region in
Patients With Chronic Mechanical Neck Pain
Roy La Touche,*y Cesar Fernandez-de-las-Penas,zx{ Josue Fernandez-Carnero,zx{
Santiago Dıaz-Parreno,*y Alba Paris-Alemany,*y and Lars Arendt-Nielsenz
*Faculty of Medicine, Department of Physical Therapy.yUniversity Center for Clinical Research of the Craneal-Cervical-Mandibular System, Universidad San Pablo CEU,Madrid, Spain.zDepartment of Physical Therapy, Occupational Therapy, Rehabilitation and Physical Medicine.xEsthesiology Laboratory, Universidad Rey Juan Carlos, Alcorcon, Madrid, Spain.{Centre for Sensory-Motor Interaction (SMI), Department of Health Science and Technology, Aalborg University,Aalborg, Denmark.
ReceivedAddressde Ciencs/n, 2892
1526-590
ª 2010 b
doi:10.10
256
Abstract: The aim of this study was to investigate bilateral pressure-pain sensitivity over the tri-
geminal region, the cervical spine, and the tibialis anterior muscle in patients with mechanical chronic
neck pain. Twenty-three patients with neck pain (56% women), aged 20 to 37 years old, and 23
matched controls (aged 20 to 38 years) were included. Pressure pain thresholds (PPTs) were bilaterally
assessed over masseter, temporalis, and upper trapezius muscles, the C5-C6 zygapophyseal joint, and
the tibialis anterior muscle in a blinded design. The results showed that PPT levels were significantly
decreased bilaterally over the masseter, temporalis, and upper trapezius muscles, and also the C5-C6
zygapophyseal joint (P < .001), but not over the tibialis anterior muscle (P = .4) in patients with
mechanical chronic neck pain when compared to controls. The magnitude of PPT decreases was
greater in the cervical region as compared to the trigeminal region (P < .01). PPTs over the masseter
muscles were negatively correlated to both duration of pain symptoms and neck-pain intensity (P <
.001). Our findings revealed pressure-pain hyperalgesia in the trigeminal region in patients with
mechanical chronic neck pain, suggesting spreading of sensitization to the trigeminal region in
this patient population.
Perspective: This article reveals the presence of bilateral pressure-pain hypersensitivity in the
trigeminal region in patients with idiopathic neck pain, suggesting a sensitization process of the tri-
gemino-cervical nucleus caudalis in this population. This finding has implications for development of
management strategies.
ª 2010 by the American Pain Society
Key words: Neck pain, trigeminal sensitization, pressure pain threshold.
Chronic mechanical neck pain is a significant clinicalproblem. It seems that the prevalence of neck painis as high as the prevalence of low back pain. A sys-
tematic review reported a 1-year prevalence for neckpain ranging from 16.7 to 75.1%, with a mean of37.2%.11 A best-evidence synthesis showed an incidencerate for self-reported neck pain in the general popula-tion between 146 and 213 per 1,000 patients per year.21
Nearly half of neck-pain patients develop chronic symp-
May 31, 2009; Revised June 29, 2009; Accepted July 22, 2009.reprint requests to Cesar Fernandez de las Penas, Facultadias de la Salud, Universidad Rey Juan Carlos, Avenida de Atenas2 Alcorcon, Madrid, Spain. E-mail: [email protected]
0/$36.00
y the American Pain Society
16/j.jpain.2009.07.003
toms,4 and many will continue to exhibit moderatedisability at long-term follow-up.17 The economicburden associated with the management of neck painis second only to low back pain in annual workers’ com-pensation costs in the United States.44
Although the aetiology of insidious mechanical neckpain is under debate, it is clear that neck pain is multifac-torial in nature, with both physical and psychosocial con-tributors.38 In recent years, there has been an increasinginterest in the study of nociceptive-pain processing indifferent musculoskeletal-pain conditions. For instance,pressure pain thresholds5,32 have been extensively usedfor investigating mechanical pain hypersensitivity inseveral chronic pain conditions, eg, whiplash,36 fibro-myalgia,9 unilateral migraine,14 repetitive strain injury,18
tension-type headache,13 osteoarthritis,1 low back

La Touche et al 257
pain,27 or carpal tunnel syndrome.15 Nevertheless, thephenomenon of sensory hypersensitivity has been rela-tively recently investigated in mechanical nontraumaticneck pain.37
Scott et al33 found that the hypersensitivity present inindividuals with idiopathic neck pain seems to be con-fined to the neck area with little evidence of spread tomore remote body regions, eg, the tibialis anterior mus-cle, as opposite happens in chronic whiplash. The pres-ence of hypersensitivity restricted to the neck regionmay reflect segmental local sensitization, but not wide-spread central sensitization, in patients with idiopathicneck pain.
Several studies have reported that patients with neckpain also suffered from symptoms in the orofacialregion,7,8,23 and headaches.29 The expansion of symp-toms from the neck area to the trigeminal region maybe related to the convergence of the nociceptive sec-ond-order neurons receiving both trigeminal and cervi-cal inputs into the trigemino-cervical nucleus caudalisin the spinal gray matter of the spinal cord.25 To thebest of our knowledge, no previous study has investi-gated the pressure hypersensitivity over the trigeminalregion in chronic mechanical neck pain. Further, Rhudyand Meagher31 demonstrated that psychological states,particularly anxiety and depression, induce an increasedeffect on pressure-pain sensitivity. Therefore, the aim ofthe present study was to investigate trigeminal sensitiza-tion in patients with chronic mechanical neck pain con-trolling psychological aspects, such as depression andanxiety.
Methods
SubjectsPatients presenting with mechanical insidious neck
pain referred by their primary-care physicians to a spe-cialized physical-therapy clinic between September2007 and February 2008 were screened for possible eligi-bility criteria. Mechanical neck pain was defined as gen-eralized neck and/or shoulder pain with symptomsprovoked by neck postures, neck movement, or palpa-tion of the cervical musculature. Symptoms had to be bi-lateral and present for at least 6 months. Patients wereexcluded if they exhibited any of the following: 1) unilat-eral neck pain; 2) diagnosis of fibromyalgia;43 3) previouswhiplash; 4) cervical spine surgery; 5) clinical diagnosis ofcervical radiculopathy or myelopathy; 6) history of previ-ous physical-therapy intervention for the cervical region;7) presence of severe degenerative arthritis (confirmedby cervical radiography taken for all patients over theage of 30 years); 8) less than 18 years; 9) diagnosis ofany TMD, according to the Research Diagnostic Criteriafor TMD (RDC/TMD)10; or 10) concomitant diagnosis ofprimary headache.
Demographic and Clinical DataDemographic data including age, gender, height,
weight, location, and nature of the symptoms was col-lected. An 11-point numerical point rate scale22 (NPRS;
0 = no pain, 10 = maximum pain) was used to assess cur-rent level of neck pain. Patients also completed the NeckDisability Index (NDI) to measure perceived disability,42
the Beck Depression Inventory (BDI-II) to assess symp-toms of depression,2 and the State-Trait Anxiety Inven-tory (STAI) for assessing state and trait anxiety.34
The NDI consist of 10 questions measured on a 6-pointscale (0 = no disability, 5 = full disability).42 The numericscore for each item is summed for a score varying from0 to 50, where higher scores reflect greater disability.The NDI has demonstrated to be a reliable (intraclass cor-relation coefficients ranging from .50 to .98)24 and validself-assessment of disability in chronic neck pain.19,39
The BDI-II is a 21-item self-report measure assessingaffective, cognitive, and somatic symptoms of depres-sion.2 Patients choose from a group of sentences thatbest describe how they have been feeling in the past 2weeks. Higher scores indicate higher levels of depressivesymptoms.2 The BDI-II showed good internal consistency(alpha coefficient .90) and adequate divergent validity.41
The STAI is a self-report assessment device whichincludes separate measures of state and trait anxiety.34
In the present study, the trait-anxiety subscale whichdenotes relatively stable anxiety proneness and refersto a general tendency to respond with anxiety to per-ceived threats in the environment was used. Participantsuse a 4-point response scale ranging from ‘‘almost never’’to ‘‘almost always’’, indicating the extent to which theyexperience each emotion. The State-Trait questionnairehas shown good internal consistency (a = .83). Higherscores indicate greater trait anxiety.34
Finally, healthy controls were recruited from volunteerwho responded to a local announcement and were ex-cluded if they exhibited a history of neck, facial, orhead pain (infrequent episodic tension-type headachewas permitted), any systemic disease or any history oftraumatic event (whiplash).
The study was conducted in accordance with the Hel-sinki Declaration, and all subjects provided informed con-sent which was approved by the local ethics committee.
Sample Size DeterminationThe sample-size determination and power calculations
were performed with an appropriate software (Tamanode la Muestra, v.1.1, Universidad de Medicina, Madrid,Spain). The calculations were based on detecting, atthe least, significant clinical differences of 20% on pres-sure pain threshold (PPT) between both groups,28 withan alpha level of .05 and a desired power of 80%, andan estimated interindividual coefficient of variation forPPT measures of 20%. This generated a sample size ofat least 16 participants per group.
PPT AssessmentPPT is defined as the minimal amount of pressure
where a sensation of pressure first changes to pain.40 Amechanical pressure algometer (Pain Diagnosis andTreatment Inc, Great Neck, NY) was used in this study.The device consists of a round rubber disk (1 cm2)attached to a pressure gauge. The gauge displays values

258 Trigeminal Pain Sensitivity in Neck Pain
in kg/cm2, ranging from 0 to 10 kg. The mean of 3 trials(intraexaminer reliability) was calculated and used forthe main analysis. A 30-second resting period wasallowed between each trial. The reliability of pressure al-gometry has been found to be high in both asymptom-atic subjects6 (ICC .91 [95% CI .82–.97]) and neck painpatients45 (ICC .78–.93; 95% CI .53–.97).
Study ProtocolThe study protocol was the same for neck-pain pa-
tients and healthy controls. All examinations weredone in a quiet, draught-free, temperature- and humid-ity-controlled laboratory (24�C 6 1�C, relative humidity25–35%). All participants were restricted from vigorousexercise from the day prior to the examination. Noneof the patients were taking any preventive drug at thetime the study was performed. Participants were not al-lowed to take analgesics or muscle relaxants throughthe 72 hours prior to the examination. PPTs were mea-sured bilaterally over masseter and temporalis muscles,the articular pillar of C5-C6 zygapophyseal joint (basedon palpation of C6-C7 spinous processes), the upper tra-pezius muscle (midway between C7 and acromion), andtibialis anterior muscle (upper one-third of the musclebelly) by an assessor blinded to the subject’s condition.The masseter and temporalis muscles were chosen as tri-geminal areas, the articular pillar of C5-C6 and the uppertrapezius muscle were chosen as the most common sitesof involvement in idiopathic neck pain, and the tibialisanterior was chosen as a remote distant site. The orderof assessment was randomized between the participants.
Pressure Pain Threshold DataManagement
In the current study, the magnitude of sensitizationwas investigated by assessing the differences of absoluteand relative PPT values between both groups. For rela-tive values, we calculated a ‘‘PPT Index,’’ dividing thePPT of each patient at each point by the mean of PPTscore of the control group at the same point. PPT indiceswere only calculated in those PPT levels significantly dif-ferent between patients and controls. A greater PPT In-dex (%) indicates lower degree of sensitization.
Statistical AnalysisData were analysed with the SPSS statistical package
(SPSS v.16.0; SPSS, Inc, Chicago, IL). Results are expressedas mean, standard deviation (SD), and 95% confidenceinterval (95% CI). The Kolmogorov-Smirnov test wasused to analyze the normal distribution of the variables(P > .05). Quantitative data without a normal distribution(ie, pain history, current level of pain, and NDI) were an-alyzed with nonparametric tests, whereas data witha normal distribution (PPT levels, BDI-II, and STAI) wereanalyzed with parametric tests. The intraclass correlationcoefficient (ICC) was used to evaluate the intraexaminerreliability of PPT data. A 2-way ANCOVA was used to in-vestigate the differences in PPT assessed over each point(masseter, temporalis, upper trapezius, tibialis anteriormuscles, and the C5-C6 zygapophyseal joint) with side
(dominant or nondominant) as within-subject factorand group (patients or controls) as the between-subjectfactor. A 2-way ANCOVA test was used for assessing thedifferences in PPT Index with side (dominant, nondomi-nant) as within-patient factor, point (masseter, tempora-lis, upper trapezius, tibialis anterior muscles, and theC5-C6 joint) as between-patient factor, and age, sex,BDI-II, and STAI scores as covariates. Post hoc compari-sons were conducted with the Bonferroni test. Finally,the Spearman’s rho (rs) test was used to analyze the asso-ciation between PPTs and the clinical variables relating tosymptoms, disability, anxiety, and depression. The statis-tical analysis was conducted at a 95% confidence leveland a P value less than .05 was considered statisticallysignificant.
Results
Demographic and Clinical Data of thePatients
Forty consecutive patients presenting with neck painbetween January and May 2009 were screened for possi-ble eligibility criteria. Seventeen patients were excluded:concomitant diagnosis RDC/TMD (n = 8), migraine (n = 5),and previous whiplash (n = 4). Finally, 23 patients (10men and 13 women) with mechanical neck pain, aged20 to 37 years (mean, 28 6 5 years; mean weight, 70 6
10 kg; mean height, 168 6 10 cm), and 23 matched con-trols, aged 20 to 38 years old (mean, 28 6 6 years; meanweight, 66 6 11 kg; mean height, 168 6 9 cm) were in-cluded. No significant differences between both groupsfor age (P = .9), weight (P = .3) and height (P = .8) werefound. Patients with neck pain showed greater levels(P < .001) of depression (BDI-II, 7.5 6 3) and anxiety(STAI, 22.4 6 3.2) as compared to controls (BDI-II, 3 6 3;STAI, 10 6 8, respectively).
Within the patient group, mean duration of neck painhistory was 10 6 4.6 months (95% CI 7.8–11.7 months),the mean intensity (NPRS) of neck pain was 3.6 6 1.5(95% CI 3.2–4.8), the mean NDI was 18.5 6 3.3 (95% CI17–20), the mean BDI-II was 7.5 6 1.6 (95% CI 6–9), andthe STAI was 22 6 3 (95% CI 21–24). Furthermore, posi-tive correlations between duration of pain history withcurrent level of pain (rs = .55, P = .007 [Fig 1A]) andBDI-II (rs =.58, P = .004 [Fig 1B]) were found: the longerthe duration of the symptoms, the greater the intensityof the perceived pain and the greater the self-reporteddepression. Further, current level of pain was also posi-tively correlated to disability (rs = .57, P = .004 [Fig 2A])and to BDI-II (rs = .64; P = .001, [Fig 2B]): the greater theintensity of the perceived pain, the greater the self-re-ported disability and the greater the self-reporteddepression.
Pressure Pain Sensitivity Over theTrigeminal Region
The intraexaminer repeatability of PPTreadings for themasseter and temporalis muscle was .9 and .92 for themost painful side and .91 for the contralateral side. Thestandard error of measurement (SEM) was .14 kg/cm2

Figure 1. Scatter plots of relationships between duration of history of neck pain and NPRS values (A) and between history ofneck pain and Beck Depression Inventory (B) A positive linear regression line is fitted to the data (NPRS: numerical pain rate scale,range 0 to 10).
La Touche et al 259
for the most painful side and .11 kg/cm2 for the contra-lateral side.
The ANOVA revealed significant differences betweenboth groups, but not between sides, for PPT levels overthe masseter (group: F = 257.3, P < .001; side: F = .58,P = .447) and temporalis (group: F = 124.8, P < .001;side: F = .06, P = .803) muscles. Over both muscles, pa-tients showed bilateral lower PPT levels than healthycontrols (P < .001). Table 1 summarizes PPT assessedover the masseter and temporalis muscles for both sideswithin each study group.
Pressure Pain Sensitivity Over theCervical Region
The intraexaminer repeatability of PPT over the C5-C6joint and the upper trapezius muscle was .91 for the mostpainful side and .89 for the contralateral side, respec-tively. The SEM was .11 and .13 kg/cm2 for the most pain-ful side and .15 kg/cm2 for the contralateral side.
The ANOVA revealed significant differences betweenboth groups, but not between sides, for PPT levels overthe upper trapezius muscle (group: F = 355.9, P < .001;side: F = .03, P = .851), and the C5-C6 zygapophyseal joint(group: F = 291.5, P < .001; side: F = .08, P = .776). Again,
Figure 2. Scatter plots of relationships between duration of NPRS pvalues and Beck Depression Inventory (B) A positive linear regression0 to 10).
patients showed bilateral lower PPT levels in both pointsas compared to healthy controls (P < .001). Table 1 showsPPT over the upper trapezius muscle and the C5-C6 zyga-pophyseal joint for both sides within each group.
Pressure Pain Sensitivity Over the TibialisAnterior Muscle
The intraexaminer repeatability of PPT over tibialis an-terior muscle was .93 for the most painful side and .91 forthe contralateral side, whereas the SEM was .18 and .2kg/cm2, respectively.
The ANOVA did not find significant differencesbetween groups and sides for PPT levels over the tibialisanterior muscle (group: F = 1.49, P = .461; side: F = .05, P =.824). Table 1 shows PPT over the tibialis anterior musclefor both sides within each group.
There was no effect of age, BDI-II, or STAI score on PPTlevels (P > .2), although there was an effect of sex at thetibialis anterior with females having lower PPTs (F = 8.8,P = .005) than males.
Pressure Pain Threshold IndicesThe ANOVA revealed significant differences for PPT
indices between sites (F = 8.7, P < .001), but not between
ain values and Neck Disability Index (A) and between NPRS painline is fitted to the data (NPRS: numerical pain rate scale, range

Table 1. Pressure Pain Thresholds (PPTs) in Patients With Mechanical Neck Pain (n = 23) andMatched Control Subjects (n = 23). Mean Values 6 Standard Deviation and 95% ConfidenceIntervals in Parenthesis (kg/cm2)
MECHANICAL NECK PAIN HEALTHY CONTROLS
DOMINANT SIDE NON-DOMINANT SIDE DOMINANT SIDE NON-DOMINANT SIDE
Trigeminal Area
Masseter* 2 6 .4 (1.8–2.2) 2 6 .5 (1.8–2.2) 3.4 6 .5 (3.2–3.6) 3.5 6 .4 (3.3–3.7)
Temporalis* 2.2 6 .5 (1.9–2.5) 2.1 6 .5 (1.9–2.4) 3.7 6 .6 (3.4–3.9) 3.6 6 .8 (3.4–3.9)
Joint
C5–C6* 1.7 6 .4 (1.5–1.9) 1.6 6 .3 (1.4–1.8) 3.2 6 .4 (3.1–3.4) 3.2 6 .6 (3.1–3.5)
Muscle
Upper trapezius* 1.8 6 .4 (1.6–2) 1.8 6 .3 (1.6–2) 3.8 6 .7 (3.6–4) 3.7 6 .5 (3.5–3.9)
Tibialis anterior 5.0 6 .8 (4.6–5.3) 5 6 .9 (4.6–5.4) 5.2 6 .7 (4.9–5.6) 5.3 6 .8 (5–5.7)
*Indicates significant difference between neck pain and control subjects (ANOVA, P < .001).
260 Trigeminal Pain Sensitivity in Neck Pain
sides (F = .03, P = .859). The post hoc analysis showedsignificant differences between both masseter and tem-poralis muscles with the upper trapezius muscle (P < .001)and between the temporalis muscles with the C5-C6 joint(P = .02). In such a way, the cervical region (upper trape-zius muscle and C5-C6 joint) showed lower PPT indices(greater degree of sensitization) compared to the tri-geminal region (masseter and temporalis muscles) forboth sides (Fig 3).
Pressure Sensitivity and Clinical Featuresin Patients with Mechanical Neck Pain
Finally, a significant negative correlation between his-tory of symptoms and PPT levels over both masseter mus-cles (dominant side: rs = –.64, P < .001 [Fig 4A];nondominant side: rs = –.42, P = .04 [Fig 4B]) was found:the longer the duration of the symptoms, the lower thePPT levels over both masseter muscles. In addition, cur-rent level of pain intensity was also negatively correlatedwith bilateral PPT levels over the masseter muscles (dom-inant side: rs = –.62, P < .001 [Fig 5A]; nondominant side:rs = –.51, P = .02 [Fig 5B]): the greater the pain intensity,the lower the bilateral PPT levels. No significant correla-tions between NDI, BDI-II, and PPT levels were found.
Figure 3. Pressure pain threshold indices in both trigeminaland cervical points. The boxes represent the mean and percen-tile scores, and the error bars represent the standard deviation.
DiscussionThis study showed bilateral pressure-pain hyperalgesia
in both the trigeminal and cervical region, but not overthe tibialis anterior muscle, in patients with mechanicalchronic neck pain as compared to healthy controls. Thedecrease in PPT levels over the trigeminal region was as-sociated with the intensity and duration of pain symp-toms, supporting a role of the peripheral nociceptiveinput as an important factor driving the developmentof spreading sensitization.
Current results of cervical, but not widespread, pressure-pain hypersensitivity in patients with idiopathic neck painare very similar to those previously found by Scott et al.33
The findings from both studies support the idea that me-chanical nontraumatic neck pain is characterized by pres-sure-pain hyperalgesia in the cervical spine, probably
reflecting peripheral nociceptor sensitization. Further-more, our study increases evidence that pressure-pain hy-peralgesia is not only restricted to cervical joints (C5–C6 orC2–C3 as previously reported) but also to cervical muscles(upper trapezius). This is expected since the upper trape-zius muscle receives nerve innervation from the C2–C4level. Nevertheless, lower PPT levels over the upper trape-zius may also be related to muscle spasm residing in theneck muscles in this patient population.
The present study demonstrated that patients withmechanical chronic neck pain also have pressure-pain hy-peralgesia in the trigeminal region. This finding may re-flect a sensitization process of the trigemino-cervicalnucleus caudalis due to the convergence of inputs from
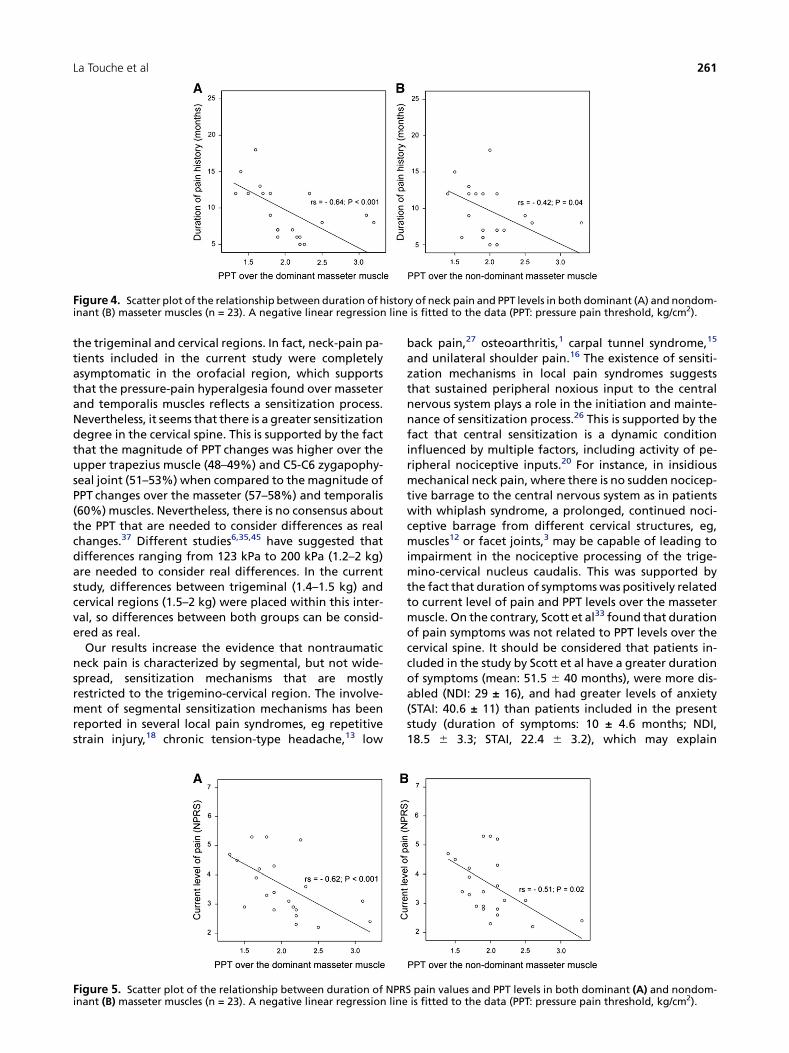
Figure 4. Scatter plot of the relationship between duration of history of neck pain and PPT levels in both dominant (A) and nondom-inant (B) masseter muscles (n = 23). A negative linear regression line is fitted to the data (PPT: pressure pain threshold, kg/cm2).
La Touche et al 261
the trigeminal and cervical regions. In fact, neck-pain pa-tients included in the current study were completelyasymptomatic in the orofacial region, which supportsthat the pressure-pain hyperalgesia found over masseterand temporalis muscles reflects a sensitization process.Nevertheless, it seems that there is a greater sensitizationdegree in the cervical spine. This is supported by the factthat the magnitude of PPT changes was higher over theupper trapezius muscle (48–49%) and C5-C6 zygapophy-seal joint (51–53%) when compared to the magnitude ofPPT changes over the masseter (57–58%) and temporalis(60%) muscles. Nevertheless, there is no consensus aboutthe PPT that are needed to consider differences as realchanges.37 Different studies6,35,45 have suggested thatdifferences ranging from 123 kPa to 200 kPa (1.2–2 kg)are needed to consider real differences. In the currentstudy, differences between trigeminal (1.4–1.5 kg) andcervical regions (1.5–2 kg) were placed within this inter-val, so differences between both groups can be consid-ered as real.
Our results increase the evidence that nontraumaticneck pain is characterized by segmental, but not wide-spread, sensitization mechanisms that are mostlyrestricted to the trigemino-cervical region. The involve-ment of segmental sensitization mechanisms has beenreported in several local pain syndromes, eg repetitivestrain injury,18 chronic tension-type headache,13 low
Figure 5. Scatter plot of the relationship between duration of NPRinant (B) masseter muscles (n = 23). A negative linear regression line
back pain,27 osteoarthritis,1 carpal tunnel syndrome,15
and unilateral shoulder pain.16 The existence of sensiti-zation mechanisms in local pain syndromes suggeststhat sustained peripheral noxious input to the centralnervous system plays a role in the initiation and mainte-nance of sensitization process.26 This is supported by thefact that central sensitization is a dynamic conditioninfluenced by multiple factors, including activity of pe-ripheral nociceptive inputs.20 For instance, in insidiousmechanical neck pain, where there is no sudden nocicep-tive barrage to the central nervous system as in patientswith whiplash syndrome, a prolonged, continued noci-ceptive barrage from different cervical structures, eg,muscles12 or facet joints,3 may be capable of leading toimpairment in the nociceptive processing of the trige-mino-cervical nucleus caudalis. This was supported bythe fact that duration of symptoms was positively relatedto current level of pain and PPT levels over the massetermuscle. On the contrary, Scott et al33 found that durationof pain symptoms was not related to PPT levels over thecervical spine. It should be considered that patients in-cluded in the study by Scott et al have a greater durationof symptoms (mean: 51.5 6 40 months), were more dis-abled (NDI: 29 ± 16), and had greater levels of anxiety(STAI: 40.6 ± 11) than patients included in the presentstudy (duration of symptoms: 10 ± 4.6 months; NDI,18.5 6 3.3; STAI, 22.4 6 3.2), which may explain
S pain values and PPT levels in both dominant (A) and nondom-is fitted to the data (PPT: pressure pain threshold, kg/cm2).

262 Trigeminal Pain Sensitivity in Neck Pain
differences between both studies. Finally, we do notknow if sensitization mechanisms found in this studyare mediated via a deregulation of second-order neu-rons in a segmental fashion or via glia30 and other im-mune cells that reside in the trigeminal-cervical region.Future studies are needed to further elucidate the mech-anisms involved in trigemino-cervical sensitization inneck pain.
It has been suggested that anxiety and depression mayinfluence pressure-pain hypersensitivity.31 Our resultswere independent of levels of depression (BDI-II) andthe state anxiety (STAI). Additionally, patients includedin the present study showed scores < 8 points in theBDI-II, which are considered normal.2 Our results agreewith those previously reported by Scott et al33 in whichanxiety appears not to influence pressure-pain sensitivityin patients with insidious mechanical neck pain. Never-
theless, further studies investigating the influence ofpsychological factors are required.
ConclusionBilateral pressure-pain hyperalgesia was detected in
both trigeminal and cervical regions in patients with me-chanical chronic neck pain. The decrease in pressure painthresholds in the trigeminal region was associated withthe intensity and duration of the neck-pain symptoms,supporting a role of the peripheral nociceptive input asa driving factor for inducing sensitization. Our study fur-ther supports that nontraumatic neck pain shows sensiti-zation in the trigemino cervical region, which has clinicalimplications in terms of spreading symptomatology tothis body area.
References
1. Bajaj P, Bajaj P, Graven-Nielsen T, Arendt-Nielsen L: Oste-oarthritis and its association with muscle hyperalgesia: Anexperimental controlled study. Pain 93:107-114, 2001
2. Beck AT, Steer RA, Brown GK: Beck Depression Inventory,(2nded.) SanAntonio.TX,ThePsychologicalCorporation,1996
3. Bogduk N, Marsland A: The cervical zygapophysial jointsas a source of neck pain. Spine 13:610-617, 1988
4. Borghouts JA, Koes BW, Bouter LM: The clinical courseand prognostic factors of non-specific neck pain: A system-atic review. Pain 77:1-13, 1998
5. Chesterton LS, Barlas P, Foster NE, Baxter GD, Wright CC:Gender differences in pressure pain threshold in healthyhumans. Pain 101:259-266, 2003
6. Chesterson LS, Sim J, Wright CC, Foster NE: Inter-rater re-liability of algometry in measuring pressure pain thresholdsin healthy humans, using multiple raters. Clin J Pain 23:760-766, 2007
7. Ciancaglini R, Testa M, Radaelli G: Association of neckpain with symptoms of temporomandibular dysfunction inthe general adult population. Scand J Rehabil Med 31:17-22, 1999
8. De Wijer A, De Leeuw JR, Steenks MH, Bosman F: Tempo-romandibular and cervical spine disorders. Self-reportedsigns and symptoms. Spine 21:1638-1646, 1996
9. Desmeules JA, Cedraschi G, Rapiti E, Baumgartner E,Finckh A, Cohen P, Daver P, Vischer TL: Neurophysiologic ev-idence for central sensitization in patients with fibromyal-gia. Arthritis Rheum 48:1420-1429, 2003
10. Dworkin SF, LeResche L: Research diagnostic criteria fortemporomandibular disorders: Review, criteria, examina-tions and specifications, critique. J Craniomandib Disord 6:301-355, 1992
11. Fejer R, Ohm-Kyvik K, Hartvigsen J: The prevalence ofneck pain in the world population: A systematic critical re-view of the literature. Eur Spine J 15:834-848, 2006
12. Fernandez-de-las-Penas C, Alonso-Blanco C,Miangolarra JC: Myofascial trigger points in subjectspresenting with mechanical neck pain: A blinded, controlledstudy. Man Ther 12:29-33, 2007
13. Fernandez-de-las-Penas C, Cuadrado ML, Ge HY, Arendt-Nielsen L, Pareja JA: Increased peri-cranial tenderness, de-creased pressure pain threshold and headache clinical pa-rameters in chronic tension type headache patients. ClinPain 23:346-352, 2007
14. Fernandez-de-las-Penas C, Cuadrado ML, Arendt-Nielsen L, Pareja JA: Side-to-side differences in pressurepain thresholds and pericranial muscle tenderness in strictlyunilateral migraine. Eur J Neurol 15:162-168, 2008
15. Fernandez-de-las-Penas C, de la Llave-Rincon AI, Fernan-dez-Carnero J, Cuadrado ML, Arendt-Nielsen L, Pareja JA: Bi-lateral widespread mechanical pain sensitivity in carpaltunnel syndrome: Evidence of central processing in unilat-eral neuropathy. Brain 132:1472-1479, 2009
16. Ge HY, Fernandez-de-las-Penas C, Madeleine P, Arendt-Nielsen L: Screening for myofascial trigger points bilaterallyin the infraspinatus muscles in patients with unilateralshoulder pain. Eur J Pain 12:859-865, 2008
17. Gore DR, Sepic SB, Gardner GM, Murray MP: Neck pain:A long-term follow-up of 205 patients. Spine 12:1-5, 1987
18. Greening J, Lynn B: Vibration sense in the upper limb inpatients with repetitive strain injury and a group of at-riskoffice workers. Int Arch Occup Environ Health 71:29-34,1998
19. Hains F, Waalen J, Mior S: Psychometric properties of theneck disability index. J Manipul Physiol Ther 21:75-80, 1998
20. Herren-Gerber R, Weiss S, Arendt-Nielsen L, Petersen-Felix S, Stefano G, Radanov B, Curaloto M: Modulation ofcentral hypersensitivity by nociceptive input in chronicpain after whiplash injury. Pain Med 5:366-376, 2004
21. Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW,Cassidy JD, Guzman J, Cote P, Haldeman S, Ammendolia C,Carragee E, Hurwitz E, Nordin M, Peloso P: Bone and JointDecade 2000-2010 Task Force on Neck Pain and Its Associ-ated Disorders. The burden and determinants of neck painin the general population. Spine 33:S39-S51, 2008
22. Jensen MP, Turbner JA, Romano JM, Fisher L: Compara-tive reliability and validity of chronic pain intensity mea-sures. Pain 83:157-162, 1999
23. Lobbezoo F, Visscher C, Naeije M: Impaired health status,sleep disorders, and pain in the craniomandibular and cervi-cal spinal regions. Eur J Pain 8:23-30, 2004

La Touche et al 263
24. Macdemid JC, Walton DM, Avery S, Blanchard A,Etruw E, Mcalpine C, Goldsmith CH: Measurement proper-ties of the neck disability index: A systematic review.J Orthop Sports Phys Ther 39:400-417, 2009
25. Marfurt CF, Rajchert DM: Trigeminal primary afferentprojections to ‘non-trigeminal’ areas of the rat central ner-vous system. J Comp Neurol 303:489-511, 1991
26. Mendell LM, Wall PD: Responses of single dorsal cordcells to peripheral cutaneous unmyelinated fibres. Nature206:97-99, 1965
27. O’Neill S, Manniche C, Graven-Nielsen T, Arendt-Nielsen L: Generalized deep-tissue hyperalgesia in patientswith chronic low-back pain. Eur J Pain 11:415-420, 2007
28. Prushansky T, Dvir Z, Defron-Assa R: Reproducibilityindices applied to cervical pressure pain threshold mea-surements in healthy subjects. Clin J Pain 20:341-347,2004
29. Rantala MA, Ahlberg J, Suvine TI, Nissine M, Lindholm H,Savolainen A, Kononen M: Temporomandibular joint re-lated painless symptoms, orofacial pain, neck pain, head-ache, and psychosocial factors among non-patients. AcOdontol Scand 61:217-222, 2003
30. Ren K, Dubner R: Neuron-glia crosstalk gets serious: Rolein pain hyper-sensitivity. Curr Opin Anaesthesiol 21:570-579,2008
31. Rhudy JL, Meagher M: Fear and anxiety: Divergenteffects on human pain thresholds. Pain 84:65-75, 2000
32. Rolke R, Andrews Campbell K, Magerl W, Treede RD:Deep pain thresholds in the distal limbs of healthy humansubjects. Eur J Pain 9:39-48, 2005
33. Scott D, Jull G, Sterling M: Widespread sensory hyper-sensitivity is a feature of chronic whiplash-associated disor-der but not chronic idiopathic neck pain. Clin J Pain 21:175-181, 2005
34. Spielberger CD, Jacobs G, Crane R: State-Trait Personal-ity Inventory. Tampa, University of South Florida, Human Re-sources Institute, 1979
35. Sterling M, Carllson Y, Crommert L, Jull G: Are cervicalphysical outcome measures influenced by the presence ofsymptomatology. Physiother Res Int 7:113-121, 2002
36. Sterling M, Jull G, Vicenzino B, Kenardy J: Sensory hyper-sensitivity occurs soon after whiplash injury and associatedwith poor recovery. Pain 104:509-517, 2003
37. Sterling M: Testing for sensory hypersensitivity or centralhyperexcitability associated with cervical spine pain. J Ma-nipulative Physiol Ther 31:534-539, 2008
38. Sterling M: Neck pain: Much more than a psychosocialcondition. J Orthop Sports Phys Ther 39:309-311, 2009
39. Stratford PW, Riddle DL, Binkley JM, Spadoni G,Westaway MD, Padfield B: Using the Neck Disability Indexto make decisions concerning individual patients. Physi-other Canada 51:107-112, 1999
40. Vanderweeen L, Oostendorp RB, Vaes P, Duquet W: Pres-sure algometry in manual therapy. Man Ther 1:258-265, 1996
41. VanVoorhis WCR, Blumentritt TL: Psychometric proper-ties of the Beck Depression inventory-II in a clinically-identi-fied sample of Mexican American adolescents. J Child FamilyStudies 5:789-798, 2007
42. Vernon H, Mior S: The neck disability index: A study ofreliability and validity. J Manipul Physiol Ther 14:409-415,1991
43. Wolfe F, Smythe HA, Yunus MB, Bennett RM,Bombardier C, Goldenberg DL, Tugwell P, Campbell SM,Abeles M, Clark P: The American College of Rheumatology1990 criteria for clasification of fibromyalgia: Report ofthe multicenter criteria committee. Arthritis and Rheum33:160-170, 1990
44. Wright A, Mayer TG, Gatchel RJ: Outcomes of disablingcervical spine disorders in compensation injuries: A prospec-tive comparison to tertiary rehabilitation response tochronic lumbar spine disorders. Spine 24:178-183, 1999
45. Ylinen J, Nykanen M, Kautainen H, Hakkinen A: Evalua-tion of repeatability of pressure algometry on the neck mus-cles for clinical use. Man Ther 12:192-197, 2007

123
5.4 Estudio IV
La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-Díaz-Parreño S,
Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero J. Craniofacial pain and disability
inventory (CF-PDI): development and psychometric validation of a new questionnaire. Pain
Physician. 2014 Jan-Feb;17(1):95-108.
Objetivo del estudio
El propósito de este estudio es presentar el desarrollo, el análisis de la estructura factorial y
propiedades psicométricas de un nuevo cuestionario auto-administrado (Inventario de dolor y
discapacidad craneofacial; IDD-CF), dirigido a medir el dolor, la discapacidad y el estado
funcional de la mandíbula y la región craneofacial.
Resultados
La versión final del IDD-CF consta de 21 ítems, el análisis factorial exploratorio reveló dos
factores ("El dolor y la discapacidad" y "el estado funcional de mandíbula"), ambos factores con
valor propio mayor que uno, que explican 44,77% de la varianza. No se observaron efectos
suelo o techo. Se confirmó una alta consistencia interna de la IDD-CF (α de Cronbach: 0,88) y
también para las dos subescalas (0,80 a 0,86 α de Cronbach). Basándose en el resultado de CCI
=0,90 (IC del 95% 0,86 hasta 0,93) fue considerado como una excelente fiabilidad test-retest. El
EEM y el MCD se calcularon como 2,4 y 7 puntos respectivamente. En la puntuación total
IDD-CF se observó una correlación moderada con la mayoría de los cuestionarios evaluados (r
= desde 0,36 hasta 0,52) y una fuerte correlación con el IDC (r = 0,65, p <0,001). El IDC, la
EVA y la TSK-11 fueron predictores del IDD-CF.
Conclusiones
El IDD-CF mostró buenas propiedades psicométricas. Con base en los hallazgos de este estudio,
el IDD-CF se puede utilizar en la investigación y la práctica clínica para la evaluación de los
pacientes con DCF.

Background: Orofacial pain, headaches, and neck pain are very common pain conditions in the general population and might be associated in their pathophysiology, although this is not yet clarified. The development and validation of a prediction inventory is important to minimize risks. Most recent questionnaires have not focused on pain, but pain is the common symptom in temporomandibular disorders, headaches, and neck pain. It is necessary to provide tools for these conditions.
Objectives: The purpose of this study is to present the development and analysis of the factorial structure and psychometric properties of a new self-administered questionnaire (Craniofacial Pain and Disability Inventory [CF-PDI]) designed to measure pain, disability, and functional status of the mandibular and craniofacial regions.
Study Design: Multicenter, prospective, cross-sectional, descriptive survey design. A secondary analysis of the reliability of the measures was a longitudinal, observational study.
Setting: A convenience sample was recruited from a hospital and 2 specialty clinics in Madrid, Spain.
Methods: The study sample consisted of 192 heterogeneous chronic craniofacial pain patients. A sub-sample of 106 patients was asked to answer the questionnaire a second time, to assess the test-retest reliability. The development and validation of the CF-PDI were conducted using the standard methodology, which included item development, cognitive debriefing, and psychometric validation. The questionnaire was assessed for the following psychometric properties: internal consistency (Cronbach’s α); floor and ceiling effects; test-retest reliability (Intraclass Correlation Coefficient [ICC]; Bland and Altman method); construct validity (exploratory factor analysis); responsiveness (standard error of measurement [SEM] and minimal detectable change [MDC]); and convergent validity (Pearson correlation coefficient), by comparing visual analog scale (VAS), the Tampa Scale for Kinesiophobia (TSK-11), the Pain Catastrophizing Scale (PCS), the Neck Disability Index (NDI), and the Headache Impact Test-6 (HIT-6). Multiple linear regression analysis was used to estimate the strength of the associations with theoretically similar constructs.
Results: The final version of the CF-PDI consists of 21 items. Exploratory factor analysis revealed 2 factors (“pain and disability” and “jaw functional status”), both with an eigenvalue greater than one, explaining 44.77% of the variance. Floor or ceiling effects were not observed. High internal consistency of the CF-PDI (Cronbach’s α: 0.88) and also of the 2 subscales (Cronbach’s α: 0.80 – 0.86) was confirmed. ICC was found to be 0.90 (95% confidence interval [CI] 0.86 – 0.93), which was considered to be excellent test-retest reliability. The SEM and MDC were 2.4 and 7 points, respectively. The total CF-PDI score showed a moderate correlation with most of the assessed questionnaires (r = 0.36 – 0.52) and a strong correlation with the NDI (r = 0.65; P < 0.001). The NDI, VAS, and TSK-11 were predictors of CF-PDI.
Limitations: Only self-reported measures were considered for convergent validity. Future research should use physical tests to explore the clinical signs relating to pain and disability.
Prospective Evaluation
Craniofacial Pain and Disability Inventory (CF-PDI): Development and Psychometric Validation of a New Questionnaire
From: 1Department of Physiotherapy, Faculty of Health Science, The Center
for Advanced Studies University La Salle. Universidad Autónoma de Madrid, Aravaca, Madrid, Spain;
2Research Group on Movement and Behavioral Science and Study of Pain,
The Center for Advanced Studies University La Salle, Universidad
Autónoma de Madrid; 3Institute of Neuroscience and Craniofacial Pain
(INDCRAN), Madrid, Spain; 4Hospital La Paz Institute for Health Research (IdiPAZ), Madrid, Spain; 5Faculty of
Medicine, Universidad San Pablo CEU, Madrid, Spain; 6Department
of Methodology of the Behavioural Sciences, Faculty of Psychology,
Universidad Nacional de Educación a Distancia, Madrid, Spain;
7Department of Neurology, Hospital Universitario La Paz, Madrid, Spain;
8Department of Physical Therapy, Occupational Therapy, Rehabilitation
and Physical Medicine, Universidad Rey Juan Carlos, Alcorcón, Madrid,
Spain
Address Correspondence: Roy La Touche
Facultad de Ciencias de la SaludCentro Superior de Estudios
Universitarios La SalleCalle la Salle, 10
28023 Madrid SPAINEmail: [email protected]
Disclaimer: There was no external funding in the preparation of this
manuscript. Conflict of interest: Each author certifies that he or she, or a
member of his or her immediate family, has no commercial
association (i.e., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that
might pose a conflict of interest in connection with the submitted
manuscript.
Manuscript received: 06-21-2013 Accepted for publication: 08-25-2013
Free full manuscript:www.painphysicianjournal.com
Roy La Touche, PT, MSc1-3, Joaquín Pardo-Montero PhD1-3, Alfonso Gil-Martínez PT, MSc1-4, Alba Paris-Alemany PT, MSc2,3, Santiago Angulo-Díaz-Parreño MSc2,5, Juan Carlos Suárez-Falcón PhD6, Manuel Lara-Lara, MD7, and Josué Fernández-Carnero, PT, PhD2,8
www.painphysicianjournal.com
Pain Physician 2014; 17:95-108 • ISSN 1533-3159

Conclusion: The CF-PDI showed good psychometric properties. Based on the findings of this study, the CF-PDI can be used in research and clinical practice for the assessment of patients with craniofacial pain.
Key words: Craniofacial pain, temporomandibular disorders, headache, neck pain, disability, development, questionnaire, reliability, psychometric validation, minimal detectable change
Pain Physician 2014; 17:95-108
Pain Physician: January/February 2014; 17:95-108
96 www.painphysicianjournal.com
disability or dysfunction but not on pain, even though pain is the common symptom in TMD, headaches, and neck pain. Additionally, pain is been addressed by other validated scales (19).
For clinical practice and research, it is necessary to have tools to measure neck pain and the associated dis-ability (20). In addition, the development and validation of a prediction inventory allows the minimization of risks and helps prevent the development of the disease.
The purpose of this study is to present the de-velopment and analysis of the factorial structure and psychometric properties of a new self-administered questionnaire (Craniofacial Pain and Disability Inven-tory [CF-PDI]) designed to measure pain, disability, and functional status of the mandibular and craniofacial regions.
Methods
The development and validation of the CF-PDI was conducted in a standardized manner, using an accepted measure development methodology that included 3 phases (21): a) item development and identification of domains; b) pilot testing on a small number of patients with
cognitive debriefing; and c) psychometric validation.
Item DevelopmentItems were generated through a multi-step process
(21): 1) literature review; 2) patient interviews and focus group; 3) examination by the research group; 4) item writing and selection; and 5) examination of the inventory by independent
experts.
The relevant scientific literature search was con-ducted using electronic databases (Medline, Embase, CINAHL). The extracted information was related to the diagnosis, pathophysiology, comorbidities, and psycho-
Chronic orofacial pain and temporomandibular disorders (TMD) are commonly associated but may also arise from other sources (1). Orofacial
pain is a common pain condition associated with the hard and soft tissues of the face and mouth. Its prevalence in the general population is approximately 13% (2). Headache and neck pain are also 2 of the most common symptoms seen in the general population (3,4).
TMD, headaches, and neck pain are related dis-eases and share signs and symptoms (5-7). Some clinical evidence of the interconnection between the cervical spine and TMD has been demonstrated (8). Plesh et al (9) showed that 53% of patients with TMD had severe headache and 54% had neck pain. Besides, 59% with TMD reported at least 2 comorbid pains, and women reported more comorbid pain than men (9). This rela-tionship between headache and a causative disorder is a criterion for secondary headache diagnoses (10).
Although it has been suggested that TMD and headaches may be related in their pathophysiology (7,11) and that headache could be a possible risk factor for the development of neck pain (12), the pathophysi-ological mechanisms underlying these pain conditions are still not fully clarified. However, a biopsychosocial approach to the etiology, assessment, and treatment of chronic pain is widely advocated (13).
Nearly 60% of both men and women reported recent pain of moderate-to-severe intensity, with a quarter of them indicating interference or termination of work-related activities (14). Therefore, the correct diagnosis of these diseases is very important to reduce their huge economic impact (15,16).
A useful scale is the Jaw Functional Limitation Scale (JFLS), which consists of 3 constructs comprising a total of 20 items identified along a global scale (17). At present, there are no questionnaires in Spanish to as-sess these characteristics. This fact is especially relevant considering that Spain is one of the European Union countries with a high cost for these disabilities (18).
Moreover, most questionnaires have focused on

www.painphysicianjournal.com 97
Psychometric Validation of the Craniofacial Pain and Disability Inventory
social and disability factors associated with craniofacial pain. We found 5 published questionnaires that assess orofacial pain and jaw function (22-26). All of them were only validated in the English language. On the ba-sis of the existing literature, a semi-structured interview guide was developed focusing on the following 3 main areas: 1) perception of physical and psychosocial health in
relation to craniofacial pain; 2) patient-perceived physical impacts of the condition
(including impacts on general physical functioning and specific jaw function); and
3) perception of disability and pain associated with their condition.
A total of 13 patients with chronic craniofacial pain underwent the semi-structured interview and 5 patients with the same condition participated in the focus group. Both processes ended with the question: “Do you think there are any other aspects of craniofacial pain we have not discussed?” The research group proceeded to ana-lyze and compare the information extracted from semi-structured interviews, focus group, and review of the relevant literature to generate the construct concept of the CF-PDI and subsequently to write the items. A list of 30 draft items was generated. The research group then selected 22 items based on a finely structured consensus process (27) to not omit any necessary concepts.
The 22 items of the inventory were subjected to an external assessment by a group of experts in cra-niofacial pain (3 physiotherapists, one dentist, and one medical doctor). The 5 experts assessed whether each of the items had a relationship with the conditions of craniofacial pain and TMD, through a 3-level Likert scale (complete disagreement, neither agreement nor disagreement, and complete agreement).
Cognitive DebriefingCognitive debriefing of the preliminary CF-PDI
was conducted with a small number of patients to as-sess their interpretations of the questions (24 patients with craniofacial pain in the pilot test). Patients were selected from 3 different educational levels (primary school, secondary school, and university) and the total response time for all items of the CF-PDI was calculated. These patients were asked to complete the preliminary CF-PDI, and were then interviewed about its compre-hensiveness, relevance, and clarity of expression. This led to some minor alterations to the questionnaire.
Psychometric Validation
Sample/PatientsThis study employed a prospective, cross-sectional,
descriptive design. A consecutive convenience sample was recruited from outpatients of the Hospital Univer-sitario La Paz (Madrid, Spain) and 2 private clinics spe-cializing in craniofacial pain and TMD (Madrid, Spain). Patients were selected if they met all of the following criteria: 1) headache and facial pain, the diagnosis of which was made according to the guidelines of the In-ternational Classification of Headache Disorders (10); 2) headache or facial pain attributed to TMD (10), the di-agnosis of which was based on the Research Diagnostic Criteria for TMD (28,29) to classify patients with painful TMD (myofascial pain, temporomandibular joint [TMJ] arthralgia, or TMJ osteoarthritis); 3) pain history of at least 6 months prior to the study; 4) at least 18 years of age; and 5) good understanding of the Spanish language. The exclusion criteria were as follows: cogni-tive impairment; the presence of psychiatric limitations that impede participation in the study assessments; and poor knowledge of the Spanish language. To assess the test-retest reliability of the CF-PDI, a sub-sample of 106 patients whose clinical conditions were stable were asked to answer the inventory a second time, after an interval of 12 days.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee of the Hospital Universitario La Paz (PI-1241). Prior to their participation, subjects gave written informed consent.
After consenting to the study, recruited patients were given a battery of questionnaires to complete on the day of the visit. These included various self-reports for demographic and pain-related variables, including the CF-PDI to be validated, a visual analog scale (VAS) for pain intensity, and the validated Spanish versions of the Tampa Scale for Kinesiophobia (TSK-11), the Pain Catastrophizing Scale (PCS), the Neck Disability Index (NDI), and the impact associated with headache was assessed using the Headache Impact Test-6 (HIT-6). The sociodemographic questionnaire collected information about gender, date of birth, marital status, living ar-rangements, education level, and work status.
Pain intensity was measured with the VAS. The VAS consists of a 100 mm line, on the left side of which represents “no pain” and the right side represents “the worst pain imaginable.” The patients placed a mark on

Pain Physician: January/February 2014; 17:95-108
98 www.painphysicianjournal.com
the line where they felt best represented their pain intensity (30).
The Spanish version of the TSK-11 is a self-reported questionnaire that assesses fear of re-injury due to movement (31). The TSK-11 is an 11-item questionnaire that eliminates psychometrically poor items from the original version of the TSK (32) to create a shorter ques-tionnaire with comparable internal consistency. The TSK-11 has a 2-factor structure: activity avoidance and harm, and has demonstrated acceptable psychometric properties (31).
The Spanish version of the PCS assesses the degree of pain catastrophization (33,34). The PCS has 13 items and a 3-factor structure: rumination, magnification, and helplessness. The theoretical range is between 0 and 52, with lower scores indicating less catastrophizing. The PCS has demonstrated acceptable psychometric proper-ties (33).
The Spanish version of the NDI measures perceived neck disability (20,35). This questionnaire consists of 10 items, with 6 possible answers that represent 6 levels of functional capacity, ranging from 0 (no disability) to 5 (complete disability) points. The NDI has demonstrated acceptable psychometric properties (20).
The Spanish version of the HIT-6 (36,37) is a 6-item questionnaire that measures the severity and impact of headache on the patient’s life. The HIT-6 has demon-strated acceptable psychometric properties (38).
Statistical AnalysisSocio-demographic and clinical variables of the pa-
tients were analyzed. Analysis of variance (ANOVA) was used to test for differences in socio-demographic and clinical characteristics between the groups of patients.
Weighted kappa statistics (39) were calculated to assess the percentage agreement between external expert evaluators. Kappa statistics were calculated for each item. The Kappa coefficient varies from -1 (com-plete disagreement) to +1 (complete agreement), with 0 representing neither agreement nor disagreement.
Factor AnalysisThe factor structure was investigated using an
explorative factor analysis (ie, principal component analysis [PCA]) with Oblimin rotation. The number of factors for extraction was based on Kaiser’s eigenvalue criterion (eigenvalue ≥1) and evaluation of the scree plot (40). The quality of the factor analysis models was assessed using Bartlett’s test for sphericity and the Kai-ser-Meyer-Olkin (KMO) test. Bartlett’s test is a measure
of the probability that the initial correlation matrix is an identity matrix and should be < 0.05 (41). The KMO test measures the degree of multicollinearity and varies between 0 and 1 (should be greater than 0.50 – 0.60) (42).
Reliability For reliability, internal consistency and reproduc-
ibility were examined. Internal consistency was estimat-ed using Cronbach’s α and item total correlation coef-ficients. For a questionnaire to be internally consistent, α levels should be above 0.7 (43).
The test-retest reliability (repeatability) was evalu-ated using the Intraclass Correlation Coefficient (ICC). An ICC value above 0.70 is considered acceptable (44). We also constructed a Bland Altman Plot by calculating the mean difference between 2 measurements and the standard deviation (SD) of the difference (45). In this plot, 95% of the differences are expected to be less than 2 SDs.
Floor and Ceiling EffectsPotential floor and ceiling effects were measured
by calculating the percentage of patients indicating the minimum or maximum possible scores in the question-naires. Floor and ceiling effects are considered to be present if more than 15% of respondents achieved the highest or lowest possible total score (44).
Responsiveness AnalysesMeasurement error is the systematic and random
error of a patient’s score that is not attributable to true changes in the construct to be measured (46). Measure-ment error is expressed as a standard error of measure-ment (SEM), which is calculated as:
SD where SD is the SD of values from all participants
and ICC is the reliability coefficient (47,48). Ostelo et al (49) suggested that the percentage of the SEM in rela-tion to the total score of a questionnaire is an impor-tant indicator of agreement, and can be interpreted as follows: ≤ 5% very good; > 5% and ≤ 10% good; > 10% and ≤ 20% doubtful; and > 20% negative. Responsive-ness was assessed with the Minimal Detectable Change (MDC). The MDC expresses the minimal magnitude of change required to be 95% confident that the observed change between the 2 measures reflects real change and not just measurement error (50). It is calculated as SEM × × 1.96 (50,51).

www.painphysicianjournal.com 99
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Convergent Validity The convergent validity was assessed by the Pear-
son correlation coefficient between the CF-PDI and the other questionnaires: VAS, TSK-11, PCS, NDI, and HIT-6. A strong correlation was considered to be over 0.60; a moderate correlation between 0.30 and 0.60; and a low (very low) correlation below 0.30 (44).
Linear RegressionMultiple linear regression analysis was used to esti-
mate the strength of the associations with theoretically similar constructs, so multiple linear regression analyses were also performed including CF-PDI as a criterion variable to estimate the strength of the association between CF-PDI and NDI, PVAS, TSK, and PCS as pre-dictor variables. As a measure of multicollinearity, the variance inflation factor (VIF) is presented (VIF < 10 indicates no problem with multicollinearity).
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 20 (IBM company, USA) except for the SEM and MDC values, which were calculated using Microsoft Excel. The critical value for significance was P < 0.05.
Results
Item Development and Cognitive DebriefingA total of 18 patients with chronic craniofacial
pain participated in the focus group and were also interviewed in May 2011 and July 2011, and 30 items were pooled as potential questions. After a review by the research group, some questions were added, and 22 items covering 4 aspects (quality of life, jaw functional status, avoidance behavior, and pain) were finally gen-erated. There was agreement among the expert evalu-ators who reviewed the items, with a kappa coefficient of 0.83. The greatest disagreement occurred in items 8 and 20.
A pilot test for cognitive debriefing was performed in 24 patients in September 2011 to examine the con-tent validity of the preliminary questionnaire in regards to relevance and clarity of the language. The mean ± SD age of the patients was 45.7 ± 13.5 years (range: 19 – 61), and 17 of the participants were women (70.8%). The time required to answer all the questions was 8.4 ± 3.1 minutes (range: 5.4 – 12.6). More than 96% of the patients could easily answer the questionnaire.
Characteristics of the SampleThe final study sample consisted of 192 heteroge-
neous chronic craniofacial pain patients (68.8% women, one patient was of unknown gender) aged 19 – 78 years (mean ± SD: 46.00 ± 13.06). The vast majority of patients (28.1%) had myofascial pain diagnoses; other patients suffered from TMJ arthralgia (15.1%), headache or fa-cial pain attributed to TMD (myofacial pain/TMJ osteo-arthritis or arthralgia) (24.5%), combined tension-type headache and myofascial pain (16.7%), and migraine (15.6 %). The mean time of pain was 130.46 ± 151.44 months (range: 15 – 888), and 19 patients (9.9%) had received disability benefits. Educational levels in our sample were primary (23.4%), secondary (36.5%), and university graduates (25.0%); there was no information for 15.1% of our sample.
Distribution of Total CF-PDI ScoresThe distribution of CF-PDI scores did not differ
significantly from a normal symmetric distribution (skewness = 0.43, SE = 0.18; kurtosis = -0.36; SE = 0.35), Kolmogorov-Smirnov Z = 1.11 (P = 0.172). There were no significant differences in scoring between men (19.46 ± 9.04) and women (20.52 ± 9.22). There was no significant association between CF-PDI scores and age, marital status, average duration of pain, education level, or work status.
Only the type of diagnosis showed differences in the median score of CF-PDI, headache or facial pain attributed to the TMD (myofacial pain/TMJ osteoarthri-tis or arthralgia) group presented higher scores 28.62 ± 7.10; TMJ arthralgia, 14.2 ± 5.24; migraine, 17.93 ± 12.30; myofascial pain, 18.17 ± 6.44; combined tension-type headache and myofascial pain, 19.00 ± 7.05. The distribution of CF-PDI total scores and other principal scales are shown in Table 1.
Table 1. Descriptive statistics and estimates of internal consistency (N = 192).
Instrument Mean (SD) Range Alpha
CF–PDI 20.24 (9.15) 2–48 0.88
Pain and Disability 15.43 (6.77) 1–34 0.86
Jaw Functional Status 4.81 (3.57) 0–14 0.80
HIT–6 54.48 (7.67) 36–74 0.85
NDI 16.96 (6.00) 0–42 0.74
TSK–11 25.40 (7.08) 11–44 0.88
PCS 23.86 (8.90) 7–52 0.84
VAS 52.94 (13.83) 15–85 –––
CF-PDI, craniofacial pain and disability inventory; VAS, visual analogue scale; TSK-11, Tampa Scale for Kinesiophobia; PCS, pain catastrophizing scale; NDI, Neck Dibility Index; HIT-6, headache impact test-6

Pain Physician: January/February 2014; 17:95-108
100 www.painphysicianjournal.com
Internal ConsistencyCronbach’s α coefficient was 0.88 (95% CI = 0.86 –
0.91), indicating a high degree of internal consistency. The item-to-total correlation coefficients ranged from 0.32 to 0.73; no item dominated with an especially high correlation and no item appeared to be redun-dant. The previous item 20, “How long have you had pain?” was deleted in the final version and it increased slightly the Cronbach’s α coefficient. This item showed a strong positive skew, refers to the time of pain in our population, and shows limited information because all patients suffered from chronic pain. It was removed it; other results in Table 2.
Factor AnalysisIn order to explore the factorial structure of the
instrument, a PCA without rotation was conducted on the scores of our sample. We also attempted to con-struct one-, 2-, and 3-factor structures. A 2-factor solu-tion emerged in our sample using a PCA that explained 40.8% of the variance. The KMO was found to be 0.85, which exceeds the recommended minimum value of 0.60. Bartlett’s Test of Sphericity was highly significant (Chi square = 1467.10 P < 0.001), supporting the suit-ability of the data for PCA.
When factor loading smaller than 0.30 was sup-pressed, but there were no cases. The first factor (30.43% of the explanatory variance) was composed of 14 items (1, 2, 3, 4, 5, 6, 7, 8, 16, 17, 18, 19, 20 (previously 21), and 21 (previously 22); the second factor (10.39% of the explanatory variance) was composed of 7 items (9, 10, 11, 12, 13, 14, and 15). With these results and a visual inspection of the scree plot, a 2-factor solution was considered suitable (Fig. 1).
Regarding factor analysis, item 9 was not clearly classified into the assumed factor (with loadings un-der 0.35 in each of them). The results showed similar weights for both factors. Despite the unexpected load-ing of this item, the CF-PDI still showed appropriate internal consistency; therefore, we incorporated it into the jaw functional status domain for theoretical rea-sons. Results of the PCA are shown in Table 3.
Floor and Ceiling EffectsNo floor or ceiling effects were identified for the
whole scale. Only 9.3% of the respondents scored the lowest possible score of 0 in the jaw functional status subscale, and none of the craniofacial pain patients scored the highest possible score of 63 points on the CF-PDI.
Table 2. Corrected item-total between CF-PDI items (N = 192)
Scale mean if item deleted
Corrected item-total correlation
Squared multiple correlation
Cronbach's α if item deleted
1 18.65 0.73 0.63 0.87
2 18.72 0.46 0.37 0.88
3 18.58 0.54 0.55 0.88
4 19.61 0.47 0.56 0.88
5 19.82 0.53 0.51 0.88
6 19.88 0.34 0.31 0.88
7 19.19 0.50 0.36 0.88
8 19.56 0.35 0.23 0.88
9 19.49 0.32 0.21 0.88
10 19.30 0.59 0.57 0.87
11 19.34 0.53 0.54 0.88
12 19.41 0.41 0.48 0.88
13 19.70 0.55 0.54 0.88
14 19.79 0.40 0.50 0.88
15 19.83 0.43 0.46 0.88
16 18.29 0.64 0.56 0.87
17 18.58 0.57 0.46 0.87
18 19.33 0.44 0.30 0.88
19 19.30 0.44 0.37 0.88
20 19.22 0.47 0.36 0.88
21 19.19 0.38 0.25 0.88
Fig. 1. Scree plot of the 21 items of the CF-PDI.

www.painphysicianjournal.com 101
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Test-Retest ReliabilityThe response to the CF-PDI provided by a random
subsample of 106 patients (gender women: 70, 66.7%; age: 45.6 ± 12.9 years; duration of the disorders: 69.0 ± 46.2 months) showed satisfactory temporal stability of
the scale after 12 days. ICC based on absolute agree-ment measures was 0.90 (95% CI: 0.86 – 0.93). The con-structed Bland and Altman plot for test-retest agree-ment showed a good reliability for total CF-PDI score
Table 3. Items of CF-PDI distribution and factor loadings according to principal component analysis with Oblimin rotation including Kaiser correction (N = 192).
Factor 1 Factor 2
1 ¿Presenta dolor en la cara? Do you feel any pain in your face? 0.79 0.45
2 ¿Se ha visto afectada su calidad de vida por esta dolencia? Is your quality of life affected by this pain? 0.58 0.21
3 Intensidad de dolor en la cara. Pain intensity on your face. 0.68 0.23
4 Le incapacita su dolor a la hora de tener relaciones afectuosas del tipo: besos, abrazos, relaciones sexuales… Does the pain make you unable to have emotional relationships, such as: kisses, embraces, or sexual relationships?
0.69 0.06
5 ¿Tiene dolor al reír? Do you feel any pain when you laugh? 0.68 0.19
6 ¿Su dolencia hace que evite el sonreír, hablar o masticar?Does your condition make you avoiding smiling, talking or chewing? 0.44 0.13
7. ¿Tiene dolor en la mandíbula?Do you feel any pain in your jaw? 0.53 0.38
8 ¿Escucha algún ruido al mover la mandíbula?Do you hear any noise when you move your jaw? 0.40 0.23
9. ¿Nota que su mandíbula se le sale o se le traba?Do you feel your jaw getting out of place or getting stuck? 0.33 0.31
10. Intensidad de dolor al masticarPain intensity when chewing 0.47 0.72
11. ¿Siente cansancio en la mandíbula, al hablar o al comer?Do you feel any tiredness in your jaw when you talk or eat? 0.38 0.73
12. ¿Tiene dificultad para abrir la boca?Do you have any trouble when you open your mouth? 0.23 0.73
13. Intensidad de dolor al hablarPain intensity when talking. 0.40 0.74
14. ¿Tiene miedo de mover la mandíbula?Do you fear moving your jaw? 0.20 0.73
15. Alimentación.Nutrition 0.24 0.72
16. ¿Con qué frecuencia tiene dolor en el cuello?How often have you got any neck pain? 0.76 0.31
17.¿Con qué frecuencia tiene dolor de cabeza?How often do you have a headache? 0.61 0.41
18. ¿Con qué frecuencia tiene dolor de oído?How often do you have an earache? 0.47 0.34
19. ¿Qué siente al tocarse la zona dolorosa?What do you feel when you touch the painful area? 0.53 0.23
20 ¿Su dolor le altera el sueño?Does the pain disrupts your sleep? 0.59 0.21
21 ¿El dolor le interfiere a la hora de desempeñar su actividad laboral?Does the pain interfere in your work? 0.38 0.36

and 2 subscales (Figs. 2-4). The results of reliability and responsiveness analy-ses are summarized in Table 4.
Convergent ValidityThe total CF-PDI score was signifi-
cantly associated with all the assessed questionnaires (Table 5), but the cor-relation with the NDI, was the most important in our sample.
Linear RegressionThe resulting beta coefficients,
ranging from 0.50 to 0.17, indicate independent contribution of each scale to the prediction of CF-PDI, the criteri-on variable. NDI, VAS, and TSK-11 were predictors of CF-PDI, significance < 0.05 (as illustrated by the higher standard-ized coefficients [beta] and P-values). NDI was the most important variable (Table 6). PCS and HIT-6 were excluded as predictor variables this time.
discussion The present study describes a
methodical approach to the develop-ment and validation of a new self-ad-ministered questionnaire to measure disability, pain, and functional status of the mandibular and craniofacial region in patients with craniofacial pain. Our results demonstrate that the CF-PDI is psychometrically valid and reliable. In addition, the instrument has proven to be easy to complete, and only requires a relatively short time to administer. The CF-PDI was de-veloped in Spain for Spanish patients with craniofacial pain and TMD. How-ever, since the CF-PDI does not contain items that are specifically related to Spanish culture, it could be translated and used internationally.
The design of the CF-PDI was based on a biopsychosocial approach. This conceptual model, recommended by the International Classification of Functioning Disability and Health (52,53), can assess the disease from a
Fig. 2. Bland Altman plot illustrating the test-retest reliability of the CF-PDI. A total of 106 patients participated in the test-retest assessment. The central line representing the mean difference between test and retest scores, which was - 2.22, and the 95% limits of agreement are presented as flanking lines.
Fig. 3. Bland Altman plot illustrating the test-retest reliability of the Pain and Disability subscale. A total of 106 patients participated in the test-retest assessment. The central line representing the mean difference between test and retest scores, which was -1,73, and the 95% limits of agreement are presented as flanking lines.
Pain Physician: January/February 2014; 17:95-108
102 www.painphysicianjournal.com

www.painphysicianjournal.com 103
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Fig. 4. Bland Altman plot illustrating the test-retest reliability of the Jaw Functional Status subscale. A total of 106 patients participated in the test-retest assessment. The central line representing the mean difference between test and retest scores, which was -0.49, and the 95% limits of agreement are presented as flanking lines.
Table 4. Descriptive statistics, test-retest reliability, and responsiveness results (N = 106)
DomainsTest Retest
ICC 95% CI SEM MDCMean SD Mean SD
CF-PDI 20.57 8.42 22.79 7.80 0.90 0.86-0.93 2.48 6.87
Pain and Disability 15.37 6.13 17.10 5.26 0.86 0.81-0.90 2.10 5.82
Jaw Functional Status 5.20 3.39 5.69 3.93 0.86 0-80-0.90 1.35 3.75
CF-PDI, craniofacial pain and disability inventory; SD, standard deviation; ICC, intraclass correlation coefficient; 95% CI, 95% confidence interval; SEM, standard error of measurement; MDC, minimal detectable change
broader perspective, and provides an understanding of health, functioning, and disability. In addition, research sup-ports that clinical diagnosis is sometimes insufficient to explain patients’ pain and disability (54-56).
The scree plot and exploratory fac-tor analysis revealed a 2-factor solution. Both factors had eigenvalues greater than 1. PCA indicated that a satisfactory percentage of total variance (40.8%) was explained by the 2 factors. The CF-PDI contains 21 items divided into 2 subscales according to their content and exploratory factor analysis: “pain and disability” and “jaw functional status.”
High internal consistency was shown for the CF-PDI (Cronbach’s α: 0.88) and also for the 2 subscales (Cron-bach’s α: 0.80 – 0.86). These data are similar to the results from other research questionnaires used to assess facial pain and mandibular function (22-25,57,58).
Table 5. Pearson Correlation Coefficient of our principles scales (N = 192).
CF-PDI Pain and Disability Jaw Functional Status
VAS 0.46** 0.50** 0.23**
NDI 0.65** 0.69** 0.37**
PCS 0.46** 0.50** 0.25**
PCS rumiation 0.34** 0.35** 0.22**
PCS magnification 0.51** 0.52** 0.32**
PCS Helplessness 0.39** 0.45** 0.16*
TSK-11 0.40** 0.41** 0.26**
HIT6 0.38** 0.46** 0.09
** P < 0.01; * P < 0.05Abbreviations: CF-PDI, craniofacial pain and disability inventory; VAS, visual analogue scale; TSK-11, Tampa Scale for Kinesiophobia; PCS, pain catastrophizing scale; NDI, Neck Disability Index; HIT-6, headache impact test-6
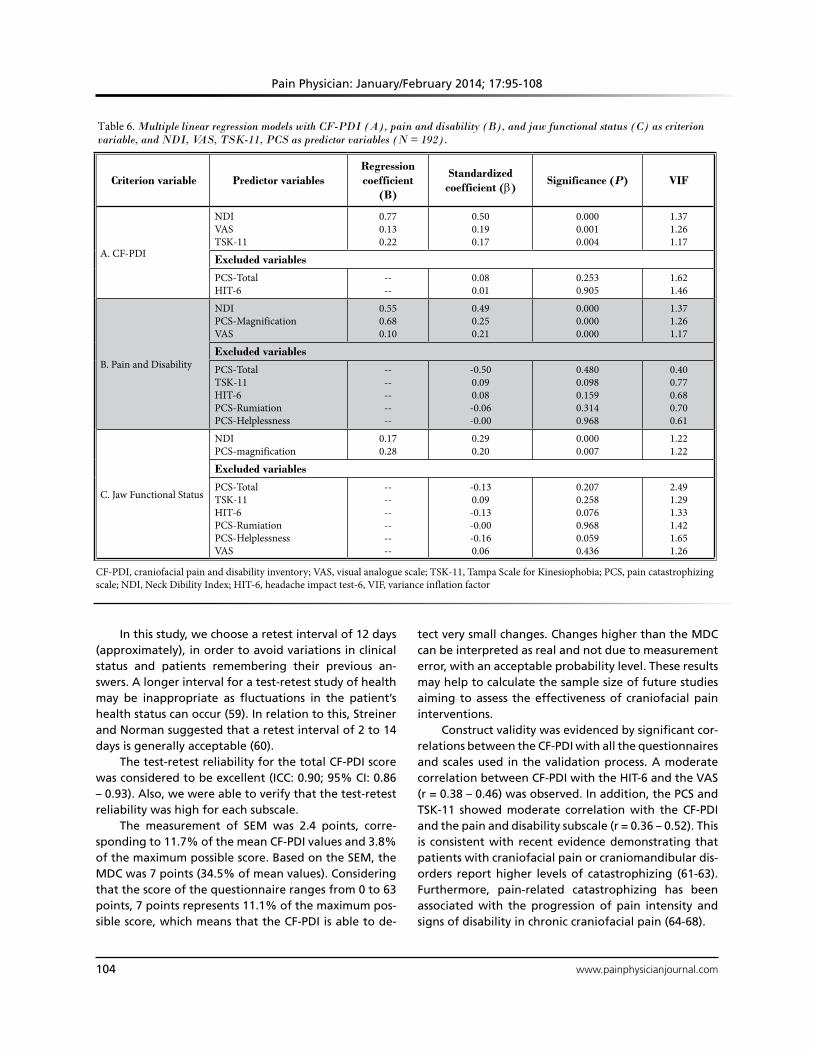
Pain Physician: January/February 2014; 17:95-108
104 www.painphysicianjournal.com
In this study, we choose a retest interval of 12 days (approximately), in order to avoid variations in clinical status and patients remembering their previous an-swers. A longer interval for a test-retest study of health may be inappropriate as fluctuations in the patient’s health status can occur (59). In relation to this, Streiner and Norman suggested that a retest interval of 2 to 14 days is generally acceptable (60).
The test-retest reliability for the total CF-PDI score was considered to be excellent (ICC: 0.90; 95% CI: 0.86 – 0.93). Also, we were able to verify that the test-retest reliability was high for each subscale.
The measurement of SEM was 2.4 points, corre-sponding to 11.7% of the mean CF-PDI values and 3.8% of the maximum possible score. Based on the SEM, the MDC was 7 points (34.5% of mean values). Considering that the score of the questionnaire ranges from 0 to 63 points, 7 points represents 11.1% of the maximum pos-sible score, which means that the CF-PDI is able to de-
tect very small changes. Changes higher than the MDC can be interpreted as real and not due to measurement error, with an acceptable probability level. These results may help to calculate the sample size of future studies aiming to assess the effectiveness of craniofacial pain interventions.
Construct validity was evidenced by significant cor-relations between the CF-PDI with all the questionnaires and scales used in the validation process. A moderate correlation between CF-PDI with the HIT-6 and the VAS (r = 0.38 – 0.46) was observed. In addition, the PCS and TSK-11 showed moderate correlation with the CF-PDI and the pain and disability subscale (r = 0.36 – 0.52). This is consistent with recent evidence demonstrating that patients with craniofacial pain or craniomandibular dis-orders report higher levels of catastrophizing (61-63). Furthermore, pain-related catastrophizing has been associated with the progression of pain intensity and signs of disability in chronic craniofacial pain (64-68).
Table 6. Multiple linear regression models with CF-PDI (A), pain and disability (B), and jaw functional status (C) as criterion variable, and NDI, VAS, TSK-11, PCS as predictor variables (N = 192).
Criterion variable Predictor variablesRegression coefficient
(B)
Standardized coefficient (β)
Significance (P) VIF
A. CF-PDI
NDIVASTSK-11
0.770.130.22
0.500.190.17
0.0000.0010.004
1.371.261.17
Excluded variables
PCS-TotalHIT-6
----
0.080.01
0.2530.905
1.621.46
B. Pain and Disability
NDIPCS-MagnificationVAS
0.550.680.10
0.490.250.21
0.0000.0000.000
1.371.261.17
Excluded variables
PCS-TotalTSK-11HIT-6PCS-RumiationPCS-Helplessness
----------
-0.500.090.08-0.06-0.00
0.4800.0980.1590.3140.968
0.400.770.680.700.61
C. Jaw Functional Status
NDIPCS-magnification
0.170.28
0.290.20
0.0000.007
1.221.22
Excluded variables
PCS-TotalTSK-11HIT-6PCS-RumiationPCS-HelplessnessVAS
------------
-0.130.09-0.13-0.00-0.160.06
0.2070.2580.0760.9680.0590.436
2.491.291.331.421.651.26
CF-PDI, craniofacial pain and disability inventory; VAS, visual analogue scale; TSK-11, Tampa Scale for Kinesiophobia; PCS, pain catastrophizing scale; NDI, Neck Dibility Index; HIT-6, headache impact test-6, VIF, variance inflation factor

www.painphysicianjournal.com 105
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Previous research demonstrated the relationship between fear of jaw movements and craniofacial pain (69,70), but only limited evidence supports it. However, there is higher evidence showing that pain-related fear is associated with reduced activities in daily life and is also a strong predictor of disability in other chronic musculoskeletal disorders (71-75).
Pain catastrophizing and pain-related fear are 2 constructs that have been linked to the chronicity of musculoskeletal pain through the “fear avoidance model” (76). Based on the results of multiple linear regression analysis, pain intensity (VAS: β = 0.19, P = 0.001) and fear of pain and movement (TSK-11: β = 0.17, P = 0.004) were predictors of CF-PDI. For jaw functional status, and pain and disability, the variable predictor was pain catastrophizing (PCS-Magnification: β = 0.25, P < 0.001; β = 0.20, P = 0.007).
The principal predictor for CF-PDI and the 2 sub-scales was the variable of neck disability (NDI: β = 0.29 – 0.50, P < 0.001). In addition, a strong correlation was observed between CF-PDI and pain and disability factor with NDI (r = 0.65 – 0.69). This is in line with the results of Olivo et al (77) who described a strong relationship between neck disability and jaw disability (r = 0.82). Several studies have reported the high prevalence and comorbidity between orofacial pain, TMD, headache, and neck pain (65,78-81). Our findings suggest the importance of taking into account the neck disability questionnaires when assessing patients with craniofa-cial pain.
Limitations Our study has several limitations. First, there is
a gender disproportion as the sample had a smaller proportion of men. However, our findings showed no significant differences in scoring between genders. The evidence suggests that the prevalence of craniofacial pain is higher in women (82).
The second limitation of this study is that we did not assess the CF-PDI in healthy subjects; the sample consisted of patients with chronic pain. Further
studies will need to be performed to assess the dis-criminant power of the CF-PDI for specific diagnostic entities.
The sample size was sufficient to test the new in-strument’s reliability, convergence validity, and explor-atory factor analysis. However, it was too small to be able to carry out confirmatory factor analysis. Kline has suggested a sample size of 10 – 15 subjects per item to perform this statistical analysis (83). It should be noted that statisticians disagree on the issue of appropriate sample size for confirmatory factor analyses. In relation to this, DeVellis stated that as the sample size becomes larger, the relative number of respondents per item can diminish (84), and that a sample of 200 is adequate in most studies (85).
Another limitation is that only self-reported mea-sures were considered for convergent validity. Future research should use physical tests to explore the clinical signs relating to pain and disability, and assess whether these are associated with the CF-PDI.
The last limitation of the study is the cross-sectional design, which prevented us from investigating the abili-ty of the CF-PDI to detect responsiveness to change over time. Although in this study we investigated in a short period of time the reproducibility and the MDC, a longi-tudinal study or one with an experimental design with a follow-up period would be required to understand how CF-PDI scores change over time. Furthermore, such a study would allow us to obtain information such as the Minimum Clinically Important Difference.
conclusion Evidence has shown that the CF-PDI has a good
structure, internal consistency, reproducibility, and construct validity, and provides an objective tool for as-sessing pain and disability in craniofacial pain patients. Neck disability showed a strong association with the CF-PDI, and is also a significant predictor of the construct. Based on the findings of this study, the CF-PDI could be used in research and clinical practice for the assessment of treatment outcomes.
RefeRences
1. Fillingim RB, Wallace MR, Herbstman DM, Ribeiro-Dasilva M, Staud R. Ge-netic contributions to pain: A review of findings in humans. Oral Dis 2008; 14:673-682.
2. Macfarlane TV, Glenny AM, Worthing-
ton HV. Systematic review of population-based epidemiological studies of oro-fa-cial pain. J Dent 2001; 29:451-467.
3. Stuginski-Barbosa J, Macedo HR, Bigal ME, Speciali JG. Signs of temporoman-dibular disorders in migraine patients: A
prospective, controlled study. Clin J Pain 2010; 26:418-421.
4. Shan CL, Bin Adon MY, Rahman AB, Hassan ST, Ismail KB. Prevalence of neck pain and associated factors with per-sonal characteristics, physical workloads

Pain Physician: January/February 2014; 17:95-108
106 www.painphysicianjournal.com
and psychosocial among male rubber workers in FELDA settlement Malaysia. Glob J Health Sci 2012; 4:94-104.
5. Anderson GC, John MT, Ohrbach R, Nixdorf DR, Schiffman EL, Truelove ES, List T. Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 2011; 152:765-771.
6. Glaros AG, Urban D, Locke J. Headache and temporomandibular disorders: Evi-dence for diagnostic and behavioural overlap. Cephalalgia 2007; 27:542549.
7. Svensson P. Muscle pain in the head:O between temporomandibular disorders and tension-type headaches. Curr Opin Neurol 2007; 20:320-325.
8. Lobbezoo F, Visscher CM, Naeije M. Impaired health status, sleep disorders, and pain in the craniomandibular and cervical spinal regions. Eur J Pain 2004; 8:23-30.
9. Plesh O, Adams SH, Gansky SA. Tem-poromandibular joint and muscle disor-der-type pain and comorbid pains in a national US sample. J Orofac Pain 2011; 25:190-198.
10. The International Classification of Headache Disorders: 2nd edition. Ceph-alalgia 2004; 24 Suppl:9-160.
11. Ashina S, Bendtsen L, Ashina M, Magerl W, Jensen R. Generalized hyperalgesia in patients with chronic tension-type headache. Cephalalgia 2006; 26:940-948.
12. Leclerc A, Niedhammer I, Landre MF, Ozguler A, Etore P, Pietri-Taleb F. One-year predictive factors for various as-pects of neck disorders. Spine (Phila Pa 1976) 1999; 24:1455-1462.
13. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial ap-proach to chronic pain: Scientific ad-vances and future directions. Psychol Bull 2007; 133:581-624.
14. Hoffmann RG, Kotchen JM, Kotchen TA, Cowley T, Dasgupta M, Cowley Jr. AW. Temporomandibular disorders and as-sociated clinical comorbidities. Clin J Pain 2011; 27:268-274.
15. Volcy-Gomez M. [The impact of mi-graine and other primary headaches on the health system and in social and economic terms]. Rev Neurol 2006; 43:228-235.
16. Shimshak DG, DeFuria MC. Health care utilization by patients with temporo-mandibular joint disorders. Cranio 1998; 16:185-193.
17. Ohrbach R, Larsson P, List T. The jaw functional limitation scale: Develop-
ment, reliability, and validity of 8-item and 20-item versions. J Orofac Pain 2008; 22:219-230.
18. Bloudek LM, Stokes M, Buse DC, Wil-cox TK, Lipton RB, Goadsby PJ, Varon SF, Blumenfeld a M, Katsarava Z, Pascual J, Lanteri-Minet M, Cortelli P, Martelletti P. Cost of healthcare for patients with migraine in five European countries: Results from the International Burden of Migraine Study (IBMS). J Headache Pain 2012; 13:361-378.
19. Salo P, Ylinen J, Kautiainen H, Arkela-Kautiainen M, Hakkinen A. Reliability and validity of the Finnish version of the neck disability index and the modi-fied neck pain and disability scale. Spine (Phila Pa 1976) 2010; 35:552-556.
20. Andrade Ortega JA, Delgado Martinez AD, Almecija Ruiz R. Validation of the Spanish version of the Neck Disabil-ity Index. Spine (Phila Pa 1976) 2010; 35:E114-118.
21. Schmidt S, Bullinger M. Current issues in cross-cultural quality of life instru-ment development. Arch Phys Med Re-habil 2003; 84:S29-34.
22. Aggarwal VR, Lunt M, Zakrzewska JM, Macfarlane GJ, Macfarlane T V. Develop-ment and validation of the Manchester orofacial pain disability scale. Communi-ty Dent Oral Epidemiol 2005; 33:141-149.
23. Lee JYK, Chen HI, Urban C, Hojat A, Church E, Xie SX, Farrar JT. Develop-ment of and psychometric testing for the Brief Pain Inventory-Facial in pa-tients with facial pain syndromes. J Neu-rosurg 2010; 113:516-523.
24. Johnson J, Carlsson S, Johansson M, Pauli N, Rydén A, Fagerberg-Mohlin B, Finizia C. Development and validation of the Gothenburg Trismus Questionnaire (GTQ). Oral Oncol 2012; 48:730-736.
25. Nixdorf DR, John MT, Wall MM, Fricton JR, Schiffman EL. Psychometric proper-ties of the modified Symptom Severity Index (SSI). J Oral Rehabil 2010; 37:11-20.
26. Ohrbach R, Granger C, List T, Dworkin S. Preliminary development and valida-tion of the Jaw Functional Limitation Scale. Community Dent Oral Epidemiol 2008; 36:228-236.
27. Jones J, Hunter D. Consensus meth-ods for medical and health services re-search. BMJ (Clinical research ed.) 1995; 311:376-380.
28. Dworkin SF, LeResche L. Research diag-nostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J Cranio-
mandib Disord 1992; 6:301-355.29. Schiffman EL, Ohrbach R, Truelove EL,
Tai F, Anderson GC, Pan W, Gonzalez YM, John MT, Sommers E, List T, Velly AM, Kang W, Look JO. The Research Di-agnostic Criteria for Temporomandibu-lar Disorders. V: Methods used to estab-lish and validate revised Axis I diagnostic algorithms. J Orofac Pain 2010; 24:63-78.
30. Bijur PE, Silver W, Gallagher EJ. Reliabil-ity of the visual analog scale for mea-surement of acute pain. Acad Emerg Med 2001; 8:1153-1157.
31. Gómez-Pérez L, López-Martínez AE, Ruiz-Párraga GT. Psychometric proper-ties of the Spanish version of the Tam-pa Scale for Kinesiophobia (TSK). J Pain 2011; 12:425-435.
32. Kori SH, Miller RP, Todd DD. Kinesio-phobia: A new view of chronic pain be-havior. Pain Manag 1990; 3:35-43.
33. García Campayo J, Rodero B, Alda M, Sobradiel N, Montero J, Moreno S. Validación de la versión española de la escala de la catastrofización ante el dolor (Pain Catastrophizing Scale) en la fibromialgia. Med Clin (Barc) 2008; 131:487-492.
34. Sullivan MJL, Bisop SC, Pivik J. The pain catastrophizing scale: Development and validation. Psychol Assess 1995; 7:524-532.
35. Vernon H, Mior S. The Neck Disabil-ity Index: A study of reliability and va-lidity. J Manipulative Physiol Ther 1991; 14:409-415.
36. Bjorner JB, Kosinski M, Ware JE. Cali-bration of an item pool for assessing the burden of headaches: An application of item response theory to the headache impact test (HIT). Qual Life Res 2003; 12:913-933.
37. Gandek B, Alacoque J, Uzun V, Andrew-Hobbs M, Davis K. Translating the Short-Form Headache Impact Test (HIT-6) in 27 countries: Methodological and conceptual issues. Qual Life Res 2003; 12:975-979.
38. Martin M, Blaisdell B, Kwong JW, Bjorner JB. The Short-Form Headache Impact Test (HIT-6) was psychometri-cally equivalent in nine languages. J Clin Epidemiol 2004; 57:1271-1278.
39. Cohen J. Weighted kappa: Nominal scale agreement with provision for scaled dis-agreement or partial credit. Psychol Bull 1968; 70:213-220.
40. Ferguson E, Cox T. Exploratory factor analysis: A users’ guide. Int J Select As-sess 1993; 1:84-94.
41. Bartlett MS. A note on the multiply-

Psychometric validation of the Craniofacial Pain and Disability Inventory
www.painphysicianjournal.com 107
ing factors for various Chi-square ap-proximations. J Royal Stat Soc B 1954; 16:296-298.
42. Kaiser H. Analysis of factorial simplicity. Psychometrika 1974; 39:31-36.
43. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika 1951; 16:297-334.
44. Terwee CB, Bot SDM, De Boer MR, Van der Windt DAWM, Knol DL, Dekker J, Bouter LM, De Vet HCW. Quality criteria were proposed for measurement prop-erties of health status questionnaires. J Clin Epidemiol 2007; 60:34-42.
45. Bland JM, Altman DG. Statistical meth-ods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1:307-310.
46. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, Bouter LM, De Vet HCW. The COSMIN study reached international consensus on tax-onomy, terminology, and definitions of measurement properties for health-re-lated patient-reported outcomes. J Clin Epidemiol 2010; 63:737-745.
47. Weir JP. Quantifying test-retest reliabil-ity using the intraclass correlation coef-ficient and the SEM. J Strength Cond Res 2005; 19:231-240.
48. Harvill L. Standard error of measure-ment. Educ Meas 1991; 10:33-41.
49. Ostelo RWJG, De Vet HCW, Knol DL, Van den Brandt PA. 24-item Roland-Morris Disability Questionnaire was preferred out of six functional status question-naires for post-lumbar disc surgery. J Clin Epidemiol 2004; 57:268-276.
50. Haley SM, Fragala-Pinkham MA. Inter-preting change scores of tests and mea-sures used in physical therapy. Phys Ther 2006; 86:735-743.
51. Wyrwich KW. Minimal important differ-ence thresholds and the standard error of measurement: Is there a connection? J Biopharm Stat 2004; 14:97-110.
52. Stucki G, Boonen A, Tugwell P, Cieza A, Boers M. The World Health Organ-isation International Classification of Functioning, Disability and Health: A conceptual model and interface for the OMERACT process. J Rheumatol 2007; 34:600-606.
53. Stucki G, Cieza A, Melvin J. The Inter-national Classification of Functioning, Disability and Health (ICF): A unifying model for the conceptual description of the rehabilitation strategy. J Rehab Med 2007; 39:279-285.
54. Turner JA, Franklin G, Turk DC. Pre-
dictors of chronic disability in injured workers: A systematic literature synthe-sis. Am J Ind Med 2000; 38:707-722.
55. Brage S, Sandanger I, Nygård JF. Emo-tional distress as a predictor for low back disability: A prospective 12-year popula-tion-based study. Spine 2007; 32:269-274.
56. Waddell G. Preventing incapacity in people with musculoskeletal disorders. Br Med Bull 2006; 77-78:55-69.
57. Ohrbach R, Larsson P, List T. The jaw functional limitation scale: Develop-ment, reliability, and validity of 8-item and 20-item versions. J Orofac Pain 2008; 22:219-230.
58. Stegenga B, De Bont LG, De Leeuw R, Boering G. Assessment of mandibular function impairment associated with temporomandibular joint osteoarthro-sis and internal derangement. J Orofac Pain 1993; 7:183-195.
59. Holt AE, Shaw NJ, Shetty A, Greenough CG. The reliability of the Low Back Out-come Score for back pain. Spine 2002; 27:206-210.
60. Streiner DL, Norman GR. Health Mea-surement Scales: A Guide to Their Develop-ment and Use. Oxford University Press, Oxford, 1989.
61. Campbell CM, Kronfli T, Buenaver LF, Smith MT, Berna C, Haythornthwaite JA, Edwards RR. Situational versus dis-positional measurement of catastroph-izing: Associations with pain respons-es in multiple samples. J Pain 2010; 11:443-453.
62. Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Dubner R, Bair E, Baraian C, Slade GD, Maixner W. Potential psycho-social risk factors for chronic TMD: De-scriptive data and empirically identified domains from the OPPERA case-control study. J Pain 2011; 12:T46-60.
63. Quartana PJ, Buenaver LF, Edwards RR, Klick B, Haythornthwaite JA, Smith MT. Pain catastrophizing and salivary cor-tisol responses to laboratory pain test-ing in temporomandibular disorder and healthy participants. J Pain 2010; 11:186-194.
64. Rantala MA, Ahlberg J, Suvinen TI, Nis-sinen M, Lindholm H, Savolainen A, Ko-nonen M. Temporomandibular joint re-lated painless symptoms, orofacial pain, neck pain, headache, and psychosocial factors among non-patients. Acta Odon-tol Scand 2003; 61:217-222.
65. Buenaver LF, Edwards RR, Smith MT, Gramling SE, Haythornthwaite JA. Cata-strophizing and pain-coping in young adults: Associations with depressive
symptoms and headache pain. J Pain 2008; 9:311-319.
66. Buenaver LF, Quartana PJ, Grace EG, Sarlani E, Simango M, Edwards RR, Hay-thornthwaite JA, Smith MT. Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial tem-poromandibular disorder participants: The mediating role of sleep disturbance. Pain 2012; 153:1159-1166.
67. Holroyd KA, Drew JB, Cottrell CK, Ro-manek KM, Heh V. Impaired function-ing and quality of life in severe mi-graine: The role of catastrophizing and associated symptoms. Cephalalgia 2007; 27:1156-1165.
68. Velly AM, Look JO, Carlson C, Lenton PA, Kang W, Holcroft CA, Fricton JR. The effect of catastrophizing and depression on chronic pain – a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 2011; 152:2377-2383.
69. Visscher CM, Ohrbach R, Van Wijk AJ, Wilkosz M, Naeije M. The Tampa Scale for Kinesiophobia for Temporomandib-ular Disorders (TSK-TMD). Pain 2010; 150:492-500.
70. Rollman A, Visscher CM, Gorter RC, Naeije M. Care seeking for orofacial pain. J Orofac Pain 2012; 26:206-214.
71. Buer N, Linton SJ. Fear-avoidance be-liefs and catastrophizing: Occurrence and risk factor in back pain and ADL in the general population. Pain 2002; 99:485-491.
72. Crombez G, Vlaeyen JW, Heuts PH, Ly-sens R. Pain-related fear is more dis-abling than pain itself: Evidence on the role of pain-related fear in chronic back pain disability. Pain 1999; 80:329-339.
73. Kamper SJ, Maher CG, Menezes Costa L da C, McAuley JH, Hush JM, Sterling M. Does fear of movement mediate the relationship between pain intensity and disability in patients following whiplash injury? A prospective longitudinal study. Pain 2012; 153:113-119.
74. Walton D, Elliott JM. A higher-order analysis supports use of the 11-item ver-sion of the tampa scale for kinesiopho-bia in people with neck pain. Phys Ther 2013; 93:60-68.
75. Vlaeyen JW, Seelen HA, Peters M, De Jong P, Aretz E, Beisiegel E, Weber WE. Fear of movement/(re)injury and mus-cular reactivity in chronic low back pain patients: An experimental investigation. Pain 1999; 82:297-304.
76. Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS.

Pain Physician: January/February 2014; 17:95-108
108 www.painphysicianjournal.com
The fear-avoidance model of musculo-skeletal pain: Current state of scientific evidence. J Behav Med 2007; 30:77-94.
77. Olivo SA, Fuentes J, Major PW, Warren S, Thie NMR, Magee DJ. The association between neck disability and jaw disabil-ity. J Oral Rehabil 2010; 37:670-679.
78. Marklund S, Wiesinger B, Wanman A. Reciprocal influence on the incidence of symptoms in trigeminally and spi-nally innervated areas. Eur J Pain 2010; 14:366-371.
79. Mienna CS, Wanman A. Self-reported impact on daily life activities related to temporomandibular disorders, head-
aches, and neck-shoulder pain among women in a Sami population living in Northern Sweden. J Orofac Pain 2012; 26:215-224.
80. Storm C, Wänman A. Temporoman-dibular disorders, headaches, and cer-vical pain among females in a Sami population. Acta Odontol Scand 2006; 64:319-325.
81. Wiesinger B, Malker H, Englund E, Wänman A. Back pain in relation to musculoskeletal disorders in the jaw-face: A matched case-control study. Pain 2007; 131:311-319.
82. Macfarlane TV, Blinkhorn AS, Davies
RM, Kincey J, Worthington H V. Oro-fa-cial pain in the community: Prevalence and associated impact. Community Dent Oral Epidemiol 2002; 30:52-60.
83. Rex B. Kline. Principles and Practice of Structural Equation Modeling (Methodol-ogy in the Social Sciences). Kenny DA, edi-tor. Guilford Press. New York, 1998.
84. DeVellis RF. Scale Development Theory and Applications. Sage Publications. Newbury Park, CA, 1991.
85. Comrey AL. Factor-analytic methods of scale development in personality and clinical psychology. J Consult Clin Psychol 1988; 56:754-761.

138
5.5 Estudio V
La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-Díaz-Parreño S,
Fernández-Carnero J. The Influence of Neck Disability and Pain Catastrophizing about
Trigeminal Sensory-Motor System in Patients with Headache Attributed to Temporomandibular
Disorders. (En revisión)
Objetivos de estudio
Nuestro objetivo fue estudiar la influencia de la discapacidad y el dolor de cuello sobre las
variables sensoriales y motoras del trigémino en pacientes con cefalea atribuida a TCM.
Resultados
Los resultados de EVAF fueron mayores a 6 minutos (media 51,7, IC 95%: 50,15-53,26) y 24
horas después (21.08, IC 95%: 18,6-23,5) para las pruebas en el grupo que muestran
discapacidad moderada cuello en comparación con el grupo de discapacidad leve cuello (6
minutos, 44,16, IC del 95%: 42,65 a 45,67 / 24 horas después, 14,3; IC del 95%: 11,9-16,7) y el
grupo de control (6 minutos, 29.92, IC 95% 28,29-31,55 / 24 horas después, 4,65; IC del 95%:
2.5 a 7.24). El análisis muestra una disminución en el MAI sin dolor inmediatamente después de
las pruebas de todos los grupos y se observó que esta disminución sólo se mantuvo en el grupo
de discapacidad moderada 24 horas después de la prueba. Los UDPs de la región del trigémino
se redujeron inmediatamente en todos los grupos, mientras que a las 24 horas se observó una
disminución sólo en los grupos de pacientes. Los UDPs de la región cervical disminuyeron sólo
en el grupo con discapacidad cuello moderado 24 horas después de la prueba. La correlación
negativa más fuerte se encontró entre MAI sin dolor inmediatamente después de la prueba y el
IDC en ambos grupos: grupo de discapacidad leve (r = -0.49, P <0,001) y grupo de discapacidad
moderada (r = -0.54, P <0,001).
Conclusiones
Nuestros resultados sugieren que la discapacidad y dolor de cuello tienen una influencia en las
variables sensomotrices evaluados en pacientes con cefalea atribuida a TCM.

1
The Influence of Neck Disability and Pain Catastrophizing about Trigeminal
Sensory-Motor System in Patients with Headache Attributed to
Temporomandibular Disorders
Roy La Touche,1-4, Alba Paris-Alemany 1-4, Alfonso Gil-Martínez1-4, Joaquín Pardo-
Montero1-4, Santiago Angulo-Díaz-Parreño, Josué Fernández-Carnero,2,4,6.
1. Department of Physiotherapy, Faculty of Health Science, The Center for Advanced Studies
University La Salle. Universidad Autónoma de Madrid, Aravaca, Madrid, Spain.
2. Motion in Brains Research Group, The Center for Advanced Studies University La Salle,
Universidad Autónoma de Madird.
3. Institute of Neuroscience and Craniofacial Pain (INDCRAN), Madrid, Spain
4. Hospital La Paz Institute for Health Research, IdiPAZ. Madrid, Spain.
Madrid, Spain
5. Faculty of Medicine, Universidad San Pablo CEU, Madrid, Spain
6. Department of Physical Therapy, Occupational Therapy, Rehabilitation and Physical
Medicine, Universidad Rey Juan Carlos, Alcorcón, Madrid, Spain.
Address for reprint requests / Corresponding author:
Roy La Touche
Facultad de Ciencias de la Salud
Centro Superior de Estudios Universitarios La Salle.
Calle la Salle, 10
28023 Madrid
SPAIN
Telephone number: + 34 91 7401980 (EXT.256)
Fax number:
Email address: [email protected]

2
ABSTRACT
OBJECTIVE: Our purpose was to investigate the influence that neck pain and disability
may have on trigeminal sensory-motor variables in patients with headache attributed to
TMD.
METHODS: An experimental case-control study comprising 83 patients with headache
attributed to TMD and 39 healthy controls was done. Patients were grouped according
to their scores on the neck disability index (NDI) (mild and moderate neck disability).
Initial assessment included the visual analogue scale (VAS), pain catastrophizing scale,
NDI and the Headache Impact Test-6. The protocol consisted of baseline measurements
of pressure pain thresholds (PPT) for mechanical pain sensitivity in the trigeminal and
cervical region and the pain-free maximum mouth opening (MMO), performance of the
provocation chewing test, immediately after data collection and 24 hours after. During
the provocation chewing test, patients were assessed for subjective feelings of fatigue
(VAFS) and pain intensity, immediately and 24 hours after completion.
RESULTS: The VAFS were higher at 6 minutes (mean 51.7; 95% CI: 50.15-53.26) and
24 hours after (21.08; 95% CI: 18.6-23.5) for tests in the group showing moderate neck
disability compared with the mild neck disability group (6 minutes, 44.16; 95% CI
42.65-45.67/ 24 hours after, 14.3; 95% CI: 11.9-16.7) and the control group (6 minutes,
29.92; 95% CI 28.29-31.55/ 24 hours after, 4.65; 95% CI: 2.05-7.24). The analysis
shows a decrease in the pain-free MMO immediately after the tests for all groups and
this decrease was observed only in the group of moderate disability 24 hours after the
test. PPTs of the trigeminal region were decreased immediately in all groups, whereas at
24 hours a decrease was observed only in the groups of patients. PPTs of the cervical
region decreased only in the group with moderate neck disability 24 hours after the test.
The strongest negative correlation was found between pain-free MMO immediately

3
after the test and NDI in both groups: mild (r=-0.49; P<0.001) and moderate (r=-0.54;
P<0.001) neck disability group.
CONCLUSION: Neck pain and disability have an influence on the sensory-motor
variables evaluated in patients with headache attributed to TMD.
KEYWORDS: Temporomandibular disorders, headache, neck pain, pain
catastrophizing, disability.

4
.INTRODUCTION
Temporomandibular disorders (TMD), headaches and neck pain are very closely
related diseases[1]. Several studies have reported the overlapping signs and symptoms
among patients with TMD, headaches and neck pain, respectively[2, 3]. It has been
shown that neck pain complaints were also significantly associated with TMD[4, 5] and
that psychosocial factors have an influence on the presence of head, neck and orofacial
pain[3].
The prevalence of temporomandibular joint (TMJ) symptoms, orofacial pain,
neck pain and headache was assessed in 1339 non-patients. Often painless TMJ
symptoms were found in 10% of subjects, orofacial pain in 7%, headache in 15% and
neck pain in 39%[3]. Plesh et al. showed that 53% of patients with TMD had severe
headache and 54% had neck pain[6]. It has been suggested that TMD and headaches
may be involved in their pathophysiology[7, 8] and this headache could be a possible
risk factor for developing neck pain[9].
Recent research has shown a strong relationship between craniomandibular
disability and pain with cervical disability[10, 11]. Several experimental studies have
described functional connections between the craniofacial and cervical afferent fibres
via patterns of neural convergence of the trigeminal nucleus and the upper cervical
nociceptive neurons, which form a functional unit, the trigeminocervical complex[12–
18]. In relation to this, it has been observed in experimental studies that the pain
induced by the infiltration of algogenic substances in the masticatory or cervical
muscles can bi-directionally modify the activity of the stretch reflexes[13, 15]. Also, in
basic research, a reflex relationship has been observed between the activity of the
nociceptors of the TMJ and the activity of the fusimotor-muscle spindle system of the
cervical muscles[17]. This information is useful for proposing theories about the
5
influence of the cervical region over the possible nociceptive and sensory-motor
mechanisms involved in masticatory fatigue, pain and alterations in motor behaviour. At
present, there is insufficient information demonstrating the influence of neck pain and
disability in the sensory-motor activity in patients with trigeminal headache attribute to
TMD. This could be a key issue, since improvements could be made by changing the
diagnostic and therapeutic approach to these patients. We used the primary hypothesis
that neck disability is a factor influencing masticatory sensory-motor activity in patients
with headache attributed to TMD.
Headache attributed to TMD is classified as a secondary headache caused by a
disorder that affects the temporomandibular region[19]. The pain may be unilateral or
bilateral and is represented in the facial region, at the masseter and temporal region[19].
An important criterion for clinical diagnosis is that the headache occurs or is aggravated
by provocative manoeuvres (such as the palpatory pressure on the TMJ and masticatory
muscles) and/or mandibular active or passive movements[19, 20]. Recently, it has been
found that the diagnostic criteria that have greater sensitivity and specificity for this
type of headache are: 1) the provocation of pain by palpation of the temporalis muscle
or jaw movements and 2) the fact that pain changes with the movements of the jaw in
the function or parafunction[20, 21].
From the clinical point of view, it is important to identify changes in motor
behaviour that may be present in patients suffering TMD, especially knowing that a
percentage of these patients develop painful chewing[22, 23], difficulty performing jaw
movements[24] and masticatory fatigue[25, 26].
During the last decades, the relationship between masticatory muscle pain and
disordered jaw motor behaviour has been studied widely; see for example the review by
Svensson and Graven-Nielsen[27]. Pain may influence the characteristics of the

6
masticatory sensory-motor system[28]. Furthermore, Kurita et al. found a positive
correlation between chewing ability and TMJ pain and reduced mouth opening[29].
According to some researchers, fatigue and fatigue-related symptoms are reported
significantly more often by chronic TMD patients than by healthy volunteers[30]. In
addition, a recent study in patients with chronic orofacial pain demonstrated that fatigue
is mediated by psychosocial factors[31]. In this connection, Brandini et al. found a
positive association in TMD patients between mandibular kinematic variables and
psychological factors such as stress and depression[32].
Research or assessments based on a biobehavioural approach may offer a better
alternative for identifying patients with chronic TMD[33]; a biobehavioural approach to
the assessment and treatment of chronic pain is widely accepted[34]. A key point to
note about patients with headache attributed to TMD is that an association between
emotional functioning and increased frequency of headache has been found[35]. This
and previous findings lead us to propose integrating the assessment of psychological
factors with pain and disability associated with trigeminal sensory-motor variables in
this research. A significant amount of scientific evidence has shown the influence of
pain catastrophizing on several variables related to TMD[36–41]. This suggests the
hypothesis that pain catastrophizing has an association or is a predictor of some of the
trigeminal sensory-motor variables studied in this research.
The primary objective of this research is to investigate the influence that pain and
disability of the neck may have on trigeminal sensory-motor variables in patients with
headache attributed to TMD, and as a secondary objective we propose identifying
whether the psychological or disability variables have any association with the studied
sensory-motor variables.

7
MATERIALS AND METHODS
Study Design
This was an experimental case-control study. The assessor of sensory-motor
measurements was blinded. One researcher administered the participant appointments
and questionnaires, and also instructed the participant not to say anything that could
reveal their pain, disability trait or state. The reporting of the study follows the
“Strengthening the Reporting of Observational studies in Epidemiology” (STROBE
statement) [42].
After receiving detailed information about the experiment, the volunteers gave
their written informed consent. All of the procedures used in this study were planned
under the ethical norms of the Helsinki Declaration and were approved by the local
ethics committee.
Participants
A consecutive convenience sample of 83 patients with chronic headache
attributed to TMD and 39 healthy controls were recruited for the study. The sample was
recruited from outpatients of a Public Health Centre (Madrid, Spain) and two private
clinics specializing in craniofacial pain and TMD (Madrid, Spain). Patients were
selected if they met all of the following criteria: 1) Headache and facial pain attributed
to TMD, diagnosis was made according to the guidelines of the International
Classification of Headache Disorders[19]; 2) TMD diagnosis based on the Research
Diagnostic Criteria for TMD[43, 44] to classify patients with painful TMD (myofascial
pain, TMJ arthralgia and TMJ osteoarthritis); 3) pain symptoms history of at least the 6
months previous to the study; 4) pain in the jaw, temples, face, neck, pre-auricular area,
or in the ear during rest or function; 5) neck pain and disability and quantified according
to neck disability index (NDI)[45]; and 6) At least 18 years of age.

8
There were 83 patients categorized into two groups according to their scores on the
NDI[45]: 1) mild neck disability (NDI 5-14), and; 2) moderate neck disability (NDI 15-
24). The criteria for exclusion were: 1) a history of traumatic injuries (e.g., contusion,
fracture, or whiplash injury); 2) presence of fibromyalgia or other chronic pain disorder;
3) neuropathic pain (e.g., trigeminal neuralgia); 4) unilateral neck pain; 5) cervical spine
surgery, and; 6) clinical diagnosis of cervical radiculopathy or myelopathy.
Healthy controls were recruited from our academic university campus and the
local community through flyers, posters, and social media. Healthy participants were
examined and were included in the study only if they had no history of craniofacial
pain, headache or neck pain and had been free of any other painful disorders for the six
months prior to the experiment. All subjects had complete dentition, did not use any
medication, had no dental pathology and none were regular gum chewers. Subjects who
reported oral parafunctions (i.e., tooth grinding, tooth clenching) were excluded.
Experimental Protocol
After consenting for the study, recruited patients were given a battery of
questionnaires to complete on the first day of the experiment. These included various
self-reports for sociodemographic, psychological and pain-related variables, including
the visual analogue scale (VAS) for pain intensity and the validated Spanish versions of
the pain catastrophizing scale (PCS), the NDI and the impact associated with headache
was assessed using the Headache Impact Test-6 (HIT-6). The experimental protocol
consisted of baseline measurements, a provocation chewing test, and data collection
immediately after, and 24 hours after, the provocation chewing test. Participants
underwent standardized measurement of pressure pain thresholds (PPT) for mechanical
pain sensitivity at the trigeminal and cervical region and the pain-free maximum mouth
opening (MMO). The PPT and MMO measures have been employed in previous

9
studies[46] and are further described below. During the performance of the provocation
chewing test, data were collected regarding the subjective feelings of fatigue and pain
intensity every minute, immediately and 24 hours after completion.
Provocation Chewing Test
The provocation chewing test consisted of 6 minutes of unilateral chewing of eight
grams of hard gum; this protocol was modified from Karibe et al.[47]. Chewing gum
was employed to elicit pain and muscle fatigue. The participants performed the test in
the sitting position, which was attained by instructing the patient to sit in a comfortable
upright position, with the thoracic spine in contact with the back of the chair, but
without contact of the craniocervical region with the seat. The feet were positioned flat
on the floor with knees and hips at 90 degrees and arms resting freely alongside.
Tests were carried out by exclusively using the right side for chewing; the
metronome was set at 80 beats per minute to indicate chewing rate, as documented in a
previous study[48]. The participants were instructed to chew gum initially for 60
seconds to soften its initial hardness, then after 70 seconds of rest, the signal was given
to start the test.
Questionnaires
The Spanish version of the PCS assesses the degree of pain catastrophizing[49, 50]. The
PCS has 13 items and a 3-factor structure: rumination, magnification and helplessness.
The theoretical range is between 0 and 52, with lower scores indicating less
catastrophizing. The PCS has demonstrated acceptable psychometric properties[50].
The Spanish version of the NDI measures perceived neck disability[45, 51]: This
questionnaire consists of 10 items, with 6 possible answers that represents 6 levels of
functional capacity, ranging from 0 (no disability) to 5 (complete disability) points. The
addition of all of the points obtained from each of the items gave the level of disability,

10
with higher scores indicating greater perceived disability. The NDI has demonstrated
acceptable psychometric properties[51].
The Spanish version of the HIT-6[52, 53] consists of a six-item questionnaire measuring
the severity and impact of headache on the patient’s life. The results of HIT-6 are
stratified into four grade-based classes: little or no impact (HIT-6 score: 36-49),
moderate impact (HIT-6 score: 50-55), substantial impact (HIT-6 score: 56-59), and
severe impact (HIT-6 score: 60-78)[52]. The HIT-6 has demonstrated acceptable
psychometric properties[54].
Pain intensity
Pain intensity was measured with the VAS. The VAS consists of a 100 mm line, on
which the left side represents “no pain” and the right side “the worst pain imaginable”.
The patients placed a mark where they felt it represented their pain intensity[55].
The VAS scale was used to quantify two different situations:
a) Habitual and spontaneously perceived pain intensity.
b) Pain intensity perceived at different times during the course of the chewing
provocation test and at 24h after completion.
Subjective perception of fatigue.
The visual analogue fatigue scale (VAFS) was used to quantify fatigue at
different times during the course of the chewing provocation test and at 24h after
completion. The VAFS consists of a 100-mm vertical line on which the bottom
represents “no fatigue” (0 mm), and the top represents “maximum fatigue” (100
mm)[56]. The researcher registered the mark in mm.
Pressure pain thresholds

11
A digital algometer (FDX 25, Wagner Instruments, Greenwich, CT, USA),
comprised of a rubber head (1 cm2) attached to a pressure gauge, was used to measure
PPTs. Force was measured in kilograms (kg); therefore, thresholds were expressed in
kg/cm2. The protocol used was a sequence of 3 measurements, with an interval of 30
seconds between each of the measurements. An average of the 3 measurements was
calculated to obtain a single value for each of the measured points in each of the
assessments. PPTs were assessed at one point in the masseter muscle (2.5 cm anterior to
the tragus and 1.5 cm inferior to the zygomatic arch), one point in the temporalis muscle
(anterior fibres of the muscle; 3 cm superior to the zygomatic arch in the middle point
between the end of the eye and the anterior part of the helix of the ear), in the
suboccipital muscles (2 cm inferior and lateral to the external occipital protuberance)
and in the upper trapezius muscle (2.5 cm above the superior medial angle of the
scapula). The device was applied perpendicular to the skin. The patients were asked to
raise their hands at the moment the pressure started to change to a pain sensation, at
which point the assessor stopped applying pressure. Compression pressure was
gradually increased at a rate of approximately 1 kg/s. This algometric method has high
intra-rater reliability (ICC=0.94-0.97) for measuring PPT[57].
Pain-free MMO
MMO was measured with the patients in a supine position. The patients were
asked to open their mouths as wide as they could without pain. The distance between
the superior incisor and the opposite inferior incisor was measured in mm with a
Craniomandibular scale (CMD scale. Pat. No. ES 1075174 U, INDCRAN: 2011.
INDCRAN, Madrid, Spain). The inter-rater reliability of this procedure has been found
to be high (ICC = 0.95 – 0.96)[58].

12
Sample size
The sample size was estimated with the G*Power Program 3.1.7 for Windows
(G*Power© from University of Dusseldorf, Germany)[59]. The sample size calculation
was considered a power calculation to detect between-group differences in the primary
outcome measures (fatigue and pain intensity). To obtain 80% statistical power (1-β
error probability) with an α error level probability of 0.05, using analysis of variance
(ANOVA) of repeated measures, within-between interaction and an medium effect size
of 0.3, we considered 3 groups and 7 measurements for primary outcomes. This
generated a sample size of 31 participants per group. Allowing a dropout rate of 20%
and aiming to increase the statistical power of the results, we planned to recruit at least a
minimum of 112 participants to provide sufficient power to detect significant group
differences.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS 21, SPSS Inc., Chicago, IL
USA) software was used for statistical analysis. The independent t-test and one-way
ANOVA was used for analysis of the self-report psychological and pain-related
variables (NDI, PCS and HIT-6), as well as pain duration and the subjects’
sociodemographic data (age, weight, height), comparing the baseline data for the three
groups. Results are presented as mean, standard deviation (±SD), range and 95%
confidence interval (CI).
For primary outcome variables (fatigue and pain intensity), we performed a 3-
way repeated-measures ANOVA, including within-between interaction factors. The
factors analysed were group (i.e., moderate neck disability group, mild neck disability
group and healthy group), sex (i.e., female and male) and time (measurement per minute
13
during the test and after 24 hours). The hypothesis of interest was the group vs. time
interaction.
The 2-way repeated-measures models of ANOVA were used to test the effect of
the task on the outcome secondary variables (i.e., PPTs and pain-free MMO). The
factors analysed were group and time (baseline, immediately after and after 24 hours),
and also the interactions group vs. time interactions were analysed. In the analysis,
repeated-measures ANOVAs, when the assumption of sphericity was violated (as
assessed using the Mauchly sphericity test), the number of degrees of freedom against
which the F-ratio was tested was corrected by the value of the Greenhouse–Geisser
adjustment. Post hoc analysis with Bonferroni corrections was performed in the case of
significant ANOVA findings for multiple comparisons between variables. Effect-sizes
(Cohen’s d) were calculated for outcome secondary variables. According to Cohen’s
method, the magnitude of the effect was classified as small (0.20 to 0.49), medium (0.50
to 0.79), and large (≥0.8)[60].
The relationship between pain-related measures after completion of the chewing
provocation test and self-reports for pain-related and psychological measures were
examined using Pearson correlation coefficients. Multiple linear regression analysis was
performed to estimate the strength of the associations between the results of VAS
[model 1], VAFS [model 2] and pain-free MMO [model 3] (criterion variables) after 24
hours following completion of the provocation chewing test and NDI, PCS, HIT-6 and
VAS were used as predictor variables. Variance inflation factors (VIFs) were calculated
to determine whether there were any multi-collinearity issues in any of the three models.
The strength of association was examined using regression coefficients (β), P
values and adjusted R2. Standardized beta coefficients were reported for each predictor
14
variable included in the final reduced models to allow for direct comparison between
the predictor variables in the regression model and the criterion variable being studied.
For regression analysis, the 10 cases per variable rule was applied in order to obtain
reasonably stable estimates of the regression coefficients[61]. The significance level for
all tests was set to P < 0.05.
RESULTS
Baseline characteristics of sociodemographic, psychological and pain-related variables
of the sample are summarized in Table 1. Finally, the total study sample consisted of
122 participants (77 females and 45 males). Table 1 shows no statistically significant
differences among the three groups in relation to sociodemographic variables. There
were no differences in the duration of pain and perceived pain intensity on a regular or
spontaneous basis in specific groups of patients, but differences were observed in NDI,
PCS and Hit-6 (p<0.05). The different diagnosis for TMD of the included patients were
as follows: 28 patients (33.7%) were diagnosed with myofascial pain, 8 patients (9.6%)
with arthralgia, 13 patients (15.6%) with osteoarthritis and 34 patients (40.9%) with a
combined diagnosis (myofascial pain with arthralgia or osteoarthritis).
In the group of healthy participants, there were no withdrawals during the
provocation chewing test; in the group of patients with moderate neck disability, nine
participants (21.9%) withdrew between minutes 5 and 6 of the test as well as six
participants in the group of patients with mild neck disability (14.2%). All of the
participants were evaluated 24 hours after the test.
Gender Differences in Response to Provocation Chewing Test
The interaction of group vs. sex showed significant differences in VAS
(F=10.86; P<0.001), VAFS (F=4.06; P=0.02) and PPTs of the trapezius muscle

15
(F=3.96; P=0.022). Post hoc analysis showed higher values of VAS and VAFS in
women compared to men for the three groups (P<0.05). PPTs in the trapezius muscle
values were lower in women than in men (P<0.05) for the two groups of patients; in the
control group there was no difference in this value. No differences (group vs. sex
interaction) were observed for the other variables.
Pain and Fatigue
The ANOVA revealed a significant group vs. time interaction (F=35.77;
P<0.001), and significant differences for the group factor (F=416.65; P<0.001)
regarding the VAS results during the provocation chewing test. VAS behaviour during
the tests can be seen in Figure 1-A. Post hoc analysis revealed that higher values on the
VAS during provocation chewing test for the moderate neck disability group compared
to the mild neck disability group and the control group. The results obtained 24 hours
after the test showed no differences between the groups of patients, but there were
differences with the control group (Figure 2-A).
For fatigue perceived during tests, the ANOVA showed a significant effect for
group vs. time interaction (F=13.05; P<0.001) and for the group factor (F=371.12;
P<0.001). VAFS behaviour during the tests can be seen in Figure 1-B. VAFS values
were higher at 6 minutes and 24 hours after the test in the group of moderate neck
disability compared with the other two groups. The post hoc analysis shows the
differences between the three groups (Figure 2-B).
Pain-free MMO
Regarding the pain-free MMO ANOVA revealed a significant effect for group
vs. time interaction (F=2.75; P=0.02) and for the group factor (F=65.74; P<0.001). The
post hoc analysis shows a decrease in the pain-free MMO immediately after the tests for

16
the three groups, but this decrease was observed only in the group of moderate disability
at 24 hours after the test (Table 2).
Pressure pain thresholds
The PPTs for all points of the trigeminal and cervical region showed statistically
significant differences by ANOVA in the group vs. time interaction and group factor
(P<0.001). According to the post hoc analysis of the PPT masseter muscle, the results
showed a decrease in all groups for measurements both immediately and 24 hours after
the test (P<0.05); however, this decrease was greater in the group showing moderate
neck disability (d>0.8). Changes in temporalis muscle PPT’s were observed in both
measures for the group of moderate neck disability (P<0.001; d>0.8). In the group of
mild neck disability, changes were only observed immediately after the test (P=0.002;
d=0.19). No changes were observed in the group of healthy subjects (P>0.05).
For PPT in the cervical region (trapezius muscle and suboccipital muscles), the
post hoc analysis shows a decrease of values measures immediately and 24 hours after
the test (P<0.001) for group of moderate neck disability. This decrease in PPT can be
considered large for the suboccipital region (d>0.9) and small-medium for the trapezius
muscle (d=0.27 and 0.61). In the group with mild neck disability, changes were
observed only in the trapezius muscle PPT measurement immediately after the test
(P=0.028; d=0.09) and no statistically significant differences were observed in any of
the PPT measurements in the cervical region in the group of healthy subjects (P>0.05).
Correlations Analysis
Table 3 shows the results of correlation analysis examining the bivariate
relationships among self-reports for pain-related and psychological measures and
MMO, VAS and VAFS measured immediately and 24 hours after the tests for the

17
groups with moderate and mild neck disability. The strongest correlations were found in
the analysis for the group with moderate neck disability, where the pain-free MMO
immediately after the test was negatively associated with NDI (r=-0.54; P<0.001). For
the mild neck disability group, the greater correlation was between the MMO results
after 24 hours and NDI, which had a negative association (r=-0.49; P<0.001).
Multiple linear regression analysis
A linear regression analysis was performed to evaluate contributors to VAFS,
VAS and pain-free MMO after 24 hours regarding all of the self-report results for pain-
related and psychological measures in the patient groups with moderate and mild neck
disability; the results are presented in Table 4.
In the first model, the criterion variable VAFS was predicted by pain
catastrophizing (for both groups), explaining 17% and 12% of variance, respectively.
The following variables, VAS (moderate neck disability, β=-0.001; P=0.10, mild neck
disability, β=-0.053; P=0.72), HIT-6 (moderate neck disability, β=0.004; P=-0.97, mild
neck disability, β=-0.071; P=0.63), and NDI (moderate neck disability, β=-0.082;
P=0.59, mild neck disability, β=-0.070; P=0.67) were not significant predictors.
In the second model, the VAS after 24 hours was predicted by HIT-6 (moderate
neck disability group) and pain catastrophizing (mild neck disability group), explaining
22% and 14% of the variance, respectively. The VAS (moderate neck disability, β=-
0.27; P=0.06, mild neck disability, β=-0.13; P=0.41), NDI (moderate neck disability,
β=0.19; P=0.17, mild neck disability, β=0.24; P=0.13) and PCS (moderate neck
disability, β=0.16; P=0.25) and HIT-6 (mild neck disability, β=-0.054; P=0.71) were not
significant predictors.
18
In a third model, the pain-free MMO was predicted by NDI for both groups;
these models accounted for between 14% and 21% of the variance. The PCS (moderate
neck disability, β=0.20; P=0.19, mild neck disability, β=0.13; P=0.39), the VAS
(moderate neck disability, β=-0.34; P=0.85, mild neck disability, β=-0.26; P=0.13) and
HIT6 (moderate neck disability, β=-0.24; P=-0.066, mild neck disability, β=0.20;
P=0.64) were not significant predictors.
DISCUSION
The results of this study demonstrate that a protocol of masticatory provocation
can induce pain, fatigue and other trigeminal sensory-motor changes in patients with
headache attributed to temporomandibular disorders. Our findings are consistent with
previous studies which have also observed sensory changes induced experimentally by
the masticatory provocation test[47, 62–64]. The duration of the masticatory
provocation test used in our study was similar to other investigations[47, 63, 65].
However, some studies have used longer and also shorter durations for the masticatory
test, reporting significant changes in both situations for both patients and healthy
subjects[48, 62, 64, 66–68]. It is important to mention that group changes were found in
the healthy subjects, but these were smaller than in the other groups, this could be
explained by the observation that exercise can induce pain and increased
hyperalgesia[69]. In addition, other authors have suggested that experimentally-induced
pain during the test may be due to masticatory muscle ischemia followed by the
accumulation of metabolic products in these muscles[70–72]. We also need to take into
account that there is sufficient evidence to suggest fatigue as a factor that increases the
pain perception[73].

