





Bahasa
Halaman
Hukum


Asian Journal of Water Environment Vol.1 No. 2 (2014) 19-30
Available online at http://www.geneares.org/publication.html
* Corresponding author – Morshed Hossan Molla
SUPPLY WATER USING PATTERNS AND HEALTH IMPACTS ON URBAN DWELLERS: A
CASE STUDY OF RESIDENTS PERCEPTIONS IN CHITTAGONG METROPOLITAN CITY,
BANGLADESH
Morshed Hossan Molla1*, Mohammad Abu Taiyeb Chowdhury
2, Kazi Md. Barkat Ali
3 and
Muhammad Muhibbullah4
Department of Geography and Environmental Studies,
University of Chittagong, Chittagong-4331, Bangladesh
Email: [email protected], [email protected]
3 ,
ABSTRACT
The study attempts to explore the supply water using patterns in Chittagong Metropolitan City (CMC),
and its perceived health impacts on urban dwellers. This is an empirical work based on field data,
obtained through a structured questionnaire survey designed for the two distinct study areas of CMC. The
study reveals that the major using patterns of supply water in Chittagong city are necessarily those of
drinking, cooking, bathing, laundry- cloth washing, cleaning- dish washing, personal hygiene, gardening,
and toilet use purposes. Piped water is the main source of drinking water for majority of the respondents.
Among the various types of pollutants present in Chittagong Water Supply and Sewerage Authority’s
(CWASA) supply water, bad odour, bad colour, bacteria, insects, bleaching powder, salt and iron are
prominent that were widely perceived by the respondents. Total 64 percent of the respondents are found
to be aware of the relationship that exists between water quality and various water-borne diseases in the
city. About 56 percent of the respondents have reported that their family members have exposed to
diarrhea, dysentery, cholera, typhoid or skin diseases at least once. Female and children are found to be
more affected by the said diseases than their male counterparts. It is suggested that CWASA should
supply safe water and people should drink it only after further treatment- boiling, filtering etc. It is also
urged that people keep water saving appliances in their houses- clean water holding pot, reservoir tanks
etc., and raise people awareness in the city. A reorientation in the management system- co-management is
strongly urged.
Keyword: Environment, water quality, contamination, health impacts and coping mechanisms
1. Introduction
The quality of supply water is closely associated with human health. The World Health Organization
(WHO, 2006) estimated that approximately 80 percent of all sickness and diseases in developing
countries are caused by the consumption of contaminated drinking water. Unfortunately, few people in
developing countries have access to clean water supply (Gleick, 1996; WHO, 2002 and UNICEF, 2006).
According to an estimate, more than 31 million people in Bangladesh collect drinking water from unsafe
sources. Total 15 percent of the urban population does not have access to improved sources of drinking
water (Ahmed, 2000). Thus, providing safe drinking water is one of the public health priorities for most
governments including Bangladesh. The provision of safe supply water means acceptable level of quality
and as well as quantity for domestic uses including food preparation, drinking, dishwashing, cleaning,
bathing, laundry, watering animals and plants etc.. However, being a port city, Chittagong is heavily
influenced by the tidal surges and saline intrusions. Thus, the provision of safe drinking water is likely to

