







Bahasa
Halaman
Hukum

Legal and Criminological Psychology (2013)
© 2013 The British Psychological Society
www.wileyonlinelibrary.com
Responding to repetitive, non-suicidal self-harm inan English male prison: Staff experiences,reactions, and concerns
Lisa Marzano*, Joanna R. Adler and Karen CiclitiraDepartment of Psychology, Middlesex University, London, UK
Objectives. This study considers how those who work in prisons are affected by andrespond to repetitive self-harm of male prisoners. The perspectives of correctional staffare often overlooked in research that considers self-harming prisoners. As prison staffhave regular, potentially daily contact with prisoners who self-harm, it is important toconsider the ways in which they respond to this aspect of their job, both in terms of theirown and prisoners’ well-being.
Design. Semi-structured interviews were conducted with prison staff and exploredusing techniques of thematic analysis.
Methods. Semi-structured face-to-face interviews were conducted with 30 correc-tional staff – 15 custodial officers and 15 health care staff – to explore their experiences,responses to, and ways of coping with non-suicidal, repetitive self-harm.
Result. Findings indicate high levels of frustration, tensions between health care andcustodial staff, feelings of powerlessness, and low sense of job control.
Conclusion. We set the tasks of prison staff within the wider contexts of work-stressliterature and forensic practice. The implications of these findings are discussed in termsof prisoner and officer well-being, secure custody, and the potential limitations both ofinstitutional resourcing and the methodology employed within this study.
Exploring the perspectives ofworkers, carers, and service providers is an important, oftenoverlooked, component when studying self-harm. This is particularly the case in prisons,where rates of self-harm are high (Ministry of Justice, 2013), and staff have regular,potentially daily, contact with prisoners who self-harm. Previous research repeatedlyconcludes that professionals dealing with self-harm experience a range of anxieties andnegative emotions (Taylor, Hawton, Fortune, & Kapur, 2009). These are not onlydetrimental to staff welfare butmay also have negative implications for the people in theircare (Marzano, Ciclitira, & Adler, 2012). Hostile, distancing or stigmatizing attitudes, andassociated poor practices, may limit support sought by self-harming individuals,potentially exacerbating distress and risk levels.
Despite some exploration of the nature and impact of workers’ and carers’ (mostlynegative) attitudes towards self-harm, there has been little focus onwhy staffmay respondto self-harm negatively, how they may be affected by such behaviours, and what, ifanything, could be done to prevent hostile reactions. The organizational health literature
*Correspondence should be addressed to Lisa Marzano, Middlesex University, The Burroughs, London NW4 4BT, UK (e-mail:[email protected]).
DOI:10.1111/lcrp.12025
1
offers a relevant theoretical framework. By focusing on dynamic interactions betweenindividuals and their environments, transactional models of work stress (Lazarus &Folkman, 1984) locate staff’s cognitive and emotional reactions to self-harm within thebroader context and content of their work.
Within this framework, potential strains of working with people who self-harm havebeen discussed with reference to staff roles and responsibilities. For instance, Hayward,Tilley, Derbyshire, Kuipers, and Grey (2005, p. 299) argued that ‘the self-harming client isengaging in socially unacceptable behaviours, behaviours which staff may feel respon-sible for, but which they are in fact relatively powerless to prevent’. Such feelings ofhelplessness have been described as potentially traumatizing (Deiter & Pearlman, 1998),and may challenge staff views of autonomy, competency, and role (Rayner, Allen, &Johnson, 2005). This, alongwith the potential trauma of the actual injury (Fish, 2000) andthe stress of witnessing and learning about difficult feelings and experiences, may set inmotion individual coping and defence mechanisms, including complex, ambivalent, andoften ‘split’ counter-transference reactions that serve to reject the ‘other’ and distancethemselves from the client, ultimately locating the source of difficulty within the client,not themselves, their skills, or abilities (Huband & Tantam, 2000).
From a cognitive–emotional perspective, these reactions are especially likely inrelation to low-severity, repetitive, seemingly non-suicidal self-harm, which may beperceived by staff as relatively trivial in nature, challenging (Stanley & Standen, 2000), orcontrollable (Weiner, 1986), and thus the responsibility of the individual concerned.Dominant conceptualizations of low-severity, non-suicidal forms of self-harm as essen-tially a female teenage activity (see e.g., Brickman, 2004)may additionally causemenwhoself-harm to be viewed as disingenuous. In these situations, especially when staff have aduty of care towards clients, workers may feel coerced, or even manipulated, to expressconcern and provide attention. That sense of obligation can be experienced as a form ofbullying or aggression from the client (Bowers, 2003; Fish, 2000), leading to feelings ofanger and subsequent behavioural reactions, such as reduced willingness to help,neglecting, reprimanding, or even retaliatory behaviour (Pannell, Howells, & Day, 2003).
Perceived or actual accountability for the behaviour of clients who self-harm can also‘raise anxiety in professional staff arising from fear [for their own] safety, from concernabout repercussions if [the client] makes “one cut too many”’ (Fieldman, 1998, p. 258).This can create a climate of blame and fear, potentially contributing to professionalburnout, a ‘syndrome of emotional exhaustion, depersonalisation and reduced personalaccomplishment that can occur among individuals who do “people work” of some kind’(Maslach & Jackson, 1986, p. 2).
Although the reactions described above appear to be common among staff workingwith people who self-harm (in a variety of roles and occupational settings, Taylor et al.,2009), the pressures and difficulties experienced by prison staff are arguably acute and inmanywaysunique. Inwhathas longbeendescribedasaninherentlystressfulworkcontext,dealingwith self-harmmaybeespecially challenging forprison staff, not least as reductionsin suicide and self-harm rates are repeatedly stated Prison Service priorities (see e.g., HMPrison Service, 2007) and are increasingly considered to be the responsibility of staff.
Prisonofficershavecrucial responsibilities in the identificationof risk and theprovisionof support, despite often feeling unqualified, untrained, or unskilled for this kind of work(Towl & Forbes, 2002), and despite the limited support available for staff dealing withself-harm in prisons (Home Office, 2007), especially with regards to repetitive self-harm(Marzano & Adler, 2007). In addition, dealing with people who self-harm may highlighttensions between officers’ custody and care roles (Home Office, 1991; Towl & Forbes,
2 Lisa Marzano et al.
2002), requiring them to ‘balance authority with a large amount of understanding andcompassion’ (HMPrison Service, 2004, p. 1). This can result in role conflict and ambiguity(Triplett, Mullings, & Scarborough, 1996), consistent predictors of psychological strain,and low job satisfaction (Cox, 1993; Mackay, Cousins, Kelly, Lee, & McCaig, 2004).