19
In this regard, our findings show strong positive correlations between fatigue
and perceived pain associated with the masticatory provocation test in the three assessed
groups. These results may explain in a general way the observed sensory-motor
changes, although they are not sufficient to justify neither the between-groups
differences nor the influence of cervical disability. Reflections and discussion of these
issues are presented in the following section in an effort to clarify and achieve a better
understanding of the matter.
One of the hypotheses proposed in this study is that cervical disability has an
influence over the trigeminal sensory-motor variables, modifying them. The results
obtained support this hypothesis because we observed greater changes in the moderate
cervical disability group immediately and 24 hours after the test. In addition, it was
hypothesized that the psychosocial factors would have a relationship with the results of
the masticatory provocation test and specifically with the pain and fatigue variables.
This relationship was proved after observing an association with pain catastrophizing.
Gender Differences
Regarding pain perception and fatigue during the test, our data show that gender
influences the results of the three groups: women presented with the greater perception
of pain intensity and masticatory fatigue. These results are consistent with previous
studies of experimentally-induced pain in patients[63] and healthy subjects[47, 68];
however, other investigations have not observed the interaction of gender factors with
experimentally-induced pain or masticatory fatigue [65, 74]. This research has not been
designed to identify the physiologic or psychological mechanisms which may explain
the differences in the results of men and women, although it is important to state that
there are many studies which present evidence-based results regarding the response that

20
women have to other painful clinical situations, adding the evidence of experimentally-
induced pain studies which indicate that women have a greater pain sensitivity than men
regarding several somatosensory tests[75].
Influence of the cervical disability over the trigeminal sensory-motor activity.
In this study, we have identified that patients with mild to moderate cervical
disability present a greater perception levels of pain and fatigue compared with healthy
subjects. It is important to mention that the group with moderate cervical disability
presented the greatest changes at the sensorial variables measured along the test,
immediately after and 24 hours after the test, with the exception of the pain intensity
perception after 24 hours, in which no statistically significant differences were found
between groups.
Although there are many studies that have used a provocative test to induce
masticatory pain and fatigue, we have only found one study similar to ours, in which
Haggman-Henrikson et al.[63] observed that patients with whiplash-associated
disorders presented greater masticatory pain and fatigue induced by the test compared to
TMD patients and healthy subjects.
We note recent scientific evidence that injuries to the cervical region may alter
the masticatory motor control and normal mandibular open-close function[76–78]. The
findings of this study may be related to this issue, because our results show that the
masticatory provocation test reduces the pain-free MMO at the end of the test, as seen in
the three groups assessed; these results are similar to previous studies[47, 72]. However,
we need to point out that the reduction was greater in both patient’s groups and it was
maintained at 24 hours only in the moderate cervical disability group. Also, it is

21
important to highlight that the regression analysis showed that cervical disability is a
predictor of the pain-free MMO (after 24 hours) in both groups of patients.
At present, the scientific evidence suggests the existence of cervical and
trigeminal motor patterns that act in a coordinated manner in the performance of
masticatory activities (chewing)[79–82], plus recent studies also support that the neck
muscles are activated during jaw-clenching tasks tasks assessed electromyographically
[83–85] and it seems that the activity of the neck muscles is increased as the demand for
masticatory work is greater[86]. Although most of these studies have been performed in
healthy subjects, we believe that these data are useful to try to explain some of the
results of this research. In this sense, we propose the theory that the masticatory motor
patterns are more altered with the presence of greater cervical pain or disability. This
situation would generate the activation of maladaptive compensatory mechanisms that
might alter the behaviour, recruitment and coordination of the neck and mandibular
motor systems, thus generating higher levels of fatigue and pain during the provocation
test and retaining these feelings 24 hours later.
This same theory could explain the results of decreased PPTs at the trigeminal and
cervical regions, noting that the PPTs changes were higher in the patient groups and that
most changes in the cervical PPTs at 24 hours occurred in the group of moderate
cervical disability. As a contributing factor to this situation, the presence of neck pain
must be considered, as this can lead to lower values of trigeminal PPTs compared to
healthy subjects [87]. Although we believe that there may be a direct relationship
between the trigeminal sensory-motor changes with cervical pain and disability, we
must also consider the possibility that the changes seen in patients would have been
mainly influenced by pre-established neuroplastic changes in the central nervous
system. Patients with chronic pain may be more susceptible to develop a central

22
sensitization process[88]. Wolf et al. suggest that in painful conditions where there is a
comorbidity, such as in the sample of patients in this study, it can be a determining
factor in the pathophysiology of central sensitization[89]. In relation to this, Gaff-
Radford proposed that in central sensitization, changes appear in afferent pathways that
enable the communication of cervical and orofacial nociceptive neurons in the
trigeminal nucleus[90]. In addition, there are many studies in TMD patients that have
found peripheral and central mechanisms compatible with a process of central
sensitization[91–97].
Influence of pain catastrophizing over trigeminal sensory-motor activity.
In this research, we have used self-reports of psychological and pain-related
variables to identify possible associations with sensory-motor variables. Through linear
regression analysis, we have observed that pain catastrophizing and the impact of
headache on the quality of life (HIT-6) were associated with the pain perception and
fatigue variables 24 hours after performing the masticatory provocation test.
Specifically, analysing the pain catastrophizing as a psychological factor resulted in a
predictor for fatigue at 24 hours after the test in the moderate cervical disability group,
and in the mild cervical disability group it was a predictor for perceived cervical
disability and fatigue after 24 hours. Pain catastrophizing is defined as a cognitive factor
that implies a mental negative perception or exaggeration of the perceived threat of
either a real or anticipated pain experience[98, 99]. It has been described that in patients
with TMD, catastrophizing contributes to the chronification of pain and disability [100].
It has also been associated with a greater use of health system services, with greater
clinical findings at assessment associated with a negative mood[40, 41] and with
alterations of the functional mandibular status[10]. Regarding the perceived fatigue and
pain catastrophizing, we did not find any clinical or experimental trials that have

23
examined their association in patients with craniofacial pain and TMD; but we found
one study researching the relationship of pain catastrophizing with masticatory
kinematic variables (i.e., amplitude, velocity, frequency cycle) which were measured
with a procedure using very short exposure times (15 seconds of chewing)[32]. In this
study, no associations of the kinematic variables measured with respect to catastrophism
were observed; however, we must take into account that the purpose of that study was
not to induce pain or fatigue to observe the response, as we did in this research. It is
important to note that a recent systematic review concluded that there is an association
between catastrophizing and fatigue and that the former influences the latter
proportionately; these results were observed in various clinical populations[101]. This
has also been demonstrated in other musculoskeletal disorders where pain
catastrophizing is associated with motor disturbances, such as decreased function,
performance of activities of daily living and limitation of exercise capacity[102–104].
The relationship between psychological factors, motor activity and pain seems to
be present in various cases of musculoskeletal pain, but the explanation for this is
complex and limited so far. Peck et al.[105] and Murray and Peck[106] have proposed a
possible explanation for this and have created a new Integrated Pain Adaptation Model
(IPAM). This model basically explains that the influence of pain on motor activity
depends on the interaction of multidimensional characteristics (biological and
psychosocial) of pain with the sensory-motor system of an individual, which results in a
new motor recruitment strategy in order to minimize pain. However, this motor
response may be associated with the appearance of another pain or worsening of the
existing pain[105, 106]. This model is based on the multidimensional features (sensory
discriminative, affective-emotional, cognitive) of the pain experience and how it affects
the sensory-motor system through the peripheral and central connections that this

24
system has with the autonomous nervous system, the limbic system and other higher
centres[105, 107].
Clinical and scientific implications
According to the results of this research, we found that neck pain and disability
can influence sensory and motor variables of the masticatory system. These findings
lead us to reflect on the importance of including a clinically specific assessment of the
cervical region in the diagnostic protocols for TMD and headache attributed to TMD. It
is noteworthy that the most commonly used diagnostic and classification methods for
patients with TMD do not include a specific assessment of neck pain and disability[20,
44, 108]. A diagnostic criterion observed recently in patients with headache attributed to
TMD is that mandibular movement, function or parafunction modify headache in the
temporal region[21]. We have observed an association between cervical disability with
pain-free MMO and have also found that patients with greater neck disability have
increased fatigue and pain induced by the masticatory test. These findings lead us to
assume that the cervical region may have an important role for this type of headache,
but this has to be confirmed in future research, as these data can be extrapolated only to
patients with this type of headache who also associate neck disability.
From the point of view of treatment, we propose an approach to reduce cervical
pain and disability as part of the overall therapeutic strategy, as this could be beneficial
to reduce the negative sensory symptoms and improve masticatory motor control. We
believe that this approach should be investigated in future studies, but it must be taken
into account that we have recent evidence that therapeutic exercise and manual therapy
to the cervical region produce positive effects on pain modulation in trigeminal areas
and improving pain-free MMO[46, 109].
25
In this study and other longitudinal or transversal studies, we have shown the
influence of psychosocial factors on patients with TMD[36, 110, 111]; specifically, our
results show an association between catastrophizing and perceived fatigue induced by
the masticatory activity. This finding shows the interaction between sensory-type
variables with psychological variables, which should be considered a crucial issue when
performing the assessment or designing of therapeutic interventions. In patients with
chronic pain, it is essential to recognize psychosocial factors that may be perceived as
obstacles to recovery[112]; achieving a reduction of pain catastrophizing is the best
predictor of successful rehabilitation in pain conditions[113].
The integration of a biopsychosocial perspective in clinical reasoning and
decision-making could be a key point in the management of pain and motor
rehabilitation of patients with headache attributed to TMD. It has been shown that
cognitive-behavioural therapy reduces pain intensity, depressive symptoms, improves
chewing function[114], reduces pain catastrophizing in patients with chronic TMD[115]
and, furthermore, it has been found that it causes neuroplastic adaptive changes
associated with decreased pain catastrophism in cases of chronic pain[116]. Prescribing
therapeutic exercise may be a good alternative to take into consideration; it has been
observed that exercise causes a reduction of catastrophizing and depressive symptoms;
these results were similar to cognitive behavioural therapy in patients with chronic
lower back pain[117].
Limitations
The results of this study should be discussed with the consideration that there are
several limitations. Although the sample size was calculated to have adequate power
and further losses were less than 20%, the results were not compared with a group with
26
headache attributed to TMD but without the presence of neck pain and disability. To
extrapolate the results to a clinical population would require similar but future studies to
be implemented using patient sample protocols with and without neck pain and
disability. Another limitation to consider is that pain catastrophizing was assessed as the
only psychological variable. It would be interesting to investigate the association of
other variables such as anxiety, depression, kinesiophobia and self-efficacy with
trigeminal sensory-motor variables.
As the only motor variable measured in this research was pain-free MMO, other
kinematic variables should be taken into consideration in future research as they may
provide more information. Moreover, we believe that measuring motor variables of the
cervical region could also be useful to analyse possible correlations with masticatory
variables.
CONCLUSION
The results of this study suggest that neck pain and disability have an influence
on the sensory-motor variables evaluated in patients with headache attributed to TMD.
In particular, it was observed that patients with moderate neck disability showed greater
changes immediately and 24 hours after the masticatory provocation test. Our data
provide new evidence about the possible neurophysiologic mechanisms of interaction
between the craniocervical region and the craniomandibular region. Regarding pain
catastrophizing, an association with perceived masticatory fatigue in both patient groups
was observed. These findings support the need to recognize the interaction between
sensory-motor and psychological aspects of headache attributed to TMD rather than
being assessed in isolation.

27
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
RL, AP, AG, JF participated in the study design, manuscript preparation and editing and
data acquisition. JP, SA, RL participated in the performed the statistical analysis,
database management and manuscript preparation. All authors read and approved the
final manuscript.
REFERENCES
1. Storm C, Wänman A (2006) Temporomandibular disorders, headaches, and cervical pain among females in a Sami population. Acta Odontol Scand 64:319–25. doi: 10.1080/00016350600801915
2. Anderson GC, John MT, Ohrbach R, et al. (2011) Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 152:765–71. doi: 10.1016/j.pain.2010.11.007
3. Rantala MA, Ahlberg J, Suvinen TI, et al. (2003) Temporomandibular joint related painless symptoms, orofacial pain, neck pain, headache, and psychosocial factors among non-patients. Acta Odontol Scand 61:217–222.
4. Ciancaglini R, Testa M, Radaelli G (1999) Association of neck pain with symptoms of temporomandibular dysfunction in the general adult population. Scand J Rehabil Med 31:17–22.
5. Nilsson I-M, List T, Drangsholt M (2013) Headache and co-morbid pains associated with TMD pain in adolescents. J Dent Res 92:802–7. doi: 10.1177/0022034513496255
6. Plesh O, Adams SH, Gansky S a (2011) Temporomandibular joint and muscle disorder-type pain and comorbid pains in a national US sample. J Orofac Pain 25:190–8.
7. Svensson P (2007) Muscle pain in the head: overlap between temporomandibular disorders and tension-type headaches. Curr Opin Neurol 20:320–325. doi: 10.1097/WCO.0b013e328136c1f9

28
8. Ashina S, Bendtsen L, Ashina M, et al. (2006) Generalized hyperalgesia in patients with chronic tension-type headache. Cephalalgia 26:940–948. doi: 10.1111/j.1468-2982.2006.01150.x
9. Leclerc A, Niedhammer I, Landre MF, et al. (1999) One-year predictive factors for various aspects of neck disorders. Spine (Phila Pa 1976) 24:1455–1462.
10. La Touche R, Pardo-Montero J, Gil-Martínez A, et al. (2014) Craniofacial pain and disability inventory (CF-PDI): development and psychometric validation of a new questionnaire. Pain Physician 17:95–108.
11. Olivo SA, Fuentes J, Major PW, et al. (2010) The association between neck disability and jaw disability. J Oral Rehabil 37:670–9. doi: 10.1111/j.1365-2842.2010.02098.x
12. Torisu T, Tanaka M, Murata H, et al. (2013) Modulation of neck muscle activity induced by intra-oral stimulation in humans. Clin Neurophysiol. doi: 10.1016/j.clinph.2013.10.018
13. Wang K, Sessle BJ, Svensson P, Arendt-Nielsen L (2004) Glutamate evoked neck and jaw muscle pain facilitate the human jaw stretch reflex. Clin Neurophysiol 115:1288–95. doi: 10.1016/j.clinph.2004.01.006
14. Svensson P, Wang K, Arendt-Nielsen L, et al. (2005) Pain effects of glutamate injections into human jaw or neck muscles. J Orofac Pain 19:109–18.
15. Ge H-Y, Wang K, Madeleine P, et al. (2004) Simultaneous modulation of the exteroceptive suppression periods in the trapezius and temporalis muscles by experimental muscle pain. Clin Neurophysiol 115:1399–408. doi: 10.1016/j.clinph.2004.01.017
16. Dessem D, Luo P (1999) Jaw-muscle spindle afferent feedback to the cervical spinal cord in the rat. Exp brain Res 128:451–9.
17. Hellström F, Thunberg J, Bergenheim M, et al. (2002) Increased intra-articular concentration of bradykinin in the temporomandibular joint changes the sensitivity of muscle spindles in dorsal neck muscles in the cat. Neurosci Res 42:91–9.
18. Hu JW, Sun K-Q, Vernon H, Sessle BJ (2005) Craniofacial inputs to upper cervical dorsal horn: implications for somatosensory information processing. Brain Res 1044:93–106. doi: 10.1016/j.brainres.2005.03.004
19. (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33:629–808. doi: 10.1177/0333102413485658
20. Schiffman E, Ohrbach R, Truelove E, et al. (2014) Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J oral facial pain headache 28:6–27.

29
21. Schiffman E, Ohrbach R, List T, et al. (2012) Diagnostic criteria for headache attributed to temporomandibular disorders. Cephalalgia 32:683–92. doi: 10.1177/0333102412446312
22. Winocur E, Gavish A, Finkelshtein T, et al. (2001) Oral habits among adolescent girls and their association with symptoms of temporomandibular disorders. J Oral Rehabil 28:624–9.
23. Gavish A, Halachmi M, Winocur E, Gazit E (2000) Oral habits and their association with signs and symptoms of temporomandibular disorders in adolescent girls. J Oral Rehabil 27:22–32.
24. Bevilaqua-Grossi D, Chaves TC, de Oliveira AS, Monteiro-Pedro V (2006) Anamnestic index severity and signs and symptoms of TMD. Cranio 24:112–8.
25. Wänman A, Agerberg G (1986) Relationship between signs and symptoms of mandibular dysfunction in adolescents. Community Dent Oral Epidemiol 14:225–30.
26. Mao J, Stein RB, Osborn JW (1993) Fatigue in human jaw muscles: a review. J Orofac Pain 7:135–42.
27. Svensson P, Graven-Nielsen T (2001) Craniofacial muscle pain: review of mechanisms and clinical manifestations. J Orofac Pain 15:117–145.
28. Lobbezoo F, van Selms MKA, Naeije M (2006) Masticatory muscle pain and disordered jaw motor behaviour: Literature review over the past decade. Arch Oral Biol 51:713–20. doi: 10.1016/j.archoralbio.2006.03.012
29. Kurita H, Ohtsuka A, Kurashina K, Kopp S (2001) Chewing ability as a parameter for evaluating the disability of patients with temporomandibular disorders. J Oral Rehabil 28:463–465.
30. De Leeuw R, Studts JL, Carlson CR (2005) Fatigue and fatigue-related symptoms in an orofacial pain population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:168–74. doi: 10.1016/j.tripleo.2004.03.001
31. Boggero IA, Kniffin TC, Leeuw R De, Carlson CR (2014) Fatigue Mediates the Relationship Between Pain Interference and Distress in Patients with Persistent Orofacial Pain. 28:38–45. doi: 10.11607/jop.1204
32. Brandini D a, Benson J, Nicholas MK, et al. (2011) Chewing in temporomandibular disorder patients: an exploratory study of an association with some psychological variables. J Orofac Pain 25:56–67.
33. Palla S (2011) Biopsychosocial pain model crippled? J Orofac Pain 25:289–90.
34. Gatchel RJ, Peng YB, Peters ML, et al. (2007) The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull 133:581–624. doi: 10.1037/0033-2909.133.4.581

30
35. List T, John MT, Ohrbach R, et al. (2012) Influence of temple headache frequency on physical functioning and emotional functioning in subjects with temporomandibular disorder pain. J Orofac Pain 26:83–90.
36. Fillingim RB, Ohrbach R, Greenspan JD, et al. (2011) Potential psychosocial risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J Pain 12:T46–60. doi: 10.1016/j.jpain.2011.08.007
37. Buenaver LF, Quartana PJ, Grace EG, et al. (2012) Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial temporomandibular disorder participants: the mediating role of sleep disturbance. Pain 153:1159–66. doi: 10.1016/j.pain.2012.01.023
38. Velly AM, Look JO, Carlson C, et al. (2011) The effect of catastrophizing and depression on chronic pain--a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 152:2377–83. doi: 10.1016/j.pain.2011.07.004
39. Quartana PJ, Buenaver LF, Edwards RR, et al. (2010) Pain catastrophizing and salivary cortisol responses to laboratory pain testing in temporomandibular disorder and healthy participants. J Pain 11:186–94. doi: 10.1016/j.jpain.2009.07.008
40. Turner JA, Brister H, Huggins K, et al. (2005) Catastrophizing is associated with clinical examination findings, activity interference, and health care use among patients with temporomandibular disorders. J Orofac Pain 19:291–300.
41. Turner JA, Dworkin SF, Mancl L, et al. (2001) The roles of beliefs, catastrophizing, and coping in the functioning of patients with temporomandibular disorders. Pain 92:41–51.
42. Von Elm E, Altman DG, Egger M, et al. (2008) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61:344–9. doi: 10.1016/j.jclinepi.2007.11.008
43. Dworkin SF, LeResche L (1992) Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 6:301–55.
44. Schiffman EL, Ohrbach R, Truelove EL, et al. (2010) The Research Diagnostic Criteria for Temporomandibular Disorders. V: methods used to establish and validate revised Axis I diagnostic algorithms. J Orofac Pain 24:63–78.
45. Vernon H, Mior S (1991) The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 14:409–15.
46. La Touche R, París-Alemany A, Mannheimer JS, et al. (2012) Does Mobilization of the Upper Cervical Spine Affect Pain Sensitivity and Autonomic Nervous System

31
Function in Patients With Cervico-craniofacial Pain?: A Randomized-controlled Trial. Clin J Pain. doi: 10.1097/AJP.0b013e318250f3cd
47. Karibe H, Goddard G, Gear RW (2003) Sex differences in masticatory muscle pain after chewing. J Dent Res 82:112–6.
48. Farella M, Bakke M, Michelotti A, Martina R (2001) Effects of prolonged gum chewing on pain and fatigue in human jaw muscles. Eur J Oral Sci 109:81–5.
49. Sullivan MJL, Bisop SC, Pivik J (1995) The pain catastrophizing scale: development and validation. Psychol Assess 7:524–532.
50. García Campayo J, Rodero B, Alda M, et al. (2008) [Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia]. Med Clin (Barc) 131:487–92.
51. Andrade Ortega JA, Delgado Martínez AD, Almécija Ruiz R (2010) Validation of the Spanish version of the Neck Disability Index. Spine (Phila Pa 1976) 35:E114–8.
52. Bjorner JB, Kosinski M, Ware JE (2003) Calibration of an item pool for assessing the burden of headaches: an application of item response theory to the headache impact test (HIT). Qual Life Res 12:913–33.
53. Gandek B, Alacoque J, Uzun V, et al. (2003) Translating the Short-Form Headache Impact Test (HIT-6) in 27 countries: methodological and conceptual issues. Qual Life Res 12:975–9.
54. Martin M, Blaisdell B, Kwong JW, Bjorner JB (2004) The Short-Form Headache Impact Test (HIT-6) was psychometrically equivalent in nine languages. J Clin Epidemiol 57:1271–8. doi: 10.1016/j.jclinepi.2004.05.004
55. Bijur PE, Silver W, Gallagher EJ (2001) Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med 8:1153–7.
56. Tseng BY, Gajewski BJ, Kluding PM (2010) Reliability, responsiveness, and validity of the visual analog fatigue scale to measure exertion fatigue in people with chronic stroke: a preliminary study. Stroke Res Treat. doi: 10.4061/2010/412964
57. Walton DM, Macdermid JC, Nielson W, et al. (2011) Reliability, standard error, and minimum detectable change of clinical pressure pain threshold testing in people with and without acute neck pain. J Orthop Sports Phys Ther 41:644–50. doi: 10.2519/jospt.2011.3666
58. Alacreu-Beltran H, Lopez-de-Uralde-Villanueva I, Paris-Alemany A, et al. (2014) Intra-rater and Inter-rater Reliability of Mandibular Range of Motion Measures Considering a Neutral Craniocervical Position. J Phys Ther Sci 26:1–6.

32
59. Faul F, Erdfelder E, Lang A-G, Buchner A (2007) G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39:175–91.
60. Cohen J. (1988) Statistical power analysis for the behavioral sciences. Hillsdale
61. Peduzzi P, Concato J, Kemper E, et al. (1996) A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol 49:1373–9.
62. Gavish A, Winocur E, Menashe S, et al. (2002) Experimental chewing in myofascial pain patients. J Orofac Pain 16:22–8.
63. Haggman-Henrikson B, Osterlund C, Eriksson P-O (2004) Endurance during Chewing in Whiplash-associated Disorders and TMD. J Dent Res 83:946–950. doi: 10.1177/154405910408301211
64. Dao TTT, Lund JP, Lavigne GJ (1994) Pain Responses to Experimental Chewing in Myofascial Pain Patients. doi: 10.1177/00220345940730060601
65. Van Selms MKA, Wang K, Lobbezoo F, et al. (2005) Effects of masticatory muscle fatigue without and with experimental pain on jaw-stretch reflexes in healthy men and women. Clin Neurophysiol 116:1415–23. doi: 10.1016/j.clinph.2005.02.017
66. Koutris M, Lobbezoo F, Naeije M, et al. (2009) Effects of intense chewing exercises on the masticatory sensory-motor system. J Dent Res 88:658–62. doi: 10.1177/0022034509338573
67. Christensen L V, Tran KT, Mohamed SE (1996) Gum chewing and jaw muscle fatigue and pains. J Oral Rehabil 23:424–37.
68. Plesh O, Curtis DA, Hall LJ, Miller A (1998) Gender difference in jaw pain induced by clenching. J Oral Rehabil 25:258–63.
69. Yokoyama T, Lisi TL, Moore SA, Sluka KA (2007) Muscle fatigue increases the probability of developing hyperalgesia in mice. J Pain 8:692–9. doi: 10.1016/j.jpain.2007.05.008
70. Stohler CS (1999) Craniofacial pain and motor function: pathogenesis, clinical correlates, and implications. Crit Rev Oral Biol Med 10:504–18.
71. Nicol C, Kuitunen S, Kyröläinen H, et al. (2003) Effects of long- and short-term fatiguing stretch-shortening cycle exercises on reflex EMG and force of the tendon-muscle complex. Eur J Appl Physiol 90:470–9. doi: 10.1007/s00421-003-0862-y
72. Svensson P, Burgaard A, Schlosser S (2001) Fatigue and pain in human jaw muscles during a sustained, low-intensity clenching task. Arch Oral Biol 46:773–7.

33
73. Cote JN, Hoeger Bement MK Update on the relation between pain and movement: consequences for clinical practice. Clin J Pain 26:754–62. doi: 10.1097/AJP.0b013e3181e0174f
74. Koutris M, Lobbezoo F, Sümer NC, et al. (2013) Is myofascial pain in temporomandibular disorder patients a manifestation of delayed-onset muscle soreness? Clin J Pain 29:712–6. doi: 10.1097/AJP.0b013e318270fa59
75. Fillingim RB, King CD, Ribeiro-Dasilva MC, et al. (2009) Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain 10:447–85. doi: 10.1016/j.jpain.2008.12.001
76. Eriksson P-O, Zafar H, Häggman-Henrikson B (2004) Deranged jaw-neck motor control in whiplash-associated disorders. Eur J Oral Sci 112:25–32.
77. Eriksson P-O, Häggman-Henrikson B, Zafar H (2007) Jaw-neck dysfunction in whiplash-associated disorders. Arch Oral Biol 52:404–8. doi: 10.1016/j.archoralbio.2006.12.016
78. Zafar H, Nordh E, Eriksson P-O (2006) Impaired positioning of the gape in whiplash-associated disorders. Swed Dent J 30:9–15.
79. Eriksson PO, Zafar H, Nordh E (1998) Concomitant mandibular and head-neck movements during jaw opening-closing in man. J Oral Rehabil 25:859–70.
80. Eriksson PO, Häggman-Henrikson B, Nordh E, Zafar H (2000) Co-ordinated mandibular and head-neck movements during rhythmic jaw activities in man. J Dent Res 79:1378–84.
81. Zafar H, Nordh E, Eriksson PO (2000) Temporal coordination between mandibular and head-neck movements during jaw opening-closing tasks in man. Arch Oral Biol 45:675–82.
82. La Touche R, París-Alemany A, Von Piekartz H, et al. (2011) The influence of cranio-cervical posture on maximal mouth opening and pressure pain threshold in patients with myofascial temporomandibular pain disorders. Clin J Pain 27:48–55. doi: 10.1097/AJP.0b013e3181edc157
83. Giannakopoulos NN, Hellmann D, Schmitter M, et al. (2013) Neuromuscular interaction of jaw and neck muscles during jaw clenching. J Orofac Pain 27:61–71.
84. Hellmann D, Giannakopoulos NN, Schmitter M, et al. (2012) Anterior and posterior neck muscle activation during a variety of biting tasks. Eur J Oral Sci 120:326–34. doi: 10.1111/j.1600-0722.2012.00969.x
85. Giannakopoulos NN, Schindler HJ, Rammelsberg P, et al. (2013) Co-activation of jaw and neck muscles during submaximum clenching in the supine position. Arch Oral Biol 58:1751–60. doi: 10.1016/j.archoralbio.2013.09.002

34
86. Häggman-Henrikson B, Nordh E, Eriksson P-O (2013) Increased sternocleidomastoid, but not trapezius, muscle activity in response to increased chewing load. Eur J Oral Sci 121:443–9. doi: 10.1111/eos.12066
87. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, et al. (2010) Bilateral mechanical-pain sensitivity over the trigeminal region in patients with chronic mechanical neck pain. J pain Off J Am Pain Soc 11:256–263.
88. Henry DE, Chiodo AE, Yang W (2011) Central nervous system reorganization in a variety of chronic pain states: a review. PM R 3:1116–25. doi: 10.1016/j.pmrj.2011.05.018
89. Woolf CJ (2011) Central sensitization: implications for the diagnosis and treatment of pain. Pain 152:S2–15. doi: 10.1016/j.pain.2010.09.030
90. Graff-Radford SB (2012) Facial pain, cervical pain, and headache. Continuum (Minneap Minn) 18:869–82. doi: 10.1212/01.CON.0000418648.54902.42
91. Ayesh EE, Jensen TS, Svensson P (2007) Hypersensitivity to mechanical and intra-articular electrical stimuli in persons with painful temporomandibular joints. J Dent Res 86:1187–92.
92. Anderson GC, John MT, Ohrbach R, et al. (2011) Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 152:765–771. doi: 10.1016/j.pain.2010.11.007
93. Park JW, Clark GT, Kim YK, Chung JW (2010) Analysis of thermal pain sensitivity and psychological profiles in different subgroups of TMD patients. Int J Oral Maxillofac Surg 39:968–74. doi: 10.1016/j.ijom.2010.06.003
94. Feldreich A, Ernberg M, Lund B, Rosén A (2012) Increased β-endorphin levels and generalized decreased pain thresholds in patients with limited jaw opening and movement-evoked pain from the temporomandibular joint. J Oral Maxillofac Surg 70:547–56. doi: 10.1016/j.joms.2011.09.013
95. Chaves TC, Nagamine HM, de Sousa LM, et al. (2013) Differences in pain perception in children reporting joint and orofacial muscle pain. J Clin Pediatr Dent 37:321–7.
96. Raphael KG, Janal MN, Anathan S, et al. (2009) Temporal summation of heat pain in temporomandibular disorder patients. J Orofac Pain 23:54–64.
97. Sarlani E, Grace EG, Reynolds MA, Greenspan JD (2004) Evidence for up-regulated central nociceptive processing in patients with masticatory myofascial pain. J Orofac Pain 18:41–55.
98. Turner JA, Aaron LA (2001) Pain-related catastrophizing: what is it? Clin J Pain 17:65–71.

35
99. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. (2001) Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 17:52–64.
100. Velly AM, Look JO, Carlson C, et al. (2011) The effect of catastrophizing and depression on chronic pain--a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 152:2377–83. doi: 10.1016/j.pain.2011.07.004
101. Lukkahatai N, Saligan LN (2013) Association of catastrophizing and fatigue: a systematic review. J Psychosom Res 74:100–9. doi: 10.1016/j.jpsychores.2012.11.006
102. Nijs J, Van de Putte K, Louckx F, et al. (2008) Exercise performance and chronic pain in chronic fatigue syndrome: the role of pain catastrophizing. Pain Med 9:1164–72.
103. Nijs J, Meeus M, Heins M, et al. (2012) Kinesiophobia, catastrophizing and anticipated symptoms before stair climbing in chronic fatigue syndrome: an experimental study. Disabil Rehabil 34:1299–305. doi: 10.3109/09638288.2011.641661
104. Meeus M, Nijs J, Van Mol E, et al. (2012) Role of psychological aspects in both chronic pain and in daily functioning in chronic fatigue syndrome: a prospective longitudinal study. Clin Rheumatol 31:921–9. doi: 10.1007/s10067-012-1946-z
105. Peck CC, Murray GM, Gerzina TM (2008) How does pain affect jaw muscle activity? The Integrated Pain Adaptation Model. Aust Dent J 53:201–7. doi: 10.1111/j.1834-7819.2008.00050.x
106. Murray GM, Peck CC (2007) Orofacial pain and jaw muscle activity: a new model. J Orofac Pain 21:263–78; discussion 279–88.
107. Craig AD (2003) A new view of pain as a homeostatic emotion. Trends Neurosci 26:303–7.
108. Benoliel R, Svensson P, Heir GM, et al. (2011) Persistent orofacial muscle pain. Oral Dis 17 Suppl 1:23–41. doi: 10.1111/j.1601-0825.2011.01790.x
109. La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, et al. (2009) The effects of manual therapy and exercise directed at the cervical spine on pain and pressure pain sensitivity in patients with myofascial temporomandibular disorders. J Oral Rehabil 36:644–52. doi: 10.1111/j.1365-2842.2009.01980.x
110. Fillingim RB, Ohrbach R, Greenspan JD, et al. (2013) Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain 14:T75–90. doi: 10.1016/j.jpain.2013.06.009
111. Chen H, Nackley A, Miller V, et al. (2013) Multisystem dysregulation in painful temporomandibular disorders. J Pain 14:983–96. doi: 10.1016/j.jpain.2013.03.011

36
112. Main CJ (2013) The importance of psychosocial influences on chronic pain. Pain Manag 3:455–66. doi: 10.2217/pmt.13.49
113. Sullivan MJ (2013) What is the clinical value of assessing pain-related psychosocial risk factors? Pain Manag 3:413–6. doi: 10.2217/pmt.13.55
114. Turner JA, Mancl L, Aaron LA (2006) Short- and long-term efficacy of brief cognitive-behavioral therapy for patients with chronic temporomandibular disorder pain: a randomized, controlled trial. Pain 121:181–94. doi: 10.1016/j.pain.2005.11.017
115. Turner JA, Mancl L, Aaron LA (2005) Brief cognitive-behavioral therapy for temporomandibular disorder pain: effects on daily electronic outcome and process measures. Pain 117:377–87. doi: 10.1016/j.pain.2005.06.025
116. Seminowicz DA, Shpaner M, Keaser ML, et al. (2013) Cognitive-Behavioral Therapy Increases Prefrontal Cortex Gray Matter in Patients With Chronic Pain. J Pain. doi: 10.1016/j.jpain.2013.07.020
117. Smeets RJEM, Vlaeyen JWS, Kester ADM, Knottnerus JA (2006) Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain 7:261–71. doi: 10.1016/j.jpain.2005.10.011

37
Figure 1. Data represent mean value and error bars with 95% confidence intervals of
the mean of the pain intensity score (A), and the visual analogue fatigue scale scores
(B). Recorded during the 6 min and 24 hours after provocation chewing test. Level of
significance (multiple comparisons for each group): Moderate disability, *P<0.05;
**P<0.01; Mild disability, °P<0.05; °°P<0.01; and Healthy, ^P<0.05; ^^P<0.01.
Figure 2. Comparison between groups of the pain intensity (A) and perceived fatigue
(B) immediately (6 min) and 24 hours after the provocation chewing test. Data represent
mean value, error bars with 95% confidence intervals of the mean and effect size (d).
Level of significance: *P<0.05; **P<0.01.

38
Table 1. Summary of Demographic, Pain and Psychological Variables
Moderate Neck Disability (N=41)
Mild Neck Disability (N=42)
Healthy (N=39)
t / F P Value
Variables Mean±SD Range Mean±SD Range Mean±SD Range Sex (female/male) 26/15 - 25/17 - 26/13 - - -
Weight (kg)
69.56±12.47 51-103 67.76±14.03 50-97 64.84±10.2 48-90 1.4 0.23
Heigth (cm)
167.56±12.4
7
152-183 165.54±12.09 150-185 169.97±8.51 156-189 1.98 0.14
Age (years)
44.31±10.9 22-59 40.95±12.89 19-60 40.61±10.01 30-65 1.3 0.27
Pain duration
(months)
19.73±12.66 6-60 22.19±13.36 6-48 - - -0.8 0.39
NDI (points) 17.58±2.69 15-24 11.42±2.48 7-14 - - 10.8 0.01
PCS (points) 17.09±3.75 7-23 15.8±4.02 7-22 5.46±1.75 2-9 143 0.01
HIT-6 (points) 55.31±4.9 49-65 53.16±4.74 43-59 - - 2 0.04
VAS (mm) 40.75±9.17 21-58 37.04±9.16 19-54 - - 1.8 0.06
Abbreviations: NDI, Neck Disability Index; PCS, Pain Catastrophizing Scale; HIT-6, headache impact test-6; Visual Analog Scale, VAS; SD, standard deviation
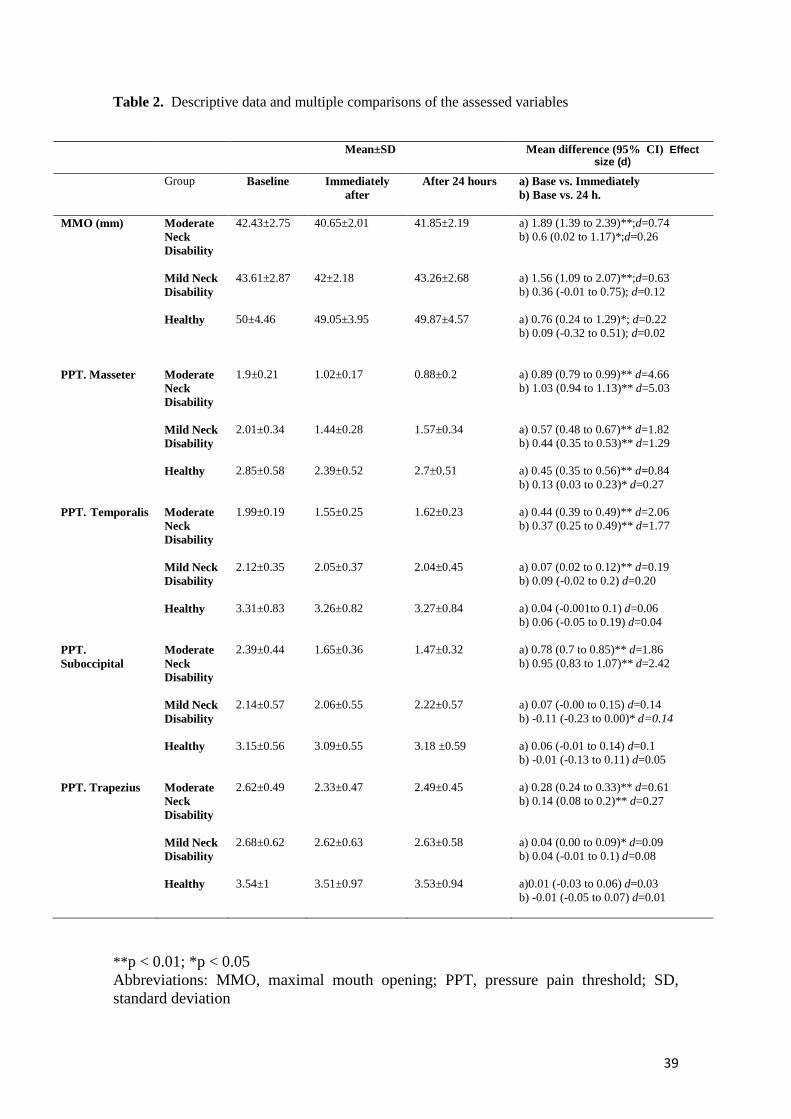
39
Table 2. Descriptive data and multiple comparisons of the assessed variables
** p < 0.01; *p < 0.05 Abbreviations: MMO, maximal mouth opening; PPT, pressure pain threshold; SD, standard deviation
Mean±SD Mean difference (95% CI) Effect size (d)
Group Baseline Immediately after
After 24 hours a) Base vs. Immediately b) Base vs. 24 h.
MMO (mm)
Moderate Neck Disability
42.43±2.75 40.65±2.01 41.85±2.19 a) 1.89 (1.39 to 2.39)**;d=0.74 b) 0.6 (0.02 to 1.17)*;d=0.26
Mild Neck Disability
43.61±2.87 42±2.18 43.26±2.68 a) 1.56 (1.09 to 2.07)**; d=0.63 b) 0.36 (-0.01 to 0.75); d=0.12
Healthy 50±4.46 49.05±3.95 49.87±4.57
a) 0.76 (0.24 to 1.29)*; d=0.22 b) 0.09 (-0.32 to 0.51); d=0.02
PPT. Masseter Moderate Neck Disability
1.9±0.21 1.02±0.17 0.88±0.2 a) 0.89 (0.79 to 0.99)** d=4.66 b) 1.03 (0.94 to 1.13)** d=5.03
Mild Neck Disability
2.01±0.34 1.44±0.28 1.57±0.34 a) 0.57 (0.48 to 0.67)** d=1.82 b) 0.44 (0.35 to 0.53)** d=1.29
Healthy 2.85±0.58 2.39±0.52 2.7±0.51
a) 0.45 (0.35 to 0.56)** d=0.84 b) 0.13 (0.03 to 0.23)* d=0.27
PPT. Temporalis Moderate Neck Disability
1.99±0.19 1.55±0.25 1.62±0.23 a) 0.44 (0.39 to 0.49)** d=2.06 b) 0.37 (0.25 to 0.49)** d=1.77
Mild Neck Disability
2.12±0.35 2.05±0.37 2.04±0.45 a) 0.07 (0.02 to 0.12)** d=0.19 b) 0.09 (-0.02 to 0.2) d=0.20
Healthy 3.31±0.83 3.26±0.82 3.27±0.84
a) 0.04 (-0.001to 0.1) d=0.06 b) 0.06 (-0.05 to 0.19) d=0.04
PPT. Suboccipital
Moderate Neck Disability
2.39±0.44 1.65±0.36 1.47±0.32 a) 0.78 (0.7 to 0.85)** d=1.86 b) 0.95 (0.83 to 1.07)** d=2.42
Mild Neck Disability
2.14±0.57 2.06±0.55 2.22±0.57 a) 0.07 (-0.00 to 0.15) d=0.14 b) -0.11 (-0.23 to 0.00)* d=0.14
Healthy 3.15±0.56
3.09±0.55 3.18 ±0.59
a) 0.06 (-0.01 to 0.14) d=0.1 b) -0.01 (-0.13 to 0.11) d=0.05
PPT. Trapezius Moderate Neck Disability
2.62±0.49 2.33±0.47 2.49±0.45 a) 0.28 (0.24 to 0.33)** d=0.61 b) 0.14 (0.08 to 0.2)** d=0.27
Mild Neck Disability
2.68±0.62 2.62±0.63 2.63±0.58 a) 0.04 (0.00 to 0.09)* d=0.09 b) 0.04 (-0.01 to 0.1) d=0.08
Healthy 3.54±1 3.51±0.97 3.53±0.94 a)0.01 (-0.03 to 0.06) d=0.03 b) -0.01 (-0.05 to 0.07) d=0.01
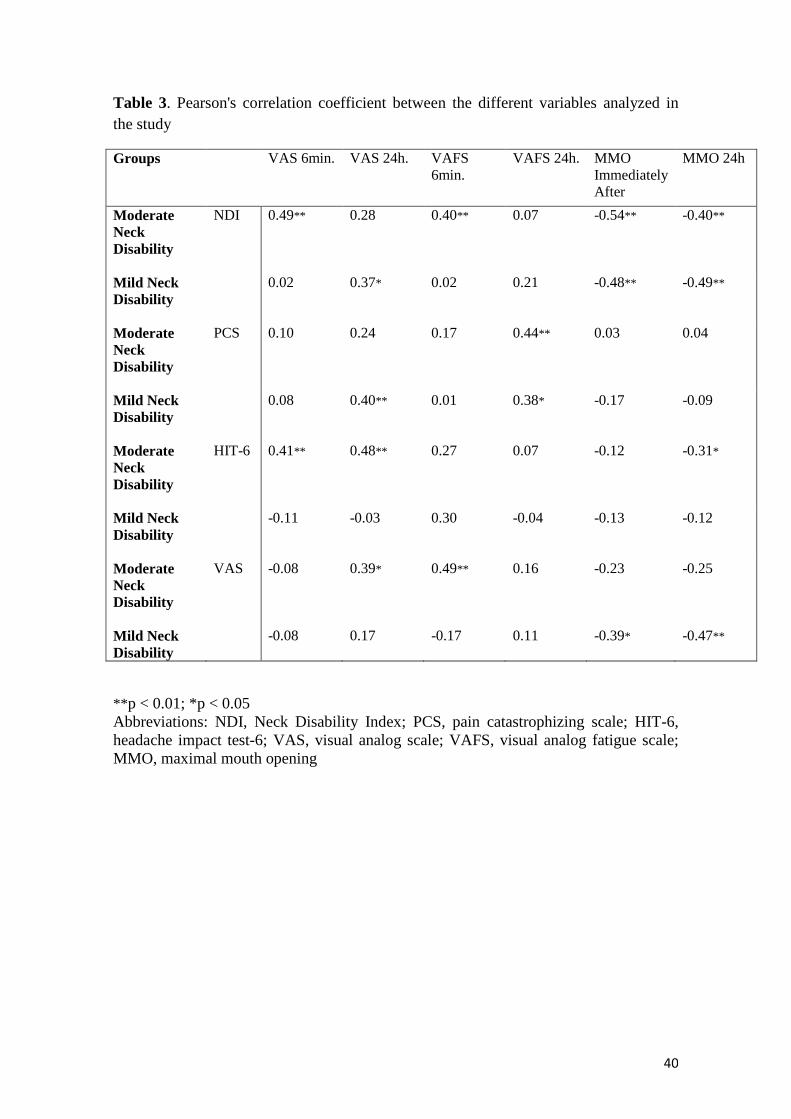
40
Table 3. Pearson's correlation coefficient between the different variables analyzed in the study
Groups VAS 6min. VAS 24h. VAFS 6min.
VAFS 24h. MMO Immediately After
MMO 24h
Moderate Neck Disability
NDI 0.49** 0.28 0.40** 0.07 -0.54** -0.40**
Mild Neck Disability
0.02 0.37* 0.02 0.21 -0.48** -0.49**
Moderate Neck Disability
PCS 0.10 0.24 0.17 0.44** 0.03 0.04
Mild Neck Disability
0.08 0.40** 0.01 0.38* -0.17 -0.09
Moderate Neck Disability
HIT-6 0.41** 0.48** 0.27 0.07 -0.12 -0.31*
Mild Neck Disability
-0.11 -0.03 0.30 -0.04 -0.13 -0.12
Moderate Neck Disability
VAS -0.08 0.39* 0.49** 0.16 -0.23 -0.25
Mild Neck Disability
-0.08 0.17 -0.17 0.11 -0.39* -0.47**
** p < 0.01; *p < 0.05 Abbreviations: NDI, Neck Disability Index; PCS, pain catastrophizing scale; HIT-6, headache impact test-6; VAS, visual analog scale; VAFS, visual analog fatigue scale; MMO, maximal mouth opening

41
Table 4. Multiple linear regression analysis
Moderate Neck Disability
criterion variable
predictor variables
Regression coefficient (B)
Standardized coefficient (β)
Significance (p)
VIF Adjusted R2
VAFS24 PCS 0.84 0.44 0.004 1.00 0.17
VAS24 HIT-6 0.93 0.48 0.001 1.00 0.22
MMO24 NDI -0.35 -0.40 0.01 1.12 0.14
Mild Neck Disability
VAFS24 PCS 0.98 0.38 0.013 1.00 0.12
VAS24 PCS 0.67 0.40 0.009 1.00 0.14
MMO24 NDI -0.53 -0.49 0.001 1.00 0.21
Abbreviations: NDI, Neck Disability Index; PCS, pain catastrophizing scale; HIT-6, headache impact test-6; VAS, visual analog scale; VAFS, visual analog fatigue scale; MMO, maximal mouth opening; 24, 24 hours after of tests
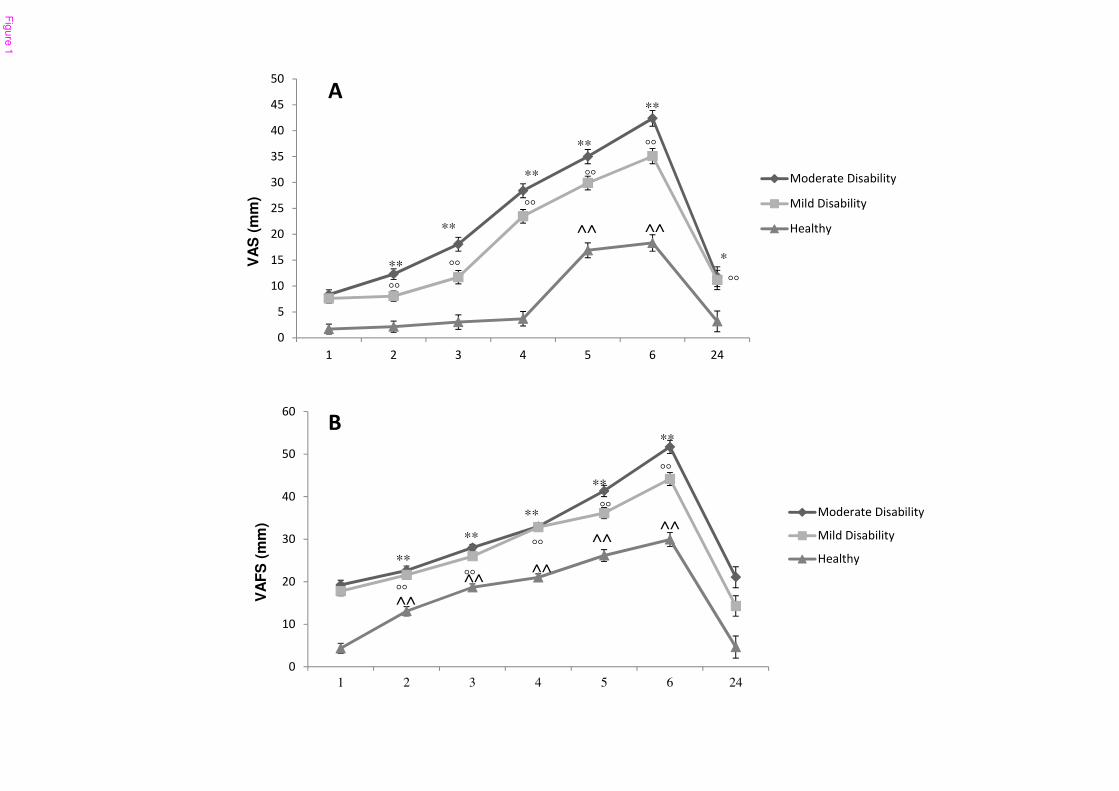
�
��
��
��
��
��
��
1 2 3 4 5 6 24
VA
FS
(m
m)
∆�� ������ ������
∆������ ������
,� ����
�
�
��
��
��
��
��
��
��
��
��
� � � � � � ��
VA
S (
mm
)
∆�� ������ ������
∆������ ������
,� ����
**
**
**
**
**
*
��
��
��
��
��
��
^^ ^^
**
**
**
**
**
��
��
��
��
��
^^
^^^^
^^^^
�
�
Fig
ure
1

0
5
10
15
20
25
30
35
40
45
50
6 24
VA
S (
mm
)
Time: 6 min and 24 hours
Moderate Disability
Mild Disability
Healthy
�
** (d=3.5)
** (d=1.22)
** (d=2.93) ** (d=1.54)
(d=0.27)
** (d=1.59)
�
0
10
20
30
40
50
60
6 24
VA
FS
(m
m)
Time: 6 min and 24 hours
Moderate Disability
Mild Disability
Healthy
** (d=3.16)
** (d=1.15)
** (d=3.47) ** (d=2.47)
** (d=0.69)
** (d=1.17)
Fig
ure
2
182
5.6 Estudio VI
La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K, Angulo-Díaz-
Parreño S, Paris-Alemany A, Cleland JA. The effects of manual therapy and exercise directed at
the cervical spine on pain and pressure pain sensitivity in patients with myofascial
temporomandibular disorders. J Oral Rehabil. 2009 Sep;36(9):644-52.
Objetivos del estudio
Nuestro objetivo fue investigar los efectos de la terapia manual y el ejercicio dirigido a la
columna cervical en la intensidad del dolor, la MAI y los UDPs de músculos masticatorios en
pacientes con TCM.
Resultados
El modelo mixto de ANOVA 2X3 reveló un efecto significativo en el factor tiempo (F = 77,8; P
<0,001), pero no para el factor lado (F = 0,2; P = 0,7) para los cambios en los UDPs sobre el
músculo masetero y más músculo temporal (tiempo: F = 66,8; P <0,001; lado: F = 0,07; P =
0,8). Las pruebas post hoc revelaron diferencias significativas entre pre-intervención y la post-
intervención y período de seguimiento (P <0,001), pero no entre la post-intervención y el
periodo seguimiento (P = 0,9) para ambos músculos. Los tamaños del efecto eran grandes (d>
1,0) para ambos períodos de seguimiento en los UDPS musculares. El ANOVA encontró un
efecto significativo de tiempo (F = 78,6; P <0,001) los cambios en la intensidad del dolor y la
MAI sin dolor (F = 17,1; P <0,001). Se encontraron diferencias significativas entre la pre-
intervención y dos periodos post-intervención (P <0.001), pero no entre la medida post-
intervención y el periodo de seguimiento (P> 0.7). Dentro del grupo tamaños del efecto eran
grandes (d> 0,8) para los resultados post-intervención y los períodos de seguimiento.
Conclusión
La aplicación de tratamiento dirigido a la columna vertebral cervical puede ser beneficioso en la
disminución de la intensidad del dolor, el aumento de los UDPS en los músculos de la
masticación y en la MAI libre de dolor en pacientes con TCM.

The effects of manual therapy and exercise directed at the
cervical spine on pain and pressure pain sensitivity in
patients with myofascial temporomandibular disorders
R. LA TOUCHE*, †, C. FERNANDEZ-DE-LAS-PENAS‡, §, J . FERNANDEZ-CARNERO‡, §,
K. ESCALANTE¶, S. ANGULO-DIAZ-PARRENO†, A. PARIS-ALEMANY† &
J. A. CLELAND** , ††, ‡‡*Faculty of Medicine, Department of Physical Therapy, Universidad San Pablo CEU, Madrid, †University
Center for Clinical Research of the Craneal-Cervical-Mandibular System of Universidad San Pablo CEU, Madrid, ‡Department of Physical
Therapy, Occupational Therapy, Rehabilitation and Physical Medicine, Universidad Rey Juan Carlos, Alcorcon, Madrid, §Esthesiology
Laboratory of Universidad Rey Juan Carlos, Alcorcon, Madrid, ¶Faculty of Psychology, Department of Personality Assessment and Psychology
Treatment, Universidad Complutense, Madrid, Spain, **Department of Physical Therapy, Franklin Pierce University, Concord, ††Physical
Therapist, Rehabilitation Services, Concord Hospital, Concord, NH and ‡‡Faculty, Manual Therapy Fellowship Program, Regis University,
Denver, CO, USA
SUMMARY No studies have investigated the effects of
the treatments directed at the cervical spine in
patients with temporomandibular disorders (TMD).
Our aim was to investigate the effects of joint
mobilization and exercise directed at the cervical
spine on pain intensity and pressure pain sensitivity
in the muscles of mastication in patients with TMD.
Nineteen patients (14 females), aged 19–57 years,
with myofascial TMD were included. All patients
received a total of 10 treatment session over a 5-
week period (twice per week). Treatment included
manual therapy techniques and exercise directed at
the cervical spine. Outcome measures included
bilateral pressure pain threshold (PPT) levels over
the masseter and temporalis muscles, active pain-
free mouth opening (mm) and pain (Visual Ana-
logue Scale) and were all assessed pre-intervention,
48 h after the last treatment (post-intervention) and
at 12-week follow-up period. Mixed-model ANOVAS
were used to examine the effects of the intervention
on each outcome measure. Within-group effect sizes
were calculated in order to assess clinical effect. The
2 · 3 mixed model ANOVA revealed significant effect
for time (F = 77Æ8; P < 0Æ001) but not for side (F = 0Æ2;
P = 0Æ7) for changes in PPT over the masseter muscle
and over the temporalis muscle (time: F = 66Æ8;
P < 0Æ001; side: F = 0Æ07; P = 0Æ8). Post hoc revealed
significant differences between pre-intervention
and both post-intervention and follow-up periods
(P < 0Æ001) but not between post-intervention and
follow-up period (P = 0Æ9) for both muscles. Within-
group effect sizes were large (d > 1Æ0) for both
follow-up periods in both muscles. The ANOVA
found a significant effect for time (F = 78Æ6;
P < 0Æ001) for changes in pain intensity and active
pain-free mouth opening (F = 17Æ1; P < 0Æ001). Sig-
nificant differences were found between pre-inter-
vention and both post-intervention and follow-up
periods (P < 0Æ001) but not between the post-
intervention and follow-up period (P > 0Æ7).
Within-group effect sizes were large (d > 0Æ8) for
both post-intervention and follow-up periods. The
application of treatment directed at the cervical
spine may be beneficial in decreasing pain intensity,
increasing PPTs over the masticatory muscles and an
increasing pain-free mouth opening in patients with
myofascial TMD.
KEYWORDS: cervical spine, temporomandibular dis-
order, pressure pain sensitivity
Accepted for publication 25 June 2009
ª 2009 Blackwell Publishing Ltd doi: 10.1111/j.1365-2842.2009.01980.x
Journal of Oral Rehabilitation 2009 36; 644–652

Introduction
Temporomandibular disorder (TMD) is a term which
includes several conditions involving the temporoman-
dibular joint and the muscles of mastication. The most
common symptoms of TMD include pain located over
the facial region and tenderness to palpation of the
masticatory structures. Some studies have shown
prevalence rate of TMD to be between 3% and 15%
in the Western population (1), with an incidence
between 2% and 4% (2). A recent survey determined
that the overall prevalence of TMD was 6Æ3% for
women and 2Æ8% for men (3).
It appears that an intimate functional relationship
exists between the mandibular and the head-neck
systems, as suggested by their anatomical and bio-
mechanical inter-relationships, although current
evidence is conflicting (4). Several epidemiological
studies have reported that patients with TMD often
experience symptoms of neck pain and that patients
with neck pain also suffered from symptoms in the
orofacial region (5–8). In addition, Eriksson et al. (9)
reported that mouth opening was accompanied by
head-neck extension and mouth closing by head-neck
flexion, with a precise temporal coordination between
jaw-neck movements dependent on the speed of the
movement (10).
The neuro-anatomical basis for the relationship
between the head and neck may be related to the
trigemino-cervical nucleus caudalis in the spinal grey
matter of the spinal cord at the C1–C3 level, where
there is a convergence on the nociceptive second order
neurons receiving trigeminal and cervical inputs (11).
The topographic arrangement of the trigeminal nucleus
caudalis allows the interchange of nociceptive infor-
mation between the cervical spine and the trigeminal
nerve (12). Studies have demonstrated that stimulation
of trigeminal-innervated structures evoked painful
sensations in the neck and vice versa (13, 14). In
addition, it has been reported that injection of an
inflammatory irritant into deep paraspinal tissues
results in a sustained activation of both jaw and neck
muscles (15, 16).
Several localized therapeutic modalities are often
used in the management of TMD, including mobiliza-
tion (17–19) or exercises (20, 21) of the temporoman-
dibular joint. As there is a connection between the neck
and the temporomandibular region, it can be hypo-
thesized that interventions targeted to the cervical spine
may also have an effect on patients with TMD.
Catanzariti et al. (22) suggested that neck pain patients
may respond to intervention applied to the temporo-
mandibular joint and that techniques applied to the
cervical spine may also have effect on the temporo-
mandibular system. To the best of our knowledge no
previous studies have investigated the effects of treat-
ment directed solely at the cervical spine in patients
with TMD. The purpose of this study was to investigate
the effects of joint mobilization directed at the cervical
spine plus an exercise protocol targeting the deep
cervical flexor muscles on intensity of pain and pressure
pain sensitivity in the muscles of mastication in patients
with myofascial TMD.
Materials and methods
Patients
Consecutive patients referred from four private dental
clinics between October 2007 and June 2008 partici-
pated in this study. Participants were eligible to partic-
ipate if they met the following criteria: (i) a primary
diagnosis of myofascial pain according to Axis I,
category Ia and Ib (i.e. myofascial pain with or without
limited opening) of the Research Diagnostic Criteria for
TMD (RDC ⁄ TMD) (23); (ii) bilateral pain involving the
masseter and temporal regions; (iii) presence of at least
one trigger point (TrP) in the masseter or temporalis
muscles; (iv) pain symptoms history of at least the
3 months previous to the study; and (v) intensity of the
pain of at least 30 mm on a 100 mm Visual Analogue
Scale (VAS). Trigger points were diagnosed following
the criteria described by Simons et al. (24): (i) presence
of a palpable taut band in a skeletal muscle; (ii)
presence of a hypersensitive tender spot within the
taut band; (iii) local twitch response elicited by the
snapping palpation of the taut band; and (iv) repro-
duction of the referred pain pattern of the TrP in
response to palpation. These criteria have demonstrated
good inter-examiner reliability (j) ranging from 0Æ84 to
0Æ88 (25).
Participants were excluded if they presented with any
of the following: (i) sign or symptoms of disc displace-
ment, arthrosis, or arthritis of the temporomandibular
joint, according to categories II and III of the
RDC ⁄ TMD; (ii) history of traumatic injuries (e.g.
fracture, whiplash); (iii) fibromyalgia syndrome (26);
(iv) diagnosis of systemic disease (rheumatoid arthritis,
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 645
ª 2009 Blackwell Publishing Ltd

systemic lupus erythematosus, or psoriatic arthritis); (v)
presence of neurological disorders (e.g. trigeminal
neuralgia); (vi) concomitant diagnosis of any primary
headache (tension-type headache or migraine); (vii)
subjects who had received any form of treatment
(physiotherapy, splint therapy and acupuncture) with-
in 3 months of the study. The study was conducted in
accordance with the Helsinki Declaration, and all
participants provided informed consent which was
approved by the local ethics committee.
Pain intensity
The VAS was used to record the patient’s level of pain at
baseline, 48 h after the last treatment (post-interven-
tion) and at 12-week follow-up period. The VAS is a
10 cm line anchored with a ‘0’ at one end representing
‘no pain’ and ‘10’ at the other end representing ‘the
worst pain imaginable’. Patients placed a mark along
the line corresponding to the intensity of their symp-
toms, which was scored to the nearest millimetre. The
VAS has been shown to be a reliable and valid
instrument for measuring pain intensity (27). It exhib-
its a minimal clinically important difference (MCID)
between 9 and 11 mm (28, 29).
Pressure pain threshold assessment
Pressure pain threshold (PPT) is defined as the amount
of pressure where the sense of pressure first changes to
pain (30). A mechanical pressure algometer (Pain
Diagnosis and Treatment Inc, Great Neck, NY, USA)
was used. This device consisted of a round rubber disc
(1 cm2) attached to a pressure (force) gauge. The gauge
displayed values in kilograms. As the surface of the
rubber tip was 1 cm2, the readings were expressed in
kg cm)2. The mean of three trials (intra-examiner
reliability) was calculated and used for the main
analysis. A 30-second resting period was allowed
between trials. The reliability of pressure algometry
was found to be high (ICC = 0Æ91 [95% confidence
intervals (CI): 0Æ82–0Æ97] (31). Pressure pain threshold
was assessed over bilateral masseter and the temporalis
muscles. The masseter point was located 1 cm superior
and 2 cm anterior from the mandibular angle, and the
temporal point was located on the anterior fibres of
temporal muscle, 2 cm above the zygomatic arch in the
middle part between lateral edge of the eye and the
anterior part of the helix. Pressure pain threshold levels
were assessed at pre-intervention, 48 h after the last
treatment (post-intervention) and at 12-week follow-
up period.
Active pain-free mouth opening
In a supine position, participants were asked to ‘open
the mouth as wide as possible without causing pain’. At
the end position of pain-free mouth opening, the
distance between upper-lower central incisors was
measured in millimetres. The intra-tester reliability of
this procedure was found to be high (ICC = 0Æ9–0Æ98)
(32). The mean of three trials was calculated and used
for the main analysis. Active pain-free mouth opening
was assessed pre-intervention, 48 h after the last
treatment (post-intervention) and at 12-week follow-
up period.
Treatment protocol
The treatment protocol included only interventions
directed at the cervical spine. The treatment techniques
were applied by the same physical therapist with
6 years of experience specializing in manipulative
therapy. All patients received a total of 10 sessions
over a 5-week period (twice a week). During the 10
treatment sessions all patients were treated with the
following techniques:
1 Upper cervical flexion mobilization: The patient was
supine with the cervical spine in a neutral position. The
therapist brought about a contact of the occipital bone
with the first finger and medial aspect of the hand, and
other hand over the frontal region of the patient’s head.
The mobilizing force was delivered by flexing the upper
cervical region using a combination of cephalic traction
with the occipital hand and caudal pressure with the
frontal hand (Fig. 1). The mobilization was applied at a
slow rate of one oscillation per 2 s (0Æ5 Hz) for a total
time of 10 min. This rate of mobilization was previously
used in another study (33).
2 C5 central posterior-anterior mobilization (34): The
patient was prone with the cervical spine in a neutral
position. The therapist placed the tips of his thumbs on
the posterior surface of the C5 spinous process, while the
other fingers rested gently around the patients’ neck
(Fig. 2). A grade III (large amplitude movement that
moved into the resistance limiting the range of move-
ment) posterior-anterior technique was applied centrally
to the C5 spinous process. The mobilization was applied
R . L A T O U C H E et al.646
ª 2009 Blackwell Publishing Ltd

at a rate of two oscillations per second (2 Hz). The
mobilizations were performed for a total of 9 min,
divided into 3-min intervalswith a 1 min rest in between.
3 Cranio-cervical flexor stabilization exercise: With the
aim to focus on the deep flexor muscles of the cervical
region, we followed the protocol described by Jull et al.
(35). Patients performed a cranio-cervical flexion exer-
cise in the supine position, which involved flexion of
the cranium (head) on the cervical spine (neck) while
ensuring that the back of the head remained in contact
with the supporting surface, in an effort to facilitate
activation of the deep cranio-cervical flexor muscula-
ture (particularly the longus capitis muscle) with
minimal activity of the superficial cervical flexors
(sternocleidomastoid and scalene muscles) (Fig. 3).
The contraction was graded through feedback from a
pressure biofeedback device (Stabilizer; Chattanooga
Group Inc., Chattanooga, TN, USA) that monitored the
flattening of the cervical lordosis due to the cranio-
cervical flexion movement from contraction of the deep
cervical flexor muscles (36). Falla et al. (37) demon-
strated that the cranio-cervical flexion test was accom-
panied by increased electromyographic activity in the
deep cervical flexor muscles. Additionally, increases in
the electromyographic activity of the deep cervical
flexors did not occur during other neck or jaw move-
ments, supporting the specificity of this test (38).
Patients first performed the correct cranio-cervical
flexion action with the following instructions: gently
nod your head as though you were saying ‘yes’ (Fig. 3).
The therapist monitored the superficial muscles by
palpation and identified the target level of the biofeed-
back where the patient could hold 10 s without use of
superficial neck flexor muscles, and without a quick or
jerky movement. Once the subject could perform the
movement correctly, the target level was established
and training began at this point. The baseline pressure
in the biofeedback device was 20 mmHg and the
patient was instructed to contract the deep neck flexors
to reach five pressure targets in increments of 2 mmHg
(35). The pressure increments were determined by
the level the patient could hold comfortably while
Fig. 1. Upper cervical flexion mobilization. Within one hand over
the occipital bone and the other hand over the frontal region of
the patient’s head, the therapist applies a mobilization force
inducing an upper cervical flexion using a combination of cephalic
traction with the occipital hand and caudal pressure with the
frontal hand.
Fig. 2. C5 central posterior-anterior mobilization. The therapist
placed the thumbs over the posterior surface of the C5 spinous
process and a posterior-anterior mobilization force is applied.
Fig. 3. Cranio-cervical flexor stabilization exercise.
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 647
ª 2009 Blackwell Publishing Ltd

maintaining a 10-second contraction with no pain.
Participants sustained the contraction for 10 repetitions
of 10-second duration, with a 10-second rest interval
between each contraction. Once this target was
achieved, the exercise progressed to the next pressure
target, repeating the process at the new pressure target,
first increasing the holding time and then the repeti-
tions. This exercise protocol has been used in previous
studies in patients with neck pain (39–41).
Statistical analysis
Statistical analysis was conducted with the SPSS 14.5
package.* Mean, s.d., or 95% CI of the values were
presented. The Kolmogorov–Smirnov test showed a
normal distribution of the data (P > 0Æ05). A 2 · 3
mixed model analysis of variance (ANOVA) with time
(pre-intervention, post-intervention and follow-up)
and side (right or left) as the within-subjects variables
was used to examine the effects of the treatment on PPT
over the masseter or the temporalis muscles. A one-way
repeated measure ANOVA with time (pre-intervention,
post-intervention and follow-up) as within-subject
variable was used to investigate the effects of the
treatment on spontaneous pain and active mouth
opening. The Bonferroni test was used for post hoc
analysis. Within-group effect size was calculated using
Cohen’s coefficient (d) (42). An effect size greater than
0Æ8 was considered large; around 0Æ5, moderate; and less
than 0Æ2, small. A P-value less than 0Æ05 was considered
as statistically significant for all analyses.
Results
A total of 19 patients, 14 females and 5 males, aged 19–
57 years old (mean age � s.d.: 37 � 10 years) partici-
pated. All subjects were right hand dominant. None of
the patients started drug therapy during the time of the
study. In this sample of patients with TMD the average
duration of symptoms was 9Æ2 months (95% CI: 7Æ7–
10Æ6 months), and the mean intensity of spontaneous
pain was 55Æ53 (95% CI: 51Æ4–59Æ6).
Pressure pain threshold levels
The 2 · 3 mixed model ANOVA revealed a significant
effect for time (F = 77Æ8; P < 0Æ001) but not for side
(F = 0Æ2; P = 0Æ7) for changes in PPT over the masseter
muscle. Post hoc testing revealed significant differences
between pre-intervention and both post-intervention
and follow-up periods (P < 0Æ001). However, no signif-
icant difference was identified between the post-inter-
vention and follow-up period (P = 0Æ9) for both
masseter muscles. Within-group effect sizes were large
(d > 1Æ0) for both follow-up periods in bilateral masse-
ter muscles. Table 1 details pre-intervention, post-
intervention, follow-up, and change scores of PPT
levels bilateral in both masseter and temporalis
muscles.
The mixed model ANOVA also found a significant effect
for time (F = 66Æ8; P < 0Æ001) but not for side (F = 0Æ07;
P = 0Æ8) for changes in PPT levels over the temporalis
muscle. The post hoc analysis found significant differ-
ences between pre-intervention and both post-inter-
vention and follow-up periods (P < 0Æ001). However,
no significant difference was identified between the
Table 1. Changes in pressure pain thresholds (kg cm)2) over the
masseter and temporalis muscles
Pressure pain threshold (kg cm)2)
in the right masseter muscle
Pre-intervention 2Æ8 � 0Æ7 (2Æ5 ⁄ 3Æ1)
Post-intervention 3Æ9 � 0Æ5 (3Æ7 ⁄ 4Æ2)
Follow-up 3Æ9 � 0Æ6 (3Æ6 ⁄ 4Æ2)
Pre- ⁄ post-differences 1Æ1 � 0Æ8 (0Æ8 ⁄ 1Æ6)
Pre ⁄ follow-up differences 1Æ1 � 0Æ7 (0Æ7 ⁄ 1Æ4)
Pressure pain threshold (kg cm)2)
in the left masseter muscle
Pre-intervention 2Æ3 � 0Æ6 (1Æ9 ⁄ 2Æ6)
Post-intervention 3Æ6 � 0Æ8 (3Æ4 ⁄ 3Æ9)
Follow-up 3Æ5 � 0Æ7 (3Æ1 ⁄ 3Æ8)
Pre- ⁄ post-differences 1Æ3 � 0Æ7 (1Æ0 ⁄ 1Æ6)
Pre ⁄ follow-up differences 1Æ2 � 0Æ8 (0Æ8 ⁄ 1Æ5)
Pressure pain threshold (kg cm)2)
in the right temporalis muscle
Pre-intervention 2Æ4 � 0Æ6 (2Æ1 ⁄ 2Æ7)
Post-intervention 3Æ7 � 0Æ5 (3Æ4 ⁄ 3Æ9)
Follow-up 3Æ5 � 0Æ7 (3Æ2 ⁄ 3Æ8)
Pre- ⁄ post-differences 1Æ3 � 0Æ7 (0Æ9 ⁄ 1Æ6)
Pre ⁄ follow-up differences 1Æ1 � 0Æ7 (0Æ7 ⁄ 1Æ4)
Pressure pain threshold (kg cm)2)
in the left temporalis muscle
Pre-intervention 3Æ0 � 0Æ7 (2Æ7 ⁄ 3Æ3)
Post-intervention 3Æ9 � 0Æ6 (3Æ6 ⁄ 4Æ2)
Follow-up 4Æ0 � 0Æ6 (3Æ6 ⁄ 4Æ3)
Pre- ⁄ post-differences 0Æ9 � 1Æ0 (0Æ4 ⁄ 1Æ4)
Pre ⁄ follow-up differences 1Æ0 � 0Æ8 (0Æ6 ⁄ 1Æ4)
Scores are expressed as mean � s.d. (95% confidence interval).*SPSS, Chicago, IL, USA.
R . L A T O U C H E et al.648
ª 2009 Blackwell Publishing Ltd

post-intervention and follow-up period (P = 0Æ9) for
both muscles. Within-group effect sizes were large
(d > 0Æ9) for both follow-up periods in bilateral tempo-
ralis muscles.
Pain
The ANOVA found a significant effect for time (F = 78Æ6;
P < 0Æ001) for changes in pain. Post hoc revealed
significant differences between pre-intervention and
both post-intervention and follow-up periods
(P < 0Æ001). However, no significant difference was
identified between the post-intervention and follow-up
period (P = 0Æ9). Within-group effect sizes were large
(d > 3Æ0) for both post-intervention and follow-up
periods. Table 2 shows pre-intervention, post-interven-
tion, follow-up and differences in scores of pain.
Active pain-free mouth opening
The ANOVA found a significant effect for time (F = 17Æ1;
P < 0Æ001) for changes in active mouth opening. Post
hoc analysis found significant differences between pre-
intervention and both post-intervention (P < 0Æ001)
and follow-up periods (P = 0Æ006). However, no signif-
icant difference was identified between the post-inter-
vention and follow-up period (P = 0Æ7). Within-group
effect sizes were large for both post-intervention
(d > 1Æ0) and follow-up (d > 0Æ8) periods. Table 2 sum-
marizes pre-intervention, post-intervention and follow-
up and change scores for VAS and active pain-free
mouth opening.
Discussion
The results of our study demonstrated that patients
with myofascial TMD treated with manual therapy and
exercise directed at the cervical spine experienced an
immediate decrease (48 h after 10 treatment sessions)
in facial pain, an increase in PPTs over the masticatory
muscles and an increase in pain-free mouth opening.
Additionally, these changes were maintained 12 weeks
after discharge. However, as this was a single cohort
design we could not say if these outcomes were the
result of treatment directed at the cervical spine or
some other variable.
The effect sizes were large for all of outcomes at both
immediate and the 12-week follow-up period. Addi-
tionally, it should be noted that the reduction in pain
was not only statistically significant but also clinically
meaningful as it exceeded the MCID on the VAS,
identified as 9–11 mm (28, 29). The relatively narrow
CI provide greater assurance when making clinical
decisions regarding the treatment effect identified in
this study (43). It should also be noted that even the
lower bound estimates for the 95% CI fell above the
MCID and provided evidence that cervical spine inter-
ventions might be beneficial in the management of
patients with TMD. Mellick and Mellick (44) reported
that treatment of the cervical spine with intra-muscular
injections was effective for reducing symptoms in
patients with orofacial pain. However, our study is the
first to provide preliminary evidence that manual
therapy and exercise directed at the cervical spine
may be beneficial in decreasing facial pain in these
patients.
The increases in PPT levels over both masseter and
temporalis muscles suggests that a hypoalgesic effects
may be induced by treatment of the cervical spine.
Previous evidence suggests that the hypoalgesic effects
occur after manual therapy interventions because of
the activation of the descending inhibitory pathways
(45, 46). It has been demonstrated that joint mobiliza-
tion of the cervical spine produced an increase of 25%
in PPTs in patients with lateral epicondylalgia (47) and
in patients with neck pain (48). In fact, O’Leary et al.
(49) found that the application of the cranio-cervical
flexor exercise protocol used in the current study
induced an immediate local hypoalgesic response in
patients with neck pain. Although the activation of
descending inhibitory pathways following the applica-
tion of manual procedures has not been demonstrated
Table 2. Changes in spontaneous pain (VAS) and active mouth
opening (mm)
Spontaneous orofacial pain
(Visual Analogue Scale)
Pre-intervention 55Æ5 � 8Æ6 (51Æ4 ⁄ 59Æ6)
Post-intervention 20Æ9 � 7Æ1 (17Æ5 ⁄ 24Æ4)
Follow-up 18Æ7 � 7Æ1 (15Æ3 ⁄ 22Æ1)
Pre- ⁄ post-differences )34Æ6 � 8Æ9 ()38Æ9 ⁄ )30Æ3)
Pre ⁄ follow-up differences )36Æ8 � 12Æ0 ()42Æ6 ⁄ )31Æ1)
Active mouth opening (mm)
Pre-intervention 38Æ3 � 5Æ0 (35Æ8 ⁄ 40Æ7)
Post-intervention 42Æ8 � 2Æ7 (41Æ5 ⁄ 44Æ1)
Follow-up 43Æ1 � 2Æ9 (41Æ7 ⁄ 44Æ5)
Pre- ⁄ post-differences 4Æ5 � 3Æ8 (2Æ8 ⁄ 6Æ4)
Pre ⁄ follow-up differences 4Æ8 � 5Æ8 (2Æ1 ⁄ 7Æ6)
Scores are expressed as mean � s.d. (95% confidence interval).
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 649
ª 2009 Blackwell Publishing Ltd

in patients with TMD this neurophysiological mecha-
nism seems plausible for explaining the bilateral hypo-
algesic effects that occurred in the trigeminal region
with interventions targeted to the cervical spine.
Nevertheless, as no signs of neck dysfunctions and ⁄ or
neck symptoms reported by the patients with TMD
were included in this study, it was difficult to establish a
relationship between the treatment of the cervical spine
and the orofacial effects found in the current study. As
we have discussed, it may be that the effects of cervical
interventions are more generalized rather than specific
for the trigeminal area. Future studies should investi-
gate these neurophysiological mechanisms between the
cervical spine and the orofacial region in patients with
myofascial TMD.
We also found an increase of 4Æ5 mm in pain-free
mouth opening after the treatment of the cervical
spine, which was slightly superior to the results of some
studies investigating changes in active mouth opening
after the treatment of masseter muscle TrPs which
ranged from 2 mm (50) to 4 mm (51). A recent study
has reported that the application of a thrust manipu-
lation targeted to the upper cervical spine resulted in an
increase in active mouth opening (3Æ5 mm) in women
with mechanical neck pain (52). As the application of
cervical interventions induced similar improvements in
mouth opening when compared with treatment of the
masseter muscle, perhaps cervical techniques might be
used as a complementary approach to manage pain in
patients with myofascial TMD. In addition, in patients
with allodynic responses in the facial region, in whom
the manual application of local interventions are often
extremely painful, an indirect approach directed to the
upper cervical spine may be beneficial.
One possible explanation for the increase in pain-free
mouth opening may be related to changes in the
positional afferent inputs of the cervical spine induced
by the protocol. Some studies have demonstrated that
position of the upper cervical spine modifies range of
motion of the mouth (53, 54) Others have shown that
the position of the cervical spine is influenced by the
masticatory muscles (55, 56). De Laat et al. (57) found
that a high percentage of patients with TMD also have
limited movement of the upper cervical spine. There-
fore, it is possible that the protocol applied in the
current study can improve the biomechanical adapta-
tion of the cervical spine with relation to the tempo-
romandibular joint, increasing pain-free mouth
opening. It is also plausible that the reduction in
spontaneous pain in the orofacial region will also
increase pain-free mouth opening.
Our study had several limitations. First, the sample
size was small. Second, we did not include a control
group, so we could not infer a direct cause and effect
relationship between the outcomes and the interven-
tions directed at the cervical spine. It is plausible that
the improvements seen in the patients may be related
to the passage of time. However, we would expect this
to be unlikely given the current duration of symptoms
(9Æ2 months). Furthermore, it was not possible to assess
gender differences because the size of the sample was
small. Future randomized controlled trials with a
greater number of participants and including a control
group which received traditional treatment for myo-
fascial TMD should be conducted in order to further
elucidate the effectiveness interventions directed at the
cervical spine for patients with TMD.
Conclusions
The results of our study demonstrated that patients
with myofascial TMD treated manual therapy and
exercise directed at the cervical spine might be bene-
ficial in decreasing facial pain, increasing PPTs over the
masticatory muscles and increasing pain-free mouth
opening. Furthermore, these changes were maintained
12 weeks after discharge in our population. The effect
sizes were large for all of outcomes at both the 48 h and
12 weeks follow-up periods. Future randomized studies
should investigate the potential of a cause and effect
relationship.
References
1. LeResche L. Epidemiology of temporomandibular disorders:
implications for the investigation of etiologic factors. Crit Rev
Oral Biol Med. 1997;8:291–305.
2. Drangsholt M, LeResche L. Temporomandibular disorder pain.
In: Crombie IK, Croft PR, Linton SJ et al., eds. Epidemiology of
pain. Seattle: IASP Press; 1999:203–233.
3. Isong U, Gansky SA, Plesh O. Temporomandibular joint and
muscle disorder-type pain in US adults: the National Health
Interview Survey. J Orofac Pain. 2008;22:317–322.
4. Olivo SA, Bravo J, Magee DJ, Thie NM, Major PW, Flores-Mir
C. The association between head and cervical posture and
temporomandibular disorders: a systematic review. J Orofac
Pain. 2006;20:9–23.
5. De Wijer A, De Leeuw JR, Steenks MH, Bosman F. Tempo-
romandibular and cervical spine disorders. Self-reported signs
and symptoms. Spine. 1996;21:1638–1646.
R . L A T O U C H E et al.650
ª 2009 Blackwell Publishing Ltd

6. De Wijer A, Steenks MH, De Leeuw JR, Bosman F, Helders PJ.
Symptoms of the cervical spine in temporomandibular and
cervical spine disorders. J Oral Rehabil. 1996;23:742–750.
7. Ciancaglini R, Testa M, Radaelli G. Association of neck pain
with symptoms of temporomandibular dysfunction in the
general adult population. Scand J Rehabil Med. 1999;31:17–
22.
8. Lobbezoo F, Visscher C, Naeije M. Impaired health status,
sleep disorders, and pain in the craniomandibular and cervical
spinal regions. Eur J Pain. 2004;8:23–30.
9. Eriksson PO, Zafar H, Nordh E. Concomitant mandibular and
head-neck movements during jaw opening-closing in man.
J Oral Rehabil. 1998;25:859–870.
10. Zafar H, Nordh E, Eriksson PO. Temporal coordination
between mandibular and head-neck movements during jaw
opening-closing tasks in man. Arch Oral Biol. 2000;45:675–
682.
11. Marfurt CF, Rajchert DM. Trigeminal primary afferent pro-
jections to ‘non-trigeminal’ areas of the rat central nervous
system. J Comp Neurol. 1991;303:489–511.
12. Goadsby PJ, Hoskin KL. The distribution of trigemino-vascular
afferents in the nonhuman primate brain Macaca nemestrina: a
c-fos immunocytochemical study. J Anat. 1997;190:367–375.
13. Bartsch T, Goadsby PJ. Stimulation of the greater occipital
nerve induces increased central excitability of dural afferent
input. Brain. 2002;125:1496–1509.
14. Bartsch T, Goadsby PJ. Increased responses in trigemino-
cervical nociceptive neurons to cervical input after stimulation
of the dura mater. Brain. 2003;126:1801–1813.
15. Hu JW, Yu XM, Vernon H, Sessle BJ. Excitatory effects on
neck and jaw muscle activity of inflammatory irritant applied
to cervical paraspinal tissues. Pain. 1993;55:243–250.
16. Yu XM, Sessle BJ, Vernon H, Hu JW. Effects of inflammatory
irritant application to the rat temporomandibular joint on jaw
and neck muscle activity. Pain. 1995;60:143–149.
17. Foster ME, Gray RJ, Davies SJ, Macfarlane TV. Therapeutic
manipulation of the temporomandibular joint. Br J Oral
Maxillofac Surg. 2000;38:641–644.
18. Jagger RG. Mandibular manipulation of anterior disc displace-
ment without reduction. J Oral Rehabil. 1991;18:497–500.
19. Kurita H, Kurashina K, Ohtsuka A. Efficacy of a mandibular
manipulation technique in reducing the permanently dis-
placed temporomandibular joint disc. J Oral Maxillofac Surg.
1999;57:784–787.
20. Nicolakis P, Erdogmus B, Kopf A, Djaber-Ansari A, Piehslinger
E, Fialka-Moser V. Exercise therapy for craniomandibular
disorders. Arch Phys Med Rehabil. 2000;81:1137–1142.
21. Nicolakis P, Erdogmus B, Kopf A, Ebenbichler G, Kollmitzer J,
Piehslinger E et al. Effectiveness of exercise therapy in patients
with internal derangement of the temporomandibular joint.
J Oral Rehabil. 2001;28:1158–1164.
22. Catanzariti JF, Debuse T, Duquesnoy B. Chronic neck pain and
masticatory dysfunction. Joint Bone Spine. 2005;72:515–519.
23. Dworkin SF, LeResche L. Research diagnostic criteria for
temporomandibular disorders: review, criteria, examinations
and specifications, critique. J Craniomandib Disord. 1992;
6:301–355.
24. Simons D, Travell J, Simons P. Travell & Simons’ myofascial
pain & dysfunction: the trigger point manual: the upper half of
body. Baltimore (MD): Williams & Wilkins; 1999.
25. Gerwin RD, Shannon S, Hong CZ, Hubbard D, Gevirtz R.
Interrater reliability in myofascial trigger point examination.
Pain. 1997;69:65–73.
26. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C,
Goldenberg DL et al. The American College of Rheumatology
1990 criteria for clasification of fibromyalgia: Report of the
multicenter criteria committee. Arthritis Rheum. 1990;
33:160–170.
27. Bijur P, Silveer W, Gallagher JE. Reliability of the visual
analogue scale for measurement of acute pain. Acad Emerg
Med. 2001;8:1153–1157.
28. BirdSB,DicksonEW.Clinically significant changes in pain along
the visual analogue scale. Ann Emerg Med. 2001; 36:639–643.
29. Gallagher EJ, Liebman M, Bijur PE. Prospective validation of
clinically important changes in pain severity measured on a
visual analogue scale. Ann Emerg Med. 2001;38:633–638.
30. Fischer AA. Application of pressure algometry in manual
medicine. J Man Med. 1990;5:145–150.
31. Chesterson LS, Sim J, Wright CC, Foster NE. Inter-rater
reliability of algometry in measuring pressure pain thresholds
in healthy humans, using multiple raters. Clin J Pain. 2007;
23:760–766.
32. Goulet JP, Clark GT, Flack VF, Liu C. The reproducibility of
muscle and joint tenderness detection methods and maximum
mandibular movement measurement for the temporoman-
dibular system. J Orofac Pain. 1998;12:17–26.
33. Chiu TW, Wright A. To compare the effects of different rates of
application of a cervical mobilisation technique on sympa-
thetic outflow to the upper limb in normal subjects. Man Ther.
1996;1:198–203.
34. Maitland G, Hengeveld E, Banks K, English K. Maitland’s
vertebral manipulation. 6th ed. London, England: Butter-
worth Heineman; 2000.
35. Jull G, Falla D, Treleaven J, Sterling M, O’Leary S. A
therapeutic exercise approach for cervical disorders. In:
Boyling JD, Jull GA, eds. Grieves’ modern manual therapy:
the vertebral column, 3rd ed. Edinburgh: Churchill Living-
stone; 2004; 451–469.
36. Mayoux-Benhamou MA, Revel M, Vallee C. Selective elec-
tromyography of dorsal neck muscles in humans. Exp Brain
Res. 1997;113:353–360.
37. Falla D, Jull G, Dall’Alba P, Rainoldi A, Merletti R. An
electromyographic analysis of the deep cervical flexor muscles
in performance of cranio-cervical flexion. Phys Ther. 2003;
83:899–906.
38. Falla D, Jull G, O’Leary S, Dall’alba P. Further evaluation of
and EMG technique for assessment of the deep cervical flexor
muscles. J Electromyogr Kinesiol. 2006;16:621–628.
39. Falla D, Jull G, Russell T, Vicenzino B, Hodges P. Effect of neck
exercise on sitting posture in patients with chronic neck pain.
Phys Ther. 2007;87:408–417.
40. O’Leary S, Jull G, Kim M, Vicenzino B. Specificity in
retraining craniocervical flexor muscle performance. J Orthop
Sports Phys Ther. 2007;37:3–9.
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 651
ª 2009 Blackwell Publishing Ltd

41. Falla D, Jull G, Hodges P. Training the cervical muscles with
prescribed motor tasks does not change muscle activation
during a functional activity. Man Ther. 2008;13:507–512.
42. Cohen J. Statistical power analysis for the behavioural
sciences. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988.
43. Noteboom JT, Allison SC, Cleland JA, Whitman JM. A primer
on selected aspects of evidence-based practice to questions of
treatment part II: Interpreting results, applying to clinical
practice, and self-evaluation. J Orthop Sports Phys Ther.
2008;38:485–501.
44. Mellick LB, Mellick GA. Treatment of acute orofacial pain
with lower cervical intramuscular bupivacaine injections:
a 1-year retrospective review of 114 patients. J Orofac Pain.
2008;22:57–64.
45. Souvlis T, Vicenzino B, Wright A. Neuro-physiological effects
of spinal manual therapy. In: Boyling JD, Jull G, eds. Grieves’
modern manual therapy: the vertebral column, 3rd ed.
Edinburgh: Churchill-Livingstone; 2004:367–379.
46. Wright A. Pain-relieving effects of cervical manual therapy.
In: Grant R, ed. Physical therapy of the cervical and thoracic
spine. New York: Churchill-Livingstone; 2002:217–238.
47. Vicenzino B, Collins D, Wright A. The initial effects of a
cervical spine manipulative physiotherapy treatment on the
pain and dysfunction of lateral epicondylalgia. Pain.
1996;68:69–74.
48. Sterling M, Jull G, Wright A. Cervical mobilisation: concurrent
effects on pain, sympathetic nervous system activity and
motor activity. Man Ther. 2001;6:72–81.
49. O’Leary S, Falla D, Hodges PW, Jull G, Vicenzino B. Specific
therapeutic exercise of the neck induces immediate local
hypoalgesia. J Pain. 2007;8:832–839.
50. Rodrıguez-Blanco C, Fernandez-de-las-Penas C, Hernandez-
Xumet JE, Pena-Algaba C, Fernandez-Rabadan M, Lillo-de-la-
Quintana MC. Changes in active mouth opening following a
single treatment of latent myofascial trigger points in the
masseter muscle involving post-isometric relaxation or
strain ⁄ counter-strain. J Bodyw Mov Ther. 2006;10:197–205.
51. Ibanez-Garcıa J, Alburquerque-Sendın F, Rodrıguez-Blanco C,
Girao D, Atienza-Meseguer A, Planella-Abella S et al. Changes
in masseter muscle trigger points following strain-counter ⁄ -strain or neuro-muscular technique. J Bodyw Mov Ther.
2009;13:2–10.
52. Mansilla-Ferragut P, Fernandez-de-las-Penas C, Alburquer-
que-Sendın F, Cleland JA, Bosca-Gandıa JJ. The immediate
effects of atlanto-occipital joint manipulation on active
mouth opening and pressure pain sensitivity in women
with mechanical neck pain. J Man Physiol Ther. 2009;32:
101–106.
53. Makofsky HW, Sexton TR. The effect of cranio-vertebral
fusion on occlusion. Cranio. 1994;12:38–46.
54. Solow B, Sonnesen L. Head posture and malocclusions. Eur J
Orthop. 1998;20:685–693.
55. Moya H, Miralles R, Zuniga C, Carvajal R, Rocabado M,
Santander H. Influence of stabilization occlusal splint on
cranio-cervical relationship. Part 1: Cephalometric analysis.
Cranio. 1994;12:47–51.
56. Miralles R, Moya H, Ravera MJ, Santander H, Zuniga C,
Carvajal R et al. Increase of the vertical occlusal dimension by
means of removable orthodontic appliance and its effects on
cranio-cervical relationships and position of the cervical spine
in children. Cranio. 1997;18:205–219.
57. De Laat A, Meuleman H, Stevens A, Verbeke G. Correlation
between cervical spine and temporomandibular disorders.
Clin Oral Investig. 1998;2:54–57.
Correspondence: Roy La Touche Arbizu, Facultad de Medicina,
Universidad San Pablo CEU, Calle Tutor, 35, 28008 Madrid, Spain.
E-mail: [email protected]
R . L A T O U C H E et al.652
ª 2009 Blackwell Publishing Ltd
192
5.7 Estudio VII
La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S, Bishop MD,
Lopéz-Valverde-Centeno A, von Piekartz H, Fernández-Carnero J. Does mobilization of
the upper cervical spine affect pain sensitivity and autonomic nervous system function
in patients with cervico-craniofacial pain?: A randomized-controlled trial. Clin J Pain.
2013 Mar;29(3):205-15.
Objetivos del estudio
Los objetivos de este estudio fueron investigar los efectos de la movilización antero-
posterior de la región cervical superior en la modulación del dolor en las regiones
craneofacial y cervical y su influencia en el sistema nervioso simpático.
Resultados
Los UDPs en las regiones craneofacial y cervical aumentó significativamente (P
<0,001) y la intensidad del dolor disminuyó significativamente (P <0,001) en el grupo
de tratamiento en comparación con placebo. La movilización produjo una respuesta
simpatoexcitatoria demostrado por un aumento significativo de la conductancia de la
piel, la frecuencia respiratoria y la frecuencia cardíaca (p <0,001), pero no en la
temperatura de la piel (P = 0,071), después de la aplicación de la técnica en
comparación con el placebo.
Conclusiones
Este estudio proporciona una evidencia preliminar del efecto hipoalgésico a corto plazo
de la movilización articular de la región cervical en las regiones craneofacial y cervical
de pacientes con DCCF de origen miofascial, lo que sugiere que la movilización puede
causar una modulación nociceptiva inmediata en el CTC. Se observó una respuesta
simpatoexcitatoria, lo que podría estar relacionado con el efecto hipoalgésico inducido
por la técnica, aspecto a ser confirmado en estudios futuros.

Does Mobilization of the Upper Cervical Spine Affect PainSensitivity and Autonomic Nervous System Function
in Patients With Cervico-craniofacial Pain?
A Randomized-controlled Trial
Roy La Touche, PT, MSc,*wz Alba Parıs-Alemany, PT, MSc,zJeffrey S. Mannheimer, PT, PhD, CCTT,y Santiago Angulo-Dıaz-Parreno, MSc,wz8
Mark D. Bishop, PT, PhD,z# Antonio Lopez-Valverde-Centeno, MD, PhD,**Harry von Piekartz, PT, PhD,ww and Josue Fernandez-Carnero, PT, PhDwzz
Objectives: The aims were to investigate the effects of anterior-posterior upper cervical mobilization (APUCM) on pain modu-lation in craniofacial and cervical regions and its influence on thesympathetic nervous system.
Methods: Thirty-two patients with cervico-craniofacial pain ofmyofascial origin were randomly allocated into experimental orplacebo groups. Each patient received 3 treatments. Outcomemeasures included bilateral pressure pain thresholds assessed atcraniofacial and cervical points preintervention, after the secondintervention and after the final treatment. Pain intensity andsympathetic nervous system variables (skin conductance, breathingrate, heart rate, and skin temperature) were assessed before andimmediately after each intervention.
Results: The pressure pain thresholds in the craniofacial and cer-vical regions significantly increased (P<0.001) and pain intensitysignificantly decreased (P<0.001) in the treatment group com-pared with placebo. APUCM also produced a sympathoexcitatoryresponse demonstrated by a significant increase in skin con-ductance, breathing rate, and heart rate (P<0.001), but not in skintemperature (P=0.071), after application of the technique com-pared with placebo.
Discussion: This study provided preliminary evidence of a short-term hypoalgesic effect of APUCM on craniofacial and cervicalregions of patients with cervico-craniofacial pain of myofascialorigin, suggesting that APUCM may cause an immediate noci-ceptive modulation in the trigeminocervical complex. We also ob-served a sympathoexcitatory response, which could be related to
the hypoalgesic effect induced by the technique, but this aspectshould be confirmed in future studies.
Key Words: manual therapy, neck pain, temporomandibular
disorders, orofacial pain, craniofacial pain
(Clin J Pain 2013;29:205–215)
Discomfort resulting from temporomandibular disorders(TMDs) is representative of many chronic craniofacial
pain (CCFP) conditions.1 TMD demographics usuallyconsist of working women in the 3rd decade of life withhigh stress levels.2 TMDs are characterized by a focal site oftenderness that provokes nociceptive input and, whenchronic, contributes to the development of central sensiti-zation. Patients with TMDs are known to have greatertemporal summation of pain, suggesting hyperexcitabilityof the central nociceptive system.3,4 More specifically,chronic muscular TMD pain is associated with a generaldysfunction of the central nociceptive system that is con-comitant with central nociceptive neuronal hyperexcitabilityand dysfunction of the descending inhibitory pain systems.5
Women have a 3 times greater risk of experiencing chronicmasticatory myofascial pain than men.6 Patients with TMDsof myofascial origin are also characterized by a general hy-persensibility to mechanical pain stimuli, presenting lowercraniofacial pressure pain thresholds (PPT) of both thepainful and nonpainful side compared with healthy controls.7
Some studies suggest a functional relationship betweenthe jaw and head-neck with regard to craniofacial and cer-vical spine and a concomitance between craniofacial painand neck pain.2,8–10 Patients with craniofacial pain are attwice the risk of experiencing neck pain than the generalpopulation.2 Restricted segmental movements of the uppercervical vertebrae (C0-C3) with a greater percentage of up-per trapezius and sternocleidomastoid tender points exist inpatients with TMDs compared with a control group.11
In addition, Eriksson et al8 demonstrated coordi-nated articular patterns of movement between the temporo-mandibular, atlanto-occipital, and cervical joints, joints thatalso have known sensory-motor interaction via the trige-minocervical complex (TCC). Disturbance of this con-nection between jaw and head-neck movements has beenidentified in patients with whiplash-associated disorders.12
Spinal manual therapy (SMT) is used by physicaltherapists (PTs) to treat chronic musculoskeletal pain.13
Received for publication June 21, 2011; revised February 14, 2012;accepted February 17, 2012.
From the *Department of Physical Therapy, La Salle UniversityCenter, Faculty of Health Science, Aravaca; wResearch Group ofMusculoskeletal Pain and Motor Control, Universidad Europea deMadrid, Villaviciosa de Odon; zInstitute of Neuroscience andCraniofacial Pain (INDCRAN); 8Faculty of Experimental Science,Universidad San Pablo CEU; zzDepartment of Physical Therapy,Occupational Therapy, Rehabilitation and Physical Medicine,Universidad Rey Juan Carlos, Alcorcon, Madrid; **Departmentof Surgery, Faculty of Medicine and Dentistry, Universidad deSalamanca, Salamanca, Spain; yProgram in Physical Therapy,Columbia University, NY; zDepartment of Physical Therapy;#Center for Pain Research and Behavioral Health, University ofFlorida, Gainesville, FL; and wwFaculty of Business, Managementand Social Science, University of Applied Science, Osnabruck,Germany.
The authors declare no conflict of interest.Reprints: Roy La Touche, PT, MSc, INDCRAN, C/Canos del Peral
11, Bajo Izquierdo, 28013 Madrid, Spain (e-mail: [email protected]).
Copyright r 2012 by Lippincott Williams & Wilkins
ORIGINAL ARTICLE
Clin J Pain � Volume 29, Number 3, March 2013 www.clinicalpain.com | 205

Various techniques such as passive manipulation and mo-bilization, active mobilization, neuromuscular facilitation,and articular glides are included under the general term ofSMT.14–17 Many SMTs have demonstrated hypoalgesiceffects. This hypoalgesic effect is not antagonized by na-loxone and does not exhibit tolerance,18 supporting thetheory that SMTs activate a nonopioid inhibitory system.In addition, a concomitant activation of the sympatheticnervous system (SNS) occurs after SMT, with the degree ofactivation depending on the technique.19,20
Many studies have investigated the effects of SMT onlower cervical pain,14–16,21 but there is no randomized-controlled trial in which SMT is used to diminish cranio-facial pain. George et al22 compared cervical manipulationwith a soft tissue technique at the cervical-cranial junctionto improve mouth opening in healthy controls, but no sig-nificant results were obtained. Another study examined amanual therapy and therapeutic exercise protocol appliedat the cervical spine, to treat craniofacial pain of myofascialorigin in a cohort intervention study, which resulted in anincrease in the PPT in the masticatory muscles and in-creased mouth opening.23
Consequently, the aims of this study were to extendprevious work by investigating the neurophysiologicaleffects of SMT in patients with CCFP of myofascial origin.Specifically, we studied passive anterior-posterior uppercervical mobilization (APUCM). We expected pain sensi-tivity in the craniofacial and cervical regions to decrease inresponse to treatment. In addition, we expected to observethe sympathetic influence of this technique on skin con-ductance (SC), breathing rate (BR), heart rate (HR), and skintemperature (ST).
MATERIALS AND METHODS
Selection and Description of ParticipantsThirty-two patients with CCFP of myofascial origin
referred from 2 private dental clinics and 3 universities inMadrid, Spain, were recruited from January 2009 to May2010. We defined the term CCFP of myofascial origin aspain and dysfunction located at the cervical and mastica-tory muscles. Patients were selected if they met all of thefollowing criteria: (1) a primary diagnosis of myofascialpain as defined by axis I, category Ia and Ib (eg, myofascialpain with or without limited opening of the mouth) of theResearch Diagnostic Criteria for Temporomandibular Dis-orders24; (2) bilateral pain involving the masseter, temporalis,upper trapezius, and suboccipital muscles; (3) a duration ofpain of at least 3 months; (4) a pain intensity correspondingto a weekly average of at least 30mm on a 100-mm visualanalog scale (VAS); (5) neck and/or shoulder pain withsymptoms provoked by neck postures or neck movement;(6) Neck Disability Index (NDI)25,26 Z15 points; and (7)presence of bilateral trigger points (TrPs) in masseter, tem-poralis, upper trapezius, and suboccipital muscles. TrPs werediagnosed according to the following criteria27: (1) presenceof a palpable taut band in the skeletal muscle; (2) presence ofa hypersensitive tender spot within the taut band; (3) localtwitch response elicited by the snapping palpation of the tautband; and (4) reproduction of referred pain in response toTrP compression.
All patients in the study were examined by a physi-otherapist with 7 years of experience managing craniofacialand cervical disorders. Patients were excluded if they pre-sented any signs, symptoms, or history of the following
diseases: (1) intra-articular temporomandibular disk displace-ment, osteoarthrosis, or arthritis of the temporomandibularjoint, according to categories II and III of the ResearchDiagnostic Criteria for Temporomandibular Disorders24,28;(2) history of traumatic injuries (eg, contusion, fracture, orwhiplash injury); (3) systemic diseases such as fibromyalgia,systemic erythematous lupus, or psoriatic arthritis; (4) neu-rological disorders (eg, trigeminal neuralgia); (5) concomitantmedical diagnosis of any primary headache (tension type ormigraine); (6) unilateral neck pain; (7) cervical spine surgery;(8) clinical diagnosis of cervical radiculopathy or myelopathy;and (9) history of previous physical therapy intervention forthe cervical region. Each participant received a thorough ex-planation of the content and purpose of the treatment beforesigning an informed consent form related to the procedures,which was approved by the local ethics committee in ac-cordance with the Helsinki Declaration.
Research DesignA randomized, double-blind placebo-controlled study
was performed. Patients were blind to which interventionthey received, and an independent assessor, blind to inter-vention assignment made the measurements and registeredthe data. Patients were randomly allocated to either treat-ment intervention or sham intervention. Randomizationwas performed by a computer generated random-sequencetable created with Graphpad software (GraphPad SoftwareInc., CA) before the beginning of the study. The random-ization sequence used a balanced block design in whichrandomization occurred in blocks of 2.
Sample Size CalculationA pilot study was performed with 5 patients in the
treatment group and 5 patients in the sham group to cal-culate the sample size. We used data indicative of the per-cent change in the PPT of the 2 assessed points: 1 at themasseter muscle and 1 at the trapezius muscle.
Sample sizes were calculated to obtain a power of 80%to detect changes in the bilateral contrast of the null hy-pothesis of equal means between the 2 groups, with 5%significance, taking into account the possibility that the SDsof the groups could be different. According to the samplecalculations which took into account the fact that the cal-culation was based on 2 different variables, we obtained 2possible results: 14 patients in each group or 16 patients ineach group. We decided to include 16 patients per group toanticipate the possible loss of patients.
Demographic and Clinical DataEach of the participants completed a questionnaire
to determine if they met the criteria for inclusion or ex-clusion. This questionnaire included demographic data,screening questions for TMDs from the American Acad-emy of Orofacial Pain,29 a body chart on which patientsmarked the location of their pain, and several questionsabout the characteristics of their pain such as “whendid it start?,” “what makes your pain worse?,” “what makesit better?,” and “what kind of pain is it?” To meetthe criteria to participate in the study, patients had to passan initial physical examination performed by a single in-vestigator to rule out the presence of nerve root com-pression.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
206 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

Instrumentation and Measurements
Self-reported VariablesPatients completed the Beck Depression Inventory
(BDI),30 the State-Trait Anxiety Inventory (STAI),31 andthe NDI25,26 to quantify their psychophysical state. TheBDI is a 21-item self-report instrument intended to assessthe existence and severity of symptoms of depression. Thereis a 4-point scale for each item ranging from 0 to 3. The resultsof each item, corresponding to a symptom of depression, aresummed to yield a single score for the BDI. A total score of0 to 13 is considered minimal, 14 to 19 mild, 20 to 28 mod-erate, and 29 to 63 severe depression. The BDI showed goodinternal consistency (a coefficient 0.86).30
The STAI31 is a 40-item self-report questionnaire de-signed to assess symptoms of anxiety. It consists of 2 in-dependent scales, a state anxiety scale and a trait anxietyscale, with 20 items each, resulting in a score between 20and 80. Higher scores indicate greater levels of anxiety. Thestate and trait scales explore anxiety as a current emotionalstate and as a personality trait, respectively.
The NDI,25,26 which measures perceived neck disability,consists of 10 items that assess different functional activitiesand uses a 6-point scale ranging from 0 (no disability) to 5(complete disability). The overall score (out of 100) is ob-tained by adding the score for each item and multiplyingby 2. A higher score indicates greater pain and disability. Thevalidity, reliability, and responsiveness of the NDI have beendemonstrated.26
Pain IntensityThe VAS was used to measure pain intensity of the
cervico-craniofacial region at rest and before and after eachtreatment. The VAS is comprised of a 100mm horizontalline in which the left side represents “no pain” and the rightside represents “worst pain.” The patient placed a mark onthe line at the point that they felt represented the intensityof their pain at the time. Pain intensity was quantified bythe assessor in millimeters. This scale has proven its reli-ability and validity for measuring pain intensity.32
Pressure Pain ThresholdPPT is defined as the minimum amount of pressure
needed to provoke a pain sensation.33 We used a digitalalgometer (Model FDX 10; Wagner Instruments, Greenwich,CT) comprised of a rubber head (1 cm2) attached toa pressure gauge, which measures in kg with thresholds ex-pressed in kg/cm2. The protocol consisted of 3 measurementswith an interval of 30 seconds between each measurement.The average of the 3 measurements was calculated to obtain asingle value for each one of the measured points in each ofthe assessments. This algometric method has high reliability(ICC=0.91, 95% CI, 0.82-0.97) for measuring PPT.34 PPTswere assessed bilaterally at 2 points in the masseter muscle(M1 and M2), 2 points in temporalis muscle (T1 and T2),suboccipital muscles, C5 zygapophyseal joint, and uppertrapezius muscle. The device was applied perpendicular to theskin, and the patients were asked to raise their hand themoment when the pressure started to change to a pain sen-sation, at which point the assessor stopped applying pressure.This procedure was performed 3 times: before the firsttreatment session (pretreatment outcome), after the secondtreatment session, and after the third treatment session(2 posttreatment outcomes).
Anatomic references for the algometric measurementsincluded the following: M1—2.5 cm anterior to the tragusand 1.5 cm inferior to the zygomatic arch; M2—1 cm su-perior and 2 cm anterior from the angle of the jaw; T1(anterior fibers of the muscle)—3 cm superior to the zy-gomatic arch in the middle point between the end of the eyeand the anterior part of the helix of the ear; T2 (middlefibers of the muscle)—2.5 cm superior from the helix of theear; suboccipital muscles—2 cm inferior to the occipitalcondyles; C5 zygapophyseal joint—2 cm lateral to the spi-nous process of C6; trapezius muscle—2.5 cm above thesuperior medial angle of the scapula.
Changes in the SNSSeveral characteristics were measured to assess the
SNS: SC, HR, BR, and ST. Measurements were taken be-fore and after each of the 3 treatment sessions. The re-cording device used was I-330-C2+ 6-channel biofeedbacksystem (J&J Engineering Inc., Poulsbo, WA) the MC-6SYsensor was used to measure SC and ST. During the meas-urements 2 electrodes were placed on the tip of the secondand third fingers of the left hand to measure the SC with thetemperature sensor attached to the tip of the fourth fingeralso at the left hand. The MC-5D electrodes used to meas-ure HR were applied longitudinally at the anterior and ra-dial aspect of the wrists and held with bracers. To measureBR, an MC-3MY breathing sensor was placed around thechest like a belt passing over the xiphoid process.
ProcedureThe experiment consisted of 3 treatment sessions. Each
patient received 3 sessions over 2 weeks, and the entire ex-periment lasted approximately 8 months.
The evaluator was a PT with extensive experience intaking the experimental measurements. During the first as-sessment, pretreatment data were obtained; after measuringthe PPT and VAS, the sensors were applied, and the patientwas instructed to lie down on a couch and relax. The roomtemperature was controlled at 251C. After 10 minutes (timedetermined for the patient to come to a normal baseline),the first record of the sympathetic parameters was regis-tered. The patient was then randomly assigned to 1 of the 2intervention groups, and the therapeutic technique wasapplied. Immediately after finishing the technique, SNSvariables were measured, and 5 minutes after the technique,VAS results were registered again. In the second and thirdtreatment session, the SNS variables and VAS were meas-ured using the same protocol (pretreatment and posttreat-ment data), but PPTs were taken only 5 minutes after theend of the treatment (posttreatment data). Therefore, weobtained 3 pretreatment and 3 posttreatment measurementsof SNS and VAS parameters and 1 pretreatment and 2posttreatment measurements (after the second and thirdsessions) of PPT.
Treatment TechniqueAPUCM directly influences the 3 upper cervical seg-
ments (C0-C3). The patient was placed in a supine positionwith a neutral position of the cervical spine. The PT heldthe occipital region of the patient with both hands to stabilizeand maintain the position of the upper cervical structures,while applying a posterior directed force on the frontal re-gion of the patient (anterior to posterior force) with the an-terior part of the shoulder. The mobilization was applied at aslow rate of 1 oscillation per 2 seconds (0.5Hz) controlled
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 207

with an MA-30 digital metronome (Korg Inc., Japan). Thisoscillation rate has been used previously with a differentmanual therapy technique.19 The total time of mobilizationwas 6 minutes. Mobilization was applied in 3 intervals of2 minutes, with 30 seconds of rest in between, resulting in atotal of 7 minutes.
Sham TechniqueTo simulate the treatment technique, the PT applied
the same grips used with the treatment technique: 2 handsunder the occipital bone with the anterior part of 1 shoulderpositioned anterior to the frontal bone, with the patient insupine position. However, mobilization was not applied tothe cervical spine. The contact with the patient was held for3 intervals of 2 minutes with 30 seconds of rest in between.
Both techniques (treatment and sham) were applied bythe same PT, and each participant received the followingexplanation about the intervention: “A physical therapistwill apply a technique on your neck with one hand placedon the posterior part of your neck and the other one onyour forehead. The purpose is to obtain changes in yourneck and craniofacial pain.”
StatisticsStatistical analysis was performed with SPSS version
15.0. A Kolmogorow-Smirnov test was used to determinewhether the sample was consistent with a normal distri-bution (P>0.05). Student t test was used to analyze self-reported psycophysical variables (NDI, STAI, and BDI)and pain duration by comparing the preintervention datafor the treatment and sham groups.
The SNS variables (ST, HR, BR, SC) and VAS weretested with a 2�3 repeated measures analysis of variance(ANOVA); the factors analyzed were time (pre-post) andgroup (treatment and sham). Time�group interactions werealso analyzed. Post hoc analysis with Bonferroni correctionswas performed for specific comparisons between variables.
To determine differences between sessions in VAS andSNS variables, a 2-way ANOVA was used, which analyzedintersession factor and group� intersession interaction(presession 1, presession 2, presession 3). The percentchange for the SNS variables and VAS was obtained rela-tive to the percent change between each session and thepercent of the total of the means in both groups. A 1-wayANOVA was used to analyze the percent change in groupfactor and time factor between sessions (% change session1, % change session 2, % change session 3). The percentchange of the total of the means of the 3 sessions in thetreatment and placebo groups was analyzed with a Studentt test.
A 3�3 mixed-model ANOVAwas used to determine thePPT variables (M1, M2, T1, T2, suboccipital, C5, trapezius);the factors were group (treatment or sham), time (pre, post 1,and post 2) and side (right and left). Bonferroni correctionswere used for post hoc analysis of specific comparisons be-tween variables. Student t test determined the percent changebetween groups between the first session (pretreatment) andlast session (posttreatment 2) outcomes. Throughout allanalyses, statistical significance was set at P<0.05.
RESULTSThirty-two patients (21 females and 11 males) with
CCFP of myofascial origin were included in this study. Nopatients dropped out during the study, and no adverseevents occurred with the APUCM. The t test did not revealany significant differences between groups with regard todemographic details and clinical data (P>0.05), as shownin Table 1. A normal distribution was confirmed with theKolmogorov-Smirnov test (P>0.05).
Pain IntensityThe ANOVA revealed a significant group�time inter-
action (F=135.81; P<0.001), and significant differencesfor the time factor (F=261.7; P<0.001) and group factor(F=32.59; P=0.003) regarding the VAS results. Post hocanalysis also revealed significant differences for the treatmentgroup (P<0.001), but not for the sham group (P=0.3) forthe descriptive data shown in Table 2. A 2-way repeated-measures ANOVA found significant intersession differences(F=11.86; P<0.001) and a group� intersession interaction(F=17.09; P<0.001), indicating that the change fromsession to session was larger for 1 group.
Regarding the percentage of change, a 2-way repeated-measures ANOVA revealed significant differences for groupfactor (F=94.24; P<0.001) and time factor (F=11.3;P<0.001), represented in Figure 1A. The t test also re-vealed significant differences between the percent change ofthe total of the means for the treatment and sham groups(t= �10.03; P<0.001).
Pain Sensitivity
Craniofacial RegionAnalysis of the PPT within the craniofacial region was
performed by a 3�3 mixed-model ANOVA, which revealeda significant effect of time factor [M1 (F=83.65; P<0.001);M2 (F=67.44; P<0.001); T1 (F=98.05; P<0.001); T2(F=18.81; P<0.001)], group factor [M1 (F=12.27; P=0.001); M2 (F=18.35; P<0.001); T1 (F=16; P<0.001);T2 (F=15.85; P<0.001)] and group� time interaction [M1(F=59.65; P<0.001); M2 (F=48.45; P<0.001); T1
TABLE 1. Descriptive Data of the 2 Intervention Groups: Treatment and Sham Groups
Treatment (N=16) Sham (N=16)
Mean SD Mean SD Mean Difference
95% CI for
Mean Difference t P
Age 33.19 9.49 34.56 7.84 �1.37 �7.64 to 4.68 �0.48 0.65NDI 15.69 3.26 16.75 3.94 �1.06 �3.67 to 1.54 �0.83 0.41Pain duration 11.31 6.74 10.69 5.79 0.62 �5.16 to 3.91 �0.28 0.78BDI 13.63 3.64 12.38 4.41 1.25 �2.67 to 3.17 �0.17 0.86STAI 25.75 5.63 24.75 4.66 1 �2.73 to 4.73 �0.54 0.58
BDI indicates Beck Depression Inventory; CI, confidence interval; NDI, Neck Disability Index; STAI, State-Trait Anxiety Inventory; t, t test value.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
208 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

F=83.57; P<0.001); T2 (F=16.48; P<0.001)], but notfor side factor [M1 (F=0.94; P=0.76); M2 (F=0.13;P=0.72); T1 (F=0.009; P=0.92); T2 (F=0.64; P=0.43)]. Post hoc testing revealed significant differences be-tween the 3 sessions for the treatment group (P<0.001) butnot for the sham group (P>0.05) at all craniofacial points;descriptive data are shown in Table 3.
The t test revealed significant differences in the percentchange in PPT at the right and left craniofacial points. Figure 2shows the percent change in PPT from the pretreatment andfinal posttreatment assessment.
Cervical RegionA 3�3 mixed-model ANOVA revealed a significant
time effect of the suboccipital musculature (F=96.33; P<0.001), C5 zygapophyseal joint (F=52.37; P<0.001),trapezius muscle (F=57.41; P<0.001), and a group�timeinteraction at the suboccipital region (F=64.12; P<0.001),C5 zygapophyseal joint (F=46.84; P<0.001), and tra-pezius muscle (F=65.3; P<0.001). However, this was notthe case for side factor [suboccipital muscles (F=1.22; P=0.27); C5 zygapophyseal joint (F=1.8; P=0.18); trapeziusmuscle (F=1.57; P=0.22)]. Post hoc analysis revealedsignificant differences in the PPT for the 3 sessions of thetreatment group (P<0.001), but not the sham group(P>0.05), at each cervical point. Descriptive data of PPTfor the cervical region are shown in Table 3.
The t test revealed significant differences in the percentchange in PPT in the right and left cervical points for thetreatment group. Figure 3 shows the percent change in PPTof these measurements from pretreatment and final post-treatment points.
SNS
Skin ConductanceThe ANOVA revealed a significant group�time in-
teraction (F=107.55; P<0.001), an effect of time (F=118; P<0.001), and an effect of group (F=10.45; P=0.003) for changes in SC. Post hoc analysis revealed sig-nificant differences in the treatment group (P<0.001), but
not the sham group (P=0.73). The descriptive data of theSC are shown in Table 2. A 1-way repeated-measuresANOVA found no significant intersession differences (F=0.001; P=0.97) or group by intersession interaction (F=0.32; P=0.57).
ANOVA revealed significant differences in the percentchange between treatment sessions for the group factor(F=31.02; P<0.001), but not the time factor (F=0.72;P=0.48), as shown in Figure 4A. The t test revealed sig-nificant differences between percent change of the totalof the means of treatment and sham groups (t=6.11;P<0.001).
Breathing RateANOVA revealed a significant group�time interaction
(F=8.91; P=0.006) and a main effect of group (F=4.36;P=0.045), but not time (F=0.22; P=0.63), for changesin BR. Post hoc analysis revealed significant differences forthe treatment group (P=0.02), but not the sham group(P=0.08). The descriptive data of the BR are shownin Table 2. A 1-way repeated-measures ANOVA found nosignificant differences for intersession (F=0.13; P=0.87)or for group� intersession interaction (F=0.29; P=0.74).
TABLE 2. Descriptive Statistics for Sympathetic Nervous System Parameters and Pain Intensity, for Pretreatment and PosttreatmentAssessments
Mean±SD
Session 1 Session 2 Session 3
Pre Post Pre Post Pre Post
SCTreatment 1.84±0.61 3.33±0.43 2.10±0.78 3.45±0.38 1.88±0.59 3.4±0.53Sham 2.2±0.58 2.25±0.61 2.21±0.61 2.27±0.55 2.15±0.58 2.20±0.57
HRTreatment 69.56±6.3 73.16±5 71.25±4.39 75.1±2.88 72.05±6.84 77.12±4.12Sham 67.87±7.35 63.81±7.56 67.31±6 63.31±6.73 69.37±5.09 66.12±7.01
RRTreatment 15.31±2.76 16.31±4.13 15.63±1.9 18.38±3.7 15.88±2.56 16.7±3.6Sham 16.58±2.37 14.9±2.99 15.38±1.4 14.28±2.7 15.45±2.2 13.95±2.6
STTreatment 31.45±3.45 28.42±4.39 32.44±3.21 27.53±5.1 30.46±3.67 27.18±4.33Sham 31.71±3.19 29.11±4.07 32.03±2.7 29.56±3.76 31.06±3.26 28.57±3.61
VASTreatment 43.88±7.3 29.66±8.97 31.06±8.83 18.31±9.18 29.31±11.8 14.75±11.8Sham 42.38±9.41 41.5±7.9 45.13±7.9 42.56±6.88 44.31±8.51 42±9.05
BR indicates breathing rate; HR, heart rate; SC, skin conductance; ST, skin temperature; VAS, visual analog scale.
0
10
-20
-10
Treatment
-50
-40
-30
Ch
ang
e in
VA
S (
%)
Sham
-70
-60
-80Session 1 Session 2 Session 3
FIGURE 1. Visual analog scale (VAS) percentage change betweenthe 3 sessions (mean of preintervention and postintervention) fortreatment and sham groups.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 209