20
be more acute in Chittagong city than any other areas. The city is presently inhabited by some 5 million
people. Further, as the commercial capital of Bangladesh, the city is growing by leaps and bounds.
CWASA is able to meet only one-fourth of the total demand of supply water of the port city. According to
an estimate, the city requires some 585 million litters (ML) per day, but CWASA has the capacity of
supplying only 175 ML (Amin, 2006 and MPWS, 2009).
2. Objectives
The main objective of the study is to identify the supply water using patterns in Chittagong Metropolitan
city and its perceived health impacts on city dwellers. The underlying objective is to explore the coping
mechanisms associated with supply water crisis (shortages) in the study area.
3. Materials and Methods
3.1 Selection of the study area
The City of Chittagong is situated on the right bank of the Karnaphuli River, and lies Latitudinally
between 22º14 and 22º24 North, and Longitudinally between 91º46 and 91º53 East It is the second
largest metropolitan area of Bangladesh covering an area of about 1,145 square kilometers. The area of
Chittagong City Corporation covers 168 sq km; there are 41 wards and 11 Metropolitan Police Station
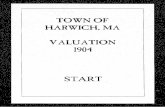
(Thana) in the area (Amin, 2006; BBS, 2008 and population census, 2001). For the convenience of the
study, the city corporation area has been taken into consideration and is divided into two broad (Figure 1)
zones: Northern Study Area-I (treated surface water) and Southern Study Area II (ground water from
deep tube wells).
3.2 Description of the Sampling Area Selection
The selection of the sample area was made in keeping pace with the Chittagong Water Supply and
Sewerage Authority’s (CWASA) current water distribution system. The research has been largely based
on primary data, obtained through a field survey (conducted during the months of February to October
2011), consisting of two components: questionnaire survey on at household level and institutional in-
depth interview on supply water users and providers in CMC. In the later approach, a total of 200 samples
and some representative in-depth interviews were taken from both the zones: Northern 70 respondents,
and Southern 170 respondents in CMC (Table 1). Sample sizes were determined on the basis of
residential structure of the city. A Chi-square ( ) test was performed after cross tabulation of the data to
see if there is any significant relationship between the supply water using patterns and its perceived health
impacts on city dwellers. Secondary information was collected from different sources including local
authority, government organizations, research cells, university libraries, and NGOs to support the
background of the study.

21
Figure 1: Location of the study area (Bangladesh, Chittagong district & Chittagong City Corporation)
Source: Base Map Collected from CDA & CWASA, 2011
Table 1: Sampling selection at CWASA networking area in CMC
Study Areas (Location of the sampling station) Residential
Structure*
Sample
Size**
Are
a-I
(Su
rfa
ce
wa
ter) BAKALIA THANA 41410 20
CHANDGAON THANA 36064 17
PANCHLIASH THANA 34079 16
BAYEJID BOSTAMI THANA 35208 17
Total Residential Structure 146761 70
Are
a-I
I (G
rou
nd
wa
ter)
KOTWALI THAN 57179 27
DOUBLE MOORING THANA 53849 26
KHULSHI THANA 52011 25
PAHARTALI THANA 25768 12
HALISHAHAR THANA 24763 12
CHITTAGONG PORT 41466 20
PATENGA 15542 8
Total Residential Structure 270578 130
Study Area-I and Study Area-II 417339 200
Source: Population Census, 2001 & Master plan for water supply CWASA, 2009.
*Residential structure is to be considered as population census, 2001 & Master plan for water supply
CWASA, 2010.
**Sample size selected by the Stratified random sampling.

