







Bahasa
Halaman
Hukum


Spectrum of HNF1B Mutations in a Large Cohort of PatientsWho Harbor Renal Diseases
Laurence Heidet,* Stephane Decramer,† Audrey Pawtowski,‡ Vincent Moriniere,*‡
Flavio Bandin,† Bertrand Knebelmann,§ Anne-Sophie Lebre,‡ Stanislas Faguer,†�
Vincent Guigonis,¶ Corinne Antignac,*‡**†† and Remi Salomon* **††
*Service de Nephrologie Pediatrique, Centre de Reference des Maladies Renales Hereditaires de l’Enfant et de l’Adulte,‡Departement de Genetique, and §Service de Nephrologie, Hopital Necker-Enfants Malades, Assistance Publique–Hopitaux de Paris, Paris, France; †Centre de Reference du Sud Ouest des Maladies Renales Rares, Service deNephrologie Pediatrique, Hopital Purpan, Toulouse, France; �Service de Nephrologie et Immunologie Clinique, HopitalRangueil, Toulouse, France; ¶Service de Pediatrie, Centre Hospitalier Universitaire de Limoges, Limoges, France;**INSERM, U574, Hopital Necker, Paris, France; and ††Universite Paris Descartes, Paris, France
Background and objectives: Hepatocyte nuclear factor 1� (HNF1�) is a transcription factor that is critical for the develop-ment of kidney and pancreas. In humans, mutations in HNF1B lead to congenital anomalies of the kidney and urinary tract,pancreas atrophy, and maturity-onset diabetes of the young type 5 and genital malformations.
Design, setting, participants, & measurements: We report HNF1B screening in a cohort of 377 unrelated cases with variouskidney phenotypes (hyperechogenic kidneys with size not more than �3 SD, multicystic kidney disease, renal agenesis, renalhypoplasia, cystic dysplasia, or hyperuricemic tubulointerstitial nephropathy not associated with UMOD mutation).
Results: We found a heterozygous mutation in 75 (19.9%) index cases, consisting of a deletion of the whole gene in 42,deletion of one exon in one, and small mutations in 32. Eighteen mutations were novel. De novo mutations accounted for 66%of deletions and 40% of small mutations. In patients who carried HNF1B mutation and for whom we were able to studyprenatal ultrasonography (56 probands), isolated hyperechogenic kidneys with normal or slightly enhanced size were themore frequent (34 of 56) phenotype before birth. Various other prenatal renal phenotypes were associated with HNF1Bmutations, at a lesser frequency. Diabetes developed in four probands. Hyperuricemia and hypomagnesemia, although notsystematically investigated, were frequently associated.
Conclusions: This large series showed that the severity of the renal disease associated with HNF1B mutations was extremelyvariable (from prenatal renal failure to normal renal function in adulthood) and was not correlated with the genotype.
Clin J Am Soc Nephrol 5: 1079–1090, 2010. doi: 10.2215/CJN.06810909
H epatocyte nuclear factor 1� gene (HNF1B) encodes atranscription factor that binds DNA as homodimeror as heterodimer with the related factor HNF1�.
Heterozygous mutations of HNF1B were first described in ma-turity-onset diabetes of the young type 5 (1). Renal manifesta-tions are frequently observed in patients with maturity-onsetdiabetes of the young type 5 and include a wide spectrum ofphenotypes (2). More recently, HNF1B mutations were found tobe associated with a subset of fetal bilateral hyperechogenickidneys (3) and other kidney diseases diagnosed before birth(4). Besides diabetes, nonrenal anomalies involving Mullerianand Wolffian derivatives, liver and pancreas abnormalities,
hyperuricemia with or without gout (5), and hypomagnesemia(6) have been reported.
HNF1B plays a crucial role in early development (7) andthereafter is involved in the organogenesis of several tissues,such as gut, pancreas, liver, lung, and kidney. The gene isalso transiently expressed in the neural tube and in theepididymis, vas deferens, seminal vesicle, prostate, uterus,and oviduct (7,8). During kidney development, the gene isexpressed in the ureteric bud, in the comma- and S-shapedbodies, and then in the proximal and distal tubules but not inthe glomerulus (9). Kidney-specific inactivation of Hnf1B inthe mouse leads to cystic disease, and HNF1� was shown tobind directly DNA elements that regulate the expression ofgenes whose mutations are responsible for cystic kidneydiseases (Nphp1, polaris, Umod, Pkhd1, and Pkd2) (10) or of agene identified as a candidate modifier in a mouse model ofcystic kidney disease (Kif12) (11). Here we report on HNF1Bmutation screening in a series of 377 unrelated patients whopresented with various kidney phenotypes, giving specialattention to the prenatal renal phenotypes.
Received September 24, 2009. Accepted March 5, 2010.
Published online ahead of print. Publication date available at www.cjasn.org.
L.H. and S.D. contributed equally to this work.
Correspondence: Dr. Laurence Heidet, Service de Nephrologie Pediatrique, Ho-pital Necker-Enfants Malades, 149 rue de Sevres, 75015 Paris, France. Phone:�33-1-44-49-43-82; Fax: �33-1-71-19-64-45; E-mail: [email protected]
Copyright © 2010 by the American Society of Nephrology ISSN: 1555-9041/506–1079

Materials and MethodsPatients
This is a retrospective study in which we included all cases that werenot previously reported and were tested for HNF1B mutations in tworeference centers for rare kidney diseases in France. Criteria for inclu-sion were hyperechogenic kidneys (but with size not more than �3 SD),uni- or bilateral multicystic kidney disease (MCD), renal agenesis, renalhypoplasia, cystic dysplasia, or hyperuricemic tubulointerstitial ne-phropathy not associated with UMOD mutation. Patients’ samples,medical records, genealogy, and written informed consent from patientand/or parents were sent from Pediatric, Pediatric Nephrology, Ne-phrology, or Obstetric Departments. Genomic DNA was extracted fromvenous blood or tissues collected from 377 unrelated cases (271 chil-dren, 57 adults, and 49 fetuses), 221 male and 156 female.
Prenatal ultrasonographs were available for 245 probands (usuallyperformed at 12, 22, and 32 weeks of amenorrhea) and had beenconsidered as normal in only 11 cases. Renal phenotypes before birthwere isolated hyperechogenic kidneys (not larger than �3 SD in size) in55 cases, bilateral MCD (13 cases), unilateral MCD (74 cases), unilateralagenesis (34 cases), bilateral agenesis (13 cases), renal hypoplasia (25cases), urinary tract dilation (11 cases), and cystic disease (nine cases).In 132 patients, either the result of the prenatal ultrasound was notknown or ultrasound was not performed (patients born before 1980).Renal phenotypes after birth were hyperechogenic kidneys (23 cases),unilateral MCD (12 cases), unilateral agenesis (8 cases), renal hypopla-sia (33 cases), urinary tract dilation (2 cases), hyperuricemic tubuloin-terstitial nephritis (18 cases), unclassified cystic disease (35 cases), andonly extrarenal symptoms (diabetes and uterine abnormalities; onecase).