Similar pressures are likely to affect prison nurses and doctors (Walsh, 2005),compounded by the historical isolation of forensic nursing and medicine (Doyle, 2001),the difficulties of working in an environment where security concerns and riskmanagement often take priority over individual health needs, and the stress of havingto treat wounds (self-inflicted or otherwise) in a population at high risk of communicabledisease (Watson, Stimpson, & Hostick, 2004).
Theways inwhichprisonofficers andhealth care staff dealwith thesepressures remainunclear and may be multi-faceted. Albeit limited, the literature on how prison officersapproach prison work in general suggests that they mainly use passive, indirect, andpalliative coping strategies, which then become dominant elements of their occupationalculture (Schaufeli & Peeters, 2000). Perhaps unsurprisingly, these have been found to belargely ineffective in termsof reducingwork stress, andmayalso ‘inhibit direct and indirectformsof support forprisoners at riskof suicide [and self-harm]’ (Liebling,Tait,Durie, Stiles,& Harvey, 2005, p. 155). Examples include ‘laying low’ (which may lead to a reactiveapproach to prisoner care), distrust of outsiders and managers (which may hinder teamwork), and machismo and social distance from prisoners (with clear implications for theapproachabilityof officers and their ability andwillingness todemonstrate care, sympathy,and concern for prisoners). These types of responses also appear to become commonamong health care staff, who reportedly copewith the anxiety ofworkingwith and caringfor prisoners by assimilating officers’ traditional culture, which then facilitates theirrelationships and integration with officers. According to Weiskopf (2005), nurses anddoctors deal with their struggle of caring for prisoners by not caring for them.
The present studyDespite apparently higher rates of self-harm among women prisoners (cf. Maden,Chamberlain, & Gunn, 2000), most incidents of self-harm in custody are carried out withno apparent suicidal intent, by prisoners who self-harm onmultiple occasions, andwho –given their over-representation in the prison population – are men (Ministry of Justice,2013). Furthermore, the number of recorded self-harm incidents in male prisoners hasincreased by over 50% in recent years (10,277 in September 2005 cf. 16,138 in September2012), with further increases in observed rates of self-harm incidents (145–195 per 1,000prisoners in 2005 cf. 2012), numbers and rates of self-harming male prisoners(respectively, 4,290 vs. 5,797, and 60 vs. 70 per 1,000 prisoners in 2005 cf. 2012), andhospital attendances bymen in custody (950 in 2005 cf. 1,315 in 2012). The reverse trendhas been reported in relation to women prisoners (Ministry of Justice, 2013). However,research in this area has focused almost exclusively on female prisoners (and staffworkingin women’s prisons – see e.g., Kenning et al., 2010; Short et al., 2009), and to date therehas been no systematic, in-depth examination of the impact on prison staff of workingwith male prisoners who repeatedly self-harm, without apparent suicidal intent. Inaddition, despite some exploration of prison officers’ attitudes towards (male and female)prisoners who self-harm (Ireland & Quinn, 2007; Liebling & Krarup, 1993; Pannell et al.,2003; Snow, 1997), the responses of health care staff have received limited attention in theliterature. Although landing-based officers have more day-to-day contact with prisoners,
Prison staff experiences of prisoner self-harm 3
prison nurses and doctors are those who deal with prisoners’ self-inflicted wounds, andare often the first to discuss with them the circumstances surrounding their self-harming.
This study aimed to increase knowledge and awareness of the effect(s) of repetitive,non-suicidal, male, self-harm on prison officers and health care staff, on both personal andprofessional levels. The broad research areas addressed are as follows:!What are the experiences, views, and reactions of prison staff working with adult,male, prisoners who repeatedly self-harm, with no apparent suicidal intent?
! How do prison staff deal with this area of work?!What coping methods do prison staff adopt?!What impact does dealing with male self-harming prisoners have on prison staff,personally and professionally?
Method
As part of a wider study into male prisoner self-harm, semi-structured interviews wereconductedwith 15 officers, 13 nurses and 2 doctors, from a local prison1 in the South Eastof England. The research was carried out in consultation with the then Safer CustodyGroup, and with approval from the National Offender Management Service AppliedPsychology Group, the Psychology Ethics Committee at Middlesex University, and theGovernor of the prison where the interviews were conducted.
ParticipantsParticipant recruitment was opportunistic, largely dictated by staff availability andconvenience. Officers and health care staff from all grades, locations within the prison,minority ethnic groups, and both genders were approached and invited to take part in aninterview about their issues, needs, and concerns about working with prisoners whorepeatedly self-harm. Information about the study was also posted within the prisonbulletin, together with an invitation to take part.
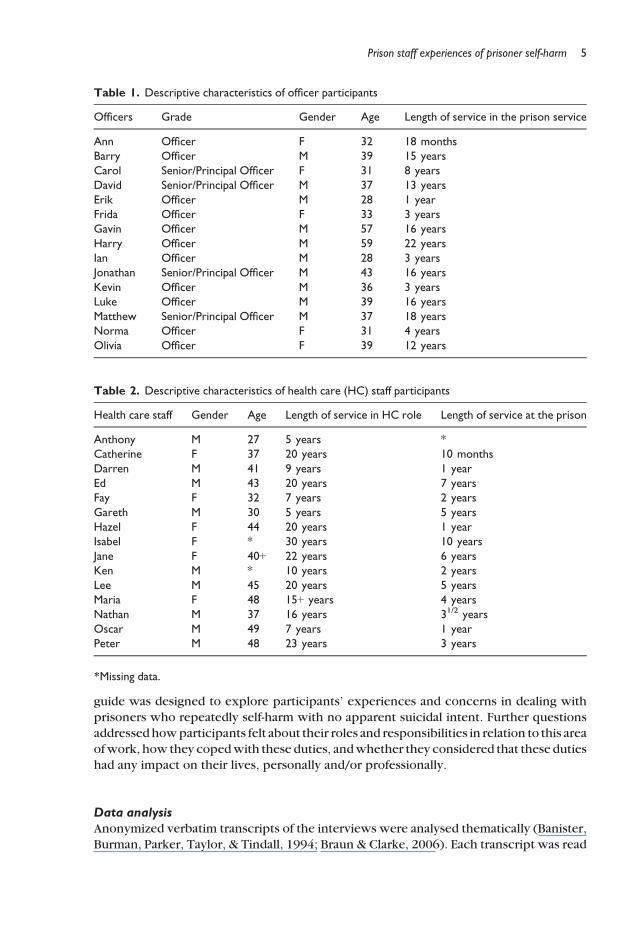
Details of participants’ personal and professional backgrounds are presented below(pseudonyms are used throughout to protect participants’ confidentiality). One officerparticipantwasaprincipalofficer (highestwing-basedrank)andthreewereseniorofficers.This information is presented in a collated form in Table 1, to protect participant identity.