A 1-way ANOVA revealed significant differences inpercent change of BR for the group factor (F=11.34;P=0.002) but not for time (F=1.03; P=0.36) as shownin Figure 4B. The t test revealed significant differences be-tween the percent change of the total of the means for thetreatment and sham groups (t=3.07; P=0.004).
Heart RateANOVA revealed a significant group� time inter-
action (F=54.14; P<0.001) and a main effect of group(F=19.4; P<0.001), but not time (F=0.14; P=0.71),for changes in HR. Post hoc analysis revealed significantdifferences in the treatment group (P<0.001) and the shamgroup (P<0.001); HR data are shown in Table 2. A 1-wayrepeated-measures ANOVA found no significant inter-session differences (F=1.5; P=0.23) or group� interses-sion interaction (F=0.45; P=0.63).
Regarding the percent change in HR, a 1-way re-peated-measures ANOVA revealed significant differencesfor group factor (F=53.66; P<0.001), but not time factor
(F=1.02; P=0.36), as shown in Figure 4C. Significantdifferences between the percent change of the total of themeans for the treatment and sham groups (t=7.37; P<0.001) were observed.
Skin TemperatureThe ANOVA did not reveal any significant group�
time interaction (F=3.49; P=0.071), time factor effect(F=1.62; P=0.2), or group factor effect (F=0.53; P=0.46) for changes in ST. The descriptive data of the ST areshown in Table 2. A 1-way repeated-measures ANOVAfound no significant intersession differences (F=2.84;P=0.06) or group� intersession interaction (F=0.25;P=0.77).
Regarding percent change in ST, a 1-way repeated-measures ANOVA did not reveal a significant difference ingroup factor (F=3.25; P=0.08) or time factor (F=2.74; P=0.07), as shown in Figure 4D. The t test did notreveal a significant difference in the percent change of the
TABLE 3. Descriptive Statistics of PPT Assessed Pretreatment, Posttreatment 1 After the Second Session, and Posttreatment 2 After theThird Session, Taken Bilaterally
Treatment Sham
Right Left Right Left
Pre Post 1 Post 2 Pre Post 1 Post 2 Pre Post 1 Post 2 Pre Post 1 Post 2
Orofacial region
M1 2.13±0.37 3.03±0.5 3.46±0.45 2.12±0.43 2.91±0.53 3.5±0.44 2.29±0.54 2.32±0.48 2.39±0.55 2.28±0.37 2.31±0.62 2.42±0.6
M2 2.12±0.44 2.88±0.44 3.4±0.38 2.09±0.39 2.94±0.36 3.59±0.45 2.18±0.49 2.27±0.56 2.37±0.63 2.12±0.61 2.21±0.45 2.15±0.66
T1 2.76±0.49 3.52±0.5 4.11±0.55 2.69±0.5 3.66±0.54 4.19±0.53 2.81±0.47 2.85±0.46 2.97±0.32 2.89±0.51 2.78±0.57 2.82±0.59
T2 2.97±0.48 3.59±0.51 3.95±0.58 2.8±0.56 3.77±0.47 3.98±0.66 3.04±0.46 2.91±0.61 3.06±0.55 2.86±0.58 2.9±0.46 2.97±0.46
Cervical region
Suboccipital 2.36±0.34 3.33±0.29 3.95±0.22 2.28±0.35 3.38±0.32 3.99±0.22 2.31±0.44 2.43±0.52 2.48±0.63 2.25±0.39 2.35±0.49 2.41±0.54
C5 2.47±0.42 3.09±0.65 3.63±0.52 2.46±0.45 3.26±0.69 3.69±0.49 2.52±0.44 2.55±0.38 2.6±0.4 2.64±0.44 2.74±0.61 2.63±0.43
Trapezius 2.61±0.38 3.51±0.42 4.13±0.67 2.66±0.37 3.62±0.41 4.24±0.5 2.85±0.29 2.82±0.44 2.87±043 2.69±0.4 2.53±0.56 2.6±0.58
Mean±SD.PPT indicates pressure pain thresholds.
100.00
120.00 Treatment/Right SideTreatment/Left SideSham/Right SideSham/Left Side
60.00
80.00
40.00
0.00
20.00
Ch
ang
e in
PP
T (
%)
M1 M2 T1 T2
-20.00
FIGURE 2. Percent change in pressure pain thresholds (PPTs) ofthe craniofacial region (M1 and M2 points of masseter muscleand T1 and T2 of temporal muscle) for treatment and sham in-terventions at right and left sides (mean of preintervention andfinal postintervention). Error bars represent 95% confidence in-tervals of the mean.
Treatment/Right SideTreatment/Left SideSham/Right SideSham/Left Side
Ch
ang
e in
PP
T (
%)
120.00
80.00
100.00
60.00
40.00
20.00
-20.00
0.00
Sub-occipital C5 Trapezius
FIGURE 3. Percent change in pressure pain thresholds (PPTs) ofthe cervical region (suboccipital muscles, C5, and trapeziusmuscles) for treatment and sham interventions on the right andleft sides (mean of preintervention and final postintervention).Error bars represent 95% confidence intervals of the mean.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
210 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins
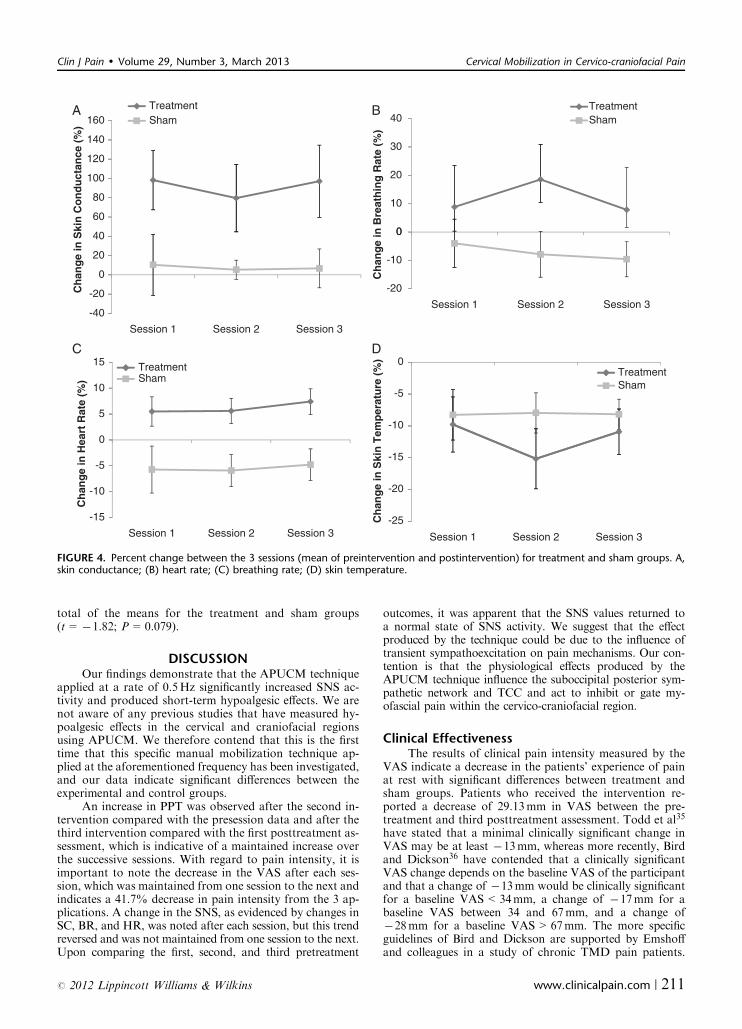
total of the means for the treatment and sham groups(t= �1.82; P=0.079).
DISCUSSIONOur findings demonstrate that the APUCM technique
applied at a rate of 0.5Hz significantly increased SNS ac-tivity and produced short-term hypoalgesic effects. We arenot aware of any previous studies that have measured hy-poalgesic effects in the cervical and craniofacial regionsusing APUCM. We therefore contend that this is the firsttime that this specific manual mobilization technique ap-plied at the aforementioned frequency has been investigated,and our data indicate significant differences between theexperimental and control groups.
An increase in PPT was observed after the second in-tervention compared with the presession data and after thethird intervention compared with the first posttreatment as-sessment, which is indicative of a maintained increase overthe successive sessions. With regard to pain intensity, it isimportant to note the decrease in the VAS after each ses-sion, which was maintained from one session to the next andindicates a 41.7% decrease in pain intensity from the 3 ap-plications. A change in the SNS, as evidenced by changes inSC, BR, and HR, was noted after each session, but this trendreversed and was not maintained from one session to the next.Upon comparing the first, second, and third pretreatment
outcomes, it was apparent that the SNS values returned toa normal state of SNS activity. We suggest that the effectproduced by the technique could be due to the influence oftransient sympathoexcitation on pain mechanisms. Our con-tention is that the physiological effects produced by theAPUCM technique influence the suboccipital posterior sym-pathetic network and TCC and act to inhibit or gate my-ofascial pain within the cervico-craniofacial region.
Clinical EffectivenessThe results of clinical pain intensity measured by the
VAS indicate a decrease in the patients’ experience of painat rest with significant differences between treatment andsham groups. Patients who received the intervention re-ported a decrease of 29.13mm in VAS between the pre-treatment and third posttreatment assessment. Todd et al35
have stated that a minimal clinically significant change inVAS may be at least �13mm, whereas more recently, Birdand Dickson36 have contended that a clinically significantVAS change depends on the baseline VAS of the participantand that a change of �13mm would be clinically significantfor a baseline VAS<34mm, a change of �17mm for abaseline VAS between 34 and 67mm, and a change of�28mm for a baseline VAS>67mm. The more specificguidelines of Bird and Dickson are supported by Emshoffand colleagues in a study of chronic TMD pain patients.
120
140
160TreatmentA B
C D
Sham
30
40TreatmentSham
60
80
100
0
10
20
-20
0
20
40
Ch
ang
e in
Ski
n C
on
du
ctan
ce (
%)
-20
-10
0
Ch
ang
e in
Bre
ath
ing
Rat
e (%
)15 Treatment
-40
Session 1 Session 2 Session 3
Session 1 Session 2 Session 3
Treatment
0
5
10Sham
Sham
-10
-5
-15
Session 1 Session 2 Session 3
Ch
ang
e in
Hea
rt R
ate
(%)
0
-10
-5
-20
-15
-25
Session 1 Session 2 Session 3
Ch
ang
e in
Ski
n T
emp
erat
ure
(%
)
FIGURE 4. Percent change between the 3 sessions (mean of preintervention and postintervention) for treatment and sham groups. A,skin conductance; (B) heart rate; (C) breathing rate; (D) skin temperature.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 211

They established that to be clinically significant, patientswith a higher pain baseline must demonstrate a greater VASreduction than those with a lower baseline, and the minimalchange should be of �19.5mm or �37.9% of the VAS.37
Our findings are clinically significant according to theguidelines of Todd et al, Bird and Dickson, or Emshoffet al.35–37
SNS ResponsePrevious studies have noted similar effects in the variables
that we measured after SMT in the cervical region.15,17,19,20,38
We observed an increase of 83.75% in SC, which is similar tothat observed by Chiu and Wright19 and Sterling et al15 whoobserved increases of approximately 50% to 60% and 16%,respectively. Studies in which SMT was applied to other bodylocations also noted similar changes in SC. A 16.85% increasein SC was observed after a thoracic mobilization applied toT4,39 and a 13.5% increase in SC was observed after lumbarmobilization.40
A similar effect was noted for HR. We observed an in-crease of 6.06% compared with previous studies that reportedchanges of 10.5%,38 13%,20 and 4.5%.17 A significant changein HR in the sham group was also noted. HR decreased by�5.5% in the sham group, which could indicate that thetreatment can increase HR, whereas the sham application issimilar to a touch massage technique that results in a decreaseof SNS activity.41
Previous studies of BR have reported increases of44%38 and 36%.20 In our study, we observed a 10.4% in-crease in BR in the experimental group. This discrepancycould be due to the type of mobilization that we applied.Previous studies that used lateral cervical glides or poste-rior-anterior mobilization techniques at a frequency of2Hz. A significant change was not obtained in ST despitea downward trend in both treatment and sham groups, asnoted by Chiu and Wright.19 However, a significant de-crease of 2.5% in ST was obtained in another study.15
The results of Sterling et al15 correlate with our datawith respect to the tendency of ST to decrease and the notedchange in SC. Furthermore, significant changes in bloodpressure, which we did not record, have been observed byPaungmali et al,17 Vicenzino et al,20 and McGuiness et al.38
These results confirm that gentle manual mobilizationtechniques on the cervical spine can confer positive phys-iological effects.
Hypoalgesic EffectsOur data indicate that the APUCM technique pro-
duces hypoalgesic effects, as demonstrated by PTT meas-urements made by an algometer, and support a significantdifference between the treatment and sham groups. Sterlinget al15 demonstrated that a unilateral posterior-anteriormobilization applied on the side of pain increased the PPTby 23% on the side of treatment in patients with chronicidiopathic neck pain. We observed increases in PPTbetween 64% and 77% for the masseter muscle points,between 38% and 59% at temporal muscle points and be-tween 47% and 79% for the cervical points after 3 treat-ments of APUCM. The greater change in PPT observed inour study and others may be because our study investigatedshort-term outcomes (3 treatment sessions) instead of im-mediate outcomes (1 treatment session), due to the appliedtechnique and the frequency of mobilization and is in-dicative of a real bilateral hypoalgesic effect at both regions.
Previous research has investigated the effect of spinalmobilization on cervical and lumbar regions and reportedpositive results.15,20,40,42 Sterling et al15 noted a differencebetween the improved PPT in the painful side and thenonpainful side, indicating a unilateral effect from a uni-lateral technique. Our study demonstrates a bilateral in-crease in PPT in both cervical and craniofacial regions. Thisdifference could be due to the central application of thetechnique in this study as opposed to the unilateral appli-cation of Sterling et al.
Manual Therapeutic NeurophysiologyResearch in SMT has focused on the neurophysio-
logical effects of manual manipulation and mobilizationswith data suggesting activation of descendent pain inhibitorysystems upon short-term (initial) hypoalgesic effects.43–45
Skyba et al46 showed that mobilization of the hyperalgesicknee joint in rats produced an antihyperalgesic effect. Thiseffect, which maintained after spinal blockage of opioid orGABA receptors, could be due to descending serotoninergicor noradrenergic inhibitory mechanisms via corticospinalprojections from the periacueductal gray matter (PAG).46
Implications relate to noradrenaline, a PGA neurotransmitterthat is more effective at inhibiting mechanical nociceptionthan thermal nociception, which seems to be serotoninergi-cally mediated.47,48 Others have demonstrated that SMTmight be the ideal stimulus for PAG mediated nonopioidanalgesia, hypoalgesia, sympathoexcitatory effects, and changesin motor activity.15,17,20,49 In the present study, we obtainedboth a sympathoexcitation and hypoalgesic effect after theAPUCM technique, which supports the fact that the d-PAG isinfluenced by the SMT technique.
One controversial issue surrounding manual therapy iswhether a localized segmental and/or extrasegmental effectis produced by SMT. Previous research has shown thatSMT improves symptoms distal to the segment where it isapplied; that is, manipulation applied at the thoracic spinehas positive effects when performed on patients with frommechanical neck pain,14,21 and cervical SMT can result inhypoalgesia at the elbow.50 However, other clinical studieshave shown only segmental effects causing diminished neckpain and PPT after ipsilateral cervical mobilization.15,16
We applied a mobilization technique at the upper cer-vical spine and observed changes in the craniofacial andcervical region as well as hypoalgesic effects further awayfrom the segment to which it was applied, suggesting thatmanual therapy has a general central or at least supra-medullar effect. A physiological or sympathoexcitatoryeffect has also been demonstrated in the upper extremityafter cervical or thoracic SMT,15,39 and in the lower ex-tremities after lumbar mobilization.40
It is clear that SMT activates central structures that con-currently activate sympathoexcitatory and hypoalgesic effectsas demonstrated in our research and in that of others.15,20 Thepresence of an extrasegmental effect may indicate activation ofthe d-PAG and could be mediated by various descending paininhibitory pathways and associated tracts of the TCC thatallow for afferent and efferent transmission between the cer-vical and craniofacial regions.51,52
Nociceptive Modulation and the TCCThe increase in PPT caused by the APUCM technique
on the craniofacial region provides additional clinical
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
212 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

support for pain modulatory mechanisms in the TCC.A review performed in 1998 outlined neurophysiologicalcoupling between craniofacial and cervical systems.53
It has been observed that manual therapeutic applica-tions to the cervical region provoked a pain reducing effectin the head and face. Mellick and Mellick54 and Mellicket al55 observed that applying a bilateral intramuscular in-jection of small amounts of 0.5% bupivacaine at the cervicalregion caused a decrease in facial pain and headaches. Inaddition, Carlson et al56 demonstrated that an infiltration of2% lidocaine on an active TrP of the trapezius muscle sig-nificantly reduced pain and electromyographical activity ofthe ipsilateral masseter.
The only previous study of manual interventions to thecervical spine to manage craniofacial pain was performedby La Touche et al. This study reported similar results toour study: improved PPT at the masseter and temporalismuscles after a manual therapy protocol directed to thecervical spine combined with a deep neck flexors train-ing program.23
Convergence pathways between cervical and trigemi-nal sensory afferents in the TCC are fully supported.52,57,58
Stimulation of an upper cervical root, such as manipulationof the greater occipital nerve has produced changes in theTCC neurons. This supports the concept that perception ofcranial pain is due to a functional convergence betweentrigeminal and cervical fibers in the TCC59,60 and provides apotential rationale for the relationship between headachesand arm and trunk pain.61
Direct stimulation of the greater occipital nerve (cer-vical input) increases metabolic activity of the TCC62 andtrigeminal nociceptors release neuropeptides, such as sub-stance P, from laminas I and II that diffuse to laminas III toV depending on the intensity of the stimulus.63 The TCCitself is formed by the upper cervical dorsal horns and thetrigeminal nucleus caudalis, which allows nociceptive inputto be transmitted from the TCC to higher centers.64 Painmodulatory structures such as the PAG, dorsolateral pon-tomesencephalic tegmentum, and rostral ventromedial me-dulla control the TCC-mediated generation of antinociceptiveor pronociceptive states.57,58,65
In summary, we propose a neurobiomechanical hypo-thesis to explain the possible mechanism by which a manualtherapeutic technique causes a hypoalgesic effect in cranio-facial and cervical regions. This technique primarily influen-ces the upper cervical region (C1-C3), which is anatomicallyrelated to the occipital bone. We believe that an anterior-posterior glide of the upper cervical structures provokes animproved arthrokinematic relationship of the target regionthereby generating improved pain-free range of movementand concomitant suboccipital muscle relaxation. A secondaryeffect might reduce mechanical forces on the upper cervicalneurovascular structures, thereby interrupting or inhibitinginput and reducing TCC sensitization by activating de-scendent pain inhibitory systems.
In addition, the TCC is the main nucleus that receivesnociceptive information from the face, head, and neck.66
Neurons inside the nuclei are considered multimodal neu-rons and can receive 2 or more inputs from different ori-gins, such as cervical nerve roots, when manual therapy isbeing applied. The input generated from the cervical regioncan alter the nociceptive processing in the TCC and, as aresult, produce a hypoalgesic effect at the facial region.Finally, another possible mechanism to explain the effect ofour manual intervention is that descending pain inhibitory
systems can be activated by SMT on the cervical spine byspinal noradrenergic and serotoninergic pathways from thedorsolateral pons and rostral ventral medulla.45,46
Study LimitationsAlthough the results of our research are positive, we
only measured short-term changes without follow-up testing.We only measured SC and ST on the right side. Other studiesinvestigating sympathetic activation after SMT treatmentonly measured one side of the body, usually the treated side.Perry and colleagues applied a unilateral lumbar mobilizationand measured sympathetic activity at both lower extremities.They only observed significant activation in the treated sidebut did observe a tendency toward sympathetic activation inthe untreated side.40 It would have been interesting to observeif central mobilization activates SNS with the same intensityin both upper extremities and if it has any effect on lowerextremities. It also could have been interesting to measure SCand ST directly on the facial region. We did not measure distalPPT; therefore, due to a lack of information, we cannot pro-vide a complete discussion about the general or segmental ef-fect of the APUCM technique.
This is the first time this type of mobilization at afrequency of 0.5Hz has been used in a clinical randomized-controlled trial. Because different techniques require differ-ent frequencies of application to provoke stronger changes,it would be of interest to test the same mobilization at dif-ferent frequencies of application.
Clinical ImplicationsWe have demonstrated that craniofacial pain can be
modulated through an upper cervical treatment (mobilization).The presence of craniofacial pain is a predictor factor for neckpain.9,67 It is interesting to treat this type of patient with atechnique that has proven effects at the craniofacial segmentthat can also treat a possible neck dysfunction. This techniquemight be contraindicated in patients with craniocervical hy-permobility syndrome due to the movement the APUCMprovokes at the upper cervical spine and the risk this entails.68
Chronic pain can be maintained by SNS modulationthrough the peripheric adrenorreceptor excitation of cat-echolamine.69 Chronic TMD patients seem to present adysregulation of b-adrenergic activity, which contributes toaltered cardiovascular and catecholamine responses.70 Thedysregulation of SNS can contribute to the severity andmaintenance of pain. The influence of APUCM on SNSactivity makes this technique an interesting tool to treatpatients with CCFP of myofascial origin and patients withfacial allodynia, in which other techniques applied directlyon the face would be contraindicated.
CONCLUSIONSWe demonstrate that APUCM reduces pain intensity
and increases PPT in the cervical and craniofacial regions.APUCM also causes sympathoexcitation, which confirms asympathetic effect. These results indicate an influence of themobilization on the CNS (medullar or supramedullar effect).This study provides preliminary evidence of the short-termhypoalgesic effect on the craniofacial and cervical regions ofpatients with CCFP of myofascial origin, suggesting thatAPUCM may cause an immediate nocioceptive modulationat the TTC.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 213

REFERENCES
1. LeResche L. Epidemiology of orofacial pain. In: Lund J,Lavigne G, Dubner R, Sessle B, eds. Orofacial Pain: FromBasic Science to Clinical Management. Chicago: QuintessencePublishing Co; 2000:15–25.
2. Ciancaglini R, Testa M, Radaelli G. Association of neckpain with symptoms of temporomandibular dysfunction inthe general adult population. Scand J Rehabil Med. 1999;31:17–22.
3. Vierck CJ. Mechanisms underlying development of spatiallydistributed chronic pain (fibromyalgia). Pain. 2006;3:242–263.
4. Sarlani E, Greenspan JD. Why look in the brain for answers totemporomandibular disorder pain? Cells Tissues Organs.2005;180:69–75.
5. Turp JC, Kowalski CJ, O’Leary N, et al. Pain maps from facialpain patients indicate a broad pain geography. J Dent Res.1998;77:1465–1472.
6. Velly AM, Gornitsky M, Philippe P. Contributing factors tochronic myofascial pain: a case-control study. Pain. 2003;104:491–499.
7. Carlson CR, Reid KI, Curran SL, et al. Psychological andphysiological parameters of masticatory muscle pain. Pain.1998;76:297–307.
8. Eriksson PO, Haggman-Henrikson B, Zafar H. Jaw-neckdysfunction in whiplash-associated disorders. Arch Oral Biol.2007;52:404–408.
9. Wiesinger B, Malker H, Englund E, et al. Does a dose-responserelation exist between spinal pain and temporomandibulardisorders? BMC Musculoskelet Disord. 2009;10:28.
10. Ries LG, Berzin F. Analysis of the postural stability inindividuals with or without signs and symptoms of tempor-omandibular disorder. Braz Oral Res. 2008;22:378–383.
11. De Laat A, Meuleman H, Stevens A, et al. Correlation betweencervical spine and temporomandibular disorders. Clin OralInvestig. 1998;2:54–57.
12. Haggman-Henrikson B, Osterlund C, Eriksson PO. Enduranceduring chewing in whiplash-associated disorders and TMD.J Dent Res. 2004;83:946–950.
13. Bokarius AV, Bokarius V. Evidence-based review of manualtherapy efficacy in treatment of chronic musculoskeletal pain.Pain Pract. 2010;10:451–458.
14. Cleland JA, Childs JD, McRae M, et al. Immediate effects ofthoracic manipulation in patients with neck pain: a random-ized clinical trial. Man Ther. 2005;10:127–135.
15. Sterling M, Jull G, Wright A. Cervical mobilisation: con-current effects on pain, sympathetic nervous system activityand motor activity. Man Ther. 2001;6:72–81.
16. Sterling M, Pedler A, Chan C, et al. Cervical lateral glideincreases nociceptive flexion reflex threshold but not pressureor thermal pain thresholds in chronic whiplash associateddisorders: a pilot randomised controlled trial. Man Ther.2010;15:149–153.
17. Paungmali A, O’Leary S, Souvlis T, et al. Hypoalgesic andsympathoexcitatory effects of mobilization with movement forlateral epicondylalgia. Phys Ther. 2003;83:374–383.
18. Paungmali A, O’Leary S, Souvlis T, et al. Naloxone fails toantagonize initial hypoalgesic effect of a manual therapy treat-ment for lateral epicondylalgia. J Manipulative Physiol Ther.2004;27:180–185.
19. Chiu TW, Wright A. To compare the effects of different ratesof application of a cervical mobilisation technique on sym-pathetic outflow to the upper limb in normal subjects. ManTher. 1996;1:198–203.
20. Vicenzino B, Collins D, Benson H, et al. An investigation ofthe interrelationship between manipulative therapy-inducedhypoalgesia and sympathoexcitation. J Manipulative PhysiolTher. 1998;21:448–453.
21. Cleland JA, Glynn P, Whitman JM, et al. Short-term effects ofthrust versus nonthrust mobilization/manipulation directed atthe thoracic spine in patients with neck pain: a randomizedclinical trial. Phys Ther. 2007;87:431–440.
22. George JW, Fennema J, Maddox A, et al. The effect of cervicalspine manual therapy on normal mouth opening in asympto-matic subjects. J Chiropr Med. 2007;6:141–145.
23. La Touche R, Fernandez-de-las-Penas C, Fernandez-Carnero J,et al. The effects of manual therapy and exercise directed at thecervical spine on pain and pressure pain sensitivity in patients withmyofascial temporomandibular disorders. J Oral Rehabil. 2009;36:644–652.
24. Dworkin SF, LeResche L. Research diagnostic criteria fortemporomandibular disorders: review, criteria, examinationsand specifications, critique. J Craniomandib Disord. 1992;6:301–355.
25. Andrade Ortega JA, Delgado Martinez AD, Almecija Ruiz R.Validation of a Spanish version of the Neck Disability Index.Med Clin (Barc). 2008;130:85–89.
26. Vernon H, Mior S. The Neck Disability Index: a study ofreliability and validity. J Manipulative Physiol Ther. 1991;14:409–415.
27. Simons DG, Travel JG, Simons LS. Myofascial Pain andDysfunction: The Trigger Point Manual. Vol 1. 2nd ed.Baltimore: Lippincott Williams & Wilkins; 1999.
28. Dworkin SF, Sherman J, Mancl L, et al. Reliability, validity,and clinical utility of the research diagnostic criteria forTemporomandibular Disorders Axis II Scales: depression,non-specific physical symptoms, and graded chronic pain.J Orofac Pain. 2002;16:207–220.
29. de Leeuw R. (ed) The American Academy of Orofacial Pain.Orofacial Pain: Guidelines for Assessment, Diagnosis, andManagement. 4th ed. Chicago: Quintessence; 2008:25–27.
30. Beck AT, Steer RA. Internal consistencies of the original andrevised Beck Depression Inventory. J Clin Psychol. 1984;40:1365–1367.
31. Spielberg CDG, Lushene RL, E. R. State Anxiety Inventory.Cuestionario de ansiedad estado-rasgo. Adaptacion espanola.Madrid: TEA; 1982.
32. Bijur PE, Silver W, Gallagher EJ. Reliability of the visualanalog scale for measurement of acute pain. Acad Emerg Med.2001;8:1153–1157.
33. Svensson P, Arendt-Nielsen L, Nielsen H, et al. Effect ofchronic and experimental jaw muscle pain on pain-pressurethresholds and stimulus-response curves. J Orofac Pain.1995;9:347–356.
34. Chesterton LS, Sim J, Wright CC, et al. Interrater reliability ofalgometry in measuring pressure pain thresholds in healthyhumans, using multiple raters. Clin J Pain. 2007;23:760–766.
35. Todd KH, Funk KG, Funk JP, et al. Clinical significance ofreported changes in pain severity. Ann Emerg Med.1996;27:485–489.
36. Bird SB, Dickson EW. Clinically significant changes in painalong the visual analog scale. Ann Emerg Med. 2001;38:639–643.
37. Emshoff R, Emshoff I, Bertram S. Estimation of clinicallyimportant change for visual analog scales measuring chronictemporomandibular disorder pain. J Orofac Pain. 2010;24:262–269.
38. McGuiness J, Vicenzino B, Wright A. Influence of a cervicalmobilization technique on respiratory and cardiovascularfunction. Man Ther. 1997;2:216–220.
39. Jowsey P, Perry J. Sympathetic nervous system effects in thehands following a grade III postero-anterior rotatory mobi-lisation technique applied to T4: a randomised, placebo-controlled trial. Man Ther. 2010;15:248–253.
40. Perry J, Green A. An investigation into the effects of aunilaterally applied lumbar mobilisation technique on periph-eral sympathetic nervous system activity in the lower limbs.Man Ther. 2008;13:492–499.
41. Lindgren L, Rundgren S, Winso O, et al. Physiological res-ponses to touch massage in healthy volunteers. Auton Neurosci.2010;158:105–110.
42. Goodsell M, Lee M, Latimer J. Short-term effects of lumbarposteroanterior mobilization in individuals with low-back pain.J Manipulative Physiol Ther. 2000;23:332–342.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
214 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins
43. Schmid A, Brunner F, Wright A, et al. Paradigm shift inmanual therapy? Evidence for a central nervous systemcomponent in the response to passive cervical joint mobilisa-tion. Man Ther. 2008;13:387–396.
44. Vicenzino B, Wright A. Effects of a novel manipulativephysiotherapy technique on tennis elbow: a single case study.Man Ther. 1995;1:30–35.
45. Wright A. Hypoalgesia post-manipulative therapy: a reviewof a potential neurophysiological mechanism. Man Ther. 1995;1:11–16.
46. Skyba DA, Radhakrishnan R, Rohlwing JJ, et al. Jointmanipulation reduces hyperalgesia by activation of mono-amine receptors but not opioid or GABA receptors in thespinal cord. Pain. 2003;106:159–168.
47. Kuraishi Y, Harada Y, Aratani S, et al. Separate involvementof the spinal noradrenergic and serotonergic systems inmorphine analgesia: the differences in mechanical and thermalalgesic tests. Brain Res. 1983;273:245–252.
48. Kuraishi Y, Kawamura M, Yamaguchi T, et al. Intrathecalinjections of galanin and its antiserum affect nociceptive res-ponse of rat to mechanical, but not thermal, stimuli. Pain.1991;44:321–324.
49. Vicenzino B, Cartwright T, Collins D, et al. Cardiovascularand respiratory changes produced by lateral glide mobilizationof the cervical spine. Man Ther. 1998;3:67–71.
50. Vicenzino B, Collins D, Wright A. The initial effects of acervical spine manipulative physiotherapy treatment on thepain and dysfunction of lateral epicondylalgia. Pain. 1996;68:69–74.
51. Piovesan EJ, Kowacs PA, Tatsui CE, et al. Referred pain afterpainful stimulation of the greater occipital nerve in humans:evidence of convergence of cervical afferences on trigeminalnuclei. Cephalalgia. 2001;21:107–109.
52. Piovesan EJ, Kowacs PA, Oshinsky ML. Convergence ofcervical and trigeminal sensory afferents. Curr Pain HeadacheRep. 2003;7:377–383.
53. Browne PA, Clark GT, Kuboki T, et al. Concurrent cervicaland craniofacial pain. A review of empiric and basic scienceevidence. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.1998;86:633–640.
54. Mellick LB, Mellick GA. Treatment of acute orofacial painwith lower cervical intramuscular bupivacaine injections: a1-year retrospective review of 114 patients. J Orofac Pain.2008;22:57–64.
55. Mellick LB, McIlrath ST, Mellick GA. Treatment of head-aches in the ED with lower cervical intramuscular bupivacaineinjections: a 1-year retrospective review of 417 patients.Headache. 2006;46:1441–1449.
56. Carlson CR, Okeson JP, Falace DA, et al. Reduction of painand EMG activity in the masseter region by trapezius triggerpoint injection. Pain. 1993;55:397–400.
57. Sessle BJ. Acute and chronic craniofacial pain: brainstemmechanisms of nociceptive transmission and neuroplasticity, andtheir clinical correlates. Crit Rev Oral Biol Med. 2000;11:57–91.
58. Mason P. Deconstructing endogenous pain modulations.J Neurophysiol. 2005;94:1659–1663.
59. Pfaller K, Arvidsson J. Central distribution of trigeminal andupper cervical primary afferents in the rat studied byanterograde transport of horseradish peroxidase conjugatedto wheat germ agglutinin. J Comp Neurol. 1988;268:91–108.
60. Scheurer S, Gottschall J, Groh V. Afferent projections of therat major occipital nerve studied by transganglionic transportof HRP. Anat Embryol (Berl). 1983;167:425–438.
61. Kajander KC, Giesler GJ Jr. Responses of neurons in thelateral cervical nucleus of the cat to noxious cutaneous stimu-lation. J Neurophysiol. 1987;57:1686–1704.
62. Goadsby PJ, Knight YE, Hoskin KL. Stimulation of thegreater occipital nerve increases metabolic activity in thetrigeminal nucleus caudalis and cervical dorsal horn of the cat.Pain. 1997;73:23–28.
63. Li JL, Wang D, Kaneko T, et al. The relationship betweenneurokinin-1 receptor and substance P in the medullary dorsalhorn: a light and electron microscopic immunohistochemicalstudy in the rat. Neurosci Res. 2000;36:327–334.
64. Bartsch T, Goadsby PJ. Stimulation of the greater occipitalnerve induces increased central excitability of dural afferent input.Brain. 2002;125:1496–1509.
65. Hjornevik T, Jacobsen LM, Qu H, et al. Metabolic plasticity inthe supraspinal pain modulating circuitry after noxiousstimulus-induced spinal cord LTP. Pain. 2008;140:456–464.
66. Hu JW, Sun KQ, Vernon H, et al. Craniofacial inputs to uppercervical dorsal horn: implications for somatosensory informa-tion processing. Brain Res. 2005;1044:93–106.
67. Marklund S, Wiesinger B, Wanman A. Reciprocal influence onthe incidence of symptoms in trigeminally and spinallyinnervated areas. Eur J Pain. 2010;14:366–371.
68. Aspinall W. Clinical testing for the craniovertebral hyper-mobility syndrome. J Orthop Sports Phys Ther. 1990;12:47–54.
69. Ren Y, Zou X, Fang L, et al. Sympathetic modulation ofactivity in Adelta- and C-primary nociceptive afferents afterintradermal injection of capsaicin in rats. J Neurophysiol.2005;93:365–377.
70. Light KC, Bragdon EE, Grewen KM, et al. Adrenergicdysregulation and pain with and without acute beta-blockadein women with fibromyalgia and temporomandibular disorder.J Pain. 2009;10:542–552.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 215

205
DISCUSIÓN

206
6. DISCUSIÓN
Los hallazgos mostrados en esta tesis coinciden con una gran cantidad de estudios
recientes publicados en las últimas dos décadas. En estas investigaciones de carácter
básico y clínico se ha comprobado como las estructuras cervicales pueden influir sobre
características sensoriales y motoras de la regiones craneofacial y craneomandibular y
viceversa (Armijo-Olivo and Magee, 2007, 2013; Dessem and Luo, 1999; Eriksson et
al., 2004, 2007; Ge et al., 2004; Giannakopoulos, Hellmann, et al., 2013;
Giannakopoulos, Schindler, et al., 2013; Häggman-Henrikson and Eriksson, 2004;
Häggman-Henrikson et al., 2013; Haggman-Henrikson et al., 2004; Hellmann et al.,
2012; Hellström et al., 2002; Hu et al., 2005; Olivo et al., 2010; Svensson et al., 2005;
Torisu et al., 2014). La investigación básica en torno a la neurofisiología del CTC ha
servido para establecer hipótesis y teorías relacionadas con los mecanismos
nociceptivos periféricos y centrales implicados en (Bartsch and Goadsby, 2002, 2003a;
Bereiter et al., 2005; Chiang et al., 1998, 2005; Hu et al., 1993; Lam et al., 2009; Salter,
2004; Sessle et al., 1986; Yu et al., 1995): 1) las comorbilidades entre las dolencias
cervicales y craneofaciales; 2) en la concomitancia motora entre la región
craneomadibular y craneocervical; 3) en las respuestas motoras alteradas; y 4) en las
posibles intervenciones terapéuticas sobre la región cervical que pudieran influir sobre
la región craneofacial. Los resultados de las investigaciones presentadas en esta tesis
ofrecen algunos hallazgos importantes que fortalecen la investigación previa en relación
con esto cuatro puntos. A continuación se discute en profundidad los resultados
obtenidos según los objetivos planteados en la tesis.

207
6.1 Diferencias de Género en la Variables Somatosensoriales.
En el análisis del efecto del género sobre variables somatosensoriales en pacientes con
DCCF hay que partir de una premisa epidemiológica y es que como está representado
en nuestros estudios, la prevalencia de estas dolencias es mayor en la población
femenina (Adèrn et al., 2014; Carlsson, 1999; LeResche, 1997; Macfarlane, Blinkhorn,
Davies, Kincey, et al., 2002). Hemos encontrado en el estudio III (La Touche et al.,
2010) y en el estudio V (La Touche, Paris-Alemany, et al., 2014) influencias del género
sobre variables somatosensoriales.
En relación al estudio V (La Touche, Paris-Alemany, et al., 2014) los resultados
mostraron que la percepción del dolor y la fatiga durante el test masticatorio de
provocación estuvo influenciada por el género en los tres grupos evaluados, se observó
que las mujeres presentan una mayor percepción de intensidad de dolor y fatiga
masticatoria, estos resultados coinciden con estudios previos de dolor inducido
experimentalmente realizados con pacientes (Haggman-Henrikson et al., 2004) y
sujetos sanos (Karibe et al., 2003; Plesh et al., 1998), sin embargo es importante
mencionar que otras investigaciones no han observado la interacción del factor genero
sobre el dolor o la fatiga masticatoria inducida experimentalmente (Koutris et al., 2013;
van Selms et al., 2005). El estudio V no está diseñado con el objetivo de identificar los
mecanismos fisiológicos o psicológicos que puedan explicar las diferencias en los
resultados entre mujeres y hombres, sin embargo es importante destacar que la
evidencia de estudios experimentales relacionados con dolor inducido indica que las
mujeres presentan mayor sensibilidad al dolor que los hombres en diferentes pruebas
somatosensoriales (Fillingim et al., 2009). Finalmente destacar que en el estudio III (La
Touche et al., 2010), solo se identificó una interacción con el género en los UDPS del

208
músculo tibial anterior, mostrando unos valores significativamente menores en mujeres
respecto a la población masculina del estudio.
6.2 Postura Craneocervical, Dinámica Mandibular y Dolor Craneofacial.
Dos investigaciones (I, (La Touche et al., 2011) y II (Lopez-de-Uralde-Villanueva et
al., 2014) de esta tesis han estudiado la influencia de la postura craneocervical sobre la
función mandibular y las posibles interacciones con mecanismos nociceptivos
trigeminales. Los resultados demuestran que las posturas craneocervicales inducidas
experimentalmente producen modificaciones en MAI presentándose menor o mayor
rango articular según la postura en que se realice el gesto (La Touche et al., 2011), estos
hallazgos también fueron comprobados por Higbie y cols. en 1999 (Higbie et al., 1999).
Además, evidencia previa refuerza estos hallazgos, ya que se han descrito las
modificaciones intra-articulares que se producen en ATM con diferentes posturas
craneocervicales o movimientos cervicales (Ohmure et al., 2008; Solow and Tallgren,
1976; Visscher et al., 2000).
Otro resultado que consideramos relevante en el estudio I, fue que los UDPS de áreas
trigeminales se vieron modificados según las diferentes posturas craneocervicales
siendo el menor UDP registrado en la postura de protracción. Este resultado es difícil
discutirlo ya que no hay estudios similares en esta línea, nosotros plantemos
teóricamente que esto puede suceder debido a cambios o ajustes que realiza el sistema
nervioso bajo diferentes condiciones del entorno y demandas de la región cervical,
creemos que estos ajustes se producen en mecanismos sensoriales pero también en los
motores. En relación a esto, debemos mencionar que contamos con evidencia previa que
describe que los movimientos cervicales o las posturas craneocervicales inducidas
experimentalmente modifican la actividad de la musculatura masticatoria

209
incrementándola (Ballenberger et al., 2012; Forsberg et al., 1985; McLean, 2005;
Ohmure et al., 2008).
En el estudio II (Lopez-de-Uralde-Villanueva et al., 2014) se encontraron diferencias en
la postura craneocervical medido con dos instrumentos entre el grupo de pacientes con
DCCF y los sujetos asintomáticos, sin embargo es fundamental tener en cuenta que esos
cambios fueron muy pequeños y en una de la mediciones no superó el MCD y en la otra
los superó pero por muy poco, estos resultados se han encontrado prácticamente con las
mismas similitudes en investigaciones realizadas en pacientes con dolor de cuello
(Silva et al., 2009) y con TCM (Armijo-Olivo et al., 2011) comparada con sujetos
asintomáticos. Por otra parte, cabe mencionar que no se encontró asociación entre la
postura craneocervical con las variables de discapacidad cervical y craneofacial, datos
de otras investigaciones apoyan este resultado (Armijo-Olivo et al., 2011; Cheung et al.,
2010) aunque otros lo contradicen (Lau et al., 2010). La relación entre la postura y los
TCM es controvertida y no está clara según datos extraídos de dos revisiones
sistemáticas recientes (Armijo Olivo et al., 2006; Rocha et al., 2013), además ambas
revisiones coinciden en recalcar que los estudios analizados en relación a esta temática
presentan serias dificultades metodológicas y complica la posibilidad de extraer
conclusiones.
6.3 Influencia del Dolor y la Discapacidad Cervical sobre la Actividad
Sensoriomotora Trigeminal.
En los estudios III (La Touche et al., 2010) y V (La Touche, Paris-Alemany, et al.,
2014) se han obtenido resultados importantes entorno a la influencia del dolor y la
discapacidad de cuello sobre la región craneofacial, específicamente en el estudio V
hemos identificado que los pacientes con moderada y leve discapacidad cervical
210
presentan mayores niveles de percepción de dolor y fatiga frente a los sujetos sanos
sometidos al test de provocación masticatorio, es importante mencionar que entre los
grupos de pacientes, el de moderada discapacidad cervical fue el que presentó mayores
cambios en las variables sensoriales medidas durante el test, inmediatamente después y
las 24 horas, La única excepción de esto ha sido en el resultado de la percepción de
intensidad dolor a las 24 horas en que entre ambos grupos no se presentaron diferencias
estadísticamente significativas. A pesar de que existen muchos estudios que utilizan los
test provocación masticatorias para inducir dolor y fatiga (Christensen et al., 1996; Dao
et al., 1994; Farella et al., 2001; Gavish et al., 2002; Karibe et al., 2003; Koutris et al.,
2009; Plesh et al., 1998), solo hemos encontrado un estudio similar al nuestro (estudio
V), (La Touche, Paris-Alemany, et al., 2014), en este Haggman-Henrikson y cols.
(Haggman-Henrikson et al., 2004) observaron que los pacientes con latigazo cervical
presentaron mayores niveles de dolor y fatiga masticatoria inducida por el test que los
pacientes con TCM y sujetos asintomáticos. Diversos estudios experimentales y clínicos
han descrito conexiones funcionales entre las regiones craniofacial y cervical a través de
patrones de convergencia neural en el CTC (Dessem and Luo, 1999; Ge et al., 2004;
Hellström et al., 2002; Hu et al., 2005; Svensson et al., 2005; Torisu et al., 2013; Wang
et al., 2004), en relación con esto se ha observado en estudios experimentales que el
dolor inducido por la infiltración de sustancias algógenas en músculos masticatorios o
cervicales modifican de forma bidireccional la actividad de los reflejos de estiramiento
(Ge et al., 2004; Wang et al., 2004) además, en investigaciones básicas con animales se
ha observado una relación refleja entre la actividad de los nociceptores de la ATM y
actividad del sistema fusimotor de los músculos de cuello (Hellström et al., 2002), esta
información es útil para plantear teorías acerca de la influencia de la región cervical

211
sobre los posibles mecanismos nociceptivos (sensoriales) y motores implicados en el
dolor y la fatiga masticatoria.
Contamos con evidencia científica reciente que demuestra que lesiones sobre la región
cervical pueden alterar el control motor masticatorio y la función mandibular normal de
apertura-cierre (Eriksson et al., 2004, 2007; Zafar et al., 2006), los hallazgos de estudio
V se pueden relacionar con esta cuestión ya que nuestros resultados muestran que el test
de provocación masticatorio reduce la MAI libre de dolor al finalizar el test en los tres
grupos, este resultados son similares a la de otros estudios (Karibe et al., 2003;
Svensson et al., 2001), sin embargo hay que tomar en cuenta que esta disminución fue
mayor en los grupos de pacientes y se mantuvo a las 24 horas únicamente en el grupo de
moderada discapacidad cervical, además es importante destacar que el análisis de
regresión mostró que la discapacidad cervical es un predictor de la MAI libre de dolor
(después de 24 horas) en los dos grupos de pacientes. Planteamos la teoría de que los
patrones motores masticatorios estén más alterados a medida que se tenga mayor dolor
o discapacidad cervical, esta situación generaría la activación de mecanismos
compensatorios des-adaptativos que alterarían la conducta, el reclutamiento y la
coordinación de los sistemas motores del cuello y la mandíbula generando mayores
niveles de fatiga y dolor durante los test de provocación y manteniendo estas
sensaciones 24 horas después. Esta misma teoría podría servir para explicar los
resultados de la disminución de los umbrales del dolor a la presión de regiones
trigeminales y cervicales, cabe destacar que los cambios UDPs fueron mayores en los
grupos de pacientes y que la mayoría de cambios en los UDPs de la región cervical a las
24 horas se produjeron en el grupo de moderada discapacidad cervical, como factor
coadyuvante a este situación hay que considerar que la presencia de dolor cuello puede
provocar menores valores de UDPs en puntos trigeminales en comparación con sujetos

212
sanos como se observó en el estudio III (La Touche et al., 2010). Aunque consideramos
que puede haber una relación directa entre los cambios sensoriomotores trigeminales
con el dolor y la discapacidad cervical, también tenemos que tener en cuenta la
posibilidad de que en los pacientes los cambios se hubieran visto influenciados
mayoritariamente por la presencia de cambios neuroplásticos ya establecidos a nivel
central; se conoce actualmente que los pacientes con dolor crónico pueden tener mayor
susceptibilidad de presentar un proceso de sensibilización central (Henry et al., 2011),
Wolf y cols. sugieren que en condiciones dolorosas en donde existe una comorbilidad
como es el caso de la muestra de pacientes de este estudio, puede ser un factor
determinante en la pato-fisiología de la sensibilización central (Woolf, 2011). En
relación con esto, Gaff-Radford propone que en la sensibilización central se producen
cambios en las vías aferentes que hacen posible la comunicación de las neuronas
nociceptivas cervicales y orofaciales en el núcleo trigeminal (Graff-Radford, 2012). A
esto hay que añadir que son muchos los estudios que han encontrado en pacientes con
TCM mecanismos periféricos y centrales compatibles con un proceso de sensibilización
central (Anderson et al., 2011; Ayesh et al., 2007; Chaves et al., 2013; Feldreich et al.,
2012; Park et al., 2010; Raphael et al., 2009; Sarlani et al., 2004), sin embargo es
importante destacar que en el grupo de pacientes con dolor de cuello crónico mecánico
del estudio III solo se encontraron diferencias en UDPs en áreas trigeminales y
cervicales pero no en zonas distales, estos nos lleva a pensar que en este tipo de
pacientes hay una posible sensibilización central especifica del CTC.

213
6.4. Asociación entre la Discapacidad Cervical y la Discapacidad
Craneofacial/craneomandibular.
En los estudios II (Lopez-de-Uralde-Villanueva et al., 2014) y IV (La Touche, Pardo-
Montero, et al., 2014) se demostró una correlación positiva fuerte-moderada entre la
discapacidad cervical y la discapacidad craneofacial (r=0,79 y r=0,65 respectivamente),
es posible que el resultado del estudio II fuese mejor por la especificidad de la muestra
de pacientes con DCCF seleccionados, hay que tomar en cuenta que la muestra del
estudio IV la conformaron pacientes con diversos tipos de DCF en donde posiblemente
la discapacidad y estatus funcional mandibular no tenga tanto peso, pero esta es una
suposición que se tendrá que comprobar futuras investigaciones. Los resultados de los
estudios II y IV son apoyados por la investigación de Olivo y cols., en esta se encontró
una correlación positiva muy fuerte entre las dos variables de discapacidad (r=0,82)
(Olivo et al., 2010).
6.5 Factores Bioconductuales Implicados en las Alteraciones Sensoriomotoras
Trigeminales y la Discapacidad Craneofacial.
En los estudios III (La Touche et al., 2010), IV (La Touche, Pardo-Montero, et al.,
2014) y V (La Touche, Paris-Alemany, et al., 2014) se utilizaron medidas de auto-
registro relacionadas con el dolor, la discapacidad y factores psicológicos para analizar
las posibles asociaciones con variables sensoriomotoras.
En el estudio V, el análisis de regresión lineal múltiple mostró que el catastrofismo del
dolor y el impacto de la cefalea sobre la calidad de vida (HIT-6) se asociaron a las
variables de percepción de dolor y fatiga 24 horas después de haber realizado el test de
provocación masticatoria. Específicamente en el estudio V el catastrofismo ante el dolor
fue un factor psicológico analizado y mostró ser un predictor de la fatiga a las 24 horas

214
en el grupo de moderada discapacidad cervical y en el grupo de leve discapacidad
cervical también fue predictor para la fatiga y la intensidad de dolor percibido 24 horas
después del test provocación masticatorio. El catastrofismo ante dolor se define como
un factor cognitivo que implica una percepción mental negativa o exagerada de la
amenaza percibida tanto real como anticipada de la experiencia de dolor (Sullivan et al.,
2001; Turner and Aaron, 2001).
En cuanto a la fatiga percibida y el catastrofismo no encontramos estudios clínicos o
experimentales en los que hayan estudiado la asociación en pacientes con DCF o TCM,
pero si hemos encontrado dos estudios sobre la relación del catastrofismo del dolor con
variables cinemáticas masticatorias (Akhter et al., 2014; Brandini et al., 2011). En el
estudio realizado por Akhter y cols. se investigó el efecto de un dolor experimental
agudo en una muestra dividida en sujetos con poco catastrofismo y alto catastrofismo,
los resultados de esta investigación mostraron que la intensidad del dolor percibida fue
más alta en los sujetos con mayor catastrofismo y además en este mismo grupo se
observó una velocidad más lenta y mayor variabilidad en los movimientos mandibulares
repetidos, los autores de este estudio sugieren que los cambios en la coordinación
motora son un ejemplo de conducta de evitación que afectan la función del sistema
motor mandibular (Akhter et al., 2014). En la otra investigación, Brandini y cols.
estudiaron variables cinemáticas masticatorias durante un procedimiento de exposición
muy corto (15 segundos) en pacientes con TMC atribuidas a dolor miofascial, en este
estudio no se observaron asociaciones de las variables cinemáticas medidas con
respecto al catastrofismo, sin embargo hay que tomar en cuenta que el propósito del
estudio no era inducir dolor o fatiga para observar la respuesta como si lo hemos hecho
en el estudio V (La Touche, Pardo-Montero, et al., 2014).

215
Se debe destacar que en una revisión sistemática muy reciente se concluye que hay una
asociación entre el catastrofismo y la fatiga y que el primero influye proporcionalmente
sobre la segunda y estos resultados se observaron en diversas poblaciones clínicas
(Lukkahatai and Saligan, 2013), también se ha demostrado que en otras dolencias
musculoesqueléticas el catastrofismo del dolor se vio asociado a alteraciones motoras
como la disminución del funcionamiento y rendimiento de las actividades de la vida
diaria y limitación de la capacidad para realizar ejercicio (Meeus et al., 2012; Nijs et al.,
2008, 2012). Además este constructo se ha asociado con una mayor utilización de los
servicios de salud, con la aparición de mayores hallazgos clínicos en la valoración, con
un estado de ánimo negativo (Turner et al., 2001; Turner, Brister, et al., 2005) y con
una alteración estatus funcional mandibular (La Touche, Pardo-Montero, et al., 2014)
como hemos comparado en el estudio IV.
En el estudio IV se evaluó la validez del constructo realizando un análisis de
correlaciones entre la discapacidad craneofacial medida con el IDD-CF con otras
medidas de auto-registro psicológicas y de discapacidad. Se observó una correlación
moderada entre IDD-CF con el HIT-6 y la EVA (r = 0,38 hasta 0,46). Además, ECD y
TSK-11 mostraron una correlación moderada con el IDD-CF y con la sub-escala de
dolor y la discapacidad (r = 0,36 hasta 0,52). Esto es coherente con los datos recientes
que demuestran que los pacientes con DCF y TCM reportaron mayores niveles de
catastrofismo (Campbell et al., 2010; Fillingim et al., 2011; Quartana et al., 2010).
Además el catastrofismo ante el dolor se ha asociado con la progresión hacia altos
niveles de intensidad del dolor y de discapacidad en pacientes con DCF crónica
(Buenaver et al., 2008, 2012; Holroyd et al., 2007; Rantala et al., 2003; Velly et al.,
2011).

216
Evidencia previa ha demostrado la relación entre el miedo a los movimientos de la
mandíbula y el DCF (Rollman et al., 2012; Visscher et al., 2010), pero la evidencia
hasta el momento se consideraba limitada. Sin embargo, hay estudios que demuestran
que el miedo al dolor y al movimiento se asocia a una disminución de las actividades de
la vida diaria y también ha sido identificado como un fuerte predictor de discapacidad
en otros trastornos musculoesqueléticos crónicos (Buer and Linton, 2002; Crombez et
al., 1999; Kamper et al., 2012; Vlaeyen et al., 1999; Walton and Elliott, 2013). El
catastrofismo ante el dolor y el miedo relacionado con el dolor son dos constructos que
se han vinculado a la cronicidad del dolor musculoesquelético a través del "Modelo de
miedo-evitación" (Leeuw et al., 2007). En el estudio IV se realizó un análisis de
regresión lineal múltiple en donde se identificó que la intensidad del dolor (EVA: β =
0,19; P = 0,001) y el miedo al dolor y al movimiento (TSK-11: β = 0,17; P = 0,004)
fueron predictores del DCF. Para el estado funcional de la mandíbula y la discapacidad
craneofacial el predictor fue el catastrofismo del dolor (ECD-magnificación: β = 0,25; P
<0,001; β = 0,20; P = 0,007).
La relación entre los factores psicosociales, la actividad motora y el dolor parece estar
presente en diversos casos de dolor musculoesquelético, sin embargo la explicación para
la misma es compleja y limitada hasta el momento. Peck y cols. (Peck et al., 2008) y
Murray y Peck (Murray and Peck, 2007) han planteado una posible explicación y para
ello han generado un nuevo modelo explicativo denominado Modelo integrado de
adaptación al dolor (MIAD). Este modelo explica básicamente que la influencia del
dolor sobre la actividad motora depende de la interacción de las características
multidimensionales (biológicas y psicosociales) del dolor con el sistema sensoriomotor
de un individuo que termina generando una nueva estrategia de reclutamiento motor con
el objetivo de minimizar el dolor, sin embargo esta respuesta motora puede asociarse a
217
la aparición de otra dolencia o al empeoramiento del dolor existente (Murray and Peck,
2007; Peck et al., 2008). Este modelo se apoya en el carácter multidimensional
(sensorial discriminativa, afectiva-emocional, cognitiva) que presenta la experiencia de
dolor y cómo este influye sobre el sistema sensoriomotor a través de las conexiones
periféricas y centrales que tiene este sistema con el sistema nervioso autónomo, el
sistema límbico y otros centros superiores (Craig, 2003; Peck et al., 2008).
Recientes estudios de neuroimagen han comprobado como el catastrofismo ante el dolor
(rumiación y desesperanza) puede influir sobre diversas áreas de la corteza cerebral en
pacientes con TCM (Kucyi et al., 2014; Salomons et al., 2012). Salomons y cols.
(Salomons et al., 2012) encontraron en pacientes con TCM una correlación entre la
desesperanza (sub-escala de la ECD) y el grosor cortical del área motora suplementaria
(AMS) y la corteza cingulada media (CCM), los autores de esa investigación sugieren
que la activación de esas áreas en los pacientes con TCM podrían tener una implicación
en aspectos cognitivos de la conducta motora incluyendo las alteraciones de la respuesta
motora, hay que tomar en cuenta que el AMS neurofisiologicamente está implicada en
la planificación del acto motor (Nachev et al., 2007, 2008) y el CCM se ha asociado con
la selección óptima de respuestas motoras en condiciones de incertidumbre (Shackman
et al., 2011). En relación a los pacientes con TCM que presentaron altos niveles de
rumiación (sub-escala de la ECD), Kucyi y cols. (Kucyi et al., 2014) encontraron una
correlación positiva de aumento de la conectividad funcional del córtex prefrontal
medial con la corteza cingulada posterior, el tálamo medial, la corteza retroespinal y la
sustancia gris periacueductal/periventricular, estos resultados indican que la rumiación
ante el dolor podría influir sobre áreas relacionadas con aspectos afectivos y
emocionales de la experiencia dolorosa y con áreas del sistema inhibitorio descendente
del dolor. Parece ser que los cambios funcionales o estructurales en áreas cerebrales no
218
solo se presentan en pacientes catastrofistas con TCM, también en otro estudio de
neuroimagen, pero en este caso en pacientes con fibromialgia que presentaban
considerables niveles de catastrofismo, se observó un incremento de actividad en áreas
cerebrales relacionadas con la anticipación del dolor, la atención al dolor, aspectos
emocionales del dolor y el control motor (Gracely et al., 2004), similares resultados se
han encontrado en otras dolencias musculoesqueléticas (Brown et al., 2014).
En el estudio III (La Touche et al., 2010) no se encontraron asociaciones entre los UDPs
de áreas trigeminales o cervicales con las medidas de síntomas depresivos o de
ansiedad. Introducir en esta investigación la valoración de estos síntomas lo
consideramos de gran interés teniendo en cuenta que estos dos factores emocionales se
han relacionado con diferentes situaciones de dolor (Castillo et al., 2013; Roddy et al.,
2013; Simons et al., 2014), a pesar de esto no hemos encontrado ningún tipo de
asociación de los síntomas de ansiedad con otras variables relacionadas con el dolor y la
discapacidad de este estudio. En relación con los síntomas depresivos sí encontramos
una asociación positiva con la intensidad (rho=0,65; P= 0,001) y la cronicidad del dolor
(rho=0,54; P=0.004) y este es un hecho que es recogido por una amplia parte de la
literatura científica (Salama-Hanna and Chen, 2013; Yalcin and Barrot, 2014).
6.6 Efecto del Tratamiento en la Región Cervical sobre el Dolor Craneofacial.
Los resultados de los estudios VI y VII (La Touche et al., 2009, 2012) demuestran que
el tratamiento de fisioterapia en la región cervical produce cambios en los UDPs de
áreas trigeminales y además una disminución en la intensidad del dolor de forma
inmediata y a corto plazo (3 meses), este es un hallazgo que consideramos relevante
teniendo en cuenta que son las primeras investigaciones que estudian estas
intervenciones sobre pacientes con TCM. Otros estudios en pacientes con cefaleas han

219
encontrado resultados similares en cuanto a la modulación del dolor con métodos
aplicados en la región cervical como técnicas de neuro-estimulación periférica del
nervio occipital (Jasper and Hayek, 2008; Lee and Huh, 2013; Saper et al., 2011; Serra
and Marchioretto, 2012; Silberstein et al., 2012; Slavin et al., 2006), infiltraciones
locales (Ashkenazi and Levin, 2007; Mellick and Mellick, 2003, 2008; Mellick et al.,
2006; Saracco et al., 2010) o tratamientos de terapia manual (Castien et al., 2011, 2012,
2013; Espí-López and Gómez-Conesa, 2014; Espí-López et al., 2014; van Ettekoven
and Lucas, 2006; Hall et al., 2007; Mongini et al., 2012; Ylinen et al., 2010).
Otro resultado a destacar, en relación al estudio VI (La Touche et al., 2009) es que el
tratamiento sobre la región cervical basado en terapia manual y ejercicio mejora la MAI
libre de dolor. Este hallazgo es interesante ya que estudios experimentales previos
demostraron que una fijación inducida experimentalmente sobre la región cervical altera
la dinámica mandibular disminuyendo el movimiento y la coordinación mandibular
(Häggman-Henrikson et al., 2006). A partir de estos datos, nosotros planteamos
teóricamente que la mejora de la función de la región cervical a través del tratamiento
de fisioterapia puede evocar mecanismos de modulación del dolor en el CTC que
regularían los efectos nociceptivos periféricos y centrales mejorando a su vez la
dinámica mandibular y las estrategias motoras concomitantes cérvico-
craneomandibulares.
6.7 Implicaciones Científicas y Clínicas
De acuerdo al conjunto de resultados de los estudios de esta tesis podemos afirmar que
la discapacidad y el dolor cervical pueden influir sobre variables sensoriales y motoras
del sistema masticatorio; estos hallazgos nos llevan a reflexionar acerca de la
importancia de incluir a nivel clínico una valoración específica de la región cervical
para los protocolos diagnósticos de los TCM. Cabe destacar que los métodos
220
diagnósticos y de clasificación más utilizados para los pacientes con TCM no incluyen
una valoración especifica del dolor y la discapacidad cervical (Benoliel et al., 2011;
Schiffman et al., 2010, 2014). Un criterio diagnóstico recientemente observado en los
pacientes con cefalea atribuida a TCM es que los movimientos mandibulares, la función
o la parafunción modifican el dolor sobre la región temporal (Schiffman et al., 2012).
Nosotros hemos observado la asociación de la discapacidad cervical con la MAI libre de
dolor, además hemos identificado que los pacientes con mayor discapacidad cervical
presentan mayor fatiga y dolor inducido por el test masticatorio. Estos hallazgos nos
llevan a suponer que la región cervical puede tener un papel importante sobre este tipo
de cefalea, pero esto tiene que confirmarse en futuras investigaciones ya que estos datos
se pueden extrapolar únicamente a los pacientes con cefalea atribuida a TCM que
además presentaban dolor y discapacidad de cuello. Sabemos en la actualidad que la
prevalencia de dolor de cuello en los pacientes con TCM es muy alta, pero no sabemos
en la actualidad la influencia que tiene la región cervical en aquellos pacientes que no
presentan dolor cuello.
Desde el punto de vista del tratamiento, el plantear un abordaje para reducir el dolor y
la discapacidad cervical como parte de la estrategia terapéutica global podría ser
beneficioso para reducir los síntomas sensoriales negativos y mejorar el control motor
masticatorio, consideramos que este planteamiento debe seguir siendo investigado en
futuros estudios. Parte de los hallazgos de esta tesis demuestran que tratamientos de
fisioterapia basados en terapia manual y ejercicio terapéutico sobre la región cervical
producen efectos positivos sobre la modulación del dolor en áreas trigeminales y sobre
la mejora de la MAI libre de dolor (La Touche et al., 2009, 2012), con los cual
consideramos que es positivo integrarlos en los protocolos actuales para este tipo de
pacientes.
221
En varios de los estudios de esta tesis y en otros estudios longitudinales o transversales
se ha observado la influencia de factores psicosociales sobre pacientes con TCM (Chen
et al., 2013; Fillingim et al., 2011, 2013). Específicamente nuestros resultados muestran
una asociación entre el catastrofismo y la kinesiofobia con variables funcionales, de
discapacidad y DCF, estos hallazgos ponen en manifiesto la interacción entre variables
de tipo sensorial con variables psicológicas y esto debería considerarse como una
cuestión determinante a la hora de plantear la valoración o de diseñar las intervenciones
terapéuticas; en pacientes con dolor crónico es fundamental reconocer factores
psicosociales que pueden ser percibidos como obstáculos para la recuperación (Main,
2013): se ha observado que lograr una disminución del catastrofismo del dolor es un
buen predictor de éxito de la rehabilitación en condiciones de dolor (Sullivan, 2013).
La integración de una perspectiva bioconductual en el razonamiento clínico y en la toma
de decisiones podría ser un punto clave en el manejo del dolor y la reeducación motora
en pacientes con DCF y TCM. Se ha demostrado que el tratamiento cognitivo-
conductual disminuye la intensidad del dolor, los síntomas depresivos, mejora la
función masticatoria (Turner et al., 2006), reduce el catastrofismo en pacientes que
sufren TCM crónicos (Turner, Mancl, et al., 2005) y además se ha observado que en
casos de dolor crónico provoca cambios neuroplásticos adaptativos asociados a una
disminución del catastrofismo del dolor (Seminowicz et al., 2013). Prescribir ejercicio
terapéutico puede ser una buena alternativa a tener en cuenta: en relación a esto se ha
observado que el ejercicio en pacientes con dolor lumbar crónico produce una reducción
del catastrofismo y de los síntomas depresivos y estos resultados fueron similares al
tratamiento cognitivo-conductual (Smeets et al., 2006)
222
6.8 Limitaciones y Futuras Investigaciones
Los resultados de esta tesis se han discutido con la consideración de que hay varias
limitaciones que hemos tenido en cuenta y que presentamos a continuación. En los
estudios que conforman esta tesis se han tenido en cuenta algunas variables relacionadas
con la discapacidad y el dolor en la región cervical, sin embargo consideramos que aún
es necesario cuantificar más aspectos de las posibles alteraciones funcionales de la
región cervical como por ejemplo, los rangos de movimiento, la resistencia muscular, la
propiocepción craneocervical y analizar si estas alteraciones pueden tener alguna
relevancia clínica sobre las alteraciones motoras craneomandibulares o sobre el DCF;
sería necesario que futuros estudios precisaran aún más estos aspectos ya que podrían
generar nuevos datos que puedan servir para plantear alternativas diagnósticas y
terapéuticas.
Otra limitación a tener en cuenta, es que en los estudios en donde se ha planteado
intervenciones terapéuticas (VI, VII) solo se han medido los efectos inmediatos y a
corto plazo. Futuros estudios deberían investigar si estas intervenciones tienen un efecto
mantenido a medio y a largo plazo, por otra parte sería necesario realizar estudios de
efectividad de este tipo de intervenciones frente a tratamientos farmacológicos, férulas
oclusales o inclusive otros tratamientos de fisioterapia basados en agentes físicos o
tratamientos de electroterapia.
En esta tesis se han identificado algunos factores psicológicos que han presentado
asociación con la función mandibular y con la discapacidad y el DCF. Desde el
planteamiento neurobiológico de la experiencia multidimensional del dolor (sensorial-
discriminativa, emocional-afectiva, cognitiva) creemos que el haber incluido estas
variables es un acierto ya que ofrece una perspectiva más global de la problemática. A

223
pesar de esto y haciendo una reflexión profunda consideramos que hay otras variables
que son necesarias identificar como por ejemplo la autoeficacia o el tipo de estrategias
de afrontamiento ante el dolor, entre otras. Además sería necesario que los factores
psicológicos identificados como relevantes se sigan estudiando pero con diseños tipo
cohorte, de esta forma se podría establecer relaciones causa efecto. Finalmente y en
relación con la anterior reflexión, creemos que es importante realizar ensayos clínicos
aleatorizados controlados con un enfoque bioconductual donde las intervenciones que se
utilicen se establecieran de forma multimodal para de esta forma intentar influir sobre
variables psicosociales, sensoriales y motoras.

224

225
CONCLUSIONES

226
7. CONCLUSIONES.
1. Las posturas craneocervicales inducidas experimentalmente modifican la
dinámica mandibular y alteran los umbrales de dolor a la presión en áreas
trigeminales en pacientes con trastornos craneomandibulares.
2. Existen pequeñas diferencias en la postura craneocervical entre pacientes con
dolor cérvico-craneofacial y sujetos asintomáticos, pero no se encontraron
asociaciones entre la postura craneocervical y la discapacidad cervical y
craneofacial.
3. Los pacientes con cefalea atribuida a trastornos craneomandibulares con
moderada discapacidad cervical presentan mayores niveles de intensidad de
dolor y fatiga en el test de provocación masticatorio, así como menores umbrales
de dolor a la presión trigeminales y cervicales y una disminución de la máxima
apertura interincisal libre de dolor a las 24 horas posteriores al test de
provocación masticatorio, que los pacientes con leve discapacidad cervical y
sujetos asintomáticos.
4. Los pacientes con dolor de cuello crónico mecánico presentan una hiperalgesia
mecánica en áreas cervicales y trigeminales pero no en áreas extra-trigeminales,
por tanto la sensibilización central en el complejo trigeminocervical podría ser
un mecanismo involucrado en el mantenimiento del dolor de estos pacientes.
5. Existe una asociación entre la discapacidad cervical y la discapacidad
craneofacial en pacientes con dolor craneofacial.
6. La discapacidad cervical es un predictor de la disminución de la máxima
apertura interincisal libre de dolor.
7. La kinesiofobia y catastrofismo ante el dolor son predictores del dolor, la
discapacidad craneofacial y el estatus funcional mandibular.

227
8. El catastrofismo ante el dolor es un predictor de la fatiga masticatoria en
pacientes con cefalea atribuida a trastornos craneomandibulares.
9. Los síntomas depresivos presentan una asociación con la cronicidad y la
intensidad del dolor en pacientes con dolor de cuello crónico mecánico.
10. Las intervenciones fisioterápicas de terapia manual y ejercicio terapéutico sobre
la región cervical provocan efectos hipoalgesicos en áreas cervicales y
trigeminales y mejoran la máxima apertura interincisal libre del dolor en
pacientes con trastornos craneomandibulares.

228

229
BIBLIOGRAFÍA
230
8. BIBLIOGRAFÍA
Adèrn B, Stenvinkel C, Sahlqvist L, Tegelberg A. Prevalence of temporomandibular
dysfunction and pain in adult general practice patients. Acta Odontol. Scand. 2014: 1–6.
Aggarwal A, Keluskar V. Physiotherapy as an adjuvant therapy for treatment of TMJ
disorders. Gen. Dent. 2012; 60: e119–22.
Akerman S, Holland PR, Goadsby PJ. Diencephalic and brainstem mechanisms in
migraine. Nat. Rev. Neurosci. 2011; 12: 570–84.
Akhter R, Benson J, Svensson P, Nicholas MK, Peck CC, Murray GM. Experimental
jaw muscle pain increases pain scores and jaw movement variability in higher pain
catastrophizers. J. oral facial pain headache 2014; 28: 191–204.
Alix ME, Bates DK. A proposed etiology of cervicogenic headache: the
neurophysiologic basis and anatomic relationship between the dura mater and the rectus
posterior capitis minor muscle. J. Manipulative Physiol. Ther. 1999; 22: 534–9.
Alonso-Blanco C, Fernández-de-Las-Peñas C, De-la-Llave-Rincón AI, Zarco-Moreno
P, Galán-Del-Río F, Svensson P. Characteristics of referred muscle pain to the head
from active trigger points in women with myofascial temporomandibular pain and
fibromyalgia syndrome. J. Headache Pain 2012; 13: 625–37.
Anderson GC, John MT, Ohrbach R, Nixdorf DR, Schiffman EL, Truelove ES, et al.
Influence of headache frequency on clinical signs and symptoms of TMD in subjects
with temple headache and TMD pain. Pain 2011; 152: 765–71.
Andrade Ortega JA, Delgado Martínez AD, Almécija Ruiz R. Validation of the Spanish
version of the Neck Disability Index. Spine (Phila. Pa. 1976). 2010; 35: E114–8.
Appelgren L, Janson M, Nitescu P, Curelaru I. Continuous intracisternal and high
cervical intrathecal bupivacaine analgesia in refractory head and neck pain.
Anesthesiology 1996; 84: 256–72.
231
Aprill C, Dwyer A, Bogduk N. Cervical zygapophyseal joint pain patterns. II: A clinical
evaluation. Spine (Phila. Pa. 1976). 1990; 15: 458–61.
Arendt-Nielsen L, Laursen RJ, Drewes AM. Referred pain as an indicator for neural
plasticity. Prog. Brain Res. 2000; 129: 343–56.
Armijo Olivo S, Magee DJ, Parfitt M, Major P, Thie NMR. The association between the
cervical spine, the stomatognathic system, and craniofacial pain: a critical review. J.
Orofac. Pain 2006; 20: 271–87.
Armijo-Olivo S, Magee D. Cervical musculoskeletal impairments and
temporomandibular disorders. J. oral Maxillofac. Res. 2013; 3: e4.
Armijo-Olivo S, Magee DJ. Electromyographic activity of the masticatory and cervical
muscles during resisted jaw opening movement. J. Oral Rehabil. 2007; 34: 184–94.
Armijo-Olivo S, Rappoport K, Fuentes J, Gadotti IC, Major PW, Warren S, et al. Head
and cervical posture in patients with temporomandibular disorders. J. Orofac. Pain
2011; 25: 199–209.
Ashina S, Bendtsen L, Ashina M, Magerl W, Jensen R. Generalized hyperalgesia in
patients with chronic tension-type headache. Cephalalgia 2006; 26: 940–948.
Ashkenazi A, Levin M. Greater occipital nerve block for migraine and other headaches:
is it useful? Curr. Pain Headache Rep. 2007; 11: 231–5.
Ashkenazi A, Matro R, Shaw JW, Abbas MA, Silberstein SD. Greater occipital nerve
block using local anaesthetics alone or with triamcinolone for transformed migraine: a
randomised comparative study. J. Neurol. Neurosurg. Psychiatry 2008; 79: 415–7.
Ayesh EE, Jensen TS, Svensson P. Hypersensitivity to mechanical and intra-articular
electrical stimuli in persons with painful temporomandibular joints. J. Dent. Res. 2007;
86: 1187–92.
Ballenberger N, von Piekartz H, Paris-Alemany A, La Touche R, Angulo-Diaz-Parreño
S. Influence of different upper cervical positions on electromyography activity of the
masticatory muscles. J. Manipulative Physiol. Ther. 2012; 35: 308–18.

232
Bartlett M. A note on the multiplying factors for various Chi-square approximations. J
R. Stat Soc B 1954; 16: 296–298.
Bartsch T, Goadsby PJ. Stimulation of the greater occipital nerve induces increased
central excitability of dural afferent input. Brain 2002; 125: 1496–509.
Bartsch T, Goadsby PJ. Increased responses in trigeminocervical nociceptive neurons to
cervical input after stimulation of the dura mater. Brain 2003a; 126: 1801–13.
Bartsch T, Goadsby PJ. The trigeminocervical complex and migraine: current concepts
and synthesis. Curr. Pain Headache Rep. 2003b; 7: 371–6.
Bartsch T, Knight YE, Goadsby PJ. Activation of 5-HT(1B/1D) receptor in the
periaqueductal gray inhibits nociception. Ann. Neurol. 2004; 56: 371–81.
Bartsch T, Levy MJ, Knight YE, Goadsby PJ. Differential modulation of nociceptive
dural input to [hypocretin] orexin A and B receptor activation in the posterior
hypothalamic area. Pain 2004; 109: 367–78.
Bartsch T, Levy MJ, Knight YE, Goadsby PJ. Inhibition of nociceptive dural input in
the trigeminal nucleus caudalis by somatostatin receptor blockade in the posterior
hypothalamus. Pain 2005; 117: 30–9.
Bartsch T. Migraine and the neck: new insights from basic data. Curr. Pain Headache
Rep. 2005; 9: 191–6.
Batlle-Gualda E, Jovani Casano V, Ivora Cortés J. Musculoskeletal diseases in Spain.
Magnitude and specialised human resources. Rev Esp Reum. 1998: 91–105.
Becker N, Bondegaard Thomsen A, Olsen AK, Sjøgren P, Bech P, Eriksen J. Pain
epidemiology and health related quality of life in chronic non-malignant pain patients
referred to a Danish multidisciplinary pain center. Pain 1997; 73: 393–400.
Becker WJ. Cervicogenic headache: evidence that the neck is a pain generator.
Headache 2010; 50: 699–705.
233
Beitz AJ, Clements JR, Ecklund LJ, Mullett MM. The nuclei of origin of brainstem
enkephalin and cholecystokinin projections to the spinal trigeminal nucleus of the rat.
Neuroscience 1987; 20: 409–25.
Beitz AJ. The nuclei of origin of brainstem serotonergic projections to the rodent spinal
trigeminal nucleus. Neurosci. Lett. 1982; 32: 223–8.
Beltran-Alacreu H, Lopez-de-Uralde-Villanueva I, Paris-Alemany A, Angulo-Díaz-
Parreño S, La Touche R. Intra-rater and Inter-rater Reliability of Mandibular Range of
Motion Measures Considering a Neutral Craniocervical Position. J Phys Ther Sci 2014;
26: 1–6.
Benjamin L, Levy MJ, Lasalandra MP, Knight YE, Akerman S, Classey JD, et al.
Hypothalamic activation after stimulation of the superior sagittal sinus in the cat: a Fos
study. Neurobiol. Dis. 2004; 16: 500–5.
Benoliel R, Svensson P, Heir GM, Sirois D, Zakrzewska J, Oke-Nwosu J, et al.
Persistent orofacial muscle pain. Oral Dis. 2011; 17 Suppl 1: 23–41.
Bereiter DA, Okamoto K, Tashiro A, Hirata H. Endotoxin-induced uveitis causes long-
term changes in trigeminal subnucleus caudalis neurons. J. Neurophysiol. 2005; 94:
3815–25.
Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement
of acute pain. Acad. Emerg. Med. 2001; 8: 1153–7.
Bjorner JB, Kosinski M, Ware JE. Calibration of an item pool for assessing the burden
of headaches: an application of item response theory to the headache impact test (HIT).
Qual. Life Res. 2003; 12: 913–33.
Bogduk N, Windsor M, Inglis A. The innervation of the cervical intervertebral discs.
Spine (Phila. Pa. 1976). 1988; 13: 2–8.
Bogduk N. The anatomy of occipital neuralgia. Clin. Exp. Neurol. 1981; 17: 167–84.
Bogduk N. The clinical anatomy of the cervical dorsal rami. Spine (Phila. Pa. 1976).
1982; 7: 319–30.
234
Bogduk N. Cervicogenic headache: anatomic basis and pathophysiologic mechanisms.
Curr. Pain Headache Rep. 2001; 5: 382–6.
Bogduk N. The anatomy and pathophysiology of neck pain. Phys. Med. Rehabil. Clin.
N. Am. 2003; 14: 455–72, v.
Borghouts JA, Koes BW, Vondeling H, Bouter LM. Cost-of-illness of neck pain in The
Netherlands in 1996. Pain 1999; 80: 629–36.
Borsook D, DaSilva AFM, Ploghaus A, Becerra L. Specific and somatotopic functional
magnetic resonance imaging activation in the trigeminal ganglion by brush and noxious
heat. J. Neurosci. 2003; 23: 7897–903.
Brandini D a, Benson J, Nicholas MK, Murray GM, Peck CC. Chewing in
temporomandibular disorder patients: an exploratory study of an association with some
psychological variables. J. Orofac. Pain 2011; 25: 56–67.
Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in
Europe: prevalence, impact on daily life, and treatment. Eur. J. Pain 2006; 10: 287–333.
Brodie AG. Anatomy and physiology of head and neck musculature. Am. J. Orthod.
1950; 36: 831–44.
Bron C, Dommerholt J, Stegenga B, Wensing M, Oostendorp RAB. High prevalence of
shoulder girdle muscles with myofascial trigger points in patients with shoulder pain.
BMC Musculoskelet. Disord. 2011; 12: 139.
Brown CA, El-Deredy W, Jones AKP. When the brain expects pain: common neural
responses to pain anticipation are related to clinical pain and distress in fibromyalgia
and osteoarthritis. Eur. J. Neurosci. 2014; 39: 663–72.
Buenaver LF, Edwards RR, Smith MT, Gramling SE, Haythornthwaite JA.
Catastrophizing and pain-coping in young adults: associations with depressive
symptoms and headache pain. J. Pain 2008; 9: 311–9.
Buenaver LF, Quartana PJ, Grace EG, Sarlani E, Simango M, Edwards RR, et al.
Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial

235
temporomandibular disorder participants: the mediating role of sleep disturbance. Pain
2012; 153: 1159–66.
Buer N, Linton SJ. Fear-avoidance beliefs and catastrophizing: occurrence and risk
factor in back pain and ADL in the general population. Pain 2002; 99: 485–91.
Burstein R, Yamamura H, Malick A, Strassman AM. Chemical stimulation of the
intracranial dura induces enhanced responses to facial stimulation in brain stem
trigeminal neurons. J. Neurophysiol. 1998; 79: 964–82.
Busch V, Jakob W, Juergens T, Schulte-Mattler W, Kaube H, May A. Functional
connectivity between trigeminal and occipital nerves revealed by occipital nerve
blockade and nociceptive blink reflexes. Cephalalgia 2006; 26: 50–5.
Byers MR, Närhi M V. Dental injury models: experimental tools for understanding
neuroinflammatory interactions and polymodal nociceptor functions. Crit. Rev. Oral
Biol. Med. 1999; 10: 4–39.
Cairns BE, Gambarota G, Svensson P, Arendt-Nielsen L, Berde CB. Glutamate-induced
sensitization of rat masseter muscle fibers. Neuroscience 2002; 109: 389–99.
Cairns BE, Sessle BJ, Hu JW. Characteristics of glutamate-evoked temporomandibular
joint afferent activity in the rat. J. Neurophysiol. 2001; 85: 2446–54.
Camacho JGDD, Oltramari-Navarro PVP, Navarro R de L, Conti AC de CF, Conti MR
de A, Marchiori LL de M, et al. Signs and symptoms of temporomandibular disorders in
the elderly. CoDAS 2014; 26: 76–80.
Campbell CM, Kronfli T, Buenaver LF, Smith MT, Berna C, Haythornthwaite JA, et al.
Situational versus dispositional measurement of catastrophizing: associations with pain
responses in multiple samples. J. Pain 2010; 11: 443–453.e2.
Campos JADB, Carrascosa AC, Bonafé FSS, Maroco J. Epidemiology of severity of
temporomandibular disorders in Brazilian women. J. oral facial pain headache 2014; 28:
147–52.

236
Capra NF, Dessem D. Central connections of trigeminal primary afferent neurons:
topographical and functional considerations. Crit. Rev. Oral Biol. Med. 1992; 4: 1–52.
Carlson CR. Psychological considerations for chronic orofacial pain. Oral Maxillofac.
Surg. Clin. North Am. 2008; 20: 185–95, vi.
Carlsson GE. Epidemiology and treatment need for temporomandibular disorders. J.
Orofac. Pain 1999; 13: 232–7.
Carroll LJ, Cassidy JD, Peloso PM, Giles-Smith L, Cheng CS, Greenhalgh SW, et al.
Methods for the best evidence synthesis on neck pain and its associated disorders: the
Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated
Disorders. Spine (Phila. Pa. 1976). 2008; 33: S33–8.
Castien R, Blankenstein A, van der Windt D, Heymans MW, Dekker J. The working
mechanism of manual therapy in participants with chronic tension-type headache. J.
Orthop. Sports Phys. Ther. 2013; 43: 693–9.
Castien RF, van der Windt DAWM, Blankenstein AH, Heymans MW, Dekker J.
Clinical variables associated with recovery in patients with chronic tension-type
headache after treatment with manual therapy. Pain 2012; 153: 893–9.
Castien RF, van der Windt DAWM, Grooten A, Dekker J. Effectiveness of manual
therapy for chronic tension-type headache: a pragmatic, randomised, clinical trial.
Cephalalgia 2011; 31: 133–43.
Castillo RC, Wegener ST, Heins SE, Haythornthwaite JA, Mackenzie EJ, Bosse MJ.
Longitudinal relationships between anxiety, depression, and pain: results from a two-
year cohort study of lower extremity trauma patients. Pain 2013; 154: 2860–6.
Català E, Reig E, Artés M, Aliaga L, López JS, Segú JL. Prevalence of pain in the
Spanish population: telephone survey in 5000 homes. Eur. J. Pain 2002; 6: 133–40.
Ceneviz C, Mehta NR, Forgione A, Sands MJ, Abdallah EF, Lobo Lobo S, et al. The
immediate effect of changing mandibular position on the EMG activity of the masseter,
temporalis, sternocleidomastoid, and trapezius muscles. Cranio 2006; 24: 237–44.
237
Chapman CR, Donaldson GW, Davis JJ, Bradshaw DH. Improving individual
measurement of postoperative pain: the pain trajectory. J. Pain 2011; 12: 257–62.
Chaves TC, Nagamine HM, de Sousa LM, de Oliveira AS, Regalo SCH, Grossi DB.
Differences in pain perception in children reporting joint and orofacial muscle pain. J.
Clin. Pediatr. Dent. 2013; 37: 321–7.
Chen CK, Nizar AJ. Myofascial pain syndrome in chronic back pain patients. Korean J.
Pain 2011; 24: 100–4.
Chen H, Nackley A, Miller V, Diatchenko L, Maixner W. Multisystem dysregulation in
painful temporomandibular disorders. J. Pain 2013; 14: 983–96.
Chen X, Tanner K, Levine JD. Mechanical sensitization of cutaneous C-fiber
nociceptors by prostaglandin E2 in the rat. Neurosci. Lett. 1999; 267: 105–8.
Cheung CH, Shum ST, Tang SF, Yau PC, Chiu TTW. The correlation between
craniovertebral angle, backpack weights, and disability due to neck pain in adolescents.
J. Back Musculoskelet. Rehabil. 2010; 23: 129–36.
Chiang CY, Park SJ, Kwan CL, Hu JW, Sessle BJ. NMDA receptor mechanisms
contribute to neuroplasticity induced in caudalis nociceptive neurons by tooth pulp
stimulation. J. Neurophysiol. 1998; 80: 2621–31.
Chiang CY, Zhang S, Xie YF, Hu JW, Dostrovsky JO, Salter MW, et al. Endogenous
ATP involvement in mustard-oil-induced central sensitization in trigeminal subnucleus
caudalis (medullary dorsal horn). J. Neurophysiol. 2005; 94: 1751–60.
Christensen L V, Tran KT, Mohamed SE. Gum chewing and jaw muscle fatigue and
pains. J. Oral Rehabil. 1996; 23: 424–37.
Ciancaglini R, Testa M, Radaelli G. Association of neck pain with symptoms of
temporomandibular dysfunction in the general adult population. Scand. J. Rehabil. Med.
1999; 31: 17–22.
Cimmino MA, Ferrone C, Cutolo M. Epidemiology of chronic musculoskeletal pain.
Best Pract. Res. Clin. Rheumatol. 2011; 25: 173–83.

238
Clark GT, Browne PA, Nakano M, Yang Q. Co-activation of sternocleidomastoid
muscles during maximum clenching. J. Dent. Res. 1993; 72: 1499–502.
Clatworthy A, Williams JH, Barasi S. Intrathecal 5-hydroxytryptamine and electrical
stimulation of the nucleus raphe magnus in rats both reduce the antinociceptive potency
of intrathecally administered noradrenaline. Brain Res. 1988; 455: 300–6.
Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: 1988.
Cooper G, Bailey B, Bogduk N. Cervical zygapophysial joint pain maps. Pain Med.
2007; 8: 344–53.
Côté P, Cassidy JD, Carroll L. The Saskatchewan Health and Back Pain Survey. The
prevalence of neck pain and related disability in Saskatchewan adults. Spine (Phila. Pa.
1976). 1998; 23: 1689–98.
Côté P, Kristman V, Vidmar M, Van Eerd D, Hogg-Johnson S, Beaton D, et al. The
prevalence and incidence of work absenteeism involving neck pain: a cohort of Ontario
lost-time claimants. Spine (Phila. Pa. 1976). 2008; 33: S192–8.
Couppé C, Torelli P, Fuglsang-Frederiksen A, Andersen KV, Jensen R. Myofascial
trigger points are very prevalent in patients with chronic tension-type headache: a
double-blinded controlled study. Clin. J. Pain 2007; 23: 23–7.
Craig AD. A new view of pain as a homeostatic emotion. Trends Neurosci. 2003; 26:
303–7.
Crombez G, Vlaeyen JW, Heuts PH, Lysens R. Pain-related fear is more disabling than
pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain
1999; 80: 329–39.
Curatolo M, Arendt-Nielsen L, Petersen-Felix S. Central hypersensitivity in chronic
pain: mechanisms and clinical implications. Phys. Med. Rehabil. Clin. N. Am. 2006; 17:
287–302.
Dallel R, Raboisson P, Auroy P, Woda A. The rostral part of the trigeminal sensory
complex is involved in orofacial nociception. Brain Res. 1988; 448: 7–19.
239
Dallel R, Raboisson P, Woda A, Sessle BJ. Properties of nociceptive and non-
nociceptive neurons in trigeminal subnucleus oralis of the rat. Brain Res. 1990; 521:
95–106.
Dao TTT, Lund JP, Lavigne GJ. Pain Responses to Experimental Chewing in
Myofascial Pain Patients. 1994
Davies PL. Electromyographic study of superficial neck muscles in mandibular
function. J. Dent. Res. 1979; 58: 537–8.
Dessem D, Luo P. Jaw-muscle spindle afferent feedback to the cervical spinal cord in
the rat. Exp. brain Res. 1999; 128: 451–9.
Dixon AD. FINE STRUCTURE OF NERVE-CELL BODIES AND SATELLITE
CELLS IN THE TRIGEMINAL GANGLION. J. Dent. Res. 1963; 42: 990–9.
Le Doaré K, Akerman S, Holland PR, Lasalandra MP, Bergerot A, Classey JD, et al.
Occipital afferent activation of second order neurons in the trigeminocervical complex
in rat. Neurosci. Lett. 2006; 403: 73–7.
Dostrovsky JO, Davis KD, Kawakita K. Central mechanisms of vascular headaches.
Can. J. Physiol. Pharmacol. 1991; 69: 652–8.
Dougherty PM, Sluka KA, Sorkin LS, Westlund KN, Willis WD. Neural changes in
acute arthritis in monkeys. I. Parallel enhancement of responses of spinothalamic tract
neurons to mechanical stimulation and excitatory amino acids. Brain Res. Brain Res.
Rev. 1992; 17: 1–13.
Dougherty PM, Willis WD. Enhanced responses of spinothalamic tract neurons to
excitatory amino acids accompany capsaicin-induced sensitization in the monkey. J.
Neurosci. 1992; 12: 883–94.
Dreyfuss P, Michaelsen M, Fletcher D. Atlanto-occipital and lateral atlanto-axial joint
pain patterns. Spine (Phila. Pa. 1976). 1994; 19: 1125–31.
Dubner R, Bennett GJ. Spinal and trigeminal mechanisms of nociception. Annu. Rev.
Neurosci. 1983; 6: 381–418.

240
Dubner R, Ren K. Brainstem mechanisms of persistent pain following injury. J. Orofac.
Pain 2004; 18: 299–305.
Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular
disorders: review, criteria, examinations and specifications, critique. J. Craniomandib.
Disord. 1992; 6: 301–55.
Dwyer A, Aprill C, Bogduk N. Cervical zygapophyseal joint pain patterns. I: A study in
normal volunteers. Spine (Phila. Pa. 1976). 1990; 15: 453–7.
Ebersberger A, Schaible HG, Averbeck B, Richter F. Is there a correlation between
spreading depression, neurogenic inflammation, and nociception that might cause
migraine headache? Ann. Neurol. 2001; 49: 7–13.
Edelmayer RM, Vanderah TW, Majuta L, Zhang E-T, Fioravanti B, De Felice M, et al.
Medullary pain facilitating neurons mediate allodynia in headache-related pain. Ann.
Neurol. 2009; 65: 184–93.
Elliott AM, Smith BH, Penny KI, Smith WC, Chambers WA. The epidemiology of
chronic pain in the community. Lancet 1999; 354: 1248–52.
Enthoven P, Skargren E, Oberg B. Clinical course in patients seeking primary care for
back or neck pain: a prospective 5-year follow-up of outcome and health care
consumption with subgroup analysis. Spine (Phila. Pa. 1976). 2004; 29: 2458–65.
Eriksson PO, Häggman-Henrikson B, Nordh E, Zafar H. Co-ordinated mandibular and
head-neck movements during rhythmic jaw activities in man. J. Dent. Res. 2000; 79:
1378–84.
Eriksson P-O, Häggman-Henrikson B, Zafar H. Jaw-neck dysfunction in whiplash-
associated disorders. Arch. Oral Biol. 2007; 52: 404–8.
Eriksson P-O, Zafar H, Häggman-Henrikson B. Deranged jaw-neck motor control in
whiplash-associated disorders. Eur. J. Oral Sci. 2004; 112: 25–32.
Eriksson PO, Zafar H, Nordh E. Concomitant mandibular and head-neck movements
during jaw opening-closing in man. J. Oral Rehabil. 1998; 25: 859–70.

241
Espí-López G, Rodríguez-Blanco C, Oliva-Pascual-Vaca A, Benítez-Martínez J, Lluch
E, Falla D. The effect of manual therapy techniques on headache disability in patients
with tension-type headache. Eur. J. Phys. Rehabil. Med. 2014
Espí-López G V, Gómez-Conesa A. Efficacy of manual and manipulative therapy in the
perception of pain and cervical motion in patients with tension-type headache: a
randomized, controlled clinical trial. J. Chiropr. Med. 2014; 13: 4–13.
Van Ettekoven H, Lucas C. Efficacy of physiotherapy including a craniocervical
training programme for tension-type headache; a randomized clinical trial. Cephalalgia
2006; 26: 983–91.
Farella M, Bakke M, Michelotti A, Martina R. Effects of prolonged gum chewing on
pain and fatigue in human jaw muscles. Eur. J. Oral Sci. 2001; 109: 81–5.
Feldreich A, Ernberg M, Lund B, Rosén A. Increased β-endorphin levels and
generalized decreased pain thresholds in patients with limited jaw opening and
movement-evoked pain from the temporomandibular joint. J. Oral Maxillofac. Surg.
2012; 70: 547–56.
Ferguson E, Cox T. Exploratory factor analysis: a users’ guide. Int J Sel. Assess 1993;
1: 84–94.
Fernández-Carnero J, Fernández-de-Las-Peñas C, de la Llave-Rincón AI, Ge H-Y,
Arendt-Nielsen L. Prevalence of and referred pain from myofascial trigger points in the
forearm muscles in patients with lateral epicondylalgia. Clin. J. Pain 2007; 23: 353–60.
Fernández-de-Las-Peñas C, Cuadrado ML, Pareja JA. Myofascial trigger points, neck
mobility and forward head posture in unilateral migraine. Cephalalgia 2006; 26: 1061–
70.
Fernández-de-Las-Peñas C, Galán-Del-Río F, Alonso-Blanco C, Jiménez-García R,
Arendt-Nielsen L, Svensson P. Referred pain from muscle trigger points in the
masticatory and neck-shoulder musculature in women with temporomandibular
disoders. J. Pain 2010; 11: 1295–304.

242
Fernández-de-las-Peñas C, Hernández-Barrera V, Alonso-Blanco C, Palacios-Ceña D,
Carrasco-Garrido P, Jiménez-Sánchez S, et al. Prevalence of neck and low back pain in
community-dwelling adults in Spain: a population-based national study. Spine (Phila.
Pa. 1976). 2011; 36: E213–9.
Ferrario VF, Tartaglia GM, Galletta A, Grassi GP, Sforza C. The influence of occlusion
on jaw and neck muscle activity: a surface EMG study in healthy young adults. J. Oral
Rehabil. 2006; 33: 341–8.
Fields HL, Heinricher MM, Mason P. Neurotransmitters in nociceptive modulatory
circuits. Annu. Rev. Neurosci. 1991; 14: 219–45.
Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex,
gender, and pain: a review of recent clinical and experimental findings. J. Pain 2009;
10: 447–85.
Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Diatchenko L, Dubner R, et al.
Psychological factors associated with development of TMD: the OPPERA prospective
cohort study. J. Pain 2013; 14: T75–90.
Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Dubner R, Bair E, et al. Potential
psychosocial risk factors for chronic TMD: descriptive data and empirically identified
domains from the OPPERA case-control study. J. Pain 2011; 12: T46–60.
Forsberg CM, Hellsing E, Linder-Aronson S, Sheikholeslam A. EMG activity in neck
and masticatory muscles in relation to extension and flexion of the head. Eur. J. Orthod.
1985; 7: 177–84.
Fricton J. Temporomandibular disorders: a human systems approach. J. Calif. Dent.
Assoc. 2014; 42: 523–33; discussion 531, 533–5.
Fricton JR, Kroening R, Haley D, Siegert R. Myofascial pain syndrome of the head and
neck: a review of clinical characteristics of 164 patients. Oral Surg. Oral Med. Oral
Pathol. 1985; 60: 615–23.

243
Funakoshi M, Fujita N, Takehana S. Relations between occlusal interference and jaw
muscle activities in response to changes in head position. J. Dent. Res. 1976; 55: 684–
90.
Gandek B, Alacoque J, Uzun V, Andrew-Hobbs M, Davis K. Translating the Short-
Form Headache Impact Test (HIT-6) in 27 countries: methodological and conceptual
issues. Qual. Life Res. 2003; 12: 975–9.
García Campayo J, Rodero B, Alda M, Sobradiel N, Montero J, Moreno S. Validación
de la versión española de la escala de la catastrofización ante el dolor (Pain
Catastrophizing Scale) en la fibromialgia. Med. Clin. (Barc). 2008; 131: 487–492.
Gavish A, Winocur E, Menashe S, Halachmi M, Eli I, Gazit E. Experimental chewing
in myofascial pain patients. J. Orofac. Pain 2002; 16: 22–8.
Ge H-Y, Wang K, Madeleine P, Svensson P, Sessle BJ, Arendt-Nielsen L.
Simultaneous modulation of the exteroceptive suppression periods in the trapezius and
temporalis muscles by experimental muscle pain. Clin. Neurophysiol. 2004; 115: 1399–
408.
Gesch D, Bernhardt O, Alte D, Schwahn C, Kocher T, John U, et al. Prevalence of signs
and symptoms of temporomandibular disorders in an urban and rural German
population: results of a population-based Study of Health in Pomerania. Quintessence
Int. 2004; 35: 143–50.
Giannakopoulos N, Hellmann D, Schmitter M, Krüger B, Hauser T, Schindler HJ.
Neuromuscular interaction of jaw and neck muscles during jaw clenching. J. Orofac.
Pain 2013; 27: 61–71.
Giannakopoulos N, Schindler HJ, Rammelsberg P, Eberhard L, Schmitter M, Hellmann
D. Co-activation of jaw and neck muscles during submaximum clenching in the supine
position. Arch. Oral Biol. 2013; 58: 1751–60.
Gillies GT, Broaddus WC, Stenger JM, Taylor AG. A biomechanical model of the
craniomandibular complex and cervical spine based on the inverted pendulum. J. Med.
Eng. Technol. 1998; 22: 263–9.

244
Goadsby PJ, Bartsch T, Dodick DW. Occipital nerve stimulation for headache:
mechanisms and efficacy. Headache 2008; 48: 313–8.
Goadsby PJ, Hoskin KL. The distribution of trigeminovascular afferents in the
nonhuman primate brain Macaca nemestrina: a c-fos immunocytochemical study. J.
Anat. 1997; 190 ( Pt 3: 367–75.
Goadsby PJ, Knight YE, Hoskin KL. Stimulation of the greater occipital nerve increases
metabolic activity in the trigeminal nucleus caudalis and cervical dorsal horn of the cat.
Pain 1997; 73: 23–8.
Gómez-Pérez L, López-Martínez AE, Ruiz-Párraga GT. Psychometric Properties of the
Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011; 12: 425–
35.
Gore DR, Sepic SB, Gardner GM, Murray MP. Neck pain: a long-term follow-up of
205 patients. Spine (Phila. Pa. 1976). 1987; 12: 1–5.
Gracely RH, Geisser ME, Giesecke T, Grant MAB, Petzke F, Williams DA, et al. Pain
catastrophizing and neural responses to pain among persons with fibromyalgia. Brain
2004; 127: 835–43.
Graff-Radford SB. Temporomandibular disorders and other causes of facial pain. Curr.
Pain Headache Rep. 2007; 11: 75–81.
Graff-Radford SB. Facial pain, cervical pain, and headache. Continuum (Minneap.
Minn). 2012; 18: 869–82.
Graven-Nielsen T, Arendt-Nielsen L. Assessment of mechanisms in localized and
widespread musculoskeletal pain. Nat. Rev. Rheumatol. 2010; 6: 599–606.
Graven-Nielsen T. Fundamentals of muscle pain, referred pain, and deep tissue
hyperalgesia. Scand. J. Rheumatol. Suppl. 2006; 122: 1–43.
Guenther S, Reeh PW, Kress M. Rises in [Ca2+]i mediate capsaicin- and proton-
induced heat sensitization of rat primary nociceptive neurons. Eur. J. Neurosci. 1999;
11: 3143–50.

245
Guzman J, Hurwitz EL, Carroll LJ, Haldeman S, Côté P, Carragee EJ, et al. A new
conceptual model of neck pain: linking onset, course, and care: the Bone and Joint
Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. J.
Manipulative Physiol. Ther. 2009; 32: S17–28.
Häggman-Henrikson B, Eriksson P-O. Head movements during chewing: relation to
size and texture of bolus. J. Dent. Res. 2004; 83: 864–8.
Häggman-Henrikson B, Nordh E, Eriksson P-O. Increased sternocleidomastoid, but not
trapezius, muscle activity in response to increased chewing load. Eur. J. Oral Sci. 2013;
121: 443–9.
Häggman-Henrikson B, Nordh E, Zafar H, Eriksson P-O. Head immobilization can
impair jaw function. J. Dent. Res. 2006; 85: 1001–5.
Haggman-Henrikson B, Osterlund C, Eriksson P-O. Endurance during Chewing in
Whiplash-associated Disorders and TMD. J. Dent. Res. 2004; 83: 946–950.
Häggman-Henrikson B, Rezvani M, List T. Prevalence of whiplash trauma in TMD
patients: a systematic review. J. Oral Rehabil. 2014; 41: 59–68.
Haldeman S, Carroll LJ, Cassidy JD. The empowerment of people with neck pain:
introduction: the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its
Associated Disorders. Spine (Phila. Pa. 1976). 2008; 33: S8–S13.
Haley SM, Fragala-Pinkham MA. Interpreting change scores of tests and measures used
in physical therapy. Phys. Ther. 2006; 86: 735–43.
Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K. Efficacy of a C1-
C2 self-sustained natural apophyseal glide (SNAG) in the management of cervicogenic
headache. J. Orthop. Sports Phys. Ther. 2007; 37: 100–7.
Hargreaves KM. Orofacial pain. Pain 2011; 152: S25–32.
Harris E, Budd R, Genovese M, Firestein G, Sargent J, Sledge C. Kelley’s Textbook of
Rheumatology. 7th ed. Philadelphia, Pa: Saunders Elsevier; 2006.

246
Hellmann D, Giannakopoulos NN, Schmitter M, Lenz J, Schindler HJ. Anterior and
posterior neck muscle activation during a variety of biting tasks. Eur. J. Oral Sci. 2012;
120: 326–34.
Hellström F, Thunberg J, Bergenheim M, Sjölander P, Djupsjöbacka M, Johansson H.
Increased intra-articular concentration of bradykinin in the temporomandibular joint
changes the sensitivity of muscle spindles in dorsal neck muscles in the cat. Neurosci.
Res. 2002; 42: 91–9.
Hellström F, Thunberg J, Bergenheim M, Sjölander P, Pedersen J, Johansson H.
Elevated intramuscular concentration of bradykinin in jaw muscle increases the
fusimotor drive to neck muscles in the cat. J. Dent. Res. 2000; 79: 1815–22.
Henry DE, Chiodo AE, Yang W. Central nervous system reorganization in a variety of
chronic pain states: a review. PM R 2011; 3: 1116–25.
Van den Heuvel SG, Heinrich J, Jans MP, van der Beek AJ, Bongers PM. The effect of
physical activity in leisure time on neck and upper limb symptoms. Prev. Med. (Baltim).
2005; 41: 260–7.
Higbie EJ, Seidel-Cobb D, Taylor LF, Cummings GS. Effect of head position on
vertical mandibular opening. J. Orthop. Sports Phys. Ther. 1999; 29: 127–30.
Hill J, Lewis M, Papageorgiou AC, Dziedzic K, Croft P. Predicting persistent neck
pain: a 1-year follow-up of a population cohort. Spine (Phila. Pa. 1976). 2004; 29:
1648–54.
Hinkle D, Jurs S, Wiersma W. Applied statistics for the behavioral sciences. 2nd ed.
Boston: Houghton Mifflin; 1988.
Hochberg MC, Altman RD, Brandt KD, Clark BM, Dieppe PA, Griffin MR, et al.
Guidelines for the medical management of osteoarthritis. Part I. Osteoarthritis of the
hip. American College of Rheumatology. Arthritis Rheum. 1995; 38: 1535–40.
Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW, Cassidy JD, Guzman J, et al.
The burden and determinants of neck pain in the general population: results of the Bone

247
and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. J.
Manipulative Physiol. Ther. 2009; 32: S46–60.
Holroyd KA, Drew JB, Cottrell CK, Romanek KM, Heh V. Impaired functioning and
quality of life in severe migraine: the role of catastrophizing and associated symptoms.
Cephalalgia 2007; 27: 1156–65.
Hoskin KL, Zagami AS, Goadsby PJ. Stimulation of the middle meningeal artery leads
to Fos expression in the trigeminocervical nucleus: a comparative study of monkey and
cat. J. Anat. 1999; 194 ( Pt 4: 579–88.
Hu JW, Sun K-Q, Vernon H, Sessle BJ. Craniofacial inputs to upper cervical dorsal
horn: implications for somatosensory information processing. Brain Res 2005; 1044:
93–106.
Hu JW, Tatourian I, Vernon H. Opioid involvement in electromyographic (EMG)
responses induced by injection of inflammatory irritant into deep neck tissues.
Somatosens. Mot. Res. 1996; 13: 139–46.
Hu JW, Vernon H, Tatourian I. Changes in neck electromyography associated with
meningeal noxious stimulation. J. Manipulative Physiol. Ther. 1995; 18: 577–81.
Hu JW, Yu XM, Vernon H, Sessle BJ. Excitatory effects on neck and jaw muscle
activity of inflammatory irritant applied to cervical paraspinal tissues. Pain 1993; 55:
243–50.
Hucho T, Levine JD. Signaling pathways in sensitization: toward a nociceptor cell
biology. Neuron 2007; 55: 365–76.
Igarashi N, Yamamura K, Yamada Y, Kohno S. Head movements and neck muscle
activities associated with the jaw movement during mastication in the rabbit authors.
Brain Res. 2000; 871: 151–5.
IHS. The International Classification of Headache Disorders, 3rd edition (beta version).
Cephalalgia. 2013; 33: 629–808.

248
Jacquin MF, Renehan WE, Mooney RD, Rhoades RW. Structure-function relationships
in rat medullary and cervical dorsal horns. I. Trigeminal primary afferents. J.
Neurophysiol. 1986; 55: 1153–86.
Jasper JF, Hayek SM. Implanted occipital nerve stimulators. Pain Physician 2008; 11:
187–200.
Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity
measurement in chronic pain patients. Pain 1993; 55: 195–203.
Jensen MP, Turner JA, Romano JM, Fisher LD. Comparative reliability and validity of
chronic pain intensity measures. Pain 1999; 83: 157–62.
Ji R-R, Kohno T, Moore KA, Woolf CJ. Central sensitization and LTP: do pain and
memory share similar mechanisms? Trends Neurosci. 2003; 26: 696–705.
Johnston MM, Jordan SE, Charles AC. Pain referral patterns of the C1 to C3 nerves:
implications for headache disorders. Ann. Neurol. 2013; 74: 145–8.
Kääriä S, Laaksonen M, Rahkonen O, Lahelma E, Leino-Arjas P. Risk factors of
chronic neck pain: a prospective study among middle-aged employees. Eur. J. Pain
2012; 16: 911–20.
Kaiser H. Analysis of factorial simplicity. Psychometrika 1974; 39: 31–36.
Kamel HA, Toland J. Trigeminal nerve anatomy: illustrated using examples of
abnormalities. AJR. Am. J. Roentgenol. 2001; 176: 247–51.
Kamisaka M, Yatani H, Kuboki T, Matsuka Y, Minakuchi H. Four-year longitudinal
course of TMD symptoms in an adult population and the estimation of risk factors in
relation to symptoms. J. Orofac. Pain 2000; 14: 224–32.
Kamper SJ, Maher CG, Menezes Costa L da C, McAuley JH, Hush JM, Sterling M.
Does fear of movement mediate the relationship between pain intensity and disability in
patients following whiplash injury? A prospective longitudinal study. Pain 2012; 153:
113–9.

249
De Kanter RJ, Truin GJ, Burgersdijk RC, Van ’t Hof MA, Battistuzzi PG, Kalsbeek H,
et al. Prevalence in the Dutch adult population and a meta-analysis of signs and
symptoms of temporomandibular disorder. J. Dent. Res. 1993; 72: 1509–18.
Kapur N, Kamel IR, Herlich A. Oral and craniofacial pain: diagnosis, pathophysiology,
and treatment. Int. Anesthesiol. Clin. 2003; 41: 115–50.
Karibe H, Goddard G, Gear RW. Sex differences in masticatory muscle pain after
chewing. J. Dent. Res. 2003; 82: 112–6.
Karibe H, Goddard G, Kawakami T, Aoyagi K, Rudd P, McNeill C. Comparison of
subjective symptoms among three diagnostic subgroups of adolescents with
temporomandibular disorders. Int. J. Paediatr. Dent. 2010; 20: 458–65.
Katsarava Z, Lehnerdt G, Duda B, Ellrich J, Diener HC, Kaube H. Sensitization of
trigeminal nociception specific for migraine but not pain of sinusitis. Neurology 2002;
59: 1450–3.
Kaube H, Katsarava Z, Przywara S, Drepper J, Ellrich J, Diener H-C. Acute migraine
headache: possible sensitization of neurons in the spinal trigeminal nucleus? Neurology
2002; 58: 1234–8.
Kaube H, Keay KA, Hoskin KL, Bandler R, Goadsby PJ. Expression of c-Fos-like
immunoreactivity in the caudal medulla and upper cervical spinal cord following
stimulation of the superior sagittal sinus in the cat. Brain Res. 1993; 629: 95–102.
Kerr FW. THE DIVISIONAL ORGANIZATION OF AFFERENT FIBRES OF THE
TRIGEMINAL NERVE. Brain 1963; 86: 721–32.
Kindler S, Samietz S, Houshmand M, Grabe HJ, Bernhardt O, Biffar R, et al.
Depressive and anxiety symptoms as risk factors for temporomandibular joint pain: a
prospective cohort study in the general population. J. Pain 2012; 13: 1188–97.
King CD, Wong F, Currie T, Mauderli AP, Fillingim RB, Riley JL. Deficiency in
endogenous modulation of prolonged heat pain in patients with Irritable Bowel
Syndrome and Temporomandibular Disorder. Pain 2009; 143: 172–8.
250
Knight YE, Bartsch T, Kaube H, Goadsby PJ. P/Q-type calcium-channel blockade in
the periaqueductal gray facilitates trigeminal nociception: a functional genetic link for
migraine? J. Neurosci. 2002; 22: RC213.
Knight YE, Goadsby PJ. The periaqueductal grey matter modulates trigeminovascular
input: a role in migraine? Neuroscience 2001; 106: 793–800.
Kobayashi A, Shinoda M, Sessle BJ, Honda K, Imamura Y, Hitomi S, et al.
Mechanisms involved in extraterritorial facial pain following cervical spinal nerve
injury in rats. Mol. Pain 2011; 7: 12.
Kohno S, Kohno T, Medina R. Rotational head motion concurrent to rhythmical
mandibular opening movements. J. Oral Rehabil. 2001; 28: 740–7.
Kohno S, Matsuyama T, Medina RU, Arai Y. Functional-rhythmical coupling of head
and mandibular movements. J. Oral Rehabil. 2001; 28: 161–7.
Komiyama O, Arai M, Kawara M, Kobayashi K, De Laat A. Pain patterns and
mandibular dysfunction following experimental trapezius muscle pain. J. Orofac. Pain
2005; 19: 119–26.
Koolstra JH, van Eijden TMGJ. Functional significance of the coupling between head
and jaw movements. J. Biomech. 2004; 37: 1387–92.
Von Korff M, Dunn KM. Chronic pain reconsidered. Pain 2008; 138: 267–76.
Kori S, Miller R, Todd D. Kinesiophobia: a new view of chronic pain behavior. Pain
Manag 1990; 3: 35–43.
Koutris M, Lobbezoo F, Naeije M, Wang K, Svensson P, Arendt-Nielsen L, et al.
Effects of intense chewing exercises on the masticatory sensory-motor system. J. Dent.
Res. 2009; 88: 658–62.
Koutris M, Lobbezoo F, Sümer NC, Atiş ES, Türker KS, Naeije M. Is myofascial pain
in temporomandibular disorder patients a manifestation of delayed-onset muscle
soreness? Clin. J. Pain 2013; 29: 712–6.

251
Kucyi A, Moayedi M, Weissman-Fogel I, Goldberg MB, Freeman B V, Tenenbaum
HC, et al. Enhanced medial prefrontal-default mode network functional connectivity in
chronic pain and its association with pain rumination. J. Neurosci. 2014; 34: 3969–75.
Kuroda K, Saitoh I, Inada E, Takemoto Y, Iwasaki T, Iwase Y, et al. Head motion may
help mouth opening in children. Arch. Oral Biol. 2011; 56: 102–7.
Lam DK, Sessle BJ, Hu JW. Glutamate and capsaicin effects on trigeminal nociception
II: activation and central sensitization in brainstem neurons with deep craniofacial
afferent input. Brain Res. 2009; 1253: 48–59.
Lambert GA, Hoskin KL, Zagami AS. Cortico-NRM influences on trigeminal neuronal
sensation. Cephalalgia 2008; 28: 640–52.
Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by
central neural plasticity. J. Pain 2009; 10: 895–926.
Lau KT, Cheung KY, Chan KB, Chan MH, Lo KY, Chiu TTW. Relationships between
sagittal postures of thoracic and cervical spine, presence of neck pain, neck pain
severity and disability. Man. Ther. 2010; 15: 457–62.
Leclerc A, Niedhammer I, Landre MF, Ozguler A, Etore P, Pietri-Taleb F. One-year
predictive factors for various aspects of neck disorders. Spine (Phila Pa 1976) 1999; 24:
1455–1462.
Lee P, Huh BK. Peripheral nerve stimulation for the treatment of primary headache.
Curr. Pain Headache Rep. 2013; 17: 319.
Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS. The
fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J.
Behav. Med. 2007; 30: 77–94.
Leiser SC, Moxon KA. Relationship between physiological response type (RA and SA)
and vibrissal receptive field of neurons within the rat trigeminal ganglion. J.
Neurophysiol. 2006; 95: 3129–45.

252
LeResche L. Epidemiology of temporomandibular disorders: implications for the
investigation of etiologic factors. Crit. Rev. Oral Biol. Med. 1997; 8: 291–305.
Leroux E, Ducros A. Occipital injections for trigemino-autonomic cephalalgias:
evidence and uncertainties. Curr. Pain Headache Rep. 2013; 17: 325.
Licini F, Nojelli A, Segù M, Collesano V. Role of psychosocial factors in the etiology
of temporomandibular disorders: relevance of a biaxial diagnosis. Minerva Stomatol.;
58: 557–66.
Liu F, Steinkeler A. Epidemiology, diagnosis, and treatment of temporomandibular
disorders. Dent. Clin. North Am. 2013; 57: 465–79.
Loeser JD, Treede R-D. The Kyoto protocol of IASP Basic Pain Terminology. Pain
2008; 137: 473–7.
Look JO, Schiffman EL, Truelove EL, Ahmad M. Reliability and validity of Axis I of
the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) with
proposed revisions. J. Oral Rehabil. 2010; 37: 744–59.
Lopez-de-Uralde-Villanueva I, Alacreu-Beltran H, Paris-Alemany A, Angulo-Díaz-
Parreño S, La Touche R. Reliability, Standard Error, and Minimal Detectable Change of
Two Measurements for Craniocervical Posture Assessment in Asymptomatic Subjects
and Chronic Neck/craniofacial Pain Patients. (En proceso) 2014
Lukkahatai N, Saligan LN. Association of catastrophizing and fatigue: a systematic
review. J. Psychosom. Res. 2013; 74: 100–9.
Lundborg C, Dahm P, Nitescu P, Biber B. High intrathecal bupivacaine for severe pain
in the head and neck. Acta Anaesthesiol. Scand. 2009; 53: 908–13.
Macfarlane T V, Blinkhorn AS, Davies RM, Kincey J, Worthington H V. Oro-facial
pain in the community: prevalence and associated impact. Community Dent. Oral
Epidemiol. 2002; 30: 52–60.

253
Macfarlane T V, Blinkhorn AS, Davies RM, Ryan P, Worthington H V, Macfarlane GJ.
Orofacial pain: just another chronic pain? Results from a population-based survey. Pain
2002; 99: 453–8.
Macfarlane T V, Glenny AM, Worthington H V. Systematic review of population-based
epidemiological studies of oro-facial pain. J. Dent. 2001; 29: 451–67.
Main CJ. The importance of psychosocial influences on chronic pain. Pain Manag.
2013; 3: 455–66.
Maixner W, Fillingim R, Sigurdsson A, Kincaid S, Silva S. Sensitivity of patients with
painful temporomandibular disorders to experimentally evoked pain: evidence for
altered temporal summation of pain. Pain 1998; 76: 71–81.
Majoie CB, Verbeeten B, Dol JA, Peeters FL. Trigeminal neuropathy: evaluation with
MR imaging. Radiographics 1995; 15: 795–811.
Makowska A, Panfil C, Ellrich J. Long-term potentiation of orofacial sensorimotor
processing by noxious input from the semispinal neck muscle in mice. Cephalalgia
2005; 25: 109–16.
Malick A, Burstein R. Cells of origin of the trigeminohypothalamic tract in the rat. J.
Comp. Neurol. 1998; 400: 125–44.
Malick A, Jakubowski M, Elmquist JK, Saper CB, Burstein R. A neurohistochemical
blueprint for pain-induced loss of appetite. Proc. Natl. Acad. Sci. U. S. A. 2001; 98:
9930–5.
Malick A, Strassman RM, Burstein R. Trigeminohypothalamic and
reticulohypothalamic tract neurons in the upper cervical spinal cord and caudal medulla
of the rat. J. Neurophysiol. 2000; 84: 2078–112.
Manfredini D, Arveda N, Guarda-Nardini L, Segù M, Collesano V. Distribution of
diagnoses in a population of patients with temporomandibular disorders. Oral Surg. Oral
Med. Oral Pathol. Oral Radiol. 2012; 114: e35–41.

254
Marklund S, Wiesinger B, Wänman A. Reciprocal influence on the incidence of
symptoms in trigeminally and spinally innervated areas. Eur. J. Pain 2010; 14: 366–71.
Martin M, Blaisdell B, Kwong JW, Bjorner JB. The Short-Form Headache Impact Test
(HIT-6) was psychometrically equivalent in nine languages. J. Clin. Epidemiol. 2004;
57: 1271–8.
Mason P, Fields HL. Axonal trajectories and terminations of on- and off-cells in the cat
lower brainstem. J. Comp. Neurol. 1989; 288: 185–207.
Matsuka Y, Yatani H, Kuboki T, Yamashita A. Temporomandibular disorders in the
adult population of Okayama City, Japan. Cranio 1996; 14: 158–62.
McLean L. The effect of postural correction on muscle activation amplitudes recorded
from the cervicobrachial region. J. Electromyogr. Kinesiol. 2005; 15: 527–35.
Meeus M, Nijs J, Van Mol E, Truijen S, De Meirleir K. Role of psychological aspects in
both chronic pain and in daily functioning in chronic fatigue syndrome: a prospective
longitudinal study. Clin. Rheumatol. 2012; 31: 921–9.
Meeus M, Nijs J, Van de Wauwer N, Toeback L, Truijen S. Diffuse noxious inhibitory
control is delayed in chronic fatigue syndrome: an experimental study. Pain 2008; 139:
439–48.
Mellick GA, Mellick LB. Regional head and face pain relief following lower cervical
intramuscular anesthetic injection. Headache 2003; 43: 1109–11.
Mellick LB, McIlrath ST, Mellick GA. Treatment of headaches in the ED with lower
cervical intramuscular bupivacaine injections: a 1-year retrospective review of 417
patients. Headache 2006; 46: 1441–9.
Mellick LB, Mellick GA. Treatment of acute orofacial pain with lower cervical
intramuscular bupivacaine injections: a 1-year retrospective review of 114 patients. J.
Orofac. Pain 2008; 22: 57–64.
Mellick LB, Pleasant MR. Do pediatric headaches respond to bilateral lower cervical
paraspinous bupivacaine injections? Pediatr. Emerg. Care 2010; 26: 192–6.

255
Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965; 150: 971–9.
Melzack R. Pain: past, present and future. Can. J. Exp. Psychol. 1993; 47: 615–29.
Melzack R. From the gate to the neuromatrix. Pain 1999; Suppl 6: S121–6.
Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain
Syndromes and Definitions of Pain Terms. Seattle:: IASP Press; 1994.
Mienna CS, Wanman A. Self-reported impact on daily life activities related to
temporomandibular disorders, headaches, and neck-shoulder pain among women in a
Sami population living in Northern Sweden. J. Orofac. Pain 2012; 26: 215–24.
Milidonis MK, Kraus SL, Segal RL, Widmer CG. Genioglossi muscle activity in
response to changes in anterior/neutral head posture. Am. J. Orthod. Dentofacial
Orthop. 1993; 103: 39–44.
Miyaoka S, Hirano H, Miyaoka Y, Yamada Y. Head movement associated with
performance of mandibular tasks. J. Oral Rehabil. 2004; 31: 843–50.
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The
COSMIN study reached international consensus on taxonomy, terminology, and
definitions of measurement properties for health-related patient-reported outcomes. J.
Clin. Epidemiol. 2010; 63: 737–45.
Mongini F, Evangelista A, Milani C, Ferrero L, Ciccone G, Ugolini A, et al. An
educational and physical program to reduce headache, neck/shoulder pain in a working
community: a cluster-randomized controlled trial. PLoS One 2012; 7: e29637.
Moses HL. Comparative fine structure of the trigeminal ganglia, including human
autopsy studies. J. Neurosurg. 1967; 26: Suppl:112–26.
Murray GM, Peck CC. Orofacial pain and jaw muscle activity: a new model. J. Orofac.
Pain 2007; 21: 263–78; discussion 279–88.
Nachev P, Kennard C, Husain M. Functional role of the supplementary and pre-
supplementary motor areas. Nat. Rev. Neurosci. 2008; 9: 856–69.

256
Nachev P, Wydell H, O’neill K, Husain M, Kennard C. The role of the pre-
supplementary motor area in the control of action. Neuroimage 2007; 36 Suppl 2:
T155–63.
Nijs J, Van Houdenhove B, Oostendorp RAB. Recognition of central sensitization in
patients with musculoskeletal pain: Application of pain neurophysiology in manual
therapy practice. Man. Ther. 2010; 15: 135–41.
Nijs J, Meeus M, Heins M, Knoop H, Moorkens G, Bleijenberg G. Kinesiophobia,
catastrophizing and anticipated symptoms before stair climbing in chronic fatigue
syndrome: an experimental study. Disabil. Rehabil. 2012; 34: 1299–305.
Nijs J, Van de Putte K, Louckx F, Truijen S, De Meirleir K. Exercise performance and
chronic pain in chronic fatigue syndrome: the role of pain catastrophizing. Pain Med.
2008; 9: 1164–72.
Nilsson I-M, List T, Drangsholt M. Headache and co-morbid pains associated with
TMD pain in adolescents. J. Dent. Res. 2013; 92: 802–7.
Nishimori T, Sera M, Suemune S, Yoshida A, Tsuru K, Tsuiki Y, et al. The distribution
of muscle primary afferents from the masseter nerve to the trigeminal sensory nuclei.
Brain Res. 1986; 372: 375–81.
Nordin M, Carragee EJ, Hogg-Johnson S, Weiner SS, Hurwitz EL, Peloso PM, et al.
Assessment of neck pain and its associated disorders: results of the Bone and Joint
Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila.
Pa. 1976). 2008; 33: S101–22.
Ohmure H, Miyawaki S, Nagata J, Ikeda K, Yamasaki K, Al-Kalaly A. Influence of
forward head posture on condylar position. J. Oral Rehabil. 2008; 35: 795–800.
Okamoto K, Kimura A, Donishi T, Imbe H, Senba E, Tamai Y. Central serotonin 3
receptors play an important role in the modulation of nociceptive neural activity of
trigeminal subnucleus caudalis and nocifensive orofacial behavior in rats with persistent
temporomandibular joint inflammation. Neuroscience 2005; 135: 569–81.