Patients with renal cavity dilation and/or recurrent acute pyelone-phritis had voiding cystourethrogram. GFR was estimated by the Mod-ification of Diet in Renal Disease (MDRD) formula for adults and by theSchwartz formula for children who were younger than 16.
Molecular AnalysisQuantitative multiplex PCR amplification of short fluorescence frag-
ments (12) was performed as described previously (13) for the search ofdeletion. When deletion was not found, the nine exons and the exon–intron boundaries of the gene were screened for mutations by directsequencing as described previously (1).
Statistical AnalysisTesting for difference in proportions was performed using the �2. All
tests were two sided. P � 0.05 was considered significant.
ResultsMutations
Heterozygous HNF1B alterations, which are thought to bepathogenic, were found in 75 probands (41 male and 34 fe-male), leading to a mutation detection rate of 19.9% of testedindex cases. They consisted of a heterozygous deletion of theentire gene in 42 cases (Table 1). Parent status was studied for21 probands: deletions were de novo in 14 of 21 cases andinherited in seven of 21. Mutations that were not deletions ofthe entire gene are shown in Table 2. One patient was carryinga de novo heterozygous deletion of exon 4, which was previ-ously reported (3,13). Twenty-four different heterozygoussmall mutations (11 missense, five nonsense, five frameshift,and three splice site mutations) were found in 32 probands.Parent status was studied for 20 of them. Mutation were shown
to be de novo in eight of 20 cases and to be inherited in 12 of 20cases; 18 were novel. Except for the mutation affecting theinitiator codon, all missense mutations were localized in theDNA binding domain (Figure 1), were modifying a conservedamino acid, and were predicted to be probably damaging bythe Polyphen program (14). In some families, there was afather-to-son transmission, in agreement with an autosomaldominant mode of inheritance (see proband 64 as an example).
Renal and Extrarenal PhenotypePatients for Whom Prenatal Ultrasound Was AvailableIn 245 cases tested for HNF1B mutation, we were able to go
back to the prenatal ultrasound. Mutations were identified in 56of them.
Prenatal phenotype in patients with HNF1B mutation wasisolated bilateral hyperechogenic kidneys with normal or mod-erately enlarged size in 34 cases, including one termination ofpregnancy (TOP) because of an associated oligo-anamnios.Evaluation of these patients at last follow-up showed renalfailure with GFR �80 ml/min per 1.73 m2 (range 32 to 61ml/min per 1.73 m2) in eight patients (1 months to 14 yearsold), GFR �80 ml/min per 1.73 m2 in 20 patients (1 to 17 yearsold), and unknown in five patients. Five patients experiencedtransitory renal failure at birth, and one developed diabetes atthe age of 17.
Other prenatal phenotypes in patients with HNF1B mutationwere bilateral MCD (leading to TOP) in two patients, unilateralMCD in eight patients, unilateral renal agenesis (with hypopla-sia and/or cysts on the single kidney) in four patients, unilat-eral renal hypoplasia in one patient, renal macrocysts in threepatients (with urinary tract dilation, pancreas hypoplasia, andTOP in one patient), and isolated upper urinary tract dilation inone patient (who developed small cortical cysts after birth). Inthree patients who presented with severe cystic dysplasia onearly ultrasound, the prenatal ultrasounds were considered asnormal. In all cases with unilateral MCD, patients developedpostnatal anomalies on the contralateral kidney. In the casewith unilateral hypoplasia, cysts developed on the hypoplastickidney after birth
Patients for Whom Prenatal Ultrasound Was not AvailableIn 132 patients who were tested for HNF1B mutation, we
were not able to go back to prenatal ultrasound (either theresult of it was not known, or ultrasound was not performed).We found an HNF1B mutation in 19 of them, including 10 whowere tested during adulthood, six of whom had a family his-tory of renal diseases. Four adult probands had cystic renalhypoplasia (associated with hypomagnesemia, gout, and a di-abetes that occurred at 42 years in one and with gestationaldiabetes in another). Two had hyperechogenic kidneys withmicrocysts. One had solitary kidney and early gout, and an-other one had hyperuricemic interstitial nephropathy. One fe-male born from consanguineous parents developed unclassi-fied renal cystic dysplasia with uterus agenesis, imperforatedvagina, cleft palate, and mental retardation. One presentedwith diabetes at the age of 31 and bicornuate uterus. Fouradults (aged 29 to 35 years) had normal renal function and five(aged 28 to 33 years) had reduced GFR (65 ml/min per 1.73 m2
1080 Clinical Journal of the American Society of Nephrology Clin J Am Soc Nephrol 5: 1079–1090, 2010

Tab
le1.
Phen
otyp
esin
prob
and
sw
ith
com
plet
eH
NF1
Bd
elet
ions
Prob
and
sPr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Del
etio
nIn
heri
tanc
e
1N
orm
alul
tras
ound
Lar
geki
dne
ysw
ith
num
erou
sbi
late
ral
cyst
s,pr
eter
min
alre
nal
failu
reat
8m
onth
s;fa
ther
wit
hre
nal
hypo
plas
ia,G
FRun
know
n
ND
(par
ents
not
test
ed)
2N
orm
alul
tras
ound
Hyp
erec
hoge
nic
and
cyst
icki
dne
ys,n
orm
alG
FRat
6ye
ars
De
novo
3B
ilate
ral
hype
rech
ogen
icki
dne
ysH
yper
echo
geni
c,no
rmal
-siz
edki
dne
ys,n
orm
alG
FRat
10m
onth
sN
D(p
aren
tsno
tte
sted
)
4B
ilate
ral
hype
rech
ogen
icki
dne
ysH
yper
echo
geni
cki
dne
ys,m
ulti
ple
mic
rocy
sts,
CR
F(G
FR29
at6
year
s);m
othe
rw
ith
rena
lcy
sts.