Four of the health care staff interviewed were general nurses, six were mental healthnurses, twowere substancemisuse nurses, onewas a substancemisuse andmental healthnurse, and two were General Practitioners. Four health care staff participants weretemporary, agency staff, and the remaining 11 were permanent members of staff (ofwhom two were appointed on a part-time basis) (Table 2).
InterviewsSemi-structured face-to-face interviews were conducted by the first author, under thesupervision of the other authors (Ciclitira is a clinician and Adler is a forensicpsychologist). Interviews lasted between 45 and 90 min, were audio recorded, and wereconducted in private, with participants’ prior written informed consent. The interview
1 Local prisons deal with men and young offenders who are sent directly from the courts, either when remanded in custody beforetrial or after conviction or sentence. These establishments can hold prisoners for the duration of their sentences, or only for theinitial assessment and classification of convicted prisoners before their allocation to another prison to serve their sentences.
4 Lisa Marzano et al.
guide was designed to explore participants’ experiences and concerns in dealing withprisoners who repeatedly self-harm with no apparent suicidal intent. Further questionsaddressedhowparticipants felt about their roles and responsibilities in relation to this areaofwork, how they copedwith these duties, andwhether they considered that these dutieshad any impact on their lives, personally and/or professionally.
Data analysisAnonymized verbatim transcripts of the interviews were analysed thematically (Banister,Burman, Parker, Taylor, & Tindall, 1994; Braun & Clarke, 2006). Each transcript was read
Table 2. Descriptive characteristics of health care (HC) staff participants
Health care staff Gender Age Length of service in HC role Length of service at the prison
Anthony M 27 5 years *Catherine F 37 20 years 10 monthsDarren M 41 9 years 1 yearEd M 43 20 years 7 yearsFay F 32 7 years 2 yearsGareth M 30 5 years 5 yearsHazel F 44 20 years 1 yearIsabel F * 30 years 10 yearsJane F 40+ 22 years 6 yearsKen M * 10 years 2 yearsLee M 45 20 years 5 yearsMaria F 48 15+ years 4 yearsNathan M 37 16 years 31/2 yearsOscar M 49 7 years 1 yearPeter M 48 23 years 3 years
*Missing data.
Table 1. Descriptive characteristics of officer participants
Officers Grade Gender Age Length of service in the prison service
Ann Officer F 32 18 monthsBarry Officer M 39 15 yearsCarol Senior/Principal Officer F 31 8 yearsDavid Senior/Principal Officer M 37 13 yearsErik Officer M 28 1 yearFrida Officer F 33 3 yearsGavin Officer M 57 16 yearsHarry Officer M 59 22 yearsIan Officer M 28 3 yearsJonathan Senior/Principal Officer M 43 16 yearsKevin Officer M 36 3 yearsLuke Officer M 39 16 yearsMatthew Senior/Principal Officer M 37 18 yearsNorma Officer F 31 4 yearsOlivia Officer F 39 12 years
Prison staff experiences of prisoner self-harm 5
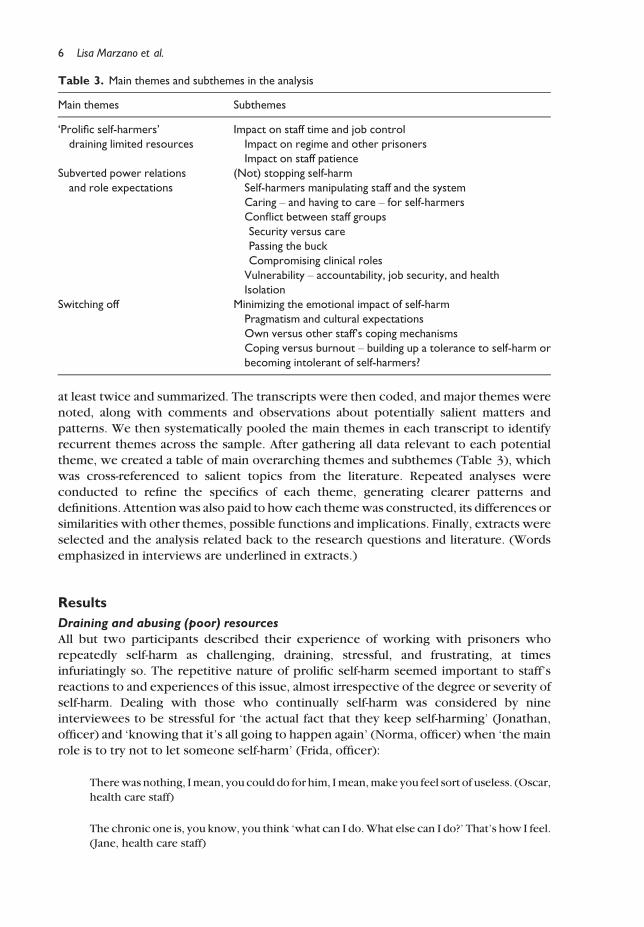
at least twice and summarized. The transcripts were then coded, and major themes werenoted, along with comments and observations about potentially salient matters andpatterns. We then systematically pooled the main themes in each transcript to identifyrecurrent themes across the sample. After gathering all data relevant to each potentialtheme, we created a table of main overarching themes and subthemes (Table 3), whichwas cross-referenced to salient topics from the literature. Repeated analyses wereconducted to refine the specifics of each theme, generating clearer patterns anddefinitions. Attentionwas also paid to how each themewas constructed, its differences orsimilarities with other themes, possible functions and implications. Finally, extracts wereselected and the analysis related back to the research questions and literature. (Wordsemphasized in interviews are underlined in extracts.)