257
Okeson JP, de Leeuw R. Differential diagnosis of temporomandibular disorders and
other orofacial pain disorders. Dent. Clin. North Am. 2011; 55: 105–20.
Okeson JP. Current terminology and diagnostic classification schemes. Oral Surg. Oral
Med. Oral Pathol. Oral Radiol. Endod. 1997; 83: 61–4.
Olivo SA, Fuentes J, Major PW, Warren S, Thie NMR, Magee DJ. The association
between neck disability and jaw disability. J Oral Rehabil 2010; 37: 670–9.
Ouaknine G, Nathan H. Anastomotic connections between the eleventh nerve and the
posterior root of the first cervical nerve in humans. J. Neurosurg. 1973; 38: 189–97.
Park JW, Clark GT, Kim YK, Chung JW. Analysis of thermal pain sensitivity and
psychological profiles in different subgroups of TMD patients. Int. J. Oral Maxillofac.
Surg. 2010; 39: 968–74.
Peck CC, Murray GM, Gerzina TM. How does pain affect jaw muscle activity? The
Integrated Pain Adaptation Model. Aust. Dent. J. 2008; 53: 201–7.
Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the
number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996;
49: 1373–9.
Penley JA, Wiebe JS, Nwosu A. Psychometric properties of the Spanish Beck
Depression Inventory-II in a medical sample. Psychol. Assess. 2003; 15: 569–77.
Pernold G, Mortimer M, Wiktorin C, Tornqvist EW, Vingård E. Neck/shoulder
disorders in a general population. Natural course and influence of physical exercise: a 5-
year follow-up. Spine (Phila. Pa. 1976). 2005; 30: E363–8.
Piovesan EJ, Kowacs PA, Oshinsky ML. Convergence of cervical and trigeminal
sensory afferents. Curr. Pain Headache Rep. 2003; 7: 377–83.
Piovesan EJ, Kowacs PA, Tatsui CE, Lange MC, Ribas LC, Werneck LC. Referred pain
after painful stimulation of the greater occipital nerve in humans: evidence of
convergence of cervical afferences on trigeminal nuclei. Cephalalgia 2001; 21: 107–9.

258
Plesh O, Adams SH, Gansky S a. Temporomandibular joint and muscle disorder-type
pain and comorbid pains in a national US sample. J. Orofac. Pain 2011; 25: 190–8.
Plesh O, Curtis DA, Hall LJ, Miller A. Gender difference in jaw pain induced by
clenching. J. Oral Rehabil. 1998; 25: 258–63.
Poletti CE. C2 and C3 pain dermatomes in man. Cephalalgia 1991; 11: 155–9.
Porreca F, Ossipov MH, Gebhart GF. Chronic pain and medullary descending
facilitation. Trends Neurosci. 2002; 25: 319–25.
Portney LG WM. Foundations of Clinical Research; Applications to Practice. New
Jersey: 2009.
Quartana PJ, Buenaver LF, Edwards RR, Klick B, Haythornthwaite JA, Smith MT. Pain
catastrophizing and salivary cortisol responses to laboratory pain testing in
temporomandibular disorder and healthy participants. J. Pain 2010; 11: 186–94.
Raboisson P, Dallel R, Clavelou P, Sessle BJ, Woda A. Effects of subcutaneous
formalin on the activity of trigeminal brain stem nociceptive neurones in the rat. J.
Neurophysiol. 1995; 73: 496–505.
Rantala MA, Ahlberg J, Suvinen TI, Nissinen M, Lindholm H, Savolainen A, et al.
Temporomandibular joint related painless symptoms, orofacial pain, neck pain,
headache, and psychosocial factors among non-patients. Acta Odontol Scand 2003; 61:
217–222.
Raphael KG, Janal MN, Anathan S, Cook DB, Staud R. Temporal summation of heat
pain in temporomandibular disorder patients. J. Orofac. Pain 2009; 23: 54–64.
Reid KI, Greene CS. Diagnosis and treatment of temporomandibular disorders: an
ethical analysis of current practices. J. Oral Rehabil. 2013; 40: 546–61.
Ren K, Dubner R. Descending modulation in persistent pain: an update. Pain 2002; 100:
1–6.

259
Rocabado M. Biomechanical relationship of the cranial, cervical, and hyoid regions. J.
Craniomandibular. Pract. 1983; 1: 61–6.
Rocha CP, Croci CS, Caria PHF. Is there relationship between temporomandibular
disorders and head and cervical posture? A systematic review. J. Oral Rehabil. 2013;
40: 875–81.
Roddy E, Zwierska I, Jordan KP, Dawes P, Hider SL, Packham J, et al. Musculoskeletal
clinical assessment and treatment services at the primary-secondary care interface: an
observational study. Br. J. Gen. Pract. 2013; 63: e141–8.
Rodríguez K, Miralles R, Gutiérrez MF, Santander H, Fuentes A, Fresno MJ, et al.
Influence of jaw clenching and tooth grinding on bilateral sternocleidomastoid EMG
activity. Cranio 2011; 29: 14–22.
Rollman A, Visscher CM, Gorter RC, Naeije M. Care seeking for orofacial pain. J.
Orofac. Pain 2012; 26: 206–14.
Salama-Hanna J, Chen G. Patients with chronic pain. Med. Clin. North Am. 2013; 97:
1201–15.
Salomons T V, Moayedi M, Weissman-Fogel I, Goldberg MB, Freeman B V,
Tenenbaum HC, et al. Perceived helplessness is associated with individual differences
in the central motor output system. Eur. J. Neurosci. 2012; 35: 1481–7.
Salter MW. Cellular neuroplasticity mechanisms mediating pain persistence. J. Orofac.
Pain 2004; 18: 318–24.
Sanders RD. The Trigeminal (V) and Facial (VII) Cranial Nerves: Head and Face
Sensation and Movement. Psychiatry (Edgmont). 2010; 7: 13–6.
Saper JR, Dodick DW, Silberstein SD, McCarville S, Sun M, Goadsby PJ. Occipital
nerve stimulation for the treatment of intractable chronic migraine headache: ONSTIM
feasibility study. Cephalalgia 2011; 31: 271–85.
Saracco MG, Valfrè W, Cavallini M, Aguggia M. Greater occipital nerve block in
chronic migraine. Neurol. Sci. 2010; 31 Suppl 1: S179–80.

260
Sarlani E, Grace EG, Reynolds MA, Greenspan JD. Evidence for up-regulated central
nociceptive processing in patients with masticatory myofascial pain. J. Orofac. Pain
2004; 18: 41–55.
Schepelmann K, Ebersberger A, Pawlak M, Oppmann M, Messlinger K. Response
properties of trigeminal brain stem neurons with input from dura mater encephali in the
rat. Neuroscience 1999; 90: 543–54.
Schiffman E, Ohrbach R, List T, Anderson G, Jensen R, John MT, et al. Diagnostic
criteria for headache attributed to temporomandibular disorders. Cephalalgia 2012; 32:
683–92.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet J-P, et al. Diagnostic
Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research
Applications: recommendations of the International RDC/TMD Consortium Network*
and Orofacial Pain Special Interest Group†. J. oral facial pain headache 2014; 28: 6–27.
Schiffman EL, Ohrbach R, Truelove EL, Tai F, Anderson GC, Pan W, et al. The
Research Diagnostic Criteria for Temporomandibular Disorders. V: methods used to
establish and validate revised Axis I diagnostic algorithms. J. Orofac. Pain 2010; 24:
63–78.
Schmid-Schwap M, Bristela M, Kundi M, Piehslinger E. Sex-specific differences in
patients with temporomandibular disorders. J. Orofac. Pain 2013; 27: 42–50.
Schofferman J, Garges K, Goldthwaite N, Koestler M, Libby E. Upper cervical anterior
diskectomy and fusion improves discogenic cervical headaches. Spine (Phila. Pa. 1976).
2002; 27: 2240–4.
Van Selms MKA, Wang K, Lobbezoo F, Svensson P, Arendt-Nielsen L, Naeije M.
Effects of masticatory muscle fatigue without and with experimental pain on jaw-stretch
reflexes in healthy men and women. Clin. Neurophysiol. 2005; 116: 1415–23.
Seminowicz DA, Shpaner M, Keaser ML, Krauthamer GM, Mantegna J, Dumas JA, et
al. Cognitive-behavioral therapy increases prefrontal cortex gray matter in patients with
chronic pain. J. Pain 2013; 14: 1573–84.

261
Serra G, Marchioretto F. Occipital nerve stimulation for chronic migraine: a randomized
trial. Pain Physician 2012; 15: 245–53.
Sessle BJ, Hu JW, Amano N, Zhong G. Convergence of cutaneous, tooth pulp, visceral,
neck and muscle afferents onto nociceptive and non-nociceptive neurones in trigeminal
subnucleus caudalis (medullary dorsal horn) and its implications for referred pain. Pain
1986; 27: 219–35.
Sessle BJ, Hu JW. Mechanisms of pain arising from articular tissues. Can. J. Physiol.
Pharmacol. 1991; 69: 617–26.
Sessle BJ. The neurobiology of facial and dental pain: present knowledge, future
directions. J. Dent. Res. 1987; 66: 962–81.
Sessle BJ. Mechanisms of trigeminal and occipital pain. Pain Rev. 1996; 3: 91–116.
Sessle BJ. Neural mechanisms and pathways in craniofacial pain. Can. J. Neurol. Sci.
1999; 26 Suppl 3: S7–11.
Sessle BJ. Acute and chronic craniofacial pain: brainstem mechanisms of nociceptive
transmission and neuroplasticity, and their clinical correlates. Crit. Rev. Oral Biol. Med.
2000; 11: 57–91.
Sessle BJ. Recent insights into brainstem mechanisms underlying craniofacial pain. J.
Dent. Educ. 2002; 66: 108–12.
Sessle BJ. Orofacial Pain. In: The Paths of Pain 1975-2005. Seattle: IASP Press; 2005.
a.
Sessle BJ. Peripheral and central mechanisms of orofacial pain and their clinical
correlates. Minerva Anestesiol. 2005b; 71: 117–36.
Sessle BJ. Peripheral and central mechanisms of orofacial inflammatory pain. Int. Rev.
Neurobiol. 2011; 97: 179–206.

262
Shackman AJ, Salomons T V, Slagter HA, Fox AS, Winter JJ, Davidson RJ. The
integration of negative affect, pain and cognitive control in the cingulate cortex. Nat.
Rev. Neurosci. 2011; 12: 154–67.
Shephard MK, Macgregor EA, Zakrzewska JM. Orofacial pain: a guide for the
headache physician. Headache 2014; 54: 22–39.
Sherman SE, Luo L, Dostrovsky JO. Spinal strychnine alters response properties of
nociceptive-specific neurons in rat medial thalamus. J. Neurophysiol. 1997; 78: 628–37.
Shigenaga Y, Sera M, Nishimori T, Suemune S, Nishimura M, Yoshida A, et al. The
central projection of masticatory afferent fibers to the trigeminal sensory nuclear
complex and upper cervical spinal cord. J. Comp. Neurol. 1988; 268: 489–507.
Shin JH, Song HK, Lee JH, Kim WK, Chu MK. Paroxysmal stabbing headache in the
multiple dermatomes of the head and neck: a variant of primary stabbing headache or
occipital neuralgia? Cephalalgia 2007; 27: 1101–8.
Shin P, Vernon H, Sessle BJ, Hu JW. Neck muscle length modulates nociceptive reflex
evoked by noxious irritant application to rat neck tissues. Exp. brain Res. 2005; 163:
314–23.
Silberstein SD, Dodick DW, Saper J, Huh B, Slavin K V, Sharan A, et al. Safety and
efficacy of peripheral nerve stimulation of the occipital nerves for the management of
chronic migraine: results from a randomized, multicenter, double-blinded, controlled
study. Cephalalgia 2012; 32: 1165–79.
Silva AG, Punt TD, Sharples P, Vilas-Boas JP, Johnson MI. Head posture and neck pain
of chronic nontraumatic origin: a comparison between patients and pain-free persons.
Arch. Phys. Med. Rehabil. 2009; 90: 669–74.
Simons D, Travell J, Simons L. Myofascial pain and dysfunction: The trigger point
manual. Vol 1. 2nd. Baltimore: Williams & Wilkins; 1999.
Simons D. Clinical and Etiological Update of Myofascial Pain from Trigger Points. J.
Musculoskelet. Pain 1996: 93–122.

263
Simons LE, Elman I, Borsook D. Psychological processing in chronic pain: a neural
systems approach. Neurosci. Biobehav. Rev. 2014; 39: 61–78.
Sipilä K, Zitting P, Siira P, Laukkanen P, Järvelin M-R, Oikarinen KS, et al.
Temporomandibular disorders, occlusion, and neck pain in subjects with facial pain: a
case-control study. Cranio 2002; 20: 158–64.
Slavin K V, Colpan ME, Munawar N, Wess C, Nersesyan H. Trigeminal and occipital
peripheral nerve stimulation for craniofacial pain: a single-institution experience and
review of the literature. Neurosurg. Focus 2006; 21: E5.
Smeets RJEM, Vlaeyen JWS, Kester ADM, Knottnerus JA. Reduction of pain
catastrophizing mediates the outcome of both physical and cognitive-behavioral
treatment in chronic low back pain. J. Pain 2006; 7: 261–71.
So K, Komiyama O, Arai M, Kawara M, Kobayashi K. Influence of occlusal contact on
cervical muscle activity during submaximal clenching. J. Oral Rehabil. 2004; 31: 417–
22.
Solow B, Tallgren A. Head posture and craniofacial morphology. Am. J. Phys.
Anthropol. 1976; 44: 417–35.
Spielberg C, Lushene R. State Anxiety Inventory. Cuestionario de ansiedad estado-
rasgo. Adaptación Española. Madrid: TEA; 1982.
Storm C, Wänman A. Temporomandibular disorders, headaches, and cervical pain
among females in a Sami population. Acta Odontol. Scand. 2006; 64: 319–25.
Strassman AM, Mineta Y, Vos BP. Distribution of fos-like immunoreactivity in the
medullary and upper cervical dorsal horn produced by stimulation of dural blood
vessels in the rat. J. Neurosci. 1994; 14: 3725–35.
Strassman AM, Raymond SA, Burstein R. Sensitization of meningeal sensory neurons
and the origin of headaches. Nature 1996; 384: 560–4.

264
Stuginski-Barbosa J, Macedo HR, Bigal ME, Speciali JG. Signs of temporomandibular
disorders in migraine patients: a prospective, controlled study. Clin J Pain 2010; 26:
418–421.
Sugiyo S, Takemura M, Dubner R, Ren K. Trigeminal transition zone/rostral
ventromedial medulla connections and facilitation of orofacial hyperalgesia after
masseter inflammation in rats. J. Comp. Neurol. 2005; 493: 510–23.
Sullivan MJ, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al.
Theoretical perspectives on the relation between catastrophizing and pain. Clin. J. Pain
2001; 17: 52–64.
Sullivan MJ. What is the clinical value of assessing pain-related psychosocial risk
factors? Pain Manag. 2013; 3: 413–6.
Suzuki S, Matsubara N, Hisano M, Soma K. Investigation of cervical muscle
mechanisms during jaw movement--using a prototype head-jaw-neck model--. J. Med.
Dent. Sci. 2003; 50: 285–90.
Svensson P, Burgaard A, Schlosser S. Fatigue and pain in human jaw muscles during a
sustained, low-intensity clenching task. Arch. Oral Biol. 2001; 46: 773–7.
Svensson P, Wang K, Arendt-Nielsen L, Cairns BE, Sessle BJ. Pain effects of glutamate
injections into human jaw or neck muscles. J. Orofac. Pain 2005; 19: 109–18.
Svensson P, Wang K, Sessle BJ, Arendt-Nielsen L. Associations between pain and
neuromuscular activity in the human jaw and neck muscles. Pain 2004; 109: 225–32.
Svensson P. Muscle pain in the head: overlap between temporomandibular disorders
and tension-type headaches. Curr Opin Neurol 2007; 20: 320–325.
Takemura M, Sugiyo S, Moritani M, Kobayashi M, Yonehara N. Mechanisms of
orofacial pain control in the central nervous system. Arch. Histol. Cytol. 2006; 69: 79–
100.
265
Terwee CB, Bot SDM, de Boer MR, van der Windt DAWM, Knol DL, Dekker J, et al.
Quality criteria were proposed for measurement properties of health status
questionnaires. J. Clin. Epidemiol. 2007; 60: 34–42.
Thompson J, Brodie A. Factors in the position of the mandible. J. Am. Dent. Assoc.
1942; 29: 925–941.
Torisu T, Suenaga H, Yoshimatsu T, Kanaoka R, Yamabe Y, Fujii H. Anticipatory and
reflexive neck muscle activities during voluntary rapid jaw opening and passive jaw
depression in humans. J. Oral Rehabil. 2002; 29: 961–8.
Torisu T, Tanaka M, Murata H, Wang K, Arendt-Nielsen L, De Laat A, et al.
Modulation of neck muscle activity induced by intra-oral stimulation in humans. Clin.
Neurophysiol. 2013
Torisu T, Tanaka M, Murata H, Wang K, Arendt-Nielsen L, De Laat A, et al.
Modulation of neck muscle activity induced by intra-oral stimulation in humans. Clin.
Neurophysiol. 2014; 125: 1006–11.
Torisu T, Yamabe Y, Hashimoto N, Yoshimatsu T, Fujii H. Head movement properties
during voluntary rapid jaw movement in humans. J. Oral Rehabil. 2001; 28: 1144–52.
La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-Parreño S, Paris-
Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain sensitivity over the trigeminal
region in patients with chronic mechanical neck pain. J. pain Off. J. Am. Pain Soc.
2010; 11: 256–263.
La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K, Angulo-
Díaz-Parreño S, Paris-Alemany A, et al. The effects of manual therapy and exercise
directed at the cervical spine on pain and pressure pain sensitivity in patients with
myofascial temporomandibular disorders. J. Oral Rehabil. 2009; 36: 644–52.
La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-Díaz-
Parreño S, Suárez-Falcón JC, et al. Craniofacial pain and disability inventory (CF-PDI):
development and psychometric validation of a new questionnaire. Pain Physician 2014;
17: 95–108.

266
La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-Díaz-
Parreño S, Fernández-Carnero J. The Influence of Neck Disability and Pain
Catastrophizing about Trigeminal Sensory-Motor System in Patients with Headache
Attributed to Temporomandibular Disorders. (En proceso) 2014
La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S, Bishop MD,
Lopéz-Valverde-Centeno A, et al. Does Mobilization of the Upper Cervical Spine
Affect Pain Sensitivity and Autonomic Nervous System Function in Patients With
Cervico-craniofacial Pain?: A Randomized-controlled Trial. Clin. J. Pain 2012
La Touche R, París-Alemany A, Von Piekartz H, Mannheimer JS, Fernández-Carnero J,
Rocabado M. The influence of cranio-cervical posture on maximal mouth opening and
pressure pain threshold in patients with myofascial temporomandibular pain disorders.
Clin. J. Pain 2011; 27: 48–55.
Tseng BY, Gajewski BJ, Kluding PM. Reliability, responsiveness, and validity of the
visual analog fatigue scale to measure exertion fatigue in people with chronic stroke: a
preliminary study. Stroke Res. Treat. 2010; 2010
Turk DC, Rudy TE. Toward an empirically derived taxonomy of chronic pain patients:
integration of psychological assessment data. J Consult Clin Psychol 1988; 56: 233–8.
Turner JA, Aaron LA. Pain-related catastrophizing: what is it? Clin. J. Pain 2001; 17:
65–71.
Turner JA, Brister H, Huggins K, Mancl L, Aaron LA, Truelove EL. Catastrophizing is
associated with clinical examination findings, activity interference, and health care use
among patients with temporomandibular disorders. J. Orofac. Pain 2005; 19: 291–300.
Turner JA, Dworkin SF, Mancl L, Huggins KH, Truelove EL. The roles of beliefs,
catastrophizing, and coping in the functioning of patients with temporomandibular
disorders. Pain 2001; 92: 41–51.
Turner JA, Mancl L, Aaron LA. Brief cognitive-behavioral therapy for
temporomandibular disorder pain: effects on daily electronic outcome and process
measures. Pain 2005; 117: 377–87.

267
Turner JA, Mancl L, Aaron LA. Short- and long-term efficacy of brief cognitive-
behavioral therapy for patients with chronic temporomandibular disorder pain: a
randomized, controlled trial. Pain 2006; 121: 181–94.
Velly AM, Look JO, Carlson C, Lenton PA, Kang W, Holcroft CA, et al. The effect of
catastrophizing and depression on chronic pain--a prospective cohort study of
temporomandibular muscle and joint pain disorders. Pain 2011; 152: 2377–83.
Venegas M, Valdivia J, Fresno MJ, Miralles R, Gutiérrez MF, Valenzuela S, et al.
Clenching and grinding: effect on masseter and sternocleidomastoid electromyographic
activity in healthy subjects. Cranio 2009; 27: 159–66.
Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J.
Manipulative Physiol. Ther. 1991; 14: 409–15.
Vernon H, Sun K, Zhang Y, Yu X-M, Sessle BJ. Central sensitization induced in
trigeminal and upper cervical dorsal horn neurons by noxious stimulation of deep
cervical paraspinal tissues in rats with minimal surgical trauma. J. Manipulative
Physiol. Ther. 2009; 32: 506–14.
Visscher CM, Huddleston Slater JJ, Lobbezoo F, Naeije M. Kinematics of the human
mandible for different head postures. J. Oral Rehabil. 2000; 27: 299–305.
Visscher CM, Ohrbach R, van Wijk AJ, Wilkosz M, Naeije M. The Tampa Scale for
Kinesiophobia for Temporomandibular Disorders (TSK-TMD). Pain 2010; 150: 492–
500.
Vlaeyen JW, Seelen HA, Peters M, de Jong P, Aretz E, Beisiegel E, et al. Fear of
movement/(re)injury and muscular reactivity in chronic low back pain patients: an
experimental investigation. Pain 1999; 82: 297–304.
Waite P, Ashwell K. The Human Nervous Sytem. San Diego: Elsevier Academic Press;
2004.

268
Walsh NE, Brooks P, Hazes JM, Walsh RM, Dreinhöfer K, Woolf AD, et al. Standards
of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-
2010). Arch. Phys. Med. Rehabil. 2008; 89: 1830–45.
Walton D, Elliott JM. A higher-order analysis supports use of the 11-item version of the
tampa scale for kinesiophobia in people with neck pain. Phys. Ther. 2013; 93: 60–8.
Walton DM, Macdermid JC, Nielson W, Teasell RW, Chiasson M, Brown L.
Reliability, standard error, and minimum detectable change of clinical pressure pain
threshold testing in people with and without acute neck pain. J. Orthop. Sports Phys.
Ther. 2011; 41: 644–50.
Wang K, Sessle BJ, Svensson P, Arendt-Nielsen L. Glutamate evoked neck and jaw
muscle pain facilitate the human jaw stretch reflex. Clin. Neurophysiol. 2004; 115:
1288–95.
Wänman A. Longitudinal course of symptoms of craniomandibular disorders in men
and women. A 10-year follow-up study of an epidemiologic sample. Acta Odontol.
Scand. 1996; 54: 337–42.
Watson DH, Drummond PD. Head pain referral during examination of the neck in
migraine and tension-type headache. Headache 2012; 52: 1226–35.
Weber P, Corrêa ECR, Ferreira F dos S, Soares JC, Bolzan G de P, Silva AMT da.
Cervical spine dysfunction signs and symptoms in individuals with temporomandibular
disorder. J. Soc. Bras. Fonoaudiol. 2012; 24: 134–9.
Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient
and the SEM. J. Strength Cond. Res. 2005; 19: 231–40.
Wiebe JS, Penley JA. A psychometric comparison of the Beck Depression Inventory-II
in English and Spanish. Psychol. Assess. 2005; 17: 481–5.
Wiesinger B, Häggman-Henrikson B, Hellström F, Wänman A. Experimental masseter
muscle pain alters jaw-neck motor strategy. Eur. J. Pain 2013; 17: 995–1004.

269
Wiesinger B, Malker H, Englund E, Wänman A. Back pain in relation to
musculoskeletal disorders in the jaw-face: a matched case-control study. Pain 2007;
131: 311–9.
Wiesinger B, Malker H, Englund E, Wänman A. Does a dose-response relation exist
between spinal pain and temporomandibular disorders? BMC Musculoskelet. Disord.
2009; 10: 28.
Woolf CJ, Costigan M. Transcriptional and posttranslational plasticity and the
generation of inflammatory pain. Proc. Natl. Acad. Sci. U. S. A. 1999; 96: 7723–30.
Woolf CJ. Pain: moving from symptom control toward mechanism-specific
pharmacologic management. Ann. Intern. Med. 2004; 140: 441–51.
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain.
Pain 2011; 152: S2–15.
Wright EF. Referred craniofacial pain patterns in patients with temporomandibular
disorder. J. Am. Dent. Assoc. 2000; 131: 1307–15.
Xie Y. Glial involvement in trigeminal central sensitization. Acta Pharmacol. Sin. 2008;
29: 641–5.
Yalcin I, Barrot M. The anxiodepressive comorbidity in chronic pain. Curr. Opin.
Anaesthesiol. 2014; 27: 520–7.
Yamabe Y, Yamashita R, Fujii H. Head, neck and trunk movements accompanying jaw
tapping. J. Oral Rehabil. 1999; 26: 900–5.
Yekkalam N, Wänman A. Prevalence of signs and symptoms indicative of
temporomandibular disorders and headaches in 35-, 50-, 65- and 75-year-olds living in
Västerbotten, Sweden. Acta Odontol. Scand. 2014
Ylinen J, Nikander R, Nykänen M, Kautiainen H, Häkkinen A. Effect of neck exercises
on cervicogenic headache: a randomized controlled trial. J. Rehabil. Med. 2010; 42:
344–9.

270
Yoshida K. [Electromyographical analysis of function of sternocleidomastoid muscle
during occlusal function]. Kokubyo Gakkai Zasshi. 1988; 55: 53–70.
Yu XM, Sessle BJ, Haas DA, Izzo A, Vernon H, Hu JW. Involvement of NMDA
receptor mechanisms in jaw electromyographic activity and plasma extravasation
induced by inflammatory irritant application to temporomandibular joint region of rats.
Pain 1996; 68: 169–78.
Yu XM, Sessle BJ, Vernon H, Hu JW. Effects of inflammatory irritant application to
the rat temporomandibular joint on jaw and neck muscle activity. Pain 1995; 60: 143–9.
Zafar H, Nordh E, Eriksson PO. Temporal coordination between mandibular and head-
neck movements during jaw opening-closing tasks in man. Arch. Oral Biol. 2000; 45:
675–82.
Zafar H, Nordh E, Eriksson P-O. Spatiotemporal consistency of human mandibular and
head-neck movement trajectories during jaw opening-closing tasks. Exp. brain Res.
2002; 146: 70–6.
Zafar H, Nordh E, Eriksson P-O. Impaired positioning of the gape in whiplash-
associated disorders. Swed. Dent. J. 2006; 30: 9–15.
Zafar H. Integrated jaw and neck function in man. Studies of mandibular and head-neck
movements during jaw opening-closing tasks. Swed. Dent. J. Suppl. 2000: 1–41.

I
UNIVERSIDAD REY JUAN CARLOS
FACULTAD DE CIENCIAS DE LA SALUD
TESIS DOCTORAL
Aspectos neurofisiológicos y biomecánicos de la región
cervical sobre el dolor cérvico-craneofacial:
Implicaciones del tratamiento y el diagnóstico
Departamento Bioquímica, Fisiología y Genética Molecular, Farmacología y
Nutrición, Anatomía y Embriología Humana e Histología Humana y Anatomía
Patológica
Roy La Touche Arbizu
MADRID, 2014

II

Facultad de Ciencias de la Salud Departamento de Bioquímica, Fisiología y Genética Molecular,
Farmacología y Nutrición, Anatomía y Embriología Humana e Histología Humana y Anatomía Patológica
III Avda. de Atenas s/n E 28922 Alcorcón Madrid España Tel. 34 91 4888855 Fax 34 91 4888831
Don Carlos Goicoechea García, Profesor Titular de Farmacología del Dpto. de
Bioquímica, Fisiología y Genética Molecular, Farmacología y Nutrición, Anatomía y
Embriología Humana e Histología Humana y Anatomía Patológica y D. Josué
Fernández Carnero, Profesor Colaborador del Dpto. de Fisioterapia, Terapia
Ocupacional, Rehabilitación y Medicina Física de la Universidad Rey Juan Carlos,
CERTIFICAN:
Que el Trabajo de investigación titulado “Aspectos neurofisiológicos y biomecánicos
de la región cervical sobre el dolor cérvico-craneofacial: Implicaciones del tratamiento
y el diagnóstico” ha sido realizado por Don. Roy La Touche Arbizu (D.N.I.: 50349803
C) bajo nuestra supervisión y dirección y cumple con los requisitos necesarios para
optar al grado de Doctor.
Y para que así conste a los efectos oportunos, firmamos el presente certificado en
Madrid, a 3 de Noviembre de 2014
Fdo. D. C. Goicoechea García Fdo. D. J. Fernández-Carnero

IV

V
A mis papás, Hilda y Melvin por su amor incondicional, esfuerzo constante y sacrificios
realizados durante toda la vida para que yo pudiera llegar hasta aquí, sin ellos este
proyecto no se hubiera podido realizar, gracias por ser mi ejemplo de vida y por las
enseñanzas en torno al esfuerzo, la perseverancia y la paciencia
A mis 5 hermanos y a todos mis sobrinos por estar ahí y comprender mi ausencia en
momentos importantes, a pesar de la distancia siempre están en mi mente y en mi
corazón

VI

VII
AGRADECIMIENTOS
Este proyecto al que he dedicado tiempo y esfuerzo, no se hubiera podido
concluir sin la inestimable ayuda y colaboración de muchas personas que han aportado
sus esfuerzos desinteresadamente en las investigaciones que conforman esta tesis, a
todos ellos quisiera expresarles mi más sincera gratitud.
En mi primer lugar quisiera agradecer a mis dos directores de tesis, el Dr. Carlos
Goicoechea García y el Dr. Josué Fernández Carnero por su ayuda y orientación durante
la elaboración de este trabajo.
Al Dr. Carlos Goicochea García quisiera agradecerle especialmente la
motivación que me ofreció para realizar la tesis una vez que terminé el Máster en
Estudio y Tratamiento del Dolor que él dirigía. Tanto el Dr. Carlos Goicochea como
Dra. Mª Isabel Martín Fontelles y todo su equipo han sido referentes para mí por su
dedicación, rigurosidad, humildad y vocación en la investigación del tratamiento del
dolor. Conocerles y que hayan sido mis profesores ha sido un privilegio que me ha
ayudado a orientar mi actividad investigadora y profesional. Siempre estaré agradecido
con ellos…
Al Dr. Josué Fernández Carnero tengo muchas cosas que agradecerle y algunas
van más allá de este mismo proyecto. Durante todos los años que he tardado en finalizar
este proyecto Josué siempre ha estado detrás de cada paso que di, aportando nuevas
ideas, motivándome y dedicando toda su capacidad y conocimiento en cada una de las
investigaciones. Para mí es un premio haberle conocido y poder establecer una
verdadera relación de amistad, tengo el orgullo de decir que además de conseguir
terminar la tesis he conseguido un gran amigo. Gracias al profesor, gracias al tutor y
sobre todo gracias al amigo que has sido durante estos años.

VIII
Haciendo una retrospectiva de lo que han sido estos años y el proceso para llegar
a conseguir este proyecto, tengo que reconocer que hay personas que han facilitado mi
adaptación a un país diferente al mío, pero el que considero un gran país del cual ya
formo parte, y en este sentido quiero agradecer especialmente al Dr. José Antonio
Martín Urrialde de la Universidad San Pablo CEU, quien me tendió una mano
desinteresadamente y me ayudó en todo momento para venir y estar en España y
conseguir finalmente este sueño. Muchas gracias por todo y más…
Hay varios profesores e investigadores de reconocido prestigio internacional que
han participado en algunas de las investigaciones de esta tesis, quiero agradecer su
colaboración al Dr. Mariano Rocabado Seaton de la Universidad Andrés Bello de Chile,
al Dr. Jeffrey Mannheimer de Columbia University de Estados Unidos de América, al
Dr. Harry Von Piekartz de la University of Applied Science Osnabruck de Alemania y
al Dr. Mark Bishop de la University of Florida de Estados Unidos de América.
Agradezco a mis compañeros y amigos del grupo de investigación Motion in
Brains de CSEU La Salle, los profesores Joaquín Pardo, Alfonso Gil, Ibai López de
Uralde y Héctor Beltrán por su colaboración en las últimas investigaciones de esta tesis.
Quiero agradecer a mi amigo el profesor Santiago Angulo Díaz-Parreño de la
Universidad San Pablo CEU por su ayuda y enseñanzas entorno al tratamiento y análisis
estadístico, su aporte a las investigaciones de esta tesis es incalculable. Muchas gracias
amigo por tu conocimiento, dedicación y amistad…
Si el título de doctor se pudiera compartir yo lo haría con mi pareja Alba París,
ella ha sido mi punto de apoyo en todo momento, ha entendido mi dedicación a la
investigación y ha estado implicada en todas los estudios que conforman esta tesis, su
aporte e implicación científica ha sido excepcional y sus palabras de motivación, su

IX
amor y cariño han sido suficientes para seguir adelante cuando se presentaron las
dificultades. Gracias mi vida por todo y porque cada día es único a tu lado…
A mis cinco hermanos, John, Vivian, Marco, Mayela y Dennis, y todos mis
sobrinos a los que amo mucho y añoro a diario, quiero dedicar esta tesis. Ellos han
sabido comprender mis muchas ausencias en momentos especiales en los que aunque
hubiera querido estar no me ha sido posible, sé que ellos se alegran de los éxitos que he
podido conseguir y yo me alegro de que sean mi familia del cual estoy muy orgulloso
de cada uno de ellos.
Finalmente quiero dedicar este proyecto a mis papás Hilda y Melvin que son
personas excepcionales, bondadosas, esforzadas a las cuales yo tengo una gran
admiración. Ambos con sus actos me han enseñado lecciones de vida impagables, son
pocas las palabras de gratitud que podría escribir en estas frases para expresar mi
profundo agradecimiento, todo y cada una de las cosas he podido conseguir se lo debo a
ellos.
Mi mamá lamentablemente no ha podido ver concluida esta fase profesional que
finalizo con esta tesis, a pesar de esto, en su memoria he querido darle este pequeño
homenaje que en su día le hice la promesa que lo finalizaría con el máximo esfuerzo.
Ella me apoyó en todo momento, sobre todo en los momentos difíciles y me arropó con
sus palabras de amor constantes. Gracias Mami te recuerdo todos los días y te voy a
querer siempre, esto es para ti…
A mi papá Melvin le debo muchas cosas, su vida es ejemplar y ha estado dedicada al
esfuerzo y trabajo por sus seis hijos, su vida es ejemplo de lucha diaria y en todo
momento, sea cual sea la adversidad. La honradez, la dignidad, la constancia y el
esfuerzo son principios que he podido aprender de mi papá, estos me han servido para
entender que el camino hacia un objetivo no siempre es fácil y que las metas no son lo

X
más importante sino el esfuerzo que dediques a ello. Gracias Papi por todo, te quiero
mucho y esto para ti…
En toda investigación clínica los pacientes son determinantes y sin duda alguna
lo más importante, quiero agradecer a todos los pacientes que amablemente accedieron
a participar en los estudios que conforman esta tesis, espero que el conocimiento que
hemos generado sirva de alguna manera para mejorar la atención que reciban o en
motivar a otros investigadores que continúen con estas líneas. Gracias a todos los
pacientes con dolor craneofacial, muchas gracias…

XI
ÍNDICE GENERAL
RESUMEN…………………………………………………………………………...XV
Lista de publicaciones originales………………………………………………...…XIX
Abreviaturas………………………………………………………………..…...…..XXI
1. INTRODUCCIÓN…………………………………………………………………..1
1.1 Aspectos Básicos del Dolor…………………………………………………....2
1.1.1 Proceso de sensibilización periférica………………………………….....4
1.1.2 Proceso de sensibilización central…………………………………….....6
1.2 Dolor Musculoesquelético Crónico…………………………………………...7
1.2.1 Epidemiología…………………………………………………………....7
1.3 Dolor Cervical Crónico………………………………………………………..8
1.3.1 Epidemiología…………………………………………………………..10
1.4 Dolor Craneofacial de Origen Musculoesquelético……………….………..12
1.4.1 Trastornos craneomandibulares………………………………………...12
1.4.2 Epidemiología…………………………………………………………..14
1.4.3 Epidemiología y comorbilidad entre trastornos craneomandibulares,
cefalea y dolor de cuello………………………………………………..16
1.5 Dolor Referido de la Región Cervical hacia la Región
Craneofacial…………………………………………………………………..18
1.6 Aspectos Anatomofuncionales de la Región Craneomandibular y la Región
Craneocervical………………………………………………………………..20
1.6.1 Modelos biomecánicos de la región craneomandibular/craneocervical..21
1.6.2 Estudios in-vivo de la relación craneomandibular/craneocervical……..23
1.6.3 Influencia de la región craneocervical sobre la dinámica mandibular…23

XII
1.6.4 Sinergias neuromusculares cervicales y masticatorias…………….……24
1.6.5 Cinemática y concomitancia craneocervical/craneomandibular………..27
1.7 Neurofisiología del Dolor Cérvico-craneofacial…………………………….28
1.7.1 Sistema sensorial trigeminal…………………………………………....29
1.7.2 Neuroanatomía de los segmentos cervicales superiores………………..35
1.7.3 Complejo trigeminocervical…………………………………………....37
1.7.4 Sensibilización del complejo trigeminocervical………………………..39
1.8 Modulación del Dolor en el Complejo Trigeminocervical…………………41
1.8.1 Influencia de las aplicaciones terapéuticas sobre el dolor craneofacial..43
2. JUSTIFICACIÓN DEL TRABAJO REALIZADO……………………………..47
3. OBJETIVOS……………………………………………………………….……….51
4. MATERIAL Y MÉTODOS……………………………………………………….57
4.1 Participantes……………………………………………………………….….60
4.2 Variables y Pruebas de Medición…………………………………………....62
4.2.1 Medidas de auto-registro…………………………………………….64
4.2.2 Instrumentos de medición…………………………………………...66
4.3 Resumen de los Procedimientos……………………………………………..70
4.4 Análisis Estadístico…………………………………………………………...72
5. RESULTADOS…………………………………………………………………….77
5.1 Estudio I…………………………………………………………………….....78
5.2 Estudio II……………………………………………………………………...87
5.3 Estudio III………………………………………………...………….……...114
5.4 Estudio IV…………………………………………………………………....123
5.5 Estudio V………………………………………………………………….…138
5.6 Estudio VI………………………………………………………………..…..182

XIII
5.7 Estudio VII……………………………………………………………..……192
6. DISCUSIÓN………………………………………………………………………205
6.1 Diferencias de Género en las Variables Somatosensoriales………….…...207
6.2 Postura Craneocervical, Dinámica Mandibular y
Dolor Craneocervical……………………………………………….………208
6.3 Influencia del Dolor y la Discapacidad Cervical sobre la Actividad
Sensoriomotora Trigeminal………………………………………………...209
6.4 Asociación entre la Discapacidad Cervical y la Discapacidad
Craneofacial/craneomandibular…………………………………………...213
6.5 Factores Bioconductuales Implicados en las Alteraciones Sensoomotoras
Trigeminales y la Discapacidad Craneofacial……………………………..213
6.6 Efecto del Tratamiento en la Región Cervical
sobre el Dolor Craneofacial…………………………………….…………..218
6.7 Implicaciones Científicas y Clínicas………………………………………..219
6.8 Limitaciones y Futuras Investigaciones…………………………………....222
7. CONCLUSIONES……………………………………………………………..…225
8. BIBLIOGRAFÍA………………………………………………………………....229

XIV

XV
RESUMEN
Introducción: El dolor craneofacial (DCF) de origen musculoesquelético, representa la
causa más común de DCF de origen no dental y puede afectar a la musculatura
masticatoria, la articulación temporomandibular y otras estructuras orofaciales. Entre
los diferentes tipos de DCF de origen musculoesquelético el más prevalente son los
denominados trastornos craneomandibulares (TCM) atribuidos o relacionados con el
dolor miofascial. Diversos estudios han descrito la presencia de comorbilidades entre la
cefalea, el dolor de cuello y los TCM, además se ha comprobado que el dolor de cuello
se asocia significativamente con los TCM y que la gravedad de estos se incrementa con
la gravedad del dolor de cuello. Evidencia científica reciente sugiere la existencia de
mecanismos neurofisiológicos trigeminocervicales implicados en las alteraciones
motoras craneomandibulares y en el DCF, a pesar de esto se necesitan más estudios
clínicos que aporten información más precisa en cuanto a la posible repercusión clínica
de características sensoriales y motoras cervicales que afectan a pacientes con DCF.
Objetivo general: Determinar la influencia biomecánica y neurofisiológica de la región
cervical sobre la discapacidad y el DCF, además se pretende identificar como
determinados factores bioconductuales influyen sobre la función craneomandibular, la
discapacidad y el DCF.
Métodos: Se realizaron 4 estudios transversales, un estudio de casos y controles, una
serie de casos y un ensayo clínico aleatorio controlado que incluyeron a pacientes con
dolor de cuello crónico mecánico, pacientes con TCM atribuido a dolor miofascial,
pacientes con dolor cérvico-craneofacial (DCCF) y pacientes con cefalea atribuida a
TCM. En tres de los estudios se realizaron comparaciones con sujetos asintomáticos.
En los estudios se evaluaron características sensoriales, motoras y factores psicológicos
implicados en el DCF mediante:

XVI
- Medidas de auto-registro psicológicas, de dolor y discapacidad (inventario de
dolor y discapacidad craneofacial, IDD-CF; índice de dolor de cuello, IDC;
inventario de depresión BECK, BDI; escala de catastrofismo ante el dolor, ECD;
escala tampa de kinesiofobia, TSK-11; Escala visual analógica del dolor, EVA;
escala visual analógica de la fatiga, EVAF).
- Mediciones de los umbrales de dolor a la presión (UDPs) en áreas trigeminales,
cervicales y extra-trigeminales mediante algometría digital.
- Medición de la máxima apertura interincisal (MAI) libre de dolor.
- Mediciones de la postura craneocervical.
En todos los estudios se realizó un análisis descriptivo e inferencial, y en algunos casos
se utilizaron análisis complementarios a los contrastes de significación como el tamaño
del efecto o el mínimo cambio detectable para determinar la relevancia clínica de los
resultados.
Resultados:
En la comparación de los resultados de los sujetos asintomáticos con respecto a los
pacientes se presentaron los siguientes hallazgos: 1) hay diferencias estadísticamente
significativas en la postura craneocervical en los pacientes con DCCF frente a los
sujetos asintomáticos, sin embargo estas diferencias son pequeñas; 2) Se identificó que
los pacientes con dolor de cuello crónico mecánico presentan hiperalgesia mecánica en
áreas trigeminales y cervicales pero no en otras áreas anatómicas a distancia; 3) Los
pacientes con cefalea atribuida a TCM con moderada discapacidad cervical presentaron
mayores niveles de dolor y fatiga masticatoria, y menores UDPS en áreas trigeminales y
cervicales y menor MAI libre de dolor. En las comparaciones intra-grupos se encontró
una fuerte correlación entre la discapacidad cervical y la discapacidad
craneofacial/craneomandibular en pacientes con TCM atribuido a dolor miofascial. Se

XVII
comprobó que distintas posturas craneocervicales inducidas experimentalmente
modifican la dinámica mandibular y alteran los UDPs de áreas trigeminales y
cervicales. Por otra parte, se identificó que el catastrofismo ante el dolor y la
kinesiofobia fueron predictores del estado funcional mandibular y de la discapacidad y
DCF. Finalmente, en los estudios en donde se realizó una intervención en pacientes con
TMC atribuido a dolor miofascial y en pacientes con DCCF se comprobó que el
ejercicio terapéutico en combinación de terapia manual o únicamente la aplicación de
terapia manual sobre la región cervical producen un efecto inmediato y a corto plazo en
la mejora MAI libre de dolor, una disminución de la intensidad de dolor y un aumento
de los UDPS en áreas trigeminales y cervicales.
Conclusiones:
Los resultados obtenidos en esta tesis sugieren la influencia de mecanismos
neurofisiológicos y biomecánicos de la región cervical sobre la función mandibular, las
alteraciones somatosensoriales en áreas trigeminales y sobre la discapacidad
craneofacial. Se ha demostrado que factores bioconductuales como el catastrofismo ante
el dolor y la kinesiofobia deben ser tomados en cuenta ya que son predictores de las
alteraciones funcionales craneomandibulares y el DCF. A nivel terapéutico se presentan
los primeros hallazgos sobre el efecto del tratamiento de fisioterapia específico sobre la
región cervical en la mejora de la dinámica mandibular y en la modulación del DCF.
Esta tesis aporta nuevos datos que pueden contribuir clínicamente al diagnóstico, la
valoración y el tratamiento de los TCM y el DCF.

XVIII

XIX
LISTA DE PUBLICACIONES ORIGINALES
Esta tesis está basada en las siguientes publicaciones originales que forman parte de una
línea de investigación que estudia los mecanismos neurofisiológicos, biomecánicos y
bioconductuales de la región cervical en pacientes con dolor craneofacial, las cuales se
presentan de forma completa en el apartado de resultados. En diferentes apartados del
texto se hace referencia a las publicaciones originales mediante números romanos:
I. La Touche R, París-Alemany A, von Piekartz H, Mannheimer JS,
Fernández-Carnero J, Rocabado M. The influence of cranio-cervical posture
on maximal mouth opening and pressure pain threshold in patients with
myofascial temporomandibular pain disorders. Clin J Pain. 2011
Jan;27(1):48-55
II. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A,
Angulo-Díaz-Parreño S, La Touche R. Reliability, Standard Error, and
Minimal Detectable Change of Two Tests for Craniocervical Posture
Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial Pain
Patients. (En revisión).
III. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-
Parreño S, Paris-Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain
sensitivity over the trigeminal region in patients with chronic mechanical
neck pain. J Pain. 2010 Mar;11(3):256-63
IV. La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-
Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero J.
Craniofacial pain and disability inventory (CF-PDI): development and

XX
psychometric validation of a new questionnaire. Pain Physician. 2014 Jan-
Feb;17(1):95-108.
V. La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-
Díaz-Parreño S, Fernández-Carnero J. The Influence of Neck Disability and
Pain Catastrophizing about Trigeminal Sensory-Motor System in Patients
with Headache Attributed to Temporomandibular Disorders. (En revision)
VI. La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K,
Angulo-Díaz-Parreño S, Paris-Alemany A, Cleland JA. The effects of
manual therapy and exercise directed at the cervical spine on pain and
pressure pain sensitivity in patients with myofascial temporomandibular
disorders. J Oral Rehabil. 2009 Sep;36(9):644-52.
VII. La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S,
Bishop MD, Lopéz-Valverde-Centeno A, von Piekartz H, Fernández-
Carnero J. Does mobilization of the upper cervical spine affect pain
sensitivity and autonomic nervous system function in patients with cervico-
craniofacial pain?: A randomized-controlled trial. Clin J Pain. 2013
Mar;29(3):205-15.

XXI
ABREVIATURAS
ATM Articulación temporomandibular
BDI Inventario de depresión Beck
CP Conductancia de la piel
CTC Complejo trigeminocervical
DCCF Dolor cérvico-craneofacial
DCF Dolor craneofacial
DMC Dolor musculoesquelético crónico
ECD Escala de catastrofismo ante el dolor
EMG Electromiografía
END Escala numérica del dolor
ETCM Ejercicio terapéutico de control motor
EVA Escala visual analógica del dolor
EVAF Escala visual analógica de fatiga
FC Frecuencia cardíaca
FR Frecuencia respiratoria
GC Grupo control
GE Grupo experimental
HIT-6 Cuestionario de impacto de la cefalea
IDC Índice de dolor cervical
IDD-CF Inventario de dolor y discapacidad craneofacial
MAI Máxima apertura interincisal
MC Migraña crónica
ME Migraña episódica

XXII
MIAD Modelo integrado de adaptación al dolor
NE Neuronas nociceptivas específicas
NMDA N-metil-D-aspartato
PMG Puntos gatillos miofasciales
RDA Neuronas de rango dinámico amplio
SDM Síndrome de dolor miofascial
STAI Cuestionario de ansiedad estado-rasgo
SVc Sub-núcleo trigeminal caudal
SVi Sub-núcleo trigeminal interpolar
SVo Sub-núcleo trigeminal oral
TC Temperatura cutánea.
TCM Trastornos craneomandibulares
TMO Terapia manual ortopédica
TSK-11 Escala de Tampa de Kinesiofobia
UDP Umbral de dolor a la presión
VPM Núcleo ventral posteromedial del tálamo

1
INTRODUCCIÓN

2
1. INTRODUCCIÓN
1.1 Aspectos Básicos del Dolor
En el modelo biomédico general, el dolor ha sido considerado como un síntoma
producido por un daño tisular, de manera que la experiencia de dolor se ha
simplificado a que, si no había daño no había dolor, si había daño tendría que
haber dolor y a mayor daño mayor dolor. El conocimiento sobre el dolor
evolucionó a partir de la compresión del procesamiento neurofisiológico del dolor
a nivel medular. Melzack y Wall (Melzack and Wall, 1965) tuvieron una
destacada labor en esta cuestión al proponer la teoría de la regulación del umbral
también conocida como la teoría de la puerta de entrada, básicamente esta teoría
explicaba el mecanismo en que el dolor estaba representado neuralmente en el asta
dorsal de la médula espinal, donde se podía facilitar o inhibir la puerta de entrada
de estímulos dolorosos hacia centros superiores. Esta teoría cobró mucha
importancia hace unas décadas a pesar de no poder explicar fisiológicamente la
situación del dolor crónico (Melzack, 1993), sin embargo lo que si permitió fue la
consideración de los factores psicológicos como parte integral del procesamiento
del dolor.
La teoría de regulación del umbral evolucionó hacia la teoría de la neuromatriz, en
esta se amplía el concepto del dolor integrando las influencias que puedan tener las
funciones cognitivas del cerebro, los sistemas de regulación del estrés y los
estímulos sensoriales (Melzack, 1999), además se expone que el dolor es una
experiencia multidimensional compuesta por la interacción de tres dimensiones:

3
- Dimensión sensorial-discriminativa: identifica, evalúa, valora y modifica
todos aquellos factores relacionados con la percepción sensorial del dolor
(intensidad, localización, cualidad, factores temporales y espaciales)
- Dimensión motivacional-afectiva: comporta el aspecto emocional del
dolor. En esta dimensión estarían implicadas estructuras troncoenfálicas y
límbicas.
- Dimensión cognitivo-evaluativa: analiza e interpreta el dolor en función de
la sensación y lo que puede ocurrir.
En la actualidad el dolor se mira desde la óptica del paradigma biopsicosocial, con
lo cual los factores fisiológicos, psicológicos y sociales son tomados en cuenta, así
lo muestra la descripción de dolor definida por la Asociación Internacional para el
Estudio del Dolor:
“Es una experiencia sensorial y emocional desagradable asociada a un daño
tisular real o potencial, o descrita en términos del daño” (Merskey and Bogduk,
1994).
Existen diversas clasificaciones del dolor basadas en el origen, la evolución, los
mecanismos fisiológicos y en la estructura anatómica implicada. Con frecuencia y
desde un punto de vista clínico el dolor musculoesquéletico se clasifica en agudo y
crónico, esta clasificación toma en cuenta la evolución del dolor desde el punto de
vista del tiempo y los aspectos neurofisiológicos relacionados con la génesis y el
mantenimiento.
El dolor agudo tiene un curso temporal relacionado con los procesos de reparación
(Chapman et al., 2011) y representa una señal de alarma disparada por los
sistemas protectores del organismo (Loeser and Treede, 2008). La ineficacia en el

4
tratamiento o en la recuperación del dolor agudo puede generar que este se
mantenga en el tiempo convirtiéndose en un dolor crónico y adquiriendo las
complicaciones que este presenta.
Se define el dolor crónico como “el que persiste más allá del tiempo normal de
reparación de los tejidos, que se supone en el dolor no maligno es de 3 meses…,
pero para fines de investigación se prefiere elegir un tiempo de 6 meses” (Merskey
y Bogduk, 1994). El tiempo (días, meses…) en el que se tiene dolor es el
parámetro más utilizado para definir la diferencia entre el dolor agudo y el dolor
crónico, esta clasificación tiene sus limitaciones teniendo en cuenta que el dolor
crónico presenta una naturaleza multifactorial (Turk and Rudy, 1988). En este
sentido Von Korff y Dunn (Von Korff and Dunn, 2008), han comprobado que un
modelo de clasificación de los pacientes basado en los niveles de discapacidad,
calidad vida, intensidad de dolor, síntomas depresivos y toma de medicamentos
tiene mayor valor predictivo que solo la clasificación basada en el tiempo de dolor
(Von Korff and Dunn, 2008).
1.1.1 Proceso de sensibilización periférica
Desde el punto de vista de la neurofisiología, el dolor agudo es considerado como
una respuesta sensorial de la activación del sistema nociceptivo a consecuencia de
un daño tisular que produce una respuesta inflamatoria que sensibiliza los
nociceptores periféricos (Loeser and Treede, 2008; Woolf, 2004); la
sensibilización se produce a consecuencia de la acción de mediadores químicos de
origen inflamatorio que se liberan en el área del daño tisular, tales como la
sustancia P y el péptido relacionado con el gen de la calcitonina que se liberan en
la periferia y se unen a otros mediadores como neutrófilos, mastocitos y basófilos;
esta unión produce a su vez la liberación de sustancias pro-inflamatorias

5
(citoquinas, bradiquinina, histamina) que favorecen la síntesis de la enzima
ciclooxigenasa-2 (COX-2) que conduce a la producción y secreción
de prostaglandinas (Woolf, 2004). Este mediador actúa como un sensibilizador
que altera la sensibilidad al dolor por el incremento de la capacidad de respuesta
de los nociceptores periféricos (Woolf, 2004).
La sensibilización periférica se define como un proceso en donde hay una
reducción del umbral y una amplificación de la capacidad de respuesta de los
nociceptores, que se produce cuando las terminales periféricas de las neuronas
sensoriales primarias de alto umbral están expuestos a mediadores de inflamación
en el tejido dañado (Chen et al., 1999; Guenther et al., 1999; Hucho and Levine,
2007).
Es un hecho más que contrastado que la sensibilización periférica contribuye a la
sensibilización del sistema nociceptivo y provoca dolor e hipersensibilidad en las
áreas en donde se produce inflamación (hiperalgesia primaria) (Latremoliere and
Woolf, 2009), este fenómeno representa una acción protectora del organismo con
el fin de evitar el uso de estructuras dañadas (Nijs et al., 2010). A la sensación
dolorosa que se extiende más allá del área de la lesión y abarca zonas no afectadas
por la lesión original, se la conoce como hiperalgesia secundaria, pero este no es
un proceso únicamente de carácter periférico, lleva implícitos mecanismos
centrales (Latremoliere and Woolf, 2009; Woolf, 2011).
El proceso de sensibilización periférica se asocia a una alteración en la
sensibilidad térmica, pero no se observa una alteración de la sensibilización
mecánica que parece ser una característica importante de la sensibilización central
(Latremoliere and Woolf, 2009; Woolf, 2004).

6
1.1.2 Proceso de sensibilización central
El dolor crónico está asociado a cambios neuroplásticos sobre mecanismos
periféricos y centrales, estos cambios pueden mantener la percepción de dolor a
pesar de la ausencia de un daño potencial (Woolf and Costigan, 1999); por otra
parte, la característica defensiva propia del dolor agudo no está presente en esta
condición.
Un estímulo doloroso mantenido crónicamente produce una excitación excesiva de
las neuronas medulares y supramedulares, la producción de este proceso hace que
aparezca el mecanismo de la sensibilización central (Latremoliere and Woolf,
2009). La sensibilización central se manifiesta como una reducción prolongada del
umbral y un aumento en la sensibilidad y extensión de las áreas receptoras del asta
dorsal de la medula espinal (Ji et al., 2003), además se ha observado una
ineficiencia en los mecanismos inhibitorios encargados de la modulación del dolor
(Meeus et al., 2008).
Desde el punto de vista clínico la sensibilización central puede provocar que la
percepción de un estímulo no doloroso se convierta en un estímulo doloroso
(alodinia), por otra parte los estímulos dolorosos serían percibidos como una
sensación de dolor desproporcionado (hiperalgesia). Se ha sugerido que la
sensibilización central puede ser el mecanismo por el cual los factores
psicológicos y somáticos se correlacionan desde el punto de vista neurobiológico.
Además, se plantea que el distrés psicológico resultante del proceso de dolor
crónico contribuye al mecanismo de sensibilización central, lo que produce una
amplificación del dolor (Curatolo et al., 2006).

7
1.2 Dolor Musculoesquelético Crónico
Se considera dolor musculoesquelético crónico (DMC) cuando el dolor se
mantiene entre 3 y 6 meses (Walsh et al., 2008). El DMC se producen alteraciones
neurales, somáticas, cognitivas y conductuales (Walsh et al., 2008), que generan
una disminución de la calidad de vida del paciente y de su desempeño laboral.
El dolor musculoesquelético es descrito usualmente por los pacientes como una
sensación firme y de presión, de características difusas y que a menudo se
acompaña de hiperalgesia muscular profunda o alodinia (Graven-Nielsen, 2006),
este tipo de dolor puede manifestarse de forma localizada, regional y generalizado
(Graven-Nielsen and Arendt-Nielsen, 2010). El síndrome de dolor miofascial
(SDM), es un ejemplo de una condición de dolor regional muscular que se
caracteriza por la presencia de bandas tensas y dolor referido característico
causado por puntos gatillo miofasciales (PGM) (Simons, 1996).
La transición de dolor agudo musculoesquelético localizado a dolor crónico
generalizado está probablemente relacionada con la progresión de la
sensibilización periférica y central (Graven-Nielsen and Arendt-Nielsen, 2010). La
neurofisiología del DMC podría explicarse a través del proceso de sensibilización
central (Graven-Nielsen and Arendt-Nielsen, 2010).
1.2.1 Epidemiología
El dolor crónico es muy prevalente en la población general (Elliott et al., 1999) y
genera impacto negativo sobre la calidad de vida, el desempeño laboral y la
interacción psicosocial del paciente (Becker et al., 1997; Breivik et al., 2006).

8
El DMC se ha convertido en el principal motivo de consulta de dolor crónico en
atención primaria en la geografía española (Batlle-Gualda et al., 1998; Català et
al., 2002).
En una reciente revisión se ha descrito que la prevalencia del DMC se encuentra
entre el 13.5% y 47% de la población general y la del DMC generalizado varía
entre 11.4% y 24% (Cimmino et al., 2011).
En relación al SDM se ha sugerido que es el tipo de dolor más prevalente de entre
los de origen musculoesquelético (Simons, 1996), pero no hay datos precisos en
cuanto a la prevalencia de este en relación a la población general; a pesar de esto
en la actualidad clínica se tiene muy en cuenta al SDM, aún más conociendo que
en muchas investigaciones se ha demostrado que los PG son muy prevalentes en
diversos trastornos musculoesqueléticos como la cefalea tensional crónica
(Couppé et al., 2007), el dolor orofacial (Fernández-de-Las-Peñas et al., 2010), los
dolores relacionados con el raquis (Chen and Nizar, 2011), el dolor de hombro
(Bron et al., 2011) o la epicondilalgia lateral (Fernández-Carnero et al., 2007).
1.3 Dolor Cervical Crónico
La Neck Pain Task Force define el dolor cervical como un evento episódico a lo largo
de la vida que presenta una recuperación variable entre los diferentes episodios
(Guzman et al., 2009).
El dolor cervical frecuentemente denominado como no específico, de tejidos blandos o
dolor cervical mecánico se puede definir como aquel localizado en el territorio situado
entre la línea nucal superior y la línea de la espina de la escápula, en la parte posterior
del cuerpo, y en la parte anterior por encima del borde superior de la clavícula y el
esternón dejando fuera el contorno facial; con o sin irradiación a la cabeza, tronco y

9
miembros superiores (Guzman et al., 2009). Los signos de irradiación del dolor son
contemplados por esta definición, en relación con esto Bogduk (Bogduk, 2003) sugiere
que los signos de irradiación hacia la extremidad superior no deben asumirse como
parte del dolor cervical ya que estos son más propios del dolor cervical radicular y
fisiopatológicamente estas dos condiciones son muy distintas, además añade que la
confusión de estas dos entidades clínicas puede llevar a errores en el diagnóstico y
planteamientos de investigación y tratamiento poco adecuados (Bogduk, 2003).
Más acorde con la sugerencia de Bogduk (Bogduk, 2003) es la definición propuesta por
Merskey y Bogduk (Merskey and Bogduk, 1994), en esta, el dolor cervical se define
como el dolor que surge en una región limitada superiormente por la línea nucal
superior, lateralmente por los márgenes laterales del cuello, e inferiormente por una
línea imaginaria transversal a través de la apófisis espinosa T1.
El dolor cervical puede considerarse como un síntoma muy frecuente en la mayoría de
trastornos que afectan al cuadrante superior, aunque rara vez es síntoma de la presencia
de tumor, infección u otra afección grave (Bogduk, 2003). El dolor cervical puede
coexistir junto a otros trastornos musculoesqueléticos (Harris et al., 2006). Y puede
estar provocado o asociado a una patología local o una enfermedad sistémica tales como
lesiones de la piel, alteraciones de la laringe, tumores, infección, fracturas y
dislocaciones, traumatismos, mielopatías, artritis reumatoide u otras enfermedades
reumáticas (Haldeman et al., 2008).
El dolor cervical tiene una etiología multifactorial, con factores de riesgo no
modificables como la edad y el sexo (Hogg-Johnson et al., 2009). En estudios
realizados en población general relacionados con la edad, se ha observado que los
sujetos más jóvenes tienen mejor pronóstico de recuperación de la discapacidad cervical
(Hogg-Johnson et al., 2009). También se ha demostrado que otros trastornos

10
musculoesqueléticos y problemas psicológicos pueden considerarse factores de riesgo
del dolor cervical, y frecuentemente se asocian a él (Carroll et al., 2008; Hogg-Johnson
et al., 2009).
Entre los factores psicológicos asociados a un mal pronóstico de dolor cervical que se
han descrito son los estados de angustia, sufrimiento, enfado o frustración en respuesta
al dolor (Hill et al., 2004), en contraposición a esto se ha observado que el positivismo
y la alta autoestima estuvieron asociados con un mejor pronóstico (Haldeman et al.,
2008).
Existe mucha literatura que avala que los cambios degenerativos cervicales van
unidos a la presencia de dolor cervical persistente e incapacitante, pero no hay evidencia
de que los cambios degenerativos obtenidos con RMN cervical se correlacionen con
síntomas de dolor cervical. Tampoco hay evidencia suficiente para demostrar que la
degeneración de disco sea un factor de riesgo para tener dolor de cuello (Nordin et al.,
2008).
Un factor positivo es el hecho de practicar ejercicio, se ha visto que si se practicaba
ejercicio físico, ante la presencia de un dolor de cuello, éste tendrá mejor pronóstico que
si el paciente es sedentario (Hogg-Johnson et al., 2009), e incluso otro estudio sugiere
que el ejercicio puede tener un efecto protector contra el dolor cervical (van den Heuvel
et al., 2005).
Entre los factores predictivos relacionados con el dolor crónico se han encontrado, el
acoso laboral, trastornos de sueño, el índice de masa corporal en la mujeres, el trabajo
relacionado con el agotamiento emocional en los hombres, presentar dolor cervical
agudo con anterioridad y dolor crónico lumbar (Kääriä et al., 2012).
1.3.1 Epidemiología
El dolor de cuello es una de las condiciones de dolor más frecuente, la prevalencia de

11
dolor de cuello en la población general se ha estimado entre 10% y 15%, siendo más
común en mujeres que en hombres (Borghouts et al., 1999). En un reciente estudio de la
prevalencia de dolor en el cuello en la población española se ha estimado que indica un
19.5% anual entre los adultos españoles (Fernández-de-las-Peñas et al., 2011).
Un 70% aproximadamente de las personas, puede que experimenten un dolor cervical
en algún momento de sus vidas (Côté et al., 1998). En la población que sufre dolor
cervical se ha encontrado que a la hora de cualificarlo se representa en forma de
pirámide, en la que la base es conformada por un gran número de casos de dolor leve,
por encima pocos casos que consultan por su dolor y en la punta solo unos pocos casos
de dolor invalidante (Côté et al., 1998; Hogg-Johnson et al., 2009). Cote y cols.
encontraron que el 39.4 % de los individuos han tenido dolor cervical en los últimos 6
meses (Côté et al., 1998).
La literatura sugiere que entre el 50-80% de la población general que ha experimentado
dolor cervical, lo volverán a sufrir entre 1 -5 años más tarde y la mayor parte no se
recuperan totalmente del problema (Carroll et al., 2008). En general en la literatura se
dividen los grupos de edad en dos grandes grupos: jóvenes y mayores, siendo los de
peor pronóstico estos últimos. Hill y cols. (Hill et al., 2004) realizaron un estudio en el
que los sujetos se dividen en tres grupos de edades; se observó que en el grupo de edad
de entre 45-59 años, existe una tendencia 4 veces mayor a que el dolor cervical se
cronifique, recurra o sea continuo comparado con edades menores y mayores.
Más de 1/3 de los pacientes desarrollan síntomas crónicos que durarán más de 6 meses
(Côté et al., 2008). Entre un 15-32% de los individuos continúan experimentando
síntomas 5 años después del primer episodio de dolor de cuello (Enthoven et al., 2004;
Pernold et al., 2005). Después de 10 años, aproximadamente un 32% de los que
experimentan un primer episodio continuarán presentando síntomas moderados o

12
graves y un 79% mejoran del dolor pero no desaparece completamente (Gore et al.,
1987).
1.4 Dolor Craneofacial de Origen Musculoesquelético
El dolor craneofacial (DCF) es una denominación general que es utilizada para describir
la presencia de dolor en la cara, cabeza y estructuras asociadas, puede estar originado
por una variedad de condiciones, estructuras o etiologías (Armijo Olivo et al., 2006;
Kapur et al., 2003). El DCF se puede clasificar en neuropático, neurovascular y
musculoesquéletico (Benoliel et al., 2011). El DCF de origen musculoesquelético,
representa la causa más común de DCF de origen no dental y puede afectar la
musculatura masticatoria, la articulación temporomandibular (ATM) y estructuras
orofaciales (Okeson and de Leeuw, 2011). Los signos y síntomas más prevalentes que
se han observado en los pacientes con DCF son: dolor al abrir la boca, dolor a la
palpación muscular y dolor articular (Macfarlane et al., 2001), y por orden de
porcentaje, las áreas de expansión del dolor que se han descrito como más prevalentes
son: alrededor de los ojos, alrededor de la región temporal, en la zona anterior a la oreja
y en la ATM y alrededores de esta (Macfarlane, Blinkhorn, Davies, Kincey, et al.,
2002). Los factores psicológicos están muy presentes en el DCF y se han observado
múltiples comorbilidades con otras dolencias y patologías (Macfarlane et al., 2001).
El DCF de origen musculoesquelético según la Asociación Internacional para el Estudio
del Dolor se clasifica en cefalea tensional crónica, trastornos craneomandibulares
(TCM) dolorosos, TCM causados por artritis o artrosis, distonías y discinesias faciales y
traumatismos craneofaciales (Merskey and Bogduk, 1994).
1.4.1 Trastornos craneomandibulares
El término TCM se refiere a una serie de signos y síntomas que afectan a la musculatura
masticatoria, la ATM y estructuras asociadas o ambas (Okeson and de Leeuw, 2011;

13
Okeson, 1997), se considera un proceso patológico multifactorial causado posiblemente
por hiperactividad muscular o por parafunciones, lesiones traumáticas, influencias
hormonales y cambios a nivel articular (Liu and Steinkeler, 2013). Estos trastornos se
caracterizan por: (a) dolor orofacial y/o en la ATM o en los músculos masticatorios; (b)
alteraciones en el movimiento mandibular y/o limitación del rango de movimiento
mandibular; y (c) presencia de ruidos articulares durante la función mandibular (Liu
and Steinkeler, 2013; Okeson and de Leeuw, 2011).
Los factores psicosociales tienen un papel relevante en los TCM, en un reciente estudio
cohorte se identificó que el estrés, la afectividad negativa y las estrategias de
afrontamiento ante el dolor presentan una repercusión importante sobre los TMD
(Fillingim et al., 2011), por otra parte, Kindler y cols. (Kindler et al., 2012)
encontraron que los síntomas depresivos están más presentes en pacientes con TCM
articulares mientras la ansiedad estuvo más asociado con TCM de origen muscular.
Características psicológicas incluyendo la somatización, depresión y la ansiedad
relacionados con el género parecen tener un impacto significativo en la prevalencia de
TCM (Licini et al., n.d.). Evidencia reciente describe que las pacientes femeninas con
TCM presentan mayor percepción de intensidad del dolor y sensibilidad muscular a la
palpación que pacientes masculinos (Schmid-Schwap et al., 2013).
Existen diversos criterios diagnósticos para clasificar los TCM (Benoliel et al., 2011;
Schiffman et al., 2010), sin embargo la clasificación más utilizada en la actualidad son
los Criterios diagnósticos de investigación para TCM (en inglés, Research Diagnostic
Criteria for Temporomandibular Disorders; RDC/TMD) (Dworkin and LeResche, 1992;
Schiffman et al., 2010), estos criterios presentan una fiabilidad y validez contrastada
englobado en un protocolo sistematizado de valoración, diagnóstico y clasificación de
los subtipos más comunes de TCM (Look et al., 2010). Los Criterios diagnósticos de

14
investigación para TCM establecen la clasificación en dos grandes secciones definidos
en dos ejes: Eje I: Diagnóstico del dolor; y el Eje II Estatus psicosocial (Schiffman et
al., 2014). Es importante destacar que estos criterios han sido recientemente revisados y
el Eje I de diagnóstico ha sido dividido en dos grandes grupos de trastornos, TCM
relacionados con dolor y trastornos del disco y patología degenerativa de la ATM
(Tabla 1) (Schiffman et al., 2014).
Tabla 1. Clasificación diagnóstica de los trastornos craneomandibulares (Schiffman et
al., 2014).
Trastornos craneomandibulares
relacionados con dolor
Trastornos del disco y patología
degenerativa de la articulación
temporomandibular.
Mialgia Luxación del disco con reducción
Mialgia local Luxación del disco con reducción y con
bloqueos intermitentes
Dolor miofascial Luxación del disco sin reducción y con
limitación de la apertura
Dolor miofascial referido Luxación del disco sin reducción y sin
limitación de la apertura
Artralgia Trastornos degenerativos
Cefalea atribuida a trastornos
craneomandibulares
Subluxación
1.4.2 Epidemiología
El DCF es una dolencia muy prevalente en la población general en torno a un 17-26%
de los cuales el 11,7% llega a convertirse en condición crónica (Macfarlane, Blinkhorn,

15
Davies, Ryan, et al., 2002). En relación al sexo es más prevalente en mujeres y el rango
de edad donde se presenta con mayor frecuencia es entre los 18-25 años y los 56-65
años (Macfarlane, Blinkhorn, Davies, Kincey, et al., 2002). La presencia de dolor en la
región temporomandibular se produce en aproximadamente un 10% de la población
adulta (LeResche, 1997). Las mujeres presentan en general más signos y síntomas de
TCM y además estos son frecuentes y más severos que en los hombres (Adèrn et al.,
2014; Carlsson, 1999; LeResche, 1997), por otra parte las mujeres tienen menos
probabilidades de recuperarse de sus síntomas (Wänman, 1996) y son más propensas a
buscar tratamiento (Carlsson, 1999). En un reciente estudio se encontró que el 26.8% de
mujeres con TCM evaluadas se clasificaron como trastornos moderados frente a un
9.3% de TCM graves (Campos et al., 2014). En pacientes ancianos se encontró mayor
prevalencia de TCM en mujeres y los trastornos se clasificaron en un 43% leves, 13%
moderados y 4.5% en graves (Camacho et al., 2014).
De Kanter y cols. en un meta-análisis de 51 estudios epidemiológicos encontraron una
prevalencia del 30% de síntomas de TCM (De Kanter et al., 1993), en otro estudio se
observó el 10% de la población estudiada presentaba TCM y de estos el 50% presentó
más de un signo de TCM (Gesch et al., 2004). Se ha observado una mayor prevalencia
de signos y síntomas en edades intermedias (Carlsson, 1999; Yekkalam and Wänman,
2014), Yekkalan y Wanman en un estudio reciente encontraron mayor prevalencia de
signos entre los sujetos de 35 y 50 años (Yekkalam and Wänman, 2014) y la evidencia
muestra una prevalencia menor en edades adultas (Carlsson, 1999; Matsuka et al., 1996;
Yekkalam and Wänman, 2014). Manfredini y cols. en un estudio epidemiológico con
pacientes con TCM encontraron que el 56.4% de los pacientes presentaron un
diagnóstico de dolor muscular, el 42% de luxación del disco y 57.5% otros trastornos
articulares (Manfredini et al., 2012).

16
En cuanto a la incidencia, Kamisaka y cols. realizaron un estudio longitudinal en un
espacio temporal de 4 años y encontraron una incidencia del 6% para el dolor en la
ATM y un 12.9% para ruidos articulares en la ATM, en esta misma investigación se
encontró en los sujetos menores de 40 años un mayor riesgo de presentar ruidos en
ATM y las mujeres presentaban un aumento en el riesgo de perpetuación de dolor en la
ATM (Kamisaka et al., 2000).
1.4.3 Epidemiología y comorbilidad entre trastornos craneomandibulares, cefalea
y dolor de cuello
Los TCM, las cefaleas y el dolor de cuello son trastornos muy relacionados (Sipilä et
al., 2002; Storm and Wänman, 2006; Wiesinger et al., 2007). Varios estudios han
informado que los signos y síntomas se superponen entre los pacientes con TCM,
cefaleas y dolor en el cuello respectivamente (Anderson et al., 2011; Rantala et al.,
2003), se ha demostrado que el dolor de cuello se asocia significativamente con los
TCM y que la gravedad de éstos se incrementa con la gravedad del dolor de cuello
(Ciancaglini et al., 1999; Nilsson et al., 2013; Wiesinger et al., 2009), adicionalmente,
se ha comprobado que los factores psicosociales a su vez están relacionados con la
presencia de cefalea, dolor de cuello y dolor orofacial (Rantala et al., 2003). Stuginski-
Barbosa investigaron recientemente los signos de TCM en pacientes con migraña
crónica (MC) y episódica (ME), en esta investigación se identificó que el 73% de los
pacientes con MC presentaron dolor a la palpación en la musculatura masticatoria, 63%
presentaron dolor a la palpación articular y 64% presentaron dolor a la palpación del
cuello (Stuginski-Barbosa et al., 2010), otras estudios similares, pero realizados en
pacientes adolecentes con cefalea han observado una alta comorbilidad con los TCM
dolorosos, además se encontró una asociación significativa con el dolor de cuello
(Nilsson et al., 2013), además en pacientes adolescentes con TCM, encontraron que los

17
pacientes que presentaban alteraciones musculares y alteraciones musculares y
articulares tuvieron mayores niveles de dolor mandibular y orofacial, cefalea, dolor de
cuello y dificultad para comer alimentos blandos (Karibe et al., 2010).
Se ha sugerido que los TCM, las cefaleas y el dolor de cuello pueden tener una base
fisiopatológica similar (Ashina et al., 2006; Marklund et al., 2010; Svensson, 2007), por
otra parte se ha identificado que la cefalea podría ser un factor de riesgo de sufrir dolor
de cuello (Leclerc et al., 1999).
Rantala y cols. describió que de entre 1339 sujetos evaluados la prevalencia de signos
relacionados con la ATM fue del 10%, el dolor orofacial fue del 7%, la cefalea del 15%
y el dolor de cuello el 39% (Rantala et al., 2003), por otra parte, Plesh y cols. mostró
que el 53% de los pacientes con TCM que presentaron dolor de cabeza severo, el 54%
tenía dolor de cuello (Plesh et al., 2011). Un estudio realizado con 487 mujeres Sami
encontró que un 17% de estas presentó dolor en la regiones mandibular y orofacial que
además lo asociaban a una limitación de su calidad de vida, y en este mismo estudio se
describe que la duración del dolor en la región mandibular, las molestias al realizar la
apertura, el dolor de cuello y un nivel educativo bajo estaban relacionados cuando los
síntomas de TCM influían en la vida cotidiana (Mienna and Wanman, 2012), en
relación con esto dato, Weber y cols. encontraron que el 88,24% de los pacientes con
TCM presentaron a su vez dolor cervical, en esta investigación se sugiere que esta
situación está generada principalmente por factores neurofisiológicos y no por factores
biomecánicos como la postura (Weber et al., 2012).
La prevalencia del latigazo cervical en pacientes con TCM ha sido estudiada en una
revisión sistemática reciente (Häggman-Henrikson et al., 2014), en esta se describe que
la prevalencia del latigazo cervical en pacientes con TCM varía entre 8,4% a un 70%,
este resultado se comparó con la población general sin TCM en donde la prevalencia de

18
latigazo cervical se encuentra entre 1,7% y 13%, además en esta revisión se señala que
los pacientes con TCM con antecedentes de haber sufrido un latigazo cervical presentan
más signos de alteración de la ATM como limitación de la apertura bucal, más dolor
articular, cefalea y síntomas de estrés. Los autores de esta revisión sugieren que el
latigazo cervical puede ser un iniciador y/o un factor agravante, así como una condición
comórbida con los TCM (Häggman-Henrikson et al., 2014)
1.5 Dolor Referido de la Región Cervical hacia la Región Craneofacial
Diversas estructuras de la región cervical pueden provocar dolor referido hacia la región
craneofacial, la literatura científica describe que las articulaciones cervicales, los
ligamentos y los músculos son estructuras relevantes a tener en cuenta en la
identificación de los patrones del dolor que pueden afectar al cráneo, la región
craneomandibular y la región orofacial. Son muchos los estudios que demuestran que
los PGM del trapecio, el esplenio, el esternocleidomastoideo y los músculos sub-
occipitales producen dolor referido hacia la región craneofacial en pacientes con TCM y
cefaleas (Alonso-Blanco et al., 2012; Fernández-de-Las-Peñas et al., 2006, 2010;
Fricton et al., 1985; Wright, 2000). Muchos de estos patrones de dolor referido
evocados por PGM fueron descritos por Simons y cols. (Simons et al., 1999) (Figura
1).

19
Figura 1. Representación modificada de los patrones de dolor referido hacia la región craneofacial provocado por
PGM de músculos de la región cervical.
A nivel de las estructuras articulares de la región cervical, la investigación relacionada
con la infiltración de sustancias algógenas y estudios relacionados con el diagnóstico
estructural han identificado patrones o mapas de dolor referido hacia la región
craneofacial, específicamente Dreyfuss y cols. comprobaron en sujetos sanos que la
infiltración de sustancias algógenas sobre la articulación atlanto-occipital y la
articulación atlanto-axial lateral provocaban patrones de dolor referido sobre la región
cervical superior y la cabeza (Dreyfuss et al., 1994), también Dwyer y cols. con un
procedimiento similar en sujetos sanos identificaron que las articulaciones
zigoapofisarias C2-C3 provocan patrones de dolor referido hacia la región cervical y la
cabeza (Dwyer et al., 1990), estos patrones fueron confirmados con gran similitud en
pacientes (Aprill et al., 1990; Cooper et al., 2007). Se ha sugerido que el patrón de dolor
de las articulaciones zigoapofisarias C3-C4 ocasionalmente puede estar relacionado con

20
la cefalea cevicogénica (Cooper et al., 2007), sin embargo en el caso del disco
intervertebral C2-C3 sí se ha identificado como una fuente importante de dolor referido
hacia la cabeza en pacientes con cefalea cervicogénica (Schofferman et al., 2002)
(Figura 2).
Figura 2. Representación, según la evidencia científica de los patrones de dolor referido de estructuras articulares
cervicales hacia áreas craneocervicales (Aprill et al., 1990; Cooper et al., 2007; Dreyfuss et al., 1994; Dwyer et al.,
1990).
Destacar como hallazgo científico reciente, que Watson y Drummond encontraron
patrones de dolor referido hacia la cabeza muy similares al valorar la articulación
atlanto-occipital y las articulaciones zigoapofisarias C2-C3 en pacientes con migraña y
cefalea tensional (Watson and Drummond, 2012).
1.6 Aspectos Anatomofuncionales de la Región Craneomandibular y la Región
Craneocervical
La asociación entre la región craneomandibular y la región craneocervical ha sido
estudiada en las últimas décadas desde diversos paradigmas, incluyendo enfoques
anatómicos, biomecánicos, neurofisiológicos, y patofisiológicos (Armijo Olivo et al.,
2006), en este apartado se pretende hacer una descripción detallada de la evidencia

21
disponible relacionada con las posibles relaciones entre estas regiones tomando en
cuenta los enfoques anatómicos y biomecánicos desde la función normal.
1.6.1 Modelos biomecánicos de la relación cranemandibular/craneocervical
Uno de los primeros planteamientos teóricos de la dinámica craneomandibular
/craneocervical fue el desarrollado por Brodie (Brodie, 1950), este autor desarrolló un
esquema gráfico (Figura 3), que explicaba cómo la postura erguida de la cabeza se
mantenía mediante el equilibrio neuromuscular de los músculos anteriores y posteriores
de la región craneocervical y cervical. Otro postulado importante que proponía este
modelo es que una actividad mandibular como el apretar isométricamente tendría que
estar equilibrada por la activación de los músculos cervicales cuando la cabeza está
erguida (Brodie, 1950; Thompson and Brodie, 1942), Rocabado desarrolló un modelo
similar al anterior, en este se señala que la estabilidad craneomandibular se mantiene
entre el equilibrio de las fuerzas anteriores (músculos masticatorios, músculos supra e
infrahiodeos, y los músculos cervicales anteriores) y posteriores (músculos cervicales
posteriores), ambos grupos musculares junto a otras estructuras de la región
craneomandibular trabajan de forma sinérgica en una cadena funcional; por otra parte
este autor sugiere que la posición de la mandíbula y del hueso hiodes depende de la
curvatura cervical (Rocabado, 1983).

22
Figura 3. Esta figura representa el esquema diseñado por Brodie, para explicar el equilibrio mecánica neuromuscular
entre las regiones craneocervical y craneomandibular (Brodie, 1950; Thompson and Brodie, 1942).
Resultados de estudios basados en modelos matemáticos apoyan en gran medida las
tesis teóricas anteriormente descritas (Gillies et al., 1998; Suzuki et al., 2003), un
ejemplo de esto es el estudio de Suzuki y cols. en este se generó un sistema mecánico de
análisis dinámico del sistema estomatognático en condiciones de normalidad, se
observó como resultado principal que la actividad muscular de la región cervical influye
sobre la actividad mecánica de la mandíbula, además sugieren que los músculos
cervicales coordinan y resisten los cambios en la postura de la cabeza durante los
movimientos mandibulares (Suzuki et al., 2003). Otro de los modelos biomecánicos
relacionados con la dinámica mandibular, señala que el movimiento de extensión
craneocervical facilita la apertura mandibular y sugieren que esta situación se da para
lograr una mejor activación de los músculos que realizan la apertura y para generar una
posición más favorable para el movimiento (Koolstra and van Eijden, 2004).

23
1.6.2 Estudios in-vivo de la relación craneomandibular/craneocervical
La mayoría de estudios in-vivo en torno a las hipótesis de la relación
craneomandibular/craneocervical se han realizado con electromiografía (EMG), análisis
cinemático y estudios radiológicos; estas investigaciones se han diseñado con el
objetivo de comprobar la influencia mutua de ambas regiones en la dinámica articular
mandibular, en la estabilidad postural y en los aspectos funcionales más generales en los
que participa la ATM y las estructuras asociadas, como por ejemplo la deglución y la
masticación.
1.6.3 Influencia de la región craneocervical sobre la dinámica mandibular
En cuanto a la dinámica mandibular, Visscher y cols. demostraron pequeñas
variaciones en la posición del cóndilo mandibular según la postura craneocervical, sus
hallazgos mostraron que la distancia intra-articular en la ATM en el movimiento de
cierre es menor con retracción craneocervical y mayor con protrusión craneocervical
(Visscher et al., 2000), en relación con esto, Omure y cols. observaron que al inducir
experimentalmente la posición de protrusión craneocervical, el cóndilo mandibular se
posteriorizaba en comparación a la posición neutra (Ohmure et al., 2008), estos
hallazgos confirmarían las observaciones de Solow y Tallegren que en 1976 ya
describieron que el movimiento de extensión craneocervical se asocia a una retrusión
mandibular (Solow and Tallgren, 1976). Otro de los aspectos importantes que se han
investigado sobre la dinámica de la ATM es que la apertura mandibular se ve
directamente influenciada por la posición craneocervical, observándose un aumento de
la apertura mandibular en la posición de protracción craneocervical y una disminución
en la posición de retracción craneocervical cuando se comparan con la posición neutra
(Higbie et al., 1999). Un esquema de la relación de la postura craneocervical y la
dinámica intra-articular de la ATM es representada en la figura 4.

24
Figura 4. Este esquema representa el efecto de la postura de protracción craneocervical sobre la dinámica mandibular
y la musculatura masticatoria según la evidencia científica de estudios experimentales. La imagen A señala un
aumento de la actividad electromiográfica cuando se induce la postura de protracción craneocervical. La imagen B
representa una posteriorización del cóndilo mandibular asociado a la postura de protracción craneocervical.
1.6.4 Sinergias neuromusculares cervicales y masticatorias
La electromiografía ha sido uno de los instrumentos más utilizados para investigar las
acciones coordinadas, sinérgicas o asociadas entre la musculatura de la región
craneomandibular (musculatura masticatoria) y la musculatura del cuello. Diversos
estudios han comprobado la activación del músculo esternocleidomastoideo durante el
apretamiento (Clark et al., 1993; Davies, 1979; Hochberg et al., 1995; Rodríguez et al.,
2011; So et al., 2004; Venegas et al., 2009; Yoshida, 1988) (Figura 5) y el
rechinamiento dentario (Rodríguez et al., 2011; Venegas et al., 2009), en relación con
esto Clark y cols. describieron que para lograr un 5% de la contracción del
esternocleidomastoideo durante el apretamiento dentario se necesita una activación del
A
B

25
50% del músculo masetero (Clark et al., 1993), evidencia reciente demuestra que
durante la masticación se produce una acción concomitante entre los músculos masetero
y esternocleidomastoideo y el nivel activación de estos músculos se modula de acuerdo
a la demanda del elemento que se esté masticando (Häggman-Henrikson et al., 2013);
otras investigaciones realizadas con electromiografía profunda y superficial han
comprobado que durante diversas tareas de apretamiento dentario varios músculos de la
región cervical (esternocleidomastoideo, semiespinales del cuello y la cabeza,
multífidos cervical, elevador de la escápula, esplenio de la cabeza) son activados y este
reclutamiento se produce en torno al 2% y al 14% de la contracción voluntaria máxima
(Giannakopoulos, Hellmann, et al., 2013; Giannakopoulos, Schindler, et al., 2013;
Hellmann et al., 2012). Al contrario de la mayoría de los estudios que se han realizado
con la función de apretamiento dentario, Armijo-Olivo y Magee estudiaron la apertura
mandibular realizada contra resistencia, los resultados mostraron un aumento similar de
la actividad electromiográfica de los músculos masetero, temporal, esplenio de la
cabeza y de las fibras superiores del músculo trapecio. (Armijo-Olivo and Magee,
2007).
A B

26
Figura 5. Esta figura representa un esquema diseñado según la evidencia científica que muestra que el apretamiento
dentario modifica la actividad electromiográfico de músculos cervicales (A). En la figura B se muestra una
concomitancia entre los movimientos craneocervicales y craneomandibulares (el movimiento de apertura bucal se
asocia un movimiento de extensión craneocervical y el movimiento de cierre al movimiento de flexión
craneocervical).
Un hallazgo importante a destacar es que se ha observado que en posiciones de reposo
mandibular se produce un descenso en la actividad electromiográfica de los músculos
trapecio y esternocleidomastoideo (Ceneviz et al., 2006), sin embargo parece ser que los
diferentes tipos de oclusión no influyen sobre la actividad eletromiográfica de la
musculatura del cuello (Ferrario et al., 2006). La figura 5 representa un esquema de la
elevación de la actividad electromiográfica de los músculos cervicales durante el
apretamiento dentario.
En cuanto a la influencia del movimiento craneocervical sobre la actividad
electromiográfica de la musculatura masticatoria, Funakoshi y cols. observaron que se
producía una gran activación del músculo temporal y una moderada activación del
músculo masetero al realizar una extensión craneocervical (Funakoshi et al., 1976), a
diferencia de este estudio, Ballenberger y cols. investigaron la influencia de los
movimientos de la región cervical superior (rotación, extensión, flexión e inclinación
lateral) y encontraron diferencias estadísticamente significativas sobre la actividad
electromiográfica del músculo masetero pero no sobre el músculo temporal, además en
este estudio se señala que la actividad electromiográfica se incrementa más en extensión
que la flexión craneocervical (Ballenberger et al., 2012), en relación con esto, Forsberg
y cols. determinaron que el incremento de actividad de masetero durante la extensión
craneocervical se produce entre 10º y los 20º (Forsberg et al., 1985). Estudios en donde
se ha inducido experimentalmente la posición de protracción craneocervical han
descrito un aumento de la actividad de los músculos masetero (McLean, 2005; Ohmure

27
et al., 2008), digástrico (Ohmure et al., 2008) y geniogloso (Milidonis et al., 1993).
1.6.5 Cinemática y concomitancia craneocervical/craneomandibular
Los estudios que valoran específicamente la cinemática craneomandibular/
craneocervical han encontrado patrones de movimiento con un alto nivel de
coordinación espacio-temporal (Eriksson et al., 1998, 2000; Kohno, Matsuyama, et al.,
2001; Zafar, 2000; Zafar et al., 2000, 2002), estos hallazgos sugieren que las funciones
mandibulares comprenden acciones sincronizadas de la ATM y la región
craneocervical (articulación atlanto-occipital y las articulaciones vertebrales cervicales),
y esta coordinación es mayor en los movimientos más rápidos (Zafar et al., 2000) y en
general el movimiento craneocervical es sincrónico o se anticipa al movimiento
mandibular (Eriksson et al., 2000). Entre los movimientos que presentan una
concomitancia se encuentra, el de apertura mandibular que se acompaña de una
extensión craneocervical y el movimiento de cierre que se acompaña de una flexión
craneocervical (Eriksson et al., 1998) (Figura 5). Resultados similares se han obtenido
en otros estudios (Kohno, Kohno, et al., 2001; Torisu et al., 2002; Yamabe et al., 1999);
es importante destacar que Eriksson y cols. comprobaron que el movimiento
craneocervical es mayor en la apertura (entorno al 50%) y significativamente menor en
el cierre mandibular (entorno al 30-40%) (Eriksson et al., 1998). Un estudio reciente ha
demostrado que el movimiento concomitante de extensión craneocervical al realizar la
apertura mandibular fue significativamente mayor en los niños que en los adultos, los
autores de esta investigación sugieren que esa situación se genera en los niños como
mecanismos para aumentar la magnitud de la apertura mandibular (Kuroda et al., 2011).
Dos de las funciones orales en donde participa la ATM son la fonación y la masticación,
el movimiento de la región craneocervical también está implicado en estas funciones

28
(Häggman-Henrikson and Eriksson, 2004; Miyaoka et al., 2004), específicamente se ha
demostrado que el movimiento de flexo-extensión craneocervical acompaña los ciclos
masticatorios, pero además de acuerdo a como sea el tamaño del bolo alimenticio que se
mastique, el movimiento de extensión craneocervical se ve modificado (Häggman-
Henrikson and Eriksson, 2004); en cuanto a la fonación se ha observado que diversas
tareas en donde se articulan palabras y se realiza apertura-cierre están asociada a
movimientos de la región craneocervical (Miyaoka et al., 2004).
En la actualidad contamos con evidencia científica muy abundante que demuestra las
relaciones anatomofuncionales entre la regiones craneomandibular y la craneocervical,
sin embargo esta información no es suficiente para demostrar los aspectos
neurofisiológicas implicados en ambas funciones; resultados de investigación básica en
conejos han descrito mecanismos neurales supramedulares implicadas en las acciones
rítmicas cervicales y craneomandibulares (Igarashi et al., 2000), otros autores han
teorizado que las acciones concomitantes son comandos pre-programados a nivel central
(Torisu et al., 2001; Zafar, 2000) y que las funciones vienen moduladas por
mecanismos sensoriomotores trigeminocervicales (Eriksson et al., 1998; Zafar, 2000).
El conocimiento entorno a la neurofisiología trigeminocervical puede ayudar a
comprender las situaciones comorbilidad del dolor de cuello y el DCF o las alteraciones
disfuncionales motoras craneocervicales/craneomandibulares; estos aspectos
neurofisiológicos se desarrollan en el siguiente apartado.
1.7 Neurofisiología del Dolor Cérvico-craneofacial
La base neurofisiológica del dolor referido de la región cervical hacia el área
craneofacial se puede explicar mediante un fenómeno anatómico y fisiológico de
convergencia de aferencias nociceptivas trigeminales y cervicales que confluyen en el
núcleo trigeminal espinal y en los segmentos cervicales superiores (Bartsch and

29
Goadsby, 2003a, 2003b; Bartsch, 2005; Piovesan et al., 2003), este centro de
procesamiento del dolor se ha denominado complejo trigeminocervical (CTC). Este
complejo es el responsable de transmitir información sensorial visceral e información
nociceptiva de la cabeza y la región orofacial hacia otros centros superiores como el
tálamo, el hipotálamo y la corteza somatosensorial primaria (Benjamin et al., 2004;
Malick and Burstein, 1998; Malick et al., 2000, 2001) (Figura 6) e inclusive tiene
conexiones neurales con áreas del diencéfalo y el tronco encefálico relacionadas con la
modulación del dolor (Akerman et al., 2011).
1.7.1 Sistema sensorial trigeminal
El sistema sensorial trigeminal lo conforman: a) el nervio trigémino (y sus tres
divisiones: oftálmica, V1; maxilar, V2; y mandibular, V3); b) el ganglio del trigémino
(Gasser); c) la raíces nerviosas trigeminales; y d) los componentes centrales
trigeminales del tronco encefálico (los núcleos trigeminales, los tractos trigeminales y
las vías tálamo-trigeminales) (Sessle, 2005b; Waite and Ashwell, 2004) (Figura 6). El
nervio trigémino es el más grande de los nervios craneales y es considerado un nervio
mixto ya que tiene una división sensorial y una motora (Majoie et al., 1995; Sanders,
2010), además es importante destacar que proporciona la inervación sensorial principal
de la cara, la cavidad oral y parte de cráneo (Majoie et al., 1995; Sessle, 2005a).

30
Figura 6. La imagen representa la organización neuroanatómica del sistema trigeminal desde la periferia hasta las
conexiones neurofisiológicas a nivel central. S1, corteza somatensorial primaria; VMP, núcleo ventral posteromedial
del tálamo; NTE, núcleo trigeminal espinal; GT ganglio trigeminal.
El ganglio de Gasser es una estructura fina, considerado como un análogo craneal de los
ganglios de la raíz dorsal en el sistema nervioso periférico, pero es significativamente
más grande anatómicamente (Dixon, 1963; Kerr, 1963; Moses, 1967). La mayoría de
los cuerpos celulares de aferencias primarias trigeminales procedentes de la tres
divisiones del nervio trigémino (V1, V2 y V3) residen en el ganglio de Gasser, en donde
se encuentran organizadas de manera somatotópica (Borsook et al., 2003; Byers and
Närhi, 1999; Jacquin et al., 1986; Leiser and Moxon, 2006), pero hay que tomar en
cuenta que los cuerpos celulares de algunas aferencias periodontales y de los husos
musculares residen en el núcleo mesencefálico (Capra and Dessem, 1992).
Las fibras aferentes primarias trigeminales terminan en los tejidos craneofaciales como

31
terminaciones nerviosas libres y funcionan como nociceptores, estos pueden activarse
con estímulos nocivos mecánicos, térmicos y químicos. Su activación puede resultar en
la excitación de fibras de pequeño diámetro y de conducción lenta (A-delta o C) (Sessle,
1999, 2005b, 2011; Takemura et al., 2006). Una serie de componentes neuroquímicos
(por ejemplo, la sustancia P, 5-HT, prostaglandinas, bradiquininas) están involucrados
en la activación de estas terminaciones periféricas por estimulación nociva o en su
sensibilización periférica; la sensibilidad de las terminaciones puede aumentar después
de una lesión leve, y esta sensibilización de las terminaciones nociceptivas es un
mecanismo periférico que ayuda a proteger los tejidos lesionados de repetidos agravios
(Sessle, 2000, 2005b, 2011).
La división V1 inerva la región nasal y peri-orbital (incluyendo la córnea y la
conjuntiva), la duramadre supratentorial, así como la frente y la parte superior de la
cabeza que se superpone con el dermatoma C2. La división V2 suministra inervación al
área cigomática, el labio superior, una parte de la cavidad nasal y oral (incluyendo los
dientes del maxilar y su periodonto asociado), y la división V3 inerva a las estructuras
extra e intra-orales restantes en el tercio inferior de la cara (incluyendo los dientes de la
mandíbula y su periodonto), el labio inferior, la piel de la mejilla, y dos tercios
anteriores de la lengua, el mentón, la ATM, además de la piel cubre la mandíbula y el
lado de la cabeza (parte de la región temporal) a excepción de el ángulo de la mandíbula
que es la parte del dermatoma C2 (Majoie et al., 1995; Sanders, 2010). Las fibras
eferentes motoras del V3 inervan los cuatro músculos de la masticación (masetero,
temporal y pterigoideo medial y lateral), el músculo milohiodeo, el fascículo anterior
del músculo digástrico, el músculo tensor del tímpano y el músculo tensor del velo
palatino (Kamel and Toland, 2001; Majoie et al., 1995). En la figura 7 se representan
gráficamente los dermatomas trigeminales (Figura 7).

32
Figura 7. Representación gráfica de los dermatomas trigeminales y cervicales.
El nervio trigémino tiene cuatro núcleos centrales en el tronco encefálico (un núcleo
motor y 3 sensoriales): a) el núcleo mesencefálico trigeminal, que media la
propiocepción; b) el núcleo sensitivo principal, que media la sensación táctil
(principalmente tacto epicrítico y en menor medida tacto protopático); c) el núcleo
motor que proporciona inervación motora: y d) el núcleo espinal trigeminal, que media
el dolor, la sensibilidad térmica y táctil (Majoie et al., 1995; Sessle, 2000) (Figura 8).
El núcleo espinal trigeminal consiste en la división de tres sub-núcleos: a) oral (SVo);
b) interpolar (SVi); y c) caudal (SVc) (Sessle, 1999, 2000, 2005b, 2011). Los sub-
núcleos SVo y SVi se asocian con la transmisión de la percepción táctil; por otra parte,
están implicados principalmente en mecanismos nociceptivos orofaciales relacionados
especialmente con el dolor intra-oral y peri-oral (Dallel et al., 1988, 1990; Raboisson et
al., 1995). Los núcleos trigeminales se representan en la figura 8.

33
Figura 8. Representación gráfica de los núcleos trigeminales, también se muestra la subdivisión del núcleo trigeminal
espinal en sus 3 sub-núcleos: SVo, sub-núcleo trigeminal oral; SVi, sub-núcleo trigeminal interpolar; SVc, sub-
núcleo trigeminal caudal.
El sub-núcleo SVc se extiende desde el nivel de la OBEX (bulbo raquídeo) hasta el
nivel de C3 de la médula espinal cervical. Este sub-núcleo es el homólogo de la
sustancia gelatinosa del asta de posterior de la medula espinal ya que sus neuronas
tienen morfología celular similar, así como las conexiones sinápticas, y sus funciones.
Dado que el sub-núcleo SVc se encuentra inmediatamente superior a la sustancia
gelatinosa de los niveles de la médula espinal cervical, también se le denomina como el
"asta dorsal medular" (Sessle and Hu, 1991; Sessle, 1987; Sessle et al., 1986). El sub-
núcleo SVc es considerado como la principal área relacionada con la información
nociceptiva de los tejidos craneofaciales superficiales y profundos (Dubner and Bennett,
1983; Ebersberger et al., 2001; Schepelmann et al., 1999; Sessle and Hu, 1991; Sessle,

34
1987, 2005b).
En las láminas superficiales y profundas del SVc predominan dos tipos de neuronas
nociceptivas (neuronas nociceptivas específicas [NE] y neuronas de rango dinámico
amplio [RDA]), estas neuronas trasmiten información aferente nociceptiva hacia centros
superiores (núcleo ventral posteromedial del tálamo [VPM]) (Sessle, 1987, 2000,
2005a, 2011). Las neuronas NE sólo responden a estímulos nocivos (por ejemplo,
pellizcar, estímulos térmicos nocivos) aplicados a un campo receptivo craneofacial
localizado y reciben impulsos aferentes de fibras de diámetro pequeño (fibras A delta
y/o C); las neuronas RDA son excitadas por estímulos no nocivos (por ejemplo
estímulos táctiles), así como por estímulos nocivos, y pueden recibir impulsos aferentes
de fibras de gran diámetro (fibras A) y de pequeño diámetro (fibras C) (Sessle, 1999).
La mayoría de neuronas NE y RDA, también pueden ser excitadas por otros tipos de
entradas aferentes periféricas de diversas regiones como las meninges, tejido vascular,
los dientes, la ATM o en los músculos masticatorios (Burstein et al., 1998; Dostrovsky
et al., 1991; Sessle, 1996, 1999, 2000). Los extensos patrones convergentes de entradas
aferentes que son característicos de la ATM o de la duramadre son activados por
neuronas NE y RDA en el SVc, este fenómeno podría explicar la mala localización del
dolor profundo, así como la difusión del dolor referido que es condición típica de
dolencias que implican la ATM y la musculatura asociada (Sessle, 1999, 2011).
Las neuronas trigeminales somatosensoriales del tronco encefálico proyectan a otras
estructuras de esta misma región anatómica como la formación reticular y los núcleos
motores de otros nervios craneales; estas conexiones proporcionan respuestas
autonómicas y motoras ante estímulos craneofaciales (Sessle, 1987, 1996, 1999).
Específicamente las neuronas del SVc proyectan hacia el núcleo VPM del tálamo a
través de una vía multisináptica denominada tracto lemnisco trigeminal dorsal (tracto

35
trigeminotalámico dorsal) (Dougherty and Willis, 1992; Dougherty et al., 1992; Sessle,
1999; Sherman et al., 1997) (Figura 9). Las neuronas nociceptivas del núcleo VPM
tienen conexiones con la corteza somatosensorial (Sherman et al., 1997), representando
la dimensión sensorial-discriminativa del dolor. También se ha observado otras
conexiones como por ejemplo con la corteza cingulada anterior, situando a estos
circuitos neurales como parte de la dimensión afectivo-emocional del dolor (Sessle and
Hu, 1991; Sessle, 1999).
Figura 9. Representación gráfica del tracto trigeminotalámico dorsal. GT, ganglio trigeminal; NTE, núcleo
trigeminal espinal; SVc; sub-núcleo trigeminal caudal; VPM, Núcleo ventral posteromedial del tálamo; S1, corteza
somatosensorial primaria.
1.7.2 Neuroanatomía de los segmentos cervicales superiores
La médula espinal cervical superior incluye los segmentos espinales C1 y C2 en donde
emergen periféricamente los tres primeros nervios cervicales que se distribuyen en un
ramo dorsal, un ramo ventral y los nervios sinovertebrales (Alix and Bates, 1999;

36
Bogduk, 1981), estos nervios inervan a nivel motor y sensitivo diversas estructuras de la
parte posterior de la cabeza y el cuello (Bogduk, 2001) que pueden generar dolor
referido hacia la cabeza y la región orofacial (Johnston et al., 2013). El nervio C1
presenta un ganglio de la raíz dorsal ectópico, se ha observado que en algunos casos
(20%) este nervio carece de raíz dorsal y en estos casos las células ganglionares se
pueden encontrar entre las raíces del nervio espinal accesorio (Ouaknine and Nathan,
1973). Este nervio carece de distribución sensitiva cutánea, sin embargo a través de su
rama dorsal inerva sensitivamente a nivel profundo los músculos cortos del triángulo
suboccipital (Bogduk, 1982), su ramo ventral pasa por detrás y debajo de articulación
atlanto-occipital a la que suministra inervación (Bogduk, 2001)
El nervio C2 da inervación sensitiva a las articulaciones atlantoaxoideas laterales y
mediales; la duramadre de la fosa craneal posterior y de la médula espinal superior; y la
arteria carótida y vertebral. La rama ventral de este nervio inerva los músculos
paravertebrales, el músculo esternocleidomastoideo y el trapecio y la rama dorsal los
músculos semiespinales de la cabeza y el músculo esplenio de la cabeza. El nervio
sinovertebral de C2 se une a los de C1 y C3 para suministrar inervación a los
ligamentos transversal, alar y a la membrana tectoria (Bogduk, 2001). La rama ventral
de C3 se une al plexo cervical e inerva los músculos paravertebrales. La rama medial
del ramo dorsal de C3 inerva el músculo semiespinoso cervical y el músculo multifidus
y además inerva las articulaciones cigapofisiarias de C2-C3. El nervio sinovertebral de
C3 inerva el disco intervertebral C2-3 en su cara posterior (Bogduk, 2001; Bogduk et
al., 1988).
A nivel cutáneo la inervación sensitiva de la región craneocervical la suministran los
nervios occipital menor, occipital mayor y el nervio auricular mayor (Poletti, 1991; Shin
et al., 2007), estos tres nervios sensitivos más la zona cutánea que inervan conformarían

37
los dermatomas de la región craneocervical, estos dermatomas (C2, C3) tienen una
representación que incluye la parte posterior del cráneo (cuero cabelludo), el ángulo de
mandíbula, la región sub-occipital, la parte posterior de la oreja y la garganta (Poletti,
1991). Es importante destacar que la mayor distribución cutánea del nervio C2 está
representada por el nervio occipital mayor (Poletti, 1991).
1.7.3 Complejo trigeminocervical
El CTC es una unidad anatómica-funcional que forman las astas dorsales de los dos
segmentos superiores de la médula cervical y el SVc del núcleo espinal trigeminal
(Becker, 2010; Hoskin et al., 1999; Hu et al., 2005; Piovesan et al., 2003). Estudios
anatómicos en animales han encontrado que el CTC se extiende hasta el segmento
cervical C2-C3 (Goadsby and Hoskin, 1997; Kaube et al., 1993; Strassman et al., 1994).
En el CTC se produce una convergencia de neuronas nociceptivas de segundo orden que
reciben aferencias nociceptivas primarias trigeminales y de los tres primeros nervios
cervicales (Bartsch and Goadsby, 2003b; Bartsch, 2005; Bogduk, 2001; Goadsby et al.,
2008; Hu et al., 1995, 2005; Piovesan et al., 2003) (Figura 10). Evidencia científica de
estudios básicos en animales ha demostrado este fenómeno de convergencia (Bartsch
and Goadsby, 2002, 2003a; Hu et al., 1993; Sessle et al., 1986; Yu et al., 1995), y
también se tiene evidencia de este mecanismo en seres humanos (Busch et al., 2006;
Piovesan et al., 2001).

38
Figura 10. Representación gráfica del complejo trigeminocervical (CTC).
El CTC puede ser sensibilizado por aferencias nociceptivas primarias provenientes del
músculo masetero y de la ATM (Cairns et al., 2001, 2002; Nishimori et al., 1986;
Shigenaga et al., 1988), además se ha descrito que las aferencias primarias nociceptivas
provenientes de la piel y de los músculos cervicales son capaces de excitar neuronas del
CTC (Bartsch and Goadsby, 2003a; Le Doaré et al., 2006; Sessle et al., 1986), sin
embargo parece ser que la principal contribución aferente cervical hacia este complejo
neural está mediada por la raíz de C2, representada periféricamente por el nervio
occipital mayor (Bartsch, 2005), en relación con esto, Goadsby y cols. demostraron que
la activación de las fibras aferentes del nervio occipital mayor aumentan la actividad
metabólica de neuronas del CTC (Goadsby et al., 1997), por otra parte, Le Doare y cols.
observaron que los receptores N-metil-D-aspartato (NMDA) glutamatérgicos están

39
implicados en estas sinapsis (Le Doaré et al., 2006), varios estudios han demostrado que
los receptores NMDA son importantes en el desarrollo de la sensibilización central del
SVc (Chiang et al., 1998; Yu et al., 1996), así como los receptores de la neuroquinina y
purinérgicos (Dubner and Ren, 2004). Recientemente se ha comprobado en modelo
animal, que la lesión sobre un nervio espinal superior provoca alodinia mecánica y la
hiperalgesia térmica en la piel de la cara, los resultados de esta investigación también
sugieren que la fosforilación de la kinasa de regulación extracelular en el SVc y en las
neuronas de C1-C2 y la activación de las células astrogliales están involucradas en el
dolor orofacial extraterritorial producido después de una lesión (Kobayashi et al., 2011).
Xie describe que en la sensibilización central trigeminal las células gliales tienen una
importante implicación incluyendo la interacción con los receptores NMDA
glutamatérgicos y purinérgicos (Xie, 2008).
1.7.4 Sensibilización central del complejo trigeminocervical
Neurofisiológicamente la recepción de entradas de aferencias nociceptivas en el sistema
nervioso central forma parte de la sensibilización central que es un proceso fundamental
en el desarrollo y mantenimiento del dolor referido y el dolor crónico (Arendt-Nielsen
et al., 2000; Salter, 2004). En la sensibilización central trigeminal se produce una
expansión de los campos receptivos profundos y cutáneos neuronales, y además se han
observado otros cambios en las propiedades de las neuronas del trigeminales y en las
vías nociceptivas medulares (Bereiter et al., 2005; Chiang et al., 1998, 2005; Lam et al.,
2009; Salter, 2004; Vernon et al., 2009), específicamente se ha demostrado que la
aplicación experimental de una “sopa inflamatoria” en la duramadre puede inducir una
sensibilización central de las neuronas trigeminales nociceptivas de segundo orden en el
SVc, generando una mayor capacidad de respuesta a la estimulación cutánea de la
región facial y en la duramadre (Burstein et al., 1998), en relación con este hallazgo,

40
Bartsch y Goadsby encontraron que la estimulación del nervio occipital mayor podía
causar una sensibilización central con un aumento de la excitabilidad de la entrada de la
duramadre (Bartsch and Goadsby, 2002), además, se ha observado que la activación de
los nociceptores meníngeos por mediadores pro-inflamatorios sensibilizan a las
neuronas de primer orden en el ganglio trigeminal (Strassman et al., 1996) y las
neuronas de segundo orden trigeminovasculares en el CTC (Burstein et al., 1998).
En el proceso de sensibilización central se producen salidas eferentes que involucran
conexiones entre motoneuronas y aferencias nociceptivas neuronales que su vez generan
respuestas motoras (Bartsch, 2005; Sessle, 2002). Evidencia científica basada en
estudios realizados con modelos animales han demostrado que la estimulación química
nociceptiva de estructuras profundas paravertebrales musculares de la región cervical
evocan efectos reflejos, incluyendo un aumento de la actividad electromiográfica en los
músculos masticatorios y cervicales ipsilaterales (Hu et al., 1993, 1996; Shin et al.,
2005) y alteraciones en los reflejos de apertura mandibular (Makowska et al., 2005).
Similares resultados se han observado en la estimulación nociceptiva de las meninges
posteriores de la rata (Hu et al., 1995). Por otra parte, se ha demostrado que la inyección
de bradiquinina en el músculo masetero en conejos provoca un aumento de la actividad
fusimotora de los husos musculares paravertebrales de la región cervical, estos
hallazgos sugieren que existe una potente conexión refleja entre el sistema trigeminal y
el sistema neuromuscular cervical (Hellström et al., 2000, 2002), resultados similares se
han descrito en estudios realizados en sujetos sanos, en donde se observó que un dolor
provocado experimentalmente en el músculo masetero provoca un aumento de la
actividad electromiográfica en los músculos esternocleidomastoideo y el esplenio del
cuello (Svensson et al., 2004), además de un aumento del reflejo de estiramiento de
estos músculos (Wang et al., 2004); otra de las manifestaciones motoras a nivel

41
mandibular que se han observado es la limitación momentánea de la apertura
mandibular después de provocar un dolor experimental en el músculo trapecio mediante
la infiltración de suero salino hipertónico (Komiyama et al., 2005). Un hallazgo
importante observado recientemente es que al provocar un dolor experimental sobre el
músculo masetero se produce una alteración del control motor de las acciones
integradas de la región craneocervical y craneomandibular al realizar los movimientos
de apertura y cierre (Wiesinger et al., 2013).
La sensibilización central del CTC se manifiesta clínicamente con un aumento de las
áreas de expansión del dolor en territorios trigeminales y cervicales, una mala
localización del dolor, hiperalgesia, alodinia mecánica (Katsarava et al., 2002; Kaube et
al., 2002; Sessle, 1999, 2002, 2011) y una disfunción de la activación del sistema
inhibitorio descendente (King et al., 2009; Maixner et al., 1998; Sarlani et al., 2004)
1.8 Modulación del Dolor en el Complejo Trigeminocervical
La recepción de los estímulos nociceptivos por las neuronas de segundo orden del CTC
está modulada por proyecciones inhibitorias descendentes de estructuras del tronco
encefálico, el diencéfalo y la corteza somatosensorial (Akerman et al., 2011; Bartsch
and Goadsby, 2003b; Sessle, 1999, 2000), se ha demostrado que la manipulación de las
neuronas ventrolaterales de la sustancia gris periacueductal (Bartsch, Knight, et al.,
2004; Knight and Goadsby, 2001; Knight et al., 2002), el núcleo magno del rafe
(Edelmayer et al., 2009) y el bulbo rostroventral (Lambert et al., 2008) pueden modular
la actividad nociceptiva evocada en el CTC, evidencia previa ha demostrado que la
estimulación de estas áreas produce un importante efecto inhibitorio anti-nociceptivo
(Fields et al., 1991) (Figura 11), sin embargo es importante destacar que la activación
del bulbo rostroventral también puede facilitar la hiperalgesia, el dolor neuropático y el
dolor crónico (Porreca et al., 2002; Ren and Dubner, 2002; Sugiyo et al., 2005; Venegas

42
et al., 2009). Otros estudios en donde se ha estimulado químicamente la región posterior
del hipotálamo han demostrado que esta región también influye en la modulación
nociceptiva del CTC (Bartsch et al., 2005; Bartsch, Levy, et al., 2004).
Figura 11. Representación gráfica del sistema inhibitorio descendente y las estructuras implicadas en la modulación
de la actividad nociceptiva. SVc, sub-núcleo trigeminal cervical; NTE, núcleo trigeminal espinal; BRV, bulbo
rostroventral; vlPAG; área ventrolateral de la sustancia gris periacueductal; HT, hipotálamo; S1, corteza
somatosensorial primaria.
En el proceso de activación del sistema inhibitorio descendente se producen diversos
mecanismos que incluyen la participación de los receptores opioides y de
neurotransmisores como el GABA y la serotonina (5-HT) (Sessle, 1999, 2002). El SVc
recibe proyecciones serotoninérgicas y encefalinérgicas del núcleo magno del rafe
(Beitz, 1982; Beitz et al., 1987) que tienen una actuación en la modulación del dolor
(Mason and Fields, 1989). Por otra parte, se ha demostrado que en la médula espinal y
en el SVc el principal neurotransmisor que actúa en la actividad eferente inhibitoria en

43
el bulbo rostroventral es la 5-HT (Beitz, 1982; Clatworthy et al., 1988; Fields et al.,
1991), en relación con esto, Okamato y cols. comprobaron en un modelo animal de
dolor inflamatorio persistente de la ATM que los receptores 5-HT3 en el CTC están
involucrados en los circuitos inhibitorios serotoninérgicos centrales que modulan la
actividad nociceptiva profunda y superficial (Okamoto et al., 2005).
Acciones terapéuticas relacionadas con los cambios del comportamiento, intervenciones
farmacológicas y otros tratamientos que actúan a nivel estructural, influyen sobre
mecanismos tronco encefálicos relacionados con la modulación descendente del dolor
craniofacial (Sessle, 2002).
1.8.1 Influencia de las aplicaciones terapéuticas sobre el dolor craneofacial
A partir de los resultados de estudios experimentales sobre mecanismos
neurofisiológicos implicados en la modulación de dolor en el CTC, muchos
investigadores han planteado estrategias terapéuticas para influir sobre estructuras de la
región cervical y a su vez modular el dolor de cabeza y orofacial. Las intervenciones
sobre el nervio occipital han sido de las más utilizadas en las últimas décadas, son
varios los estudios que se sugieren que la neuro-estimulación periférica del nervio
occipital es efectiva en la disminución del dolor orofacial y la cefalea en un porcentaje
importante de los pacientes en los que se aplica este tratamiento (Jasper and Hayek,
2008; Lee and Huh, 2013; Saper et al., 2011; Serra and Marchioretto, 2012; Silberstein
et al., 2012; Slavin et al., 2006). Siguiendo con las intervenciones sobre el nervio
occipital, hay que destacar que Leroux y Ducros en una recientemente revisión de
ensayos clínicos y series de casos, describen que la infiltración mediante cortico-
esteroides con o sin adición de anestésicos locales sobre el nervio occipital en pacientes
con cefalea en racimos produce efectos inmediatos en la disminución de la frecuencia
de los ataques, sin embargo varios estudios describen que el dolor local tras la

44
intervención es un efecto secundario muy común pero no considerado grave (Leroux
and Ducros, 2013), en otra revisión narrativa se sugiere que la infiltración del nervio
occipital mayor presenta efectos positivos sobre los pacientes con migraña pero se
señala que estos datos se interpreten con precaución ya que se han extraído de estudios
con pobres diseños metodológicos (Ashkenazi and Levin, 2007). Posterior a esta
revisión, se publicaron dos ensayos clínicos aleatorizados en donde se pretendía
comprobar el efecto de una infiltración del nervio occipital mayor y de puntos gatillo de
músculos paravertebrales y del trapecio utilizando anestésicos locales con y sin cortico-
esteroides en pacientes con migraña, los resultados de ambas investigaciones
demostraron la efectividad de ambas intervenciones en la reducción del dolor de cuello
y el dolor de cabeza pero no hubo diferencia en la comparación de los dos tratamientos
(Ashkenazi et al., 2008; Saracco et al., 2010). Evidencia científica proveniente de
estudios de series de casos retrospectivos describen que la infiltración intramuscular de
bupivacaina en la musculatura paravertebral reduce el dolor en pacientes adultos
(Mellick and Mellick, 2003, 2008; Mellick et al., 2006) y en niños (Mellick and
Pleasant, 2010) que presentan dolor orofacial y/o cefalea.
La evidencia sobre la administración de bupivacaina intratecal en la región cervical para
dolores refractarios cervicales, de cabeza y orofaciales es limitada, sin embargo las
series de casos publicadas describen una eficacia en la analgesia producida y una
disminución de la utilización de fármacos opiáceos (Appelgren et al., 1996; Lundborg
et al., 2009) por otra parte, los efectos adversos descritos fueron pocos y la mayoría de
los casos transitorios (Lundborg et al., 2009).
Intervenciones específicas de fisioterapia aplicadas al tratamiento de la región cervical
para modular el dolor en pacientes con cefalea han sido muy investigadas en las últimas
dos décadas, específicamente se debe destacar que un gran número de ensayos clínicos

45
muestran que la terapia manual, el ejercicio terapéutico o la combinación de ambas
enfocadas a tratar estructuras musculoesqueléticas de la región cervical han demostrado
efectividad en las disminución de la intensidad y la frecuencia del dolor en pacientes
con cefalea tensional y cefalea cervicogénica (Castien et al., 2011, 2012, 2013; Espí-
López and Gómez-Conesa, 2014; Espí-López et al., 2014; van Ettekoven and Lucas,
2006; Hall et al., 2007; Mongini et al., 2012; Ylinen et al., 2010).

46

47
JUSTIFICACIÓN

48
2. JUSTIFICACIÓN DEL TRABAJO REALIZADO
La región orofacial y el cráneo, que a su vez incluyen estructuras orales y dentales
representan una de las zonas anatómicas más complejas del organismo, esta situación
conlleva a una difícil compresión de los mecanismos fisiopatológicos de los trastornos
que afectan a la región craneofacial como por ejemplo los TCM, las cefaleas y el dolor
orofacial (Fricton, 2014). La comprensión de la clínica, la patogénesis y el tratamiento
es esencial para ayudar a los pacientes que presentan estos problemas (Graff-Radford,
2007).
Es manifiesto que en la últimas décadas se ha incrementado de manera exponencial la
investigación en torno al DCF, estos estudios en su mayoría se han enfocado en estudiar
los mecanismos biológicos periféricos y centrales relacionados con la transmisión y
modulación nociceptiva, así como los sistemas de clasificación del paciente y los
factores psicosociales implicados (Hargreaves, 2011), los resultados de algunas
investigaciones en esta línea sugieren, que áreas extra-trigeminales como la región
cervical parecen tener un papel relevante en la fisiopatología de las cefaleas y el dolor
orofacial (Graff-Radford, 2012), a pesar de esto, consideramos que aún es necesario
contar con más estudios que apoyen los hallazgos demostrados y que además terminen
de identificar con mayor exactitud las implicaciones biomecánicas y neurofisiológicas
de la región cervical sobre el DCF, por otra parte, creemos que es importante aclarar
cómo estos datos se pueden utilizar para el diagnóstico clínico y el planteamiento
terapéutico de fisioterapia. En los últimos años el tratamiento de fisioterapia ha
adquirido un estatus importante en el tratamiento de los TCM y el DCF (Aggarwal and
Keluskar, 2012), sin embargo no contamos con evidencia científica suficiente que
demuestre la relevancia o el papel del tratamiento de fisioterapia sobre la región cervical
en los pacientes con TCM, este es uno de los motivos centrales que justifica esta tesis

49
doctoral y que nos lleva a plantear diversos objetivos entorno a esta cuestión.
La evidencia científica contemporánea nos ha llevado a la reflexión sobre las
limitaciones que presentan los estudios y los abordajes clínicos basados en modelos
mecanicistas o que toman en cuenta únicamente la dimensión sensorial-discriminativa
del DCF (Reid and Greene, 2013), en una parte de esta tesis hemos intentado contestar
interrogantes desde un punto de vista más integral utilizando un enfoque bioconductual
en el que planteamos las posibles interacciones entre el dolor y la discapacidad
craneofacial, con variables motoras, de discapacidad cervical y variables psicológicas.
El enfoque bioconductual para el tratamiento, el diagnóstico y la valoración del DCF
reconoce la importancia de los factores psicosociales, como antecedentes de dolor, los
estados emocionales en curso, el estatus cognitivo, las creencias de salud, y las
habilidades de afrontamiento, que interactúan con las alteraciones fisiológicas en la
determinación de la experiencia del dolor para los pacientes (Carlson, 2008; Shephard et
al., 2014).