Del
etio
nin
the
mot
her
5B
ilate
ral
hype
rech
ogen
icki
dne
ysH
yper
echo
geni
c,no
rmal
-siz
edki
dne
ys,m
icro
cyst
s,no
rmal
GFR
at5
year
sN
D(p
aren
tsno
tte
sted
)
6U
nila
tera
lhy
popl
asia
Uni
late
ral
hypo
plas
iaw
ith
cyst
s,no
rmal
GFR
at2
year
sD
eno
voFa
ther
and
pate
rnal
gran
dm
othe
rw
ith
rena
lcy
sts
7B
ilate
ral
hype
rech
ogen
icki
dne
ysSm
all
cyst
icki
dne
ys,n
orm
alG
FRat
3ye
ars
ND
(par
ents
not
test
ed)
8B
ilate
ral
hype
rech
ogen
icki
dne
ysN
orm
al-s
ized
kid
ney
wit
hco
rtic
alcy
sts
�le
ftPU
JOhy
peru
rice
mia
,nor
mal
GFR
at5
year
sN
D(p
aren
tsno
tte
sted
)
9U
nila
tera
lM
CD
,con
tral
ater
alcy
sts
Uni
late
ral
MC
D,c
orti
cal
cyst
son
cont
rala
tera
lki
dne
y,hy
peru
rice
mia
,ele
vate
dliv
eren
zym
es,n
orm
alG
FRat
10ye
ars
ND
(par
ents
not
test
ed)
10B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
cort
ical
cyst
s,no
rmal
-siz
edki
dne
y,no
rmal
GFR
at17
mon
ths;
fath
erw
ith
rena
lhy
pod
yspl
asia
,GFR
unkn
own;
pate
rnal
gran
dfa
ther
has
CR
F;pr
evio
usT
OP
for
MC
Dan
dan
amni
osin
the
mot
her
ND
(par
ents
not
test
ed)
11N
DD
iabe
tes,
bico
rnua
teut
erus
TO
Pin
the
past
beca
use
ofan
amni
os,n
orm
alG
FRat
adul
tag
e;d
iabe
tes
insi
ster
san
dfa
ther
Del
etio
nin
the
fath
er
12B
ilate
ral
hype
rech
ogen
icki
dne
ysFe
wcy
sts,
unkn
own
GFR
De
novo
13U
nila
tera
lM
CD
,con
tral
ater
alhy
pere
chog
enic
kid
ney
Cys
tsin
the
sing
leki
dne
y,no
rmal
GFR
at9
year
sN
D(p
aren
tsno
tte
sted
)
14B
ilate
ral
hype
rech
ogen
icki
dne
ys,o
neco
rtic
alcy
stH
yper
echo
geni
cla
rge
(�2
SD)
kid
neys
,CR
F(u
nkno
wn
GFR
)at
1m
onth
De
novo
15N
DC
ysti
cki
dne
yd
isea
se,u
teri
neag
enes
is,i
mpe
rfor
ated
vagi
na,
men
tal
reta
rdat
ion,
norm
alG
FRat
29ye
ars
ND
(par
ents
not
test
ed)
16B
ilate
ral
pelv
icd
ilati
onB
ilate
ral
PUJO
,uni
late
ral
smal
lco
rtic
alcy
sts,
norm
alG
FRat
14m
onth
sD
eno
vo
17B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
cort
ical
cyst
s,no
rmal
GFR
at3
year
s;br
othe
rw
ith
pelv
icki
dne
yan
dPU
JO;m
othe
rw
ith
norm
alki
dne
ysan
dno
rmal
GFR
,lef
the
pati
cag
enes
is,p
ancr
eas
head
hypo
plas
ia,b
icor
nuat
eut
erus
Del
etio
nin
the
mot
her
Clin J Am Soc Nephrol 5: 1079–1090, 2010 Renal Phenotypes and HNF1B Mutations 1081

Tab
le1.
cont
inue
d
Prob
and
sPr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Del
etio
nIn
heri
tanc
e
18B
ilate
ral
hype
rech
ogen
icki
dne
ysFe
wcy
sts,
norm
al-s
ized
hype
rech
ogen
icki
dne
ys,n
eona
tal
rena
lfa
ilure
,nor
mal
GFR
at20
mon
ths;
mot
her
wit
hcy
sts
and
gest
atio
nal
dia
bete
s
Del
etio
nin
the
mot
her
19B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
cort
ical
cyst
s,no
rmal
GFR
at5
year
s;m
othe
rw
ith
rena
lcy
sts
and
seve
rech
oles
tasi
sD
elet
ion
inth
em
othe
r
20N
DB
ilate
ral
cyst
s,no
rmal
GFR
at11
year
sN
D(p
aren
tsno
tte
sted
)21
Bila
tera
lhy
pere
chog
enic
kid
neys
,cor
tica
lcy
sts
(MR
I),d
iaph
ragm
atic
hern
ia
Ded
iffe
rent
iate
dki
dne
ys(5
4an
d58
mm
)w
ith
cyst
s,ac
ute
rena
lfa
ilure
atbi
rth,
GFR
40m
l/m
inpe
r1.
73m
2at
2m
onth
s
De
novo
22B
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
cyst
s,ol
igoa
mni
os
TO
P;re
nal
hist
olog
ysh
owed
cyst
icd
ilati
onof
near
lyal
lgl
omer
uli
wit
hco
llaps
edfl
ocul
us,g
lom
erul
arcy
sts
wer
elin
edby
fibr
osis
,int
erst
itia
lfi
bros
isw
ith
rare
fied
tubu
les
De
novo
23N
DB
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
mic
rocy
sts,
norm
alG
FRat
17ye
ars
De
novo
24N
DB
ilate
ral
cort
ical
mic
rocy
sts,
bico
rnua
teut
erus
,dia
bete
s,no
rmal
GFR
at20
year
sN
D(p
aren
tsno
tte
sted
)
25N
DB
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
mic
rocy
sts,
norm
alG
FRat
3ye
ars
ND
(par
ents
not
test
ed)
26B
ilate
ral
hype
rech
ogen
icki
dne
ys,p
elvi
cd
ilati
onB
ilate
ral
hype
rech
ogen
ichy
popl
asti
cki
dne
ys,u
nkno
wn
GFR
,m
icro
cyst
sin
mot
her
Del
etio
nin
the
mot
her
27N
DB
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
mic
rocy
sts,
CR
F(G
FR65
at30
year
s)N
D(p
aren
tsno
tte
sted
)
28B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
hype
rech
ogen
icki
dne
ysC
RF
(GFR
40at
3ye
ars)
ND
(par
ents
not
test
ed)
29N
DB
ilate
ral
hype
rech
ogen
icki
dne
ysco
rtic
alm
icro
cyst
s,no
rmal
GFR
at35
year
s;m
othe
rw
ith
type
2d
iabe
tes
ND
(par
ents
not
test
ed)
30N
DB
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
mic
rocy
sts,
norm
alG
FRat
6ye
ars;
mic
rocy
stic
sole
kid
ney
inm
othe
rN
D(p
aren
tsno
tte
sted
)
31B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
hype
rech
ogen
icki
dne
ys,C
RF
(GFR
35at
1ye
ar)
ND
(par
ents
not
test
ed)
32B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
hype
rech
ogen
icki
dne
ys,d
iabe
tes
at17
year
s,no
rmal
GFR
at20
year
sN
D(p
aren
tsno
tte
sted
)
33B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
hype
rech
ogen
icki
dne
ys,n
orm
alG
FRat
1ye
arD
eno
vo
34U
nila
tera
lM
CD
,oth
erki
dne
yhy
pere
chog
enic
Uni
late
ral
MC
D,o
ther
kid
ney
hype
rech
ogen
icw
ith
pelv
icd
ilati
on,n
orm
alG
FRat
3ye
ars
De
novo
35B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
hype
rech
ogen
icki
dne
ys,n
orm
alG
FRat
15ye
ars
De
novo
1082 Clinical Journal of the American Society of Nephrology Clin J Am Soc Nephrol 5: 1079–1090, 2010

to end-stage renal failure), and renal function was unknown forone.
We found an HNF1B mutation in nine patients who weretested during childhood, two of whom had a family history ofrenal disease. Eight probands had hyperechogenic kidney andcysts and one hypoplastic kidney and/or uterus anomalies (n �
2) and/or pancreatic hypoplasia (n � 1). One developed dia-betes at the age of 20 years. Renal function was normal in sixpatients (aged 3 to 20 years) and altered three times (aged 4 to15 years).