Results
Draining and abusing (poor) resourcesAll but two participants described their experience of working with prisoners whorepeatedly self-harm as challenging, draining, stressful, and frustrating, at timesinfuriatingly so. The repetitive nature of prolific self-harm seemed important to staff’sreactions to and experiences of this issue, almost irrespective of the degree or severity ofself-harm. Dealing with those who continually self-harm was considered by nineinterviewees to be stressful for ‘the actual fact that they keep self-harming’ (Jonathan,officer) and ‘knowing that it’s all going to happen again’ (Norma, officer) when ‘the mainrole is to try not to let someone self-harm’ (Frida, officer):
Therewas nothing, Imean, you could do for him, Imean,make you feel sort of useless. (Oscar,health care staff)
The chronic one is, you know, you think ‘what can I do.What else can I do?’ That’s how I feel.(Jane, health care staff)
Table 3. Main themes and subthemes in the analysis
Main themes Subthemes
‘Prolific self-harmers’draining limited resources
Impact on staff time and job controlImpact on regime and other prisonersImpact on staff patience
Subverted power relationsand role expectations
(Not) stopping self-harmSelf-harmers manipulating staff and the systemCaring – and having to care – for self-harmersConflict between staff groupsSecurity versus carePassing the buckCompromising clinical rolesVulnerability – accountability, job security, and healthIsolation
Switching off Minimizing the emotional impact of self-harmPragmatism and cultural expectationsOwn versus other staff’s coping mechanismsCoping versus burnout – building up a tolerance to self-harm orbecoming intolerant of self-harmers?
6 Lisa Marzano et al.
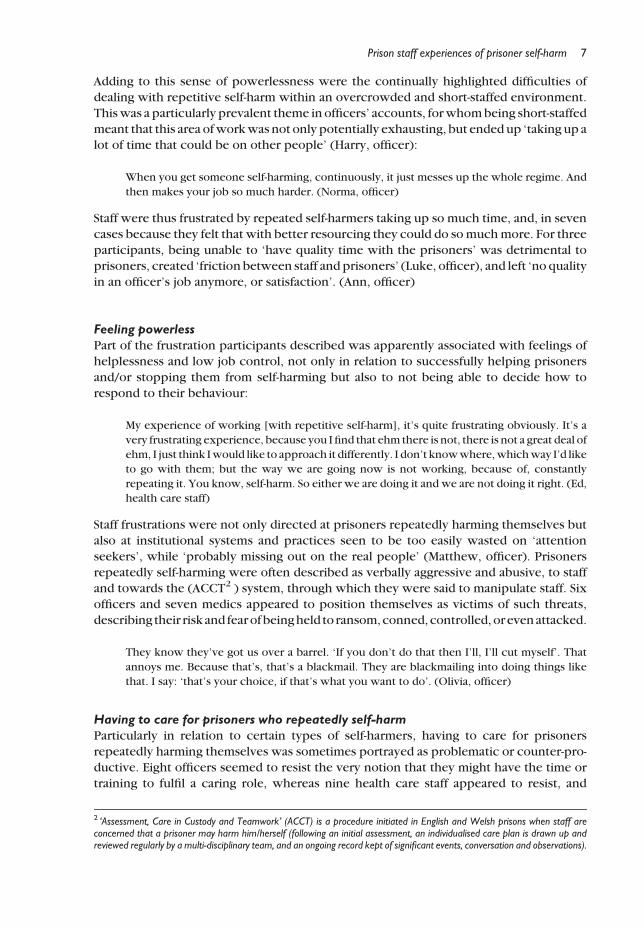
Adding to this sense of powerlessness were the continually highlighted difficulties ofdealing with repetitive self-harm within an overcrowded and short-staffed environment.Thiswas a particularly prevalent theme in officers’ accounts, forwhombeing short-staffedmeant that this area ofworkwas not only potentially exhausting, but endedup ‘taking up alot of time that could be on other people’ (Harry, officer):
When you get someone self-harming, continuously, it just messes up the whole regime. Andthen makes your job so much harder. (Norma, officer)
Staff were thus frustrated by repeated self-harmers taking up so much time, and, in sevencases because they felt that with better resourcing they could do somuchmore. For threeparticipants, being unable to ‘have quality time with the prisoners’ was detrimental toprisoners, created ‘friction between staff and prisoners’ (Luke, officer), and left ‘no qualityin an officer’s job anymore, or satisfaction’. (Ann, officer)
Feeling powerlessPart of the frustration participants described was apparently associated with feelings ofhelplessness and low job control, not only in relation to successfully helping prisonersand/or stopping them from self-harming but also to not being able to decide how torespond to their behaviour:
My experience of working [with repetitive self-harm], it’s quite frustrating obviously. It’s avery frustrating experience, because you I find that ehm there is not, there is not a great deal ofehm, I just think Iwould like to approach it differently. I don’t knowwhere,whichway I’d liketo go with them; but the way we are going now is not working, because of, constantlyrepeating it. You know, self-harm. So either we are doing it and we are not doing it right. (Ed,health care staff)
Staff frustrations were not only directed at prisoners repeatedly harming themselves butalso at institutional systems and practices seen to be too easily wasted on ‘attentionseekers’, while ‘probably missing out on the real people’ (Matthew, officer). Prisonersrepeatedly self-harming were often described as verbally aggressive and abusive, to staffand towards the (ACCT2 ) system, through which they were said to manipulate staff. Sixofficers and seven medics appeared to position themselves as victims of such threats,describing their risk and fearofbeingheld to ransom,conned, controlled, orevenattacked.
They know they’ve got us over a barrel. ‘If you don’t do that then I’ll, I’ll cut myself’. Thatannoys me. Because that’s, that’s a blackmail. They are blackmailing into doing things likethat. I say: ‘that’s your choice, if that’s what you want to do’. (Olivia, officer)
Having to care for prisoners who repeatedly self-harmParticularly in relation to certain types of self-harmers, having to care for prisonersrepeatedly harming themselves was sometimes portrayed as problematic or counter-pro-ductive. Eight officers seemed to resist the very notion that they might have the time ortraining to fulfil a caring role, whereas nine health care staff appeared to resist, and
2 ‘Assessment, Care in Custody and Teamwork’ (ACCT) is a procedure initiated in English and Welsh prisons when staff areconcerned that a prisoner may harm him/herself (following an initial assessment, an individualised care plan is drawn up andreviewed regularly by a multi-disciplinary team, and an ongoing record kept of significant events, conversation and observations).