50

51
OBJETIVOS

52
3. OBJETIVOS
El objetivo general de esta investigación es determinar la influencia biomecánica y
neurofisiológica de la región cervical sobre el dolor y la discapacidad craneofacial
crónica. Además se pretende identificar como determinados factores bioconductuales
influyen sobre la función craneomandibular, la discapacidad y el dolor craneofacial.
A continuación se detallan los objetivos específicos:
1- Evaluar la influencia de la postura craneocervical sobre la discapacidad
craneofacial, la dinámica mandibular y el umbral de dolor a la presión,
además se pretende analizar las diferencias de postura craneocervical entre
sujetos asintomáticos y pacientes con dolor cérvico-craneofacial (DCCF)
crónico.
Este objetivo se ha abordado en las publicaciones originales I y II:
I. La Touche R, París-Alemany A, von Piekartz H, Mannheimer JS,
Fernández-Carnero J, Rocabado M. The influence of cranio-cervical posture
on maximal mouth opening and pressure pain threshold in patients with
myofascial temporomandibular pain disorders. Clin J Pain. 2011
Jan;27(1):48-55
II. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A,
Angulo-Díaz-Parreño S, La Touche R. Reliability, Standard Error, and
Minimal Detectable Change of Two Tests for Craniocervical Posture

53
Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial Pain
Patients. 2014 (En revisión).
2- Determinar la influencia del dolor y la discapacidad cervical sobre la función
sensoriomotora trigeminal.
Este objetivo se ha abordado en las publicaciones originales III y V:
III. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-
Parreño S, Paris-Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain
sensitivity over the trigeminal region in patients with chronic mechanical
neck pain. J Pain. 2010 Mar;11(3):256-63
V. La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-
Díaz-Parreño S, Fernández-Carnero J. The Influence of Neck Disability and
Pain Catastrophizing about Trigeminal Sensory-Motor System in Patients
with Headache Attributed to Temporomandibular Disorders. 2014 (En
revision)
3- Estudiar la asociación entre la discapacidad craneofacial y la discapacidad
cervical en pacientes con trastornos craneomandibulares, cefaleas y dolor
craneofacial crónico.
Este objetivo se ha abordado en las publicaciones originales II y IV:
II. López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A,
Angulo-Díaz-Parreño S, La Touche R. Reliability, Standard Error, and

54
Minimal Detectable Change of Two Tests for Craniocervical Posture
Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial Pain
Patients. 2014 (En revisión).
IV. La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A,
Angulo-Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero
J. Craniofacial pain and disability inventory (CF-PDI): development and
psychometric validation of a new questionnaire. Pain Physician. 2014 Jan-
Feb;17(1):95-108.
4- Analizar la asociación de factores psicológicos como la depresión, el miedo
al movimiento y el catastrofismo ante el dolor con variable motoras, de dolor
y discapacidad cervical y craneofacial.
Este objetivo se ha abordado en las publicaciones originales III, IV y V:
III. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-
Parreño S, Paris-Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain
sensitivity over the trigeminal region in patients with chronic mechanical
neck pain. J Pain. 2010 Mar;11(3):256-63
IV. La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A,
Angulo-Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero
J. Craniofacial pain and disability inventory (CF-PDI): development and
psychometric validation of a new questionnaire. Pain Physician. 2014 Jan-
Feb;17(1):95-108.
V. La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-
Díaz-Parreño S, Fernández-Carnero J. The Influence of Neck Disability and
Pain Catastrophizing about Trigeminal Sensory-Motor System in Patients

55
with Headache Attributed to Temporomandibular Disorders. 2014 (En
revision)
5- Determinar el efecto del tratamiento de fisioterapia aplicado en la región
cervical sobre la función mandibular y el dolor craneofacial.
Este objetivo se ha abordado en las publicaciones originales VI y VII:
VI. La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J,
Escalante K, Angulo-Díaz-Parreño S, Paris-Alemany A, Cleland JA. The
effects of manual therapy and exercise directed at the cervical spine on pain
and pressure pain sensitivity in patients with myofascial temporomandibular
disorders. J Oral Rehabil. 2009 Sep;36(9):644-52.
VII. La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S,
Bishop MD, Lopéz-Valverde-Centeno A, von Piekartz H, Fernández-
Carnero J. Does mobilization of the upper cervical spine affect pain
sensitivity and autonomic nervous system function in patients with cervico-
craniofacial pain?: A randomized-controlled trial. Clin J Pain. 2013
Mar;29(3):205-15.

56

57
MATERIAL Y MÉTODOS

58
4. MATERIAL Y MÉTODOS
Se realizaron un total de 7 estudios con diferentes diseños metodológicos (Tabla 2). Los
pacientes fueron reclutados de dos clínicas odontológicas privadas de la Comunidad de
Madrid (Estudios VI y VII), dos clínicas privadas especializadas en dolor orofacial y
TCM (Estudios II, III, IV y V), una clínica universitaria de la Comunidad de Madrid
(Estudio I) y el Hospital Universitario La Paz de la Comunidad de Madrid (Estudio IV),
en los estudios donde se realizaron comparaciones con sujetos asintomáticos los
pacientes fueron reclutados en tres campus universitarios de la comunidad de Madrid
(Estudios II, III y V). Los procedimientos utilizados en las investigaciones de esta tesis
doctoral se realizaron bajo las directrices de la Declaración del Helsinki. Todos los
participantes de los estudios dieron su consentimiento informado por escrito antes de
comenzar con las investigaciones y estas fueron aprobadas previamente por los
respectivos comités de ética locales. Una visión general de los diseños de estudio,
características de la muestra, los métodos de recogida de datos e instrumentos de
medición se presentan en la Tabla 2.
Tabla 2. Descripción general de los diseños, características de la muestra, variables e
intervenciones.
Estudio I Estudio II Estudio III Estudio IV Estudio V Estudio VI Estudio VII
Tamaño de la
muestra
N=29
(19 mujeres; 10
hombres)
N=60 GE
(32 mujeres; 28
hombres)
N=53 GC
(30 mujeres; 23
hombres)
N=23 GE
(13 mujeres; 10
hombres)
N=23 GC
(15 mujeres; 8
hombres)
N=192
(132 mujeres; 60
hombres)
N=41 GE1
(26 mujeres; 15
hombres)
N=42 GE2
(25 mujeres; 17
hombres)
N=39 GC
(26 mujeres; 13
hombres)
N=19
(14 mujeres; 5
hombres)
N=16 GE
(10 mujeres; 5
hombres)
N=16 GC
(11 mujeres; 4
hombres)
Características de
los Participantes
Pacientes con TCM/
dolor miofascial
GE= pacientes con
TCM/ dolor miofascial
GE=dolor de
cuello crónico
Pacientes con
DCF
GE1=Cefalea
atribuida a TCM
Pacientes con
TCM/ dolor
Pacientes con
TCM/ dolor

59
crónico crónico y dolor de cuello
crónico mecánico
(DCCF)
GC=sujetos
asintomáticos
mecánico
GC=sujetos
asintomáticos
a.TCM/ dolor
miofascial crónico
b.TCM/ artralgia
c.Cefalea
atribuida por
TCM
d.Cefalea
tensional
e. Migraña
con moderada
discapacidad
cervical
GE2= Cefalea
atribuida a TCM
con leve
discapacidad
cervical
GC=Sujetos
asintomáticos
miofascial
crónico
miofascial
crónico y dolor
de cuello crónico
mecánico
(DCCF)
Media y Desviación
Típica de la Edad
34.69 ±10.83 GE=41,7±11,7
GC=38,1±10,5
GE=28±5
GC=28±6
46±13.06 GE1=44.31±10.9
GE2=40.95±12.8
9
GC=40.61±10.01
37±10 GE=33,19±9,49
GC=34,56±7,84
Diseño del Estudio Estudio prospectivo
transversal
Estudio prospectivo
transversal de fiabilidad
intra e inter-examinador
Estudio
prospectivo
transversal
Estudio
multicéntrico
prospectivo
transversal de un
diseño de un
cuestionario
Estudio
longitudinal de
casos y controles
Estudio
prospectivo de
casos
Ensayo clínico
aleatorio
controlado
Variables Somato-
sensoriales y
motoras
- UDP
- MAI
- EVA
-Postura de cabeza
-Distancia mentón-
esternón
- UDP
- END
- - UDP
-MAI
- EVA
- EVAF
-UDP
-MAI
- EVA
-UDP
-EVA
[Variable
simpáticas: CP,
FC, TC, FR]
Medidas de auto-
registro
IDC
IDD-CF
IDC
BDI
STAI
IDC
IDD-CF
HIT-6
ECD
TSK-11
IDC
HIT-6
ECD
- - IDC
- BDI
- STAI
Intervenciones - - - - - -TMO en la
región cervical
(a. Rol anterior
de la región
cervical
superior; b.
movilización
postero-anterior
de C5)
-ETCM
-TMO en la
región cervical
(movilización
antero-posterior
de la región
cervical superior)
Abreviaturas: TCM, trastornos craneomandibulares; DCF, dolor craneofacial; DCCF, dolor cérvico-craneofacial; UDP, umbral de

60
dolor a la presión; MAI, máxima apertura interincisal; EVA, escala visual analógica del dolor; END, escala numérica del dolor; GE,
grupo experimental; GC, grupo control; IDC, índice de dolor cervical; IDD-CF, inventario de dolor y discapacidad craneofacial;
BDI, inventario de depresión Beck; STAI, cuestionario de ansiedad estado-rasgo; HIT-6, cuestionario de impacto de la cefalea;
ECD; escala de catastrofismo ante el dolor; TSK-11, escala de Tampa de Kinesiofobia; EVAF, escala visual analógica de fatiga;
TMO, terapia manual ortopédica; ETCM, ejercicio terapéutico de control motor; CP, conductancia de la piel; FC, frecuencia
cardíaca; FR, frecuencia respiratoria; TC, temperatura cutánea.
4.1 Participantes
La muestra de los estudios I y VI estuvo conformada por pacientes que presentaban
TCM atribuido a dolor miofascial, esta denominación se extrae de los Criterios
diagnósticos de investigación para TCM (Dworkin and LeResche, 1992; Schiffman et
al., 2010), aunque es importante mencionar que además se establecieron otros criterios
de inclusión que se exponen a continuación: a) diagnóstico primario de dolor miofascial
de acuerdo a los Criterios diagnósticos de investigación para TCM; (Dworkin and
LeResche, 1992; Schiffman et al., 2010); b) dolor bilateral en los músculos masetero y
temporal; c) duración del dolor mayor a 6 meses; d) intensidad del dolor mayor a 30mm
según la escala visual analógica (EVA); y e) presencia de PGM en la musculatura
masticatoria. Los criterios de exclusión adoptados en estos estudios fueron los
siguientes: a) TCM atribuidos a disfunciones articulares o enfermedades degenerativos
de acuerdo a los Criterios diagnósticos de investigación para TCM (Dworkin and
LeResche, 1992; Schiffman et al., 2010); b) lesiones traumáticas como fracturas o
latigazo cervical; c) enfermedades sistémicas reumatológicas como fibromialgia y
artritis; c; dolor neuropático; y d) concomitancia con cefaleas primarias.
El estudio III contó con una muestra de pacientes con dolor de cuello crónico mecánico
inespecífico. Conceptualmente esta dolencia se define como una afectación que presenta
signos y síntomas de disfunción muscular como empeoramiento de dolor con el
mantenimiento de la postura, limitación del rango del movimiento y dolor a la palpación
de la musculatura cervical. Además los pacientes incluidos en este estudio tenían que

61
tener el dolor en un periodo superior a 6 meses. Los criterios de exclusión adoptados en
este estudio fueron los siguientes: a) dolor de cuello unilateral; b) enfermedades
reumáticas; c) latigazo cervical; d) cirugías previas de la región cervical; e) diagnóstico
de radiculopatía cervical; f) diagnóstico de TCM.
La muestra del estudio IV estuvo representada por pacientes con distintos tipos de DCF
como los siguientes, cefalea tensional, migraña, cefalea atribuida a TCM, artralgia y
dolor miofascial. Los criterios de inclusión fueron los siguientes: a) pacientes mayores
de 18 años; b) diagnóstico de dolor facial o cefalea de acuerdo a los criterios de la
Clasificación Internacional de las Cefaleas (IHS, 2013); c) diagnóstico de TCM de
acuerdo a los Criterios diagnósticos de investigación para TCM; (Dworkin and
LeResche, 1992; Schiffman et al., 2010); d) presencia de los síntomas dolorosos de más
de 6 meses; y e) buena compresión del idioma español. Los criterios de exclusión
adoptados en este estudio fueron los siguientes: a) dificultad en la compresión del
idioma español; b) deterioro cognitivo; y trastornos psiquiátricos.
El estudio V fue conformado por pacientes con cefalea atribuida a TCM de acuerdo a
los criterios de la Clasificación Internacional de las Cefaleas (IHS, 2013) y los criterios
clínicos y de investigación para TCM (Schiffman et al., 2014), además se incluyeron
los siguientes criterios de inclusión: a) presencia de dolor superior a 6 meses; b) dolor
en mandíbula, zona temporal, cara y cuello en reposo o en movimiento; c) ser mayor de
18 años; y d) discapacidad de cuello cuantificado de acuerdo al índice de discapacidad
cervical (IDC) (Andrade Ortega et al., 2010), por otra parte se debe mencionar que en
este estudio los pacientes se subdividieron de acuerdo a los niveles de discapacidad
cervical según el IDC (discapacidad leve y moderada) (Andrade Ortega et al., 2010).
Los criterios de exclusión adoptados en estos estudios fueron los siguientes: a) TCM
atribuidos a disfunciones articulares o enfermedades degenerativos de acuerdo los

62
Criterios diagnósticos de investigación para TCM (Dworkin and LeResche, 1992;
Schiffman et al., 2010); b) lesiones traumáticas como fracturas o latigazo cervical; c)
enfermedades sistémicas reumatológicas como fibromialgia y artritis; c; dolor
neuropático; d) concomitancia con cefaleas primarias; e) dolor de cuello unilateral; f)
procedimientos quirúrgicos previos en la región cervical; y g) radiculopatía cervical.
Los estudios II y VII contaron con una muestra de pacientes con DCCF crónico, estos
pacientes integran clínicamente una comorbilidad entre el dolor de cuello crónico
mecánico inespecífico (descrito en estudio III) y TCM atribuido a dolor miofascial
(descrito en los estudios I y VI). Definimos DCCF como un dolor de origen muscular
que presenta mecanismos disfuncionales como limitación del movimiento, movimientos
in-coordinados y debilidad y falta de resistencia en el cuello y la mandíbula, estos
síntomas pueden exacerbarse con posturas mantenidas generando dolor en la región
cervical y craneofacial. Los criterios de exclusión adoptados en estos estudios fueron los
mismos que en los estudios I, III y VI.
También es importante destacar que en los estudios II, III y V se realizaron
comparaciones con participantes asintomáticos.
4.2 Variables y Pruebas de Medición
En todos los estudios se registraron diversos tipos de variables sociodemográficas como
la edad, peso, altura, sexo y la duración de los síntomas, además en el estudio V se
cuantifico el nivel de estudios y el estado laboral. A parte de las variables
sociodemográficas en los estudios también se evaluaron variables somatosensoriales,
motoras y psicológicas mediante la utilización de diversos instrumentos y otras
herramientas de auto-registro especializadas. En la tabla 3 se presenta un resumen de la
variables e instrumentos de medición utilizadas en cada estudio.
Tabla 3. Variables e instrumentos utilizados en los estudios.

63
Variables Medidas Estudios
I II III IV V VI VII
Intensidad del dolor
a. Escala visual
analógica del dolor
b. Escala numérica de
dolor
X-a X-b X-a X-a X-a
Máxima apertura interincisal a. Escala therabite
b. Escala CMD
c.
X-a X-b X-a
Umbral de dolor a la presión Algométro
X X X X X
Postura craneocervical a. Distancia mentón
esternón medido con
un calibre digital.
b. Postura de cabeza
medido con CROM
X-ab
Percepción de fatiga Escala visual analógica de fatiga
X
Discapacidad cervical Índice de discapacidad cervical
X X X X X
Discapacidad craneofacial y
función mandibular
Inventario de dolor y
discapacidad craneofacial
X X
Síntomas depresivos Inventario de depresión Beck
X
Estado de ansiedad Cuestionario de ansiedad
estado/rasgo
X X
Miedo al movimiento Escala Tampa de Kinesiofobia
X
Catastrofismo ante el dolor Escala de catastrofismo ante el
dolor
X X
Impacto de la cefalea en la
vida diaria
Cuestionario de impacto de la
cefalea HIT-6
X X

64
4.2.1 Medidas de auto-registro
Catastrofismo ante el Dolor
Se utilizó la versión española de la escala de catastrofismo ante el dolor (ECD) para
evaluar el nivel de catastrofismo (García Campayo et al., 2008). La ECD está
compuesta por 13 ítems, cada ítem puntúa del 0 al 4. El rango de puntuación total se
encuentra de 0 a 52, donde puntuaciones mayores indican mayor nivel de catastrofismo.
Este instrumento presentó la misma estructura factorial original presentando tres
factores (rumiación, magnificación y desesperanza), así como unas adecuadas
propiedades psicométricas (García Campayo et al., 2008).
Miedo al Movimiento
La versión en español de la escala Tampa de kinesiofobia (TSK-11) mide el miedo al
dolor y al movimiento (Gómez-Pérez et al., 2011). La TSK-11 contiene 11 ítems en su
versión española, tras el análisis factorial se eliminaron algunos ítems de la versión
original que fueron psicométricamente pobres (Gómez-Pérez et al., 2011; Kori et al.,
1990). La puntuación total del TSK-11 se encuentra entre 11 – 44 puntos y cada ítem
presenta una escala likert que puntúa del 1 al 4 (1 = totalmente en desacuerdo, 4 =
totalmente de acuerdo). Puntuaciones más altas indican mayor miedo al movimiento y
al dolor. El TSK-11 tiene dos sub-escalas: evitación de actividad y daño, además esta
escala ha demostrado aceptables propiedades psicométricas (Gómez-Pérez et al., 2011).
Intensidad del Dolor
La intensidad del dolor se midió con la escala visual analógica del dolor (EVA). La
EVA consiste en una línea de 100 mm, en el que el lado izquierdo representa "ningún
dolor" y el lado derecho "el peor dolor imaginable". Los pacientes colocan una marca
donde se sentían que representan la intensidad del dolor. Se ha comprobado que este
instrumento tiene una buena fiabilidad (Bijur et al., 2001).

65
En la medición de la intensidad del dolor también se utilizó la escala numérica del dolor
(END), esta escala presenta 11 puntos posibles representados en números del 0 (sin
dolor) al 10 (máximo dolor). Se ha demostrado que END presenta una buena fiabilidad
y validez en pacientes crónicos (Jensen and McFarland, 1993; Jensen et al., 1999).
Percepción de Fatiga
La escala visual analógica de fatiga (EVAF) se utilizó para cuantificar la fatiga
percibida. La EVAF consiste en una línea vertical de 100 mm en la que la parte inferior
representa "ninguna fatiga" (0 mm), y la parte superior representa la "fatiga máxima"
(100 mm). El investigador registra el resultado en mm. Se ha comprobado que este
instrumento tiene una buena fiabilidad (Tseng et al., 2010).
Discapacidad Cervical
La versión española del índice de discapacidad cervical (IDC) es instrumento utilizado
para evaluar la discapacidad percibida en relación a la dolencia en el cuello (Andrade
Ortega et al., 2010; Vernon and Mior, 1991). Este cuestionario consta de 10 ítems, con
6 posibles respuestas que representa 6 niveles de capacidad funcional, que van desde 0
(sin discapacidad) a 5 (discapacidad total) puntos. Las puntuaciones más altas indican
mayor discapacidad percibida. El IDC ha demostrado propiedades psicométricas
aceptables (Andrade Ortega et al., 2010).
Impacto de la Cefalea en la Vida Diaria
La versión española del HIT-6 (Bjorner et al., 2003; Gandek et al., 2003) consiste en un
cuestionario de seis ítems que evalúa la gravedad y el impacto del dolor de cabeza en la
vida del paciente. Los resultados de HIT-6 están estratificados en cuatro clases basadas
en el grado de impacto: poco o ningún impacto (HIT-6 puntuación de: 36-49), impacto
moderado (HIT-6 puntuación de: 50-55), impacto sustancial (HIT-6 puntuación de: 56-
59), y el impacto severo (HIT-6 puntuación de: 60-78) (Bjorner et al., 2003). El HIT-6

66
ha demostrado propiedades psicométricas aceptables (Martin et al., 2004).
Síntomas de Ansiedad
La versión española del cuestionario de ansiedad estado-rasgo (STAI) es una medida de
auto-informe de 40 ítems, diseñado para evaluar los síntomas de la ansiedad (Spielberg
and Lushene, 1982). Consta de 2 escalas independientes, una escala de ansiedad estado
y una escala de ansiedad rasgo, con 20 puntos cada uno, lo que resulta en una
puntuación entre 20 y 80. Superiores puntuaciones indican un mayor nivel de ansiedad.
Las escalas de estado y rasgo evalúan la ansiedad como un estado emocional actual y
como un rasgo de la personalidad, respectivamente. El STAI ha demostrado
propiedades psicométricas aceptables en su versión en español (Spielberg and Lushene,
1982).
Síntomas Depresivos
Los síntomas depresivos se evaluaron con el Inventario de Depresión Beck (BDI-II),
este instrumento de auto-registro evalúa síntomas afectivos, cognitivos y somáticos de
depresión. Se ha comprobado en estudios con población general y clínica que el BDI-II
presenta adecuadas propiedades psicométricas (Penley et al., 2003; Wiebe and Penley,
2005)
4.2.2 Instrumentos de medición
Máxima Apertura Interincisal
La máxima apertura interincisal (MAI) es la capacidad de abrir la boca tan amplio
como se pueda sin dolor. Esta distancia se mide en milímetros entre el incisivo superior
y el incisivo inferior. La MAI se midió con la escala TheraBite (Model CPT 95851;
Atos Medical AB; Sweden) y con la escala craneomandibular (Escala CMD. Patente.
No. ES 1075174 U, INDCRAN: 2011. INDCRAN, Madrid, Spain) (Figura 12). El
procedimiento para medir la MAI ha demostrado una buena fiabilidad inter-evaluador

67
(ICC = 0,95 - 0,96) (Beltran-Alacreu et al., 2014).
Figura 12. Medición de máxima apertura interincisal con la escala CMD.
Umbral de Dolor a la Presión
Un algómetro digital (FDX 25, Wagner Instruments, Greenwich, CT, EE.UU.),
compuesto por un cabezal de goma (1 cm2) unido a un manómetro, se utilizó para medir
UDPs (Figura 13). La presión ejercida se mide en kilogramos (kg); por lo tanto, los
UDPs se expresaron en kg /cm2. El protocolo utilizado fue una secuencia de 3
mediciones, con un intervalo de 30 segundos entre cada una de las mediciones. Un
promedio de las 3 mediciones se calculó para obtener un único valor para cada uno de
los puntos medidos en cada una de las evaluaciones. Los UDPs se evaluaron en varios
puntos de la región craneofacial y craneomandibular (Figura 14). El dispositivo se
aplica perpendicular a la piel. Se pidió a los pacientes que levantasen la mano en el
momento en que la presión comenzara a cambiar a una sensación de dolor, y en ese
momento el evaluador dejó de aplicar presión. La presión aplicada en la prueba se
aumentó gradualmente a una velocidad de aproximadamente 1 kg/s. Este procedimiento
de algometría tiene alta fiabilidad intra-evaluador (ICC = 0,94 a 0,97) para la medición

68
de los UDPs (Walton et al., 2011).
Figura 13. Medición del umbral de dolor a la presión con el algómetro digital.
Figura 14. Puntos de áreas trigeminales y cervicales en donde se midieron los umbrales de dolor a la presión en los
diferentes estudios.
Postura Craneocervical
Utilizamos el dispositivo CROM para medir la postura de cabeza (PC). Este dispositivo

69
tiene tres partes: a) una estructura plástica con forma de gafas; b) tres inclinómetros,
uno para cada plano de movimiento; y c) un brazo plástico para medir la de cabeza
hacia adelante y un localizador de vértebra (Figura 15). La medición de la PC está
graduada en el instrumento en 0,5 cm, que indican la distancia horizontal entre el puente
de la nariz y el localizador de vértebras. El localizador de vértebras tiene un nivel de
burbuja en la parte superior para ayudar a la colocación exacta. Los inclinómetros no se
utilizaron debido a los movimientos del cuello no se evaluaron.
Figura 15. Medición de la postura craneocervical
Para medir la distancia mentón-esternón (DME) se utilizó un calibre digital. El
dispositivo está hecho de plástico con una pantalla LCD de 5 dígitos y se puede medir
en pulgadas o en milímetros (mm) con un rango de 0,01 mm a 150 mm.
El evaluador explica en primer lugar que la medición se llevará a cabo mientras está

70
acostado en una camilla. En este momento, el evaluador mostró los calibradores
digitales al tema y dijo: "Usted sentirá que el instrumento contactará con su esternón y
en la barbilla; en ese momento no se debe mover”. Una vez en su lugar, la medición fue
tomada de la escotadura yugular del esternón a la protuberancia de la barbilla (Figura
16). La medida fue tomada en dos ocasiones.
Figura 16. Medición de la distancia mentón-esternón.
4.3 Resumen de los Procedimientos
Estudio I
Se registraron inicialmente las variables sociodemográficas y la intensidad del dolor y
después se procedió a medir los UDPs y la MAI en tres posturas craneocervicales
inducidas experimentalmente (posición neutra craneocervical, retracción craneocervical
y protracción craneocervical)
Estudio II
Se seleccionaron a los pacientes y los sujetos asintomáticos del grupo control, después
se registraron las variables sociodemográficas y las medidas de auto-registro (IDC y
IDD-CF) y finalmente se realizaron las mediciones de la postura craneocervical.

71
Estudio III
Se registraron las variables sociodemográficas y las medidas de auto-registro y después
se procedió a realizar mediciones del UDP en los puntos trigeminales.
Estudio IV
Se seleccionaron a los pacientes y después se procedió a registrar las variables
sociodemográficas y una batería de medidas de auto-registro de variables psicológicas,
dolor y discapacidad.
Estudio V
Una vez seleccionados los pacientes y el grupo control se procedió al registro de
variables sociodemográficas y las medidas de auto-registro, después de esa fase se
realizó el test masticatorio de provocación durante 6 minutos en donde se evaluó la
fatiga y la intensidad del dolor. Al finalizar el test masticatorio de provocación se
procedió a realizar las mediciones de la MAI y los UDPs.
Estudio VI
Se realizó un tratamiento sobre los pacientes seleccionados durante 10 sesiones, este
tratamiento estaba enfocado a la región cervical y específicamente se utilizó un
protocolo de estabilización cervical y un tratamiento de terapia manual sobre la región
cervical, además se realizaron mediciones de variables somatosensoriales y motoras
pre-intervención, post-intervención y tres meses después.
Estudio VII
Se seleccionaron un grupo de pacientes que se subdividen aleatoriamente en dos grupos,
un grupo recibe un tratamiento placebo y el otro un tratamiento manual sobre la región
cervical superior. Se realizaron mediciones de variables somatosensoriales y del sistema
nervioso simpático pre-intervención y post-intervención.

72
4.4 Análisis Estadístico
En el análisis de datos se ha utilizado estadística descriptiva para mostrar los datos de
las variables continuas que se presentan como media ± desviación típica (DT), intervalo
de confianza del 95% (IC) y frecuencia relativa (porcentaje). Prueba de Chi-cuadrado,
se utilizó para comparar las diferencian entre las variables categóricas (nominales). Se
realizo la prueba de Kolmogorov Smirnov para comprobar la normalidad.
Se utilizó la t de Student para la comparar las variables continuas entre los dos grupos.
Cuando las comparaciones se realizaron con más de dos grupos o se intentó analizar la
interacción con otras variables se aplicó una ANOVA de una, dos o tres vías según
procediese, seguido de un test post hoc de Bonferroni para analizar las comparaciones
múltiples. En uno de los estudios se realizó un análisis con una ANCOVA de dos vías
para identificar múltiples interacciones entre variables.
Se calculó el tamaño del efecto (d de Cohen) para las variables principales estudiadas.
De acuerdo con el método de Cohen, la magnitud del efecto fue considerado como
pequeño (0,20 a 0,49), medio (0,50 a 0,79), y grande (0,8) (Cohen, 1988).
La estructura factorial se analizó mediante un análisis factorial exploratorio (es decir,
análisis de componentes principales, ACP) con la rotación Oblimin. El número de
factores para la extracción se basa en el criterio de valor propio de Kaiser (valor propio
≥1) y la evaluación del gráfico de sedimentación (Ferguson and Cox, 1993). La calidad
de los modelos de análisis factorial se evaluó mediante la prueba de Bartlett para la
esfericidad y la prueba de Kaiser-Meyer-Olkin (KMO). Prueba de Bartlett es una
medida de la probabilidad de que la matriz de correlación inicial es una matriz de
identidad y debe ser <0,05 (Bartlett, 1954). La prueba de KMO mide el grado de
multicolinealidad y varía entre 0 y 1 (debe ser mayor que 0,50-0,60) (Kaiser, 1974).
El efecto suelo-techo se midieron mediante el cálculo del porcentaje de pacientes que

73
indican los puntajes mínimos y máximos posibles en los cuestionarios. El efecto suelo-
techo se considera que está presente si más del 15% de los encuestados logró el mayor o
menor puntuación total posible (Terwee et al., 2007).
La fiabilidad intra e inter-evaluador se analizo mediante coeficiente de correlación intra-
clase (CCI). Niveles de fiabilidad se definieron en base a la siguiente clasificación:
buena fiabilidad: ICC ≥ 0,75; fiabilidad moderada: ICC ≥ 0,50 y <0,75; y escasa
fiabilidad: ICC <0,50 (Portney LG, 2009).
El error de medición se expresa como un error estándar de medición (EEM), que se
calcula como 𝐷𝑇 × √1 − 𝐶𝐶𝐼, donde DT es la de los valores de todos los participantes,
y el CCI es el coeficiente de fiabilidad (Weir, 2005). El error de medición es el error
sistemático y aleatorio de la puntuación de un paciente que no es atribuible a los
cambios reales en el constructo a medir (Mokkink et al., 2010). Capacidad de respuesta
se evaluó utilizando el mínimo cambio detectable (MCD). MCD expresa el cambio
mínimo necesario para identificar el 90% de confianza de que el cambio observado
entre las dos medidas refleja un cambio real y no un error de medición (Haley and
Fragala-Pinkham, 2006). Se calcula como 𝐸𝐸𝑀 × √2 × 1,96 (Haley and Fragala-
Pinkham, 2006).
La asociación entre las variables se determinó mediante el coeficiente de correlación de
Pearson. Un coeficiente de correlación de Pearson mayor que 0,60 indica una fuerte
correlación, un valor entre 0,30 y 0,60 indica una correlación moderada, y uno por
debajo de 0,30 indica una correlación baja o muy baja (Hinkle et al., 1988). También se
utilizó en uno de los estudios el coeficiente de correlación de Spearman.
Se realizó un análisis de regresión lineal múltiple para estimar la fuerza de las
asociaciones entre los resultados variables primarias (variables criterio) con las
secundarias (variables predictoras). Se calcularon los factores de inflación de varianza

74
(FIV) para determinar si existían problemas de multicolinealidad en cualquiera de los
modelos analizados.
La fuerza de asociación se examinó utilizando los coeficientes de regresión (β), los
valores de P y r2 ajustado. Coeficientes beta estandarizados fueron reportados para cada
variable de predicción incluida en los modelos finales reducidas para permitir una
comparación directa entre las variables predictoras en el modelo de regresión y la
variable criterio que se está estudiando. Para el análisis de regresión, se utilizó la regla
de 10 casos por variable con el fin de obtener estimaciones razonablemente estables de
coeficientes de regresión (Peduzzi et al., 1996).
En la tabla 4 se presenta un resumen de los test estadísticos utilizados en cada uno de
los estudios.
El programa estadístico para Ciencias Sociales (SPSS 21, SPSS Inc., Chicago, IL
EE.UU.) se utilizó para el análisis estadístico. El nivel de significación para todas las
pruebas se estableció a un nivel de P <0,05.

75
Tabla 4. En esta tabla se puede observar las pruebas estadísticas utilizadas en cada uno
de los estudios.
Pruebas estadísticas Estudios
I II III IV V VI VII
- Análisis descriptivo X X X X X X X
- Pruebas de normalidad (test de Kolmogorov Smirnov) X X X X X X X
- t de student X X X
- ANOVA X X X X X
- ANCOVA X
- Calculo del tamaño del efecto (d) X X
- Análisis factorial exploratorio X
- Efecto suelo-techo X
- Coeficiente de correlación intra-clase X X X
- Error estándar de medición X X X X
- Mínimo cambio detectable X X
- Coeficiente de correlación de Pearson X X X
- Coeficiente de correlación de Spearman X
- Análisis de regresión lineal múltiple X X

76

77
RESULTADOS

78
5. RESULTADOS
5.1 Estudio I
La Touche R, París-Alemany A, von Piekartz H, Mannheimer JS, Fernández-Carnero J,
Rocabado M. The influence of cranio-cervical posture on maximal mouth opening and
pressure pain threshold in patients with myofascial temporomandibular pain disorders. Clin
J Pain. 2011 Jan;27(1):48-55.
Objetivo del estudio
El objetivo de este estudio fue evaluar la influencia de la postura craneocervical sobre la
MAI y el UDP en pacientes TCM atribuidos a dolor miofascial.
Resultados
Las comparaciones indicaron diferencias significativas en los UDPs de los 3 puntos
musculares con inervación trigeminal [masetero (M1 y M2) y temporal anterior (T1)] entre
las 3 posturas de cabeza [M1 (F = 117.78, p <0,001), M2 (F = 129.04, p <0,001), y T1 (F =
195,44, p <0,001)]. También hubo diferencias significativas en la MAI medidas en las 3
posturas de cabeza (F = 208.06, p <0,001). La fiabilidad intra-evaluador en base a pruebas
realizadas día a día fue buena, presentando un coeficiente de correlación intra-clase en los
rangos de 0,89-0,94 y 0,92 hasta 0,94 para UDP y la MAI, respectivamente, entre las
diferentes posturas craneocervicales.
Conclusiones
Los resultados de este estudio muestran que la inducción experimental de diferentes
posturas craneocervicales influye en los valores de la MAI y los UDPS de la ATM y
músculos de la masticación que reciben inervación motora y sensitiva por el nervio
trigémino. Nuestros resultados proporcionan información que respalda la relación
biomecánica entre la región craneocervical y la dinámica de la ATM, así como las
modificaciones en el procesamiento nociceptivo trigeminal en diferentes posturas
craneocervicale.

The Influence of Cranio-cervical Posture on Maximal MouthOpening and Pressure Pain Threshold in Patients With
Myofascial Temporomandibular Pain Disorders
Roy La Touche, PT, MSc,*w z Alba Parıs-Alemany, PT, MSc,w Harry von Piekartz, PT, PhD,yJeffrey S. Mannheimer, PT, PhD, CCTT,J Josue Fernandez-Carnero, PT, PhD,w z
and Mariano Rocabado, PT, DPT#
Objective: The aim of this study was to assess the influence ofcranio-cervical posture on the maximal mouth opening (MMO)and pressure pain threshold (PPT) in patients with myofascialtemporomandibular pain disorders.
Materials and Methods: A total of 29 patients (19 females and 10males) with myofascial temporomandibular pain disorders, aged19 to 59 years participated in the study (mean years±SD;34.69±10.83 y). MMO and the PPT (on the right side) of patientsin neutral, retracted, and forward head postures were measured. A1-way repeated measures analysis of variance followed by 3 pair-wise comparisons were used to determine differences.
Results: Comparisons indicated significant differences in PPT at 3points within the trigeminal innervated musculature [masseter (M1and M2) and anterior temporalis (T1)] among the 3 head postures[M1 (F=117.78; P<0.001), M2 (F=129.04; P<0.001), and T1(F=195.44; P<0.001)]. There were also significant differencesin MMO among the 3 head postures (F=208.06; P<0.001). Theintrarater reliability on a given day-to-day basis was good with theinterclass correlation coefficient ranging from 0.89 to 0.94 and 0.92to 0.94 for PPT and MMO, respectively, among the different headpostures.
Conclusions: The results of this study shows that the experimentalinduction of different cranio-cervical postures influences the MMOand PPT values of the temporomandibular joint and musclesof mastication that receive motor and sensory innervation by thetrigeminal nerve. Our results provide data that supports thebiomechanical relationship between the cranio-cervical region andthe dynamics of the temporomandibular joint, as well as trigeminalnociceptive processing in different cranio-cervical postures.
Key Words: temporomandibular disorders, myofascial pain, posture,
cervical spine, orofacial pain
(Clin J Pain 2011;27:48–55)
Pain in the masticatory muscles and arthralgia of thetemporomandibular joints are some of the features of
the term temporomandibular disorders (TMD) that havebeen categorized into 3 major groups by the ResearchDiagnostic Criteria (RDC) that is most commonly used toclassify symptomatology of TMD.1,2 Myofascial pain, discdisplacements, and arthralgia/osteoarthrosis constitute thisdiagnostic grouping. TMD of myofascial origin is categor-ized by episodic pain with periods of exacerbation andremission.3 Nevertheless, some patients may suffer persis-tent pain, and their prognosis is determined by psycho-metric evaluation (Axis II of the RDC/TMD). Myofascialpain is frequently associated with the presence of triggerpoints (TrPs) and the discomfort is considered to representa taut and painful disturbance of muscle and fascia that canbe local or referred with tenderness and pressure uponpalpation.4,5
It is well known that cervical spine tissues can referpain to the head and orofacial region.6,7 Comorbidity ofTMD and cervical spine disorders is quite common andconsists of a composite of functional limitation, pain,tender points, and hyperalgesia indigenous to the upperquarter.8 Some authors believe that neuronal plasticity,local interactions, and general predisposing musculoskeletalfactors might be behind this coexistence, but the relation-ship between the orofacial and cervical region is stronglyrooted by dense neuromusculoskeletal and neurophysiolo-gic connections.8,9 The trigeminal brainstem sensorynuclear complex located within the suboccipital spine,represents the prime neurophysiologic region where theconvergence of sensory information from the first 3 cervicalspinal nerves converge with trigeminal afferents, whereassome fibers descend to lower segmental levels.10–15 There-fore ascending cervicogenic and descending trigeminalreferral is mediated through the trigeminal brainstemsensory nuclear complex.15,16 The convergence of differenttypes of afferent and efferent neurotransmission on thetrigeminal nucleus together with the good evidence forneuronal plasticity that is known to occur in chronic painstates17–19 may account for the concomitant pain anddysfunction of the cervical, temporomandibular joints, andmasticatory system because of changes in head posture.17,20
Forward positioning of the head may contribute toor occur concomitantly with TMD,21,22 cervicogenic head-ache,23 and tension-type headache.24 Some authors supportthe connection between TMD and head posture,20–22,25
whereas others do not.26,27 The mechanism whereby headposture might be related to craniofacial signs and symptomsis unclear. The neuroplastic changes associated withCopyright r 2010 by Lippincott Williams & Wilkins
Received for publication April 7, 2010; revised June 9, 2010; acceptedJune 14, 2010.
From the *School of Health Science, Department of Physical Therapy;wGroup for Musculoskeletal Pain and Motor Control ClinicalResearch; zOrofacial Pain Unit of the Policlınica Universitaria,Universidad Europea de Madrid, Villaviciosa de Odon; zDepart-ment of Physical Therapy, Occupational Therapy, Rehabilitationand Physical Medicine, Universidad Rey Juan Carlos, Alcorcon,Madrid, Spain; yFaculty of Business, Management and SocialScience, University of Applied Science Osnabruck, Osnabruck,Germany; JProgram in Physical Therapy, Columbia University,New York, NY; and #Faculty of Rehabilitation Science, UniversidadAndres Bello, Santiago, Chile.
Reprints: Roy La Touche, PT, MSc, Facultad de Ciencias de la Salud/Departamento de Fisioterapia, Universidad Europea de Madrid,C/Tajo s/n, 28670 Villaviciosa de Odon, Madrid, Espana (e-mail:[email protected]).
ORIGINAL ARTICLE
48 | www.clinicalpain.com Clin J Pain � Volume 27, Number 1, January 2011

convergent afferent inputs mentioned above might play aconsiderable role. Further, it is noteworthy that changes inhead posture can alter the position of the mandible28,29 andthe activity of the masticatory muscles.30 Higbie et al31
demonstrated increased mouth opening in a forward headposition as compared with the neutral or retracted headposition, in healthy individuals. Furthermore, postural anddeep cervical flexor training as well as cervical manualtherapy have been shown to improve TMD signs andsymptoms.21,32,33
Although Visscher et al27 did obtain a wide rangeof head postures in both patients with craniomandibulardysfunction and healthy ones, their results data did notsupport the suggestion that craniomandibular dysfunctionis related to abnormal head posture, even in the presence ofcervical spine dysfunction. On the basis of their findings,Olivo et al34 found that the association between head andcervical posture with intra-articular or muscular TMD isnot clear.
Given the conflict in the literature as to whether thereis an association between head posture might be relatedto craniofacial signs and symptoms; the aim of this study isto assess the influence of cranio-cervical posture on themaximal mouth opening (MMO) and pressure pain thresh-old (PPT) of the trigeminal region in patients withmyofascial TMD pain.
MATERIALS AND METHODS
PatientsTMD patients were recruited from November 2008 to
March 2009 and were referred from 3 private dental clinicsin Madrid, Spain. Patients were selected if they met all ofthe following criteria: (1) a primary diagnosis of myofascialpain as defined by the Axis I, category Ia and Ib (ie,myofascial pain with or without limited opening), of theRDC/TMD,2 (2) bilateral pain involving the masseter andtemporalis, (3) a duration of pain of at least 6 months, (4) apain intensity corresponding to a weekly average of at least30mm on a 100mm visual analog scale, and (5) a presenceof bilateral TrPs in both the masseter and temporalismuscles diagnosed following the criteria described bySimons et al.35 TrPs were diagnosed according to thefollowing criteria: (1) presence of a palpable taut band inskeletal muscle, (2) presence of a hypersensitive tender spotwithin the taut band, (3) local twitch response elicited bythe snapping palpation of the taut band, and (4) reproduc-tion of referred pain in response to TrP compression. Thesecriteria have shown good interrater reliability (k) rangingfrom 0.84 to 0.88.36
All patients included in the study were examined byan experienced TMD specialist, with more than 4 years ofclinical practice, from the University Center of ClinicalResearch of the Cranial-Cervical-Mandibular System,Faculty of Medicine, San Pablo CEU University.
Patients were excluded if they presented any signs,symptoms, or history of the following diseases: (1) intra-articular disc displacement, ostheoarthrosis, or arthritis ofthe temporomandibular joint (TMJ), according to cate-gories II and III of the RDC/TMD2; (2) history of trauma-tic injuries (eg, contusion, fracture, and whiplash injury);(3) systemic diseases: (fibromyalgia, systemic lupus erythe-matosus, and psoriatic arthritis); (4) neurologic disorders(eg, trigeminal neuralgia); (5) concomitant diagnosis ofany primary headache (tension type or migraine); and
(6) current or recent therapy for the disorder within theprevious 2 months.
Each participant received a thorough explanationabout the content and purpose of the treatment beforesigning an informed consent relative to the procedures. Allprocedures were approved by the local ethics committee inaccordance with the Helsinki Declaration.
Experimental ProceduresEach patient with myofascial TMD pain were
subjected to a protocol for assessing maximum activeopening and PPT in 3 different cranio-cervical postures asfollows and illustrated in Figure 1:
Neutral head posture (NHP) defined as the positionassumed when the individual was told to sit and maintaintheir head in a vertical position. This position was furtherconfirmed as neutral if the tragus of the ear and acromionwere bisected by a plumb line.Forward head posture (FHP) defined as anteriortranslation of the head with or without lower cervicalflexion. It is claimed that the FHP is associated with anincrease in upper-cervical extension.37,38
Retracted head posture (RHP) defined as posteriortranslation of the head over the trunk associated withupper cranio-cervical flexion and extension of the low-to-mid cervical spine.39
All measurements were conducted by 2 physiothera-pists who had experience in research evaluations, one incharge of placing the patient in the measurement positionand the other responsible for the recording of MMOand PPT. All patients underwent 3 measurements of eachvariable in the 3 head positions on 3 different days. Awashout period of 24 hours was incorporated between eachmeasurement day.
A software program was used to obtain blockedrandomization of the size to arrange the order of measure-ment (GraphPad Software, Inc, CA). An average of 15minutes per patient was required to perform the random-ized measurements of MMO and PPT in NHP, FHP, andRHP. Every patient maintained their head in each positionfor 5 seconds during these measurements.
Establishment of the Measurement PositionsA plumb line hanging from the ceiling and a cervical
range of motion (CROM) device (Performance AttainmentAssociates, 958 Lydia DR, Roseville, MN) was usedto determine each patients’ cranio-cervical postures. TheCROM instrument measured the degree of FHP or RHPand the active cervical range of movement. The CROMinstrument uses a clear plastic eyeglass-like frame with 2dial-angle meters, a head arm that includes a vertebrallocator and bubble leveller (Fig. 2). The head arm wasplaced in the frame of the CROM horizontally to the head.The base of the vertebral locator was placed on the C-7spinous process so that the bubble leveller was centeredwithin the 2 vertical lines on the dial with the examinerstanding to the left of the patient to read the sagittal planemeter (Fig. 2). When the sagittal plane meter read zero andwith the head arm horizontal (parallel to the floor), theintersection of the head arm and vertebral locator wasrecorded as the head posture measurement in centimeters.Excellent reliability has been showed for the measurementof FHP using the CROM instrument [intrarater reliability
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 49

(interclass correlation coefficient, ICC=0.93) and interraterreliability (ICC=0.83)].40
Cranio-cervical postures were measured in the sittingposition attained by instructing the patient to sit in acomfortable upright position with the thoracic spine incontact with the back of the chair. The feet were positionedflat on the floor with knees and hips at 90 degrees and armsresting freely alongside.
Forward and retruded head postures were achieved byinitial placement into the NHP using the plumb line asexplained earlier. Movement into a FHP was performedwith the CROM after verbal instruction to position thehead forward in a horizontal plane allowing the tragus to bealigned to a target plumb line placed 8 cm anterior to thebase plumb line. Each patient was instructed to continuallymaintain their eyes at the same horizontal level while being
told to “slide your jaw and head forward until the examinertells you to stop” upon reaching the target plum line (Fig. 1).
Movement into a RHP was also performed with theCROM by instruction to position the head posteriorly ina horizontal plane allowing the tragus to be aligned to thetarget plumb line placed 4 cm posterior to the base plumbline. Each patient was instructed to continually maintaintheir eyes at the same horizontal level while being told to“slide your jaw and head backward until the examiner tellsyou to stop” upon reaching the target plum line (Fig. 1).
Measurement of MMOThe MMO was measured with a TheraBite range of
motion scale (Model CPT 95851; Atos Medical AB;Sweden) (Fig. 2). The patients were told to: “Open yourmouth as wide as possible without causing pain or
FIGURE 1. Measurement of maximum mouth opening with TheraBite, controlling the head position with the CROM device and plumline: A, retracted head posture. B, Forward head position. Measurement of pressure pain thresholds at masseter and temporalis muscleswith a mechanical algometer, controlling head position with CROM device: C, forward head position. D, Neutral head position. CROMindicates cervical range of motion.
FIGURE 2. Description and representation of measurement devices: TheraBite scale (A); CROM device: plastic eyeglass-like frame with 2dial-angle meters (B), head arm (C), and vertebral locator and bubble leveller (D).
La Touche et al Clin J Pain � Volume 27, Number 1, January 2011
50 | www.clinicalpain.com r 2010 Lippincott Williams & Wilkins

discomfort.” Interincisal distance was then recorded byplacing one end of the TheraBite scale against the incisaledge of one central mandibular incisor with the other endagainst the incisal edge of the opposing maxillary centralincisor (Fig. 1). Earlier research has shown excellentintrarater (0.92 to 0.97) and interrater (0.92 to 0.93)reliability when assessing MMO in 3 different cranio-cervical positions.33
Measurement of PPTThe PPT was defined as the amount of pressure that
a patient would initially perceive as painful.41 PPTs havebeen assessed with a mechanical pressure algometer (PainDiagnosis and Treatment Inc, Great Neck, NY) whichwas used in this study. The instrument consists of a 1 cmdiameter hard rubber tip, attached to the plunger of apressure (force) gauge. The dial of the gauge is calibratedin kg/cm2 and the range of the algometer is 0 to 10 kgwith 0.1 kg divisions. Earlier research has shown that thereliability of pressure algometry is as high as [ICC=0.91(95% confidence interval, CI 0.82-0.97)].42
Before the evaluation, 3 specific cutaneous regionsoverlying the masseter and temporalis were marked with apencil. Algometric measurements were then performed at 2masseteric sites and 1 temporalis site as delineated by:masseter muscle (M1 and M2) and temporalis muscle (T1)(Fig. 3). During the measurements, the algometer was heldperpendicular to the skin (Fig. 1) and the patient was toldto immediately alert the assessor when the pressure turned
into a sensation of pain, at which point the mechanicalstimulus was stopped. Three consecutive measurementswere obtained by the same assessor, with a pause of 30seconds between measurements. The mean of 3 measureswas calculated and used for analysis. All measurementswere performed on the right side because of the disturbanceinduced by the dial-angle meter of the CROM at the leftside (Fig. 1).
Statistical AnalysisData are expressed as mean, SD, and 95% CI. The
Kolmogorov-Smirnov test was used to determine the normaldistribution of the variables (P<0.05). A 1-way repeatedmeasures analysis of variance (ANOVA) followed by 3 pair-wise comparisons was used to determine differences in MMOand PPT among the 3 different head postures. Post-hoccomparisons were conducted with the Bonferroni test.Intrarater reliability of repeated measures was determinedfrom the ICC by means of the 2-way model, the 95% CI,and the standard error of the measurement (SEM). Thestrength of the ICC was interpreted as <0.50=poor; 0.50<0.75=moderate; 0.75 <0.90=good; and >0.90=excel-lent. The ICC and SEM convey different information aboutreliability of a measure. The analysis was conducted at 95%CI and P value less than 0.05 was considered to bestatistically significant. Statistical analyses were carried outusing the Statistical Package for Social Sciences, Version 15.0(SPSS, Chicago, IL).
RESULTSThe general demographic data and pain-related data
are shown in Table 1. Figure 4 represents the study samplesize and the reasons for exclusion of the patients. All thepatients who started the study were analyzed, and therewere no dropouts or losses.
FIGURE 3. Pressure pain threshold measurement sites attemporalis and masseter muscles. T1: located 3 cm above theline between the lateral edge of the eye and the anterior part ofthe helix on the anterior fibers of temporalis muscle. M1: located2.5 cm anterior to the tragus and 1.5 cm inferiorly. M2: located1 cm superior and 2 cm anterior from the mandibular angle.
TABLE 1. General Data of the Analyzed Patients
Demographic and Clinical Data Mean SD
Age (y) 34.69 10.83Weight (kg) 68.83 7.87Height (cm) 166.72 8.52Duration of pain (mo) 9 2.44VAS (mm) 39.7 1.78
SD indicates standard deviation; VAS, visual analog scale.
51 patients screened
Causes for exclusion
29 patients included(19 females)(10 males)
22 patients excluded
29 patients analysed0 losses or dropouts
FIGURE 4. Flow diagram of the patients in this study. RDCindicates Research Diagnostic Criteria; TMD, temporomandibulardisorders.
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 51

MMOThe intrarater reliability on a given day-to-day basis
was excellent with ICC ranging from 0.92 to 0.94 for MMOamong the 3 cranio-cervical postures. Reliability coeffi-cients, ICC associated 95% CI, and SEM values for MMOare presented in Table 2. A 1-way repeated measuresANOVA followed by 3 pair-wise comparisons indicated asignificant difference in MMO among the 3 cranio-cervicalpostures (F=208.06; P<0.001). Post-hoc results revealedthat the MMO was higher in FHP compared with the NHP(difference between means=2.81 cm) and the RHP (differ-ence between means=6.81 cm) (P<0.001). Furthermore,the MMO of the NHP was higher when compared with theRHP (difference between means=4cm) (P<0.001). Table 2summarizes MMO assessed among the 3 cranio-cervicalpostures.
PPTThe intrarater reliability on a given day-to-day basis
was good with ICC ranging from 0.89 to 0.94 for PPTamong the 3 cranio-cervical postures. Reliability coeffi-cients, ICC associated 95% CI, and SEM values for PPTare presented in Table 3. A 1-way repeated measuresANOVA followed by 3 pair-wise comparisons indicated asignificant difference in PPT of the 3 measurement pointsamong the 3 cranio-cervical postures [M1 (F=117.78;P<0.001); M2 (F=129.04; P<0.001); and T1 (F=195.44;P<0.001)]. Results of the post-hoc test for multiplecomparisons between PPT among the 3 cranio-cervicalpostures are presented in Figure 5. Table 4 summarizes thePPT among the 3 head postures.
DISCUSSIONThe experimental posture model used in this study
showed that MMO and PPT values become modifiedamong the induced cranio-cervical postures. MMO andPPT values in the NHP were between those obtained in theFHP and RHP. We observed the highest MMO in the FHP
and the lowest in the RHP. However, the PPT values didnot correspond with those obtained for the MMO as theywere lower in the FHP. In addition, the intrarater reliabilityof the model used to assess MMO and PPT was good.
MMOThe results obtained in the assessment of MMO in
the 3 different postures (NHP 40.8mm, RHP 36.8mm, andFHP 43.7mm) correspond with the results obtained byHigbie et al31 with healthy individuals (NHP 41.5mm,RHP 36.2mm, and FHP 44.5mm). The coincident valuessupport the existence of a functional integration betweenthe anatomic and biomechanical relationship of thetemporomandibular and cranio-cervical regions that hasbeen tested earlier by static and dynamic means. Erikssonet al43 and Zafar et al44 have demonstrated parallel andcoordinated head-neck movements during concomitant jawmovements. Haggman-Henrikson et al45 found a limitationof jaw movement and a shorter duration of jaw opening/closing cycles when experimental fixation of the neck wasperformed.
The variations of MMO in different head positions canbe explained by different actions of the masticatory andcervical muscles as well as intra-articular variations ofcondylar motion. Visscher et al46 found small changes inthe intra-articular distance of the TMJ when it wasmeasured in different cranio-cervical postures. RecentlyOhmure et al47 observed posterior condylar positioning inthe presence of a forced FHP, which may be a predisposingfactor toward intrinsic TMJ disorders resulting fromcumulative muscular and ligamental microtrauma ofabnormal postural origin.48 However, this factor has yetto be supported by clinical research.49,50 Olmos, et al51
demonstrated that after a TMJ treatment in symptomatic
TABLE 2. Descriptive and Intrarater Reliability Statistics forMeasurements of MMO in Patients With Myofascial TMD Pain(N=29) in the 3 Cranio-cervical Postures
Posture Mean±SD 95% CI ICC 95% CI for ICC SEM
NHP 40.8±3.12 39.69-42.07 0.93 0.89-0.96 0.78RHP 36.8±3.6 35.69-38.25 0.93 0.85-0.96 0.92FHP 43.7±2.93 42.58-44.81 0.94 0.90-0.97 0.68
CI indicates confidence interval; FHP, forward head posture; ICC,intraclass correlation coefficient; MMO, maximal mouth opening; NHP,neutral head posture; RHP, retracted head posture; SEM, standard error ofthe measurement; TMD, temporomandibular disorders.
TABLE 3. Descriptive Statistics for Measurements of PPT (kg/cm2) in Patients With Myofascial TMD Pain (N=29)
NHP RHP FHP
Measurement Points Mean±SD 95% CI Mean±SD 95% CI Mean±SD 95% CI
M1 2.2±0.61 1.97-2.44 1.91±0.52 1.71-2.11 1.73±0.48 1.55-1.92M2 2.4±0.61 2.17-2.64 2.1±0.55 1.91-2.35 1.91±0.55 1.7-2.12T1 2.43±0.58 2.2-2.65 2±0.58 1.84-2.28 1.82±053 1.62±2
CI indicates confidence interval; FHP, forward head posture; NHP, neutral head posture; PPT, pressure pain threshold; RHP, retracted head posture; SD,standard deviation; TMD, temporomandibular disorders.
3,50
NHP* * ** *
*2,50
3,00 RHPFHP
** * *
1,00
1,50
2,00
PP
T (
kg/c
m2 )
0,00
0,50
T1M1 M2
FIGURE 5. Comparison of the means of pressure pain thresholds(PPT) measures at masseter and temporalis muscles in relation to3 cranio-cervical postures: neutral head posture (NHP), retractedhead posture (RHP), and forward head posture (FHP). Error barsindicate SD and *P < 0.001.
La Touche et al Clin J Pain � Volume 27, Number 1, January 2011
52 | www.clinicalpain.com r 2010 Lippincott Williams & Wilkins

patients there seemed to be an increase in the retrodiscalspace and decrease in the distance between the shoulder andexternal auditory meatus. Therefore, an improved condylefossa relationship was apparent as the resting condylarposition became more anterior in conjunction with areduction of the FHP.
Recent evidence and the results of this study support theexistence of a relationship between the biomechanical actionof the cranio-cervical region and jaw movements, but ourresults do not show the degree of clinical implication that thedifferent postures have specific to intrinsic TMJ disorders.
PPTOur findings show that PPT values modify depending
upon the head posture in which they are measured. Thisvariability could be because of increased excitability ofthe trigeminal muscular nociceptors induced by differentcranio-cervical postures within which the PPT was mea-sured. In relation to orofacial nociception, an interactionbetween somatosensory processing and sensory-motorfunction is supported by our data.52
The results of our research cannot determine thereason by which the PPT decreases in the RHP and FHP ascompared with the NHP values. However, if our datais added to the findings of others it may lead to thedevelopment of different theories that offer additionalexplanations. We suggest that the PPT variations may bebecause of experimental biomechanical modifications ofmuscle and soft tissue that were produced when the patientstried to hold the FHP and the RHP, which generatedaugmented electromyography (EMG) activity and masti-catory reflexes. Modification of the activity produced ateach of the aforementioned postures could be causing PPTalteration. Furthermore, increased jaw-reflex activity maybe triggered by enhanced fusimotor drive, thereby elevatingmuscle spindle discharge resulting in reflex facilitation.Elevated fusimotor drive may in turn lead to increased TMJstiffness and pain. Earlier research has supported thepremise that experimental pain can augment masticatoryreflex activity.53–56
A recent study has shown that masseteric EMGactivity increases in the presence of a forced FHP.48 Inaddition, EMG changes in the suprahyoid muscles havebeen observed in experimentally induced FHP.57 However,in direct contrast, earlier studies have found increasedmasticatory EMG activity in head extension,58 which isa component of the RHP. Johansson and Sojka59 haveproposed a model to explain the spread of muscle painbased on the g-motoneuron system in which muscle stiffnessand pain are increased by enhanced activity of primarymuscle spindle afferents. This hypothesis may explain someof the results of this study, however, such thoughts are only
theoretical reflections and future research needs to provewhether postural changes truly alter the nociceptive trigem-inal mechanism.
Study LimitationsThe results of this study must be taken with caution
because the objective measurements were performed inan experimentally forced posture and not a natural one. Itwould also be interesting to determine in future researchwhether the PPT is modified with different natural posturesand whether postural alterations may affect or may be anaggravating factor in the development of orofacial pain. Itis also important to state that our participant sample onlyincluded patients with myofascial TMD. Therefore, it isimperative that future research apply the same method-ology with healthy individuals and other cohorts of TMDto determine whether the results can be replicated.
Clinical ImplicationsThe anatomic and physiological interaction between
the cranio-cervical and temporomandibular regions asshowed in this research supports the concept of a functionaltrigeminocervical coupling during jaw activities that influ-ences the inherent modifications that we observed in MMOand PPT. This factor must be taken into account duringpatient evaluation to control for variations in measurement.
The methodology that we used can result in a morestructured assessment of the MMO and PPT in neutralposition, within which we observed that average values wereobtained with excellent intrarater reliability. Postural treat-ment has already been shown to be useful for reducing TMDmyofascial pain and improving MMO.33,60 We have demon-strated experimentally that pain thresholds at the trigeminalarea can be modified only by changing the cranio-cervicalposture. As PPT values diminish in FHP and RHP, it wouldbe useful to consider new therapeutic strategies to improvethe cranio-cervical posture toward a NHP and futureresearch should determine whether postural treatments canhelp to modulate pain in myofascial TMD patients.
CONCLUSIONSThe results of this study shows that the experimental
induction of different cranio-cervical postures influencesthe MMO and PPT values of masticatory and joint func-tion of the temporomandibular complex. Our observationssupport the concept of a biomechanical relationship andinteraction within the trigeminocervical complex as well asinherent nociceptive processing in different cranio-cervicalpostures. Why or how postural modifications influence thePPT and MMO values are issues that are beyond the scopeof this study.
TABLE 4. Intrarater Reliability Statistics for Measurements of PPT in Patients With Myofascial TMD Pain (N=29) in the 3 Cranio-cervicalPostures
NHP RHP FHP
Measurement Points ICC 95% CI for ICC SEM ICC 95% CI for ICC SEM ICC 95% CI for ICC SEM
M1 0.93 0.87-0.96 0.16 0.9 0.82-0.94 0.16 0.93 0.87-0.96 0.12M2 0.91 0.84-0.95 0.18 0.92 0.86-0.96 0.16 0.92 0.87-0.96 0.15T1 0.89 0.82-0.94 0.19 0.94 0.89-0.97 0.14 0.92 0.86-0.96 0.13
CI indicates confidence interval; FHP, forward head posture; ICC, intraclass correlation coefficient; NHP, neutral head posture; PPT, pressure painthreshold; RHP, retracted head posture; SD, standard deviation; SEM, standard error of the measurement; TMD, temporomandibular disorders.
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 53

ACKNOWLEDGMENT
The authors thank Dr Greg Murray (Professor ofDentistry, Jaw Function and Orofacial Pain Research Unit,Faculty of Dentistry, University of Sydney, Australia) for hishelpful contribution in this article.
REFERENCES
1. Okeson JP. Management of Temporomandibular Disorders andOcclusion. 6 th ed. St. Louis: Mosby; 2007:300.
2. Dworkin SF, LeResche L. Research diagnostic criteria fortemporomandibular disorders: review, criteria, examinations andspecifications, critique. J Craniomandib Disord. 1992;6:301–355.
3. Dworkin SF, Huggins KH, Wilson L, et al. A randomizedclinical trial using research diagnostic criteria for temporoman-dibular disorders-axis II to target clinic cases for a tailored self-care TMD treatment program. J Orofac Pain. 2002;16:48–63.
4. Mense S, Simons DG. Muscle Pain: Understanding Its Nature,Diagnosis, and Treatment. Philadelphia: Lippincott Williams &Wilkins; 2001:253–259.
5. Shindler HJ, Svensson P. Myofascial temporomandibulardisorder pain. In: Turp JC, Sommer C, Hugger A. Pathophy-siology and Management. Basel: Karger; 2007:91–123.
6. Sessle BJ, Hu JW, Amano M, et al. Convergence of cutaneous,tooth pulp, visceral, neck and muscle afferents onto nociceptiveand non-nociceptive neurons in trigeminal subnucleus caudalis(medullary dorsal horn) and its implications for referred pain.Pain. 1986;27:219–235.
7. Bogduk N. The neck and headaches. Neurol Clin. 2004;22:151–171.
8. De Laat A, Meuleman H, Stevens A, et al. Correlation betweencervical spine and temporomandibular disorders. Clin OralInvestig. 1998;2:54–57.
9. De Laat A. Reflexes elicitable in jaw muscles and their roleduring jaw function and dysfunction: a review of the literature.Part II. Central connections of orofacial afferents. Cranio.1987;5:246–253.
10. Bogduk N. The anatomical basis for cervicogenic headache.J Manipulative Physiol Ther. 1992;15:67–70.
11. Kerr FW. Structural relation of the trigeminal spinal tract toupper cervical roots and the solitary nucleus in the cat. ExpNeurol. 1961;4:134–148.
12. Marfurt CF. The central projections of trigeminal primaryafferent neurons in the cat as determined by the tranganglionictransport of horseradish peroxidase. J Comp Neurol. 1981;203:785–798.
13. Jacquin MF, Rhoades RW, Enfiejian HL, et al. Organisationand morphology of masticatory neurons in the rat: a retro-grade HRP study. J Comp Neurol. 1983;218:139–156.
14. Bogduk N. Cervical causes of headache and dizziness. In:Grieve G, ed. Modern Manual Therapy. Edinburgh (UK):Churchill Livingstone; 1994:317–331.
15. Hu JW, Sun KQ, Vernon H, et al. Craniofacial inputs to uppercervical dorsal horn: implications for somatosensory informa-tion processing. Brain Res. 2005;1044:93–106.
16. Michler RP, Bovim G, Sjaastad O. Disorders in the lowercervical spine. A cause of unilateral headache? A case report.Headache. 1991;31:550–551.
17. Coderre TJ, Katz J, Vaccarino AL, et al. Contribution ofcentral neuroplasticity to pathological pain: review of clinicaland experimental evidence. Pain. 1993;52:259–285.
18. Latremoliere A, Woolf CJ. Central sensitization: a generator ofpain hypersensitivity by central neural plasticity. J Pain. 2009;10:895–926.
19. Costigan M, Scholz J, Woolf CJ. Neuropathic pain: amaladaptive response of the nervous system to damage. AnnuRev Neurosci. 2009;32:1–32.
20. Huggare JA, Raustia AM. Head posture and cervicovertebraland craniofacial morphology in patients with craniomandibu-lar dysfunction. Cranio. 1992;10:173–177.
21. Mannheimer JS. Prevention and restoration of abnormalupper quarter posture. In: Gelb H, Gelb M, eds. PosturalConsiderations in the Diagnosis and Treatment of Cranio-Cervical-Mandibular and Related Chronic Pain Disorders.London: Mosby-Wolfe; 1994:277–323.
22. Gonzalez HE, Manns A. Forward head posture: its structuraland functional influence on the stomatognathic system,a conceptual study. Cranio. 1996;14:71–80.
23. Watson DH, Trott PH. Cervical headache: an investigation ofnatural head posture and upper cervical flexor muscleperformance. Cephalagia. 1993;13:272–284.
24. Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML,et al. Trigger points in the suboccipital muscles and forwardhead posture in tension-type headache. Headache. 2006;46:454–460.
25. Nicolakis P, Nicolakis M, Piehslinger E, et al. Relationshipbetween craniomandibular disorders and poor posture. Cranio.2000;18:106–112.
26. Darlow LA, Pesco J, Greenberg MS. The relationship ofposture to myofascial pain dysfunction syndrome. J Am DentAssoc. 1987;114:73–75.
27. Visscher CM, De Boer W, Lobbezoo F, et al. Is there arelationship between head posture and craniomandibular pain?J Oral Rehabil. 2002;29:1030–1036.
28. Darling DW, Kraus S, Glasheen-Wray MB. Relationship ofhead posture and the rest position of the mandible. J ProsthetDent. 1984;52:111–115.
29. Goldstein DF, Kraus SL, Williams WB, et al. Influence ofcervical posture on mandibular movement. J Prosthet Dent.1984;52:421–426.
30. Forsberg CM, Hellsing E, Linder-Aronson S, et al.EMG activity in neck and masticatory muscles in relation toextension and flexion of the head. Eur J Orthod. 1985;7:177–184.
31. Higbie E, Seidel-Cobb D, Taylor LF, et al. Effect of headposition on vertical mandibular opening. J Orthop Sports PhysTher. 1999;29:127–130.
32. La Touche R, Fernandez-de-las-Penas C, Fernandez-CarneroJ, et al. The effects of manual therapy and exercise directed atthe cervical spine on pain and pressure pain sensitivity inpatients with myofascial temporomandibular disorders. J OralRehabil. 2009;36:644–652.
33. Wright EF, Domenech MA, Fischer JR Jr. Usefulness ofposture training for patients with temporomandibular dis-orders. J Am Dent Assoc. 2000;131:202–210.
34. Olivo SA, Bravo J, Magee DJ, et al. The association betweenhead and cervical posture and temporomandibular disorders:a systematic review. J Orofac Pain. 2006;20:9–23.
35. Simons DG, Travell J, Simons LS. Myofascial Pain andDysfunction: The Trigger Point Manual. 2nd ed. Vol. 1.Baltimore: Williams & Wilkins; 1999:11–28.
36. Gerwin RD, Shanon S, Hong CZ, et al. Interrater reliabilityin myofascial trigger point examination. Pain. 1997;69:65–73.
37. Hanten WP, Lucio RM, Russell JL, et al. Assessment of totalhead excursion and resting head posture. Arch Phys MedRehabil. 1991;71:877–880.
38. Enwemeka CS, Bonet IM, Ingle JA, et al. Postural correctionin persons with neck pain. II. Integrated electromyography ofthe upper trapezius in three simulated neck positions. J OrthopSports Phys Ther. 1986;8:240–242.
39. Lentell G, Kruse M, Chock B, et al. Dimensions of the cervicalneural foramina in resting and retracted positions usingmagnetic resonance imaging. J Orthop Sports Phys Ther. 2002;32:380–390.
40. Garrett TR, Youdas JW, Madson TJ. Reliability of measuringforward head posture in a clinical setting. J Orthop Sports PhysTher. 1993;17:155–160.
41. Svensson P, Arendt-Nielsen L, Nielsen H, et al. Effect ofchronic and experimental jaw muscle pain on pressure painthresholds and stimulus response curves. J Orofac Pain.1995;9:347–356.
La Touche et al Clin J Pain � Volume 27, Number 1, January 2011
54 | www.clinicalpain.com r 2010 Lippincott Williams & Wilkins

42. Chesterson LS, Sim J, Wright CC, et al. Inter-rater reliabilityof algometry in measuring pressure pain thresholds in healthyhumans, using multiple raters. Clin J Pain. 2007;23:760–766.
43. Eriksson PO, Zafar H, Nordh E. Concomitant mandibular andhead-neck movements during jaw opening-closing in man.J Oral Rehabil. 1998;25:859–870.
44. Zafar H, Nordh E, Eriksson PO. Temporal coordinationbetween mandibular and head-neck movements during jawopening-closing tasks in man. Arch Oral Biol. 2000;45:675–682.
45. Haggman-Henrikson B, Nordh E, Zafar H, et al. Headimmobilization can impair jaw function. J Dent Res. 2006;85:1001–1005.
46. Visscher CM, Huddleston Slater JJ, Lobbezoo F, et al.Kinematics of the human mandible for different head postures.J Oral Rehabil. 2000;27:299–305.
47. Ohmure H,Miyawaki S, Nagata J, et al. Influence of forward headposture on condylar position. J Oral Rehabil. 2008;35:795–800.
48. Rocabado M. Arthrokinematics of the temporomandibularjoint. Dent Clin North Am. 1983;27:573–594.
49. Hackney J, Bade D, Clawson A. Relationship between forwardhead posture and diagnosed internal derangement of thetemporomandibular joint. J Orofac Pain. 1993;7:386–390.
50. MunhozWC, Marques AP, de Siqueira JT. Evaluation of bodyposture in individuals with internal temporomandibular jointderangement. Cranio. 2005;23:269–277.
51. Olmos SR, Kritz-Silverstein D, Halligan W, et al. The effect ofcondyle fossa relationships on head posture. Cranio. 2005;23:48–52.
52. Sessle BJ. Mechanisms of oral somatosensory and motorfunctions and their clinical correlates. J Oral Rehabil. 2006;33:243–261.
53. Svensson P, Macaluso GM, De Laat A, et al. Effects of localand remote muscle pain on human jaw reflexes evoked by faststretches at different clenching levels. Exp Brain Res.2001;139:495–502.
54. Wang K, Svensson P, Arendt-Nielsen L. Effect of tonic musclepain on short-latency jaw-stretch reflexes in humans. Pain.2000;88:189–197.
55. Wang K, Arendt-Nielsen L, Svensson P. Excitatory actions ofexperimental muscle pain on early and late components ofhuman jaw stretch reflexes. Arch Oral Biol. 2001;46:433–442.
56. Wang K, Arendt-Nielsen L, Svensson P. Capsaicin-inducedmuscle pain alters the excitability of the human jawstretchreflex. J Dent Res. 2002;81:650–654.
57. Milidonis MK, Kraus SL, Segal RL, et al. Genioglossi muscleactivity in response to changes in anterior/neutral headposture. Am J Orthod Dentofacial Orthop. 1993;103:39–44.
58. Funakoshi M, Fujita N, Takehana S. Relations betweenocclusal interference and jaw muscle activities in response tochanges in head position. J Dent Res. 1976;55:684–690.
59. Johansson H, Sojka P. Pathophysiological mechanisms in-volved in genesis and spread of muscular tension in occupa-tional muscle pain. Med Hypotheses. 1991;135:196–203.
60. Komiyama O, Kawara M, Arai M, et al. Posture correction aspart of behavioural therapy in treatment of myofascial painwith limited opening. J Oral Rehabil. 1999;26:428–435.
Clin J Pain � Volume 27, Number 1, January 2011 Influence of Cranio-cervical Posture on TMD Pain
r 2010 Lippincott Williams & Wilkins www.clinicalpain.com | 55

87
5.2 Estudio II
López-de-Uralde-Villanueva I, Beltran-Alacreu H, Paris-Alemany A, Angulo-Díaz-Parreño S,
La Touche R. Reliability, Standard Error, and Minimal Detectable Change of Two Tests for
Craniocervical Posture Assessment in Asymptomatic Subjects and Chronic Neck/craniofacial
Pain Patients. (En revisión).
Objetivo del Estudio
Nuestro objetivo fue examinar la fiabilidad de dos mediciones para evaluar la postura
craneocervical (PC y DME). Además, se evaluó una posible asociación entre las variables
registradas. Como objetivo final, tenemos la intención de evaluar si existen diferencias en la
postura craneocervical entre sujetos asintomáticos y pacientes con dolor cérvico- craneofacial.
Resultados
La fiabilidad intra-evaluador de la medición de PC fue alta para los sujetos asintomáticos y
pacientes DCCF (CCI = 0,93 y 0,81, respectivamente) y para DME (rango CCI entre 0,78-0,99).
La fiabilidad intra-evaluador se mantuvo alta cuando se evaluó 9 días más tarde. Los resultados
de fiabilidad inter-evaluador fue alta para la PC (rango CCI entre 0,94 a 0,96) y fue justa para la
DME (rango CCI entre 0,78 a 0,79). El EEM de PC fue de 0,41 hasta 0,75 cm, mientras que el
MCD fue 0,96 a 1,74 cm. El SEM para la DME fue 1,61 a 7,06 mm, mientras que el MCD fue
3,76 a 16,47 mm. Se observó una correlación positiva moderada en ambos grupos entre HP y
SCD (sujetos asintomáticos, r = 0,447; pacientes con DCCF, r = 0,52). Análisis realizado con
una t de student mostró diferencias estadísticamente significativas entre los grupos para las
medidas de la postura craneocervical, pero estas diferencias eran muy pequeñas. Se encontró
una correlación positiva fuerte entre la discapacidad cervical y la craneofacial.
Conclusiones
Las mediciones para evaluar la postura craneocervical son fiables cuando se realizan por uno o
por dos evaluadores en sujetos asintomáticos o pacientes con DCCF.

1
Reliability, Standard Error, and Minimal Detectable Change of Two Tests for
Craniocervical Posture Assessment in Asymptomatic Subjects and Chronic
Neck/craniofacial Pain Patients
Ibai López-de-Uralde-Villanueva, PT, MSc1-4
, Hector Beltran-Alacreu, PT, MSc 2,3
,
Alba Paris-Alemany, PT, MSc1-4
, Santiago Angulo-Díaz-Parreño, MSc2,3,5
, Roy La
Touche, PT, MSc1-4
,
1. Department of Physiotherapy, Faculty of Health Science, The Center for
Advanced Studies University La Salle, Universidad Autónoma de Madrid,
Aravaca, Madrid, Spain.
2. Research Group on Movement and Behavioral Science and Study of Pain, The
Center for Advanced Studies University La Salle, Universidad Autónoma de
Madrid.
3. Institute of Neuroscience and Craniofacial Pain (INDCRAN), Madrid, Spain
4. Hospital La Paz Institute for Health Research, IdiPAZ. Madrid, Spain.
Madrid, Spain
5. Faculty of Medicine, Universidad San Pablo CEU, Madrid, Spain
Address for reprint requests / Corresponding author:
Roy La Touche
Facultad de Ciencias de la Salud
Centro Superior de Estudios Universitarios La Salle.
Calle la Salle, 10
28023 Madrid
SPAIN
Telephone number: + 34 91 7401980 (EXT.256)
Fax number:
Email address: [email protected]
The study protocol was approved by the local ethics committee of the Center for
Advanced Studies University La Salle, Madrid (Spain).

2
Reliability, Standard Error, and Minimal Detectable Change of Two Tests for
Craniocervical Posture Assessment in Asymptomatic Subjects and Chronic
Neck/craniofacial Pain Patients
ABSTRACT
PURPOSE:
Is recommended to quantifying the craniocervical posture as part of the assessment of
patients with neck and craniofacial pain to facilitate diagnosis and determine
treatment strategies. There is insufficient research regarding the intra-rater and inter-
rater reliability of craniocervical posture measurement using a CROM device and a
Digital Calliper.
OBJETIVE:
Determine the intra-rater and inter-rater reliability of two craniocervical posture
measurements on asymptomatic subjects and chronic neck/craniofacial pain (chronic
cervico-craniofacial pain, CCFP).
METHODS:
Two-groups repeated measures for inter- and intra-rater reliability study. 53
asymptomatic adult subjects and 60 CCFP patients who volunteered for the study.
Two raters measured head posture (HP) and the sternomental distance (SMD) using
the CROM device and Digital Calliper respectively.
RESULTS:
Intra-rater reliability of the HP measurement was high for asymptomatic subjects and
CCFP patients (Intraclass Correlation Coefficients (ICC)=0.93 and 0.81 respectively)
and for SMD (ICC range between 0.78-0.99), the intra-rater reliability remained high

3
when evaluated 9 days later. Inter-rater reliability was high for HP (ICC range
between 0.94-0.96) and fair for SMD (ICC range between 0.78-0.79). The HP
standard error of measurement (SEM) was 0.41–0.75cm while the minimal detectable
change (MDC) was 0.96–1.74cm. The SMD SEM was 1.61-7.06mm while the MDC
was 3.76-16.47mm. A moderate positive correlation for both groups was observed
between HP and SCD (asymptomatic subjects, r=0.447; CCFP patients, r=0.52).
Analysis with an independent t-test showed statistically significant differences
between groups for measures of craniocervical posture, but these differences were
very small. No statistically significant correlations between the HP and SMD with the
disabilities variables. Neck disability is strong positively correlated with the
craniofacial disability (r=0.79, p<0.001, n=60).
CONCLUSION:
The CROM device and Digital Calliper were reliable means of measuring HP and
SMD when performed by two or one raters in asymptomatic subjects and CCFP
patients.
KEYWORDS:
Reliability, Posture, Reproducibility of Results, Rehabilitation, Measurement, Neck
Pain, Temporomandibular disorders
INTRODUCTION
The optimal position of the head is the one in which the cranium is not inclined,
retracted, rotated, or extended. This position minimizes the muscle forces needed to
compensate the tendency of the head to tilt forward.[1] Currently, many professions
(office workers, clerks, carriers, etc.) require workers to spend much of their work day
sitting. In this situation one may adopt an excessive forward head posture (FHP).[2]

4
This head posture (HP) may occur due to a front translation of the head, a flexion of
the lower cervical spine, or both, and is also associated with an increase in extension
of the upper cervical spine.[3] It has been suggested that FHP increases the
compressive forces of the cervical zygapophyseal joint and those in the rear of the
vertebrae,[4] causing changes in the length and strength of the connective tissue
leading to stretching of the anterior neck structures and shortening of the posterior
neck muscles, all leading to pain.[5]
It is recommended that HP is quantified as part of the examination of patients with
neck pain to facilitate the diagnosis and determine treatment strategies. In addition, it
is very important to monitor a patient’s progress.[5] This growing interest around the
importance of the HP by researchers and clinicians is due to the belief that FHP is
associated with the development and persistence of certain disorders, such as cervical
headaches and migraines,[6] myofascial pain syndrome,[7] and woman with
craniofacial pain.[8] Regarding the association between the FHP and pain, there are
numerous studies with conflicting results: some showed differences in the HP of
patients with neck pain versus asymptomatic subjects,[9] while others do not.[10]
Attempts have been made to quantify FHP in many ways, both objectively and
subjectively. Subjective methods are described by some authors,[11] while objective
methods use photographs (to measure the tragus-C7-horizontal angle),[12]
radiographic images,[13] or the Cervical Range of Motion instrument (CROM),[14]
among others.
The CROM was designed to measure cervical range of motion but it can also measure
protraction and retraction of the head.[14] In the trial conducted by Garret et al.[14],
HP was measured in a sitting position with the CROM. The authors found high intra-

5
examiner reliability (ICC=0.93) while inter-examiner reliability was good
(ICC=0.83).
Another measurement that may be of interest is the sternomental distance (SMD). We
hypothesize a direct association between the SMD and the HP. We found only two
studies that evaluated the SMD, but they did not association it with HP.[15, 16]
There is little evidence concerning the reliability of intra-examiner and inter-examiner
measurement of HP using the CROM, therefore our purpose was to examine this
reliability and of using a Digital Calliper to measure the SMD. In addition, we
assessed a possible association between the variables recorded by these instruments
and as ultimate objective, we intend to assess whether there are differences in
craniocervical posture between asymptomatic subjects and patients with chronic
cervico-craniofacial pain (CCFP).
METHODS
Study design
We employed two-group repeated measures for intra- and inter-rater reliability
design. This study was planned and conducted in accordance with the Guidelines for
Reporting Reliability and Agreement Studies (GRRAS).[17]
Sample size
Sample size was calculated using the method described by Walter et al.[18]. This
method is recommended for estimating of sample size based on the Intraclass
Correlation Coefficient (ICC). The minimally acceptable ICC value (ρ1 = 0.7) versus
an alternative ICC reflecting the expected value (ρ1 = 0.8) was chosen. To obtain a
power of 80% (β = 0.2) and significance level of 5%, we determined that a sample of
at least 53 healthy subjects was required for intra-rater and inter-rater reliability (two
sets of 2 measurements were performed each day for two days). In addition, under the

6
same conditions, we determined that a sample of at least 57 symptomatic subjects was
required for intra-rater reliability (1 set of 2 measurements were performed each day
for three days). To estimate sample size we used the Power Analysis & Sample Size
Software (PASS 12).
Subjects
Two convenience samples of asymptomatic subjects were obtained from our
university campus and the local community through flyers, posters, and social media.
To participate in this study, the asymptomatic subjects were required to be between
18 and 65 years of age and must not have experienced: (1) neck or face pain during
data collection, or (2) a history of neck or face pain in the prior six months.
The second convenience sample of symptomatic subjects consisted in chronic
cervico-craniofacial pain patients. The sample was recruited two private clinics
specialized in spine, craniofacial pain and temporomandibular disorders (TMD)
(Madrid, Spain). A diagnosis of CCFP of muscular origin was the first inclusion
criterion. We defined CCFP of muscular origin as the presence of mechanical signs of
dysfunction and muscular pain (e.g. limited movement, uncoordinated movement,
weakness and lack of endurance in the neck and jaw) that were exacerbated by
maintained postures and movement, generating pain at the cervical and craniofacial
regions [19]. The specific inclusion criteria were: a) signs of disability and pain in the
orofacial and craniomandibular region, according to the Craniofacial pain and
disability inventory (CF-PDI) [20]; b) a primary diagnosis of myofascial pain
following Axis 1 (myofascial pain) of the Research Diagnostic Criteria for
Temporomandibular Disorders[21]; c) ≥ 6 months with the presence of the pain; d) ≥
5 points on the Neck Disability Index (NDI)[22]; f) bilateral pain of the temporal,
masseter, suboccipital and trapezius muscles. Patients were excluded if they had any

7
"red flags,"[23] a rheumatologic disease, any type of cancer, cervical radiculopathy,
myelopathy, a history of cervical surgery or whiplash trauma. The study was
conducted in accordance with the Declaration of Helsinki and was approved by the
local ethics committee. Prior to their participation, subjects gave written informed
consent.
Evaluators
The assessments were made by two physical therapists with more than three years of
clinical experience using the CROM to measure range of movement (ROM) and head
posture (HP) in clinical practice. Both therapists received a 120-minute training
session on how to use the Digital Calliper and how to measure the SMD.
Instrumentation
In this study we used the CROM equipped to measure the HP. The device used was
the CROM 3. It has the appearance of eyeglasses and is made from a lightweight
plastic with three inclinometers, one for each plane of motion. It is adjusted using a
hook-and-loop strap. The part of the device used to measure HP includes the forward
head arm and the vertebra locator. The forward head arm is equipped with a ruler
marked in 0.5 cm units, indicating the horizontal distance between the bridge of the
nose and the vertebra locator. The vertebra locator has a leveler bubble on top to
assist with accurate positioning. In this study the inclinometers were not used because
neck movements were not evaluated.
The digital calliper was used to quantify the SMD. The device is made of plastic with
a 5-digit LCD display, and can measure in inches or millimeters (mm) and with a
range of 0.01 mm to 150 mm. It also includes a ruler provided with a nonius, for
accurate measurement of lengths or angles. The one used for measuring length
comprised of a rule divided into equal parts on which a nonius slides such that n-1

8
divisions of the rule are divided into n equal parts of the nonius. It has two tips for
controlling internal and external measurements. The digital calliper is used for direct
measurement. Also, it is a fast and accurate instrument.
Procedures
The assessments were made between May and June of 2012 in our university
laboratory for asymptomatic subjects and between July and September of 2014 for
symptomatic subjects. Each healthy subject visited the laboratory on two different
occasions separated by a space of 48 hours. On the first day, rater A performed the
first assessment followed by rater B. On the second day, rater B performed the first
assessment followed by rater A. Moreover, each symptomatic subject visited the
laboratory on three different occasions separated by a space of 48 hours (between trial
1 and trial 2) and 9 days (between trial 2 and trial 3). In symptomatic subjects, the
assessment always was performed by the same rater. In both samples of subjects, each
rater used a data collection sheet on which to record the measurements. Before the
assessments, subjects removed eyeglasses, caps, and any jewelry. The measurements
in this study were taken twice, and the order in which they were performed was as
follows:
1. Head Posture
To quantify HP, the subjects were told to stay in the starting position: sitting in a chair
with a back rest, feet flat on the floor, and arms hanging alongside the body. The
evaluator placed the CROM on the subject’s head like a pair of eyeglasses and
adjusted it with the strap. The evaluator then located the spinous process of C7 and
placed the vertebra locator on it, adjusting the pressure until the subject indicated that
the pressure of the device was felt. Once the subject felt the pressure over C7, the

9
evaluator stated, “From this moment you should not move”. This was performed as a
means for the subject to become familiar with the test.
Then the subject was asked to stand up and then sit back into the starting position.
The evaluator standing to the left side of the subject, found the spinous process of C7
and placed the vertebra locator such that it formed a 90° angle with the head arm of
the CROM with the bubble indicating the instrument was level (Figure 1. A). This
measurement was made twice, and between the first and the second measurements the
subjects were asked to stand up and sit back into the starting position again,
whereupon the evaluator completed the procedure.
2. Sternomental Distance
The evaluator first explained to the subject that the measurement would take place
while lying on a couch. Also at this time the evaluator showed the Digital Calliper to
the subject and said: “You will notice contact on your sternum and on your chin; at
the moment you notice that you should not move.” When the subject understood the
statement and gave the evaluator permission to proceed, the subject was asked to lie
in a supine position on the couch, looking at the ceiling. When the subject was in
position the evaluator gave the instruction: “Don’t move your head.” Once in place,
the measurement was taken from the jugular notch of the sternum to the chin
protuberance (Figure 1. B). The measurement was taken twice between the subject
was instructed to roll to a right lateral position and then return to the supine position.
DATA ANALYSIS
Data were analysed with the SPSS statistical package (SPSS v.20.0; SPSS, Inc,
Chicago, IL). The Kolmogorov-Smirnov test was used to analyze the normal
distribution of the variables (P>0.05).

10
The intra-rater and inter-rater reliability was evaluated using the Intraclass Correlation
Coefficient (ICC). Reliability levels were defined based on the following
classification: good reliability, ICC ≥ 0.75; moderate reliability, ICC ≥ 0.50 and
<0.75; and poor reliability, <0.50 [24].
Bland-Altman analysis were performed by calculating the mean difference between
two measurements and the standard deviation (SD) of the difference.[25] A 95% of
the differences is expected to be less than two SDs. The closer the mean difference
was to 0 and the smaller the SD of this difference, the better was the agreement.[25]
The Bland–Altman analysis was used to compare the values of HP and SMD obtained
by the two raters separately. Similarly, comparisons were made to confirm the
reproducibility by analyzing the measurements values obtained on two trials. Bland-
Altman analysis was performed using MedCalc for Windows, version 12.5.0.0
(MedCalc Software, Mariakerke, Belgium).
Measurement error is expressed as a standard error of measurement (SEM), which is
calculated as , where SD is the SD of values from all participants and
ICC is the reliability coefficient.[26] Measurement error is the systematic and random
error of a patient’s score that is not attributable to true changes in the construct to be
measured.[27]
Responsiveness was assessed using the Minimal Detectable Change (MDC). The
MDC90 expresses the minimal change required to be 90% confident that the observed
change between the two measures reflects real change and not measurement error.[28]
It is calculated as .[28]
The Pearson correlation coefficient was used to analyze the association between HP
and SMD in the two samples of subjects, also used to analyze the correlations
between the variables of disability with the data HP and SMD in patients with CCFP.

11
A Pearson correlation coefficient greater then 0.60 indicated a strong correlation,
between 0.30 and 0.60 indicated a moderate correlation, and below 0.30 indicated a
low or very low correlation.[29]
Finally, the independent t-test was used for the analysis of HP and SMD variables
(using the mean of the trial 1 and 2), comparing the collection data for the two
samples.
RESULTS
The asymptomatic subjects sample consisted of 53 participants, 30 of whom were
women; the subjects were between 18 and 53 years of age (mean=38.1, SD=10.5
years). The symptomatic subjects sample consisted of 60 CCFP patients, 32 of whom
were women; the subjects were between 19 and 61 years of age (mean=41.7, SD=11.7
years). No statistically significant differences between the general characteristics of
both groups are presented. The group of symptomatic subjects presented a mean of
14.78 ±4.04 of neck disability and 16.30±7.11 of craniofacial disability. All variables
were normally distributed according to the Kolmogorov-Smirnov test (P>0.05). No
subjects were excluded from the study based on the inclusion and exclusion criteria.
Asymptomatic subjects
The ICC value for intra-rater reliability of single measures separated by a space of 48
hours was 0.93 for HP and ranged from 0.95 to 0.99 for SMD. Descriptive statistics,
ICCs and associated 95% CIs, SEMs and MDC90 between each evaluator´s trials are
presented in Table 1.
ICC values for interrater reliability of single measures ranged from 0.78 to 0.79 for
SMD and from 0.94 to 0.96 for HP. Descriptive statistics, ICCs and associated 95%
CIs, SEMs, and MDC90 between each rater´s trials are presented in Table 1.

12
The Bland-Almand analysis for the intra-rater and inter-rater performances are shown
for assessement of HP and SMD in Table 2. The mean differences in all Bland-
Almand analysis were close to zero, suggesting that appropriate intra-rater and inter-
rater reliability. Inter-rater performances of SMD at the 95% confidence intervals
showed large variability, would indicate error and suggesting that SMD assessment is
reliable but not precise (Table 2).
The scatter diagram (Figure 2. A) shows a moderate positive correlation between HP
and the SMD (r=0.44, p=0.001, n=53).
Chronic cervico-craniofacial pain patients
The ICC value for intra-rater reliability of single measures separated by a space of 48
hours was 0.88 for HP and 0.79 for SMD. When the singles measures were separated
by a space of 9 days, the ICC value for intra-rater reliability was 0.81 for HP and 0.76
for SMD. Descriptive statistics, ICCs and associated 95% CIs, SEMs and MDC90
between trials are presented in Table 3.
The Bland-Almand analysis for the intra-rater performances are shown for
assessement of HP and SMD in Table 4. The mean differences in all Bland-Almand
analysis were close to zero, suggesting that appropriate intra-rater and inter-rater
reliability. Inter-rater performances of SMD at the 95% confidence intervals showed
large variability, would indicate error and suggesting that SMD assessment is reliable
but not precise. (Table 4).
The scatter diagram (Figure 2. B) shows a moderate positive correlation between HP
and the SMD (r=0.56, p<0.001, n=60). No statistically significant correlations
between the HP and SMD with the disabilities variables. Neck disability is strong
positively correlated with the craniofacial disability (r=0.79, p<0.001, n=60).

13
Asymptomatic subjects versus chronic cervico-craniofacial pain patients
The independent t-test for comparison between the asymptomatic and symptomatic
samples, using the mean of the trial 1 and 2 (separated by 48 hours), found
statistically significant differences for HP and SMD (p<0.05). Descriptive statistics,
mean differences and associated 95% CIs between the two samples are presented in
Table 5.
DISCUSSION
The evaluation of HP is a variable to consider evaluating in clinical practice due to its
influence on the pathophysiology of the cervical region.[4, 30] Our results show
strong intra- and inter-rater reliability when measuring HP with the CROM device. As
for the examination of the SMD, results obtained with the Digital Calliper reflected
strong reliability.
Recently, several studies have measured HP using different methods and
instruments,[1, 11–13] but disadvantages were low reliability,[11, 31] high cost, and
difficulty in transporting the equipment.[13, 32, 33] Furthermore, where a
radiological diagnosis was used, the risk of radiation exposure to the subject must be
considered.
In the literature we found only one study in which the intra- and inter-rater
reliabilities were evaluated in measuring HP using CROM; results showed a good
intra and inter-rater reliability.[14] If we compare this data with our own, we find
strong intra-rater reliability in both investigations, while our inter-rater reliability was
superior to that obtained by Garrett et al.[14] for asymptomatic subjects but not for
CCFP patients. Both investigations followed a rigorous standardized protocol using
similar samples. An important aspect to note is that the time did not influence the

14
intra-rater reliability and the results were very similar at 48 hours and 9 days later. It
has been suggested that a range of 2 to 14 days is generally acceptable for analyzing
test reliability.[34]
As we mentioned, the SMD measured by the Digital Calliper showed high intra-rater
reliability where it showed acceptable inter-rater reliability. Again, we find only one
article that mentions the SMD, but that investigation was designed to generate a
prediction rule for the degree of difficulty when performing a laryngoscopy.[15, 16]
The SMD measurement used in a study by Al Ramadhani et al.[15], was of 142.8
(SD=1.50), whereas we found SMD to be between 107.5 and 113.57 of our study.
This difference could be explained by the fact that their measurement protocol was
performed measuring the cervical extension. It is also worth mentioning that the
measure was performed using a ruler with an accuracy of 5 mm rather than a Digital
Calliper with a resolution of 0.01 mm. We feel this fact supports a contention that our
investigation is more rigorous and reliable.
We found the intra-rater MDC of HP varied from 1.27 cm to 1.74 cm but that the
inter-rater MDC was between 0.96 cm and 1.30 cm. We also found that the intra-rater
MDC of the SMD was between 3.76 mm and 14.55 mm while the inter-rater MDC
was between 16.13 mm and 16.47 mm. Is considered MDC the smallest quantity
above the SEM, although it should not be assumed that this change has reached the
threshold of clinically significant improvement.[35]
With regard to the comparison of the means of the 2 measurements of the
craniocervical posture, the results show that there are statistically significant
differences between both groups, with higher measures in the group of CCFP,
however you have to take into account that the differences are very small and exceed
slightly the MDC in the HP measurement (mean difference -1.27 cm), nor for the

15
SMD (mean difference -5.01 mm), other studies have found similar results to ours,
finding very small differences between measurements of craniocervical posture in
asymptomatic subjects versus symptomatic subjects with neck pain [30] and
TMD.[36] We did not find association between measurements of craniocervical
posture and disability variables, this result is supported by recent evidence [36, 37],
being this issue controversial.[38] We have found a strong correlation between neck
disability and craniofacial disability (r=0.79), other studies have also found similar
results to our findings. [20, 36]
Furthermore, the Pearson correlation coefficient between HP and the SMD is 0.447
for asymptomatic subject and 0.56 for symptomatic subjects, suggesting a moderate
correlation. We believe this is the first study to determine this association; we found
that the previous studies measuring the SMD do not correlate it to HP. Thus, we can
assume that there is a relationship between HP in the sitting position and SMD in
supine position in healthy subjects.
Limitations
This study has several limitations that must be discussed. We agree with Garret et
al.[14] that a limitation exists in the head arm of the CROM in that it is marked in
increments of 0.5 cm, making it hard to determine a measurement when the indicator
is between two marks. We believe that the reliability and data collection could be
improved if the head arm was marked in mm. Lastly, we calculated the MDC but not
the minimal clinically relevant change (MCRC), which we believe is of special
interest in clinical practice. We must remember that the MDC is not the same as the
MCRC, which is the grade of clinically significant improvement and is normally
associated with an external criteria that indicates when that change has occurred.[35]
We have not calculated the MCRC, so we do not know the grade of clinically

16
significant improvement. Future randomized controlled trials should identify
interventions that influence the HP and SMD, this could help assess the performance
of this test when subjected to clinical interventions and also with those results could
calculate the MCRC.
CONCLUSIONS
The CROM and the Digital Calliper are reliable instruments for measuring HP and the
SMD in healthy subjects and CCFP patients. Furthermore, there is a moderate
correlation between HP and the SMD and strong correlation between neck disability
and craniofacial disability. We did not find association between measurements of
craniocervical posture and disability variables. We also believe further studies should
consider the MCRC and the influence of longer periods between examinations on the
measures.

17
REFERENCES
1. Silva AG, Johnson MI (2012) Does forward head posture affect postural control in
human healthy volunteers? Gait Posture. doi: 10.1016/j.gaitpost.2012.11.014
2. Seghers J, Jochem A, Spaepen A (2003) Posture, muscle activity and muscle
fatigue in prolonged VDT work at different screen height settings. Ergonomics
46:714–30. doi: 10.1080/0014013031000090107
3. Enwemeka CS, Bonet IM, Ingle JA, et al. (1986) Postural Correction in Persons
with Neck Pain (II. Integrated Electromyography of the Upper Trapezius in
Three Simulated Neck Positions). J Orthop Sports Phys Ther 8:240–2.
4. Bonney RA, Corlett EN (2002) Head posture and loading of the cervical spine.
Appl Ergon 33:415–7.
5. Cheung Lau HM, Wing Chiu TT, Lam T-H (2009) Clinical measurement of
craniovertebral angle by electronic head posture instrument: a test of reliability
and validity. Man Ther 14:363–8. doi: 10.1016/j.math.2008.05.004
6. Fernández-de-Las-Peñas C, Cuadrado ML, Pareja JA (2006) Myofascial trigger
points, neck mobility and forward head posture in unilateral migraine.
Cephalalgia 26:1061–70. doi: 10.1111/j.1468-2982.2006.01162.x
7. Cimbiz A, Beydemir F, Manisaligil U (2006) Evaluation of Trigger Points in
Young Subjects. J Musculoskelet Pain 14:27–35.
8. Braun BL (1991) Postural differences between asymptomatic men and women and
craniofacial pain patients. Arch Phys Med Rehabil 72:653–6.
9. Haughie LJ, Fiebert IM, Roach KE (1995) Relationship of forward head posture
and the cervical backward bending to neck pain. J Man Manip Ther 3:91–7.
10. Hanten WP, Olson SL, Russell JL, et al. (2000) Total head excursion and resting
head posture: normal and patient comparisons. Arch Phys Med Rehabil 81:62–6.
11. Silva AG, Punt TD, Johnson MI (2010) Reliability and validity of head posture
assessment by observation and a four-category scale. Man Ther 15:490–5. doi:
10.1016/j.math.2010.05.002
12. Horton SJ, Johnson GM, Skinner MA (2010) Changes in head and neck posture
using an office chair with and without lumbar roll support. Spine (Phila Pa 1976)
35:E542–8. doi: 10.1097/BRS.0b013e3181cb8f82
13. Gadotti IC, Magee D (2013) Assessment of intrasubject reliability of radiographic
craniocervical posture of asymptomatic female subjects. J Manipulative Physiol
Ther 36:27–32. doi: 10.1016/j.jmpt.2012.12.009

18
14. Garrett TR, Youdas JW, Madson TJ (1993) Reliability of measuring forward head
posture in a clinical setting. J Orthop Sports Phys Ther 17:155–60.
15. Al Ramadhani S, Mohamed LA, Rocke DA, Gouws E (1996) Sternomental
distance as the sole predictor of difficult laryngoscopy in obstetric anaesthesia.
Br J Anaesth 77:312–6.
16. Khan ZH, Mohammadi M, Rasouli MR, et al. (2009) The diagnostic value of the
upper lip bite test combined with sternomental distance, thyromental distance,
and interincisor distance for prediction of easy laryngoscopy and intubation: a
prospective study. Anesth Analg 109:822–4. doi:
10.1213/ane.0b013e3181af7f0d
17. Kottner J, Audige L, Brorson S, et al. (2011) Guidelines for Reporting Reliability
and Agreement Studies (GRRAS) were proposed. Int J Nurs Stud 48:661–71.
doi: 10.1016/j.ijnurstu.2011.01.016
18. Walter SD, Eliasziw M, Donner A (1998) Sample size and optimal designs for
reliability studies. Stat Med 17:101–10.
19. La Touche R, París-Alemany A, Mannheimer JS, et al. (2013) Does mobilization
of the upper cervical spine affect pain sensitivity and autonomic nervous system
function in patients with cervico-craniofacial pain?: A randomized-controlled
trial. Clin J Pain 29:205–15. doi: 10.1097/AJP.0b013e318250f3cd
20. La Touche R, Pardo-Montero J, Gil-Martínez A, et al. (2014) Craniofacial pain
and disability inventory (CF-PDI): development and psychometric validation of
a new questionnaire. Pain Physician 17:95–108.
21. Dworkin SF, LeResche L (1992) Research diagnostic criteria for
temporomandibular disorders: review, criteria, examinations and specifications,
critique. J Craniomandib Disord 6:301–55.
22. Andrade Ortega JA, Delgado Martínez AD, Almécija Ruiz R (2010) Validation of
the Spanish version of the Neck Disability Index. Spine (Phila Pa 1976)
35:E114–8. doi: 10.1097/BRS.0b013e3181afea5d
23. Greenhalgh S, Selfe J (2009) A qualitative investigation of Red Flags for serious
spinal pathology. Physiotherapy 95:224–7. doi: 10.1016/j.physio.2009.04.006
24. Portney LG WM. (2009) Foundations of Clinical Research; Applications to
Practice. New Jersey
25. Bland JM, Altman DG (1986) Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet 1:307–10.
26. Weir JP (2005) Quantifying test-retest reliability using the intraclass correlation
coefficient and the SEM. J Strength Cond Res 19:231–40. doi: 10.1519/15184.1

19
27. Mokkink LB, Terwee CB, Patrick DL, et al. (2010) The COSMIN study reached
international consensus on taxonomy, terminology, and definitions of
measurement properties for health-related patient-reported outcomes. J Clin
Epidemiol 63:737–45. doi: 10.1016/j.jclinepi.2010.02.006
28. Haley SM, Fragala-Pinkham MA (2006) Interpreting change scores of tests and
measures used in physical therapy. Phys Ther 86:735–43.
29. Hinkle D, Jurs S, Wiersma W (1988) Applied statistics for the behavioral
sciences, 2nd ed. Houghton Mifflin, Boston
30. Silva AG, Punt TD, Sharples P, et al. (2009) Head posture and neck pain of
chronic nontraumatic origin: a comparison between patients and pain-free
persons. Arch Phys Med Rehabil 90:669–74. doi: 10.1016/j.apmr.2008.10.018
31. Juul-Kristensen B, Hansson GA, Fallentin N, et al. (2001) Assessment of work
postures and movements using a video-based observation method and direct
technical measurements. Appl Ergon 32:517–24.
32. Harrison DE, Haas JW, Cailliet R, et al. (2005) Concurrent validity of flexicurve
instrument measurements: sagittal skin contour of the cervical spine compared
with lateral cervical radiographic measurements. J Manipulative Physiol Ther
28:597–603. doi: 10.1016/j.jmpt.2005.08.012
33. Van Niekerk S-M, Louw Q, Vaughan C, et al. (2008) Photographic measurement
of upper-body sitting posture of high school students: a reliability and validity
study. BMC Musculoskelet Disord 9:113. doi: 10.1186/1471-2474-9-113
34. Streiner DL, Norman GR (1989) Health Measurement Scales: a Guide to Their
Development and Use. Oxford Oxford Univ. Press
35. Fletcher JP, Bandy WD (2008) Intrarater reliability of CROM measurement of
cervical spine active range of motion in persons with and without neck pain. J
Orthop Sports Phys Ther 38:640–5. doi: 10.2519/jospt.2008.2680
36. Armijo-Olivo S, Rappoport K, Fuentes J, et al. (2011) Head and cervical posture
in patients with temporomandibular disorders. J Orofac Pain 25:199–209.
37. Cheung CH, Shum ST, Tang SF, et al. (2010) The correlation between
craniovertebral angle, backpack weights, and disability due to neck pain in
adolescents. J Back Musculoskelet Rehabil 23:129–36. doi: 10.3233/BMR-2010-
0259
38. Lau KT, Cheung KY, Chan KB, et al. (2010) Relationships between sagittal
postures of thoracic and cervical spine, presence of neck pain, neck pain severity
and disability. Man Ther 15:457–62. doi: 10.1016/j.math.2010.03.009

20
FIGURES AND LEGENDS
Figure 1. A) Placement of CROM with the head arm for the measure of Head Posture
with the vertebra locator. B) Evaluator taking measure from the jugular notch of the
sternum to the chin protuberance to quantitative the Sternomental Distance.

21
Figure 2. Scatter Diagram showing correlation between Head Posture and the
Sternomental Distance. A) Scatter diagram for asymptomatic subjects (n=53); B)
scatter diagram for chronic cervico-craniofacial pain patients (n=60).

22
Table 1. Intra-rater and Inter-rater reliability and descriptive statistics for
measurements in asymptomatic subjects.
Abbreviations: CI, confidence interval; ICC 3,1, intraclass correlation coefficient,
model 3,1; HP, head posture; MDC90, minimal detectable change at the 90%
confidence level; SMD, sternomental distance; SD, standard deviation; SEM,
standard error of the measurement.
Rater A Rater B
Trial 1
(Mean
± SD)
Trial 2
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90 Trial 1
(Mean
± SD)
Trial 2
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90
HP (cm) 18.97 ±
2.47
19.07
± 2.19
0.93 0.88 –
0.96
0.60 1.40 18.77
± 2.35
18.96
± 2.19
0.93 0.89 –
0.96
0.55 1.30
SMD
(mm)
108.50
± 16.55
109.03
±
16.14
0.99
0.98 –
0.99
1.61 3.76 105.07
±
14.55
107.54
±
14.21
0.95 0.85 –
0.97
2.75 6.42
Trial 1
Trial 2
Rater A
(Mean
± SD)
Rater
B
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90 Rater
A
(Mean
± SD)
Rater
B
(Mean
± SD)
ICC
3,1
95%
CI for
ICC
SEM MDC90
HP (cm) 18.97 ±
2.47
18.77
± 2.35
0.94 0.90 –
0.96
0.56 1.30 19.07
± 2.19
18.96
± 2.19
0.96 0.93 –
0.98
0.41 0.96
SMD
(mm)
108.50
± 16.55
105.07
±
14.55
0.78 0.63 –
0.87
7.06 16.47 109.03
±
16.14
107.54
±
14.21
0.79 0.66 –
0.87
6.91 16.13

23
Table 2. Statistical metrics from Bland-Altman analysis of the intra-rater and inter-
rater measurements in asymptomatic subjects.
Intra-rater
Rater A Rater B
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
HP (cm) -0.10 ± 0.85 -0.34 to 0.15 -1.76 to 1.57 -0.19 ± 0.79 -0.41 to 0.04 -1.73 to 1.36
SMD (mm) -0.53 ± 2.28 -1.18 to 0.12 -4.99 to 3.94 -2.47 ± 3.89 -3.58 to -1.37 -10.10 to 5.16
Inter-rater
Trial 1 Trial 2
HP (cm)
0.19 ± 0.79 -0.03 to 0.42 -1.35 to 1.74 0.10 ± 0.59 -0.06 to 0.27 -1.05 to 1.25
SMD (mm) 3.43 ± 9.99 0.59 to 6.27 -16.14 to 23 1.49 ± 9.78 -1.29 to 4.26 -17.68 to 20.65
Abbreviations: CI, confidence interval; HP, head posture; LOA, limits of agreement;
SMD, sternomental distance; SD, standard deviation.

24
Table 3. Intra-rater reliability and descriptive statistics for measurements in chronic
cervico-craniofacial pain patients.
Abbreviations: CI, confidence interval; ICC 3,1, intraclass correlation coefficient,
model 3,1; HP, head posture; MDC90, minimal detectable change at the 90%
confidence level; SMD, sternomental distance; SD, standard deviation; SEM,
standard error of the measurement.
Rater A
Trial 1
(Mean
± SD)
Trial 2
(Mean
± SD)
Trial 3
(Mean
± SD)
48 hours between trials
(Trial 1-Trial 2)
9 days between trials
(Trial 2-Trial 3)
ICC
3,1
95% CI
for ICC
SEM MDC90 ICC
3,1
95% CI
for ICC
SEM MDC90
HP (cm) 20.40 ±
1.50
20.23
± 1.58
20.03 ±
1.84
0.88 0.80 –
0.92
0.54 1.27 0.81 0.70 –
0.88
0.75 1.74
SMD
(mm)
111.53
± 12.41
113.57
±
11.83
112.73
± 13.78
0.79
0.67 –
0.87
5.60 13.07 0.76 0.63 –
0.85
6.24 14.55

25
Table 4. Statistical metrics from Bland-Altman analysis of the intra-rater
measurements in chronic cervico-craniofacial pain patients.
Intra-rater
48 hours (Trial 1 – Trial 2) 9 days (Trial 2 – Trial 3)
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
Mean
differences
± SD
95% CI for
mean
differences
LOA (Lower
limit-Upper
limit)
HP (cm) 0.17 ± 0.77 -0.03 to 0.37 -1.34 to 1.67 0.21 ± 1.06 -0.06 to 0.48 -1.86 to 2.28
SMD (mm) -2.03 ± 7.92 -4.08 to 0.01 -17.56 to 13.49 0.83 ± 8.82 -1.45 to 3.11 -16.46 to 18.12
Abbreviations: CI, confidence interval; HP, head posture; LOA, limits of agreement;
SMD, sternomental distance; SD, standard deviation.

26
Table 5. Comparison between the asymptomatic subjects and chronic cervico-
craniofacial pain patients samples for measurements.
Asymptomatic
subjects (Mean ± SD)
CCFP patients (Mean
± SD)
Mean differences (95% CI)
HP (cm) 18.95 ± 2.25 20.32 ± 1.49 -1.37 (-2.11 to -0.63)**
SMD (mm) 107.54 ± 14.53 112.55 ± 11.46 -5.01 (-9.92 to -0.1)*
Abbreviations: CI, confidence interval; HP, head posture; SMD, sternomental
distance; SD, standard deviation.
* p<0.05
** p<0.01

114
5.3 Estudio III
La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-Parreño S, Paris-
Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain sensitivity over the trigeminal region
in patients with chronic mechanical neck pain. J Pain. 2010 Mar;11(3):256-63
Objetivos del estudio
El objetivo del presente estudio fue investigar la sensibilización del trigémino en pacientes con
dolor de cuello crónico mecánico, además se observaron la interacción de los resultados con
variables psicológicos, como la depresión y la ansiedad.
Resultado
Los resultados mostraron que los niveles de UDPS son significativamente menores
bilateralmente sobre los puntos musculares del masetero, temporal, los del trapecio superior, y
también los puntos medidos en las articulaciones cigapofisiarias de C5-C6 (P <0,001), pero no
sobre los puntos del músculo tibial anterior (P = 0,4) en pacientes con dolor de cuello crónico
mecánico, en comparación con los controles. La magnitud de la disminución de los UDPs fue
mayor en la región cervical, en comparación con la región del trigeminal (P <0,01). Los UDPs
en los músculos maseteros se correlacionaron negativamente tanto a la duración de los síntomas
de dolor y la intensidad del dolor (P <0,001). Además se encontraron correlaciones positivas
entre la intensidad de dolor con la discapacidad de cuello y los síntomas depresivos.
Conclusiones
Nuestros resultados revelaron la presencia de hiperalgesia mecánica en la región trigeminal en
pacientes con dolor de cuello crónico mecánico, lo que sugiere la difusión de la sensibilización a
la región del trigémino en esta población de pacientes. Los resultados de este estudio sugieren
que existe la presencia de un proceso de sensibilización del NCT en esta población. Este
hallazgo tiene implicaciones para el desarrollo de estrategias de gestión.