Genotype–Phenotype CorrelationThe severity of the renal disease that is associated with
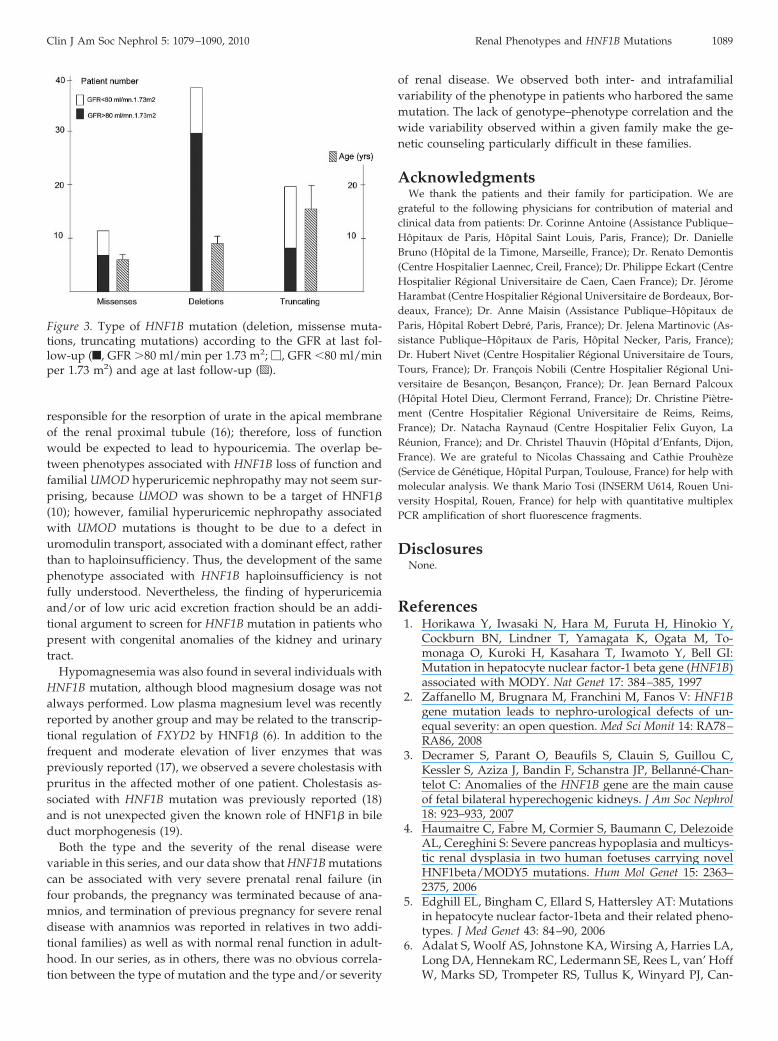
HNF1B mutation was extremely variable (from prenatal severerenal failure to normal renal function in adulthood). The type ofmutation (deletion of the whole gene; missense mutation; ortruncating mutation because of nonsense, frameshift, or splicemutation) was analyzed according to the renal phenotype forthe 75 probands who carried an HNF1B mutation, as well as forother affected family members when their kidney phenotypewas known (Figure 2). The percentage of each type of mutationwas not statistically different when the group of patients whohad prenatal hyperechogenic kidneys was compared with agroup that included all other patients. We also looked for arelation between the type of mutation and the severity of thedisease in terms of renal failure, independent of the type ofrenal disease. The patients with severe and early renal failure(six patients with TOP for oligohydramnios and six patientswith terminal or preterminal renal failure that occurred beforethe age of 4 years) were associated either with deletions (sevenpatients), truncating mutation (three patients), or missense mu-tations (two patients), a figure that is not different from theproportion of each type of mutation in all patients. Figure 3shows the number of patients with and without renal failure foreach type of mutation. The proportion of patients with renalfailure at last follow-up was significantly (P � 0.012) higher inpatients who carried a truncating mutation than in patientswho carried an HNF1B deletion; however, for unknown rea-sons, patients with truncating mutation were older than pa-tients with gene deletion at last follow-up. This age differencemay account, at least in part, for the different severity of therenal failure.
DiscussionTo our knowledge, we report here the largest series of phe-
notypic and genetic analysis of patients who harbor renal dis-eases that are associated with HNF1B mutations. We screened377 unrelated patients and identified an HNF1B mutation ordeletion in 75 unrelated cases: 10 adults and 65 children orfetuses. This rate of mutation (19.9%) is not significantly differ-ent from that (23%) recently reported in a smaller cohort ofchildren with renal malformation (6). Going back to the prena-tal ultrasound when available, we report the renal phenotypesbefore birth in patients with HNF1B mutation and analyzed theevolution of their renal function.
We had information regarding prenatal ultrasound for 245patients, and this study confirms our previous finding thatT
able
1.co
ntin
ued
Prob
and
sPr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Del
etio
nIn
heri
tanc
e
36B
ilate
ral
hype
rech
ogen
icki
dne
ys�
unila
tera
lm
acro
cyst
s
Bila
tera
lhy
pere
chog
enic
kid
neys
�un
ilate
ral
mac
rocy
sts,
CR
F(G
FR55
at3
year
s)D
eno
vo
37U
nila
tera
lM
CD
,oth
erki
dne
yhy
pere
chog
enic
Uni
late
ral
MC
D,h
yper
echo
geni
cki
dne
y,no
rmal
GFR
at6
year
sD
eno
vo
38B
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
mic
rocy
sts
Bila
tera
lhy
pere
chog
enic
kid
neys
,cor
tica
lm
icro
cyst
s,no
rmal
GFR
at6
year
sD
eno
vo
39U
nila
tera
lag
enes
isSi
ngle
hype
rech
ogen
icki
dne
y,co
rtic
alm
icro
cyst
s,no
rmal
GFR
at10
year
sN
D(p
aren
tsno
tte
sted
)
40U
nila
tera
lag
enes
is,
hype
rech
ogen
icki
dne
yw
ith
mic
rocy
sts
Sing
lehy
pere
chog
enic
kid
ney,
mic
rocy
sts,
CR
F(G
FR23
at1
year
);si
ngle
kid
ney
wit
hcy
sts
inth
em
othe
r(G
FR75
at30
year
s)
Del
etio
nin
the
mot
her
41B
ilate
ral
hype
rech
ogen
icki
dne
ysB
ilate
ral
hype
rech
ogen
icki
dne
ys,u
nila
tera
lV
UR
,unk
now
nG
FRN
D(p
aren
tsno
tte
sted
)
42N
DB
ilate
ral
hype
rech
ogen
icki
dne
ys,c
orti
cal
mic
rocy
sts,
norm
alG
FRat
3ye
ars
ND
(par
ents
not
test
ed)
CR
F,ch
roni
cre
nal
failu
re;M
RI,
mag
neti
cre
sona
nce
imag
ing;
ND
,not
don
e;PU
JO,p
elvi
-ure
teri
cju
ncti
onob
stru
ctio
n;V
UR
,ves
icou
rete
ral
refl
ux.
Clin J Am Soc Nephrol 5: 1079–1090, 2010 Renal Phenotypes and HNF1B Mutations 1083

Tab
le2.