Prison staff experiences of prisoner self-harm 7
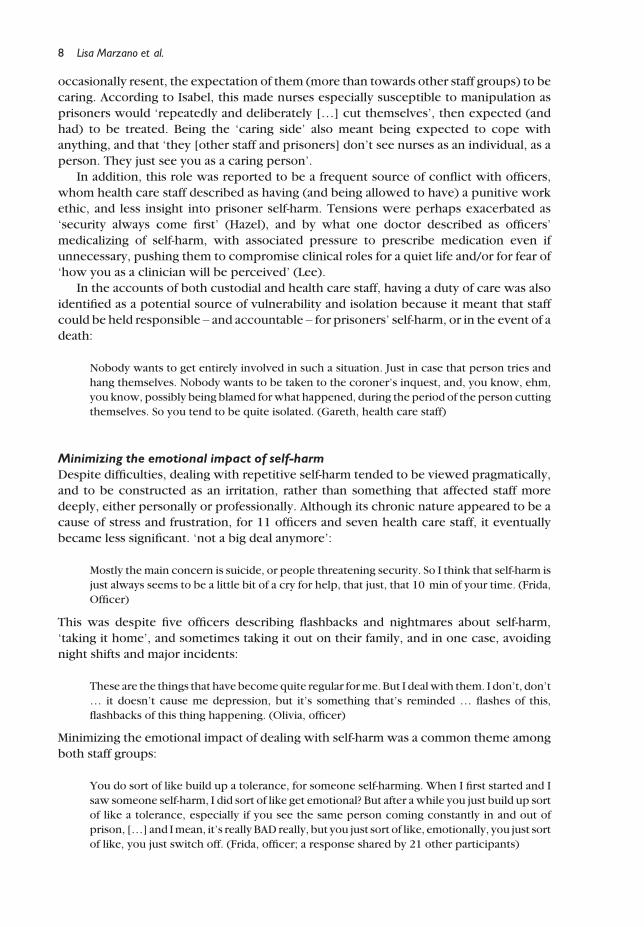
occasionally resent, the expectation of them (more than towards other staff groups) to becaring. According to Isabel, this made nurses especially susceptible to manipulation asprisoners would ‘repeatedly and deliberately […] cut themselves’, then expected (andhad) to be treated. Being the ‘caring side’ also meant being expected to cope withanything, and that ‘they [other staff and prisoners] don’t see nurses as an individual, as aperson. They just see you as a caring person’.
In addition, this role was reported to be a frequent source of conflict with officers,whom health care staff described as having (and being allowed to have) a punitive workethic, and less insight into prisoner self-harm. Tensions were perhaps exacerbated as‘security always come first’ (Hazel), and by what one doctor described as officers’medicalizing of self-harm, with associated pressure to prescribe medication even ifunnecessary, pushing them to compromise clinical roles for a quiet life and/or for fear of‘how you as a clinician will be perceived’ (Lee).
In the accounts of both custodial and health care staff, having a duty of care was alsoidentified as a potential source of vulnerability and isolation because it meant that staffcould be held responsible – and accountable – for prisoners’ self-harm, or in the event of adeath:
Nobody wants to get entirely involved in such a situation. Just in case that person tries andhang themselves. Nobody wants to be taken to the coroner’s inquest, and, you know, ehm,you know, possibly being blamed forwhat happened, during the period of the person cuttingthemselves. So you tend to be quite isolated. (Gareth, health care staff)
Minimizing the emotional impact of self-harmDespite difficulties, dealing with repetitive self-harm tended to be viewed pragmatically,and to be constructed as an irritation, rather than something that affected staff moredeeply, either personally or professionally. Although its chronic nature appeared to be acause of stress and frustration, for 11 officers and seven health care staff, it eventuallybecame less significant. ‘not a big deal anymore’:
Mostly the main concern is suicide, or people threatening security. So I think that self-harm isjust always seems to be a little bit of a cry for help, that just, that 10 min of your time. (Frida,Officer)
This was despite five officers describing flashbacks and nightmares about self-harm,‘taking it home’, and sometimes taking it out on their family, and in one case, avoidingnight shifts and major incidents:
These are the things that have becomequite regular forme. But I dealwith them. I don’t, don’t… it doesn’t cause me depression, but it’s something that’s reminded … flashes of this,flashbacks of this thing happening. (Olivia, officer)
Minimizing the emotional impact of dealing with self-harm was a common theme amongboth staff groups:
You do sort of like build up a tolerance, for someone self-harming. When I first started and Isaw someone self-harm, I did sort of like get emotional? But after awhile you just build up sortof like a tolerance, especially if you see the same person coming constantly in and out ofprison, […] and Imean, it’s really BAD really, but you just sort of like, emotionally, you just sortof like, you just switch off. (Frida, officer; a response shared by 21 other participants)
8 Lisa Marzano et al.
Being emotionally detachedwas often constructed as being both a practical necessity anda cultural expectation:
There is stigma attached to being a, ehm, a care bear, they call them in here – in the PrisonService – officers who care too much. Ehm, it’s almost uncool to care too much […] Peoplelike to be, ehm hard, and, and unaffected … (Erik, officer)
The whole ethos in this prison seems to be ‘IT’S HAPPENED. GET OVER IT. CARRY ON’because we’ve got to, we’ve got to let them out for feeding or, or exercise, or something.(Barry, officer)
In addition, some discussed resorting to gallows humour to ‘leave work at work’.Rationalizing that ‘it’s their choice… you will not stop them, because that’s the way theyare’ (Harry, officer). Resisting one’s role with prisoners who self-harm and referring on toanother department also appeared to help staff manage their difficulties in relation to thiswork. For example, it was common for officers to argue that ‘if he’s continually cuttinghimself he should be in hospital … it’s not my job’ (Luke), whereas for health care staff(many) prisoners who repeatedly self-harm were not ‘unwell as such’ (Hazel), and weretherefore a ‘problem’ for officers and psychologists, rather than doctors and nurses:
It’s a management thing more than anything […] ehm, basically the officers are mainlyinvolved with the daily management of the prisoners. (Anthony, health care staff)
However, mostly when referring to how other staff dealt with this area of work,interviewees also mentioned turning to drink, and avoiding dealing with or talking aboutprisoners who self-harm repeatedly. A related theme was that these reactions can beindicative of work stress and burnout, and be associated with absenteeism, depression,flashbacks, and even staff self-harm.
Switching off: Coping or burnout?Rather than always being offered as a sign of coping with this area of work, shutting offwas sometimes described as a symptom of burnout, emotional blunting, and of not beingable to deal with or to understand self-harm:
So if you don’t understand, you, you shut off from it. (Luke, officer)
Whether switching off was described as a sign of successfully coping or, quite theopposite, it was clear from the interviews that staff’s work, the regime, their energies,compassion, and patience could suffer as a result of dealing with prisoners repeatedlyinjuring themselves. Implicit within many accounts was the idea that becomingdesensitized to self-harm did not mean having no thoughts or feelings about it, butpotentially becoming intolerant of self-harmers, angry, cynical, or blas!e. Comments suchas ‘if you are going to do it, do it properly’ (David, officer), ‘it’s your own skin, so dowhatever you like’ (Kevin, officer), ‘pull yourself together’ (Luke, officer), and ‘YOU AREAMAN, for god’s sake… just dealwith it’ (Norma, officer)were not uncommon. Althoughthis may have been a way of coping, some other participants questioned its implicationsfor prisoners and staff.