22
3.3 In-depth interview survey
A pre-coded in-depth interview questionnaire survey was conducted to collect information the volume of
supply water, improve service delivery, promote linkage management, ensure getting portable water and
especially reduce contaminated paths in CWASA authorize, water related NGOs and local authority
(ward member) level.
3.4 Data processing, Analysis and Presentation
The collected data were processed and analyzed with the help of selected computer software ( i.e.
Statistical Package for Social Science/SPSS, version 18; MS Word and MS Excel) using various
statistical tools and techniques e.g. Chi-square ( ) test, tables, diagrams and figures. To show the
sampling stations of the study area, base maps (2011) were collected from the GIS section of CDA and
CWASA. Collected maps were modified and digitized using Arc View 3.3 and Arc GIS 9.1 software.
4. Results and Discussions
Supply water using patterns in Chittagong City varies widely at different levels: individuals, households
and economic classes. Moreover, the dwellers could hardly provide us with the correct estimation of their
daily domestic water uses. The following discussion discloses the water supply using patterns and its
perceived health impacts on city dwellers and also explores the coping mechanisms associated with
supply water crisis (shortages) in the study area.
4.1 Daily supply water using patterns in CMC at household level
Supply water using patterns in CMC depend to a large extent on the type of users and the availability of
water from various sources. Consumption patterns of supply water, in turn, depend on user’s style of
livings, income level, family structure, religious activities, population density and understanding of the
value of scarce resources- an ethical stand. As shown in Table 2, type of uses of supply water by different
groups in CMC at household level includes drinking, cooking, bathing, dish washing, cloth washing,
personal hygienic, toilet use, gardening, house cleaning, vehicles clearing and showering and vehicle
cleaning. The following table depicts that the total supply water in CMC are used mostly in bathing (24)
cooking (17 percent), toilet use (13 percent), personal hygienic (about 11 percent), drinking (9 percent)
and dish washing (about 9 percent), and cloth washing (7 percent), and very little amount are used for
showering, gardening, vehicles clearing and house cleaning in the study area.
Table 2: Supply water using patters in CMC at household level Sectors of supply water uses Area-I
(N=70)
Area-II
(N=130)
Total
(N=200)
Drinking 12.00 11.00 9.00
Cooking 17.00 16.50 17.50
Bathing 21.00 25.50 24.50
Dish Washing 9.90 14.00 8.50
Cloth Washing 14.00 7.50 7.00
Toilet Use 8.00 11.50 13.00
Personal Hygienic 10.00 7.50 10.50
House cleaning 5.00 3.00 4.00
Gardening 0.10 0.10 1.00
Vehicles clearing 2.00 0.50 2.00
Showering purpose 1.00 2.90 2.50
Total 100.0 100.0 100.0
Source: Field Survey, 2011

23
4.2 Major water sources in CMC for domestic use purposes
The dwellers of Chittagong city never get water according to their demand due to the scarcity of supply.
For domestic use purposes, the city dwellers collect water from a number of sources including pipe line
water, rain water harvesting, railway supply water, Tube-well and pond. Figure 2 depicts the major
sources of water supply for CMC at household level. It is evident that piped water is the main (85 per
cent) source of water for city dwellers followed by Tube-well- the second major source of drinking water
for city dwellers. Only a small portion (varies from 2 to 9 percent) of inhabitants collect rain water for
their household purposes in both the study areas: I and II. The other mentionable sources of water for
household purposes in CMC are railway supply water and community pond.
Figure 2: Sources of water in Chittagong Metropolitan city (CMC) at household level. Source: Field
Survey, 2011
4.3 Pollutants Contain in CWASA Supply Water
Quality of supply water is acceptable near the treatment plant. A variety of physical, chemical and
biological pollutants entry in the distribution network by the help of installation to unauthorized pumps in
the service line, leaks in the old pipes and absence of pressure or negative pressure in water mains during
non-supply hours (Lahlou, 2002; Choudhury et. al., 1997 & Ahmad, 1998). From current investigation
explore that, various types of pollutants like iron, sand, insects, bad odour, bacteria, bad colour, salts,
blessing powder and unfamiliar etc. present in CWASA supplying water in Chittagong metropolitan city.
Following Table 3 easily depict the different pollutants presence in the CWASA supply water networks in
CMC.

24
Table 3: Pollutants Contain in CWASA Supply Water
Type of pollutants Area-I
(N=70)
Area-II
(N=387)
Total
(N=549)
Sand 14.90 14.20 14.38
Insects 9.31 13.69 12.38
Bacteria 8.69 11.62 10.74
Bad odour 11.80 13.69 12.93
Bad colour 7.45 12.14 10.92
Iron 23.60 19.63 20.76
Salty 13.66 8.01 9.83
Blessing powder ….....
0.25 0.18
Not applicable 11.18 6.45 7.83
Total 100.0 100.0 100.0
Source: Field Survey, 2011
4.4 Perceived health impacts of CMC dwellers connected to supply water
The quality of drinking water is closely associated with human health, and providing safe drinking water
is one of the public health priorities (WHO, 1984). Out of 200 respondents in total in CMC, some 56
percent residents reported that they suffered from water borne disease in the city. In both the study areas,
the percentage of city dwellers reporting experience of water-borne diseases is above 50 percent (Figure
3).
Figure 3: Chittagong Metropolitan city (CMC) dwellers reporting perceived health impacts. Source: Field
Survey, 2011
4.5 Water borne diseases among male, female and children residents of city
There is also a gender and demographic dimension of water-borne diseases in CMC as this varies by sex
and age structure of the population. Table 4 depicts the reported variation of water-borne diseases in
CMC by male, female and children categories. As the Table shows, the CMC dwellers suffer from
different types of water borne diseases i.e. diarrhoea, dysentery, cholera, typhoid, skin disease and fever,