Mut
atio
nsan
dph
enot
ypes
inpa
tien
tsw
ith
HN
F1B
mut
atio
nsth
atar
eno
tco
mpl
ete
del
etio
ns
Prob
and
sN
ucle
otid
eC
hang
ePr
otei
nC
hang
eE
xon
(Int
ron)
Ref
eren
cePr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Mut
atio
nIn
heri
tanc
e
43c.
3G3
Ap.
Met
1Ile
1T
his stud
yB
ilate
ral
cort
ical
cyst
sB
ilate
ral
cort
ical
mic
rocy
sts,
norm
alG
FRat
7ye
ars;
fath
erw
ith
rena
lcy
sts
Mut
atio
nin
the
fath
er
44c.
3G3
Ap.
Met
1Ile
Bila
tera
lco
rtic
alcy
sts
Bila
tera
lco
rtic
alm
icro
cyst
s,no
rmal
GFR
at7
year
s;fa
ther
wit
hd
iabe
tes
and
rena
lcy
sts
Mut
atio
nin
the
fath
er
45c.
211
del
AA
GG
GC
Cp.
Lys
71fs
1T
his stud
yN
DH
ypod
yspl
asti
cki
dne
ysw
ith
mic
rocy
sts,
GFR
45at
28ye
ars;
fath
erw
ith
hype
ruri
cem
icne
phro
path
y(G
FRun
know
n)
Mut
atio
nin
the
fath
er
46c.
232G3
Tp.
Glu
78X
1T
his stud
yN
orm
alul
tras
ound
Bila
tera
lco
rtic
alcy
sts,
ESR
Fat
3m
onth
sD
eno
vo
47c.
232G3
Tp.
Glu
78X
1M
CD
�2
TO
P;se
ptat
edut
erus
ND
48c.
322
del
Gp.
Ala
108f
s1
Thi
s stud
yN
DH
yper
uric
emic
neph
ropa
thy,
ESR
Fat
33ye
ars;
fath
erw
ith
hype
ruri
cem
icne
phro
path
y(w
ith
kid
ney
graf
t)an
dd
iabe
tes
Mut
atio
nin
the
fath
er
49IV
S134
5–1G3
A(1
)T
his stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lco
rtic
alcy
sts,
neon
atal
rena
lfa
ilure
,no
rmal
GFR
at8
year
s
ND
50IV
S134
5–1G3
A(1
)U
nila
tera
lag
enes
is�
hype
rech
ogen
icki
dne
y
Sing
lehy
pere
chog
enic
kid
ney
�C
RF
(GFR
25at
17ye
ars)
ND
(par
ents
not
test
ed)
51c.
452C3
Gp.
Ser1
51C
ys2
Thi
s stud
yU
nila
tera
lM
CD
Uni
late
ral
MC
Dan
dco
rtic
alcy
sts
onth
eot
her
kid
ney,
norm
alG
FRat
6ye
ars
ND
52c.
476C3
Tp.
Pro1
59L
eu2
Thi
s stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Isol
ated
hype
rech
ogen
icki
dne
ys,u
ltra
soun
dno
rmal
ized
(siz
ean
dec
hoge
nici
ty)
at10
mon
ths,
norm
alG
FRat
10m
onth
s
ND
1084 Clinical Journal of the American Society of Nephrology Clin J Am Soc Nephrol 5: 1079–1090, 2010

Tab
le2.
cont
inue
d
Prob
and
sN
ucle
otid
eC
hang
ePr
otei
nC
hang
eE
xon
(Int
ron)
Ref
eren
cePr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Mut
atio
nIn
heri
tanc
e
53c.
494
G3
Ap.
Arg
165H
is2
(20)
ND
Smal
lhy
pere
chog
enic
kid
neys
,CR
F(G
FR16
at4
year
s);f
athe
rw
ith
rena
lfa
ilure
and
dia
bete
s
ND
54c.
494G3
Cp.
Arg
165P
ro2
Thi
s stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lhy
pere
chog
enic
hypo
plas
tic
kid
neys
CR
F(G
FR32
at10
year
s)�
panc
reat
ichy
popl
asia
De
novo
55c.
513G3
Ap.
Trp
171X
2T
his stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lco
rtic
alcy
sts,
norm
alG
FRat
11m
onth
sN
D
56IV
S254
4�
3del
AA
GT
(2)
(6)
ND
Ren
alcy
sts
and
VU
R,
norm
alG
FRat
6ye
ars;
mot
her
wit
hun
ilate
ral
cyst
san
dge
stat
iona
ld
iabe
tes,
norm
alG
FRat
30ye
ars
Mut
atio
nin
the
mot
her
57IV
S254
4�
3del
AA
GT
(2)
ND
Sing
leki
dne
y,go
ut,C
RF
(GFR
25at
65ye
ars)
;m
othe
ran
dm
ater
nal
cous
inw
ith
rena
lfa
ilure
;d
augh
ter
wit
hsi
ngle
kid
ney
ND
58IV
S254
4�
3del
AA
GT
(2)
ND
Cys
ts,C
RF
(GFR
60at
33ye
ars)
,dia
bete
s,hy
peru
rice
mia
,ele
vate
dliv
eren
zym
es,
hypo
mag
nesa
emia
;fat
her
wit
hE
SRF
ND
59c.
544C3
Tp.
Gln
182X
2(2
0)N
DH
yper
echo
geni
cki
dne
ys,
CR
F(b
utun
know
nG
FR);
dia
bete
sin
the
mot
her.
Mut
atio
nin
the
mot
her
60c.
544C3
Tp.
Gln
182X
2U
nila
tera
lM
CD
,oth
erki
dne
yw
ith
cyst
sU
nila
tera
lM
CD
,oth
erki
dne
yw
ith
cort
ical
cyst
s,no
rmal
GFR
at3
mon
ths
ND
61c.
544C3
Tp.
Gln
182X
2U
nila
tera
lag
enes
isSi
ngle
hypo
plas
tic
hype
rech
ogen
icki
dne
y,C
RF
(GFR
55at
7ye
ars)
ND
Clin J Am Soc Nephrol 5: 1079–1090, 2010 Renal Phenotypes and HNF1B Mutations 1085
Tab
le2.