Discussion
Fifteen officers and 15 health care staff were interviewed about their experiences ofworking with male prisoners who repeatedly harm themselves with no apparent
Prison staff experiences of prisoner self-harm 9
suicidal intent. Consistent with previous literature (e.g., McAllister, Creedy, Moyle, &Farrugia, 2002; Ramon, 1980), participants described a range of concerns, feelings, andannoyances, some of which were constructed as being inherent to this work (or to‘self-harmers’), others as precipitated and/or exacerbated by institutional requirementsand limited resources. Being short-staffed and over-stretched seemed to be particularlycentral to officers’ responses to repetitive self-harm, with some making direct linksbetween resourcing/staffing and their reactions to these behaviours. Concerns seemedto relate to low job control (Cox, 1993; Karasek, 1979) and to be associated withfeelings of powerlessness and helplessness that mirror those frequently reported inphenomenological accounts of why individuals self-harm, and how they are affected bynegative staff reactions (Marzano et al., 2012). Officers felt limited by time andresources available with low influence over systems that seemingly let ‘attentionseekers’ manipulate them, diverting them away from ‘real people’, and facedbehaviours that they neither always understood nor knew how to manage, but hadto try to stop.
Trying to prevent further self-harm, described by some as an unrealistic and potentiallycounter-productive role (e.g., Shaw & Shaw, 2007), appeared to be a greater source ofconflict than tensions between officers’ dual caring and security roles. Doctors’ andnurses’ main difficulties in dealing with repetitive self-harm were also considered inrelation to their professional roles with self-harmers, and especially to their having to carefor them. Lack of training or resources were not particularly salient to health careprofessionals, nor were the pressures of stopping self-harm. Rather, being – and beingexpected to be – the caring ones seemed to be resisted, and occasionally resented. In thiscontext, feelings of vulnerability were frequently mentioned, both with regards to being(and being held) accountable and to being pressurized by both prisoners and officers.
These findings suggest that a fundamental question of what is meant by care hasperhaps been overlooked. Implied in the accounts of both prisoners (Marzano et al.,2012) and staff was the idea that medical staff should also care for prisoners on anemotional level, while remaining themselves unemotional. However, more than half ofthe health care staff in the sample were not trained to deal with psychological or mentalhealth issues. Rather, they had been trained to provide physical care, in relation to generalpractice and substance-related complaints.
These findings add to the previous literature in suggesting that working with peoplewho self-harm can be challenging (HMCIP, 1999; Liebling et al., 2005; Paton, Harrison, &Jenkins, 2000), and that these difficulties may be usefully conceptualized within thecontext and content of one’s work. As highlighted in the accounts of staff, negativereactions to self-injury may not only affect prisoners’ welfare, but can also be indicative ofstaff stress and burnout. These may be especially recurrent whenworking with prisonerswho repeatedly self-harm. Previous research has shown that perceived likelihood ofrepetition may be negatively associated with staff optimism (Mackay & Barrowclough,2005), which in turn has been found to be linkedwithworkers’ willingness to help clients(see Weiner, 1986). Although qualitative data from a relatively small interview study maynot allowone to test this chain of reactions, these results clearly suggest that the frequencyor repetition of self-harm is an important, often overlooked, dimension for understandingthe possible impact of this behaviour on staff. Furthermore, the findings of this study mayadd to thework-stress literatureby reaffirming that these reactions areparticularly likely inan environment where staff are already stretched and under-resourced, poorly/inadequately trained, and yet accountable for the client group’s behaviour.
10 Lisa Marzano et al.

On the other hand, some staff seemed almost to play down the impact of this area ofwork, particularly when discussing their own reactions (as opposed to other people’s)and when considering how prisoner self-harm affected them on a personal (rather thanprofessional) level. Implicit in the accounts of 12 officers and 11 health care staff were theideas that working with prisoners repeatedly self-harming could be challenging, draining,and frustrating, but neither traumatic nor stressful per se. Indeed, in some cases dealingwith self-harm was described as being relatively minor when compared to the otherpressures and difficulties faced by staff in prisons, especially assaults and self-inflicteddeaths. In addition, many interviewees implied that they had – and had to – becomedesensitized to self-harm.
At the same time, some of the tensions and inconsistencies in participants’ accountssuggest that this process of switching offmay not be as clear-cut nor as positive as implied,neither for staff themselves nor for the prisoners in their care. Being emotionally detachedwas for some, indicative of staff stress and burnout, associated with absenteeism,depression, and flashbacks, as well as angry, blas!e, and resigned attitudes towardsself-harming prisoners. Rationalizing self-harm as a prisoner’s conscious choice and/or theresponsibility of another department also appeared to free staff of their responsibilities inrelation to self-harm, but further contributed to the feelings of learned helplessness(Petersen, Maier, & Seligman, 1995), thus exacerbating their difficulties in dealing withthese behaviours.
Concentrating specifically on dealing with how staff experience and react torepetitive, non-suicidal, self-harm among adult, male, prisoners was especially informa-tive, as this appears to be an area which could benefit from further understanding.Although rates of self-harm appear to be higher among women prisoners, the number ofprisoners and staff affected by this issue ismuchhigher inmale than female establishments(in part of course due to the sheer size of the male estate). Furthermore, male self-harm islikely to raise different challenges for prison staff than female self-harm, owing todifferences in the work environment (not least in terms of types of establishments andprisoner populations), and to the common conception that self-harm is a ‘femaleproblem’. Our findings, and the ways in which they were analysed, cannot fully answerthese questions nor enable conclusions as to whether a prisoner’s gender is in itself afactor in how prison staff respond to their self-harm. Wewill be reporting separately on adiscourse analytic study of staff’s constructions ofmale self-harm (including as a genderedissue), but further quantitative work may also be warranted.