25
and these are perceived to be related with the contaminated supply water in the city area. It is striking to
note that of the total respondents, children are exposed to be mostly affected by dysentery (67 percent),
Diarrhoea (59 percent), and skin disease (52 percent). The percentages of female reporting exposure to
these water-borne diseases in CMC are nevertheless striking. As shown in Table3, female reporting
exposure to water-borne diseases includes Skin diseases (51 percent,) Dysentery (49 percent) and
Diarrhoea (41 percent). Very small portion of the people are found to suffer from cholera, typhoid and
fever in the study area.
Table 4: Water borne diseases among male, female and children residents of city
Disease pattern Area-I
(N=70)
Area-II
(N=130)
Total
(N=200)
Male Female Children Male Female Children Male Female Children
Diarrhoea Yes 34.5 51.4 55.7 27.7 49.5 60.8 25.0 41.2 59.0
No 65.5.0 48.6 44.3 72.3 50.5 39.2 75.0 58.8 41.0
Dysentery Yes 17.1 55.9 30.2 9.2 64.6 46.2 12.0 48.5 66.6
No 82.9 41.1 69.8 90.8 35.4 53.8 88.0 51.5 33.4
Cholera Yes 1.4 1.4 ……..
1.5 1.5 1.5 1.5 1.5 1.0
No 98.6 98.6 100.0 98.5 98.5 98.5 98.5 98.5 99.0
Typhoid Yes 7.1 4.3 2.9 5.4 6.9 6.2 6.0 6.0 5.0
No 92.9 95.7 97.1 94.6 93.1 93.8 94.0 94.0 95.0
Skin
disease
Yes 22.9 53.2 17.1 17.7 59.6.0 48.7.0 19.5 51.0 52.0
No 77.1 46.8 82.9 82.3 40.4 51.3 80.5 49.0 48.0
Fever Yes 4.3 4.3 4.3 7.7 8.5 7.7 6.5 7.0 6.5
No 95.7 95.7 95.7 92.3 91.5 92.3 93.5 93.0 93.5
Total 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0
Source: Field Survey, 2011
4.6 Relationship between supply water uses and health impacts of CMC dwellers
In order to analyze the data more strictly an attempt has been made to statistically interpret the
relationship between supply water uses and various diseases in CMC. For this aspect a null hypothesis is
as, Ho : there is no association between supply water uses and human health (diseases) in CWASA in
CMC.
Chi square ( ) test has been performed after cross tabulation. Table 5 shows the results with the
levels of significance for the chi-square ( ) test. Rejecting the null hypothesis- there is no association or
significant difference of frequency occurring between perception of supply water uses and disease pattern
of CMC, the chi-square ( ) test results indicate that significant difference exists between uses of supply
water and water-borne disease patterns in CMC. The following table 5 shows that, diarrhoea in male,
female and children, dysentery in female, cholera in female , typhoid in children, skin disease in male,
female and children and family suffer due to water borne disease are significant with supply water uses in
study area-I. on the other hand, diarrhoea in male and female, dysentery in children, typhoid in children,
skin disease and family suffer due to water borne disease are significant with supply water uses in the
study area-II. Rest of disease is insignificant with supply water uses in both areas of Chittagong. Thus,
the results suggested that water quality is correlated and significant with different water borne diseases
like diarrhoea, cholera, typhoid and skin disease due to water borne disease in Chittagong metropolitan
city. Supply water is good for northern zone; study area-II than southern zone; study area-I.