cont
inue
d
Prob
and
sN
ucle
otid
eC
hang
ePr
otei
nC
hang
eE
xon
(Int
ron)
Ref
eren
cePr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Mut
atio
nIn
heri
tanc
e
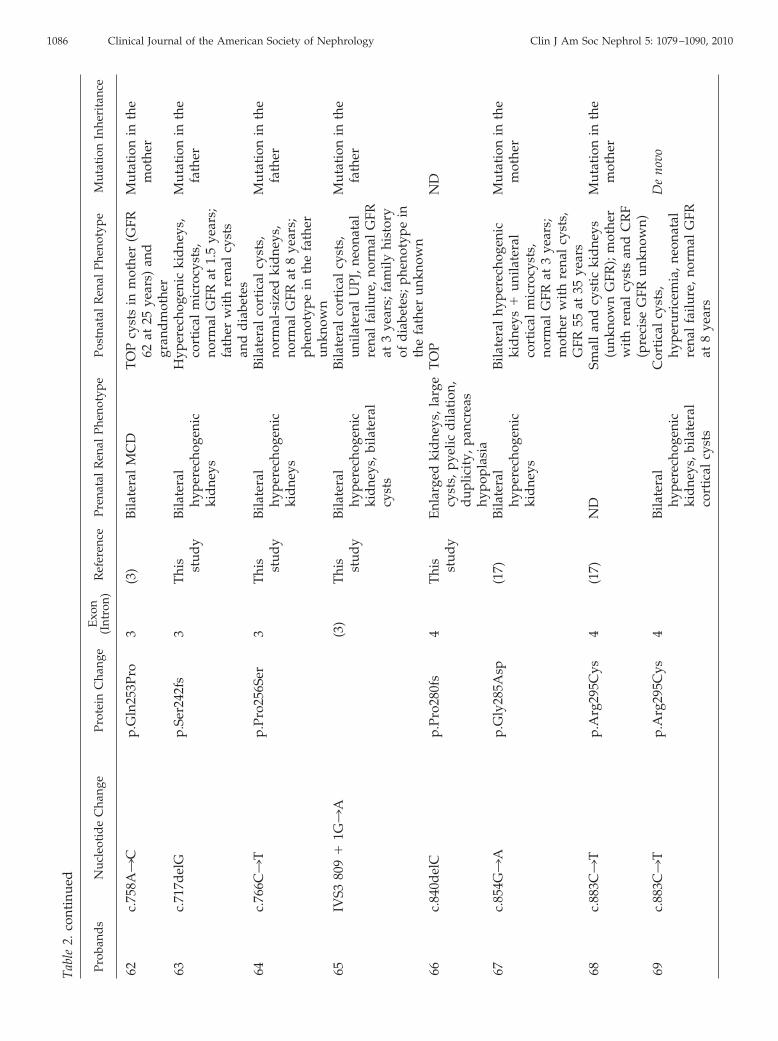
62c.
758A3
Cp.
Gln
253P
ro3
(3)
Bila
tera
lM
CD
TO
Pcy
sts
inm
othe
r(G
FR62
at25
year
s)an
dgr
and
mot
her
Mut
atio
nin
the
mot
her
63c.
717d
elG
p.Se
r242
fs3
Thi
s stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Hyp
erec
hoge
nic
kid
neys
,co
rtic
alm
icro
cyst
s,no
rmal
GFR
at1.
5ye
ars;
fath
erw
ith
rena
lcy
sts
and
dia
bete
s
Mut
atio
nin
the
fath
er
64c.
766C3
Tp.
Pro2
56Se
r3
Thi
s stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lco
rtic
alcy
sts,
norm
al-s
ized
kid
neys
,no
rmal
GFR
at8
year
s;ph
enot
ype
inth
efa
ther
unkn
own
Mut
atio
nin
the
fath
er
65IV
S380
9�
1G3
A(3
)T
his stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys,b
ilate
ral
cyst
s
Bila
tera
lco
rtic
alcy
sts,
unila
tera
lU
PJ,n
eona
tal
rena
lfa
ilure
,nor
mal
GFR
at3
year
s;fa
mily
hist
ory
ofd
iabe
tes;
phen
otyp
ein
the
fath
erun
know
n
Mut
atio
nin
the
fath
er
66c.
840d
elC
p.Pr
o280
fs4
Thi
s stud
yE
nlar
ged
kid
neys
,lar
gecy
sts,
pyel
icd
ilati
on,
dup
licit
y,pa
ncre
ashy
popl
asia
TO
PN
D
67c.
854G3
Ap.
Gly
285A
sp(1
7)B
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lhy
pere
chog
enic
kid
neys
�un
ilate
ral
cort
ical
mic
rocy
sts,
norm
alG
FRat
3ye
ars;
mot
her
wit
hre
nal
cyst
s,G
FR55
at35
year
s
Mut
atio
nin
the
mot
her
68c.
883C3
Tp.
Arg
295C
ys4
(17)
ND
Smal
lan
dcy
stic
kid
neys
(unk
now
nG
FR);
mot
her
wit
hre
nal
cyst
san
dC
RF
(pre
cise
GFR
unkn
own)
Mut
atio
nin
the
mot
her
69c.
883C3
Tp.
Arg
295C
ys4
Bila
tera
lhy
pere
chog
enic
kid
neys
,bila
tera
lco
rtic
alcy
sts
Cor
tica
lcy
sts,
hype
ruri
cem
ia,n
eona
tal
rena
lfa
ilure
,nor
mal
GFR
at8
year
s
De
novo
1086 Clinical Journal of the American Society of Nephrology Clin J Am Soc Nephrol 5: 1079–1090, 2010

Tab
le2.
cont
inue
d
Prob
and
sN
ucle
otid
eC
hang
ePr
otei
nC
hang
eE
xon
(Int
ron)
Ref
eren
cePr
enat
alR
enal
Phen
otyp
ePo
stna
tal
Ren
alPh
enot
ype
Mut
atio
nIn
heri
tanc
e
70c.
895T3
GpT
rp29
9Gly
4T
his stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys,b
ilate
ral
cort
ical
mic
rocy
sts
Bila
tera
lhy
pere
chog
enic
kid
neys
,cor
tica
lm
icro
cyst
sC
RF
(GFR
51at
3ye
ars)
ND
71c.
766C3
Tp.
Asn
302L
ys4
Thi
s stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lco
rtic
alcy
sts,
CR
F(G
FR60
at7
year
s)N
D
72E
xon
4d
elet
ion
c.81
0_10
45d
el23
6p.
Arg
270f
s4
(3,1
3)U
nila
tera
lM
CD
Abs
ence
ofhy
pert
roph
yof
the
cont
rala
tera
lki
dne
y,V
UR
,CR
F(G
FR65
at4
year
s)
De
novo
73c.
1136
C3
Ap.
Ser3
79X
5T
his stud
yN
DH
yper
echo
geni
cki
dne
ys,
cort
ical
mic
rocy
sts,
CR
F(G
FR61
at15
year
s),
did
elph
icut
erus
�pa
ncre
atic
hypo
plas
ia
De
novo
74c.
1360
C3
Tp.
Gln
454X
7T
his stud
yU
nila
tera
lM
CD
,oth
erki
dne
yhy
pere
chog
enic
Uni
late
ral
MC
D,o
ther
kid
ney
hype
rech
ogen
icw
ith
cort
ical
mic
rocy
sts,
norm
alG
FRat
2ye
ars
De
novo
75c.
del
AG
1363
–136
4p.
Ser4
55fs
7T
his stud
yB
ilate
ral
hype
rech
ogen
icki
dne
ys
Bila
tera
lco
rtic
alcy
sts,
left
hypo
plas
tic
kid
ney
CR
F(G
FR80
at14
year
s)
ND
CR
F,ch
roni
cre
nal
failu
re;E
SRF,
end
-sta
gere
nal
failu
re;U
PJ,u
rete
rope
lvic
junc
tion
.