The Journal of Pain, Vol 11, No 3 (March), 2010: pp 256-263Available online at www.sciencedirect.com
Bilateral Mechanical-Pain Sensitivity Over the Trigeminal Region in
Patients With Chronic Mechanical Neck Pain
Roy La Touche,*y Cesar Fernandez-de-las-Penas,zx{ Josue Fernandez-Carnero,zx{
Santiago Dıaz-Parreno,*y Alba Paris-Alemany,*y and Lars Arendt-Nielsenz
*Faculty of Medicine, Department of Physical Therapy.yUniversity Center for Clinical Research of the Craneal-Cervical-Mandibular System, Universidad San Pablo CEU,Madrid, Spain.zDepartment of Physical Therapy, Occupational Therapy, Rehabilitation and Physical Medicine.xEsthesiology Laboratory, Universidad Rey Juan Carlos, Alcorcon, Madrid, Spain.{Centre for Sensory-Motor Interaction (SMI), Department of Health Science and Technology, Aalborg University,Aalborg, Denmark.
ReceivedAddressde Ciencs/n, 2892
1526-590
ª 2010 b
doi:10.10
256
Abstract: The aim of this study was to investigate bilateral pressure-pain sensitivity over the tri-
geminal region, the cervical spine, and the tibialis anterior muscle in patients with mechanical chronic
neck pain. Twenty-three patients with neck pain (56% women), aged 20 to 37 years old, and 23
matched controls (aged 20 to 38 years) were included. Pressure pain thresholds (PPTs) were bilaterally
assessed over masseter, temporalis, and upper trapezius muscles, the C5-C6 zygapophyseal joint, and
the tibialis anterior muscle in a blinded design. The results showed that PPT levels were significantly
decreased bilaterally over the masseter, temporalis, and upper trapezius muscles, and also the C5-C6
zygapophyseal joint (P < .001), but not over the tibialis anterior muscle (P = .4) in patients with
mechanical chronic neck pain when compared to controls. The magnitude of PPT decreases was
greater in the cervical region as compared to the trigeminal region (P < .01). PPTs over the masseter
muscles were negatively correlated to both duration of pain symptoms and neck-pain intensity (P <
.001). Our findings revealed pressure-pain hyperalgesia in the trigeminal region in patients with
mechanical chronic neck pain, suggesting spreading of sensitization to the trigeminal region in
this patient population.
Perspective: This article reveals the presence of bilateral pressure-pain hypersensitivity in the
trigeminal region in patients with idiopathic neck pain, suggesting a sensitization process of the tri-
gemino-cervical nucleus caudalis in this population. This finding has implications for development of
management strategies.
ª 2010 by the American Pain Society
Key words: Neck pain, trigeminal sensitization, pressure pain threshold.
Chronic mechanical neck pain is a significant clinicalproblem. It seems that the prevalence of neck painis as high as the prevalence of low back pain. A sys-
tematic review reported a 1-year prevalence for neckpain ranging from 16.7 to 75.1%, with a mean of37.2%.11 A best-evidence synthesis showed an incidencerate for self-reported neck pain in the general popula-tion between 146 and 213 per 1,000 patients per year.21
Nearly half of neck-pain patients develop chronic symp-
May 31, 2009; Revised June 29, 2009; Accepted July 22, 2009.reprint requests to Cesar Fernandez de las Penas, Facultadias de la Salud, Universidad Rey Juan Carlos, Avenida de Atenas2 Alcorcon, Madrid, Spain. E-mail: [email protected]
0/$36.00
y the American Pain Society
16/j.jpain.2009.07.003
toms,4 and many will continue to exhibit moderatedisability at long-term follow-up.17 The economicburden associated with the management of neck painis second only to low back pain in annual workers’ com-pensation costs in the United States.44
Although the aetiology of insidious mechanical neckpain is under debate, it is clear that neck pain is multifac-torial in nature, with both physical and psychosocial con-tributors.38 In recent years, there has been an increasinginterest in the study of nociceptive-pain processing indifferent musculoskeletal-pain conditions. For instance,pressure pain thresholds5,32 have been extensively usedfor investigating mechanical pain hypersensitivity inseveral chronic pain conditions, eg, whiplash,36 fibro-myalgia,9 unilateral migraine,14 repetitive strain injury,18
tension-type headache,13 osteoarthritis,1 low back

La Touche et al 257
pain,27 or carpal tunnel syndrome.15 Nevertheless, thephenomenon of sensory hypersensitivity has been rela-tively recently investigated in mechanical nontraumaticneck pain.37
Scott et al33 found that the hypersensitivity present inindividuals with idiopathic neck pain seems to be con-fined to the neck area with little evidence of spread tomore remote body regions, eg, the tibialis anterior mus-cle, as opposite happens in chronic whiplash. The pres-ence of hypersensitivity restricted to the neck regionmay reflect segmental local sensitization, but not wide-spread central sensitization, in patients with idiopathicneck pain.
Several studies have reported that patients with neckpain also suffered from symptoms in the orofacialregion,7,8,23 and headaches.29 The expansion of symp-toms from the neck area to the trigeminal region maybe related to the convergence of the nociceptive sec-ond-order neurons receiving both trigeminal and cervi-cal inputs into the trigemino-cervical nucleus caudalisin the spinal gray matter of the spinal cord.25 To thebest of our knowledge, no previous study has investi-gated the pressure hypersensitivity over the trigeminalregion in chronic mechanical neck pain. Further, Rhudyand Meagher31 demonstrated that psychological states,particularly anxiety and depression, induce an increasedeffect on pressure-pain sensitivity. Therefore, the aim ofthe present study was to investigate trigeminal sensitiza-tion in patients with chronic mechanical neck pain con-trolling psychological aspects, such as depression andanxiety.
Methods
SubjectsPatients presenting with mechanical insidious neck
pain referred by their primary-care physicians to a spe-cialized physical-therapy clinic between September2007 and February 2008 were screened for possible eligi-bility criteria. Mechanical neck pain was defined as gen-eralized neck and/or shoulder pain with symptomsprovoked by neck postures, neck movement, or palpa-tion of the cervical musculature. Symptoms had to be bi-lateral and present for at least 6 months. Patients wereexcluded if they exhibited any of the following: 1) unilat-eral neck pain; 2) diagnosis of fibromyalgia;43 3) previouswhiplash; 4) cervical spine surgery; 5) clinical diagnosis ofcervical radiculopathy or myelopathy; 6) history of previ-ous physical-therapy intervention for the cervical region;7) presence of severe degenerative arthritis (confirmedby cervical radiography taken for all patients over theage of 30 years); 8) less than 18 years; 9) diagnosis ofany TMD, according to the Research Diagnostic Criteriafor TMD (RDC/TMD)10; or 10) concomitant diagnosis ofprimary headache.
Demographic and Clinical DataDemographic data including age, gender, height,
weight, location, and nature of the symptoms was col-lected. An 11-point numerical point rate scale22 (NPRS;
0 = no pain, 10 = maximum pain) was used to assess cur-rent level of neck pain. Patients also completed the NeckDisability Index (NDI) to measure perceived disability,42
the Beck Depression Inventory (BDI-II) to assess symp-toms of depression,2 and the State-Trait Anxiety Inven-tory (STAI) for assessing state and trait anxiety.34
The NDI consist of 10 questions measured on a 6-pointscale (0 = no disability, 5 = full disability).42 The numericscore for each item is summed for a score varying from0 to 50, where higher scores reflect greater disability.The NDI has demonstrated to be a reliable (intraclass cor-relation coefficients ranging from .50 to .98)24 and validself-assessment of disability in chronic neck pain.19,39
The BDI-II is a 21-item self-report measure assessingaffective, cognitive, and somatic symptoms of depres-sion.2 Patients choose from a group of sentences thatbest describe how they have been feeling in the past 2weeks. Higher scores indicate higher levels of depressivesymptoms.2 The BDI-II showed good internal consistency(alpha coefficient .90) and adequate divergent validity.41
The STAI is a self-report assessment device whichincludes separate measures of state and trait anxiety.34
In the present study, the trait-anxiety subscale whichdenotes relatively stable anxiety proneness and refersto a general tendency to respond with anxiety to per-ceived threats in the environment was used. Participantsuse a 4-point response scale ranging from ‘‘almost never’’to ‘‘almost always’’, indicating the extent to which theyexperience each emotion. The State-Trait questionnairehas shown good internal consistency (a = .83). Higherscores indicate greater trait anxiety.34
Finally, healthy controls were recruited from volunteerwho responded to a local announcement and were ex-cluded if they exhibited a history of neck, facial, orhead pain (infrequent episodic tension-type headachewas permitted), any systemic disease or any history oftraumatic event (whiplash).
The study was conducted in accordance with the Hel-sinki Declaration, and all subjects provided informed con-sent which was approved by the local ethics committee.
Sample Size DeterminationThe sample-size determination and power calculations
were performed with an appropriate software (Tamanode la Muestra, v.1.1, Universidad de Medicina, Madrid,Spain). The calculations were based on detecting, atthe least, significant clinical differences of 20% on pres-sure pain threshold (PPT) between both groups,28 withan alpha level of .05 and a desired power of 80%, andan estimated interindividual coefficient of variation forPPT measures of 20%. This generated a sample size ofat least 16 participants per group.
PPT AssessmentPPT is defined as the minimal amount of pressure
where a sensation of pressure first changes to pain.40 Amechanical pressure algometer (Pain Diagnosis andTreatment Inc, Great Neck, NY) was used in this study.The device consists of a round rubber disk (1 cm2)attached to a pressure gauge. The gauge displays values

258 Trigeminal Pain Sensitivity in Neck Pain
in kg/cm2, ranging from 0 to 10 kg. The mean of 3 trials(intraexaminer reliability) was calculated and used forthe main analysis. A 30-second resting period wasallowed between each trial. The reliability of pressure al-gometry has been found to be high in both asymptom-atic subjects6 (ICC .91 [95% CI .82–.97]) and neck painpatients45 (ICC .78–.93; 95% CI .53–.97).
Study ProtocolThe study protocol was the same for neck-pain pa-
tients and healthy controls. All examinations weredone in a quiet, draught-free, temperature- and humid-ity-controlled laboratory (24�C 6 1�C, relative humidity25–35%). All participants were restricted from vigorousexercise from the day prior to the examination. Noneof the patients were taking any preventive drug at thetime the study was performed. Participants were not al-lowed to take analgesics or muscle relaxants throughthe 72 hours prior to the examination. PPTs were mea-sured bilaterally over masseter and temporalis muscles,the articular pillar of C5-C6 zygapophyseal joint (basedon palpation of C6-C7 spinous processes), the upper tra-pezius muscle (midway between C7 and acromion), andtibialis anterior muscle (upper one-third of the musclebelly) by an assessor blinded to the subject’s condition.The masseter and temporalis muscles were chosen as tri-geminal areas, the articular pillar of C5-C6 and the uppertrapezius muscle were chosen as the most common sitesof involvement in idiopathic neck pain, and the tibialisanterior was chosen as a remote distant site. The orderof assessment was randomized between the participants.
Pressure Pain Threshold DataManagement
In the current study, the magnitude of sensitizationwas investigated by assessing the differences of absoluteand relative PPT values between both groups. For rela-tive values, we calculated a ‘‘PPT Index,’’ dividing thePPT of each patient at each point by the mean of PPTscore of the control group at the same point. PPT indiceswere only calculated in those PPT levels significantly dif-ferent between patients and controls. A greater PPT In-dex (%) indicates lower degree of sensitization.
Statistical AnalysisData were analysed with the SPSS statistical package
(SPSS v.16.0; SPSS, Inc, Chicago, IL). Results are expressedas mean, standard deviation (SD), and 95% confidenceinterval (95% CI). The Kolmogorov-Smirnov test wasused to analyze the normal distribution of the variables(P > .05). Quantitative data without a normal distribution(ie, pain history, current level of pain, and NDI) were an-alyzed with nonparametric tests, whereas data witha normal distribution (PPT levels, BDI-II, and STAI) wereanalyzed with parametric tests. The intraclass correlationcoefficient (ICC) was used to evaluate the intraexaminerreliability of PPT data. A 2-way ANCOVA was used to in-vestigate the differences in PPT assessed over each point(masseter, temporalis, upper trapezius, tibialis anteriormuscles, and the C5-C6 zygapophyseal joint) with side
(dominant or nondominant) as within-subject factorand group (patients or controls) as the between-subjectfactor. A 2-way ANCOVA test was used for assessing thedifferences in PPT Index with side (dominant, nondomi-nant) as within-patient factor, point (masseter, tempora-lis, upper trapezius, tibialis anterior muscles, and theC5-C6 joint) as between-patient factor, and age, sex,BDI-II, and STAI scores as covariates. Post hoc compari-sons were conducted with the Bonferroni test. Finally,the Spearman’s rho (rs) test was used to analyze the asso-ciation between PPTs and the clinical variables relating tosymptoms, disability, anxiety, and depression. The statis-tical analysis was conducted at a 95% confidence leveland a P value less than .05 was considered statisticallysignificant.
Results
Demographic and Clinical Data of thePatients
Forty consecutive patients presenting with neck painbetween January and May 2009 were screened for possi-ble eligibility criteria. Seventeen patients were excluded:concomitant diagnosis RDC/TMD (n = 8), migraine (n = 5),and previous whiplash (n = 4). Finally, 23 patients (10men and 13 women) with mechanical neck pain, aged20 to 37 years (mean, 28 6 5 years; mean weight, 70 6
10 kg; mean height, 168 6 10 cm), and 23 matched con-trols, aged 20 to 38 years old (mean, 28 6 6 years; meanweight, 66 6 11 kg; mean height, 168 6 9 cm) were in-cluded. No significant differences between both groupsfor age (P = .9), weight (P = .3) and height (P = .8) werefound. Patients with neck pain showed greater levels(P < .001) of depression (BDI-II, 7.5 6 3) and anxiety(STAI, 22.4 6 3.2) as compared to controls (BDI-II, 3 6 3;STAI, 10 6 8, respectively).
Within the patient group, mean duration of neck painhistory was 10 6 4.6 months (95% CI 7.8–11.7 months),the mean intensity (NPRS) of neck pain was 3.6 6 1.5(95% CI 3.2–4.8), the mean NDI was 18.5 6 3.3 (95% CI17–20), the mean BDI-II was 7.5 6 1.6 (95% CI 6–9), andthe STAI was 22 6 3 (95% CI 21–24). Furthermore, posi-tive correlations between duration of pain history withcurrent level of pain (rs = .55, P = .007 [Fig 1A]) andBDI-II (rs =.58, P = .004 [Fig 1B]) were found: the longerthe duration of the symptoms, the greater the intensityof the perceived pain and the greater the self-reporteddepression. Further, current level of pain was also posi-tively correlated to disability (rs = .57, P = .004 [Fig 2A])and to BDI-II (rs = .64; P = .001, [Fig 2B]): the greater theintensity of the perceived pain, the greater the self-re-ported disability and the greater the self-reporteddepression.
Pressure Pain Sensitivity Over theTrigeminal Region
The intraexaminer repeatability of PPTreadings for themasseter and temporalis muscle was .9 and .92 for themost painful side and .91 for the contralateral side. Thestandard error of measurement (SEM) was .14 kg/cm2

Figure 1. Scatter plots of relationships between duration of history of neck pain and NPRS values (A) and between history ofneck pain and Beck Depression Inventory (B) A positive linear regression line is fitted to the data (NPRS: numerical pain rate scale,range 0 to 10).
La Touche et al 259
for the most painful side and .11 kg/cm2 for the contra-lateral side.
The ANOVA revealed significant differences betweenboth groups, but not between sides, for PPT levels overthe masseter (group: F = 257.3, P < .001; side: F = .58,P = .447) and temporalis (group: F = 124.8, P < .001;side: F = .06, P = .803) muscles. Over both muscles, pa-tients showed bilateral lower PPT levels than healthycontrols (P < .001). Table 1 summarizes PPT assessedover the masseter and temporalis muscles for both sideswithin each study group.
Pressure Pain Sensitivity Over theCervical Region
The intraexaminer repeatability of PPT over the C5-C6joint and the upper trapezius muscle was .91 for the mostpainful side and .89 for the contralateral side, respec-tively. The SEM was .11 and .13 kg/cm2 for the most pain-ful side and .15 kg/cm2 for the contralateral side.
The ANOVA revealed significant differences betweenboth groups, but not between sides, for PPT levels overthe upper trapezius muscle (group: F = 355.9, P < .001;side: F = .03, P = .851), and the C5-C6 zygapophyseal joint(group: F = 291.5, P < .001; side: F = .08, P = .776). Again,
Figure 2. Scatter plots of relationships between duration of NPRS pvalues and Beck Depression Inventory (B) A positive linear regression0 to 10).
patients showed bilateral lower PPT levels in both pointsas compared to healthy controls (P < .001). Table 1 showsPPT over the upper trapezius muscle and the C5-C6 zyga-pophyseal joint for both sides within each group.
Pressure Pain Sensitivity Over the TibialisAnterior Muscle
The intraexaminer repeatability of PPT over tibialis an-terior muscle was .93 for the most painful side and .91 forthe contralateral side, whereas the SEM was .18 and .2kg/cm2, respectively.
The ANOVA did not find significant differencesbetween groups and sides for PPT levels over the tibialisanterior muscle (group: F = 1.49, P = .461; side: F = .05, P =.824). Table 1 shows PPT over the tibialis anterior musclefor both sides within each group.
There was no effect of age, BDI-II, or STAI score on PPTlevels (P > .2), although there was an effect of sex at thetibialis anterior with females having lower PPTs (F = 8.8,P = .005) than males.
Pressure Pain Threshold IndicesThe ANOVA revealed significant differences for PPT
indices between sites (F = 8.7, P < .001), but not between
ain values and Neck Disability Index (A) and between NPRS painline is fitted to the data (NPRS: numerical pain rate scale, range

Table 1. Pressure Pain Thresholds (PPTs) in Patients With Mechanical Neck Pain (n = 23) andMatched Control Subjects (n = 23). Mean Values 6 Standard Deviation and 95% ConfidenceIntervals in Parenthesis (kg/cm2)
MECHANICAL NECK PAIN HEALTHY CONTROLS
DOMINANT SIDE NON-DOMINANT SIDE DOMINANT SIDE NON-DOMINANT SIDE
Trigeminal Area
Masseter* 2 6 .4 (1.8–2.2) 2 6 .5 (1.8–2.2) 3.4 6 .5 (3.2–3.6) 3.5 6 .4 (3.3–3.7)
Temporalis* 2.2 6 .5 (1.9–2.5) 2.1 6 .5 (1.9–2.4) 3.7 6 .6 (3.4–3.9) 3.6 6 .8 (3.4–3.9)
Joint
C5–C6* 1.7 6 .4 (1.5–1.9) 1.6 6 .3 (1.4–1.8) 3.2 6 .4 (3.1–3.4) 3.2 6 .6 (3.1–3.5)
Muscle
Upper trapezius* 1.8 6 .4 (1.6–2) 1.8 6 .3 (1.6–2) 3.8 6 .7 (3.6–4) 3.7 6 .5 (3.5–3.9)
Tibialis anterior 5.0 6 .8 (4.6–5.3) 5 6 .9 (4.6–5.4) 5.2 6 .7 (4.9–5.6) 5.3 6 .8 (5–5.7)
*Indicates significant difference between neck pain and control subjects (ANOVA, P < .001).
260 Trigeminal Pain Sensitivity in Neck Pain
sides (F = .03, P = .859). The post hoc analysis showedsignificant differences between both masseter and tem-poralis muscles with the upper trapezius muscle (P < .001)and between the temporalis muscles with the C5-C6 joint(P = .02). In such a way, the cervical region (upper trape-zius muscle and C5-C6 joint) showed lower PPT indices(greater degree of sensitization) compared to the tri-geminal region (masseter and temporalis muscles) forboth sides (Fig 3).
Pressure Sensitivity and Clinical Featuresin Patients with Mechanical Neck Pain
Finally, a significant negative correlation between his-tory of symptoms and PPT levels over both masseter mus-cles (dominant side: rs = –.64, P < .001 [Fig 4A];nondominant side: rs = –.42, P = .04 [Fig 4B]) was found:the longer the duration of the symptoms, the lower thePPT levels over both masseter muscles. In addition, cur-rent level of pain intensity was also negatively correlatedwith bilateral PPT levels over the masseter muscles (dom-inant side: rs = –.62, P < .001 [Fig 5A]; nondominant side:rs = –.51, P = .02 [Fig 5B]): the greater the pain intensity,the lower the bilateral PPT levels. No significant correla-tions between NDI, BDI-II, and PPT levels were found.
Figure 3. Pressure pain threshold indices in both trigeminaland cervical points. The boxes represent the mean and percen-tile scores, and the error bars represent the standard deviation.
DiscussionThis study showed bilateral pressure-pain hyperalgesia
in both the trigeminal and cervical region, but not overthe tibialis anterior muscle, in patients with mechanicalchronic neck pain as compared to healthy controls. Thedecrease in PPT levels over the trigeminal region was as-sociated with the intensity and duration of pain symp-toms, supporting a role of the peripheral nociceptiveinput as an important factor driving the developmentof spreading sensitization.
Current results of cervical, but not widespread, pressure-pain hypersensitivity in patients with idiopathic neck painare very similar to those previously found by Scott et al.33
The findings from both studies support the idea that me-chanical nontraumatic neck pain is characterized by pres-sure-pain hyperalgesia in the cervical spine, probably
reflecting peripheral nociceptor sensitization. Further-more, our study increases evidence that pressure-pain hy-peralgesia is not only restricted to cervical joints (C5–C6 orC2–C3 as previously reported) but also to cervical muscles(upper trapezius). This is expected since the upper trape-zius muscle receives nerve innervation from the C2–C4level. Nevertheless, lower PPT levels over the upper trape-zius may also be related to muscle spasm residing in theneck muscles in this patient population.
The present study demonstrated that patients withmechanical chronic neck pain also have pressure-pain hy-peralgesia in the trigeminal region. This finding may re-flect a sensitization process of the trigemino-cervicalnucleus caudalis due to the convergence of inputs from

Figure 4. Scatter plot of the relationship between duration of history of neck pain and PPT levels in both dominant (A) and nondom-inant (B) masseter muscles (n = 23). A negative linear regression line is fitted to the data (PPT: pressure pain threshold, kg/cm2).
La Touche et al 261
the trigeminal and cervical regions. In fact, neck-pain pa-tients included in the current study were completelyasymptomatic in the orofacial region, which supportsthat the pressure-pain hyperalgesia found over masseterand temporalis muscles reflects a sensitization process.Nevertheless, it seems that there is a greater sensitizationdegree in the cervical spine. This is supported by the factthat the magnitude of PPT changes was higher over theupper trapezius muscle (48–49%) and C5-C6 zygapophy-seal joint (51–53%) when compared to the magnitude ofPPT changes over the masseter (57–58%) and temporalis(60%) muscles. Nevertheless, there is no consensus aboutthe PPT that are needed to consider differences as realchanges.37 Different studies6,35,45 have suggested thatdifferences ranging from 123 kPa to 200 kPa (1.2–2 kg)are needed to consider real differences. In the currentstudy, differences between trigeminal (1.4–1.5 kg) andcervical regions (1.5–2 kg) were placed within this inter-val, so differences between both groups can be consid-ered as real.
Our results increase the evidence that nontraumaticneck pain is characterized by segmental, but not wide-spread, sensitization mechanisms that are mostlyrestricted to the trigemino-cervical region. The involve-ment of segmental sensitization mechanisms has beenreported in several local pain syndromes, eg repetitivestrain injury,18 chronic tension-type headache,13 low
Figure 5. Scatter plot of the relationship between duration of NPRinant (B) masseter muscles (n = 23). A negative linear regression line
back pain,27 osteoarthritis,1 carpal tunnel syndrome,15
and unilateral shoulder pain.16 The existence of sensiti-zation mechanisms in local pain syndromes suggeststhat sustained peripheral noxious input to the centralnervous system plays a role in the initiation and mainte-nance of sensitization process.26 This is supported by thefact that central sensitization is a dynamic conditioninfluenced by multiple factors, including activity of pe-ripheral nociceptive inputs.20 For instance, in insidiousmechanical neck pain, where there is no sudden nocicep-tive barrage to the central nervous system as in patientswith whiplash syndrome, a prolonged, continued noci-ceptive barrage from different cervical structures, eg,muscles12 or facet joints,3 may be capable of leading toimpairment in the nociceptive processing of the trige-mino-cervical nucleus caudalis. This was supported bythe fact that duration of symptoms was positively relatedto current level of pain and PPT levels over the massetermuscle. On the contrary, Scott et al33 found that durationof pain symptoms was not related to PPT levels over thecervical spine. It should be considered that patients in-cluded in the study by Scott et al have a greater durationof symptoms (mean: 51.5 6 40 months), were more dis-abled (NDI: 29 ± 16), and had greater levels of anxiety(STAI: 40.6 ± 11) than patients included in the presentstudy (duration of symptoms: 10 ± 4.6 months; NDI,18.5 6 3.3; STAI, 22.4 6 3.2), which may explain
S pain values and PPT levels in both dominant (A) and nondom-is fitted to the data (PPT: pressure pain threshold, kg/cm2).

262 Trigeminal Pain Sensitivity in Neck Pain
differences between both studies. Finally, we do notknow if sensitization mechanisms found in this studyare mediated via a deregulation of second-order neu-rons in a segmental fashion or via glia30 and other im-mune cells that reside in the trigeminal-cervical region.Future studies are needed to further elucidate the mech-anisms involved in trigemino-cervical sensitization inneck pain.
It has been suggested that anxiety and depression mayinfluence pressure-pain hypersensitivity.31 Our resultswere independent of levels of depression (BDI-II) andthe state anxiety (STAI). Additionally, patients includedin the present study showed scores < 8 points in theBDI-II, which are considered normal.2 Our results agreewith those previously reported by Scott et al33 in whichanxiety appears not to influence pressure-pain sensitivityin patients with insidious mechanical neck pain. Never-
theless, further studies investigating the influence ofpsychological factors are required.
ConclusionBilateral pressure-pain hyperalgesia was detected in
both trigeminal and cervical regions in patients with me-chanical chronic neck pain. The decrease in pressure painthresholds in the trigeminal region was associated withthe intensity and duration of the neck-pain symptoms,supporting a role of the peripheral nociceptive input asa driving factor for inducing sensitization. Our study fur-ther supports that nontraumatic neck pain shows sensiti-zation in the trigemino cervical region, which has clinicalimplications in terms of spreading symptomatology tothis body area.
References
1. Bajaj P, Bajaj P, Graven-Nielsen T, Arendt-Nielsen L: Oste-oarthritis and its association with muscle hyperalgesia: Anexperimental controlled study. Pain 93:107-114, 2001
2. Beck AT, Steer RA, Brown GK: Beck Depression Inventory,(2nded.) SanAntonio.TX,ThePsychologicalCorporation,1996
3. Bogduk N, Marsland A: The cervical zygapophysial jointsas a source of neck pain. Spine 13:610-617, 1988
4. Borghouts JA, Koes BW, Bouter LM: The clinical courseand prognostic factors of non-specific neck pain: A system-atic review. Pain 77:1-13, 1998
5. Chesterton LS, Barlas P, Foster NE, Baxter GD, Wright CC:Gender differences in pressure pain threshold in healthyhumans. Pain 101:259-266, 2003
6. Chesterson LS, Sim J, Wright CC, Foster NE: Inter-rater re-liability of algometry in measuring pressure pain thresholdsin healthy humans, using multiple raters. Clin J Pain 23:760-766, 2007
7. Ciancaglini R, Testa M, Radaelli G: Association of neckpain with symptoms of temporomandibular dysfunction inthe general adult population. Scand J Rehabil Med 31:17-22, 1999
8. De Wijer A, De Leeuw JR, Steenks MH, Bosman F: Tempo-romandibular and cervical spine disorders. Self-reportedsigns and symptoms. Spine 21:1638-1646, 1996
9. Desmeules JA, Cedraschi G, Rapiti E, Baumgartner E,Finckh A, Cohen P, Daver P, Vischer TL: Neurophysiologic ev-idence for central sensitization in patients with fibromyal-gia. Arthritis Rheum 48:1420-1429, 2003
10. Dworkin SF, LeResche L: Research diagnostic criteria fortemporomandibular disorders: Review, criteria, examina-tions and specifications, critique. J Craniomandib Disord 6:301-355, 1992
11. Fejer R, Ohm-Kyvik K, Hartvigsen J: The prevalence ofneck pain in the world population: A systematic critical re-view of the literature. Eur Spine J 15:834-848, 2006
12. Fernandez-de-las-Penas C, Alonso-Blanco C,Miangolarra JC: Myofascial trigger points in subjectspresenting with mechanical neck pain: A blinded, controlledstudy. Man Ther 12:29-33, 2007
13. Fernandez-de-las-Penas C, Cuadrado ML, Ge HY, Arendt-Nielsen L, Pareja JA: Increased peri-cranial tenderness, de-creased pressure pain threshold and headache clinical pa-rameters in chronic tension type headache patients. ClinPain 23:346-352, 2007
14. Fernandez-de-las-Penas C, Cuadrado ML, Arendt-Nielsen L, Pareja JA: Side-to-side differences in pressurepain thresholds and pericranial muscle tenderness in strictlyunilateral migraine. Eur J Neurol 15:162-168, 2008
15. Fernandez-de-las-Penas C, de la Llave-Rincon AI, Fernan-dez-Carnero J, Cuadrado ML, Arendt-Nielsen L, Pareja JA: Bi-lateral widespread mechanical pain sensitivity in carpaltunnel syndrome: Evidence of central processing in unilat-eral neuropathy. Brain 132:1472-1479, 2009
16. Ge HY, Fernandez-de-las-Penas C, Madeleine P, Arendt-Nielsen L: Screening for myofascial trigger points bilaterallyin the infraspinatus muscles in patients with unilateralshoulder pain. Eur J Pain 12:859-865, 2008
17. Gore DR, Sepic SB, Gardner GM, Murray MP: Neck pain:A long-term follow-up of 205 patients. Spine 12:1-5, 1987
18. Greening J, Lynn B: Vibration sense in the upper limb inpatients with repetitive strain injury and a group of at-riskoffice workers. Int Arch Occup Environ Health 71:29-34,1998
19. Hains F, Waalen J, Mior S: Psychometric properties of theneck disability index. J Manipul Physiol Ther 21:75-80, 1998
20. Herren-Gerber R, Weiss S, Arendt-Nielsen L, Petersen-Felix S, Stefano G, Radanov B, Curaloto M: Modulation ofcentral hypersensitivity by nociceptive input in chronicpain after whiplash injury. Pain Med 5:366-376, 2004
21. Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW,Cassidy JD, Guzman J, Cote P, Haldeman S, Ammendolia C,Carragee E, Hurwitz E, Nordin M, Peloso P: Bone and JointDecade 2000-2010 Task Force on Neck Pain and Its Associ-ated Disorders. The burden and determinants of neck painin the general population. Spine 33:S39-S51, 2008
22. Jensen MP, Turbner JA, Romano JM, Fisher L: Compara-tive reliability and validity of chronic pain intensity mea-sures. Pain 83:157-162, 1999
23. Lobbezoo F, Visscher C, Naeije M: Impaired health status,sleep disorders, and pain in the craniomandibular and cervi-cal spinal regions. Eur J Pain 8:23-30, 2004

La Touche et al 263
24. Macdemid JC, Walton DM, Avery S, Blanchard A,Etruw E, Mcalpine C, Goldsmith CH: Measurement proper-ties of the neck disability index: A systematic review.J Orthop Sports Phys Ther 39:400-417, 2009
25. Marfurt CF, Rajchert DM: Trigeminal primary afferentprojections to ‘non-trigeminal’ areas of the rat central ner-vous system. J Comp Neurol 303:489-511, 1991
26. Mendell LM, Wall PD: Responses of single dorsal cordcells to peripheral cutaneous unmyelinated fibres. Nature206:97-99, 1965
27. O’Neill S, Manniche C, Graven-Nielsen T, Arendt-Nielsen L: Generalized deep-tissue hyperalgesia in patientswith chronic low-back pain. Eur J Pain 11:415-420, 2007
28. Prushansky T, Dvir Z, Defron-Assa R: Reproducibilityindices applied to cervical pressure pain threshold mea-surements in healthy subjects. Clin J Pain 20:341-347,2004
29. Rantala MA, Ahlberg J, Suvine TI, Nissine M, Lindholm H,Savolainen A, Kononen M: Temporomandibular joint re-lated painless symptoms, orofacial pain, neck pain, head-ache, and psychosocial factors among non-patients. AcOdontol Scand 61:217-222, 2003
30. Ren K, Dubner R: Neuron-glia crosstalk gets serious: Rolein pain hyper-sensitivity. Curr Opin Anaesthesiol 21:570-579,2008
31. Rhudy JL, Meagher M: Fear and anxiety: Divergenteffects on human pain thresholds. Pain 84:65-75, 2000
32. Rolke R, Andrews Campbell K, Magerl W, Treede RD:Deep pain thresholds in the distal limbs of healthy humansubjects. Eur J Pain 9:39-48, 2005
33. Scott D, Jull G, Sterling M: Widespread sensory hyper-sensitivity is a feature of chronic whiplash-associated disor-der but not chronic idiopathic neck pain. Clin J Pain 21:175-181, 2005
34. Spielberger CD, Jacobs G, Crane R: State-Trait Personal-ity Inventory. Tampa, University of South Florida, Human Re-sources Institute, 1979
35. Sterling M, Carllson Y, Crommert L, Jull G: Are cervicalphysical outcome measures influenced by the presence ofsymptomatology. Physiother Res Int 7:113-121, 2002
36. Sterling M, Jull G, Vicenzino B, Kenardy J: Sensory hyper-sensitivity occurs soon after whiplash injury and associatedwith poor recovery. Pain 104:509-517, 2003
37. Sterling M: Testing for sensory hypersensitivity or centralhyperexcitability associated with cervical spine pain. J Ma-nipulative Physiol Ther 31:534-539, 2008
38. Sterling M: Neck pain: Much more than a psychosocialcondition. J Orthop Sports Phys Ther 39:309-311, 2009
39. Stratford PW, Riddle DL, Binkley JM, Spadoni G,Westaway MD, Padfield B: Using the Neck Disability Indexto make decisions concerning individual patients. Physi-other Canada 51:107-112, 1999
40. Vanderweeen L, Oostendorp RB, Vaes P, Duquet W: Pres-sure algometry in manual therapy. Man Ther 1:258-265, 1996
41. VanVoorhis WCR, Blumentritt TL: Psychometric proper-ties of the Beck Depression inventory-II in a clinically-identi-fied sample of Mexican American adolescents. J Child FamilyStudies 5:789-798, 2007
42. Vernon H, Mior S: The neck disability index: A study ofreliability and validity. J Manipul Physiol Ther 14:409-415,1991
43. Wolfe F, Smythe HA, Yunus MB, Bennett RM,Bombardier C, Goldenberg DL, Tugwell P, Campbell SM,Abeles M, Clark P: The American College of Rheumatology1990 criteria for clasification of fibromyalgia: Report ofthe multicenter criteria committee. Arthritis and Rheum33:160-170, 1990
44. Wright A, Mayer TG, Gatchel RJ: Outcomes of disablingcervical spine disorders in compensation injuries: A prospec-tive comparison to tertiary rehabilitation response tochronic lumbar spine disorders. Spine 24:178-183, 1999
45. Ylinen J, Nykanen M, Kautainen H, Hakkinen A: Evalua-tion of repeatability of pressure algometry on the neck mus-cles for clinical use. Man Ther 12:192-197, 2007

123
5.4 Estudio IV
La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-Díaz-Parreño S,
Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero J. Craniofacial pain and disability
inventory (CF-PDI): development and psychometric validation of a new questionnaire. Pain
Physician. 2014 Jan-Feb;17(1):95-108.
Objetivo del estudio
El propósito de este estudio es presentar el desarrollo, el análisis de la estructura factorial y
propiedades psicométricas de un nuevo cuestionario auto-administrado (Inventario de dolor y
discapacidad craneofacial; IDD-CF), dirigido a medir el dolor, la discapacidad y el estado
funcional de la mandíbula y la región craneofacial.
Resultados
La versión final del IDD-CF consta de 21 ítems, el análisis factorial exploratorio reveló dos
factores ("El dolor y la discapacidad" y "el estado funcional de mandíbula"), ambos factores con
valor propio mayor que uno, que explican 44,77% de la varianza. No se observaron efectos
suelo o techo. Se confirmó una alta consistencia interna de la IDD-CF (α de Cronbach: 0,88) y
también para las dos subescalas (0,80 a 0,86 α de Cronbach). Basándose en el resultado de CCI
=0,90 (IC del 95% 0,86 hasta 0,93) fue considerado como una excelente fiabilidad test-retest. El
EEM y el MCD se calcularon como 2,4 y 7 puntos respectivamente. En la puntuación total
IDD-CF se observó una correlación moderada con la mayoría de los cuestionarios evaluados (r
= desde 0,36 hasta 0,52) y una fuerte correlación con el IDC (r = 0,65, p <0,001). El IDC, la
EVA y la TSK-11 fueron predictores del IDD-CF.
Conclusiones
El IDD-CF mostró buenas propiedades psicométricas. Con base en los hallazgos de este estudio,
el IDD-CF se puede utilizar en la investigación y la práctica clínica para la evaluación de los
pacientes con DCF.

Background: Orofacial pain, headaches, and neck pain are very common pain conditions in the general population and might be associated in their pathophysiology, although this is not yet clarified. The development and validation of a prediction inventory is important to minimize risks. Most recent questionnaires have not focused on pain, but pain is the common symptom in temporomandibular disorders, headaches, and neck pain. It is necessary to provide tools for these conditions.
Objectives: The purpose of this study is to present the development and analysis of the factorial structure and psychometric properties of a new self-administered questionnaire (Craniofacial Pain and Disability Inventory [CF-PDI]) designed to measure pain, disability, and functional status of the mandibular and craniofacial regions.
Study Design: Multicenter, prospective, cross-sectional, descriptive survey design. A secondary analysis of the reliability of the measures was a longitudinal, observational study.
Setting: A convenience sample was recruited from a hospital and 2 specialty clinics in Madrid, Spain.
Methods: The study sample consisted of 192 heterogeneous chronic craniofacial pain patients. A sub-sample of 106 patients was asked to answer the questionnaire a second time, to assess the test-retest reliability. The development and validation of the CF-PDI were conducted using the standard methodology, which included item development, cognitive debriefing, and psychometric validation. The questionnaire was assessed for the following psychometric properties: internal consistency (Cronbach’s α); floor and ceiling effects; test-retest reliability (Intraclass Correlation Coefficient [ICC]; Bland and Altman method); construct validity (exploratory factor analysis); responsiveness (standard error of measurement [SEM] and minimal detectable change [MDC]); and convergent validity (Pearson correlation coefficient), by comparing visual analog scale (VAS), the Tampa Scale for Kinesiophobia (TSK-11), the Pain Catastrophizing Scale (PCS), the Neck Disability Index (NDI), and the Headache Impact Test-6 (HIT-6). Multiple linear regression analysis was used to estimate the strength of the associations with theoretically similar constructs.
Results: The final version of the CF-PDI consists of 21 items. Exploratory factor analysis revealed 2 factors (“pain and disability” and “jaw functional status”), both with an eigenvalue greater than one, explaining 44.77% of the variance. Floor or ceiling effects were not observed. High internal consistency of the CF-PDI (Cronbach’s α: 0.88) and also of the 2 subscales (Cronbach’s α: 0.80 – 0.86) was confirmed. ICC was found to be 0.90 (95% confidence interval [CI] 0.86 – 0.93), which was considered to be excellent test-retest reliability. The SEM and MDC were 2.4 and 7 points, respectively. The total CF-PDI score showed a moderate correlation with most of the assessed questionnaires (r = 0.36 – 0.52) and a strong correlation with the NDI (r = 0.65; P < 0.001). The NDI, VAS, and TSK-11 were predictors of CF-PDI.
Limitations: Only self-reported measures were considered for convergent validity. Future research should use physical tests to explore the clinical signs relating to pain and disability.
Prospective Evaluation
Craniofacial Pain and Disability Inventory (CF-PDI): Development and Psychometric Validation of a New Questionnaire
From: 1Department of Physiotherapy, Faculty of Health Science, The Center
for Advanced Studies University La Salle. Universidad Autónoma de Madrid, Aravaca, Madrid, Spain;
2Research Group on Movement and Behavioral Science and Study of Pain,
The Center for Advanced Studies University La Salle, Universidad
Autónoma de Madrid; 3Institute of Neuroscience and Craniofacial Pain
(INDCRAN), Madrid, Spain; 4Hospital La Paz Institute for Health Research (IdiPAZ), Madrid, Spain; 5Faculty of
Medicine, Universidad San Pablo CEU, Madrid, Spain; 6Department
of Methodology of the Behavioural Sciences, Faculty of Psychology,
Universidad Nacional de Educación a Distancia, Madrid, Spain;
7Department of Neurology, Hospital Universitario La Paz, Madrid, Spain;
8Department of Physical Therapy, Occupational Therapy, Rehabilitation
and Physical Medicine, Universidad Rey Juan Carlos, Alcorcón, Madrid,
Spain
Address Correspondence: Roy La Touche
Facultad de Ciencias de la SaludCentro Superior de Estudios
Universitarios La SalleCalle la Salle, 10
28023 Madrid SPAINEmail: [email protected]
Disclaimer: There was no external funding in the preparation of this
manuscript. Conflict of interest: Each author certifies that he or she, or a
member of his or her immediate family, has no commercial
association (i.e., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that
might pose a conflict of interest in connection with the submitted
manuscript.
Manuscript received: 06-21-2013 Accepted for publication: 08-25-2013
Free full manuscript:www.painphysicianjournal.com
Roy La Touche, PT, MSc1-3, Joaquín Pardo-Montero PhD1-3, Alfonso Gil-Martínez PT, MSc1-4, Alba Paris-Alemany PT, MSc2,3, Santiago Angulo-Díaz-Parreño MSc2,5, Juan Carlos Suárez-Falcón PhD6, Manuel Lara-Lara, MD7, and Josué Fernández-Carnero, PT, PhD2,8
www.painphysicianjournal.com
Pain Physician 2014; 17:95-108 • ISSN 1533-3159

Conclusion: The CF-PDI showed good psychometric properties. Based on the findings of this study, the CF-PDI can be used in research and clinical practice for the assessment of patients with craniofacial pain.
Key words: Craniofacial pain, temporomandibular disorders, headache, neck pain, disability, development, questionnaire, reliability, psychometric validation, minimal detectable change
Pain Physician 2014; 17:95-108
Pain Physician: January/February 2014; 17:95-108
96 www.painphysicianjournal.com
disability or dysfunction but not on pain, even though pain is the common symptom in TMD, headaches, and neck pain. Additionally, pain is been addressed by other validated scales (19).
For clinical practice and research, it is necessary to have tools to measure neck pain and the associated dis-ability (20). In addition, the development and validation of a prediction inventory allows the minimization of risks and helps prevent the development of the disease.
The purpose of this study is to present the de-velopment and analysis of the factorial structure and psychometric properties of a new self-administered questionnaire (Craniofacial Pain and Disability Inven-tory [CF-PDI]) designed to measure pain, disability, and functional status of the mandibular and craniofacial regions.
Methods
The development and validation of the CF-PDI was conducted in a standardized manner, using an accepted measure development methodology that included 3 phases (21): a) item development and identification of domains; b) pilot testing on a small number of patients with
cognitive debriefing; and c) psychometric validation.
Item DevelopmentItems were generated through a multi-step process
(21): 1) literature review; 2) patient interviews and focus group; 3) examination by the research group; 4) item writing and selection; and 5) examination of the inventory by independent
experts.
The relevant scientific literature search was con-ducted using electronic databases (Medline, Embase, CINAHL). The extracted information was related to the diagnosis, pathophysiology, comorbidities, and psycho-
Chronic orofacial pain and temporomandibular disorders (TMD) are commonly associated but may also arise from other sources (1). Orofacial
pain is a common pain condition associated with the hard and soft tissues of the face and mouth. Its prevalence in the general population is approximately 13% (2). Headache and neck pain are also 2 of the most common symptoms seen in the general population (3,4).
TMD, headaches, and neck pain are related dis-eases and share signs and symptoms (5-7). Some clinical evidence of the interconnection between the cervical spine and TMD has been demonstrated (8). Plesh et al (9) showed that 53% of patients with TMD had severe headache and 54% had neck pain. Besides, 59% with TMD reported at least 2 comorbid pains, and women reported more comorbid pain than men (9). This rela-tionship between headache and a causative disorder is a criterion for secondary headache diagnoses (10).
Although it has been suggested that TMD and headaches may be related in their pathophysiology (7,11) and that headache could be a possible risk factor for the development of neck pain (12), the pathophysi-ological mechanisms underlying these pain conditions are still not fully clarified. However, a biopsychosocial approach to the etiology, assessment, and treatment of chronic pain is widely advocated (13).
Nearly 60% of both men and women reported recent pain of moderate-to-severe intensity, with a quarter of them indicating interference or termination of work-related activities (14). Therefore, the correct diagnosis of these diseases is very important to reduce their huge economic impact (15,16).
A useful scale is the Jaw Functional Limitation Scale (JFLS), which consists of 3 constructs comprising a total of 20 items identified along a global scale (17). At present, there are no questionnaires in Spanish to as-sess these characteristics. This fact is especially relevant considering that Spain is one of the European Union countries with a high cost for these disabilities (18).
Moreover, most questionnaires have focused on

www.painphysicianjournal.com 97
Psychometric Validation of the Craniofacial Pain and Disability Inventory
social and disability factors associated with craniofacial pain. We found 5 published questionnaires that assess orofacial pain and jaw function (22-26). All of them were only validated in the English language. On the ba-sis of the existing literature, a semi-structured interview guide was developed focusing on the following 3 main areas: 1) perception of physical and psychosocial health in
relation to craniofacial pain; 2) patient-perceived physical impacts of the condition
(including impacts on general physical functioning and specific jaw function); and
3) perception of disability and pain associated with their condition.
A total of 13 patients with chronic craniofacial pain underwent the semi-structured interview and 5 patients with the same condition participated in the focus group. Both processes ended with the question: “Do you think there are any other aspects of craniofacial pain we have not discussed?” The research group proceeded to ana-lyze and compare the information extracted from semi-structured interviews, focus group, and review of the relevant literature to generate the construct concept of the CF-PDI and subsequently to write the items. A list of 30 draft items was generated. The research group then selected 22 items based on a finely structured consensus process (27) to not omit any necessary concepts.
The 22 items of the inventory were subjected to an external assessment by a group of experts in cra-niofacial pain (3 physiotherapists, one dentist, and one medical doctor). The 5 experts assessed whether each of the items had a relationship with the conditions of craniofacial pain and TMD, through a 3-level Likert scale (complete disagreement, neither agreement nor disagreement, and complete agreement).
Cognitive DebriefingCognitive debriefing of the preliminary CF-PDI
was conducted with a small number of patients to as-sess their interpretations of the questions (24 patients with craniofacial pain in the pilot test). Patients were selected from 3 different educational levels (primary school, secondary school, and university) and the total response time for all items of the CF-PDI was calculated. These patients were asked to complete the preliminary CF-PDI, and were then interviewed about its compre-hensiveness, relevance, and clarity of expression. This led to some minor alterations to the questionnaire.
Psychometric Validation
Sample/PatientsThis study employed a prospective, cross-sectional,
descriptive design. A consecutive convenience sample was recruited from outpatients of the Hospital Univer-sitario La Paz (Madrid, Spain) and 2 private clinics spe-cializing in craniofacial pain and TMD (Madrid, Spain). Patients were selected if they met all of the following criteria: 1) headache and facial pain, the diagnosis of which was made according to the guidelines of the In-ternational Classification of Headache Disorders (10); 2) headache or facial pain attributed to TMD (10), the di-agnosis of which was based on the Research Diagnostic Criteria for TMD (28,29) to classify patients with painful TMD (myofascial pain, temporomandibular joint [TMJ] arthralgia, or TMJ osteoarthritis); 3) pain history of at least 6 months prior to the study; 4) at least 18 years of age; and 5) good understanding of the Spanish language. The exclusion criteria were as follows: cogni-tive impairment; the presence of psychiatric limitations that impede participation in the study assessments; and poor knowledge of the Spanish language. To assess the test-retest reliability of the CF-PDI, a sub-sample of 106 patients whose clinical conditions were stable were asked to answer the inventory a second time, after an interval of 12 days.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee of the Hospital Universitario La Paz (PI-1241). Prior to their participation, subjects gave written informed consent.
After consenting to the study, recruited patients were given a battery of questionnaires to complete on the day of the visit. These included various self-reports for demographic and pain-related variables, including the CF-PDI to be validated, a visual analog scale (VAS) for pain intensity, and the validated Spanish versions of the Tampa Scale for Kinesiophobia (TSK-11), the Pain Catastrophizing Scale (PCS), the Neck Disability Index (NDI), and the impact associated with headache was assessed using the Headache Impact Test-6 (HIT-6). The sociodemographic questionnaire collected information about gender, date of birth, marital status, living ar-rangements, education level, and work status.
Pain intensity was measured with the VAS. The VAS consists of a 100 mm line, on the left side of which represents “no pain” and the right side represents “the worst pain imaginable.” The patients placed a mark on

Pain Physician: January/February 2014; 17:95-108
98 www.painphysicianjournal.com
the line where they felt best represented their pain intensity (30).
The Spanish version of the TSK-11 is a self-reported questionnaire that assesses fear of re-injury due to movement (31). The TSK-11 is an 11-item questionnaire that eliminates psychometrically poor items from the original version of the TSK (32) to create a shorter ques-tionnaire with comparable internal consistency. The TSK-11 has a 2-factor structure: activity avoidance and harm, and has demonstrated acceptable psychometric properties (31).
The Spanish version of the PCS assesses the degree of pain catastrophization (33,34). The PCS has 13 items and a 3-factor structure: rumination, magnification, and helplessness. The theoretical range is between 0 and 52, with lower scores indicating less catastrophizing. The PCS has demonstrated acceptable psychometric proper-ties (33).
The Spanish version of the NDI measures perceived neck disability (20,35). This questionnaire consists of 10 items, with 6 possible answers that represent 6 levels of functional capacity, ranging from 0 (no disability) to 5 (complete disability) points. The NDI has demonstrated acceptable psychometric properties (20).
The Spanish version of the HIT-6 (36,37) is a 6-item questionnaire that measures the severity and impact of headache on the patient’s life. The HIT-6 has demon-strated acceptable psychometric properties (38).
Statistical AnalysisSocio-demographic and clinical variables of the pa-
tients were analyzed. Analysis of variance (ANOVA) was used to test for differences in socio-demographic and clinical characteristics between the groups of patients.
Weighted kappa statistics (39) were calculated to assess the percentage agreement between external expert evaluators. Kappa statistics were calculated for each item. The Kappa coefficient varies from -1 (com-plete disagreement) to +1 (complete agreement), with 0 representing neither agreement nor disagreement.
Factor AnalysisThe factor structure was investigated using an
explorative factor analysis (ie, principal component analysis [PCA]) with Oblimin rotation. The number of factors for extraction was based on Kaiser’s eigenvalue criterion (eigenvalue ≥1) and evaluation of the scree plot (40). The quality of the factor analysis models was assessed using Bartlett’s test for sphericity and the Kai-ser-Meyer-Olkin (KMO) test. Bartlett’s test is a measure
of the probability that the initial correlation matrix is an identity matrix and should be < 0.05 (41). The KMO test measures the degree of multicollinearity and varies between 0 and 1 (should be greater than 0.50 – 0.60) (42).
Reliability For reliability, internal consistency and reproduc-
ibility were examined. Internal consistency was estimat-ed using Cronbach’s α and item total correlation coef-ficients. For a questionnaire to be internally consistent, α levels should be above 0.7 (43).
The test-retest reliability (repeatability) was evalu-ated using the Intraclass Correlation Coefficient (ICC). An ICC value above 0.70 is considered acceptable (44). We also constructed a Bland Altman Plot by calculating the mean difference between 2 measurements and the standard deviation (SD) of the difference (45). In this plot, 95% of the differences are expected to be less than 2 SDs.
Floor and Ceiling EffectsPotential floor and ceiling effects were measured
by calculating the percentage of patients indicating the minimum or maximum possible scores in the question-naires. Floor and ceiling effects are considered to be present if more than 15% of respondents achieved the highest or lowest possible total score (44).
Responsiveness AnalysesMeasurement error is the systematic and random
error of a patient’s score that is not attributable to true changes in the construct to be measured (46). Measure-ment error is expressed as a standard error of measure-ment (SEM), which is calculated as:
SD where SD is the SD of values from all participants
and ICC is the reliability coefficient (47,48). Ostelo et al (49) suggested that the percentage of the SEM in rela-tion to the total score of a questionnaire is an impor-tant indicator of agreement, and can be interpreted as follows: ≤ 5% very good; > 5% and ≤ 10% good; > 10% and ≤ 20% doubtful; and > 20% negative. Responsive-ness was assessed with the Minimal Detectable Change (MDC). The MDC expresses the minimal magnitude of change required to be 95% confident that the observed change between the 2 measures reflects real change and not just measurement error (50). It is calculated as SEM × × 1.96 (50,51).

www.painphysicianjournal.com 99
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Convergent Validity The convergent validity was assessed by the Pear-
son correlation coefficient between the CF-PDI and the other questionnaires: VAS, TSK-11, PCS, NDI, and HIT-6. A strong correlation was considered to be over 0.60; a moderate correlation between 0.30 and 0.60; and a low (very low) correlation below 0.30 (44).
Linear RegressionMultiple linear regression analysis was used to esti-
mate the strength of the associations with theoretically similar constructs, so multiple linear regression analyses were also performed including CF-PDI as a criterion variable to estimate the strength of the association between CF-PDI and NDI, PVAS, TSK, and PCS as pre-dictor variables. As a measure of multicollinearity, the variance inflation factor (VIF) is presented (VIF < 10 indicates no problem with multicollinearity).
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 20 (IBM company, USA) except for the SEM and MDC values, which were calculated using Microsoft Excel. The critical value for significance was P < 0.05.
Results
Item Development and Cognitive DebriefingA total of 18 patients with chronic craniofacial
pain participated in the focus group and were also interviewed in May 2011 and July 2011, and 30 items were pooled as potential questions. After a review by the research group, some questions were added, and 22 items covering 4 aspects (quality of life, jaw functional status, avoidance behavior, and pain) were finally gen-erated. There was agreement among the expert evalu-ators who reviewed the items, with a kappa coefficient of 0.83. The greatest disagreement occurred in items 8 and 20.
A pilot test for cognitive debriefing was performed in 24 patients in September 2011 to examine the con-tent validity of the preliminary questionnaire in regards to relevance and clarity of the language. The mean ± SD age of the patients was 45.7 ± 13.5 years (range: 19 – 61), and 17 of the participants were women (70.8%). The time required to answer all the questions was 8.4 ± 3.1 minutes (range: 5.4 – 12.6). More than 96% of the patients could easily answer the questionnaire.
Characteristics of the SampleThe final study sample consisted of 192 heteroge-
neous chronic craniofacial pain patients (68.8% women, one patient was of unknown gender) aged 19 – 78 years (mean ± SD: 46.00 ± 13.06). The vast majority of patients (28.1%) had myofascial pain diagnoses; other patients suffered from TMJ arthralgia (15.1%), headache or fa-cial pain attributed to TMD (myofacial pain/TMJ osteo-arthritis or arthralgia) (24.5%), combined tension-type headache and myofascial pain (16.7%), and migraine (15.6 %). The mean time of pain was 130.46 ± 151.44 months (range: 15 – 888), and 19 patients (9.9%) had received disability benefits. Educational levels in our sample were primary (23.4%), secondary (36.5%), and university graduates (25.0%); there was no information for 15.1% of our sample.
Distribution of Total CF-PDI ScoresThe distribution of CF-PDI scores did not differ
significantly from a normal symmetric distribution (skewness = 0.43, SE = 0.18; kurtosis = -0.36; SE = 0.35), Kolmogorov-Smirnov Z = 1.11 (P = 0.172). There were no significant differences in scoring between men (19.46 ± 9.04) and women (20.52 ± 9.22). There was no significant association between CF-PDI scores and age, marital status, average duration of pain, education level, or work status.
Only the type of diagnosis showed differences in the median score of CF-PDI, headache or facial pain attributed to the TMD (myofacial pain/TMJ osteoarthri-tis or arthralgia) group presented higher scores 28.62 ± 7.10; TMJ arthralgia, 14.2 ± 5.24; migraine, 17.93 ± 12.30; myofascial pain, 18.17 ± 6.44; combined tension-type headache and myofascial pain, 19.00 ± 7.05. The distribution of CF-PDI total scores and other principal scales are shown in Table 1.
Table 1. Descriptive statistics and estimates of internal consistency (N = 192).
Instrument Mean (SD) Range Alpha
CF–PDI 20.24 (9.15) 2–48 0.88
Pain and Disability 15.43 (6.77) 1–34 0.86
Jaw Functional Status 4.81 (3.57) 0–14 0.80
HIT–6 54.48 (7.67) 36–74 0.85
NDI 16.96 (6.00) 0–42 0.74
TSK–11 25.40 (7.08) 11–44 0.88
PCS 23.86 (8.90) 7–52 0.84
VAS 52.94 (13.83) 15–85 –––
CF-PDI, craniofacial pain and disability inventory; VAS, visual analogue scale; TSK-11, Tampa Scale for Kinesiophobia; PCS, pain catastrophizing scale; NDI, Neck Dibility Index; HIT-6, headache impact test-6

Pain Physician: January/February 2014; 17:95-108
100 www.painphysicianjournal.com
Internal ConsistencyCronbach’s α coefficient was 0.88 (95% CI = 0.86 –
0.91), indicating a high degree of internal consistency. The item-to-total correlation coefficients ranged from 0.32 to 0.73; no item dominated with an especially high correlation and no item appeared to be redun-dant. The previous item 20, “How long have you had pain?” was deleted in the final version and it increased slightly the Cronbach’s α coefficient. This item showed a strong positive skew, refers to the time of pain in our population, and shows limited information because all patients suffered from chronic pain. It was removed it; other results in Table 2.
Factor AnalysisIn order to explore the factorial structure of the
instrument, a PCA without rotation was conducted on the scores of our sample. We also attempted to con-struct one-, 2-, and 3-factor structures. A 2-factor solu-tion emerged in our sample using a PCA that explained 40.8% of the variance. The KMO was found to be 0.85, which exceeds the recommended minimum value of 0.60. Bartlett’s Test of Sphericity was highly significant (Chi square = 1467.10 P < 0.001), supporting the suit-ability of the data for PCA.
When factor loading smaller than 0.30 was sup-pressed, but there were no cases. The first factor (30.43% of the explanatory variance) was composed of 14 items (1, 2, 3, 4, 5, 6, 7, 8, 16, 17, 18, 19, 20 (previously 21), and 21 (previously 22); the second factor (10.39% of the explanatory variance) was composed of 7 items (9, 10, 11, 12, 13, 14, and 15). With these results and a visual inspection of the scree plot, a 2-factor solution was considered suitable (Fig. 1).
Regarding factor analysis, item 9 was not clearly classified into the assumed factor (with loadings un-der 0.35 in each of them). The results showed similar weights for both factors. Despite the unexpected load-ing of this item, the CF-PDI still showed appropriate internal consistency; therefore, we incorporated it into the jaw functional status domain for theoretical rea-sons. Results of the PCA are shown in Table 3.
Floor and Ceiling EffectsNo floor or ceiling effects were identified for the
whole scale. Only 9.3% of the respondents scored the lowest possible score of 0 in the jaw functional status subscale, and none of the craniofacial pain patients scored the highest possible score of 63 points on the CF-PDI.
Table 2. Corrected item-total between CF-PDI items (N = 192)
Scale mean if item deleted
Corrected item-total correlation
Squared multiple correlation
Cronbach's α if item deleted
1 18.65 0.73 0.63 0.87
2 18.72 0.46 0.37 0.88
3 18.58 0.54 0.55 0.88
4 19.61 0.47 0.56 0.88
5 19.82 0.53 0.51 0.88
6 19.88 0.34 0.31 0.88
7 19.19 0.50 0.36 0.88
8 19.56 0.35 0.23 0.88
9 19.49 0.32 0.21 0.88
10 19.30 0.59 0.57 0.87
11 19.34 0.53 0.54 0.88
12 19.41 0.41 0.48 0.88
13 19.70 0.55 0.54 0.88
14 19.79 0.40 0.50 0.88
15 19.83 0.43 0.46 0.88
16 18.29 0.64 0.56 0.87
17 18.58 0.57 0.46 0.87
18 19.33 0.44 0.30 0.88
19 19.30 0.44 0.37 0.88
20 19.22 0.47 0.36 0.88
21 19.19 0.38 0.25 0.88
Fig. 1. Scree plot of the 21 items of the CF-PDI.

www.painphysicianjournal.com 101
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Test-Retest ReliabilityThe response to the CF-PDI provided by a random
subsample of 106 patients (gender women: 70, 66.7%; age: 45.6 ± 12.9 years; duration of the disorders: 69.0 ± 46.2 months) showed satisfactory temporal stability of
the scale after 12 days. ICC based on absolute agree-ment measures was 0.90 (95% CI: 0.86 – 0.93). The con-structed Bland and Altman plot for test-retest agree-ment showed a good reliability for total CF-PDI score
Table 3. Items of CF-PDI distribution and factor loadings according to principal component analysis with Oblimin rotation including Kaiser correction (N = 192).
Factor 1 Factor 2
1 ¿Presenta dolor en la cara? Do you feel any pain in your face? 0.79 0.45
2 ¿Se ha visto afectada su calidad de vida por esta dolencia? Is your quality of life affected by this pain? 0.58 0.21
3 Intensidad de dolor en la cara. Pain intensity on your face. 0.68 0.23
4 Le incapacita su dolor a la hora de tener relaciones afectuosas del tipo: besos, abrazos, relaciones sexuales… Does the pain make you unable to have emotional relationships, such as: kisses, embraces, or sexual relationships?
0.69 0.06
5 ¿Tiene dolor al reír? Do you feel any pain when you laugh? 0.68 0.19
6 ¿Su dolencia hace que evite el sonreír, hablar o masticar?Does your condition make you avoiding smiling, talking or chewing? 0.44 0.13
7. ¿Tiene dolor en la mandíbula?Do you feel any pain in your jaw? 0.53 0.38
8 ¿Escucha algún ruido al mover la mandíbula?Do you hear any noise when you move your jaw? 0.40 0.23
9. ¿Nota que su mandíbula se le sale o se le traba?Do you feel your jaw getting out of place or getting stuck? 0.33 0.31
10. Intensidad de dolor al masticarPain intensity when chewing 0.47 0.72
11. ¿Siente cansancio en la mandíbula, al hablar o al comer?Do you feel any tiredness in your jaw when you talk or eat? 0.38 0.73
12. ¿Tiene dificultad para abrir la boca?Do you have any trouble when you open your mouth? 0.23 0.73
13. Intensidad de dolor al hablarPain intensity when talking. 0.40 0.74
14. ¿Tiene miedo de mover la mandíbula?Do you fear moving your jaw? 0.20 0.73
15. Alimentación.Nutrition 0.24 0.72
16. ¿Con qué frecuencia tiene dolor en el cuello?How often have you got any neck pain? 0.76 0.31
17.¿Con qué frecuencia tiene dolor de cabeza?How often do you have a headache? 0.61 0.41
18. ¿Con qué frecuencia tiene dolor de oído?How often do you have an earache? 0.47 0.34
19. ¿Qué siente al tocarse la zona dolorosa?What do you feel when you touch the painful area? 0.53 0.23
20 ¿Su dolor le altera el sueño?Does the pain disrupts your sleep? 0.59 0.21
21 ¿El dolor le interfiere a la hora de desempeñar su actividad laboral?Does the pain interfere in your work? 0.38 0.36

and 2 subscales (Figs. 2-4). The results of reliability and responsiveness analy-ses are summarized in Table 4.
Convergent ValidityThe total CF-PDI score was signifi-
cantly associated with all the assessed questionnaires (Table 5), but the cor-relation with the NDI, was the most important in our sample.
Linear RegressionThe resulting beta coefficients,
ranging from 0.50 to 0.17, indicate independent contribution of each scale to the prediction of CF-PDI, the criteri-on variable. NDI, VAS, and TSK-11 were predictors of CF-PDI, significance < 0.05 (as illustrated by the higher standard-ized coefficients [beta] and P-values). NDI was the most important variable (Table 6). PCS and HIT-6 were excluded as predictor variables this time.
discussion The present study describes a
methodical approach to the develop-ment and validation of a new self-ad-ministered questionnaire to measure disability, pain, and functional status of the mandibular and craniofacial region in patients with craniofacial pain. Our results demonstrate that the CF-PDI is psychometrically valid and reliable. In addition, the instrument has proven to be easy to complete, and only requires a relatively short time to administer. The CF-PDI was de-veloped in Spain for Spanish patients with craniofacial pain and TMD. How-ever, since the CF-PDI does not contain items that are specifically related to Spanish culture, it could be translated and used internationally.
The design of the CF-PDI was based on a biopsychosocial approach. This conceptual model, recommended by the International Classification of Functioning Disability and Health (52,53), can assess the disease from a
Fig. 2. Bland Altman plot illustrating the test-retest reliability of the CF-PDI. A total of 106 patients participated in the test-retest assessment. The central line representing the mean difference between test and retest scores, which was - 2.22, and the 95% limits of agreement are presented as flanking lines.
Fig. 3. Bland Altman plot illustrating the test-retest reliability of the Pain and Disability subscale. A total of 106 patients participated in the test-retest assessment. The central line representing the mean difference between test and retest scores, which was -1,73, and the 95% limits of agreement are presented as flanking lines.
Pain Physician: January/February 2014; 17:95-108
102 www.painphysicianjournal.com

www.painphysicianjournal.com 103
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Fig. 4. Bland Altman plot illustrating the test-retest reliability of the Jaw Functional Status subscale. A total of 106 patients participated in the test-retest assessment. The central line representing the mean difference between test and retest scores, which was -0.49, and the 95% limits of agreement are presented as flanking lines.
Table 4. Descriptive statistics, test-retest reliability, and responsiveness results (N = 106)
DomainsTest Retest
ICC 95% CI SEM MDCMean SD Mean SD
CF-PDI 20.57 8.42 22.79 7.80 0.90 0.86-0.93 2.48 6.87
Pain and Disability 15.37 6.13 17.10 5.26 0.86 0.81-0.90 2.10 5.82
Jaw Functional Status 5.20 3.39 5.69 3.93 0.86 0-80-0.90 1.35 3.75
CF-PDI, craniofacial pain and disability inventory; SD, standard deviation; ICC, intraclass correlation coefficient; 95% CI, 95% confidence interval; SEM, standard error of measurement; MDC, minimal detectable change
broader perspective, and provides an understanding of health, functioning, and disability. In addition, research sup-ports that clinical diagnosis is sometimes insufficient to explain patients’ pain and disability (54-56).
The scree plot and exploratory fac-tor analysis revealed a 2-factor solution. Both factors had eigenvalues greater than 1. PCA indicated that a satisfactory percentage of total variance (40.8%) was explained by the 2 factors. The CF-PDI contains 21 items divided into 2 subscales according to their content and exploratory factor analysis: “pain and disability” and “jaw functional status.”
High internal consistency was shown for the CF-PDI (Cronbach’s α: 0.88) and also for the 2 subscales (Cron-bach’s α: 0.80 – 0.86). These data are similar to the results from other research questionnaires used to assess facial pain and mandibular function (22-25,57,58).
Table 5. Pearson Correlation Coefficient of our principles scales (N = 192).
CF-PDI Pain and Disability Jaw Functional Status
VAS 0.46** 0.50** 0.23**
NDI 0.65** 0.69** 0.37**
PCS 0.46** 0.50** 0.25**
PCS rumiation 0.34** 0.35** 0.22**
PCS magnification 0.51** 0.52** 0.32**
PCS Helplessness 0.39** 0.45** 0.16*
TSK-11 0.40** 0.41** 0.26**
HIT6 0.38** 0.46** 0.09
** P < 0.01; * P < 0.05Abbreviations: CF-PDI, craniofacial pain and disability inventory; VAS, visual analogue scale; TSK-11, Tampa Scale for Kinesiophobia; PCS, pain catastrophizing scale; NDI, Neck Disability Index; HIT-6, headache impact test-6

Pain Physician: January/February 2014; 17:95-108
104 www.painphysicianjournal.com
In this study, we choose a retest interval of 12 days (approximately), in order to avoid variations in clinical status and patients remembering their previous an-swers. A longer interval for a test-retest study of health may be inappropriate as fluctuations in the patient’s health status can occur (59). In relation to this, Streiner and Norman suggested that a retest interval of 2 to 14 days is generally acceptable (60).
The test-retest reliability for the total CF-PDI score was considered to be excellent (ICC: 0.90; 95% CI: 0.86 – 0.93). Also, we were able to verify that the test-retest reliability was high for each subscale.
The measurement of SEM was 2.4 points, corre-sponding to 11.7% of the mean CF-PDI values and 3.8% of the maximum possible score. Based on the SEM, the MDC was 7 points (34.5% of mean values). Considering that the score of the questionnaire ranges from 0 to 63 points, 7 points represents 11.1% of the maximum pos-sible score, which means that the CF-PDI is able to de-
tect very small changes. Changes higher than the MDC can be interpreted as real and not due to measurement error, with an acceptable probability level. These results may help to calculate the sample size of future studies aiming to assess the effectiveness of craniofacial pain interventions.
Construct validity was evidenced by significant cor-relations between the CF-PDI with all the questionnaires and scales used in the validation process. A moderate correlation between CF-PDI with the HIT-6 and the VAS (r = 0.38 – 0.46) was observed. In addition, the PCS and TSK-11 showed moderate correlation with the CF-PDI and the pain and disability subscale (r = 0.36 – 0.52). This is consistent with recent evidence demonstrating that patients with craniofacial pain or craniomandibular dis-orders report higher levels of catastrophizing (61-63). Furthermore, pain-related catastrophizing has been associated with the progression of pain intensity and signs of disability in chronic craniofacial pain (64-68).
Table 6. Multiple linear regression models with CF-PDI (A), pain and disability (B), and jaw functional status (C) as criterion variable, and NDI, VAS, TSK-11, PCS as predictor variables (N = 192).
Criterion variable Predictor variablesRegression coefficient
(B)
Standardized coefficient (β)
Significance (P) VIF
A. CF-PDI
NDIVASTSK-11
0.770.130.22
0.500.190.17
0.0000.0010.004
1.371.261.17
Excluded variables
PCS-TotalHIT-6
----
0.080.01
0.2530.905
1.621.46
B. Pain and Disability
NDIPCS-MagnificationVAS
0.550.680.10
0.490.250.21
0.0000.0000.000
1.371.261.17
Excluded variables
PCS-TotalTSK-11HIT-6PCS-RumiationPCS-Helplessness
----------
-0.500.090.08-0.06-0.00
0.4800.0980.1590.3140.968
0.400.770.680.700.61
C. Jaw Functional Status
NDIPCS-magnification
0.170.28
0.290.20
0.0000.007
1.221.22
Excluded variables
PCS-TotalTSK-11HIT-6PCS-RumiationPCS-HelplessnessVAS
------------
-0.130.09-0.13-0.00-0.160.06
0.2070.2580.0760.9680.0590.436
2.491.291.331.421.651.26
CF-PDI, craniofacial pain and disability inventory; VAS, visual analogue scale; TSK-11, Tampa Scale for Kinesiophobia; PCS, pain catastrophizing scale; NDI, Neck Dibility Index; HIT-6, headache impact test-6, VIF, variance inflation factor

www.painphysicianjournal.com 105
Psychometric Validation of the Craniofacial Pain and Disability Inventory
Previous research demonstrated the relationship between fear of jaw movements and craniofacial pain (69,70), but only limited evidence supports it. However, there is higher evidence showing that pain-related fear is associated with reduced activities in daily life and is also a strong predictor of disability in other chronic musculoskeletal disorders (71-75).
Pain catastrophizing and pain-related fear are 2 constructs that have been linked to the chronicity of musculoskeletal pain through the “fear avoidance model” (76). Based on the results of multiple linear regression analysis, pain intensity (VAS: β = 0.19, P = 0.001) and fear of pain and movement (TSK-11: β = 0.17, P = 0.004) were predictors of CF-PDI. For jaw functional status, and pain and disability, the variable predictor was pain catastrophizing (PCS-Magnification: β = 0.25, P < 0.001; β = 0.20, P = 0.007).
The principal predictor for CF-PDI and the 2 sub-scales was the variable of neck disability (NDI: β = 0.29 – 0.50, P < 0.001). In addition, a strong correlation was observed between CF-PDI and pain and disability factor with NDI (r = 0.65 – 0.69). This is in line with the results of Olivo et al (77) who described a strong relationship between neck disability and jaw disability (r = 0.82). Several studies have reported the high prevalence and comorbidity between orofacial pain, TMD, headache, and neck pain (65,78-81). Our findings suggest the importance of taking into account the neck disability questionnaires when assessing patients with craniofa-cial pain.
Limitations Our study has several limitations. First, there is
a gender disproportion as the sample had a smaller proportion of men. However, our findings showed no significant differences in scoring between genders. The evidence suggests that the prevalence of craniofacial pain is higher in women (82).
The second limitation of this study is that we did not assess the CF-PDI in healthy subjects; the sample consisted of patients with chronic pain. Further
studies will need to be performed to assess the dis-criminant power of the CF-PDI for specific diagnostic entities.
The sample size was sufficient to test the new in-strument’s reliability, convergence validity, and explor-atory factor analysis. However, it was too small to be able to carry out confirmatory factor analysis. Kline has suggested a sample size of 10 – 15 subjects per item to perform this statistical analysis (83). It should be noted that statisticians disagree on the issue of appropriate sample size for confirmatory factor analyses. In relation to this, DeVellis stated that as the sample size becomes larger, the relative number of respondents per item can diminish (84), and that a sample of 200 is adequate in most studies (85).
Another limitation is that only self-reported mea-sures were considered for convergent validity. Future research should use physical tests to explore the clinical signs relating to pain and disability, and assess whether these are associated with the CF-PDI.
The last limitation of the study is the cross-sectional design, which prevented us from investigating the abili-ty of the CF-PDI to detect responsiveness to change over time. Although in this study we investigated in a short period of time the reproducibility and the MDC, a longi-tudinal study or one with an experimental design with a follow-up period would be required to understand how CF-PDI scores change over time. Furthermore, such a study would allow us to obtain information such as the Minimum Clinically Important Difference.
conclusion Evidence has shown that the CF-PDI has a good
structure, internal consistency, reproducibility, and construct validity, and provides an objective tool for as-sessing pain and disability in craniofacial pain patients. Neck disability showed a strong association with the CF-PDI, and is also a significant predictor of the construct. Based on the findings of this study, the CF-PDI could be used in research and clinical practice for the assessment of treatment outcomes.
RefeRences
1. Fillingim RB, Wallace MR, Herbstman DM, Ribeiro-Dasilva M, Staud R. Ge-netic contributions to pain: A review of findings in humans. Oral Dis 2008; 14:673-682.
2. Macfarlane TV, Glenny AM, Worthing-
ton HV. Systematic review of population-based epidemiological studies of oro-fa-cial pain. J Dent 2001; 29:451-467.
3. Stuginski-Barbosa J, Macedo HR, Bigal ME, Speciali JG. Signs of temporoman-dibular disorders in migraine patients: A
prospective, controlled study. Clin J Pain 2010; 26:418-421.
4. Shan CL, Bin Adon MY, Rahman AB, Hassan ST, Ismail KB. Prevalence of neck pain and associated factors with per-sonal characteristics, physical workloads

Pain Physician: January/February 2014; 17:95-108
106 www.painphysicianjournal.com
and psychosocial among male rubber workers in FELDA settlement Malaysia. Glob J Health Sci 2012; 4:94-104.
5. Anderson GC, John MT, Ohrbach R, Nixdorf DR, Schiffman EL, Truelove ES, List T. Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 2011; 152:765-771.
6. Glaros AG, Urban D, Locke J. Headache and temporomandibular disorders: Evi-dence for diagnostic and behavioural overlap. Cephalalgia 2007; 27:542549.
7. Svensson P. Muscle pain in the head:O between temporomandibular disorders and tension-type headaches. Curr Opin Neurol 2007; 20:320-325.
8. Lobbezoo F, Visscher CM, Naeije M. Impaired health status, sleep disorders, and pain in the craniomandibular and cervical spinal regions. Eur J Pain 2004; 8:23-30.
9. Plesh O, Adams SH, Gansky SA. Tem-poromandibular joint and muscle disor-der-type pain and comorbid pains in a national US sample. J Orofac Pain 2011; 25:190-198.
10. The International Classification of Headache Disorders: 2nd edition. Ceph-alalgia 2004; 24 Suppl:9-160.
11. Ashina S, Bendtsen L, Ashina M, Magerl W, Jensen R. Generalized hyperalgesia in patients with chronic tension-type headache. Cephalalgia 2006; 26:940-948.
12. Leclerc A, Niedhammer I, Landre MF, Ozguler A, Etore P, Pietri-Taleb F. One-year predictive factors for various as-pects of neck disorders. Spine (Phila Pa 1976) 1999; 24:1455-1462.
13. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial ap-proach to chronic pain: Scientific ad-vances and future directions. Psychol Bull 2007; 133:581-624.
14. Hoffmann RG, Kotchen JM, Kotchen TA, Cowley T, Dasgupta M, Cowley Jr. AW. Temporomandibular disorders and as-sociated clinical comorbidities. Clin J Pain 2011; 27:268-274.
15. Volcy-Gomez M. [The impact of mi-graine and other primary headaches on the health system and in social and economic terms]. Rev Neurol 2006; 43:228-235.
16. Shimshak DG, DeFuria MC. Health care utilization by patients with temporo-mandibular joint disorders. Cranio 1998; 16:185-193.
17. Ohrbach R, Larsson P, List T. The jaw functional limitation scale: Develop-
ment, reliability, and validity of 8-item and 20-item versions. J Orofac Pain 2008; 22:219-230.
18. Bloudek LM, Stokes M, Buse DC, Wil-cox TK, Lipton RB, Goadsby PJ, Varon SF, Blumenfeld a M, Katsarava Z, Pascual J, Lanteri-Minet M, Cortelli P, Martelletti P. Cost of healthcare for patients with migraine in five European countries: Results from the International Burden of Migraine Study (IBMS). J Headache Pain 2012; 13:361-378.
19. Salo P, Ylinen J, Kautiainen H, Arkela-Kautiainen M, Hakkinen A. Reliability and validity of the Finnish version of the neck disability index and the modi-fied neck pain and disability scale. Spine (Phila Pa 1976) 2010; 35:552-556.
20. Andrade Ortega JA, Delgado Martinez AD, Almecija Ruiz R. Validation of the Spanish version of the Neck Disabil-ity Index. Spine (Phila Pa 1976) 2010; 35:E114-118.
21. Schmidt S, Bullinger M. Current issues in cross-cultural quality of life instru-ment development. Arch Phys Med Re-habil 2003; 84:S29-34.
22. Aggarwal VR, Lunt M, Zakrzewska JM, Macfarlane GJ, Macfarlane T V. Develop-ment and validation of the Manchester orofacial pain disability scale. Communi-ty Dent Oral Epidemiol 2005; 33:141-149.
23. Lee JYK, Chen HI, Urban C, Hojat A, Church E, Xie SX, Farrar JT. Develop-ment of and psychometric testing for the Brief Pain Inventory-Facial in pa-tients with facial pain syndromes. J Neu-rosurg 2010; 113:516-523.
24. Johnson J, Carlsson S, Johansson M, Pauli N, Rydén A, Fagerberg-Mohlin B, Finizia C. Development and validation of the Gothenburg Trismus Questionnaire (GTQ). Oral Oncol 2012; 48:730-736.
25. Nixdorf DR, John MT, Wall MM, Fricton JR, Schiffman EL. Psychometric proper-ties of the modified Symptom Severity Index (SSI). J Oral Rehabil 2010; 37:11-20.
26. Ohrbach R, Granger C, List T, Dworkin S. Preliminary development and valida-tion of the Jaw Functional Limitation Scale. Community Dent Oral Epidemiol 2008; 36:228-236.
27. Jones J, Hunter D. Consensus meth-ods for medical and health services re-search. BMJ (Clinical research ed.) 1995; 311:376-380.
28. Dworkin SF, LeResche L. Research diag-nostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J Cranio-
mandib Disord 1992; 6:301-355.29. Schiffman EL, Ohrbach R, Truelove EL,
Tai F, Anderson GC, Pan W, Gonzalez YM, John MT, Sommers E, List T, Velly AM, Kang W, Look JO. The Research Di-agnostic Criteria for Temporomandibu-lar Disorders. V: Methods used to estab-lish and validate revised Axis I diagnostic algorithms. J Orofac Pain 2010; 24:63-78.
30. Bijur PE, Silver W, Gallagher EJ. Reliabil-ity of the visual analog scale for mea-surement of acute pain. Acad Emerg Med 2001; 8:1153-1157.
31. Gómez-Pérez L, López-Martínez AE, Ruiz-Párraga GT. Psychometric proper-ties of the Spanish version of the Tam-pa Scale for Kinesiophobia (TSK). J Pain 2011; 12:425-435.
32. Kori SH, Miller RP, Todd DD. Kinesio-phobia: A new view of chronic pain be-havior. Pain Manag 1990; 3:35-43.
33. García Campayo J, Rodero B, Alda M, Sobradiel N, Montero J, Moreno S. Validación de la versión española de la escala de la catastrofización ante el dolor (Pain Catastrophizing Scale) en la fibromialgia. Med Clin (Barc) 2008; 131:487-492.
34. Sullivan MJL, Bisop SC, Pivik J. The pain catastrophizing scale: Development and validation. Psychol Assess 1995; 7:524-532.
35. Vernon H, Mior S. The Neck Disabil-ity Index: A study of reliability and va-lidity. J Manipulative Physiol Ther 1991; 14:409-415.
36. Bjorner JB, Kosinski M, Ware JE. Cali-bration of an item pool for assessing the burden of headaches: An application of item response theory to the headache impact test (HIT). Qual Life Res 2003; 12:913-933.
37. Gandek B, Alacoque J, Uzun V, Andrew-Hobbs M, Davis K. Translating the Short-Form Headache Impact Test (HIT-6) in 27 countries: Methodological and conceptual issues. Qual Life Res 2003; 12:975-979.
38. Martin M, Blaisdell B, Kwong JW, Bjorner JB. The Short-Form Headache Impact Test (HIT-6) was psychometri-cally equivalent in nine languages. J Clin Epidemiol 2004; 57:1271-1278.
39. Cohen J. Weighted kappa: Nominal scale agreement with provision for scaled dis-agreement or partial credit. Psychol Bull 1968; 70:213-220.
40. Ferguson E, Cox T. Exploratory factor analysis: A users’ guide. Int J Select As-sess 1993; 1:84-94.
41. Bartlett MS. A note on the multiply-

Psychometric validation of the Craniofacial Pain and Disability Inventory
www.painphysicianjournal.com 107
ing factors for various Chi-square ap-proximations. J Royal Stat Soc B 1954; 16:296-298.
42. Kaiser H. Analysis of factorial simplicity. Psychometrika 1974; 39:31-36.
43. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika 1951; 16:297-334.
44. Terwee CB, Bot SDM, De Boer MR, Van der Windt DAWM, Knol DL, Dekker J, Bouter LM, De Vet HCW. Quality criteria were proposed for measurement prop-erties of health status questionnaires. J Clin Epidemiol 2007; 60:34-42.
45. Bland JM, Altman DG. Statistical meth-ods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1:307-310.
46. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, Bouter LM, De Vet HCW. The COSMIN study reached international consensus on tax-onomy, terminology, and definitions of measurement properties for health-re-lated patient-reported outcomes. J Clin Epidemiol 2010; 63:737-745.
47. Weir JP. Quantifying test-retest reliabil-ity using the intraclass correlation coef-ficient and the SEM. J Strength Cond Res 2005; 19:231-240.
48. Harvill L. Standard error of measure-ment. Educ Meas 1991; 10:33-41.
49. Ostelo RWJG, De Vet HCW, Knol DL, Van den Brandt PA. 24-item Roland-Morris Disability Questionnaire was preferred out of six functional status question-naires for post-lumbar disc surgery. J Clin Epidemiol 2004; 57:268-276.
50. Haley SM, Fragala-Pinkham MA. Inter-preting change scores of tests and mea-sures used in physical therapy. Phys Ther 2006; 86:735-743.
51. Wyrwich KW. Minimal important differ-ence thresholds and the standard error of measurement: Is there a connection? J Biopharm Stat 2004; 14:97-110.
52. Stucki G, Boonen A, Tugwell P, Cieza A, Boers M. The World Health Organ-isation International Classification of Functioning, Disability and Health: A conceptual model and interface for the OMERACT process. J Rheumatol 2007; 34:600-606.
53. Stucki G, Cieza A, Melvin J. The Inter-national Classification of Functioning, Disability and Health (ICF): A unifying model for the conceptual description of the rehabilitation strategy. J Rehab Med 2007; 39:279-285.
54. Turner JA, Franklin G, Turk DC. Pre-
dictors of chronic disability in injured workers: A systematic literature synthe-sis. Am J Ind Med 2000; 38:707-722.
55. Brage S, Sandanger I, Nygård JF. Emo-tional distress as a predictor for low back disability: A prospective 12-year popula-tion-based study. Spine 2007; 32:269-274.
56. Waddell G. Preventing incapacity in people with musculoskeletal disorders. Br Med Bull 2006; 77-78:55-69.
57. Ohrbach R, Larsson P, List T. The jaw functional limitation scale: Develop-ment, reliability, and validity of 8-item and 20-item versions. J Orofac Pain 2008; 22:219-230.
58. Stegenga B, De Bont LG, De Leeuw R, Boering G. Assessment of mandibular function impairment associated with temporomandibular joint osteoarthro-sis and internal derangement. J Orofac Pain 1993; 7:183-195.
59. Holt AE, Shaw NJ, Shetty A, Greenough CG. The reliability of the Low Back Out-come Score for back pain. Spine 2002; 27:206-210.
60. Streiner DL, Norman GR. Health Mea-surement Scales: A Guide to Their Develop-ment and Use. Oxford University Press, Oxford, 1989.
61. Campbell CM, Kronfli T, Buenaver LF, Smith MT, Berna C, Haythornthwaite JA, Edwards RR. Situational versus dis-positional measurement of catastroph-izing: Associations with pain respons-es in multiple samples. J Pain 2010; 11:443-453.
62. Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Dubner R, Bair E, Baraian C, Slade GD, Maixner W. Potential psycho-social risk factors for chronic TMD: De-scriptive data and empirically identified domains from the OPPERA case-control study. J Pain 2011; 12:T46-60.
63. Quartana PJ, Buenaver LF, Edwards RR, Klick B, Haythornthwaite JA, Smith MT. Pain catastrophizing and salivary cor-tisol responses to laboratory pain test-ing in temporomandibular disorder and healthy participants. J Pain 2010; 11:186-194.
64. Rantala MA, Ahlberg J, Suvinen TI, Nis-sinen M, Lindholm H, Savolainen A, Ko-nonen M. Temporomandibular joint re-lated painless symptoms, orofacial pain, neck pain, headache, and psychosocial factors among non-patients. Acta Odon-tol Scand 2003; 61:217-222.
65. Buenaver LF, Edwards RR, Smith MT, Gramling SE, Haythornthwaite JA. Cata-strophizing and pain-coping in young adults: Associations with depressive
symptoms and headache pain. J Pain 2008; 9:311-319.
66. Buenaver LF, Quartana PJ, Grace EG, Sarlani E, Simango M, Edwards RR, Hay-thornthwaite JA, Smith MT. Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial tem-poromandibular disorder participants: The mediating role of sleep disturbance. Pain 2012; 153:1159-1166.
67. Holroyd KA, Drew JB, Cottrell CK, Ro-manek KM, Heh V. Impaired function-ing and quality of life in severe mi-graine: The role of catastrophizing and associated symptoms. Cephalalgia 2007; 27:1156-1165.
68. Velly AM, Look JO, Carlson C, Lenton PA, Kang W, Holcroft CA, Fricton JR. The effect of catastrophizing and depression on chronic pain – a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 2011; 152:2377-2383.
69. Visscher CM, Ohrbach R, Van Wijk AJ, Wilkosz M, Naeije M. The Tampa Scale for Kinesiophobia for Temporomandib-ular Disorders (TSK-TMD). Pain 2010; 150:492-500.
70. Rollman A, Visscher CM, Gorter RC, Naeije M. Care seeking for orofacial pain. J Orofac Pain 2012; 26:206-214.
71. Buer N, Linton SJ. Fear-avoidance be-liefs and catastrophizing: Occurrence and risk factor in back pain and ADL in the general population. Pain 2002; 99:485-491.
72. Crombez G, Vlaeyen JW, Heuts PH, Ly-sens R. Pain-related fear is more dis-abling than pain itself: Evidence on the role of pain-related fear in chronic back pain disability. Pain 1999; 80:329-339.
73. Kamper SJ, Maher CG, Menezes Costa L da C, McAuley JH, Hush JM, Sterling M. Does fear of movement mediate the relationship between pain intensity and disability in patients following whiplash injury? A prospective longitudinal study. Pain 2012; 153:113-119.
74. Walton D, Elliott JM. A higher-order analysis supports use of the 11-item ver-sion of the tampa scale for kinesiopho-bia in people with neck pain. Phys Ther 2013; 93:60-68.
75. Vlaeyen JW, Seelen HA, Peters M, De Jong P, Aretz E, Beisiegel E, Weber WE. Fear of movement/(re)injury and mus-cular reactivity in chronic low back pain patients: An experimental investigation. Pain 1999; 82:297-304.
76. Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS.

Pain Physician: January/February 2014; 17:95-108
108 www.painphysicianjournal.com
The fear-avoidance model of musculo-skeletal pain: Current state of scientific evidence. J Behav Med 2007; 30:77-94.
77. Olivo SA, Fuentes J, Major PW, Warren S, Thie NMR, Magee DJ. The association between neck disability and jaw disabil-ity. J Oral Rehabil 2010; 37:670-679.
78. Marklund S, Wiesinger B, Wanman A. Reciprocal influence on the incidence of symptoms in trigeminally and spi-nally innervated areas. Eur J Pain 2010; 14:366-371.
79. Mienna CS, Wanman A. Self-reported impact on daily life activities related to temporomandibular disorders, head-
aches, and neck-shoulder pain among women in a Sami population living in Northern Sweden. J Orofac Pain 2012; 26:215-224.
80. Storm C, Wänman A. Temporoman-dibular disorders, headaches, and cer-vical pain among females in a Sami population. Acta Odontol Scand 2006; 64:319-325.
81. Wiesinger B, Malker H, Englund E, Wänman A. Back pain in relation to musculoskeletal disorders in the jaw-face: A matched case-control study. Pain 2007; 131:311-319.
82. Macfarlane TV, Blinkhorn AS, Davies
RM, Kincey J, Worthington H V. Oro-fa-cial pain in the community: Prevalence and associated impact. Community Dent Oral Epidemiol 2002; 30:52-60.
83. Rex B. Kline. Principles and Practice of Structural Equation Modeling (Methodol-ogy in the Social Sciences). Kenny DA, edi-tor. Guilford Press. New York, 1998.
84. DeVellis RF. Scale Development Theory and Applications. Sage Publications. Newbury Park, CA, 1991.
85. Comrey AL. Factor-analytic methods of scale development in personality and clinical psychology. J Consult Clin Psychol 1988; 56:754-761.

138
5.5 Estudio V
La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-Díaz-Parreño S,
Fernández-Carnero J. The Influence of Neck Disability and Pain Catastrophizing about
Trigeminal Sensory-Motor System in Patients with Headache Attributed to Temporomandibular
Disorders. (En revisión)
Objetivos de estudio
Nuestro objetivo fue estudiar la influencia de la discapacidad y el dolor de cuello sobre las
variables sensoriales y motoras del trigémino en pacientes con cefalea atribuida a TCM.
Resultados
Los resultados de EVAF fueron mayores a 6 minutos (media 51,7, IC 95%: 50,15-53,26) y 24
horas después (21.08, IC 95%: 18,6-23,5) para las pruebas en el grupo que muestran
discapacidad moderada cuello en comparación con el grupo de discapacidad leve cuello (6
minutos, 44,16, IC del 95%: 42,65 a 45,67 / 24 horas después, 14,3; IC del 95%: 11,9-16,7) y el
grupo de control (6 minutos, 29.92, IC 95% 28,29-31,55 / 24 horas después, 4,65; IC del 95%:
2.5 a 7.24). El análisis muestra una disminución en el MAI sin dolor inmediatamente después de
las pruebas de todos los grupos y se observó que esta disminución sólo se mantuvo en el grupo
de discapacidad moderada 24 horas después de la prueba. Los UDPs de la región del trigémino
se redujeron inmediatamente en todos los grupos, mientras que a las 24 horas se observó una
disminución sólo en los grupos de pacientes. Los UDPs de la región cervical disminuyeron sólo
en el grupo con discapacidad cuello moderado 24 horas después de la prueba. La correlación
negativa más fuerte se encontró entre MAI sin dolor inmediatamente después de la prueba y el
IDC en ambos grupos: grupo de discapacidad leve (r = -0.49, P <0,001) y grupo de discapacidad
moderada (r = -0.54, P <0,001).
Conclusiones
Nuestros resultados sugieren que la discapacidad y dolor de cuello tienen una influencia en las
variables sensomotrices evaluados en pacientes con cefalea atribuida a TCM.

1
The Influence of Neck Disability and Pain Catastrophizing about Trigeminal
Sensory-Motor System in Patients with Headache Attributed to
Temporomandibular Disorders
Roy La Touche,1-4, Alba Paris-Alemany 1-4, Alfonso Gil-Martínez1-4, Joaquín Pardo-
Montero1-4, Santiago Angulo-Díaz-Parreño, Josué Fernández-Carnero,2,4,6.
1. Department of Physiotherapy, Faculty of Health Science, The Center for Advanced Studies
University La Salle. Universidad Autónoma de Madrid, Aravaca, Madrid, Spain.
2. Motion in Brains Research Group, The Center for Advanced Studies University La Salle,
Universidad Autónoma de Madird.
3. Institute of Neuroscience and Craniofacial Pain (INDCRAN), Madrid, Spain
4. Hospital La Paz Institute for Health Research, IdiPAZ. Madrid, Spain.
Madrid, Spain
5. Faculty of Medicine, Universidad San Pablo CEU, Madrid, Spain
6. Department of Physical Therapy, Occupational Therapy, Rehabilitation and Physical
Medicine, Universidad Rey Juan Carlos, Alcorcón, Madrid, Spain.
Address for reprint requests / Corresponding author:
Roy La Touche
Facultad de Ciencias de la Salud
Centro Superior de Estudios Universitarios La Salle.
Calle la Salle, 10
28023 Madrid
SPAIN
Telephone number: + 34 91 7401980 (EXT.256)
Fax number:
Email address: [email protected]

2
ABSTRACT
OBJECTIVE: Our purpose was to investigate the influence that neck pain and disability
may have on trigeminal sensory-motor variables in patients with headache attributed to
TMD.
METHODS: An experimental case-control study comprising 83 patients with headache
attributed to TMD and 39 healthy controls was done. Patients were grouped according
to their scores on the neck disability index (NDI) (mild and moderate neck disability).
Initial assessment included the visual analogue scale (VAS), pain catastrophizing scale,
NDI and the Headache Impact Test-6. The protocol consisted of baseline measurements
of pressure pain thresholds (PPT) for mechanical pain sensitivity in the trigeminal and
cervical region and the pain-free maximum mouth opening (MMO), performance of the
provocation chewing test, immediately after data collection and 24 hours after. During
the provocation chewing test, patients were assessed for subjective feelings of fatigue
(VAFS) and pain intensity, immediately and 24 hours after completion.
RESULTS: The VAFS were higher at 6 minutes (mean 51.7; 95% CI: 50.15-53.26) and
24 hours after (21.08; 95% CI: 18.6-23.5) for tests in the group showing moderate neck
disability compared with the mild neck disability group (6 minutes, 44.16; 95% CI
42.65-45.67/ 24 hours after, 14.3; 95% CI: 11.9-16.7) and the control group (6 minutes,
29.92; 95% CI 28.29-31.55/ 24 hours after, 4.65; 95% CI: 2.05-7.24). The analysis
shows a decrease in the pain-free MMO immediately after the tests for all groups and
this decrease was observed only in the group of moderate disability 24 hours after the
test. PPTs of the trigeminal region were decreased immediately in all groups, whereas at
24 hours a decrease was observed only in the groups of patients. PPTs of the cervical
region decreased only in the group with moderate neck disability 24 hours after the test.
The strongest negative correlation was found between pain-free MMO immediately

3
after the test and NDI in both groups: mild (r=-0.49; P<0.001) and moderate (r=-0.54;
P<0.001) neck disability group.
CONCLUSION: Neck pain and disability have an influence on the sensory-motor
variables evaluated in patients with headache attributed to TMD.
KEYWORDS: Temporomandibular disorders, headache, neck pain, pain
catastrophizing, disability.

4
.INTRODUCTION
Temporomandibular disorders (TMD), headaches and neck pain are very closely
related diseases[1]. Several studies have reported the overlapping signs and symptoms
among patients with TMD, headaches and neck pain, respectively[2, 3]. It has been
shown that neck pain complaints were also significantly associated with TMD[4, 5] and
that psychosocial factors have an influence on the presence of head, neck and orofacial
pain[3].
The prevalence of temporomandibular joint (TMJ) symptoms, orofacial pain,
neck pain and headache was assessed in 1339 non-patients. Often painless TMJ
symptoms were found in 10% of subjects, orofacial pain in 7%, headache in 15% and
neck pain in 39%[3]. Plesh et al. showed that 53% of patients with TMD had severe
headache and 54% had neck pain[6]. It has been suggested that TMD and headaches
may be involved in their pathophysiology[7, 8] and this headache could be a possible
risk factor for developing neck pain[9].
Recent research has shown a strong relationship between craniomandibular
disability and pain with cervical disability[10, 11]. Several experimental studies have
described functional connections between the craniofacial and cervical afferent fibres
via patterns of neural convergence of the trigeminal nucleus and the upper cervical
nociceptive neurons, which form a functional unit, the trigeminocervical complex[12–
18]. In relation to this, it has been observed in experimental studies that the pain
induced by the infiltration of algogenic substances in the masticatory or cervical
muscles can bi-directionally modify the activity of the stretch reflexes[13, 15]. Also, in
basic research, a reflex relationship has been observed between the activity of the
nociceptors of the TMJ and the activity of the fusimotor-muscle spindle system of the
cervical muscles[17]. This information is useful for proposing theories about the

5
influence of the cervical region over the possible nociceptive and sensory-motor
mechanisms involved in masticatory fatigue, pain and alterations in motor behaviour. At
present, there is insufficient information demonstrating the influence of neck pain and
disability in the sensory-motor activity in patients with trigeminal headache attribute to
TMD. This could be a key issue, since improvements could be made by changing the
diagnostic and therapeutic approach to these patients. We used the primary hypothesis
that neck disability is a factor influencing masticatory sensory-motor activity in patients
with headache attributed to TMD.
Headache attributed to TMD is classified as a secondary headache caused by a
disorder that affects the temporomandibular region[19]. The pain may be unilateral or
bilateral and is represented in the facial region, at the masseter and temporal region[19].
An important criterion for clinical diagnosis is that the headache occurs or is aggravated
by provocative manoeuvres (such as the palpatory pressure on the TMJ and masticatory
muscles) and/or mandibular active or passive movements[19, 20]. Recently, it has been
found that the diagnostic criteria that have greater sensitivity and specificity for this
type of headache are: 1) the provocation of pain by palpation of the temporalis muscle
or jaw movements and 2) the fact that pain changes with the movements of the jaw in
the function or parafunction[20, 21].
From the clinical point of view, it is important to identify changes in motor
behaviour that may be present in patients suffering TMD, especially knowing that a
percentage of these patients develop painful chewing[22, 23], difficulty performing jaw
movements[24] and masticatory fatigue[25, 26].
During the last decades, the relationship between masticatory muscle pain and
disordered jaw motor behaviour has been studied widely; see for example the review by
Svensson and Graven-Nielsen[27]. Pain may influence the characteristics of the

6
masticatory sensory-motor system[28]. Furthermore, Kurita et al. found a positive
correlation between chewing ability and TMJ pain and reduced mouth opening[29].
According to some researchers, fatigue and fatigue-related symptoms are reported
significantly more often by chronic TMD patients than by healthy volunteers[30]. In
addition, a recent study in patients with chronic orofacial pain demonstrated that fatigue
is mediated by psychosocial factors[31]. In this connection, Brandini et al. found a
positive association in TMD patients between mandibular kinematic variables and
psychological factors such as stress and depression[32].
Research or assessments based on a biobehavioural approach may offer a better
alternative for identifying patients with chronic TMD[33]; a biobehavioural approach to
the assessment and treatment of chronic pain is widely accepted[34]. A key point to
note about patients with headache attributed to TMD is that an association between
emotional functioning and increased frequency of headache has been found[35]. This
and previous findings lead us to propose integrating the assessment of psychological
factors with pain and disability associated with trigeminal sensory-motor variables in
this research. A significant amount of scientific evidence has shown the influence of
pain catastrophizing on several variables related to TMD[36–41]. This suggests the
hypothesis that pain catastrophizing has an association or is a predictor of some of the
trigeminal sensory-motor variables studied in this research.
The primary objective of this research is to investigate the influence that pain and
disability of the neck may have on trigeminal sensory-motor variables in patients with
headache attributed to TMD, and as a secondary objective we propose identifying
whether the psychological or disability variables have any association with the studied
sensory-motor variables.

7
MATERIALS AND METHODS
Study Design
This was an experimental case-control study. The assessor of sensory-motor
measurements was blinded. One researcher administered the participant appointments
and questionnaires, and also instructed the participant not to say anything that could
reveal their pain, disability trait or state. The reporting of the study follows the
“Strengthening the Reporting of Observational studies in Epidemiology” (STROBE
statement) [42].
After receiving detailed information about the experiment, the volunteers gave
their written informed consent. All of the procedures used in this study were planned
under the ethical norms of the Helsinki Declaration and were approved by the local
ethics committee.
Participants
A consecutive convenience sample of 83 patients with chronic headache
attributed to TMD and 39 healthy controls were recruited for the study. The sample was
recruited from outpatients of a Public Health Centre (Madrid, Spain) and two private
clinics specializing in craniofacial pain and TMD (Madrid, Spain). Patients were
selected if they met all of the following criteria: 1) Headache and facial pain attributed
to TMD, diagnosis was made according to the guidelines of the International
Classification of Headache Disorders[19]; 2) TMD diagnosis based on the Research
Diagnostic Criteria for TMD[43, 44] to classify patients with painful TMD (myofascial
pain, TMJ arthralgia and TMJ osteoarthritis); 3) pain symptoms history of at least the 6
months previous to the study; 4) pain in the jaw, temples, face, neck, pre-auricular area,
or in the ear during rest or function; 5) neck pain and disability and quantified according
to neck disability index (NDI)[45]; and 6) At least 18 years of age.

8
There were 83 patients categorized into two groups according to their scores on the
NDI[45]: 1) mild neck disability (NDI 5-14), and; 2) moderate neck disability (NDI 15-
24). The criteria for exclusion were: 1) a history of traumatic injuries (e.g., contusion,
fracture, or whiplash injury); 2) presence of fibromyalgia or other chronic pain disorder;
3) neuropathic pain (e.g., trigeminal neuralgia); 4) unilateral neck pain; 5) cervical spine
surgery, and; 6) clinical diagnosis of cervical radiculopathy or myelopathy.
Healthy controls were recruited from our academic university campus and the
local community through flyers, posters, and social media. Healthy participants were
examined and were included in the study only if they had no history of craniofacial
pain, headache or neck pain and had been free of any other painful disorders for the six
months prior to the experiment. All subjects had complete dentition, did not use any
medication, had no dental pathology and none were regular gum chewers. Subjects who
reported oral parafunctions (i.e., tooth grinding, tooth clenching) were excluded.
Experimental Protocol
After consenting for the study, recruited patients were given a battery of
questionnaires to complete on the first day of the experiment. These included various
self-reports for sociodemographic, psychological and pain-related variables, including
the visual analogue scale (VAS) for pain intensity and the validated Spanish versions of
the pain catastrophizing scale (PCS), the NDI and the impact associated with headache
was assessed using the Headache Impact Test-6 (HIT-6). The experimental protocol
consisted of baseline measurements, a provocation chewing test, and data collection
immediately after, and 24 hours after, the provocation chewing test. Participants
underwent standardized measurement of pressure pain thresholds (PPT) for mechanical
pain sensitivity at the trigeminal and cervical region and the pain-free maximum mouth
opening (MMO). The PPT and MMO measures have been employed in previous

9
studies[46] and are further described below. During the performance of the provocation
chewing test, data were collected regarding the subjective feelings of fatigue and pain
intensity every minute, immediately and 24 hours after completion.
Provocation Chewing Test
The provocation chewing test consisted of 6 minutes of unilateral chewing of eight
grams of hard gum; this protocol was modified from Karibe et al.[47]. Chewing gum
was employed to elicit pain and muscle fatigue. The participants performed the test in
the sitting position, which was attained by instructing the patient to sit in a comfortable
upright position, with the thoracic spine in contact with the back of the chair, but
without contact of the craniocervical region with the seat. The feet were positioned flat
on the floor with knees and hips at 90 degrees and arms resting freely alongside.
Tests were carried out by exclusively using the right side for chewing; the
metronome was set at 80 beats per minute to indicate chewing rate, as documented in a
previous study[48]. The participants were instructed to chew gum initially for 60
seconds to soften its initial hardness, then after 70 seconds of rest, the signal was given
to start the test.
Questionnaires
The Spanish version of the PCS assesses the degree of pain catastrophizing[49, 50]. The
PCS has 13 items and a 3-factor structure: rumination, magnification and helplessness.
The theoretical range is between 0 and 52, with lower scores indicating less
catastrophizing. The PCS has demonstrated acceptable psychometric properties[50].
The Spanish version of the NDI measures perceived neck disability[45, 51]: This
questionnaire consists of 10 items, with 6 possible answers that represents 6 levels of
functional capacity, ranging from 0 (no disability) to 5 (complete disability) points. The
addition of all of the points obtained from each of the items gave the level of disability,

10
with higher scores indicating greater perceived disability. The NDI has demonstrated
acceptable psychometric properties[51].
The Spanish version of the HIT-6[52, 53] consists of a six-item questionnaire measuring
the severity and impact of headache on the patient’s life. The results of HIT-6 are
stratified into four grade-based classes: little or no impact (HIT-6 score: 36-49),
moderate impact (HIT-6 score: 50-55), substantial impact (HIT-6 score: 56-59), and
severe impact (HIT-6 score: 60-78)[52]. The HIT-6 has demonstrated acceptable
psychometric properties[54].
Pain intensity
Pain intensity was measured with the VAS. The VAS consists of a 100 mm line, on
which the left side represents “no pain” and the right side “the worst pain imaginable”.
The patients placed a mark where they felt it represented their pain intensity[55].
The VAS scale was used to quantify two different situations:
a) Habitual and spontaneously perceived pain intensity.
b) Pain intensity perceived at different times during the course of the chewing
provocation test and at 24h after completion.
Subjective perception of fatigue.
The visual analogue fatigue scale (VAFS) was used to quantify fatigue at
different times during the course of the chewing provocation test and at 24h after
completion. The VAFS consists of a 100-mm vertical line on which the bottom
represents “no fatigue” (0 mm), and the top represents “maximum fatigue” (100
mm)[56]. The researcher registered the mark in mm.
Pressure pain thresholds

11
A digital algometer (FDX 25, Wagner Instruments, Greenwich, CT, USA),
comprised of a rubber head (1 cm2) attached to a pressure gauge, was used to measure
PPTs. Force was measured in kilograms (kg); therefore, thresholds were expressed in
kg/cm2. The protocol used was a sequence of 3 measurements, with an interval of 30
seconds between each of the measurements. An average of the 3 measurements was
calculated to obtain a single value for each of the measured points in each of the
assessments. PPTs were assessed at one point in the masseter muscle (2.5 cm anterior to
the tragus and 1.5 cm inferior to the zygomatic arch), one point in the temporalis muscle
(anterior fibres of the muscle; 3 cm superior to the zygomatic arch in the middle point
between the end of the eye and the anterior part of the helix of the ear), in the
suboccipital muscles (2 cm inferior and lateral to the external occipital protuberance)
and in the upper trapezius muscle (2.5 cm above the superior medial angle of the
scapula). The device was applied perpendicular to the skin. The patients were asked to
raise their hands at the moment the pressure started to change to a pain sensation, at
which point the assessor stopped applying pressure. Compression pressure was
gradually increased at a rate of approximately 1 kg/s. This algometric method has high
intra-rater reliability (ICC=0.94-0.97) for measuring PPT[57].
Pain-free MMO
MMO was measured with the patients in a supine position. The patients were
asked to open their mouths as wide as they could without pain. The distance between
the superior incisor and the opposite inferior incisor was measured in mm with a
Craniomandibular scale (CMD scale. Pat. No. ES 1075174 U, INDCRAN: 2011.
INDCRAN, Madrid, Spain). The inter-rater reliability of this procedure has been found
to be high (ICC = 0.95 – 0.96)[58].

12
Sample size
The sample size was estimated with the G*Power Program 3.1.7 for Windows
(G*Power© from University of Dusseldorf, Germany)[59]. The sample size calculation
was considered a power calculation to detect between-group differences in the primary
outcome measures (fatigue and pain intensity). To obtain 80% statistical power (1-β
error probability) with an α error level probability of 0.05, using analysis of variance
(ANOVA) of repeated measures, within-between interaction and an medium effect size
of 0.3, we considered 3 groups and 7 measurements for primary outcomes. This
generated a sample size of 31 participants per group. Allowing a dropout rate of 20%
and aiming to increase the statistical power of the results, we planned to recruit at least a
minimum of 112 participants to provide sufficient power to detect significant group
differences.
Statistical Analysis
The Statistical Package for Social Sciences (SPSS 21, SPSS Inc., Chicago, IL
USA) software was used for statistical analysis. The independent t-test and one-way
ANOVA was used for analysis of the self-report psychological and pain-related
variables (NDI, PCS and HIT-6), as well as pain duration and the subjects’
sociodemographic data (age, weight, height), comparing the baseline data for the three
groups. Results are presented as mean, standard deviation (±SD), range and 95%
confidence interval (CI).
For primary outcome variables (fatigue and pain intensity), we performed a 3-
way repeated-measures ANOVA, including within-between interaction factors. The
factors analysed were group (i.e., moderate neck disability group, mild neck disability
group and healthy group), sex (i.e., female and male) and time (measurement per minute

13
during the test and after 24 hours). The hypothesis of interest was the group vs. time
interaction.
The 2-way repeated-measures models of ANOVA were used to test the effect of
the task on the outcome secondary variables (i.e., PPTs and pain-free MMO). The
factors analysed were group and time (baseline, immediately after and after 24 hours),
and also the interactions group vs. time interactions were analysed. In the analysis,
repeated-measures ANOVAs, when the assumption of sphericity was violated (as
assessed using the Mauchly sphericity test), the number of degrees of freedom against
which the F-ratio was tested was corrected by the value of the Greenhouse–Geisser
adjustment. Post hoc analysis with Bonferroni corrections was performed in the case of
significant ANOVA findings for multiple comparisons between variables. Effect-sizes
(Cohen’s d) were calculated for outcome secondary variables. According to Cohen’s
method, the magnitude of the effect was classified as small (0.20 to 0.49), medium (0.50
to 0.79), and large (≥0.8)[60].
The relationship between pain-related measures after completion of the chewing
provocation test and self-reports for pain-related and psychological measures were
examined using Pearson correlation coefficients. Multiple linear regression analysis was
performed to estimate the strength of the associations between the results of VAS
[model 1], VAFS [model 2] and pain-free MMO [model 3] (criterion variables) after 24
hours following completion of the provocation chewing test and NDI, PCS, HIT-6 and
VAS were used as predictor variables. Variance inflation factors (VIFs) were calculated
to determine whether there were any multi-collinearity issues in any of the three models.
The strength of association was examined using regression coefficients (β), P
values and adjusted R2. Standardized beta coefficients were reported for each predictor

14
variable included in the final reduced models to allow for direct comparison between
the predictor variables in the regression model and the criterion variable being studied.
For regression analysis, the 10 cases per variable rule was applied in order to obtain
reasonably stable estimates of the regression coefficients[61]. The significance level for
all tests was set to P < 0.05.
RESULTS
Baseline characteristics of sociodemographic, psychological and pain-related variables
of the sample are summarized in Table 1. Finally, the total study sample consisted of
122 participants (77 females and 45 males). Table 1 shows no statistically significant
differences among the three groups in relation to sociodemographic variables. There
were no differences in the duration of pain and perceived pain intensity on a regular or
spontaneous basis in specific groups of patients, but differences were observed in NDI,
PCS and Hit-6 (p<0.05). The different diagnosis for TMD of the included patients were
as follows: 28 patients (33.7%) were diagnosed with myofascial pain, 8 patients (9.6%)
with arthralgia, 13 patients (15.6%) with osteoarthritis and 34 patients (40.9%) with a
combined diagnosis (myofascial pain with arthralgia or osteoarthritis).
In the group of healthy participants, there were no withdrawals during the
provocation chewing test; in the group of patients with moderate neck disability, nine
participants (21.9%) withdrew between minutes 5 and 6 of the test as well as six
participants in the group of patients with mild neck disability (14.2%). All of the
participants were evaluated 24 hours after the test.
Gender Differences in Response to Provocation Chewing Test
The interaction of group vs. sex showed significant differences in VAS
(F=10.86; P<0.001), VAFS (F=4.06; P=0.02) and PPTs of the trapezius muscle

15
(F=3.96; P=0.022). Post hoc analysis showed higher values of VAS and VAFS in
women compared to men for the three groups (P<0.05). PPTs in the trapezius muscle
values were lower in women than in men (P<0.05) for the two groups of patients; in the
control group there was no difference in this value. No differences (group vs. sex
interaction) were observed for the other variables.
Pain and Fatigue
The ANOVA revealed a significant group vs. time interaction (F=35.77;
P<0.001), and significant differences for the group factor (F=416.65; P<0.001)
regarding the VAS results during the provocation chewing test. VAS behaviour during
the tests can be seen in Figure 1-A. Post hoc analysis revealed that higher values on the
VAS during provocation chewing test for the moderate neck disability group compared
to the mild neck disability group and the control group. The results obtained 24 hours
after the test showed no differences between the groups of patients, but there were
differences with the control group (Figure 2-A).
For fatigue perceived during tests, the ANOVA showed a significant effect for
group vs. time interaction (F=13.05; P<0.001) and for the group factor (F=371.12;
P<0.001). VAFS behaviour during the tests can be seen in Figure 1-B. VAFS values
were higher at 6 minutes and 24 hours after the test in the group of moderate neck
disability compared with the other two groups. The post hoc analysis shows the
differences between the three groups (Figure 2-B).
Pain-free MMO
Regarding the pain-free MMO ANOVA revealed a significant effect for group
vs. time interaction (F=2.75; P=0.02) and for the group factor (F=65.74; P<0.001). The
post hoc analysis shows a decrease in the pain-free MMO immediately after the tests for

16
the three groups, but this decrease was observed only in the group of moderate disability
at 24 hours after the test (Table 2).
Pressure pain thresholds
The PPTs for all points of the trigeminal and cervical region showed statistically
significant differences by ANOVA in the group vs. time interaction and group factor
(P<0.001). According to the post hoc analysis of the PPT masseter muscle, the results
showed a decrease in all groups for measurements both immediately and 24 hours after
the test (P<0.05); however, this decrease was greater in the group showing moderate
neck disability (d>0.8). Changes in temporalis muscle PPT’s were observed in both
measures for the group of moderate neck disability (P<0.001; d>0.8). In the group of
mild neck disability, changes were only observed immediately after the test (P=0.002;
d=0.19). No changes were observed in the group of healthy subjects (P>0.05).
For PPT in the cervical region (trapezius muscle and suboccipital muscles), the
post hoc analysis shows a decrease of values measures immediately and 24 hours after
the test (P<0.001) for group of moderate neck disability. This decrease in PPT can be
considered large for the suboccipital region (d>0.9) and small-medium for the trapezius
muscle (d=0.27 and 0.61). In the group with mild neck disability, changes were
observed only in the trapezius muscle PPT measurement immediately after the test
(P=0.028; d=0.09) and no statistically significant differences were observed in any of
the PPT measurements in the cervical region in the group of healthy subjects (P>0.05).
Correlations Analysis
Table 3 shows the results of correlation analysis examining the bivariate
relationships among self-reports for pain-related and psychological measures and
MMO, VAS and VAFS measured immediately and 24 hours after the tests for the

17
groups with moderate and mild neck disability. The strongest correlations were found in
the analysis for the group with moderate neck disability, where the pain-free MMO
immediately after the test was negatively associated with NDI (r=-0.54; P<0.001). For
the mild neck disability group, the greater correlation was between the MMO results
after 24 hours and NDI, which had a negative association (r=-0.49; P<0.001).
Multiple linear regression analysis
A linear regression analysis was performed to evaluate contributors to VAFS,
VAS and pain-free MMO after 24 hours regarding all of the self-report results for pain-
related and psychological measures in the patient groups with moderate and mild neck
disability; the results are presented in Table 4.
In the first model, the criterion variable VAFS was predicted by pain
catastrophizing (for both groups), explaining 17% and 12% of variance, respectively.
The following variables, VAS (moderate neck disability, β=-0.001; P=0.10, mild neck
disability, β=-0.053; P=0.72), HIT-6 (moderate neck disability, β=0.004; P=-0.97, mild
neck disability, β=-0.071; P=0.63), and NDI (moderate neck disability, β=-0.082;
P=0.59, mild neck disability, β=-0.070; P=0.67) were not significant predictors.
In the second model, the VAS after 24 hours was predicted by HIT-6 (moderate
neck disability group) and pain catastrophizing (mild neck disability group), explaining
22% and 14% of the variance, respectively. The VAS (moderate neck disability, β=-
0.27; P=0.06, mild neck disability, β=-0.13; P=0.41), NDI (moderate neck disability,
β=0.19; P=0.17, mild neck disability, β=0.24; P=0.13) and PCS (moderate neck
disability, β=0.16; P=0.25) and HIT-6 (mild neck disability, β=-0.054; P=0.71) were not
significant predictors.

18
In a third model, the pain-free MMO was predicted by NDI for both groups;
these models accounted for between 14% and 21% of the variance. The PCS (moderate
neck disability, β=0.20; P=0.19, mild neck disability, β=0.13; P=0.39), the VAS
(moderate neck disability, β=-0.34; P=0.85, mild neck disability, β=-0.26; P=0.13) and
HIT6 (moderate neck disability, β=-0.24; P=-0.066, mild neck disability, β=0.20;
P=0.64) were not significant predictors.
DISCUSION
The results of this study demonstrate that a protocol of masticatory provocation
can induce pain, fatigue and other trigeminal sensory-motor changes in patients with
headache attributed to temporomandibular disorders. Our findings are consistent with
previous studies which have also observed sensory changes induced experimentally by
the masticatory provocation test[47, 62–64]. The duration of the masticatory
provocation test used in our study was similar to other investigations[47, 63, 65].
However, some studies have used longer and also shorter durations for the masticatory
test, reporting significant changes in both situations for both patients and healthy
subjects[48, 62, 64, 66–68]. It is important to mention that group changes were found in
the healthy subjects, but these were smaller than in the other groups, this could be
explained by the observation that exercise can induce pain and increased
hyperalgesia[69]. In addition, other authors have suggested that experimentally-induced
pain during the test may be due to masticatory muscle ischemia followed by the
accumulation of metabolic products in these muscles[70–72]. We also need to take into
account that there is sufficient evidence to suggest fatigue as a factor that increases the
pain perception[73].

19
In this regard, our findings show strong positive correlations between fatigue
and perceived pain associated with the masticatory provocation test in the three assessed
groups. These results may explain in a general way the observed sensory-motor
changes, although they are not sufficient to justify neither the between-groups
differences nor the influence of cervical disability. Reflections and discussion of these
issues are presented in the following section in an effort to clarify and achieve a better
understanding of the matter.
One of the hypotheses proposed in this study is that cervical disability has an
influence over the trigeminal sensory-motor variables, modifying them. The results
obtained support this hypothesis because we observed greater changes in the moderate
cervical disability group immediately and 24 hours after the test. In addition, it was
hypothesized that the psychosocial factors would have a relationship with the results of
the masticatory provocation test and specifically with the pain and fatigue variables.
This relationship was proved after observing an association with pain catastrophizing.
Gender Differences
Regarding pain perception and fatigue during the test, our data show that gender
influences the results of the three groups: women presented with the greater perception
of pain intensity and masticatory fatigue. These results are consistent with previous
studies of experimentally-induced pain in patients[63] and healthy subjects[47, 68];
however, other investigations have not observed the interaction of gender factors with
experimentally-induced pain or masticatory fatigue [65, 74]. This research has not been
designed to identify the physiologic or psychological mechanisms which may explain
the differences in the results of men and women, although it is important to state that
there are many studies which present evidence-based results regarding the response that

20
women have to other painful clinical situations, adding the evidence of experimentally-
induced pain studies which indicate that women have a greater pain sensitivity than men
regarding several somatosensory tests[75].
Influence of the cervical disability over the trigeminal sensory-motor activity.
In this study, we have identified that patients with mild to moderate cervical
disability present a greater perception levels of pain and fatigue compared with healthy
subjects. It is important to mention that the group with moderate cervical disability
presented the greatest changes at the sensorial variables measured along the test,
immediately after and 24 hours after the test, with the exception of the pain intensity
perception after 24 hours, in which no statistically significant differences were found
between groups.
Although there are many studies that have used a provocative test to induce
masticatory pain and fatigue, we have only found one study similar to ours, in which
Haggman-Henrikson et al.[63] observed that patients with whiplash-associated
disorders presented greater masticatory pain and fatigue induced by the test compared to
TMD patients and healthy subjects.
We note recent scientific evidence that injuries to the cervical region may alter
the masticatory motor control and normal mandibular open-close function[76–78]. The
findings of this study may be related to this issue, because our results show that the
masticatory provocation test reduces the pain-free MMO at the end of the test, as seen in
the three groups assessed; these results are similar to previous studies[47, 72]. However,
we need to point out that the reduction was greater in both patient’s groups and it was
maintained at 24 hours only in the moderate cervical disability group. Also, it is

21
important to highlight that the regression analysis showed that cervical disability is a
predictor of the pain-free MMO (after 24 hours) in both groups of patients.
At present, the scientific evidence suggests the existence of cervical and
trigeminal motor patterns that act in a coordinated manner in the performance of
masticatory activities (chewing)[79–82], plus recent studies also support that the neck
muscles are activated during jaw-clenching tasks tasks assessed electromyographically
[83–85] and it seems that the activity of the neck muscles is increased as the demand for
masticatory work is greater[86]. Although most of these studies have been performed in
healthy subjects, we believe that these data are useful to try to explain some of the
results of this research. In this sense, we propose the theory that the masticatory motor
patterns are more altered with the presence of greater cervical pain or disability. This
situation would generate the activation of maladaptive compensatory mechanisms that
might alter the behaviour, recruitment and coordination of the neck and mandibular
motor systems, thus generating higher levels of fatigue and pain during the provocation
test and retaining these feelings 24 hours later.
This same theory could explain the results of decreased PPTs at the trigeminal and
cervical regions, noting that the PPTs changes were higher in the patient groups and that
most changes in the cervical PPTs at 24 hours occurred in the group of moderate
cervical disability. As a contributing factor to this situation, the presence of neck pain
must be considered, as this can lead to lower values of trigeminal PPTs compared to
healthy subjects [87]. Although we believe that there may be a direct relationship
between the trigeminal sensory-motor changes with cervical pain and disability, we
must also consider the possibility that the changes seen in patients would have been
mainly influenced by pre-established neuroplastic changes in the central nervous
system. Patients with chronic pain may be more susceptible to develop a central

22
sensitization process[88]. Wolf et al. suggest that in painful conditions where there is a
comorbidity, such as in the sample of patients in this study, it can be a determining
factor in the pathophysiology of central sensitization[89]. In relation to this, Gaff-
Radford proposed that in central sensitization, changes appear in afferent pathways that
enable the communication of cervical and orofacial nociceptive neurons in the
trigeminal nucleus[90]. In addition, there are many studies in TMD patients that have
found peripheral and central mechanisms compatible with a process of central
sensitization[91–97].
Influence of pain catastrophizing over trigeminal sensory-motor activity.
In this research, we have used self-reports of psychological and pain-related
variables to identify possible associations with sensory-motor variables. Through linear
regression analysis, we have observed that pain catastrophizing and the impact of
headache on the quality of life (HIT-6) were associated with the pain perception and
fatigue variables 24 hours after performing the masticatory provocation test.
Specifically, analysing the pain catastrophizing as a psychological factor resulted in a
predictor for fatigue at 24 hours after the test in the moderate cervical disability group,
and in the mild cervical disability group it was a predictor for perceived cervical
disability and fatigue after 24 hours. Pain catastrophizing is defined as a cognitive factor
that implies a mental negative perception or exaggeration of the perceived threat of
either a real or anticipated pain experience[98, 99]. It has been described that in patients
with TMD, catastrophizing contributes to the chronification of pain and disability [100].
It has also been associated with a greater use of health system services, with greater
clinical findings at assessment associated with a negative mood[40, 41] and with
alterations of the functional mandibular status[10]. Regarding the perceived fatigue and
pain catastrophizing, we did not find any clinical or experimental trials that have

23
examined their association in patients with craniofacial pain and TMD; but we found
one study researching the relationship of pain catastrophizing with masticatory
kinematic variables (i.e., amplitude, velocity, frequency cycle) which were measured
with a procedure using very short exposure times (15 seconds of chewing)[32]. In this
study, no associations of the kinematic variables measured with respect to catastrophism
were observed; however, we must take into account that the purpose of that study was
not to induce pain or fatigue to observe the response, as we did in this research. It is
important to note that a recent systematic review concluded that there is an association
between catastrophizing and fatigue and that the former influences the latter
proportionately; these results were observed in various clinical populations[101]. This
has also been demonstrated in other musculoskeletal disorders where pain
catastrophizing is associated with motor disturbances, such as decreased function,
performance of activities of daily living and limitation of exercise capacity[102–104].
The relationship between psychological factors, motor activity and pain seems to
be present in various cases of musculoskeletal pain, but the explanation for this is
complex and limited so far. Peck et al.[105] and Murray and Peck[106] have proposed a
possible explanation for this and have created a new Integrated Pain Adaptation Model
(IPAM). This model basically explains that the influence of pain on motor activity
depends on the interaction of multidimensional characteristics (biological and
psychosocial) of pain with the sensory-motor system of an individual, which results in a
new motor recruitment strategy in order to minimize pain. However, this motor
response may be associated with the appearance of another pain or worsening of the
existing pain[105, 106]. This model is based on the multidimensional features (sensory
discriminative, affective-emotional, cognitive) of the pain experience and how it affects
the sensory-motor system through the peripheral and central connections that this

24
system has with the autonomous nervous system, the limbic system and other higher
centres[105, 107].
Clinical and scientific implications
According to the results of this research, we found that neck pain and disability
can influence sensory and motor variables of the masticatory system. These findings
lead us to reflect on the importance of including a clinically specific assessment of the
cervical region in the diagnostic protocols for TMD and headache attributed to TMD. It
is noteworthy that the most commonly used diagnostic and classification methods for
patients with TMD do not include a specific assessment of neck pain and disability[20,
44, 108]. A diagnostic criterion observed recently in patients with headache attributed to
TMD is that mandibular movement, function or parafunction modify headache in the
temporal region[21]. We have observed an association between cervical disability with
pain-free MMO and have also found that patients with greater neck disability have
increased fatigue and pain induced by the masticatory test. These findings lead us to
assume that the cervical region may have an important role for this type of headache,
but this has to be confirmed in future research, as these data can be extrapolated only to
patients with this type of headache who also associate neck disability.
From the point of view of treatment, we propose an approach to reduce cervical
pain and disability as part of the overall therapeutic strategy, as this could be beneficial
to reduce the negative sensory symptoms and improve masticatory motor control. We
believe that this approach should be investigated in future studies, but it must be taken
into account that we have recent evidence that therapeutic exercise and manual therapy
to the cervical region produce positive effects on pain modulation in trigeminal areas
and improving pain-free MMO[46, 109].

25
In this study and other longitudinal or transversal studies, we have shown the
influence of psychosocial factors on patients with TMD[36, 110, 111]; specifically, our
results show an association between catastrophizing and perceived fatigue induced by
the masticatory activity. This finding shows the interaction between sensory-type
variables with psychological variables, which should be considered a crucial issue when
performing the assessment or designing of therapeutic interventions. In patients with
chronic pain, it is essential to recognize psychosocial factors that may be perceived as
obstacles to recovery[112]; achieving a reduction of pain catastrophizing is the best
predictor of successful rehabilitation in pain conditions[113].
The integration of a biopsychosocial perspective in clinical reasoning and
decision-making could be a key point in the management of pain and motor
rehabilitation of patients with headache attributed to TMD. It has been shown that
cognitive-behavioural therapy reduces pain intensity, depressive symptoms, improves
chewing function[114], reduces pain catastrophizing in patients with chronic TMD[115]
and, furthermore, it has been found that it causes neuroplastic adaptive changes
associated with decreased pain catastrophism in cases of chronic pain[116]. Prescribing
therapeutic exercise may be a good alternative to take into consideration; it has been
observed that exercise causes a reduction of catastrophizing and depressive symptoms;
these results were similar to cognitive behavioural therapy in patients with chronic
lower back pain[117].
Limitations
The results of this study should be discussed with the consideration that there are
several limitations. Although the sample size was calculated to have adequate power
and further losses were less than 20%, the results were not compared with a group with

26
headache attributed to TMD but without the presence of neck pain and disability. To
extrapolate the results to a clinical population would require similar but future studies to
be implemented using patient sample protocols with and without neck pain and
disability. Another limitation to consider is that pain catastrophizing was assessed as the
only psychological variable. It would be interesting to investigate the association of
other variables such as anxiety, depression, kinesiophobia and self-efficacy with
trigeminal sensory-motor variables.
As the only motor variable measured in this research was pain-free MMO, other
kinematic variables should be taken into consideration in future research as they may
provide more information. Moreover, we believe that measuring motor variables of the
cervical region could also be useful to analyse possible correlations with masticatory
variables.
CONCLUSION
The results of this study suggest that neck pain and disability have an influence
on the sensory-motor variables evaluated in patients with headache attributed to TMD.
In particular, it was observed that patients with moderate neck disability showed greater
changes immediately and 24 hours after the masticatory provocation test. Our data
provide new evidence about the possible neurophysiologic mechanisms of interaction
between the craniocervical region and the craniomandibular region. Regarding pain
catastrophizing, an association with perceived masticatory fatigue in both patient groups
was observed. These findings support the need to recognize the interaction between
sensory-motor and psychological aspects of headache attributed to TMD rather than
being assessed in isolation.

27
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
RL, AP, AG, JF participated in the study design, manuscript preparation and editing and
data acquisition. JP, SA, RL participated in the performed the statistical analysis,
database management and manuscript preparation. All authors read and approved the
final manuscript.
REFERENCES
1. Storm C, Wänman A (2006) Temporomandibular disorders, headaches, and cervical pain among females in a Sami population. Acta Odontol Scand 64:319–25. doi: 10.1080/00016350600801915
2. Anderson GC, John MT, Ohrbach R, et al. (2011) Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 152:765–71. doi: 10.1016/j.pain.2010.11.007
3. Rantala MA, Ahlberg J, Suvinen TI, et al. (2003) Temporomandibular joint related painless symptoms, orofacial pain, neck pain, headache, and psychosocial factors among non-patients. Acta Odontol Scand 61:217–222.
4. Ciancaglini R, Testa M, Radaelli G (1999) Association of neck pain with symptoms of temporomandibular dysfunction in the general adult population. Scand J Rehabil Med 31:17–22.
5. Nilsson I-M, List T, Drangsholt M (2013) Headache and co-morbid pains associated with TMD pain in adolescents. J Dent Res 92:802–7. doi: 10.1177/0022034513496255
6. Plesh O, Adams SH, Gansky S a (2011) Temporomandibular joint and muscle disorder-type pain and comorbid pains in a national US sample. J Orofac Pain 25:190–8.
7. Svensson P (2007) Muscle pain in the head: overlap between temporomandibular disorders and tension-type headaches. Curr Opin Neurol 20:320–325. doi: 10.1097/WCO.0b013e328136c1f9

28
8. Ashina S, Bendtsen L, Ashina M, et al. (2006) Generalized hyperalgesia in patients with chronic tension-type headache. Cephalalgia 26:940–948. doi: 10.1111/j.1468-2982.2006.01150.x
9. Leclerc A, Niedhammer I, Landre MF, et al. (1999) One-year predictive factors for various aspects of neck disorders. Spine (Phila Pa 1976) 24:1455–1462.
10. La Touche R, Pardo-Montero J, Gil-Martínez A, et al. (2014) Craniofacial pain and disability inventory (CF-PDI): development and psychometric validation of a new questionnaire. Pain Physician 17:95–108.
11. Olivo SA, Fuentes J, Major PW, et al. (2010) The association between neck disability and jaw disability. J Oral Rehabil 37:670–9. doi: 10.1111/j.1365-2842.2010.02098.x
12. Torisu T, Tanaka M, Murata H, et al. (2013) Modulation of neck muscle activity induced by intra-oral stimulation in humans. Clin Neurophysiol. doi: 10.1016/j.clinph.2013.10.018
13. Wang K, Sessle BJ, Svensson P, Arendt-Nielsen L (2004) Glutamate evoked neck and jaw muscle pain facilitate the human jaw stretch reflex. Clin Neurophysiol 115:1288–95. doi: 10.1016/j.clinph.2004.01.006
14. Svensson P, Wang K, Arendt-Nielsen L, et al. (2005) Pain effects of glutamate injections into human jaw or neck muscles. J Orofac Pain 19:109–18.
15. Ge H-Y, Wang K, Madeleine P, et al. (2004) Simultaneous modulation of the exteroceptive suppression periods in the trapezius and temporalis muscles by experimental muscle pain. Clin Neurophysiol 115:1399–408. doi: 10.1016/j.clinph.2004.01.017
16. Dessem D, Luo P (1999) Jaw-muscle spindle afferent feedback to the cervical spinal cord in the rat. Exp brain Res 128:451–9.
17. Hellström F, Thunberg J, Bergenheim M, et al. (2002) Increased intra-articular concentration of bradykinin in the temporomandibular joint changes the sensitivity of muscle spindles in dorsal neck muscles in the cat. Neurosci Res 42:91–9.
18. Hu JW, Sun K-Q, Vernon H, Sessle BJ (2005) Craniofacial inputs to upper cervical dorsal horn: implications for somatosensory information processing. Brain Res 1044:93–106. doi: 10.1016/j.brainres.2005.03.004
19. (2013) The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 33:629–808. doi: 10.1177/0333102413485658
20. Schiffman E, Ohrbach R, Truelove E, et al. (2014) Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J oral facial pain headache 28:6–27.