There are issues regarding the transferability/generalizability of findings to othermen’sprisons as this study was conducted in a large and overcrowded local establishment, witha predominately male staff sample. Interviewing more female participants and/or staffdealingwith a less transient population, in a smaller and better resourcedprison,mayhaveresulted in a less negative picture of staff’s responses to self-harm (see e.g., Ireland &Quinn, 2007). Although rates of self-harm are disproportionately high in local establish-ments, and the majority of those working in prisons are men, further research couldinvestigate the experiences and responses to self-harm (anddifferent types of self-harm) ofprison officers and health care staff in more diverse settings, and include the perspectivesof other individuals and staff groups involved in the care of prisoners who self-harm.Further studies could also usefully explore and evaluateways of improving staff responsesto self-harm, including training, clinical supervision, and other support and prob-lem-focused interventions that seek to develop and strengthen the skills, cognitivereappraisal strategies, and resilience required for this demanding area of work.
Prison staff experiences of prisoner self-harm 11
ConclusionsThe majority of staff commented that dealing with this issue was challenging andfrustrating, that they did not have the practical resources and/or skills to deal with it, andthat levels of prisoner care may suffer as a result of staff becoming cynical and angry. Ourfindings suggest that staff’s responses to prisoners’ repetitive self-harm – whatever thestaff’s motivations – contravene policies and guidelines that emphasize supportiveconversations, proactive care, and non-judgmental attitudes (e.g., HMPrison Service, n.d.;NICE, 2004; Royal College of Psychiatrists, 2006).
Amore encouraging implication of the data presented here is that negative reactions toself-harm are not inevitable. Staff’s responses to self-harm are likely to have beeninfluenced by a variety of factors. These include staff’s (mis)understandings of self-harm,their personal experiences of this issue, and the practicalities of dealing with suchbehaviours over and over again with inadequate facilities and resourcing. Evenwhen staffseemed to consider self-harmers to be inherently difficult or frustrating, it was clear thatthese constructions could not be isolated from their roles and responsibilities within anunder-resourced, overcrowded environment.
The current findings reiterate the need to better support staff dealing with prisonerswho self-harm (Marzano & Adler, 2007), as well as those who may themselvesself-harm. For a policy so heavily reliant on good staff–prisoner relationships, care, andteamwork (HM Prison Service, 2005), the current suicide and self-harm strategy paystoo little attention to the needs of staff, particularly in relation to repetitive, non-suicidalforms of self-harm. As implied by many participants, with more time and understanding,staff’s reactions to self-harming prisoners may greatly improve, as will their jobsatisfaction.
References
Banister, P., Burman, E., Parker, I., Taylor, M., & Tindall, C. (1994). Qualitative methods inpsychology: A research guide. Buckingham, UK: Open University Press.
Bowers, L. (2003). Manipulation: Description, identification and ambiguity. Journal of Psychiatricand Mental Health Nursing, 10, 323–328. doi:10.1046/j.1365-2850.2003.00602.x
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in
Psychology, 3, 77–101. doi:10.1191/1478088706qp063oaBrickman, B. J. (2004). ‘Delicate’ cutters: Gendered self-mutilation and attractive flesh in medical
discourse. Body and Society, 10, 87–111. doi:10.1177/1357034X04047857Cox, T. (1993). Stress research and stress management: Putting theory to work. HSE Contract
Research Report No 61/1993. Sudbury, ON: HSE Books.Deiter, P., & Pearlman, L. (1998). Responding to self-injurious behaviour. In P. Kleespies (Ed.),
Emergencies in mental health practice: Evaluation and management (pp. 235–257). NewYork, NY: The Guilford Press.
Doyle, J. (2001). Forensic nursing: A review of the literature. Australian Journal of AdvancedNursing, 18, 32–39. Retrieved from http://www.ajan.com.au/Vol18/Vol18.3-4.pdf
Fieldman, M. D. (1998). The challenge of self-mutilation: A review. Comprehensive Psychiatry, 29,252–269. doi:10.1016/0010-440X(88)90048-X
Fish, R. M. (2000). Working with people who harm themselves in a forensic learning disabilityservice: Experiences of direct care staff. Journal of Learning Disabilities, 4, 193–207. doi:10.1177/146900470000400302
Hayward, P., Tilley, F., Derbyshire, C., Kuipers, E., & Grey, S. (2005). ‘The ailment’ revisited: Are‘manipulative’ patients really themost difficult? Journal of Mental Health, 14, 291–303. doi:10.1080/09638230500136423
12 Lisa Marzano et al.
HM Prison Service. (2004). Prison officer: The role. Retrieved from http://hmprisonservice.gov.uk/careersandjobs
HM Prison Service. (2005). Prison Service Order 18/2005: Introducing ACCT (assessment, care incustody & teamwork) – The replacement for the F2052SH (risk of self-harm). London, UK:HMSO.
HM Prison Service. (2007). Prison Service Order 2700: Suicide Prevention and Self-HarmManagement. London, UK: HMSO.
HMPrison Service. (n.d.). TheACCT approach: Caring for people at risk in prison. Pocket guide forstaff. Retrieved from http://www.hmprisonservice.gov.uk/assets/documents/10000C1BACCTStaffGuide.pdf
HMCIP. (1999). Suicide is everyone’s concern: A thematic review byHMChief Inspector of Prisonsfor England and Wales. London, UK: HMSO.
HomeOffice. (1991).Custody, care and justice: Thewayahead for thePrison Service EnglandandWales. London, UK: HMSO.
Home Office. (2007). Prison Service Staff Surveys 2002 to 2006. Retrieved from http://www.ohcsportal.co.uk/safercustody/managersandspcs/index.cfm
Huband, N., & Tantam, D. (2000). Attitudes to self-injury within a group of mental health staff.British Journal of Medical Psychology, 73, 495–504. doi:10.1348/000711200160688
Ireland, J. L., & Quinn, K. (2007). Officer attitudes towards adult male prisoners who self-harm:Development of an attitudinal measure and investigation of sex differences. AggressiveBehavior, 33, 63–72. doi:10.1002/ab.20168
Karasek, R. A. (1979). Job demands, job decision latitude, and mental strain: Implications for jobredesign. Administrative Science Quarterly, 24, 285–308. doi:10.2307/2392498
Kenning, C., Cooper, J., Short, V., Shaw, J., Abel, K., & Chew-Graham, C. (2010). Prison staffand women prisoner’s views on self-harm; their implications for service delivery anddevelopment: A qualitative study. Criminal Behaviour and Mental Health, 20, 274–284.doi:10.1002/cbm.777
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal and coping. New York, NY: Springer.Liebling, A., & Krarup, H. (1993). Suicide attempts and self-injury in male prisons: A report
commissioned by theHomeOfficeResearchandPlanningUnit for the Prison Service. London,UK: Home Office. ISBN: 1858930650.