Clin J Am Soc Nephrol 5: 1079–1090, 2010 Renal Phenotypes and HNF1B Mutations 1087

isolated bilateral hyperechogenic fetal kidneys with normal orslightly enlarged (��3 SD) size were the most frequent phe-notype observed before birth in patients who carried an HNF1Bmutation (3); however, one limit of our study is that our pop-ulation represents patients who had congenital anomalies ofthe kidney and urinary tract and whose samples were receivedfor HNF1B testing in France during a certain period of time.Thus, it will be of interest to perform a prospective study that
includes all hyperechogenickidneys with normal or slightlyenlarged size diagnosed beforebirth and test them for HNF1Bmutation. Almost all patientswith HNF1B mutation andmoderately enlarged hypere-chogenic kidneys before birthdisplayed normal-sized or smallkidneys with hyperechogenic-ity and/or cortical cysts in thepostnatal period, suggesting aslow-down in kidney growthafter birth.
Besides hyperechogenic kid-neys, HNF1B mutations wereassociated with several otherprenatal renal abnormalitiesbut far less frequently: bilateralor unilateral MCD, unilateralrenal agenesis, kidney hypopla-sia, isolated pyelic dilation, orkidneys with individualizedcysts. Because unilateral renalagenesis has been reported inassociation with HNF1B abnor-malities only in adults so far (5),it had been suggested that these
cases may be due to involution of overlooked MCD (13). Ourstudy shows that genuine renal unilateral agenesis can be as-sociated with HNF1B mutation. The absence of cases of bilateralagenesis may be due to the small number of patients tested. Inall cases of renal unilateral agenesis associated with HNF1Bmutation, the single kidney was abnormal. More generally,except for one patient with unilateral hypoplasia and normalcontralateral kidney, all probands who carried HNF1B muta-tion displayed bilateral kidney abnormalities. Regarding extra-renal symptoms, no patient with HNF1B mutation developeddiabetes during early childhood. Only four presented diabetesat 17, 20, 31, and 42 years, respectively, and one developedgestational diabetes. Six other probands had family history ofdiabetes, but the type of diabetes in relatives was not alwaysknown.
Twelve patients with HNF1B mutation had early goutand/or hyperuricemia, a feature that has been reported inpatients with HNF1B mutations (15), but this frequency must beunderestimated because the uricemia dosage was not availablefor many patients in our cohort. Only one adult proband whopresented with tubulointerstitial nephropathy and early hyper-uricemia that was previously shown not to be associated withUMOD mutation was carrying an HNF1B mutation. The asso-ciation of familial hyperuricemic nephropathy with HNF1Bmutation has been reported previously (5,15), but the mecha-nisms responsible for the reduced fractional excretion of uricacid are not well understood. HNF1�/HNF1� heterodimershave been shown to bind and positively regulate the proximalpromoter region of SLC22A12, encoding a transporter that is
Figure 1. HNF1� protein and localization of the various mutations identified in this study.The N-terminal portion of the protein consists of a short dimerization domain (dim). TheDNA-binding domain is characterized by a region distantly related to the POU box-specificdomain and an atypical homeodomain structure. The residues required for HNF1� trans-activation have been mapped to the carboxy-terminal region. Deletions are indicated by asolid line. *Novel mutation.
Figure 2. Type of HNF1B mutation (�, deletion of the entiregene; u, missense mutations; f, truncating mutations) accord-ing to the renal phenotype in patients and affected relatives. 1,prenatal hyperechogenic kidneys; 2, hyperechogenic kidneydiagnosed after birth; 3, MCD; 4, unilateral renal agenesis; 5,cystic disease; 6, renal hypoplasia; 7, tubulointerstitial nephri-tis; 8, pyeloureteral junction; 9, pelvic kidney; 10, lack of renalanomaly.
1088 Clinical Journal of the American Society of Nephrology Clin J Am Soc Nephrol 5: 1079–1090, 2010
responsible for the resorption of urate in the apical membraneof the renal proximal tubule (16); therefore, loss of functionwould be expected to lead to hypouricemia. The overlap be-tween phenotypes associated with HNF1B loss of function andfamilial UMOD hyperuricemic nephropathy may not seem sur-prising, because UMOD was shown to be a target of HNF1�
(10); however, familial hyperuricemic nephropathy associatedwith UMOD mutations is thought to be due to a defect inuromodulin transport, associated with a dominant effect, ratherthan to haploinsufficiency. Thus, the development of the samephenotype associated with HNF1B haploinsufficiency is notfully understood. Nevertheless, the finding of hyperuricemiaand/or of low uric acid excretion fraction should be an addi-tional argument to screen for HNF1B mutation in patients whopresent with congenital anomalies of the kidney and urinarytract.
Hypomagnesemia was also found in several individuals withHNF1B mutation, although blood magnesium dosage was notalways performed. Low plasma magnesium level was recentlyreported by another group and may be related to the transcrip-tional regulation of FXYD2 by HNF1� (6). In addition to thefrequent and moderate elevation of liver enzymes that waspreviously reported (17), we observed a severe cholestasis withpruritus in the affected mother of one patient. Cholestasis as-sociated with HNF1B mutation was previously reported (18)and is not unexpected given the known role of HNF1� in bileduct morphogenesis (19).
Both the type and the severity of the renal disease werevariable in this series, and our data show that HNF1B mutationscan be associated with very severe prenatal renal failure (infour probands, the pregnancy was terminated because of ana-mnios, and termination of previous pregnancy for severe renaldisease with anamnios was reported in relatives in two addi-tional families) as well as with normal renal function in adult-hood. In our series, as in others, there was no obvious correla-tion between the type of mutation and the type and/or severity
of renal disease. We observed both inter- and intrafamilialvariability of the phenotype in patients who harbored the samemutation. The lack of genotype–phenotype correlation and thewide variability observed within a given family make the ge-netic counseling particularly difficult in these families.
AcknowledgmentsWe thank the patients and their family for participation. We are
grateful to the following physicians for contribution of material andclinical data from patients: Dr. Corinne Antoine (Assistance Publique–Hopitaux de Paris, Hopital Saint Louis, Paris, France); Dr. DanielleBruno (Hopital de la Timone, Marseille, France); Dr. Renato Demontis(Centre Hospitalier Laennec, Creil, France); Dr. Philippe Eckart (CentreHospitalier Regional Universitaire de Caen, Caen France); Dr. JeromeHarambat (Centre Hospitalier Regional Universitaire de Bordeaux, Bor-deaux, France); Dr. Anne Maisin (Assistance Publique–Hopitaux deParis, Hopital Robert Debre, Paris, France); Dr. Jelena Martinovic (As-sistance Publique–Hopitaux de Paris, Hopital Necker, Paris, France);Dr. Hubert Nivet (Centre Hospitalier Regional Universitaire de Tours,Tours, France); Dr. Francois Nobili (Centre Hospitalier Regional Uni-versitaire de Besancon, Besancon, France); Dr. Jean Bernard Palcoux(Hopital Hotel Dieu, Clermont Ferrand, France); Dr. Christine Pietre-ment (Centre Hospitalier Regional Universitaire de Reims, Reims,France); Dr. Natacha Raynaud (Centre Hospitalier Felix Guyon, LaReunion, France); and Dr. Christel Thauvin (Hopital d’Enfants, Dijon,France). We are grateful to Nicolas Chassaing and Cathie Prouheze(Service de Genetique, Hopital Purpan, Toulouse, France) for help withmolecular analysis. We thank Mario Tosi (INSERM U614, Rouen Uni-versity Hospital, Rouen, France) for help with quantitative multiplexPCR amplification of short fluorescence fragments.