29
21. Schiffman E, Ohrbach R, List T, et al. (2012) Diagnostic criteria for headache attributed to temporomandibular disorders. Cephalalgia 32:683–92. doi: 10.1177/0333102412446312
22. Winocur E, Gavish A, Finkelshtein T, et al. (2001) Oral habits among adolescent girls and their association with symptoms of temporomandibular disorders. J Oral Rehabil 28:624–9.
23. Gavish A, Halachmi M, Winocur E, Gazit E (2000) Oral habits and their association with signs and symptoms of temporomandibular disorders in adolescent girls. J Oral Rehabil 27:22–32.
24. Bevilaqua-Grossi D, Chaves TC, de Oliveira AS, Monteiro-Pedro V (2006) Anamnestic index severity and signs and symptoms of TMD. Cranio 24:112–8.
25. Wänman A, Agerberg G (1986) Relationship between signs and symptoms of mandibular dysfunction in adolescents. Community Dent Oral Epidemiol 14:225–30.
26. Mao J, Stein RB, Osborn JW (1993) Fatigue in human jaw muscles: a review. J Orofac Pain 7:135–42.
27. Svensson P, Graven-Nielsen T (2001) Craniofacial muscle pain: review of mechanisms and clinical manifestations. J Orofac Pain 15:117–145.
28. Lobbezoo F, van Selms MKA, Naeije M (2006) Masticatory muscle pain and disordered jaw motor behaviour: Literature review over the past decade. Arch Oral Biol 51:713–20. doi: 10.1016/j.archoralbio.2006.03.012
29. Kurita H, Ohtsuka A, Kurashina K, Kopp S (2001) Chewing ability as a parameter for evaluating the disability of patients with temporomandibular disorders. J Oral Rehabil 28:463–465.
30. De Leeuw R, Studts JL, Carlson CR (2005) Fatigue and fatigue-related symptoms in an orofacial pain population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:168–74. doi: 10.1016/j.tripleo.2004.03.001
31. Boggero IA, Kniffin TC, Leeuw R De, Carlson CR (2014) Fatigue Mediates the Relationship Between Pain Interference and Distress in Patients with Persistent Orofacial Pain. 28:38–45. doi: 10.11607/jop.1204
32. Brandini D a, Benson J, Nicholas MK, et al. (2011) Chewing in temporomandibular disorder patients: an exploratory study of an association with some psychological variables. J Orofac Pain 25:56–67.
33. Palla S (2011) Biopsychosocial pain model crippled? J Orofac Pain 25:289–90.
34. Gatchel RJ, Peng YB, Peters ML, et al. (2007) The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull 133:581–624. doi: 10.1037/0033-2909.133.4.581

30
35. List T, John MT, Ohrbach R, et al. (2012) Influence of temple headache frequency on physical functioning and emotional functioning in subjects with temporomandibular disorder pain. J Orofac Pain 26:83–90.
36. Fillingim RB, Ohrbach R, Greenspan JD, et al. (2011) Potential psychosocial risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J Pain 12:T46–60. doi: 10.1016/j.jpain.2011.08.007
37. Buenaver LF, Quartana PJ, Grace EG, et al. (2012) Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial temporomandibular disorder participants: the mediating role of sleep disturbance. Pain 153:1159–66. doi: 10.1016/j.pain.2012.01.023
38. Velly AM, Look JO, Carlson C, et al. (2011) The effect of catastrophizing and depression on chronic pain--a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 152:2377–83. doi: 10.1016/j.pain.2011.07.004
39. Quartana PJ, Buenaver LF, Edwards RR, et al. (2010) Pain catastrophizing and salivary cortisol responses to laboratory pain testing in temporomandibular disorder and healthy participants. J Pain 11:186–94. doi: 10.1016/j.jpain.2009.07.008
40. Turner JA, Brister H, Huggins K, et al. (2005) Catastrophizing is associated with clinical examination findings, activity interference, and health care use among patients with temporomandibular disorders. J Orofac Pain 19:291–300.
41. Turner JA, Dworkin SF, Mancl L, et al. (2001) The roles of beliefs, catastrophizing, and coping in the functioning of patients with temporomandibular disorders. Pain 92:41–51.
42. Von Elm E, Altman DG, Egger M, et al. (2008) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61:344–9. doi: 10.1016/j.jclinepi.2007.11.008
43. Dworkin SF, LeResche L (1992) Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 6:301–55.
44. Schiffman EL, Ohrbach R, Truelove EL, et al. (2010) The Research Diagnostic Criteria for Temporomandibular Disorders. V: methods used to establish and validate revised Axis I diagnostic algorithms. J Orofac Pain 24:63–78.
45. Vernon H, Mior S (1991) The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 14:409–15.
46. La Touche R, París-Alemany A, Mannheimer JS, et al. (2012) Does Mobilization of the Upper Cervical Spine Affect Pain Sensitivity and Autonomic Nervous System

31
Function in Patients With Cervico-craniofacial Pain?: A Randomized-controlled Trial. Clin J Pain. doi: 10.1097/AJP.0b013e318250f3cd
47. Karibe H, Goddard G, Gear RW (2003) Sex differences in masticatory muscle pain after chewing. J Dent Res 82:112–6.
48. Farella M, Bakke M, Michelotti A, Martina R (2001) Effects of prolonged gum chewing on pain and fatigue in human jaw muscles. Eur J Oral Sci 109:81–5.
49. Sullivan MJL, Bisop SC, Pivik J (1995) The pain catastrophizing scale: development and validation. Psychol Assess 7:524–532.
50. García Campayo J, Rodero B, Alda M, et al. (2008) [Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia]. Med Clin (Barc) 131:487–92.
51. Andrade Ortega JA, Delgado Martínez AD, Almécija Ruiz R (2010) Validation of the Spanish version of the Neck Disability Index. Spine (Phila Pa 1976) 35:E114–8.
52. Bjorner JB, Kosinski M, Ware JE (2003) Calibration of an item pool for assessing the burden of headaches: an application of item response theory to the headache impact test (HIT). Qual Life Res 12:913–33.
53. Gandek B, Alacoque J, Uzun V, et al. (2003) Translating the Short-Form Headache Impact Test (HIT-6) in 27 countries: methodological and conceptual issues. Qual Life Res 12:975–9.
54. Martin M, Blaisdell B, Kwong JW, Bjorner JB (2004) The Short-Form Headache Impact Test (HIT-6) was psychometrically equivalent in nine languages. J Clin Epidemiol 57:1271–8. doi: 10.1016/j.jclinepi.2004.05.004
55. Bijur PE, Silver W, Gallagher EJ (2001) Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med 8:1153–7.
56. Tseng BY, Gajewski BJ, Kluding PM (2010) Reliability, responsiveness, and validity of the visual analog fatigue scale to measure exertion fatigue in people with chronic stroke: a preliminary study. Stroke Res Treat. doi: 10.4061/2010/412964
57. Walton DM, Macdermid JC, Nielson W, et al. (2011) Reliability, standard error, and minimum detectable change of clinical pressure pain threshold testing in people with and without acute neck pain. J Orthop Sports Phys Ther 41:644–50. doi: 10.2519/jospt.2011.3666
58. Alacreu-Beltran H, Lopez-de-Uralde-Villanueva I, Paris-Alemany A, et al. (2014) Intra-rater and Inter-rater Reliability of Mandibular Range of Motion Measures Considering a Neutral Craniocervical Position. J Phys Ther Sci 26:1–6.

32
59. Faul F, Erdfelder E, Lang A-G, Buchner A (2007) G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39:175–91.
60. Cohen J. (1988) Statistical power analysis for the behavioral sciences. Hillsdale
61. Peduzzi P, Concato J, Kemper E, et al. (1996) A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol 49:1373–9.
62. Gavish A, Winocur E, Menashe S, et al. (2002) Experimental chewing in myofascial pain patients. J Orofac Pain 16:22–8.
63. Haggman-Henrikson B, Osterlund C, Eriksson P-O (2004) Endurance during Chewing in Whiplash-associated Disorders and TMD. J Dent Res 83:946–950. doi: 10.1177/154405910408301211
64. Dao TTT, Lund JP, Lavigne GJ (1994) Pain Responses to Experimental Chewing in Myofascial Pain Patients. doi: 10.1177/00220345940730060601
65. Van Selms MKA, Wang K, Lobbezoo F, et al. (2005) Effects of masticatory muscle fatigue without and with experimental pain on jaw-stretch reflexes in healthy men and women. Clin Neurophysiol 116:1415–23. doi: 10.1016/j.clinph.2005.02.017
66. Koutris M, Lobbezoo F, Naeije M, et al. (2009) Effects of intense chewing exercises on the masticatory sensory-motor system. J Dent Res 88:658–62. doi: 10.1177/0022034509338573
67. Christensen L V, Tran KT, Mohamed SE (1996) Gum chewing and jaw muscle fatigue and pains. J Oral Rehabil 23:424–37.
68. Plesh O, Curtis DA, Hall LJ, Miller A (1998) Gender difference in jaw pain induced by clenching. J Oral Rehabil 25:258–63.
69. Yokoyama T, Lisi TL, Moore SA, Sluka KA (2007) Muscle fatigue increases the probability of developing hyperalgesia in mice. J Pain 8:692–9. doi: 10.1016/j.jpain.2007.05.008
70. Stohler CS (1999) Craniofacial pain and motor function: pathogenesis, clinical correlates, and implications. Crit Rev Oral Biol Med 10:504–18.
71. Nicol C, Kuitunen S, Kyröläinen H, et al. (2003) Effects of long- and short-term fatiguing stretch-shortening cycle exercises on reflex EMG and force of the tendon-muscle complex. Eur J Appl Physiol 90:470–9. doi: 10.1007/s00421-003-0862-y
72. Svensson P, Burgaard A, Schlosser S (2001) Fatigue and pain in human jaw muscles during a sustained, low-intensity clenching task. Arch Oral Biol 46:773–7.

33
73. Cote JN, Hoeger Bement MK Update on the relation between pain and movement: consequences for clinical practice. Clin J Pain 26:754–62. doi: 10.1097/AJP.0b013e3181e0174f
74. Koutris M, Lobbezoo F, Sümer NC, et al. (2013) Is myofascial pain in temporomandibular disorder patients a manifestation of delayed-onset muscle soreness? Clin J Pain 29:712–6. doi: 10.1097/AJP.0b013e318270fa59
75. Fillingim RB, King CD, Ribeiro-Dasilva MC, et al. (2009) Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain 10:447–85. doi: 10.1016/j.jpain.2008.12.001
76. Eriksson P-O, Zafar H, Häggman-Henrikson B (2004) Deranged jaw-neck motor control in whiplash-associated disorders. Eur J Oral Sci 112:25–32.
77. Eriksson P-O, Häggman-Henrikson B, Zafar H (2007) Jaw-neck dysfunction in whiplash-associated disorders. Arch Oral Biol 52:404–8. doi: 10.1016/j.archoralbio.2006.12.016
78. Zafar H, Nordh E, Eriksson P-O (2006) Impaired positioning of the gape in whiplash-associated disorders. Swed Dent J 30:9–15.
79. Eriksson PO, Zafar H, Nordh E (1998) Concomitant mandibular and head-neck movements during jaw opening-closing in man. J Oral Rehabil 25:859–70.
80. Eriksson PO, Häggman-Henrikson B, Nordh E, Zafar H (2000) Co-ordinated mandibular and head-neck movements during rhythmic jaw activities in man. J Dent Res 79:1378–84.
81. Zafar H, Nordh E, Eriksson PO (2000) Temporal coordination between mandibular and head-neck movements during jaw opening-closing tasks in man. Arch Oral Biol 45:675–82.
82. La Touche R, París-Alemany A, Von Piekartz H, et al. (2011) The influence of cranio-cervical posture on maximal mouth opening and pressure pain threshold in patients with myofascial temporomandibular pain disorders. Clin J Pain 27:48–55. doi: 10.1097/AJP.0b013e3181edc157
83. Giannakopoulos NN, Hellmann D, Schmitter M, et al. (2013) Neuromuscular interaction of jaw and neck muscles during jaw clenching. J Orofac Pain 27:61–71.
84. Hellmann D, Giannakopoulos NN, Schmitter M, et al. (2012) Anterior and posterior neck muscle activation during a variety of biting tasks. Eur J Oral Sci 120:326–34. doi: 10.1111/j.1600-0722.2012.00969.x
85. Giannakopoulos NN, Schindler HJ, Rammelsberg P, et al. (2013) Co-activation of jaw and neck muscles during submaximum clenching in the supine position. Arch Oral Biol 58:1751–60. doi: 10.1016/j.archoralbio.2013.09.002

34
86. Häggman-Henrikson B, Nordh E, Eriksson P-O (2013) Increased sternocleidomastoid, but not trapezius, muscle activity in response to increased chewing load. Eur J Oral Sci 121:443–9. doi: 10.1111/eos.12066
87. La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, et al. (2010) Bilateral mechanical-pain sensitivity over the trigeminal region in patients with chronic mechanical neck pain. J pain Off J Am Pain Soc 11:256–263.
88. Henry DE, Chiodo AE, Yang W (2011) Central nervous system reorganization in a variety of chronic pain states: a review. PM R 3:1116–25. doi: 10.1016/j.pmrj.2011.05.018
89. Woolf CJ (2011) Central sensitization: implications for the diagnosis and treatment of pain. Pain 152:S2–15. doi: 10.1016/j.pain.2010.09.030
90. Graff-Radford SB (2012) Facial pain, cervical pain, and headache. Continuum (Minneap Minn) 18:869–82. doi: 10.1212/01.CON.0000418648.54902.42
91. Ayesh EE, Jensen TS, Svensson P (2007) Hypersensitivity to mechanical and intra-articular electrical stimuli in persons with painful temporomandibular joints. J Dent Res 86:1187–92.
92. Anderson GC, John MT, Ohrbach R, et al. (2011) Influence of headache frequency on clinical signs and symptoms of TMD in subjects with temple headache and TMD pain. Pain 152:765–771. doi: 10.1016/j.pain.2010.11.007
93. Park JW, Clark GT, Kim YK, Chung JW (2010) Analysis of thermal pain sensitivity and psychological profiles in different subgroups of TMD patients. Int J Oral Maxillofac Surg 39:968–74. doi: 10.1016/j.ijom.2010.06.003
94. Feldreich A, Ernberg M, Lund B, Rosén A (2012) Increased β-endorphin levels and generalized decreased pain thresholds in patients with limited jaw opening and movement-evoked pain from the temporomandibular joint. J Oral Maxillofac Surg 70:547–56. doi: 10.1016/j.joms.2011.09.013
95. Chaves TC, Nagamine HM, de Sousa LM, et al. (2013) Differences in pain perception in children reporting joint and orofacial muscle pain. J Clin Pediatr Dent 37:321–7.
96. Raphael KG, Janal MN, Anathan S, et al. (2009) Temporal summation of heat pain in temporomandibular disorder patients. J Orofac Pain 23:54–64.
97. Sarlani E, Grace EG, Reynolds MA, Greenspan JD (2004) Evidence for up-regulated central nociceptive processing in patients with masticatory myofascial pain. J Orofac Pain 18:41–55.
98. Turner JA, Aaron LA (2001) Pain-related catastrophizing: what is it? Clin J Pain 17:65–71.

35
99. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. (2001) Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 17:52–64.
100. Velly AM, Look JO, Carlson C, et al. (2011) The effect of catastrophizing and depression on chronic pain--a prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 152:2377–83. doi: 10.1016/j.pain.2011.07.004
101. Lukkahatai N, Saligan LN (2013) Association of catastrophizing and fatigue: a systematic review. J Psychosom Res 74:100–9. doi: 10.1016/j.jpsychores.2012.11.006
102. Nijs J, Van de Putte K, Louckx F, et al. (2008) Exercise performance and chronic pain in chronic fatigue syndrome: the role of pain catastrophizing. Pain Med 9:1164–72.
103. Nijs J, Meeus M, Heins M, et al. (2012) Kinesiophobia, catastrophizing and anticipated symptoms before stair climbing in chronic fatigue syndrome: an experimental study. Disabil Rehabil 34:1299–305. doi: 10.3109/09638288.2011.641661
104. Meeus M, Nijs J, Van Mol E, et al. (2012) Role of psychological aspects in both chronic pain and in daily functioning in chronic fatigue syndrome: a prospective longitudinal study. Clin Rheumatol 31:921–9. doi: 10.1007/s10067-012-1946-z
105. Peck CC, Murray GM, Gerzina TM (2008) How does pain affect jaw muscle activity? The Integrated Pain Adaptation Model. Aust Dent J 53:201–7. doi: 10.1111/j.1834-7819.2008.00050.x
106. Murray GM, Peck CC (2007) Orofacial pain and jaw muscle activity: a new model. J Orofac Pain 21:263–78; discussion 279–88.
107. Craig AD (2003) A new view of pain as a homeostatic emotion. Trends Neurosci 26:303–7.
108. Benoliel R, Svensson P, Heir GM, et al. (2011) Persistent orofacial muscle pain. Oral Dis 17 Suppl 1:23–41. doi: 10.1111/j.1601-0825.2011.01790.x
109. La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, et al. (2009) The effects of manual therapy and exercise directed at the cervical spine on pain and pressure pain sensitivity in patients with myofascial temporomandibular disorders. J Oral Rehabil 36:644–52. doi: 10.1111/j.1365-2842.2009.01980.x
110. Fillingim RB, Ohrbach R, Greenspan JD, et al. (2013) Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain 14:T75–90. doi: 10.1016/j.jpain.2013.06.009
111. Chen H, Nackley A, Miller V, et al. (2013) Multisystem dysregulation in painful temporomandibular disorders. J Pain 14:983–96. doi: 10.1016/j.jpain.2013.03.011

36
112. Main CJ (2013) The importance of psychosocial influences on chronic pain. Pain Manag 3:455–66. doi: 10.2217/pmt.13.49
113. Sullivan MJ (2013) What is the clinical value of assessing pain-related psychosocial risk factors? Pain Manag 3:413–6. doi: 10.2217/pmt.13.55
114. Turner JA, Mancl L, Aaron LA (2006) Short- and long-term efficacy of brief cognitive-behavioral therapy for patients with chronic temporomandibular disorder pain: a randomized, controlled trial. Pain 121:181–94. doi: 10.1016/j.pain.2005.11.017
115. Turner JA, Mancl L, Aaron LA (2005) Brief cognitive-behavioral therapy for temporomandibular disorder pain: effects on daily electronic outcome and process measures. Pain 117:377–87. doi: 10.1016/j.pain.2005.06.025
116. Seminowicz DA, Shpaner M, Keaser ML, et al. (2013) Cognitive-Behavioral Therapy Increases Prefrontal Cortex Gray Matter in Patients With Chronic Pain. J Pain. doi: 10.1016/j.jpain.2013.07.020
117. Smeets RJEM, Vlaeyen JWS, Kester ADM, Knottnerus JA (2006) Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain 7:261–71. doi: 10.1016/j.jpain.2005.10.011

37
Figure 1. Data represent mean value and error bars with 95% confidence intervals of
the mean of the pain intensity score (A), and the visual analogue fatigue scale scores
(B). Recorded during the 6 min and 24 hours after provocation chewing test. Level of
significance (multiple comparisons for each group): Moderate disability, *P<0.05;
**P<0.01; Mild disability, °P<0.05; °°P<0.01; and Healthy, ^P<0.05; ^^P<0.01.
Figure 2. Comparison between groups of the pain intensity (A) and perceived fatigue
(B) immediately (6 min) and 24 hours after the provocation chewing test. Data represent
mean value, error bars with 95% confidence intervals of the mean and effect size (d).
Level of significance: *P<0.05; **P<0.01.

38
Table 1. Summary of Demographic, Pain and Psychological Variables
Moderate Neck Disability (N=41)
Mild Neck Disability (N=42)
Healthy (N=39)
t / F P Value
Variables Mean±SD Range Mean±SD Range Mean±SD Range Sex (female/male) 26/15 - 25/17 - 26/13 - - -
Weight (kg)
69.56±12.47 51-103 67.76±14.03 50-97 64.84±10.2 48-90 1.4 0.23
Heigth (cm)
167.56±12.4
7
152-183 165.54±12.09 150-185 169.97±8.51 156-189 1.98 0.14
Age (years)
44.31±10.9 22-59 40.95±12.89 19-60 40.61±10.01 30-65 1.3 0.27
Pain duration
(months)
19.73±12.66 6-60 22.19±13.36 6-48 - - -0.8 0.39
NDI (points) 17.58±2.69 15-24 11.42±2.48 7-14 - - 10.8 0.01
PCS (points) 17.09±3.75 7-23 15.8±4.02 7-22 5.46±1.75 2-9 143 0.01
HIT-6 (points) 55.31±4.9 49-65 53.16±4.74 43-59 - - 2 0.04
VAS (mm) 40.75±9.17 21-58 37.04±9.16 19-54 - - 1.8 0.06
Abbreviations: NDI, Neck Disability Index; PCS, Pain Catastrophizing Scale; HIT-6, headache impact test-6; Visual Analog Scale, VAS; SD, standard deviation

39
Table 2. Descriptive data and multiple comparisons of the assessed variables
** p < 0.01; *p < 0.05 Abbreviations: MMO, maximal mouth opening; PPT, pressure pain threshold; SD, standard deviation
Mean±SD Mean difference (95% CI) Effect size (d)
Group Baseline Immediately after
After 24 hours a) Base vs. Immediately b) Base vs. 24 h.
MMO (mm)
Moderate Neck Disability
42.43±2.75 40.65±2.01 41.85±2.19 a) 1.89 (1.39 to 2.39)**;d=0.74 b) 0.6 (0.02 to 1.17)*;d=0.26
Mild Neck Disability
43.61±2.87 42±2.18 43.26±2.68 a) 1.56 (1.09 to 2.07)**; d=0.63 b) 0.36 (-0.01 to 0.75); d=0.12
Healthy 50±4.46 49.05±3.95 49.87±4.57
a) 0.76 (0.24 to 1.29)*; d=0.22 b) 0.09 (-0.32 to 0.51); d=0.02
PPT. Masseter Moderate Neck Disability
1.9±0.21 1.02±0.17 0.88±0.2 a) 0.89 (0.79 to 0.99)** d=4.66 b) 1.03 (0.94 to 1.13)** d=5.03
Mild Neck Disability
2.01±0.34 1.44±0.28 1.57±0.34 a) 0.57 (0.48 to 0.67)** d=1.82 b) 0.44 (0.35 to 0.53)** d=1.29
Healthy 2.85±0.58 2.39±0.52 2.7±0.51
a) 0.45 (0.35 to 0.56)** d=0.84 b) 0.13 (0.03 to 0.23)* d=0.27
PPT. Temporalis Moderate Neck Disability
1.99±0.19 1.55±0.25 1.62±0.23 a) 0.44 (0.39 to 0.49)** d=2.06 b) 0.37 (0.25 to 0.49)** d=1.77
Mild Neck Disability
2.12±0.35 2.05±0.37 2.04±0.45 a) 0.07 (0.02 to 0.12)** d=0.19 b) 0.09 (-0.02 to 0.2) d=0.20
Healthy 3.31±0.83 3.26±0.82 3.27±0.84
a) 0.04 (-0.001to 0.1) d=0.06 b) 0.06 (-0.05 to 0.19) d=0.04
PPT. Suboccipital
Moderate Neck Disability
2.39±0.44 1.65±0.36 1.47±0.32 a) 0.78 (0.7 to 0.85)** d=1.86 b) 0.95 (0.83 to 1.07)** d=2.42
Mild Neck Disability
2.14±0.57 2.06±0.55 2.22±0.57 a) 0.07 (-0.00 to 0.15) d=0.14 b) -0.11 (-0.23 to 0.00)* d=0.14
Healthy 3.15±0.56
3.09±0.55 3.18 ±0.59
a) 0.06 (-0.01 to 0.14) d=0.1 b) -0.01 (-0.13 to 0.11) d=0.05
PPT. Trapezius Moderate Neck Disability
2.62±0.49 2.33±0.47 2.49±0.45 a) 0.28 (0.24 to 0.33)** d=0.61 b) 0.14 (0.08 to 0.2)** d=0.27
Mild Neck Disability
2.68±0.62 2.62±0.63 2.63±0.58 a) 0.04 (0.00 to 0.09)* d=0.09 b) 0.04 (-0.01 to 0.1) d=0.08
Healthy 3.54±1 3.51±0.97 3.53±0.94 a)0.01 (-0.03 to 0.06) d=0.03 b) -0.01 (-0.05 to 0.07) d=0.01

40
Table 3. Pearson's correlation coefficient between the different variables analyzed in the study
Groups VAS 6min. VAS 24h. VAFS 6min.
VAFS 24h. MMO Immediately After
MMO 24h
Moderate Neck Disability
NDI 0.49** 0.28 0.40** 0.07 -0.54** -0.40**
Mild Neck Disability
0.02 0.37* 0.02 0.21 -0.48** -0.49**
Moderate Neck Disability
PCS 0.10 0.24 0.17 0.44** 0.03 0.04
Mild Neck Disability
0.08 0.40** 0.01 0.38* -0.17 -0.09
Moderate Neck Disability
HIT-6 0.41** 0.48** 0.27 0.07 -0.12 -0.31*
Mild Neck Disability
-0.11 -0.03 0.30 -0.04 -0.13 -0.12
Moderate Neck Disability
VAS -0.08 0.39* 0.49** 0.16 -0.23 -0.25
Mild Neck Disability
-0.08 0.17 -0.17 0.11 -0.39* -0.47**
** p < 0.01; *p < 0.05 Abbreviations: NDI, Neck Disability Index; PCS, pain catastrophizing scale; HIT-6, headache impact test-6; VAS, visual analog scale; VAFS, visual analog fatigue scale; MMO, maximal mouth opening

41
Table 4. Multiple linear regression analysis
Moderate Neck Disability
criterion variable
predictor variables
Regression coefficient (B)
Standardized coefficient (β)
Significance (p)
VIF Adjusted R2
VAFS24 PCS 0.84 0.44 0.004 1.00 0.17
VAS24 HIT-6 0.93 0.48 0.001 1.00 0.22
MMO24 NDI -0.35 -0.40 0.01 1.12 0.14
Mild Neck Disability
VAFS24 PCS 0.98 0.38 0.013 1.00 0.12
VAS24 PCS 0.67 0.40 0.009 1.00 0.14
MMO24 NDI -0.53 -0.49 0.001 1.00 0.21
Abbreviations: NDI, Neck Disability Index; PCS, pain catastrophizing scale; HIT-6, headache impact test-6; VAS, visual analog scale; VAFS, visual analog fatigue scale; MMO, maximal mouth opening; 24, 24 hours after of tests

�
��
��
��
��
��
��
1 2 3 4 5 6 24
VA
FS
(m
m)
∆�� ������ ������
∆������ ������
,� ����
�
�
��
��
��
��
��
��
��
��
��
� � � � � � ��
VA
S (
mm
)
∆�� ������ ������
∆������ ������
,� ����
**
**
**
**
**
*
��
��
��
��
��
��
^^ ^^
**
**
**
**
**
��
��
��
��
��
^^
^^^^
^^^^
�
�
Fig
ure
1

0
5
10
15
20
25
30
35
40
45
50
6 24
VA
S (
mm
)
Time: 6 min and 24 hours
Moderate Disability
Mild Disability
Healthy
�
** (d=3.5)
** (d=1.22)
** (d=2.93) ** (d=1.54)
(d=0.27)
** (d=1.59)
�
0
10
20
30
40
50
60
6 24
VA
FS
(m
m)
Time: 6 min and 24 hours
Moderate Disability
Mild Disability
Healthy
** (d=3.16)
** (d=1.15)
** (d=3.47) ** (d=2.47)
** (d=0.69)
** (d=1.17)
Fig
ure
2

182
5.6 Estudio VI
La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K, Angulo-Díaz-
Parreño S, Paris-Alemany A, Cleland JA. The effects of manual therapy and exercise directed at
the cervical spine on pain and pressure pain sensitivity in patients with myofascial
temporomandibular disorders. J Oral Rehabil. 2009 Sep;36(9):644-52.
Objetivos del estudio
Nuestro objetivo fue investigar los efectos de la terapia manual y el ejercicio dirigido a la
columna cervical en la intensidad del dolor, la MAI y los UDPs de músculos masticatorios en
pacientes con TCM.
Resultados
El modelo mixto de ANOVA 2X3 reveló un efecto significativo en el factor tiempo (F = 77,8; P
<0,001), pero no para el factor lado (F = 0,2; P = 0,7) para los cambios en los UDPs sobre el
músculo masetero y más músculo temporal (tiempo: F = 66,8; P <0,001; lado: F = 0,07; P =
0,8). Las pruebas post hoc revelaron diferencias significativas entre pre-intervención y la post-
intervención y período de seguimiento (P <0,001), pero no entre la post-intervención y el
periodo seguimiento (P = 0,9) para ambos músculos. Los tamaños del efecto eran grandes (d>
1,0) para ambos períodos de seguimiento en los UDPS musculares. El ANOVA encontró un
efecto significativo de tiempo (F = 78,6; P <0,001) los cambios en la intensidad del dolor y la
MAI sin dolor (F = 17,1; P <0,001). Se encontraron diferencias significativas entre la pre-
intervención y dos periodos post-intervención (P <0.001), pero no entre la medida post-
intervención y el periodo de seguimiento (P> 0.7). Dentro del grupo tamaños del efecto eran
grandes (d> 0,8) para los resultados post-intervención y los períodos de seguimiento.
Conclusión
La aplicación de tratamiento dirigido a la columna vertebral cervical puede ser beneficioso en la
disminución de la intensidad del dolor, el aumento de los UDPS en los músculos de la
masticación y en la MAI libre de dolor en pacientes con TCM.

The effects of manual therapy and exercise directed at the
cervical spine on pain and pressure pain sensitivity in
patients with myofascial temporomandibular disorders
R. LA TOUCHE*, †, C. FERNANDEZ-DE-LAS-PENAS‡, §, J . FERNANDEZ-CARNERO‡, §,
K. ESCALANTE¶, S. ANGULO-DIAZ-PARRENO†, A. PARIS-ALEMANY† &
J. A. CLELAND** , ††, ‡‡*Faculty of Medicine, Department of Physical Therapy, Universidad San Pablo CEU, Madrid, †University
Center for Clinical Research of the Craneal-Cervical-Mandibular System of Universidad San Pablo CEU, Madrid, ‡Department of Physical
Therapy, Occupational Therapy, Rehabilitation and Physical Medicine, Universidad Rey Juan Carlos, Alcorcon, Madrid, §Esthesiology
Laboratory of Universidad Rey Juan Carlos, Alcorcon, Madrid, ¶Faculty of Psychology, Department of Personality Assessment and Psychology
Treatment, Universidad Complutense, Madrid, Spain, **Department of Physical Therapy, Franklin Pierce University, Concord, ††Physical
Therapist, Rehabilitation Services, Concord Hospital, Concord, NH and ‡‡Faculty, Manual Therapy Fellowship Program, Regis University,
Denver, CO, USA
SUMMARY No studies have investigated the effects of
the treatments directed at the cervical spine in
patients with temporomandibular disorders (TMD).
Our aim was to investigate the effects of joint
mobilization and exercise directed at the cervical
spine on pain intensity and pressure pain sensitivity
in the muscles of mastication in patients with TMD.
Nineteen patients (14 females), aged 19–57 years,
with myofascial TMD were included. All patients
received a total of 10 treatment session over a 5-
week period (twice per week). Treatment included
manual therapy techniques and exercise directed at
the cervical spine. Outcome measures included
bilateral pressure pain threshold (PPT) levels over
the masseter and temporalis muscles, active pain-
free mouth opening (mm) and pain (Visual Ana-
logue Scale) and were all assessed pre-intervention,
48 h after the last treatment (post-intervention) and
at 12-week follow-up period. Mixed-model ANOVAS
were used to examine the effects of the intervention
on each outcome measure. Within-group effect sizes
were calculated in order to assess clinical effect. The
2 · 3 mixed model ANOVA revealed significant effect
for time (F = 77Æ8; P < 0Æ001) but not for side (F = 0Æ2;
P = 0Æ7) for changes in PPT over the masseter muscle
and over the temporalis muscle (time: F = 66Æ8;
P < 0Æ001; side: F = 0Æ07; P = 0Æ8). Post hoc revealed
significant differences between pre-intervention
and both post-intervention and follow-up periods
(P < 0Æ001) but not between post-intervention and
follow-up period (P = 0Æ9) for both muscles. Within-
group effect sizes were large (d > 1Æ0) for both
follow-up periods in both muscles. The ANOVA
found a significant effect for time (F = 78Æ6;
P < 0Æ001) for changes in pain intensity and active
pain-free mouth opening (F = 17Æ1; P < 0Æ001). Sig-
nificant differences were found between pre-inter-
vention and both post-intervention and follow-up
periods (P < 0Æ001) but not between the post-
intervention and follow-up period (P > 0Æ7).
Within-group effect sizes were large (d > 0Æ8) for
both post-intervention and follow-up periods. The
application of treatment directed at the cervical
spine may be beneficial in decreasing pain intensity,
increasing PPTs over the masticatory muscles and an
increasing pain-free mouth opening in patients with
myofascial TMD.
KEYWORDS: cervical spine, temporomandibular dis-
order, pressure pain sensitivity
Accepted for publication 25 June 2009
ª 2009 Blackwell Publishing Ltd doi: 10.1111/j.1365-2842.2009.01980.x
Journal of Oral Rehabilitation 2009 36; 644–652

Introduction
Temporomandibular disorder (TMD) is a term which
includes several conditions involving the temporoman-
dibular joint and the muscles of mastication. The most
common symptoms of TMD include pain located over
the facial region and tenderness to palpation of the
masticatory structures. Some studies have shown
prevalence rate of TMD to be between 3% and 15%
in the Western population (1), with an incidence
between 2% and 4% (2). A recent survey determined
that the overall prevalence of TMD was 6Æ3% for
women and 2Æ8% for men (3).
It appears that an intimate functional relationship
exists between the mandibular and the head-neck
systems, as suggested by their anatomical and bio-
mechanical inter-relationships, although current
evidence is conflicting (4). Several epidemiological
studies have reported that patients with TMD often
experience symptoms of neck pain and that patients
with neck pain also suffered from symptoms in the
orofacial region (5–8). In addition, Eriksson et al. (9)
reported that mouth opening was accompanied by
head-neck extension and mouth closing by head-neck
flexion, with a precise temporal coordination between
jaw-neck movements dependent on the speed of the
movement (10).
The neuro-anatomical basis for the relationship
between the head and neck may be related to the
trigemino-cervical nucleus caudalis in the spinal grey
matter of the spinal cord at the C1–C3 level, where
there is a convergence on the nociceptive second order
neurons receiving trigeminal and cervical inputs (11).
The topographic arrangement of the trigeminal nucleus
caudalis allows the interchange of nociceptive infor-
mation between the cervical spine and the trigeminal
nerve (12). Studies have demonstrated that stimulation
of trigeminal-innervated structures evoked painful
sensations in the neck and vice versa (13, 14). In
addition, it has been reported that injection of an
inflammatory irritant into deep paraspinal tissues
results in a sustained activation of both jaw and neck
muscles (15, 16).
Several localized therapeutic modalities are often
used in the management of TMD, including mobiliza-
tion (17–19) or exercises (20, 21) of the temporoman-
dibular joint. As there is a connection between the neck
and the temporomandibular region, it can be hypo-
thesized that interventions targeted to the cervical spine
may also have an effect on patients with TMD.
Catanzariti et al. (22) suggested that neck pain patients
may respond to intervention applied to the temporo-
mandibular joint and that techniques applied to the
cervical spine may also have effect on the temporo-
mandibular system. To the best of our knowledge no
previous studies have investigated the effects of treat-
ment directed solely at the cervical spine in patients
with TMD. The purpose of this study was to investigate
the effects of joint mobilization directed at the cervical
spine plus an exercise protocol targeting the deep
cervical flexor muscles on intensity of pain and pressure
pain sensitivity in the muscles of mastication in patients
with myofascial TMD.
Materials and methods
Patients
Consecutive patients referred from four private dental
clinics between October 2007 and June 2008 partici-
pated in this study. Participants were eligible to partic-
ipate if they met the following criteria: (i) a primary
diagnosis of myofascial pain according to Axis I,
category Ia and Ib (i.e. myofascial pain with or without
limited opening) of the Research Diagnostic Criteria for
TMD (RDC ⁄ TMD) (23); (ii) bilateral pain involving the
masseter and temporal regions; (iii) presence of at least
one trigger point (TrP) in the masseter or temporalis
muscles; (iv) pain symptoms history of at least the
3 months previous to the study; and (v) intensity of the
pain of at least 30 mm on a 100 mm Visual Analogue
Scale (VAS). Trigger points were diagnosed following
the criteria described by Simons et al. (24): (i) presence
of a palpable taut band in a skeletal muscle; (ii)
presence of a hypersensitive tender spot within the
taut band; (iii) local twitch response elicited by the
snapping palpation of the taut band; and (iv) repro-
duction of the referred pain pattern of the TrP in
response to palpation. These criteria have demonstrated
good inter-examiner reliability (j) ranging from 0Æ84 to
0Æ88 (25).
Participants were excluded if they presented with any
of the following: (i) sign or symptoms of disc displace-
ment, arthrosis, or arthritis of the temporomandibular
joint, according to categories II and III of the
RDC ⁄ TMD; (ii) history of traumatic injuries (e.g.
fracture, whiplash); (iii) fibromyalgia syndrome (26);
(iv) diagnosis of systemic disease (rheumatoid arthritis,
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 645
ª 2009 Blackwell Publishing Ltd

systemic lupus erythematosus, or psoriatic arthritis); (v)
presence of neurological disorders (e.g. trigeminal
neuralgia); (vi) concomitant diagnosis of any primary
headache (tension-type headache or migraine); (vii)
subjects who had received any form of treatment
(physiotherapy, splint therapy and acupuncture) with-
in 3 months of the study. The study was conducted in
accordance with the Helsinki Declaration, and all
participants provided informed consent which was
approved by the local ethics committee.
Pain intensity
The VAS was used to record the patient’s level of pain at
baseline, 48 h after the last treatment (post-interven-
tion) and at 12-week follow-up period. The VAS is a
10 cm line anchored with a ‘0’ at one end representing
‘no pain’ and ‘10’ at the other end representing ‘the
worst pain imaginable’. Patients placed a mark along
the line corresponding to the intensity of their symp-
toms, which was scored to the nearest millimetre. The
VAS has been shown to be a reliable and valid
instrument for measuring pain intensity (27). It exhib-
its a minimal clinically important difference (MCID)
between 9 and 11 mm (28, 29).
Pressure pain threshold assessment
Pressure pain threshold (PPT) is defined as the amount
of pressure where the sense of pressure first changes to
pain (30). A mechanical pressure algometer (Pain
Diagnosis and Treatment Inc, Great Neck, NY, USA)
was used. This device consisted of a round rubber disc
(1 cm2) attached to a pressure (force) gauge. The gauge
displayed values in kilograms. As the surface of the
rubber tip was 1 cm2, the readings were expressed in
kg cm)2. The mean of three trials (intra-examiner
reliability) was calculated and used for the main
analysis. A 30-second resting period was allowed
between trials. The reliability of pressure algometry
was found to be high (ICC = 0Æ91 [95% confidence
intervals (CI): 0Æ82–0Æ97] (31). Pressure pain threshold
was assessed over bilateral masseter and the temporalis
muscles. The masseter point was located 1 cm superior
and 2 cm anterior from the mandibular angle, and the
temporal point was located on the anterior fibres of
temporal muscle, 2 cm above the zygomatic arch in the
middle part between lateral edge of the eye and the
anterior part of the helix. Pressure pain threshold levels
were assessed at pre-intervention, 48 h after the last
treatment (post-intervention) and at 12-week follow-
up period.
Active pain-free mouth opening
In a supine position, participants were asked to ‘open
the mouth as wide as possible without causing pain’. At
the end position of pain-free mouth opening, the
distance between upper-lower central incisors was
measured in millimetres. The intra-tester reliability of
this procedure was found to be high (ICC = 0Æ9–0Æ98)
(32). The mean of three trials was calculated and used
for the main analysis. Active pain-free mouth opening
was assessed pre-intervention, 48 h after the last
treatment (post-intervention) and at 12-week follow-
up period.
Treatment protocol
The treatment protocol included only interventions
directed at the cervical spine. The treatment techniques
were applied by the same physical therapist with
6 years of experience specializing in manipulative
therapy. All patients received a total of 10 sessions
over a 5-week period (twice a week). During the 10
treatment sessions all patients were treated with the
following techniques:
1 Upper cervical flexion mobilization: The patient was
supine with the cervical spine in a neutral position. The
therapist brought about a contact of the occipital bone
with the first finger and medial aspect of the hand, and
other hand over the frontal region of the patient’s head.
The mobilizing force was delivered by flexing the upper
cervical region using a combination of cephalic traction
with the occipital hand and caudal pressure with the
frontal hand (Fig. 1). The mobilization was applied at a
slow rate of one oscillation per 2 s (0Æ5 Hz) for a total
time of 10 min. This rate of mobilization was previously
used in another study (33).
2 C5 central posterior-anterior mobilization (34): The
patient was prone with the cervical spine in a neutral
position. The therapist placed the tips of his thumbs on
the posterior surface of the C5 spinous process, while the
other fingers rested gently around the patients’ neck
(Fig. 2). A grade III (large amplitude movement that
moved into the resistance limiting the range of move-
ment) posterior-anterior technique was applied centrally
to the C5 spinous process. The mobilization was applied
R . L A T O U C H E et al.646
ª 2009 Blackwell Publishing Ltd

at a rate of two oscillations per second (2 Hz). The
mobilizations were performed for a total of 9 min,
divided into 3-min intervalswith a 1 min rest in between.
3 Cranio-cervical flexor stabilization exercise: With the
aim to focus on the deep flexor muscles of the cervical
region, we followed the protocol described by Jull et al.
(35). Patients performed a cranio-cervical flexion exer-
cise in the supine position, which involved flexion of
the cranium (head) on the cervical spine (neck) while
ensuring that the back of the head remained in contact
with the supporting surface, in an effort to facilitate
activation of the deep cranio-cervical flexor muscula-
ture (particularly the longus capitis muscle) with
minimal activity of the superficial cervical flexors
(sternocleidomastoid and scalene muscles) (Fig. 3).
The contraction was graded through feedback from a
pressure biofeedback device (Stabilizer; Chattanooga
Group Inc., Chattanooga, TN, USA) that monitored the
flattening of the cervical lordosis due to the cranio-
cervical flexion movement from contraction of the deep
cervical flexor muscles (36). Falla et al. (37) demon-
strated that the cranio-cervical flexion test was accom-
panied by increased electromyographic activity in the
deep cervical flexor muscles. Additionally, increases in
the electromyographic activity of the deep cervical
flexors did not occur during other neck or jaw move-
ments, supporting the specificity of this test (38).
Patients first performed the correct cranio-cervical
flexion action with the following instructions: gently
nod your head as though you were saying ‘yes’ (Fig. 3).
The therapist monitored the superficial muscles by
palpation and identified the target level of the biofeed-
back where the patient could hold 10 s without use of
superficial neck flexor muscles, and without a quick or
jerky movement. Once the subject could perform the
movement correctly, the target level was established
and training began at this point. The baseline pressure
in the biofeedback device was 20 mmHg and the
patient was instructed to contract the deep neck flexors
to reach five pressure targets in increments of 2 mmHg
(35). The pressure increments were determined by
the level the patient could hold comfortably while
Fig. 1. Upper cervical flexion mobilization. Within one hand over
the occipital bone and the other hand over the frontal region of
the patient’s head, the therapist applies a mobilization force
inducing an upper cervical flexion using a combination of cephalic
traction with the occipital hand and caudal pressure with the
frontal hand.
Fig. 2. C5 central posterior-anterior mobilization. The therapist
placed the thumbs over the posterior surface of the C5 spinous
process and a posterior-anterior mobilization force is applied.
Fig. 3. Cranio-cervical flexor stabilization exercise.
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 647
ª 2009 Blackwell Publishing Ltd

maintaining a 10-second contraction with no pain.
Participants sustained the contraction for 10 repetitions
of 10-second duration, with a 10-second rest interval
between each contraction. Once this target was
achieved, the exercise progressed to the next pressure
target, repeating the process at the new pressure target,
first increasing the holding time and then the repeti-
tions. This exercise protocol has been used in previous
studies in patients with neck pain (39–41).
Statistical analysis
Statistical analysis was conducted with the SPSS 14.5
package.* Mean, s.d., or 95% CI of the values were
presented. The Kolmogorov–Smirnov test showed a
normal distribution of the data (P > 0Æ05). A 2 · 3
mixed model analysis of variance (ANOVA) with time
(pre-intervention, post-intervention and follow-up)
and side (right or left) as the within-subjects variables
was used to examine the effects of the treatment on PPT
over the masseter or the temporalis muscles. A one-way
repeated measure ANOVA with time (pre-intervention,
post-intervention and follow-up) as within-subject
variable was used to investigate the effects of the
treatment on spontaneous pain and active mouth
opening. The Bonferroni test was used for post hoc
analysis. Within-group effect size was calculated using
Cohen’s coefficient (d) (42). An effect size greater than
0Æ8 was considered large; around 0Æ5, moderate; and less
than 0Æ2, small. A P-value less than 0Æ05 was considered
as statistically significant for all analyses.
Results
A total of 19 patients, 14 females and 5 males, aged 19–
57 years old (mean age � s.d.: 37 � 10 years) partici-
pated. All subjects were right hand dominant. None of
the patients started drug therapy during the time of the
study. In this sample of patients with TMD the average
duration of symptoms was 9Æ2 months (95% CI: 7Æ7–
10Æ6 months), and the mean intensity of spontaneous
pain was 55Æ53 (95% CI: 51Æ4–59Æ6).
Pressure pain threshold levels
The 2 · 3 mixed model ANOVA revealed a significant
effect for time (F = 77Æ8; P < 0Æ001) but not for side
(F = 0Æ2; P = 0Æ7) for changes in PPT over the masseter
muscle. Post hoc testing revealed significant differences
between pre-intervention and both post-intervention
and follow-up periods (P < 0Æ001). However, no signif-
icant difference was identified between the post-inter-
vention and follow-up period (P = 0Æ9) for both
masseter muscles. Within-group effect sizes were large
(d > 1Æ0) for both follow-up periods in bilateral masse-
ter muscles. Table 1 details pre-intervention, post-
intervention, follow-up, and change scores of PPT
levels bilateral in both masseter and temporalis
muscles.
The mixed model ANOVA also found a significant effect
for time (F = 66Æ8; P < 0Æ001) but not for side (F = 0Æ07;
P = 0Æ8) for changes in PPT levels over the temporalis
muscle. The post hoc analysis found significant differ-
ences between pre-intervention and both post-inter-
vention and follow-up periods (P < 0Æ001). However,
no significant difference was identified between the
Table 1. Changes in pressure pain thresholds (kg cm)2) over the
masseter and temporalis muscles
Pressure pain threshold (kg cm)2)
in the right masseter muscle
Pre-intervention 2Æ8 � 0Æ7 (2Æ5 ⁄ 3Æ1)
Post-intervention 3Æ9 � 0Æ5 (3Æ7 ⁄ 4Æ2)
Follow-up 3Æ9 � 0Æ6 (3Æ6 ⁄ 4Æ2)
Pre- ⁄ post-differences 1Æ1 � 0Æ8 (0Æ8 ⁄ 1Æ6)
Pre ⁄ follow-up differences 1Æ1 � 0Æ7 (0Æ7 ⁄ 1Æ4)
Pressure pain threshold (kg cm)2)
in the left masseter muscle
Pre-intervention 2Æ3 � 0Æ6 (1Æ9 ⁄ 2Æ6)
Post-intervention 3Æ6 � 0Æ8 (3Æ4 ⁄ 3Æ9)
Follow-up 3Æ5 � 0Æ7 (3Æ1 ⁄ 3Æ8)
Pre- ⁄ post-differences 1Æ3 � 0Æ7 (1Æ0 ⁄ 1Æ6)
Pre ⁄ follow-up differences 1Æ2 � 0Æ8 (0Æ8 ⁄ 1Æ5)
Pressure pain threshold (kg cm)2)
in the right temporalis muscle
Pre-intervention 2Æ4 � 0Æ6 (2Æ1 ⁄ 2Æ7)
Post-intervention 3Æ7 � 0Æ5 (3Æ4 ⁄ 3Æ9)
Follow-up 3Æ5 � 0Æ7 (3Æ2 ⁄ 3Æ8)
Pre- ⁄ post-differences 1Æ3 � 0Æ7 (0Æ9 ⁄ 1Æ6)
Pre ⁄ follow-up differences 1Æ1 � 0Æ7 (0Æ7 ⁄ 1Æ4)
Pressure pain threshold (kg cm)2)
in the left temporalis muscle
Pre-intervention 3Æ0 � 0Æ7 (2Æ7 ⁄ 3Æ3)
Post-intervention 3Æ9 � 0Æ6 (3Æ6 ⁄ 4Æ2)
Follow-up 4Æ0 � 0Æ6 (3Æ6 ⁄ 4Æ3)
Pre- ⁄ post-differences 0Æ9 � 1Æ0 (0Æ4 ⁄ 1Æ4)
Pre ⁄ follow-up differences 1Æ0 � 0Æ8 (0Æ6 ⁄ 1Æ4)
Scores are expressed as mean � s.d. (95% confidence interval).*SPSS, Chicago, IL, USA.
R . L A T O U C H E et al.648
ª 2009 Blackwell Publishing Ltd

post-intervention and follow-up period (P = 0Æ9) for
both muscles. Within-group effect sizes were large
(d > 0Æ9) for both follow-up periods in bilateral tempo-
ralis muscles.
Pain
The ANOVA found a significant effect for time (F = 78Æ6;
P < 0Æ001) for changes in pain. Post hoc revealed
significant differences between pre-intervention and
both post-intervention and follow-up periods
(P < 0Æ001). However, no significant difference was
identified between the post-intervention and follow-up
period (P = 0Æ9). Within-group effect sizes were large
(d > 3Æ0) for both post-intervention and follow-up
periods. Table 2 shows pre-intervention, post-interven-
tion, follow-up and differences in scores of pain.
Active pain-free mouth opening
The ANOVA found a significant effect for time (F = 17Æ1;
P < 0Æ001) for changes in active mouth opening. Post
hoc analysis found significant differences between pre-
intervention and both post-intervention (P < 0Æ001)
and follow-up periods (P = 0Æ006). However, no signif-
icant difference was identified between the post-inter-
vention and follow-up period (P = 0Æ7). Within-group
effect sizes were large for both post-intervention
(d > 1Æ0) and follow-up (d > 0Æ8) periods. Table 2 sum-
marizes pre-intervention, post-intervention and follow-
up and change scores for VAS and active pain-free
mouth opening.
Discussion
The results of our study demonstrated that patients
with myofascial TMD treated with manual therapy and
exercise directed at the cervical spine experienced an
immediate decrease (48 h after 10 treatment sessions)
in facial pain, an increase in PPTs over the masticatory
muscles and an increase in pain-free mouth opening.
Additionally, these changes were maintained 12 weeks
after discharge. However, as this was a single cohort
design we could not say if these outcomes were the
result of treatment directed at the cervical spine or
some other variable.
The effect sizes were large for all of outcomes at both
immediate and the 12-week follow-up period. Addi-
tionally, it should be noted that the reduction in pain
was not only statistically significant but also clinically
meaningful as it exceeded the MCID on the VAS,
identified as 9–11 mm (28, 29). The relatively narrow
CI provide greater assurance when making clinical
decisions regarding the treatment effect identified in
this study (43). It should also be noted that even the
lower bound estimates for the 95% CI fell above the
MCID and provided evidence that cervical spine inter-
ventions might be beneficial in the management of
patients with TMD. Mellick and Mellick (44) reported
that treatment of the cervical spine with intra-muscular
injections was effective for reducing symptoms in
patients with orofacial pain. However, our study is the
first to provide preliminary evidence that manual
therapy and exercise directed at the cervical spine
may be beneficial in decreasing facial pain in these
patients.
The increases in PPT levels over both masseter and
temporalis muscles suggests that a hypoalgesic effects
may be induced by treatment of the cervical spine.
Previous evidence suggests that the hypoalgesic effects
occur after manual therapy interventions because of
the activation of the descending inhibitory pathways
(45, 46). It has been demonstrated that joint mobiliza-
tion of the cervical spine produced an increase of 25%
in PPTs in patients with lateral epicondylalgia (47) and
in patients with neck pain (48). In fact, O’Leary et al.
(49) found that the application of the cranio-cervical
flexor exercise protocol used in the current study
induced an immediate local hypoalgesic response in
patients with neck pain. Although the activation of
descending inhibitory pathways following the applica-
tion of manual procedures has not been demonstrated
Table 2. Changes in spontaneous pain (VAS) and active mouth
opening (mm)
Spontaneous orofacial pain
(Visual Analogue Scale)
Pre-intervention 55Æ5 � 8Æ6 (51Æ4 ⁄ 59Æ6)
Post-intervention 20Æ9 � 7Æ1 (17Æ5 ⁄ 24Æ4)
Follow-up 18Æ7 � 7Æ1 (15Æ3 ⁄ 22Æ1)
Pre- ⁄ post-differences )34Æ6 � 8Æ9 ()38Æ9 ⁄ )30Æ3)
Pre ⁄ follow-up differences )36Æ8 � 12Æ0 ()42Æ6 ⁄ )31Æ1)
Active mouth opening (mm)
Pre-intervention 38Æ3 � 5Æ0 (35Æ8 ⁄ 40Æ7)
Post-intervention 42Æ8 � 2Æ7 (41Æ5 ⁄ 44Æ1)
Follow-up 43Æ1 � 2Æ9 (41Æ7 ⁄ 44Æ5)
Pre- ⁄ post-differences 4Æ5 � 3Æ8 (2Æ8 ⁄ 6Æ4)
Pre ⁄ follow-up differences 4Æ8 � 5Æ8 (2Æ1 ⁄ 7Æ6)
Scores are expressed as mean � s.d. (95% confidence interval).
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 649
ª 2009 Blackwell Publishing Ltd

in patients with TMD this neurophysiological mecha-
nism seems plausible for explaining the bilateral hypo-
algesic effects that occurred in the trigeminal region
with interventions targeted to the cervical spine.
Nevertheless, as no signs of neck dysfunctions and ⁄ or
neck symptoms reported by the patients with TMD
were included in this study, it was difficult to establish a
relationship between the treatment of the cervical spine
and the orofacial effects found in the current study. As
we have discussed, it may be that the effects of cervical
interventions are more generalized rather than specific
for the trigeminal area. Future studies should investi-
gate these neurophysiological mechanisms between the
cervical spine and the orofacial region in patients with
myofascial TMD.
We also found an increase of 4Æ5 mm in pain-free
mouth opening after the treatment of the cervical
spine, which was slightly superior to the results of some
studies investigating changes in active mouth opening
after the treatment of masseter muscle TrPs which
ranged from 2 mm (50) to 4 mm (51). A recent study
has reported that the application of a thrust manipu-
lation targeted to the upper cervical spine resulted in an
increase in active mouth opening (3Æ5 mm) in women
with mechanical neck pain (52). As the application of
cervical interventions induced similar improvements in
mouth opening when compared with treatment of the
masseter muscle, perhaps cervical techniques might be
used as a complementary approach to manage pain in
patients with myofascial TMD. In addition, in patients
with allodynic responses in the facial region, in whom
the manual application of local interventions are often
extremely painful, an indirect approach directed to the
upper cervical spine may be beneficial.
One possible explanation for the increase in pain-free
mouth opening may be related to changes in the
positional afferent inputs of the cervical spine induced
by the protocol. Some studies have demonstrated that
position of the upper cervical spine modifies range of
motion of the mouth (53, 54) Others have shown that
the position of the cervical spine is influenced by the
masticatory muscles (55, 56). De Laat et al. (57) found
that a high percentage of patients with TMD also have
limited movement of the upper cervical spine. There-
fore, it is possible that the protocol applied in the
current study can improve the biomechanical adapta-
tion of the cervical spine with relation to the tempo-
romandibular joint, increasing pain-free mouth
opening. It is also plausible that the reduction in
spontaneous pain in the orofacial region will also
increase pain-free mouth opening.
Our study had several limitations. First, the sample
size was small. Second, we did not include a control
group, so we could not infer a direct cause and effect
relationship between the outcomes and the interven-
tions directed at the cervical spine. It is plausible that
the improvements seen in the patients may be related
to the passage of time. However, we would expect this
to be unlikely given the current duration of symptoms
(9Æ2 months). Furthermore, it was not possible to assess
gender differences because the size of the sample was
small. Future randomized controlled trials with a
greater number of participants and including a control
group which received traditional treatment for myo-
fascial TMD should be conducted in order to further
elucidate the effectiveness interventions directed at the
cervical spine for patients with TMD.
Conclusions
The results of our study demonstrated that patients
with myofascial TMD treated manual therapy and
exercise directed at the cervical spine might be bene-
ficial in decreasing facial pain, increasing PPTs over the
masticatory muscles and increasing pain-free mouth
opening. Furthermore, these changes were maintained
12 weeks after discharge in our population. The effect
sizes were large for all of outcomes at both the 48 h and
12 weeks follow-up periods. Future randomized studies
should investigate the potential of a cause and effect
relationship.
References
1. LeResche L. Epidemiology of temporomandibular disorders:
implications for the investigation of etiologic factors. Crit Rev
Oral Biol Med. 1997;8:291–305.
2. Drangsholt M, LeResche L. Temporomandibular disorder pain.
In: Crombie IK, Croft PR, Linton SJ et al., eds. Epidemiology of
pain. Seattle: IASP Press; 1999:203–233.
3. Isong U, Gansky SA, Plesh O. Temporomandibular joint and
muscle disorder-type pain in US adults: the National Health
Interview Survey. J Orofac Pain. 2008;22:317–322.
4. Olivo SA, Bravo J, Magee DJ, Thie NM, Major PW, Flores-Mir
C. The association between head and cervical posture and
temporomandibular disorders: a systematic review. J Orofac
Pain. 2006;20:9–23.
5. De Wijer A, De Leeuw JR, Steenks MH, Bosman F. Tempo-
romandibular and cervical spine disorders. Self-reported signs
and symptoms. Spine. 1996;21:1638–1646.
R . L A T O U C H E et al.650
ª 2009 Blackwell Publishing Ltd

6. De Wijer A, Steenks MH, De Leeuw JR, Bosman F, Helders PJ.
Symptoms of the cervical spine in temporomandibular and
cervical spine disorders. J Oral Rehabil. 1996;23:742–750.
7. Ciancaglini R, Testa M, Radaelli G. Association of neck pain
with symptoms of temporomandibular dysfunction in the
general adult population. Scand J Rehabil Med. 1999;31:17–
22.
8. Lobbezoo F, Visscher C, Naeije M. Impaired health status,
sleep disorders, and pain in the craniomandibular and cervical
spinal regions. Eur J Pain. 2004;8:23–30.
9. Eriksson PO, Zafar H, Nordh E. Concomitant mandibular and
head-neck movements during jaw opening-closing in man.
J Oral Rehabil. 1998;25:859–870.
10. Zafar H, Nordh E, Eriksson PO. Temporal coordination
between mandibular and head-neck movements during jaw
opening-closing tasks in man. Arch Oral Biol. 2000;45:675–
682.
11. Marfurt CF, Rajchert DM. Trigeminal primary afferent pro-
jections to ‘non-trigeminal’ areas of the rat central nervous
system. J Comp Neurol. 1991;303:489–511.
12. Goadsby PJ, Hoskin KL. The distribution of trigemino-vascular
afferents in the nonhuman primate brain Macaca nemestrina: a
c-fos immunocytochemical study. J Anat. 1997;190:367–375.
13. Bartsch T, Goadsby PJ. Stimulation of the greater occipital
nerve induces increased central excitability of dural afferent
input. Brain. 2002;125:1496–1509.
14. Bartsch T, Goadsby PJ. Increased responses in trigemino-
cervical nociceptive neurons to cervical input after stimulation
of the dura mater. Brain. 2003;126:1801–1813.
15. Hu JW, Yu XM, Vernon H, Sessle BJ. Excitatory effects on
neck and jaw muscle activity of inflammatory irritant applied
to cervical paraspinal tissues. Pain. 1993;55:243–250.
16. Yu XM, Sessle BJ, Vernon H, Hu JW. Effects of inflammatory
irritant application to the rat temporomandibular joint on jaw
and neck muscle activity. Pain. 1995;60:143–149.
17. Foster ME, Gray RJ, Davies SJ, Macfarlane TV. Therapeutic
manipulation of the temporomandibular joint. Br J Oral
Maxillofac Surg. 2000;38:641–644.
18. Jagger RG. Mandibular manipulation of anterior disc displace-
ment without reduction. J Oral Rehabil. 1991;18:497–500.
19. Kurita H, Kurashina K, Ohtsuka A. Efficacy of a mandibular
manipulation technique in reducing the permanently dis-
placed temporomandibular joint disc. J Oral Maxillofac Surg.
1999;57:784–787.
20. Nicolakis P, Erdogmus B, Kopf A, Djaber-Ansari A, Piehslinger
E, Fialka-Moser V. Exercise therapy for craniomandibular
disorders. Arch Phys Med Rehabil. 2000;81:1137–1142.
21. Nicolakis P, Erdogmus B, Kopf A, Ebenbichler G, Kollmitzer J,
Piehslinger E et al. Effectiveness of exercise therapy in patients
with internal derangement of the temporomandibular joint.
J Oral Rehabil. 2001;28:1158–1164.
22. Catanzariti JF, Debuse T, Duquesnoy B. Chronic neck pain and
masticatory dysfunction. Joint Bone Spine. 2005;72:515–519.
23. Dworkin SF, LeResche L. Research diagnostic criteria for
temporomandibular disorders: review, criteria, examinations
and specifications, critique. J Craniomandib Disord. 1992;
6:301–355.
24. Simons D, Travell J, Simons P. Travell & Simons’ myofascial
pain & dysfunction: the trigger point manual: the upper half of
body. Baltimore (MD): Williams & Wilkins; 1999.
25. Gerwin RD, Shannon S, Hong CZ, Hubbard D, Gevirtz R.
Interrater reliability in myofascial trigger point examination.
Pain. 1997;69:65–73.
26. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C,
Goldenberg DL et al. The American College of Rheumatology
1990 criteria for clasification of fibromyalgia: Report of the
multicenter criteria committee. Arthritis Rheum. 1990;
33:160–170.
27. Bijur P, Silveer W, Gallagher JE. Reliability of the visual
analogue scale for measurement of acute pain. Acad Emerg
Med. 2001;8:1153–1157.
28. BirdSB,DicksonEW.Clinically significant changes in pain along
the visual analogue scale. Ann Emerg Med. 2001; 36:639–643.
29. Gallagher EJ, Liebman M, Bijur PE. Prospective validation of
clinically important changes in pain severity measured on a
visual analogue scale. Ann Emerg Med. 2001;38:633–638.
30. Fischer AA. Application of pressure algometry in manual
medicine. J Man Med. 1990;5:145–150.
31. Chesterson LS, Sim J, Wright CC, Foster NE. Inter-rater
reliability of algometry in measuring pressure pain thresholds
in healthy humans, using multiple raters. Clin J Pain. 2007;
23:760–766.
32. Goulet JP, Clark GT, Flack VF, Liu C. The reproducibility of
muscle and joint tenderness detection methods and maximum
mandibular movement measurement for the temporoman-
dibular system. J Orofac Pain. 1998;12:17–26.
33. Chiu TW, Wright A. To compare the effects of different rates of
application of a cervical mobilisation technique on sympa-
thetic outflow to the upper limb in normal subjects. Man Ther.
1996;1:198–203.
34. Maitland G, Hengeveld E, Banks K, English K. Maitland’s
vertebral manipulation. 6th ed. London, England: Butter-
worth Heineman; 2000.
35. Jull G, Falla D, Treleaven J, Sterling M, O’Leary S. A
therapeutic exercise approach for cervical disorders. In:
Boyling JD, Jull GA, eds. Grieves’ modern manual therapy:
the vertebral column, 3rd ed. Edinburgh: Churchill Living-
stone; 2004; 451–469.
36. Mayoux-Benhamou MA, Revel M, Vallee C. Selective elec-
tromyography of dorsal neck muscles in humans. Exp Brain
Res. 1997;113:353–360.
37. Falla D, Jull G, Dall’Alba P, Rainoldi A, Merletti R. An
electromyographic analysis of the deep cervical flexor muscles
in performance of cranio-cervical flexion. Phys Ther. 2003;
83:899–906.
38. Falla D, Jull G, O’Leary S, Dall’alba P. Further evaluation of
and EMG technique for assessment of the deep cervical flexor
muscles. J Electromyogr Kinesiol. 2006;16:621–628.
39. Falla D, Jull G, Russell T, Vicenzino B, Hodges P. Effect of neck
exercise on sitting posture in patients with chronic neck pain.
Phys Ther. 2007;87:408–417.
40. O’Leary S, Jull G, Kim M, Vicenzino B. Specificity in
retraining craniocervical flexor muscle performance. J Orthop
Sports Phys Ther. 2007;37:3–9.
C E R V I C A L S P I N E I N M Y O F A S C I A L T E M P O R O M A N D I B U L A R D I S O R D E R 651
ª 2009 Blackwell Publishing Ltd

41. Falla D, Jull G, Hodges P. Training the cervical muscles with
prescribed motor tasks does not change muscle activation
during a functional activity. Man Ther. 2008;13:507–512.
42. Cohen J. Statistical power analysis for the behavioural
sciences. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988.
43. Noteboom JT, Allison SC, Cleland JA, Whitman JM. A primer
on selected aspects of evidence-based practice to questions of
treatment part II: Interpreting results, applying to clinical
practice, and self-evaluation. J Orthop Sports Phys Ther.
2008;38:485–501.
44. Mellick LB, Mellick GA. Treatment of acute orofacial pain
with lower cervical intramuscular bupivacaine injections:
a 1-year retrospective review of 114 patients. J Orofac Pain.
2008;22:57–64.
45. Souvlis T, Vicenzino B, Wright A. Neuro-physiological effects
of spinal manual therapy. In: Boyling JD, Jull G, eds. Grieves’
modern manual therapy: the vertebral column, 3rd ed.
Edinburgh: Churchill-Livingstone; 2004:367–379.
46. Wright A. Pain-relieving effects of cervical manual therapy.
In: Grant R, ed. Physical therapy of the cervical and thoracic
spine. New York: Churchill-Livingstone; 2002:217–238.
47. Vicenzino B, Collins D, Wright A. The initial effects of a
cervical spine manipulative physiotherapy treatment on the
pain and dysfunction of lateral epicondylalgia. Pain.
1996;68:69–74.
48. Sterling M, Jull G, Wright A. Cervical mobilisation: concurrent
effects on pain, sympathetic nervous system activity and
motor activity. Man Ther. 2001;6:72–81.
49. O’Leary S, Falla D, Hodges PW, Jull G, Vicenzino B. Specific
therapeutic exercise of the neck induces immediate local
hypoalgesia. J Pain. 2007;8:832–839.
50. Rodrıguez-Blanco C, Fernandez-de-las-Penas C, Hernandez-
Xumet JE, Pena-Algaba C, Fernandez-Rabadan M, Lillo-de-la-
Quintana MC. Changes in active mouth opening following a
single treatment of latent myofascial trigger points in the
masseter muscle involving post-isometric relaxation or
strain ⁄ counter-strain. J Bodyw Mov Ther. 2006;10:197–205.
51. Ibanez-Garcıa J, Alburquerque-Sendın F, Rodrıguez-Blanco C,
Girao D, Atienza-Meseguer A, Planella-Abella S et al. Changes
in masseter muscle trigger points following strain-counter ⁄ -strain or neuro-muscular technique. J Bodyw Mov Ther.
2009;13:2–10.
52. Mansilla-Ferragut P, Fernandez-de-las-Penas C, Alburquer-
que-Sendın F, Cleland JA, Bosca-Gandıa JJ. The immediate
effects of atlanto-occipital joint manipulation on active
mouth opening and pressure pain sensitivity in women
with mechanical neck pain. J Man Physiol Ther. 2009;32:
101–106.
53. Makofsky HW, Sexton TR. The effect of cranio-vertebral
fusion on occlusion. Cranio. 1994;12:38–46.
54. Solow B, Sonnesen L. Head posture and malocclusions. Eur J
Orthop. 1998;20:685–693.
55. Moya H, Miralles R, Zuniga C, Carvajal R, Rocabado M,
Santander H. Influence of stabilization occlusal splint on
cranio-cervical relationship. Part 1: Cephalometric analysis.
Cranio. 1994;12:47–51.
56. Miralles R, Moya H, Ravera MJ, Santander H, Zuniga C,
Carvajal R et al. Increase of the vertical occlusal dimension by
means of removable orthodontic appliance and its effects on
cranio-cervical relationships and position of the cervical spine
in children. Cranio. 1997;18:205–219.
57. De Laat A, Meuleman H, Stevens A, Verbeke G. Correlation
between cervical spine and temporomandibular disorders.
Clin Oral Investig. 1998;2:54–57.
Correspondence: Roy La Touche Arbizu, Facultad de Medicina,
Universidad San Pablo CEU, Calle Tutor, 35, 28008 Madrid, Spain.
E-mail: [email protected]
R . L A T O U C H E et al.652
ª 2009 Blackwell Publishing Ltd

192
5.7 Estudio VII
La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S, Bishop MD,
Lopéz-Valverde-Centeno A, von Piekartz H, Fernández-Carnero J. Does mobilization of
the upper cervical spine affect pain sensitivity and autonomic nervous system function
in patients with cervico-craniofacial pain?: A randomized-controlled trial. Clin J Pain.
2013 Mar;29(3):205-15.
Objetivos del estudio
Los objetivos de este estudio fueron investigar los efectos de la movilización antero-
posterior de la región cervical superior en la modulación del dolor en las regiones
craneofacial y cervical y su influencia en el sistema nervioso simpático.
Resultados
Los UDPs en las regiones craneofacial y cervical aumentó significativamente (P
<0,001) y la intensidad del dolor disminuyó significativamente (P <0,001) en el grupo
de tratamiento en comparación con placebo. La movilización produjo una respuesta
simpatoexcitatoria demostrado por un aumento significativo de la conductancia de la
piel, la frecuencia respiratoria y la frecuencia cardíaca (p <0,001), pero no en la
temperatura de la piel (P = 0,071), después de la aplicación de la técnica en
comparación con el placebo.
Conclusiones
Este estudio proporciona una evidencia preliminar del efecto hipoalgésico a corto plazo
de la movilización articular de la región cervical en las regiones craneofacial y cervical
de pacientes con DCCF de origen miofascial, lo que sugiere que la movilización puede
causar una modulación nociceptiva inmediata en el CTC. Se observó una respuesta
simpatoexcitatoria, lo que podría estar relacionado con el efecto hipoalgésico inducido
por la técnica, aspecto a ser confirmado en estudios futuros.

Does Mobilization of the Upper Cervical Spine Affect PainSensitivity and Autonomic Nervous System Function
in Patients With Cervico-craniofacial Pain?
A Randomized-controlled Trial
Roy La Touche, PT, MSc,*wz Alba Parıs-Alemany, PT, MSc,zJeffrey S. Mannheimer, PT, PhD, CCTT,y Santiago Angulo-Dıaz-Parreno, MSc,wz8
Mark D. Bishop, PT, PhD,z# Antonio Lopez-Valverde-Centeno, MD, PhD,**Harry von Piekartz, PT, PhD,ww and Josue Fernandez-Carnero, PT, PhDwzz
Objectives: The aims were to investigate the effects of anterior-posterior upper cervical mobilization (APUCM) on pain modu-lation in craniofacial and cervical regions and its influence on thesympathetic nervous system.
Methods: Thirty-two patients with cervico-craniofacial pain ofmyofascial origin were randomly allocated into experimental orplacebo groups. Each patient received 3 treatments. Outcomemeasures included bilateral pressure pain thresholds assessed atcraniofacial and cervical points preintervention, after the secondintervention and after the final treatment. Pain intensity andsympathetic nervous system variables (skin conductance, breathingrate, heart rate, and skin temperature) were assessed before andimmediately after each intervention.
Results: The pressure pain thresholds in the craniofacial and cer-vical regions significantly increased (P<0.001) and pain intensitysignificantly decreased (P<0.001) in the treatment group com-pared with placebo. APUCM also produced a sympathoexcitatoryresponse demonstrated by a significant increase in skin con-ductance, breathing rate, and heart rate (P<0.001), but not in skintemperature (P=0.071), after application of the technique com-pared with placebo.
Discussion: This study provided preliminary evidence of a short-term hypoalgesic effect of APUCM on craniofacial and cervicalregions of patients with cervico-craniofacial pain of myofascialorigin, suggesting that APUCM may cause an immediate noci-ceptive modulation in the trigeminocervical complex. We also ob-served a sympathoexcitatory response, which could be related to
the hypoalgesic effect induced by the technique, but this aspectshould be confirmed in future studies.
Key Words: manual therapy, neck pain, temporomandibular
disorders, orofacial pain, craniofacial pain
(Clin J Pain 2013;29:205–215)
Discomfort resulting from temporomandibular disorders(TMDs) is representative of many chronic craniofacial
pain (CCFP) conditions.1 TMD demographics usuallyconsist of working women in the 3rd decade of life withhigh stress levels.2 TMDs are characterized by a focal site oftenderness that provokes nociceptive input and, whenchronic, contributes to the development of central sensiti-zation. Patients with TMDs are known to have greatertemporal summation of pain, suggesting hyperexcitabilityof the central nociceptive system.3,4 More specifically,chronic muscular TMD pain is associated with a generaldysfunction of the central nociceptive system that is con-comitant with central nociceptive neuronal hyperexcitabilityand dysfunction of the descending inhibitory pain systems.5
Women have a 3 times greater risk of experiencing chronicmasticatory myofascial pain than men.6 Patients with TMDsof myofascial origin are also characterized by a general hy-persensibility to mechanical pain stimuli, presenting lowercraniofacial pressure pain thresholds (PPT) of both thepainful and nonpainful side compared with healthy controls.7
Some studies suggest a functional relationship betweenthe jaw and head-neck with regard to craniofacial and cer-vical spine and a concomitance between craniofacial painand neck pain.2,8–10 Patients with craniofacial pain are attwice the risk of experiencing neck pain than the generalpopulation.2 Restricted segmental movements of the uppercervical vertebrae (C0-C3) with a greater percentage of up-per trapezius and sternocleidomastoid tender points exist inpatients with TMDs compared with a control group.11
In addition, Eriksson et al8 demonstrated coordi-nated articular patterns of movement between the temporo-mandibular, atlanto-occipital, and cervical joints, joints thatalso have known sensory-motor interaction via the trige-minocervical complex (TCC). Disturbance of this con-nection between jaw and head-neck movements has beenidentified in patients with whiplash-associated disorders.12
Spinal manual therapy (SMT) is used by physicaltherapists (PTs) to treat chronic musculoskeletal pain.13
Received for publication June 21, 2011; revised February 14, 2012;accepted February 17, 2012.
From the *Department of Physical Therapy, La Salle UniversityCenter, Faculty of Health Science, Aravaca; wResearch Group ofMusculoskeletal Pain and Motor Control, Universidad Europea deMadrid, Villaviciosa de Odon; zInstitute of Neuroscience andCraniofacial Pain (INDCRAN); 8Faculty of Experimental Science,Universidad San Pablo CEU; zzDepartment of Physical Therapy,Occupational Therapy, Rehabilitation and Physical Medicine,Universidad Rey Juan Carlos, Alcorcon, Madrid; **Departmentof Surgery, Faculty of Medicine and Dentistry, Universidad deSalamanca, Salamanca, Spain; yProgram in Physical Therapy,Columbia University, NY; zDepartment of Physical Therapy;#Center for Pain Research and Behavioral Health, University ofFlorida, Gainesville, FL; and wwFaculty of Business, Managementand Social Science, University of Applied Science, Osnabruck,Germany.
The authors declare no conflict of interest.Reprints: Roy La Touche, PT, MSc, INDCRAN, C/Canos del Peral
11, Bajo Izquierdo, 28013 Madrid, Spain (e-mail: [email protected]).
Copyright r 2012 by Lippincott Williams & Wilkins
ORIGINAL ARTICLE
Clin J Pain � Volume 29, Number 3, March 2013 www.clinicalpain.com | 205

Various techniques such as passive manipulation and mo-bilization, active mobilization, neuromuscular facilitation,and articular glides are included under the general term ofSMT.14–17 Many SMTs have demonstrated hypoalgesiceffects. This hypoalgesic effect is not antagonized by na-loxone and does not exhibit tolerance,18 supporting thetheory that SMTs activate a nonopioid inhibitory system.In addition, a concomitant activation of the sympatheticnervous system (SNS) occurs after SMT, with the degree ofactivation depending on the technique.19,20
Many studies have investigated the effects of SMT onlower cervical pain,14–16,21 but there is no randomized-controlled trial in which SMT is used to diminish cranio-facial pain. George et al22 compared cervical manipulationwith a soft tissue technique at the cervical-cranial junctionto improve mouth opening in healthy controls, but no sig-nificant results were obtained. Another study examined amanual therapy and therapeutic exercise protocol appliedat the cervical spine, to treat craniofacial pain of myofascialorigin in a cohort intervention study, which resulted in anincrease in the PPT in the masticatory muscles and in-creased mouth opening.23
Consequently, the aims of this study were to extendprevious work by investigating the neurophysiologicaleffects of SMT in patients with CCFP of myofascial origin.Specifically, we studied passive anterior-posterior uppercervical mobilization (APUCM). We expected pain sensi-tivity in the craniofacial and cervical regions to decrease inresponse to treatment. In addition, we expected to observethe sympathetic influence of this technique on skin con-ductance (SC), breathing rate (BR), heart rate (HR), and skintemperature (ST).
MATERIALS AND METHODS
Selection and Description of ParticipantsThirty-two patients with CCFP of myofascial origin
referred from 2 private dental clinics and 3 universities inMadrid, Spain, were recruited from January 2009 to May2010. We defined the term CCFP of myofascial origin aspain and dysfunction located at the cervical and mastica-tory muscles. Patients were selected if they met all of thefollowing criteria: (1) a primary diagnosis of myofascialpain as defined by axis I, category Ia and Ib (eg, myofascialpain with or without limited opening of the mouth) of theResearch Diagnostic Criteria for Temporomandibular Dis-orders24; (2) bilateral pain involving the masseter, temporalis,upper trapezius, and suboccipital muscles; (3) a duration ofpain of at least 3 months; (4) a pain intensity correspondingto a weekly average of at least 30mm on a 100-mm visualanalog scale (VAS); (5) neck and/or shoulder pain withsymptoms provoked by neck postures or neck movement;(6) Neck Disability Index (NDI)25,26 Z15 points; and (7)presence of bilateral trigger points (TrPs) in masseter, tem-poralis, upper trapezius, and suboccipital muscles. TrPs werediagnosed according to the following criteria27: (1) presenceof a palpable taut band in the skeletal muscle; (2) presence ofa hypersensitive tender spot within the taut band; (3) localtwitch response elicited by the snapping palpation of the tautband; and (4) reproduction of referred pain in response toTrP compression.
All patients in the study were examined by a physi-otherapist with 7 years of experience managing craniofacialand cervical disorders. Patients were excluded if they pre-sented any signs, symptoms, or history of the following
diseases: (1) intra-articular temporomandibular disk displace-ment, osteoarthrosis, or arthritis of the temporomandibularjoint, according to categories II and III of the ResearchDiagnostic Criteria for Temporomandibular Disorders24,28;(2) history of traumatic injuries (eg, contusion, fracture, orwhiplash injury); (3) systemic diseases such as fibromyalgia,systemic erythematous lupus, or psoriatic arthritis; (4) neu-rological disorders (eg, trigeminal neuralgia); (5) concomitantmedical diagnosis of any primary headache (tension type ormigraine); (6) unilateral neck pain; (7) cervical spine surgery;(8) clinical diagnosis of cervical radiculopathy or myelopathy;and (9) history of previous physical therapy intervention forthe cervical region. Each participant received a thorough ex-planation of the content and purpose of the treatment beforesigning an informed consent form related to the procedures,which was approved by the local ethics committee in ac-cordance with the Helsinki Declaration.
Research DesignA randomized, double-blind placebo-controlled study
was performed. Patients were blind to which interventionthey received, and an independent assessor, blind to inter-vention assignment made the measurements and registeredthe data. Patients were randomly allocated to either treat-ment intervention or sham intervention. Randomizationwas performed by a computer generated random-sequencetable created with Graphpad software (GraphPad SoftwareInc., CA) before the beginning of the study. The random-ization sequence used a balanced block design in whichrandomization occurred in blocks of 2.
Sample Size CalculationA pilot study was performed with 5 patients in the
treatment group and 5 patients in the sham group to cal-culate the sample size. We used data indicative of the per-cent change in the PPT of the 2 assessed points: 1 at themasseter muscle and 1 at the trapezius muscle.
Sample sizes were calculated to obtain a power of 80%to detect changes in the bilateral contrast of the null hy-pothesis of equal means between the 2 groups, with 5%significance, taking into account the possibility that the SDsof the groups could be different. According to the samplecalculations which took into account the fact that the cal-culation was based on 2 different variables, we obtained 2possible results: 14 patients in each group or 16 patients ineach group. We decided to include 16 patients per group toanticipate the possible loss of patients.
Demographic and Clinical DataEach of the participants completed a questionnaire
to determine if they met the criteria for inclusion or ex-clusion. This questionnaire included demographic data,screening questions for TMDs from the American Acad-emy of Orofacial Pain,29 a body chart on which patientsmarked the location of their pain, and several questionsabout the characteristics of their pain such as “whendid it start?,” “what makes your pain worse?,” “what makesit better?,” and “what kind of pain is it?” To meetthe criteria to participate in the study, patients had to passan initial physical examination performed by a single in-vestigator to rule out the presence of nerve root com-pression.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
206 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

Instrumentation and Measurements
Self-reported VariablesPatients completed the Beck Depression Inventory
(BDI),30 the State-Trait Anxiety Inventory (STAI),31 andthe NDI25,26 to quantify their psychophysical state. TheBDI is a 21-item self-report instrument intended to assessthe existence and severity of symptoms of depression. Thereis a 4-point scale for each item ranging from 0 to 3. The resultsof each item, corresponding to a symptom of depression, aresummed to yield a single score for the BDI. A total score of0 to 13 is considered minimal, 14 to 19 mild, 20 to 28 mod-erate, and 29 to 63 severe depression. The BDI showed goodinternal consistency (a coefficient 0.86).30
The STAI31 is a 40-item self-report questionnaire de-signed to assess symptoms of anxiety. It consists of 2 in-dependent scales, a state anxiety scale and a trait anxietyscale, with 20 items each, resulting in a score between 20and 80. Higher scores indicate greater levels of anxiety. Thestate and trait scales explore anxiety as a current emotionalstate and as a personality trait, respectively.
The NDI,25,26 which measures perceived neck disability,consists of 10 items that assess different functional activitiesand uses a 6-point scale ranging from 0 (no disability) to 5(complete disability). The overall score (out of 100) is ob-tained by adding the score for each item and multiplyingby 2. A higher score indicates greater pain and disability. Thevalidity, reliability, and responsiveness of the NDI have beendemonstrated.26
Pain IntensityThe VAS was used to measure pain intensity of the
cervico-craniofacial region at rest and before and after eachtreatment. The VAS is comprised of a 100mm horizontalline in which the left side represents “no pain” and the rightside represents “worst pain.” The patient placed a mark onthe line at the point that they felt represented the intensityof their pain at the time. Pain intensity was quantified bythe assessor in millimeters. This scale has proven its reli-ability and validity for measuring pain intensity.32
Pressure Pain ThresholdPPT is defined as the minimum amount of pressure
needed to provoke a pain sensation.33 We used a digitalalgometer (Model FDX 10; Wagner Instruments, Greenwich,CT) comprised of a rubber head (1 cm2) attached toa pressure gauge, which measures in kg with thresholds ex-pressed in kg/cm2. The protocol consisted of 3 measurementswith an interval of 30 seconds between each measurement.The average of the 3 measurements was calculated to obtain asingle value for each one of the measured points in each ofthe assessments. This algometric method has high reliability(ICC=0.91, 95% CI, 0.82-0.97) for measuring PPT.34 PPTswere assessed bilaterally at 2 points in the masseter muscle(M1 and M2), 2 points in temporalis muscle (T1 and T2),suboccipital muscles, C5 zygapophyseal joint, and uppertrapezius muscle. The device was applied perpendicular to theskin, and the patients were asked to raise their hand themoment when the pressure started to change to a pain sen-sation, at which point the assessor stopped applying pressure.This procedure was performed 3 times: before the firsttreatment session (pretreatment outcome), after the secondtreatment session, and after the third treatment session(2 posttreatment outcomes).
Anatomic references for the algometric measurementsincluded the following: M1—2.5 cm anterior to the tragusand 1.5 cm inferior to the zygomatic arch; M2—1 cm su-perior and 2 cm anterior from the angle of the jaw; T1(anterior fibers of the muscle)—3 cm superior to the zy-gomatic arch in the middle point between the end of the eyeand the anterior part of the helix of the ear; T2 (middlefibers of the muscle)—2.5 cm superior from the helix of theear; suboccipital muscles—2 cm inferior to the occipitalcondyles; C5 zygapophyseal joint—2 cm lateral to the spi-nous process of C6; trapezius muscle—2.5 cm above thesuperior medial angle of the scapula.
Changes in the SNSSeveral characteristics were measured to assess the
SNS: SC, HR, BR, and ST. Measurements were taken be-fore and after each of the 3 treatment sessions. The re-cording device used was I-330-C2+ 6-channel biofeedbacksystem (J&J Engineering Inc., Poulsbo, WA) the MC-6SYsensor was used to measure SC and ST. During the meas-urements 2 electrodes were placed on the tip of the secondand third fingers of the left hand to measure the SC with thetemperature sensor attached to the tip of the fourth fingeralso at the left hand. The MC-5D electrodes used to meas-ure HR were applied longitudinally at the anterior and ra-dial aspect of the wrists and held with bracers. To measureBR, an MC-3MY breathing sensor was placed around thechest like a belt passing over the xiphoid process.
ProcedureThe experiment consisted of 3 treatment sessions. Each
patient received 3 sessions over 2 weeks, and the entire ex-periment lasted approximately 8 months.
The evaluator was a PT with extensive experience intaking the experimental measurements. During the first as-sessment, pretreatment data were obtained; after measuringthe PPT and VAS, the sensors were applied, and the patientwas instructed to lie down on a couch and relax. The roomtemperature was controlled at 251C. After 10 minutes (timedetermined for the patient to come to a normal baseline),the first record of the sympathetic parameters was regis-tered. The patient was then randomly assigned to 1 of the 2intervention groups, and the therapeutic technique wasapplied. Immediately after finishing the technique, SNSvariables were measured, and 5 minutes after the technique,VAS results were registered again. In the second and thirdtreatment session, the SNS variables and VAS were meas-ured using the same protocol (pretreatment and posttreat-ment data), but PPTs were taken only 5 minutes after theend of the treatment (posttreatment data). Therefore, weobtained 3 pretreatment and 3 posttreatment measurementsof SNS and VAS parameters and 1 pretreatment and 2posttreatment measurements (after the second and thirdsessions) of PPT.
Treatment TechniqueAPUCM directly influences the 3 upper cervical seg-
ments (C0-C3). The patient was placed in a supine positionwith a neutral position of the cervical spine. The PT heldthe occipital region of the patient with both hands to stabilizeand maintain the position of the upper cervical structures,while applying a posterior directed force on the frontal re-gion of the patient (anterior to posterior force) with the an-terior part of the shoulder. The mobilization was applied at aslow rate of 1 oscillation per 2 seconds (0.5Hz) controlled
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 207

with an MA-30 digital metronome (Korg Inc., Japan). Thisoscillation rate has been used previously with a differentmanual therapy technique.19 The total time of mobilizationwas 6 minutes. Mobilization was applied in 3 intervals of2 minutes, with 30 seconds of rest in between, resulting in atotal of 7 minutes.
Sham TechniqueTo simulate the treatment technique, the PT applied
the same grips used with the treatment technique: 2 handsunder the occipital bone with the anterior part of 1 shoulderpositioned anterior to the frontal bone, with the patient insupine position. However, mobilization was not applied tothe cervical spine. The contact with the patient was held for3 intervals of 2 minutes with 30 seconds of rest in between.
Both techniques (treatment and sham) were applied bythe same PT, and each participant received the followingexplanation about the intervention: “A physical therapistwill apply a technique on your neck with one hand placedon the posterior part of your neck and the other one onyour forehead. The purpose is to obtain changes in yourneck and craniofacial pain.”
StatisticsStatistical analysis was performed with SPSS version
15.0. A Kolmogorow-Smirnov test was used to determinewhether the sample was consistent with a normal distri-bution (P>0.05). Student t test was used to analyze self-reported psycophysical variables (NDI, STAI, and BDI)and pain duration by comparing the preintervention datafor the treatment and sham groups.
The SNS variables (ST, HR, BR, SC) and VAS weretested with a 2�3 repeated measures analysis of variance(ANOVA); the factors analyzed were time (pre-post) andgroup (treatment and sham). Time�group interactions werealso analyzed. Post hoc analysis with Bonferroni correctionswas performed for specific comparisons between variables.
To determine differences between sessions in VAS andSNS variables, a 2-way ANOVA was used, which analyzedintersession factor and group� intersession interaction(presession 1, presession 2, presession 3). The percentchange for the SNS variables and VAS was obtained rela-tive to the percent change between each session and thepercent of the total of the means in both groups. A 1-wayANOVA was used to analyze the percent change in groupfactor and time factor between sessions (% change session1, % change session 2, % change session 3). The percentchange of the total of the means of the 3 sessions in thetreatment and placebo groups was analyzed with a Studentt test.
A 3�3 mixed-model ANOVAwas used to determine thePPT variables (M1, M2, T1, T2, suboccipital, C5, trapezius);the factors were group (treatment or sham), time (pre, post 1,and post 2) and side (right and left). Bonferroni correctionswere used for post hoc analysis of specific comparisons be-tween variables. Student t test determined the percent changebetween groups between the first session (pretreatment) andlast session (posttreatment 2) outcomes. Throughout allanalyses, statistical significance was set at P<0.05.
RESULTSThirty-two patients (21 females and 11 males) with
CCFP of myofascial origin were included in this study. Nopatients dropped out during the study, and no adverseevents occurred with the APUCM. The t test did not revealany significant differences between groups with regard todemographic details and clinical data (P>0.05), as shownin Table 1. A normal distribution was confirmed with theKolmogorov-Smirnov test (P>0.05).
Pain IntensityThe ANOVA revealed a significant group�time inter-
action (F=135.81; P<0.001), and significant differencesfor the time factor (F=261.7; P<0.001) and group factor(F=32.59; P=0.003) regarding the VAS results. Post hocanalysis also revealed significant differences for the treatmentgroup (P<0.001), but not for the sham group (P=0.3) forthe descriptive data shown in Table 2. A 2-way repeated-measures ANOVA found significant intersession differences(F=11.86; P<0.001) and a group� intersession interaction(F=17.09; P<0.001), indicating that the change fromsession to session was larger for 1 group.
Regarding the percentage of change, a 2-way repeated-measures ANOVA revealed significant differences for groupfactor (F=94.24; P<0.001) and time factor (F=11.3;P<0.001), represented in Figure 1A. The t test also re-vealed significant differences between the percent change ofthe total of the means for the treatment and sham groups(t= �10.03; P<0.001).
Pain Sensitivity
Craniofacial RegionAnalysis of the PPT within the craniofacial region was
performed by a 3�3 mixed-model ANOVA, which revealeda significant effect of time factor [M1 (F=83.65; P<0.001);M2 (F=67.44; P<0.001); T1 (F=98.05; P<0.001); T2(F=18.81; P<0.001)], group factor [M1 (F=12.27; P=0.001); M2 (F=18.35; P<0.001); T1 (F=16; P<0.001);T2 (F=15.85; P<0.001)] and group� time interaction [M1(F=59.65; P<0.001); M2 (F=48.45; P<0.001); T1
TABLE 1. Descriptive Data of the 2 Intervention Groups: Treatment and Sham Groups
Treatment (N=16) Sham (N=16)
Mean SD Mean SD Mean Difference
95% CI for
Mean Difference t P
Age 33.19 9.49 34.56 7.84 �1.37 �7.64 to 4.68 �0.48 0.65NDI 15.69 3.26 16.75 3.94 �1.06 �3.67 to 1.54 �0.83 0.41Pain duration 11.31 6.74 10.69 5.79 0.62 �5.16 to 3.91 �0.28 0.78BDI 13.63 3.64 12.38 4.41 1.25 �2.67 to 3.17 �0.17 0.86STAI 25.75 5.63 24.75 4.66 1 �2.73 to 4.73 �0.54 0.58
BDI indicates Beck Depression Inventory; CI, confidence interval; NDI, Neck Disability Index; STAI, State-Trait Anxiety Inventory; t, t test value.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
208 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

F=83.57; P<0.001); T2 (F=16.48; P<0.001)], but notfor side factor [M1 (F=0.94; P=0.76); M2 (F=0.13;P=0.72); T1 (F=0.009; P=0.92); T2 (F=0.64; P=0.43)]. Post hoc testing revealed significant differences be-tween the 3 sessions for the treatment group (P<0.001) butnot for the sham group (P>0.05) at all craniofacial points;descriptive data are shown in Table 3.
The t test revealed significant differences in the percentchange in PPT at the right and left craniofacial points. Figure 2shows the percent change in PPT from the pretreatment andfinal posttreatment assessment.
Cervical RegionA 3�3 mixed-model ANOVA revealed a significant
time effect of the suboccipital musculature (F=96.33; P<0.001), C5 zygapophyseal joint (F=52.37; P<0.001),trapezius muscle (F=57.41; P<0.001), and a group�timeinteraction at the suboccipital region (F=64.12; P<0.001),C5 zygapophyseal joint (F=46.84; P<0.001), and tra-pezius muscle (F=65.3; P<0.001). However, this was notthe case for side factor [suboccipital muscles (F=1.22; P=0.27); C5 zygapophyseal joint (F=1.8; P=0.18); trapeziusmuscle (F=1.57; P=0.22)]. Post hoc analysis revealedsignificant differences in the PPT for the 3 sessions of thetreatment group (P<0.001), but not the sham group(P>0.05), at each cervical point. Descriptive data of PPTfor the cervical region are shown in Table 3.
The t test revealed significant differences in the percentchange in PPT in the right and left cervical points for thetreatment group. Figure 3 shows the percent change in PPTof these measurements from pretreatment and final post-treatment points.
SNS
Skin ConductanceThe ANOVA revealed a significant group�time in-
teraction (F=107.55; P<0.001), an effect of time (F=118; P<0.001), and an effect of group (F=10.45; P=0.003) for changes in SC. Post hoc analysis revealed sig-nificant differences in the treatment group (P<0.001), but
not the sham group (P=0.73). The descriptive data of theSC are shown in Table 2. A 1-way repeated-measuresANOVA found no significant intersession differences (F=0.001; P=0.97) or group by intersession interaction (F=0.32; P=0.57).
ANOVA revealed significant differences in the percentchange between treatment sessions for the group factor(F=31.02; P<0.001), but not the time factor (F=0.72;P=0.48), as shown in Figure 4A. The t test revealed sig-nificant differences between percent change of the totalof the means of treatment and sham groups (t=6.11;P<0.001).
Breathing RateANOVA revealed a significant group�time interaction
(F=8.91; P=0.006) and a main effect of group (F=4.36;P=0.045), but not time (F=0.22; P=0.63), for changesin BR. Post hoc analysis revealed significant differences forthe treatment group (P=0.02), but not the sham group(P=0.08). The descriptive data of the BR are shownin Table 2. A 1-way repeated-measures ANOVA found nosignificant differences for intersession (F=0.13; P=0.87)or for group� intersession interaction (F=0.29; P=0.74).
TABLE 2. Descriptive Statistics for Sympathetic Nervous System Parameters and Pain Intensity, for Pretreatment and PosttreatmentAssessments
Mean±SD
Session 1 Session 2 Session 3
Pre Post Pre Post Pre Post
SCTreatment 1.84±0.61 3.33±0.43 2.10±0.78 3.45±0.38 1.88±0.59 3.4±0.53Sham 2.2±0.58 2.25±0.61 2.21±0.61 2.27±0.55 2.15±0.58 2.20±0.57
HRTreatment 69.56±6.3 73.16±5 71.25±4.39 75.1±2.88 72.05±6.84 77.12±4.12Sham 67.87±7.35 63.81±7.56 67.31±6 63.31±6.73 69.37±5.09 66.12±7.01
RRTreatment 15.31±2.76 16.31±4.13 15.63±1.9 18.38±3.7 15.88±2.56 16.7±3.6Sham 16.58±2.37 14.9±2.99 15.38±1.4 14.28±2.7 15.45±2.2 13.95±2.6
STTreatment 31.45±3.45 28.42±4.39 32.44±3.21 27.53±5.1 30.46±3.67 27.18±4.33Sham 31.71±3.19 29.11±4.07 32.03±2.7 29.56±3.76 31.06±3.26 28.57±3.61
VASTreatment 43.88±7.3 29.66±8.97 31.06±8.83 18.31±9.18 29.31±11.8 14.75±11.8Sham 42.38±9.41 41.5±7.9 45.13±7.9 42.56±6.88 44.31±8.51 42±9.05
BR indicates breathing rate; HR, heart rate; SC, skin conductance; ST, skin temperature; VAS, visual analog scale.
0
10
-20
-10
Treatment
-50
-40
-30
Ch
ang
e in
VA
S (
%)
Sham
-70
-60
-80Session 1 Session 2 Session 3
FIGURE 1. Visual analog scale (VAS) percentage change betweenthe 3 sessions (mean of preintervention and postintervention) fortreatment and sham groups.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 209

A 1-way ANOVA revealed significant differences inpercent change of BR for the group factor (F=11.34;P=0.002) but not for time (F=1.03; P=0.36) as shownin Figure 4B. The t test revealed significant differences be-tween the percent change of the total of the means for thetreatment and sham groups (t=3.07; P=0.004).
Heart RateANOVA revealed a significant group� time inter-
action (F=54.14; P<0.001) and a main effect of group(F=19.4; P<0.001), but not time (F=0.14; P=0.71),for changes in HR. Post hoc analysis revealed significantdifferences in the treatment group (P<0.001) and the shamgroup (P<0.001); HR data are shown in Table 2. A 1-wayrepeated-measures ANOVA found no significant inter-session differences (F=1.5; P=0.23) or group� interses-sion interaction (F=0.45; P=0.63).
Regarding the percent change in HR, a 1-way re-peated-measures ANOVA revealed significant differencesfor group factor (F=53.66; P<0.001), but not time factor
(F=1.02; P=0.36), as shown in Figure 4C. Significantdifferences between the percent change of the total of themeans for the treatment and sham groups (t=7.37; P<0.001) were observed.
Skin TemperatureThe ANOVA did not reveal any significant group�
time interaction (F=3.49; P=0.071), time factor effect(F=1.62; P=0.2), or group factor effect (F=0.53; P=0.46) for changes in ST. The descriptive data of the ST areshown in Table 2. A 1-way repeated-measures ANOVAfound no significant intersession differences (F=2.84;P=0.06) or group� intersession interaction (F=0.25;P=0.77).
Regarding percent change in ST, a 1-way repeated-measures ANOVA did not reveal a significant difference ingroup factor (F=3.25; P=0.08) or time factor (F=2.74; P=0.07), as shown in Figure 4D. The t test did notreveal a significant difference in the percent change of the
TABLE 3. Descriptive Statistics of PPT Assessed Pretreatment, Posttreatment 1 After the Second Session, and Posttreatment 2 After theThird Session, Taken Bilaterally
Treatment Sham
Right Left Right Left
Pre Post 1 Post 2 Pre Post 1 Post 2 Pre Post 1 Post 2 Pre Post 1 Post 2
Orofacial region
M1 2.13±0.37 3.03±0.5 3.46±0.45 2.12±0.43 2.91±0.53 3.5±0.44 2.29±0.54 2.32±0.48 2.39±0.55 2.28±0.37 2.31±0.62 2.42±0.6
M2 2.12±0.44 2.88±0.44 3.4±0.38 2.09±0.39 2.94±0.36 3.59±0.45 2.18±0.49 2.27±0.56 2.37±0.63 2.12±0.61 2.21±0.45 2.15±0.66
T1 2.76±0.49 3.52±0.5 4.11±0.55 2.69±0.5 3.66±0.54 4.19±0.53 2.81±0.47 2.85±0.46 2.97±0.32 2.89±0.51 2.78±0.57 2.82±0.59
T2 2.97±0.48 3.59±0.51 3.95±0.58 2.8±0.56 3.77±0.47 3.98±0.66 3.04±0.46 2.91±0.61 3.06±0.55 2.86±0.58 2.9±0.46 2.97±0.46
Cervical region
Suboccipital 2.36±0.34 3.33±0.29 3.95±0.22 2.28±0.35 3.38±0.32 3.99±0.22 2.31±0.44 2.43±0.52 2.48±0.63 2.25±0.39 2.35±0.49 2.41±0.54
C5 2.47±0.42 3.09±0.65 3.63±0.52 2.46±0.45 3.26±0.69 3.69±0.49 2.52±0.44 2.55±0.38 2.6±0.4 2.64±0.44 2.74±0.61 2.63±0.43
Trapezius 2.61±0.38 3.51±0.42 4.13±0.67 2.66±0.37 3.62±0.41 4.24±0.5 2.85±0.29 2.82±0.44 2.87±043 2.69±0.4 2.53±0.56 2.6±0.58
Mean±SD.PPT indicates pressure pain thresholds.
100.00
120.00 Treatment/Right SideTreatment/Left SideSham/Right SideSham/Left Side
60.00
80.00
40.00
0.00
20.00
Ch
ang
e in
PP
T (
%)
M1 M2 T1 T2
-20.00
FIGURE 2. Percent change in pressure pain thresholds (PPTs) ofthe craniofacial region (M1 and M2 points of masseter muscleand T1 and T2 of temporal muscle) for treatment and sham in-terventions at right and left sides (mean of preintervention andfinal postintervention). Error bars represent 95% confidence in-tervals of the mean.
Treatment/Right SideTreatment/Left SideSham/Right SideSham/Left Side
Ch
ang
e in
PP
T (
%)
120.00
80.00
100.00
60.00
40.00
20.00
-20.00
0.00
Sub-occipital C5 Trapezius
FIGURE 3. Percent change in pressure pain thresholds (PPTs) ofthe cervical region (suboccipital muscles, C5, and trapeziusmuscles) for treatment and sham interventions on the right andleft sides (mean of preintervention and final postintervention).Error bars represent 95% confidence intervals of the mean.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
210 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

total of the means for the treatment and sham groups(t= �1.82; P=0.079).
DISCUSSIONOur findings demonstrate that the APUCM technique
applied at a rate of 0.5Hz significantly increased SNS ac-tivity and produced short-term hypoalgesic effects. We arenot aware of any previous studies that have measured hy-poalgesic effects in the cervical and craniofacial regionsusing APUCM. We therefore contend that this is the firsttime that this specific manual mobilization technique ap-plied at the aforementioned frequency has been investigated,and our data indicate significant differences between theexperimental and control groups.
An increase in PPT was observed after the second in-tervention compared with the presession data and after thethird intervention compared with the first posttreatment as-sessment, which is indicative of a maintained increase overthe successive sessions. With regard to pain intensity, it isimportant to note the decrease in the VAS after each ses-sion, which was maintained from one session to the next andindicates a 41.7% decrease in pain intensity from the 3 ap-plications. A change in the SNS, as evidenced by changes inSC, BR, and HR, was noted after each session, but this trendreversed and was not maintained from one session to the next.Upon comparing the first, second, and third pretreatment
outcomes, it was apparent that the SNS values returned toa normal state of SNS activity. We suggest that the effectproduced by the technique could be due to the influence oftransient sympathoexcitation on pain mechanisms. Our con-tention is that the physiological effects produced by theAPUCM technique influence the suboccipital posterior sym-pathetic network and TCC and act to inhibit or gate my-ofascial pain within the cervico-craniofacial region.
Clinical EffectivenessThe results of clinical pain intensity measured by the
VAS indicate a decrease in the patients’ experience of painat rest with significant differences between treatment andsham groups. Patients who received the intervention re-ported a decrease of 29.13mm in VAS between the pre-treatment and third posttreatment assessment. Todd et al35
have stated that a minimal clinically significant change inVAS may be at least �13mm, whereas more recently, Birdand Dickson36 have contended that a clinically significantVAS change depends on the baseline VAS of the participantand that a change of �13mm would be clinically significantfor a baseline VAS<34mm, a change of �17mm for abaseline VAS between 34 and 67mm, and a change of�28mm for a baseline VAS>67mm. The more specificguidelines of Bird and Dickson are supported by Emshoffand colleagues in a study of chronic TMD pain patients.
120
140
160TreatmentA B
C D
Sham
30
40TreatmentSham
60
80
100
0
10
20
-20
0
20
40
Ch
ang
e in
Ski
n C
on
du
ctan
ce (
%)
-20
-10
0
Ch
ang
e in
Bre
ath
ing
Rat
e (%
)15 Treatment
-40
Session 1 Session 2 Session 3
Session 1 Session 2 Session 3
Treatment
0
5
10Sham
Sham
-10
-5
-15
Session 1 Session 2 Session 3
Ch
ang
e in
Hea
rt R
ate
(%)
0
-10
-5
-20
-15
-25
Session 1 Session 2 Session 3
Ch
ang
e in
Ski
n T
emp
erat
ure
(%
)
FIGURE 4. Percent change between the 3 sessions (mean of preintervention and postintervention) for treatment and sham groups. A,skin conductance; (B) heart rate; (C) breathing rate; (D) skin temperature.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 211

They established that to be clinically significant, patientswith a higher pain baseline must demonstrate a greater VASreduction than those with a lower baseline, and the minimalchange should be of �19.5mm or �37.9% of the VAS.37
Our findings are clinically significant according to theguidelines of Todd et al, Bird and Dickson, or Emshoffet al.35–37
SNS ResponsePrevious studies have noted similar effects in the variables
that we measured after SMT in the cervical region.15,17,19,20,38
We observed an increase of 83.75% in SC, which is similar tothat observed by Chiu and Wright19 and Sterling et al15 whoobserved increases of approximately 50% to 60% and 16%,respectively. Studies in which SMT was applied to other bodylocations also noted similar changes in SC. A 16.85% increasein SC was observed after a thoracic mobilization applied toT4,39 and a 13.5% increase in SC was observed after lumbarmobilization.40
A similar effect was noted for HR. We observed an in-crease of 6.06% compared with previous studies that reportedchanges of 10.5%,38 13%,20 and 4.5%.17 A significant changein HR in the sham group was also noted. HR decreased by�5.5% in the sham group, which could indicate that thetreatment can increase HR, whereas the sham application issimilar to a touch massage technique that results in a decreaseof SNS activity.41
Previous studies of BR have reported increases of44%38 and 36%.20 In our study, we observed a 10.4% in-crease in BR in the experimental group. This discrepancycould be due to the type of mobilization that we applied.Previous studies that used lateral cervical glides or poste-rior-anterior mobilization techniques at a frequency of2Hz. A significant change was not obtained in ST despitea downward trend in both treatment and sham groups, asnoted by Chiu and Wright.19 However, a significant de-crease of 2.5% in ST was obtained in another study.15
The results of Sterling et al15 correlate with our datawith respect to the tendency of ST to decrease and the notedchange in SC. Furthermore, significant changes in bloodpressure, which we did not record, have been observed byPaungmali et al,17 Vicenzino et al,20 and McGuiness et al.38
These results confirm that gentle manual mobilizationtechniques on the cervical spine can confer positive phys-iological effects.
Hypoalgesic EffectsOur data indicate that the APUCM technique pro-
duces hypoalgesic effects, as demonstrated by PTT meas-urements made by an algometer, and support a significantdifference between the treatment and sham groups. Sterlinget al15 demonstrated that a unilateral posterior-anteriormobilization applied on the side of pain increased the PPTby 23% on the side of treatment in patients with chronicidiopathic neck pain. We observed increases in PPTbetween 64% and 77% for the masseter muscle points,between 38% and 59% at temporal muscle points and be-tween 47% and 79% for the cervical points after 3 treat-ments of APUCM. The greater change in PPT observed inour study and others may be because our study investigatedshort-term outcomes (3 treatment sessions) instead of im-mediate outcomes (1 treatment session), due to the appliedtechnique and the frequency of mobilization and is in-dicative of a real bilateral hypoalgesic effect at both regions.
Previous research has investigated the effect of spinalmobilization on cervical and lumbar regions and reportedpositive results.15,20,40,42 Sterling et al15 noted a differencebetween the improved PPT in the painful side and thenonpainful side, indicating a unilateral effect from a uni-lateral technique. Our study demonstrates a bilateral in-crease in PPT in both cervical and craniofacial regions. Thisdifference could be due to the central application of thetechnique in this study as opposed to the unilateral appli-cation of Sterling et al.
Manual Therapeutic NeurophysiologyResearch in SMT has focused on the neurophysio-
logical effects of manual manipulation and mobilizationswith data suggesting activation of descendent pain inhibitorysystems upon short-term (initial) hypoalgesic effects.43–45
Skyba et al46 showed that mobilization of the hyperalgesicknee joint in rats produced an antihyperalgesic effect. Thiseffect, which maintained after spinal blockage of opioid orGABA receptors, could be due to descending serotoninergicor noradrenergic inhibitory mechanisms via corticospinalprojections from the periacueductal gray matter (PAG).46
Implications relate to noradrenaline, a PGA neurotransmitterthat is more effective at inhibiting mechanical nociceptionthan thermal nociception, which seems to be serotoninergi-cally mediated.47,48 Others have demonstrated that SMTmight be the ideal stimulus for PAG mediated nonopioidanalgesia, hypoalgesia, sympathoexcitatory effects, and changesin motor activity.15,17,20,49 In the present study, we obtainedboth a sympathoexcitation and hypoalgesic effect after theAPUCM technique, which supports the fact that the d-PAG isinfluenced by the SMT technique.
One controversial issue surrounding manual therapy iswhether a localized segmental and/or extrasegmental effectis produced by SMT. Previous research has shown thatSMT improves symptoms distal to the segment where it isapplied; that is, manipulation applied at the thoracic spinehas positive effects when performed on patients with frommechanical neck pain,14,21 and cervical SMT can result inhypoalgesia at the elbow.50 However, other clinical studieshave shown only segmental effects causing diminished neckpain and PPT after ipsilateral cervical mobilization.15,16
We applied a mobilization technique at the upper cer-vical spine and observed changes in the craniofacial andcervical region as well as hypoalgesic effects further awayfrom the segment to which it was applied, suggesting thatmanual therapy has a general central or at least supra-medullar effect. A physiological or sympathoexcitatoryeffect has also been demonstrated in the upper extremityafter cervical or thoracic SMT,15,39 and in the lower ex-tremities after lumbar mobilization.40
It is clear that SMT activates central structures that con-currently activate sympathoexcitatory and hypoalgesic effectsas demonstrated in our research and in that of others.15,20 Thepresence of an extrasegmental effect may indicate activation ofthe d-PAG and could be mediated by various descending paininhibitory pathways and associated tracts of the TCC thatallow for afferent and efferent transmission between the cer-vical and craniofacial regions.51,52
Nociceptive Modulation and the TCCThe increase in PPT caused by the APUCM technique
on the craniofacial region provides additional clinical
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
212 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

support for pain modulatory mechanisms in the TCC.A review performed in 1998 outlined neurophysiologicalcoupling between craniofacial and cervical systems.53
It has been observed that manual therapeutic applica-tions to the cervical region provoked a pain reducing effectin the head and face. Mellick and Mellick54 and Mellicket al55 observed that applying a bilateral intramuscular in-jection of small amounts of 0.5% bupivacaine at the cervicalregion caused a decrease in facial pain and headaches. Inaddition, Carlson et al56 demonstrated that an infiltration of2% lidocaine on an active TrP of the trapezius muscle sig-nificantly reduced pain and electromyographical activity ofthe ipsilateral masseter.
The only previous study of manual interventions to thecervical spine to manage craniofacial pain was performedby La Touche et al. This study reported similar results toour study: improved PPT at the masseter and temporalismuscles after a manual therapy protocol directed to thecervical spine combined with a deep neck flexors train-ing program.23
Convergence pathways between cervical and trigemi-nal sensory afferents in the TCC are fully supported.52,57,58
Stimulation of an upper cervical root, such as manipulationof the greater occipital nerve has produced changes in theTCC neurons. This supports the concept that perception ofcranial pain is due to a functional convergence betweentrigeminal and cervical fibers in the TCC59,60 and provides apotential rationale for the relationship between headachesand arm and trunk pain.61
Direct stimulation of the greater occipital nerve (cer-vical input) increases metabolic activity of the TCC62 andtrigeminal nociceptors release neuropeptides, such as sub-stance P, from laminas I and II that diffuse to laminas III toV depending on the intensity of the stimulus.63 The TCCitself is formed by the upper cervical dorsal horns and thetrigeminal nucleus caudalis, which allows nociceptive inputto be transmitted from the TCC to higher centers.64 Painmodulatory structures such as the PAG, dorsolateral pon-tomesencephalic tegmentum, and rostral ventromedial me-dulla control the TCC-mediated generation of antinociceptiveor pronociceptive states.57,58,65
In summary, we propose a neurobiomechanical hypo-thesis to explain the possible mechanism by which a manualtherapeutic technique causes a hypoalgesic effect in cranio-facial and cervical regions. This technique primarily influen-ces the upper cervical region (C1-C3), which is anatomicallyrelated to the occipital bone. We believe that an anterior-posterior glide of the upper cervical structures provokes animproved arthrokinematic relationship of the target regionthereby generating improved pain-free range of movementand concomitant suboccipital muscle relaxation. A secondaryeffect might reduce mechanical forces on the upper cervicalneurovascular structures, thereby interrupting or inhibitinginput and reducing TCC sensitization by activating de-scendent pain inhibitory systems.
In addition, the TCC is the main nucleus that receivesnociceptive information from the face, head, and neck.66
Neurons inside the nuclei are considered multimodal neu-rons and can receive 2 or more inputs from different ori-gins, such as cervical nerve roots, when manual therapy isbeing applied. The input generated from the cervical regioncan alter the nociceptive processing in the TCC and, as aresult, produce a hypoalgesic effect at the facial region.Finally, another possible mechanism to explain the effect ofour manual intervention is that descending pain inhibitory
systems can be activated by SMT on the cervical spine byspinal noradrenergic and serotoninergic pathways from thedorsolateral pons and rostral ventral medulla.45,46
Study LimitationsAlthough the results of our research are positive, we
only measured short-term changes without follow-up testing.We only measured SC and ST on the right side. Other studiesinvestigating sympathetic activation after SMT treatmentonly measured one side of the body, usually the treated side.Perry and colleagues applied a unilateral lumbar mobilizationand measured sympathetic activity at both lower extremities.They only observed significant activation in the treated sidebut did observe a tendency toward sympathetic activation inthe untreated side.40 It would have been interesting to observeif central mobilization activates SNS with the same intensityin both upper extremities and if it has any effect on lowerextremities. It also could have been interesting to measure SCand ST directly on the facial region. We did not measure distalPPT; therefore, due to a lack of information, we cannot pro-vide a complete discussion about the general or segmental ef-fect of the APUCM technique.
This is the first time this type of mobilization at afrequency of 0.5Hz has been used in a clinical randomized-controlled trial. Because different techniques require differ-ent frequencies of application to provoke stronger changes,it would be of interest to test the same mobilization at dif-ferent frequencies of application.
Clinical ImplicationsWe have demonstrated that craniofacial pain can be
modulated through an upper cervical treatment (mobilization).The presence of craniofacial pain is a predictor factor for neckpain.9,67 It is interesting to treat this type of patient with atechnique that has proven effects at the craniofacial segmentthat can also treat a possible neck dysfunction. This techniquemight be contraindicated in patients with craniocervical hy-permobility syndrome due to the movement the APUCMprovokes at the upper cervical spine and the risk this entails.68
Chronic pain can be maintained by SNS modulationthrough the peripheric adrenorreceptor excitation of cat-echolamine.69 Chronic TMD patients seem to present adysregulation of b-adrenergic activity, which contributes toaltered cardiovascular and catecholamine responses.70 Thedysregulation of SNS can contribute to the severity andmaintenance of pain. The influence of APUCM on SNSactivity makes this technique an interesting tool to treatpatients with CCFP of myofascial origin and patients withfacial allodynia, in which other techniques applied directlyon the face would be contraindicated.
CONCLUSIONSWe demonstrate that APUCM reduces pain intensity
and increases PPT in the cervical and craniofacial regions.APUCM also causes sympathoexcitation, which confirms asympathetic effect. These results indicate an influence of themobilization on the CNS (medullar or supramedullar effect).This study provides preliminary evidence of the short-termhypoalgesic effect on the craniofacial and cervical regions ofpatients with CCFP of myofascial origin, suggesting thatAPUCM may cause an immediate nocioceptive modulationat the TTC.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 213

REFERENCES
1. LeResche L. Epidemiology of orofacial pain. In: Lund J,Lavigne G, Dubner R, Sessle B, eds. Orofacial Pain: FromBasic Science to Clinical Management. Chicago: QuintessencePublishing Co; 2000:15–25.
2. Ciancaglini R, Testa M, Radaelli G. Association of neckpain with symptoms of temporomandibular dysfunction inthe general adult population. Scand J Rehabil Med. 1999;31:17–22.
3. Vierck CJ. Mechanisms underlying development of spatiallydistributed chronic pain (fibromyalgia). Pain. 2006;3:242–263.
4. Sarlani E, Greenspan JD. Why look in the brain for answers totemporomandibular disorder pain? Cells Tissues Organs.2005;180:69–75.
5. Turp JC, Kowalski CJ, O’Leary N, et al. Pain maps from facialpain patients indicate a broad pain geography. J Dent Res.1998;77:1465–1472.
6. Velly AM, Gornitsky M, Philippe P. Contributing factors tochronic myofascial pain: a case-control study. Pain. 2003;104:491–499.
7. Carlson CR, Reid KI, Curran SL, et al. Psychological andphysiological parameters of masticatory muscle pain. Pain.1998;76:297–307.
8. Eriksson PO, Haggman-Henrikson B, Zafar H. Jaw-neckdysfunction in whiplash-associated disorders. Arch Oral Biol.2007;52:404–408.
9. Wiesinger B, Malker H, Englund E, et al. Does a dose-responserelation exist between spinal pain and temporomandibulardisorders? BMC Musculoskelet Disord. 2009;10:28.
10. Ries LG, Berzin F. Analysis of the postural stability inindividuals with or without signs and symptoms of tempor-omandibular disorder. Braz Oral Res. 2008;22:378–383.
11. De Laat A, Meuleman H, Stevens A, et al. Correlation betweencervical spine and temporomandibular disorders. Clin OralInvestig. 1998;2:54–57.
12. Haggman-Henrikson B, Osterlund C, Eriksson PO. Enduranceduring chewing in whiplash-associated disorders and TMD.J Dent Res. 2004;83:946–950.
13. Bokarius AV, Bokarius V. Evidence-based review of manualtherapy efficacy in treatment of chronic musculoskeletal pain.Pain Pract. 2010;10:451–458.
14. Cleland JA, Childs JD, McRae M, et al. Immediate effects ofthoracic manipulation in patients with neck pain: a random-ized clinical trial. Man Ther. 2005;10:127–135.
15. Sterling M, Jull G, Wright A. Cervical mobilisation: con-current effects on pain, sympathetic nervous system activityand motor activity. Man Ther. 2001;6:72–81.
16. Sterling M, Pedler A, Chan C, et al. Cervical lateral glideincreases nociceptive flexion reflex threshold but not pressureor thermal pain thresholds in chronic whiplash associateddisorders: a pilot randomised controlled trial. Man Ther.2010;15:149–153.
17. Paungmali A, O’Leary S, Souvlis T, et al. Hypoalgesic andsympathoexcitatory effects of mobilization with movement forlateral epicondylalgia. Phys Ther. 2003;83:374–383.
18. Paungmali A, O’Leary S, Souvlis T, et al. Naloxone fails toantagonize initial hypoalgesic effect of a manual therapy treat-ment for lateral epicondylalgia. J Manipulative Physiol Ther.2004;27:180–185.
19. Chiu TW, Wright A. To compare the effects of different ratesof application of a cervical mobilisation technique on sym-pathetic outflow to the upper limb in normal subjects. ManTher. 1996;1:198–203.
20. Vicenzino B, Collins D, Benson H, et al. An investigation ofthe interrelationship between manipulative therapy-inducedhypoalgesia and sympathoexcitation. J Manipulative PhysiolTher. 1998;21:448–453.
21. Cleland JA, Glynn P, Whitman JM, et al. Short-term effects ofthrust versus nonthrust mobilization/manipulation directed atthe thoracic spine in patients with neck pain: a randomizedclinical trial. Phys Ther. 2007;87:431–440.
22. George JW, Fennema J, Maddox A, et al. The effect of cervicalspine manual therapy on normal mouth opening in asympto-matic subjects. J Chiropr Med. 2007;6:141–145.
23. La Touche R, Fernandez-de-las-Penas C, Fernandez-Carnero J,et al. The effects of manual therapy and exercise directed at thecervical spine on pain and pressure pain sensitivity in patients withmyofascial temporomandibular disorders. J Oral Rehabil. 2009;36:644–652.
24. Dworkin SF, LeResche L. Research diagnostic criteria fortemporomandibular disorders: review, criteria, examinationsand specifications, critique. J Craniomandib Disord. 1992;6:301–355.
25. Andrade Ortega JA, Delgado Martinez AD, Almecija Ruiz R.Validation of a Spanish version of the Neck Disability Index.Med Clin (Barc). 2008;130:85–89.
26. Vernon H, Mior S. The Neck Disability Index: a study ofreliability and validity. J Manipulative Physiol Ther. 1991;14:409–415.
27. Simons DG, Travel JG, Simons LS. Myofascial Pain andDysfunction: The Trigger Point Manual. Vol 1. 2nd ed.Baltimore: Lippincott Williams & Wilkins; 1999.
28. Dworkin SF, Sherman J, Mancl L, et al. Reliability, validity,and clinical utility of the research diagnostic criteria forTemporomandibular Disorders Axis II Scales: depression,non-specific physical symptoms, and graded chronic pain.J Orofac Pain. 2002;16:207–220.
29. de Leeuw R. (ed) The American Academy of Orofacial Pain.Orofacial Pain: Guidelines for Assessment, Diagnosis, andManagement. 4th ed. Chicago: Quintessence; 2008:25–27.
30. Beck AT, Steer RA. Internal consistencies of the original andrevised Beck Depression Inventory. J Clin Psychol. 1984;40:1365–1367.
31. Spielberg CDG, Lushene RL, E. R. State Anxiety Inventory.Cuestionario de ansiedad estado-rasgo. Adaptacion espanola.Madrid: TEA; 1982.
32. Bijur PE, Silver W, Gallagher EJ. Reliability of the visualanalog scale for measurement of acute pain. Acad Emerg Med.2001;8:1153–1157.
33. Svensson P, Arendt-Nielsen L, Nielsen H, et al. Effect ofchronic and experimental jaw muscle pain on pain-pressurethresholds and stimulus-response curves. J Orofac Pain.1995;9:347–356.
34. Chesterton LS, Sim J, Wright CC, et al. Interrater reliability ofalgometry in measuring pressure pain thresholds in healthyhumans, using multiple raters. Clin J Pain. 2007;23:760–766.
35. Todd KH, Funk KG, Funk JP, et al. Clinical significance ofreported changes in pain severity. Ann Emerg Med.1996;27:485–489.
36. Bird SB, Dickson EW. Clinically significant changes in painalong the visual analog scale. Ann Emerg Med. 2001;38:639–643.
37. Emshoff R, Emshoff I, Bertram S. Estimation of clinicallyimportant change for visual analog scales measuring chronictemporomandibular disorder pain. J Orofac Pain. 2010;24:262–269.
38. McGuiness J, Vicenzino B, Wright A. Influence of a cervicalmobilization technique on respiratory and cardiovascularfunction. Man Ther. 1997;2:216–220.
39. Jowsey P, Perry J. Sympathetic nervous system effects in thehands following a grade III postero-anterior rotatory mobi-lisation technique applied to T4: a randomised, placebo-controlled trial. Man Ther. 2010;15:248–253.
40. Perry J, Green A. An investigation into the effects of aunilaterally applied lumbar mobilisation technique on periph-eral sympathetic nervous system activity in the lower limbs.Man Ther. 2008;13:492–499.
41. Lindgren L, Rundgren S, Winso O, et al. Physiological res-ponses to touch massage in healthy volunteers. Auton Neurosci.2010;158:105–110.
42. Goodsell M, Lee M, Latimer J. Short-term effects of lumbarposteroanterior mobilization in individuals with low-back pain.J Manipulative Physiol Ther. 2000;23:332–342.
La Touche et al Clin J Pain � Volume 29, Number 3, March 2013
214 | www.clinicalpain.com r 2012 Lippincott Williams & Wilkins

43. Schmid A, Brunner F, Wright A, et al. Paradigm shift inmanual therapy? Evidence for a central nervous systemcomponent in the response to passive cervical joint mobilisa-tion. Man Ther. 2008;13:387–396.
44. Vicenzino B, Wright A. Effects of a novel manipulativephysiotherapy technique on tennis elbow: a single case study.Man Ther. 1995;1:30–35.
45. Wright A. Hypoalgesia post-manipulative therapy: a reviewof a potential neurophysiological mechanism. Man Ther. 1995;1:11–16.
46. Skyba DA, Radhakrishnan R, Rohlwing JJ, et al. Jointmanipulation reduces hyperalgesia by activation of mono-amine receptors but not opioid or GABA receptors in thespinal cord. Pain. 2003;106:159–168.
47. Kuraishi Y, Harada Y, Aratani S, et al. Separate involvementof the spinal noradrenergic and serotonergic systems inmorphine analgesia: the differences in mechanical and thermalalgesic tests. Brain Res. 1983;273:245–252.
48. Kuraishi Y, Kawamura M, Yamaguchi T, et al. Intrathecalinjections of galanin and its antiserum affect nociceptive res-ponse of rat to mechanical, but not thermal, stimuli. Pain.1991;44:321–324.
49. Vicenzino B, Cartwright T, Collins D, et al. Cardiovascularand respiratory changes produced by lateral glide mobilizationof the cervical spine. Man Ther. 1998;3:67–71.
50. Vicenzino B, Collins D, Wright A. The initial effects of acervical spine manipulative physiotherapy treatment on thepain and dysfunction of lateral epicondylalgia. Pain. 1996;68:69–74.
51. Piovesan EJ, Kowacs PA, Tatsui CE, et al. Referred pain afterpainful stimulation of the greater occipital nerve in humans:evidence of convergence of cervical afferences on trigeminalnuclei. Cephalalgia. 2001;21:107–109.
52. Piovesan EJ, Kowacs PA, Oshinsky ML. Convergence ofcervical and trigeminal sensory afferents. Curr Pain HeadacheRep. 2003;7:377–383.
53. Browne PA, Clark GT, Kuboki T, et al. Concurrent cervicaland craniofacial pain. A review of empiric and basic scienceevidence. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.1998;86:633–640.
54. Mellick LB, Mellick GA. Treatment of acute orofacial painwith lower cervical intramuscular bupivacaine injections: a1-year retrospective review of 114 patients. J Orofac Pain.2008;22:57–64.
55. Mellick LB, McIlrath ST, Mellick GA. Treatment of head-aches in the ED with lower cervical intramuscular bupivacaineinjections: a 1-year retrospective review of 417 patients.Headache. 2006;46:1441–1449.
56. Carlson CR, Okeson JP, Falace DA, et al. Reduction of painand EMG activity in the masseter region by trapezius triggerpoint injection. Pain. 1993;55:397–400.
57. Sessle BJ. Acute and chronic craniofacial pain: brainstemmechanisms of nociceptive transmission and neuroplasticity, andtheir clinical correlates. Crit Rev Oral Biol Med. 2000;11:57–91.
58. Mason P. Deconstructing endogenous pain modulations.J Neurophysiol. 2005;94:1659–1663.
59. Pfaller K, Arvidsson J. Central distribution of trigeminal andupper cervical primary afferents in the rat studied byanterograde transport of horseradish peroxidase conjugatedto wheat germ agglutinin. J Comp Neurol. 1988;268:91–108.
60. Scheurer S, Gottschall J, Groh V. Afferent projections of therat major occipital nerve studied by transganglionic transportof HRP. Anat Embryol (Berl). 1983;167:425–438.
61. Kajander KC, Giesler GJ Jr. Responses of neurons in thelateral cervical nucleus of the cat to noxious cutaneous stimu-lation. J Neurophysiol. 1987;57:1686–1704.
62. Goadsby PJ, Knight YE, Hoskin KL. Stimulation of thegreater occipital nerve increases metabolic activity in thetrigeminal nucleus caudalis and cervical dorsal horn of the cat.Pain. 1997;73:23–28.
63. Li JL, Wang D, Kaneko T, et al. The relationship betweenneurokinin-1 receptor and substance P in the medullary dorsalhorn: a light and electron microscopic immunohistochemicalstudy in the rat. Neurosci Res. 2000;36:327–334.
64. Bartsch T, Goadsby PJ. Stimulation of the greater occipitalnerve induces increased central excitability of dural afferent input.Brain. 2002;125:1496–1509.
65. Hjornevik T, Jacobsen LM, Qu H, et al. Metabolic plasticity inthe supraspinal pain modulating circuitry after noxiousstimulus-induced spinal cord LTP. Pain. 2008;140:456–464.
66. Hu JW, Sun KQ, Vernon H, et al. Craniofacial inputs to uppercervical dorsal horn: implications for somatosensory informa-tion processing. Brain Res. 2005;1044:93–106.
67. Marklund S, Wiesinger B, Wanman A. Reciprocal influence onthe incidence of symptoms in trigeminally and spinallyinnervated areas. Eur J Pain. 2010;14:366–371.
68. Aspinall W. Clinical testing for the craniovertebral hyper-mobility syndrome. J Orthop Sports Phys Ther. 1990;12:47–54.
69. Ren Y, Zou X, Fang L, et al. Sympathetic modulation ofactivity in Adelta- and C-primary nociceptive afferents afterintradermal injection of capsaicin in rats. J Neurophysiol.2005;93:365–377.
70. Light KC, Bragdon EE, Grewen KM, et al. Adrenergicdysregulation and pain with and without acute beta-blockadein women with fibromyalgia and temporomandibular disorder.J Pain. 2009;10:542–552.
Clin J Pain � Volume 29, Number 3, March 2013 Cervical Mobilization in Cervico-craniofacial Pain
r 2012 Lippincott Williams & Wilkins www.clinicalpain.com | 215

205
DISCUSIÓN

206
6. DISCUSIÓN
Los hallazgos mostrados en esta tesis coinciden con una gran cantidad de estudios
recientes publicados en las últimas dos décadas. En estas investigaciones de carácter
básico y clínico se ha comprobado como las estructuras cervicales pueden influir sobre
características sensoriales y motoras de la regiones craneofacial y craneomandibular y
viceversa (Armijo-Olivo and Magee, 2007, 2013; Dessem and Luo, 1999; Eriksson et
al., 2004, 2007; Ge et al., 2004; Giannakopoulos, Hellmann, et al., 2013;
Giannakopoulos, Schindler, et al., 2013; Häggman-Henrikson and Eriksson, 2004;
Häggman-Henrikson et al., 2013; Haggman-Henrikson et al., 2004; Hellmann et al.,
2012; Hellström et al., 2002; Hu et al., 2005; Olivo et al., 2010; Svensson et al., 2005;
Torisu et al., 2014). La investigación básica en torno a la neurofisiología del CTC ha
servido para establecer hipótesis y teorías relacionadas con los mecanismos
nociceptivos periféricos y centrales implicados en (Bartsch and Goadsby, 2002, 2003a;
Bereiter et al., 2005; Chiang et al., 1998, 2005; Hu et al., 1993; Lam et al., 2009; Salter,
2004; Sessle et al., 1986; Yu et al., 1995): 1) las comorbilidades entre las dolencias
cervicales y craneofaciales; 2) en la concomitancia motora entre la región
craneomadibular y craneocervical; 3) en las respuestas motoras alteradas; y 4) en las
posibles intervenciones terapéuticas sobre la región cervical que pudieran influir sobre
la región craneofacial. Los resultados de las investigaciones presentadas en esta tesis
ofrecen algunos hallazgos importantes que fortalecen la investigación previa en relación
con esto cuatro puntos. A continuación se discute en profundidad los resultados
obtenidos según los objetivos planteados en la tesis.