26
Undesired quantity, restricted use and no alternate without supply water in the lower class
residential areas and middle class residential areas few people developed ground and roof reserve tank
(Bakalia and Bayejid Bostami thana residential areas in the study area-I and Pahartali, Double Mooring,
Halishahar, Kotwali, Bandor and Patenga thana residential areas in the study area-II). Availability of
supply water in the higher class residential areas (Chandgaon and Panchlaish thana residential areas in the
study area-I and Khulshi thana residential area in the study area-II) because people have developed
ground and roof reserve tank inside their house. The lower class residential areas are affected by various
water borne diseases than higher and middle class residential areas in Chittagong Metropolitan city.
Table 5: Relationships between supply water uses and health impacts of CMC dwellers
1st Variable 2
nd Variable
Study Area-I Study Area-II
df Sig.* df Sig.*
Su
pp
ly w
ate
r U
ses
Diarrhoea
Male 5.143 1 S 5.436 1 S
Female 6.182 1 S 6.588 1 S
Children 8.631 1 S 1.231 1 NS
Dysentery
Male 0.17 1 NS 0.228 1 NS
Female 6.389 1 S 8.532 1 S
Children 0.177 1 NS 0.402 1 NS
Cholera
Male 0.676 1 NS 0.190 1 NS
Female 8.676 1 S 0.190 1 NS
Children …. …. … 1.112 1 NS
Typhoid
Male 0.897 1 NS 0.181 1 NS
Female 0.929 1 NS 0.347 1 NS
Children 3.088 1 S 5.851 1 S
Skin
disease
Male 7.143 1 S 5.460 1 S
Female 9.375 1 S 7.074 1 S
Children 10.291 1 S 9.729 1 S
Fever
Male 0.058 1 NS 0.137 1 NS
Female 0.058 1 NS 0.346 1 NS
Children 0.058 1 NS 0.137 1 NS
*S= Significant *NS = Not Significant df = degree of freedom, Significance at the level of 0.025
5 Management techniques
5.1 Dealing with supply water scarcity
Supply water using pattern in CMC at household level depends on a number of things including family
size, income, occupation and lifestyles of the users. High class income groups use huge amount of water
for bathing, washing machine, flushing toilet and also abuse of water for gardening and vehicles clearing.
Middle class income group also have similar patterns of using supply water but in limited quantity. It is,
however, the lower class people who face water scarcity in the city at all time. If we can ensure public
awareness in managing supply water in CMC, especially in managing the water by above mentioned
categories than the situation can hopefully be improved. In general, the following (Table 6) categories are
found to be more irresponsible in supply water uses:

27
Table 6: Abuse of supply water in CMC by categories of uses
SI.No. Water using sector Rank*
01 Ablution (Muslim) (Lower, Middle and Higher R/A**) 1
02 Personal Hygienic (Lower, Middle and Higher R/A)
Face wash
2 Tooth brushing
Shave
Hand wash
03 Showering (Middle and Higher R/A) 3
04 Bathing (Lower, Middle and Higher R/A) 4
05 Bath tab (High R/A) 5
06 Flashing Toilet (High R/A) 6
07 Cloth washing (Lower, Middle and Higher R/A) 7
Source: In-depth interview, 2011
*Rank size considered by the respect of percentage
R/A**- Residential area
5.2 Demand and supply analysis
CWASA immediately take attempts to create and implement data base management practices such as
Demand Assessment, Population Assessment etc. The demand assessment for the present and future years
with respect to water supply should be based on present and future population estimates of the project
area i.e. equation, Qf = Pf ×q. Where, Qf, is the quantity of water requirement per day; Pf, is the projected
population estimated at the end of the design period; q, is the rate of consumption per capita per day. In
population assessment, the most widely used method is geometric progressive method. This is also known
as empirical method suggested by Hardenberg. The future population can be estimated by this method
using the following equation Pf = Pp (1+r), where, Pf, is the estimate of future population; Pp, is the
estimate of present population; r, rate of early growth; n, Number of year to be considered.
5.3 Online quality control assessment
CWASA should be promoting online quality control assessment from treatment plant to consumer,
households, and it should operate minimum two times in a day.
5.4 Setup overhead and reservoir
Chittagong city is situated on the undulating area. As a result, supplied water does not move optimally. It
is strongly recommended that in future setup, all types of overhead and reservoir should be built on the
hill tops (Figure 4). It helps the distribution of gravity flows; no need to lift pump, only need small boost
pump, easy operation and strong to electrical shortage etc.
Figure 4: Authors suggested above types of overhear setup on the hill tops or upland area in CMC.