Liebling, A., Tait, S., Durie, L., Stiles, A., & Harvey, J. (2005). An evaluation of the Safer LocalsProgramme: Final report. Cambridge,UK:Cambridge Institute ofCriminology, PrisonResearchCentre.
Mackay, N., & Barrowclough, C. (2005). Accident and emergency staff’s perceptions of deliberateself-harm: Attributions, emotions and willingness to help. British Journal of ClinicalPsychology, 44, 255–267. doi:10.1348/014466505X29620
Mackay, C., Cousins, R., Kelly, P. J., Lee, S., & McCaig, R. H. (2004). ‘Management standards’ andwork-related stress in the UK: Policy background and science. Work and Stress, 18, 91–112.doi:10.1080/02678370410001727474
Maden, A., Chamberlain, S., & Gunn, J. (2000). Deliberate self-harm in sentenced male prisoners inEngland andWales: Some ethnic factors.Criminal Behaviour andMentalHealth, 10, 199–204.doi:10.1002/cbm.357
Marzano, L., & Adler, J. (2007). Supporting staff working with prisoners who self-harm: A survey ofsupport services for staff dealing with self-harm in prisons in England and Wales. InternationalJournal of Prisoner Health, 3, 268–282. doi:10.1080/17449200701682501
Marzano, L., Ciclitira, K., & Adler, J. (2012). The impact of prison staff responses on self-harmingbehaviours: Prisoners’ perspectives. British Journal of Clinical Psychology, 51, 4–18. doi:10.1111/j.2044-8260.2010.02007.x
Maslach, C.,& Jackson, S. E. (1986).Maslachburnout inventory (2nded.). PaloAlto, CA:ConsultingPsychologists Press.
McAllister, M., Creedy, D., Moyle, W., & Farrugia, C. (2002). Nurses’ attitudes towards clients whoself-harm. Journal of Advanced Nursing, 40, 578–586. doi:10.1046/j.1365-2648.2002.02412.x
Prison staff experiences of prisoner self-harm 13
Ministry of Justice. (2013). Safety in custody statistics. Quarterly update to September 2012-England and Wales. London, UK: Ministry of Justice.
NICE. (2004). Self-harm – The short termphysical and psychologicalmanagement and secondaryprevention of self-harm in primary and secondary care. London, UK: National Institute forClinical Excellence.
Pannell, J., Howells, K., & Day, A. (2003). Prison officers’ beliefs regarding self-harm in prisoners: anempirical investigation. International Journal of Forensic Psychology, 1, 103–110. Retrievedfrom http://tle.tafevc.com.au/toolbox/file/ee24706c-8648-e4fe-feac-7f2408aeab03/1/701_c3_task32617.zip/docs/pris_officers_beliefs_re_self_harm.pdf
Paton, J., Harrison,M., & Jenkins, R. (2000). TrainingNeeds of PrisonOfficers in relation toMentalHealth and Personality Disorders. Report to Prison Service. Unpublished.
Petersen, C., Maier, S. F., & Seligman, M. E. P. (1995). Learned helplessness: A theory for the age of
personal control. Oxford, UK: Oxford University Press.Ramon, S. (1980). Attitudes of doctors and nurses to self-poisoning patients. Social Science and
Medicine, 14, 317–324. doi:10.1016/S0271-7123(80)90248-5Rayner, G. C., Allen, S. L., & Johnson, M. (2005). Countertransference and self-injury: A cognitive
behavioural cycle. Journal of Advanced Nursing, 50, 12–19. doi:10.1111/j.1365-2648.2005.03344.x
Royal College of Psychiatrists. (2006). Better services for people who self-harm: Quality standardsfor healthcare professionals. London, UK: Royal College of Psychiatrists Centre for QualityImprovement.
Schaufeli, W. B., & Peeters, M. C. W. (2000). Job stress and burnout among correctional officers: Aliterature review. International Journal of Stress Management, 7, 19–48. doi:10.1023/A:1009514731657
Shaw, C., & Shaw, T. (2007). A dialogue of hope and survival. In H. Spandler & S. Warner (Eds.),Beyond fear and control: Working with young people who self-harm (pp. 25–36).Ross-on-Wye, UK: PCCS Books.
Short, V., Cooper, J., Shaw, J., Kenning, C., Abel, K., & Chew-Graham, C. (2009). Custody vs care:attitudes of prison staff to self-harm in women prisoners – A qualitative study. Journal ofForensic Psychiatry & Psychology, 20, 408–426. doi:10.1080/14789940802377114
Snow, L. (1997). A pilot study of self-injury amongst women prisoners. Issues in Criminological &
Legal Psychology, 28, 50–59.Stanley, B., & Standen, P. J. (2000). Carers’ attributions for challenging behaviour.British Journal of
Clinical Psychology, 39, 157–168. doi:10.1348/014466500163185Taylor, T. L., Hawton, K., Fortune, S., & Kapur, N. (2009). Attitudes towards clinical services among
people who self-harm: Systematic review. British Journal of Psychiatry, 194, 104–110. doi:10.1192/bjp.bp.107.046425
Towl, G., & Forbes, D. (2002). Working with suicidal prisoners. In G. Towl, L. Snow & M. McHugh(Eds.), Suicide in prison (pp. 93–101). Oxford, UK: BPS Blackwell.
Triplett, R., Mullings, J. L., & Scarborough, K. E. (1996). Work-related stress and coping amongcorrectional officers: implications from organizational literature. Journal of Criminal Justice,24, 291–308. doi:10.1016/0047-2352(96)00018-9
Walsh, L. (2005). Developing prison health care through reflective practice. In C. Johns & D.Freshwater (Eds.), Transforming nursing through reflective practice (2nd ed., pp. 65–84).London, UK: Blackwell Publishing Ltd..
Watson, R., Stimpson, A., & Hostick, T. (2004). Prison health care: a review of the literature.International Journal of Nursing Studies, 41, 119–128. doi:10.1016/S0020-7489(03)00128-7
Weiner, B. (1986). An attributional theory of motivation and emotion. New York, NY:Springer-Verlag.
Weiskopf, C. S. (2005). Nurses’ experience of caring for inmate patients. Journal of AdvancedNursing, 49, 336–343. doi:10.1111/j.1365-2648.2004.03297.x
Received 23 August 2012; revised version received 26 June 2013
14 Lisa Marzano et al.
Top Related
Copyright © 2022 FDOKUMEN