207
6.1 Diferencias de Género en la Variables Somatosensoriales.
En el análisis del efecto del género sobre variables somatosensoriales en pacientes con
DCCF hay que partir de una premisa epidemiológica y es que como está representado
en nuestros estudios, la prevalencia de estas dolencias es mayor en la población
femenina (Adèrn et al., 2014; Carlsson, 1999; LeResche, 1997; Macfarlane, Blinkhorn,
Davies, Kincey, et al., 2002). Hemos encontrado en el estudio III (La Touche et al.,
2010) y en el estudio V (La Touche, Paris-Alemany, et al., 2014) influencias del género
sobre variables somatosensoriales.
En relación al estudio V (La Touche, Paris-Alemany, et al., 2014) los resultados
mostraron que la percepción del dolor y la fatiga durante el test masticatorio de
provocación estuvo influenciada por el género en los tres grupos evaluados, se observó
que las mujeres presentan una mayor percepción de intensidad de dolor y fatiga
masticatoria, estos resultados coinciden con estudios previos de dolor inducido
experimentalmente realizados con pacientes (Haggman-Henrikson et al., 2004) y
sujetos sanos (Karibe et al., 2003; Plesh et al., 1998), sin embargo es importante
mencionar que otras investigaciones no han observado la interacción del factor genero
sobre el dolor o la fatiga masticatoria inducida experimentalmente (Koutris et al., 2013;
van Selms et al., 2005). El estudio V no está diseñado con el objetivo de identificar los
mecanismos fisiológicos o psicológicos que puedan explicar las diferencias en los
resultados entre mujeres y hombres, sin embargo es importante destacar que la
evidencia de estudios experimentales relacionados con dolor inducido indica que las
mujeres presentan mayor sensibilidad al dolor que los hombres en diferentes pruebas
somatosensoriales (Fillingim et al., 2009). Finalmente destacar que en el estudio III (La
Touche et al., 2010), solo se identificó una interacción con el género en los UDPS del

208
músculo tibial anterior, mostrando unos valores significativamente menores en mujeres
respecto a la población masculina del estudio.
6.2 Postura Craneocervical, Dinámica Mandibular y Dolor Craneofacial.
Dos investigaciones (I, (La Touche et al., 2011) y II (Lopez-de-Uralde-Villanueva et
al., 2014) de esta tesis han estudiado la influencia de la postura craneocervical sobre la
función mandibular y las posibles interacciones con mecanismos nociceptivos
trigeminales. Los resultados demuestran que las posturas craneocervicales inducidas
experimentalmente producen modificaciones en MAI presentándose menor o mayor
rango articular según la postura en que se realice el gesto (La Touche et al., 2011), estos
hallazgos también fueron comprobados por Higbie y cols. en 1999 (Higbie et al., 1999).
Además, evidencia previa refuerza estos hallazgos, ya que se han descrito las
modificaciones intra-articulares que se producen en ATM con diferentes posturas
craneocervicales o movimientos cervicales (Ohmure et al., 2008; Solow and Tallgren,
1976; Visscher et al., 2000).
Otro resultado que consideramos relevante en el estudio I, fue que los UDPS de áreas
trigeminales se vieron modificados según las diferentes posturas craneocervicales
siendo el menor UDP registrado en la postura de protracción. Este resultado es difícil
discutirlo ya que no hay estudios similares en esta línea, nosotros plantemos
teóricamente que esto puede suceder debido a cambios o ajustes que realiza el sistema
nervioso bajo diferentes condiciones del entorno y demandas de la región cervical,
creemos que estos ajustes se producen en mecanismos sensoriales pero también en los
motores. En relación a esto, debemos mencionar que contamos con evidencia previa que
describe que los movimientos cervicales o las posturas craneocervicales inducidas
experimentalmente modifican la actividad de la musculatura masticatoria

209
incrementándola (Ballenberger et al., 2012; Forsberg et al., 1985; McLean, 2005;
Ohmure et al., 2008).
En el estudio II (Lopez-de-Uralde-Villanueva et al., 2014) se encontraron diferencias en
la postura craneocervical medido con dos instrumentos entre el grupo de pacientes con
DCCF y los sujetos asintomáticos, sin embargo es fundamental tener en cuenta que esos
cambios fueron muy pequeños y en una de la mediciones no superó el MCD y en la otra
los superó pero por muy poco, estos resultados se han encontrado prácticamente con las
mismas similitudes en investigaciones realizadas en pacientes con dolor de cuello
(Silva et al., 2009) y con TCM (Armijo-Olivo et al., 2011) comparada con sujetos
asintomáticos. Por otra parte, cabe mencionar que no se encontró asociación entre la
postura craneocervical con las variables de discapacidad cervical y craneofacial, datos
de otras investigaciones apoyan este resultado (Armijo-Olivo et al., 2011; Cheung et al.,
2010) aunque otros lo contradicen (Lau et al., 2010). La relación entre la postura y los
TCM es controvertida y no está clara según datos extraídos de dos revisiones
sistemáticas recientes (Armijo Olivo et al., 2006; Rocha et al., 2013), además ambas
revisiones coinciden en recalcar que los estudios analizados en relación a esta temática
presentan serias dificultades metodológicas y complica la posibilidad de extraer
conclusiones.
6.3 Influencia del Dolor y la Discapacidad Cervical sobre la Actividad
Sensoriomotora Trigeminal.
En los estudios III (La Touche et al., 2010) y V (La Touche, Paris-Alemany, et al.,
2014) se han obtenido resultados importantes entorno a la influencia del dolor y la
discapacidad de cuello sobre la región craneofacial, específicamente en el estudio V
hemos identificado que los pacientes con moderada y leve discapacidad cervical

210
presentan mayores niveles de percepción de dolor y fatiga frente a los sujetos sanos
sometidos al test de provocación masticatorio, es importante mencionar que entre los
grupos de pacientes, el de moderada discapacidad cervical fue el que presentó mayores
cambios en las variables sensoriales medidas durante el test, inmediatamente después y
las 24 horas, La única excepción de esto ha sido en el resultado de la percepción de
intensidad dolor a las 24 horas en que entre ambos grupos no se presentaron diferencias
estadísticamente significativas. A pesar de que existen muchos estudios que utilizan los
test provocación masticatorias para inducir dolor y fatiga (Christensen et al., 1996; Dao
et al., 1994; Farella et al., 2001; Gavish et al., 2002; Karibe et al., 2003; Koutris et al.,
2009; Plesh et al., 1998), solo hemos encontrado un estudio similar al nuestro (estudio
V), (La Touche, Paris-Alemany, et al., 2014), en este Haggman-Henrikson y cols.
(Haggman-Henrikson et al., 2004) observaron que los pacientes con latigazo cervical
presentaron mayores niveles de dolor y fatiga masticatoria inducida por el test que los
pacientes con TCM y sujetos asintomáticos. Diversos estudios experimentales y clínicos
han descrito conexiones funcionales entre las regiones craniofacial y cervical a través de
patrones de convergencia neural en el CTC (Dessem and Luo, 1999; Ge et al., 2004;
Hellström et al., 2002; Hu et al., 2005; Svensson et al., 2005; Torisu et al., 2013; Wang
et al., 2004), en relación con esto se ha observado en estudios experimentales que el
dolor inducido por la infiltración de sustancias algógenas en músculos masticatorios o
cervicales modifican de forma bidireccional la actividad de los reflejos de estiramiento
(Ge et al., 2004; Wang et al., 2004) además, en investigaciones básicas con animales se
ha observado una relación refleja entre la actividad de los nociceptores de la ATM y
actividad del sistema fusimotor de los músculos de cuello (Hellström et al., 2002), esta
información es útil para plantear teorías acerca de la influencia de la región cervical

211
sobre los posibles mecanismos nociceptivos (sensoriales) y motores implicados en el
dolor y la fatiga masticatoria.
Contamos con evidencia científica reciente que demuestra que lesiones sobre la región
cervical pueden alterar el control motor masticatorio y la función mandibular normal de
apertura-cierre (Eriksson et al., 2004, 2007; Zafar et al., 2006), los hallazgos de estudio
V se pueden relacionar con esta cuestión ya que nuestros resultados muestran que el test
de provocación masticatorio reduce la MAI libre de dolor al finalizar el test en los tres
grupos, este resultados son similares a la de otros estudios (Karibe et al., 2003;
Svensson et al., 2001), sin embargo hay que tomar en cuenta que esta disminución fue
mayor en los grupos de pacientes y se mantuvo a las 24 horas únicamente en el grupo de
moderada discapacidad cervical, además es importante destacar que el análisis de
regresión mostró que la discapacidad cervical es un predictor de la MAI libre de dolor
(después de 24 horas) en los dos grupos de pacientes. Planteamos la teoría de que los
patrones motores masticatorios estén más alterados a medida que se tenga mayor dolor
o discapacidad cervical, esta situación generaría la activación de mecanismos
compensatorios des-adaptativos que alterarían la conducta, el reclutamiento y la
coordinación de los sistemas motores del cuello y la mandíbula generando mayores
niveles de fatiga y dolor durante los test de provocación y manteniendo estas
sensaciones 24 horas después. Esta misma teoría podría servir para explicar los
resultados de la disminución de los umbrales del dolor a la presión de regiones
trigeminales y cervicales, cabe destacar que los cambios UDPs fueron mayores en los
grupos de pacientes y que la mayoría de cambios en los UDPs de la región cervical a las
24 horas se produjeron en el grupo de moderada discapacidad cervical, como factor
coadyuvante a este situación hay que considerar que la presencia de dolor cuello puede
provocar menores valores de UDPs en puntos trigeminales en comparación con sujetos

212
sanos como se observó en el estudio III (La Touche et al., 2010). Aunque consideramos
que puede haber una relación directa entre los cambios sensoriomotores trigeminales
con el dolor y la discapacidad cervical, también tenemos que tener en cuenta la
posibilidad de que en los pacientes los cambios se hubieran visto influenciados
mayoritariamente por la presencia de cambios neuroplásticos ya establecidos a nivel
central; se conoce actualmente que los pacientes con dolor crónico pueden tener mayor
susceptibilidad de presentar un proceso de sensibilización central (Henry et al., 2011),
Wolf y cols. sugieren que en condiciones dolorosas en donde existe una comorbilidad
como es el caso de la muestra de pacientes de este estudio, puede ser un factor
determinante en la pato-fisiología de la sensibilización central (Woolf, 2011). En
relación con esto, Gaff-Radford propone que en la sensibilización central se producen
cambios en las vías aferentes que hacen posible la comunicación de las neuronas
nociceptivas cervicales y orofaciales en el núcleo trigeminal (Graff-Radford, 2012). A
esto hay que añadir que son muchos los estudios que han encontrado en pacientes con
TCM mecanismos periféricos y centrales compatibles con un proceso de sensibilización
central (Anderson et al., 2011; Ayesh et al., 2007; Chaves et al., 2013; Feldreich et al.,
2012; Park et al., 2010; Raphael et al., 2009; Sarlani et al., 2004), sin embargo es
importante destacar que en el grupo de pacientes con dolor de cuello crónico mecánico
del estudio III solo se encontraron diferencias en UDPs en áreas trigeminales y
cervicales pero no en zonas distales, estos nos lleva a pensar que en este tipo de
pacientes hay una posible sensibilización central especifica del CTC.

213
6.4. Asociación entre la Discapacidad Cervical y la Discapacidad
Craneofacial/craneomandibular.
En los estudios II (Lopez-de-Uralde-Villanueva et al., 2014) y IV (La Touche, Pardo-
Montero, et al., 2014) se demostró una correlación positiva fuerte-moderada entre la
discapacidad cervical y la discapacidad craneofacial (r=0,79 y r=0,65 respectivamente),
es posible que el resultado del estudio II fuese mejor por la especificidad de la muestra
de pacientes con DCCF seleccionados, hay que tomar en cuenta que la muestra del
estudio IV la conformaron pacientes con diversos tipos de DCF en donde posiblemente
la discapacidad y estatus funcional mandibular no tenga tanto peso, pero esta es una
suposición que se tendrá que comprobar futuras investigaciones. Los resultados de los
estudios II y IV son apoyados por la investigación de Olivo y cols., en esta se encontró
una correlación positiva muy fuerte entre las dos variables de discapacidad (r=0,82)
(Olivo et al., 2010).
6.5 Factores Bioconductuales Implicados en las Alteraciones Sensoriomotoras
Trigeminales y la Discapacidad Craneofacial.
En los estudios III (La Touche et al., 2010), IV (La Touche, Pardo-Montero, et al.,
2014) y V (La Touche, Paris-Alemany, et al., 2014) se utilizaron medidas de auto-
registro relacionadas con el dolor, la discapacidad y factores psicológicos para analizar
las posibles asociaciones con variables sensoriomotoras.
En el estudio V, el análisis de regresión lineal múltiple mostró que el catastrofismo del
dolor y el impacto de la cefalea sobre la calidad de vida (HIT-6) se asociaron a las
variables de percepción de dolor y fatiga 24 horas después de haber realizado el test de
provocación masticatoria. Específicamente en el estudio V el catastrofismo ante el dolor
fue un factor psicológico analizado y mostró ser un predictor de la fatiga a las 24 horas

214
en el grupo de moderada discapacidad cervical y en el grupo de leve discapacidad
cervical también fue predictor para la fatiga y la intensidad de dolor percibido 24 horas
después del test provocación masticatorio. El catastrofismo ante dolor se define como
un factor cognitivo que implica una percepción mental negativa o exagerada de la
amenaza percibida tanto real como anticipada de la experiencia de dolor (Sullivan et al.,
2001; Turner and Aaron, 2001).
En cuanto a la fatiga percibida y el catastrofismo no encontramos estudios clínicos o
experimentales en los que hayan estudiado la asociación en pacientes con DCF o TCM,
pero si hemos encontrado dos estudios sobre la relación del catastrofismo del dolor con
variables cinemáticas masticatorias (Akhter et al., 2014; Brandini et al., 2011). En el
estudio realizado por Akhter y cols. se investigó el efecto de un dolor experimental
agudo en una muestra dividida en sujetos con poco catastrofismo y alto catastrofismo,
los resultados de esta investigación mostraron que la intensidad del dolor percibida fue
más alta en los sujetos con mayor catastrofismo y además en este mismo grupo se
observó una velocidad más lenta y mayor variabilidad en los movimientos mandibulares
repetidos, los autores de este estudio sugieren que los cambios en la coordinación
motora son un ejemplo de conducta de evitación que afectan la función del sistema
motor mandibular (Akhter et al., 2014). En la otra investigación, Brandini y cols.
estudiaron variables cinemáticas masticatorias durante un procedimiento de exposición
muy corto (15 segundos) en pacientes con TMC atribuidas a dolor miofascial, en este
estudio no se observaron asociaciones de las variables cinemáticas medidas con
respecto al catastrofismo, sin embargo hay que tomar en cuenta que el propósito del
estudio no era inducir dolor o fatiga para observar la respuesta como si lo hemos hecho
en el estudio V (La Touche, Pardo-Montero, et al., 2014).

215
Se debe destacar que en una revisión sistemática muy reciente se concluye que hay una
asociación entre el catastrofismo y la fatiga y que el primero influye proporcionalmente
sobre la segunda y estos resultados se observaron en diversas poblaciones clínicas
(Lukkahatai and Saligan, 2013), también se ha demostrado que en otras dolencias
musculoesqueléticas el catastrofismo del dolor se vio asociado a alteraciones motoras
como la disminución del funcionamiento y rendimiento de las actividades de la vida
diaria y limitación de la capacidad para realizar ejercicio (Meeus et al., 2012; Nijs et al.,
2008, 2012). Además este constructo se ha asociado con una mayor utilización de los
servicios de salud, con la aparición de mayores hallazgos clínicos en la valoración, con
un estado de ánimo negativo (Turner et al., 2001; Turner, Brister, et al., 2005) y con
una alteración estatus funcional mandibular (La Touche, Pardo-Montero, et al., 2014)
como hemos comparado en el estudio IV.
En el estudio IV se evaluó la validez del constructo realizando un análisis de
correlaciones entre la discapacidad craneofacial medida con el IDD-CF con otras
medidas de auto-registro psicológicas y de discapacidad. Se observó una correlación
moderada entre IDD-CF con el HIT-6 y la EVA (r = 0,38 hasta 0,46). Además, ECD y
TSK-11 mostraron una correlación moderada con el IDD-CF y con la sub-escala de
dolor y la discapacidad (r = 0,36 hasta 0,52). Esto es coherente con los datos recientes
que demuestran que los pacientes con DCF y TCM reportaron mayores niveles de
catastrofismo (Campbell et al., 2010; Fillingim et al., 2011; Quartana et al., 2010).
Además el catastrofismo ante el dolor se ha asociado con la progresión hacia altos
niveles de intensidad del dolor y de discapacidad en pacientes con DCF crónica
(Buenaver et al., 2008, 2012; Holroyd et al., 2007; Rantala et al., 2003; Velly et al.,
2011).

216
Evidencia previa ha demostrado la relación entre el miedo a los movimientos de la
mandíbula y el DCF (Rollman et al., 2012; Visscher et al., 2010), pero la evidencia
hasta el momento se consideraba limitada. Sin embargo, hay estudios que demuestran
que el miedo al dolor y al movimiento se asocia a una disminución de las actividades de
la vida diaria y también ha sido identificado como un fuerte predictor de discapacidad
en otros trastornos musculoesqueléticos crónicos (Buer and Linton, 2002; Crombez et
al., 1999; Kamper et al., 2012; Vlaeyen et al., 1999; Walton and Elliott, 2013). El
catastrofismo ante el dolor y el miedo relacionado con el dolor son dos constructos que
se han vinculado a la cronicidad del dolor musculoesquelético a través del "Modelo de
miedo-evitación" (Leeuw et al., 2007). En el estudio IV se realizó un análisis de
regresión lineal múltiple en donde se identificó que la intensidad del dolor (EVA: β =
0,19; P = 0,001) y el miedo al dolor y al movimiento (TSK-11: β = 0,17; P = 0,004)
fueron predictores del DCF. Para el estado funcional de la mandíbula y la discapacidad
craneofacial el predictor fue el catastrofismo del dolor (ECD-magnificación: β = 0,25; P
<0,001; β = 0,20; P = 0,007).
La relación entre los factores psicosociales, la actividad motora y el dolor parece estar
presente en diversos casos de dolor musculoesquelético, sin embargo la explicación para
la misma es compleja y limitada hasta el momento. Peck y cols. (Peck et al., 2008) y
Murray y Peck (Murray and Peck, 2007) han planteado una posible explicación y para
ello han generado un nuevo modelo explicativo denominado Modelo integrado de
adaptación al dolor (MIAD). Este modelo explica básicamente que la influencia del
dolor sobre la actividad motora depende de la interacción de las características
multidimensionales (biológicas y psicosociales) del dolor con el sistema sensoriomotor
de un individuo que termina generando una nueva estrategia de reclutamiento motor con
el objetivo de minimizar el dolor, sin embargo esta respuesta motora puede asociarse a

217
la aparición de otra dolencia o al empeoramiento del dolor existente (Murray and Peck,
2007; Peck et al., 2008). Este modelo se apoya en el carácter multidimensional
(sensorial discriminativa, afectiva-emocional, cognitiva) que presenta la experiencia de
dolor y cómo este influye sobre el sistema sensoriomotor a través de las conexiones
periféricas y centrales que tiene este sistema con el sistema nervioso autónomo, el
sistema límbico y otros centros superiores (Craig, 2003; Peck et al., 2008).
Recientes estudios de neuroimagen han comprobado como el catastrofismo ante el dolor
(rumiación y desesperanza) puede influir sobre diversas áreas de la corteza cerebral en
pacientes con TCM (Kucyi et al., 2014; Salomons et al., 2012). Salomons y cols.
(Salomons et al., 2012) encontraron en pacientes con TCM una correlación entre la
desesperanza (sub-escala de la ECD) y el grosor cortical del área motora suplementaria
(AMS) y la corteza cingulada media (CCM), los autores de esa investigación sugieren
que la activación de esas áreas en los pacientes con TCM podrían tener una implicación
en aspectos cognitivos de la conducta motora incluyendo las alteraciones de la respuesta
motora, hay que tomar en cuenta que el AMS neurofisiologicamente está implicada en
la planificación del acto motor (Nachev et al., 2007, 2008) y el CCM se ha asociado con
la selección óptima de respuestas motoras en condiciones de incertidumbre (Shackman
et al., 2011). En relación a los pacientes con TCM que presentaron altos niveles de
rumiación (sub-escala de la ECD), Kucyi y cols. (Kucyi et al., 2014) encontraron una
correlación positiva de aumento de la conectividad funcional del córtex prefrontal
medial con la corteza cingulada posterior, el tálamo medial, la corteza retroespinal y la
sustancia gris periacueductal/periventricular, estos resultados indican que la rumiación
ante el dolor podría influir sobre áreas relacionadas con aspectos afectivos y
emocionales de la experiencia dolorosa y con áreas del sistema inhibitorio descendente
del dolor. Parece ser que los cambios funcionales o estructurales en áreas cerebrales no

218
solo se presentan en pacientes catastrofistas con TCM, también en otro estudio de
neuroimagen, pero en este caso en pacientes con fibromialgia que presentaban
considerables niveles de catastrofismo, se observó un incremento de actividad en áreas
cerebrales relacionadas con la anticipación del dolor, la atención al dolor, aspectos
emocionales del dolor y el control motor (Gracely et al., 2004), similares resultados se
han encontrado en otras dolencias musculoesqueléticas (Brown et al., 2014).
En el estudio III (La Touche et al., 2010) no se encontraron asociaciones entre los UDPs
de áreas trigeminales o cervicales con las medidas de síntomas depresivos o de
ansiedad. Introducir en esta investigación la valoración de estos síntomas lo
consideramos de gran interés teniendo en cuenta que estos dos factores emocionales se
han relacionado con diferentes situaciones de dolor (Castillo et al., 2013; Roddy et al.,
2013; Simons et al., 2014), a pesar de esto no hemos encontrado ningún tipo de
asociación de los síntomas de ansiedad con otras variables relacionadas con el dolor y la
discapacidad de este estudio. En relación con los síntomas depresivos sí encontramos
una asociación positiva con la intensidad (rho=0,65; P= 0,001) y la cronicidad del dolor
(rho=0,54; P=0.004) y este es un hecho que es recogido por una amplia parte de la
literatura científica (Salama-Hanna and Chen, 2013; Yalcin and Barrot, 2014).
6.6 Efecto del Tratamiento en la Región Cervical sobre el Dolor Craneofacial.
Los resultados de los estudios VI y VII (La Touche et al., 2009, 2012) demuestran que
el tratamiento de fisioterapia en la región cervical produce cambios en los UDPs de
áreas trigeminales y además una disminución en la intensidad del dolor de forma
inmediata y a corto plazo (3 meses), este es un hallazgo que consideramos relevante
teniendo en cuenta que son las primeras investigaciones que estudian estas
intervenciones sobre pacientes con TCM. Otros estudios en pacientes con cefaleas han

219
encontrado resultados similares en cuanto a la modulación del dolor con métodos
aplicados en la región cervical como técnicas de neuro-estimulación periférica del
nervio occipital (Jasper and Hayek, 2008; Lee and Huh, 2013; Saper et al., 2011; Serra
and Marchioretto, 2012; Silberstein et al., 2012; Slavin et al., 2006), infiltraciones
locales (Ashkenazi and Levin, 2007; Mellick and Mellick, 2003, 2008; Mellick et al.,
2006; Saracco et al., 2010) o tratamientos de terapia manual (Castien et al., 2011, 2012,
2013; Espí-López and Gómez-Conesa, 2014; Espí-López et al., 2014; van Ettekoven
and Lucas, 2006; Hall et al., 2007; Mongini et al., 2012; Ylinen et al., 2010).
Otro resultado a destacar, en relación al estudio VI (La Touche et al., 2009) es que el
tratamiento sobre la región cervical basado en terapia manual y ejercicio mejora la MAI
libre de dolor. Este hallazgo es interesante ya que estudios experimentales previos
demostraron que una fijación inducida experimentalmente sobre la región cervical altera
la dinámica mandibular disminuyendo el movimiento y la coordinación mandibular
(Häggman-Henrikson et al., 2006). A partir de estos datos, nosotros planteamos
teóricamente que la mejora de la función de la región cervical a través del tratamiento
de fisioterapia puede evocar mecanismos de modulación del dolor en el CTC que
regularían los efectos nociceptivos periféricos y centrales mejorando a su vez la
dinámica mandibular y las estrategias motoras concomitantes cérvico-
craneomandibulares.
6.7 Implicaciones Científicas y Clínicas
De acuerdo al conjunto de resultados de los estudios de esta tesis podemos afirmar que
la discapacidad y el dolor cervical pueden influir sobre variables sensoriales y motoras
del sistema masticatorio; estos hallazgos nos llevan a reflexionar acerca de la
importancia de incluir a nivel clínico una valoración específica de la región cervical
para los protocolos diagnósticos de los TCM. Cabe destacar que los métodos

220
diagnósticos y de clasificación más utilizados para los pacientes con TCM no incluyen
una valoración especifica del dolor y la discapacidad cervical (Benoliel et al., 2011;
Schiffman et al., 2010, 2014). Un criterio diagnóstico recientemente observado en los
pacientes con cefalea atribuida a TCM es que los movimientos mandibulares, la función
o la parafunción modifican el dolor sobre la región temporal (Schiffman et al., 2012).
Nosotros hemos observado la asociación de la discapacidad cervical con la MAI libre de
dolor, además hemos identificado que los pacientes con mayor discapacidad cervical
presentan mayor fatiga y dolor inducido por el test masticatorio. Estos hallazgos nos
llevan a suponer que la región cervical puede tener un papel importante sobre este tipo
de cefalea, pero esto tiene que confirmarse en futuras investigaciones ya que estos datos
se pueden extrapolar únicamente a los pacientes con cefalea atribuida a TCM que
además presentaban dolor y discapacidad de cuello. Sabemos en la actualidad que la
prevalencia de dolor de cuello en los pacientes con TCM es muy alta, pero no sabemos
en la actualidad la influencia que tiene la región cervical en aquellos pacientes que no
presentan dolor cuello.
Desde el punto de vista del tratamiento, el plantear un abordaje para reducir el dolor y
la discapacidad cervical como parte de la estrategia terapéutica global podría ser
beneficioso para reducir los síntomas sensoriales negativos y mejorar el control motor
masticatorio, consideramos que este planteamiento debe seguir siendo investigado en
futuros estudios. Parte de los hallazgos de esta tesis demuestran que tratamientos de
fisioterapia basados en terapia manual y ejercicio terapéutico sobre la región cervical
producen efectos positivos sobre la modulación del dolor en áreas trigeminales y sobre
la mejora de la MAI libre de dolor (La Touche et al., 2009, 2012), con los cual
consideramos que es positivo integrarlos en los protocolos actuales para este tipo de
pacientes.

221
En varios de los estudios de esta tesis y en otros estudios longitudinales o transversales
se ha observado la influencia de factores psicosociales sobre pacientes con TCM (Chen
et al., 2013; Fillingim et al., 2011, 2013). Específicamente nuestros resultados muestran
una asociación entre el catastrofismo y la kinesiofobia con variables funcionales, de
discapacidad y DCF, estos hallazgos ponen en manifiesto la interacción entre variables
de tipo sensorial con variables psicológicas y esto debería considerarse como una
cuestión determinante a la hora de plantear la valoración o de diseñar las intervenciones
terapéuticas; en pacientes con dolor crónico es fundamental reconocer factores
psicosociales que pueden ser percibidos como obstáculos para la recuperación (Main,
2013): se ha observado que lograr una disminución del catastrofismo del dolor es un
buen predictor de éxito de la rehabilitación en condiciones de dolor (Sullivan, 2013).
La integración de una perspectiva bioconductual en el razonamiento clínico y en la toma
de decisiones podría ser un punto clave en el manejo del dolor y la reeducación motora
en pacientes con DCF y TCM. Se ha demostrado que el tratamiento cognitivo-
conductual disminuye la intensidad del dolor, los síntomas depresivos, mejora la
función masticatoria (Turner et al., 2006), reduce el catastrofismo en pacientes que
sufren TCM crónicos (Turner, Mancl, et al., 2005) y además se ha observado que en
casos de dolor crónico provoca cambios neuroplásticos adaptativos asociados a una
disminución del catastrofismo del dolor (Seminowicz et al., 2013). Prescribir ejercicio
terapéutico puede ser una buena alternativa a tener en cuenta: en relación a esto se ha
observado que el ejercicio en pacientes con dolor lumbar crónico produce una reducción
del catastrofismo y de los síntomas depresivos y estos resultados fueron similares al
tratamiento cognitivo-conductual (Smeets et al., 2006)

222
6.8 Limitaciones y Futuras Investigaciones
Los resultados de esta tesis se han discutido con la consideración de que hay varias
limitaciones que hemos tenido en cuenta y que presentamos a continuación. En los
estudios que conforman esta tesis se han tenido en cuenta algunas variables relacionadas
con la discapacidad y el dolor en la región cervical, sin embargo consideramos que aún
es necesario cuantificar más aspectos de las posibles alteraciones funcionales de la
región cervical como por ejemplo, los rangos de movimiento, la resistencia muscular, la
propiocepción craneocervical y analizar si estas alteraciones pueden tener alguna
relevancia clínica sobre las alteraciones motoras craneomandibulares o sobre el DCF;
sería necesario que futuros estudios precisaran aún más estos aspectos ya que podrían
generar nuevos datos que puedan servir para plantear alternativas diagnósticas y
terapéuticas.
Otra limitación a tener en cuenta, es que en los estudios en donde se ha planteado
intervenciones terapéuticas (VI, VII) solo se han medido los efectos inmediatos y a
corto plazo. Futuros estudios deberían investigar si estas intervenciones tienen un efecto
mantenido a medio y a largo plazo, por otra parte sería necesario realizar estudios de
efectividad de este tipo de intervenciones frente a tratamientos farmacológicos, férulas
oclusales o inclusive otros tratamientos de fisioterapia basados en agentes físicos o
tratamientos de electroterapia.
En esta tesis se han identificado algunos factores psicológicos que han presentado
asociación con la función mandibular y con la discapacidad y el DCF. Desde el
planteamiento neurobiológico de la experiencia multidimensional del dolor (sensorial-
discriminativa, emocional-afectiva, cognitiva) creemos que el haber incluido estas
variables es un acierto ya que ofrece una perspectiva más global de la problemática. A

223
pesar de esto y haciendo una reflexión profunda consideramos que hay otras variables
que son necesarias identificar como por ejemplo la autoeficacia o el tipo de estrategias
de afrontamiento ante el dolor, entre otras. Además sería necesario que los factores
psicológicos identificados como relevantes se sigan estudiando pero con diseños tipo
cohorte, de esta forma se podría establecer relaciones causa efecto. Finalmente y en
relación con la anterior reflexión, creemos que es importante realizar ensayos clínicos
aleatorizados controlados con un enfoque bioconductual donde las intervenciones que se
utilicen se establecieran de forma multimodal para de esta forma intentar influir sobre
variables psicosociales, sensoriales y motoras.

224

225
CONCLUSIONES

226
7. CONCLUSIONES.
1. Las posturas craneocervicales inducidas experimentalmente modifican la
dinámica mandibular y alteran los umbrales de dolor a la presión en áreas
trigeminales en pacientes con trastornos craneomandibulares.
2. Existen pequeñas diferencias en la postura craneocervical entre pacientes con
dolor cérvico-craneofacial y sujetos asintomáticos, pero no se encontraron
asociaciones entre la postura craneocervical y la discapacidad cervical y
craneofacial.
3. Los pacientes con cefalea atribuida a trastornos craneomandibulares con
moderada discapacidad cervical presentan mayores niveles de intensidad de
dolor y fatiga en el test de provocación masticatorio, así como menores umbrales
de dolor a la presión trigeminales y cervicales y una disminución de la máxima
apertura interincisal libre de dolor a las 24 horas posteriores al test de
provocación masticatorio, que los pacientes con leve discapacidad cervical y
sujetos asintomáticos.
4. Los pacientes con dolor de cuello crónico mecánico presentan una hiperalgesia
mecánica en áreas cervicales y trigeminales pero no en áreas extra-trigeminales,
por tanto la sensibilización central en el complejo trigeminocervical podría ser
un mecanismo involucrado en el mantenimiento del dolor de estos pacientes.
5. Existe una asociación entre la discapacidad cervical y la discapacidad
craneofacial en pacientes con dolor craneofacial.
6. La discapacidad cervical es un predictor de la disminución de la máxima
apertura interincisal libre de dolor.
7. La kinesiofobia y catastrofismo ante el dolor son predictores del dolor, la
discapacidad craneofacial y el estatus funcional mandibular.

227
8. El catastrofismo ante el dolor es un predictor de la fatiga masticatoria en
pacientes con cefalea atribuida a trastornos craneomandibulares.
9. Los síntomas depresivos presentan una asociación con la cronicidad y la
intensidad del dolor en pacientes con dolor de cuello crónico mecánico.
10. Las intervenciones fisioterápicas de terapia manual y ejercicio terapéutico sobre
la región cervical provocan efectos hipoalgesicos en áreas cervicales y
trigeminales y mejoran la máxima apertura interincisal libre del dolor en
pacientes con trastornos craneomandibulares.

228

229
BIBLIOGRAFÍA

230
8. BIBLIOGRAFÍA
Adèrn B, Stenvinkel C, Sahlqvist L, Tegelberg A. Prevalence of temporomandibular
dysfunction and pain in adult general practice patients. Acta Odontol. Scand. 2014: 1–6.
Aggarwal A, Keluskar V. Physiotherapy as an adjuvant therapy for treatment of TMJ
disorders. Gen. Dent. 2012; 60: e119–22.
Akerman S, Holland PR, Goadsby PJ. Diencephalic and brainstem mechanisms in
migraine. Nat. Rev. Neurosci. 2011; 12: 570–84.
Akhter R, Benson J, Svensson P, Nicholas MK, Peck CC, Murray GM. Experimental
jaw muscle pain increases pain scores and jaw movement variability in higher pain
catastrophizers. J. oral facial pain headache 2014; 28: 191–204.
Alix ME, Bates DK. A proposed etiology of cervicogenic headache: the
neurophysiologic basis and anatomic relationship between the dura mater and the rectus
posterior capitis minor muscle. J. Manipulative Physiol. Ther. 1999; 22: 534–9.
Alonso-Blanco C, Fernández-de-Las-Peñas C, De-la-Llave-Rincón AI, Zarco-Moreno
P, Galán-Del-Río F, Svensson P. Characteristics of referred muscle pain to the head
from active trigger points in women with myofascial temporomandibular pain and
fibromyalgia syndrome. J. Headache Pain 2012; 13: 625–37.
Anderson GC, John MT, Ohrbach R, Nixdorf DR, Schiffman EL, Truelove ES, et al.
Influence of headache frequency on clinical signs and symptoms of TMD in subjects
with temple headache and TMD pain. Pain 2011; 152: 765–71.
Andrade Ortega JA, Delgado Martínez AD, Almécija Ruiz R. Validation of the Spanish
version of the Neck Disability Index. Spine (Phila. Pa. 1976). 2010; 35: E114–8.
Appelgren L, Janson M, Nitescu P, Curelaru I. Continuous intracisternal and high
cervical intrathecal bupivacaine analgesia in refractory head and neck pain.
Anesthesiology 1996; 84: 256–72.

231
Aprill C, Dwyer A, Bogduk N. Cervical zygapophyseal joint pain patterns. II: A clinical
evaluation. Spine (Phila. Pa. 1976). 1990; 15: 458–61.
Arendt-Nielsen L, Laursen RJ, Drewes AM. Referred pain as an indicator for neural
plasticity. Prog. Brain Res. 2000; 129: 343–56.
Armijo Olivo S, Magee DJ, Parfitt M, Major P, Thie NMR. The association between the
cervical spine, the stomatognathic system, and craniofacial pain: a critical review. J.
Orofac. Pain 2006; 20: 271–87.
Armijo-Olivo S, Magee D. Cervical musculoskeletal impairments and
temporomandibular disorders. J. oral Maxillofac. Res. 2013; 3: e4.
Armijo-Olivo S, Magee DJ. Electromyographic activity of the masticatory and cervical
muscles during resisted jaw opening movement. J. Oral Rehabil. 2007; 34: 184–94.
Armijo-Olivo S, Rappoport K, Fuentes J, Gadotti IC, Major PW, Warren S, et al. Head
and cervical posture in patients with temporomandibular disorders. J. Orofac. Pain
2011; 25: 199–209.
Ashina S, Bendtsen L, Ashina M, Magerl W, Jensen R. Generalized hyperalgesia in
patients with chronic tension-type headache. Cephalalgia 2006; 26: 940–948.
Ashkenazi A, Levin M. Greater occipital nerve block for migraine and other headaches:
is it useful? Curr. Pain Headache Rep. 2007; 11: 231–5.
Ashkenazi A, Matro R, Shaw JW, Abbas MA, Silberstein SD. Greater occipital nerve
block using local anaesthetics alone or with triamcinolone for transformed migraine: a
randomised comparative study. J. Neurol. Neurosurg. Psychiatry 2008; 79: 415–7.
Ayesh EE, Jensen TS, Svensson P. Hypersensitivity to mechanical and intra-articular
electrical stimuli in persons with painful temporomandibular joints. J. Dent. Res. 2007;
86: 1187–92.
Ballenberger N, von Piekartz H, Paris-Alemany A, La Touche R, Angulo-Diaz-Parreño
S. Influence of different upper cervical positions on electromyography activity of the
masticatory muscles. J. Manipulative Physiol. Ther. 2012; 35: 308–18.

232
Bartlett M. A note on the multiplying factors for various Chi-square approximations. J
R. Stat Soc B 1954; 16: 296–298.
Bartsch T, Goadsby PJ. Stimulation of the greater occipital nerve induces increased
central excitability of dural afferent input. Brain 2002; 125: 1496–509.
Bartsch T, Goadsby PJ. Increased responses in trigeminocervical nociceptive neurons to
cervical input after stimulation of the dura mater. Brain 2003a; 126: 1801–13.
Bartsch T, Goadsby PJ. The trigeminocervical complex and migraine: current concepts
and synthesis. Curr. Pain Headache Rep. 2003b; 7: 371–6.
Bartsch T, Knight YE, Goadsby PJ. Activation of 5-HT(1B/1D) receptor in the
periaqueductal gray inhibits nociception. Ann. Neurol. 2004; 56: 371–81.
Bartsch T, Levy MJ, Knight YE, Goadsby PJ. Differential modulation of nociceptive
dural input to [hypocretin] orexin A and B receptor activation in the posterior
hypothalamic area. Pain 2004; 109: 367–78.
Bartsch T, Levy MJ, Knight YE, Goadsby PJ. Inhibition of nociceptive dural input in
the trigeminal nucleus caudalis by somatostatin receptor blockade in the posterior
hypothalamus. Pain 2005; 117: 30–9.
Bartsch T. Migraine and the neck: new insights from basic data. Curr. Pain Headache
Rep. 2005; 9: 191–6.
Batlle-Gualda E, Jovani Casano V, Ivora Cortés J. Musculoskeletal diseases in Spain.
Magnitude and specialised human resources. Rev Esp Reum. 1998: 91–105.
Becker N, Bondegaard Thomsen A, Olsen AK, Sjøgren P, Bech P, Eriksen J. Pain
epidemiology and health related quality of life in chronic non-malignant pain patients
referred to a Danish multidisciplinary pain center. Pain 1997; 73: 393–400.
Becker WJ. Cervicogenic headache: evidence that the neck is a pain generator.
Headache 2010; 50: 699–705.

233
Beitz AJ, Clements JR, Ecklund LJ, Mullett MM. The nuclei of origin of brainstem
enkephalin and cholecystokinin projections to the spinal trigeminal nucleus of the rat.
Neuroscience 1987; 20: 409–25.
Beitz AJ. The nuclei of origin of brainstem serotonergic projections to the rodent spinal
trigeminal nucleus. Neurosci. Lett. 1982; 32: 223–8.
Beltran-Alacreu H, Lopez-de-Uralde-Villanueva I, Paris-Alemany A, Angulo-Díaz-
Parreño S, La Touche R. Intra-rater and Inter-rater Reliability of Mandibular Range of
Motion Measures Considering a Neutral Craniocervical Position. J Phys Ther Sci 2014;
26: 1–6.
Benjamin L, Levy MJ, Lasalandra MP, Knight YE, Akerman S, Classey JD, et al.
Hypothalamic activation after stimulation of the superior sagittal sinus in the cat: a Fos
study. Neurobiol. Dis. 2004; 16: 500–5.
Benoliel R, Svensson P, Heir GM, Sirois D, Zakrzewska J, Oke-Nwosu J, et al.
Persistent orofacial muscle pain. Oral Dis. 2011; 17 Suppl 1: 23–41.
Bereiter DA, Okamoto K, Tashiro A, Hirata H. Endotoxin-induced uveitis causes long-
term changes in trigeminal subnucleus caudalis neurons. J. Neurophysiol. 2005; 94:
3815–25.
Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement
of acute pain. Acad. Emerg. Med. 2001; 8: 1153–7.
Bjorner JB, Kosinski M, Ware JE. Calibration of an item pool for assessing the burden
of headaches: an application of item response theory to the headache impact test (HIT).
Qual. Life Res. 2003; 12: 913–33.
Bogduk N, Windsor M, Inglis A. The innervation of the cervical intervertebral discs.
Spine (Phila. Pa. 1976). 1988; 13: 2–8.
Bogduk N. The anatomy of occipital neuralgia. Clin. Exp. Neurol. 1981; 17: 167–84.
Bogduk N. The clinical anatomy of the cervical dorsal rami. Spine (Phila. Pa. 1976).
1982; 7: 319–30.

234
Bogduk N. Cervicogenic headache: anatomic basis and pathophysiologic mechanisms.
Curr. Pain Headache Rep. 2001; 5: 382–6.
Bogduk N. The anatomy and pathophysiology of neck pain. Phys. Med. Rehabil. Clin.
N. Am. 2003; 14: 455–72, v.
Borghouts JA, Koes BW, Vondeling H, Bouter LM. Cost-of-illness of neck pain in The
Netherlands in 1996. Pain 1999; 80: 629–36.
Borsook D, DaSilva AFM, Ploghaus A, Becerra L. Specific and somatotopic functional
magnetic resonance imaging activation in the trigeminal ganglion by brush and noxious
heat. J. Neurosci. 2003; 23: 7897–903.
Brandini D a, Benson J, Nicholas MK, Murray GM, Peck CC. Chewing in
temporomandibular disorder patients: an exploratory study of an association with some
psychological variables. J. Orofac. Pain 2011; 25: 56–67.
Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in
Europe: prevalence, impact on daily life, and treatment. Eur. J. Pain 2006; 10: 287–333.
Brodie AG. Anatomy and physiology of head and neck musculature. Am. J. Orthod.
1950; 36: 831–44.
Bron C, Dommerholt J, Stegenga B, Wensing M, Oostendorp RAB. High prevalence of
shoulder girdle muscles with myofascial trigger points in patients with shoulder pain.
BMC Musculoskelet. Disord. 2011; 12: 139.
Brown CA, El-Deredy W, Jones AKP. When the brain expects pain: common neural
responses to pain anticipation are related to clinical pain and distress in fibromyalgia
and osteoarthritis. Eur. J. Neurosci. 2014; 39: 663–72.
Buenaver LF, Edwards RR, Smith MT, Gramling SE, Haythornthwaite JA.
Catastrophizing and pain-coping in young adults: associations with depressive
symptoms and headache pain. J. Pain 2008; 9: 311–9.
Buenaver LF, Quartana PJ, Grace EG, Sarlani E, Simango M, Edwards RR, et al.
Evidence for indirect effects of pain catastrophizing on clinical pain among myofascial

235
temporomandibular disorder participants: the mediating role of sleep disturbance. Pain
2012; 153: 1159–66.
Buer N, Linton SJ. Fear-avoidance beliefs and catastrophizing: occurrence and risk
factor in back pain and ADL in the general population. Pain 2002; 99: 485–91.
Burstein R, Yamamura H, Malick A, Strassman AM. Chemical stimulation of the
intracranial dura induces enhanced responses to facial stimulation in brain stem
trigeminal neurons. J. Neurophysiol. 1998; 79: 964–82.
Busch V, Jakob W, Juergens T, Schulte-Mattler W, Kaube H, May A. Functional
connectivity between trigeminal and occipital nerves revealed by occipital nerve
blockade and nociceptive blink reflexes. Cephalalgia 2006; 26: 50–5.
Byers MR, Närhi M V. Dental injury models: experimental tools for understanding
neuroinflammatory interactions and polymodal nociceptor functions. Crit. Rev. Oral
Biol. Med. 1999; 10: 4–39.
Cairns BE, Gambarota G, Svensson P, Arendt-Nielsen L, Berde CB. Glutamate-induced
sensitization of rat masseter muscle fibers. Neuroscience 2002; 109: 389–99.
Cairns BE, Sessle BJ, Hu JW. Characteristics of glutamate-evoked temporomandibular
joint afferent activity in the rat. J. Neurophysiol. 2001; 85: 2446–54.
Camacho JGDD, Oltramari-Navarro PVP, Navarro R de L, Conti AC de CF, Conti MR
de A, Marchiori LL de M, et al. Signs and symptoms of temporomandibular disorders in
the elderly. CoDAS 2014; 26: 76–80.
Campbell CM, Kronfli T, Buenaver LF, Smith MT, Berna C, Haythornthwaite JA, et al.
Situational versus dispositional measurement of catastrophizing: associations with pain
responses in multiple samples. J. Pain 2010; 11: 443–453.e2.
Campos JADB, Carrascosa AC, Bonafé FSS, Maroco J. Epidemiology of severity of
temporomandibular disorders in Brazilian women. J. oral facial pain headache 2014; 28:
147–52.

236
Capra NF, Dessem D. Central connections of trigeminal primary afferent neurons:
topographical and functional considerations. Crit. Rev. Oral Biol. Med. 1992; 4: 1–52.
Carlson CR. Psychological considerations for chronic orofacial pain. Oral Maxillofac.
Surg. Clin. North Am. 2008; 20: 185–95, vi.
Carlsson GE. Epidemiology and treatment need for temporomandibular disorders. J.
Orofac. Pain 1999; 13: 232–7.
Carroll LJ, Cassidy JD, Peloso PM, Giles-Smith L, Cheng CS, Greenhalgh SW, et al.
Methods for the best evidence synthesis on neck pain and its associated disorders: the
Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated
Disorders. Spine (Phila. Pa. 1976). 2008; 33: S33–8.
Castien R, Blankenstein A, van der Windt D, Heymans MW, Dekker J. The working
mechanism of manual therapy in participants with chronic tension-type headache. J.
Orthop. Sports Phys. Ther. 2013; 43: 693–9.
Castien RF, van der Windt DAWM, Blankenstein AH, Heymans MW, Dekker J.
Clinical variables associated with recovery in patients with chronic tension-type
headache after treatment with manual therapy. Pain 2012; 153: 893–9.
Castien RF, van der Windt DAWM, Grooten A, Dekker J. Effectiveness of manual
therapy for chronic tension-type headache: a pragmatic, randomised, clinical trial.
Cephalalgia 2011; 31: 133–43.
Castillo RC, Wegener ST, Heins SE, Haythornthwaite JA, Mackenzie EJ, Bosse MJ.
Longitudinal relationships between anxiety, depression, and pain: results from a two-
year cohort study of lower extremity trauma patients. Pain 2013; 154: 2860–6.
Català E, Reig E, Artés M, Aliaga L, López JS, Segú JL. Prevalence of pain in the
Spanish population: telephone survey in 5000 homes. Eur. J. Pain 2002; 6: 133–40.
Ceneviz C, Mehta NR, Forgione A, Sands MJ, Abdallah EF, Lobo Lobo S, et al. The
immediate effect of changing mandibular position on the EMG activity of the masseter,
temporalis, sternocleidomastoid, and trapezius muscles. Cranio 2006; 24: 237–44.

237
Chapman CR, Donaldson GW, Davis JJ, Bradshaw DH. Improving individual
measurement of postoperative pain: the pain trajectory. J. Pain 2011; 12: 257–62.
Chaves TC, Nagamine HM, de Sousa LM, de Oliveira AS, Regalo SCH, Grossi DB.
Differences in pain perception in children reporting joint and orofacial muscle pain. J.
Clin. Pediatr. Dent. 2013; 37: 321–7.
Chen CK, Nizar AJ. Myofascial pain syndrome in chronic back pain patients. Korean J.
Pain 2011; 24: 100–4.
Chen H, Nackley A, Miller V, Diatchenko L, Maixner W. Multisystem dysregulation in
painful temporomandibular disorders. J. Pain 2013; 14: 983–96.
Chen X, Tanner K, Levine JD. Mechanical sensitization of cutaneous C-fiber
nociceptors by prostaglandin E2 in the rat. Neurosci. Lett. 1999; 267: 105–8.
Cheung CH, Shum ST, Tang SF, Yau PC, Chiu TTW. The correlation between
craniovertebral angle, backpack weights, and disability due to neck pain in adolescents.
J. Back Musculoskelet. Rehabil. 2010; 23: 129–36.
Chiang CY, Park SJ, Kwan CL, Hu JW, Sessle BJ. NMDA receptor mechanisms
contribute to neuroplasticity induced in caudalis nociceptive neurons by tooth pulp
stimulation. J. Neurophysiol. 1998; 80: 2621–31.
Chiang CY, Zhang S, Xie YF, Hu JW, Dostrovsky JO, Salter MW, et al. Endogenous
ATP involvement in mustard-oil-induced central sensitization in trigeminal subnucleus
caudalis (medullary dorsal horn). J. Neurophysiol. 2005; 94: 1751–60.
Christensen L V, Tran KT, Mohamed SE. Gum chewing and jaw muscle fatigue and
pains. J. Oral Rehabil. 1996; 23: 424–37.
Ciancaglini R, Testa M, Radaelli G. Association of neck pain with symptoms of
temporomandibular dysfunction in the general adult population. Scand. J. Rehabil. Med.
1999; 31: 17–22.
Cimmino MA, Ferrone C, Cutolo M. Epidemiology of chronic musculoskeletal pain.
Best Pract. Res. Clin. Rheumatol. 2011; 25: 173–83.

238
Clark GT, Browne PA, Nakano M, Yang Q. Co-activation of sternocleidomastoid
muscles during maximum clenching. J. Dent. Res. 1993; 72: 1499–502.
Clatworthy A, Williams JH, Barasi S. Intrathecal 5-hydroxytryptamine and electrical
stimulation of the nucleus raphe magnus in rats both reduce the antinociceptive potency
of intrathecally administered noradrenaline. Brain Res. 1988; 455: 300–6.
Cohen J. Statistical power analysis for the behavioral sciences. Hillsdale: 1988.
Cooper G, Bailey B, Bogduk N. Cervical zygapophysial joint pain maps. Pain Med.
2007; 8: 344–53.
Côté P, Cassidy JD, Carroll L. The Saskatchewan Health and Back Pain Survey. The
prevalence of neck pain and related disability in Saskatchewan adults. Spine (Phila. Pa.
1976). 1998; 23: 1689–98.
Côté P, Kristman V, Vidmar M, Van Eerd D, Hogg-Johnson S, Beaton D, et al. The
prevalence and incidence of work absenteeism involving neck pain: a cohort of Ontario
lost-time claimants. Spine (Phila. Pa. 1976). 2008; 33: S192–8.
Couppé C, Torelli P, Fuglsang-Frederiksen A, Andersen KV, Jensen R. Myofascial
trigger points are very prevalent in patients with chronic tension-type headache: a
double-blinded controlled study. Clin. J. Pain 2007; 23: 23–7.
Craig AD. A new view of pain as a homeostatic emotion. Trends Neurosci. 2003; 26:
303–7.
Crombez G, Vlaeyen JW, Heuts PH, Lysens R. Pain-related fear is more disabling than
pain itself: evidence on the role of pain-related fear in chronic back pain disability. Pain
1999; 80: 329–39.
Curatolo M, Arendt-Nielsen L, Petersen-Felix S. Central hypersensitivity in chronic
pain: mechanisms and clinical implications. Phys. Med. Rehabil. Clin. N. Am. 2006; 17:
287–302.
Dallel R, Raboisson P, Auroy P, Woda A. The rostral part of the trigeminal sensory
complex is involved in orofacial nociception. Brain Res. 1988; 448: 7–19.

239
Dallel R, Raboisson P, Woda A, Sessle BJ. Properties of nociceptive and non-
nociceptive neurons in trigeminal subnucleus oralis of the rat. Brain Res. 1990; 521:
95–106.
Dao TTT, Lund JP, Lavigne GJ. Pain Responses to Experimental Chewing in
Myofascial Pain Patients. 1994
Davies PL. Electromyographic study of superficial neck muscles in mandibular
function. J. Dent. Res. 1979; 58: 537–8.
Dessem D, Luo P. Jaw-muscle spindle afferent feedback to the cervical spinal cord in
the rat. Exp. brain Res. 1999; 128: 451–9.
Dixon AD. FINE STRUCTURE OF NERVE-CELL BODIES AND SATELLITE
CELLS IN THE TRIGEMINAL GANGLION. J. Dent. Res. 1963; 42: 990–9.
Le Doaré K, Akerman S, Holland PR, Lasalandra MP, Bergerot A, Classey JD, et al.
Occipital afferent activation of second order neurons in the trigeminocervical complex
in rat. Neurosci. Lett. 2006; 403: 73–7.
Dostrovsky JO, Davis KD, Kawakita K. Central mechanisms of vascular headaches.
Can. J. Physiol. Pharmacol. 1991; 69: 652–8.
Dougherty PM, Sluka KA, Sorkin LS, Westlund KN, Willis WD. Neural changes in
acute arthritis in monkeys. I. Parallel enhancement of responses of spinothalamic tract
neurons to mechanical stimulation and excitatory amino acids. Brain Res. Brain Res.
Rev. 1992; 17: 1–13.
Dougherty PM, Willis WD. Enhanced responses of spinothalamic tract neurons to
excitatory amino acids accompany capsaicin-induced sensitization in the monkey. J.
Neurosci. 1992; 12: 883–94.
Dreyfuss P, Michaelsen M, Fletcher D. Atlanto-occipital and lateral atlanto-axial joint
pain patterns. Spine (Phila. Pa. 1976). 1994; 19: 1125–31.
Dubner R, Bennett GJ. Spinal and trigeminal mechanisms of nociception. Annu. Rev.
Neurosci. 1983; 6: 381–418.

240
Dubner R, Ren K. Brainstem mechanisms of persistent pain following injury. J. Orofac.
Pain 2004; 18: 299–305.
Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular
disorders: review, criteria, examinations and specifications, critique. J. Craniomandib.
Disord. 1992; 6: 301–55.
Dwyer A, Aprill C, Bogduk N. Cervical zygapophyseal joint pain patterns. I: A study in
normal volunteers. Spine (Phila. Pa. 1976). 1990; 15: 453–7.
Ebersberger A, Schaible HG, Averbeck B, Richter F. Is there a correlation between
spreading depression, neurogenic inflammation, and nociception that might cause
migraine headache? Ann. Neurol. 2001; 49: 7–13.
Edelmayer RM, Vanderah TW, Majuta L, Zhang E-T, Fioravanti B, De Felice M, et al.
Medullary pain facilitating neurons mediate allodynia in headache-related pain. Ann.
Neurol. 2009; 65: 184–93.
Elliott AM, Smith BH, Penny KI, Smith WC, Chambers WA. The epidemiology of
chronic pain in the community. Lancet 1999; 354: 1248–52.
Enthoven P, Skargren E, Oberg B. Clinical course in patients seeking primary care for
back or neck pain: a prospective 5-year follow-up of outcome and health care
consumption with subgroup analysis. Spine (Phila. Pa. 1976). 2004; 29: 2458–65.
Eriksson PO, Häggman-Henrikson B, Nordh E, Zafar H. Co-ordinated mandibular and
head-neck movements during rhythmic jaw activities in man. J. Dent. Res. 2000; 79:
1378–84.
Eriksson P-O, Häggman-Henrikson B, Zafar H. Jaw-neck dysfunction in whiplash-
associated disorders. Arch. Oral Biol. 2007; 52: 404–8.
Eriksson P-O, Zafar H, Häggman-Henrikson B. Deranged jaw-neck motor control in
whiplash-associated disorders. Eur. J. Oral Sci. 2004; 112: 25–32.
Eriksson PO, Zafar H, Nordh E. Concomitant mandibular and head-neck movements
during jaw opening-closing in man. J. Oral Rehabil. 1998; 25: 859–70.

241
Espí-López G, Rodríguez-Blanco C, Oliva-Pascual-Vaca A, Benítez-Martínez J, Lluch
E, Falla D. The effect of manual therapy techniques on headache disability in patients
with tension-type headache. Eur. J. Phys. Rehabil. Med. 2014
Espí-López G V, Gómez-Conesa A. Efficacy of manual and manipulative therapy in the
perception of pain and cervical motion in patients with tension-type headache: a
randomized, controlled clinical trial. J. Chiropr. Med. 2014; 13: 4–13.
Van Ettekoven H, Lucas C. Efficacy of physiotherapy including a craniocervical
training programme for tension-type headache; a randomized clinical trial. Cephalalgia
2006; 26: 983–91.
Farella M, Bakke M, Michelotti A, Martina R. Effects of prolonged gum chewing on
pain and fatigue in human jaw muscles. Eur. J. Oral Sci. 2001; 109: 81–5.
Feldreich A, Ernberg M, Lund B, Rosén A. Increased β-endorphin levels and
generalized decreased pain thresholds in patients with limited jaw opening and
movement-evoked pain from the temporomandibular joint. J. Oral Maxillofac. Surg.
2012; 70: 547–56.
Ferguson E, Cox T. Exploratory factor analysis: a users’ guide. Int J Sel. Assess 1993;
1: 84–94.
Fernández-Carnero J, Fernández-de-Las-Peñas C, de la Llave-Rincón AI, Ge H-Y,
Arendt-Nielsen L. Prevalence of and referred pain from myofascial trigger points in the
forearm muscles in patients with lateral epicondylalgia. Clin. J. Pain 2007; 23: 353–60.
Fernández-de-Las-Peñas C, Cuadrado ML, Pareja JA. Myofascial trigger points, neck
mobility and forward head posture in unilateral migraine. Cephalalgia 2006; 26: 1061–
70.
Fernández-de-Las-Peñas C, Galán-Del-Río F, Alonso-Blanco C, Jiménez-García R,
Arendt-Nielsen L, Svensson P. Referred pain from muscle trigger points in the
masticatory and neck-shoulder musculature in women with temporomandibular
disoders. J. Pain 2010; 11: 1295–304.

242
Fernández-de-las-Peñas C, Hernández-Barrera V, Alonso-Blanco C, Palacios-Ceña D,
Carrasco-Garrido P, Jiménez-Sánchez S, et al. Prevalence of neck and low back pain in
community-dwelling adults in Spain: a population-based national study. Spine (Phila.
Pa. 1976). 2011; 36: E213–9.
Ferrario VF, Tartaglia GM, Galletta A, Grassi GP, Sforza C. The influence of occlusion
on jaw and neck muscle activity: a surface EMG study in healthy young adults. J. Oral
Rehabil. 2006; 33: 341–8.
Fields HL, Heinricher MM, Mason P. Neurotransmitters in nociceptive modulatory
circuits. Annu. Rev. Neurosci. 1991; 14: 219–45.
Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex,
gender, and pain: a review of recent clinical and experimental findings. J. Pain 2009;
10: 447–85.
Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Diatchenko L, Dubner R, et al.
Psychological factors associated with development of TMD: the OPPERA prospective
cohort study. J. Pain 2013; 14: T75–90.
Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Dubner R, Bair E, et al. Potential
psychosocial risk factors for chronic TMD: descriptive data and empirically identified
domains from the OPPERA case-control study. J. Pain 2011; 12: T46–60.
Forsberg CM, Hellsing E, Linder-Aronson S, Sheikholeslam A. EMG activity in neck
and masticatory muscles in relation to extension and flexion of the head. Eur. J. Orthod.
1985; 7: 177–84.
Fricton J. Temporomandibular disorders: a human systems approach. J. Calif. Dent.
Assoc. 2014; 42: 523–33; discussion 531, 533–5.
Fricton JR, Kroening R, Haley D, Siegert R. Myofascial pain syndrome of the head and
neck: a review of clinical characteristics of 164 patients. Oral Surg. Oral Med. Oral
Pathol. 1985; 60: 615–23.

243
Funakoshi M, Fujita N, Takehana S. Relations between occlusal interference and jaw
muscle activities in response to changes in head position. J. Dent. Res. 1976; 55: 684–
90.
Gandek B, Alacoque J, Uzun V, Andrew-Hobbs M, Davis K. Translating the Short-
Form Headache Impact Test (HIT-6) in 27 countries: methodological and conceptual
issues. Qual. Life Res. 2003; 12: 975–9.
García Campayo J, Rodero B, Alda M, Sobradiel N, Montero J, Moreno S. Validación
de la versión española de la escala de la catastrofización ante el dolor (Pain
Catastrophizing Scale) en la fibromialgia. Med. Clin. (Barc). 2008; 131: 487–492.
Gavish A, Winocur E, Menashe S, Halachmi M, Eli I, Gazit E. Experimental chewing
in myofascial pain patients. J. Orofac. Pain 2002; 16: 22–8.
Ge H-Y, Wang K, Madeleine P, Svensson P, Sessle BJ, Arendt-Nielsen L.
Simultaneous modulation of the exteroceptive suppression periods in the trapezius and
temporalis muscles by experimental muscle pain. Clin. Neurophysiol. 2004; 115: 1399–
408.
Gesch D, Bernhardt O, Alte D, Schwahn C, Kocher T, John U, et al. Prevalence of signs
and symptoms of temporomandibular disorders in an urban and rural German
population: results of a population-based Study of Health in Pomerania. Quintessence
Int. 2004; 35: 143–50.
Giannakopoulos N, Hellmann D, Schmitter M, Krüger B, Hauser T, Schindler HJ.
Neuromuscular interaction of jaw and neck muscles during jaw clenching. J. Orofac.
Pain 2013; 27: 61–71.
Giannakopoulos N, Schindler HJ, Rammelsberg P, Eberhard L, Schmitter M, Hellmann
D. Co-activation of jaw and neck muscles during submaximum clenching in the supine
position. Arch. Oral Biol. 2013; 58: 1751–60.
Gillies GT, Broaddus WC, Stenger JM, Taylor AG. A biomechanical model of the
craniomandibular complex and cervical spine based on the inverted pendulum. J. Med.
Eng. Technol. 1998; 22: 263–9.

244
Goadsby PJ, Bartsch T, Dodick DW. Occipital nerve stimulation for headache:
mechanisms and efficacy. Headache 2008; 48: 313–8.
Goadsby PJ, Hoskin KL. The distribution of trigeminovascular afferents in the
nonhuman primate brain Macaca nemestrina: a c-fos immunocytochemical study. J.
Anat. 1997; 190 ( Pt 3: 367–75.
Goadsby PJ, Knight YE, Hoskin KL. Stimulation of the greater occipital nerve increases
metabolic activity in the trigeminal nucleus caudalis and cervical dorsal horn of the cat.
Pain 1997; 73: 23–8.
Gómez-Pérez L, López-Martínez AE, Ruiz-Párraga GT. Psychometric Properties of the
Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011; 12: 425–
35.
Gore DR, Sepic SB, Gardner GM, Murray MP. Neck pain: a long-term follow-up of
205 patients. Spine (Phila. Pa. 1976). 1987; 12: 1–5.
Gracely RH, Geisser ME, Giesecke T, Grant MAB, Petzke F, Williams DA, et al. Pain
catastrophizing and neural responses to pain among persons with fibromyalgia. Brain
2004; 127: 835–43.
Graff-Radford SB. Temporomandibular disorders and other causes of facial pain. Curr.
Pain Headache Rep. 2007; 11: 75–81.
Graff-Radford SB. Facial pain, cervical pain, and headache. Continuum (Minneap.
Minn). 2012; 18: 869–82.
Graven-Nielsen T, Arendt-Nielsen L. Assessment of mechanisms in localized and
widespread musculoskeletal pain. Nat. Rev. Rheumatol. 2010; 6: 599–606.
Graven-Nielsen T. Fundamentals of muscle pain, referred pain, and deep tissue
hyperalgesia. Scand. J. Rheumatol. Suppl. 2006; 122: 1–43.
Guenther S, Reeh PW, Kress M. Rises in [Ca2+]i mediate capsaicin- and proton-
induced heat sensitization of rat primary nociceptive neurons. Eur. J. Neurosci. 1999;
11: 3143–50.

245
Guzman J, Hurwitz EL, Carroll LJ, Haldeman S, Côté P, Carragee EJ, et al. A new
conceptual model of neck pain: linking onset, course, and care: the Bone and Joint
Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. J.
Manipulative Physiol. Ther. 2009; 32: S17–28.
Häggman-Henrikson B, Eriksson P-O. Head movements during chewing: relation to
size and texture of bolus. J. Dent. Res. 2004; 83: 864–8.
Häggman-Henrikson B, Nordh E, Eriksson P-O. Increased sternocleidomastoid, but not
trapezius, muscle activity in response to increased chewing load. Eur. J. Oral Sci. 2013;
121: 443–9.
Häggman-Henrikson B, Nordh E, Zafar H, Eriksson P-O. Head immobilization can
impair jaw function. J. Dent. Res. 2006; 85: 1001–5.
Haggman-Henrikson B, Osterlund C, Eriksson P-O. Endurance during Chewing in
Whiplash-associated Disorders and TMD. J. Dent. Res. 2004; 83: 946–950.
Häggman-Henrikson B, Rezvani M, List T. Prevalence of whiplash trauma in TMD
patients: a systematic review. J. Oral Rehabil. 2014; 41: 59–68.
Haldeman S, Carroll LJ, Cassidy JD. The empowerment of people with neck pain:
introduction: the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its
Associated Disorders. Spine (Phila. Pa. 1976). 2008; 33: S8–S13.
Haley SM, Fragala-Pinkham MA. Interpreting change scores of tests and measures used
in physical therapy. Phys. Ther. 2006; 86: 735–43.
Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K. Efficacy of a C1-
C2 self-sustained natural apophyseal glide (SNAG) in the management of cervicogenic
headache. J. Orthop. Sports Phys. Ther. 2007; 37: 100–7.
Hargreaves KM. Orofacial pain. Pain 2011; 152: S25–32.
Harris E, Budd R, Genovese M, Firestein G, Sargent J, Sledge C. Kelley’s Textbook of
Rheumatology. 7th ed. Philadelphia, Pa: Saunders Elsevier; 2006.

246
Hellmann D, Giannakopoulos NN, Schmitter M, Lenz J, Schindler HJ. Anterior and
posterior neck muscle activation during a variety of biting tasks. Eur. J. Oral Sci. 2012;
120: 326–34.
Hellström F, Thunberg J, Bergenheim M, Sjölander P, Djupsjöbacka M, Johansson H.
Increased intra-articular concentration of bradykinin in the temporomandibular joint
changes the sensitivity of muscle spindles in dorsal neck muscles in the cat. Neurosci.
Res. 2002; 42: 91–9.
Hellström F, Thunberg J, Bergenheim M, Sjölander P, Pedersen J, Johansson H.
Elevated intramuscular concentration of bradykinin in jaw muscle increases the
fusimotor drive to neck muscles in the cat. J. Dent. Res. 2000; 79: 1815–22.
Henry DE, Chiodo AE, Yang W. Central nervous system reorganization in a variety of
chronic pain states: a review. PM R 2011; 3: 1116–25.
Van den Heuvel SG, Heinrich J, Jans MP, van der Beek AJ, Bongers PM. The effect of
physical activity in leisure time on neck and upper limb symptoms. Prev. Med. (Baltim).
2005; 41: 260–7.
Higbie EJ, Seidel-Cobb D, Taylor LF, Cummings GS. Effect of head position on
vertical mandibular opening. J. Orthop. Sports Phys. Ther. 1999; 29: 127–30.
Hill J, Lewis M, Papageorgiou AC, Dziedzic K, Croft P. Predicting persistent neck
pain: a 1-year follow-up of a population cohort. Spine (Phila. Pa. 1976). 2004; 29:
1648–54.
Hinkle D, Jurs S, Wiersma W. Applied statistics for the behavioral sciences. 2nd ed.
Boston: Houghton Mifflin; 1988.
Hochberg MC, Altman RD, Brandt KD, Clark BM, Dieppe PA, Griffin MR, et al.
Guidelines for the medical management of osteoarthritis. Part I. Osteoarthritis of the
hip. American College of Rheumatology. Arthritis Rheum. 1995; 38: 1535–40.
Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW, Cassidy JD, Guzman J, et al.
The burden and determinants of neck pain in the general population: results of the Bone

247
and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. J.
Manipulative Physiol. Ther. 2009; 32: S46–60.
Holroyd KA, Drew JB, Cottrell CK, Romanek KM, Heh V. Impaired functioning and
quality of life in severe migraine: the role of catastrophizing and associated symptoms.
Cephalalgia 2007; 27: 1156–65.
Hoskin KL, Zagami AS, Goadsby PJ. Stimulation of the middle meningeal artery leads
to Fos expression in the trigeminocervical nucleus: a comparative study of monkey and
cat. J. Anat. 1999; 194 ( Pt 4: 579–88.
Hu JW, Sun K-Q, Vernon H, Sessle BJ. Craniofacial inputs to upper cervical dorsal
horn: implications for somatosensory information processing. Brain Res 2005; 1044:
93–106.
Hu JW, Tatourian I, Vernon H. Opioid involvement in electromyographic (EMG)
responses induced by injection of inflammatory irritant into deep neck tissues.
Somatosens. Mot. Res. 1996; 13: 139–46.
Hu JW, Vernon H, Tatourian I. Changes in neck electromyography associated with
meningeal noxious stimulation. J. Manipulative Physiol. Ther. 1995; 18: 577–81.
Hu JW, Yu XM, Vernon H, Sessle BJ. Excitatory effects on neck and jaw muscle
activity of inflammatory irritant applied to cervical paraspinal tissues. Pain 1993; 55:
243–50.
Hucho T, Levine JD. Signaling pathways in sensitization: toward a nociceptor cell
biology. Neuron 2007; 55: 365–76.
Igarashi N, Yamamura K, Yamada Y, Kohno S. Head movements and neck muscle
activities associated with the jaw movement during mastication in the rabbit authors.
Brain Res. 2000; 871: 151–5.
IHS. The International Classification of Headache Disorders, 3rd edition (beta version).
Cephalalgia. 2013; 33: 629–808.

248
Jacquin MF, Renehan WE, Mooney RD, Rhoades RW. Structure-function relationships
in rat medullary and cervical dorsal horns. I. Trigeminal primary afferents. J.
Neurophysiol. 1986; 55: 1153–86.
Jasper JF, Hayek SM. Implanted occipital nerve stimulators. Pain Physician 2008; 11:
187–200.
Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity
measurement in chronic pain patients. Pain 1993; 55: 195–203.
Jensen MP, Turner JA, Romano JM, Fisher LD. Comparative reliability and validity of
chronic pain intensity measures. Pain 1999; 83: 157–62.
Ji R-R, Kohno T, Moore KA, Woolf CJ. Central sensitization and LTP: do pain and
memory share similar mechanisms? Trends Neurosci. 2003; 26: 696–705.
Johnston MM, Jordan SE, Charles AC. Pain referral patterns of the C1 to C3 nerves:
implications for headache disorders. Ann. Neurol. 2013; 74: 145–8.
Kääriä S, Laaksonen M, Rahkonen O, Lahelma E, Leino-Arjas P. Risk factors of
chronic neck pain: a prospective study among middle-aged employees. Eur. J. Pain
2012; 16: 911–20.
Kaiser H. Analysis of factorial simplicity. Psychometrika 1974; 39: 31–36.
Kamel HA, Toland J. Trigeminal nerve anatomy: illustrated using examples of
abnormalities. AJR. Am. J. Roentgenol. 2001; 176: 247–51.
Kamisaka M, Yatani H, Kuboki T, Matsuka Y, Minakuchi H. Four-year longitudinal
course of TMD symptoms in an adult population and the estimation of risk factors in
relation to symptoms. J. Orofac. Pain 2000; 14: 224–32.
Kamper SJ, Maher CG, Menezes Costa L da C, McAuley JH, Hush JM, Sterling M.
Does fear of movement mediate the relationship between pain intensity and disability in
patients following whiplash injury? A prospective longitudinal study. Pain 2012; 153:
113–9.

249
De Kanter RJ, Truin GJ, Burgersdijk RC, Van ’t Hof MA, Battistuzzi PG, Kalsbeek H,
et al. Prevalence in the Dutch adult population and a meta-analysis of signs and
symptoms of temporomandibular disorder. J. Dent. Res. 1993; 72: 1509–18.
Kapur N, Kamel IR, Herlich A. Oral and craniofacial pain: diagnosis, pathophysiology,
and treatment. Int. Anesthesiol. Clin. 2003; 41: 115–50.
Karibe H, Goddard G, Gear RW. Sex differences in masticatory muscle pain after
chewing. J. Dent. Res. 2003; 82: 112–6.
Karibe H, Goddard G, Kawakami T, Aoyagi K, Rudd P, McNeill C. Comparison of
subjective symptoms among three diagnostic subgroups of adolescents with
temporomandibular disorders. Int. J. Paediatr. Dent. 2010; 20: 458–65.
Katsarava Z, Lehnerdt G, Duda B, Ellrich J, Diener HC, Kaube H. Sensitization of
trigeminal nociception specific for migraine but not pain of sinusitis. Neurology 2002;
59: 1450–3.
Kaube H, Katsarava Z, Przywara S, Drepper J, Ellrich J, Diener H-C. Acute migraine
headache: possible sensitization of neurons in the spinal trigeminal nucleus? Neurology
2002; 58: 1234–8.
Kaube H, Keay KA, Hoskin KL, Bandler R, Goadsby PJ. Expression of c-Fos-like
immunoreactivity in the caudal medulla and upper cervical spinal cord following
stimulation of the superior sagittal sinus in the cat. Brain Res. 1993; 629: 95–102.
Kerr FW. THE DIVISIONAL ORGANIZATION OF AFFERENT FIBRES OF THE
TRIGEMINAL NERVE. Brain 1963; 86: 721–32.
Kindler S, Samietz S, Houshmand M, Grabe HJ, Bernhardt O, Biffar R, et al.
Depressive and anxiety symptoms as risk factors for temporomandibular joint pain: a
prospective cohort study in the general population. J. Pain 2012; 13: 1188–97.
King CD, Wong F, Currie T, Mauderli AP, Fillingim RB, Riley JL. Deficiency in
endogenous modulation of prolonged heat pain in patients with Irritable Bowel
Syndrome and Temporomandibular Disorder. Pain 2009; 143: 172–8.

250
Knight YE, Bartsch T, Kaube H, Goadsby PJ. P/Q-type calcium-channel blockade in
the periaqueductal gray facilitates trigeminal nociception: a functional genetic link for
migraine? J. Neurosci. 2002; 22: RC213.
Knight YE, Goadsby PJ. The periaqueductal grey matter modulates trigeminovascular
input: a role in migraine? Neuroscience 2001; 106: 793–800.
Kobayashi A, Shinoda M, Sessle BJ, Honda K, Imamura Y, Hitomi S, et al.
Mechanisms involved in extraterritorial facial pain following cervical spinal nerve
injury in rats. Mol. Pain 2011; 7: 12.
Kohno S, Kohno T, Medina R. Rotational head motion concurrent to rhythmical
mandibular opening movements. J. Oral Rehabil. 2001; 28: 740–7.
Kohno S, Matsuyama T, Medina RU, Arai Y. Functional-rhythmical coupling of head
and mandibular movements. J. Oral Rehabil. 2001; 28: 161–7.
Komiyama O, Arai M, Kawara M, Kobayashi K, De Laat A. Pain patterns and
mandibular dysfunction following experimental trapezius muscle pain. J. Orofac. Pain
2005; 19: 119–26.
Koolstra JH, van Eijden TMGJ. Functional significance of the coupling between head
and jaw movements. J. Biomech. 2004; 37: 1387–92.
Von Korff M, Dunn KM. Chronic pain reconsidered. Pain 2008; 138: 267–76.
Kori S, Miller R, Todd D. Kinesiophobia: a new view of chronic pain behavior. Pain
Manag 1990; 3: 35–43.
Koutris M, Lobbezoo F, Naeije M, Wang K, Svensson P, Arendt-Nielsen L, et al.
Effects of intense chewing exercises on the masticatory sensory-motor system. J. Dent.
Res. 2009; 88: 658–62.
Koutris M, Lobbezoo F, Sümer NC, Atiş ES, Türker KS, Naeije M. Is myofascial pain
in temporomandibular disorder patients a manifestation of delayed-onset muscle
soreness? Clin. J. Pain 2013; 29: 712–6.

251
Kucyi A, Moayedi M, Weissman-Fogel I, Goldberg MB, Freeman B V, Tenenbaum
HC, et al. Enhanced medial prefrontal-default mode network functional connectivity in
chronic pain and its association with pain rumination. J. Neurosci. 2014; 34: 3969–75.
Kuroda K, Saitoh I, Inada E, Takemoto Y, Iwasaki T, Iwase Y, et al. Head motion may
help mouth opening in children. Arch. Oral Biol. 2011; 56: 102–7.
Lam DK, Sessle BJ, Hu JW. Glutamate and capsaicin effects on trigeminal nociception
II: activation and central sensitization in brainstem neurons with deep craniofacial
afferent input. Brain Res. 2009; 1253: 48–59.
Lambert GA, Hoskin KL, Zagami AS. Cortico-NRM influences on trigeminal neuronal
sensation. Cephalalgia 2008; 28: 640–52.
Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by
central neural plasticity. J. Pain 2009; 10: 895–926.
Lau KT, Cheung KY, Chan KB, Chan MH, Lo KY, Chiu TTW. Relationships between
sagittal postures of thoracic and cervical spine, presence of neck pain, neck pain
severity and disability. Man. Ther. 2010; 15: 457–62.
Leclerc A, Niedhammer I, Landre MF, Ozguler A, Etore P, Pietri-Taleb F. One-year
predictive factors for various aspects of neck disorders. Spine (Phila Pa 1976) 1999; 24:
1455–1462.
Lee P, Huh BK. Peripheral nerve stimulation for the treatment of primary headache.
Curr. Pain Headache Rep. 2013; 17: 319.
Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS. The
fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J.
Behav. Med. 2007; 30: 77–94.
Leiser SC, Moxon KA. Relationship between physiological response type (RA and SA)
and vibrissal receptive field of neurons within the rat trigeminal ganglion. J.
Neurophysiol. 2006; 95: 3129–45.

252
LeResche L. Epidemiology of temporomandibular disorders: implications for the
investigation of etiologic factors. Crit. Rev. Oral Biol. Med. 1997; 8: 291–305.
Leroux E, Ducros A. Occipital injections for trigemino-autonomic cephalalgias:
evidence and uncertainties. Curr. Pain Headache Rep. 2013; 17: 325.
Licini F, Nojelli A, Segù M, Collesano V. Role of psychosocial factors in the etiology
of temporomandibular disorders: relevance of a biaxial diagnosis. Minerva Stomatol.;
58: 557–66.
Liu F, Steinkeler A. Epidemiology, diagnosis, and treatment of temporomandibular
disorders. Dent. Clin. North Am. 2013; 57: 465–79.
Loeser JD, Treede R-D. The Kyoto protocol of IASP Basic Pain Terminology. Pain
2008; 137: 473–7.
Look JO, Schiffman EL, Truelove EL, Ahmad M. Reliability and validity of Axis I of
the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) with
proposed revisions. J. Oral Rehabil. 2010; 37: 744–59.
Lopez-de-Uralde-Villanueva I, Alacreu-Beltran H, Paris-Alemany A, Angulo-Díaz-
Parreño S, La Touche R. Reliability, Standard Error, and Minimal Detectable Change of
Two Measurements for Craniocervical Posture Assessment in Asymptomatic Subjects
and Chronic Neck/craniofacial Pain Patients. (En proceso) 2014
Lukkahatai N, Saligan LN. Association of catastrophizing and fatigue: a systematic
review. J. Psychosom. Res. 2013; 74: 100–9.
Lundborg C, Dahm P, Nitescu P, Biber B. High intrathecal bupivacaine for severe pain
in the head and neck. Acta Anaesthesiol. Scand. 2009; 53: 908–13.
Macfarlane T V, Blinkhorn AS, Davies RM, Kincey J, Worthington H V. Oro-facial
pain in the community: prevalence and associated impact. Community Dent. Oral
Epidemiol. 2002; 30: 52–60.

253
Macfarlane T V, Blinkhorn AS, Davies RM, Ryan P, Worthington H V, Macfarlane GJ.
Orofacial pain: just another chronic pain? Results from a population-based survey. Pain
2002; 99: 453–8.
Macfarlane T V, Glenny AM, Worthington H V. Systematic review of population-based
epidemiological studies of oro-facial pain. J. Dent. 2001; 29: 451–67.
Main CJ. The importance of psychosocial influences on chronic pain. Pain Manag.
2013; 3: 455–66.
Maixner W, Fillingim R, Sigurdsson A, Kincaid S, Silva S. Sensitivity of patients with
painful temporomandibular disorders to experimentally evoked pain: evidence for
altered temporal summation of pain. Pain 1998; 76: 71–81.
Majoie CB, Verbeeten B, Dol JA, Peeters FL. Trigeminal neuropathy: evaluation with
MR imaging. Radiographics 1995; 15: 795–811.
Makowska A, Panfil C, Ellrich J. Long-term potentiation of orofacial sensorimotor
processing by noxious input from the semispinal neck muscle in mice. Cephalalgia
2005; 25: 109–16.
Malick A, Burstein R. Cells of origin of the trigeminohypothalamic tract in the rat. J.
Comp. Neurol. 1998; 400: 125–44.
Malick A, Jakubowski M, Elmquist JK, Saper CB, Burstein R. A neurohistochemical
blueprint for pain-induced loss of appetite. Proc. Natl. Acad. Sci. U. S. A. 2001; 98:
9930–5.
Malick A, Strassman RM, Burstein R. Trigeminohypothalamic and
reticulohypothalamic tract neurons in the upper cervical spinal cord and caudal medulla
of the rat. J. Neurophysiol. 2000; 84: 2078–112.
Manfredini D, Arveda N, Guarda-Nardini L, Segù M, Collesano V. Distribution of
diagnoses in a population of patients with temporomandibular disorders. Oral Surg. Oral
Med. Oral Pathol. Oral Radiol. 2012; 114: e35–41.

254
Marklund S, Wiesinger B, Wänman A. Reciprocal influence on the incidence of
symptoms in trigeminally and spinally innervated areas. Eur. J. Pain 2010; 14: 366–71.
Martin M, Blaisdell B, Kwong JW, Bjorner JB. The Short-Form Headache Impact Test
(HIT-6) was psychometrically equivalent in nine languages. J. Clin. Epidemiol. 2004;
57: 1271–8.
Mason P, Fields HL. Axonal trajectories and terminations of on- and off-cells in the cat
lower brainstem. J. Comp. Neurol. 1989; 288: 185–207.
Matsuka Y, Yatani H, Kuboki T, Yamashita A. Temporomandibular disorders in the
adult population of Okayama City, Japan. Cranio 1996; 14: 158–62.
McLean L. The effect of postural correction on muscle activation amplitudes recorded
from the cervicobrachial region. J. Electromyogr. Kinesiol. 2005; 15: 527–35.
Meeus M, Nijs J, Van Mol E, Truijen S, De Meirleir K. Role of psychological aspects in
both chronic pain and in daily functioning in chronic fatigue syndrome: a prospective
longitudinal study. Clin. Rheumatol. 2012; 31: 921–9.
Meeus M, Nijs J, Van de Wauwer N, Toeback L, Truijen S. Diffuse noxious inhibitory
control is delayed in chronic fatigue syndrome: an experimental study. Pain 2008; 139:
439–48.
Mellick GA, Mellick LB. Regional head and face pain relief following lower cervical
intramuscular anesthetic injection. Headache 2003; 43: 1109–11.
Mellick LB, McIlrath ST, Mellick GA. Treatment of headaches in the ED with lower
cervical intramuscular bupivacaine injections: a 1-year retrospective review of 417
patients. Headache 2006; 46: 1441–9.
Mellick LB, Mellick GA. Treatment of acute orofacial pain with lower cervical
intramuscular bupivacaine injections: a 1-year retrospective review of 114 patients. J.
Orofac. Pain 2008; 22: 57–64.
Mellick LB, Pleasant MR. Do pediatric headaches respond to bilateral lower cervical
paraspinous bupivacaine injections? Pediatr. Emerg. Care 2010; 26: 192–6.

255
Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965; 150: 971–9.
Melzack R. Pain: past, present and future. Can. J. Exp. Psychol. 1993; 47: 615–29.
Melzack R. From the gate to the neuromatrix. Pain 1999; Suppl 6: S121–6.
Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain
Syndromes and Definitions of Pain Terms. Seattle:: IASP Press; 1994.
Mienna CS, Wanman A. Self-reported impact on daily life activities related to
temporomandibular disorders, headaches, and neck-shoulder pain among women in a
Sami population living in Northern Sweden. J. Orofac. Pain 2012; 26: 215–24.
Milidonis MK, Kraus SL, Segal RL, Widmer CG. Genioglossi muscle activity in
response to changes in anterior/neutral head posture. Am. J. Orthod. Dentofacial
Orthop. 1993; 103: 39–44.
Miyaoka S, Hirano H, Miyaoka Y, Yamada Y. Head movement associated with
performance of mandibular tasks. J. Oral Rehabil. 2004; 31: 843–50.
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The
COSMIN study reached international consensus on taxonomy, terminology, and
definitions of measurement properties for health-related patient-reported outcomes. J.
Clin. Epidemiol. 2010; 63: 737–45.
Mongini F, Evangelista A, Milani C, Ferrero L, Ciccone G, Ugolini A, et al. An
educational and physical program to reduce headache, neck/shoulder pain in a working
community: a cluster-randomized controlled trial. PLoS One 2012; 7: e29637.
Moses HL. Comparative fine structure of the trigeminal ganglia, including human
autopsy studies. J. Neurosurg. 1967; 26: Suppl:112–26.
Murray GM, Peck CC. Orofacial pain and jaw muscle activity: a new model. J. Orofac.
Pain 2007; 21: 263–78; discussion 279–88.
Nachev P, Kennard C, Husain M. Functional role of the supplementary and pre-
supplementary motor areas. Nat. Rev. Neurosci. 2008; 9: 856–69.

256
Nachev P, Wydell H, O’neill K, Husain M, Kennard C. The role of the pre-
supplementary motor area in the control of action. Neuroimage 2007; 36 Suppl 2:
T155–63.
Nijs J, Van Houdenhove B, Oostendorp RAB. Recognition of central sensitization in
patients with musculoskeletal pain: Application of pain neurophysiology in manual
therapy practice. Man. Ther. 2010; 15: 135–41.
Nijs J, Meeus M, Heins M, Knoop H, Moorkens G, Bleijenberg G. Kinesiophobia,
catastrophizing and anticipated symptoms before stair climbing in chronic fatigue
syndrome: an experimental study. Disabil. Rehabil. 2012; 34: 1299–305.
Nijs J, Van de Putte K, Louckx F, Truijen S, De Meirleir K. Exercise performance and
chronic pain in chronic fatigue syndrome: the role of pain catastrophizing. Pain Med.
2008; 9: 1164–72.
Nilsson I-M, List T, Drangsholt M. Headache and co-morbid pains associated with
TMD pain in adolescents. J. Dent. Res. 2013; 92: 802–7.
Nishimori T, Sera M, Suemune S, Yoshida A, Tsuru K, Tsuiki Y, et al. The distribution
of muscle primary afferents from the masseter nerve to the trigeminal sensory nuclei.
Brain Res. 1986; 372: 375–81.
Nordin M, Carragee EJ, Hogg-Johnson S, Weiner SS, Hurwitz EL, Peloso PM, et al.
Assessment of neck pain and its associated disorders: results of the Bone and Joint
Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila.
Pa. 1976). 2008; 33: S101–22.
Ohmure H, Miyawaki S, Nagata J, Ikeda K, Yamasaki K, Al-Kalaly A. Influence of
forward head posture on condylar position. J. Oral Rehabil. 2008; 35: 795–800.
Okamoto K, Kimura A, Donishi T, Imbe H, Senba E, Tamai Y. Central serotonin 3
receptors play an important role in the modulation of nociceptive neural activity of
trigeminal subnucleus caudalis and nocifensive orofacial behavior in rats with persistent
temporomandibular joint inflammation. Neuroscience 2005; 135: 569–81.

257
Okeson JP, de Leeuw R. Differential diagnosis of temporomandibular disorders and
other orofacial pain disorders. Dent. Clin. North Am. 2011; 55: 105–20.
Okeson JP. Current terminology and diagnostic classification schemes. Oral Surg. Oral
Med. Oral Pathol. Oral Radiol. Endod. 1997; 83: 61–4.
Olivo SA, Fuentes J, Major PW, Warren S, Thie NMR, Magee DJ. The association
between neck disability and jaw disability. J Oral Rehabil 2010; 37: 670–9.
Ouaknine G, Nathan H. Anastomotic connections between the eleventh nerve and the
posterior root of the first cervical nerve in humans. J. Neurosurg. 1973; 38: 189–97.
Park JW, Clark GT, Kim YK, Chung JW. Analysis of thermal pain sensitivity and
psychological profiles in different subgroups of TMD patients. Int. J. Oral Maxillofac.
Surg. 2010; 39: 968–74.
Peck CC, Murray GM, Gerzina TM. How does pain affect jaw muscle activity? The
Integrated Pain Adaptation Model. Aust. Dent. J. 2008; 53: 201–7.
Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the
number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996;
49: 1373–9.
Penley JA, Wiebe JS, Nwosu A. Psychometric properties of the Spanish Beck
Depression Inventory-II in a medical sample. Psychol. Assess. 2003; 15: 569–77.
Pernold G, Mortimer M, Wiktorin C, Tornqvist EW, Vingård E. Neck/shoulder
disorders in a general population. Natural course and influence of physical exercise: a 5-
year follow-up. Spine (Phila. Pa. 1976). 2005; 30: E363–8.
Piovesan EJ, Kowacs PA, Oshinsky ML. Convergence of cervical and trigeminal
sensory afferents. Curr. Pain Headache Rep. 2003; 7: 377–83.
Piovesan EJ, Kowacs PA, Tatsui CE, Lange MC, Ribas LC, Werneck LC. Referred pain
after painful stimulation of the greater occipital nerve in humans: evidence of
convergence of cervical afferences on trigeminal nuclei. Cephalalgia 2001; 21: 107–9.

258
Plesh O, Adams SH, Gansky S a. Temporomandibular joint and muscle disorder-type
pain and comorbid pains in a national US sample. J. Orofac. Pain 2011; 25: 190–8.
Plesh O, Curtis DA, Hall LJ, Miller A. Gender difference in jaw pain induced by
clenching. J. Oral Rehabil. 1998; 25: 258–63.
Poletti CE. C2 and C3 pain dermatomes in man. Cephalalgia 1991; 11: 155–9.
Porreca F, Ossipov MH, Gebhart GF. Chronic pain and medullary descending
facilitation. Trends Neurosci. 2002; 25: 319–25.
Portney LG WM. Foundations of Clinical Research; Applications to Practice. New
Jersey: 2009.
Quartana PJ, Buenaver LF, Edwards RR, Klick B, Haythornthwaite JA, Smith MT. Pain
catastrophizing and salivary cortisol responses to laboratory pain testing in
temporomandibular disorder and healthy participants. J. Pain 2010; 11: 186–94.
Raboisson P, Dallel R, Clavelou P, Sessle BJ, Woda A. Effects of subcutaneous
formalin on the activity of trigeminal brain stem nociceptive neurones in the rat. J.
Neurophysiol. 1995; 73: 496–505.
Rantala MA, Ahlberg J, Suvinen TI, Nissinen M, Lindholm H, Savolainen A, et al.
Temporomandibular joint related painless symptoms, orofacial pain, neck pain,
headache, and psychosocial factors among non-patients. Acta Odontol Scand 2003; 61:
217–222.
Raphael KG, Janal MN, Anathan S, Cook DB, Staud R. Temporal summation of heat
pain in temporomandibular disorder patients. J. Orofac. Pain 2009; 23: 54–64.
Reid KI, Greene CS. Diagnosis and treatment of temporomandibular disorders: an
ethical analysis of current practices. J. Oral Rehabil. 2013; 40: 546–61.
Ren K, Dubner R. Descending modulation in persistent pain: an update. Pain 2002; 100:
1–6.

259
Rocabado M. Biomechanical relationship of the cranial, cervical, and hyoid regions. J.
Craniomandibular. Pract. 1983; 1: 61–6.
Rocha CP, Croci CS, Caria PHF. Is there relationship between temporomandibular
disorders and head and cervical posture? A systematic review. J. Oral Rehabil. 2013;
40: 875–81.
Roddy E, Zwierska I, Jordan KP, Dawes P, Hider SL, Packham J, et al. Musculoskeletal
clinical assessment and treatment services at the primary-secondary care interface: an
observational study. Br. J. Gen. Pract. 2013; 63: e141–8.
Rodríguez K, Miralles R, Gutiérrez MF, Santander H, Fuentes A, Fresno MJ, et al.
Influence of jaw clenching and tooth grinding on bilateral sternocleidomastoid EMG
activity. Cranio 2011; 29: 14–22.
Rollman A, Visscher CM, Gorter RC, Naeije M. Care seeking for orofacial pain. J.
Orofac. Pain 2012; 26: 206–14.
Salama-Hanna J, Chen G. Patients with chronic pain. Med. Clin. North Am. 2013; 97:
1201–15.
Salomons T V, Moayedi M, Weissman-Fogel I, Goldberg MB, Freeman B V,
Tenenbaum HC, et al. Perceived helplessness is associated with individual differences
in the central motor output system. Eur. J. Neurosci. 2012; 35: 1481–7.
Salter MW. Cellular neuroplasticity mechanisms mediating pain persistence. J. Orofac.
Pain 2004; 18: 318–24.
Sanders RD. The Trigeminal (V) and Facial (VII) Cranial Nerves: Head and Face
Sensation and Movement. Psychiatry (Edgmont). 2010; 7: 13–6.
Saper JR, Dodick DW, Silberstein SD, McCarville S, Sun M, Goadsby PJ. Occipital
nerve stimulation for the treatment of intractable chronic migraine headache: ONSTIM
feasibility study. Cephalalgia 2011; 31: 271–85.
Saracco MG, Valfrè W, Cavallini M, Aguggia M. Greater occipital nerve block in
chronic migraine. Neurol. Sci. 2010; 31 Suppl 1: S179–80.

260
Sarlani E, Grace EG, Reynolds MA, Greenspan JD. Evidence for up-regulated central
nociceptive processing in patients with masticatory myofascial pain. J. Orofac. Pain
2004; 18: 41–55.
Schepelmann K, Ebersberger A, Pawlak M, Oppmann M, Messlinger K. Response
properties of trigeminal brain stem neurons with input from dura mater encephali in the
rat. Neuroscience 1999; 90: 543–54.
Schiffman E, Ohrbach R, List T, Anderson G, Jensen R, John MT, et al. Diagnostic
criteria for headache attributed to temporomandibular disorders. Cephalalgia 2012; 32:
683–92.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet J-P, et al. Diagnostic
Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research
Applications: recommendations of the International RDC/TMD Consortium Network*
and Orofacial Pain Special Interest Group†. J. oral facial pain headache 2014; 28: 6–27.
Schiffman EL, Ohrbach R, Truelove EL, Tai F, Anderson GC, Pan W, et al. The
Research Diagnostic Criteria for Temporomandibular Disorders. V: methods used to
establish and validate revised Axis I diagnostic algorithms. J. Orofac. Pain 2010; 24:
63–78.
Schmid-Schwap M, Bristela M, Kundi M, Piehslinger E. Sex-specific differences in
patients with temporomandibular disorders. J. Orofac. Pain 2013; 27: 42–50.
Schofferman J, Garges K, Goldthwaite N, Koestler M, Libby E. Upper cervical anterior
diskectomy and fusion improves discogenic cervical headaches. Spine (Phila. Pa. 1976).
2002; 27: 2240–4.
Van Selms MKA, Wang K, Lobbezoo F, Svensson P, Arendt-Nielsen L, Naeije M.
Effects of masticatory muscle fatigue without and with experimental pain on jaw-stretch
reflexes in healthy men and women. Clin. Neurophysiol. 2005; 116: 1415–23.
Seminowicz DA, Shpaner M, Keaser ML, Krauthamer GM, Mantegna J, Dumas JA, et
al. Cognitive-behavioral therapy increases prefrontal cortex gray matter in patients with
chronic pain. J. Pain 2013; 14: 1573–84.

261
Serra G, Marchioretto F. Occipital nerve stimulation for chronic migraine: a randomized
trial. Pain Physician 2012; 15: 245–53.
Sessle BJ, Hu JW, Amano N, Zhong G. Convergence of cutaneous, tooth pulp, visceral,
neck and muscle afferents onto nociceptive and non-nociceptive neurones in trigeminal
subnucleus caudalis (medullary dorsal horn) and its implications for referred pain. Pain
1986; 27: 219–35.
Sessle BJ, Hu JW. Mechanisms of pain arising from articular tissues. Can. J. Physiol.
Pharmacol. 1991; 69: 617–26.
Sessle BJ. The neurobiology of facial and dental pain: present knowledge, future
directions. J. Dent. Res. 1987; 66: 962–81.
Sessle BJ. Mechanisms of trigeminal and occipital pain. Pain Rev. 1996; 3: 91–116.
Sessle BJ. Neural mechanisms and pathways in craniofacial pain. Can. J. Neurol. Sci.
1999; 26 Suppl 3: S7–11.
Sessle BJ. Acute and chronic craniofacial pain: brainstem mechanisms of nociceptive
transmission and neuroplasticity, and their clinical correlates. Crit. Rev. Oral Biol. Med.
2000; 11: 57–91.
Sessle BJ. Recent insights into brainstem mechanisms underlying craniofacial pain. J.
Dent. Educ. 2002; 66: 108–12.
Sessle BJ. Orofacial Pain. In: The Paths of Pain 1975-2005. Seattle: IASP Press; 2005.
a.
Sessle BJ. Peripheral and central mechanisms of orofacial pain and their clinical
correlates. Minerva Anestesiol. 2005b; 71: 117–36.
Sessle BJ. Peripheral and central mechanisms of orofacial inflammatory pain. Int. Rev.
Neurobiol. 2011; 97: 179–206.

262
Shackman AJ, Salomons T V, Slagter HA, Fox AS, Winter JJ, Davidson RJ. The
integration of negative affect, pain and cognitive control in the cingulate cortex. Nat.
Rev. Neurosci. 2011; 12: 154–67.
Shephard MK, Macgregor EA, Zakrzewska JM. Orofacial pain: a guide for the
headache physician. Headache 2014; 54: 22–39.
Sherman SE, Luo L, Dostrovsky JO. Spinal strychnine alters response properties of
nociceptive-specific neurons in rat medial thalamus. J. Neurophysiol. 1997; 78: 628–37.
Shigenaga Y, Sera M, Nishimori T, Suemune S, Nishimura M, Yoshida A, et al. The
central projection of masticatory afferent fibers to the trigeminal sensory nuclear
complex and upper cervical spinal cord. J. Comp. Neurol. 1988; 268: 489–507.
Shin JH, Song HK, Lee JH, Kim WK, Chu MK. Paroxysmal stabbing headache in the
multiple dermatomes of the head and neck: a variant of primary stabbing headache or
occipital neuralgia? Cephalalgia 2007; 27: 1101–8.
Shin P, Vernon H, Sessle BJ, Hu JW. Neck muscle length modulates nociceptive reflex
evoked by noxious irritant application to rat neck tissues. Exp. brain Res. 2005; 163:
314–23.
Silberstein SD, Dodick DW, Saper J, Huh B, Slavin K V, Sharan A, et al. Safety and
efficacy of peripheral nerve stimulation of the occipital nerves for the management of
chronic migraine: results from a randomized, multicenter, double-blinded, controlled
study. Cephalalgia 2012; 32: 1165–79.
Silva AG, Punt TD, Sharples P, Vilas-Boas JP, Johnson MI. Head posture and neck pain
of chronic nontraumatic origin: a comparison between patients and pain-free persons.
Arch. Phys. Med. Rehabil. 2009; 90: 669–74.
Simons D, Travell J, Simons L. Myofascial pain and dysfunction: The trigger point
manual. Vol 1. 2nd. Baltimore: Williams & Wilkins; 1999.
Simons D. Clinical and Etiological Update of Myofascial Pain from Trigger Points. J.
Musculoskelet. Pain 1996: 93–122.

263
Simons LE, Elman I, Borsook D. Psychological processing in chronic pain: a neural
systems approach. Neurosci. Biobehav. Rev. 2014; 39: 61–78.
Sipilä K, Zitting P, Siira P, Laukkanen P, Järvelin M-R, Oikarinen KS, et al.
Temporomandibular disorders, occlusion, and neck pain in subjects with facial pain: a
case-control study. Cranio 2002; 20: 158–64.
Slavin K V, Colpan ME, Munawar N, Wess C, Nersesyan H. Trigeminal and occipital
peripheral nerve stimulation for craniofacial pain: a single-institution experience and
review of the literature. Neurosurg. Focus 2006; 21: E5.
Smeets RJEM, Vlaeyen JWS, Kester ADM, Knottnerus JA. Reduction of pain
catastrophizing mediates the outcome of both physical and cognitive-behavioral
treatment in chronic low back pain. J. Pain 2006; 7: 261–71.
So K, Komiyama O, Arai M, Kawara M, Kobayashi K. Influence of occlusal contact on
cervical muscle activity during submaximal clenching. J. Oral Rehabil. 2004; 31: 417–
22.
Solow B, Tallgren A. Head posture and craniofacial morphology. Am. J. Phys.
Anthropol. 1976; 44: 417–35.
Spielberg C, Lushene R. State Anxiety Inventory. Cuestionario de ansiedad estado-
rasgo. Adaptación Española. Madrid: TEA; 1982.
Storm C, Wänman A. Temporomandibular disorders, headaches, and cervical pain
among females in a Sami population. Acta Odontol. Scand. 2006; 64: 319–25.
Strassman AM, Mineta Y, Vos BP. Distribution of fos-like immunoreactivity in the
medullary and upper cervical dorsal horn produced by stimulation of dural blood
vessels in the rat. J. Neurosci. 1994; 14: 3725–35.
Strassman AM, Raymond SA, Burstein R. Sensitization of meningeal sensory neurons
and the origin of headaches. Nature 1996; 384: 560–4.

264
Stuginski-Barbosa J, Macedo HR, Bigal ME, Speciali JG. Signs of temporomandibular
disorders in migraine patients: a prospective, controlled study. Clin J Pain 2010; 26:
418–421.
Sugiyo S, Takemura M, Dubner R, Ren K. Trigeminal transition zone/rostral
ventromedial medulla connections and facilitation of orofacial hyperalgesia after
masseter inflammation in rats. J. Comp. Neurol. 2005; 493: 510–23.
Sullivan MJ, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al.
Theoretical perspectives on the relation between catastrophizing and pain. Clin. J. Pain
2001; 17: 52–64.
Sullivan MJ. What is the clinical value of assessing pain-related psychosocial risk
factors? Pain Manag. 2013; 3: 413–6.
Suzuki S, Matsubara N, Hisano M, Soma K. Investigation of cervical muscle
mechanisms during jaw movement--using a prototype head-jaw-neck model--. J. Med.
Dent. Sci. 2003; 50: 285–90.
Svensson P, Burgaard A, Schlosser S. Fatigue and pain in human jaw muscles during a
sustained, low-intensity clenching task. Arch. Oral Biol. 2001; 46: 773–7.
Svensson P, Wang K, Arendt-Nielsen L, Cairns BE, Sessle BJ. Pain effects of glutamate
injections into human jaw or neck muscles. J. Orofac. Pain 2005; 19: 109–18.
Svensson P, Wang K, Sessle BJ, Arendt-Nielsen L. Associations between pain and
neuromuscular activity in the human jaw and neck muscles. Pain 2004; 109: 225–32.
Svensson P. Muscle pain in the head: overlap between temporomandibular disorders
and tension-type headaches. Curr Opin Neurol 2007; 20: 320–325.
Takemura M, Sugiyo S, Moritani M, Kobayashi M, Yonehara N. Mechanisms of
orofacial pain control in the central nervous system. Arch. Histol. Cytol. 2006; 69: 79–
100.

265
Terwee CB, Bot SDM, de Boer MR, van der Windt DAWM, Knol DL, Dekker J, et al.
Quality criteria were proposed for measurement properties of health status
questionnaires. J. Clin. Epidemiol. 2007; 60: 34–42.
Thompson J, Brodie A. Factors in the position of the mandible. J. Am. Dent. Assoc.
1942; 29: 925–941.
Torisu T, Suenaga H, Yoshimatsu T, Kanaoka R, Yamabe Y, Fujii H. Anticipatory and
reflexive neck muscle activities during voluntary rapid jaw opening and passive jaw
depression in humans. J. Oral Rehabil. 2002; 29: 961–8.
Torisu T, Tanaka M, Murata H, Wang K, Arendt-Nielsen L, De Laat A, et al.
Modulation of neck muscle activity induced by intra-oral stimulation in humans. Clin.
Neurophysiol. 2013
Torisu T, Tanaka M, Murata H, Wang K, Arendt-Nielsen L, De Laat A, et al.
Modulation of neck muscle activity induced by intra-oral stimulation in humans. Clin.
Neurophysiol. 2014; 125: 1006–11.
Torisu T, Yamabe Y, Hashimoto N, Yoshimatsu T, Fujii H. Head movement properties
during voluntary rapid jaw movement in humans. J. Oral Rehabil. 2001; 28: 1144–52.
La Touche R, Fernández-de-Las-Peñas C, Fernández-Carnero J, Díaz-Parreño S, Paris-
Alemany A, Arendt-Nielsen L. Bilateral mechanical-pain sensitivity over the trigeminal
region in patients with chronic mechanical neck pain. J. pain Off. J. Am. Pain Soc.
2010; 11: 256–263.
La Touche R, Fernández-de-las-Peñas C, Fernández-Carnero J, Escalante K, Angulo-
Díaz-Parreño S, Paris-Alemany A, et al. The effects of manual therapy and exercise
directed at the cervical spine on pain and pressure pain sensitivity in patients with
myofascial temporomandibular disorders. J. Oral Rehabil. 2009; 36: 644–52.
La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-Díaz-
Parreño S, Suárez-Falcón JC, et al. Craniofacial pain and disability inventory (CF-PDI):
development and psychometric validation of a new questionnaire. Pain Physician 2014;
17: 95–108.

266
La Touche R, Paris-Alemany A, Gil-Martínez A, Pardo-Montero J, Angulo-Díaz-
Parreño S, Fernández-Carnero J. The Influence of Neck Disability and Pain
Catastrophizing about Trigeminal Sensory-Motor System in Patients with Headache
Attributed to Temporomandibular Disorders. (En proceso) 2014
La Touche R, París-Alemany A, Mannheimer JS, Angulo-Díaz-Parreño S, Bishop MD,
Lopéz-Valverde-Centeno A, et al. Does Mobilization of the Upper Cervical Spine
Affect Pain Sensitivity and Autonomic Nervous System Function in Patients With
Cervico-craniofacial Pain?: A Randomized-controlled Trial. Clin. J. Pain 2012
La Touche R, París-Alemany A, Von Piekartz H, Mannheimer JS, Fernández-Carnero J,
Rocabado M. The influence of cranio-cervical posture on maximal mouth opening and
pressure pain threshold in patients with myofascial temporomandibular pain disorders.
Clin. J. Pain 2011; 27: 48–55.
Tseng BY, Gajewski BJ, Kluding PM. Reliability, responsiveness, and validity of the
visual analog fatigue scale to measure exertion fatigue in people with chronic stroke: a
preliminary study. Stroke Res. Treat. 2010; 2010
Turk DC, Rudy TE. Toward an empirically derived taxonomy of chronic pain patients:
integration of psychological assessment data. J Consult Clin Psychol 1988; 56: 233–8.
Turner JA, Aaron LA. Pain-related catastrophizing: what is it? Clin. J. Pain 2001; 17:
65–71.
Turner JA, Brister H, Huggins K, Mancl L, Aaron LA, Truelove EL. Catastrophizing is
associated with clinical examination findings, activity interference, and health care use
among patients with temporomandibular disorders. J. Orofac. Pain 2005; 19: 291–300.
Turner JA, Dworkin SF, Mancl L, Huggins KH, Truelove EL. The roles of beliefs,
catastrophizing, and coping in the functioning of patients with temporomandibular
disorders. Pain 2001; 92: 41–51.
Turner JA, Mancl L, Aaron LA. Brief cognitive-behavioral therapy for
temporomandibular disorder pain: effects on daily electronic outcome and process
measures. Pain 2005; 117: 377–87.

267
Turner JA, Mancl L, Aaron LA. Short- and long-term efficacy of brief cognitive-
behavioral therapy for patients with chronic temporomandibular disorder pain: a
randomized, controlled trial. Pain 2006; 121: 181–94.
Velly AM, Look JO, Carlson C, Lenton PA, Kang W, Holcroft CA, et al. The effect of
catastrophizing and depression on chronic pain--a prospective cohort study of
temporomandibular muscle and joint pain disorders. Pain 2011; 152: 2377–83.
Venegas M, Valdivia J, Fresno MJ, Miralles R, Gutiérrez MF, Valenzuela S, et al.
Clenching and grinding: effect on masseter and sternocleidomastoid electromyographic
activity in healthy subjects. Cranio 2009; 27: 159–66.
Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J.
Manipulative Physiol. Ther. 1991; 14: 409–15.
Vernon H, Sun K, Zhang Y, Yu X-M, Sessle BJ. Central sensitization induced in
trigeminal and upper cervical dorsal horn neurons by noxious stimulation of deep
cervical paraspinal tissues in rats with minimal surgical trauma. J. Manipulative
Physiol. Ther. 2009; 32: 506–14.
Visscher CM, Huddleston Slater JJ, Lobbezoo F, Naeije M. Kinematics of the human
mandible for different head postures. J. Oral Rehabil. 2000; 27: 299–305.
Visscher CM, Ohrbach R, van Wijk AJ, Wilkosz M, Naeije M. The Tampa Scale for
Kinesiophobia for Temporomandibular Disorders (TSK-TMD). Pain 2010; 150: 492–
500.
Vlaeyen JW, Seelen HA, Peters M, de Jong P, Aretz E, Beisiegel E, et al. Fear of
movement/(re)injury and muscular reactivity in chronic low back pain patients: an
experimental investigation. Pain 1999; 82: 297–304.
Waite P, Ashwell K. The Human Nervous Sytem. San Diego: Elsevier Academic Press;
2004.

268
Walsh NE, Brooks P, Hazes JM, Walsh RM, Dreinhöfer K, Woolf AD, et al. Standards
of care for acute and chronic musculoskeletal pain: the Bone and Joint Decade (2000-
2010). Arch. Phys. Med. Rehabil. 2008; 89: 1830–45.
Walton D, Elliott JM. A higher-order analysis supports use of the 11-item version of the
tampa scale for kinesiophobia in people with neck pain. Phys. Ther. 2013; 93: 60–8.
Walton DM, Macdermid JC, Nielson W, Teasell RW, Chiasson M, Brown L.
Reliability, standard error, and minimum detectable change of clinical pressure pain
threshold testing in people with and without acute neck pain. J. Orthop. Sports Phys.
Ther. 2011; 41: 644–50.
Wang K, Sessle BJ, Svensson P, Arendt-Nielsen L. Glutamate evoked neck and jaw
muscle pain facilitate the human jaw stretch reflex. Clin. Neurophysiol. 2004; 115:
1288–95.
Wänman A. Longitudinal course of symptoms of craniomandibular disorders in men
and women. A 10-year follow-up study of an epidemiologic sample. Acta Odontol.
Scand. 1996; 54: 337–42.
Watson DH, Drummond PD. Head pain referral during examination of the neck in
migraine and tension-type headache. Headache 2012; 52: 1226–35.
Weber P, Corrêa ECR, Ferreira F dos S, Soares JC, Bolzan G de P, Silva AMT da.
Cervical spine dysfunction signs and symptoms in individuals with temporomandibular
disorder. J. Soc. Bras. Fonoaudiol. 2012; 24: 134–9.
Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient
and the SEM. J. Strength Cond. Res. 2005; 19: 231–40.
Wiebe JS, Penley JA. A psychometric comparison of the Beck Depression Inventory-II
in English and Spanish. Psychol. Assess. 2005; 17: 481–5.
Wiesinger B, Häggman-Henrikson B, Hellström F, Wänman A. Experimental masseter
muscle pain alters jaw-neck motor strategy. Eur. J. Pain 2013; 17: 995–1004.

269
Wiesinger B, Malker H, Englund E, Wänman A. Back pain in relation to
musculoskeletal disorders in the jaw-face: a matched case-control study. Pain 2007;
131: 311–9.
Wiesinger B, Malker H, Englund E, Wänman A. Does a dose-response relation exist
between spinal pain and temporomandibular disorders? BMC Musculoskelet. Disord.
2009; 10: 28.
Woolf CJ, Costigan M. Transcriptional and posttranslational plasticity and the
generation of inflammatory pain. Proc. Natl. Acad. Sci. U. S. A. 1999; 96: 7723–30.
Woolf CJ. Pain: moving from symptom control toward mechanism-specific
pharmacologic management. Ann. Intern. Med. 2004; 140: 441–51.
Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain.
Pain 2011; 152: S2–15.
Wright EF. Referred craniofacial pain patterns in patients with temporomandibular
disorder. J. Am. Dent. Assoc. 2000; 131: 1307–15.
Xie Y. Glial involvement in trigeminal central sensitization. Acta Pharmacol. Sin. 2008;
29: 641–5.
Yalcin I, Barrot M. The anxiodepressive comorbidity in chronic pain. Curr. Opin.
Anaesthesiol. 2014; 27: 520–7.
Yamabe Y, Yamashita R, Fujii H. Head, neck and trunk movements accompanying jaw
tapping. J. Oral Rehabil. 1999; 26: 900–5.
Yekkalam N, Wänman A. Prevalence of signs and symptoms indicative of
temporomandibular disorders and headaches in 35-, 50-, 65- and 75-year-olds living in
Västerbotten, Sweden. Acta Odontol. Scand. 2014
Ylinen J, Nikander R, Nykänen M, Kautiainen H, Häkkinen A. Effect of neck exercises
on cervicogenic headache: a randomized controlled trial. J. Rehabil. Med. 2010; 42:
344–9.

270
Yoshida K. [Electromyographical analysis of function of sternocleidomastoid muscle
during occlusal function]. Kokubyo Gakkai Zasshi. 1988; 55: 53–70.
Yu XM, Sessle BJ, Haas DA, Izzo A, Vernon H, Hu JW. Involvement of NMDA
receptor mechanisms in jaw electromyographic activity and plasma extravasation
induced by inflammatory irritant application to temporomandibular joint region of rats.
Pain 1996; 68: 169–78.
Yu XM, Sessle BJ, Vernon H, Hu JW. Effects of inflammatory irritant application to
the rat temporomandibular joint on jaw and neck muscle activity. Pain 1995; 60: 143–9.
Zafar H, Nordh E, Eriksson PO. Temporal coordination between mandibular and head-
neck movements during jaw opening-closing tasks in man. Arch. Oral Biol. 2000; 45:
675–82.
Zafar H, Nordh E, Eriksson P-O. Spatiotemporal consistency of human mandibular and
head-neck movement trajectories during jaw opening-closing tasks. Exp. brain Res.
2002; 146: 70–6.
Zafar H, Nordh E, Eriksson P-O. Impaired positioning of the gape in whiplash-
associated disorders. Swed. Dent. J. 2006; 30: 9–15.
Zafar H. Integrated jaw and neck function in man. Studies of mandibular and head-neck
movements during jaw opening-closing tasks. Swed. Dent. J. Suppl. 2000: 1–41.
Copyright © 2022 FDOKUMEN