28
5.5 Improve supply water quality
CMC dwellers assume that CWASA provide supplies of safe water in the City but it is contaminated on
the way by a number of means- inefficient distribution networks, illegal linkages, entrance of unexpected
materials during non-suction period, and unwise household practices e.g. keeping pot and underground
reservoirs. Present investigation reveals that of the remedial measures, about 38 percent respondents
believe enhancements of the system efficiency could be achieved by raising conscientiousness of
CWASA authority to ensure safe supply water from point (centre) of production to consumption-
households. About 28 percent respondents understood that filtering of supply water before drinking is
undoubtedly a safe method that can be used widely. About 17 percent of the respondents are found to be
in favour of boiling supply water before drinking (Table 7). Rest of the sample respondents believe that
supply water quality in the city could be further improved by the use of appropriate chemicals reduce
severity and magnitude of water borne diseases
Table 7: Improve supply water quality in CMC
Remedial measures Area-I
(N=70)
Area-II
(N=120)
Total
(N=200)
Boiling of supply water before drinking 22.22 13.33 16.66
Filtering of supply water before drinking 29.62 42.96 27.31
Use of safe water 4.93 7.40 6.48
Enhance responsibility of CWASA authority to ensure safe
supply water from production center to households
23.45 29.62 37.96
Use of proper chemical 6.17 0.7 2.77
Quality ensure by online …. 2.22 1.38
No answer 13.58 3.70 7.40
Total 100.0 100.0 100.0
Source: Field Survey, 2011
5.6 Provisions for staff training
CWASA should arrange training camps and workshops for laboratory level (scientific officer) to ensure
acceptable water quality, mechanical level (engineering) to ensure site selection, selection of pipe (metal
or plastic). Training of GIS map division, field personnel to ensure proper service connection,
rehabilitation of old pipe and setup new pipe, sluice valves and chamber repair including leakage or fault
line identification and repairing.
5.7 Reorientation in management approach: Bottom-up
This approach mainly put emphasis on stakeholder and users of supply water in the city. CWASA should
organized different programs/ types of initiatives like seminar, symposium, advertisement and campaign
etc. to ensure the participation all stakeholders. These are expected to be helpful for awareness building
which, in turn, will discourage unauthorized connection in city area. Some behavioural changes are also
expected from the supply water users; every morning before using the water for drinking or cooking
purposes, some water from the taps should get run for several minutes. Consumer should also be very
careful in storing water i.e. to store water safe and hygienically. pot should be washed out by bleaching
powder on a regular basis.