DisclosuresNone.
References1. Horikawa Y, Iwasaki N, Hara M, Furuta H, Hinokio Y,
Cockburn BN, Lindner T, Yamagata K, Ogata M, To-monaga O, Kuroki H, Kasahara T, Iwamoto Y, Bell GI:Mutation in hepatocyte nuclear factor-1 beta gene (HNF1B)associated with MODY. Nat Genet 17: 384–385, 1997
2. Zaffanello M, Brugnara M, Franchini M, Fanos V: HNF1Bgene mutation leads to nephro-urological defects of un-equal severity: an open question. Med Sci Monit 14: RA78–RA86, 2008
3. Decramer S, Parant O, Beaufils S, Clauin S, Guillou C,Kessler S, Aziza J, Bandin F, Schanstra JP, Bellanne-Chan-telot C: Anomalies of the HNF1B gene are the main causeof fetal bilateral hyperechogenic kidneys. J Am Soc Nephrol18: 923–933, 2007
4. Haumaitre C, Fabre M, Cormier S, Baumann C, DelezoideAL, Cereghini S: Severe pancreas hypoplasia and multicys-tic renal dysplasia in two human foetuses carrying novelHNF1beta/MODY5 mutations. Hum Mol Genet 15: 2363–2375, 2006
5. Edghill EL, Bingham C, Ellard S, Hattersley AT: Mutationsin hepatocyte nuclear factor-1beta and their related pheno-types. J Med Genet 43: 84–90, 2006
6. Adalat S, Woolf AS, Johnstone KA, Wirsing A, Harries LA,Long DA, Hennekam RC, Ledermann SE, Rees L, van’ HoffW, Marks SD, Trompeter RS, Tullus K, Winyard PJ, Can-
Figure 3. Type of HNF1B mutation (deletion, missense muta-tions, truncating mutations) according to the GFR at last fol-low-up (f, GFR �80 ml/min per 1.73 m2; �, GFR �80 ml/minper 1.73 m2) and age at last follow-up (p).
Clin J Am Soc Nephrol 5: 1079–1090, 2010 Renal Phenotypes and HNF1B Mutations 1089
sick J, Mushtaq I, Dhillon HK, Bingham C, Edghill EL,Shroff R, Stanescu H, Ryffel GU, Ellard S, Bockenhauer D:HNF1B mutations associate with hypomagnesemia andrenal magnesium wasting. J Am Soc Nephrol 20: 1123–1131,2009
7. Barbacci E, Reber M, Ott MO, Breillat C, Huetz F, Ce-reghini S: Variant hepatocyte nuclear factor 1 is requiredfor visceral endoderm specification. Development 26: 4795–4805, 1999
8. Reber M, Cereghini S: Variant hepatocyte nuclear factor 1 ex-pression in the mouse genital tract. Mech Dev 100: 75–78, 2001
9. Coffinier C, Barra J, Babinet C, Yaniv M: Expression of thevHNF1/HNF1beta homeoprotein gene during mouse or-ganogenesis. Mech Dev 89: 211–213, 1999
10. Gresh L, Fischer E, Reimann A, Tanguy M, Garbay S, ShaoX, Hiesberger T, Fiette L, Igarashi P, Yaniv M, Pontoglio M:A transcriptional network in polycystic kidney disease.EMBO J 23: 1657–1668, 2004
11. Gong Y, Ma Z, Patel V, Fischer E, Hiesberger T, PontoglioM, Igarashi P: HNF-1beta regulates transcription of thePKD modifier gene Kif12. J Am Soc Nephrol 20: 41–47, 2009
12. Charbonnier F, Raux G, Wang Q: Detection of exon dele-tions and duplications of the mismatch repair genes inhereditary nonpolyposis colorectal cancer families usingmultiplex polymerase chain reaction of short fluorescentfragments. Cancer Res 60: 2760–2763, 2000
13. Ulinski T, Lescure S, Beaufils S, Guigonis V, Decramer S,Morin D, Clauin S, Deschenes G, Bouissou F, Bensman A,Bellanne-Chantelot C: Renal phenotypes related to hepa-tocyte nuclear factor-1beta (HNF1B) mutations in a pedi-atric cohort. J Am Soc Nephrol 17: 497–503, 2006
14. Sunyaev S, Ramensky V, Koch I, Lathe W 3rd, KondrashovAS, Bork P: Prediction of deleterious human alleles. HumMol Genet 10: 591–597, 2001
15. Bingham C, Ellard S, van’t Hoff WG, Simmonds HA, Mari-naki AM, Badman MK, Winocour PH, Stride A, LockwoodCR, Nicholls AJ, Owen KR, Spyer G, Pearson ER, Hatter-sley AT: Atypical familial juvenile hyperuricaemic ne-phropathy associated with a hepatocyte nuclear factor-1beta gene mutation. Kidney Int 63: 1645–1651, 2003
16. Kikuchi R, Kusuhara H, Hattori N, Kim I, Shiota K, Gonza-lez FJ, Sugiyama Y: Regulation of tissue-specific expressionof the human and mouse urate transporter 1 gene byhepatocyte nuclear factor 1 alpha/beta and DNA methyl-ation. Mol Pharmacol 72: 1619–1625, 2007
17. Bellanne-Chantelot C, Clauin S, Chauveau D, Collin P,Daumont M, Douillard C, Dubois-Laforgue D, DusselierL, Gautier JF, Jadoul M, Laloi-Michelin M, Jacquesson L,Larger E, Louis J, Nicolino M, Subra JF, Wilhem JM,Young J, Velho G, Timsit J: Large genomic rearrange-ments in the hepatocyte nuclear factor-1beta (HNF1B)gene are the most frequent cause of maturity-onsetdiabetes of the young type 5. Diabetes 54: 3126 –3132,2005
18. Beckers D, Bellanne-Chantelot C, Maes M: Neonatal cho-lestatic jaundice as the first symptom of a mutation in thehepatocyte nuclear factor-1beta gene (HNF-1beta). J Pediatr150: 313–314, 2007
19. Coffinier C, Gresh L, Fiette L, Tronche F, Schutz G, BabinetC, Pontoglio M, Yaniv M, Barra J: Bile system morphogen-esis defects and liver dysfunction upon targeted deletion ofHNF1beta. Development 129: 1829–1838, 2002
20. Bellanne-Chantelot C, Chauveau D, Gautier JF, Dubois-Laforgue D, Clauin S, Beaufils S, Wilhelm JM, Boitard C,Noel LH, Velho G, Timsit J: Clinical spectrum associatedwith hepatocyte nuclear factor-1beta mutations. Ann InternMed 140: 510–517, 2004
Access to UpToDate on-line is available for additional clinical informationat http://www.cjasn.org/
1090 Clinical Journal of the American Society of Nephrology Clin J Am Soc Nephrol 5: 1079–1090, 2010
Top Related
Copyright © 2022 FDOKUMEN