29
5.8 Community- based co-management governing system
The essential idea of community-based co-management system is the idea sharing of decision making and
management functions between CWASA, primary stakeholders (supply water users in the dwellers of
CMC) and other appropriate Government agencies. These approach not only put emphasis on the
collaborative and participatory process of regulatory decision- making among representatives of user
groups, CWASA governing agencies and research institutions but also empower the focused of groups
(lower and middle class income groups) who can easily play a vital role about sustainable uses of supply
water in CMC. It is strongly suggested that ‘community- based co-management governing system’
approach practices in CWASA should receive a priority, because these are helpful to improve quality,
reduce miss-management, ensure effective use of scarce water, knowledge-based analysis of demand and
supply, and directly integrate the governing body and primary stakeholders to reform and restructure of
every planning agenda at CWASA.
6. Conclusion
The overall finding of the study is that the various aspects of supply water quality in CMC including its
diverse use patterns and perceived health impacts are important factors to be considered for improved
water supply management in the city. In socio-economic terms, the lower class income group is more
affected (disadvantaged) by the water borne diseases than middle and upper class income groups in the
study area. Although regular water supply in the city is hindered by seasonality, there are other causes
such as electricity crises, load shading, system loss, and lack of network etc. that are responsible for
shortage or irregularity in the supply. It is suggested that CWASA should do everything possible on its
behalf to ensure regular supply of adequate and safe drinking water in the city. People then should drink
water after further treatment- boiling, filtering, using purifying tablet, fitcary- potassium alma etc. It is
also urged that people keep water saving appliances in their houses- clean water holding pot, reservoir
tanks etc., and raise people awareness in the city through campaigns. A reorientation in the management
policy (from top-down to bottom-up centered on community-based co-management approaches) can pave
the way for all concerned.
References
Ahmad, Q.K. 2000. Bangladesh Water Vision 2025 towards a sustainable water world In Q. K. Ahmad
(ed.). Bangladesh water vision. Bangladesh water partnership (BWP) -2000. pp, 3-32, Dhaka,
Bangladesh.
Ahmed, M.F. 1998. Problems of water supply in Dhaka metropolitan city. Present of the workshop on
problems and prospect of water supply in Dhaka metropolitan city. Dhaka, Bangladesh.
Amin, M. O. 2006. Status of Water and Sanitation Services in Chittagong Water Supply and Sewerage
Authority Bangladesh. Capacity Building Workshop on Partnerships for Improving the
Performance of Water Utilities in the Asia and the Pacific Region. UNCC, Bangkok. 25-27 July.
BBS 2008. Bangladesh Bureau of Statistic. Peoples Republic of Bangladesh. Dhaka. Bangladesh.
CDA. 2011. Chittagong Development Authority. Department of Geographical Information System.
Andarkilla, Chittagong, Bangladesh.
Choudhury, M.A.I, Ahmed, M. F, Bhuyan, M. A., Rahaman, M. H. 1997. Unaccounted- for water
management status in Bangladesh. Journal of water SRI-Aqua, U.K, Vol.46, p.no5.
CWASA . 2010. Preparation of Master plan for water supply and wastewater Management of the detailed
planned area of Chittagong. Chittagong, Bangladesh.
Gleick, P.H. 1996. Basic Water Requirements for Human Activities: Meeting Basic Needs. Water
International, Vol.21 No.2, Pp.83-92.
Lahlou, Z. M. 2002. Water quality in distribution system. Tech Brief, A National drinking water
clearinghouse fact sheet. West Virginia University.

30
Master plan for water supply (MPWS). 2009. Preparation of Master plan for water supply and
wastewater Management of the Detailed planned area of Chittagong. Chittagong, Bangladesh.
Population census. 2001. Population census, Ministry of Planning. People’s Republic of Bangladesh.
Dhaka, Bangladesh
UNICEF. 2006. UNICEF Handbook on Water Quality. United Nations Children's Fund (UNICEF). New
York, UNICEF, 3 UN Plaza, New York, NY 10017, New York.
http://www.unicef.org/publications/files/UNICEF_EFH_2005.pdf
WHO. 2002. Global water supply and sanitation Assessment 2000 Report. Iseman Creative, Washington
DC.
WHO. 2006. Water and Sanitation. Joint Monitoring Programme. USA,
http//www.wssinfo.org/who_2006.
WHO. 1984. Guidelines for Drinking Water Quality: Drinking water quality Control in Small Community
Supplies. World Health Organization, Geneva.
Top Related
Copyright © 2022 FDOKUMEN

